
Improving the Outcomes Of Patients with ANCA Associated ...
355
Improving the Outcomes Of Patients with ANCA Associated Vasculitis Dr Nina Brown A thesis submitted to the University of Manchester for the degree of Doctor of Philosophy (PhD) in the Faculty of Biology, Medicine and Health School of Medical Sciences 2016
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Improving the Outcomes Of Patients with ANCA Associated ...

Improving the Outcomes
Of Patients with
ANCA Associated Vasculitis
Dr Nina Brown
A thesis submitted to the University of Manchester for the
degree of Doctor of Philosophy (PhD) in the Faculty of Biology,
Medicine and Health
School of Medical Sciences
2016

2
CONTENTS
Abstract .................................................................................................................................... 9
Declaration and Copyright ..................................................................................................... 11
Preface ................................................................................................................................... 12
Definition of my role in this work .......................................................................................... 12
Collaborations and Acknowledgements ................................................................................ 13
Publications and abstracts ..................................................................................................... 15
Abbreviations ......................................................................................................................... 17
Introduction ........................................................................................................................... 21
1.1 Background ...................................................................................................................... 21
1.1.1 What is ANCA Associated Vasculitis? An overview of disease pathogenesis 21
1.1.2 PR3 versus MPO: the role of antigens and antibodies................................... 22
Figure 1. Putative representation of AAV disease pathogenesis343 ............................... 23
1.1.3 Neutrophils and NETs in AAV ......................................................................... 24
1.1.4 The role of B cells, T cells and complement ................................................... 24
1.2 Epidemiology of AAV .............................................................................................. 26
1.2.1 Genetics of AAV ............................................................................................. 26
1.2.2 Environmental exposure and epigenetics ...................................................... 27
1.3 The role of infection in disease pathogenesis ....................................................... 28
1.4 Diagnosis and classification ................................................................................... 30
Table 1. Description of AAV according to ANCA positivity and organ involvement6 ..... 30
Table 2. Chapel Hill Consensus Conference classification of AAV 201263 ...................... 31
1.5 Treatment .............................................................................................................. 32
Table 3. Definition of disease severity according to EULAR72 ........................................ 33
1.6 Prognosis ................................................................................................................ 37
1.6.1 Mortality ........................................................................................................ 37
1.6.2 Relapse ........................................................................................................... 39
1.6.3 Biomarkers to predict disease activity ........................................................... 40
1.7 Treatment and disease associated morbidity ........................................................ 41
1.7.1 Infection as a significant complication of therapy ......................................... 42
Table 4. Summary of infections reported in the 4 combined EUVAS trials90 ................. 43
1.7.2 Cardiovascular disease ................................................................................... 43
1.7.3 Bone Health .................................................................................................... 44
1.7.4 Malignancy ..................................................................................................... 44
1.7.5 Sexual health and fertility .............................................................................. 45

3
1.8 Current challenges to care for patients with AAV ................................................. 45
2 The Pathway of the UK Vasculitis Patient- from symptoms to diagnosis and beyond .. 47
2.1 Introduction ........................................................................................................... 47
2.2 Materials and Methods .......................................................................................... 48
2.2.1 Patient questionnaire..................................................................................... 48
2.2.2 Subjects .......................................................................................................... 49
2.2.3 Statistical analysis .......................................................................................... 49
2.3 Results .................................................................................................................... 49
2.3.1 Responder characteristics .............................................................................. 49
Table 1. Presenting symptoms ....................................................................................... 50
2.3.2 Symptoms ...................................................................................................... 50
Table 2. Relationship of patient characteristics to time to diagnosis (** statistically
significant when compared with time to diagnosis for those with skin symptoms) ..... 51
Table 3. Alternative diagnoses received prior to vasculitis ........................................... 52
2.3.3 Utilisation of healthcare ................................................................................. 52
Figure 1. Vasculitis patient health care utilisation ........................................................ 53
2.4 Discussion ............................................................................................................... 53
3 Vasculitis patient awareness of medication side- effects and uptake of preventative/
prophylactic measures: a UK questionnaire study ................................................................ 66
3.1 Background ...................................................................................................................... 66
3.2 Patients and Methods ............................................................................................ 67
3.3 Results .................................................................................................................... 68
3.3.1 Pilot/validity check ......................................................................................... 68
3.3.2 Main study ..................................................................................................... 68
Table 1. Characteristics of the Sample .................................................................... 69
Figure 1: Reported exposure to immunosuppression ................................................... 70
Figure 2. Patient reported awareness of potential medication side effects ................. 71
Figure 3. Patient reported uptake of preventative therapy .......................................... 73
3.4 Discussion ............................................................................................................... 73
4 A Delphi study to Assess Prevention of Treatment and disease related morbidity In
Vasculitis (ADAPTIV): Delphi methodology ............................................................................ 77
4.1 Introduction ........................................................................................................... 77
4.1.1 Objective ........................................................................................................ 78
4.1.2 Target Audience ............................................................................................. 78
4.1.3 Stakeholder groups ........................................................................................ 78
4.1.4 Co-ordination Team ....................................................................................... 78

4
4.1.5 Expert panel members (Delphi contributors) ................................................ 79
4.1.6 Other Stakeholder representatives................................................................ 80
4.2 Delphi Study ........................................................................................................... 80
4.3 Results .................................................................................................................... 82
4.4 Discussion ............................................................................................................... 84
4.5 Appendix 1. Round 1 questions ............................................................................. 85
4.6 Appendix 2: Statements generated following Round 1 ......................................... 88
4.7 Appendix 3. Consensus Statements ..................................................................... 102
4.8 Appendix 4. Summary of main consensus statement and levels of consensus ... 112
5 Literature review: methods and results ....................................................................... 118
5.1 Search strategy .................................................................................................... 118
5.2 Results .................................................................................................................. 119
5.2.1 Section 1: Bone health ................................................................................. 119
5.2.2 Section 2: Cardiovascular and thromboembolic risk ................................... 121
5.2.3 Section 3: Cancer Risk .................................................................................. 123
5.2.4 Section 4: Fertility ........................................................................................ 124
5.2.5 Section 5: Vaccination .................................................................................. 125
5.2.6 Section 6: Infection Prophylaxis ................................................................... 127
5.3 Summary .............................................................................................................. 129
5.4 Appendix 1: Search strategies .............................................................................. 130
5.4.1 Bone Health search strategy ........................................................................ 130
5.4.2 Cardiovascular/ thromboembolic risk search strategy ................................ 133
5.4.3 Cancer screening search strategy ................................................................ 138
5.4.4 Fertility preservation search strategy ......................................................... 140
5.4.5 Vaccination search strategy ......................................................................... 142
5.4.6 Pneumocystis search strategy...................................................................... 145
5.4.7 Viral and fungal prophylaxis search strategy ............................................... 150
Appendix: Evidence Tables .................................................................................................. 154
6 A Delphi study to Assess the Prevention of Treatment and disease related morbidity In
Vasculitis (ADAPTIV): recommendations ............................................................................. 229
6.1 Bone Health.......................................................................................................... 230
6.2 Cardiovascular risk modification .......................................................................... 232
6.3 Fertility preservation ............................................................................................ 234
6.4 Cancer recommendations .................................................................................... 236
6.5 Infection prevention ............................................................................................ 239
6.6 Education and monitoring ................................................................................... 243

5
6.7 Applicability and utility ........................................................................................ 243
6.7.1 A statement of potential organizational barriers to introduction ............... 243
6.7.2 Potential costs implications for introduction of guideline ........................... 243
6.7.3 Suggested audit measures ........................................................................... 243
7 Development of a Vasculitis Care Optimisation Tool .................................................. 246
7.1 Part A: Concept development and user engagement .......................................... 246
7.1.1 Introduction ................................................................................................. 246
7.1.2 Identification and engagement of stakeholders .......................................... 247
7.1.3 Methods ....................................................................................................... 247
Table 1. Characteristics of patients selected for interview ......................................... 250
1.1.1 Figure 1. VasCOT user map .......................................................................... 252
1.1.2 Figure 2. VasCOT concept ............................................................................ 253
Table 2. Themes from patient interviews .................................................................... 256
Table 3. Clinician “problem” and “wish” list ................................................................ 258
Table 4. Patient “problem” and “wish” list .................................................................. 259
Table 5. Survey responder characteristics ................................................................... 260
7.2 Section B: Design of patient and clinician interfaces ........................................... 261
7.2.1 Patient data capture .................................................................................... 261
7.2.2 Clinical data capture..................................................................................... 261
7.2.3 Frequency and scope of use ........................................................................ 263
7.3 Part C: Development of VasCOT ‘Engine’ (Functional Specification) ................... 264
7.3.1 Platform and Strategy .................................................................................. 264
7.3.2 Audit ............................................................................................................. 264
7.3.3 Security and Authentication ........................................................................ 265
7.3.4 Data Protection ............................................................................................ 265
7.3.5 Feature Access ............................................................................................. 265
7.3.6 Settings ......................................................................................................... 266
7.3.7 Role Editor .................................................................................................... 266
7.3.8 User Editor ................................................................................................... 266
7.3.9 Patient Creation ........................................................................................... 266
7.3.10 User Verification .......................................................................................... 266
7.3.11 Self-Registration ........................................................................................... 267
7.3.12 Patient Queues ............................................................................................. 267
7.3.13 Requesting Patient Access ........................................................................... 267
7.3.14 Accepting / Rejecting Patient Access Requests ........................................... 268

6
7.3.15 Access, Data Input and Versioning ............................................................... 268
7.3.16 Patient Editor ............................................................................................... 268
7.4 Discussion ............................................................................................................. 269
Appendix 1. Patient questionnaire and results .................................................................... 272
Appendix 2. Clinical data specifications……………………………………………………………………………275
Appendix 3: Patient view wireframes .................................................................................. 283
Appendix 4. Clinician view wireframes ................................................................................ 289
Appendix 5. Detailed Functional specifications ................................................................... 296
8 Discussion ..................................................................................................................... 315
8.1 Recognition and identification of disease ............................................................ 315
8.2 Initial management .............................................................................................. 317
8.3 Longer term management ................................................................................... 317
8.4 Further work ........................................................................................................ 319
8.5 Future therapies ................................................................................................... 320
8.6 Epigenetics ........................................................................................................... 321
8.7 Summary .............................................................................................................. 321
9 Publications .................................................................................................................. 322
10 Bibliography ................................................................................................................. 328
Word count 82 083

7
TABLES AND FIGURES
Chapter 1
Table 1. Description of AAV according to ANCA positivity and organ involvement6 ..... 30
Table 2. Chapel Hill Consensus Conference classification of AAV 201263 ...................... 31
Table 3. Definition of disease severity according to EULAR72 ........................................ 33
Table 4. Summary of infections reported in the 4 combined EUVAS trials90 ................. 43
Chapter 2
Table 1. Presenting symptoms ....................................................................................... 50
Table 2. Relationship of patient characteristics to time to diagnosis) ........................... 51
Table 3. Alternative diagnoses received prior to vasculitis ........................................... 52
Figure 1. Vasculitis patient health care utilisation ........................................................ 53
Chapter 3
Table 1. Characteristics of the Sample .................................................................... 69
Figure 1: Reported exposure to immunosuppression ................................................... 70
Figure 2. Patient reported awareness of potential medication side effects ................. 71
Figure 3. Patient reported uptake of preventative therapy .......................................... 73
Chapter 5
Appendix 1: Search strategies .............................................................................................. 130
Bone Health search strategy ........................................................................................ 130
Cardiovascular/ thromboembolic risk search strategy ................................................ 133
Cancer screening search strategy ................................................................................ 138
Fertility preservation search strategy ......................................................................... 140
Vaccination search strategy ........................................................................................ 142
Pneumocystis search strategy ..................................................................................... 145
Viral and fungal prophylaxis search strategy ............................................................... 150
Appendix: Evidence Tables .................................................................................................. 154
Chapter 7
Table 1. Characteristics of patients selected for interview ......................................... 250
Figure 1. VasCOT user map .......................................................................................... 252
Figure 2. VasCOT concept ............................................................................................ 253
Table 2. Themes from patient interviews .................................................................... 256
Table 3. Clinician “problem” and “wish” list ................................................................ 258
Table 4. Patient “problem” and “wish” list .................................................................. 259

8
Table 5. Survey responder characteristics ................................................................... 260
Appendix 1. Patient questionnaire and results .................................................................... 272
Appendix 2. Clinical data specifications……………………………………………………………………………275
Appendix 3: Patient view wireframes .................................................................................. 283
Appendix 4. Clinician view wireframes ................................................................................ 289
Appendix 5. Detailed Functional specifications ................................................................... 296

9
ABSTRACT
For submission to the University of Manchester, for the degree of Doctor of
Philosophy (PhD)
Title: Improving Outcomes for Patients with ANCA Associated Vasculitis
Dr Nina Brown, December 2016
Background: ANCA Associated Vasculitis (AAV) is a relatively rare autoimmune
condition with the potential to cause life-threatening organ inflammation and
failure. Due to the relative rarity, and the heterogenous way in which the disease
may present, delay to diagnosis is common. Although initial immunosuppressive
treatment is usually effective at controlling disease, morbidity associated with
treatment is high and disease relapses frequent, necessitating further
immunosuppression exposure.
Aims and Objectives: This body of work therefore seeks to address 2 of the main
challenges faced by the AAV population; 1) identifying factors that may contribute
to a delay to diagnosis and disease recognition 2) reducing morbidity associated
with the disease and the treatment.
Methods: Patient pathways, knowledge and uptake of protective therapy were
explored through a national patient report study. Patient care guidelines to assist
with morbidity prevention were informed through Delphi consensus methodology
and comprehensive literature review. The development of software to support
implementation of a rigorous systematic approach to the assessment of the
vasculitis patients was achieved through collaboration with information technology,
business development and system architecture and design experts.
Results: Patient presentation including symptoms, initial mis-diagnosis and eventual
diagnosis appear to influence time to diagnosis. There is substantial delay from
symptom onset to diagnosis demonstrating the need for increased awareness and
education. Equally patient awareness of treatment related morbidity is low with
variable uptake of protective therapy.

10
A Delphi study has produced consensus on which guidelines can be based to
address some of these inadequacies. A software programme: “Vasculitis Care
Optimisation Tool (VasCOT)”, has been designed to support implementation of
these guidelines.
Discussion: The various approaches used in this body of work have so far allowed
evaluation of areas where patient care needs to be improved. This in part will be
addressed through the publication of national vasculitis care guidelines, informed
by this work and the ongoing development of VasCOT.

11
DECLARATION AND COPYRIGHT
No portion of the work referred to in the thesis has been submitted in support of an
application for another degree or qualification of this or any other university or other
institute of learning.
i. The author of this thesis (including any appendices and/or schedules to this thesis) owns
certain copyright or related rights in it (the “Copyright”) and s/he has given The University
of Manchester certain rights to use such Copyright, including for administrative purposes.
ii. Copies of this thesis, either in full or in extracts and whether in hard or electronic copy,
may be made only in accordance with the Copyright, Designs and Patents Act 1988 (as
amended) and regulations issued under it or, where appropriate, in accordance with
licensing agreements which the University has from time to time. This page must form part
of any such copies made.
iii. The ownership of certain Copyright, patents, designs, trade marks and other intellectual
property (the “Intellectual Property”) and any reproductions of copyright works in the
thesis, for example graphs and tables (“Reproductions”), which may be described in this
thesis, may not be owned by the author and may be owned by third parties. Such
Intellectual Property and Reproductions cannot and must not be made available for use
without the prior written permission of the owner(s) of the relevant Intellectual Property
and/or Reproductions.
iv. Further information on the conditions under which disclosure, publication and
commercialisation of this thesis, the Copyright and any Intellectual Property University IP
Policy (see http://documents.manchester.ac.uk/display.aspx?DocID=24420), in any
relevant Thesis restriction declarations deposited in the University Library, The University
Library’s regulations (see http://www.library.manchester.ac.uk/about/regulations/) and in
The University’s policy on Presentation of Theses.

12
PREFACE
This report will follow the alternative (journal paper) thesis format. This is felt to be
appropriate for this body of work due to the various methodologies used and as
some sections have been published, with others submitted for publication, or
shortly about to be.
DEFINITION OF MY ROLE IN THIS WORK
Chapters 2 and 3: I led on the development of the questionnaire with support from
the steering group outlined below. I wrote the application to the Research and
Ethics committee for approval of the pilot work and carried out this pilot along with
the data collection and analysis from patient health records for validation. With
regards to the full questionnaire study, I performed the majority of data entry and
analysis with assistance from those outlined below. The manuscripts were prepared
by me with acknowledgement of those involved below.
Chapter 4, 5 and 6: The idea for the Delphi study was generated by me. I assisted in
the identification and recruitment of panel members and stakeholders. I created
the original questions for Round 1 of the Delphi. I supported and supervised DT (see
below) in the administration of the rounds 2 and 3 of the Delphi and in
streamlining/ clarifying statements between rounds. I led in the organisation and
chairing of the 2 consensus conferences and was responsible for documenting and
translating the outcomes into written format.
I conducted the literature reviews in chapter 5 with assistance as outlined below.
I was responsible for the creation of the guidelines from the combination of
consensus statements and evidence.
Chapter 7: The idea for VasCOT was generated and developed by me, with support
as outlined below. I worked with information technology, business development
and design experts to translate my vision into something more tangible.

13
I produced the clinical data specifications, with input as listed below. I produced the
content of all the wire frames seen in the Appendix, which were translated into the
patient and clinician views by the design team. I obtained industry support for the
initial development phases through presentation of the concept in various forums. I
directed the IT team to produce the functional specifications, based the anticipated
requirements of the software.
COLLABORATIONS AND ACKNOWLEDGEMENTS
Chapters 2 and 3: The initial questionnaire development was supported by a
steering group consisting of;
• Dr Michael Venning, Renal Unit, Manchester Royal Infirmary
• Professor Ian Bruce, Arthritis Research Epidemiology Unit, University of
Manchester
• Professor Paul Brenchley, Chair of renal immunology, University of
Manchester
• Professor Ann Louise Caress, School of Nursing and Midwifery, University of
Manchester
• Dr Ed O’Riordan, Renal Unit, Salford Royal
• Dr Jon Sussman, Neurology, Salford Royal
• Dr Ajay Dhaygude, Renal Unit, Royal Preston Hospital
• Shelley Harris, Renal Research, Manchester Royal Infirmary
• With input from the patient support group Vasculitis UK.
• Dr Faisal Ali (trainee in dermatology) contributed the questions on skin
monitoring for the questionnaire.
• Dr Zoe Cousland and Dr Heather Arya assisted with data entry.
Chapter 2: Some of the data analysis and figure production in this section was
completed by Dr. Zoe Cousland under my direction. She has also been involved in
the drafting of this article planned for submission shortly.

14
Chapter 3: In addition to those mentioned in the steering group, Dr. Matthew
Helbert was involved in the preparation of this article.
Chapter 4, 5 and 6: The ADAPTIV study was carried out under the auspice of the UK
and Ireland Vasculitis Rare Disease Group, with Professor Mark Little and Professor
Richard Watts as chair. Access to the Delphi 7comms software was enabled though
the creator of this software, Professor Kevin Mackway-Jones. David Tooth, then
medical student, carried out the co-ordination of the Delphi study using the
software under my supervision. Angela Summers provided support in addition,
particularly during my absence for maternity leave. The literature review was
undertaken with assistance from David Tooth, Dimitrios Chanouzas and Patrick
Hamilton. Professor Mark Little and Dr Matthew Morgan provided guidance in the
latter part of the process, particularly the drafting of the guidelines.
Chapter 7: Bruce Magill, previously Northwest ehealth, now SAP, helped with the
development of the design for VasCOT into a product from initial concept. Hitachi
carried out the detailed patient and physician interviews and questionnaire and
analysed the results to produce the “wish-lists”. In addition, the product schema
and wireframes were produced by Hitachi Design Centre Europe under direct
instruction from myself. Central Manchester Foundation Trust IT department, Chris
Anderson (Xibble Ltd) and Chris Lee (OBEC ltd), produced the functional
specification for VasCOT, under my direction. The UK and Ireland Vasculitis RDG
provided clinical expertise to review the content of the clinical dashboards.
Dr Mike Venning, has provided input into all aspects of this work. In particular he
was actively involved with development of the questionnaire, he actively supported
the Delphi process and was involved with the development of the concept and
content of VasCOT.
Professors Paul Brenchley and Ian Bruce have provided guidance and comment on
the entire thesis, with additional independent review from Professor Rick Body.

15
PUBLICATIONS AND ABSTRACTS
Medication-related side effects in vasculitis: a patient self-report survey of
awareness and reported uptake of protective therapy. Brown N, Bruce IN,
O'Riordan E, Dhaygude A, Helbert M, Caress AL, Sussman JD, Venning MC.
Rheumatology 2016;55:186-189.
Lack of awareness of skin cancer amongst immunocompromised patients with
ANCA-associated vasculitis: a questionnaire survey. Ali FR*, Brown N*, Lear J,
Helbert M, Bruce I N, Venning M C. British Journal of Dermatology (2014) 171,
pp193-5.(*joint first authorship)
Development of a Vasculitis Care Optimisation Tool (VasCOT), in Collaboration with
Hitachi Europe. Brown N, Magill B, Mills J, Luqmani R, Venning M. Nephron
2015;129(suppl2):47
A Delphi Study for Assessing Prevention of Disease and Treatment Related
Morbidities in ANCA Associated Vasculitis (ADAPTIV). Brown N, Tooth D, Morgan M,
Little M, Venning M. Nephron 2015;129(suppl2):128
Vasculitis care in the UK: How do patients perceive the care provided and what
should the future hold? Arya H, Brown N, Venning M, Bruce I. Annals Rheumatic
Diseases 2014; 71(Suppl 3):627-62
ADAPTIV: A Delphi study to assess morbidity prevention and treatment in vasculitis.
Brown N, Tooth D, Summers A, Venning M. La Presse Médicale 04/2013; 42(4):746-
747.
Prevention of treatment related morbidity in ANCA-associated vasculitis: the
patient’s perspective. Brown N, Bruce IN, Venning MC. EDTA Conference. Paris, May
2012

16
Skin cancer awareness and surveillance in vasculitis patients: the lost tribe? Ali F,
Brown N, Lear J, Bruce IN, Venning MC. British Association Dermatology.
Birmingham, June 2012.
ANCA-associated vasculitis: the patient’s perspective on the route to diagnosis.
Cousland Z, Brown N, Bruce IN, Venning MC. Renal Association. Gateshead, June
2012

17
ABBREVIATIONS
AAV ANCA Associated Vasculitis
ACR American College of Rheumatology
ANCA Anti-neutrophil cytoplasmic antibody
ANOVA Analysis of variance
BCG Bacillus Calmette–Guérin
Blys B lymphocyte stimulator
Bregs regulatory B cells
BMD Bone mineral density
c-ANCA cytoplasmic ANCA
CIN Cervical intra-epithelial neoplasia
CKD Chronic Kidney Disease
CMV Cytomegalovirus
CPG 5’-C-phosphate-G-3’
cPR3 Complementary PR3
CRP C reactive protein
CSS Churg Strauss syndrome
CVD Cardiovascular disease
CYC cyclophosphamide
DEXA Dual-energy X-ray absorptiometry
eGFR Estimated glomerular filtration rate
EGPA Eosinophilic Granulomatosis with Polyangiitis
ELISA enzyme-linked immunosorbent assay

18
EMEA European Medicines Agency
ENT Ear Nose and Throat
ESRD End stage renal disease
EULAR European League against Rheumatism
EUVAS European Vasculitis Study Group
GP General Practice
GPA Granulomatosis with Polyangiitis
GWAS Genome wide association study
HR Hazard Ratio
HSV Herpes simplex virus
HZV Herpes zoster virus
Ig Immunoglobulin
IL interleukin
IQR Interquartile range
I.v. intravenous
LAMP2 Lysosomal-associated membrane protein 2
MMF Mycophenolate mofetil
MPA Microscopic Polyangiitis
MPO myeloperoxidase
MTX methotrexate
NET neutrophil extracellular traps
NMSC Non-melanomatous skin cancer
OR Odds Ratio
p-ANCA peri-nuclear ANCA

19
PBMC Peripheral blood mononuclear cells
PCP Pneumocystis pneumonia
PCT Procalcitonin
PHE Public Health England
PjP Pneumocystis jirovecii pneumonia
PMN Polymorphonuclear leucocyte
PR3 proteinase-3
RCT randomised controlled trial
ROS Reactive oxygen species
RTX rituximab
SNP Single nucleotide polymorphism
SLE Systemic Lupus Erythematosus
TB tuberculosis
Th T helper
Tregs regulatory T cells
TREM Triggering receptor expressed on myeloid cells
UTI Urinary tract infection
VTE venous thromboembolism
WCC white cell count

20
DEDICATION
This thesis is dedicated to my boys, Ewan and Finlay, who were both born during the course
of this PhD. They have been my inspiration and sunshine throughout it all.
Thank you to my incredibly patient husband, Ross, whose support and encouragement
enabled me to keep going.
To my parents who have always been there for me.
Thank you to my supervisors and advisor, Ian, Paul and Mike who provided so much
guidance.
And finally, to the patients who it is a privilege to care for, without whom none of this
would be possible.

21
INTRODUCTION
1.1 BACKGROUND
ANCA (anti-neutrophil cytoplasmic antibody) associated vasculitis (AAV) is an umbrella
term for a group of rare, multi- system autoimmune diseases causing potentially life-
threatening inflammation of small blood vessels. Although it appears that outcomes from
this disease are generally improving, morbidity and mortality is still high. This thesis aims to
identify some of the contributors to this morbidity and to describe possible barriers to
improving outcomes for this population including how these barriers may be overcome.
To better identify the possible contributory factors to this morbidity and mortality, this
introduction will give an overview of the disease, from diagnosis to treatment and longer
term outcomes.
1.1.1 What is ANCA Associated Vasculitis? An overview of disease pathogenesis
AAV is an autoimmune disorder that causes small to medium sized blood vessel
inflammation leading to organ damage and possibly failure. Histologically, vascular damage
and destruction may be visualised but classically the lesions are pauci-immune. However, it
is now firmly established that the pathogenesis of this disease is linked with formation of
anti- neutrophil cytoplasmic antibodies (ANCA). ANCA was first described in association
with glomerulonephritis in an Australian case series in 19891. These antibodies were
observed in a cohort of patients with what we now recognise to be ANCA Associated
Vasculitis and the aetiology of the antibodies was postulated to be linked with exposure of
the patients to Ross river virus (a group A arbovirus) due to the geographical clustering.
Following this initial discovery their pathogenic potential for causing vascular injury was
first described by Falk et al in 19902. This work originated from the observation that ANCA
were present in the serum of around 80% of patients with pauci-immune systemic
vasculitis or glomerulonephritis. The group went on to demonstrate, in an in vitro setting,
that ANCA could activate neutrophils resulting in release of reactive oxygen species (ROS)
and postulated that this was the mechanism by which tissue damage was effected in AAV.
Since then there has been a growing body of evidence supporting the pathogenic nature of
ANCA including animal models and a case report of trans placental transfer of these
antibodies causing neonatal disease3–5.

22
On immunofluorescence, these antibodies are classified as c-ANCA (cytoplasmic) or p-
ANCA (peri- nuclear) depending on their pattern of staining. Through ELISA we can now test
specifically for ANCA directed against the antigenic components expressed on the
neutrophil membrane, proteinase 3 (PR3) and myeloperoxidase (MPO). These antigen
specific antibodies tend to segregate with clinical phenotype. Granulomatosis with
polyangiitis (GPA) is predominantly linked with c-ANCA antibodies formed against PR3
(70%) and Microscopic Polyangiitis with p-ANCA against MPO (50%)6.
1.1.2 PR3 versus MPO: the role of antigens and antibodies
It has relatively recently been demonstrated that MPO and PR3 associated disease are
genetically different (discussed later)7. This was likely unsurprising to the majority of
clinicians who, for many years, have observed that patients with different antibodies
appear to have different diseases, both phenotypically and prognostically. Both MPO and
PR3 are neutrophil membrane proteins that are expressed predominantly in the earlier
stages of neutrophil development, promyelocyte and myeloblast stages8, in the healthy
population. It has been demonstrated that level of expression of PR3 on neutrophil
membranes appears to be under genetic regulation, and that patients with GPA have a
higher percentage of membrane PR3 expressing neutrophils, compared with healthy
controls9.
Current opinion on the pathogenesis of this disease is that an inflammatory stimulus, such
as infection, primes these neutrophils, leading to membrane expression of MPO or PR310.
IgG ANCA are produced by B cells against these neutrophil membrane antigens, under the
stimulus of inflammatory cytokines and T cell dysregulation. Binding of the antibody to
antigen on the neutrophil surface causes neutrophil activation, in the setting of priming by
certain inflammatory cytokines, which may result in adherence to and migration through
the vessel wall, activation of reactive oxygen species, neutrophil degranulation and enzyme
release. It is through these mechanisms, further perpetuated by complement activation,
that tissue damage occurs11,12(see Figure 1).
The role of MPO in disease development has been the most extensively studied with Xiao’s
successful animal model of MPO associated pauci-immune glomerulonephritis and
pulmonary capilleritis13 contributing significantly to understanding of pathogenesis. Indeed,
it was the MPO murine model that uncovered the role of the alternative complement

23
pathway in induction of disease14, in turn leading to clinical trials of a C5a receptor inhibitor
in ANCA associated glomerulonephritis (discussed below). Essentially, activation of
neutrophils can cause relocation of MPO from azurophilic granules within the neutrophil to
the surface of the cell membrane, whereby anti- MPO antibodies can bind causing
neutrophil degranulation. However, in addition, MPO is released extracellularly within
Neutrophil Extracellular Traps (NETS), the role of which are discussed subsequently.
One of the most recent descriptions of the potential role of MPO in disease development
includes a schema in which not just MPO targeted antibodies are pathogenic but also with
possible roles for MPO reactive T cells and even direct MPO toxicity15. Low level anti- MPO
ANCA has been demonstrated in the healthy population, but further work has elucidated
that this appears to be a different epitope than the one present in active disease16.
PR3 associated disease has proven to be a much more difficult entity to replicate with the
most successful model resulting from creation of a human-mouse chimeric immune system
prior to passive transfer of human IgG from patients with PR3. This produced vasculitic lung
and renal injury in a substantial proportion of the mice adding further weight to the
evidence for the pathogenic nature of ANCA17.
Figure 1. Putative representation
of AAV disease pathogenesis343.

24
1.1.3 Neutrophils and NETs in AAV
Adding to the models for disease development, there has been recent suggestion that
Neutrophil Extracellular Traps (NETs) may have a role to play in pathogenesis. NETs are a
chromatin mesh containing cytoplasmic components including MPO and PR318. There are
two models of NET production. In the first, termed NETosis, NETs are formed through
release of cytoplasmic contents, this being a form of cell death. The second involves DNA
and enzyme extrusion but does not appear to result in cell death19. NETs have been
identified in the kidneys (through analysis of renal biopsy samples) of patients with AAV. In
addition, abnormally shaped NETs can be shown in animal models to induce MPO ANCA
formation and pulmonary capilleritis20.
1.1.4 The role of B cells, T cells and complement
Plasma cells are obviously implicated in the pathogenesis of disease through production of,
predominantly IgG, ANCA. However, the role of B cells in this disease appears to extend
beyond this, supported by the efficacy of the anti CD20 monoclonal antibody Rituximab in
the treatment of AAV. Studies have explored the potential role of B regulatory (Bregs) cells
(which may have a role in T cell regulation) in AAV, finding that regulatory B cells (classed
as IL10+ B cells) were significantly diminished in patients with AAV compared with healthy
controls21. Another group has demonstrated that in active disease Bregs (in this study
identified as CD5+ cells) were lower in those AAV patients with active disease22. However,
subsequent studies have failed to demonstrate the use of CD5+ Bregs as biomarkers for
disease activity with further phenotyping of these cells required23.
B lymphocyte stimulator (Blys), a neutrophil produced B-cell survival signal24 is another area
of research interest, with Belimumab, an anti-Blys monoclonal antibody having been shown
to be effective in the treatment of Systemic Lupus Erythematosus25. It has been
demonstrated that AAV patients with active disease have higher levels of Blys, and that
Blys release from primed neutrophils may be stimulated by the presence of PR3 ANCA24.
The currently underway phase III clinical trial BREVAS (ClinicalTrials.gov Identifier:
NCT01663623) aims to evaluate the efficacy/safety of Belimumab in combination with
azathioprine for maintenance of remission in AAV (versus azathioprine alone).
T cells have been known for some time to play a significant role in the pathogenesis of GPA
with the presence of over-active peripheral T cells, as well as the presence of T cells in

25
granulomatous lesions in GPA being previously reported12. However, the discovery of Th17,
which secretes the pro-inflammatory IL-17 has reawakened interest in this area.
Increased presence of Th-17 cells has been demonstrated in patients with GPA26, with
higher levels of IL-17 present during acute vasculitic episodes27. IL-23 is an upstream
cytokine vital for Th17 lineage induction. In the previous study, IL-23 levels were found to
correspond with disease activity27. It has been shown that infections such as
Staphylococcus aureus may influence development of the Th17 lineage through IL-23
production28.
The production of these Th17 cells may also be dependent on regulatory T cells (Tregs). A
number of groups have demonstrated that Tregs from patients with AAV are unable to
suppress T –cell proliferation12,29. It may be that increased Th17 cell development in part
follows this diminished suppressive action of Tregs or indeed that Th17 cells are possibly
even able to develop directly from Tregs30. AAV is predominantly a disease of the elderly
with the peak age of incidence being 65-74 years31. It is well established that the risk of
autoimmunity increases with age with theories such as involution of the thymus with
compensatory T cell proliferation and changes in T cell apoptosis suggested in explanation
of this phenomenon. However, from cohort studies of those with “limited” GPA it can be
noted that this is a disease in which the age of onset appears to be earlier. Limited GPA has
been found to be associated with a predominantly Th1 helper response and systemic
disease with a Th2 response32. With increasing age, the cytokine response to stimulus shifts
from Th1 to Th2, perhaps explaining why the elderly are more prone to development of
systemic versus local disease.
There has been recent focus on the role of the alternative complement pathway in the
pathogenesis of vasculitis, with data supporting that this occurs through neutrophil
activation generating C5. C5 then appear to not only cause chemotaxis of neutrophils but
also further primes neutrophils 33. Inhibition of C5 using monoclonal antibodies provided a
protective effect against the development of glomerulonephritis in a murine model of MPO
IgG induced glomerulonephritis34. Following this a C5a receptor antagonist has been
developed as a potential therapeutic agent and is undergoing Phase 2 trials with early
results suggesting a potential therapeutic role in ANCA vasculitis glomerular disease35.

26
1.2 EPIDEMIOLOGY OF AAV
ANCA associated vasculitis is a rare disease with a combined incidence of between 13 and
20 per million in Europe36. Of these GPA is the predominant disorder in Northern Europe
with an annual incidence in one study of 11.3/million compared with 5.9/million for MPA37.
This trend is reversed in Southern Europe and Southern Asia with MPA representing the
majority of disease in these areas38. This pattern of distribution supports two theories
concerning the development of AAV. The first, that this is a disease with genetic
contribution to susceptibility and secondly, that environmental factors are likely to play a
role in disease development. Both theories now have substantial evidence in their support.
1.2.1 Genetics of AAV
The first work looking at genetic predisposition to development of AAV was published in
1992 when a highly significant association between HLA DR1 and disease was reported in
those with GPA compared with healthy controls39. Subsequently in 2003, Schreiber et al.
published research revealing that the general population appeared to be divided into 2
subgroups- those with high levels of PR3 expressed on neutrophil membranes and those
with low levels9, and that the level of expression appeared to remain stable over time (12
months). They then investigated a group of patients with GPA and discovered that these
patients had a significantly higher number of neutrophils expressing membrane PR3.
Comparison of PR3 membrane expression in monozygotic twins, compared with dizygotic,
demonstrated significant correlation between expression levels in the monozygotic twins.
This supported the argument that the degree of PR3 expression on neutrophil membranes
appeared to be under genetic control. This link was further strengthened by the
observation that first-degree relatives of those with GPA had a relative risk of developing
the disease of 1.5640.
Following this, increasing availability of gene array testing has allowed identification of
Single Nucleotide Polymorphisms (SNPs) which appear to confer risk to the individual of
developing AAV. There have been two Genome Wide Association Studies (GWAS) in AAV
published in recent years. The first European identified a strong association in a SNP at
HLA- DPB1 with the presence of disease. This study also demonstrated significant
differences at several loci including SERPINA1, MHC and PRTN3, associated with PR3
positive but not MPO positive disease7. The US GWAS41, including only patients with GPA,

27
also identified the same HLA association, but in addition identified a SNP near SEMA6A
associated with the presence of GPA.
1.2.2 Environmental exposure and epigenetics
Genetic predisposition in isolation is obviously insufficient to lead to disease development
as vasculitis is not a “classically” inherited disease, and remains relatively rare. For many
autoimmune diseases, epigenetics (the study of “mechanisms that determine and/or
perpetuate heritable genomic functions without changes in DNA sequence”42) has helped
to explain the “two hit theory” of disease susceptibility and disease development following
environmental exposure. In AAV the environmental exposure that leads to development of
disease is far from certain and is likely to differ according to patient. However, there have
been several well described associations which deserve some focus here.
Exposure to silica has been reported as a trigger for AAV in addition to other autoimmune
and respiratory diseases. A systematic review of the literature examining the possible
association with AAV was published in 201343. This found an association with “ever” having
been exposed to silica and subsequent development of AAV with a summary OR of 2.56.
Hypotheses to explain this association include the causation of neutrophil apoptosis by
silica and trapping of silica in alveoli leading to a systemic inflammatory response through T
cell activation. However, to prove a definite association prospective longitudinal studies are
ideally required which remain unlikely due to the disease rarity.
Other possible occupational exposures associated with AAV development include farming.
A recent German questionnaire study found a strong association between reported regular
farm exposure and development of GPA, with the strongest association for those with
regular exposure to cattle44. Both of these possible environmental risk factors were
detailed in a New Zealand case- control study, with reported associations to disease (GPA)
development including exposure to silica and grain dust, occupation as a farm worker or
having undertaken specific gardening activities45.

28
1.3 THE ROLE OF INFECTION IN DISEASE PATHOGENESIS
Although occupational exposure may well for some be the trigger for disease development,
perhaps the most extensively observed and explored hypothesis is the link between
infection and AAV. Sixty-three percent of patients with GPA, compared with 25% of healthy
controls, have been found to have chronic nasal carriage of Staphylococcus aureus46. The
persistence of nasal carriage of S. aureus has been found to strongly increase the risk of
relapse in this population47. Several mechanisms have been suggested to explain this
including S.aureus super- antigen stimulus of B and T cells, neutrophil priming and
molecular mimicry46. The use of anti-staphylococcal agents including co- trimoxazole has
been shown to support disease control with reduction in the rate of relapses48. The
protective mechanism of this anti-microbial is uncertain but one possibility is that it may be
mediated through an alteration of the balance of nasal flora49. Others had postulated that
perhaps S.aureus proteins and ANCA target epitopes were homologous, with a theory of
molecular mimicry. However, this was found to not be the case.
In 2004, an alternative “theory of autoantigen complementarity” was investigated.
Prendergraft et al. discovered that a proportion of their patients with AAV appeared to
additionally be producing an antibody against an epitope present in the central portion of
the PR3 antigen, an antibody they named “complementary PR3” (cPR3). They
demonstrated that not only did mice injected with the cPR3 antigen produce cPR3
antibodies but they also produced PR3 antibodies50. The discovery that the cPR3 epitope
shared homology with pathogens including Staph.aureus gave rise to the theory that the
formation of cPR3 antibodies may provide the missing link between infection and the
pathogenesis of vasculitis. Subsequently Tadema et al.51 were unable to find any
association between levels of complementary PR3 and disease activity in those with AAV,
and conversely actually found that levels of cPR3 activity appeared to be lower in those
with vasculitis than healthy controls. They were also unable to find any association
between cPR3 levels and exposure to S. aureus (as defined by being a nasal carrier of S.
aureus). However, they did accept that it was possible that the formation of anti- cPR3 and
anti- PR3 complexes may be masking true measurement of cPR3 activity. Adding strength
to these theories is the observation that Staph. aureus has been shown to trigger NET
formation52.

29
Multiple other pathogens have been described in association with ANCA production53. Kain
et al. have focused on a possible mechanism of molecular mimicry between a protein
(FimH) on the fimbriae of gram- negative pathogens and the antibody LAMP-2. They
postulated that other, currently unmeasured antigen targets, aside from MPO and PR3,
may be responsible for inducing ANCA production. They discovered that antibodies to the
heavily glycosylated protein LAMP-2 were detectable by immunofluorescence in 95% of
their AAV population54, but absent in their healthy controls. They went on to demonstrate
the potential pathogenic nature of these antibodies by inducing glomerulonephritis in rats
through injection of LAMP-2 antibodies, and further showed that immunisation of the rats
with FimH protein not only induced LAMP-2 antibody formation but was also capable of
stimulating the development of a clinical picture of glomerulonephritis and pulmonary
haemorrhage compatible with vasculitis. However, work attempting to validate these
findings in other cohorts has yet to be successful. Investigators from Chapel Hill, North
Carolina have attempted to replicate this work in a cohort of 329 patients with AAV
glomerulonephritis, healthy controls and patients with Gram-negative urinary tract
infections (UTIs)55. They found that LAMP-2 antibodies were present in only 21% of their
patients with AAV but also in 16% of patients with UTIs. They were also unable to replicate
induction of glomerulonephritis in the rats through immunisation of the LAMP-2
antibodies.
Two individual groups have demonstrated a less specific link between infection and
vasculitis by stimulating B cells in from patients with AAV in vitro with bacterial DNA56,57.
Both groups demonstrated that ANCA production could be provoked by B cell exposure to
CpG deoxynucluotides (hypomethylated DNA found in bacteria and viruses). In both
studies, however, these responses were more pronounced in those PR3 positive patients
than MPO positive, reinforcing the link between this particular AAV and infection.
Essentially further work is required to try to elucidate this link between exposure to
infectious agents and development of vasculitis.

30
1.4 DIAGNOSIS AND CLASSIFICATION
Once disease has developed in a genetically predisposed individual, the greatest challenge
perhaps for the patient, is receiving timely and accurate diagnosis and classification of their
disorder, allowing for appropriate treatment. It is clinically relevant to ensure the correct
immunological and clinical subtype are identified as this has significant prognostic
implications. AAV may be categorised as Microscopic Polyangiitis (MPA), Granulomatosis
with Polyangiitis (GPA) or Eosinophilic Granulomatosis with Polyangiitis (EGPA). However,
due to increasing evidence that EGPA comprises a uniquely different spectrum of disorders
it is only the two most common of these, MPA and GPA, shall be considered here.
Granulomatosis with Polyangiitis (formally known as Wegener’s Granulomatosis) causes
small vessel inflammation in association with granuloma formation. It is associated with
initial upper airway disease in over 70% of patients and may remain limited to these
organs. However, in the multi- system form it can affect the lungs, causing granulomatous
disease or pulmonary haemorrhage, renal failure or nerve and skin involvement, amongst
other rarer manifestations58.
Vessel
size
Granulomas ANCA positivity Organ
involvement
%renal
involvement
GPA Small Yes 95 %
70% PR3/cANCA
25% MPO/pANCA
ENT
Lungs
Renal
systemic
80
MPA Small No 90%
40% PR3/cANCA
50% MPO/pANCA
Lungs
Renal
systemic
90
Table 1. Description of AAV according to ANCA positivity and organ involvement6
Granulomatosis with Polyangiitis was first described by Klinger in 193159 as a form of
polyarteritis nodosa and then defined as a distinct clinical entity by Wegener in 1936 and
193960. For 80 years, this inflammatory condition, characterised by granulomatous
inflammation with a predilection for the renal and respiratory tract (commonly including
the ear and nose) was known as Wegener’s Granulomatosis. This condition has recently

31
been renamed as Granulomatosis with Polyangiitis (GPA) by the Board of Directors for the
American College of Rheumatology (ACR), the American Society of Nephrology and the
European League against Rheumatism (EULAR) partly in keeping with the movement away
from eponymous syndromes and following concerns regarding potential affiliations Dr.
Wegener may have had with the Nazi Party in the Second World War61.
Microscopic Polyangiitis was first recognised as a condition causing rapidly progressive
glomerulonephritis, in association with systemic illness, chest and abdominal signs. The
glomerulonephritis was identified by the presence of fibrinoid necrosis and crescents in the
kidney at autopsy in a case series published in 194862 and the term “microscopic
periarteritis” was coined. Prior to this there had been debate as to whether patients
suffering from this form of vasculitis actually had periarteritis nodosa (polyarteritis nodosa)
with an “independent” glomerulonephritis. MPA is differentiated from GPA pathologically
by the absence of granulomas and phenotypically by the (usual) absence of upper
respiratory tract involvement. Current disease classification criteria are outlined in Table 2.
ANCA-associated vasculitis (AAV) Necrotizing vasculitis, with few or no immune
deposits, predominantly affecting small vessels (i.e.,
capillaries, venules, arterioles, and small arteries),
associated with myeloperoxidase (MPO) ANCA or
proteinase 3 (PR3) ANCA. Not all patients have ANCA.
Add a prefix indicating ANCA reactivity, e.g., MPO-
ANCA, PR3-ANCA, ANCA-negative.
Microscopic polyangiitis (MPA) Necrotizing vasculitis, with few or no immune
deposits, predominantly affecting small vessels (i.e.,
capillaries, venules, or arterioles). Necrotizing arteritis
involving small and medium arteries may be present.
Necrotizing glomerulonephritis is very common.
Pulmonary capillaritis often occurs. Granulomatous
inflammation is absent.
Granulomatosis with polyangiitis (Wegener's) (GPA) Necrotizing granulomatous inflammation usually
involving the upper and lower respiratory tract, and
necrotizing vasculitis affecting predominantly small to
medium vessels (e.g., capillaries, venules, arterioles,
arteries and veins). Necrotizing glomerulonephritis is
common.
Table 2. Chapel Hill Consensus Conference classification of AAV 201263

32
As a complex and heterogenous group of disorders, with a myriad of presentations,
diagnosis and classification of AAV can be challenging. Although there is suggestion that
time to recognition and diagnosis of these disorders may be improving64 there is still recent
documentation of significant delay to diagnosis65,66. A recent publication of the combined
outcomes of EUVAS clinical trials showed that 34.5% of patients had at least 1 item of
damage at baseline (as measured by the Vasculitis Damage Index), likely reflecting damage
accruing from disease manifestations prior to diagnosis67.
Classification of disease has been historically challenging with the first American College of
Rheumatology classification system omitting MPA68. Due to a need for accurate
classification for inclusion of patients in clinical trials and epidemiological studies, the EMEA
classification algorithm was developed and published in 2007 which was validated to
successfully classify patients into a single category69. Since then disease classification has
moved on, with the publication of the GWAS study and the suggestion of MPO positive and
PR3 positive disease as distinct entities7 and with the publication of the updated 2012
classification criteria63. The ongoing Diagnostic and Classification in Vasculitis (DCVAS)
international study aims to assist in this area by assisting with development and validation
of diagnostic and classification criteria for all, not just small vessel, vasculitis70.
1.5 TREATMENT
Following accurate diagnosis and classification of disease, timely and appropriate
treatment can be delivered. Treatment strategies for AAV can be divided into “induction”
and “maintenance” phases. Induction therapy conventionally involves high dose steroid
therapy e.g. prednisolone at 1mg/kg of body weight and may include one to three initial
intravenous steroid infusions, depending on disease severity (See Table 3). Steroid dose is
then tapered down after the first month, with recommendations that the steroid dose is
not reduced to less than 15mg for the first 3 months then tapered to 10mg or less during
remission57. Remission can be defined as the absence of disease activity attributable to
vasculitis as measured by a standardised, validated scoring system such as the Birmingham
Vasculitis Activity Score (BVAS)71.Disease category

33
Table 3. Definition of disease severity according to EULAR72
Patients with severe organ or life threatening disease may also be treated with plasma
exchange, supported by evidence from the MEPEX trial73 which showed that the use of 7
plasma exchange sessions for patients presenting with AAV and serum creatinine >
500µmol/l had a reduction in risk of 24% of progression to end stage renal failure at 12
months, when compared with those treated with 3 pulses of intravenous
methylprednisolone (1g).
Alongside steroid treatment, patients with organ or life-threatening disease should be
treated with cyclophosphamide which can be administered as daily oral or pulsed
intravenous (i.v.) therapy, until remission is reached (usually at 3 to 6 months). The
publication of initial outcomes from the CYCLOPS clinical trial comparing pulsed
intravenous cyclophosphamide therapy to daily oral, supported pulsed therapy, allowing a
much lower total cyclophosphamide dose to be administered. The CYCLOPS study indicated
that the two regimens were equivalent for time to remission but with fewer leucopenic
episode in the pulsed intravenous group, indicating perhaps a safety advantage74. However,
longer term follow-up data (median follow-up 4.3 years) has suggested that those receiving
a lower cumulative dose of cyclophosphamide are more likely to relapse (20.8% daily oral
Definition
Localised Upper and/or lower respiratory tract disease
without any other systemic involvement or
constitutional symptoms
Early systemic Any, without organ threatening or life-
threatening disease
Generalised Renal or other organ threatening disease, serum
creatinine <500 µmol/ litre (5.6 mg/dl)
Severe Renal or other vital organ failure, serum
creatinine >500 µmol/litre (5.6 mg/dl)
Refractory Progressive disease unresponsive to
glucocorticoids and cyclophosphamide

34
versus 39.5% i.v.) although the increased relapse rate was not associated with an increase
in morbidity or mortality75.
For patients in whom preservation of fertility is desirable, or with significant previous
cyclophosphamide exposure, the other first-line option (in keeping with FDA approval and
NICE guidance) is Rituximab. Rituximab was first developed as an adjunct to chemotherapy
for treatment of B cell lymphomas. In AAV, it has been found that higher numbers of
activated B cells can correlate with disease activity76, therefore logically leading to the
potential use of Rituximab as a therapy for AAV. Initially Rituximab was used in patients
with refractory, relapsing disease77 but the publication of two Randomised Controlled Trials
have demonstrated non- inferiority to cyclophosphamide for induction of disease
remission. The American “RAVE” trial78 compared administration of Rituximab (375mg/m2,
weekly for four weeks) with daily oral cyclophosphamide converted to oral azathioprine at
remission (3- 6 months). The steroid regime was the same in both groups (tapered and
discontinued by 5 months in those remaining without disease flare). 130/ 197 patients
(66%) had renal involvement. 63/99 patients (64%) who had received Rituximab met the
primary end point of no disease activity plus no steroids at 6 months, compared with 52/98
(53%) in the cyclophosphamide group. This allowed the authors to conclude that Rituximab
was non- inferior to cyclophosphamide for induction of remission, including for those
patients with severe disease. In terms of adverse events, leucopenia was more common in
the group treated with cyclophosphamide (10% versus 3%) but infection rates were
identical between the two groups (occurring in 7% of the patients). The European
RITUXIVAS study79 differed in that all the patients included had renal involvement. The
treatment protocols also varied in that this trial used pulsed intravenous cyclophosphamide
for the control arm, and the patients in the Rituximab group also received two doses of
cyclophosphamide (15mg/kg) with the first and third doses of Rituximab. The steroid dose
was tapered but patients remained on 5mg prednisolone/ day from 6 months. This was an
unblinded study and the follow- up period was longer than the RAVE trial at 12 months.
Sustained remission was achieved in 25/33 (76%) of the patients receiving Rituximab and
9/11 (82%) of the control group. 36% of patients receiving Rituximab had at least 1
infectious episode compared with 27% of the cyclophosphamide group. The authors
therefore concluded that in their trial, Rituximab was not superior in inducing remission or
at avoiding treatment related toxicity in this population, compared with cyclophosphamide.

35
This may be explained by the fact that some of the adverse events such as infectious
episodes may be related to the steroid regimes which were identical between intervention
and control arms. Indeed, it can be noted that the RAVE trial, which aimed to have patients
off steroids completely by 6 months, had a much lower reported infection rate than
RITUXIVAS.
It has been suggested that patients treated with Rituximab do not appear to be at
increased risk of serious infection despite their complete B cell depletion due to reasonably
well preserved IgG levels (but a fall in IgM levels)80. However, repeated courses are likely to
affect the ability of the humoral immunity to fight new pathogens. A cohort study of 29
patients with GPA evaluated immunoglobulin levels in patients receiving pre-emptive
“maintenance” Rituximab therapy (1g biannually or 2g annually, median dose 9g
received)81. Of these patients, eight discontinued therapies due to
hypogammaglobulinaemia, defined as total IgG levels < 6g/L. Five of these had severe or
recurrent infections. This paper described risk factors for severe hypogammaglobulinaemia
requiring treatment withdrawal as being male, having renal involvement and receiving the
1g biannual regime. The Cambridge group have subsequently described the use of
replacement intravenous immunoglobulins (IvIg) in patients with recurrent infections and
hypogammaglobulinaemia following Rituximab therapy82. Of these, six continued to receive
Rituximab alongside the IvIg replacement, for disease control.
These issues become more relevant as the evidence gathers to support the use of
Rituximab in maintenance of remission. For patients having received cyclophosphamide,
once remission is achieved the patient can be switched to maintenance
immunosuppression, first-line with azathioprine, or with mycophenolate mofetil,
methotrexate or leflunomide as other possibilities83. However, it is less clear-cut how to
continue or alter treatment for those patients initiated on Rituximab. Equally, for patients
who relapse on maintenance oral therapy, and require Rituximab to induce remission,
there is little evidence to guide whether to continue their oral agent. Recommendations for
the use of Rituximab in AAV, published in 2011, did not issue firm guidance with regards to
this area, stating the available evidence to be that whilst many published series had
continued other agents alongside Rituximab, the RCTs had not84. However, these patients
would require pre-emptive Rituximab to ensure maintenance of remission. Whilst this is
supported by the current NHS England funding policy for relapsing/ refractory patients

36
requiring Rituximab, maintenance therapy with Rituximab is not commissioned for patients
receiving it first-line85.
However, this position may alter in future as evidence builds. The MAINRITSAN study was a
non-blinded randomized controlled trial comparing Rituximab (5 x 500mg doses over 18
months) with azathioprine (2 mg per kilogram per day for 12 months, and then 1.5 mg per
kilogram per day for 6 months and 1 mg per kilogram per day for 4 months), following
achievement of remission with standard cyclophosphamide and steroid therapy. Both arms
received tapering prednisolone doses as part of their maintenance therapy86. This study
reported superiority of Rituximab over azathioprine for prevention of major relapses over
28 months’ follow-up with 29% of patients in the azathioprine group relapsing compared
with 5% in the rituximab group (HR for relapse 6.61). A follow-up study, MAINRITSAN 2
(ClinicalTrials.gov Identifier: NCT01731561) is currently underway aiming to assess whether
Rituximab for maintenance therapy is best administered at regular time points or based
upon returning B cells and ANCA titres. This will further contribute to how this treatment is
best used in control of AAV.
The ongoing UK study RITAZAREM (ClinicalTrials.gov Identifier: NCT01697267) will provide
additional data, comparing 4 monthly 1g Rituximab infusions, over 20 months with
Azathioprine (withdrawn by month 27) following induction of remission with Rituximab for
relapsing disease. The primary outcome is time to relapse with a follow-up period of 4
years.
Other agents have been considered for treatment of AAV. Following on from the success of
B cell depleting therapies for this disease, as mentioned above the BREVAS study
(Clinicaltrials.gov Identifier: NCT01663623) is a phase 3 clinical trial comparing Belimumab,
with placebo, alongside azathioprine for maintenance of remission. Belimumab has
recently received NICE approval for treatment of active lupus with some evidence for
clinical effectiveness from 2 clinical trials87. Abatacept inhibits T cell activation by blocking
engagement of CD-28 with its ligand. Based on this mechanism of action and the known
roles of T cells in GPA, an open label trial of Abatacept was undertaken in 20 patients with
relapsing non-severe GPA88. Patients were continued in addition on their maintenance
immunosuppression agent. Eighty percent of patients achieved remission, with a median
time to remission of 1.9 months. An acceptable adverse event profile in addition suggests
that this may be a drug warranting further investigation for this population.

37
The mainstay of new clinical trials in AAV involves minimization of steroid exposure due to
the significant side effect profile from these agents. However, until new treatments are
available it remains prudent to maintain vigilance for possible complications of
immunosuppression due to the associated possible morbidity and mortality.
1.6 PROGNOSIS
1.6.1 Mortality
The average time to death prior to the development of modern treatment strategies for
patients with AAV was 5 months89, yet with advances in treatment, mortality rates have
significantly improved with recent data for 1 year mortality reported as 11%90.
Historically, reported outcomes for this patient group was largely confined to single-centre
experience. However, in more recent years collaboration between centres on a national
and international level has allowed for wider experience, with larger patient numbers to be
published.
The first of these by the “Pan- Thames” group included patients presenting to 7 London
hospitals with a new diagnosis of renal vasculitis between 1995 and 200091. 313 patients
were included with the majority having a diagnosis of MPA 120 (49%) or GPA 82 (33%).
Survival rates at 1 and 5 years were 84% and 76% respectively. Predictors for mortality
were poorer renal function at presentation (with those presenting with end stage renal
failure having a 5-year survival of 53%, p= 0.01) and age greater than 60 years (p=0.0002).
Infection and leucopenia were the most common adverse events, with treatment induced
leucopenia occurring in 99 (41%) of patients and being strongly associated with sepsis (p<
0.001). Seventy- three episodes of sepsis were reported (although it is not stated in how
many patients they occurred), the presence of which were a predictor of mortality (p=
0.048) with the most common infection being pneumonia at 23 episodes (31.5%), followed
by neutropenic sepsis at 12 episodes (16.4%) then herpes zoster virus at 11 episodes
(15.1%). It should be noted that this study only included patients with renal involvement,
and therefore this is likely to have had an impact upon mortality and possibly adverse
events. There was no mention of adjustment of cyclophosphamide dose for renal function,
but the majority of centres used oral therapy, compared with intravenous (2/7). Similarly,
the French Vasculitis Group retrospectively analysed 595 patients with a diagnosis of MPA,
Eosinophilic Granulomatosis with Polyangiitis or Polyarteritis Nodosa diagnosed and

38
treated between 1953 and 199992. 60 patients (10%) died in the first year following
diagnosis with 33 (55%) of these deaths related to active vasculitis and 27 (45%) to
infection. They also found that older age, renal involvement, and central nervous system
involvement was predictive of mortality. Of note in this study is the extensive time period
from which these patients were recruited, meaning that therapy was variable depending
on the era in which patients were treated. Analysis by time of diagnosis showed that
mortality has improved significantly since 1990, compared with patients presenting prior to
this date (p< 0.01).
In 2007 the European League Against Rheumatism (EULAR) Systemic Vasculitis Task Force
also published a systematic review of outcome data from patients with AAV that included
44 studies. They reported 1-year survival rates of 85-97% in GPA, 82-92% in MPA and 93-
94% in EGPA. Five- year survival rates were only available for patients with GPA and
reported as 75-88%93. Age and renal function were found once again to predict mortality
but also the presence of damage, as measured by the Vasculitis Damage Index (VDI). The
VDI is a validated assessment tool which records damage accrued not only due to vasculitis,
but also due to treatment for the condition94.
In recent years, the European Vasculitis Study Group (EUVAS) have completed a number of
randomised controlled trials in patients with AAV to answer questions with regards to the
efficacy of specific therapeutic options; CYCLOPS74, NORAM95, CYCAZAREM96, MEPEX73 and
IMPROVE97 in addition to the Rituximab study outlined above. A combined review of
outcomes for the first 4 of these studies has provided follow- up data for a median duration
of 5.2 years in 535 patients98. The leading cause of death in the first year was infection at
47.5 % of deaths followed by active vasculitis at 18.6% then cardiovascular disease at
15.3%. After the first year, cardiovascular disease became the commonest cause of death
at 25.7% followed by malignancy at 21.6%, with infection still contributing significantly at
20.3%. Significant predictors of mortality were the presence of both MPO and PR3 ANCA
(dual positivity), age greater than 75 years and estimated glomerular filtration rate (eGFR) <
15mls/min (chronic kidney disease stage 5). There is currently data collection underway for
the 10 year follow- up for this study which will provide more valuable long-term data for
this cohort.
Specific to those patients with renal involvement, the Chapel Hill group has recently
published outcomes for 554 patients with AAV with a median follow- up of 31 months99.

39
This study, encompassing outcomes for patients diagnosed between 1985 and 2009,
reported that renal function at diagnosis has improved over time; patients having a median
eGFR of 11 ml/min/1.73 m2 in the earliest time period and 23 ml/min/1.73 m2 in the latest
period. This would explain the observation that significantly fewer patients developed ESRD
over time. There was no significant difference in the adjusted relapse rate over time with
no factors identified associated with relapse (including ANCA type or duration of
cyclophosphamide therapy). The authors suggested that this may be due to the inclusion of
only those with renal involvement having received cyclophosphamide, therefore excluding
many patients perhaps with airway limited PR3 associated disease. Data from other
sources additionally supports that generally outcomes from AAV are improving with a
decline in Standardised Mortality Ratios from 2.1 to 1.03, in subsequent German vasculitis
cohorts over a 36 years period64. However, it is clear that morbidity from treatment is still
significant and ways of approaching prevention of this shall be addressed in later sections.
1.6.2 Relapse
The risk of disease relapse for patients with AAV appears to be in the order of
50%100,101(with follow- up over 44 months in 2 cohorts). One group’s reports have
suggested that relapse rates may be reducing, with a relapse rate of 35.3% in patients
diagnosed from 1999 to 2002, compared with 51.2% of those diagnosed between 1994 and
199864. As mentioned above, however, the Chapel Hill study did not report an
improvement in relapse rates with their 5-year relapse rate being 35%. Furthermore,
longer term follow-up data from the CYCLOPS trial has shown that those treated with
pulsed i.v. therapy were significantly more likely to have relapsed at follow-up (median
duration 4.3 years) but this was not associated with a difference in mortality or morbidity
between the two arms75. Other studies have shown the pattern of organ involvement to
help predict relapse risk with respiratory involvement, cardiac involvement and lack of
significant renal involvement (creatinine clearance >60ml/min) all being risk factors for
relapse93,101. PR3 positivity has been recurrently demonstrated to be a risk factor for
relapse102, however, the relationship between ANCA titres and relapse is complex and is
discussed in more detail below.
Nasal carriage of Staph.aureus has been shown to be associated with a higher rate of
disease relapse47 with treatment with co-trimoxazole shown to be efficacious in reducing
relapse rates48.

40
The mechanism behind this association is not as yet fully understood with roles for
molecular mimicry, Toll Like receptors and Neutrophil Extracellular Traps all suggested as
potential explanations103.
1.6.3 Biomarkers to predict disease activity
However, although ANCA type has become an important part of disease classification, it is
still an inexact tool to predict disease activity including relapse, in addition not being
helpful for disease monitoring in the 5-10% of GPA/MPA ANCA negative patients6.
In ANCA positive patients, the sensitivity and positive predictive value of ANCA rises in
predicting disease relapses have been reported at anything from 20 to almost 100%104. One
publication evaluated ANCA titres in relapsers and non- relapsers in the NORAM trial using
9 different ELISAs. However, although a PR3 peak could be identified to correspond with
disease activity in all relapsers, the monthly increment in PR3 levels prior to the peak was
the same for relapsers and non- relapsers105.
There does appear to be MPO detectable in healthy populations, however, it is likely that
the type of ANCA antibody i.e. the epitope, determines the pathogenicity. The Chapel Hill
group has published data on varying MPO ANCA epitopes. They were able to identify a
pathogenic MPO ANCA epitope in ANCA negative patients along with demonstration of the
presence of a masking protein present in sera, preventing routine antibody detection16.
In summary, although commercially available ANCA titres may in some cases correlate with
disease activity, they cannot be relied upon to distinguish active disease from other
pathology. At present the management of AAV is challenging with uncertainty as to the
balance between drug-maintained disease control, with drug-related morbidity and
mortality and, on the other hand, the risks of relapse with attendant morbidity and
mortality if drug therapy is reduced or withdrawn. Thus, other biomarkers of active disease
are needed to enable improved long term disease management. In addition, earlier
diagnosis and prompt treatment of AAV is needed to reduce damage accruing early on in
disease.
Due to the similarities of presentation between flares of disease activity and possible
infection (e.g. affecting the renal tract, chest or sinuses) some researchers have focused on
serological markers which potentially could be used to distinguish active vasculitis from
infection.

41
The first of these was procalcitonin (PCT), a peptide precursor of the hormone calcitonin,
the levels of which were compared with other inflammatory markers such as CRP and IL-6
in patients with SLE or AAV106,107. It was found that in the absence of infection the PCT
levels were normal in 95 of 98 samples from patients with AAV. However, in the presence
of infection (16 episodes) PCT became markedly elevated. The authors concluded that PCT
appeared to have a specificity of 84% and sensitivity of 100% for the detection of systemic
infection in patients with autoimmune disease such as AAV. However, subsequent studies
have commented that PCT may be raised in patients with active vasculitis and additionally
may be normal in patients with localised, rather than systemic, infection108.
Other markers which have been evaluated include anti-β-glucan antibody109, with a study
demonstrating, perhaps unsurprisingly, that patients on immunosuppressive treatment for
AAV had lower titres of this antibody, and the mean was further lowered in 3 patients who
developed the infectious complications of Pneumocystis pneumonia (PjP) or aspergillus.
However, it did not appear that level of this antibody could be used as a diagnostic marker
of infection. Another marker which perhaps suggests more promise is the serum level of
soluble triggering receptor expressed on myeloid cells-1 (TREM-1). The presence of this
receptor has been shown to be up regulated in the presence of bacterial and fungal
infection, however investigation of levels in patients with AAV failed to distinguish between
those with inactive vasculitis and infection and those with active vasculitis and no
infection110. However, the ratio of serum TREM-1 to serum creatinine appeared to be
higher in those with infectious complications. Overall, the above studies all conclude that
some of these markers may be useful but ultimately further investigation is required in
these areas.
1.7 TREATMENT AND DISEASE ASSOCIATED MORBIDITY
The majority of patients now survive their initial disease episode. However, this means that
vasculitis has shifted from being an acute life limiting disease to a chronic relapsing
condition. Due to the paucity of prospective data as to which patients are at higher risk
from the initial disease and subsequent relapse, patients are often treated aggressively
with high dose immunosuppression. Equally, there is uncertainty as to how long
maintenance immunosuppression should be continued meaning that patients often
continue for years on treatment. Although there have been risk factors for relapse

42
identified (as previously discussed), it remains a challenge to ascertain the optimal time
and regimen for withdrawal of immunosuppression. Leading from this, morbidity
associated with drug exposure is not uncommon, and in fact now may be linked to the
majority of deaths in this population.
1.7.1 Infection as a significant complication of therapy
The risk of infection in vasculitis is likely predominantly linked with immunosuppression
exposure. However, other possible contributory factors in this population may include
susceptibility to infection due to previous organ damage from vasculitis or even an
aberrant immune response.
Hoffman’s series of 158 patients with GPA reported in 1992 included 140 serious infections
in 73 patients (46%), resulting in a rate of 0.11 infections per patient year. The most
commonly presenting infections were bacterial pneumonias at 57 episodes (39%), followed
by skin infections at 38 episodes (26%)100. A full breakdown of the nature of the infections
reported in the combined EUVAS clinical trials is outlined in Table 490. A further review of
240 consecutive patients with AAV presenting to a Birmingham centre over 10 years
reported 91 deaths, of which 33 (36%) were attributable to infection. Patients attending
this centre were treated with a regime of oral cyclophosphamide 2mg/kg until remission
was achieved, with the dose reduced by 25% if the patient became leucopenic (WCC<4.0
x109L) or if the patient was greater than 65 years old. Those patients presenting with
pulmonary haemorrhage or serum creatinine > 500µmol/L were also treated with pulsed
methylprednisolone plus seven sessions of plasma exchange over 14 days. Maintenance
therapy was with azathioprine 1.5mg/kg plus prednisolone tapered to 7.5 mg and
maintenance therapy was continued for 5 years. This study reported identified risk factors
for infection in this population as older age and leucopenia111 .

43
Infection Number(%) of infections % of total
population
Respiratory:
Lower
Upper
40 (24)
7 (4)
7.6
1.3
Hepatitis B 2 (1) 0.4
Urine 9 (5) 1.7
Miscellaneous 37 (22) 7.1
Unknown 22 (13) 4.2
Opportunistic: 48 (29)
Pneumocystis carinii 5* (3) 0.9
CMV 12 (7) 2.2
Candidiasis 16 (10) 3.1
HSV 7 (4) 1.3
Epstein Barr virus 1 (0.6) 0.2
Clostridium difficile 3 (2) 0.6
Parvovirus 1 (0.6) 0.2
HZV 5 (3) 0.9
Table 4. Summary of infections reported in the 4 combined EUVAS trials90
1.7.2 Cardiovascular disease
It has been known for some time that patients with AAV have an increased risk of
thromboembolic disease, particularly associated with periods of active disease112. This
initially was thought to be due to endothelial changes and hypercoagulability associated
with both the disease and the treatment. However, more recently the presence of anti-
plasminogen antibodies has been demonstrated in patients with AAV. In addition, the
presence of these antibodies has been shown to retard fibrinolysis in vitro113.

44
With regards to cardiovascular disease, matched cohort studies have demonstrated an
increased incidence of events in AAV patients, with an observed to expected ratio of 1.9 in
one study compared with the background population and a hazard ratio of 2.23 compared
with a CKD population114,115. This observation has led to the development of a model for
predicting cardiovascular events in AAV patients with age, diastolic hypertension and
absence of PR3 antibodies being identified as risk factors for cardiovascular events in newly
diagnosed AAV116. However, as yet there is no evidence or consensus as to whether
patients with AAV should be treated any differently from patients with traditional
cardiovascular risk factors.
1.7.3 Bone Health
Due to the ongoing reliance on immunosuppressive regimens with significant corticosteroid
exposure this population is at risk from steroid induced osteoporosis. In addition, there is a
likely contributory effect from cytokines involved in the inflammatory disease117.
The only study into bone density in AAV reported a prevalence of 57% osteopenia and 21%
osteoporosis in 99 patients118. There is no study reporting fracture rates as a complication
of bone disease in this population but due to current lack of steroid- sparing treatment
regimens available for this population, awareness of, and the need for assessment and
modification of this risk, is required.
1.7.4 Malignancy
Early studies in AAV, with a substantially greater cyclophosphamide load for patients
reported a 2.4-fold increase for all malignancies, with higher rates of bladder cancer and
lymphoma100. Since the introduction of a switch from cyclophosphamide to maintenance
therapy at 3 to 6 months and a trend towards pulsed intravenous therapy rather than daily
oral, resulting in a much lower total cyclophosphamide dose, this risk appears to have
diminished somewhat. A recent analysis of the available data suggests a SIR of malignancy
of 1.6-2.0 compared with the general population. The majority of this risk can be attributed
to the increased incidence of skin malignancy in this population. With studies supporting
the preferential use of azathioprine for maintaining remission in AAV, an agent which has
shown to be associated with increased risk of skin cancer119, it is prudent that these
patients receive appropriate education and screening.

45
1.7.5 Sexual health and fertility
Other considerations of possible complications of therapy in these patients include the
effect of treatment on fertility and cervical cytology. In the lupus population, it has been
demonstrated that there appears to be a relationship between intravenous
cyclophosphamide dose and development of cervical intraepithelial neoplasia (CIN). This
appears to reverse following cessation of therapy 120.
Similarly, the majority of data on the effect of cyclophosphamide exposure on fertility is
derived from the lupus population, with a rate of around 30% of cessation of menstruation
following exposure to cyclophosphamide121. However, this risk varies depending on
cumulative cyclophosphamide exposure and age at cyclophosphamide administration.
It is also well established that exposure to cyclophosphamide in men causes significant
sperm abnormalities associated with a reduction in fertility122. Therefore, the possible
ramifications of exposure to cyclophosphamide for those of child-bearing potential should
be considered when choosing the optimal treatment strategy for an individual patient.
1.8 CURRENT CHALLENGES TO CARE FOR PATIENTS WITH AAV
In summary, it can be seen that the major challenges for patients with AAV are; firstly,
receiving a correct and timely diagnosis, with historical difficulty in disease classification.
This may be compounded by a lack of awareness of vasculitis as a potential diagnosis due
to the rarity and heterogeneous presentation of the disease. Secondly, even following
appropriate treatment, the patient remains at significant risk of relapse, with monitoring
often dependent on inexact immunological markers. This is in part due to the lack of
complete understanding of the underlying disease pathogenesis. Delays to both
identification of initial disease and subsequent flares may result in accrual of damage and
may necessitate higher exposure to immunosuppression than would have been necessary
with earlier identification of disease activity. Again, treatment of relapse commensurate
with the severity of disease activity is also important in maintaining the balance between
disease damage and treatment complications. Thirdly, no matter how timely the diagnosis
and appropriate the treatment, as outlined above current immunosuppression regimens
carry with them significant morbidity. Until there are significant changes in
immunosuppression strategy it is essential that there is vigilance regarding side effects of
these agents. There is the need for awareness and for clinicians to work with the patient to
optimise preventative approaches to try to limit disease and treatment related morbidity.

46
Alongside this there is a parallel need to focus on identification of alternative future
therapeutic targets which could have reduced treatment complication profiles. This body of
work will use a variety of approaches to explore potential contributors to these obstacles
faced by patients and to attempt to provide means of addressing some of the challenges
faced.

47
2 THE PATHWAY OF THE UK VASCULITIS PATIENT- FROM
SYMPTOMS TO DIAGNOSIS AND BEYOND
2.1 INTRODUCTION
The ANCA- Associated Vasculitides (AAV) are a heterogeneous group of conditions that may
cause small to medium vessel inflammation in a number of different organ systems. The
three AAV are classified as Granulomatosis with Polyangiitis (GPA, formally known as
Wegener’s Granulomatosis), Microscopic Polyangiitis (MPA) and Eosinophilic
Granulomatosis with Polyangiitis (EGPA, formerly known as Churg- Strauss Syndrome).
Historically, interventions and outcomes for this diverse patient group have often been
studied together, in part due to their rarity. However, data is emerging to support that
these are definite distinct disease entities with different disease courses and outcomes,
including differing underlying genetic predispositions7.These conditions are often treated
with initial aggressive “induction” therapy followed by long-term maintenance
immunosuppression, which has served to improve mortality but carries with it substantial
morbidity itself93.
Depending on the disease type, organ involvement may vary meaning that patients can
present with a wide spectrum of initial symptoms and, therefore, to multiple clinical
disciplines. This can provide significant challenges for the diagnosing clinician, particularly if
the patient presents to a discipline which may not commonly see these conditions.
There have been some reports of time from first symptoms to diagnosis in the
Granulomatosis with Polyangiitis cohort. Holle et al. compared a number of parameters
and outcomes across a single centre cohort, stratified according to date of presentation.
They reported that the median time to diagnosis did appear to be improving over time,
from 8 months for those patients diagnosed between 1966 and 1993, to 5 months between
1994 and 1998, and 4 months from 1999 to 200264. A similar pattern was reported in a
Finnish study of GPA patients with median time from onset to diagnosis improving from 17
months from 1981 to 1985 to 4 months between 1996 to 2000123. A further Scandinavian
study reported characteristics of patients with GPA but also MPA, EGPA and polyarteritis

48
nodosa diagnosed between 1997 and 2006. The median “diagnostic delay” was reported
here as 2 months for those with GPA, 1.5 months for MPA and 2.5 months for those with
EGPA124.
Providing comprehensive ongoing care for this patient group is a further challenge.
Alongside variable initial presentation, these patients have the potential for other organ
manifestations to subsequent evolve in the future. In addition, the burden of
immunosuppressive treatment means that patients may develop local or systemic
complications of therapy, such as bone disease, immune deficiencies or cardiovascular
disease, which requires specialist management and support.
Currently, the majority of care for these patients is provided in secondary and tertiary
centres. Due to evolving care models, with a greater focus on utilisation of primary care
resources, those planning future care for this population may look to see whether aspects
of vasculitis care can be devolved to primary care. Although there are some models in
place, such as shared care monitoring of blood tests for those on immunosuppression, this
is a practice which is not uniformly implemented at present.
We sought to gain an overview of the UK vasculitis patients’ pathway, from presenting
symptoms, through diagnosis and including post diagnosis care.
2.2 MATERIALS AND METHODS
The intention was firstly to establish how and where patients with vasculitis present in the
UK to explore factors influencing time to diagnosis. Secondly, we wished to evaluate where
patient care continues to be provided after a diagnosis has been made, and how patients
view the role of their different care providers, including primary care, in managing their
health and disease.
2.2.1 Patient questionnaire
To achieve this, a multi-disciplinary research group including clinicians with expertise in
vasculitis care, qualitative and nursing researchers and a patient representative was
assembled. This group collaborated to produce a self-report patient questionnaire

49
encompassing areas including: experience surrounding presentation and diagnosis, current
medical care and therapy (full questionnaire available in Appendix 1).
2.2.2 Subjects
This questionnaire was distributed to all 700 members of the UK national patient support
group, Vasculitis UK, using their established mailing list. Ethical approval was not required
(confirmed in writing by Preston REC) as participants were identified by the patient support
group and remained anonymous to the researchers.
2.2.3 Statistical analysis
Simple descriptive statistics were used to analyse the majority of the data. Kruskal- Wallis
analysis or Mann-Whitney testing was used to compare the medians between patient
groups. Thematic analysis was used for the semi- qualitative data describing symptoms. All
statistical analysis was carried out using GraphPad Prism (v.7).
2.3 RESULTS
2.3.1 Responder characteristics
Three hundred and seventy-eight completed questionnaires were returned, giving a
response rate of 54%. Within these, responses were excluded if there was no diagnosis
stated, or any diagnosis other than systemic vasculitis, ANCA-associated vasculitis,
Wegener’s Granulomatosis, Granulomatosis with Polyangiitis, Microscopic Polyangiitis or
Churg-Strauss syndrome (now known as Eosinophilic Granulomatosis with Polyangiitis). In
total, 306 patient questionnaires (81% of those returned) were analysed.
Of the analysed questionnaires, the mean responder age was 61.7 (range 21-87) years.
Responders were predominantly white British (93%) with 62% being female.

50
% patients
GPA(n=24
1)
EGPA(n=
41)
MPA
(n=15)
Other (disease not
specified)(n=9)
Nasal/sinus 34.1 40.3 17.1 6.7 0
Fatigue 26.6 24.8 36.6 33.3 28.6
Musculoskeletal joint
symptoms
25.6 27.7 14.6 14.6 0
Respiratory 24.3 21 48.8 26.7 0
Ear 22.6 27.7 7.3 0 0
Other pain 11.2 9.7 19.5 13.3 14.3
Flu/cold/viral 10.2 10.5 9.8 13.3 0
Skin 9.9 9.2 17.1 6.7 0
Eyes 9.2 10.1 0 20 0
Weight loss 6.9 7.6 7.3 0 0
Headaches 5.6 6.3 4.9 0 0
Peripheral nerve 3.0 2.1 12.2 0 0
Musculoskeletal muscle
symptoms
3.0 2.9 2.4 6.7 0
Haematuria/renal 1.6 2.1 0 0 14.3
Mood/cognitive 1.6 1.7 2.4 0 0
Table 1. Presenting symptoms
2.3.2 Symptoms
The most common initial symptoms for all patients were categorised as nasal/sinus
(34.1%), followed by fatigue (26.6%). When analysed according to eventual diagnoses,
patients with GPA most commonly presented with nasal/sinus symptoms (40.3%), EGPA
with respiratory symptoms (48.8%) and MPA with fatigue (33.3%). Median time to
diagnosis was reported as being 6 months ().

51
Characteristics Median time to diagnosis
(IQR) months
P value
Diagnosis
GPA (n=217) 6 (13.75) 0.0793 (comparing
across all gps)
MPA (n=13) 13.5 (24)
EGPA (n=38) 13.5 (32)
Predominant presenting symptom
Ears/Nasal/sinus (n=155) 6 (17.5)
Fatigue (n=74) 6 (12.25)
Musculoskeletal symptoms (n=80) 6 (20.25)
Respiratory symptoms (n= 66) 10 (17.5) 0.0013**
Skin (n=28) 4 (6.5)
Eye (n=25) 9 (19)
Neurological (n=10) 7 (14)
Discipline seen pre-diagnosis
Rheumatology (n=71) 8.5 (26.5) 0.9699
Nephrology (n=25) 9 (56.5)
ENT (n=117) 10 (22.5)
Chest (n=60) 9 (31)
Table 2. Relationship of patient characteristics to time to diagnosis (** statistically
significant when compared with time to diagnosis for those with skin symptoms)
Time to diagnosis appeared to differ (though not significantly) by eventual diagnosis
received but not by initial clinical discipline consulted. Those patients presenting with skin
manifestations had the shortest reported time to diagnosis (median 4 months), this was
significantly shorted than those who reported the longest time to diagnosis following
presentation with chest symptoms (p=0.0013). The majority, 70.9%, of patients reported
receiving an initial alternative diagnosis before later being given a diagnosis of vasculitis.
Most commonly, this was infection, followed by sinusitis/rhinitis in the GPA population,

52
asthma (which is acknowledged to often precede the onset of EGPA) followed by
psychological disorders in EGPA and viral infection in MPA.
% All
patients
GPA EGPA MPA Other
Sinusitis/rhinitis 11.7 13.7 4.9 6.7 0
Viral infection 10.8 11.2 9.8 13.3 0
Other infection 13.0 15.8 4.9 0 0
Psychological 7.2 6.6 12.2 6.7 0
Asthma 5.2 2.0 26.8 0 0
Malignancy 4.9 6.2 0 0 0
Tuberculosis 4.2 5.0 2.4 0 0
Allergy 2.9 3.7 0 0 0
Polymyalgia rheumatica 2.9 2.9 2.4 6.7 0
Other rheumatological disease (e.g. RA, SLE, connective tissue disorder)
13.7 12.5 9.8 46.7 14.3
Other 21.5 20.3 24.4 26.7 42.9
Table 3. Alternative diagnoses received prior to vasculitis
2.3.3 Utilisation of healthcare
The majority of patients (73.2%) initially consulted their general practitioner (GP), and
81.8% patients reported attending a hospital specialist appointment before their diagnosis
of vasculitis was made. Many patients reported being seen by more than one discipline
with the median number of disciplines consulted prior to receipt of diagnosis being two.
The most common clinics attended prior to diagnosis were ENT (26.2%), in keeping with the
most common presenting symptoms of nasal and sinus disease, followed by rheumatology
(15.8%).
Subjects were asked who they viewed as the main person looking after their vasculitis from
a list of hospital doctor, specialist nurse and GP, with the majority, 259 (84.6%), choosing
hospital doctor. Patients were then asked to report how often they had seen this individual
in the preceding year. 245 patients gave a numerical answer (with the remainder answering
non- specifically e.g. “often” or “a lot”). The median frequency was 3 (IQR 2-5). The specific

53
clinics attended can be seen in Figure 2, and are primarily rheumatology (49.5%) and
nephrology (41%).
Finally, patients were asked to describe how they perceived the role of their GP in the
management of their condition. 51.3% stated they would see their GP as the first point of
contact for any health problem, 64.1% for any health problem not relating to vasculitis,
36.9% for blood tests and 35.6% for blood pressure monitoring. Only 12.1% reported that
they saw their GP as having no role in their disease management. When asked about more
specific medical scenarios, the majority would contact their GP in the first instance for each
of the following; for a chest infection (79.6%), other infection (80.3%), joint problem
(59.9%), eye problem (62.5%), skin problem (75%) or ENT/sinus problem (58.6%).
Figure 1. Vasculitis patient health care utilisation
2.4 DISCUSSION
In this patient reported historical study we novelly explore the alternative diagnoses often
received by vasculitis patients prior to their definitive diagnosis. We report that a majority
of patients initially present to primary care and their symptoms are attributed to more
common disease processes.
Our data is in keeping with previous published time to diagnosis of between 4 and 8
months, depending on era of diagnosis64. However, our study attempts to further evaluate
other factors contributing to length to diagnosis, with this time period appearing to vary
0
50
100
150
Pat
ien
t n
um
ber
s
Clinical discipline
Disciplines accessed pre and post diagnosis
Pre Post

54
according to initial presentation, but not by the discipline patients first present to. Our data
suggests that those patients who present with a visible manifestation of their disease such
as a skin rash are significantly more likely to receive a timely diagnosis than those who
present with respiratory symptoms. This study highlights the need for increased education
and awareness of vasculitis as a possible diagnosis in the broader medical community, in
light of the fact that the majority of patients initially present to primary care. We have also
identified those initial diagnoses that may alert health care providers of the need to
potentially seek an alternative explanation for persistent patient symptoms.
Contrary to the perhaps anticipated opinion that vasculitis patients would wish to
predominantly be managed in secondary care we report that patients appear to have
confidence in their primary care providers and the majority would see their GP as the first
point of contact in any health scenario. However, it is unclear whether the patients
recognised some of the given health scenarios as potentially being linked with their
vasculitic illness, which may highlight the need for better patient education regarding
symptom recognition.
This work has significant implications for the planning of future health care delivery for this
patient population. The British Society of Rheumatology guidelines suggest that patients
with vasculitis be managed within networks of care, involving expert vasculitis centres83. It
may be that future care models would allow patients to have designated parts of their care
carried out in a community setting (e.g. blood monitoring, co-morbidity prevention) under
guidance from expert centres. This may allow remote monitoring to become a possibility
for some patients with stable disease, avoiding unnecessary travel and clinic waiting times
and allowing prioritisation of vasculitis out- patient appointments for those with unstable
or challenging disease.
We acknowledge this study has limitations. Firstly, it was necessary to design a new
questionnaire for our purposes meaning that only limited validation of the questions in this
survey could be undertaken prior to the full study. Although this was a lengthy
questionnaire, pilot testing showed that the questions were predominantly completed in
full.

55
One of the major limits of a historical questionnaire study is that it relies on retrospective
patient report which is not infallible. With regards to time from first symptom as recalled
by the patient to diagnosis, it is unclear and impossible to verify whether this truly was a
manifestation of the vasculitis. This is likely to apply particularly to those patients with
EGPA with a preceding diagnosis of asthma. Equally this study only included members of a
national patient support group and were furthermore self-selected by being responders.
This is likely to have had an impact on the demographic as noted in the gender and
ethnicity of those included. There also was a predominance of GPA in our surveyed
population, meaning that there were insufficient numbers of the other vasculitides
involved from which to draw robust conclusions. However, whilst this will be relevant for
the symptomatology related data, information regarding areas such as utilisation of
healthcare pathways, may be transferrable across other groups. It also may be that
patients had been misclassified, leading to an over reporting of GPA and an under reporting
of MPA. However, patients with GPA are more likely to relapse and are more likely to have
ongoing difficult to control symptoms originating from ENT or respiratory systems, meaning
that this particular disease group may be more likely to be members of a patient support
group. The strengths of this study are the inclusion of a large number of patients with a
rare disease and across a wide geographical area. In addition, this study contributes
previously unreported possible contributory factors to diagnostic delay, including the most
frequent “misdiagnoses” received by this patient group.
We therefore feel that the results are important in highlighting the need for improved
awareness and recognition of vasculitis, identifying ways in which patients may present and
acknowledging that that this may influence time to diagnosis. In addition, defining current
pathways pre-and post diagnosis can help to inform those involved in planning of services
for this diverse and challenging patient population.

56
Appendix 1. Full Questionnaire
From the North- West Vasculitis
Group
In association with
Vasculitis UK
Questionnaire for people living with
vasculitis
To help us improve diagnosis and care provided

57

58

59

60

61

62

63

64

65
66
3 VASCULITIS PATIENT AWARENESS OF MEDICATION SIDE-
EFFECTS AND UPTAKE OF PREVENTATIVE/ PROPHYLACTIC
MEASURES: A UK QUESTIONNAIRE STUDY
3.1 BACKGROUND
ANCA- associated vasculitis (AAV) is a small to medium vessel systemic vasculitis with a
combined annual incidence in the UK of 10- 15 per million31. This umbrella term currently
refers to patients with a diagnosis of Granulomatosis with Polyangiitis (GPA), Microscopic
Polyangiitis (MPA) and Eosinophilic Granulomatosis with Polyangitiis (EGPA, formerly Churg
Strauss Syndrome).
While these are genetically and phenotypically distinct disease entities, when evaluating
non- disease related factors it is still reasonable to group these patients together for study
due to their rarity and exposure to similar therapeutic regimes. Early descriptive data
reports the average survival for GPA following diagnosis as just 5 months89. Since the
introduction of immunosuppressive agents to treat this spectrum of diseases, this has
significantly improved with 5 year survival currently at 75%125. Most patients now survive
their initial vasculitic episode suggesting that AAV now needs to be viewed not only as an
acute life- threatening illness, but increasingly as a chronic relapsing / remitting disease.
Although developments in care have resulted in improved patient survival, there remains
substantial morbidity and mortality associated with the disease and the treatment125. Care
for this complex group of patients may be delivered in a number of care settings including
single specialty Rheumatology, Nephrology, Neurology, Respiratory, and multi-disciplinary
clinics. The physician faces challenges in maintaining awareness of all possible
manifestations of this multi- system disease, as well as awareness of the wide spectrum of
complications of immunosuppressive therapy to which this population is susceptible.
Current evidence-based induction therapy for acute, organ or life- threatening disease
consists of high dose corticosteroids and cyclophosphamide or Rituximab. This is followed
by a period (which may continue for many years) of maintenance therapy, with oral
steroids often continuing alongside other immunosuppressive agents such as azathioprine

67
or mycophenolate. All of these are associated with possible long-term adverse events
including infection, bone disease, increased cardiovascular and malignancy risk. The aims of
the work reported here were to assess patients’ level of knowledge and awareness of
potential side effects of their therapy. Alongside this we evaluated uptake of protective and
prophylactic measures aiming to reduce disease and therapy related complications.
3.2 PATIENTS AND METHODS
A multi-disciplinary expert panel including clinicians with expertise in vasculitis
(nephrology, rheumatology, neurology, ENT and ophthalmology), research methodologists
and patient representatives was assembled. This group developed a self-report patient
questionnaire addressing patients’ experience surrounding presentation and diagnosis,
current medical care and therapy. The topics to be covered in this questionnaire were
identified through clinical experience and published literature and questions were
reviewed and modified by patient representatives prior to distribution. It was necessary to
design a new questionnaire for this study as none existed which addressed the areas of
patient knowledge and reported care we wished to evaluate. This paper focuses on data
relating to vasculitis treatment, patients’ knowledge of side effects and adoption of
measures aimed at reducing disease and treatment-related side effects.
Questionnaire piloting and assessment of validity of self-reports was undertaken with a
local cohort of patients with AAV and Systemic Lupus Erythematosus prior to use. The
main study was a national questionnaire survey using the already established mailing list
from the UK national patient support group, Vasculitis UK. This questionnaire was
distributed to all 700 members across the UK. Ethical approval was not required for the
main study (confirmed in writing by the NRES Committee North West, Preston) as
participants were identified by the patient support group and remained anonymous to the
researchers.
Statistical analysis: Simple descriptive statistics were used to analyse the majority of the
data. Unpaired t- tests were used for comparison of unmatched data sets e.g. the
characteristics of those reporting knowledge of side effects compared with those without.
Fisher’s exact test was used for comparison of proportions of patients within a group
reporting certain behavior. Thematic analysis was used for responses to open-ended
questions (e.g. those describing side-effects).

68
3.3 RESULTS
3.3.1 Pilot/validity check
The questionnaire was piloted with a sample of 30 local patients with AAV or Systemic
Lupus Erythematosus. Patients were asked to complete the questionnaire designed for the
above study and answers were validated by case note review. As these were recruited via
NHS hospitals, ethical approval for this stage of the study was granted by the NRES
committee North West, Preston. Full medical information was available on 73% of patients.
Of these, the diagnosis given by the patient was confirmed using ACR criteria and EMEA
algorithm in 94.4% of cases. Regarding exposure to immunosuppressive medication, there
was agreement between patient reporting and medical notes in 76% of cases. With regards
to receipt of prophylactic/ preventative measures, patient responses could be corroborated
in the medicines history in 78.9% of cases. This level of agreement was considered
acceptable.
3.3.2 Main study
For the main postal survey, a response rate of 54% (378 completed questionnaires) was
achieved. Analysis included only those with a self- reported diagnosis of “Systemic
Vasculitis”, “ANCA Associated Vasculitis”, “Wegener’s Granulomatosis” (now known as
Granulomatosis with Polyangiitis), “Microscopic Polyangiitis” or “Churg Strauss Syndrome”
(306 patients). Of the 306 eligible questionnaires, the majority were completed by women
(62%) with the mean age of the population 61.7 years (range 21 to 87). (See Table 1 for
sample demographics). Given the study methodology we do not have demographic data on
those who did not complete and return the questionnaire. The responding population
differs from the profile typically seen in practice by the female preponderance. Also,
although GPA is accepted to be twice as common as MPA in Northern Europe, 79% of our
questionnaire respondents reported a diagnosis of GPA. However, this study aim was to
assess patient knowledge. Therefore, due to common drug exposure for the differing
disease subtypes, the diagnosis although of interest, is not of particular importance.

69
Demographics Patient numbers (%)
Granulomatosis with Polyangiitis
(previously Wegener’s Granulomatosis)
241 (79%)
Churg Strauss Syndrome 41 (13%)
Microscopic Polyangiitis 15 (5%)
Other "Systemic vasculitis/ANCA
Associated Vasculitis"
Total
9 (3%)
306
Female
Male
Not specified
190 (62%)
112 (37%)
4 (1%)
Age 61.7 years (range 21-87)
White British
White other
Other
Not specified
285 (93%)
5 (2%)
10 (3%)
6 (2%)
Table 1. Characteristics of the Sample
3.3.2.1 Awareness of side effects of therapy
Patients were asked to choose the drugs they had been prescribed to treat their vasculitis
from a list, with room for expansion for those not included. They were then asked to
describe any potential side- effects of therapy of which they were aware. This was done in
a free text format so as not to influence possible answers.
The most frequently reported drug received by 295 (96%) patients at some point in their
disease course was oral steroids. The next most frequent drug to which they had been
exposed was cyclophosphamide at 74.5% (oral and intravenous combined) followed by
azathioprine at 69%. Further information on drug exposure is provided in Figure 1. The
majority of patients (74.8%) reported awareness of at least one potential drug side effect.
However, some patients commented that awareness of these side- effects had only come

70
through experiencing them, rather than being counselled regarding them prior to drug
exposure.
Figure 1: Reported exposure to immunosuppression
The most commonly recognised side effects were those associated with steroid exposure,
with 27% of patients recognising bone thinning/ osteoporosis as a potential steroid related
problem. The next most common group of adverse effects recognised appeared to be those
that the patients would be aware of having experienced, such as weight gain with steroids
and hair loss with cyclophosphamide. The most common themes in the “other” category
were fatigue, headaches, dizziness and cognitive impairment. Only 4% of patients reported
symptoms that were unlikely to be attributed to their medication. There was generally low
awareness of the increased infection risk associated with immunosuppression and
potential increased long- term cancer risk. There was also very little awareness of the
increased cardiovascular disease associated with steroid exposure (Figure 2).
A sensitivity analysis was performed in addition for patients with current exposure to drugs
versus all (current versus previous). This was carried out for patients exposed to
azathioprine and the associated awareness of skin damage (defined by warts, sun damage
or skin cancer) as a potential side effect of the drug.

71
Twelve of 98 patients currently taking azathioprine (12.2%) had an awareness of these side
effects, versus 18 of 212 (8.5%) having ever taken it (p=ns).
The most frequent source of drug information reportedly used by patients was their
hospital doctor (56.6%) followed by the drug information leaflets inside the medication box
(52%). Following this, the internet was the third most frequent source of information, with
a trend for those under 60 years old to utilise this resource compared with those over 60,
but this did not reach statistical significance (p=0.06). Further investigation of the
characteristics of the group who reported no awareness of any possible medication side
effect showed a mean age of 76 years (compared with 59 years in the group with
awareness of side effects and a longer time since diagnosis, 5217 days, compared with
4398 days (p=ns)). This may simply reflect that due to the longer time lapse since diagnosis,
information regarding drug side effects may have been forgotten. However, the focus on
patient education has increased over the years making those diagnosed recently perhaps
more likely to be better informed.
Figure 2. Patient reported awareness of potential medication side effects
(GI= gastrointestinal, CVD= cardiovascular disease).

72
Men made up 56% of the group with no awareness of side effects, compared with only 31%
of the group reporting awareness. This may highlight men as being a group who potentially
need more dedicated education regarding drug counselling. Of those men who did report
an awareness of side-effects, the majority utilised the secondary care clinician as a source
of information (62.8%) followed by the drug information leaflet accompanying the
medication (51.3%) and the internet (26.9%). Men were least likely to use patient
information leaflets (such as those provided in clinic) as information sources. The women
surveyed in this study were less likely, although not statistically significantly, to report using
a specialist nurse (p= 0.23) but more likely to use a patient information leaflet (p= 0.07) as
an information source, when compared with men. We were unable to perform any analysis
between the level of education/ socioeconomic status and knowledge levels, as the
majority of patients reported their employment status as retired, and did not specify
previous occupation. 123 (40.2%) of patients reported having had to discontinue a therapy
at some point due to side- effects.
3.3.2.2 Reported uptake of prophylaxis/ screening
We explored patient reported practice regarding therapy aiming to reduce the
complications of immunosuppressive therapy using a list of potential prophylaxis or
screening measures which may have been recommended by a health care professional.
Patients were asked to indicate which of these they had received.

73
Figure 3. Patient reported uptake of preventative therapy
Our results showed that, in line with the awareness reported above, uptake of bone
protection was good. Other steroid prophylaxis such as gastro-protection was also
commonly reported.
Current Department of Health recommendations are that those over 65 years or in “at risk”
groups, including those on immunosuppression, should receive influenza and
pneumococcal vaccination85.The majority of patients had received ‘flu vaccine (85%), with
further analysis demonstrating that 50% of these having received the vaccine were less
than 65 years old. This may demonstrate awareness amongst primary care of the need for
‘flu vaccination in the younger immunosuppressed population. However, pneumococcal
vaccine was less frequently delivered at 40.2%. Use of skin protection in the sun was low
(17.6%) considering the high percentage of these patients (69%) that had been exposed to
azathioprine.
3.4 DISCUSSION
Patient outcomes from vasculitis are improving but, particularly until steroid sparing
regimes can be identified, treatment continues to carry high levels of morbidity. Provision

74
of care for vasculitis patients is becoming increasingly complex as patients survive longer
with multiple co- morbidities. Although research for this patient group has primarily
focused on improving outcomes from active disease, it is important to also remain aware of
other areas where patient care could potentially be improved.
The strengths of this study include the large number of respondents; particularly for a rare
disease such as vasculitis. Validation of self-report in our local cohort demonstrated
generally good concordance with what is documented in hospital records. However, we
accept the limitations associated with a patient reported questionnaire study. The
responders were mainly female (a characteristic not generally reflected in the disease
population). Also the majority of patients reported their clinical diagnosis as GPA. This may
reflect some misclassification of disease or potentially that patients who may have
“limited” GPA have a better prognosis and therefore were more likely to survive to
participate in this study. The responding group are likely to represent a more motivated
population, potentially being better informed about their disease and treatment. However,
this means that the results from this study probably represent a “best- case scenario”. As
participants were anonymous to the researchers we were not able to identify those a priori
for whom English was not their first language who may have required translated material.
This is likely to mean that non- English speakers were excluded from this study. Some
questionnaires were completed by relatives/ spouses of those who were not able to
complete the questionnaire for other reasons (e.g. visual impairment). However, we
appreciate that the requirement for self- reporting of data in this study have excluded
those who with disability or severe illness.
Our study has highlighted that there are deficiencies in patient knowledge regarding
potential adverse effects associated with vasculitis treatment. This will reflect patient recall
as well as initial imparting of information by health care providers. This is supported by the
sensitivity analysis which showed that more patients currently taking azathioprine were
aware of skin side effects compared with the population who had ever taken azathioprine
(12.2% versus 8.5%), though not significantly so. However, overall, this was still a very ow
level of awareness of a potentially serious but preventable adverse effect.This study also
potentially highlights that men and women may prefer to access information in different
ways and that this may need to be taken into consideration during drug counselling.

75
There are relatively few studies evaluating patient knowledge of drug side-effects. Those
that have been carried out in populations with osteoarthritis, inflammatory bowel disease
and lymphoma re-iterate our findings that knowledge of potential drug side- effects is
poor126–128. It is important to bear in mind that valid consent for treatment includes patient
awareness of potential adverse effects. This is particularly important, as studies in other
groups of patients receiving immunosuppressive therapy have found that side-effects can
have a significant impact on patients’ quality of life, the impact of which may be under-
estimated by health professionals129,130. Furthermore, as some patients may largely self-
manage their condition and may have only infrequent contact with specialists, good
awareness of side effects is essential in enabling patients to accurately recognise problems
early and take appropriate action. The data highlight areas where improved patient
information and self-management education may be required.
It is likely that overall cancer risk is reducing in the vasculitis population, due to a trend to
move towards pulsed intravenous cyclophosphamide resulting in a lower total dose.
However, it may be some years before this reduced risk filters through and until current
long- term data is available as to what this absolute risk is, surveillance and awareness of
potential malignancy in this population should be maintained. Of particular concern is the
lack of awareness of skin cancer, which is potentially preventable if appropriate sun
avoidance/ protection strategies are adopted. It has long been common practice for solid
organ transplant clinics to provide annual skin surveillance for their patients on long- term
immunosuppressive agents. As the data starts to suggest that vasculitis patients may need
to remain on their maintenance phase of therapy for longer (with current evidence
favouring azathioprine as the agent of choice for maintenance72), it may be time to ensure
that other patient groups on chronic immunosuppression are afforded the same level of
vigilance.
Infection continues to be a significant problem in this population, with vaccine preventable
organisms such as Pneumococcus a major cause of morbidity and mortality. There have
been some studies in recent years that have sought to evaluate the immune response of
this patient group to influenza vaccination131,132. However, these studies have been small
and primarily have excluded patients on significant immunosuppression- those most at risk
from infection. Further studies evaluating both the efficacy and the clinical effectiveness of
vaccination in this patient population are required. However, until this evidence is available

76
it would seem reasonable to extrapolate from recommended practice for other groups with
immunodeficiencies133.
In summary, our study demonstrates that vasculitis patient awareness of potential adverse
effects of therapy is low. Patient reported practice regarding uptake of measures to reduce
these adverse effects is variable. This may indicate that there is room for improvement in
the care we deliver for patients with vasculitis. Future work should focus on long-term
studies to evaluate on going treatment related morbidity in this population including
identification of risk factors and potential prevention strategies. Alongside this, clinical
services should be developed to include comprehensive and systematic regular assessment
of the vasculitis patient. This would enable identification and monitoring of therapy-related
complications and provide patient information and self-management education. With
these strategies, it would be hoped that the mortality and morbidity of patients diagnosed
with vasculitis can continue to fall.

77
4 A DELPHI STUDY TO ASSESS PREVENTION OF TREATMENT
AND DISEASE RELATED MORBIDITY IN VASCULITIS (ADAPTIV):
DELPHI METHODOLOGY
4.1 INTRODUCTION
Primary systemic vasculitis (PSV) is a multi-organ, life-threatening, inflammatory disease
requiring aggressive initial immunosuppressive therapy. Even following treatment of the
presenting episode, due to the risk of relapse (approximately 50% over 5 years)134,135 long-
term immunosuppression is often required. The most common group of PSV seen in the UK
is ANCA Associated Vasculitis (AAV), with a prevalence of around 220/million in 200838.
Whilst mortality from initial disease is improving; only 14% of deaths at 1 year following
diagnosis from active disease90, patients now increasingly survive to experience side effects
of the both the disease and the therapy. Initial life or organ threatening disease is treated
with cyclophosphamide or Rituximab, a B cell depleting agent, and high dose steroids,
whilst once remission has been achieved the patient may require years of therapy with low
dose corticosteroids and a steroid sparing agent such a azathioprine or mycophenolate (see
British Society of Rheumatology publication 2014 for full treatment guidelines)83.
Due to the often intensive immunosuppressive regimen, this population has a high level of
treatment related morbidity and mortality. Infection accounts for 50% of deaths in the first
year following diagnosis of AAV90. Beyond the first year, this risk continues, though at a
lower level (20% of deaths), with the risks of cancer and cardiovascular disease increasing
along with the cumulative immunosuppressive burden98. Other problems frequently faced
by this population include steroid related bone disease and sub-fertility or infertility as a
result of cytotoxic therapy. Due to the relative rarity of these diseases, there is a paucity of
evidence for best practice in the prevention/ reduction of these co-morbidities. Although
some evidence can be extrapolated from other disease groups, it is increasingly apparent
that the risks of co-morbidities relate not only to drug exposure but also to the underlying
disease pathogenesis. Therefore, these guidelines have been produced, using both the

78
available evidence and expert consensus, by the UK and Ireland Rare Disease Group for
Vasculitis to inform clinical care for this population.
4.1.1 Objective
To produce comprehensive, clinically relevant guidelines to inform the screening for and
prevention of co-morbidities of patients with ANCA Associated Vasculitis (AAV). Although
these guidelines do focus particularly on this disease group, they may equally be applicable
to other patients on chronic immunosuppression for whom robust guidelines in this area
are not available.
4.1.2 Target Audience
Any primary care or secondary clinician involved in the care of patients with AAV including
but not limited to; rheumatologists, nephrologists, Ear, Nose and Throat (ENT) specialists,
respiratory physicians, neurologists, and specialty trainees and specialist nurses in these
fields.
4.1.3 Stakeholder groups
The following were identified as key stakeholders to contribute to the guideline
development
• Primary care
• Patients
• Nephrologists
• Rheumatologists
• Immunologists
• Virologists
• Vaccinologists/Public Health England
• Cardiologists
• Endocrinologists
• Oncologists
• Fertility specialists
4.1.4 Co-ordination Team
The below were responsible for the organisation and running of the Delphi process.

79
Dr Nina Brown
Dr David Tooth
Dr Angela Summers
Dr Michael Venning
4.1.5 Expert panel members (Delphi contributors)
Professor Richard Watts, Rheumatologist, Norwich
Professor Mark Little, Nephrologist, Dublin
Professor David Scott, Rheumatologist, Norwich
Dr David Jayne, Nephrologist, Cambridge
Professor Ray Borrow, Vaccinologist, HPA
Dr Ken Mutton, Virologist, HPA
Dr Matt Morgan, Nephrologist, Birmingham
Dr Oliver Flossman, Nephrologist, Reading
Dr Peter Andrews, Nephrologist, St. Helier’s, London
Dr Joanne Ledingham, Rheumatologist, Portsmouth
Professor John Lear, Dermatologist, Manchester
Professor Peter Selby, Endocrinologist, Manchester
Professor Alistair Hutchison, Nephrologist, Manchester
Dr Ajay Dhaygude, Nephrologist, Preston
Dr Jaqueline Andrews, Rheumatologist, Leeds
Dr Sara Mackie, Rheumatologist, Leeds
Dr Yasmin Sajjid, Fertility consultant, Manchester
Dr Cheryl Fitzgerald, Fertility consultant, Manchester
Dr Yousef Karim, Immunologist, Frimley
Dr Louise Mercer, Rheumatologist, Manchester
Professor Alan Salama, Nephrologist, Royal Free, London
Dr Alison Brown, Nephrologist, Newcastle
Dr Chetan Mukhtyar, Rheumatologist, Norwich
Professor Ian Bruce, Rheumatologist, Manchester
Professor David Wheeler, Nephrologist, Royal Free, London
Dr James Galloway, Rheumatologist, King’s London.
Dr Michael Venning, Nephrologist, Manchester

80
4.1.6 Other Stakeholder representatives
Provided feedback regarding applicability/ practicality of study
John Mills, Patient chair of Vasculitis UK
Dr Ivan Bennet, General practitioner and Central Manchester CCG lead
Involved in consensus conferences to provide additional expertise
Dr Alex Richter, Clinical immunologist, Birmingham
Dr Tomaz Garcez, Immunologist, Manchester
Professor Lorraine Harper, Nephrologist, Birmingham
Professor Alistair Hall, Cardiologist, Leeds
Professor Derek Crowther, Oncologist, Manchester
4.2 DELPHI STUDY
The Delphi technique can be described as “a method of combining the judgements of
knowledgeable individuals”136. The process was originally developed by the RAND
corporation (an American not for profit think tank) in the 1940s as a way of more
effectively using group information137. The three key elements that are today understood
to comprise a Delphi study are the same as those described by the RAND corporation in
1969; a) anonymity (between panel members) 2) controlled feedback and 3) a statistical
group response136. Essentially, a Delphi study uses an expert panel to reach consensus on
areas where evidence or consensus are not available. This is usually done through
structured questioning with iterative feedback from the panel members between rounds.
The level of consensus required is set “a priori” and statements are removed from the
process once they achieve this level of consensus. If further consensus is required to be
reached following completion of the rounds, then consensus conferences can be held to
achieve final resolution.
The Delphi technique is often used to create national and international guidelines for
health management138–140. The reason for this is that guidelines are required usually where
the evidence to support clinical practice is limited or unclear. The ideal alternative to a
Delphi would be randomised controlled trials (RCTs) to provide the evidence required to
inform practice. However, the cost of RCTs is substantial and even then may not provide
the answers sought. Particularly in a rare disease such as vasculitis, patient recruitment, as
well as cost, adds an additional obstacle to conducting robust clinical trials. The breadth of

81
clinical areas to be covered by these guidelines is therefore unlikely to be supported by
definitive evidence in the near future. Therefore, an alternative method has to be sought to
produce guidance for the care of this vulnerable population.
We chose to conduct a three round Delphi survey with two further subsequent consensus
conferences held. Experts were identified from the stakeholder groups highlighted above.
Expertise was defined through; clinical expertise, involvement in guideline creation or
involvement in service development on a national level. Initial questions for generating
statements were informed by the literature including existing guidelines for clinical care
(see Appendix 1 for initial questions). Initial questions additionally focussed on the areas of
treatment and monitoring. However, following liaison with the British Society of
Rheumatology who were conducting a parallel Delphi study covering these areas83, these
topics were removed. Twenty- seven experts accepted the invitation to participate in the
study and submitted comments in response to the questions in Round 1. They are listed
above. Of the participants who answered round 1, 20 took part in round 2.
Responses to the initial questions were reviewed by 2 members of the co-ordination team
(NB, DT) and edited into statements to which the panel could express agreement or
disagreement. Following formation of initial questions to guide the clinicians, subsequent
rounds were carried out with the assistance of the Delphi software. This software provided
analysis of responses enabling automatic identification of statements which had reached
consensus and could be removed from the process. This programme also subsequently
generated the following round, with these statements removed.
Two hundred and eighty statements were generated in the first round (see Appendix 2).
The panel were asked to rank statements according to level of agreement using a Likert
scale from 1-7 (1 being “I strongly disagree” and 7 being “I strongly agree”). The panel
members were also given the option of selecting not to answer particular questions due to
insufficient knowledge. The decision was taken to include this response due to the wide
range of specialties covered by this study. For statements to reach consensus a level of
agreement of 80% was required. Statements that reached consensus following round 2
were removed. Remaining statements continued to round 3 where panel members could
view other participants (anonymised) responses from the previous round to aid the
decision making process. Clarification was also offered if feedback had indicated that a

82
decision had not been reached in the previous round due to ambiguity of a statement.
Some statements which were very similar or contained no additional information were
removed between rounds 2 and 3.
Following Round 3, remaining areas of non- consensus were discussed at two subsequent
consensus conferences to which all panel members were invited. Round 4 consisted of two
consensus conferences, the first attended by 14 of the expert panel members, covering the
spectrum of clinical disciplines. During this round, results from the 2 previous rounds were
reviewed along with any outstanding areas of non- consensus according to category. One
further conference was held specific to the area of infection risk/ immune monitoring as
there were ongoing areas of non- consensus. This was attended by nephrologists with a
specialist interest in infection risk (MM, LH, ML), with representatives from Public Heath
England (RB, KM) and immunology (AR). Final consensus statements were then further
circulated for review and confirmation of agreement from the participants. The final
guidelines document will be additionally reviewed by the UK and Ireland Vasculitis Rare
Disease Group members (including patient representatives) for ratification prior to
publication.
4.3 RESULTS
Following Round 2, 69 statements reached consensus and were therefore removed from
the process as having already attained a level of “expert consensus”. A further 24
statements reached consensus in Round 3 (see Appendix 3 for consensus statements).
Some of these statements were combined where similar into single statements to avoid
repetition. Further consensus was reached during the consensus conferences.
As mentioned previously, due to the parallel study conducted by the British Society for
Rheumatology to produce guidelines for management of disease, including therapy and
monitoring, these areas were excluded from the final recommendations. A summary of all
consensus statements can be found in Appendix 3. The resulting recommendations, level of
consensus and supporting evidence can be viewed in the ADAPTIV recommendations
section.

83
Bone health
There was general agreement that steroid exposure should be minimised and that patients
should be formally assessed with regards to risk of glucocorticoids. However, areas that
were more contentious included the use of more novel agents and the surveillance and
treatment of the subset of patients with significant renal disease.
Cardiovascular health
Similarly, the panel were quick to reach agreement with regards to the notion that patients
with vasculitis have an augmented CV and thromboembolic risk and therefore conventional
risk factors should be aggressively modified. Areas where agreement was more difficult to
reach included to what degree patients’ risk was elevated and therefore, whether this
group should be treated any differently to the general population for primary prevention of
CVD.
Similarly, a particularly contentious issue was that of anti-coagulation for patients having
had one episode of VTE. There were those who felt that due to the reported risk in the
literature of VTE in AAV, these patients would warrant life- long anti-coagulation following
a single VTE episode. However, there was also generalised agreement that the major risk
appeared to be associated with episodes of disease activity and therefore this would seem
excessive in times of disease remission.
Cancer
There was uniform consensus that patients were at increased risk of skin cancers and
therefore should be more vigilant with regards to this risk. There was less agreement with
regards to the use of Mesna and bladder cancer but the recommendation for its use still
reached consensus. An area of contention was that of cervical screening frequency,
particularly for patients during the intensive phases of immunosuppression.
Infection
This was one of the most challenging areas to reach consensus, with infection perhaps
posing one of the biggest clinical threats to this population. Once again, the panel were
quick to agree with regards to the increased risk faced by this patient group and the fact
that increased vigilance and surveillance was required. During the initial rounds, no
consensus could be reached on how to identify those at the highest risk for infection and

84
thresholds for commencing protective anti-infective prophylaxis (with the exception of PJP
prophylaxis for those on cyclophosphamide and “high dose” steroids). For this reason, and
due to the lack of supportive evidence in the literature recommendations in this section are
fairly generic with a clear need identified for information to guide practice in this area.
4.4 DISCUSSION
During this study, a Delphi methodology has been successfully used to reach expert
consensus on a national level for holistic management of the vasculitis patient. The
recommendations derived from this process are presented elsewhere (please see Chapter
6). However, for those areas above where consensus could not be reached and evidence is
not available to inform guidance, the default position of the recommendations made are in
line with population guidance (e.g. for primary CV prevention, anti-coagulation following
VTE, population cancer screening). This clearly highlights the need for at minimum, high
quality longitudinal data for this population, in the likely ongoing absence of clinical trials to
address these issues.
We accept that the Delphi methodology is not perfect. It is a time- consuming process,
requiring commitment from a large group of busy experts. In addition, this method has
come under scrutiny in the past with regards to reliability and validity141. We have sought
to address these potential issues through using a large, heterogeneous expert panel,
including the use of consensus conferences to clarify more difficult areas and, in parallel,
conducting a comprehensive literature review to support the consensus reached and
subsequent recommendations made.
One of the advantages of using the Delphi process, particularly when reaching the
consensus conference stage, is that we found it encouraged further collaboration in driving
similar work forward in the vasculitis community. This study has also aided in identification
of the most pressing areas where better evidence is required to improve the safety and
quality of patient care. In summary, the use of a large “classical” Delphi study has enabled
consensus to be reached to provide guidance in some of the grey areas of clinical practice
for this population

85
4.5 APPENDIX 1. ROUND 1 QUESTIONS
1) How often should a patient with stable vasculitis be seen for supervision of the
vasculitis in secondary/ tertiary care?
2) Is there a role for primary care in supervision of the vasculitis patient?
3) How frequently should a patient have BVAS assessed?
4) How frequently should a patient have VDI assessed?
5) How frequently should ANCA levels be tested?
6) Do you have anything to add to standard UK guidelines (NICE/BHS/RA) for primary
prevention of cardiovascular disease with regards to lifestyle and blood pressure control in
vasculitic patients?
7) Do you think that standard national guidelines for aspirin/ lipid therapy should be
modified for patients with vasculitis?
8) Do you think that patients with vasculitis should be treated with standard or
augmented thromboembolic risk measures?
9) Do you have any additional comments to add to current guidelines for prevention
of glucocorticoid induced osteoporosis (vitamin d/calcium/bisphosphonate use) (NOS 2002,
NICE guidelines due June 2012)
10) What frequency of routine DEXA scans indicated for patients with vasculitis?
11) What should be the recommendation for vaccination of vasculitis patients in
addition to annual flu vaccine? With particular reference to pneumococcal and Hib
vaccines?

86
12) When and how often should vasculitis patients receive pneumococcal and Hib
vaccines?
13) How should a patient’s response to vaccine be assessed?
14) What are the indications for co-trimoxazole prophylaxis in vasculitis patients?
15) What are the indications for co-trimoxazole use in the treatment of vasculitis?
16) What are the indications for fungal and viral prophylaxis (e.g.aciclovir and
fluconazole use) in vasculitis patients?
17) Would you recommend any additional routine monitoring of patients’ immune
profiles to assess infection risk (e.g. lymphocyte subsets, immunoglobulins)?
18) Would you set thresholds for altering immunotherapy based on the patient’s
immune profile (neutrophil count, lymphocyte count, CD4 count, IgG level etc.)?
19) Should any group of patients with vasculitis be screened at presentation, for
underlying malignancy (e.g. gastroscopy; colonoscopy; CT chest/abdo/pelvis; blood
markers)?
20) Should vasculitis patients under follow- up undergo any additional cancer screening
compared with an age and sex matched population? (including breast, bowel and
prostate)?
21) What is your opinion on cervical cancer screening in vasculitis patients?
22) What should the recommendations be for bladder cancer screening and mesna use
in patients exposed to cyclophosphamide?
23) Do you recommend additional sun protection or regular skin cancer screening for
vasculitis patients?

87
24) Should cyclophosphamide use be avoided in any patient group with regards to
preservation of fertility or other factors?
25) What is the maximum dose of cyclophosphamide that can be administered
concerning;
a) the preservation of fertility?
b) malignancy risk?
26) What is the role of sperm banking/ oocyte retrieval in vasculitis patients?
27) What is the role of GnRH antagonists to preserve fertility? What other therapeutic
options would you recommend?
Sources
(1) Vaccinations in the Immunocompromised Person. Guidelines for the Patient taking
Immunosupppressants, Steroids and New Biological Therapies142.
(2) EULAR Recommendations for vaccination in the adult patients with autoimmune
inflammatory rheumatic diseases143.
(3) BSR and BHPR Guidelines for the management of adults with ANCA associated
vasculitis144.
(4) Glucocorticoid-induced osteoporosis. A concise guide to the prevention and
treatment145.
(5) EULAR Recommendations for the management of primary small and medium vessel
vasculitis72.
(6) Immunisation against infectious disease: The Green Book146.
(7) Hypertension in adults; diagnosis and management147.
(8) Chronic Kidney Disease: Early identification and management of chronic kidney disease
in adults in primary and secondary care148.

88
4.6 APPENDIX 2: STATEMENTS GENERATED FOLLOWING ROUND 1
Question and Statement
1) Do you have any suggestions for approaches to therapy to add to existing EULAR/BSR guidelines for
vasculitis?
1.1 EULAR and BSR guidelines need to be updated.
1 .2 EULAR and BSR treatment algorithms and protocols need to be devised.
1 .3 Treatment of relapsing disease needs to be updated.
1.4 'Fixed dose' protocol based therapy may result in over immunosuppression of some patients
and under treatment of some patients.
1.5 Rituximab should be used for induction and remission therapy, instead of cyclophosphamide
or methotrexate.
1.6 Rituximab is the first line therapy for patients with relapsing/persistent disease.
1.7 Rituximab shouldn’t be recommended as first line therapy until long term safety data is
available.
1.8 Pulsed cyclophosphamide leads to an increase in relapse rate.
1.9 Dose reduction of cyclophosphamide for the elderly is not needed.
1.10 A high dose of 0.8g/m2 cyclophosphamide given every 3-4 weeks is safe.
1.11 Current guidelines focus on total WBC and neutrophil count, as cyclophosphamide
predominantly affect lymphocyte counts, effect of lymphocyte count should be taken in to
account while prescribing cyclophosphamide dose.
1.12 Before cyclophosphamide therapy, pre-dose lymphocyte count should be maintained above
0.4 x10^9/L; during maintenance therapy lymphocyte count should be maintained above 0.7
x10^9/L.
1.13 The roles of methotrexate, mycophenolate and leflunomide should be included in the
guidelines.
1.14 Methotrexate can be used at a maximum dose of 35mg/week.
1.15 Use of Methotrexate for less severe disease leads to an increased risk of relapse.
1.16 If initial pulsed intravenous steroids are used then oral steroids can be started as low as
0.5mg/Kg.
1.17 There is no evidence to support continuation of high dose oral steroids for 3 months.
1.18 Current recommendations for plasma exchange should be reduced as there is insufficient
evidence to support them.

89
1.19 Supervision of treatment should be by expert centres.
1) How often should a patient with stable vasculitis be seen for supervision of the vasculitis in
secondary/ tertiary care?
2.1 No change to BSR 2006 guidelines (Follow-up after 12 months should be as dictated by the
clinical condition of the patient, but should not be less frequent than every 6 months).
2.2 Frequency of follow up depends on risk of relapse, previous immunotherapy and current
immunosuppression.
2.3 Once every 2 weeks while on induction therapy.
2.4 In remission and on maintenance therapy once a month for 3 months then every 3 months for
the first 2 years.
2.5 Every 3 months if still on med-high steroids / MMF.
2.6 After 2 years, every 3-6 months.
2.7 If on small dose steroid without relapse for several years - annually
2.8 If off all immunosuppression and clinically stable for > 12 months, not at all.
2.9 Efforts should be made to engage patient in follow up care. Teaching them how to dipstick
their own urine and appropriate use of self-referral pathways if unwell.
2) Is there a role for primary care in supervision of the vasculitis patient?
3.1 Primary care has no role in the supervision of the vasculitis patient.
3.2 Primary care should be involved, especially with stable patients.
3.3 Primary carers should be aware of the immunosuppressive medications the patient is taking.
3.4 Primary care should be responsible for cardiovascular risk assessment.
3.5 Primary care should be responsible for drug monitoring.
3.6 Primary care should be responsible for urine and blood testing.
3.7 Primary care should be responsible for screening for skin and bladder malignancy.
3.8 Primary care should be responsible for lifestyle (diet, alcohol intake and exercise) advice.
3.9 Primary care physicians are key to advising patients how to avoid intercurrent infection and
picking up infections at an early stage.
3.10 This process should only be used in areas where primary care has the appropriate IT facilities
to view and communicate results with secondary care.
3.11 Solid shared care protocols are needed.
3.12 Unwell vasculitis patients should have a direct route to secondary care.
3) How frequently should a patient have BVAS assessed?
4.1 Informally, the questions can be asked at every visit but a score need not be recorded.

90
4.2 Each clinical encounter.
4.3 Current recommendations for initial score, then monthly including at 3 months to confirm
response, then as dictated clinically subsequently.
4.4 If the patient is stable every 3-6 months after induction.
4.5 If the patient is unstable every 1-3 months.
4.6 No role outside research studies, a recording tool rather than an assessment tool. Although it
can be useful as an aide-memoire for less common disease manifestations in inexperienced
clinicians.
4) How frequently should a patient have VDI assessed?
5.1 Informally every visit, the questions may be asked but no need to calculate a score.
5.2 Formally at time points dictated by trials or at induction then at 3 and 6 months.
5.3 Every 3-6months.
5.4 Every 6-12 months.
5.5 Every clinical visit.
5.6 Research tool only. Would be a useful guideline addition to enable comparison between
different units.
5.7 VDI can be carried out by a specialist nurse.
5) How frequently should ANCA levels be tested?
6.1 No more frequently than every 4-6weeks as half-life of IgG is 3 weeks.
6.2 Every 2-3 weeks until remission.
6.3 Every 3 months for the first 2 years then every 4-6 months thereafter.
6.4 Every 3 months for the first 5 years once stable.
6.5 Annually.
6.6 As per clinical symptoms.
6.7 If clinically stable no need to check.
6.8 At each clinical visit if ANCA-positive.
6.9 If ANCA negative, measure if new clinical evidence of Vasculitis develops.
6.10 Should be tested by both ANCA immunofluorescence and MPO/PR3 antigen specific tests.
7)Do you have anything to add to standard UK guidelines (NICE/BHS/RA) for primary prevention of
cardiovascular disease with regards to lifestyle and blood pressure control in vasculitic patients?
7.1 Vasculitis appears to be a risk factor for cardiovascular disease therefore treatment threshold
should be lowered.

91
7.2 Steroids/immunosuppression appear to be risk factors for cardiovascular disease therefore
treatment threshold should be lowered.
7.3 Given the increase risk in Vasculitis patients, they should be started on “stage 1” of the
hypertension treatment ladder according to NICE guidelines.
7.4 Lower BP targets, typically below 130/80.
7.5 Treating inflammation is more important than treating cholesterol.
7.6 Stopping smoking is critical.
7.7 PR3 is a possible risk factor for cardiovascular disease.
7.8 There is a new cardiovascular risk calculator for use in AAV which modifies the Framingham
calculator, this needs to be taken into account
7.9 Annual assessment of CVD risk.
7.10 No specific interventions that have been demonstrated to be efficacious in clinical trials.
8)Do you think that standard national guidelines for aspirin/ lipid therapy should be modified for
patients with vasculitis?
8.1 Current guidelines for aspirin/lipid therapy should not be modified for patients with vasculitis
8.2 Further evidence for the need for modification of these guidelines in a large cohort study is
needed.
8.3 Yes with some sort of adjustment made (e.g. as per Rheumatoid Arthritis guidelines
multiplication of risk of CVD by 1.5).
8.4 Overemphasized, focus on BP.
8.5 Consider all Vasculitis patients on steroid therapy for aspirin treatment.
8.6 Caution about statins as the side effects can mimic systemic symptoms (myalgia).
8.7 Treat all patients as being high risk for cardiovascular disease.
9)Do you think that patients with vasculitis should be treated with standard or augmented
thromboembolic risk measures?
9.1 Augmented all the time.
9.2 Augmented if active, normal if stable.
9.3 Augmented if any loss of mobility or history of thromboembolic event.
9.4 Standard measures at presentation only, no measures after.
9.5 Standard due to risk of pulmonary haemorrhage.
9.6 Aspirin only for most patients.
10)Do you have any additional comments to add to current guidelines for prevention of glucocorticoid
induced osteoporosis (vitamin D/calcium/bisphosphonate use) (NOS 2002, NICE guidelines due June

92
2012)?
10.1 Follow the RCP guidance- nothing to add to current guidelines.
10.2 Minimise steroid exposure.
10.3 The 2006 BSR guidelines should be used in preference to current NOS guidelines (higher
steroid dose used for vasculitis treatment compared to studies informing NOS guidelines).
10.4 Measuring bone turnover markers at 3-6 months to check compliance with oral
bisphosphonates.
10.5 Add DEXA to guide therapy and therapy withdrawal.
10.6 Monitoring of vitamin D level can be incorporated.
10.7 Stop bisphosphonates in advanced renal disease. Pressing need for evidence based
intervention that is effective for patients with GFR<30.
10.8 Calcichew D3 is an appropriate alternative to bisphosphonates especially in pregnant
Vasculitis patients.
10.9 Denosumab should be considered as an alternative in patients whom bisphosphonates have
been contraindicated.
10.10 Denosumab therapy needs evidence before being used in immunosuppressed patients due to
infection risk.
10.11 Patients should be counselled regarding potential bisphosphonate side effects prior to
commencing therapy (osteonecrosis of the jaw, avascular necrosis of the hip, and "frozen
bone"/sub trochanteric hip fracture).
10.12 Patients should have dentition assessed prior to commencing bisphosphonates.
11)What frequency of routine DEXA scans indicated for patients with vasculitis?
11.1 The following patients should have DEXA scans (applies to the next 8 statements);
All patients should have DEXA scan at baseline.
11.2 Patients on steroids- every 2-3 years
11.3 Patients only on prednisolone greater than 10mg/day- every 2-3 years.
11.4 If on steroids and older than 50 years.
11.5 If greater than 65 years.
11.6 Every 3-5 years dependent on results.
11.7 No more than once every 5 years if already on bisphosphonates and no fracture.
11.8 In young patients who bisphosphonate therapy doesn’t work very well e.g. premenopausal
women.
11.9 Patients should have overall fracture risk assessed rather than just BMD.

93
12)What should be the recommendation for vaccination of vasculitis patients in addition to annual flu
vaccine? With particular reference to pneumococcal and Hib vaccines?
12.1 Avoid live vaccines in the severely immunosuppressed.
12.2 Patients should have every vaccine available on the market.
12.3 An individual risk assessment should be undertaken for a number of vaccines which may be
given if low immunosuppression, e.g. MMR and VZV.
12.4 One-off Pneumococcal (unconjugated) prior to start of treatment. If low titres try a booster
with conjugated vaccine.
12.5 VZV prior to treatment.
12.6 BCG should only be given before immunosuppression.
12.7 HPV if at risk and in licensed age range.
12.8 Consider Hep A/Hep B (particularly for any one with renal involvement).
12.9 Use inactivated polio only.
12.10 Dual vaccination may be required if on rituximab.
13)When and how often should vasculitis patients receive pneumococcal and Hib vaccines?
13.1 5 yearly.
13.2 5 yearly is inappropriate. Need for vaccine should be assessed on antibody levels taken every
1-2 years.
13.3 Pneumococcal once, repeat if titres are inadequate.
13.4 Pneumococcal and Hib vaccine as soon as possible at presentation, preferable before
immunotherapy starts.
13.5 If already immunosuppressed then vaccinate after immunosuppressive therapy has finishes
e.g. 6 months after rituximab, shorter for other agents.
14)How should a patients response to vaccine be assessed?
14.1 No point-not cost effective.
14.2 Antibody levels at 4-6 weeks.
14.3 Specific antibody titre testing including type specific antibody.
14.4 Need for vaccine should be assessed on antibody levels taken every 1-2 years.
14.5 If initial vaccine response to pneumococcus is inadequate Prevenar13, a conjugate vaccine
may be considered.
14.6 Annual check of pneumococcal and Hib antibody status if antibody deficient 2 months post
vaccine.
14.7 3-yearly check of pneumococcal and Hib antibody status if antibody status okay 2 months

94
post vaccine
15) What are the indications for co-trimoxazole prophylaxis in vasculitis patients?
15.1 Give to everyone.
15.2 Give if starting high dose immunosuppressive especially in GPA.
15.3 Give for 3 months if treatment with induction of cyclophosphamide or MMF therapy.
15.4 Give for the first 6 months especially if on high dose cyclophosphamide or MMF.
15.5 Continue indefinitely in those with sino-nasal granulomatous disease.
15.6 Continue for 6months after cyclophosphamide therapy.
15.7 Give if on Prednisolone 20mg/day for greater than 4 weeks plus additional
immunosuppressant.
15.8 Give if on Prednisolone greater than 40mg/day for greater than 12 weeks.
15.9 During high dose steroid therapy >60mg/day.
15.10 Give during initial therapy and then tailor co-trimoxazole therapy to CD4 counts.
15.11 Patients with previous PJP infection.
15.12 Blanket guidelines are unlikely to work.
15.13 If lymphocyte count <0.6 x10^9/L, or if consistently <0.7 x10^9/L
15.14 If CD4 count <200 x10^6/L.
15.15 If other opportunistic infections (e.g. warts, shingles, thrush, chest infections) and CD4 of
<400x 10^6/L or lymphocytes <1.0 x10^9/L.
15.16 Guidelines are needed for PJP prophylaxis in patients treated with Rituximab which is being
used more frequently.
15.17 Consideration of additional prophylaxis options for Pneumocystis jirovecii e.g. azithromycin,
atovaquone
16) What are the indications for co-trimoxazole treatment in vasculitis patients?
16.1 There are no indications for co-trimoxazole in the treatment of vasculitis.
16.2 Do not use as monotherapy in any circumstances.
16.3 ENT disease in general warrants antibiotic prophylaxis. Could be macrolides or Septrin.
16.4 Can be used alone as “treatment” for limited GPA or with low dose steroids.
16.5 All patients with ENT disease should be treated with Septrin
16.6 All GPA should be treated with Septrin
16.7 Persistent disease should be treated with Septrin
16.8 Remission maintenance in a few if they have local disease and cannot tolerate methotrexate,
leflunomide or azathioprine.

95
16.9 The highest dose tolerated should be used (960-1920mg daily).
16.10 Control of respiratory tract infection.
17)What are the indications for fungal and viral prophylaxis (e.g.aciclovir and fluconazole use) in
vasculitis patients?
17.1 Fungal and viral prophylaxis should be initiated before starting high-dose
immunosuppression.
17.2 Fungal and viral prophylaxis should be used in patients receiving cyclophosphamide and high
dose steroids or rituximab or TNFa blockers.
17.3 There are no indications for viral prophylaxis as it is not cost effective.
17.4 Viral prophylaxis if frequent recurrent HSV infections.
17.5 CMV prophylaxis with valganciclovir and VZ prophylaxis after rituximab.
17.6 If previous history of fungal or Zoster infection then consider prophylaxis if intense therapy is
repeated.
17.7 Fungal prophylaxis should be offered to high risk patients (those living in endemic
histoplasmosis areas, or those that go caving in the Cheddar gorge).
17.8 The incidence of invasive fungal disease doesn’t warrant the risk of fluconazole therapy.
17.9 Fluconazole when on high dose steroids.
17.10 No regular prophylaxis outside nystatin use.
17.11 Topical oral anti-fungal (nystatin pastilles) for ten days of first treatment or when pred
>20mg.
17.12 Aciclovir only if symptoms/signs/ past history of recurrent herpes.
17.13 If lymphocyte <0.6 x10^9/L or persistently <0.7 x10^9/L.
17.14 If CD4 count <200 x10^6/L.
17.15 If other opportunistic infections (warts, shingles, thrush, chest infections), and CD4 < 400
x10^6/L or lymphs < 1.0 x10^6/L.
17.16 A role for hepatitis B screening and prophylaxis or monitoring.
18)Would you recommend any additional routine monitoring of patients immune profiles to assess
infection risk (e.g. lymphocyte subsets, immunoglobulins)?
18.1 There is no role for routine monitoring of immune profiles to assess infection risk (e.g.
lymphocyte subsets/ Igs).
18.2 Only if there are infectious complications.
18.3 Immunoglobulin levels should measure yearly.
18.4 Lymphocytes or immunoglobulins should be measured if on cyclophosphamide or rituximab

96
therapy.
18.5 CD4 count should be measured if lymph <1.0 x10^6/L
18.6 Measure CD 19 and 20 if rituximab considered.
18.7 Lymph count is useful to detect if abnormalities are drug related or pre existing
18.8 There is no evidence that measuring lymphocyte subsets is any better than peripheral blood
lymphocyte count.
18.9 IgGs at start of treatment and subsequently if recurrent infection.
18.10 Patients that require >1 induction therapies should have additional monitoring.
18.11 Patients on long term maintenance e.g. >2 years should have additional monitoring.
18.12 Immunoglobulin monitoring if repeated rituximab use.
18.13 PJP prophylaxis should not be titrated to CD4 counts.
18.14 More evidence is required re: the use of these to validate.
19)Would you set thresholds for altering immunotherapy based on the patient’s immune profile
(neutrophil count, lymphocyte count, CD4 count, IgG level etc.)?
19.1 The aim should be to use the minimum necessary immunosuppression in an individual patient
according to their clinical history.
19.2 Thresholds should be for individual patients.
19.3 If thresholds can be agreed, prophylaxis regimens and vaccine recommendations should be
adjusted according to CD4.
19.4 Antimicrobial and antifungal prophylaxis should be adjusted with neutrophil count.
19.5 The significance of lymphopenia has not been established.
19.6 Immunosuppression should be based on neutrophil count alone.
19.7 The following should guide alterations to immunotherapy (applies to the next 6 statements);
Total WCC
19.8 Neutrophils.
19.9 IgG levels.
19.10 CD4+.
19.11 CD19.
19.12 Total lymphocyte count.
19.13 Lymphocyte count <0.6 x109/L or consistently <0.7 x10^9/L or CD4 count < 200 x10^6/L or
Other opportunistic infections (warts, shingles, thrush, chest infections), and CD4 < 400
x10^6/L or lymphocytes < 1.0 x10^6 or IgG < 3 g/L.
19.14 The infection history is more important rather than the absolute IgG level.

97
19.15 Immunoglobulin monitoring will need to be explored for rituximab in the future if this
becomes the choice for remission maintenance.
20)Should any group of patients with vasculitis be screened at presentation, for underlying
malignancy (e.g. gastroscopy; colonoscopy; CT chest/abdo/pelvis; blood markers)?
20.1 Not unless clinically indicated (e.g. change in bowel habit, or with major weight loss/night
sweats).
20.2 CXR in smokers.
20.3 Yes all (as in Membranous Glomerulonephritis).
20.4 Patients presenting outside the "usual" age groups, with unusual presentations or who have
not responded to treatment as expected.
20.5 Patients should have CXR and abdo USS rather than CT chest/abdo/pelvis (due to high
radiation dose) unless there is a high index of suspicion.
20.6 Iron deficiency/hypercalcaemia might raise the index of suspicion.
20.7 Blood tumour markers are not very helpful, even as a screening tool.
21)Should vasculitis patients under follow- up undergo any additional cancer screening compared
with an age and sex matched population? (including breast, bowel and prostate)?
21.1 Patients with vasculitis shouldn’t have any additional cancer screening but there is a need for
enhanced awareness of malignancy risk during follow-up.
21.2 Due to increased immunosuppression, patients with vasculitis should have additional cancer
screening.
21.3 Such screening is not cost effective (avoid feeding a screening industry dominated by zealots
and big pharma).
21.4 Not routine but lower threshold for further investigations if patients are symptomatic or have
abnormal findings such as worsening anaemia.
21.5 Patients should be encouraged to attend for the routine population screening.
21.6 Due to increased immunosuppression, patients with vasculitis should have additional cancer
screening.
21.7 Vasculitis patients should have periodic urine analysis and cytology if they have received
significant cyclophosphamide load to screen for bladder cancer.
21.8 Skin cancer surveillance.
22)What should the recommendations be for bladder cancer screening and mesna use in patients
exposed to cyclophosphamide?
22.1 Always use mesna during cyclophosphamide therapy.

98
22.2 Mesna and screening if received > 10g cyclophosphamide.
22.3 No need for mesna in pulsed cyclophosphamide therapy.
22.4 Any cyclophosphamide patient with persistent micro haematuria needs a cystoscopy and
cytology assessment of urine.
22.5 Check urinalysis for blood at every hospital visit.
22.6 Patients with significant cyclophosphamide exposure in the past should have regular
monitoring of urine with dipsticks (6-12 monthly).
23)What is your opinion on cervical cancer screening in vasculitis patients?
23.1 Cervical cancer screening should be as per the general population.
23.2 At risk women should have a smear annually for the first 3 years after induction therapy.
23.3 Cervical screening should be undertaken dependent on age and degree of
immunosuppression.
23.4 Recommend all female patients should attend for a cervical screening update after 3 months
of treatment when in remission, screening thereafter as per national guidelines.
23.5 HPV vaccination makes the cost effectiveness of screening even less favourable.
24)Do you recommend additional sun protection or regular skin cancer screening for vasculitis
patients?
24.1 All patients on immunosuppression require sun protection and regular screening if on
immunosuppressants.
24.2 Only patients on azathioprine- require sun protection and regular screening.
24.3 Only for patients who require long-term immunosuppression (>5years)-should undergo skin
screening.
24.4 Avoidance of tanning beds is wise.
24.5 Patients should be educated to perform self-checking for skin cancer.
24.6 GPs should perform six-monthly visual check of "moles" / other skin lesions.
24.7 Examination of the skin for suspicious lesions should be part of an annual review.
24.8 Take into account patient’s history including family history and repeated episodes of sun-burn
/ high levels UV exposure earlier in life (e.g. living abroad).
24.9 Research related to non-melanoma skin cancer is flawed.
24.10 Regular screening is unnecessary as data arises from cohorts who were over-
immunosuppressed in an era when sunbathing was the norm.
25)Should cyclophosphamide use be avoided in any patient group with regards to preservation of
fertility or other factors?

99
25.1 Rituximab should be substituted for those who fear risk of infertility e.g. young women and
men unable to undergo sperm banking/retrieval.
25.2 Rituximab may be used in those felt to be at high risk of infectious complications, those with
active infection or those with evidence of marrow fragility.
25.3 After Rituximab exposure, pregnancy should be avoided for a year.
25.4 Advice should be given regarding the severe effect that kidney failure has on fertility and of
the importance of not using a "soft touch" for organ threatening disease.
25.5 Cyclophosphamide should never be avoided in life threatening disease.
25.6 Cyclophosphamide avoidance or minimisation in pre-menopausal females.
25.7 In female patients who are above 35 years of age, do not have organ threatening
involvement, and want children, cyclophosphamide should be avoided.
25.8 Avoid cyclophosphamide (or at least markedly reduce the dose) in those with GFR< 60.
25.9 Large previous cyclophosphamide load is a relative contraindication to further
cyclophosphamide use; e.g. >15g.
26)What is the maximum dose of cyclophosphamide that can be administered concerning;
a) the preservation of fertility?
b) malignancy risk?
26.1
(a)
There is no minimum safe dose that would completely eradicate risk.
26.2
(a)
6g is the minimum modern dose of cyclophosphamide.
26.3
(a)
10g if >25 years.
26.4
(a)
<12g.
26.5
(a)
7-14g depending on age.
26.6
(a)
1.2g per pulse.
26.7
(a)
Depends on sperm and ovarian viability before treatment begins.
26.8
(a)
Depends on body surface area.

100
26.9
(a)
Depends on patient age.
26.10
(a)
Evidence here is not robust.
26.11
(a)
The effects of cyclophosphamide on fertility are not related to the strength of dose but to
duration of treatment (small doses over a long period are more damaging to fertility than
several big heavy doses).
26.12
(b)
36g.
26.13
(b)
An increased risk of leukaemia / MDS or bladder cancer is only seen with cumulative dose
>30g.
26.14
(b)
25-35g depending on age.
26.15
(b)
20g-30g for depending on age.
26.16
(b)
20g but needs to be corrected for body surface area.
26.17
(b)
15 g/m2.
26.18
(b)
Up to 10 g
26.19
(b)
Recent EUVAS data suggests no increased risk of cancer with the current low doses of
cyclophosphamide although further follow up will be necessary.
27)What is the role of sperm banking/ oocyte retrieval in vasculitis patients ?
27.1 Men should be offered the chance to store sperm if they wish before starting
cyclophosphamide (as long as it does not interfere with medically urgent therapy).
27.2 Any man under 55 should be actively encouraged to bank even if he feels that he will not
want to use the sperm as his thoughts may change.
27.3 Any women wanting to start a family or <42 years with a partner should be offered the
opportunity to (applies to the next 3 statements):
Store fertilised eggs prior to starting therapy (procedure takes possible three weeks).
27.4 To store vitrilised eggs (better success rates than storing fertilised eggs. Takes about 3
weeks).

101
27.5 To freeze a wedge section of the ovary containing the immature eggs and the supporting
cells.
27.6 Should be performed if possible in anyone being treated with cyclophosphamide of
childbearing age.
27.7 Oocyte retrieval in unwell females with active vasculitis is not currently feasible.
27.8 Links with the appropriate local reproductive health departments should be established.
28)What is the role of GnRH antagonists to preserve fertility? What other therapeutic options would
you recommend?
28.1 Should be offered to younger women at risk of ovarian damage from cyclophosphamide.
28.2 There is a role for Goserelin (Gonaderelin analogue) to preserve fertility.
28.3 Anti-mullerian hormone level should be checked prior to commencing treatment (predictor of
ovarian reserve.)
28.4 The oral contraceptive pill or long acting hormone injection can be used instead of GnRH
agonists (less side effects).
28.5 There is insufficient evidence for other options such as the OCP.
28.6 There is no role for the use of GnRH antagonists.
28.7 We would ask national experts e.g. David Jayne
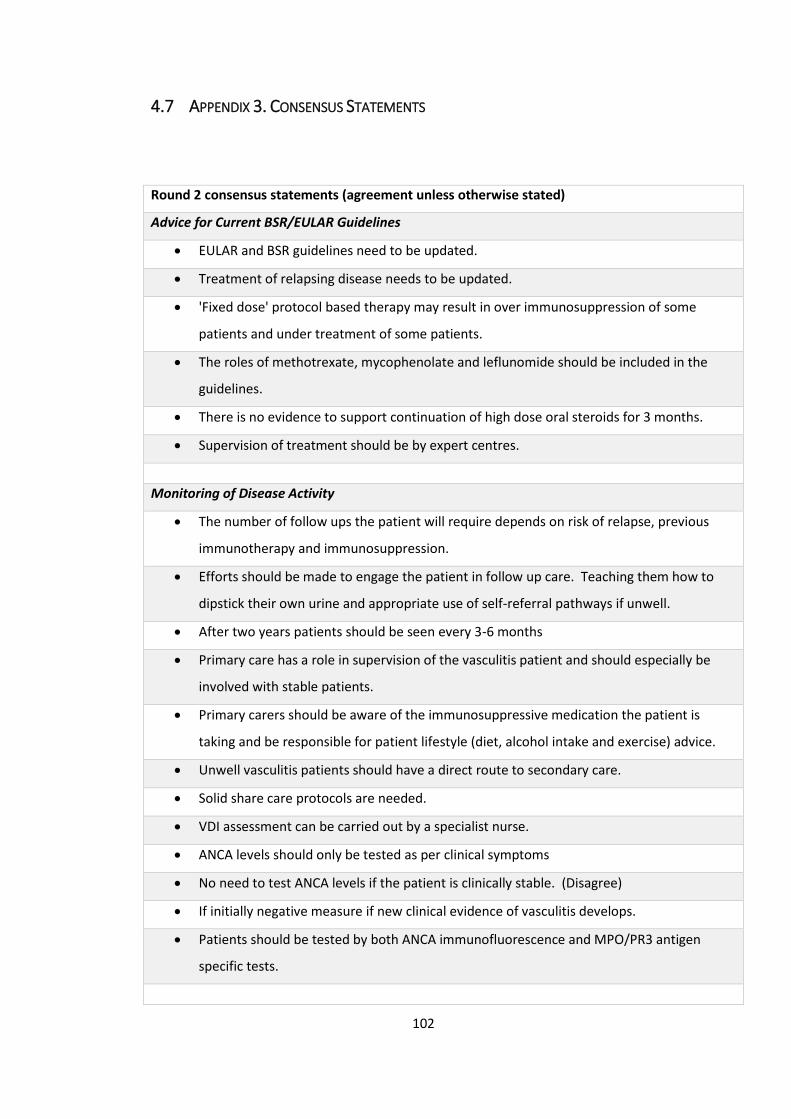
102
4.7 APPENDIX 3. CONSENSUS STATEMENTS
Round 2 consensus statements (agreement unless otherwise stated)
Advice for Current BSR/EULAR Guidelines
• EULAR and BSR guidelines need to be updated.
• Treatment of relapsing disease needs to be updated.
• 'Fixed dose' protocol based therapy may result in over immunosuppression of some
patients and under treatment of some patients.
• The roles of methotrexate, mycophenolate and leflunomide should be included in the
guidelines.
• There is no evidence to support continuation of high dose oral steroids for 3 months.
• Supervision of treatment should be by expert centres.
Monitoring of Disease Activity
• The number of follow ups the patient will require depends on risk of relapse, previous
immunotherapy and immunosuppression.
• Efforts should be made to engage the patient in follow up care. Teaching them how to
dipstick their own urine and appropriate use of self-referral pathways if unwell.
• After two years patients should be seen every 3-6 months
• Primary care has a role in supervision of the vasculitis patient and should especially be
involved with stable patients.
• Primary carers should be aware of the immunosuppressive medication the patient is
taking and be responsible for patient lifestyle (diet, alcohol intake and exercise) advice.
• Unwell vasculitis patients should have a direct route to secondary care.
• Solid share care protocols are needed.
• VDI assessment can be carried out by a specialist nurse.
• ANCA levels should only be tested as per clinical symptoms
• No need to test ANCA levels if the patient is clinically stable. (Disagree)
• If initially negative measure if new clinical evidence of vasculitis develops.
• Patients should be tested by both ANCA immunofluorescence and MPO/PR3 antigen
specific tests.

103
Cardiovascular and Thromboembolic Risk
• Stopping smoking in the vasculitis patient is critical.
• They should have an annual assessment of CVD risk and the new cardiovascular risk
calculator, which modifies the Framingham calculator for use in AAV, needs to be taken
into account.
• The national guidelines for aspirin/lipid should be modified for patients with vasculitis
with some sort of adjustment made (e.g.as per Rheumatoid Arthritis guidelines
multiplication of risk of CVD by 1.5).
• Further evidence for the need for modification of these guidelines in a large cohort study
is needed.
• Patients with vasculitis should be treated with augmented thromboembolic risk measure
if any loss of mobility or history of thromboembolic event.
Bone Health
• Minimise steroid exposure.
• Patients should be counselled regarding potential bisphosphonate side effects prior to
commencing therapy (osteonecrosis of the jaw, avascular necrosis of the hip, and "frozen
bone"/subtrochanteric hip fracture).
• Denosumab should be considered as an alternative in patients whom bisphosphonates
have been contraindicated.
• Patients should have overall fracture risk assessed rather than just BMD.
Infection Risk
• Avoid live vaccines in the severely immunosuppressed.
• Use inactivated polio only.
• Give co-trimoxazole if starting high dose immunosuppressive especially in GPA.
• Give co-trimoxazole to patients with previous PJP infection.
• Guidelines are needed for PJP prophylaxis in patients treated with Rituximab which is
being used more frequently.
• Consideration of additional prophylaxis options for Pneumocystis jirovecii eg
azithromycin, atovaquone.
• There are indications for co-trimoxazole in the treatment of vasculitis.

104
• Viral prophylaxis if frequent recurrent HSV infections.
• If previous history of fungal or Zoster infection then consider prophylaxis if intense
therapy repeated.
• Aciclovir only if symptoms/signs/ past history of recurrent herpes.
• Lymphocytes or immunoglobulins should be measured if on cyclophosphamide or
rituximab therapy.
• Immunoglobulin monitoring if repeated rituximab use.
• The aim should be to use the minimum necessary immunosuppression in an individual
patient according to their clinical history.
• The following should guide alterations to immunotherapy-neutrophils, total lymphocyte
count.
• The infection history is very important rather than the absolute IgG level.
• Immunoglobulin monitoring will need to be explored for rituximab in the future if this
becomes the choice for remission maintenance.
• Thresholds should be for individual patients
• Immunosuppression should not be based on neutrophil count alone.
Cancer Risk
• Vasculitis patients should not be screened for malignancy prior to treatment unless
clinically indicated (e.g. change in bowel habit, or with major weight loss/night sweats).
• CXR in smoker.
• Iron deficiency/hypercalcaemia might raise the index of suspicion.
• Follow-up patients should be encouraged to attend for the routine population screening
• Periodic urine analysis and cytology if significant cyclophosphamide load to screen for
bladder cancer.
• Skin cancer surveillance.
• Any cyclophosphamide patient with persistent micro haematuria needs a cystoscopy and
cytology assessment of urine.
• Check urinalysis for blood at every hospital visit.
• Patients with significant cyclophosphamide exposure in the past should have regular
monitoring of urine with dipsticks (6-12 monthly).
• Avoidance of tanning beds is wise.
• Patients should be educated to perform self checking for skin cancer.

105
• Take into account patient’s history including family history and repeated episodes of sun-
burn / high levels UV exposure earlier in life (eg living abroad)
• Only if on azathioprine- avoid sun exposure, and use sun cream if sun-exposure is
unavoidable. (disagree)
Fertility
• Cyclophosphamide avoidance or minimisation in pre-menopausal females.
• Rituximab may be used in those felt to be at high risk of infectious complications, or those
with active infection, or those with evidence of marrow fragility.
• Advice should be given regarding the severe effect that kidney failure has on fertility and
of the importance of not using a "soft touch" for organ threatening disease.
• There is no minimum safe dose of cyclophosphamide that would completely eradicate risk
of infertility.
• The maximum dose of cyclophosphamide that would preserve fertility depends on patient
age.
• Evidence on maximum dose of cyclophosphamide that would preserve fertility here is not
robust.
• Recent EUVAS data suggests no increased risk of cancer with the current low doses of
cyclophosphamide although further follow up will be necessary.
• Men should be offered the chance to store sperm if they wish before starting
cyclophosphamide (as long as it does not interfere with medically urgent therapy).
• Oocyte retrieval in unwell females with active vasculitis is not currently feasible.
• Links with the appropriate local reproductive health departments should be established.
• There is insufficient evidence for other options such as the OCP.
Round 3 consensus
Disagree
How often should a patient with stable vasculitis be seen for supervision of the vasculitis in
secondary/ tertiary care?
· If off all immunosuppression and clinically stable for > 12 months, not at all.
How frequently should a patient have VDI assessed?
· Every clinical visit.
How frequently should ANCA levels be tested?

106
· Every 2-3 weeks until remission.
· Every 3 months for the first 5 years once stable.
Do you think that standard national guidelines for aspirin/ lipid therapy should be modified for
patients with vasculitis?
· Caution about statins as the side effects can mimic systemic symptoms (myalgia)
Do you think that patients with vasculitis should be treated with standard or augmented
thromboembolic risk measures?
· Standard due to risk of pulmonary haemorrhage.
What should be the recommendation for vaccination of vasculitis patients in addition to annual
flu vaccine? With particular reference to pneumococcal and Hib vaccines?
· Patients should have every vaccine available on the market.
What are the indications for co-trimoxazole prophylaxis in vasculitis patients?
· Give to everyone.
· Continue for 6months after cyclophosphamide therapy
Do you recommend additional sun protection or regular skin cancer screening for vasculitis
patients?
Regular screening is unnecessary as data arises from cohorts who were over-immunosuppressed
in an era when sunbathing was the norm.
What is the maximum dose of cyclophosphamide that can be administered concerning malignancy
risk?
An increased risk of leukaemia / MDS or bladder cancer is only seen with cumulative dose >30g.
25-35g depending on age
Agree
How often should BVAS be assessed?
· Informally, the questions can be asked at every visit but a score need not be recorded.
What should be the recommendation for vaccination of vasculitis patients in addition to annual flu
vaccine? With particular reference to pneumococcal and Hib vaccines?
BCG should only be given before immunosuppression
Consider Hep A/Hep B (particularly for any one with renal involvement).
Would you recommend any additional routine monitoring of patients immune profiles to assess
infection risk (e.g. lymphocyte subsets, immunoglobulins)?

107
· More evidence is required re: the use of these to validate.
Would you set thresholds for altering immunotherapy based on the patients immune profile
(neutrophil count, lymphocyte count, CD4 count, IgG level etc)?
· The following should guide alterations to immunotherapy ;
Total WCC
What is your opinion on cervical cancer screening in vasculitis patients?
· Cervical screening should be undertaken dependent on age and degree of
immunosuppression
Do you recommend additional sun protection or regular skin cancer screening for vasculitis
patients?
· All patients on immunosuppression require sun protection and regular screening if on
immunosuppressants.
· Examination of the skin for suspicious lesions should be part of an annual review.
Should cyclophosphamide use be avoided in any patient group with regards to preservation of
fertility or other factors?
· In female patients who are above 35 years of age, do not have organ threatening
involvement, and want children, cyclophosphamide should be avoided.
· Large previous cyclophosphamide load is a relative contraindication to further
cyclophosphamide use; eg: >15g.
What is the role of sperm banking/ oocyte retrieval in vasculitis patients?
· Any man under 55 should be actively encouraged to bank even if he feels that he will not
want to use the sperm as his thoughts may change.
What is the role of GnRH antagonists to preserve fertility? What other therapeutic options would
you recommend?
· Should be offered to younger women at risk of ovarian damage from cyclophosphamide.
Round 4 Consensus
In the absence of life threatening disease cyclophosphamide should be avoided in women and
men of child-bearing potential.
There is emerging data that pregnancy may be safe in the months following Rituximab exposure
However, until more data is available patients should be counselled to avoid pregnancy post
Rituximab exposure for 12 months.

108
Patients exposed to Rituximab in the preceding 12 months should be referred for discussion in a
specialised joint obstetric/ rheum or renal clinic.
All vasculitis patients of future child- bearing potential should be considered for referral for
sperm banking/ egg retrieval including those treated with Rituximab due to the potential for
future exposure to cyclophosphamide.
Individual cases, such as sperm banking following exposure to 1 or 2 doses of cyclophosphamide
or for patients who are physically incapable of sperm banking should be discussed with the local
reproductive health department
There is insufficient evidence to routinely recommend the use of GnRH agonists/ GnRH
analogues/or OCP to protect fertility. This requires prospective studies
Patients with non- life threatening relapsing disease and previous treatment with
cyclophosphamide should avoid further exposure to cyclophosphamide i.e. consider Rituximab
treatment. This is supported by current funding policies for Rituximab.
Patients exposed to pulsed intravenous cyclophosphamide should receive:
· Mesna
The educated patient and GP may be better placed to perform regular (annual) skin screening
than the clinician in the vasculitis clinic. However, patients with skin lesions require regular
appropriate follow- up (i.e. dermatology).
Cervical screening should be carried out annually for first 3 years then as per population (see
BSR guidelines).
Patients should be warned in advance of cyclophosphamide exposure regarding the potential
increase in CIN changes on cervical screening.
The rheumatoid arthritis model of multiplying traditional CV risk by 1.5 may not be appropriate
for this population. AAV may be more comparable to the lupus population but more data is
required.
Vasculitis and the therapy, particularly steroids appear to be risk factors for cardiovascular
disease. Therefore to manage these risk factors the disease should be appropriately treated and
unnecessary steroid exposure avoided
Early identification of CKD in this group is imperative due to the additional risk of cardiovascular
disease this confers
Awareness of increased CVD risk in Vasculitis should be raised in both primary and secondary
care and to the patient.

109
Vasculitis patients should receive standard therapy after assessment of traditional risk factors
as there is currently no evidence to support escalation of therapy in this population. However,
the awareness of the higher risk status of CVD in these patients means that risk factors should
be rigorously addressed and modified. (exercise/ weight/ BP/ smoking/ cholesterol)
Due to steroid exposure in this population the increased risk of GI blood loss associated with
concurrent aspirin prescription should be borne in mind.
Awareness of the risk of the increased risk of VTEs is important in this population, with standard
VTE prophylaxis being used if there is any loss of mobility.
Vasculitis patients having had more than one VTE should receive life-long anticoagulation.
There is no evidence to support the role of aspirin in VTE prophylaxis
Vitamin D levels should be checked at baseline with replacement and maintenance therapy
prescribed as required. Recheck levels 3-6 months post replacement, thereafter not required.
Awareness is required in interpreting results for the seasonal variation in vitamin D levels.
In pts with advanced renal impairment (CKD 4 and 5) there is limited safety data for
bisphosphonates which should not be routinely used.
Specialist management of their (CKD 4 and 5) bone disease is required.
Other unlicensed treatments for steroid induced osteoporosis may be considered.
Teriperatide may be considered within the remit of the NICE guidelines
Caution should be advised in the prescription of bisphosphonates to women of childbearing
age- it is unusual for pre- menopausal females to require bisphosphonates.
Ensure adequate calcium and vitamin D nutrition in pregnancy.
Outside of pregnancy (where they are contra-indicated), if bisphosphonates are prescribed
ensure adequate calcium and vitamin D by checking levels and nutritional intake. Dietetic
review may be required to ensure this.
DEXA scanning in CKD 4/5 may not provide valid information
DEXA should be performed:
· If assessing risk with a view to starting bisphosphonate therapy
· If > 50 on steroids/ no fracture
· Repeat 18-36 months following above.* or according to NOGG recommendations 2014
PJP prophylaxis is recommended during induction therapy and with reintroduction of therapy
for relapse

110
Co-trimoxazole should be first line (with discussion of other options if not tolerated/
contraindicated in text)
There are no evidence based biomarkers of risk of PJP in AAV, however, prolonged high dose
steroids should be recognised as a risk factor.
Education of pts with regards to risk of infection and potential symptoms is key in conjunction
with prescription of prophylaxis
PJP prophylaxis should be continued for 6 months post Rituximab.
There is no consensus as to the duration of continuation of prophylaxis post cyclophosphamide
however it would seem reasonable to follow the guidance for Rituximab (i.e. consider
continuing for 6 months post cessation of cyclophosphamide in those felt to be high risk).
Clinicians should be aware of other potential markers of immunosuppressed status, including
the development of opportunistic infections such as warts, thrush and shingles. These patients
may benefit from more detailed profiling of their immune status such as measurement of
lymphocyte subsets.
However, there is no evidence in this population to support a CD4 count below which PJP
prophylaxis is recommended.
Vaccination ('flu, pneumococcal, other as indicated) should be undertaken where possible,
ideally 6 weeks and at least 2 weeks prior to Rituximab
We recommend ‘flu vaccination for all pts- including those undergoing induction therapy with
Rx/cyclophos (where usual ‘flu vaccination season falls during the pts induction regime)
There is good evidence that vaccination does not cause disease relapse
We advise education of patients and primary care to encourage early presentation and
treatment for immunosuppressed pts at risk during flu epidemic with ‘flu like symptoms.
Latent TB- screening and treatment as per BTS guidelines
Monitoring of Ig levels pre/ post induction therapy may be helpful in those pts who develop
infections as a complication of therapy.
Individual investigation of the pt who declares themselves at risk of recurrent infection should
be assessed with regards to immunosuppression and immune status
The evidence in other immunosuppressed pts does not support topical, non- absorbed fungal
prophylaxis, such as topical nystatin and amphotericin.
For pts on induction therapy immunosuppression (or high dose steroids for relapse) or pts with
an episode of candidiasis/previous candidiasis may require prophylaxis with a therapy of
proven efficacy such as fluconazole.

111
Pretesting of varicella zoster immunity should be carried out prior to commencement of
immunotherapy. However, one should be aware that pts immune status may change following
exposure to immunosuppression.
Exposure to varicella in the immunosuppressed pt should necessitate early presentation for
assessment of varicella immune status and need for pre-emptive therapy (VZV Ig hyperimmune
or consideration of antivirals in situations where Ig cannot be used)
Current UK recommendations from the Green Book state Varicella Zoster vaccine is
contraindicated in immunosuppressed patient as a live vaccine, however, there is evidence to
suggest administration may be safe in those on low dose immunosuppression ( e.g. less than
20mg/ day prednisolone)
Measurement of Haemophilus iinfluenzae B immunity (ab) may not be helpful as this is against
non- typable strains. We therefore do not recommend routine ab measurement and
immunisations but there may be benefits for those travelling overseas. The Hib vaccine is
immunogenic and safe.
Serotype-specific Pneumococcal IgG antibody monitoring may be relevant for assessing immune
response to vaccination.
WHO guidelines state that protective antibody levels to pneumococcus are regarded as
antibodies to 2/3 of serotypes ≥ 0.35 µg/mL. However, there is no evidence base or consensus
as to whether this is useful in guiding further immunisation.

112
4.8 APPENDIX 4. SUMMARY OF MAIN CONSENSUS STATEMENT AND LEVELS OF
CONSENSUS
Statement Round reaching consensus
Level of consensus
%
There is no robust evidence that there is a safe dose of cyclophosphamide that would completely eradicate risk of infertility
2 87
In the absence of life threatening disease cyclophosphamide should be avoided in women and men of child-bearing potential.
4
Advice should be given regarding the severe effect that kidney failure has on fertility and of the importance of not using a "soft touch" for organ threatening disease
2 88
There is emerging data that pregnancy may be safe in the months following Rituximab exposure
4
However, until more data is available patients should be counselled to avoid pregnancy post Rituximab exposure for 12 months.
4
Patients exposed to Rituximab in the preceding 12 months should be referred for discussion in a specialised joint obstetric/ rheum or renal clinic.
4
Links with the appropriate local reproductive health departments should be established, including urgent referral pathways should be available, particularly for sperm banking for those patients who present acutely requiring rapid treatment.
2 94
Men should be offered the chance to store sperm if they wish before starting cyclophosphamide (as long as it does not interfere with medically urgent therapy).
2 94
Oocyte retrieval in unwell females with active vasculitis is not currently feasible.
2 92
All vasculitis patients of future child- bearing potential should be considered for referral for sperm banking/ egg retrieval including those treated with Rituximab due to the potential for future exposure to cyclophosphamide.
4
Individual cases, such as sperm banking following exposure to 1 or 2 doses of cyclophosphamide or for patients who are physically incapable of sperm banking should be discussed with the local reproductive health department
4
There is insufficient evidence to routinely recommend the use of GnRH agonists/ GnRH analogues/or OCP to protect fertility. This requires prospective studies
4

113
Statement Round reaching consensus
Level of consensus
A large previous cyclophosphamide load (e.g.>15g) is a relative contraindication to further cyclophosphamide treatment
3 92%
Patients with non- life threatening relapsing disease and previous treatment with cyclophosphamide should avoid further exposure to cyclophosphamide i.e. consider Rituximab treatment. This is supported by current funding policies for Rituximab.
4
Patients exposed to pulsed intravenous cyclophosphamide should receive:
4
· Pre-hydration where possible
· Mesna 4
Recent EUVAS data suggests no significant increase risk of cancer *with the current low doses of cyclophosphamide although further follow up will be necessary. *except non- melanoma skin cancer
2 85
All patients should be encouraged to attend for routine age and gender determined population cancer screening
2 94
All patient on immunosuppression require sun protection and regular (annual) skin screening
3 94
The patient’s history (including family and repeated history of high level of UV exposure early in life e.g. living abroad) should be taken into account regarding skin cancer risk
2 88
The avoidance of tanning beds should be advised. 2 94
Patients should be educated to perform self-checking for skin cancer with knowledge of the appropriate place to present to for further investigation.
2 89
The educated patient and GP may be better placed to perform regular (annual) skin screening than the clinician in the vasculitis clinic. However, patients with skin lesions require regular appropriate follow- up (i.e. dermatology).
4
Urinalysis for blood at every hospital visit (at least 12 monthly) 2 94
with cystoscopy and cytology assessment in any cyclophosphamide patient with persistent haematuria
2 88
Cervical screening should be carried out annually for first 3 years then as per population (see BSR guidelines).
4
Patients should be warned in advance of cyclophosphamide exposure regarding the potential increase in CIN changes on cervical screening.
4

114
Statement Round reaching consensus
Level of consensus
CVD assessment should be carried out annually 2 94
with smoking cessation critical. 2 95
The rheumatoid arthritis model of multiplying traditional CV risk by 1.5 may not be appropriate for this population. AAV may be more comparable to the lupus population but more data is required.
4
Vasculitis and the therapy, particularly steroids appear to be risk factors for cardiovascular disease. Therefore to manage these risk factors the disease should be appropriately treated and unnecessary steroid exposure avoided
4
Early identification of CKD in this group is imperative due to the additional risk of cardiovascular disease this confers
4
Awareness of increased CVD risk in Vasculitis should be raised in both primary and secondary care and to the patient.
4
Vasculitis patients should receive standard therapy after assessment of traditional risk factors as there is currently no evidence to support escalation of therapy in this population. However, the awareness of the higher risk status of CVD in these patients means that risk factors should be rigorously addressed and modified. (exercise/ weight/ BP/ smoking/ cholesterol)
4
Due to steroid exposure in this population the increased risk of GI blood loss associated with concurrent aspirin prescription should be borne in mind.
4
Awareness of the risk of the increased risk of VTEs is important in this population, with standard VTE prophylaxis being used if there is any loss of mobility.
4
There is no evidence to support the role of aspirin in VTE prophylaxis.
4

115
Statement Round reaching consensus
Level of consensus
Steroid exposure should be minimised. 2 94
Vitamin D levels should be checked at baseline with replacement and maintenance therapy prescribed as required. Recheck levels 3-6 months post replacement, thereafter not required.
4
Awareness is required in interpreting results for the seasonal variation in vitamin D levels.
4
Patients should have overall fracture risk assessed rather than just BMD.
2 81
DEXA scanning in CKD 4/5 may not provide valid information 4
DEXA should be performed:
· If assessing risk with a view to starting bisphosphonate therapy:
4
· If > 50 on steroids/ no fracture 4
· Repeat 18-36 months following above.* or according to NOGG recommendations 2014
4
Treatment with Denosumab (not licensed) should be considered for use in patients where bisphosphonates have been contraindicated
2 86
Patients should always be counselled regarding the potential side effect of bisphosphonates (osteonecrosis of the jaw, avascular necrosis of the hip and “frozen bone”/subtrochanteric hip fracture) prior to commencing therapy.
2 94
In pts with advanced renal impairment (CKD 4 and 5) there is limited safety data for bisphosphonates which should not be routinely used.
4
Specialist management of their (CKD 4 and 5) bone disease is required.
4
Other unlicensed treatments for steroid induced osteoporosis may be considered.
4
Teriperatide may be considered within the remit of the NICE guidelines
4
Caution should be advised in the prescription of bisphosphonates to women of childbearing age- it is unusual for pre- menopausal females to require bisphosphonates.
4
Ensure adequate calcium and vitamin D nutrition in pregnancy. 4
Outside of pregnancy (where they are contra-indicated), if bisphosphonates are prescribed ensure adequate calcium and vitamin D by checking levels and nutritional intake. Dietetic review may be required to ensure this.
4

116
Statement Round reaching consensus
Level of consensus
Rituximab may be used in those felt to be at high risk of infectious complications or those with evidence of marrow fragility.
2 85
PJP prophylaxis is recommended during induction therapy and with reintroduction of therapy for relapse
4
Co-trimoxazole should be first line (with discussion of other options if not tolerated/ contraindicated in text)
4
There are no evidence based biomarkers of risk of PJP in AAV, however, prolonged high dose steroids should be recognised as a risk factor.
4
Education of pts with regards to risk of infection and potential symptoms is key in conjunction with prescription of prophylaxis
4
PJP prophylaxis should be continued for 6 months post Rituximab.
4
There is no consensus as to the duration of continuation of prophylaxis post cyclophosphamide however it would seem reasonable to follow the guidance for Rituximab (i.e. consider continuing for 6 months post cessation of cyclophosphamide in those felt to be high risk).
4
Clinicians should be aware of other potential markers of immunosuppressed status, including the development of opportunistic infections such as warts, thrush and shingles. These patients may benefit from more detailed profiling of their immune status such as measurement of lymphocyte subsets.
4
However, there is no evidence in this population to support a CD4 count below which PJP prophylaxis is recommended.
4
Vaccination ('flu, pneumococcal, other as indicated) should be undertaken where possible, ideally 6 weeks and at least 2 weeks prior to Rituximab
4
BCG vaccine should only be give prior to immunosuppression 3 80
Hepatitis A/B vaccine should be administered for anyone with renal involvement
3 81
We recommend ‘flu vaccination for all pts- including those undergoing induction therapy with Rx/cyclophos (where usual ‘flu vaccination season falls during the pts induction regime)
4
There is good evidence that vaccination does not cause disease relapse
4
We advise education of patients and primary care to encourage early presentation and treatment for immunosuppressed pts at risk during flu epidemic with ‘flu like symptoms.
4
Latent TB- screening and treatment as per BTS guidelines 4

117
Monitoring of Ig levels pre/ post induction therapy may be helpful in those pts who develop infections as a complication of therapy.
4
Individual investigation of the pt who declares themselves at risk of recurrent infection should be assessed with regards to immunosuppression and immune status
4
The evidence in other immunosuppressed pts does not support topical, non- absorbed fungal prophylaxis, such as topical nystatin and amphotericin.
4
For pts on induction therapy immunosuppression (or high dose steroids for relapse) or pts with an episode of candidiasis/previous candidiasis may require prophylaxis with a therapy of proven efficacy such as fluconazole.
4
Pretesting of varicella zoster immunity should be carried out prior to commencement of immunotherapy. However, one should be aware that pts immune status may change following exposure to immunosuppression.
4
Exposure to varicella in the immunosuppressed patient should necessitate early presentation for assessment of varicella immune status and need for pre-emptive therapy (VZV Ig hyperimmune or consideration of antivirals in situations where Ig cannot be used)
4
Current UK recommendations from the Green Book state Varicella Zoster vaccine is contraindicated in immunosuppressed patient as a live vaccine, however, there is evidence to suggest administration may be safe in those on low dose immunosuppression ( e.g. less than 20mg/ day prednisolone)
4
Measurement of Haemophilus influenza B immunity (ab) may not be helpful as this is against non- typeable strains. We therefore do not recommend routine ab measurement and immunisations but there may be benefits for those travelling overseas. The Hib vaccine is immunogenic and safe.
4
Serotype-specific Pneumococcal IgG antibody monitoring may be relevant for assessing immune response to vaccination.
4
WHO guidelines state that protective antibody levels to pneumococcus are regarded as antibodies to 2/3 of serotypes ≥ 0.35 µg/mL. However, there is no evidence base or consensus as to whether this is useful in guiding further immunisation.
4

118
5 LITERATURE REVIEW: METHODS AND RESULTS
5.1 SEARCH STRATEGY
In parallel to the Delphi study, a review of the available literature was undertaken. This
review was undertaken with a formal search strategy as outlined below. Articles were
reviewed in a structured format for methodological and reporting quality as well as
summarising the principle findings. Articles were not graded (e.g. according to STROBE
criteria) due to the volume, breadth and heterogeneity of articles covered by this review.
The search was conducted using Ovid Medline and Embase (1946- 2016) along with a
review of the Cochrane database, National Institute for Health and Care Excellence (NICE),
Royal College of Physicians (RCP), Scottish Intercollegiate Guidelines Network (SIGN), BSR
and EULAR guidelines that may be relevant.
The searches were conducted between May and August 2016. Where searches were
conducted prior to this, they were updated during this window. The search was limited to
English language and human subjects. Single case reports and letters were discarded.
Conference abstracts were discarded if there was insufficient data to include. The full
search strategy and evidence table for each area is included below. Search strategies varied
slightly depending on the volume of literature available within the subject area. Where
data was scarce, the disease categories were widened to include others such as Systemic
Lupus Erythematosus, from which possible analogies may be drawn relevant to the
vasculitis population. Where literature was in abundance, the search terms were narrowed
in specificity to ensure only the most relevant articles were included and that the volume of
literature to be reviewed was manageable.
Literature searches were performed by three of the authors NB, DT and DC. All literature
searches, review of titles and abstracts for suitability for inclusion and extraction of
relevant data from articles will be performed by two independent reviewers prior to
publication (currently underway). Final analysis for data inclusion was performed by NB.
119
5.2 RESULTS
5.2.1 Section 1: Bone health
The questions to be answered by this section were;
1. What is the prevalence of osteoporosis in patients with ANCA Associated
Vasculitis?
2. What screening or prophylactic bone protection strategies should be carried out in
this population?
3. What treatment should patients with AAV and GIOP receive?
It was not possible to undertake a review of all the evidence for prevention and treatment
of Glucocorticoid Induced Osteoporosis (GIOP) as part of this process. Review of available
guidelines identified the following relevant national/ international guidelines.
1) National Osteoporosis Guideline Group: Guideline for the diagnosis and management of
osteoporosis in postmenopausal women and men from the age of 50 years in the UK.
Updated March 2014149.
2) Scottish Intercollegiate Guidelines Network: Management of osteoporosis and the
prevention of fragility fractures A national clinical guideline. Updated March 2015150.
3) EULAR evidence-based recommendations on the management of systemic glucocorticoid
therapy in rheumatic diseases151.
Review of references revealed that the NOGG report contained the most up –to – date
evidence with their systematic review informing the guidelines including articles published
up to and including 2012.
Therefore, the majority of recommendations were taken from this document, with a
further literature review encompassing 2012- 2016 undertaken. The evidence table from
this process is included below.
Results
The prevalence of osteoporosis in the AAV population appears to be in the region of 14-
16%67,152. However, this is likely to be in patients on prophylaxis as at least one of the
studies providing this data included compulsory use of calcium, vitamin D and
bisphosphonate therapy. Earlier data, prior to the routine use of bisphosphonates in the
prevention of GIOP reported higher rates at 21%118, perhaps indicating the possible
effectiveness of these preventative strategies.

120
Current recommendations
Patients should have overall fracture risk assessed rather than just Bone Mineral Density
(BMD) using a validated risk prediction model. The National Osteoporosis Guidelines Group
advise the following adjustments to fracture risk (multiples of FRAX probabilities) based on
UK data;
For postmenopausal women and men aged ≥50 years;
For hip fracture
• adjust by 0.65 for daily doses <2.5 mg/day prednisolone or its equivalent
• adjust by 1.20 for daily doses ≥7.5 mg/day prednisolone or its equivalent
For major osteoporotic fracture
• adjust by 0.8 for daily doses <2.5 mg/day prednisolone or its equivalent
• adjust by 1.15 for daily doses ≥7.5 mg/day prednisolone or its equivalent
Higher doses of steroids (e.g. ≥15mg prednisolone/day) may require further upward
adjustment of fracture probability.
Algorithms for determining whether BMD measurements are required are available from
the NOGG guidelines: Osteoporosis clinical guideline for prevention and treatment.
However, in general the following groups exceed the intervention threshold and should be
considered for bone protective therapy;
• women > 70yrs
• women with previous fragility fracture
• women taking >15mg prednisolone /day.
Therefore, BMD measurement is likely to be indicated prior to treatment for younger
women and men and following the recommended treatment duration (see below) for
those not in a high risk category.
GIOP prevention options include alendronic acid, risedronate or zolendronic acid for which
there is clinical trial evidence for all three150. There is now RCT evidence to support the
safety and tolerability of once yearly zolendronic acid infusion for patients on
glucocorticoids. However, this study was only above to demonstrate a significant difference
when compared with risedronate at preserving or increasing bone mineral density in men
as a subgroup153. Treatment review is recommended after 5 years for alendronate,
risedronate or ibandronate or 3 years for zolendronic acid. However, those who are high
risk should generally continue treatment without the need for review, including; those over

121
age 75 years, those with previous hip/vertebral fracture and those continuing on
prednisolone doses greater than 7.5mg/day.
5.2.2 Section 2: Cardiovascular and thromboembolic risk
The questions to be answered in this section are;
1) What is the incidence of Venous Thromboembolism (VTE) in the AAV population?
2) What is the incidence of Cardiovascular disease (CVD) in the AAV population?
3) What are the risk factors for VTE in the AAV population?
4) What are the risk factors for CVD in the AAV population?
5) Is there any evidence for strategies to reduce this risk specific to this population?
It is well recognised that all of the AAV may present or relapse with cardiac involvement.
This can range from direct inflammation of the coronary arteries to eosinophilic or
granulomatous infiltration of the myocardium in EGPA or GPA. Due to the high rate of
cardiac involvement in EGPA, to include cardiac involvement as part of the primary disease
manifestations is not possible within this review. Therefore, articles were limited for
inclusion in the below narrative synthesis of evidence if cardiovascular disease was
reported as an outcome rather than a disease manifestation.
Thromboembolic Risk
The rate of VTE has been reported variably in the literature with interest in this area having
been primarily provoked by the observation of a high number of VTEs in the WGET clinical
trial154. This study reported 29 of 180 patients (16%) with GPA developing a VTE. Of these,
16 occurred in patients with no history of VTE giving an incidence rate of 7.0 per
100/person years. In addition, this was one of the first studies to report the observation
between VTEs and vasculitis disease activity, with the median time from active disease to
VTE being 2.07 months in this trial. Subsequent reports of VTE rates in this population
range from 1.84/100/person years in all follow up increasing to 7.26/100/person years in
periods of disease activity155, with significant associations to VTE development reported as
older age at time of vasculitis diagnosis, male sex, previous VTE, nephrotic range
proteinuria >3 g/24 h and/or stroke with motor deficit. A further study has reported

122
outcomes corresponding to an incidence rate of 4.3 per 100 person- years during all follow-
up156. However, it must be noted that these studies are retrospective cohort studies.
Some have attempted to draw comparisons of the rate of VTEs with other “at risk”
populations with a systemic lupus VTE incidence rate of 1.0 per 100/person years and those
having had a previous VTE having an incidence rate of recurrent VTE of 7.20 per 100/
person years. However, the definitions and methods of identification of VTEs in these
studies were different making them unsuitable for direct comparison154. One systematic
review has specifically addressed the rate of arterial and venous thromboembolism in EGPA
reporting arterial event rates at between 3.1 and 18.7% and VTEs at 5.8- 30%157.
In summary it is now widely accepted and clearly reported that patient with AAV have a
higher rate of VTE than anticipated and that this risk is highest during periods of disease
activity. Postulated mechanisms to explain this include the contribution of endothelial cell
dysfunction, neutrophil activation (NETosis), and the demonstrated presence of anti-
plasminogen antibodies associated with active disease113,158.
Cardiovascular risk
The first studies to evaluate the relationship between AAV and CVD disease included small
groups of patients, usually with a matched control population, and looked at surrogate
markers for cardiovascular disease such as common carotid intimal medical thickness,
ultrasound vascular plaque detection and Ankle-brachial pressure index (ABPI)159–161. These
all showed that patients with vasculitis had higher rates of atherosclerotic disease, as
detected by these surrogate methods. Some, in addition, were able to demonstrate a
relationship with cumulative relapses and atherosclerotic burden.
Although there was initial data reported at conferences in 2002-3 of an increased incidence
of CVD in vasculitis patients, perhaps the most convincing data was published as recently as
2009. This year saw data from a UK cohort with AAV, matched to CKD controls,
demonstrating a HR for CV events of 2.23. Risk factors for events included a history of CVD,
ever having required dialysis, ever having smoked, male sex, age, and (lower)cholesterol at
presentation115. Alongside this, a large Danish retrospective cohort study reported an
observed to expected event rate of 1.9 for patients with GPA compared with the
background population114.

123
The recent reporting of the EUVAS combined clinical trials contributed further data by
reporting that after the first year (following diagnosis) CVD is primary cause of death at
25.7% in this population98.
Subsequent analysis of the events in these trials has served to produce a model for
predicting CV events in the AAV population from the time of diagnosis. This model
identified independent risk factors as age> 72.4 years, absence of PR3 antibody and
diastolic hypertension >90mmHg116. It should be borne in mind that the reason for data
being available on diastolic as opposed to systolic hypertension is that the presence of
diastolic hypertension is a scoring item on the Birmingham Vasculitis Activity Score.
Therefore, all patients being scored as having diastolic hypertension had this attributed to
active vasculitis. It is possible that there were patients with pre-existing hypertension who
would not have been captured by this categorisation.
For both VTE and CVD events, there is no trial based evidence to support prophylactic
measures over and above current recommendations for the general population.
5.2.3 Section 3: Cancer Risk
1) What is the risk of cancer for patients diagnosed with AAV?
2) Is there a “safe” dose of cyclophosphamide with regards to cancer risk?
3) Do patients with AAV require additional screening for cancer, over and above
population cancer screening?
Historical data regarding the incidence of cancer in AAV stems from Hoffman’s reported
series of outcomes for 158 patients with GPA100. Cumulative cyclophosphamide doses were
high in this series, e.g. 2mg/kg/day oral therapy continued for at least 1 year after achieving
remission; this would equate to around 60g of cyclophosphamide being administered to a
60kg patient over 18 months. This study reported a 2.4-fold increase in all malignancies
(compared with the background population), with a 33-fold increase in bladder cancer and
an 11-fold increase in lymphomas. However, the most recent data from this population
suggests that this risk has significantly diminished with more recent SIRs of 3.6- 7.2
reported for bladder cancer and SIR of only 1.1 for lymphoma162 . There is, in addition, a
significant increase in non- melanomatous skin cancer which the patient should be

124
counselled about with regards to appropriate sun protection and skin monitoring (SIR 2.8-
10.4)162. This apparent reduction in cancer rates would logically follow from the reduction
in cumulative cyclophosphamide exposure over time.
With regards to cyclophosphamide and bladder cancer, it has been reported that each 10g
increment in cyclophosphamide dose is associated with a doubling of the risk of bladder
cancer development, with cumulative doses of greater than 25g being associated with a
5-fold risk163. However, with regards to bladder cancer, the long latency (11-16 years after
first cyclophosphamide exposure164) needs to be borne in mind.
In addition, other populations with immune mediated disease treated with
cyclophosphamide have been reported to have a significantly increased risk of cervical
intra-epithelial neoplasia (CIN). In a study of women with SLE treated with i.v.
cyclophosphamide, the overall 3-year incidence of CIN was 9.8%. A dose relationship was
observed between cumulative cyclophosphamide dose and CIN with each increase of 1g
corresponding to a 13% increased risk of CIN (p=0.04)120. Whether this is predominantly
contributed to by the disease or the drug is not established. There is currently no data on
the rate on CIN in AAV compared with the background population. However, it would seem
prudent to ensure patients are counselled regarding the importance of attending routine
cervical screening.
5.2.4 Section 4: Fertility
1) Is there a “safe” dose of cyclophosphamide with regards to preservation of fertility
for women?
2) Is there evidence to support the recommendation of measures to try to protect
fertility for those receiving cyclophosphamide?
The risk of amenorrhea following cyclophosphamide exposure has been repeatedly
demonstrated to relate to cumulative dose and age at exposure. Ioannidis calculated the
risk of amenorrhoea for a patient receiving 15 g of CYC (5 to 10% for patients <25 years,
30% for patients aged 25 to 31 years and 90% for patients >32 years)165. Boumpas reported
100% of those with a long course of CYC (pulsed every 1-3 months, up to 24 doses) plus >

125
31 years of age developed sustained amenorrhoea versus 0% of those age < 25yrs plus
short course CYC(7 monthly pulses)166.
A comprehensive systematic review of the effectiveness of gonadotropin-releasing
hormone agonist (GnRHa) therapy for women undergoing chemotherapy for breast cancer
or lymphoproliferative disorders or those receiving cyclophosphamide for SLE was
undertaken in 2010. This included a meta-analysis of 19 prospective studies167. Fifteen of
these, including 681 patients, evaluated “fertility preservation” as defined by regular
menses or by FSH levels, following GnRHa. This analysis yielded a significant benefit for
GnRHa in preserving the menstrual cycle (RR 0.26, 95% CI 0.22–0.34). However, the three
RCTs that included pregnancy rates as outcomes failed to show an advantage for the use of
GnRHas. This review acknowledged though that the studies included had many limitations
including lack of stratification by age, different chemotherapy regimens and inaccurate
definitions of preservation of ovarian reserve.
The only data published subsequent to this is a retrospective case study of patients with
SLE, reporting a non- statistically significant increase in preservation of menses following
co-administration of GnRHas with cyclophosphamide121.
In summary, there may be benefits of co-administration of GnRHas with cyclophosphamide
but there is limited data to support this, with further RCTs required.
5.2.5 Section 5: Vaccination
1) Which vaccinations should patients with AAV routinely receive?
2) What is the optimal timing of vaccination for patients undergoing induction
therapy with cyclophosphamide or Rituximab?
Guidance for vaccination is predominantly derived from the Green Book as it is not possible
to identify and review the evidence for recommending population wide vaccination for
those on immunosuppression.
Influenza vaccine is recommended annually, within the ‘flu season. Pneumococcal
vaccination, in the form of Pneumococcal Polysaccharide Vaccine (PPV) is recommended

126
once. However, a booster after 5 years is recommended in those with “chronic renal
disease”168.
With regards to timing of vaccination, the Green Book recommends “individuals due to
commence immunosuppressive treatments, inactivated vaccines should ideally be
administered at least two weeks before commencement. In some cases this will not be
possible and therefore vaccination may be carried out at any time and re-immunisation
considered after treatment is finished and recovery has occurred”133.
Studies in the vasculitis population have evaluated firstly the safety of vaccination in
patients and secondly the response to vaccination. With regards to safety, concerns have
been raised regarding the possibility of triggering disease activity with several case reports
detailing patients who presented for the first time with vasculitis following an
immunisation169.
However, there have been 2 clinical trials (one specifically designed to answer the question
of vaccination safety) that have reported no increase in disease activity in a vasculitis
population with stable disease following vaccination against ‘flu, pneumococcus,
Haemophilus influenza and meningococcal disease170,171.
With regards to effectiveness of vaccination, initial studies evaluated the immune response
(antibody and cell mediated) to influenza vaccination in patients with AAV, finding it to be
comparable to that of a healthy control population131,172.
However, these studies excluded patients on high dose immunosuppression (prednisolone
> 30mg/day or cyclophosphamide). There is no data with regards to the effectiveness of
vaccination following cyclophosphamide in this population. However, there is significant
literature regarding the effect of Rituximab on the response to vaccination, including, at
which point following treatment, vaccination response reconstitutes.
Generally, as expected, most studies report an impaired response to vaccination following
Rtx, however, this was often not statistically significant173. One study reported that at 6 to
10 months following Rituximab patients mounted a moderate IgG response to ‘flu
vaccine174. However, one study specifically compared antibody responses in those patients

127
immunised 6 days pre-Rtx versus those immunised 6 months post-Rtx, finding that those
immunised pre- had a better B cell response to ‘flu vaccine175.
Therefore, despite PHE recommendations to immunise 2 weeks prior to therapy it might be
that vaccines given within a week prior to induction therapy will be more effective than
waiting until after therapy has completed, and in addition may provide some protection for
patients during their most vulnerable period.
5.2.6 Section 6: Infection Prophylaxis
1) Which patients should receive PJP prophylaxis and what should they receive?
2) Do patients require routine fungal or viral prophylaxis?
A recent Cochrane review concluded that PJP prophylaxis is justified for any patient
population with an event rate of greater than 6.2%176. It is difficult to ascertain the true
incidence of PJP in AAV as the more recent studies, with larger patient numbers and better
data quality recommend PJP prophylaxis (although uptake of this is not reported, making
interpretation of the rate of infection during these studies challenging)90.
However, historical data, prior to the routine recommendation of prophylaxis suggests an
incidence of 20%135. Although it could be argued that immunosuppression exposure was
much higher in this era, a more recent single study of rheumatology patients receiving
cyclophosphamide reported an annual incidence rate of 9.5% in those not receiving
prophylaxis versus 5.3% in those who did177. The 2009 EULAR guidelines “encouraged”
prophylaxis against PJP72, with the 2014 BSR guidelines suggesting prophylaxis should be
considered83. However, the more recent Canadian guidelines recommend that “prophylaxis
against pneumocystis jiroveci infection should be given to patients receiving
cyclophosphamide or Rituximab”178. With regards to recommendations for prophylaxis
following Rituximab therapy, there have been multiple case reports of PJP following
Rituximab administration. Indeed, the head to head trials of Rituximab versus
cyclophosphamide showed no significant difference in infection rates between the 2 arms
(although there were no reported cases of PJP in the RITUXVAS trial with detail of infection
not provided in the RAVE trial78,79. However, extrapolating from this, PJP prophylaxis, for at
least 6 months from the date of administration of rituximab would seem reasonable and

128
indeed this is what the FDA advises in the licensing agreement for the use of Rituximab in
AAV179.
Risk factors for the development of PjP have been reported as exposure to “high dose
steroids” (defined in some series as > 15mg day and in some as > 30mg day), low
lymphocytes (mean lymphocyte count 495/mm3 in one series180 in the patient cohort who
developed infection) or low CD4 counts, older age, worse renal function/ dialysis
dependency and lung involvement180–185.
There is the most evidence to support co-trimoxazole as a first-line agent for the prevent of
PjP176. A review of evidence appears to support that there is no significant difference in
outcome between those patients receiving “full dose” (960mg/day) and those on “low
dose” (480mg/day or 960mg alternate days) co-trimoxazole prophylaxis186.
With regards to requirements for additional prophylaxis against fungal or viral infection in
this immunocompromised population there is very little data to guide practice. Coming
back once more to the results from the combined EUVAS clinical trials, details of the
infections experienced by this population demonstrated 10% of infection was attributable
to candidiasis, 7% CMV, 4% HSV and 3% HZV90. In the French series of 113 patients with
GPA, 13 of 53 serious infections were viral (HZV, HSV, CMV) with only one candidiasis187.
With regards to data for efficacy of primary preventative viral or fungal prophylaxis, this
has to be extrapolated from other immunosuppressed populations. A review of the
evidence for prevention of candidiasis in people with immunosuppression following cancer
treatment, found that absorbed (e.g. fluconazole) or partially absorbed antifungal drugs
prevented oropharyngeal candidiasis compared with non-absorbed antifungal drugs
(nystatin or amphotericin B) which may be no more effective than placebo188. There were
insufficient studies in tissue transplant recipients to draw any conclusions. A separate
systematic review of antifungal prophylaxis in solid organ transplant recipients showed no
reduction in mortality but demonstrated a significant reduction in invasive fungal infections
for fluconazole (RR 0.28, 95% CI 0.13 to 0.57) in liver transplant recipients. The overall rate
of proven invasive fungal infections in the control arm (i.e. no prophylaxis) of these four
studies was 13% (range 4 to 23%) therefore perhaps more comparable to the AAV
population than those receiving haemopoetic stem cell transplants(HSCTs) who receive a
higher burden of immunosuppression189. However, the only data for anti-viral prophylaxis

129
arises from the HSCT population, with an RCT of acyclovir versus prophylaxis showing a
highly significant reduction in VZV disease, with no difference in adverse effects between
the 2 groups190.
In summary, the evidence supports the prescription of PjP prophylaxis for patients
receiving high dose immunosuppression, with risk factors for infection appearing to be
steroid dose, older age, worse renal function, low lymphocyte/CD4 counts and lung
involvement. There appears to be a significant burden of fungal and viral infections in this
population in addition. Although there is little evidence to support routine prescription of
prophylaxis, those at risk would likely benefit from an absorbed/ partially absorbed anti-
fungal. Equally, the prescription of acyclovir as an anti-viral appears safe and effective but
data are absent in the AAV or comparable populations.
5.3 SUMMARY
A comprehensive and structured review of the literature has been undertaken in parallel to
the Delphi study. This will allow the recommendations made to be strengthened with the
best available evidence. The guidelines formed from the combination of Delphi and
literature review are outlined in the following section.

130
5.4 APPENDIX 1: SEARCH STRATEGIES
5.4.1 Bone Health search strategy

131

132

133
5.4.2 Cardiovascular/ thromboembolic risk search strategy

134

135
A total of 24 articles were included in the evidence table for review

136

137
From these a total of 15 articles were found to be relevant for inclusion in the evidence
table below

138
5.4.3 Cancer screening search strategy

139

140
5.4.4 Fertility preservation search strategy

141

142
5.4.5 Vaccination search strategy

143

144

145
5.4.6 Pneumocystis search strategy

146

147

148

149

150
5.4.7 Viral and fungal prophylaxis search strategy

151

152

153
Search repeated with Embase. No new articles identified. After review, 9 articles were
found to be relevant and are included in the evidence tables

154
APPENDIX: EVIDENCE TABLES
Article Population Study design Comparisons Outcome Comments/quality
Long-term follow-up of a
randomized trial on 118
patients with polyarteritis
nodosa or microscopic
polyangiitis without poor-
prognosis factors. Samson M et
al.
Autoimmunity reviews. 13
(2):197-205, 2014152.
118 pts between
November 1993 and
January
2005, and treated in
France and the UK with
PAN or MPA
Long-term
outcomes
reported from
RCT
Mean ± SD overall follow-up was 98.2 ±
41.9 months. Primary outcomes, relapse,
remission, death. No comparisons between
groups made. Patients received initial
treatment with oral prednisone (1
mg/kg/day for 3 weeks tapered by 5 mg
every 10 days to a dosage of 0.5 mg/kg/day,
then by 2.5 mg every 10 days
until a dosage of 15 mg/day was obtained
and, finally, by 1 mg
every 10 days to the minimal effective dose
or, when possible,
until definitive withdrawal.
Calcium, vitamin D3, and
Bisphosphonates adjuvant treatment was
compulsory.
16% of patients had osteoporosis documented
at follow-up
Population are those with
non- severe disease. Also
57/124 had PAN. Need to
refer to original article for
steroid regime and
prophylaxis. Little discussion
of limitations.
Damage in the ANCA-associated
vasculitides: long-term data
from the European vasculitis
study group (EUVAS)
therapeutic trials.
Robson J et al.
Annals of the Rheumatic
Diseases. 74(1):177-84, 201567 .
GPA /MPA pts
recruited to 4 RCTs
Long-term
follow- up
reporting from
RCTs
Outcomes reported according GPA vs MPA
mean length of glucocorticoid use being
40.4 months
Osteoporosis in 15.6% (MPA) and 14.4% (GPA)
pts at LTFU (mean 87 months). Four hundred
and sixty-seven patients (87.3% of the 535) had
data at LTFU.
Good discussion of study
limitations and
acknowledgement of absent
LTFU data. No data on
steroid doses just duration
or osteoporosis prophylaxis
Bone protection evidence

155
Prevalence of reduced bone
mineral density in patients with
anti-neutrophil cytoplasmic
antibody associated vasculitis
and the role of
immunosuppressive therapy: a
cross-sectional study.
Boomsma M et al. Osteoporosis
International. 13(1):74-82,
2002118.
Ninety-nine
consecutive patients
(48 men, 51 women)
with a mean (SD) age
of 55 (16) years Pts
with MPO or PR3
assoc. vasculitis in
single centre under
follow-up between
January 1998 and
December 1999 During
high-dose CS
treatment, all patients
received calcium
carbonate combined
with alphacalcidol or
dihydrotachysterol
therapy
Cross-sectional
cohort study
Measurement of
BMD of the proximal femur, lumbar spine
and radius were measured by DXA .Sixty-
nine patients were treated with 10.7 g
(median cumulative dose; range 0.4–67.2g)
of CS
Overall, 21 of 99 (21%) patients had BMD values
indicating osteoporosis as defined by the WHO
criteria (BMD T-score: <–2.5 SD) and 56 of 99
(57%) patients had osteopenia (WHO; BMD T-
score: –1 SD to –2.5 SD) at least at one site. In 22
of 99 (22%) patients normal BMD (WHO; BMD T-
score >–1.0 SD) values were measured at all
three sites.
Fracture rate 8%
Control values for
comparison extracted from
the general population
(no study control data)
A meta-analysis of alendronate
for the prevention and
treatment of glucocorticoid-
induced osteoporosis. Yang L,
Tian JH, He ZY, Tang XL, Yang
KH. Chinese Journal of Internal
Medicine. 2013;52(10):838-
843191.
(DARE abstract only as article in
Chinese)
Seven studies with
1111 patients were
included
Meta-analysis
PubMed,
EMBASE,
Cochrane
Library, Web of
Science,
Chinese
BioMedical
Literature
Database (CBM)
and Wanfang
Alendronate vs placebo on the outcomes of
BMD and fracture rate
Compared with placebo, alendronate
significantly increased bone mineral density
(BMD) at the lumbar spine[MD = 3.35, 95%CI
(2.67-4.02), P = 0.000] and the femoral neck[MD
= 1.90, 95%CI (0.89-2.92), P = 0.000] after 12
months of therapy. After 24 months of therapy,
alendronate significantly increased BMD at the
lumbar spine[MD = 3.91, 95%CI (2.37-5.45), P =
0.000], but not at the femoral neck[MD = 1.91,
95%CI (-1.15-5.02), P = 0.22]. Compared with
placebo, no significant reduction was found by

156
Data were
searched for all
randomized
controlled trials
(RCT) of
alendronate vs.
placebo.
the use of alendronate in the incidence of
vertebral fractures [RR = 1.00, 95%CI (0.49-2.07),
P = 0.99] or nonvertebral fractures [RR = 1.02,
95%CI (0.49-2.14), P = 0.95]. No difference was
shown with the adverse event between the two
groups[RR = 0.97, 95%CI (0.90-1.05), P = 0.47].
Effect on bone turnover
markers of once-yearly
intravenous infusion of
zoledronic acid versus daily oral
risedronate in patients treated
with glucocorticoids.
Devogelaer JP, Sambrook P,
Reid DM, Goemaere S, Ish-
Shalom S, Collette J, Su G, Bucci-
Rechtweg C, Papanastasiou P,
Reginster JY
Rheumatology (Oxford,
England). 52(6):1058-69,
2013192.
833 patients (771
completed trial) 18 and
85 years (54 centres/16
countries) being
treated with at least
7.5 mg oral prednisone
daily (or equivalent)
and expected to
continue GCs for at
least another 12
months.
Pts with creat
clearance < 30mls/min
were excluded
Randomised
controlled trial
(double blind-
double dummy)
Non- inferiority study comparing once-
yearly i.v. infusion of ZOL 5mg and daily oral
placebo capsules or daily oral RIS 5mg
capsules and a once-yearly i.v. infusion of
placebo infusion and continuing throughout
the trial. Patients classified according to
duration pre-study GC therapy (prevention
subpopulation <=3 months, treatment
subpopulation >3 months), gender (male
and female) and menopausal status in
females (pre- menopausal and post-
menopausal).
Outcomes- bone turnover markers 3,6,12
months
Once-yearly i.v. infusion of ZOL 5 mg was well
tolerated in different subgroups of GIO patients.
ZOL was non-inferior to RIS and even superior to
RIS in the response of BTMs in GIO patients.
Post hoc analysis of original
RCT. Randomisation
methods not discussed but
have been in original article.
Limitations: short duration
and not designed to evaluate
bone turnover markers in
primary analysis.
Unlikely to have direct
influence on clinical practice.
Authors comment that bone
turnover markers in these
pts suggested that
underlying inflammatory
condition rather than GCs
causing bone resorption in
this population
Bisphosphonates and
glucocorticoid osteoporosis in
men: results of a randomized
controlled trial comparing
zoledronic acid with
risedronate.
Same study as above-
subgroup analysis of
men (265 pts)
BMD and bone turnover markers- subgroup
analysis of “prevention” and treatment
arms
In the treatment subpopulation, ZOL increased L-
spine (LS) BMD by 4.7% vs. 3.3% for RIS and at
total hip (TH) the percentage changes were 1.8%
vs. 0.2%, respectively. In the prevention
subpopulation, bone loss was prevented by both
treatments. At LS the percentage changes were
“Once-yearly ZOL preserves
or increases BMD within 1
year to a greater extent than
daily RIS in men receiving
glucocorticoid therapy.”

157
Sambrook PN, Roux C,
Devogelaer JP, Saag K, Lau CS,
Reginster JY, Bucci-Rechtweg C,
Su G, Reid DM
Bone. 50(1):289-95, 2012153 .
2.5% vs. -0.2% for ZOL vs. RIS and at TH the
percentage changes were 1.1% vs. -0.4%,
respectively. ZOL significantly increased lumbar
spine BMD more than RIS at Month 12 in both
the prevention population (p=0.0024) and the
treatment subpopulation (p=0.0232) in men
Post hoc analysis of a single IV
infusion of zoledronic acid
versus daily oral risedronate on
lumbar spine bone mineral
density in different subgroups
with glucocorticoid-induced
osteoporosis.
Roux C, Reid DM, Devogelaer JP,
Saag K, Lau CS, Reginster JY,
Papanastasiou P, Bucci-
Rechtweg C, Su G, Sambrook PN
Osteoporosis international :
23(3):1083-90, 2012193
Same study as above
Once-monthly oral ibandronate
provides significant
improvement in bone mineral
density in postmenopausal
women treated with
glucocorticoids for
inflammatory rheumatic
diseases: a 12-month,
randomized, double-blind,
placebo-controlled trial.
Hakala M, Kroger H, Valleala H,
140 post menopausal
women with any
rheumatic disease
receiving 5-15mg/day
pred
Randomized,
double-blind,
placebo-
controlled,
parallel-group
study
Patients were randomized 1:1 to receive
either monthly oral ibandronate 150mg or
placebo for 12months. Primary endpoint
was the relative change in mean LS BMD
from baseline to 12 months.
Significant increases in mean LS BMD of 2.6%
and 3.2% with ibandronate and 0.3% and –0.1%
with placebo from baseline to 6 and 12 months
Reports same adverse events (rx vs placebo),
more SAE in treatment group but no single type
No discussion of those who
did not complete study.
As this was placebo
controlled, those with
severe osteopenia or
osteoporosis were excluded.
No comparison with other
bisphosphonates. Not
powered to evaluate effect
in fracture rate
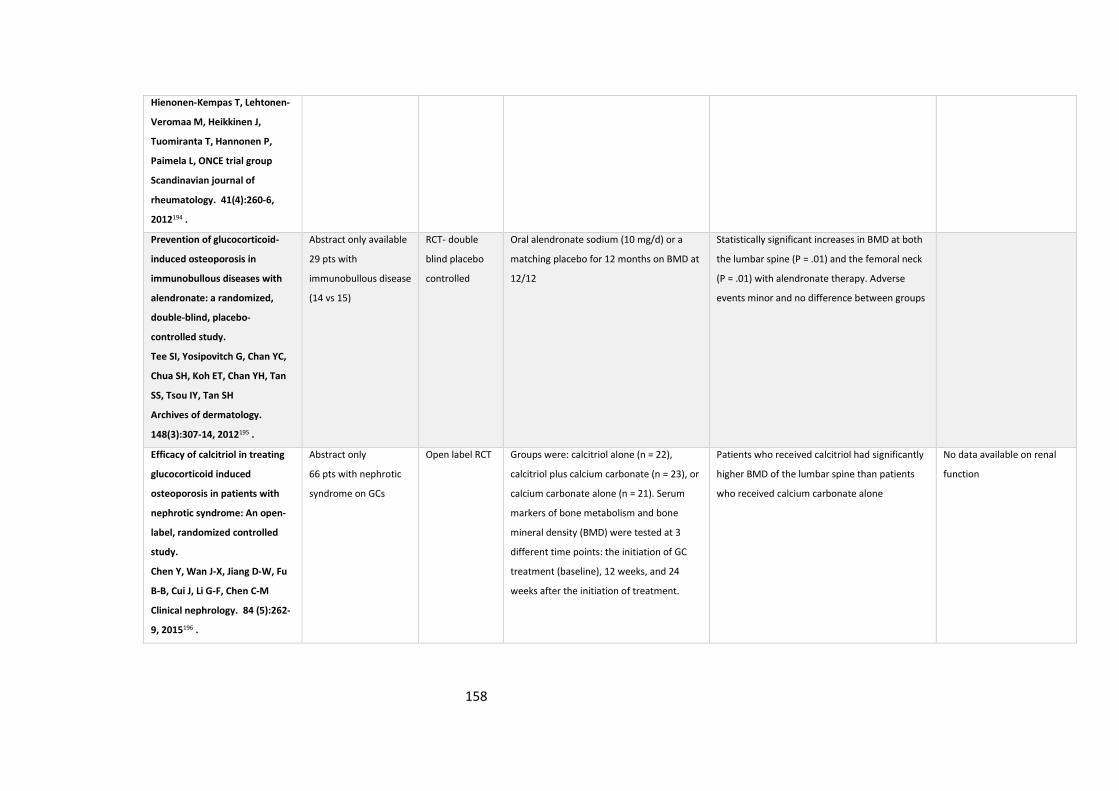
158
Hienonen-Kempas T, Lehtonen-
Veromaa M, Heikkinen J,
Tuomiranta T, Hannonen P,
Paimela L, ONCE trial group
Scandinavian journal of
rheumatology. 41(4):260-6,
2012194 .
Prevention of glucocorticoid-
induced osteoporosis in
immunobullous diseases with
alendronate: a randomized,
double-blind, placebo-
controlled study.
Tee SI, Yosipovitch G, Chan YC,
Chua SH, Koh ET, Chan YH, Tan
SS, Tsou IY, Tan SH
Archives of dermatology.
148(3):307-14, 2012195 .
Abstract only available
29 pts with
immunobullous disease
(14 vs 15)
RCT- double
blind placebo
controlled
Oral alendronate sodium (10 mg/d) or a
matching placebo for 12 months on BMD at
12/12
Statistically significant increases in BMD at both
the lumbar spine (P = .01) and the femoral neck
(P = .01) with alendronate therapy. Adverse
events minor and no difference between groups
Efficacy of calcitriol in treating
glucocorticoid induced
osteoporosis in patients with
nephrotic syndrome: An open-
label, randomized controlled
study.
Chen Y, Wan J-X, Jiang D-W, Fu
B-B, Cui J, Li G-F, Chen C-M
Clinical nephrology. 84 (5):262-
9, 2015196 .
Abstract only
66 pts with nephrotic
syndrome on GCs
Open label RCT Groups were: calcitriol alone (n = 22),
calcitriol plus calcium carbonate (n = 23), or
calcium carbonate alone (n = 21). Serum
markers of bone metabolism and bone
mineral density (BMD) were tested at 3
different time points: the initiation of GC
treatment (baseline), 12 weeks, and 24
weeks after the initiation of treatment.
Patients who received calcitriol had significantly
higher BMD of the lumbar spine than patients
who received calcium carbonate alone
No data available on renal
function

159
Author, Date and Title. Target Population. Study Design. Comparisons. Outcomes. Comments and quality of evidence
Cardiovascular disease due
to accelerated
atherosclerosis in systemic
vasculitides.
Best Practice & Research
Clinical Rheumatology 27
(2013) 33–44
Terveart197
Systemic vasculitis Review (not
systematic)with
focus on
mechanisms
HDL generally decreased in systemic
vasculitis but quantative measures not
predictive of atherosclerosis in these
conditions
Pro-inflammatory HDL is increased
during prednisolone therapy of >7.5
mg day, all cholesterol (HDL/LDL and
total) increased by steroids
RR of CHD in AAV is 2-4x that of
controls. Odds ratio of CVA 3-4
Impaired endothelial function,
abnormal ABPI and increased arterial
stiffness reported in AAV
Active disease seems to correlate
with increased atherosclerosis with
this returning to normal in disease
control
Recommends most pts with systemic
vasculitis should be treated with
statins. Treatable risk factors for
statin-induced myopathy should be
addressed (e.g., vitamin D deficiency
and hypothyroidism)
“Preventive therapy for accelerated
atherosclerosis in vasculitis includes
aggressive therapy of inflammation
and an aggressive approach against
classic risk factors for cardiovascular
disease such as smoking, lack of
physical activity, obesity and
unhealthy diet”
Accelerated atherosclerosis
in patients with Wegener's
granulomatosis.
K de Leeuw et al.
Ann Rheum Dis
2005;64:753–759159.
Case control study
29 GPA pts- consecutive,
in remission, 26 controls
(age and sex matched)
Common carotid
intimal medial
thickness (IMT)
assessed by USS
Plus sCRP and
traditional CV RF
Increased IMT was a sign of
accelerated development of
atherosclerosis in WG patients,
assessed during inactive disease,
compared with controls, not
accounted for by conventional risk
factors. Interestingly number of
exacerbations of disease negatively
Overall disease burden measured by
“cumulative BVAS” not VDI.
Limited number of patients and
controls meant that multi-variate
analysis could not be undertaken.
The clinical relevance of a raised IMT
was not explored
Cardiovascular risk evidence table

160
assoc with IMT in pt group. No diff in
cumulative pred dose between those
with and without raised IMT.
Increased Incidence of
Cardiovascular Events in
Patients With
Antineutrophil Cytoplasmic
Antibody – Associated
Vasculitides A Matched-Pair
Cohort Study. Morgan et al.
Arthritis and Rheumatism.
Vol. 60, No. 11, November
2009, pp 3493–3500115.
113 AAV pts matched to
CKD patients in single
centre
Retrospective
matched cohort
study
Matched to CKD controls- age at
diagnosis within 5 years, same sex,
smoking status as ever smoked or
never smoked, previous history of a
cardiovascular disease (prior to
diagnosis of CKD or AAV), and same
CKD stage (at time of presentation for
CKD patients and at 1 year for AAV
patients).
23 cardiovascular events in the AAV
group compared with 16 events in the
CKD group. HR 2.23
Preexisting history of cardiovascular
disease ever required dialysis, ever
having smoked, male sex, age, and
(lower)cholesterol at presentation
were significant risk factors for CVD in
AAV
Matching used to address majority
of confounders.
Increased morbidity from
ischemic heart disease in
patients with Wegener's
granulomatosis.
Arthritis and Rheumatism.
M Faurschou et al.Vol. 60,
No. 4, April 2009, pp 1187–
1192114 .
Cohort of 293 Danish
patients diagnosed as
having WG between
1973 and 1999
Retrospective
cohort study
WG patients were found to have a 3.6-
fold increased risk of acute MI
occurring
<5.0 years after the date of the WG
diagnosis
2.2-fold, significantly increased risk of
IHD-associated cardiovascular events
occurring >=10 years after the
diagnosis of WG. Significantly
Acknowledges lack of statistical
power in evaluating risk IHD in
women and the young with WG.
Data not available on cumulative
steroid dose and disease activity.

161
increased risks of IHD and acute MI
were found in elderly WG patients
(defined as patients>=50 years old at
the time of WG diagnosis), in male
patients, and in patients who received
a cumulative dose of>36 gm of CYC.
The risk of IHD from the fifth to the
ninth year of follow-up matched the
risk in the background population
Long-term patient survival
in ANCA-associated
vasculitis. Flossmann et al.
Ann Rheum Dis
2011;70:488–49498.
535 MPA/GPA from 4
EUVAS clinical trials
Retrospective
analysis of
combined RCT
outcomes.
After 1st year CVD primary cause of
death 25.7%
Study quality assessed elsewhere.
A model to predict
cardiovascular events in
patients with newly
diagnosed Wegener's
granulomatosis and
microscopic polyangiitis.
Suppiah et al. Arthritis Care
& Research Vol. 63, No. 4,
April 2011, pp 588–596116.
535 pts from combined
EUVAS clinical trials
Retrospective
analysis of
combined RCT data
to produce risk
prediction model.
CVD events in first 5 years of f/u
reviewed
Then prognostic tool created and
validated in WGET cohort
(events= non-fatal MI or CVA)
74(13.8%) of 535 patients had at least
1 CV event: 3.7 x higher than the
background population
independent risk factors established=
age> 72.4 years, absence of PR3 (MPO
positive) diastolic HTN >90
Note that diastolic HTN was defined
as being attributed to active
vasculitis (due to BVAS scoring) for
the purpose of the EUVAS studies,
but not for validation cohort.
Data not available to allow inclusion
of cholesterol or CV meds in model.
108 pts could not be included in the
development of the model due to
pre-existing CVD or missing values.
Mortality in Wegener's
granulomatosis: a bimodal
pattern. Luqmani et al.
255 pts from GPRD Retrospective
cohort study
Mortality rate, cause and pattern Identified increased risk of mortality,
highest in first year from diagnosis
then again 10-15 years from diagnosis.
Deaths at > 5 years, numbers too
small to draw any conclusions

162
Rheumatology 2011;50:697-
702198.
Major causes of death > 5years
malignancy, MI, renal and resp failure.
Translational Mini-Review
Series on Immunology of
Vascular Disease:
Accelerated atherosclerosis
in vasculitis. JC Terveart.
Clinical and Experimental
Immunology, 156: 377–385.
2009199.
Review of
association/
pathophysiology of
atherosclerosis in
vasculitis.
Not systematic r/v
no search strategy
Zaenker et al. reported that patients
with Wegener’s granulomatosis had a
higher frequency of cardiovascular
diseases compared with healthy
controls [odds ratio (OR) 6·7}In line
with these findings, patients with
ANCA-associated vasculitis more often
had stroke and/or myocardial
infarction (OR 3–4)
Conflicting reports in IMT studies
and vasodilatation studies reported.
Abnormal ABPI and arterial stiffness
reported- seems to correlate with
periods of active inflammation.
Increase in HTN DM and weight gain
all reported in AAV (likely in assoc
with GC exposure). Other RF;, CKD,
proteinuria and persistently raised
CRP.
Author suggests primary prevention
with aspirin, ACE/RB and statin.
Increased prevalence of
subclinical atherosclerosis in
patients with small-vessel
vasculitis. Chironi et al.
Heart 2007;93:96–99160.
50 consecutive pts with
PSV (mixed disease
group) recruited
between 2002-2005
matched with 2 controls
from database of 1881
pts referred to CV
preventative medicine
centre (age sex, hx of
CVD)
Case control study Pts underwent ultrasonography of
fem, carotid and aorta (abd)
looking for plaque/IMT
Traditional CV RF and inflamm
markers also measured in all pts
Following adjustment for high risk
status, plaques sig. more common in
the pts at aortic and combined 3 vessel
sties. The odds ratio of having three-
vessel plaques was 1.34 (95%
confidence interval (CI) 1.09 to 1.68)
by presence of vasculitis, 1.27 (95% CI
1.02 to 1.60) by presence of high-risk
status and 1.75 (95% CI 1.08 to 3.02)
by each increase of 1SD in CRP level.
No difference between carotid IMT
between cases and controls but diff
technique used in comparison with
other study.
Interestingly no increase in % “high
risk” pts in vasculitis group when
compared with controls suggesting
that mechanism may not be
corticosteroid mediated.
Confounders acknowledged.
However; heterogenous disease gp,
under powered and outcome
dichotomous (plaque or no- plaque)
Clinical outcomes of ANCA-
associated vasculitis in
93 consecutive AAV pts
between1998 and 2012
Retrospective single
centre cohort study.
Those over 65years compared with
those less than 65yrs
Treatment comparable across whole
cohort
Event numbers, particularly in the
younger group were low. Study
163
elderly patients. A Haris et
al.
Int Urol Nephrol (2014)
46:1595–1600200.
primary end points were all cause
mortality, mortality due to
cardiovascular disease, active vasculitis
or infections. HTN and DM more
prevalent in elderly. Main cause of
death in the elderly was CVD- this
likely due to increased prevalence of
CVD at baseline
aimed to report efficacy of a reduced
immunosuppression strategy in the
elderly not CV event rates.
Cardiac involvement in
systemic inflammatory
diseases. DC Knockaert
European Heart Journal
(2007) 28, 1797–1804201.
Systematic review
MEDLINE database
was searched for
the period January
1, 1990 through
September 2005,
using PubMed for
articles containing
‘cardiac’,
‘cardiovascular’,
‘heart disease’, and
the SIDs discussed
in this review
Search terms not fully
comprehensive and no MESH terms
used. Encompassed many SIDs so
only the data for those of interest
examined.
Predominantly reports on cardiac
involvement due to active disease
rather than CVD risk as a composite
outcome, therefore data not
included.
Risks of treatments and
long-term outcomes of
systemic ANCA-associated
vasculitis. O Flossman.
Presse Medicale. 44(6 Pt
2):e251-7, 2015202.
Informal review of
lit (conference
paper)
Studies reported are covered
elsewhere.
Factors associated with
major cardiovascular events
in patients with systemic
Forty-two patients (27
males, age 54 ± 15 yrs)
were included. SNV
Retrospective single
centre cohort
review
To identify factors predictive
of major CV events (MCVE) in
patients with SNV by analysing the
After a mean follow-up of 7.1 ± 2.6
years, 8 patients (19%) with SNV had
MCVE: 4 had myocardial infarction or
“this longitudinal follow-up indicated
that patients with SNV had 2-fold to
3-fold accelerated atherosclerosis”

164
necrotizing vasculitides:
results of a longterm
followup study.
B Terrier et al. Journal of
Rheumatology. 41(4):723-9,
2014203.
diagnoses were GPA in
20 patients, EGPA in 9,
MPA in 8, and PAN in 5.
long-term follow-up for CV risk and
subclinical atherosclerosis.
hospitalization for unstable angina, 2
underwent arterial revascularization, 1
had a stroke, and 1 died of CV causes.
Respective 5-year and 10-year MCVE
rates of 9.5% and 26.8% markedly
exceeded the expected 10-year
Framingham CV risk score (9%). PR3
neg more likely to have CVD but not
stat sig. plaque detection in abdo aorta
and CIMT was assoc with MCVE as was
being “high risk” or BMI >30
Note HTN defined in addition as “use
of antihypertensive drugs”.
Acknowledges heterogeneous group,
small numbers and lack of controls
as limitations (uses Framingham risk
scores for “expected data”)
The interface of
inflammation and
subclinical atherosclerosis in
granulomatosis with
polyangiitis (Wegener's): a
preliminary study. Hajj-Ali,
Rula A. et al. Translational
Research: The Journal Of
Laboratory & Clinical
Medicine.166(4):366-74,
2015204
N=46 GPA pts (38 in
remission, 8 with active
disease)
Case control study
(28 healthy
controls)
Classic atherosclerotic risk factors,
platelet aggregation responses, and
circulating micro- particle (MP)
levels were recorded. All patients
underwent carotid artery intima-
media thickness (IMT)
measurement as outcome for
subclinical atherosclerosis
Number of disease relapses, diastolic
blood pressure, and age at disease
onset independently correlated with
IMT in patients with GPA
Authors comment that the
correlation with disease relapses and
subclinical atherosclerosis could be
because of glucocorticoid use and
not the inflammatory process in
GPA, giving the inherent bias that
exists with the use of glucocorticoid
with each relapse.
Damage in the ANCA-
associated vasculitides:
long-term data from the
European vasculitis study
group (EUVAS) therapeutic
trials. Robson J et al.
Annals of the Rheumatic
Diseases. 74(1):177-84,
735 AAV pts enrolled in
EUVAS clinical trials
Review of combined
LTFU (up to 7 years)
data from 6
combined EUVAS
RCTs
Comparison of damage at baseline
compared with at f/u
+ 36.7% increase in HTN from baseline.
+ 4.1% in MI, + 7.4% angina/CABG, +
3.7% CVA

165
2015205.
Atherosclerotic factors in
PR3 pulmonary vasculitis.
Zycinska, K et al. Advances
in Experimental Medicine &
Biology. 755:283-6, 2013206.
21 GPA pts Cross-sectional case
control study
Comparison of the prevalence of
traditional CV RFs between pts and
controls
Prevalence of traditional risk factors
differed significantly between the WG
patients and control subject. Patients
had higher blood pressure and body
mass index, and had a family history of
cardiovascular disease. Total
cholesterol, LDL, and TG
concentrations were all higher and
HDL was lower in the WG group
No CV outcome data provided.
Simply cross- sectional.
Risk of subsequent coronary
heart disease in patients
hospitalized for immune-
mediated diseases: a
nationwide follow-up study
from Sweden. Zöller, B et al.
PLoS ONE. 7(3):e33442,
2012207.
333 GPA pts 40 PAN Retrospective
cohort study
CHD All individuals in Sweden
hospitalized with a main diagnosis
of an IMD (n = 336,479) without
previous or coexisting, between
January 1, 1964 and December 31
2008, were followed for first
hospitalization for CHD
SIR CHD in 1st year after hospitalisation
polyarteritis nodosa 3.81 (95% CI 2.72-
5.19), GPA 2.21(1.98-2.46)
Association of cigarette
smoking with organ damage
in primary systemic
vasculitis. Mohammad, A J
Segelmark, M
Scandinavian Journal of
Rheumatology. 40(1):51-6,
2011208.
86 PSV pts (46 WG, 27
MPA, four CSS, and nine
PAN)- 77 included in
analysis
Retrospective case
control study
median f/u 10
(smoker)/9.5 (non-
smoker) yrs
Comparison of damage accrual as
per VDI in AAV pts who had been
ever vs never smokers
MI- 15% of smokers/ex- smokers 0%
of never smokers
Outcomes reported for whole group
but likely to be different amongst
the disease subgroups.
Patients with Wegener's
granulomatosis: a long-term
follow-up study. De Leeuw,
K. Clinical & Experimental
23 GPA pts Prospective case
control study
Comparison IMT in pts vs controls
at 2 time points
IMT increased at both entry and f/u
but no evidence of accelerated
progression compared with controls.
Equally no evidence of increased rate
Outcomes may be explained by low
disease activity in pt group and good
control of traditional CV risk factors.
No adjustment of confounders such

166
Rheumatology. 28(1 Suppl
57):18-23, 2010209.
of progression in those with relapses
vs none.
as smoking possible due to small
numbers
Ankle-brachial pressure
index: a simple tool for
assessing cardiovascular risk
in patients with systemic
vasculitis.
Sangle, SR et al.
Rheumatology. 47(7):1058-
60, 2008161.
54 consecutive vasculitis
pts
Case control study Measurement of ABPI compared
with healthy controls
Hypertension, family history of CV
events, the elevated BMI (>25) were
significantly more common in
vasculitis patients.
The ABPI was abnormal in 11/54
(20.4%) of the SV patients and 2/49
(4%) of the control group
ABPI has been used in other
populations to predict CV outcomes
Too heterogenous a disease
population to draw any meaningful
conclusions
Atherosclerosis in ANCA-
associated vasculitides.
Pagnoux C et al.
Annals of the New York
Academy of Sciences.
1107:11-21, 2007210.
Review Zaenker and coworkers reported
(compared to healthy
controls/patients with fibromyalgia or
OA), 50 GPA patients had higher
frequency of CVD (coronary artery
disease, stroke, peripheral arterial
occlusive disease), OR 6.7 (95% CI:
1.6–31.8), and wider
ultrasonographically measured intima–
media thicknesses of common carotid
arteries and carotid bulb(previously
proven to be predictive of
cardiovascular events in other
populations).
50 patients with systemic necrotizing
vasculitides, compared to 100 sex- and
age-matched “healthy” controls.
Found no significantly different carotid
intima–media thicknesses for patients

167
and controls (0.60 vs. 0.59mm,
respectively), but patients had a higher
frequency of ultrasonographically
detected plaques in, aorta, and/or
femoral arteries, independently of
other cardiovascular risk factors
Cardiovascular events were also more
frequent, but not always significantly,
2 studies by the group on patients with
AAV reported incidence of coronary
artery disease higher (587/105
patients) in their first study on 265
patients compared to local “healthy”
subjects (133/105 inhabitants), but
was not strikingly different from that
of individuals included in the MONICA
cohort study (554/105 subjects). In
second study on 116 patients, the
odds ratio of MI was 4.0 (95% CI: 0.5–
14), stroke incidence was 414/105 for
the patients versus 130/105 for the
local “healthy” controls. Booth and
colleagues demonstrated aorta and
systemic arteries were significantly
stiffer in patients with active AAV than
controls
Accelerated atherogenesis
in autoimmune rheumatic
diseases. Bacon, Stevens,
Carruthers, Young, & Kitas.
Includes PSV plus RA and
SLE
review Reports endothelial cell dysfunction in
PSV, this has been widely reported in
other populations to be a marker of
CAD
Not systematic so not formally
appraised

168
Autoimmunity Reviews.
1(6):338-47, 2002211
Enhanced endothelium-
dependent microvascular
responses in patients with
Wegener's granulomatosis.
Neinhuis et al.
Journal of Rheumatology.
34(9):1875-81, 2007212.
28 WG patients with
inactive disease and 28
age and sex matched
controls
Case control study IMT measurement WG patients had increased IMT
compared to controls. IMT correlated
positively with age and BMI.
Abstract only available
Inflammation and arterial
stiffness in systemic
vasculitis: a model of
vascular inflammation.
Booth AD, Wallace S,
McEniery CM, Yasmin,
Brown J, Jayne DR, et al.
Arthritis and Rheumatism
2004;50:581-8213
Thirty-one patients with
AASV (15 with
active disease) and 32
age-matched controls
Case control study Pulse wave velocity (PWV) and the
augmentation index (AIx)
No sig difference in PWV and AIx
between pts in remission and controls.
AIx was sig different between patients
with active disease and in remission
Authors conclude that arterial
stiffness in AAV may be “modifiable”
as correlates with inflammation as
opposed to disease.
Small numbers, controls matched on
age only but no sig difference across
groups reported.

169
Author, Date and Title. Target Population. Study Design. Comparisons. Outcomes. Comments and quality of evidence
Best Practice & Research
Clinical Rheumatology 27
(2013) 57–67. Thrombosis in
vasculitis, Gaffo214.
AAV pts Review of the
literature. Not
systematic- no
search strategy
detailed. Reviews 4
studies in AAV- see
comments
7 VTEs over 100 pt/yrs in WGET
trial sparked interest- VTEs
usually occurring during
episodes of active disease.
Weidner 2006, 4.3
episodes/100pt yrs. 81% during
active episodes. Stassen-
1.8/100ptyrs increasing to
6.7/100/pt years if only periods
of active disease included.
French study 1.58 increasing to
7.26 for active disease. Risk
factors: older age at diagnosis,
male sex, history of prior VTE
and history of stroke with
motor deficiency
Bham CV events HR 2.23 when
c/ CKD matched controls- CVD
papers reviewed elsewhere
Multiple references obtained .
Not a systematic review so not formally
appraised
Venous thromboembolism
with concurrent pulmonary
haemorrhage in systemic
vasculitis
E de Sousa et al. Nephrol
Dial Transplant (2012) 27:
Retrospective cohort
study. (sequential pts
with PH referred to a
single unit)35 pts with
PH. 7/35 (20%) had VTE.
(AAV in 4/7)
Majority of concurrent PH and
VTEs were in initial
presentations responding to
PLEX. No worsening of PH
occurred in 5/6 with anti-coag
but precipitated PH in the 6th.
Small descriptive study highlighting a clinical
conundrum
Thromboembolic risk evidence table

170
4357–4361215. Anti-plasminogen antibodies
may explain this increased risk.
Conventional
immunomodulation and anti-
coag effective in all but 1
High frequency of venous
thromboembolic events in
Churg-Strauss syndrome,
Wegener's granulomatosis
and microscopic polyangiitis
but not polyarteritis
nodosa: a systematic
retrospective study on 1130
patients. Y Allenbach et al.
Ann Rheum Dis
2009;68:564–567155.
1130 pts EGPA,GPA,PAN
and MPA enrolled in
FVSG between 1989 and
2006
Retrospective
cohort study. VTE
included if in 6/12
prior to or following
diag. Events and
characteristics of
study group clearly
defined.
Characteristics of non VTE gp vs
VTE gp using multi and univariate
analyses.
83 VTEs in 74 pts (6.5% of all
pts).Fifty-seven (68.7%) of the
VTE occurred within 3 months
before the SNV diagnosis or 6
months after (n=42), or a
relapse (n=15). Rate of 7.26 per
100 person-years for AAV
during this period (1.84
throughout all f/up). At first
VTE diagnosis, mean BVAS was
12.6 (10.5) and mean CRP was
67.0 (80.9) mg/l. Older age at
SNV diagnosis (p=0.002), male
sex (p=0.04), previous VTE
(p=0.02), nephrotic range
proteinuria >3 g/24 h (p=0.03)
and/or stroke with motor
deficit (p=0.03) were
significantly associated with
VTE.
Reports increased risk of VTE in AAV, assoc.
with periods of disease activity and risk
factors identified through multi-variate
analysis.
Eosinophilia and
thrombophilia in Churg
Strauss syndrome: a clinical
and pathogenetic overview.
Ames, P. R. J.
Reviewed all literature
1951 to 2010 reported
thrombotic episodes in
EGPA
Systematic review.
Pubmed, Embase
and google search.
Search strategy
clearly defined. Case
18 case series,
24 pt case reports. However,
primary aim of all bar one series
was to report clinical
manifestations of disease therefore
Reported prevalence of 3.1-
30% arterial or venous TE in
EGPA.
Arterial 3.1-18.7, venous 5.8-
30%
Fairly robust review of all VTEs reported in
associated with EGPA. Suggestion that VTEs
may be more prevalent in ANCA negative
disease with tissue infiltration by eosinophils.
Highlight that VTEs likely underreported

171
Margaglione, M.
Mackie, S.
Delgado Alves, J.
Clinical and Applied
Thrombosis/Hemostasis
16(6) 628-636. 2010157
reports and series
reviewed.
likely underestimating prevalence before possible association with AAV became
known
Brief communication: high
incidence of venous
thrombotic events among
patients with Wegener
granulomatosis: the
Wegener’s Clinical
Occurrence of Thrombosis
(WeCLOT) Study. Merkel PA,
Lo GH, Holbrook JT Ann
Intern Med. 2005;142:620–
6154.
180 pts enrolled in the
WGET trial
RCT (subgroup
analysis- cohort
study)
29 of 180 patients (16%) with
WG had had a VTE at some
point. The 16 new VTEs in 167
patients with no history VTE
occurred over 228 person-years
(incidence rate 7.0 per 100
person-years).
Median time fromm active
disease to VTE was 2.07
months.
For 13 of 16 patients (81%) who
had VTEs during WGET, AAV
was active at the time of the
event or within 2 months
before the event.
Otherwise age was only risk
factor for VTE.
Comparison with baseline in
population- healthy same age
Swedes incidence rate of first
VTE of 0.31 per 100 person-
years.
Lupus VTE incidence rate of 1.0
per 100 person-years
However, rate of VTEs in comparison
populations were defined and identified
differently so not truly comparable.

172
Previous VTE: incidence rate of
recurrent VTE of 7.20 per 100
person-years
Thromboembolic events as
a complication of
antineutrophil cytoplasmic
antibody- associated
vasculitis. Weidner S,
Hafezi-Rachti S, Rupprecht
HD. Arthritis Rheum.
2006;55:146–9156.
Review of records of 105
incident pts with SVV in
a single centre 1986-
2001.
All pts had renal
involvement.
Retrospective
cohort review
13 VTEs in 105 pts in active
phase of disease (3 Pes when
pts in remission).
In summary, during
retrospective follow-up of 105
patients, 16 VTEs occurred over
367.5 person-years of
observation, corresponding to
an incidence rate of 4.3 per 100
person- years (95% confidence
interval 1.6–10.2).
Patients observed to be
predominantly PR3 positive
No data available on those pts who did not
develop VTEs making derivation of
associations impossible.
Small numbers and essentially a descriptive
case series
Venous thromboembolism
in ANCA-associated
vasculitis—incidence and
risk factors. Stassen et al.
Rheumatology 2008;47:530–
534112.
198 AAV pts diagnosed
1990-2005
Retrospective
cohort study plus
patient
questionnaire
VTEs counted if 3/12 prior to or
after diagnosis.
52% VTEs occurred in 3/12
prior- 3/12 post diagnosis (total
no VTEs= 23)
The incidence of VTE during
Those with GPA/PR3 were less likely to have
VTEs in this study.
Some acknowledgement of limitations
through retrospective study design and an
attempt to address this through pt
questionnaire though no comment on the

173
active disease was 6.7/100
person-years compared with
1.0/100 person-years inactive.
Overall found an increased
incidence of VTE just prior to
and after the diagnosis of AAV
of 1.8/100 person-years,
compared with 0.3 in a healthy
population of the same age
fallibility of pt recollection.
Consensus task force
recommendations for
evaluation and
management of eosinophilic
granulomatosis with
polyangiitis syndrome.
(Churg-Strauss). Groh et al.
Europ J Int Med. 28 (4) (pp
321-326), 2015216
Venous thromboembolic
events (VTE) and pulmonary
embolism
should be treated according to
general guidelines for the
management
of thromboembolic disease; it
is unknown whether
anticoagulation should be
prolonged in selected patients
with persistent
or recurring disease activity
Do neutrophil extracellular
traps contribute to the
heightened risk of
thrombosis in inflammatory
diseases? Rao et al.
World Journal of Cardiology.
7 (12) (pp 829-842), 2015217
Mechanistic review New ref. NETs may contribute
to thrombosis is AAV and other
diseases
A meta-analysis of the risk
of venous
Meta-analysis up to
June 2014
4 studies of AAV(N =16,295)
resulted in VTE cumulative
No new refs
Search limited to full text English language

174
thromboembolism in
inflammatory rheumatic
diseases. Lee JJ, Pope
JE.Arthritis Res Ther.
2014;16:435218
MEDLINE,
Embase, PubMed
and the Cochrane
databases
incidence of 7.97% (95% CI:
5.67% to 10.28%). (compared
with 7.29% for SLE)
papers.
Descriptive statistics only on AAV pts- not
included in meta-analysis
Thrombosis in vasculitis:
From pathogenesis to
treatment. Emmi et al.
Thrombosis Journal. 13 (1),
2015. Article Number: 15158
NETs are able to promote
thrombosis by inhibiting the TF
pathway inhibitor and by
recruiting platelets Engelmann
B, Massberg S. Thrombosis as
an intravascular effector of
innate immunity. Nat Rev
Immunol. 2013;13:34–45.
Thrombosis in vasculitic
disorders-clinical
manifestations,
pathogenesis and
management. Katz, Brenner
& Horowitz.
Thrombosis Research.
136(3):504-12, 2015219
1 new ref
High risk of pulmonary
embolism and deep venous
thrombosis but not of
stroke in granulomatosis
with polyangiitis
(Wegener's). Faurschou,
Obel, & Baslund. Arthritis
care & research.
66(12):1910-4, 2014220.
180 prevalent Danish
GPA pts 1993-2011
Case control study Controls 19:1 age and sex matched The occurrence of VTEs was
substantially increased in GPA
patients during first 2 years of
followup, with IRR estimates
for PE and DVT of 25.7 and
20.2, respectively. No increase
in CVA compared with controls

175
Risk of pulmonary embolism
in patients with
autoimmune disorders: a
nationwide follow-up study
from Sweden. Zöller, Li,
Sundquist, & Sundquist.
Lancet. 379(9812):244-9,
2012221.
Pts without VTE at
inception and
autoimmune disease
15085 GPA
Retrospective case
control study
Incidence PE in autoimmune
disorders compared with reference
group (remainder of population)
SIR for hospital admission for
PE in GPA 6.57 in 1st year
Clinical and laboratory
characteristics of 19
patients with Churg-Strauss
syndrome from a single
South Australian centre.
Whyte AF, Smith WB, Sinkar
SN, Kette FE, Hissaria P.
Intern Med J. 2013;43:784–
90222
EGPA case series Single centre case
series
Thrombosis was a feature at
diagnosis in six patients
(31.6%): two patients had PE,
one had
thrombosis of subclavian,
internal jugular and external
jugular veins, one had internal
capsule ischaemic
stroke, one had internal jugular
and lower limb deep vein
thrombosis (DVT) and one had
lower limb DVT only.
Two had recurrence of DVT
with relapse of vasculitis. One
patient had a past history
of DVT.

176
Article Study population Study Design Comparisons Outcomes Comments
Rituximab versus
Azathioprine for
maintenance in ANCA-
associated vasculitis.
Guillevin et al. NEJM
2014;371(19):1771-178086.
115 patients with newly
diagnosed or relapsing AAV in
complete remission after
combined treatment with GC
and pulse CYC
Open label randomized
controlled trial
1:1 randomisation to
maintenance treatment with
Rtx (every 6 months until
month 18) or AZA (daily oral
until month 22). Follow up
until month 28.
2 patients developed a
malignancy in the AZA group
and 1 patient in the Rtx
treated group
Small number of malignancies
and short duration of follow
up preclude adequate
conclusions to be drawn in
terms of risk of malignancy
associated with AZA versus
Rtx in AAV.
Survival of patients with
ANCA-associated vasculitis
on chronic dialysis: data from
the French REIN registry from
2002 to Romeu et al.
2011.QJM 2014;107(7):545-
55223.
425 patients with MPA or
GPA that commenced chronic
dialysis between 2002 and
2011 – single centre.
Prospective observational
data collection
Matched non-AAV dialysis
group of 794 patients
Higher percentage of deaths
from malignancy in control
group compared to AAV
group (15% vs. 4%, p=0.001)
Cancer under-represented in
AAV group potentially due to
short follow up (median 23
months). No information
provided on type / duration
of immunosuppressive
therapy received.
Caveolin-1 single nucleotide
polymorphism in
antineutrophil cytoplasmic
antibody associated
vasculitis. Chand et al. PLOS
One 2013;8(7):e69022224.
187 patients with AAV from
single centre in the UK
(Birmingham)
Association of a single
nucleotide polymorphism of
caveolin-1 with outcome in
AAV. Retrospective analysis
Validation of results sought
from 589 AAV patients from 2
European cohorts
Presence of a CC genotype is
associated with reduced
incidence of cancer in the
Birmingham cohort (HR 5.55,
p=0.007). This was not
replicated in the validation
cohort.
Over a median follow-up
period of 9.2 years the
incidence of cancer in the
Birmingham cohort was
11.8% and over a median
follow-up period of 7.4 years
2.9% in the European cohort
(NMSC excluded).
Caveolin-1 has been
associated with prognosis in
several cancers. However,
further research is necessary
Cancer evidence table

177
before these results can be of
clinical relevance in AAV.
Paraneoplastic
rheumatologic syndromes.
Azar et al. Curr Opin
Rheumatol 2013;25(1):44-
9225.
Review. Review of rheumatic
syndromes that can be a
paraneoplastic manifestation
of an underlying malignancy.
The association between
cancer and vasculitis is
uncommon and difficult to
establish. Overall,
paraneoplastic vasculitides
are estimated to represent
about 2-5% of all vasculitides.
However, descriptions of AAV
as paraneoplastic
manifestations are even more
exceedingly rare.
ANCA-associated vasculitis
and malignancy: current
evidence for cause and
consequence relationships.
Mahr et al. Best Pract Res
Clin Rheumatol
2013;27(1):45-56162.
Review Review of the relationship of
AAV with malignancy
specifically looking at de novo
overall and specific cancer
incidence, role of specific
immunosuppressive agents in
cancer development and
cancer as a trigger or cause of
AAV
Overall cancer incidence
SIR ranges from 1.6 to 3.8.
Cancer SMR estimated at 2.2.
Most data from GPA rather
than MPA. Cancer incidence
may have decreased over
time due to use of CYC
sparing regimes.
Specific cancer-type
incidences
Urinary – long latency (6.9 -
18.5 years) after 1st CYC
exposure. Early studies show
SIR of 31-33 whilst recent
studies show SIR of 3.6 – 7.2
potentially reflecting lower
Recommendations made by
authors: Systematically co-
prescribe mesna and
hyperhydration with IV CYC.
Consider mesna with
prolonged oral CYC (> 4-6
months). Patients exposed to
CYC should have 6-12
monthly urine cytology; non-
glomerular haematuria
should be investigated. CYC
contraindicated in patients
with CYC induced
haemorrhagic cystitis and
those patients should have
routine cystoscopy once or
twice yearly.

178
CYC doses and potentially
also reflecting the use of
mesna.
Leukaemia – dose dependent
complication of CYC.
NMSC – SIR 2.8 – 10.4.
Lymphoma – equivocal
results.
Cancer as trigger of vasculitis
Inadequate evidence to
suggest this – but numbers is
studies very small.
NMSC – avoid sun exposure,
use sun blockers. Annual skin
examination advocated.
Adherence to regular cervical
screening.
Encouragement to quit
smoking.
In GPA with atypical disease
or inadequate response to
therapy, investigations for
cancer should be considered
on a case-to-case basis.
Cancer incidence in
pulmonary vasculitis.
Zycinska et al. Adv Exp Med
Biol 2013;788:349-53226.
[Full text not available
therefore limited
information]
117 patients with biopsy
proven pulmonary vasculitis
treated with CYC between
1990 and 2008 in Warsaw,
Poland.
Observational SIRs were calculated based on
general population incidence
of the cancers examined.
During the observation period
15 cancers occurred. A
significantly increased SIR was
observed for NMSC (SIR 5.2;
CI 2.3- 8.7), AML (SIR 4.3; 2.1
– 11.2) and bladder cancer
(SIR 3.4; 1.6 – 5.2).
Full text not available
therefore limited information
however this study suggests
an increased risk of NMSC,
AML and bladder cancer
following CYC treatment in
patients with pulmonary
vasculitis.
Long-term outcome of
antineutrophil cytoplasmic
antibody-associated small
vessel vasculitis after renal
transplantation. Marco et al.
Clin Transplant
2013;27(3):338-47227.
51 patients with AAV that
received a kidney transplant
between 1984 and 2007
(pooled data from 6 units in
Barcelona).
Retrospective observational
study.
Matched control group
(kidney transplant recipients),
n=49.
Probability of developing a
malignancy was similar in
both groups (10% in AAV vs.
12.8% in control group at 5-
year follow up; p=0.65)
Data suggests no excess risk
of cancer incidence in AAV
following transplantation
compared to a matched
cohort. However, the
relatively young age of
patients (median 52.9) and
medium duration of follow up
(median 5.2 years) has to be

179
taken into account.
TNF-alpha blocker therapy
and solid malignancy risk in
ANCA associated vasculitis.
Silva F et al. Curr Rheumatol
Rep 2012;14(6):501-508.
Review Review of the risk of solid
malignancies with TNF-alpha
blocker therapies in AAV
The authors discuss the short
and long-term follow up of
the WGET trial.
They suggest that etanercept
should be avoided in patients
with AAV, particularly in cases
with long-standing relapse
history, CYC exposure and
previous history of
malignancy.
Myelodysplasia and
malignancy-associated
vasculitis Agha et al. Curr
Rheumatol Rep
2012;14(6):526-31228.
Review The authors review available
evidence suggesting a link
between malignancy and
vasculitis as a secondary
phenomenon. They suggest
that myelodysplasia is more
commonly associated with
vasculitis than are solid
tumours. However in both
cases the most common
manifestation is
leukocytoclastic vasculitis.
There remains uncertainty
about the nature of the
association between vasculitis
and malignancy.
They suggest that in atypical
cases of AAV that do not
respond to standard
treatment, clinical suspicion
for an underlying malignancy
should be high.
Complications of long-term
therapy for ANCA-associated
systemic vasculitis. Wall &
Harper Nat Rev Nephrol
2012;8(9):523-32229.
Review Cytotoxic therapy increases
malignancy risk by greater
than two-fold compared to
the background incidence.
Increased risk varies
The authors make the
following recommendations:
Routine surveillance for non-
glomerular haematuria
(urinalysis every 3-6 months),

180
according to organ affected:
4.8-33-fold increase in
bladder cancer, 10-fold
increase in NMSC, and 4.2-11-
fold increase in lymphoma.
Additionally there are reports
of a predisposition to
malignancy inherent of AAV
itself although this is
controversial.
Recent publications are
contradictory about the risk
of malignancy using current
CYC regimes: at 5 years follow
up, risk was increased only for
NMSC for patients enrolled in
4 EUVAS trials that employed
lower CYC cumulative doses
than previously; however a
French study suggested still a
5-fold increase in urinary tract
cancer compared to the
background population
although oral administration
and cumulative dose were
important predictors of risk in
that study.
which should be continued
indefinitely in patients that
have ever received CYC.
Urine microscopy, culture and
cytology should be performed
if haematuria is detected and
clinicians should have a low
threshold for urology referral
and cystoscopy.
Mesna and adequate
hydration should employed.
AAV patients should receive
education about increased
NMSC risk, reduce exposure
to UV light and use sunscreen
– low threshold for
dermatology referral for
suspected skin lesions.
Patients should be
encouraged to participate in
age and gender appropriate
national cancer screening
programs as, for example,
cervical neoplasia has been
shown to be increased with
immunosuppression.
Pulse versus daily oral
cyclophosphamide for
induction of remission in
Long-term follow up of the
CYCLOPS study. Median
duration of follow up 4.3
Long-term follow up of
randomized controlled non-
blinded clinical trial
Pulse CYC versus daily CYC
No difference in the incidence
of malignancy between the 2
groups.
Relatively short follow up.

181
ANCA-associated vasculitis:
long-term follow up. Harper
et al. Ann Rheum Dis
2012;71(6):955-6075.
years.
[Identified from the
references from paper 10]
Long-term patient survival in
ANCA-associated vasculitis.
Flossmann et al. Ann Rheum
Dis 2011;70(3):488-9498.
535 patients who had been
recruited at the time of
diagnosis to four randomized
controlled trials between
1995 and 2002.
Prospectively collected
baseline data. Outcome data
were collected via
questionnaires sent to
participating doctors.
After the 1st year of diagnosis,
malignancy was the second
most common cause of death
accounting for 22% of deaths
in this cohort.
Out of 16 malignancies
recorded, 12 were solid organ
cancers and 4 haematological
malignancies.
Unfortunately this study does
not contain detail in relation
to treatment characteristics
or SIRs, which would have
been useful given the
relatively recent nature of the
clinical trials involved.
[Identified from the
references from paper 10]
Improved outcome in 445
patients with Wegener’s
granulomatosis in a German
vasculitis center over four
decades. Holle et al.
Arthritis Rheum
2011;63(1):257-6664.
167 patients diagnosed with
GPA between 1999 and 2002
were compared to 123
patients diagnosed between
1994 and 1998. The two
cohorts were compared to a
historical cohort diagnosed
between 1966 and 1993.
Retrospective analysis. Incidence of malignancies and
mortality related malignancy
was examined and compared
to cancer incidence and
cancer mortality in the
general population.
18 malignancies were
documented in 445 patients
overall. In the 3 cohorts
together, there was neither
an increased SIR nor SMR
compared to the general
population.
Incidence of malignancy in
this study was much lower
than previously reported.
The authors suggest that this
might have been due to
universal administration of
mesna irrespective of route of
CYC administration (i.e. oral
and pulse).
Interestingly there was a
reduction of total CYC dose
moving from the oldest to the
newest cohort (median CYC
dose 67 vs. 36 vs. 24g),
however this was not
associated with any
differences in the incidence of

182
malignancy or CYC induced
cystitis amongst the 3 cohorts
(p=0.233 and 0.228
respectively).
Incidence of malignancy in
patients treated for
antineutrophil cytoplasm
antibody-associated
vasculitis: follow-up data
from European Vasculitis
Study Group clinical trials.
Heijl et al. Ann Rheum Dis
2011; 70(8):1415-21230.
535 with newly diagnosed
AAV from 15 countries
enrolled between 1995 and
2002 in 4 European clinical
trials
Observational prospective
collection of additional data
between 2004 and 2007.
SIRs for different types of
cancer were calculated.
SIRs (95% CI) were 1.58 (1.17
to 2.08) for cancers at all
sites, 1.30 (0.90 to 1.80) for
cancers at all sites excluding
NMSC, 2.41 (0.66 to 6.17) for
bladder cancer, 3.23 (0.39 to
11.65) for leukaemia, 1.11
(0.03 to 6.19) for lymphoma
and 2.78 (1.56 to 4.59) for
NMSC – importantly, the only
significantly increased SIR was
found to be that for NMSC.
Cancer rates for AAV patients
treated with conventional
immunosuppressive therapy
exceeded those expected for
the general population. This
cancer excess was largely
driven by an increased
incidence of NMSC. The
smaller cancer risk magnitude
in this cohort, compared with
previous studies, might
reflect less extensive use of
CYC in current treatment
protocols.
[Identified from the
references from paper 10]
Incidence and predictors of
urotoxic adverse events in
cyclophosphamide-treated
patients with systemic
necrotizing vasculitides.
Arthritis Rheum Le Guenno
et al. 2011;63(5):1435-45231.
805 CYC treated patients with
GPA, MPA, CSS or PAN with a
mean follow up period of 5.3
years.
Retrospective analysis. The observed incidence of
urinary tract cancer was
compared to the expected
incidence in the general
population by calculating
SIRs.
Amongst 27 patients there
were 22 episodes of
haemorrhagic cystitis and 7
episodes of urinary tract
cancer. The SIR for urinary
tract cancer was 5.00.
Cumulative CYC dose, ever
oral use of CYC as well as GPA
diagnosis were predictors of
haemorrhagic cystitis and / or
urinary tract cancer after
multivariate adjustment.
There was a wide range of
CYC cumulative dose of 0.72 –
463g (mean +/- SD, 25.1 +/-
38g).

183
Having ever smoked also
predicted the above
outcomes on univariate
analysis only.
Life expectancy, standardized
mortality ratios, and causes
of death in six rheumatic
diseases in Hong Kong, China
Mok et al. . Arthritis Rheum
2011;63(5):1182-9232.
Hospital registry analysis
(1999 – 2008) – 1636 patients
with systemic vasculitis
included.
Hospital registry analysis.
SMRs calculated.
SMRs calculated. SMR for systemic vasculitis
was 2.64. Loss of life
expectancy was 19.3 – 28.3
years.
Suggests a high incidence of
malignancy in systemic
vasculitis although this was
not standardized / compared
to the general population.
Mycophenolate mofetil vs
azathioprine for remission
maintenance in
antineutrophil cytoplasmic
antibody-associated
vasculitis. Hiemstra et al.
JAMA 2010;304(21):2381-897.
156 patients with AAV
assigned to AZA (n=80) or
MMF (n=76) and were
followed up for a median of
39 months.
Open label randomized
controlled clinical trial
AZA vs MMF for maintenance
of remission.
No difference between the
incidences of malignancy in
the 2 groups.
Limited by short follow-up
but would suggest no
difference in malignancy rates
when MMF is used in place of
AZA.
[Identified from the
references from paper 10]
EULAR recommendations for
the management of primary
small and medium vessel
vasculitis Mukhtyar et al.
Ann Rheum Dis
2009;68(3):310-1772.
Modified Delphi technique.
Expert panel group comprised
of rheumatologists,
nephrologists, immunologists
and general physicians.
In relation to CYC
administration the authors
suggested that pulse therapy
has been associated with a
higher likelihood of remission
and lower risk of side effects
but with a higher risk of
relapse compared to daily
oral CYC. They recommended
hydration and Mesna for
pulse CYC administration.
A recommendation was made
to investigate persistent
The level of evidence for the
recommendation to
investigate persistent
unexplained haematuria in
patients with prior CYC
exposure was 2B and the
grade of recommendation C.

184
unexplained haematuria in
patients with prior CYC
exposure. Specifically they
suggested periodic urine
analysis for the duration of
follow up and urgent
urological opinion in the
presence of non-glomerular
haematuria.
Cancer preceding Wegener’s
granulomatosis: a case
control study. Faurschou et
al. Rheumatology (Oxford)
2009;48(4):421-4233.
293 patients with GPA. 10
gender and age matched
controls were selected
randomly for each GPA
patient from the Danish
Central Population Registry.
Retrospective case control
study.
Occurrence of malignancies
before GPA diagnosis among
patients and before GPA
diagnosis of their matched
case among controls
(reference date) was
compared by calculation of
prevalence OR.
The OR for a prior cancer at
any site was not significantly
increased. A significantly
increased prevalence was
found for testis cancer on the
basis of 2 GPA patients
(cancer diagnosed 10.8 and
19.6 years prior to GPA
diagnosis). An increased
prevalence was also found for
malignancies listed as kidney
cancers. NMSC prevalence
within 2 years prior to GPA
diagnosis was increased
compared to the reference
group.
The authors conclude that
there is no clear evidence of
an increased prevalence of
preceding cancer in their GPA
cohort, suggesting that
shared risk factors for cancer
and GPA are of minor
importance for the excess of
malignancies that occur in
GPA patients after the
diagnosis of vasculitis.
They postulate that the
increased prevalence of
NMSC within 2 years of
diagnosis may represent a
state of acquired
immunological dysfunction
that predisposes to both
conditions.
Their data does not support
that patients with newly

185
diagnosed GPA should be
examined for the presence of
serious underlying
malignancy.
[Identified from the
references from paper 10]
Malignancies in Wegener’s
granulomatosis: incidence
and relation to
cyclophosphamide therapy in
a cohort of 293 patients.
Faurschou et al. J
Rheumatol 2008;35(1):100-
5234.
293 patients diagnosed with
GPA in a Danish hospital
between 1973 and 1999.
Retrospective analysis. Cancer incidence in the
cohort was assessed through
2003 by linkage to the Danish
Cancer Registry and
compared to that of the
general population by
calculation of SIR. Analyses
were stratified according to
low (<36g) or high (>36g)
cumulative CYC doses.
SIR of cancer overall was 2.1.
Significantly elevated SIR
were observed for AML (19.6
CI 4.0-57), bladder cancer (3.6
CI 1.2-8.3), and NMSC (4.7 CI
2.8-7.3).
Latency period for bladder
cancer and AML was 6.9 to
18.5 years after first CYC
exposure.
Risk of these malignancies
was not increased in patients
that had never received CYC
or had received < 36g
cumulative dose, with the
exception of NMSC.
In contrast, patients in the
>36g group had very high
rates of both bladder cancer
(SIR 9.5 CI 2.6-24) and AML
(SIR 59 CI 12-172).
Azathioprine or
methotrexate maintenance
for anca-associated
vasculitis. Pagnoux et al. N
Engl J Med
2008;359(26):2790-803235
126 patients with AAV were
assigned on a 1:1 basis to
receive either AZA or MTX for
maintenance of AAV and
were followed up for a mean
period of 29 months.
Open label randomized
controlled clinical trial
AZA vs MTX for maintenance
of remission
No difference between the
incidence of malignancy in
the 2 groups
Very low event rate for
malignancy (total of 3) and
short duration of follow up
precludes any firm
conclusions.
Vasculitides associated with
malignancies: analysis of
sixty patients Fain et al.
Arthritis Rheum
2007;57(8):1473-80236.
60 patients with a mean
follow up duration of 45.2
months. Vasculitides were
cutaneous leukocytoclastic
(45%), PAN (36.7%), GPA
(6.7%), MPA (5%) and HSP
(5%).
Retrospective analysis Vasculitides were diagnosed
concurrently with malignancy
in 38% of cases. Independent
of subtype patients with
vasculitides associated with
MDS more frequently, had
renal manifestations (p=0.02),
steroid dependence (p=0.04)
and achieved remission less
Not very helpful for this
process.

186
often (p=0.04) compared with
vasculitides associated with
other malignancies.
[Identified from the
references from paper 10]
Urinary bladder cancer in
Wegener’s granulomatosis;
risk and relation to
cyclophosphamide. Knight et
al. Ann Rheum Dis 2004;
63(10):1307-11163.
1065 patients with GPA were
identified from the
nationwide Swedish Inpatient
Register (1969 – 1995).
Cases of bladder cancer were
identified through linkage
with the Swedish Cancer
Register.
Each bladder cancer case was
then matched with 3 controls
from the same cohort in a
nested matched case control
study.
There were 11 confirmed
incident cases of bladder
cancer with a diagnosis of
GPA – 10 of those had been
treated with CYC.
20 of the 25 controls had
been exposed to CYC.
Median cumulative CYC dose
was 113g in cases as opposed
to 25g amongst controls.
Each 10g increment in CYC
dose was associated with a
doubling of bladder cancer
development. Cumulative
doses > 25g were associated
with a 5-fold risk.
8 of the 1065 patients had
developed bladder cancer
before the GPA diagnosis –
this amounted to a relative
risk of 2.1 (CI 0.6 – 3.6)
compared to the expected
prevalence of bladder cancer
in Sweden, suggesting a risk
factor different than CYC
administration in GPA;
however this association was
not significant.
Haemorrhagic cystitis did not
precede bladder cancer in
these cases – however only 1
of the cases had had a
previous cystoscopy prior to
the cancer diagnosis.
The authors suggest that the
two conditions may not arise
from the same mechanisms.
Particularly, the toxic
metabolite acrolein that
causes haemorrhagic cystitis
can be protected against by
mesna whereas it is possible
that the carcinogenic

187
properties are mediated
through molecular changes
cause by the alkylating
properties of CYC. In that
respect, haemorrhagic cystitis
may not be a good marker of
bladder cancer risk and
mesna may not necessarily be
cancer protective.
Malignancy is increased in
ANCA associated vasculitis.
Pankhurst et al.
Rheumatology (Oxford)
2004;43(12):1532-5237.
200 consecutive patients with
GPA or MPA
Retrospective analysis.
Malignancies preceding or
concurrent with vasculitis (up
to 6 months following
diagnosis of vasculitis) were
recorded
The incidence of malignancy
was compared with those in a
population of 129 patients
with HSP, 333 patients with
SLE and a control population
in the West Midlands, UK.
Patients with AAV had an
increased risk of malignancy
compared with HSP patients
(RR 0.85, CI 0.69-1.05,
p=0.034) and SLE patients (RR
0.31, CI 0.14-0.7, p<0.0001).
The rate of malignancy
compared with an age
matched control group was
increased in AAV (RR 6.02, CI
3.72-9.74). The presence of
ANCA was not predictive of
malignancy.
Authors suggest that
malignancy should be
considered as part of the
differential diagnosis in
patients with ANCA-
associated vasculitis
[Identified from references
from paper 6]
Increased incidence of
cervical intraepithelial
neoplasia in women with
systemic lupus
erythematosus treated with
intravenous
61 women with SLE under
active follow up. Study
excluded women that were
treated with oral
cyclophosphamide, had an
abnormal cervical smear at
screening or had no previous
sexual exposure.
Observational prospective
study. Cervical smears were
obtained at baseline and at 3
and 7 years. Results were
analysed according to
treatment received for SLE.
The overall 3-year incidence
of CIN was 9.8%. A dose
relationship was observed
between cumulative
intravenous CYC exposure
and CIN with each increase of
1g of IV CYC exposure
corresponding to 13%
Suggests a risk of CIN with
CYC exposure.

188
cyclophosphamide
Ognenovski et al. J
Rheumatol 2004;31(9):1763-
7120.
increased risk of CIN (p=0.04).
[Identified from the
references from paper 10]
Cancer incidence in a
population based cohort of
patients with Wegener’s
granulomatosis. Knight et al.
Int J Cancer 2002;100(1):82-
5238.
All individuals (n=1176)
discharged with the diagnosis
of GPA within the Swedish
Inpatient Register were
identified.
A total of 1065 patients had
complete data.
The cohort was linked to the
Nationwide registers
including the Swedish Cancer
Register.
SIRs and SMRs were
constructed.
Among 1065 patients, 110
incident cancers were
registered during 5708
person-years of follow up (SIR
2.0 CI 1.7-2.5). SMR due to
cancer (2.2 CI 1.7-2.8).
Bladder cancer SIR 4.80 (CI
2.6-8.1).
Squamous skin cancer SIR 5.7
(CI 2.3-12). Leukaemia SIR 5.7
(CI 2.3-12). Lymphoma SIR 4.2
(1.8 – 8.3). Hepatic cancer SIR
3.8 (CI 1.2-8.8).
Increased risk of cancer noted
overall, particularly for
bladder cancer, NMSC and
lymphoma / leukaemia.
However, this suggests a
lower risk compared to
previous studies.
Unfortunately, this study does
not provide treatment details
such as CYC dose.
Relapse rate, renal survival,
and cancer morbidity in
patients with Wegener’s
granulomatosis or
microscopic polyangiitis with
renal involvement Westman
et al. J Am Soc Nephrol
1998;9(5):842-52239.
Consecutive series of 123
patients with GPA (n=56) or
MPA (n=67) with biopsy
proven renal involvement,
followed up for a median of
55 months (range 0.1 – 273.2
months).
Retrospective analysis. Standardised morbidity ratios
were calculated using
expected values from the
health care region.
There was a 10.4 times higher
risk of developing skin cancer.
When calculating
standardized morbidity ratios
for malignancy with a latency
period of greater than 60
months, treatment with CYC
for greater than 12 months
resulted in a standardized
morbidity ratio for overall
cancer of 3.7, 181.3 for vulva
cancer and 20.2 for bladder
cancer.
Standardised morbidity ratios
were constructed on the basis
of only a few cases for each
cancer type.

189
Skin carcinoma had the
strongest relationship with
AZA > 12 months (24.7 times
more likely) and GC > 48
months (20.8 times more
likely).
Side-effects of intravenous
cyclophosphamide pulse
therapy Martin et al. Lupus
1997;6(3):254-7240.
75 patients with a variety of
autoimmune disorders that
received pulse CYC monthly
and were followed up for 26.7
+/- 22.1 months.
Retrospective analysis. Examined rates of adverse
effects during the follow up
period.
Haemorrhagic cystitis was not
observed.
Only 4 patients developed a
neoplastic condition.
Mean cumulative CYC dose
was low at 4.7g. Follow up
was relatively short therefore
it is difficult to draw accurate
conclusion with regards to
malignancy risk that has
previously been shown to
have a potentially long
latency period.
[Identified from references
from paper 6]
Cyclophosphamide induced
cystitis and bladder cancer in
patients with Wegener’s
granulomatosis. Talar-
Williams et al. Ann Intern
Med 1996;124(5):477-84241.
145 patients who received
CYC for the treatment of GPA
and were followed up for 0.5
to 27 years
Retrospective observational
analysis
50% of patients developed
non-glomerular haematuria.
Bladder cancer developed in
5% of the cohort representing
a 31-fold increase in
incidence. Estimated
incidence of bladder cancer at
15 years after first exposure
to CYC was 16%. Only
microscopic non-glomerular
haematuria was found to be a
significant risk factor for the
development of bladder
cancer (p=0.02). Smokers
developed non-glomerular
Patients in this cohort
received large doses of CYC
(13.8 % received cumulative
doses > 200g). CYC was
continued a minimum of 12
months in all patients.
Authors recommended
urinalysis every 3-6 months
even after cyclophosphamide
is discontinued. As urine
cytology is useful for
detecting higher grade
bladder cancer they suggest
doing this every 6-12 months.

190
haematuria and / or bladder
cancer with shorter duration
and lower dosage of CYC
exposure.
However, the authors make
the point that urine cytology
is relatively insensitive for
detecting lower grade
malignant lesions and
therefore recommend routine
cystoscopy every 1-2 years for
all patients with CYC induced
haematuria.
[Identified from the
references from paper 10]
Wegener’s granulomatosis –
an analysis of 158 patients.
Hoffman et al. Ann Intern
Med 1992;116(6):488-98100.
158 patients enrolled in the
National Institutes of Health
(NIH) cohort
Retrospective analysis The malignancy rate among
patients with GPA was
compared to the National
Cancer Institute Registry for
the general population
2.4-fold overall increase in
malignancies
33-fold increase in bladder
cancer
11-fold increase in lymphoma
Latency period – 7 months to
12 years
Large doses of
cyclophosphamide –
2mg/kg/day as standard dose
but some patients received 3-
5mg/kg/day
[Identified from the
references from paper 18]
Cyclophosphamide induced
bladder toxicity in Wegener’s
granulomatosis. Stillwell et
al. Arthritis Rheum
1988;31(4):465-70242.
111 patients with GPA and
prior CYC exposure seen at
the Mayo Clinic from 1966 to
1985.
Retrospective analysis 17 patients developed
haemorrhagic cystitis.
Bladder cancer developed in 3
patients with haemorrhagic
cystitis.
Incidence of toxicity was not
correlated to CYC dose.
Incidence of Malignancies in
Patients With Antineutrophil
Cytoplasmic Antibody-
Associated Vasculitis
Diagnosed Between 1991
and 2013. Rahmattulla et al.
138 pts with
histopathologically confirmed
AAV (68% GPA, 32% MPA)
Single centre retrospective
cohort review
Primary malignancies were
identified via the Dutch
National Pathology Database-
compared with expected
number of malignancies
(defined as the person-years
Thirty-six patients developed
malignancies (total of 85
malignancies) during the
followup period (mean 9.7
years) 61 were NMSCs, in 22
patients.

191
Arthritis & Rheumatology.
67(12):3270-8, 2015243.
at risk multiplied by the
national cancer incidence
rate)
Subgroup analysis diagnosed
pre vs post 2003
sex-, age-, and calendar year–
adjusted malignancy risk was
2.21-fold higher than the risk
in the general population
(95% CI 1.64–2.92) Increased
risk was attributable solely to
an increased risk of
developing NMSC SIR 4.23
Risk was sig increased in
those diagnosed pre 2003
(cycazarem) compared with
gen population whereas was
not for those post 2003.
Also duration CYC directly
assoc with ca risk but risk not
increased among patients
who had been exposed to CYC
for <1year.
Incidence of Cancer in ANCA-
Associated Vasculitis: A
Meta-Analysis of
Observational Studies. Shang
W et al.
PLoS ONE 10(5):e0126016,
2015244.
258 cases of cancers
identified in a total cohort of
2,578 individuals
Meta- analysis of 6 studies- all
already identified by search
cohort studies that estimate
the influence of AASV on
cancer risk with odds ratio
(OR), risk ratio (RR), hazard
ratio (HR), or standardized
incidence/mortality
rate(SIR/SMR) (2) defined
AASV as one of the exposure
interests and cancer as one of
the out- come of interests
SIR of cancers within the six
individual study populations
ranged between 0.8 and 2.5,
with an overall meta-
analytical SIR of 1.74 NMSC,
leukaemia and bladder cancer
more frequently observed in
patients with AASV with SIR
of 5.18 ,4.89 and 3.84
respectively
(risk of lymphoma, liver and
lung ca also increased)
Moderate heterogeneity
noted

192
ANCA-associated diseases
and lung carcinomas: a five-
case series. Chemouny et al.
Clinical Nephrology.
81(2):132-7, 2014
Five patients with ANCA-
associated diseases who had
associated lung carcinomas or
were diagnosed within 2
years after vasculitis onset.
Abstract only
Wegener's granulomatosis
associated with renal cell
carcinoma. Tatsis, Reinhold-
Keller, Steindorf, Feller, &
Gross,
Arthritis & Rheumatism.
42(4):751-6, 1999245.
477 patients with biopsy-
proven WG
Retrospective case control
study
Pts compared with control
group of 479 patients with
(RA) for the frequencies and
types of malignant neoplasms
occurring before or
simultaneously with the
diagnosis of the rheumatic
disorder.
4.8 % pts vs 3.8% controls
developed ca. 7 cases of renal
ca vs 1 control. Simultaneous
occurrence of cancer and WG
was observed in 14 patients
in the WG group compared
with 1 patient in the control
group
Authors suggest a link
between GPA and RCC
Incidence and prevention of
bladder toxicity from
cyclophosphamide in the
treatment of rheumatic
diseases: a data-driven
review. Monach PA, Arnold
LM, Merkel PA (2010)
Arthritis Rheum 62: 9–21164
PubMed search:search terms
[cyclophosphamide AND
(cystitis OR bladder cancer)
AND (vasculitis OR arteritis
OR granulomatosis OR
rheumatoid OR lupus OR
scleroderma OR non-
Hodgkin’s)]
Then
[(cyclophosphamide
ifosfamide) AND cystitis AND
mesna]
Plus references reviewed
Review- see search strategy Conclusions:
1)daily oral
cyclophosphamide is
associated with an increased
risk of haemorrhagic cystitis
and bladder cancer, in a dose-
dependent and/or duration-
dependent manner (mean
cyclophosphamide exposure
of pts with haemorrhagic
cystitis was >100 gm over a
mean of>30 months;
increased risk of bladder
cancer associated with
cyclophosphamide treatment
was observed in all studies
(OR range 3.6–100) 2)
In summary- low dose pulsed
iv CYC is likely to be assoc
with a low risk of cystitis and
bladder ca. there is little
evidence to support the use
of mesna in this setting,
However, as there may be
some benefit and mesna is
well tolerated, expert
consensus is that the use of
mesna may be considered in
this setting

193
haemorrhagic cystitis ( during
cyc treatment) is associated
with an increased risk of
bladder cancer years later
(11-16 yrs); 3)pulsed IV
cyclophosphamide therapy
carries a low risk of cystitis
and probably also of bladder
cancer; 4) evidence for the
effectiveness of mesna in
preventing cystitis is based
largely on its use with
ifosfamide in patients with
cancer and on data from
animal models, both of which
are of uncertain relevance to
the use of cyclophosphamide
in patients with rheumatic
diseases; 5) there is no direct
evidence for the effectiveness
of mesna in preventing
bladder cancer in humans.
High risk of human
papilloma- virus type 16
infections and of
development of cervical
squamous intraepithelial
lesions in systemic lupus
erythematosus patients.
Nath R, Mant C, Luxton J,
30 women with SLE, 67 with
abnormal smears from
colposcopy clinics, and 15
community subjects with
normal smears
Prospective case control
study
Polymerase chain reaction
results for viral DNA and HPV-
16 sequencing data were
correlated to cytology and
colposcopic findings
SLE patients were more likely
to be both HPV DNA positive
and HPV-16 DNA positive (i.e.,
have a high viral load:
colposcopy patients were
more likely to be only HPV
DNA positive. (both more
likely to be positive compared
Study notes that although
more HPV 16 in SLE vs
colposcopy group they were
ethnically diff which is
relevant for HPV
epidemiology
“60% of patients with SLE had
a history or

194
Hughes G, Raju KS, Shepherd
P, et al. (2007) Arthritis
Rheum 57: 619–625246.
with controls)
Ten (36%) SLE patients had a
high HPV-16 viral load, 7 of
these patients had current
abnormal histology. No assoc
between HPV status and
current or previous drug
therapy. HCQ appeared to
exert a protective effect-
(?confounding by disease
severity as this is used for
milder disease therefore
cervical disease likely to be
assoc with more aggressive
disease or therapy) when this
was removed from analysis
other immunosupp were
assoc with OR 1.4 on
presence SIL (squamous
intraepithelial lesions). SIL
rate 27%
current evidence of cervical
disease”
Multiple other references
here for lupus and CIN
The below ref selected for
inclusion as most recent and
relevant.
Factors associated with
abnormal Pap results in
systemic lupus
erythematosus. Bernatsky S,
Ramsey-Goldman R, Gordon
C, Joseph L, Boivin JF, Rajan
R, et al. Rheumatology
(Oxford) 2004;43:1386–9247.
1015 pts with SLE from 3
centres
Cross-sectional cohort study
(pt self- report survey)
To determine the factors
associated with lifetime
occurrence of an abnormal
Pap test in women with SLE,
and to determine the
influence of immunosup-
pressive exposure on the
odds of abnormal Pap test
results occurring after
13.3% had abn smear, with
half occurring after diag SLE.
mean duration of SLE at the
time of the abnormal test was
12.1 yr
STD and OC assoc with abn
smear
OR for the effect of
immunosuppressive exposure
Limitations of a self- report
survey acknowledged

195
diagnosis of SLE. on abnormal results occurring
after diagnosis of SLE, when
adjusted for smoking,
nulliparity, OC use, STD
history, age, race and centre,
was 1.6.

196
Article Study population Study Design Comparisons Outcomes Comments
Fertility, ovarian failure, and
pregnancy outcome in SLE
patients treated with
intravenous
cyclophosphamide in Saudi
Arabia.
Alarfaj A.S., Khalil N.
Clinical Rheumatology. 33
(12) (pp 1731-1736), 2014248
Saudi Arabian women with SLE
treated with IV CYC (188) vs.
not (347) over 26 year period
Retrospective analysis Rates of amenorrhoea.
Rates of conception, abortion,
foetal loss and pre-term births.
Higher rate of amenorrhoea
in the IV CYC group.
Older age at time of
receiving IV CYC and higher
cumulative dose of IV CYC
were risk factors.
Rates of conception, foetal
loss and live birth similar
between 2 groups but IV CYC
group had more pre-term
births.
Older age at time of CYC
exposure and cumulative
dosage correlated with rates
of amenorrhoea.
Pharmacological
interventions for fertility
preservation during
chemotherapy: A systematic
review and meta-analysis.
Ben-Aharon I., Gafter-Gvili
A., Leibovici L., Stemmer
S.M.
Breast Cancer Research and
Treatment. 122 (3) (pp 803-
811), 2010167.
Cancer and SLE patients
treated with chemotherapy
agents at risk of chemotherapy
induced ovarian failure
Meta-analysis and
systematic review
Randomised controlled and
observational studies that
assessed GnRH analogs
(GnRHa) or the oral
contraceptive pill for fertility
preservation prior to
chemotherapy.
GnRHa effective in reducing
amenorrhoea in all patients.
Pregnancy rate higher in the
GnRHa arm.
However, the advantage of
GnRHa was only shown in
observational studies and
not in clinical trials.
Inconclusive results from
studies evaluating use of oral
contraceptive pill.
Preservation of fertility and
ovarian function and
minimizing gonad toxicity in
young women with systemic
Women of reproductive age
with severe connective tissue
disease
Observational study 8 women that received GhRHa
together with chemotherapy
versus 9 women that did not.
None of the women treated
with GnRHa developed pre-
mature ovarian failure
whereas 5 out of 9 of the
Study was not controlled.
Mean age as well as mean
total dose of
cyclophosphamide was
Fertility preservation evidence table

197
lupus erythematosus
treated by chemotherapy.
Blumenfeld Z., Shapiro D.,
Shteinberg M., Avivi I.,
Nahir M.
Lupus. 9 (6) (pp 401-405),
2000249.
women that did not receive
GnRHa did experience pre-
mature ovarian failure.
higher in the group that did
not receive GnRHa.
Hormonal Strategies for
Fertility Preservation in
Patients Receiving
Cyclophosphamide to Treat
Glomerulonephritis: A
Nonrandomized Trial and
Review of the Literature.
Cigni et al. American
Journal of Kidney Diseases.
52 (5) (pp 887-896), 2008250 .
28 consecutive patients (11
men, 17 women) with various
forms of glomerulonephritis
treated with CYC
Clinical Trial 11 men: all received
testosterone with CYC
17 women: 13 patients
received CYC plus GnRHa and 4
patients received only CYC
All 4 patients in group B of
the female patients (CYC
only) developed sustained
amenorrhoea as opposed to
group A.
Authors suggest a protective
effect of testosterone and
triptorelin against CYC
induced gonadal damage.
Very small numbers in this
study.
The sub-study in men was
not controlled i.e. all men
received testosterone.
The sub-study in women was
not randomized.
Furthermore the group that
did not receive GnRHa was
comprised only of 4 patients.
Therapy Insight: Preserving
fertility in
cyclophosphamide-treated
patients with rheumatic
disease.
Dooley M.A., Nair R.
Nature Clinical Practice
Rheumatology. 4 (5) (pp
250-257), 2008251.
CYC treated patients with
rheumatic disease
Review Patient's age at treatment
and the cumulative dose
received are important risk
factors for CYC-induced
gonadal failure in both males
and females.
Storing male gametes prior
to chemotherapy widely
practiced and technically
successful.
Questionable benefit of oral
contraceptives for females
and testosterone for males.

198
Fertility preservation
treatment for young women
with autoimmune diseases
facing treatment with
gonadotoxic agents.
Elizuret al.
Rheumatology. 47 (10) (pp
1506-1509), 2008252.
7 patients that required CYC
treatment and underwent
fertility preservation
treatments. One of the
patients had MPA.
Case series. Describes successful fertility
preservation in 7 female
patients prior to
commencing CYC therapy.
Authors suggest that oocyte
or embryo cryopreservation
should be considered for
fertility preservation in
young women with systemic
autoimmune rheumatic
diseases who face imminent
gonadotoxic treatment.
The impact of
cyclophosphamide on
menstruation and
pregnancy in women with
rheumatologic disease.
Harward L.E., Mitchell K.,
Pieper C., Copland S.,
Criscione-Schreiber L.G.,
Clowse M.E.B.
Lupus. 22 (1) (pp 81-86),
2013121.
Women diagnosed with SLE,
scleroderma or vasculitis prior
to the age of 35.
Case series. Comparison of patients with
CYC exposure versus not.
Comparison of patients with
GnRH co-therapy and CYC
versus not.
Amenorrhoea was related to
CYC use, older age at time of
therapy as well as CYC
dosage received.
More women with GnRHa
co-therapy had maintained
menses however this value
did not reach statistical
significance.
Higher conception rates in
women that received
GnRHa.
All pregnancies after CYC
exposure resulted in elective
termination, miscarriage or
pre-term birth.
Does not provide sufficient
evidence to routinely
recommend GnRHa.
Fertility preservation Total of 2836 patients within Retrospective analysis of Most patients opted for a Advocates for GnRHa co-

199
methods in young women
with systemic lupus
erythematosus prior to
cytotoxic therapy:
Experiences from the
FertiProtekt network.
Henes M., Henes J.C.,
Neunhoeffer E., Von Wolff
M., Schmalzing M., Kotter I.,
Lawrenz B.
Lupus. 21 (9) (pp 953-958),
2012253.
the FertiPROTEKT network.
Out of those 68 were
counselled for severe SLE.
prospectively collected data.
Also literature review.
fertility preservation
method. The largest
proportion (91.2%) opted for
GnRHa co-therapy. Ovarian
tissue removal for
cryoconservation (25%) and
stimulation therapy for
cryoconservation of fertilized
egg cells (4.4%) was also
performed.
therapy although does not
provide any data for GnRHa
effectiveness.
Authors suggest
cryoconservation of ovarian
tissue if no active disease.
Causes and management of
infertility in systemic lupus
erythematosus.
Hickman R.A., Gordon C.
Rheumatology. 50 (9) (pp
1551-1558), 2011254.
Review of causes and
management of infertility in
SLE.
Literature review. Advocates for GnRHa use in
female patients and use of
testosterone in male
patients.
Risk of ovarian failure and
fertility after intravenous
cyclophosphamide. A study
in 84 patients.
Huong D.L.T., Amoura Z.,
Duhaut P., Sbai A.,
Costedoat N., Wechsler B.,
Piette J.-C.
Journal of Rheumatology. 29
(12) (pp 2571-2576), 2002255.
Study of 84 women that
received CYC.
Approximately one third of the
patients had GPA or other
systemic vasculitis.
Retrospective analysis. Confirms that the risk of
ovarian failure depends on
the age of the woman at the
time of CYC therapy.
It is possible to conceive
during CYC therapy;
however, the outcome is
almost always negative
therefore efficient
contraception during CYC
therapy is mandatory.
In this cohort, after iv CYC

200
withdrawal pregnancy was
possible with favourable
outcome in two thirds of
cases.
Ovarian failure in systemic
lupus erythematosus
patients treated with pulsed
intravenous
cyclophosphamide.
Katsifis G.E., Tzioufas A.G.
Lupus. 13 (9) (pp 673-678),
2004256.
Review of ovarian failure in SLE
patients treated with CYC.
Review. Supports the evidence that
premature ovarian failure
after CYC therapy depends
on the age of the patient at
the time of treatment and
the CYC dosage.
Advocates consideration of
ovarian banking prior to CYC
therapy in selected patients.
Prevention of gonadal
toxicity and preservation of
gonadal function and
fertility in young women
with systemic lupus
erythematosus treated by
cyclophosphamide: the
PREGO-Study.
Manger K., Wildt L., Kalden
J.R., Manger B.
Autoimmunity reviews. 5 (4)
(pp 269-272), 2006257.
63 pre-menopausal women
with SLE without ovarian
protection that received CYC.
Prospective study. Tested concentrations of FSH
and LH before and after CYC
treatment.
60% of patients treated with
CYC suffered from pre-
mature ovarian failure.
Again, the age and dosage
were found to be crucial
determinants of pre-mature
ovarian failure.
Absence of conclusive
evidence for the safety and
efficacy of gonadotropin-
releasing hormone analogue
treatment in protecting
against chemotherapy-
Comment on the impact of
gonadotoxic therapy on
women with malignant and
non-malignant diseases.
Review and commentary. Comprehensive review of
literature on the
effectiveness and safety of
GnRHa therapy.
Most studies that show
benefit have used control

201
induced gonadal injury.
Oktay K., Sonmezer M.,
Oktem O., Fox K., Emons G.,
Bang H.
Oncologist. 12 (9) (pp 1055-
1066), 2007258.
groups retrospectively
selected from historical
patients treated with similar
regimens. In some studies,
the mean follow-up was
longer in the control group
and dosage of CYC in the two
groups was not clear.
Concerns exist on the safety
of administering GnRHa
during chemotherapy.
Fertility and pregnancy in
vasculitis.
Pagnoux C., Mahendira D.,
Laskin C.A.
Best Practice and Research:
Clinical Rheumatology. 27
(1) (pp 79-94), 2013259.
Review of fertility and
pregnancy in vasculitis
Review. No systematic so not
formally appraised
Ovarian failure and
strategies for fertility
preservation in patients
with systemic lupus
erythematosus.
Raptopoulou A.,
Sidiropoulos P., Boumpas
D.T.
Embase Lupus. 13 (12) (pp
887-890), 2004260.
Editorial. Comments on current
literature (up to 2004).
Ovarian toxicity an important
consideration for CYC
treatment. Drug toxicity
cumulative and dose
dependent therefore
advocates use of small
effective dose and shortest
duration.
Advocates use of GnRHa.
In terms of male fertility,

202
sperm banking is the only
proven method for male
fertility preservation.
Adverse effects of therapy
for ANCA-associated
vasculitis.
Turnbull J., Harper L.
Embase Best Practice and
Research: Clinical
Rheumatology. 23 (3) (pp
391-401), 2009261.
Review of adverse effects of
therapy in AAV.
Review. Includes section on fertility
although limited.
No new information with
regards to CYC.
Methotrexate also
associated with infertility
particularly in men.
Recommends informed
discussion before
commencement of therapy.
Suggests that
cryopreservation of sperm is
done when time allows prior
to CYC therapy and possibly
also methotrexate.
Suggests GnRHa may be able
to protect female fertility.
Impact of systemic lupus
erythematosus on ovarian
reserve in premenopausal
women: evaluation by using
anti-Muellerian hormone.
Lawrenz B et al.
Lupus. 20(11):1193-7,
2011262.
33 premenopausal SLE patients
without previous
cyclophosphamide- treatment
compared with 33 age-
matched healthy controls
Not relevant as pts not
exposed to CYC and not
disease group of interest
Cyclophosphamide-induced
gonadal toxicity: a
Review (not systematic) 6 studies reviewed
examining relationship
Most relevant ref
Ioannidis JPA, Katsifis GE,

203
treatment dilemma in
patients with lupus
nephritis? Wetzels et al.
Netherlands Journal of
Medicine. 62(10):347-52,
2004263.
between CYC dose/ age and
amenorrhea.
cumulative dosages CYC of
12 to 25 g. mean age of the
patients was 28 years. Risk of
amenorrhoea ranged from
27 to 60%)sustained in >
80%). Generally developed
average of four months after
starting CYC.
Risk of sustained
amenorrhea dependent on
dose and age.
Ioannidis calculated the risk
of amenorrhoea for 15 g CYC
(5 to 10%
for patients <25 years, 30%
for patients aged 25 to 31
years and 90% for patients
>32 years). V low risk if
<10g/ young.
Male data extrapolated from
pts usually treated pre-
puberty- concludes dose of
12g appears safe for 70kg
adult
Occurred 2-3 months
following exposure and
recovery occurred and 3
years (70% of those <
Tzioufas AG, Moutsopoulos
HM. Predictors of sustained
amenorrhea from pulsed
intravenous
cyclophosphamide in
premenopausal women with
systemic lupus
erythematosus. J Rheumatol
2002;29:2129-35.
10.

204
7.5g/m2)
Mentions lack of evidence
for OCP, possible benefit of
GnRH agonists (but RCTs
needed and may be
associated with disease
flares). Mentioned one study
showing possible benefit of
concurrent testosterone for
preserving fertility in men.
Predictors of sustained
amenorrhea from pulsed
intravenous
cyclophosphamide in
premenopausal women
with systemic lupus
erythematosus. Ioannidis
JPA, Katsifis GE, Tzioufas
AG, Moutsopoulos HM. J
Rheumatol 2002;29:2129-
35165.
67 premenopausal women
with SLE who were treated
with a monthly regimen of IC
pulses for lupus nephritis or
other indications at the
Department of
Pathophysiology, National
University of Athens, between
January 1992 and June 2001
Retrospective cohort study Predictors of CYC induced
sustained amenorrhoea(AM)
including cox Ph models to
predict dose of CYC that would
result in amenorrhoea
Twenty-one women (31%)
developed sustained
amenorrheoa of at least 12
months’ duration during
followup. For those >=32yrs,
90% expected to develop
sustained AM by 12g CYC.
Confirms dose/duration CYC
and age as determinants of
amenorrheoa
Risk for sustained
amenorrhea in patients with
systemic lupus
erythematosus receiving
intermittent pulse
cyclophosphamide therapy.
Boumpas, D T. et al.
Annals of Internal Medicine.
119(5):366-9, 1993166.
Pts with SLE < 40yrs old,
participating in two
prospective therapeutic trials
for lupus nephritis from 1973
to 1990 and in a retrospective
study for neuropsychiatric
lupus.
Retrospective cohort study Risk of sustained amenorrhea
(defined as > 12/12) in those
with short course (7 doses
n=16) vs long course (at least
15 doses, n=23)
100% of those with long
course CYC plus > 31 yrs. age
developed sustained
amenorrhoea vs 0% of those
age < 25yrs plus short course

205
The effect of
cyclophosphamide pulses
on fertility in patients with
lupus nephritis. Langevitz,P
et al.
American Journal of
Reproductive Immunology.
28(3-4):157-8, 1992264.
17 females with LN, mean age
29.4 years. Receiving 2-13
pulses CYC, some requiring
repeat therapy.
Retrospective cohort study Descriptive outcomes Menopause appeared in four
females, three of them
44-45 years old. Early
menopause occurred in one
28-year- old female who
received a total of 11 g of
cyclophosphamide. The
menstrual cycle remained
unchanged in 11 females,
14-33 years old, who
received between 2.4 and 9
g of cyclophosphamide
Authors conclude < 10g
appears safe for those <
40yrs

206
Article Patients Design Comparisons Outcomes Comments/refs
Effect of methotrexate,
anti-tumor necrosis factor
alpha, and rituximab on the
immune response to
influenza and
pneumococcal vaccines in
patients with rheumatoid
arthritis: a systematic
review and meta-analysis.
Hua, Barnetche, Combe, &
Morel.
Arthritis care & research.
66(7):1016-26, 2014173.
Pts with RA Meta-analysis for studies of
human subjects published in
English or French up to
March 2013 in Medline (via
PubMed), EMBase, Cochrane
Library, and databases for
the American College of
Rheumatology (ACR) and
European League Against
Rheumatism (EULAR) annual
meetings. The key- words
were “influenza vaccines,”
“pneumococcal vac- cines,”
and “rheumatoid arthritis,”
with no limit on the date of
publication.
12 studies included in meta-
analysis: 6 of influenza vaccine,
5 of pneumococcal vaccine, 1
both
Two studies assessed the
humoral response to
influenza vaccine with
(experimental group) and
without (control group) RTX
treatment. The response
rate was reduced with RTX,
but the pooled OR was not
significant for the H1N1
strain.
For the 2 studies evaluating
the response to
pneumococcal vaccine in
patients receiving RTX,
response rate was reduced
for both serotypes in the
experimental group with RTX
treatment as compared with
the control group, but the
pooled OR did not reach
significance for serotype 23F
Rituximab impairs
immunoglobulin (Ig)M and
IgG (subclass) responses
after influenza vaccination
in rheumatoid arthritis
23 RA patients on RTX
(treatment of 11 patients 4–8
weeks before vaccination and
of 12 patients 6–10 months
before vaccination. Controls on
RCT Ab levels measured before and
28 days following vaccination
Reduced IgG and particularly
IGM response to vaccine in
RTX pts. However, there was
a modest IgG response in
those 6-10 months since RTX
Conclusion regarding BAFF
and T cell response
somewhat confusing
Vaccination evidence table

207
patients.
Westra et al Clinical &
Experimental Immunology.
178(1):40-7, 2014174.
MTX and healthy controls
Efficient boosting of the
antiviral T cell response in B
cell-depleted patients with
autoimmune rheumatic
diseases following influenza
vaccination. Muller RB et al.
Clinical & Experimental
Rheumatology. 31(5):723-
30, 2013265
Abstract only available
16 pts having received Rtx
Prospective cohort study Influenza virus-specific
immune responses were
analysed after the first and a
booster vaccination with
PandemrixTM
2/7 with low (<10%) and 4/9
with normal (>10%) B cells
developed significant
antibody responses after first
vaccination. Booster
vaccination led to an
antibody response in one
additional patient. After the
first vaccination, virus-
specific CD4+ and CD8+ T cell
responses were significantly
lower in patients with low B
cells than in those with
normal B cells. Of
importance, the booster
vaccination stimulated the
antiviral T cell response only
in patients with low B cells.
T cell response to vaccine
may help compensate for
those who are B cell deplete
Rituximab-treated patients
have a poor response to
influenza vaccination.
Eisenberg et al.
Journal of Clinical
Immunology. 33(2):388-96,
2013266.
17 pts anticipated to receive
RTX
Prospective case control
study
Seroconversion (4 fold increase
in ab titres) following ‘flu
vaccination measured.
Vaccinated at 7-9/12 following
RTX
2/12 vs 10/12 controls had
seroconversion following
vaccination
Patients with B cell counts of
>1 cell/mm3 did have some
response to vaccine (2 fold
rise in titre to one serotype),
while those subjects who
had B cell counts <1
cell/mm3 did not respond
Immunization responses in N= 69 RA pts with MTX plus RCT Ab responses post vaccine Response to tetanus toxoid “to maximize response,

208
rheumatoid arthritis
patients treated with
rituximab: results from a
controlled clinical trial.
Bingham et al.
Arthritis & Rheumatism.
62(1):64-74, 2010267.
RTX vs MTX alone vaccine same across groups
and no evidence of impaired
DTH response.
Reduced response to
pneumococcal vaccine
(secondary outcome)
polysaccharide and primary
immunizations should be
administered prior to
rituximab infusions”
Vaccination response to
protein and carbohydrate
antigens in patients with
rheumatoid arthritis after
rituximab treatment.
Rehnberg et al.
Arthritis Research &
Therapy. 12(3):R111,
2010175
19 RA pts with RTX
patients were vacci- nated 6
months after RTX treatment
(post-RTX group, n = 11), or 6
days before RTX treatment
(pre-RTX group, n = 8). As a
control group, 10 patients
never treated with RTX were
included.
Prospective case control
study
Vaccine specific B cells at 0, 6,
21 days
Pts immunised 6 days pre-
RTX had a better response at
21 days than those receiving
RTX 6 months previously.
Formation of influenza-
specific B cells was lower in
post-RTX group at day 6
compared with the pre-RTX
group and controls (P =
0.04). Polysaccharide-specific
B cells were found in 27% to
50%, being equally
distributed between the
groups. On day 21,
impairment of humoral
responses was more
pronounced for influenza
compared with
pneumococcal vaccine
(affecting both IgG and light-
chain production). Total
absence of influenza-specific
IgG production was observed
It is prob better to immunise
6 days before than 6 months
after RTX

209
in 55% of the post-RTX group
The Green Book- chapter
7133
“individuals due to
commence
immunosuppressive
treatments, inactivated
vaccines should ideally be
administered at least two
weeks before
commencement. In some
cases this will not be possible
and therefore
vaccination may be carried
out at any time and re-
immunisation considered
after treatment is finished
and recovery has occurred”
Rituximab and abatacept
but not tocilizumab impair
antibody response to
pneumococcal conjugate
vaccine in patients with
rheumatoid arthritis. Crnkic
Kapetanovic, Saxne,
Jönsson, Truedsson, &
Geborek.
Arthritis Research &
Therapy. 15(5):R171,
2013268
55 RA pts with RTX Prospective case control
study
Ab response 4-6 weeks post
vacc
Pts with RTX had sig
diminished ab response
following pneum vaccine. no
statistically significant
differences in antibody
responses between patients
vaccinated within ≤180 days
compared to those receiving
vaccination >180 days after
the last rituximab treatment
Time from RTX to vaccine
very variable. (Range 0-894
days)
Randomized trial
investigating the safety and
31 GPA/MPA pts in remission
for > 3 /12 (24 vacc, 7 unvacc)
Open prospective
randomised study
Comparing ab response of AAV
vacc vs not vacc and non AAV
>70% AAV vac achieved
seroprotection at 28 days
No significant change in CRP,
disease activity as measured

210
efficacy of influenza
vaccination in patients with
antineutrophil cytoplasmic
antibody-associated
vasculitis. Jeffs et al.
Nephrology. 20(5):343-51,
2015170
vacc post vac to 2/3 strains by BVAS activity scores or
ANCA titres post- vaccination
Risk factors for severe
bacterial infections in
patients with systemic
autoimmune diseases
receiving rituximab.
Heusele et al. Clinical
Rheumatology. 33(6):799-
805, 2014269.
AI pts having received RTX Retrospective case controls
study
Risk factors for infection History of pneumococcal
vaccination significantly
decreased the risk of Serious
bacterial Infections
(OR=0.11, 95%CI= 0.03–0.41,
p=0.0009)
ANCA-associated vasculitis
following influenza
vaccination: causal
association or mere
coincidence? Birck, Kaelsch,
Schnuelle, Flores-Suárez, &
Nowack.
Journal of Clinical
Rheumatology. 15(6):289-
91, 2009169.
Abstract only available 4 cases of new onset or
relapsing antineutrophil
cytoplasmic antibodies
associated vasculitis
occurring in “timely
association” with influenza
vaccination
Wegener's granulomatosis
patients show an adequate
antibody response to
influenza vaccination.
Holvast et al. Annals of the
GPA pts in randomly assigned
to receive influenza
vaccination (n = 49) or to
participate as controls (n = 23)
remission. 47% of vacc not on
RCT Ab response to vaccination at
0,1 and 3-4 months
WG patients achieved high
seroprotection rates to all
three influenza strains,
comparable with healthy
controls
No evidence of an increase
in ANCA or disease activity
following vaccination
Pts excluded if “active
disease” pred>30 mg/od or

211
Rheumatic Diseases.
68(6):873-8, 2009172.
IS cyc.
Cell-mediated immune
responses to influenza
vaccination in Wegener’s
granulomatosis. Holvast et
al.
Ann Rheum Dis
2010;69:924–927131
24 pts with GPA- all in
remission. 45.8% on
immunosuppression
Prospective case control
study
Vaccine response at 28 days Found no differences in cell-
mediated immune responses
to subunit influenza
vaccination between
patients with WG and
controls
Responses were, at least
largely, independent of
previous vaccination status
and the use of
immunosuppressive drugs.
Antibody response to
inactivated subunit
influenza vaccine in
patients with Wegener's
Granulomatosis. Zycinska et
al.
Journal of Physiology and
Pharmacology. 2007, 58
suppl 5, p819-828270.
35 GPA pts in remission vacc
compared with 28 pts not vacc
(plus 35 healthy controls)
Prospective case control
study
Ab response at 1 month >70% vac pts ab
seroprotection rate to 2/3
strains (compared with >85%
healthy subjects)
EULAR recommendations
for vaccination in adult
patients with autoimmune
inflammatory rheumatic
diseases. van Assen et al.
414 Ann Rheum Dis
2011;70:414–422143.
Systematic lit review plus
Delphi
The vaccination status
should be assessed in the
initial investigation of
patients with AIIRD
Vaccination in patients with
AIIRD should ideally be
administered during stable
disease
Live attenuated vaccines
should be avoided whenever
possible in
immunosuppressed patients

212
with AIIRD
Vaccination in patients with
AIIRD can be administered
during the use of DMARDs
and TNFα blocking agents,
but should ideally be
administered before starting
B cell- depleting biological
therapy
Influenza vaccination should
be strongly considered for
patients with AIIRD
23-valent polysaccharide
pneumococcal vaccination
should be strongly
considered
for patients with AIIRD
Influenza vaccination does
not result in an increase in
relapses in patients with
ANCA-associated vasculitis.
Stassen PM, Sanders JS,
Kallenberg CG, Stegeman
CA Nephrol Dial Transplant
2008; 23: 654–658271
All consecutive AAV patients
from one centre who had a
follow-up of at least 1 year
between 1999 and 2004.
Retrospective nested case
control study
Relapses occurring within 1
year of the vaccination were
attributed to that vaccination
The relapse rate per 100
patients at risk over the
period 1999–2004 was lower
in patients who had been
vaccinated within the
previous year (3.4) than in
patients who had not been
vaccinated against influenza
(6.3).

213
Article Patients Design Comparisons Outcomes Comments/refs
Cochrane review
Prophylaxis for
Pneumocystis pneumonia
(PCP) in non-HIV
immunocompromised
patients. Stern, A
Green, H
Paul, M
Vidal, L
Leibovici, L. 2015176
Cancer patients
(haematological and solid
organ malignancy) • Bone
marrow recipients • Solid
organ transplant patients •
Patients receiving
corticosteroids • Patients
receiving other
immunosuppressive
medications
(for connective tissue disease,
chronic lung disease,
inflammatory bowel disease) •
Severe malnutrition • Primary
immune-deficiency diseases
Electronic searches of the
Cochrane Central Register
of Controlled
Trials(CENTRAL)
(TheCochraneLibrary2014,
Issue 1),MEDLINE and
EMBASE (to March 2014),
LILACS (to March 2014),
relevant conference
proceedings; and
references of identified
trials
Thirteen trials performed
between the years 1974
and 2008 were included,
involving 1412 patients.
Any chemoprophylaxis
administered for the
prevention of Pneu-
mocystis infections versus
placebo, no intervention,
or an antibiotic(s) with no
activity against
Pneumocystis pneumonia.
Trials that compared
different antibiotics for the
prevention of
Pneumocystis infections
also included
Compared to no treatment or
treatment with fluoroquinolones
(inactive against Pneumocystis)
there was an 85% reduction in
the occurrence of PCP in
patients receiving prophylaxis
with
trimethoprim/sulfamethoxazole,
RR of 0.15 (95% CI 0.04 to 0.62;
10 trials, 1000 patients). The
evidence was graded as
moderate due to possible risk of
bias.
No significant differences in
overall adverse events or events
requiring discontinuation were
seen comparing
trimethoprim/sulfamethoxazole
to no treatment or placebo (four
trials, 470 patients, moderate
quality evidence)
Given an event rate of 6.2% in
the control groups of the
included trials, prophylaxis for
PCP using
trimethoprim/sulfamethoxazole
is highly effective among non-
HIV immunocompromised
patients, with a number needed
to treat to prevent PCP of 19
patients (95% CI 17 to 42).
Prophylaxis should be
considered for patients with a
similar baseline risk of PCP.
A Systematic Review of Two
Different Trimethoprim–
Sulfamethoxazole
Regimens Used to Prevent
576 solid organ transplant
recipients
Electronic searches of
MEDLINE, EMBASE and
Cochrane reviews Key
words were prophyl*,
4 studies comparing full-
dose
prophylaxis (160/800 mg/d
every day), low-dose
Incidence of PJP among patients
undergoing full- dose
prophylaxis was 0% (0/181),
1% in those undergoing
There appeared to be no sig
difference in incidence of
infection between those on full
or low dose prophylaxis.
Pneumocystis evidence table

214
Pneumocystis jirovecii and
No Prophylaxis
at All in Transplant
Recipients: Appraising the
Evidence. Di Cocco et al.
Transplantation
Proceedings, 41, 1201–1203
(2009)186
transpl*, trimethophrim,
sulfamethoxazole,
Pneumocystis carinii
and jiroveci, prevent*, and
pneumonia. Quality of
studies assessed using
GRADE system
prophylaxis (80/400 mg/d
every day or 160/800
mg/d every other day) , or
no prophylaxis at all were
analysed
low-dose prophylaxis (1/105;
range, 0%–2%);
and 11%
in those who did not receive
prophylaxis (31/284; range, 4%–
41%).
Pneumocystis jirovecci
pneumonia in connective
tissue diseases: Comparison
with other
immunocompromised
patients. Teichtahl et al.
Seminars in Arthritis &
Rheumatism. 45(1):86-90,
2015183.
90 subjects who fulfilled the
diagnostic criteria of
either a positive P. jirovecii PCR
(64%) or toludine blue O stain
(36%) with a concurrent
respiratory illness were
included in the study. 11 of
these had CTDs
Single centre retrospective
case control study.
(i) to examine the
contribution of CTDs to the
total number of PJP
diagnoses and (ii) to
determine any between
group differences in
subject characteristics and
basic laboratory
parameters between
people with non-CTDs and
CTDs who had been
diagnosed with PJP
Around the time of PJP
diagnosis, people with CTDs
were significantly older, had
greater lymphopaenia and worse
renal function than non-CTD
subjects and were more likely to
have been exposed to
corticosteroids or other
immunosuppression
Small study (i.e. numbers of
CTD patients) but interesting
results.
CTD pts contributed 21.6% of
the PJP cases in this centre
once HIV population had been
excluded. Mortality from PJP
27.3 % vs 2.5% in the non- CTD
population
Pneumocystis jirovecii
pneumonia in patients with
autoimmune disease on
high-dose glucocorticoid.
Chew, Maceda-Galang, Tan,
Chakraborty, & Thumboo.
Journal of Clinical
Rheumatology. 21(2):72-5,
2015272.
1063 pts hospitalised to
Singapore General Hospital
between January 2003 and
December 2007. Patients with
concomitant diagnosis of
HIV/AIDS were excluded
Single centre retrospective
cohort study
Patient demographics,
mean glucocorticoid dose
(in the last 1 month), and
the outcomes of patients
who developed PCP were
analysed.
4 pts developed PJP, none of
whom had received prophylaxis.
Authors conclude that the RR of
developing PJP on high dose
(>30mg/day) pred vs low dose is
19 as ¾ pts who developed PJP
were on high dose.
Overall incidence of PJP in this
study in AI disease was 0.075%
Small numbers
Predisposing factors, clinical 62 HIV-negative adult patients Single centre retrospective The aim of this study was 50% had haematological

215
characteristics and outcome
of Pneumonocystis jirovecii
pneumonia in HIV-negative
patients. Kofteridis et al.
Journal of Infection &
Chemotherapy. 20(7):412-
6, 2014273.
admitted to
the University Hospital of
Heraklion, Crete, Greece and
diagnosed with PCP from
January 2004 through to May
2013
cohort study to investigate the
predisposing factors,
clinical features and
outcome of Pneumocystis
pneumonia in HIV-
negative patients
malignancies, 26% solid tumour
and 24% chronic inflammatory
disease. 34% of those
developing PCP had received co-
trimoxazole prophylaxis.
Mortality rate 29%.
Pneumocystis jirovecii
pneumonia in HIV-negative
patients: a prospective
study with focus on
immunosuppressive drugs
and markers of immune
impairment. Roblot et al.
Scandinavian Journal of
Infectious Diseases.
46(3):210-4, 2014274
Abstract only Low lymph/CD4 and high
corticosteroid exposure seem to
be risk factors for development
of PJP
A dose-escalation regimen
of trimethoprim-
sulfamethoxazole is
tolerable for prophylaxis
against Pneumocystis
jiroveci pneumonia in
rheumatic diseases.
Takenaka, Komiya, Ota,
Yamazaki, & Nagasaka.
Modern Rheumatology.
23(4):752-8, 2013275
41 pts with rheumatic diseases
receiving co-trimoxazole as
prophylaxis due to (1)
treatment with 0.8 mg/kg/day
or more of prednisolone (PSL),
(2) 0.5 mg/kg/day or more of
PSL with immuno- suppressive
agents, (3) 0.5 mg/kg/day or
more of PSL in patients with
pulmonary complications, (4)
20 mg/day or more of PSL in
patients over 80 years of age
Retrospective single centre
cohort study
Dose escalation of
TMP/SMX from 10% to
100% over > 3 days vs
starting on full dose
6 month retention rate on
TMP/SMX higher in the
incremental group but not stat
sig. Almost half pts were on
smaller doses than
recommended. 1 case of PJP in
the routine group after cessation
of TMP/SMX
Dose escalation may be helpful
to increase tolerability. Small
doses than recommended of
TMP/SMX may protect against
PJP.
Pneumocystis jirovecii 8 patients with RA who Case series and review R/v- discussed RF for This describes PJP outbreak in

216
pneumonia in rheumatoid
arthritis patients: Risks and
prophylaxis
recommendations.
Mori S., Sugimoto M.
Clinical Medicine Insights:
Circulatory, Respiratory and
Pulmonary Medicine. 9 (pp
29-40), 2015182.
developed PJP in a single
centre between March 2005
and October 2009
development- older, steroids,
higher dose, pre-existing lung
disease lymphopenia, carriage of
PJP.The Japanese Ministry of
Health, Labor and Welfare Study
Group recommended the use of
TMP-SMX or pentamidine as a
prophylactic against PCP for
patients with inflammatory
rheumatic diseases over the age
of 50 receiving steroids
equivalent to 1.2 mg/kg/day of
prednisolone or more, 0.8
mg/kg/day of prednisolone or
more plus immunosuppressives,
or peripheral lymphocyte counts
<500/mL during
immunosuppressive therapy.
pts on methotrexate only.
Suggests short term prophylaxis
for all those on IS if new case
identified in dept (i.e. 5-7 days)
Increasing Pneumocystis
pneumonia, England, UK,
2000-2010. Maini R et al.
Emerging Infectious
Diseases. 19(3):386-92,
2013276.
All patients coded in HES as
having had PJP between 2000
and 2010. 2258 cases identified
Retrospective cohort study Number of cases 2000 till
2010 and proportion of
disease groups
contributing
HIV related PJP reducing but
incidence PJP increasing. Largely
contributed to by haem
malignancy and transplant
patients
Pneumocystis jirovecii
pneumonia in two patients
with systemic lupus
erythematosus after
rituximab therapy. Bonilla-
Abadia, F. et al.
2 pts with lupus Case reports 1 pt developed PJP with
refractory lupus requiring 2g RTX
every 9 months over 4 years plus
pred 5 and aza 50mg- survived.
2nd pt developed PJP 6 weeks
after first dose RTX- died

217
Clinical Rheumatology.
33(3):415-8, 2014277.
Should Pneumocystis
jiroveci prophylaxis be
recommended with
Rituximab treatment in
ANCA-associated vasculitis?
Besada & Nossent
Clinical Rheumatology.
32(11):1677-81, 2013181
67 yo male GPA, previous CYC,
MTX relapsed on MMF. Given
RTX and developed PCP 3/12
later
Case study and review Review includes 6 pts with PCP
following RTX with AAV. PJP
reported at developing 2,3
months but also as late as 32
months following last RTX. 50%
on RTX monotherapy
Retrospective study from a
single centre—Mayo Clinic
Rochester between 1998 and
2011—identifies 30 patients that
developed PCP after RTX
treatment: 90 % had
haematological malignancies.
10% on RTX monotherapy.
Patients mostly older males—73
% males with a median age of 70
years—and 27 % have chronic
renal disease. PCP occurred after
a median of four RTX Cycles and
a mean of 77 days after its last
administration. Patients have
low lymphocytes (0.38×109/L),
CD4 (0.025× 109/L) and CD8
(0.077×109/L) counts at PCP
onset with undetectable B cell
counts.
In summary, a thorough
assessment of the patient’s
net state of immunodeficiency
before administering RTX can
help stratify the risk for both
colonisation and PCP
development. Risk factors to be
considered are age, renal or
lung involvement, previous
infections due to T cell-
mediated immunity
dysfunction, blood tests
(lymphocytopenia, low CD4 cell
count and inverted ratio) and
concomitant therapy
Pneumocystis pneumonia in
patients treated with
30 patients who received
rituximab and developed PcP
Single centre retrospective
cohort review
To establish the underlying
conditions, clinical course,
Only 1 pt had GPA, majority had
haem malignancy. The mean
3 patients developing PcP were
on single immunosuppression

218
rituximab. Martin-Garrido,
Carmona, Specks, & Limper.
Chest. 144(1):258-65,
2013278.
at Mayo Clinic Rochester over
the years 1998 to 2011
possible risk factors, and
potential association
between RTX and PcP
number of days from last
administration of rituximab to
development of PcP was 76.8 +/-
21.6 day. Only 1 pt had received
prophylaxis. Mortality was 30%
with RTX
Increased risk of
Pneumocystis carinii
pneumonia in patients with
Wegener's granulomatosis.
Jarrousse et al . Clin Exp
Rheumatol. 1993 Nov-
Dec;11(6):615-21180
6 cases of Pneumocystis carinii
pneumonia (PCP) in 23 patients
with biopsy-proven WG and
renal involvement over 10
months (pts were in clinical
trial of either intermittent
high-dose pulse Cy or daily oral
low-dose Cy in combination
with oral prednisone.)
Full text not available-
therefore abstract
reviewed
Mean delay of onset of PCP was
2.5 months after the beginning
of the immunosuppressive
therapy. None of the patients
experienced severe leukopenia
at the time of diagnosis, but the
mean lymphocyte count
decreased to 495/mm3 (range
100 to 830/mm3) and 2 patients
had inverted CD4/CD8 T-cell
ratios. Renal function was
significantly impaired (creatinine
= 493.5 vs 195.4 micromol/l; p =
0.03) in the 6 patients
presenting PCP vs those without.
High-dose co-trimoxazole
therapy was successful in 3
patients, but 3 others who
required mechanical ventilation
died.
26% over 10 months= 31% over
12 months
Fact or fiction: does the
non-HIV/AIDS
immunosuppressed patient
need Pneumocystis jiroveci
pneumonia prophylaxis? An
A review to answer the
questions (1) at what level of
immunosuppression should
one initiate prophylaxis, and
(2) what is the best type of
Search was conducted
with “appropriate MeSH
terms”, using PubMed,
Medline, and The
Cochrane Database. MeSH
Included 7 articles, with
199 patients who
developed PJP (cancer,
transplant, inflammatory
conditions)
25% of patients developed PJP
after 8 wk of therapy with dose
equivalent of 30 mg prednisone.
Median duration of
corticosteroid therapy before
Vague search strategy

219
updated literature
review.Grewal & Brassard.
Journal of Cutaneous
Medicine & Surgery.
13(6):308-12, 2009279.
prophylaxis to use for non- HIV
immunosuppressed pts
terms included PJP, PCP,
prophylaxis, Pneumocystis,
non-HIV, non-AIDS, and
immunosuppression.
the development of PJP was 12
wk
Corticosteroid use, whether it
was stable or being tapered, was
a risk factor in 77% of patients
developing PJP
Audit of pneumocystis
pneumonia in patients seen
by the Christchurch Hospital
rheumatology service over
a 5-year period. Meuli et al.
Internal Medicine Journal.
37(10):687-92, 2007177.
Rheumatology pts having been
prescribed MTX (n=547, 50
randomly selected for more
detailed case review) or
Cyclophos (n=50)
Single centre retrospective
case review
Comparison for the risk of
developing PJP whilst on
CYC vs MTX
4/597 pts develop PJP, 2 on MTX
and 2 on CYC
Only 14 of 47 (29.7%) CYC-
treated patients received PCP
prophylaxis. The annual
incidence of PCP was 0.17%
(95% confidence interval (CI)
0.02–0.63) and 5.33% (95%CI
0.65–19.24) in patients
prescribed MTX and CYC,
respectively. For the 33 patients
receiving CYC without
concomitant PCP prophylaxis the
annual incidence was 9.50%
(95%CI 1.15–34.33).
Infection-related morbidity
and mortality in patients
with connective tissue
diseases: a systematic
review. Falagas, Manta,
Betsi, & Pappas. Clinical
Rheumatology. 26(5):663-
70, 2007280.
CTD patients with infections Systematic review. Search
terms=
“systemic lupus
erythematosus”,
“rheumatoid arthritis”,
”dermatomyositis”,
“polymyositis”,
“Wegener’s
granulomatosis”, “Sjogren
7 articles included with PJP
reported as an outcomes,
of these 64 patients had
GPA
Mortality in this population
reported as between 41 and
61.3%.All pts for whom there
was data for were on high dose
steroid (1mg/kg/day or 60mg)
plus additional IS

220
syndrome”,
“systemic
sclerosis/scleroderma”,
“connective tissue
disease”,
“steroid treatment”,
“methylprednisolone”,
“infection”,
“prophylaxis”,
“Pneumocystis carinii
jiroveci”
Autoimmune inflammatory
disorders, systemic
corticosteroids and
pneumocystis pneumonia: a
strategy for prevention.
Sowden & Carmichael.
BMC Infectious Diseases.
4:42, 2004 Oct 16184.
Pts with AID and PJP General review(not
structured)
Risk factors for PJP in this
population mentioned as
steroids, > 15mg/day steroid,
other immunosuppression, low
lymphs, low CD4, ? presence of
underlying lung disease but
likely presence of steroids plus
inflammation.
They suggest the following
approach to prophylaxis
Given the laboratory costs, we
would argue in favour of
performing CD4+ counts after
one month's
immunosuppression only on
patients who satisfy the
following three screening
criteria:
• Steroid dosage >15 mg
prednisolone or equivalent/day
• >three months corticosteroid
treatment proposed • total
lymphocyte count <600
cells/mm3
A CD4+ count <200 cells/mm3
might then warrant the use of
prophylactic co-trimoxazole, if

221
the annual risk of PCP in these
patients is greater than 9%.
Most cases of PCP in patients
with AID would be captured by
these criteria, according to
published series.
Adverse events and
infectious burden, microbes
and temporal outline from
immunosuppressive
therapy in antineutrophil
cytoplasmic antibody-
associated vasculitis with
native renal function.
McGregor et al. Nephrology
Dialysis Transplantation. 30
Suppl 1:i171-81, 2015281
Biopsy-proven AAV patients
(diagnosed 1/1991–6/ 2011)
followed in an inception
cohort.
374 pts with 2 years f/u
Prospective cohort study Description of infection
rate and type, adverse
events, ESKD, death
Cumulative incidence infection
(any) at 5 years 65% 9severe
infection 26%.
1 PJP 6/52 post induction
therapy. This patient had not
received prophylaxis
Adds little to PJP data but good
for infection overall
Frequency, risk factors and
prophylaxis of infection in
ANCA-associated vasculitis.
Kronbichler, Jayne, &
Mayer. European Journal of
Clinical Investigation.
45(3):346-68, 2015282.
Includes 17 articles with
opportunistic infection
described as an outcomes
Review Description of infections as
outcome
Number of cases of PJP within
reviewed articles (ND=not
documented)
1. PJP 3/133- Flossman
2. Charlier ND
3. PJP 12/38- Bligny
4. PJP 6 Aasarod
5. PJP 2 Goupil
6. PJP 1 Harper
7. PJP 1.4% Booth
8. Weldanz ND
9. Lionaki ND
10. PJP 1 Charles
Risk factors (for infection)
identified as being: older age,
high creat/dialysis, lung
disease, steroids, leucopenia,
lymphopaenia, neg/falling
ANCA, IS on dialysis,
Total n=47 (plus from Booth n=
? unable to find raw data)
Authors recommend PJP
prophylaxis on CYC, on RTX
until pred < 10mg, or when

222
11. PJP 1 Cartin Ceba
12. Chen ND
13. Itabashi ND (but 4
deaths due to PJP)
14. PJP 8 Palsson
15. PJP 1 Uezono
16. Matsumoto ND
17. PJP 12 Godeau
lymph count <300
Incidence of Pneumocystis
jiroveci pneumonia among
groups at risk in HIV-
negative patients. Fillatre
et al. American Journal of
Medicine.
127(12):1242.e11-7, 2014283
All pts with PJP in 20 yr period,
HIV neg
Single centre retrospective
cohort review
From 1990 to 2010, 293 cases of
PJP documented, of which 154
(52.6%) tested negative for HIV.
The main underlying conditions
were haematological
malignancies (32.5%), solid
tumours (18.2%), inflammatory
diseases (14.9%), solid organ
transplant (12.3%), and vasculitis
(9.7%).
GPA pts ranked as high risk
(incidence rates >45 cases per
100,000 patient- year)
Value of anti-infective
chemoprophylaxis in
primary systemic vasculitis:
what is the evidence?
Moosig, Holle, & Gross.
Arthritis Research &
Therapy. 11(5):253, 2009284
Review Recommends PJP proph as TMX
for all those receiving pred >
15mg/day plus additional IS or
pentamadine for those with
intolerance
Cost-effectiveness of
prophylaxis against
Hypothetical cohort A Markov state-transition
model was developed to
1) no prophylaxis; 2)
trimethoprim/sulfamethox
Prophylaxis using TMP/SMX
alone increased life expectancy

223
Pneumocystis carinii
pneumonia in patients with
Wegner's granulomatosis
undergoing
immunosuppressive
therapy. Chung, Armstrong,
Schwartz, Albert, & Al.
Arthritis & Rheumatism.
43(8):1841-8, 2000.285.
follow a hypothetical
cohort of WG patients
over their lifetimes
starting from the time of
initial exposure to the
immunosuppressive
therapy
azole (TMP/SMX) 160
mg/800 mg 3 times a
week, which is
discontinued if patients
experience an adverse
drug reaction (ADR); and
3) TMP/SMX 160 mg/800
mg 3 times a week, which
is replaced by monthly
aerosolized pentamidine
(300 mg) if patients
experience an ADR
and reduced cost for patients
with WG receiving
immunosuppressive therapy.
Replacing TMP/SMX with
monthly aerosolized
pentamidine in cases of ADR
further increased life
expectancy, although at an
increased cost.
Pulmonary complications of
combination therapy with
Cyclophosphamide and
prednisone. Sen, Walsh,
Fisher, & Brock. Chest.
99(1):143-6, 1991.286
Case series HIV neg PJP (4 pts) Single centre case series Risk factors identified as;
hypoalbuminemia (serum
albumin level less than 3.0 g/dl)
and daily (pred plus CYC) therapy
were associated with increased
risk for development of PCP (p
less than 0.05). None of the
patients had leukopenia (less
than 3,500/cu mm) or
neutropenia
Note n=4
Factors associated with
Pneumocystis carinii
pneumonia in Wegener's
granulomatosis. Godeau et
al.
Annals of the Rheumatic
Diseases. 54(12):991-4,
1995.185
12 pts with GPA and PJP
compared with 32 pts with
GPA and without PCP (1984-
1992 in 4 centres)
Retrospective case control
study
Pt characteristics PCP vs
no PCP compared.
Excluded if has received
primary prophylaxis
Mean delay before onset of PCP
was 128 (SD 127) days after the
beginning of immunosuppressive
therapy (median 90 days, range
50-510)
smallest lymphocyte count was
significantly less in the PCP
group (244 (362)/mm3 (range 0-
Threshold of 600 lymphocytes
per mm3 during the first three
months after diagnosis
suggested to define the group
of patients at greater risk of
PCP.

224
1200) v 738
(543)/mm3 (range 60-2400); p =
0001).
Mean cum CYC dose higher in
PJP gp (may represent more
aggressive disease though)
Pneumocystis carinii
pneumonia: a major
complication of
immunosuppressive
therapy in patients with
Wegener's granulomatosis.
Ognibene FP et al. Am J
Respir Crit Care Med 1995,
151:795-799287
Abstract only available.
11 cases of GPA in 180 pts
Retrospective cohort
review
All patients were receiving daily
steroids and a second
immunosuppressive therapy.
Lymphocytopaenia was noted in
all patients, with a mean +/- SEM
total lymphocyte count of 303
+/- 69 cells/microL
A prospective, multicenter,
randomized trial comparing
steroids and pulse
cyclophosphamide versus
steroids and oral
cyclophosphamide in the
treatment of generalized
Wegener’s granulomatosis.
Guillevin L, et al. Arthritis
Rheum 1997, 40:2187-
2198135.
50 pts with GPA Prospective RCT Pulsed iv cyc vs daily oral
cyc, remission at 6 months
and longer follow up
compared
Pneumocystis carinii pneumonia
was higher in oral CYC-treated
patients (30.4%) than in pulse
CYC-treated patients (11.1%).
Total of 10/50 cases 20%
(prophylaxis added after first 12
pts due to high rate PCP)

225
Population Study design Comparisons Outcomes Comments
Mould-active compared with fluconazole
prophylaxis to prevent invasive fungal
diseases in cancer patients receiving
chemotherapy or haematopoietic stem-
cell transplantation: a systematic review
and meta-analysis of randomised
controlled trials. Ethier et al. Br J Cancer.
2012 May 8;106(10):1626-37
288.
Cancer pts receiving
chemotherapy or
haematopoetic SCT
Systematic review and
meta-analysis of RCTs from
984 reviewed articles, 20
were included in this review
Primary outcome
was proven/probable
invasive fungal
infections (IFI)
Mould-active compared with fluconazole
prophylaxis significantly reduced the number
of proven/probable IFI (RR 0.71, 95% CI 0.52 to
0.98; P=0.03). Mould-active prophylaxis also
decreased the risk of invasive aspergillosis (IA;
RR 0.53, 95% confidence interval (CI) 0.37–
0.75; P=0.0004) and IFI-related mortality (RR
0.67, 95% CI 0.47–0.96; P=0.03) but is also
associated with an increased risk of adverse
events (AEs) leading to antifungal
discontinuation (RR 1.95, 95% CI 1.24–3.07;
P=0.004). There was no decrease in overall
mortality (RR 1.0; 95% CI 0.88–1.13; P=0.96).
Baseline incidence IFI on
fluconazole in HSCT seems to be
around 15%, higher that in AAV
as “candidiasis” (not qualified as
invasive or not) in combined
EUVAS only 10%. No aspergillosis
mentioned
Candidiasis (oropharyngeal). C
Pankhurst. British Medical Journal:
Clinical Evidence. 2013 188.
Oropharyngeal candidiasis
affects between 15% and
60% of people with
haematological or
oncological malignancies
during periods of
immunosuppression
What are the effects
of interventions to
prevent and treat
oropharyngeal
candidiasis in adults
undergoing
treatments that
cause
immunosuppression?
In people with immunosuppression following
cancer treatment, absorbed (ketoconazole,
itraconazole, or fluconazole) or partially
absorbed antifungal drugs (miconazole,
clotrimazole) prevent oropharyngeal
candidiasis compared with placebo or non-
absorbed antifungal drugs.
• Non-absorbed antifungal drugs (nystatin or
amphotericin B) may be no more effective
than placebo at preventing candidiasis
Too few studies in those pts
having tissue transplants to draw
conclusions.
Antifungal agents for preventing fungal
infections in solid organ transplant
Fourteen unique trials
with 1497 randomised
Systematic r/v Invasive Fungal
Infections (IFI) rates
Antifungal prophylaxis did not reduce
mortality (RR 0.90, 95% CI 0.57 to 1.44). In
The overall rate of proven
infections (IFI) in the control arm
Viral and fungal prophylaxis evidence table

226
recipients. Playford, Webster, Sorell, &
Craig.
EBM Reviews - Cochrane Database of
Systematic Reviews
Cochrane Database of Systematic
Reviews. 4, 2009189.
participants were
included, SOT
liver tx recipients, a significant reduction in
IFIs was demonstrated for fluconazole (RR
0.28, 95% CI 0.13 to 0.57). Although less data
was available for itraconazole and liposomal
amphotericin B, indirect comparisons and one
direct comparative trial suggested similar
efficacy. Fluconazole prophylaxis did not
significantly increase invasive infections or
colonisation with fluconazole-resistant fungi.
In renal and cardiac transplant recipients,
neither ketoconazole nor clotrimazole
significantly reduced invasive infections.
Overall, strength and precision of comparisons
were limited by paucity of data.
i.e. no prophylaxis, of these four
studies was 13%(range 4 to 23%)-
therefore perhaps a rate more
comparable to the AAV
population rather than HSCT
Asymptomatic cytomegalovirus viremia
is associated with increased risk of
pneumocystis and fungal infections.
Poglajen G.et al.
Journal of Heart and Lung
Transplantation. Conference: 34th
Annual Meeting and Scientific Sessions of
the International Society for Heart and
Lung Transplantation, ISHLT 2014 San
Diego, CA United States.
70 consecutive adult heart
transplant recipients
To investigate the
aetiology and time
course of
opportunistic
infections in pts with
asymptomatic CMV
viraemia
In CMV Group, we found a significantly higher
incidence of PJP (45% vs. 2%, P< 0.001) and
fungal infections (27% vs. 1%; P< 0.001). On
average, PJP infections occurred 4.2+/-3.1
months after CMV viremia, and fungal
infections occurred 1.4+/-0.7 months after
CMV
Mean time from transplantation
to CMV viremia was 10.4+/-1.5
months (PJP, CMV and fungal
prophylaxis continued for 6
months post-transplant)
Duration of prophylaxis against fungal
infection in kidney transplant recipients
Guerra C Formica R Kulkarni S et. al.
Progress in Transplantation, 2015289.
84 KTR recipients Single centre retrospective
case-control study
Compare the efficacy
of two strategies
prophylaxis with
nystatin suspension
(NPx) in kidney
transplant recipients
Primary outcome was the incidence of thrush
and Candida esophagitis within 3 months post-
transplantation
Limiting the administration of NPx to the
duration of admission after tx appears
sufficient for prophylaxis of fungal infections in

227
(KTR). (KTR prior to
the protocol change
received NPx
500,000 units swish
and swallow for 2
month (pre group)
and KTR after the
change received NPx
for the duration of
admission (post
group)
KTR.
Risk factors for invasive fungal disease in
heart transplant recipients.
Rabin A.S., Givertz M.M., Couper G.S.,
Shea M.M., Peixoto D., Yokoe D.S.,
Baden L.R., Marty F.M., Koo S.
Journal of Heart and Lung
Transplantation. 34 (2) (pp 227-232),
2015290.
Not so relevant as risk factors are
drugs not used in vasculitis and
the surgery itself
Efficacy and safety of measles, mumps,
rubella and varicella live viral vaccines in
transplant recipients receiving
immunosuppressive drugs.
Danerseau A, Robinson J. World Journal
of Pediatrics
2008 vol: 4 (4) pp: 254-258291.
Six case series studies
(n=112 children) and 2
case reports (adults)- SOT
Systematic review Post-immunisation titres were in the immune
range in 57% (82/145) of situations where they
were measured (17-100%) following a single
dose of vaccine, in 68% (15/22) of situations
following two doses and in two of two cases
following three doses. Three cases of mild
varicella There was one case of rejection three
weeks post-immunisation of MMR and
measles vaccines
Insufficient published data to
derive evidence-based guidelines
for use of live viral vaccines in
transplant recipients on
immunosuppression. Preliminary
data on efficacy and safety
suggested that the use of these
vaccines in transplant recipients
still on immunosuppression could
be a reasonable strategy.
Long-term acyclovir for prevention of 77 hematopoietic cell Double blind placebo VZV disease at 1 year Highly significant reduction of VZV disease was Authors conclude “acyclovir given

228
varicella zoster virus disease after
allogeneic hematopoietic cell
transplantation--a randomized double-
blind placebo-controlled study.
Boeckh M, Kim HW, Flowers ME, Meyers
JD, Bowden RA
Blood. 107(5):1800-5, 2006190.
transplant recipients at
risk for VZV reactivation
were randomized to
acyclovir 800 mg twice
daily (38) or placebo (39)
given from 1 to 2 months
until 1 year after
transplantation.
controlled RCT was the primary end
point
seen in acyclovir recipients. no sig diff in
adverse effects
at 800 mg twice daily until 1 year
after transplantation is a safe and
highly effective strategy to
prevent clinical VZV infections in
hematopoietic cell transplant
recipient”
B Cell Therapies, Approved and
Emerging: A Review of Infectious Risk
and Prevention During Use. Md Yusof,
Vital, & Buch. Current Rheumatology
Reports. 17(10):65, 2015292.
Non- systematic review Data from RCTs and LTE studies in 3194
patients with RA
reported 108 cases of herpes zoster in 100
patients (including
two cases of ophthalmic herpes zoster and five
SAEs) in the all exposure group compared to
13 cases in the placebo+MTX group, rates of
9/1000 and 11.7/1000 patient-years,
respectively. This is comparable to the rate in
the general RA population, 11.5/1000 patient-
years.

229
6 A DELPHI STUDY TO ASSESS THE PREVENTION OF
TREATMENT AND DISEASE RELATED MORBIDITY IN VASCULITIS
(ADAPTIV): RECOMMENDATIONS Overarching Recommendations
1. Patients should be educated to engage in follow up care. This may include the
appropriate use of self-referral pathways to secondary care when unwell.
2. Primary care should be involved with stable patients, being aware of the
immunosuppressive medication they are taking and be responsible for lifestyle advice.
3. With regards to maintaining bone health, patients should have overall fracture risk
assessed rather than just Bone Mineral Density (BMD). Patients with CKD 4/5 should
have bone disease managed in conjunction with specialist centres (renal/ endocrine).
4. Patients with vasculitis have a higher cardiovascular (CV) risk than the general
population and therefore CV risk assessment should be carried out on an at least annual
basis. Awareness of increased CVD risk in vasculitis should be raised in both primary and
secondary care and to the patient.
5. There is a need for recognition of the increased infection risk of patients with ANCA
associated vasculitis. We recommend vaccination against ‘flu and pneumococcus for this
population and Pneumocystic jiroveci prophylaxis for those on “induction” therapy.
6. There should be awareness of the possible effects of cyclophosphamide therapy on
both female and male fertility. Therefore, in the absence of life/organ threatening
disease alternatives should be considered. Where alternative therapies are not possible,
strong links with the local reproductive health unit should be in place to enable gamete
storage where appropriate.
7. Patients should be counselled and educated with regards to possible increased cancer
risk. These patients should be strongly encouraged to attend routine population cancer
screening and should undergo regular skin surveillance.

230
Level of evidence
Grading of recommendations and evidence levels
Levels of evidence for studies of intervention are defined as follows:
Ia from meta-analysis of randomised controlled trials (RCTs)
Ib from at least one RCT
IIa from at least one well designed controlled study without randomization
IIb from at least one other type of well-designed quasi-experimental study
III from well-designed non-experimental descriptive studies, e.g. comparative studies,
correlation studies, case-control studies
IV from expert committee reports or opinions and/or clinical experience of authorities
The quality of the guideline recommendations is similarly graded to indicate the levels of
evidence on which they are based:
grade A: evidence levels Ia and Ib
grade B: evidence levels IIa, IIb and III
grade C: evidence level IV
6.1 BONE HEALTH
ANCA Associated Vasculitis is predominantly a disease of the older population with peak
age of onset being 65-74 years38. In addition, due to the ongoing reliance on
immunosuppressive regimens with a significant corticosteroid exposure, these patients are
at risk from glucocorticoid-induced osteoporosis (GIOP). The disease process itself likely
contributes further to this risk through effects from cytokines involved in the inflammatory
process 117.
Fracture risk increases early on during glucocorticoid exposure (the first 3 to 6 months) and
reduces again following steroid withdrawal. The risk increases to be most significant for
those taking a dose of greater than or equal to 7.5 mg/day prednisolone and it is the risk of
vertebral fractures that increases most293. The following recommendations are therefore
made for preservation of bone health in patients with AAV. The recommendations here

231
mirror the currently available national/ international guidelines for prevention and
treatment of GIOP, which will require updating on a regular basis.
1) Patients should have overall fracture risk assessed rather than just Bone Mineral
Density (BMD) using a validated risk prediction model (Evidence A, 1a) (expert consensus
level 81%)
Currently validated assessment tools include FRAX and QFracture 2012. However, FRAX has
limitations in that it assumes an average dose of prednisolone of between 2.5 and 7.5mg
per day149. Adjustments are recommended for those taking prednisolone doses outside this
range (see NOGG for details). Algorithms for determining whether BMD measurements are
required are available from the NOGG. However, in general women over 70 years, or with
previous fragility fracture or taking > 15mg prednisolone/day should be considered for
bone protective therapy. Preventative therapy options for GIOP includes; alendronic acid,
risedronate or zolendronic acid for those patients who are intolerant of oral
bisphosphonates and in whom adherence to oral therapy may be difficult150. Treatment
review is recommended after 5 years (alendronate, risedronate or ibandronate) or 3 years
(zolendronic acid) but those who are high risk should generally continue treatment (over
age 75 years, those with previous hip/vertebral fracture and those continuing on
prednisolone doses greater than 7.5mg/day).149
2) Specialist management of bone disease in patients with stage Chronic Kidney Disease
(CKD) Stages 4 and 5 is required (Evidence IV).
In patients with advanced renal impairment (CKD 4 and 5) there is limited safety data for
bisphosphonates. Alendronate is not recommended in patients with a creatinine clearance
of <35mls/min and risendronate is contraindicated with a creatinine clearance <30mls/min.
The use of ibandronate is recommended with caution at creatinine clearance <30mls/min
and zolendronate at <35mls/min. In addition, it should be borne in mind that DEXA
scanning in patient with CKD stage 3 to 5 may not provide valid information in the presence
of metabolic bone disease294.
3) All patients should be counselled regarding risks prior to bisphosphonate therapy
including osteonecrosis of the jaw, avascular necrosis of the hip and “frozen
bone”/subtrochanteric hip fracture (Grade C, Evidence IV) (expert consensus level
94%)

232
Dental assessment and pre-emptive treatment is recommended prior to commencement
with bisphosphonates due to the risks of non-healing following extraction if on therapy.
However, dental treatment on bisphosphonate therapy is not contra-indicated if it is
required149.
4) Vitamin D levels should be checked at baseline with replacement and maintenance
therapy prescribed as required (Grade A, Evidence 1b).
More frequent lower dose vitamin D should be considered as annual high dose vitamin D
has shown an increase in falls and fractures. There should be awareness of seasonal
variation in vitamin D levels. Increased dietary calcium may be preferable to calcium
supplementation due to concerns regarding increased cardiovascular event rates in a study
of calcium supplementation, although the majority of studies have reported calcium as
having a neutral or beneficial effect on CV event rates295.
5) Treatment with Denosumab should be considered for use in patients where
bisphosphonates have been contraindicated (Grade A, Evidence 1a) (expert consensus
86%).
Denosumab is NICE approved in this scenario for the primary prevention and treatment of
osteoporosis in post-menopausal women296. Denosumab should never be administered in
the presence of hypocalcaemia. Patients with eGFR less than 30ml/min are at higher risk of
hypocalcaemia and therefore should have regular calcium monitoring whilst on
Denosumab297.
6.2 CARDIOVASCULAR RISK MODIFICATION
It is acknowledged that patients with AAV have an increased risk of thromboembolic
disease, particularly associated with periods of active disease112. In more recent years
epidemiological cohort studies and analysis of the EUVAS clinical trial follow- up data has
supported that this patient population has a higher rate of CVD in addition, with this
contributing to later death in the bimodal pattern of mortality seen in this population198.

233
1) Patients with vasculitis have a higher cardiovascular risk than the general
population and therefore cardiovascular (CV) risk assessment should be carried out on an
at least annual basis (Grade B, Evidence III)(expert consensus level 94%)
Matched cohort studies have demonstrated an increased incidence of CV events in AAV
patients, with an observed to expected ratio of 1.9 in one study compared with the
background population 114 and a hazard ratio of 2.23 compared with a CKD population 115.
This observation has led to the development of a model for predicting cardiovascular
events in AAV patients with age, diastolic hypertension and absence of PR3 antibodies
being identified as risk factors for cardiovascular events in newly diagnosed AAV 116. A
smaller French study has recently suggested that the risk of cardiovascular events in this
population may be 2- 3 times that which may be anticipated through conventional risk
factor stratification203. However, as yet there is insufficient evidence to support that
patients with AAV should be treated differently to other patient groups with regards to
primary prevention of CVD.
There are multiple smaller studies in addition, reporting abnormal surrogate markers for CV
outcomes such as intimal medial thickness (IMT) on USS or Ankle-brachial Pressure Index
(ABPI) in patients with vasculitis 159–161. It should also be noted that patients with AAV may
have cardiac involvement as a manifestation of their disease that may be asymptomatic
and not detectable using conventional cardiac imaging such as echocardiography298,299.
2) Awareness of increased CVD risk in vasculitis should be raised in both primary
and secondary care and to the patient (Grade C, Evidence IV).
Although there is currently no evidence for augmented primary prevention in this
population, the awareness of the higher risk status of CVD means that known risk factors
should be rigorously addressed and modified, including attention to exercise, BMI, blood
pressure control, and lipid monitoring with smoking cessation critical (expert consensus
level 95%) BMI has been shown to predict major cardiovascular events in this population
203, with smoking status associated with MI and progression to ESRD in patients with
vasculitis208.
In addition, early identification of Chronic Kidney Disease (CKD)/ proteinuria in this group is
imperative due to the additional significant risk of cardiovascular disease this confers300.

234
3) Awareness of the increased risk of Venous Thromboembolism (VTEs) is important
in this population, with standard VTE prophylaxis being used if there is any loss of
mobility (Grade B, Evidence III).
VTEs are much more frequent in AAV than the background population. The rate varies from
1.58 episodes/ 100 patient years increasing to 7.26/ 100 patient years during active disease
in one study155. Other risk factors aside from periods of disease activity for the
development of VTEs include, older age, male, previous VTE, CVA with motor deficit and
nephrotic range proteinuria 214.
Vasculitis patients having had more than one VTE should receive long-term anticoagulation,
as per other populations301. There is a clear need for further research to determine the
relationship between VTE risk, disease activity and autoantibodies (including non-ANCA
autoantibodies). There is no evidence to support the role of aspirin in primary or secondary
VTE prophylaxis.
6.3 FERTILITY PRESERVATION
1) In the absence of life or severe organ threatening disease, the routine use of
cyclophosphamide should be avoided in women of child-bearing potential (Grade A,
Evidence level 1b- i.e. Rituximab versus cyclophosphamide).
The majority of data on the effect of cyclophosphamide exposure on fertility is derived
from the lupus population, with a rate of around 30% of cessation of menstruation
following exposure to cyclophosphamide121. However, this risk varies depending on
cumulative cyclophosphamide exposure and age at cyclophosphamide administration. It
has been reported that premature ovarian failure can be induced with a dose of 20.4g for
women 20-30 years old or 5.2g for women >40259. However, there is no robust evidence
that there is a safe dose of cyclophosphamide that would completely eradicate the risk of
infertility (expert consensus level 87%).
It is also well established that exposure to cyclophosphamide in men causes significant
sperm abnormalities associated with a reduction in fertility 122. Therefore, careful
consideration should be given to the use in men (with non- life or severe organ threatening
disease) who have not completed their family. However, it should equally be noted that
kidney failure due to inadequately treated disease would have a significant effect on

235
fertility, and therefore it is prudent to ensure organ threatening disease is treated
appropriately (expert consensus level 88%).
Links with the appropriate local reproductive health departments should be established,
including urgent referral pathways should be available, particularly for sperm banking for
those patients who present acutely requiring rapid treatment (expert consensus level 94%).
Men should be offered the chance to store sperm before starting cyclophosphamide (if it
does not interfere with medically urgent therapy) (expert consensus level 94%). Individual
cases, such as sperm banking following exposure to 1 or 2 doses of cyclophosphamide or
for patients who are physically incapable of sperm banking should be discussed with the
local reproductive health department. Oocyte retrieval in unwell females with active
vasculitis is not currently feasible (expert consensus level 92%).
It should be borne in mind that all vasculitis patients may have the potential for future
cyclophosphamide exposure (in severe relapse) and therefore may wish to explore the
option of gamete storage (sperm banking or oocyte retrieval) prospectively.
2) Current recommendations are that patients should be counselled to avoid
pregnancy for 12 months following Rituximab exposure179(Grade C, Evidence IV)
However, there is emerging data that patients can have successful pregnancy outcomes in
the months following Rituximab exposure. A reported series of 8 pregnancies in 6 such
vasculitis patients with Rituximab exposure between 1 week and 16.5 months prior to
conception demonstrated successful outcomes in 7 of the 8 pregnancies. In addition, of
interest, foetal CD20+ B lymphocytes measured in cord blood at time of delivery did not
appear to be affected 302. Therefore, the patient who becomes pregnant following
Rituximab exposure should be referred for counselling /management in a specialist joint
vasculitis- obstetric clinic. Ideally, all patients with vasculitis who are pregnant or
considering pregnancy should be referred to a specialist joint clinical service.
3) There may be some benefit in preservation of fertility from GnRH agonists/ GnRH
analogues to protect fertility. However, there is insufficient current evidence to
recommend routine use with this requiring prospective studies.(Grade B, evidence level
III)

236
There are multiple examples in the literature of GnRH analogues used to help maintain
fertility and aid pregnancy after cyclophosphamide therapy121,253,303 but these are typically
small, retrospective studies. Literature reviews generally support the use of GnRH
analogues but meta-analyses are conflicted254,260,304,167. The most recent of these does
conclude that GnRHas appear effective in reducing amenorrhoea in all patients, with
pregnancy rates higher in the GnRHa arm. However, these were observational studies with
clinical trial evidence not available167.
6.4 CANCER RECOMMENDATIONS
1. Patients with non- life threatening relapsing disease and previous treatment with
cyclophosphamide should avoid further exposure to cyclophosphamide i.e. consider
Rituximab treatment. This is supported by current funding policies for Rituximab. (Grade
B, Evidence level III)(expert consensus level 92%)
Early studies, with a substantially greater cyclophosphamide load for patients reported a
2.4 fold increase for all malignancies, with this increase predominantly being accounted for
by bladder cancer and lymphoma134. Since the introduction of a switch from
cyclophosphamide to maintenance therapy at 3 to 6 months and a trend towards pulsed
intravenous therapy rather than daily oral, resulting in a much lower total
cyclophosphamide dose, it is hoped that this risk has diminished somewhat. However, data
from the long-term follow-up (median 4.3 years) of the CYCLOPS trial (comparing daily oral
to pulsed intravenous cyclophosphamide) showed no difference in malignancy rates75. This
suggests that it may be many more years before this change in practice translates to an
actual reduction in malignancy rates.
With regards to cumulative cyclophosphamide dose, one series of 293 GPA patients
reported no increased in cancer risk (with the exception of Non Melanomatous Skin
Cancers NMSC) for those patients receiving less than 36g in total305. However, with regards
to bladder cancer, a series of 1065 GPA patients reported that cumulative
cyclophosphamide doses of greater than 25g were associated with a 5-fold risk of bladder
cancer, with each 10g increment associated with a doubling of cancer risk163.

237
A recent meta-analysis of the risk of cancer in AAV included 6 observational studies. This
study reported that NMSC, leukemia and bladder cancer were more frequently observed in
patients with AASV with SIRs of 5.18 ,4.89 and 3.84 respectively and with rates of
lymphoma, liver and lung also increased. However, evidence is accumulating for the
reported increased incidence of cancer in AAV to be predominantly attributable to the
increased risk of NMSC230,243.
In summary, patients with previous significant cyclophosphamide exposure are likely to
have increased ongoing cancer risk that requires continued vigilance. In particular, patients
should receive education and advice with regards to prevention and screening for skin
cancer (see below).
2. Patients should be encouraged to attend for age and gender appropriate routine
population cancer screening (Grade B, Evidence level III/IV) (expert consensus level 94%)
3. CXRs should be carried out in smokers but no other routine cancer, aside from
population screening should be carried out unless otherwise clinically indicated (e.g.
change in bowel habit, major weight change or night sweats). (Grade B, Evidence level
III).
Clinicians should have a high degree of suspicion for investigating for possible malignancy
in atypical cases of AAV not responding to treatment. However, there is no clear evidence
that cancer predisposes to develop of AAV233.
4. Cervical screening should be carried out as per the population screening
There is currently insufficient evidence to support annual cervical screening of this
population. However, in other populations with autoimmune disease an increased
incidence of CIN has been described120,246. It is unclear whether this risk relates to an
association with more aggressive disease or more aggressive therapy. Therefore, patients
should be counselled in advance of immunosuppression exposure regarding the potential
increase in CIN changes on cervical screening and the need to attend routine population
screening re-enforced.
Clinicians should be aware of patient’s HPV status/ immunisation status, with HPV positivity
being well established as a risk factor for CIN and cervical cancer.

238
5. All patients on immunosuppression require counselling regarding the need for sun
protection and regular (annual) skin screening (Grade C, Evidence level IV)(expert
consensus level 94%)
The recent data for malignancy in AAV suggests that the only truly significant increase in
cancer risk in this population may be in non-melanomatous skin cancer230. Both
azathioprine and cyclophosphamide are likely to be significant in terms of risk for
NMSC306,307. The patient’s history (including family and repeated history of high level of UV
exposure early in life e.g. living abroad) should be taken into account regarding skin cancer
risk (expert consensus level 88%). The avoidance of tanning beds should be advised (expert
consensus level 94%). Patients should be educated to perform self-checking for skin cancer
with knowledge of the appropriate place to present to for further investigation (expert
consensus level 89%). Skin protection and vigilance should be led through education of the
patient, with support from primary care and appropriate links to secondary care when
required.
6. Patients exposed to cyclophosphamide should be considered for: (Grade C, Evidence
level IV)
· Pre-hydration where possible (prior to pulsed intravenous cyclophosphamide)
· Mesna
It has been well reported that very high doses of cyclophosphamide leads to a significant
increase in the risk of bladder cancer163, with one series reporting a substantial increase in
the rate of bladder cancer in those receiving more than 36g cyclophosphamide
cumulatively (SIR 9.5)234. However, a more recent review of the data available for the use of
cyclophosphamide to treat rheumatic disease concluded that low dose pulsed intravenous
cyclophosphamide is likely to be associated with a low risk of cystitis and bladder cancer164.
In this setting, there is little evidence to support the use of mesna. However, as there may
be some benefit and mesna is well tolerated, expert consensus is that the use of mesna
may be considered. Patients with a previous history of cyclophosphamide exposure should
in addition have urinalysis for blood at every relevant hospital visit (at least 12 monthly)
(expert consensus 94%) with cystoscopy and cytology assessment in any cyclophosphamide
patient with persistent non- glomerular haematuria (expert consensus level 88%).

239
6.5 INFECTION PREVENTION
Nearly half of all deaths accounting for the 11%, 1 year mortality for patients with AAV are
now attributable to infection, with the majority of these being lower respiratory tract
infections 90. A recent review of infections within this population reports between 20 and
60% of patients with AAV experiencing significant infections, depending on the cohort,
immunosuppression exposure and prophylaxis282. Again, the majority of articles reviewed
report LRTI as the most frequent but opportunistic infections are not insignificant with
Cytomegalovirus, Pneumocystis jirovecii, Candidiasis and herpes/varicella zoster all being
reported.
1) There is a need for recognition of the increased infection risk of patients with
ANCA associated vasculitis (Grade C, Evidence IV).
The risk of infection within this population is likely to arise from both the
immunosuppression and the underlying disease pathology itself.
We advise education of patients and primary care with regards to this increased infection
risk to encourage early presentation and treatment for immunosuppressed patients with
infective symptoms.
2) PJP prophylaxis is recommended during induction therapy and with
reintroduction of therapy for major relapse. (i.e. during treatment with high dose
steroids/Rituximab/cyclophosphamide) (Grade A, evidence level 1a)
A meta- analysis of evidence for PJP prophylaxis in immunocompromised patients
concluded that the rate of PJP infection within a population needs to be around 6.2% for
prophylaxis to be effective308. There are few large studies on the rate of infection in the
AAV population without prophylaxis. In recent years, the protocols for EUVAS trials have
included suggested PJP prophylaxis but data is not available as to how many received this,
and the effect on infection rates. However, earlier trial data suggests an incidence of PJP in
this population during induction therapy of around 20%309.
Known risk factors for PJP development in this population include; lymphopenia, low CD4
count, steroid use, higher dose steroid use, and cytotoxic therapy272,279,177,185,183. In addition,
a substantial number of cases of PJP have been reported following treatment with
rituximab, as early as days to weeks following exposure and up to 32 months from last

240
administration310,181,277. In acknowledgement of this risk, the FDA licensing for the use of
Rituximab in the US for GPA and MPA includes advisement of concurrent PJP prophylaxis
prescribing for at least 6 months following the last Rituximab infusion179.
Co-trimoxazole should be first line prophylaxis as there is the most data to support safety
and efficacy308 (Evidence 1b). If the patient is unable to take co-trimoxazole, sulfonamide or
trimethoprim then other options include dapsone, atovaquone and nebulised
pentamadine. If using dapsone there should be awareness of the possible side- effect of
methaemogloginaemia 311, and this should be screened for if there is any clinical suspicion
(symptoms or an unexplained drop in haemoglobin). There is very little data directly
comparing the effectiveness of these alternative prophylactic agents, with no evidence in
favour of a particular agent in the small number of comparisons that have been made308.
Awareness should be maintained of the potential serious interaction between
methotrexate and co-trimoxazole, with fatalities due to cytopaenias reported312.
There is no evidence on which to base a recommendation for continuation of prophylaxis
for any given time period post cyclophosphamide treatment. PJP risk may continue post
cessation of cyclophosphamide with cases being reported up to 24 months in a patient
treated with rituximab and cyclophosphamide as part of chemotherapy regimen for
haematological malignancy313, although this patient had received an investigational drug
shortly prior to development of PJP.
Education of patients and primary care with regards to the risk of PJP infection and
potential symptoms is key in conjunction with prescription of prophylaxis.
3) Clinicians should be aware of markers of potential over- immunosuppression in
patients.(Grade C, evidence level IV)
Clinical markers such as the development of previous opportunistic infections may be
helpful in the identification of potentially over immunosuppression, and as a predictor for
future infection. Frequency of infection has been shown to be associated with an increased
risk of future severe infection, and in turn, all-cause mortality281. Other risk factors for
infection in this population include; leucopenia, lymphopenia, older age, female gender,
higher steroid exposure and dialysis dependency111,187,281,314. These patients may benefit

241
from more detailed profiling of their immune status such as measurement of lymphocyte
subsets and immunoglobulin levels, and consideration of reduction in immunosuppression.
Low CD4 count, B cells and IgG levels have been demonstrated to correlate with infection
rate in this population171.
4) We recommend ‘flu and pneumococcal vaccination for immunosuppressed
patients with vasculitis.
In patients who have not yet commenced immunosuppression, inactive vaccinations should
ideally be administered at least 2 weeks prior to initiation of therapy133.
For patients having received Rituximab, there is some evidence that there may be an
antibody response to vaccination >6 months following administration for those in whom B
cell reconstitution has begun to occur174,266. However, patients should be counselled that
vaccine response is still likely to be suboptimal.
For those where usual ‘flu vaccination season falls during the patient’s induction regime
(i.e. within the first 6 months following initiation of rituximab or cyclophosphamide)
individual risk- benefit analysis should be undertaken as to whether to administer ‘flu
vaccine during this time period. There is no evidence that vaccination will trigger disease
relapse in patients with stable disease171,172,271.
Pneumococcal vaccination should be with Pneumococcal Polysaccharide Vaccine (PPV 23)
as per the Green Book. Where possible PPV should be given 4-6 weeks prior to initiation of
immunosuppression but where not possible, at least 2 weeks before or delay until 3
months following cessation of “induction therapy”. Patients with chronic renal disease
should be re-immunised every 5 years with PPV 23.168. Serotype-specific Pneumococcal IgG
antibody monitoring may be relevant for assessing immune response to vaccination.
5) Prior to commencement of immunosuppressive therapy patients should be screened/
treated for latent TB as per British Thoracic Society guidelines315
Current BTS guidelines recommend: “In adults who are anticipated to be or are currently
immunocompromised, a risk assessment is undertaken to establish whether testing should
be offered, taking into account:
1)risk of progression to active TB based on how severely they are immunocompromised

242
and for how long they have been immunocompromised
2)risk factors for TB infection, such as country of birth or recent contact with an index
case with suspected infectious or confirmed pulmonary or laryngeal TB.
For adults who are immunocompromised, consider an interferon-gamma release assay
alone or an interferon-gamma release assay with a concurrent Mantoux test. If either test
is positive (for Mantoux, this is an induration of 5 mm or larger, regardless of BCG history),
assess for active TB.
If this assessment is negative then patients should be offered treatment for latent TB
infection.”
6) Patients on induction therapy immunosuppression (or high dose steroids for relapse)
or patients with an episode of candidiasis/previous candidiasis may require fungal
prophylaxis (Grade B, evidence level III).
This should be with a therapy of proven efficacy such as fluconazole as the evidence in
other immunosuppressed patients does not support non- absorbed fungal prophylaxis,
such as topical nystatin and amphotericin 188.
Equally, anti-viral prophylaxis (acyclovir) should be considered for prophylaxis against
herpes simplex/zoster if there is evidence of previous infection or if the patient is thought
to be at high risk of opportunistic infection (Grade C, evidence level IV).
7) Ideally, routine pretesting of varicella zoster immunity should be carried out prior to
commencement of immunotherapy. (Grade C. Level IV))
However, clinicians should be aware that patients’ immune status may change following
exposure to immunosuppression. Exposure to varicella in the immunosuppressed patient
should necessitate early presentation for re-assessment of varicella immune status and
need for pre-emptive therapy. Varicella Zoster Immunoglobulin G (VZIG) prophylaxis is
recommended for individuals who fulfil all of the following three criteria:316
1) significant exposure to chickenpox or herpes zoster
2) a clinical condition that increases the risk of severe varicella (includes
immunosuppressed patients)
3) no antibodies to VZ virus (VZIG administration should not be
delayed past seven days after initial contact while an antibody test is done.
Under these circumstances, VZIG should be given on the basis of a negative
history of chickenpox).

243
Current UK recommendations from the Green Book state Varicella Zoster vaccine is
contraindicated in the immunosuppressed patient as a live vaccine316.
6.6 EDUCATION AND MONITORING
1) All vasculitis patients, including those off immunosuppression and clinically stable for
more than 12 months, should continue to receive secondary care follow- up (Grade C,
Level IV)
The frequency of secondary/ tertiary care review for a patient with stable vasculitis
depends upon risk of relapse, previous immunotherapy, and current degree of
immunosuppression. However, after 2 years, every 3-6 months may be reasonable (if
clinically stable).
2) Patients should be educated to engage in follow up care. This may include the
appropriate use of self-referral pathways to secondary care when unwell (Grade C, Level
IV).
3) Primary care should be involved with stable patients, being aware of the
immunosuppressive medication they are taking and be responsible for lifestyle advice
(Grade C, Level IV).
6.7 APPLICABILITY AND UTILITY
6.7.1 A statement of potential organizational barriers to introduction
Vasculitis patients are complex often requiring input from multiple, cross-specialty care
providers. The development of cohesive networks of care, involving all relevant stake-
holders, on a regional and national level will support optimal delivery of care for this
population. This is in line with current recommendations for this population83.
6.7.2 Potential costs implications for introduction of guideline
There should be no major cost implications for the introduction of these guidelines as the
majority of the recommendations reflect best clinical practice.
6.7.3 Suggested audit measures
Cumulative dose cyclophosphamide

244
Indications for use of Rituximab
Compliance with NOGG for GIOP prevention and management
Compliance with Green Book recommendations for vaccinations
Compliance with BTS guidelines for pre- treatment TB screening
Documentation of patient drug education prior to initiation of therapy

245
Following on from the process to define standards of care for this population, the next
logical step was to consider how these standards could be best applied.
This initially took the form of a checklist, covering the areas outlined in the Delphi and
subsequent recommendations.
However, following extensive discussions with those involved in electronic healthcare this
“checklist” soon evolved into the concept of software which would allow efficient use of all
currently available relevant healthcare data, in addition to aiding with the systematic
review of the required areas. This concept was named the “Vasculitis Care Optimisation
Tool” or VasCOT.

246
7 DEVELOPMENT OF A VASCULITIS CARE OPTIMISATION TOOL
7.1 PART A: CONCEPT DEVELOPMENT AND USER ENGAGEMENT
7.1.1 Introduction
Vasculitis is a rare autoimmune inflammatory condition that may affect multiple organ
systems. The severity of the disease can vary greatly from patient to patient, as can
treatment and assessment within the NHS. Untreated, life- expectancy averages 5 months89
but advances in immunosuppressive therapy has resulted in a 75% survival at 5 years98.
However, beyond initial aggressive treatment, long- term therapy to control the disease is
often required.
Evidence has shown that some of the most significant ongoing problems for this population
are infections, cardiovascular disease and cancer, with these accounting for the majority of
deaths 90,98. Despite this, systematic assessment of these risks and application of
preventative measures are not widely implemented and patients remain relatively unaware
of these risks 317,318. Variable awareness is made worse by the fragmented nature of the
information systems used in the NHS.
Clinics for patients with vasculitis may have no access to advanced information on patient
health and as a consequence clinics are not running at maximum efficiency. To address
these problems we have designed the Vasculitis Care Optimisation Tool (VasCOT). VasCOT
is a web- based package designed to improve the comprehensive nature of patient care
and to be applicable and usable at every Vasculitis centre in the UK. It provides a method of
structured assessment with co-ordination of available electronic patient data (primary/
secondary care and patient entered). This is initially intended to facilitate identification of
patients at risk of developing disease and treatment related co-morbidities. However, once
established, it could also assist with patient self-reporting of disease status, enabling better
prioritisation of patient appointments. This tool may be used across the spectrum of
vasculitis care providers, to facilitate seamless care and efficient communication to all,
including the patient themselves. Indeed, the patient will be able to input and edit
information including reporting of health events and quality of life measures.

247
In other complex chronic disease groups, a structured approach using an electronic health
record has shown improved clinical outcomes, in addition to high levels of patient and
clinician satisfaction319–9. It is anticipated that the benefits of this system will include
improving patient safety and involvement in their care, and improving the efficiency of care
delivered.
7.1.2 Identification and engagement of stakeholders
The first stage within this process was to identify all key parties for involvement in both
initial development and building of the prototype but also those who may be involved in
future use and dissemination of the product.
The following were consulted and contributed to this development process:
• Primary care: Dr Ivan Bennet: Chair Central Manchester CCG
• Secondary care clinicians: Rheumatology and nephrology
• UK and Ireland Vasculitis Rare Disease Group
• Patients: Vasculitis UK and individual patients locally (see patient interviews)
• Specialised Service Commissioning (SSC)
• NorthWest EHealth: business analysis: requirements elicitation, wire framing and
solution feasibility and commercialisation consultancy
• Hitachi Design Centre Europe: user experience design, commercialisation
• Trusttech: commercialisation
• Central Manchester Foundation Trust Information Technology, Chris Anderson
(Xibble Ltd) and Chris Lee (OBEC ltd): functional specification.
7.1.3 Methods
Concept (the concept was developed by Dr Brown, with support from Dr Venning. All
development leading from the concept was supervised and guided by input from Dr Brown)
The idea for VasCOT initially developed from the observation that due to the number and
complexity of areas for review in a clinical encounter it would be helpful to have a
structured method of assessment (e.g. a checklist). This was noted alongside the use of an
established model of “annual review” in the local renal transplant population323. Following
initial exploratory discussions with local clinicians and patients, alongside a dialogue in the
wider vasculitis community through the UK and Ireland Rare Disease Group network, the
concept of VasCOT was developed and the user map outlined (represented in Figure 1. and
2.)

248
In summary:
1. The patient, attending a secondary care clinic for their vasculitis management is
invited to participate in VasCOT and their account is created and linked to a primary and
secondary care provider, and a named vasculitis clinician.
2. An automated data feed from primary to secondary care is then established with
events and data required predefined using primary care (READ/SNOMED) codes (following
consent from patient and primary care). This data is limited to relevant items including
prescriptions, vaccinations, cancer screening attendance/ results and events such as
infections.
3. This data prepopulates some of the fields in the “health review” pages.
4. Prior to clinic review the patient is invited to log-in and to verify demographic data,
medication, lifestyle and family history and to complete a quality of life assessment (EQ-
5D). This further populates some of the data fields. The patient also has the opportunity to
highlight any particular issues that they would like addressing within the upcoming clinical
encounter.
5. On attending the clinic, the clinician logs in to the system with the patient present.
The clinician can then validate events entered by the patient or primary care. The clinician
can then perform a detailed “health review” for the patient covering the areas of
cardiovascular risk, infection prevention, bone health, fertility and cancer screening and
steroid “other”. Each area has its own screen with the existing information from primary
care and the patient available to view. Fields containing missing data or values outside pre-
set limits will be flagged. Disease assessment scoring is not included in VasCOT but it is
envisaged that this will be provided through a link to the validated Birmingham Vasculitis
Activity Score324 which is currently being updated.
6. Following review, a summary is generated which will form part of the patient’s
hospital record (Electronic Patient Record or paper). In addition; the patient, primary care
and other nominated care providers will receive a copy.
7.1.3.1 Identification of existing products and intellectual property
Vasculitis patients are predominantly cared for by nephrologists and rheumatologists.
Therefore, a search of existing health informatics systems used by these two departments
within the NHS in the UK was undertaken. Two products of interest were identified and are
reviewed below.

249
1. 4S-DAWN
4S-DAWN is a clinical software company that produces software designed for the
monitoring of rheumatology patients (as well as other disease groups). The primary
function of this software appears to be monitoring of disease activity of common
rheumatic diseases (e.g. Rheumatoid Arthritis) as well as facilitating monitoring of required
blood tests for patients on immunosuppression. It does provide a configurable option to
add relevant screening test for your population such as DEXA or TB screening. However, the
main focus is to support safety of drug monitoring and it does not have longer-term
sequelae of immunosuppression grouped into systematic review. In addition, it is only a
secondary care clinician portal, with no patient or primary care access.
2. (Renal) Patient View (RPV)
RPV was established in 2004 to provide patients with renal disease access to their health
information. It has since undergone rebranding as “generic” PatientView with a plan to
make it accessible to patients with other diagnoses, starting with Inflammatory Bowel
Disease and Diabetes in 2014. RPV is well established and accepted by the majority of renal
units in the UK with over 11 000 renal patients having been reported as registered by
2009325. It enables patients to view blood results, clinic letters and to enter symptoms and
parameters such as blood pressure readings. In summary, PatientView fulfils the criteria for
the patient section of VasCOT. However, PV does not offer the functionality for clinicians to
review data and does not organise and present data in the format envisaged will be
provided by VasCOT.
In summary, although there are systems in existence that provide some of the functionality
required for VasCOT, there is no identified system that appears to provide both clinician
and patient access to primary, secondary care and patient entered data, amalgamated and
presented to facilitate review of risk factors for patients on long-term immunosuppression.

250
Patient id Gender Age Diagnosis Duration
Disease
Disease
manifestations
1
2
3
4
5
6
7
8
Male
Male
Male
Female
Male
Female
Male
Female
54
64
60
76
78
41
56
73
MPA
MPA
GPA
GPA
MPA
GPA
GPA
MPA
1 year
4.5 years
14 years
9 years
4 years
13 years
24 years
7 years
Renal
Renal
Renal, nerve, ENT
Renal, lung
Renal, lung
ENT
Eye, renal, ENT
Renal, lung
Table 1. Characteristics of patients selected for interview
7.1.3.2 User engagement
Following identification of the need for this product a user-centred iterative design
approach was taken in collaboration with Hitachi Design Centre Europe to develop the
patient and clinician user interfaces. In order to ascertain whether the proposed solution
was applicable and relevant to the user groups, initial detailed interviews were conducted.
Patients (n=8) were selected by the project lead (Dr Brown) to represent a broad age and
socioeconomic spread. In addition, patients were selected with a wide variety of disease
manifestations and duration (see Table 1 for patient characteristics). A team of two people
conducted the interviews; a member of the Hitachi Design Centre Europe and an external
ethnographic researcher. The purpose of the investigation was to understand patients’
experiences, feelings and needs of their everyday life with vasculitis. In order to understand
the role of the supportive network and their perspectives, partners or family members of
the vasculitis patients were invited to join. The individual interviews were approximately
one hour, audio-recorded and were semi-structured with open-ended questions. All

251
information was treated as strictly confidential and anonymised prior to presentation or
publication. Interviews covered the following areas
• General health history
• Vasculitis diagnosis, treatment and maintenance
• Everyday life
• Mental states, motivation and influences
• Tools and Information.

252
1.1.1 Figure 1. VasCOT user map

253
1.1.2 Figure 2. VasCOT concept

254
Thematic analysis informed by grounded theory and phenomenological approaches was
used to identify recurring and significant areas of concern to the patient326,327. These are
detailed in Table 2.
Areas
Overarching themes
Individual vasculitis
Vasculitis type and severity varies significantly among patients. Patients experience individual treatment journeys and care. Rare disease: Lack of knowledge from healthcare professionals. Some patients feel alone: ‘guest in a ward’ Some patients feel ‘special’. “There is no solution” - patients are aware of trial and error approach.
Accepting vasculitis
Most patients experience frustration towards different care providers before the diagnosis. Accepting the disease is a process and takes time. With increasing years, patients seem to be more okay with it. Patients show different approaches for accepting it: religion, engagement, education, pragmatism.
Learning a new lifestyle
Patients have to learn a new language, medication, symptoms and body systems. With changing medication patients continue to adapt. Over time they become their own expert. Medication becomes part of their life - and with it the risk for side effects. Patients develop their own routines and organisation systems. Some patients face temporary diets; some struggle with weight gain. Patients face limitations in activities, energy, holiday planning. “You have to learn to pace yourself”. Some patients struggle with depression and disconnection.
Not taking over life
All patients emphasise that they don’t want vasculitis to take over their life. Many patients have no need to talk about the disease with friends or peers. With growing experience some patients get bored of it. They don’t want reminders.

255
Unpredictable life
Patients experience good phases and relapses of different severities. Unpredictability and uncertainty is one of the biggest challenges. Fatigue/exhaustion is a key symptom. Patients have good days and bad days.
Looking forward
Future thoughts include fear, restrictions and uncertainty. Patients look forward to get off certain medication (steroids) and/or overcoming symptoms/relapses. Patients often focus on the ‘now’; “grateful for every day I get”.
Partner In some cases, the partner becomes the main supporter; emotionally and practically. There can be a high emotional impact on the partner due to the unpredictability and limitations. The role of the partner seems to depend on the individual case.
Having a champion Patients have the desire to have a lead clinician = a ‘champion’. They want someone they can trust in regards to treatment and medication, coordination, managing fears, motivation, advice. Patients who have a champion seem to worry less and be more satisfied with their care.
Feeling lucky All patients describe themselves as ‘lucky’. They know they could be ‘worse off’. All patients show a positive life attitude. Their vasculitis journey gives them a sense of strength, uniqueness and achievement. They are grateful for the treatment they received, and for kind people they met.
Being in control Patients want to be in control in regard to living with the disease and treatment decisions. Education and experience influence this striving for control. Patients want to be involved in decisions. The individuality and lack of general knowledge strengthen the need for control. The management of the disease is a ‘balancing act’ of:

256
- emotions - medication - symptoms - life. They don’t want to give up routines when being an in-patient. All patients emphasise to ‘self-medicate’
Care co-ordination
The coordination of different care providers and medication is a big challenge. Processes are slow, not supportive and increase complications. There is too little exchange of the GP, different clinics, consultants and hospitals.
Reassurance touch points Several patients take regular measurements on their own (blood pressure, blood tests, morning routine) for self-monitoring. Phone numbers of their clinicians give them a sense of security. Although they never/rarely use it. The regular check-ups give patients reassurance. Some (who are in control) feel it is “a bit of waste of time”. Some patients have access their blood results to keep track.
Emotional bonding with medication Patients feel grateful for medication, despite the physical and emotional impact of steroid or chemotherapy treatment. Changing medication after several years makes patients feel vulnerable. Medication becomes part of their life and life test.
Table 2. Themes from patient interviews
7.1.3.3 Clinician interviews
Following this, six clinicians were interviewed. All were chosen by the project team as
having involvement in the care of patients with vasculitis and were as follows; consultant
nephrologist tertiary centre n=3, consultant rheumatologist tertiary centre n=3. Interview
questions involved exploration of current clinical and information systems in use and the
challenges involved in the care of the vasculitis patient. In addition, draft wireframes of
some of the proposed clinician view pages were presented for review.

257
The results from both the patient and clinician interviews were analysed to produce a
patient and clinician “problem list” and “wish list” (See Tables 3 and 4).
7.1.3.4 Patient questionnaire
Once it had been identified that the proposed solution appeared to align with the needs of
patients and clinicians, further information was sought with regards to the proposed
method of patients entering and accessing information and to the level of clinical
information accessible to patients. This was undertaken through a larger national patient
questionnaire. All patients attending a national vasculitis patient conference were invited
to participate. N= 66 responses were analysed with responder characteristics outlined in
Table 5. The questionnaire and results can be viewed in Appendix 1. In summary, the
results from this supported that the majority of patients completing this questionnaire
currently used the internet to access health information with a substantial majority
wanting complete access to their own health data. This is in keeping with studies
supporting the patient perceived benefits of an “open notes” or “shared record”
system328,329,330.

258
Clinician “problem list” Central Care (CC) expertise- Local care delivery, missing links Letter system: filtered (incomplete) information data access only if in CC (need for) common way of information capture and exchange Incomplete information: difficult to get external information and results currently: chasing information; different systems no official way to get results from GP tertiary referrals often incomplete Disempowered patients: different specialists create lack of holistic care educated patients better to manage Leader and supporter: (need for) coordination between vasculitis lead and supporters (need for) clear distinction of roles Information collection: patient medication intake might differ from prescription medication therapy = key data cause for co-morbidities need for original documents/results; vasculitis interpretation different specific tools measure specific aspects at specific places trends are important (renal, inflammation) blood test results (not available until) 1 day after check-up need for better data overview/collection (raw data, specific links, verification, decision reasoning) Standardising Vasculitis Care: scores needed to justify actions (currently) no triggers/reminders for long-term risk assessments
Clinician “wish list”
Key data overview pulling together all data streams (specialists, GP, patient) objective raw data (diagnosis, medication, results) key data only; incl. relevant trends/changes GP data (events, medication) validated by patient Complementing care no conflict with established systems/routines (letters) no double work/administrative effort aligning care activities data transparency Long-term risk control reminder/trigger for actions (scans, reviews, results) links to proven (specific) tools scores/standardisation to justify actions providing context for risk assessment VasCOT elements diagnosis medication (current, immunosuppression, history) patient report (symptoms, medication, lifestyle) long-term risk dimensions (infection, malignancy, medication, cardiovascular, bone health, woman’s health) Patient role empowering patients preparing for check-up confirming GP data reminding and reporting symptoms and incidents well-being (lifestyle and mental health) education: what to look for, how to take care
Table 3. Clinician “problem” and “wish” list

259
Patient “problem list” Unpredictable life risk for relapses risk for side effects fatigue “it never stops” Care coordination frustration due to little data exchange/patient knowledge slow processes, waiting for letters care not aligned, different medication advice no vasculitis lead; feeling alone many appointments at different places Medication Patients bond with long-term medication and feel vulnerable when it changes Patients self-medicate (no data capture of actual in-take) Patients lose control over their medication as in-patients Individuality ‘trial and error’ approach rare disease: feeling alone versus feeling special Learning and accepting “you have to learn to pace yourself” accepting process takes time impact on work and private life Patient “wish list” Trust in care clear vasculitis leader - ‘champion’ information and education better coordination between different specialist fields and GP reassurance through touchpoints (results, check-ups, contacts) Being in control being involved in decisions, team effort respect for their own methods and routines access and understanding of key data (blood results) reading signs, knowing what to do balancing act: emotions, medication, symptoms, life Data availability access to vasculitis data for other clinicians/health care providers key information at hand (medication, diagnosis) better vasculitis knowledge of healthcare providers Taking worries accepting living with vasculitis learning a new lifestyle Not taking over life living a ‘normal’ life not constantly thinking/talking of vasculitis looking forward (holidays, family, hobbies) Individuality receiving personalised care GP privileges
Table 4. Patient “problem” and “wish” list

260
Table 5. Survey responder characteristics
Patient characteristics N=66
Number responders
Age in years
< 30 5
31-40 1
41-50 6
51-60 19
62-70 25
>70 10
Gender
Female 38
Male 22
Not specified 6
Diagnosis
GPA 31
MPA 6
EGPA 11
HSP 2
GCA 6
AAV not specified 1
Other 9
Year of diagnosis
Before 2000 6
2000-2005 10
2006-2010 15
2011 onwards 30
Not yet 2
Country of diagnosis
England 16
Scotland 1
Wales 1
UK not specified 46

261
7.2 SECTION B: DESIGN OF PATIENT AND CLINICIAN INTERFACES
7.2.1 Patient data capture
Following patient consultation, the initial drafts of the patient view pages were produced.
The wireframes of this interface can be viewed in Appendix 3.
The following areas will be included
Demographics: Patients will be asked to update demographics if they change
Relevant family history: in order to facilitate accurate calculation of fracture and CV risk
scores relevant family history will be requested
Lifestyle: Including smoking status, alcohol intake and weight.
Medication: The record will be pre-populated with the patient’s most recent primary care
prescription. Patients will be required to corroborate/ amend this as appropriate as it is
widely accepted that medication adherence may be poor in those with chronic
conditions331.
EQ-5D: This quality of life measure has been chosen for several reasons. Firstly, it is short
and therefore not too onerous for the patient to complete, Secondly, it has been shown to
have some relationship with improvement following treatment in a sub-group of
vasculitis332. In addition, data from the EQ-5D can be used in health economic
calculations333, which will be essential to support wider diffusion of the use of VasCOT.
“Significant events”: Patients will be asked to select health events that have occurred since
previous review from a drop down list. The comprehensive list is included in Appendix 2
but will include items such as infection, cardiovascular events, fracture and other steroid
related events.
Topics for review: Patients will be able to highlight areas of particular concern that they
would like to focus on in their upcoming clinic encounter.
Education: Patients will be able to request links to disease, lifestyle and health topics that
can then be added by their clinician.
7.2.2 Clinical data capture
The clinical data screens are split into relevant systems for review. The topics included
were informed by systematic literature review and a Delphi study performed with UK
expert members to inform “standards of care” for this population (full methodology and
results reported elsewhere). The five health review areas are defined as; Bone health,
cardiovascular risk, infection risk, cancer screening/fertility and steroid “other”.

262
The specifics of which data to include and the data sources (e.g. primary, secondary care or
patient entered) were determined by Dr Brown with input from Dr Venning, with advise on
availability and access to data from North-west Ehealth. Following this, the list of data
items was circulated to the UK and Ireland Vasculitis RDG for review and feedback
incorporated. A full list of data specifications including data source can be viewed in
Appendix 2. but the main areas for review covered by each page are outlined below.
Wireframes for these pages can be viewed in Appendix 4.
Bone Health: Patients will input some of the data required to inform fracture risk
assessment (to be undertaken using FRAX calculator334). Other data, such as DEXA reports
may have to be manually entered, unless present in the primary care record.
Infection risk: Data from primary care will include vaccination types and dates and
infection events. The page will include triggers for secondary care to consider prophylaxis
for PJP, fungal, viral infections where relevant.
Cardiovascular risk: This section will include data from primary care including blood
pressure readings cholesterol, and patient entered risk factors such as smoking status and
family history. This will enable a validated risk score such as the Qrisk score335 to be
undertaken but with information regarding the likely increased risk of CVD in the vasculitis
population highlighted.
Cancer risk: This section will include information on cumulative cyclophosphamide dose to
allow an awareness of previous exposure when continuing vigilance with regards to cancer
screening. Urinalysis in addition to population cancer screening data (breast, cervical,
bowel) from primary care will be displayed here.
Steroid other: This section will allow screening for and to prompt an awareness of steroid
related side effects including easy bruising, thin skin, raised blood glucose and glaucoma or
cataracts.
Following completion of the health review a summary can be produced which can be
communicated electronically to the patient and all relevant health care providers with any
pertinent recommendations highlighted. It is intended that there will in addition be an
education section with links to topics either suggested by the clinician or requested by the
patient.

263
7.2.3 Frequency and scope of use
Initial consultations with both patients and clinicians (including interview feedback) suggest
that this tool will be of most value in the chronic phase of disease management i.e. 6
months plus from presentation. It is therefore intended that the pilot of this will only
include prevalent vasculitis patients and that the use of the tool initially be piloted for 6
monthly use with a view for it to be used at 6 to 12 monthly intervals. Patients will be
invited to contribute data in the 2 weeks leading up to their clinical review but will be able
to enter data as they feel relevant at any time point. Equally, other clinicians and primary
care (once registered as linked with a patients account) will be able to view the records
whenever required but there will be no mandatory manual data entry from any sources
apart from the patient and lead vasculitis clinician. This is to encourage engagement with
the tool, particularly by the already overburdened primary care providers.

264
7.3 PART C: DEVELOPMENT OF VASCOT ‘ENGINE’ (FUNCTIONAL SPECIFICATION)
Following identification and specification of the content of both the clinical and patient
view pages the next stage was to consider the functional specification for the software.
This stage was undertaken by Chris Anderson (Xibble Ltd) and Chris Lee (OBEC ltd) on
behalf of Central Manchester Foundation Trust Information Technology product
development department. Consultation regarding the functionality of the product was
provided throughout by Dr Brown.
The below solutions to the following areas are proposed. The full requirements for each
area can be viewed in Appendix 5.
7.3.1 Platform and Strategy
The VasCOT solution will be an independent application existing within its own framework
and platform, although it will have the ability to consume data from other sources. With
this in mind, the solution will be capable of defining and maintaining its own security –
including access, users and roles, any required system metadata and implementation
methodology.
Uptake of the VasCOT solution by Providers and Patients will be gradual and the solution
will support this phased approach to achieving a National Diffusion. System Administrators
will be granted the ability to create these entities dynamically, supported by any Standard
Operating Procedures (SOP’s) used to validate the creation.
7.3.2 Audit
All CRUD (Create, Review, Update and Delete) actions will be audited and stored by VasCOT
in such a way as to be readable by a System Administrator. All audit entries will be date /
time stamped and if applicable, include: a username, action performed, value change from
/ to and the patient ID. A front end user interface will be provided to interrogate the audit
data.

265
Consideration should be given to the storage of audit log data due to sheer volume. It may
be necessary to archive sections of logs after defined amounts of time, to ensure the logs
do not grow to a size which may impact core operations.
7.3.3 Security and Authentication
User authentication and access to patient information will be a key concern of the VasCOT
solution. Enough flexibility will exist for the system to be usable, whilst ensuring the
security of confidential information.
7.3.4 Data Protection
As the VasCOT solution will be accessible via the internet, the necessary technical design
must seek to reduce vulnerabilities and inhibit attacks designed to access or steal patient
information, including but not limited to: Cross Site Scripting (XSS) attacks, SQL injections,
unauthorised redirects and man-in-the-middle attacks. In addition, guidelines published by
the HSCIC dictate that all transfers of patient data must be encrypted and preferably to
AES256 (Advanced Encryption Standard).
7.3.5 Feature Access
The solution itself will offer Role Based Access Control (RBAC) as a way of managing and
maintaining user access to the features and data. Although a role editor will be required to
define privileges at a granular level, there will be certain ‘Roles’ which will be integral to the
way in which the system works. First of all, there will be the ability to create overarching
System Administrators. These users will have the ability to create other System
Administrators and access all system functionality – most important of which will be the
ability to create Providers and Super Users. ‘Providers’ is the term used to describe a
healthcare facility (a Trust, GP Practice, etc). Users will belong to a Provider and nominated
users within a Provider will be identified as Super Users. These Super Users will be the local
administrators for that Provider, devolving system maintenance to a local level and
removing the responsibility from the System Administrators.

266
7.3.6 Settings
The Settings Menu will be restricted to System Administrators and Super Users. It is a
dedicated sub-menu into the various Editors required to setup and maintain the system.
Although Super Users will have access to this screen, they will be further restricted to only
the functions which are applicable to their Role and again, restricted to Settings for their
own Provider.
7.3.7 Role Editor
The introduction of a Role Editor will future proof the system for further scope and roll out,
past the pilot phase. The editor will offer the ability to define new roles, as well as making
all system features available to be assigned to a Role, thus providing complete flexibility
whilst maintaining governed access and control.
7.3.8 User Editor
The User Editor will be available to System Administrators and Super Users (as defined by
role). The difference being that System Administrators will be able to view and maintain a
Global list of Users, whereas Super Users will be restricted to a list of Users local to their
own Provider. In addition, although Patients could also technically exist in VasCOT as Users,
they will not be created and maintained here. Instead, they will be created by the Lead
Clinician and maintained via their Patient Record, to which they will also have access to for
self-maintenance. Therefore, the User Editor is used only for creation and maintenance of
Administrative and Clinical users.
7.3.9 Patient Creation
Patients will be created by the Lead Provider (as defined by Role) as there will not (initially)
be an integrated demographic service. The patient demographic details will be entered, as
will the association to any Providers available in the system.
7.3.10 User Verification
Whenever a new user is setup and enabled - regardless of whether they are a Patient or a
Clinician – a verification email will be sent to the registered email address of that User. The
email will contain a secure link, valid for a predetermined amount of time, which the user

267
will need to click. Following the link will allow the user create a password for their account
and complete the User Creation process. The purpose of this is ensure that the user has
access to the email address they have registered and so that they are forced to create a
personalised password before accessing VasCOT.
7.3.11 Self-Registration
The Registration form offers a self-service approach to sign up for clinical users; whether
the potential user belongs to a ‘known Provider’ or not. The behaviour of the Registration
screen will change depending on the information entered. If the domain of the email
address entered is recognised as a ‘known Provider’, then the Provider information on the
right hand side of the screen will remain hidden and upon submission, the access request
will be sent to the Super User of that Provider – as they are more likely to be able to
validate the access the request. If the domain is unrecognised, the new user will be
required to complete all of the Provider information too. This request will be sent to the
System Administrator, as the new Provider will need to be validated and created.
Patients will be registered by their Lead Provider during consultation once as identified as
being a suitable candidate and as a way of authenticating the patient-user
7.3.12 Patient Queues
Patient Queues will become the default Home Screen for clinical users (as defined by role).
The queue will be split into tabs – “My” and “Our” Patient. The “Our” tab will present all
patients to which the Provider (not the individual) is associated. The “My” tab will be a
further refined list of the “Our” patients, filtered to only show patients where the logged in
user is also the Named Clinician on the Provider tab of the Patient Editor. This ensures that
we provide a user specific list of patients for convenience but also provides a full provider
specific list of patients, in order to mitigate any bottlenecks caused by only associating a
patient to an individual clinician. In addition, we will also highlight patient specific
notifications within the Patient Queues to identify the number of notifications awaiting
acknowledgment by the Provider.
7.3.13 Requesting Patient Access
Until a Provider is associated to a Patient, then the Patient will not appear in the Patient
Queues and the Provider will not have access to Clinical information. Therefore, the system

268
needs to provide a mechanism to request patient access, as well as the ability to approve
or reject this request.
In addition, a Provider may want to change their association to a patient – such as a
Satellite Clinic taking over as the Lead Provider. In both of these scenarios, a “Handshake”
process will need to exist to facilitate the handover of patient access.
7.3.14 Accepting / Rejecting Patient Access Requests
Access to patient data will trigger a notification to be routed to the Lead Provider. A user
within this Provider has the ability to review these requests and decide whether to accept
or reject the request. Depending on the request and the action taken, the user may or may
not grant access to the patient information – in the same way clinicians today approve
patient data requests manually via phone, fax or email.
7.3.15 Access, Data Input and Versioning
Access to the Patient Record will be defined through an association to a Provider. Users
within that Provider will have access and the ability to the Patient Record as a result –
unless explicitly defined through Roles. However, if a Provider hands over responsibility to
another E.g. A GP Practice change or a switch in Lead Provider, the original Provider will still
require access to the information they contributed to the Record, even though they may no
longer be able to contribute or view information captured since their handover.
The system will need to maintain versions of the Patient Record and attribute those
versions to the appropriate Provider, as and when the Record is modified. This will ensure
that Providers can always access information they are (or have been) responsible for.
7.3.16 Patient Editor
The Patient Editor will be available to all users with patient access, including the Patients
themselves. It is the same screen as used during the Patient Creation process but provides
access to update patient information as well as Provider Association. Roles will determine
exactly which fields can be updated.

269
7.4 DISCUSSION
Here it has been outlined how the idea of a “checklist” approach to co-morbidity
prevention for patients has undergone extensive development, with input from many areas
of expertise to become a fully specified and designed concept.
During this process, involvement has been sought from those with the technical and design
knowledge to guide and inform this process. In addition, the content and format has been
driven in the majority by the target audience, patients and clinicians. We have worked
extensively with individual patients locally, alongside seeking feedback from larger national
patient groups to ensure the resulting product will meet the needs of this population. It is
hoped that VasCOT will facilitate patients in chronic disease self- management and
promoting their health as well as providing an educational resource.
Alongside this, it is paramount to ensure that within the constraints of a busy NHS clinic,
this tool will add value for the clinician, by aiding in a more efficient and comprehensive
assessment of the patient, and not just providing more boxes to be ticked. Through the
planned use of existing, mainly primary care, data, organised and displayed in a relevant
and systematic fashion it is hoped that VasCOT will facilitate holistic care in a user- friendly
way. In addition, VasCOT will aid in communication between the often many clinical
disciplines that may be involved in a single patient’s care.
It is highly likely that further adjustments will be required to both the content/ design and
functional specification. However, this next stage will be informed through pilot testing of
the product with small numbers of patients and clinicians. Funding is required for the initial
product development, with several avenues currently being explored.
Once we have a successful first version of this product the next stage will involve ensuring
that clinical and patient outcomes can be captured to start to support a health economic
model for wider scale use. It will be difficult, initially, to demonstrate a significant
difference in hard end-points and it is likely that surrogate parameters such as patient
satisfaction, quality of life and care quality indicators will be useful in this stage. It is
possible, however, that an impact on the more frequent complications such as infection or
even hospital admissions may be able to be demonstrated.

270
It has taken a significant amount of work to develop the concept and design of this
innovation to the point where it can now undergo product development for field testing.
Alongside this process this tool has garnered substantial support from clinicians,
commissioners, patients and industry which will hopefully translate to success in the
clinical testing phase.
VasCOT has been supported by the UK and Ireland Vasculitis Rare Disease Group which will
aid in increasing awareness on a national level of this project, and eventually will support
national diffusion.
As this product is essentially a long-term immunosuppression management tool (as
opposed to being disease specific) VasCOT can readily be adapted for use in other disease
groups. It is therefore intended that alongside the initial clinical pilot, the software will
undergo slight adaption for use in patients with Systemic Lupus Erythematosus (another
multi-system autoimmune disease requiring long-term immunosuppression). It is
anticipated that future work will include further adaption for use in other renal and
rheumatology autoimmune disease groups, Inflammatory Bowel Disease (IBD) and the solid
organ transplantation population.
Although outcomes from vasculitis are improving, data over recent years has supported
that we need to move from viewing vasculitis as an acute life- limiting illness to a chronic
disease. Alongside this shift in perception, a change in how care is delivered to this
population is required. It is clear that areas such as cardiovascular disease, cancer and
infection could be better addressed and that the key to achieving this is to define and
consistently apply standards of care to this population. In an already stretched system
caring for a complex heterogeneous patient group, the use of a web-based platform to
support holistic care could provide the ideal solution.
The 5-year forward view for the NHS focuses on giving patients greater autonomy over
their healthcare, breaking down the barriers between primary and secondary care and
supporting innovation to develop new models of care336. In this changing landscape of
healthcare provision, an innovation such as VasCOT fulfils all of these requirements, in
addition to providing the basis for standardising care in this, and other complex,
populations.

271
Here I have outlined results from initial scoping work involving key stakeholders (patients
and clinicians) which support the design of our solution. I have also detailed work that has
been carried out to define the clinical content, initial user interfaces of both the clinician
and patient view and the functional specification. Subsequent stages of development and
testing will allow further improvements to these initial designs following user testing.
Future work will include collection of clinical outcome and health economic data to support
the business model for wide spread adoption within the NHS to enable improvement of
outcomes for this challenging population.

272
APPENDIX 1. PATIENT QUESTIONNAIRE AND RESULTS
5%21%
74%
1) Do you use the internet to access information about
your health?
a) never
b) rarely
c) often
54
13
37
18
37
21
2) Which websites do you use for information about your health?
31 34 37
16
3) What devices do you use for accessing health information online?
14%
86%
4) Do you use renal patient view?
Yes
No 67%
33%
5) If so, how often?
a) onlyimmediatelyfollowingclinicsappointments
b) regularly toupdate myinformation 89%
11%
6) If not, would you like the option of being able to see your
blood tests online?
Yes
No

273
69%
25%
6%
7) Do you receive copies of hospital correspondence following your
visit to the vasculitis clinic?
Yes
No
sometimes
100%
0%
8) If not, would you like to?
Yes
No
1%25%
74%
9) How much information do you like to receive about your health?
a) on a need to knowbasis only
b) enough so Iunderstand what is goingon but not every detail
c) as much as possible
82%
15%3%
10) If you could log into your hospital records would you like to
be able to view;
a) everything (thesame informationyour doctor sees)
b) a summary ofyour health andcurrent issues
c) I would not liketo access mymedical records
54%
5%
41%
11) Do you think that more information about your health
would make you;
a) less worriedabout your health
b) More worriedabout your health
c) Have no effect
19%
51%
22%
8%
12) How do you currently organise and manage your
health information?
a) Diary
b) Folder
c) Computer
d) I don't collecthealth information

274
APPENDIX 2: CLINICAL DATA SPECIFICATIONS
Data type
Input source
Automated or manual
Notes
PAGE 1
Patient name Auto populated by login GP Records or Hospital Records A
Patient postcode Patient M
Patient DOB Patient M
Ethnicity Patient M
Date of registration Auto populated by system System A
GP name/code Auto populated by GP system or
select from list
GP
GP practice name/code GP record A
Hospital Name
Hospital clinician name Auto populated from login Hospital A
Diagnosis - Manual from hospital
records/UKIVAS
Hospital/GP A/M
Year of diagnosis per
diagnosis
Manual from hospital
records/UKIVAS
Hospital/GP A/M
Induction regime Manual from hospital
records/UKIVAS
Hospital A/M
Previous maintenance
exposure
Manual from hospital
records/UKIVAS
A/M

275
Current
immunosuppression
Drop down list Pt/hospital M
Steroids Y/N Pt/hospital M
dose
Immunosuppression
monitoring frequency =
Number picker, frequency picker-
day/week/month/year
Pt/hosp M
PAGE 2- CVD RISK
BP target <140/90 2y care entered M
or <130/80 if proteinuria
BP actual Double free numeric fields GP Records A
Cholesterol total Free numeric field GP Records A
Cholesterol HDL Free numeric field GP Records A
Cholesterol LDL Free numeric field GP Records A
Cholesterol HDL/LDL ratio Free numeric field Calculated from above A
Smoker current: light < 10/day patient
moderate 10-19/day
heavy > 20 /day
previous
never
Pack years? Free text GP Records
CV/thromboembolic
history
Drop down:
MI
GP records A Code in GP records needs to be
translated to one of dropdown

276
IHD
DVT
PE
CVA
TIA
AF
options
1 degree Family CV
history<60 yrs
Drop down:
Heart Attack
Angina
None
Patient entered
CKD (if CKD 3/ above) 2y care entered Associated further information
available (e.g., have 'I' button
which displays info when click
on it)
Urine PCR/ACR Numeric value GP or 2y care entered M If PCR>30 or ACR>50 then BP
target should become <130/80
CV meds Anti-platelets GP extracted/ patient entered M/A Code in GP records/text from
patient needs to be translated
to one of options
Ace/ARB
Statin
Other anti-hypertensive
Other lipid lowering drugs
Link to Qrisk calculator GP/2y care A

277
(http://www.qrisk.org/)
PAGE 3- BONE HEALTH
DEXA result T score GP or 2y care entered M
L spine
Fem neck
forearm
Vit D level Free numeric field GP/2y care M
Vit D status adequate/inadequate/borderline 2y care M Red if 'Inadequate'
Bisphosphonate Date commenced GP A At 3 or 5 years from 'Date', need
to flag that 'biphosphonate
holiday' should be considered.
The time period is dependent on
'Other medication'.
Fracture history Read/medcode GP A Translate from codes
Steroid exposure (graphed
over time)
Monthly dose (mean) Patient entered M
Post-menopausal Y/N Patient entered/2y care entered M
Alcohol intake units/week Patient entered M Flag if >14 for female, >21 for
male
Parent hip fracture Y/N Patient entered M
Link to FRAX
calculator(http://www.she
f.ac.uk/FRAX/tool.jsp)

278
PAGE 4 CANCER
SCREENING/FERTILITY
Cyclophosphamide
exposure
y/n 2y care entered Flag if Dose (cumulative) >15g
dates UKIVAS
cumulative dose
Urine RBC (graphed over
time)
0-3+ 2y care M
cystoscopy Date GP A
Action required:
No action required
Repeat
Treatment
2y care M If Action = Repeat then need to
enter a date
USS KUB Date 2y care M
Action required:
No action required
Repeat
Treatment
2y care If Action = Repeat then need to
enter a date
Skin check Y/N GP Records/hospital/ patient M
Date Date is autopopulated with date
entered Y but allow clinician to
change it. Flag if over a year
since last check

279
skin awareness education Y/N GP Records/hospital/ patient M Link to the relevant site should
appear in this table and also in
Patient's Education tab.
Date Date is autopopulated with date
clicked the link on Eduation tab
but allow clinician to change it.
Flag if 'Y' over a year since last
had it.
Cancer screening for Attended: Y/N GP records A Translation to
bowel/breast/cervical cancer
bowel, breast, cervical Result A This is not needed
Action required:
No action required
Repeat
Treatment
2y care If no action required then
generate next screening date.
Next due A
PAGE 5 STEROID OTHER
BMI Graphical over time vs target BMI Calculated Generate flag
if sig change
occurs
between visits
Flag if move from one band to
another and put links to diet and
lifestyle on Education Topics
page in patient application
Target BMI Range
Last recorded weight Patient entered/2y care M

280
Height Patient entered M
Blood glucose Numeric value (random or fasting) GP or Hospital records A
Status: Set status and action according
to rules on Diabetes and IGR
Action required:
No action required
Repeat
Treatment
HbA1c (graph over time) Numeric value GP or hospital records A
Bruising Y/N Patient M
Site of bruising Drop down selector or body map Patient
Other steroid side effects Drop down: M
Cataracts
Glaucoma
Skin tears
Mood change
PAGE 6 INFECTION RISK
Episode infection Read code/medcode Patient entered A/M
GP Display READ code as well as
term translated to
Action required Antimicrobial translation required as patient
entered
Hospital admission

281
nil
PJP prophylaxis Co-trimoxazole 2y care M
Dapsone
Atovaquone
pentamidine
Indication Induction 2ycare M
Previous infection
Other
Anti-viral prophylaxis Acyclovir 2y care M
other
indication As above
Anti-fungal prophylaxis Fluconazole
other 2ycare M
Indication As above
Flu vaccination date GP A
Date Repeat Required 365 days
Pneumococcal vaccine Date GP A
Date Repeat Required If CKD = Y then need booster in 5
years
Episode leucopenia last
12 months
Lymph Gp/2y care M
Neut
both

282
Action required Nil 2y care/patient M
Meds withheld
Dose reduced
Meds changed
Immunoglobulins IgA 2y care M
IgM
IgG If <6 flag
Date picker
Varicella ab status Positive 2y care M
Negative
date
HPV immunisation Y/N GP A

283
APPENDIX 3: PATIENT VIEW WIREFRAMES

284

285

286

287

288

289
APPENDIX 4. CLINICIAN VIEW WIREFRAMES

290

291

292

293

294

295

296
ID Requirement Comments
1. VasCOT landing page will provide functionality to navigate through different sections of the website.
It is envisaged that users can visit the ‘VasCOT’ website for information / guidance / updates before choosing the Log In or Register
2. Website content design and content will be defined by Hitachi
3. From the landing page, the user will have the option to:
• Login – routed to “Login” page
• Register – routed to “Registration” page.
4. Clicking “Register” will route the user to the Registration Page See Self-Registration
5. Clicking “Login” will route to a dedicated Login Page. Here the user will have 3 options:
• Register
• Login
• Forgotten Password
6. Clicking “Register” will route the user to the Registration Page See Self-Registration
7. “Forgotten Password” – Clicking this link button will guide the user to a dedicated screen. No wireframes available.
7.1. “Cancel” - User will be routed back to the System Login page.
7.2. On this screen the user will be prompted to enter the email address they use to access VasCOT
7.3. Once an email address has been entered the user will be able to click a “Submit” button
7.4. Validation will check that the email is recognised. If not, the user will be presented with an on-screen message.
7.5. If the email address is recognised, the submit button will trigger an on-screen message to the user to notify the user that a “Reset password” email has been sent to their email address and will be valid for 48 hours.
7.6. An email with a secure URL, valid for 48 hours will be generated and emailed for the user See User Verification
7.7. The URL will take the user to a dedicated password reset screen which will prompt the user to enter a new password and confirm that password. The user will submit this information.
7.7.1. .......................................................................................................................................................... The system will need to check that the passwords entered match, if they do not, an on-screen message will be displayed.
7.8. After submission, if the passwords match, the user will be presented with a “Log In” button which will route them back to the Log In screen
7.9. If the 48 hour expiry on the URL has passed, the system will prompt the user to acknowledge this and be routed back to the Forgotten Password screen to initiate the process again.
APPENDIX 5. DETAILED FUNCTIONAL SPECIFICATIONS

297
8. Log In - If a user enters a username and password, they will have the ability to click the “Log In” button
8.1. If incorrect, an on-screen notification will be displayed informing the user of the number of attempts left.
8.1.1. .......................................................................................................................................................... This defined number of attempts should be defined as a variable within the system to allow for easy configuration
8.1.2. .......................................................................................................................................................... If an incorrect username and password combination is entered x times (defined above), the account will become locked and a notification will be sent to the Provider’s Super User (if the username is identified correctly)
See Notifications
8.2. If correct, the system will direct the user to appropriate Home Page defined by Role:
8.2.1. .......................................................................................................................................................... • Clinical User – Patient Queues
• System Administrator - Dashboard
• Super User – Provider Specific Dashboard
• Patient – Patient Summary
See Dashboards, See Patient Queues and Patient Summary as defined by Hitachi
ID Requirement Comments
9. The system will offer a “Settings” menu located on the Dashboard Toolbar. The “Settings Screen” will provide access to administrative type functions, including:
• A User editor
• A Role editor
• A Provider editor
• Notification Settings
10. There will be the ability to restrict the “Settings” menu to specific roles
10.1. System Administrators and Super Users will have access to the Settings Menu. However, Super Users will only have access to the “User Editor”.
11. Breadcrumbs will detail the user navigation to the Settings screen from the Home Page, providing a way back.

298
ID Requirement Comments
12. The system will offer a Role Editor in order to attribute system wide and screen specific CRUD Features to Roles. These Roles will then be attributed to users.
CRUD = Create, Review, Update and Delete
13. There will be some system defined / default Roles available within the system.
• Clinical User
• System Administrator
• Patient
• Super User
• Read Only
13.1. System Administrator – Has complete CRUD access to all users and providers within the VasCOT community but cannot view Patient Data. A System Administrator can create another System Administrator and has full access to the Settings menu
13.2. Super User – Is restricted to a single Provider but has complete CRUD access to all users within that Provider. Can create other Super Users but cannot create System Administrators or Providers. Limited access to the Settings menu.
13.3. Patient – Has no access to anything other than their own data.
13.4. Read Only – Will have access to the screens as defined by roles but will supersede the ability to Create, Update or Delete
13.5. Clinical User – Has access to view and add information to patient records associated to their Provider.
14. Features will include but will not be limited to: as follows

299
ID Requirement Comments
15. Clicking into the Provider Editor from the “Settings” screen will allow the System Administrator to search for an existing Provider or create a new Provider.
16. Breadcrumbs will display the path taken to reach this screen as well as provide navigation functionality to return to previous screens.
17. Search – The system will perform a text match search based on the entered string compared with all existing Provider names.
17.1. There will be validation to ensure a minimum of 3 characters are entered prior before a search can begin
17.2. The user will be required to click / touch the search button to initiate the search
17.3. This will be a Global search across all Providers
18. Search results will appear in the table below, detailing:
• Provider name
• Domain
• Type
• Address
• Telephone number
18.1. Pagination controls will be presented at the bottom of the screen to limit the number of results per ‘page’
Guidance required on the number of results to be display on each page.
19. The user will be able to click / touch a search result to navigate through to the details of that particular Provider, providing options to Edit, Delete or Cancel.
UI guidance required by Hitachi – Will use a link, a row select, a dedicated button, etc
19.1. When viewing an individual Provider, it will be initially displayed in read only mode. The available action buttons on this screen will include:
19.2. “Cancel” button – return to Provider Search screen without saving
19.3. “Edit” button – Makes fields editable and presents “Save” and “Cancel” buttons
19.4. “Delete” button – Deletes the provider from visible view (deactivates) but not from the database for reporting purposes
19.4.1. ........................................................................................................................................................ It will not be possible to delete a Provider if there are associated Users (including patients)
19.4.2. ........................................................................................................................................................ “Delete” – Modal window for user to confirm if they wish to delete record. “Yes” – Record deleted and will no longer be available. “No” – Return to provider overview page.
19.4.3. ........................................................................................................................................................ The system will not allow the Provider to be deleted if there are patients associated to it
19.5. “Edit” – Selecting edit will enable changes to be made to the below fields:

300
• Provider name
• Type
• Address
• Telephone number
19.5.1. ........................................................................................................................................................ Domain field will not be editable.
19.5.2. ........................................................................................................................................................ When ”Edit” is selected the below button options will become available: “Save” – All changes made to record will be saved, overwriting original information. “Cancel”- Return user to “Provider Overview” page
ID Requirement Comments
20. To create a new Provider the User will select the “New” button on the Search screen. Selecting “New” will route the User to “Provider Editor” screen.
21. To create a new Provider the User will be required to populate the following fields:
21.1. Provider Enabled – A non-mandatory Boolean value which dictates whether the Provider is active or not
21.1.1. ........................................................................................................................................................ If disabled, it will not be possible to create Users under this Provider or associate Patients to it
21.1.2. ........................................................................................................................................................ It will not be possible to disable the Provider if there are Users (patients or clinical users) associated with it.
21.1.3. ........................................................................................................................................................ This field is of particular use when a user attempts self-registration and their Provider is unknown by VasCOT. The system will populate the Provider information but will not enable it, so that the System Admin can review and enable once verified as a true Provider
See Self-Registration
21.2. Type – Mandatory combo box selection containing: o Hospital o GP Practice o Satellite Clinic
21.3. Code – All providers will have a unique national code available to them. Free text. Mandatory.
21.4. Name – Free text field. Mandatory
21.5. Domain – The email domain associated to that Provider and the same domain users at that Provider will use when they sign up using their email address. Mandatory.
21.6. Telephone Number – Number field
21.7. 1st line of address – free text. No lookup
21.8. 2nd line of address – free text. No lookup
21.9. 3rd line of address – free text. No lookup

301
21.10. ......................................................................................................................................................... 4th line of address – free text. No lookup
21.11. ......................................................................................................................................................... Postcode – free text. No lookup.
22. Cancel button – will return the user to the search screen without saving changes
23. Save button – will save the provider, when all fields are completed.
23.1. Validation will check that a Provider with this domain does not already exist
23.2. Save Successful confirmation message. The modal window will confirm successful creation of the New provider and in addition feature two buttons:
• Close
• Create New User
UI / UX guidance if appropriate
23.2.1. ........................................................................................................................................................ The Provider cannot be used with a User. Therefore, the system will attempt to guide the System Administrator to complete the process correctly by taking them to the User Editor to create a User under this Provider. It is important to note that the first User added to a newly created provider will always system default to be a Super User role, whilst allowing for other roles to be added too. This will ensure a Provider can always be self-maintained
23.3. Close – User routed back to “Provider Editor” Search screen.
23.4. Create New User – User routed to the “User Editor” screen. See User Editor

302
ID Requirement Comments
24. Clicking into the User Editor will allow the System Administrator to search for an existing User or create a new User.
25. Search – The system will perform a text match search based on the entered string compared with the entered text.
25.1. There will be validation to ensure a minimum of 3 characters are entered
25.2. The user will be required to click / touch the search button to initiate the search
26. Search results will appear in the table below, detailing:
• Name
• Provider
• Role
26.1. Pagination controls will be presented at the bottom of the screen to limit the number of results per ‘page’
27. The user will be able to click / touch a search result to navigate through to the details of that particular Provider, providing options to Edit or Delete.
UI guidance required by Hitachi – Will use a link, a row select, a dedicated button, etc
28. When viewing an individual User, it will initially be displayed in read only mode. The available action buttons on this screen will include:
29. “Cancel” button – return to User Search screen without saving
30. “Edit” button – Makes fields editable and presents “Save” and “Cancel” buttons
31. “Delete” button – Deletes the User from visible view (deactivates) but not from the database for reporting purposes
31.1. It will not be possible to delete a User if they are associated to patients
31.1.1. ........................................................................................................................................................ A administrative function will be available to bulk move patients from one clinician to another See Admin Functions
31.2. “Delete” – Modal window for user to confirm if they wish to delete record. “Yes” – Record deleted and will no longer be available. “No” – Return to provider overview page.
31.3. The system will not allow the User to be deleted if there are patients associated to it
32. “Edit” – Selecting edit will enable changes to be made to all fields
32.1. When ”Edit” is selected the action buttons options will become available:
32.1.1. ........................................................................................................................................................ “Save” – All changes made to record will be saved, overwriting original information.
32.1.2. ........................................................................................................................................................ “Cancel”- Return to “User” page in read only view
33. System Administrators will have the ability to view the global user list. However, Super Users will only have the ability to view and search local users within their own Provider
34. New – The New button will initiate the creation of a new User in a dedicated screen

303
ID Requirement Comments
35. System Administrators and Super Users can create New Users through the “User Editor” tile within the VasCot settings screen.
36. Selecting “User Editor” will route the user to the “User Search” screen. This screen gives the user the functionality to search for an existing patient or select the “New” button to create a new user.
Search functionality will follow the same conventions as Provider Search.
37. Selecting “New” will route the user to “User Editor” screen.
38. Creating a new user will require the following information to be completed:
38.1. Account enabled – Selecting this option will activate the account and send the user an email to create a password. Tick box. Not mandatory.
This will be actioned at the point of selecting “Save”
38.1.1. ........................................................................................................................................................ If the Account is disabled, it will not be possible to create / associate Patients to this user as a named Clinician
38.1.2. ........................................................................................................................................................ It will not be possible to disable the User if there are Patients associated with it.
38.1.3. ........................................................................................................................................................ This field is of particular use when a user attempts self-registration and the User is unknown by VasCOT. The system will populate the User information but will not enable it, so that the System Admin can review and enable once verified as a true User
See Self-Registration
38.2. Account locked – Selecting this option will add the account details to the VasCOT database but upon login attempt, the user will be informed that the Account is locked.
38.2.1. ........................................................................................................................................................ The account will be locked by the System automatically if the number of login attempts is surpassed
38.2.2. ........................................................................................................................................................ Can also be manually set by a Super User to restrict access to the account without needing to disable.
38.3. Force Password Reset – If selected, a password reset email with a secure link will be sent to the User. Tick box.
This will be actioned at the point of selecting “Save”
38.3.1. ........................................................................................................................................................ User will not be able to sign in until they change their password
38.4. Role – Role(s) will be set for the user. It will be possible to assign a user to multiple roles Multi-select combo box used in wireframes to facilitate many roles being available in the future
38.5. Provider – Combo box. The Provider to which the user belongs. System Administrators will be able to select from the full list. Super Users will be restricted to their own Provider and will not be able to change this.
May require a search and suggest type implementation if there is large number of Providers
38.6. Title – combo box. Containing: o Mr o Miss o Mrs o Ms o Dr

304
o Prof
38.7. Forename – free text field. Mandatory.
38.8. Surname – free text field. Mandatory.
38.9. Email – free text field. Validation required to ensure the domain used matches the domain of the Provider
38.10. ......................................................................................................................................................... Telephone number – number field
38.11. ......................................................................................................................................................... 1st Line of Address – free text. No lookup.
38.12. ......................................................................................................................................................... 2nd Line of Address – free text. No lookup.
38.13. ......................................................................................................................................................... 3rd Line of Address – free text. No lookup.
38.14. ......................................................................................................................................................... 4th Line of Address – free text. No lookup.
38.15. ......................................................................................................................................................... Post code – free text. No lookup.
38.16. ......................................................................................................................................................... Secretary / team email – Free text field Requires review for notifications
39. Cancel – will return the user to the search screen without saving changes
40. Save – will save the provider, if all mandatory fields are completed.
40.1. Save Successful confirmation message UI / UX guidance if appropriate
40.2. If the User has had their account enabled, the “Successful Save” will trigger the sending of an email to the User for them verify registration and create their password.
See User Verification

305
ID Requirement
41. Patient creation will not be completed from the User editor and instead will be completed from within the “Patient Folder” screen, which means the user creating the patient will need to have access to patient data – likely to be a clinician but to be determined by Role.
42. Patient entries will be selectable. Selecting a patient will route User to “Patient Overview”
43. The Patient Folder offers the ability to search for a patient. In the event of the patient not being found, the system will suggest that the patient can be created, using a dedicated “Create New Patient” button.
44. “Create New Patient” will route the User to “Patient Folder – Editor”
45. “Patient Folder – Editor” will be displayed in tab format:
• Patient – Patient details
• Provider – Provider details
45.1. User will be required to input the below information on the “Patient” tab:
• NHS Number – Number field. Mandatory.
• Title – Drop down menu (Miss, Ms, Mrs, Mr, Dr). Mandatory.
• Forename – Free text field. Mandatory. Middle Name(s) – Free text field Surname – Free text field. Mandatory.
• Date of Birth – Date Picker. Mandatory.
• Email Address – Free text field. Mandatory.
• Telephone Number – Number Field. Mandatory.
• 1st Line of Address – Free test field. Mandatory.
• 2nd Line of Address – Free test Field. Mandatory.
• 3rd Line of Address – Free text Field
• 4th Line of Address – Free text Field. Mandatory.
• Preferred Method of Communication – Tick box (Email, Post). Mandatory.
• Consent – The Consent field will be disabled during Patient creation as the Patient will need to provide this when they verify and login.
45.1.1. ........................................................................................................................................................ NHS Number validation algorithm will check that the NHS number is in the correct format and a valid number but will not check that this number belongs to the created patient unless otherwise specified.
45.1.2. ........................................................................................................................................................ Without consent, users of the creating Provider can begin to populate patient data but it will not be shared with the wider VasCOT community (users associated to providers other than the creating Provider) until consent is provided by the patient. If this consent is removed only the Lead Provider will have access until Consent is granted again.
45.2. Cancel – Returns user to “Patient Folder” without saving
45.3. Next Button – Will route the user to the “Providers” tab in a wizard style approach

306
46. On the Providers tab, the patient will need to be associated with:
46.1. A Lead Provider – The user will select from a list of currently existing Providers of Types “Hospital” or “Clinic”. Mandatory.
46.1.1. ........................................................................................................................................................ The “Lead Provider” will automatically populate the details of the Provider associated with the currently logged in User.
46.1.2. ........................................................................................................................................................ When Lead Provided is inputted the “Clinician” field will be enabled for the user to select a user associated to this Provider. Optional.
46.2. GP Practice – The user will select from a list of currently existing Providers of Type “Practice”. Optional.
46.2.1. ........................................................................................................................................................ When GP Practice is inputted the “GP” field will be enabled for the user to select a user associated to this Provider. Optional.
46.3. Satellite Clinic – The user will select from a list of currently existing Providers of Types “Hospital” or “Clinic”. Optional.
46.3.1. ........................................................................................................................................................ When Satellite Clinic is inputted the “Clinician” field will be enabled for the user to select a user associated to this Provider. Optional.
46.4. All of these Providers will already need to exist in the system in order to associate them to a patient using the combo boxes.
47. There will be controls to add / remove multiple satellite sites, as required.
48. Cancel Button – Will return to the search screen without saving
49. Back Button – Will move the user back to the “Patient” tab / wizard screen.
50. Save Button – Will save the patient (subject to mandatory fields being completed correctly)
51. Selecting “Save” will trigger the Patient verification email.
52. A “Save Successful” message will be presented in a modal window.
53. “OK” Button – Route user back to “Patient Folder” with the patient present in the Patient Queues

307
ID Requirement
54. Enabling a new User will trigger the sending of a verification email to the email address inputted.
54.1. The email will contain instructions and a secure VasCOT URL which allows the user to create a password for their account
54.1.1. ........................................................................................................................................................ The URL will only be valid for ‘x’ amount of time (will need to be defined as a variable / config setting for flexible changes in the future)
54.1.2. ........................................................................................................................................................ If this time elapses before the user has verified their email, the URL should present a screen informing the user of this fact and provide the ability for the user to request a new URL, which will trigger the same verification email but with a new URL, to be delivered to their registered email address
55. Upon accessing the verification email (within the allowed time limit) and following the URL link provided, the User will have the ability to create a password.
56. The User will be required to input:
• Email – Free text field
• Create Password – Free text field
• Re-enter Password – Free text field
56.1. Password will be entered twice so that matching validation can confirm that the password was entered the same on both occasions.
56.1.1. ........................................................................................................................................................ Password criteria validation will also be enforced (E.g. min characters, upper case, etc)
57. Depending on whether the user verifying their account is a Patient or not, the screen will either a present Disclaimer information (not a patient) or Consent information (patient).
57.1. It will be a mandatory requirement that the user confirms that they either give consent or acknowledge the disclaimer before they can submit to verify their account.
57.2. Guidance and wording to be provided for Disclaimer
57.3. Guidance and wording to be provided for Consent
57.3.1. ........................................................................................................................................................ Consent can later be revoked by the Patient within their own Patient Details section
58. “Submit” – Selecting submit will validate the details entered
58.1. If the details are correct a modal window will appear confirming successful registration. Close – Routes User to the Login page
58.2. If the details are incorrect, the fields will be cleared and the User instructed to re-enter.

308
ID Requirement
59. The system will offer the ability for new users to register directly from the home screen of the solution via the “Register” button.
60. If the user enters an email address with a domain already belonging to a Provider, the request will be sent to the Provider Super User(s) and the “Provider” details on the right hand side of the registration screen will be hidden.
61. If the user enters an email address with a domain which does not belong to a known Provider, the “Provider” details on the right of the screen will be shown and made mandatory. The request will be sent to the System Administrator for review and for a Provider to be setup.
62. To register, the user will complete the below mandatory fields:
63. Title – Drop down menu
• Miss
• Mrs
• Ms
• Mr
• Dr
• Other
64. Forename – Free text field
65. Surname – Free text field
66. Email Address – Free Text field
67. Domain checking will be performed on the email address to show / hide the Provider details as required
68. Unique ID – string
69. Telephone Number – Number field
70. Reason for access request – Free text field
71. If the email domain is unrecognised, the following mandatory information will be completed:
72. Provider type: Drop down menu
• Trust / Hospital
• GP Practice
• Clinic
73. Code – String
74. Provider Name – Free text field
75. 1st Line of Address – Free text field
76. 2nd Line of Address – Free text field
77. 3rd Line of Address – Free text field
78. 4th Line of Address – Free text field
79. Postcode – Free text field
80. Telephone Number – Number field
81. “Cancel” button will not commit the information inputted and route the user back to the VasCOT landing page.

309
82. “Submit” button will register details to the system and a modal window will appear explaining the next steps.
83. The submission will trigger a notification to the relevant VasCOT Users to authorise the request.
ID Requirement
84. The Dashboard will provide full visibility across all Providers to System Administrators.
85. The Dashboard will display Provider Specific information to Super Users of that Provider.
86. The Dashboard will display KPI information in the main body of the screen. This will include:
• No. of user login in the last 24 hours
• No. of hits the website received in 24 hours
• No. of users online
87. The VasCOT dashboard will include a fixed toolbar that will feature across the top of the screen.
88. The toolbar will display user credentials with a “User Profile” button.
89. “Logout” button when selected will end the Users current session and route back to “Login” screen.
90. “Settings” button will direct users to the “Settings” page. From this page four options will be available:
• User Editor
• Role Editor
• Provider Editor
• Notification Settings
ID Requirement
91. Clinical Users will be routed to “Patients” screen upon login (as defined by Role)
92. The main body of the screen will be split into two tabs listing patients
92.1. • My Patients: List of patients associated with the User identified as the Named Clinician
• Our Patients: List of patients associated with the Provider
92.2. Each tab header will contain:
• Tab Title
• A Patient Count: This is the number of patients on that list.
• Notification Count: This is the total number of notifications awaiting acknowledgement from that Provider, on that list.
93. Patient information will be displayed in a table including the following columns:
93.1. • Patient Name
• Date of Birth
• NHS number
• Last Patient Update (Date / Time)

310
• Next Appointment
• Lead Clinician (Named clinician of lead Provider)
• Consent (Yes / No)
• Notification Count
94. Users will be able to navigate between the tabs freely
95. Selecting a patient row from the list will route the User to the “Patient Overview”.
ID Requirement
96. If the User belongs to a Provider which is not associated to any patients, then the Patient Queues will be empty with a count of zero.
97. The system will provide a search feature from the Patient Folder, for the user to find patients using a combination of names or NHS Number.
98. The system will return results based on the search or offer to create a new patient, depending on Role.
99. Upon selecting a patient from the search results, the system will determine whether the current User’s Provider is associated to the patient or not.
99.1. If it is, the user will be able to access the Patient Overview information.
99.2. If it is not, all clinical information will be hidden and the user will be informed that they do not currently have access but may request it
100. The user will be required to select how they would like to be associated to the Patient from a drop down menu, consisting of:
• Lead Provider
• GP Practice
• Satellite Clinic
100.1. ......................................................................................................................................................... The available options in the dropdown will intelligently be restricted based on the current user. If the user belongs to a GP Practice, then the option will default and be restricted to “GP Practice”. If the user belongs to any other type of Provider, they will have the options to select “Lead Provider” or “Satellite Clinic”
100.2. ......................................................................................................................................................... If “Lead Provider” is selected, a warning will appear under the field informing the user that if they are granted access, they will replace the current Lead Provider for that patient, as only one Provider can be identified as the Lead.
100.3. ......................................................................................................................................................... If “GP Practice” is selected, a warning will appear under the field informing the user that if they are granted access, they will replace the current GP Practice for that patient, as only one GP Practice can be associated to the patient.
100.4. ......................................................................................................................................................... If “Satellite” is selected, a note will appear under the field informing the user that if they are granted access, they will be added as another satellite provider without replacing any of the other providers.
101. The User will be required to select who they are requesting access on behalf of, from a drop down list. The list should contain all of the Users for their Provider with the current user defaulted into the box.
102. The system will offer a mandatory dropdown menu of coded reasons
102.1. ......................................................................................................................................................... The system will also offer a supplementary but optional free text box to capture additional information for requesting access.
103. The Request Access screen will offer two control buttons:
• Request Access
• Cancel

311
103.1. ......................................................................................................................................................... “Request Access” – Will present a “Submission Success” message.
103.1.1........................................................................................................................................................ This will also trigger a notification to the Lead Provider in order for them to approve or reject the request
Requirement
104. To request a change to Provider Type, a User will need existing access to patient data (via their Provider asscociated), in order to access the “Edit Patient Details” Screen from the “Patient Overview”.
105. “Edit Patient Details” will feature:
• Patient Tab – Patient details
• Provider Tab – Provider details
106. The Provider tab will display all current provider information (Lead, Satelite, GP etc.)
107. If the logged in user is not the current Lead Provider and is not a GP Practice a check box should be displayed labelled “Send request to become Lead Provider”.
107.1. ......................................................................................................................................................... Checking this box and saving the changes will trigger a notification to the current Lead Provider for review.
107.2. ......................................................................................................................................................... No changes in Provider Type will take effect until the request has been “Accepted”
108. Within the Patient Editor, Satellite Providers will also have the ability to relinquish access to the patient, using the same add / remove controls available to the Super User but restricted by RBAC to only allow removal of themselves.
ID Requirement
109. To request a change to Provider Type, a User will need existing access to patient data (via their Provider asscociated), in order to access the “Edit Patient Details” Screen from the “Patient Overview”.
110. “Edit Patient Details” will feature:
• Patient Tab – Patient details
• Provider Tab – Provider details
111. The Provider tab will display all current provider information (Lead, Satelite, GP etc.)
112. If the logged in user is not the current Lead Provider and is not a GP Practice a check box should be displayed labelled “Send request to become Lead Provider”.
112.1. Checking this box and saving the changes will trigger a notification to the current Lead Provider for review.
112.2. No changes in Provider Type will take effect until the request has been “Accepted”
113. Within the Patient Editor, Satellite Providers will also have the ability to relinquish access to the patient, using the same add / remove controls available to the Super User but restricted by RBAC to only allow removal of themselves.

312
ID Requirement
114. The notification will route the user to Patient Editor upon selection. However, the user can also access the Patient Editor manually, via the Patient Overview screen.
115. Requested Provider changes will present themselves next to the current Provider information for easy comparison
115.1. ......................................................................................................................................................... In some instances the current Provider information will be blank for GP Practices and Satellite Clinics, if they have not been previously set.
116. A dedicated control container will surround the current provider and the requested changes with two action buttons:
• Approve
• Reject
116.1. ......................................................................................................................................................... “Reject” button. Rejecting the change would trigger a notification to the satellite clinic and provider status would remain the same.
116.2. ......................................................................................................................................................... “Accept” button - Accepting the change will populate the fields in the “Provider” tab accordingly by updating the current Provider information with the requested Provider information.
116.2.1........................................................................................................................................................ A notification will be triggered to the requesting Provider to confirm the change.
117. The system will still require the user to Save the changes by using the dedicated Patient Editor Controls:
117.1. ......................................................................................................................................................... Cancel – Route back to “Notifications”
117.2. ......................................................................................................................................................... Save – Save will open a modal window asking user if they wish to become a satellite provider:
117.2.1........................................................................................................................................................ If the request was to change the Lead Provider and the Lead Provider approves this change, they will effectively be removing their own association to the patient and will no longer have the ability to contribute to the patient record – although they will have access to any past information they have been responsible for. Therefore, in this scenario, an additional check should prompt the user with a modal window with two actions buttons.
117.2.2........................................................................................................................................................ The modal should ask the user : “Do you also wish to set the previous Lead Provider as a Satellite Provider now? This will ensure that this Provider can still contribute to the Patient Record. Yes – Provider details will automatically set as Satellite for this patient No – Provider details will be removed from the patient record and the ability to contribute will be removed
117.2.3........................................................................................................................................................ Any current workflows, data input or record contributions will be completed prior to the Lead Provider before accepting another Provider as the Lead. Incomplete workflow / information will be attributed to the new Provider under their responsibility.
118. “Patient folder” will be displayed in read only again to reflect the change in Providers agreed.

313
ID Requirement
119. The notification will route the user to Patient Editor upon selection. However, the user can also access the Patient Editor manually, via the Patient Overview screen.
120. Requested Provider changes will present themselves next to the current Provider information for easy comparison
120.1. ......................................................................................................................................................... In some instances the current Provider information will be blank for GP Practices and Satellite Clinics, if they have not been previously set.
121. A dedicated control container will surround the current provider and the requested changes with two action buttons:
• Approve
• Reject
121.1. ......................................................................................................................................................... “Reject” button. Rejecting the change would trigger a notification to the satellite clinic and provider status would remain the same.
121.2. ......................................................................................................................................................... “Accept” button - Accepting the change will populate the fields in the “Provider” tab accordingly by updating the current Provider information with the requested Provider information.
121.2.1........................................................................................................................................................ A notification will be triggered to the requesting Provider to confirm the change.
122. The system will still require the user to Save the changes by using the dedicated Patient Editor Controls:
122.1. ......................................................................................................................................................... Cancel – Route back to “Notifications”
122.2. ......................................................................................................................................................... Save – Save will open a modal window asking user if they wish to become a satellite provider:
122.2.1........................................................................................................................................................ If the request was to change the Lead Provider and the Lead Provider approves this change, they will effectively be removing their own association to the patient and will no longer have the ability to contribute to the patient record – although they will have access to any past information they have been responsible for. Therefore, in this scenario, an additional check should prompt the user with a modal window with two actions buttons.
122.2.2........................................................................................................................................................ The modal should ask the user : “Do you also wish to set the previous Lead Provider as a Satellite Provider now? This will ensure that this Provider can still contribute to the Patient Record. Yes – Provider details will automatically set as Satellite for this patient No – Provider details will be removed from the patient record and the ability to contribute will be removed
122.2.3........................................................................................................................................................ Any current workflows, data input or record contributions will be completed prior to the Lead Provider before accepting another Provider as the Lead. Incomplete workflow / information will be attributed to the new Provider under their responsibility.
123. “Patient folder” will be displayed in read only again to reflect the change in Providers agreed.

314
ID Requirement
124. “Notifications Settings” will only be available for System Administrators.
125. System Administrators will use notification settings to define role types.
126. The screen will detail the “Notification Type” and the recipient of such notification type.
127. All recipient types will be listed in a dropdown/tick box menu:
• Patient
• Clinical User
• Receiving Provider
• Super User
• System Administrator
• Administrator
128. Several recipient types can be selected per notification type.
129. Users will access this screen from the Patient Overview.
130. As per the other editors, the fields will be first displayed as read-only with the following actions:
131. Cancel – Returns to the Patient Overview
132. Edit – Enables the fields for editing (Role dependant)
133. Replaces the current action buttons with just two: Save – Save changes and return to read only view of the Patient Editor Cancel – Do not save any changes and return to read only view of the Patient Editor

315
8 DISCUSSION
Although mortality from ANCA associated vasculitis itself is improving, this body of work
looks beyond treating the disease, to managing the patient in the longer-term through
acknowledging the morbidity that may accrue through chronic disease and
immunosuppression exposure. Identification of potential factors contributing towards
current morbidity in this population was undertaken through an initial literature review
followed by the broad patient questionnaire study. This study highlighted that there are
several hurdles patients face on their route through diagnosis, initial treatment and long
term management that must be overcome to optimise their outcomes.
8.1 RECOGNITION AND IDENTIFICATION OF DISEASE
One of the major challenges for patients with vasculitis is correct and timely identification
of the disease. Data from the patient questionnaire study has shown there is often
substantial delay to diagnosis with this likely to translate into accrual of organ damage. This
is more prominent in patients presenting with more unusual disease manifestations
perhaps highlighting the need for increased awareness of the disease and its spectrum in
the wider clinical community. The majority of patients surveyed were diagnosed from the
year 2000 onwards (59%) meaning that this data reflects relatively recent patient
experience. This is supported by data from the combined EUVAS studies reporting that
34.5% of patients had more than one item of damage, as identified through the Vasculitis
Damage Index, at baseline (being enrolment to clinical trial)205.
The Chapel Hill group conducted a study with some parallels, examining the pathway to
renal biopsy of patients with small vessel vasculitis diagnosed in the United States. They
identified that contributory factors to delay to biopsy (and therefore usually definitive
diagnosis) included a delay from the patient in seeking care, and those presenting with
upper respiratory tract involvement or ‘flu like prodrome66.
One approach to improving the patient’s pathway to diagnosis will be in having clearer
diagnostic and classification criteria for vasculitis. This will be provided by the previously

316
mentioned DCVAS study which has so far recruited around 4000 patients worldwide,
aiming to not only revise the classification criteria for vasculitis but for the first time to
provide diagnostic criteria.
The questionnaire study novelly reports diagnoses that patients had their vasculitis
symptoms attributed to prior to receiving their diagnosis of vasculitis. Understandably,
patients were assigned commoner diagnoses, usually in primary care, initially.
Education and raising awareness of vasculitis is undoubtedly part of the challenge to
improve routes to diagnosis. However, due to the rarity of the disease it is not appropriate
to focus these efforts on primary care as predominantly the patients presenting with
symptoms of nasal congestion or arthralgia will not have vasculitis.
Equally with an increasing burden on primary care, it is not reasonable to expect primary
care physicians to not only be aware of the full spectrum of vasculitis disorders, but also to
dedicate their time and resources to defining and diagnosing these rare and challenging
conditions. One approach however, may be to examine constellations of presenting
symptoms and to use this to develop algorithms to allow generation of red flags for ANCA
testing and secondary care referral should these arise within a certain time period in a
patient. In order to inform this sort of algorithm large numbers of well phenotyped patients
are required. Once again, this is something that may be supported by the DCVAS data set
following completion of this study.
Another possible source of data to contribute to such a development would be the Clinical
Practice Research Datalink (CPRD). This is a resource with over 11 million UK patient
primary care records, including around 6.9% of the population337. This dataset provides
complete primary care records, allowing identification of the most common initial
presenting complaints to primary care, prior to the diagnosis of AAV. This would also allow
the findings of the most frequent “misdiagnoses” in AAV to be validated using a different
approach.

317
8.2 INITIAL MANAGEMENT
For patients for whom the suspicion of disease has been raised the next step is ensuring
that patients are rapidly referred to a centre with the capacity and experience to facilitate
timely and appropriate therapy. The way care is delivered within the NHS is evolving. Finite
resources and increasing patient numbers means that the structure of care is changing to
ensure the most efficient models are used. For many specialties this is resulting in “centres
of expertise” being formed to concentrate both resources and clinicians with the
knowledge and experience in these particular areas. With regards to provision of vasculitis
care, current recommendations are that patients should be managed “by a nominated
clinician within clinical networks linked with centres of expertise and other specialities
within the local organisation”83. One way of defining these “centres of expertise” is through
the designation of “Specialised Centres” through Specialised Service Commissioning.
However, these services are provided through individual clinical disciplines, being
Rheumatology for vasculitis care. Patients with vasculitis clearly can have multi- organ
involvement and as such may need clinical input from multiple disciplines. This can make
planning for delivery of care to these patients challenging.
However, through close collaboration and establishment of networks of care involving the
relevant clinicians across a region, these challenges can be overcome. In the case of the
patient with life- threatening disease, initial care needs to be provided in a centre with
critical care support and plasma exchange facilities. For patients who require treatment
with Rituximab as opposed to cyclophosphamide, current NHS England commissioning
requires patients to be entered onto the UKIVAS national disease registry. Therefore,
although patients do not necessarily need to be managed in UKIVAS registered centres,
they will need to be managed in collaboration with such a centre to enable registry entry if
NHS England criteria is to be met.
8.3 LONGER TERM MANAGEMENT
Once initial therapy has been decided upon and arranged then the longer-term treatment
strategy becomes important. It is important for patients with vasculitis to remain under
life-long follow-up due to the risk of future disease relapse, or complications that may arise
from the disease or the therapy. Currently, that long-term surveillance is usually carried out

318
in secondary or tertiary centres. However, the questionnaire study and the Delphi results
suggest there is a role for primary care in the long-term management of this patient group.
Indeed, the population appears to have confidence in their GP, seeing them as the first
point of contact for scenarios including infection but also clinical manifestations that could
represent vasculitis disease activity.
Equally, one of the major parts of managing this condition long-term is managing the risks
associated with damage and therapy. There are none better placed than primary care to
undertake cardiovascular risk assessment, ensure vaccination uptake and cancer
surveillance.
What is vital, is to provide the support and education to facilitate this. Primary care need to
be empowered with the information regarding the augmented risk of cardiovascular
disease, infection, and cancer amongst others, in order to provide appropriate screening
and prophylaxis.
However, prospectively collected data would provide a much more valid way of answering
these questions. Within the UK and Ireland, the national vasculitis registry (UKIVAS) aims to
eventually provide a comprehensive repository for longitudinal data on all patient within
these countries. There are also well established disease registries in Poland and
Germany338 amongst other countries . In the future, combination of these large datasets
may allow us better information to inform our patients of their likely outcomes.
In addition, a tool such as VasCOT has a role, through providing prompts to secondary care
to evaluate for risk factors, through improving two- way communication with primary care,
and in addition providing an educational resource, both for the patient, but also for other
clinicians. The principle of VasCOT fits well within the “5 year forward view” of NHS
England336 which focuses in part on emerging models of care with creating integrated
networks of care a key principle. This report outlines the concept of patients having access
to specialist centres at pivotal points in their management but in parallel acknowledging
that creation and maintenance of care networks for conditions will enable a significant
proportion of patient care to be delivered closer to their home.

319
8.4 FURTHER WORK
Following publication of the ADAPTIV guidelines it is hoped that these will provide a
valuable resource for all clinicians involved in the care of this patient group. The idea is that
these guidelines will provide a comprehensive point of reference to allow safe and holistic
management of the patient, without clinicians having to access multiple documents to
guide them in the different facets of long-term vasculitis care. The guidelines will in
addition, provide standards against which care can be audited to ensure ongoing
improvement of quality.
The major section of this work which is ongoing, is that of VasCOT. Initial development (of
the stages so far outlined within this thesis) was undertaken with resource support from
Hitachi Europe. There has been subsequent interest from other software developers, with
discussions underway as to how to best move this project forward. The next step, following
development, is clinical testing in a single centre, for user acceptability. This will include
detailed feedback from both clinicians and patients to ensure that the data input
requirements are sustainable and will not lead to user fatigue and that the outputs are
valid and relevant. This project is fully supported by the UK and Ireland Rare Disease Group
for Vasculitis and with collaboration with the leading vasculitis centres across the UK
already, this secures participation in more wide scale testing to allow initial outcome and
health economic data to be collected. Alongside this, there is substantial interest in
developing this product for the monitoring of other populations requiring long-term
immunosuppression. The initial plan is to, in conjunction with developing the vasculitis
software, adapt and pilot this tool for patients with Systemic Lupus Erythematosus. These
are patients with many parallels with vasculitis. Not only is lupus an autoimmune disease
with the ability to affect multiple systems, but in addition, these patients may receive
similar induction therapy (in the form of cyclophosphamide or Rituximab and steroids) and
continue to need long-term immunosuppression. This is a population for whom the major
causes of morbidity and mortality include infection, VTE, CVD and bone disease339,
therefore there is significant reason to think that a similar approach will translate well.
In addition to lupus, other conditions requiring long-term immunosuppression, including
immune mediated renal and rheumatological conditions, inflammatory bowel disease and
the transplant population would be suitable to consider adaptation of this software.

320
As electronic health records continue to develop across the UK, this will in turn improve the
functionality of VasCOT and the possible scope for future use. Once there is a validated
method for patients to perform their own disease activity scoring, then VasCOT could aid in
distance monitoring of patients, allowing self- reporting of symptoms and prioritisation of
those to be seen in specialist centres. Other possible opportunities include testing of
VasCOT in a different healthcare setting overseas, with initial steps towards future
collaboration with the Monash Institute in Melbourne, Australia, already taken.
It is hoped that with the approaches outlined in this thesis, the major complications of
infection, cardiovascular disease, and osteoporosis can be raised in the conscious level of
the community, and hopefully diminished. In addition, the longer-term cancer risks seen in
this population will hopefully continue to dwindle with more controlled, and evidence
based, use of cyclophosphamide.
8.5 FUTURE THERAPIES
However, moving forwards, better future outcomes for these patients will largely depend
on more targeted and steroid sparing immunosuppressive regimes. The PEXIVAS study340,
which evaluates the role of plasma exchange for those with moderate renal impairment
secondary to AAV, in addition randomises patients to receive a modified steroid protocol
equating to approximately half that prescribed by “standard” protocols340. This will allow
better definition of both the sub population of vasculitis patients who may benefit from
PLEX whilst hopefully allowing patients to be exposed to fewer steroids, with an evidence
base to support this.
One of the most promising new therapeutic agents currently undergoing clinical trials is the
C5a receptor inhibitor, CCX168. In a Phase II randomised controlled trial of this agent
compared 1) standard care (cyclophosphamide or rituximab) and prednisolone starting at
60mg a day, 2) CCX168 plus CYC or RTX and prednisolone starting at 20 mg a day with 3)
CCX168 and CYC or RTX plus no prednisolone. At week 12, the patients who received the
study drug had better outcomes, in terms of a reduction in disease activity and patient
reported outcomes, than those on standard therapy35. This therapeutic agent shows great
promise, with Phase III trials now underway.

321
8.6 EPIGENETICS
Another strategy which will allow us to provide more personalised medicine to our
patients, therefore hopefully reducing unnecessary immunosuppression exposure, is the
field of epigenetics. Epigenetics can be defined as “mechanisms that register, signal or
perpetuate gene activity states”341. Essentially epigenetic processes affect gene expression
without affecting gene sequences. It is thought that these processes of epigenetic
modification occur in response to environmental changes, either the environment of the
cell, or the entire organism. Therefore, it is thought that this may be the missing link that
explains why there is significant disconcordance, even amongst genetically identical twins,
in patterns of disease development. Epigenetics has started to explain the “two-hit” model
of autoimmune disease with regards to the interaction between genetic predisposition and
environmental trigger in other conditions such as Inflammatory Bowel Disease and Lupus.
Although there is limited data regarding the epigenetics of AAV so far, there is some
suggestion that it will aid with allowing distinction early on between those patients who
will relapse and those who will attain drug free remission342. This will allow
immunosuppression strategies to be more commensurate with the risk of future disease
activity. In addition, it is likely that the study of epigenetics will enable us to further
understand this complex disease pathogenesis and identify new therapeutic targets.
8.7 SUMMARY
In summary, the landscape of care for those with vasculitis has and is undergoing some
significant changes. As clinicians, we must remain focused on optimising outcomes for our
patients despite increasing financial constraints and evolving models of care. Although this
will be challenging, the vasculitis community continues to work together, with
collaboration bringing the possibility of more robust longitudinal data for outcomes in this
population. In addition, this collaboration increases the power for meaningful clinical trial
data.
Therefore, despite tough times ahead for the healthcare system in this country, the
ongoing enthusiasm and drive of both the clinical and patient communities promise that
outcomes for patients with ANCA associated vasculitis can, and will, continue to improve.

322
9 PUBLICATIONS

323

324

325

326

327

328
10 BIBLIOGRAPHY
1. Davies, D. J., Moran, J. E., Niall, J. F. & Ryan, G. B. Segmental necrotising
glomerulonephritis with antineutrophil antibody: possible arbovirus aetiology? Br.
Med. J. (Clin. Res. Ed). 285, 606 (1982).
2. Falk, R. J., Terrell, R. S., Charlest, L. A. & Jennettet, J. C. Anti-neutrophil cytoplasmic
autoantibodies induce neutrophils to degranulate and produce oxygen radicals in
vitro. Proc. Natl. Acad. Sci. USA 87, 4115–4119 (1990).
3. Jennette, J. C., Xiao, H., Falk, R. & Gasim, A. M. H. Experimental models of vasculitis
and glomerulonephritis induced by antineutrophil cytoplasmic autoantibodies.
Contrib. Nephrol. 169, 211–20 (2011).
4. Salama, A. D. & Little, M. A. Animal models of ANCA associated vasculitis. Curr. Opin.
Rheumatol. 24, 1–7 (2012).
5. Schlieben, D. J., Korbet, S. M., Kimura, R. E., Schwartz, M. M. & Lewis, E. J.
Pulmonary-renal syndrome in a newborn with placental transmission of ANCAs. Am.
J. Kidney Dis. 45, 758–61 (2005).
6. Falk, R. & Jennette, C. in Comprehensive clinical nephrology (eds. Feehally, J., Floege,
J. & Johnson, R.) 275–89 (Mosby, 2007).
7. Lyons, P. a et al. Genetically distinct subsets within ANCA-associated vasculitis. N.
Engl. J. Med. 367, 214–23 (2012).
8. Cowland, J. B. & Borregaard, N. The individual regulation of granule protein mRNA
levels during neutrophil maturation explains the heterogeneity of neutrophil
granules. J. Leukoc. Biol. 66, 989–95 (1999).
9. Schreiber, A., Busjahn, A., Luft, F. & Kettritz, R. Membrane Expression of Proteinase
3 Is Genetically Determined. J. Am. Soc. Nephrol. 14, 68–75 (2003).
10. Witko-Sarsat, V. L34. Neutrophils in ANCA-associated vasculitis: still under
investigation. Presse Med. 42, 595–7 (2013).
11. Flint, J., Morgan, M. D. & Savage, C. O. S. Pathogenesis of ANCA-associated
Vasculitis. Rheum. Dis. Clin. North Am. 36, 463–477 (2010).
12. Abdulahad, W. H., Stegeman, C. A. & Kallenberg, C. G. Review article: The role of
CD4(+) T cells in ANCA-associated systemic vasculitis. Nephrol. 14, 26–32 (2009).
13. Xiao, H. et al. The role of neutrophils in the induction of glomerulonephritis by anti-

329
myeloperoxidase antibodies. Am. J. Pathol. 167, 39–45 (2005).
14. Xiao, H., Schreiber, A., Heeringa, P., Falk, R. J. & Jennette, J. C. Alternative
complement pathway in the pathogenesis of disease mediated by anti-neutrophil
cytoplasmic autoantibodies. Am. J. Pathol. 170, 52–64 (2007).
15. Couser, W. G. & Johnson, R. J. What is myeloperoxidase doing in ANCA-associated
glomerulonephritis? Kidney Int. 88, 938–940 (2015).
16. Roth, A. J. et al. Epitope specificity determines pathogenicity and detectability in
ANCA-associated vasculitis. J. Clin. Invest. 123, 1773–83 (2013).
17. Little, M. A. et al. Anti-Proteinase 3 Anti-Neutrophil Cytoplasm Autoantibodies
Recapitulate Systemic Vasculitis in Mice with a Humanized Immune System. PLoS
One 7, 1–11 (2012).
18. Furuta, S. & Jayne, D. R. W. Antineutrophil cytoplasm antibody-associated vasculitis:
recent developments. Kidney Int. 84, 244–9 (2013).
19. Kaplan, M. J. & Radic, M. Neutrophil extracellular traps: double-edged swords of
innate immunity. J. Immunol. 189, 2689–95 (2012).
20. Nakazawa, D. et al. Abnormal conformation and impaired degradation of
propylthiouracil-induced neutrophil extracellular traps: implications of disordered
neutrophil extracellular traps in a rat model of myeloperoxidase antineutrophil
cytoplasmic antibody-associated vasculiti. Arthritis Rheum. 64, 3779–87 (2012).
21. Wilde, B. et al. Regulatory B cells in ANCA-associated vasculitis. Ann. Rheum. Dis. 72,
1416–9 (2013).
22. Bunch, D. O. et al. Decreased CD5+ B cells in active ANCA vasculitis and relapse after
rituximab. Clin. J. Am. Soc. Nephrol. 8, 382–91 (2013).
23. Unizony, S. et al. Peripheral CD5+ B cells in antineutrophil cytoplasmic antibody-
associated vasculitis. Arthritis Rheumatol. (Hoboken, N.J.) 67, 535–44 (2015).
24. Holden, N. J. et al. ANCA-stimulated neutrophils release BLyS and promote B cell
survival: a clinically relevant cellular process. Ann. Rheum. Dis. 70, 2229–33 (2011).
25. Manzi, S. et al. Effects of belimumab, a B lymphocyte stimulator-specific inhibitor,
on disease activity across multiple organ domains in patients with systemic lupus
erythematosus: combined results from two phase III trials. Ann. Rheum. Dis. 71,
1833–8 (2012).
26. Abdulahad, W. H., Stegeman, C. a, Limburg, P. C. & Kallenberg, C. G. M. Skewed
distribution of Th17 lymphocytes in patients with Wegener’s granulomatosis in
remission. Arthritis Rheum. 58, 2196–205 (2008).

330
27. Nogueira, E. et al. Serum IL-17 and IL-23 levels and autoantigen-specific Th17 cells
are elevated in patients with ANCA-associated vasculitis. Nephrol. Dial. Transplant
25, 2209–17 (2010).
28. Wang, J., Roderiquez, G. & Norcross, M. A. Control of adaptive immune responses
by Staphylococcus aureus through IL-10, PD-L1, and TLR2. Sci. Rep. 2, 606 (2012).
29. Rimbert, M. et al. Decreased numbers of blood dendritic cells and defective function
of regulatory T cells in antineutrophil cytoplasmic antibody-associated vasculitis.
PLoS One 6, e18734 (2011).
30. Lepse, N., Abdulahad, W. H., Kallenberg, C. G. M. & Heeringa, P. Immune regulatory
mechanisms in ANCA-associated vasculitides. Autoimmun. Rev. 1–7 (2011).
doi:10.1016/j.autrev.2011.08.002
31. Ntatsaki, E., Watts, R. A. & Scott, D. G. I. Epidemiology of Vasculitis. Rheum. Dis. Clin.
North Am. 36, 447–461 (2010).
32. Lamprecht, P. et al. Research article Heterogeneity of CD4 + and CD8 + memory T
cells in localized and generalized Wegener ’ s granulomatosis. Arthritis Res. Ther.
25–31 (2003). doi:10.1186/ar610
33. Charles Jennette, J., Xiao, H. & Hu, P. Complement in ANCA-Associated Vasculitis.
Semin. Nephrol. 33, 557–64 (2013).
34. Huugen, D. et al. Inhibition of complement factor C5 protects against anti-
myeloperoxidase antibody-mediated glomerulonephritis in mice. Kidney Int. 71,
646–54 (2007).
35. Jayne, D. et al. Successful steroid replacement in ANCA-associated vasculitis with
C5a receptor inhibitor CCX168 in phase 2 randomised trial (CLEAR). Nephrol. Dial.
Transplant. 31, i45- (2016).
36. Watts, R. A. et al. Classification, epidemiology and clinical subgrouping of
antineutrophil cytoplasmic antibody ( ANCA ) -associated vasculitis. Nephrol Dial
Transpl. 30, i14–i22 (2015).
37. Watts, R. A., Mooney, J., Skinner, J., Scott, D. G. I. & Macgregor, A. J. The contrasting
epidemiology of granulomatosis with polyangiitis (Wegener’s) and microscopic
polyangiitis. Rheumatology (Oxford). 51, 926–31 (2012).
38. Ntatsaki, E., Watts, R. A. & Scott, D. G. I. Epidemiology of ANCA-associated vasculitis.
Rheum. Dis. Clin. North Am. 36, 447–61 (2010).
39. Papiha, S. S., Murty, G. E., Ad’Hia, A., Mains, B. T. & Venning, M. Association of
Wegener’s granulomatosis with HLA antigens and other genetic markers. Ann.

331
Rheum. Dis. 51, 246–8 (1992).
40. Knight, A., Sandin, S. & Askling, J. Risks and relative risks of Wegener’s
granulomatosis among close relatives of patients with the disease. Arthritis Rheum.
58, 302–7 (2008).
41. Xie, G. et al. Association of granulomatosis with polyangiitis (Wegener’s) with HLA-
DPB1*04 and SEMA6A gene variants: Evidence grom genome-wide analysis. Arthritis
Rheum. 65, 2457–2468 (2013).
42. Meda, F., Folci, M., Baccarelli, A. & Selmi, C. The epigenetics of autoimmunity. Cell.
Mol. Immunol. 8, 226–36 (2011).
43. Gomez-Puerta, J. A., Gedmintas, L. & Costenbader, K. H. The association between
silica exposure and development of ANCA-associated vasculitis: Systematic review
and meta-analysis. Autoimmun. Rev. 12, 1129–1135 (2013).
44. Willeke, P. et al. Farm Exposure as a Differential Risk Factor in ANCA-Associated
Vasculitis. PLoS One 10, e0137196 (2015).
45. Stamp, L. K. et al. Association between environmental exposures and
granulomatosis with polyangiitis in Canterbury, New Zealand. Arthritis Res. Ther. 17,
333 (2015).
46. Kallenberg, C. G. M. & Tadema, H. Autoimmunity Reviews Vasculitis and infections :
Contribution to the issue of autoimmunity reviews devoted to ‘ autoimmunity and
infection ’. Arthritis Rheum. 8, 29–32 (2008).
47. Stegeman, C. A. et al. Association of chronic nasal carriage of Staphylococcus aureus
and higher relapse rates in Wegener granulomatosis. Ann. Intern. Med. 120, 12–7
(1994).
48. Stegeman, C. A., Tervaert, J. W., de Jong, P. E. & Kallenberg, C. G. Trimethoprim-
sulfamethoxazole (co-trimoxazole) for the prevention of relapses of Wegener’s
granulomatosis. Dutch Co-Trimoxazole Wegener Study Group. N. Engl. J. Med. 335,
16–20 (1996).
49. Laudien, M. et al. Nasal carriage of Staphylococcus aureus and endonasal activity in
Wegener s granulomatosis as compared to rheumatoid arthritis and chronic
Rhinosinusitis with nasal polyps. Clin. Exp. Rheumatol. 28, 51–5
50. Pendergraft, W. F. et al. Autoimmunity is triggered by cPR-3(105-201), a protein
complementary to human autoantigen proteinase-3. Nat. Med. 10, 72–9 (2004).
51. Tadema, H., Kallenberg, C. G. M., Stegeman, C. a & Heeringa, P. Reactivity against
complementary proteinase-3 is not increased in patients with PR3-ANCA-associated

332
vasculitis. PLoS One 6, e17972 (2011).
52. Pilsczek, F. H. et al. A novel mechanism of rapid nuclear neutrophil extracellular trap
formation in response to Staphylococcus aureus. J Immunol 185, 7413–7425 (2010).
53. Konstantinov, K. N., Ulff-Moller, C. J. & Tzamaloukas, A. H. Infections and
antineutrophil cytoplasmic antibodies: Triggering mechanisms. Autoimmun. Rev. 14,
201–203 (2015).
54. Kain, R. et al. Molecular mimicry in pauci-immune focal necrotizing
glomerulonephritis. Nat. Med. 14, 1088–96 (2008).
55. Roth, A. J. et al. Anti-LAMP-2 Antibodies Are Not Prevalent in Patients With
Antineutrophil Cytoplasmic Autoantibody Glomerulonephritis. J. Am. Soc. Nephrol.
1–11 (2011). doi:10.1681/ASN.2011030273
56. Tadema, H. et al. Bacterial DNA motifs trigger ANCA production in ANCA-associated
vasculitis in remission. Rheumatology (Oxford). 50, 689–96 (2011).
57. Hurtado, P. R. et al. CpG oligodeoxynucleotide stimulates production of anti-
neutrophil cytoplasmic antibodies in ANCA associated vasculitis. BMC Immunol. 9,
34 (2008).
58. Langford, C. & Hoffman, G. S. Wegener granulomatosis. Am. J. Med. Sci. 321, 76–82
(2001).
59. Klinger, H. Grenzformen der Periarteriitis nodosa. Frankfurt Ztschr Path 42, 455–80
(1931).
60. Wegener, F. Uber eine eigenartige rhinogene Granulomatose mit besonderer
Beteiligung des Arteriensystems und der Nieren. Beitr path Anat 102, 36–68 (1939).
61. Falk, R. J. et al. Granulomatosis with Polyangiitis (Wegener’s): An alternative name
for Wegener’s Granulomatosis. Arthritis Rheum. 63, 863–4 (2011).
62. Davson, J., Ball, J. & Platt, R. The kidney in periarteritis nodosa. Q. J. Med. 17, 175–
202 (1948).
63. Jennette, J. C. et al. 2012 revised International Chapel Hill Consensus Conference
Nomenclature of Vasculitides. Arthritis Rheum. 65, 1–11 (2013).
64. Holle, J. U. et al. Improved outcome in 445 patients with Wegener’s granulomatosis
in a German vasculitis center over four decades. Arthritis Rheum. 63, 257–66 (2011).
65. Sokołowska, B. et al. Effect of delayed diagnosis on disease course and management
of Churg-Strauss syndrome: a retrospective study. Clin. Rheumatol. 32, 349–54
(2013).
66. Poulton, C. J. et al. Pathways to renal biopsy and diagnosis among patients with

333
ANCA small-vessel vasculitis. Clin Exp Rheumatol 31, 1–13 (2013).
67. Robson, J. et al. Damage in the ANCA-associated vasculitides: Long-term data from
the European Vasculitis Study Group therapeutic trials. Ann Rheum Dis 74, 177–84
(2015).
68. Jennette, J. C., Falk, J. R. & Al., E. Nomenclature of Systemic Vasculitides. Arthritis
Rheum. 37, 187–192 (1994).
69. Watts, R. et al. Development and validation of a consensus methodology for the
classification of the ANCA-associated vasculitides and polyarteritis nodosa for
epidemiological studies. Ann Rheum Dis 66, 222–227 (2007).
70. Craven, A. et al. ACR/EULAR-endorsed study to develop Diagnostic and Classification
Criteria for Vasculitis (DCVAS). Clin. Exp. Nephrol. 17, 619–21 (2013).
71. Suppiah, R. et al. Measurement of damage in systemic vasculitis : a comparison of
the Vasculitis Damage Index with the Combined Damage Assessment Index
Measurement of damage in systemic vasculitis : a comparison of the Vasculitis
Damage Index with the Combined Damage Assess. Ann. Rheum. Dis. 70, 80–5
(2011).
72. Mukhtyar, C. et al. EULAR recommendations for the management of primary small
and medium vessel vasculitis. Ann. Rheum. Dis. 68, 310–17 (2009).
73. Jayne, D. R. W. et al. Randomized trial of plasma exchange or high-dosage
methylprednisolone as adjunctive therapy for severe renal vasculitis. J. Am. Soc.
Nephrol. 18, 2180–8 (2007).
74. De Groot, K. et al. Pulse Versus Daily Oral Cyclophosphamide for Induction of
Remission in Antineutrophil Cytoplasmic Antibody—Associated Vasculitis. Ann.
Intern. Med. 150, 670 (2009).
75. Harper, L. et al. Pulse versus daily oral cyclophosphamide for induction of remission
in ANCA-associated vasculitis: long-term follow-up. Ann. Rheum. Dis. 71, 955–60
(2012).
76. Popa, E. R., Stegeman, C. A., Bos, N. A., Kallenberg, C. G. & Tervaert, J. W.
Differential B- and T-cell activation in Wegener’s granulomatosis. J. Allergy Clin.
Immunol. 103, 885–94 (1999).
77. Seo, P., Specks, U. & Keogh, K. A. Efficacy of Rituximab in Limited Wegener ’ s
Granulomatosis with Refractory Granulomatous Manifestations. J. Rheumatol.
2017–2023 (2008).
78. Stone, J. H. et al. Rituximab versus cyclophosphamide for ANCA-associated

334
vasculitis. N. Engl. J. Med. 363, 221–32 (2010).
79. Jones, R. B. et al. Rituximab versus Cyclophosphamide in ANCA- Associated Renal
Vasculitis. N. Engl. J. Med. 363, 211–220 (2010).
80. Cambridge, G. et al. Serologic changes following B lymphocyte depletion therapy for
rheumatoid arthritis. Arthritis Rheum. 48, 2146–54 (2003).
81. Besada, E., Koldingsnes, W. & Nossent, J. C. Serum immunoglobulin levels and risk
factors for hypogammaglobulinaemia during long-term maintenance therapy with
rituximab in patients with granulomatosis with polyangiitis. Rheumatology (Oxford).
1–7 (2014). doi:10.1093/rheumatology/keu194
82. Roberts, D. M. et al. Immunoglobulin G replacement for the treatment of infective
complications of rituximab-associated hypogammaglobulinemia in autoimmune
disease: a case series. J. Autoimmun. 57, 24–9 (2015).
83. Ntatsaki, E. et al. BSR and BHPR guideline for the management of adults with ANCA-
associated vasculitis. Rheumatology (Oxford). (2014).
doi:10.1093/rheumatology/ket445
84. Guerry, M.-J. C. J. et al. Recommendations for the use of rituximab in anti-
neutrophil cytoplasm antibody-associated vasculitis. Rheumatology (Oxford). 1–10
(2011). doi:10.1093/rheumatology/ker150
85. NHS England. Clinical Commissioning Policy: Rituximab for the treatment of ANCA-
associated vasculitis in adults. NHS England website (2015). at
<https://www.england.nhs.uk/commissioning/wp-
content/uploads/sites/12/2015/01/a13-ritux-anca-vascul.pdf>
86. Guillevin, L. et al. Rituximab versus azathioprine for maintenance in ANCA-
associated vasculitis. N Engl J Med 371, 1771–1780 (2014).
87. NICE. Belimumab for treating active auto-antibody positive systemic lupus
erythematosus. (2016).
88. Langford, C. a et al. An open-label trial of abatacept (CTLA4-IG) in non-severe
relapsing granulomatosis with polyangiitis (Wegener’s). Ann. Rheum. Dis. 73, 1376–
9 (2014).
89. Walton, E. W. Giant Cell Granuloma of Respiratory Tract. BMJ 265–270 (1958).
90. Little, M. A. et al. Early mortality in systemic vasculitis: relative contribution of
adverse events and active vasculitis. Ann Rheum Dis 69, 1036–1043 (2010).
91. Booth, A. D. et al. Outcome of ANCA-associated renal vasculitis: a 5-year
retrospective study. Am J Kidney Dis 41, 776–784 (2003).

335
92. Bourgarit, A. et al. Deaths occurring during the first year after treatment onset for
polyarteritis nodosa, microscopic polyangiitis, and Churg-Strauss syndrome: a
retrospective analysis of causes and factors predictive of mortality based on 595
patients. Medicine(Baltimore) 84, 323–30 (2005).
93. Mukhtyar, C. et al. Outcomes from studies of antineutrophil cytoplasm antibody
associated vasculitis : a systematic review by the European League Against
Rheumatism systemic vasculitis task force Outcomes from studies of antineutrophil
cytoplasm antibody associated vasculiti. Ann. Rheum. Dis. (2008).
doi:10.1136/ard.2007.071936
94. Seo, P. et al. The future of damage assessment in vasculitis. J. Rheumatol. 34, 1357–
71 (2007).
95. De Groot, K. et al. Randomized trial of cyclophosphamide versus methotrexate for
induction of remission in early systemic antineutrophil cytoplasmic antibody-
associated vasculitis. Arthritis Rheum. 52, 2461–9 (2005).
96. Jayne, D., Rasmussen, N., Andrassy, K. & Bacon, P. A Randomized Trial of
Maintenance Therapy for Vasculitis Associated with Antineutrophil Cytoplasmic
Autoantibodies. N. Engl. J. Med. 349, 36–44 (2003).
97. Hiemstra, T. F. et al. Mycophenolate Mofetil vs Azathioprine for Remission
Maintenance in Antineutrophil Cytoplasmic Antibody–Associated Vasculitis. JAMA
304, 2381 (2010).
98. Flossmann, O. et al. Long-term patient survival in ANCA-associated vasculitis. Ann.
Rheum. Dis. 70, 488–94 (2011).
99. Rhee, R. L. et al. Trends in long-term outcomes among patients with ANCA-
associated vasculitis with renal disease. Arthritis Rheumatol. n/a-n/a (2016).
doi:10.1002/art.39614
100. Hoffman, G. S. et al. Wegener Granulomatosis: An analysis of 158 patients. Ann.
Intern. Med. 116, 488–98 (1992).
101. Pagnoux, C., Hogan, S. L., Chin, H., Jennette, J. C. & Falk, R. J. Predictors of
Treatment Resistance and Relapse in Antineutrophil Cytoplasmic Antibody –
Associated Small-Vessel Vasculitis Comparison of Two Independent Cohorts.
Arthritis Rheum. 58, 2908–2918 (2008).
102. Boomsma, M. M. et al. Prediction of relapses in Wegener’s granulomatosis by
measurement of antineutrophil cytoplasmic antibody levels: a prospective study.
Arthritis Rheum. 43, 2025–33 (2000).

336
103. Tadema, H., Heeringa, P. & Kallenberg, C. G. M. Bacterial infections in Wegener’s
granulomatosis: mechanisms potentially involved in autoimmune pathogenesis.
Curr. Opin. Rheumatol. 23, 366–71 (2011).
104. Stegeman, C. a. Predictive value of antineutrophil cytoplasmic antibodies in small-
vessel vasculitis: is the glass half full or half empty? J. Rheumatol. 32, 2075–7 (2005).
105. Rasmussen, N. et al. Changes in proteinase 3 anti-neutrophil cytoplasm
autoantibody levels in early systemic granulomatosis with polyangiitis (Wegener’s)
may reflect treatment rather than disease activity. Clin. Exp. Rheumatol. 31, S38-44
106. Brunkhorst, R., Eberhardt, O. K., Haubitz, M. & Brunkhorst, F. M. Procalcitonin for
discrimination between activity of systemic autoimmune disease and systemic
bacterial infection. Intensive Care Med 26 Suppl 2, S199-201 (2000).
107. Eberhard, O. K. et al. Usefulness of procalcitonin for differentiation between activity
of systemic autoimmune disease (systemic lupus erythematosus/systemic
antineutrophil cytoplasmic antibody-associated vasculitis) and invasive bacterial
infection. Arthritis Rheum. 40, 1250–1256 (1997).
108. Zycinska, K. et al. Procalcitonin as an indiator of systemic response to infection in
ative pulmonary Wegener’s. J. Physiol. Pharmacol. 59, 839–844 (2008).
109. Yoshida, M. et al. Rapid decrease of anti-beta-glucan antibody as an indicator for
early diagnosis of carinii pneumonitis and deep mycotic infections following
immunosuppressive therapy in antineutrophil cytoplasmic antibody-associated
vasculitis. Clin Rheumatol 28, 565–571 (2009).
110. Hirayama, K., Nagai, M., Ebihara, I., Shimohata, H. & Kobayashi, M. Serum ratio of
soluble triggering receptor expressed on myeloid cells-1 to creatinine is a useful
marker of infectious complications in renal vasculitis. Nephrol Dial Transpl. 1–6
(2010). doi:10.1093/ndt/gfq506
111. Harper, L. & Savage, C. O. ANCA-associated renal vasculitis at the end of the
twentieth century — a disease of older patients. Rheumatology 44, 495–501 (2005).
112. Stassen, P. M., Derks, R. P. H., Kallenberg, C. G. M. & Stegeman, C. A. Venous
thromboembolism in ANCA-associated vasculitis--incidence and risk factors.
Rheumatology (Oxford). 47, 530–4 (2008).
113. Berden, A. E. et al. Anti-plasminogen antibodies compromise fibrinolysis and
associate with renal histology in ANCA-associated vasculitis. J. Am. Soc. Nephrol. 21,
2169–79 (2010).
114. Faurschou, M. et al. Increased morbidity from ischemic heart disease in patients

337
with Wegener’s granulomatosis. Arthritis Rheum. 60, 1187–92 (2009).
115. Morgan, M. D. et al. Increased Incidence of Cardiovascular Events in Patients With
Antineutrophil Cytoplasmic Antibody – Associated Vasculitides A Matched-Pair
Cohort Study. Arthritis Rheum. 60, 3493–3500 (2009).
116. Suppiah, R. et al. A model to predict cardiovascular events in patients with newly
diagnosed Wegener’s granulomatosis and microscopic polyangiitis. Arthritis Care
Res. (Hoboken). 63, 588–96 (2011).
117. Ginaldi, L., Di Benedetto, M. C. & De Martinis, M. Osteoporosis, inflammation and
ageing. Immun. Ageing 2, 14 (2005).
118. Boomsma, M. M. et al. Prevalence of reduced bone mineral density in patients with
anti-neutrophil cytoplasmic antibody associated vasculitis and the role of
immunosuppressive therapy: a cross-sectional study. Osteoporos. Int. 13, 74–82
(2002).
119. Meggitt, S. J., Anstey, a V, Mohd Mustapa, M. F., Reynolds, N. J. & Wakelin, S.
British Association of Dermatologists’ guidelines for the safe and effective
prescribing of azathioprine 2011. Br. J. Dermatol. 165, 711–34 (2011).
120. Ognenovski, V. M. et al. Increased incidence of cervical intraepithelial neoplasia in
women with systemic lupus erythematosus treated with intravenous
cyclophosphamide. J. Rheumatol. 31, 1763–7 (2004).
121. Harward, L. E. et al. The impact of cyclophosphamide on menstruation and
pregnancy in women with rheumatologic disease. Lupus 22, 81–6 (2013).
122. Rabelo-Júnior, C. N. et al. Penile alterations with severe sperm abnormalities in
antiphospholipid syndrome associated with systemic lupus erythematosus. Clin.
Rheumatol. 32, 109–13 (2013).
123. Takala, J. H., Kautiainen, H., Malmberg, H. & Leirisalo‐Repo, M. Wegener’s
granulomatosis in Finland in 1981–2000: clinical presentation and diagnostic delay.
Scand. J. Rheumatol. 37, 435–438 (2008).
124. Mohammad, A. J., Jacobsson, L. T. H., Westman, K. W. A., Sturfelt, G. & Segelmark,
M. Incidence and survival rates in Wegener’s granulomatosis, microscopic
polyangiitis, Churg-Strauss syndrome and polyarteritis nodosa. Rheumatology
(Oxford). 48, 1560–5 (2009).
125. Mukhtyar, C. et al. Outcomes from studies of antineutrophil cytoplasm antibody
associated vasculitis: a systematic review by the European League Against
Rheumatism systemic vasculitis task force. Ann. Rheum. Dis. 67, 1004–10 (2008).

338
126. Yilmaz, H., Gürel, S. & Ozdemir, O. Turkish patients with osteoarthritis: their
awareness of the side effects of NSAIDs. Turk. J. Gastroenterol. 16, 89–92 (2005).
127. Cullen, G., Donnellan, F., Long, S., Forry, M. & Murray, F. E. Perceptions of
medication safety among patients with inflammatory bowel disease. Scand. J.
Gastroenterol. 45, 1076–83 (2010).
128. Hess, S. L. et al. Adult survivors of childhood malignant lymphoma are not aware of
their risk of late effects. Acta Oncol. 50, 653–9 (2011).
129. Peters, T. et al. Differences in patient and transplant professional perceptions of
immunosuppression-induced cosmetic side effects. Transplantation 78, 537–43
(2004).
130. de Geest, S. & Moons, P. The patient’s appraisal of side effects: the blind spot in
quality of life assessments in transplant recipients. Nephrol. Dial. Transplant. 15,
457–459 (2000).
131. Holvast, A. et al. Cell-mediated immune responses to infl uenza vaccination in
Wegener ’ s granulomatosis. Ann. Rheum. Dis. 924–927 (2010).
doi:10.1136/ard.2009.112813
132. Assen, S. Van et al. Humoral Responses After Influenza Vaccination Are Severely
Reduced in Patients With Rheumatoid Arthritis Treated With Rituximab. Arthritis
Rheum. 62, 75–81 (2010).
133. Department of Health. Chapter 7: Immunisation of individuals with underlying
medical conditions. Immunisation against infectious disease - Green Book (2014). at
<https://www.gov.uk/government/publications/immunisation-of-individuals-with-
underlying-medical-conditions-the-green-book-chapter-7>
134. Hoffman, G. S. et al. Wegener granulomatosis: an analysis of 158 patients. Ann.
Intern. Med. 116, 488–98 (1992).
135. Guillevin, L. et al. A prospective, multicenter, randomized trial comparing steroids
and pulse cyclophosphamide versus steroids and oral cyclophosphamide in the
treatment of generalized wegener’s granulomatosis. Arthritis Rheum. 40, 2187–
2198 (1997).
136. Dalkey, N. The Delphi Method: An Experimental Study of Group Opinion. Futures 1,
408–426 (1969).
137. Keeney, S., Hasson, F. & McKenna, H. P. A critical review of the Delphi technique as
a research methodology for nursing. Int. J. Nurs. Stud. 38, 195–200 (2001).
138. Bond, K. S., Jorm, A. F., Kitchener, B. A., Kelly, C. M. & Chalmers, K. J. Development

339
of guidelines for family and non-professional helpers on assisting an older person
who is developing cognitive impairment or has dementia: a Delphi expert consensus
study. BMC Geriatr. 16, 129 (2016).
139. Carsons, S. E. et al. Treatment Guidelines for Rheumatologic Manifestations of
Sjögren’s: Use of Biologics, Management of Fatigue and Inflammatory
Musculoskeletal Pain. Arthritis Care Res. (Hoboken). (2016). doi:10.1002/acr.22968
140. Duru, N. et al. EULAR evidence-based recommendations on the management of
systemic glucocorticoid therapy in rheumatic diseases. Ann. Rheum. Dis. 66, 1–9
(2013).
141. Hasson, F. & Keeney, S. Enhancing rigour in the Delphi technique research. Technol.
Forecast. Soc. Chang. 78, 1695–1704 (2011).
142. British Society for Rheumatology. Vaccinations in the immunocompromised person.
Guidelines for the patient taking immunosupressants, steroids and the new biologic
therapies. (2009).
143. van Assen, S. et al. EULAR recommendations for vaccination in adult patients with
autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 70, 414–22 (2011).
144. Lapraik, C. et al. BSR and BHPR guidelines for the management of adults with ANCA
associated vasculitis. Rheumatology 46, 1–11 (2007).
145. Royal College of Physicians. Glucocorticoid-induced osteoporosis: guidelines for
prevention and treatment. (2002).
146. Department of Health. The Green Book: Immunisation against infectious disease.
147. National Institute for Clinical Excellence. Hypertension in adults: diagnosis and
management. (2011).
148. National Institute for Clinical Excellence. Chronic Kidney Disease: Early identification
and management of chronic kidney disease in adults in primary and secondary care.
(2008).
149. National Osteoporosis Guideline Group. Guideline for the diagnosis and
management of osteoporosis. (2014). doi:10.1016/j.icrp.2009.12.007
150. Gyle, S. Scottish Intercollegiate Guidelines Network. Management of osteoporosis
and the preventon of fragility fractures. (2015).
151. Hoes, J. N. et al. EULAR evidence-based recommendations on the management of
systemic glucocorticoid therapy in rheumatic diseases. Ann. Rheum. Dis. 66, 1560–7
(2007).
152. Samson, M. et al. Long-term follow-up of a randomized trial on 118 patients with

340
polyarteritis nodosa or microscopic polyangiitis without poor-prognosis factors.
Autoimmun. Rev. 13, 197–205 (2014).
153. Sambrook, P. N. et al. Bisphosphonates and glucocorticoid osteoporosis in men:
results of a randomized controlled trial comparing zoledronic acid with risedronate.
Bone 50, 289–295 (2012).
154. Merkel, P. A., Lo, G. H., Holbrook, J. T., Tibbs, A. K. & Allen, N. B. Brief
Communication : High Incidence of Venous Thrombotic Events among Patients with
Wegener Granulomatosis:The Wegener’s Clinical Occurrence of Thrombosis
(WeCLOT) Study. Ann. Intern. Med. 142, 620–626 (2005).
155. Allenbach, Y. et al. High frequency of venous thromboembolic events in Churg-
Strauss syndrome, Wegener’s granulomatosis and microscopic polyangiitis but not
polyarteritis nodosa: a systematic retrospective study on 1130 patients. Ann.
Rheum. Dis. 68, 564–7 (2009).
156. Weidner, S., Hafezi-Rachti, S. & Rupprecht, H. D. Thromboembolic events as a
complication of antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis
Care Res. 55, 146–149 (2006).
157. Ames, P. R. J., Margaglione, M., Mackie, S. & Alves, J. D. Eosinophilia and
thrombophilia in churg strauss syndrome: a clinical and pathogenetic overview. Clin.
Appl. Thromb. Hemost. 16, 628–36 (2010).
158. Emmi, G. et al. Thrombosis in vasculitis: from pathogenesis to treatment. Thromb. J.
13, 15 (2015).
159. de Leeuw, K. et al. Accelerated atherosclerosis in patients with Wegener’s
granulomatosis. Ann. Rheum. Dis. 64, 753–9 (2005).
160. Chironi, G. et al. Increased prevalence of subclinical atherosclerosis in patients with
small-vessel vasculitis. Heart 93, 96–9 (2007).
161. Sangle, S. R. et al. Ankle-brachial pressure index: a simple tool for assessing
cardiovascular risk in patients with systemic vasculitis. Rheumatology (Oxford). 47,
1058–60 (2008).
162. Mahr, A., Heijl, C., Le Guenno, G. & Faurschou, M. ANCA-associated vasculitis and
malignancy: current evidence for cause and consequence relationships. Best Pract.
Res. Clin. Rheumatol. 27, 45–56 (2013).
163. Knight, A., Askling, J., Granath, F., Sparen, P. & Ekbom, A. Urinary bladder cancer in
Wegener’s granulomatosis: risks and relation to cyclophosphamide. Ann. Rheum.
Dis. 63, 1307–11 (2004).

341
164. Monach, P. A., Arnold, L. M. & Merkel, P. A. Incidence and Prevention of Bladder
Toxicity From Cyclophosphamide in the Treatment of Rheumatic Diseases. Arthritis
Rheum. 62, 9–21 (2010).
165. Ioannidis, J. P. A., Katsifis, G. E., Tzioufas, A. G. & Moutsopoulos, H. M. Predictors of
sustained amenorrhea from pulsed intravenous cyclophosphamide in
premenopausal women with systemic lupus erythematosus. J. Rheumatol. 29,
2129–2135 (2002).
166. Boumpas, D. T. et al. Risk for sustained amenorrhea in patients with systemic lupus
erythematosus receiving intermittent pulse cyclophosphamide therapy. Ann. Intern.
Med. 119, 366–369 (1993).
167. Ben-Aharon, I., Gafter-Gvili, A., Leibovici, L. & Stemmer, S. M. Pharmacological
interventions for fertility preservation during chemotherapy: a systematic review
and meta-analysis. Breast Cancer Res. Treat. 122, 803–11 (2010).
168. Department of Health. Chapter 25: Pneumococcal. Immunisation against infectious
disease - Green Book (2013).
169. Birck, R., Kaelsch, I., Schnuelle, P., Flores-Suárez, L. F. & Nowack, R. ANCA-associated
vasculitis following influenza vaccination: causal association or mere coincidence? J.
Clin. Rheumatol. 15, 289–91 (2009).
170. Jeffs, L., Peh, C. A., Jose, M., Lange, K. & Hurtado, P. Randomized trial investigating
the safety and efficacy of influenza vaccination in patients with antineutrophil
cytoplasmic antibody-associated vasculitis. Nephrology 20, 343–351 (2015).
171. David Morgan, M. et al. Association of Low B Cell Count and IgG Levels With
Infection, and Poor Vaccine Response With All-Cause Mortality in an
Immunosuppressed Vasculitis Population. Arthritis Care Res. (Hoboken). 68, 853–
860 (2016).
172. Holvast, A. et al. Wegener ’ s granulomatosis patients show an adequate antibody
response to influenza vaccination. Ann. Rheum. Dis. 873–878 (2009).
doi:10.1136/ard.2008.092924
173. Hua, C., Barnetche, T., Combe, B. & Morel, J. Effect of methotrexate, anti-tumor
necrosis factor α, and rituximab on the immune response to influenza and
pneumococcal vaccines in patients with rheumatoid arthritis: a systematic review
and meta-analysis. Arthritis Care Res. (Hoboken). 66, 1016–26 (2014).
174. Westra, J. et al. Rituximab impairs immunoglobulin (Ig)M and IgG (subclass)
responses after influenza vaccination in rheumatoid arthritis patients. Clin. Exp.

342
Immunol. 178, 40–47 (2014).
175. Rehnberg, M. et al. Vaccination response to protein and carbohydrate antigens in
patients with rheumatoid arthritis after rituximab treatment. Arthritis Res. 2008, 1–
8 (2010).
176. Stern, A., Green, H., Paul, M., Vidal, L. & Leibovici, L. Prophylaxis for Pneumocystis
pneumonia ( PCP ) in non-HIV immunocompromised patients ( Review). Cochrane
Database Syst. Rev. (2015).
doi:10.1002/14651858.CD005590.pub3.www.cochranelibrary.com
177. Meuli, K., Chapman, P., O’Donnell, J., Frampton, C. & Stamp, L. Audit of
pneumocystis pneumonia in patients seen by the Christchurch Hospital
rheumatology service over a 5-year period. Intern. Med. J. 37, 687–692 (2007).
178. McGeoch, L. et al. CanVasc Recommendations for the Management of
Antineutrophil Cytoplasm Antibody-associated Vasculitides. J. Rheumatol. 43, 97–
120 (2016).
179. FDA Rituximab licensing information. (2012). at
<www.accessdata.fda.gov/drugsatfda_docs/label/2012/103705s5362lbl.pdf>
180. Jarrousse, B. et al. Increased risk of Pneumocystis carinii pneumonia in patients with
Wegener’s granulomatosis. Clin. Exp. Rheumatol. 11, 615–21 (1993).
181. Besada, E. & Nossent, J. C. Should Pneumocystis jiroveci prophylaxis be
recommended with Rituximab treatment in ANCA-associated vasculitis? Clin.
Rheumatol. (2013). doi:10.1007/s10067-013-2293-4
182. Mori, S. & Sugimoto, M. Pneumocystis jirovecii pneumonia in rheumatoid arthritis
patients: Risks and prophylaxis recommendations. Clin. Med. Insights Circ. Respir.
Pulm. Med. 9, 29–40 (2015).
183. Teichtahl, A. J. et al. Pneumocystis jirovecci pneumonia in connective tissue
diseases: Comparison with other immunocompromised patients. Semin. Arthritis
Rheum. 45, 86–90 (2015).
184. Sowden, E. & Carmichael, A. J. Autoimmune inflammatory disorders, systemic
corticosteroids and pneumocystis pneumonia: a strategy for prevention. BMC Infect.
Dis. 4, 42 (2004).
185. Godeau, B. et al. Factors associated with Pneumocystis carinii pneumonia in
Wegener’s granulomatosis. Ann. Rheum. Dis. 991–994 (1995).
186. Di Cocco, P. et al. A Systematic Review of Two Different Trimethoprim-
Sulfamethoxazole Regimens Used to Prevent Pneumocystis jirovecii and No

343
Prophylaxis at All in Transplant Recipients: Appraising the Evidence. Transplant.
Proc. 41, 1201–1203 (2009).
187. Charlier, C. et al. Risk factors for major infections in Wegener granulomatosis :
analysis of 113 patients. Ann. Rheum. Dis. 68, 658–663 (2009).
188. Pankhurst, C. Clinical Evidence: Candidiasis ( oropharyngeal ). Br. Med. J. Clin. Evid.
1–39 (2013).
189. Playford, E. G., Webster, a C., Sorell, T. C. & Craig, J. C. Antifungal agents for
preventing fungal infections in solid organ transplant recipients. Cochrane Database
Syst. Rev. CD004291 (2004). doi:10.1002/14651858.CD004291.pub2
190. Boeckh, M. Long-term acyclovir for prevention of varicella zoster virus disease after
allogeneic hematopoietic cell transplantation--a randomized double-blind placebo-
controlled study. Blood 107, 1800–1805 (2006).
191. Yang, L., Tian, J., He, Z., Tang, X. & Yang, K. A Meta-analysis of alendronate for the
prevention and treatment of glucocorticoid-induced osteoporosis. Chinese J. Intern.
Med. 52, 838–43 (2013).
192. Devogelaer, J. P. et al. Effect on bone turnover markers of once-yearly intravenous
infusion of zoledronic acid versus daily oral risedronate in patients treated with
glucocorticoids. Rheumatol. (United Kingdom) 52, 1058–1069 (2013).
193. Roux, C. et al. Post hoc analysis of a single IV infusion of zoledronic acid versus daily
oral risedronate on lumbar spine bone mineral density in different subgroups with
glucocorticoid-induced osteoporosis. Osteoporos. Int. 23, 1083–1090 (2012).
194. Hakala, M. et al. Once-monthly oral ibandronate provides significant improvement
in bone mineral density in postmenopausal women treated with glucocorticoids for
inflammatory rheumatic diseases: a 12-month, randomized, double-blind, placebo-
controlled trial. Scand J Rheumatol 41, 260–266 (2012).
195. Tee, S.-I. et al. Prevention of glucocorticoid-induced osteoporosis in immunobullous
diseases with alendronate: a randomized, double-blind, placebo-controlled study.
Arch. Dermatol. 148, 307–14 (2012).
196. Chen, Y. et al. Efficacy of calcitriol in treating glucocorticoidinduced osteoporosis in
patients with nephrotic syndrome: an open-label, randomized controlled study. Clin.
Nephrol. 84, 262–9 (2015).
197. Cohen Tervaert, J. W. Cardiovascular disease due to accelerated atherosclerosis in
systemic vasculitides. Best Pract. Res. Clin. Rheumatol. 27, 33–44 (2013).
198. Luqmani, R. et al. Mortality in Wegener’s granulomatosis: a bimodal pattern.

344
Rheumatology (Oxford). 50, 697–702 (2011).
199. Tervaert, J. W. C. Translational mini-review series on immunology of vascular
disease: accelerated atherosclerosis in vasculitis. Clin. Exp. Immunol. 156, 377–85
(2009).
200. Haris, A. et al. Clinical outcomes of ANCA-associated vasculitis in elderly patients.
Int. Urol. Nephrol. 46, 1595–600 (2014).
201. Knockaert, D. C. Cardiac involvement in systemic inflammatory diseases. Eur. Heart
J. 28, 1797–804 (2007).
202. Flossmann, O. Risks of treatments and long-term outcomes of systemic ANCA-
associated vasculitis. Presse Med. 44, e251-7 (2015).
203. Terrier, B. et al. Factors associated with major cardiovascular events in patients with
systemic necrotizing vasculitides: Results of a longterm followup study. J.
Rheumatol. 41, 723–729 (2014).
204. Hajj-Ali, R. A. et al. The interface of inflammation and subclinical atherosclerosis in
granulomatosis with polyangiitis (Wegener’s): a preliminary study. Transl. Res. 166,
366–374 (2015).
205. Robson, J. et al. Damage in the ANCA-associated vasculitides: long-term data from
the European Vasculitis Study group (EUVAS) therapeutic trials. Ann. Rheum. Dis. 74,
177–84 (2015).
206. Zycinska, K., Wardyn, K., Zielonka, T. M., Nitsch-osuch, A. & Smolarczyk, R.
Atherosclerotic factors in PR3 pulmonary vasculitis. Respir. Regul. - Clin. Adv. 755,
283–286 (2013).
207. Zöller, B., Li, X., Sundquist, J. & Sundquist, K. Risk of subsequent coronary heart
disease in patients hospitalized for immune-mediated diseases: A nationwide
follow-up study from Sweden. PLoS One 7, 1–8 (2012).
208. Mohammad, A. J. & Segelmark, M. Association of cigarette smoking with organ
damage in primary systemic vasculitis. Scand. J. Rheumatol. 40, 51–56 (2011).
209. De Leeuw, K. et al. Patients with Wegener ’ s granulomatosis : a long-term follow-up
study. Clin Exp Rheumatol 28, S18-23 (2010).
210. Pagnoux, C., Chironi, G., Simon, A. & Guillevin, L. Atherosclerosis in ANCA-associated
vasculitides. Ann. N. Y. Acad. Sci. 1107, 11–21 (2007).
211. Bacon, P. A., Stevens, R. J., Carruthers, D. M., Young, S. P. & Kitas, G. D. Accelerated
atherogenesis in autoimmune rheumatic diseases. Autoimmun. Rev. 1, 338–347
(2002).

345
212. Nienhuis, H. L. A. et al. Enhanced endothelium-dependent microvascular responses
in patients with Wegener’s granulomatosis. J. Rheumatol. 34, 1875–81 (2007).
213. Booth, A. D. et al. Inflammation and Arterial Stiffness in Systemic Vasculitis: A Model
of Vascular Inflammation. Arthritis Rheum. 50, 581–588 (2004).
214. Gaffo, A. L. Thrombosis in vasculitis. Best Pract. Res. Clin. Rheumatol. 27, 57–67
(2013).
215. De Sousa, E., Smith, R., Chaudhry, A., Willcocks, L. & Jayne, D. Venous
thromboembolism with concurrent pulmonary haemorrhage in systemic vasculitis.
Nephrol. Dial. Transplant 27, 4357–61 (2012).
216. Groh, M. et al. Eosinophilic granulomatosis with polyangiitis (Churg-Strauss) (EGPA)
Consensus Task Force recommendations for evaluation and management. Eur. J.
Intern. Med. 26, 545–553 (2015).
217. Rao, A. N. Do neutrophil extracellular traps contribute to the heightened risk of
thrombosis in inflammatory diseases? World J. Cardiol. 7, 829 (2015).
218. Lee, J. J. & Pope, J. E. A meta-analysis of the risk of venous thromboembolism in
inflammatory rheumatic diseases. Arthritis Res. Ther. 16, 435 (2014).
219. Katz, O. B., Brenner, B. & Horowitz, N. A. Thrombosis in vasculitic disorders-clinical
manifestations, pathogenesis and management. Thromb. Res. 136, 504–12 (2015).
220. Faurschou, M., Obel, N. & Baslund, B. High risk of pulmonary embolism and deep
venous thrombosis but not of stroke in granulomatosis with polyangiitis
(Wegener’s). Arthritis Care Res. 66, 1910–1914 (2014).
221. Zöller, B., Li, X., Sundquist, J. & Sundquist, K. Risk of pulmonary embolism in patients
with autoimmune disorders: A nationwide follow-up study from Sweden. Lancet
379, 244–249 (2012).
222. Whyte, A. F., Smith, W. B., Sinkar, S. N., Kette, F. E. & Hissaria, P. Clinical and
laboratory characteristics of 19 patients with Churg-Strauss syndrome from a single
South Australian centre. Intern. Med. J. 43, 784–790 (2013).
223. Romeu, M. et al. Survival of patients with ANCA-associated vasculitis on chronic
dialysis: data from the French REIN registry from 2002 to 2011. QJM 107, 545–55
(2014).
224. Chand, S. et al. Caveolin-1 Single Nucleotide Polymorphism in Antineutrophil
Cytoplasmic Antibody Associated Vasculitis. PLoS One 8, e69022 (2013).
225. Azar, L. & Khasnis, A. Paraneoplastic rheumatologic syndromes. Curr. Opin.
Rheumatol. 25, 44–9 (2013).

346
226. Zycinska, K., Kostrzewa-Janicka, J., Nitsch-Osuch, A. & Wardyn, K. Cancer incidence
in pulmonary vasculitis. Adv. Exp. Med. Biol. 788, 349–53 (2013).
227. Marco, H. et al. Long-term outcome of antineutrophil cytoplasmic antibody-
associated small vessel vasculitis after renal transplantation. Clin. Transplant. 27,
338–47 (2013).
228. Agha, A., Bateman, H., Sterrett, A. & Valeriano-Marcet, J. Myelodysplasia and
malignancy-associated vasculitis. Curr. Rheumatol. Rep. 14, 526–31 (2012).
229. Wall, N. & Harper, L. Complications of long-term therapy for ANCA-associated
systemic vasculitis. Nat. Rev. Nephrol. 8, 523–32 (2012).
230. Heijl, C. et al. Incidence of malignancy in patients treated for antineutrophil
cytoplasm antibody-associated vasculitis: follow-up data from European Vasculitis
Study Group clinical trials. Ann. Rheum. Dis. 70, 1415–21 (2011).
231. Le Guenno, G., Mahr, A., Pagnoux, C., Dhote, R. & Guillevin, L. Incidence and
predictors of urotoxic adverse events in cyclophosphamide-treated patients with
systemic necrotizing vasculitides. Arthritis Rheum. 63, 1435–45 (2011).
232. Mok, C. C., Kwok, C. L., Ho, L. Y., Chan, P. T. & Yip, S. F. Life expectancy, standardized
mortality ratios, and causes of death in six rheumatic diseases in Hong Kong, China.
Arthritis Rheum. 63, 1182–9 (2011).
233. Faurschou, M. et al. Cancer preceding Wegener’s granulomatosis: a case-control
study. Rheumatology (Oxford). 48, 421–4 (2009).
234. Faurschou, M. et al. Malignancies in Wegener’s granulomatosis: incidence and
relation to cyclophosphamide therapy in a cohort of 293 patients. J. Rheumatol. 35,
100–5 (2008).
235. Pagnoux, C. et al. Azathioprine or Methotrexate Maintenance for ANCA-Associated
Vasculitis. N. Engl. J. Med. 359, 2790–2803 (2008).
236. Fain, O. et al. Vasculitides associated with malignancies: Analysis of sixty patients.
Arthritis Rheum. 57, 1473–1480 (2007).
237. Pankhurst, T., Savage, C. O. S., Gordon, C. & Harper, L. Malignancy is increased in
ANCA-associated vasculitis. Rheumatology (Oxford). 43, 1532–5 (2004).
238. Knight, A., Askling, J. & Ekbom, A. Cancer incidence in a population-based cohort of
patients with Wegener’s granulomatosis. Int. J. Cancer 100, 82–5 (2002).
239. Westman, K. W., Bygren, P. G., Olsson, H., Ranstam, J. & Wieslander, J. Relapse rate,
renal survival, and cancer morbidity in patients with Wegener’s granulomatosis or
microscopic polyangiitis with renal involvement. J. Am. Soc. Nephrol. 9, 842–52

347
(1998).
240. Martin, F., Lauwerys, B., Lefèbvre, C., Devogelaer, J. P. & Houssiau, F. A. Side-effects
of intravenous cyclophosphamide pulse therapy. Lupus 6, 254–7 (1997).
241. Talar-Williams, C. et al. Cyclophosphamide-induced cystitis and bladder cancer in
patients with Wegener granulomatosis. Ann. Intern. Med. 124, 477–84 (1996).
242. Stillwell, T. J., Benson, R. C., DeRemee, R. A., McDonald, T. J. & Weiland, L. H.
Cyclophosphamide-induced bladder toxicity in Wegener’s granulomatosis. Arthritis
Rheum. 31, 465–70 (1988).
243. Rahmattulla, C. et al. Incidence of malignancies in patients with antineutrophil
cytoplasmic antibody-associated vasculitis diagnosed between 1991 and 2013.
Arthritis Rheumatol. 67, 3270–3278 (2015).
244. Shang, W. et al. Incidence of cancer in ANCA-associated vasculitis: A meta-analysis
of observational studies. PLoS One 10, 1–11 (2015).
245. Tatsis, E., Reinhold-Keller, E., Steindorf, K., Feller, A. C. & Gross, W. L. Wegener’s
granulomatosis associated with renal cell carcinoma. Arthritis Rheum 42, 751–6.
(1999).
246. Nath, R. et al. High risk of human papillomavirus type 16 infections and of
development of cervical squamous intraepithelial lesions in systemic lupus
erythematosus patients. Arthritis Rheum. 57, 619–25 (2007).
247. Bernatsky, S. et al. Factors associated with abnormal Pap results in systemic lupus
erythematosus. Rheumatology 43, 1386–1389 (2004).
248. Alarfaj, A. S. & Khalil, N. Fertility, ovarian failure, and pregnancy outcome in SLE
patients treated with intravenous cyclophosphamide in Saudi Arabia. Clin.
Rheumatol. 33, 1731–1736 (2014).
249. Blumenfeld, Z., Shapiro, D., Shteinberg, M., Avivi, I. & Nahir, M. Preservation of
fertility and ovarian function and minimizing gonadotoxicity in young women with
systemic lupus erythematosus treated by chemotherapy. Lupus 9, 401–5 (2000).
250. Cigni, A. et al. Hormonal strategies for fertility preservation in patients receiving
cyclophosphamide to treat glomerulonephritis: a nonrandomized trial and review of
the literature. Am. J. Kidney Dis. 52, 887–96 (2008).
251. Dooley, M. A. & Nair, R. Therapy Insight: preserving fertility in cyclophosphamide-
treated patients with rheumatic disease. Nat. Clin. Pract. Rheumatol. 4, 250–257
(2008).
252. Elizur, S. E. et al. Fertility preservation treatment for young women with

348
autoimmune diseases facing treatment with gonadotoxic agents. Rheumatology
(Oxford). 47, 1506–9 (2008).
253. Henes, M. et al. Fertility preservation methods in young women with systemic lupus
erythematosus prior to cytotoxic therapy: experiences from the FertiPROTEKT
network. Lupus 21, 953–8 (2012).
254. Hickman, R. A. & Gordon, C. Causes and management of infertility in systemic lupus
erythematosus. Rheumatology (Oxford). 50, 1551–8 (2011).
255. Huong, D. L. T. et al. Risk of ovarian failure and fertility after intravenous
cyclophosphamide. A study in 84 patients. J. Rheumatol. 29, 2571–6 (2002).
256. Katsifis, G. E. & Tzioufas, A. G. Ovarian failure in systemic lupus erythematosus
patients treated with pulsed intravenous cyclophosphamide. Lupus 13, 673–8
(2004).
257. Manger, K., Wildt, L., Kalden, J. R. & Manger, B. Prevention of gonadal toxicity and
preservation of gonadal function and fertility in young women with systemic lupus
erythematosus treated by cyclophosphamide: The PREGO-Study. Autoimmun. Rev.
5, 269–272 (2006).
258. Oktay, K. et al. Absence of conclusive evidence for the safety and efficacy of
gonadotropin-releasing hormone analogue treatment in protecting against
chemotherapy-induced gonadal injury. Oncologist 12, 1055–66 (2007).
259. Pagnoux, C., Mahendira, D. & Laskin, C. A. Fertility and pregnancy in vasculitis. Best
Pract. Res. Clin. Rheumatol. 27, 79–94 (2013).
260. Raptopoulou, A., Sidiropoulos, P. & Boumpas, D. Ovarian failure and strategies for
fertility preservation in patients with systemic lupus erythematosus. Lupus 13, 887–
90 (2004).
261. Turnbull, J. & Harper, L. Adverse effects of therapy for ANCA-associated vasculitis.
Best Pract. Res. Clin. Rheumatol. 23, 391–401 (2009).
262. Lawrenz, B. et al. Impact of systemic lupus erythematosus on ovarian reserve in
premenopausal women: evaluation by using anti-Muellerian hormone. Lupus 20,
1193–7 (2011).
263. Wetzels, J. F. M. Cyclophosphamide-induced gonadal toxicity: A treatment dilemma
in patients with lupus nephritis? Neth. J. Med. 62, 347–352 (2004).
264. Langevitz, P., Klein, L., Pras, M. & Many, A. The effect of cyclophosphamide pulses
on fertility in patients with lupus nephritis. Am. J. Reprod. Immunol. 28, 157–158
(1992).

349
265. Muller, R. B. et al. Efficient boosting of the antiviral T cell response in B cell-depleted
patients with autoimmune rheumatic diseases following influenza vaccination. Clin.
Exp. Rheumatol. 31, 723–30
266. Eisenberg, R. A. et al. Rituximab-Treated Patients Have a Poor Response to Influenza
Vaccination. J. Clin. Immunol. 4, 388–396 (2011).
267. Bingham, C. O. et al. Immunization responses in rheumatoid arthritis patients
treated with rituximab: Results from a controlled clinical trial. Arthritis Rheum. 62,
64–74 (2010).
268. Crnkic Kapetanovic, M., Saxne, T., Jönsson, G., Truedsson, L. & Geborek, P.
Rituximab and abatacept but not tocilizumab impair antibody response to
pneumococcal conjugate vaccine in patients with rheumatoid arthritis. Arthritis Res.
Ther. 15, R171 (2013).
269. Heusele, M. et al. Risk factors for severe bacterial infections in patients with
systemic autoimmune diseases receiving rituximab. Clin. Rheumatol. 33, 799–805
(2014).
270. Zycinska, K., Romanowska, M., Now, I., Rybicka, K. & Brydak, L. B. Antibody response
to inactivated subunit influenza vaccine in patients with Wegener’s Granulomatosis.
J. Physiol. Pharmacol. 58, 819–828 (2007).
271. Stassen, P. M., Sanders, J. F., Kallenberg, C. G. M. & Stegeman, C. A. Influenza
vaccination does not result in an increase in relapses in patients with ANCA-
associated vasculitis. Nephrol Dial Transpl. 654–658 (2008).
doi:10.1093/ndt/gfm640
272. Chew, L.-C., Maceda-Galang, L. M., Tan, Y. K., Chakraborty, B. & Thumboo, J.
Pneumocystis jirovecii pneumonia in patients with autoimmune disease on high-
dose glucocorticoid. J. Clin. Rheumatol. 21, 72–75 (2015).
273. Kofteridis, D. P. et al. Predisposing factors, clinical characteristics and outcome of
Pneumonocystis jirovecii pneumonia in HIV-negative patients. J. Infect. Chemother.
20, 412–416 (2014).
274. Roblot, F. et al. Pneumocystis jirovecii pneumonia in HIV-negative patients: A
prospective study with focus on immunosuppressive drugs and markers of immune
impairment. Scand. J. Infect. Dis. 46, 210–4 (2014).
275. Takenaka, K., Komiya, Y., Ota, M., Yamazaki, H. & Nagasaka, K. A dose-escalation
regimen of trimethoprim-sulfamethoxazole is tolerable for prophylaxis against
Pneumocystis jiroveci pneumonia in rheumatic diseases. Mod. Rheumatol. 23, 752–

350
758 (2013).
276. Maini, R. et al. Increasing Pneumocystis pneumonia, England, UK, 2000-2010.
Emerg. Infect. Dis. 19, 386–392 (2013).
277. Bonilla-Abadia, F. et al. Pneumocystis jirovecii pneumonia in two patients with
systemic lupus erythematosus after rituximab therapy. Clin. Rheumatol. 33, 415–
418 (2014).
278. Martin-Garrido, I., Carmona, E. M., Specks, U. & Limper, A. H. Pneumocystis
pneumonia in patients treated with rituximab. Chest 144, 258–265 (2013).
279. Grewal, P. & Brassard, A. Fact or fiction: does the non-HIV/AIDS immunosuppressed
patient need Pneumocystis jiroveci pneumonia prophylaxis? An updated literature
review. J. Cutan. Med. Surg. 13, 308–312 (2009).
280. Falagas, M. E., Manta, K. G., Betsi, G. I. & Pappas, G. Infection-related morbidity and
mortality in patients with connective tissue diseases: A systematic review. Clin.
Rheumatol. 26, 663–670 (2007).
281. McGregor, J. A. G. et al. Adverse events and infectious burden, microbes and
temporal outline from immunosuppressive therapy in antineutrophil cytoplasmic
antibody-associated vasculitis with native renal function. Nephrol. Dial. Transplant.
30, i171–i181 (2015).
282. Kronbichler, A., Jayne, D. R. W. & Mayer, G. Frequency, risk factors and prophylaxis
of infection in ANCA-associated vasculitis. Eur. J. Clin. Invest. 45, 346–368 (2015).
283. Fillatre, P. et al. Incidence of pneumocystis jiroveci pneumonia among groups at risk
in HIV-negative patients. Am. J. Med. 127, 1242.e11-1242.e17 (2014).
284. Moosig, F., Holle, J. U. & Gross, W. L. Value of anti-infective chemoprophylaxis in
primary systemic vasculitis: what is the evidence? Arthritis Res. Ther. 11, 253 (2009).
285. Chung, J. B., Armstrong, K., Schwartz, J. S., Albert, D. & Al, C. E. T. Cost-effectiveness
of prophylaxis against pneumocystis carinii pneumonia in patients with Wegener’s
Granulomatosis undergoing immunosuppressive therapy. Arthritis Rheum. 43,
1841–1848 (2000).
286. Sen, R. P., Walsh, T. E., Fisher, W. & Brock, N. Pulmonary complications of
combination therapy with cyclophosphamide and prednisone. Chest 99, 143–146
(1991).
287. Ognibene, F. P. et al. Pneumocystis carinii pneumonia: a major complication of
immunosuppressive therapy in patients with Wegener’s granulomatosis. Am. J.
Respir. Crit. Care Med. 151, 795–9 (1995).

351
288. Ethier, M. C. et al. Mould-active compared with fluconazole prophylaxis to prevent
invasive fungal diseases in cancer patients receiving chemotherapy or
haematopoietic stem-cell transplantation: a systematic review and meta-analysis of
randomised controlled trials. Br. J. Cancer 106, 1626–1637 (2012).
289. Guerra, C. M., Formica, R. N., Kulkarni, S., Asch, W. S. & Tichy, E. M. Duration of
prophylaxis against fungal infection in kidney transplant recipients. Prog.
Transplant. 25, 311–315 (2015).
290. Rabin, A. S. et al. Risk factors for invasive fungal disease in heart transplant
recipients. J Hear. Lung Transpl. 34, 229–262 (2015).
291. Danerseau, A. M. & Robinson, J. L. Efficacy and safety of measles, mumps, rubella
and varicella live viral vaccines in transplant recipients receiving immunosuppressive
drugs. World J. Pediatr. 4, 254–258 (2008).
292. Md Yusof, M. Y., Vital, E. M. & Buch, M. H. B Cell Therapies, Approved and Emerging:
a Review of Infectious Risk and Prevention During Use. Curr. Rheumatol. Rep. 17, 65
(2015).
293. Lekamwasam, S. et al. A framework for the development of guidelines for the
management of glucocorticoid-induced osteoporosis. Osteoporos. Int. 23, 2257–
2276 (2012).
294. West, S. L., Patel, P. & Jamal, S. a. How to predict and treat increased fracture risk in
chronic kidney disease. J. Intern. Med. 278, 19–28 (2015).
295. Challoumas, D., Stavrou, A., Pericleous, A. & Dimitrakakis, G. Effects of combined
vitamin D – Calcium supplements on the cardiovascular system: Should we be
cautious? Atherosclerosis 238, 388–398 (2015).
296. Scotland, G. et al. Denosumab for the prevention of osteoporotic fractures in post-
menopausal women. NICE technology appraisal guidance 204. (2011).
doi:10.2165/11589310-000000000-00000
297. British National Formulary. (2016).
298. Mavrogeni, S. et al. Cardiac tissue characterization and the diagnostic value of
cardiovascular magnetic resonance in systemic connective tissue diseases. Arthritis
Care Res. (Hoboken). 66, 104–12 (2014).
299. Mavrogeni, S. et al. Detection of coronary artery lesions and myocardial necrosis by
magnetic resonance in systemic necrotizing vasculitides. Arthritis Care Res. 61,
1121–1129 (2009).
300. Hemmelgam, B. et al. Relation between kidney function, proteinuria, and adverse

352
outcomes. JAMA 303, 423–9 (2010).
301. National Institute for Clinical Excellence. Clinical Knowledge Summary: Oral
Anticoagulation. at <http://cks.nice.org.uk/anticoagulation-oral>
302. Pendergraft, W. F. et al. Fetal outcomes after rituximab exposure in women with
autoimmune vasculitis. Ann. Rheum. Dis. 72, 2051–3 (2013).
303. Marder, W. et al. Adjunctive GnRH-a treatment attenuates depletion of ovarian
reserve associated with cyclophosphamide therapy in premenopausal SLE patients.
Gynecol. Endocrinol. 28, 624–7 (2012).
304. Clowse, M. E. B. et al. Ovarian preservation by GnRH agonists during chemotherapy:
a meta-analysis. J. Womens. Health (Larchmt). 18, 311–9 (2009).
305. Faurschou, M. et al. cyclophosphamide therapy in a cohort of 293 patients .
Malignancies in Wegener ’ s Granulomatosis : Incidence and Relation to
Cyclophosphamide Therapy in a Cohort of 293 Patients. 35, (2008).
306. Faurschou, M. et al. Prolonged risk of specific malignancies following
cyclophosphamide therapy among patients with granulomatosis with polyangiitis.
Rheumatology 54, 1345–1350 (2015).
307. Pedersen, E. G. et al. Risk of non-melanoma skin cancer in myasthenia patients
treated with azathioprine. Eur. J. Neurol. 21, 454–458 (2014).
308. Stern, A., Green, H., Paul, M., Vidal, L. & Leibovici, L. Prophylaxis for Pneumocystis
pneumonia ( PCP ) in non-HIV immunocompromised patients ( Review ). Cochrane
Database Syst. Rev. (2015).
doi:10.1002/14651858.CD005590.pub3.www.cochranelibrary.com
309. Guillevin, L. et al. A prospective, multicenter, randomized trial comparing steroids
and pulse cyclophosphamide versus steroids and oral cyclophosphamide in the
treatment of generalized Wegener’s granulomatosis. Arthritis Rheum. 40, 2187–98
(1997).
310. Tsai, M.-J., Chou, C.-W., Lin, F.-C. & Chang, S.-C. Pneumocystis jiroveci pneumonia in
patients with systemic lupus erythematosus after rituximab therapy. Lupus 21, 914–
918 (2012).
311. Mitsides, N. et al. Dapsone-induced methemoglobinemia in renal transplant
recipients: More prevalent than previously thought. Transpl. Infect. Dis. 16, 37–43
(2014).
312. Al-Quteimat, O. M. & Al-Badaineh, M. A. Methotrexate and trimethoprim-
sulphamethoxazole: Extremely serious and life-threatening combination. J. Clin.

353
Pharm. Ther. 38, 203–205 (2013).
313. Haeusler, G. M. et al. Late-onset Pneumocystis jirovecii pneumonia post-
fludarabine, cyclophosphamide and rituximab: implications for prophylaxis. Eur. J.
Haematol. 91, 157–63 (2013).
314. Uezono, S. et al. Outcome of ANCA-associated primary renal vasculitis in Miyazaki
Prefecture. Intern Med 46, 815–822 (2007).
315. Tuberculosis. NICE guideline. (2016).
316. Department of Health. Chapter 34: Varicella. Immunisation against infectious
disease - Green Book (2015).
317. Brown, N. et al. Medication-related side effects in vasculitis: a patient self-report
survey of awareness and reported uptake of protective therapy. Rheumatology
(Oxford). 55, 185–6 (2016).
318. Brown, N. et al. Lack of awareness of skin cancer amongst immunocompromised
patients with ANCA-associated vasculitis: a questionnaire survey. Br. J. Dermatol.
(2014). doi:10.1111/bjd.12861
319. Ralston, J. D. et al. Web-based collaborative care for type 2 diabetes: a pilot
randomized trial. Diabetes Care 32, 234–9 (2009).
320. Vollmer, W. M. et al. Improving adherence to cardiovascular disease medications
with information technology. Am. J. Manag. Care 20, SP502-10 (2014).
321. O’Connor, P. J. et al. Impact of electronic health record clinical decision support on
diabetes care: a randomized trial. Ann. Fam. Med. 9, 12–21 (2011).
322. Earnest, M. A., Ross, S. E., Wittevrongel, L., Moore, L. A. & Lin, C.-T. Use of a patient-
accessible electronic medical record in practice for congestive heart failure: Patient
and physician experiences. J. Am. Med. Informatics Assoc. 11, 410–418 (2004).
323. Short, C. D., Russell, S. & Valentine, A. Clinical audit and long-term evaluation of
renal transplant recipients. Transplantation 72, S94-8 (2001).
324. Flossmann, O. et al. Development of comprehensive disease assessment in systemic
vasculitis. Ann. Rheum. Dis. 66, 283–92 (2007).
325. Phelps, R. G., Taylor, J., Simpson, K., Samuel, J. & Turner, A. N. Patients’ continuing
use of an online health record: a quantitative evaluation of 14,000 patient years of
access data. J. Med. Internet Res. 16, e241 (2014).
326. Braun, V. & Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 3,
77–101 (2006).
327. Fereday, J. & Muir-Cochrane, E. Demonstrating Rigor Using Thematic Analysis: A

354
Hybrid Approach of Inductive and Deductive Coding and Theme Development. Int. J.
Qual. Methods 5, 80–92 (2006).
328. Walker, J. et al. Inviting patients to read their doctors’ notes: patients and doctors
look ahead: patient and physician surveys. Ann. Intern. Med. 155, 811–9 (2011).
329. Delbanco, T. et al. Inviting patients to read their doctors’ notes: A quasi-
experimental study and a look ahead. Ann. Intern. Med. 157, 461–470 (2012).
330. Ross, S. E. et al. Expectations of patients and physicians regarding patient-accessible
medical records. J. Med. Internet Res. 7, e13 (2005).
331. Osterberg, L. & Blaschke, T. Adherence to Medication. N. Engl. J. Med. 353, 487–497
(2005).
332. Quartuccio, L. et al. Health-related quality of life in severe cryoglobulinaemic
vasculitis and improvement after B-cell depleting therapy. Clin. Exp. Rheumatol. 31,
S9-14 (2013).
333. Rabin, R. & de Charro, F. EQ-5D: a measure of health status from the EuroQol
Group. Ann. Med. 33, 337–43 (2001).
334. Cummins, N. M., Poku, E. K., Towler, M. R., O’Driscoll, O. M. & Ralston, S. H. clinical
risk factors for osteoporosis in Ireland and the UK: a comparison of FRAX and
QFractureScores. Calcif. Tissue Int. 89, 172–7 (2011).
335. Hippisley-Cox, J. et al. Derivation and validation of QRISK, a new cardiovascular
disease risk score for the United Kingdom: prospective open cohort study. BMJ 335,
136 (2007).
336. NHS England. Five Year Forward View. (2014).
337. Herrett, E. et al. Data Resource Profile: Clinical Practice Research Datalink (CPRD).
Int. J. Epidemiol. 44, 827–836 (2015).
338. Reinhold-Keller, E., Herlyn, K., Wagner-Bastmeyer, R. & Gross, W. L. Stable incidence
of primary systemic vasculitides over five years: Results from the German vasculitis
register. Arthritis Rheum. 53, 93–99 (2005).
339. Cervera, R. et al. Morbidity and Mortality in Systemic Lupus Erythematosus During a
10-Year Period A Comparison of Early and Late Manifestations in a Cohort of.
Mortality 82, 299–308 (2003).
340. Walsh, M. et al. Plasma exchange and glucocorticoid dosing in the treatment of anti-
neutrophil cytoplasm antibody associated vasculitis (PEXIVAS): protocol for a
randomized controlled trial. Trials 14, 73 (2013).
341. Bird, A. Perceptions of epigenetics. Nature 447, 396–8 (2007).

355
342. Jones, B. E. et al. Gene-Specific DNA Methylation Changes Predict Remission in
Patients with ANCA-Associated Vasculitis. J. Am. Soc. Nephrol. (2016).
doi:10.1681/ASN.2016050548
343. Jennette, J. C., Falk, R. J., Hu, P. & Xiao, H. Pathogenesis of antineutrophil
cytoplasmic autoantibody-associated small-vessel vasculitis. Annu. Rev. Pathol. 8,
139–60 (2013).




















