Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 in non-small cell...
8
ORIGINAL ARTICLE Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 in non-small cell lung cancer patients: Prognostic value and impact on survival Gehan H. Abo El-Magd a, * , Omnia Abd El-Fattah b , Eman M. Saied c a Department of Chest, Faculty of Medicine, Tanta University, Egypt b Department of Clinical Oncology, Faculty of Medicine, Tanta University, Egypt c Department of Pathology, Faculty of Medicine, Tanta University, Egypt Received 14 October 2013; accepted 7 November 2013 Available online 11 December 2013 KEYWORDS Immuohistochemistry; COX-2; NF-jB; Non-small cell lung cancer Abstract Introduction: Nuclear factor kappa B/p65 (NF-jB/p65) regulates the expression of various molecules important in tumorigenesis as cyclooxygenase-2 (COX-2). Aim: To study the immunohistochemical expression of NF-jB/p65 and COX-2 in NSCLC, investigate the relationship between their expression and the clinicopathological parameters, evalu- ate their prognostic value and clarify their impact on survival. Patients and methods: Fifty NSCLC patients were enrolled in this study and subjected to: full med- ical history and physical examination, routine laboratory tests and CT chest. Fiberoptic bronchos- copy was done and biopsies were taken from visible masses and 20 mucosal biopsies of the same patients (as control); sent for histopathological and immunohistochemical examination using anti- COX2 and anti-NF-jB/p65 antibodies. The median follow up of patients was 13 (range 4–22 months). Results: Thirty six (72%) showed positive NF-jB/p65 expression, it was higher in squamous cell carcinoma and adenocarcinoma than in normal biopsies. Adenocarcinoma showed higher NF-jB/ p65 positivity compared to squamous and large cell carcinomas. A significant relationship was found between NF-jB/p65 expression and overall survival. Forty five (90%) showed positive COX-2 expression, no expression was detected in normal biopsies. COX-2 expression was significantly higher in adenocarcinoma compared to squamous and large cell carcinomas. NF-jB/p65 and COX-2 expression was significantly correlated with advanced tumor * Corresponding author. E-mail address: [email protected] (G.H. Abo El-Magd). Peer review under responsibility of The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier Egyptian Journal of Chest Diseases and Tuberculosis (2014) 63, 193–200 The Egyptian Society of Chest Diseases and Tuberculosis Egyptian Journal of Chest Diseases and Tuberculosis www.elsevier.com/locate/ejcdt www.sciencedirect.com 0422-7638 ª 2013 The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier B.V. http://dx.doi.org/10.1016/j.ejcdt.2013.11.007 Open access under CC BY-NC-ND license.
Transcript of Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 in non-small cell...
Egyptian Journal of Chest Diseases and Tuberculosis (2014) 63, 193–200
The Egyptian Society of Chest Diseases and Tuberculosis
Egyptian Journal of Chest Diseases and Tuberculosis
www.elsevier.com/locate/ejcdtwww.sciencedirect.com
ORIGINAL ARTICLE
Immunohistochemical expression of nuclear factor
kappa-B/p65 and cyclooxygenase-2 in non-small cell
lung cancer patients: Prognostic value and impact
on survival
Gehan H. Abo El-Magd a,*, Omnia Abd El-Fattah b, Eman M. Saied c
a Department of Chest, Faculty of Medicine, Tanta University, Egyptb Department of Clinical Oncology, Faculty of Medicine, Tanta University, Egyptc Department of Pathology, Faculty of Medicine, Tanta University, Egypt
Received 14 October 2013; accepted 7 November 2013
Available online 11 December 2013
*
E-
Pe
D
04Op
KEYWORDS
Immuohistochemistry;
COX-2;
NF-jB;Non-small cell lung cancer
Corresponding author.mail address: gehan19@yaho
er review under responsibil
iseases and Tuberculosis.
Production an
22-7638 ª 2013 The Egyptiaen access under CC BY-NC-ND l
o.com (G
ity of Th
d hostin
n Society
httpicense.
Abstract Introduction: Nuclear factor kappa B/p65 (NF-jB/p65) regulates the expression of
various molecules important in tumorigenesis as cyclooxygenase-2 (COX-2).
Aim: To study the immunohistochemical expression of NF-jB/p65 and COX-2 in NSCLC,
investigate the relationship between their expression and the clinicopathological parameters, evalu-
ate their prognostic value and clarify their impact on survival.
Patients and methods: FiftyNSCLCpatients were enrolled in this study and subjected to: full med-
ical history and physical examination, routine laboratory tests and CT chest. Fiberoptic bronchos-
copy was done and biopsies were taken from visible masses and 20 mucosal biopsies of the same
patients (as control); sent for histopathological and immunohistochemical examination using anti-
COX2 and anti-NF-jB/p65 antibodies. Themedian followupof patientswas 13 (range 4–22 months).
Results: Thirty six (72%) showed positive NF-jB/p65 expression, it was higher in squamous cell
carcinoma and adenocarcinoma than in normal biopsies. Adenocarcinoma showed higher NF-jB/p65 positivity compared to squamous and large cell carcinomas. A significant relationship was found
between NF-jB/p65 expression and overall survival.
Forty five (90%) showedpositiveCOX-2 expression, no expressionwas detected in normal biopsies.
COX-2 expression was significantly higher in adenocarcinoma compared to squamous and large cell
carcinomas. NF-jB/p65 and COX-2 expression was significantly correlated with advanced tumor
.H. Abo El-Magd).
e Egyptian Society of Chest
g by Elsevier
of Chest Diseases and Tuberculosis. Production and hosting by Elsevier B.V.
://dx.doi.org/10.1016/j.ejcdt.2013.11.007

194 G.H. Abo El-Magd et al.
stage, lymph node metastasis and grade. A significant positive relationship was found between NF-
jB/p65 and COX-2 expression.
Conclusion: NF-jB/P65 and COX-2 expression has a prognostic value in NSCLC, they are suit-
able targets for development of new lung cancer therapies; inhibition of NF-jB and COX-2 will aug-
ment the efficacy of anticancer therapy.
ª 2013 The Egyptian Society of Chest Diseases and Tuberculosis. Production and hosting by Elsevier
B.V. Open access under CC BY-NC-ND license.
Introduction
Lung cancer is the leading cause of death worldwide. The non-small cell lung cancer (NSCLC) accounts for 75–85% among
all lung cancers. The conventional treatment e.g. surgery,radiotherapy and chemotherapy yields a dismal overall 5-yearsurvival of 14% which necessitates the development of new
treatment options [1].An interesting implication for the presence of high levels of
nuclear factor kappa-B (NF-jB)/p65 expression in epithelial
tumors such as lung cancer is the finding reported from severalin vivo and in vitro studies that NF-jB inhibits chemotherapy-induced apoptosis of tumor cells by regulating either directlyor indirectly the transcription of several genes whose protein
products have an antiapoptotic effect [2]. In particular, p65activation is a predictive factor of resistance to neoadjuvantchemotherapy in breast cancer patients [3].
The most common form of NF-jB is a heterodimer consist-ing of p65 and p50. In most quiescent normal cells; the NF-jBdimers are bound with and kept in the cytoplasm by inhibitor
of NF-jB that mask the nuclear localization sequence (NLS)in the NF-jB proteins [4].
NF-jB regulates the expression of various molecules
important in tumorigenesis, such as matrix metalloproteinases,cyclooxygenase-2 (COX-2), iNOS, chemokines, and inflamma-tory cytokines, all of which promote tumor cell invasion andangiogenesis [5].
With advances in cytogenetic and molecular biology, thedetection and analysis of tumor suppressor genes and onco-genes may provide predictive values for prognosis and treat-
ment choice for NSCLC. Among these molecular markers,COX-2 over expression is common in NSCLC [6].
Cyclooxygenase-2 is an inducible enzyme that can be acti-
vated by cytokines, growth factors, oncogenes and chemicalcarcinogens. COX-2 is related to inflammation and carcino-genesis. It has been shown that COX-2 contributes to carcino-
genesis by increasing the angiogenesis and invasiveness, andinhibiting apoptosis. The carcinogenic effect of COX-2 ismainly exerted through the increase of prostaglandin levelse.g. PGE2 [7].
COX-2 inhibitor has been investigated in both pre-clinicaland clinical studies, and has shown synergistic effects withradiation and chemtoxic drugs on tumor [1].
Aim of the work
To study the immunohistochemical expression of NF-jB/p65protein and COX-2 in NSCLC patients, investigate the rela-tionship between their expression and the clinicopathologicalparameters, evaluate their prognostic value and clarify theirimpact on survival in such patients.
Patients and methods
Patients
This study was carried out on 50 cases of NSCLC and 20 nor-mal bronchial mucosal biopsies taken from the same patients
(as control) at Chest and Clinical Oncology Departments,Tanta university hospital and the patients were treated and fol-lowed up during the period from December 2010 to April
2013. Written, informed consent was obtained from each pa-tient before enrollment into the study.
All patients were subjected to the following:
(1) Complete medical history and physical examinationincluding a full neurologic examination, documentationof the Eastern Cooperation Oncology Group (ECOG)
performance and weight loss.(2) Routine laboratory tests: complete blood picture, liver,
kidney functions and biochemical testing
(3) Plain chest X ray postero-anterior view.(4) Spirometry.(5) CT chest with contrast (peripheral tumors were diag-
nosed by CT guided biopsy and sent for histopatholo-gical examination).
(6) Fiberoptic bronchoscopy for inspection of the tracheo-bronchial tree for vocal cord paralysis, subcarinal wid-
ening for staging, and biopsy taking.
The fiberoptic bronchoscopy (Model: Olympus BF type
P10, Tokyo, Japan) was done for diagnosis of central tumorsas follows:
� After fasting overnight, premedications were taken in theform of 0.6 mg atropine sulfate intramuscular 30 min beforethe procedure.
� Xylocaine spray 10% was used for local anesthesia forupper airways.� It was done via nasal route; Xylocaine solution 2% wasused to anesthetize vocal cords, trachea and lower airways.
� Visible tumor was biopsied, also multiple endobronchialbiopsies were taken from the other side of the bronchial tree(as control); any biopsy with proved dysplastic changes was
discarded. The biopsies were obtained by forceps underdirect vision, carefully removed and placed in 10% forma-line fixative.
(7) Histopathological study: using hematoxylin and eosinstaining for routine evaluation of the histopathologicalcharacteristics and grading of the studied tumors.
(8) Immunohistochemical study: 3 lm sections were depa-raffinized in xylene for 30 min and rehydrated withgraded alcohol series. Sections were then subjected to

Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 195
antigen retrieval by boiling the tissue sections in 10 mM
citrate buffer, pH 6.0 (Lab Vision catalog # AP-9003),for 10 min followed by cooling at room temperaturefor 20 min and rinsing with phosphate buffered saline
(PBS) for one minute. Endogenous peroxidase wasblocked by immersion of the sections in 3% hydrogenperoxide solution for 10 min, then washing them inPBS. Immunohistochemical staining was performed
using the UltraVision Detection Kit (TP-015-HD, LabVision, USA) according to the manufacturer’s protocol.Sections were incubated for 10 min with Ultra V block
to prevent non-specific background staining, followedby rinsing the sections with PBS. Afterward, an over-night incubation was done in a humidity chamber with
rabbit monoclonal anti-COX-2 antibody (Clone SP21,Cat. No. RM-9121-R7, Ready to use, Lab Vision),and rabbit polyclonal anti-NFkB/p65 (Rel A) Ab-1 anti-body (Cat. No. RB-1638-R7, Ready to use, Lab Vision),
followed by washing in PBS.
Sections were then covered with 4–5 drops of UltraVision
biotinylated goat anti-polyvalent secondary antibody, incu-bated at room temperature for 10 min, then washed in PBS, fol-lowed by incubation with streptavidin peroxidase solution for
10 min at room temperature, then rinsing with PBS. Sectionswere then covered for 15 min by adding one drop of 3-30-diami-no-benzidine-tetra-hydrochloride (DAB) chromogen mixed
with 2 ml of DAB substrate. Finally, sections were counter-stained with Mayer’s hematoxylin, dehydrated in alcohol andmounted in di-n-butyl-phthalate-polystyrene-xylene (DPX).As positive controls, sections from a case of colonic carcinoma
known to show over-expression of COX-2 antibody, and sec-tions from a case of prostatic carcinoma known to showover-expression of NF-jB/p65 antibody were used. Negative
controls were prepared by omission of the primary antibodies.
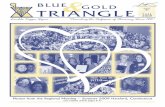
Figure 1 NF-jB/p65 staining of a case of bronchogenic adeno-
carcinoma, showing nuclear expression in >10% of tumor cells
(Immunoperoxidase ·400).
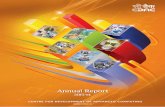
Figure 2 NF-jB/p65 staining of a case of bronchogenic squa-
mous cell carcinoma, showing nuclear expression in >10% of
tumor cells (Immunoperoxidase ·400).
Immunohistochemical evaluation and scoring
COX-2 expression was evaluated semiquantitatively accordingto the gross percentage of cells demonstrating a distinct cyto-plasmic immunohistochemical reaction.[8] The immunostained
samples were scored to display absent (0), weak (+), moderate(++), or strong (+++) immunoreactivity [9].
Positivity of the tumor for NF-jB expression was defined asonly distinct nuclear immunostaining, which is considered as
activated NF-jB [10].Nuclear localization ofNF-jBwas categorized as positive or
negative, aswell as an overall proportion of cells (<1%, 1–10%,
and>10%) with positive nuclear staining in the studied field at100 magnification. A minimum of five different areas for eachspecimen was evaluated, and the mean was assessed [11].
(9) Patients underwent computed tomographic scans of theabdomen, magnetic resonance imaging of the brain andradionuclide bone scans were performed when clinically
indicated. Each patient had a performance status of 2 orlower on the ECOG scale and adequate hematologicparameters were included in this study.
The clinical and pathological staging was determinedaccording to the international staging system [12] and accord-
ingly standard treatment protocols and follow up schedulesbased on published guidelines were selected [13].
Statistical analysis
The data were analyzed using SPSS 13.0 software package.The correlation of NF-jB and COX-2 expression with differ-
ent clinicopathologic characteristics was analyzed with chi-square test. The Kaplan–Meier method and Log-rank testwere used to analyze the correlation of patient survival with
NF-jB and COX-2 expression. Overall-survival was definedas the time from diagnosis to the date of death from any causeor last follow-up. A significance level of P < 0.05 was used.
Results
In the fifty patients who were enrolled in this study; only three
out of 20 patients with early stage disease (stages I, II, IIIA)underwent lobectomy while the remaining were medicallyinoperable or refused surgery. Nine patients were assigned toreceive thoracic radiotherapy alone. Seventeen patients re-
ceived concurrent carboplatin/paclitaxel and thoracic radio-therapy. While the majority of patients ([21]; stage IV)received chemotherapy alone in the form of platinum-based
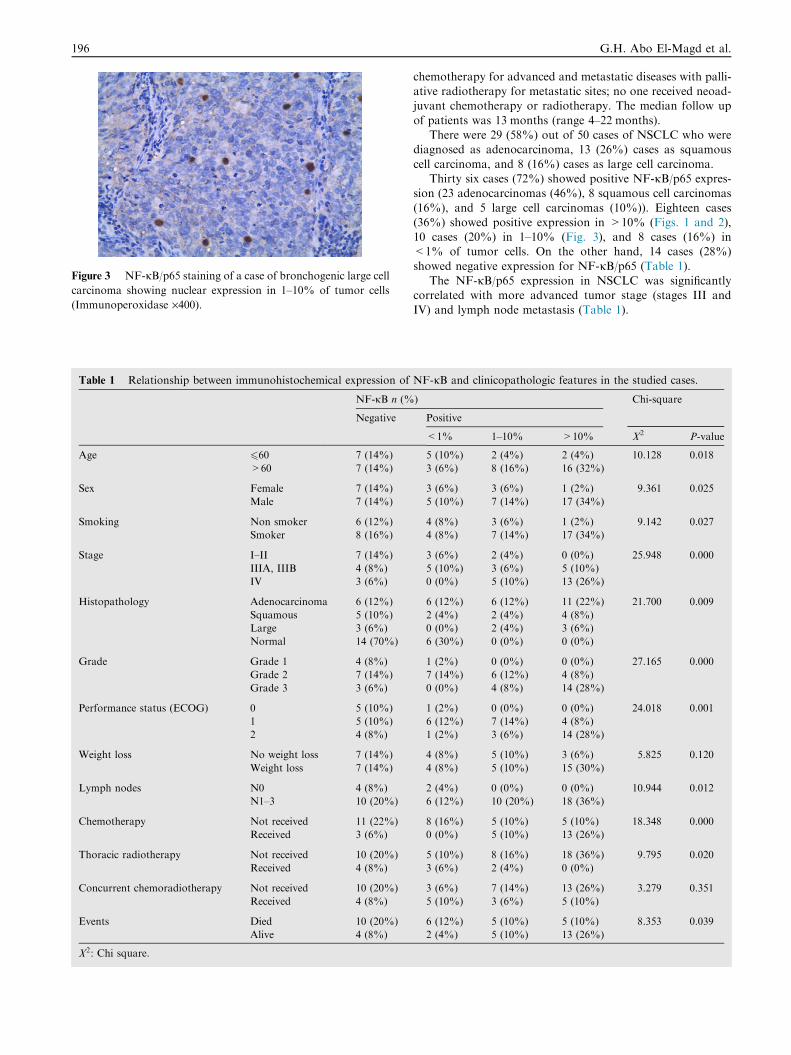
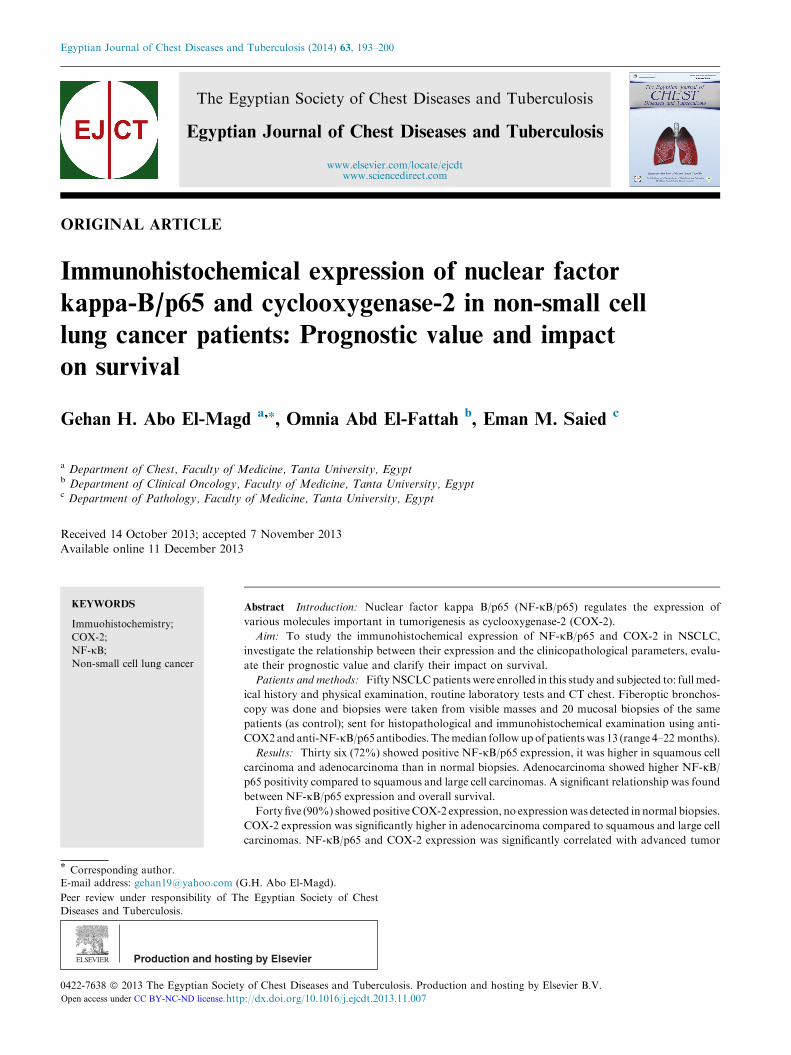
Figure 3 NF-jB/p65 staining of a case of bronchogenic large cellcarcinoma showing nuclear expression in 1–10% of tumor cells
(Immunoperoxidase ·400).
Table 1 Relationship between immunohistochemical expression of
NF-jB n (%
Negative
Age 660 7 (14%)
>60 7 (14%)
Sex Female 7 (14%)
Male 7 (14%)
Smoking Non smoker 6 (12%)
Smoker 8 (16%)
Stage I–II 7 (14%)
IIIA, IIIB 4 (8%)
IV 3 (6%)
Histopathology Adenocarcinoma 6 (12%)
Squamous 5 (10%)
Large 3 (6%)
Normal 14 (70%)
Grade Grade 1 4 (8%)
Grade 2 7 (14%)
Grade 3 3 (6%)
Performance status (ECOG) 0 5 (10%)
1 5 (10%)
2 4 (8%)
Weight loss No weight loss 7 (14%)
Weight loss 7 (14%)
Lymph nodes N0 4 (8%)
N1–3 10 (20%)
Chemotherapy Not received 11 (22%)
Received 3 (6%)
Thoracic radiotherapy Not received 10 (20%)
Received 4 (8%)
Concurrent chemoradiotherapy Not received 10 (20%)
Received 4 (8%)
Events Died 10 (20%)
Alive 4 (8%)
X2: Chi square.
196 G.H. Abo El-Magd et al.
chemotherapy for advanced and metastatic diseases with palli-ative radiotherapy for metastatic sites; no one received neoad-juvant chemotherapy or radiotherapy. The median follow up
of patients was 13 months (range 4–22 months).There were 29 (58%) out of 50 cases of NSCLC who were
diagnosed as adenocarcinoma, 13 (26%) cases as squamous
cell carcinoma, and 8 (16%) cases as large cell carcinoma.Thirty six cases (72%) showed positive NF-jB/p65 expres-
sion (23 adenocarcinomas (46%), 8 squamous cell carcinomas
(16%), and 5 large cell carcinomas (10%)). Eighteen cases(36%) showed positive expression in >10% (Figs. 1 and 2),10 cases (20%) in 1–10% (Fig. 3), and 8 cases (16%) in<1% of tumor cells. On the other hand, 14 cases (28%)
showed negative expression for NF-jB/p65 (Table 1).The NF-jB/p65 expression in NSCLC was significantly
correlated with more advanced tumor stage (stages III and
IV) and lymph node metastasis (Table 1).
NF-jB and clinicopathologic features in the studied cases.
) Chi-square
Positive
<1% 1–10% >10% X2 P-value
5 (10%) 2 (4%) 2 (4%) 10.128 0.018
3 (6%) 8 (16%) 16 (32%)
3 (6%) 3 (6%) 1 (2%) 9.361 0.025
5 (10%) 7 (14%) 17 (34%)
4 (8%) 3 (6%) 1 (2%) 9.142 0.027
4 (8%) 7 (14%) 17 (34%)
3 (6%) 2 (4%) 0 (0%) 25.948 0.000
5 (10%) 3 (6%) 5 (10%)
0 (0%) 5 (10%) 13 (26%)
6 (12%) 6 (12%) 11 (22%) 21.700 0.009
2 (4%) 2 (4%) 4 (8%)
0 (0%) 2 (4%) 3 (6%)
6 (30%) 0 (0%) 0 (0%)
1 (2%) 0 (0%) 0 (0%) 27.165 0.000
7 (14%) 6 (12%) 4 (8%)
0 (0%) 4 (8%) 14 (28%)
1 (2%) 0 (0%) 0 (0%) 24.018 0.001
6 (12%) 7 (14%) 4 (8%)
1 (2%) 3 (6%) 14 (28%)
4 (8%) 5 (10%) 3 (6%) 5.825 0.120
4 (8%) 5 (10%) 15 (30%)
2 (4%) 0 (0%) 0 (0%) 10.944 0.012
6 (12%) 10 (20%) 18 (36%)
8 (16%) 5 (10%) 5 (10%) 18.348 0.000
0 (0%) 5 (10%) 13 (26%)
5 (10%) 8 (16%) 18 (36%) 9.795 0.020
3 (6%) 2 (4%) 0 (0%)
3 (6%) 7 (14%) 13 (26%) 3.279 0.351
5 (10%) 3 (6%) 5 (10%)
6 (12%) 5 (10%) 5 (10%) 8.353 0.039
2 (4%) 5 (10%) 13 (26%)
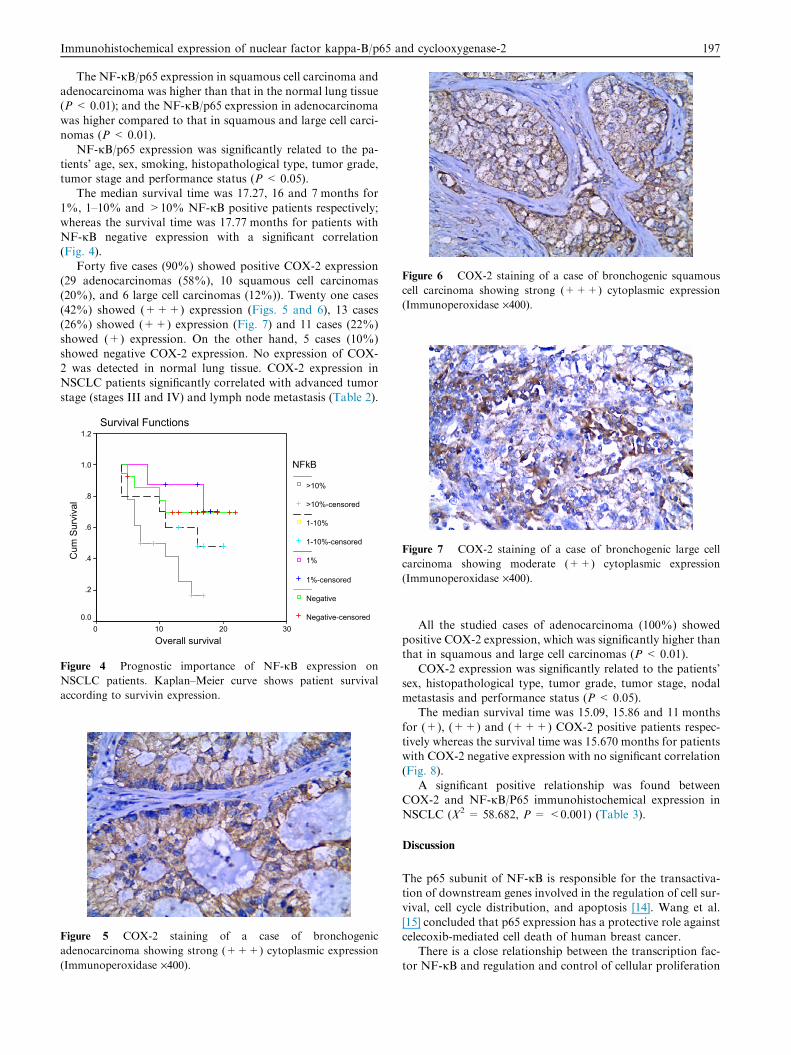
Figure 6 COX-2 staining of a case of bronchogenic squamous
cell carcinoma showing strong (+++) cytoplasmic expression
(Immunoperoxidase ·400).
Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 197
The NF-jB/p65 expression in squamous cell carcinoma andadenocarcinoma was higher than that in the normal lung tissue(P < 0.01); and the NF-jB/p65 expression in adenocarcinoma
was higher compared to that in squamous and large cell carci-nomas (P < 0.01).
NF-jB/p65 expression was significantly related to the pa-
tients’ age, sex, smoking, histopathological type, tumor grade,tumor stage and performance status (P < 0.05).
The median survival time was 17.27, 16 and 7 months for
1%, 1–10% and >10% NF-jB positive patients respectively;whereas the survival time was 17.77 months for patients withNF-jB negative expression with a significant correlation(Fig. 4).
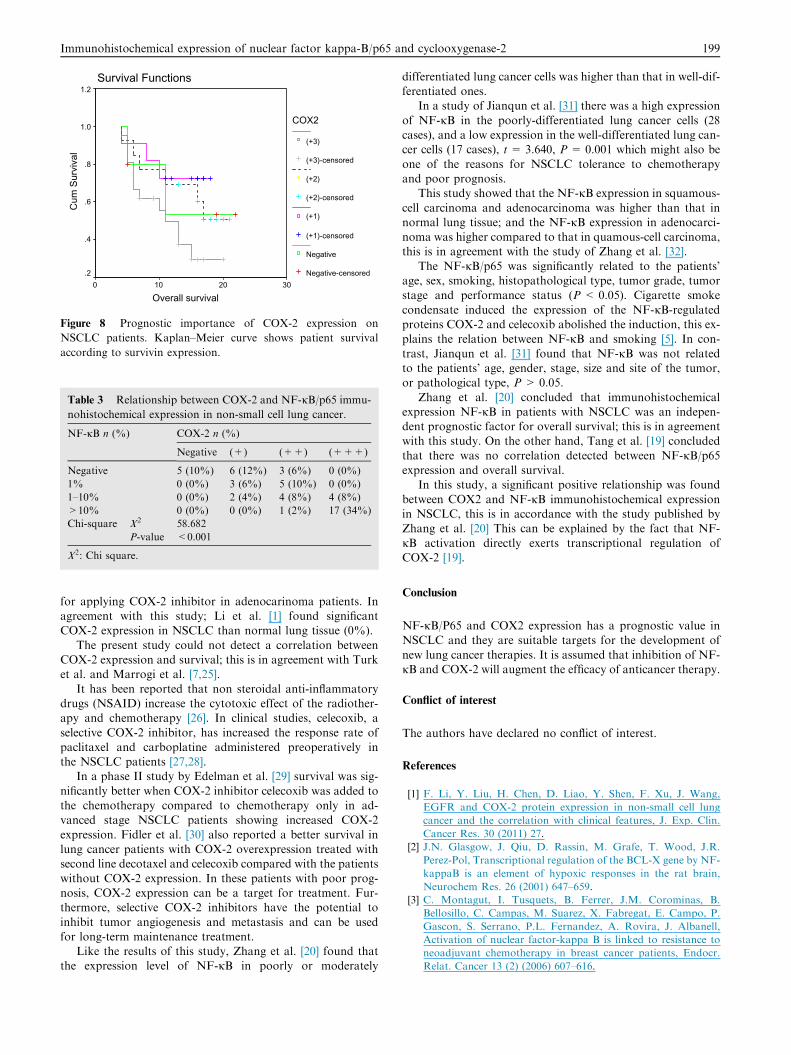
Forty five cases (90%) showed positive COX-2 expression(29 adenocarcinomas (58%), 10 squamous cell carcinomas(20%), and 6 large cell carcinomas (12%)). Twenty one cases
(42%) showed (+++) expression (Figs. 5 and 6), 13 cases(26%) showed (++) expression (Fig. 7) and 11 cases (22%)showed (+) expression. On the other hand, 5 cases (10%)
showed negative COX-2 expression. No expression of COX-2 was detected in normal lung tissue. COX-2 expression inNSCLC patients significantly correlated with advanced tumor
stage (stages III and IV) and lymph node metastasis (Table 2).
Survival Functions
Overall survival3020100
Cum
Sur
viva
l
1.2
1.0
.8
.6
.4
.2
0.0
NFkB
>10%
>10%-censored
1-10%
1-10%-censored
1%
1%-censored
Negative
Negative-censored
Figure 4 Prognostic importance of NF-jB expression on
NSCLC patients. Kaplan–Meier curve shows patient survival
according to survivin expression.
Figure 5 COX-2 staining of a case of bronchogenic
adenocarcinoma showing strong (+++) cytoplasmic expression
(Immunoperoxidase ·400).
Figure 7 COX-2 staining of a case of bronchogenic large cell
carcinoma showing moderate (++) cytoplasmic expression
(Immunoperoxidase ·400).
All the studied cases of adenocarcinoma (100%) showedpositive COX-2 expression, which was significantly higher thanthat in squamous and large cell carcinomas (P < 0.01).
COX-2 expression was significantly related to the patients’sex, histopathological type, tumor grade, tumor stage, nodalmetastasis and performance status (P < 0.05).
The median survival time was 15.09, 15.86 and 11 months
for (+), (++) and (+++) COX-2 positive patients respec-tively whereas the survival time was 15.670 months for patientswith COX-2 negative expression with no significant correlation
(Fig. 8).A significant positive relationship was found between
COX-2 and NF-jB/P65 immunohistochemical expression in
NSCLC (X2 = 58.682, P = <0.001) (Table 3).
Discussion
The p65 subunit of NF-jB is responsible for the transactiva-tion of downstream genes involved in the regulation of cell sur-vival, cell cycle distribution, and apoptosis [14]. Wang et al.
[15] concluded that p65 expression has a protective role againstcelecoxib-mediated cell death of human breast cancer.
There is a close relationship between the transcription fac-tor NF-jB and regulation and control of cellular proliferation
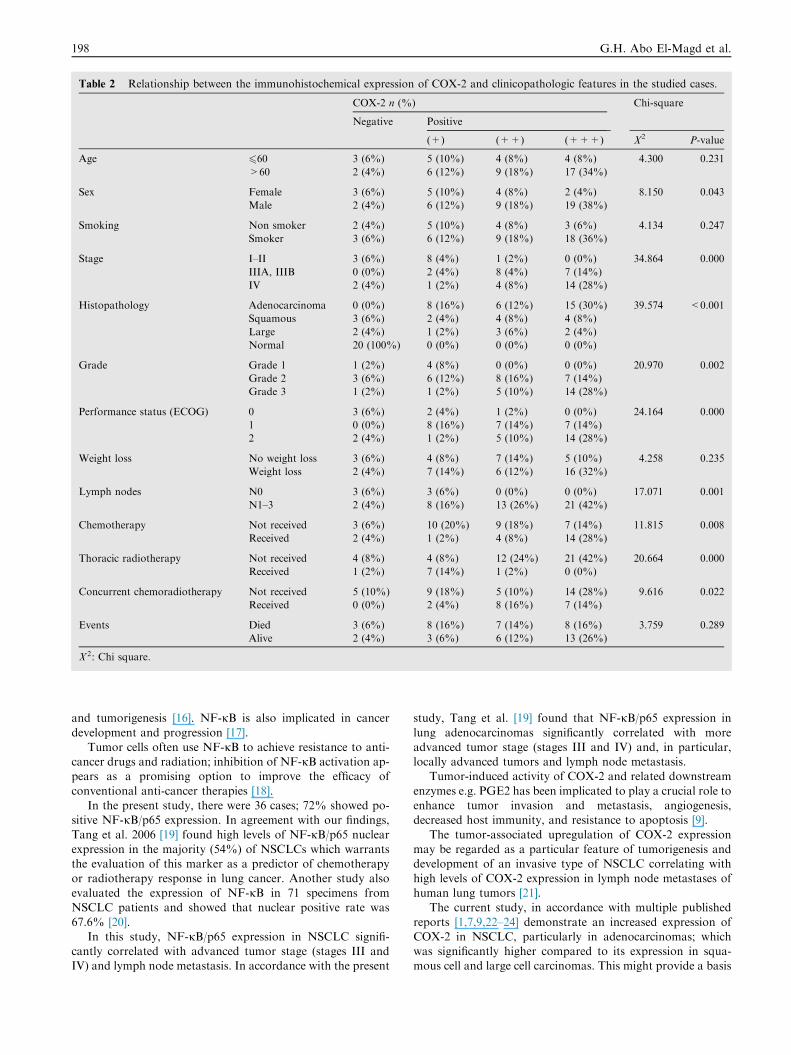
Table 2 Relationship between the immunohistochemical expression of COX-2 and clinicopathologic features in the studied cases.
COX-2 n (%) Chi-square
Negative Positive
(+) (++) (+++) X2 P-value
Age 660 3 (6%) 5 (10%) 4 (8%) 4 (8%) 4.300 0.231
>60 2 (4%) 6 (12%) 9 (18%) 17 (34%)
Sex Female 3 (6%) 5 (10%) 4 (8%) 2 (4%) 8.150 0.043
Male 2 (4%) 6 (12%) 9 (18%) 19 (38%)
Smoking Non smoker 2 (4%) 5 (10%) 4 (8%) 3 (6%) 4.134 0.247
Smoker 3 (6%) 6 (12%) 9 (18%) 18 (36%)
Stage I–II 3 (6%) 8 (4%) 1 (2%) 0 (0%) 34.864 0.000
IIIA, IIIB 0 (0%) 2 (4%) 8 (4%) 7 (14%)
IV 2 (4%) 1 (2%) 4 (8%) 14 (28%)
Histopathology Adenocarcinoma 0 (0%) 8 (16%) 6 (12%) 15 (30%) 39.574 <0.001
Squamous 3 (6%) 2 (4%) 4 (8%) 4 (8%)
Large 2 (4%) 1 (2%) 3 (6%) 2 (4%)
Normal 20 (100%) 0 (0%) 0 (0%) 0 (0%)
Grade Grade 1 1 (2%) 4 (8%) 0 (0%) 0 (0%) 20.970 0.002
Grade 2 3 (6%) 6 (12%) 8 (16%) 7 (14%)
Grade 3 1 (2%) 1 (2%) 5 (10%) 14 (28%)
Performance status (ECOG) 0 3 (6%) 2 (4%) 1 (2%) 0 (0%) 24.164 0.000
1 0 (0%) 8 (16%) 7 (14%) 7 (14%)
2 2 (4%) 1 (2%) 5 (10%) 14 (28%)
Weight loss No weight loss 3 (6%) 4 (8%) 7 (14%) 5 (10%) 4.258 0.235
Weight loss 2 (4%) 7 (14%) 6 (12%) 16 (32%)
Lymph nodes N0 3 (6%) 3 (6%) 0 (0%) 0 (0%) 17.071 0.001
N1–3 2 (4%) 8 (16%) 13 (26%) 21 (42%)
Chemotherapy Not received 3 (6%) 10 (20%) 9 (18%) 7 (14%) 11.815 0.008
Received 2 (4%) 1 (2%) 4 (8%) 14 (28%)
Thoracic radiotherapy Not received 4 (8%) 4 (8%) 12 (24%) 21 (42%) 20.664 0.000
Received 1 (2%) 7 (14%) 1 (2%) 0 (0%)
Concurrent chemoradiotherapy Not received 5 (10%) 9 (18%) 5 (10%) 14 (28%) 9.616 0.022
Received 0 (0%) 2 (4%) 8 (16%) 7 (14%)
Events Died 3 (6%) 8 (16%) 7 (14%) 8 (16%) 3.759 0.289
Alive 2 (4%) 3 (6%) 6 (12%) 13 (26%)
X2: Chi square.
198 G.H. Abo El-Magd et al.
and tumorigenesis [16]. NF-jB is also implicated in cancer
development and progression [17].Tumor cells often use NF-jB to achieve resistance to anti-
cancer drugs and radiation; inhibition of NF-jB activation ap-pears as a promising option to improve the efficacy of
conventional anti-cancer therapies [18].In the present study, there were 36 cases; 72% showed po-
sitive NF-jB/p65 expression. In agreement with our findings,
Tang et al. 2006 [19] found high levels of NF-jB/p65 nuclearexpression in the majority (54%) of NSCLCs which warrantsthe evaluation of this marker as a predictor of chemotherapy
or radiotherapy response in lung cancer. Another study alsoevaluated the expression of NF-jB in 71 specimens fromNSCLC patients and showed that nuclear positive rate was
67.6% [20].In this study, NF-jB/p65 expression in NSCLC signifi-
cantly correlated with advanced tumor stage (stages III andIV) and lymph node metastasis. In accordance with the present
study, Tang et al. [19] found that NF-jB/p65 expression in
lung adenocarcinomas significantly correlated with moreadvanced tumor stage (stages III and IV) and, in particular,locally advanced tumors and lymph node metastasis.
Tumor-induced activity of COX-2 and related downstream
enzymes e.g. PGE2 has been implicated to play a crucial role toenhance tumor invasion and metastasis, angiogenesis,decreased host immunity, and resistance to apoptosis [9].
The tumor-associated upregulation of COX-2 expressionmay be regarded as a particular feature of tumorigenesis anddevelopment of an invasive type of NSCLC correlating with
high levels of COX-2 expression in lymph node metastases ofhuman lung tumors [21].
The current study, in accordance with multiple published
reports [1,7,9,22–24] demonstrate an increased expression ofCOX-2 in NSCLC, particularly in adenocarcinomas; whichwas significantly higher compared to its expression in squa-mous cell and large cell carcinomas. This might provide a basis
Survival Functions
Overall survival3020100
Cum
Sur
viva
l
1.2
1.0
.8
.6
.4
.2
COX2
(+3)
(+3)-censored
(+2)
(+2)-censored
(+1)
(+1)-censored
Negative
Negative-censored
Figure 8 Prognostic importance of COX-2 expression on
NSCLC patients. Kaplan–Meier curve shows patient survival
according to survivin expression.
Table 3 Relationship between COX-2 and NF-jB/p65 immu-
nohistochemical expression in non-small cell lung cancer.
NF-jB n (%) COX-2 n (%)
Negative (+) (++) (+++)
Negative 5 (10%) 6 (12%) 3 (6%) 0 (0%)
1% 0 (0%) 3 (6%) 5 (10%) 0 (0%)
1–10% 0 (0%) 2 (4%) 4 (8%) 4 (8%)
>10% 0 (0%) 0 (0%) 1 (2%) 17 (34%)
Chi-square X2 58.682
P-value <0.001
X2: Chi square.
Immunohistochemical expression of nuclear factor kappa-B/p65 and cyclooxygenase-2 199
for applying COX-2 inhibitor in adenocarinoma patients. Inagreement with this study; Li et al. [1] found significantCOX-2 expression in NSCLC than normal lung tissue (0%).
The present study could not detect a correlation betweenCOX-2 expression and survival; this is in agreement with Turket al. and Marrogi et al. [7,25].
It has been reported that non steroidal anti-inflammatorydrugs (NSAID) increase the cytotoxic effect of the radiother-apy and chemotherapy [26]. In clinical studies, celecoxib, a
selective COX-2 inhibitor, has increased the response rate ofpaclitaxel and carboplatine administered preoperatively inthe NSCLC patients [27,28].
In a phase II study by Edelman et al. [29] survival was sig-
nificantly better when COX-2 inhibitor celecoxib was added tothe chemotherapy compared to chemotherapy only in ad-vanced stage NSCLC patients showing increased COX-2
expression. Fidler et al. [30] also reported a better survival inlung cancer patients with COX-2 overexpression treated withsecond line decotaxel and celecoxib compared with the patients
without COX-2 expression. In these patients with poor prog-nosis, COX-2 expression can be a target for treatment. Fur-thermore, selective COX-2 inhibitors have the potential to
inhibit tumor angiogenesis and metastasis and can be usedfor long-term maintenance treatment.
Like the results of this study, Zhang et al. [20] found thatthe expression level of NF-jB in poorly or moderately
differentiated lung cancer cells was higher than that in well-dif-ferentiated ones.
In a study of Jianqun et al. [31] there was a high expression
of NF-jB in the poorly-differentiated lung cancer cells (28cases), and a low expression in the well-differentiated lung can-cer cells (17 cases), t= 3.640, P = 0.001 which might also be
one of the reasons for NSCLC tolerance to chemotherapyand poor prognosis.
This study showed that the NF-jB expression in squamous-
cell carcinoma and adenocarcinoma was higher than that innormal lung tissue; and the NF-jB expression in adenocarci-noma was higher compared to that in quamous-cell carcinoma,this is in agreement with the study of Zhang et al. [32].
The NF-jB/p65 was significantly related to the patients’age, sex, smoking, histopathological type, tumor grade, tumorstage and performance status (P < 0.05). Cigarette smoke
condensate induced the expression of the NF-jB-regulatedproteins COX-2 and celecoxib abolished the induction, this ex-plains the relation between NF-jB and smoking [5]. In con-
trast, Jianqun et al. [31] found that NF-jB was not relatedto the patients’ age, gender, stage, size and site of the tumor,or pathological type, P > 0.05.
Zhang et al. [20] concluded that immunohistochemicalexpression NF-jB in patients with NSCLC was an indepen-dent prognostic factor for overall survival; this is in agreementwith this study. On the other hand, Tang et al. [19] concluded
that there was no correlation detected between NF-jB/p65expression and overall survival.
In this study, a significant positive relationship was found
between COX2 and NF-jB immunohistochemical expressionin NSCLC, this is in accordance with the study published byZhang et al. [20] This can be explained by the fact that NF-
jB activation directly exerts transcriptional regulation ofCOX-2 [19].
Conclusion
NF-jB/P65 and COX2 expression has a prognostic value inNSCLC and they are suitable targets for the development of
new lung cancer therapies. It is assumed that inhibition of NF-jB and COX-2 will augment the efficacy of anticancer therapy.
Conflict of interest
The authors have declared no conflict of interest.
References
[1] F. Li, Y. Liu, H. Chen, D. Liao, Y. Shen, F. Xu, J. Wang,
EGFR and COX-2 protein expression in non-small cell lung
cancer and the correlation with clinical features, J. Exp. Clin.
Cancer Res. 30 (2011) 27.
[2] J.N. Glasgow, J. Qiu, D. Rassin, M. Grafe, T. Wood, J.R.
Perez-Pol, Transcriptional regulation of the BCL-X gene by NF-
kappaB is an element of hypoxic responses in the rat brain,
Neurochem Res. 26 (2001) 647–659.
[3] C. Montagut, I. Tusquets, B. Ferrer, J.M. Corominas, B.
Bellosillo, C. Campas, M. Suarez, X. Fabregat, E. Campo, P.
Gascon, S. Serrano, P.L. Fernandez, A. Rovira, J. Albanell,
Activation of nuclear factor-kappa B is linked to resistance to
neoadjuvant chemotherapy in breast cancer patients, Endocr.
Relat. Cancer 13 (2) (2006) 607–616.
200 G.H. Abo El-Magd et al.
[4] W. Chen, Z. Li, L. Bai, Y. Lin, NF-kappaB, a mediator for lung
carcinogenesis and a target for lung cancer prevention and
therapy, Front Biosci. 16 (2011) 1172–1185.
[5] S. Shishodia, B.B. Aggarwal, Cyclooxygenase (COX)-2 inhibitor
celecoxib abrogates activation of cigarette smoke-induced
nuclear factor (NF)-jB by suppressing activation of I-jB akinase in human non-small cell lung carcinoma correlation with
suppression of cyclin D1, COX-2, and matrix metalloproteinase-
9, Cancer Res. 64 (2004) 5004.
[6] M. Sahin, E. Sahin, S. Gumuslu, Cyclooxygenase-2 in cancer
and angiogenesis, Angiology 60 (2) (2009) 242–253.
[7] H.M. Turk, C. Camci, A. Sevinc, S. Bukyukberber, I. Sari, M.
Adli, Cyclooxygenase-2 expression is not a marker of poor
survival in lung cancer, Asian Pac. J. Cancer Prev. 13 (1) (2012)
315–318.
[8] S. Hastu, B. Kemp, S.K. Kalapurakal, J.M. Kurie, W.K. Hong,
J.S. Lee, Expression of cyclooxygenase-1 and cyclooxygenase-2
in bronchial epithelium and non small cell lung carcinoma,
Cancer 94 (4) (2002) 1023–1031.
[9] L. Ermert, C. Dierkes, M. Ermert, Immunohistochemical
expression of COX-2 isoenzymes and downstream enzymes in
human lung, Clin. Cancer Res. 9 (2003) 1604–1610.
[10] M. Scartozzi, I. Bearzi, C. Pierantoni, A. Mandolesi, F.
Loupakis, A. Zaniboni, V. Catalano, A. Quadri, F. Zorzi, R.
Berardi, T. Biscotti, R. Labianca, A. Falcone, S. Cascinu,
Nuclear factor-kB tumor expression predicts response and
survival in irinotecan-refractory metastatic colorectal cancer
treated with cetuximab–irinotecan therapy, J. Clin. Oncol. 25
(25) (2007).
[11] H.A. Ismail, L. Lessard, A.M. Mes-Masson, F. Saad,
Expression of NF-jB in prostate cancer lymph node
metastases, Prostate 58 (2004) 308–313.
[12] American Joint Committee on Cancer, Lung, in: AJCC Cancer
Staging Manual, seventh ed., Springer, New York, 2010, pp.
253–270.
[13] National Comprehensive Cancer Network, Clinical Practices
Guidelines in, Oncology V.1, 2012, www.nccn.org.
[14] J.M. O’Shea, N.D. Perkins, Regulation of the RelA (p65)
transactivation domain, Biochem. Soc. Trans. 36 (4) (2008) 603–
608.
[15] L. Wang, F. Kang, J. Li, J. Zhang, B. Shan, Overexpression of
p65 attenuates celecoxib-induced cell death in MDA-MB-231
human breast cancer cell line, Cancer Cell Int. 13 (2013) 14.
[16] R.Z. Orlowski, A.S. Baldwin Jr., NF-j B as a therapeutic target
in cancer, Trends Mol. Med. 8 (2002) 385–389.
[17] A. Gastonguay, T. Berg, A.D. Hauser, N. Schuld, E. Lorimer,
C.L. Williams, The role of Rac1 in the regulation of NF-jBactivity, cell proliferation, and cell migration in non-small cell
lung carcinoma, Cancer Biol. Ther. 13 (8) (2012) 647–656.
[18] V. Baud, M. Karin, Is NF-kappaB a good target for cancer
therapy? Hopes and pitfalls, Nat. Rev. Drug Discov. 8 (1) (2009)
33–40.
[19] X. Tang, D. Liu, S. Shishodia, N. Ozburn, C. Behrens, J.J. Lee,
W.K. Hong, B. Aggarwal, I. Wistuba, Overall, lung cancers
demonstrated high levels of activated nuclear NF-jB p65
expression, Cancer 107 (11) (2006) 2637–2645.
[20] Z. Zhang, J. Ma, N. Li, C. Wang, Expression of nuclear factor-
jB and its clinical significance in nonsmall-cell lung cancer, Ann.
Thorac. Surg. 82 (1) (2006) 243–248.
[21] T. Hida, Y. Yatabe, H. Achiwa, H. Muramatsu, K. Kozaki, S.
Nakamura, M. Ogawa, T. Mitsudomi, T. Sugiura, T.
Takahashi, Increased expression of cyclooxygenase 2 occurs
frequently in human lung cancers, specifically adenocarcinomas,
Cancer Res. 58 (1998) 3761–3764.
[22] Y. Hosomi, T. Yokose, Y. Hirose, R. Nakajima, K. Nagai, Y.
Nishiwaki, A. Ochiai, Increased cyclooxygenase 2 (COX-2)
expression occurs frequently in precursor lesions of human
adenocarcinoma of the lung, Lung Cancer 30 (2000) 73–81.
[23] J.L. Masferrer, K.M. Leahy, A.T. Koki, B.S. Zweifel, S.L.
Settle, M. Woerner, D.A. Edwards, A.G. Flickinger, R.J.
Moore, K. Seibert, Antiangiogenic and antitumor activities of
cyclooxygenase-2 inhibitors, Cancer Res. 60 (2000) 1306–1311.
[24] F.L. Khuri, H. Wu, J.L. Lee, B.L. Kemp, R. Lotan, S.M.
Lippman, L. Feng, W.K. Hong, X.C. Xu, Cyclooxygenase-2
overexpression is a marker of poor prognosis in stage I non-
small cell lung cancer, Clin. Cancer Res. 7 (2001) 861–867.
[25] A.J. Marrogi, W.D. Travis, J.A. Welsh, et al, Nitric oxide
synthase, cyclooxigenase 2, and vascular endothelial growth
factor in the angiogenesis of non-small cell lung carcinoma, Clin.
Cancer Res. 6 (2000) 4739–4744.
[26] O.C. Trifan, W.F. Durham, V.S. Salazar, et al,
Cyclooxygenase-2 inhibition with celecoxib enhances
antitumor efficacy and reduces diarrhea side effect of CPT- 11,
Cancer Res. 62 (2002) 5778–5784.
[27] N.K. Altorki, R.S. Keresztes, J.L. Port, et al, Celecoxib, a
selective cyclo-oxygenase-2 infibitor, enhances the response to
preoperative paclitaxel and carboplatin in early-stage non small
cell lung cancer, J. Clin. Oncol. 21 (2003) 2645–2650.
[28] C. Mascaux, B. Martin, M. Paesmans, et al, Has Cox-2 a
prognostic role in non-small-cell lung cancer? A systematic
review of the literature with meta-analysis of the survival results,
Br. J. Cancer 9 (2006) 139–145.
[29] M.J. Edelman, D. Watson, X. Wang, et al, Eicosanoid
modulation in advanced lung cancer: cyclooxygenase-2
expression is a positive predictive factor for
celecoxib + chemotherapy–Cancer and Leukemia Group B
Trial 30203, J. Clin. Oncol. 26 (2008) 848–855.
[30] M.J. Fidler, A. Argiris, J.D. Patel, et al, The potential predictive
value of cyclooxygenase-2 expression and increased risk of
gastrointestinal hemorrhage in advanced non-small cell lung
cancer patients treated with erlotinid and celecoxib, Clin. Cancer
Res. 14 (2008) 2088–2094.
[31] M.A. Jianqun, Z. Zhenfa, X. Shidong, Relationship between the
expression of NF-kappa B and apoptosis in non-small cell lung
cancer, Chin. J. Clin. Oncol. 5 (3) (2008) 187–190.
[32] J. Zhang, Y.J. Xu, Z.X. Zhang, D.L. DU, L.F. Qiao, W. Ni,
S.X. Chen, Nuclear factor-kappaB activity and its correlation
with cell proliferation in non-small cell lung cancer tissues,
Zhonghua Jie He He Hu Xi Za Zhi 30 (10) (2007) 771–775.