
Aggressivity, inattention, hyperactivity, and impulsivity in boys at high and low risk for substance...
27
Journal of Abnormal Child Psychology, Pot 22, No. 2, 1994 Aggressivity, Inattention, Hyperactivity, and Impulsivity in Boys at High and Low Risk for Substance Abuse Christopher S. Martin, 1~ Mitchell Earleywine,2 Timothy C. Blackson, 1 Michael M. Vanyukov, 1 Howard B. Moss, 1 and Ralph E. Tarter I Aggressivity, inattention, hyperactivity, and impulsivity are cardinal dimensions of externalizing behavior problems of childhood. They are diagnostic and clinical features of childhood disorders, and are thought to be linked to the subsequent development Of adult disorders such as substance abuse (SA). Little is known, however, about the convergent and discriminant validity of these four constructs. We used multiple measures to develop indices of aggressivity, inattention, hyperactivity, and impulsivity in a sample of 10- to 12-year-old boys (N = 183) with and without a family history of SA. Data were taken from mother reports, child reports, teacher reports, and laboratory tasks. The study aims were (1) to test the convergent and discriminant validity of aggressivity, inattention, hyperactivity, and impulsivity; (2) to examine whether the data were consistent with a model specifying the four constructs as indicators of one superordinate factor; and (3) to differentiate boys with and without a family history of SA in construct scores. The results supported the convergent and discriminant validity of the four constructs~ Although discriminable, the constructs covaried strongly and were consistent with a model specifying them as indicators of a single superordinate factor. Boys with a family history of substance abuse scored higher than control boys on aggressivity, inattention, and impulsivity scores, but the groups did not differ on hyperactivity scores. The results are discussed in terms of the role of childhood behavior problems in vulnerability to SA. Manuscript received in final form August 25, 1993. This work was supported by the National Institute on Drug Abuse grant No. DA 05605. 1C.enter for Education and Drug Abuse Research, A consortium between the University of Pittsburgh and St. Francis Medical Center, Pittsburgh, Pennsylvania. 2Department of Psychology, University of Southern California, Los Angeles, California. 3Address all correspondence to Christopher S. Martin, Ph.D., Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, 3811 O'Hara St., Pittsburgh, Pennsylvania 15213-2593. 177 0091-.o627/94/040o-0177507.0o/0 1994 plenum Publishing Corporation
Transcript of Aggressivity, inattention, hyperactivity, and impulsivity in boys at high and low risk for substance...

Journal of Abnormal Child Psychology, Pot 22, No. 2, 1994
Aggressivity, Inattention, Hyperactivity, and Impulsivity in Boys at High and Low Risk for Substance Abuse
Christopher S. Martin, 1~ Mitchell Earleywine, 2 Timothy C. Blackson, 1 Michael M. Vanyukov, 1 Howard B. Moss, 1 and Ralph E. Tarter I
Aggressivity, inattention, hyperactivity, and impulsivity are cardinal dimensions of externalizing behavior problems of childhood. They are diagnostic and clinical features of childhood disorders, and are thought to be linked to the subsequent development Of adult disorders such as substance abuse (SA). Little is known, however, about the convergent and discriminant validity of these four constructs. We used multiple measures to develop indices of aggressivity, inattention, hyperactivity, and impulsivity in a sample of 10- to 12-year-old boys (N = 183) with and without a family history of SA. Data were taken from mother reports, child reports, teacher reports, and laboratory tasks. The study aims were (1) to test the convergent and discriminant validity of aggressivity, inattention, hyperactivity, and impulsivity; (2) to examine whether the data were consistent with a model specifying the four constructs as indicators of one superordinate factor; and (3) to differentiate boys with and without a family history of SA in construct scores. The results supported the convergent and discriminant validity of the four constructs~ Although discriminable, the constructs covaried strongly and were consistent with a model specifying them as indicators of a single superordinate factor. Boys with a family history of substance abuse scored higher than control boys on aggressivity, inattention, and impulsivity scores, but the groups did not differ on hyperactivity scores. The results are discussed in terms of the role of childhood behavior problems in vulnerability to SA.
Manuscript received in final form August 25, 1993. This work was supported by the National Institute on Drug Abuse grant No. DA 05605. 1C.enter for Education and Drug Abuse Research, A consortium between the University of Pittsburgh and St. Francis Medical Center, Pittsburgh, Pennsylvania.
2Department of Psychology, University of Southern California, Los Angeles, California. 3Address all correspondence to Christopher S. Martin, Ph.D., Western Psychiatric Institute and Clinic, University of Pittsburgh School of Medicine, 3811 O'Hara St., Pittsburgh, Pennsylvania 15213-2593.
177
0091-.o627/94/040o-0177507.0o/0 �9 1994 plenum Publishing Corporation

178 Martin et al,
Little is known about the mechanisms underlying vulnerability to and the development of substance abuse (SA), as defined by the presence of a DSM-III-R psychoactive substance use disorder. Disruptive behavior dis- orders of childhood and adolescence have been linked to the subsequent development of SA (eft Sher, 1991), particularly attention-deficit hyperac- tivity disorder (ADHD) and conduct disorder (CD). Inattention, impulsiv- ity, and hyperactivity are central diagnostic and clinical features of ADHD. CD involves illegal acts and a pervasive history of antisocial, criminal, or violent behaviors (American Psychiatric Association, 1987). The features of CD include aggressivity and impulsivity.
Substance abusers retrospectively report more symptoms of childhood behavior problems associated with CD and ADHD (Robins & Price, 1991; Tarter, McBride, Buonpane, & Schneider, 1977). Adopted children with symptoms of ADHD are more likely to have an alcoholic biologic father than controls (Morrison & Stewart, 1973). Prospective studies of children and adolescents have documented that ADHD and CD are predictive of delinquency in adolescence (Loeber, 1988), adult antisocial personality dis- order (ASP) (Farrington, 1991), and adult SA (Gittleman, Mannuzza, Shenker, & Bongura, 1985; Mannuzza, Klein, Bonagura, Malloy, Giampino, & Addalli, 1991; Mendelson, Johnson, & Stewart, 1971).
The disorders of ADHD, CD, and ASP have overlapping symptoms, which suggests the possibility of common underlying mechanisms in the development of these disorders (e.g., Abikoff & Klein, 1992). In view of the association of these disorders with SA, the shared symptomatology fur- ther suggests that the study of specific aggregates of symptoms may prove informative in explicating mechanisms of vulnerability to SA. Aside from aggressivity (Loeber, 1988; Moss, Mezzich, Yao, Gavaler, & Martin, in press), the roles of particular symptoms in SA risk have not yet been dis- entangled.
This report addresses four dimensions of externalizing child behavior problems: (1) aggressivity, (2) inattention, (3) hyperactivity, and (4) impul- sivity. The selection of these dimensions stems from their widespread use in the childhood psychopathology literature and their putative associations with SA. There has been little agreement, however, about the definition of these four terms. The descriptive psychopathology of childhood disorders sometimes has used these terms without definition. When provided, defi- nitions are often inconsistent with each other. In the present paper, the four constructs are conceptualized as traits that show some degree of cross- situational consistency. That is, stable individual differences in these be- havioral propensities are postulated. A description and working definition of each construct is given below.

Aggressivity, Inattention, Hyperactivity, and Impulsivity 179
Aggressivity is defined by the likelihood and severity of acts of physical violence deliberately designed to hurt or damage other persons or their property, and nonviolent acts deliberately designed to threaten, provoke, or incite other persons (e.g., verbal aggression) (Valzelli, 1981). Aggressive behaviors are amenable to topographical classification (Moyer, 1968; Valzelli, 1981). Nevertheless, there is considerable evidence for the cross- situational consistency and developmental stability of aggressive behaviors (Olweus, 1979). Childhood aggressivity has been demonstrated to be an important risk factor for later SA (Kelam, Brown, Rubin, & Ensminger, 1983; MeCord & McCord, 1960).
Inattention is defined by a relatively low ability to sustain concentration on particular environmental stimuli. Inattentive children are easily distracted by extraneous stimuli, and are relatively unable to sustain performance on tasks that require concentration. The conceptualization of inattention as a psychopathological characteristic is supported by its heuristic role in explain- ing many aspects of information processing (e.g., Shiffrin, 1988). While symptoms of ADHD are predictive of later SA, it is not clear whether this association holds for particular symptoms that reflect inattention.
Hyperactivity is defined as relatively high motor activity, including ver- bal behavior (the term does not denote ADHD or earlier formulations of this diagnostic category). Several lines of evidence indicate that hyperac- tivity may augment risk for SA. Greater motor activity has been reported among adult and prepubescent offspring of alcoholics and substance abuse, using instruments that objectively quantify motor activity (Moss, Blackson, Martin, & Tarter, 1992; Newlin & Thomson, 1991). Heightened motor ac- tivity in animals predicts heightened behavioral sensitivity to amphetamine (Piazza, Deminiere, Le Moal, & Simon, 1989), cocaine, and scopolamine (Hooks, Jones, Smith, & Neill, 1991). Rats selectively bred for alcohol pref- erence have higher motor activity in an alcohol-naive state, and after al- cohol ingestion, compared to their nonpreferring counterparts (e.g., Murphy, McBride, Wlodarek & McBride, 1992). Psychomotor stimulant ef- fects of drugs are theorized to be mechanistically related to drug reinforce- ment (Wise & Bozarth, 1987). Both motor activity and drug reinforcement appear to be subserved by central dopaminergic systems (Wise, 1988).
Impulsivity is one of the most widely studied, yet inconsistently de- fined, behavioral dimensions of childhood psychopathology. Some investi- gators have defined impulsivity as performance on delay of gratification, response perseveration, or resistance to temptation tasks (e.g., Gordon, 1979; Kagan, Rosman, Day, Albert, & Phillips, 1964; Porteus, 1965). Others have provided a set of descriptions for impulsivity, such as poor self control, lack of foresight for consequences, and inability to inhibit behavior (Milich

180 Martin et al.
& Kramer, 1984). The DSM-III-R contains a set of behavioral descriptors of ADHD that appear to reflect impulsivity, but lacks a comprehensive definition of the term.
Impulsivity is defined herein as a tendency to emit behaviors in situ- ations in which the delay or inhibition of these behaviors would provide benefit. Impulsivity is therefore reflected by errors of commission with re- gard to the consequences of behavior. Some investigators have suggested that impulsivity is too broad to be useful as a construct for research, and that more specific constructs should be developed (e.g., Milich & Kramer, 1984). However, the concept of impulsivity has proved heuristic for psy- chopathology research. Both drug taking and impulsivity can be conceptu- alized in terms of the choice of short-term over long-term reinforcers. Peer relations, accidents, and academic and legal difficulties have all been as- sociated with impulsivity (Blackman & Goldstein, 1982; Milich & Landau, 1982).
The four constructs often have been regarded as distinct. Some re- search has supported the discriminant validity of aggressivity and hyperac- tivity (Milich, Loney, & Landau, 1981; Tryon, 1991). Hinshaw (1992) postulated that inattention and aggressivity are distinct but often comorbid. Using factor analysis of sociometric ratings, Pope, Bierman, and Mumma (1991) found three factors related to aggression, hyperactivity, and inatten- tion/immaturity in third- to sixth-grade boys. Numerous investigators, how- ever, have reported covariation among aggressivity, hyperactivity, in- attention, and impulsivity, as well as similar constructs such as disinhibition and sensation seeking (Zuckerman, 1983). Aggressive and delinquent be- haviors have been associated with impulsivity, although mechanisms have not been dearly specified (Camp, 1977; Dodge & Newman, 1981). Few studies have used multiple measures from different data sources to examine the convergent and discriminant validity of these constructs. The results have important implications for understanding the role of these behavior problems in psychopathological disorders of childhood and adulthood.
The primary purposes of the present project were (1) to test the con- vergent and discriminant validity of aggressivity, hyperactivity, inattention, and impulsivity in 10- to 12-year-old boys, using multiple measures from each of several data sources; (2) to test the hypothesis that these four di- mensions of problem behavior, while discriminable, also fit a second-order model in which they serve as indicators of a single superordinate construct; and (3) to determine differences in construct scores between boys with and without a family history of SA.

Aggressi~ty, Inattention, Hyperactivity, and ImpulslvJty 181
METHOD
Subjects.
The sample consisted of 183 10- to 12-year-old boys and their bio- logical parents. Families were recruited through the fathers via multiple sources in the community, including social service agencies, substance abuse treatment programs, and newspaper advertisements. Advertisements were made in a variety of media, including radio and daily and community news- papers. All persons were invited to participate for pay in a family study. The 183 subjects were classified in four groups based on parental psychi- atric diagnoses. The first group had no history of psychiatric disorder, in- eluding substance abuse, in either parent (SA-; n = 78). The second group had a history of substance abuse in the father that was not limited to al- cohol diagnoses (SA+; n = 67). The third group had a history of psychiatric disorder in the father (psychiatric control, n = 16). The fourth group had a parental history of alcohol abuse with no other substance abuse diagnosis (alcohol only; n = 22). SA and other psychiatric diagnoses were made using an expanded version of the Structured Clinical Interview for DSM-III-R (SCID) given to the parents (Spitzer & Williams, 1983). Interviews were given by a trained research associate and a consensual diagnosis was made during a clinical conference.
Boys from all groups were used to develop indices of the constructs of interest, in order to assess behavior problems across a broad range of severity in a large sample of boys with and without a family history of psy- chopathology, including SA. All subjeets were members of families who participated in the first wave of a longitudinal study of the development of SA, conducted by the Center for Education and Drug Abuse Research (CEDAR). The CEDAR protocol affords the opportunity to characterize putative SA risk characteristics across a wide range of measures and data sources.
The boys' mean age was 10.9 years (SD = .84), and their mean grade level was 4.52 (SD = 1.1). The sample was 92% Caucasian and 8% Afri- can-American. None of these variables differentiated the four groups. In the SA+ group, fathers had significantly lower socioeconomic status com- pared to the other groups. Table I presents rates of lifetime psychiatric disorders for the four groups. Percentages are provided for five general categories: no diagnosis, ADHD, oppositional defiant disorder (ODD), anxiety disorders, and mood disorders. Generally, the percentage of sub- jeets with these psychiatric disorders was higher in the SA+ group eom-

182 Martin et al.
Table I. Rates of Psychiatric Disorders of Childhood in the Four Groups of Subjects: SA+, 8A-, Psychiatric Control, and Alcohol-only a
Family history group
SA+ SA- Psychiatric Alcohol-only (n ffi 67) (n = 78) (n = 16) (n = 22)
No diagnosis 35.8% 70.5% 62.5% 54.5% ADHD 23.9% 9.0% 12.5% 9.1% ODD 28.4% 6.4% 25.0% 18.2% Anxiety disorders 34.3% 16.7% 18.7% 40.9% Affective disorders 26.9% 3.8% 0% 4.5%
aThe sum of percentages within groups exceeds 100% due to comorbidity. SA = substance abuse; ADHD ffi attention-deficit hyperactivity disorder; ODD -- oppositional defiant disorder.
pared to the SA- group. Rates of disorders in the psychiatric control and alcohol-only groups must be interpreted cautiously due to the low n sizes.
Procedure
Male 10- to 12-year-old index cases and their mothers participated in a day-long protocol, which included questionnaires, interviews, and labo- ratory tasks. Teachers of the index cases were asked to report on child behavior using several rating scales. This study used mother and teacher reports on the index cases, laboratory task data, and reports of index cases on their own behavior. Because participation of fathers in the protocol was more limited, data were not used from father reports in developing indices of problem behavior.
Selection of Potential Measures of Aggressivity, Inattention, Hyperactivity, and Impulsivity. Using the working definitions provided above, the investi- gators selected potential measures for each construct by consensual agree- ment. Potential measures for the four constructs were selected from each of four data sources: the child's report on self, mother's report on the child, teacher's report on the child, and laboratory task data. Measures were se- lected if they appeared to assess one of the four constructs based on pub- lished data, and in some cases face validity. Some of the laboratory measures, and some of the behavior ratings scales, were specifically de- signed to measure a particular construct (e.g., the Porteus Mazes impulsive errors score; the aggression subscale of the Child Behavior Checklist). Sets of symptoms from diagnostic interviews were selected by the investigators as measures of a particular construct, so long as these items appeared to specifically assess that construct.

Aggressivity, Inattention, Hyperactivity, and Impulsivity 183
Mother reports on the child were taken from the Kiddie-Schedule for Affeetive Disorders and Schizophrenia-Expanded (K-SADS-E), a struc- tured clinical interview with versions designed to provide reports on both current (past 6 months) and lifetime DSM-III-R symptoms and disorders of childhood (Orvaschel, Puig-Antieh, Chambers, Fabrizi, & Johnson, 1982). Mother reports also were taken from the Child Behavior Checklist (CBCL: Achenbach & Edelbrock, 1983) and the Minimal Brain Dysfunc- tion (MBD) questionnaire (Tarter et al., 1977). Child reports were primar- ily taken from current and lifetime symptoms endorsed in the K-SADS-E (Orvasehel et al., 1982). Teacher reports on the child were taken from re- sponses to three questionnaires: the Child Behavior Checklist--Teacher Version, and the Disruptive Behavior Disorders (DBD) rating scale (Pel- ham & Murphy, 1987), and the Conners Behavior Rating Scale (CBRS; Conners, 1969). Laboratory data were taken from a variety of tasks, in- eluding a provocation to aggression task (Pelham et al., 1991), a vigilance task (Schneider & Detweiler, 1987), several subtests from the Wechsler In- telligence Scale for Children (WISC; Wechsler, 1991), and an actigraph measure of motor activity (el. Tryon, 1991).
Data Reduction. This project employed a structural approach to data reduction that prevented any one measure or informant from exerting un- due influence on resultant construct scores. First, the covariation of items was examined within each instrument, test, or interview that assessed a par- tieular construct using a particular data source. Second, the covariation of all measures within a data source for a particular construct was examined. These measures were standardized and averaged to compute a trait~method indicator, i.e., a summary index for a construct from a data source. Third, the covariation of trait/method indicators for a particular construct was ex- amined. Items were retained at each step of the data reduction procedure if item deletion did not improve internal consistency.
Missing Data. There were differences among variables in the number of subjects with available data. Given the large number of variables used in this research, we developed a conservative strategy for missing data. Co- variation of items and indicators was examined using only subjects with complete data for these variables. Subjects received summary scores for a trait/method indicator only if most or all measures were available. If a vari- able had relatively few subjects, it was not selected as a potential measure in the development of construct scores. Instead, these variables were used in the concurrent validation of the constructs of interest.
The derivation of each trait/method indicator is described below. Measures are described in the text. For each construct, a table provides n sizes and internal consistency values at each level of the data reduction process. Internal consistency is described for most measures using Cron-

184 Martin et al.
bach's alpha. Unless otherwise noted, alpha values did not improve with the deletion of items. Alpha coefficients were not computed for measures if high internal consistency had previously been established (e.g., CBCL subscales; Achenbach & Edelbrock, 1983). Concurrent validation analyses for each construct are described in the text.
Aggressivity
Mother's Report. The first and second measures were current (past 6 months) and lifetime counts of oppositional defiant disorder symptoms from the K-SADS-E: "often argues with adults," "often actively defies adult re- quests or rules," is often touchy or easily annoyed by others," "is often spiteful and vindicative," "often loses temper," "often deliberately does things which annoy other people," and "is often angry and resentful." The third and fourth measures were current and lifetime counts of (CD) symptoms from the K- SADS-E: "carded a weapon," "was disorderly and rowdy," "destroying prop- erty," "setting fires," "starting fights," "using a weapon to hurt somebody," "hitting somebody with the intention of hurting them," "gang fights," "hurting people," and "hurting animals." The fifth measure was a count of items en- dorsed by mothers on the Minimal Brain Dysfunction questionnaire: "fights," "destructive," "temper tantrums," and "overly aggressive." The sixth and sev- enth measures were mother reports on the Aggression and Delinquency subscales of the CBCL (Achenbach & Edelbrock, 1983).
Child's Report. The first and second measures were counts of current and lifetime ODD symptoms (described above) endorsed by boys in the K-SADS-E interview. The third and fourth measures were counts of current and lifetime CD symptoms (described above) from the K-SADS-E inter- view with the boys.
Teacher's Report. Two measures were employed. The first was the score on the teacher CBCL aggression subscale. The second measure was the sum of four items from the Connors Behavior Rating Scale: "quarrel- some," "acts smart," "defiant," and "uncooperative."
Laboratory Measures. Laboratory measures of aggressivity were taken from the child's performance on a provocation to aggression task (Pelham et al., 1991). Subjects competed in a reaction time task against a presumed opponent to earn points that could be exchanged for money. No opponent was actually involved, and the experiment was controlled by a computer. The task involves a total of 48 reaction time trials, of which the subject wins 32 times. The 16 loss trials are randomly distributed along the 48. The winner of each trial takes 0 to 100 points from the opponent. Half of the trials in which the subject loses are high-provocation trials (opponent

Aggressivlty, Inattention, Hyperactivlty, and lmpulsivity 18S
takes away many points), and half are low-provocation trials (opponent takes away few points). Dependent measures were computed as (1) the total number of points taken away from opponents, and (2) the difference between the number of points taken following high- versus low-provocation loss trials.
Table II summarizes the results of data reduction for aggressivity con- struet scores. Sample sizes and measures of internal consistency are given at each step of the data reduction process: measures, trait/method indicators, and construct scores. Measures of a construct from a data source were stand- ardized and averaged to compute trait/method indicators. Trait/method in- dicators that covaried were standardized and averaged to compute construct scores.
As shown in Table II, the internal consistency of most aggressivity measures was moderate to high. Internal consistency measures also were moderate to high for each of the four trait/method indicators. The covaria- tion of the four aggressivity trait/method indicators was examined using sub- jects who had complete data (n = 143). The item-total correlation of the laboratory indicator was .20, which was substantially lower than the other item total correlations (range = .35 to .47). Therefore, the laboratory/ag- gressivity indicator was dropped. As shown in Table II, the three remaining trait/method indicators showed a moderate level of internal consistency. These three indicators were standardized and averaged to compute aggres- sivity construct scores, which were available for 156 subjects.
Concurrent Validation. Aggressivity construct scores were significantly correlated with mother reports on the hostile withdrawal subscale of the CBCL (r = .27; n -- 62, p < .05). A second concurrent validator was the sum of four aggresivity items from the Disruptive Behavior Disorders (DBD) scale (Pelham & Murphy, 1987), completed by teachers: "is often angry and resentful," "often initiates physical fights," "often swears or uses obscene language," and "has been physically cruel to people." This measure was significantly correlated with aggressivity construct scores (r --- .42, n = 130, p < .001).
Inattention
Mother's Report. Two measures were taken from the K-SADS-E, using five symptoms of inattention: "is easily distracted by extraneous stimuli," "has difficulty following through on instructions from others (not due to incom- prehension or defiance)," "has difficulty sustaining attention in tasks or play activities," "often does not seem to listen to what is being said to him or her," and "often loses things necessary for tasks or activities." The first meas-

Mea
sure
s n
Mot
her
repo
rt
OD
D s
ympt
oms
(cur
rent
) 17
9 0c
=
.75
OD
D s
ympt
oms
(lif
etim
e)
179
cc -
- .8
0 C
D s
ympt
oms
(cur
rent
) 17
9 oc
=
.40
CD
sym
ptom
s (l
ifet
ime)
17
9 0c
--
.40
MB
D
169
~ =
.67
Que
stio
nnai
re i
tem
s 17
1 C
BC
L A
ggre
ssio
n 17
1 --
C
BC
L D
elin
quen
cy
Chi
ld r
epor
t O
DD
sym
ptom
s (c
urre
nt)
179
cx =
.7
2 O
DD
sym
ptom
s (l
ifet
ime)
17
9 r
.69
CD
sym
ptom
s (c
urre
nt)
179
cr
.53
CD
sym
ptom
s (l
ifet
ime)
17
9 0c
..5
1 T
each
er r
epor
t C
BR
S i
tem
s 17
0 c~
=
.91
'[
CB
CL
Agg
ress
ion
158
--
J L
abor
ator
y m
easu
res c
P
rovo
cati
on (
tota
l)
169
--
| P
rovo
cati
on (
high
vs.
low
) 16
9 /
Tab
le l
I. D
ata
Red
ucti
on f
or A
ggre
ssiv
ity
Con
stru
ct S
core
s a
Tra
it-m
etho
d in
dica
tor
Inte
rnal
con
sist
ency
n
Inte
rnal
con
sist
ency
Mot
her/
aggr
essi
vity
17
1 b
r162
= .8
5/'
Chi
ld/a
ggrc
ssiv
ity
179
oc =
.8
2
Tea
cher
/agg
ress
ivit
y 15
8 r
= .7
7
Lab
orat
ory/
aggr
essi
vity
c 16
9 r
= .6
3
Con
stru
ct
n In
tern
al c
onsi
sten
cy
Agg
ress
ivit
y c
156
cr -
- .5
9
aOD
D
= op
posi
tion
al d
efia
nt d
isor
der;
CD
=
cond
uct
diso
rder
; M
BD
=
Min
imia
l B
rain
Dys
func
tion
; C
BC
L =
C
hild
Beh
avio
r C
heck
list
; C
BR
S
= C
onno
rs B
ehav
ior
Rat
ing
Sca
le.
bTra
it-m
etho
d in
dica
tor
scor
es w
ere
com
pute
d fo
r su
bjec
ts w
ith
data
on
four
(n
= 6)
, fi
ve (
n --
3).
Six
(n
= 7)
, an
d se
ven
(n =
16
3) o
f th
e se
ven
tota
l m
easu
res.
Alp
ha s
tati
stic
bas
ed o
n n
= 16
3. c
~ =
Cro
nbac
h's
alph
a; r
=
Pea
rson
pro
duct
-mom
ent
corr
elat
ion.
C
The
la
bora
tory
/agg
ress
ivit
y in
dica
tor
was
not
use
d to
com
pute
con
stru
ct s
core
s du
e to
its
wea
k as
soci
atio
n w
ith
othe
r in
dica
tors
of
this
co
nstr
uct.
F.
as a. as

Aggressivity, Inattention, Hyperactivity, and lmpulsivity 187
ure was a count of lifetime symptoms, and the second was a count of current symptoms. The third measure was a sum of two items on the Minimal Brain Dysfunction questionnaire: "short attention span" and "daydreams."
Child's Report. Two measures were used from the K-SADS-E inter- view with index cases: the number of current inattention symptoms, and the number of lifetime inattention symptoms (described above).
Teacher's Report. The first measure was the score on the inattention subscale of the CBCL. The second measure was the sum of two items from the CBRS: "fails to finish things he or she starts" and "inattentive/easily distracted."
Laboratory Measures. Four measures were employed. The first measure was the digit span subtest of the Wechsler Intelligence Scale for Children. Subjects are read a series of digits and are then required to repeat the digits in the correct sequence. The dependent measure is the largest number of digits correctly recalled. The second measure was an interference score on a computerized version of the Stroop task (Stroop, 1938). Subjects report the ink color of words shown on a computer by moving a joystick to an appropriate position. Interference scores were defined as the difference in average response latency in trials that used neutral words, and trials that used words that denoted a color other than the ink color of the item. In- terference errors were chosen as an inattention measure because they may reflect an inability to sustain attention on relevant stimulus attributes. The third measure was the number of true positive responses on a computerized vigilance task. Subjects scan changing computer displays of two letters and two dummy characters in a 2 x 2 matrix while searching for the appearance of either of two specific target letters. Subjects are instructed to press a computer key when a target appears on a screen, and to inhibit a response when a nontarget appears (Schneider & Detweiler, 1987). The fourth meas- ure was the number of completed task items during a forbidden toy task. In this task, the subject is put alone in a room with a number of interesting toys, but is told to ignore these toys and complete a set of symbol matching worksheets. Subjects are given 15 min to complete the worksheets.
Table III summarizes the results of data reduction for inattention con- struct scores. Sample sizes and measures of internal consistency are given at the level of measures, trait/method indicators, and construct scores. Measures for a construct from a data source were standardized and aver- aged to compute trait/method indicators. Trait/method indicators were in turn standardized and averaged to compute construct scores.
Table III indicates that the internal consistency of inattention meas- ures was moderate to high. Internal consistency measures also were mod- erate to high for each of the four trait/method indicators. The four trait/method indicators, in turn, showed a moderate level of internal con-

Tab
le I
lL D
ata
Red
ucti
on f
or I
natt
enti
on C
onst
ruct
Sco
res a
G
O
Mea
sure
s n
Inte
rnal
con
sist
ency
n
Mot
her
repo
rt
K-S
AD
S-E
sym
ptom
s (c
urre
nt)
179
K-S
AD
S-E
sym
ptom
s (l
ifet
ime)
17
9 2
MB
D Q
uest
ionn
aire
ite
ms
169
a=.8
1 }
a =
.82.
r
= .3
2 16
6
Tra
it-m
etho
d in
dica
tor
Inte
rnal
con
sist
ency
Mot
her/
inat
tent
ion
r --
.84
Con
stru
ct
n In
tern
al c
onsi
sten
cy
Chi
ld r
epor
t K
-SA
DS-
E s
ympt
oms
(cur
rent
) 17
9 a
-- .
71
]. C
hild
/ina
tten
tion
K
-SA
DS-
E s
ympt
oms
(lif
etim
e)
179
a =
.70
.I 17
9 r
= .7
2
Tea
cher
rep
ort
CB
CL
Ina
tten
tion
Sca
le
158
--
I T
each
er/i
natt
enti
on
2 It
ems
from
Con
nors
Beh
avio
r I
158
r =
.80
Rat
ing
Scal
e 17
0 r
= .7
8
Lab
orat
ory
mea
sure
s b
WIS
C d
igit
spa
n 17
8 m
St
roop
tas
k in
terf
eren
ce
164
m
/ L
abor
ator
y/in
atte
ntio
n V
igil
ance
tas
k sc
ore
179
--
179/
' a
= .5
3 b
Forb
idde
n to
y ta
sk s
core
18
0
Inat
tent
ion
146
a =
.66
aa
= C
ronb
ach'
s al
pha;
r
= Pe
arso
n pr
oduc
t-m
omen
t co
rrel
atio
n;
MB
D
= M
inim
al B
rain
Dys
func
tion
; C
BC
L
-- C
hild
Beh
avio
r C
heck
list
; W
ISC
=
Wec
hsle
r In
tell
igen
ce S
cale
for
Chi
ldre
n; K
-SA
DS-
E
= K
iddi
e-Sc
hedu
le f
or A
ffec
tive
Dis
orde
rs a
nd S
chiz
ophr
enia
-Exp
ande
d.
bThe
lab
orat
ory/
inat
tent
ion
scor
es w
ere
com
pute
d fo
r su
bjec
ts w
ith
thre
e (n
=
27)
or f
our
(n
= 15
2) o
f th
e fo
ur m
easu
res
avai
labl
e. A
lpha
st
atis
tic
base
d on
n
= 15
2.
to
gl

Aggressivity, Inattention, Hyperactivity, and Impulsivity 189
sisteney. Alpha-if-item-deleted values indicated that if the laboratory indi- cators were deleted, alpha would increase by .02. However, the laboratory indicator of inattention was retained, as the small increase in alpha was judged as less important than the use of laboratory data. The four indica- tors were standardized and averaged to compute inattention construct scores, which were available for 146 subjects.
Concurrent Validation. One measure was used for the concurrent vali- dation of inattention construct scores. This measure was the sum of two items completed by teachers on the DBD: "often shifts from one uncom- pleted activity to another" and "has difficulty following through on instruc- tions from others, e.g., fails to finish chores." The sum of these two items correlated (r = .70, n = 145, p < .001) with inattention construct scores.
Hyperactivity
Mother's Report. The first measure was a count of three current symp- toms taken from the K-SADS-E: "often fidgets with hands or feet or squirms in seat," "has difficulty remaining seated when required to do so," and "often talks excessively." The second measure was a count of the same symptoms for the child's lifetime. The third measure was mother's report on the CBCL hyperactivity scale. The fourth measure was mother's report on the General Activity subscale of the Dimensions of the Temperament Survey (DOTS; Lerner, Palermo, Spiro, & Nesselroade, 1982). The fifth measure was the sum of the following hyperactivity items from the Minimal Brain Dysfunction Questionnaire: "overactive," "can't sit still, . . . . talks too much and/or too loudly," "wears out toys, shoes, and clothes," "fidgets," and "constantly touches other people or things."
Child's Report. Two measures were employed: a count of current and of lifetime symptoms of hyperactivity (described above) taken from the K- SADS-E interview with the child.
Teacher's Report. One measure of the teacher/hyperactivity indicator was employed. This measure was the sum of two items on the CBRS: "rest- less or overactive" and "constantly fidgeting."
Laboratory Measures. The laboratory measures of hyperactivity em- ployed the motionlogger actigraph activity monitor (Ambulatory Monitor- ing, Inc.), a wearable device that records motor activity in real time. Subjects wear the activity monitor during the entire CEDAR protocol. Ac- tivity is measured as total activity per unit time for particular behavioral tasks. Six measures of motor activity during particular activities were used: vigilance task, Porteus Mazes task, forbidden toy task, motor restraint task, reactivity to violence task, and total activity during the entire protocol.

190 Martin et ai.
Table IV summarizes the results of data reduction for inattention con- struct scores. Sample sizes and measures of internal consistency are pro- vided for measures, trait/method indicators, and construct scores. Measures for a construct from a data source were standardized and averaged to com- pute trait/method indicators. Trait/method indicators that covaried were standardized and averaged to compute construct scores.
Table IV indicates that the internal consistency of hyperactivity meas- ures was moderate to high. Internal consistency measures were fairly high for each of the trait/method indicators. The four trait/method indicators showed a low-to-moderate level of internal consistency (n = 143, alpha = .56). Item analysis indicated that the laboratory indicator showed by far the least covariation with other indicators, and that if this indicator were deleted, internal consistency would improve. Therefore, hyperactivity con- struct scores were computed by standardizing and averaging three trait/method indicators: mother, child, and teacher report. As can be seen in Table IV, these indicators had a moderate level of internal consistency, and were available for 157 subjects.
Concurrent Validation. Hyperactivity construct scores were signifi- cantly correlated with the sum of three DBD items completed by teachers: "has difficulty remaining seated when required to," "has difficulty playing quietly," and "often talks excessively" (r = .53, n = 132, p < .001).
Impulsivity
Mother's Report. Three measures were used. The first and second measures were current and lifetime counts for three symptoms of impul- sivity from the K-SADS-E: "often blurts out answers to questions before they have been completed," "often interrupts and intrudes on others," and "often engages in physical dangerous activities without considering possible consequences (not for the purpose of thrill seeking)." The third measure was mother's report on the task persistence subscale of the Dimensions of Temperament Scale (DOTS; Lerner et al., 1982). This subscale assesses a child's ability to complete particular tasks.
Child's Report. Three measures were employed. The first and second measures were current and lifetime counts of hyperactivity symptoms from the K-SADS-E (described above). The third measure was the child's report on the task persistence suhscale of the DOTS. The child/impulsivity indi- cator was computed by standardizing and averaging the three measures.
Teacher's Report. Only one measure of impulsivity from teacher re- ports was used: the item "excitable, impulsive" from the CBRS. This item

Mea
sure
s
Mo
ther
rep
ort
K-S
AD
S-E
sy
mp
tom
s (c
urre
nt)
179
r =
.87
K-S
AD
S-E
sy
mp
tom
s (l
ifet
ime)
17
9 (x
=
.69
DO
TS
Act
ivit
y 17
7 M
BD
Que
stio
nnai
re i
tem
s 16
9 0~
=
.84
CB
CL
Hyp
erac
tivi
ty
171
--
Tab
le I
V.
Dat
a R
educ
tion
for
Hyp
erac
tivi
ty C
onst
ruct
Sco
res a
Tra
it-m
etho
d in
dica
tor
n In
tern
al c
onsi
sten
cy
n In
tern
al c
onsi
sten
cy
Mot
her/
aggr
essi
vity
16
3 b
r =
.89 ~
Con
stru
ct
n In
tern
al e
nnxi
sten
cy
Chi
ld r
epor
t K
-SA
DS
-E s
ym
pto
ms
(cur
rent
) 17
9 K
-SA
DS
-E s
ym
pto
ms
(lif
etim
e)
179
= .5
5 [
Chi
ld/h
yper
acti
vity
H
yper
acti
vity
c (x
.5
3 .I
179
r =
.73
157
a --
.63
Tea
cher
rep
ort
Tea
cher
/hyp
erac
tivi
ty
CB
CL
ite
ms
169
r =
.74
} 16
9 r
= .7
4
Lab
orat
ory
mea
sure
s c
Lab
orat
ory/
hype
ract
ivit
yC
Act
ivit
y m
onit
or
169
o~ =
.8
9 }
169
o~ =
.8
9
aDO
TS
=
Dim
ensi
ons
of
Tem
per
amen
t S
urve
y; M
BD
=
Min
imia
l B
rain
Dys
func
tion
; C
BC
L =
C
hild
Beh
avio
r C
heck
list
; K
-SA
DS
-E =
K
iddi
e S
ched
ule
for
Aff
ecti
ve D
isor
ders
and
Sch
izop
hren
ia-E
xpan
ded.
/~
l'rai
t-m
etho
d in
dica
tor
scor
es w
ere
com
pute
d fo
r su
bjec
ts w
ith
data
on
four
(n
= 4)
and
fiv
e (n
=
159)
of
the
five
mea
sure
s. A
lpha
sta
tist
ic
base
d on
n
= 15
9. o
~ --
Cro
nbac
h's
alph
a; r
=
Pea
rson
pro
du
ct-m
om
ent
corr
elat
ion.
C
The
lab
orat
ory/
hype
ract
ivit
y in
dica
tor
was
not
use
d to
co
mp
ute
con
stru
ct s
core
s du
e to
its
wea
k as
soci
atio
n w
ith
othe
r in
dica
tors
of
this
con
stru
ct.
qlQ
*e
m g O
Ig
gg
gg

192 Mar t in et al.
showed a reasonable distribution and was retained for subsequent analyses as the teaeher/impulsivity indicator.
Laboratory Tasks. Two measures were examined. The first was the total number of impulsive errors on the Porteus Mazes test (Porteus, 1965). In this task, subjects are required to carefully trace a path through a maze with a pen. Impulsive errors are those that involve tracing outside the lines and shortcuts. The second measure was the false alarm rate on a vigilance task (Schneider & Detweiler, 1987). Subjects are required to press a key when a target appears on a keyboard, and to inhibit this response when a nontarget appears. The percentage of the nontarget trials in which the sub- ject pressed the key is the false alarm rate.
Table V summarizes the results of data reduction for inattention con- struct scores. Measures of this construct from a particular data source were standardized and averaged to compute trait/method indicators. Trait/method indicators were in turn standardized and averaged to compute construct s c o r e s .
Table V shows that the internal consistency of impulsivity measures was moderate. Internal consistency measures also were moderate for the trait/method indicators, and quite modest for the laboratory/impulsivity in- dicator. The four trait/method indicators showed a moderate level of internal consistency. Impulsivity construct scores were computed by standardizing and averaging the four trait/method indicators. Construct scores were avail- able for 147 subjects.
Concurrent Validation. Impulsivity construct scores were significantly correlated with an item from the teacher DBD selected to indicate impul- sivity, "has difficulty awaiting turn in games or group situations" (r = .39, n = 129, p < .001). A second variable used for concurrent validation was scores on a computerized motor restraint task. Subjects are required to draw on the computer screen a 180 ~ arc as slowly as possible using a light pen. Scores are the total number of seconds taken to complete the task; lower numbers are taken to reflect more impulsivity. Motor restraint scores correlated (r = .29, n = 145, p < .001) with impulsivity construct scores.
RESULTS
Multi-Trait Multi-Method Matrix Analysis Using Confimnatory Factor Analysis.
The reliability analyses indicated a reasonable level of covariation among indicators for each construct. Measures of concurrent validity pro- vided some support for the construct scores. However, these analyses have

Mea
sure
s
Tab
le V
. D
ata
Red
ucti
on f
or I
mpu
lsiv
ity
Con
stru
ct S
core
s a
Tra
it-m
etho
d in
dica
tor
n In
tern
al c
onsi
sten
cy
n In
tern
al c
onsi
sten
cy
Mot
her
repo
rt
K-S
AD
S-E
sym
ptom
s (c
urre
nt)
176
r =
.74
| K
-SA
DS-
E s
ympt
oms
(lif
etim
e)
176
oc =
.6
8 D
OT
S T
ask
Pers
iste
nce
Scal
e 17
8 M
othe
r/im
puls
ivit
y 16
3 (x
=
.76
Chi
ld r
epor
t K
-SA
DS-
E s
ympt
oms
(cur
rent
) 17
6 0~
=
.53
] C
hild
/im
puls
ivit
y K
-SA
DS-
E s
ympt
oms
(lif
etim
e)
176
Gt =
.5
3 I
173
ot =
.7
2 D
OT
S T
ask
Pers
iste
nce
Scal
e 17
8
Tea
cher
rep
ort
Tea
cher
/im
puls
ivit
y C
BR
S i
tem
15
8 --
)
158
Con
stru
ct
n In
tern
al c
onsi
sten
cy
lmpu
lsiv
ity
147
tx =
.5
9
Lab
orat
ory
mea
sure
s Po
rteu
s M
aze
impu
lsiv
e er
rors
17
8 --
~
Lab
orat
ory/
impu
lsiv
ity
Vig
ilan
ce t
ask
fals
e al
arm
rat
e 18
0 --
J
175
r --
.26
aDO
'IS
--
D
imen
sion
s of
Tem
pera
men
t Su
rvey
; C
BR
S
= C
onno
rs
Beh
avio
r R
atin
g Sc
ale;
K
-SA
DS-
E
= K
iddi
e Sc
hedu
le
for
Aff
ecti
ve
Dis
orde
rs a
nd S
chiz
ophr
enia
-Exp
ande
d;
~ --
Cro
nbac
h's
alph
a; r
=
Pear
son
prod
uct-
mom
ent
corr
elat
ion.
g | m
gS
m
O g gfl
m

194 Martin et al.
several limitations. The convergent and discriminant validity of constructs is best examined in a unified analytic framework. It is important to examine whether the data suggest four separable constructs, or if they are better explained by a single-factor model. Covariation among the four constructs is best estimated after accounting for the influence of method variance.
To address these issues, a confirmatory factor analysis approach using the multi-trait multi-method (MTMM) framework was conducted. Devel- oped by Campbell and Fiske (1959), this framework examines convergent and discriminant validity as a function of the extent to which measures of the same construct using different methods converge, relative to the con- vergence of measures of different constructs that use the same method. The original procedures designed to assess MTMM properties suffered from restrictive assumptions, such as uncorrelated error variance between measures and orthogonal constructs (Campbell & Fiske, 1959). In the con- firmatory factor analysis procedures designed to address these issues, these assumptions are not required. Variation in each test score is partitioned into variation due to a trait, variation due to method, and unique (or error) variance (Bagozzi, 1991; Joreskog & Sorbom, 1989; Loehlin; 1987). Each of these sources of variance is estimated, as is the fit of this MTMM model to the data. The MTMM model posits method factors and trait constructs that contribute to scores on each variable. The significance of each indi- cator to its related trait construct and method factor is tested, and relations among the four latent trait constructs and among the four method factors are estimated. This specific MTMM model was compared to four alterna- tive models: (1) a single-factor model, where each measure served as an indicator of a single first-order factor; (2) a null model, specifying that each indicator reflects one of 14 covarying but distinguishable factors; (3) a four- trait model, in which only four latent traits are hypothesized; and (4) a four-method model, in which only four method factors are hypothesized.
Each model was tested using subjects with complete data for all 14 indicators (n = 135). Summary statistics for model comparisons are provided in Table III. Chi-square values are given for each model; lower values in- dicate a better fit of the data to a model. The difference in Chi squares between the MTMM and alternative models are provided; significant effects demonstrate that the MTMM model provided a statistically significant im- provement in fit over an alternative. The ratio of Chi square to degrees of freedom (df) is also provided as a goodness of fit measure (Joreskog & Sorbom, 1979). A smaller ratio suggests a better fit relative to the number of hypothesized parameters. Although no specific value of the ratio has proven an infallible indicator of adequate fit, ratios of 2 or less are often considered satisfactory (Loehlin, 1987). Finally, normed fit and parsimonious fit indices are provided to assess the relative increase in fit from an alter-

A~gresslvity, Inattention, Hyperactivity, and lmpulsivity 195
native model to the MTMM. The normed fit index compares the change in Chi square from an alternative model to the MTMM. Normed fit indices range from 0 to 1.0, with higher numbers suggesting larger increases in fit (Bentler & Bennett, 1980). The parsimonious fit index multiplies the normed fit index by the ratio of the df of the MTMM model to that of an alternative (James, Mulaik, & Brett, 1982). Any model's improvement in fit is weighted according to the number of additional hypothesized parameters.
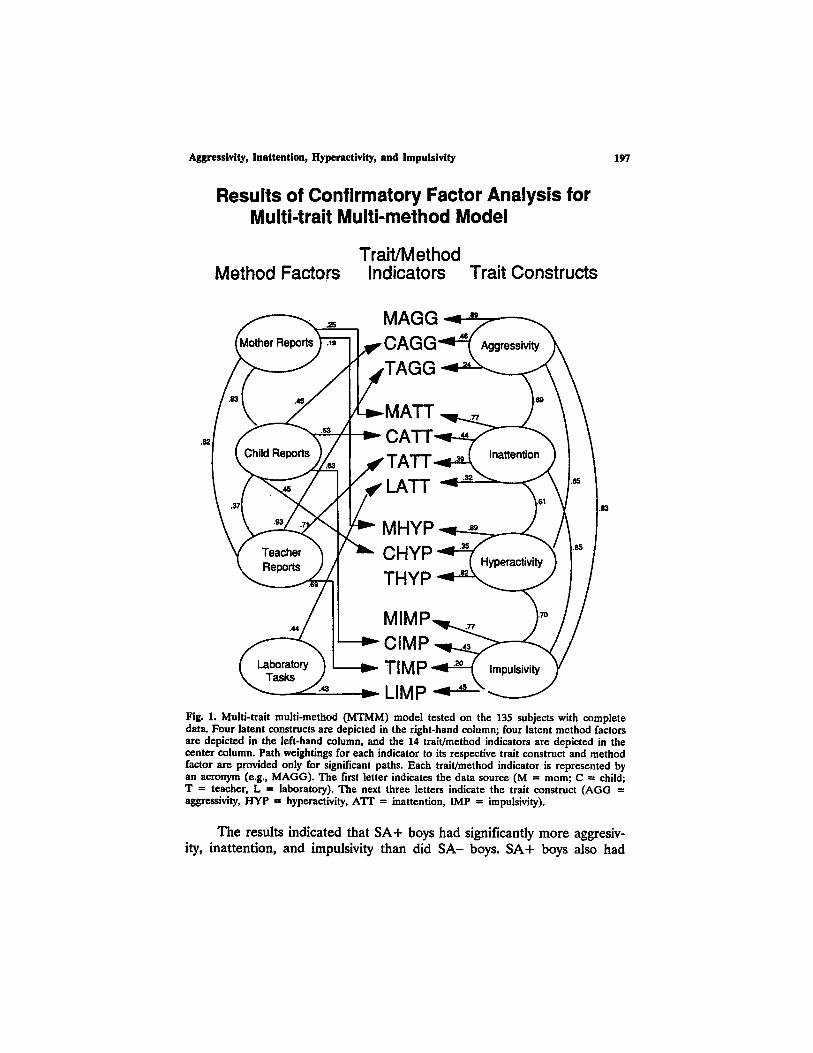
The data in Table VI indicate that the MTMM provides a better fit to the data than alternative models. The increased fit is evident even when accounting for the increased number of hypothesized parameters in the MTMM (James, Mulaik, & Brett, 1982; Joreskog & Sorbom, 1979). The results indicate that the covariance among the 14 indicators is best repre- sented by the four specified traits and the four specified methods, and sug- gest reasonable convergent and discriminant validity of the aggressivity, inattention, hyperactivity, and impulsivity constructs. The MTMM model is presented in Fig. 1. 4 Significant paths from trait/method indicators to their associated trait constructs and method factors are indicated by arrows and path loadings. Significant associations among the four trait constructs and among the four method factors are provided.
As can be seen in Fig. 1, associations among the four trait constructs were estimated to be quite high even when the influence of method vari- ance was accounted for. Correlations among the trait constructs ranged from .60 to .83. The majority of significant factor loadings stemmed from the underlying traits rather than the method factors, providing further evi- dence for the validity of the four traits.
The strong covariation among the four latent trait constructs suggests that they could be conceptualized as multiple indicators of a single, sec- ond-order factor. This proposition was tested using a second-order model. This model was similar to the MTMM except that it used each of the trait
4Kenny and Kashy (1992) suggested that this type of confirmatory factor analysis of MTMM matrices makes estimation procedures difficult, and that the assumption of method factors that exert consistent effects across traits is often unwarranted. Also discussing these issues, Marsh (1989) proposed a correlated uniqueness model as an alternative. This model posits latent traits but no method factors. Instead of assuming uneorrelated error (uniqueness), this model permits correlated errors for indicators that use the same method. We have presented the MTMM and related models because they (1) provide tests of the structure of the data related to the clear conceptual framework of Campbell and Fiske (1959), and (2) provide more direct estimates of the influence of method variance (within the context of assumptions about the presence of method factors). Nevertheless, the fit of the correlated uniqueness model to the data was examined. The Chl-square value (81.8, 52 d o was comparable to that of the MTMM model, and results regarding associations among the four traits were very similar. Therefore, we conclude that the MTMM model provides a reasonable description of the data, especially with regard to the discriminant and convergent validity of the four traits.

196 Mart in et al.
Table VI. Comparison of MTMM, Null, Single-Factor, Trait-Only, and Method-Only Models*
Difference in Chi
square from Model Chi square (dr) Chi square/df MTMM n.f.i, p.f.i.
MTMM 80.18 (53) b 1.5 - - - - - - Null 876.36 (77) r 5.0 796.18 c .91 .63 Single-factor 388.73 (77) c 11.4 308.55 c .79 .55 Trait-only r 305.87 (71) c 4.3 225.69 c .74 .55 Method-only 260.20 (71) r 3.7 180.02 c .69 .52
aMTMM = multi-trait, multi-method; df = degrees of freedom; n.f.i. -- normed fit index; p.f.i. -- parsimonious fit index. ~ < .05.
"p < .001.
constructs as indicators of a second-order, superordinate factor. Given their similarities, the MTMM and second-order models should not be seen as competing with one another. Instead, tests of the second-order model against the same four alternative model~ null, one-factor, trait-only, and method-only--provide tests of the specific hypothesis that the covariation among the four constructs is consistent with a single second-order factor.
The second-order model fit the data better than the alternative models. The second-order model provided a significantly lower Chi square (80.99, 55 f) compared to the other models (all p < .001). The ratio of Chi square to df was 1.5, much lower than that of the other models (range of Chi square/dr = 3.7 to 11.4). Normed fit and parsimonious fit indices also sup- ported the superior fit of the second-order model compared to the alterna- tive models after accounting for the number of hypothesized parameters. These results are consistent with the conceptualization of aggressivity, inat- tention, hyperactivity, and impulsivity as four facets of a second-order factor, and at the least suggest a highly associated constellation of behavior prob- lems.
Differences in Construct Scores Between Boys With and Without a Family History of SA.
Boys with construct scores from the SA+ and SA- groups were con- trasted on the aggressivity, inattention, hyperactivity, and impulsivity construct scores. Construct scores were computed as the average of standardized indi- cators for that construct. A second-order factor score also was computed as the average of the four construct scores. Differences between the SA+ and SA- groups in this index were tested. The data are provided in Table VII.
Aggressivity, Inattention, Hyperactivity, and Impulsivity
Results of Confirmatory Factor Analysis for Multi-trait Multi-method Model
Trait/Method Method Factors Indicators Trait Constructs
197
.83
Fig. 1. Multi-trait mult i -method (MTMM) model tested on the 135 subjects with complete data. Four la tent constructs are depicted in the r ight-hand column; four latent method factors are depicted in the left-hand column, and the 14 trai t /method indicators are depicted in the center column. Path weightings for each indicator to its respective trait construct and method factor are provided only for significant paths. Each trai t /method indicator is represented by an acronym (e.g., M A G G ) . The first letter indicates the data source (M = morn; C = child; T -- teacher, L = laboratory). The next three letters indicate the trait construct ( A G G = aggressivity, HYP - hyperactivity, A ' fT -- inattention, IMP = impulsivity).
The results indicated that SA+ boys had significantly more aggresiv- ity, inattention, and impulsivity than did SA- boys. SA+ boys also had

198 Martin et al.
Table Vii. Comparisons of SA+ and SA- Boys on Aggressivity, Inattention, Hyperactivity, Impulsivity, and Second-Order Factor Scores ~
SA+ SA- Construct (n) Mean (SD) (n) Mean (SD) t-Value p-Value
Aggressivity (65) .163 (.63) (75) -.133 (.58) 2.90 .004 Inattention (65) .227 (.73) (76) -.159 (.62) 3.39 .001 Hyperactivity (66) .107 (.80) (77) -.060 (.75) 1.28 n.s. Impulsivity (58) .248 (.67) (71) -.116 (.63) 3.19 .002 Second-order factor (58) .712 (2.3) (70) -.318 (2.1) 2.67 .009
aSA = substance abuse.
significantly higher scores on the second-order factor. The two groups did not differ in hyperactivity scores. These results must be interpreted cau- tiously, however, as the subjects in these analyses were a subset of those used to develop the construct scores.
DISCUSSION
The results suggest reasonable convergent and discriminant validity of the constructs aggressivity, inattention, hyperactivity, and impulsivity in 10- to 12-year-old boys. The sample provided a broad range in the severity of behavior problems. The construct scores developed in this report used multiple data sources, thereby minimizing any undue influence of a par- ticular measure or data source. The MTMM model allowed examination of the data using the conceptual framework of Campbell and Fiske (1959) in conjunction with more recent advances in statistical methodology. The MTMM fit the data better than did alternative models. The modeling pro- cedures allowed method variance to be estimated, and revealed a strong association among the constructs after the influence of method variance was estimated. Moreover, the second-order model was consistent with the hypothesis that aggressivity, inattention, hyperactivity, and impulsivity rep- resent four indicators of a superordinate factor.
We propose a heuristic framework for understanding the strong as- sociation among the four constructs. Aggressivity, inattention, hyperactivity, and impulsivity are all hypothesized to be determined, in part, by dysregu- lation of executive cognitive functions. Executive cognitive functions are defined as self-regulatory, i.e., those needed to plan, execute, and evaluate goal-directed behavior (Miller & Brown, 1991; Tarter, Kabene, Escallier, Laird, & Jacob, 1990). Deficits in executive functions are hypothesized to create an overall behavioral dysregulation, an impaired executive self-regu-

Aggressivity, Inattention, Hyperactivity, and Impulsivity 199
lation that is manifested in a constellation of observable behaviors. Aggres- sivity, inattention, hyperactivity, and impulsivity all can be conceptualized as reflecting deficits in the planning, execution and evaluation of goal-di- rected behavior. There is substantial evidence from neuropsychology and cognitive psychology that executive functions are important determinants of many behaviors (e.g., Stuss, 1992; Tarter, Alterman, & Edwards, 1985). Each construct involves both behavior as well as maladaptive cognitive di- rection and control of this behavior (e.g., behavioral goals, foresight for consequences, emission of behaviors, responses to punishment).
Many others have reported covariation of behavior problems, and some have postulated second-order factors of problem behavior. The strong asso- ciations among the four constructs are important, but are amenable to other interpretations. Nevertheless, we have chosen to label the superordinate fac- tor behavioral dysregulation, to highlight potential functional similarities be- tween these behavior problems and drug-taking behavior. Specifically, we postulate that aggressivity, inattention, hyperactivity, and impulsivity are as- sociated with SA because both are determined in part by dysregulation of executive cognitive functions. The initiation and maintenance of drug use has been conceptualized as involving cognitive determinants of goal-directed be- havior (Maisto, Connors, & Sachs, 1981). Self-regulation of affective and cog- nitive states via drug consumption has received considerable research attention (Miller & Brown, 1991). The potential role of dysfunction in ex- ecutive cognitive processing in SA is consistent with conceptual models link- ing deficits in frontal neuropsychological functioning to SA and ASP (Gorenstein & Newman, 1980). Behavioral dysregulation is a broad construct intended to promote heuristic research on the role of executive cognitive functions in vulnerability to SA (cf. Tarter et al., 1990).
Several limitations of this research should be emphasized. First, our data did not meet the criterion for an ideal multi-trait multi-method matrix as described by Campbell and Fiske (1959). The covariation of indices of the same construct from different data sources usually was moderate, and measures of different constructs using the same data source often were associated. As noted by Fiske and Campbell (1992), few data sets in the behavioral sciences have ideal matrix properties. In particular, our labora- tory measures of hyperactivity and aggression were not highly associated with other indicators of these constructs. Using confirmatory factor analysis procedures designed to address the MTMM framework, we were able to estimate both method and error variance. Nevertheless, problems of dis- entangling trait-method units and developing more valid measures of con- structs are highly relevant to this research (Campbell & Fiske, 1959).
Another limitation involves the use of only male subjects who are 10 to 12 years old. It is unclear the extent to which these results apply to

200 Martin et aL
females. It remains to be determined whether associations amount the four constructs would be the same if assessed at later stages of development. In the CEDAR project, we plan to use different methods and measures to assess the four constructs in the current sample when subjects are age 16. If there is a strong relation of a construct as measured at 10 to 12 and at 16 years, this will lend support for the validity of the four constructs as traits.
Boys with family history of substance abuse scored higher than their family history counterparts on the aggressivity, impulsivity, and inattention scores. These differences, however, must be interpreted cautiously. It is preferable to develop indices and to test for group differences using inde- pendent samples. Because our purpose was to examine the convergent and discriminant validity of the four constructs, we used all available subjects to provide adequate power. We present the family history results as pre- liminary in nature. The best evidence for the role of aggressivity, impulsiv- ity, inattention, and hyperactivity in SA vulnerability will be to examine the ability of these constructs to predict future substance use, abuse, and de- pendence.
Further research on the validity and limitations of the construct of behavioral dysregulation will increase knowledge of vulnerability to SA. The role of executive cognitive functions in the initiation and maintenance of drug-using behaviors requires explication. A greater understanding of neuropsychological structures and functions associated with cognitive ex- ecutive processes will likely increase our knowledge of biological mecha- nisms in aggressivity, hyperactivity, inattention, and impulsivity. The specific aspects of the development of SA that are influenced by these behavior problems, and the mechanisms involved, are largely unknown. A greater understanding of the nature of these associations will increase knowledge of the etiology of substance abuse.
REFERENCES
Abikoff, H., & Kelin, R. (1992). Attention-deficit hyperactivity and conduct disorder: Comorbidity and implications for treatment. Journal of Consulting and Clinical Psychology, 60, 881-892.
Achenhach, T., & Edelbrock, C. (1983). Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Burlington, University of Vermont.
American Psychiatric Association (1987). Diagnostic and statistical manual of mental disorders (3rd ed., rev.). Washington, D.C.: Author.
Bagozzi, R. (1991). Further thoughts on the validity of measures of elation, gladness, and joy. Journal of Personality and Social Psychology, 61, 98-104.
Bentler, P., & Bonnet, D. (1980). Significance tests and goodness of fit in the analysis of covariance structures. Psychological Bulletin, 88, 588-606.

Aggressivity, Inattention, Hyperactivity, and Impulsivity 201
Blackman, S., & Ooidstein, K. (1982). Cognitive styles and learning disabilities. Journal of Learning Disabilities, 15, 105-115.
Camp, B. (1977). Verbal mediation in young aggressive boys. Journal of Abnormal Psychology, 86, 145-153.
Campbell, D., & Fiske, D. (1959). Convergent and discriminant validation by the multi-trait multi-method matrix. Psychological Bulletin, 56, 81-105.
Conners, C. (1969). A teacher rating scale for use in drug studies with children. American Journal of Psychiatry, 126, 152-156.
Dodge, K., & Newman, J. (1981). Biased decision-making processes in aggressive boys. Journal of Abnormal Psychology, 90, 375-379.
Farrington, D. (1991). Antisocial personality from childhood to adulthood. The Psychologist: Bulletin of the British Psychological Society, 4, 389-394.
Fiske, D., & Campbell, D. (1992). Citations do not solve problems. Psychological Bulletin, 112, 393-395.
Gittleman, R., Mannuzza, S., Shenker, R., & Bongura, N. (1985). Hyperactive boys almost grown up: Psychiatric status. Archives of General Psychiatry, 42, 937-947.
Gordon, M. (1979). The assessment of impulsivity and mediating behaviors in hyperactive and nonhyperactive boys. Journal of Abnormal Child Psychology, 7, 317-326.
Gorenstein, E., & Newman, J. (1980). Disinhlbitory psychopathology: A new perspective as a model for research. Psychological Review, 87, 301-315.
Hinshaw, S. (1992). Academic underachievement, attention deficits, and aggression: comorbidity and implications for intervention. Journal of Consulting and Clinical Psychology, 60, 893-903.
Hooks, M., Jones, G., Smith, A., & Neil, D. (1991). Individual differences in locomotor activity and sensitization. Pharmacology, Biochemistry, and Behavior, 38, 467-470.
James, L., Mulaik, S., & Brett, J. (1982). Causal analysis: Assumptions, models, and data. Beverley Hills: Sage.
Joreskog, K., & Sorbom, D. (1979). Advances in factor ana&sls and structural equation models. Cambridge, MA: ABT Books.
Joreskog, K., & Sorbom, D. (1989). LISREL-VII users reference guide. Mooresville, In: Scientific Software, Inc.
Kagan, J., Rosman, B., Day, D., Albert, J. & Phillips, W. (1964). Information processing in the child: Significance of analytic and reflective attitudes. Psychological Monographs, 76, 78-92.
Kellam, S., Brown, C., Rubin, B., & Ensminger, M. (1983). Paths leading to teenage psychiatric symptoms and substance use: Developmental epidemiological studies in Woodiawn. In S. Guze & J. Barrett (Eds.), Childhood psychopathology and development (pp. 17-51). New York: Raven Press.
Kenny, D., & Kashy, D. (1992). Analysis of the multitrait-multimetbod matrix by confirmatory factor analysis. Psychological Bulletin, 112, 165-172.
Lerner, R., Palermo, M., Spiro, A., & Nesseiroade, A. (1982). Assessing the dimensions of temperamental individuality across the life span: The Dimensions of Temperament Survey (DOTS). Child Development, 53, 149-157.
Loeber, R. (1988). Natural histories of conduct problems, delinquency, and associated substance use: Evidence for developmental progressions. In B. Lahey & A. Kazdin (Eds.), Advances in clinical child psychology (Vol. II, pp. 73-124). New York: Plenum Press.
Loehlin, J. (1987). Latent variable models. (pp. 87-91). Hilisdale, NJ: Erlbaum. Maisto, S., Connors, G., & Sachs, P. (1981). Expectation as a mediator in alcohol intoxication:
A reference-level model. Behavior Research and Therapy, 5, 1-18. Mannuzza, S., Klein, R., Bonagura, N., Malloy, P., Giampino, T., & Addalli, K. (1991).
Hyperactive boys almost grown up: IV. Replication of psychiatric status. Archives of General Psychiatry, 48, 77-83.
Marsh, H. (1989). Confirmatory factor analyses of multitrait-multimethod data: Many problems and a few solutions. Applied Psychological Measurement, 20, 335-361.
McCord, W., & McCord, J. ~(1960). Origins ofaicoholism. Stanford: Stanford University Press.

202 Martin et al.
Mendelson, W., Johnson, N., & Stewart, M. (1971). Hyperactive children as teenagers: A follow-up study. Journal of Nervous and Mental Disease, 153, 273-279.
Milich, R., & Kramer, J. (1984). Reflections on impnlsivity: An empirical investigation of impulsivity as a construct. In K. Gadow & L Bialer (Eds.), Advances in learning and behavioral disabilities (Vol. 3, pp. 57-94). Greenwich, CT: JAI Press.
Milich, R., & Landau, S. (1982). Socialization and peer relations in hyperactive children. In K. Gadow & I. Bialer (Eds.), Advances in learning and behavioral disabilities (VoL 1, pp. 283-339). Greenwich, CT: JAI Press.
Milich, R., Loney, H., & Landau, S. (1981). Independent dimensions of hyperactivity and aggression: A validation with playroom observation data. Journal of Abnormal Psychology, 91, 183-198.
Miller, W., & Brown, J. (1991). Self-regulation as a conceptual basis for the prevention of addictive behaviours. In N. Heather, W. Miler, & J. Greeley (Eds.), Self.control and the addictive behaviours (pp. 3-79). Sydney: Maxwell Macmillan Publishing Australia.
Moss, H., Blackson, T., Martin, C., & Tarter, R. (1992). Heightened motor activity level in male offspring of substance abusing fathers. Biological Psychiatry, 32, 1135-1147.
Moss, H., Mezzich, A., Yao, J., Gavaler, J., & Martin, C. (in press). Aggressivity among sons of substance abusing fathers: Association with psychiatric disorder in the father and son, paternal personality, pubertal development and socioeconomic status. American Journal of Drug and Alcohol Abuse.
Morrison, J., & Stewart, M. (1973). The psychiatric status of the legal families of adopted hyperactive children. Archives of General Psychiatry, 28, 888-891.
Moyer, K. (1968). Kinds of aggression and their physiological basis. Community Behavior and Biology, 2, 65-87.
Murphy, J., McBride, A., Wlodarek, W., & McBride, L. (1992). Differences in the ontogeny of locomotor activity between the alcohol-preferring P and -nonpreferring NP rats. Alcoholism: Clinical and Experimental Research, 16, 406 (abstract).
Newlin, D., & Thomson, H. (1991). Chronic tolerance and sensitization to alcohol in sons of alcoholics. Alcoholism: Clinical and Experimental Research, 15, 399-405.
Olweus, D. (1979). The stability of aggressive reaction patterns in human males: A review. Psychological Bulletin, 85, 852-875.
Orvaschel, H., Puig-Antich, H., Chambers, W., Fabrizi, M., & Johnson. R. (1982). Retrospective assessment of prepubertal major depression with the Kiddie-SADS-E. Journal of the American Society of Child Psychiatry, 21, 392-397.
Pelham, W., Milich, R., Cummings, E., Murphy, D., Schaughency, E., & Greiner, A. (1991). Effects of background anger and methylphenidate on emotional arousal and aggressive responding in attention deficit/hyperactivity disordered boys with and without concurrent aggressiveness. Journal of Abnormal Child Psychology, 19, 407-426.
Pelham, W., & Murphy, D. (1987). The DBD rating scale: A parent and teacher rating scale for the disruptive behavior disorders of childhood in DSM-III-R. Unpublished manuscript, Department of Psychiatry, University of Pittsburgh School of Medicine.
Piazza, P., Deminiere, J., Le Moal, M., & Simon, H. (1989). Factors that predict individual vulnerability to amphetamine administration. Science, 245, 1511-1513.
Pope, A., Bierman, K., & Mumma, G. (1991). Aggression, hyperactivity, and inattention- immaturity: Behavior dimensions associated with peer rejection in elementary school boys. Developmental Psychology, 27, 663-671.
Porteus, S. (1965). Porteus Mazes Tests: Fifty years' application. Palo Alto: Pacific Books. Robins, L., & Price, R. (1991). Adult disorders predicted by childhood conduct problems:
Results from the NIMH epidemiologic catchment area project. Psychiatry, 54, 116-132. Schneider, W., & Detweiler, M. (1987). A connectionist/control architecture for working
memory. In G. H. Bower (Ed.), The psychology of learning and motivation (Vol. 21, pp. 54-119). New York: Academic Press.
Sher, K. (1991). Children of alcoholics: A critical appraisal of theory and research. Chicago: University of Chicago Press.

Aggressivity, Inattention, Hyperactivity, and lmpulsivity 203
Shiffrin, R. (1988). Attention. In R. Atkinson, R. Herrnstein, G. Lidzey, & R. Luce (Eds.), Stevens handbook of erperimentalpsychology: VoL II. Learning and cognition. (pp. 739-811) New York: Wiley.
Spitzer, R., & Williams, J. (1983). Structured clinical interview for DSM-III-R. New York: New York State Psychiatric Institute.
Stroop, J. (1938). Factors affecting speed in serial verbal reactions. Psychological Monographs, 50, 38-48.
Stuss, D. (1992). Biological and psychological development of executive functions. Brain and Cognition, 20, 8-23.
Tarter, R., Alterman, A., & Edwards, K. (1985). Vulnerability to alcoholism in men. A behavior genetic perspective. Journal of Studies on Alcohol, 46, 329-356.
Tarter, R., Kabene, M., Escallier, E., Laird, S., & Jacob, T. (1990). Temperament deviation and risk for alcoholism. Alcoholism: Clinical and Experimental Research, 14, 380-382.
Tarter, R., McBride, H., Buonpane, N., & Schneider, D. (1977). Differentiation of alcoholics: Childhood history of minimal brain dysfunction, family history, and drinking patterns. Archives of General Psychiatry, 34, 761-768.
Tryon, W. (1991). Activity measurement in psychology and medicine. New York: Plenum Press. Vaizelli, L. (1981). Psychobiology of aggression and violence. New York: Raven Press. Wechsler, D. (1991). Wechsler Intelligence Scale for Children--Third Edition: Manual. San
Antonio, TX: The Psychological Corporation. Wise, R. (1988). The neurobiology of craving: implications for the understanding and
treatment of addiction. Journal of Abnormal Psychology, 97, 118-132. Wise, R., & Bozarth, M. (1987). A psychomotor stimulant theory of addiction. Psychological
Review, 94, 469-492. Zuckerman, M. (1983). Biological bases of sensation seeking, impulsivity, and anxiety. HiUsdale,
N J: Edbaum.




















