The association of complex liver disorders with HBV genotypes prevalent in Pakistan

HC
TGA*GDa
BttauiulWatscvaHw605wCvpHtpdat
HcpH
GASTROENTEROLOGY 2004;126:102–110
epatitis B Virus Maintains Its Pro-oncogenic Properties in thease of Occult HBV Infection
ERESA POLLICINO,* GIOVANNI SQUADRITO,* GIOVANNI CERENZIA,* IRENE CACCIOLA,*IUSEPPINA RAFFA,* ANTONIO CRAXI,‡ FABIO FARINATI,§ GABRIELE MISSALE,¶
NTONINA SMEDILE,� CLAUDIO TIRIBELLI,# ERICA VILLA,** and GIOVANNI RAIMONDO*Unit of Clinical and Molecular Hepatology, Department of Internal Medicine, University of Messina, Messina; ‡Department ofastroenterology, University of Palermo, Palermo; §Department of Gastroenterology, University of Padova, Padova; ¶Division of Infectiousiseases, Hospital of Parma, Parma; �Department of Gastroenterology, University of Torino, Torino; #Centro Studi Fegato, AREA Science Parknd Department BBCM, University of Trieste, Trieste; and **Department of Gastroenterology, University of Modena, Modena, Italy
cciccmtiiflhddctp
lHbicatppHc
rH
Dr
See editorial on page 347.
ackground & Aims: Occult hepatitis B virus (HBV) infec-ion is characterized by persistence of HBV DNA into theissue of hepatitis B surface antigen–negative individu-ls. The clinical relevance of this peculiar infection is stillnder debate. In particular, the impact of occult HBVnfection in cases of hepatocellular carcinoma (HCC) isncertain. We investigated the prevalence and molecu-ar status of occult HBV in patients with HCC. Methods:e tested tumor tissues from 107 patients with HCCnd the corresponding nontumor liver tissue from 72 ofhese patients for HBV DNA. We also examined liverpecimens from 192 patients with chronic hepatitis. Allases were hepatitis B surface antigen negative. Co-alently closed circular HBV genomes, HBV transcripts,nd viral integrated forms were investigated in cases ofCC found positive for occult HBV. Results: Viral DNAas detected in 68 of 107 cases of HCC (63.5%) and in3 of 192 cases of chronic hepatitis (32.8%) (P <.0001; odds ratio, 3.6; 95% confidence interval, 2.2–.9). The significant association of occult HBV with HCCas irrespective of age, sex, and contemporary hepatitisvirus infection. Both integrated viral DNA and co-
alently closed circular HBV genomes were detected inatients with occult HBV. Moreover, the presence of freeBV genomes was associated with persistence of viralranscription and replication. Conclusions: Our findingsrovide clear evidence that occult HBV is a risk factor forevelopment of HCC and show that the potential mech-nisms whereby overt HBV might induce tumor forma-ion are mostly maintained in cases of occult infection.
epatitis B virus (HBV) infection is a major healthproblem worldwide; it is one of the 10 leading
auses of mortality, with an estimated 400 million peo-le chronically infected at the turn of this millennium.1,2
BV infection may associate with a large spectrum of
linical forms, ranging from very mild and asymptomaticlinical pictures to the most severe liver diseases includ-ng fulminant hepatitis, cirrhosis, and hepatocellular car-inoma (HCC).1 In particular, chronic HBV infection isommonly considered a primary risk factor for develop-ent of HCC,3 exerting its pro-oncogenic properties
hrough both indirect and direct mechanisms.4–7 Thendirect mechanisms are related to its propensity tonduce continuous or recurrent phases of liver necroin-ammation and to promote the progression of chronicepatitis to cirrhosis, which is the step preceding theevelopment of HCC in most cases.8 Schematically, theirect carcinogenic mechanisms have been related to theapacity of HBV to integrate into the host’s genome ando produce proteins (X protein and truncated preS-Srotein) provided of potential transforming properties.9
HBV infection is usually diagnosed when the circu-ating hepatitis B surface antigen (HBsAg) is detected.owever, the availability of highly sensitive molecular
iology techniques has allowed the identification of HBVnfection in HBsAg-negative individuals with or withoutirculating antibodies to HBsAg and/or hepatitis B corentigen (anti-HBc).10–15 Much evidence suggests thathis so-called occult or cryptic HBV infection is highlyrevalent and may have a relevant clinical impact.16–18 Inarticular, we and others previously showed that occultBV infection significantly correlates with cirrhosis in
hronic hepatitis C virus (HCV) carriers.15,19–21
Since the early 1980s, a certain number of studies haveeported the detection of HBV DNA in liver tissue ofBsAg-negative patients with HCC.22,23 With the ad-
Abbreviations used in this paper: cccDNA, covalently closed circularNA; CLD, chronic liver disease; PCR, polymerase chain reaction;cDNA, relaxed circular DNA.
© 2004 by the American Gastroenterological Association0016-5085/04/$30.00
doi:10.1053/j.gastro.2003.10.048

v(fimlnosau
ls
catgptdm1ptmcata
n
1hthiccm
1wHHwln
po
ew(sacpdbpTae
dw4arpDesoit
oacD
FSg
January 2004 OCCULT HBV AND HCC 103
ent of the most sensitive polymerase chain reactionPCR) techniques, this observation has been con-rmed24–26; however, extensive studies performed in ho-ogeneous populations and evaluating the real preva-
ence of this event are still lacking.17 Another aspect thateeds to be highlighted is the molecular status of theccult HBV in patients with HCC, which is an essentialupport for understanding the possible pathogenic mech-nisms through which the cryptic HBV might contrib-te to hepatocellular transformation.In this study, we investigated the presence and mo-
ecular features of HBV DNA in liver tissues from a largeeries of HBsAg-negative patients with HCC.
Patients and MethodsPatients
We studied liver specimens from 107 HBsAg-negativeirrhotic patients with HCC (81 men and 26 women; meange, 63.7 � 10 years) randomly collected from January 1999o December 2000 at 7 Italian liver units located in distincteographic areas of the country. Seventy-three of the 107atients were antibody to HCV (anti-HCV) positive; amonghe 34 anti-HCV–negative individuals, 5 had alcoholic liverisease and 29 had cryptogenic liver disease (Figure 1). Serumarkers of previous HBV infection were available for 82 of the
07 patients. Twenty-five of these 82 patients were anti-HBcositive and 11 of them were also antibody to HBsAg positive;he remaining 57 cases were negative for all HBV serumarkers. Tumor liver specimens from the 107 patients and the
orresponding nontumor tissue from 72 of the patients werevailable for molecular analysis. Tissue samples had been ob-ained by surgical resection or percutaneous needle liver biopsynd immediately frozen and stored at �80°C.
A total of 192 frozen liver biopsy specimens from HBsAg-egative patients (125 men and 67 women; mean age, 48.2 �
igure 1. Schematic representation of the study populations. (A)tudy group (HBsAg-negative cirrhotic patients with HCC). (B) Controlroup (HBsAg-negative patients with CLD).
1.5 years) with chronic liver disease (CLD) (143 with chronicepatitis and 43 with cirrhosis) were available for inclusion inhis study as a control group. A total of 153 of the 192 patientsad an HCV-related CLD; among the 39 anti-HCV–negativendividuals, 7 had alcohol-related liver disease and 32 hadryptogenic liver disease (Figure 1). These specimens wereollected from June 1999 to May 2000 at 3 of the previouslyentioned Italian centers (Messina, Palermo, and Turin).Serum markers of previous HBV infection were available for
19 of the 192 patients. Thirty-three of these 119 patientsere anti-HBc positive and 18 of them were also antibody toBsAg positive; the remaining 86 cases were negative for allBV serum markers. None of these patients had been treatedith antiviral or immunosuppressive drugs before undergoing
iver biopsy, and none were infected with the human immu-odeficiency virus.The study protocol was performed according to the princi-
les of the Declaration of Helsinki, and informed consent wasbtained from all patients.
HBV DNA Analyses
DNA was extracted from the frozen liver specimens ofach case by standard procedures.27 In brief, tissue specimensere homogenized in 150 mmol/L NaCl, 50 mmol/L Tris-HCl
pH 7.4), 10 mmol/L ethylenediaminetetraacetic acid, and 1%odium dodecyl sulfate and incubated overnight with protein-se K (800 �g/mL) at 37°C. After extraction with phenol/hloroform, the nucleic acids were precipitated in 2 vol ofure, cold ethanol. Nucleic acids were then resuspended andigested with pancreatic ribonuclease (100 �g/mL) followedy extraction with phenol/chloroform and reprecipitation inure cold ethanol. The DNA was resuspended in 10 mmol/Lris-HCl (pH 7.4) and 1 mmol/L ethylenediaminetetraaceticcid, and its concentration was determined by spectrophotom-try at 260 nm.
Occult HBV infection had been identified as previouslyescribed with slight modification.15 All liver DNA extractsere analyzed for the presence of HBV genomes by performingdifferent in-house single-step or nested PCR amplification
ssays to detect preS-S (S), precore-core (C), Pol, and X viralegions, respectively. We considered the cases that showedositivity in at least 2 different viral genomic regions as HBVNA positive. Appropriate negative controls were included in
ach PCR. Moreover, direct sequencing of all amplified HBVequences confirmed the specificity of the reactions. The limitf sensitivity of our single-step and nested PCR methods wasn the range of 103 and 10 genome equivalents/mL, respec-ively. The 4 sets of primers used are reported in Table 1.
Detection of HBV Covalently Closed CircularDNA
Paired tumor and nontumor liver tissues from 30ccult HBV-positive cases and tumor specimens from 12dditional positive cases were tested for the presence of HBVovalently closed circular DNA (cccDNA) by digestion of liverNA extracts with mung bean nuclease and subsequent nested

Pbprb6oarHtnDo
rofgd
tHgagfi
facsaebasaum
T
HHHHHHHHHHHHH
HHHAH
HHS
SSHHHHH
Na
b
104 POLLICINO ET AL. GASTROENTEROLOGY Vol. 126, No. 1
CR analysis.28 The primers used were selected to discriminateetween relaxed circular DNA (rcDNA) genome of HBVarticles and HBV cccDNA present in the infected cells. HBVcDNA contains 2 regions sensitive to digestion with mungean nuclease: the single-stranded area, covering about 10%–0% of the genome length, and a nick within the minus strandf the direct repeat region. When the sense primers HBV P23nd HBV P25 (Table 1), located within the single-strandedegion of HBV, are used together with the antisense primersBV P24 and HBV P26 (Table 1), amplification runs across
he minus strand nick of HBV rcDNA in both rounds ofested PCR. After digestion with mung bean nuclease of liverNA extracts used as PCR templates, positive signals are
btained only from samples containing HBV cccDNA.
Southern Blot Analysis
We analyzed both tumor and nontumor tissue from 10andomly selected occult HBV-positive cases for the presencef integrated HBV sequences. Southern blot analysis was per-ormed following standardized procedures.29 Briefly, 25 �g ofenomic DNA isolated from each liver tissue specimen wasigested with HindIII restriction enzyme, separated by elec-
able 1. Oligonucleotides Used as PCR Primers, Hybridizatio
Sense primers
Name Nucleotide sequence Positiona Na
BV 1 5�-GGTCACCATATTCTTGGGAA-3� 2815–2834 HBVBV 3b 5�-AATCCAGATTGGGACTTCAA-3� 2932–2951 HBVBV 5 5�-GCCTTAGAGTCTCCTGAGCA-3� 2021–2040 HBVBV 7b 5�-CCTCACCATACTGCACTCA-3� 2048–2066 HBVBV 9 5�-CGTCGCAGAAGATCTCAATC-3� 2416–2436 HBVBV 11b 5�-CCTTGGACTCATAAGGT-3� 2457–2473 HBVBV 13 5�-CCATACTGCGGAACTCCTAGC-3� 1266–1286 HBVBV 15b 5�-GCTAGGCTGTGCTGCCAACTG-3� 1380–1400 HBVBV P23 5�-CTGAATCCTGCGGACGACCC-3� 1441–1460 HBVBV P25b 5�-GTCTGTGCCTTCTCATCTGCC-3� 1551–1571 HBVBV 17 5�-TTGGGGTGGAGCCCTCAGGCT-3� 3037–3057 HBVBV 18b 5�-CCTGCTGGTGGCTCCAGTTCA-3� 56–76 HBVBV 5 5�-GCCTTAGAGTCTCCTGAGCA-3� 2021–2040 HBV
BV 7b 5�-CCTCACCATACTGCACTCA-3� 2048–2066 HBVBV 15 5�-GCTAGGCTGTGCTGCCAACTG-3� 1380–1400 HBV1BV 20b 5�-CGCGGGACGTCCTTTGTTTACG-3� 1408–1429 HBVCT 1 5�-GATGCATTGTTACAGGAAGT-3� 1465–1484 ACT 2BV P1 5�-CCGGAAAGCTTGGCTCTTC HBV
TTTTTCACCTCTGCCTAATCA-3� 1821–1841BV P5b 5�-CTTTTTCACCTCTGCCTAATCA-3� 1821–1841 HBVBV 17b 5�-TTGGGGTGGAGCCCTCAGGCT-3� 3037–3057 HBVEQ 1 5�-GTCTAGACTCGTGGTGGACTT-3� 246–266 SEQ
EQ 3 5�-TGTGCACTTCGCTTCACCTCT-3� 1578–1598 SEQEQ 5 5�-GTGGTATTGGGGGCCAAG-3� 748–765 HBVBV 9 5�-CGTCGCAGAAGATCTCAATC-3� 2414–243 HBVBV P23 5�-CTGAATCCTGCGGACGACCC-3� 1441–1460 HBVBV 18 5�-CCTGCTGGTGGCTCCAGTTCA-3� 56–76BV P5 5�-CTTTTTCACCTCTGCCTAATCA-3� 1821–1841 HBVBV 1 5�-GGTCACCATATTCTTGGGAA-3� 2815–2834
OTE. Heterologous nucleotides containing restriction enzyme SstI aNucleotide positions of the primers are numbered from the unique EApplied in the second round of amplification of the nested PCR.
rophoresis in a 0.8% agarose gel, and blotted onto a nylonybond N� membrane (Amersham, Buckinghamshire, En-
land). The membrane was hybridized overnight at 65°C with32P random prime-labeled (Amersham) full-length HBV
enome probe and then was washed and exposed to X-Omatlm (Kodak, Rochester, NY) at �80°C.
Isolation of Total RNA and Reverse-Transcription PCR Amplification
Good-quality material for RNA analysis was availablerom 10 pairs of tumor and nontumor tissue and from 4dditional tumor samples, all of which were positive for HBVccDNA. Total RNA was extracted from 50 mg of each liverpecimen using TRIzol reagent (Invitrogen, Paisley, Scotland)s recommended by the manufacturer. Five micrograms ofxtracted RNA was digested with ribonuclease-free deoxyri-onuclease I (Promega, Madison, WI) at 70°C for 10 minutesnd used as a template for first-strand complementary DNAynthesis by SuperScript Reverse Transcriptase (Invitrogen)nd oligo(dT) primers. The housekeeping gene �-actin wassed as an internal standard. Equilibrated amounts of comple-entary DNA were taken for HBV transcript nested PCR
bes, and Sequencing Primers
Antisense primers
Primer setdesignationNucleotide sequence Positiona
5�-AATGGCACTAGTAAACTGAG-3� 690–671 PreS-S5�-CCTTGATAGTCCAGAAGAAC-3� 459–4405�-GTCCAAGGAATACTAAC-3� 2464–2448 Precore-core5�-GAGGGAGTTCTTCTTCTAGG-3� 2385–23665�-CCTGATGTGATGTTCTCCATG-3� 174–155 Pol5�-TTGAAGTCCCAATCTGGATT-3 2951–29325�-CGTTCACGGTGGTCTCCAT-3� 1628–1608 X5�-CGTAAAGAGAGGTGCGCCCCG-3� 1540–15205�-CCCAAGGCACAGCTTGGAGG-3� 1889–1869 cccDNA5�-AGAGATGATTAGGCAGAGGTG-3� 1846–18265�-AATGGCACTAGTAAACTGAG-3� 690–672 S mRNA5�-CCTTGATAGTCCAGAAGAAC-3� 459–4405�-GTCCAAGGAATACTAAC-3� 2464–2448 Precore-core
mRNA5�-GAGGGAGTTCTTCTTCTAGG-3� 2385–23665�-GGGGAGTCCGCGTAAAGAGAGG-3� 1550–1529 X mRNA5�-GGTCGGTCGGAACGGCAGACGG-3� 1518–14975�-TCATACATCTCAAGTTGGGGG-3� 1706–1686 �-actin5�-CCGGAAAGCTTGGCTCTTC Full-length HBVAAAAAGTTGCATGGTGCTGG-3� 1796–18255�-CCTTGATAGTCCAGAAGAAC-3� 459–4405�-AAAAAGTTGCATGGTGCTGG-3� 1796–18255�-GGAGTGCGAATCCACAC-3� 2286–2270 Probes and
sequencingprimer set
5�-TTCCCAAGAATATGGTGACC-3� 2834–28155�-CGTTCACGGTGGTCTCCAT-3� 1628–16085�-CCTTGATAGTCCAGAAGAAC-3� 459–4405�-GTCCAAGGAATACTAAC-3� 2464–2448
5�-AAAAAGTTGCATGGTGCTGG-3� 1796–1825
pI sites are underlined.site.
n Pro
me
24b
68b
1012b
1416b
P24P26b
24b
6
8b
921b
P2
4b
P6b
2
41446
P6
nd SacoRI

auXtpvic
wbopesH
TtceRtrG
Kfis
AA
q
nppgeegc(Pwo2bo(teitv((cpo0iwwbHap64rau
T
HC
a
T
O
a
b
c
d
January 2004 OCCULT HBV AND HCC 105
mplification. HBV RNA expression was analyzed with these of 3 different sets of primers (Table 1) specific for S, C, and
transcript, respectively. In all experiments, 2 negative con-rol samples were subjected to all steps. The PCR amplificationroducts were separated by 1% agarose gel electrophoresis andisualized by ethidium bromide staining. Southern blot exper-ments were performed to show the specificity of the amplifi-ation products.
Full-Length and Subgenomic HBVAmplification
HBV DNA isolates from tissue specimens of 5 casesere full-length amplified following the method describedy Gunther et al.30 Because the first-round PCR yieldednly weak or no bands on a 1% agarose gel after electro-horesis, we performed a second-round PCR with 2 differ-nt primer pairs yielding the amplification of 2 overlappingubgenomic fragments that cover the whole length of theBV genome (Table 1).
Cloning and Sequencing of PCR Products
Cloning of PCR products was performed using theOPO TA cloning kit (Invitrogen) according to the manufac-
urer’s protocol. Nucleotide sequences of PCR products andloned DNA fragments were determined using specific prim-rs (Table 1) and the BigDye Terminator Cycle Sequencingeady Reaction Kit (Applera, Foster City, CA) according to
he manufacturer’s instructions. The sequencing products wereesolved in an automatic DNA sequencer (ABI PRISM 310enetic Analyzer; Applera).
Statistical Analysis
Data were analyzed statistically by means of �2 test,endall’s rank correlation test, and odds ratio and 95% con-dence interval test. P � 0.05 (2 tailed) was consideredignificant.
Accession Numbers
The GenBank accession numbers of HBV areY230111–AY230128, AY232836–AY232840, andY236160–AY236169.
ResultsIdentification of Occult HBV Infection inLiver Tissue
We investigated the presence of HBV DNA se-uences in liver tissue specimens from 107 HBsAg-
able 2. Prevalence of Occult HBV Infection in Patients WithHCC and in Patients With CLD
No. of cases Occult HBV positive (%)
CC 107 68a (63.5)LD 192 63a (32.8)
P � 0.0001.
egative patients with HCC and 192 HBsAg-negativeatients with CLD by nested PCR and the use of 4rimer sets, each specific for S, C, Pol, and X viralenomic regions, respectively. As we previously report-d15 and as also recommended by others,17,18 we consid-red cases in which sequences of at least 2 different HBVenomic regions were detected as occult HBV-positiveases. In this way, 68 of the 107 patients with HCC63.5%) and 63 of the 192 patients with CLD (32.8%;
� 0.0001) were positive for occult HBV (Table 2),ith a univariate odds ratio for the association betweenccult HBV and HCC of 3.6 (95% confidence interval,.2–5.9). When we divided the study populations on theasis of anti-HCV positivity, we found HBV DNA in 45f the 73 anti-HCV–positive patients with HCC61.6%) and in 56 of the 153 anti-HCV–positive pa-ients with CLD (36.6%; P � 0.001), resulting in anstimated univariate odds ratio of 2.9 (95% confidencenterval, 1.6–5.1). Among the anti-HCV–negative pa-ients (34 with HCC and 39 with CLD), we detectediral sequences in the liver of 23 patients with HCC67.6%) and 7 patients with CLD (18%; P � 0.0001)Table 3) and the univariate odds ratio was 9.6 (95%onfidence interval, 3.2–28.4). Notably, in the group ofatients with HCC, we found no correlation betweenccult HBV infection and anti-HCV positivity (P .5); in the group of patients with CLD, the presence ofntrahepatic HBV sequences was significantly associatedith HCV infection (P 0.03) (Table 3), in accordanceith previous data reported by us and others (reviewedy Torbenson and Thomas18). The prevalence of occultBV infection did not differ with sex or age either
mong patients with HCC or those with CLD. As ex-ected, the patients with HCC were older (mean age,3.7 � 10 years) than those with CLD (mean age,8.2 � 11.5 years). Consequently, to verify whether theelationship of occult HBV infection with HCC wasffected by age, we performed multivariate analysis bysing the Kendall’s rank correlation test on the total of
able 3. Prevalence of Occult HBV in Anti-HCV–Positive andAnti-HCV–Negative Patients With HCC or CLD
Anti-HCV–positivepatients (%)
Anti-HCV–negativepatients (%)
HCC(n 73)
CLD(n 153)
HCC(n 34)
CLD(n 39)
ccult HBVpositive 45 (61.6)a,b 56 (36.6)a,c 23 (67.6)b,d 7 (18)c,d
P � 0.001.P 0.5.P 0.03.P � 0.0001.

2CH(HH0
cgsottoa0
8A2HomopqoTfsHpsi
atppr
oswogidersabpbmcomefcooboccaistmwaAniAttoed
T
N
N
N
106 POLLICINO ET AL. GASTROENTEROLOGY Vol. 126, No. 1
99 cases (107 patients with HCC and 192 patients withLD). There was a correlation between age and occultBV ( 0.2; P 0.00002), between age and HCC
0.46; P � 0.000001), and between occult HBV andCC ( 0.3; P � 0.0001). Of note, occult HBV andCC were associated regardless of age ( 0.23; P �
.000001).As previously mentioned, all patients with HCC had
irrhosis, as did 43 of the 192 individuals in the controlroup. HBV DNA was detected in 19 of these 43ubjects (44.2%). The comparison of the prevalence ofccult HBV between HCC and non-HCC cirrhotic pa-ients showed the persistence of the significant associa-ion between HBV and liver cancer (P 0.03). More-ver, the Kendall’s test showed that occult HBV isssociated with HCC independently of cirrhosis ( .18; P 0.015).Data on serum anti-HBc reactivity were available for
2 patients with HCC and 119 patients with CLD.mong patients with HCC, occult HBV was detected in1 of 25 anti-HBc–positive (84%) and 32 of 57 anti-Bc–negative cases (56.1%; P 0.01). Therefore, not
nly most of the anti-HBc–positive individuals but alsoore than half of subjects negative for all serum markers
f HBV infection carried occult HBV. The analysis ofatients with CLD showed the presence of HBV se-uences in 15 of 33 anti-HBc–positive (45.5%) and 22f 86 anti-HBc–negative patients (25.6%; P 0.04).hese results are in accordance with data that emerged
rom a recent review of the literature that, besides theignificant association between occult HBV and anti-Bc positivity, also showed that more than 20% of
atients with chronic hepatitis and negative for all HBVerum markers prove to be carriers of cryptic HBVnfection.18
Molecular Analyses of Occult HBV Infectionin Patients With HCC
Besides the tumor specimens, we were able tonalyze the corresponding nontumor liver tissue of 72 ofhe 107 patients with HCC. Fifty-two of these 72 wereositive for occult HBV. In particular, 17 cases showedositive reactivity for 3 or all 4 tested HBV genomicegions both in tumor and nontumor specimens, 8 cases
able 4. Distribution of 68 Patients With HCC Based on theand Nontumor Liver Specimens by 4 Different Prime
o. of HBV-positive regionsin tumor/nontumor liver specimens 4/4 4/3 3/4 4/2 2/4
o. of cases 4 3 2 3 3
A, not available.
nly in tumor samples, and 12 cases only in nontumorpecimens (Table 4). In addition, 16 of the 35 cases fromhich only tumor tissue was available tested positive forccult HBV, showing positivity for all 4 genomic re-ions in 7 cases, for 3 regions in 6 cases, and for 2 regionsn 3 cases (Table 4). In summary, occult HBV could beetected in most cases independently of the set of prim-rs used, suggesting the presence of viral genomes car-ying no gross rearrangements. To further confirm thepecificity of our results, we performed direct sequencingnalysis of all the PCR products. Such examination,esides the diversity of HBV DNA sequences betweenatients, showed a certain degree of sequence divergenceetween isolates from tumor and nontumor liver speci-ens of individual cases. This observation was largely
onfirmed when the entire S-gene sequences of isolatesbtained from paired tumor and nontumor tissue speci-ens of 5 randomly chosen patients were compared with
ach other, showing a nucleotide divergence rangingrom 1.5% to 3%. However, it must be noted that in noase was mutation(s) potentially responsible for the lackf serum HBsAg reactivity found. In this context, an-ther relevant finding was the presence of HBV strains ofoth genotype D and A in the tumor specimen from onef these 5 patients and only viruses of genotype A in theorresponding nontumor tissue. To study this peculiarase in depth, we performed HBV DNA full-lengthmplification, cloning, and sequencing analysis of HBVsolates from both tumor and nontumor specimens. Theequencing of 10 clones from each specimen confirmedhat only genotype A strains were present in the nontu-or tissue, whereas 6 of the clones from tumor isolatesere of genotype D and 4 of genotype A (GenBank
ccession numbers AY230111–AY230120, AY236165–Y236169, and AY232836–AY232840). Of relevance,o viral clone carried a mutation apparently able tonterfere with the HBV replication and gene expression.mplifying full-length viral genomes, we clearly showed
hat free HBV forms might infect HBsAg-negative pa-ients with HCC. Indeed, we showed that this was not anccasional event because we succeeded in amplifying thentire HBV genome in liver DNA extracts from 4 ad-itional cases randomly selected among those that were
ber of Positively Amplified HBV Genomic Regions in Tumorts
1/4 3/3 3/2 2/3 1/3 2/2 2/1 1/2 4/NA 3/NA 2/NA2 8 4 3 4 11 1 3 7 6 3
Numr Se
4/11

pPA
Dogbmcfip
natPdusasisHndctamnss
csGcRda1wrooCR
wmAlasHrwCtcomentiswwosa
rwwcraah
T
C
NpT
January 2004 OCCULT HBV AND HCC 107
ositive for all of the virus genomic regions tested byCR amplification (GenBank accession numbersY236160–AY236164).Integration of viral DNA sequences into the cellular
NA of patients with HCC with occult HBV is a knownccurrence.22,23,26,31 In this study, we could detect inte-rated HBV in 2 of 10 tumor tissues tested by Southernlot analysis (data not shown). In addition, when theost sensitive PCR amplification technique was used, we
onsidered the failure of 2 or 3 sets of primers in ampli-ying viral DNA from individual cases as indicative ofnterrupted and possibly integrated HBV genomes, asreviously suggested.32
Succeeding in the isolation of complete HBV ge-omes, we focused our attention on the molecular formsllowing occult HBV to persist as free genome withinhe liver of patients with HCC. We applied a nestedCR approach28 to discriminate between the partiallyouble-stranded HBV rcDNA present in virions that isnable to accomplish RNA transcription and the double-tranded HBV cccDNA essential for HBV expressionnd replication. By the use of this highly sensitive andpecific approach, we were able to detect HBV cccDNAn 20 of the 30 cases examined that were randomlyelected among those showing positivity for 3 or all 4BV genomic regions tested by PCR in both tumor and
ontumor tissue. In particular, HBV cccDNA could beetected both in tumor and nontumor specimens in 14ases, whereas it was shown only in tumor or nontumorissue in 4 and 2 cases, respectively. To rule out possiblertefacts, we included several controls in each experi-ent; HBV DNA–negative liver tissues were always
egative, and DNA from serum HBV particles gave noignal after digestion with mung bean nuclease. We nextought to assess the HBV transcriptional activity in
able 5. Detection of S, X, and C Transcripts by Reverse-Transcription PCR and the Use of Specific Primersin Paired Tumor and Nontumor Tissues From 10Cases Positive for HBV cccDNA
ases Tissues S RNA X RNA C RNA
1 T/NT �/� �/� �/�2 T/NT �/� �/� �/�3 T/NT �/� �/� �/�4 T/NT �/� �/� �/�5 T/NT �/� �/� �/�6 T/NT �/� �/� �/�7 T/NT �/� �/� �/�8 T/NT �/� �/� �/�9 T/NT �/� �/� �/�
10 T/NT �/� �/� �/�
OTE. Nucleotide sequences of primers used to determine the ex-ression of S, X, and C transcripts are reported in Table 1., tumor; NT, nontumor.
ccDNA-positive tumor and nontumor paired liver tis-ues by performing reverse-transcription PCR analysis.ood-quality liver RNA was available from 10 of the 14
ases showing the presence of HBV cccDNA, and HBVNA was detected in all of them. In particular, weetected transcripts corresponding to S gene in 9 tumornd 8 nontumor specimens, X transcripts were found in0 tumors and 8 nontumor specimens, and C transcriptsere found in 2 tumor and 5 nontumor specimens,
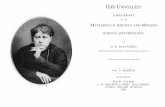
espectively (Table 5 and Figure 2). These data show thatccult HBV persisting as cccDNA maintains low levelsf transcriptional activity. Moreover, the detection of-gene transcripts corresponding to the pregenomicNA indicates ongoing viral replication.
Discussion
HCC is one of the most common cancers world-ide, and its incidence appears to be increasing in theore industrialized areas of North America, Europe, andsia.2,33 Human HCCs mostly occur in patients with
ong-lasting chronic hepatitis due to infection with HBVnd/or HCV.34–36 However, while this malignancy istill mainly related to an overt (namely, HBsAg positive)BV infection in developing countries, the increasing
ate of HCC observed in the past decade in the westernorld seems to be more frequently linked with cirrhosis.37,38 Much evidence indicates that cryptic HBV infec-
ion is a phenomenon often occurring in chronic HCVarriers, and we previously reported that about one thirdf individuals with type C CLD in our area have aasked HBV coinfection.15 In the present study, our
xamination of a large series of liver tissues from HBsAg-egative individuals with HCC showed that most ofhese patients carry occult HBV infection, with a signif-cantly higher prevalence compared with that observed inubjects with HBsAg-negative CLD; this significanceas also maintained when the comparison was performedith the subgroup of non-HCC cirrhotic patients. More-ver, the statistical analysis showed that occult HBVtrongly associated with liver cancer independently ofge, sex, and contemporary HCV infection.
Our results indicate that cryptic HBV infection is aisk factor for development of HCC. This is in agreementith data obtained in animal models showing that bothoodchucks and ground squirrels, once infected by the
orresponding hepadnaviruses (woodchuck hepatitis vi-us and ground squirrel hepatitis virus, respectively), aret high risk of developing HCC after the apparent clear-nce of the virus.39,40 The mechanisms responsible forepatocellular transformation in these rodents are essen-

ti
teilpilamwlohtokHailnte(mpaerrca
ncivilsgnHutwcntmsuMrat(eaiH
ogiiHh
Fnc(r
108 POLLICINO ET AL. GASTROENTEROLOGY Vol. 126, No. 1
ially related to the propensity of the viruses to act as annsertional mutagen of the host’s myc family genes.41,42
However, it was shown that besides integrating intohe host DNA, the viral genomes may also persist as freepisomal forms during occult woodchuck hepatitis virusnfection42; an interesting study on woodchucks conva-escent from acute viral hepatitis showed the lifelongersistence of small amounts of replicating virus thatnduce a mild liver necroinflammation continuing forife.43 Also, occult HBV may persist as episomal DNAfter HBsAg seroclearance,44–46 and it is able to induceild inflammation persisting for decades.47,48 Moreover,hen occult HBV infection coexists with other causes of
iver disease (HCV, alcohol abuse, iron overload, and son), it might be a cofactor in the pathogenesis of theepatic injury.17,49,50 In this context, we have to mentionhat occult HBV infection seems to favor the progressionf chronic hepatitis toward cirrhosis,15,20,21 which isnown to be the main precancerous lesion of the liver.owever, our present data indicate that occult HBV is
ssociated with HCC independently of cirrhosis. Of note,n our series of patients with HCC developed on cirrhoticivers, we found free viral genomes in a considerableumber of cases. These viruses maintain low levels ofranscription and replication, as indicated by the pres-nce of HBV cccDNA and viral messenger RNAsmRNAs) that, interestingly, were detected in both tu-or and nontumor samples. Although we cannot com-
letely rule out possible contamination between tumornd surrounding nontumor liver tissues, several consid-rations suggest that free replicative forms of HBV wereeally present in neoplastic cells: (1) all 4 HBV genomicegions were amplified in tumor extracts but not in theorresponding nontumor specimen from several cases; (2)nalogously, some cases had HBV cccDNA in tumor but
igure 2. Expression of the HBV core mRNA in liver tissues of patieontumor (NT) liver specimens of 3 individual cases (A, B, and C) wasore mRNA expression. (B) �-actin mRNA was amplified as an internA and B) M, DNA molecular-weight marker (sizes along left margin). (esults. �, positive control; �, negative control.
ot in the paired nontumor samples; (3) a discrete nu-leotide divergence was found between HBV sequencessolated from tumor and nontumor specimens of indi-idual patients; and (4) in one case, viral strains belong-ng to 2 different genotypes were detected in the tumoraliver whereas only one HBV genotype was shown in theurrounding nontumoral tissue. The sequence diver-ences observed between viral isolates from tumor andontumor tissues might reflect the heterogeneity of theBV infecting the liver in toto and tempts us to spec-
late on a possible segregation of some viral strains inransformed and clonally expanded cells. In any case,hat clearly emerged from our study is that ongoing
overt HBV replication frequently occurs in HBsAg-egative cirrhotic patients who develop HCC. The long-erm persistence of cryptic yet productive HBV infectionight exert an indirect oncogenic role by chronically
ustaining a mild necroinflammation that may contrib-te to the development of cirrhosis and liver cancer.oreover, occult HBV might play a direct oncogenic
ole through both its integration into the host genomend the maintained transcriptional activity that, al-hough at low levels, may allow the synthesis of proteinssuch as X protein) with potential pro-oncogenic prop-rties. In summary, our data show that the directnd indirect mechanisms whereby overt HBV mightnduce tumor formation are mostly maintained by occultBV.HBV has been classified as a group 1 human carcin-
gen and is considered the second most important onco-enic agent after smoking tobacco.4,51 Our study defin-tively shows that HBV also maintains its oncogenic rolen the case of occult infection. Consequently, testingBsAg-negative individuals with progressive chronic
epatitis or frank cirrhosis for HBV DNA seems to be of
ith occult HBV infection. (A) Total RNA isolated from tumor (T) andzed by reverse-transcription PCR and the use of specific primers forntrol for the integrity of the RNA and the quantity loaded per lane.uthern blot analysis was performed to confirm the specificity of the
nts wanalyal coC) So

pw
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
January 2004 OCCULT HBV AND HCC 109
rimary importance for the identification of patientsith a higher risk of developing liver cancer.
References1. Lee WM. Hepatitis B virus infection: a review. N Engl J Med
1997;324:1733–1745.2. Bergsland EK, Venook AP. Hepatocellular carcinoma. Curr Opin
Oncol 2000;12:357–361.3. Beasley RP, Hwang LY. Overview on the epidemiology of hepato-
cellular carcinoma. In: Hollinger FB, Lemon SM, Margolis HS,eds. Viral hepatitis and liver disease. Baltimore: Williams &Wilkins, 1991:532–535.
4. Hillman MR. Overview of the pathogenesis, prophylaxis and ther-apeusis of viral hepatitis B, with focus on reduction to practicalapplications. Vaccine 2001;19:1837–1848.
5. Chisari FV. Viruses, immunity, and cancer: lessons from hepatitisB. Am J Pathol 2000;156:1118–1132.
6. Chen PJ, Chen DS. Hepatitis B virus infection and hepatocellularcarcinoma: molecular genetics and clinical perspectives. SeminLiver Dis 1999;19:253–262.
7. Buendia MA, Pineau P. The complex role of hepatitis B virus inhuman hepatocarcinogenesis. In: Barbanti-Brodano, ed. DNA tu-mor viruses: oncogenic mechanisms. New York: Plenum, 1995:171–193.
8. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Bur-roughs AK, Christensen E, Pagliaro L, Colombo M, Rodes J.Clinical management of hepatocellular carcinoma: Conclusionsof the Barcelona-2000 EASL conference. J Hepatol 2001;35:421–430.
9. Brechot C, Gozuacik D, Murakami Y, Paterlini-Brechot P. Molecu-lar basis for the development of the hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC). Semin Cancer Biol2000;10:211–231.
0. Kaneko S, Miller RH, Feinstone SM, Unoura M, Kobayashi K,Hattori N, Purcell RH. Detection of serum hepatitis B virus DNA inpatients with chronic hepatitis using the polymerase chain reac-tion assay. Proc Natl Acad Sci U S A 1989;86:312–316.
1. Wang JT, Wang TH, Sheu JC, Shih LN, Lin JT, Chen DS. Detectionof hepatitis B virus DNA by polymerase chain reaction in plasmaof volunteer blood donors negative for hepatitis B surface anti-gen. J Infect Dis 1991;163:397–399.
2. Zhang YY, Hansson BG, Kuo LS, Widell A, Nordenfelt E. HepatitisB virus DNA in serum and liver is commonly found in Chinesepatients with chronic liver disease despite the presence of anti-bodies to HBsAg. Hepatology 1993;17:538–544.
3. Liang TJ, Baruch Y, Ben-Porath E, Enat R, Bassan L, Brown NV,Rimon N, Blum HE, Wands JR. Hepatitis B virus infection inpatients with idiopathic liver disease. Hepatology 1991;13:1044–1051.
4. Koike K, Kobayashi M, Gondo M, Hayashi I, Osuga T, Takada S.Hepatitis B virus DNA is frequently found in liver biopsy samplesfrom hepatitis C virus-infected chronic hepatitis patients. J MedVirol 1998;54:249–255.
5. Cacciola I, Pollicino T, Squadrito G, Cerenzia G, Orlando ME,Raimondo G. Occult hepatitis B virus infection in patients withchronic hepatitis C liver disease. N Engl J Med 1999;341:22–26.
6. Raimondo G, Balsano C, Craxi A, Farinati F, Levrero M, MondelliM, Pollicino T, Squadrito G, Tiribelli C. Occult hepatitis B virusinfection. Dig Liver Dis 2000;32:822–826.
7. Brechot C, Thiers V, Kremsdorf D, Nalpas B, Pol S, Paterlini-Brechot P. Persistent hepatitis B virus infection in subjects with-out hepatitis B surface antigen: clinically significant or purely“occult”? Hepatology 2001;34:194–203.
8. Torbenson M, Thomas DL. Occult hepatitis B. Lancet Infect Dis2002;2:479–486.
9. De Maria N, Colantoni A, Friedlander L, Leandro G, Idilman R,
Harig J, Van Thiel DH. The impact of previous HBV infection onthe course of chronic hepatitis C. Am J Gastroenterol 2000;95:2272–2273.
0. Sagnelli E, Coppola N, Scolastico C, Mogavero AR, Filippini P,Piccinino F. HCV genotype and “silent” HBV coinfection: two mainrisk factors for a more severe liver disease. J Med Virol 2001;64:350–355.
1. Chemin I, Zoulim F, Merle P, Arkhis A, Chevallier M, Kay A, CovaL, Chevallier P, Mandrand BCT. High incidence of hepatitis Binfections among chronic hepatitis cases of unknown aetiology.J Hepatol 2001;34:447–454.
2. Brechot C, Hadchouel M, Scotto J, Fonck M, Potet F, Vyas GN,Tiollais P. State of hepatitis B virus DNA in hepatocytes ofpatients with hepatitis B surface antigen-positive and -negativeliver diseases. Proc Natl Acad Sci U S A 1981;78:3906–3910.
3. Shafritz DA, Shouval D, Sherman HI, Hadziyannis SJ, Kew MC.Integration of hepatitis B virus DNA into the genome of liver cellsin chronic liver disease and hepatocellular carcinoma: Studies inpercutaneous liver biopsies and post-mortem tissue specimens.N Engl J Med 1981;305:1067–1073.
4. Paterlini P, Gerken G, Nakajima E, Terre S, D’Errico A, Grigion W,Nalpas B, Franco D, Wands JR, Kew MC, Brechot C. Polymerasechain reaction to detect hepatitis B virus DNA and RNA se-quences in primary liver cancers from patients negative for hep-atitis B surface antigen. N Engl J Med 1990;323:80–85.
5. Sheu JC, Huang GT, Shih LN, Lee WC, Chou HC, Wang JT, Lee PH,Lai MY, Wang CY, Yang PM, Lee H-S, Chen D-S. Hepatitis C andB viruses in hepatitis B surface antigen-negative hepatocellularcarcinoma. Gastroenterology 1992;103:1322–1327.
6. Tamori A, Nishiguchi S, Kubo S, Koh N, Moriyama Y, Fujimoto S,Takeda T, Shomi S, Hirohashi K, Kinoshita H, Otani S, Kuroki T.Possible contribution to hepatocarcinogenesis of X transcript ofhepatitis B virus in Japanese patients with hepatitis C virus.Hepatology 1999;29:1429–1434.
7. Cacciola I, Pollicino T, Squadrito G, Cerenzia G, Villari D, deFranchis R, Santantonio T, Brancatelli S, Colucci G, Raimondo G.Quantification of intrahepatic hepatitis B virus (HBV) DNA inpatients with chronic HBV infection. Hepatology 2000;31:507–512.
8. Stoll-Becker S, Repp R, Glebe D, Schaefer S, Kreuder J, Kann M,Lampert F, Gerlich WH. Transcription of hepatitis B virus in pe-ripheral blood mononuclear cells from persistently infected pa-tients. J Virol 1997;71:5399–5407.
9. Raimondo G, Burk RD, Lieberman HM, Muschel J, Hadziyannis S,Will H, Kew MC, Dusheiko GM, Shafritz DA. Interrupted replica-tion of hepatitis B virus in liver tissue of HBsAg carriers withhepatocellular carcinoma. Virology 1988;166:103–112.
0. Gunther S, Li BC, Miska S, Kruger DH, Meisel H, Will H. A novelmethod for efficient amplification of whole hepatitis B virus ge-nome permits rapid functional analysis and reveals deletion mu-tants in immunosuppressed patients. J Virol 1995;69:5437–5444.
1. Paterlini P, Poussin K, Kew M, Franco D, Brechot C. Selectiveaccumulation of the X transcript of hepatitis B virus in patientsnegative for hepatitis B surface antigen with hepatocellular car-cinoma. Hepatology 1995;21:313–321.
2. Poussin K, Dienes H, Sirma H, Urban S, Beaugrand M, Franco D,Schirmacher P, Brechot C, Paterlini Brechot P. Expression ofmutated hepatitis B virus X genes in human hepatocellular car-cinomas. Int J Cancer 1999;80:497–505.
3. El-Serag HB, Mason AC. Rising incidence of hepatocellular carci-noma in the United States. N Engl J Med 1999;340:745–750.
4. Tsukuma H, Hiyama T, Tanaka S, Nakao M, Yabuchi T, KitamuraT, Nakanishi K, Fujimoto I, Inoue A, Yamazaki H. Risk factors forhepatocellular carcinoma among patients with chronic liver dis-ease. N Engl J Med 1993;328:1797–1801.

3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
CPr
R
a
110 POLLICINO ET AL. GASTROENTEROLOGY Vol. 126, No. 1
5. Bosch FX, Ribes J, Borras J. Epidemiology of primary liver cancer.Semin Liver Dis 1999;19:271–285.
6. Tagger A, Donato F, Ribero ML, Chiesa R, Portera G, Gelatti U,Albertini A, Fasola M, Boffetta PGN. Case-control study on hepa-titis C virus (HCV) as a risk factor for hepatocellular carcinoma:the role of HCV genotypes and the synergism with hepatitis Bvirus and alcohol. Brescia HCC Study. Int J Cancer 1999;81:695–699.
7. Colombo M. Hepatitis C virus and hepatocellular carcinoma.Semin Liver Dis 1999;19:263–269.
8. El-Serag HB. Hepatocellular carcinoma and hepatitis C in theUnited States. Hepatology 2002;36:S74–S83.
9. Korba BE, Wells FV, Baldwin B, Cote PJ, Tennant BC, Popper H,Gerin JL. Hepatocellular carcinoma in woodchuck hepatitis virus-infected woodchucks: presence of viral DNA in tumor tissue fromchronic carriers and animals serologically recovered from acuteinfections. Hepatology 1989;9:461–470.
0. Marion PI. Ground squirrel hepatitis virus. In: McLachlan A, ed.Molecular biology of hepatitis B virus. Boca Raton: CRC, 1991:39–51.
1. Fourel G, Trepo C, Bougueleret L, Henglein B, Ponzetto A, TiollaisP, Buendia MA. Frequent activation of N-myc genes by hepadna-virus insertion in woodchuck liver tumors. Nature 1990;347:294–298.
2. Buendia MA. Hepatitis B viruses and liver cancer: the woodchuckmodel. In: Minson AC, Neil JC, McRae MA, eds. Viruses andcancer. Cambridge: Cambridge University Press, 1994:173–187.
3. Michalak TI, Pardoe IU, Coffin CS, Churchill ND, Freake DS, SmithP, Trelegan CL. Occult lifelong persistence of infectious hepad-navirus and residual liver inflammation in woodchucks convales-cent from acute viral hepatitis. Hepatology 1999;29:928–938.
4. Michalak TI, Pasquinelli C, Guilhot S, Chisari FV. Hepatitis B viruspersistence after recovery from acute viral hepatitis. J Clin Invest
1994;94:907. t5. Penna A, Artini M, Cavalli A, Levrero M, Bertoletti A, Pilli M,Chisari FV, Rehermann B, Del Prete G, Fiaccadori F, Ferrari C.Long-lasting memory T cell responses following self-limited acutehepatitis B. J Clin Invest 1996;98:1185–1194.
6. Yotsuyanagi H, Yasuda K, Iino S, Moriya K, Shintani Y, Fujie H,Tsutsumi T, Kimura S, Koike K. Persistent viremia after recoveryfrom self-limited acute hepatitis B. Hepatology 1998;27:1377–1382.
7. Huo TI, Wu JC, Lee PC, Chau GY, Lui WY, Tsay SH, Ting LT, ChangFY, Lee SD. Sero-clearance of hepatitis B surface antigen inchronic carriers does not necessarily imply a good prognosis.Hepatology 1998;28:231–236.
8. Blackberg J, Kidd-Ljunggren K. Occult hepatitis B virus after acuteself-limited infection persisting for 30 years without sequencevariation. J Hepatol 2000;33:992–997.
9. Conjeevaram HS, Lok AS. Occult hepatitis B virus infection: ahidden menace? Hepatology 2001;34:204–206.
0. Raimondo G. Occult hepatitis B virus infection and liver disease:fact or fiction? J Hepatol 2001;34:471–473.
1. Stuver SO. Towards global control of liver cancer? Semin CancerBiol 1998;8:299–306.
Received April 22, 2003. Accepted October 2, 2003.Address requests for reprints to: Giovanni Raimondo, M.D., Unit oflinical and Molecular Hepatology, Department of Internal Medicine,oliclinico Universitario di Messina, 98124 Messina, Italy. e-mail:[email protected]; fax: (39) 0-90-293-5162.Supported in part by a grant from the Associazione Italiana per laicerca sul Cancro.The authors thank Pierfrancesco Cacciola, M.Sc., for the statisticalnalyses as well as Prof. Cesare Campello and Dr. Marina Crovatto for
heir contribution to the collection of the samples.Copyright © 2022 FDOKUMEN