Improving the mental health of the population - Parliament ...
179
HOUSE OF LORDS European Union Committee 14th Report of Session 2006–07 “Improving the mental health of the population”: can the European Union help? Volume II: Evidence Ordered to be printed 27 March 2007 and published 24 April 2007 Published by the Authority of the House of Lords London : The Stationery Office Limited £price HL Paper 73-II
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Improving the mental health of the population - Parliament ...
HOUSE OF LORDS
European Union Committee
14th Report of Session 2006–07
“Improving the mental health of the
population”: can the European Union
help?
Volume II: Evidence
Ordered to be printed 27 March 2007 and published 24 April 2007
Published by the Authority of the House of Lords
London : The Stationery Office Limited
£price
HL Paper 73-II
CONTENTS
Oral Evidence European Commission Oral Evidence, 6 July 2006 1 Professor Martin Knapp, Mr David McDaid, Professor Elias Mossialos and Professor Graham Thornicroft Written Evidence 10 Oral Evidence, 20 July 2006 13 Supplementary Written Evidence, Professor Thornicroft 22 Department of Health Written Evidence 28 Written Evidence 30 Oral Evidence, 19 October 2006 34 Mr John Bowis MEP Oral Evidence, 2 November 2006 44 Mind, Rethink Written Evidence, Mind 54 Written Evidence, Rethink 60 Oral Evidence, 23 November 2006 64 Ms Camilla Parker Oral Evidence, 30 November 76 World Health Organization (WHO) Written Evidence 86 Oral Evidence, 7 December 2006 87 Rt Hon Rosie Winterton MP, Department of Health Oral Evidence, 14 December 2006 98 Supplementary Written Evidence 107
Written Evidence Age Concern 108 British Geriatrics Society 110 British Medical Association 111 Christian Council on Ageing 112 Department of Health’s Older People’s Mental Health Programme Delivery Board 113 European Public Health Alliance 115 Finance & Leasing Association 117 Professor Tamara Hervey and Professor Peter Bartlett, University of Nottingham 118 International Longevity Centre UK 120 Kent County Council 123 King’s Fund 124
Law Reform Committee of the Bar Council of England and Wales 127 Marylebone Healing and Counselling Centre 128 Medical Ethics Alliance 130 Mencap 132 Mental Disability Advocacy Center 134 Mental Health Foundation 140 NHS Confederation 144 NHS London EU Unit 145 Northern Ireland Association of Mental Health 148 Open Society Mental Health Initiative 155 Professor Stefan Priebe 159 Royal College of Psychiatrists 161 Samaritans 164 SAMH 167 Professor Norman Sartorius 170 Shift and Social Inclusion Programme 171 Turning Point 172 UK Mental Health Research Network 174 West Sussex County Council 174 NOTE: The Report of the Committee is published in Volume I, HL Paper No 73-I The Evidence of the Committee is published in Volume II, HL Paper No 73-II

3564222001 Page Type [Ex 1] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
Minutes of EvidenceTAKEN BEFORE THE SELECT COMMITTEE ON THE EUROPEAN UNION
(SUB-COMMITTEE G)
THURSDAY 6 JULY 2006
Present Colwyn, L Morgan of Huyton, BDundee, E Moser, LGale, B Neuberger, BGreengross, B Thomas of Walliswood, BHarrison, L (Chairman)Howarth of Breckland, B Trefgarne, L
Examination of Witness
Witness: Mr Jurgen Scheftlein, DG Health and Consumer Protection, European Commission, examined.
Q1 Chairman: Welcome to our session. We are veryglad that you could come and assist us with ourinquiry at rather short notice—I am sorry about that.I would also like to express my thanks to yourDirectorate for letting you come over and speak withus. To start with housekeeping points, the session isopen to the public. Although I do not think there areany members of the public here, it is a public session,and it will be recorded for possible broadcasting orwebcasting. A verbatim transcript will be taken andit will be sent to you so that if you feel you have beenmisrepresented, or you feel you need to changesomething, you can do that and then it will beattached to our evidence should we do a report andpublish the report. If you feel, during the course ofour hour, that you have not been able to fully explainsomething we are very happy to receivesupplementary evidence from you by e-mail or letter.That would be most welcome. You should have hador seen a register of Members’ interests. Going on tothe substance of the matter, this is a paper which hascaused us, it is fair to say, a certain amount ofconcern. The inquiry is only just starting and we arestill trying to get to grips with the subject. It willcontinue when Parliament resumes in October, andwe may want to invite more evidence from theCommission at that stage. What we wanted toachieve today was to get a briefing from you as theoYcial closely connected with the drafting of theGreen Paper and so on, so that you can set the scenefor us and we can understand what the Commission’sobjectives are in publishing this paper. Obviously, itis a consultative document and we have seen some ofthe responses which have gone to you. You may not,therefore, be able to give definitive answers as to whatis going to happen next, but the scope of somethingcalled mental health policy is extremely wide. Wehave several people in the room who know quite a lotabout it. It also includes some very sensitive issues
and it raises issues of competence and subsidiarity aswell. We hope that you will be able to give us a cleareridea of what the mental health strategy is likely toinvolve in practice, what the priorities are and whatthe roles of the Member States and the Commissionare going to be. I hope you understand where we arecoming from. It is not so much that we are critical, itis more that we want to know what the main thrust ofthe Commission’s ideas and of this consultationpaper really are. Could you start by stating yourname for the recording, and if you want to make anopening statement we would be very happy to hearthat. Otherwise we will move straight into questions.Have you been able to understand and hear what Ihave been saying?Mr Scheftlein: Yes, I understood you very well, andwe can begin. My name is Jurgen Scheftlein, I amworking with the European Commission DirectorateGeneral for Health and Consumer Protection in aunit which is dealing with health determinants. I amthe administrator in charge of the Green PaperImproving the Mental Health of the Population,Towards a strategy on mental health for the EuropeanUnion which the Commission adopted on 14 Octoberlast year. The idea behind publishing this paper was,in principle, that we saw, through work that we havebeen undertaking through projects under the publichealth programme, that the burden of mental illnessis increasing and that this is creating challenges forMember States and, also, for the attainment of thestrategic policy objectives of the European Union.We wanted, in the aftermath of the WHO MinisterialConference in Copenhagen in January 2005, to makea contribution to identifying the challenges and thenaddressing it commonly, and to do this together onthe basis of this document. The document objectivewas first to raise the visibility of mental health as anarea of concern for public health and, also, for otherpublic policies, and then to launch a debate about
3564222001 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
2 commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
whether the European Union should get involvedand should develop a strategic approach on this ornot. Since the launch of this document in October2005 we have organised a high-level launchconference in Luxembourg with ministers andmembers of parliament and others involved, and thenwe had three meetings at technical level from Januaryto May. Since 31 May the consultation has beenclosed oYcially but, of course, we still receivecomment and reactions. For instance, the EuropeanParliament will only adopt its report on the GreenPaper in October. I am very pleased and honoured bythis invitation to discuss this document with you, andlook forward to the discussion that we will have.
Q2 Chairman: Thank you for that backgroundintroduction; it was rather useful to get the timingand programming of the whole thing clear. If I canstart oV, can you explain a little bit more about theway in which the Green Paper relates to the WHOMental Health Action Plan for Europe, and can youalso outline the main features of the WHO Plan andthe role which it apparently envisages for theCommission?Mr Scheftlein: Yes. It is no coincidence that the GreenPaper was published a few months after the WHOMinisterial Conference on Mental Health inHelsinki. Mr Markos Kyprianou, the EuropeanCommissioner for Health and Consumer Protection,participated in this conference, together with therepresentatives of Member States, and theCommission service also worked together with theWHO in preparing this conference. The new featureof the WHO declaration and action plan was that itbrought mental health up to the highest level ofpolicy-making, on the one hand, and it created acommitment which has not been existing beforehandand, at the same time, it developed a verycomprehensive strategic approach, ranging frompromotion and prevention through care andtreatment to rehabilitation. So it covered a very widerange of areas and one area which was certainly new,as an work area for the WHO was the one ofpromotion and prevention, which is the startingpoint of the Commission’s work on mental health.The Commission has been a co-organiser, even acollaborative partner in this conference. It was onlyreasonable then, after the conference, to be involvedin the follow-up to the conference because theconference is only a starting point of work, and whathappens afterwards is much more important. There isa sentence in the conference declaration inviting theCommission to support the implementation of thedeclaration action plan—within its scope ofcompetences, of course. So that is how things arerelated. The Commission will have to focus on thosefields in the WHO action plan—the 12 fields rangingon the points I mentioned—in which we are working,
and where we have the competences to act, and thatis mainly promotion and prevention, supportingvulnerable groups, information and research, andaddressing discrimination and stigma. Thecomplicated thing about mental health is that itcovers so many diVerent policy areas. It concernspractically the whole range of community policies:Ourselves in the Directorate-General for Health andConsumer Protection address issues like promotionand prevention. Stigma and discrimination is thework area of the colleagues in the Directorate-General for Employment, Social AVairs and EqualOpportunities. Then the Commission also financesresearch under the framework programme onresearch. Our colleagues from Eurostat but, also,ourselves (under the public health programme)collect information and data about the status ofmental health of the population. In summary ourGreen Paper initiative, is a response to the WHOAction Plan. It is an oVer to the WHO and to theother actors whom we want to involve, includingMember States, to work together with us indeveloping and implementing a strategy at EU-level.We published it as a Green Paper because we believeif the Commission would have come out with aproposal for a strategy it would have been a kind ofartificial product. Through this discussion we hope todevelop a consensus on the direction of our work andon the objectives together with the WHO but mainly,also, with Member States to have a mandate foraction in the future.Chairman: Thank you for that. I think we have gonea step further along the way.
Q3 Lord Trefgarne: While the aspirations of theCommission in this matter are, of course, entirelygood, is there not a risk of confusion between theactivities of the WHO, the activities of MemberStates and, now, the activities of the Commission aswell?Mr Scheftlein: I would not see it like that. On theother hand, I agree that the working areas and thebalance of work has shifted after the WHOMinisterial Conference. For instance, you can see itfrom the fact that before the conference we had aclear division of work. Member States had their ownwork; organised their mental health systems anddelivered mental health services in their own right, ofcourse, and the Commission would, on the basis ofthe provisions in the Treaty, support this in the fieldsof promotion and prevention and collection ofinformation. The role of the WHO had been to focuson treatment aspects and to advise Member States onthis. After the conference the WHO said wherepromotion and prevention is part of our action planso we also have to work on this ourselves.

3564222001 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
3commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
Q4 Lord Trefgarne: Is the EU a member of theWHO in its own right?Mr Scheftlein: No, no. The EU is not a member ofWHO.
Q5 Lord Trefgarne: It is the Member States.Mr Scheftlein: Yes, but we had a commonunderstanding of the roles of the Council of Europe,the WHO and the Commission versus MemberStates. This has shifted a bit towards more co-operation across the working fields of theseorganisations.
Q6 Lord Trefgarne: A common understandingbetween the WHO, the Commission and theMember States?Mr Scheftlein: Yes, we are mainly promoting acommon understanding between the threeorganisations. We have regular meetings betweenthese three organisations, in which we co-ordinateour line of work.
Q7 Chairman: That is the WHO, the Communityand the Council of Europe?Mr Scheftlein: And the WHO, yes.
Q8 Chairman: Those three?Mr Scheftlein: Yes, plus, of course, the Commissionis participating in regional committee meetings whereMember States are meeting with the WHO. So wehad a rather clear division of work, but now we aremoving more towards working together inpartnership, and that means that WHO helps us inthe Commission in working on promotion andprevention, for instance.
Q9 Earl of Dundee: You mentioned the three bodies,the Council of Europe, WHO and the Commission,and the allocation of tasks and the division of work.Could you say, just very generally, what kind of focuswould be given by the Council of Europe, by theWHO and by the Commission?Mr Scheftlein: Yes. Very generally, the task of theWHO would be to advise Member States on issues ofhealth services and treatment—aspects whereas therole of the Council of Europe would be to work onhuman rights aspects, and the Commission’s rolewould be in the rather innovative field of mentalhealth promotion and prevention, plus collection ofhealth information and health status data. The latteris also a field of work of the WHO. One could say thatWHO has with its Mental Health Atlas established aninventory of resources invested in mental health andof service organisation, whereas the Commissionthen would focus on aspects of the health status in thepopulation, on determinants, and on preventive andpromotion policies, so to say.
Q10 Lord Trefgarne: Very great care is going to beneeded to avoid confusion between these diVerentroles.Mr Scheftlein: Yes, but the most important necessityis certainly to have a common philosophy and towork together. I can say that I have a very good andclose co-operation with colleagues at WHO Europe,the regional adviser Matt Muijen and hiscollaborator Dr Jane-Llopis, and so we feel that thereis a scope of mutual strengthening by workingtogether. The WHO can contribute its expertise intoour work. Also, since recently we have a strandreserved for co-operation with internationalorganisations under the public health programme. Soa certain share of the money under the public healthprogramme is reserved for WHO, and there, forinstance, now the WHO is doing a project, abenchmarking exercise, to identify the state of play inMember States versus the WHO Action Plan.Furthermore, as the European Commission, we canoVer more regular meetings with all the MemberStates together. So WHO advises Member Statesbilaterally whereas we have the possibility to bringtogether all Member States plus WHO which meansthat the work from WHO can be disseminated in amore eYcient way, not only bilaterally.
Q11 Baroness Gale: I have got two questions to putto you, as they are linked, on definitions. The first oneis: does the Commission foresee practical diYcultiesin the very broad definitions of mental health andmental ill-health, which are used by the WHO?Secondly, we have received written evidencesuggesting that “emotional well-being” would be auseful definition. Does the Commission have viewson that definition?Mr Scheftlein: Yes. Concepts and definitions arecertainly an important aspect in this work and whenyou have them then you need also to clarify what youwant to cover and what you want to segregate fromthe work. Now, for mental health and mental ill-health as definitions, we thought, in the sense ofpartnership that I have just described but, also, in asense of referring to consensual terms, that it was themost logical step to use the WHO’s definition onmental health and mental ill-health. In fact, we hadmuch discussion about what term we could use:mental illness, mental ill-health, mental disorder—there are so many and there is always one groupwhich is suggesting it is a politically incorrect one.Then we decided to refer to mental ill-health. Theseare very broad definitions, I know, but, on the otherhand, they fit to the approach of the paper, I wouldsay, because what we propose in our Green Paper isa public health approach to mental health and we donot limit it and present it as a medical issue alone. Itis very much a medical issue, but not only, and for uswe want to look first into health and only then into

3564222001 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
4 commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
disorders. We do not want to adopt a medicalapproach and focus on severe disorders or clinically-defined disorders as they are classified in ICD 10, aninternational system classifying mental disorders.Therefore for the purpose of early prevention and ofthe promotion of wide definition issues, like stress inthe workplace—“strain” I think is the true Englishword—
Q12 Chairman: Stress.Mr Scheftlein: Yes, caused by strain. That may not bea clinical disorder but it may lead to one if nointervention takes place. So this attempts to useagreed definitions, and then the wide scope of ourwork were the reasons to use these definitions. “Well-being” as such is certainly a good term because wethink what we address is very much about quality oflife and well-being. “Emotional well-being”, yes, isinteresting as a term. Possibly it might excludedisorders with an organic background. While we donot focus on them, is it possible to fully exclude themfrom the work? Sometimes there is also a lot ofinteraction between social aspects and biologicalaspects. Therefore, it could be a term that we coulduse to describe what we are talking about, forinstance, in the school environment, where it could bea very valuable concept in addressing children andadolescents.Lord Colwyn: I think I would like to see the word“distress” as a definition.Chairman: Mental distress.
Q13 Lord Colwyn: Mental distress. This is such avast subject we are getting into. You talk about itaVecting every fourth citizen; 27 per cent of adultEuropeans are estimated to experience some form ofmental ill-health. It is such a massive subject. This ismy concern with this inquiry; I just do not know howwe are going to be able to cope with it.Mr Scheftlein: There are diVerent figures. There arefigures suggesting that at any point in time a quarterof the population are aVected, and there are otherWHO statements that at one moment during lifeevery fourth citizen is aVected by it. I do not thinkthat every mental health problem needs medicalintervention; our objective is mainly to raiseawareness of how important this is for life and thatpromotion and prevention are possible, and thatonce a person has a problem that it should seek help,and that its surroundings should show understandingand avoid for instance, stigma. People with mentalhealth problems try to hide that very often, andemployers have no understanding or theirenvironment has no understanding. But showing thatmental health problems are a common part of realityhelps people who have problems to feel normalcitizens and to accept that they should seek help andcan get help. So we have a very successful project
called European Alliance against Depression underthe public health programme. It is not a big one but itis one that finds a lot of interest. It is about informingmedia, teachers, priests, police and doctors aboutdepression as a sickness, as an illness, which is oftennot detected, so that people have to see whether thereare signs of that. That has led, in a pilot case of aGerman research project in a region, to a decrease ofsuicidal acts by around 25 per cent. The project leadertold me that one of the most important aspects is thatpeople, when they see campaigns, feel understandingand that helps them to go to a doctor and tell themabout their mental health problems.
Q14 Earl of Dundee: Has that scheme graduatedbeyond the pilot stage?Mr Scheftlein: It was developed as a German researchproject, and then it was taken up at EU level underthe public health programme. It was implemented in15 Member States during the one-and-a-half years,and now it has been extended to all Member States,but not fully covered—it is only implemented in thoseregions which are interested. It is very much ademand-led project. So you need to find personalitieswho are interested in this and who are ready to investsome of their time into it, and then they getstandardised material and there are meetings toexchange, so there is a framework that helps them todevelop their activities.
Q15 Baroness Howarth of Breckland: This really getsto the heart of whether or not we should pursue ourinquiry. The issue has been very well demonstratedby the little debate that has just gone before. TheBamford report, as you will know, says that positivemental health cannot be gained by treating mentaldisorders alone. That is what we have beendiscussing. However, it does lead us into saying whatis it that we can do—indeed, what is it that theCommission can do—that adds value to what theMember States can do for themselves. Therefore,where should we be placing our energies, because wecannot possibly look at the whole of the mentalhealth/mental illness scenario? If we are going to dosomething useful what would you see that as being?Mr Scheftlein: Firstly, of course, we do not want tointervene into Member States’ actions. However, weunderstood from the WHO Ministerial Conferencethat mental health has become a field of interest, apriority, in many Member States. We know thatsituations in Member States are diVerent and theywill never be equal because they reflect cultures andtraditions and many factors, but we think that theremight be an interest in Member States in exchangingand seeing whether they can work together andidentify common recommendations on some fields ofhigh priority. In fact, in the past we have workedtogether only with researchers when we implemented

3564222001 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
5commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
our public health programme. We felt that it is notsuYcient to develop research and then not tocommunicate it to the actors in Member States. Thatis another reason why we did develop the GreenPaper.Baroness Howarth of Breckland: If there were twoquestions you wanted this Committee to address—Lord Trefgarne: Or even one!
Q16 Baroness Howarth of Breckland: —that wouldenable you to further your work in the Green Paper,what do you think they would be?Mr Scheftlein: My interest would be what you woulddefine as those priorities where you would wish toshare knowledge with other Member States.
Q17 Baroness Howarth of Breckland: It is aboutinformation and dissemination that you would reallylike the focus?Mr Scheftlein: No, I would like to go further. I thinkit would be the involvement of many other societyactors, like the business environment, like the schoolenvironment—so the public health approach. Howcan we demonstrate the value of positive mentalhealth to other policy areas, and how can we convincethem to invest in better mental health and to integrateit into their actions?
Q18 Baroness Howarth of Breckland: So it is insituations of employment, education, generalcommunity situations and how one conveysinformation to those communities about positivemental health programmes?Mr Scheftlein: Yes, information, but also thenconsensus building with them. Not only sendingrecommendations to them but involving them inwork. May I add one point? I also think it is crucial,then, not only to do this from the point of view ofpublic health policy but, also, to consider theobjectives of the other elements. So, for business, it isproductivity; for instance, to show that mental healthhas an impact on productivity, and that promotingmental health and boosting productivity is possible,and that promoting life skills in children is possiblefor success in later life.
Q19 Baroness Greengross: Following on very wellfrom that, I think we are in danger, and you are indanger, if I may say so, of giving very positive, nicemessages, but we hear those all the time. It seems tome that it is the economic arguments that are reallygoing to change people’s behaviour. One of the moststrong of those might be that if you invest incombating mental ill-health (or mental distress, asmy colleague called it) in the workplace, for example,what the results would be and, therefore, theeconomic consequences of mental ill-health and theinvestment needed to combat it in hard data would
seem to me to be something you could do whichwould be extremely helpful. I understood earlier thatDavid McDaid, who I worked with quite a lot, isdoing some work with you as an economist here atthe LSE. That interests me because I think that iswhere you could make such a diVerence, with harddata to business, to employers, to educationalists orwhoever. Is there a possibility that you could look atnot just the economic consequences but the economicinvestment and what the return on that investmentmight be, in hard terms?Mr Scheftlein: Yes. We have projects looking into theeconomics of mental health, led by the LondonSchool of Economics, and these projects could beused to develop this evidence. At the moment theevidence is very striking about the increase of theproblem. There is less knowledge about the success ofpromotion aspects in companies and preventativeaction. But that is something we would have todeliver, that is true. Recently, two weeks ago,colleagues of mine participated in a business meetingcalled “CSR (Corporate Social Responsibility)marketplace” where companies exchanged bestpractice, including towards their employees. Wethink that this work on corporate socialresponsibility could also be an avenue fordisseminating information and, also, for involvingcompanies in mental health promotion. So we havenetworks of healthy enterprises, and the best thingwould be if, once there was the scientific data, likethrough the projects from David McDaid, businessesthemselves would be present and say: “We have donethis and we have learned it works. It is possible.”That is something that we will try to do through themental health strategy and in commonality with thecolleagues working on health and safety at work andin Commission service for Employment policy.
Q20 Baroness Greengross: May I follow up on that?I Chair the all-party group here on CSR (CorporateSocial Responsibility) and I know that there issomebody in the Commission who has responsibilityfor that. If that unit was involved with you in gettingout these hard messages, would that not be veryhelpful?Mr Scheftlein: Of course.Baroness Greengross: I think it might be. I would bevery happy to take that further from this end. WhatI am saying is it is so vague and we need hard,convincing data, economic data, which would bevery, very welcome, I think, from the businesscommunity. Thank you.
Q21 Lord Moser: It really continues the same themeraised by my colleagues either side of me: we are at aloss where to focus our energies in this Committee.That is our problem, in a sense. However, the GreenPaper, which I have studied quite carefully, is very

3564222001 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
6 commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
interesting, and it covers almost everything one canthink of, but I want to focus on this issue ofawareness, which takes us back to facts andknowledge. Obviously, in the Green Paper it is clearyou are very interested in the issue of publicawareness of mental health problems—however theyare defined. If you take Alzheimer’s, I speak assomebody slightly involved with the Alzheimer’sSociety in this country. Everybody knows it is aterrible aZiction.Mr Scheftlein: Yes.
Q22 Lord Moser: At a low level everybody is aware,but that does not get one anywhere because people donot know the facts at any level. For example, in thecase of Alzheimer’s or dementia, we believe that inthis country there are 150,000 new cases every year.That is one every three minutes. That kind ofdramatic fact gets the headlines but, again, it is notvery solid. Question one: as an input to raisingawareness, how good is Europe now, in your view, onhard facts on the incidence, first of all, of variouskinds of mental illness? Question two: how well-informed is Europe (the diVerent countries andBrussels) on the state of medical knowledge, which issomething quite diVerent—not the incidence but thestate of the medical knowledge? Most people thinkthat Alzheimer’s is totally incurable. Somebody saidto me at lunch yesterday: “You do know there is anew pill?” I did not know there was a new pill and itmay not be true anyway. So there are hard facts onthe medical side and then there are hard facts on curesand care, etc, etc. I am interested—and, I think, weare interested—in what Brussels can contribute andwhat we can contribute and work on in helping toimprove the state of awareness via these variouslevels of knowledge. Hard facts on the incidence,hard facts of medical knowledge, hard facts on careand cures, etc, etc. Do you get my drift?Mr Scheftlein: First, I would like to say that throughthe meetings that we organise and through thereactions that we receive I also understand thatraising awareness is very important, and that it mightget in a possible strategy even a higher priority thanit has in the Green Paper. We would have to findadequate ways for ensuring that. The Green Paperitself is certainly already an initiative to raiseawareness. Regarding your questions aboutAlzheimer’s, that is not my field of expertise but Ihave a colleague who is working on this and I knowthat we are doing projects on Alzheimer’s. So it is notsomething that would be included in the routine datacollection system of the EU, through Eurostat, but itis something that we address in our annual calls forprojects under the public health programmeexplicitly and we have good contacts to Alzheimer’sEurope and to the European Brain Council. So wewill certainly be at the state of play of research.
Q23 Lord Moser: I used Alzheimer’s as an example.Mr Scheftlein: Mental health data is a bit diYcultarea, I must say. We have invested quite a lot offunding into information projects but we do not yethave the complete picture. That is also why I quoteWHO figures and studies of the European BrainCouncil. We are telling Europe that we aredeveloping systems of indicators on which datashould be collected, and we have some data available.There are some mental health indicators in our mainlist that we have developed—the list of EuropeanCommunity Health Indicators (ECHI)—but formany we have problems in getting the data. That hasto grow. That is also something that needs thevisibility of the issue and awareness in Eurostat, forinstance, and more psychological indicators will bepart of an European household survey in the future.Also, under the EU’s Labour Force Survey there willbe more mental health indicators. So this is clearlygrowing. The information will become better, but weare clearly not where we would like to be at themoment because it is diYcult to cope with it. Asregards the state of medical knowledge, we rely onsupport from the WHO. Our field of work is mainlythe promotion and prevention side—so what ishappening around the medical intervention but notthe treatment issues as such, and also not in detailwhat is behind the illness in medical terms.
Q24 Earl of Dundee: We presume that gatheringmore information and exchanging best practicewill be handled through the Open Method ofCo-ordination. How might this activity in fact beco-ordinated and the results disseminated?Mr Scheftlein: I would say that we need to define ourstrategy and, in fact, the principal decision aboutwhether our strategy would be developed has not yetbeen made. The Open Method of Co-ordination is, atthis stage, not an instrument which would be used inthe health policy context. So I do not think that wewould do it here. The Open Method of Co-ordinationwould also require that Member States agree to this.It is an eVective tool, certainly. On the other hand, itis one that requires a lot of resource investment. Ithink we would try to find a looser way of co-operation in the form of a Platform on MentalHealth.
Q25 Earl of Dundee: Even if that policy weredeployed, up until now other OMC exercises perhapsprovide a useful guide?Mr Scheftlein: Maybe. The Open Method of Co-ordination as a tool where guidelines and targets aredefined and then Member States report on theiractions and achievements is a very valid one, and weshould certainly learn from it. We also have one onlong-term health care which is, however, operatedunder the responsibility of the colleagues in DG

3564222001 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
7commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
Employment, and we contribute to it. Perhaps itcould also look into some aspects of mental health, itis possible, yes, but for ourselves it is not really anoption in our reflections to launch an Open Methodof Co-ordination. However, there might be someelements of that approach in our work. So, of course,we need to agree on some principles and on someobjectives when we work together, but certainly theimplementation of a mental health strategy willnot be as fixed as other Open Methods ofCo-ordination are.
Q26 Baroness Neuberger: I think we have all readwhat there is in the Green Paper about the EUPlatform on Mental Health, and I can see it is co-ordinating policy makers and experts and it isdrawing together, if you like, health people andpeople interested in civil society. I have two bits tothis question: first, I am not clear what theCommission brings that is additional to what theWorld Health Organisation can already do and,indeed, to some extent, does already do. Secondly, ifyou are going to go down this path and, presumably,therefore, do more than the World HealthOrganisation does, what would it mean in practice?What would it look like?Mr Scheftlein: One has to see that the structuresexplained in the Green Paper mainly relate to theconsultation itself. This is over now; so it has been anexperimental phase. However, what we want to do iswe want to launch a platform on mental health nextyear, and that will replace the former working partyon mental health that we had. That will probably bethe main structure for the implementation of astrategy on mental health. At least, as far as thehealth policy context is concerned.
Q27 Baroness Neuberger: With the World HealthOrganisation in partnership?Mr Scheftlein: The WHO will be involved in it, yes, inpartnership, but the Commission will be the owner ofthe platform, so to say. We will invite the WHO. Theidea will be there to bring people together like we didin the consultation process from Member States: onthe one hand, from the economic world, from thehealth context, from the social field and from civilsociety. So a mixture of key actors in that field. In thepast we had only researchers there, plus some NGOs,but that does not lead to action; it leads to research,yes, knowledge but not to implementation. There Isee the contribution, the value, that the Commissioncan add in partnership with WHO. WHO is a sectoralorganisation, so to say, it is a health organisation,whereas we, as the Commission, have our colleaguesin the other departments who we can invite, and theycame to our consultation meetings from DGResearch, from Employment and from others. So wecan involve them, and that means we also have access
to other sectors, which is key in this public healthapproach that we are pursuing. Secondly, we havemore of a sustainability dimension. Platformmeetings could take place once or twice every year,whereas for WHO it is not possible to involvedelegates from Member States every year. So thatmeans we can add a continuity to the work on mentalhealth. This we can use to monitor the progress inimplementing the commitment at the Helsinkiconference. So that is our starting point. Our ownstrategy would remain within the ranges of thatstrategy, but it would be tailored towards the needs ofthe EU, what Member States identified together withus, and then we can establish a monitoring process.WHO cannot do that alone. At least, they can do itmuch better if they do it together with us.
Q28 Baroness Neuberger: And the result of thatmonitoring and the result of that platform is that youmight make recommendations for legislation?Mr Scheftlein: Legislation, or recommendations inthe sense of encouragement. Most of these areas areout of the mandate for legislative action atCommunity level.
Q29 Chairman: So it is exchange of good practice?Mr Scheftlein: Yes.
Q30 Chairman: Perhaps a better technical base, abetter statistical base—that kind of thing?Mr Scheftlein: Yes. As a brief idea of how this couldwork we could use our projects and our researchnetworks that have been growing to put together astate-of-the-art on a theme like suicide prevention.We could have a discussion paper, we could agreewith Member States and the other actors involved inthe Platform on Mental Health that this is an issue ofcommon interest, where we believe we can learn fromeach other, and that action at a Community levelmakes sense. There could be a paper prepared puttingtogether the existing knowledge and proposals foraction. It could be presented for discussion. Aconsensus could be built on the key measures to betaken at community level and in Member States.That could then be the material for a Councilrecommendation. Then there could be somereporting about how this has been implemented inCommunity policies in Member States. So everythingwould be there; you could even think of legislation onthe size of packages of sleeping drugs, but the key ofthe approach is to promote more informed action.
Q31 Chairman: Understanding, informing andexchanging?Mr Scheftlein: Yes.Chairman: We are getting to the end of our time and,also, your time.

3564222001 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
8 commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
Q32 Lord Harrison: Good morning, Mr Scheftlein.Thank you very much for answering our questions. Iwonder if I could just ask you about paragraph 6.2,where you raise the question of some initiatives thatmight be done at a Community level, including thequestion of social inclusion, but also theFundamental Rights Agency. What kind of initiativemight arise there? My final question is: in answer toBaroness Neuberger about possible legislation, yougave a reply, but would the Commission perhaps goas far—other than being a swap-shop for good ideasand best practice—as to try and think aboutminimum good standards which should operatethroughout the European Union in the field ofmental health? Or would you stand back from that?Mr Scheftlein: This is a very tricky issue.
Q33 Chairman: That is why we are asking it!Mr Scheftlein: Regarding social inclusion that maynot be so tricky, to begin with this. We would have towork together with colleagues in the Directorate-General for Employment and we would certainly notwish to reinvent the wheel. We would work togetherwith them and would see how we could give morepriority, more attention to mental health and mentaldisability or disability resulting from mental healthwithin the processes that already exist on socialinclusion. That would be there and then we could seeabout further additional actions. Regarding theFundamental Rights Agency, that is a matter ofdiscussion with Member States, and a mandate willarrive from that. Whether there will then, in the end,be a mandate to look into issues relating to humanrights in mental health, I do not know. The idea weput into the Green Paper was that it could be a placefor collection of information about conditions ininstitutions in all Member States, not only the newMember States, because we believe there could bedeficits in all of them. Whether Member States areready to accept that, I do not know. Regardingminimum standards on human rights in health care. Iwould certainly not see the emergence of harmonisedand not legally binding ones. But one could thinkabout developing good practice and guidelines forhealth promotion in such institutions, and you couldalso link it to quality management. In one of theconsultation meetings we had a colleague from theCouncil of Europe, so we worked together with them,similarly to how we work with WHO. We can alsohelp in monitoring what is happening on the basis ofthe Council of Europe’s recommendations, but Idon’t expect binding instruments. The whole projectof a mental health strategy is certainly a long-termendeavour. We could now enter into a kind of testphase now. We would see how it develops and then itcould grow into something more settled, but it is nowimportant to start up with this action.
Q34 Chairman: I am aware that we are beginning tolose some Members and I am watching our quorum.May I butt in at this point. Am I right when I thinkthat the actions which would be taken at Communitylevel would lie in the field of stimulatingunderstanding which results in action amongstpractitioners, as it were, providing and collectingdata, the exchange of best practice and perhapsawareness-raising as a result of the improved data,the exchange of best practice and so on, those are thesorts of activities from the Commission’s point ofview that you are thinking about?Mr Scheftlein: Mainly, yes, but at this stage I wouldalso think of consensus building and then oVeringmedia to monitor actions, so not only saying, “Thisis important”, but also agreeing on what should bedone and then asking what has been done. I hope thatwill also be an element of the strategy.Chairman: Thank you. That was a very helpfulanswer.
Q35 Baroness Morgan of Huyton: This is just onfunding and, in a sense, it partly relates to that. Is thisabout better use of existing funding in the communityof research and structural funds? Is it taking the samemoney that is there now and using it diVerently, or isit also going to change the priority which is given toother cross-cutting issues, like drugs or alcoholabuse?Mr Scheftlein: It is about encouraging that anadequate part of funding from existing communityinstruments is used for mental health. If you look intostructural funds, that is an area where theCommission can only highlight its priorities. It is upto Member States to ask for funding for mentalhealth. We cannot impose this. It is also aboutintegrating mental health as a context into theresearch framework programme. I think that workswell and there is interest in this.
Q36 Chairman: Thank you very much. You havealready explained to us that your deadline for thereceipt of consultation responses has now finished.Can you give us any indication about what the futuretimetable of this paper might be?Mr Scheftlein: The deadline for contributions inprinciple ended on 31 May. We have received about250/260 reactions and a few further ones are stillexpected. Over the Summer, into the Autumn, we willperform an analysis of these contributions, and thenduring the Autumn we should publish a workdocument providing a summary of the outcomes.Also, hopefully during the next few days, if notduring the next few weeks, all the contributions willbe published on our website to make themtransparent. Then in the Autumn we will publish ourown analysis and then we will make the decisionsabout the follow-up steps, including the strategy, and

3564222001 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
9commission green paper on eu mental health strategy: evidence
6 July 2006 Mr Jurgen Scheftlein
we hope it will be ready for the spring of 2007.Because of the good feedback to the Green Paper,and also the delays in the replies from some of themain actors, for example the European Parliamentwill only send in its report in September, we havedecided that we will give it more time and have a newdeadline in the spring of 2007.Chairman: Thank you very much for coming. Youwill understand that our interlocutor is our owngovernment, so our report will be made to them. Youhave been extremely helpful in clarifying particularlywhat the potential activities and actions of theCommission might be. We were getting ourselves alittle bit worried that in such a wide field there might
be something rather peculiar going on, but I think weare much clearer now as to what your paper is movingtowards and what your aims and objectives so far are.Obviously they may change as you respond to theconsultation. Thank you very much for coming andhelping us to clarify our own minds, and I hope youhave had an interesting session as well. I can see thatsometimes our questions took you into territory thatyou were not always happy about, but never mind,you coped with all our questions, and we are verygrateful for all your help.Mr Scheftlein: Thank you very much for oVering methis opportunity. If it helped to clarify our objectives,it was a good investment from my side.Chairman: Thank you.

3564222002 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
10 commission green paper on eu mental health strategy: evidence
THURSDAY 20 JULY 2006
Present Colwyn, L Moser, LGreengross, B Neuberger, BHarrison, L (Chairman) Trefgarne, LHowarth of Breckland, B
Memorandum by Martin Knapp, David McDaid, Elias Mossialos and Graham Thornicroft
Note: Much of the material for this submission is drawn from the forthcoming book Mental Health Policy andPractice Across Europe edited by Martin Knapp, David McDaid, Elias Mossialos and Graham Thornicroft.Open University Press/McGraw-Hill, November 2006.
1. Would an EU Strategy on Mental Health would be Appropriate?
1.1 One in four of the European population can expect to experience a mental health problem during theirlifetime. Nearly all of us will know someone either in our families, at our workplaces or in our localcommunities with a mental health problem. Good mental health is a critical aspect of public health. The riskof poor physical health is significantly higher in those individuals experiencing mental health problems. Theconsequences of poor mental health go beyond health, impacting on all aspects of life. Other consequencescan include loss of employment and housing, deterioration of family relationships, and increased contact withthe criminal justice system. The level of stigma experienced by those with mental health problems can beprofound.
1.2 The Green Paper was the European Commission’s response to the 2005 Helsinki WHO European RegionMinisterial Declaration and Action Plan for Mental Health. Greater visibility for mental health at an EU levelcan help challenge the low priority it receives in some European countries. Both the development of nationalpolicies and the level of funding for mental health services or initiatives have been disappointing across almostthe length and breadth of Europe. Most countries now do have national or regional mental health policies inplace. Some have a long pedigree, and are revised quite regularly, but others are rather dated and clearly inneed of reform.
1.3 Funding in some EU Member States remains below 5 per cent of the total public health expenditure,despite poor mental health accounting for as much as 20 per cent of the total burden of ill health. This ishowever much variation in funding and service provision across Europe. Data from the Mental HealthEconomics European Network indicates, for instance, that the UK allocates one of the highest known sharesof health budget to mental health (around 13 per cent in England alone).
1.4 Despite growing policy attention, as well as advances in recognition and treatment, there are concerns thatthe situation in some parts of Europe could get worse before it gets better, widening inequalities in health.Rapid economic and social change in central and eastern Europe has been accompanied by a decline inpopulation mental health, with increasing rates of alcohol problems, violence and suicide. The mental healthneeds of people displaced through conflict, persecution or economic migration pose further challenges. Thechanging demography of Europe will clearly generate growth in age-related needs over the next few decades.
1.5 The EU also has an important role to play in promoting good mental health. There is a small but growingbody of robust evidence indicating that there are eVective promotion and prevention interventions availableto reduce the risks of poor mental health. Examples include parent training programmes and interventions forthe early identification of mental health problems in schools, flexible practices and access to counselling andsupport in the workplace, and bereavement counselling and social activities to reduce isolation and the riskof depression in older age. Despite the growth in this evidence base, mental health promotion continues toreceive little attention in most countries; recent EC sponsored action however through the ImplementingMental Health Promotion Action network has had some success in raising the profile of mental healthpromotion.
1.6 The EU can also play an important role, perhaps through the proposed Fundamental Rights Agency, inhelping to address and draw attention to human rights violations, stigma, discrimination and social exclusion.Few other health problems are characterised by such disadvantages. Violations of rights have been reported
3564222002 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
11commission green paper on eu mental health strategy: evidence
20 July 2006
across Europe, but are most visible in the psychiatric institutions and social care homes that remain themainstay of mental health systems in parts of central and Eastern Europe. In some countries, individualsadmitted to institutional settings still have a very low probability of ever returning to live in the community.
2. What Elements Might an EU Strategy Contain?
2.1 Intelligence gathering might be one crucial element of the strategy. This would not simply be a question ofregularly collecting comparable data on the level of mental well-being and poor mental health across Europe(in the same way that data on physical health is collected), but also collecting some basic information aboutservices and structures in countries. Ideally this would not be confined to the health system but would look atthe provision of services and development of national and regional strategies in other sectors. Currently thereis a lack of information on the pervasiveness of stigma towards mental disorders. The EU could also play agreater role in collecting information Europe-wide on public attitudes, as well as looking at the success oflegislation and other strategies to tackle stigma and discrimination.
2.2.1 Enhancing the evidence base. There are already many national and international organisations lookingat the eVectiveness of health care interventions such as anti-psychotics and anti-depressants. The EU Strategycould concentrate on areas where the evidence base is more limited and where research funding is more diYcultto obtain. Primarily through the EU’s Research Framework Programme, but also through individualdirectorates, more work could be done to enhance our understanding of eVective interventions and strategiesfor the promotion of mental well-being and prevention of mental disorders. Another area for research wouldbe to look at interventions intended improve public attitudes and reduce stigma towards people with mentalhealth problems. A first step would be to synthesise the existing evidence base rather than reinventing thewheel. A second step would be the commissioning of additional research in areas where it is clear thatknowledge is very limited.
2.2.2 While there is a small but growing evidence base for non health care interventions, much of thisinformation has been published in the United States and its applicability to diVerent European contexts maybe questioned. The EU should not only look at issues of eVectiveness but also consider what resources andinfrastructures would need to be in place to deliver interventions. For instance more work could be done tolook at the cost eVectiveness of workplace mental health promotion strategies in Europe or on the eVectivenessof strategies to help people with more severe mental health problems return to work. The perspectives ofservice users are important. Outcomes of importance to service users, such as self esteem, reduction in socialisolation, and greater sense of empowerment may not necessarily be identified by professional groups.
2.3 Making the evidence base accessible. Evidence on what interventions and strategies work, in what context,and at what cost, needs to be easily accessible. This might perhaps be through a database placed on the EU’sHealth Portal, but information also needs to be available in other formats to promote accessibility to policymakers, service users and other stakeholders.
2.4 Both the research capacity to produce evidence on what works, as well the capacity of the policy makingcommunity to interpret diVerent source of evidence, are limited in some Member States. Training and capacitybuilding initiatives to address these limitations might also form one element of the strategy.
2.5 An EU strategy might also encourage Member States to think about the consequences of shifting theresponsibility for supporting people with mental health problems out of the health sector. The availability ofand entitlement to services outside the health sector can be very variable and subject to means testing. Forinstance in some provinces of Austria, individuals and/or their families have to pay up to one third of the costsof social care services out of pocket.
2.6. Actions in the workplace are important. Occupational health and safety actions could more explicitlyaddress mental health in the workplace. The strategy could also help promote workplace/employmentintegration for people with mental health problems. Helping individuals return to/enter the workforce canhelp reduce stigma and discrimination and promote social inclusion. Employment also helps reduce povertyand thus empower individuals.
2.7 Promoting better coordination between parts of government and communities. To take child and adolescentmental health as just one example—there is a need to coordinate schools, general medical services, social care,social welfare, criminal justice, and housing services with those specialist mental health services. This canpromote better identification of and responses to emotional and behavioural problems in childhood/adolescence. Similar actions might take place in other sectors, for instance building on the recent agreementbetween the European Social Partners on Stress in the Workplace.

3564222002 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
12 commission green paper on eu mental health strategy: evidence
20 July 2006
2.8 The EU might also facilitate better recognition that the psychological challenges faced by older people arenot just to be accepted as inevitable consequences of the ageing process. They can devastate quality of life andoften treatable. Depression is not well recognised; older age groups can also have relatively high rates ofsuicide.
2.9 Promote awareness of and information campaigns related to mental health. Stigma distinguishes mentalhealth disorders from most other health problems and is the major reason for discrimination and socialexclusion. Fear of stigmatisation reduces an individual’s willingness to seek help. There are no easy solutions,but long-term actions such as intervention in schools to raise awareness of mental health, and constructiveengagement with the media (who can reinforce negative social attitudes by sensationalist and inaccurateportrayals of mental illness) appear to be eVective if concerted and prolonged.
3. How Might an EU Strategy Complement and Add Value to the Strategies of Member States and
the Activities of the World Health Organisation and Other International Bodies?
3.1 Unlike most other pertinent international agencies, such as the World Health Organisation or theInternational Labour Organisation, the EU has the advantage of having jurisdiction across many diVerentsectors; this multi-sectoral involvement is essential to any mental health strategy. It has already taken actionsthat promoting good mental health as well as addressing social exclusion and discrimination through anumber of diVerent Directorates. An EU Strategy could also help to improve co-ordination of actions andcommunication within the European Commission.
3.2 There have been some very positive development in national policies for mental health and well-being inEurope, as for instance in Scotland, where mental health policy enjoys a high profile. But there has been littledevelopment and/or implementation of modern mental health policies in some EU Member States, as well asin Candidate and neighbouring countries. A higher profile for mental health at an EU level, coupled withmonitoring arrangements on the state of mental health, issues of social exclusion and discrimination, as wellas on service provision, might act as a catalyst to promote an appropriate level of attention to mental healthin these countries.
3.3 The development of community based services to help shift the balance of care away from a predominanceof institutional care is expensive. Community services must be in place before institutions can be phased out.Raised visibility and a strategy for mental health might encourage Member States whose resources are morelimited to apply for European Structural Funds for mental health reforms. A good example of this might beseen in Greece, where international concerns about institutional care in the 1980s, and subsequent access toEU funds, have acted as a catalyst for ongoing system reform.
3.4 It is clear that many actions remain the responsibility of individual Member States. The EU strategy mighthowever through the open method of co-ordination, facilitate a process, by which Member States can if theyso choose, come together to work on common goals related to mental health that go beyond the competenceof the EU.
On behalf of all four editors of the book—Dated: 5 June 2006.
David McDaid, Research Fellow, PSSRU, LSE Health & Social Care & European Observatory on HealthSystems & Policies, London School of Economics & Political Science.
Professor Martin Knapp, PSSRU, & Co-Director, LSE Health & Social Care, London School of Economics& Political Science & Centre for the Economics of Mental Health, Institute of Psychiatry, King’s College,London.
Professor Graham Thornicroft, Head of Health Services Research Department, Institute of Psychiatry,King’s College, London.
Professor Elias Mossialos, Co-Director, LSE Health and Social Care and & European Observatory on HealthSystems & Policies, London School of Economics & Political Science.

3564222003 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
13commission green paper on eu mental health strategy: evidence
20 July 2006
Examination of Witnesses
Witnesses: Professor Graham Thornicroft, Professor of Community Psychiatry, Head of Health ServicesResearch Development, Institute of Psychiatry, and Mr David McDaid, Research Fellow, LSE Health and
Social Care and European Observatory on Health Systems and Policies, examined.
Q37 Chairman: Good morning, gentlemen. A verywarm welcome to Professor Graham Thornicroftand Mr David McDaid. We are grateful to you forcoming in. We are sorry about your colleague,Professor Knapp, being unavailable, but at suchshort notice and at the end of term, as it were, it is sohelpful to have you here. This is, of course, an openmeeting of the Committee so there may be hordes ofthe general public who will come sweeping in throughthose doors, but I am sure they will sit down veryquietly. A verbatim transcript will be made. As ever,when you leave the room if you think there are otherthings you wanted to say or wanted to correct, orwhatever, please let us know. We will send you a copyof the transcript. Please do feel free if you feel youhave made a material error or whatever to correct itand change what might have been misunderstood.Equally, you may feel there were items that you hadwanted to say which you had not said and we wouldbe most grateful if you jotted us a note and told usmore. Our purpose today is to get as much out of youto help us in this particular Inquiry. You have had anote of the members’ interests but I think somecolleagues will feel happier to say so on the record.You may know about the acoustics of this room.These rooms were designed for politicians whodeclaimed and threw their voices over large crowds,so if you could speak up it would be extremelyhelpful. I now turn to the main purpose of thismorning’s hour, which is that we have embarkedupon this Inquiry and we recognise it is at an earlystage. It is a Green Paper, but we think it importantto bring in colleagues like yourselves to give us a feelfor the area that we are talking about and to test thatdiYcult question about where the European Unioncan bring, as it were, added value so that what we dois worthwhile, and particularly worthwhile to you,your colleagues, your patients and those who youserve. That would be very helpful, especially right atthe end of term when we can think about what wehear from you over the Summer. I would like to askyou this. It could be argued that, with some 52countries signed up to the World HealthOrganisation Action Plan for Europe, a separatestrategy for the European Union is not really needed.Could you summarise what you think about thatand, in inviting you to summarise, for the purposes ofthe transcript could you please say who you are andwhere you are from right at the beginning. ProfessorThornicroft, do you want to start first? If either ofyou want to make a brief opening statement, pleasedo, but otherwise if you would like to take that firstquestion.
Professor Thornicroft: My Lord Chairman, thank youvery much for inviting me this morning. First I willintroduce myself to the Committee. I come from botha clinical and research background. I am a consultantpsychiatrist at South London and Maudsley NHSTrust. I have worked in psychiatry for the last 20years, most of that time in community mental healthteams. Secondly, at the same trust I am Director ofResearch and Development so I have an overallresponsibility for managing our research and seeingthat it gets through to be implemented for the publicgood. Thirdly, I am Head of the Health ServiceResearch Department at the Institute of Psychiatry atKing’s College, London, so I am the head of a largeresearch team investigating which treatments andservices are eVective and cost-eVective. To turn toyour question, my starting point would be the biggerpicture about mental health in Europe. We know thatthe large majority of people with mental illnessesreceive no treatment at all. I think our starting pointis that it is not at all the case that even in the bestorganised and funded countries in Europe that we aredoing even a half-way decent service. I have broughtsome background material that I can pass on to theCommittee to reference some evidence points that Ishall make. In terms of the simple occurrence ofmental illness, we know that in the best-financedsystem in the world, namely the United States, betterprovided even than the European countries, the mostrecent surveys show that the occurrence of mentalillness in a year is about 29–30 per cent. It dependshow you measure it. We know that of all those peoplein any one year only about 30 per cent will actuallyreceive any treatment at all for their mental illnesses.To turn this round the other way, we know that overtwo-thirds of all people, where we have studied this,with mental illness receive no treatment at all. Thestarting point is quite shocking levels of neglect andfailure to treat people with treatable mental illnesses.Shall I pass the materials to you later or as we goalong?Chairman: You could pass them to our assistant.
Q38 Lord Colwyn: Do those people who have amental illness know they have a mental illness or arethese people who do not know?Professor Thornicroft: This will vary a lot. In terms ofthe public understanding about mental healthproblems, I would say it is a mixture of lack ofinformation and gross misinformation. This bringsus on to the stigma area to some extent. Most peoplereceive no formal teaching at any stage of their livesabout any types of mental illness, so there is very

3564222003 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
14 commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
widespread misunderstanding about, for example,features that would indicate that someone may havedepression. So if a man who has become unemployedis irritable and drinking more, most people would notthink “perhaps this is depression”, including thatperson, “maybe I should seek an assessment andtreatment”. There are very widespread levels ofmisunderstanding and ways in which misinformationis put out into the public domain, mostly through thepress, broadcast and cinematographic media.
Q39 Chairman: We will come on to stigma, BaronessHowarth in particular will take that up later.Professor Thornicroft: My first general point is I thinkthe large majority of people in all of our Europeancountries simply go wholly untreated. My secondpoint is that for many of those people who are treatedwithin mental health care systems in Europe, thestandards of care are poor or very poor indeed. In thefirst case we may look at some countries in EasternEurope, including some accession and, indeed, pre-accession countries, to see the worst excesses. Therehave been recent reports by Amnesty Internationalon some of these countries and also by the MentalDisability Rights International Group showing, forexample, that in some of these countries peoplereceive electroconvulsive treatment withoutanaesthetic modification. In some of these countriesit is clear that there is good evidence that people diewithin psychiatric hospitals at a higher rate than youwould expect largely because of malnutrition andhypothermia in Winter for a series of institutionalreasons. The standards of care at present in some, Iwould say in many, Eastern European countriesespecially, are not up to what I would say is areasonably basic acceptable standard. To come backto your main point, I think that one reason to say thatwe do need a pan-European strategy is because thecurrent situation left to members alone is not at anacceptable level.
Q40 Chairman: Given that the WHO has got thisplan for the 52 countries with a much broader andbigger Europe, is there a danger of duplication? In asense, why should it be under the umbrella of theEuropean Union?Professor Thornicroft: I think two main reasons. Firstof all, the World Health Organisation Europeanregion, as you know, covers 52 nations spreadingfrom Iceland to Vladivostok and necessarily theirfocus is on the most deprived and economicallyunderdeveloped countries, which would be the SovietUnion and Central Asian republics. That means evenwithin some of the recent EU10, you might say theCzech Republic, Estonia and the Baltic States, theyhave relatively little contribution because their smallresources are focused elsewhere. The first issue is oneof focus, it cannot be the case that the WHO can
simply assist all of those Member States in the sameway because of the spread of countries and becausetheir focus is on the most deprived countries whichare outside the European Union. The second is thequestion of resource. If you think about the resource,in fact in the Mental Health OYce of the WHOEuropean region there is a small number, a handful,of people. They simply do not have the capacity torender material assistance to all of those countriessimultaneously whereas the budgets of theDirectorates-General of the European Union havemany millions of euros to be able to render assistancewhere required, especially for the new accessioncountries through infrastructural support. That canbe vital, for example, in de-institutionalising. Thathas been fundamental in changing the structure ofservices in Portugal, Spain and Greece and is alreadymaking a contribution in many Eastern Europeancountries.
Q41 Chairman: Those were two very interestinganswers. Mr McDaid, I saw you nodding. Do youwant to do a little introduction and then respond tothat first question?Mr McDaid: Yes. Thank you. In terms of mybackground, I am a health economist and healthpolicy analyst based at the London School ofEconomics where I work in the Health and SocialCare unit. I also work as a Research Fellow at theEuropean Observatory on Health Systems andPolicies looking at broader European health systemissues. Another relevant part of background is that Iedit a journal called EuroHealth Journal which looksat European health policy issues. Just a very briefopening statement, which echoes much of whatGraham has said, to highlight the fact that mentalhealth has long been the Cinderella in terms of issuesrelated to health. In many countries in Europe it isgrossly under-funded if you compare that to therelative burden that poor mental health contributesto the overall disease burden. It is almost unique inthese issues around stigma and discrimination whichtend to mean that it remains at the bottom of the pile,so to speak. There is less focus on mental healthperhaps than might be the case in other areas becauseit is not seen as a sexy area, for want of a better term.In terms of your first question, I would emphasisethat I believe the European Commission’s approachshould not be seen as an alternative but ascomplementary and part of the Commission’sresponse to the Action Plan declaration by the WHO.It is important to recognise the level of resourceswithin WHO Europe. They are limited bothfinancially and in terms of capacity where they aredealing with 52 countries. It must also beremembered that their primary focus is to responddirectly to the needs of individual Member States, soif an individual Member State approaches them with

3564222003 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
15commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
a specific issue they have to respond to that. It meansthat they have less time perhaps to look at over-arching issues across all European countries. It isreasonable to say as well that a lot of their focus willbe on those Member States further East, for want of abetter term, because the issues there are more obviousand more profound. Another important reason forEC involvement in this approach is that, unlike theWHO, the EU crosses across a number of diVerentareas, so we are not just talking here about the healthcare system, and I think that is very important. Thereare important issues about ways and means ofintegrating individuals back into the community,issues around promoting good health in theworkplace and also protecting the health ofvulnerable people returning to the workplace, issuesaround access to housing, issues arounddiscrimination, issues around education and supportfor carers. Many of these issues’ remits go beyondhealth and there are questions, perhaps, as to theextent that the WHO can influence sectors other thanhealth. I think the European Union can have a verypositive role to play in that respect. It is probablyreasonable to say if progress is made within theEuropean Union it will have some influence onaccession countries and neighbouring states as well.
Q42 Chairman: I find those two sets of answers veryhelpful indeed in answering the question about theadded value. What advice would you give aboutensuring that we do not cross wires with the WHO,the Commission and what is done in Member States?How can you help us there?Professor Thornicroft: Perhaps if I could first add oneitem of detail that Mr McDaid mentioned. In termsof expenditure, I have information that may help theCommittee on the proportion of healthcareexpenditure on mental health in diVerent Europeancountries.
Q43 Chairman: Are there other items that you willbe handing in?Professor Thornicroft: We have got a few items tohelp you.
Q44 Chairman: If you give them to us as a packagewe will circulate them to the Committee.Professor Thornicroft: The main point is this: if westart with the question what proportion of alldisability in Europe is attributable to mental illness,the answer is about 12 per cent. If we then ask is ittrue that 12 per cent of the health budgets as a wholeof European countries are spent on mental illness, theanswer is no, it is about three or four per cent. I wouldsee this as a material example of how there issystemic, some might say institutional, neglect anddiscrimination against the category of people whohave mental illness in all European countries.
Q45 Chairman: Thank you. Do you want to addanything, Mr McDaid?Mr McDaid: Just a small caveat in terms of funding,and that is always to be aware that there is fundingoutside the health system, particularly in social caresystems, that often does not get reported when welook at funding statements. It is just to be a littlecareful about that.
Q46 Baroness Howarth of Breckland: I will tell youa bit more about who I am when I come to myproper question. I know that we are going to havea lot of discussion about definitions but in terms offunding and coming to a conclusion about theproportion of funds that go to mental health, oneof the diYculties is the spectrum of mental illness/mental health and what other budgets contribute tomental well-being that therefore contribute tomental health. Is that not a complexity that isdiYcult to come to and, therefore, a straightforward12 per cent/3 per cent is really an inappropriate sortof response? I do not know how to put that kindly.Professor Thornicroft: This is a fair point. In termsof the mandate of the EC here, part of the diYcultythe Committee may be grappling with is by virtue ofthe delegation to Member States on issues regardingtreatment and services, so there is an open questionabout what issues may be taken at the pan-European level. This is usually restricted topromotion, prevention and those issues within therealm of public health, but also they will addressquestions of access to healthcare and human rightsand social exclusion, for example in the workplace.I think we can see it in the broader realm, asMr McDaid mentioned, not just in pure healthterms. With respect to definition, I can take thatnow or later when we come to that item.
Q47 Baroness Greengross: As you were talkingabout other ways of dealing with this problem, I justwondered about the budget which might be veryhelpful in something like this, which is the socialexclusion budget, and whether that is something wecould look at.Mr McDaid: I can come back on that. Certainly Ithink it is important to try to capture all theelements of funding, including social exclusion, butit is extremely diYcult to do. Just to illustrate withone simple example: the WHO in Geneva producean atlas on mental health of all the countries in theworld and it is very helpful. If you turn to thesection on Norway and look at the funding ofmental health in Norway you will see that theyspend 0.1 of 1 per cent on mental health in Norway.Clearly that is not true, they spend a lot more, butbecause it is not specifically earmarked for mentalhealth it is very diYcult to identify. That is justlooking at funding within the health care system. It

3564222003 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
16 commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
is an incredibly challenging issue and I do think itis something where the European Union, because itworks across diVerent sectors, can try and improveour understanding and knowledge of total fundingfor mental in other sectors, but it is diYcult to doand there are no easy answers to that.Chairman: I saw Lord Moser’s head nodding whenyou were talking about the diYculty of comparinglike with like. Let us move on to definitions.
Q48 Lord Trefgarne: You have described at somelength the diYculties of definition of funding andProfessor Thornicroft explained how large numbersof people suVer from mental ill-health, but would younot agree that the numbers of people are whollydependent upon the definition of what is mental ill-health. The Green Paper quotes the WHO definitionsof mental health and mental ill-health, which areexceedingly broad, and if you make it broader I thinkyou could include almost every member of thepopulation. Are you happy with the definitions thatthe WHO, and hence the EU, are relying upon? Icannot resist quoting from Katherine Mansfield, whowas an author from the 1920s, who wrote abouthealth rather than ill-health: “By health I mean thepower to live a full, adult, living, breathing life inclose contact with what I love. I want to be all that Iam capable of becoming”. That is a wonderfuldefinition of health, I wonder if you could producesuch an elegant one for mental ill-health.Professor Thornicroft: Thank you very much. As ahumble researcher I could not compete with thelyricism of that quotation. I think what I would sayis this: clearly the frequency of mental illness whollydepends upon how widely or narrowly you definethose particular definitions. Nevertheless, we nowhave an international consensus on what forms ofsuVering should be included within the broad remitof mental illnesses and when you apply those criteriato any populations in the world you find veryconsistent findings. You find roughly between 25–30per cent of people have such problems which areserious enough to aVect work, social relations oreveryday functioning within any year. If you say howmany people in their lifetimes suVer from theseproblems, the answer is half. They are bothremarkably common and do have impacts onpeople’s everybody lives. A paradox—we will comelater to the stigmatisation—is why it is that we shouldhave such adverse reactions when these are socommon. If you ask in general population surveys,“Do you know someone directly who has beenaVected by mental illness (including yourself)” theanswer is 75 per cent. The large majority of peoplehave direct family experience of these problems, so Iam afraid the plain fact is they are that common.
Mr McDaid: The only thing I would add is that theGreen Paper deliberately takes a broad definition toemphasise the importance of promoting mental well-being. I am not a psychiatrist but I do know that is amore diYcult concept to measure. There is no doubtabout that, but it does reflect partly the politicalreality of the Commission having competence overpublic health and health promotion but not so much,other than what Professor Thornicroft has alreadysaid, in terms of looking at treatments. There is aphilosophy within the Commission, in my view,which is partly about dealing with mental ill-healthbut also about trying to promote good mental well-being, which is more challenging.
Q49 Lord Trefgarne: We all know whathypochondria means. It means I want every kind ofpill I can find. Is there such a thing as mental healthhypochondria?Professor Thornicroft: Yes, there is, but I do not thinkit would be at all helpful to the Committee’sconsiderations to think that out of that 25 per cent ofthe population a proportion of those are malingeringor suVering from hypochondria in any way.
Q50 Lord Trefgarne: None at all?Professor Thornicroft: Not of those people. These arepeople who meet diagnostic criteria, in the technicaljargon. To expand upon your point: if we considernot the broad range of people mostly suVeringanxiety or depression, or both, but the much smallerproportion who have what we would call severemental illnesses, essentially psychotic disorders suchas schizophrenia or bipolar disorder, that wouldprobably come to about 1 per cent of the wholepopulation in European countries. Although the careof those is properly the remit of the Member Statesthere are aspects of the wider social participation ofthose people which are clearly within the remit of theEC. One example is work. Recently I conducted astudy in several European countries and one of thequestions was simply among people withschizophrenia, typical people with schizophrenia infive European countries, how many are working, andthe largest proportion was in Italy with 23 per cent.The smallest proportion was in London with 5 percent.
Q51 Chairman: In London?Professor Thornicroft: In London it was 5 per cent. Ican pass this information to the Committee. Thesewere otherwise remarkably similar people. It is nottrue that it is somehow inherent that such peopleshould be excluded from the workforce. It is truethere are huge variations between countries and itappears to be true that in this country we are the bestat excluding such people from the general workforceand all that that implies.

3564222003 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
17commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
Q52 Chairman: Without asking you why thatdiscrepancy is the case, that would typify why it isuseful perhaps to embark upon the research that weare doing in this report because when you comparethose kinds of statistics it begins to ask why that isthe case.Professor Thornicroft: It then leads us into anti-discrimination laws, disability laws, andarrangements to make the necessary adjustments inaccommodation for disabled people to enter and stayin the workforce, which we might come on tosubsequently.Chairman: I am going to invite Lord Moser toput his question on information-gathering anddissemination but I know that he was interested in thequestion of definition.
Q53 Lord Moser: First of all, to declare an interest:I have various links with the Alzheimer’s Society. Myfield is statistics. I note in your joint paper you stressthat from the point of the view of the EU strategyimproving the information base, the evidence base,improving the data would be an important element.I was pleased to see that but slightly puzzled. TheCommission has said that although they have spent alot of money on improving information, data, thereare many gaps. From my own experience—I used tobe in charge of statistics in this country, I was onEurostat, UN statistics, the WHO, et cetera—Iremember endless concern about improving healthstatistics, including mental health statistics. I am alsoaware that in ONS, as it is now called—I was lookingup the statistics yesterday—there is a lot ofinformation on mental health, including agediVerentials, social class diVerentials, regionaldiVerentials, so it does not seem to me, as astatistician, to be a field that is lacking ininformation. But clearly you experts think that thereare big gaps, so it would be very helpful to us to getyour assessment on the state of play on theinformation and what should and could be done.Mr McDaid: In terms of what we understand aboutthe prevalence of mental health problems in Europe,there was a very interesting report produced by theEuropean Brain Council recently. I think you haveseen the figure quoted of one-quarter of peoplehaving mental health problems at any point in theirlifetime. That came from a survey of surveys lookingacross Europe and the interesting thing was in 12 ofthe 28 countries that were covered there is noinformation at all. I agree, the UK is a good exampleand we have good information, relatively speaking,but there are parts of Europe where the informationbase is very limited.
Q54 Lord Moser: You are not referring to theaccession countries?
Mr McDaid: I am referring to the accessioncountries, but not exclusively. If my recollection iscorrect, Ireland and Portugal were two of thecountries where no information was available. I doknow in Ireland, for instance, there is quite a lot ofinformation on use of beds and so forth, but not interms of other things. There are clear issues aroundthe spread and access to information across Europe.In terms of what the Commission can provide I thinkwe have to be pragmatic about that. I do not think itis possible for the EU to try to impose on all countriesa common system of data collection using the samestandard. I think that is going to be very diYcult todo, but what they can do, and are doing now throughEurostat, is they are trying to increase the amount ofinformation on mental health they do collect, andthat is a process that I believe is ongoing at themoment. I am sure Eurostat can provide moreinformation on that. There is also a role for trying tocollect, or even fund, specific surveys and perhapslong-term studies looking at trends over smallertimescales across a number of diVerent countries. Aswe have seen here in the UK, if you follow children,for instance, over a very long period of time that canprovide very powerful evidence on the consequencesof poor mental health. That may be a more targetedway of doing things rather than trying to doeverything that national statistics agencies should bedoing. It is a question of working with them but thereare things on which the European Union can helpand also the sharing of good practice about datacollection and perhaps coming to more comparablemeasuring methods.
Q55 Lord Moser: If I can go on for one more minute,and welcome to you from the LSE, in your reply wereyou thinking specifically of incidence or also care?Mr McDaid: I think it is important to haveinformation on the utilisation of services, access toservices, the availability of services, as well as theincidence and prevalence of poor mental healthacross Europe. These surveys could look atpopulations that have been identified as havingmental health problems, to what extent they do comeinto contact with services and not just emphasisehealthcare services necessarily but also broaderservices that may be appropriate as well.
Q56 Lord Moser: My final point on this: obviouslyfrom our point of view the key question is, is theCommission, and that really means Eurostat, in yourjoint professional view well-equipped to do what weare talking about, in other words fill the gap both onincidence and care throughout the European Union?Professor Thornicroft: I cannot answer that directlybecause I am not very familiar with the workings ofEurostat and perhaps that says a lot about the extent

3564222003 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
18 commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
to which their information reaches the researchcommunity.Mr McDaid: I would echo that. One thing which isrelevant to all of these discussions is communicationwithin the Commission. Although there are goodlinks between some of the DGs there are always waysin which communication can be improved, andperhaps communication between public health andEurostat, and indeed between researchers and whatEurostat is doing, is an interesting area to look at. Icannot directly answer that question, I do not havethe competence.Professor Thornicroft: I think there is a lot ofinformation collected within Europe but much of it isnot very informative. A lot of it is about inputs, forexample investments, or processes, for example thenumbers of beds, and I have got material here thatmay help the Committee on these things, but you willhave seen this. Relatively little is on helpful processessuch as the extent to which these are servicesdelivered in ways that are acceptable to the patientsthey are intended to benefit and very little usefulinformation on the outcomes of care, including theextent to which the needs of people with mentalillnesses are met in their own judgment, for example.Lord Moser: I am left with the conclusion our expertsfeel that not only in what is available there are majorgaps but also it does not reach the researchers, etcetera. I think that is something for us to talk about,but not now.Chairman: My comment was going to be that thisCommittee is learning a lot which is very useful thismorning. I am going to pass on to BaronessNeuberger to talk about research.
Q57 Baroness Neuberger: Good morning, Graham,it is very nice to see you. I ought to declare an interest:I am an adviser to Trustees to the Sainsbury’s Centrefor Mental Health, as you well know, Graham, andalso a newly elected Honorary Fellow of the RoyalCollege of Psychiatrists. I think in a sense you haveanswered part of the question about the prioritiesthat you would like to see for using the EU researchbudget to make a positive contribution to the EUMental Health Strategy because part of that is clearlyabout pulling together some of the data that you havebeen talking about that is not properly available. Isuppose the question I would like to ask is have yougot a view between you on doing more than that andmore than drilling down into what already exists andsome fairly basic primary research that needs to bedone that could make a positive contribution to thestrategy?Professor Thornicroft: If I could start with a slightlybroader statement and then focus down on the detail.It seems to me that what the EC can contribute heremore generally are three domains: namely, ethics,evidence and experience. What I mean by “ethics” is
making it clear to all concerned throughout Europewhat already their obligations are under varioustreaties and covenants in relation to human rights ofpeople with mental illness. By “evidence”, I meangathering and then using research to the best eVect.By “experience” I mean trading examples of bestpractice between nations but particularly carefullyassembling information from people with mentalillnesses, from their experience, what helps them thebest. I come on to the research point in particular.Most of the important questions we simply do notknow the answers to within the wider Europe. Wehave some detailed information about the occurrenceof mental illness but, the second point, the extent towhich such people are treated at all we do not know,then the extent to which those people are receivinganything resembling eVective care we do not know.We do have some worrying background informationin, again, the Kessler paper that I will pass to you thatin some, perhaps many, countries, of those peoplewho are treated within the mental health system up tohalf do not have a mental illness. They are notnecessarily malingering, or whatever we may call it,but perhaps they have recovered and no longer needactive treatment. The coverage of our mental healthsystems in Europe we know will miss at least two-thirds of people with mental illness. In terms of thetargeting it suggests that up to half of the people whoare actually treated do not or no longer requiretreatment, so we are actually misusing the scarceresources that we have. More particularly, it is clearto me that I would like the Committee to considercarefully the extent to which the general frameworkFP7 focuses on mental illness. In the current FP6programme, the two core themes are genomics andthe information society and it was essentially verydiYcult to find any category under which one couldbid for mental health or mental illness relatedresearch despite the clear public health impact ofthese disorders. I think it would be very helpful if youwere to recommend that FP7 should have a clearcommitment to mental illness and mental healthresearch within its forward remit.
Q58 Chairman: Is FP forward planning?Mr McDaid: The Framework Programme.Professor Thornicroft: It is the five year funding spendfor research throughout the European Commission.
Q59 Baroness Neuberger: Can I just follow that up?You said a lot about looking at who is actuallyreceiving treatment who do not need it and peoplewho do need it not getting their treatment. Clearlyyou can deal with part of that under access and thequestion of human rights, but is there an area aroundthe public health and promotion area which youthink also requires research? Is that an area that is asurgent given how widely the Green Paper is drafted?

3564222003 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
19commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
Professor Thornicroft: I would interpret this in relationto the access question, therefore the need to pass onclear information to all of the publics throughout theEuropean Union about what are the features ofmental illness, if you may have such a condition, orsomebody within your family may have suchsymptoms or signs, what do you do, where do you gofor help, are these conditions treatable, should we beless embarrassed and not ashamed to seek contact atall. I would frame it in terms of the access questionprimarily.
Q60 Chairman: Mr McDaid, do you want to addto that?Mr McDaid: Yes. I think there are important areaswithin public health and health promotion thatresearch could focus on. Let us be honest, it may beone of the few sources of funding for public healthand health promotion in later research. As ProfessorThornicroft has indicated, the evidence base in thisarea is not as good as it could be. But there is a lot ofevidence in the United States in several areas: issuesaround early interventions for children in school andalso in the workplace and promoting mental healthwithin the workplace. One modest research agendamight be to look at to what extent that research couldbe applicable within a European context. I say it ismodest because I talked about funding but withincertain streams of funding in the European Union,the public health programme, that is limited, theSeventh Framework is where there is more scope.The second thing that might be important is goingback to this point about the longitudinal studies,cohort studies, following people over a period oftime. If we could fund that, that would be veryvaluable, but the challenge is we are talking abouttime-limited funding for research programmes. Ifthere is a way that is possible to think beyond two orthree years and think about a longer term approachto actually generating the evidence, so that instead ofsaying we do not know what the answers are toquestions we can come up with some answers, thatwould be helpful, but it is a diYcult thing to do.Certainly I would have thought the EuropeanCommission may have more scope to do that thanperhaps national governments can.Professor Thornicroft: One more detailed point inrelation to promotion, which is promoting thephysical health of people with mental illnesses. Weknow that death rates are much higher than for thegeneral population. We know that people withschizophrenia on average die eight years youngerthan their otherwise equivalent counterparts and weknow that rates of smoking and diabetes are higher,essentially across the board, are higher and we seepoorer physical health and poorer physicalhealthcare for people with mental illness. There isstrong evidence of discrimination against people with
mental illnesses when they seek investigation ortreatment for physical problems, essentially it isascribed to being all in the mind. These are issuesfairly and squarely within the health promotiondomain.Chairman: I am anxious to use our final 15 minutes aswell as we might. Lord Colwyn, I think we havepartly moved into the area that you were going to talkabout. Would you like to just put the question.
Q61 Lord Colwyn: I think everything you are sayingis enormously useful but it is making me realise thevast task we have got and what a wide subject it is.When we saw Mr Scheftlein from the Commission hetalked about promotion and prevention as being veryimportant goals and we are hearing from you of vastnumbers who have mental health problems, vastnumbers not knowing they have got it, and now vastnumbers who have got it and are not being treated,and yet infants, children, young people and olderpeople are particularly at risk from social,psychological, biological and environmental factors.I am getting a bit lost here. What does it mean inpractice and what should the practice be? Can youhelp us?Professor Thornicroft: We will try to be helpful, I amsure. It is true that this is a vast domain and one hasto try very hard not to become lost because of themagnitude of the task. It would be helpful if theCommittee wished to focus on very specificrecommendations, for example the extent to whichthe mental health of the workforce may be promotedand protected. We know that in all Europeancountries there are two main issues. One is access tothe workforce for those people who have, or havehad, mental illness. The second is re-entry into theworkforce of people who are on sick leave by virtueof mental illnesses. Both issues are dealt with badlyeverywhere that we have got evidence about. Wecould make specific recommendations with respect,for example, to identifying people who are becomingstressed or depressed or anxious at any early stage;with respect to employers employing good practicefor psychological treatments for people who havedeveloped, for example, anxiety and depression; andfor good practice in flexible arrangements in re-entryto work, return to work, for people who have had aperiod of sick leave by virtue of anxiety or depression,for example.
Q62 Lord Colwyn: Should we be trying to identifythe causes of mental illness?Professor Thornicroft: Certainly. There is a very largeamount of research, including from my ownInstitute, on that, but at present relatively little isclearly understood about the causes and, therefore, itis diYcult to be precise about whether the current

3564222003 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
20 commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
evidence allows us primary prevention, if you like, tostop mental disorders developing in the first place.Chairman: Because of what Professor Thornicrofthas said about mental health in the workplace, I amgoing to invite Lady Greengross to put her questionbecause I think it is particularly relevant toMr McDaid’s work.
Q63 Baroness Greengross: Exactly, and I know MrMcDaid because of that. I should just declare aninterest as co-Chair of the Alliance for Health in theFuture which works across Europe. I am alsoinvolved in two organisations which promote healthin the workplace, including mental health, but it ispeople with disabilities of all sorts. I was going tofocus on the economic aspects of mental ill-healthand ask particularly Mr McDaid, but both of you ifyou will, to tell us more about the work that is beingdone in collaboration with the Commission and howthe hard work that the data and economic analysiscan provide us in looking at how better mental healthin the workplace and more employability andretention of people with mental illness in theworkplace could help the European Union regardingthe Lisbon Agenda particularly, hard economic data?Mr McDaid: There is a challenge with hard economicdata, I have to say. I should say I co-ordinate withcolleagues at the London School of Economics onthe Mental Health Economics European Network,which is a 31-country network funded by theCommission and it is on its second phase of funding,which is quite unusual by Commission standards. Wehave extended the number of countries involved. Oneof our key areas of work is looking at the economicsof prevention and promotion in the area of mentalhealth and there we are focusing on two areasspecifically, one in terms of early childhoodinterventions, the other in terms of the workplace.We are hostages to fortune in the sense that most ofthe evidence of eVectiveness is US-based evidence sowe are looking at two things: the potential for usinginterventions that have been shown to work within aUS context within the European context, and theseinclude things like employee assistance programmesand also some of the things that ProfessorThornicroft mentioned around flexible workingarrangements, et cetera, for people in the workplaceas well. We are trying to combine that with evidenceon the extent to which mental health problemsimpact on absenteeism, early retirement from theworkforce, and something called presenteeism, whereyou are at work but you are not productive. We aretrying to put an economic cost on that loss ofproductivity, for want of a better term. We are alsolooking at the potential requirement for disabilitybenefits and so forth to be paid out earlier, looking atthe costs of delivering interventions to promotemental health in the workplace and then to try to
have some crude, but hopefully quite helpful, figuresin terms of the potential benefits of investing more inpromotion of mental health within the workplace.We are constructing models for various countriesaround Europe. We cannot do it for all of them butwe are trying to think of diVerent contexts to showthe potential benefits of doing this. I have to say it isinteresting that many of the interventions in this areamay not necessarily be funded by public money. Theymay be funded by companies and enterprises, whichis another stakeholder we have to think about in thisequation. There are some interesting issues there but,hopefully, at the end of the day we can say somethingabout the potential costs and benefits of actuallyinvesting in workplace health promotion and otherareas as well.
Q64 Baroness Greengross: Could I just follow thatup very quickly by saying I was at a breakfast meetingthis morning with somebody from the Royal Mail,and this was regarding disability including mentalillness and mental health, who was saying that onemillion invested got them a return of five million, andthat was very impressive. Would you agree that is theright sort of calculation? That would include alldisability.Mr McDaid: The one thing I will say is despite beingan economist, of course, we should not makedecisions just on the basis of whether it is value formoney.
Q65 Baroness Neuberger: Gosh!Mr McDaid: That is terrible, is it not?
Q66 Lord Moser: Very brave!Mr McDaid: I do think it is terribly important toemphasise the benefits of having a healthy workforce.There are some people who argue you can replacepeople by others who are unemployed and so forth,but in fact you can take that argument apart to alarge extent. There are strong economic benefits inhaving good mental health in the workforce if the USevidence is to be believed. There is good evidencefrom the Boeing company, for example, of a long-standing programme, not just for mental healthpromotion but physical health promotion as wellwithin the company.Baroness Greengross: This data I am quoting fromwas on physical health but it was one to five and thiswas a big pilot that they had done.
Q67 Chairman: Professor Thornicroft, do you haveanything to add to that?Professor Thornicroft: Not on that point, no.
Q68 Chairman: So it is not outlandish to say whenthe Commission talk about the Lisbon Strategy it isnot as fanciful as it might at first seem?

3564222003 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
21commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
Mr McDaid: No, it is not. The Lisbon Strategy didoriginally talk about social inclusion much more thanit does now and, of course, there is an importantelement of integrating people into the workforce orother activities.
Q69 Lord Moser: Is Richard Layard’s recent stuV onthe cost of depression to the economy part of your—Mr McDaid: It is not part of our unit’s work althoughmy colleague, Professor Martin Knapp, has beenworking with Lord Layard on that. That is aninteresting and important area because he is lookingat broader issues in terms of income levels and someof these macroeconomic determinants which are veryimportant.
Q70 Baroness Howarth of Breckland: The Chairmanwants the question on the record, so I am going toread it in a minute. I am a social worker by trainingand background with 40 years in social care, and I donot look or feel that old but I started young. I amconcerned about what progress we have made inwhat time and in doing this investigation whether ornot you believe that the EU can really make somesort of step change across the whole piece. You put itvery much in terms of changing things aroundstigma, ignorance, discrimination and understanding,and those are things that may have moved somewhatbut are still fairly well engrained in this country,never mind Eastern Europe as some of your statisticshave said. So that we have got the question on therecord: we were very impressed by what you saidabout overcoming stigma. Bringing mental illnessout of the dark corners where it has been consignedby fear, prejudice and ignorance is potentially amassive long-term task requiring sustained politicaldetermination and a sense of clear priorities, and mywork in the child-care field has shown that has notmoved substantially in paediatric mental health. Inyour paper you have outlined levels of action thatwould be needed. Do you detect, because this is thewhole point about what we are doing, a receptiveclimate for constructive progress among EU MemberStates? Is the level of public awareness suYcient togenerate political momentum for change?Professor Thornicroft: I shall be brief. I have recentlywritten a book on this question so I have informationabout that for the Committee, but I will try toencapsulate that in a small statement. We can seethese as three related problems: the problem ofignorance, that is a knowledge problem; the problemof attitudes, namely prejudice against people withmental illness; and the problem of behaviour. In myown judgment it is the behaviour problem, namelydiscrimination, which is the worst and the mosturgent to tackle. I think we can look to Europeaninstitutions and the Council of Europe, but also those
framing and implementing human rights and civilliberties arrangements, to take a lead on this. In termsof preparedness, I think we now see for the first timesigns that the European Union, EuropeanCommission and the World Health Organisation/Europe are taking these issues seriously and they arenamed amongst the five highest priorities in theWHO/EC European Declaration and Action Plan. Inanswer to your question have we made progress inthese areas, no. Is there now a receptive frameworkwhere we can make a serious and long-termcommitment, I think yes.Chairman: That is very helpful. I wonder whether wecan take the last two questions together.Baroness Neuberger: To a large extent I think myquestion has been answered in what ProfessorThornicroft just said.
Q71 Chairman: Just on the EU Platform on MentalHealth, which is mentioned in the Green Paper, doesthat mean something or is there a danger of a talkingshop developing here?Mr McDaid: With all platforms there is always thepotential for them not to be as eVective as they couldbe. It will depend a lot on whether or not there aregood links between those working on the platformand those that actually influence policy and theMember States. I do not have any knowledge on howthat is going to work. One thing I will say is that it isimportant that all stakeholders do take part andthere have been some practical issues in the past withrepresentatives from service users and service userorganisations not necessarily being able toparticipate simply because of cash flow issues. It isnot that there is not funding to allow them to attendbut the funding is retrospective so they find it diYcultto get there. In terms of involving more stakeholders,that is important but it is the links that will determinewhether or not the platform is eVective or not.Professor Thornicroft: I would make two brief points.It is meaningful if it leads to real investmentdecisions, probably requiring hypothecated funds,for mental illness because given the competition withcancer or people in wheelchairs, we always lose out.Within that investment I think there needs to be aclear-cut budget, again probably hypothecated, tosupport patient services and consumers and familyorganisations to establish themselves because at themoment they are operating on a shoestring and withcentral investment they could play a much morerealistic role in the long-term.Chairman: In concluding this session can I invite youagain just to think if there is anything you wereunable to answer in your questions because of thelack of time or, indeed, the additional informationthat Professor Thornicroft has, if that could beadvanced to our oYcers. Can I say, ProfessorThornicroft and Mr McDaid, rarely have I had such
3564222003 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
22 commission green paper on eu mental health strategy: evidence
20 July 2006 Professor Graham Thornicroft and Mr David McDaid
an interesting and informative session on aCommittee like this and I believe that I do speak forthe rest of the Committee. Also, the quality andeconomy of your answers were very helpful indeedfor us pondering this issue, which is a very importantissue, over the summer break. We are extremelythankful.
Supplementary written evidence by Professor Graham Thornicroft, Institute of Psychiatry,King’s College London
1. Introduction
It is now beyond doubt that widespread discrimination adds to the disability of people with mental illness. Thebasic problem is this: many people with mental illness are subjected to systematic disadvantages in most areasof their lives. These forms of social exclusion occur at home, at work, in personal life, in social activities, inhealthcare, and in the media.
2. From Stigma to Ignorance, Prejudice and Discrimination
What is stigma? The concept of stigma is necessary to develop an understanding of experiences of socialexclusion, but it is not suYcient to grasp the whole picture, nor to know what practical steps need to be takento promote social inclusion. Stigma is best seen as three related problems:
— The problem of knowledge: Ignorance— The problem of attitudes: Prejudice— The problem of behaviour: Discrimination
2.1 Ignorance: strong evidence is presented here that most people have little knowledge about mental illnesses,and much of this information is factually incorrect. There is a pressing need to convey more usefulinformation, for example about how to recognise the features of mental illness and where to get help, both tothe whole population and to specific groups such as teenagers.
2.2 Prejudice: fear, anxiety and avoidance are common feelings both for people who do not have mentalillness (when reacting to those who have), and for people with mental illness who anticipate rejection anddiscrimination and therefore impose upon themselves a form of “self-stigma”.
2.3 Discrimination: the scientific evidence and the strong message from service users and their advocates areclear that discrimination blights life for many people with mental illness, making marriage, childcare, work,and a normal social life much more diYcult. Actions are needed to specifically redress the social exclusion ofpeople with mental illness, and to use the legal measures intended to support all disabled people (such as theUK Disability Discrimination Act) for physical and mental disabilities on the basis of parity.
3. Action to Support Service User Advocacy Groups
Empowerment has been described as the opposite of self-stigmatisation. Policy makers can therefore providespecific financial support for ways in which individuals with mental illness can empower themselves or beempowered include the following:
— Participating in formulating care plans and crisis plans.
— Using cognitive-behavioral therapy to reverse negative self-stigma.
— Running regular assessments of consumer satisfaction with services.
— Creating user-led and user-run services.
— Developing peer support worker roles in mainstream mental health care.
— Advocating for employers to give positive credit for experience of mental health illness.
— Taking part in treatment and service evaluation and research.
Q72 Lord Colwyn: How many years do you think weneed to undertake this Inquiry?Professor Thornicroft: I believe in short reports andlong-term commitment and to change things aroundwith respect to discrimination in ethnicity or physicaldisabilities has taken about 15 years to see realprogress, and I think that is the perspective. Thankyou for your interest in this field.Chairman: Thank you very much.
3564222004 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
23commission green paper on eu mental health strategy: evidence
20 July 2006
4. Action to Support Individuals and Their Families
A series of changes are necessary to assist individual people with mental illness and their carers and familymembers:
Action By
Develop new ways to oVer diagnoses Mental health staV
Have information packages for family members that explain causes, nature and Mental health staV,treatments of diVerent types of mental illness consumer and families
Actively provide factual information against popular myths Mental health staV
Develop and rehearse accounts of mental illness experiences which do not Mental health staV andalienate other people consumer groups
5. Action to Support People With Mental Illness at Work
For some people with mental illness, allowance needs to be made at work for their personal requirements(1–3). In parallel with the modifications made for people with physical disabilities, people with mental illness-related disabilities may need what are called “reasonable adjustments” in relation to the anti-discriminationlaws. In practice this can include the following measures:
— for people with concentration problems, having a quieter work place with fewer distractions ratherthan a noisy open plan oYce, with a rest area for breaks;
— more or more frequent supervision than usual to give feedback and guidance on job performance;
— allow a person to use headphones to block out distracting noise;
— flexibility in work hours so that they can attend their healthcare appointments, or work when notimpaired by medication;
— provide an external job coach for counselling and support, and to mediate between employee andemployer;
— buddy/mentor scheme to provide on-site orientation, and assistance;
— clear person specifications, job descriptions and task assignments to assist people who find ambiguityor uncertainty hard to cope with;
— for people likely to become unwell for prolonged periods it may be necessary to make contractmodifications to specifically allow whatever sickness leave they need;
— a more gradual induction phase, for example with more time to complete tasks, for those who returnto work after a prolonged absence, or who may have some cognitive impairment;
— improved disability awareness in the workplace to reduce stigma and to underpin all otheraccommodations;
— reallocation of marginal job functions which are disturbing to an individual; and
— allow use of accrued paid and unpaid leave for periods of illness.
6. Actions Needed at the Local Level
In local communities or health and social care economies these initiatives are needed to promote the socialinclusion of people with mental illness:
Action By
Introduction supported work schemes Mental health services with specialistindependent sector providers
Psychological treatments to improve cognition, self-esteem Mental health and general health servicesand confidentHealth and social care explicitly give credit to applicants with Health and social care agenciesa history of mental illness when hiring staVProvision of reasonable adjustments/accommodations at Mental health providers engaging withwork employers and business confederations
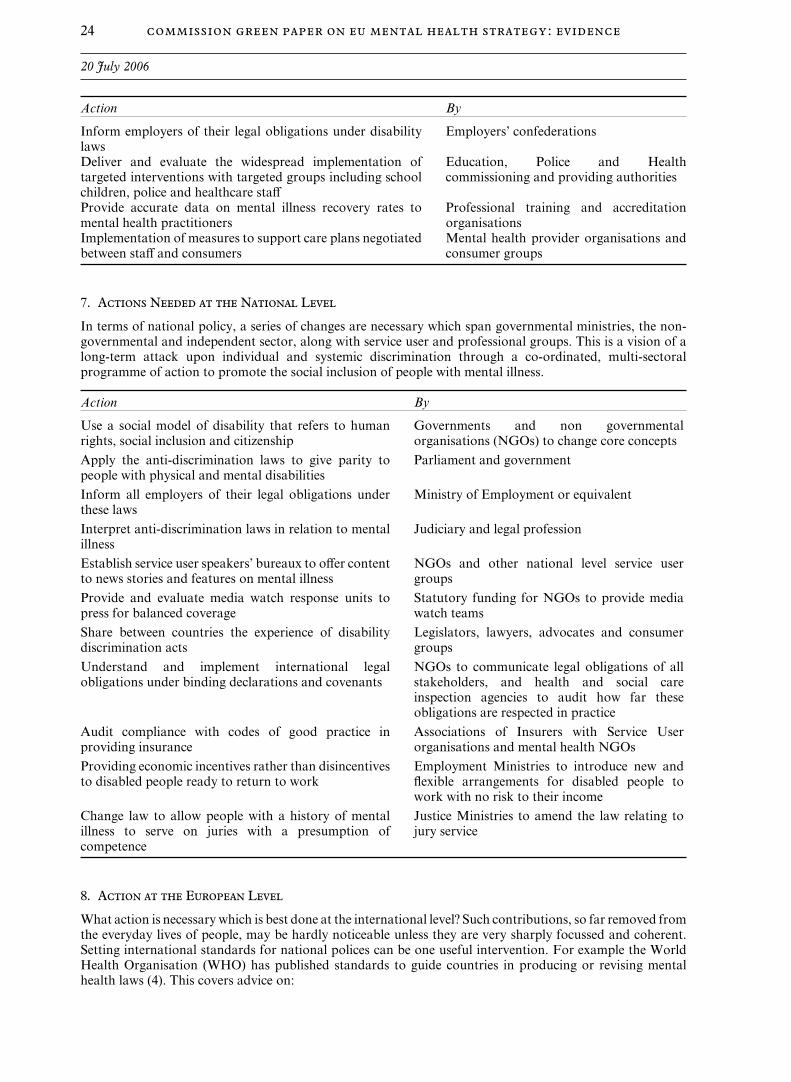
3564222004 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
24 commission green paper on eu mental health strategy: evidence
20 July 2006
Action By
Inform employers of their legal obligations under disability Employers’ confederationslawsDeliver and evaluate the widespread implementation of Education, Police and Healthtargeted interventions with targeted groups including school commissioning and providing authoritieschildren, police and healthcare staVProvide accurate data on mental illness recovery rates to Professional training and accreditationmental health practitioners organisationsImplementation of measures to support care plans negotiated Mental health provider organisations andbetween staV and consumers consumer groups
7. Actions Needed at the National Level
In terms of national policy, a series of changes are necessary which span governmental ministries, the non-governmental and independent sector, along with service user and professional groups. This is a vision of along-term attack upon individual and systemic discrimination through a co-ordinated, multi-sectoralprogramme of action to promote the social inclusion of people with mental illness.
Action By
Use a social model of disability that refers to human Governments and non governmentalrights, social inclusion and citizenship organisations (NGOs) to change core concepts
Apply the anti-discrimination laws to give parity to Parliament and governmentpeople with physical and mental disabilities
Inform all employers of their legal obligations under Ministry of Employment or equivalentthese laws
Interpret anti-discrimination laws in relation to mental Judiciary and legal professionillness
Establish service user speakers’ bureaux to oVer content NGOs and other national level service userto news stories and features on mental illness groups
Provide and evaluate media watch response units to Statutory funding for NGOs to provide mediapress for balanced coverage watch teams
Share between countries the experience of disability Legislators, lawyers, advocates and consumerdiscrimination acts groups
Understand and implement international legal NGOs to communicate legal obligations of allobligations under binding declarations and covenants stakeholders, and health and social care
inspection agencies to audit how far theseobligations are respected in practice
Audit compliance with codes of good practice in Associations of Insurers with Service Userproviding insurance organisations and mental health NGOs
Providing economic incentives rather than disincentives Employment Ministries to introduce new andto disabled people ready to return to work flexible arrangements for disabled people to
work with no risk to their income
Change law to allow people with a history of mental Justice Ministries to amend the law relating toillness to serve on juries with a presumption of jury servicecompetence
8. Action at the European Level
What action is necessary which is best done at the international level? Such contributions, so far removed fromthe everyday lives of people, may be hardly noticeable unless they are very sharply focussed and coherent.Setting international standards for national polices can be one useful intervention. For example the WorldHealth Organisation (WHO) has published standards to guide countries in producing or revising mentalhealth laws (4). This covers advice on:
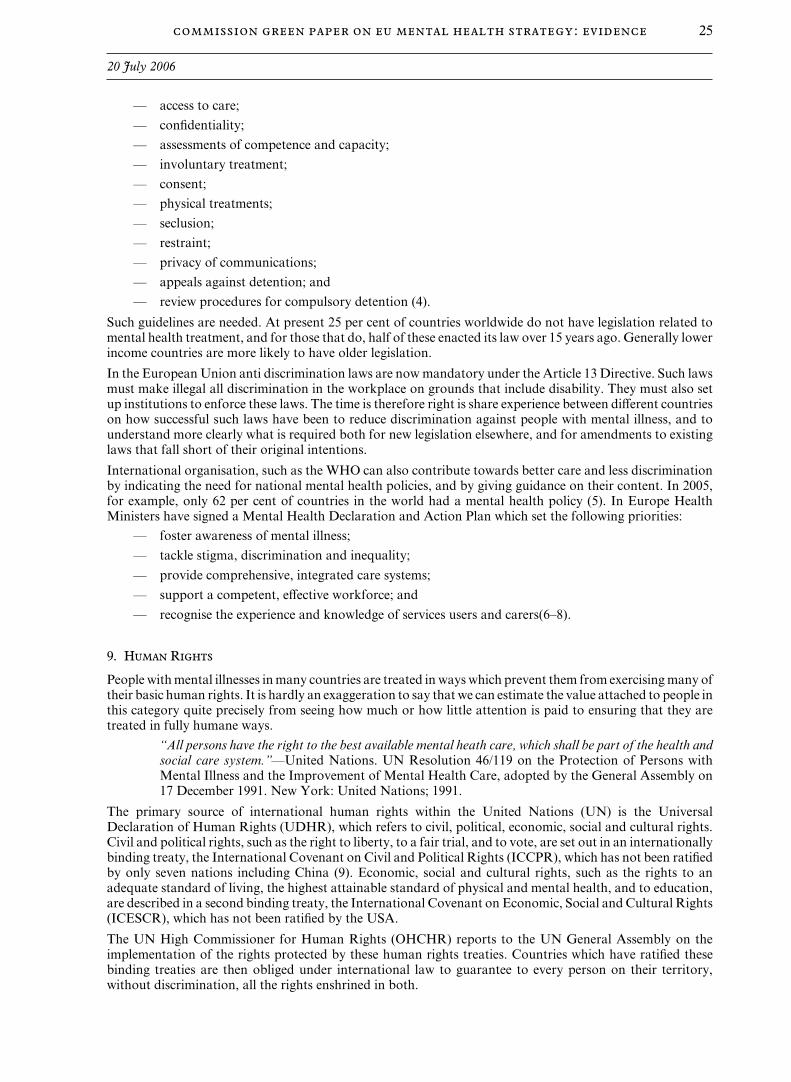
3564222004 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
25commission green paper on eu mental health strategy: evidence
20 July 2006
— access to care;
— confidentiality;
— assessments of competence and capacity;
— involuntary treatment;
— consent;
— physical treatments;
— seclusion;
— restraint;
— privacy of communications;
— appeals against detention; and
— review procedures for compulsory detention (4).
Such guidelines are needed. At present 25 per cent of countries worldwide do not have legislation related tomental health treatment, and for those that do, half of these enacted its law over 15 years ago. Generally lowerincome countries are more likely to have older legislation.
In the European Union anti discrimination laws are now mandatory under the Article 13 Directive. Such lawsmust make illegal all discrimination in the workplace on grounds that include disability. They must also setup institutions to enforce these laws. The time is therefore right is share experience between diVerent countrieson how successful such laws have been to reduce discrimination against people with mental illness, and tounderstand more clearly what is required both for new legislation elsewhere, and for amendments to existinglaws that fall short of their original intentions.
International organisation, such as the WHO can also contribute towards better care and less discriminationby indicating the need for national mental health policies, and by giving guidance on their content. In 2005,for example, only 62 per cent of countries in the world had a mental health policy (5). In Europe HealthMinisters have signed a Mental Health Declaration and Action Plan which set the following priorities:
— foster awareness of mental illness;
— tackle stigma, discrimination and inequality;
— provide comprehensive, integrated care systems;
— support a competent, eVective workforce; and
— recognise the experience and knowledge of services users and carers(6–8).
9. Human Rights
People with mental illnesses in many countries are treated in ways which prevent them from exercising many oftheir basic human rights. It is hardly an exaggeration to say that we can estimate the value attached to people inthis category quite precisely from seeing how much or how little attention is paid to ensuring that they aretreated in fully humane ways.
“All persons have the right to the best available mental heath care, which shall be part of the health andsocial care system.”—United Nations. UN Resolution 46/119 on the Protection of Persons withMental Illness and the Improvement of Mental Health Care, adopted by the General Assembly on17 December 1991. New York: United Nations; 1991.
The primary source of international human rights within the United Nations (UN) is the UniversalDeclaration of Human Rights (UDHR), which refers to civil, political, economic, social and cultural rights.Civil and political rights, such as the right to liberty, to a fair trial, and to vote, are set out in an internationallybinding treaty, the International Covenant on Civil and Political Rights (ICCPR), which has not been ratifiedby only seven nations including China (9). Economic, social and cultural rights, such as the rights to anadequate standard of living, the highest attainable standard of physical and mental health, and to education,are described in a second binding treaty, the International Covenant on Economic, Social and Cultural Rights(ICESCR), which has not been ratified by the USA.
The UN High Commissioner for Human Rights (OHCHR) reports to the UN General Assembly on theimplementation of the rights protected by these human rights treaties. Countries which have ratified thesebinding treaties are then obliged under international law to guarantee to every person on their territory,without discrimination, all the rights enshrined in both.

3564222004 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
26 commission green paper on eu mental health strategy: evidence
20 July 2006
The body which monitors implementation of the ICESCR is the Committee on Economic, Social and CulturalRights (CESCR). In a special report explaining how the ECESCR relates specifically to the rights of peoplewith disabilities, the Committee stated:
“The obligation of States parties to the Covenant to promote progressive realisation of the relevantrights to the maximum of their available resources clearly requires Governments to do much more thanmerely abstain from taking measures which might have a negative impact on persons with disabilities.The obligation in the case of such a vulnerable and disadvantaged group is to take positive action toreduce structural disadvantages and to give appropriate preferential treatment to people with disabilitiesin order to achieve the objectives of full participation and equality within society for all persons withdisabilities. This almost invariably means that additional resources will need to be made available forthis purpose and that a wide range of specially tailored measures will be required.”
More specifically in relation to mental illness, the UN Principles for the Protection of Persons with MentalIllness and for the Improvement of Mental Health Care were adopted in 1991, and elaborate the basic rightsand freedoms of people with mental illness that must be secured if states are to be in full compliance with theICESCR. The “The Right to Mental Health” is stated in Article 12 of the ICESCR, which provides the rightof everyone to the “enjoyment of the highest attainable standard of physical and mental health”, and identifiessome of the measures states should take “to achieve the full realisation of this right”.
These “Mental Illness Principles” apply to all people with mental illness, and to all people admitted topsychiatric facilities, whether or not they are diagnosed as having a mental illness. They provide criteria forthe determination of mental illness, protection of confidentiality, standards of care, the rights of people inmental health facilities, and the provision of resources. Mental Illness Principle 1 lays down the basicfoundation upon which nations’ obligations towards people with mental illness are built: that “all persons witha mental illness, or who are being treated as such persons, shall be treated with humanity and respect for theinherent dignity of the human person”, and “shall have the right to exercise all civil, political, economic, socialand cultural rights as recognised in the Universal Declaration of Human Rights, the International Covenanton Economic, Social and Cultural Rights, the International Covenant on Civil and Political Rights and inother relevant instruments”. It also provides that “all persons have the right to the best available mental healthcare”. As the United Nations’ health agency, the World Health Organisation (WHO) gives substance to theUN’s understanding of what is meant by “the best available mental health care” (4;10).
In addition to these agreements, 46 member states of the Council of Europe are bound or guided by a seriesof arrangements (11;12). These include the 1950 European Convention on Human Rights and FundamentalFreedoms (ECHR), and the European Committee for the Prevention of Torture and Inhuman or DegradingTreatment or Punishment (CPT). It is now time for EU nations to recognise and to fully implement theseobligations (13).
Reference List
(1) Pinfold V, Thornicroft G, Huxley P, Farmer P. Active ingredients in anti-stigma programmes in mentalhealth. International Review of Psychiatry 2005;17(2):123–31.
(2) Pinfold V, Huxley P, Thornicroft G, Farmer P, Toulmin H, Graham T. Reducing psychiatric stigma anddiscrimination: evaluating an educational intervention with the police force in England. Soc PsychiatryPsychiatr Epidemiol 2003 June;38(6):337–44.
(3) Pinfold V, Toulmin H, Thornicroft G, Huxley P, Farmer P, Graham T. Reducing psychiatric stigma anddiscrimination: evaluation of educational interventions in UK secondary schools. Br J Psychiatry2003;182:342–6.
(4) World Health Organisation. WHO Resource Book on Mental Health, Human Rights and Legislation.Geneva: World Health Organisation; 2005.
(5) World Health Organisation. Mental Health Atlas 2005. Geneva: World Health Organisation; 2005.
(6) World Health Organisation. Mental Health Declaration for Europe. Copenhagen: World HealthOrganisation; 2005.
(7) World Health Organisation. Mental Health Action Plan for Europe. Copenhagen: World HealthOrganisation; 2005.
(8) Thornicroft G, Rose D. Mental health in Europe. BMJ 2005 March 19;330(7492):613–4.

3564222004 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
27commission green paper on eu mental health strategy: evidence
20 July 2006
(9) United Nations. International Covenant on Civil and Political Rights. Adopted by the UN GeneralAssembly Resolution 2200A (XXI) of 16 December 1966. New York: United Nations(http://www.ohchr.org/english/countries/ratification/4.htm); 1966.
(10) Thornicroft G. Actions Speak Louder: Tackling Discrimination against People with Mental Illness.London: Mental Health Foundation; 2006.
(11) Kingdon D, Jones R, Lonnqvist J. Protecting the human rights of people with mental disorder: newrecommendations emerging from the Council of Europe. Br J Psychiatry 2004 October;185:277–9.
(12) Bindman J, Maingay S, Szmukler G. The Human Rights Act and mental health legislation. Br JPsychiatry 2003 February;182:91–4.
(13) Thornicroft G. Shunned: Discrimination against People with Mental Illness. Oxford: Oxford UniversityPress; 2006.
3564222005 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
28 commission green paper on eu mental health strategy: evidence
THURSDAY 19 OCTOBER 2006
Present Colwyn, L Moser, LDundee, E Neuberger, BGale, B Thomas of Walliswood, B (Chairman)Greengross, B Trefgarne, LHarrison, L
Explanatory memorandum on European Community Document
GREEN PAPER: IMPROVING THE MENTAL HEALTH OF THE POPULATION TOWARDS ASTRATEGY ON MENTAL HEALTH FOR THE EUROPEAN UNION
Submitted by the Department of Health on 31 October 2005
Subject Matter
The stated purpose of the green paper is to launch a debate about “the relevance of mental health for the EU,the need for a strategy at EU level, and its possible priorities.” The paper was adopted by the Commission on14 October.
Key messages
The green paper’s key messages are that:
— mental health is important for key EU policy objectives—eg health, quality of life, economic andsocial welfare;
— there are serious challenges—eg mental ill-health leading to suicide or absenteeism, stigma anddiscrimination; and
— there is a need for a stronger evidence base for action.
The need for an EU strategy
The paper suggests that an EU-wide strategy would add value by:
— creating a framework for exchange and co-operation between member states;
— increasing the coherence of actions in diVerent policy sectors; and
— opening a new platform for involving service users.
Priorities
The paper identifies three basic priorities, and in each case some options for action based on good practiceidentified through EU projects:
— promoting mental health and addressing mental ill health through preventive action;
— promoting the social inclusion of mentally ill or disabled people and protecting their fundamentalrights and dignity; and
— improving information and knowledge on mental health in the EU.
Consultation
The consultation will happen in three main ways:
— by creating a dialogue on mental health with member states;
— by launching an EU platform on mental health (to promote consensus and co-operation across thevarious sectors and stakeholders involved); and
— by developing an interface between mental health policy and research (to overcome gaps in data andensure better-informed policy making).
3564222005 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
29commission green paper on eu mental health strategy: evidence
19 October 2006
The questions that the consultation will focus on are:
— how relevant is mental health for the EU’s strategic policy objectives?
— would an EU mental health strategy add value, and does the green paper identify the rightpriorities? and
— are the initiatives that the paper proposes appropriate and suYcient?
The results of the consultation process may be developed into a Council Recommendation on the promotionof mental health and another on the reduction of depression and suicidal behaviour.
Ministerial Responsibility
The Secretary of State for Health has lead responsibility. Ministers of the Scottish Executive and the WelshAssembly have an interest relating to their responsibilities for health care provision. Whilst the NorthernIreland Assembly and Executive are suspended the Secretary of State for Northern Ireland has these functions.
Legal and Procedural Issues
(i) Legal basis
Some of the proposals for action in the green paper fall under Community competence in accordance with theprovisions of Article 152 of the EC Treaty. The paper recognises that other proposals will be the exclusivecompetence of Member States.
(ii) European Parliament Procedure
None. This is a consultation document only.
(iii) Voting Procedure
None.
(iv) Impact on United Kingdom law
None.
(v) Application to Gibraltar
None.
Policy Implications
This is a consultation document only. However, the paper’s main proposals and priorities are in line withcurrent UK policy: for example on combatting the social exclusion and stigma associated with mental health,and reducing suicide rates.
Financial Implications
None.
Timing
The consultation period was launched formally on 24 October. The consultation period will run until the endof May 2006. Depending on the outcome of the consultation, there may be Council Recommendations and aCommission proposal for an EU mental health strategy by the end of 2006.
Minister for Health Services,Department of Health
3564222006 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
30 commission green paper on eu mental health strategy: evidence
19 October 2006
Memorandum by the Department of Health
EUROPEAN COMMISSION GREEN PAPER—“IMPROVING THE MENTAL HEALTH OF THEPOPULATION: TOWARDS A STRATEGY ON MENTAL HEALTH FOR THE EUROPEAN UNION”
I am writing further to my letter of 20 December 2005, when I discussed the concerns about the Green Paperthat your Committee had raised and said that I would let you see the Government’s response to theCommission as soon as it was ready.
I have enclosed a copy of the document that we have just sent to the Commission. It represents the views ofthe UK Government, including the devolved administrations. It, together with this letter, also constitutes ourformal written evidence to your Committee’s inquiry into the Green Paper.
I hope the response is reasonably self-explanatory. To summarise, it generally concurs with the Green Paper’sproposals subject to two clear principles:
— that any EU strategy that emerges must serve as a contribution to the Helsinki Declaration’simplementation, not as an alternative to it; and
— that it must accommodate and support Member States’ own local priorities (insofar as they areconsistent with Helsinki and the strategy).
The main extra points it makes are:
— the need for the strategy to address inequalities in mental health—this maintains consistency withthe themes of last year’s UK Presidency of the EU;
— the need for a strategy that integrates health and social care with other policy sectors—for exampleemployment and education—that have a role in promoting mental health and social inclusion; and
— the need for the strategy to be clear about what specific action the EU will take and who will beaccountable for it.
We expect the Commission to consider the outcome of its consultation over the coming months, and that wewill have a proposal for an EU mental health strategy by the end of the year.
Let us know if you need more information. I look forward to discussing the issues with the Committee soon.
THE RESPONSE OF THE UNITED KINGDOM GOVERNMENT31 MAY 2006
Context
1. The UK Government and its devolved administrations welcome the European Commission’s Green Paperand the opportunity to comment.
2. In the UK, health policy is a devolved function for the Scottish Parliament, the National Assembly forWales and the Northern Ireland Assembly. Each of these home nations has therefore developed its ownstrategic approach to mental health. Wales, for example, developed a national strategy in 2001 followed by anational service framework which was revised and republished with an action plan in 2005.
3. This means that we have considered the Green Paper from a position that has made mental health one ofthe top three clinical priorities across the UK for improvement and reform (along with cancer and coronaryheart disease).
4. There are good reasons for giving that level of priority to mental health. For example, in the UK:
— one in every four family doctor consultations is about a mental health problem;
— one in six adults report a neurotic disorder at any one time; and
— over a million of the people out of work and claiming incapacity benefits in England list mental orbehavioural illnesses as their main disability.
5. This situation is far from unique—the Green Paper sets out broadly similar figures for the EU as a whole.
6. Raising the priority of mental health has led to some significant changes in mental health care in the UK.In England alone, planned spending on mental health services has risen by over 25 per cent since 1999, andthere are 50 per cent more psychiatrists and 20 per cent more psychiatric nurses than in 1997.
3564222006 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
31commission green paper on eu mental health strategy: evidence
19 October 2006
7. There are now over 700 new, specialised teams working for mental health outside hospitals in thecommunity. Since the 1990s, we have seen a four-fold increase in the use of modern anti-psychotic medication.The suicide rate in England has fallen to its lowest recorded level. About 75 per cent of mental health patientsrate the care they receive as either good, very good or excellent.
8. So, as the Green Paper says (section 1, page 3), improvement is possible. But while real progress has beenmade, we know that there is much more to do.
9. Social exclusion, discrimination and stigma still add to the suVering of people with mental health problems(and of those close to them). Less than a quarter of adults with long-term mental health problems are in work.They are nearly three times more likely to be in debt, and can struggle for basic requirements of modern lifelike good housing or transport. There are persistent inequalities in mental health and in services, includingthose for black and minority ethnic communities. Over 4,000 people still take their own life each year.
10. We believe that services, quality of life and social inclusion for people experiencing mental ill health canall be improved further. We also believe that the promotion of mental health and well-being now needs toembrace whole communities, and move beyond specialised services for those immediately and directlyaVected.
11. This is why, during the UK Presidency of the EU, Minister of State Rosie Winterton welcomed theCommission’s Green Paper as a potentially valuable contribution to our shared objectives for mental health.Our response sets out our views on how the Green Paper could develop into an EU strategy that supportsimprovements in mental health across Europe.
Consultation
12. Before preparing its response the UK Government invited views from a range of networks representinga diverse selection of governmental and non-governmental agencies, as well as users of mental health servicesand those who care for them. The general public were able to comment through a web site that also publicisedthe Commission’s own consultation exercise. The UK Government is grateful for the contributions it receivedand considered them all before producing this response.
The Questions
13. The Green Paper (pages 13–14) asks for views on three specific questions that we will address directly.
A. How relevant is the mental health of the population for the EU’s strategic policy objectives?
14. The Green Paper (page 3) suggests that the most pertinent of these strategic objectives are:
— putting Europe back on the path to long-term prosperity; and
— sustaining Europe’s commitment to solidarity and social justice; and bringing tangible, practicalbenefits to the quality of life for European citizens.
15. The UK believes that the mental health and well-being of the population are directly relevant to all threeof those objectives.
16. The Green Paper itself explains the relationship clearly, and the relationship in the UK is equally clearfrom facts such as those we set out at the beginning of this document. it has been estimated that the cost ofmental ill-health in the UK is the equivalent of 2 per cent of Gross Domestic Product. Mental illnesssignificantly increases the risk of unemployment, poverty, poor physical health and substance misuse (and viceversa). The injustices of stigma, discrimination and social exclusion are still associated with mental illness andare still blighting the lives of tens of millions of EU citizens and their families.
17. The close relevance of mental health to the EU’s wider strategic objectives has implications for the scopeof an EU mental health strategy. In particular, it demonstrates the need—recognised by the Green Paper—for an integrated strategy that involves agencies beyond the traditionally perceived boundaries of health andsocial care. For example:
— a strategy should explicitly support positive action on employment for people with experience ofmental ill health—both in terms of their employability and the benefits to mental health of the rightkind of work;
3564222006 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
32 commission green paper on eu mental health strategy: evidence
19 October 2006
— encouraging social inclusion means addressing participation and citizenship in every aspect ofcommunity life—including arts, culture, recreation, sport and education; and
— the human rights of those experiencing mental illness may need special attention and protection.
B. Would the development of a comprehensive EU strategy on mental health add value to the existing and envisagedactions and does section 5 [of the Green Paper] propose adequate priorities?
Added value
18. The Green Paper (page 7) suggests that an EU strategy could add value in three ways:
— by creating a framework for exchange and co-operation between Member States;
— by helping to increase the coherence of action in diVerent policy sectors; and
— by opening up a platform for involving stakeholders, including patient and civil societyorganisations into building solutions.
19. The UK agrees that each of these has potential for added value. We have already expressed the view thatan eVective mental health strategy needs to engage policy sectors beyond health (including employment,education, inclusion, regeneration and human rights), and the EU is obviously well placed to facilitate thatengagement at a European level. This leads to another potential benefit of a strategy—to help raise the profileof mental health and improve understanding of the issues across the EU, its directorates and departments, andMember States.
20. We address the ideas of exchange and co-operation, and of a platform for stakeholders, later in thisresponse.
21. Underlying these questions, though, we believe there are two fundamental tests of whether an EU strategywould add value:
— would it complement, rather than duplicate or confuse, existing European activity on mentalhealth—in particular, the World Health Organisation’s Helsinki Declaration? And
— would it be flexible enough to recognise and accommodate Member States’ varying startingpositions, and to support them in addressing their local priorities?
22. The UK is investing significant resources in developing mental health policies and services that matchthe ambitions of the WHO action plan for mental health in Europe, agreed by Ministers at Helsinki in January2005. The action plan’s priorities overlap with those that the Green Paper suggests for an EU strategy,including their focus on:
— promotion of good mental health and the prevention of mental ill-health;
— tackling stigma and discrimination; and
— establishing good mental health information.
23. An EU strategy must make sure that this overlap does not result in duplication of eVort and confusionover roles and responsibilities, but instead builds eYciency, co-ordination and co-operation around a sharedset of objectives.
24. We see no conflict here with the Green Paper’s expressed intentions. We welcome the Green Paper’sdescription of itself as a contribution to the implementation of the WHO action plan (section 1, page 3). Thisis also how we believe an EU strategy should be positioned—as a strategy for the practical support that theEU can give to the Helsinki Declaration.
25. To add real value, an EU strategy should oVer support to all Member States as they work towards localobjectives that are consistent with the strategy (and the WHO plan), even though the choice of priorities, thepace of progress and the resources available for the work may vary between Member States.
26. Again, we see no conflict with the ambitions of the Green Paper. As it says (page 5), Member States areexclusively competent for the organisation of health services, and Community action should complementnational policies on health. We also share the Green Paper’s recognition (page 7) that Member States’ diversitymakes it impossible to draw simple conclusions or propose uniform solutions.
3564222006 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
33commission green paper on eu mental health strategy: evidence
19 October 2006
Priorities
27. The Green Paper (page 8) proposes four priorities for an EU strategy:
— to promote the mental health of all;
— to address mental ill health through preventive action;
— to improve the quality of life of people with mental ill health or disability through social inclusionand the protection of their rights and dignity; and
— to develop a mental health information, research and knowledge system for the EU.
28. These priorities are suYciently broadly defined to allow for local variations in emphasis. As we havenoted, the priorities are also among those of the Helsinki action plan, to which the UK and other MemberStates are already committed. We believe that confirming unity of purpose between the WHO and the EU inthis way is helpful, but that identifying additional—or competing—priorities in an EU strategy would becounter-productive.
29. The UK has agreed to assist the WHO European OYce by developing programmes of European worklinked to the action plan. The focus for these programmes will be on:
— cross government action to tackle inequalities and reduce social exclusion;
— addressing stigma and discrimination;
— the development and implementation of new service models for community mental health; and
— mental health care research.
30. The emphasis on tackling inequalities and social exclusion is one in particular that we would like an EUstrategy to support. The Green Paper acknowledges the issues, and further action to address them would beentirely consistent with the stated priorities of both the Green Paper and the WHO action plan.
C. Are the initiatives proposed in sections 6 and 7 [of the Green Paper] appropriate to support the co-ordination ofmental health into health and non-health policies and stakeholder action, and to better liaise research and policy onmental health aspects?
31. The initiatives that the Green Paper (pages 8–13) proposes are:
— promoting mental health and addressing mental ill health through preventive action;
— promoting the social inclusion of mentally ill or disabled people and protecting their fundamentalrights and dignity;
— improving information and knowledge on mental health in the EU;
— creating a dialogue with Member States on mental health;
— launching an EU Platform on mental health; and
— developing an interface between policy and research on mental health.
32. To a large extent these proposals arise naturally from the Green Paper’s priorities, which we have alreadyendorsed. We believe that it is whether, and how, the initiatives are delivered as part of an EU strategy thatwill determine how much value the strategy adds in practice.
33. Mental health promotion, for example, should recognise the strong relationships between mental health,physical health and general well-being. EVective promotion and prevention should take place in a variety ofsettings, including communities, schools, universities and workplaces, as well as across the stages of life fromchildhood to old age. A strategy must also take care not to widen inequalities by inadvertently favouring ordiscriminating against any sector of society, regardless of factors such as ethnic origin, age or socio-economic status.
34. Promoting social inclusion eVectively would provide another opportunity to break down the traditionalboundaries between governmental agencies in policy sectors such as housing, employment, education,recreation and income.
35. The EU Platform on mental health could avoid any risk of a strategy being seen as a bureaucratic oracademic exercise by keeping it firmly rooted in the needs and aspirations of real people (and comprehensibleto them). It could also have an important part to play in disseminating ideas and information, and in helpingto understand the diVerent cultures and sensitivities of stakeholders and citizens across the EU.

3564222007 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
34 commission green paper on eu mental health strategy: evidence
19 October 2006
36. Successfully widening the availability of high quality information and knowledge, and developing theinterface between policy and mental health, would provide a solid foundation for the other initiatives and areamong the most important benefits that an EU strategy could oVer. Shared evidence and expertise on issueslike the mental health of migrants, for example, is likely to become increasingly valuable.
37. There is a need for more research in these areas, and we welcome the inclusion of mental health in theCommission’s proposals for Framework Programme 7. Larger scale studies across the EU would be especiallywelcome as a means of developing a more robust evidence base for these relatively underdeveloped areas ofknowledge, and larger routine datasets across Member States would be valuable to regular research and themonitoring of mental health.
Conclusion
38. The UK welcomes the Green Paper as the foundation of an EU mental health strategy that:
— directly supports implementation of the WHO Helsinki action plan and rationalises the relationshipbetween the WHO and the EU in the field of mental health; and
— supports Member States in taking action on local priorities that are consistent with the strategy andthe action plan.
39. We believe the development of the strategy presents an opportunity for the EU to adopt a more integratedapproach to improving mental health. A strategy will add real value if it:
— sets out specific actions, identifies who will be responsible for them and describes clear governancearrangements for the strategy; and
— delivers better co-ordination across relevant policy sectors including EU directorates-general anddepartments in employment, social living and social funds, public health, and education.
40. We look forward to continuing our involvement in the strategy’s development.
May 2006
Examination of Witnesses
Witnesses: Mrs Kathryn Tyson, Programme Director, Mental Health, Ms Susannah Rix, UK NationalCounterpart for Mental Health to WHO, and Mr Jim Fowles, Senior Policy Manager, Mental Health
Programme, Department of Health, examined.
Q73 Chairman: First of all I would like to thank youon behalf of the Sub-Committee for coming today. Itis obviously quite a diYcult inquiry for us coming tothe subject rather new. We have got our headsaround it more or less but I am sure you will be ableto help us to do that. I think, Mrs Tyson, you want tomake a statement later on but if you do not mind I amgoing to go through a few things first which we needto remind ourselves and you of. You have seen thetranscripts, I think. We have had a lot of otherresponses from people who have written to us and wewant to make a timely report and a constructivecontribution to the Commission strategy byconcentrating on desirable, practical andproportionate public policy objectives where the EUcan have a worthwhile role. We are hoping that thismorning you are going to help us get a clearer idea ofwhat the Government thinks the EU strategy can andshould try to achieve and how the Member States andthe Commission can work together with the WHO inachieving those objectives. We also would be glad ofyour views on some of the evidence which we havealready received and to know what issues have beenraised in the Government’s own consultations on the
Green Paper. We hope that towards the end of theinquiry your Minister will be able to come before usand sum up the Government’s position and commenton some of the subsequent evidence that we have tohave. That is where we are, as it were, in the story ofthe inquiry. This meeting is open to the public and, asyou can see, is being recorded for broadcasting orwebcasting and a verbatim transcript will also bemade. That will be published on the parliamentarywebsite and in an annex to the inquiry report. Shortlyafter this meeting you will receive a copy of that sothat if you wish to correct it because you have beenmisrepresented in some way or something does notsound quite like what you really wanted to say orthere are accuracy problems please advise us of thatas soon as possible and those corrections will betaken on board before publication. If we get to theend of our time and, as quite often happens, there isextra information that you would have wished topass on to us, we would be very happy for you tosubmit supplementary evidence in writing. I thinkyou have in front of you a note of members’ interests.With no further ado please would you make your firststatement?

3564222007 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
35commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
Mrs Tyson: Shall I start, my Lord Chairman, byintroducing my colleagues and myself?
Q74 Chairman: Please do.Mrs Tyson: I am Kathryn Tyson, as you can see, andI am Programme Director for Mental Health in theDepartment of Health, which means that all mattersto do with the mental health of working age adults,and by extension and co-operation with other partsof the department, all other adults beyond workingage, are part of my concerns. Jim Fowles is a memberof my team. He is Senior Policy Manager and he has aparticular interest in matters about equalities, humanrights and European and international aspects.Susannah Rix is our UK counterpart to the WorldHealth Organisation on mental health issues. As yousee, we come from the mental health policy area and,with the possible exception of Susannah, ourunderstanding of the intricacies of Europeaninstruments and so forth is perhaps not all that wewould need to be able to help you through everythingyou want to say, but we can, of course, find things outand come back to you and we will do our best toanswer your questions. On the EU strategy, I havesome very brief opening remarks. Of course, thestrategy itself has not been drafted, much lesspublished, so we are still working on the basis of theGreen Paper and what we know of the consultationresponses, including our own Government response,but we have welcomed the Green Paper and what itsuggests it will set out to do in terms of being a helpfuladdition to the ways in which Member States canhelp take forward implementation of their particularaspects of the Helsinki Declaration. That is the waywe have approached the Green Paper. That is all Iwanted to say by way of opening.
Q75 Chairman: Thank you for that. I am going toexplore that a little further. Obviously, in letters andin the response to the Green Paper there were severalprinciples and approaches which have been laiddown about the EU mental health strategy, it shouldbe a contribution to the Helsinki Declaration’simplementation and not an alternative, it shouldaccommodate and support Member States’ ownpriorities, it should not duplicate or confuse existingEuropean activity and particularly it should act inaccordance with and not in order to confuse theHelsinki approach. It should be flexible enough torecognise and accommodate Member States andtheir diVerent starting positions in relation to thiskind of topic. Following the consultations of theDepartment does the Government believe that theseprinciples and tests can be met? Are they satisfied,broadly speaking, that the new approach, the mentalhealth strategy, is going to go along the lines that theywould like to see in this context and can you see
anything which might go wrong? Are there anypitfalls which might lie ahead?Mrs Tyson: Yes, we think that the principles and testscan be met. From what we have observed of theprocesses and the degree of co-operative consultationthat has gone on in the period towards the drawingup of the Green Paper itself and following thatthroughout the whole consultation we do see that asgiving some indication that that is the way things willwork out. As you probably know, the HelsinkiDeclaration and the Green Paper, by the quirks ofthese things, did end up being published at roundabout the same time, and in fact they cross-refer toone another in the ways in which we set out that wewould wish to see that they did. Our observations ofthe way that oYcials involved in both work streamshave worked together show that there has been lotsof cross-membership, cross-attendance of eachother’s meetings, significant involvement in eachother’s discussions and a significant eVort to ensurethat the one feeds into and supports the other. We dofeel that the tests and principles could well be met bythe strategy that arises, and I suppose in a small waythis is mirrored by the approach that we take here. Itis the same team that deals with mental healthmatters for the Helsinki Declaration and for thestrategies in the Green Paper, so we are not sayingone thing to one set of people and another thing toanother set; we are approaching it as if that is thecase. Of course, largely our approach to theimprovement of mental health services is what is setout in our National Health Service Frameworkpublished in 1999 and we continually look to that tosee in what ways it expresses our intentions to fulfilthe Helsinki Declaration and we will use it again asour central platform for the ways in which we wouldpursue things set out in the EU strategy. With regardto possible pitfalls, I suppose that, like anyconsultation of this kind, it gives a lot of people theopportunity to dust oV hobby-horses and raise issuesagain that we perhaps rather thought had been put tobed. We clearly will deal with these in the usual way.We will give them due consideration and take fromthem the things that we need to apply to the way inwhich we seek to implement Helsinki and anyrelevant parts of an EU strategy, and, of course, theEU oYcials will want to strike their own balance asthey continue to conduct the analysis of theconsultation responses that they are nowundertaking. They will need to take that intoconsideration.
Q76 Chairman: Thank you. Mr Scheftlein of theEuropean Commission came before us and I must saygave us very careful evidence in which he emphasisedon more than one occasion the way in which what theEuropean Union was doing was intended to fit inwith the WHO strategies. I do not think he was in any

3564222007 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
36 commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
doubt as to where the positioning of his paper was. Ithink he was to a large extent the author of the paper.On the other hand there are some other diYculties.Health is obviously what the WHO does. TheCommission has a much wider remit and can bringtogether several directorates at the same time. WHOcovers 52 countries with a small secretariat andrelatively small resources, mainly focused, of course,on deprived countries outside the European Union,or the rest of Europe as well for that matter. Are youconfident that despite everyone wanting this tohappen these three diVerent levels—the WHO, theEuropean Union and the Member States—can find amodus operandi which will really bring added value toall the things that you want it to? It is a moremechanical question, if you like, rather than aphilosophical question.Ms Rix: Our understanding of the correspondingroles of the WHO and the European Commission isthat WHO, which is the UN agency with theresponsibility for health, tends to have more of a rolein advising Member States on matters of healthservices and treatment and providing technicalguidance, gathering information and servicesresources. They published a global atlas of mentalhealth resources around the world, for example. Formental health the European Commission tends to bemore focused around population and public healthmatters and, as you pointed out, has the advantage ofhaving a wider number of directorates withresponsibilities for other areas which are alsorelevant to this broader remit. Our experience so faris that the European oYce of WHO and theEuropean Commission and Member States haveworked together very positively, harmoniously andeVectively. There has been positive two-waycommunication both within the consultationmeetings but also outside those meetings. It has alsobeen our experience that where representatives fromWHO’s European oYce and from the EuropeanCommission have been at the same event or meetingthey have both been able to make positive andcomplementary contributions to the discussions.Regarding the relationship with Member States,WHO Europe has developed this system of havingnational counterparts who are able to represent andliaise both between individual Member States andalso with WHO on specific things, and mental healthis one. It seems that on the whole it has been thenational counterpart who has also representedindividual Member States at the consultationmeetings with the European commission, so this is agroup of people who have got to know each otherquite well and there are good active workingrelationships. As Kathryn Tyson says, within theDepartment of Health there is also taken a veryconsistent and common approach to working in bothorganisations, the European Commission and WHO
Europe, with common representation at both sets ofmeetings. The other thing to say is that across the 52Member States in what WHO defines as Europe thereis, of course, a wide variety of experiences andstarting places or stages of development for mentalhealth policy and systems. WHO, in taking forwardthe very early stages of the implementation workaround the Helsinki Declaration, has been verysensitive in addressing this issue in how they haveworked with Member States and a good example ofthis would be the last meeting of Europeancounterparts which took place in April this year,where the discussions with Member States werestructured so that participants were divided intogroups and the United Kingdom was part of the firstgroup of 12 Member States who were identified ashaving the most advanced mental health policy andsystems.
Q77 Chairman: That rather suggests that there is arecognition that some European states, if you takethe broad Europe, will have diVerent needs thanother European states. Is that what you were saying,that the groups reflected that, so that you were tryingto get from the WHO perspective the maximumbenefit to all Member States in accordance with whattheir current eVectiveness and competence is in thisfield? Is that the sort of approach that you are taking?Ms Rix: Yes, certainly in terms of the focus thatWHO has had in its relationship to diVerent MemberStates and obviously discussions about theimplications of the Helsinki Declaration in theUnited Kingdom, Holland or France will be ratherdiVerent from perhaps Latvia and Lithuania. Thesorts of issues would be that perhaps for ourselves weare now focusing more on public health issues, moreadvanced issues, whereas maybe in countries ingroups C and D they may be working on more basicissues of de-institutionalisation and human rights.
Q78 Chairman: Does the Council of Europe playany role in this as well?Ms Rix: Less so at the moment. I have to say that itis much harder for us to comment on relations withthe Council of Europe because we have not had anyrecent direct contact with the Council of Europe.
Q79 Lord Trefgarne: May I ask a supplementary toall of that? In the Department’s response two moreprinciples were established. We have talked about theHelsinki accord, where all this stuV is. We have beentalking about the open method of co-ordination andwe look forward to that. Nowhere in this is therereference to the patients. Are they going to derive anybenefit from all of this or is it just going to lead tosome huge new European infrastructure?

3564222007 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
37commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
Mr Fowles: There is a thing at the moment called theEU Platform on Mental Health and that is thechannel or the avenue for people who use mentalhealth services and people who care for those peopleas well as possibly for providers of servicesthemselves. It is their chance to have a say in thestrategies that take shape and in the way they aremanaged and taken forward once it is published.
Q80 Lord Trefgarne: There will be nationalrepresentatives on it. I was going to ask you about theEU platform. Do you see that as an improvement onthe Open Method of Co-ordination and, as I guessfrom what you have just been saying, there will beuser representatives on that platform?Mr Fowles: Yes. The first thing I have to say is thatmy understanding of the Open Method of Co-ordination is very limited but, based on what I doknow, we are not sure that it is directly applicable, orshould be, to the sort of strategy that we areexpecting. The objectives that Member States will beworking towards will be what they are now, whichare those of the Helsinki Declaration and, as Kathrynwas saying, we do not expect an EU strategy tochange that, and the World Health Organisationthemselves are currently considering how they canbest gather in information from Member States toenable them to judge what is happening and whatprogress is being made, so I think there is a risk ofsetting up the sorts of duplicate systems that we weretrying to avoid in our response to the Green Paper.The platform on the other hand does bring togethernon-governmental representatives, I think, who arestakeholders in terms of people from independentsector organisations and service users andprofessionals. That gives the opportunity for adiVerent sort of scrutiny or monitoring of progress,the holding to account of the sort that you weresuggesting is needed in keeping this centred on theneeds of real people rather than turning it into atotally academic discussion between bureaucrats orclinicians.
Q81 Lord Trefgarne: I am right in thinking, am Inot, that the provision of mental health carethroughout the EU at present is very variable and insome cases no doubt pretty poor?Mr Fowles: Yes.
Q82 Lord Trefgarne: Will the end result be a raisingof the standard all round or is that too much tohope for?Mr Fowles: It is not too much to hope for. I doubt ifthe strategy itself will set new standards to be workedtowards that Member States do not already havethrough the Helsinki Declaration or through humanrights legislation or disability legislation, but we hopethat just the very fact that there is an EU strategy will
help to raise the profile of the subject and bring it outfrom the darkness into the light in those places whereit does still remain in the darkness, if you see what Imean.
Q83 Baroness Gale: When the Government talksabout real people and that the platform will be usedto bring in these real people, I am aware, and I amsure everybody else is, that Scotland and Wales willhave their own mental health strategy, but how is thatgoing to work as far as the UK is concerned becauseas I understand it what we are looking at is what isgoing on in England rather than in Wales andScotland? How will all of those people be brought into reflect what has gone on in Wales and Scotland aswell as in England?Mr Fowles: It is true that we all represent the EnglishDepartment of Health but the response that we gaveto the Commission on their Green Paper was a jointagreed UK response and colleagues from Scotlandand Wales have been involved in the build-up to thepublication of the Green Paper and in theconsultation exercise since. I do not know but Isuspect that there are representatives from Scotlandand Wales on the platform now and if there are notthat is something that we can certainly pursue andmake sure the Commission realises that that is a gapthey need to fill.Mrs Tyson: If I may add to that, we do not expect thatEngland, Wales or Scotland will stop doing their ownconsulting and involving of real people, service usersand carers and families as they seek to develop andimplement their own policies but we do see that theplatform may add an extra dimension and an extraencouragement to that, so we fully see the importanceof continuing that involvement through our owncountries’ implementation of service development.
Q84 Lord Moser: My question also in a sense relatesto Open Method of Co-ordination. My particularinterest is in the statistical information base.Obviously, it is one of the roles of the Commission toimprove that. I hope that in the course of our inquirywe will get some understanding of how adequate thestatistics are in the diVerent countries but that is notfor now. Presumably the Statistical OYce inLuxembourg will be responsible together with WHOand I hope not too much duplication will result. Thebasic issue is the Government’s view and MrScheftlein told us that he had no doubt that the OpenMethod of Co-ordination was important and thatindividual Member States would be required tosupport it and go with it. He also indicated that a lessformal process might be just as helpful, so I would beinterested to know what you feel about that. In otherwords, have you any comments on the informationbase in general and the Government’s particularapproach to improving it?

3564222007 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
38 commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
Mrs Tyson: Building on Jim’s remarks earlier, that wedo not have a very great understanding of the OpenMethod of Co-ordination but we can find out somemore, you asked about the state of the informationbase in general. I expect that, just as the state ofmental health care varies across Member States, sothe state of their information about both theperformance of those services and the general state ofmental health of their populations will varyconsiderably. We have something called the mentalhealth minimum data set which you may knowabout. That is a very comprehensive tool. It is notquite as widely implemented and used as we mighthope and there is continuing work to do to roll it outbetter. Where it is fully implemented it has provideda very rich set of data about what services are doing,how they are helping people, how many people andso on. Public health observatories, particularly, Ithink, the one in Yorkshire, the northern one, have alead on mental health public health data, and againprovide a very rich variety of things for us. Just asthere is work continuing for us to do, so there will befor the other Member States and we do think thateven Mr Scheftlein’s less formal means of swappingand comparing data will be helpful for MemberStates to compare where they are at to learn fromeach other’s models of collection of statistics and soforth. I am sorry if that is a bit of a waZy answer. Iam very happy to write if there is some more detailthat you would like.
Q85 Lord Moser: No, just two quicksupplementaries. So far Brussels, or ratherLuxembourg for statistics, seems happy with ourstatistics.Mr Fowles: Yes.
Q86 Lord Moser: I know from my days that they arepretty comprehensive, are they not?Mr Fowles: Yes, they are.
Q87 Lord Moser: Here are you looking mainly toONS or to the Department of Health for mentalhealth data? That is not very relevant but it isinteresting to me.Mrs Tyson: There are periodic surveys for theprevalence of mental illness and those are, as Iunderstand it, run for us by the ONS, but mostly thestatistical base that we use is the Department ofHealth’s and the NHS’s own.Mr Fowles: That, for example, gives us plenty ofinformation to tell us whether we are meeting theWorld Health Organisation’s Helsinki Declaration.Whatever questions they choose to ask us about thatwe will certainly have the information to be able toanswer them.
Q88 Earl of Dundee: Turning to promotion andprevention, might these really be best done byMember States themselves at national, local andsectoral level rather than by the Commission?Mrs Tyson: We do clearly believe that we should becarrying out our own mental health promotion andprevention activities to tackle the particular range ofproblems and causes in the particular context of thiscountry, and clearly other Member States will feel thesame, that they know their local situation best andcan best carry it forward. Having said that, they arenot straightforward activities and their eVectivenessis diYcult to track, by which I mean that it is diYcultto know if you have prevented something, if you arebeing successful in your promotion activities. We aretherefore very alive to the possibility that input froman EU strategy might help with our own nationalpromotion and prevention agenda. This might bethrough further raising of the profile of mental healthissues and the actions that people can take in theireveryday lives to preserve and promote their ownmental health. It might be through the sharing ofgood practice and we have got an example. There is avery helpful publication that accompanied the GreenPaper called Country Stories and that had acollection of, as it says on the tin, stories aboutsuccessful activities around promoting mental healthfrom diVerent Member States. That sort of thing ishelpful. It can be a bit of a long and lonely hard slogin the world of mental health promotion andprevention precisely because it is diYcult to point tosomething and say, “Look what we have achieved”.A lack of something is diYcult to evidence, and soevidence that you are not alone, that there are otherpeople doing this and finding evidence that certainthings succeed better than others in certain contextsthat may be similar across diVerent states, is alwaysuseful.
Q89 Earl of Dundee: So you would like to see a jointeVort, would you, between the Commission andMember States?Mrs Tyson: I would like to see whatever the strategysays supporting the idea that there is a Member State-specific lead to these activities because the contextand the particular state of aVairs with the MemberStates’ populations are unique but I would like to seemore of the sharing of things that have workedbetween Member States and more sharing ofevidence about prevalence and what we know aboutthe causes and the possible prevention of thosethings.
Q90 Earl of Dundee: These diVerentials are reallyrather obvious. One would not expect the MemberStates to be party to something where theCommission rode roughshod over that. Would youagree?
3564222007 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
39commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
Mrs Tyson: Indeed, yes.
Q91 Earl of Dundee: So it will fall into place on itsown and that will be satisfactory?Mrs Tyson: If that was the case I think we would notneed to be paying the attention that we are, but weare. We do not perceive it as an imminent large threatbut we will be looking in our support for ministersand how they react to this to see that that is preciselyhow this fits in.
Q92 Baroness Greengross: It is extremely interestingto hear about the platform and the close workingrelationships at diVerent levels but, perhapsparticularly in the area that Mr Fowles covers, legalinstruments legislation can do an enormous amountand if we are to have a lasting eVect in these verydiYcult areas is there a need for some legalinstruments or at least regulations and, if so, whatsort of thing do you envisage?Mrs Tyson: We have a bit of diYculty with thisquestion. We do not think that the strategy, when itcomes, will be the sort of thing that ends up beingenacted through legal instruments at all. We just donot think it is that kind of thing. I believe there issomething called a Council recommendation which isa sort of one-star “It would be a jolly good idea if youdid this, chaps”, and we think that there might besome areas where that sort of thing is developed.Mr Fowles: The Green Paper itself says that it isdiYcult to come up with a one-size-fits-all solutionand, as I understand it, legislation would be anattempt at the one-size-fits-all solution that we do notthink would work.
Q93 Baroness Greengross: But you will use theHuman Rights Convention and so on and thelegislation there to implement whatever isrecommended, will you?Mrs Tyson: Indeed, and a country’s own mentalhealth legislation where it exists.
Q94 Lord Colwyn: I want to move on to attitudes tomental health. I am sure that you would agree thatmany people with mental health problems also havea range of other health conditions and care needs,and the media are widely to blame, I think, forimplying a link between violence and mental healthconditions which I imagine probably does lead tosome form of discrimination. We are aware of theDepartment’s five-year shift programme to tacklestigma and discrimination. Can you say whether thisEU Mental Health Strategy is going to be utilised andwill do any more to overcome a change in attitudes tomental health, and also could it cover the problemsfaced by the learning disabled?
Mrs Tyson: My answer to this is going to be verysimilar to my answer to the question about mentalhealth promotion and prevention in terms ofdescribing what we think the contribution of any newstrategy will be. It is about further raising the profileand the more that can be done to give a high publicprofile to the ways in which people who have suVeredor are suVering some form of mental health problem,the diYculties that they have even when they arerecovered, picking up the pieces of their lives andregaining employment, fitting back into theircommunities and where this is ascribed todiscriminatory attitudes through the media, byemployers and in people’s own communities then Ithink the more fuel that can be added to that fire thebetter and so I would welcome what an EU strategyhad to say about this as a significant barrier to peopleregaining the running of their normal lives. I wouldsay again that tackling stigma and discrimination,like prevention and promotion, is a very diYcultthing to do, so again all the help and all the learningthat we can get (and I am aware that there are othercountries that have tried diVerent approaches andhave had diVering degrees of success), anyinformation sharing, good practice sharing, platformand facilitation that we can have through the EUStrategy and in other places will be extremelywelcome. There is a small and growing body ofexpertise on what works, but it does need nurturingand helping by contacts. It is also clear that this is notsomething that the health sector can do on its own.You will know that there is a Government strategycalled Health, Work and Wellbeing which bringstogether the Department for Work and Pensions forthe benefits end of things, the Health and SafetyExecutive for support to employees in the workplace,and the Department of Health. Ministers alsolaunched the Action on Stigma campaign on WorldMental Health Day last week, which again seeks toengage major employers, starting with NHSemployers, in helping to tackle this together.
Q95 Chairman: That was what we thought, did wenot?Mrs Tyson: We should get our own house in orderfirst!
Q96 Chairman: Several minds are thinking alike onthat one!Mrs Tyson: Looking wider, we have a national socialinclusion programme as part of the mental healthprogramme and that is based on the work of theSocial Exclusion Unit in 2003. It involves folk from alot of government departments and delivery agencies,local government, housing, DWP again, the HomeOYce around homeless people, oVenders, asylumseekers and so forth. The EU does work in this wayand we talked earlier about it being a cross-sectoral

3564222007 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
40 commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
organisation, and so it can, for instance, verypowerfully bring their employment spokesperson tothings that look at first sight to be a health event and,both through encouraging by example and throughsimply the knock-on eVect of, “Oh, the employmentspokesperson is there; the employment people hadbetter come and join the discussion”, can be quitepowerful in helping that sort of cross-sectoral eVort. Ihave not talked about your learning disability point.When we think about the practical things, thestrategies that might be employed to tackle stigmaand discrimination, those might well look verysimilar for whatever group of people it is that is beingstigmatised and discriminated against, but I do thinkit probably is not fair to lump together with alearning disability or other sorts of disability a groupof people with mental health problems because Ithink their particular concerns and some of thespecific ways in which they experience diYculties inintegrating into communities and taking upemployment again are suYciently diVerent andindividual that they need a separate approach. Thereis practical use in making sure that lots of work doesnot go into reinventing the same sorts of strategiesthat are at a process level but we must be alive to thediVerent concerns of diVerent groups of people.
Q97 Lord Colwyn: I must say I am attracted by theview of professionals being available in places likechurches or council leisure centres, libraries, etcetera, and I am sure you probably agree with that.Anyhow, the two of you agree that the strategy willwork, are you?Mrs Tyson: Absolutely, yes.
Q98 Chairman: One of the things which alwaysconcerns me is that employers do not seem to see thevalue of early approaches to people who areobviously having health problems of any kind. If youhave trained somebody to do whatever job it is youwould have thought that you would want to noticestraightaway if there was something wrong so thatyou could deal with it with the minimum amount ofdisruption in the workplace, leaving out anythingcharitable, nothing to do with that, but the sheerpractical reason for doing that. Do you think thatkind of topic is going to get spoken about in thecontext of this exchange of information and betterpractice and so forth? I am going to leave the nextquestion as it comes into what Lord Harrison wantsto say, but I just wondered whether you felt that thatwas something you could get at through this processwe are just starting now.Mrs Tyson: Through the process with the EUstrategy?
Q99 Chairman: Yes.Mrs Tyson: I think it will, and it will be part of whatwe in the UK, in England, will want to bring to thediscourse. You will know about the work led by LordLayard around identifying relatively cheap andsimple interventions that can help people not only getback to work but also stay there and work through awobbly patch in the first place. On the back of that weare pursuing some demonstration work to show howthat can be done in the context of local services andwith real people rather than on the basis of aneconomic model, and that is indeed showing that partof the enormous benefit of this is that it can be usedto stop people from having to leave work in the firstplace, that you can pick up these early signs, you canoVer help in a non-stigmatising way and people canbe supported and continue working. The Health,Work and Wellbeing Strategy also, throughengagement of the Health and Safety Executive, doesaim to do more for helping people to handleworkplace stress, so we will certainly be bringingthose pieces of evidence to the discourse and wewould expect a number of other Member States to bedoing the same sorts of things.
Q100 Lord Harrison: Good morning to you all. Ithink you have been very frank in saying that you donot demonstrate any great knowledge of finding yourway around the warren of EU business and the waythings are transacted there, but, of course, theCommittee is looking at this issue in terms of whatadded value an EU dimension can bring to this verydiYcult area. Doubtless when you first saw theLisbon Strategy you wondered what that had to dowith mental health but what I am sure you will deeplyunderstand is the aZiction that mental health hasbrought on people who are trying to lead industriousand proper, fulfilling lives, especially in theworkplace. It is that area that I want to go intobecause I wonder whether you share with me thefeeling that this area of the economic consequences ofhaving good practice throughout the EuropeanUnion, of vibrant and innovative mental healthstrategies, can bring in terms of the practical resultsof people being in their jobs and doing those verythings that we want. What is the state of play at themoment in the discussions that you have, say, withbusiness organisations, trade unions and so on togauge what they feel about the importance orotherwise of having good policies for mental health?Do you see that there can be added value by havingthat European dimension so that we help to mobilisethose who might otherwise be left on the sidelinesbecause strategies which may have been successfulelsewhere, which you talked about earlier, are notnecessarily practised in this country or indeed in oneof the other 24 countries of the European Union?

3564222007 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
41commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
Ms Rix: The first thing to say is that the link betweeneconomic prosperity and good mental health hasbeen well made in the report on mental health fromour Social Exclusion Unit. The European UnionCommission asked a number of Member States tomake contributions to the consultation meetings byoVering a presentation on a particular innovation orthe progress that was being made in an individualMember State. The United Kingdom was asked inparticular to contribute to the programme for thesecond of the consultation meetings which was inVienna in March and that was on the theme of socialinclusion. At that meeting myself and anotherrepresentative from the National Institute for MentalHealth in England provided a presentation on thatSocial Exclusion Unit report on mental health. Ourexperience there was and has been at other times thatthat particular specific development in mental healthpolicy in this country has been of interest to otherMember States. Building on that, the Department ofHealth has agreed to develop a special documentwhich will summarise our experience in England onsocial inclusion and the work so far to implement thatreport that can be disseminated through WHOEurope to other Member States as part of the workaround the Helsinki Declaration. Looking at theresponses that the European Commission appears tohave received so far in response to this consultationon the Green Paper, it is interesting that theCommission does not appear to have received anydirect responses from business or industry colleaguesin response to the Green Paper other than perhapsthe pharmaceutical industry, but perhaps thecomment to make about that is whether or not thosewere sought.
Q101 Lord Harrison: The pharmaceutical industrybut not the actual employers which might benefit inthe end—how interesting.Ms Rix: Yes. We have noticed that. Perhaps I canhand over to Jim to talk about our own experience.Mr Fowles: Perhaps our own experience here could behelpful to the strategy in terms of demonstrating thatthis sort of participation can happen and can work.The anti-stigma programme that we talked aboutearlier involves representatives from business as doeswork being taken forward to implement the SocialExclusion Unit’s report on mental health. There isalso a piece of work just beginning that Kathrynmight have referred to earlier between ourselves, theTreasury and the Department for Work and Pensionson improving employment outcomes for people withmental illness, keeping them in work and gettingthem back to work more quickly than can happennow, and organisations like the CBI are deeplyinvolved in formulating that policy. We candemonstrate precedents here domestically that mightbe of interest to a wider European strategy.
Q102 Lord Harrison: So, to put words into yourmouth, you can see how this would be an additionthat could add value to the work that you do here inour country by having this EU dimension and thatthis is a question that we need to satisfy ourselvesabout here?Mr Fowles: Yes. The Green Paper recognises that,and in our conversations with the Commission this isanother gap that they recognise needs to be filled. Weall accept now that we cannot tackle all theseproblems from within the health sector alone. It ismuch bigger than that.Ms Rix: I attended a meeting with somepresentations on tackling social inclusion aroundEurope and at that there were some interestingcontributions on projects from Germany. I thinkthere was one from a large car manufacturingcompany—it might have been VW, it might havebeen BMW, I cannot remember, but it was talkingabout a corporate response on mental health.Obviously, that could have wider benefits if thatcompany has a base in the UK as well.
Q103 Baroness Neuberger: I wish to declare aninterest. I am an adviser to the trustees of theSainsbury Centre for Mental Health, so I have beenfairly involved in some of these issues over the years.I have to say I was slightly disappointed by yourresponse to Baroness Greengross’s question on legalinstruments, particularly when you said that it isalmost like a one-star piece of advice that might comeout as opposed to using the directives or otherinstruments that are there. Our evidence suggests thatthe Green Paper is itself raising expectations of whatcould be done by setting some EU minimumstandards and using obligations under human rightslegislation and disability legislation, if you like. Thereare pretty good examples in this country under thedisability discrimination legislation. I suppose thefirst question I would like to put to you is whether,given what you said before, the Government sees thiskind of use of the human rights legislation, thefundamental rights perspective, possibly a Europeanfundamental rights agency, as a desirable and feasibleoutcome of the strategy because so far you have notsuggested that it does?Mr Fowles: First of all, I do not think there isanything wrong with raising expectations.
Q104 Baroness Neuberger: I presume not!Mr Fowles: It is a necessary precedent to raising thequality of service and care, but I have to echo whatKathryn was saying earlier, which is that we do notexpect this strategy document, when it appears, toadd to the standards that you can argue already existthrough mental health instruments like the HelsinkiDeclaration or human rights legislation or disabilitylegislation. That is not to say that the strategy will not

3564222007 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
42 commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
have a beneficial eVect, as I say, by raisingexpectations and by giving more attention to thesubject, and I think there are some precedents forEurope using structural funds to help improvemental health services but in the context of humanrights rather than mental health or whatever. Recentfunds have been used in Greece that have had theeVect of improving mental health services but takenfrom the approach of human rights rather than ahealth service approach.
Q105 Baroness Neuberger: One of the things thathas been put to us is that in a sense raisingexpectations and using human rights legislation andfundamental rights thinking from that perspectivecould also have an eVect on candidate MemberStates. Is that something as far as you know thatthe Government is keen on and would want topromote?Mrs Tyson: I do not feel informed enough tocomment on that.Baroness Neuberger: That is fine. Thank you.
Q106 Chairman: The scope of the strategy issomething which people who have responded to ushave spoken about at some length and people havesuggested that there should be more emphasis onsuicide reduction or young people or elderly personsor alcohol and drugs and other things. Spiritualneeds, for example, comes in several times. Severalrespondents have urged more involvement of serviceusers, so how might the strategy reconcile theseclaims and set sensible priorities, or is thatsuggestion slightly beside the point of the strategyas it is developing?Mr Fowles: The Green Paper sets four broadpriorities which we express support for in ourresponse and those are to promote good mentalhealth, to prevent mental ill health, to promotesocial inclusion and to develop a better informationsystem, and we feel that that is as detailed as astrategy needs to be, the priorities you were justtalking about, and we can point to activity in everyone of those within the UK and they are all entirelyconsistent with the Helsinki Declaration. Ourapproach is that Member States will have their owndiVering priorities depending on their startingposition and it is the job of a strategy to supportMember States in delivering those priorities insofaras they are consistent with Helsinki and otherexisting practice. We do not think it would behelpful for a strategy to try and set that level ofdetail of objective for Member States.
Q107 Chairman: I think probably we are ratherglad that that was the answer you gave becausewhen we first tackled this paper we were deeplyconcerned that we might get ourselves bogged down
in diVerent professional views as to what the besttreatment was for A or B aspect of mental health.We simply feel ourselves competent to—well, someof us are competent, as you have seen, but most ofus are not competent to deal with that sort ofsubject. Some of us are greatly above our pay grade,not just slightly. The sorts of things you have beentalking about are much more accessible and indeedimportant in terms of the development of theEuropean Union and our scrutiny of what goes onduring that kind of process.Mrs Tyson: If I could just add to the answer, I dothink it might well be helpful if the strategy couldmake it clear that it was concerned about mentalhealth as it manifests itself in all of these sorts ofareas, really reminding Member States that there aremental health issues pervading a lot of other aspectsof the care of their population.
Q108 Chairman: I think that is absolutely right. Itis when we got down to detailed consideration of thecorrect treatment for A or B that we felt we might begetting rather lost in that whole area. Mr Scheftleintold us that he was expecting to publish an analysisof the responses to the Green Paper in the autumnand proposals in the spring. What is theGovernment’s latest information about theCommission’s plans and when do you expect theCommission’s proposals to be published, and howsoon after that do you foresee the need for theCouncil to take a decision because in the end therewill be a Council of Ministers decision? I wonderedif you had an idea of how that programme waslikely to develop.Ms Rix: Our latest information from the EuropeanCommission—I think you heard this from Ju£rgenScheftlein—is that they received a lot moreresponses than they originally anticipated inresponse to the consultation, so it has taken a littlelonger to work through them than they originallyplanned. At the moment they are working throughthose and they are expecting to produce quite ahigh-level analysis of the main themes of emergingconsultation and they think that might be availablein November. Apparently that is currently inproduction and they have had some assistance fromFinland, I think, in producing that. The EuropeanCommission have also told us that they will beconducting something called “an impact assessmentexercise” on the Green Paper and we are told thatthis is a standard procedure which has two aims:first, to consider the eVects of policy proposals intheir economic, social and environmentaldimensions and, secondly, to try to simplify andimprove the regulatory environment. Thisassessment will consider the impact of the policy atboth EU and Member State level and its aims are totry to consider whether there is a need for strategy at

3564222007 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
43commission green paper on eu mental health strategy: evidence
19 October 2006 Mrs Kathryn Tyson, Ms Susannah Rix and Mr Jim Fowles
EU level at all. Following that impact assessmentexercise the Commission say that they still expect topublish their proposals in spring 2007 and youwould expect that then to be considered by theCouncil shortly following that.
Q109 Chairman: Thank you, that was very helpful.Is there anything that you have not said which youcame here wanting to say? I always think I do notwant to miss the thing when someone said, “Youmust tell them this”, or, “You must express a viewon that”.Ms Rix: Maybe one. One of the points that we tookpains to make at the consultation meetings was tourge the involvement of service users and carers inthe meetings. At the consultation meetings I thinkthe most moving part for me was hearing theexperience of an Austrian service user who reallywas able to make people laugh and cry in the spaceof 10 minutes and that was a very consistent theme
that might not be explicit in this document butcertainly was a very live issue at the meetings thatI attended.Chairman: Thank you very much for that, andthank you for being with us. I think you did say youwould send some additional information?
Q110 Lord Harrison: Could I just say on that lastpoint that was made and also the earlier point aboutthe German car manufacturer that it would be veryinteresting to have some of those examples if youhave got them ready to hand just to give us an ideaof what might be done in a practical way.Ms Rix: Okay.Chairman: I think that you felt you might have someadditional information for Lord Moser on theinformation collection issue, so we look forward toseeing that. As I say, thank you very much for beingwith us, all three of you, and assisting us in ourinquiry.

3564222008 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
44 commission green paper on eu mental health strategy: evidence
THURSDAY 2 NOVEMBER 2006
Present Colwyn, L Howarth of Breckland, BDundee, E Moser, LGale, B Neuberger, BGreengross, B Thomas of Walliswood, B (Chairman)Harrison, L Trefgarne, L
Examination of Witness
Witness: Mr John Bowis, a Member of the European Parliament, examined.
Q111 Chairman: First of all we would like to thankyou very much for coming to see us. I am sure you aregoing to make an extremely valuable input into ourconsiderations of this matter. When we first looked atthe paper we were conscious that the potential scopeof what was being considered was extremely wide andwe want to focus our inquiry so that we can producea timely report and make a constructive contributionto the next part of the discussion by concentrating ondesirable, practical and proportionate public policyobjectives where the European Union has anappropriate and valuable role to play. That is the waywe are trying to focus the report. We have beenassisted in our report by Professor Martin Knapp —sitting on my right here—who is Co-Director ofHealth and Social Care at the LSE. We have had oralevidence from the European Commission and fromthe UK Health Department as well as havingreceived quite a lot of written evidence. We havecertainly studied the very comprehensive text of theEuropean Parliament Resolution on Mental Healthin its form as adopted on 6 September. We want toexplore that with you today. Just on a matter of somehousekeeping, this session is open to the public; thereare in fact no members of the public sitting here butit is an open meeting. It will be recorded forbroadcasting or web casting. A verbatim transcriptof your evidence will also be taken and that will bepublished on the parliamentary website and in anannexe to the report that we will eventually write.You have a right to look at that transcript and tocorrect it if you have been misrepresented or for anyother reason. Also, as sometimes we do not manageto get all the points out in these conversations, it isalso an opportunity for you to add anything else youfeel has somehow been overlooked during ourconversation. You should have a note of members’interests before you. The last point I need to make isthat the acoustics in this room are very bad so if youcan speak in the traditional manner, ie with yourhead up, it helps enormously for us to be able to hearwhat you are saying. Perhaps for the recording andfor the script you could state your name and youroYcial title and then you might wish to make anopening statement and if so you are most welcome todo so.
Mr Bowis: Thank you very much, and thank you forinviting me. My name is John Bowis; I am a Memberof the European Parliament representing Londonand I am Rapporteur in the Parliament for the GreenPaper on Mental Health amongst others includingpatient mobility and perhaps other related issues. Iam also spokesman and coordinator for the EPPgroup in the Parliament. Formerly for three years Iwas responsible for mental health in the Departmentof Health and went on, when the electors gave usleave of absence, to work with the World HealthOrganisation on its Nations for Mental Healthcampaign which then led into my work initially withthe Finnish Presidency in 1998 to 1999 and by then Iwas in the Parliament and could take a part from theother side of that particular counter. By way ofintroduction I can be very brief because myintroduction really is my report. I think mental healthis a fascinating area and I do not think that anyonehas got it right yet. I always said when I went into theDepartment of Health that I thought I knew it all;after a year I knew I did not; after two years I knewnobody else did either and that is when I reallystarted to enjoy exploring the options and thesolutions and the problems of mental health, but alsothe opportunities which have been largelyunderplayed to promote mental wellbeing andthereby have a fit community and hence a fiteconomy under the Lisbon Agenda for Europe andso forth. I list here the background; I do not needremind you of the cost of ill health and mentaldisorder to our society and our economies and Iwould just highlight perhaps the five areas of deficitthat I identify: the inadequacy of communityservices; the failure to listen to the service users andtheir carer; the inability or unwillingness of agenciesto work together; serious under-funding; and little, ifany, interest in policy making in the healthpromotion area.
Q112 Chairman: Thank you. That leads straight intothe first question on our list. You have produced anextremely interesting document which has anenormous number of diVerent points in it, all ofwhich are important and interesting points. Is there a

3564222008 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
45commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
sense of prioritising not so much in terms of the pre-considerations but in the actual recommendationsthat the document makes between these variouspoints? Where would you like the focus of theCommission’s eVorts to lie?Mr Bowis: I apologise for the length of the document;if you saw my initial draft it would have been rather aslimmer version but as you probably know Europeanlegislation is like a Christmas tree and everyone pinstheir bits on. We see how much of that we can acceptand it goes through and we hope it will eventually beof use in diVerent ways. I think to me thefundamental issue is how we put the individual centrestage—the individual patient, the individual serviceuser and the individual carer—both in terms ofmanaging his/her own health but also in the planningof services. If we get that right then I think anunderstanding in government of the cost of mentaldisorder and the potential benefits to everyone ofinvesting in good health, would be of benefit. I thinkif you asked me which of the specific areas of actionare the most important I would say defeating stigmais fundamental (we are a long way fromunderstanding either what causes it or how we cureit). The second is suicide, the most unnecessary wasteof lives—very often young lives—and if governmentsand societies understood that that cost in death washigher than for road accidents and higher than forHIV Aids then I think they would see the need totackle what is in eVect an epidemic. Then there are thethree areas which were highlighted in the originalFinnish Presidency in the WHO EU document inJanuary and in this Green Paper which are: how welook after children and avoid some of the behaviouralproblems, the eating disorders and those sorts ofthings; how we look after people at work (that is avery direct responsibility of the European Union,ever since the Treaty of Rome we have hadresponsibility for health and safety in that area butwe have tended to neglect the health side as opposedto the accident prevention side and we have certainlyneglected the mental health side as opposed to thephysical health side); then of course the challenge ofthe ageing population with more people happilyliving longer lives—I have a mother of 101—but bythen you become frail either physically or mentallyand the cost of neuro-degenerative disease isenormous. We spend more now on drugs forParkinson’s Disease than for cancer. It is the bigchallenge for the future, how we prevent some of thedementia and cope with it when it is there.
Q113 Baroness Howarth of Breckland: We have beentold—and some of us know from experience—thatstandards across the European Union varyenormously. We wondered what perspective you hadon those diVerences and how realistic is it for us to tryto reach some common standards across Europe
both in dealing with mental illness and looking atwellbeing, but also if we accept that that may not berealistic in the short term do you think that we couldfind some minimum standards for countries to aimfor?Mr Bowis: I think we can find minimum standards insome areas; we certainly could in terms ofemployment law and we certainly could in terms ofhuman rights and the UN Convention in that area isgoing to be very helpful. Yes, you are right, we arelooking for good practice and that is what Europe israther good at actually. It is finding and sharing goodpractice and then describing that rather thanprescribing it so that there is pressure on MemberStates because their citizens, their media and theirprofessionals know what is possible in other MemberStates and can put pressure to raise standards there.
Q114 Baroness Howarth of Breckland: Do you havea time perspective in terms of what might beachieved?Mr Bowis: I think the time perspective is theCommission’s proposals, which is unusual, that wedo move towards recommendations (which is a typeof legislation). There has been considerablediscussion as to whether that should also take theform of a framework directive rather as we have donefor clinical trials which is, again, finding thatcompendium of good practice and setting it out, a bitlike the Highway Code, again not prescribing thatevery Member State has to do everything in it but justto say that here is good practice. If I think of the goodpractice and the bad practice that I have seen withinEurope I think of some of the work in Italy wherethere has been a tremendous amount of work to closeinstitutions, to move people into the community—aswe have done here since the 60s—perhaps sometimesdoing it too fast before there are adequatecommunity services ready. Nevertheless they haveput the boat out to move in that direction. I have seensome of the worst, of course, in Leros, the GreekIsland, which had to be tackled and closed withGreece moving towards a more humane society. Ihave seen in incoming Member States, in Bulgaria forexample, some of the most appalling conditions inhospitals and particularly in hospitals where they linkto the justice system. However, I have seen goodpractice in many parts of Europe and I think theconcept which the WHO has of the demonstrationsites—I have seen that at work, I have pinched theidea for my Report to say that we should dosomething like that in Europe—is a good way oftelling each other how to tackle a particular problem(Lithuania’s suicide; how to do better than the CzechRepublic’s use of the caged bed and so forth). I thinkthere is a lot there. I do not think any Member Statehas got it all right but some are doing better thanothers.

3564222008 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
46 commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
Q115 Baroness Greengross: The Commission weknow would like to see a Platform to take thisdiscussion forward and I wondered what youthought about that and what you think about theopen method of coordination, and whether you thinkthat is—as the Commission have suggested—terriblyresource intensive? I feel so strongly about this and Ijust want to know what you think would be the bestway forward and then we might argue aboutresources later. How do you think we could bestmake sure this is a really eVective strategy?Mr Bowis: Platforms are flavour of the month in theCommission; they set them up for everything. Themost alarming one they set up was the ObesityPlatform (we just hoped it was strong enough!). Wealso have things called High Level ReflectionGroups; I have been on one of those and it wasamazing. The concept of the Platform I have noproblem with if it is bringing people together. Whatthey do do is bring together not just the policy makersbut the NGOs and the experts (no doubt people likeMartin Knapp would be sitting on a Platformadvising the Commission as well as yourselves). Ifthat is gathering together good practice and if that ismonitoring how diVerent problems are tackled indiVerent Member States, that is fine as long as that isnot the end of the story. It has to be a tool for furtheraction. My preferred further action is the FrameworkDirective with or without the specificrecommendation areas. The open method ofcoordination is, I think, a cop out (if I may use un-Parliamentary language). It is very much linked tothe employment policies of the European Union it isnot something we have used in the health orenvironment areas, and it is a way of sidelining theParliament; Parliament has no role at all in the openmethod of coordination. The Commission has verylittle role apart from surveillance, and it is just anagreement by Member States on the Council to say,“Let’s get round this; we’ll have this open method ofcoordination and we will talk to each other abouthow we are doing things.” I have no problem withthat in itself, but it is seen as being the end of thestory; that is why Parliament does not like themethod. I think if you have an elected Parliament itsrole is to have eYcient scrutiny; its role is to reviseand advise and to push increasingly for areas wherewe can move forward in legislation. I am not happyand I think Parliament feels very strongly on issues ofcomitology and throughout health and environmenton my Committee in the Parliament where I amspokesman we go for co-decision and I think thatworks eVectively. It puts pressure on governmentsand sometimes governments do not like that but thatis what they are there for, to be challenged.
Q116 Earl of Dundee: What do you think about theproposal for a directive on mental health and how isthat likely to be received among Parliamentarymembers?
Mr Bowis: As I say, I think it should be a frameworkdirective; I am not looking for a directive which setstargets and dates and so forth. I think it should laydown reasonable standards of practice and I do citethe Clinical Trials Directive because I think that hasbeen a good way forward. We have been looking todo something like that in the areas of diabetes andcancer screening and so on. I think that would be mypreferred way and it would link to the idea of thedemonstration site where you provide opportunitiesfor Member States to go and look at anotherMember State’s experiment maybe or what they seeas good practice (it could be in looking after childrenand behavioural problems; it could be caring for theelderly; it could be the Czechs looking for a betterway of managing disturbed people than locking theminto a bed with bars on it).
Q117 Earl of Dundee: The focus is on standards andgood practice of course, but can you say how, in yourview, if the directive proposal comes to fruition, itwould add value to results otherwise engendered bythe Platform approach?Mr Bowis: It gives it a little more strength than justsharing good practice. It is like the Highway Code inthat it could be brought in evidence if a Member Stateis being questioned as to its eVectiveness in an area.It is possible that it could be developed so that theindividual citizen would be able to cite it as goodpractice when, for example, looking for access to hisor her rights under the patient mobility laws as theynow stand. At the moment the assumption is that weare talking about physical health when we are talkingabout patients’ rights to go to another Member Stateif they are facing undue delay; there is nothing in thelegislation or the judgments which suggests it shouldnot also apply to mental health delays. That is an areawhere we could raise the standards, but I think Iwould also be looking—and it may be separate fromthe framework directive—for some amendinglegislation to require employers to report each yearon their mental health at work policy and that wouldput pressure on them to look around and to see whatis good practice and to then put it into eVect. Thenthe requirements of international conventions onhuman rights and so on could be added on.
Q118 Earl of Dundee: Could the latter come to beincorporated within the terms of the directive?Mr Bowis: They could do but there is a complicationin that within the European Union you are dealingwith diVerent directorates and diVerent committeesand therefore you tend to have employmentlegislation dealt with by the Employment Committeeand my committee might have an opinion on it ratherthan a comprehensive directive which wouldprobably come to the Environment and HealthCommittee. I am open minded as to whether one

3564222008 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
47commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
should have a single framework directive or abroadish framework directive plus some specificpieces of legislation, particularly on employment andhuman rights.
Q119 Earl of Dundee: Whichever it may be, whatcaveats would you give about its composition?Mr Bowis: The caveat always is that we can go as faras we can or dare within the treaties. I have to say thatI am one who believes that we should always test thatlimit and I do not accept that just because somebodytells me a treaty says we cannot do something weshould not be able to do it. We have to find waysthrough the treaty. To give an example, it isimpossible to do anything about tobacco under thehealth aspect of the treaty so it is done under thesingle market legislation. It is impossible to doanything about giving people patient mobility rightsunder the health criteria, but it is under the rights ofmobility. I am not saying that you should ignore thetreaties; I am saying that sometimes you have to lookat the treaties as a whole. My answer to Lord Dundeeis that we have to be careful all the time that we arenot trespassing on the rights of the Member States.Article 152 of the Treaty gives us a broadrequirement that we should do our best for the healthof the citizens of the European Union but says thatwe should not impinge on the individual State’s rightsto run its own health services and so forth. That hasto be right and has to be how we manage it, but thingsdo move on. I am not one who supported theEuropean Constitution but had that gone throughand our Government was willing to advocate it, thatwould have given a stronger health competence thanis the case now. That may well come back in anyfuture treaty because I suspect there is going to be atreaty rather than a constitution in the future, but Iam getting into dangerous constitutional groundshere.
Q120 Baroness Neuberger: You have obviously beenvery strongly involved in the World HealthOrganisation and in the Helsinki Declaration itself. Isuppose what we are interested in is both your viewpersonally and the view—as much as you can say itis—of MEPs more generally on how the Commissionand WHO Europe can actually work together andadd value separately and jointly in developing thisstrategy and, indeed, you then pushing for newlegislation?Mr Bowis: It is something that I very much support.When I started in 1999 in the Parliament there was astand-oV between WHO Europe and the EU whichwas very jealous of its competencies and so on. Ithought that was ridiculous and because I had hadthat link I tried to use it and bring people together ina variety of ways, and I think it is now accepted. I amalso on the Development Committee and I have
brought WHO into a lot of their discussions as wellas on European health. When it came to my report Ihad a hearing in the European Parliament and one ofthe people I asked to come and speak was MattMuijen who is the Adviser on Mental Health toWHO Europe. We worked with another memberfrom Geneva on their report on violence and healthto see how that has links to mental health. I think thathas to be good and it also extends the scope of ourhorizons in some areas. WHO Europe obviouslycovers the whole of Europe and a bit more and sothey are looking at our new neighbours in a way thatwe cannot, although we have tried to work with themunder the Neighbourhood Policy of the EuropeanUnion. For example, one of the areas I have beenquite involved with personally is the GenevaInitiative—Global Initiative as it is now called—onPsychiatry initially to campaign against the abuse ofpsychiatry in the old Soviet bloc and then to helpthem to introduce reforms in that area. Certainlythree of those countries are now in the EuropeanUnion (the Baltic trio) and others within the newEuropean Union—or just about to be—were verymuch influenced by Soviet psychiatry. That is an areawhere we can work together to overcome that policyon the whole aspect of looking after people who donot fit into society—which is essentially where it wasbeing abused—but then moving on to helping themto de-institutionalise because that is very, very slow inmost of the new Member States. I have been quiteinvolved with Slovenia and even there, where it is avery progressive country—they spend more percapita on health than many current Member Stateswhich is very unusual in that new group of in-comingcountries—there I pushed and pushed for them toclose a castle which was where they tucked theirpatients away, those with severe illness, andeventually they invited me to come to the closureceremony. So we do get there bit by bit.
Q121 Baroness Gale: The European Parliamentresolution “Considers that the gender dimension hasnot been duly taken into account in the Green Paper”and it calls “for this dimension to be systematicallyconsidered.” That is one aspect. Then ProfessorKnapp has said that this issue gets much moreattention than he would have expected but on themental health debate in the UK we are, he says,rightly exercised by ethnicity and mental healthwhich does not get a mention. In what particularways would you expect the MEPs to think about thepriority of distinguishing the separate issues relatingto mental health for women and men? What would betheir views about the relative priority of gender issuesand the mental health issues relating to the diVerentgroups in the population from diVerent ethnicbackgrounds?

3564222008 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
48 commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
Mr Bowis: I would hesitate to challenge the statementthat there is no reference; it is there but I agree it is avery small reference in paragraph 14 where it specifiesethnic and other minority groups. You are right inboth respects. There are bits in here which are notmine, I have to say. I am not ducking the challengebecause it is my report and I accept responsibility forthe whole, but I was under considerable pressurefrom other colleagues to include aspects of the genderdiVerences and in the end I agreed to include some ofthem. I remember a Greek colleague was verystrongly of the belief that we should recognise thediVerence in the brain between men and women. Hesaid that is scientifically proven. I said that I did notwant that.
Q122 Baroness Gale: What did it prove, I wonder?Mr Bowis: There are clearly diVerences such as theobvious one of pre- and post-natal depression whichis a woman’s issue. There is clear evidence, I think,that if we can promote good mental health amongmothers then their children are more likely to growup without some of the diYculties that otherwiseensue. I well recall, when I had responsibility for thehigh security hospitals, coming away very uneasythat we were putting women into this very intensivesecurity and you only had to look at their arms for thecigarette burns and the stabbings to see that self-harm is very much a woman’s issue (not entirely butvery much so). It is not just women, there are men’sdiVerences too. I was speaking recently in theParliament on breast cancer and where 88,000women in Europe die each year from breast cancer,so do a thousand men. Nobody knows that but if youare one of those thousand and you are diagnosed andyou have to go home and try to tell your family thatyou have breast cancer or down to the pub to tell yourmates, that puts enormous pressure on men and Iknow of cases where suicide has been the solution.That is a men’s problem because we do not screenmen, we do not give them the counselling after sucha diagnosis that they need, so there are areas wherewe could do much more to link into mental health toensure that they can cope. That is what mentalwellbeing is all about being able to cope with stress incrises. I think we need to do a lot more.
Q123 Baroness Gale: Could I just follow that up, thediVerence between men and women and theirattitudes to health? We see now that women are quitewilling now to talk quite openly about breast cancerand other cancers whereas men are still very reluctantto discuss these issues because of embarrassment andso on. There is a lot of eVort being put into this now,for men to talk much more openly about it; there area lot of promotions going on to make them comeforward, as it were, and go to their doctors to seekhelp and advice. How do you think this strategy
could be brought about to get rid of this sort ofstigma?Mr Bowis: It is a stigma, and part of that is ensuringthey all have access to the services, that men in thatcase have the same access to the counselling andcancer screening services that women expect to have.I think we have to look for good practice in some ofthe areas aVecting women to see how we can sharethat in all parts of Europe to make a diVerence. Asianwomen have very specific health problems, includingmental health problems, and we need to look atthose. That links into the ethnic minority issue whereI am convinced we need to do a lot more. It may bethat we understand that better in this country than inmost. I remember one of the first initiatives I had inthe Department of Health was to establish andreceive a report on black mental health and the factthat black males in particular were more likely to bediagnosed with schizophrenia and more likely to bein custody or compulsory care and more likely toreceive high dosages of medication and so forth. Thequestion was whether that was because they neededthat or because society was in some way labellingthem as needing that. There was an institutionalisedstigmatisation with or without racial connotationthat we needed to look at. Those are certainly areaswe need to develop and I think that Britain canactually send quite a helpful message to othercountries—perhaps France—which are beginning tolook in these areas. Certainly when I go to speak atEuropean conferences on these sorts of issues I amimpressed at how often it is a British speaker who hascome as the expert.
Q124 Baroness Howarth of Breckland: I would liketo go to the question of definitions, which is a diYcultone. In paragraph nine of the European Resolutionthere is a stress about the need to be careful in the useof various terms: “Mental Ill Health”, “MentalHealth Disorders”, “Severe Mental Illness” and“Personality Disorder”. We have had some concernin our evidence that mental ill health embracing as awide group as 25 per cent of the population might notbe helpful. The concern we have developed is thisrecommendation to include people with learningdisabilities on the basis that in the UK these peopleare treated very diVerently. Indeed, the organisationsthat deal with people with learning disabilities andthe users themselves do not see themselves asmentally ill; this is a condition they have had frombirth, they have come to live with it and many of themlive very successful, mentally ill free lives. We justwondered what views the Parliament members haveabout the need to distinguish elements of mentalhealth strategies specifically applying to the cases of“Mental Ill Health”, “Mental Health Disorders” and“Severe Mental Illness” as well as “PersonalityDisorders” (one that foxes most of us who are

3564222008 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
49commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
working in these fields), and what arguments arethere for including people with learning disabilitieswithin the strategy when the users particularlythemselves may have a very diVerent view?Mr Bowis: You are right, we included both thosereferences. One is what I would call the NormanSartorious school of thought which is that there is alot of muddled thinking over definitions andtherefore we should try to find common definitions,at least throughout Europe, on what is a mentaldisorder and what is a mental illness and so forth. Ithink he would probably put under the disordercategory the diagnosed and treatable conditions asopposed to the ability to cope with stresses andchallenges of life which, if you are not able to cope,then you have an illness but not necessarily adisorder. I think the issue of personality disorder issomething we have wrestled with since the Reidreports—there was a sequence of them—in the early1990s and it was how we should care for people whohave diVerent types of disorder for which it wasquestioned whether there was a treatmentprogramme and therefore within the Mental HealthAct whether you could detain them for treatment andso forth, whether or not there was some perceivedrisk of self-harm or harm to others. That has been adiYcult one. I met a lot of those people again in highsecurity institutions and they are clearly diVerentfrom the average severely ill user of those services. Ithink nobody has yet found the solution as to how wemanage people. Personally I am certain we do notmanage them by just locking them up and if I haveany advice it would be to try to make sure that it is theHealth Department which manages such people andnot the Home OYce, but that is a personal beliefwhich I actually gave in evidence to Lord Carlile’sinvestigation in that area. That is one of the areaswhere we need a lot more research and we can learnfrom each other. The definition of who comes intothat category, perhaps at the back of my mind isagain Soviet psychiatry and meeting psychiatristswho have said to me, “What do you about peoplewith sluggish schizophrenia?” and I said that I didnot think we had a definition called sluggishschizophrenia. They said, “You must have, otherwisewhat do you do with those terrorists in NorthernIreland?” It dawned on me that actually these weresociety’s problems all being labelled in this way andit might well be a personality disorder. I met anotheryoung man in the Ukraine who had absconded fromthe then Red Army with his weapons and so,perfectly correctly should have been taken to courtunder the laws of the land and put in prison to bepunished. But he was not because it was deemed thatno sane person could have absconded from theglorious Red Army so therefore they put him in ahospital, pumped him full of drugs and notsurprisingly he became a zombie and certainly very
ill. There is an argument to say that learningdisability is very diVerent; it has a definition problemtoo. There is a term used in many parts of Europeother than learning disability (mental diYculty insome places; mental handicap it used to be called).My experience of that is that there are diVerentdegrees of disability and very often there is a dualdiagnosis of having that learning disability but alsohaving a mental health problem. If we are going to tryto separate them, then where goes your policy ondual diagnosis and treatment?
Q125 Baroness Howarth of Breckland: It does notnecessarily follow, does it?Mr Bowis: No, but if you ask people like the OpenSociety who deal a lot with the new Member States,they will tell you that it is normal practice for them allto be institutionalised in the same institution and thatin a way we are trying to introduce the more humaneservices, the ability to be cared for in the communityand to give a degree of independence, dignity andrespect which applies to both. I think it is closeenough for us to say, in this Green Paper at least, thatwe think you must not forget that side of this world.
Q126 Baroness Howarth of Breckland: You weresaying that this was much more a Europeanperspective because in the UK I think we have sortedthis pretty well—although not perfectly—andpresumably there is something that one could sayabout what the UK could demonstrate in terms ofhaving clearly separated this issue and how youtherefore treat across the spectrum because there arepeople with learning diYculties who are never goingto be mentally ill.Mr Bowis: Yes, and there are people who arealcoholic or drug addicts who do not need someaspects of the mental health services, but there aremany mentally ill people who do need addictionservices. I do think that is maybe something wherethe UK can help to spread better practice but alwaysremembering that in no case that I am aware of do wereally have that respect for the individuals and thatinvolvement of the individual in his own case and inthe primary services, for example, which applies toboth. We must be very careful that we do not assumethat people with learning disabilities cannot think,cannot express themselves and cannot have a say justas we must make sure that people with severe mentalillness have rights—within limits maybe—to choosehow they live, where they live, have some say in theirtreatment and medication, their therapies and soforth. In all countries in both those areas I think weare woefully behind best practice.
Q127 Lord Colwyn: The Green Paper recognisesthat people with mental ill health or disability or thisdual diagnosis you have just been talking about meet

3564222008 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
50 commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
fear and prejudice and they can suVer discriminationin many ways. This is fuelled by a lack of publicinformation and mis-information in the media.When you said the main problem is stigma and thatcan lead to suicide, how do you see a Europeanstrategy helping existing eVorts of the Member Statesand do you think they really are going to be able towork together bearing in mind the diVerent ways theydeal with this matter?Mr Bowis: I think stigma is an added burden to anillness which is wholly unnecessary and therefore wemust tackle it as a human rights abuse. That impliesboth that we should give people some legalprotections in terms of access to work, to play, toservices and so forth; that is part of it. I think themore we are able to help the public to understandwhat a mental illness really is, I find that the publicare remarkably tolerant of people living in their midstwho have a mental health problem so long as theyknow what that person needs, so long as they knowthat the services are available in the community tocare for those needs and so long as they know who toturn to if there is a crisis. A woman in Battersea oncetold me that she worried rather when the lady wholived underneath her flat went out and left the gascooker burning. I think she had a point when shesaid, “Who do I ring because I think she’s wanderedoV and I can smell burning?” She was not saying,“Take this woman away, lock her up”. She wassaying, “Tell me who I turn to when there’s a crisis.”I think we can do more in that field to reassure thepublic and reassure them that the policy is possible.The media also has a responsibility in this. Every timewe had a problem like one man in the lion’s den atLondon Zoo or the Christopher Clunis case on theLondon Underground and a number other cases likethat, they were reported three times in the press—once when the incident took place, secondly when thecourt report was made and thirdly when the Inquiryconclusions were published—and the public thoughtthere were three of them every time. That is nothelpful. Of course it is right to identify and change theprocedures that have gone wrong and so forth. Ofcourse it is right to make sure we have the careservices in place in the community and of course it isright that we ensure that the agencies work together.It is one of my criticisms that getting doctors andsocial workers to work together is diYcult: “It is notmy responsibility; I am not trained to shareinformation on my patients with X, Y or Z”. Wecould get housing oYcers to be aware that actuallythe housing environment in which you placesomebody who has come out from a period ofhospitalisation is fundamental in helping that personto recover. That is important. The employmentservices, the training services, the social securityservices, all these need to work together which is whyI have often advocated a one-stop-shop so that one
person purchases all the care needs and the providerscan be from a variety of places but if somebody, likea good key worker (beyond just health and socialcare) is looking after the individual, that I thinkwould help to defeat stigma. Then I think we have torecognise that this stigma is in all of us; it is in thehealth service. The attitude “I’m a doctor and I knowbest” (with apologies to doctors present) is there inthe health service and it is certainly there ingovernment and in Parliament who respond to thetabloid headlines leading to letters coming in fromfrightened or worried constituents. We have to domore to undermine that ignorance.
Q128 Lord Colwyn: You are describing a situationhere but is it possible that all Member States canthink along those lines?Mr Bowis: I think so. Italy, as I said, has movedfurther than we have I think in some of these areas.Denmark is a good example of where things aregoing; Slovenia is moving in that direction; Finlandhas some good practice; some of the French practiceis moving that way. I think there is a willingness to tryto overcome this. It was the Greek Presidency whichlaunched an initiative on defeating stigma. I think itis there but it will be much more diYcult when wecome to the Czech Republic, Hungary, Slovakia andthose countries.
Q129 Chairman: Yes, because of the Sovietbackground where, if you oppose the state, you mustbe mad. You had a mental illness if you were, in anysense, an opponent of anything that was run by thestate so you were sent to a mental institution. Then ofcourse you did become mentally ill naturally; you lostyour own sense of reality at that point. I am suremany of them did become mentally disturbed ormentally ill but their sin was that they opposedsomething or disagreed with something or whateverit was. That was a terrible method of punishinganybody; I cannot think of anything worse actually.Mr Bowis: That is absolutely right. That was the statediagnosis and then the state with its authoritariansolutions and that combination was disastrous.
Q130 Lord Harrison: I would like to turn to MentalHealth at Work policies now and I have threequestions. First of all, how would you fit those in withthe Lisbon Agenda which you mentioned right at thebeginning in your opening statement which I regardas an extremely important aspect of this issue?Secondly, could you help the Committee understandhow operating at an EU level would add value otherthan simply Member States doing these things bythemselves? The third question relates to smallbusinesses. You mentioned an interesting idea ofasking employers perhaps to report on their mentalhealth at work policies as a way of reminding them,

3564222008 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
51commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
nudging them and encouraging them to have suchpolicies. I think it was small business and the addedbureaucracy that they might say was the outcome ofmaking that kind of requirement so how can weconstructively help small businesses to engage inpolicies of the kind that you describe that wouldwork and operate at EU level to the benefit ofemployees, employers and ultimately for theEuropean Union and its prosperity andcompetitiveness?Mr Bowis: I think those points and your concerns arecorrect, so is your reference to the Lisbon Agenda. Ithink when we look at our development of policiesfor Africa or wherever we clearly understand that ifyou do not have a healthy people then you cannothave a healthy economy and so health becomes apriority within our development strategy. When itcomes to Europe I think we are learning that againand two of the pillars of Lisbon are a healthy peopleand a healthy environment and both are actuallyingredients in a healthy economy. In fact I would saythey are a prerequisite to it. It avoids some of thecosts, obviously, to the community if you can have ahealthier people and it gives great potential benefitsnot just to the country but to the firms that areinvolved. Just as there is a market out there thatAmerica is beginning to understand that we areahead of the game on having a cleaner environmentin our policy making including our product design, soI think they will come to learn that if we are showingthe way in terms of ensuring we have healthy peopleat work then that will give us something of acompetitive advantage in the market place. I thinkone should do it where possible by encouragementand carrots rather than sticks not least because of thesmall firm issue which is why my specific suggestionwas that we should require firms to report as they doon their attitude to the environment and theirworkforce in general, the community and so forth.Why not on this? I was a judge some months ago inthe national Health and Safety at Work awards andI sat for a day listening to multi-nationals and smallfirms all coming up and telling me how few accidentsthey had had. We were able to cross-question themand say, “That’s fine, we understand the safety bit,now what about the health bit?” A lot of them hadnot really understood what that meant and whensomebody did show that they understood what itmeant I said, “Well, what about the mental healthbit?” and they looked blank. That is why we need toeducate employers and unions to work more in thisdirection. If, for example, you have a non-threatening counselling service within a firm—I amtalking about a bigger firm now—so that if somebodyfeels they have a problem or they have had a problemand are returning to work and they feel a bit of a crisiscoming on, they can go and talk to somebodywithout feeling that it is line management and it is
going to be put on the employee’s record. Then Ithink that helps both to give opportunities to theindividual but also helps the firm to manage the riskthat is there. The same goes if you are a carer. If youare trying to look after somebody maybe withlearning disabilities, maybe with an eating disorder athome and your firm is inflexible, you are going to findit very tough going both at home and at work. If afirm is flexible in terms perhaps of working hours andit makes sure that the person is not havingunnecessary worries on top of the job responsibilities,then you can help the employee be both a betteremployee—and therefore help make the companymore productive—and a better carer at home andtherefore maybe avoiding society having to step inand provide that care. That is the sort of thing I wantto see and if we can require people to publish whattheir policies are then of course somebody—maybethe Health and Safety Executive—should come upwith some guidelines of the sorts of things they mightinclude. I do recall when I was in the Department ofHealth going to some awards for firms that do well inthis area. I remember going down to Marks andSpencer’s headquarters at Baker Street to make theseawards and before I went I asked our permanentsecretary if I could have a look at the Department ofHealth’s Mental Health at Work policy and he said,“I think it is just being finalised”. I do not knowwhether it is there now. Public service has to set anexample and not just require everything to come fromthe private sector. In terms of the small firms it is verydiVerent. Some of the pressures of working in a bigfirm will not be there; you will be more part of a teamand have a better relationship with the managers andso on. However, even in a small firm there should beopportunities for people who have had mental healthproblems to come and work there in an appropriatecapacity, and people who work there and developsuch problems should be looked after, givenappropriate leave and helped back to full workinglife. It is more diYcult and they may need more helpparticularly if it is a key worker whom the firmcannot operate without. We know there arediYculties but I do not think that is an excuse forsaying that small firms should not be included in this,although the requirements on publishing yourcompany policy each year is restricted at the momentto the larger firms rather than the small partnerships.
Q131 Lord Trefgarne: Could I just ask whether youthink that the Human Rights Protection which willbe in place—particularly as it applies to what wewould regard as the less careful nations in thisregard—is adequate? Am I right in thinking that notonly do we have the benefit of the UniversalDeclaration of Human Rights but also the EuropeanConvention on Human Rights?

3564222008 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
52 commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
Mr Bowis: Yes, although the European Conventionon Human Rights is not the responsibility of theEuropean Union, it comes under the Council ofEurope. The Council of Europe, let me stress, has arole in this as well to ensure human rights. The recentUN Declaration on Disabilities is going to be anotherplayer in that, as are the children’s rights and soforth. I think rights are not perfect in any country butthey are even less perfect in the countries you referredto and that is where we have to put pressure onpolitically—and we are doing so—to get them to stopthe practices which we find unacceptable. In terms ofall of us, I think the right of access to services is afundamental right we need to look at. Thinking back,when I was reviewing the Mental Health Act—LouisBlom-Cooper was very much involved in reviewingthat—to see what we should be doing about it and wewere very conscious that our other legislationcovered people in institutions but not in thecommunity. With a service moving increasinglytowards the community we had to make sure that itwas both giving them rights of access but also givingthem rights to be treated or not to be treated in thecommunity in the same sort of way.
Q132 Lord Trefgarne: The particular issue is theright of compulsory detention and compulsorytreatment which we, of course, allow only verysparingly but no doubt in some of the newcountries—as you have said and others have said—ismuch more widespread and we need to look to themto modify their position on that.Mr Bowis: Yes, and in our law we have some very oddconcepts like the constables who have the right tocome and take you to a place for assessment. The oldlegislation was very good. The Mental Health ActCommission was actually seen as a demonstrationsite by the WHO to show other countries how tomanage that aspect of human rights. If you are goingto have more people treated in the community andsome of them treated compulsorily in the communitythat is where the gaps are.
Q133 Lord Moser: I am very interested in theresearch and statistical backup to all you have beentalking about. We have been told that the Parliamenthas talked about the research funding and that thereis a framework in place for it. On the assumption thatyou can get access to that funding is that the kind ofbackup that you feel you really need for your work onmental health, coupled with, are the statistics goodenough?Mr Bowis: Certainly we have established mentalhealth in the FP6 and 7 policy for research under DGresearch’s work in a way that it probably was notbefore. That is good. We also have neurology thereincidentally, in the sense that the two work together.I think in terms of the statistics our worry is that
diVerent Member States calculate in a diVerentnumerical language as well as linguistic and that iswhere we want to see the research done in terms ofhaving comparable data. I think we also—it is notjust the European Union—want to have bettermeasurements of the outcomes, particularly formental health promotion. I believe that we need toinvest more in enabling people to have mentalwellbeing. I cannot prove that to the Treasury. Icannot prove that if you invest in A, B or C you willproduce this outcome and thereby you will makesavings in terms of the cost or free up money whichyou could spend in other areas of health. There arevarious ways of calculating this. We have the DALYs(Disability Adjusted Life Years) and we need theHealthy Life Years (the HELYs or WELLYsperhaps) to be the other side of that coin. I think thatwould be extremely helpful. The other areas really arein the areas we have talked about like personalitydisorder and in suicide prevention and in the stigmathat causes and how you tackle it.
Q134 Lord Moser: In a sense the MEPs and theCommission are in the hands of the EuropeanStatistical OYce in Luxembourg for a lot of this stuV.Everybody knows it has been through a terrible crisis.In a word, has it recovered from that suYciently tohelp you?Mr Bowis: Not noticeably.
Q135 Chairman: I take your point about inter-comparability or at least inter-understandabilityeven if they are not strictly speaking comparable.Could you do some of that statistical work on thebasis of Member States by a collaborative process?Mr Bowis: You could if you could trust them to giveyou an objective picture. One of the eVective tools wedo have is the Health Observatory and thepublications it has on each country in the EU andoutside the EU. I think it needs the objective eyebased, of course, on what governments and healthservices will tell you as to how eVective a policy is.
Q136 Chairman: We are all extremely grateful toyou for giving us your time and also for the veryinteresting light you have shed on several aspects ofthis matter. We do have some questions which Ithink I would have asked Professor Knapp to askhad we had the time. I apologise, we had a diYcultmorning this morning; we started late and of courseas a result we have ended late. What I would behappy to do, if you could accept it, is to askProfessor Knapp to send a letter to you with hisquestions. I think you have actually touched onmost of them so if you think there are still thingsyou might be able to feed into us on that particularlittle set of questions we would be extremelygrateful. I do not want to increase your workload;
3564222008 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
53commission green paper on eu mental health strategy: evidence
2 November 2006 Mr John Bowis
I know that MEPs do actually work. Contrary towhat most people suppose, they do actually workquite hard. You are obviously completely on top ofthis subject so while it is all fresh in your mind youmight be able to dash oV a few answers that that
would be very helpful to us. If it is too much of aburden we will find out another way.Mr Bowis: I am happy to do that.Chairman: On behalf of the Committee I reallywould like to thank you most sincerely for yourevidence today.
3564222009 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
54 commission green paper on eu mental health strategy: evidence
THURSDAY 23 NOVEMBER 2006
Present Dundee, E Morgan of Huyton, BGale, B Neuberger, BGreengross, B Thomas, B (Chairman)Howarth of Breckland, B Trefgarne, L
Memorandum by Mind
Mind’s vision is of a society that promotes and protects good mental health for all, and that treats people withexperience of mental distress fairly, positively, and with respect.
The needs and experiences of people with mental distress drive our work and we make sure their voice is heardby those who influence change.
Our independence gives us the freedom to stand up and speak out on the real issues that aVect daily lives.
We provide information and support, campaign to improve policy and attitudes and, in partnership withindependent local Mind associations, develop local services.
We do all this to make it possible for people who experience mental distress to live full lives, and play theirfull part in society.
Being informed, diversity, partnership, integrity and determination are the values underpinning Mind’s work.
1. Introduction
1.1 Mind welcomes the European Commission’s Green Paper on mental health and the intention to developa strategy on mental health for the European Union.
1.2 We also welcome the opportunity to submit evidence to the House of Lords Committee on the EuropeanUnion for its inquiry into the Green Paper.
1.3 This submission is based on our response to the Green Paper and follows the questions posed in it.
1.4 We would be happy to supply further evidence if required.
2. How Relevant is the Mental Health of the Population for the EU’s Strategic Policy Objectives?
2.1 Mind believes that safeguarding and promoting good mental health is essential to achieving the EU’sstrategic policy objectives. Protecting and promoting the mental health of the European population must bea central component of the EU’s strategy to put Europe back on the path to long-term prosperity.
Economic costs
2.2 As the Green Paper states, mental ill health costs the EU an estimated 3 per cent to 4 per cent of GDP. Inthe UK, the Sainsbury Centre for Mental Health calculates that the total economic and social costs of mentalillness in England alone in 2002–03 were £77 billion. This is broken down into £12.5 billion in health and socialcare costs, £23 billion in output losses and £41.8 billion in human costs, which were calculated by putting amonetary value on the suVering, pain, disability and distress associated with mental ill health (SainsburyCentre 2003).
2.3 This means that only 15 per cent of this total expenditure of £77 billion was actually invested in mentalhealth and related services, while 85 per cent was accounted for by lost productivity and human suVering. Thisis despite the fact that the UK invests a higher proportion of its total health budget in mental health servicesthan any other EU country with the exception of Luxembourg (Annex 6 of the Green Paper).
2.4 To our knowledge the human costs of mental ill health have never been calculated in the way used by theSainsbury Centre at European level—if they were the figure would run to many hundreds of billion Euro. Sucha calculation could be useful in informing the EU’s mental health strategy.
3564222009 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
55commission green paper on eu mental health strategy: evidence
23 November 2006
2.5 We know that properly resourced mental health and social support services can significantly reduce theoverall costs of mental ill health—to individuals, families and society as a whole. Greater investment in serviceprovision and the promotion of mental well-being across the EU could significantly reduce the economic cost,with a substantial positive impact on the economic performance of European countries. But, to achieve this,the development of mental health policy must be sensitive to the needs of people with mental health problems,informed by their voices, evidence based and well-resourced.
Mainstreaming mental well-being
2.6 The EU could play a major role in promoting mental well-being as a mainstream public health concernacross Europe—helping to transform the way that EU countries think about the issue of mental health. Thepress release that accompanies the European Commission’s Green Paper rightly highlights the fact that onein four adults in Europe suVer from mental health problems each year. Annex 2 reprints the findings of a 2005study by Wittchen and Jacobi that concluded that 27.4 per cent of the general EU population aged 18 to 65had been aVected directly by mental disorders in the previous 12 months—nearly 83 million people.
2.7 Depression and anxiety are not marginal to the lives of European citizens. They are part of the day-to-dayreality of their lives. The economic costs are substantial. Nearly 10 per cent of GNP in the UK is lost each yeardue to job-related stress. The Confederation of British Industry (CBI) estimates that 30 times as many workingdays are lost due to mental ill-health as from industrial disputes. Half of all days lost through mental ill healthare due to anxiety and stress conditions (cited in Gray P 2000, see Mind 2005).
Stigma and exclusion
2.8 One of the main barriers to the participation of people with experience of mental health problems in thework place is the stigma that is still associated with mental illness—especially the most serious disorders—andthe lack of flexibility among employers.
2.9 In the UK, the Social Exclusion Unit (SEU)’s report Mental Health and Social Exclusion concluded that“fewer than four in 10 employers would consider employing someone with a history of mental healthproblems, compared to more than six in 10 for physical disability”. It added that “three quarters of employersbelieve that it would be diYcult or impossible to employ someone with schizophrenia, even thoughschizophrenia can be controlled with medication and would not require physical adaptations to the workenvironment (SEU 2004).
2.10 More recently, the Chartered Institute of Personnel and Development (CIPD) found that more than 60per cent of 755 employers surveyed disregarded applications from people with drug or alcohol problems,criminal records, a history of mental health problems or incapacity. Fifty five per cent of respondents saidnothing would persuade them to recruit from these “core jobless” groups (CIPD 2005).
2.11 It is likely that attitudes to mental health are more progressive in the UK than in some other EU countries,where experience of stigma and exclusion may be greater still.
Benefits
2.12 Some people are not able to contribute to economic prosperity because of ill health. They are entitled toa fair share of prosperity through welfare benefits. Condemning people to poverty simply because they are tooill to work is contrary to the basic principles of justice and community of the EU. Interventions for theunemployed to enter the labour market are cost eVective, as the Green Paper states. But care must be takento ensure that people with mental health problems are not coerced into work and that adequate andappropriate support is available to those for whom work is not a realistic option. It is also important to makework more flexible, and increase opportunities for people on welfare benefits to supplement their income byworking part time.
2.13 The World Health Organisation identifies the main protective factors for mental health as empowerment,ethnic minority integration, positive personal interactions, social participation, social responsibility andtolerance, social services and social support and community networks (Annex 7 of the Green Paper). Wherepeople are not able to participate in paid work they can potentially get many of these benefits frominvolvement in voluntary work—as well as from drop-in and social centres, art and music therapy groups,

3564222009 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
56 commission green paper on eu mental health strategy: evidence
23 November 2006
opportunities to participate in outdoor activities and so on. These kinds of projects make a vital contributionto the well-being and social inclusion of people with mental health problems, and it is important that they areproperly funded as part of a comprehensive European mental health strategy.
Marginalisation
2.14 The Social Exclusion Unit report on mental health begins by stating that “adults with mental healthproblems are one of the most excluded groups in society” (SEU 2004). A strategy that seeks to addressdeprivation and marginalisation among people with experience of mental illness is essential to underpin theEU’s wider commitment to solidarity, community and social justice. In order to do so eVectively it must alsoaddress issues of race, gender, disability, age and sexual orientation.
2.15 People in prison should be added to the Green Paper’s list of marginalised groups to be targeted. In theUK, the SEU has estimated that 72 per cent of male prisoners and 70 per cent of female prisoners suVer fromtwo or more mental disorders, respectively 14 and 35 times the level in the general population (SEU 2002). Amore recent report from the Prison Reform Trust found that up to three quarters of men in prison suVeredfrom two or more mental disorders; about one in 10 had a functional psychosis; and an estimated 3,000 to3,700 prisoners at any time have problems suYciently serious as to require urgent transfer to secure NHSfacilities (Rickford and Edgar 2005).
Quality of life
2.16 Good mental health is an essential component of a good quality of life. Conversely, a good quality oflife protects and enhances mental well-being. Impact on mental health must be a central consideration for allinitiatives intended to bring tangible practical benefits to the quality of life of European citizens—as, indeed,it should be in initiatives right across the EU’s policy portfolio.
2.17 The development of an EU strategy on mental health would help to ensure that impact on mental well-being is a central consideration in the development and implementation of all EU policies. A good exampleis the potential link with the European Commission’s environmental action plan and agricultural policies.There is growing empirical evidence that exposure to nature has substantial mental health benefits. Promotingactivities such as walking, fishing and conservation work as part of a mental well-being strategy could alsocontribute to the regeneration of rural economies across the EU.
2.18 In 2004, green “care farms” were developing across Europe, with 500 farms in Norway, 430 in theNetherlands, 300 in Italy, 300 in Germany, 250 in Austria, 140 in Belgium and 15 in Slovenia (Pretty J). Thisis a good example of an area where it would be useful to monitor the development of diVerent approaches tomental health policy across Europe and for the EU to play a role in supporting promising initiatives,evaluating them and disseminating good practice.
2.19 Other areas of policy with clear links to a mental well-being agenda would include sport and exercise,nutrition and health and safety at work.
3. Would the Development of a Comprehensive EU Strategy on Mental Health Add Value to
Existing and Envisaged Actions and Does Section Propose Adequate Priorities?
Whole more than parts
3.1 Historically, EU initiatives on mental health have been restricted to specific initiatives in separate policyareas. Although these initiatives are all welcome, they may not complement and underpin each other aseVectively as they might if they were part of a coherent, strategic whole. For example, investment in initiativesto reduce the stigma of mental illness are unlikely to succeed if governments pursue policies, or indulge inrhetoric, that portrays people in mental distress as a threat to public safety, as is happening at present inEngland and Wales, as exemplified by the debate over how the 1983 Mental Health Act should be reformed.
3.2 If an EU mental health strategy results in a more coherent approach, and increases the prominence given toconsiderations of mental well-being across the policy spectrum—this will add value to existing and envisagedinitiatives.
3564222009 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
57commission green paper on eu mental health strategy: evidence
23 November 2006
A social model
3.3 Mind endorses the priorities set out in section 5. The EU strategy must ensure that due regard is given tothe enormous diversity of the EU population. A recent report by the National Institute for Mental Health forEngland (NIMHE) on race equality and mental health in England concludes that black and minority ethnicpeople are more likely to experience a whole range of problems with mental health services, including problemswith accessing services; lower satisfaction with services; higher rates of transfer to medium and high securefacilities; higher voluntary admission rates to hospital; lower satisfaction with hospital care; longer stays inhospital; higher rates of readmission; more coercive treatments and lower access to talking treatments(NIMHE 2003). Refugees and asylum seekers are exceptionally vulnerable to developing mental healthproblems, both as a result of their past experience and, too often, of their present experiences of abuse,exclusion and marginalisation.
3.4 The consideration of action to prevent mental ill health must be based on a thorough understanding andcomprehensive knowledge of the many diVerent factors that can contribute to mental ill health, as identified bythe World Health Organisation in Annex 7 of the Green Paper: exposure to drugs and alcohol, displacement,isolation and alienation, lack of education, transport and housing, neighbourhood disorganisation, peerrejection, poor social circumstances, poor nutrition, poverty, racial injustice and discrimination, socialdisadvantage, urbanisation, violence and delinquency, war, work stress and unemployment.
3.5 Medical models of mental health are still dominant in many of the EU countries. They obscure the socialcauses and contexts of mental distress. For example, medication—while it can be eVective in controllingsymptoms—is clearly not an answer to lack of housing, racial injustice or excessive work stress. But it isobvious that these factors have a profound psychological eVect.
3.6 Given this “mental well-being” is perhaps a more useful term to use than “mental (ill) health”. The conceptof well-being is something that all European citizens can readily relate to their own lives and experiences. It isnaturally associated with a whole range of life factors and events, not with a narrow set of clinical and forensicinterventions.
Rights and welfare
3.7 The third proposed priority could usefully be broken into two priorities: (i) bringing about social inclusionand (ii) protecting people’s rights and dignity. Although very closely linked—and both essential to improvingquality of life—they are not necessarily synonymous.
3.8 People with mental health problems should have rights to ensure they are not unnecessarily orinappropriately submitted to compulsory treatment. More generally, the World Health Organisation hasstated that “all people with mental disorders have a right to receive high quality treatment and care deliveredthrough responsive health care services. They should be protected against any form of inhuman treatment ordiscrimination” (WHO 2003).
3.9 It is essential that these rights are protected and promoted by the EU, but they will not necessarily have adirect impact on social exclusion. Conversely, eVective policies to combat exclusion will require more thansimply the protection of basic rights. For example, the stigma associated with mental health problems can actas a barrier to employment, even if a formal “right to work” is recognised.
4. Are the Initiatives Proposed in Sections 6 and 7 Appropriate to Support the Coordination
Between the Member States, to Promote the Integration of Mental Health into Health and Non-health Policies and Stakeholder Action, and to Better Liaise Research and Policy on Mental
Health Aspects?
4.1 Mind believes the initiatives are appropriate.
Participation and empowerment
4.2 A proposal by the Commission for a Council Recommendation on the promotion of mental health wouldbe welcome, but would need to include, as well as all the areas covered in the Green Paper, a substantial inputfrom those who have experienced mental distress. In identifying best practice for promoting the socialinclusion of people with mental health problems, the EU strategy should put in place specific, easily accessiblechannels whereby people with experience of mental distress can contribute to the development and
3564222009 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
58 commission green paper on eu mental health strategy: evidence
23 November 2006
implementation of a mental health strategy. The voluntary and community sector should be included as muchas possible, and organisations in diVerent member states should be encouraged to share their experience andexpertise.
4.3 This would build on and develop the work currently being undertaken by Mental Health Europe (MHE),with support from the EU. The membership of MHE is drawn from right across Europe, and brings togetherindividuals and organisations with diVerent kinds of mental health interests, experiences, expertise andresponsibilities, who form an equal partnership. The membership includes user organisations, volunteers andprofessional organisations working at the regional, national and European level. MHE’s core belief is that“the burden caused by mental illness for individuals, families and society is too heavy, and that the stigma andtaboos are too great, to leave mental health development only to politicians and professionals”.
Depression and suicidal behaviour
4.4 A proposal by the European Commission for a Council Recommendation on the reduction of depressionand suicidal behaviour should include as wide a range of factors as possible, including access to (and fundingfor) support networks, early intervention (including work place interventions supported by employers),employment policies, alternatives to drug treatments—such as talking treatments (not only cognitivebehavioural therapy)—exercise, diet and environment.
4.5 There is a need to investigate further the links between some drug treatments and suicidal behaviour.
4.6 The EU is also uniquely placed to conduct research to explain why suicide rates vary so much across theEU countries. Why, for example, is the death rate from suicide per 100,000 people more that seven times higherin Lithuania than the UK? (Annex 3 of the Green Paper.) Is it related to the fact that the proportion of theLithuanian health budget spent on mental health is only about half that of the UK? (Annex 6 of the GreenPaper.) Or are there wider environmental or societal causes? Addressing these sorts of questions can improveour understanding of mental distress, its causes and remedies, and contribute to the development of anevidence-based approach in Europe.
Rights and institutionalisation
4.7 Regarding the protection of the rights of people with mental health and disability, Mind welcomes themove away from institutionalisation. Mind agrees that compulsory treatment must only ever be a last resort.
4.8 The World Health Organisation has stated that “where there is a potential for voluntary admission, this[ie compulsory treatment] should only be used in very specific circumstances and in accordance with the law.Public misconceptions about the dangerousness of people with mental disorders lead to an undue emphasison protecting society” (WHO 2003).
4.9 The WHO concludes that involuntary admission should be permissible only if two criteria are both met:
1. there is evidence of a mental disorder of suYcient severity as defined by internationally acceptedstandards; and
2. there is a likelihood of self-harm or harm to others and/or a deterioration in the patient’s conditionif treatment is not given.
The promotion of these safeguards across all EU member states would be a positive step forward. Mind wouldlike to see more stringent criteria. There should, for example, be a requirement that proposed treatment hasa therapeutic benefit and there needs to be an appropriate threshold for risk of harm or self-harm. (Forfurther discussion of these issues, see Mind’s comments on the draft Mental Health Bill on our website at http://www.mind.org.uk/.
Fundamental rights
4.10 We welcome the proposal in the Green Paper to include people with mental ill health or disability andthe situation in psychiatric institutions in the activities of the Fundamental Rights Agency of the EU, whichbecomes operational on 1 January 2007. The role of this new agency is to be an independent centre of expertiseon fundamental rights issues, and to undertake analysis and data collection. It will also provide input on howto prepare and implement legislation in the area of fundamental rights. The inclusion of mental ill health andpsychiatric institutions within its remit is, therefore, not optional, but essential.
3564222009 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
59commission green paper on eu mental health strategy: evidence
23 November 2006
Research and dissemination
4.11 The development of a mental health information, research and knowledge system for the EU is essentialto the success of the EU mental health strategy. The strategy should also ensure that mental health practiceis monitored and evaluated, and best practice is shared between member states, as the Green Paper indicateswill be the case.
4.12 By supporting research and introducing safeguards, the EU can also help to prevent policy beingdominated by special interests—such as pharmaceutical companies—whose economic power can mean thatthey have undue influence over research agendas and information flow.
4.13 A number of EU institutions could potentially play a role in data analysis and policy development. Theseinclude the Fundamental Rights Agency (see above), the European Foundation for Improvement of Livingand Working Conditions, European Agency for the Evaluation of Medicinal Products, European MonitoringCentre for Drugs and Drug Addiction and the European Parliament’s Disability Intergroup and Intergroupon Ageing.
4.14 In October 2005, the final report to the European Commission from the Implementing Mental HealthPromotion Action (IMHPA) project concluded that “most programs implemented across Member States arenot considered to have suYcient evidence base to be good practice. Countries are in need of information oneVective practices and guidelines for eVective policy and program development and implementation”(IMPHA 2005).
4.15 In developing an interface between policy and research, the Commission might consider creating anagency similar to the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) with a mentalhealth remit. The EMCDDA has made a significant contribution to evidence based drug policy andcontributed to the development of more eVective drug services across the EU. It is recognised as a centralsource of comprehensive and reliable information on drugs and drug addiction.
4.16 A dialogue with member states on mental health, and the launch of an EU platform, would help to ensurethat best practice is not only identified, but also shared. Policy, practice, investment in and attitudes to mentalhealth vary widely within the EU. It is questionable whether the approach to mental health in all member statesis compliant with the European Convention of Human Rights, particularly since the expansion of the EU.
5. Conclusion
5.1 The WHO Mental Health Action Plan for Europe (Facing the Challenges, Building Solutions) was agreedin Helsinki in January 2005, and endorsed by the UK government.
5.2 It identifies five key priorities for the coming decade:
1. To foster awareness of the importance of mental health.
2. To collectively tackle stigma, discrimination and inequality, and empower and support people withmental health problems and their families to be actively engaged in the process.
3. To design and implement, comprehensive, integrated and eYcient mental health systems that coverpromotion, prevention, treatment and rehabilitation, care and recovery.
4. To address the need for a competent work force, eVective in all these areas.
5. To recognise the experience and knowledge of service users and carers as an important basis forplanning and developing services.
An EU strategy that took forward these priorities and promoted them across Europe would be a major stepforward. But it is important that good intentions translate into progressive policy, evidence based practice andeVective implementation. For example, it is important that service users are engaged in a systematic, and nota tokenistic, way—and that the EU strategy fully engages with the social, cultural and experiential diversityamong people who experience mental distress.
5.3 The pursuit of mental well-being cannot be isolated from wider EU policy to tackle risk factors such asdrug and alcohol misuse, poverty, exclusion, work stress, displacement and experience of racial injustice anddiscrimination. Nor will the strategy deliver on its promises unless mental health and social support servicesare properly resourced. As argued above, this makes economic sense too.
5.4 Finally, and to repeat, Mind would urge as full a role as possible for mental health service users and non-governmental organisations in the process of developing an EU strategy.

3564222009 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
60 commission green paper on eu mental health strategy: evidence
23 November 2006
Mind’s report on stress in the workplace is available on our website at http://www.mind.org.uk/Mindweek/report.htm
Mind’s current campaign highlighting the neglected problem of mental distress in later life is at http://www.mind.org.uk/News!policy!and!campaigns/Campaigns/ages/
References
CIPD (2005) at www.cipd.co.uk/news/—articles/employersexcludecorejobless.htm.
Gray P (2000), Mental Health in the Work Place, Mental Health Foundation, London.
IMHPA (2005), Final report to the European Commission, DG SANCO/G (at http://ec.europa.eu/comm/health/ph—projects/2002/promotion/fp—promotion—2002—annexe1—16—en.pdf).
Mind (2005), Stress and mental health problems in the workplace, Mind, London.
NIMHE (2003), Delivering race equality: A framework for Action, Department of Health, London.
Pretty J (2006), From Green Exercise to Green Care:A New Opportunity for Agriculture in the UK?,University of Essex, Unpublished.
Dora Rickford & Kimmett Edgar (2005), Troubled Inside: Responding to the Mental Health Needs of Menin Prison, PRT, London.
SEU (2002), Reducing Re-oVending by ex-prisoners, ODPM publications, London.
SEU (2004), Mental health and social exclusion, ODPM Publications, London.
World Health Organisation (2003), Mental health legislation and human rights, Mental Health Policy andService Guidance Package, WHO.
World Health Organisation (2005), Mental Health Action Plan for Europe—Facing the challenges, buildingsolutions, EUR/04/5047810/7, 14 January 2005.
Websites
Mind’s website is at http://www.mind.org.uk/.
The Sainsbury Centre for Mental Health website is at http://www.scmh.org.uk/.
The Mental Health Europe website is at http://www.mhe-sme.org/.
Memorandum by Rethink
1. Rethink is the leading national mental health membership charity in the United Kingdom; supportingaround 7,500 people every day of the year and working together to help everyone aVected by severe mentalillness recover a better quality of life. Our aim is to make a practical and positive diVerence by providing hopeand empowerment through eVective services and support to all those who need us. We believe that people whoexperience severe mental illness are entitled to be treated with respect and as equal citizens. We activelycampaign for change through greater awareness and understanding and we are dedicated to creating a worldwhere prejudice and stigma are eliminated.
2. Rethink believes mental health is a prerequisite to achieving the strategic policy objectives of the EuropeanUnion because long term prosperity within the European Union rests on the health and wellbeing of itscitizens. Mental health is an integral part of the overall wellbeing of individuals and communities. As suchRethink, together with EUFAMI (European Union Federation of Associations of Families of People withMental Illness) wanted to contribute to the European Union consultation process by gathering the views ofpeople who have experienced mental ill health, their families and carers. We did this by creating an onlinesurvey. The results of which have informed our response.
3. The concern for the European Union is that mental ill health is becoming increasingly prevalent and theconsequences of developing a mental illness are far-reaching. “Mental health problems are increasingsignificantly. Some countries register up to 6 per cent of the population as having serious mental disorders.Mental ill health accounts for up to 30 per cent of consultations with general practitioners in Europe.”1 Theincreased prevalence of mental illness within the European Union will have significant consequences for the1 World Health Organisation. (2002). “European Health Report.” http://www.euro.who.int/document/e76907.pdf
3564222010 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
61commission green paper on eu mental health strategy: evidence
23 November 2006
Lisbon agenda of improving the competitiveness of Europe within the world economy. “Mental ill health coststhe UK £77 billion a year through the costs of care, economic losses and premature death.”2
4. Any EU mental health strategy would sit within the overall EU strategic objectives of prosperity, securityand solidarity. Thus, mental health should be integrated within other work programmes. Embedding mentalhealth issues within the work of other departments is essential to ending the social exclusion currentlyexperienced by people with mental illness. This would contribute to the work of the British governments’Social Exclusion Unit and the Strategy Unit’s aim of improving the life chances of people with mental illness.This is particularly important in the context of employment for people with mental illness. The Departmentfor Work and Pensions has outlined an ambitious programme of work aimed at reducing the number of peoplereceiving incapacity benefit by 1million. Given that 40 per cent of Incapacity Benefits claimants have a primarydiagnosis of mental illness; it is essential that employers’ understanding of mental illness improves in order toachieve this goal. An EU strategy could help to ensure that mental illness becomes part of cross-Europeaninitiatives on employment.
5. An EU strategy would particularly contribute towards the goals of mental health promotion and stigmareduction expressed in Standard One of the National Service Framework for Mental Health and the Shift anti-discrimination programme. Both these goals require extensive cross-departmental working and an EUstrategy would help ensure that a coherent approach is taken across all UK Government departments,especially the Department for Education and Skills, the Department for Work and Pensions and theDepartment for Trade and Industry as well as local government. In bringing together people who accessservices and civil society organisations, an EU strategy would help to embed mental health within the cultureof these organisations.
6. Finally, Rethink believes that the creation of an EU strategy on mental health would help to ensure thatresearch priorities among the member states are better coordinated, that good practice is shared moreeVectively and a wider evidence-base for mental health interventions is built up. This will help to ensure thatassessment of mental illness, under Standard 2 of the National Service Framework, is more eVective andaccurate. It will also help to facilitate the provision of “care which optimises engagement, anticipates orprevents a crisis, and reduces risk” under standard three of the National Service Framework.
7. A European strategy for mental health should address the following issues Unemployment, Poverty, Poorphysical health, Poor quality of life and Social exclusion to build mental health into it’s population.
8. Unemployment—Economic prosperity within the European Union significantly relies on the health andhappiness of its workforce. The burden of mental ill heath has a significant impact on the productivity of acountry’s workforce. “People with long term mental health problems are less likely to be in employment thanpeople with other disabilities (21 per cent compared to 49 per cent of all people with disabilities).”3
9. Though for some mental illness is a barrier preventing them returning to, or gaining employment, themajority of people with mental ill health wish to return to work. It is necessary that the European Unionensures employers consider the needs of people with mental ill health; principally the need for ongoing supportduring occasional periods of illness or diYculty. The European Union should actively encourage theemployment of people with mental ill health, should they wish to pursue employment, particularly throughinitiatives such as flexible working hours, part time work, job sharing, and voluntary work. The stigma anddiscrimination of employers is a barrier to bring about social inclusion of those with mental ill health.
10. Poverty and Social exclusion—Social cohesion relies on the fulfillment of an individual’s human rights andthe social inclusion of an individual as a citizen of the European Community as well as community acceptanceof individual diVerence. People with mental ill health often express feelings of isolation and exclusion fromthings such as employment, quality housing, social networks and education. Some groups are more vulnerablethan others; particularly women who are single parents or experience domestic violence, BAME (Black Asianand Ethnic Minority) groups, the homeless and unemployed. Withdrawal from society, particularly throughunemployment has been closely linked to mental ill health. “Social isolation is an important risk factor fordeteriorating mental health and suicide. Two thirds of men under the age of 35 with mental health problemswho die (in the UK) by suicide are unemployed.”4
2 The Sainsbury Centre for Mental Health, Policy Paper 3: The Economic and Social Costs of Mental Illness. (2003) London, TheSainsbury Centre for Mental Health.
3 Department for Work and Pensions 2001.4 OYce of the Deputy Prime Minister. (2004). “Mental Health and Social Exclusion”. Social Exclusion Unit Report Summary. Page 3.
ODPM Publications.
3564222010 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
62 commission green paper on eu mental health strategy: evidence
23 November 2006
11. The stigma surrounding mental illness often prevents people with mental ill health forming close personalrelationships, compounding their isolation. Social exclusion and mental ill heath are a vicious cycle—eachperpetuating the other.
12. Poor physical health—Mental health is fundamentally linked to physical health. “People with severemental illness die 10 years younger than the rest of the population, not because of suicide or self-harm, butbecause of physical health problems”.5 Regular physical health checks can help tackle many of the physicalaliments that aVect people with mental ill health. Many of these physical ailments are the result of theirmedication.
13. Service users with severe mental illness often cite improving the side eVects of their medication assomething they would like to change. Continued investment in drug research is necessary as part of a holisticapproach to tackling the burden of mental ill health on the Community.
14. It is necessary to ensure that primary care workers are trained and have adequate resources to address thephysical needs of those with mental illness.
15. Poor quality of life—Poor quality of life is a significant problem for people who have mental healthproblems. Access to education, housing, transport, employment, leisure facilities and social networks canvastly improve the quality of life of service users.
16. Tackling the discrimination surrounding mental ill health requires a concerted eVort to uphold people’shuman rights—particularly with reference to Article 14 of the European Convention of Human Rights—theprohibition of discrimination. Education can further awareness of mental health and build mental health intosociety, thus easing the burden of mental ill health on society.
17. And… Mental ill health not only aVects those who experience it but those who provide informal care forthem; their friends and families. “There are 1.5 million carers in UK”.6 Comparable data for other EuropeanUnion Member States was not available. Supporting these informal social networks is extremely important,not only to create an atmosphere of social inclusion for individuals experiencing mental ill health, but to ensurethat these informal networks are encouraged and maintained.
18. Support and acknowledgement is something that carers often feel they lack. “1 in 6 carers have no carersservices in their area despite government commitments.”7 Examining the needs of carers is as important asfulfilling the needs of those with mental ill health. It must be recognised that providing round the clock careand support has many impacts on an individual’s health and wellbeing. “Involved and supported carers havea better experience and are more eVective carers than those who are uninvolved and without access to supportand information”.8 Informal carers require better information, communication and support. They must notfeel excluded from the formal care system. Informal carers need to be recompensed financially for their time.Respite care for both informal carers and those with mental ill health is a necessity. The European Union’sstrategy should include recommendations for supporting carers
19. Rethink believes the European Green Paper sets out a positive approach to tackling mental ill health inEurope and that these solutions will have a great impact on mental ill health across European Union MemberStates provided they are accompanied by adequate funding and the mechanism to distribute it. With regardto specific points Rethink would like to highlight the following aspects which it feels should be prioritised.
20. Promoting the mental health of the population—European Union wide public health campaigns should bein line with other European Union health competencies. Health promotion campaigns should not only focuson mental health specifically but health and wellbeing in general. Health promotion campaigns need to belocally and nationally based.
21. Addressing mental ill health through preventative action—Preventative action and the dissemination ofgood practice should be coordinated within the European Union network. Of particular concern to us isdeveloping and facilitating good practice on issues such as cannabis and suicide interventions. Though thepaper expresses that “mental ill health” will be addressed through preventative action the importance of bothproactive and reactive approaches to mental ill health must be recognised.5 Harris, J (2006). “A win-win situation. Making life easier for GP practices and people with mental illness.” Page 1. Rethink.6 V Pinfold and P Corry. June 2003. “Who Cares? The Experiences of Mental Health Carers Accessing Services and Information”. Page
2. Rethink.7 V Pinfold and P Corry. June 2003. “Who Cares? The Experiences of Mental Health Carers Accessing Services and Information”. Page
2. Rethink.8 V Pinfold & P Corry. 2003. “Under Pressure”. Rethink.

3564222010 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
63commission green paper on eu mental health strategy: evidence
23 November 2006
22. Promoting the social inclusion of mentally ill or disabled people and protecting their fundamental rights anddignity—The promotion of mental health and building mental health, through public education, into theEuropean Community is an important aspect of tackling both mental ill health and the stigma associated withit. It is necessary to stress every individual’s right to good health.
23. The European Union should undertake a broad piece of work on social inclusion, to promote theawareness of rights under European Convention of Human Rights for all people including those experiencingmental ill health.
24. Mental health service users do not only require the protection of civil society. More importantly those withmental ill health require empowerment. By enabling involvement within society through correct medication,adequate support in accessing services, and reducing barriers to accessing services, not only in mental healthservices but all services, particularly housing, education, those with mental ill health can be enabled toparticipate within wider society. It is extremely important to enable service users and carers’ voices to be heardby involving stakeholders who vocalise the needs of those involved. Bringing together patient and civil societyorganisations will perpetuate the building of long term solutions. Enabling participation, and maintaininginvolvement, in society helps people with mental ill health to remain active citizens.
25. Improving information and knowledge on mental health in the EU—The European Union’s desire toconfront mental health creates a considerable opportunity to create a knowledge base that can communicateand implement ‘best practice’ within mental health. The European Union should give priority to mental healthresearch. Funding needs to be proportionate to spending on other areas of public health.
26. Rethink considers a comprehensive European Union strategy would add value to the existing andenvisaged actions and strategies of other Member States and international bodies such as the WHO.
27. A framework to facilitate exchange and cooperation between member states would aid the developmentof research and investment in mental ill health; thus enabling the European Community to tackle those issuesmost important to service users and carers. This framework would be particularly of use if it was accessibleto both to mental health professionals, researchers and mental health service users and carers. Accessibleinformation for service users and carers aids the empowerment of both groups.
28. Facilitating the increase in the coherence of actions in diVerent policy sectors is extremely importantnamely because people experiencing mental ill health have a multiplicity of needs—not only in terms ofaccessing the correct treatments but also accessing the services they require to function as a citizen withinsociety including adequate housing and employment services and education. Synergies need to be created bothbetween departments within member states governments, and between members states themselves.
29. The paper does not explicitly expand upon “mental ill health”. Mental ill health has a variety of formsand levels of severity. Mental ill health is also extremely complex in its causes and outcomes. For example co-morbidity, or dual diagnosis seriously impact upon mental ill health, either by causing, or aggravating, mentalhealth disorders. “Suicide is the second most common cause of death after road traYc accidents for Europeansaged between 15 and 35. Alcohol use and co-morbidity heighten the risk of suicide”.9 Rethink believes thatthe definition of mental illness should clearly state the inclusion of personality disorders.
30. Though the paper mentions the link between physical health and mental health, the connection should beexpanded upon, as physical health has an important part to play. Mental ill health can be expressed throughphysical manifestations, particularly stress. Improving the physical health of the population can impact uponmental health and vice versa. It is important that co-morbidity between physical health and mental health isrecognized. “The side eVects of medication can have serious detrimental eVects on a person’s physical health.Promoting healthy eating, regular exercise and the use of complimentary therapies will impact significantly onpeople’s mental wellbeing and physical fitness.”10
9 Jane-Llopis, E & Anderson, P. 2005. Mental Health Promotion and Mental Disorder Prevention. A Policy for Europe.Nijmegen:Radboud University Nijmegen.
10 Harris, J & Corry, P. 2005. Make a Fresh Start: An Action Pack for the Forgotten Generation. Page 20. Rethink.

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
64 commission green paper on eu mental health strategy: evidence
23 November 2006
Examination of Witnesses
Witnesses: Dr Marcus Roberts, Head of Policy and Parliamentary Unit, Mr David Stone, ParliamentaryOfficer, of Mind, Mrs Alexandra Burner, Senior Campaigns Officer and Mr Paul Corry, Director of Public
Affairs, Rethink, examined.
Q137 Chairman: Welcome to our inquiry, which weare doing at as a great a speed as we can manage.Obviously your two organisations are very importantwitnesses in this particular inquiry, and we have seenyour written evidence. We realise that the potentialscope of this inquiry is very wide and we are trying tokeep it limited, in a way, to a very strictunderstanding of what it is the Commission is tryingto do and why it is trying to do it, and what the limitsof its actions are, rather than allowing ourselves towander down a very wide consideration of diVerentMember States’ national health systems and howthey aVect mental health. You can think of 20 othersubjects that we can discuss in this context, but we aretrying not to do that. We are being assisted in ourwork by Professor Knapp, whom I am sure youprobably all know, and we want to particularly studythe views about the Green Paper proposals andrepresentatives of mental health service users, andthere is a question on that and your evidence was veryuseful in that respect. A few, what we call,housekeeping points. This session is open to thepublic and it will be recorded for possiblebroadcasting or web casting, and a verbatim scriptwill be taken of your evidence as well, and that willbe published on the Parliamentary website and in anannex to the report. You will be sent a copy of thescript—you have probably done all this already, butto make sure it is on the record—and you canobviously check it for accuracy, and if you do haveany concerns please get in touch immediately withour Secretary and we will deal with that. If you wantto submit supplementary evidence after ourdiscussion—and that is something very useful and tothe people who have given us evidence—of course wewill be absolutely delighted to receive it. You shouldhave a notice of Members’ interests. The last thing isthe question of acoustics. This room has a horribleacoustic; it seems to disappear up there somewhere,so if you could, when you are speaking to us, lift yourheads as much as you can oV the printed page. I knowit is nice to have your notes as your comfort blanket,but you probably know what you want to say wellenough and not really need it! So please speak asclearly as you can. I would like you to start by givingyour oYcial names and titles for the record, and ifanybody wants to make an opening statement we willbe happy to hear that as well. If you could start oV,Mr Stone.Mr Stone: My name is David Stone and I am aParliamentary OYcer at Mind.Dr Roberts: I am Marcus Roberts and I am Head ofthe Policy Unit at Mind.
Mrs Burner: I am Alexandra Burner; I am SeniorCampaigns OYcer at Rethink.Mr Corry: I am Paul Corry, Director of PublicAVairs at Rethink.
Q138 Chairman: Thank you. Does anybody want tomake an opening statement?Dr Roberts: Yes. Thank you, my Lord Chairman, andthank you for giving us the opportunity to come andshare our thoughts with you about the EuropeanGreen Paper and the prospects for a Europeanmental health strategy. I would like to say two thingsin introduction. Firstly, I think that is whathappening at European level is very encouraging interms of the way that Europe is starting to thinkabout mental health as a core European issue.Basically the Green Paper and the World HealthOrganisation’s action plan for Europe on mentalhealth are recent signs of this. I would like to say veryquickly what we think is good about the approachthat is being taken, and then a little bit about what Ithink you were referring to in terms of thepracticalities of what this means for us, working onthe ground in the UK. Very briefly on the things wewelcome, I think it is great to see Europe adopting asocial model of mental health, which recognises theclose relationships between mental well being andthings like poverty, exclusion, lack of socialconnectedness, isolation and so on, not as simply adisease of the brain, as it were, but as something thatis very much bound up with relationships and so on.Secondly, I think it is really good to see Europerecognising the sheer scale and significance of thisproblem for European populations. They estimatethat three to four per cent of European GDP is theeconomic cost of mental health, but if you add in thewider human cost then that figure is going to beastronomical. The Sainsbury Centre for mentalhealth calculates that in England alone it is about£77 billion a year, so if you think of that acrossEurope it is a very big figure in terms of the humancosts there are 58,000 suicides a year in Europe—suicide causes more premature death than, forexample, road accidents; so that we welcome. And wewelcome the emphasis on deinstitutionalisation andwe welcome the commitment to well resourced,evidence-based mental health services, whichcombine health and social care and also respect thebasic human rights and liberties of people caught upin the system, and we like the commitment to tacklingstigma, and of course we like the commitment topromoting service user involvement. So that is thecase for. Just a couple of very brief disclaimers. What

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
65commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
we have at the moment from the World HealthOrganisation and the European Union are some verypromising statements of good intention. How theyactually translate into resource and eVective changeon the ground is something that we are not entirelyclear about and we do not come here with a clearsense of how that would happen. Linked to that, Iguess, is a bit of a disclaimer that Mind’s focus is verymuch domestic—we do not do a huge amount ofEuropean work and we do not have a sophisticatedknowledge of the way in which EU institutions work.But I think that is a point in itself that is worth notingat the outset. I think there is a reason thatorganisations like Mind in the UK are quite insularand quite focused on domestic policy. It is partlyabout not being clear what the benefits are ofinvesting resource on and engaging with Europeaninstitutions; there is a skills deficit in terms of howEurope works and how you can eVectively work in it,and there is a general lack of clarity about what thebenefits of EU engagement are. So I think that is botha disclaimer about our knowledge but also therecould be a role for the European Union there inskilling-up and thinking about how it can moreeVectively engage with organisations like Mind.Mr Corry: If I may add a few words from Rethink’sperspective? In terms of the evidence that Mind andRethink are giving today, we will not waste theCommittee’s time by repeating things, so we willendorse many of each other’s comments, I think, andwe would certainly associate ourselves with all thecomments that Marcus has made. Perhaps the slightdiVerence between ourselves and Mind on this is thatRethink historically has tried to engage with Europeboth in terms of making connections with othervoluntary sector organisations but also with theinstitutions of Europe, and it is actually quite adiYcult thing to do in terms of mental health,certainly up until recent years. I think that is for tworeasons. I think there is a cultural diVerence betweenthe way voluntary sector organisations operate inthis country and those in Europe. Rethink is amember of an organisation called EUFAMI, whichrepresents organisations, such as Rethink itself, whoare member-based organisations made up of peopleexperienced in severe mental illness, and their familymembers. But it would be fair to say that of all theorganisations in EUFAMI Rethink is by far thelargest, the best resourced and the most connectedwith both the political will in this country and withcivil society itself. The feedback that we get fromvoluntary sector organisations in Europe is veryoften that they feel marginalised, under-resourcedand lack eVectiveness in the political process. So Ithink in looking at an across-European approach tomental health there is something to be said for theEuropean Union institutions making it easier for the
voluntary sector organisations to actually work andconnect with the institutions in Europe. Where wehave had success in the past—and it is somethingworth pursuing in the future—is in the area ofacademic research. Rethink works in associationwith the Institute of Psychiatry on a number of cross-European projects to do with discrimination andstigma, and one of them is called Indigo, which is astudy of 26 diVerent countries, looking at the day-to-day living experiences of people with all kinds ofmental health conditions, and the barriers that theyfeel are put in the way of full social inclusion, and theevidence that you will hear from both Mind andRethink this morning will show that at the top oftheir list of concerns is the issue of discrimination andstigma and public understanding, and if we can lookat it from slightly diVerent points of view. I think ifthere is a consistent message from people using theservice across Europe that they very muchappreciate—and this is perhaps what the EuropeanUnion’s contribution can be—is a wider public spacein which mental health issues can be freely discussed.I do not think we should underestimate theimportance of getting services right and gettinginvestment right, but it is also particularly true ofmental health where there is so much for individualsand organisations and governments to talk about it,and we should not underestimate the importance ofcreating that public space, and it is one of thevaluable things of the work of this Committee that, inEurope more generally, I hope in future years we willbe able to have the debate more openly aboutpeople’s personal experience.
Q139 Baroness Howarth of Breckland: Mr Corry isdropping his voice. My disability is a slight hearingimpediment! I am very interested in what you aresaying.Mr Corry: I have a feeling that I was repeating myselftowards the end anyway! I was just trying to make thepoint that it is extremely important that we have thepublic space available to us to talk about mentalhealth, and although we all have concerns about howmuch the European Union can do to influence thetypes of services and the investment going intoservices in a particular country, we still think it isextraordinarily important that strategy documentsand principles and so on are being discussed at thatEuropean level.
Q140 Chairman: One of the mechanisms that theCommission is talking about is the well-wornmechanisms that they use quite a lot, of bringingvarious sorts of organisations together, both thoseinvolved in delivering services and those, like you,working from civil society. I do not think thisquestion is on our list but would you consider that

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
66 commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
applying that methodology to the whole question ofmental health would in fact be quite valuable? I thinkthey tend to discuss a relatively limited agenda so youmight meet four times a year or twice a year andconcentrate once on stigma and once on some aspectof treatment—diVerent things each time. Do youthink that would be something that would enlivenand enable you all to get in better touch with what isgoing on across the Channel in continental Europe?Mr Corry: Certainly from our perspective,absolutely. We hosted the annual general meeting ofEUFAMI two years ago and we broughtorganisations from around Europe together and itwas fantastic to be able to be in the same roomtogether for a day sharing experiences.Dr Roberts: We are a member of an organisationcalled Mental Health Europe, which is an umbrellaorganisation for voluntary sector provider andservice user organisations across Europe and acts asan information hub. It does very good work but it isnot particularly well resourced. So it may be thatthere is no need to invent a new platform level butthat investing in that platform would be better. Theother thing is that bringing people together to discussissues is important but there has to be some clearagendas and some clear purposes.
Q141 Chairman: I think that these meetings can be,as it were, clerked by the Commission, is that notcorrect? That is my impression. So that might givethem that kind of continuity and also reduce theexpenditure from the point of view of theorganisations involved if that was the way it wasgoing to function, but I think that is a question wemight address in our report because it is obviously avery important aspect of the work. I have goneoutside my remit, so we will get back to the properquestions now. Mind in particular gave us evidenceof the importance of prevention and the largenumbers who are involved, and you have repeatedthat again in your statement today. So what measureswould you regard as the most important forpreventing against the impact of the factors inmodern life which can lead to mental health; and howwould you see a European Union health strategyhelping with these measures?Dr Roberts: I think that is a very good question. Whenyou look at the World Health Organisation’s list ofsome of the causes and contexts of people developingmental health problems it is about addressing somereally very big and diYcult problems—problemsabout inequality and poverty, problems aboutisolation and lack of community and integration, andof course things like war and conflict, and all thoseare contributors to people’s mental health, and thequestion of how much and in what ways theEuropean Union can impact on those as part of the
mental health strategy is something that needsthinking about in practical terms. I would suggestthat there are two or three things that spring to mind.I think the first thing, just as a note, is that it isinteresting that the European Union has becomemore interested in mental health exactly at the timewhen we become more aware of its social andeconomic causes and the way it is bound up with allthese things, because of course the EU does notactually have competence about this area of policy—that lies with the Member States. But once mentalhealth is seen as a mainstream public policy issue thathas enormous implications for citizens acrossEurope, it creates the space for Europe to becomeinvolved, and the question then is what sort of thingsit could do? It could be approached all those otherpolicy areas in a way that reflected considerationsabout mental health. For example, it may be thatEuropean legislation, reports, etc, across a certainspectrum could be “mental health-proofed” so thatlegislation and reports would be checked and therewould be some sort of reporting about their likelyimpact on mental well being as part of the process ofdebate right across the range of policy areas the EUis concerned with. Another question is whether a setamount of funds available for Europeanregeneration, could be directed at projects that havea clear mental health component. So when theEuropean Union is investing in measures to tacklesocial exclusion, integrate communities, it wouldactually be required to devote some of that resourcealways to projects that are about mental health andwell being. The final thing is that I think there arevarious obvious areas of existing European policywhere there are more direct ways that it can helptackle causes of mental health problems and promotemental well being. Two obvious examples: I do notthink the European Union drugs strategy has muchto say about mental health at the moment—its drugand alcohol strategies are much more fixated oncrime and physical health, blood-borne illness and soon—but the mental health issues around substancemisuse are enormous. The second example is theEU’s responsibility for employment and health andsafety at work, and the possibility that the EuropeanUnion can play a role in mainstream mental health asa core health and safety issue again would help totackle a lot of those causal issues around theworkplace stress and so on. There will be otherexamples, as well.Mr Corry: We would agree with that approach.Chairman: Thank you. Lady Morgan.
Q142 Baroness Morgan of Huyton: I want to ask youabout quality of life issues. You have both put inevidence that has covered quality of life. Our anxietyas a Committee is to try and work out where is the

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
67commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
value added of European action on a whole range ofissues, but particularly it seems to strike me on thequality of life, as distinct from action by nationalgovernments on quality of life. Can you pin down inany way how you think European mental healthstrategy could seek to promote improvements inquality of life, which could help with mental healthwellbeing?Dr Roberts: I think that certainly in this country theissues about the quality of life—issues about mentalwell being, the benefits of good food, of green space,of access to nature, of physical exercise there is moreand more awareness of those issues and we arecertainly doing a lot of work to encourage and to seeactive participation in nature as a core mental wellbeing issue. I think there are a couple of other waysthat the EU could add value. Firstly, one of the thingsthat I do know about the European Union is that ithas a lot to do with agricultural matters—andworking time directives—those are areas ofEuropean policy, that spring to mind! What I think isinteresting about promoting green exercise activity asa source of mental well being and quality of life isactually that it is also quite a useful way ofregenerating rural economies so that people who aregoing out into the countryside to do all these thingsare also helping regeneration, and I would havethought that was something that could be integratedinto European policy in that area. I think the otherobvious thing is that Europe could do a lot to supportthe emerging evidence base and, as Paul said earlier,to help to invest in research and good practice sharingacross the Union about the quality of life initiatives.A good example, I think, is the development of greencare farms in lots of European countries which areactually mainstreamed into health and social careprovision, and are places where people go where it isnice to be and where they get involved in variousactivities with therapeutic value—conservation workand so on. The European Union could potentiallyplay a useful role in looking at how eVective they arein funding the research and also disseminating it.Mr Corry: If I could just add something completelydiVerent to the mix. Rethink works with amembership charity that works with people mostlywith severe mental illness—schizophrenia, bi-polardisorder and severe personality disorder—and thequality of life issue that people come back to us withtime and time again is the side eVects of themedications they use, and I think there is aninteresting tension that exists at the moment betweensome of the European regulatory measures aroundthe use of medicines and our own regulatory systeminside the UK, and I know that Rethink, unlikeMind, works with the pharmaceutical industry interms of some of these issues. I know that fromtalking to some of the pharmaceutical companies
they certainly look to Europe or the UK to seewhether they may get most advantage beforeintroducing new medicines and putting throughdiVerent regulatory processes, and for us, Rethink,there is a definite need to get common standardsacross the European Union and the UK and for agreater concentration on governments to work withthe pharmaceutical industry to minimise the sideeVects of the medication that people use.Chairman: That is very interesting. BaronessNeuberger.
Q143 Baroness Neuberger: You have alreadyanswered to some extent the question about thestigma and what you think the European mentalhealth strategy could do and Lady Thomas asked youthe question about possibly bringing together groupsfrom the UK and around Europe for some kind ofsummit. Do you feel that there is more that theEuropean Union could do? If you had a blank sheetof paper—and you are not very aware about how theEU works or indeed you can influence it—is theresomething that you would like to happen at aEuropean level, a statement, whatever, that youcould see making a diVerence to stigma, which youhave both written about and given a lot of evidenceabout, both here and in the past?Mr Corry: One thing in a dream world is hard to pickon. It sounds simplistic to say this but I think it isabout creating that public space; it is about makingsure that governments across the piece recognise thatstigma and discrimination is a huge issue for peoplewith mental health problems, and if there was onething that any government or indeed any Europeaninstitution could do it would be to enforce some ofthe very good practice that we have arounddiscrimination issues in the disability field, and toenforce those in the mental health field. I think thatis the one thing I would pick up.
Q144 Baroness Neuberger: So that is bringing, as hashappened to some extent in this country, mentalhealth or mental illness into the frame of disability?Mr Corry: Yes.
Q145 Baroness Neuberger: And that would be aEuropean-led statement?Mr Corry: Yes.
Q146 Baroness Neuberger: Thank you very much,that is very helpful. Is there anything you want to addDr Roberts?Dr Roberts: I have. I will say it very briefly. I think thecrucial thing is, exactly as Paul said, the mainstreamof good mental health is a core disability rights issue.I think people are sceptical about changes inlanguage, but I think it would be quite helpful if

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
68 commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
mental health was not just assimilated within“disability” as a legal term, because I think if peopleare told that the policy is about disability theynaturally think about physical disabilities. I alsothink there is a role for the European Union infunding a really good pan-European anti-stigmacampaign. There is a campaign called SHIFT in theUK, which is something you might know about, butit is only funded to around £873,000.
Q147 Baroness Morgan of Huyton: When you say“funding”, do you mean European money going tonational governments to run campaigns that work inindividual countries, or do you mean someEuropean-wide campaign?Dr Roberts: I think the answer to that would bewhichever one seems to be the most eVective way toget the message across actually—both of thosemodels could work. We know from the experience of,for example, New Zealand, that if you invest realserious money in anti-stigma work it significantlychanges attitude.
Q148 Baroness Neuberger: I know about this, as youprobably know—I think you gave me the evidence.Could you tell the rest of the Committee about thatbecause I think that is important, about how muchthey invested and how it worked?Dr Roberts: I know it was 20 times as much as we did.Mr Corry: I can remember oV the top of my heads thefigures that I carry around with me that made thebiggest impact with me. In New Zealand it is agovernment-funded five-year campaign. So the firstimportant thing about it is that it is sustainable overa long period of time; in England it is from year toyear and we have already had two diVerentincarnations, one called “Mind Out for MentalHealth” and now the SHIFT one, with a year gapbetween the two. So that is the first point to make. InScotland they have a campaign that is called “SeeMe”, which, interestingly, is funded through theScottish Executive, but it is funded by monies thatthey raised through tobacco levy. I think that is aninteresting thing about mental health as well; I thinkwe are guilty in the mental health world of living in abit of a ghetto sometimes, when we do not look forsome of those other opportunities that are out therewhich present themselves to look for other areas.There is a distinct link between smoking and mentalhealth anyway, and I think that a legitimate use of atax on tobacco would be to use it in thediscrimination world. But the figures that made theimpact on me are that in New Zealand they spend theequivalent of 34 pence per head of population ontheir anti-discrimination work; in Scotland it is about13 pence per head; and in England, shockingly, it is1.44 pence per head. So the scale of diVerence is
tremendous. The other factor that I would put on thetable is when you talk about the European Unionperhaps giving money to governments to do this,what works in New Zealand and what works inScotland is the longevity of the funding, but theactual programmes are delivered by coalitions of thevoluntary sector and I think that is an importantelement.
Q149 Baroness Neuberger: That is something thatyou would like us to say to you.Mr Corry: Absolutely.Dr Roberts: Could I add one quick thing? I think oneof the important things about stigma is that itsometimes seems quite soft in terms of policy, but itis not at all because so many of the concrete costsassociated with mental health are rooted with stigma;it is stigma that keeps people out of work, it is stigmathat stops them approaching services when they needhelp, and it is stigma that keeps people isolatedbecause they do not integrate into their community,and therefore it perpetuates—in a vicious circle—those wider causes of mental health we were talkingabout earlier. So I think it is important to make outthat there is a hard, practical case for stigma work fortackling economic, social and human costs, well aschanging attitude as an inherently desirable thing todo.Chairman: Lady Gale’s question was about stigma inthe workplace.
Q150 Baroness Gale: When Mind gave evidence toour Committee you did speak about the stigma ofmental illness in the workplace and that employersare reluctant and avoid people who they know suVermental illness. So what do you feel are the mostserious issues faced by mentally ill people in theworkplace and how could these be eVectivelyaddressed? Are there particular problems for smallbusinesses, which need to be considered?Dr Roberts: This is a really important issue for us andI think there are three issues about mental health andwell being and employment. The first is the issue ofstigma. The Social Exclusion Unit report that onlyfour in 10 employers would be willing to employsomeone with a mental health problem—this isfrankly a shocking figure. Second there are issuesabout access to employment and employers dutiesunder the Disability Discrimination Act to facilitateaccess for people with disabilities. A lot of employerssee that, as I said, in terms of wheelchair ramps andso on; they are not so clear on what theirresponsibilities are to facilitate access for people withmental health problems, which may be about stagedreturn to work; it may be about providing facilitiesand opportunities where people can leave their desks,those sorts of things. I do not think it is just about

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
69commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
stigma with employers, I think a lot of it is aboutsupport, information and advice to know how tohandle mental health as an issue. The third thing isbad working practices as a source of stress andmental health problems and what we do about them.On what we could do I have three things to say. Iwonder if there is a room for a European Directive,or something along those lines, which would actuallyrequire all businesses above a certain size to haveproper mental health policies. Secondly, in the UKthe Department of Work and Pensions runs a schemecalled Access to Work, which helps to providefunding to make adjustments in the workplace tohelp people with disabilities, including mental healthproblems, back into the workplace, so, in theory,financial issues should not be a barrier to peoplegetting into work because they can apply to thatfund, and that will speak to the issue about smallbusinesses as well. Perhaps something similar couldbe done at European level. I think on small businessesthere are obviously issues about size and resources. Ifyou are a three-person business then it can be hard tobe as flexible as a bigger organisation. I think it isabout the public purse stepping in to give somesupport, but also I think potentially as well socialenterprise models are very good models forreintegrating people into work. So support formental health service users to set up their ownbusinesses and to make those businesses work isanother thing that we would want to support andencourage.Mr Corry: I do think there is a particular issue withsmall employers and I think the first thing to do is toget a couple of facts across to small employers aboutthe productivity rates of people who have a history ofmental health problems, that when they are actuallyin work their productivity rates tend to be higherthan the general workforce anyway; their motivationrates are higher, so there is a good reason foremploying somebody with mental health problems.In terms of when they are in the workplace, the fearon the part of the employer would be: what is thesickness rate going to be like? DiVerent schemes havebeen tried, even with the voluntary sector or inlimited ways through the statutory sector, of havingreplacement workers that can go in and fill the placefor somebody at short notice. They have tended toprove to be quite expensive and they are notparticularly popular with service users either becauseit makes them feel that there is always someonestanding behind them ready to take over, althoughthey seem to work very well on the West End stage!So there is a kind of model there that perhaps couldbe tested further. There are issues but there are notissues that are insurmountable.
Q151 Baroness Gale: This access, especially to smallbusinesses, do you know how eVective that has been?And is there anything going on between employers
and trade unions in working together to tackle thisproblem of the stigma of getting people back intowork when they have suVered mental illness?Dr Roberts: I think on the Access to Work scheme andhow that is being used—I would have to check this—my understanding is that there is an issue about howaware employers are about that scheme and how toget the money, and I think it tends to have been usedmore for people with physical disabilities and thosesorts of adjustments than mental health, is myunderstanding.
Q152 Baroness Greengross: Just a quicksupplementary, if I may? How widespread is thepractice with people who suVer, for example, fromdepressive illness, in flexible working and having a setof goals which need to be done in a month, forexample, which give people that sort of flexibility?Does that seem sensible because within anorganisation there are jobs like that to be done, andpeople cannot always say they will be in from nine tofive but can take on a certain amount of tasks to bedone in a month? Is that widespread?Mr Corry: Just to use the example of Rethink;Rethink employs 1,400 people and 20 per cent ofthose have a declared mental health problem. We liketo think of ourselves as quite a successfulorganisation in terms of the services that we provide,and so on, so in terms of a business model it worksand you can employ large numbers of people withmental health problems and still be successful, and Ithink one of the keys to it is flexibility in workingpractices, and I think it is good working practiceanyway to have flexible hours and, as you describe it,workloads that can be spread over a day, a week, amonth, and diVerent targets that are set. It is alsogood management practice to use systems, whichcertainly Rethink use, around monthly supervisionsessions, one-to-one sessions to check back on workand workloads. I suppose the other thing to mentionis just to emphasise that the world Rethink works inis not all soft and fluVy, we run 350 services in thecommunity which are largely funded by the statutorysector and they are only funded against certainoutcomes and targets on which we have to deliver. Sothere is pressure on us as an organisation as well todeliver in the same way that there would be pressureon a private sector organisation to deliver. I am sureit is the same at Mind. I do think that we have asuccessful model that is built around flexible workingand close, supportive supervision with ouremployees.Dr Roberts: I think the model that you have sketchedout is eminently sensible. I think one of the questionsis how widespread is that. I do not have a figure infront of me but my guess is that it is pretty rare fromwhat we know about employers’ attitudes and how

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
70 commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
many businesses have proper mental health policies.The other point I would make is the issue of what thelegal requirements are under the DisabilityDiscrimination Act, and whether that kind ofpractice would count as reasonable adjustment, andI think there is also quite low awareness of legalresponsibility under the Disability DiscriminationAct, as applied to mental health.
Q153 Lord Trefgarne: My Lord Chairman, ourwitnesses have referred to the existing legal structuresin all this, but then they went further and were talkingof new European Directives. Are you really sure thatthe small and medium-sized companies are going towelcome a directive that they must employ even morepeople of one kind or another? That will be deeplyresented.Dr Roberts: The proposal, when I mentionedEuropean Directives, was that it would be allemployers above a certain size, and the requirementwould be simply that they have a mental healthpolicy.
Q154 Lord Trefgarne: But a directive would be hard.Dr Roberts: It might not be a directive; it might besome other mechanism of achieving that end.Lord Trefgarne: When people talk about EuropeanDirectives the alarm bells start ringing!Chairman: Lord Dundee.
Q155 Earl of Dundee: Good morning. How do youthink that a European mental health strategy can bestdevelop a consistent and coherent approach forpolicies impacting on mental health?Mr Corry: For us it is about sharing good practiceacross a number of countries. We would see theEuropean Union as being instrumental in taking bestpractice in one country and being able to spread itfurther through a strategy for mental health, which iswhat is being developed. I think from Rethink’sperspective, perhaps picking up the earlier point, wehave to recognise the real limitations of the EuropeanUnion as it exists and perhaps even the theoreticallimitations of what the future European Union maylook like. I do not think we can get to a stage wherewe have a national service framework for mentalhealth, which we have in England, which sets outcertain standards for service delivery. I could notenvisage a future where we could roll that out acrossthe European Union. But particularly on those largepublic health issues that we have talked about,mental health and health well being in general and—I am sorry to keep harping on about this—the stigmaand discrimination question, I think that is where theEuropean Union could be instrumental in spreadinggood practice.
Q156 Earl of Dundee: Let us take the desirable aimof best practice. How consistent do you think the1983 Mental Health Act is with just that?Mr Corry: Across the European Union?
Q157 Earl of Dundee: Yes.Mr Corry: I think it varies enormously. The researchthat I referred to before that we are doing with theInstitute of Psychiatry about mental healthexperience across the European Union produced—Iwill not go through the statistics—a photographfrom Romania of a caged bed still being used in apsychiatric hospital. We can argue about how wellthe government has done it in this country, butcompare that to the new services that we have overhere around early intervention services, aroundgetting 15 to 18 year olds before they develop seriousmental health problems, crisis services that are aimedat engaging with people in the community to preventthem going into hospital in the first place, there is ahuge gap between the practice on the ground. Interms of compulsion—I think I can speak for Mindwhen I say this as well—we do believe that as faradvanced as we think many of the services on theground are in England, we are about to take a verygreat step in reforming the 1983 Mental Health Act—and I believe it is coming to the House of Lords nextTuesday—and we are stepping back into a culture ofcrisis and compulsion, where in fact what we shouldbe doing is stepping forward into an era of recovery,hope and optimism. I think I have dodged answeringyour question in detail about diVerent legislations ineach country because I do not know in detail what thediVerent legislations are.
Q158 Earl of Dundee: Thank you. Dr Roberts, youmade a point earlier on that while of course mentalhealth is a national responsibility, neverthelessbuilding onto European strategy is much to bewelcomed, and we would all agree with that. I wonderhow you would encourage contributions within thatstrategy, coming from the European Union on theone hand and from the Council of Europe on theother.Dr Roberts: That is an interesting question and it maybe around some of what Paul said, because I thinkthat traditionally the role of trans-national andinternational organisations has been more theenforcement of minimum standards than achievingconsistency of practice, which would not be realistic,and I think the EU could potentially have animportant role in ensuring that certain minimumstandards are upheld within mental health systemsright across the European Union. I found out fromour legal unit earlier in the week that there already isa recommendation—No 10-2004—of the Committeeof Ministers of the Council of Europe to Member

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
71commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
States concerning human rights and protection of theperson with mental health. That, as I understand it,does not have legal force, it is not binding, but it hasa certain moral authority and political clout, and thatsort of set of minimum requirements might be whatwe should be looking for rather than consistency.Very quickly, if you would allow me, on the MentalHealth Bill because it is such an important issue for usat the moment, I would make three very quick pointsabout that. The first thing—and this is why I think itis an issue that should be engaged by Europe—is thesheer fundamental nature of the rights and libertiesthat mental health legislation is dealing with. It isabout withdrawing from people some of the mostfundamental rights of all—about bodily integrity,about freedom of movement—so we need to be very,very careful about safeguards and rights there. Ithink the second thing is that the mental healthsystem is a health system and hospitals are hospitals,they are not places that you should look to forpreventative detention for diYcult people. So if weare going to deprive people of their liberty the quidpro quo for that has to be that we can give themtreatment with a demonstrable therapeutic benefit,and the government seems reluctant to accept that asa criterion. The third and final point I quickly makeis about the European role in making sure that policyis based on evidence, and the proposals in the MentalHealth Bill to increase compulsion in the communityas a way of stopping people relapsing after releasefrom hospital. These proposals have raised rightsissues but they are also not evidence based; all theevidence tells us that the way that you prevent relapsewhen people leave hospital is about good after careprovision, good support services in the community,assertive outreach, and so on. So Europe can help toensure that minimum standards are complied with;they can do so against a background of recognisingthat this engages with the sort of fundamental rightsthat Europe has traditionally championed and it canalso be a bastion and informer of evidence-basedpractice.Mr Corry: Could I add one very quick point on theevidence-based practice? We do know, in particularin relation to the Mental Health Bill andgovernment’s present attempts to amend the 1983Act, that there has been a very large Department ofHealth funded study done on the use of compulsorytreatment orders around the world and theireVectiveness, which we would be very interested tosee published at this moment in time, as it is an issuethat is being hotly debated shortly in both Houses.The Department of Health at the moment seemsreluctant to release it publicly, but we would be veryencouraged if Members of the Committee requestedto see it in the context of what it actually says aboutcompulsory treatment orders and their use within the
European Union. That was probably a bit cheeky,sorry!Baroness Neuberger: But useful.Chairman: Lady Gale will take the next question.
Q159 Baroness Gale: My next question is onimproving information and knowledge about mentalhealth. Could you expand upon the types ofinformation about mental health issues that you feelhave been most deficient, and which you think shouldbe a priority for improvement in the EU knowledgebase that you envisage?Mrs Burner: I think at the moment the mental healtharena in Europe is quite a fragmented thing, and Ithink the greatest problem is finding information.Information is increasingly available throughEurostat and the WHO, but the types of informationthat are available are quite limited. I know when wecame to do our response to the Green Paperconsultation that obtaining information about whatservices and carers felt was important to them wasvery diYcult, so we had to carry out our own researchreport. I think the most significant aspect is the lackof service user and carer involvement within Europe,and I think that the EU platform that is proposed inthe consultation paper would be a useful mechanismfor giving service users and carers a voice withinEurope.
Q160 Chairman: So you want better statistics, morecomprehensive, but also particularly with a focus oncarers and users, as an origin, as an originator ofdata?Mrs Burner: Yes.Dr Roberts: We would entirely endorse that. The onlything briefly to add is that there might be room forsomething along the lines of the EuropeanMonitoring Centre for Drugs and Drug Addiction,which was set up to monitor the progress on theEuropean drug strategy. One of the helpful thingsabout the EMCDDA is that it has also improveddata collection within the Member States. So, in theUK, to take one example, we currently have nonationally collected and published data on waitingtimes for talking therapy, so it would help toimprove that.Chairman: Yes, there are great gaps, are there not, inthe information right across the European Union;there is diVerent information in diVerent countries,which is not there. Lady Neuberger.
Q161 Baroness Neuberger: I really wanted to askyou a question that I suppose is fairly obvious. Wehave some figures quoted about better mental healthservices in the UK, and you have actually raised someof that and said that, although you can be verycritical, in fact compared with caged beds that we

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
72 commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
have seen in Romania and the Czech Republic and soon it is very much better. But if you look at that andyou say, “Okay, we are maybe extremely critical ofsome of the proposals in the Bill but the serviceprovision here is better,” what is there about the UKmental health services that you think a Europeanmental health strategy could make even better, couldstimulate even further, and is there a way, do youthink, that something at a European level could pushare government to doing better still?Dr Roberts: I think the first thing to say is just a noteon the facts about how well we are doing. It is basedon not a huge amount of data, but, for example, weknow that the UK is near the top of the league forinvestment in mental health provision and we knowthat it is near the bottom of the league for suicides, sothose sorts of quite rough figures are indicative. Alsoit is quite low in terms of use of compulsoryhospitalisation compared with some other countrieslike Germany or France. So what I think we couldexport is that we may be slightly further down theroad in providing more eVective care in thecommunity than some of our European partners. Ithink in terms of what the European Union can do todrive up performance here, we have a lot to learnfrom other countries. Just one quick example, I wasreading about some really good service userinvolvement work that was going on in Estonia,which was engaging with local communities, wherethey showed the film of Beautiful Mind in a localcinema. So all across Europe there are things we canlearn from—green care farms that I mentionedearlier. We really do not know all that much; there isnot all that much evidence and research there aboutwhat is going on. The final thing is that although wehave taken an important step over the last 30 or 40years towards deinstitutionalisation there is now asense that we are back-pedalling again, and althoughwe are near the bottom compared with Germany orFrance in our reliance on institutions, we are startingto climb back up and we need to look at that.Mr Corry: Rethink would endorse those points. I donot want to sound too miserable about this becausethat is what the voluntary sector often does, but incomparing our mental health services with thoseacross Europe, yes, I think we can be proud of someof the services that we have developed, but there aretwo warnings on that. One is that the information weare getting back from the comprehensive spendingreview at the moment is that, “Come 2008 that is it—you have had your day.” If you look at the evidencefrom the mental health tsar, Louis Appleby, in hisreview of the first five years of reform, all the evidenceis that the job is very much only half done, and if wewere to take our foot oV the accelerator of investmentand reform in the future we would have missed agolden opportunity to do what the government set
out to do in the Wittchen Report, which was to havea gold standard, world standard mental healthservice in the future. So that is the first warning—thatthe job is only half done. Secondly, I think it is alsoimportant that we compare the experience of usingthe mental health services in this country to theexperience of using physical health services in thiscountry, and there is still a large gap there. If youlook at evidence from the Healthcare Commission,patient surveys of diVerent kinds, it is a consistentlylower positive response rate than people using mentalhealth services. So, yes, we are a long way ahead ofmany countries but we are not where we should be.
Q162 Baroness Howarth of Breckland: We havetalked a lot about the need to ensure that people withmental health problems can get employment andretain employment, but in your evidence you alsotalk about those people who are dependent uponbenefits. One quote that struck us was that, “Caremust be taken to ensure that people with mentalhealth problems are not coerced into work.” It isoften a very diYcult balance to achieve and wewondered how the best balance can be found in theUK between those two things and how the EuropeanMental health strategy would help in that area.Dr Roberts: I think the first thing to say is that therewill be a group of people with mental health problemswho cannot work and are not ready for work at thatparticular time, and it is important that we havebenefits for that group to enable them not only to livebut to participate in the things that we knowcontribute to quality of life and help to improvemental well being. I think for the group of people whocould get into work with the right support and helpand the right job, the question is: what is the bestbalance of things to get them into the workplace? Wehave done a lot of campaigning on the WelfareReform Bill domestically. There simply is not aproblem in relation to fraud in relation to incapacitybenefit—there is not. Fraud rates are about 0.05 percent; fraud is not a significant issue. Actually theOECD has said that we have some of the toughestgateways to disability benefits in the world. Thequestion then is the balance between sanction andsupport, carrot and stick. Do you need to sanctionpeople into work or is about supporting people andencouraging people? There is no evidence thatsanctions work and what sanctions do, if you arerequired to attend a work-focused interview, orwhatever, for a lot of the people we work with, this isa very worrying experience; people become panickedand they often take unsuitable jobs. They do not needsanctions, they are ready to work; what they need issupport, condition management, and so on, to getthem back in the workplace, and a lot of that isalready provided in the voluntary sector. Mind in

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
73commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
particular has some excellent services. It is not onlyproviding support and encouragement and trainingand building self-esteem to get people back into theworkplace, but also stopping people dropping out ofthe workplace in the first place. I was at Croydonlocal Mind association the other week and they havea very close relationship with their local GP surgery,and when people are developing problems they canhelp to ensure that they retain their jobs and do notfall out of their job in the first place. So there are lotsof things you can do. What is the right balancebetween coercion and support? You do not need anycoercion apart from the obvious laws about fraudand proper benefit administration. What you need iscondition management and help and less stigma.
Q163 Baroness Howarth of Breckland: How do youthink that the EU Strategy could help?Dr Roberts: I think that the European Parliament’sdisability integration, its disability action plan couldbe looking at employment as an issue. I think its anti-stigma campaign that we earlier talked about, thepotential for that could make attitudes amongemployers a key target. I think that there is a wholerange of work the European Union could do acrossits responsibilities—across the areas where it hascompetencies—which would help to make inroadsinto that—health and safety at work responsibilities,for example, should include mental health as a coreissue.Mr Corry: We would endorse that again and just addperhaps one point to that, which is the whole workfocus, employment focus. It is also proving achallenge to the voluntary sector as well.Historically—and I do not think this is true of Mind,and I would not ask them to associate themselveswith the following comment—certainly for Rethinkwe were founded by family members of people whowere coming out of long-stay psychiatric hospitalsand moving back into the community, and I stillthink that for us there is a challenge about therelationship that we have with people using ourservices and how much of that is a dependencyculture in which we say, yes, we want to encouragepeople back into work but that there are risksinvolved and we are perhaps a little conservative—with a small “c”—in encouraging people to engagewith that. However, I would also make the point thatas a membership charity we have to listen carefully toour members and one of the big issues for ourmembers is—do not force us back into work if we arenot capable or we are not willing or we are not readyto go back into work. OVer a gradation of choicesbetween a life on benefits and a life of full-time work;everything from the therapeutic benefit that exists atthe moment where people can go to work for periodsof time and earn a certain amount of money, to when
you move back into the workplace to protect yourposition in the benefits ladder in case the work doesnot work out and you have to go back onto benefits.So it is quite a complex area with diVerent tensions.Dr Roberts: Can I mention one point that we wouldlike to put on the record? You may be aware of LordLayard’s work, which makes a strong economic casefor investment in cognitive behaviour therapy andnotes that we lose about £20 billion a year in lostoutput and benefits by not providing talkingtreatments that we know are a factor in gettingpeople back into work. So we would also say thatbetter access to psychological therapies is a key partof solving the employment issue, but also that this isnot just an employment issue, and not just aboutcognitive behaviour therapy. We recognise that thereare very powerful arguments about work, but, asPaul said, there is too much emphasis onemployment—it is also about elderly people, aboutyoung people and so on; it is about access for all toevidence-based therapies that we know can beeVective.Chairman: Strictly speaking we only have fiveminutes left of your hour. We have two questionsfrom Lady Greengross and then another two that wehave not covered. What tends to happen,unfortunately, is that the Membership beginsslipping away as the hour approaches because theyhave other things they need to get on to. We may beable to maintain a quorum, but if there is any dangerthat we do not maintain a quorum—which is onlythree essentially—perhaps you could respond to ourquestions by letter or whatever. Having made thatproviso, Lady Greengross, your question onvulnerable populations, please.
Q164 Baroness Greengross: Dr Roberts what youhave just said in your last sentence, most EuropeanUnion countries now are very diverse in theirpopulation and do you think that there is a role forEurope in identifying particularly vulnerablegroups—and you mentioned two—and particularlyethnic minority diVerences—and we know there aresignificant diVerences—in the type of mental healthproblems from which diVerent groups suVer. Howcould Europe help with the mental health strategy todo something like that?Dr Roberts: It feels to me, particularly in terms ofethnic diversity, that Europe should have a core roleto play because the European Union is partly aboutpeople moving between countries and the problemsand issues they confront in new societies. The pointto make is that there are two general issues. One is anissue about access people have to appropriatecultural services, which might be about language, butit also might be about wanting to talk to someonewho shares your cultural presuppositions. There is

3564222011 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
74 commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
also the problem about the shocking over-representation of some minority groups among thosewho are in the mental health system under forcefuldetention in secure units and so on. I think there is anissue there which is about stigma, but I also think thatit might be a core European Union work stream tolook at the mental health issues that arise given themovement of population between diVerent countries,and to provide financial and other support fordeveloping culturally appropriate services and, quitesimple practical things like the availability of talkingtreatments in a range of languages, or of mentalhealth resources more generally in languages that areappropriate in what are often very diversecommunities.Mr Corry: Particularly in the field of severe mentalillness it is crucially important that as the labourmarket opens up across Europe that this issue istaken on board. All the evidence suggests that theincidents of prevalence of severe mental illness aremuch higher in what you might describe as secondgeneration groups in society. It does not matterwhere their first generation comes from—Africa,Caribbean, Eastern Europe, Ireland or faithcommunities—there is no doubt that the secondgeneration experiences significantly higher rates ofsevere mental illness. I do not think it is fullyunderstood why that is the case; a lot of it has to dowith living in two cultures and the tensions andstresses that are involved in that, but I do not thinkthat is the whole picture, but as we get very largepopulation movements across Europe to diVerentwork places it is going to be very important for thosegroups who settle that services are in place for theirchildren.
Q165 Baroness Greengross: I think we have talkedabout this to some extent, but in terms of humanrights and institutionalisation, that is not really theCommission’s job, human rights, as such, is it, it iswider? But is there a role for the Commission to dosomething about that, in your view?Dr Roberts: I think there is a role for the Commissionin upholding the principle of proper human rightsprotection and safeguards within the mental healthsystem. In broader European Union terms there areissues about the application of the EuropeanConvention on Human Rights within the mentalhealth system. It is extremely diYcult to pursue caseswithin the ECHR framework. The most obviouslyrelevant Article would be Article 3—inhuman anddegrading treatment. What happens to people in themental health system in any other context wouldqualify as inhuman—being pinned down and injectedwith drugs, for example. But there is an issue aboutmedical necessity. My understanding from ourlawyers at Mind is that what cases have been
brought, however extreme the treatment has seemed,none of them have been successful because there hasalways been a defence of medical necessity.
Q166 Baroness Greengross: My main question was,was that the Commission’s role as opposed to thelawyers at Mind’s role?Dr Roberts: Yes, absolutely.Chairman: Except that sometimes you can get acourse in the European Court and of course that thensets a precedent. Talking about the legal cases as faras the Court is concerned and what happened to themwhen they did get there, if there were a diVerentattitude and there were a couple of good cases, whichwere good from your point of view, that would ofcourse have a knock-on eVect, certainly throughoutthe British legal system because we take the decisionsof the Court extremely seriously, and I am sure wewill continue to do so. I cannot speak for other legalsystems but I know that we do take that veryseriously, so it is an interesting point.
Q167 Baroness Howarth of Breckland: I cancompact the last two questions very quickly. We havetalked a bit about the platform anyway, and reallywhat I want to know is what would be most useful tousers and services in terms of a platform acrossEurope. And whilst you are answering that, also tosay a bit about what could be done across Europe interms of the needs of carers and the kind of supportthat families and other members would have in caringfor people with mental illness.Dr Roberts: The first thing to say is we would like tosee mental health services at the very heart of thedevelopment of the European Strategy, and it is notclear from this document that that is really there yet,and there is a lot to be done. There are existing pan-European service user networks—there is a networkcalled Users, Ex-Users and Survivors of Psychiatry,so I think the European Union as part of this processshould be identifying and engaging with existingnetworks. There is also something about sharinggood practice on user involvement across theEuropean Union; there is something about providingsupport information to enable service users toparticipate in a meaningful way where they aresupported and paid properly for their services andtheir expenses are paid promptly—quite simplepractical things. I think there is also something aboutpotential for consultancy style support across theUnion in developing service user involvement. I thinkthis is, an area where the UK can play a part becausethe work of organisations like Mind and Rethink isquite well down the road and we have good practicewe could be sharing with other people, and we can belearning from them too. I think it is important thatservice users are not presented with documents that

3564222011 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
75commission green paper on eu mental health strategy: evidence
23 November 2006 Dr Marcus Roberts, Mr David Stone, Mrs Alexandra Burner andMr Paul Corry
have largely been worked out by other people to sayyeah or nay to; it is about proper service userinvolvement in strategic decision-making, inplanning, in design and in monitoring the delivery ofservices, and that should be absolutely at the core ofEuropean work.Mrs Burner: I would agree that everything DrRoberts has said basically applies to carers as well.Carers’ organisations do exist, such as EUFAMI. Wespoke about these pan-European umbrellaorganisations however what is often ignored is thatthe fact that they are very, very small and they havevery limited funding. I think the necessity of havingthis platform, as Dr Roberts said, is to create a spacefor research and funding, it would be very importantto have a single point of access to information aboutservice users and carers and from service users andcarers as well.
Q168 Chairman: Would that be a website type singlesource of information? Is that the way you would go?That is a natural thing to do at a European level isit not?
Mrs Burner: Yes, I think that would be a goodpotential source. There already exists the EU Portalon health, which is a good source but then there areissues around people’s access to the internet and useof computers and technology. But that would be agood foundation.Mr Corry: My Lord Chairman, we are coming backto visit you again in slightly larger numbers nextTuesday as part of our work around the MentalHealth Bill, so if any of you wanted to come andspeak to service users and carers about any of theissues that are in front of you at the moment or anyother issues, we will be in and around Parliament onTuesday from one o’clock.Chairman: On behalf of the Sub-Committee I wouldlike to thank you very much indeed for your veryinteresting contribution. As I say, if there is anythingthat you wish you had said but did not, we would bedelighted to receive it. Look carefully at the record tomake sure that you have not been misquoted in anyway and thank you very much for your examinationin this inquiry.

3564222012 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
76 commission green paper on eu mental health strategy: evidence
THURSDAY 30 NOVEMBER 2006
Present Dundee, E Neuberger, BGreengross, B Thomas of Walliswood, B (Chairman)Howarth of Breckland, L Trefgarne, LMoser, L
Examination of Witness
Witness: Ms Camilla Parker, Mental Health and Human Rights Consultant, examined.
Q169 Chairman: Ms Parker, it is very good of you tocome and give us the benefit of your wisdom on thisrather complicated matter. I have been looking atyour CV and the things that you are interested in, andyou seem to be perfectly located in what you do inhelping us through this rather special way of lookingat mental health from the point of view of what theEuropean Commission and the European Union cando, which is not quite the same thing as what MemberState governments can do obviously. Thank you verymuch for being with us. We want to focus our inquiryon the strategy set out by the Commission’s GreenPaper so it makes a constructive contribution todealing with these issues at EU level. You knowProfessor Martin Knapp and he is assisting us in ourinquiry. Obviously the human rights aspects ofmental health are a major element in the EuropeanUnion approach to this because human rights is somuch part of the European Union locus and theyhave a real right to operate in that area. Thank youvery much also for the tables that you sent us. I do notthink I have quite absorbed every bit of them, but Ithink they are going to be extremely useful to us as akind of check-list to make sure that we have coveredas many of the angles and as many of the aspects ofthis rather diYcult question as we possibly can. If youwant to refer to those, we do have them before us.Before we start, I need to do a bit of housekeeping.This is an open public session of this Committee andit will be recorded for broadcasting and webcasting.A verbatim transcript will also be taken and this willbe published on the parliamentary website and it willalso be published in the annex to the report once wehave published it. You will be sent a copy of thattranscript in a few days’ time. If you wish to correctit, please do. We do not wish to misquote you orassign the wrong opinions to you because we havenot heard quite correctly, but please advise us ofthose corrections as soon as possible. We would bedelighted if we do not get to the end of questions orif there are wider issues than we can manage withinour hour, which I think there might be, for you tosubmit supplementary evidence by letter if you areable to do that. Could you start for the record bystating your name and your professional title and ifyou wish to do so you can make an opening statementat that point. Thank you once again for being with us.
Ms Parker: Thank you. My name is Camilla Parkerand I am a legal and policy consultant working in thefield of mental health disability and human rights. Iam hoping that I will be able to cover all the points Iwant to make within the questions you ask.
Q170 Chairman: I am going to start now on thehuman rights background to all of this. Of course weunderstand how it is that the European Union hascome to make this initiative. Could you describe howyou think the issue of human rights should berecognised in the development of the proposedEuropean strategy for mental health?Ms Parker: First of all, I would like to make a generalpoint which is that human rights instruments, bothinternationally and within the European area, areuniversal and apply to everyone. That was really whyI thought it might be useful just to give a fewexamples of human rights instruments in one of thetables (marked Human Rights Instruments) to reallygive a flavour of the range of human rights, and reallyemphasise that all of those will apply to people withmental health problems, so that is the first point.Therefore it will not, I am sure, come as a surprise toyou when I say that human rights are integral to themental health strategy that the EuropeanCommission has put forward in the Green Paper, andhopefully will develop. First of all, I think it isimportant that we recognise that people with mentalhealth problems face widespread human rightsabuses, ranging from unjustified institutionalisation,particularly in parts of Europe, to unfairdiscrimination, which I think is worldwide. Thesecond point is that it is important to recognise thatall activities described within the strategy should beplanned and implemented within the human rightscontext, for example, ensuring that the strategyenhances respect for the individual, promotesequality and social inclusion, and ensuring thatpeople with mental health problems are able toparticipate in the planning and implementation ofmental health policies. The third point is it isimportant to recognise that human rights are not justabout ensuring that states refrain from arbitraryinterference with people’s rights. There arecircumstances where states are expected to do muchmore than that and actually take positive action to

3564222012 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
77commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
ensure that their citizens’ rights are protected. Withinthe mental health context we are very clear that inmental health legislation we need to ensure that thedecisions on the circumstances in which people maybe subject to involuntary admission and/orcompulsory treatment are made within a humanrights context and are respecting those individuals’rights. Also looking at this from a human rightscontext, it is very important to ensure that we haveanti-discrimination legislation which includes peoplewith mental health problems. I would argue whenlooking at the strategy, that the human rights contexttakes us yet further, in terms of thinking about how,for example, states should develop community-basedalternatives to institutions. That is something whichI think is very key when you are looking at the issuesfrom a European-wide context rather than justlooking at the United Kingdom, where we see in partsof Europe people are still placed in institutions, oftenfor life.Chairman: You have really covered both the first andthe second question. I think it would be more sensibleto leave this matter at this point because I suspect wewill come back to it again as we go through the restof the paper. I am going to ask Lady Howarth to getdown to some of the nitty-gritty and talk about theEuropean Commission’s platform approach.
Q171 Baroness Howarth of Breckland: Before I dothat can I ask a follow-up which may not be where Iam normally coming from. Because you are talkingabout rights, what about the rights of people to beprotected from those who are dangerous? It is anissue that has become a great cause of debate at themoment. It would be useful if you took a moment toexpand on that balance between the rights of peoplewho have mental illness and the right of thecommunity to be protected.Ms Parker: Thank you very much for asking thatquestion because clearly it is a very important one,particularly at the moment when we are looking at anew Mental Health Bill for England and Wales. Itclearly is a matter of great importance and I thinkthat is where, looking at human rights, what is helpfulis recognising that what needs to happen is a balancebetween individual rights and the interests of thecommunity. I think it would be wrong to suggest thatthere are clear answers on that, but what the humanrights framework can do is oVer a mechanism forreally engaging in very, very diYcult and complexmatters and trying to weigh up the interests of theindividual against the interests of the community. Itis a process of doing that in a way that one isrespecting the individuals’ rights, for example theright to liberty, the right to private and family life,which within the European Convention contextincludes personal autonomy and integrity and wouldinclude issues such as compulsory treatment. So it is
engaging in those very diYcult areas and trying toensure that the process balances those two aspects;the individual rights and the rights of the community.I do not know whether that has answered yourquestion, but I cannot give an answer in terms ofwhat is right and wrong because it would very muchbe in terms of looking at the individualcircumstances. What human rights can oVer is amechanism for going through that process andmaking sure that the ultimate decision did respectthose two interests and balance them and come to adecision that can be seen to be fair and reasonableand there are good grounds for making whicheverdecision it is.
Q172 Baroness Howarth of Breckland: That leads meneatly to the problem we have which is what is it thatthe EU mental health strategy is going to add to thegeneral debate? As you know, the Commission hasseen the strategy having a platform where there canbe some of these discussions across the whole of theUnion. How eVective do you think the concept of theplatform for discussion will be in taking this forward?Ms Parker: I think it will be a huge challenge and onethat I think is needed to be engaged with, butthinking about how to include all the relevantstakeholders, particularly people who use mentalhealth services and their families, and ensuring thatall of those with an interest in developing a strategycan meet and discuss and everyone has their voicesheard, ensuring that those discussions are focusedand then can conclude with some concrete action,and ensuring that that then can be taken forward. Ithink it is a very welcome step, but I think it would bewrong to pretend that it will be easy.
Q173 Baroness Howarth of Breckland: Which takesme again nicely into the next problem which is thatstandards across Europe vary so hugely, and weunderstand that you have a lot of experience acrossEurope. How realistic do you think would be the aimof achieving minimum standards in mental healthacross the European Union and how could theplatform approach achieve that aim? We areparticularly concerned that there might be a wholerange of legal instruments, Directives andRegulations. How useful do you think that might be?Ms Parker: Again, I think that that is a very diYcultquestion to answer. My first point would be the issueabout minimum standards, and I think we wouldneed to be very clear about what we are looking atbecause there is a very broad range of issues that thestrategy covers. I think while yes, in theory, havingminimum standards is a good idea, there is clearly adanger that those countries that are providingservices which are of a higher standard may feel thatthey do not need to try quite so hard to progress, andI think that is something that would need to be very

3564222012 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
78 commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
clearly stated; that these are minimum standards andthe goal is that much further than those minimumstandards would suggest. So that would be my firstpoint. Secondly, coming with some experience oflooking at what is happening in Eastern and CentralEurope, my view is the first thing we would reallyneed to do is to have a commitment across Europe toensure that governments work with the stakeholderswithin their countries to close institutions anddevelop alternative community-based services. Thatfor me would be the key thing to come out of thisstrategy, which I think is not expressed stronglyenough. While there is some reference to institutionsand how that has a contribution to stigma, my viewis that it is far worse than that. If we continue to haveinstitutions where people are placed for long periods,as I said, often for life, that is going to perpetrate thesocial exclusion of people with mental healthproblems, and it is going to perpetrate the fear andignorance which then leads to stigma anddiscrimination. If we are serious about trying to dosomething to promote mental health that has to be,for me, the first step in a European-wide strategy; tomake that commitment and make it very clear thatthere must be work to ensure that the long-stayinstitutions are closed and community-based servicesare developed, with the involvement of service users,to ensure that people can live in the community andcan be supported within the community and haverespect for their human rights. So that would be forme the first step. I think it would be interesting toengage then in terms of minimum standards of howwe take that forward, but that would be the first andforemost point that I would want to see.
Q174 Baroness Howarth of Breckland: In a word areyou suggesting that there really should be a set ofprinciples rather than minimum standards? You weredescribing the dangers of minimum standards andthen what you are describing is a set of principles. Ifthat could be worked out through the EU it wouldactually give us a way forward?Ms Parker: Yes, and again human rights are a goodstarting point for thinking about those principles. Inthe second table that I gave to you I suggested somekey principles right at the top: protection againstdiscrimination; the promotion of equality and socialinclusion, the promotion of personal autonomy andindependence; least restrictive alternative. Youtalked about the issue of people who presented adanger and what action should be taken in order toprotect the community. That principle would bepicked up in there in assessing someone’s risk andidentifying those risks and then thinking about howto address those risks. Within that process you wouldbe thinking about the least restrictive alternative,which means how can you address those risks in away that is the least intrusive, so you address the risk
but you do not—the expression that is used in theEuropean Convention—use a sledgehammer tocrack a nut. It is thinking about what is the mostappropriate action to take. I think that is a verycrucial principle within mental health. Then theprovision of care on the basis of individual needs andthen, finally, I have suggested participation in policydevelopment for service users. Yes, that might be thestarting point which the platform could then look atand decide what principles they think would bevaluable. For me the underlying point is that what weneed to do is have a shift from the idea that peoplewith mental health problems and people withlearning disabilities should be placed in institutions,and move towards providing the appropriate supportwithin the community.
Q175 Chairman: Can I ask a question which isperhaps not quite so straightforward from your pointof view. During the process of enlargement, theincoming states are supposed to acquire theaccumulated fruit of all treaties but they are alsosupposed to show that they are on the right path asfar as human rights are concerned. That usuallymeans the justice system works well, the police areunder control, the military does not take too muchpart in public life and all that kind of thing. There aresome other major human rights issues of which thismight be one where we might want to be a little bitmore fierce—not that the British have a particularlystrong platform on which to stand in this particularrespect—but the Community might wish to be a littlebit more exigent in this kind of matter. What wouldyou think about that?Ms Parker: Yes, I think that would be very helpfuland extremely important. That is certainly somethingthat people have tried to highlight within theEuropean Commission, the need to look at thehuman rights of people with mental health problemsand intellectual disabilities (learning disabilities as wecall them in the UK). That is certainly something thatdoes need to be raised as an issue. Again thinkingabout the debate around institutionalised care andcommunity-based care, I think that is something thatwould be important for all European Members todiscuss.Chairman: That is why I said I do not think we havea particularly strong platform here on which to standon and criticise other people, because although weare putting people out of institutions, I am not so surethat we are supplying the mental health care in thecommunity that people need. I have got twosupplementaries, one from Lady Greengross and onefrom Lord Trefgarne.
Q176 Baroness Greengross: It follows on, Chairman,from what you have just said. We must learn fromhistory as well. I would have thought that closing

3564222012 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
79commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
down institutions before adequate provision has beenset up in the community would be a total abuse ofhuman rights. We know what happened in Italy, weknow what happened in some parts of the US, andeven here when one assumed there was a communitycare pattern which was widespread which in fact didnot exist. I just think if we are doing this in thecontext of human rights it is sometimes a very slowprocess and the disaster of institutionalisation couldbe exchanged for something even worse, because theyare totally insecure if we chuck people out into thecommunity when they have been institutionalised fora long time.Ms Parker: I completely agree with you and I thinkthat is why when the word “deinstitutionalisation” isused, which for non-native English speakers is alwaysa very diYcult word to say, but also it is a verydiYcult thing to achieve. For me deinstitutionalisationis not just about closing the institutions; it is aboutdeveloping the alternatives, and they have to go inparallel. I think that is one of the points arising fromthe UK experience—and we have not got everythingright—but we can perhaps highlight the things thatwe have not done so well. Looking at where countrieshave closed institutions, the point is that alternativesmust be developed at the same time, and thatobviously has cost implications but I do not thinkthat is something that governments should shirkfrom. It is very complex and that for me is why we doneed to address it, because it is about sharingexperience and thinking about the complexity ofshifting from institutionalised care to community-based care and thinking how the financial, the legaland other mechanisms need to be thought through,and it is very complex. Where perhaps othercountries that have not started that process as yetmight be in a better position than the UK was, is thatthere is now, a very strongly feeling that people whoare receiving services and their families and othersupporters should be very much engaged in thatprocess of shifting from institutional care tocommunity-based care. What I am concerned aboutis that there is not suYcient impetus to make thatchange, and that is what for me really does need tocome out of a mental health strategy for Europe: tosay that we need to close the institutions but in orderto do so we need to ensure that alternatives aredeveloped so that we are not in a situation wherepeople are removed from the institutions and thenhave no support. That is not at all what I wouldargue for.
Q177 Lord Trefgarne: May I agree very stronglywith what Baroness Greengross has been saying andour witness has been confirming about the need forthe development of in-the-community arrangementsin parallel with the closure of the huge institutions.We seem to take it as read that the standards of
human rights observance in the Eastern Europeancountries and the new members of the EU aregenerally much worse than ours, and on the whole Ibelieve they are. How far, however, I am anxious tobe lectured on these matters by the EuropeanCommission is another matter. I do not think that wewould take that very kindly, particularly as many ofthe Commissioners themselves come from thoseEastern European countries, and if one of them werestanding up to lecture us on some shortcomings hehad seen here I would take that rather amiss, as I daresay we all would. I was going to ask whether youthink that the overall observance of human rightshere—and charity begins at home does it not—withregard to the human rights field is, in your view,adequate?Ms Parker: The short answer is no. I should reallytalk about England rather than other parts of theUnited Kingdom. We have made the shift from thelarge institutions to community-based services, but Ithink we still struggle with the fact that people whodevelop mental health problems do face a hugeamount of stigma. In England what we see isinsuYcient service provision for people. Too often wesee that people have to reach crisis point beforesomething is done, and that then means that they areperhaps placed in hospital under the Mental HealthAct. I think what we really do need to be looking atis how to ensure we can provide appropriate supportto people and ensure that that is timely and issomething that they are involved in in terms ofplanning their own care, and also families areinvolved as appropriate. I think that is for us the realchallenge to ensure that we provide mental healthservices in a way that is accessible and is appropriateto people’s needs.
Q178 Lord Trefgarne: Do you think that it too easyfor a family to get, say, an elderly relative who hasgone potty locked up?Ms Parker: I would perhaps think about it in anotherway, which is that people trying to get services forthemselves or for their relatives sometimes find itincredibly frustrating. One of the challenges in thiscountry in terms of the provision, particularly ofsocial care support, is that we are looking at localauthorities who say they have got very restrictedbudgets so the eligibility criteria for receiving servicestend to be very high. Then there are issues around theprovision of care. I think one of the things that hascaused concern for disabled people generally is that,too often, a placement in residential accommodationis suggested rather than providing people withsupport in their own homes. That is how I woulddescribe the scenario, rather than families trying toput their relatives in an institution. It is much morethe frustration of not getting suitable support forpeople so they can live at home, if that is what they

3564222012 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
80 commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
choose to do. Clearly people should be able to choosewhether they want to receive support in their ownhomes or want to go into residential care.Chairman: I think I am going to bring us back to ourlist of questions; thank you for those interventions.Lord Dundee on defining mental health and mentalill health.
Q179 Earl of Dundee: Within the context of humanrights how important do you think it is to clarify thedefinitions of mental health and mental ill health?Ms Parker: Again, I think it will really depend onwhat context we are talking about. In terms of mentalhealth promotion, having some very broad conceptsof mental health—and I know you talked aboutissues such as emotional well-being—and being asinclusive as possible would be good in that context,but clearly, going back to the previous questionabout people who are perceived to be dangerous andwhat needs to be done, what you need to have then issome very clear criteria, which would include anassessment that somebody does have some form ofmental illness, alongside other criteria to ensure thatonly in limited circumstances do people becomesubject to compulsion. That is why I am saying itdepends on the circumstances.
Q180 Earl of Dundee: But how would you deal withthe concept of well-being, for example? Well-being isa sine qua non obviously but here it could come to bea tricky customer. For within a strategy of mentalhealth it has got a foot in both camps. A man who ismentally ill, wants to get better, and when he getsbetter he wants to take on well-being; yet converselya man who is not mentally ill also wants to developwell-being. Therefore well-being itself has a foot inboth camps. However, we are told that a strategywhich gives too much prominence to well-being isgoing to include 25 per cent of the population, sothere is a dichotomy here. How would you deal withthis and how would you sharpen up on a definition ofwell-being to help that strategy?Ms Parker: I am not sure that at this moment I couldcome up with a definition of well-being. What Iwould say is that when we are looking at those issueswhat we are talking about is prevention and trying tothink about how people can really think about theirmental health, in the same way as they think abouttheir physical health, and the need to ensure that welook after both. So I think that is important in termsof having a broad concept. In that context, thatworks well because it is trying to almost shift people’sattitudes from mental health or mental illness asbeing something that happens to other people and isvery scary, whereas if you start thinking aboutmental well-being and how that is just as importantas looking after our own physical health, then thatmight start to engage people with this concept and
have some success in minimising the stigma anddiscrimination. I am sorry, but I do not think I cancome up with a definition of well-being other than toput it in those broad terms as to why I think it wouldbe useful to have that.
Q181 Earl of Dundee: Those broad terms that youhave just expressed could be very useful in helping adefinition or clarification come into being. Perhapsone does not have to think of particular definitionsnecessarily; what we want to achieve is a gooddirection to the strategy.Ms Parker: Yes, absolutely.
Q182 Earl of Dundee: What you have said might bevery helpful I should have thought.Ms Parker: As I said, a concept of well-being isincredibly important in terms of thinking about howwe can promote mental health and how we can ensurethat people are more willing to seek help at an earlierstage because they recognise that as being important.We would minimise the stigma so that that enablespeople to feel less uncomfortable about seeking help,so looking at it from that point of view, a broad termof mental well-being is a very useful one but, as I said,you then also have to think about other contextswhen we are thinking about the use of compulsion. Iwould want to ensure that the criteria are reallytightened up in that area so that we have muchclearer, discrete definitions in terms of when wewould use compulsion, but that is trying to addresssomething slightly diVerent to the well-beingconcept.Chairman: We had some interesting evidence lastweek from MIND about what people had discoveredabout the various aspects of our lives that actuallycontribute to our feeling of well-being. There wassome interesting evidence and I am sure you will findit interesting when the report comes out. However, Iam not going to distract us by going down that pathnow. Lord Moser, we are talking here about peoplewith learning disabilities and the grouping of themwith people who have mental health problems.
Q183 Lord Moser: In a way, it is the samedefinitional problem once again. I have to confessever since we have started on this inquiry I have beentotally uncertain and confused as to what is in andwhat is out (and Professor Knapp will presumably indue course tell us what the answer to that is) so I wasvery surprised that in the Green Paper learningdisabilities make an appearance. This is a field that Iused to have some connection with so I know a littleabout learning disabilities, and I know very littleabout mental ill health, but I find it very diYcult tounderstand—and you did mention learningdisabilities a moment ago—whether our inquirydeals with learning disabilities. I do not believe it

3564222012 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
81commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
does. Within this context what is interesting iswhether from the human rights point of view theseare two related things that interest you and, if so,why?Ms Parker: Yes, I would agree with you that that isone of the areas where the Green Paper is not clearwhether it includes people with learning disabilitiesor not. I think, on balance, I would like to seelearning disabilities included in that, and that againreally goes back much more to thinking about thisbeing a strategy for Europe. It seems to be the casethat in some countries there is insuYcient distinctionbetween the two groups, people with mental healthproblems and people with learning disabilities, andindeed in some countries institutions house both, sofrom a human rights perspective and from aEuropean perspective I would suggest that it isimportant to have both groups in the strategybecause both groups are the most marginalised of analready margionalised group of people, ie peoplewith disabilities. I think it is really important to havesomething in the strategy to recognise that those twogroups of people do face very severe human rightsabuses, going back to the point about institutionsand being placed in institutions, such as the stigmaand discrimination that they face and the problemsthat they would have if living in the community interms of being able to work and to make a wholerange of decisions that many of us take for grantedsuch as the right to vote. So there are a whole host ofhuman rights aspects that are similar for people withmental health and for people with intellectualdisabilities. If I may go back again to a Europeanconcern particularly for Central and Eastern Europe,in many of those countries they have a system ofguardianship, which is nothing like our guardianshipunder the existing Mental Health Act. It is aboutpeople being deemed to lack capacity, and in somecases they are deemed no longer to have a legal entityof their own. A guardian is appointed who then willmake a whole range of decisions on that person’sbehalf. Sometimes that might be agreeing that theperson goes into an institution. Another examplewould be the barriers to employment that thosepeople who are placed under guardianship face.There is a lot of confusion in many of the countriesabout whether or not someone under guardianshipcan actually work or whether the guardian can agreeto them working, and clearly that is a major barrierfor people who are subject to guardianship to then goback into the community and actually enter intoemployment. So I think there are very major barriersthat both groups face in terms of human rights abusesand also being included in the community, which Ithink it would be very useful to recognise in a strategysuch as this. That is not to say that their needs are thesame but in terms of the barriers I think they aresimilar.
Lord Moser: The last thing I wanted is to argue withyou but I found this rather confusing. From ourpoint of view, in my view at least, the more specific wecan be the better. What is true is that learningdisabilities are disabilities, so are mental healthdisabilities, so are a million other things. What theyhave in common is that they are disabilities, but thatis no reason for including them. Secondly, it isobvious to me that some learning disabilities arecaused by mental ill health, but so are many otherthings. It is again no argument for including thembecause they are an eVect of mental health. Mostlearning disabilities that I know about have nothingwhatever to do with mental ill health, such as dyslexiawhich is the most common learning disability. So Iunderstand what you are saying but I still do notunderstand really why it makes sense, certainly fromour point of view, to be all inclusive. However, I thinkI had better leave it at that as just one reaction.
Q184 Baroness Howarth of Breckland: I am justtrying to get a greater clarity on this one. The learningdisability lobby in this country would argue veryfiercely that to include people with learningdisabilities—and I mean with the more severelearning disabilities than the ones Lord Moser istalking about—is contravening their human rightsbecause they are not mentally ill. They might bementally ill, like anybody else might be mentally ill,but they are not mentally ill per se. However, Iunderstand what you are saying, that people arealready lumped together in other parts of Europe andwe have a diVerent position here. I just wondered interms of taking a EU perspective in trying to dealwith that issue whether you had a way of taking thatforward because it is quite a polarised situation.Ms Parker: I agree, it is a very diYcult one. Onbalance, I would suggest at this point (and because itis Europe we are looking at) it would be good to havelearning disabilities within that strategy. Equally, Irecognise the reasons for not doing so because we aretalking about a diVerent group of people. Going backagain to the European aspect, one of the otherconcerns I have about this strategy is that it does notseem to me to relate as strongly as I would havehoped to the work that other parts of the EuropeanCommission are doing on disability generally, ie theDisability Unit and the Disability Action Plan, whichvery much promotes the concept of independentliving and access to social care and support, which Iwould want to see including people with mentalhealth problems. However, it may be that peoplefrom the learning disability sector would much preferlearning disabilities to be placed within the DisabilityAction Plan. I would not have an argument with that.I suppose my only point is to really ensure that we allrecognise what happens in relation toinstitutionalisation, aVects people, whether they have

3564222012 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
82 commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
mental health problems or whether they havelearning disabilities, and this is what happens topeople in some parts of Europe, and to try andaddress that. If people feel it would be far better to dothat within the Disability Action Plan, I would bevery supportive. I just do not want them to be left out,and that is what happens too often with people withlearning disabilities.
Q185 Baroness Neuberger: You have partlyanswered the question about stigma and you havemade it clear that some understanding of the humanrights of people with mental health problems, if youactually have a human rights base for understandingthat, it might help them integrate better into thecommunity. You have certainly argued that makinga statement of the principles would make that veryclear. Do you think there is something else morespecific that could be done within an EU platform,particularly when you look at the issue ofemployment? Do you think there is something morespecific that could be done given the diYculty ofreporting across Europe and the diYculties of peoplewith mental health in getting and indeed staying inwork?Ms Parker: I think that would be a very useful area ofwork for the platform to look at, because I thinkthere is a will to try and make changes across theboard. If we could look at something as specific asemployment, that could really engage people and getpeople thinking about how we can move forward.One example we do have is the European Directiveon employment which should already have beentransposed within states’ legislation ie, they havetaken the Directive and they now have legislationwhich incorporates the requirements of thatDirective. Where I think it would be very useful, andcould be a specific piece of work for the platform tolook at, is whether the legislation within each countrydoes, first of all, take on board the Directive and,more specifically, does it ensure that people withmental health problems are covered and then what ishappening in terms of reasonable accommodation,this concept of enabling people to get intoemployment and getting employers to work with theemployees about how to—
Q186 Baroness Neuberger: You mean thatflexibility?Ms Parker: Yes, reasonable accommodation. Oftenpeople think of it as making buildings accessible topeople with physical disabilities. Where it is morediYcult, and obviously from our point of view veryimportant, is to think about reasonableaccommodation in terms of flexibility for people withmental health problems. I think that would be a veryuseful piece of work for the platform to discuss andengage in and come up with some very clear ideas for
helping employers to do that and ensuring thatindividuals are aware of their rights and can seek towork with employers in ensuring that there are moreflexible working practices, so I think that would be avery useful piece of work to be done.
Q187 Baroness Greengross: Obviously we are a verydiverse society from an ethnic minority point of viewbut also in terms of age and gender and so on, anddiVerent groups of people have diVerent experiences.So what do you feel are the most important thingsthat the strategy should include to cover thosediVerences or should it just be one general strategy?Ms Parker: Certainly in terms of looking at thediVerent groups that you might want to be thinkingabout in terms of the mental health strategy, I thinkit is absolutely crucial that we look at children andyoung people. Again just looking at what ishappening in the UK, I think there are figuressuggesting one in 10 children develop mental healthproblems, so that is something that we do need to betaking seriously. If you get into young people in careor in custody then those figures rise very steeply, andthat is something that should be of concern to us.Again, I think looking at it from a Europeanperspective, we see children and young people placedin institutions, and that is something of seriousconcern. That is because of a whole range of thingsbut one of the reasons is there is no support forparents for caring for their children in thecommunity. Women—yes we need to look at thatgroup in terms of mental health, but again then youstart having a very long check-list. Equally, weshould be aware of the issues relating to men andmental health and the high rates of suicide we see, andI think that is across Europe. Certainly there is a highrate of young men in the UK who take their own livesunder 25. While I am obviously conscious that wecould have a very long check-list, I think somehowwithin the strategy there does need to be somerecognition of the particular issues that relate toparticular groups. If we could do that in a way that ismanageable then I think that would be a very usefulpoint to include. Also in terms of ethnic minorities,again knowing the situation in England where thereis a high proportion of young black men who areplaced in hospital, often in seclusion and such like,thinking about that as something that we do need tolook at and think about what is happening and howcan we address that. There are various areas that Ithink could be usefully highlighted within a strategy,but clearly what that needs to do is highlight those asissues and then really help states to look at what isgoing on in their own particular country and thinkabout what is important to them. That is why, goingback to the platform and participation, it is going tobe really important to involve stakeholders becausewe are talking about a European strategy. In order

3564222012 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
83commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
for this to be meaningful, it then needs to be carriedforward into each country and people need to takethose points seriously and work to address the areasof concern that have been identified.
Q188 Earl of Dundee: It certainly does and youmentioned young people in prison but generally theprison population and their human rights and indeedthe strategy for people in prison with mental healthproblems is obviously a priority, or should be, buthow do you feel this issue should be addressed?Should it be a specific area of concern? Should it bedealt with in terms of human rights?Ms Parker: Yes, it is an area of concern and I think itshould be in the strategy. I know that it is a seriousconcern in the UK; I am not so aware of what thesituation is in other countries, but I suspect that wewould find (if there was any work around) that it is asimilar concern in other countries, so it is something,if that was the case, that needs to be addressed both atnational level and also within the European strategy.From a human rights point of view, I think therewould be questions around how appropriate it is toplace people with mental health problems in a prisonenvironment and should there not be a moreappropriate placement for those people, thinkingabout the adequacy of care for prisoners and whetherthat is something that we do need to address. I thinkwork is going on at the moment to look at what ishappening within our prisons, but I think more canbe done and, as I say, from a human rightsperspective one would challenge whether or notpeople with severe mental health problems should bein prison at all.
Q189 Chairman: A point which occurred to me is ifyou start talking about specific groups with specificmental health problems, is there a danger that thewhole group gets stigmatised? I have been drivingthrough the streets of London regularly and it isremarkable how often you see people from aCaribbean background behaving in peculiar ways inthe street. I do not want to say more than thatbecause I do not know what the basis of theirbehaviour is. I have certainly seen a couple of peoplewho seem to me to be suVering from some kind ofmental disorder. You could see it, could you not, inthe Daily Mail “Persons of Afro-Caribbeanbackground are much more likely to have mentalhealth problems than the rest of us”, and that couldbe used in a stigmatising way. I know you have totreat people and it is a useful way of concentrating themind on where resources and action should betargeted, but how could you escape from that kind ofresponse in the general community? It is a hard one,is it not?
Ms Parker: I think probably it is trying to go backagain to this idea—well, it is not an idea it is factualin terms of one in four people may have mental healthproblems at any time in their lives. I suppose thestarting point is trying somehow to get across thatthis is not something that happens to “others”. Anyone of us or people one is close to could developmental health problems but that does not mean theyare no longer a person. It means they are having todeal with some crises and could be very distressed,but they are still a human being. How can we get thatacross, but then also recognise that there areparticular groups within our society who face, on topof that, particular discrimination? I think that iswhere when we are going into discrimination in thissense. We should recognise that, again, we are allhuman and somebody may face discrimination onthe basis of their disability but they may also facediscrimination on the basis they are a woman or onthe basis of their sexuality, and it is recognising thatpeople can face multi-faceted discrimination andtrying to work on a basis that what we need to do isrespond to individual needs, not make blanketdecisions and not have prejudice against peoplebecause of, for example, their background, the colourof their skin, or the fact they use a wheelchair. I amnot sure I am answering your question.
Q190 Chairman: I understand what you are saying.Ms Parker: It is a very complex question and it needsto be unravelled how we all perceive each other and,coming back to the human rights point, how we needto respect each other as individuals.Baroness Howarth of Breckland: And it could be thatblack people are more noticeable because we noticethem.Chairman: It could be that; I am simply reporting anexperience I have had.
Q191 Baroness Howarth of Breckland: It leads neatlyto my question because those are issues about how weimprove knowledge and understanding about mentalhealth generally in the EU context. It is said thismight provide a considerable opportunity forlooking at knowledge right across the spectrum. Youhave talked a lot about gaps and about things that wedo not know. If you had the opportunity to say whattype of information you would think was currentlymost deficit, what do you think would be the priorityfor the EU? If you had a research budget what wouldyou spend it on?Ms Parker: Top of my list would be looking at howto develop best practice and disseminate best practicein relation to the transition from institutional care tocommunity-based services. I think that is essential.Again, I am looking at it from a Europeanperspective. It seems to me that even when there is awill on governments’ part, there may be a lack of

3564222012 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
84 commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
expertise. This is a really huge transition, and in theUK we took a long time in achieving that transition.I think trying to engage with governments and shareexpertise, share learning, and again I would like tostress that we have not got it all right in this countryand so it would be very much an exchange ofinformation, but if we could do something on thatand really assist that shift, I think that would be avery valuable and important piece of work.
Q192 Baroness Howarth of Breckland: You are oneof the few people we have had before us who hasmentioned children and young people. It happens tobe my passion in mental health. The transition forthem is very diVerent to the transition for adultsbecause it involves alternative forms of care otherthan just accommodation and support; it involvesgood parenting issues. How would you see theEuropean Union getting into best practice in thoseareas? We are not very good at it even here, where weare putting young people into prisons with all of theeVects that has on them.Ms Parker: Again, I guess my starting point would beabout exchanging information and best practice, andyou could have another piece of research looking atwhat is going on in other parts of Europe and what isworking and what is not working. I certainly wouldagree with you that in this country we have veryserious problems at the moment in terms of ensuringthat children and young people who develop mentalhealth problems get services early on. Too often,things are left until they reach crisis point. I realise Isaid that about adults but I think it is a worsesituation for children and young people. I think thegap is the transition between children and adolescentmental health services and adult mental healthservices. My understanding is that for a lot of youngpeople they find that they are not considered to beeligible for adult mental health services and they getleft without support. From a legislative point of viewthere are also issues around the Children Act 1989and then looking at the community care legislationthat we have and again whether agencies such associal care services are willing to take on and engagewith young people who perhaps received services as achild or young person and then the question is arethey eligible for support as an adult. I would notpretend to be an expert on that, but it does seem to methat is another area that we are struggling with, and itwould be interesting to find out whether othercountries in Europe have similar problems, andperhaps some of them might have solved some ofthose very diYcult issues.
Q193 Chairman: It is a question of diVerent modelsof mental health care provision and that is one of thethings we might find out more about and, as you say,the transition between one model and another is
always diYcult in any health care system. We havehad this in other parts of the health care system, sothat is complicated in itself, to say nothing of thefunding problems of the transition, which is usuallyvery expensive. I think that is interesting. I think wehave one last question which is like asking you toreinvent everything you have said really because whatwe are asking is how you view the human rights issuessurrounding the Government’s intention to updatethe 1983 Mental Health Act. When we were lookingat this question before we started I suggested wemight ask you to give a one paragraph reply and ifyou wanted to write another 15 paragraphs, orwhatever it was, we would be very happy to have thatfrom you. Some people sitting around this table arejust beginning to struggle with this as it is just cominginto the House of Lords now and we had the secondreading this week. So what do you feel about thatparticular hot potato?Ms Parker: I guess on the whole it is quitedisappointing that we have reached this point aftermany years of consultation and people are still veryunhappy with what is being proposed. We have got aslimmer bill but it is not that slim and I think manypeople are really very disappointed with the fact thatthe proposals that have been taken forward are notthe ones that many people working within the mentalhealth sector would want. A lot of the good points ofthe draft 2004 bill have been dropped, such asadvocacy. Again, picking up on children and youngpeople; that is a huge concern in that there are nosafeguards, whereas there were at least somesafeguards for children and young people before. Interms of one of the core proposals, the communitytreatment or supervision orders, this is somethingthat raises for me quite a lot of concern, and I thinkit is really about how that would be put into practice,and I think in terms of human rights how that wouldbe implemented. I realise I am repeating myself but Iguess for me what is really crucial is ensuring thatpeople have access to the services that they need. ThisBill does not do that, the Government is very clearthat it does not do that, but that is where I think wecould usefully do more, given our focus, and I thinkin terms of human rights that is something that willneed to be looked at in closer detail, particularly inrelation to the implementation of the Act. I know theGovernment has brought in some revisions that pickup on areas that have been shown to be contrary tothe European Convention on Human Rights, and tothat extent it is welcome but I am concerned that thisis not really going to address the real needs of peoplewith mental health problems.
Q194 Chairman: Thank you very much for a veryinteresting evidence session. I think we have beenvery lucky with all the people who have appeared

3564222012 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
85commission green paper on eu mental health strategy: evidence
30 November 2006 Ms Camilla Parker
before us so far, and you are certainly one of a rathera distinguished group and you have given us a lot ofmeat to think about. As I say, if there are things thatyou wish you had said or things that you feel youwould like to say when you get back to your oYce, asit were, do not hesitate to write us a letter and we can
add that into the evidence. Meanwhile on behalf ofthe Committee I would like to thank you very, verysincerely for what you have given us here thismorning.Ms Parker: Thank you very much for giving me theopportunity to speak to you.
3564222013 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
86 commission green paper on eu mental health strategy: evidence
THURSDAY 7 DECEMBER 2006
Present Dundee, E Moser, LGale, B Thomas of Walliswood, B (Chairman)Greengross, B Uddin, BMorgan of Huyton, B Wade of Chorlton, L
Memorandum by WHO Mental Health Programme
The World Health Organization (WHO) Regional OYce for Europe welcomed the European Commission(EC) proposal for the development of an European Union (EU) Strategy for Mental Health, which followedthe Ministerial Conference in Helsinki.
WHO has long supported the development of mental health in the European Region, with one of its lateroutcomes being the European Ministerial Conference on Mental Health, held in Helsinki, January 2005. Thisconference, with the support and co-sponsorship of the European Commission and the Council of Europe,gathered political support for mental health across 52 European Member States which have signed andendorsed the European WHO Declaration and Action Plan for Mental Health.
In support and further development of some lines of the WHO Declaration and Action Plan, the Green Paperhighlights the importance of developing areas of mental health within the competence of the EU, includingthe improvement of quality of life and protecting the rights and dignity of people with mental health problems,the promotion of mental health and prevention of mental ill-health, and the provision of a European systemon mental health information. These are all also central aspects in the WHO Action Plan.
1. Strengthening the Points put Forward by the WHO Declaration and Action Plan
The role of the WHO and its accountability framework diVers considerably from the EU. Its health mandateis broader than the EU, including support to countries to develop health systems and services.
However the WHO Declaration and Action Plan on Mental Health also stress the importance of mentalhealth, the centrality of mental health for human, social and economic development and the importance andimpact of positive mental health as part of other public policies such as education, justice, social care oremployment. These aspects that contribute to population’s mental health and are outlined in the WHO ActionPlan are central to the European Commissions’ role.
The WHO Declaration and Action Plan outline a framework for a comprehensive approach to mental health.The initiative of the European Commission strengthens the points put forward by the WHO, and suggestsactions in the areas of competency of the EC, highlighting that mental health is central to health and socio-economic development and key to achieving the EU’s strategic policy objectives such as those envisaged in theLisbon Strategy.
2. Added Value of the Green Paper and EU Strategy
We hope that the EU strategy on Mental Health will add value as a supporting mechanism at the Communitylevel towards the implementation of the WHO Declaration and Action Plan for Mental Health. I may alsostimulate inter-sectoral policy development through the engagement of the non-health policy sector.
In principle, WHO supports the proposed actions and priorities identified in the Green Paper, which are basedon the current evidence, are supportive and complementary to those proposed in the WHO Action Plan onMental Health, and provide a comprehensive approach. The four actions prioritised in the Green Paper:promotion of mental health, prevention of mental disorders, improvement of quality of life and protectinghuman rights and dignity of people with mental health problems and a developed mental health information,research and knowledge system for the EU are essential. In addition the two areas of action proposed by theEC Green paper at the European level, the creation of a coordination mechanism and the inclusion of the non-health sector on mental health issues are welcome by the WHO, as these bring value added to the ongoinginitiatives:

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
87commission green paper on eu mental health strategy: evidence
7 December 2006
Coordination mechanism. The proposed actions and initiatives by the EC Green Paper, such as the creationof a European Platform and an information system for mental health could be an asset for the developmentof mental health across European countries. It could support exchange at the Community level by providinga platform for an eYcient approach to implementation. The support to co-ordination across countries iscrucial along with the involvement of key European and International stakeholders and organizations thathave a direct or indirect relation to mental health development, also as stressed in the WHO Declaration andAction Plan. The presence of WHO as a partner in the coordination mechanisms may ensure collaborationand information sharing as well as avoid duplication.
Inclusion of non-health sector. The inclusion of other non-health sectors in the proposed European Platformand other actions proposed in the EU strategy supports the development of action for mental health acrosspublic policy, potentially broadening opportunities for improving the mental health in the European Region.
3. EC and WHO Working Together
In order to ensure complementarity of approaches and actions the WHO Mental Health Programme and theMental Health division of the European Commission have been working closely together in the discussion anddrafting of the EC Green Paper on Mental Health.
Actions proposed in the Green Paper are compatible with those proposed in the WHO Action Plan, andprovide a description of what can be achieved in the four areas of the WHO Action Plan that the EC GreenPaper encompasses.
The WHO has also been actively involved in the preparation and course of the Consultation Process on theGreen Paper, and the organisation of the three Invited Consultation meetings organised by the EC. The WHOProgramme, as member in the main committee of the EC to support the consultation process, has been activelyinvolved in the consultation meetings themselves and in providing support for the outcomes of the meetings.
The WHO is currently involved in the brainstorming sessions and drafting of the EU Strategy following theconsultation phase, furthering the recommendations in the Green Paper.
We hope that this synergy will be perceived by Member States as a strengthening mechanism for the field ofmental health. The partnership between the two organisations could ensure that the European futureguidelines for mental health development are perceived as a joint and complementary action.
Challenges
A key challenge for the EC is the production of a meaningful strategy that can make a positive impact onmental health of the population of Member States, and to follow up the strategy with activities that willfacilitate change.
The WHO will need to muster its resources in order to make the greatest impact in areas of greatest need. Allof its poorest Member States are outside the EU, and the balance of action between the needs of people withmental illness and the wellbeing of the population as a whole is very challenging.
Finally, the EC and the WHO are discussing how best to complement each others’ activities in order to avoidoverlap. Member States, mandates and implementation mechanisms are not identical, and the organisationsneed to be constantly aware to add value, rather than to duplicate eVorts.
Examination of Witness
Witness: Dr Matt Muijen, World Health Organisation, examined.
Q195 Chairman: Good morning, Dr Muijen.Thank you very much for coming to help us. Youare extremely welcome here. Obviously, from yourperspective as European WHO representative youare just the person we need to fit this all into theinternational strategy. I have a number of pointsthat I need to make before we start this session. Weare sorry that we had to rearrange the date. I hopethat has not inconvenienced you too much but it isone of these things which happen occasionally. We
have heard from a number of very helpful witnessesabout the issues raised by the Commission’s GreenPaper. Indeed, I think we have had an exceptionalset of witnesses so far to this inquiry and I am sureyou are going to be just such another one and weare keen to explore how all this fits into a moreinternational approach to this whole matter ofmental health and its costs and the stigma attachedto it. You may already know Professor MartinKnapp. He is here to help us write a good report

3564222014 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
88 commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
and I am going to say in public what I said to himin private at our last session, that if he does wish tointervene or ask a further question he should nothesitate. We have some housekeeping points. Theacoustic in this room is abominable. If you couldspeak with your head up that would help us all. Itis what opera singers call singing out. I am sorryabout that but it can be quite diYcult. A verbatimtranscript will be taken of your evidence and thiswill be published on the parliamentary website andalso in an annex to the report. You may have seenHouse of Lords reports already. A few days afterthis session you will be sent a copy of your evidence.Do please correct it if you feel you have beenmisrepresented. Also, if you wish on reflection tosubmit additional evidence when you return home,or if we did not manage to cover all the topics in thehour which we allow ourselves, your supplementaryevidence will be extremely welcome to theCommittee. Could you start by stating your nameand your professional title for the record, and if youwish to make a statement about how you see theinteraction between the Commission work and theWorld Health Organisation work we would be veryhappy to listen to that. I should say that there willbe a small number of OYcers of the KenyanParliament who are in the House today. Over to younow, Dr Muijen.Dr Muijen: Thank you. Let me start by saying thatI am Dr Matt Muijen, Regional Adviser for MentalHealth at the European Region of the World HealthOrganisation. Previously I worked for many yearsin England and it is very nice to have theopportunity to report back to the country that hasbeen my home for so many years. Let me make ashort statement to explain the diVerent roles of theWorld Health Organisation and the EuropeanCommission in their dealings with health andspecifically mental health in Europe. First of all,there is an important diVerence in geography. TheEuropean Region of the World Health Organizationaddresses the health needs of 53 countries, includingthe Central Asian Republics, so in some ways onecould simplify it by saying the new EU plus all thecountries of the former Eastern Europe and SovietUnion. The EU is essentially responsible for its ownMember States. Also, the role of the EC is morediverse. We have a role to work with the ministriesof health of our Member States to optimise healthaccording to our mandate as set out in 1948. TheEC acts on behalf of its citizens, according to anumber of treaties, and is responsible within thosetreaties for public health but not for health services,which are explicitly excluded. It has a broadmandate which will, of course, make an impact onhealth via human rights and issues that are relatedto the productivity of the citizens, whereas we havea straight mandate to deal with health, including
health services. There is at times a very confusingdiVerentiation of responsibilities towards MembersStates resulting from our diVerent remits, which nodoubt will come out in the discussion and has greatrelevance to discussing the role of both the HelsinkiDeclaration and the EC Green Paper.
Q196 Chairman: Thank you. That was a usefulopening statement. The Declaration of theConference held in Helsinki in January 2005 hasbeen very influential in setting the agenda for thedebate in Europe about the future direction ofmental health policy, but how confident are you thatdevelopments since the Helsinki conference havebeen positive in building momentum towardsactions for improvements in mental health care inEurope?Dr Muijen: I can say that I have been positivelysurprised by the impact it has made so far. I wasvery concerned that, following the very successfulministerial conference in Helsinki, this would havebeen perceived as a piece of paper that was non-binding, and Member States moving on to otherpriorities. That has not at all been the case. Insteadthere have been a large number of countries whichhave compared their existing policies and legislationwith the Declaration they endorsed in Helsinki andthere has also been a tremendous amount of policyand legislation work across the whole of Europe.Countries such as Romania and Bulgaria have beenvery active in working with us, but also countriessuch as Spain used the Helsinki Declaration to lookat their existing sets of policies. Much work has beenhappening, particularly in the poorer MemberStates, and it has retained its momentum. At themoment we are undertaking a benchmark studyacross the whole of the EU, to which countries againhave been remarkably committed, so mental healthhas remained high on the agenda. It has not becomea marginalised, stigmatised area to whichgovernments are not showing any real commitment,not at all.Chairman: Thank you. That is a rather reassuringreply.
Q197 Baroness Morgan of Huyton: Obviously, youhave a lot of experience of mental health strategy andprogrammes in Britain, having worked here for awhile. We are interested, because of your experience,in what you think in a sense we do well here and whatother parts of the EU could learn from us, but alsowhat we could learn from other parts of the EU.What are the best practice areas around that we couldshare more eVectively?Dr Muijen: Let me start this oV by saying howdiVerent mental healthcare is across Europe andhealthcare in general. Certainly one has had to learnvery fast how important context is, particularly

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
89commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
diVerences in health service funding and traditions.An important factor I did not realise at the time wasthe degree of centralisation in England. England isprobably the most centralised country in Europe.What I mean by that is that policy and guidance butalso standards set by the Government are validthroughout the country and are taken seriously, anddo not underestimate the importance of this last bit.Germany has 17 diVerent health policies, as doesSpain. Switzerland is tremendously decentralised.Most countries in Europe have forms of governmentwhich allow a far greater degree of freedom at theperiphery, for good and bad. Some of the strength ofEngland follows from that, and the national serviceframework was a massive achievement in this respect.I took part in it and, if I may mention my Guardianinterview, my position was largely based on that.Only in retrospect did I realise the achievements ofthis, ie to develop a visionary strategy documentsupported by funding and driven through byidentifying the need for policy, legislation, workforceas well as standards. This was unique and I do notthink has happened, with the possible exception ofparts of Australia, anywhere in the world on thisscale. I do not know anywhere in the world with thenumber of specialist services in each catchment areawhich have been introduced in England, maybe notall perfect but at least they are there, so in a structuralway England is remarkably impressive. Also, theworkforce reform that has taken place here, thechanges in staV roles, the introduction of newprofessional groups in the primary care, again I donot know of any country with such a highlydeveloped form of primary care related to mentalhealth. This is an area where England is very farahead, with the development of teams of primarycare staV and mental health specialists workingtogether. There is a negative side to this, which is thepotential lack of flexibility, which is a clearproblematic aspect of centralisation. Whether ruralShropshire should have the same global outline ofservices as Lambeth in London is highly debatable,and maybe at some stage a greater degree offlexibility might be helpful. Another, probably moreimportant, diVerence is the consequences of healthservice funding, and I am thinking about the elementof choice here. England, because of its central budgetraised by taxes, distributes this budget in a way whichcreates salaried staV who are given specified jobs todo and on the whole are linked to catchment areas.Patients go to a specified psychiatrist and other staVand receive ongoing care from these staV. What doesnot exist here in the public sector is the opportunityfor people to go in particular to therapists of theirown choosing, receive the care they want and decidewhat else they might require. What this means incombination is that, if one suVers from a severemental illness requiring continuity of care possibly
involving multiple agencies, England might well beone of the best countries to be in. However, if onesuVers from more common mental disorders, such asdepression, which may need short, sharpinterventions in a one-to-one relationship, I wouldprefer not to be in England because one does not havechoice as one has in countries such as Germany andFrance.
Q198 Baroness Uddin: The Commission’s GreenPaper makes clear that the proposed Europeanmental health strategy has the aim of lendingpractical support to the implementation of the WHOHelsinki Declaration and Action Plan. In theirevidence to our inquiry also the Commission haveexplained that they are closely working with theWHO in taking forward the development of theproposed strategy through their Platform approach.Largely you have explained to us some of the issuesthat I would want you to address, but why could notthe objective of the WHO’s Helsinki Declaration andAction Plan be achieved by individual countriesworking together with the WHO without the need foran EU-led mental health strategy? Also, how eVectiveis the Platform approach adopted by the EUCommission likely to be in your view, given thediscrepancies in services and strategies at this currentmoment in place?Dr Muijen: In essence, of course, you are asking ahighly political question of why the EuropeanCommission requires its own strategy, and in a wayit is not quite for me to answer. I suggest that one ofthe answers might be because is the issue was there forthe EC, so it needed a strategy. Obviously, myconcerns at the very beginning were indeed that wemight find ourselves in a competitive position, twostrategies, two champions, so we start competing forour Member States. That has not at all happened,largely due to very strong personal partnerships butalso because I think the EC has made great eVorts toinvolve us, which have been genuinely impressive.They made a special point of inviting us and for us toopen some of the key events, in order to underlinethat we work together. We also have been veryclosely involved in drafting many of these papers. Ihave seen all the papers well before they werepublished and have commented on all of thembeforehand, and our contributions were takenseriously. In reality the EC commitment is verywelcome to us because of the single fact that it keepsmental health on the agenda. It is still constantlybeing discussed by Member States who need to lookat some aspects, such as the benchmarking exercisewe are currently undertaking. This is an indicator ofthe importance given since it is co-funded betweenthe EC and the World Health Organisation. MemberStates also meet at the EC Green Paper and nowstrategy events where we are also represented. An

3564222014 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
90 commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
important point which I have already referred to isthe diVerent remit of the two organisations. The ECis very strongly focused on mental health promotionand prevention, which sits within our remit, butneither organisation has the capacity to deal with thisalone. The potential impact of the EC is massive. Onthis point, we have found that we can make thegreatest impact in countries that are striving tobecome EU members. We have noticed a strongdiVerence, particularly in Romania and Bulgaria inthe last few years, because they had to work towardsmeeting non-explicit EU standards, and often askedus to assist them to do so, which has also beenencouraged by the EC itself. The partnership canwork very eVectively if parties choose to do so, which,not only in mental health but also in other areas, is onthe whole working well. If we were set up against eachother it would be very diYcult.
Q199 Chairman: What about the eVectiveness of thePlatform approach? Do you have any experience ofthat?Dr Muijen: It has yet to be demonstrated because youthey are part of the Plan as outlined in the GreenPaper. So far there have been a few discussionmeetings that were helpful towards formulating thecontent, particularly of the strategy, but I think it isa plan for the future, which is very challengingbecause, of course, the real concern is that it couldbecome a talking shop for a very limited group ofpeople. At its best it will create an ongoingcommunication and agreement on further work.Chairman: Certainly the voluntary associations whohave come before us, “civil society” I think is thephrase, were very happy that these platforms allowthem to interact, and in one case interact on behalf ofthe suVerers of mental health problems as well, whichthey obviously found very useful.
Q200 Lord Wade of Chorlton: We have receivedevidence regarding the human rights aspect of mentalhealth and it has been suggested that an agreed basisof key principles for human rights in the sphere ofmental health might be a better basis for makingprogress with Member States than one of settingminimum standards for mental health. We would begrateful to know how realistic you feel would be theaim of achieving minimum standards for mentalhealth across the European Union, and what do youthink of the alternative approach based on agreeinga set of key principles?Dr Muijen: First of all, I do not think they aremutually exclusive. One of the strengths of thenational service framework was that in eVect it wasbased on principles which then were reinforced bystandards, not minimum standards but standards. Ithink that principles or standards on their own canoperate somewhat in a vacuum—what do you do
with principles that are invariably well-meaning?They need to be followed through with quite hard-hitting policies and legislation supported by funding.Neither EC nor WHO, by the way, has a mandate tocome up with binding principles or standards, so itwould be at best advisory, which in itself might beworthwhile. Why I am always slightly struggling withprinciples is that they nearly always refer towonderful ideals about human rights and otheraspects of care but can almost be seen as a substitutefor the real thing. The other danger of it is that,certainly across Europe, words can mean so manydiVerent things in diVerent countries. If one talksabout least restrictive care in some of our newerMember States, it means something very diVerentfrom what it means in the UK, which already impliesthat in that case principles need to be translated intovery specific statements of what is required, whichthen invariably leads to a common denominatorwhich is adjusted to the least developed MemberStates. What has been interesting in the HelsinkiDeclaration exercise, however, was that the leastdeveloped countries were least worried about theimplications because they often did not understandquite what the meaning was, whereas thegovernments of England and other highly developedcountries were highly concerned because theyunderstood very much what was meant by some ofthe more complex statements. It does not necessarilymean that countries will resist principles but it mightmean that they certainly will not follow themthrough. The same could be said about minimumstandards, not that minimum standards imply thatcountries will not go beyond minimum standards,but again how do you phrase them in such a way thatthey have a clear meaning. And how do you inspectthem afterwards across Europe with no organisationhaving a mandate to both impose them and reinforcethem? I am not against principles. I think principlesare important, but on their own we would yet againget many of these strategy documents which I receiveon an almost daily basis. It makes me exasperatedbecause they include all these wonderful standardsand then none of them will be implemented.
Q201 Lord Wade of Chorlton: On that basis you aresuggesting that the minimum standard would be amore sensible way, at least to start. Would you preferto see a system in which you could start with aminimum standard that might be accepted over abroad area but you could then ratchet it up as timeprogressed, because clearly, from what you aresuggesting, some of the minimum standards thatmight be accepted would not be terribly good?Dr Muijen: If I had to choose I would go forminimum standards. If I did not have to choose Iwould have both. I think that principles areimportant as statements of intent but they have to be

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
91commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
followed by some quite clear explicit descriptions ofthe care that is required in a more detailed manner.Besides, these services need to be costed, and I meanservice in its broadest meaning here.
Q202 Baroness Greengross: Could we start bylooking at deinstitutionalisation? Do you think thatthe EU has competence to look at care in thecommunity and so on, and what are the main issuesthat it might have competence to deal with?Dr Muijen: Let me answer the last question first. TheEuropean Commission (and the European Union, ofcourse) does not have competence to deal withservices, but it does have competence to deal withissues that have impact on services, such as humanrights, and also public health and those can betranslated in ways which can bring it very close to, ifnot directly aVecting services by directives that couldshape some of the foundations of services. This cancause tension with Member States but CommissionerKyprianou is always very explicit in his statements, iethat there is no mandate to impose any servicedirective. That is very clear.
Q203 Baroness Greengross: Taking that a bit furtherinto the issue of compulsory treatment and humanrights and so on, could you set out for us the keyissues relating to that, not just in institutions but alsofor compulsory treatment in the community becausethat is very important to us at the moment as a Bill isgoing through Parliament now on mental health?Dr Muijen: And also since your Bill will have majorimplications for the rest of Europe because Englandin particular is seen as taking a leadership role. I havealready been to meetings where communitytreatment orders were perceived as a good ideabecause there was a belief that they had already beenintroduced in England, so any decision that is madein England will have consequences for the rest ofEurope, something England is not always aware of.It is still seen as the model country in terms of mentalhealthcare, and healthcare as a whole, I believe. Whatone finds around Europe is a lot of diversity inlegislation similar to the diversity I referred to earlieron in services. Again, it has been delegated in manycountries to a lower level. There is no German mentalhealth law. There are laws in each of the diVerentlandler. The same is true in Spain and in Switzerland,I believe, as well. There is considerable diVerence inthe principles of legislation around Europe. Somecountries use a competence principle at the point atwhich people are being admitted, and I am talking, ofcourse, here about legislation which takes awayfreedom from a person with mental illness andenforces treatment. I assume that that is the kind oflegislation you refer to here. There is, as I just said, adiVerentiation in many countries betweencompetence and risk. Some countries use the
competence principle and so someone can beadmitted against their will if they are deemed to beincompetent. In other countries, as in the UK, it isbased on the risk of an individual suVering from amental illness with very diVerent definitions of whatmental illness is. The problem invariablyencountered with competence is the definition ofcompetence. Competence has at least five diVerentmeanings and in the end what it means is often that apsychiatrist has to give a judgment on what theybelieve competence is. What also diVers is that inmany countries magistrates will make the finaldecision about whether someone should be admitted,rather than, as in some countries such as the UK,psychiatrists on their own, although often requiringapproval by a third party such as a social worker,being allowed to make this decision. Anotherimportant distinction is that some countries,including Holland, only allow people to be taken toa place of safety following the imposition of an orderrather than treatment being given against their will,which is another specific step in addition to someonebeing hospitalised. The direct link between peoplebeing placed in a place of safety and then being giventreatment is not automatic in some countries, whichcan lead to very perverse situations of people havingto stay in hospital for weeks without treatment beinggiven because they meet the criteria for one but notthe other. At the moment there is no country I amaware of in Europe, but again I have to be carefulbecause there are so many diVerent legislations,which has a proper community treatment order in thepure sense of the meaning, and what I mean by thatis that people can be treated against their will in thecommunity. Countries are very much looking to theUK. Recall is possible in some countries, so thatpeople are temporarily allowed conditional dischargeinto the community, but there is as yet no example ofthe American form of community treatment orders.One observation I always make is that the whole issueof choice can be ignored in these debates. To givemyself as an example, if someone were to judge thatI needed treatment against my will I would prefer theoption of receiving that in a place of my own choicerather than immediately and without alternativebeing taken to hospital, of course, with dueprocedures in place.Baroness Greengross: You have been talking moreabout competence than risk and the big issue whichis all over the red tops at the moment here is, ofcourse, risk.Chairman: Risk to other people.
Q204 Baroness Greengross: It is the risk to otherpeople, not to the patient, and in that case it isprobably in relation to the taking of medication.Would that come under this competence?

3564222014 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
92 commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
Dr Muijen: That is precisely the problem, and that iswhy many countries in the end decide on risk,because the risk may not be very easy to judge but itis easier; at least you know what one refers to. Thereare many diVerent dimensions of competence andthey are very rarely explicit. They have advantagesand disadvantages. The risk to others no doubt willweigh heavily when determining competence becauseit is clearly related to competence when judgingwhether behaviour is responsible. It could always beformulate in terms of competence. On philosophicalhuman right grounds no doubt competence is theproper way to go. On the other hand, if one looks atcommunity protection, I can well see that risk is ashortcut to decide what should happen. I also have tosay that when one looks at the evaluation ofintroductions of mental health acts which create adiVerent basis for admission, there can be littlechange. When numbers were evaluated in Holland, itwas found that through one mechanism or the otheron the whole the same number of people are admittedagainst their will, although it should be added thatthis is not a good argument not to develop optimallegislation.
Q205 Earl of Dundee: What are your views onpreventative measures and the part that these canusefully play in protecting against mental ill health?Dr Muijen: It is, of course, a highly complex question.Let me make one point that is relevant to everyquestion, which is the question of terminology. Thisis not unique to this House, but already in thesequestions “mental health”, “mental ill health”,“mental wellbeing”, “mental illness”, “lack of mentalwellbeing” are all being used, and we all assume weare talking about the same group and the sameconcepts. It is very dangerous. In the HelsinkiDeclaration we consistently used either “mentalwellbeing” to talk about positive mental health, or“mental health problems” to talk about negativemental health, and already this could lead to debatesabout the meaning of those concepts. Theimportance of it is that clearly prevention refers tovery diVerent groups from those when we discusscommunity treatment order. The other issue, and thiswill come back later in the debate about stigma, isthat there are diVerent shades. We cluster together awhole group of disorders and a whole group ofpeople who actually have nothing in common. It is abit like talking about infectious diseases as onegroup, and I do not mean this in any other way as aparallel. We talk about people with, let us say,relatively minor anxiety states and people with verymajor forms of schizophrenia as part of the samegroup. It is unhelpful because they need very diVerentinterventions leading to diVerent outcomes. That isrelated to prevention because there is already thechallenge here of prevention at the population level,
which is particularly relevant to, let us say, stress-related disorders, anxiety and depression, rather thanlooking at prevention for very specific high-riskgroups, for example, children with two parents withschizophrenia. Everyone is on the side of preventionbut in practice it is very often secondary to otherforms of government action. Think about buildingroads, building new housing, school development, allof which have major implications for the mentalwellbeing of the population and potentially thedevelopment of stress and anxiety disorders. Thereare some specifically targeted prevention strategies ina country such as Finland which is very strong onthat. Holland has a very well developed preventionnetwork, including specific prevention workers. Theevidence for very high level prevention strategies isnot very strong, for the obvious reason that they costa lot and they are quite non-specific. The evidence formore targeted specific interventions is well beyondthis discussion because one then, of course, has tobreak it down into individual groups. Just in passingI want to say a few words about the Commission forSocial Determinants, which has been started at theWorld Health Organisation, chaired by ProfessorMarmot, who is probably well known to you. It looksat the implications of diVerent structures of societyfor exposure to risk factors, which then leads todiVerential disease burden and also to diVerences inaccess to care. Mental health is very important in thiscycle because mental ill health is associated with avery high level of co-morbidity. The joint prevalenceof depression and cancer and the link with survivalrates is very important and as such I think mentalhealth deserves a far stronger and more explicit placein many policy-making areas.
Q206 Earl of Dundee: But do you consider that wemight be at risk of falling between two stools here,because, as you point out, it may be very unhelpful tobe too loose with a definition of what mental healthis or to extend it so much to include wellbeing that weare not really, by including wellbeing in preventativemeasures, achieving very much at all? On the otherhand, if we learn, which we do, that in a given yearas many as one in four people suVer a lack of mentalwellbeing, then even if we begin with a rather non-targeted collection of preventative measures perhapsthat will still serve a useful purpose. For if Europeanpolicy and deployment start like this in a rather looseway then arguably proper methodology andtargeting might develop all the better later on. Whatdo you think about that? Will this approach fallbetween two stools? Or instead, will it yield the bestresult?Dr Muijen: I take the point that in an ideal worldwhere we prevent—and I do not quite know the rightterm—poor wellbeing, we would have societalintervention which means that everyone is going to

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
93commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
be happy all the time, which would prevent all formsof mental illness and which would be well worth theinvestment. Sadly, I cannot think of any interventionthat would meet any of these kinds of aspirations,except maybe in an absolutely equal society. It wasattempted to create such societies in some countriesearly in the last century, but we do not support theseforms of intervention and when they were tried theyfailed. EYciency is far higher when we target highrisk groups. It is even higher when we deal withpeople who already have developed some early stagesof these diseases. Again, I am with you if you say thatwe need to combine these two approaches, which is,of course, always a desirable compromise position,but I would insist on some hard evidence from healtheconomists, such as Professor Knapp, who leads theworld in this area, that it will pay for itself becauseany pound spent on prevention is a pound not spenton people suVering from very bad conditions. Onecan add to this that sometimes the very bestinterventions are non-specific mental healthinterventions, such as improving conditions at work.
Q207 Chairman: That was what I was going to askyou. What about working practices, for example? Iam sorry to interrupt you, and I do not know howtechnical the evidence is but there seems to be quite alot of evidence that there are certain ways of workingand atmosphere in the workplace now which can bedirectly inimical to mental wellbeing and thereforelead to things like depression and all the more minorthings which do cost the economy—and this is aninterest of the European Union, of course—a lot ofmoney. I do not know whether you have had anythoughts about how the European Union cansomehow get into that area because it might make adiVerence, not perhaps to schizophrenia, that sort ofillness, but to the ones which are more general mentalillness, the depressive diseases, in eVect.Dr Muijen: Exactly, and a lot of work has been donein this country in some of these areas. If I am thinkingabout stress at work, let me just say that the 28 percent mentioned in the Green Paper I findastonishingly low; that must be referring topathological stress because I am no doubt included inthe people who have some stress at work sometimes,as I suspect many of you would agree with. Nor isthat necessarily a bad thing, but I suspect that issueslike working environment, management styles,enforced breaks, enforced holidays, would have avery beneficial eVect. Sometimes these simple generalinterventions are far more important than mentalhealth specific strategies in the workplace, which Ifind, if anything, rather stigmatising.
Q208 Earl of Dundee: Earlier on you pointed outthat the newer applicants to the European Union aremore receptive than some other countries in these
matters. Just now you mentioned the beneficial eVectof friendly working conditions, enforced breaks andso on. Improved access to education, housing andtransport forms another example. There arecountless other simple remedies to reduce stress. Allof them are fairly obvious. No great studies arerequired. How strongly and frequently, therefore, doyou and your organisation advocate this commonsense approach?Dr Muijen: I would say that I do not need to go toLithuania to give advice about stress and transport.Taking the train into work is very stressful. Certainlyone of the lessons I learned when I started workingacross Europe was how much many of these newercountries are struggling economically. We are nottalking about wealthy countries that have theopportunity to fund research. These are countriesthat are fighting for their economic life and with veryhigh levels of unemployment, high levels ofinequality, and they are struggling to spend everydollar in a way that is directly linked to a bettereconomy and growth and wealth. I think many ofthese issues we are talking about here are not quite ontheir agenda yet. Also, you would be surprised howbackward—and I use this word advisedly—many ofthese countries are in their services. Most countriesoutside western Europe, not just outside the EU, arestill dominated by institutions, so when we advise onfirst steps we look at issues such as people sometimessharing a bed, and if they are lucky they have ablanket each to cover them. In some countriesoutside the EU membership they are fortunate if theyreceive any medication at all, not just newmedication. There was one hospital I visited whereonly 20 per cent of the patients were able to receivethe medication they needed.
Q209 Chairman: It is almost like the developingworld, in fact.Dr Muijen: Some are, yes. Even countries which arenow members of the European Union are still verymuch struggling even to provide basic facilities inmental hospitals, so to deal with prevention at asocietal level is hard. What does happen in thesecountries is micro initiatives. We talked earlier aboutcivil society. There are some very fascinating small-scale initiatives wherever you go, nearly alwaysinspired by charismatic local leaders who take aninitiative and make it happen. Everywhere you gothey are there, and that is an area of real potential, inEngland as much as anywhere in Europe.
Q210 Chairman: Thank you. We ought to move onto stigma. You have had the question. I would like toknow how you think the stigma issue should beaddressed in respect of mental health. It is obviouslya very severe problem, particularly for those peoplewho go in and out, let us say, of the workforce or who

3564222014 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
94 commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
are sometimes ill and sometimes well and areconscious of the stigma, as it were, of it being heldagainst them. What examples have you seen acrossEurope where promotional activities have helpedwith this problem?Dr Muijen: I have seen promotional activities. WhatI have not seen are well evaluated national activities.I have been to countries where I saw posters on thebus, like, “Your neighbour may suVer from mentalillness”. That was in France. I am not sure whether ithelps or not, by the way. There are quite a fewinitiatives around Europe but evaluation is nearlyalways rather soft. Of course, it is very hard becausehow do you measure these kinds of nationalinitiatives? I very much liked the activities in Greecewhere famous singers were involved and othernational personalities. Finland has been very active.Holland has done some good work and Scotland hasbeen very active, amongst the leaders in its level ofactivity, but good evaluation has not taken place. Iam always a bit concerned about stigma because ithas become so popular a theme that it is almost anexcuse these days. Whenever I talk to politicians theyuse the word “stigma”, and, rather than coming upwith solutions, it tends to be a reason why it is all sodiYcult. It has emerged as the key theme over the lastcouple of years and not particularly in a helpfulfashion. There is also tremendous attention beinggiven to addressing stigma of mental illness, andsometimes it actually makes situations worse. Iremember once seeing a video that tried to de-stigmatise mental illness, and if anything it probablywould have increased racism as well as stigma at thesame time by constantly showing the link between avery mean-looking big black man and schizophrenia,which probably was not the intention. It is not alwaysvery professional and well thought through,although always with the best intent. What interestsme much more is discrimination, the behaviourallevel of stigma. That is where some more interestingactivities can take place. The other concern ispromoting stigma as a solution. It sometimes createsa kind of sense of mental illness being a myth: if onlywe de-stigmatise it, it will disappear. Mental illnesscan be a very serious conditions with people needinga lot of support, and de-stigmatisation would notmean that support could be taken away.
Q211 Chairman: Or gets any better, no.Dr Muijen: Exactly. Stigma is everywhere. Let us notbelittle it. I have been to many countries where peopledo not want to work in mental health because ofstigma. Some of our Member States have majorproblems recruiting staV. Trained staV go to the UKbecause salaries are higher. I know of one countrywhere one per cent of medical students specialise inpsychiatry and then they often do not becomepsychiatrists because they go for better paid jobs in
the local economy. Stigma has a direct role there. Itis a theme well beyond just people at work.
Q212 Chairman: I quite like your idea ofconcentrating on discrimination rather than onstigma. Discrimination is something you can dealwith. There is a legal framework for dealing with it.In this country we are supposed not to discriminateagainst people for various reasons. One might addother categories to that, so that is helpful, thank you,the use of that word.Dr Muijen: Can I add to that by anticipating aquestion a bit later on, since we are now talking aboutdiscrimination? The other important aspect is that itmight be counter-productive to specifically deal withmental illness as an isolated theme, and that weshould mainstream as much as we can. I think bysingling out legislation to protect people with mentalillness we may create a kind of gaming by employersto avoid employing people with mental illnessaltogether.Chairman: It has happened in other areas. There wasa reluctance to take on people with physicaldisabilities because they had a responsibility towardsthem. I hope it is passing over now but that would bethe same sort of problem.
Q213 Baroness Uddin: Just before I come to myquestion, which is about dealing with vulnerablegroups, particularly minority groups, I welcomewhat you said about de-stigmatisation, particularlyof groups who are suVering in that way. As a socialworker in this field many years ago, workingparticularly with women, I think that the way itmakes them out to be some kind of demon in societywhen they have been through institutions is a reallyvalid point and I wish you every success in de-stigmatising this and getting into that kind of arenaof acceptability. I am very interested in yourreference to the demonisation of black men and whatthat entails and now Muslims being demonised asterrorists. Given that there is recognition that somegroups in our society are suVering more strenuouslythan the general population, triggered by conflict orprejudice or discrimination, and an example ischildren and very high suicide rates and self harmamong Asian women in this country, which could bebecause of discrimination and conflict, lack ofemployment, all those points you mentioned, as wellas racism and Islamaphobia, what do you think arethe specific things that can be done to handle thisissue at an European Union mental health strategylevel? I would be very interested to hear from youabout your experiences of good practice in Europe,and if England is as good as you say, and I know it is,whether you have sighted any good examples inEngland about this particular issue.

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
95commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
Dr Muijen: Let me start with the second part of thequestion which in some sense is easier. I was veryimpressed with the report of the Social ExclusionCommittee. It showed what can be done when peoplefrom a more generalist perspective look at a specialistarea, because they look for mainstreaming—and Ihave used that word earlier—rather than singling outand providing very specific interventions, whichalways alarms me. I think mainstreaming is veryimportant in any form of discrimination. You wantto integrate people. You talked about specific sub-groups. I think the danger is precisely that they canbe marginalised and as a consequence do not reachany of the support that is required. Europe has verydiVerent challenges. I remember very well from beingin England, and also when I now talk to Englishfriends, that there is strong concern about first of allrace and ethnicity and, secondly, Islamophobia.What is interesting is that the former is not so muchof an issue elsewhere. Religion is often far moreimportant. There are very diVerent sub-groups incountries, for example juxtaposing Hungarians inRomania and Romanians in Bulgaria, in TurkeyChristians and Muslims. There are rather diVerentchallenges in many diVerent countries. I think thereis a real danger for organisations like WHO to planthis top-downwards. We believe we can come up witha strategy for the whole of Europe, which isimpossible. I believe we need to think in countries atthe level of Blackburn and a sub-part of Londonrather than Europe as a whole. It is too diverse. Thisis an area where England again has been very activeand I think that many other countries increasinglyrealise that they also have to deal with thesechallenges. This is however a question way beyondmy remit. You are talking about the whole of societyrather than mental illness. The consequences aredirectly aVecting mental health, and, again, the socialdeterminants for health are relevant here but also thesocial stratification with nearly always immigrantgroups, and particularly ethnic immigrant groups, atthe very bottom living in unhealthy circumstancesand having poor access to care with all thepredictable consequences.
Q214 Baroness Uddin: I understand that that may bewell beyond your remit but does that remit belongto anyone?Dr Muijen: That is a very good question. The mentalhealth remit belongs to me but I am talking about thesocial determinants of health. There I feel anownership, but where I always get very nervous iswhen mental health specialists start giving advice onthe economic running of a country because Iprobably do not know really what I am talkingabout.
Chairman: I am sure you could have a good stab at itbut I think we appreciate your ability to pick whatyou feel comfortable with in giving us your expertadvice.
Q215 Lord Moser: If I may turn to discrimination inthe workplace, I find it very puzzling why the mentalhealth strategy of WHO, and therefore the EU,covers learning disabilities. It is a field that I know alittle bit about. I realise that people with learningdisabilities need help; I am not questioning that. Ialso realise that mental health problems can causelearning disabilities, et cetera, but mental health is abig enough and confusing enough subject anyhow.Why throw in learning disabilities?Dr Muijen: We did not. That is actually a questionwhich should be the other way round, and I willanswer it in a moment as if it were the other wayround. Learning disability is not included in theHelsinki Declaration and as far as I am aware it isalso not included in the Green Paper. There arereferences to disability; I do not think there arereferences to learning disability, unless I am verywrong. I can certainly talk authoritatively about theHelsinki Declaration, which explicitly excludedlearning disability.
Q216 Lord Moser: When we asked last week’switness he strongly defended its inclusion.Dr Muijen: Who was this? In what? In Helsinki or inthe Green Paper?Chairman: No, I think in the work that we are doing.Lord Moser: Perhaps Professor Knapp will be able totell us.
Q217 Chairman: In the Commission strategy.Dr Muijen: The Commission strategy is notsomething I am willing to take responsibility for, butbased on this question, I actually read it through andit is not mentioned. The word “disability” ismentioned but it was mentioned as disability in theworkplace.
Q218 Lord Moser: Sorry to interrupt, but theCommission Green Paper does include it.Dr Muijen: I am surprised because it has never comeup in any discussions, nor does it come up in thedocument itself. Can I answer it? What deeplyembarrasses me is our lack of activity in relation todisability. That is probably a more importantquestion. I am very ashamed about having nodiscernible activity in the area of learning disabilitywhen those are probably the people who suVer mostin institutions in many of our Member States. Ofcourse, the obvious follow-up question is why is thereno activity, which is my lack of resources. I amworking with three technical staV and two secretariesin 53 countries. I have to assist with the

3564222014 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
96 commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
implementation of the Helsinki Declaration and twotop priorities I cannot address, which are learningdisability and dementia.Lord Moser: I am very happy with your reply aboutthat. Professor Knapp can sort this out for us.Something is funny.Chairman: Thank you very much indeed.Discrimination in the workplace, Lady Gale.
Q219 Baroness Gale: I think you have partlyanswered this in your earlier remarks aboutdiscrimination in the workplace. Do you think thereis a need for some new anti-discriminatory legislationrelating to mental health in the workplace? We knowthat many employers would not employ someone ifthey knew they had poor mental health. Do you thinkemployers ought to have some sort of code ofpractice that they follow and do you know anyexamples of this good practice in Europe?Dr Muijen: The second half is easier than the first, butlet me start with the first. To some extent I am alwaysvery reluctant to recommend legislation because firstof all it needs to be enforced and secondly people lookfor ways of bypassing it. We can hardly recommendaYrmative action to make you employ five per centof your staV with mental illness because who is goingto determine what mental illness is? What is moreimportant is to oVer support for people in theworkplace, particularly supporting people to getback to work and stay at work, but, of course,prevention is highly relevant here. It is probably farmore eVective at the workplace to prevent high levelsof stress rather than cure. I was asked a question notthat long ago about why we do not give specialprotection to people with mental illness in theworkplace, like giving them oYces, to which mypoint was, “I am in quite a stressful situation becauseI am in an open space myself”, and it is very diYcultto come out with guidance which specifies protectionto a relatively undefined group, like people suVeringfrom stress. It seems to me that this is an area wheregeneral good practice is probably more importantthan specifically targeting a few people. With regardto people with diagnosed mental health problems it isa question of who to target. There are many examplesof very good practice in several countries, such asongoing support after people go back to work, job-seeking support, for example the clubhouse modelbut also the social club, particularly in Italy, whichgives tax advantages if one employs a certainproportion of people with disabilities includingmental illness, which is much appreciated by thepeople attending them. I have also seen excellentexamples of modern forms of industrial workshops incountries such as Israel and France. At a nationallevel legislation is more complex. It might well be bycarrots rather than sticks that action will be most
helpful, such as giving subsidies or tax breaks forgood practice.
Q220 Baroness Morgan of Huyton: I have a finalquestion on a very vulnerable group. We are awarethat there are disproportionate numbers of people inprison with mental health problems and we areinterested in what lessons you have for us, what doesand does not work here but in particular are there anyexamples in other parts of the EU or anywhere elseyou have seen of good practice in this area, because itis clearly the poor relation?Dr Muijen: Yes. I have consulted my colleague LarsMoller who is responsible for the Health in Prisonnetwork at WHO Europe, and we looked at the bestpractice website to identify good examples of practicein prisons, and we came up with one, which is inHolland. In essence it is a specialised mental hospitalfor people in prisons, which is probably not the mostimaginative but it is the best we know of. Theproblems are the same everywhere—very high levelsof depression, very high levels of severe mental illnessall together with very poor treatment conditions. Mymost upsetting visit in the last two and a half yearswas a visit to a prison in a country I will not name butit was an EU member, where we saw a few units forpeople with mental illness and these were the worstcells—dark, mediaeval, where people were supposedto stay for weeks and they had stayed for three yearsin some circumstances. It is not just that that nopositive care is taking place in many countries butthat you get a worse deal if you are identified withmental illness, with what could only be described asa Stalinist prison doctor showing a remarkable lackof care for patients. It was a very frightening exampleof bad practice. There are examples of good practicewhich are on the whole in modern forensic units. Tosome extent it is obvious, but if one looks at a moreinclusive form of care, again, you do not need to gobeyond England. There are excellent liaison schemesbetween prison and the community and there is at themoment quite a bit of build-up of specialist supportin prisons. It is no doubt not enough but it is a start.Sadly, there are not a lot of additional inspiringexamples from elsewhere.
Q221 Baroness Gale: Could I just ask you if there aregood examples in other parts of the world?Dr Muijen: Unfortunately I do not know manydetails from elsewhere in the whole world. I do noteven know the whole of Europe, and, of course,prison care is not my special area. The main concernin prisons is HIV and TB. Mental health ismarginalised. I think that leads to the sameconsequences as being stigmatised. It is marginalisedtogether with many other disorders. I suspect thatcare is mostly rather ad hoc and if one is lucky therewill be special units with a few beds.

3564222014 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
97commission green paper on eu mental health strategy: evidence
7 December 2006 Dr Matt Muijen
Chairman: Thank you very much for a very usefulsession. We have already kept you here longer thanwe should but if any of the things that we have saidto you, or that you perhaps have not been able to sayto us because of shortness of time, do come to youplease give us the benefit of your thoughts because Ithink it has been a very stimulating session, especiallylooked at from your particular perspective, and hashelped us to see things in that structural context in a
rather reassuring way. We know a little bit moreabout how all that works now, and obviously yourexperience and knowledge of what is going on in therest of your own patch has been very helpful to us. Onbehalf of the Committee please let me thank you mostsincerely for your evidence today. If necessary we willbe in contact with you but I think you recognise thatyou are what we call a very busy person, so we mustnot impose too much on your time and kindattention.

3564222015 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
98 commission green paper on eu mental health strategy: evidence
THURSDAY 14 DECEMBER 2006
Present Dundee, E Neuberger, BGreengross, B Thomas of Walliswood, B (Chairman)Howarth of Breckland, B Trefgarne, LMoser, L Wade of Chorlton, L
Examination of Witness
Witness: Rt Hon Rosie Winterton, a Member of the House of Commons, Minister of State for HealthServices, Department of Health, examined.
Q222 Chairman: Thank you very much for comingbefore us on this mental health strategy which is ourmain inquiry at the present moment. This isobviously a very interesting and important matterand we are grateful to you for coming to see us andhelp us on it. We have heard from a number ofwitnesses and in fact I think that most members of theCommittee would agree that we have had a reallyvery excellent series of witness statements so far froma wide range of diVerent people.Ms Winterton: Good.
Q223 Chairman: They have all been of a very highquality, including your staV who came earlier, so weare happy that we are getting very good advice,including, as I say, from your own staV who came tosee us on 19 October. We have focused our inquiry onthe strategy set out by the Commission, hoping thatwe could make a constructive contribution byconcentrating on the policy objectives where the EUmay have a worthwhile and appropriate role and Iam sure that, as a Minister in the Government, youwill be equally concerned that there is not, as it were,an improper overlapping between the national andthe European role. We are being assisted in our workby Professor Martin Knapp who, as you may know,is the Co-Director of Health and Social Care at theLSE. I should give you a few housekeeping points.You are aware, I am sure, that this is a public sessionand it will be recorded for broadcasting andwebcasting. A verbatim transcript will also be takenand this will be published on the parliamentarywebsite and in an annex to the inquiry report. Youwill receive a copy of that a few days after this sessionand, if there is anything you feel ought to be alteredeither for clarity or to make sure that the point youwanted to make has been correctly recorded and soon, please do correct it, but make sure that is done assoon as possible because we have to move fairlyquickly. If you, for any reason, want to submitsupplementary evidence after the end of the session,we would of course be delighted to receive it.Sometimes questions do not get quite as wellanswered as the witness would like or something getsleft out, so we would be delighted to hear anysupplementary points you want to make. Could you
start by stating your name and your oYcial positionfor the record and then, if you want to make astatement, we would be very happy to listen to whatyou have to say before we go into our questions.Ms Winterton: I am Rosie Winterton, Minister ofState at the Department of Health. I would just makesome very brief remarks to say that I am very gladthat you are conducting this inquiry because I knowthat you do not always look into every singledocument that comes out of the EU and I thinkpersonally that this is a very good indication of thenew level of interest that there is mental health. Therehave been some, I think, quite remarkable changes inour delivery of mental health services in this country,but we just need to continue to move to make surethat we get that kind of cultural change in attitudetowards mental health services and see mental healthpromotion as part of not only a kind of nationalagenda, but an international one as well. As I say, Iam very pleased that this is taking place and also,looking back at some of the evidence that my oYcialsgave and others have given, I can see that you areconducting a very wide-ranging and in-depthdiscussion about it which I think is very good.
Q224 Chairman: Thank you for that and it leadsvery neatly into the first questions which are aboutmental health services in England. I think we havereceived the impression that in some ways we are, asit were, ahead of the field in terms of the delivery ofmental health services as compared with otherMember States, particularly of course the newerentrants. On the other hand, a number of seriousconcerns have been expressed to us, such as the lackof understanding of mental health issues amongst thepopulation in general. Also that suVerers frommental health issues can be the subject ofdiscrimination in the workplace, for example, andthat the cost of mental health or mental ill-health tothe economy, which is something, of course, that theEuropean Union itself has commented upon. Whatdo you see as the biggest successes in the developmentof mental health policies in recent times and what arethe main problem areas for us now? Perhaps youcould tell us something about how the Government
3564222015 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
99commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
is developing that approach on the basis of what hasalready been done.Ms Winterton: I think the biggest successes have comethrough the National Service Framework for MentalHealth which was issued in 1999 and I think duringthat time in terms of additional investment, if youlook at health and social care together, we are talkingabout something like £1° billion more investmentnow which goes into mental health services thanpreviously. I think in the way we have been able todevelop some of the community teams, there aresomething like 700 new community teams now upand running and that includes things like crisisresolution teams and early intervention teams so thatwe can help support people in the community as faras possible, but also to get help to people at an earlystage with early intervention teams and also to havethat support in crisis times. The reason why I thinkthat is important is because we have wanted to moveaway, and I think this is very much the contrastbetween how we are looking at delivering care andhow in some of the other European countries it is stillvery much institutionalised, if I can put it that way,so what we have tried to do is get teams out there sothat we can support people to remain within thecommunity with their families and with their carersas opposed to going into the institutional setting.Within that, there is obviously still a long way to goand we do need to make sure that the very good teamsthat are in some parts of the country are actually inall parts of the country. That is a challenge, but I dothink we have been quite successful, through themanagement from the Department and through thestrategic health authorities and so on, in actuallyencouraging people to set up these teams. One of thebig challenges that we face is stigma anddiscrimination, as you said, very much againstmental health in general, but particular groups,people from black and minority ethnic communities,suVer considerable discrimination and I think thereare various aspects to that. One is the ability to talkmore about mental health issues which we have triedto do through the media with some of the Shiftcampaigns that we have got, talking with youngpeople about mental health problems and trying towork with the media in how they portray mentalhealth problems. I think the community aspect of theway we deliver services is an important part of thatbecause it is about saying that yes, people withmental health problems can live within thecommunity and there is not this necessity for themalways to have to be removed, so that is a generalapproach which I think helps in that. In terms ofwhat I sometimes call the ‘choice agenda in mentalhealth’, it is not necessarily about people havingtreatment in diVerent parts of the country, it is abouthaving diVerent types of treatment and making surethat what we are doing is oVering people, for
example, more talking therapies, something we arehearing a lot about at the moment, which are notalways an alternative to medication, but they canassist people very greatly and that is why we have anumber of programmes at the moment in order toincrease the kind of CBT and so on. That is achallenge, but we are, through the pilot sites in placeslike Doncaster and Newham, actually looking at howwe can demonstrate that this works and what the bestmethods of delivery of that should be so that we canthen move towards rolling that out more nationally.Therefore, there has been a lot of progress, but thereis a lot more to do and particularly through things aswell like the Delivering Race Equality programme,looking at how we really tackle some of those issuesabout people from BME communities not feelingthat they are getting access to services and perhapsnot coming forward for services because of a feelingthat there might be discrimination there. It is tacklingit on all those fronts and also in the workplacethrough things like our action on stigma and ourHealth, Work and Wellbeing programme which islooking at how we get employers to play their part inacknowledging mental health problems in theworkplace, being willing to deal with those problemsand not making people feel excluded or that theyhave to leave work, but that they will be givensupport in work.
Q225 Chairman: I would just like to ask one morething and that is that when we were listening to thevoluntary sector, the people who came before us,raised the matter of the input from the patientsthemselves to the style and organisation of theservices to which they could get access. Now, I do notknow whether that is something to which yourDepartment has given thought because I think someof them felt that it was kind of oVered to them on a‘take it or leave it’ basis. I am going rather furtherthan what the evidence actually said, but I think thatis what they were getting at, that they were not ableto make enough contribution to how they werebeing treated.Ms Winterton: I think there are two issues there. Oneis the individual service-user or patient and whetherthere is the degree of discussion with patients thatthere ought to be. It is certainly an emphasis where Iknow increasingly clinicians are adopting that kindof approach because I think mental health again is areal area where, if there is not a proper explanationand discussion with the individual about the type oftreatment they are being given, why it is, what side-eVects there might be, then really it is incrediblydiYcult to get a buy-in. I think we are changing a lotof that culture and I know, through a lot of theinternational work that I do, that actually we arequite a long way down the line in getting over thatmessage. I think as well that the kind of community

3564222015 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
100 commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
team approach has helped in that because with thecommunity teams, when you are actually bringingtogether the psychiatric nurse, the consultant andothers who all work in the team, they develop, Ithink, a much more open attitude to what it is that theindividual is needing in their particular instance andthere is more discussion of that and, therefore, thereis more involvement. In a wider sense, I know verywell that the best services are delivered if there hasbeen proper service-user input in a wider sense and Ithink that mental health services have been quitegood at that actually, maybe not to perfection, but Iknow that particularly there is quite an input fromcarers as well in the delivery of services. If you lookat where some of the care trusts are operating andlook at how they will try to involve service-users inthe design of services, I think there are some verygood examples of how it can be done and we do try toassist in spreading that best practice. Where we couldfurther improve on that, I believe very strongly that,as we move to the future, there is an even greater rolefor the voluntary sector as, for example, service-providers and I do not think that we haveacknowledged that enough. I launched a documenttwo years ago which talked about the ability of thevoluntary sector to join with other service-providersin the design and provision of services and there wasthis kind of feeling, I think, within the NHS thatperhaps the voluntary sector was really badlyorganised and badly managed and how would theydeliver properly. The reality, when you looked at theevidence, was that they were very well organised andvery well managed, but they were also very good atreaching out to people who sometimes got worried bycontact with the statutory sector, so what I have beentrying to look at, and encourage, is that bringing in ofthe voluntary sector to work with the statutory sectorin the actual provision of services. I think, if we cando a lot more of that, we will have that greater input.
Q226 Baroness Greengross: Minister, I think we allwant to see the Helsinki Declaration implementedwell, and I just want to ask you really whether youthink that the EU should be involved in this way inhelping to make that happen and whether there is alot of added value in that or whether just individualcountries working with the WHO would get the sameeVect? In other words, is there a lot of added valueto this?Ms Winterton: I think that anything that sends outthe message that this is a very important area that weneed to address can only help, frankly, and Ilaunched the Green Paper during our Presidency, soperhaps you might say, “Well, she would say that,wouldn’t she?”, but I do think we can back up theWHO and use some of the structures that we havejust to give that added impetus to it. They are verysimilar conclusions in a sense, the importance of
good mental health for wider society, links withoverall prosperity, the tragic waste that there is, ifpeople do not have help, to the economy as a wholeand the eVect on the whole, wider society, so I thinkit can actually give a lot in terms of sending out thatmessage that yes, this is something that allinstitutions take very seriously.
Q227 Baroness Greengross: Do you think that thisplatform approach, which is the one which theCommission is taking, is eVective or will be eVective?Ms Winterton: I know that during the consultationprocess there have been a number of meetings thathave taken place and that has given the opportunityagain for service-users to be able to put their viewsforward. I think that it will be, if it is decided tocontinue that process, a good way of exchanginginformation and ideas. Just going back to the pointsthat you were making about the input of service-users, actually there is quite a lot where it would beimportant for service-users to know what happens inother countries as well and I think there is quite a lotof empowerment that could happen through thatprocess and particularly in trying perhaps toencourage service-users in other countries to push forsome of the changes that we have seen and whichhave been successful and probably vice versa as thereare other countries that have done good preventioncampaigns, for example, that we could perhapslearn from.
Q228 Earl of Dundee: What has the Governmentdone to advise people about the qualities of lifestylethat can best help to maintain mental health?Ms Winterton: Well, we have in many senses a lot ofwork which takes place at local level as opposed tokind of big, national campaigns, but what we havetried to do, through things like the Choosing HealthWhite Paper and through the Work, Health andWellbeing Paper, is to draw attention to theimportance of good mental health. Also, throughthings like Delivering Race Equality, we have actuallyissued guidance about promoting mental healthwellbeing amongst the BME communities. Themessage that we are really trying to get across is thatthis is a widespread problem and that we have tochange the attitude of people feeling that they cannotcome forward to seek assistance, so we can put in placethe services and we can look at, and I think this isimportant as well, rolling out things like talkingtherapies where we talk about things like mild tomoderate depression where again people may notalways feel that they can share that. Then, at the locallevel, through things like public health strategies, it isabout how we can get people to do things like moreexercise and to eat well, all of which is actually linkedto good mental health. Therefore, in a sense it is abouta general message of wellbeing for the individual and

3564222015 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
101commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
of preventing people getting into situations where, forwhatever reason, their mental health can deteriorateand that can often be linked to lifestyle, but, as I havesaid, rather than big, national campaigns, we aretrying to encourage people to work out what is goingto work best in their local area, but again importantwork with employers to start talking to theiremployees about having a healthy workplace,including a healthy mental health workplace.
Q229 Earl of Dundee: In your evidence to theCommission, you rank mental health as one of yourtop three clinical priorities, the others being coronaryheart disease and cancer. In addition to what you arealready doing, whether it is at local or national level,and the message you are sending out, do you feel thatso far your communication to the public on mentalhealth is as strong as you would like and that it is asstrong as you may be already giving a message aboutin order to help people against cancer and coronaryheart disease?Ms Winterton: I think it could be stronger. I think wealways need to learn whether there is more that we cando. The National Service Frameworks for olderpeople and for younger people do have promotinggood mental health as part of their strategies as well. Ithink there is a real diYculty in really getting itabsolutely right as to how you can make it as eVective,for example, as a stop smoking policy because some ofit is so much about individual circumstances and howan individual is at any particular time. I think that themessage that we really have to get over, if we were tosay, “How do you promote mental wellbeing mosteVectively?”, is to talk about the fact that this issomething that for many, many people, it does happento people at various points in their lives and, therefore,coming forward and talking about it should not be aproblem. Those are some of the ways in which I thinkyou can promote it. There is a lot of talk at themoment, is there not, about the kind of ‘happinessculture’, how you promote happiness. I think there areother things that we could do, for example, throughthe kind of Social Exclusion Unit work that we havedone which is about looking at the impact that poorhousing will have on mental health, the impact ofbeing unemployed, the fact that that will contributetowards mental ill-health, so it is about emphasisinghow all these outside factors can impact on a person’smental health and making sure that, through veryoften local strategies, whether it is urban renewal orjust generally, trying to improve people’s quality of lifewill, therefore, improve mental health as well.
Q230 Earl of Dundee: What examples of goodpractice in the prevention of mental ill-health acrossEurope are you aware of and for which Englandcompares well?
Ms Winterton: In other countries?
Q231 Earl of Dundee: Yes.Ms Winterton: Well, I know that Spain has had somevery good preventative mental health projects and Ithink France has as well, particularly in theemployment field. I think we need to look at some ofthose examples and see whether they would applywithin our country as well and learn from some ofthose.
Q232 Earl of Dundee: Is the Government in theprocess of studying these examples?Ms Winterton: Yes, we do have exchanges ofinformation the other way too and I was last nightwith people from some of the big mental health trusts.The people from Oxleas Mental Health Trust weretelling me that there were people from Germany andSpain who were actually taking jobs with the Trust sothat they could learn about community mental healthservices because they wanted to take the experienceback home. I think Italy have sent people over to lookat what we are doing in the Essex Partnership Trust interms of employment practices and how they havemanaged to get people back to work. There areexamples where we can learn from each othercertainly.
Q233 Lord Trefgarne: I would like to ask you, if Imay, about care in the community. Care in thecommunity, I think it is fair to say, has been the sortof flavour of the month for a very great many years,but you have rightly pointed, and justifiably pointed,to the increased impetus which you and yourcolleagues have given it in comparatively recent times.All the same, care in the community has never been atotal success. One of the problems is of course that afew of the people whom we are concerned with areprobably not suitable for care in the community, andI am thinking, for example, of people who have beenin an institution for a very long time and just are notcapable of taking any sort of individual place in thecommunity. Therefore, I wonder what your view is asto the adequacy of the present provision of communitycare facilities within your area of responsibility andwhether there is anything further we need to do inthat regardMs Winterton: I am sure there is more that we need todo. As I said earlier, I think in terms of the teams thatwe have been able to put in the community, that hasbeen a success story and, as I say, particularly thingslike early intervention teams and crisis resolutionteams and so on, there is a lot that we can point to tosay that has almost revolutionised the way that wedeliver care. That was sort of a battle for quite a longtime because I think people were worried aboutmaking those sorts of changes, but now, when youactually sit down with teams and where, dare I say it,

3564222015 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
102 commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
psychiatrists are actually themselves going out topeople’s homes, it just suddenly seems to make somuch sense because you are actually seeing peoplewithin their own environment and not in a sensesummoning people to somewhere which is totally aliento them, but actually going out into the community.Where I think we need to look—
Q234 Lord Trefgarne: But for some people of course,they are in environment which is an institution.Ms Winterton: Of course, and where I think we need todo even more work is when we look at things like howwe can get supported housing, for example, for peoplewho want to live in the community or who perhaps, asyou say quite rightly, have been living in institutionsfor many, many years, some of them for really quitetragic reasons when you look at the background, andit is about how we make sure that people can makethat transition and make it successfully. I have seen anumber of schemes, as I say, where people have movedinto, for example, supported housing, have beenhelped through employment schemes to do perhaps asmall amount of work, but something which actuallybrings some structure to people’s lives and I think thatis the area that we need to continue to move into. It isimportant, I have to say, to make sure that, in doingthat, we continue to work on reducing stigma anddiscrimination because sometimes there are some verydiYcult issues around actually placing people in thecommunity because people can have really quite thewrong impression of what people are going to be like,and that is a very important part of the stigma anddiscrimination reduction as well that we need to makesure is there.
Q235 Lord Trefgarne: My Lord Chairman, I cannothelp but mention it, that in 1982 I was theParliamentary Secretary for the Department of Healthand Social Security and I visited Leavesden, which wasthen, I think, the largest mental hospital in thecountry. It had been opened in 1915 and there weresome women in there who went in in 1915, and thiswas in 1982, only because they were unmarriedmothers.Ms Winterton: I have met the same. It is terrible.Lord Trefgarne: I do not know if there are still anythere.Baroness Neuberger: There are a few.
Q236 Baroness Howarth of Breckland: I want to ask asupplementary. Clearly we are ahead of Europe in theinstitutionalisation in much of Europe, but I want toput this in the context of the Mental Health Bill whichis coming forward and the concern that there is animbalance between community care and theassessment of dangerousness which clearly is there inthe Bill. I just wondered whether there was anythingthat we see in Europe or what your view is about how
we can move forward because dangerousness is whatmakes people worried about stigma if we look at whathas happened in the press in terms of a few cases whichhave caused huge concern, and how, as Europeans, wecan really tackle that imbalance and if we could givea lead.Ms Winterton: It is quite interesting when you look atwhere there is mental health legislation in place acrossEurope and, in terms of the detention rates perhundred thousand, I think we are kind of in the middlewhen it comes to detention. I know that there arecountries like Spain at the moment who do not haveany mental health legislation, but who are actuallylooking in the future actually to bring some in becauseof the problems of maybe people going through thecriminal justice system instead of through the mentalhealth system because there is not appropriatelegislation in place. We at the moment, and this is, Ithink, one of the very important changes in terms ofthe Mental Health Bill itself, are lagging behind someother countries in terms of having the ability tosupport people in the community under mental healthlegislation. You probably know, for example, and Iknow they are not entirely separate, that Scotland hasjust recently brought in legislation which supportspeople in the community. I think that there are twothings that we have to remember on that. When welook at the support which is available in thecommunity, I think it is absolutely vital that ourmental health legislation keeps up with the changesthat there are in service provision and that we canadequately support people in a community setting, butprevent some of the kind of ‘revolving door’ syndromewhich occurs when people are perhaps detained, goout into the community, do not take medication, donot stay in touch with mental healthcare professionals,deteriorate, go back into hospital and go out again. Ihave psychiatrists who say to me, “I know thatsomebody is going into the community and they willbe back again in two months’ time”, and I think insome instances that does lead people to deteriorate tosuch an extent that they either become a danger tothemselves more seriously or, in a very few cases, adanger to other people. Now, if we can, through theMental Health Bill, provide that support in thecommunity so that we can make sure that peoplecontinue to take medication, continue to stay in touchwith the services, then we can do two things: (a) we canhelp manage risk more eVectively; and (b) we canreduce stigma and discrimination. One of the thingsthat I think is the most diYcult is that, if people feelthat they have a mental health legislation systemwhich is not robust enough to handle risk and to beable to say that it can give support to people in thecommunity, then people feel, and some people havesaid to me, that they start to think that anyone withschizophrenia is really dangerous, and of course thatis not true. It is about saying, “Yes, we have a system

3564222015 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
103commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
which can ensure that we get treatment to people whoneed it”, and I think that is the crucial part whichsometimes gets left out of this debate. It is not all aboutpublic safety, it is actually about making sure thatpeople get the treatment that they need and thetragedies that you see, the parents and the carers thatI meet who say, “Why can’t you do more to actuallyhelp me manage my son”, daughter, husband orwhatever, “who is going through this terribledeterioration? There is nothing you can do to help meunless you say that they have got to be taken back intoa hospital situation”, so I think it is getting thosebalances right that will help to reduce stigma anddiscrimination and looking too at how some of thesesituations are managed in other countries as well.
Q237 Baroness Neuberger: That leads directly intothe question that I want to put to you. I have to say,however, that I think that some of us would say thatthe emphasis on dangerousness in the mental healthlegislation might conceivably add to questions ofstigma and I would like you to address that, but Iwanted to ask you more particularly where do youthink the advances have actually been made intackling stigma and discrimination by the Five-YearShift programme over the past two years and wherehave we done better than Europe? It was veryinteresting hearing from the voluntary sectororganisations where they thought we had done better,but equally where they thought we had not spentenough on anti-stigma programmes, so perhaps youcould say whether you think that we could teach themthings in Europe about anti-stigma programmes.Ms Winterton: In terms of some of the real successes inthe Shift programme, I think a lot of the work with themedia has been quite successful and some of thecampaigns that, for example, the BBC have done,particularly targeted at young people, have beeneVective. I think the work that we are doing withemployers as well has been a good thing because wehave had some really quite high-profile businesspeople who have been good enough to share their ownkind of personal experiences and then put togetheradvice for managers, for example, on how to just be somuch more open about the whole issue of mentalhealth. Big employers, like Royal Mail and BT, havebeen very good in talking about how they have dealtwith those issues and it has become something, Ibelieve, that people actually talk about now asopposed to thinking that they cannot approachsomebody whom they know may be having a problemin the workplace because it is embarrassing or ofcourse they would not want anybody to know, but itis about encouraging people to be able to comeforward and say, “Yes, I do have this issue”, and,instead of people saying, “Well, the best thing for youto do is go home and have a rest”, they say, “What canwe do to make your working life easier? Maybe you
need a change of oYce at the moment or just tell us ifyou want to have some time oV to have counselling.We can handle it”. Those kinds of things make a realdiVerence. I think sometimes there is an issue aboutwhether you can have huge, as I have said, nationalcampaigns, advertising campaigns or whatever, whichsometimes people feel would work, but I feel morestrongly that you have got to actually have somethingthat tackles what is happening to people in theireveryday lives and get through it that way and that iswhy I think the workplace is extremely important. Ithink changing the attitude of clinicians in talking topeople and involving them much more in theirtreatment so that people do not kind of run away fromit and moving services into the community is all partof that. I think there are things that we can learn fromother countries and, as I say, I think Spain has donesome good work on mental health promotion andlinking it with substance mis-use, and again some ofthe employment work that has gone on in France issomething that we do need to look at. In terms ofdangerousness and the Mental Health Bill, it is alwaysdiYcult to try to get the balance right here. We do tryto talk about the fact that this is about gettingappropriate treatment to people, but we cannot runaway from the fact that there are some of those issuesout there, like if people deteriorate to the extent, and Ialways do emphasise that this is usually about, wherethey are a risk to themselves, not a risk to other people.What we cannot do is ignore the fact that there havebeen some of these cases and, if we did, I think it wouldlook as though we were kind of neglecting a duty totackle it. We have tried to put it in the context of howwe can not only use mental health legislation,although that is an important part of it, but we look atthe issue of treatability. I know people feel verystrongly about personality disorder and whether weare trying to bring thousands more people under theMental Health Bill detention, and that is certainly notthe case, but we cannot run away from the fact thatthere have been times when people have said, “I amnot treatable” and, therefore, they cannot be detained.That is an issue we need to tackle, but it is also an issuewhereby under the Mental Health Alliance lobby lastweek, some of my constituents came down andincidentally one of them actually said, “I have actuallylooked at the Bill”, and he said, “I do think it is quiteimportant that you do tackle some of these issuesabout the revolving door and make sure that peopledo not feel that there is not a strong system because,otherwise, I get discriminated against because I have amental health problem”. Also one woman there said,“Rosie, I am constantly told that, because I have apersonality disorder, I can’t be treated, and I am notgetting treatment”. I think we do need to use theMental Health Bill and the changes that we aremaking about treatability to say that there aretreatments available and to overcome some of that

3564222015 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
104 commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
culture which is about denying people treatment for,quite frankly, some of the wrong reasons.
Q238 Lord Wade of Chorlton: During the evidencethat we took from your Department, they told us thenabout the proposals for the Health, Work andWellbeing programme and we have also had in theevidence the suggestion that some employers shouldbe required to formulate a policy for handling mentalhealth issues at their place of work. We would begrateful if you could bring us up to date with how thisHealth, Work and Wellbeing programme isprogressing and in what ways can this help to generatea code of good practice for employers for handlingmental health issues at their place of work and arethose examples that other Member States might beable to use?Ms Winterton: I think one of the successes of theprogramme, although there is a still a long way to go,has been to bring my Department, the DWP and theHealth and Safety Commission together to really kindof make sure we have got joined-up strategies on this.Through our stakeholder council, where we have gotbusiness, we have got trade unions, we have gotvoluntary organisations and others, they are allsaying, “What part can we play in getting over thismessage?”, which I think has been a very diYcult one,but I am quite surprised that there has been areceptiveness to the idea that work is good for you. Myconstituency is an ex-mining constituency and therewas a time, because there were massively higher ratesof unemployment when the pits closed, when peoplewould go on incapacity benefit and there was certainlya feeling that people were doing that because there wasnot really anything else to do and people felt that thatwas the only way that they could cope with some ofthese problems. I think in changing the culture, first ofall, through the Pathways to Work projects which aresaying that so many people on incapacity benefitactually have a mental health problem and, if they donot start oV with one, they are probably going todevelop one after six months simply because of thekind of lack of structure and the problems that thereare with self-esteem and so on, carrying that throughto the Health, Work and Wellbeing programme has,therefore, been easier than it might otherwise havebeen, and the message, saying that work is good formental health, but also in times like this, when we dowant to maximise everyone’s potential and skills andkeep them at work, employers are increasinglyrecognising that, if they do give assistance to peopleand can get over the message about talking to peopleabout their mental health and providing them withsupport, the loyalty is tremendous from those peoplewho feel that they have had support at a very diYculttime in their lives. I think in terms of taking thatthrough to a code of practice, the first thing we havedone is to try to put out our action on stigma which is
about encouraging employers to have a healthyworkplace, starting with the NHS and governmentdepartments that we are encouraging to take part inthis, but also some of the big employers, getting peopleto kind of sign up to saying, “We are adopting theguidance to say this is how we can have a mentalhealth strategy for our workplace”. Beyond that, ofcourse I think that the Disability Discrimination Actwith mental health becoming part of that will actuallyplay quite a good part in ensuring that employers signup to it.
Q239 Lord Wade of Chorlton: Just as a follow-on tothat: clearly, as far as physical disability is concerned,there are now codes of good practice of variousindustrial systems you can use to prevent physicalillness from happening in the place of workparticularly. Do you see a similar code of practicebeing established in mental health, oVering guidanceto employers of the sorts of approaches which can betaken to avoid their employees developing mentalhealth problems?Ms Winterton: Well, it would be interesting to seewhether, as a result of the Disability DiscriminationAct, that leads automatically to a code of practice, andthat is something that I would like to look further into.Certainly, as I say, the guidance that we are puttingout is obviously voluntary at the moment and I thinkit will be quite interesting to see how many employersgo along with that and how easy, or otherwise, theyfind it to implement. I think one of the issues we reallyneed to explore is that, because with mental healththere is so much that is about the individual, you mighthave to have something which was really quite broad,so it did not necessarily capture everything that youwanted it to, but it is something that I would like totake away and look at certainly.
Q240 Lord Trefgarne: Is it not the case though that somany mental health problems are in fact the result ofeither alcohol problems or drug-abuse problemswhich of course add to the stigma which has to beovercome in the wider context?Ms Winterton: Yes, I think that there have clearly beenindications and sometimes this can be a two-wayprocess, I guess, in that if somebody has a mentalhealth problem, they might turn to drugs or alcohol orin some cases drugs and alcohol can perhaps leadcertainly to some quite serious depressions and so on.I think that taking action on both of those issues isreally quite important and, as I say, that is somethingthat I know, certainly in terms of mental healthpromotion and drug-abuse, Spain has looked at quiteeVectively
Q241 Baroness Howarth of Breckland: Minister,although many of those who have any of thoseproblems could fall foul of mental health problems, we

3564222015 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
105commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
also know that it is more likely in vulnerable groups,that they are triggered by many of the things youdescribed earlier in terms of housing and the like. I justwondered how do you think the mental health issuesabout these specific groups in the population shouldbe handled in a European context? We are particularlyinterested, and I personally am, in the position ofchildren who seem to be missed out of the strategiclook in the Green Paper in any great depth byclinicians and how can you actually ensure thatchildren from black and minority ethnic groups arealso looked at in terms of the European strategy?Ms Winterton: If I just address the BME situation tostart with, that is a whole programme of work whichwe have undertaken through Delivering RaceEquality, and one of those things has been aboutmonitoring. Obviously in some European countries, Ithink in France and Germany, the kind of collectionof data in Germany is illegal and in France it isunconstitutional, I believe, so it is quite interesting tolook at how we would capture some of thatinformation. What we have tried to do through thingslike the Count Me In census is to look, for example, atdetention rates amongst people from BMEcommunities and we have set in train a whole range ofmeasures through our focused implementation siteswhich are particular areas which are focusing on howto implement our Delivering Race Equality strategy.Very often, that is about getting to particularcommunities and one of the things we have pushedvery hard there is community development workersbecause sometimes the real issue is about comingforward at the appropriate time, feeling that theservices are going to be sympathetic and not feelingkind of frightened of services and leaving it until toolate, or not too late obviously, but until somebody canbe quite severely ill before coming forward. That islooking at some of the cultural barriers that theremight be, some of the perhaps fear of discriminationthat there might be and making sure, and this is wherecommunity teams come into it again, that the teams goout to particular communities, and there is a lot ofgood work that has been done through the focusedimplementation sites in terms of analysing what theproblem is and then working out how to overcome it.I do not know whether any of our people from thefocused implementation sites have given you anyevidence or perhaps we might ask for some to be sentforward, if that would help.
Q242 Chairman: That would be helpful, yes.Ms Winterton: There are some very interesting projectsthat are going on in that area. I think in the wider senseof children, there are some very, very real issuesobviously around that and there have been someimprovements, monetary-wise and personnel-wise,that have certainly taken place, however, there is nodoubt that there is still a long way to go. I actually
think that in terms of the NHS becoming muchstronger in its commissioning abilities, having to showwhat the needs are of the local population and thenlooking at providing services accordingly can beactually something of a driver for looking at groupswhich have perhaps traditionally not had theseservices which they should be having and it is aboutgetting people to focus on that. I also think, probablybecause it is one of my other areas in terms of patientand public involvement, that we really do need tostrengthen that and get a specific focus within that onchildren saying what services are available locally andhow can we improve on those. There is no doubt thereis much further to go in terms of the issues aroundchildren. We have tried to address some of them but Iknow there is more that we need to do.
Q243 Baroness Howarth of Breckland:Commissioning has been recognised as a weakness inboth local authorities and the National HealthService. Are there things we could learn from Europeabout doing that in a better way or do you think theyare even further behind than we are in terms of properleadership in commissioning?Ms Winterton: In a sense, because of some of thediVerences in the system through things like socialinsurance and the way that operates, it is slightlydiYcult to draw too many parallels. I hope thatcommissioning will improve as well through thingslike the Local Area Agreements because when it comesto things like children’s services and the specificemphasis in local authorities on the Children’sDirectorate and what we have tried to do throughLocal Area Agreements, getting social servicesdepartments and health authorities to work togetherto commission services, the ability to have pooledbudgets, in some cases pooled teams, will help with theemphasis that can go towards children’s services.
Q244 Chairman: Minister, I am getting a littleconcerned because it is now two minutes past eleven.Ms Winterton: Am I talking too much?
Q245 Chairman: Not at all, no, it is just that you havegiven us very full answers. I am concerned from yourpoint of view, I do not know what your timetable is. Iam afraid that at about this time the Committee beginsto slightly dissolve at the edges because people have togo oV and do other things. How would you like tohandle this? One way of handling it would be to put acouple of questions on the side, as it were, for you togive us written answers, if that would be more helpfulto us, or we can battle on. I am concerned about yourtimetable.Ms Winterton: I have a meeting with some Members ofParliament at 11.30 that I would like to get to.

3564222015 Page Type [E] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
106 commission green paper on eu mental health strategy: evidence
14 December 2006 Rt Hon Rosie Winterton MP
Q246 Chairman: So you have not got to go very farperhaps for that.Ms Winterton: I have to have a slight briefing. If Icould maybe go at quarter past.Chairman: That would be very generous. Let us presson and see where we get to by quarter past and if thereis something left over then we might ask you to sendus a note or something about what has been left out.
Q247 Baroness Greengross: You did talk aboutcollaboration in answer to one of the other questionsand the collaborative approach with your teamscoming from diVerent areas, but would you say overallthis has been very successful in the UK? If it has, doyou think that this Green Paper approach canstimulate collaboration which is much more diYcult,I think, across the diVerent EU Commission policyareas?Ms Winterton: I think what is going to be quiteimportant in terms of the Green Paper is the way thatit sets out very clearly some of the issues about theimportance of employment, the importance to theeconomy of good mental health strategies. I know thatunder the Finnish Presidency—it was not just mentalhealth, it was health in general—we had somemeetings together with employment ministers, or DTI,and we had a meeting which looked across all sectorsand the diVerent roles that people could play. I suspectthat the more that message gets out, the more it isimportant at national and, by the way, local level aswell. I suspect that one of the main ways that thestrategy will stimulate that kind of discussion and thatkind of collaboration is by showing how in diVerentcountries there is best practice and being a platformfor that exchange of ideas as to what has worked welland looking at how in some of the work that I hopewould be un-siloed, if you like, if that is a word,between diVerent parts of the Commission to look atwhat employers have done in terms of healthyworkplaces, what social security has done toencourage work as a means of stimulating betterquality of life, better health promotion in general.Chairman: Thank you. I think it is back to LadyHowarth.Baroness Howarth of Breckland: I would like to get tothe next two questions.Chairman: I felt the same myself. Lord Wade onminimum standards.
Q248 Lord Wade of Chorlton: I would like to raisewith you the question of minimum standards formental health and ask you how realistic do you feelwould be the aim of achieving minimum standards formental health across the European Union? How farcould the Platform approach achieve this aim? What
would be your view on the need for European legalinstruments, which might be a Directive, a Regulationor a Resolution?Ms Winterton: I am not sure that minimum standardssetting would be particularly helpful. The generalattitude that we have in health service matters, as I amsure you know, is that this is something that wecertainly do try to keep within the Member States’remit, if you like, because of some of the very realdiVerences in healthcare systems and legislation is notgenerally considered to be something that we wouldwant to be particularly tied to at a European levelbecause we do want to make sure that we have theability to decide our health systems, particularlybecause of the uniqueness of the National HealthService. I know that the WHO at the moment arecollecting some baseline information about what isprovided in terms of mental health services in diVerentcountries. I would say that in terms of UK provisionwe would be at quite a high standard so I cannot seeit as being something that would necessarily alter thestandard that we would be oVering. I am not sure Iwould go for the standards approach. The platformfor exchange of ideas will act, as I said earlier, as a kindof stimulus for people to be able to go back—thiscomes again to the point of the service users—and say,“This is what is available, how can we look to copythese?”Chairman: Thank you. Lord Moser has a question onpeople with learning disabilities.Lord Moser: Chairman, I would have thought wecould skip this one. It is just the question whetherlearning disabilities should be part of our generalconcern. We have been advised diVerently: theCommission puts it in in its Green Paper; the WHOsays it is not in. Unless you particularly want to talkabout this, Minister, we could save time on this one.
Q249 Chairman: What I would suggest, Minister, iswhen your oYcials look at what has been said andperhaps what has not been said and the questions wehave left out, if there is something that you feel fromyour own point of view you want to tell us about,either on the question about the co-ordination ofactivities across the countries of the UK or people withlearning disabilities, we would be very grateful to hearthat. Obviously you are now very near your deadlineand rather than go on about that now, it would bemuch nicer to be able to say thank you very muchindeed for being with us for such a long time and forbeing so open, frank and willing to discuss theinnermost bits of how these things are done. We haveall valued your evidence, thank you very much forbeing with us.Ms Winterton: Thank you very much.
3564222016 Page Type [O] 03-04-07 21:28:16 Pag Table: LOENEW PPSysB Unit: PAG1
107commission green paper on eu mental health strategy: evidence
14 December 2006
Supplementary memorandum submitted by Department of Health
COMMISSION GREEN PAPER ON EU MENTAL HEALTH STRATEGY
It was a pleasure to meet you and the Committee members on 14 December and I hope you found the sessionuseful. I said I would write with comments on two questions that we did not have time to discuss, and withsome more information about our plan for race equality in mental health care. I would also like to expandslightly on what I said about codes of practice for dealing with mental illness in the workplace.
Co-ordination of Activity Across the Countries of the UK
The Committee was interested in the scope for formalising co-operation between England, Scotland andWales, and whether co-operation within the context of an EU strategy would aVect that relationship.
In the post-devolution world it is, of course, entirely appropriate for the UK countries to have their ownmental health strategies. My colleagues in the Welsh Assembly and the Scottish Executive independently playa very active and constructive role on health issues within Europe and I am sure they will continue to do so.At the same time, we still collaborate successfully between ourselves—on our response to the Green Paper,for example—and we do have some mechanisms for co-operation more generally. There have been two UKgovernmental conferences on mental health and I believe another is planned for 2008. Occasionally we takea UK-wide approach: Scotland has a good programme called Mental Health First Aid, which raises awarenessof mental health issues and is about to be spread to England and Wales.
People With Learning Disabilities
The Committee wanted to ask whether we felt that the needs of people with learning disabilities should beembraced by the EU mental health strategy.
There are clear links and connections between the issues facing people with a mental illness and those with alearning disability. For example, the Department of Health is currently working on its response to a reportproduced here by the Disability Rights Commission that highlights the serious and unnecessary inequalitiesin physical health that both groups experience. But ultimately they are two diVerent conditions, and we don’tthink that service users would necessarily appreciate being bracketed together in a single strategy.
Delivering Race Equality in Mental Health Care
We spoke about the delivering race equality action plan that we launched in January 2005, and the focusedimplementation sites (FISs) that are leading the development of good practice. There are currently 17 FISsacross England, each of which has set its own local priorities for reaching the national objectives set out in theaction plan. It is still relatively early days, but I have been genuinely impressed with the amount of verypromising work they have begun.
For example, in Plymouth the FIS is establishing an entirely new counselling service for the local BMEcommunities, helping to extend a wider choice in services to people who may not have been able to choosebefore; in TraVord, the FIS has helped to set up a new support service for carers from the African Caribbeancommunity, oVering access to culturally sensitive support groups, access to training and opportunities to takeshort breaks; and in Birmingham the FIS is helping to redesign the processes for commissioning mental healthservices to make sure they reflect all patients’ perspectives and needs.
Employers’ Code of Practice
I thought I should reiterate that the Action on Stigma document that we launched in October sets out ourlatest guidance to employers on promoting mental health and ending discrimination at work. While some ofit is voluntary, it will certainly help employers to comply with their new duties under the DisabilityDiscrimination Act. The Act includes mental illness in its definition of disability, and requires public sectorbodies to produce equality schemes demonstrating how they will protect and promote the rights of disabledemployees.
December 2006
3564223001 Page Type [SE] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
108 commission green paper on eu mental health strategy: evidence
Written Evidence
Memorandum by Age Concern
1. Introduction
1.1 Age Concern welcomes the opportunity to submit evidence to the Select Committee Inquiry into policyissues related to the European Commission Green Paper on Improving the mental health of the population.
1.2 Age Concern England (the National Council on Ageing) brings together Age Concern organisationsworking at a local level and 100 national bodies, including charities, professional bodies and representationalgroups with an interest in older people and ageing issues. Through our national information line, whichreceives 225,000 telephone and postal enquiries a year, and the information services oVered by local AgeConcern organisations, we are in day-to-day contact with older people and their concerns.
1.3 Age Concern England has set up an independent Inquiry into Mental Health and Well-Being in Later Life,in partnership with the Mental Health Foundation. The Inquiry is a UK-wide project running until 2007. Todate it has reviewed existing evidence and gathered new information from over 1,000 older people and 200organisations and professionals. The Inquiry will publish two reports of recommendations—one on thepromotion of mental health and well-being in later life (due June 2006) and the other on the provision ofservices and support to older people with mental health problems and their carers (expected Spring 2007).
2. Summary
2.1 Age Concern welcomes the European Commission Green Paper and the proposal to establish a strategyon mental health for the EU. We particularly welcome the Green Paper’s emphasis on promoting mentalhealth and preventing mental illness.
2.2 An EU strategy on mental health would be appropriate but it must include people of all ages. Mentalhealth in later life is a much neglected area in policy, practice and research. In the UK, this neglect has resultedin the development of an unfair system that disadvantages older people.1 Much more work is needed to ensurethat older people’s mental health receives the attention it deserves.
3. Would an EU Strategy on Mental Health be Appropriate?
3.1 Age Concern supports the development of an EU strategy on mental health. Mental health and well-beingare very relevant in achieving the common objectives of economic prosperity, social justice and equality as setout in the Lisbon Agenda. As noted in the Green Paper, mental health problems are a growing challenge forthe EU. In the UK, mental illness has been called “our biggest social problem—bigger than unemploymentand bigger than poverty”.2 Mental health problems are also a growing challenge for citizens of all ages.Discrimination is a major barrier to social inclusion and quality of life for people with mental health problems,and even associated with shorter life expectancy.3
3.2 An EU strategy on mental health must be considered in the context of demographic change andpopulation ageing, which are growing challenges for all Member States and already regarded by theCommission as strategically important for economic growth and social protection. In particular, a strategythat includes actions to improve mental health in later life is needed at this time.
3.3 Mental health problems in later life pose a challenge for the EU and for citizens of all ages. Depression isthe most common mental health problem in later life, aVecting up to one in four people aged 65 and over,4 or2.4 million people in the UK,5 at any one time. As the older population grows, this number will rise to 3.1million over the next 15 years6 if prevalence rates of depression stay the same; in fact they are expected to rise.7
1 Healthcare Commission, Audit Commission and Commission for Social Care Inspection, Living well in later life: A review of progressagainst the National Service Framework for Older People, Commission for Healthcare Audit and Inspection, 2006.
2 Layard, R, Therapy for all on the NHS, Sainsbury Centre Lecture 6 September 2005, Sainsbury Centre for Mental Health, 2005.3 Social Exclusion Unit, Mental health and social exclusion, OYce of the Deputy Prime Minister, 2004. Life expectancies for people with
schizophrenia are 10 years less than the average.4 Godfrey, M et al, Literature and policy review on prevention and services, UK Inquiry into Mental Health and Well-Being in Later Life,
2005. Godfrey et al estimate that one in seven people aged 65 and over have “major” depression which is severe and persistent anddisrupts day-to-day functioning. The proportion rises to one in four if we include all depressions which are severe enough to impairquality of life.
5 Based on Government Actuary’s Department estimates, there are currently 9.7 million people aged 65 and over in the UK.6 Based on Government Actuary’s Department projections, the number of people aged 65 and over in the UK will increase by nearly
30 per cent to 12.5 million in 2020.7 Sainsbury Centre for Mental Health, The economic and social costs of mental illness, 2003.
3564223001 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
109commission green paper on eu mental health strategy: evidence
There are 5 million people with dementia in the EU and this number is expected to double by 2040.8 The costsof care, including related pressures on the supply of informal support from family and friends, will increase.
3.4 Mental health problems are not an inevitable part of ageing. The majority of older people are in goodmental health and they make significant contributions to the economy and to society. In the UK, workers aged50 and over account for a quarter of the nation’s economic output.9 Older people add £24.2 billion in unpaidcontributions as volunteers, carers and grandparents.10 They boost the economy by a further £239 billion inconsumer spending.11 As the older population outgrows the younger population, society will becomeincreasingly reliant on older people’s contributions. Good mental health is crucial to enabling thesecontributions.
3.5 It is thus in the public interest to promote good mental health and well-being in later life. The opportunityto maximise older people’s contributions and to minimise the costs of care is one that no country in the EUcan aVord to ignore.
3.6 To date, mental health in later life has been much neglected in policy, practice and research. In the UK,it is recognised that the issue has fallen in the gaps between mental health and ageing, with mental health policytending to focus on younger people and adults “of working age” (meaning up to age 65), and ageing policytending to focus on physical health. More work is needed to ensure that older people’s mental health receivesthe attention it deserves, and to better integrate the issue into existing national policies.
4. What Elements Might an EU Strategy on Mental Health Contain?
4.1 An EU strategy on mental health must address the mental health needs of people of all ages, includingolder people. It should incorporate a life course perspective on ageing and mental health, and ensure thatmental health promotion and the prevention of mental illness are given priority.
4.2 The Strategy should incorporate the findings of the UK Inquiry into Mental Health and Well-Being inLater Life, which show that the following themes impact on mental health for people of all ages, butparticularly older people:
— Discrimination. Age discrimination is the most common type of prejudice experienced by people aged55 and over in the UK. Our evidence from older people has shown that it has a very negative impacton mental health and must be tackled as a matter of priority. Age discrimination within mentalhealth policy is a particular problem. The Strategy could help to tackle this by ensuring that it doesnot discriminate against older people, directly (eg by excluding them from consideration) orindirectly (eg by presenting ageing negatively).
— Participation. Older people want to make contributions to society and be recognised for them, butthey face barriers to participation in many areas of public and private life.
— Relationships. Strengthening positive relationships will help to promote mental health and well-beingfor people of all ages. Isolation and loneliness are a particular risk in later life and must be tackled.Intergenerational contact should be encouraged.
— Physical health. Physical health and mental health are inextricably linked. Improving physical healthwill help to improve mental health as well. There is overwhelming evidence for the mental healthbenefits of physical activity, and older people also stress the importance of a healthy diet. Improvedplanning, for example in the development of communities with good local facilities which promotesafe walking and cycling, would fall within the remit of Regional Policy.
— Poverty. Poverty is a risk factor for poor mental health. Nearly 2 million older people in the UK livein poverty. Money is important for the things it can provide to make people feel included in society.Confidence about future financial security is important for mental health and well-being.
5. How might an EU Strategy on Mental Health Complement and Add Value to Other Strategies
and Activities?
5.1 A strategy that pays particular attention to mental health promotion and the prevention of mental illnesswill complement and add value to strategies and activities being undertaken by Member States and otherinternational bodies. The promotion of good mental health and well-being for people of all ages requiresco-ordinated action across many diVerent areas of public policy, such as health, social inclusion, income8 Ferri, CP, et al “Global prevalence of dementia: a Delphi consensus study”, The Lancet 2005 Dec 17;366(9503):2112–7.9 Age Concern England, The ageing workforce, forthcoming.10 Meadows, P, The economic contribution of older people, Age Concern England, 2004.11 OYce of National Statistics, Household expenditure by age of household reference person 2004–05, Family Spending Survey, 2005.
3564223001 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
110 commission green paper on eu mental health strategy: evidence
support, housing, transport, employment and education. An EU strategy will provide a platform for sharingexamples of good practice within the UK and create opportunities for learning from others.
5.2 A strategy that pays equal attention to older people will complement and add value to strategies that arebeing developed for ageing populations across the EU. The UK strategy for an ageing population, OpportunityAge, aims to promote well-being in later life and enhance older people’s contributions to society. Improvingthe mental health of older people can play an important role in realising these aims.
5.3 Other policy developments in the UK that would be enhanced by the development of a strategy on mentalhealth include:
— Strategies to promote equality and human rights, for example in the establishment of theCommission for Equality and Human Rights, which will tackle discrimination, including agediscrimination and stigma experienced by people with mental health problems.
— Strategies to tackle physical health inequalities, which are often experienced by people with mentalhealth problems.12
— Strategies to tackle mental health inequalities, which are often experienced by older people.13
— Strategies to tackle social exclusion, which is experienced both by people with mental healthproblems14 and by older people.15
6. Recommendations
Age Concern recommends that the European Commission should:
6.1 Prioritise the mental health needs of older people, as they have been much neglected across the spectrumof mental health services, including promotion, prevention, treatment and care.16
6.2 Use the findings of the UK Inquiry into Mental Health and Well-Being in Later Life to develop a strategyon mental health promotion in later life.
6.3 Ensure that the strategy is “age proofed” to take older people’s needs into account. Specifically, theCommission should further develop the following parts of the Green Paper:
— Pages 4–5: By acknowledging the costs to society of mental ill health in later life.
— Page 8: By identifying a setting for action for older people, similar to the settings that have beenidentified for children (schools) and working adults (workplaces).
— Page 10: By recognising that suicide is an important issue for older people, as suicide rates tend toincrease with age; globally the highest rates are among men aged 75 and over17.
— Page 16: By ensuring that all statistics and figures include adults aged 65 and over.
6.4 Eliminate the use of age discriminatory language such as the distinction between “the workingpopulation” and “older people”. Many older people still work. With the EU employment directive on AgeDiscrimination coming into eVect in the UK in October 2006, the term “working age” will become outdatedand meaningless.
Memorandum by British Geriatrics SocietySpecialist Medical Society for Health in Old Age
The British Geriatrics Society
The British Geriatrics Society (BGS) is the only professional association, in the United Kingdom, for doctorspractising geriatric medicine. The 2,200 members worldwide are consultants in geriatric medicine, thepsychiatry of old age, public health medicine, general practitioners, allied health professionals, and scientistsengaged in the research of age-related disease. The Society oVers specialist medical expertise in the whole rangeof health care needs of older people, from acute hospital care to high quality long-term care in the community.12 Disability Rights Commission, Equal treatment: Closing the gap, Interim report of a formal investigation into health inequalities, 2005.13 Healthcare Commission, Audit Commission and Commission for Social Care Inspection, Living well in later life: A review of progress
against the National Service Framework for Older People, Commission for Healthcare Audit and Inspection, 2006.14 Social Exclusion Unit, Mental health and social exclusion, OYce of Deputy Prime Minister, 2004.15 Social Exclusion Unit, A sure start to later life: Ending inequalities for older people, OYce of the Deputy Prime Minister, 2006.16 National Institute for Mental Health in England, Making it possible: Improving mental health and well-being in England, Care Services
Improvement Partnership and the National Institute for Mental Health in England, 2005.17 Bertolote, JM and Fleischmann, A, “A global perspective in the epidemiology of suicide”, Suicidologi 2002;7(2):6–8.
3564223002 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
111commission green paper on eu mental health strategy: evidence
Geriatric Medicine
Geriatric Medicine (Geriatrics) is that branch of general medicine concerned with the clinical, preventive,remedial and social aspects of illness of older people. Their high morbidity rates, diVerent patterns of diseasepresentation, slower response to treatment and requirements for social support, call for special medical skills.The purpose is to restore an ill and disabled person to a level of maximum ability and, wherever possible,return the person to an independent life at home.
The Society is delighted to be given the opportunity to contribute to this debate and would comment asfollows:
1. How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed in section 1?
1.1 Mental health is clearly relevant to a number of EU strategic policy objectives, but the Green paper failsto outline how these objectives diVer from those of the individual nations that comprise the EU. In short howEU-level policy objectives add in any way to those already in place at national level.
2. Would the development of a comprehensive EU-strategy on mental health add value to the existing and envisagedactions and does section 5 propose adequate priorities?
2.1 Section 4 acknowledges widespread mental health inequalities within and between member states,illustrating this point with regard to national suicide rates. The Green paper states that there are no uniformsolutions and restricts its aim to “exchange and cooperation between Member States and the opportunity tolearn from each other”. Section 5 lays out the reasons for an EU-wide strategy:
(a) Creating a framework for exchange and cooperation between Member States.
(b) Helping to increase the coherence of actions in diVerent policy sectors.
(c) To open up a platform for involving stakeholders including patient and civil society organisationsinto building solutions.
2.2 Aim (a) appears sensible since the EU possesses appropriate resources and experience in setting upframeworks to enhance exchange and cooperation between member states.
2.3 Aim (b) is appropriate insofar as it relates to EU institutions, in particular ensuring coherence of policiesproposed by the EU Commission in diVerent spheres (eg trade, environment, education etc).
2.4 Aim (c) is less clearly defined. Many platforms already exist within individual nations to take forwardsolutions locally. It is unclear how an EU-wide platform would add to this, especially since it is unclear howrepresentation at such a platform could be equitably organised. Otherwise, those organisations with thegreatest resources within the EU may end up over-represented compared with less well-resourcedorganisations, perhaps from newer EU members. The EU needs to address this issue before such a platformcould be supported as adding value.
3. Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between Member States, topromote the integration of mental health into the health and non-health policies and stakeholder action, and to betterliaise research and policy on mental health aspects?
3.1 Numerous initiatives are proposed in Sections 6 and 7. Many overlap with current EU member statepriorities. It is unclear how far practices in one state are relevant to very diVerent cultural traditions andeconomic circumstances in other states. A guide here would be to use available resources to focus on thoseinitiatives where the EU can clearly add value rather than merely replicate nationally established programmes.There is a role for the EU to provide guidance based on the EC Treaty and European Human Rights legislationas interpreted by the European Court of Human Rights. There are initiatives, such as those relating to themental health of migrant workers, which may be addressed better at an EU than at a national level. Similarlythe EU has a clear role in promoting collaborative research between member states into mental health.
Memorandum by British Medical Association
Thank you for giving the British Medical Association the opportunity to contribute to the inquiry by theCommittee. The BMA supports the Green Paper, and the recognition central to it that good mental health isvital to physical well being.

3564223003 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
112 commission green paper on eu mental health strategy: evidence
It is essential that the proposals in the Green Paper are adequately funded for it to achieve its aims. The BMAis also concerned that discrepancies between mental health legislation in member states could potentiallyhamper the Green Paper.
The BMA would like to highlight the need for better pay and conditions and other incentives in somecountries, in order to encourage the mental health workforce to remain where they are most needed. We wouldalso like to see more EU support of mental health non-governmental organisations in the central Europeanmember countries to further improve mental healthcare provision.
The BMA feels that the following points are not suYciently covered in the Green Paper:
— That those suVering from mental health problems often need State financial support.
— Alcohol and/or substance misuse. This should be included on page 4, section 2.
— The benefits of good nutrition and regular exercise should be addressed on page 8, section 6.1.1.
— Stress caused by career or loss of income. Page 9, paragraph 1 fails to mention the adverse eVects ofstress in the workplace on cardiovascular disease.18
— The state of mental health institutions, which is relatively poor in many countries.
— Prisons and mental health.
— Alzheimers disease.
Memorandum by the Christian Council on Ageing
Introduction
Since its inception in 1982 the ecumenical Christian Council on Ageing (CCOA) has worked to ensure thatolder people remain high on the agenda of the churches and to provide a corporate voice in consultations suchas that promoted by the European Green Paper on EU Mental Health Strategy. This response has been drawnup by Dr Daphne Wallace, chair of the CCOA Dementia Group and herself an old age psychiatrist, afterconsultation with the acting chair of CCOA and members of its executive committee.
1. We would urge that older people be given a significant place in this consultation and in the strategy andoptions for action that may emerge. The population of UK is ageing and the same is true of many otherEuropean countries. Dementia is estimated to aVect some 750,000 persons in UK and one in four of those over80. Clinical depression in older people is also widespread, though not always recognised or diagnosed as such,either as a concomitant of dementia or otherwise.
2. Progress in the EU as a whole in relation to mental health of the population will only be possible if thereis, as suggested in the green paper, a comprehensive strategy on mental health. Such a strategy should givegoals towards which all member states can aspire and work together to improve situations which impair themental health of its citizens. Such a strategy would also serve to address the inequalities between the situationsin diVerent member states.
3. Such a strategy would need to encompass promotion of mental health, prevention of mental ill health and,importantly, the promotion of appropriate, flexible, person-centred care for those with mental healthproblems especially severe mental illness. The importance of the recognition of spiritual needs and the evidenceregarding its impact on positive mental health should also be taken into account. Use of appropriatemedications should not be influenced purely by cost. Care would also have to promote appropriate dignityand rights for those with such illnesses and only then would stigma be reduced.
4. The causes of inequalities and deficiencies are many and complex. DiVerences in proportion of healthbudgets spent on mental health aVect mental health status but there is not a direct correlation. How moneyis spent and on whom is also important. It must be that cultural and other factors influence what is appropriateand acceptable in diVerent member states. A comprehensive strategy as proposed should facilitate mutualcooperation and learning, together with promotion of research, which can only be beneficial.
5. The proposals in section 5 rightly promote involvement of stakeholders, including patients, in buildingsolutions. Many groups have been seen in the past as being unable, because of their mental illnesses, tocontribute usefully to any such discussions. The changing attitude to people with dementia in many EU stateshas increased their ability to make a contribution to planning their care. Other groups of elderly with mentalhealth problems have also often been neglected in the face of the needs of those who are of working age—neglecting the valuable contribution of the older members of the population to the overall community.18 Hemingway H & Marmot M (1999) Evidence based cardiology: Psychosocial factors in the aetiology and prognosis of coronary heart
disease: systematic review of prospective cohort studies BMJ 318: 1460–7.
3564223004 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
113commission green paper on eu mental health strategy: evidence
6. It often seems that the needs of those, young or old, with enduring mental health problems are regardedas too expensive, whether long term care is available to people in their own homes or through 24-hour care.Long-term “warehousing” of problems is not unknown as a way of ignoring needs and rights of people whocan be hidden away. Even the abolition of the worst of the old institutions does not prevent unsatisfactoryprovision for the need for “asylum” for those most adversely aVected and damaged by enduring mental illness.Not everyone can “recover” completely but that does not mean that they cannot contribute to their societygiven the appropriate support and care. This is part of the third focus proposed for the EU strategy. Socialinclusion, rights and dignity are important for all.
7. In section 6.1.1 of the paper the proposals for preventative action are very important. Promotion of mentalhealth in older people often takes a back seat in provision despite the known stressors leading to mental ill-health. Support interventions, as suggested, can improve mental well-being but are all too often ratherneglected in this age group. CCOA has particular concerns at present with the current situation in UK withregard to prescription of drugs for dementia. The current view of NICE seems to be that although it acceptsthat at least three of those currently available can be eVective, they should not be prescribed, at least until thesymptoms are “bad enough”. There are already areas in UK where people with Alzheimer’s disease have neverhad access to these medications causing distress and more rapid deterioration in symptoms. It is importantthat decisions of this sort are not made purely in relation to cost.
8. The proposals in section 6.2 with regard to social inclusion are very important but it needs to be recognisedthat not only does the community have to accept those with mental health problems without stigma, but someof those with enduring mental health problems cannot cope with the demands of life in our modern societies.No-one likes to be in an institution, including those with dementia or severe mental illness, but some aspectsof the institutions were beneficial. A sheltered environment with easy access to recreation and useful activitymay be the most satisfactory way of preserving the rights and dignity of some individuals. This does not haveto be in an “institution” but does need to alleviate isolation fear and anxiety. Support should not meandisempowerment.
9. The use of Compulsory Admission and Involuntary treatment should be strictly regulated and kept to aminimum. It should be recognised that within such a legal framework the rights of the individual may beprotected. The Bournewood case in Britain is an example of these issues. In UK statutory rights under mentalhealth legislation may help to ensure finance for appropriate provision which may be less easily available forthose who are not subject to statutory responsibilities. Residential environments may be very guilty ofneglecting the rights and dignity of residents, whether young or old, especially those with impaired mentalcapacity. These issues are powerful examples of subjects appropriate for consideration in an EU strategy withmuch scope for exchange of knowledge and expertise and cooperation in research.
10. It is important that the proposed Dialogue between states, while concerned initially with mental healthpromotion and depression and suicide, should eventually extend to the many other areas of concern I havetouched upon above.
Memorandum by Department of Health’s Older People’s Mental Health Programme Delivery Board
GOVERNMENT RESPONSE TO THE EUROPEAN COMMISSION GREEN PAPERIMPROVING THE MENTAL HEALTH OF THE POPULATION: TOWARDS A STRATEGY ON
MENTAL HEALTH FOR THE EUROPEAN UNION
General
The Green Paper (although it does touch on OPMH issues) seems to focus predominantly on services forworking age adults (WAA).
Sections 1 through 5 focus predominantly on issues relating to WAA.
The focus is also mainly on functional and not organic illness. It would be useful for example to refer in the“Introduction” and, particularly, in Section 3 under the heading “Mental Health, A Growing Challenge forthe EU” to the pressures created on public services by the growing population of older people.
Pressures created by an ageing population are well-documented, most recently in the Wanless Social CareReview: Securing Good Care for Older People. In the next 10 years, the number of people aged over 65 willincrease by 15 per cent, and the number of people aged over 85 will increase by 27 per cent. We are thereforelikely to see a significant increase in the incidence of age-related mental health problems.
Current figures show:
— Depression is present in about 12 to 15 per cent of people aged over 65.
— Dementia aVects one person in 20 aged over 65 and one person in five over the age of 85
3564223005 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
114 commission green paper on eu mental health strategy: evidence
4.1 The European Community, its mandate and activities in the field of mental health
The Green Paper states that the DAPHNE II programme combats violence against children, young peopleand women. There is no reference to how the Community handles issues relating to the protection of othervulnerable adults, and particularly what measures it has taken to confront the issue of elder abuse.
It might be worth referring to the No Secrets guidance launched in the UK in 2000 to improve the levels ofsupport and protection for adults considered vulnerable to abuse; and the recently-released, DH-commissioned study into Adult Protection Recording Systems in England, carried out by Action on ElderAbuse.
The issue of elder abuse should also be included in section 6.2 “Promoting the social inclusion of mentally illor disabled people and protecting their fundamental rights and dignity”.
4.2 Mental Health in Member States
The figures given for suicide rates are not disaggregated according to age but again it is worth mentioning thesignificant proportion of suicides in the at-risk group of men aged 75!.
6.1.1 Promoting mental health in older people
Everybody’s Business (DH/CSIP 2005), DH’s new service development guide which outlines the elements ofa comprehensive older people’s mental health (OPMH) service, identifies promoting good mental health forolder people as a cross-cutting issue.
It is worth including access to advocacy and specialist advice; lifelong learning; volunteering; transport;finance and benefits; housing and safety and environment alongside health, social care and social activities inthe list of essential pre-requisites for ensuing good mental health for this client group.
Useful research has been done on key drivers of quality of life in older people, for example Adding quality toquantity. Older people’s views on quality of life and its enhancement (Bowling and Keneally).
The Commission may wish to be aware of the work of the UK Inquiry into Mental Health and Well-Being inLater Life which is being conducted by Age Concern and the Mental Health Foundation.
The Inquiry has undertaken work to raise awareness and create better understanding of mental healthpromotion in later life. Work to date has included:
— A review of literature and policy.
— Gathering evidence from older people. This was done via a written questionnaire which generatednearly 900 responses; focus groups with Black and minority ethnic older people and older lesbians,gay men and bisexuals; and various consultation events.
— Gathering evidence from organisations and professionals. This was done via a written questionnairewhich generated nearly 200 responses; roundtable discussion groups; and various presentations andworkshops.
Reports of this work are available on the Inquiry website at www.mhilli.org.
It is also worth noting that the National Institute for Clinical Excellence (NICE) are considering promotinggood mental health as one of a range of possible candidate topics for public health guidance.
Annexes
The Green Paper’s supporting annexes also focus on WAA or on children’s transition into adult services.
As noted before, the information on suicide is not disaggregated according to age but it is worth noting thatthe second highest at risk group for suicide is men aged 75!.
The table detailing the financial costs of social exclusion has a clear focus on WWA. The economic case forpreventative services and activities in relation to older people is well set out in Making Life Better for OlderPeople (Social Exclusion Unit, ODPM).
For example, for an annual cost of £1.5 million, Manchester City Council forecast the following potentialbenefits:
— Supporting older people to live at home: Estimated benefit of £1.4 million per year.
— Preventing the need for higher intensity care: Forecast benefit of £1.4 million per year.
3564223005 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
115commission green paper on eu mental health strategy: evidence
— Reducing avoidable, emergency admissions and bed days: Forecast benefit of £11k per year.
— The net present value of benefits minus costs: £25 million over 10 years (base case scenario).
Partnerships for Older People Projects (POPPs) grants aim to encourage councils in England to deviseinnovative approaches with their NHS, local government, voluntary and community sector partners toestablishing sustainable arrangements for supporting older people in active and healthy living.
Conclusion
DH OPMH Programme Board members welcome the suggestion of an EU-strategy on mental health, but feelsthat further work is necessary to ensure that this strategy is properly age-inclusive.
Memorandum by European Public Health Alliance (EPHA)
1. The European Public Health Alliance welcomes the adoption of the Green Paper on Mental Health, andespecially the approach of the European Commission in its consultation, which goes beyond the borders ofhealth actors and aims to involve other relevant stakeholders. The Green Paper constitutes an important steptowards a strategy to tackle mental health issues in a comprehensive, sustainable and harmonised way acrossthe EU.
2. Addressing mental health and well-being requires therefore a multi-faceted public policy approach, whichis what EPHA advocates for. As EPHA focuses on activities at EU level, our response aims to highlightCommunity activities and actions that could feed into an EU strategy on mental health and well-being.19
I. The Relevance of Good Mental Health of the Population for the EU’s Strategic Policy
Objectives
3. One in four Europeans experience a significant episode of mental illness during their lifetime, according tothe World Health Organisation (WHO). Mental health problems hamper all aspects of EU’s social, economic,educational, justice and health care systems. They are also wide-ranging, long-lasting and usually source ofdiscrimination, challenging European values at their core. Mental health and well-being depends on variousfactors ranging from poverty, unemployment, housing, physical environment, social networks, social capita,stigma, discrimination, and opportunities. Therefore, EPHA strongly recommends to promote good mentalhealth for the EU population as to allow the EU to comply with its core values and goals: achieving asustainable knowledge-based growth without ignoring its commitment to protect Human Rights andstrengthening social inclusion (EU Treaty article 13). An EU strategy will be key to underpin the EU’s widercommitment to solidarity, community and social justice.
II. The Added Value of an EU-Strategy on Mental Health and its Components
4. An EU Strategy on mental health and well-being would add value by creating a framework for exchangebetween Member States, increase the coherence between policies at European level, and between theEuropean, national and regional level, as well as improve communication between the diVerent actors.
5. EPHA calls for a EU strategy that allows an horizontal approach to mental health, extend its scope beyondthe health sector and impact on other EU public policies. In EPHA’s view, the EU strategy should put moreemphasis on the promotion and prevention of mental health, as required by the article 152 of the TreatyEstablishing the European Community, which states: “a high level of human health protection shall beensured in the definition and implementation of all Community policies and activities”.
III. Mainstreaming Mental Health into Other European Policy Sectors
6. The Green Paper reviews the eVects of mental health on the European society and it aims to broaden theperspective from an healthcare point of view to a wider public health approach, especially focusing onprevention and promotion of mental health in various settings (poverty, violation of human rights, stigma anddiscrimination, and the workplace). EPHA welcomes the approach chosen by the European Commission andwould like to add some Community policy areas where mental health and well-being should be mainstreamed.19 A complete version of EPHA response can be downloaded at:
http://www.epha.org/IMG/pdf/EPHA–response–Green–Paper–mental–health.pdf
3564223006 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
116 commission green paper on eu mental health strategy: evidence
3.1 Promoting mental health and addressing mental ill health through preventive action
7. Access to healthy diets and the practice of regular physical activity shall be highlighted in the Green Paper.EPHA believes that our agri-food system holds a key to the growing burden of mental and physical ill healthin the recent decades. Agriculture policy development (namely the Common Agriculture Policy—CAP)should be reformed to take into account its tremendous impact on health.
8. EPHA welcomes the intention outlined in the Green Paper of drawing together work that has already beenundertaken at EU level on drugs, alcohol and substance abuse disorders. We also welcome the will to examinethe use and application of harm-reduction strategies in this domain, in particular with relation to the situationof homelessness. We would like to point out that a strategy on drug and alcohol shall NOT focus only onchildren and young people but must target the environment and conditions which are associated withdrinking.
9. As such, the future EU Strategy on mental health could draw on the coming Strategy on alcohol. Inaddition, we would recommend the EU strategy to build on the existing international alcohol policy initiatives.In addition, the use of health or nutrition claims on alcoholic products should not be allowed: Europe’sconsumption of alcohol is already high and causing considerable health damage.
10. With regard to vulnerable groups as mentioned in the Green Paper, EPHA believes that it may beappropriate to call for “individuals in community and settings”, rather than targeting vulnerable groups. Asetting-based approach (eg family life, school life, work life, housing conditions) could be more flexible andprevent from further stigmatising vulnerable groups.
11. Furthermore, EPHA calls for the emergence of a consistent and coherent approach to children’s heathacross EU policies and programmes. Evidence shows that targeted interventions in school and communitysettings should be supported. The role of the European Commission has to be to coordinate eVorts and topromote exchange of best practice between Member States.
12. Gender is a missing issue from the Green Paper, although this determinant should be taken into accountwhen designing and reforming mental health services, which should be gender-sensitive.
13. The workplace is of particular importance in order to improve good mental health and prevent mental illhealth. The Green Paper mentions changes to work patterns such as sensible working hours. It is importantto mention here the EU Working Time Directive as a tool towards the mental well-being of the Europeanworkforce. Similarly, the elimination of stigma and discrimination associated with mental health problems inemployment practices could fall under the European Employment Strategy.
14. The European Agency for Health and Safety at Work (OSHA) could help incorporating mental health inoccupational health and safety (eg dedicating a year to good mental health promotion at the workplace,developing guidelines to improve the monitoring of work-related mental health through appropriateindicators and instruments).
15. A better social inclusion of people living with Mental Health disorders can also draw on the EuropeanDirective of Equal Opportunities which sets out conditions for employment and the obligation for MemberStates to provide an independent financial support for everyone who needs it.
3.2 Promoting the social inclusion of mentally ill or disabled people
16. Education is key to alleviate the burden of Mental health on children and young people. EU programmesfor Education and Culture can further encourage the integration of children and young people with mentalhealth problems and disabilities in the regular education and vocational training schemes.
17. The EU strategy could as well use resources available in sport programmes in order to encourageinitiatives to include children living with mental disorders in regular school programmes and activities. Thiswould hinder stigma at an early age.
18. The EU Social Inclusion strategy should include provisions to facilitate the access to social housing ofpeople with mental health problems. The same does apply to homeless people whose mental health conditionsprevent them from social reinsertion. A strong framework for exchange and learning in the area of mentalhealth will certainly feed into the Open Method of Coordination’s objectives such as objectives on theeradication of poverty and social exclusion, as well as objectives on ensuring accessible, high-quality andsustainable healthcare and long-term care.
19. Structural Funds could be used to plan and fund pilot programmes, develop guidelines for good practiceand monitor their implementation, establishing partnership across sectors. Structural Funds are all the moreimportant as regional and local levels play an increasing role in the provision of health and social care. Theycould also fund the establishment of community based services rather than the building of closed doorinstitutions.
3564223006 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
117commission green paper on eu mental health strategy: evidence
3.3 Protecting fundamental rights, dignity and combating stigma
20. A right-based approach can be used to combat discrimination (art 13 of the EU Treaty), although itslimitations shall be acknowledged: people that are treated for mental health problems have a right to healthand are protected by human rights conventions. However, the enactment of those rights requires an activeparticipation of a provider.
21. The future European Agency on Fundamental Rights could play an active role in promoting rights ofpeople with mental conditions. However, this would imply an extension of its remit towards the inclusion ofhuman rights abuses occurring under national laws. In this line, the European Council could adopt a CouncilRecommendation on civil detention to provide clear guidelines on compulsory treatment. TheRecommendation, based on current Human Right instruments, could clarify the definition of compulsorytreatment, as well as the criteria used for civil detention. It could provide guidelines on the definition andtraining of experts for assessment and decision making, on the timeframe for emergency detention, healthreporting standards, the inclusion of patient counselling.
22. As mentioned in the Green Paper and in the WHO Action Plan, it is of critical importance to scrutinisedisability rights legislation to ensure that it covers mental health equitably.
23. Another policy area which can play a significant and powerful role in promoting mental health andreducing stigma is audio-visual policy. The current revision of the Television without Frontiers Directivecould provide a momentum to include mentally healthy programmes.
3.4 Improving information and knowledge on mental health in the EU
24. The implementation of eYcient and outcome-driven policies will depend on the availability of data anduseful indicators. The current status of mental health indicators is fragmented and incomplete: it is coveredby several Directorate General of the European Commission, pan-European survey, local and regional data,national indicators, World Health Organisation initiatives.
25. There is agreement that we have already important amount of information about the state of mentalhealth of the EU. However, there are still some information needs/gaps more specifically on the eVectivenessof measures to promote good mental health that could be addressed by the European Union 7th ResearchFramework Programme: Information needs also target mental health in children, mental health in the elderly,longitudinal mental health, health determinants, geographical, economic and social diVerences, vulnerablegroups. There is a need to collect data on positive mental health, as well as on protective factors.
Memorandum by Finance & Leasing Association
1. FLA (Finance & Leasing Association) is the main representative organisation for the UK consumer credit,motor finance and asset finance sectors. Our members comprise banks, subsidiaries of banks and buildingsocieties, the finance arms of leading retailers and manufacturing companies, and a range of independentfirms.
2. The facilities provided by FLA members include finance leasing, operating leasing, hire purchase,conditional sale, personal contract purchase plans, personal lease plans, secured and unsecured personalloans, credit cards and store cards.
3. FLA members achieved £87.3 billion of new business in 2005. Of this, £27.2 billion was provided to thebusiness sector and UK public services, representing over 30 per cent of all fixed capital investment in the UKin 2005 (excluding real property). The remaining £60.1 billion was provided to the consumer sector, and FLAmembers represented 25.5 per cent of all unsecured lending in the UK. In the above total is £18.6 billion offinance provided to the motor sector. FLA members financed at least 50 per cent of all new car registrationsin the UK in 2005.
4. FLA, as part of the UK Cross-Industry Group, twice gave evidence to the Sub- Committee Inquiry intothe EU Consumer Credit Directive in 2005 and 2006.
5. FLA welcomes the opportunity to contribute to the Sub-Committee’s Inquiry. According to the OYce ofNational Statistics, one in six people experience some kind of mental health problem at any one time. This cancause many diYculties, especially in managing finances and debt.
6. FLA is well placed to help promote to the lending industry the interests of vulnerable groups. In November2005, FLA produced a film and training materials entitled “Money Worries” aimed at improving the adviceand support oVered by finance providers to those with mental health diYculties and debt problems. This waslaunched in Parliament at an event hosted by Mark Lazarowicz, MP. Produced in partnership with CitizensAdvice the package highlights what lenders can do to ensure they respond sensitively, appropriately and fairly

3564223007 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
118 commission green paper on eu mental health strategy: evidence
to those in financial diYculty and how best to raise awareness with front-line staV and those engaged in debtcollection.
7. This initiative was our response to Citizens Advice’s April 2004 report “Out of the Picture”, whichhighlighted the experiences of people with mental health problems in a variety of social contexts includingaccess to the benefits system, employment and financial problems. The material is primarily aimed at raisingthe profile of the issue of mental health and debt problems with lenders and Citizens Advice Bureaux andenabling them to adopt a more practical approach to making the experience better for consumers.
8. We believe that the initiative also played a role in helping raising the profile of the inter-action that canexist between mental health and debt problems. Mentalhealth diYculties can lead to a range of problems insomeone’s life and their relationships with others. It will often cause problems with their employment and theirability to manage their money. For many people, debt problems can arise as a result of their illness, for othersdebt problems can cause stress anxiety and lead to health problems.
9. We enclose a copy of the pack, press release and frequently asked questions together with FLA’s LendingCode, section 1C.5 (on page 13) of which requires FLA members to take particular care if the consumer issuVering from health problems, including mental health diYculties. As far as we know, such a commitmentis unique to the Lending Code.
10. FLA has also sponsored a booklet on mental health and financial diYculty (enclosed), launched on20 July 2006, and produced by the Royal College of Psychiatrists. It aims to provide sound and practical advicefor psychiatric nurses on dealing with client debt. This initiative acknowledges FLA’s growing commitmentto meeting the needs of customers with mental health problems. We have recently committed to funding asecond print run of 18,000 copies due to overwhelming demand for the first 13,500 copies.
Memorandum by Professor Peter Bartlett, Nottinghamshire Healthcare NHS TrustProfessor of Mental Health Law and Professor Tamara Hervey, Professor of European Law,
School of Law, University of Nottingham
Whether an EU Strategy on Mental Health would be Appropriate
1. As the Commission’s Green Paper (COM (2005) 484) admits, the European Union has limited competencein matters relating to mental health. Notwithstanding, to date, the EU has used various diVerent legal basesand various diVerent type of governance intervention in mental health matters. The Commission’s proposaleVectively amounts to a proposal to “join up” these various disparate activities into a coherent EU mentalhealth strategy. We note that this proposal fits within the Commission’s increased interest in health mattersgenerally over the last five years or so, and that this in turn may relate to the need (in the light of the dramaticrejection of the Treaty establishing a Constitution for Europe in a number of referenda) for the EU to find away to connect its activities with matters that are important to the population of the EU, among which healthis one of the highest (Eurobarometer 61, 2004).
2. Nevertheless, the EU has only a limited amount of resources available to it in the health field, includingmental health. This position is unlikely to change significantly. Even if the Commission were to use theemergence of an EU mental health strategy to argue for increased resources, and the European Parliamentwere to support this, the Council is unlikely to agree to a major increase in the EU’s budgetary settlement. Inthe light of this, it is our view that an EU mental health strategy would be appropriate only if it is based on acareful consideration of the best use of scarce resources. Therefore an EU mental health strategy should behighly focussed upon the areas of greatest need.
3. In our view, the areas of greatest need for an EU mental health strategy should be determined by referenceto the fundamental values and principles upon which the EU itself (Article 6 Treaty on European Union) andits Member States are based. Among these, the most important for these purposes is the respect forfundamental rights.
4. By fundamental rights in this context, we mean both the “civil liberties” approach to fundamental rightsas “freedoms from state interference” and the “positive rights” approach, which sees fundamental rights asrights that must be promoted within civilised societies. We do not wish to enter into the debate about thedistinction between “civil and political” and “economic and social” rights here, noting simply that state of theart thinking on human rights law and practice finds these types of fundamental rights interdependent andindivisible. If human rights most urgently need defending where they are most denied, a rights agenda is bydefinition aspirational; but this does not necessarily reduce it to mere rhetoric.
5. We are aware that the EU does not have an independent human rights competence, in the sense of a powerto adopt binding EU laws that aim to protect fundamental rights. In Europe, the main institution holding thisresponsibility is the Council of Europe, with in particular the European Convention on Human Rights and

3564223008 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
119commission green paper on eu mental health strategy: evidence
European Social Charter. However, we note that the European Court of Justice has recognised fundamentalhuman rights as “general principles of EU law” since the late 1960s20 and that, more recently, the EU hasexplicitly recognised both “civil and political” and “economic and social” rights in its own Charter ofFundamental Rights, which has been agreed by all the Member States. Moreover, the establishment of an EUFundamental Rights Agency will cement the EU’s commitment to human rights in all its governance activities,including the open method of coordination and “governance by dominium” (the use of funding to achievedesired regulatory aims).
If So, What Elements it Might Contain
6. In much of Europe, institutional care remains common. In Poland alone, for example, there are around50,000 people with mental health problems and intellectual disabilities living in around 400 institutions, oftenfor long periods of time or for life.21 These patterns of institutional care are often the inheritance of formerSoviet systems, and do not reflect current human rights norms. It is not merely a question of long-stay, large-scale institutionalisation, a human rights issue in itself, but also the conditions of care in those institutions.The reports of the European Committee for the Prevention of Torture and Inhuman or Degrading Treatmentor Punishment (CPT) provide numerous examples of conditions falling well short of current internationalstandards. “Cage beds” or “net beds”—beds with wire or mesh enclosures that do not allow the occupant toleave the bed—are still used in central European countries including the Czech Republic, Hungary, Slovakiaand, at least until recently, Germany and Austria. Treatment regimes may not meet international standards.“Unmodified” ECT, for example (that is, ECT without anaesthetics or muscle relaxants, placing the patientat significantly increased risk of bone fractures and making the process considerably more unpleasant for thepatient) is still practised in some countries. StaYng levels and staV training are not always adequate. In partas a result, violence on wards, either between residents or, less frequently, exerted on residents by members ofstaV remains an issue.
7. The problem is exacerbated by limited legal rights aVorded to persons in these facilities. Many Europeanguardianship regimes, both inside and outside the former Soviet Union, remove all rights from the individual,even in areas where he or she may continue to have capacity. Of particular importance, the individual losesthe right to pursue any action in the domestic courts, or to retain and instruct legal counsel. There is thereforeno practical way in which he or she can challenge the conditions of the institution. In theory, such a challengecould be mounted by the guardian, but often the guardian will be the director of the instititution in question.There appears to be no legal mechanism to challenge such conflicts of interest.
8. The problems associated with institutionalisation will increase as the current accession states join the EU.In a 2002 visit to Bulgaria, for example, the CPT found that the per capita allocation for food in one institutionwas less than half a Euro per day. Heating in the institution was minimal, with a temperature of 12 degreesCelsius recorded at mid-day on the day of the Committee’s visit.
9. The way forward for these countries does not lie primarily in better institutions. Certainly, it is unlikely thatinstitutional options for people with mental disabilities should be done away with entirely,22 and within thoseinstitutions, it is appropriate to ensure reasonable standards of care. Nonetheless, the direction in careinternationally is away from long-stay institutions and towards community alternatives. The provision of suchalternatives in the newer EU states is not merely impeded by financial concerns; it is also impeded by a lackof knowledge and experience of those community alternatives by professional carers in those jurisdictions.Overall, both the problems with care conditions in institutional structures and the lack of community-basedalternatives may be seen to stem from a failure to link these matters to fundamental human rights protection.
10. It follows that the elements of an EU mental health strategy would need to focus on these greatestchallenges for the EU in terms of respect for and promotion of the fundamental rights of those with mentalill health and intellectual disability. This implies the following:
— Focus the use of the EU’s structural funds on the creation of meaningful community-based mentalhealth care services, as an alternative to the large institution-based care that is the only optionavailable at present in many parts of the EU;
— Focus the use of the EU’s research funding (both under the Public Health Programme and under thehealth strand of Framework Programme 7) on the determination of best practice in terms ofcommunity-based provisions;
20 Case 29/69 Stauder v City of Ulm [1969] ECR 419.21 G FreyhoV, et al, eds, Included in Society, Results and Recommendations of the European Research Initiative on Community-Based
Residential Alternatives for Disabled People (Brussels: Inclusion Europe, Autism Europe, Mental Health Europe and the Open SocietyMental Health Initiative, 2005).
22 See G Thornicroft and M Tansella, “Components of a modern mental health service: a pragmatic balance of community and hospitalcare”, 185 British Journal of Psychiatry (2004) 283.
3564223008 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
120 commission green paper on eu mental health strategy: evidence
— Use of the EU’s “open method of coordination” or similar governance strategy to mandate sharingand dissemination of best practice among Member States, regional and local authorities, health careorganisations of various types and indeed civil society; and
— All of the above EU governance strategies, and others that might be envisaged in the future(including, for instance, any “scoreboard” or league table created and disseminated by the EU in thisrespect) must take explicit account of fundamental rights—both as “freedom from” and as“entitlement to”—not only in terms of the formal legal position in national law, but also the positionin practice.
How it might complement and add value to the strategies of the Member States and the activities of the World HealthOrganisation and other international bodies
11. An EU mental health strategy on the terms we envisage would imply the movement of resources withinthe EU (essentially from Western Europe to eastern and Central Europe), using the institutional mechanismsof the structural funds, and to a smaller extent, the EU’s research funding. It would generate a much widerpool of good practice from which Member States, and the providers of health care within them, could drawin developing their own mental health care strategies. The approach suggested here fits squarely with theWorld Health Organisation’s view that the best approach to mental health care is community-basedtreatment. It also fits with the Council of Europe’s Action Plan for Disability.
12. The EU has been instrumental in creating the conditions and incentives for policy change in central andeastern European states seeking membership of the EU. Of course, this is principally concerned with creatingthe conditions of a market-based economy. But it is also concerned with the conditions of democracy, the ruleof law and respect for fundamental rights. The EU mental health strategy proposed here could therefore berolled out, via the EU’s “neighbourhood policy”, to promote policy change in aspirant states in EasternEurope, whose mental health policies are in need of urgent reform.
Memorandum by The International Longevity Centre UK
The International Longevity Centre-UK believes that the European Commission 2005 Green Paper“Improving the mental health of the population—Towards a strategy on mental health for the EuropeanUnion” represents an excellent framework for action and will hopefully lead to a new generation of policyreforms across Europe.
The Green Paper makes the point clearly that mental ill-health is poorly recognised and that politicians,professionals and the general public are poorly aware of the burden it poses. The point that mental ill-healthin Europe is second only to cardiovascular disease in its toll on morbidity and mortality may make a powerfuladdition to the Green Paper.
We are particularly interested in contributing to this consultation as we have recently published a reportentitled “Severe mental illness in Europe—from policy to practice” Green Paper consultation. The report isavailable on:http://www.ilcuk.org.uk/downloads/Severe%20mental%20illness%20report%20pdf%20Mar%2006.PDF.
The purpose of this report is to highlight the particular issues relevant people with severe mental illness. Werecognise that the Green Paper aims to keep a broad scope and encompass all mental ill-health, however wewould argue that the focus is too much on depression and that too little mention is made of some of the lessprevalent but very severe mental disorders, such as schizophrenia and bipolar disorder. It may be worthmentioning that, whilst in many cases actions and policies may address all mental ill-health, however in somecases, disease-specific approaches may be needed.
We have endeavoured to address the three questions specifically posed by the Green Paper and to providefurther comments thereafter.
Answers to the 3 Questions Posed in the Green Paper:
1. How relevant is the mental health of the population for the EU’s strategic policy objectives?
The Green Paper states that “there is no health without mental health”. The magnitude of mental health—with one person in four being aVected—means that none of the EU’s strategic goals can be achieved if mentalhealth is not improved across Europe.
3564223009 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
121commission green paper on eu mental health strategy: evidence
To ensure that its proposals lead to concrete actions across Europe, the Commission may wish to emphasisefurther in the Green Paper the severe burden that mental ill-health poses on individuals aVected, their familiesand society as a whole. For example, severe mental illness reduces life expectancy by between eight to 20 yearsin those aVected. The Green Paper should clearly state that the social and economic burden posed by mentalill-health is growing across all European countries. If this burden is left unaddressed, Europe will fall short ofachieving sustainable health and social care systems, achieving optimal prosperity and productivity, andensuring that our populations achieve the best possible quality of life:
— The Green Paper may further underline the high prevalence of mental ill-health, the burden it poseson health and social care systems, individuals and their families and society at large.
— It should also make clear that governments, the public and professionals need to recognise that, likeobesity, mental ill-health has a profound impact on all aspects of society and that targeting resourcestowards its prevention and appropriate health and social responses is both urgent and necessary ifwe are to achieve EU strategic goals.
2a. Would the development of a comprehensive EU-strategy on mental health add value to existing and envisagedactions?
We strongly support the development of a comprehensive EU strategy on mental health. Whilst existinginitiatives on mental health supported by the Commission as well as by the WHO represent significant progressin enabling people with mental ill-health to achieve better health and social inclusion, much still remains tobe done.
Moreover, significant discrepancies exist between countries in the place accorded to mental health in policypriorities and resource allocation, as is made evident in the WHO Mental Health Atlas. Guidance and, to acertain extent, pressure from the EU may help harmonise the approach to mental health across member statesand ensure that it is given suitable attention across all countries.
We recognise that member states are exclusively competent for the financing and organisation of healthservices and care. Nonetheless, the EU plays a critical role in motivating and validating national levelinitiatives, particularly when non-governmental stakeholders are seeking to instigate policy reform. Thus thecreation of an EU strategy on mental health will provide a powerful steer to national initiatives.
Furthermore, the creation of a comprehensive EU-strategy that bridges across diVerent sectors anddepartments will provide an important example to guide national policy development. One of the keychallenges with mental health, and particularly severe mental illness, faces is to know where to “place” it withinoverarching debates about the future of health and social care, user empowerment, social inclusion anddiscrimination. Some countries consider mental ill-health (and hence severe mental illness) as a disability,whereas others treat it as a chronic disease within policy frameworks:
— We welcome the creation of a comprehnsive EU-platform on mental health.
— We hope that the creation of this platform may encourage similar initiatives at the national level,and may help the EU engage diVerent national policymakers on the topic of mental health totranslate EU goals into national agendas.
2b. Does Section 5 propose adequate priorities?
The priorities outlined in Section 5 are comprehensive, however we feel that further priorities to be added are:
— raise awareness of the burden of mental ill-health, and of particular mental health conditions suchas severe mental illness, across European institutions, professionals, and civil society;
— recognise that mental health is a critical component of physical health, and vice versa; and
— provide guidance and encourage better practices in the care of people with mental ill-health acrossEurope.
These are addressed further in Question 3 below.
3564223009 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
122 commission green paper on eu mental health strategy: evidence
3. Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between member states, topromote the integration of mental health into the health and non-health policies and stakeholder action, and to betterliaise research and policy on mental health aspects?
The initiatives proposed in sections 6 and 7 are appropriate, however we would make the followingamendments and suggestions:
(i) Targeting vulnerable groups in society (Section 6.1.1, p 9)
Amongst vulnerable groups, we believe it is important to include those aVected by severe mentalillness. People with severe mental illness face particular challenges to social inclusion. These include:
— Poor understanding of severe mental illness by professionals, patients, carers, policy-makersand the general public.
— Increased risk of stigma and social inclusion.
— Barriers to access to eVective treatments in many settings.
— Significant risks of relapse in the case of treatment failure.
— Lack of patient choice and empowerment.
— Significant human rights issues.
Whilst many of these challenges are common to all those facing mental ill-health, people with severemental illness are particularly vulnerable to these challenges.
— The Green Paper should make mention that promotion and prevention programmes must takeinto account the particular circumstances and barriers that are faced by the individuals orpopulations they are addressing. Targeted solutions will be most eVective and engagement ofthose with particular conditions and from particular communities in devising these solutions isessential.
(ii) Addressing mental ill health through preventive action
We welcome the preventive actions proposed by the Green Paper, however we would argue that theseactions can only be achieved if suYcient resources are devolved to their achievement, if professionalsreceive adequate training to recognise their role in enabling prevention.
Moreover, whilst we recognise that treatment of mental ill-health falls beyond the direct remit of theEU, we urge the Green Paper for the sake of completeness to include in this section a call for betteraccess and information on available treatments for all mental conditions. The barriers to treatmentthat exist across member states need to be overcome if we are to reduce the burden of mental ill-health in our communities. Access to appropriate care is a critical component and goes hand-in-handwith social inclusion.
We urge the Commission through the Green Paper:
— to make explicit the need for targeted resources and investment in mental health prevention andtreatment; and
— to recognise that significant barriers to treatment exist across Member States and that eVorts toeliminate these barriers are critical to allowing the social inclusion and quality of life of thoseaVected by mental ill-health.
(iii) Promoting the social inclusion of mentally ill or disabled people and protecting their fundamentalrights and dignity (section 6.2)
Individual and carer empowerment:
We feel that this chapter of the Green Paper would benefit from a dedicated section which underlines thecritical role that patient/family engagement plays in advancing social inclusion and human rights for peoplewith mental ill-health.
This section should also mention the critical role of joint training of patients, family members, professionalsand policymakers in advancing social inclusion. The Leonardo programme, supported by the EuropeanCommission, provides an excellent example of such an initiative. Other examples include Prospect, developedby Eufami, and Profamille, run in Switzerland.
— We urge the Commission to recommend explicitly the engagement of persons with mental and theirfamilies in the development of policies, information materials and service provision as a vital stepto reform.
3564223009 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
123commission green paper on eu mental health strategy: evidence
— We also urge the Commission to high the critical role that joint training programmes that bridgeacross diVerent sectors and stakeholder groups may play to foster removal of stigma and increasedsocial acceptance and understanding of mental ill-health.
A change in paradigm:
We share the Commission’s goal of increasing de-institutionalisation and moving the nexus of care for peoplewith mental ill-health to the community. However, we feel that, particularly in the case of severe mental illness,it is important to acknowledge that this switch has often been ill-managed and that considerable gaps intreatment still persist today. The development of appropriate mental health services in the community has notbeen achieved in many countries. The greatest shortage in most countries appears to be in services that bridgeacross social care and healthcare.
Thus we urge the green paper to recommend:
— The provision of improved training for all specialist and non-specialist health and social care staVworking with people in the community and facilitate these strategies via EU-level initiatives.
— The good coverage of sheltered housing and community schemes for the entire populationcorresponding to local need.
— Investment in social reintegration programmes for people with severe mental illness at the crucialstage of re-entering the community following specialist treatment.
Evolution of local support services
Local solutions to the challenges of severe mental illness have made an enormous diVerence within localcommunities. These local partnerships will, to some extent, need to evolve organically if they are to be eVective.National and regional policy makers can make the diVerence by ensuring those local actors who “dare to care”are resourced, connected to others, listened to, and above all, respected.
— We recommend that Member states are encouraged to provide and facilitate flexible and long-termfunding for local level schemes, recognising the crucial role of NGOs and other non-governmentalcare providers in working for the public good.
C. Summary
Mental ill-health in Europe is second only to cardiovascular disease in its toll on morbidity and mortality. Wewelcome the Green Paper as an important vehicle for communicating the importance of addressing mentalhealth at EU- and national level with utmost urgency. Mental health and physical health are linked. Actionsand approaches to reduce the burden of mental health may learn from eVorts aimed at reducing the burdenof physical health.
Most importantly, at the heart of all initiatives aimed at improving the health and quality of life of people withmental ill-health lies the issue of their empowerment and social integration. Access to appropriate prevention,health and social care is a critical component and vehicle towards social inclusion and the destigmatisation ofpeople with mental ill-health.
Memorandum by Kent County Council
1. Kent County Council (KCC) welcomes the opportunity to respond to the Green Paper. It is supportive ofthe economic approach being taken to the analysis of the costs of mental ill-health to the Member States. Theemphasis placed on prosperity, solidarity and social justice sets a framework within which issues can beunderstood and actions taken.
2. The economic emphasis is in line with UK domestic policy in the area of seeking to return people who haveexperienced mental illness to meaningful economic activity. Central Government have set targets in this regardfor Local Government services to achieve. To that end KCC works in partnership with voluntary sector (non-State) partners to deliver specialist employment services to steer people towards “mainstream” services orprovide the extra more intensive support that some people require.
3. Considerable eVort is being expended at UK Government level to attempt to get people who have beenmentally ill back into the workforce. There are more people who have been mentally ill on long-term sicknesswelfare benefits than any other category. In the past, the diYculty in making the transition from these benefitsto paid employment has amounted to what has been termed the “benefit trap”. Through its ground-breaking“Supporting Independence Programme” KCC has struck an agreement with Central Government which
3564223010 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
124 commission green paper on eu mental health strategy: evidence
removes the “benefit trap” by changing the regulations surrounding the payment of benefits so that no loss ofincome is experienced when a person begins to work—often on a part-time basis, at first.
4. The phrase “there can be no health without mental health” used in the Green Paper is both striking andprofoundly true. Indeed this could well be the key slogan for the pan-European campaign(s) that will followadoption of the proposed strategy on mental health.
5. Turning to the questions raised in section 8 of the document: The mental health of the population is vitalto the policy objectives around prosperity, solidarity and social justice outlined in section 1. The creation ofa comprehensive EU strategy will add value to the actions envisaged in section 5. The priorities cited areappropriate as are the actions outlined in section 7 and 8.
6. KCC wishes to raise again the issues raised on its behalf at the meeting with Jurgen Scheftlein (EuropeanCommission, Directorate General on Health and Consumer Protection) who is leading on the Green Paperfor the Commission. KCC notes that the huge issue of older people and dementia is not included in the GreenPaper. This should be explained and clarified. The reasoning conveyed by Jurgen Scheftlein was clear andunderstandable and it should be available to all who take an interest in the Green Paper and any future actionsfollowing from it.
7. The diVerent attitudes and level of development to “immigrant populations” (usually referred to in the UKas “ethnic minorities”) is acknowledged. However, it is the case that mental illness exists at a higher rate amongsuch minorities than it does in the more established indigenous population. Encouragement should, therefore,be given to the Member States to consider carefully how to address this issue, while acknowledging thatdiVerent States will be at diVerent stages of development in this area. This is merely to fall into line with theHuman Rights Legislation.
8. It would be useful to acknowledge the huge amount of resource that is represented by people who care forpeople with mental illness and the debt that society owes them. The Commission should ensure that theirpresence and influence is reflected in the outcomes from the Green Paper. The provision of assessment ofCarers’ needs and services to help them to continue to care is a priority in the UK.
Memorandum by King’s Fund
1. The King’s Fund is an independent charitable foundation working for better health, especially in London.We carry out research, policy analysis and development activities, working on our own, in partnerships, andthrough funding.
Background
2. On 18 October 2005 the European Commission published a consultative Green Paper entitled “Improvingthe mental health of the population: towards a strategy on mental health for the European Union”(Commission document 13442/05 reference COM (2005) 484 final. Consultation on the Green Paper closes on31 May 2006).
3. Sub Committee G of the House of Lords European Select Committee has decided to hold an Inquiry intothe policy issues relating to the Green Paper. Views were invited on:
— whether an EU strategy on mental health would be appropriate;
— if so, what elements it might contain; and
— how it might complement and add value to the strategies of Member States and the activities of theworld Health organisation and other international bodies.
Is an EU Strategy on Mental Health Appropriate?
4. Yes, but it is vital that the strategy does not duplicate work already being carried out by Member Statesand that it has limited and clearly defined objectives.
5. We agree with the Green Paper view that a strategy would provide a useful framework to gather togetherthe various disparate pieces of pan-European mental health work currently being undertaken. Across Europe,the development of national policies and the level of funding for mental health are limited [1]. However it isimportant not to reinvent the wheel or waste time . . . on strategic blue sky thinking that does not impact onpractice. The WHO European Ministerial Conference on Mental Health’s Mental Health Action Plan forEurope, published in January 2005,[2] presents a succinct but comprehensive plan to develop and implementmental health policies and services in 12 key areas. (The Green Paper acknowledges this Action Plan as apossible model at 7.1.) The commitment from Ministers was that countries of the WHO European Region,

3564223011 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
125commission green paper on eu mental health strategy: evidence
which covers EU Member States, would reflect these policies in their own mental health strategies and plans,to determine what will be delivered in the next five to 10 years. In focusing on raising awareness of theimportance of mental wellbeing, tackling stigma and discrimination, implementing eVective services,addressing workforce issues and involving service users and carers in planning process, this Action Planalready sets out a template for some of the priority issues that the EU strategy might cover.
6. It is also worth bearing in mind the potential for a number of Eastern European countries—and Turkey—to join the European Union in the next few years. These countries tend to have less well developed mentalhealth services with an emphasis on institutionalisation. It would be helpful to have in place an EU strategyfor mental health that those countries could use as a template for developing their own mental health systemsas and when they become EU member States.
What Elements Might an EU Strategy Contain?
7. The Green Paper invites debate on the priorities for an EU strategy. This does pose certain diYculties asEU-wide priorities may or may not reflect the priorities within individual Member States. For example, in theUnited Kingdom, the Government’s current priority for the next five years is on developing communityservices for the wider population rather than specialist services for the few.[3] However other Member Statesmay well feel their first priority is to develop better services for those with the greatest need.
8. In February 2005 a two day event in London organised jointly by the King’s Fund, the LondonDevelopment Centre for Mental Health (now part of the Care Services Improvement Partnership, CSIP) andQueen Mary College, University of London brought together experts from seven European capital cities—London, Paris, Rome, Belgrade, Prague, Berlin and Madrid—to share the experience of mental health systemsin order to identify common factors influencing service provision and policy.
9. A number of common themes emerged from this event that we suggest are pointers to the priorities thatmight inform an EU mental health strategy:
— the move from institutional to community care should continue, though it was essential thatadequate resources were allocated to the development of eVective community services;
— mental health problems are on the rise, especially within primary care services; a significantproportion of this is due to people presenting with complex needs involving drug and alcohol misuse;
— stigma remains a major burden on service users and carers;
— refugees and migrant communities provided a challenge across all countries;
— older and younger populations were mentioned as particularly high risk groups vulnerable to mentalhealth problems;
— service user involvement was underdeveloped in many cities; and
— the fragility of governments and frequent changes in health ministers made implementation ofreform diYcult.
Resources
10. The issue of resources is a crucial one. It is worth noting that the WHO European Ministerial ConferenceAction Plan[2] supported the implementation of the Plan “in accordance with each country’s needs andresources” . This takes into account the reality of current and future funding of mental health in diVerentcountries and the enormous variety of service provision across diVerent countries in areas such as inpatientbeds, community facilities and workforce levels. Some EU Member States spend less than 5% of their healthbudget on mental health; others (including the UK) spend over 10%.[4]
11. We suggest that the strategy should acknowledge the resource pressures on health spending, but shouldencourage all Member States to provide adequate resources to meet assessed needs of their populations andto consider how they might achieve both cost and health benefits by shifting resources from institutionalisedcare to a range of community-based services (a process already under way in EU Member States, though notin many European countries currently outside the EU), and to increased evidence-based mental healthpromotion activity.
3564223011 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
126 commission green paper on eu mental health strategy: evidence
The priorities
12. We believe an EU strategy should consider the following as possible priorities:
(a) a multiagency approach: mental health is not just an issue for health and social care services. As theGreen Paper rightly point out, mental ill health causes significant losses and burdens to theeconomic, social, educational as well as criminal justice systems. It would be important for the EUstrategy to target Ministers and organisations responsible for these areas within all Member States—especially schools, employment and housing authorities, and police and court services.
(b) mental health promotion and prevention: the WHO Action Plan focuses strongly on the need for thebetter promotion of good mental health and more preventative strategies, such as developingprogrammes for parenting support and education and the emotional wellbeing of children andyoung people. It is becoming increasingly clear that the high prevalence of mental health problemsacross Europe must partly be tackled through a focus on prevention as well as the development ofbetter treatment and care services. Such an approach accords with the Green Paper’s remit to“improve the mental health of the population” , and not just provide better services for those alreadysuVering from a mental disorder. It will be important, though, to ensure that the evidence base forany promotion and prevention programmes is clear and that limited resources are focused on high-risk groups.
(c) tackling stigma: Governments should lead on tackling the stigma and discrimination faced by peoplewith mental health problems, common throughout Europe (and the rest of the world). This stigmais a major barrier facing people trying to recover from mental health problems, and can deter peoplefrom seeking help when they first develop problems.
(d) children and older people: mental health resources across Europe are primarily concentrated onadults of working age with enduring mental health needs. While it is important to ensure thispopulation has access to a range of appropriate treatment and care, the strategy should emphasisethe need to provide support both for children and older people, where the prevalence of mentalhealth problems is rising.
(e) refugees and immigrant populations: evidence from the London event (see above) suggests that inmany European countries there are high levels of mental health problems among refugee andimmigrant populations. This is likely to remain an issue over the coming years with the greatermobility of the population within Europe, and increasing numbers of people entering Europe fromother parts of the world. The stigma of a mental disorder may also be compounded for these groupsby the stigma of being from a minority ethnic community. The strategy should encourage EUMember States to develop culturally appropriate services for such populations.
(f) service user and carer engagement: the strategy should emphasise the benefits of involving serviceusers and carers in planning and developing local mental health services so that services reflect whatthey want rather than just what professionals think they need.
(g) information and data exchange: good policies and appropriate resource allocations rely on havinggood data. The reporting and analysis of mental health data varies considerably across EU MemberStates and leaves much to be desired.[5] The strategy should point out the need for good data andencourage Member Sates to develop information systems and share comparable data across countryboundaries.
How Might an EU Strategy Add Value to the Strategies of Member States and the Activities of the
World Health Organisation and Other International Bodies?
The Green Paper suggests added value would come with establishing a framework for exchange andcooperation between Member States; by helping to increase the coherence of actions in the health and non-health policy sectors; and by allowing involvement of a broad range of relevant stakeholders into buildingsolutions.
We believe an EU strategy for mental health would have the potential to add value in these areas if it is activelypromoted by the European Commission and Ministers and policy-makers within Member States. It will begood to have the strategic thinking brought together within a European Commission document—butimplementing the strategy will require not only political will but also the availability of resources.
3564223011 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
127commission green paper on eu mental health strategy: evidence
For an EU strategy to be eVective it will need some resources to help Member States work individually andcollectively to gather and exchange good practice and to support service user and carer organisations—whichoften have limited means—to be involved in strategic thinking and planning at national and local level. It willalso require funds to develop further a programme of comparable data collection across Member States.
References
[1] WHO. European Observatory on Health Systems and Policies: Policy Brief: Mental Health I: Key issuesin the development of policy and practice across Europe (2005).
[2] WHO. European Ministerial Conference on Mental Health: Mental Health Action Plan for Europe: Facingthe Challenges, Building Solutions, January 2005.
[3] Department of Health. The National Service Framework for Mental Health—Five Years On, December2004.
[4] WHO. European Observatory on Health Systems and Policies: Policy Brief: Mental Health III: Fundingmental health in Europe (2005).
[5] Marusic, Andrej. Mental health in the enlarged European Union: need for relevant public mental healthaction, British Journal of Psychiatry (2004), 184, 450–451.
Memorandum by the Law Reform Committee of the Bar Council of England and Wales
1. The Law Reform Committee of the Bar Council for England and Wales welcomes the call for evidence bySub-Committee G of the House of Lords Select Committee on the European Union and the opportunity tocomment on the European Commission Green Paper on EU Mental Health Strategy.
2. The Law Reform Committee also appreciates the extended deadline of 5 June 2006 given to it to respond(rather than the original deadline of 22 May 2006).
3. The European Commission Green Paper is a consultative document designed to launch a policy debateabout the relevance of mental health for the EU, the need for a strategy at EU level and possible priorities. Itacknowledges that, while some public health aspects of mental health would fall under Communitycompetence, others would be the exclusive competence of Member States.
4. The Commission point out in the Green Paper that:
— Mental ill health aVects every fourth citizen of the EU, costs the EU an estimated 3–4 per cent ofGDP, mainly through lost productivity, and causes many suicides.
— Mental disorders are a leading cause of early retirement and disability pensions.
— Mental ill health and conduct and behavioural disorders in childhood incur costs for the social,educational, criminal and justice systems.
— Further intangible costs concern how society treats mentally ill or disabled persons who stillexperience social exclusion, stigmatisation, discrimination or non-respect of their fundamentalrights and dignity.
5. Against that background, the Commission states that mental health is an important issue for the EuropeanCommunity because of:
— the contribution that good mental health of the population can make to some of the EU’s strategicpolicy objectives;
— the role of the Community to encourage and support cooperation between Member States and toaddress inequalities between them; and
— the obligation for the Community to contribute to a high level of human health protection throughall its policies and activities.
6. The Green Paper suggests that an EU-level strategy on mental health could add value by:
(1) creating a framework for exchange and cooperation between Member States;
(2) helping to increase the coherence of actions in diVerent policy sectors; and
(3) opening a platform for involving stakeholders, including patient and civil society organisations, inbuilding solutions.
7. Among the options for action outlined by the Green Paper are:
— promoting mental health and addressing mental health though preventive action;
3564223012 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
128 commission green paper on eu mental health strategy: evidence
— promoting the social inclusion of mentally ill or disabled people and protecting their fundamentalrights and dignity; and
— improving information and knowledge on mental health in the EU.
8. Sub-Committee G of the House of Lords is seeking views on:
— whether an EU strategy on mental health would be appropriate;
— if so, what elements it might contain; and
— how it might complement and add value to the strategies of Member States and the activities of theWorld Health Organisation and other international bodies.
9. The LRC believes the EU Strategy on Mental Health set out in the Green Paper is appropriate. It bothsupports and advances the World Health Organisation (WHO) Declaration and Action Plan.
10. The LRC notes that a number of recent European Community initiatives on mental health have arisenindependently and suggests that—to prevent the development of conflicting programmes and consequentialdissipated eVort—a single integrating strategy with strong co-ordination would make progress in this areamore eVective.
11. There will always be diVerent mental health needs within specific target populations (such as children,adolescents, adults of working age and older adults) and whatever strategy is adopted it should reflect theincreasing age distribution of the population.
12. The LRC commends the considerable eVort which has been devoted to reform of Mental Healthlegislation in the United Kingdom.
13. The Mental Capacity Act 2005 will shortly come into force.
14. The LRC notes, however, that the details of the reform of the Mental Health Act 1983—contained in thedetailed provisions of the Mental Health Bill 2004—remain unclear since the Government abandoned the Billat the end of March 2006.
15. The Mental Health Bill 2004 and the Mental Capacity Act 2005 were part of a unified package ofsignificant reform in this area. After eight years of preliminary legislative work on this topic all that is currentlyknown is that some elements of the Bill will be grafted on to other Department of Health legislation expectedin October or November 2006.
16. Until the final detail of that proposed legislation is available it is diYcult to measure how elements of theEU Green Paper are or may be reflected in this proposed legislation.
17. For this reason the LRC would appreciate the opportunity for further comment or the giving of directevidence to the House of Lords Sub-Committee G, if appropriate, when details of this domestic legislation areavailable.
Memorandum by Marylebone Healing and Counselling Centre
A statement prepared by the Reverend Christopher MacKenna, Director of St Marylebone Healing andCounselling Centre, London, and Chair of the Westminster Christian Mental Health Forum.
1. I welcome the publication of the Green Paper. It rightly highlights the importance of mental health for thewell-being of individuals, communities, and nations, and—given the high incidence of mental illness withinthe EU—the need for strategic thinking in this area.
2. The Green paper suggests that “There is widespread agreement that the human, social and economicdimension of mental health need wider recognition by policy makers and greater public awareness”. (p 13,paragraph 8). My contention is that the spiritual dimension of mental health needs also to be recognised inpublic policy and mental health care.
3. The “spiritual dimension” may manifest in religious, or non-religious forms. Either way, it has to do withachieving a sense of meaning and purpose in life. Human beings need to have something to live for. Excellentmedical care and social provision are both crucial but, in themselves, are not enough: human beings do notlive by bread alone. This has long been recognised within the broad tradition of European psychiatry, forexample in the work of Dr Viktor Frankli and Dr Carl Jung.ii A growing body of research evidence nowsupports this contention.
4. The Handbook of Religion and Health (edited by Koenig, McCullough, and Larson. Oxford UniversityPress: Oxford & New York. 2001) helpfully draws together a large body of medical research on the eVects of

3564223013 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
129commission green paper on eu mental health strategy: evidence
religious belief on all forms of health, including mental health. The overall findings are that those who believein a higher power, who pray regularly, and associate with others for worship are statistically likely to enjoybetter health and longevity than those who do not.
5. The findings of the Somerset Project, conducted by the Mental Health Foundation among mental healthservice users, revealed that a large percentage of people living with chronic mental illness report that their faith/spirituality is the most important factor in enabling them to cope with their condition.
6. The importance of spirituality in mental health care is recognised and endorsed by the English RoyalCollege of Psychiatrists: see their documents Spirituality and Mental Health Care: Advice for NHS Trusts,and Spirituality and Mental Health, both prepared by the Spirituality and Psychiatry Special Interest Groupof the Royal College of Psychiatrists.
7. Croydon MIND has recently commissioned a DVD/video Hard to Believe, which allows three mentalhealth service users to explain how their spirituality was (too often mis-)understood by mental health services,and the role which it has played in their recovery. The film also features work being undertaken at the SouthLondon and Maudsley NHS Trust, and by Dr Andrew Copsey and his Multi-Faith Team, in East London,to incorporate spirituality/religious adherence in their overall care for their patients. Given the tensionsbetween many ethnic/religious minorities and majority populations in diVerent parts of Europe this approachcan only become more necessary, as well as contributing directly to the integration and improvement ofspiritual and professional mental health care.
8. Many faith communities are already seeking to play a part in mental health care and education. Forexample, at the St Marylebone Healing and Counselling Centre, we have a team of 16 professional counsellorsand psychotherapists, all equipped to work in the interface between spirituality and mental health. We alsorun a mental health support group, for service users, which explicitly allows discussion of religious andspiritual issues. And we run a rolling programme of conferences and seminars for mental health professionals,which address diVerent aspects of the spirituality/mental health divide.
9. I trust that these points are suYcient to support my contention that the European Commission Green Paperon European Union Mental Health Strategy ought to make explicit reference to the importance of spiritualityand liaision with Faith Communities in mental health provision and care.
References:
i For example, in 1961 Frankl wrote, “A psychiatrist today is confronted more and more with a new type ofpatient, a new class of neurosis, a new sort of suVering, the most remarkable characteristic of which is the factthat it does not represent a disease in the proper sense of the term. This phenomenon has brought about achange in the function—or should I say mission?—of present-day psychiatry. In such cases, the traditionaltechniques of treatment available to the psychiatrist prove themselves to be less and less applicable:
“I have called this phenomenon, which the psychiatrist now has to deal with so frequently, ‘theexistential vacuum’. What I mean thereby is the experience of a total lack, or loss, of an ultimatemeaning to one’s existence that would make life worthwhile. The consequent void, the state of inneremptiness, is at present one of the main challenges to psychiatry.” Psychiatry and Man’s Quest forMeaning, p 71. Reprinted in Psychotherapy and Existentialism, Selected Papers on Logotherapy, byViktor E Frankl Simon and Schuster: New York, 1967.
Of course, in our health system, many patients suVering in this way do not get as far as seeing apsychiatrist. Instead, they clog the GP’s surgery, presenting many vague psychosomatic typesymptoms.
ii For example, in 1932 Jung wrote, “I should like to call attention to the following facts. During the past thirtyyears, people from all the civilized countries of the earth have consulted me. Many hundreds of patients havepassed through my hands, the greater number being Protestants, a lesser number Jews, and not more than fiveor six believing Catholics. Among all my patients in the second half of life—that is to say, over thirty-five—there has not been one whose problem in the last resort was not that of finding a religious outlook on life. Itis safe to say that every one of them fell ill because he had lost what the living religions of every age have givento their followers, and none of them has been really healed who did not regain his religious outlook. This ofcourse has nothing whatever to do with a particular creed or membership of a church”. (Psychotherapists orthe Clergy, reprinted in C G Jung, The Collected Works, vol.xi, Psychology and Religion West and East,paragraph 509. (Edited by Read, Fordham, and Adler. Routledge and Kegan Paul: London, secondedition, 1969).
3564223014 Page Type [E] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
130 commission green paper on eu mental health strategy: evidence
Memorandum by Dr G M Craig MD, FRCP on behalf of the Medical Ethics Alliance
This response will touch on the following points raised in the Call for Evidence.
A. How society treats mentally ill or disabled persons who still experience social exclusion, stigmatisation,discrimination or non-respect of their fundamental rights and dignity; and
B. Promoting mental health and addressing mental health through preventive action
A. Discrimination with Respect to the Provision of Food and Water
1. The EU strategy on mental health should address the fact that food and water, howsoever given, shouldbe regarded as a basic human need without which no person can survive. The view that food and water whengiven by means such as tube feeding can be regarded as medical treatment is controversial and unsatisfactory.It puts at risk the lives of many disabled and mentally incompetent patients who cannot make decisions forthemselves.
2. Guidance issued by the British Medical Association in 1999 allows doctors to withhold or withdraw socalled “artificial nutrition and hydration” (ANH) under some circumstances if patients are deemed to lack self-awareness.
3. Guidance issued by the General Medical Council (GMC) in 2002 allows doctors to withhold or withdrawlife-prolonging medical treatment including ANH under some circumstances if patients are mentallyincapacitated.
4. When the draft Mental Incapacity Bill was under scrutiny by a Joint Committee of the House of Lords andHouse of Commons in 2002–03, many doctors advised the Committee that ANH should be regarded as basiccare and not medical treatment. See for example evidence given by:
— The Medical Ethics Alliance (Draft Mental Incapacity Bill, Joint Committee Report, Session2002–03 Volume II, Oral and Written Evidence. Ev 162 para 13. HMSO) and by
— Dr David Kingsley (Ibid Ev 321, para 2.2.1.) and by
— Dr P J Howard. (Ibid. Ev 165, para 7.)
5. Disturbing cases. In 2002 the Medical Ethics Alliance (MEA) gave the Joint Committee on the draft MentalIncapacity Bill brief information about cases where ANH had been withheld from dying patients or terminallyill elderly patients. (See Ev 163, Committee Report Vol II Oral and Written Evidence.)
6. In 2006 the MEA drew these cases to the attention of Appeal Court Judges in the Burke case (vide infra).The Judges found the information “disturbing” but did not accept it as admissible evidence. (R [Burke] vGeneral Medical Council [2005] EWCA 1003. In the Supreme Court of Judicature Court of Appeal (CivilDivision) on Appeal from the High Court. Paragraphs 60, 61 and 63)
7. The case of Mr Lesley Burke. Mr Lesley Burke is a man who suVers from a progressive neurologicaldisorder that will eventually render him incapable of speaking or swallowing. He challenged the legality of theGMC guidance on “Withholding and Withdrawing Life-prolonging Treatments: Good practice in decision-making”. He wanted to ensure that when the time came he would receive ANH to prevent him from dying ofdehydration and starvation. Mr Justice Munby found in favour of Burke, and ruled that the GMC Guidancewas unlawful in several respects. His judgment was overturned on Appeal in July 2005.
8. Appeal Court Judges were swayed by concerns expressed by the Intensive Care Society, and feared that theCourts might be swamped with cases if, as Judge Munby had advised, Court supervision of controversial end-of-life decisions involving the withdrawal of ANH was increased. Yet Dr Bruce Taylor, the Consultant whonow chairs the Intensive Care Society Standards Committee, writing in GMC today in April 2006, stated:
“. . . in critical care medicine ANH is generally a basic pre-requisite of supportive care. Even whenit is clear that treatment is futile, its withdrawal or withholding is seldom (if ever) contemplated asa means of allowing nature to take its course.”
9. Mr John Reid, then Secretary of State for Health, wrote to Appeal Court Judges to express concern aboutthe cost implications of keeping patients alive. (Daily Mail 5 February 2005). Yet given the favourablecontracts oVered to the NHS by firms that supply liquid feeds, nutrients required to tube feed an inpatient fora year cost less than one MRI scan of the knee. Thus to withhold ANH from the elderly on grounds of expenseis unacceptable. Moreover once a feeding tube is in place ANH provision can be managed in the communityif carers are given the necessary training and supervision.
10. Mr Burke was refused leave to take matters to the House of Lords. He has now applied for his case to beheard in the European Court of Human Rights. Patients should not have to go to these lengths to ensure thatthey do not die of dehydration or starvation at the end of life.
3564223014 Page Type [O] 03-04-07 21:33:34 Pag Table: LOENEW PPSysB Unit: PAG2
131commission green paper on eu mental health strategy: evidence
11. The right to receive food and water. During the House of Lords Debate at the second reading of thePatients’ Protection Bill in 2003, Earl Howe said:
“. . . The issue for us is whether food and water should be regarded as separate and distinct fromconventional medical treatment, and whether the right for every patient, however ill, to receive foodand water should be protected by law.” (Hansard 12 March 2003, col 1426)
Many people believe that the answer to these questions should be yes.
12. Since the right of patients to refuse treatment including food and water is well established, the right ofpatients to receive food and water, howsoever given, should also be recognised and protected by law. The EUGreen Paper provides an opportunity to address this crucial matter.
13. Basic care and human rights. All people whether mentally ill or not should have certain rights safeguarded,in particular:
— The right to receive food and water by any reasonable, appropriate and proportional means that donot cause unacceptable discomfort.
— Basic nursing care and bodily comfort provision as necessary.
— Warmth, clean dry clothes and clean bedding.
— Shelter and friendly human support in safe surroundings.
— Pain relief when necessary, short of deliberate ending of a life.
14. Assessment of Mental Incapacity. Mental Capacity may be temporary and reversible, slowly progressiveor permanent, depending on the cause. Therefore skilled medical input is required before a person is labelled“mentally incapacitated” or “lacking in self-awareness” with dangerous consequences.
15. When the question of withholding or withdrawing ANH arises in a person who is thought to be in apermanent vegetative state, a Judge requires evidence that this diagnosis is correct before a decision to permitwithdrawal of ANH is made. Patients with lesser degrees of brain damage should have similar safeguards inlaw, before ANH is withdrawn or withheld.
16. The case of Miss X. Miss X was a woman who suVered a severe traumatic head injury. Her family thoughtfrom comments made prior to the injury, that she would not want to live, so ANH withdrawal was considered.Arrangements were made to bring the case to Court, but specialist neuropsychological assessment byProfessor T M McMillan of Glasgow University showed that she wanted to live. Therefore ANH was notwithdrawn. Over the course of the next decade her condition improved progressively. Ten years post injuryshe was living in a modified bungalow, able to feed herself with a spoon, independent in an electric wheel chairand able to walk 16 metres with two helpers. (McMillan and Herbert, Brain Injury 2004, 18:9 935–940).
17. Professor McMillan is of the opinion that:
“Where there is any possibility of a locked in state and the issue of cognitive ability or will to live isin doubt, an expert and independent neuropsychological assessment is essential and should bemandatory.” (Brain Injury 1996; 11:481–490)
18. Lasting power of attorney. When the Mental Capacity Act (2005) comes into operation the currentEnduring Power of Attorney (EPA) will be replaced with a Lasting Power of Attorney (LPA). The Law Societyis worried that the LPA will create new problems, for capacity will have to be assessed in relation to a particulardecision at the time that the decision has to be made, rather than at the point when control is handed over tothe attorney. Solicitors foresee problems for banks for example (Law Society Gazette 4 May 2006 page 8).However since LPAs can apply to irrevocable life and death decisions such as withholding or withdrawingANH, it is obviously important to reassess the patient’s mental capacity and wishes very carefully before afinal decision is made. No doctor should be obliged to comply with an advance directive that is clearly suicidalin intent. Intentional killing of patients by act or omission should not be permitted.
19. Parliament should refrain from passing laws that undermine the moral basis of medicine. Assisted suicideshould remain unlawful in the UK, irrespective of what goes on in other member states in the EU.
20. EU strategy on Mental Health should restrain member states from making unethical decisions on politicalor economic grounds.
21. Doctors and nurses working in the EU must be given the resources needed to practice a high standard ofmedicine.
22. EU strategy on Mental Health should promote the social inclusion of mentally ill and/or disabled peopleand should protect their fundamental rights and dignity.
3564223014 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
132 commission green paper on eu mental health strategy: evidence
B. Promoting Mental Health and Addressing Mental Health through Preventive Action
23. Many major causes of mental illness are potentially preventable. For example dementia due tocerebrovascular disease (multi-infarct dementia) could be reduced by careful attention to diet during life, bycutting down on smoking, and by medication that reduces risk factors such as a high cholesterol.
24. The basic pathology of Alzheimers Disease is known. Grants to support good research could ultimatelyfind a cure. Unfortunately in the UK the provision of medication that may slow the progress of thisdevastating illness is being limited for financial reasons. This matter should be addressed as it discriminatesagainst the vulnerable elderly.
25. Excessive consumption of alcohol increases the risk of mental illness through head injuries when drunk,and through vitamin deficiencies due to inadequate diet. Chronic alcoholism causes loss of memory, blindnessand damage to peripheral nerves. It disables people and families. Treatment of liver failure due to alcoholismis a considerable financial burden on the National Health Service. Alcoholism puts at risk the health of theyounger generation and increases vandalism in inner cities. There are far too many licensed premises in ourcities. In addition our young people are having a bad influence worldwide, for the habit of drinking is nowspreading to places such as India. Measures to reduce alcohol consumption must be addressed with greaterurgency.
26. Misuse of Drugs. Criminal activity by drug addicts who are short of money to fuel their habit results inburglaries and muggings that reduce the quality of life for law-abiding citizens. Young drug addicts sometimessteal from their own family members causing grief, distress and their eviction from the family home.
27. Drug addicts are at risk of premature death from hepatitis, septicaemia and AIDS. In addition drugs suchas cannabis increase the risk of mental illness. Anything that the EU can do to help the police control drugtraYc would be welcome.
28. Stress due to the frenetic pace of modern life is a major cause of illness and days oV work. Human beingsshould have time to relax with their families.
29. Spiritual aspects of life are vitally important. People must have freedom to worship and to speak freelyabout their personal faith in the privacy of their own homes and in public places. The importance of religiousfaith to mental health should never be underestimated.
30. Nations should protect and preserve buildings that are an important part of their spiritual heritage. In theUK many churches are in need of repair and restoration that their congregations cannot aVord. Churches andcathedrals, synagogues and mosques add dignity and stability to life. At times of crisis people go to their placesof worship for comfort and reassurance. The spiritual heritage of Europe must be cherished for generationsto come.
31. Music is an important part of religious expression. Church organs are an important part of our musicaland spiritual heritage. EU laws that prevent the manufacture or repair of pipe organs because their pipes orelectrical components contain some lead represent bureaucracy gone mad. The loss to our musical heritagewill far outweigh any conceivable health danger due to lead in the pipes.
32. Elderly people who cannot attend places of worship should be visited at their homes. Simple religiousservices with hymns should be arranged at residential and nursing homes. There are many example of goodpractice in this field eg the work of the Christian Council on Ageing in the UK, and of organisations such asPARCHE, based in Eastbourne, Sussex, UK.
33. EU strategy on mental health should recognize that faith is an important factor in mental health andwellbeing.
In Conclusion. The Medical Ethics Alliance consider that an EU strategy on mental health could be helpfuland appropriate. Such a strategy might usefully include some of the points made in this brief paper.
The Medical Ethics Alliance is an association of World Faith organisation and individuals who share acommon ethos as stated in the Hippocratic Oath or Code of Practice and the Declaration of Geneva of 1948.www.medethics-alliance.org. Address PO Box 11582, Edgbaston, Birmingham B16 9XE (UK).
Memorandum by Mencap
1. Mencap is the leading UK charity working with children and adults with a learning disability and theirfamilies and carers. We welcome the opportunity to contribute to this consultation. We have chosen not toanswer directly the three questions in the consultation paper, but to comment on the issues we think are mostimportant to the people we work with.

3564223015 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
133commission green paper on eu mental health strategy: evidence
Terminology
2. Learning disability is not the same as mental ill health. A learning disability is lifelong and untreatable, andaVects the way people learn, understand, communicate and interact with others. The Green Paper rightlydefines mental ill health to include “mental health problems and strain, impaired functioning associated withdistress, symptoms, and diagnosable mental disorders, such as schizophrenia and depression” (para 2). Peoplewith a learning disability face diVerent challenges from people with a mental illness, and have diVerent needs.
3. In general, the Green Paper limits its discussion to issues related to mental ill health. However, it also refersfrequently to “mentally ill or disabled people” and “people with mental ill health or disability” (eg at para 6.2).This is an ambiguous phrase in English, but a look at versions of the Green Paper in other languages suggestsstrongly that it is intended to refer both to people with mental ill health and people with a mental disability,including learning disability. It is not clear why a Green Paper on mental health strategy mentions learningdisability in passing on so many occasions without making any reference whatever to the factors whichdistinguish it from mental ill health.
4. Given the distinction between mental ill health and learning disability, the Green Paper should do one oftwo things. It should either limit itself to a discussion of mental ill health and its eVects, dropping theoccasional confusing references to unrelated disabilities, or it should be explicit about the fact that its scopeis wider than just mental ill health. If the latter, it needs to discuss learning disability in much greater detailthan it does. This would involve rewriting the document substantially.
5. The authors of the Green Paper are not alone in blurring the distinction between mental ill health andlearning disability. The distinction is widely misunderstood, perhaps because of the fact that both mental illhealth and learning disability are non-physical and invisible, because both involve the brain, and also becauseof confusions in terminology. Learning disability is still sometimes referred to as “mental handicap”, and theword “mental” is sometimes used as a term of abuse against both people with mental ill health and people witha learning disability. Given this common confusion, it is vitally important that the distinction is kept clearwhen making public policy.
Stigma and Discrimination
6. Para 6.2, on social inclusion, appears to refer both to people with mental ill health and people with alearning disability. Stigma, discrimination and misunderstanding are indeed problems for both groups. Oneelement of this misunderstanding is the confusion between mental ill health and learning disability, asdiscussed above. While both groups do experience stigma and discrimination, the stigma and discriminationthey experience often takes diVerent forms. Putting the groups together, as this document does, and thendiscussing solutions almost exclusively in terms of mental ill health might in itself be seen as a form ofdiscrimination.
7. Mencap agrees that there is a need for a shift in public attitudes, for an improvement in public awarenessabout mental ill health and treatment options, and for encouraging the integration of people with mentalhealth problems and learning disabilities across society. This must include a recognition of the distinctionsbetween mental ill health and learning disability, and the distinct needs of these separate groups.
8. Para 6.2 also discusses the replacement of large hospitals or asylums with community-based services.People with a learning disability, as well as people with mental health problems, have historically been placedin long-stay institutions. Mencap strongly supports the closure of such long-stay institutions, both in the UKand in Member States in general, and their replacement with community-based supported living serviceswhich enable people to exercise as much control as possible over where they live and who they live with.
Employment
9. Para 6.1.1 rightly notes that vulnerability to mental ill health increases with low social and economic status,and with job loss and unemployment. People with a learning disability are more likely to be unemployed thanthe general population, and indeed than other disabled groups. In the UK, only around 11 per cent of peopleof working age with a learning disability are employed, even though around 65 per cent want to work; wewould not be surprised to see similarly low employment rates among people with a learning disability acrossMember States. People with a learning disability need properly tailored employment support which recognisestheir distinct needs.
3564223016 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
134 commission green paper on eu mental health strategy: evidence
Memorandum by Mental Disability Advocacy Center
The Mental Disability Advocacy Center (MDAC) is an international non-governmental organisation based inBudapest that promotes and protects the human rights of people with mental health problems and intellectualdisabilities across central and eastern Europe and central Asia. MDAC works to improve the quality of lifefor people with mental disabilities through litigation, research and international advocacy. MDAC hasparticipatory status at the Council of Europe and is a cooperating organization of the International HelsinkiFederation for Human Rights.
Summary
As a response to the Green Paper, “Promoting the Mental Health of the Population. Towards a Strategy onMental Health for the European Union”, MDAC recommends:
— As a cross-cutting issue, Fundamental Rights should be mainstreamed across all policies andprogrammes in the proposed EU Strategy on Mental Health.
— More emphasis should be placed on consultation with users of mental health services and theirfamilies.
— The issues of legal capacity, institutionalisation and involuntary hospitalisation and treatment mustbe addressed in a European Strategy on Mental Health.
1. Introduction
MDAC welcomes the development of a comprehensive EU strategy on mental health as proposed by theGreen Paper and is in agreement that the mental health of the European population can be improvedsignificantly. While this positive initiative on behalf of the EU certainly merits enthusiasm, there are someareas of concern in the paper which MDAC addresses in this commentary. MDAC makes a series of generalcomments before addressing specific concerns which merit more discussion, namely (a) fundamental rightsand mental health, (b) legal capacity and guardianship, (c) institutionalisation and (d) forced treatment.
2. General Comments
2.1 Fundamental Rights Dimension
MDAC considers the almost total absence of a fundamental rights dimension to the paper to be a seriousomission. Fundamental rights are a cross-cutting issue in mental health and cannot be treated as a separatequestion. The Green Paper appears to endorse a traditional medical model of mental health rather than asocial one. This can be observed, for example, in the sections on the provision of eVective care and treatmentservices.23 In contrast, the improvement of the quality of life of persons with mental health problems ordisability is relegated to third position in the list of priorities.24
2.2 Emphasise Importance of Empowerment and Involvement of Users of Mental Health Services
The Green Paper lacks emphasis on the involvement and empowerment of users of mental health services.Users and ex-users of mental health services are in an expert position to contribute to the development of afuture EU strategy on mental health. Consultation with users should therefore be mainstreamed across anyEuropean research, policy development, and service/programme development dealing with mental health.25
23 “. . . there is agreement that a first priority is to provide eVective and high-quality mental health care and treatment services, accessibleto those with mental ill-health.” See Green Paper, Section 4 “Developing Responses: Policy Iniatives on Mental Health”, page 5.
24 See Section 5 “The need for an EU Strategy on Mental Health,” page 8.25 Such involvement of users has already been emphasised strongly by the WHO European Ministerial Conference on Mental Health,
Mental Health Declaration for Europe, Helsinki, Finland, January 2005 EUR/04/5047810/6 at paragraph 11 and also paragraphs 7(ii),8(iii) and 10(iv); UN Standard Rules on the Equalization of Opportunities for Persons with Disabilities, rules 14 and 18; Report of theSpecial Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, PaulHunt, February 2005, paragraphs 59–61; Conclusions of the Commissioner, Seminar organized by the Council of EuropeCommissioner for Human Rights and hosted by the World Health Organization Regional OYce for Europe, Copenhagen, Denmark5–7 February 2003.
3564223016 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
135commission green paper on eu mental health strategy: evidence
2.3 Expand Definition of “Vulnerable Groups”
The reference to “vulnerable groups” in society is too narrow. The Green Paper refers to “migrants and othermarginalised groups”.26 Marginalised and isolated populations (eg ethnic minorities, indigenous populations,Roma, adolescents, children, and women)27 who also suVer from mental health problems are at an even greaterrisk of suVering stigma and discrimination. In particular, research has shown that experiences of women inthe mental health system diVer significantly from men and that they are more vulnerable to discriminationand abuse.28 Within the mental disability group, persons with intellectual disabilities have been particularlyneglected and excluded.29 In addition, prisoners30 and persons in social care homes with mental healthproblems are more vulnerable to abuse and mistreatment. Vulnerable groups need to be explicitly mentionedand included in the consultation process to the Green Paper and in any further strategic planning.
2.4 Include tangible action points
The initiatives outlined in the Green Paper are pragmatically weak. In order to achieve any real change, theproposals for action need to become more concrete and tangible, with substantive, achievable and measurableactions set out. In line with a cross-cutting approach, all actions should have a fundamental rights basis andinvolve users of mental health services and their families.
3. Specific Areas of Concern
3.1 Fundamental Rights and Mental Health
The first major weakness in the Green Paper is that fundamental rights are treated as a separate and distinctissue.31 From the outset, it must be recognised that in the area of mental health, fundamental rights are a cross-cutting issue which apply to all areas mentioned in the Green Paper, including promotion of good mentalhealth, prevention of mental health problems, care and treatment services and research.
The section in the Green Paper on fundamental rights is weak and MDAC is concerned that it does notemphasise strongly enough the uncontentious fact that there continue to be serious fundamental rights abusescaused by mental health and social care services.32 Such basic fundamental rights violations throughout theEU have been well documented. In particular, the European Committee for the Prevention of Torture (CPT)has raised human rights concerns during visits to psychiatric facilities in many EU Member States.33 Suchinstances of fundamental rights violations need to be acknowledged in the Green Paper.
Further, concrete measures to promote fundamental rights and to prevent abuses should be laid out. Theremust be a clear statement on the absolute prohibition of inhuman and degrading treatment and punishment,which still exists in many mental health systems within the EU. In addition, the mechanisms necessary toprotect persons from fundamental rights abuses in mental health care should be further elaborated. MDACproposes the following:
— State-funded independent inspectorate systems.34
For example, a properly resourced Ombudsman oYce, a specialised permanent commission, orother inspectorate systems.35
26 See Section 6 “Seeking Solutions-Options for Action” , page 9.27 See the reference to vulnerable groups in the Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest
attainable standard of physical and mental health, Paul Hunt, February 2005, paragraph 12.28 See Grobe, Jeanine, “Beyond Bedlam: Contemporary Women Psychiatric Survivors Speak out”, Third Side Press, Chicago IL, 1995
and Beresford, Peter and Wallcraft, Jan, “Psychiatric System Survivors and Emancipatory Research: Issues, Overlaps and DiVerences”in “Doing Disability Research”, Colin Barnes and Geof Mercer (Eds.). Leeds, The Disability Press 1997 at pp 66–87.
29 See Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical andmental health, Paul Hunt, February 2005, where he states “For many years persons with intellectual disabilities were placed at the edgesof the margins.”, paragraphs 77–82.
30 See Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical andmental health, Ibid at paragraph 11.
31 See page 8 of the Green Paper where the Commission proposes that an EU-strategy could focus on 4 distinct aspects: 1) promotion ofthe mental health of all; 2) address mental ill health through preventive action; 3) improve the quality of life of people with mental illhealth or disability through social inclusion and the protection of their rights and dignity; 4) the development of a mental healthinformation, research and knowledge system for the EU. See also Section 6.2 “Promoting the Social Inclusion of Mentally Ill orDisabled People and Protecting their Fundamental Rights and Dignity”, page 11.
32 See Section 6.2 of the Green Paper, ibid, page 11.33 See http://www.cpt.coe.int/en/states.htm to view CPT country reports.34 The European Committee for the Prevention of Torture in its “Standards”, states:
The CPT also attaches considerable importance to psychiatric establishments being visited on a regular basis by an independentoutside body (eg a judge or supervisory committee) which is responsible for the inspection of patients’ care. This body should beauthorised, in particular, to talk privately with patients, receive directly any complaints which they might have and make anynecessary recommendations. (para 55)
35 MDAC will be issuing a report on inspectorate mechanisms later in 2006.
3564223016 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
136 commission green paper on eu mental health strategy: evidence
— Lay advocacy in institutions
By this, MDAC means non-lawyers providing advocacy services in institutional settings in order toensure that patients receive information about their rights, and about other agencies andprofessionals that can assist.36
— Adequate legal representation in mental health cases.
It is a requirement under the European Convention on Human Rights that lawyers represent peoplewith mental health diYculties where detention in psychiatric settings is concerned.37 MDAC isconcerned that in many cases, this legal representation is purely cosmetic.38
In the framework of a strategy to develop a mental health information, research and knowledge system forthe EU,39 information should also be gathered on the state of fundamental rights in the mental health field,including information on the existence of fundamental rights abuses and whether and how human rightsconsiderations are implemented into policies.40
In summary, an approach that separates fundamental rights from other mental health issues will prove to beineVective and will only serve to reinforce the unfortunate prevailing attitude in many Member States offundamental rights being an optional extra.
3.2 Legal Capacity and Guardianship
The issues of legal capacity and guardianship are ignored in the Green Paper. Legal incapacitation removesrecognition of a person before the law and often results in the withdrawal of a number of fundamental rights:the right to decide on residence, the right to manage property, the right to respect for family life, to marry andto found a family and the right to vote. Guardianship also prevents people from working, which has aneconomic impact on individuals, families and Member States as a whole. With the demographics of Europeindicating that people are living longer, guardianship is becoming an increasing concern.41
Adults with mental health problems are commonly deprived of their legal capacity because they may (or areperceived to) require assistance in decision-making. To address such circumstances, most Member Statesoperate a system of substitute decision-making, by which the legal capacity of the person is removed by ajudicial authority and decision-making authority is vested in another person. This type of system is commonlycalled “guardianship” .
However, guardianship is too often used to remove a person’s rights and autonomy. Guardianship systemsdo not comply with international due process guarantees, are susceptible to abuse and frequently lead to arange of other fundamental rights violations.42 Some of the more commonly occurring abuses are: lack of fairtrial in the deprivation of legal capacity, lack of suYcient legal flexibility to allow the person any meaningfulparticipation in decision-making once guardianship is established, and lack of regular review of capacity orguardianship. Once under guardianship, an individual can be “placed” in a social care institution for theirentire life, on the decision of the guardian: the person is de facto detained but enjoys none of the legalguarantees provided to people who are detained in law.
Adults under guardianship in some countries are also stripped of their right to access courts. This blocks accessto justice to remedy any rights violations or to modify or terminate guardianship.
In order to tackle this growing issue, MDAC suggests that the future EU strategy on mental health should,at a minimum, require all Member States to bring guardianship laws into compliance with internationalhuman rights standards. This means that Member States must make every eVort to ensure respect for the rightsof the person concerned at every stage of the guardianship process from incapacitation to establishment of theguardianship arrangement to oversight of the guardianship and finally to termination of guardianships when36 See for example, the right to advocacy contained in the Mental Health Bill, England and Wales, 2005.37 See Article 5 ECHR, discussion in Mental Disability Advocacy Center, Training Pack on ECHR and Mental Disability, (Budapest:
MDAC, 2003).38 See Mental Disability Advocacy Center, Liberty Denied: Human Rights Violations in Criminal Psychiatric Detention Reviews in
Hungary, (Budapest: MDAC, 2004).39 See Section 6.3 “Improving Information and Knowledge on Mental Health in the EU”, page 12.40 There are established research and monitoring tools now used widely, including the WHO’s Resource Book on Mental Health, Human
Rights and Legislation, WHO, 2005, available athttp://www.who.int/entity/mental health/policy/who rb mnh hr leg FINAL 11 07 05.pdf.
41 See Green Paper “Confronting Demographic Change: a new solidarity between the generations” 2005.Available at http://ec.europa.eu/employment social/news/2005/mar/comm2005-94 en.pdf
42 See forthcoming publications on the findings of MDAC’s Guardianship Assessment Project.
3564223016 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
137commission green paper on eu mental health strategy: evidence
no longer appropriate. Member States should move laws towards a system of supported decision-making withguardianship to be increasingly used only as a protective measure of last resort.43 In order to achieve thesechanges, Member States must commit to provision of community-based services rather than institutional care.
3.3 Institutionalisation
The Green Paper’s position on institutions is unclear. By institution, MDAC means “any place in whichpeople who have been labelled as having a disability are isolated, segregated and/or compelled to live together.An institution is also any place in which people do not have, or are not allowed to exercise control over theirlives and their day-to-day decisions. An institution is not defined merely by its size”.44 While the focus on thecommunity as the ideal setting for mental health services is welcomed,45 the Green Paper lacks a clear visionabout how mental health systems should be reformed. There is ample evidence to show that large institutionssuch as psychiatric hospitals, social care homes and large residential establishments are no longer acceptablein modern day Europe.46 Essentially, they do not meet modern European standards of core fundamentalrights. As referenced above, fundamental rights abuses in such institutions have been extensively documented.Fundamental rights violations caused and exacerbated by institutions include: deprivation of liberty, inhumanand degrading treatments and punishments (physical and chemical restraints and solitary confinement), lackof healthcare, overcrowding, physical and sexual abuse and neglect.47
The European Union is in a powerful position to encourage governments to show leadership and pledge tofind an appropriate balance of hospital and community services. Across Europe, especially in the new MemberStates, there is a lack of political will to commit to a process of closure of institutions and establishment ofcommunity-based services.
MDAC recommends that the mental health strategy include:
— An EU commitment to fund research on the experiences, including successes, limitations andfailings, of Member States which have already established community care services. Such an actionis clearly within the competencies of the EU as it will involve access to healthcare, education,cooperation across Member States, EU wide coalition-building and planning. This research woulddevelop joint strategies to address the successes and failures of European mental health systems andto provide information on which to base more eVective health policies, strategies and actions atMember State and EU levels.48
— A timeframe within which to achieve appropriate closure of large institutions and eVectivemonitoring of the process.49
— Biennial meetings of all Member States, WHO, UN Special Rapporteur on the Right to Health andcivil society to discuss progress.
— A commitment to include examination of mental health systems into annual progress reports onaccession States.
Despite recognising that the community is the key location for mental health services, the Green Paperincongruously encourages Member States to “assess with the regions and the Commission how the StructuralFunds can be better used to improve long-term care facilities and health infrastructure in the field of mentalhealth”.50 The Green Paper therefore appears to support the continued existence of institutions and long termsocial care homes. This is an alarming direction, maintaining and expanding lifelong social exclusion, and onewhich runs counter to a modern community-based approach already endorsed by the EU.51 MDAC suggeststhat the Commission should instead insist that structural funds be used to create and promote diverse43 Supported decision-making provides an alternative to guardianship because it is premised on the notion that decision-making generally
is an interdependent activity as opposed to an independent activity and therefore with proper support and assistance a person whomight be otherwise deemed to lack capacity is in fact able to make personal decisions on his or her own behalf.
44 This is the definition of “Institution” used by the European Coaliton for Community Living, of which MDAC is a member organisation.See http://www.community-living.info/?page%205
45 “The deinstitutionalisation of mental health services and the establishment of services in primary care, community centres and generalhospitals, in line with patient and family needs, can support social inclusion.” See Section 6.3 of the Green Paper “ImprovingInformation and Knowledge on Mental Health in the EU”, page 11.
46 See “Included in Society”. Results and Recommendations of the European Research Initiative on Community-Based ResidentialAlternatives for Disabled People. European Commission 2003.
47 See Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical andmental health, supra note 7, paragraph 9.
48 See http://ec.europa.eu/comm/dgs/health consumer/general info/mission en.html49 See Interaction OYcial Response to European Union Green Paper on Mental Health, page 3.50 See Section 5 “The need for an EU- Strategy on Mental Health”, page 7.51 See WHO Mental Health Declaration for Europe, Helsinki, Finland, January 2005 EUR/04/5047810/6 at paragraph 10 (xi) where the
Ministers of Health of the Member States in the WHO European Region, committed themselves to “develop community-based servicesto replace care in large institutions for those with severe mental health problems”.

3564223016 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
138 commission green paper on eu mental health strategy: evidence
community-based services, such as recovery-oriented services, self-help groups, sheltered and supportedaccommodation, supported employment schemes, peer-run drop-in centres and community-based crisisservices.
Finally, MDAC would like to draw attention to the current fundamental rights situation of people with mentalhealth problems in EU accession countries, Bulgaria52 and Romania.53 During the last wave of accession in2004, disability rights issues were not high on the agenda despite the existence of the Copenhagen criteria.54
The fundamental rights situation of people with mental health problems in Bulgaria and Romania is evenworse than in previous accession countries. MDAC urges the Commission to take seriously this continuinghuman crisis when considering membership.55
3.4 Forced Treatment
Compulsory admission to psychiatric hospitals and involuntary treatment remain commonplace throughoutEurope. Persons with mental health problems in Europe are routinely subjected to forced medical treatmentand drugging on the basis that it is in the person’s best interests. The unregulated and severe use of methodssuch as electroconvulsive therapy (ECT), psychosurgery and the forced administration of chemical drugs oftenresults in violations of human rights and dignity and can amount to inhuman and degrading treatment underinternational law.56 All of these interventionist methods can have severe physical, neurological andpsychological side eVects, including significant memory loss, depression, apathy, anxiety, vomiting, muscleparalysis, the lethal Malignant Neuroleptic Syndrome and the frequently occurring tardive dyskinesia andmetabolic syndrome. The pain and suVering often caused by such methods is well documented by users andsurvivors of psychiatric services themselves.57 Research has shown that coercion, including forced treatment,is counterproductive in treating mental health problems and a wide range of alternative and non-medicaltreatments have proved successful for many persons.58
While the Green Paper acknowledges that “compulsory placement of patients in psychiatric institutions andinvoluntary treatment aVects severely their rights”,59 there is no further discussion on this serious topic. TheGreen Paper states that “a first priority is to provide eVective and high-quality mental health care andtreatment services, accessible to those with mental ill-health”,60 without addressing the fact that many of themedical interventions used to “treat” persons with mental health problems are highly controversial andcontested. MDAC recommends that the EU co-ordinate research on the availability and eVectiveness ofalternative voluntary treatment services. Such research would probably illustrate what existing research hasconvincingly shown: that the need for forced interventions is significantly less when a range of alternativetreatments are readily available.52 In its May 2006 Monitoring Report on Bulgaria, the European Commission noted that, “[b]asic conditions in institutions caring for
the elderly, the physically and mentally handicapped and children are appalling. The legal basis for their institutionalisation, along withthe slow and sometimes badly planned process towards real de-institutionalisation are unsatisfactory and still give cause forconsiderable concern. Continued increased eVorts are still needed.” Available at http://ec.europa.eu/comm/enlargement/report 2006/pdf/monitoring report bg en.pdf. See also the Amnesty International Annual Report 2006 at http://web.amnesty.org/report2006/index-eng and Amnesty International, “Bulgaria. Far from the Eyes of Society. Systematic Discrimination against People with MentalDisabilities.” 2001. Available at http://web.amnesty.org/library/Index/ENGEUR150052002.
53 The European Commission recently highlighted the lack of progress made by Romania in the area of social policy and inclusion in itsMonitoring Report reviewing pre-accession progress in May 2006 and referred in particular to institutionalisation: “Increased eVortsare needed to close or restructure large residential institutions for people with disabilities by developing alternative community-basedservices, support to families and smaller residential units.” See http://ec.europa.eu/comm/enlargement/report 2006/pdf/monitoring report ro en.pdf. See also the Amnesty International Annual Report 2006 at http://web.amnesty.org/report2006/index-eng and the recent report by Mental Disability Rights International, Hidden SuVering: Romania’s Segregation and Abuse of Infants andChildren with Disabilities, MDRI: Washington DC: May 2006. Available at http://www.mdri.org/projects/romania/romania-May%209%20final.pdf.
54 See http://europa.eu/scadplus/glossary/accession criteria copenhague en.htm55 A requirement of basic human rights standards in mental health should also be applied to the candidate countries of Turkey, Croatia
and Macedonia and also to future potential candidate countries.56 See Report of the Special Rapporteur on the right of everyone to the enjoyment of the highest attainable standard of physical and
mental health, supra note 7, paragraph 9.57 See for example, Peter Lehmann “Schone Neue Psychiatrie” (Peter Lehmann Publishing, Berlin) and the academic references therein.
See also Cobb A, Darton K & Juttla K “Mind’s Yellow Card for Reporting Drug Side EVects. A Report of Users’ Experiences.” MindPublications: London 2001.
58 For European research on coercion in psychiatry, see the EC-funded EUNOMIA project, available at http://www.eunomia-study.net.See also Hoyer G et al “Paternalism and Autonomy: a presentation of a Nordic study on the use of coercion in the mental health caresystem.” Int. Journal of Law and Psychiatry 2002 Mar–April 25(2):93-108. On the consequences of coercion, see for example “FromPrivileges to Rights: People labelled with Psychiatric Disabilities speak for themselves.” Report by the U.S. National Council onDisability, available at http://www.ncd.gov/newsroom/publications/2000/privileges.htm. See also Lidz, C W et al, “Factual Sources ofPsychiatric Patients’ Perceptions of Coercion in the Hospital Admission Process” , Am J Psychiatry 155:1254–1260, September 1998,and the references therein.
59 See Section 6.2 “Promoting the Social Inclusion of Mentally Ill or Disabled People and Protecting their Fundamental Rights andDignity”, page 11.
60 See Green Paper, Section 4 “Developing Responses: Policy Iniatives on Mental Health”, page 5.

3564223016 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
139commission green paper on eu mental health strategy: evidence
In addition to involuntary treatment in hospitals, there is also the issue of involuntary outpatient commitment.In some European countries where de-institutionalisation has already been initiated, community treatmentorders (or outpatient commitments) exist, which force a person to receive medication in the community.61
MDAC contends that such treatment is inconsistent with the aim of deinstitutionalisation and the purpose ofcommunity-based services, which is to enable and empower persons with mental health problems to live insociety to the best of his/her ability. The introduction of community treatment orders merely relocatescompulsion from an institution into the community.
It is important to note that the right to physical and mental integrity and the right to be protected frominhuman and degrading treatment are enshrined in the European Charter of Fundamental Rights.62 While theCharter of Fundamental Rights does not yet have any legally binding force,63 the European Court of Justicehas held that “the Charter has undeniably placed the rights which form its subject-matter at the highest levelof values common to the Member States”.64
All Member States have ratified the European Convention on Human Rights,65 a legally binding documentwhich explicitly prohibits inhuman and degrading treatment and punishment in Article 3 and protects the rightto respect for private and family life in Article 8, concepts which include physical and moral integrity of theperson,66 and compulsory medical treatment.67
MDAC contends that the lack of a serious discussion on forced hospitalisation and treatment is a seriousomission in the Green Paper, which needs to be rectified and adequately tackled in a European strategy onmental health.
4. MDAC Response to Questions Posed by the Commission
In this section MDAC summarises its views in response to specific questions posed by the Commission.68
1. How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed in section 1?
The improvement of the mental health of European citizens is clearly relevant to the policy aims and objectivesof the EU. It is important for social justice, non-discrimination and the socio- economic development of theEuropean population. However, it is not possible to achieve these aims without an underlying basis offundamental rights. Achieving non-discrimination for such a heavily stigmatised and marginalised “group”requires positive and pro-active measures in order to ensure that persons with mental health problems enjoytheir rights on an equal basis with other European citizens. In this context, MDAC recommends that theCommission finally commit itself to a Disability Specific Directive.69
2. Would the development of a comprehensive EU strategy on Mental Health add value to the existing and envisagedactions and does section 5 propose adequate priorities?
As mental health services diVer greatly between Member States, a comprehensive EU strategy on MentalHealth would have the potential to harmonise and link existing policies and strategies in order to make themmore eVective. However, the priorities of the proposed EU strategy outlined in section 5 are questionable.Primacy is given to the promotion of mental health and prevention of mental ill health. MDAC believes thatthe quality of life of persons who have experience of mental health problems should be a dominant priority.The empowerment of users of mental health services and their families is the key to the improvement of theirquality of life and the process of empowerment itself will give such persons ownership over their mental health,61 For example, such laws have been introduced in the Netherlands and in some federal States in Germany. There is an ongoing debate
in the UK. On the contrary, Ireland provides an example of where a conscious decision was made not to open up coercive treatmentin the community.
62 Article 3(1) states “Everyone has the right to respect for his or her physical and mental integrity”. Article 3(2) goes on to state that “inthe fields of medicine and biology, the following must be respected in particular: the free and informed consent of the person concerned,according to the procedures laid down by law. . . .”. Article 4 states “No one shall be subjected to torture or to inhuman or degradingtreatment or punishment.”
63 The Charter has been incorporated into the Treaty establishing a Constitution for Europe, which if ratified would give the Charterbinding legal force. See http://europa.eu.int/constitution/. However, there is also nothing to prevent the Charter from being adoptedas a stand alone document.
64 Advocates-General Tizzano, Leger and Mischo. See http://europa.eu/scadplus/leg/en/lvb/l33501.htm65 Convention for the Protection of Human Rights and Fundamental Freedoms, Rome, 4. XI. 1950.66 X & Y v. The Netherlands, judgement of 26 March 1985, para. 22.67 Herczegfalvy v. Austria, judgement of 24 September 1992.68 See Section 8 “Next Steps” at page 13.69 For more information on the EU wide campaign for a Disability Specific Directive, see the website of the European Disability Forum.
EDF has also drafted a proposal for a Disability Specific Directive. See http://www.edf-feph.org/en/welcome.htm.
3564223016 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
140 commission green paper on eu mental health strategy: evidence
which is also keeping in line with the European ideal of active citizenship. MDAC contends that improvementof the quality of life of persons with mental health problems as well as the promotion and prevention of mentalhealth problems will remain impossible without proactive measures to promote fundamental rights in the fieldof mental health. The promotion of fundamental rights should be a first priority, which applies throughoutthe realm of mental health.
3. Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between Member States, topromote the integration of Mental Health into the health and non-health policies and stakeholder action, and to betterliaise research and policy on Mental Health aspects?
The initiatives proposed on page 12 of the Green Paper with regard to social inclusion and fundamental rightsare pragmatically weak and inappropriate to achieve the above aims. The first proposal to identify “bestpractice for promoting the social inclusion and protecting the rights of people with mental ill health anddisability” lacks any substantive content. Secondly, the proposal to include people with mental ill health ordisability and the situation in psychiatric institutions in the activities of the future Fundamental Rights Agencyis quite a basic and rudimentary suggestion from the Commission as it would be grossly discriminatory notto include disability within the competencies of the FRA. Furthermore, this type of proposal embodies thetop-down approach for which the Commission has often been criticised. In order to achieve long term impact,clear guidance is needed on all levels in order to ensure that mental health services comply withfundamental rights.
MDAC looks forward to further consultation with the European Commission during the process ofdeveloping a Mental Health Strategy for Europe.
Memorandum by Mental Health Foundation
1. Introduction
The Mental Health Foundation welcomes the opportunity to submit evidence to the Select Committee on theEuropean Union.
Our mission is to help people survive, recover from and prevent mental health problems. We use innovativeresearch and community projects to address issues of mental well-being for the whole population as well as toimprove the support, services, rights and social inclusion for people with mental health problems. People whouse mental health services are at the heart of all our work—as employees, advisors, volunteers, and supporters.We gather and provide information for anyone who is experiencing mild to severe mental health problems,and people with dementia. We also provide information for their friends, families, carers and providers ofmental health services. Our work encompasses children, adults of working age, and older people.
2. Would an EU Strategy on Mental Health be Appropriate?
An EU strategy designed to facilitate exchange and collaboration between member states would be of valueto individual states and contribute to a greater understanding and consensus in regard to mental health policyand practice across the EU. In the UK alone, costs incurred as a result of mental health problems areapproximately £93 billion per annum. One in four people will be aVected by mental health problems at somepoint each year, yet discrimination against people with mental health problems is still a pan-Europeanproblem. We therefore regard the promotion of mental health and the prevention of mental health problemsas key priorities in keeping with the goals of prosperity, solidarity and social justice and quality of life forall citizens.
A European Union Strategy on Mental Health will have the potential to increase understanding andinformation-sharing across member states and complement existing national policies as laid out in documentssuch as the Department of Health’s Choosing Health White Paper and Making it Possible, a framework forthe implementation of a public mental health strategy in England.
We welcome the recognition in the Green Paper of the importance of exchange between member states, ofworking vertically at all levels, from individual to EU Community level, and of working across sectors. Mentalhealth should not be perceived as a distinct health or a social issue, but as an underpinning factor whichimpacts across all areas of society. We stress the importance of policies which encourage integrated workingand information sharing across sectors encompassing areas such as education, employment, business and theenvironment.

3564223017 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
141commission green paper on eu mental health strategy: evidence
The Green Paper attempts to cover all aspects of need in terms of both public mental health and mental healthservices for people with diagnosed mental health problems. However we would like to see more clarity andfocus in regard to the role of a population-wide EU mental health strategy. We believe that at EU level, it maybe more useful initially to distinguish between these interrelated, but separate areas of concern.
As set out in the Mental Health Foundation’s report “Choosing Mental Health”, public mental health isconcerned with improving the mental health of a whole population. It needs to take a view across the lifespanof all members of the population and take into account gender, ethnicity, disability, social class, sexuality andspirituality. It is our view that a clearly defined European strategy on mental health is entirely appropriate totackling public mental health. This would usefully support member states” national strategies on the secondarea of concern—the provision of services for people already experiencing mental health problems.
3. What Elements Might it Contain?
We agree with the four priority areas set out in the EU green paper: promotion, prevention, social inclusionand further research. However we would like to see a more detailed strategy or action plan to drive forwardimplementation throughout the community.
3.1 Investment
In order to reduce the human and economic costs of mental ill health, investment is required in long termstrategies to raise awareness, tackle discrimination, reduce social exclusion and promote mentally healthylifestyles amongst member states’ populations. These will be key components in producing a prosperouscommunity in which all citizens experience good quality of life. It has been calculated that the cost benefit ofbetter mental health care would be a net saving across government as a whole of some £3.1 billion a year(Making it Possible, p 9). This does not take into account the savings from promoting mental health andpreventing problems in the first place. An EU strategy should be backed up by a robust economic analysisshowing potential savings through investment. Member states with fragile economies should be supported inimplementing priority areas of an EU mental health strategy.
3.2 Children and Young People
Strategies should include a focus on whole-school approaches to mental health promotion, the reduction ofbullying within schools, the provision of universal support to parenting and mechanisms to monitor progresson promoting children’s mental health. Young people in their teens and early twenties need services designedto address their particular needs and issues. There needs to be less reliance on medication and further researchinto identifying eVective ways of building resilience. Early intervention is a crucial component of mental healththat can significantly reduce the human and economic costs of mental ill health across the life course. Thisshould be suYciently resourced. (See Lifetime Impacts, The Mental Health Foundation 2005)
3.3 Workplace
Employers and employees should be made aware of their duties and rights under EU and national law aroundwork/life balance and disabilities issues. If member states laws are inadequate in this regard, they should beencouraged and supported to implement legislation. Strategies are needed to tackle discrimination byemployers against people with mental health problems through national, regional and local initiatives. TheEuropean Commission could lead by example in this regard by implementing positive and proactiveemployment initiatives for staV with experience of mental health problems. Agencies responsible for theprovision of financial support for people out work as a consequence of mental health problems should takeaccount of the fluctuating nature of mental health problems and enable a flexible and non-punitive re-entryinto the workplace through return to work approaches such as transitional employment and individualplacement and support.
3.4 Lifestyle
The Green Paper places emphasis on prioritising “high quality mental health and treatment services”. Whilewe wholly endorse policies which support the continued development and improvement in availability andquality of services for people with mental health problems, we would urge the Commission to also incorporatewithin any mental health promotion strategy a strong focus on core lifestyle factors such as diet, physicalactivity and alcohol/substance use.

3564223017 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
142 commission green paper on eu mental health strategy: evidence
3.4.1 Diet
The links between diet and mental health are being increasingly understood. Studies have ranged fromexamining individual responses to diet changes in randomised controlled trials, to population-based cross-cultural comparisons of mental health and food intake. Dietary changes have been found to have a significantimpact on problems such as anxiety and depression, schizophrenia, Alzheimers disease and Attention DeficitHyperactivity Disorder. We propose the promotion of healthy eating at all levels and across sectors. Any suchstrategies will need to link up with member states food and industry sectors in order to make healthy foodattainable and aVordable for all members of society. (See Feeding Minds, Mental Health Foundation, 2006)
3.4.2 Physical Activity
There is also a substantial body of evidence to show that physical exercise can be as eVective as anti-depressants in treating mild or moderate depression. In April 2004, a report by the Chief Medical OYcer onthe impact of physical activity and its relationship to health stated that: “Physical activity is eVective in thetreatment of clinical depression and can be as successful as psychotherapy or medication, particularly in thelonger term”. In December 2004 the National Institute for Clinical Excellence recommended in its guidelinesfor treating depression in primary and secondary care that: “Patients of all ages should be advised of thebenefits of following a structured and supervised exercise programme of typically up to three sessions per weekof moderate duration”.
In view of this, there are strong reasons for promoting exercise therapy as a first-line treatment. In contrastto the negative side eVects of medication, exercise has coincidental benefits and can be used to treat a mix ofphysical and mental health problems. It is a sustainable recovery choice; less costly, it promotes socialinclusion and it is popular. Treatment completion rates are often much higher than with medication. However,research carried out by the Mental Health Foundation found that although exercise referral schemes are inplace in the UK, only 5 per cent of general practitioners use them as their first line of treatment. We proposeexercise be promoted both amongst the general population at local, regional and national level and thatpolicies targeted at prevention and treatment are comprehensively communicated to healthcare practitionersthrough the use of “exercise champions”. (See Up and Running, Mental Health Foundation, 2005) There isa need for further action research on the most eVective ways of increasing exercise uptake and reducing thebarriers to physical activity among the most vulnerable and disadvantaged groups including low income,people with mental health problems and older people. Practical solutions for enabling participation areneeded.
3.4.3 Alcohol
Little has been said in public policy documents about the way the general population relies on alcohol.However alcohol can have a significantly detrimental eVect on mental health. We recommend that all alcohol-related public health materials, training and teaching should cover mental health aspects of alcohol misuse/use. Increased education about the association between alcohol use and mental health in schools should beused to alert people to the potential risks of using alcohol.
3.5 Mobility
The strategy should take into account the increased migration between states and issues around culturalsensitivity, language and state responsibility.
3.6 Research and Monitoring
The Green Paper acknowledges the importance of developing a mental health information, research andknowledge system to underpin Community actions on improving mental health.
A European public mental health observatory based on the UK regional models would provide a usefulplatform for the setting of over-arching key public mental health indicators, data collection and evaluation.This would enable all European countries to collect comparable data and track changes over time. Otherinitiatives might include:
— The identification of cost benefits arising from mental health promotion.
— A standardised toolkit that can be applied across all settings.
3564223017 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
143commission green paper on eu mental health strategy: evidence
— Any process involving the setting of indicators, monitoring and evaluation should incorporateservice user defined outcomes as a core element.
— Service user involvement at local, national and community level should be measured.
3.7 Service User Involvement
It is crucial that people who use mental health services and their carers are central to any thinking about anEU mental health strategy that sets out plans for mental health service provision, however this is not a strongfocus in the Green Paper. There is a need to consider ways in which to build capacity for a high degree of serviceuser and carer involvement at community and member state level. Commissioners may find it useful to linkin to the NGO Service User involvement Group established following the World Health Organisation’sDeclaration on Mental Health in 2005.
3.8 Social Inclusion
People with mental health problems often experience isolation and exclusion from fundamental aspects of lifesuch as employment, quality housing, social networks and education. In order to meet the policy priority ofequality and social justice set out in the Green Paper, it is important the strategy sets out practical ways inwhich to recognise and support diverse needs. Under the theme of social inclusion, we would like to see a realfocus on reducing stigma and discrimination and on recovery orientated approaches such as flexible supportsand phased approaches towards community development and involvement, such as the clubhouse model.
The media plays a central role in contributing to public perceptions of mental illness. However in the vastmajority of cases it serves only to reinforce the most negative misperceptions. The media therefore play a keyrole in challenging stigma and raising public awareness. Consideration and planning should be given to waysof disseminating the most eVective delivery of social inclusion.
4. How Might it Complement and Add Value to the Strategies of Member States and the Activities
of the World Health Organisation and Other International Bodies?
4.1 Health and Social Care Policy in England
A European Strategy on Mental Health would complement Department of Health policy by providing anunderpinning framework linking key health and social care policy initiatives, which otherwise appeardisconnected and do not maximise opportunities for cross-agency working, for example:
— Standard One of the National Service Framework for Mental Health—Promoting Mental Healthand Tackling Stigma and Discrimination. This requires the NHS in England in partnership withother agencies to promote the mental health of their local population, and to tackle the stigma,discrimination and exclusion experienced by people with mental health problems.
— The National Service Framework for Children and Young People sets out standards and strategieswhich include the promotion of mental health and well-being, prevention and early intervention,including parenting support and the protection of maternal mental health.
— The Choosing Health White Paper outlines the agenda for public health over the next three to fiveyears. It identifies mental health as a priority issue and is part of a growing awareness of both theeconomic and public health case for a greater focus on promotion and prevention.
There would be similar benefits in relation to policy in Scotland, Wales, and Northern Ireland.
4.2 Equality and Social Inclusion Policy
Other key areas in which a European strategy would add value to UK policy are:
— Social Inclusion agenda—An EU mental health strategy would support the programme set out inMental Health and Social Exclusion which covers discrimination, employment, mental healthpromotion and access to fundamental rights such as decent housing and education.
— The Disability Discrimination Act clearly legislates that people should not be discriminated againston the grounds of disability including disability as a consequence of poor mental health. An EUstrategy may help to ensure all member states implement similar legislation.
3564223017 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
144 commission green paper on eu mental health strategy: evidence
— General Medical Services Contract—A European Strategy on Mental Health will complement andpotentially place greater emphasis on the need to make general mental health promotion andscreening a priority within the Quality Outcomes Framework guidance within the GMS contract.
4.3 WHO Policy
An EU strategy would directly support the priorities set out in the World Health Organisation’s Declarationon mental heath, namely to:
(i) foster awareness of the importance of mental well-being;
(ii) collectively tackle stigma, discrimination and inequality, and empower and support people withmental health problems and their families to be actively engaged in this process;
(iii) design and implement comprehensive, integrated and eYcient mental health systems that coverpromotion, prevention, treatment and rehabilitation, care and recovery;
(iv) address the need for a competent workforce, eVective in all these areas; and
(v) recognise the experience and knowledge of service users and carers as an important basis forplanning and developing mental health services. (Helsinki Declaration 2005)
5. Conclusion
The Mental Health Foundation supports the intention to develop an EU-level strategy on mental health andfeels this would add value to the work done by member states. In particular, elements relating to public mentalhealth should be enhanced, as these have the greatest opportunity to promote the wellbeing of the wholepopulation and address many of the issues relating to disability, social exclusion and stigmatisation currentlyexperienced.
Memorandum by the NHS Confederation
Introduction
1. The NHS Confederation welcomes the inquiry on the European Commission Green Paper on EU MentalHealth Strategy
2. The NHS Confederation is a membership body that represents over 93 per cent of all statutory NHSorganisations across the UK, including 90 per cent of Primary Care Trusts (PCTs) and 100 per cent of StrategicHealth Authorities (SHAs). Our role is to provide a voice for the management and leadership of the NHS andto represent the interests of NHS organisations. We are independent of the UK Government although, ofcourse, we work closely with the Department of Health and the devolved administrations.
3. Our evidence sets out our general views, based on feedback from our members.
4. The NHS Confederation also leads the UK delegation to HOPE, the European hospital and healthcarefederation. We have therefore made a similar contribution to HOPE’s submission on this strategy.
Overview
5. Mental health problems cause diYculties in almost every aspect of society. Economic prosperity is aVectedby absenteeism and poor productivity, insurance costs for disability insurance claims are increasingly onerousand welfare benefits to support the unemployed place a huge burden on the tax-payer.
6. Mental illness undermines social cohesion, especially for those excluded from the workplace. People withmental health problems suVer from community isolation even after de-institutionalisation. This is notameliorated by public concern about risk, and the reality that many criminal oVenders have diagnosablemental illness.
7. Most importantly, however, mental health problems severely reduce the quality of life of those who are ill.The eVects are felt in their personal relationships and social networks, and more systemically in terms of theirdownward occupational mobility.
8. The UK and other member states have made great strides in improving the way in which mental healthproblems are addressed. However, there is much more to be done. We look forward to the advances to be madefrom taking a Community approach to mental health.
3564223018 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
145commission green paper on eu mental health strategy: evidence
Whether an EU strategy on mental health would be appropriate. If so, what elements might it contain?
9. A great deal has been achieved at member state level to combat the eVects of mental health problems andto tackle the determinants of mental illness. An EU strategy that enables information-sharing and cross-pollination of ideas will, wherever possible, permit common responses to common problems. The openmethod of co-ordination is an ideal tool for such exchange.
10. Given the EU’s existing competence in health promotion, it is sensible to tackle the promotion of mentalwell-being. However, there is much more that could be done in schools and for young people. Theidentification and prevention of problems before adulthood is now acknowledged as a major priority for re-organising mental health services. It should therefore be the cornerstone of service change across memberstates.
11. We already know how to reduce suicide and depression and we are rapidly improving our knowledge ofsubstance abuse. However, it is likely that prevention could be much more eVective if knowledge was sharedacross member states.
12. Tackling stigma, social exclusion, discrimination and the myths of mental illness is absolutely crucial.Instrumental to this would be national commitments to raise the employment rate of those with mental illness.When considering the contribution that social inclusion makes to dynamic and competitive economies, it isclear that mental health is relevant to more than just health-related policy initiatives. The business case forincreased labour market participation is a compelling one.
13. Research and information is essential, as is access to a common data-set to enable cross-border learningand policy exchange. Learning should centre on policy and practice based on the best available evidence. Wesuggest that the European Commission support a more pro-active, research-based strategy for mental health.This would include a multi-phase and long-term attempt to gather evidence and promote research into mentalhealth issues. An evidence base supported by social, scientific and policy related research will create a robustplatform for an evolving and maturing mental health strategy for the EU.
14. The proposed strategy refers to health inequalities within as well as between member states. We urge theEuropean Commission to focus particularly on the diVerential use of services by diVerent ethnic groups. Wehave much to learn about improving access for black and minority ethnic users across the European Union.
15. We would also suggest that a Community strategy pay attention to the workforce requirements implicitin each proposal. Professional roles and the degree to which staV are substituted varies between member states.However, multi-disciplinary teams play a pivotal role in health service organisation and can be used to deliverservices in pro-active and creative ways.
Conclusion
16. We are aware of the diYculties in mainstreaming mental health services in a climate of increasing pressureon health budgets. However, we believe that a collective approach to prevention, promotion and inclusion,under-pinned by robust evidence-based research will only be positive for citizens of the EU.
17. Finally, we would like to thank the House of Lords for the opportunity to comment on the EU MentalHealth Strategy.
May 2006
Memorandum by NHS London EU Unit
“By health I mean the power to live a full, adult, living, breathing life in close contact with what I love . . . I wantto be all that I am capable of becoming” Katherine Mansfield70
Key Recommendations
The EU should:
— Use its role in relation to employment and workplaces to:
— Promote awareness of Emotional Wellbeing.
— Encouraging the better management of mental illness at work.
— Increase the employment rates of people with mental illness.
70 The Journal of Katherine Mansfield, 1927, Constable.
3564223019 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
146 commission green paper on eu mental health strategy: evidence
— Promote the development of “one stop shops” where people can access information about andassistance with emotional wellbeing and mental illness, and related issues (eg housing, finance,physical healthcare) in non-stigamitising settings.
— Support the active engagement of people who use mental illness services in their design and delivery.
— Encourage the exchange of information to support eVective and culturally sensitive help for migrantsand others from minority ethnic groups who have mental health problems or mental illness.
— Support local initiatives to challenge stigma and discrimination about mental illness.
— Promote the use of emotional wellbeing impact assessments in policy development andimplementation.
Preparation of this Contribution
This contribution on behalf of the NHS and Regional Public Health Group London and other stakeholdersis based on discussions with individuals, and following a seminar in April 2006. A list of contributors isincluded as Appendix A.
Responses to the Committee’s Questions
1. Is an EU strategy on Mental Health appropriate?
1.1 An EU strategy is ethically, socially and economically appropriate.
1.2 People with mental illness experience varying degrees of exclusion and ill treatment. Stigma,discrimination and exclusion in relation to employment aVect the prosperity of individuals and nations.Increasing sickness absence due to mental illness limits the ability of the EU to deliver the Lisbon Agenda.
1.3 The Commission should:
1.3.1 Recognise the importance of dignity and humanity in a future Emotional Wellbeing (EW) strategy.
1.3.2 Challenge stigma, discrimination and social exclusion due to Mental Illness (MI).
1.3.3 Consider EW as central to achieving the Lisbon agenda (including an employment rate of 70 per centfor adults of working age).
2. What elements might an EU Mental Health strategy contain?
2.1 Promotion of mental health of all:
2.1.1 The EU should promote evidence-based guidance for improving young people’s EW.
2.1.2 The EU should use its role in relation to health and safety at work, and its procurement practice to:
2.1.2.1 Support innovations and promote awareness of EW through the workplace.
2.1.2.2 Encourage employers to design and implement interventions to support employees with MentalHealth Problems (MHP) and MI.
2.1.3 The EU should encourage provision better information to older people to promote their EW.
2.1.4 The EU should encourage the sharing of information about cultural attitudes to MI, and how to workwith ethnic minorities to help member states promote EW with them.
2.1.5 An EW strategy should pay attention to the EW and MI needs of prisoners, and training for thoseworking in the criminal justice system.
2.1.6 The EU should help member states to share their experience of challenging stigma and discriminationeVectively.
2.2 Tackle mental illness:
2.2.1 An EW strategy should consider the resources needed to build the capacity of non-statutoryorganisations who provide EW and MI services.
2.2.2 An EW strategy should promote the development of “one stop shops” for emotional wellbeing andmental illness in non-stigmatising settings.
2.3 Increase social inclusion, and equality of opportunity and health care for people with mental illness.
2.4 The EU should support locally designed and delivered campaigns to challenge stigma.
2.4.1 The EU should:
2.4.1.1 continue to support schemes which help people with mental illness gain and retain work; and

3564223019 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
147commission green paper on eu mental health strategy: evidence
2.4.1.2 promote procurement initiatives which encourage employing people with a mental illness.
2.4.2 The EU should promote equality of public health interventions and physical healthcare for people withmental illness.
2.4.3 The Commission should use the Daphne II Programme of the DG Employment and Social AVairs(which considers domestic violence) as a good example of how EW needs can be considered across policyareas.
2.4.4 An EW strategy should support pan-EU networks of service users and carers, and promote theirinvolvement in designing and delivering services.
2.5 Improve knowledge and information sharing between members states and regions
2.5.1 An EU EW strategy should include:
2.5.1.1 EU wide networks to share good practice and research, and support exchange visits.
2.5.1.2 The development of a web based EU portal for EW.
2.5.2 An EU EW strategy should encourage networks of EU capital cities to consider EW and the needs ofmigrants.
2.5.3 Eurostat should consider making comparisons on EW indicators between cities only, towns only andrural areas only across the EU.
3. How might a Mental Health Strategy compliment and add value to the strategies of member states, the WorldHealth Organisation, and other international bodies?
3.1 The EU should:
3.1.1 Lead by example on EW by ensuring all Directorates General use an EW impact assessment of newpolicies.
3.1.2 Consider how EW impact assessment might be integrated within the wider Strategic EnvironmentalAssessment (SEA) directive.
3.1.3 Actively engage in dialogue on EW with a range of organisations across the EU including business andcommunity groups.
3.2 The EU should continue and use existing platforms for EW supported by an expert advisory group.
APPENDIX A
Contributions are gratefully acknowledged from the following:
Name Organisation
Alexandra Turney RethinkSuzanne Collins London Development Centre (Core User Survivor Group)Brian Dawn Mind in CamdenMark Brangwyn Association for London GovernmentDavid Shaer Oxleas MH TrustJoan Penrose CarerSanja Stevic Learning and Skills Council—London SouthAideen Silke London Development AgencyEric Carrington CarerGrant Pettitt Greater London AuthorityRebecca Smith Greater London AuthorityHilary Guite Greenwich Primary Care TrustStuart Bell South London and Maudsley NHS TrustJagadish Jha London Development Centre (Core User Survivor Group)Claire Helman Community Service VolunteersRabbia Khan Enfield Primary Care TrustCaroline Reid North West London Strategic Health AuthorityPeter Spelman Redbridge Primary Care TrustTony Jones London FirstPaul Gocke London Development CentrePhilip Cohen London Borough of CroydonJohn Bowis MEP (London)Jose Westgeest NHS London EU Unit
3564223019 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
148 commission green paper on eu mental health strategy: evidence
Name Organisation
Jenny Lee Spencer NHS London EU UnitSean Duggan Health and Criminal Justice ProgrammePaul de Ponte London Health Observatory
Memorandum by The Northern Ireland Association of Mental Health
The Bamford Review of Mental Health and Learning Disability (Northern Ireland) See footnote
MENTAL HEALTH PROMOTION
The Need For a Cross-sectoral Approach
The Report of the Expert Working Committee of The Bamford Review of Mental Health and LearningDisability (Northern Ireland) “Mental Health Improvement and well-being—a personal, public and politicalissue” (Full Report attached) recommends the implementation of a cross sectoral approach and partnershipworking rather than the siloing of mental health promotion into the health portfolio as has been the case inthe past.
To Realise the Vision for Mental Health Promotion there is the need for a focused, resourced, centrally driven,cross-sectoral, cross-departmental and prioritised approach. Collaborative work among key agencies andcentral government departments—partnerships between health and social services and education agencieshold particular potential. Mental health should be promoted in the context of social justice, equality andcitizenship.
The coordination between member states to promote the integration of mental health into the health and non-health policies and stakeholder action is essential to the well-being and prosperity of the EuropeanCommunity.
The questions set out in the Green Paper have been addressed as follows:
(1) How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed insection 1?
Mental Health is a Resource
The Green paper referres to The Mental Health of the population of Europe as a Resource.
This view is endorsed by the Expert working Committee on Mental Health Promotion of the Bamford Reviewof Mental Health and Learning Disability under the chairmanship of Prof Alan Ferguson, Chief Executive ofthe Northern Ireland Association for Mental Health.
“Mental Health Improvement and well Being—A personal, public and political issue”
The foreword to the report states:
“Mental Health is as important as physical health. Mental health promotion is not just for those with mentalhealth problems. Mental well-being underpins all health and well-being: it is a resource which must be protectedand promoted” .
Under the heading Vision and Principles the Expert Working Committee express the view that the followingvision is central to the success of a mental health improvement strategy for Northern Ireland.
There must be a recognition at all levels in Northern Ireland that:
— everyone has mental health needs;
— mental well-being underpins all aspects of health and well-being; and
— mental health, like physical health, is a resource to be promoted and protected.
The Costs of Mental Ill-health and the need for Investment in Mental Health Promotion
The Green paper referres to the fact that Mental ill health causes significant losses and burdens to theeconomic, social, educational as well as criminal and justice systems.
3564223020 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
149commission green paper on eu mental health strategy: evidence
The Northern Ireland Association in Collaboration with the Sainsbury Centre for Mental Health produceda policy document on Counting the Cost, the economic and social costs of mental illness in Northern Ireland(Document enclosed). The economic and social costs of mental illness in Northern Ireland amounted to nearly£3 billion in 2002–03—more than the total spend on all health and social care for all health conditions.
The Mental Health Promotion report refers to the burden of disease as follows and makes reference to thefigures pertaining to Northern Ireland.
Over 19 per cent of the total burden of disease in Western European countries was attributable tomental illness compared with 17 per cent for cardiovascular disease and 16 per cent for cancer. In2002 no other condition exceeded 8 per cent (World Health Organisation, WHO 2004).
Of the total disease burden in Western Europe, just over half is attributable to non-fatal outcomesof morbidity and disability, of which mental ill health accounts for over 30 per cent. No other healthcondition accounts for more than 10 per cent. In Northern Ireland we are only spendingapproximately 9.3 per cent of our Health AND Social Services Budget on mental health.
The 2001 Northern Ireland Health and Well-Being Survey found that 21 per cent of our populationaged over 16 considers themselves to be depressed and a similar percentage had a potentialpsychiatric disorder. The Department of Health, Social Services and Public Safety (DHSSPS)estimate that in terms of the scale of the problem, prevalence figures for mental health problems inNorthern Ireland are 25 per cent higher than in England.
Addressing these challenges for the whole community in Northern Ireland, as exemplified by theWHO Action Plan for Europe (WHO 2005), as a long-term investment. That investment must reflectthe growing body of evidence that positive mental health cannot be gained by treating mentaldisorders alone (Cp Green Paper Section 4 ).
Suicide rates for Northern Ireland Suicides in Northern Ireland soared by almost 50 per cent lastyear. 213 people there took their lives in 2005.
The Economic Case for Mental Health Promotion
The Northern Ireland Association for Mental Health is in the process of commissioning a study on theeconomic case for mental health promotion with the help of an expert on mental health promotion and anexpert in health economics. The feasibility study will apply economic analysis to mental health promotion Thestudy will complement the earlier publication.
The promotion of Mental Health and well-being for all is seen by the Review Committee as a long terminvestment, an investment which must be predictable and sustainable.
In addressing the challenge mention is made of the WHO action plan (2005) which cites certain actions asbeneficial, such as the adoption of mental health as a long term investment, with education and informationprogrammes having a long time frame.
(2) Would the development of a comprehensive EU-strategy on mental health add value to the existing andenvisaged actions and does section 5 propose adequate priorities?
EU Mental Health Strategy for Europe
The Green Paper in Section 5 refers to the need for an EU mental health strategy and the establishment of astrategy on mental health at EU-level would add value by:
(1) Creating a framework for exchange and cooperation between Member States.
(2) Helping to increase the coherence of actions in diVerent policy sectors.
(3) To open up a platform for involving stakeholders including patient and civil society organisations intobuilding solutions.
Investment in Mental Health Promotion Throughout Europe
The Green Paper refers to structural funds and how these can be better used to improve long term care facilitiesand health infrastructure in the field of mental health/
Whilst there is the need to provide eVective and high quality mental health care and treatment services,accessible to those with mental ill health, tackling mental ill-health on its own cannot address and changesocial determinants.
3564223020 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
150 commission green paper on eu mental health strategy: evidence
The Bamford Report on Mental Health Promotion fully endorses this approach—“Investment must reflectthe growing body of evidence that positive mental health cannot be gained by treating mental disorders alone”.
The Mental health Promotion Report of the Bamford review emphasises the need to invest in mental healthpromotion for the whole of society to prevent the occurrence of mental ill-health and to tackle the issues ofstigma and social exclusion.
The Bamford Report referres to the growing body of evidence that positive mental health cannot be gainedby treating mental disorders alone (WHO2004). For example, providing the most eVective evidence basedtreatment for one half of all people with depression would only reduce the current burden of depression byless than one quarter. On the other hand, evidence demonstrates that mental health promotion and preventioncan lead to health, social and economic gain, increases in social inclusion and economic productivity,reductions in the risks for mental and behavioral disorders and decreased social welfare and help costs (JaneLlopis & Anderson 2005, WHO 2005).
The Need for Cross-sectoral Working
The main thrust of the report is similar to the emphasis in the Green Paper that there is a need for a crosssectoral approach and partnership working rather than the siloing of mental health promotion into the healthportfolio as has been the case in the past.
To Realise the Vision for Mental Health Promotion there is the need for a focused, resourced, centrally driven,cross-sectoral, cross-departmental and prioritised approach.
The experience in Northern Ireland has been that whilst there have been many initiatives on mental healthpromotion and these are happening at a local level. Indeed the hard work and commitment of individuals andgroups must be commended. However a single Department approach has not delivered on a focused outcome.There is the lack of an eVective, focused regional structure, properly resourced, sustainable and able to driveforward and build on existing policy such as the current strategy and action plan 03/08.
Vision—Underpinning Principles
The Bamford Mental Health Promotion Report notes that such a Vision must be underpinned by thefollowing principles.
To achieve a society where everyone plays a role in and takes action to create an environment that promotesthe mental well-being and improvement of individuals, families, organizations and communities, there is aneed for:
— increased cross-sectoral, collaborative work among key agencies and central governmentdepartments—partnerships between health and social services and education agencies holdparticular potential.
The Primary Recommendation of the Bamford Review Report on Mental Health Promotion is The
Creation of a Regional Mental Health Promotion Directorate at the Heart of Government
The Review, having agreed and recommended a Directorate as necessary for providing strategic, coordinated,cross-sectoral and multi-agency action on mental health promotion, then considered the appropriatestructures and siting to achieve this function.
The Review considered where the centre of gravity should be for this recommendation. Should it be focusedwithin the health sphere or if we are looking to wider contributions, including those of education, culture andemployment to produce the change we want, what mechanism and approach is most eVective in making thoselinkages.
The Review considers that it is necessary, in order to achieve this strategic vision, to place the Mental HealthPromotion Directorate at the heart of Government. The Review’s recommendation is that to ensure mentalhealth promotion is a policy priority across the whole of the public sector the Directorate would best be placedwithin the OYce of the First Minister and Deputy First Minister (OFMDFM).
The assigning of the Directorates to a single department or Quango should be avoided to ensure thatownership of mental health promotion is not perceived as being the sole responsibility of a single department,such as health and personal social services. The assigning of a Directorate for Mental Health Promotion toOFMDFM fits in well with the portfolio of responsibilities already assumed by this Department. Theseinclude such issues as equality, children and young people, disability, human rights, as well as the
3564223020 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
151commission green paper on eu mental health strategy: evidence
Department’s responsibility for promoting co-operation between Government Departments in NorthernIreland.
The Creation of a Framework for exchange and cooperation between Member States would be welcomed bythe Steering Committee of the Bamford Review and also by the Northern Ireland Association for MentalHealth.
(3) Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between MemberStates, to promote the integration of mental health into the health and non-health policies and stakeholder action,and to better liaise research and policy on mental health aspects?
Support and Co-ordination Between Member States
The Bamford Report on Mental Health Promotion fully is in full agreement with the development of theinitiatives as set out in the Green Paper with regard to the need for coordination between member states. Thereport notes the need for a regional, national and international approach to mental health promotion andquotes from the resolution passed by the council of the European Union in November 1999 calling on theEuropean Commission to recognise the importance of promoting mental health and to access the mentalimpact of policy.
The coordination between member states to promote the integration of mental health into the health and non-health policies and stakeholder action is essential to the well-being and prosperity of the EuropeanCommunity.
The development of a EU policy on mental health needs to take into account the matter of social capital whichrefers to such features as social organisation to include networks, norms, and social trust that facilitatecoordination and cooperation for mutual benefit.
Primary Recommendation: The Creation of a Regional Mental Health Promotion Directorate at
the Heart of Government
Recommendation 1 of the Report considers settings, stages and levels for actions
— Settings for Action: Schools, Primary Care, Workplace, further and higher education, communities,including marginalized groups and faith communities.
— Stages of Life: Children and Adolescents, older people, people in receipt of statutory mentalhealth services.
— Levels of Action: Regional level/capacity building.
Recommendation 2 Deals with the identification of resources and recommends a resource allocation(Northern Ireland) in the region of £5–6 million over the initial three year period.
Recommendation 3 Suicide prevention is an integral part of mental health promotion and therecommendation is that suicide prevention needs to be placed as a public health priority and a RegionalMental Health Promotion Directorate needs to ensure that a separate suicide prevention strategy isimplemented as part of its overall responsibility
The initiatives proposed in the Green Paper on seeking solutions—options for action which includes:
— Promoting mental health and addressing mental ill health through preventive action.
— Promoting the mental health of the population.
— Addressing mental ill health through preventive action.
— Promoting the social inclusion of mentally ill or disabled people and protecting their fundamentalrights and dignity.
— Improving information and knowledge on mental health in the EU.
The Bamford Report on Mental Health Promotion has addressed the above issues and has identified three keydomains for action (See chapter 3 “The Action”).
Key Domains for Action
— The promotion of mental health and well-being for all the population at large.
— The prevention of mental health problems in key risk groups:
— children and adolescents;

3564223020 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
152 commission green paper on eu mental health strategy: evidence
— people who are deaf or hard of hearing;
— people with a learning disability;
— ethnic minorities;
— older people;
— people aVected by unemployment;
— people with physical illness;
— people with gender and sexuality issues;
— people traumatized by sexual abuse; and
— people within the criminal justice system.
— Improving the quality of life for people who have experienced mental health problems:
— people with enduring mental illness;
— people with eating disorders;
— people at risk of suicide;
— people emotionally and physically traumatized due to the NI “Troubles”; and
— people involved in substance abuse/dual diagnosis.
The Green Paper
A Consultation Process for the Development of an EU-strategy on Mental Health
The crosscutting relevance of mental health makes it appropriate to develop an EU-strategy on mental healthbased on a broad and inclusive consultation process.
The following activities are envisaged:
7.1 Creating a Dialogue with Member States on Mental Health.
7.2 Launching an EU-Platform on Mental Health.
7.3 Developing an interface between policy and research on mental health.
Given the extensive work on mental health and learning disability which has been undertaken in NorthernIreland by the Bamford Review which includes nine detailed reports—A review which will shape the natureof services in Northern Ireland for the next 20–30 years—The Expert working Committee on Mental Healthimprovement and well-being invite the Commission to consider a Belfast Conference on Mental HealthPromotion in Europe to take place in to include :
— Papers on mental health promotion initiatives.
— Examples of good practice.
— Development a mental health strategy for Europe and the necessary structures to achieve this.
— Consolidation and the future.
The Bamford Review of Mental Health and Learning Disability (Northern Ireland)
See Strategic framework, Terms of Reference and list of the expert working Committees below.
Four reports have been concluded (Mental Health Promotion Report is the fourth to be published) with theothers coming to fruition later this year.
A Strategic Framework for Mental Health and Learning Disability
A New Vision for Mental Health and Learning Disability Services
The vision behind this strategic framework is to give a real and meaningful priority to the challenges of mentalhealth and learning disability, embracing a reduction in the incidence and prevalence, a reduction in mortalityand in the extent and severity of problems associated with mental ill-health and learning disability. Central tothe vision is a valuing of people with mental health needs or a learning disability, their rights to full citizenship,equality of opportunity and self-determination. It anticipates a process of reform, renewal and modernisationof services.
3564223021 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
153commission green paper on eu mental health strategy: evidence
The strategic framework embraces the complementary challenges of mental health and learning disability. Italso recognises the requirement for:
— a balanced response to the need for better services for people with mental health and learningdisability; and
— a clear framework to promote positive mental health and reduce stigma.
Values and Principles
The framework is based on a set of fundamental values and guiding principles. People with mental healthneeds, learning disability and their carers should look forward to a response from services which:
— respects their individual autonomy—through openness and honesty in the providing of information,respect and courtesy in individual interactions with service users, partnership and empowerment inservice planning and delivery—with Government, providers and wider society each accepting theirrespective responsibilities; and
— demonstrates justice and fairness—resources for services should be allocated and managedaccording to criteria which are transparent, and which demonstrate equity.
The framework for service development and service provision is based on the following principles:
— partnership with users and carers in the development, evaluation and monitoring of services;
— partnership with users in the individual assessment process, and in the development of theirprogramme of treatment and care and support;
— delivery of high quality, eVective treatment, care and support;
— provision of services which are readily accessible;
— delivery of continuity of care and support for as long as is needed;
— provision of a comprehensive and co-ordinated range of services and accommodation based onindividual needs;
— take account of the needs and views of carers, where appropriate, in relation to assessment,treatment, care and support;
— provision of comprehensive and equitable advocacy support, where required or requested;
— promotion of independence, self-esteem and social interaction through choice of services andopportunities for meaningful employment;
— promotion of safety of service users, carers, providers and members of the public;
— staV are provided with the necessary education, training and support; and
— services are subject to quality control, informed by the evidence.
Framework Goals and High Level Objectives
Informed by these values and principles, the service review provides a unique opportunity to address the fullspectrum of issues relating to mental ill-health and learning disability. The Review goes beyond specific mentalhealth problems or individual groupings, to include, for example, mental health promotion, public healthmeasures to reduce mental ill-health and suicide, and the challenges of stigma. In responding to the needs ofindividual service users and their carers, there is a need for clear specification of models and standards.
To ensure a balanced and inclusive framework, the following high level objectives have been set:
1. recommend specific reforms of service for each of the following user groups—children, young people, menand women with mental health needs or a learning disability; [Service reforms will specify models of care andstandards of provision in relation to the quality, comprehensiveness, eVectiveness, accessibility andacceptability of provision. They will include detailed consideration of primary and secondary care services,the interface between these services, the linkages and interfaces between health and social care, education,culture arts and leisure, employment and housing, the complementary roles of statutory and non-statutoryservices, and the issues surrounding multi-disciplinary and multi-agency working.]
2. review the strategy for mental health promotion, embracing public health measures to reduce mental illhealth and suicide;
3564223021 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
154 commission green paper on eu mental health strategy: evidence
3. review of the law:
1. review of relevant legislation and other requirements relating to human rights, equality ofopportunity and social inclusion of people with mental health needs or learning disability andtheir carers;
2. review of the Mental Health Order (NI) 1986; and
3. make recommendations regarding future legislation to reflect the needs of users and carers in thecontext of the framework values and principles.
All proposals will be evidence-based, noting the quality of evidence presently available.
Terms of Reference
1. To carry out an independent review of the eVectiveness of current policy and service provision relating tomental health and learning disability, and of the Mental Health (Northern Ireland) Order 1986.
2. To take into account:
— the need to recognise, preserve, promote and enhance the personal dignity of people with mentalhealth needs or a learning disability and their carers;
— the need to promote positive mental health in society;
— relevant legislative and other requirements, particularly relating to human rights, discrimination andequality of opportunity;
— evidence—based best practice developments in assessment, treatment and care regionally, nationallyand internationally;
— the need for collaborative working among all relevant stakeholders both within and outside thehealth and personal social services sector;
— the need for comprehensive assessment, treatment and care for people with a mental health need ora learning disability who have oVended or are at risk of oVending; and
— issues relating to incapacity.
3. To make recommendations regarding future policy, strategy, service priorities and legislation, to reflect theneeds of users and carers.
Social Justice and Citizenship:Convenor: Bill Halliday, Praxis
To consider relevant legislative and other requirements, particularly relating to human rights, discriminationand equality of opportunity; and how best to promote the social inclusion of people with a mental healthproblem or learning disability and their carers, taking account of employment, housing, education, socialsecurity, personal finance and other social issues.
Legal Issues:Convenor: Master Brian Hall, Master of Care and Protection
To include a review of the Mental Health (N Ireland) Order 1986; the Mental Health Commission; the MentalHealth Review Tribunal; the procedures for the transfer of patients to and from N Ireland; issues relating topeople who are not able to look after their own property and aVairs as a result of a mental health problem orlearning disability; and issues relating to people with a mental health problem or a learning disability who arein contact with the criminal justice system.
3564223021 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
155commission green paper on eu mental health strategy: evidence
Learning Disability:Convenor: Siobhan Bogues, Manager, ARC (NI)
To review policy and services for children and adults with learning disabilities.
Adult Mental Health:Convenor: Professor Roy McClelland, Deputy Chair of the Review
To include consideration of primary care provision, acute services, rehabilitation and community care foradults with a mental health problem.
Mental Health Promotion:Convenor: Professor Alan Ferguson, Chief Executive, N Ireland Association for Mental Health
To include consideration of how best to promote positive mental health in society, with particular referenceto the impact of the recently-published Mental Health Promotion Strategy, and how best to meet the needsof people at risk of suicide.
Child and Adolescent Mental Health:Convenor: Moira Davren, Royal College of Nursing
To include consideration of primary care provision, acute services, rehabilitation and community care forchildren and adolescents.
Dementia and Mental Health Issues of Older People:Convenor: Nevin Ringland, Praxis
To include consideration of primary care provision, acute services, rehabilitation and community care forolder people with a mental health problem or dementia.
Alcohol and Substance Misuse:Convenor: Dr Diana Patterson, Shaftesbury Square Hospital
To include consideration of the links between mental health and alcohol and substance misuse, and theprovision of the most appropriate assessment, treatment and care for those involved.
Forensic Services:Convenor: Dr Fred Browne, Chief Clinician, Shannon Clinic.
To consider the assessment, care and treatment of people with a categorical mental illness, severe personalitydisorder or who engage in dangerous or persistently challenging, aggressive behaviour, and who may be incontact with the criminal justice system.
Needs and Resources:Convenor: Glenn Houston, Chief Executive of Craigavon and Banbridge HSS Trust.
To support other working committees in assessing the financial implications of their recommendations.
Memorandum by Open Society Mental Health Initiative (MHI)
1. The Open Society Mental Health Initiative (MHI)
MHI is a program of the Open Society Institute. It seeks to ensure that people with mental disabilities (mentalhealth problems and/or intellectual disabilities) are able to live as equal citizens in the community and toparticipate in society with full respect for their human rights and currently works in Central and EasternEurope and the former Soviet Union. MHI promotes the social inclusion of people with mental disabilities bysupporting the development of community-based alternatives to institutionalization and by actively engagingin policy based advocacy. MHI is both a grant making and an operational program, providing training andtechnical assistance to its partner organisations.
3564223022 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
156 commission green paper on eu mental health strategy: evidence
The focus of MHI’s activities is to end the unjustified and inappropriate institutionalization of people withmental disabilities by advocating for the closure of institutions and for the development of community-basedalternatives. Over the past 12 years MHI has provided sustained and strategic financial and technical supportfor the development of community-based alternatives to institutionalisation in the region.
2. General Comments on the Green Paper
MHI welcomes and supports the European Commission’s initiative in establishing an EU-strategy on mentalhealth. The mental health of the EU population is of crucial relevance to the EU’s strategic policy objectivessuch as bringing tangible practical benefits to the quality of life for European Citizens (question 1, page 13).As the Green Paper makes clear, there are many areas in which the mental health of the EU population canbe improved and it is of crucial importance that steps are taken to address the causes and eVects of mental illhealth. Thus MHI considers that the development of a comprehensive EU-strategy would “add value to theexisting and envisaged actions” (first part of question 2, page 13). However, MHI has two major concerns withthe Green Paper:
— Greater emphasis on deinstitutionalisation71 is required: there is insuYcient emphasis on the need toensure that all EU Member States commit to, and implement, deinstitutionalisation policies. Unlesspolicy and practice is focused on the development of comprehensive community-based services,resources will continue to be tied up long-stay institutions. This will perpetuate the social exclusionof people with mental disabilities. It will also limit the opportunities to initiate action to address whatthe Green Paper acknowledges as “a first priority”, namely “to provide eVective and high-qualitymental health care and treatment services, accessible to those with mental ill health”.Deinstitutionalisation should be included in the priorities of the EU-strategy (second part ofquestion 2, page 13).
— Lack of clarity on the target group: it is not clear whether people with intellectual disabilities(described as people with learning disabilities or learning diYculties in the UK) are included in theseproposals. MHI advocates for including people with intellectual disabilities in the target group ofthe Green Paper. In the new Central and Eastern European Member States of the European Union,people with mental health problems and people with intellectual disabilities are often relegated tothe same long-stay institutions. Because people with intellectual disabilities make up a substantialportion of the population in long-stay institutions, it is crucial that EU mental health policy alsoaddresses the needs of this group. If people with intellectual disabilities are to be included in thisstrategy, then this needs to be made explicit and those organisations working in the intellectualdisability field should be invited to participate in the consultation process.
Set out below is a more detailed explanation of MHI’s concerns and additional comments on various aspectsof the Green Paper, including the appropriateness of the initiatives outlined in sections 6 and 7 of the GreenPaper (question 3, page 14).
3. Greater Emphasis on Deinstitutionalisation is Required
Context
Traditionally, governmental policy across Central and Eastern Europe (CEE) has been to segregate peoplewith mental disabilities in long-term residential institutions, such as psychiatric facilities, social care homesand orphanages. Children and adults with mental disabilities who are isolated in institutions, regardless oftheir age, sex, or type of disability are often subjected to the most severe forms of cruel, inhuman and degradingtreatment and other human rights violations.
Despite many positive political and economic developments across CEE in the last 15 years, the situation forpeople with mental disabilities has received little attention and is largely unchanged. To date, membership in,or candidacy for membership of, the European Union has done little to promote the social inclusion of peoplewith mental disabilities. In the Member States of the European Union, new institutions for people with mentaldisabilities continue to be built despite the fact that some governments have stated their intent to closeinstitutions. None of the new EU Member States have concrete plans or financing mechanisms to developnetworks of community-based alternatives. While there are pockets of high quality community-based servicesin the region, and a number of governments have stated their intentions to move toward a community-basedmodel, tens of thousands of people with mental disabilities are still living in institutions.71 We use this term to mean the process by which the closure of long-stay institutions is planned and implemented in conjunction with
the development of a range of community-based services as alternatives to institutional care.

3564223022 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
157commission green paper on eu mental health strategy: evidence
Segregating people, barring them from access to education and employment, denying them the right to choosewhere and how they live and who they associate with, solely on the basis of a mental disability label isunacceptable. The nature of institutions is, in itself, dehumanising. The existence of institutions is an anathemato the concept of a civil and open society in which the rights of all citizens are respected.
Deinstitutionalisation must be a priority for the EU-strategy on mental health
While MHI welcomes the reference to deinstitutionalisation in the Green Paper, the Paper fails to make clearthat the unjustified segregation of people with mental disabilities in long-stay institutions is not acceptable andconstitutes a severe human rights violation. Governments must, as a priority, develop and implement policiesthat require the closure of long-stay institutions and the development of community based alternatives.
The Green Paper mentions psychiatric facilities and mental health reforms in connection with the move awayfrom institutions towards community-based services. This is only part of the picture. Many people with“chronic conditions”, or those who are elderly, are placed in social care homes. Children and young peoplewith mental disabilities are commonly placed in orphanages, often because there is no support available totheir parents to be able to provide for them at home. Thus action is required to assist governments in reformingtheir social welfare systems and in developing legal and financial mechanisms which underpin the transfer ofall types of institutional care to the provision of community-based services.
A further concern is that the Green Paper refers to an assessment by Member States and the Commission on“how the Structural Funds can be better used to improve long-term care facilities and health infrastructure inthe field of mental health” (page 7). It is not clear what is meant by “long-term care facilities” or who wouldbe considered to need them. MHI’s view is that it would be a grave error for EU policy to promote theimprovement of long-term care facilities, since, with the exception of some forensic patients, people withmental disabilities do not need long term care, but rather need support that that is community-based.
MHI believes that in many countries the lack of knowledge and expertise within governments about how todevelop capacity in the community and close institutions is a major disincentive to such work being carriedout. Thus the development of an EU-strategy is a timely opportunity not only for the crucial importance ofdeinstitutionalisation to be highlighted but also for initiatives at EU level to be proposed. MHI thereforesuggests that deinstitutionalisation should be one of the focus areas of the EU-strategy, in addition to the otherfour areas identified on page 8 of the Green Paper (mental health promotion; addressing mental healththrough preventative action; improving the quality of life of people with mental ill health or disability throughsocial inclusion and the protection of their rights and dignity and the development of mental healthinformation, research and knowledge system for the EU). Deinstitutionalisation is crucial step towardsaddressing these four areas. Unless policy and practice is focused on the development of comprehensivecommunity-based services, resources will continue to be tied up long-stay institutions. This will perpetuate thesocial exclusion of people with mental disabilities. It will also limit the opportunities to initiate action toaddress what the Green Paper acknowledges as “a first priority”, namely “to provide eVective and high-qualitymental health care and treatment services, accessible to those with mental ill health”.
MHI suggests that the Commission proposes a Council Recommendation on the need for long-stayinstitutions to be closed in conjunction with the development of alternative community-based services.
4. Lack of Clarity on Target Group
It is not clear whether the Green Paper is intended to address the needs and interests of people with intellectualdisabilities. Much of the paper appears to be focused on issues relating to mental health, such as action toprevent suicide and references to mental health reforms. However there are parts of the paper which suggestthat people with intellectual disabilities may be included. For example, page 6 refers to “the social inclusionof people with mental disabilities” and on page 11 it is suggested that the EU-Platform on Mental Health willbe able to “identify best practice for promoting the social inclusion of people with mental ill health anddisability . . .”. If people with intellectual disabilities are to be included in this strategy then this needs to bemade clear and those organisations working in the intellectual disability field should be invited to participatein the consultation process.
MHI would argue that people with intellectual disabilities should be included in this strategy. While there aresignificant diVerences between people with intellectual disabilities and people with mental health problems,many of the issues faced by both these groups of people are similar—such as serious human rights abuses,social exclusion, stigma and prejudice.

3564223022 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
158 commission green paper on eu mental health strategy: evidence
5. Additional Comments
The need for a comprehensive approach
MHI welcomes the Green Paper’s emphasis on the need to take a comprehensive approach to the developmentof mental health policy and ensure that all stakeholders are engaged in the process (page 5). However, MHIwould like to see this approach reflected more clearly in the suggested areas of action. For example, while theGreen Paper refers to reforms within psychiatric services, little attention is given to social welfare reform whichwill be of crucial importance to the development of community-based services. Action to facilitate themeaningful participation of people with mental health problems (and if the strategy relates to them, peoplewith intellectual disabilities) will be crucial. Furthermore, it will be vital that the work initiated under the EU-strategy for mental health is closely linked to—informs, and is informed by—EU initiatives on widerdisability issues.
Protecting the rights of people with mental disabilities
The Green Paper refers to compulsory placement in psychiatric institutions, pointing out that this should onlyhappen as a last resort. Again, it should be noted that people are placed in a variety of institutions, not justpsychiatric institutions, without their consent. While MHI agrees that such placements should only occur asa last resort, the European Convention on Human Rights sets out further conditions that should be met beforea person can be lawfully detained.72 Furthermore, the concept of “last resort” is arguably meaningless if thereis no support available to individuals with mental disabilities living in the community.
Many countries in CEE have a system of “guardianship” under which a court can appoint a person to havethe power to make decisions on behalf of a person deemed to lack the capacity to make decisions for him/herself. The guardian often has extensive powers, for example the power to require the person subject toguardianship to move into an institution thereby circumventing any legal formalities which would have beenotherwise required if the person did not consent to the admission.
The activities of the new Fundamental Rights Agency of the EU should not be limited to addressing thesituation in psychiatric institutions. Rather, its work should include all long-stay institutions and other areasin which the rights of people with mental disabilities are being violated, such as guardianship which allowothers to exercise arbitrary and invasive powers over people with mental disabilities.
Action to address stigma and discrimination
The Green Paper rightly acknowledges the problems caused by the stigma and discrimination faced by peoplewith mental health problems. Such widespread and severe stigma and discrimination is a serious andsubstantial barrier to the social inclusion of people with mental disabilities. Member States must take concretesteps to address these barriers if they are to succeed in the first three of the suggested priorities (promotingmental health, addressing mental ill health through preventative action and improving the quality of life ofpeople with mental ill health or disability through social inclusion and the protection of their rights anddignity).
The possible initiative to identify, through the consultation process, “best practice for promoting the socialinclusion and protecting the rights of people with mental ill health and disability” (page 12) would hopefullygenerate a range of activities that could address stigma and discrimination and promote the social inclusionof people with mental disabilities. For example:
— Awareness raising in schools, among employers and the wider population—this could be part ofbroader work on disability issues.
— Ensuring that people with mental disabilities are aware of their rights. For example the EUEmployment Framework Directive73 requires that Member States introduce legislation whichoutlaws the discrimination of disabled people in employment. People with mental disabilities shouldbe protected by such legislation.
— Providing information and advice to employers to assist them in meeting requirements to provide“reasonable accommodation” at the workplace for people with mental disabilities.
72 See, for example Winterwerp v the Netherlands (1979).73 Council Directive 2000/78/EC, 27 November 2000—established a “general framework for equal treatment in employment and
occupation”. It covers discrimination on the grounds of age, disability, religion or belief and sexual orientation in employment andoccupation.

3564223022 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
159commission green paper on eu mental health strategy: evidence
— Considering barriers to social inclusion and taking steps to address these. For example, as mentionedabove, in some CEE countries the guardian for a person with mental disabilities deemed to lackcapacity has extensive powers. The ward has no right to make important and personal decisions suchas to vote or to marry, irrespective of his or her actual capacity to make such decisions.
People with mental health problems and intellectual disabilities must be involved at every stage of theconsultation on, and the development and implementation of, such proposed activities.
Open Society Mental Health Initiative
1 February 2006
Memorandum by Professor Stefan Priebe
Thanks for asking me to comment on the EU Green Paper on Mental Health Strategy for the House of LordsEU Select Committee enquiry.
The EU Green Paper touches on so many fundamental issues of a mental health strategy that the evidencerelated to it would fill whole libraries. In my view, the EU Green Paper is most welcome to shift publicattention to the most important subject of mental health. At the same time, it suggests ways forward on whichone might have diVerent views. This applies in particular to the tendencies to a) define distress in a society interms of individual mental disorders requiring medical or psychological treatment of the individual concerned,and b) consider general issues of societal importance such as unemployment and social isolation as specificmental health issues. For your information, I attach a commentary on the EU Green Paper that I was askedto write for Psychiatric Bulletin. It will probably be published in August and explains the two points above.
If you have any specific queries or would like me to elaborate on any of the above or other points, I will bemore than happy to be contacted at any time.
Sign of Progress or Confusion? A Commentary on the European Commission Green Paper on
Mental Health
In the history of psychiatry in Europe, there have been several texts and documents inspiring new ideas,influencing the way professionals and the Public think about mental health care and, subsequently, impactingon every day practice. Examples for such texts maybe the Psychiatrie-Enquete in Germany, and the law 180initiated by Franco Basaglia in Italy. It is unlikely that future generations will count the recent green paperon mental health, published by the European Commission (Commission of the European Communities 2005),among such seminal texts. Nevertheless, it is worth noticing. It illustrates important challenges to mentalhealth care at the beginning of the 21st century and highlights issues that might change the direction for thefuture.
The paper came out in October 2005 following the WHO European Ministerial Conference on Mental Healthin the same year. It has the noble intention “to launch a debate with the European institutions, governments,health professionals, stakeholders and other sectors about the relevance of mental health for the EU, the needfor a strategy at EU—level and its possible priorities.” It portrays “mental ill health” as a growing problemin the EU with wide economic consequences, and suggests preventive action, social inclusion of mentally illpeople, and more data on mental health across the EU. In the paper, the Commission invited everyone in theEU to contribute to a consultation process, which ended in May 2006. The results of the consultation processare not yet known in detail, but one can expect that most of the contributors will have agreed that mentalhealth is relevant indeed, that a comprehensive EU strategy on mental health is welcome, and that an interfacebetween policy and research should be developed to improve prevention and care. Yet, whether theconsultation process will also yield a clear concept of how mental health should be best promoted, anagreement on achievable priorities, and specific ideas for actions is less certain.
The paper reflects a general dilemma in psychiatry about the concept of “mental ill health” and the scope ofmental health care. It begins with quoting an epidemiological study estimating that more than 27 per cent ofadult Europeans experience at, least one form of mental ill health within a year. This is in line with variousfindings of epidemiological research in industrialised countries showing a prevalence of mental disorders of25 per cent or more. These figures have rarely been challenged in the psychiatric literature. However, does aconcept of mental disorder or “mental ill health” really make sense if it applies to 27 per cent of the population?Why have psychiatrists not taken these figures as a reason to re-consider the definition of mental disordersor—at least—the methods employed to identify them? The definitions of health and illness will always be fuzzyat the edges, but are essential to define the scope of medicine and professional mental health care. The greenpaper, which is surely not to be blamed for the dilemma that it highlights, states that “there is agreement thata first priority is to provide eVective and high-quality mental health care and treatment services to those with

3564223023 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
160 commission green paper on eu mental health strategy: evidence
mental ill health”. Putting this and the previous wisdom about the prevalence of mental ill health in thepopulation together would lead to the conclusion that mental health services should be established for 27 percent of the population, a suggestion which will be regarded as ludicrous by many in both professional groupsand the public. What “high-quality mental health care and treatment services” can be developed—andfunded—for more than a quarter of the population? Neither does the paper explicitly ask for new armies ofpsychotherapists and other mental health professionals to provide such care, nor does it specify whatapproaches other than conventional services might deliver eVective treatment for 27 per cent of the populationevery year. Either the concept of mental ill health or that of eVective treatment may require revising. Anyuseful debate on the future of mental health care cannot avoid this dilemma. Using an inconsistentterminology that mixes the terms mental illness, mental disorder, mental ill health, poor mental health andmental health problems on the one hand, and medical treatment, health and social care, professional help,psychosocial support andtherapy on the other without meaningful and consistent definitions for any of themwill not be a solution in the long term.
The green paper mentions a number of possible preventive actions and—in doing so—touches on anotherdilemma. The suggestions for actions include reducing the social isolation of older people, interventions forthe unemployed to re-enter the labour market, prevention of bullying throughout society, and strengtheningof social cohesion. All these are certainly important tasks for European societies, and achievements on any ofthem may have a positive impact on the mental health of the groups concerned. A society with an increasingdisparity between the rich and the poor, less social cohesion and a lower degree of general trust is likely to bebad for the mental health of the population. Yet, should all of these wider social problems be tackled underthe banner of “prevention of mental ill health”? Changing the fabric of society is not mainly a matter ofimproving health indicators, but foremost of social and political values. Reducing economic inequalities withall its consequences may therefore be regarded as a primarily political task, and not one for specific mentalhealth policies or care. Clarifying this might help to decide on the most appropriate action, and avoidoverloading mental health care with issues that it alone cannot shoulder.
The paper asks for comparable information across Europe. The diVerences among European countries intraditions of psychiatry, attitudes to and philosophy of health care, organisation of the health care systems,and funding arrangements can be used as a naturalistic experiment, and comparative data might help allcountries to learn from each other and understand how diVerent factors impact on the mental health of thepopulation as a whole and specific sub-groups (Priebe 2005). Whoever has tried to put data from diVerentcountries together, will have found the experience more diYcult than anticipated. Reliable information onsimple parameters such as the provision of diVerent types of services, let alone more sophisticated indicators,can be extremely diYcult to obtain, and comparisons are further complicated by diVerent definitions andconnotations. Additionally, there are various language problems which are hard to overcome, even if andwhen all documents and data are translated into English. Cynics might say that it will probably take another20 years of European collaboration before the participants understand to what extent they misunderstandeach other. Despite these problems, communication and exchange of ideas and information are important andworthwhile. Better collection, accessibility and comparisons of data across Europe are both feasible andpromising. Such data should feed into a wider debate on the future of mental health care addressing the above-mentioned issues.
So, if we are going to have a debate, where is that debate supposed to happen? There is no obvious Europeanforum for it. On national levels, some countries such as Germany and Italy have begun to organise largenational psychiatric congresses, which are held at the same place and time every year and attract more than4–5,000 participants. In the UK, such a congress does not exist, but there are excellent journals which mighttake the debate forward. For instance, the Psychiatric Bulletin recently published a full series of debate paperson future directions of mental health care (Priebe 2004). Perhaps, discussions on future challenges anddirections can also be held in local services, although—for whatever reasons—this currently does not oftenhappen.
The green paper does not contain new ideas and gives rather confusing signals about the direction of travelfor mental health care. Yet, it might reflect a new interest in mental health in the wider society and on a politicallevel. If this is the case, it could herald exciting times for developing and improving mental health care. Onemay conclude from history that major reforms of psychiatry were possible only when psychiatric issuesreceived wider public attention and political interest. Is the green paper a sign that we are at the beginning ofa new era of such public interest in mental health and innovative reforms of care? As always, the future will tell.
3564223023 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
161commission green paper on eu mental health strategy: evidence
References
Commission of the European Commission: Green Paper—Improving the mental health of the population.Towards a strategy on mental health for the European Union. Brussels, 14.10.2005 COM(2005) 484 final.
Priebe, S (2004) Psychiatry in the future. Where is mental health going? A European perspective. PsychiatricBulletin, 28, 315–316.
Priebe, S (ed) (2005) Mental Health Care in European Capitals. European Psychiatry, 20, Supplement 2,S265–S300.
Stefan PriebeProfessor of Social & Community Psychiatry, Queen Mary, University of London, Newham Centre forMental Health, London E13 8SP, e-mail: s.priebewqmul.ac.uk
Memorandum by The Royal College of Psychiatrists
The Royal College of Psychiatrists is the leading medical authority on mental health in the United Kingdomand the Republic of Ireland and is the professional and educational organisation for doctors specialising inpsychiatry.
The Royal College of Psychiatrists warmly welcomes this Green Paper as a prospective contribution to theWHO Declaration and Action Plan, and commends the work that has been done to develop and promote thestrategy.
The case for an integrated mental health strategy is well made in the paper, and the dual emphasis uponpromotion of positive mental wellbeing and the prevention and treatment of mental illness is stronglysupported. Pressures to which every fourth citizen succumbs at some stage must be so prevalent that they arefelt by almost everyone. The strategy should therefore include the right mix of measures for improving themental health of the whole population, and for providing a social, psychological or medical remedy for groupsof people who are particularly at risk of incapacitating mental illnesses.
Responsibility for detecting and responding to mental ill health is shared not only between patients and healthworkers, but also by staV in social, educational, occupational, housing, criminal justice and other settings—and of course by their carers and by members of the public. All of these people need to understand their rolesand feel able to act.
In most countries individuals and agencies who are striving to improve the lot of those with mental healthproblems experience a lack of political and financial resource. The mental health lobby is small in comparisonwith its competitors. Where mental health is a part of general health provision it is our experience that it willrarely come first on the list for action. Unfortunately, negative attitudes or indiVerence towards the care ofpeople with mental health problems is often as commonplace amongst health workers and administrators asin the general population. This EU strategy should help to overcome those barriers to progress. The Collegetherefore particularly welcomes the suggestion that a stakeholder’s platform be set up to provide anopportunity for views and expertise to be received, in the expectation that support and empowerment will bereturned.
The Green Paper includes two proposals for Council Recommendations, which address the numerically largest groupsaffected:
A Council Recommendation on the promotion of mental health should encourage positive attitudes towardssocial and family cohesion, and creativity and empowerment within society as a whole. There is a commonview that modern lifestyles are becoming less conducive to a sense of well-being and therefore to good mentalhealth. The strategy cannot ignore that view, but should actively investigate these conflicted issues, and withinits competency create a practical framework of mechanisms for change.
A Council Recommendation on the reduction of depression and suicidal behaviour would have the potentialto influence the largest diagnostic group, as well as those who are most at risk—and suicide and deliberate selfharm rates are elevated in all mental illnesses. There is now enough reliable evidence upon which to basestrategic decisions. As indicated in the Green Paper, new strategies for prevention can be built upon practicesthat have proven eVectiveness, in diVerent States, various age groups and in diverse settings.
So far as treatment is concerned, at the base of the pyramid of severity of depression, psychosocialinterventions and lifestyle changes may be recommended by a range of people with limited specialist training.However there is a shortage of professionals able to treat moderately severe cases, for whom the initialtreatment of choice is formalised psychological therapy such as a cognitive behavioural approach.
3564223024 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
162 commission green paper on eu mental health strategy: evidence
Treatment of severe depression and other mental illnesses may require medical and nursing care in hospital,not least to preserve the physical health and safety of patients and those around them until their mental stateimproves. Reliance upon hospitalisation varies between Member States. Although the College supports theleast restrictive approaches to care, and is fully aware of the potential for institutionalisation and ill-treatmentin badly run hospitals, nevertheless a balance must be struck, for closing hospital facilities without adequatealternatives can result in increased risk and stigmatisation in the community, and eVective re-incarceration in“mini-institutions”.
The College’s Responses to the Three Consultation Questions are as Follows:
How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed in section 1?
Mental health is highly relevant to the EU’s strategic policy objectives, and the EC is well placed to make anumber of valuable interventions.
The need for change is well summarised in Section 1, and the secondary benefits of improved mental healthto other policy areas, including economics, are enumerated and clear. We wish to emphasise also the increasingcapacity for change, due not least to the recent expansion in knowledge about mental health and mental illness:about risk and protective factors, primary, secondary and tertiary prevention, and improvements in a widerange of medical treatments and psychological therapies. This more optimistic view of what can be done torelieve mental health problems and improve recovery is slowly replacing traditional associations withsequestered custodial care. A wide-reaching and authoritative strategy, with an eVective means ofdissemination, should accelerate the acceptance of this positive view.
Would the development of a comprehensive EU-strategy on mental health add value to the existing and envisagedactions and does section 5 propose adequate priorities?
The College agrees that added value would flow most readily from initiatives that facilitate inter-agency andinter-state collaboration; co-ordinate parallel developments between policy areas; and facilitate the provisionof appropriate information for users at all organisational levels.
Satisfactory mental health in a community will depend in part upon economic and political stability and onsettings that promote family life, good schooling, cohesion, rewarding work and care of the elderly. Thestrategy should encourage the richness of local diversity as well as oVering standard approaches.
The College also agrees that provision of eVective mental health care is a first priority, and suggests that thestrategy should address the problems faced by all Member States in setting realistic threshold criteria for entryto services. Although states are exclusively competent for organisation of their own mental health care andpsychiatric services, nonetheless supportive actions might be taken by the EC to promote discussion andunderstanding of the principles involved. Those most mildly aVected by mental health problems often havethe greater personal resources, are the most articulate, and the most numerous; while the long term severelymentally ill have the greatest need. Variations in local prevalence and social deprivation should also aVect thedistribution of services. This introduces particular pressures upon state intervention. Added value wouldaccrue from shared research and development on epidemiology and resourcing mechanisms.
As indicated in Section 4.1 of the Green Paper, recent Community initiatives on mental health have so fararisen independently from a variety of policy areas. The strategy should not hinder such initiatives from arisingwherever they are required. However, there is a risk that a series of independently-generated projects will notfully cover the ground, that eVorts may be duplicated, and that initiatives may turn out to be incompatible.The College therefore strongly supports the plan for a single integrating strategy, with a strong co-ordinatinginfluence.
Such a complex strategy must nonetheless be structured into a number of elements, and the question arises asto whether those should be denoted by existing policy areas. An alternative might be to recognise the diVeringneeds within specific target populations, with sub-strategies (implemented by linked programmes or teams)as follows:
A. Promoting mental health in the whole population (but separating Children, Adolescents, Adults ofWorking Age, and Older Adults).
For children, schools programmes, parental support, city planning and dealing with conductdisorders deserve special attention.
The strategy should respond to the increasing age distribution of the population.
3564223024 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
163commission green paper on eu mental health strategy: evidence
B. Preventing mental illness and its eVects in target vulnerable groups, such as:
— Those with a past or family history of mental illness (including alcohol and drug abuse).
— Those with a history of psychological trauma (including abuse at any age, combat andterrorism).
— Those with learning/intellectual disabilities (including specific and pervasive developmentaldisorders).
— Those with long-term physical illnesses and disabilities.
— Migrants.
— Prisoners (pre- and post-conviction).
— Those at risk from discrimination or exploitation.
Each programme would need to work across policy areas and consider a number of facets (which may or maynot coincide with existing policy) including:
— Promotion and Prevention.
— Supporting carers.
— Knowledge and Information.
— Legislation.
— Research.
— Training.
— Social Inclusion.
— Health Economics.
— Ethics and Human Rights.
The fourth stated priority, the development of a mental health information, research and knowledge systemfor the EU is a complex and specialised task. Technological advances have implications for many aspects ofthe organisation and delivery of mental healthcare. They also demand significant financial investment. AEuropean perspective would therefore be extremely valuable.
Each of the specialist programmes would also benefit the Community through joint work with the WHO andCouncil of Europe.
Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between Member States, topromote the integration of mental health into the health and non-health policies and stakeholder action, and to betterliaise research and policy on mental health?
The proposed initiatives set an ambitious and far-reaching agenda. The WHO Network of PromotingHospitals and the European Alliance against Depression seem to provide good examples.
Co-ordination between Member States should take place at all levels and the proposals in Section 7 seem likelyto ensure that.
Integration of mental health into general health and non-health policies would be assisted by a strengthenedcentral Mental Health presence, rather than the domain being represented by a scattering of unconnectedprojects and stakeholder champions. Hopefully this will provide the energy, breadth of understanding andinfluence required. Those involved in the strategy may need to avoid becoming fragmented into interest groupscorresponding to each policy area.
Successful implementation of the strategy will not occur without extensive training and re-training. This willneed to extend through mental health professions to primary and secondary health staV, the wide range ofworkers already mentioned, to carers and the general public.
Greater clarity is perhaps required in the areas of knowledge and information, and with respect to the goal ofimproving the liaison between research and policy. The knowledge and information required for setting andmonitoring strategies, for managing services, and for patient care are of diVerent types but are frequently inter-dependent—or else they may be presented by using diVerent analysis of the same raw data. Information maybe gathered through original research initiated for a set purpose, or as a by-product of routinely collectedinformation. Information is required about mental health problems in general, about services, and about
3564223024 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
164 commission green paper on eu mental health strategy: evidence
individuals. And it is required by the public, policy makers, commissioners, service managers, careprofessionals, carers and service users. In view of these inter-dependencies and the diYculty in obtaining goodquality data, it may be inappropriate to focus too much upon research and policy.
In conclusion, the College will be keen to be active in publicizing and promoting the policies and initiatives ofthe proposed EU Strategy.
Memorandum submitted by Samaritans
A. Introduction: Samaritans
Samaritans is a non-religious, non-partisan organisation representing 202 organisations across the UK andIreland working under a constitution that seeks to support people in distress and despair, including thoseconsidering suicide.
Befrienders Worldwide, for which Samaritans runs the secretariat, extends this mission to a further 200organisations, in 38 countries, across the world.
Samaritans was founded by the Reverend Chad Varah in 1953 and is regarded as the UK/I’s first “helpline”,providing support to people in distress and despair, including those considering suicide. Samaritans is avolunteer led organisation, headed by a small board of trustees and an association made up of the leadvolunteer from each of the 202 autonomous federated branches. Samaritans network of branches developedslowly as a community led initiative wherever suicide was recognised as an issue.
Communities outside the UK/I began to develop similar activities and in 1974 they came together to formBefrienders International, which was also founded by Chad Varah. In 2003 Samaritans took on theco-ordination of the network which now aims to provide an exchange of support, knowledge and experiencewhilst linking externally for mutual learning and influencing. The Befrienders Worldwide multi-languagewebsite is the principal global resource for people in emotional distress, with up to 80,000 “hits” every month.
The other activities of the, newly named, Befrienders Worldwide network include providing advice andresources to members and potential members in setting up services and a long running twinning scheme tofoster visits and exchanges. The twinning project has a record of success showing the benefits of eVectivelistening across language and culture.
In order to maximise impact Samaritans works closely with our sister organisations IFOTES and LifeLineInternational to extend good practice across the globe, including on the media’s portrayal of suicide. As partof this coalition we are in the process of partnership development with the World Health Organisation.
B. General Comments on the Consultation
Samaritans/Befrienders Worldwide welcomes the adoption of the Green Paper and applauds the processwhich has enabled a number of stakeholders, including our organisation, the opportunity to share its viewswith the Commission. We hope that the engagement with a diversity of actor remains a fundamental part ofthe continuing programme including its delivery.
As mental health becomes increasingly synonymous with well being it is seen by Samaritans as a subjectiveconcept and one we feel that services have to recognise as such. This is because caught up in the issue ofwhether a person accesses mental health services, is how they feel about their mental health and whether theyconsider such services relevant or helpful. Samaritans now talks about emotional health, since this is arguablya less threatening and medicalised term. In our emotional health promotion and emotional supportworkstreams we recognise that people express their needs diVerently and as such may wish to use otherlanguage to describe their mental health. In essence, it is vital that services adopt a holistic approach to mentalhealth and begin by listening to how people wish to discuss such issues.
The stigma surrounding mental health and the resulting discrimination experienced by people in distress is amajor determinant of their quality of life. The stigma and discrimination present in mental health services,other services and in the general population must be addressed as a priority.
3564223025 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
165commission green paper on eu mental health strategy: evidence
C. Specific Comments on Questions Raised in the Consultation Paper
Question 1. The relevance of good mental health of the population, and our beneficiaries, for the EU’s strategic policyobjectives
1.1 The statistics for the burden of mental health are increasingly well known, we have figures that show theforecast for those who will have an episode of mental illness (one in four74), the number of days lost in the UKdue to stress in the workplace (2975) and the fact that by 2020 Depression will be the greatest cause of morbidityin the world.76 However there is a need for more information specific to the Europe and this is the first reasonwhy we would commend the adoption of a Europe wide policy for mental health.
By drawing the research of individual states together it will be possible to assess the impact of policies,environment and societal changes and trends into the widest picture of emotional health. A basis for thisresearch can be found in the work of researchers such as Knapp and Patel. By making a case for mental healththat is linked to a strong economic argument we believe that greater eVorts will then be made to address thissituation.
1.2 The people of Europe are amongst the most mobile, thanks to the competitive nature of transport,portability of qualifications and the open borders between member states. As new states join we have seenmajor movements of their populations into the more developed areas seeking employment opportunities. Atthe other end of the scale there has long been a movement of people, often retired, from Western Europetoward the warmer, and sometimes cheaper, southern areas.
The central place of work as a part of European lifestyles means that there is an opportunity to use it as a keypart of health promotion activities but it is a necessity to ensure that a good work-life balance is promoted tothose in employment. Samaritans have recognised the central role of work and developed activities to improveemotional health and well being in the workplace which in turn also address the stigma.
The mobility, which enables Europe to remain economically buoyant and flexible, is a key priority of the EU.However we would support the view that dependent on the origin of the “patient” and the destination ofcountry in which they reside for work, the quality level of mental health accessible to these groups variessignificantly.77 There is also increasing evidence78 that wealth does not lead to an increase in happiness furthersupporting the view that an eVective work-life balance must be found.
Migrant workers are noticeable in the UK in that they often work in sectors requiring low skills and in whichpay levels are barely above the national minimum. For example in rural areas agencies such as CitizensAdvice79 have recognised that significant migrants are working as crop pickers. As migrants are often comingin from new accession countries which are those with higher rates of suicide and combined with a lack of theirnormal support networks this can bring further marginalisation and stress upon individuals. A major Englishfood manufacturer has recently been in contact with Samaritans having identified just such a support need fortheir seasonal Polish workers.
In order to make our service accessible to migrants we oVer a variety of initiatives. Samaritans advertise ourservices (available via telephone, face to face visit, letter, email, textphone and SMS text message) bothnationally and locally, in a variety of languages. Our services can also be delivered in over 50 languages viaSamaritans volunteer language bank.
1.3 However help seeking behaviour is a not a common characteristic of Europeans and cultural issuesmediating against this must be addressed. These traits can establish themselves as a part of a national, self-fulfilling, stereotype that can act against good mental health. Where a country is establishing itself as a touristlocation where vacationers “get away from it all” there can be a reluctance to accept that mental healthremains an issue. An anecdotal report from a Samaritans branch based in a country popular with retiringBritish citizens states that they receive a lot of calls from individuals, many of them widowed, who havingretired there with their partner are now alone and feel adrift in the health care system. Due to Samaritansawareness levels with British people the branch is seen as a dependable, though unoYcial, part of thehealthcare provision. However the branch receive only minimal support from the government there as thecountry wishes to portray itself as a “happy place” in order to protect the tourist industry.74 WHO—Investing in Mental Health 2003.75 HSE—Stress Management Guidelines.76 WHO—Prevention of Mental Disorders 2004.77 The State of Mental Health in the European Union. 2004.78 Happiness. Lessons from a new science. Richard Layard. Penguin Books 2005.79 Supporting migrant workers in rural areas. Citizens Advice. September 2005.
3564223025 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
166 commission green paper on eu mental health strategy: evidence
We would wish to see support for the continued provision of helplines and other support service to those indistress and despair, including those considering taking their own lives. The work of Befrienders Worldwidein conjunction with partners makes up a significant part of this support and recognition for it must be includedin any strategy. We would further welcome initiatives to increase the participation of the voluntary sector, andof service users, in the development and implementation of measures to support those in need.
1.4 If the aim of the strategy is to provide, and increase access to, quality mental health services then investingthe required resources is necessary to provide those choices. This means oVering long-term therapeuticsupport, requiring not only resource commitment but also a commitment to partnership with thosestakeholders, including agencies such as Samaritans, to develop methodologies which complement each otherand add value to the total service oVering. To achieve this level of working Samaritans would like to see anagreed standards framework covering mental health services. As a measure of good practice this would includesome form of assessment that identifies risk.
1.5 In order to overcome language and cultural barriers we would hope to see a simple EU wide mental healthpromotion campaign that would, as appropriate, overarch or fit in with members states’ own initiatives.Where member states do not have suicide prevention or mental health promotion strategies in place theyshould be encouraged to develop these and measures to enthuse and supports members states to supportinitiatives within their own countries should be made available. World Suicide Prevention Day and WorldMental Health Day (respectively the 10 of September and October) should be used as key activities in thiswork.
Question 2. The value added, to our service or our beneficiaries, through an EU strategy and its components
2.1 Through the partnership Samaritans has with IFOTES and LifeLine International (operating asVolunteer Emotional Support Helplines or VESH) we would be able to use the common reference tool of anEU wide strategy to further develop our joint working activities to optimise their impact. We currently sharea common platform at events such as at the 2005 International Association of Suicidology conference inDurban.
Our strong commitment to inter-agency collaboration reflects our recognition of an increasingly mobilesociety, and the need for services to keep pace in terms of being available across borders and with varied meansof access. Everyone is responsible and accountable for ensuring that relevant rights are respected for all groupsat risk, and especially for those facing high stigma mental health issues.
The Samaritans email service demonstrates the cross-border nature of emotional support, with up to a thirdof emails coming from outside the UK/Ireland.
2.2 The development of this partnership also oVers increased potential for the sharing of experiences and bestpractice and a chance to evaluate how successful an EU strategy is across a Pan European partnership. Wewould hope to see that any policy whilst including suicide and mental health also extends its scope to bring inother areas. As a provider of a helpline (amongst other services) we would look to the Commissions’ role indeveloping ICT as a key part of the strategy. We already foresee that further opportunities to extend andimprove our service delivery may become available due to developments in telephony and ICT:
— Voice over Internet Protocols (VOIP) would potentially enable all non face to face contacts includingemail, voice and SMS text messages into Samaritans to be channelled digitally.
— Harmonised European Short Codes (HESC) (such as 112) which connects callers to emergencyservices, such as the police, in whatever country they are in will be examined to see how they maybenefit our beneficiaries.
However there are other areas that we would also hope to see the EU strategy reflected in. As part of its workon the Department of Environment, Food and Rural AVairs’ Rural Stress Action Plan Samaritans has inputinto a checklist to “rural stress proof” policies. Given the role of the CAP in European policy and potentialreforms in the future this would be a system we would advocate for in future policy development and ofparticularly relevance to rural communities.
We would also look towards this strategy being one that proposes the need for early intervention work inschools and workplaces and one that in line with the work of Jenkins, McCulloch, Friedli and Parker80
includes both risk reduction and health promotion activities as equally valuable activities and necessary ifsuccess is to be achieved. Samaritans has, in line with the relevant strategies of the UK and Ireland, developedinterventions in both of these areas and aims to further develop our emotional health promotion work inthe future.80 Developing a Mental Health Policy. Maudsley Monograph 43. 2002.

3564223025 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
167commission green paper on eu mental health strategy: evidence
2.3 An EU strategy should aspire to simplifying and streamlining activities, building on existing agreementsand principles and avoiding duplication. This should take place at all levels ensuring that internationalagreements such as the Helsinki Declaration of 2005 feed down to individual member states and areimplemented. As has been seen in previous research81 the lack of consistency in data collection and indicatorshas made cross comparison diYcult if not impossible and the need for clear and agreed objectives, interventionand indicators are critical if eVective medium and long term evaluation is to take place.
2.4 It has been shown in some studies that there is link a between alcohol use and mental health, specificallysuicidal behaviour. But the evidence linking alcohol abuse to increased impulsivity and then suicide remains,in the view of Samaritans, inconclusive. It should also not be forgotten that these substances are also likely tobe used as a support mechanism by some people. Research into the links remains necessary and we would wishto see this continue. However until this is more conclusive we would wish to see a strategy in which thepromotion of healthy choices is a priority and where any actions to deter people from substance abuse takeplace in a supportive environment.
2.5 It is disappointing that self-harm does not figure in the Green Paper and Samaritans would point to thereport of the UK National Inquiry into Self Harm “Truth Hurts”82 to inform additional recommendations.Though self-harm is related to emotional distress, and interventions not specifically focused on self-harm canimprove emotional well-being, it remains important that interventions are based on an understanding of self-harm and respond to it as a specific issue.
2.6 The strategy fails to engage the need for Media to be engaged with both as a group to influence and achannel to utilise. Samaritans has for many years produced media guidelines on the representation of suicideand these have been the basis of many other guides. We continue to work across the UK and Ireland to developmedia guidelines and monitor media output in order to inform journalists and their audiences of positive, non-stigmatising and alternative messages on the portrayal of mental ill health and suicide. This is supported bywork with government and industry to develop codes of conduct. The EU strategy enables Samaritans todisseminate this work to a wider audience and share our best practice. We would call for Media to beincorporated in the strategy and are happy to share further information on this issue.
We would also seek to see measures in the final strategy that encompasses New Media and particularly ourconcerns over the overtly graphic portrayal of suicide methodologies that are available over the Internet. Weaspire to the promotion of positive choices and would wish to see Samaritans and our sister organisationsprioritised by Internet Service and Search Engine Providers (ISPs). The company AOL has already agreed toprioritise services like our own and we will continue to work with ISPs to enable this wherever possible. Wedo not advocate for the banning of these sites as we strongly believe that this would not prevent them fromexisting and merely drive them underground and increase stigma.
Question 3. Are the initiatives proposed appropriate to support the co-ordination between Member States, to promotethe integration of mental health into the health and non-health policies and stakeholder action, and to better liaiseresearch and policy on mental health aspects?
Samaritans are keen to see the creation of an EU wide network, but would caution that this should not be atthe expense of existing interagency networks and should seek to work with them. In addition to our own workwithin Befrienders Worldwide IFOTES, there is work underway by SME, EPHA, IASP and many others,which will be of significant value to the development of this strategy. Samaritans looks forward to the strategyand engaging further in its successful implementation, we would be willing to meet with representatives of theCommission or other implementing agency at their convenience to discuss any of these issues raised in thisresponse in greater detail and how Samaritan may contribute.
May 2006
Memorandum by SAMH
SAMH is the leading not-for-profit sector organisation in its field in Scotland providing accommodation,support, training, employment and structured day services for people with mental health and related problemsincluding homelessness, addictions and other forms of social exclusion. In addition, we operate aninformation service, oVering general mental health information and specialist legal and benefits advice.SAMH campaigns on a wide range of mental health issues, and works to challenge the stigma anddiscrimination experienced by people who live with mental health problems, influence policy and improve careservices in Scotland.81 “The State of Mental Health in the European Union.82 Truth Hurts: Report of the National Inquiry into Self-harm among Young People. Mental Health Foundation 2006.
3564223026 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
168 commission green paper on eu mental health strategy: evidence
General Comments
SAMH welcomes the opportunity to respond to the European Green Paper on mental health and stronglyendorses the European Commission’s acknowledgement that there is no health without mental health.SAMH’s response to the Green Paper will first of all consider each of the three proposed strands of an EUstrategy on mental health and will then consider the specific questions posed in the paper. Throughout thisdocument we refer to “mental health problems” rather than “mental illness” or “disorder”. We do this becausewe believe that this is a less stigmatising form of words.
Detailed Comments
Strand 1—Creating a dialogue with member states on mental health
The Commission proposes to create a forum between member states which will lead to an action plan formental health, possibly based on the January 2005 WHO Mental Health Action Plan for Europe, along withthe EU Public Health Programme’s “Mental Health Promotion and Mental Disorder Prevention: a Policy forEurope”.
SAMH would welcome such a forum and the opportunity it would provide to create pan-European debateon mental health and to learn from experiences in diVerent member states. In order to set up such a forum itwould be vital to ensure that people who have experience of mental health problems were invited andsupported to participate both in discussions about mental health and in constructing an action plan, with theattendant necessary resources.
SAMH believes that the WHO Mental Health Action Plan for Europe is a largely positive and aspirationaldocument which in general would serve as a suitable model for a European Action Plan. However, SAMHhas some reservations about the WHO plan, as follows:
1. The Plan makes no reference to recovery83 from mental health problems
This is the most significant omission from the WHO plan that SAMH has identified. Recovery as a concepthas received a significant amount of attention in recent years in the mental health field, and for good reason.Mental health services have, in the past, frequently robbed people who use them of their hope and aspirations,focusing on managing symptoms and maintaining people in illness. This has the eVect that too often, once aperson has developed a mental health problem, he or she is no longer seen as someone with the potential tobe a useful and productive member of society, but simply in the passive and recipient role of a “patient”.
A Mental Health Action Plan for Europe must be grounded in the belief that recovery from mental healthproblems is not only possible but is in fact probable for the majority of people. The belief in the ability ofpeople with mental health problems to recover is fundamental and must feed into all other aspects of the plan,including staV training, public education and the challenging of stigma and discrimination.
2. The Plan does not place sufficient importance on involving people who have experience of mental health problems
The WHO plan does emphasise the need to involve people who have experience of mental health problems inchallenging stigma and to recognise their experience and knowledge in planning services. However, SAMHfeels that it does not go far enough in requiring that people with experience of mental health problems shouldbe consulted on and involved with every aspect of mental health, including policy, stigma and training.
3. The Plan does not sufficiently emphasise the need for early intervention
Quite rightly, the Plan suggests actions for mental health promotion and for adequate primary care andcommunity-based care. However, this misses out an important element of mental health service provision: theavailability of straightforward early interventions. SAMH is aware that, all too often, people who are in theearly stages of a crisis or developing mental health problem are turned away from services because they arequite simply not considered to be “ill” enough. This leads to the person’s condition becoming worse, perhapsuntil the point when they require admission to hospital, when all that may have been required was support atan early stage. Mental health services must be provided to meet the whole spectrum of needs and with the clear83 “Recovery is happening when people can live well in the presence or absence of their problems and the many losses that may come in
their wake, such as isolation, poverty, unemployment and discrimination. Recovery does not always mean that people will return tofull health or retrieve all their losses, but it does mean that people can live well in spite of them”. Mental Health Commission ofNew Zealand.
3564223026 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
169commission green paper on eu mental health strategy: evidence
intention of providing support as early as possible. Such support will include talking therapies, user-led crisisservices and therapeutic drop-in centres, but must be based on the requirements of people who use the services.It should also be recognised that in many countries, a significant proportion of mental health services areprovided by the not-for-profit sector. The sector must therefore be a key partner in the development of astrategy on mental health.
Despite these concerns there are several suggested actions in the WHO plan that SAMH strongly welcomes,in particular:
— to make mental health an inseparable part of public health;
— to require that the impact of any new policy on the mental well-being of the population should beassessed before its introduction and evaluated thereafter; and
— to ensure parity of funding in relation to comparable health services.
SAMH also notes that the Plan proposes actions to tackle the stigma and discrimination associated withmental health problems, and would suggest that the anti-stigma programme in Scotland, “see me”, wouldform a good model for use in devising other national and local anti-stigma campaigns. Along with four othermental health organisations, SAMH campaigned for funding for “see me” to be set up and is now one of theorganisations responsible for managing the campaign. The “see me” campaign has won several awards and,more importantly, there are early signs that it is having a positive eVect.84
The Green Paper also suggests that the Forum would consider the need for Council recommendations onsuicide prevention and mental health promotion. SAMH has a particular interest in suicide prevention, giventhat Scotland has one of the highest rates of death by suicide in Western Europe.85 Any recommendations thathelped to maintain a strong focus on suicide reduction would therefore be welcome.
Similarly, a Council recommendation on mental health promotion, particularly one framed in the context ofthe WHO Plan’s emphasis on long-term investment, programmes for children and young people and healthyworkplaces, would be welcome. SAMH would hope that such a recommendation would lead to greaterrecognition of the links between physical and mental health and greater integration between public healthcampaigns focusing on physical and mental health.
Launching an EU Platform on Mental Health
SAMH believes that this is an appropriate aim of an EU strategy on mental health, and would particularlywelcome the opportunity to identify best practice in mental health services and in promoting social inclusionfrom across the EU. Again, SAMH would emphasise the need to involve people who use mental health servicesin all aspects of this area of work. Furthermore, any eVort to identify best practice in social inclusion shouldtake a holistic approach rather than simply focusing on areas relating to mental health. It is important toacknowledge that social exclusion cannot be resolved simply by focusing on a person’s mental health problem:indeed one of the underlying causes of social exclusion of people with mental health problems is the tendencyto focus exclusively on their medical symptoms rather than addressing the underlying cause of theirdiYculties86. Issues that should be explored include equality and diversity, employment opportunities, accessto both physical and mental health care, housing, social networks and skills development.
Developing an Interface Between Policy and Research on Mental Health
SAMH is not yet in a position to support or otherwise the proposed “indicator system” which would includeinformation on mental health and its determinants, impact assessment and evidence based practice. Moreinformation is needed on how this would be developed and who would be involved in this developmentprocess. SAMH anticipates that it would be necessary to involve a wide range of stakeholders including thenot-for-profit sector and people who use services, to avoid an inappropriate focus on medical models of mentalhealth problems.
SAMH supports the overall aim to ensure a better interface between research knowledge and policy-making,but cautions against an over-reliance on research into drug treatments. Equal importance should be placedon research into the eVects of diet, exercise, talking therapies and other forms of therapeutic support on mentalhealth. The strategy should encourage member states to make substantial levels of funding available for non-pharmaceutical treatments for mental health problems. It may be useful to refer to the 2004 SAMHpublication, “All You Need to Know?87” which reports on a Scotland-wide survey of people who use mental84 Well What Do You Think: The Second National Scottish Survey of Public Attitudes to Mental Health, Mental Well-Being and Mental
Health Problems, Scottish Executive, 2004.85 Scotland’s Suicide Rate Compared with 16 Western European Countries 1950–2003, Choose Life.86 Mental Health and Social Exclusion—Social Exclusion Unit Report, OYce of the Deputy Prime Minister, 2004.87 All you need to Know? SAMH, 2004.

3564223026 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
170 commission green paper on eu mental health strategy: evidence
health services on their views about psychiatric drugs. Many service users have reported significant benefitfrom alternative and complementary therapies and many would like greater access to and availability of suchtreatments.
The rest of this response will deal with the specific questions put by the Commission.
How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed in section 1?
The policy objectives outlined in section 1 of the consultation are to put Europe back on the path to long-term prosperity, to sustain Europe’s commitment to solidarity and social justice and to bring tangible practicalbenefits to the quality of life for European citizens.
SAMH believes that the mental health of the population is critical in each of these areas. The consultationidentifies that a high proportion of GDP is lost each year in the EU due to mental health problems, and it isself-evident that this will have a detrimental eVect on the prosperity of the EU. In Scotland, 79 per cent ofpeople with mental health problems are unemployed.88 This has a cost to the economy in terms of the loss ofpotential earnings and the cost of incapacity and other benefits, not to mention the negative eVect onindividuals’ self-esteem and confidence of being unemployed. Improving the population’s mental health, aswell as addressing the stigma attached to mental health problems and supporting people into work, wouldhave a positive eVect on the EU’s economy.
It is also clear that if Europe’s commitment to solidarity and social justice is to be sustained, the inequalitiesexperienced by people with mental health problems must be addressed. These inequalities range from beingunable to find work and facing stigma on a daily basis to being treated in unsuitable wards or institutionswhich are often unpleasant environments which do not provide appropriate therapeutic activities. It shouldalso be remembered that people do not experience inequalities solely in the context of their mental health:people with mental health problems may also experience discrimination because of their sexual orientation,economic status, gender, ethnic origin or religion. The needs of each individual must be considered if the EUis to maintain its commitment to social justice.
Finally, improved mental health must surely contribute positively to the quality of life of European citizens.To demonstrate this, we only have to return to the WHO’s statement that there is no health without mentalhealth. A focus on positive mental health and on early intervention to prevent unnecessary deterioration inmental health will have positive eVects on the economy, on individual well-being and on the quality of life ofthe general population.
Would the development of a comprehensive EU-strategy on mental health add value to the existing and envisagedactions and does section 5 propose adequate priorities?
SAMH supports the development of a comprehensive EU strategy on mental health, in the belief that it willlead to an EU-wide focus on mental health and to improvements in population mental health. SAMH doesbelieve that the priorities identified in section 5 are appropriate but would wish these priorities to beunderpinned by a commitment to consistently involve people with experience of mental health problems inputting these priorities into action.
Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between Member States, topromote the integration of mental health into the health and non-health policies and stakeholder action, and to betterliaise research and policy on mental health aspects?
SAMH believes that these initiatives are appropriate. It will be important in attempting to co-ordinateactivities between member states to consider the very diVerent starting points that each state has in terms ofits population mental health. It may be helpful to agree a set of principles or core values that each memberstate should commit to upholding in developing both its mental health services and its mental healthpromotion activities. SAMH would be pleased to see the EU-wide adoption of the Millan principles whichunderpin the Mental Health (Care and Treatment) (Scotland) Act 2003.
May 2006
Memorandum by Professor Norman Sartorius
I have previously given detailed comments on the Green Paper and addressed one of the EU commissions onthe topic. I shall therefore restrict my comments to the points you raised in your three questions.88 Disability and Employment in Scotland: a Review of the Evidence Base, Scottish Executive, 2005.
3564223027 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
171commission green paper on eu mental health strategy: evidence
1. Is it appropriate to formulate an EU strategy on mental health?
The answer to this question is yes provided that 1) the strategy is followed by the allocation of means for itsimplementation; and 2) provisions are made for a review of the strategy, at regular intervals involving allinterested parties.
2. What elements should be contained in the strategy?
The document deals mainly with the prevention of mental disorders and of the promotion of mental health.It would be important to add a section that will address those issues arising in the treatment and care for peoplewith mental illness that are directly relevant to the prevention of mental disorders and promotion of mentalhealth. It is of course clear that the development of guidelines for the provision of health care is not a mandateof the Commission: nevertheless the omission of their consideration weakens the document and the strategy.A mental disorder such as depression may increase the risks for cardiovascular and other physical illness aswell as for dementia: similar examples abound. It would also be useful to consider adding a part dealing withlearning disability and mental retardation to the document. In this area there are numerous possibilities foraction concerning prevention of the disorder that would not only improve the quality of life of people aVectedby it but also diminish risks for other mental and physical illnesses.
3. Is there a need for a co-coordinated mental health strategy for Europe
Yes. There are numerous issues that could be handled better at national level if an overall consensus aboutprinciples and a strategy for action in this field exists.
4. What would be the relationship between the WHO mental health plan and the EU strategy?
There are significant diVerences between the approaches of the EU and the WHO. The latter covers allcountries of Europe as well as some that are geographically and possibly in other ways distant from the EUcountries—eg the countries in Central Asia, such as Tajikistan. It deals with all aspects of mental health—treatment, prevention, promotion and the management of psychosocial issues. The administrative andgovernance structures are diVerent from those of the EU.
Yet, a coherent strategy adopted by the EU might be very helpful in the development of mental healthprogrammes not only for the European Region of the WHO but also for other regions of the WHO.
I believe therefore that it is possible to make the EU strategy and WHO plans complementary and mutuallysupportive.
Memorandum by Shift and the Social Inclusion Programme
“We endorse the key priorities of MH Promotion, Prevention, Social Inclusion, Protecting rights and dignity,Better information and knowledge within the EU Green Paper on Mental Health Strategy. These prioritiescorrespond to the existing key objectives of the National Social Inclusion Programme (NSIP) which co-ordinates the implementation of the actions arising from the Social Exclusion and Mental Health reportundertaken by the Social Exclusion Unit (SEU, ODPM, 2004; www.socialinclusion.org.uk) and Shift thenational anti-stigma and discrimination programme (launched in 2004; www.shift.org.uk)
It is essential to integrate mental health into both general health and non-health policies to address the socialexclusion, stigma and discrimination, experienced by people with mental health problems. Policies can thenmeet the needs of the whole population rather than excluding those whose needs are not currently met throughexisting non-integrated policies.
The National Social Inclusion Programme (driven by the SEU action points) works across traditionalboundaries with a range of government departments to influence policy developments and raise awareness ofthe non-health needs of people with mental health issues such as housing, employment, education, income andbenefits. NSIP also works with traditional partners within the health field to influence social inclusiveoutcomes and share good practice.
Shift works with the media, schools, private and public organizations to reduce the stigma and discriminationon mental health grounds. It is a communications driven programme using a variety of evidence-basedmethods including: multi-media communication; strategic campaigning; public events; developingpartnerships; information/educational/training; and research. People with mental health problems form a corepart of our structure.
3564223028 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
172 commission green paper on eu mental health strategy: evidence
Addressing mental health within EU strategic policy objectives is relevant as this would ensure that theobjectives were inclusive but also promote mental health and wellbeing and influence the prevention agendawithin non health related policies. For example, employer practice can have a large impact upon the mentalhealth of the staV, with a supportive and flexible environment having positive mental health outcomes.”
Memorandum by Turning Point
Turning Point is the UK’s leading social care organisation and a registered charity. We provide services forpeople with complex needs, including those aVected by drug and alcohol misuse, mental health problems orthose with a learning disability. We run services in over 200 locations in England and Wales.
Our portfolio of over 20 mental health services includes crisis support, assertive community outreachprogrammes, supported housing, residential care and specialist provision for people with personalitydisorders. Our service users are similarly diverse. In 2004–05 we worked directly with 89,736 clients of whom5,856 used mental health services. We also helped 37,479 more people through services such as needleexchanges and telephone helplines.
The majority of Turning Point clients have a combination of needs. For example, we estimate that at least onein five of the people we support with mental health issues also need help with serious substance misuse andour experience mirrors national trends that 50 per cent of people in drug or alcohol services also have a mentalhealth problem.89
(1) How relevant is the mental health of the population for the EU’s strategic policy objectives, as detailed insection 1?
Mental Health is extremely relevant to the strategic objectives outlined in section 1. The Green Paperrecognises that there are strong links between good mental health and long-term prosperity, both for countriesnationally and at an individual level. The mental health of a population is essential to the economic prosperityof the EU: for example, women provide the majority of unpaid childcare. If they are not supported in termsof their mental health, then these childcare costs will have to be met.
Evidence suggests that provided that a person is in appropriate employment, with the right support, workingcan improve a person’s mental health. Benefits include not only more financial independence and stability, butalso social interaction and increased self-esteem.
However, as the Green Paper acknowledges in its references to quality of life, Turning Point strongly believesthat in considering a country’s prosperity, it is essential to go beyond purely economic indicators, to look athow it treats its most vulnerable citizens, many of whom are not in work.
The majority of people who Turning Point works with have overlapping needs, such as mental health andsubstance use problems or mental health and a learning disability, sometimes combined with an oVendinghistory or unstable housing. Such people have valuable contributions to make to society far beyond economicterms. However, these people are being denied the right to contribute to society to their full potential becausemany social care agencies and other services in this country are not designed to support people withcomplex needs.
In England, there has also been a growing impetus for mental health to be seen from a rights based perspective.The Disability Discrimination Act 2005 broadens the definition of disability by removing the requirement thata person’s mental illness be “clinically well-recognised” in order for that person to gain protection fromdiscrimination.
The new Disability Equality Duty requires that from December 2006, public sector bodies are proactive inensuring that disabled people, including those with mental health problems are treated fairly. Therefore, thisvery relevant to the European Union’s strategic objective sustain Europe’s commitment to solidarity andsocial justice.
(2) Would the development of a comprehensive EU-strategy on mental health add value to the existing andenvisaged actions and does section 5 propose adequate priorities?
Developing a comprehensive EU strategy on mental health would have many benefits. It would help toincrease the priority given to mental health issues. As the Green Paper suggests it would constitute aframework for exchange and cooperation between member states. This would be particularly useful for thoseissues with a scope beyond individual countries which are relevant to many Member States such as the mentalhealth of migrants and asylum seekers. Furthermore, a Mental Health strategy could play a valuable role inhelping to: ensure consistency of approach and care across the EU, limit the inequalities in mental healthbetween countries and highlight the important links between mental health and the Human Rights Act.89 Royal College of Psychiatrists Dual Diagnosis Information Manual 2002.
3564223029 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
173commission green paper on eu mental health strategy: evidence
However, Turning Point sees the principle value of an EU strategy on mental health as building on existinginitiatives both across Europe (eg the WHO Ministerial Conference on Mental Health’s Mental Health ActionPlan for Europe, referred to in the Green Paper) and within individual Member States (eg in England, theNational Service Framework for Mental Health) and in sharing best practice. It should not reinvent the wheel.The focus and resources of a strategy should also be on practical applications and measures which make atangible, measurable diVerence to people’s lives.
The EU strategy should also take note of other international work and initiatives such as The InternationalInitiative of Mental Health Leadership (IIMHL)90
With regard to the priorities listed in section 5, Turning Point welcomes an emphasis on “preventive action”(2). We would also like to see specific reference to early intervention once mental health issues have becomeapparent, to prevent problems from escalating. Whilst it is important to “promote the mental health of all” (1)this is potentially such a wide area that some prioritisation will be essential to focus on areas of greatest need.
(3) Are the initiatives proposed in sections 6 and 7 appropriate to support the coordination between MemberStates, to promote the integration of mental health into the health and non-health policies and stakeholder action,and to better liaise research and policy on mental health aspects?
Turning Point believes that the initiatives proposed are appropriate. We particularly welcome the GreenPaper’s recognition that a person’s mental health is profoundly aVected by social care issues such as housing,income and employment which generally are the responsibility of diverse departments within Member States.We are also pleased that the Green Paper adopts a broad understanding of mental health which includes well-being (WHO definition) and that it mentions specifically reduction of substance use disorders (section 6.1.2).
It is important that an EU strategy highlights the value and importance of people who have direct experienceof using mental health services and their carers and families. The Green Paper makes little reference to finance,although it will be essential that the Strategy is adequately resourced at all stages including co-ordination,implementation and review. Otherwise we fear that the Strategy will have little practical impact.
With regard to mental health research and policy, it is key that mental health policy and practice acrossmember states is evidence-based. Robust, empirically sound research which compares and evaluates servicedelivery across the EU would ensure the dissemination of expertise and best practice. There could beconsiderable cost savings if research was better co-ordinated and conducted across Europe, with lessduplication of work in individual countries. This could be supported by an EU mental health research body.
It is important that lessons learnt from research are widely publicised and are made accessible. Researchprogrammes should include user involvement wherever possible in the research process.
We note that there is much to be done to improve data collection within each country and at a pan-Europeanlevel. There are many challenges. It will be useful to develop mechanisms so that data between countries canbe compared, but this must not be at the expense of ‘losing’ important distinct information. For example,currently in England, for the purposes of data collection, a learning disability comes under the category ofmental health even though the nature of these conditions and the needs of the people concerned are quitedistinct.
In Summary
— Turning Point believes that the mental health of the population is extremely relevant to the EU’sstrategic policy objectives.
— There are significant benefits to developing a comprehensive EU strategy on mental health. It shouldbuild on existing work and its focus must be practical. Its particular value would lie in researchingissues that are beyond the scope of individual countries.
— Turning Point supports a strategy which has a broad understanding of mental health and well-beingand which encompasses people of all ages and situations including children and older people.Priorities will naturally need to be established within these wide areas.
— From our experience of working with people who have complex needs, we also welcome the GreenPaper’s recognition that mental health should be seen in the wider context of housing, employment,income and other social care factors.
90 The IIMHL was launched in 2003 by three member organisations—New Zealand’s Ministry of Health, the National Institute forMental Health in England and the Substance Abuse and Mental Health Service Administration in the United States. Canada, Wales,Northern Ireland and possible Eire are likely to be next to join the IIMHL. Its Director is Fran Silvestri.
3564223030 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
174 commission green paper on eu mental health strategy: evidence
Memorandum by UK Mental Health Research Network
Please find below the UK MHRN response to this consultation. To answer your specific questions in turn:
1. How relevant is mental health for the EU’s strategic policy objectives?
UK MHRN considers mental health vital to EU’s strategic policy objectives. Mental health problems are aleading cause of illness and disability, well highlighted by WHO. Recent information from the Department ofWork & Pensions acknowledges the burden of mental health disorders on sick leave and productivity. In theUK for example, 80 million days are lost every year due to mental illness costing employers £1–2 billion eachyear (www.mentalhealth.org.uk//Vcost.htm).
2. Would an EU Mental Health Strategy add value, and does the Green Paper identify the right priorities?
Yes, an EU mental health strategy would add value and does identify the right priorities. There is a need forexchange and co-operation between key stakeholders including the involvement of service users and carersand coherence of actions in diVerent policy sectors and the promotion of a stronger evidence base that cantruly inform policy. UK MHRN would support the promotion of all mental health research of high qualitywhich has implications for prevention, services and treatments.
Now is an opportune moment for an EU mental health strategy able to capitalise on and benefit from currentactivities such as those created by UK MHRN which provides the infrastructure to support large scale,generalisable and clinically relevant high impact research externally funded through sources including the EUFramework Programmes.
3. Are the initiatives that the Paper proposes appropriate and sufficient?
Yes, the initiatives are appropriate and suYcient. UK MHRN would like to emphasise the importance ofService User centred and valued services.
4. How might an EU Mental Health Strategy support the implementation of current Government priorities (includingthe Mental Health National Service Framework)?
To support the implementation of current Government priorities an EU mental health strategy should supportresearch in:
(1) Legislation.
(2) Risk factors.
(3) Cultural issues in Mental Health.
(4) Interventions to support return to work would feed into the wealth of the nation.
Memorandum by West Sussex County Council
1. Introduction
1.1 West Sussex County Council welcomes the opportunity to contribute to the debate on the EuropeanCommission’s plans for a mental health strategy. The publication of the Green Paper in October 2005 providesscope to share current best practice and learning across the EU.
1.2 We recognise the economic and social emphasis in the Green Paper. Mental ill-health should be a realpriority for Member States as an estimated 3–4 per cent GDP is lost to economic productivity, and there areconsiderable service impacts on social and educational support systems, as well as on the work of the criminaljustice agencies. However it is not just about people in employment that an EU Strategy needs to beconcerned—the mental health needs of older people, and of (unpaid) carers, need also to be incorporated.
3564223031 Page Type [O] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
175commission green paper on eu mental health strategy: evidence
2. Is an EU Strategy Needed?
2.1 It is our belief that the development of the EU-wide strategy on mental health is needed but we must ensurethat resources are not diverted away from delivering the public health and well-being agenda in our ownlocal areas.
2.2 There is already much work underway to tackle the causes of lost productivity due to mental distress.Supported employment schemes, some funded by the EU, operate in a number of areas. These supportindividuals with mental distress in seeking and sustaining meaningful daytime activity, and gaining or re-gaining employment wherever possible. Research conducted by independent policy organisations in the UK,and also reported in the UK Government’s annual Labour Force Survey consistently confirms that peoplewith severe mental disorders are among the groups in society who have the highest rates of unemployment.The UK Government therefore has a number of existing policy objectives in this area.
2.3 Some local authorities, such as ourselves, are developing innovative approaches, focusing not so much onsupporting individuals with mental distress but rather on encouraging more progressive attitudes andapproaches by employers. For example, training companies to manage and understand better the challengesof employing people who experience mental distress will lead to companies that are better able to understandand support their workforces.
2.4 One way the UK Government can help is by changing the current disability benefit rules that have theperverse incentive of discouraging people who could work from seeking a job. A change in the rules couldunlock huge potential to fill jobs across a range of skills, get people contributing to the health and the wealthof the nation instead of being a drain on it, and also improve their own health so that they would be less likelyto require Government benefits in future. For example, work has been successfully undertaken by one of ourneighbouring county councils (Kent), to change the regulations aVecting those people making the transitionfrom being in receipt of welfare benefits to gaining a meaningful wage through paid employment.
3. What Should an EU Mental Health Strategy Contain?
3.1 Any strategy that focuses on health and wellbeing of the population needs to understand thecharacteristics of the populations of Member States. The Green Paper also highlights wide variations in thesuicide rates across the Member States. Even with a 10-year National Service Framework for Mental Healthin place (and its core emphasis on significantly reducing death by suicide), suicide rates per 100,000 populationin England are still twice the rate of Greece. It is a somewhat surprising to note that suicide kills more peoplein the EU annually than road accidents. Yet which subject is more fixed in the minds of the general public—the driving habits of fellow Europeans or the health and social care systems in place across the EU?
3.2 The proposed strategy could set out a number of preventive measures and approaches that could beadopted by Member States. One such example is how we have been working imaginatively with the UKGovernment’s Carers Grant. Some of that annual grant has been specifically earmarked to meet the assessedneeds of carers of adults with mental distress. The purpose of this specific scheme is to enable carers, knownto the local integrated health and social care mental health NHS Trust, to take a break—whether a familyholiday in Europe, paying for a pamper day at a health resort, or a city break in the UK, or paying for a rangeof complementary therapies. The scheme sustains the ability of carers to maintain good mental health whilstproviding an unpaid caring role for their loved ones.
3.3 The UK Government, through the work of its Social Exclusion Unit, has been focused on improving thequality of life of those suVering from mental distress. Programmes of work that emphasise the building ofmentally healthy local communities are essential. Local Area Agreements—with potentially challenging“stretch” targets—are essential if significant progress is to be made. Among the many target areas for qualityof life improvement set out in Local Area Agreements are subjects such as reducing domestic violence andteenage pregnancies; improving workforce skills and opportunities; and cutting death and serious injuryaccidents on our roads. It is possible that this is an approach that could be promoted across the EU.
3.4 The EU should consider developing an EU-wide mental health information, research and knowledgesystem. Information and knowledge about mental distress, as well as the evidence for change, is held by avariety of institutions and in various countries. With use of the Internet, it should be possible to create portalsfrom which access to these resources can be obtained.
3.5 The EU could consider establishing an EU-wide platform on mental health issues, to not only includepoliticians, but also those people with a personal experience of mental distress as well as specialists in this fieldand other stakeholders and institutions such as the World Health Organisation.
3564223031 Page Type [E] 03-04-07 21:33:35 Pag Table: LOENEW PPSysB Unit: PAG2
176 commission green paper on eu mental health strategy: evidence
3.6 Our children and young people should also be able to enjoy good physical and emotional health andchoose to live healthy lifestyles. Agencies are committed to working towards eradicating health inequalitiesand improving children and young people’s health by shifting the focus from the treatment of establishedhealth problems towards prevention. There is a need to continue to work in partnership to promote healthylifestyle choices, such as the provision of education, advice and guidance for parents and young people onphysical activity and balanced diet and nutrition to reduce the incidence of obesity. (Obesity can lead to mentaldistress and to experiences of exclusion). The EU can help by encouraging Member States to identify andtarget support on those people who need more help than others.
Printed in the United Kingdom by The Stationery OYce Limited4/2007 356422 19585