
Parents’ Reactions to Youths’ Hyperactivity, Impulsivity, and Attention Problems
Upload
independentCategory
view
4download
0
COMPREHENSIVE REVIEW
Impulsivity as a predictor of treatment outcome in substance usedisorders: Review and synthesis
AMY M. LOREE, LESLIE H. LUNDAHL & DAVID M. LEDGERWOOD
Department of Psychiatry and Behavioral Neurosciences, Wayne State University School of Medicine, Detroit, USA
AbstractIssues. Impulsivity is a widely studied personality trait and research construct that has been implicated as a risk factor forsubstance use, including initiating and continuing use. However, relatively few studies have examined impulsivity as a predictorof treatment outcome. Because impulsivity has been operationalised in many different ways, cross-comparisons of empiricalstudies have been difficult. Approach. The PubMed database was searched in September 2013. Reference lists of papersretrieved from this search were also manually scanned for additional resources. Studies were included if they presented data thatassessed impulsivity as a predictor of treatment outcomes. Key Findings. The body of literature reviewed in this paper suggeststhat higher pretreatment impulsivity, regardless of how it is measured, usually is associated with poorer treatment outcomes.Recent data indicate that some psychosocial and pharmacological treatments may directly impact impulsivity and thus representan interesting avenue for further research. Conclusions. Impulsivity appears to be a key predictor of substance use treatmentoutcomes and warrants more attention in the improvement of treatment outcomes. Suggestions for future research on the role ofimpulsivity in substance use treatment are provided. [Amy M. Loree AM, Leslie H. Lundahl LH, David M. LedgerwoodDM. Impulsivity as a predictor of treatment outcome in substance use disorders: Review and synthesis. Drug AlcoholRev 2014]
Key words: impulsivity, personality, relapse, substance use, treatment.
Introduction
Impulsivity, as a personality trait, is broadly defined asa tendency to act without adequate forethought [1],but as a research construct, impulsivity has beenoperationalised in many different ways. Impulsivitymeasures include primary measures of inattention,response inhibition, delay discounting, risk-taking, sen-sation seeking and others. Despite the multifacetednature of impulsivity, several studies have demonstratedthat substance use disorders are strongly associatedwith elevated impulsivity scores on various measures[2–4]. Furthermore, several studies have revealed thatimpulsivity may be an important variable in predictingtreatment outcomes and relapse risk (e.g. [5–8]).
However, there are many gaps in our understandingof the relationship between impulsivity and recovery
from substance use disorders. Thus, in this review ourmain aims are to: (i) describe the current research onimpulsivity as a predictor of treatment outcomes andrelapse; (ii) identify the important gaps in the empiricalliterature; and (iii) provide suggestions for futureresearch to address these gaps. To accomplish theseaims, we also provide a brief overview of the generalresearch on impulsivity in substance use disorders.
Operationalisation of impulsivity
The use of the term ‘impulsive’ to describe an indivi-dual’s tendency to be moved to action through emotionor sudden impulse dates back at least to the mid-1800s[9]. Since that time, the concept of impulsivity as apersonality trait has received a tremendous amountof study. Examination of the PsycInfo database, for
Amy M. Loree MA, Leslie H. Lundahl PhD., David M. Ledgerwood PhD., Correspondence to Dr David Ledgerwood, Department of Psychiatryand Behavioral Neurosciences, Wayne State University School of Medicine, 3901 Chrysler Drive, Suite 2A, Detroit, MI 48201, USA. Tel: +313993 1380; Fax: +313 993 1372; E-mail. [email protected]
Received 27 August 2013; accepted for publication 9 February 2014.
bs_bs_banner
R E V I E W
Drug and Alcohol Review (2014)DOI: 10.1111/dar.12132
© 2014 Australasian Professional Society on Alcohol and other Drugs

example, finds the terms impulsive, impulsiveness orimpulsivity have been mentioned in over 15 000 publi-cations [10].
Perhaps because of its long history of use, impulsivityas a trait has been operationalised in myriad ways, withmost studies utilising self-report measures of impulsiv-ity. Some of the more frequently used self-report meas-ures include the Barratt Impulsiveness Scale [11,12],Eysenck’s Impulsiveness Scale [13] and the UPPSImpulsive Behavior Scale [14]. Furthermore, impulsiv-ity subscales are found in several more lengthy per-sonality assessments, such as the TridimensionalPersonality Questionnaire [15] and the NEO Personal-ity Inventory-Revise [16]. Individual self-report meas-ures have also been designed to assess different aspectsof impulsivity. For example, Barratt’s measure has beenfactor analysed to devise scales to assess attention,motor and non-planning aspects of impulsiveness [12].The UPPS, which was based on the Five Factor Modelof personality and derived from a handful of impulsivitymeasures via factor analysis, includes four distinct per-sonality facets: urgency, lack of premeditation, lack ofperseverance and sensation-seeking [14]. Other con-structs, such as rash impulsivity [17] and functionaland dysfunctional impulsivity, have also been examined[18]. Self-report measures also assess closely relatedconstructs, such as sensation seeking, which is a traitcharacterised by a need for novel, varied and complexexperiences that are often associated with significantrisk taking [19]. The lack of consistency across meas-ures purporting to assess impulsivity makes it difficultto directly compare the findings of these studies.
Although self-report measures are generally acceptedas valid instruments to assess impulsivity among manypopulations, they are not without limitations.The valid-ity of self-report measures is sometimes questionedbecause these assessments are subjective and may beinfluenced by distorted perceptions of one’s own traits[20].To this end, behaviourally based impulsivity meas-ures may better capture the different dimensions ofimpulsivity because they elicit impulsive behaviourrather than relying on individuals to accurately charac-terise their behaviours through self-report.
There are several task-based measures of impulsivity,including those that assess discounting of delayedrewards, behavioural response inhibition, attention andmemory, and decision making. Delay discounting isdefined as a tendency to discount larger, delayedrewards in favour of smaller, more immediate ones[21]. In a typical monetary discounting task, partici-pants are asked to choose between a smaller rewarddelivered immediately and a larger reward deliveredafter some period of delay. As the delay duration of areward increases, the subjective value of that rewarddecreases [22]. Impulsivity is considered to be a func-
tion of the rate at which a delayed larger reward isdiscounted with greater rate of discounting associatedwith greater impulsivity [22].
Several studies have found significant congruencebetween response inhibition tasks and scores on paperand pencil measures of impulsivity [23–26]. Responseinhibition tasks measure a participant’s ability to holdback responding when required by the rules of the taskand often after receiving a signal to respond. Moreimpulsive individuals have greater difficulty inhibiting aresponse when they are presented with a ‘stop’ signal,especially as the latency between the target stimulusand the ‘stop’ signal increases [26,27].
Attention and memory measures have also been usedto assess impulsivity. Similar measures that use atten-tion and working memory operationalise impulsivity asa deficit in one’s ability to withhold responding untilaccurate processing of environmental stimuli hasoccurred [28,29]. The continuous performance task isone of the most frequently used examples of attention/memory assessments of impulsivity and has demon-strated significant relationships with attention andinhibition difficulties observed in attention deficithyperactivity disorder [30].
Laboratory measures of decision making and risktaking are also relevant to the study of impulsivity. Themost commonly used decision-making task is the IowaGambling Task, which measures a participant’s abilityto maximise positive consequences and minimise nega-tive consequences of decisions based on feedback [31].Other decision-making tasks include the CambridgeGambling Task and the Risky Gains Task [32,33].Several measures, such as the balloon analogue risk task[34,35], are computer-based measures of risk takingthat are also correlated with self-report measures ofimpulsivity and sensation seeking.
As with self-report measures, laboratory-based beha-vioural assessments of impulsivity measure severaldifferent constructs (e.g. attention, risky behaviours,decision making). Furthermore, although some studieshave found that the interrelationship among thesemeasures is modest [3,20,36,37], others have foundsignificant overlap between self-report and laboratory-based behavioural measures [38]. Thus, the variousimpulsivity measures likely reflect distinct underlyingprocesses with no single measure fully capturing thismultidimensional construct. Therefore, researchersmay want to consider choosing both laboratory-basedbehavioural measures and self-report measures basedon their guiding theoretical framework.
Impulsivity research in substance use disorders
Impulsivity has been almost invariably linked to addic-tive diseases, including both substance use disorders
2 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

and behavioural addictions (e.g. pathological gam-bling). In this paper, we provide only a brief overview.For a thorough review of the relationship betweenimpulsivity and addictive disorders, we refer the readerto several recent sources [2–4]. Although causal pro-cesses remain unclear, it is likely that impulsivity inaddictive diseases includes a component of pre-existingtrait impulsivity that acts as a risk factor for the devel-opment of addiction, as well as a component that devel-ops or intensifies as a consequence of chronic drug use[38].
Compared with control participants, higher levelsof impulsivity have been found in individualswith regular stimulant, opiate, alcohol and 3,4-methylenedioxymethamphetamine use [3]. Severalstudies, for example, have found that substancedependence is associated with greater discountingof delayed rewards among individuals dependent onalcohol [39], cocaine [40,41], opiates [41,42] andmethamphetamine [43]. However, some studies havefound that discounting levels may vary by substance,with some substances, including marijuana, heroinand cocaine, being associated with greater impulsivitythan others [41,44].
Studies examining self-report and response inhibi-tion measures of impulsivity have found similar results.Self-reported impulsivity has been found to be elevatedamong alcohol [45], cocaine [46], opiate [47] andcannabis-dependent [44] individuals. Finn et al. foundthat response inhibition was associated with impulsivitymeasures in participants with early onset alcoholismand conduct disorder [24]. Another investigationobserved response inhibition deficits in chronic meth-amphetamine users who were abstinent for 5–7 days[48]. A study using a laboratory decision-making taskalso found impaired performance among drug abusersrelative to controls [49].
Overall, higher levels of impulsivity are associatedwith substance use disorder severity across various sub-stances of abuse. For example, impulsivity is associatedwith greater self-reported quantity of cocaine use andmore severe withdrawal symptoms among cocaine-dependent individuals [8]. Recent attention has alsofocused on the relationship between impulsivity andcraving, with evidence suggesting that self-reportedimpulsivity is associated with craving among individ-uals dependent on alcohol [50,51], cocaine [52,53] andmethamphetamine [53]. Furthermore, abuse of morethan one substance is associated with greater impulsiv-ity than is abuse of a single substance [54].
Impulsivity has also been shown to be elevatedamong tobacco users. Current smokers have beenshown to discount delayed monetary rewards at signifi-cantly higher rates than never smokers and ex-smokers[55]. Indeed, a review of the smoking literature suggests
that choice measures (such as delay discounting) maymore consistently distinguish smokers from non-smokers than response inhibition measures of impul-sivity [56]. Furthermore, nicotine deprivation amongsmokers appears to increase the frequency with whichsmokers will discount delayed choices [57]. Thus,increasing withdrawal may increase impulsive decisionmaking. Impulsivity may also be positively related tosensitivity to the rewarding aspects of nicotine in non-smokers, particularly among men [58].
In summary, most studies have found that impulsiv-ity is elevated among people with addictions, regardlessof whether self-report, delay discounting, responseinhibition or other behavioural measures are used.Furthermore, some have suggested that high levels ofimpulsivity precede the development of substance usedisorders [3,56]. Therefore, impulsivity may be acommon risk factor for substance use disorders.
Treatment outcomes
Studies that examine putative pretreatment predictorsof treatment outcomes are important because they canultimately inform both the treatment type and magni-tude needed for success [59]. Below, we review studiesthat have examined impulsivity as a putative predictorof treatment outcomes among substance-abusingpopulations.
Search strategy
A comprehensive literature search was conducted onthe PubMed database for the period of 1950 to Sep-tember 2013. Key search terms were: impulsivity,impulsiveness, novelty seeking, sensation seeking, delaydiscounting and disinhibition each in combination withthe key words nicotine, tobacco, smoking, opiate,opioid, heroin, cocaine, marijuana, amphetamine andalcohol, as well as treatment terms treatment outcomeand relapse. Abstracts produced from the databasesearch were examined, and those that presented dataassessing impulsivity as a predictor of treatment out-comes were reviewed. Additional articles that were notidentified through the database search were retrievedfrom reference lists of relevant articles.
Results
According to the above criteria, a search of PubMedreturned 1828 results, of which 33 papers examiningimpulsivity as a predictor of substance use treatmentoutcomes were identified. Year of publication rangedfrom 1997 to 2012. Although studies prior to 1997examined impulsivity and substance use, prior to thisyear, no published studies appeared to directly address
Impulsivity in substance use treatment 3
© 2014 Australasian Professional Society on Alcohol and other Drugs

impulsivity as a predictor of treatment outcome. Acomprehensive list of the relevant studies for each sub-stance is presented in Tables 1–5. The studies arereviewed below, and the consistencies between them aresummarised in the section that follows.
Impulsivity as a Predictor of Substance AbuseTreatment Outcomes
In this review, we cover studies that examine pretreat-ment assessments of impulsivity as predictors of treat-ment outcomes for nicotine, marijuana, cocaine,alcohol and opioid use disorders; no studies were iden-tified for amphetamine treatment.
Nicotine studies. Fifty per cent of the studies to dateexamined nicotine dependence and the relationshipbetween impulsivity and cessation rates or relapseamong cigarette smokers. Doran et al. found that traitimpulsivity, measured using the Barratt ImpulsivenessScale (BIS-11) prior to participation in a clinical trialfor smoking cessation, predicted more rapid relapsefollowing a 48-h abstinence period [6]. Impulsivityremained a significant predictor even after controllingfor treatment condition, participant age and level ofnicotine dependence. Furthermore, negative affect,positive affect and tobacco craving did not mediate therelationship between impulsivity and relapse rate.
Krishnan-Sarin et al. examined four impulsivitymeasures (BIS-11, Kirby Delay Discounting Measure,Experiential Discounting Task and Conners’ Continu-ous Performance Task) as possible predictors ofsmoking outcomes among adolescents in a cessationprogramme [64]. At post-treatment, non-abstinent par-ticipants (n = 14) discounted more significantly on theExperiential Discounting Task and had fewer commis-sion errors on the Continuous Performance Task thandid the smoking abstinent adolescents (n = 16). Theother two impulsivity measures did not distinguishgroups. In a study utilising both self-report measuresand laboratory tasks, Sheffer et al. found that delaydiscounting and cognitive impulsivity (as measured bythe BIS-11) predicted relapse among a group of lowersocioeconomic status smokers [69].
Another study examined smoking cessation amongadolescents randomly assigned to a one-session moti-vational enhancement condition or a control tobaccopsychoeducation session [63]. Although these authorsdid not find significant differences between their twointerventions, they did find differential treatmentresponse based on impulsivity. Participants with higherlevels of impulsivity reported greater reduction in self-reported smoking in the tobacco education controlcondition than in the motivational session, whereasparticipants with lower levels of impulsivity experi-
enced the opposite effect. Thus, in some cases, impul-sivity may mediate the relationship between treatmenttype and outcome.
Rukstalis et al. examined whether increases in inatten-tion and hyperactive-impulsive attention deficit disordersymptoms during the first week of nicotine replacementtreatment predicted relapse at the end of eight weeks oftreatment [68]. End of treatment abstinence rates were41% for participants who reported either no change or adecline in their inattention and hyperactive-impulsivesymptoms, compared with 29% among those whoreported an increase in these symptoms.
A handful of other studies have examined delay dis-counting as a predictor of outcome among smokers.One study examined delay discounting rates as a pre-dictor of relapse in heavy drinking smokers who wereparticipating in a clinical trial to examine combinedbrief smoking cessation and alcohol use interventions[65]. Using survival analysis, the authors found thatgreater rates of discounting delayed dollar amountswere associated with shorter time to smoking lapse.Sensation seeking, level of nicotine dependence,income and treatment condition were then enteredalong with discounting value into a regression model.Lower rates of discounting were found for participantsabstinent at 2- and 8-weeks post-quit date but not for16- and 26-weeks after the quit date.
Yoon et al. examined whether baseline delay dis-counting predicted post-partum relapse among preg-nant smokers enrolled in a clinical trial of contingencymanagement versus non-contingent reinforcement whohad spontaneously quit smoking upon learning of theirpregnancy [70].Women who continued to abstain fromsmoking discounted delayed rewards at significantlylower rates than those who had relapsed to smoking atthe 24-week post-partum assessment. This study dif-fered from past ones in that: (i) the 24-week period wasapproximately a year after initial baseline assessment;and (ii) repeated measurements of delay discountingrevealed that this value is relatively stable across time.Thus, this study shows that delay discounting may be aparticularly robust predictor of long-term abstinence.
Two laboratory studies have also examined impulsiv-ity as a predictor of smoking relapse. In one, Powellet al. examined impulsivity, inhibitory control and cuereactivity measures as predictors of relapse to smokingduring a pharmacologically unaided quit attempt [67].Behavioural measures of behavioural-response inhibi-tion, including the Stroop interference test, anantisaccade task and the continuous performance task(as a measure of motor impulsivity) predicted relapseafter one week. Self-report measures (which includedthe Impulsivity, Venturesomeness and Empathy Ques-tionnaire,TPQ Novelty Seeking and Sensation SeekingScales) did not predict relapse. At 1- and 3-months
4 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

Tab
le1.
Nic
otin
est
udie
s
Aut
hors
Sub
stan
ceR
esea
rch
desi
gnS
ampl
esi
zean
dfo
llow
-up
Impu
lsiv
ity
mea
sure
sF
indi
ngs
Car
lton
etal
.[6
0]N
icot
ine
Cor
rela
tion
al25
smok
ers
part
icip
atin
gin
an12
0-da
yop
entr
ial
for
nico
tine
repl
acem
ent
ther
apy
SS
S(F
renc
hve
rsio
n)S
ensa
tion
seek
ing
did
not
pred
ict
smok
ing
cess
atio
n.
Dal
lery
&R
aiff
[61]
Nic
otin
eR
ando
mis
edco
ntro
lled
tria
l,la
bora
tory
anal
ogue
stud
y
30sm
oker
sw
ith
noin
tent
ion
toqu
it;
nofo
llow
-up
DD
TL
owan
dhi
ghco
ntin
genc
yco
ndit
ions
incr
ease
dla
tenc
yto
smok
ing,
but
nico
tine
patc
hdi
dno
t.In
divi
dual
sw
hosm
oked
duri
ngth
eco
ntin
genc
yco
ndit
ions
disp
laye
dhi
gher
rate
sof
disc
ount
ing.
Dor
anet
al.
[6]
Nic
otin
eR
ando
mis
edco
ntro
lled
tria
l45
regu
lar
smok
ers
wit
ha
hist
ory
ofm
ajor
depr
essi
on;
follo
w-u
p4
wee
ksaf
ter
base
line
BIS
-11
Ele
vate
dim
puls
ivit
ypr
edic
ted
shor
ter
tim
eto
rela
pse
follo
win
ga
skill
str
aini
ngw
orks
hop,
afte
rco
ntro
lling
for
trea
tmen
tco
ndit
ion,
base
line
nico
tine
depe
nden
cean
dag
e.R
elat
ions
hip
betw
een
impu
lsiv
ity
and
rapi
dre
laps
eco
uld
not
beex
plai
ned
bypo
siti
veor
nega
tive
affe
ct,
orcr
avin
g.H
all
etal
.[6
2]N
icot
ine
Pro
spec
tive
coho
rtde
sign
8845
adul
tsm
oker
sfr
omA
ustr
alia
,C
anad
a,U
nite
dK
ingd
om,
and
the
US
A;
follo
w-u
p8
mon
ths
late
r
4it
ems:
‘You
like
toex
plor
est
rang
epl
aces
;’‘Y
oulik
eto
doth
rilli
ngth
ings
;’‘Y
oulik
ene
wan
dex
citi
ngex
peri
ence
s,ev
enif
you
have
tobr
eak
the
rule
s;’‘
You
like
tobe
wit
hfr
iend
sw
hoar
eex
citi
ngan
dun
pred
icta
ble.
’
Sen
sati
onse
ekin
gdi
dno
tpr
edic
tqu
itat
tem
pts
orfa
ctor
skn
own
toen
hanc
equ
itti
ng,
such
asst
reng
thof
quit
inte
ntio
n,pe
rcei
ved
bene
fits
ofqu
itti
ng,
orhe
alth
-rel
ated
smok
ing
conc
erns
.
Hel
stro
met
al.
[63]
Nic
otin
eR
ando
mis
edco
ntro
lled
tria
l81
adju
dica
ted
adol
esce
ntsm
oker
s;fo
llow
-up
at1
and
6m
onth
spo
st-t
reat
men
t
ImpS
SP
arti
cipa
nts
wit
hlo
wer
leve
lsof
alco
hol
use
and
impu
lsiv
ity
had
asi
gnifi
cant
lygr
eate
rre
spon
seto
mot
ivat
iona
len
hanc
emen
tth
erap
y,w
here
aspa
rtic
ipan
tsw
ith
high
erra
tes
ofal
coho
lus
ean
dim
puls
ivit
yre
spon
ded
bett
erto
the
toba
cco
educ
atio
nco
ntro
l.K
rish
nan-
Sar
inet
al.
[64]
Nic
otin
eC
orre
lati
onal
32ad
oles
cent
smok
ers;
follo
w-u
pat
four
thw
eek
ofst
udy.
BIS
-11,
DD
M,
ED
T,
CP
TC
ompa
red
wit
had
oles
cent
sw
hore
mai
ned
abst
inen
tat
the
end
ofth
e4-
wee
kst
udy,
thos
eno
tac
hiev
ing
abst
inen
cedi
scou
nted
mor
em
onet
ary
rew
ards
onth
eE
DT
and
mad
em
ore
com
mis
sion
erro
rson
the
CP
T;
nogr
oup
diff
eren
ces
obse
rved
onth
eB
IS-I
Ior
DD
M.
Mac
Kill
op&
Kah
ler
[65]
Nic
otin
eR
ando
mis
edco
ntro
lled
smok
ing
cess
atio
ntr
ial
57tr
eatm
ent-
seek
ing
smok
ers;
follo
w-u
p2,
8,16
and
26w
eeks
post
-tre
atm
ent
MC
Q,
SS
S-B
Del
ayed
rew
ard
disc
ount
ing
pred
icte
dda
ysto
rela
pse
beyo
ndni
coti
nede
pend
ence
,se
nsat
ion-
seek
ing
and
inco
me.
Nie
vaet
al.
[66]
Nic
otin
eC
orre
lati
onal
103
smok
ers
part
icip
atin
gin
aw
orkp
lace
cess
atio
npr
ogra
mm
e;fo
llow
-up
at12
mon
ths.
ImpS
SH
igh
leve
lsof
impu
lsiv
ity
pred
icte
dre
laps
ein
mal
es,
but
not
fem
ales
.
Pow
ell
etal
.[6
7]N
icot
ine
Sin
gle
grou
p,pr
e-po
stde
sign
141
smok
ers;
follo
w-u
pat
1w
eek,
1m
onth
and
3m
onth
spo
st-q
uit
date
SS
S,T
PQ
-NS
,I7
-Im
p,S
troo
p,A
ntis
acca
deta
sk,
CP
T
At
the
1-w
eek
follo
w-u
p,ab
stin
ence
was
pred
icte
dby
saliv
ary
coti
nine
,at
tent
iona
lbi
asto
smok
ing
cues
,an
dan
tisa
ccad
eer
rors
.A
tth
e1-
and
3-m
onth
follo
w-u
ps,
saliv
ary
coti
nine
,C
PT
mot
orim
puls
ivit
y,an
dcu
ere
acti
vity
indi
vidu
ally
pred
icte
dab
stin
ence
.N
one
ofth
ese
lf-r
epor
tim
puls
ivit
ym
easu
res
pred
icte
dre
laps
e.R
ukst
alis
etal
.[6
8]N
icot
ine
Ran
dom
ised
smok
ing
cess
atio
ntr
ial
454
smok
ers;
follo
w-u
pat
8w
eeks
post
-qui
tda
teC
SS
Ear
lyin
crea
ses
inin
atte
ntio
nan
dhy
pera
ctiv
e-im
puls
ive
sym
ptom
sdu
ring
nico
tine
repl
acem
ent
ther
apy
pred
icte
dsm
okin
gre
laps
e.S
heff
eret
al.
[69]
Nic
otin
eC
orre
lati
onal
97ni
coti
ne-d
epen
dent
part
icip
ants
;fo
llow
-up
at4,
8,12
and
28w
eeks
afte
rta
rget
quit
date
BA
RT
,B
IS-1
1,3
DD
Ts,
I7,
Go/
No-
Go
Tas
kT
hree
mea
sure
sof
dela
ydi
scou
ntin
gpr
edic
ted
abst
inen
ce,
such
that
thos
ew
hodi
scou
nted
mor
est
eepl
yw
ere
less
likel
yto
beab
stin
ent.
Gre
ater
impu
lsiv
enes
son
the
BIS
-11
cogn
itiv
eim
puls
iven
ess
scal
eal
sopr
edic
ted
redu
ced
likel
ihoo
dof
abst
inen
ce.
Yoo
net
al.
[70]
Nic
otin
eR
ando
mis
edco
ntro
lled
tria
l48
preg
nant
wom
en;
follo
w-u
pat
24w
eeks
post
-par
tum
DD
TB
asel
ine
dela
ydi
scou
ntin
gpr
edic
ted
smok
ing
stat
usat
24w
eeks
post
-par
tum
Not
e:B
AR
T,B
allo
onA
nalo
gue
Ris
kT
ask
[34,
35];
BIS
-11,
Bar
ratt
Impu
lsiv
enes
sS
cale
[11,
12];
CS
S,C
urre
ntS
ympt
oms
Sca
le[7
1];D
DT
,Del
ayD
isco
unti
ngT
ask;
ED
T,E
xper
ient
ialD
isco
unti
ngT
ask
[72]
;Im
puls
ivit
y,V
entu
reso
men
ess,
and
Em
path
yqu
esti
onna
ire
[74]
;I7-
Imp,
Impu
lsiv
ity
scal
efr
omth
eIm
puls
ivit
y,V
entu
reso
men
ess,
and
Em
path
yqu
esti
onna
ire
[74]
;Im
pSS
,Im
puls
ivit
y/S
ensa
tion
See
king
Sca
le[7
5];D
DM
,Kir
byD
elay
Dis
coun
ting
Mea
sure
[42]
;M
CQ
,M
onet
ary
Cho
ice
Que
stio
nnai
re[4
2];
SS
S,
Sen
sati
onS
eeki
ngS
cale
[76]
;S
SS
-B,
Sen
sati
onS
eeki
ngS
cale
-Bri
ef[7
7].
Impulsivity in substance use treatment 5
© 2014 Australasian Professional Society on Alcohol and other Drugs
Tab
le2.
Alc
ohol
stud
ies
Aut
hors
Sub
stan
ceR
esea
rch
desi
gnS
ampl
esi
zean
dfo
llow
-up
Impu
lsiv
ity
mea
sure
sF
indi
ngs
Cha
rney
etal
.[5
]A
lcoh
olC
orre
lati
onal
175
pati
ents
wit
hal
coho
lus
edi
sord
ers
ente
ring
trea
tmen
t;fo
llow
-up
at12
wee
ksin
totr
eatm
ent
BIS
-11
Tho
sew
hore
laps
edw
ere
mor
elik
ely
toha
vea
high
erle
vel
ofim
puls
ivit
y(B
ISco
gnit
ive
subs
cale
),in
addi
tion
toC
lust
erB
pers
onal
ity
diso
rder
diag
nose
s,an
dm
ore
seve
reso
cial
prob
lem
sat
inta
ke.
Evr
enet
al.
[50]
Alc
ohol
Cor
rela
tion
al10
2m
ale
alco
hol-
depe
nden
tpa
tien
tsin
terv
iew
ed12
mon
ths
afte
rdi
scha
rge
BIS
-11,
TC
I-N
SA
mon
gth
ose
who
rela
psed
,m
ean
scor
eson
BIS
-11
and
nove
lty
seek
ing
subs
cale
sof
the
TC
Iw
ere
high
erco
mpa
red
wit
hth
eno
n-re
laps
edgr
oup.
BIS
-11
non-
plan
ning
and
nove
lty-
seek
ing
fact
ors
(exp
lora
tory
exci
tabi
lity
and
extr
avag
ance
)w
ere
also
sign
ifica
ntly
rela
ted
tocr
avin
g.E
win
get
al.
[78]
Alc
ohol
Ran
dom
ised
cont
rolle
dtr
ial
67em
ergi
ngad
ult
prob
lem
drin
kers
;fo
llow
-up
30da
ysaf
ter
inte
rven
tion
TP
Q-N
S,
ImpS
SP
arti
cipa
nts
low
inim
puls
ivit
yan
dno
velt
yse
ekin
gex
hibi
ted
grea
ter
beha
viou
rch
ange
,as
evid
ence
dby
taki
ngst
eps
tow
ards
redu
cing
drin
king
,fo
llow
mot
ivat
iona
len
hanc
emen
tth
erap
y.Jo
oset
al.
[103
]A
lcoh
olR
ando
mis
ed,
doub
le-b
lind,
plac
ebo-
cont
rolle
dtr
ial
83al
coho
l-de
pend
ent
pati
ents
;fo
llow
-up
3an
d6
mon
ths
post
-tre
atm
ent
BIS
-11,
Sta
teIm
puls
ivit
yQ
uest
ionn
aire
,S
ST
,D
DT
Mod
afini
lsi
gnifi
cant
lyim
prov
edsc
ores
onse
lf-r
epor
tm
easu
res
ofim
puls
ivit
y,bu
tha
dno
effe
cton
beha
viou
ral
mea
sure
sof
impu
lsiv
ity.
Mod
afina
lal
soha
dno
over
all
effe
cton
drin
king
outc
omes
(per
cent
age
ofab
stin
ent
days
,pe
rcen
tage
ofhe
avy
drin
king
days
).A
mon
gth
ose
wit
hpo
orre
spon
sein
hibi
tion
atba
selin
e,m
odafi
nil
prol
onge
dti
me
tore
laps
ean
dte
nded
toin
crea
sepe
rcen
tage
ofab
stin
ent
days
;ho
wev
er,
amon
gth
ose
wit
hbe
tter
resp
onse
inhi
biti
onat
base
line,
mod
afini
lre
duce
dpe
rcen
tage
ofab
stin
ent
days
and
incr
ease
dpe
rcen
tage
ofhe
avy
drin
king
days
.K
ravi
tzet
al.
[79]
Alc
ohol
Ran
dom
ised
,do
uble
-blin
d,pl
aceb
o-co
ntro
lled
tria
l17
0al
coho
l-de
pend
ent
men
;fo
llow
-up
6m
onth
spo
st-b
asel
ine
TP
Q-N
SD
ropo
uts
had
sign
ifica
ntly
high
erno
velt
y-se
ekin
gsc
ores
.H
ighe
rno
velt
yse
ekin
gw
asal
soas
soci
ated
wit
hin
crea
sed
risk
ofdr
oppi
ngou
tan
dea
rlie
rdr
opou
t.M
esza
ros
etal
.[8
0]A
lcoh
olR
ando
mis
edco
ntro
lled
tria
l52
1de
toxi
fied,
alco
hol-
depe
nden
tpa
tien
ts;
follo
w-u
pat
2,4,
6,8,
12,
16,
24,
32,
40an
d52
wee
ksaf
ter
base
line.
TP
QN
ovel
tyse
ekin
gw
asa
stro
ngpr
edic
tor
ofre
laps
efo
rm
ales
but
not
fem
ales
.
Mul
ler
etal
.[8
1]A
lcoh
olC
orre
lati
onal
146
alco
hol-
depe
nden
tpa
tien
ts;
follo
w-u
p12
mon
ths
afte
rtr
eatm
ent
disc
harg
e
NE
O-F
FI,
TC
I,E
PQ
,IV
E,
SS
SIn
addi
tion
tohi
ghsc
ores
onps
ycho
tici
sm,
low
scor
eson
pers
iste
nce
wer
esi
gnifi
cant
lyre
late
dto
risk
ofre
laps
e.H
igh
scor
eson
nove
lty
seek
ing
and
impu
lsiv
enes
sal
sosi
gnifi
cant
lydi
ffer
enti
ated
rela
psed
vers
usab
stin
ent
pati
ents
at12
-mon
ths
post
-tre
atm
ent.
Rub
ioet
al.
[82]
Alc
ohol
Ran
dom
ised
cont
rolle
dtr
ial
63m
ales
wit
hal
coho
lde
pend
ence
rand
omis
edto
rece
ive
topi
ram
ate
orpl
aceb
o;fo
llow
-up
at12
wee
kspo
st-b
asel
ine
CP
T,
BIS
-11,
SS
T,
DR
LR
Pat
ient
sw
hore
ceiv
edto
pira
mat
ere
port
edlo
wer
rate
sof
alco
hol
cons
umpt
ion,
decr
ease
dcr
avin
gan
dex
hibi
ted
impr
oved
perf
orm
ance
onth
eC
PT
and
SS
T.T
opir
amat
ere
duce
ddr
inki
ng,
perh
aps
via
mod
ulat
ion
ofbe
havi
oura
lin
hibi
tion
.
Sel
lman
etal
.[8
3]A
lcoh
olC
orre
lati
onal
87al
coho
l-de
pend
ent
men
wit
han
tiso
cial
pers
onal
ity
diso
rder
part
icip
atin
gin
am
ulti
mod
alth
erap
euti
cpr
ogra
mm
e;fo
llow
-up
for
6m
onth
s.
TP
QN
ovel
tyse
ekin
gw
asno
tas
soci
ated
wit
hre
laps
e.
BIS
-11,
Bar
ratt
Impu
lsiv
enes
sS
cale
[11,
12];
CP
T,
Con
tinu
ous
Per
form
ance
Tas
k;D
DT
,D
elay
disc
ount
ing
task
;D
RL
R,
Diff
eren
tial
rein
forc
emen
tof
low
-rat
ere
spon
ding
;E
PQ
,E
ysen
ckP
erso
nalit
yQ
uest
ionn
aire
[84]
;I7
,Im
puls
ivit
y,V
entu
reso
men
ess,
and
Em
path
yqu
esti
onna
ire
[74]
;Im
pSS
,Im
puls
ivit
y/S
ensa
tion
See
king
Sca
le[7
5];
NE
O-F
FI,
NE
OF
ive
Fac
tor
Inve
ntor
y[1
6];
SS
S,
Sen
sati
onS
eeki
ngS
cale
[76]
;S
ST
,S
top-
sign
alT
ask;
TC
I,T
empe
ram
ent
and
Cha
ract
erIn
vent
ory
[85]
;TC
I-N
S,
nove
lty
seek
ing
dim
ensi
onof
TC
I[8
5];T
PQ
,Tri
dim
ensi
onal
Per
sona
lity
Que
stio
nnai
re[1
5].
6 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

follow-up, only the continuous performance task waspredictive among the impulse control tasks.
In the other laboratory study, Dallery and Raiff con-ducted an analogue study of delayed discounting as apredictor of relapse in smokers who had no intention ofquitting [61]. Specifically, they assessed the relationshipbetween delay discounting and return to smoking fol-lowing a period of nicotine deprivation. They alsoassessed the effects of monetary contingency and nico-tine patch on time to ‘relapse’. Contingency conditions(both a high $20 and low $5 magnitude) increasedlatency to smoking but assignment to active (vs.placebo) nicotine patch did not. Furthermore, regard-less of group assignment, individuals who discountedmonetary rewards at a greater rate at baseline weremore likely to return to smoking.
Similar to the finding by Powell et al. [67] that sen-sation seeking did not predict relapse, several studieshave also failed to find an association between self-reported sensation seeking and treatment outcome[62,66,97]. In testing an alternative five-factor model ofpersonality applied to nicotine dependence, Nieva et al.found that gender moderated the relationship betweenimpulsivity and smoking relapse. Among a sample ofsmokers receiving combination cognitive behaviouraltherapy and medication (nicotine replacement therapy,bupropion or varenicline) as part of a workplacesmoking cessation programme, high-levels of sensationseeking assessed by the Zuckerman-Kuhlman Person-ality Questionnaire predicted relapse but only in males[66]. Another open trial study of transdermal nicotinepatches failed to find an association between sensationseeking and smoking cessation [60]. Finally, in Hallet al.’s longitudinal cohort study of adult smokers inAustralia, Canada, United Kingdom and the USA, sen-sation seeking was not a significant predictor of quitattempts or factors that have been shown to enhancequitting, including quit intention, perceived benefitsof quitting and perceived health risks to smoking.Notably, however, this survey study utilised four Likertscale items to assess sensation seeking (e.g. ‘You like toexplore strange places,’You like to do thrilling things‘)that had not undergoing rigorous validation studies[62].
Alcohol studies. Impulsivity has been linked to earlyinitiation of alcohol use as well as increased risk ofmisuse later in life [98,99]. Higher levels of self-reported impulsivity also have been linked to earlier ageof onset of alcohol-related negative consequences[100,101], and this finding itself has been found to bea robust predictor of later alcohol dependence severity[102]. Despite the clear role that impulsivity plays inalcohol use and misuse, very few studies have examinedits impact on alcohol treatment outcome.
Tab
le3.
Mar
ijuan
ast
udie
s
Aut
hors
Sub
stan
ceR
esea
rch
desi
gnS
ampl
esi
zean
dfo
llow
-up
Impu
lsiv
ity
mea
sure
sF
indi
ngs
Car
pent
eret
al.
[86]
Mar
ijuan
aC
orre
lati
onal
25m
ariju
ana-
depe
nden
tpa
rtic
ipan
ts;
follo
w-u
pva
ried
acco
rdin
gto
indi
vidu
altr
eatm
ent
com
plet
ion
Mod
ified
Str
oop
Tas
kC
ocai
ne-
and
hero
in-r
elat
edst
imul
iin
terf
eren
cesc
ores
wer
eas
soci
ated
wit
ha
sign
ifica
ntly
grea
ter
prop
orti
onof
mar
ijuan
apo
siti
veur
ine
drug
scre
ens
and
asi
gnifi
cant
lylo
wer
prop
orti
onof
trea
tmen
tw
eeks
com
plet
ed.
Sta
nger
etal
.[8
7]M
ariju
ana
Ran
dom
ised
clin
ical
tria
l16
5ad
oles
cent
sm
eeti
ngcr
iter
iafo
rm
ariju
ana
abus
eor
depe
nden
ce;
follo
w-u
pth
roug
h14
wee
ks
DD
TD
elay
disc
ount
ing
ofhi
gher
mon
eyre
war
ds($
1000
)pr
edic
ted
abst
inen
ceou
tcom
esov
eran
dab
ove
type
oftr
eatm
ent
rece
ived
.H
owev
er,
disc
ount
ing
beca
me
ano
n-si
gnifi
cant
pred
icto
ron
cede
mog
raph
icco
vari
ates
(e.g
.so
cioe
cono
mic
stat
us,
race
)w
ere
incl
uded
.
DD
T,
Del
aydi
scou
ntin
gta
sk.
Impulsivity in substance use treatment 7
© 2014 Australasian Professional Society on Alcohol and other Drugs

Tab
le4.
Coc
aine
stud
ies
Aut
hors
Sub
stan
ceR
esea
rch
desi
gnS
ampl
esi
zean
dfo
llow
-up
Impu
lsiv
ity
mea
sure
sF
indi
ngs
Bal
l&
Sch
otte
nfiel
d[8
8]C
ocai
neC
orre
lati
onal
/ran
dom
ised
clin
ical
tria
l92
preg
nant
orpo
st-p
artu
mco
cain
eus
ing
wom
enpa
rtic
ipat
ing
inou
tpat
ient
trea
tmen
t;fo
llow
-up
unti
ltr
eatm
ent
com
plet
ion
ordr
opou
t
ImpS
SA
ltho
ugh
scor
eson
the
ImpS
Sw
ere
corr
elat
edw
ith
num
ber
ofdr
ugs
used
,im
puls
ivit
yw
asno
tre
late
dto
rece
ncy,
quan
tity
,fr
eque
ncy
ordu
rati
onof
use,
nor
was
itre
late
dto
trea
tmen
tou
tcom
es,
incl
udin
gpe
rce
ntpo
siti
veur
ine
drug
scre
ens,
num
ber
ofcl
inic
alco
ntac
tsor
num
ber
ofw
eeks
intr
eatm
ent.
Car
pent
eret
al.
[86]
Coc
aine
Cor
rela
tion
al45
coca
ine-
depe
nden
tpa
tien
ts;
follo
w-u
pva
ried
acco
rdin
gto
indi
vidu
altr
eatm
ent
com
plet
ion
Mod
ified
Str
oop
Tas
k
Com
pare
dw
ith
mar
ijuan
a-de
pend
ent
part
icip
ants
,co
cain
e-de
pend
ent
part
icip
ants
resp
onde
dm
ore
slow
lyto
all
stim
ulus
wor
ds.
Fur
ther
mor
e,am
ong
coca
ine-
depe
nden
tpa
rtic
ipan
ts,
mod
ified
Str
oop
perf
orm
ance
inth
epr
esen
ceof
coca
ine
stim
uli
pred
icte
dw
orse
trea
tmen
tou
tcom
es.
Hel
mus
etal
.[7
]C
ocai
neR
ando
mis
edco
ntro
lled
tria
l68
opia
te-d
epen
dent
trea
tmen
tse
eker
sw
hous
eco
cain
e;fo
llow
-up
thro
ugh
wee
k17
oftr
eatm
ent
TP
Q-N
SC
ompa
red
wit
hlo
wno
velt
yse
eker
s,hi
ghno
velt
yse
eker
sw
ere
mor
elik
ely
todr
opou
tby
the
end
oftr
eatm
ent,
but
had
high
erre
tent
ion
rate
sdu
ring
the
earl
yph
ases
oftr
eatm
ent.
Moe
ller
etal
.[8
]C
ocai
neC
orre
lati
onal
/ran
dom
ised
cont
rolle
dtr
ial
50co
cain
e-de
pend
ent
trea
tmen
tse
eker
s;fo
llow
-up
12w
eeks
into
trea
tmen
t
BIS
-11
BIS
-11
tota
lsc
ores
sign
ifica
ntly
corr
elat
edw
ith
self
-rep
ort
aver
age
daily
coca
ine
use
and
coca
ine
wit
hdra
wal
sym
ptom
s.A
mon
gth
ose
who
agre
edto
part
icip
ate
ina
sepa
rate
doub
le-b
lind
plac
ebo
cont
rolle
dtr
ial
ofm
edic
atio
nan
dgr
oup
ther
apy,
thos
ew
ith
high
erba
selin
eim
puls
ivit
ydr
oppe
dou
tsi
gnifi
cant
lyea
rlie
r.P
atka
ret
al.
[46]
Coc
aine
Cor
rela
tion
al14
1A
fric
an-A
mer
ican
coca
ine-
depe
nden
tpa
tien
tsen
teri
ngtr
eatm
ent
and
60co
ntro
ls;
follo
w-u
pat
end
of12
-wee
ktr
eatm
ent
BIS
-11
Coc
aine
-dep
ende
ntpa
rtic
ipan
tsre
port
edsi
gnifi
cant
lyhi
gher
BIS
scor
esth
anco
ntro
ls.
BIS
was
sign
ifica
ntly
asso
ciat
edw
ith
days
intr
eatm
ent
and
drop
out
rate
s.
Was
hio
etal
.[8
9]C
ocai
neR
ando
mis
edco
ntro
lled
tria
l36
coca
ine-
depe
nden
tou
tpat
ient
s;fo
llow
-up
12an
d24
wee
ksaf
ter
base
line.
DD
TD
elay
disc
ount
ing
was
rela
ted
num
ber
ofco
ntin
uous
wee
ksin
trea
tmen
t,ev
enaf
ter
cont
rolli
ngfo
rtr
eatm
ent
cond
itio
n(l
ow-
vs.
high
-mag
nitu
deC
Mvo
uche
rs).
Par
tici
pant
sin
the
low
-mag
nitu
de(b
utno
thi
gh-m
agni
tude
)vo
uche
rco
ndit
ion
who
exhi
bite
dst
eepe
rdi
scou
ntin
gac
hiev
edsh
orte
rpe
riod
sof
abst
inen
ce.
BIS
-11,
Bar
ratt
Impu
lsiv
enes
sS
cale
[11,
12];
DD
T,
Del
aydi
scou
ntin
gta
sk;
ImpS
S,
Impu
lsiv
ity/
Sen
sati
onS
eeki
ngS
cale
[75]
;TP
Q-N
S,
Nov
elty
See
king
Sca
leof
the
Tri
dim
ensi
onal
Per
sona
lity
Que
stio
nnai
re[1
5].
8 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

Tab
le5.
Opi
ate
stud
ies
Aut
hors
Sub
stan
ceR
esea
rch
desi
gnS
ampl
esi
zean
dfo
llow
-up
Impu
lsiv
ity
mea
sure
sF
indi
ngs
Car
pent
eret
al.
[86]
Opi
ates
Cor
rela
tion
al10
hero
in-d
epen
dent
pati
ents
;fo
llow
-up
vari
edac
cord
ing
toin
divi
dual
trea
tmen
tco
mpl
etio
n
Mod
ified
Str
oop
Tas
kN
osi
gnifi
cant
rela
tion
ship
sbe
twee
nm
odifi
edS
troo
ppe
rfor
man
cean
dtr
eatm
ent
outc
omes
.
Pas
sett
iet
al.
[90]
Opi
ates
Cor
rela
tion
al37
opia
te-d
epen
dent
trea
tmen
tse
eker
s;fo
llow
-up
at3
mon
ths
into
trea
tmen
t
IGT
;C
GT
;D
DT
;TO
L;
IST
;S
ST
;G
o/N
o-G
ota
sk
Per
form
ance
onde
cisi
on-m
akin
gte
sts,
but
not
plan
ning
,m
otor
inhi
biti
on,
refle
ctio
nim
puls
ivit
yor
dela
ydi
scou
ntin
g,pr
edic
ted
abst
inen
ceat
3m
onth
sin
totr
eatm
ent
wit
hhi
ghsp
ecifi
city
and
mod
erat
ese
nsit
ivit
y.P
oire
ret
al.
[91]
Opi
ates
Cor
rela
tion
al73
opia
te-d
epen
dent
pati
ents
rece
ivin
ghi
gh-d
ose
bupr
enor
phin
e;fo
llow
-up
thro
ugh
3-m
onth
trea
tmen
tpe
riod
SS
SG
ood
trea
tmen
tre
spon
se(i
.e.
75%
opia
te-n
egat
ive
urin
edr
ugsc
reen
sdu
ring
last
mon
thof
trea
tmen
tan
dpa
rtic
ipat
ion
in3-
mon
thst
udy)
was
pred
icte
dby
anu
mbe
rof
fact
ors,
incl
udin
glo
wdi
sinh
ibit
ion
and
bore
dom
susc
epti
bilit
yfa
ctor
sfr
omth
eS
SS
.R
oll
etal
.[7
3]O
piat
es&
Coc
aine
Cor
rela
tion
al21
hero
in-d
epen
dent
coca
ine
user
sin
trea
tmen
t;fo
llow
-up
at17
wee
ks/e
ndof
trea
tmen
t
TP
QT
hose
who
scor
edhi
ghon
the
TP
QN
ovel
tyS
eeki
ngS
cale
atte
nded
sign
ifica
ntly
few
ersc
hedu
led
appo
intm
ents
,m
isse
dm
ore
appo
intm
ents
and
had
shor
ter
trea
tmen
tre
tent
ion
tim
es.
Sch
mit
zet
al.
[92]
Opi
ates
Ran
dom
ised
cont
rolle
dtr
ial
75co
cain
e-de
pend
ent
trea
tmen
tse
eker
s;fo
llow
-up
aten
dof
trea
tmen
t(1
2-w
eeks
post
-bas
elin
e)
Imm
edia
tean
dD
elay
edM
emor
yT
ask,
BIS
-11,
IGT
Impu
lsiv
ity
was
not
pred
icti
veof
trea
tmen
tre
tent
ion.
Abs
tine
ntpa
rtic
ipan
tsw
ere
mor
eim
puls
ive,
asm
easu
red
byth
eB
IS-1
1,bu
tal
som
ore
likel
yto
use
adva
ntag
eous
deci
sion
-mak
ing
stra
tegi
es,
asm
easu
red
byth
eIG
T.
Zoc
cali
etal
.[9
3]O
piat
esC
orre
lati
onal
144
opia
te-d
epen
dent
pati
ents
inre
side
ntia
ltr
eatm
ent;
follo
w-u
pth
roug
h6-
mon
thst
udy
peri
od
TC
IN
ovel
tyse
ekin
gw
asno
tre
late
dto
trea
tmen
tdr
opou
t.
BIS
-11,
Bar
ratt
Impu
lsiv
enes
sS
cale
[11,
12];
CG
T,C
ambr
idge
Gam
blin
gT
ask
[94]
;CP
T,C
onti
nuou
sP
erfo
rman
ceT
ask;
DD
T,D
elay
disc
ount
ing
task
;EP
Q,E
ysen
ckP
erso
nalit
yQ
uest
ionn
aire
[84]
;I7
,Im
puls
ivit
y,V
entu
reso
men
ess,
and
Em
path
yqu
esti
onna
ire
[74]
;Im
pSS
,Im
puls
ivit
y/S
ensa
tion
See
king
Sca
le[7
5];
IGT
,Io
wa
Gam
blin
gT
ask
[95]
;IS
T,
Info
rmat
ion
Sam
plin
gT
ask;
NE
O-F
FI,
NE
OF
ive
Fac
tor
Inve
ntor
y[1
6];
SS
S,
Sen
sati
onS
eeki
ngS
cale
[76]
;S
ST
,S
top-
sign
alT
ask;
TC
I,T
empe
ram
ent
and
Cha
ract
erIn
vent
ory
[85]
;TO
L,T
ower
ofL
ondo
nT
est
[96]
;TP
Q,T
ridi
men
sion
alP
erso
nalit
yQ
uest
ionn
aire
[15]
;TP
Q-N
S,
Nov
elty
See
king
Sca
leof
the
Tri
dim
ensi
onal
Per
sona
lity
Que
stio
nnai
re[1
5].
Impulsivity in substance use treatment 9
© 2014 Australasian Professional Society on Alcohol and other Drugs

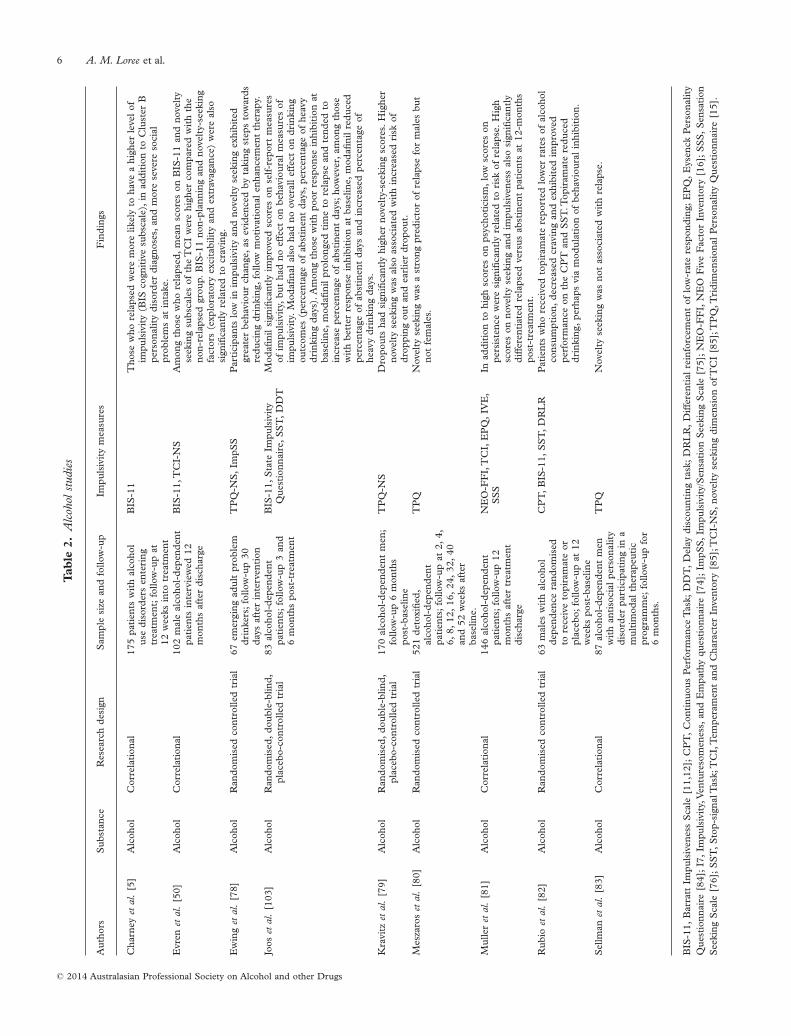
Impulsivity likely exerts an influence early in thetreatment process. In their study of 175 alcoholdependent individuals, Charney et al. found that higherscores on the BIS-11 were associated with higher ratesof slips and relapse within the first 28 days of treatment[5]. The authors hypothesised that impulsivity mayprecede the onset of alcohol problems, and one mecha-nism of action by which impulsivity might impact thecourse of alcohol treatment is via an impulsive decisionto enter treatment when not sufficiently motivated. Inaccordance with this finding, Kravitz et al. found thathigher novelty seeking was associated with increasedrisk of early treatment dropout [79]. Meszaros et al.similarly found that novelty seeking was a strong pre-dictor of relapse in detoxified male alcoholics; however,novelty seeking did not predict relapse among females[80]. Finally, Sellman et al. failed to find a relationshipbetween novelty seeking and relapse among a sample ofmales in treatment for alcohol dependence [83].
Greater impulsivity also has been associated withincreased risk for relapse after treatment in alcohol-dependent individuals. Muller et al. revealed that higherscores on the Impulsiveness subscale of the EysenckImpulsiveness-Venturesomeness-Empathy Scale (I7)distinguished between relapsed and abstinent alcohol-dependent patients one year after treatment discharge[81]. A similar finding was reported by Evren et al., whofound that higher scores on the BIS-11 differentiatedbetween relapsed and non-relapsed groups one yearafter detoxification. Interestingly, scores on the BIS-11were positively correlated with severity of self-reportedcraving for alcohol in this treatment sample, a findingthat has been reported by others (e.g. [51]). Thus, itmay be that impulsivity mediates the relationshipbetween craving and relapse [50,103].
Impulsivity may also directly mediate the effects oftreatment. Ewing et al. randomised a sample of 67emerging adult problem drinkers to receive eitheralcohol education or a single session of MotivationalEnhancement Therapy (MET) [78]. Although METincreased behaviour change during the first 30 dayspost-intervention, these effects were stronger for thoseindividuals who were lower in impulsivity, as measuredby the Impulsivity/Sensation-Seeking Scale [75]. METwas less effective for individuals with higher impulsivity.
The notion that impulsivity may mediate the effectsof pharmacotherapy on alcohol consumption was sup-ported by Rubio et al., who administered the anti-convulsant topiramate to alcohol-dependent males in a12-week, double-blind, placebo-controlled trial [82].Patients who received topiramate demonstratedimprovement on several alcohol use measures, includ-ing fewer alcohol drinks per drinking day, greaternumber of days of abstinence and reduced craving. Inaddition, topiramate significantly improved perfor-
mance on several behavioural impulsivity tasks, as wellas reduced BIS-II scores, compared with placebo. Theauthors concluded that the reduction in alcohol intakeobserved in the topiramate group may be associatedwith the medication’s effect on impulsivity. That is,topiramate may modulate alcohol use via improvementof inhibitory control. Unfortunately, it is not possible todetermine whether topiramate decreased impulsivity,which in turn decreased alcohol consumption, or viceversa.
In another pharmacotherapy treatment study, base-line impulsivity appeared to moderate the effect ofmodafinil on treatment outcome. Specifically, amongalcohol-dependent patients with poor response inhibi-tion at baseline, modafinil prolonged time to relapseand tended to increase percentage of abstinence days;however, among those with better response inhibitionat baseline, modafinil seemed to predict poorer treat-ment outcomes, including fewer abstinent days andgreater heavy drinking days [104]. These findingssuggest that modafinil may only be a useful treatmentfor alcohol dependence among individuals with greaterimpulsivity.
Marijuana studies. Fewer studies have focused on therole of impulsivity in response to treatment for mari-juana, and these reveal that other mediating or moder-ating factors may need to be included in any model ofimpulsivity and marijuana use. In one study, Carpenteret al. examined performance on a modified Stroop testamong marijuana-, cocaine-, and heroin-dependentpatients in a time-limited outpatient treatment pro-gramme utilising pharmacotherapy and cognitive-behavioural coping skills therapy [86]. Interferencescores on cocaine and heroin stimulus words (but notmarijuana or polydrug stimulus words) were signifi-cantly positively associated with a greater proportion ofmarijuana positive urine drug screens and significantlynegatively associated with the proportion of treatmentweeks completed.
Stanger et al. examined whether delay discountingpredicted treatment outcomes among adolescent mari-juana users participating in a randomised clinical trialcomparing three behavioural treatments—cognitivebehavioural therapy, cognitive behavioural therapy andcontingency management, and a combined cognitivebehavioural therapy/contingency management andfamily management curriculum [87]. Regardless oftreatment condition, delay discounting of $1000 inhypothetical money predicted treatment abstinence.However, once demographic covariates, such as socio-economic status and race, were included in regressionanalyses, discounting no longer significantly predictedto treatment outcome. Thus, there may be importantmediating and moderating relationships between
10 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

impulsivity, other patient characteristics and treatmentoutcomes that need to be further examined to betterunderstand the role of impulsivity on treatmentoutcome for marijuana use.
Cocaine studies. Moeller et al. found that higher base-line scores on the BIS-11 predicted greater treatmentdropout and lower retention among individuals seekingtreatment for cocaine dependence [8]. No significantfindings were identified for urine toxicology results butthe authors suggest that the small sample size mayaccount for this negative finding. In another study,higher impulsivity and sensation seeking were associ-ated with fewer days in treatment among patientsseeking intensive outpatient treatment for cocainedependence [46]. Higher sensation seeking was alsoassociated with fewer negative urine drug screens andhigher dropout rate.
Carpenter et al. found that cocaine-dependentpatients responded more slowly to both drug andneutral stimulus words compared with marijuana-dependent patients. Furthermore, performance on themodified Stroop task containing cocaine-related wordswas associated with worse treatment outcome forcocaine-dependent patients, including significantlymore positive urine drug screens and earlier treatmentdropout [86]. Another laboratory study examiningdelay discounting among cocaine-dependent outpa-tients receiving contingency management found thatdelay discounting was significantly associated withnumber of weeks of continuous abstinence, even aftercontrolling for treatment condition. Furthermore,among participants in the low magnitude voucher con-dition (but not the high magnitude condition), steeperdiscounting predicted shorter periods of abstinence[89].
In a contrary finding, cocaine-dependent outpatientsin a placebo-controlled trial of the selective serotoninreuptake inhibitors citalopram who were consideredabstainers (four or more consecutive cocaine-negativeurine drug screens) endorsed higher impulsivity scoreson the BIS-11 but demonstrated more advantageousdecision making on the Iowa Gambling Task than didnon-abstainers (fewer than three consecutive negativedrug screens) [92]. All participants received the samecognitive-behavioural and contingency managementtreatment regardless of medication treatment condition.The authors suggest that the contingency managementtreatment, which results in immediate reinforcementthat may circumvent problems of discounting delayedrewards, and intact decision-making resulting in anability to benefit from cognitive therapy, may account forthese somewhat counterintuitive findings.
Finally, in contrast to the above studies, one studyfocusing on pregnant and post-partum cocaine users in
outpatient treatment found no association betweenimpulsive sensation seeking (as measured by theZuckerman-Kuhlman Personality Questionnaire) andtreatment outcomes. Specifically, sensation seeking wasnot related to per cent of cocaine-positive urines,number of treatment sessions attended or duration oftreatment [88].
Opiate studies. Carpenter et al. failed to find any sig-nificant link between impulsivity and treatment-relatedoutcomes among heroin-dependent patients using amodified Stroop Task [86]; however, this may in parthave been due to their limited sample size of only 10heroin-dependent patients. Others, however, havefound impulsivity to be related to treatment outcomeamong heroin and other opiate users.
Helmus et al. examined novelty seeking as a predictorof treatment retention among opioid-dependentcocaine-abusing patients in a study examining the effi-cacy of combined buprenorphine and voucher contin-gency management treatments [7]. They found thathigh novelty seekers were significantly more likely todropout of treatment before week 17 (78%) than werelow novelty seekers (50%). Using survival analysis, theauthors demonstrated that high novelty seekers hadhigher retention rates than low novelty seekers early intreatment, but lower retention rates later in treatment.The authors suggested that the buprenorphine andcontingency management treatments may have beenexperienced as novel, which may have contributed tothe early success of high novelty-seeking participants. Asimilar study conducted by the same group [73] foundthat buprenorphine-treated opioid-dependent cocaineusers who scored high on the Novelty Seeking scale ofthe Tridimensional Personality Questionnaire attendedfewer scheduled visits, had more no-shows and werein treatment for fewer weeks than participants whoscored lower on this measure. Conversely, amonga sample of high-dosage buprenorphine opioid-dependent patients—a significant proportion of whomalso met dependence criteria for alcohol, cocaine,marijuana—Poirer et al. found that low sensationseeking (low disinhibition in particular) predicted posi-tive treatment response [91]. Finally, Zoccali et al.failed to find an association between novelty seekingand treatment dropout among opioid-dependentpatients residing in therapeutic communities [93].
In a study utilising laboratory measures of impulsiv-ity, decision making (e.g. Iowa Gambling Task), plan-ning (Tower of London), delay discounting andimpulsivity (e.g. Go-NoGo response inhibition) taskswere used to predict treatment outcome amongmethadone-maintained opioid-dependent patients[90]. At three months, participants were divided into‘abstinent’ (from all illicit drugs; n = 10) and ‘non-
Impulsivity in substance use treatment 11
© 2014 Australasian Professional Society on Alcohol and other Drugs

abstinent’ (n = 27) groups. Individuals in the non-abstinent group were more likely than those in theabstinent group to have baseline scores reflectingimpairment on the Iowa Gambling Task. On a seconddecision-making task (the Cambridge Gambling Task),all of the abstinent individuals were categorised ashaving ‘unimpaired’ decision making, compared withonly about half of those in the non-abstinent group.Non-abstinent patients discounted delayed rewards athigher rates than abstinent patients, but this differencemet only marginal significance. Group differences werenot found for theTower of London planning task, or forcognitive and motor impulsivity tasks.
Gaps in the literature and future directions
Although initial work has, for the most part, found thatimpulsivity is associated with poorer treatment out-comes among substance abusing populations, thecurrent research literature is limited in several ways.First, the total number of studies examining the rela-tionship between impulsivity and treatment outcomesis small. In this review, we identified only 33 studies ofsubstance use disorders or nicotine dependence. Thefew studies that have been conducted show that impul-sivity is likely a robust predictor of treatment outcomesand thus should be a focus of treatment development.
Second, as mentioned above, there are several diverseways of operationalising impulsivity. Although mostforms of impulsivity studied thus far have been found tobe associated with addictive disorders, there are severalfactors to consider with regard to how impulsivity ismeasured: (i) self-report measures differ from behav-ioural measures in that they fundamentally measure theindividual’s perception of their own behaviours ratherthan the actual phenotype being exhibited; (ii) impul-sivity measures are surprisingly modestly intercor-related [3,20,36]; and (iii) different measures of impul-sivity may also be associated with differential brainfunctioning [105].Thus, even though several impulsiv-ity measures may converge on similar outcomes (e.g.predicting treatment outcome or relapse), we do not yetknow whether different impulsivity measures are assess-ing the same underlying constructs that affect theseoutcomes. Indeed, several studies have found that whilesome measures predict outcomes, others that are meas-uring similar constructs do not [67,69]. Sensationseeking in particular did not appear to consistentlypredict treatment outcomes [60,62,66,67]. Further-more, others have argued the need to distinguishbetween impulsivity phenotypes [104] and endophe-notypes (e.g. [104,105]) when conducting predictivestudies [106]. Ultimately, studies of endophenotypes(e.g. underlying genetic variability to impulsivity) maybe more informative than studies of phenotypes (i.e.
observable characteristics of impulsivity) given thecomplex aetiology of addictive disorders [107].
Third, there is nearly a complete lack of researchrelated to the implications of impulsivity on the effec-tiveness of different types of treatment, or treatmentintensity. Two studies utilising MET, for example,found it to be less effective for those who had higherlevels of self-reported impulsivity [63,78]. Additionally,a pharmacotherapy trial found modafinil to be effica-cious in treating alcohol dependence but only amongindividuals with poor response inhibition [71]. Further-more, findings from two other studies examining con-tingency management indicated that level of noveltyseeking and the availability of immediate rewardsin contingency management may impact treatmentoutcome [7,92]. Clearly, more research is needed toexamine moderators and mediators of treatmentoutcome and whether there may be different treatmenttypes, treatment intensity/duration, co-occurring psy-chiatric or substance use disorders, or other factorsthat may interact with impulsivity to affect treatmentoutcomes.
Fourth, there is also a lack of data on whether certaintypes of treatments reduce state impulsivity. It is impor-tant to note, for example, whether some types of treat-ment lead to better decision making. Studies thatexamine the effect of treatment on impulsivity are rare.Dallery and Raiff found that, although nicotine replace-ment reduced negative affect among recently abstinentsmokers, this form of treatment did not affect delaydiscounting [61]. Similarly,Yoon et al. found no reduc-tions in impulsivity as a result of contingency manage-ment treatment [70]. On the other hand, topiramatewas found in one study to reduce impulsivity levelsamong individuals treated for alcohol use disorder [82].No studies, to our knowledge, have extended thesefindings on topiramate to other drugs of abuse.Furthermore, future studies may identify whether othermedications may result in similar reductions in impul-sivity.
Nevertheless, abstinence from substance use disor-ders may result in lower levels of impulsivity amongsome individuals. Some investigations, for example,show that former substance users discount delayedmoney rewards at rates much less than current users,and often comparable with never-users (e.g. [55]).Because impulsivity often is associated with higher riskof relapse, it is important to understand the interrela-tionship between impulsivity, abstinence and relapse asit pertains to treatment outcomes.
Conclusions
Impulsivity, a widely studied personality trait andresearch construct, has been implicated as a risk factor
12 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

for initiating and continuing drug use. Given thatimpulsivity has been operationalised in many differentways, cross-comparisons of empirical studies have beendifficult. In addition, relatively few studies have exam-ined the use of impulsivity as a predictor of treatmentoutcome. Taken together, the studies reviewed in thispaper reveal that higher pretreatment impulsivity,regardless of how it is measured, usually is associatedwith poorer treatment outcomes. There were only afew exceptions to this finding. Psychosocial andpharamacological treatments that may positivelyimpact impulsivity appear to be worthy of furtherexamination, including contingency management, andtopiramate. Future studies should continue to examinethe relationship between impulsivity and substance usetreatment outcomes. Finally, treatment studies shouldfurther examine the impact of impulsivity on treatmentintensity and outcome.
Acknowledgements
This paper was supported by Lycaki-Young fundingthrough the State of Michigan.
References
[1] Evanden JL. Varieties of impulsivity. Psychopharmacology(Berl) 1999;146:348–61.
[2] Petry NM, Madden GJ. Discounting and pathologicalgambling. In: Madden GJ, Bickel WK, eds. Impulsivity:the behavioral and neurological science of discounting.Washington, DC: American Psychological Association,2010:273–294.
[3] Verdejo-Garcia A, Lawrence AJ, Clark L. Impulsivity as avulnerability marker for substance-use disorders: review offindings from high-risk research, problem gamblers andgenetic association studies. Neurosci Biobehav Rev2008;32:777–810.
[4] Yi R, Mitchell SH, Bickel WK. Delay discounting andsubstance abuse-dependence. In: Madden GJ, Bickel WK,eds. Impulsivity: the behavioral and neurological science ofdiscounting. Washington, DC: American PsychologicalAssociation, 2010:191–211.
[5] Charney DA, Zikos E, Gill KJ. Early recovery from alcoholdependence: factors that promote or impede abstinence.J Subst Abuse Treat 2010;38:42–50. doi: 10.1016/j.jsat.2009.06.002.
[6] Doran N, Spring B, McChargue D, Pergadia M,Richmond M. Impulsivity and smoking relapse. NicotineTob Res 2004;6:641–7.
[7] Helmus TC, Downey KK, Arfken CL, Henderson MJ,Schuster CR. Novelty seeking as a predictor of treatmentretention for heroin dependent cocaine users. DrugAlcohol Depend 2001;61:287–95.
[8] Moeller FG, Dougherty DM, Barratt ES, Schmitz JM,Swann AC, Grabowski J. The impact of impulsivity oncocaine use and retention in treatment. J Subst AbuseTreat 2001;21:193–8.
[9] Oxford University Press. Oxford English Dictionaryonline. 2013 Available at: http://www.oed.com/view/Entry/92922?redirectedFrom=impulsive# (accessed December2013).
[10] American Psychological Association. PsychInfo. 2013Available at: http://www.apa.org/pubs/databases/psycinfo/index.aspx (accessed June 2013).
[11] Barratt ES. Impulsiveness subtraits: arousal and informa-tion processing. Motivation, emotion and personality.1985:137–46.
[12] Patton JH, Stanford MS, Barratt ES. Factor structure ofthe Barratt Impulsiveness Scale. J Clin Psychol 1995;51:768–74.
[13] Eysenck SBG, Eysenck HJ. Impulsiveness and venture-someness: their position in a dimensional system of per-sonality description. Psychol Rep 1978;43:1247–55.
[14] Whiteside SP, Lynam DR. The five factor model andimpulsivity: using a structural model of personality tounderstand impulsivity. Pers Individ Dif 2001;30:669–89.
[15] Cloninger RC. A systematic method for clinical descrip-tion and classification of personality traits: a proposal.Arch Gen Psychiatry 1987;44:573–88.
[16] Costa PT, McCrae RR. Revised NEO Personality Inven-tory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI). Odessa, FL: Psychological Assessment Resources,1992.
[17] Dawe S, Gullo MJ, Loxton NJ. Reward drive and rashimpulsiveness as dimensions of impulsivity: implicationsfor substance misuse. Addict Behav 2004;29:1389–405.
[18] Dickman SJ. Functional and dysfunctional impulsivity:personality and cognitive correlates. J Pers Soc Psychol1990;58:95–102.
[19] Zukerman M. Sensation seeking: beyond the optimal levelof arousal. Hillsdale, NJ: Lawrence Erlbaum Associates,1979.
[20] Ledgerwood DM, Alessi SM, Phoenix N, Petry NM.Behavioral assessment of impulsivity in pathological gam-blers with and without substance use disorder historiesversus healthy controls. Drug Alcohol Depend 2009;105:89–96.
[21] Rachlin H, Raineri A, Cross D. Subjective probability anddelay. J Exp Anal Behav 1991;55:233–44.
[22] Green L, Fry AF, Myerson J. Discounting of delayedrewards: a life-span comparison. Psychol Sci 1994;5:33–6.
[23] Finn PR, Justus A, Mazas C, Steinmetz JE. Workingmemory, executive processes and the effects of alcohol onGo/No-Go learning: testing a model of behavioral regula-tion and impulsivity. Psychopharmacology (Berl) 1999;146:465–72.
[24] Finn PR, Mazas CA, Justus AN, Steinmetz J. Early-onsetalcoholism with conduct disorder: go/no go learning defi-cits, working memory capacity, and personality. AlcoholClin Exp Res 2002;26:186–202.
[25] Horn N, Dolan M, Elliott R, Deakin J, Woodruff P.Response inhibition and impulsivity: an fMRI study.Neuropsychologia 2003;41:1959–66.
[26] Marsh DM, Dougherty DM, Mathias CW, Moeller FG,Hicks LR. Comparisons of women with high and lowtrait impulsivity using behavioral models of response-disinhibition and reward choice. Pers Individ Dif 2002;33:1291–310.
[27] Dougherty DM. Laboratory behavioral measures ofimpulsivity: general information manual. Houston, TX:Neurobehavioral Research Laboratory and Clinic, Univer-sity of Texas Health Science Center, 2003.
[28] Dougherty DM, Marsh DM. Immediate and delayedmemory tasks (IMT/DMT 2.0): a research tool for study-ing attention, memory, and impulsive behavior. Houston,TX: Neurobehavioral Research Laboratory and Clinic,University of Texas Health Center at Houston, 2003.
Impulsivity in substance use treatment 13
© 2014 Australasian Professional Society on Alcohol and other Drugs

[29] Swann AC, Bjork JM, Moeller FG, Dougherty DM.Two models of impulsivity: relationships to personalitytraits and psychopathology. Biol Psychiatry 2002;51:988–94.
[30] Epstein JN, Erkanli A, Connors CK, Klaric J, Costello JE,Angold A. Relations between continuous performance testperformance measures and ADHD behaviors. J AbnormChild Psychol 2003;31:543–54.
[31] Bechara A, Damasio H, Tranel D, Damasio AR. Decidingadvantageously before knowing the advantageous strategy.Science 1997;275:1293–5.
[32] Rogers RD, Everitt BJ, Baldacchino A, et al. Dissociabledeficits in the decision-making cognition of chronicamphetamine abusers, opiate abusers, patients with focaldamage to the prefrontal cortex, and tryptophan-depletednormal volunteers: evidence for monoaminergic mecha-nisms. Neuropsychopharmacology 1999;20:322–39.
[33] Rogers RD, Owen AM, Middleton HC, et al. Choosingbetween small, likely rewards and large, unlikely rewardsactivates inferior and orbital prefrontal cortex. J Neurosci1999;19:9029–38.
[34] Lejuez CW, Read JP, Kahler CW, et al. Evaluation of abehavioral measure of risk taking: the Balloon AnalogueRisk Task (BART). J Exp Psychol Appl 2002;8:75–84.
[35] Lejuez CW, Aklin WM, Zvolensky MJ, Pedulla CM.Evaluation of the Balloon Analogue Risk Task (BART) asa predictor of adolescent real-world risk-taking behaviors.J Adolesc 2003;26:475–9.
[36] Lijffijt M, Bekker EM, Quik EH, Bakker J, Kenemans JL,Verbaten MN. Differences between low and high traitimpulsivity are not associated with differences in inhibi-tory motor control. J Atten Disord 2004;8:25–32.
[37] Reynolds B, Ortengren A, Richards JB, de Wit H. Dimen-sions of impulsive behavior: personality and behavioralmeasures. Pers Individ Dif 2006;40:305–15.
[38] Meda SA, Stevens MC, Potenza MN, et al. Investigatingthe behavioural and self-report constructs of impulsivitydomains using principal components analysis. BeahvioralPharmacology 2009;20:390–9.
[39] Vuchinich RE, Simpson CA. Hyperbolic temporal dis-counting in social drinkers and problem drinkers. ExpClin Psychopharmacol 1998;6:292–305.
[40] Coffey SF, Gudleski GD, Saladin ME, Brady KT. Impul-sivity and rapid discounting of delayed hypotheticalrewards in cocaine-dependent individuals. Exp ClinPsychopharmacol 2003;11:18–25.
[41] Kirby KN, Petry NM. Heroin and cocaine abusers havehigher discount rates for delayed rewards than alcoholicsor non-drug-using controls. Addiction 2004;99:461–71.
[42] Kirby KN, Petry NM, Bickel WK. Heroin addicts havehigher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol Gen 1999;128:78–87.
[43] Hoffman WF, Moore M, Templin R, McFarland B,Hitzemann RJ, Mitchell SH. Neuropsychological functionand delay discounting in methamphetamine-dependentindividuals. Psychopharmacology (Berl) 2006;188:162–70.
[44] Johnson MW, Bickel WK, Baker F, Moore BA, Badger GJ,Budney AJ. Delay discounting in current and formermarijuana-dependent individuals. Exp Clin Psychophar-macol 2010;18:99–107.
[45] Cangemi S, Giorgi I, Bonfiglio NS, Renati R, Vittadini G.Impulsiveness and time perception in alcohol dependentpatients in alcoholic rehabilitation treatment. G Ital MedLav Ergon 2010;32(3, Suppl. B):B23–8.
[46] Patkar AA, Murray HW, Mannelli P, Gottheil E,Weinstein SP, Vergare MJ. Pre-treatment measures ofimpulsivity, aggression and sensation seeking are associ-ated with treatment outcome for African-AmericanCocaine-Dependent patients. J Addict Dis 2004;23:109–22.
[47] Nielsen DA, Ho A, Bahl A, et al. Former heroin addictswith or without a history of cocaine dependence are moreimpulsive than controls. Drug Alcohol Depend 2012;124:113–20.
[48] Monterosso JR, Aron AR, Cordova X, Xu J, London ED.Deficits in response inhibition associated with chronicmethamphetamine abuse. Drug Alcohol Depend 2005;79:273–7.
[49] Grant S, Contoreggi C, London ED. Drug abusers showimpaired performance in a laboratory test of decisionmaking. Neuropsychologia 2002;38:1180–7.
[50] Evren C, Durkaya M, Evren B, Dalbudak E, Cetin R.Relationship of relapse with impulsivity, novelty seekingand craving in male alcohol-dependent inpatients. DrugAlcohol Rev 2012;31:81–90. doi: 10.1111/j.1465-3362.00303.x.
[51] Joos L, Goudriaan AE, Schmaal L, et al. The relationshipbetween impulsivity and craving in alcohol dependentpatients. Psychopharmacology (Berl) 2013;226:273–83.doi: 10.1007/s00213-012-2905-8.
[52] Roozen HG, van der Kroft P, van Marle HJ, Franken IHA.The impact of craving and impulsivity on aggression indetoxified cocaine-dependent patients. J Subst AbuseTreat 2011;40:414–18.
[53] Tziortis D, Mahoney JJ, Kalechstein AD, Newton TF,De La Garza R. The relationship between impulsivity andcraving in cocaine- and methamphetamine-dependent vol-unteers. Pharmacol Biochem Behav 2011;98:196–202.
[54] Patkar AA, Thornton CC, Mannelli P, et al. Comparisonof pretreatment characteristics and treatment outcomesfor alcohol-, cocaine-, and multisubstance-dependentpatients. J Addict Dis 2004;23:93–109.
[55] Bickel WK, Odum AL, Madden GJ. Impulsivity and ciga-rette smoking: delay discounting in current, never andex-smokers. Psychopharmacology (Berl) 1999;146:447–54.
[56] Mitchell SH. Measuring impulsivity and modeling itsassociation with cigarette smoking. Behav Cogn NeurosciRev 2004;3:261–75.
[57] Field M, Santacangelo M, Sumnall H, Goudie A, Cole J.Delay discounting and the behavioral economics of ciga-rette purchases in smokers: the effects of nicotine depriva-tion. Psychopharmacology (Berl) 2006;186:255–63.
[58] Perkins KA, Lerman C, Coddington SB, et al. Initial nico-tine sensitivity in humans as a function of impulsivity.Psychopharmacology (Berl) 2008;200:529–44.
[59] Rounsaville BJ, Dolinsky ZS, Babor TF, Meyer RE. Psy-chopathology as a predictor of treatment outcome in alco-holics. Arch Gen Psychiatry 1987;44:505–13.
[60] Carlton S, Le Houzec J, Lagrue G, Jouvent R. Relation-ships between sensation seeking and emotional symptoma-tology during smoking cessation with nicotine patchtherapy. Addictive Behaviors 2000;25:653–62.
[61] Dallery J, Raiff BR. Delay discounting predicts cigarettesmoking in a laboratory model of abstinence reinforce-ment. Psychopharmacology (Berl) 2007;190:485–96.
[62] Hall PA, Fong GT, Young H, Sansone G, Borland R,Siahpush M. Do time perspective and sensation-seekingpredict quitting activity among smokers? Findings from
14 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs

the International Tobacco Control (ITC) Four CountrySurvey. Addict Behav 2012;37:1307–13.
[63] Helstrom A, Hutchinson K, Bryan A. Motivationalenhancement therapy for high-risk adolescent smokers.Addict Behav 2007;32:2404–10.
[64] Krishnan-Sarin S, Reynolds B, Duhig AM, et al.Behavioral impulsivity predicts treatment outcome in asmoking cessation program for adolescent smokers. DrugAlcohol Depend 2007;88:79–82.
[65] MacKillop J, Kahler CW. Delayed reward discountingpredicts treatment response for heavy drinkers receivingsmoking cessation treatment. Drug Alcohol Depend2009;104:197–203.
[66] Nieva G, Valero S, Bruguera E, et al. The alternative five-factor model of personality, nicotine dependence andrelapse after treatment for smoking cessation. AddictBehav 2011;36:965–71.
[67] Powell J, Dawkins L, West R, Powell J, Pickering A.Relapse to smoking during unaided cessation: clinical,cognitive and motivational predictors. Psychophar-macology (Berl) 2010;212:537–49.
[68] Rukstalis M, Jepson C, Patterson F, Lerman C. Increasesin hyperactive impulsive symptoms predict relapse amongsmokers in nicotine replacement therapy. J Subst AbuseTreat 2005;28:297–304.
[69] Sheffer C, MacKillop J, McGeary J, et al. Delay discount-ing, locus of control, and cognitive impulsiveness indepen-dently predict tobacco dependence treatment outcomesin a highly dependent, lower socioeconomic group ofsmokers. Am J Addict 2012;21:221–32.
[70] Yoon JH, Higgins ST, Heil SH, Sugarbaker RJ, ThomasCS, Badger GJ. Delay discounting predicts postpartumrelapse to cigarette smoking among pregnant women. ExpClin Psychopharmacol 2007;15:176–86.
[71] Murphy K, Barkley RA. Attention deficit hyperactivitydisorder adults: comorbidities and adaptive impairments.Compr Psychiatry 1996;37:393–401.
[72] Reynolds B, Schiffbauer R. Measuring state changes inhuman delay discounting: an experiential discounting task.Behav Process 2004;67:43–56.
[73] Roll JM, Saules KK, Chudzynski JE, Sodano R. Relation-ship between Tridimensional Personality Questionnairescores and clinic attendance among cocaine abusing,buprenorphine maintained outpatients. Subst Use Misuse2004;39:1025–40.
[74] Eysenck HJ, Eysenck SBG. Adult IVE. London: Hodder &Stoughton, 1991.
[75] Zuckerman M, Kuhlman DM, Joireman J, Teta P, KraftM. A comparison of three structural models for personal-ity: the big three, the big five, and the alternative five. J PersSoc Psychol 1993;65:757–68.
[76] Zuckerman M, Eysenck S, Eysenck HJ. Sensation seekingin England and America: cross-cultural age and sex com-parisons. J Consult Clin Psychol 1978;46:139–49.
[77] Stephenson MT,Hoyle RH,Palmgreen P,Slater MD.Briefmeasures of sensation seeking for screening and large-scalesurveys. Drug Alcohol Depend 2003;72:279–86.
[78] Ewing SWF, LaChance HA, Bryan A, Hutchinson KE.Do genetic and individual risk factors moderate the effi-cacy of motivational enhancement therapy? Drinking out-comes with an emerging adult sample. Addict Biol2009;14:356–65. doi: 10.1111/j.1369-1600.2009.00149.x.
[79] Kravitz HM, Fawcett J, McGuire M, Kravitz G, WhitneyM. Treatment attrition among alcohol-dependent men: is
it related to novelty seeking personality traits? J ClinPsychopharmacol 1999;19:51–6.
[80] Meszaros K, Lenzinger E, Hornik K, et al. The Tridimen-sional Personality Questionnaire as a predictor of relapsein detoxified alcohol dependents. Alcohol Clin Expe Res1999;23:483–86.
[81] Muller SE, Weijers H-G, Boning J, Wiesbeck GA. Person-ality traits predict treatment outcome in alcohol-dependent patients. Neuropsychobiology 2008;57:159–64. doi: 10.1159/000147469.
[82] Rubio G, Martinez-Gras I, Manzanares J. Modulation ofimpulsivity by topiramate: implications for the treatmentof alcohol dependence. J Clin Psychopharmacol2009;29:584–9. doi: 10.1097/JCP.0b013e3191bfdb79.
[83] Sellman JD, Mulder RT, Sullivan PF, Joyce PR. Lowpersistence predicts relapse in alcohol dependence follow-ing treatment. J Stud Alcohol 1997;58:257–63.
[84] Ruch W. The Eysenck Personality Questionnaire-Revisedand the construction of German standard and short ver-sions (EPQ-R and EPQ-RK). Z Diagn Psychol 1999;20:1–24.
[85] Cloninger CR, Pryzbeck TR, Svaric DM, Wentzel RD.The Temperament and Character Inventory (TCI): aguide to its development and use. St. Louis: WashingtonUniversity, 1994.
[86] Carpenter KM, Schreiber E, Church S, McDowell D.Drug Stroop performance: relationships with primarysubstance of use and treatment outcome in adrug-dependent outpatient sample. Addict Behav2006;31:174–81.
[87] Stanger C, Ryan SP, Hongyun F, et al. Delay discountingpredicts adolescent substance abuse treatment outcome.Exp Clin Psychopharmacol 2012;20:205–12. doi:10.1037/a0026543.
[88] Ball SA, Schottenfield RS. A five-factor model of person-ality and addiction, psychiatric, and AIDS risk severity inpregnant and postpartum cocaine misusers. Subst UseMisuse 1997;32:25–41.
[89] Washio Y, Higgins ST, Heil SH, et al. Delay discounting isassociated with treatment response among cocaine-dependent outpatients. Exp Clin Psychopharmacol2011;19:243–48.
[90] Passetti F, Clark L, Mehta MA, King JM. Neuro-psychological predictors of clinical outcome in opiateaddiction. Drug Alcohol Depend 2008;94:82–91.
[91] Poirer M, Laqueille X, Jalfre V, et al. Clinical profile ofresponders to buprenorphine as a substitution treatmentin heroin addicts: results of a multicenter study of 73patients. Prog Neuropsychopharmacol Biol Psychiatry2004;28:267–72.
[92] Schmitz JM, Mooney ME, Green CE, et al. Baselineneurocognitive profiles differentiate abstainers and non-abstainers in a cocaine clinical trial. J Addict Dis 2009;28:250–7.
[93] Zoccali R, Muscatello MRA, Bruno A, et al. Temperamentand character dimensions in opiate addicts: Comparingsubjects who completed inpatient treatment in therapeuticcommunities vs. incompleters. Am J Drug Alcohol Abuse2007;33:707–15.
[94] Bechara A, Damásio AR, Damásio H, Anderdon SW.Insensitivity to future consequences following damage tohuman prefrontal cortex. Cognition 1994;50:7–14.
[95] Manes F, Sahakian BJ, Clark L, et al. Decision-makingprocesses following damage to the prefrontal cortex. Brain2002;125:624–39.
Impulsivity in substance use treatment 15
© 2014 Australasian Professional Society on Alcohol and other Drugs
[96] Culbertson WC, Zillmer EA. TheTower of London (DX):A standardized approach to assessing executive function inchildren. Arch Clin Neuropsychol 1998;13:285–301.
[97] Rubio G, Jimenez M, Rodriguez-Jimenez R, et al. The roleof behavioral impulsivity in the development of alcoholdependence: a 4-year follow-up study. Alcohol Clin ExpRes 2008;32:1681–7.
[98] Soloff PH, Lynch KG, Moss HB. Serotonin, impulsivity,and alcohol use disorders in the older adolescent: a psycho-biological study. Alcohol Clin Exp Res 2000;24:609–19.
[99] Bjork JM, Hommer DW, Grant SJ, Danube C. Impulsivityin abstinent alcohol-dependent patients: relation tocontrol subjects and type 1-/type-2 like traits. Alcoholism2004;34:133–50.
[100] Dom G, Hulstijn W, Sabbe B. Differences in impulsivityand sensation seeking between early- and late-onset alco-holics. Addict Behav 2006;31:289–308.
[101] Irwin M, Schuckit M, Smith TL. Clinical importance ofage at onset ofType 1 andType 2 primary alcoholics. ArchGen Psychiatry 1990;47:320–4.
[102] Tracy JI. Assessing the relationship between craving andrelapse. Drug Alcohol Rev 1994;13:71–7.
[103] Joos L, Goudriaan AE, Schmaal L, et al. Effect ofmodafinil on impulsivity and relapse in alcohol-dependentpatients: a randomized placebo-controlled trial. EurNeuropsychopharmacol 2013;23:948–55.
[104] Dalley JW, Everitt BJ, Robbins TW. Impulsivity,compulsivity, and top-down cognitive control. Neuron2011;69:680–94.
[105] Chamberlain SR, Sahakian BJ. The neuropsychiatry ofimpulsivity. Curr Opin Psychiatry 2007;20:255–61.
[106] Goudriaan AE, Oosterlaan J, DeBeurs E, Van DenBrink W. The role of self-reported impulsivity and rewardsensitivity versus neurocognitive measures of disinhi-bition and decision-making in the prediction of relapsein pathological gamblers. Psychol Med 2008;38:41–50.
[107] Gottesman II, Gould TD. The endophenotype concept inpsychiatry: etymology and strategic intentions. Am J Psy-chiatry 2003;160:636–45.
16 A. M. Loree et al.
© 2014 Australasian Professional Society on Alcohol and other Drugs
Copyright © 2022 FDOKUMEN




















