
High-grade oncocytic mucoepidermoid carcinoma of the minor salivary gland origin: a case report with...
6
High-grade oncocytic mucoepidermoid carcinoma of the minor salivary gland origin: a case report with immunohistochemical study HyukIl Kwon, BS, a WonBong Lim, PhD, b YooDuk Choi, MD, PhD, c JongHee Nam, MD, PhD, c ChangWoo Han, MS, c JiSun Kim, PhD, b YoungJong Ko, MS, b InAe Kim, MS, b SeoYune Kim, MS, b MiSook Kim, PhD, b OkSu Kim, DDS, PhD, d HongRan Choi, DDS, PhD, e and OkJoon Kim, DDS, PhD, f Gwangju, Korea CHONNAM NATIONAL UNIVERSITY An oncocytic mucoepidermoid carcinoma arising from the minor salivary gland origin is extremely rare. We report on a 44-year-old man with a high-grade oncocytic mucoepidermoid carcinoma originating in the minor salivary gland of the posterior mandible. All tumor cells showed the expected pattern of immunoreactivity, with positive results for the antimitochondrial antibody and p63, and negative results for the androgenic receptor antibody. Microscopically, the tumor was considered to be a high-grade carcinoma in the grading systems of the Armed Forces Institute of Pathology and Brandwein. The patient underwent a partial mandibulectomy, and the lesion was reconstructed with a right fibula osteofasciocutaneous flap under general anesthesia. The patient is currently under long-term follow-up. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e72-e77) An oncocytic mucoepidermoid carcinoma (OMEC) of the minor salivary gland is extremely rare and occurs over a wide range of ages. Most OMECs arise in the parotid gland, whereas OMEC arising from the minor salivary gland is rare. Only 5 cases of an OMEC originating in the minor salivary gland have been re- ported. Chomette et al. 1 and Martins et al. 2 described 3 cases and 1 case, respectively. Recently, Weinreb et al. 3 reported a tumor originating from the palate in 1 case. However, an OMEC of minor salivary gland origin has been reported with incomplete information with respect to the grades, origin, outcome, and treatment. A high- grade OMEC is infrequent; only a few cases have been reported as high-grade tumors, whereas most OMECs present as low- and intermediate-grade tumors. We report a rare high-grade OMEC of the minor salivary gland with the clinical and histopathological presenta- tions. CASE REPORT In February 2009, a 44-year-old man was referred to the Department of Oral and Maxillofacial Surgery at Chonnam National University Hospital, Gwangju, Korea, from a local dental clinic. The patient displayed erythematous ulcerative swelling on the mandibular gingiva around the left lower second molar with serious mobility and slight pain (Fig. 1). The patient was otherwise healthy and re- ported no significant prior medical or other family history. Panoramic radiography (Fig. 2) and positron emission to- mography– computed tomography (Fig. 3) revealed an ap- proximately 3-cm heterogeneously enhancing, bony de- structive mass of the left mandible. Clinically, the patient was diagnosed with a malignant bone tumor. Magnetic resonance imaging revealed a lobulated and heteroge- neously enhancing mass (approximately 3.9 2.5 2.9 cm) involving the left mandibular angle, with an invasion to the left buccinators and medial pterygoid muscle. Si- nusitis was observed in both sides of the ethmoid andright maxillary sinus with mild mucosa thickening (Fig. 4). A biopsy with an immunohistochemical study yielded a pathological diagnosis of a high-grade OMEC from a minor salivary gland. Based on the OMEC diagnosis, a partial mandibulectomy was performed and the lesion was reconstructed with a right fibula osteofasciocutaneous flap under general anesthesia in March 2009. H.K., Y.J.K., and I.A.K. are supported by the second stage of Brain Korea 21. a DDS PhD candidate, 2 nd Stage of Brain Korea 21 for School of Dentistry, Dental Science Research Institute, Chonnam National Uni- versity. b Resercher, Department of Oral Pathology, Chonnam National Uni- versity School of Dentistry. c Professor, Department of Pathology, Faculty of Medicine, Chonnam National University. d Associate Professor, Department of Periodontics, Chonnam National University School of Dentistry. e Professor, Department of oral pathology, Chonnam National Uni- versity School of Dentistry. f Assistant Professor, Department of oral pathology, Chonnam Na- tional University School of Dentistry. Received for publication Jul 29, 2009; returned for revision Dec 30, 2009; accepted for publication Jan 26, 2010. 1079-2104/$ - see front matter © 2010 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2010.01.026 e72
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of High-grade oncocytic mucoepidermoid carcinoma of the minor salivary gland origin: a case report with...

High-grade oncocytic mucoepidermoid carcinoma of the minorsalivary gland origin: a case report withimmunohistochemical studyHyukIl Kwon, BS,a WonBong Lim, PhD,b YooDuk Choi, MD, PhD,c
JongHee Nam, MD, PhD,c ChangWoo Han, MS,c JiSun Kim, PhD,b YoungJong Ko, MS,b
InAe Kim, MS,b SeoYune Kim, MS,b MiSook Kim, PhD,b OkSu Kim, DDS, PhD,d
HongRan Choi, DDS, PhD,e and OkJoon Kim, DDS, PhD,f Gwangju, KoreaCHONNAM NATIONAL UNIVERSITY
An oncocytic mucoepidermoid carcinoma arising from the minor salivary gland origin is extremely rare. Wereport on a 44-year-old man with a high-grade oncocytic mucoepidermoid carcinoma originating in the minor salivarygland of the posterior mandible. All tumor cells showed the expected pattern of immunoreactivity, with positiveresults for the antimitochondrial antibody and p63, and negative results for the androgenic receptor antibody.Microscopically, the tumor was considered to be a high-grade carcinoma in the grading systems of the Armed ForcesInstitute of Pathology and Brandwein. The patient underwent a partial mandibulectomy, and the lesion wasreconstructed with a right fibula osteofasciocutaneous flap under general anesthesia. The patient is currently under
long-term follow-up. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e72-e77)An oncocytic mucoepidermoid carcinoma (OMEC) ofthe minor salivary gland is extremely rare and occursover a wide range of ages. Most OMECs arise in theparotid gland, whereas OMEC arising from the minorsalivary gland is rare. Only 5 cases of an OMECoriginating in the minor salivary gland have been re-ported. Chomette et al.1 and Martins et al.2 described 3cases and 1 case, respectively. Recently, Weinreb et al.3
reported a tumor originating from the palate in 1 case.However, an OMEC of minor salivary gland origin hasbeen reported with incomplete information with respectto the grades, origin, outcome, and treatment. A high-grade OMEC is infrequent; only a few cases have been
H.K., Y.J.K., and I.A.K. are supported by the second stage of BrainKorea 21.aDDS PhD candidate, 2nd Stage of Brain Korea 21 for School ofDentistry, Dental Science Research Institute, Chonnam National Uni-versity.bResercher, Department of Oral Pathology, Chonnam National Uni-versity School of Dentistry.cProfessor, Department of Pathology, Faculty of Medicine, ChonnamNational University.dAssociate Professor, Department of Periodontics, Chonnam NationalUniversity School of Dentistry.eProfessor, Department of oral pathology, Chonnam National Uni-versity School of Dentistry.fAssistant Professor, Department of oral pathology, Chonnam Na-tional University School of Dentistry.Received for publication Jul 29, 2009; returned for revision Dec 30,2009; accepted for publication Jan 26, 2010.1079-2104/$ - see front matter© 2010 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2010.01.026e72
reported as high-grade tumors, whereas most OMECspresent as low- and intermediate-grade tumors. Wereport a rare high-grade OMEC of the minor salivarygland with the clinical and histopathological presenta-tions.
CASE REPORTIn February 2009, a 44-year-old man was referred to the
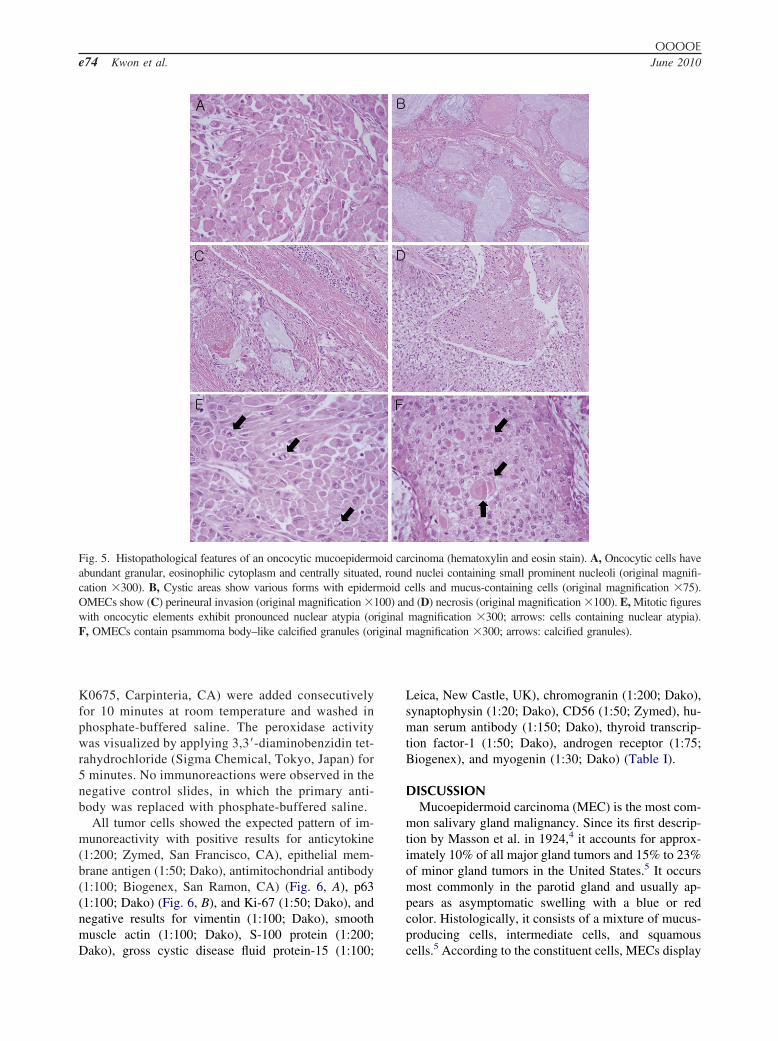
Department of Oral and Maxillofacial Surgery at ChonnamNational University Hospital, Gwangju, Korea, from alocal dental clinic. The patient displayed erythematousulcerative swelling on the mandibular gingiva around theleft lower second molar with serious mobility and slightpain (Fig. 1). The patient was otherwise healthy and re-ported no significant prior medical or other family history.Panoramic radiography (Fig. 2) and positron emission to-mography– computed tomography (Fig. 3) revealed an ap-proximately 3-cm heterogeneously enhancing, bony de-structive mass of the left mandible. Clinically, the patientwas diagnosed with a malignant bone tumor. Magneticresonance imaging revealed a lobulated and heteroge-neously enhancing mass (approximately 3.9 � 2.5 � 2.9cm) involving the left mandibular angle, with an invasionto the left buccinators and medial pterygoid muscle. Si-nusitis was observed in both sides of the ethmoid and rightmaxillary sinus with mild mucosa thickening (Fig. 4). A biopsywith an immunohistochemical study yielded a pathologicaldiagnosis of a high-grade OMEC from a minor salivary gland.Based on the OMEC diagnosis, a partial mandibulectomy wasperformed and the lesion was reconstructed with a right fibulaosteofasciocutaneous flap under general anesthesia in March
2009.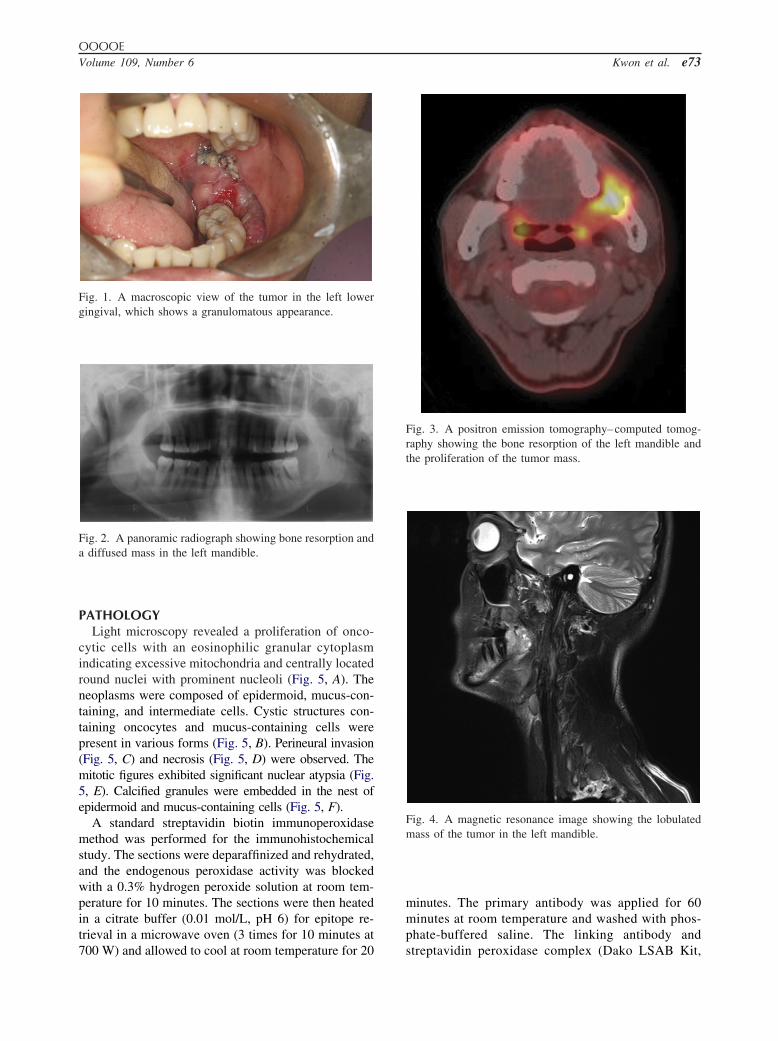
OOOOEVolume 109, Number 6 Kwon et al. e73
PATHOLOGYLight microscopy revealed a proliferation of onco-
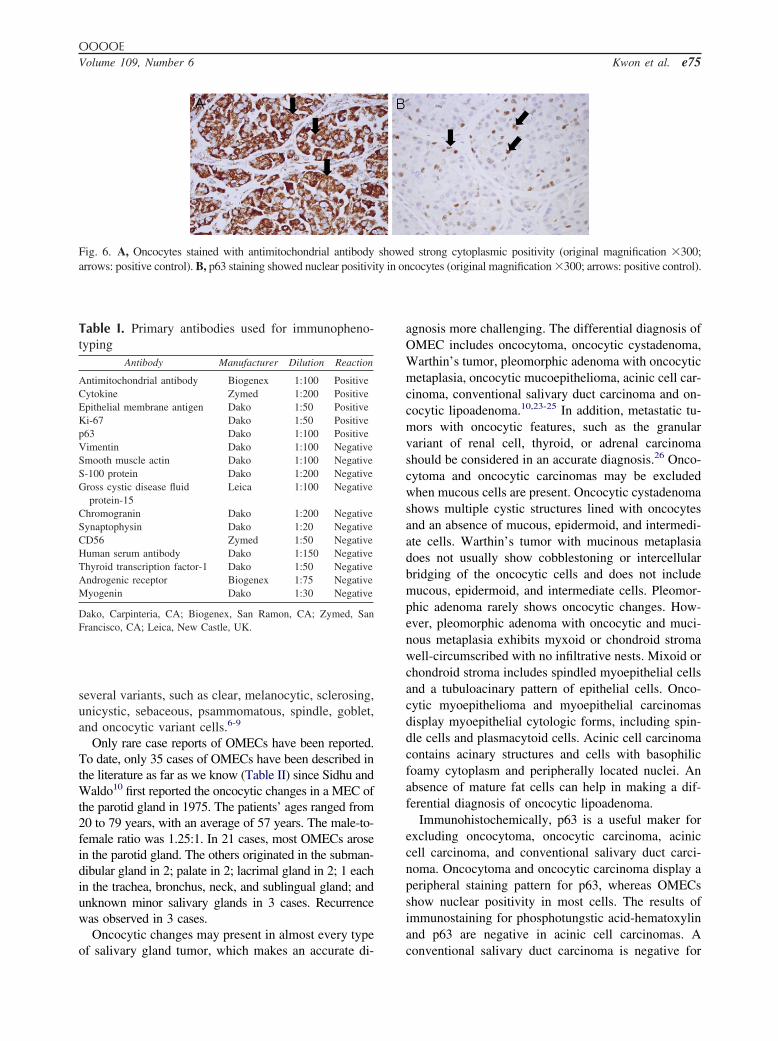
cytic cells with an eosinophilic granular cytoplasmindicating excessive mitochondria and centrally locatedround nuclei with prominent nucleoli (Fig. 5, A). Theneoplasms were composed of epidermoid, mucus-con-taining, and intermediate cells. Cystic structures con-taining oncocytes and mucus-containing cells werepresent in various forms (Fig. 5, B). Perineural invasion(Fig. 5, C) and necrosis (Fig. 5, D) were observed. Themitotic figures exhibited significant nuclear atypsia (Fig.5, E). Calcified granules were embedded in the nest ofepidermoid and mucus-containing cells (Fig. 5, F).
A standard streptavidin biotin immunoperoxidasemethod was performed for the immunohistochemicalstudy. The sections were deparaffinized and rehydrated,and the endogenous peroxidase activity was blockedwith a 0.3% hydrogen peroxide solution at room tem-perature for 10 minutes. The sections were then heatedin a citrate buffer (0.01 mol/L, pH 6) for epitope re-trieval in a microwave oven (3 times for 10 minutes at
Fig. 1. A macroscopic view of the tumor in the left lowergingival, which shows a granulomatous appearance.
Fig. 2. A panoramic radiograph showing bone resorption anda diffused mass in the left mandible.
700 W) and allowed to cool at room temperature for 20
minutes. The primary antibody was applied for 60minutes at room temperature and washed with phos-phate-buffered saline. The linking antibody and
Fig. 3. A positron emission tomography–computed tomog-raphy showing the bone resorption of the left mandible andthe proliferation of the tumor mass.
Fig. 4. A magnetic resonance image showing the lobulatedmass of the tumor in the left mandible.
streptavidin peroxidase complex (Dako LSAB Kit,
iginal
OOOOEe74 Kwon et al. June 2010
K0675, Carpinteria, CA) were added consecutivelyfor 10 minutes at room temperature and washed inphosphate-buffered saline. The peroxidase activitywas visualized by applying 3,3=-diaminobenzidin tet-rahydrochloride (Sigma Chemical, Tokyo, Japan) for5 minutes. No immunoreactions were observed in thenegative control slides, in which the primary anti-body was replaced with phosphate-buffered saline.
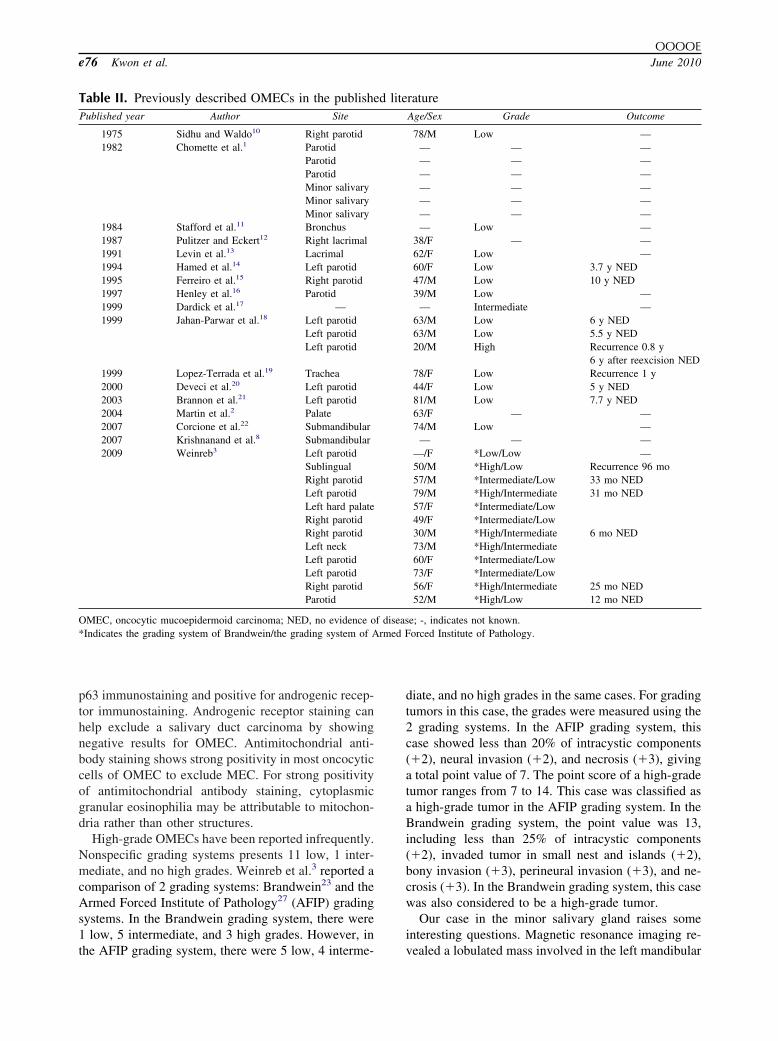
All tumor cells showed the expected pattern of im-munoreactivity with positive results for anticytokine(1:200; Zymed, San Francisco, CA), epithelial mem-brane antigen (1:50; Dako), antimitochondrial antibody(1:100; Biogenex, San Ramon, CA) (Fig. 6, A), p63(1:100; Dako) (Fig. 6, B), and Ki-67 (1:50; Dako), andnegative results for vimentin (1:100; Dako), smoothmuscle actin (1:100; Dako), S-100 protein (1:200;
Fig. 5. Histopathological features of an oncocytic mucoepidermabundant granular, eosinophilic cytoplasm and centrally situatedcation �300). B, Cystic areas show various forms with epiderOMECs show (C) perineural invasion (original magnification �1with oncocytic elements exhibit pronounced nuclear atypia (oF, OMECs contain psammoma body–like calcified granules (or
Dako), gross cystic disease fluid protein-15 (1:100;
Leica, New Castle, UK), chromogranin (1:200; Dako),synaptophysin (1:20; Dako), CD56 (1:50; Zymed), hu-man serum antibody (1:150; Dako), thyroid transcrip-tion factor-1 (1:50; Dako), androgen receptor (1:75;Biogenex), and myogenin (1:30; Dako) (Table I).
DISCUSSIONMucoepidermoid carcinoma (MEC) is the most com-
mon salivary gland malignancy. Since its first descrip-tion by Masson et al. in 1924,4 it accounts for approx-imately 10% of all major gland tumors and 15% to 23%of minor gland tumors in the United States.5 It occursmost commonly in the parotid gland and usually ap-pears as asymptomatic swelling with a blue or redcolor. Histologically, it consists of a mixture of mucus-producing cells, intermediate cells, and squamous
rcinoma (hematoxylin and eosin stain). A, Oncocytic cells haved nuclei containing small prominent nucleoli (original magnifi-ells and mucus-containing cells (original magnification �75).d (D) necrosis (original magnification �100). E, Mitotic figuresmagnification �300; arrows: cells containing nuclear atypia).magnification �300; arrows: calcified granules).
oid ca, rounmoid c00) an
riginal
cells.5 According to the constituent cells, MECs display
ty in on
OOOOEVolume 109, Number 6 Kwon et al. e75
several variants, such as clear, melanocytic, sclerosing,unicystic, sebaceous, psammomatous, spindle, goblet,and oncocytic variant cells.6-9
Only rare case reports of OMECs have been reported.To date, only 35 cases of OMECs have been described inthe literature as far as we know (Table II) since Sidhu andWaldo10 first reported the oncocytic changes in a MEC ofthe parotid gland in 1975. The patients’ ages ranged from20 to 79 years, with an average of 57 years. The male-to-female ratio was 1.25:1. In 21 cases, most OMECs arosein the parotid gland. The others originated in the subman-dibular gland in 2; palate in 2; lacrimal gland in 2; 1 eachin the trachea, bronchus, neck, and sublingual gland; andunknown minor salivary glands in 3 cases. Recurrencewas observed in 3 cases.
Oncocytic changes may present in almost every type
Fig. 6. A, Oncocytes stained with antimitochondrial antibodyarrows: positive control). B, p63 staining showed nuclear positivi
Table I. Primary antibodies used for immunopheno-typing
Antibody Manufacturer Dilution Reaction
Antimitochondrial antibody Biogenex 1:100 PositiveCytokine Zymed 1:200 PositiveEpithelial membrane antigen Dako 1:50 PositiveKi-67 Dako 1:50 Positivep63 Dako 1:100 PositiveVimentin Dako 1:100 NegativeSmooth muscle actin Dako 1:100 NegativeS-100 protein Dako 1:200 NegativeGross cystic disease fluid
protein-15Leica 1:100 Negative
Chromogranin Dako 1:200 NegativeSynaptophysin Dako 1:20 NegativeCD56 Zymed 1:50 NegativeHuman serum antibody Dako 1:150 NegativeThyroid transcription factor-1 Dako 1:50 NegativeAndrogenic receptor Biogenex 1:75 NegativeMyogenin Dako 1:30 Negative
Dako, Carpinteria, CA; Biogenex, San Ramon, CA; Zymed, SanFrancisco, CA; Leica, New Castle, UK.
of salivary gland tumor, which makes an accurate di-
agnosis more challenging. The differential diagnosis ofOMEC includes oncocytoma, oncocytic cystadenoma,Warthin’s tumor, pleomorphic adenoma with oncocyticmetaplasia, oncocytic mucoepithelioma, acinic cell car-cinoma, conventional salivary duct carcinoma and on-cocytic lipoadenoma.10,23-25 In addition, metastatic tu-mors with oncocytic features, such as the granularvariant of renal cell, thyroid, or adrenal carcinomashould be considered in an accurate diagnosis.26 Onco-cytoma and oncocytic carcinomas may be excludedwhen mucous cells are present. Oncocytic cystadenomashows multiple cystic structures lined with oncocytesand an absence of mucous, epidermoid, and intermedi-ate cells. Warthin’s tumor with mucinous metaplasiadoes not usually show cobblestoning or intercellularbridging of the oncocytic cells and does not includemucous, epidermoid, and intermediate cells. Pleomor-phic adenoma rarely shows oncocytic changes. How-ever, pleomorphic adenoma with oncocytic and muci-nous metaplasia exhibits myxoid or chondroid stromawell-circumscribed with no infiltrative nests. Mixoid orchondroid stroma includes spindled myoepithelial cellsand a tubuloacinary pattern of epithelial cells. Onco-cytic myoepithelioma and myoepithelial carcinomasdisplay myoepithelial cytologic forms, including spin-dle cells and plasmacytoid cells. Acinic cell carcinomacontains acinary structures and cells with basophilicfoamy cytoplasm and peripherally located nuclei. Anabsence of mature fat cells can help in making a dif-ferential diagnosis of oncocytic lipoadenoma.
Immunohistochemically, p63 is a useful maker forexcluding oncocytoma, oncocytic carcinoma, aciniccell carcinoma, and conventional salivary duct carci-noma. Oncocytoma and oncocytic carcinoma display aperipheral staining pattern for p63, whereas OMECsshow nuclear positivity in most cells. The results ofimmunostaining for phosphotungstic acid-hematoxylinand p63 are negative in acinic cell carcinomas. A
d strong cytoplasmic positivity (original magnification �300;cocytes (original magnification �300; arrows: positive control).
showe
conventional salivary duct carcinoma is negative for
rmed F
OOOOEe76 Kwon et al. June 2010
p63 immunostaining and positive for androgenic recep-tor immunostaining. Androgenic receptor staining canhelp exclude a salivary duct carcinoma by showingnegative results for OMEC. Antimitochondrial anti-body staining shows strong positivity in most oncocyticcells of OMEC to exclude MEC. For strong positivityof antimitochondrial antibody staining, cytoplasmicgranular eosinophilia may be attributable to mitochon-dria rather than other structures.
High-grade OMECs have been reported infrequently.Nonspecific grading systems presents 11 low, 1 inter-mediate, and no high grades. Weinreb et al.3 reported acomparison of 2 grading systems: Brandwein23 and theArmed Forced Institute of Pathology27 (AFIP) gradingsystems. In the Brandwein grading system, there were1 low, 5 intermediate, and 3 high grades. However, in
Table II. Previously described OMECs in the publishePublished year Author Site
1975 Sidhu and Waldo10 Right parotid1982 Chomette et al.1 Parotid
ParotidParotidMinor salivaryMinor salivaryMinor salivary
1984 Stafford et al.11 Bronchus1987 Pulitzer and Eckert12 Right lacrimal1991 Levin et al.13 Lacrimal1994 Hamed et al.14 Left parotid1995 Ferreiro et al.15 Right parotid1997 Henley et al.16 Parotid1999 Dardick et al.17 —1999 Jahan-Parwar et al.18 Left parotid
Left parotidLeft parotid
1999 Lopez-Terrada et al.19 Trachea2000 Deveci et al.20 Left parotid2003 Brannon et al.21 Left parotid2004 Martin et al.2 Palate2007 Corcione et al.22 Submandibular2007 Krishnanand et al.8 Submandibular2009 Weinreb3 Left parotid
SublingualRight parotidLeft parotidLeft hard palateRight parotidRight parotidLeft neckLeft parotidLeft parotidRight parotidParotid
OMEC, oncocytic mucoepidermoid carcinoma; NED, no evidence o*Indicates the grading system of Brandwein/the grading system of A
the AFIP grading system, there were 5 low, 4 interme-
diate, and no high grades in the same cases. For gradingtumors in this case, the grades were measured using the2 grading systems. In the AFIP grading system, thiscase showed less than 20% of intracystic components(�2), neural invasion (�2), and necrosis (�3), givinga total point value of 7. The point score of a high-gradetumor ranges from 7 to 14. This case was classified asa high-grade tumor in the AFIP grading system. In theBrandwein grading system, the point value was 13,including less than 25% of intracystic components(�2), invaded tumor in small nest and islands (�2),bony invasion (�3), perineural invasion (�3), and ne-crosis (�3). In the Brandwein grading system, this casewas also considered to be a high-grade tumor.
Our case in the minor salivary gland raises someinteresting questions. Magnetic resonance imaging re-
ratureAge/Sex Grade Outcome
78/M Low —— — —— — —— — —— — —— — —— — —— Low —
38/F — —62/F Low —60/F Low 3.7 y NED47/M Low 10 y NED39/M Low —
— Intermediate —63/M Low 6 y NED63/M Low 5.5 y NED20/M High Recurrence 0.8 y
6 y after reexcision NED78/F Low Recurrence 1 y44/F Low 5 y NED81/M Low 7.7 y NED63/F — —74/M Low —
— — ——/F *Low/Low —50/M *High/Low Recurrence 96 mo57/M *Intermediate/Low 33 mo NED79/M *High/Intermediate 31 mo NED57/F *Intermediate/Low49/F *Intermediate/Low30/M *High/Intermediate 6 mo NED73/M *High/Intermediate60/F *Intermediate/Low73/F *Intermediate/Low56/F *High/Intermediate 25 mo NED52/M *High/Low 12 mo NED
e; -, indicates not known.orced Institute of Pathology.
d lite
f diseas
vealed a lobulated mass involved in the left mandibular

OOOOEVolume 109, Number 6 Kwon et al. e77
angle with an invasion of the left buccinators andmedial pterygoid muscle. Several hypotheses have beenproposed to explain the pathogenesis of OMEC of aminor salivary gland origin. One theory suggests thatthey may arise from ectopic parotid tissue or othermajor salivary gland tissue that was developmentallyentrapped within the gingiva or jaw. However, therewas no evidence of ectopic major salivary tissue, suchas parotid gland or submandibular gland tissue. On theother hand, it is possible that OMEC of the mandibulargingiva may arise from the tail of the parotid gland.However, no metastasis through lymphovascular inva-sion was observed and no oncocytic lesions were foundin the biopsy specimen of the parotid and submandib-ular glands. For the purpose of this study, a metastasisof this tumor was not considered despite its likelihood.
High-grade oncocytic mucoepidermoid carcinoma ofthe minor salivary gland is extremely rare. Cervicallymph node metastasis occurs only rarely, and theprognosis is generally good. In this case, the postoper-ative course after 4 months has been uneventful; how-ever, our patient will receive long-term follow-up.
REFERENCES1. Chomette G, Auriol M, Tereau Y, Vaillant JM. Mucoepidermoid
tumors of minor salivary glands. Clinical and pathologic corre-lations. Histoenzymologic and ultrastructural studies (author’stranslation). Ann Pathol 1982;2(1):29-40.
2. Martins C, Cavaco B, Tonon G, Kaye FJ, Soares J, Fonseca I. Astudy of MECT1-MAML2 in mucoepidermoid carcinoma andWarthin’s tumor of salivary glands. J Mol Diagn 2004;6(3):205-10.
3. Weinreb I, Seethala RR, Perez-Ordonez B, Chetty R, HoscharAP, Hunt JL. Oncocytic mucoepidermoid carcinoma: clinico-pathologic description in a series of 12 cases. Am J Surg Pathol2009;33(3):409-16.
4. Masson RB, Berger L. Epiteliomas a double metaphisie de laparotide. Bull Assoc Fr Atude Cancer 1924;(13):366-73.
5. Neville B, Damm D, Allen C, Bouquot J. Oral and maxillofacialpathology. St. Louis, MO; Saunders; 2008.
6. Takeda Y, Kurose A. Pigmented mucoepidermoid carcinoma, acase report and review of the literature on melanin-pigmentedsalivary gland tumors. J Oral Sci 2006;48(4):253-6.
7. Shivapathasundharam B, Bertin AE. Clear cell variant of muco-epidermoid carcinoma. Report of a case and a review of clear celllesions of the oral cavity. Indian J Dent Res 2003;14(1):23-8.
8. Krishnanand G, Kaur M, Rao RV, Monappa V. Oncocytic vari-ant of mucoepidermoid carcinoma of submandibular gland: anunusual clinical and morphological entity. Indian J Pathol Mi-crobiol 2007;50(3):538-40.
9. Aguiar MC, Bernardes VF, Cardoso SV, Barbosa AA, MesquitaRA, Carmo MA. A rare case of sclerosing mucoepidermoidcarcinoma arising in minor salivary glands with immunohisto-chemical evaluation. Minerva Stomatol 2008;57(9):453-7.
10. Sidhu GS, Waldo ED. Oncocytic change in mucoepidermoid
carcinoma of the parotid gland. Arch Pathol 1975;99(12):663-6.11. Stafford JR, Pollock WJ, Wenzel BC. Oncocytic mucoepider-moid tumor of the bronchus. Cancer 1984;54(1):94-9.
12. Pulitzer DR, Eckert ER. Mucoepidermoid carcinoma of the lac-rimal gland. An oxyphilic variant. Arch Ophthalmol 1987;105(10):1406-9.
13. Levin LA, Popham J, To K, Hein A, Shore J, Jakobiec FA.Mucoepidermoid carcinoma of the lacrimal gland. Report of acase with oncocytic features arising in a patient with chronicdacryops. Ophthalmology 1991;98(10):1551-5.
14. Hamed G, Shmookler BM, Ellis GL, Punja U, Feldman D.Oncocytic mucoepidermoid carcinoma of the parotid gland. ArchPathol Lab Med 1994;118(3):313-4.
15. Ferreiro JA, Stylopoulos N. Oncocytic differentiation in salivarygland tumours. J Laryngol Otol 1995;109(6):569-71.
16. Henley JD, Rehan J, Oda D, Gown AM, Gnepp DR. Oncocyticmetaplastic tumors of salivary gland origin [abstract]. Oral SurgOral Med Oral Pathol Oral Radiol Endod 1997;84(2):187-8.
17. Dardick I, Birek C, Lingen MW, Rowe PE. Differentiation andthe cytomorphology of salivary gland tumors with specific ref-erence to oncocytic metaplasia. Oral Surg Oral Med Oral PatholOral Radiol Endod 1999;88(6):691-701.
18. Jahan-Parwar B, Huberman RM, Donovan DT, Schwartz MR,Ostrowski ML. Oncocytic mucoepidermoid carcinoma of thesalivary glands. Am J Surg Pathol 1999;23(5):523-9.
19. Lopez-Terrada D, Bloom MG, Cagle PT, Ostrowski ML. Onco-cytic mucoepidermoid carcinoma of the trachea. Arch Pathol LabMed 1999;123(7):635-7.
20. Deveci MS, Deveci G, Gunhan O, Finci R. Oncocytic mucoepi-dermoid carcinoma of the parotid gland: report of a case withDNA ploidy analysis and review of the literature. Pathol Int2000;50(11):905-9.
21. Brannon RB, Willard CC. Oncocytic mucoepidermoid carci-noma of parotid gland origin. Oral Surg Oral Med Oral PatholOral Radiol Endod 2003;96(6):727-33.
22. Corcione L, Giordano G, Gnetti L, Multinu A, Ferrari S. Onco-cytic mucoepidermoid carcinoma of a submandibular gland: acase report and review of the literature. Int J Oral MaxillofacSurg 2007;36(6):560-3.
23. Brandwein MS, Huvos AG. Oncocytic tumors of major salivaryglands. A study of 68 cases with follow-up of 44 patients. Am JSurg Pathol 1991;15(6):514-28.
24. Chang A, Harawi SJ. Oncocytes, oncocytosis, and oncocytictumors. Pathol Annu 1992;27(Pt 1):263-304.
25. Ilie M, Hofman V, Pedeutour F, Attias R, Santini J, Hofman P.Oncocytic lipoadenoma of the parotid gland: immunohistochem-ical and cytogenetic analysis. Pathol Res Pract 2010;206:66-72.
26. Seifert G, Brocheriou C, Cardesa A, Eveson JW. WHO interna-tional histological classification of tumours. Tentative histologi-cal classification of salivary gland tumours. Pathol Res Pract1990;186(5):555-81.
27. Ellis G, Auclair P. Atlas of tumor pathology: tumors of thesalivary glands. Washington, DC: Armed Forces Institute ofPathology; 1996. p. 468.
Reprint requests:
OkJoon Kim, DDS, PhDDepartment of Oral PathologySchool of DentistryChonnam National UniversityBug-Gu, Gwangju, 500-757, Korea
[email protected]



















