
Analysis of Colour-Magnitude Diagrams of Rich LMC Clusters: NGC 1831

www.elsevier.com/locate/ijpsycho
International Journal of Psychoph
Hostility and sex differences in the magnitude, duration, and determinants
of heart rate response to forehead cold pressor: Parasympathetic
aspects of risk
John M. Ruiz a,*, Bert N. Uchino b, Timothy W. Smith b
a Department of Psychology, Washington State University, PO Box 644820, Pullman, WA 99164-4820, USAb Department of Psychology, University of Utah, 380 South 1530 east, Room 502, Salt Lake City, UT 84112-0251, USA
Received 4 May 2005; received in revised form 25 July 2005; accepted 27 July 2005
Available online 24 August 2005
Abstract
Recent models hypothesize that hostility confers increased risk of CHD through weaker parasympathetic dampening of cardiovascular
reactivity (CVR). We tested this possibility using the forehead cold pressor task, a common maneuver which elicits the ‘‘dive reflex’’
characterized by a reflexive decrease in HR presumably through cardiac-parasympathetic stimulation. Participants were initially chosen from
the outer quartiles of a sample of 670 undergraduates screened using the hostility subscale of the Aggression Questionnaire ([Buss, A.H.,
Perry, M., 1992. The Aggression Questionnaire. Journal of Personality and Social Psychology, 63, 452-459.]). The final sample of 80
participants was evenly divided between men and women and high and low hostility. Following a 10-min baseline, participants underwent a
3-min forehead cold pressor task. The task evoked a significant HR deceleration that was mediated by PNS activation, as assessed by
respiratory sinus arrhythmia (RSA). Replicating prior research, men displayed greater decrease in HR. More important, low hostiles
maintained larger HR deceleration over time compared to high hostiles although the autonomic basis for this effect was unclear. The findings
broaden understanding of hostility and sex-related cardiovascular functioning and support the task as a method for evoking PNS-cardiac
stimulation.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Hostility; Vagal tone; Respiratory sinus arrhythmia; Forehead cold pressor; Heart rate variability; Impedance cardiography
1. Introduction
Epidemiological evidence supports individual differences
in hostility and anger as risk factors for coronary heart
disease (CHD) and all-cause mortality (Barefoot et al.,
1983, 1995). These findings are based on increasingly well-
designed cross-sectional and prospective studies (Gallo and
Matthews, 2003; Rozanski et al., 1999; Suls and Bunde,
2005). For example, individual differences in hostility and
anger predict severity of carotid atherosclerosis (Julkunen et
al., 1994; Matthews et al., 1998) and incidence of MI,
cardiac death, and stroke (Everson et al., 1999; Kawachi et
al., 1996; Williams et al., 2000). In addition, a quantitative
0167-8760/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.ijpsycho.2005.07.005
* Corresponding author. Tel.: +1 509 335 8034; fax: +1 509 335 5043.
E-mail address: [email protected] (J.M. Ruiz).
review found support for a relationship between hostility
and associated behaviors and subsequent clinical manifes-
tations of CHD (Miller et al., 1996). Cardiovascular
reactivity (CVR) is one proposed mechanism linking
psychosocial risk factors and cardiovascular disease
(CVD) (Krantz and Manuck, 1984; Manuck, 1994).
Laboratory and ambulatory studies demonstrate a reliable
relationship between hostility and larger and more frequent
cardiovascular responses (Christensen and Smith, 1993;
Guyll and Contrada, 1998; Shapiro et al., 1997). Studies
have shown these physiological responses are also associ-
ated with atherosclerosis (Kamarck et al., 1997; Matthews et
al., 1993) and myocardial ischemia in the laboratory
(Blumenthal et al., 1995; Gottdiener et al., 1994; Krantz et
al., 1991) and during daily life (Bairey et al., 1990; Gabbay
et al., 1996; Legault et al., 1995).
ysiology 60 (2006) 274 – 283

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283 275
Recent models identify autonomic imbalance as a
potentially important mechanism linking hostility to exag-
gerated CVR (Brosschot and Thayer, 1998; Sloan et al.,
1999; Rhodes et al., 2002; Williams, 1994). Specifically,
these models hypothesize that individual differences in
negative affect including hostility and trait anger are
associated with lower parasympathetic activity or vagal
tone, resulting in less attenuation or dampening of cardiac
response. Prospective investigations have demonstrated an
association between low heart rate variability (HRV: an
index of parasympathetic influence) and recurrent coronary
events and cardiovascular and all cause mortality (Bigger et
al., 1993a,b; Kleiger et al., 1987; Tsuji et al., 1996).
Investigations involving hostility and parasympathetic
control have primarily focused on acute autonomic reac-
tivity as opposed to basal differences in control capability.
For example, in a small, mixed sex sample, Sloan and
colleagues (2001) found greater decreases in respiratory
sinus arrhythmia (RSA, a non-invasive index of para-
sympathetic control of the heart) in response to traditional
mental stressors amongst high hostiles. However, the
question of whether these responses are due to differences
in situational appraisal or other psychological mechanisms
as opposed to underlying physiological differences in
parasympathetic/vagal capability remains open. Individual
differences in parasympathetic control may impair regula-
tion of cardiac responses regardless of cognitive factors,
perhaps impeding recovery following exposure to acute
stressors.
To date, only one study has investigated the relationship
between hostility and parasympathetic cardiac control in
response to reflex challenge. Reflex challenges may provide
a less ambiguous test of underlying autonomic correlates of
hostility, due to the reduced level of psychological
mediation (e.g., appraisal) compared to other laboratory
tasks. Graham and colleagues (1996) found Cook–Medley
hostility scores were inversely related to the magnitude of
change in heart period variability (HPV: R–R interbeat
interval) in response to graded trials of bilateral carotid
baroreflex stimulation, a technique for evoking carotid–
cardiac vagal influence on the heart. Similar findings among
high Type A individuals by Fukudo et al. (1992) and
Muranaka et al. (1988) suggest that constructs similar to
hostility may be associated with weaker parasympathetic
cardiac control. However, interpretation is limited by the
lack of direct assessment of parasympathetic functioning
such as RSA (for review and recommendations see Berntson
et al., 1997). In addition, these data are limited to men.
Recent findings suggest that men show less parasympathetic
withdrawal during psychological stressors (Sloan et al.,
2001; Hughes and Stoney, 2000) and larger increases in
parasympathetic outflow in response to a facial cold pressor
task (Hughes and Stoney, 2000), suggesting greater cardiac
vagal activity in men than women. Thus, hostility, sex, and
possibly their interaction may be associated with important
differences in parasympathetic cardiac control.
1.1. The forehead cold pressor as a parasympathetic task
Cold pressor tasks are widely used to examine individual
differences in pain perception and physiological response.
The tasks reliably evoke physiological responses although
the degree and character of such responses may vary with
the instructional set. For example, research suggests that
perceptions of the task mediate affective responses with
some influence on the degree of physiological response
(Baker and Kirsch, 1991; Peckerman et al., 1991; Saab et
al., 1993). In addition, the pattern of physiological response
varies by cold pressor methodology (Durel et al., 1993).
Three methods are commonly employed, foot or leg
immersion in ice water, hand immersion, and application
of cold stimulation to the forehead. Foot and hand
immersion are commonly associated with increased periph-
eral resistance (e.g., blood pressure) and increased heart rate
(Peckerman et al., 1994; Saab et al., 1993). In contrast the
forehead cold pressor is an effective method for eliciting a
simulated ‘‘dive reflex’’, characterized by a reduction in
heart rate in response to cold temperature to the forehead
region (Heath and Downey, 1990; Khurana et al., 1980;
Peckerman et al., 1994; Reyners et al., 2000; Wildenthal et
al., 1975). Blood pressure responses specifically during
forehead cold pressor are mixed (Heath and Downey, 1990;
Peckerman et al., 1991; Saab et al., 1993).
Research has demonstrated the reproducibility of cardiac
responses to the forehead cold pressor (Durel et al., 1993;
Ryan et al., 1976). The assumed anatomical pathway
involves stimulation of trigeminal afferents in the face via
cold, producing stimulation to central brainstem connections
to parasympathetic (vagal nerve) efferents that slow the
heart (Peckerman et al., 1994; White and McRitchie, 1973).
Although more evidence on the autonomic determinants of
this task is needed, Hughes and Stoney (2000) reported
concurrent HR deceleration and increased RSA in response
to forehead cold stimulation. The forehead cold pressor has
been used to investigate between group differences in
cardiac response in a number of samples including Blacks
and Whites, individual differences in pain perception
(Peckerman et al., 1994; Saab et al., 1993), and depressive
symptoms (Hughes and Stoney, 2000). However, no studies
have used the task to examine potential hostility differences
in cardiovascular functioning.
1.2. Current experiment
The aims of the current experiment were to examine
hostility, sex, and hostility by sex differences in HR
response to the forehead cold pressor task. Participants
were told that they were part of a study of temperature
effects on cardiovascular functioning. Following a baseline
period a standard ice bag was held across the forehead and
nose for 3-min. Physiological measures were taken con-
tinuously during both the baseline and task period in order
to analyze change. Participants completed ratings of mood

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283276
following both the baseline and task. Impedance cardiog-
raphy was used to examine HR and its underlying
autonomic determinants while blood pressure was assessed
each minute. It was hypothesized that the task would evoke
HR deceleration and increased RSA. Low hostiles were
expected to display larger HR deceleration and a greater
increase in RSA compared to high hostile participants in
response to the task. In addition, we sought to replicate
previous findings suggesting men display greater decreases
in HR and larger increases in RSA compared to women in
response to cold stimulation.
2. Methods
2.1. Participants
Participants were chosen from the outer quartiles scores
<13, >21) of a sample of 670 undergraduates screened
using the hostility subscale of the Aggression Question-
naire (AQ; Buss and Perry, 1992). The AQ was chosen
because of its psychometric superiority as a measure of
hostility compared to other measures such as the Buss–
Durkee Hostility Inventory (BDHI; Buss and Durkee,
1957) and the Cook Medley Hostility Scale (Cook and
Medley, 1954). Despite a lack of research examining the
AQ as a predictor of CHD, individual differences in AQ-
assessed hostility are associated with expected differences
in magnitude and duration of cardiovascular reactivity
(Smith and Gallo, 1999; Smith et al., 2004). The AQ
Hostility subscale measures hostile cognitions such as
mistrust (‘‘I am suspicious of overly friendly strangers’’) or
perceived slights (‘‘Other people always seem to get the
breaks’’). Respondents reported the extent to which items
are characteristic of them on a 5-point scale ranging from 1
(extremely uncharacteristic) to 5 (extremely characteristic).
The Hostility subscale has a reported internal consistency
of .77 and test–retest reliability of .70 (Buss and Perry,
1992), and is demonstrated to have strong associations
with interpersonal antagonism (Gallo and Smith, 1998;
Ruiz et al., 2001) and other measures of hostility (e.g.,
Cook and Medley, 1954) associated with cardiovascular
morbidity and mortality.
Trait self-report instruments, even psychometrically
sound instruments like the Aggression Questionnaire, are
not perfect assessment tools (test–retest correlations <1.0).
In order to reduce potential mischaracterization error, we
chose to reassess hostility at the conclusion of the lab
session. Only participants scoring in the expected half of a
median split distribution, derived from the original sample
pool of 670 participants, were retained for analysis. Six
participants (7%) did not meet these criteria and were
excluded from the final sample. In order to maintain equal
cell size, replacement participants were chosen based on sex
and initial hostility screening criteria. Following the task,
each replacement participant was again screened for
hostility. All 6 replacement participants met the median
split criteria.
The final sample of 80 participants was evenly divided
between men and women and high and low hostility. All
were healthy undergraduates from the University of Utah.
The mean age of participants was 21.16 years (SD=3.17),
and the mean years of education was 13.63 (SD=1.96). Of
the participants 88% identified themselves as Caucasian
with the remainder self-identifying as Asian American (9%),
Hispanic (1%), and other (3%).
2.2. Procedure
2.2.1. Baseline period
Sessions were conducted in a single-occupant chamber
with adjoining space for monitoring equipment. Except for
brief interactions with the experimenter, participants were
alone. On arrival, they listened to an audiotape introducing
the experiment as examining ‘‘cardiovascular responses to
temperature.’’ They were told that their responses would be
measured during a baseline period and while holding a
standard ice bag over their forehead and eyes. To limit
anxious anticipation during baseline, we avoided further
specific description of the task or instructions. Following
initial informed consent, four mylar band sensors were
placed on the participant and connected to an impedance
cardiograph. Participants were asked handedness prior the
attachment of a blood pressure cuff. The cuff was then
placed on the upper potion of the nondominant arm to
ensure that it would not interfere with the participants’
ability to complete questionnaires during the study. The 10-
min baseline involved a minimally demanding task (i.e.,
‘‘vanilla baseline’’; Jennings et al., 1992), in which
participants were asked to examine and rate pairs of pictures
at 1-min intervals.
2.2.2. Cold procedure
Following baseline, the audiotaped instructions intro-
duced the forehead cold pressor task. A standard latex ice
bag was placed across the bridge of the nose, covering the
forehead and eyes for 180-s (Durel et al., 1993; Saab et al.,
1993). The bag contained a mixture of 4.5 cups crushed ice
and 0.5 cups water. During the task data collection was
automated, allowing the experimenter to hold the bag to
reduce movement on the part of the participant and to
monitor the participant’s comfort level and maintain
consistency in the application.
2.3. Affect measurement
Some studies have shown the cold pressor to evoke
changes in affect although no studies have done so with
specific focus on hostility (Peckerman et al., 1991, 1994).
In order to account for any potential role of affect change
in cardiovascular response participants completed an affect
measure following the baseline and cold pressor. The

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283 277
questionnaire consisted of twelve 4-point Likert items
reflecting anger and anxiety (see Smith et al., 2004). Ten
of the 12 items were drawn from the State–Trait Person-
ality Inventory (STPI: Spielberger, Unpublished Manual).
Items were chosen based on obvious content-validity.
Anxiety was assessed with six items (four negatively
valenced: worried, tense, nervous, anxious; two positively
valenced, reverse scored: calm, relaxed) drawn from the
state anxiety scale of the STPI. Cronbach’s alpha
coefficients for the six-item anxiety scale were 0.83 for
baseline and 0.82 for the task. The anger scale was
comprised of four negatively valenced items (annoyed,
angry, irritated, aggravated) taken from the STPI anger
subscale. Due to the lack of positively worded items
(inversely associated with anger) in the STPI we added
two additional items (friendly, kindhearted) to this scale.
Cronbach’s alpha coefficients for the six-item anger scale
were 0.71 for baseline and 0.87 for the task. Total item
correlations were not adversely affected by the inclusion of
these two positively valenced items. Prior research
demonstrated this measure to correspond to expected
differences in hostility and cardiovascular reactivity (Smith
et al., 2004).
2.4. Physiological measures
A Minnesota Impedance Cardiograph Model 304B
(Surcom, Inc., Minneapolis, MN) assessed electrocardio-
gram (ECG), basal thoracic impedance (Z0), and the first
derivative of the impedance signal (dZ / dt). Four mylar
bands were placed in the tetrapolar configuration (Sherwood
et al., 1990). A 4 mA AC current at 100 kHz was passed
through the two outer bands, and Z0 and dZ / dt were
recorded from the two inner bands. The ECG, Z0, and dZ /
dt signals were digitized at 500 Hz. Data were analyzed
using ANS Suite software (Uchino et al., 1995). We
ensemble averaged these data within 1-min epochs and
verified or edited waveforms prior to analyses. Stroke
volume (SV) was estimated using the Kubicek equation
(see Sherwood et al., 1990), and CO in 1/min was
calculated by multiplying heart rate (HR) by the product
of (SV/1000). Total peripheral resistance (TPR) was
measured in resistance units (dynes-s�cm�5) on the basis
of mean arterial pressure (MAP) and CO (i.e., TPR=
MAP/CO X 80). Preejection period (PEP) was calculated
as the time interval, in milliseconds, between the Q-point
of the ECG and the B-point of the dZ / dt signal. PEP
reflects sympathetic control of the heart (see Cacioppo et
al., 1994).
RSA provides an index of parasympathetic control of the
heart. It was calculated on the basis of the digitized interbeat
intervals (IBI) and checked and edited for artifacts using the
detection algorithm of Berntson et al. (1990). A heart period
time series was created from the IBI series using a
‘‘weighted’’ beat algorithm (Berntson et al., 1995). We
detected sharp transitions in the heart period time series
(e.g., because of arrhythmia) using the Berntson et al.
(1995) algorithm and removed them by smoothing. A linear
(first order) polynomial was fit to, and subtracted from, the
heart period time series (Litvack et al., 1995). Subtraction of
this first-order polynomial (linear detrending) acted as a
high pass filter, removing very large ultralow frequency
trends (including the DC component) from the input signal.
After linear detrending, the heart period time series was
band-pass filtered from 0.12 to 0.40 Hz using an interpo-
lated finite impulse response filter (Neuvo et al., 1984). The
power spectrum of the heart period time series was
calculated using a fast Fourier transform and scaled to
ms2/Hz. RSA was calculated as a natural log of the area
under the heart period power spectrum within the corner
frequencies of the band-pass filter (see Litvack et al., 1995).
Average RSA was calculated for each minute. A Dinamap
Model 8100 monitor (Critikon Corporation, Tampa, FL)
was used to measure systolic blood pressure (SBP), diastolic
blood pressure (DBP), and MAP. It uses the oscillometric
method to estimate blood pressure. Blood pressure was
measured once per minute.
3. Results
3.1. Affective responses and baseline equivalence of groups
Self-reported anger and anxiety were measured at base-
line and immediately following the task. No baseline
differences in affect were found in 2 (hostility groups)�2
(sex) ANOVAs. The low self-reported affect values follow-
ing the baseline suggest that participants were in a relatively
relaxed state prior to the cold pressor task. Changes in affect
were calculated to determine potential differences in task
impact between groups (see Table 1). A marginal effect for
hostility was found for self-reported anger, F(1,74)=3.88,
p =.053, g2= .050, where high hostiles reported a larger
increase in anger relative to low hostiles. High hostiles also
reported a larger increase in anxiety, F(1,74)=4.71, p <.05,
g2= .060. Finally, a significant effect was found for sex
where women reported a larger increase in anxiety than men
following the task, F(1,74)=7.58, p <.01, g2= .093.Baseline values for key physiological indices are
presented in Table 2. A 2 (high vs. low hostility)�2 (men
vs. women) ANOVA was used to test between group
differences. A significant sex effect was found for two
measures: SBP and respiration rate (RR). Compared to
women, men displayed significantly higher SBP,
F(1,76)=32.60, p <.001, and lower RR at baseline. Differ-
ences between high and low hostiles were found only for
CO where high hostiles displayed larger baseline CO,
F(1,68)=4.20, p <.05. Interactions of hostility by sex were
also found for CO, F(1,68)=7.57, p < .01, and TPR,
F(1,68)=5.36, p <05. Specifically, high hostile men dis-
played larger CO compared to low hostile men at baseline,
t(36)=3.36, p <.01. High and low hostile women did not

Table 1
Baseline values and change from baseline to task in self-reported anger and anxiety
Low hostiles High hostiles Total sample
Men Women All low Men Women All high Men Women
Baseline
Anger 8.9 (3.8) 9.2 (1.7) 9.1 (2.9) 9.2 (2.2) 10.6 (2.6) 9.9 (2.5) 9.1 (3.0) 9.9 (2.5)
Anxiety 8.3 (3.8) 7.9 (2.6) 8.1 (3.2) 8.1 (3.2) 10.2 (2.9) 9.1 (2.6) 8.2 (2.9) 9.0 (2.9)
Change to task
Anger 1.80 (.92) 3.99 (.89) 2.90 (.64) 4.46 (.89) 4.89 (.91) 4.68 (.63) 3.13 (.64) 4.40 (.63)
Anxiety 1.10 (.84) 4.61 (.83) 2.85 (.59) 4.13 (.82) 5.22 (.85) 4.67 (.58) 2.62 (.59) 4.91 (.58)
J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283278
differ, t(32)=0.51, p =n.s. High hostile men also displayed
lower TPR compared to low hostile men, t(36)=2.68,
p <.05, whereas high and low hostile women did not differ,
t(32)=0.51, p =n.s.
3.2. Primary analyses
Consistent with prior recommendations (Llabre et al.,
1991), change scores (i.e., task minus baseline) were
computed for each minute of the task period. Because
baseline levels can affect degree of change (Benjamin,
1967), baseline values were included as a covariate in mixed
analyses of covariance (ANCOVAs). During the task period
we computed three-way mixed ANCOVAs (i.e., High vs.
Low Hostility�Sex�3 min) for each cardiovascular
measure. To follow-up significant effects involving the
trials factor, mean comparisons were calculated using
pooled error terms (Bernhardson, 1975). Impedance-derived
HR was considered the primary outcome. SBP and DBP
reactivity were also examined, and CO and TPR were
examined as determinants of blood pressure responses. PEP
and RSA were examined as determinants of HR responses.
Table 2
Means and standard deviations for baseline physiological measures
Measure Low hostiles H
Men Women Total M
SBP (mm/Hg) 120.30
(9.35)
106.50
(10.18)
113.40
(11.91)
1
(9
DBP (mm/Hg) 67.28
(4.79)
64.32
(8.09)
65.80
(6.73)
6
(5
TPR (dyne-s*cm�5) 1207.47
(343.16)
981.117
(283.29)
1100.25
(332.36)
9
(3
CO (l/min) 5.97
(1.31)
6.78
(1.59)
6.35
(1.48)
7
(2
HR (bpm) 70.66
(10.70)
70.39
(9.23)
70.53
(9.89)
6
(7
PEP (ms) 125.82
(17.95)
125.01
(9.12)
125.44
(14.27)
1
(1
RSA (natural log) 6.65
(.96)
6.74
(.69)
6.69
(.83)
6
(1
RR 15.1
(1.5)
16.8
(2.0)
15.9
(2.0)
1
(1
SBP = systolic blood pressure; DBP = diastolic blood pressure; TPR = total per
minute; PEP = preejection period; RSA = respiratory sinus arrhythmia; RR = res
As discussed above, the effects of cold stimulation were
expected to produce differential HR deceleration responses
accompanied by increases in RSA. No BP, TPR, or PEP
effects were expected.
3.3. Effects of cold on dive-reflex response
As expected, application of the cold pressor resulted in a
significant reduction in HR compared to baseline (69.48 vs.
64.49 bpm), F(1,71)=104.15, p <.001, g2= .595. Consis-
tent with expectations, a significant hostility by time
interaction was found for change in HR during the 3-min
task, F(2,140)=4.37, p <.02, g2= .059 (see Fig. 1). Low and
high hostile participants had similar initial HR decelerations
(see Table 3). Planned-comparisons were performed to
compare differences in HR both within each hostility group
as well as between groups at each minute. Planned
comparisons showed that for low hostiles, despite a
significant loss of HR deceleration between minutes 2 and
3, t(140)=1.97, p <.05, the overall deceleration across the
task from minute 1 to 3 was stable, t(140)= .30, p =ns). In
contrast, heart rate deceleration waned over the three minute
igh hostiles Total sample
en Women Total Men Women
18.50
.92)
108.18
(8.21)
113.34
(10.40)
119.40
(9.56)
107.34
(9.17)
6.98
.36)
66.02
(5.58)
66.50
(5.43)
67.13
(5.02)
65.17
(6.92)
25.31
01.95)
1029.34
(262.93)
974.27
(284.90)
1073.82
(350.35)
1003.81
(270.86)
.88
.15)
6.50
(1.62)
7.23
(2.02)
6.87
(1.98)
6.65
(1.59)
6.29
.98)
70.55
(7.78)
68.48
(8.07)
68.47
(9.57)
70.48
(8.35)
21.25
5.80)
117.63
(17.93)
119.55
(16.68)
123.65
(16.90)
121.54
(14.25)
.72
.09)
7.21
(1.09)
6.97
(1.16)
6.68
(1.07)
6.99
(.95)
5.1
.4)
15.9
(2.0)
15.5
(1.7)
15.1
(1.5)
16.3
(2.0)
ipheral resistance; CO = cardiac output; HR = heart rate; bpm = beats per
piration rate.

-7
-6
-5
-4
-3
-2
-1
01 2 3
Time (min)
Ch
ang
e in
HR
(b
pm
)
Low Hostile
High Hostile
p <.05
p <.05p <.05
p <.05
Fig. 1. Change in heart rate over time for high and low hostiles.
J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283 279
task for high hostiles (minutes 1 to 3, t(140)=4.73, p< .001)
with a significant loss of deceleration between minutes 2
and 3, t(140)=3.10, p <.01. Comparison between groups
revealed that high hostiles displayed significantly less HR
deceleration during the 3rd minute compared to low
hostiles, t(70)=2.21, p <.05.
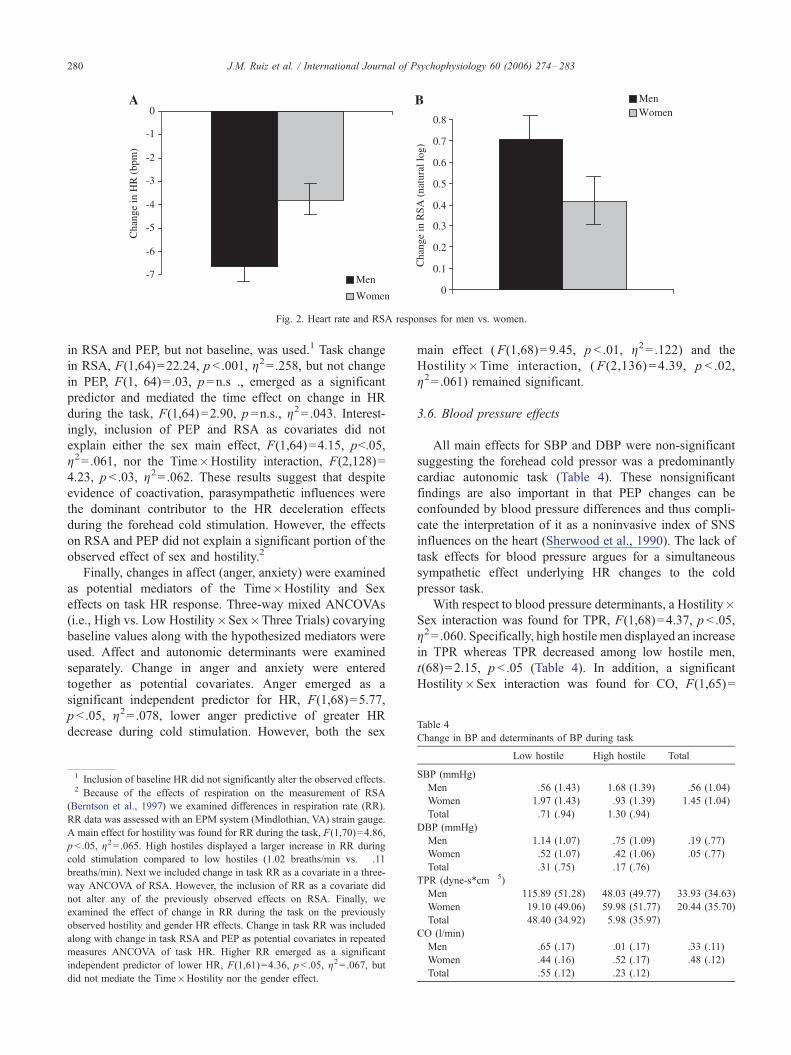
In addition to the hostility by time effect, an expected
significant sex main effect was also found, F(1,70)=11.30,
p <.001, g2= .139. As depicted in Fig. 2A, men displayed a
greater reduction in HR in response to the cold stimulation
as compared to women.
3.4. Analysis of HR determinants
Autonomic responses to cold stimulation (see Table 3)
were characterized by a significant increase in parasympa-
thetic (RSA; F(1,71)=44.57, p <.001, g2= .386) as well as
Table 3
Change in HR and determinants of HR during each minute of cold task
Measure Low hostiles High hostiles
Men Women All low Men
HR (bpm)
Min 1 �6.33 (1.01) �4.54 (1.07) �5.44 (.74) �7.53Min 2 �7.85 (1.08) �4.63 (1.14) �6.25 (.79) �6.43Min 3 �7.85 (1.08) �3.63 (1.11) �5.14 (.76) �4.66Total �6.95 (.94) �4.27 (.99) �4.36 (.65) �6.21
RSA (natural log)
Min 1 .74 (.19) .44 (.20) .59 (.14) .61
Min 2 1.01 (.17) .33 (.18) .67 (.13) .59
Min 3 .69 (.17) .11 (.18) .40 (.12) .49
Total .81 (.16) .29 (.17) .55 (.11) .57
PEP (ms)
Min 1 �5.32 (1.97) �6.79 (2.01) �6.06 (1.42) �5.34Min 2 �5.10 (2.67) � .35 (2.73) �2.72 (1.92) �2.80Min 3 �2.55 (1.48) �6.14 (1.51) �4.34 (1.06) �5.86Total �4.32 (1.64) �4.43 (1.67) �4.37 (1.18) �4.69
an unexpected increase in sympathetic activity (PEP;
F(1,68)=24.22, p <.001, g2= .263). A marginal main effect
for sex in the expected direction, was found on RSA,
F(1,70)=3.69, p <.06, g2= .050. Men displayed greater
increase in RSA in response to the cold task as compared
to women (Fig. 2B). However, no effects of hostility on
RSA were found, suggesting that the hostility differences in
HR were not mediated by differences in parasympathetic
functioning.
An unexpected three-way interaction of Time�Hosti-
Hostility�Sex was found for PEP, F(2,132) =4.37,
p <.02, g2= .062. This effect was driven by fluctuations
in low hostile women who displayed a significant loss of
PEP shortening from minute 1 to minute 2 (see Table 3),
t(132)=2.70, p <.01 and a significant increase in PEP
shortening from minute 2 to minute 3, t(132)= .30,
p <.05.
3.5. Mediational analyses
Mediational analyses were conducted in a manner
consistent with Baron and Kenny’s (1986) approach to
examining mediation. To test the hypothesis that the
forehead cold pressor is a task for evoking parasympathetic
stimulation to the heart, autonomic responses (RSA, PEP)
were examined as potential mediators of the aforementioned
task effect on HR. Raw baseline and task HR were entered
into a two-way ANCOVA with raw task PEP and RSA
entered together as covariates. Both task RSA, F(1,
64)= .12.86, p <.001, g2= .167, and PEP, F(1, 64)= .5.87,
p <.02, g2= .084, emerged as significant predictors and
explained the time effect on HR, F(1, 64)= .04, p =n.s.,
g2= .001. Second, we examined autonomic mediation
effects of HR in the context of change from baseline.
A Three-way mixed ANCOVAs (i.e., High vs. Low
Hostility�Sex�Three Trials) covarying mean task change
All
Women All high Men Women
(1.03) �3.58 (.99) �5.56 (.71) �6.93 (.72) �4.06 (.73)
(1.10) �2.85 (1.06) �4.64 (.76) �7.14 (.77) �3.75 (.78)
(1.06) �1.12 (1.02) �2.89 (.73) �5.66 (.74) �2.37 (.75)
(.95) �2.52 (.91) �5.61 (.68) �6.58 (.66) �3.40 (.67)
(.19) .58 (.19) .59 (.13) .67 (.13) .51 (.14)
(.17) .54 (.17) .56 (.12) .80 (.12) .44 (.13)
(.17) .31 (.17) .40 (.12) .59 (.12) .21 (.12)
(.16) .47 (.16) .52 (.11) .69 (.11) .38 (.11)
(2.01) �2.26 (2.16) �3.80 (1.48) �5.33 (1.40) �4.52 (1.47)
(2.73) �5.01 (2.93) �3.91 (2.01) �3.95 (1.90) �2.68 (1.99)
(1.51) �4.02 (1.62) �4.94 (1.11) �4.21 (1.05) �5.08 (1.10)
(1.67) �3.76 (1.79) �4.21 (1.23) �4.50 (1.17) �4.09 (1.22)
-7
-6
-5
-4
-3
-2
-1
0
Cha
nge
in H
R (
bpm
)
Men
Women
A
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Cha
nge
in R
SA (
natu
ral l
og)
MenWomen
B
Fig. 2. Heart rate and RSA responses for men vs. women.
Table 4
Change in BP and determinants of BP during task
J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283280
in RSA and PEP, but not baseline, was used.1 Task change
in RSA, F(1,64)=22.24, p <.001, g2= .258, but not change
in PEP, F(1, 64)= .03, p =n.s ., emerged as a significant
predictor and mediated the time effect on change in HR
during the task, F(1,64)=2.90, p =n.s., g2= .043. Interest-ingly, inclusion of PEP and RSA as covariates did not
explain either the sex main effect, F(1,64)=4.15, p<.05,
g2= .061, nor the Time�Hostility interaction, F(2,128)=
4.23, p <.03, g2= .062. These results suggest that despite
evidence of coactivation, parasympathetic influences were
the dominant contributor to the HR deceleration effects
during the forehead cold stimulation. However, the effects
on RSA and PEP did not explain a significant portion of the
observed effect of sex and hostility.2
Finally, changes in affect (anger, anxiety) were examined
as potential mediators of the Time�Hostility and Sex
effects on task HR response. Three-way mixed ANCOVAs
(i.e., High vs. Low Hostility�Sex�Three Trials) covarying
baseline values along with the hypothesized mediators were
used. Affect and autonomic determinants were examined
separately. Change in anger and anxiety were entered
together as potential covariates. Anger emerged as a
significant independent predictor for HR, F(1,68)=5.77,
p <.05, g2= .078, lower anger predictive of greater HR
decrease during cold stimulation. However, both the sex
1 Inclusion of baseline HR did not significantly alter the observed effects.2 Because of the effects of respiration on the measurement of RSA
(Berntson et al., 1997) we examined differences in respiration rate (RR).
RR data was assessed with an EPM system (Mindlothian, VA) strain gauge.
A main effect for hostility was found for RR during the task, F(1,70)=4.86,
p <.05, g2= .065. High hostiles displayed a larger increase in RR during
cold stimulation compared to low hostiles (1.02 breaths/min vs. � .11breaths/min). Next we included change in task RR as a covariate in a three-
way ANCOVA of RSA. However, the inclusion of RR as a covariate did
not alter any of the previously observed effects on RSA. Finally, we
examined the effect of change in RR during the task on the previously
observed hostility and gender HR effects. Change in task RR was included
along with change in task RSA and PEP as potential covariates in repeated
measures ANCOVA of task HR. Higher RR emerged as a significant
independent predictor of lower HR, F(1,61)=4.36, p <.05, g2= .067, but
did not mediate the Time�Hostility nor the gender effect.
main effect (F(1,68)=9.45, p < .01, g2= .122) and the
Hostility�Time interaction, (F(2,136) = 4.39, p < .02,
g2= .061) remained significant.
3.6. Blood pressure effects
All main effects for SBP and DBP were non-significant
suggesting the forehead cold pressor was a predominantly
cardiac autonomic task (Table 4). These nonsignificant
findings are also important in that PEP changes can be
confounded by blood pressure differences and thus compli-
cate the interpretation of it as a noninvasive index of SNS
influences on the heart (Sherwood et al., 1990). The lack of
task effects for blood pressure argues for a simultaneous
sympathetic effect underlying HR changes to the cold
pressor task.
With respect to blood pressure determinants, a Hostility�Sex interaction was found for TPR, F(1,68)=4.37, p <.05,
g2= .060. Specifically, high hostile men displayed an increase
in TPR whereas TPR decreased among low hostile men,
t(68)=2.15, p <.05 (Table 4). In addition, a significant
Hostility�Sex interaction was found for CO, F(1,65)=
Low hostile High hostile Total
SBP (mmHg)
Men � .56 (1.43) 1.68 (1.39) .56 (1.04)
Women 1.97 (1.43) .93 (1.39) 1.45 (1.04)
Total .71 (.94) 1.30 (.94)
DBP (mmHg)
Men �1.14 (1.07) .75 (1.09) � .19 (.77)
Women .52 (1.07) � .42 (1.06) .05 (.77)
Total � .31 (.75) .17 (.76)
TPR (dyne-s*cm� 5)
Men �115.89 (51.28) 48.03 (49.77) �33.93 (34.63)
Women 19.10 (49.06) �59.98 (51.77) �20.44 (35.70)
Total �48.40 (34.92) �5.98 (35.97)
CO (l/min)
Men .65 (.17) .01 (.17) .33 (.11)
Women .44 (.16) .52 (.17) .48 (.12)
Total .55 (.12) .23 (.12)

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283 281
4.46, p < .05, g2= .064. Specifically, high hostile men
displayed less increase in CO compared to all other
Sex�Hostility cells, ts(65)>2.00, p <.05.
4. Discussion
The current experiment supports the hypothesis that the
forehead cold pressor evokes parasympathetic cardiac
activation. Interestingly, these data suggest the task is better
characterized as evoking autonomic coactivation, although
the cardiac deceleration was accounted for by parasympa-
thetic activation. Replicating prior research, men showed a
stronger cardiac deceleration to cold stimulation, marked by
larger decreases in HR and increases in RSA, compared to
women. More important, the dive reflex responses clearly
differed between high and low hostile individuals in
response to cold stimulation. As expected, high hostile
individuals displayed a weaker dive-reflex response char-
acterized by a loss of HR deceleration over time relative to
low hostile participants.
It is important to note that two critical emotional
mediators of autonomic activity, state anger and anxiety,
were examined as potential explanations for the task effects
on HR and RSA. However, these emotional states did not
mediate the effects nor were there any noticeable differences
in HR or RSA that would suggest that ratings of anger or
anxiety influenced physiological response. Hence, these
findings suggest that the observed HR responses to the task
reflect a reflexive physiological response pattern, irrespec-
tive of negative emotional states, driven by autonomic
efferents to the heart.
This experiment contributes to the literature in three
important ways. First, this is the first experiment to
demonstrate the autonomic determinants of the forehead
cold pressor response by indexing the autonomic systems
(PEP, RSA) themselves rather than assuming their activity
through HR responses. Second, these results broaden
understanding of constitutional cardiac differences between
high and low hostile individuals. Specifically, this experi-
ment demonstrated hostility differences in duration of the
reflex cardiac response to the task. This effect could have
important implications for understanding the determinants
of hostility differences in cardiovascular reactivity and
associated health vulnerabilities. Third, this experiment
replicated previous findings by Hughes and Stoney (2000)
of larger parasympathetic response to the forehead cold
pressor in men relative to women.
4.1. Qualifications and limitations
The most obvious limitation of the current experiment
was not finding a physiological basis for the hostility by
time interaction on HR. Clearly the deceleration of HR
suggests parasympathetic involvement. However, the lack
of corresponding main effect of hostility on RSA or time
interaction suggests either that other factors obscured the
effect, a problem in measurement, or that the effect was a
result of some factor not assessed (see Berntson et al.,
1991). For example, because respiration rate contributes to
vagal outflow to the heart (see Berntson et al., 1997) it was
possible that hostility differences in respiration may have
masked any parasympathetic effect on HR. Again, despite
evidence that high hostile participants breathed at a faster
rate during the task (which would lead to decreases in
estimates of RSA), respiration rate also failed to explain the
findings. A related possibility is that differences in
respiratory tidal volume that was not assessed here may
have influenced the results. Several studies have demon-
strated that RSA magnitude is positively correlated with
tidal volume (Laude et al., 1993; Grossman et al., 1991;
Kobayashi, 1998) and that such changes may impact the
spectral-frequency range in which RSA is measured (Hirsch
and Bishop, 1981).
With respect to measurement, RSA and PEP are
estimates, and thus, imperfect indices of autonomic activity.
For example, the employed high frequency spectral range
(.12 to .40 Hz), although widely accepted (Berntson et al.,
1997), is geared toward the modal frequency range of
parasympathetic functioning and therefore not inclusive of
all possible ranges of functioning. Hence, it is plausible that
gradients in hostility-related parasympathetic functioning
produced the observed HR differences but that this para-
sympathetic activity occurred in frequency ranges outside
the modal bandwidth. In addition, error in the estimation
process can be increased for more complex associations
(e.g., combined error as a function of estimating RSA as a
function of task and hostility). Thus, power to detect more
complex interactive processes such as the Hostility�Time
interaction for RSA may have been weakened.
Finally, this task was limited to producing efferent
parasympathetic activation and therefore does not address
the possibility of hostility differences in afferent or higher
order pathways that may precede such autonomic activation.
In addition, relative weakness in the vagal system may
reflect problems of conduction or non-autonomic, humoral
factors (Berntson et al., 1997; Hainsworth, 1995). Future
research should address these issues accordingly.
4.2. Conclusions
In spite of these limitations, the HR deceleration effects
extend descriptions of hostility and sex-related cardiovas-
cular functioning to include differences in underlying
physiological mechanisms, although the lack of more direct
evidence of mediation by RSA precludes firm conclusions
about the parasympathetic basis of these differences. None-
theless, the evidence regarding autonomic mediation of HR
response to the forehead cold pressor contributes to the
literature using this task and supports the procedure as an
effective method for examining the parasympathetic-cardiac
pathway.

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283282
Acknowledgements
We would like to thank two anonymous reviewers for
their comments on an earlier draft of this manuscript. This
project was sponsored by a Student Research Award from
the Division of Health Psychology (38) of the American
Psychological Association.
References
Bairey, C.N., Yang, L., Berman, D.S., Rozanski, A., 1990. Comparison of
physiologic ejection fraction responses to activities of daily living:
implications for clinical testing. Journal of the American College of
Cardiology 16, 847–854.
Baker, S.L., Kirsch, I., 1991. Cognitive mediators of pain perception and
tolerance. Journal of Personality and Social Psychology 61, 504–510.
Barefoot, J.C., Dahlstrom, W.G., Williams Jr., R.B., 1983. Hostility, CHD
incidence, and total mortality: a 25-year follow-up study of 255
physicians. Psychosomatic Medicine 45, 59–63.
Barefoot, J.C., Larsen, S., Von der Lieth, L., Schroll, M., 1995. Hostility,
incidence of acute myocardial infarction and mortality in a sample of
older Danish men and women. American Journal of Epidemiology 142,
477–484.
Baron, R.M., Kenny, D.A., 1986. Moderator–mediator variable distinction
in social psychological research: conceptual, strategic, and statistical
considerations. Journal of Personality and Social Psychology 51,
1173–1182.
Benjamin, L., 1967. Facts and artifacts in using analysis of covariance to
‘‘undo’’ the law of initial values. Psychophysiology 4, 187–206.
Bernhardson, C.S., 1975. Type I error rates when multiple comparison
procedure follow a significant F test. Biometrics 31, 229–236.
Berntson, G.G., Quigley, K.S., Jang, J., Boysen, S.T., 1990. An approach to
artifact identification: application to heart period data. Psychophysiology
27, 586–598.
Berntson, G.G., Cacioppo, J.T., Quigley, K.S., 1991. Autonomic determin-
ism: the modes of autonomic control, the doctrine of autonomic
space, and the laws of autonomic constraint. Psychological Review 98,
459–487.
Berntson, G.G., Cacioppo, J.T., Quigley, K.S., 1995. The metrics of cardiac
chronotropism: biometric perspectives. Psychophysiology 31, 44–61.
Berntson, G.G., Bigger, J.T., Eckberg, D.L., Grossman, P., Kaufmann, P.G.,
Malik, M., Nagaraja, H.N., Porges, S.W., Saul, J.P., Stone, P.H., van Der
Molen, M.W., 1997. Heart rate variability: origins, methods, and
interpretive caveats. Psychophysiology 34, 623–648.
Bigger, J.T., Fleiss, J.L., Rolnitzky, L.M., Steinman, R.C., 1993a.
Frequency domain measures of heart period variability to assess risk
late after myocardial infarction. Journal of the American College of
Cardiology 3, 729–736.
Bigger, J.T., Fleiss, J.L., Rolnitzky, L.M., Steinman, R.C., 1993b. The
ability of several short-term measures of RR variability to predict
mortality after myocardial infarction. Circulation 88, 927–934.
Blumenthal, J.A., Jiang, W., Waugh, R.A., Frid, D.J., Morris, J.J., Coleman,
R.E., Hanson, M., Babyak, M., Thyrum, E.T., Krantz, D.S., O’Connor,
C., 1995. Mental stress-induced ischemia in the laboratory and
ambulatory ischemia during daily life. Circulation 92, 2102–2108.
Brosschot, J.F., Thayer, J.F., 1998. Anger inhibition, cardiovascular
recovery and vagal function: a model of the link between hostility and
cardiovascular disease. Annals of Behavioral Medicine 20, 326–332.
Buss, A.H., Durkee, A., 1957. An inventory for assessing different kinds of
hostility. Journal of Consulting and Clinical Psychology 21, 343–349.
Buss, A.H., Perry, M., 1992. The aggression questionnaire. Journal of
Personality and Social Psychology 63, 452–459.
Cacioppo, J.T., Berntson, G.G., Binkley, P.F., Quigley, K.S., Uchino, B.N.,
Fieldstone, A., 1994. Autonomic cardiac control: II. Basal response,
noninvasive indices, and autonomic space as revealed by autonomic
blockade. Psychophysiology 31, 586–598.
Christensen, A.J., Smith, T.W., 1993. Cynical hostility, self-disclosure, and
cardiovascular reactivity. Psychosomatic Medicine 55, 532–537.
Cook, W.W., Medley, D.M., 1954. Proposed hostility and pharisaic-virtue
scales for the MMPI. Journal of Applied Psychology 38, 414–418.
Durel, L.A., Kus, L.A., Anderson, N.B., McNeilly, M., Llabre, M.M.,
Spitzer, S., Saab, P.G., Efland, J., Williams, R., Schneiderman, N.,
1993. Patterns and stability of cardiovascular responses to variations of
the cold pressor test. Psychophysiology 30, 39–46.
Everson, S.A., Kaplan, G.A., Goldberg, D.E., Lakka, T.A., Sivenius, J.,
Salonen, J.T., 1999. Anger expression and incident stroke: prospective
evidence from the Kuopio ischemic heart disease study. Stroke 30,
523–528.
Fukudo, S., Lane, J.D., Anderson, N.B., Kuhn, C.M., Schanberg, S.M.,
McCown, N., Muranaka, M., Suzuki, J., Williams Jr., R.B., 1992.
Accentuated vagal antagonism of beta-adrenergic effects on ventricular
repolarization: evidence of weaker antagonism in hostile type A men.
Circulation 85, 2045–2053.
Gabbay, F.H., Krantz, D.S., Hedges, S.M., Kop, W.J., Klein, J.K.,
Gottdiener, J.S., Rozanski, A., 1996. Triggers of daily-life myocar-
dial ischemia inpatients of daily-life myocardial ischemia in patients
with coronary artery disease: physical activities, emotional arousal
and smoking. Journal of the American College of Cardiology 27,
585–592.
Gallo, L.C., Matthews, K.A., 2003. Understanding the association between
socioeconomic status and physical health: do negative emotions play a
role? Psychological Bulletin 129, 10–51.
Gallo, L.C., Smith, T.W., 1998. Construct validation of health-relevant
personality traits: interpersonal circumplex and five-factor model
analyses of the aggression questionnaire. International Journal of
Behavioral Medicine 5, 129–147.
Gottdiener, J.S., Krantz, D.S., Howell, R.H., Hecht, G.M., Klein, J.,
Falconer, J.J., Rozanski, A., 1994. Induction of silent myocardial
ischemia with mental stress testing: relation to the triggers of ischemia
during daily life activities and to ischemic functional severity. Journal of
the American College of Cardiology 24, 1645–1651.
Graham, R.E., Zeichner, A., Peacock, L.J., Dishman, R.K., 1996.
Bradycardia during baroreflex stimulation and active or passive stressor
tasks: cardiorespiratory fitness and hostility. Psychophysiology 33,
566–575.
Grossman, P., Karemaker, J., Wieling, W., 1991. Prediction of tonic
parasympathetic cardiac control using respiratory sinus arrhythmia: the
need for respiratory control. Psychophysiology 28, 201–216.
Guyll, M., Contrada, R.J., 1998. Trait hostility and ambulatory cardiovas-
cular activity: responses to social interaction. Health Psychology 17,
30–39.
Hainsworth, R., 1995. The control and physiological importance of heart
rate. In: Malik, M., Camm, A.J. (Eds.), Heart Rate Variability. Future
Publishing Company, Armonk, NY, pp. 3–19.
Heath, M.E., Downey, J.A., 1990. The cold face test (dive reflex) in clinical
autonomic assessment: methodological considerations and repeatability
of responses. Clinical Science 78, 139–147.
Hirsch, J.A., Bishop, B., 1981. Respiratory sinus arrhythmia in humans:
how breathing pattern modulates heart rate. American Journal of
Physiology 241, H620–H629.
Hughes, J.W., Stoney, C.M., 2000. Depressed mood is related to high-
frequency heart rate variability during stressors. Psychosomatic Med-
icine 62, 796–803.
Jennings, J.R., Kamarck, T.W., Stewart, C., Eddy, M., Johnson, P., 1992.
Alternative cardiovascular baseline assessment techniques: vanilla or
resting baseline. Psychophysiology 29, 742–750.
Julkunen, J., Salonen, R., Kaplan, G.A., Chesney, M.A., Salonen, J.T.,
1994. Hostility and the progression of carotid atherosclerosis. Psycho-
somatic Medicine 56, 519–525.
Kamarck, T.W., Everson, S.A., Kaplan, G.A., Manuck, S.B., Jennings, J.R.,
Salonen, R., Salonen, J.T., 1997. Exaggerated blood pressure responses

J.M. Ruiz et al. / International Journal of Psychophysiology 60 (2006) 274–283 283
during mental stress are associated with enhanced carotid atheroscle-
rosis in middle-aged Finnish men. Circulation 96, 3842–3848.
Kawachi, I., Sparrow, D., Spiro III, A., Vokonas, P., Weiss, S.C., 1996. A
prospective study of anger and coronary heart disease: the normative
aging study. Circulation 94, 2090–2095.
Khurana, R.K., Watabiki, S., Hebel, J.R., Toro, R., Nelson, E., 1980. Cold
face test in the assessment of trigeminal–brainstem–vagal function in
humans. Annals of Neurology 7, 144–149.
Kleiger, R.E., Miller, J.P., Bigger Jr., J.T., Moss, A.J., The Multicenter Post-
Infarction Research Group, 1987. Decreased heart rate variability and
its association with increased mortality after acute myocardial infarc-
tion. American Journal of Cardiology 59, 256–262.
Kobayashi, H., 1998. Normalization of respiratory sinus arrhythmia by
factoring in tidal volume. Applied Human Science 17, 207–213.
Krantz, D.S., Manuck, S.B., 1984. Acute psychophysiologic reactivity and
risk of cardiovascular disease: a review and methodologic critique.
Psychological Bulletin 96, 435–464.
Krantz, D.S., Helmers, K.F., Bairey, C.N., Nebel, L.E., Hedges, S.M.,
Rozanski, A., 1991. Cardiovascular reactivity and mental stress-induced
myocardial ischemia in patients with coronary artery disease. Psycho-
somatic Medicine 53, 1–12.
Laude, D., Goldman, M., Escourrou, P., Elghozi, J.L., 1993. Effect of
breathing pattern on blood pressure and heart rate oscillations in humans.
Clinical and Experimental Pharmacology and Physiology 20, 619–626.
Legault, S.E., Langer, A., Armstrong, P.W., Freeman, M.R., 1995.
Usefulness of ischemic response to mental stress in predicting silent
myocardial ischemia during ambulatory monitoring. American Journal
of Cardiology 75, 1007–1011.
Litvack, D.A., Oberlander, T.F., Carney, L.H., Saul, J.P., 1995. Time and
frequency domain methods for heart rate variability analysis: a
methodological comparison. Psychophysiology 32, 492–504.
Llabre, M.M, Spitzer, S.B., Saab, P.G., Ironson, G.H., Schneiderman, N.,
1991. The reliability and specificity of delta versus residualized change
as measures of cardiovascular reactivity to behavioral challenges.
Psychophysiology 28, 701–711.
Manuck, S.B., 1994. Cardiovascular reactivity and cardiovascular disease:
‘‘once more unto the breach’’. International Journal of Behavioral
Medicine 1, 4–31.
Matthews, K.A., Woodall, K.L., Allen, M.T., 1993. Cardiovascular
reactivity to stress predicts future blood pressure status. Hypertension
22, 479–485.
Matthews, K.A., Owens, J.F., Kuller, L.H., Sutton-Tyrrell, K., Jansen-
McWilliams, L., 1998. Are hostility and anxiety associated with carotid
atherosclerosis in healthy postmenopausal women? Psychosomatic
Medicine 60, 633–638.
Miller, T.Q., Smith, T.W., Turner, C.W., Guijarro, M.L., Hallet, A.J., 1996.
A meta-analytic review o research on hostility and physical health.
Psychological Bulletin 119, 322–348.
Muranaka, M., Lane, J.D., Suarez, E.C., Anderson, N.B., Suzuki, J.,
Williams Jr., R.B., 1988. Stimulus-specific patterns of cardiovascular
reactivity in type A and B subjects: evidence for enhanced vagal
reactivity in type B. Psychophysiology 25, 330–338.
Neuvo, Y., Cheng-Yu, D., Mitra, S., 1984. Interpolated finite impulse
response filters. I.E.E.E. Transactions on Acoustics, Speech, and Signal
Processing 32, 563–570.
Peckerman, A., Saab, P.G., MccCabe, P.M., Skyler, J.S., Winters, R.W.,
Llabre, M.M., Schneiderman, N., 1991. Blood pressure reactivity
and perception of pain during the forehead cold pressor test.
Psychophysiology 28, 485–495.
Peckerman, A., Hurwitz, B.E., Saab, P.G., Llabre, M.M., McCabe,
P.M., Schneiderman, N., 1994. Stimulus dimensions of the cold
pressor test and the associated patterns of cardiovascular response.
Psychophysiology 31, 282–290.
Reyners, A.K., Tio, R.A., Vlutters, F.G., van der Woude, G.F., Reitsma,
W.D., Smit, A.J., 2000. Re-evaluation of the cold face test in humans.
European Journal of Applied Physiology 82, 487–492.
Rhodes, R.D., Harrison, D.W., Demaree, H.A., 2002. Hostility as a
moderator of physical reactivity and recovery to stress. International
Journal of Neuroscience 112, 167–186.
Rozanski, A., Blumenthal, J.A., Kaplan, J., 1999. Impact of psychological
factors on the pathogenesis of cardiovascular disease and implications
for therapy. Circulation 99, 2192–2217.
Ruiz, J.M., Smith, T.W., Rhodewalt, F., 2001. Distinguishing narcissism
and hostility: similarities and differences in interpersonal circumplex
and five-factor correlates. Journal of Personality Assessment 76,
537–555.
Ryan, C., Hollenberg, M., Harvey, D.B., et al., 1976. Impaired para-
sympathetic responses in patients after myocardial infarction. American
Journal of Cardiology 37, 1013–1018.
Saab, P.G., Llabre, M.M., Hurwitz, B.E., Schneiderman, N., Wohlgemuth,
W., Durel, L.A., Massie, C., Nagel, J., 1993. The cold pressor test:
vascular and myocardial response patterns and their stability. Psycho-
physiology 30, 366–373.
Shapiro, D., Jamner, L.D., Goldstein, I.B., 1997. Daily mood states and
ambulatory blood pressure. Psychophysiology 34, 399–405.
Sherwood, A., Allen, M.T., Fahrenberg, J., Kelsey, R.M., Lovallo, W.R.,
van Doornen, L.J.P., 1990. Methodological guidelines for impedance
cardiography. Psychophysiology 27, 1–23.
Sloan, R.P., Shapiro, P.A., Bagiella, E., Myers, M.M., Gorman, J.M., 1999.
Cardiac autonomic control buffers blood pressure variability responses
to challenge: a psychophysiological model of coronary artery disease.
Psychosomatic Medicine 61, 58–68.
Sloan, R.P., Bagiella, E., Shapiro, P.A., Kuhl, J.P., Chernikhova, D., Berg,
J., Myers, M.M., 2001. Hostility, gender, and cardiac autonomic
control. Psychosomatic Medicine 63, 434–440.
Smith, T.W., Gallo, L.C., 1999. Hostility and cardiovascular reactivity
during marital interaction. Psychosomatic Medicine 61, 436–445.
Smith, T.W., Ruiz, J.M., Uchino, B.N., 2004. Mental activation of
supportive ties, hostility, and cardiovascular reactivity to laboratory
stress in young men and women. Health Psychology 23, 476–485.
Spielberger, C.D. Preliminary manual for the State–Trait Anger Scales
(STAS). Tampa, FL: University of South Florida Human Resources
Institute.
Suls, J., Bunde, J., 2005. Anger, anxiety, and depression as risk factors for
cardiovascular disease: the problems and implications of overlapping
affective dispositions. Psychological Bulletin 131, 260–300.
Tsuji, H., Larson, M.G., Venditti, F.J., Manders, E.S., Evans, J.C.,
Feldman, C.L., Levy, D., 1996. Impact of reduced heart rate
variability on risk for cardiac events: the Framingham heart study.
Circulation 94, 2850–2855.
Uchino, B.N., Cacioppo, J.T., Malarkey, W., Glaser, R., 1995. Individual
differences in cardiac sympathetic control predict endocrine and
immune responses to acute psychological stress. Journal of Personality
and Social Psychology 69, 736–743.
White, S.W., McRitchie, R.J., 1973. Nasopharyngeal reflexes: integrative
analysis of evoked respiratory and cardiovascular effects. Australian
Journal of Experimental Biological Medical Science 51, 17–31.
Wildenthal, K., Leshin, S.J., Atkins, J.M., et al., 1975. The diving reflex
used to treat paroxysmal atrial tachycardia. Lancet 1, 12–14.
Williams, R.B., 1994. Neurobiology, cellular and molecular biology, and
psychosomatic medicine. Psychosomatic Medicine 56, 308–315.
Williams, J.E., Paton, C.C., Siegler, I.C., Eigenbrodt, M.L., Nieto, F.J.,
Tyroler, H.A., 2000. Anger proneness predicts coronary heart disease
risk: prospective analysis from the atherosclerosis risk in communities
(ARIC) study. Circulation 101, 2034–2039.
Copyright © 2022 FDOKUMEN




















