High C-reactive protein and low paraoxonase1 in diabetes as risk factors for coronary heart disease
6
Atherosclerosis 186 (2006) 396–401 High C-reactive protein and low paraoxonase1 in diabetes as risk factors for coronary heart disease Bharti Mackness a , David Hine a , Patrick McElduff b , Michael Mackness a,∗ a University Department of Medicine, Manchester Royal Infirmary, Oxford Road, Manchester M13 9WL, UK b School of Epidemiology and Public Health, University of Manchester, Manchester, UK Received 18 March 2005; received in revised form 27 July 2005; accepted 27 July 2005 Available online 2 September 2005 Abstract Background: Paraoxonase1 (PON1) is an anti-inflammatory enzyme located on HDL, which protects against the development of atheroscle- rosis. C-reactive protein (CRP) is a marker of the inflammatory response in CHD. We hypothesised that low PON1 and high CRP found in CHD may be important markers of CHD and the CRP:PON1 ratio may be an index of the risk of developing atherosclerosis. We have, therefore, compared the levels of PON1 and CRP between control subjects, those with no diabetes and CHD, type 1 diabetes and type 2 diabetes. Methods and results: PON1 activity was different between the populations in the order: controls > type 1 diabetes > type 2 diabetes > CHD with no diabetes (P < 0.001). CRP concentration also differed between the populations in the order: controls < type 1 diabetes < type 2 diabetes < CHD with no diabetes (P < 0.001). The CRP:PON1 ratio followed the same trend as the CRP concentration (P < 0.001). Both CRP and the CRP:PON1 ratio were associated with the presence of CHD. In the control population only, PON1 was a determinant of CRP concentration. Amongst the diabetics, people with CHD had higher levels of CRP (P < 0.001) and in comparing the control group with the CHD group, the CHD group had a higher level of CRP (P < 0.001). Conclusions: Higher levels of CRP seem to be generally associated with low levels of PON1 activity, providing a mechanistic link between inflammation and the development of atherosclerosis. However, the relationship between PON1, CRP and atherosclerosis, and the usefulness of the PON1:CRP ratio as a risk factor for CHD requires further evaluation. © 2005 Elsevier Ireland Ltd. All rights reserved. Keywords: Paraoxonase1; C-reactive protein; Inflammation; Diabetes mellitus; Coronary heart disease 1. Introduction Atherosclerosis is in part an inflammatory disease. After damage to the vascular endothelium by lipoproteins or high blood pressure, the resulting inflammatory response in the arterial wall is believed to be primarily due to oxidatively modified low-density lipoprotein (LDL), which triggers a cytokine response in vascular endothelial cells [1–3] stimulating the migration of blood monocytes across the intima. This response includes the upregulation of MCP-1 and adhesion molecules such as VCAM-1 which promote the ∗ Corresponding author. Tel.: +44 161 276 8633; fax: +44 161 274 4833. E-mail address: [email protected] (M. Mackness). recruitment of monocytes in the initial stages of atheroscle- rosis and later in the actively growing shoulder regions of the mature lesion. Beneath the intima, these monocytes trans- form into macrophages which rapidly take up modified LDL through scavenger receptors to become foam cells. Cytokines produced by these and the endothelial cells attract smooth muscle cells into the lesion from the media which themselves transform into fibroblasts elaborating collagen beneath the endothelium to form a fibrous cap [4,5]. HDL-associated paraoxonase (PON1) retards the oxidation of LDL both in vitro and in vivo [reviewed in [6]]. PON1 therefore inhibits the initiation/progression of atherosclerosis and has been shown to be active in atherosclerotic plaques [7,8]. PON1 has been shown to inhibit the pro-inflammatory responses of 0021-9150/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.atherosclerosis.2005.07.028
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of High C-reactive protein and low paraoxonase1 in diabetes as risk factors for coronary heart disease
Atherosclerosis 186 (2006) 396–401
High C-reactive protein and low paraoxonase1 in diabetes asrisk factors for coronary heart disease
Bharti Mackness a, David Hine a, Patrick McElduff b, Michael Mackness a,∗a University Department of Medicine, Manchester Royal Infirmary, Oxford Road, Manchester M13 9WL, UK
b School of Epidemiology and Public Health, University of Manchester, Manchester, UK
Received 18 March 2005; received in revised form 27 July 2005; accepted 27 July 2005Available online 2 September 2005
Abstract
Background: Paraoxonase1 (PON1) is an anti-inflammatory enzyme located on HDL, which protects against the development of atheroscle-rosis. C-reactive protein (CRP) is a marker of the inflammatory response in CHD. We hypothesised that low PON1 and high CRP foundin CHD may be important markers of CHD and the CRP:PON1 ratio may be an index of the risk of developing atherosclerosis. We have,therefore, compared the levels of PON1 and CRP between control subjects, those with no diabetes and CHD, type 1 diabetes and type 2dMwdCcCCio©
K
1
dbamasia
0d
iabetes.ethods and results: PON1 activity was different between the populations in the order: controls > type 1 diabetes > type 2 diabetes > CHDith no diabetes (P < 0.001). CRP concentration also differed between the populations in the order: controls < type 1 diabetes < type 2iabetes < CHD with no diabetes (P < 0.001). The CRP:PON1 ratio followed the same trend as the CRP concentration (P < 0.001). BothRP and the CRP:PON1 ratio were associated with the presence of CHD. In the control population only, PON1 was a determinant of CRPoncentration. Amongst the diabetics, people with CHD had higher levels of CRP (P < 0.001) and in comparing the control group with theHD group, the CHD group had a higher level of CRP (P < 0.001).onclusions: Higher levels of CRP seem to be generally associated with low levels of PON1 activity, providing a mechanistic link between
nflammation and the development of atherosclerosis. However, the relationship between PON1, CRP and atherosclerosis, and the usefulnessf the PON1:CRP ratio as a risk factor for CHD requires further evaluation.
2005 Elsevier Ireland Ltd. All rights reserved.
eywords: Paraoxonase1; C-reactive protein; Inflammation; Diabetes mellitus; Coronary heart disease
. Introduction
Atherosclerosis is in part an inflammatory disease. Afteramage to the vascular endothelium by lipoproteins or highlood pressure, the resulting inflammatory response in therterial wall is believed to be primarily due to oxidativelyodified low-density lipoprotein (LDL), which triggerscytokine response in vascular endothelial cells [1–3]
timulating the migration of blood monocytes across thentima. This response includes the upregulation of MCP-1nd adhesion molecules such as VCAM-1 which promote the
∗ Corresponding author. Tel.: +44 161 276 8633; fax: +44 161 274 4833.E-mail address: [email protected] (M. Mackness).
recruitment of monocytes in the initial stages of atheroscle-rosis and later in the actively growing shoulder regions of themature lesion. Beneath the intima, these monocytes trans-form into macrophages which rapidly take up modified LDLthrough scavenger receptors to become foam cells. Cytokinesproduced by these and the endothelial cells attract smoothmuscle cells into the lesion from the media which themselvestransform into fibroblasts elaborating collagen beneath theendothelium to form a fibrous cap [4,5]. HDL-associatedparaoxonase (PON1) retards the oxidation of LDL both invitro and in vivo [reviewed in [6]]. PON1 therefore inhibitsthe initiation/progression of atherosclerosis and has beenshown to be active in atherosclerotic plaques [7,8]. PON1has been shown to inhibit the pro-inflammatory responses of
021-9150/$ – see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.atherosclerosis.2005.07.028

B. Mackness et al. / Atherosclerosis 186 (2006) 396–401 397
macrophages and endothelial cells to oxidised and minimallymodified LDL in a co-culture system [9], and has been shownto suppress oxidised-LDL induced monocytic chemotacticprotein-1 (MCP-1) production by endothelial cells [10] andis, probably, involved in the suppression of cytokine inducedexpression of adhesion molecules in endothelial cells. Theaccumulated evidence is therefore that PON1 is responsiblefor the anti-atherosclerotic/anti-inflammatory actions ofHDL [6]. Low PON1 activity is frequently found in peoplesusceptible to the development of CHD including those withdiabetes mellitus [11–13] and our studies have shown thatlow PON1 activity is an independent, predictive risk factorfor the development of CHD [14].
C-reactive protein (CRP) is a marker of the inflammatoryresponse in CHD [15–17]. Elevated CRP is associated withthe presence of CHD in population studies [15–17], indicat-ing CRP as a marker of the inflammatory state associated withCHD. It has been suggested that CRP is a stronger predic-tor of cardiovascular events than LDL-cholesterol [18] and ithas been suggested that the measurement of CRP should beadded to the other measures of cardiovascular risk [19]. It isour hypothesis that the low PON1 and high CRP levels foundin CHD may be important markers for the presence of CHD,augmenting the currently used risk factors.
It has been shown that statins reduce CRP [20,21]. How-ever, the effect of statins on PON1 is less clear. A reviewoPsah[
Farwbar
Ca
2
2
2
pDH[t
eral neuropathy, 82 with nephropathy, 101 with retinopathyand 83 with coronary artery disease). Fifty-eight patientswere receiving no drug therapy, 66 were receiving insulin,129 oral hypoglycaemic agents (11 on metformin and 118on sulphonylurea drugs), 2 were receiving �-blocker ther-apy, 3 ACE inhibitors, 1 a Ca2+ antagonist and 1 frusemide.None of the type 2 group had yet received lipid-lowering drugtherapy.
Neuropathy was diagnosed clinically on the basis oftypical neuropathic symptoms and/or at least one abnor-mal neurological sign including a decrease in light-touch,vibration, pin prick sensation or reduced/absent anklereflexes. Nephropathy was defined as urinary albumin excre-tion > 30 mg/24 h or serum creatinine > 140 �mol/l. The pres-ence of retinopathy was assessed by fundal examinationthrough dilated pupils using an ophthalmoscope. The pres-ence of CHD was defined as a history of angina, previousdefinite myocardial infarction or angiographically provenCHD which was considered severe enough (70% stenosisin at least one coronary artery) to require intervention bycoronary angioplasty or surgery.
2.1.2. Patients with type 1 diabetesThe type 1 diabetic group consisted of 152 unselected
patients who were attending the Manchester Diabetes Centre.Type 1 diabetes was diagnosed according to the 1980 WorldH[anwdh
2
pMHpeapiswtwac(7
2
w
f the literature shows that at best, statin therapy increasesON1 activity in vivo by 5%; however, many studies havehown no effect or even a reduction in PON1 expressionnd this remains an area of contention [6,22]. Studies usinguman hepatocytes have also produced conflicting results23].
The purpose of the present investigation was three-fold.irstly, we investigated whether the PON1:CRP ratio wasdiscriminating index of the risk of developing atheroscle-
osis. Secondly, whether the PON1:CRP ratio is associatedith the development of vascular complications in dia-etes and thirdly, whether statins modulated either PON1nd CRP levels and thus favourably affect the PON1:CRPatio.
We have, therefore, compared the levels of PON1 andRP between control subjects and those with no diabetesnd CHD, type 1 diabetes and type 2 diabetes.
. Methods
.1. Subjects
.1.1. Patients with type 2 diabetesThe type 2 diabetic group comprised 252 unselected
atients who were attending the Manchester Diabetes Centre.iabetes mellitus was diagnosed according to the 1980 Worldealth Organisation Expert Committee Report (WHO 1980)
24]. Ninety-three patients were free of diabetic complica-ions and 159 had one or more complication (124 with periph-
ealth Organisation Expert Committee Report (WHO 1980)24]. Fifty-nine patients were free of diabetic complicationsnd 93 had one or more complication (86 with peripheraleuropathy, 62 with nephropathy, 82 with retinopathy and 17ith CHD according to the same criteria as used for type 2iabetes). All patients were receiving insulin. None of themad yet received lipid-lowering medication.
.1.3. Patients with CHD but no diabetesThe CHD patients included in the study were all out-
atients attending the Cardiology Departments at eitheranchester Royal Infirmary, UK, or the Royal Victoriaospital, Blackpool, UK. All patients had angiographicallyroven CHD which was visually assessed, and was consid-red severe enough (70% stenosis in at least one coronaryrtery) to require intervention either by coronary angio-lasty or surgery. No patient had sustained a myocardialnfarction (MI) within 6 months prior of taking part in thetudy. CHD patients with diabetes, renal and hepatic diseaseere excluded from this group. Four hundred and seven-
een sequential patients who fulfilled the inclusion criteriaere studied. One hundred and four patients were receiving�-adrenoreceptor blocking drugs, 89 were taking a calciumhannel blocker and 154 were on lipid-lowering medication151 statins and 3 fibrates). All patients were receiving aspirin5 or 150 mg daily.
.1.4. Healthy controlsThe control population consisted of 282 healthy subjects,
ho either attended a routine health check at a general prac-
398 B. Mackness et al. / Atherosclerosis 186 (2006) 396–401
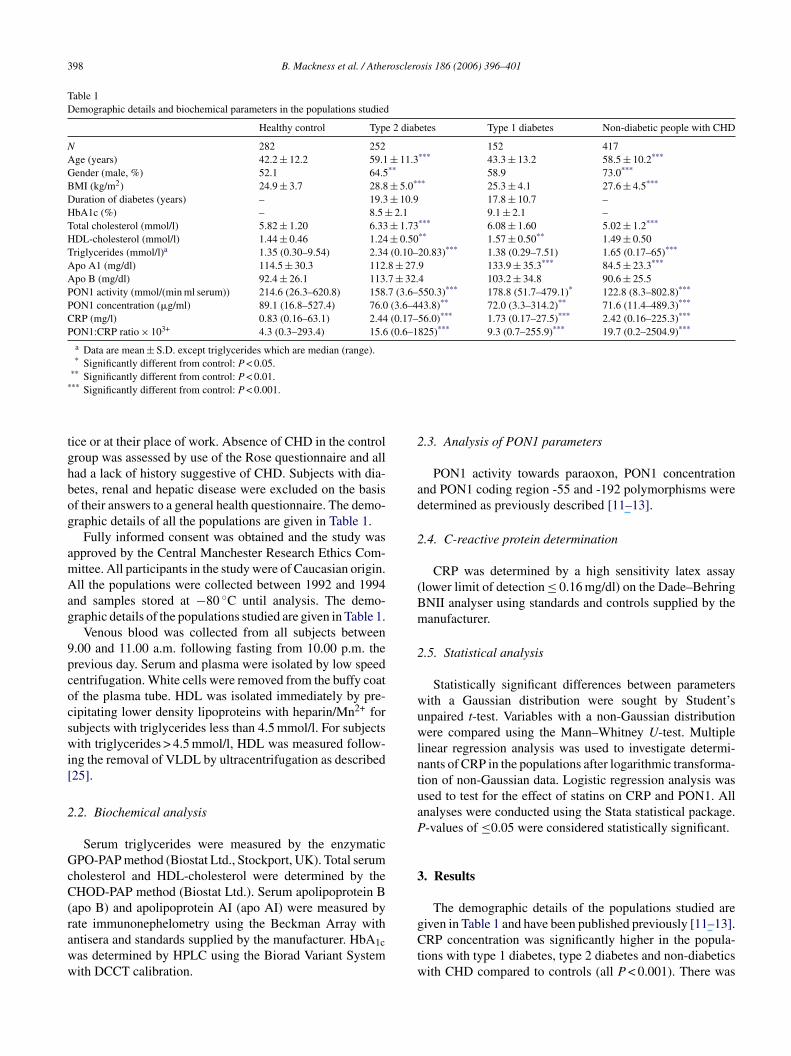
Table 1Demographic details and biochemical parameters in the populations studied
Healthy control Type 2 diabetes Type 1 diabetes Non-diabetic people with CHD
N 282 252 152 417Age (years) 42.2 ± 12.2 59.1 ± 11.3*** 43.3 ± 13.2 58.5 ± 10.2***
Gender (male, %) 52.1 64.5** 58.9 73.0***
BMI (kg/m2) 24.9 ± 3.7 28.8 ± 5.0*** 25.3 ± 4.1 27.6 ± 4.5***
Duration of diabetes (years) – 19.3 ± 10.9 17.8 ± 10.7 –HbA1c (%) – 8.5 ± 2.1 9.1 ± 2.1 –Total cholesterol (mmol/l) 5.82 ± 1.20 6.33 ± 1.73*** 6.08 ± 1.60 5.02 ± 1.2***
HDL-cholesterol (mmol/l) 1.44 ± 0.46 1.24 ± 0.50** 1.57 ± 0.50** 1.49 ± 0.50Triglycerides (mmol/l)a 1.35 (0.30–9.54) 2.34 (0.10–20.83)*** 1.38 (0.29–7.51) 1.65 (0.17–65)***
Apo A1 (mg/dl) 114.5 ± 30.3 112.8 ± 27.9 133.9 ± 35.3*** 84.5 ± 23.3***
Apo B (mg/dl) 92.4 ± 26.1 113.7 ± 32.4 103.2 ± 34.8 90.6 ± 25.5PON1 activity (mmol/(min ml serum)) 214.6 (26.3–620.8) 158.7 (3.6–550.3)*** 178.8 (51.7–479.1)* 122.8 (8.3–802.8)***
PON1 concentration (�g/ml) 89.1 (16.8–527.4) 76.0 (3.6–443.8)** 72.0 (3.3–314.2)** 71.6 (11.4–489.3)***
CRP (mg/l) 0.83 (0.16–63.1) 2.44 (0.17–56.0)*** 1.73 (0.17–27.5)*** 2.42 (0.16–225.3)***
PON1:CRP ratio × 103+ 4.3 (0.3–293.4) 15.6 (0.6–1825)*** 9.3 (0.7–255.9)*** 19.7 (0.2–2504.9)***
a Data are mean ± S.D. except triglycerides which are median (range).* Significantly different from control: P < 0.05.
** Significantly different from control: P < 0.01.*** Significantly different from control: P < 0.001.
tice or at their place of work. Absence of CHD in the controlgroup was assessed by use of the Rose questionnaire and allhad a lack of history suggestive of CHD. Subjects with dia-betes, renal and hepatic disease were excluded on the basisof their answers to a general health questionnaire. The demo-graphic details of all the populations are given in Table 1.
Fully informed consent was obtained and the study wasapproved by the Central Manchester Research Ethics Com-mittee. All participants in the study were of Caucasian origin.All the populations were collected between 1992 and 1994and samples stored at −80 ◦C until analysis. The demo-graphic details of the populations studied are given in Table 1.
Venous blood was collected from all subjects between9.00 and 11.00 a.m. following fasting from 10.00 p.m. theprevious day. Serum and plasma were isolated by low speedcentrifugation. White cells were removed from the buffy coatof the plasma tube. HDL was isolated immediately by pre-cipitating lower density lipoproteins with heparin/Mn2+ forsubjects with triglycerides less than 4.5 mmol/l. For subjectswith triglycerides > 4.5 mmol/l, HDL was measured follow-ing the removal of VLDL by ultracentrifugation as described[25].
2.2. Biochemical analysis
GcC(raww
2.3. Analysis of PON1 parameters
PON1 activity towards paraoxon, PON1 concentrationand PON1 coding region -55 and -192 polymorphisms weredetermined as previously described [11–13].
2.4. C-reactive protein determination
CRP was determined by a high sensitivity latex assay(lower limit of detection ≤ 0.16 mg/dl) on the Dade–BehringBNII analyser using standards and controls supplied by themanufacturer.
2.5. Statistical analysis
Statistically significant differences between parameterswith a Gaussian distribution were sought by Student’sunpaired t-test. Variables with a non-Gaussian distributionwere compared using the Mann–Whitney U-test. Multiplelinear regression analysis was used to investigate determi-nants of CRP in the populations after logarithmic transforma-tion of non-Gaussian data. Logistic regression analysis wasused to test for the effect of statins on CRP and PON1. Allanalyses were conducted using the Stata statistical package.P-values of ≤0.05 were considered statistically significant.
3
gCtw
Serum triglycerides were measured by the enzymaticPO-PAP method (Biostat Ltd., Stockport, UK). Total serum
holesterol and HDL-cholesterol were determined by theHOD-PAP method (Biostat Ltd.). Serum apolipoprotein B
apo B) and apolipoprotein AI (apo AI) were measured byate immunonephelometry using the Beckman Array withntisera and standards supplied by the manufacturer. HbA1cas determined by HPLC using the Biorad Variant Systemith DCCT calibration.
. Results
The demographic details of the populations studied areiven in Table 1 and have been published previously [11–13].RP concentration was significantly higher in the popula-
ions with type 1 diabetes, type 2 diabetes and non-diabeticsith CHD compared to controls (all P < 0.001). There was
B. Mackness et al. / Atherosclerosis 186 (2006) 396–401 399
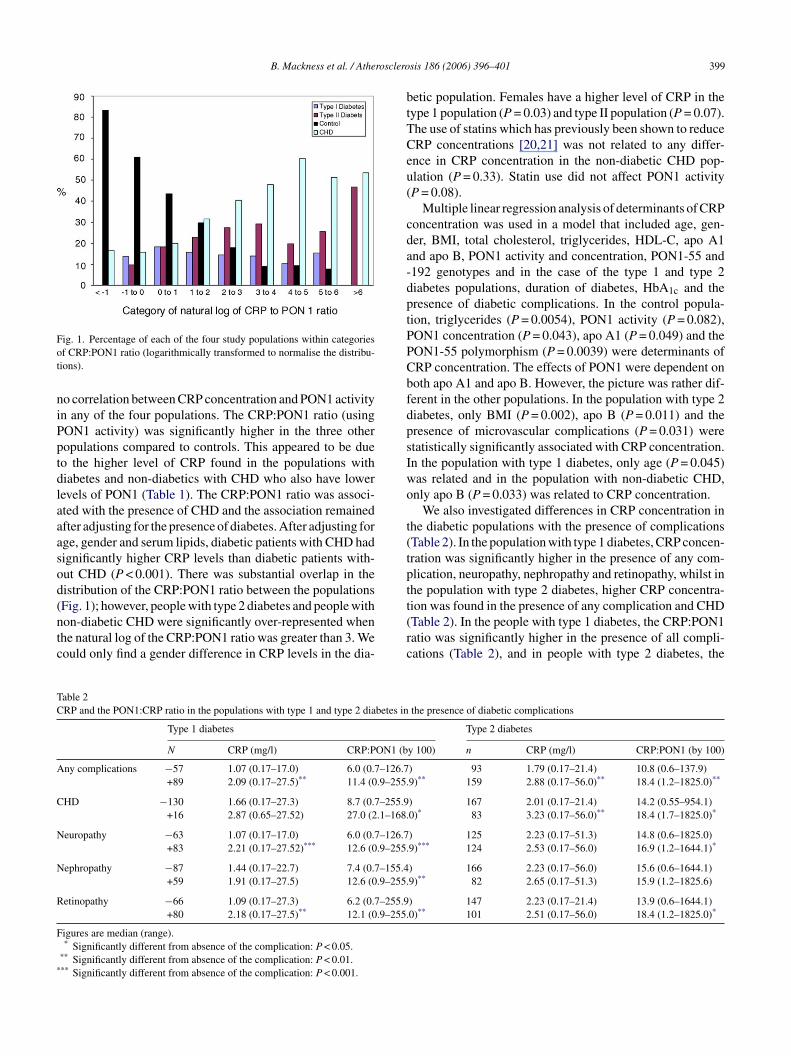
Fig. 1. Percentage of each of the four study populations within categoriesof CRP:PON1 ratio (logarithmically transformed to normalise the distribu-tions).
no correlation between CRP concentration and PON1 activityin any of the four populations. The CRP:PON1 ratio (usingPON1 activity) was significantly higher in the three otherpopulations compared to controls. This appeared to be dueto the higher level of CRP found in the populations withdiabetes and non-diabetics with CHD who also have lowerlevels of PON1 (Table 1). The CRP:PON1 ratio was associ-ated with the presence of CHD and the association remainedafter adjusting for the presence of diabetes. After adjusting forage, gender and serum lipids, diabetic patients with CHD hadsignificantly higher CRP levels than diabetic patients with-out CHD (P < 0.001). There was substantial overlap in thedistribution of the CRP:PON1 ratio between the populations(Fig. 1); however, people with type 2 diabetes and people withnon-diabetic CHD were significantly over-represented whenthe natural log of the CRP:PON1 ratio was greater than 3. Wecould only find a gender difference in CRP levels in the dia-
betic population. Females have a higher level of CRP in thetype 1 population (P = 0.03) and type II population (P = 0.07).The use of statins which has previously been shown to reduceCRP concentrations [20,21] was not related to any differ-ence in CRP concentration in the non-diabetic CHD pop-ulation (P = 0.33). Statin use did not affect PON1 activity(P = 0.08).
Multiple linear regression analysis of determinants of CRPconcentration was used in a model that included age, gen-der, BMI, total cholesterol, triglycerides, HDL-C, apo A1and apo B, PON1 activity and concentration, PON1-55 and-192 genotypes and in the case of the type 1 and type 2diabetes populations, duration of diabetes, HbA1c and thepresence of diabetic complications. In the control popula-tion, triglycerides (P = 0.0054), PON1 activity (P = 0.082),PON1 concentration (P = 0.043), apo A1 (P = 0.049) and thePON1-55 polymorphism (P = 0.0039) were determinants ofCRP concentration. The effects of PON1 were dependent onboth apo A1 and apo B. However, the picture was rather dif-ferent in the other populations. In the population with type 2diabetes, only BMI (P = 0.002), apo B (P = 0.011) and thepresence of microvascular complications (P = 0.031) werestatistically significantly associated with CRP concentration.In the population with type 1 diabetes, only age (P = 0.045)was related and in the population with non-diabetic CHD,only apo B (P = 0.033) was related to CRP concentration.
t(tptt(rc
Table 2CRP and the PON1:CRP ratio in the populations with type 1 and type 2 diabetes in
Type 1 diabetes
N CRP (mg/l) CRP:PON1 (b
Any complications −57 1.07 (0.17–17.0) 6.0 (0.7–126.7+89 2.09 (0.17–27.5)** 11.4 (0.9–255.
C –255.9.1–168.
N –126.7.9–255.
N –155.4.9–255.
R –255.9.9–255.
F
*
HD −130 1.66 (0.17–27.3) 8.7 (0.7+16 2.87 (0.65–27.52) 27.0 (2
europathy −63 1.07 (0.17–17.0) 6.0 (0.7+83 2.21 (0.17–27.52)*** 12.6 (0
ephropathy −87 1.44 (0.17–22.7) 7.4 (0.7+59 1.91 (0.17–27.5) 12.6 (0
etinopathy −66 1.09 (0.17–27.3) 6.2 (0.7+80 2.18 (0.17–27.5)** 12.1 (0
igures are median (range).* Significantly different from absence of the complication: P < 0.05.
** Significantly different from absence of the complication: P < 0.01.** Significantly different from absence of the complication: P < 0.001.
We also investigated differences in CRP concentration inhe diabetic populations with the presence of complicationsTable 2). In the population with type 1 diabetes, CRP concen-ration was significantly higher in the presence of any com-lication, neuropathy, nephropathy and retinopathy, whilst inhe population with type 2 diabetes, higher CRP concentra-ion was found in the presence of any complication and CHDTable 2). In the people with type 1 diabetes, the CRP:PON1atio was significantly higher in the presence of all compli-ations (Table 2), and in people with type 2 diabetes, the
the presence of diabetic complications
Type 2 diabetes
y 100) n CRP (mg/l) CRP:PON1 (by 100)
) 93 1.79 (0.17–21.4) 10.8 (0.6–137.9)9)** 159 2.88 (0.17–56.0)** 18.4 (1.2–1825.0)**
) 167 2.01 (0.17–21.4) 14.2 (0.55–954.1)0)* 83 3.23 (0.17–56.0)** 18.4 (1.7–1825.0)*
) 125 2.23 (0.17–51.3) 14.8 (0.6–1825.0)9)*** 124 2.53 (0.17–56.0) 16.9 (1.2–1644.1)*
) 166 2.23 (0.17–56.0) 15.6 (0.6–1644.1)9)** 82 2.65 (0.17–51.3) 15.9 (1.2–1825.6)
) 147 2.23 (0.17–21.4) 13.9 (0.6–1644.1)0)** 101 2.51 (0.17–56.0) 18.4 (1.2–1825.0)*

400 B. Mackness et al. / Atherosclerosis 186 (2006) 396–401
CRP:PON1 ratio was significantly higher in the presence ofany complication, CHD, neuropathy and retinopathy.
4. Discussion
In the present study, we have shown that CRP concen-tration is significantly elevated in diseases associated withlow PON1. The greatest elevation in CRP was in people withnon-diabetic CHD where PON1 is the lowest. PON1 has con-sistently been shown to be low in patients with type 1 andtype 2 diabetes and non-diabetic CHD [11–13]. PON1 wasfirst shown by us to inhibit the oxidation of LDL by reducingthe generation of lipid-peroxides [26,27]; these initial resultshave subsequently been confirmed in many laboratories bothin vitro, ex vivo and in animal models of atherosclerosis[8,9,28,29].
An increased pro-oxidative state is associated with dia-betes and CHD [30,31]; this in turn leads to reduced PON1due to the inhibition of PON1 by its substrates, i.e. lipid-peroxides [32]. This would lead to an increase in oxidativestress, which is pro-inflammatory, leading to an increase inCRP. This would provide a mechanistic association betweenlow PON1 and inflammation in patients susceptible to thedevelopment of CHD and may be the mechanism by whichlow PON1 levels promote atherosclerosis and is an indepen-dalter
bailscrmTnsC“iF
nHtrirt
obvious. However, a number of unspecified experimental dif-ferences, such as the isoforms used, as some PON1 isoformsare more efficient at preventing LDL-oxidation than others[8,23] could explain the different results.
One of our contentions was that the PON1:CRP ratio maybe a more accurate marker of the presence of CHD than moreusually used risk factors, although this contention requiresfurther investigation, a high PON1:CRP ratio was associatedwith the presence of CHD even after adjusting for the pres-ence of diabetes.
In conclusion, higher levels of the inflammatory markerCRP are associated with low levels of the anti-inflammatoryenzyme PON1, providing a potential mechanistic linkbetween low PON1 and the development of atherosclerosis.However, whether the low PON1:CRP ratio has clinical rel-evance for the diagnosis of CHD needs further investigation.
References
[1] Ross R. The pathogenesis of atherosclerosis: a perspective for the1990’s. Nature 1993;362:801–9.
[2] Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL.Beyond cholesterol modifications of low-density lipoprotein thatincrease its atherogenicity. N Engl J Med 1989;320:915–24.
[3] Witztum JL, Steinberg D. Role of oxidized low density lipoproteinin atherogenesis. J Clin Invest 1991;88:1785–92.
[
[
[
[
[
[
ent risk factor for CHD events [14]. The problem with thisrgument is that PON1 was a significant determinant of CRPevel only in the control population. It is therefore possiblehat at some point in the inflammatory process, the protectiveffect of PON1 is overwhelmed, due to its inhibition and theelationship between PON1 and CRP breaks down.
Alternatively, the inflammatory state associated with dia-etes and CHD could be the cause of the reduced PON1ssociated with these states. This could be because pro-nflammatory cytokines have been shown to reduce circu-ating PON1 [33,34] by inhibiting its hepatic synthesis andecretion [33,35]. Such a scenario would lead to a viciousycle of further oxidation, more inflammation and a furthereduction in PON1. Therefore, treatment to reduce inflam-ation could have the positive effect of increasing PON1.he paradox of this argument is that in the population ofon-diabetics with CHD, the use of statins, which have beenhown to reduce inflammation and CRP [20,21], did not affectRP levels in our population. It is possible that there is apoint of no return” where it is not possible to correct thenflammatory process and CHD development is inevitable.urther work in this area is clearly required.
Recently, it has been suggested that purified and recombi-ant human PON1 do not protect LDL from oxidation [36].owever, this report from one laboratory is very much in
he minority, with all other reports whether using purified orecombinant human PON1 and many in vivo studies indicat-ng that PON1 does inhibit LDL-oxidation [8,9,28,29]. Theeason(s) why the results from this laboratory are so dras-ically different from all other reports are not immediately
[4] Lusis AJ. Atherosclerosis. Nature 2000;407:233–41.[5] Chisholm GM, Penn MS. Oxidised lipoproteins and atherosclerosis.
In: Fuster V, Ross R, Topol EJ, editors. Atherosclerosis and coronaryartery disease. Philadelphia: Lippincott/Raven; 1996. p. 129–49.
[6] Durrington PN, Mackness B, Mackness MI. Paraoxonase andatherosclerosis. Arterioscler Thromb Vasc Biol 2001;21:473–80.
[7] Mackness B, Hunt R, Durrington PN, Mackness MI. Increasedimmunolocalisation of paraoxonase, clusterin and apolipoprotein AIin the human artery wall with progression of atherosclerosis. Arte-rioscler Thromb Vasc Biol 1997;17:1233–8.
[8] Aviram M, Hardak E, Vaya J, et al. Human serum paraoxonase(PON1) Q and R selectively decrease lipid peroxides in humancoronary and carotid atherosclerotic lesions: PON1 esterase andperoxidase-like activities. Circulation 2000;101:2510–7.
[9] Watson AD, Berliner JA, Hama SY, et al. Protective effect of highdensity lipoprotein associated paraoxonase—inhibition of the biolog-ical activity of minimally oxidised low-density lipoprotein. J ClinInvest 1995;96:2882–91.
10] Mackness B, Hine D, Liu Y, Mastorikou M, Mackness M. Paraox-onase 1 inhibits oxidised LDL-induced MCP-1 production byendothelial cells. BBRC 2004;318:680–3.
11] Mackness B, Davies GK, Turkie W, et al. Paraoxonase status incoronary heart disease. Are activity and concentration more impor-tant than genotype? Arterioscler Thromb Vasc Biol 2001;21:1451–7.
12] Mackness B, Durrington PN, Boulton AJM, Hine D, Mackness MI.Serum paraoxonase activity in patients with type 1 diabetes com-pared to healthy controls. Eur J Clin Invest 2002;32:259–64.
13] Mackness B, Mackness MI, Arrol S, et al. Serum paraoxonase(PON1) 55 and 192 polymorphism and paraoxonase activity andconcentration in non-insulin dependent diabetes mellitus. Atheroscle-rosis 1998;139:341–9.
14] Mackness B, Durrington P, McElduff P, et al. Low paraoxonaseactivity predicts coronary events in the Caerphilly prospective study.Circulation 2003;107:2775–9.
15] Ridker PM, Glynn RJ, Hennekens CH. C-reactive protein adds tothe predictive value of total and HDL cholesterol in determin-

B. Mackness et al. / Atherosclerosis 186 (2006) 396–401 401
ing risk of first myocardial infarction. Circulation 1998;97:2007–11.
[16] Ridker PM, Hennekens CH, Buring JE, Rifai N. C-reactive proteinand other markers of inflammation in the prediction of cardiovasculardisease in women. N Engl J Med 2000;342:836–43.
[17] Rifai N, Ridker PM. Inflammatory markers and coronary heart dis-ease. Curr Opin Lipidol 2002;13:383–9.
[18] Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparisonof C-reactive protein and low density lipoprotein cholesterol lev-els in the prediction of first cardiovascular events. N Engl J Med2002;347:1557–65.
[19] Ridker PM, Wilson PWF, Grundy SM. Should C-reactive protein beadded to metabolic syndrome and to assessment of global cardio-vascular risk? Circulation 2004;109:2818–25.
[20] Jialal I, Stein D, Balis D, et al. Effect of hydroxymethyl glutaryl,co-enzyme a reductase inhibitor therapy on high sensitive C-reactiveprotein levels. Circulation 2001;103:1933–5.
[21] Ridker PM, Rifai N, Pfeffer MA, Sacks F, Braunwald E. Long-term effects of pravastatin on plasma concentration of C-reactiveprotein. The Cholesterol and Recurrent Events (CARE) Investigators.Circulation 1999;100:230–5.
[22] Gouedard C, Koum-Besson N, Barouki R, Morel Y. Opposite reg-ulation of the human paraoxonase-1 gene PON1 by fenofibrate andstatins. Mol Pharmacol 2003;63:945–56.
[23] Mackness M, Durrington P, Mackness B. Role of paraoxonase 1 incardiovascular disease: potential for therapeutic intervention. Am JCardiovasc Drugs 2004;4:211–7.
[24] World Health Organisation Expert Committee on Diabetes Mellitus.Second report. WHO technical report series no. 646. Geneva: WHO;1980.
[25] Mackness MI, Durrington PN. Lipoprotein separation and analysis
[
[27] Mackness MI, Arrol S, Abbott CA, Durrington PN. Protec-tion of low-density lipoprotein against oxidative modification byhigh-density lipoprotein associated paraoxonase. Atherosclerosis1993;104:129–35.
[28] Ahmed Z, Ravandi A, Maguire GF, et al. Apolipoprotein AIpromotes the formation of phosphatidylcholine core aldehydesthat are hydrolysed by paraoxonase (PON1) during high densitylipoprotein oxidation with a peroxynitrite donor. J Biol Chem2001;276:24473–81.
[29] Shih DM, Gu L, Xia Y-R, et al. Mice lacking serum paraoxonase aresusceptible to organophosphate toxicity and atherosclerosis. Nature1998;394:284–7.
[30] Babiy AV, Gebicki JM, Sullivan DR, Willey K. Increased oxidizabil-ity of plasma lipoproteins in diabetic patients can be decreased byprobucol therapy and is not due to glycation. Biochem Pharmacol1992;43(S):995–1000.
[31] Liu K, Cuddy TE, Pierce GN. Oxidative status of lipoproteins incoronary disease patients. Am Heart J 1992;123:285.
[32] Aviram M, Rosenblat M, Billecke S, et al. Human serum paraox-onase (PON1) is inactivated by oxidised low density lipoproteinand preserved by antioxidants. Free Radic Biol Med 1999;26:892–904.
[33] Feingold KR, Memon RA, Moser AH, Grunfeld C. Paraoxonaseactivity in the serum and hepatic mRNA levels decrease during theacute phase response. Atherosclerosis 1998;139:307–15.
[34] Van Lenten BJ, Wagner AC, Navab M, Fogelman AM. Oxidisedphospholipids induce changes in hepatic paraoxonase and Apo Jbut not monocyte chemattractant protein-1 via interleukin-6. J BiolChem 2001;276:1923–9.
[35] Ali AB, Zhang Q, Lim YK, et al. Expression of major HDL-associated antioxidant PON1 is gender dependent and regulated
[
for clinical studies. In: Converse CA, Skinner ER, editors. Lipopro-tein analysis. Oxford University Press; 1992. p. 1–42.26] Mackness MI, Arrol S, Durrington PN. Paraoxonase prevents accu-mulation of lipoperoxides in low-density lipoprotein. FEBS Lett1991;286:152–4.
during inflammation. Free Radic Biol Med 2003;34:824–9.36] Draganov DI, Teiber JF, Speelman A, Osawa Y, Sunahara R, La
Du BN. Human paraoxonases (PON1, PON2 and PON3) are lac-tonases with overlapping and distinct substrate specificities. J LipidRes 2005;46:1239–47.