
Histogram Feature–Based Classification Improves Differentiability of Early Bone Healing Stages...
8
Histogram FeatureYBased Classification Improves Differentiability of Early Bone Healing Stages From Micro-Computed Tomographic Data Bernd Preininger, MD,* Bernhard Hesse, MSc,Þþ Daniel Rohrbach, MSc,*Þ Peter Varga, PhD,* Hinnerk Gerigk,* Max Langer, PhD,þ§ Francoise Peyrin, PhD,þ§ Carsten Perka, MD,* and Kay Raum, PhD*Þ Objective: Contrast between not fully mineralized tissues is weak and limits conventional computed tomography (CT). An automated grayscale histogram-based analysis features could improve the sensitivity to tissue alterations during early bone healing. Materials and Methods: Tissue formation in a rat osteotomy model was analyzed using in vivo micro-CT and classified histologically (min- eralized, cartilage, and connective tissues). A conventional threshold-based method including manual contouring was compared to a novel moment- based method: after removing the background peak, the histograms of each slice were characterized by their moments and analyzed as a func- tion of the position along the long bone axis. Results: The threshold-based method could differentiate between the mineralized and connective tissue (R 2 = 0.73). The moment-based ap- proach yielded a clear distinction between all 3 groups with a classifi- cation accuracy up to R 2 = 0.93. Conclusions: The moment-based evaluation outperforms the con- ventional threshold-based CT analysis in sensitivity to the healing stage, user independence, and time consumption. Key Words: bone healing, microYcomputed tomography, histogram moment (J Comput Assist Tomogr 2012;36: 469Y476) C omputed tomography (CT) is a well-established and ver- satile tool that is often used for qualitative and quantitative analysis of mineralized tissue formations, their pathologies and regeneration, both in human and in animal trials. In contrast to histological analysis, x-rayYbased analysis can be done in vivo. The advantages of CT and micro-CT in mineralized tissue re- search are excellent, that is, the strong contrast between soft and mineralized tissues provides 3-dimensional distribution and structural properties of mineralized tissue nondestructively with a high spatial resolution. Recently, it has been shown that the contrast for tissues with low mineralization and soft tissues can be greatly enhanced by using phase-contrast CT (PCCT) ima- ging. 1Y3 However, this technology has not been implemented in clinical CT or experimental micro-CT systems. Donath et al 4 expected that both preclinical and clinical phase-contrast scan- ners will be developed within the next decade. Bone healing can be divided into 4 overlapping phases: (1) inflammation, (2) soft callus formation, (3) hard callus forma- tion, and (4) remodeling. The assessment of the onset of soft callus formation is crucial for the prediction of success or failure of the healing process. 5 However, the assessment of the early healing phases is still a challenging issue, both in clinical and in experimental situations. Attenuation-based x-ray imaging cannot detect soft tissue alterations, for example, endochondral cartilage formation. Other imaging modalities, for example, magnetic re- sonance imaging, provide in principle better soft tissueYspecific contrast but have limited potential for practical application owing to the cost factor and the vicinity of metallic fixation devices that are often necessary for the stabilization of the defect. Quantitative ultrasound has been proposed as a nonionizing alternative; but particularly for small animal applications, quantitative ultrasound is still at a developmental stage. 6 The results of micro-CT analysis strongly depend on the image processing techniques. Different image segmentation approaches using thresholds have been reported, for example, the classic global, 7,8 adaptive, 9 dual, 10 and multiple thresholds, 11 among others. 12,13 The most common approach is to use a fixed global threshold. For this, the proper selection is a delicate step and is user dependent. Moreover, the use of a fixed global threshold implies the assumption of a consistent linear attenu- ation criterion to the entire reconstructed grayscale image. In addition to the threshold-based segmentation, a manual con- touring of the low mineralized callus regions is necessary, which is a very time-consuming and user-dependent procedure. The aim of this study was to increase the sensitivity of parameters derived from attenuation-based CT data with respect to soft tissue variations in the healing callus. We hypothesized that a more sensitive user-independent and faster assessment of the healing stage could be achieved by an evaluation of grayscale distributions in the repair region. To minimize the effects of beam hardening and interspecimen variability, only the relative var- iations of histogram moments derived from image slices parallel to the osteotomy gap have been evaluated with respect to slice position. The new moment-based evaluation was compared with an established threshold-based protocol for their feasibility to discriminate between early healing phases in a small animal osteotomy (OT) model. MATERIALS AND METHODS Animal Model In this pilot study, 15 representative Sprague-Dawley rats (age, 12 months) were selected from another larger cohort study. All rats received a double OT in the femoral midshaft (2-mm gap) that was stabilized with an external fixator. Without further treatment, the 2-mm OT leads to a delayed healing. A broad ORIGINAL ARTICLE J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012 www.jcat.org 469 From the *Julius Wolff Institute and Center for Musculoskeletal Surgery, Charite ´YUniversita ¨tsmedizin Berlin, Berlin, Germany, and †Berlin-Brandenburg School for Regenerative Therapies, Charite ´YUniversita ¨tsmedizin Berlin, Berlin, Germany; ‡European Synchrotron Radiation Facility, Grenoble, France; and §CNRS UMR 5220, INSERM U1044, Universite ´ de Lyon, INSA Lyon, Villeurbanne Cedex, France. Received for publication April 5, 2012; accepted May 9, 2012. Reprints: Kay Raum, PhD, Julius Wolff Institute and Center for Musculoskeletal Surgery, Charite ´ - Universita ¨tsmedizin Berlin, Augustenburger Platz 1, 13353 Berlin, Germany (e-mail: [email protected]). This work has been supported by the Deutsche Forschungsgemeinschaft in the framework of the Berlin-Brandenburg School for Regenerative Therapies GSC 203, SFB 760 (project G-2.2), and grant Ra1380/8-1. Bernd Preininger and Bernhard Hesse contributed equally to this work. The authors report no conflicts of interest. Copyright * 2012 by Lippincott Williams & Wilkins Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
-
Upload
charite-de -
Category
Documents
-
view
2 -
download
0
Transcript of Histogram Feature–Based Classification Improves Differentiability of Early Bone Healing Stages...

Histogram FeatureYBased Classification ImprovesDifferentiability of Early Bone Healing Stages From
Micro-Computed Tomographic DataBernd Preininger, MD,* Bernhard Hesse, MSc,Þþ Daniel Rohrbach, MSc,*Þ Peter Varga, PhD,*
Hinnerk Gerigk,* Max Langer, PhD,þ§ Francoise Peyrin, PhD,þ§Carsten Perka, MD,* and Kay Raum, PhD*Þ
Objective: Contrast between not fully mineralized tissues is weak andlimits conventional computed tomography (CT). An automated grayscalehistogram-based analysis features could improve the sensitivity to tissuealterations during early bone healing.Materials and Methods: Tissue formation in a rat osteotomy modelwas analyzed using in vivo micro-CT and classified histologically (min-eralized, cartilage, and connective tissues). A conventional threshold-basedmethod including manual contouring was compared to a novel moment-based method: after removing the background peak, the histograms ofeach slice were characterized by their moments and analyzed as a func-tion of the position along the long bone axis.Results: The threshold-based method could differentiate between themineralized and connective tissue (R2 = 0.73). The moment-based ap-proach yielded a clear distinction between all 3 groups with a classifi-cation accuracy up to R2 = 0.93.Conclusions: The moment-based evaluation outperforms the con-ventional threshold-based CT analysis in sensitivity to the healing stage,user independence, and time consumption.
Key Words: bone healing, microYcomputed tomography, histogrammoment
(J Comput Assist Tomogr 2012;36: 469Y476)
Computed tomography (CT) is a well-established and ver-satile tool that is often used for qualitative and quantitative
analysis of mineralized tissue formations, their pathologies andregeneration, both in human and in animal trials. In contrast tohistological analysis, x-rayYbased analysis can be done in vivo.The advantages of CT and micro-CT in mineralized tissue re-search are excellent, that is, the strong contrast between soft andmineralized tissues provides 3-dimensional distribution andstructural properties of mineralized tissue nondestructively witha high spatial resolution. Recently, it has been shown that thecontrast for tissues with low mineralization and soft tissues canbe greatly enhanced by using phase-contrast CT (PCCT) ima-ging.1Y3 However, this technology has not been implemented inclinical CT or experimental micro-CT systems. Donath et al4
expected that both preclinical and clinical phase-contrast scan-ners will be developed within the next decade.
Bone healing can be divided into 4 overlapping phases: (1)inflammation, (2) soft callus formation, (3) hard callus forma-tion, and (4) remodeling. The assessment of the onset of softcallus formation is crucial for the prediction of success or failureof the healing process.5 However, the assessment of the earlyhealing phases is still a challenging issue, both in clinical and inexperimental situations. Attenuation-based x-ray imaging cannotdetect soft tissue alterations, for example, endochondral cartilageformation. Other imaging modalities, for example, magnetic re-sonance imaging, provide in principle better soft tissueYspecificcontrast but have limited potential for practical application owingto the cost factor and the vicinity of metallic fixation devices thatare often necessary for the stabilization of the defect. Quantitativeultrasound has been proposed as a nonionizing alternative; butparticularly for small animal applications, quantitative ultrasoundis still at a developmental stage.6
The results of micro-CT analysis strongly depend on theimage processing techniques. Different image segmentationapproaches using thresholds have been reported, for example, theclassic global,7,8 adaptive,9 dual,10 and multiple thresholds,11
among others.12,13 The most common approach is to use a fixedglobal threshold. For this, the proper selection is a delicate stepand is user dependent. Moreover, the use of a fixed globalthreshold implies the assumption of a consistent linear attenu-ation criterion to the entire reconstructed grayscale image. Inaddition to the threshold-based segmentation, a manual con-touring of the low mineralized callus regions is necessary, whichis a very time-consuming and user-dependent procedure.
The aim of this study was to increase the sensitivity ofparameters derived from attenuation-based CT data with respectto soft tissue variations in the healing callus. We hypothesizedthat a more sensitive user-independent and faster assessment ofthe healing stage could be achieved by an evaluation of grayscaledistributions in the repair region. Tominimize the effects of beamhardening and interspecimen variability, only the relative var-iations of histogram moments derived from image slices parallelto the osteotomy gap have been evaluated with respect to sliceposition. The new moment-based evaluation was compared withan established threshold-based protocol for their feasibility todiscriminate between early healing phases in a small animalosteotomy (OT) model.
MATERIALS AND METHODS
Animal ModelIn this pilot study, 15 representative Sprague-Dawley rats
(age, 12 months) were selected from another larger cohort study.All rats received a double OT in the femoral midshaft (2-mm gap)that was stabilized with an external fixator. Without furthertreatment, the 2-mm OT leads to a delayed healing. A broad
ORIGINAL ARTICLE
J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012 www.jcat.org 469
From the *Julius Wolff Institute and Center for Musculoskeletal Surgery,ChariteYUniversitatsmedizin Berlin, Berlin, Germany, and †Berlin-BrandenburgSchool for Regenerative Therapies, ChariteYUniversitatsmedizin Berlin, Berlin,Germany; ‡European Synchrotron Radiation Facility, Grenoble, France;and §CNRS UMR 5220, INSERM U1044, Universite de Lyon, INSA Lyon,Villeurbanne Cedex, France.Received for publication April 5, 2012; accepted May 9, 2012.Reprints: Kay Raum, PhD, Julius Wolff Institute and Center for
Musculoskeletal Surgery, Charite - Universitatsmedizin Berlin,Augustenburger Platz 1, 13353 Berlin, Germany(e-mail: [email protected]).
This work has been supported by the Deutsche Forschungsgemeinschaft in theframework of the Berlin-Brandenburg School for Regenerative TherapiesGSC 203, SFB 760 (project G-2.2), and grant Ra1380/8-1.
Bernd Preininger and Bernhard Hesse contributed equally to this work.The authors report no conflicts of interest.Copyright * 2012 by Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

range of different healing stages after 6 weeks of consolidationwas achieved by different treatments, that is, implantation ofprogenitor cells, body morphogenetic protein 2 or blood clotsinto the OT gap.14 The animal experiments were carried outfollowing the protocol described elsewhere.15 Micro-CT scanswere conducted after 6 weeks of consolidation. Afterward, therats were euthanasized and the osteotomized femora were har-vested for histological analysis. All animal experiments werecarried out according to the policies and principles established bythe Animal Welfare Act. The design of the animal surgeries wascritically reviewed and approved by the local legal representative(Landesamt fur Arbeitsschutz, Gesundheitsschutz und technischeSicherheit, Berlin: G 0428/08).
Histological AnalysisThe femora were decalcified in EDTA and embedded in
paraffin. Four-micrometer-thick sections were cut in a longitudi-nal direction, that is, parallel to the long axis of the femur (Fig. 1).All sections were stained with Movat pentachrome, which allowsdifferentiation between fibrous tissue (light green-blue), cartilage(deep green), and bone (yellow). The types and quantities of tis-sues in the OT gap were analyzed in all slices. Based on the typeof tissue predominantly found within the OT gap, the specimenswere assigned to one of the following healing phases: 1, fibrousconnective tissue; 2, hyaline cartilage and fibrous connectivetissue; and 3, woven bone.
MicroYComputed TomographyPrior to sacrifice, in-vivo micro-CT imaging of the osteo-
tomized femora was performed using a vivaCT 40 (ScancoMedical AG, Switzerland) at a voltage of 55 kilovolt (peak) and acurrent of 145KA. The exposure time for each projection was setto 150 milliseconds. An isotropic voxel size of 35 Km was se-lected for acquisition and reconstruction. Linear attenuation datawere scaled by multiplying by 4096 and stored as 16-bit signedinteger values, which corresponds to the native units of the CTmanufacturer. Hereinafter, these integer values will be referred toas grayscale or integer values.
Conventional Threshold-Based EvaluationA cylindrical volume of interest (VOI) of 4-mm total length
was defined, covering the 2-mm gap region and 1 mm in bothproximal and distal directions of the original OT gap. Callusformed around the fixator pinswas excluded from the analysis. Afixed global threshold value that segmented mineralized callusand cortical tissue from soft tissue was defined as 50% of themean integer value found in intact cortical bone tissue. Theproper segmentation was verified by visual inspection of 10
randomly selected 2-dimensional (2D) slices from every sample.Afterward, the callus tissue was segmented from the adjacentcortical tissue by manual polygon contouring of the interface intransverse 2D sections. From the segmented 3D callus datawithin the VOI, the following parameters were calculated, asdescribedbyMehta et al15: bonevolume (BV, inmm3), total volume(TV, in mm3), bone volume fraction (BV/TV, in percent), bonemineral content (BMC) in the segmented callus tissue (BMCBV, inmgHA), and BMC in the total callus volume (BMCTV inmgHA).
Moment-Based EvaluationIn each 3D reconstructed micro-CT VOI, the pin axes were
detected and the VOI was transformed by translation and rotationoperations to align pin axes with the xz plane. Figure 2 showsrepresentative xy grayscale slices and corresponding histograms.Each histogram exhibits a peak at a value of approximately 5000corresponding to background and soft tissue pixels (Fig. 2C). Abroader distribution between 5000 and 25,000 corresponds topixels filled with mineralized tissues.
AGaussian function was fitted to the background peak, andthe fitted curve was subtracted from the histogram. Theremaining bimodal distribution was composed of mineralizedcortical and callus tissues, as illustrated in Figure 2D, where2 Gaussian functions were fitted to the histograms. However,because callus and cortical tissues cannot be assumed to benormally distributed, the jth order central moments Mj of theentire background-subtracted distributions were evaluated, wherej Z {0, 1, 2, 3, 4}. A description of the features of thesemoments is summarized in Table 1.
Subsequently, the variation ofMj was analyzed with respectto the long axis position z. The left and right boundaries of the OTgap were defined as zl and zr, respectively. The area under thecurve IMj between zl and zr characterizes the OT gap region:
IMj ¼ ~zr
z¼zl
MjðzÞ I$z; ð1Þ
where$z is the slice thickness. The values of the image momentsat the locations zl and zr approximate the cortical tissue adjacentto the OT gap. It should be noted that Mj(zl) and Mj(zr) can beinfluenced by periosteal and endosteal callus formations. Thearea under a linear function that connects Mj(zl) and Mj(zr) is anapproximation of a very advanced healing case:
Aj ¼
�MjðzlÞ þMjðzrÞ
�
2I ðzl � zrÞ: ð2Þ
The difference of the 2 areas, Dj = Aj j IMj, characterizesthe difference of the actual magnitude of Mj compared to the
FIGURE 1. Representative Movat pentachromeYstained tissue sections of the 3 healing stages (scale bar = 2 mm). A, In the earlyhealing stage (group 1), the tissue in the OT gap consists mainly of fibrous connective tissue. B, In group 2, hyaline cartilage synthesisis present. C, In the late healing stage (group 3), the entire callus has been mineralized.
Preininger et al J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012
470 www.jcat.org * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

approximated fully healed OT (Fig. 2E). Moreover, to minimizethe potential impacts of bone geometry and grayscale calibration,Dj was normalized to the respective Aj and expressed in percent:
mj ¼Dj
AjI100 ð3Þ
The resulting fractions mj were used for classification ofthe samples (Fig. 2E). Representative profiles ofM0,M1, andM2
are shown in Figure 3. Note that an important feature of theparameters mj is their invariance to linear scaling of the grayvalue units of the micro-CT images. In this study, the OTboundaries along the z-axis were determined manually fromsagittal x-ray projections reconstructed from the volume data
(not shown). To assess the sensitivity of the measured parameterswith respect to the selection of the boundary position, the pa-rameter estimations have been repeated, whereas zl and zr werevaried T5 slides from their manually selected positions.
Statistical AnalysisAssociations between the parameters determined with the
threshold and moment-based methods were evaluated using re-gression analysis. To determine healing stage-specific differ-ences of the parameters, analysis of variance (ANOVA)followed by post hoc Tukey-Kramer multiple comparison (MC)tests were used. The distributions of the parameters were testedfor normality and variance homogeneity using Lilliefors16 andBartlett test, respectively. All statistical results were considered
FIGURE 2. Summary of the moment-based evaluation method. A, Volume-rendered image showing the pins, cortical and callustissues, and the OT gap. B, Transverse sections, separated by 30 z slices. C, Corresponding histograms exhibit a sharp background peakand a broader distribution of mineralized callus and cortical tissues. The background was approximated by a Gaussian profile.D, Background-subtracted histograms reveal bimodal distributions with low and high gray values corresponding to callusand cortical tissues, respectively (the 2 Gaussian profiles are fitted to the data for illustration purposes only). E, Parameters derivedfrom the variation of the histogram moments Mj with respect to the long axis z are illustrated for j = 0.
J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012 Histogram Based Assessment of Bone Healing Stages
* 2012 Lippincott Williams & Wilkins www.jcat.org 471
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

significant at P G 0.05. To explore the sensitivity of differentparameters on the 3 healing groups, multivariate ANOVA(MANOVA) was performed with a post hoc Bonferroni ad-justment. Based on MANOVA, a canonical analysis was con-ducted to find the linear combination of the features that bestseparated the 3 groups. Hereinafter, Ck is defined as the kthcanonical component. All statistical tests were performed usingthe Statistics Toolbox of MATLAB R2010a (The MathworksInc, Natick, Mass).
ClassificationTwo different types of classifiers were used in this study, a
support vector machine (SVM) and a k-nearest neighbor (k-NN)classifier. The SVMmethod17 is suitable for 2 class problems. Toextend SVM to multiclass problems, the most common solutionsare the strategies ‘‘one against all’’ and ‘‘one against one.’’18 Forthis study, a simple approach was used consisting of a mixture ofboth techniques. For each test, the outcome of the decisionfunction was counted for each class and the decision was madefor the class with the highest count. A linear kernel was used fortraining. To confirm the results obtained using SVM, a k-NNclassifier19 was used, which belongs to the family of nonpara-metric or instance-based classifiers.20 The parameter k in thisapproach specifies the amount of neighbors taken into accountwhen classifying an unknown sample. Euclidean distance metricwas used in this study, and the accuracy of k-NN was tested fordifferent k Z {1,2,3}. The accuracy of the 2 classifiers was
assessed using an n-fold cross-validation. It has been shown thatstratified n-fold cross-validation (with n = 10) is better than othermethods, for example, bootstrapping.21 Owing to the low samplenumber in this study, we decided to use n = sample number,which is equal to a leave-one-out cross-validation.21 Accuracy,precision, and sensitivity were derived by applying a 3 � 3confusion matrix.22,23 Accuracy was defined as the ratio ofcorrectly classified samples and the total amount of samplesinvolved in the classification, whereas sensitivity gives the rateof the worst classified class.24
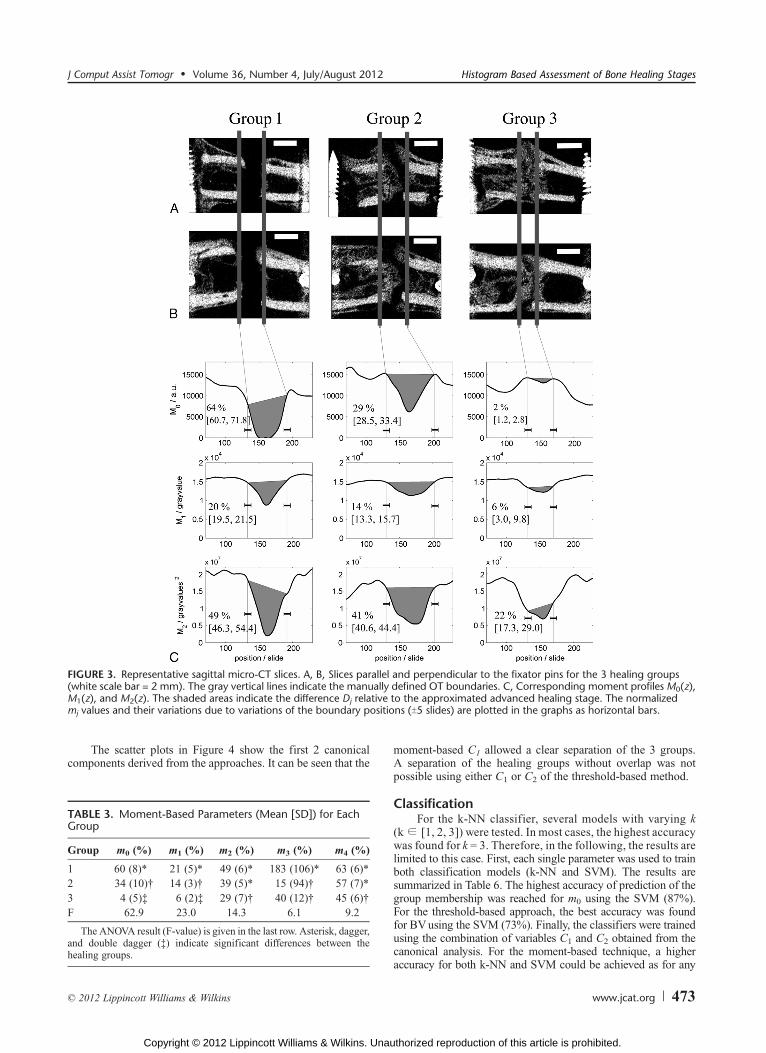
RESULTSRepresentative sagittal micro-CT images for each healing
group are shown in Figures 3A and B. In group 1, no intra-membranous callus formation could be observed. In group 2,mineralized callus was partially found in the gap region. How-ever, cartilage formation, as revealed by histologic examination,was not visible in the micro-CT images. In group 3, massivemineralized callus formation with partial to full bridging of bothends could be seen. The moment profiles Mj(z) exhibited aminimum in the central region of gap. Note that local maxima didnot necessarily occur at the OT boundaries but rather furtheraway from the gap, which was caused by the periosteal callusformations proximal and distal to the OT boundaries.
The values of the derived relative moments were slightlyinfluenced by the selection of the boundary positions. However,these variations were much smaller compared to the variationsobserved between the healing groups (Fig. 3C).
The threshold-based evaluation took approximately1.5 hours per sample, whereas the analyses using the moment-based evaluation was done within minutes per sample on astandard PC (Intel Core Duo, 3 GHz, 1.9 GB RAM). Theaverage parameters determined by both methods in eachhealing group are summarized in Tables 2 and 3.
For the threshold-based method, the segmented callus tissuevolumesTV (F = 9.8) andBV (F= 9.9) aswell as bothBMC (8.3eF e 9.3) parameters were significantly higher in healing group 3than in group 1. In contrast, the moments m0, m1, and m2 weredifferent between all healing groups (14.3 e F e 62.9; Table 3).
All threshold-based parameters were highly correlated (R2Q
0.96). Therefore, the canonical combination of threshold-basedparameters did not result in a remarkable improvement of thedifferentiability between the healing groups (Table 4).
The correlations between threshold and moment-basedparameters weremoderate or not significant (Table 5).Moreover,the correlations between the individual mi were much weakerthan those between the threshold-based parameters and in somecases not significant. Therefore, the canonical combination ofmoment-based parameters led to a further improvement of thedifferentiability between the healing groups (Table 4).
TABLE 1. Description of the Moments Mj derived From theGrayscale Histograms
ImageMoment Name Histogram Property
M0 Area Number of pixels in the histogram: corre-sponds to the amount of the mineralizedtissue
M1 Mean Mean gray value: qualitative measure of themean degree of mineralization
M2 Variance Variance of the gray value distribution:corresponds to the variance of the degreeof mineralization
M3 Skewness Asymmetry of the gray value distribution:depends on the amount andmineralizationof callus and cortical tissues
M4 Kurtosis A measure that describes the shape of thegray value distribution, for example,peaked or flat: depends on the relativeamounts and overlap of the distributionsof callus and cortical tissues
TABLE 2. Threshold-Based Parameters (Mean [SD]) for Each Healing Group
Group TV (mm3) BV (mm3) BV/TV BMCTV (mg) BMCBV (mg)
1 22.7 (6.0)* 14.9 (5.5)* 0.64 (0.11) 7.9 (3.5)* 11.0 (4.4)*2 61.5 (25.8) 47.4 (19.5) 0.77 (0.04) 28.8 (12.0) 36.2 (14.7)3 122.8 (56.4)† 91.9 (43.0)† 0.75 (0.08) 51.9 (26.7)† 67.3 (32.3)†F 9.8 9.9 n.s. 8.3 9.3
The ANOVA result (F value) is given in the last row. Asterisk (*) and dagger (†) indicate significant differences between the healing groups.
n.s. indicates nonsignificant.
Preininger et al J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012
472 www.jcat.org * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
The scatter plots in Figure 4 show the first 2 canonicalcomponents derived from the approaches. It can be seen that the
moment-based C1 allowed a clear separation of the 3 groups.A separation of the healing groups without overlap was notpossible using either C1 or C2 of the threshold-based method.
ClassificationFor the k-NN classifier, several models with varying k
(kZ [1, 2, 3]) were tested. In most cases, the highest accuracywas found for k = 3. Therefore, in the following, the results arelimited to this case. First, each single parameter was used to trainboth classification models (k-NN and SVM). The results aresummarized in Table 6. The highest accuracy of prediction of thegroup membership was reached for m0 using the SVM (87%).For the threshold-based approach, the best accuracy was foundfor BVusing the SVM (73%). Finally, the classifiers were trainedusing the combination of variables C1 and C2 obtained from thecanonical analysis. For the moment-based technique, a higheraccuracy for both k-NN and SVM could be achieved as for any
FIGURE 3. Representative sagittal micro-CT slices. A, B, Slices parallel and perpendicular to the fixator pins for the 3 healing groups(white scale bar = 2 mm). The gray vertical lines indicate the manually defined OT boundaries. C, Corresponding moment profiles M0(z),M1(z), and M2(z). The shaded areas indicate the difference Dj relative to the approximated advanced healing stage. The normalizedmj values and their variations due to variations of the boundary positions (T5 slides) are plotted in the graphs as horizontal bars.
TABLE 3. Moment-Based Parameters (Mean [SD]) for EachGroup
Group m0 (%) m1 (%) m2 (%) m3 (%) m4 (%)
1 60 (8)* 21 (5)* 49 (6)* 183 (106)* 63 (6)*2 34 (10)† 14 (3)† 39 (5)* 15 (94)† 57 (7)*3 4 (5)‡ 6 (2)‡ 29 (7)† 40 (12)† 45 (6)†F 62.9 23.0 14.3 6.1 9.2
The ANOVA result (F-value) is given in the last row. Asterisk, dagger,and double dagger (‡) indicate significant differences between thehealing groups.
J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012 Histogram Based Assessment of Bone Healing Stages
* 2012 Lippincott Williams & Wilkins www.jcat.org 473
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

single parameter of the threshold-based method. Contrarily, forthe threshold-based approach, the accuracy could not be in-creased for the canonical components compared with that ob-tained with the single parameters.
DISCUSSIONThe evaluation of the bone healing status by x-rayYbased
techniques is highly dependent on the sensitivity of themethod totissues without or with low mineralization. In this study, we haveevaluated a novel approach to analyze micro-CT data on sensi-tivity to small differences in themineral content of tissues formedwithin an OT gap after 6 weeks in a small animal model. Theproposed method is based on the analysis of grayscale histogramdistributions within and adjacent to the tissue repair region. Incontrast to conventional segmentation-based approaches, thenew method does not require manual contouring, which is a verytime-consuming and user-dependent method. Moreover, thenovel approach does not use a threshold to segment the miner-alized from nonmineralized tissues, which was hypothesized toimprove the sensitivity to tissues with very low degrees ofmineralization and to reduce the impacts of beam hardening andinterspecimen variability.
The ability of the new method to differentiate betweendifferent healing stages was compared to the one using a fixedglobal threshold reported in previous bone healing studies.15 Incontrast to the threshold-based evaluation, which requires thedefinition of a global threshold value and the manual contouringof the newly formed callus tissue, the moment-based approachproposed in this study only requires the proper alignment of thebone axis within the CT volume and the manual selection of theOT gap boundaries along the bone long axis. In processingspeed, the conventional method, including defining the VOI,contouring within the VOI, determining the threshold, rendering,and finally processing the outcomemeasurements, required up to
1.5 hours for each sample. The new method was much moreefficient and provided results within a few minutes.
The initial assignment of the samples to the 3 differenthealing stages, which was used to validate the micro-CTYbasedresults, was based on the descriptive analysis of histologicalsections by an experienced observer using well-establishedfeatures that provide clear distinction between the healing stages.It should be noted, however, that histological analysis is limitedto 2D sections and therefore may not represent the real healingstage of the entire investigated samples. In contrast, micro-CTprovides 3D access to the repair region.
The moment-based data analysis relies on the evaluation ofthe jth moments of gray value distributions with respect to theposition along the long axis of the bone. The spatial distributionwithin each slide along the long axis is therefore lost. A limi-tation of this method is therefore the assumption that the OT isperpendicular to the z axis. A potential anatomical misalignmentof the proximal and distal OT sides may alter the parametersused for the classification. Hence, only specimens fulfilling thisgeometric requirement should be evaluated using the moment-based approach.
The newmethod is independent of linear scaling of the grayvalues and therefore does not require calibration of the micro-CTimages. Therefore, data acquired using different micro-CTdevices but comparable settings are anticipated to result incomparable results as long as the correlation of gray values tothe linear attenuation coefficients follows a linear relation. Ifthis is not the case, the images must be calibrated beforecalculation of mj.
For both the moment- and threshold-based approaches,correlations between the output parameters were investigated.For the threshold-based approach, all correlation coefficientswere found to be larger than 0.9, which indicated that all para-meters describe highly redundant information. Since m0 and m1
are calculated based on the amount of mineralized volumeobtained from histograms, the observed correlations between BVand m0 as well as m1 were not unexpected. However, results ofstatistical analysis revealed a higher predictive power of thefeatures of the moment-based approach. As both parameters arerelated to the number of voxels that contain mineralized tissue,the moderate correlation between m0 and BV and the superiorpredictive value of m0 support that the histogram-based evalu-ation is more sensitive in tissues with lowmineralization than thesegmentation-based approach. Another reason may be that m0
describes a relative loss of bone volume in OT region, whereasBV describes the absolute number of mineralized voxels in theVOI regardless of their location.
TABLE 4. Variance Analyses of the Canonical VariablesDerived From the Moment- and Threshold-Based Approaches(F Value and Post Hoc Multiple Comparison [MC]Test)
F MC
Threshold-based C1 16.4 (III = II) G IThreshold-based C2 6.8 III G IIMoment-based C1 84.8 I G II G IIIMoment-based C2 5.1 II G III
TABLE 5. Correlation Coefficients (R2) for Each Pair of Features
m1 m2 m3 m4 TV BV BV/TV BMCTV BMCBV
m0 0.89 0.67 0.29 0.51 0.59 0.61 n.s. 0.60 0.61m1 0.7 n.s. 0.51 0.53 0.58 0.33 0.58 0.57m2 n.s. 0.83 0.3 0.34 n.s. 0.36 0.34m3 n.s. n.s. n.s. n.s. n.s. n.s.m4 0.24 0.24 n.s. n.s. n.s.TV 0.97 n.s. 0.90 0.96BV n.s. 0.98 90.99BV/TV n.s. n.s.BMCTV 0.99
Nonsignificant relations are denoted by ‘‘n.s.’’, and R2 values larger than 0.7 are set in boldface.
Preininger et al J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012
474 www.jcat.org * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

This study has several limitations. The most prominentlimitation of the study is the low amount of sample data, whichcould cause a low power of the statistical hypothesis tests anddegraded performance of both classifiers. The relationship be-tween the optimal training size for nonparametric classifierssuch as k-NN and the dimensionality of the features was reportedto be exponential.25 Because both classifiers used in this studyare known to be sensitive to data size and feature dimension,sophisticated statistical testing was used to address this limita-tion. Different statistical analyses (MANOVA, classifier, andregression) were performed to verify the results. Canonicalanalyses were conducted to reduce the number of features. Thelatter was especially important because it was shown that theoptimal feature size decreases strongly when the features arehighly correlated, which was the case for the threshold-basedapproach.26
Despite the fact that literature offers a rich variety onclassifiers, SVM was selected because of its top level rank inperformance compared to other popular classifiers27,28 and itswide application in medical imaging.29,30 Furthermore, SVMwas reported to be robust also with small sample sizes.26 Tominimize the effects of small sample size on the outcome, a linearkernel function was used in this study during training. Thenearest neighbor algorithm is a very intuitive approach and oneof the most and best studied classifiers in literature.20,28,31,32
In the present study, the effect of CT image resolution hasnot been investigated. During bone healing, mineralization of the
connective tissue occurs in a speculated manner, which results ina highly heterogeneous distribution of highY and lowYmineraldensity regions. The partial volume effect may therefore have aninfluence on the measured density distributions, which couldaffect the outcome of our evaluations. Incorporating the effects ofspatial resolution and voxel size with respect to the structuraldimensions of the newly formed callus tissue will be the subjectof future work.
The small sample size used in this study does not allow forgeneralization of the findings to a larger data set. Nonetheless,our results indicate that the sensitivity and precision of theclassifiers derived from the moment-based method are superiorto those derived from the threshold-based method, which will beconfirmed in future studies with an increased sample size.
CONCLUSIONSIn this study, a novel evaluation of micro-CT images is
proposed with the aim to improve the ability to differentiatebetween early healing stages. Compared to the common threshold-based approach, the moment-based data evaluation was able todistinguish better, faster, and, except for the manual definition ofthe 2 OT gap boundaries, user independent between different his-tologically identified healing stages.
By taking properties of the adjacent nonfractured bone intoaccount to normalize the measurements from the region of in-terest and by avoiding contouring as well as the use of thresholds,the sensitivity toward lowmineralized tissues could be increased,whereas time efficacy and the objectiveness could be improved.
The proposed method may help to improve the currentmicro-CTYbased evaluation protocols of fracture callus in smallanimal OT studies, to develop a diagnostic tool for better as-sessment of low mineralized tissue formations and therebyyielding valuable information about the bone regenerationprocess.
ACKNOWLEDGMENTSThe authors thank Prof Dr Stefan Posch for his comments
on the classification, Eleanor Stephenson for proofreading,Mario Thiele for supporting the micro-CT measurements, andNils Mannicke and Martin Schone for discussion.
REFERENCES
1. Langer M, Liu Y, Tortelli F, et al. Regularized phase tomography enablesstudy of mineralized and unmineralized tissue in porous bone scaffold.J Microsc. 2010;238:230Y239.
FIGURE 4. Scatter plots for the first 2 canonical components. A, Moment-based method. B, Threshold-based approach.
TABLE 6. Classification Accuracy for k-NN and SVM ClassifiersTrained by Single Parameter
k-NN SVM
m0 0.87 0.87M1 0.80 0.80m2 0.47 0.67m3 0.53 0.53m4 0.67 0.47Moment-based C1 0.93 0.93Moment-based C2 0.20 0.20TV 0.67 0.67BV 0.67 0.73BV/TV 0.40 0.13BMCTV 0.13 0.13BMCBV 0.60 0.67Threshold-based C1 0.60 0.67Threshold-based C2 0.60 0.47
J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012 Histogram Based Assessment of Bone Healing Stages
* 2012 Lippincott Williams & Wilkins www.jcat.org 475
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

2. Momose A. Recent advances in X-ray phase imaging. Jpn J Appl Phys.2005;44:6355Y6367.
3. Zhou SA, Brahme A. Development of phase-contrast X-ray imagingtechniques and potential medical applications. Phys Med.2008;24:129Y148.
4. Donath T, Pfeiffer F, Bunk O, et al. Toward clinical X-ray phase-contrastCT: demonstration of enhanced soft-tissue contrast in human specimen.Invest Radiol. 2010;45:445Y452.
5. Peters A, Schell H, Bail HJ, et al. Standard bone healing stages occurduring delayed bone healing, albeit with a different temporal onset andspatial distribution of callus tissues. Histol Histopathol.2010;25:1149Y1162.
6. Protopappas VC, Vavva MG, Fotiadis DI, et al. Ultrasonic monitoring ofbone fracture healing. IEEE Trans Ultrason Ferroelectr Freq Control.2008;55:1243Y1255.
7. Muller R, Ruegsegger P. Micro-tomographic imaging for thenondestructive evaluation of trabecular bone architecture. Stud HealthTechnol Inform. 1997;40:61Y79.
8. Muller R, Van Campenhout H, Van Damme B, et al. Morphometricanalysis of human bone biopsies: a quantitative structural comparison ofhistological sections and micro-computed tomography. Bone.1998;23:59Y66.
9. Burghardt AJ, Kazakia GJ, Majumdar S. A local adaptive thresholdstrategy for high resolution peripheral quantitative computedtomography of trabecular bone. Ann Biomed Eng. 2007;35:1678Y1686.
10. Buie HR, Campbell GM, Klinck RJ, et al. Automatic segmentation ofcortical and trabecular compartments based on a dual thresholdtechnique for in vivo micro-CT bone analysis. Bone. 2007;41:505Y515.
11. Freeman TA, Patel P, Parvizi J, et al. Micro-CT analysis with multiplethresholds allows detection of bone formation and resorption duringultrasound-treated fracture healing. J Orthop Res. 2009;27:673Y679.
12. Morgan EF, Mason ZD, Chien KB, et al. MicroYcomputed tomographyassessment of fracture healing: relationships among callus structure,composition, and mechanical function. Bone. 2009;44:335Y344.
13. Duvall CL, Taylor WR, Weiss D, et al. Quantitative microcomputedtomography analysis of collateral vessel development after ischemicinjury. Am J Physiol. 2004;287:302Y310.
14. Preininger B, Gerigk H, Bruckner J, et al. An experimental setup toevaluate innovative therapy options for the enhancement of bone healingusing BMP2 as a benchmarkVa pilot study. Eur Cell Mater.2012;23:262Y272.
15. Mehta M, Strube P, Peters A, et al. Influences of age and mechanicalstability on volume, microstructure, and mineralization of the fracture
callus during bone healing: is osteoclast activity the key to age-relatedimpaired healing? Bone. 2010;47:219Y228.
16. Lilliefors HW. On the Kolmogorov-Smirnov test for normality withmean and variance unknown. J Am Stat Assoc. 1967;62:399Y402.
17. Cortes C, Vapnik V. Support-vector networks. Machine Learning.1995;20:273Y297.
18. Chih-Wei H, Chih-Jen L. A comparison of methods for multiclasssupport vector machines. IEEE Trans Neural Netw. 2002;13:415Y425.
19. Cover T, Hart P. Nearest neighbor pattern classification. IEEE Trans
Inform Theory. 1967;13:21Y27.
20. Mitchell T. Machine Learning. New York, NY: MacGraw-Hill; 1997.
21. Kohavi R. A Study of Cross-Validation and Bootstrap for Accuracy
Estimation and Model Selection. San Francisco, CA: Morgan KaufmannPublishers Inc; 1995:1137Y1143.
22. Fawcett T. An introduction to ROC analysis. Pattern Recognition Letters.2006;27:861Y874.
23. Everson RM, Fieldsend JE. Multi-class ROC analysis froma multi-objective optimisation perspective. Pattern Recogn Lett.2006;27:918Y927.
24. Fernandez Caballero JC, Martinez FJ, Hervas C, et al. Sensitivity versusaccuracy in multiclass problems using memetic Pareto evolutionaryneural networks. IEEE Trans Neural Netw. 2010;21:750Y770.
25. Raudys SJ, Jain AK. Small sample size effects in statistical patternrecognition: recommendations for practitioners. IEEE Trans Pattern
Anal Mach Intell. 1991;13:252Y264.
26. Hua J. Optimal number of features as a function of sample size forvarious classification rules. Bioinformatics. 2004;21:1509Y1515.
27. Meyer D. The support vector machine under test. Neurocomputing.2003;55:169Y186.
28. Theodoridis S. Pattern Recognition. Amsterdam. Amsterdam; Boston:Elsevier/Academic Press; 2006.
29. El-Naqa I, Yongyi Y, Wernick MN, et al. A support vector machineapproach for detection of microcalcifications. IEEE Trans Med Imaging.2002;21:1552Y1563.
30. Zhang Z, Zhang S, Zhang C-X, et al. SVM for density estimation andapplication to medical image segmentation. J Zhejiang University
Science B. 2006;7:365Y372.
31. Duda R. Pattern Classification. New York, NY: Wiley; 2001.
32. Patrick E, Fischeriii F. A generalized nearest neighbor rule. Informationand Control. 1970;16:128Y152.
Preininger et al J Comput Assist Tomogr & Volume 36, Number 4, July/August 2012
476 www.jcat.org * 2012 Lippincott Williams & Wilkins
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.




















