
I By Dr PUSHYA A GAUTAMA Dissertation submitted to Rajiv ...
233
I A CLINICAL STUDY TO EVALUATE THE SHWASAHARA KARMA OF PARNAYAVANI (COLEUS AROMATICUS BENTH.) ARKA NEBULIZATION IN THE MANAGEMENT OF TAMAKA SHWASA WITH SPECIFIC REFERENCE TO ACUTE EXACERBATION OF BRONCHIAL ASTHMA By Dr PUSHYA A GAUTAMA Dissertation submitted to Rajiv Gandhi University Of Health Sciences, Karnataka, Bengaluru In partial fulfillment of the requirement for the award of the degree of Ayurveda Vachaspati (Doctor of Medicine) In Dravya Guna Under the Guidance of Dr HARINI A M D (Ayu.) Associate Professor DEPARTMENT OF DRAVYA GUNA SRI DHARMASTHALA MANJUNATHESHWARA COLLEGE OF AYURVEDA AND HOSPITAL HASSAN, KARNATAKA -573201 2018
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of I By Dr PUSHYA A GAUTAMA Dissertation submitted to Rajiv ...

I
A CLINICAL STUDY TO EVALUATE THE SHWASAHARA KARMA OF PARNAYAVANI
(COLEUS AROMATICUS BENTH.) ARKA NEBULIZATION IN THE MANAGEMENT OF
TAMAKA SHWASA WITH SPECIFIC REFERENCE TO ACUTE EXACERBATION OF
BRONCHIAL ASTHMA
By
Dr PUSHYA A GAUTAMA
Dissertation submitted to
Rajiv Gandhi University Of Health Sciences,
Karnataka, Bengaluru
In partial fulfillment of the requirement for the award of the degree of
Ayurveda Vachaspati (Doctor of Medicine)
In Dravya Guna
Under the Guidance of
Dr HARINI A M D (Ayu.)
Associate Professor
DEPARTMENT OF DRAVYA GUNA SRI DHARMASTHALA MANJUNATHESHWARA
COLLEGE OF AYURVEDA AND HOSPITAL
HASSAN, KARNATAKA -573201
2018

II
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
KARNATAKA, BENGALURU
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “A Clinical Study To Evaluate The Shwasahara
Karma Of Parnayavani (Coleus aromaticus Benth.) Arka Nebulization In The Management Of
Tamaka Shwasa with specific reference to acute exacerbation of Bronchial Asthma” is a
bonafide and genuine research work carried out by me under the guidance of Dr Harini A.,
Associate Professor Department of Dravya Guna, Shri Dharmasthala Manjunatheshwara
College of Ayurveda and Hospital, Hassan – 573201.
Date: 3.3.2018 Signature of the candidate
Place: Hassan Dr. Pushya A. Gautama

III
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
KARNATAKA, BENGALURU
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “A Clinical Study To Evaluate The Shwasahara
Karma Of Parnayavani (Coleus aromaticus Benth.) Arka Nebulization In The Management
Of Tamaka Shwasa with specific reference to acute exacerbation of Bronchial Asthma” is a
bonafide research work done by Dr. Pushya A. Gautama in partial fulfillment for the degree of
Ayurveda Vachaspati in Dravya Guna.
Date : 3.3.2018 SIGNATURE OF GUIDE Place: Hassan Dr. Harini A. M D (Ayu.),
Associate Professor Dept.of Dravya Guna
Shri Dharmasthala Manjunatheshwara College of Ayurveda, Hassan - 573 201

Scanned by CamScanner

V
COPYRIGHT
DECLARATION BY THE CANDIDATE
I Dr. Pushya A. Gautama of Shri Dharmasthala Manjunatheshwara college of Ayurveda and
Hospital, Hassan hereby declare that Rajiv Gandhi University of Health Sciences, Bengaluru,
Karnataka. Shall have the perpetual rights to preserve, use, and disseminate this dissertation /
thesis in print or electronic format for academic / research purpose.
Signature by the Candidate Date: 3.3.2018 Place: Hassan Dr. Pushya A. Gautama
© Rajiv Gandhi University of Health Sciences, Karnataka

VI
ACKNOWLEDGEMENT
This thesis is the culmination of two years effort in my journey towards
obtaining a Masters degree in Ayurveda. I am extremely grateful to everyone
without whom this could not have been possible.
First of all, I bow my head to Lord Ganapathi, Lord Dhanvantari and
Lord Manjunatha for their blessings.
I am grateful to Padmavibhushana Dr. D Veerendra Heggade,
Dharmadhikari Shri Kshetra Dharmasthala and President SDM Education Society,
for his legendary vision that led to the establishment of such a centre for Ayurveda
in the country.
I am deeply grateful to my beloved Principal, Dr. Prasanna N. Rao,
Principal SDMCAH, Hassan for his support, guidance, and his extraordinary
leadership.
Above all, I am extremely grateful to my guide, Dr. Harini A, Asso.
Professor, Dept of Dravyaguna, SDMCAH, for her wisdom, support and guidance in
everthing – academically and in life. Without her, this thesis would not have been
possible. It is with utmost reverence that I thank mam for making me the person I
am today, and showing me the way ahead on countless occasions.

VII
I am extremely grateful to the dynamic and amazing HOD of my
Department, Dr. Prakash L Hegde for embodying the perfection he expects from
students. Thank you sir for being a living example of excellence with humility.
I offer my sincerest thanks to the esteemed teachers of my department – Dr.
Pradeep, Dr. Anuradha K N, and Dr. Tejaswi Kiran who have taught me
everything I know, and whose guidance will always shine like a beacon.
I am sincerely grateful to Dr. Girish K J and Dr. Suhas Kumar Shetty for
their constant support and valuable suggestions.
I am grateful to my loving friends and colleagues Dr. Puneshwar Keshari,
Dr. Kopila Adhikari, Dr. Ahana Nambiar, Dr. Anju C, Dr. Supriya Araganji, –
Dr. Udayshankar, Dr. Chithira V Babu, and Dr. Shyamasundaran K. I thank all
other colleagues, seniors and juniors who were involved in the study.
Any endeavor in my life would be incomplete without the mention of my the
foundation stones of my life – my parents and brother. I am extremely grateful to
them for their constant and unwavering love.
Lastly, I would like to specially thank my patients for believing in me, and
cooperating. Without them, this study could not have taken place.
DATE:
PLACE: Hassan Dr. PUSHYA A GAUTAMA

VIII
ABBREVIATIONS
A.H. Ashtanga Hridaya
A.S. Ashtanga Sangraha
A.T. After Treatment
C.S. Charaka Samhita
S.S. Sushruta Samhita
M.N. Madhava Nidana
Y.R. Yoga Ratnakara
B.P. Bhavaprakasha
G.N. Gada Nigraha
PEFR Peak expiratory flow rate
IPD In-‐patient department
OPD Out-‐patient department
WHO World Health Organization
API Ayurvedic Pharmacoepia of India
BT Before Treatment
AT After Treatment

IX
LIST OF TABLES
Sl. No. TABLES PAGES
1. Synonyms Of Parnayavani 7
2. Vernacular Names Of Parnayavani 7
3. The Known Volatile Constituents Of Parnayavani 15
4. The Known Non-Volatile Constituents Of Parnayavani 19
5. Rasa Panchaka and Karma Of Parnayavani 21
6. Pharmacological Activity Of Different Parts Of C. Aromaticus 27
7. Nidana Classification Based On Dosha Prakopa 35
8. Vyadhi Avastha Sambandi Nidana In Tamaka Shwasa 36
9. Agantu Nidana In Tamaka Shwasa 37
10. Poorvarupa Of Tamaka Shwasa 38
11. Rupa Of Tamaka Shwasa 39
12. Samprapti Ghatakas In Tamaka Shwasa 45
13. Upashaya And Anupashaya In Tamaka Shwasa 47
14. Group Allocation In Clinical Study 78
15. Subjective Assessment Parameters (Gina) Of Acute Asthma 79
16. Gina Grading Of Subjective Parameters In Acute Asthma 79
17. Trial drug authentification, processing and manufacture 81
18. Results Of Physicochemical Analysis 88
19. Result Of Preliminary Phytochemical Tests 88
20. Summarized Results Of Preliminary Phytochemical Tests 90

X
21. Results Of Parnayavani Arka Evaluation 91
22. Ms Of Compounds Identified From Arka Of Coleus Aromaticus 92
23. Gender Distribution Of 60 Patients Of Tamaka Shwasa 93
24. Age Distribution Of 60 Patients Of Tamaka Shwasa 94
25. Marital Status Distribution Of 60 Patients Of Tamaka Shwasa 95
26. Place Wise Distribution Of 60 Patients Of Tamaka Shwasa 96
27. Religion Wise Distribution Of 60 Patients Of Tamaka Shwasa: 97
28. Socio-Economic Status Wise Distribution Of 60 Patients Of Tamaka
Shwasa
98
29. Education Wise Distribution Of 60 Patients Of Tamaka Shwasa 99
30. Presenting Complaints Of 60 Patients Of Tamaka Shwasa 100
31. Duration Of Onset In 60 Patients Of Tamaka Shwasa 101
32. Mode Of Onset In 60 Patients Of Tamaka Shwasa 102
33. Trigger Factors In 60 Patients Of Tamaka Shwasa 103
34. History Of Previous Illness In 60 Patients Of Tamaka Shwasa 104
35. History Of Previous Treatment In 60 Patients Of Tamaka Shwasa 105
36. Family History In 60 Patients Of Tamaka Shwasa 106
37. Occupation Of 60 Patients Of Tamaka Shwasa 107
38. Agni Of 60 Patients Of Tamaka Shwasa 108
39. Ahara Of 60 Patients Of Tamaka Shwasa 109
40. Nidra Of 60 Patients Of Tamaka Shwasa 110
41. Rasa Preference Of 60 Patients Of Tamaka Shwasa 111
42. Alcohol And Smoking Consumption In Patients Of Tamaka Shwasa 112

XI
43. Tea And Coffee Consumption In 60 Patients Of Tamaka Shwasa
113
44. Wheezing In 60 Patients Of Tamaka Shwasa 114
45. Nature Of Wheezing Sounds In 43 Patients Of Tamaka Shwasa 115
46. Timing Of Wheezing Sounds In 43 Patients Of Tamaka Shwasa 116
47. Rhonchi In 60 Patients Of Tamaka Shwasa 117
48. Crepitations In 60 Patients Of Tamaka Shwasa 118
49. Timing Of Crepitation In 21 Patients Of Tamaka Shwasa 119
50. Friedman’s Test To Assess Breathlessness Within Parnayavani Arka
Nebulization Group
120
51. WSR Post Hoc Test With Bonferroni’s Correction To Assess
Breathlessness Within Trial Group
121
52. Friedman’s Test To Assess Wheezing Within Parnayavani Arka
Nebulization Group
121
53. WSR Post Hoc Test With Bonferroni’s Correction To Assess
Wheezing Within Trial Group
122
54. Friedman’s Test To Assess Speech Difficulty Within Parnayavani
Arka Nebulization Group
123
55. WSR Post Hoc Test With Bonferroni’s Correction To Assess
Speech Difficulty Within Trial Group
123
56. Friedman’s Test To Assess Cough Within Parnayavani Arka
Nebulization Group
124
57. WSR Post Hoc Test With Bonferroni’s Correction To Assess Cough 125

XII
Within Trial Group
58. Friedman’s Test To Assess Sputum Expectoration Within
Parnayavani Arka Nebulization Group
125
59. WSR Post Hoc Test With Bonferroni’s Correction To Assess
Sputum Expectoration Within Trial Group
126
60. Friedman’s Test To Assess Tightness In Chest Within Parnayavani
Arka Nebulization Group
127
61. WSR Post Hoc Test With Bonferroni’s Correction To Assess Chest
Tightness Within Trial Group
128
62. Friedman’s Test To Assess Pulse Rate Within Parnayavani Arka
Nebulization Group
128
63. WSR Post Hoc Test With Bonferroni’s Correction To Assess Pulse
Rate Within Trial Group
129
64. Friedman’s Test To Assess Respiratory Rate Within Parnayavani
Arka Nebulization Group
130
65. WSR Post Hoc Test With Bonferroni’s Correction To Assess
Respiratory Rate Within Trial Group
130
66. Mann Whitney –U Test For Between The Groups Analysis 132
67. Anova With Repeated Measures With A Greenhouse-Geisser
Correction In Parnayavani Arka Nebulization Group
138
68. Tests Of Within Subjects Effects Of Pefr For Parnayavani Arka Group 138
69. Independent Samples T- Test Between The Groups Analysis Of Pefr
Immediately After Nebulization
139

XIII
70. Independent Samples T- Test Between The Groups Analysis Of Pefr
One Hour After Nebulization
140

XIV
LIST OF FIGURES
Sl. No. FIGURES PAGE NO.
1. Flow chart of Tamaka Shwasa Samprapti 46
2. Octadecane, 3-ethyl-5-(2 ethylbutyl) 92
3. Dodecyl acrylate 92
4. Octadecanal, 2-bromo- 92
5. Gender Distribution of 60 patients of Tamaka Shwasa 93
6. Age distribution of 60 patients of Tamaka Shwasa 94
7. Marital status Distribution of 60 patients of Tamaka
Shwasa
95
8. Place wise distribution of 60 patients of Tamaka Shwasa 96
9. Religion wise distribution of 60 patients of Tamaka
Shwasa:
97
10. Socio-economic status wise distribution of 60 patients of
Tamaka Shwasa
98
11. Education wise distribution of 60 patients of Tamaka
Shwasa
99
12. Presenting complaints of 60 patients of Tamaka Shwasa 100
13. Duration of onset in 60 patients of Tamaka Shwasa 101
14. Mode of onset in 60 patients of Tamaka Shwasa 102
15. Trigger factors in 60 patients of Tamaka Shwasa 103
16. History of previous illness in 60 patients of Tamaka 104

XV
Shwasa
17. History of previous treatment in 60 patients of Tamaka
Shwasa
105
18. Family History in 60 patients of Tamaka Shwasa 106
19. Occupation of 60 patients of Tamaka Shwasa 107
20. Agni of 60 patients of Tamaka Shwasa 108
21. Ahara of 60 patients of Tamaka Shwasa 109
22. Nidra of 60 patients of Tamaka Shwasa 110
23. Rasa preference of 60 patients of Tamaka Shwasa 111
24. Alcohol and Smoking consumption in patients of Tamaka
Shwasa
112
25. Tea and Coffee consumption in 60 patients of Tamaka
Shwasa
113
26. Wheezing in 60 patients of Tamaka Shwasa 114
27. Nature of Wheezing sounds in 43 patients of Tamaka
Shwasa
115
28. Timing of Wheezing sounds in 43 patients of Tamaka
Shwasa
116
29. Rhonchi in 60 patients of Tamaka Shwasa 117
30. Crepitations in 60 patients of Tamaka Shwasa 118
31. Timing of crepitation in 21 patients of Tamaka Shwasa 119
32. Macroscopy of coleus aromaticus leaf 213
33. T.S of midrib of Coleus aromaticus leaf 213

XVI
34. Midrib portion enlarged – Coleus aromaticus leaf 214
35. T.S. of lamina of Coleus aromaticus leaf 214
36. Lamina portion enlarged – coleus aromaticus leaf 215
37. Upper midrib – Coleus aromaticus leaf 216
38. Lower epidermis – Coleus aromaticus leaf 216
39. Coleus aromaticus 217
40. Shredding of leaves 217
41. Weighing of leaves 217
42. Soaking of leaves 217
43. Soxhlet distillation 217
44. Clear Arka obtained 217

1
ABSTRACT
A CLINICAL STUDY TO ASSESS THE EFFICACY OF PARNAYAVANI
(Coleus aromaticus Benth.) ARKA NEBULIZATION IN THE MANAGEMENT
OF TAMAKA SHWASA W.S.R. TO ACUTE EXACERBATION OF
BRONCHIAL ASTHMA
Background and Objectives:
Global incidence of Tamaka Shwasa, Bronchial asthma is estimated to be
around 334 million. In India, 15-20 million population are asthmatics. It is of utmost
importance to find ways to combat this disease. Parnayavani is a commonly used
folklore remedy for Tamaka Shwasa. With this perspective, the objective of the study
was to assess the Shwasahara Karma of Parnayavani Arka when administered
through nebulization and compare it with the Standard drug – Theophylline
nebulization.
Methods:
Subjects were divided in to two groups, Trial group consisting of 30 subjects
received a single dose of Parnayavani Arka nebulization (5ml). Standard group
consisting of 30 subjects received a single dose of Theophylline nebulization (5ml).
Before administration and after administration assessment was done using the
following criteria - Subjective parameters as per GINA guidelines and objective
parameter – i.e. Peak Expiratory Flow Rate, both within and between the groups.

2
Results:
With respect to subjective and objective parameters, (p=0.05), this study
found that Parnayavani Arka nebulization showed equivalent action to Theophylline
immediately after nebulization. However, there was no significant difference
between the groups (p=0.05).
Interpretation and Conclusion:
Parnayavani Arka nebulization showed equivalent action to Theophylline
immediately after nebulization, but did not show sustained action till the end of one
hour, with almost all parameters showing a non-significant decrease by the end of one
hour.
It has proven bronchodilatory, antispasmodic, tracheal and bronchial muscle
relaxant properties. Parnayavani has Katu Tikta Rasa and Ushna Veerya. Hence, it
counteracts the effects of Kapha in the Pranavaha Srotas. This proves the
Shwasahara Karma of Parnayavani Arka nebulization immediately in acute
exacerbation of bronchial asthma.
Keywords – Coleus aromaticus, Shwasahara, Parnayavani, Theophylline,
Nebulization, Bronchial asthma

3
INTRODUCTION
A CLINICAL STUDY TO ASSESS THE EFFICACY OF PARNAYAVANI (Coleus aromaticus Benth.) ARKA NEBULIZATION IN THE MANAGEMENT OF TAMAKA SHWASA W.S.R. TO ACUTE EXACERBATION OF BRONCHIAL ASTHMA
The drug Parna Yavani (Coleus aromaticus Benth.) is a large succulent herb,
fleshy and highly aromatic, much branched, possessing short, soft erect hairs, with
distinctive smelling leaves. It is Teekshna, Ushna and Laghu in Guna, Katu Tikta in
Rasa, and is said to have Deepana, Pachana, Ruchya, Malasangraha Karmas. It is
indicated in disorders such as Agnimandya, Yakrudroga, Grahani, Udarraroga,
Krimi, Visoochika, Ashmari, and Mootrakricchra, Kasa and Shwasa. (1)
Shwasa is commonly understood to mean ‘difficulty in breathing’ –
‘Shwasanaat Shwasaha’. (2) It is broadly divided into five – Kshudra Shwasa, Maha
Shwasa, Chinna Shwasa, Urdhva Shwasa and Tamaka Shwasa.
Bronchial Asthma is one of the oldest recorded respiratory disorders. It may
be correlated with Tamaka Shwasa due to similarity in their signs and symptoms.
Asthma is a common long term inflammatory disease of the airways of the lungs,
characterized by variable and recurring symptoms, reversible airflow obstruction and
bronchospasms (3)
According to the WHO, over 180,000 deaths world wide are caused due to
asthma annually. (4) India, as of 2015, is the country with the highest number of
deaths caused by respiratory causes. There has been an overall increase of incidence
of respiratory disorders in India, with a marked increase in all the metropolis,
especially Delhi. (5). Modern drugs used in the treatment of bronchial asthma are
selected on the basis of symptom frequency, severity, chronicity etc. These
medications are associated with a number of side-effects. Theophylline, the most

4
commonly used bronchodilator can be associated with nausea, diarrhea, palpitations,
tachycardia, cardiac arrhythmia and insomnia. (6) Hence, it is obvious that safer
efficacious, easily available ad affordable medication is the need of the hour. In this
regard, ParnayavaniArka (Coleus aromaticus), a drug commonly used in folklore
practice in the treatment of Kasa and Shwasa, has been selected for administration
through nebulization, to analyze its efficacy in the management of Tamaka Shwasa.
The Shwasahara karma of ParnaYavani has been well documented. (1)
A nebulizer is a drug delivery device used for the administration of medication
as mist inhaled into the lungs, commonly used in the treatment of asthma, COPD,
cystic fibrosis, and other respiratory disorders. Advantages of nebulization over
metered dose inhalers are: their ability to deliver larger doses at a greater rate,
especially in conditions of acute asthma, as well as lower doses required for clinical
result. (7)

5
OBJECTIVES OF THE STUDY
1. To evaluate the Shwasahara (bronchodilatory) Karma of
Parnayavani (Coleus aromaticus Benth. Arka nebulization in
Tamaka Shwasa.
2. To carry out pharmacognostic study of Parnayavani (Coleus aromaticus
Benth.)
3. To carry out preliminary phytochemical analysis of Parnayavani (Coleus
aromaticus Benth.)
4. To compare the Shwasahara action of Parnayavani Arka nebulization
(Coleus aromaticus Benth.) with the standard Theophylline nebulization.

6
DRUG REVIEW
In Ayurveda, a drug is called Bheshaja, or Aushadha - that which
overcomes Bhesham or Osha, i.e. disease or even fear of disease and includes any
material or means used for this purpose. Classical texts of Ayurveda have little
mention of Parnayavani, although abundant folklore uses of this drug have been
documented.
CLASSICAL REFERENCES OF PARNAYAVANI:
Literature on Parnayavani that has been obtained from various authentic texts of
Ayurveda can be presented under the following headings.
§ VEDIC PERIOD, SAMHITA PERIOD, NIGHANTU KALA:
No references are found in texts belonging to these periods.
§ CONTEMPORARY TEXTS:
Parnayavani has been mentioned in Priya Nighantu by Vaidya P V Sharma. This
drug is said to be Teekshna, Ushna and Laghu in Guna, Katu Tikta in Rasa, and is
said to have Deepana, Pachana, Ruchya, Malasangraha Karma. It is indicated in
disorders such as Agnimandya, Yakrudroga, Grahani, Udarraroga, Krimi,
Visoochika, Ashmari, and Mootrakricchra. (8)
Books of modern botany have identified this drug as follows (9),(10),(11) –
Coleus aromaticus Benth.

7
Parnayavani was initially considered as the Yavani Vishesha mentioned in
Dhanvantari Nighantu, which was eventually proven to be Khurasani Yavani
(Hyoscymus niger) – an entirely different drug. (9)
SYNONYMS: (8)
Due to its limited mention in classical texts, few synonyms of Parnayavani are
available.
TABLE 1: SYNONYMS OF PARNAYAVANI
SYNONYMS D.G.V.
Parnayavani +
Yavani +
Gandhaparnika +
Table 2: VERNACULAR NAMESOF PARNAYAVANI(8, 10-12)
S.N. Language Name
1. Hindi Patta ajwain, Amroda, Patherchur, Pathercheer
2. English Country borage, Indian mint, Indian borage
3. Bengali Patharchoor, Patechur, Amakuchi
4. Gujarati Ovapan
5. Kannada Doddapatre, Sambrani, Sambrani soppu
6. Malayalam Panikoorka
7. Marathi Panova
8. Tamil Karpooravalli, Kurpuravallai
9. Telugu Karuvacru, Suganda vallekam, Karpooravalli

8
10. French Coleus d’Afrique, Plectrianthus aromatique
11. German Cubanischer oregano, Jamaican Thymian
12. Japanese Koreusu amboinikusu, Kuuban oregano
13. Malay Daun kucin, Daun Kambing
14. Russian Plektrantus aromatryi
15. Spanish Oregano
16. Vietnamese Tan ay le
17. Mah Panova
18. Gujarathi Ovapana
19. Chinese Zuo Shou Xiang
TAXONOMICAL NOMENCLATURE:
The name is derived from the Greek word koleos meaning sheath, referring to the
manner in which the stamens are united (10); while aromaticus refers to the
aromatic volatile oils present in the leaves. (11)
Kingdom-Plantae
Phylum: Tracheophyta
Division – Magnoliopsida
Class – Eudicots
Subclass – Gamopetalae
Family- Lamiaceae
Subfamily: Nepetoideae
Genus – Coleus

9
Species – aromaticus
Botanical name – Coleus aromaticus
Synonyms:
• Plectranthus aromaticus
• Plectranthus amboinicus
• Coleus amboinicus
GEOGRAPHICAL DISTRIBUTION:
It is unclear whether the origin of this drug is Africa or India. However, this drug
is now cultivated and available pantropically. (12, 13)
The drug is found throughout India from the upper Gangetic plane to Bihar,
Orissa, West Bengal, Tripura, Gujarat, Deccan, Konkan plateau, Karnataka
plains, Andhra Pradesh, Tamil Nadu, Kerala and Lakshadweep.
FAMILY FEATURES OF LAMIACEAE (14-15)
The broad family features of Lamiaceae are as follows:
• Labiateae refers to the labia shaped petals- fused into an upper lip and a
lower lip. Although this is considered acceptable, most botanists
nowadays use the term Lamiaceae in reference to this family.
• This family consists of about 236 genera with 6900-7200 species.
Among these, the largest genera are:-
Salvia (900), Scutellaria (360), Stachys (300), Plectranthus(300), Hyptis
(280), Teucrium (250), Vitex (250),
Thymus (220), and Nepeta (200).
• It is a family of flowering plants, most of which are aromatic in nature.

10
• The flowers are bilaterally symmetrical with 3 petals united to form an
upper lip, and 2 united to form a lower lip, and 5 united sepals. They are
usually bisexual and verticillate.
• Leaves are opposite, decussate or whorled.
• The stem is frequently square in cross section.
Macroscopic Description of Coleus aromaticus Benth. (16-18)
• General description: A large succulent herb, fleshy and highly
aromatic, much branched, possessing short, soft erect hairs, with
distinctive smelling leaves.
• Stem: Fleshy, about 30-90 cm, either hispidly villous, or tomentose.
Leaves: Simple, broadly ovate to suborbicular in shape, thick, thickly
pubescent, with the lower surface possessing numerous glandular hairs
giving it a frosted appearance.
• Flowers: Shortly pedicelled, pale, purplish in dense whorls at distant
intervals in a long slender raceme. The flowers have a bell shaped calyx
and the throat is smooth inside with two lips, the upper lip being ovate
and thin, the lower lip having four narrow teeth. The corolla is pale
purplish and five times longer than the calyx, with a short tube, inflated
throat and short lips.
• Fruit – Nutlets; smooth, pale brown in colour, 0.7 mm long and 0.5mm
wide.
Microscopic Description – (19)
Leaves -
• Petiole: Transverse section of petiole of Coleus aromaticusBenth.. is
concave on the upper side and convex on the lower side. Trichomes of both

11
glandular and nonglandular type are present all over the surface. The outer
layer epidermis consist of a single layer of laterally elongated cells,
followed by 3-4 layers of cortical cells which are round &
collenchymatous. The rest of the cortical cells are polygonal to round. The
vasculature comprises of a ring of eight collateral vascular bundles, of
which the two are larger in size. The ground tissue consists of thin walled
parenchymatous cells.
• Midrib: Transverse section of leaf passing through the midrib appears
hemispherical on the ventral side and slightly depressed on the dorsal side.
Upper epidermis is single layered and consists of compactly arranged
rectangular cells. Below this layer there is palisade parenchyma which is
also continuous with the midrib. Vascular bundles are solitary, collateral
and consist of 4-6 rows of xylem and a thin arc of phloem runs along the
midrib. Lower epidermis is similar to upper epidermis and is discontinuous
due to the presence of diacytic stomata On the upper and lower epidermal
surface numerous glandular and non glandular trichomes are present.
• Lamina: Transverse section of leaf shows dorsiventral character. Upper
Epidermis consists of single layer of rectangular cells along with a thin
layer of cuticle on it. Numerous Trichomes of both glandular and non
glandular nature are present on both upper and lower epidermis.
• Mesophyll: The Mesophyll is differentiated into 2 parts – palisade
parenchyma and spongy parenchyma. The palisade parenchyma lies toward
the upper epidermis and consist of single layer of elongated columnar
parenchymatous cells. Towards the lower epidermis there lies the spongy
parenchyma which consists of 5-6 layers of loosely arranged spherical

12
cells. Beside these numerous oil globules and prismatic calcium oxalate
crystals were present in the ground tissue. Coursing through the mesophyll
vascular bundles surrounded by parenchymatous cells is present.
• Hairs: The plant is densely covered with hairs of both glandular and non
glandular type. The glandular trichomes are of capitates type which
consists of a basal epidermal cell, unicellular to bicellular stalk of variable
lengh, a neck cell and a large globular unicellular secretory head. The non
glandular trichomes are 3-6 celled, variable length uniseriate, unbranched
and progressively tapering with pointed apex.
• Powder characteristics: The moderately coarse leaf powder(40 mesh size)
is dark green in colour and when studied under different magnifications
show the presence of diacytic stomata, epidermal cell, glandular and
uniseriate trichomes etc.
PART USED:
Generally, the leaves are the used part of this plant, though the whole
plant may also be used.
PHYTOCHEMISTRY:
The literature survey has emphasized the occurrence of different classes of
phytocompounds including 76 volatiles and 30 non-volatile compounds
• Volatile Composition of C. aromaticus (20)
The essential oil obtained from the leaves and stem explants contain a total of
76 volatile constituents. The essential oil contains copious quantity of the two

13
major phenolic compounds, namely, carvacrol and thymol, which are
pharmaceutically appreciated for various properties. The quality as well as quantity
of chemical compounds occurring in the essential oil is directly related to its
biological functions.
GC and GC-MS techniques have indicated the occurrence of Thymol (94.3%),
followed by Carvacrol (1.2%), 1,8-Cineole (0.8%), p-Cymene (0.3%), Spathulenol
(0.2%) and Terpinen-4-ol (0.2%) as the major constituents of Indian C. aromaticus
leaf essential oil. Investigation of volatiles of C. aromaticus collected from
Mysore, Karnataka, India showed the existence of Carvacrol (70%), -
Caryophyllene (6.2%), p-Cymene (5.6%) and -Terpinolene (5.3%) as the main
components. (21) The volatile composition of aerial parts and flowers of C.
aromaticus growing in Belgaum, Western Ghats region of North West Karnataka,
revealed the occurrence of 12 components from aerial parts oil and 4 constituents
from flower oil and represented 94.29% and 90.25% of the total oil, respectively.
In both the essential oils, the major compound observed was Carvacrol (50.98% in
flowers and 77.16% in aerial parts oils). Yet, the presence of chemical variation in
the leaf essential oils was evident from the plants collected from the same state. A
total of 10 volatile compounds were identified with dominant constituents as
Carvacrol (50.7%), -caryophyllene (13.1%) and patchoulane (8.7%). (22-27).
The leaf essential oil obtained from Martinique, France was found to contain
Carvacrol (72%) as a chief phenolic component along with newly identified
compounds such as (Z)-1,3-Hexadiene (0.1%), (E,Z)- -Farnesene (0.2%), (Z)-3-
Hexenol (0.6%), -Muurolene (0.2%) and (E,E)- -Farnesene (0.2%) (28) C.

14
aromaticus oil from Cambodia was shown to contain largely Thymol (57.4%). (29)
Similarly, Velasco et al. (30) identified 15 volatile constituents in the essential oil
of C. aromaticus collected from Venezuela and the major component observed was
Carvacrol (65.2%). The essential oil from Uganda consisted of Linalool (50.3%),
Carvacrol (14.3%), Nerol acetate (11.6%) and Geranyl acetate (11.7%) as the
major components as revealed by GC-MS analysis (31) Essential oil of C.
aromaticus leaves from Serdang, Malaysia was shown to contain Carvacrol
(19.29%), 3-Carene (20.78%) and Camphor (17.96%) as the major volatile
constituents. (32)
The essential oil yield and its main chemical constituents are also influenced
by the environmental factors and different seasons. Mallavarupu et al. have
revealed that the quality of essential oil will be superior when collected during
September. The oil content was found to be higher in the plants harvested during
September in comparison to the plants harvested during May. Moreover, the
compositions also differed among the two harvest times. About 68% of
oxygenated monoterpenes, 11% of sesquiterpenes and 3.3% oxygenated
sesquiterpenes were found in the oil distilled from the September harvest time,
whereas, the oil obtained from the May harvest comprised higher amounts of
monoterpenes (35.7%). The major compounds such as Carvacrol (67.0%), -
Caryophyllene (7.4%), -Humulene (2.1%) and Caryophyllene oxide (2.2%) were
found to be higher in oil obtained during September, while the oil distilled during
May showed the presence of p-Cymene (12.6%), -Terpinene (15.5%), Carvacrol
(53.0%) and -Caryophyllene (4.3%). (33)

15
Table 3: The known volatile constituents of Coleus aromaticus Benth. (34)
Compound
Name Formula Plant Origin/Part
Monoterpene hydrocarbons
-3-Carene C10H16
India, Malaysia, Morocco,
Mauritius/Leaf
p-Cymene C10H14
Brazil, India, Cambodia, Malaysia,
Venezuela/Aerial parts, Leaf
Limonene C10H16 India, Mauritius/Leaf
-Myrcene C10H16 Cambodia, India, Venezuela /Leaf
Ocimene C10H16 Morocco/Leaf
-Phellandrene C10H16
India, Comoros, Mauritius,
Venezuela/Leaf
-Phellandrene C10H16 India/Leaf
-Pinene C10H16 India, CambodiRa /Leaf
-Pinene C10H16 India/Leaf
Sabinene C10H16 Cambodia,India, Morocco /Leaf
-Terpinene C10H16 India, Mauritius/Leaf
-Terpinene C10H16
Brazil, Cambodia, Malaysia,
Mauritius India, /Leaf
-Terpinolene C10H16 Morocco, Brazil/Leaf
-Thujene C10H16 India, Comoros, Venezuela/Leaf
Oxygenated monoterpenes
Camphor C10H16O Comoros, Malaysia, Mauritius/Leaf
Carvacrol C10H14O
Cambodia, India, Malaysia,
Mauritius, Venezuela/Aerial parts,

16
Leaf, Flower
Carvone C10H14O India/Leaf
1,8-Cineole C10H18O India/Leaf
Eugenol C10H12O2 Cambodia, India/Leaf
Geraniol C10H18O Mauritius/Leaf
Linalool C10H18O Comoros, Mauritius /Leaf
Methyl carvacrol C11H16O India/Leaf
Methyl eugenol C11H14O2 Cambodia/Leaf
-Terpineol C10H18O India, Comoros, Venezuela /Leaf
Terpinen-4-ol C10H18O Brazil, India, Mauritius /Leaf
Thymol C10H14O
Brazil, Cambodia, India,
Venezuela/Aerial parts, Leaf
Thymol methyl
ether C11H16O Brazil/Leaf
Sesquiterpene hydrocarbons
-Amorphene C15H24 Cambodia/Leaf
Aromadendrene C15H24 Brazil, India/Leaf
trans- -
Bergamotene C15H24
Brazil, Comoros, India, Venezuela
/Leaf, Aerial parts, Flower
trans- -
Bergamotene C15H24 Cambodia/Leaf
-Cadinene C15H24 Cambodia/Leaf
-Cadinene C15H24 India, Cambodia/Leaf
-Calacorene C15H20 India/Aerial parts
cis-Calamenene C15H22 Cambodia/Leaf
-Caryophyllene C15H24 Brazil, India, Venezuela /Leaf,

17
Flower
-Caryophyllene C15H24 India/Leaf
-Copaene C15H24 Comoros, India /Leaf
-Cubebene C15H24 India/Leaf, Aerial parts
(E,Z)- -
Farnesene C15H24 France /Leaf
Germacrene D C15H24 Cambodia/Leaf
-Gurjunene C15H24 India/Aerial parts
Humulene C15H24
Brazil, Cambodia, India, Morocco,
Venezuela/Leaf, Aerial parts
-Muurolene C15H24 Cambodia, France, Mauritius/Leaf
Patchoulene C15H24 India, Mauritius/Leaf
-Selinene C15H24 India, Comoros/Leaf
-
Sesquiphellandre
ne C15H24 Cambodia/Leaf
Compound
Name
Formula Plant Origin/Part
Oxygenated sesquiterpenes
Caryophyllene
oxide C15H24O
India, Cambodia, Venezuela /Leaf,
Aerial parts
-Cedrene
epoxide C15H24O India/Aerial parts
-Copaen-4- -ol C15H24O India/Aerial parts
1-Epi-cubenol C15H26O India/Aerial parts

18
-Eudesmol C15H26O India/Leaf
-Himachalene
oxide C15H24O India/Aerial parts
Humulene oxide C15H24O India/Leaf
Spathulenol C15H24O India/Leaf
Others (Terpenes,
phenylpropanoids, esters, fatty
acids, alcohols, aldehyde)
1,2-Benzenediol
4-(1,1
C10H14O2 India/Leaf dimethylethyl)
Chavicol C9H10O India/Leaf
Methyl chavicol C10H12O India/Aerial parts
-Corocalene C15H20 India/Aerial parts
Dihydro carveol C10H18O India/Aerial parts
Durohydroquino
ne
C10H14O
2 India/Leaf
1,4 Eicosadiene C20H38 India/Leaf
Ethyl Salicylate C9H10O3 India/Leaf
(Z)-1,3-
Hexadiene C6H10 France /Leaf
(Z)-3-Hexen-1-
ol C6H12O France/Leaf

19
Methyl
octanoate C9H18O2 India/Aerial parts
1-Octen-3-ol C8H16O India, Mauritius, Venezuela/Leaf
Oleic acid
C18H34O
2 India/Leaf
2-Phenyl ethyl
tiglate
C13H16O
2 India/Aerial parts
Phytol C20H40O India/Leaf
Squalene C30H50 India/Leaf
Tetradecanal C14H28O India/Aerial parts
3,7,11,15–
Tetramethyl-2-
hexadecen-1-ol C20H40O India/Leaf
Thymol acetate
C12H16O
2 India/Leaf
Trans-sabinene
hydrate
C12H20O
2 India/Aerial parts
Undecanal C11H22O India/Aerial parts
Table 4: The known non-volatile components of Coleus aromaticus (34)
A total of 30 non-volatile constituents have been identified from C. aromaticus
according to our literature survey (27). These non-volatile chemical components
included phenolic acids, flavonoids, monoterpene hydrocarbons, sesquiterpene
hydrocarbons, oxygenated monoterpenes and esters

20
Compound Name Plant Origin/Part
Phenolic acids
Caffeic acid India, Egypt/Leaf, stem, root (Methanol extract)
Gallic acid India/Stem (Methanol extract)
p-Coumaric acid
India, Egypt/Leaf, stem, root (Methanol and ethyl
acetate fraction)
Rosmarinic acid
India, Egypt, Thailand/Leaf, stem, root (Methanol
and ethyl acetate fraction)
Salvianolic acid A Thailand/Aerial parts (Water extract)
Shimobashiric acid Thailand/Aerial parts (Water extract)

21
Flavonoids
Table 5: RASA PANCHAKA AND KARMA OF PARNAYAVANI (8)
RASA
PANCHAKA PARNAYAVANI
Rasa Katu, Tikta
Guna Teekshna, Ushna, Laghu
Virya Usna
Vipaka Katu
Chrysoeriol Leaf, stem, root (Chloroform extract; Ethyl acetate fraction) –
Philippines/Egypt Cirsimaritin Philippines/Leaf (Chloroform extract)
Eriodictyol Egypt/Leaf, stem, root (Ethyl acetate fraction)
Luteolin Egypt/Leaf, stem, root (Ethyl acetate fraction)
Rutin India/Stem (Methanol extract)
Salvigenin Philippines/Leaf (Chloroform extract)
Thymoquinone Thailand/Aerial parts (Water extract)
Quercetin Egypt/Leaf, stem, root (Ethyl acetate fraction)
5,41 -Dihydroxy-6,7-
dimethoxy flavone
Egypt/Leaf, stem, root (Ethyl acetate fractions)
5,41 -Dihydroxy-
3,7-dimethoxy flavone
Egypt/Leaf, stem, root (Ethyl acetate fractions)
5-O-Methyl-luteolin Egypt/Leaf, stem, root (Ethyl acetate fractions)
3,5,7,31 ,41 -Pentahydroxy
flavanone Egypt/Leaf, stem, root (Ethyl acetate fractions)
41 ,5,7-Trihydroxyflavone
(apigenin)
Egypt/Leaf, stem, root (Ethyl acetate fractions)

22
Doshaghnata Kapha Vata Shamaka
Karma Deepana, Pachana, Ruchya, Malasangrahaka
Rogaghnata
Agnimandya, Yakridroga, Grahani, Udara, Krimi, Visoochika,
Ashmari, Mootrakricchra
TRADITIONAL USES:
C. aromaticus is among the most widely used herbs by traditional medicine
practitioners due to widespread availability in India and other countries. A brief
summary of its traditional uses is given below:
§ Respiratory Disorders
amboinicus is frequently cited in the treatment of chronic coughs, asthma,
bronchitis and sore throat in India and the Caribbean Islands (35). In Eastern Cuba,
essential oil from aerial parts of C. aromaticus is used to treat asthma (36).
Decoction or juice made from leaves together with other herbs is also taken orally
to control asthma. This decoction is also used to treat catarrhal infections where it
clears the excessive build-up of thick phlegm or mucus in an airway or cavity of
the body. In Brazil, a drink or a bath of C. aromaticus juice/decoction is used to
treat influenza, cough, bronchitis and throat problems (37).
• Digestive system Diseases
C. aromaticus is a popular treatment for dyspepsia, indigestion and diarrhea, and a
carminative in India and Africa. C. aromaticus juice obtained from pounded leaves
is used as a drink to cure constipation in Indonesia and Malaysia. (38) In India, the

23
leaves of C. aromaticus are consumed along with buttermilk, yogurt, or any other
probiotic sources during pathogen-induced diarrhea. (39)
• Epilepsy:
In Cuba, it is used as an anticonvulsive and antiepileptic drug (40)
§ Skin diseases
C. aromaticus has been used in Brazil since the early days for the treatment of
skin ulcerations caused by Leishmania braziliensis (41) In India, the juice of the
leaves is used to treat skin allergies. It is also used to treat burns in Asian regions
(42) When the leaf paste is baked on a flame and applied to cuts or burns, it acts as
an antiseptic and promotes healing (42)
• Animal and insect bites
Leaves of C. aromaticus are also used as a poultice for centipede and scorpion
bites in Asian regions, including Malaysia (38)
§ Lactogenic Activity
In Indonesia, C. aromaticus is used as a traditional food in soup to stimulate
lactation for the month or so following childbirth. The leaves are commonly
consumed by mothers who have given birth in North Sumatra, in particular the
Batak tribe. The leaves of this herb are believed to increase the production of
breast milk due to the high content of nutrients, especially iron and carotene.
Consumption of leaves significantly increases minerals such as iron, potassium,
zinc and magnesium in milk, thus, improving the infant’s weight and health
holistically (43)

24
• Cardiac diseases:
C. aromaticus is also used in the Caribbean, to treat congestive heart failure
(44)
§ Genitourinary diseases:
§ The leaves of C. aromaticus are frequently utilized in the treatment of
urinary diseases in the Amazon and India. (45) This species is also
reported to relieve kidney troubles and treat vaginal discharges, and is
taken as a drink after childbirth (46). The juice of C. aromaticus has been
used as a natural remedy to dilute the crystals in the urinary tract in India
from ancient times (47)
§ Analgesic activity
In Africa, C. aromaticus is used as a remedy for headaches (48)
§ Activity against Other Diseases
C. aromaticus is an important herb in Asia and South America for the
treatment of infectious diseases such as fevers cholera and meningitis. It also used
to treat sensory disorders associated with ear and eye problems. In India its leaves
are rubbed into the eyes to alleviate conjunctivitis (48).
RESEARCH PROFILE:
C. aromaticus is a widely researched herb – both for its culinary as well as
therapeutic usage. A brief research profile of the drug C. aromaticus is as follows:
§ Digestive disorders:

25
The leaves are known to have a prebiotic effect on the probiotic bacteria
Lactobacillus plantarum. They utilize the phytoconstituents of the leaves by
producing necessary metabolic enzymes. A detailed examination by Shubha and
Bhatt describes the mode of hot water extract (HWE) of C. aromaticus leaves on
growth inhibition of Escherichia coli and Salmonella typhimurium (pathogens)
while stimulating the growth of Lactobacillus plantarum. Sodium dodecyl sulfate
polyacrylamide gel electrophoresis (SDS-PAGE)gel showed the presence of
phenolic acid decarboxylase enzyme induced in the presence of HWE, which
indicated the utilization of polyphenols by the bacteria. Cells grown on HWE also
showed -galactosidase activity, indicating their ability to utilize sugars present in
HWE. This provides evidence in the traditional use of the leaves in the alleviation
of diarrhea by accelerating microbial gut balance during infection.(49)
§ Epilepsy:
Bhattacharjee and Manjumder tested the anticonvulsant activity of the leaf,
stem and root alcoholic extract separately on Swiss albino mouse models by
maximal electric shock-induced seizures and pentylenetetrazole-induced seizures.
They found significant anticonvulsant activity in both the models with alcoholic
leaf extract recording the highest activity. (50)
§ Scorpion bites:
It is reported that aqueous extracts (0.706 mg/mL and 0.406 mg/mL) of C.
aromaticus to be more than 70% efficient when tested against fibroblast cell lysis
(51) This implies the aqueous extracts to have a tendency to be scorpion
(Heterometrus laoticus) venom antidotes.

26
§ Cardiac diseases:
The aqueous extracts of the fresh leaves of C. aromaticus exhibited dose-
dependent positive inotropic activity in the isolated frog heart without affecting
the heart rate. This may be attributed to the increase in sodium influx thereby
causing greater intracellular availability of calcium. In this report the bioactivity of
the tissue-cultured extracts of C. aromaticus to the parent plant was also described.
Both extracts from tissue-cultured and parent plant produced a comparable
significant effect indicating that they both can be used as a source of biochemical
production. (52)
§ Genito-urinary diseases:
The antilithiotic activity of the concentrated fresh juice of the leaves of C.
aromaticus is proved by Jose et al. The said study on urine analysis revealed
significant reduction in calcium, oxalates and total protein level compared to the
control. Further histopathological results showed an absence of crystal and normal-
sized tubules with a single epithelial lining. He suggested this antilithiotic activity
could be associated with calcium oxalateorigin. The diuretic properties of ethanolic
and aqueous extracts of C. aromaticus were evaluated by determination of urine
volume and electrolyte concentration in male albino rats. Furosemide (10 mg/kg)
was used as a standard, while normal saline (0.9%) was used as a control. Both
ethanolic and aqueous extracts (500 mg/kg) have shown a significant increase in
the volume of urine and urinary concentration of Na, K and Cl ions and were
comparable to furosemide. This study concludes that the leaves of C. aromaticus
possess diuretic activities (53)

27
§ Analgesic activity:
The aqueous extract of C. aromaticus leaves showed an analgesic and anti-
inflammatory property, mainly modulated by controlling inhibition of
proinflammatory mediators (54).
Table 6: Pharmacological activity of different parts of C. aromaticus: (55)
Pharmacological
activity Bioactive compound Research profile
Antibacterial activity
Biogenic zinc oxide
nanoparticles
Pam-ZnO NPs control the growth of
methicillin-resistant
Staphylococcus aureus biofilm;
inhibits growth of Escherichia coli,
Salmonella typhimurium &
Mycobacterium tuberculosis.
Antiviral activity -
Exhibited antiviral activity against
viruses (VSV, HSV1 & HIV).
Activity against
Respiratory diseases -
Expectorant, smooth muscle relaxant,
bronchodilator
Lavicidal potential
Pam-ZnO NPs (zinc
oxide nanoparticles)
Exhibited up to 100% mortality in
Anopheles stephensi, Culex
Quinquefasciatus & Culex
tritaeniorhynchus.
Oral Diseases Carvacrol Antagonistic effect when used with

28
mouthwash.
Digestive diseases
(Diarrhea,
Constipation,
dyspepsia, indigestion
& as carminative) -
Stimulates growth of Lactobacillus
plantarum and inhibits growth of
selected food-borne pathogens
(Escherichia coli & Salmonella
typhimurium); relieves constipation
troubles; prevents formation of
gas in the gastrointestinal tract &
facilitates expulsion of gas
Antitumor activity
Flavone (Luteolin),
flavonols
Inhibited the growth of sarcoma 180 &
Ehrlich ascite carcinoma
tumors in mice; showed significant
anticancer activity through
inducing apoptosis in A549 (human lung
cancer) cell line.
Antiinflammatory
activity
Rosmarinic acid L, Rutin,
Thymoquinone,
Quercetin
Concentration of 0.1 mg/mL inhibited
10%–50% DNA binding to its consensus
sequence; decreased carrageenan-induced
paw edema up to 40%;
significantly increased IgG, IgM &
lysozyme activity in rats.
Analgesic activity -
Analgesia in musculo-skeletal disorders
proven
Wound healing
activities -
Increased wound healing activity in
experimentally induced

29
diabetic mice & againt murrels.
Cardiovascular
disorders -
Positive inotropic activity in the isolated
frog heart; effective for
treating congestive heart failure.
Skin disease (Anti-
dandruff, Cuts,
Skin Allergy; Burns)
Thymol, 1,8-Cineole, -
Pinene, -pinene,
phenolic compounds
Inhibits the growth of Malassezia furfur;
applied on cut as antiseptic
promoted better healing; paste was
effective against skin allergies,
skin burns.
Insect bites -
Potency as antidote for scorpion
(Heterometrus laoticus) venom
with>50% efficiency.
Lactogenic properties
Nutrient content (iron &
carotene)
Increased breast milk production in new
mothers.
Anti-epileptic activity
Alkaloids, flavonoids &
saponins
Effective as an anticonvulsive and/or
antiepileptic medicine.
Activity against
Genitourinary diseases -
Showed increased urine volume &
electrolyte concentration in
male albino rats.
Antioxidant activity Carvocrol & Thymol
Exhibited significant inhibition in DPPH
free radical & hydroxyl
radical formation.
Other diseases - Reduced free radical formation in

30
Xerophathalmia.
PROPAGATION, CULTIVATION AND COLLECTION
(56-57)
PROPAGATION:
Coleus aromaticus is propagated by terminal stem cuttings, approximately 10 cm
in size. It is rarely propagated by roots or seeds.
CULTIVATION:
It grows well in subtropical and tropical climates – especially well drained, red
loamy soil, semi shaded positions. Care should be taken to avoid water stagnation.
Ideally, the crop grows in areas receiving 70cm annual rainfall. 60 X 45cm spacing
is required for planting. Around 37,000 plants may be planted in one hectare. In
soils with low fertility, 60 X 30 cm spacing may be done. Immediatetly after
planting, irrigation should be done, and continued ideally once every week for
optimum yield. 15t/hectare of farmyard manure is added during the last ploughing.
NPK fertilizers at 30:60:50 kg/hectare is applied in two split doses. The first dose
is administered at 30 days, while the second dose is administered at 45 days after
planting. 10kg Zinc sulfate is also aopplied per hectare to avoid micronutrient
deficiency.
Likely sources of crop d estruction are : Nematode infection, Root rot, and
Bacterial wilt. 200kg of neem cake and 20kg carbofuran is applied to each hectare
before planting to prevent nematode infection.

31
COLLECTION:
The plant is collected at maturity i.e. after complete flowering and fruiting.
Usually, it is collected 5-6 months after planting. Care should be taken to avoid
damage to leaves while harvesting. For every hectare, the yield is around 15-20
tons of fresh leaves.
TRADE AND COMMERCE (58)
Rate in Indian market is Rs. 260/kg. Major drug dealers are in Karnataka,
Chandigarh, Amritsar, Delhi, Gujarat, Punjab, Tamilnadu, Maharashtra and
Orissa.

32
DISEASE REVIEW
HISTORICAL REVIEW OF SHWASA:
VEDIC AND UPANISHAD PERIOD
Available literature from the Prevedic and Vedic periods reveals the
physiology of respiration from an Indian perspective. In the Rig Veda, the terms
Prana and Vayu are used interchangeably. The term Shwasa was first used during
the Upanishad Kala. The Garuda Purana contains the earliest attempts to
scientifically assess Shwasa – and mentions the Nidana of Shwasa. (59)
SAMHITA PERIOD:
Charaka Samhita, Sushruta Samhita, Ashtanga Hridaya, Ashtanga Sangraha,
Madhava Nidana, Bhavaprakasha, Yogaratnakara etc. and all major treatises
elaborately describe the types, Nidana, Poorvaroopa, Roopa, Samprapti, Upashaya,
Anupashaya, Chikitsa and the variable presentations of Shwasa. (60-67)
ETYMOLOGICAL DERIVATIONS (NIRUKTI)
ETYMOLOGY OF TAMAKA SHWASA
The term Tamaka Shwasa consists of two words - Tamaka and Shwasa
ETYMOLOGY OF TAMAKA:
The word Tamaka is derived from Tama + Va. According to Shabda
Kalpa Druma it is defined as Tamyatyasmat anena va. Tamaka means -
oppression of the chest, to choke, to be suffocated, to be exhausted, to be
uneasy, or distressed. (68)
ETYMOLOGY OF SHWASA:
The word Shwasa is derived from the root - Shwas + Karane gnanj.
Shabda Kalpa Druma defines Shwasa as follows - Shvasiti anena iti Shwasa
which refers to the act of respiration. This derivation details the physiology of

33
breathing. But rapid or interrupted breathing is a disease, also known as
Shwasa. In the context of disease, it refers to ‘panting respiration’. (68)
TAMAKA SHWASA:
Tamaka Shwasa is defined as
· ‘Visheshat Durdine Tamyeth Shwasa sa Tamako Mataha’
Shwasa which occurs especially during Durdina is called Tamaka Shwasa.
(69).
· ‘Tamakascha Asou Shwasascha Tamaka Shwasa’
The attack of Shwasa, which occurs mainly during the Tamah kala - night
time, is called Tamaka Shwasa.
NIDANA PANCHAKA OF TAMAKA SHWASA
The Nidana Panchaka ie, Nidana, Poorvaroopa, Roopa, Samprapti,
Upashaya, Anupashaya of Tamaka Shwasa have been elaborated in various
Samhitas as mentioned above.
NIDANA
Tamaka Shwasa has been described as a Yapya Vyadhi by Charaka.
As Nidana is the Vyadhi Karana (67), Nidana Parivarjana plays an important
role in the management of diseases like Tamaka Shwasa in order to prevent
the further vitiation of Doshas. (67)
Various authors (61-68) have mentioned general etiological factors of
Shwasa These are the same for Tamaka Shwasa as well.

34
According to Chakrapani, the Nidanas of Tamaka Shwasa may be
classified into two: (69)
b) Vata Prakopaka Nidanas
c) Kapha Prakopaka Nidanas
Vata Prokopaka Nidanas: The Nidanas which cause the vitiation of Vata.
These include - Sheetapana and Sheeta Ashana, Ruksha Bhojana, Sheetavata
Sevana, Raja Sevana, Vyayama and Vegadharana, etc.
Kapha Prakopaka Nidanas: The Nidanas which cause the vitiation of Kapha.
These include - Gurubhojana, Adhyashana, Shleshmala Ahara Sevana,
Sheetapana, etc.
Another classification of Shwasa Roga Nidana is as follows :- (68)
� Bahya (extrinsic)
� Abhyantara ( intrinsic)
Bahya nidanas (69-73) like Rajas, Dhuma etc. are factors from the
external environment responsible for causation of the disease.
Abhyantara Nidanas are the Doshas. Kapha and Vata are the main
Doshas responsible for the manifestation of Tamaka Shwasa.
The vitiation of Vata and Kapha Dosha in Tamaka Shwasa, is referred
to as Sannikrista Nidana. It is the outcome of exposure to Viprakrista Nidanas
in the form of Ahita Aharas and Viharas. A summary of etiological factors of
Tamaka Shwasa are presented below:

35
Table 7: Showing Nidana classification based on Dosha Prakopa
Nidana Factors C.S74 S.S75 A.H76 A.S77 M.N78
Ahara Vatakara
Rukshanna + + + + +
Vishamashana + + - - -
Adhyashana - + - - -
Samashana - + - - -
Sheetashana - + - - +
Sheetapana + + + + +
Pittakara
Tila taila + - - -
Vidahi + + - - +
Katu - - + +
Ushna - - + + -
Amla - - + + -
Vihara Kaphakara
Jalaja Mamsa + - - - -
Anupa
Mamsa + + - - +
Dadhi + - - - -
Abhishyandi + + + + +
Vishtambhi + + - - +
Vatakara

36
Raja + + + + +
Dhuma + + + + +
Prag vata + + + + +
Sheeta Sthana + + - - +
Sheeta Ambu + + + + -
Ativyayama + + + + +
Gramya
Dharma/ Stree + + + + -
Apatarpana + + - - +
Kantha Ura
Pratighata + - - - -
Bharakarshita - + - - +
Adhwahata - + - - +
Vega nirodha - + + + +
Abhighata - + - - -
Marmabhigata - - + + -
Pittakara
Ushna Vayu - + - - +
Kaphakara
Abhishyandi
upachara + + - - -
Table 8: Showing Vyadhi Avastha Sambandi Nidana in Tamaka Shwasa
Sl. No Nidana C.S S.S A.S A.H Y.R B.P M.N G.N

37
1. Pratishyaya + + - - - - - -
2. Kasa - + + + + - - -
3. Jwara + - + + + + + -
4. Chardi + - + + + - - -
5. Kshata Ksheena + - - - - - - -
6. Atisara + - + + + + + -
7. Visuchika + - - - - - - -
8. Vibandha + - - - - - - -
9. Dourbalya + - - - - - - -
10. Udavarta + - - - - - - -
11. Raktapitta + - - - - - - -
12. Anaha + - - - - - - -
13. Pandu + - + + + - - -
14. Rukshata + - - - - - - -
15. Apatarpana + + - - + + + -
Table 9: Showing Agantu Nidana in Tamaka Shwasa
Sl. No Nidana C.S S.S A.S A.H Y.R B.P M.N G.N
1. Marmaghata + + + + + - - -
2. Visha + - + + + - - -
3. Kantorasa Pratighata + - - - - - - -

38
POORVA RUPA
The Lakshanas which appear before the onset or manifestation
of actual signs of a disease are considered as Poorva Rupa (79). No
specific Poorva Rupas have been explained for Tamaka Shwasa.
However, the general Poorva Rupas explained for Shwasa are
applicable in Tamaka Shwasa as well.
Table 10: Showing Poorvarupa of Tamaka Shwasa
Poorvarupa C.S80 S.S81 A.H82 M.N83
Anaha + + + +
Parshva Shula + + + +
Hrit pidana + + + +
Pranasya Vilomata + - + -
Adhmana - - - +
Mukha Virasata - + - +
Shankha Nistoda - - + +
Arati - + - -
Bhakta Dvesha - + - -
RUPA
The signs and symptoms which exhibit as a result of disease
manifestation in the body are called Roopas. Vata and Kapha Dosha,
Rasa Dhatu and Pranavaha srotas are the main factors concerned in the
pathogenesis of Tamaka Shwasa. Other features such as the mode of

39
onset, course, aggravating factors, and relieving factors are very typical
and are hence diagnostic of Tamaka Shwasa.
Table 11: Showing Rupa of Tamaka Shwasa
Rupa C.S84 S.S85 A.H86 M.N87
Griva Parigraha + - + +
Shira Parigraha + - + +
Shwasa + + + +
Peenasa + - + +
Ghurghuraka Shabda + + + +
Prana Prapeedaka Shwasa + - - +
Kasena Pratamyati + - - +
Kasat Pramohanam + - + +
Shleshmana Vimokshane
Sukham + - - +
Shamyati Kaphe Heena - + - -
Krichchra Bhashitam + - - +
Anidra/ Svapata Vivardhate + + - +
Asino Labhate Saukhyam + - - +
Ushnabhinandati + - - +
Ucchritaksha + - + +
Lalata Sveda + + + +
Mukha Shosha/Trishna + - + +
Muhurmuhu Shwasa + - + +

40
Sakapha Kasa - + - -
Vamana - + - -
Aruchi - - + -
Roopa of Pratamaka Shwasa
Jwara + + + +
Murcha + + + +
Udvarta Rajo Ajeerna Klinnakaya
Nirodha + - - +
Sheete shamyet - - + -
Rupa of Santamaka Shwasa
Tamasa vardhate + - - +
Sheeta prashamyati + - - +
Majjata Tamasi + - - +
Among the numerous Rupas of Tamaka Shwasa mentioned in
the table, Ati-Teevra Vega Shwasa, Ghurghura Shabda, and Sakapha
Kasa are considered to be the chief symptoms of Tamaka Shwasa.
Ghurghurkam: It is a typical sound produced, when excessive secretion of
the Kapha, causes Avarodha in the Pranavaha Srotas and thereby obstructs the
free flow of Pranavayu.
Ati Teevra Vega Shwasa: The excess secretion of mucus & sputum clogs the
path of the Pranavayu, i.e., it results in difficulty in breathing due to
obstruction to the flow of air in and out of the lungs.

41
Kasa: The excess secretion of mucus & sputum clogs the path of Pranavayu
causing Kasa. When unable to expectorate, the thick sticky sputum further
aggravates the coughing and sense of suffocation.
Greeva - Shiraso- Uraso Sangraham: These features are due to the hyper
inflation of the lungs. The subject experiences discomfort, or aching pain on
bilateral aspects of the chest.
Sleshmanam vimokshante muhurtham labhathe sukham: Once the
sputum has been expectorated, the frequency of breathlessness and coughing
reduces and there is momentary relief due to the easy flow of Prana Vayu. The
subject prefers hot things, which liquefy Kapha, and make Kapha
expectoration easier.
Kanthodhvamsa: Because of repeated coughing the patient develops
hoarseness of voice.
Shayanasya Shwasa Peeditha: When the patient lies in a recumbent position,
the space for air exchange reduces in the lungs which causes a sudden
decrease in the volume of the thoracic cavity. The air trapped cannot easily
escape and severe pain occurs.

42
Asinolabhate Saukhyam: On sitting the diaphragm is lowered and the space
for air exchange increase, and the volume of the thoracic cavity increases.
This facilitates the flow of Pranavayu.
Kricchrena Bhashate: During an episodic attack of Tamaka Shwasa the
patient can hardly speak. This is due to Shwasa Krucchrata and also due to
tenacious mucous coated in the throat including the vocal cords.
When the condition becomes severe, certain life threating symptoms or
Asadhya Lakshanas of Tamaka Shwasa will be seen in patients like -
Pramoham Kasamanashcha. The patient may go into syncope during bouts of
coughing. Other symptoms like increased respiratory distress which can be
correlated to the term Pratamyati, may also be seen. The patient becomes
motionless -Sannirudhyate.
Sometimes the patient may develop loss of consciousness – Pramoham. Some
have their eyes wide open - Ucchrita Akshata, sweating on the forehead -
Lalata Sweda, dryness of the mouth due to air hunger – Vishukasyata etc.
PRABHEDA OF TAMAKA SHWASA
2 types of Tamaka Shwasa have been explained (88).
· Pratamaka Shwasa: If Tamaka Shwasa is associated with Jvara and
Murcha, it is called Pratamaka. Udavarta, Rajas, Ajeerna, Klinnakaya and

43
Veganirodha are mentioned as the etiological factors. According to Vagbhatta,
this type of Shwasa subsides by giving Sheetala Upachara.
· Santamaka Shwasa: This type aggravates due to Tamas and is alleviated by
Sheetala Upachara. A patient with this condition feels as if he/she is being
submerged in Tamas. Some authorities correlate this condition to Cardiac
arrhythmia.
SAMPRAPTI
Samprapti is the process from Dosha Vaishamya till the expression of
the disease. Shwasa is a disease caused due to the simultaneous vitiation of
Vata and Kapha wherein either both are independent, or vitiate each other
(89). Among the two Doshas, Kapha Dosha is primarily involved in the
Tamaka Shwasa Samprapti. (90).
Samanya Samprapti
The morbid Vata which gets obstructed by Kapha, causing the vitiation
of the Prana, Udaka, and Annavaha srotas. The Vata then finally gets lodged
in the Ura pradesha causing Shwasa and Hikka. (91)
Vishista Samprapti of Shwasa
In the common Samprapti of all the five types of Shwasa, when the
Kapha and Vata obstruct the Srotas, the hindered Vayu, trying to overcome
the obstacle, moves in all directions results in Shwasa. The term
‘Vishawakvrajati’ denotes this.

44
Samprapti of Tamaka Shwasa:
Vata moving in the Pratiloma Gati pervades the Srotas (channel),
afflicts the Shiras and Griva, stimulates Kapha and causes Tamaka Shwasa.
This Kapha causes obstruction at the site of the throat Ghurguraka Shabda is
produced when Vata passes through the same region. This results in an
increase in the respiratory rate. (92)
Sthana Samshraya in Tamaka Shwasa
During this Kriyakala, the Purvarupavastha of Tamaka Shwasa is
manifested. In this stage, Khavaigunya occurs due to the already aggravated
Doshas circulating throughout the body which in turn affects the tissues of the
Pranavaha Srotas. Due to Sthana Samshraya of Doshas in the Pranavaha
Srotas, it becomes obstructed (Srotosanga) and Vata moves in all directions.
Vyakta in Tamaka Shwasa
Srotosanga due to Kapha and Ama Dosha in Pranavaha Srotas causes
Vimarga Gamana of Pranavata, results in the manifestation of the Lakshanas
of Tamaka Shwasa.
Bhedavastha in Tamaka Shwasa
The pathological process which is already ongoing in a patient reaches
this stage if the patient is a chronic sufferer, or if the disease is uncontrolled.
In long term permanent irreversible air flow obstruction, other Dhatus and
Srotas are vitiated, resulting in complications.

45
Table 11: Samprapti Ghatakas in Tamaka Shwasa
SAMPRAPTI GHATAKAS
Dosha Prana Vayu, Udana Vayu, Pachaka Pitta,
Avalambaka Kapha
Dushya Rasa
Agni Jataragni, Rasadhatwagni
Ama Jataragnijanya, Rasa dhatwagnijanya
Srotas Pranavaha Srotas, Udakavaha, Annavaha,
Rasavaha Srotas
Srotodushti Prakara Sanga, Vimargagamana
Udbhava Sthana Pitta Sthana (Adhoamasaya)
Sanchara Sthana Urah, Kanta, Shiras.
Adhishtana Uras
Vyakta Sthana Uras
Roga Marga Abhyantara

[Type the document title]
46
Figure 1: Flow chart of Samprapti in Tamaka Shwasa
Nidana Sevana
Vata Prakopaka
Vata prakopa
Kapha prakopaka
Kapha prakopa
Agnimandya
Kapha prakopa, Amotpa8
Sarva shareera
sancharana
Doshas lodge in Pranavaha
Srotas
Obstruct the movement of Prana Vayu
PraAloma gaA of Vayu
Tamaka Shwasa
Raja, Dhooma
Kha vaigunya in pranavaha
srotas
Pranavaha srotas
vaigunya

[Type the document title]
47
UPASHAYA – ANUPASHAYA
Upashaya
Any Dravya (Oushadhi, Ahara) or Adravya (Vihara) Upacharas which lead to
Sukhanubandha areUpashaya (93).
Anupashaya
Anupashaya is the opposite of Upashaya i.e. Ahara, Vihara and Oushadhis which
aggravate the condition of the disease are Anupashayas.
Table 13: Showing Upashaya and Anupashaya in Tamaka Shwasa (94)
Upashaya Anupashaya
Ushna Ahara Vihara.
Sheeta Ahara Vihara, Sheeta Ambu-
cold water
Aseeno Labhate Soukhyam – feels
comfortable to breath in a sitting
position.
Shayanasya Shwasa Piditaha –
discomfort worsens on lying.
Vimokshante Sukham –slight relief in
breathlessness on spitting out of the
sputum.
Presence of Kapha in the Pranavaha
srotas worsens difficulty in breathing.
Sunny weather relieves the symptoms.
Meghaihi Abhivardhate – cloudy
weather worsens the attack.
Quiet atmosphere is favorable. Pragvata – breeze.

[Type the document title]
48
Clear atmosphere, devoid of smoke and
dust helps in reducing the symptoms.
Exposure to dust or smoke worsens the
attack of Tamaka Shwasa.
Factors that reduces the Kapha vitiation
bring relief.
Sleshmala - Kapha increasing factors
aggravate the disease.
SADHYASADHYATA
Sadhyasadhyata refers to the prognosis of a disease i.e., whether the
disease is easily curable, difficult to cure or incurable. In Charaka Samhita it is
clearly mentioned that Tamaka Shwasa which is of recent origin is considered as
Sadhya and when it becomes chronic it is considered as Yapya. (95)
Vagbhata also supports the opinion of Charaka. He adds that if the disease
persists for less than a year in a Durbala Rogi, the disease is Kricchra Sadhya. (96)
Some authors consider Tamaka Shwasa to be Asadhya in Durbala Rogis. (97).
CHIKITSA
The term Chikitsa is derived from the root Kit Rogaapanayane.ie, the
measures adopted to remove causative factors. This also includes the break down
of the pathology involved and maintenance of Doshic equlibirum. Among the five
varieties of Shwasa - Urdhva, Maha and Chinna Shwasa are Asadhya and hence
treatment of these is not fruitful. Kshudra Shwasa is a trivial condition and does
not require any energetic treatment.
As the pathology of Tamaka Shwasa involves multiple changeable factors,
effective treatment of this illness cannot be standardized beyond a point. Vitiated
Vata and Kapha Doshas stemming from the Pitta Sthana, afflict the Rasa Dhatu
and Hridaya marma in the Pranavaha Srotas to produce the illness. Thus, the

[Type the document title]
49
procedures which aim to correct imbalance in Vata or Kapha Dosha form the main
aim of treatment in Tamaka Shwasa. (98)
Thus, drugs having Ushna veerya and which are Vatanulomaka are given
to Shwasa patients. Tamaka Shwasa is identified as a Yaapya /Kashtasaadhya
Vyadhi in which treatment has to be continued for prolonged periods with
meticulous care of the patient. (99)
NIDANA PARIVARJANA: (100)
The main Chikitsa for any disease is Nidana Parivarjana- avoidance of
causative factors. Being a Yapya Roga, avoidance of triggering factors and
provision of good quality of life with minimum medication is the aim of Tamaka
Shwasa management.
Treatment modalities used in Tamaka Shwasa may broadly be divided into two:
1. Management of Vegavastha
2. Management of Avegavastha
VEGAVASTHA
In the Vegavastha, all Acharyas have highlighted the importance of
Shodhana Chikitsa. After Poorvakarma of Snehana and Swedana, Vamana Karma
is advocated.

[Type the document title]
50
Vamana Karma in Tamaka Shwasa (101)
Vamana Karma expels the accumulated Kapha which has been liquefied by
Snehana and Swedana, thus clearing the air passages. Thus the free movement of
Vayu is restored. This is followed by Dhoomapana. In weak patients who cannot
undergo Shodhana, Dhoomapana alone can be adviced.
Nasya Prayoga in Tamaka Shwasa (102-103)
Different Yogas such as Rasona, Palandu, Grinjanaka Svarasa, and
Madhura Varga Dravya Siddha Ghrita are indicated for Nasya Karma.
AVEGAVASTHA
In between attacks treatment is given to prevent further vitiation of
Doshas.
1. Virechana Karma
2. Brimhana Chikitsa
3. Rasayana Chikitsa
Virechana Karma (104)
Virechana drugs which are Vatanulomaka, Ushna, and Kaphavataghna are
beneficial in setting right the Pratiloma Gati of Vayu. The Udbhava Sthana of
Tamaka Shwasa is the Pittasthana. Thus, Virechana which is Pittahara in nature,
cleanses the Pitta Sthana. Nityavirechana is an important therapeutic measure in
Tamaka Shwasa.

[Type the document title]
51
Brimhana and Rasayana Chikitsa (105)
Brimhana and Rasayana Chikitsa enhance the vital capacity and resistance
of the lungs, and can also act as adjuvants to the present modern treatments by
improving the quality of life of affected patients. Further, in the long run, this
disease causes emaciation of the body, which can be corrected by Brimhana
Chikitsa.
CONTEMPORARY VIEW:
HISTORICAL REVIEW OF ASTHMA:
Asthma is a Greek word derived from the verb aazein, meaning to exhale
with an open mouth, to pant, to gasp, or breathe sharply. The word first appeared
in Homer‘s Iliad. (106)
Hippocrates (460-367 B.C): He was the first person to use the term with reference
to a medical condition in his text Corpus Hippocraticum. (106)
The signs and symptoms of Tamaka Shwasa resemble those of Bronchial
Asthma in contemporary science.
DEFINITION
Bronchial Asthma is an inflammatory airway disease with episodic
occurrence of dyspnoea with wheezing. (107) The Global Initiative for Asthma has
proposed a descriptive definition of Asthma as follows - Asthma is a chronic
inflammatory disorder of the airways in which many cells and cellular elements
play a role‘.
The chronic inflammation is associated with airway hyper responsiveness
that leads to recurrent episodes of wheezing, breathlessness, chest tightness and

[Type the document title]
52
coughing, particularly at night or in the early morning. These episodes are usually
associated with widespread but variable airflow obstruction within the lung that is
often reversible either spontaneously or with treatment.
EPIDEMOLOGY (108)
The prevalence of asthma increased steadily over the latter part of the last
century, first in the developed and then in the developing countries. Current
estimates suggest that Asthma affects 300 million people worldwide, with a
predicted additional 100 million people affected by 2025. The socio-economic
impact is enormous, as poor control leads to days lost from school or work,
unscheduled health-care visits and hospital admissions.
Although the development and course of the disease, and the response to
the treatment, are influenced by genetic determinants, the rapid rise in prevalence
implies
that environmental factor are critically important in the development and
expression of the disease. To date, studies have explored the potential role of
indoor and outdoor allergens, microbial exposure, seasonal changes, diet, vitamins,
breastfeeding, tobacco smoke, air pollution and obesity but no clear consensus has
emerged. (109)
PATHOPHYSIOLOGY (110)
Airway hyper-reactivity (AHR) – the tendency for airways to narrow
excessively in response to triggers that have little or no effect in normal individuals
– is integral to the diagnosis of asthma and appears to be related, although not
exclusively, to airway inflammation. Other factors likely to be important in the
behavior of airway smooth muscle include the degree of airway narrowing and

[Type the document title]
53
neurogenic mechanisms. The relationship between atopy (the propensity to
produce IgE) and asthma is well established, and in many individuals there is a
clear relationship between sensitization and allergen exposure, as demonstrated by
skin prick reactivity or elevated serum specific IgE.
Common examples of allergens include house dust mites, pets such as cats
and dogs, pests such as cockroaches, and fungi. Inhalation of an allergen into the
airway is followed by an early and late-phase Bronchoconstrictor response.
In exercise-induced asthma, hyperventilation results in water loss from the
pericellular lining fluid of the respiratory mucosa, which, in turn, triggers mediator
release. In Persistent Asthma, a chronic and complex inflammatory response
ensues, characterized by an influx of numerous inflammatory cells, the
transformation and participation of airway structural cells, and the secretion of an
array of cytokines, chemokines and growth factors. Examination of the
inflammatory cell profile in induced sputum samples demonstrates that, although
asthma is predominantly characterized by airway eosinophilia, neutrophilic
inflammation predominates in some patients, while, in others, scant inflammation
is observed: so-called ‗pauci-granulocytic‘ asthma. With increasing severity and
chronicity of the disease, remodeling of the airway may occur, leading to fibrosis
of the airway wall, fixed narrowing of the airway and a reduced response to
bronchodialator medication.
CLINICAL FEATURES (111)
Typical symptoms include recurrent episodes of wheezing, chest tightness,
breathlessness and cough. Classical precipitants include exercise, particularly in
cold weather, exposure to airborne allergens or pollutants, and viral upper

[Type the document title]
54
respiratory tract infections. An inspection for nasal polyps and eczema should be
performed. Patients with mild intermittent asthma are usually asymptomatic
between exacerbations.
Individuals with persistent Asthma report ongoing breathlessness and
wheeze, but these are variable, with symptoms fluctuating over the course of one
day, or from day to day or month to month. Asthma characteristically displays a
diurnal pattern, with symptoms and lung function being worse in the early morning
or night. Particularly when poorly controlled symptoms such as cough and wheeze
disturbs sleep and have led to the term Nocturnal Asthma. Cough may be the
dominant symptom in some patients, and the lack of wheeze or breathlessness may
lead to a delay in reaching the diagnosis of so-called cough-variant Asthma. Some
patients with Asthma have a similar inflammatory response in the upper airway.
Careful enquiry should be made as to a history of Sinusitis, Sinus headache, a
blocked or runny nose, and loss of sense of smell.
Symptoms may occur in certain seasons or without any pattern; some
patients may remain symptomatic throughout the year. Cough is paroxysmal and
may be
accompanied by expectoration of thick and sticky sputum. Sneezing and running
nose are common and may precede and accompany with the attacks of wheezing.
The frequency and severity of symptoms and exacerbations varies from patient to
patient and also within the same patient from time to time.
AETIOLOGY (112)
Although the etiology of asthma is often elusive, an attempt should be
made to identify any agents that may contribute to the appearance or aggravation
of the condition. Particular enquiry should be made about potential allergens, such

[Type the document title]
55
as exposure to a pet cat, guinea pig, rabbit or horse, pest infestation, exposure to
moulds following water damage to a home or building, and any potential
occupational agents. In some circumstances, the appearance of asthma is triggered
by medications. Beta-blockers, even when administered topically as eye drops,
may induce bronchospasm, as may aspirin and other non-steroidal anti-
inflammatory drugs (NSAIDs). Other medications implicated include the oral
contraceptive pill, cholinergic agents and prostaglandin F2α. Betel nuts contain
arecoline, which is structurally similar to methacholine and can aggravate asthma.
Etiological factors of bronchial asthma are of two types. Some factors
called inducing factors can set initial development of asthma, whereas some other
factors provoke an episode in predisposed individuals suffering from asthma and
these are called provoking or trigger factors.
v Inducing Factors
Genetic factors are important to determine why asthma occurs in a particular
individual. Asthma occurs more commonly in relatives of atopic individuals. A
distinct gene for atopy on chromosome 11 has been identified. The frequent
clinical observation that asthma runs in families has been supported by many more
formal investigations. The genetics of production of total serum IgE have studied.
A correlation was found between the total serum IgE of parents and children,
suggesting the involvement of one or more genes. A gene for IgE response with
maternal inheritance was identified at chromosome. High level of IgE in cord
blood appears to be strong indicator of subsequent development of atopic disease.

[Type the document title]
56
v Precipitating Factors (Triggers) for Asthma (113)
1. Allergic triggers
· Indoor and outdoor moulds
· Pollen
· Insects
· Animal dander
· Dust mite particles
· Cockroach particles
· Some food and drug additives, preservatives and coloring agents (sulphites
used as a preservatives in some foods)
2. Non-allergic triggers
· Irritants: Tobacco smoke, indoor fuel (biomass) smoke, room deodorants,
fresh paint, household cleaning products, cooking odors
· Work place chemicals (occupational asthma, perfumes and cosmetics)
· Outdoor air pollution (zone, oxides of nitrogen, sulphur dioxide)
· Respiratory viral infections (para influenza in children, rhinovirus and
influenza in adults) can lead to prolonged destabilization of chronic
asthma.
· Exercise: especially in cold and dry air (free running, cycling, jogging);
swimming is least likely to precipitate
· Micro aspiration of gastric secretions (Gastro eosophageal reflux)

[Type the document title]
57
· Non-steroidal anti inflammatory drugs (aspirin, ibuprofen, indomethacin,
mefanmic acid)
· B-adrenergic antagonists (even selective agents can trigger asthma at high
doses; eye drops containing these drugs can precipitate asthma)
· Change in atmospheric conditions (pressure, humidity, temperature)
· Psychological factors; also alter perception of airways obstruction.
·
FEATURES THAT INCREASE THE PROBABILITY OF ASTHMA
(114)
More than one of the following symptoms: Wheeze, Breathlessness, Chest
tightness and Cough, particularly if:
· Symptoms worse at night and in the early morning
· Symptoms in response to exercise, allergen exposure and cold air
· Symptoms after taking aspirin or beta blockers
· History of atopic disorder
· Family history of asthma and/or atopic disorder
· Widespread wheeze heard on auscultation of the chest
· Unexplained low FEV1 or PEF
· Unexplained increased peripheral blood Eosinophilia
FEATURES THAT LOWER THE PROBABILITY OF ASTHMA (115)
· Prominent dizziness, light-headedness, peripheral tingling sensation
· Chronic productive cough in the absence of wheeze or breathlessness
· Repeatedly normal physical examination of chest when symptomatic
· Voice disturbance

[Type the document title]
58
· Symptoms with colds only
· Cardiac disease
· Normal PEFR or spirometry when symptomatic
EXACERBATIONS OF ASTHMA (116)
The course of Asthma may be punctuated by exacerbations with increased
symptoms, deterioration in lung function, and an increase airway inflammation.
Exacerbations are most commonly precipitated by viral infections, moulds
(Alternaria and Cladosporium), pollens and air pollution is also implicated. Most
attacks are characterized by a gradual deterioration over several hours to days but
some appear to occur with little or no warning: so-called Brittle Asthma. An
important minority of
patients appear to have a blunted perception of airway narrowing and fail to
appreciate the early signs of deterioration.
PROGNOSIS (117-118)
The outcome from Acute Severe Asthma is generally good. Death is
fortunately rare but a considerable. Failure to recognize the severity of an attack,
on the part of either the assessing physician or the patient, contributes to delay in
delivering appropriate therapy and to under-treatment.

[Type the document title]
59
INVESTIGATIONS (119)
Some physical examination findings increase the probability of asthma.
Nasal mucosal swelling, increased nasal secretions, and nasal polyps are often seen
in patients with allergic asthma. Eczema, atopic dermatitis, or other manifestations
of allergic skin disorders may also be present. Wheezing during normal breathing
or a prolonged forced expiratory phase correlates well with the presence of air flow
obstruction. Chest examination may be normal between exacerbations in patients
with mild asthma. During severe asthma exacerbations, airflow may be too limited
to produce wheezing and the only diagnostic clue on auscultation may be globally
reduced breath sounds with prolonged expiration. Hunched shoulders and use of
accessory muscles of respiration suggest an increased work of breathing.
PULMONARY FUNCTION TESTS (120)
The diagnosis of Asthma is predominantly clinical and based on a
characteristic history. Supportive evidence is provided by the demonstration of
variable airflow obstruction, preferably by using Spirometry to measure FEV1 and
VC. This identifies the obstructive defect, defines its severity, and provides a
baseline for bronchodilator reversibility.
PEAK EXPIRATORY FLOW RATE (121)
Definition:
Peak expiratory flow rate (PEFR) is the maximum rate at which the air
can be expired after a deep inspiration.

[Type the document title]
60
PEAK EXPIRATORY FLOW MONITORING (122)
PEF should be recorded as the best of three forced expiratory blows from
total lung capacity with a maximum pause of two seconds before blowing. The
patient can be standing or sitting. Further blows should be done if the largest two
PEF are not within 40 l/min.
PEF is best used to provide an estimate of variability of airflow from
multiple measurements made over at least two weeks. Increased variability may be
evident from twice daily readings. More frequent readings will result in a better
estimate but the improved precision is likely to be achieved at the expense of
reduced patient compliance.
OTHER INVESTIGATIONS (122)
Measurement of allergic status: The presence of atopy may be
demonstrated by skin prick tests. Similar information may be provided by
the measurement of total and allergen-specific IgE. A full blood picture
may show the peripheral blood Eosinophilia.
· Radiological examination: Chest X-ray appearances are often normal or
show hyperinflation of lung fields. Lobar collapse may be seen if mucus
occludes a large bronchus and, if accompanied by the presence of flitting
infiltrates, may suggest that Asthma has been complicated by allergic
Bronchopulmonary aspergillosis. An HRCT scan may be useful to detect
Bronchiectasis.

[Type the document title]
61
· Assessment of Eosinophilic airway inflammation: An induced sputum
differential Eosinophil count of greater than 2% or exhaled breath nitric
oxide concentration (FENO) may support the diagnosis but is non-specific.
MANAGEMENT (123)
Asthma is a chronic condition but may be controlled with appropriate
treatment in the majority of patients. Whenever possible, patients should be
encouraged to take responsibility for managing their own disease. A full
explanation of the nature of the condition, importance of key symptoms such as
nocturnal waking, the different types of medication, and, if appropriate, the use of
PEF to guide management decisions, should be given.
AVOIDANCE OF AGGRAVATING FACTORS (123)
This is particularly important in the management of Occupational Asthma
but may also be relevant in atopic patients. Smoking cessation is particularly
important, as smoking not only encourages sensitization, but also induces a
relative corticosteroid resistance in the airway.
THE STEPWISE APPROACH TO THE MANAGEMENT OF ASTHMA
(123)
· Step 1: Occasional use of inhaled short-acting β2-Adreno receptor agonist
Bronchodilators
· Step 2: Introduction of regular preventer therapy
· Step 3: Add-on therapy

[Type the document title]
62
· Step 4: Poor control on moderate dose of inhaled steroid and add-on
therapy: addition of a fourth drug
· Step 5: Continuous or frequent use of Oral Steroids
· Step-down therapy
NEBULIZATION
For treating acute symptoms, fast drug delivery and disposition is often
beneficial. Metered dose inhalers for asthma provide a prototype for rapid delivery
of drug to its site of action, as they produce beta agonist aerosols that deposit
directly onto the target tissue of the pulmonary airways. (124)
A nebulizer is a device which turns an aqueous solution of a drug into a
mist of fine particles for inhalation. (124). The aim of nebulizer therapy is to
deliver a therapeutic dose of the desired drug within a short delivery time, usually
10 minutes.
This is most beneficial when:
• Large inhaled drug doses are required
• Patients are too unwell or are unable to co-ordinate drug delivery devices
• Drugs are unavailable in hand held inhalers and a wider choice is needed
• Direct pulmonary therapy is required
A nebulizer delivers the liquid form of medication. Nebulized medications
are generally safe, as the amount of medication the child is prescribed and actually
receives is relatively small. This way of delivering the medication is relatively
easy for all age groups. The medication can be either pre-mixed or require the user

[Type the document title]
63
to dilute the medication with saline solution that is specifically manufactured for
use in the lungs. (125)
Aim of nebulizer therapy (125)
The aim of nebuliser therapy is to deliver a therapeutic dose of the desired
drug as an aerosol in the form of reparable particles within a fairly short period of
time, usually 5–10 minutes.
PROPER USE OF NEBULIZERS FOR THE PERFECT OUTPUT (126)
Driving gas:
In acute asthma while giving Salbutamol, Terbutaline, Ipratropium or
Duovent, use oxygen as the driving gas. In all other situations use air. Patients
with severe asthma are often hypoxic. Giving a bronchodilator via air may worsen
hypoxaemia. The appropriate gas should be indicated by the prescriber.
Diluents & fill volumes
All nebulizer chambers leave a residual volume of between 0.5 and 1.0ml.
The residual volume in the Intersurgical Cirrus Chamber is 0.9ml. This means that
0.9ml of the drug does not reach the patient, and this should be considered when
the dose is calculated. Increasing the fill volume by adding a diluents leads to a
decrease in the amount of active drug wasted.
Flow rates
Gas flow rate influences both nebulization time and the size of the droplets
being dispersed. An increased flow rate means that although nebulization time is

[Type the document title]
64
shorter, the size of the droplets is smaller. For efficient drug delivery to the
bronchial tree, the optimum droplet diameter is 1-5 microns.
Delivery time
The nebulizer will never run dry due to the residual volume. Dependent
upon the drug and nebulizer, up to 80% of the total dose is administered within the
first five minutes of delivery. But compliance drops with longer administration
time. The nebulizer chamber should be tapped when spluttering occurs.
Patient position
The patient should be comfortable and sitting upright. Ensure the mask fits
properly and is comfortable and encourage the patient to breathe steadily through
the mouth (not nose) where possible. The patient should avoid talking as this
reduces the efficiency of drug delivery. Leaning slightly forwards gives maximum
expansion of the lungs. It is important that the nebulizer chamber remains upright
at all times.
DRUGS USED VIA A NEBULISER (126-127)
Beta agonists, anti-cholinergics, corticosteroids and antibiotics are the main
drugs commonly administered by nebulizer. If a diluent is required, unless
otherwise stated, only Sodium Chloride 0.9% for injection should be used, as
hypotonic solutions can cause bronchospasm.

[Type the document title]
65
ARKA AS A DOSAGE FORM: (127-128)
Arka Kalpana can be defined as a liquid preparation obtained by
distillation of certain liquids or of drugs soaked in water using the Arkayantra, or
any convenient modern distillation apratus. The concept of Arka as a dosage form
is dealt with mainly in Ravana’s Arka Prakasha. Seven different types of Arka
have been mentioned in classical literature – based on contents, part used, duration
of preparation, action on the doshas, Manogunas, Rutus and Rogas.
General Method of Arka preparation:
A required quantity of water is added to the particular drug which is soaked and
kept overnight. The following day morning, it is poured into the Arka Yantra and
the remaining water is added to it and it is boiled. Recent authors add that eight
times the quantity of water must be added to the raw drug. The vapors produced
therein get condensed and are collected in a receiver. Recent authors have once
again specified that only 2/3rds of the condensed liquid must be collected.
Specifications for Arka preparation with respect to the nature of the Agni
(Deeptagni, Kharagni etc.), the concentration of the Arka required (Atyanta
Kathina, Kathina etc.), the part of the plant used (Patra, Kanda etc.), have been
mentioned.
Aim of Arka Kalpana:
The Arka kalpana is frequently used today due to its reduced dose, increased
patient compliance and increased potency. Contemporary texts provide standard
preparation methods and evaluation techniques for Arkas extracted from different
plants.

[Type the document title]
66
The main aim in this Kalpana is to extract the maximum number of active and
volatile principles from the raw ingredients. Hence, it is suitable for use as a
nebulizing agent.

67
METHODOLOGY
The objectives of the study were to evaluate the Shwasahara Karma of
Parnayavani Arka nebulization and compare its efficacy with a standard drug
– Theophylline - nebulization and carry out a preliminary phytochemical and
pharmacognostic study of Parnayavani (Coleus aromaticus Benth.). In
fulfillment of these, the study has been carried out in two phases as follows:
• Preliminary pharmacognostic and physico-chemical analysis
• Clinical study
Ø PHARMACOGNOSTIC ANALYSIS :
1. Macroscopy: The external features of the test sample was documented
using Canon IXUS digital camera.
2. Microscopy: Sample was preserved in fixative solution. The fixative used
was FAA (Formalin-5ml + Acetic acid-5ml + 70% Ethyl alcohol-90ml).
The materials were left in FAA for more than 48 hours. The preserved
specimens were cut into thin transverse section using a sharp blade and the
sections were stained with saffranine. Transverse sections were
photographed using Zeiss AXIO trinocular microscope attached with Zeiss
AxioCam camera under bright field light. Magnifications of the figures are
indicated by the scale-bars.
3. Powder microscopy: A pinch of powder was warmed with drops of
chloralhydrate on a microscopic slide and mounted in glycerine. Slides
observed under microscope and diagnostic characters were observed and
photographed using Zeiss AXIO trinocular microscope attached with Zeiss

68
AxioCam camera under bright field light. Magnifications of the figures are
indicated by the scale-bars.
Ø PHYSICO-CHEMICAL ANALYSIS:
I. PHYSICAL ANALYSIS
1) Loss on drying at 105oC
10 g of sample was placed in tarred evaporating dish. It was dried at 105˚C for 5
hours in a hot air oven and weighed. The drying was continued until the
difference between two successive weights was not more than 0.01g after
cooling in a desiccator. The percentage of moisture was calculated with
reference to the weight of the sample.
2) Total Ash
2 g of sample was incinerated in a tarred platinum crucible ata temperature not
exceeding
450˚C until carbon free ash was obtained. The percentage of ash was calculated
with reference to the weight of the sample.
3) Acid insoluble Ash:
To the crucible containing total ash, 25ml of dilute HCl was added and boiled.
The insoluble matter was collected on ashless filter paper (Whatmann 41) and
washed with hot water until the filtrate became neutral. The filter paper
containing the insoluble matter was then transferred to the original crucible,
dried on a hot plate and ignited to a constant weight. The residue was allowed
to cool in a suitable dessicator for 30 min and weighed without delay.

69
Thepercentage of acid insoluble ash was calculated with reference to the air
dried drug.
4) Water soluble ash
The ash obtained from the Total Ash experiment was boiled for 5 min with 25
ml of water; insoluble matter collected on an ashless filter paper, washed with
hot water, and ignited for 15 min at a temperature not exceeding 450˚C. The
weight of the insoluble matter was subtracted from the weight of the ash. The
difference in weight represents the water soluble ash content with reference to
the air-dried sample.
5) Alcohol soluble extractive
4 g of the sample was accurately weighed and taken in a glass stoppered flask.
100 ml of distilled Alcohol (approximately 95%) was added, and shaken
occasionally for 6 hours. It was then allowed to stand for 18 hours. It was then
filtered rapidly taking care not to lose any solvent. 25ml of the filtrate was
pipetted out in a pre-weighed 100 ml beaker and evaporated to dryness on a
water bath. It was then kept in a hot air oven at 105°C for 6 hours, cooled in a
desiccator for 30 minutes and weighed. The percentage of Alcohol extractable
matter of the sample was then calculated. The experiment was repeated twice,
and the average value taken.
6) Water soluble extractive:
4 g of the sample was accurately weighed and taken in a glass stoppered flask.
100 ml of distilled water was added and shaken occasionally for 6 hours. It
was then allowed to stand for 18 hours, then filtered rapidly taking care not to

70
lose any solvent. 25ml of the filtrate was pipetted out in a pre-weighed 100 ml
beaker and evaporated to dryness on a water bath. It was then kept in a hot air
oven at 105°C for 6 hours, cooled in a desiccator for 30 minutes and weighed.
The percentage of water extractable matter of the sample was then calculated.
The experiment was repeated twice, and the average value taken.
II. PHYTOCHEMICAL ANALYSIS
Preliminary phytochemical tests:
Preliminary Phytochemical tests are used to detect the presence of various
organic functional groups, which is indicative of the type of phytochemicals
present in the plant. These tests indicate the presence of different classes of
constituents present in the extract. Tests were performed as per the
methodologies mentioned by Harborne JB, 1973 (Phytochemical Methods.
Jackman H. (Ed.), London, p. 70.)
The following tests were carried out for the aqueous extract of the drug:
1. Tests for alkaloids
a. Dragendroff’s test: To a few mg of extract dissolved in alcohol, a few drops
ofacetic acid and Dragendroff’s reagent were added and shaken well. An
orange red precipitate formed indicates the presence of alkaloids.
b. Wagners’s test: To a few mg of extract dissolved in acetic acid, a few drops
of
Wagner’s reagent was added. A reddish brown precipitate formed indicates
the presence of alkaloids.

71
c. Mayer’s test: To a few mg of extract dissolved in acetic acid, a few drops of
Mayer’s reagent was added. A dull white precipitate formed indicates the presence of
alkaloids.
d. Hager’s test: To a few mg of extract dissolved in acetic acid, 3 ml of Hager’sreagent
was added, the formation of yellow precipitate indicates the presence of alkaloids.
2. Tests for carbohydrates
a. Molisch’s test: To the extract, 1 ml of α-naphthol solution and conc. sulphuricacid
were added along the sides of test tube. Violet colour formed at the junction of the two
liquids indicates the presence of carbohydrates.
b. Fehling’s test: A few mg of extract was mixed with equal quantities of
Fehling’s solution A and B. The mixture was warmed on a water bath. The
formation of a brick red precipitate indicates the presence of carbohydrates.
c. Benedict’s test: To 5 ml of Benedict’s reagent, a few mg of extract was added,and
boiled for two minutes and cooled. Formation of a red precipitate indicates the
presence of carbohydrates.
3. Test for steroids
a. Libermann-Burchardtest:To the extract was dissolved in chloroform, 1 ml ofacetic
acid and 1 ml of acetic anhydride were added, then heated on a water bath and
cooled. Few drops of conc. Sulphuric acid were added along the sides of the test tube.
Appearance of bluish green colour indicates the presence of steroids.

72
b. Salkowski test: The extract was dissolved in chloroform and equal volume ofconc.
Sulphuric acid was added. Formation of bluish red to cherry red colour in chloroform
layer and green fluorescence in the acid layer indicates the presence of steroids.
4. Test for saponins: To a few mg of extract, distilled water was added andshaken.
Stable froth formation indicates the presence of saponins.
5. Test for tannins: To the extract, a few drops of dilute solution of ferric chloridewas
added, formation of dark blue colour shows the presence of tannins.
6. Test for flavonoids
Shinoda’s test: To the extract in alcohol, a few magnesium turnings and fewdrops of
conc. hydrochloric acid were added and heated on a water bath. Formation of red to
pink colour indicates the presence of flavonoids.
7. Test for phenols
To the extract in alcohol, added two drops of alcoholic ferric chloride. Formation of
blue to blue black indicates the presence of phenol.
8. Test for coumarins
To the extract in alcohol, a few drops of 2 N sodium hydroxide solution was added.
Dark yellow colour formation indicates the presence of coumarins.

73
9. Test for triterpenoids
The extract was warmed with tin bits and few drops of thionyl chloride. Formation
of pink colour indicates the presence of triterpenoids.

74
CLINICAL STUDY
AIM:
To evaluate the efficacy of Parnayavani Arka nebulization in the management of Tamaka
Shwasa with special reference to Bronchial Asthma.
ETHICS:
The study was initiated after obtaining Institutional Ethics Committee (SDM/IEC/22/2015-
2016) Approval and written informed consent from participants. The study was registered
with the Clinical Trial Registry of India (CTRI/2018/03/012339)
SOURCE OF DRUG:
Parnayavani was cultivated in the Shri Dharmasthala Manjunatheshwara College of
Ayurveda and Hospital, Hassan herbal garden.
PLACE OF WORK:
(a) Parnayavani Arka was prepared at the Dept. of Dravyaguna and Rasashastra and
Bhaishjyakalpana, Shri Dharmasthala Manjunatheshwara College of Ayurveda and
Hospital, Hassan.
(b) Preliminary pharmacognostic and physic-chemical analysis was carried out at Shri
Dharmasthala Manjunatheshwara College of Ayurveda and Hospital, Kuthpady,
Udupi
(c) Clinical study was carried out at Shri Dharmasthala Manjunatheshwara College of
Ayurveda and Hospital, Hassan.

75

76
DESIGN OF THE STUDY:
A single blind double arm, active control clinical trial with pre-test - post-
test design.
Plan of Study:
The clinical study was done as follows:
Patients falling under the inclusion criteria were randomly allocated to the
study and pre and post PEFR was done to evaluate change in lung function.
Nebulization was given at a dose of 5 ml, once.
SOURCE OF DATA:
Patients of either sex diagnosed with Tamaka Shwasa, who fulfilled inclusion criteria
for the study were taken from the OPD and IPD of Shri Dharmasthala
Manjunatheshwara College of Ayurveda and Hospital, Hassan.
Methods of collection of data:
A clinical case proforma was prepared with all points of history taking,
physical signs and symptoms of Tamaka Shwasa. Accordingly patients were
subjected to detailed clinical examinations. Selected patients were randomly
allocated into one of two intervention groups based on chit method - Parnayavani
Arka nebulization group, or Theophylline nebulization group.

77
Design of the study:
The present clinical study was a double arm, active control, randomized
clinical study conducted in a tertiary Ayurveda healthcare center attached to a
teaching institute, situated at the district headquarters in Hassan, Karnataka. 60
patients suffering from Tamaka Shwasa w.s.r. to Bronchial Asthma, who signed
the informed consent form, and who fulfilled the inclusion criteria for the study
were randomly allocated into two groups – one with the trial drug of Parnayavani
Arka nebulization, and the other with the standard drug, Theophylline
nebulization.
Diagnosis
Diagnosis was made on the basis of Lakshanas of Tamaka Shwasa w.s.r. to
bronchial asthma like wheezing, tightness of chest, breathlessness and cough,
followed by a detailed respiratory system examination.
Inclusion criteria:
• Peak Expiratory Flow Rate (PEFR) 60% - 90%
• Conscious and well oriented
• Age 16 – 60 years
• Either gender
• Previously diagnosed cases of bronchial asthma
• Those patients who are ready to sign the informed consent form

78
Exclusion criteria:
• PEFR < 40%
• Patients with a history of Tuberculosis, Emphysema, Chronic airway
limitation
• History of Cardiac involvement
• Other complicated respiratory diseases having any organic lesions such as a
tumor or any anatomical defect in the airway
• Cyanosis
• Uncontrolled Hypertension,
• Uncontrolled Diabetes mellitus
Table 14: Group allocation in clinical study
Group No. Patients Drugs Dose
Dose
administration
T (Stand. Group) 30 Theophylline respule nebulization 5 ml Single time
PA (Trial Group) 30 Parnayavani Arka nebulization 5ml Single time
Assessment criteria:
1. The effect of the therapy was assessed on the basis of relief in the
following signs and symptoms of Tamaka Shwasa w.s.r. to bronchial asthma as
per GINA guidelines which were assigned suitable scores.
• Breathlessness
• Wheezing

79
• Difficulty in speech
• Chest tightness
• Cough
• Sputum expectoration
• Pulse rate
• Respiratory rate
Table 15: Subjective assessment parameters (GINA) of Acute asthma
Signs and Symptoms BT IMMEDIATELY AT 1 HOUR AT
1. Breathlessness
2. Wheeze
3. Talks in
4. Cough
5. Sputum
6. Chest Tightness
7. Pulse Rate
8. Respiratory Rate
Table 16: GINA Grading of Subjective Parameters in Acute Asthma
SL
No
ASSESSMENT
CRITERIA 0 1 2 3

80
2. Objective parameter for assessment was PEFR done before treatment,
after treatment, and one hour after treatment.
1 . Breathlessness Absent
Mild- while
walking
Can lie down
While at rest-
prefers sitting
While at rest-sits
upright
2. Wheeze Absent
Moderate -
often only at
end expiration
Loud-
throughout
expiration
Usually loud-
throughout
inhalation &
exhalation
3. Talks in Sentences Sentences Phrases Words
4. Cough Absent After exercise Continuous,
disturb work
Continuous,
disturbs normal
activity
5. Sputum Absent 1-3 times 4-5 times Continuously
6. Chest tightness Absent Mild Moderate Severe
7. Pulse/min <80 80-100 100-120 >120
8. Respiratory
rate/min 18-23 24-30 31-40 >40

81
Table 17: Table showing trial drug authentication, processing and manufacture :
Raw materials and authentication Cultivated and collected from the herb
garden of Shri Dharmasthala
Manjunatheshwara College of Ayurveda,
Hassan, and validated at the Dept. of
Dravyaguna, Shri Dharmasthala
Manjunatheshwara College of Ayurveda,
Hassan.
Parnayavani Arka preparation
To 50gms of raw Parnayavani Patra, 2
times water was added and kept for 24
hours. This mixture (drug and water)
was continuously heated in the
ArkaYantra (distillation apparatus) till
60% of distillate was collected. After
cooling, the collected Arka (distillate)
was filtered and preserved in an air
tight container.
Packaging and labelling The prepared medicine was stored in a
properly labeled airtight container,
labeled with the Name, Batch no.,

82
manufacturing date, and expiry date.
Withdrawal Criteria
The participants were allowed to withdraw from the trial if there were any
major ailments necessitating the institution of new modalities of treatment. The
decision to withdraw a participant from the trial was taken by the principal
investigator with proper justification and formal information to the Ethics Committee
within two working days.
Drop-Outs
An attempt was made to record the reason for drop outs, if any during the clinical trial.
STATISTICAL METHODS
§ Statistical analysis was done using SPSS VER. 20
§ Completed 60(30+30) patients were taken for statistical analysis.
§ Friedman’s test with Bonferroni correction was applied to analyze the
significance of change in Subjective parameters (within the group).
§ Wilcoxon sign rank test was done for post Hoc analysis with
Bonferroni correction on parameters which show significance in
Friedman’s test, to interpret the time of significant change.
§ Mann-Whitney U was done to assess the differences in time points
within the groups.

83
§ Repeated measures ANOVA was done for analyzing the different
time of significant changes between the groups.
The obtained results were interpreted in statistical terms as:
§ Significant (S): P <0.05

84
SAMPLE SIZE OF ESTIMATION
Mean population (µ0): 8
Mean, study group (µ1): 5
Probability of type I error (α) : 0.05
Probability of type II error (β): 0.2
Power: 0.8
Sample Size group 1 (N1): 29
Sample Size group 2 (N2): 29
Total: 58
N1 = (σ21 + σ2
2 / K) (z1- α/2 + z1- β)2 ∆2
= (4.12 + 4.12/1)(1.96 + 0.84)2
32
N1 = 29 N2 = K * N1 = 29 Hence, a sample size consisting of 60 volunteers was selected.

85
RESULTS
1. PHARMACOGNOSTIC ANALYSIS
2. CLINICAL STUDY
PHARMACOGNOSTIC STUDY:
Leaf of Coleus aromaticus Benth.
• Macroscopy:
Leaf:
The leaves are simple, opposite, long petioled, broadly ovate or cordate,
with an acute apex. They have a dentate margin, are very fleshy, thick and
very aromatic. They are thickly studded with hairs. On the lower surface,
glandular hairs are more numerous.
Stem:
The stem is fleshy, tomentose, hispidly villous and is about 30 cm.
• Microscopy:
• Petiole:
Transverse section of petiole is concave on the upper side and convex on
the lower side. Trichomes of both glandular and nonglandular type are
present all over the surface. The outer layer epidermis consist of a single
layer of laterally elongated cells, followed by 3-4 layers of cortical cells
which are round & collenchymatous. The rest of the cortical cells are
polygonal to round. The vasculature comprises of a ring of eight collateral
vascular bundles, of which the two are larger in size. The ground tissue
consists of thin walled parenchymatous cells.

86
• Midrib:
Transverse section of leaf passing through the midrib appears
hemispherical on the ventral side and slightly depressed on the dorsal side.
Upper epidermis is single layered and consists of compactly arranged
rectangular cells. Below this layer there is palisade parenchyma which is
also continuous with the midrib. Vascular bundles are solitary, collateral
and consist of 4-6 rows of xylem and a thin arc of phloem runs along the
midrib. Lower epidermis is similar to upper epidermis and is
discontinuous due to the presence of diacytic stomata On the upper and
lower epidermal surface numerous glandular and non glandular trichomes
are present.
• Lamina:
Upper Epidermis consists of single layer of rectangular cells along with a
thin layer of cuticle on it. Numerous trichomes of both glandular and non
glandular nature are present on both upper and lower epidermis.
The Mesophyll is differentiated into 2 parts – palisade parenchyma and
spongy parenchyma. The palisade parenchyma lies toward the upper
epidermis and consist of single layer of elongated columnar
parenchymatous cells. Towards the lower epidermis there lies the spongy
parenchyma which consists of 5-6 layers of loosely arranged spherical
cells.

87
Beside these numerous oil globules and prismatic calcium oxalate crystals
and starch cells were present in the ground tissue. Coursing through the
mesophyll vascular bundles surrounded
• Trichome:
The plant is densely covered with hairs of both glandular and non
glandular type.
The glandular trichomes are of capitates type which consists of a basal
epidermal cell, unicellular to bicellular stalk of variable lengh, a neck cell
and a large globular unicellular secretory head.
The non glandular trichomes are 3-6 celled, variable length uniseriate,
unbranched and progressively
Powder:
The powder is green, bitter to taste and has a characteristic odour. It shows
epidermal cells in the surface view with slightly wavy walls; diacyctic
stomata; both uneseriate as well as glandular trichomes; broad and narrow
vessel elements also seen, collapsed trichomes seen in the surface view of
the epidermis.

88
Table 18: RESULTS OF PHYSICOCHEMICAL ANALYSIS:
Table 19: RESULT OF PRELIMINARY PHYTOCHEMICAL TESTS:
Sl No Tests Color if positive Parnayavani
1. Alkaloids
Dragendrof’s test Orange precipitate Red precipitate
Wagners test Red precipitate Red precipitate
Mayers test Dull white precipitate Dull white precipitate
Hagers test Yellow precipitate
2. Steroids
Liebermann- buchard
test Bluish green
Greenish white at the chloroform
layer and colorless at the acid layer
Salkowski test Bluish red to cherry
red
Green solution at the upper layer and
clear at the base layer
Physico-chemical result (w/w)%
Test Parnayavani Standard (API)
Foreign matter None Not more than 2%
Loss on drying 6.24% -
Total ash 7.5% Not more than 16%
Acid insoluble acid 1.4% Not more than 2 %
Water soluble ash 2.8% -
Alcohol soluble extractive 15.2% Not less than 7%
Water soluble extractive 19.2% Not less than 23%

89
3. Carbohydrate
Molish test Violet ring Violet ring
Fehlings test Brick red precipitate Ink blue solution
Benedicts test Red precipitate Dark green solution
4. Tannin
With FeCl3 Dark blue or green or
brown Green
5. Flavanoids
Shinoda’s test Red to pink White solution
6. Saponins
With NaHCO3 Stable froth Stable froth
7. Triterpenoids
Tin and thionyl
chloride test Red White precipitate
8. Coumarins
With 2 N NaOH Yellow Brownish green
9. Phenols
With alcoholic ferric
chloride
Blue to blue black,
brown Green
10. Carboxylic acid
With water and
NaHCO3 Brisk effervescence no effervescence
11. Resin
With aqueous acetone Turbidity Turbidity

90
12. Quinone
5% NaOH Pink/purple/red Brownish green
13. Amino acids
Ninhydrine reagent Purple color Green solution
Table 20: Summarized results of preliminary phytochemical tests
Test Parnayavani
Alkaloid +
Carbohydrate +
Carboxylic acid -
Coumarins -
Flavanoids -
Phenol +
Quinone -
Resins +
Steroid -
Saponins +
Tannin +
Terpenoid -
Amino acids -

91
Table 21: RESULTS OF PARNAYAVANI ARKA EVALUATION:
Test Parnayavani
pH 6
Refractive index 1.33229
Specific gravity 63.89
Viscosity 63.89
Volatile matter
(%)
0.21
Boiling point 1000C
Total acidity 0.36
% acidity 0.021

92
RESULTS OF GC-MS EVALUATION OF ARKA:
Table 22: MS of compounds identified from Arka of Coleus aromaticus
Fig.2: Octadecane, 3-ethyl-5-(2 ethylbutyl)
Fig 3: Dodecyl acrylate
Fig 4: Octadecanal, 2-bromo-
RT Name Formula MF RMF
6.311 Octadecane, 3-ethyl-5-(2
ethylbutyl)
C26H54 882 897
6.981 Dodecyl acrylate C15H28O2 811 847
7.077 Octadecanal, 2-bromo- C13H35BrO 770 770

93
CLINICAL STUDY:
Table 23: Gender Distribution of 60 patients of Tamaka Shwasa
Gender analysis of 60 patients of Tamaka Shwasa in the current study showed that
there were 12 males and 17 females in the trial group, and 16 males and 15 females in
the control group. Totally there were 28 males and 32 females.
Figure 5: Gender Distribution of 60 patients of Tamaka Shwasa
12
16 18
14
Trial Control
Male Female
Gender Group Total Percentage (%)
Trial Control
Male 12 16 28 46.7
Female 18 14 32 53.3
Total 30 30 60 100

94
Table 24: Age distribution of 60 patients of Tamaka Shwasa:
Age-wise analysis of 60 patients of Tamaka Shwasa in the current study showed that
there was highest incidence of patients in the age group between 40-60 years, and 20-
30 years.
Figure 6: Age distribution of 60 patients of Tamaka Shwasa:
0
2
4
6
8
10
12
14
10-‐20 yrs 20-‐30 yrs 30-‐40 yrs 40-‐50 yrs 50-‐60 yrs
Trial
Control
Age Group Total Percentage (%)
Trial Control
10-20 yrs 0 0 0 0
20-30 yrs 5 8 13 21.7
30-40 yrs 2 8 10 16.7
40-50 yrs 13 5 18 30
50-60 yrs 10 9 19 31.6
Total 30 30 60 100

95
Table 25: Marital status Distribution of 60 patients of Tamaka Shwasa:
Marital status analysis of 60 patients of Tamaka Shwasa in the current study showed
that there were 2 unmarried and 28 married subjects in the trial group, and 4
unmarried and 26 married subjects in the control group. Totally, there were 6
unmarried and 54 married subjects. There were no divorced or widowed subjects.
Figure 7: Marital status Distribution of 60 patients of Tamaka Shwasa
2 4
28 26
Trial Control
Unmarried Married
Marital status Group Total Percentage (%)
Trial Control
Unmarried 2 4 6 10
Married 28 26 54 90
Total 30 30 60 100

96
Table 26: Place wise distribution of 60 patients of Tamaka Shwasa
Place wise distribution of 60 patients of Tamaka Shwasa in the current study showed
that there were 12 subjects from urban areas and 18 subjects from rural areas in the
trial group. There were 25 subjects from urban areas and 5 subjects from rural areas in
the control group.Totally, there were 37 subjects from urban areas and 23 subjects
from rural areas.
Figure 8: Place wise distribution of 60 patients of Tamaka Shwasa
12
25
18
5
Trial Control
Urban Rural
Place Group Total Percentage (%)
Trial Control
Urban 12 25 37 61.6
Rural 18 5 23 38.4
Total 30 30 60 100

97
Table 27: Religion wise distribution of 60 patients of Tamaka Shwasa:
Religion wise distribution of 60 patients of Tamaka Shwasa in the current study
showed that there were 29 Hindu subjects and 1 Muslim subject in the trial group.
There were 26 Hindu subjects, 2 Muslim subjects and 2 Christian subjects in the
control group. Totally, there were 55 Hindu subject, 3 Muslim subjects and 2
Christian subjects.
Figure 9: Religion wise distribution of 60 patients of Tamaka Shwasa
0
5
10
15
20
25
30
35
Hindu Muslim Christian
Trial
Control
Religion Group Total Percentage (%)
Trial Control
Hindu 29 26 55 91.7
Muslim 1 2 3 5
Christian 0 2 2 3.3
Total 30 30 60 100

98
Table 28: Socio-economic status wise distribution of 60 patients of Tamaka
Shwasa:
Socio-economic status wise distribution of 60 patients of Tamaka Shwasa in the
current study showed that there were 3 from poor backgrounds, 27 from lower middle
class backgrounds, 21 from middle class backgrounds, and 9 from upper middle class
backgrounds.
Figure 10: Socio-economic status wise distribution of 60 patients of Tamaka
Shwasa
3
20
7
0 0
7
14
9
Poor Lower middle class Middle Class Upper middle class
Trial Control
Socio-economic status Group Total Percentage (%)
Trial Control
Poor 3 0 3 5
Lower middle class 20 7 27 45
Middle Class 7 14 21 35
Upper middle class 0 9 9 35
Total 30 30 60 100

99
Table 29: Education wise distribution of 60 patients of Tamaka Shwasa
Education status wise distribution of 60 patients of Tamaka Shwasa in the current
study showed that there were 17 subjects who had completed Lower Secondary
education, 1 subject who had completed SSLC, 9 subjects who had completed
Undergraduation, and 3 subjects who had completed Postgraduation in the trial group.
There were 8 subjects who had completed lower secondary education, 6 subjects who
had completed SSLC, 1 subject who had completed PUC, 21 who had completed
Undergraduation and 6 who had completed Postgraduation in the control group.
Totally, there were 25 subjects who had completed Lower Secondary education, 7
subjects who had completed SSLC, 1 subject who had completed PUC, 21 subjects
who had completed Undergraduation, and 6 subjects who had completed
Postgraduation.
Figure 11: Education wise distribution of 60 patients of Tamaka Shwasa
17
1 0
9
3 8 6
1
12
3
Lower Secondary
SSLC PUC UG PG
Trial Control
Education Group Total Percentage (%)
Trial Control
Lower Secondary 17 8 25 41.7
SSLC 1 6 7 11.7
PUC 0 1 1 1.6
UG 9 12 21 35
PG 3 3 6 10
Total 30 30 60 100

100
Table 30: Presenting complaints of 60 patients of Tamaka Shwasa
In the current study, it was found that maximum number of patients presented with
Wheezing during the night (60), Chest tightness (50), Dyspnoea on exertion (42), and
cough (35).
Figure 12: Presenting complaints of 60 patients of Tamaka Shwasa
25
5 12
9
30
21
11
0
9
17 13
23
8
30 29
3 0
6
Trial Control
Presenting complaints Group Total
Trial Control
Dyspnoea on exertion 25 17 42
Dyspnea on rest and exertion 5 13 18
Cough 12 23 35
Wheezing during the day 9 8 17
Wheezing during the night 30 30 60
Chest tightness 21 29 50
Difficulty in speech 11 3 14
Confusion 0 0 0
Rhinitis 9 6 15

101
Table 31: Duration of onset in 60 patients of Tamaka Shwasa:
Analysis of duration of onset in 60 patients of Tamaka Shwasa in the current study
showed that there were 9 who complained of onset less than 5 years ago, 2 who
complained of a duration of onset between 5-10 years ago, 7 who complained of onset
between 10-15 years ago, and 5 who complained of a duration of onset between 20-25
years ago in the trial group. There were 10 who complained of onset less than 5 years
ago, 11 who complained of a duration of onset between 5-10 years ago, 13 who
complained of onset between 10-15 years ago, and 0 who complained of a duration of
onset between 20-25 years ago in the control group. Totally, there were 19 who
complained of onset less than 5 years ago, 13 who complained of a duration of onset
between 5-10 years ago, 12 who complained of onset between 10-15 years ago, 11
who complained of a duration of onset between 15-20 years ago, and 5 who
complained of a duration of onset between 20-25 years ago.
Figure 13: Duration of onset in 60 patients of Tamaka Shwasa
9
2
7 7 5
10 11
5 4
0
0-‐5 years 5-‐10 years 10-‐15 years 15-‐20 years 20-‐25 years
Trial Control
Duration Group Total Percentage (%)
Trial Control
0-5 years 9 10 19 31.7
5-10 years 2 11 13 21.7
10-15 years 7 5 12 20
15-20 years 7 4 11 18.3
20-25 years 5 0 5 8.3
Total 30 30 60 100

102
Table 32: Mode of onset in 60 patients of Tamaka Shwasa:
Analysis of mode of onset in 60 patients of Tamaka Shwasa in the current study
showed that there was no subject complained of gradual onset while all subjects
complained of sudden onset.
Figure 14: Mode of onset in 60 patients of Tamaka Shwasa
0
5
10
15
20
25
30
35
Trial Control
Gradual
Sudden
Onset Group Total Percentage (%)
Trial Control
Gradual 0 0 0 0
Sudden 30 30 60 100
Total 30 30 60 100

103
Table 33: Trigger factors in 60 patients of Tamaka Shwasa:
Analysis of trigger factors in 60 patients of Tamaka Shwasa in the current
study showed that there were 12 subjects who complained of dust as a trigger, 28
subjects who complained of cold as a trigger, 18 subjects who complained of both
dust and cold as triggers, and 2 who complained of other specific allergens.
Figure 15: Trigger factors in 60 patients of Tamaka Shwasa
7
20
3 0
5 8
15
2
Dust Cold Dust and Cold Other allergen
Trial Control
Trigger Group Total Percentage (%)
Trial Control
Dust 7 5 12 20
Cold 20 8 28 46.7
Dust and Cold 3 15 18 30
Other allergen 0 2 2 3.3
Total 30 30 60 100

104
Table 34: History of previous illness in 60 patients of Tamaka Shwasa
Analysis of trigger factors in 60 patients of Tamaka Shwasa in the current
study showed that there were 12 subjects who complained of dust as a trigger, 28
subjects who complained of cold as a trigger, 18 subjects who complained of both
dust and cold as triggers, and 2 who complained of other specific allergens.
Figure 16: History of previous illness in 60 patients of Tamaka Shwasa
10
15
0
5 5
1
6
18
Diabetes Hypertension DM and HTN Nothing signiNicant
Trial Control
Previous illness Group Total Percentage (%)
Trial Control
Diabetes 10 5 15 20
Hypertension 15 1 16 46.7
DM and HTN 0 6 6 30
Nothing significant 5 18 23 3.3
Total 30 30 60 100

105
Table 35: History of previous treatment in 60 patients of Tamaka
Shwasa:
Analysis of previous medication in 60 patients of Tamaka Shwasa in the
current study showed that there were 27 subjects who had a history of use of B2
adrenoreceptor bronchodilators such as Salbutamol or Terbutaline. 16 subjects had a
history of use of Anti-inflammatory therapy of inhaled corticosteroids such as
Beclometasone, Budesonide etc. 9 subjects had a history of use of Long acting B2
agonists such as Salmoterol, Formoterol etc. 5 subjects had a history of oral steroid
use. 3 subjects did not have significant previous treatment history.
Figure 17: History of previous treatment in 60 patients of Tamaka Shwasa
12
8
3 4 3
15
8 6
1 0
Trial Control
Treatment Group Total Percentage (%)
Trial Control
B-2 adrenoreceptor bronchodilators 12 15 27 45
Anti-inflammatory therapy - ICS 8 8 16 26.7
Long acting B2 agonists - Add on therapy 3 6 9 15
Oral steroid therapy - Prednisolone 4 1 5 8.3
Nothing significant 3 0 3 5
Total 30 30 60 100

106
Table 36: Family History in 60 patients of Tamaka Shwasa:
Analysis of family history in 60 patients of Tamaka Shwasa in the current
study showed that there were 16 subjects whose father (father’s relatives) suffered
from asthma, 11 subjects whose mother suffered from asthma (or mother’s relatives),
1 subject whose son suffers from asthma, 2 subjects whose daughter suffers from
asthma, and 30 subjects who have no significant history of asthma.
Figure 18: Family History in 60 patients of Tamaka Shwasa
5
8
0
2
15
11
3
1 0
15
Father Mother Son Daughter Nothing signiNicant
Trial Control
Family history Group Total Percentage (%)
Trial Control
Father 5 11 16 26.7
Mother 8 3 11 18.3
Son 0 1 1 1.6
Daughter 2 0 2 3.4
Nothing significant 15 15 30 50
Total 30 30 60 100

107
Table 37: Occupation of 60 patients of Tamaka Shwasa:
Analysis of occupation in 60 patients of Tamaka Shwasa in the current study
showed that 15 subjects were housewifes/homemakers, 9 were independent
businessmen, 16 were agriculturalists, 6 were students, and 14 belonged to other
occupations such as drivers, construction workers etc.
Figure 19: Occupation of 60 patients of Tamaka Shwasa
4
8
12
1
5
11
1
4 5
9
Housewife Business Agriculture Student Other
Trial Control
Occupation Group Total Percentage (%)
Trial Control
Housewife 4 11 15 25
Business 8 1 9 15
Agriculture 12 4 16 26.7
Student 1 5 6 10
Other 5 9 14 23.3
Total 30 30 60 100

108
Table 38: Agni of 60 patients of Tamaka Shwasa
Analysis of Agni in 60 patients of Tamaka Shwasa in the current study
showed that 19 subjects had Sama Agni and 41 subjects had Manda Agni.
Figure 20: Agni of 60 patients of Tamaka Shwasa
0
5
10
15
20
25
Sama Manda Teekshna Vishama
Trial
Control
Agni Group Total Percentage (%)
Trial Control
Sama 8 11 19 31.7
Manda 22 19 41 68.3
Teekshna 0 0 0 0
Vishama 0 0 0 0
Total 30 30 60 100

109
Table 39: Ahara of 60 patients of Tamaka Shwasa:
Analysis of Ahara in 60 patients of Tamaka Shwasa in the current study
showed that 19 subjects were consumed only vegetarian food, while 41 subjects
consumed a mixed diet.
Figure 21: Ahara of 60 patients of Tamaka Shwasa
7
23
0 0
12
18
0 0
Vegetarian Mixed Teekshna Vishama
Trial Control
Ahara Group Total Percentage (%)
Trial Control
Vegetarian 7 12 19 31.7
Mixed 23 18 41 68.3
Teekshna 0 0 0 0
Vishama 0 0 0 0
Total 30 30 60 100

110
Table 40: Nidra of 60 patients of Tamaka Shwasa
Analysis of Nidra in 60 patients of Tamaka Shwasa in the current study
showed that 53 of subjects reported disturbed sleep, while 7 reported sound sleep.
Fig. 22: Nidra of 60 patients of Tamaka Shwasa
26 27
4 3
Trial Control
Disturbed Sound
Nidra Group Total Percentage (%)
Trial Control
Disturbed 26 27 53 88.4
Sound 4 3 7 11.6
Total 30 30 60 100

111
Table 41: Rasa preference of 60 patients of Tamaka Shwasa
Analysis of Rasa preferred in 60 patients of Tamaka Shwasa in the current
study showed that 27 subjects preferred Madhura Rasa, 6 preferred Amla Rasa and 27
preferred Katu Rasa.
Fig. 23: Rasa preference of 60 patients of Tamaka Shwasa
14
1
15 13
5
12
Madhura Amla Katu
Trial Control
Rasa Group Total Percentage (%)
Trial Control
Madhura 14 13 27 45
Amla 1 5 6 10
Katu 15 12 27 45
Total 30 30 60 100

112
Table 42: Alcohol and Smoking consumption in patients of Tamaka Shwasa:
Analysis of Alcohol and Smoking in in 60 patients of Tamaka Shwasa in the
current study showed that 17 subjects were regular smokers, 2 were habituated to
regular alcohol intake (beer, whiskey), 7 to both, and 34 to neither.
Fig. 24: Alcohol and Smoking consumption in patients of Tamaka Shwasa
4 2
5
21
13
0 2
13
Smoking Alcohol Both None of the above
Trial Control
Habits Group Total Percentage (%)
Trial Control
Smoking 4 13 17 28.4
Alcohol 2 0 2 3.3
Both 5 2 7 11.6
None of the above 21 13 34 56.7
Total 30 30 60 100

113
Table 43: Tea and Coffee consumption in 60 patients of Tamaka Shwasa:
Analysis of Alcohol and Smoking in in 60 patients of Tamaka Shwasa in the
current study showed that 17 subjects were regular smokers, 2 were habituated to
regular alcohol intake (beer, whiskey), 7 to both, and 34 to neither.
Fig. 25: Tea and Coffee consumption in 60 patients of Tamaka Shwasa
28 30
2 0
Trial Control
Tea/Coffee Neither
Habits Group Total Percentage (%)
Trial Control
Tea/Coffee 28 30 58 96.7
Neither 2 0 2 3.3
Total 30 30 60 100

114
Table 44: Wheezing in 60 patients of Tamaka Shwasa
Analysis of wheezing sounds in 60 patients of Tamaka Shwasa in the current study
showed that 43 had wheezing sounds, while 17 subjects did not show wheezing
sounds.
Fig. 26: Wheezing in 60 patients of Tamaka Shwasa
27
16
3
14
Trial Control
Present Absent
Wheezing Group Total Percentage (%)
Trial Control
Present 27 16 43 71.6
Absent 3 14 17 28.4
Total 30 30 60 100

115
Table 45: Nature of Wheezing sounds in 43 patients of Tamaka Shwasa
Among the 43 subjects who had wheezing sounds, 41 had polyphonic wheezes
while 2 had monophonic wheezes.
Fig. 27: Nature of Wheezing sounds in 43 patients of Tamaka Shwasa
27
16
3
14
Trial Control
Present Absent
Wheeze Group Total Percentage (%)
Trial Control
Polyphonic 26 15 41 95.3
Monophonic 1 1 2 4.7
Total 27 16 43 100

116
Table 46: Timing of Wheezing sounds in 43 patients of Tamaka Shwasa
Among the 43 subjects who had wheezing sounds, 17 showed inspiratory
wheezes and 26 showed expiratory wheezing sounds.
Fig. 28: Timing of Wheezing sounds in 43 patients of Tamaka Shwasa
10
7
12
14
Trial Control
Inspiratory Expiratory
Wheeze time Group Total Percentage (%)
Trial Control
Inspiratory 10 7 17 39.5
Expiratory 12 14 26 60.5
Total 22 21 43 100

117
Table 47: Rhonchi in 60 patients of Tamaka Shwasa
Analysis of rhonchi in 60 patients of Tamaka Shwasa in the current study
showed that 17 patients had rhonchi, while 43 did not.
Fig. 29: Rhonchi in 60 patients of Tamaka Shwasa
2
15
28
15
Trial Control
Present Absent
Rhonchi Group Total Percentage (%)
Trial Control
Present 2 15 17 28.4
Absent 28 15 43 71.6
Total 30 30 60 100

118
Table 48: Crepitations in 60 patients of Tamaka Shwasa
Analysis of rhonchi in 60 patients of Tamaka Shwasa in the current study
showed that 17 patients had rhonchi, while 43 did not.
Fig. 30: Crepitations in 60 patients of Tamaka Shwasa
13
8
17
22
Trial Control
Present Absent
Ralls Group Total Percentage (%)
Trial Control
Present 13 8 21 35
Absent 17 22 39 65
Total 30 30 60 100

119
Table 49: Timing of crepitation in 21 patients of Tamaka Shwasa
Among the 21 patients who had crepitations, it was found that 16 had coarse
ralls, while 5 had fine ralls.
Fig. 31: Timing of crepitation in 21 patients of Tamaka Shwasa
4
12
0
5
Trial Control
Coarse Fine
Ralls Group Total Percentage (%)
Trial Control
Coarse 4 12 16 76.2
Fine 0 5 5 23.8
Total 4 17 21 100
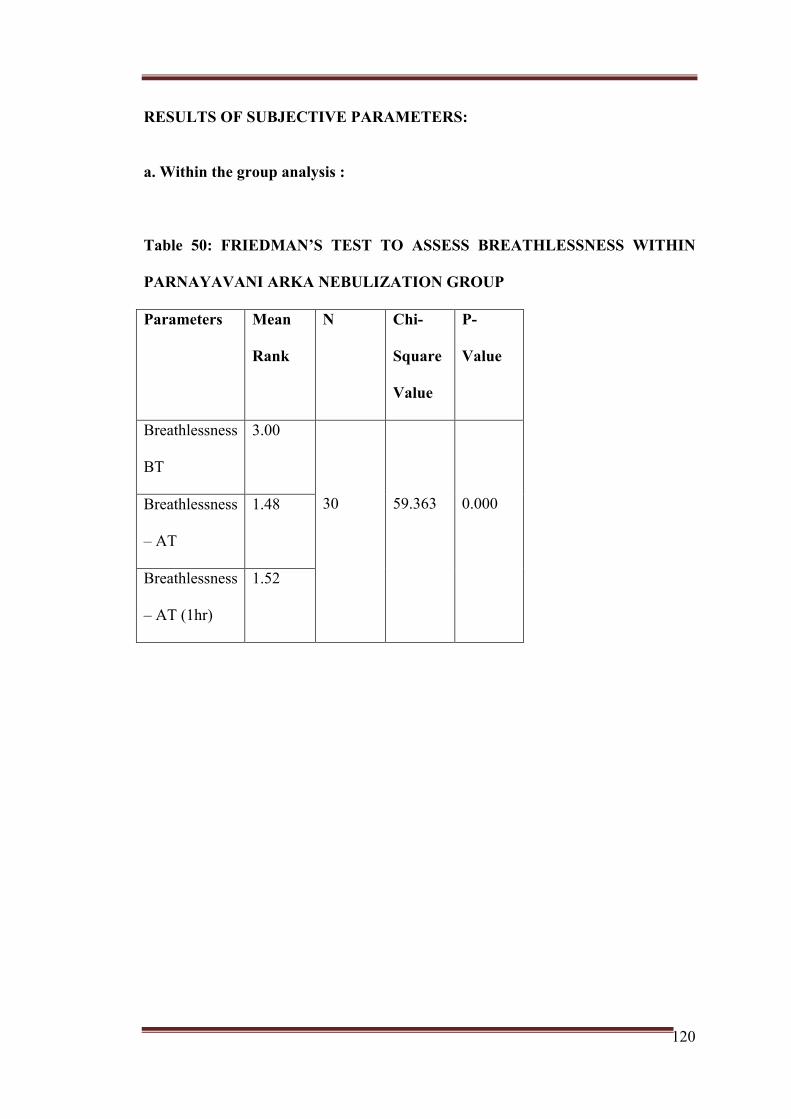
120
RESULTS OF SUBJECTIVE PARAMETERS:
a. Within the group analysis :
Table 50: FRIEDMAN’S TEST TO ASSESS BREATHLESSNESS WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-
Value
Breathlessness
BT
3.00
30
59.363
0.000 Breathlessness
– AT
1.48
Breathlessness
– AT (1hr)
1.52

121
Table 51: WSR Post hoc test with Bonferroni’s correction to assess
Breathlessness within trial group
There was a statistically significant difference in breathlessness before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
breathlessness between the BT and AT groups (Z = 4.928a a, p=0.000), and between
the BT-AT1 group (Z=-4.940a, p=0.000). There was a non-significant increase in
breathlessness between the AT-AT1 group (Z=-1.000b, p=0.157).
Table 52: FRIEDMAN’S TEST TO ASSESS WHEEZING WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Wheezing
–
BT
2.98
30
57.022
0.000 Wheezing
– AT
1.45
Wheezing 1.57
Parameters Breathlessness
(BT-AT)
Breathlessness
(BT-AT1)
Breathlessness
(AT-AT1)
Z-Value -4.928a -4.940a -1.000b
P-value 0.000 0.000 0.317
a. Based on positive ranks
b. Based on negative ranks

122
– AT (1hr)
Table 53: WSR Post hoc test with Bonferroni’s correction to assess
Wheezing within trial group
•
•
There was a statistically significant difference in wheezing before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
wheezing between the BT and AT groups (Z = -4.998a, p=0.000), and between the
BT-AT1 group (Z=--4.939, p=0.000). There was a non-significant increase in
wheezing between the AT-AT1 group (Z=-1.604, p=0.083).
Parameters Wheezing
(BT-AT)
Wheezing
(BT-
AT1)
Wheezing
(AT-
AT1)
Z-Value -4.998a -4.939a -1.604b
P-value 0.000 0.000 0.083
a. Based on positive ranks
b. Based on negative ranks

123
Table 54: FRIEDMAN’S TEST TO ASSESS SPEECH DIFFICULTY WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Speech
difficulty
– BT
3.00
30
60
0.000 Speech
difficulty
– AT
1.50
Speech
difficulty
– AT (1hr)
1.50
Table 55: WSR Post hoc test with Bonferroni’s correction to assess Speech
difficulty within trial group
Parameters Cough
(BT-AT)
Cough
(BT-
AT1)
Cough
(AT-
AT1)
Z-Value -5.007a -5.0079a -0.000b
P-value 0.000 0.000 1.000
a. Based on positive ranks
b. Based on negative ranks

124
There was a statistically significant difference in cough before and after intervention.
Post-hoc analysis with WSR was conducted with a Bonferroni correction applied,
resulting in a significance level p<0.017. There was a significant decrease in speech
difficulty between the BT and AT groups (Z = -5.007a, p=0.000), and between the
BT-AT1 group (Z=-5.007, p=0.000). There was no change in speech between AT-
AT1 groups. (Z=-0.000, p=1.000).
Table 56: FRIEDMAN’S TEST TO ASSESS COUGH WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Cough –
BT
3.00
30
60.00
0.000
Cough –
AT
1.50
Cough –
AT (1hr)
1.50

125
Table 57: WSR Post hoc test with Bonferroni’s correction to assess Cough
within trial group
•
•
There was a statistically significant difference in cough before and after intervention.
Post-hoc analysis with WSR was conducted with a Bonferroni correction applied,
resulting in a significance level p<0.017. There was a significant decrease in Cough
between the BT and AT groups (Z = -4.932a, p=0.000), and between the BT-AT1
group (Z=-4.932, p=0.000). There was no change in cough between the AT-AT1
group (Z=-0.000, p=1.000).
Table 58: FRIEDMAN’S TEST TO ASSESS SPUTUM EXPECTORATION
WITHIN PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Sputum
expectoration
2.98
Parameters Cough
(BT-AT)
Cough
(BT-
AT1)
Cough
(AT-
AT1)
Z-Value -4.932a -4.932a -0.000
P-value 0.000 0.000 1.000
a. Based on positive ranks
b. Based on negative ranks

126
–
BT
30
51.784
0.000
Sputum
expectoration
– AT
1.60
Sputum
expectoration
– AT (1hr)
1.42
Table 59: WSR Post hoc test with Bonferroni’s correction to assess Sputum
expectoration within trial group
•
There was a statistically significant difference in sputum production before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
sputum production between the BT and AT groups (Z = -4.800a, p=0.000), and
between the BT-AT1 group (Z=-4.922, p=0.000). There was a non-significant
decrease in sputum production between the AT-AT1 group (Z=-1.387, p=0.166).
Parameters Sputum
expectoration
(BT-AT)
Sputum
expectoration
(BT-AT1)
Sputum
expectoration
(AT-AT1)
Z-Value -4.800a -4.922a -1.387a
P-value 0.000 0.000 0.166
a. Based on positive ranks
b. Based on negative ranks

127
Table 60: FRIEDMAN’S TEST TO ASSESS TIGHTNESS IN CHEST WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value df
Tightness
in the
Chest –
BT
3.00
30
57.532
0.000
2
Tightness
in the
Chest –
AT
1.47
Tightness
in the
Chest –
AT (1hr)
1.53

128
Table 61: WSR Post hoc test with Bonferroni’s correction to assess Chest
tightness within trial group
Parameters Tightness
in the
chest
(BT-AT)
Tightness
in the
chest
(BT-
AT1)
Tightness
in the
chest
(AT-
AT1)
Z-Value -4.920a -4.922a -1.000b
P-value 0.000 0.000 0.317
There was a statistically significant difference in Chest Tightness before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
chest tightness between the BT and AT groups (Z = -4.920a, p=0.000), and between
the BT-AT1 group (Z=-4.922a, p=0.000). There was a non-significant increase in
chest tightness between the AT-AT1 group (Z=-1.000b, p=0.025)
Table 62: FRIEDMAN’S TEST TO ASSESS PULSE RATE WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Pulse rate
–
BT
2.92
a. Based on positive ranks
b. Based on negative ranks

129
Pulse rate
– AT
1.52 30 54.071 0.000
Pulse rate
– AT (1hr)
1.57
Table 63: WSR Post hoc test with Bonferroni’s correction to assess Pulse
rate within trial group
•
•
There was a statistically significant difference in pulse rate before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
pulse rate between the BT and AT groups (Z = -5.013a, p=0.000), and between the
BT-AT1 group (Z=-4.916, p=0.000). There was a non-significant increase in pulse
rate between the AT-AT1 group (Z=-1.000, p=0.317).
Parameters Pulse
rate
(BT-AT)
Pulse
rate
(BT-
AT1)
Pulse
rate
(AT-
AT1)
Z-Value -5.013a -4.916a -1.000b
P-value 0.000 0.000 0.317
a. Based on positive ranks
b. Based on negative ranks

130
Table 64: FRIEDMAN’S TEST TO ASSESS RESPIRATORY RATE WITHIN
PARNAYAVANI ARKA NEBULIZATION GROUP
Parameters Mean
Rank
N Chi-
Square
Value
P-Value
Respiratory
rate –
BT
2.60
30
36.000
0.000 Respiratory
rate – AT
1.70
Respiratory
rate – AT
(1hr)
1.70
Table 65: WSR Post hoc test with Bonferroni’s correction to assess
Respiratory rate within trial group
Parameters Respiratory
rate (BT-
AT)
Respiratory
rate (BT-
AT1)
Respiratory
rate (AT-
AT1)
Z-Value -4.243a -4.243a -0.000b
P-value 0.000 0.000 1.000
a. Based on positive ranks
b. Based on negative ranks

131
There was a statistically significant difference in respiratory rate before and after
intervention. Post-hoc analysis with WSR was conducted with a Bonferroni correction
applied, resulting in a significance level p<0.017. There was a significant decrease in
respiratory rate between the BT and AT groups (Z = -4.243a, p=0.000), and between
the BT-AT1 group (Z=-4.243, p=0.000). There was a no change in respiratory rate
between the AT-AT1 group (Z=-0.000, p=1.000).

132
b. Between the groups:
Table 66: MANN WHITNEY –U TEST FOR BETWEEN THE GROUPS
ANALYSIS
DEPENDANT
VARIABLE
INDEPENDENT
VARIABLE
N MEAN
RANK
ASYMP.
SIG. (2
TAILED)
P-value
INFERENCE
Breathlessness
immediately after
nebulization
Parnayavani Arka 30 30
Theophylline 30 31
Total 60 -0.399 0.690**
Breathlessness one
hour after
nebulization
Parnayavani Arka 30 29
Theophylline 30 32
Total 60 -0.993 0.321**
Wheezing
immediately after
nebulization
Parnayavani Arka 30 30
Theophylline 30 31
Total 60 -0.463 0.643**
Wheezing one
hour after
Parnayavani Arka 30 30

133
nebulization
Theophylline 30 31
Total 60 -0.000 1.000**
Speech difficulty
immediately after
nebulization
Parnayavani 30 30.50
Theophylline 30 30.50
Total 60 -0.000 1.000**
Speech difficulty
one hour after
nebulization
Parnayavani Arka 30 31.5
Theophylline 30 29.5
Total 60 -0.493 0.624**
Cough
immediately after
nebulization
Parnayavnai Arka 30 30.5
Theophylline 30 30.5
Total 60 -0.000 1.000**
Cough 1 hour after
nebulization
Parnayavani Arka 30 31.5
Theophylline
nebulization
30 29.50
Total 60 -0.753 0.451**
Sputum Parnayavani arka 30 31.5

134
expectoration
Theophylline 30 29.50
Total 60 -0.853 0.393**
Sputum
expectoration 1
hour after
nebulization
Theophylline 30 31.5
Parnayavani Arka 30 29.50
Total 60 -0.753 0.451**
Tightness in the
chest immediately
after nebulization
Parnayavani Arka 30 30.00
30 31.00
Total 60 -0.331 0.741**
Tightness in the
chest 1 hour after
nebulization
Parnayavani Arka 30 31
Theophyllinel 30 30
Total 60 -0.296 0.767**
Pulse rate
immediately after
nebulization
Parnayavani Arka 30 31.5
Theophylline 30 29.50
Total 60 -0.853 0.393**

135
Pulse rate one hour
after nebulization
Parnayavani Arka 30 31.5
Theophylline 30 29.50
Total 60 -0.753 0.451**
Respiratory rate
immediately after
nebulization
Parnayavani Arka 30 30
Theophylline 30 31
Total 60 -0.587 0.557**
Respiratory rate
one hour after
nebulization
Parnayavani Arka 30 30.5
Theophylline 30 30.5
Total 60 -0.000 1.000**
On comparing breathlessness immediately after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 435.000, W(29) = 900.000,
Z = -0.399, p = 0.690.On comparing breathlessness one hour after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 405.000, W(29) = 870.000,
Z = -0.993, p = 0.321.
On comparing wheezing immediately after nebulization in the Parnayavani
Arka nebulization group and the Theophylline nebulization group, it was found the
two groups did not differ significantly, U(29) = 435.000, W(29) = 900.000, Z = -

136
0.463, p = 0.643. On comparing wheezing one hour after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found that there was no significant change between the groups. U(29) = 450.000,
W(29) = 915.000, Z = 0.000, p = 1.000.
On comparing speech difficulty immediately after nebulization in both groups,
no significant difference was found between the two groups. U(29) = 450.000, W(29)
= 915.000, Z = -0.000, p = 1.000. On comparing speech difficulty one hour after
nebulization in both groups, there was no significant difference between the groups.
U(29) = 450.000, W(29) = 915.000, Z = -0.0001, p = 1.000
On comparing cough immediately after nebulization in both groups, there no
significant difference between the groups. U(29) = 450.000, W(29) = 915.000, Z = -
0.0001, p = 1.000. On comparing cough one hour after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 420.000, W(29) = 885.000,
Z = -0.753, p = 0.451.
On comparing the sputum expectoration immediately after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 420.000, W(29) = 885.000,
Z = -0.853, p = 0.393. On comparing sputum expectoration one hour after
nebulization in the Parnayavani Arka nebulization group and the Theophylline
nebulization group, it was found the two groups did not differ significantly, U(29) =
420.000, W(29) = 885.000, Z = -0.753, p = 0.451.
On comparing the chest tightness immediately after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 435.000, W(29) = 900.000,

137
Z = -0.331, p = 0.741. On comparing the chest tightness one hour after nebulization in
the Parnayavani Arka nebulization group and the Theophylline nebulization group, it
was found the the two groups did not differ significantly, U(29) = 435.000, W(29) =
900.000, Z = -0.296, p = 0.767.
On comparing the pulse rate immediately after nebulization in the Parnayavani
Arka nebulization group and the Theophylline nebulization group, it was found the
two groups did not differ significantly, U(29) = 420.000, W(29) = 885.000, Z = -
0.853, p = 0.393. On comparing pulse rate one hour after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 420.000, W(29) = 885.000,
Z = -0.753, p = 0.451.
On comparing respiratory rate immediately after nebulization in the
Parnayavani Arka nebulization group and the Theophylline nebulization group, it was
found the two groups did not differ significantly, U(29) = 435.000, W(29) = 900.000,
Z = -0.587, p = 0.557. On comparing the respiratory rate one hour after nebulization
in the Parnayavani Arka nebulization group and the Theophylline nebulization group,
it was found the two groups did not differ significantly, U(29) = 450.000, W(29) =
915.000, Z = -0.000, p = 1.000.

138
OBJECTIVE PARAMETER: (PEFR)
a. Within the group :
Table No. 67: ANOVA WITH REPEATED MEASURES WITH A
GREENHOUSE-GEISSER CORRECTION IN PARNAYAVANI ARKA
NEBULIZATION GROUP
b.
c.
Table 68: TESTS OF WITHIN SUBJECTS EFFECTS OF PEFR FOR
PARNAYAVANI ARKA GROUP:
Source Correction df F-Value P-Value
Greenhouse-
Geisser
56.678 1.954 349.055 0.000
Parameters Mean
Difference
(I-J)
Standard
Error
Significancea I J
1 2
3
-85.000
-80.667
3.888
3.521
0.000
0.000
2 1
3
85.000
4.333
3.888
3.447
0.000
0.656
3 1
2
80.667
-4.333
3.521
3.447
0.000
0.656
a. Adjustment for multiple comparisons: Bonferroni

139
A RM-ANOVA with a Greenhouse-Geisser correction determined that mean PEFR
values differed statistically significantly between timepoints F (1.954, 56.678) =
349.055, p < 0.000). Post hoc tests using the Bonferroni correction revealed that
PEFR After Treatment was significantly increased as compared to PEFR Before
Treatment. (p=0.000). PEFR after 1 hr (AT1hr) was significantly increased as
compared to PEFR Before Treatment. (0.000). PEFR after 1hr (AT1hr) showed a non-
significant decrease in PEFR as compared to PEFR After Treatment. Hence, we can
conclude that the intervention elicits a statistically significant increase in PEFR, both
immediately after and 1 hour after nebulization.
b. Between the groups:
Table No. 69: INDEPENDENT SAMPLES T- TEST BETWEEN THE GROUPS
ANALYSIS OF PEFR IMMEDIATELY AFTER NEBULIZATION
Intervention N Mean Std. Deviation
Parnayavani Arka 30 199.67 13.514
Theophylline 30 196.67 14.70
F P T Df Std. Error
0.341 0.562 0.823 58 3.63571
Analysis of PEFR immediately after nebulization in the Parnayavani Arka group and
Theophylline nebulization group showed a non-significant difference.

140
Table 70: INDEPENDENT SAMPLES T- TEST BETWEEN THE GROUPS
ANALYSIS OF PEFR ONE HOUR AFTER NEBULIZATION
Intervention N Mean Std. Deviation
Parnayavani Arka 30 189.33 12.57
Theophylline 30 192.33 14.54
F P T Df Std. Error
1.079 0.303 -0.855 58 3.51079
Analysis of PEFR one hour after nebulization in the Parnayavani Arka group and
Theophylline nebulization group showed a non-significant difference.

141
DISCUSSION
REGARDING DRUG, DOSAGE FORM AND MODE OF ADMINSITRATION:
Microscopy and Macroscopy:
• The findings from the micro and macroscopic studies were corroborated by
similar findings from other studies, thus proving the authenticity of the drug
sample.
Preliminary phytochemical and physicochemical analysis:
• The results from study showed that the leaves of C. aromaticus possess
alkaloids, carbohydrates, phenols, resins, tannins and saponins.
• The drug is a proven source of many volatile principles. In the current study, it
was shown that the volatile oil content in the Arka sample was 0.21%.
GC-MS:
• Three volatile compounds were elicited from the current Arka sample.
• Among these, Dodecyl acrylate (C10H28O2) was found to possess structural
similarity to Thymol and Carvacrol (C10H14O2) as per the PubChem indexing
tool.
• Thymol and Carvacrol are the chief active principles in the drug C.
aromaticus.

142
ON DEMOGRAPHIC DATA:
1. Age:
A study revealed the prevalence of asthma has been found to be maximum in children
below the age of 5 and adults above the age of 70 years. (129) An ICMR report from
2009 states the prevalence of ever-asthma in adults over 15 years of age in India to be
2.4%, while a recent report suggests that it could be as high as 3.5%. (130) An
independent study found that elderly patients were more likely to suffer from asthma
due to psychological stress and perceived lack of social support systems. (131)
However, the observations in the present study do not correlate to previous works as
patients between the age group of 16-60 years were included. In the current study, it
was found that the age group between 40-60 years, and 20-30 years showed
maximum prevalence.
2. Marital status:
In the current study, 54 subjects were married and 6 were unmarried. It has been
found that there are more reported cases of asthma in India among
divorced/widowed/separated/deserted people as compared to married or unmarried
people. (131)
3. Occupation:
There are more than 400 substances that are currently known to induce asthma in the
workplace. (132) However, the occupations that show the highest prevalence of
asthma are region specific and cannot be generalized – they include factory workers,
drug manufacturers, farmers, grain handlers etc. In India, there are relatively few
studies that attempt to evaluate preventable occupation induced causes of asthma.

143
(133) A relatively recent study found that out of 62725 men and 52995 women
surveyed, the prevalence of ‘workplace induced’ asthma was 1.9%. Men who worked
as machine operators, or in the mining, construction, manufacturing or transport
categories were found to be most prone to developing asthma, while those in trade
and business were least prone. (131) The current study found that housewives and
agriculturalists were most prone to asthma.
4. Place(Urban/Rural):
Contrary opinions exist regarding prevalence of bronchial asthma in rural and urban
areas. In 2013, Agarwal reported that there was a higher prevalence of asthma in rural
adults and children as compared to industrialized countries. (131) The same article
also states that asthma was one among the leading causes of death in rural areas, with
rural North Eastern States and Tripura having the highest prevalence. Iverson 2005
suggests that rural dwellers have ‘fewer disabilities and long term limiting illnesses’,
and are also less drug-dependent. (134) Another meta-analysis study found that
globally there was minimal difference in the incidence of asthma between urban and
rural areas.(135) Urban factors that cause bronchial asthma include indoor air
pollutants, airborne microbes, air pollution, traffic, pollen, high temperatures and
humidity etc. Rural factors that directly or indirectly cause bronchial asthma include
biomass fuel combustion, airborne microbes, pest allergens, endotoxins, and a limited
access to health care (134, 135). In this study, it was found that there were a larger
number of subjects from urban areas (61.6%) as compared to rural areas. This might
be because many of the subjects who attended the study were from Hassan city.
5. Religion

144
Two independent studies – a cohort (Agarwal 2013) (131) and a meta-analysis
(Prakash, 2017) (136) found that Muslim men and women were more likely to report
cases of asthma as compared Hindus and other sects. The reason for this has been
proposed to be a difference in dietary habits – with Muslims tending to have a higher
proportion of non-vegetarian components in their food. (131) The relationship
between a non-vegetarian diet and asthma has been independently established. (137)
In the current study, there were 55 Hindu subjects, 3 Muslim subjects and 2 Christian
subjects. This is probably because Hassan has a greater Hindu population as
compared to other religions – over 50% of subjects who enrolled for the trial were
from Hassan city.
6. Economic status:
The current study found that the highest percentage (45%) of subjects belonged to a
lower middle class background. It has been found that in India, families with the
lowest wealth quintile had a higher asthma prevalence, as compared to wealthier
families (131) – with the highest prevalence in Eastern and North-Eastern states
(136). Lower economic status households have poorer nutrition, longer work hours
for manual labour and diminished access to health care, especially in rural areas.
7. Education:
The current study found that those over 50% of enrolled subjects had studied only
upto SSLC (10th Standard). (138) Various studies have shown that the prevalence of
asthma is inversely proportional to the number of years of schooling. (139) People
who are less educated tend to be more prone to developing asthma. This is possibly
because of a greater health awareness both at home and in the work place, in more
educated groups.

145
DISCUSSION ON PATIENT HISTORY:
1. Chief complaints:
The most common clinical presentations during an episode of asthma are
breathlessness, cough and wheezing most often during the night or early hours of the
morning with or without chest tightness. (140) The wheezing is attributed to dynamic
lung hyperinflation on exposure to a specific/non-specific trigger. It tends to be
polyphonic due to its origin from diverse lung airways. (141) The cough may be dry
or expectorant with small quantities of sticky sputum – whitish/greenish in colour.
(142) However, while minimal, or asymptomatic presentations have been known, they
are beyond the purview of the current study. The current study considered only cases
which presented with exacerbation of symptoms which include use of accessory
respiratory muscles, wheezing, breathlessness etc. It was found that maximum
patients reported wheezing during the night (60), chest tightness (50), Dyspnoea on
exertion (42) and cough (35). These are the main symptoms used to diagnose
bronchial asthma.
2. History of illness:
• Duration
In the current study, it was found that maximum patients reported onset less
than 5 years ago. However, 60% of the study population mentioned a duration
of onset between 10-20 years back. One study that compared 50 patients with

146
asthma of comparable severity found that childhood-onset asthmatics showed
significantly greater sensitivity to allergens, while adult-onset asthmatics
showed worse lung function despite a shorter duration of disease. (131)
• Mode of onset
While the exact mechanism underlying the development of an acute asthma
attack is unknown, there are two phenotypes which are commonly seen
clinically: (143)
a. Gradual onset – Associated with eosinophilic infiltration, gradual
attacks are seen over 48 hours, and show slower response to
treatment.
b. Sudden onset – Associated with significant exposure to allergens.
Such attacks tend to present in the late night or early morning, is
associated with neutrophilic inflammation, and shows a swifter
response to therapy.
The following study showed that 98% of the subjects showed sudden onset of
asthma.
• Trigger factors
The following trigger-induced phenotypes of asthma have been proposed:
(144)
a. Allergic asthma

147
Most asthma attacks are caused due to allergens. While onset is
usually in childhood, a number of adult asthmatics demonstrate this
phenotype as well. Common allergens include dust, pollen, animal
dander etc. The current study showed that 20% of the subjects cited
dust as a triggering factor for asthma. While study is ongoing to
better understand the inflammatory cascade in allergic asthma, it
has been found that IgE is an important mediator of inflammatory
reactions. Anti-IgE therapy has shown significant reduction in
exacerbations. This study found that
b. Occupational asthma
‘Work-aggravated asthma’ refers to asthma that is exacerbated by
work place conditions, while ‘occupational asthma’ refers to
asthma that was caused due to workplace exposure. The current
study found that the highest percentage of subjects were
agriculturalists, where exposure to dust, and natural allergens is
high. Subjects belonging to other occupations – such as drivers,
construction and building workers, coolie workers constituted 23%
of the sample population. All of these have high exposure to
occupational triggers such as dust, rubble, extreme temperatures
etc.
c. Others:
a. Aspirin induced asthma – not seen in the current study

148
b. Exercise induced asthma – not seen in the current study.
c. Menses related asthma – not seen in the current study.
3. History of past illnesses and treatment history:
• Hypertension:
In the following study, it was found that 46.7% of patients suffered from hypertension
and were under medication for the same. Commonly seen Hypertension medication
was Amlodipine (Ca Channel Blocker), Losartan and Olmesartan (ACE inhibitor),
Atenolol (B-Blocker), While asthma has been known to increase predisposition for
adult hypertension (145) , a history of diagnosed hypertension with medication is
significant when coming to the prescription of asthma medication. Beta blockers have
been known to induce bronchial obstruction and airway reactivity, even on topical
administration. (146) Angiotensin converting enzyme (ACE) inhibitors induce cough
and airway hyperresponsiveness in certain patients (147). However, Calcium channel
blockers have been shown to have a mildly relaxant effect on bronchial tone, and
small protective effect against allergens, and exercise induced broncho-
constriction.(148)
• Diabetes:
In the current study, 20% of the patients were diabetic and under medication for the
same. Microangiopathy of the lungs is seen as a chronic complication in patients of
both Type 1 and Type 2 diabetes. (149) One cohort that examined the risk of
pulmonary disease in patients of diabetes in 1,811,288 members found that
individuals with diabetes were at increased risk of asthma. (150) Few studies exist

149
that examine the relationship between Diabetes medication and asthma. However, it
has been proven that Metformin use in Diabetes patients was associated with
significantly reduced risk of asthma exacerbations and hospitalisations. (151)
4. Family History:
Genetic predisposition is a significant cause of asthma – and plays a major role in
asthma pathogenesis in over 50% of asthma cases. Five main asthma genes and gene
complexes have been identified that predispose for asthma – ADAM33, PHF11,
DPP10, GRPA AND SPINK5. (152) The complete functions of these genes are still
being investigated. Other genes such as IL13 that modify mucus production and
FCERI-B which modify the allergic trigger on mast cells and microbial pattern
recognition receptors of the innate immune system play a significant role in the
asthma pathogenesis. (153) In the current study,
5. Ahara:
Mixed diet was the most common Ahara taken in the current study (68%).
Previous studies have shown that a non-vegetarian diet increases the likelihood of
asthma in childhood and adults.(137) Mamsahara is Guru, Manda and Kapha
Prakopakara – thus playing an important role in the Samprapti of Tamaka Shwasa.
6. Rasa:
Madhura and Katu Rasa Ahara was the most preferred in this study. The
intake of Madhura Rasa results in Kapha Prakopa which is an important factor in the

150
Samprapti of Tamaka Shwasa. The intake of Katu Rasa Ahara may be have been
observed due to Kapha predominance in the body, and a natural desire for Vipareeta
Guna.
7. Nidra:
In the current study, 88% of subjects had disturbed sleep. Mid night nocturnal
dyspnoea is one of the cardinal features in asthma diagnosis. In asthmatic patients, in
the supine position, the alveoli become obstructed by secretions due to which
respiration becomes labored. Reflex cough and dyspnea are hence observed. (154)
Classically, Charaka has corroborated that disease aggravation is observed on lying
down - ‘Na chaapi labhate nidra shayane shwasa piditam’.
8. Habits:
Tea and Coffee:
Caffeine which is the main ingredient in both tea and coffee has been proven to be a
weak bronchodilator that also transiently reduces fatigue of the respiratory muscles.
(155) In the current study, 98.7% of the subjects were regular consumers of tea and
coffee. A meta-analysis on the effect of caffeine on asthma shows that even at low
doses (less than 5 mg/kg body weight) caffeine transiently improves lung function for
upto two hours. (156) Caffeine is also chemically related to Theophylline, a drug
commonly used in the treatment of asthma. (155, 156) However, it is not
recommended to undergo a lung function test for upto 4 hours after consumption of
caffeine as the results might be influenced by it. (155)

151
Smoking:
Smoking has severe detrimental effects on asthma – it has been known to accelerate
decline of lung function (157), and alter inflammatory mechanisms in asthma to
resemble those in COPD (158) . It is also associated with a poor response to inhaled
corticosteroids which are recommended as first line anti-inflammatory medication in
asthma. (159) In this study, it was found that 28.4% of the subjects were regular
smokers.
Alcohol:
The effect of alcohol on asthma has been contradictorily described by clinical and
experimental studies – with some claiming that alcohol is beneficial while others
claim that it worsens symptoms. (160) Some studies claim that the additives in
alcoholic beverages such as Sulfite cause bronchoconstriction, while pure ethanol by
itself is a broncho-relaxant. (161) Among alcoholic beverages, wine drinkers have
maximum alcohol sensitivity. (162) In the current study 3.3% were regular drinkers –
with the most common drinks being rum, whiskey and beer. 11.6% of the subjects
were regular drinkers and smokers.

152
DISCUSSION REGARDING RESULTS:
SUBJECTIVE PARAMETERS: (GINA)
Chest Tightness:
It has been widely believed that chest tightness is only one of the cardinal
symptoms of asthma. However, recent findings suggest that chest tightness
may be the only symptom that asthmatic patients experience. (163)
Inflammation of the airways and resultant bronchoconstriction is the cause of
chest tightness. (164) Inhaled Arka was found produce to produce a
significant decrease in chest tightness in both the groups in the current study.
There was no significant difference in chest tightness immediately after
nebulization and 1 hour after nebulization between the groups showing that
both drugs have equivalent efficacy. However, in the trial group, there was a
non-significant increase in chest tightness after one hour, showing that perhaps
the action of the drug at a dose of 5 ml does not last beyond a temporary
period. Further dose dependent clinical and experimental studies will need to
be carried out to establish this.
The proven tracheo-relaxant properties, and anti-inflammatory activity
of both the chief active constituents of Parnayavani – Thymol and Carvacrol –
might be responsible for this action. Also, previous studies have proven that
inhalation is the most superior method of drug administration in acute asthma
– both in terms of efficacy of drug delivery to the lung field as well as in terms
of desired action.

153
Breathlessness:
Breathlessness is one of the cardinal symptoms of Bronchial asthma. This also
takes place due to airway inflammation and resulting bronchoconstriction.
(165) Inhaled Arka was found produce to produce a significant decrease in
breathlessness – both at rest and on exertion, in the current study. There was
no significant difference in breathlessness immediately after nebulization and
1 hour after nebulization between the groups showing that both drugs have
equivalent efficacy.
However, there was a non-significant increase in breathlessness after
one hour in the trial group, showing that perhaps the action of the drug at a
dose of 5 ml does not last beyond a temporary period. Further dose dependent
clinical and experimental studies will need to be carried out to establish this.
The proven tracheo-relaxant properties, and anti-inflammatory activity of both
the chief active constituents of Parnayavani – Thymol and Carvacrol – might
be responsible for this action. Also, previous studies have proven that
inhalation is the most superior method of drug administration in acute asthma
– both in terms of efficacy of drug delivery to the lung field as well as in terms
of desired action

154
Wheezing:
Wheezing is such a common presentation in Bronchial Asthma, that the
symptom is often used synonymously with the disease by laymen. It is
attributed to dynamic lung hyperinflation on exposure to a specific/non-
specific trigger. It tends to be polyphonic due to its origin from diverse lung
airways. (166) The current study showed a significant decrease in wheezing in
both groups. 43 out of 60 subjects complained of wheezing, while 41 of the 43
had polyphonic wheeze. There was no significant difference in wheezing
immediately after nebulization and 1 hour after nebulization between the
groups showing that both drugs have equivalent efficacy.
However, there was a non-significant increase in wheezing after one
hour in the trial group, showing that perhaps the action of the drug at a dose of
5 ml does not last beyond a temporary period. Further dose dependent clinical
and experimental studies will need to be carried out to establish this. Thymol,
a major active principle in Arka has proven antispasmodic and anti-
inflammatory effects. It has been shown to decrease recruitment of
inflammatory cells and inflammatory mediators (such as IL-13, IL-5 and IL-4)
into the airways as well as reduce airway hyperresponsiveness, both of which
play an important role in the genesis of wheeze. Carvacrol is a phenolic
monoterpene that is known to be bronchial smooth muscle relaxant. It has also
been shown to selectively reduce the release of IL-4 (cytokine that is an
inflammatory mediator released by Th2 helper cells), while stimulating INF-
gamma (IL that naturally counteracts the action of inflammatory mediators,
produced by Th1 helper cells).

155
Cough
Generally in asthma, variable airflow obstruction leads to symptoms such as
cough and dyspnea. In the current study, 35 out of 60 patients complained of
cough associated with other symptoms. There was no significant difference in
cough immediately after nebulization and 1 hour after nebulization between
the groups showing that both drugs have equivalent efficacy. Cough in asthma
is typically dry or minimally productive, but may also be associated with
hyper-secretion of mucus. In such cases, cough is a respiratory defense
mechanism to expel the accumulated mucus. Many active constituents of the
Arka are antitussive (alpha-pinene, eugenol etc.) and spasmolytic (thymol,
carvacrol etc.). Hence, the drug was found to reduce cough and sputum
production in all asthma subjects.
Pulse rate
Transient hypoxia induced by bronchoconstriction in asthma is responsible for
tachycardia in asthma. (167) This is relieved on bronchodilation. In the current
study most subjects showed mild to moderate tachypnea that significantly
reduced after nebulization. The trial group showed a significant decrease in
pulse rate before and after treatment, that persisted till the one hour followup.
This demonstrates that bronchodilatory effects of the drug last for upto an
hour after drug administration. There was no significant difference in pulse
rate immediately after nebulization and 1 hour after nebulization between the
trial and control group showing that both drugs have equivalent efficacy at
both time points.

156
Sputum expectoration
The airway epithelium is normally covered by a mucus gel layer, that, under
pathological conditions such as asthma may show hypersecretion and
manifests as increased intracellular mucin, or increased mucus in the airway
lumen. (168) In case of excessive luminal mucus, cough clearance facilitates
ciliary clearance of the airways. In asthma, the distal airways become
impacted with mucus produced by surface epithelium, thus showing minimal
sputum expectoration. (169) In the current study, it was shown that there was a
significant decrease in mucous production post nebulization, possibly due to
the reduction in cough associated with bronchodilation.
There was a further non-significant decrease in sputum expectoration
after 1 hour. This might be because after nebulization, there is usually a
residual expectoration of exudate that increases in volume with rehydration.
This is expectorated immediately, or a few minutes after nebulization. This is
however absent an hour after nebulization. There was no significant difference
in sputum expectoration immediately after nebulization and 1 hour after
nebulization between the trial and control group showing that both drugs have
equivalent efficacy at both time points.

157
Speech difficulty
Speech difficulty as a result of hyperventilation is a common finding in
asthma. (142) It reduces with bronchodilation induced by medication. In the
current study, Post nebulization, there was a significant decrease in speech
difficulty in the trial group which remained unchanged uptil the one hour
follow up. This demonstrates that the therapeutic effects of the drug last for
upto an hour after drug administration. There was no significant difference in
respiratory rate immediately after nebulization and 1 hour after nebulization
between the trial and control group showing that both drugs have equivalent
efficacy at both time points.
Respiratory rate
Subjects of acute asthma generally tend to display tachypnea born of
hyperventilation due to bronchoconstriction. It has been shown in several
studies that in asthma, the average rate of respiration is between 20-25
cycles/min. (167) This was corroborated in the current study, with most
subjects displaying moderate tachypnea. Post nebulization, there was a
significant decrease in respiratory rate, which remained unchanged uptil the
one hour follow up. This demonstrates that bronchodilatory effects of the drug
last for upto an hour after drug administration. There was no significant
difference in respiratory rate immediately after nebulization and 1 hour after
nebulization between the trial and control group showing that both drugs have

158
equivalent efficacy. As mentioned previously, the main active ingredients of
this drug have proven antispasmodic and muscle relaxant properties.
Bronchoconstriction induced hyperventilation and tachypnea will
automatically be relieved on bronchodilation.
OBJECTIVE PARAMETERS:
PEFR:
Peak flowmetry is used to measure peak velocity of air streams in forced
expiration, and is intended to determine the condition of bronchial patency.
Asthma, being an obstructive type of disordered ventilation (because of
bronchoconstriction, compression of the trachea etc.), shows a markedly
increased load on the respiratory muscles. The ability of the respiratory
apparatus to perform additional functional load decreases. Hence, fast
expiration and rapid breathing become impossible. However, after
nebulization with Arka, which is known to have bronchodilatory and anti-
inflammatory properties, and also reduce airway hyperresponsiveness, the
PEFR significantly increased. In the current study, significant increase in the
PEFR in both groups was observed immediately after treatment.
However, in the trial group, there was a non-significant decrease in
PEFR after one hour, showing that perhaps the action of the drug at a dose of
5 ml does not last beyond a temporary period. Further dose dependent clinical
and experimental studies will need to be carried out to establish this.

159
There was no significant difference in PEFR immediately after nebulization
and 1 hour after nebulization between the groups showing that both drugs have
equivalent efficacy at both time points.

160
DISCUSSION REGARDING MODE OF ACTION OF PARNAYAVANI ARKA
NEBULIZATION :
As mentioned in the drug review section, two main volatile principles in
Parnayavani are Thymol and Carvacrol. Thymol is a naturally occurring monocyclic
phenolic compound derived from the herb Thymus vulgaris, which has widely
documented antioxidant, antispasmodic and anti-inflammatory effects. It has been
shown to decrease recruitment of inflammatory cells and inflammatory mediators
(such as IL-13, IL-5 an IL-4) into the airways as well as reduce airway
hyperresponsiveness, both of which play an important role in the pathogenesis of
bronchial asthma. Carvacrol is a phenolic monoterpene that is known to be a tracheal
smooth muscle relaxant. It has also been shown to selectively reduce the release of
IL-4 (cytokine that is an inflammatory mediator released by Th2 helper cells), while
stimulating release of INF-gamma (interleukin that naturally counteracts the action of
inflammatory mediators, produced by Th1 helper cells). A double blind clinical study
of Carvacrol in asthma patients was shown improve LFTs, and reduce subjective
parameters of asthma such as dyspnea and tightness of chest, and objective parameters
such as infiltration of inflammatory cells into airways.
Thus, when administering an aqueous distillate of the drug through
nebulization – which directly targets the airways and lung fields, instantaneous relief
is observed due to its anti-inflammatory and bronchodilatory action.
In Tamaka Shwasa, there is Avarana of Vata by Kapha. So in this condition,
Vata is in Moodavastha. Parnayavani Arka does Kapha Vilayana, due to its
Teekshna, Ushna and Laghu Gunas, which helps break Avarana of Kapha. As Vata

161
attains its Prakrutavastha, and resumes its normal course in the Pranavaha Srotas, the
patient obtains relief from Shwasa Kruchrata.

162
CONCLUSION
• Parnayavani Arka nebulization at a dose of 5ml was administered in 30 subjects
who presented in Vegavastha of Tamaka Shwasa w.s.r. to acute exacerbation of
bronchial asthma.
• Parnayavani Arka nebulization showed significant decrease in chest tightness,
breathlessness, wheezing, speech difficulty, cough, sputum production, pulse rate
and respiratory rate. (p=0.05), immediately after administration. It also showed a
significant decrease in PEFR (p=0.05) immediately after nebulization proving that
it increases lung expiratory flow.
• However, there was a non-significant increase in chest tightness, breathlessness,
wheezing and respiratory rate by the end of one hour indicating that the effect at a
dose of 5 ml on single time administration does not last for one hour. Further dose
dependent studies, and studies after repeated periodic administration will need to
be done to evaluate it’s long term efficacy.
• There was a non significant difference between the two groups in both subjective
and objective parameters, indicating that Parnayavani Arka has equivalent action
to Theophylline in acute exacerbation immediately after administration.
• The pharmacognostic study helped confirm the identity of Parnayavani. Three
volatile compounds were elicited from the Arka sample on GC-MS evaluation.
Among these, Dodecyl acrylate (C10H28O2) was found to possess structural
similarity to Thymol and Carvacrol (C10H14O2) as per the PubChem indexing tool.
Thymol and Carvacrol are the chief active principles in the drug C. aromaticus.

163
• Thus, the study concludes that Parnayavani arka nebulization at a dose of 5 ml
was effective in Vegavastha of Tamaka Shwasa w.s.r. to acute exacerbation of
bronchial asthma immediately after administration.

164
SUMMARY
Title:
A Clinical Study To Evaluate The Shwasahara Karma Of Parnayavani (Coleus
Aromaticus Benth.) Arka Nebulization In The Management Of Tamaka Shwasa with
specific reference to acute exacerbation of Bronchial Asthma
Introduction:
Global incidence of Tamaka Shwasa, Bronchial asthma is estimated to be around
334 million. In India, 15-20 million population are asthmatics. It is of utmost importance
to find ways to combat this disease. Parnayavani is a commonly used folklore remedy for
Tamaka Shwasa. With this perspective, the objective of the study was to assess the
Shwasahara Karma of Parnayavani Arka when administered through nebulization and
compare it with the Standard drug – Theophylline nebulization.
Review of Literature:
Drug Review:
The drug Parna Yavani (Coleus aromaticus Benth.) is a large succulent herb,
fleshy and highly aromatic, much branched, possessing short, soft erect hairs, with
distinctive smelling leaves. It is Teekshna, Ushna and Laghu in Guna, Katu Tikta in
Rasa, and is said to have Deepana, Pachana, Ruchya, Malasangraha Karmas. It is
indicated in disorders such as Agnimandya, Yakrudroga, Grahani, Udarraroga, Krimi,
Visoochika, Ashmari, and Mootrakricchra, Kasa and Shwasa.

165
Disease Review:
Tamaka Shwasa is defined as - ‘Visheshat Durdine Tamyeth Shwasa sa
Tamako Mataha’. Shwasa which occurs especially during Durdina is called Tamaka
Shwasa. Bronchial Asthma is an inflammatory airway disease with episodic occurrence
of dyspnoea with wheezing.
Materials and Methods:
The study was carried out in two parts:
a. Physico-Chemical Analysis:
b. Clinical study
Physico-Chemical analysis: The drug was subjected to physical evaluation, chemical
investigations, and the Arka was subjected to GC-MS evaluation.
Clinical study: For the clinical study, the subjects were divided randomly into two groups
comprising of 30 patients each.
Group No. Patients Drugs Dose
T (Stand. Group) 30 Theophylline respule nebulization 5 ml
PA (Trial Group) 30 Parnayavani Arka nebulization 5ml
The duration of the study was for a single hour, with analysis done before
nebulization, immediately after nebulization and one hour after nebulization.

166
Observations and Results:
With respect to subjective and objective parameters, (p=0.05), this study found
that Parnayavani Arka nebulization showed equivalent action to Theophylline
immediately after nebulization. However, there was no significant difference between
the groups (p=0.05).
Discussion and Conclusion:
Parnayavani Arka nebulization showed significant decrease in chest tightness,
breathlessness, wheezing, speech difficulty, cough, sputum production, pulse rate and
respiratory rate. (p=0.05), immediately after administration. It also showed a significant
decrease in PEFR (p=0.05) immediately after nebulization proving that it increases lung
expiratory flow.
However, there was a non-significant increase in chest tightness, breathlessness,
wheezing and respiratory rate by the end of one hour indicating that the effect at a dose of
5 ml on single time administration does not last for upto one hour. Further dose
dependent studies, and studies after repeated periodic administration will need to be done
to evaluate it’s long term efficacy.
There was a non significant difference between the two groups in both subjective
and objective parameters, indicating that Parnayavani Arka has equivalent action to
Theophylline in acute exacerbation immediately after administration.
This proves the Shwasahara Karma of Parnayavani Arka nebulization
immediately in acute exacerbation of bronchial asthma.

167
References:
A list of sources referred to in the completion of this work is given.

169
REFERENCES:
1. Kaliappan, Nirmala Devi, & Periyanayagam Kasi Vishwanathan,
2008, 'Pharmacognostical studies on the leaves of Plectranthus
amboinicus (Lour) Spreng', International Journal of Green
Pharmacy, 2(3): 182-4,
2. Vermavandana. A review on respiratory system physiology as
described in Ayurveda. Int. J.Res. Ayurveda Pharm. 2014:5(4)-578-
581.
3. Boulet LP (April 2009). "Influence of comorbid conditions on
asthma". European Respiratory Journal.33 (4): 897–906.
4. http://www.who.int/mediacentre/factsheets/fs206/en/
5. http://www.thehindu.com/news/national/andhra-pradesh/india-tops-
world-in-lung-disease-deaths/article7372468.ece
6. http://www.mhra.gov.uk/spc-pil/
7. Clark NM, Houle C, Partridge MR, Leo HL, Paton JY (2010). "The
puzzle of continued use of nebulized therapy by those with asthma".
ChronRespir Dis. 7 (1): 3–7
8. Sharma P.V. Dravyaguna Vijnana Vol.II.1st edition, Varanasi;
Chaukhamba Bharti Academy; 2005; p.461-463
9. Shastri JLN. Dravyaguna Vijnana. 1st edition. Vol. 2. Varanasi:
Choukhamba Orientalia; 2009; p. 899.
10. Pandey, G. Dravyaguna Vijanana (Materia medica – vegetable drugs)
Part III, 1st edition, Varanasi; Krishnadas Academy; 2001; p.56
11. Ayurvedic Pharmacoepia of India 1st Edition. Vol. 6. Dept. of Ayush,
Govt. of India, Minsistry of Health and Family Welfare; 2008; p. 124.

170
12. https://en.wiktionary.org/wiki/coleus
13. Wagner et al. (1999)
14. Wagner, W.L.; Lorence, D.H. Flora of the Marquesas Islands website.
Available online:
http://botany.si.edu/pacificislandbiodiversity/marquesasflora/index.ht
m (accessed on 18 January 2016).
15. Arumugam, Geetha et al. Plectranthus amboinicus (Lour.) Spreng:
Botanical, Phytochemical, Pharmacological and Nutritional
Significance. Molecule 21; 2016; p. 369.
16. Rout, Om Prakash et al. Int. Jou. Of App Bio. And Pharm. Tech.;
Vol.3(4); 2011; p.348-355.
17. http://easyayurveda.com/2017/03/27/country-borage-parnayavani/
18. Raymond M. Harley, Sandy Atkins, Andrey L. Budantsev, Philip D.
Cantino, Barry J. Conn, Renée J. Grayer, Madeline M. Harley, Rogier
P.J. de Kok, Tatyana V. Krestovskaja, Ramón Morales, Alan J. Paton,
and P. Olof Ryding. 2004. "Labiatae" pages 167-275. In: Klaus
Kubitzki (editor) and Joachim W. Kadereit (volume editor). The
Families and Genera of Vascular Plants volume VII. Springer-
Verlag: Berlin; Heidelberg, Germany.
19. Parnell, J. and Curtis, T. 2012. Webb's An Irish Flora. Cork
University Press. 2004.
20. Kaliappan, Nirmala Devi, & Periyanayagam Kasi VISWANATHAN,
2008, 'Pharmacognostical studies on the leaves of Plectranthus
amboinicus (Lour) Spreng', International Journal of Green
Pharmacy, 2(3): 182-4

171
21. Wagner, W.L.; Lorence, D.H. Flora of the Marquesas Islands website.
Available online:
http://botany.si.edu/pacificislandbiodiversity/marquesasflora/index.ht
m (accessed on 18 January 2016).
22. Khan, M.C.P.I. Current Trends in Coleus Aromaticus: An Important
Medicinal Plant; Booktango: Bloomington, IN, USA, 2013.
23. Dutta, S. Essential oil of Coleus aromaticus of Indian origin. Indian
Oil Soap J. 1959, 25, 120.
24. Castillo, R.A.M.; Gonzalez, V.P. Plecthranthus amboinicus (Lour.)
Spreng. Rev. Cuba. Plantas Med. 1999, 4, 110–115.
25. Cartaxoa, S.L.; Souzaa, M.M.A.; Albuquerque, U.P. Medicinal plants
with bioprospecting potential used in semi-arid northeastern Brazil. J.
Ethnopharmacol. 2010, 131, 326–342.
26. Ong, H.C.; Nordiana, M. Malay ethno-medico botany in Machang,
Kelantan, Malaysia. Fitoterapia 1999, 70, 502–513.
27. Coleus amboinicus (Lour.).Int. J. Green Pharm. 2013, 7, 211–215.
28. Cano, J.H.; Volpato, G. Herbal mixtures in the traditional medicine of
Eastern Cuba. J. Ethnopharmacol. 2004, 90, 293–316.
29. Franca, F.; Lago, E.L.; Marsden, P.D. Plants used in the treatment of
leishmanial ulcers due to Leishmania (Viannia) braziliensis in an
endemic area of Bahia, Brazil. Rev. Soc. Brasil. Med. Trop. 1996, 29,
229–232.
30. Velasco et al.
31. Uganda aromatic oil

172
32. Malaysia
33. Mallavarapu et al.
34. Sharma M, Sahu S, Sapra U. K., Pharmacognostical Standardization
of Leaves of Parnayavani (Coleus Amboinicus Lour.)
35. Dutta, S. Essential oil of Coleus aromaticus of Indian origin. Indian
Oil Soap J. 1959, 25, 120.
36. Castillo, R.A.M.; Gonzalez, V.P. Plecthranthus amboinicus (Lour.)
Spreng. Rev. Cuba. Plantas Med. 1999, 4, 110–115.
37. Cartaxoa, S.L.; Souzaa, M.M.A.; Albuquerque, U.P. Medicinal plants
with bioprospecting potential used in semi-arid northeastern Brazil. J.
Ethnopharmacol. 2010, 131, 326–342.
38. Ong, H.C.; Nordiana, M. Malay ethno-medico botany in Machang,
Kelantan, Malaysia. Fitoterapia 1999, 70, 502–513.
39. Coleus amboinicus (Lour.).Int. J. Green Pharm. 2013, 7, 211–215.
40. Cano, J.H.; Volpato, G. Herbal mixtures in the traditional medicine of
Eastern Cuba. J. Ethnopharmacol. 2004, 90, 293–316.
41. Franca, F.; Lago, E.L.; Marsden, P.D. Plants used in the treatment of
leishmanial ulcers due to Leishmania (Viannia) braziliensis in an
endemic area of Bahia, Brazil. Rev. Soc. Brasil. Med. Trop. 1996, 29,
229–232.
42. Harsha, V.H.; Hebbar, S.S.; Shripathi, V.; Hedge, G.R.
Ethnomedicobotany of Uttara Kannada District in Karnataka, India;

173
plants in treatment of skin diseases. J. Ethnopharmacol. 2003, 84, 37–
40.
43. Foong SC, Tan ML, Marasco LA, Ho JJ, Foong WC. Oral
galactagogues for increasing breast-milk production in mothers of
non-hospitalised term infants (Protocol). Cochrane Database of
Systematic Reviews 2015, Issue 4.
44. Baharvand-Ahmadi B, Bahmani M, Eftekhari Z, Jelodari M,
Mirhoseini M. Overview of medicinal plants used for cardiovascular
system disorders and diseases in ethnobotany of different areas in
Iran. J HerbMed Pharmacol. 2016;5(1):39-44.
45. Muthu C, Ayyanar M, Raja N, Ignacimuthu S. Medicinal plants used
by traditional healers in Kancheepuram District of Tamil Nadu,
India. Journal of Ethnobiology and Ethnomedicine. 2006;2:43.
46. SR Ghatapanadi, Nicky Johnson, AH Rajasab. Documentation of folk
knowledge on medicinal plants of Gulbarga district, Karnataka.
Indian Journal of Traditional Knowledge. Vol. 10 (2), April 2011. Pp.
349-353.
47. S. Sankaranarayana et al. Ethnobotanical study of medicinal plants
used by traditional users in Villupuram district of Tamil Nadu, India.
Journal of Medicinal Plants Research. Vol 4(12), June, 2010. pp.
1089-1101.
48. Jhoan Rhea L. Pizon et al. Ethnobotany of Medicinal Plants used by
the Subanen tribe of Lapuyan, Zamboanga del Sur. Bulletin of
Environment, Pharmacology and Life sciences. Aprl 2016.
174
49. Shubha, J.R.; Bhatt, P. Plectranthus amboinicus leaves stimulate
growth of probiotic L. plantarum: Evidence for ethnobotanical use in
diarrhea. J. Ethnopharmacol. 2015, 166, 220–227.
50. Bhattacharjee P, Majumder P. Investigation ofphytochemicals and
anti-convulsant activity of the plant Coleus amboinicus
(lour.). Int J Green Pharm 2013;7:211-5.
51. Uawonggul, N.; Chaveerach, A.; Thammasirirak, S.; Arkaravichien,
T.; Chuachan, C.; Daduang, S. Screening of plants acting against
Heterometrus laoticus scorpion venom activity on fibroblast cell lysis.
J. Ethnopharmacol. 2006,103, 201–207.
52. R.C. Hole, et al. Positive inotropic effet of the leaf extracts of parent
and tisse culture plants of coleus amboinicus on an isolated perfused
frog heart preparation. Food Chemistry. 114(1). 2009: pp 139-141.
53. Jose, A.M.; Ibrahim; Janardhanan, S. Modulatory effect of
Plectranthus amboinicus Lour. on ethylene glycol-induced
nephrolithiasis in rats. Indian J. Pharmacol. 2005, 37, 43–44.
54. Chen, Y.S.; Yu, H.M.; Shie, J.J.; Cheng, T.J.R.; Wu, C.Y.; Fang,
J.M.; Wong, C.H. Chemical constituents of Plectranthus amboinicus
and the synthetic analogs possessing anti-inflammatory activity.
Bioorg. Med. Chem. 2014,22, 1766–1772
55. Arumugam, Geetha et al. Plectranthus amboinicus (Lour.) Spreng:
Botanical, Phytochemical, Pharmacological and Nutritional
Significance. Molecule 21; 2016; p. 369.
56. Orient Longman. Indian Medicinal Plants; Microprint: Madras, India,
1995.

175
57. Ayurvedic Pharmacoepia of India 1st Edition. Vol. 6. Dept. of Ayush,
Govt. of India, Minsistry of Health and Family Welfare; 2008; p. 126.
58. Pandey, G. Dravyaguna Vijanana (Materia medica – vegetable drugs)
Part III, 1st edition, Varanasi; Krishnadas Academy; 2001; p.57-58.
59. Garuda Purana, Acharya Baladeva Uadhya, Chaukhambha Sanskrit series,
Edition1966, PP:488.
60. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani
Datta. Chikitsa Sthana 17/1-150. Reprint ed. Varanasi (India): Chaukambha Orientalia;
2011.p.533-539.
61. Sushruta, Sushruta Samhita with Nibandhasangraha commentary by
Dalhanacharya and Nyayachandrika Panjika by Gayadasacharya on
Nidansthana, Edited by Vaidya Jadavji Trikamji Acharya & Narayan
Ramchacharya Kavyatirtha, Uttartantra 51st Chapter,Reprint 2003,
Chaukhamba Surbharti Prakashan. Pp:824, Pg No: 761
62. Vagbhata, Astangahridhaya with Sarvangasundara commentary by Arunadatta &
Ayurvedarasayana by Hemadri, Edited by Bhisagacharya Harisastri Paradakara
Vaidya, Nidanasthana 4th Chapter, 9th Edition 2005 Chaukhambha Orientalia. Pp:956,
Pg No: 472
63. Vagbhata, Ashtanga Sangraha with hindi commentary by Kaviraj Atridev Gupta.
Reprinted Edition 1993, published by Krishnadas Academy, Varanasi.
64. Acharya Madhavkara, Madhava Nidana with Madhukosha Sanskrit commentary by
Acharya vijaya Rakshit and Shrikanta Datta, Edited by Dr. Ravidatta Tripathi, 1st
Volume 12th Chapter 1st edition 1993, Varanasi Sanskrit Sansthana, Pp: 597
65. Bhavamishra (1964), Bhavaprakash 3rd edition Ed: Brhahma Shankara Mishra,

176
Varanasi: Choukambha Sanskrit Samsthana; Pg: 427-735.
66. Laxmipathi Shastry Vaidya (1988), Yogarathnakara 4th edition Ed:Brahmashankara
Shastri, Varanasi: Choukambha Sanskrit Series Pg: 149-152.
67. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani
Dutta. Chikitsa Sthana 17/11-16. Reprint ed. Varanasi (India): Chaukambha
Orientalia; 2011.p.533.
68. Yadunandan Upadhyay, Madhava Nidana, Vol-1, 1/5, 15th ed, 1985, Choukumbha
Samskrut Samsthan, Varanasi.
69. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani
Datta. Chikitsa Sthana 17/11-16. Reprint ed. Varanasi (India): Chaukambha
Orientalia; 2011.p.533.
70. Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Uttara Tantra 50/3-5. Reprint ed. Varanasi (India): Chaukambha
Sanskrit Sansthan; 2010. p. 758.
71. Paradakara HSS, Ashtanga Hrudayam with Sarvanga Sundaram commentary of
Arunadutta and Ayurveda Rasayana of Hemadri. Nidana Sthana 4/1. 10thed.
Varanasi (India): Chaukambha Orientalia; 2011. P.472
72. Sharma SP. Astanga samgraha of Vrddha Vaghbhata with Sasilekha Sanskrit
commentary of Indu. Nidana Sthana 4/2-8. Varanasi (India): Chaukambha
Orientalia; 2008.p 168-169.
73. Yadunandan Upadhyay, Madhava Nidana, Vol-1, 12/15, 15th ed, 1985,
Choukumbha Samskrut samstan, Varanasi, pp 289
74. Acharya JT. Charaka Samhita by Agnivesa, Reprint ed. Varanasi: Chaukhamba
Orientalia; 2011. p.533.
75. Acharya JT. Susruta Samhita of Susruta, Nibandhasangraha of Dalhana, Reprint ed.
177
Varanasi: Chaukhambha Surbharati prakashan; 2012.p.758.
76. Kunte AM, Sastri KR. Paradakara HS (ed). Ashtanga Hrdaya of Vagbhata, Reprint
ed. Varanasi: Chaukhambha Sanskrit Sansthan; 2011. p.472.
77. Sharma Shivaprasad (ed). Astanga Samgraha of Vagbhata, 3rd ed. Varanasi:
Chowkamba Sanskrit Series Office; 2012. p.370.
78. Sastri SS, Upadyaya Y (ed). Madhava Nidana of Madhavakara, Part 1, 22nd
ed. Varanasi: Chaukhambha Sanskrit Sansthan; 1993. p.281
79. Yadunandan Upadhyay, Madhava Nidana, Vol-1, 1/5-6, 15th ed, 1985,
Choukumbha Samskrut samstan, Varanasi, pp 32
80. Acharya JT. Charaka Samhita by Agnivesa, Reprint ed. Varanasi:
Chaukhamba Orientalia; 2011. p.533.
81. Acharya JT. Susruta Samhita of Susruta, Nibandhasangraha of Dalhana, Reprint ed.
Varanasi: Chaukhambha Surbharati Prakashan; 2012. p.761.
82. Kunte AM, Sastri KR. Paradakara HS (ed). Ashtanga Hrdaya of Vagbhata, Reprint
ed. Varanasi: Chaukhambha Sanskrit Sansthan; 2011. p.472.
83. Sastri SS, Upadyaya Y (ed). Madhava Nidana of Madhavakara, Part 1, 22nd
ed.Varanasi: Chaukhambha Sanskrit Sansthan; 1993. p.290.
84. Acharya JT. Charaka Samhita by Agnivesa, Reprint ed. Varanasi: Chaukhamba
Orientalia; 2011. p.535.
85. Acharya JT. Susruta Samhita of Susruta, Nibandhasangraha of Dalhana, Reprint ed.
Varanasi: Chaukhambha Surbharati prakashan; 2012. p.762.
86. Kunte AM, Sastri KR. Paradakara HS (ed). Ashtanga Hrdaya of Vagbhata,
Reprint ed. Varanasi: Chaukhambha Surbharati Prakashan; 2011. p.473.
87. Sastri SS, Upadyaya Y (ed). Madhava Nidana of Madhavakara, Part 1, 22nd

178
ed.Varanasi: Chaukhambha Sanskrit Sansthan; 1993. p.296.
88. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of Chakrapani
Dutta. Chikitsa Sthana 17/63. Reprint ed. Varanasi (India): Chaukhambha
Orientalia: 2011.p.535.
89. Acharya JT. Charaka Samhita by Agnivesa, Reprint ed. Varanasi: Chaukhamba
Orientalia; 2011. p.533.
90. Acharya JT. Susruta Samhita of Susruta, Nibandhasangraha of Dalhana, Reprint ed.
Varanasi: Chaukhambha Surbharati Prakashan; 2012. p.761.
91. Agnivesha, Charaka samhitha, revised by Charaka and Dridabala with
Ayurveda dipika Commentary of Chakrapanidatta, edited by Yadavji
Trikamji Acharya, Chikitsa sthana 17th chapter, 5th edition-2001,
Chaukambha Sanskrit sansthan, Pp.738, Page 535.
92. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Chikitsa Sthana 17/56. Reprint ed. Varanasi (India):
Chaukambha Orientalia; 2011.p.535.
93. Yadunandan Upadhyay, Madhava Nidana, Vol-1, 1/8, 15th ed, 1985,
Choukumbha Samskrut samstan, Varanasi, pp 32
94. Agnivesha, charakaShitaam revised by Charaka & Dridabala with Ayurveda
Dipika commentary of Chakrapanidatta edited by Yadavaji Trikamji Acharya
Chikitsa sthana chapter 17th/11t h edition 2008 Chaukamba Sanskrit
samsthana Pp. 738
95. Agnivesha, Charaka samhitha, revised by Charaka and Dridabala with
Ayurveda dipika commentary of Chakrapanidatta, edited by Yadavji Trikamji
Acharya, Chikitsa sthana 8th chapter, 5th edition-2001, Chaukambha Sanskrit

179
sansthan, Pp.738, Page 461.
96. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary of
Chakrapani Datta. Chikitsa Sthana 17/62. Reprint ed. Varanasi (India):
Chaukambha Orientalia; 2011.p.535.
97. Acharya Y T. Sushruta Samhita with Nibandhasangraha commentary of
Dalhanacharya. Uttara Tantra 51/14. Reprint ed. Varanasi (India):
Chaukambha Sanskrit Sansthan; 2010. p. 762
98. Charaka Samhita with Ayurveda Deepika Commentary of Chakrapanidatta.
Edited by Vaidya Jadavji Trikamji Acharya; 8th edition ; Chaukhamba
Sanskrit Sansthana; Varanasi;2005;Pp:738; Page No: 535
99. Charaka Samhita with Ayurveda Deepika Commentary of Chakrapanidatta.
Edited by Vaidya Jadavji Trikamji Acharya; 8th edition ; Chaukhamba
Sanskrit Sansthana; Varanasi;2005;Pp:738; Page No: 536
100. Acharya Y T. Sushruta Samhita with Nibandhasangraha
commentary of Dalhanacharya. Uttara Tantra 1/25. Reprint ed. Varanasi (India):
Chaukambha Sanskrit Sansthan; 2010. p. 597.
101. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary
of Chakrapani Datta. Chikitsa Sthana 17/75. Reprint ed. Varanasi (India):
Chaukambha Orientalia; 2011.p.536.
102. Acharya YT. Charaka Samhita with Ayurveda Dipika commentary
of Chakrapani Datta. Chikitsa Sthana 17/129-134. Reprint ed. Varanasi
(India): Chaukambha Orientalia; 2011.p.538.
103. Paradakara HSS, Ashtanga Hrudayam with Sarvanga Sundaram commentary
of Arunadutta and Ayurveda Rasayana of Hemadri. Chikitsa Sthana 4/47.

180
10thed. Varanasi (India): Chaukambha Orientalia; 2011. P.607.
104. Agnivesha, Charaka samhitha, revised by Charaka and Dridabala
with Ayurveda dipika commentary of Chakrapanidatta, edited by Yadavji Trikamji
Acharya, Sutra sthana 13th chapter, 5th edition-2001, Chaukambha Sanskrit
sansthan, Pp. 82
105. Agnivesha, Charaka samhitha, revised by Charaka and Dridabala
with Ayurveda dipika commentary of Chakrapanidatta, edited by Yadavji Trikamji
Acharya, Chikitsa sthana 17th chapter, 5th edition-2001, Chaukambha Sanskrit
sansthan, Pp.536.
106. Davidson’s Priciples and Practice of Medicine. Edited by
Christopher Haslett,Edwin.R.Chilvers,Nicholas a.Boon,NickiR.Colledge.
International editor John A.A.Hunter 19th edition 2002
107. LANGE. CMDT 2009 Current Medical Diagnosis & Treatment
McPhee Papadaki’s 48th edition. McGraw Hill.
108. Davidson’s Priciples and Practice of Medicine. Edited by
Brian.R.Walker,Ian D Penman, NickiR.Colledge et al. 22nd edition 2014.Pg.666
109. Ibid. pp 667
110. Siddarth B. Shaha ed, API Textbook of Medicine, 7th ed, 2003,
The Association of Physician’s of India, Mumbai, Pg. 291.
111. Davidson’s Priciples and Practice of Medicine. Edited by
Christopher Haslett,Edwin.R.Chilvers,Nicholas a.Boon,NickiR.Colledge.
International editor John A.A.Hunter 19th edition 2002
112. British guideline on the management of Asthma. British thoracic

181
society. 4th edition,May 2011.Pg.1
113. Ibid. Pg. 2
114. Davidson’s Priciples and Practice of Medicine. Edited by
Brian.R.Walker,Ian D Penman, NickiR.Colledge et al. 22nd edition 2014.Pg.671
115. Ibid. Pp. 673
116. A.P.I text book of medicine editor-in-chief Siddharth Shah 8th edition
volume-1, 2008.
117. Davidson’s Priciples and Practice of Medicine. Edited by
Brian.R.Walker,Ian D Penman, NickiR.Colledge et al. 22nd edition 2014.Pg.668
118. Sembulingam K, Sembulingam P. Essentials of Medical Physiology.
4th ed. New Delhi: Jayee Brothers Medical Publishers Pvt Ltd; 2006. p. 621-22.
119. Davidson’s Priciples and Practice of Medicine. Edited by
Brian.R.Walker,Ian D Penman, NickiR.Colledge et al. 22nd edition 2014.Pg.669.
120. Ibid. Pp. 670.
121. Rabinowitz. J.D,Lloyd. P.M, Munzar.P.et.al. Ultra-Fast Absorption
of Amorphous Pure Drug Aerosols Via Deep Lung Inhalation. Journal of
pharmaceutical sciences, vol. 95, no. 11, November 2006.
122. Nebulizer guidelines. Directorate of Children’s Service, 2006, Pg.1
123. EMS Authority Inhaled Medications Training, SB 1663, chapter
625, September 1998.
124. British Guidelines, Thorax1997;52(Suppl 2):S4-S16.
125. Nebulizer guidelines. Directorate of Children’s Service, 2006, Pg3-4
126. EMS Authority Inhaled Medications Training, SB 1663, chapter
625, September 1998.

182
127. Tripaty I, Arka Prakasha of langhapati ravana with hindi tikka Reprint
edition, Varanasi:Chaukambha Orientalia;2006.p.43.
128. Rahul U, GAzala Hussain, Basavaraj Y GAnti. Pharmaceutical Review of
Arka Kalpana. International Ayurvedic Medical Journal. Vol 2 (6). 2014.
129. Bröms K, Norbäck D, Eriksson M, Sundelin C, Svärdsudd K. Effect Of
Degree Of Urbanisation On Age And Sex-Specific Asthma Prevalence In Swedish
Preschool Children. Bmc Public Health. 2009;9:303.
130. Sk Jindal. Indian Study On Epidemiology Of Asthma, Respiratory
Symptoms And Chronic Bronchitis (Insearch). Final Report; Icmr, September 2010.
131. Agrawal S, Pearce N, Ebrahim S. Prevalence And Risk Factors For Self-
Reported Asthma In An Adult Indian Population: A Cross-Sectional Survey. The
International Journal Of Tuberculosis And Lung Disease. 2013;17(2):275-282.
132. Janssens T, Ritz T. Perceived Triggers Of Asthma: Key To Symptom
Perception And Management. Clinical And Experimental Allergy : Journal Of The
British Society For Allergy And Clinical Immunology. 2013;43(9):1000-1008.
133. Tarlo Sm, Liss Gm. Occupational Asthma: An Approach To Diagnosis And
Management. Cmaj: Canadian Medical Association Journal. 2003;168(7):867-871.
134. Evers U, Jones Sc, Iverson D, Caputi P. “Get Your Life Back”: Process And
Impact Evaluation Of An Asthma Social Marketing Campaign Targeting Older
Adults. Bmc Public Health. 2013;13:759.
135. Malik Hu-R, Kumar K, Frieri M. Minimal Difference In The Prevalence Of
Asthma In The Urban And Rural Environment. Clinical Medicine Insights
Pediatrics. 2012;6:33-39.
136. Kumar P, Ram U (2017) Patterns, Factors Associated And Morbidity

183
Burden Of Asthma In India. Plos One 12(10): E0185938.
137. Rosenkranz Rr, Rosenkranz Sk, Neessen Kj. Dietary Factors Associated
With Lifetime Asthma Or Hayfever Diagnosis In Australian Middle-Aged And
Older Adults: A Cross-Sectional Study. Nutrition Journal. 2012;11:84.
138. Meng Y-Y, Babey Sh, Wolstein J. Asthma-Related School Absenteeism
And School Concentration Of Low-Income Students In California. Preventing
Chronic Disease. 2012;9:E98.
139. Narayana Pp, Prasanna Mp, Narahari Sr, Guruprasad Am. Prevalence Of
Asthma In School Children In Rural India. Annals Of Thoracic Medicine.
2010;5(2):118-119. Doi:10.4103/1817-1737.62478.
140. Cavallazzi R, Hirani A, Vasu Ts, Et Al. Clinical Manifestations And
Treatment Of Adult-Onset Asthma And Periocular Xanthogranuloma. Canadian
Respiratory Journal : Journal Of The Canadian Thoracic Society. 2009;16(5):159-
162.
141. Gong H Jr.. Wheezing And Asthma. In: Walker Hk, Hall Wd, Hurst Jw,
Editors. Clinical Methods: The History, Physical, And Laboratory Examinations.
3rd Edition. Boston: Butterworths; 1990. Chapter 37.
142. Niimi A. Cough And Asthma. Current Respiratory Medicine Reviews.
2011;7(1):47-54.
143. Davoodi P, Mahesh Pa, Holla Ad, Ramachandra Nb. Family History & The
Risk For Adult Onset Asthma. The Indian Journal Of Medical Research.
2015;141(3):361-363.
144. See Kc, Phua J, Lim Tk. Trigger Factors In Asthma And Chronic
Obstructive Pulmonary Disease: A Single-Centre Cross-Sectional
Survey. Singapore Medical Journal. 2016;57(10):561-565.

184
145. B. L. Salako, S. O. Ajayi. Bronchial Asthma: A Risk Factor For
Hypertension?
Afr J Med Med Sci. 2000 Mar; 29(1): 47–50.
146. Arboe B, Ulrik Cs. Beta-Blockers: Friend Or Foe In Asthma? International
Journal Of General Medicine. 2013;6:549-555.
147. Löfdahl Cg1. Antihypertensive Drugs And Airway Function, With Special
Reference To Calcium Channel Blockade.Journal Of Cardiovascular
Pharmacology. 1989;14 Suppl 10:S40-51; Discussion S59-62.
148. Ann Twiss M, Harman E, Chesrown S, Hendeles L. Efficacy Of Calcium
Channel Blockers As Maintenance Therapy For Asthma. British Journal Of Clinical
Pharmacology. 2002;53(3):243-249.
149. Hsiao Y-T, Cheng W-C, Liao W-C, Et Al. Type 1 Diabetes And Increased
Risk Of Subsequent Asthma: A Nationwide Population-Based Cohort Study.
Xiaolin Z, Ed. Medicine. 2015;94(36):E1466.
150. Perez Mk, Piedimonte G. Metabolic Asthma: Is There A Link Between
Obesity, Diabetes And Asthma? Immunology And Allergy Clinics Of North
America. 2014;34(4):777-784.
151. Forno E. Asthma In Adults With Diabetes: Treat Their Diabetes With
Metformin, Improve Their Asthma? Respirology (Carlton, Vic). 2016;21(7):1144-
1145.
152. Ober C, Yao T-C. The Genetics Of Asthma And Allergic Disease: A
21st Century Perspective. Immunological Reviews. 2011;242(1):10-30.
153. Bijanzadeh M, Mahesh Pa, Ramachandra Nb. An Understanding Of The
Genetic Basis Of Asthma. The Indian Journal Of Medical Research.
2011;134(2):149-161.

185
154. Mukerji V. Dyspnea, Orthopnea, And Paroxysmal Nocturnal Dyspnea. In:
Walker Hk, Hall Wd, Hurst Jw, Editors. Clinical Methods: The History, Physical,
And Laboratory Examinations. 3rd Edition. Boston: Butterworths; 1990. Chapter
11.
155. Bronchodilator Effects Of Caffeine In Coffee. A Dose-Response Study Of
Asthmatic Subjects.
Chest. 1986 Mar;89(3):335-42.
156. Becker Ab, Simons Kj, Gillespie Ca, Simons Fen The Bronchodilator
Effects And Pharmacokinetics Of Caffeine In Asthma. England Journal Of
Medicine. 1984 Mar 22;310(12):743-6.
157. Sturm Jj, Yeatts K, Loomis D. Effects Of Tobacco Smoke Exposure On
Asthma Prevalence And Medical Care Use In North Carolina Middle School
Children. American Journal Of Public Health. 2004;94(2):308-313.
158. Gilliland Fd, Islam T, Berhane K, Et Al. Regular Smoking And Asthma
Incidence In Adolescents. American Journal Of Respiratory And Critical Care
Medicine. 2006;174(10):1094-1100.
159. Lazarus Sc, Chinchilli Vm, Rollings Nj, Et Al. Smoking Affects Response
To Inhaled Corticosteroids Or Leukotriene Receptor Antagonists In
Asthma. American Journal Of Respiratory And Critical Care Medicine.
2007;175(8):783-790.
160. Talbot Ja. Effect Of Alcohol On Asthma. Bmj : British Medical Journal.
1993;306(6881):854-855.
161. Vally H, Thompson Pj. Allergic And Asthmatic Reactions To Alcoholic
Drinks. Addictive Biology. 2003. Mar(; 8(1): 3-11.
162. Halper Gm, Gershwin Me, Ough C, Fletcher Mp, Nagy Sm Jr. The Effect Of

186
White Wine Upon Pulmonary Function Of Asthmatic Subjects. Annals Of Allergy.
1985 Nov; 55(5): 686-90.
163. Irwin Rs. Chest Tightness Variant Asthma (Ctva): Reconfirmed And Not
Generally Appreciated. Journal Of Thoracic Disease. 2014;6(5):405-406.
164. Https://Www.Ncbi.Nlm.Nih.Gov/Pubmedhealth/Pmh0072705/
165. Lavietes Mh. The Interpretation Of Dyspnea In The Patient With
Asthma. Pulmonary Medicine. 2015;2015:869673.
166. Martinez Fd, Helms Pj. Types Of Asthma And Wheezing. The European
Respiratory Journal. Supplement. 1998 Jul; 27:3s-8s.
167. Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical Review: Severe
Asthma. Critical Care. 2002;6(1):30-44.
168. Evans Cm, Kim K, Tuvim Mj, Dickey Bf. Mucus Hypersecretion In
Asthma: Causes And Effects. Current Opinion In Pulmonary Medicine.
2009;15(1):4-11.
169. Tanizaki Y Et Al. Clinical Features Of Bronchial Asthma With Mucus
Hypersecretion. Nihon Kyobu Shikkan Gakkai Zasshi. 1993. May;31(5):575-9.

186
CONSENT FORM 1.Title of synopsis:
A CLINICAL STUDY TO EVALUATE THE SHWASAHARA KARMA OF PARNAYAVANI (Coleus aromaticus Benth.) ARKA NEBULIZATION IN THE
MANAGEMENT OF TAMAKA SHWASA (BRONCHIAL ASTHMA) 2. Participant enrollment ID for this trial: ___________________________________
3. Name of the Investigating Physician (Research Scholar): Dr. Pushya A. Gautama
4. Name of the Guide: Dr. Harini A. M.D. (Ayu)
5. I confirm that I have read/the study has been explained to me adequately and I have
understood the information sheet for the above study and had the opportunity to ask
questions.
6. I hope to complete the study, but I understand that my participation is voluntary
and that I am free to withdraw at any time, without giving a reason, and without my
medical care or legal rights being affected.
7. I understand that my doctor will provide information about my progress, in
confidence, to the related authorities. I understand that the information held by the
Investigators and researchers and records maintained by the concerned authorities
might be used to follow up my health status.
8. I understand that the information will be used for medical research only and that I
will not be identified in any way in the analysis and reporting of the results. I
understand that sections of any of my medical notes may be looked at by the
authorities or responsible individuals from the members of the IEC, Regulatory
authorities or Court, if necessary. I give permission for these individuals to have
access to my records.
9. I understand what is involved in this trial and agree to take part in the clinical trial
for a period of 3 days.
Signature of the Subject:
Name of the Subject: Date:
Signature of the Witness:
Name of the Witness: Date:
Signature of the Research Scholar:
Name of the Research Scholar: Dr. Pushya A. Gautama Date:
Signature of the Guide:
Name of the Guide: Dr.Harini A. M.D. (Ayu) Date:

Scanned by CamScanner187

188
CLINICAL CASE PROFORMA:
Name: Serial No.
Age: yrs OPD No.
Marital status: M/UM/W/D Address
Place: U/R
Religion: H/M/Ch/Other Mob. No.
Occupation: Date of commencement:
Economic status: VP/P/L/M/U/R Date of completion
Education: L/SSC/PUC/UG/PG
MAIN COMPLAINTS:
Symptoms Duration
Dyspnoea on rest/ dyspnoea on exertion
Cough
Wheezing during the day
Wheezing during the night
Use of accessory muscles
Diffculty in speech
Confusion
Rhinitis
ASSOCIATED COMPLAINTS:
Symptoms Duration
Thirst
Fever
Anorexia
Vomitting
Fainting

189
Pain in the chest/flanks
HISTORY OF THE PRESENT ILLNESS:
HISTORY OF PAST ILLNESSES:
TREATMENT HISTORY:
FAMILY HISTORY:
Symptoms Age/Yrs Health Status
D/L
Disease Notes
Father
Mother
Brother
Sister
Son
Daughter
SOCIAL HISTORY:
OCCUPATIONAL HISTORY: Dust/Smoke/Smell/Extreme temperatures
Type of
work……………………………………………………………………………………
….Working hours………../Night
Shift………Resting day………….
Exercise: Minimum/Moderate/Heavy
PERSONAL HISTORY:
Agni: Sama/Tikshna/Vishama/Manda
Koshta: Mridu/Madhyama/Kroora
Aahara: Type: Veg/Non Veg/ Mixed
Matra: Alpa/ Madhyama/ Atipramana

190
Rasa preferred: Madhura/ Amla/ Lavana/ Katu/ Tikta/ Kashaya
Nidra: ……… Hrs. Disturbed/ Sound/ Excess
Mala: Formed/ Unformed/ Hard/ Smooth/ Regular/ Constipated
…….. Times/ Day
Mootra: Frequency: ………. /day
Regular/Increased/Incontinence/ Retention
Habit Duration Quantity
Tea
Coffee
Smoking
Alcohol
Tobacco
Snuff
Others
OBSTETRIC HISTORY:
No delivery/ Normal / Surgical intervention/ Abortion/ Last delivery
GYNAECOLOGICAL HISTORY:
Menstrual cycle: Regular/ Irregular
Menarche age:
Metrorrhagia/Dysmenorrhoea/Leucorrhoea
Menopause age:
ROGI PAREEKSHA:
Dashavidha Pareeksha;
• Prakriti
• Vikruti
• Sara
• Samhanana: P/M/A
• Vyayama shakti: P/M/A
• Vaya
• Pramana: Height……… cm. Weight …………….. kg

191
• Satva
• Abhyavaharana shakti: P/M/A
• Jarana shakti : P/M/A
• Desha: Jata J/A/S
Samvruddha: J/A/S
Vyadhita: J/A/S
Ashta sthana pareeksha:
• Nadi: Regular/Irregular/Full/Low volume/ V/P/K/VP/PK/VK
• Mala
• Mootra
• Jihva
• Shabda
• Sparsha
• Drik
• Akruti
GENERAL EXAMINATION:
• Pulse: /min. Regular/Irregular/Full/Weak
• BP: ………………… mm of Hg
• Temperature:
• Respiratory rate
• Build: Slender/ Muscular/ Obese
• Nourishment: Good/Poor
• Nails: Pink/Pallor/ Bluish
• Conjunctive: Pink/Pallor/Bluish
• Cyanosis: Extremities: Upper/Lower, Buccal mucosa, Lips, Conjunctiva
• Oedema: Foot/Ankle/Leg/Sacral region/ Hands/ Face/Pitting/ Non pitting
• Skin –
• Lymph nodes:

192
Pranavaha Sroto Pareeksha:
Inspection:
• Size and shape of the chest –
o Bilaterally symmetrical, elliptical, conical, long and flat, funnel chest,
barrel chest, kyphosis, scoliosis, local bulging
• Movement of the chest: Symmetrical, reduced in the right/left side,
Synchronicity of movement, Delayed movement in Left/Right
• Inspiratory retraction of interspaces – Exaggerated, Diminished to the
right/left.
• Movement of coastal margins during inspiration: Outward, Inward, Use of
accessory muscles
• Rate of respiration: ………./min
• Rhythm: Regular/Irregular/Periodic breathing/ Prolonged
inspiration/Prolonged both phase/Kussmauls respiration/ Ataxic breating/
Apnoetic breating/ Catch in breathing
• Type of respiration: Abodminal – thoracic, Thoraco – abdominal, Pursed lip
breathing, Shallow breathing
• Sternomastoid sign – Absent/Present
• Distended chest veins: Absent/Present
• Oedema: Unilateral/Bilateral
Palpation:
• Trachea: Slightly shifted to right/ Centrally located/ Shifted to the left
• Apex impulse
• Expansion of the chest – Unilateral/ Bilateral masses/ Sinus tract/ Tenderness/
Lymph node enlargement
• Tactile fremitus: Decreased/ Absent/ Normal in …….. lung
Percussion:
• Resonant/Hyperesonant/ Dull/ Stony dull
Auscultation:
• Breath sounds – Vesicular/Bronchovesicular/ Bronchial

193
• Adventitious sounds – rhonchi – High pitched/ low pitched/ Inspiratory,
Expiratory/ Short/ Long
• Crepitation – Early inspiratory/ Late inspiratory/ Mid inspiratory/ Expiratory
• Pleural rub site -
…………………………………………………………………………………
………
• Vocal resonance- Increased/ Decreased/ Absent/ Normal
INVESTIGATIONS:
Parameters BT AT
Hb gm%
TC
DC
Total Eosinophil count
ESR
Urine
CXR
Sputum/AFB
Spirometry
SEVERITY OF ILLNESS:
Parameters BT 1st day 2nd day 3rd day After 1
week
Attack per week
Duration of the
attack
Tightness in the
chest
Cough – Dry or
Expectorant
Dyspnoea on
rest
Dyspnoea on
exertion
Wheezing

194
Use of
accessory
muscles
Sputum colour
Sputum
quantity
Sputum
consistency
Pulse
BP
Temperature
Respiratory rate
Appetite
Digestion
Sleep
Weight /kg
PEAK FLOW METER TEST:
Parameters BT 1st day 2nd day 3rd day After 1
week
PEF
Gradings
RESULTS:
Signature of Scholar Signature of Guide Signature of HOD

195
GINA – SEVERITY OF ASTHMA EXACERBATION
Signs and Symptoms BT IMMEDIATELY AT 1 HOUR AT
1. Breathlessness 2. Wheeze 3. Talks in 4. Cough 5. Sputum 6. Chest Tightness 7. Pulse Rate 8. Respiratory Rate
1 – Mild asthma exacerbation 2 – Moderate asthma exacerbation 3 – Severe asthma exacerbation
SL No
ASSESSMENT CRITERIA 0 1 2 3
1 . Breathlessness Absent Mild-‐ while walking
Can lie down
While at rest-‐prefers sitting
While at rest-‐sits upright
2. Wheeze Absent Moderate -‐ often only at end expiration
Loud-‐throughout expiration
Usually loud-‐throughout inhalation & exhalation
3. Talks in Sentences Sentences Phrases Words
4. Cough Absent After exercise Continuous, disturb work
Continuous, disturbs normal
activity
5. Sputum Absent 1-‐3 times 4-‐5 times Continuously
6. Chest tightness Absent Mild Moderate Severe
7. Pulse/min <80 80-‐100 100-‐120 >120
8. Respiratory rate/min 18-‐23 24-‐30 31-‐40 >40

Scanned by CamScanner
196

Scanned by CamScanner197

Scanned by CamScanner198

Scanned by CamScanner199

Scanned by CamScanner200

Scanned by CamScanner
201

Scanned by CamScanner202

Scanned by CamScanner203

Scanned by CamScanner204

Scanned by CamScanner205

Scanned by CamScanner206

Scanned by CamScanner
207

Scanned by CamScanner208

Scanned by CamScanner209

Scanned by CamScanner
210

Scanned by CamScanner
211

Scanned by CamScanner
212

213
Figure1:Macroscopy of Coleus aromaticus
Fig 32. Macroscopy of Coleus aromaticus
Figure2: Microscopy of Coleus aromaticus
Fig 33. T.S of midrib
Pa→ Ph→
GT→
Xy→
VB→
Pal→
LE→
T→
SG→
UE↓
cavity; E
–
epidermis
; GT –
ground
tissue; Ph
–
phloem;
RC -
rosette
crystal;
VB –
vascular
bundle;
Xy –
xylem.
SP→

214
Fig 34. midrib portion enlarged
GT –glandular trochomes; LE – lower epidermis; Me – mesophyll;Pa – parenchyma; Pal –
palisade; Ph – phloem; SG-starch rains; SP – spongy parenchyma; UE – upperepidermis; VB –
vascular bundle; XY – xylem.
Fig 35. T.S of lamina
Pal→
↑Me↓
SP→
E→
T→
Pa→ Ph→
GT→
Xy→ VB→
Pal→
LE→
T→ UE↓
cavity; E
–
epidermis
; GT –
ground
tissue; Ph
–
phloem;
RC -
rosette
crystal;
VB –
vascular
bundle;
Xy –
xylem.

215
Fig 36.Lamina enlarged
E – epidermis; Col – collenchymas; LE – lower epidermis; Me – mesophyll;Pa – parenchyma;
Pal – palisade; Ph – phloem; ; SG-starch grains; SP – spongy parenchyma; . GT –glandular
trichomes; UE – upperepidermis; VB – vascular bundle; XY – xylem.
Pal→
↑Me↓
SP→
GT→
SG→
LE→
UE→

216
Fig 37. Upper midrib
Fig 38. Lower epidermis
GT –glandular trichomes; LE – lower epidermis;Pa – parenchyma; Ph – phloem; SG-starch
grains; SP – spongy parenchyma; UE – upperepidermis; VB – vascular bundle; XY – xylem.
Pa→
VB→
Ph→
UE↓
cavity;
E –
epider
mis;
GT –
groun
d
tissue;
Ph –
phloe
m; RC
-
rosette
crystal
; VB –
vascul
ar
bundle
; Xy –
xylem.
Xy→
LE→
T→
VB→
SG→
GT→

217
PROCESS OF ARKA PREPARATION
Fig. 39. Coleus aromaticus Benth. Fig. 40. Shredding the leaves
Fig. 41. Weighing the leaves
Fig.43. Soxhlet distillation
Fig.42. Soaking the leaves
Fig.44. Clear Arka obtained




















