
the challenge of changing family planning and child feeding ...
Upload
khangminh22Category
view
2download
0
Health Planning Procedures
DISCLAIMER
The material contained within this document was sourced from a module the Good to Great e-learning (ELMO) system.
This material is for reference only. No claim or representation is made or warranty given, express or implied, in relation to any of the material. You use the material entirely at your own risk. The material is provided as point-in-time reference documents. DCJ does not maintain the material and does not undertake to ensure that it is accurate, current, suitable or complete. Where conditions and warranties implied by law cannot be excluded, DCJ limits its liability where it is entitled to do so. Otherwise, DCJ is not liable for any loss or damage (including consequential loss or damage) to any person, however caused (including for negligence), which may arise directly or indirectly from the material or the use of such material.
Good to Great e-Learning Module

Health Planning Procedures
MODULE
Good to Great e-Learning Module

Health Planning Procedures
=========== NOTEs =========== [*]
Support workers
ADHC support workers include:
• Disability support workers; • Nurses; • Line managers.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Culturally sensitive
The traditional Aboriginal perspective of health is holistic and encompasses land, environment, physical body, community, relationships and law. Health is connected to the social, emotional, and cultural wellbeing of the whole community, and the sense of being indigenous.
Note
The Aboriginal and Torres Strait Islander health assessment Medicare item can be claimed by the GP once every nine months.
In ADHC operated or funded accommodation support services, the next health assessment appointment should be booked as soon as possible after the nine months has elapsed.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
https://lcms.elmolms.compages/images/ADHC_donut.pdf https://lcms.elmolms.compages/images/ADHC_donut.pdf https://lcms.elmolms.compages/images/ADHC_donut.pdf
Good to Great e-Learning Module

Health Planning Procedures
Advocacy
In the context of health planning with the person, health advocacy includes:
1. Support: by providing health information, encouragement and skill development to empower the person to self-advocate.
2. Assistance: by prompting the person to communicate their health needs and issues with health professionals. For instance, supporting the person during the health assessment to communicate what health treatment advice is working or not working for them.
3. Representing the person: by speaking up when the person's rights are violated and they are unable to do so for themselves. For instance, if the health professional does not engage with or provide adequate advice and support to the person during a health assessment appointment.
Important
Representing the person does not include making health decisions for them. This is the role of the person responsible.
Tip
Further information on capacity and consent can be found in the Decision Making and Consent Policy and Guidelines in the Lifestyle Policy and Practice Manual.
Good to Great e-Learning Module

Health Planning Procedures
Person responsible
The role of the person responsible is only relevant to giving or withholding consent for dental or medical treatments. The Guardianship Division of the NSW Civil and Administrative Tribunal (NCAT) provides guidance on who can be the person responsible for giving or withholding consent.
Important
At no time can you, as a support worker, provide consent for the person or be a person responsible.
Tip
Further information on decision making and consent is available in the Decision Making and Consent Policy and Guidelines in the Lifestyle Policy and Practice Manual.
Good to Great e-Learning Module

Health Planning Procedures
Not satisfactory
At an unsatisfactory appointment the health professional may:
• Refuse to provide recommendations in writing; • Refuse to provide a copy of the Annual Health Assessment; • Not act on concerns raised about the person's health and wellbeing.
Further action
If the person, person responsible, or support worker are not satisfied with the outcome of the health appointment, and have not been able to raise their concerns directly with the GP during the consultation, the matter must be referred to the line manager for further action.
It is the line manager's responsibility to escalate the matter by:
• Discussing the concerns directly with the GP; • Informing a senior manager of the issue; • Making a referral to an ADHC Clinical Nurse for advice and support with approaching the GP.
Good to Great e-Learning Module

Health Planning Procedures
Another GP
When assisting the person to choose an alternate GP, the following factors should be considered:
• The person has an affinity with the GP; • Physical accessibility of the GP for the person, especially if they have mobility issues; • The proximity of the GP to where the person lives; • The GP's knowledge of the disability sector and people with a disability.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Sections
My Health and Wellbeing Plan is split into 4 sections:
• Part A: Information About Me; • Part B: Information About My Health; • Part C: My Support Plans; • Part D: Review Record.
Important
The My Health and Wellbeing Plan should not be 'filed away' as this will discourage the person and support workers from using it.
When not in use, the plan should sit in a location where it is private and safe from damage or loss but is physically accessible to the person, support workers and others involved.
Good to Great e-Learning Module

Health Planning Procedures
By the person
In situations where the person is unable to provide personal details, the information is sourced from the person's records and from people who know the person well.
Leave no fields blank
For instance, if it is unclear if the person has received a Hepatitis B injection, then record "unknown" in the person's Immunisation Record. This information can be discussed further with the person's GP.
Note
Information in Part A is only recorded once. Changes to the person's details are updated as they occur and reviewed as part of a quarterly review cycle or sooner if any changes occur.
Sources
Possible sources of information about the person include:
Good to Great e-Learning Module

Health Planning Procedures
Source Further information
The person and the person's family
People who have known the person for a long time
Long term support workers
The Client Information System (CIS)
Information about the person from files
eHealth
When requesting information from families, support workers are to be sensitive and respectful, especially if the person has experienced a
trauma. Remember to be mindful of these sensitivities when asking questions about the person's medical and family history.
Friends and advocates
Support workers who currently or have previously supported the person
Discuss with your line manager about recording information on CIS
People who have been with ADHC for some time, and who have received support from ADHC clinicians (psychologists, speech pathologists, occupational therapists, physiotherapists) may have a hard-copy file containing personal information. Discuss with your line manager about accessing information from these files.
eHealth is a record system which stores a person's health information online. The person has control over what information is stored and who has access to it. An authorised representative can be appointed if the person does not have the capacity to apply for and manage their eHealth record.
Past documents relating to the person are stored in the Government Records Repository. If information is missing about the person it may Archived information
be contained in archived records. Discuss with your line manager about whether it is necessary to access archived information.
Good to Great e-Learning Module

Health Planning Procedures
All support workers
This includes permanent, temporary, casual and agency support workers.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
All support workers
This includes permanent, temporary, casual and agency support workers.
Changes
To determine whether a change in the person's health status has occurred, refer to:
• The person directly; • How the person communicates their health needs as outlined in Part A of the My Health and Wellbeing Plan; • Other support workers on shift or at other services the person may have attended recently, such as a day
program or work place; • Recent written records, such as the person's daily notes / shift report, the Communication Book, and
completed incident reports.
Health Action Plan
Information about the Health Action Plan will be provided in the following section of this module.
Good to Great e-Learning Module

Health Planning Procedures
Note
The Appointment Checklist is a non-mandatory tool. Where possible, a support worker who knows the person and their medical history attends the health appointment. With the person's consent, a family member or someone who knows the person well may also attend the appointment.
Use the Appointment Checklist to assist you in preparing for appointments and to keep on top of health actions prescribed by a health professional. Completion of the checklist can help support the person to receive prompt and coordinated support with their health care needs.
Example
If a person fell over and hurt their ankle:
1. Apply first aid and seek medical attention. 2. Complete an incident report outlining the situation, how it occurred, follow-up action and any
recommendations to prevent reoccurrence. 3. Make observations of the injury and record these in the Health Learning Log. 4. In the person's daily notes / shift report refer the reader to where detailed information has been recorded.
For example, 'Danny tripped on a rock and hurt his ankle when walking to the corner store. Danny went to see Dr Mathews. Refer to incident report, Health Learning Log and Health Action Plan for detailed information and further actions required.'
5. Reference to any additional support requirements also needs to be made in the Urgent Matter Alert on the Individual Shift Report.
6. Update any new information in the person's communication profile.
Good to Great e-Learning Module

Health Planning Procedures
Written record
A written record provided by the health professional will eliminate the risk of support workers transcribing and misinterpreting information.
You are not responsible for recording the advice and recommendations provided by the health professional in any format.
Hand written
If the health professional provides a hand written report, the support worker attending the appointment needs to go through it with the health professional to understand it and ensure that it is legible and clear enough for other support workers to read.
Good to Great e-Learning Module

Health Planning Procedures
Completion of actions
The Health Action Plan is NOT intended to be used to transcribe and record health information from a health professional. This is solely the responsibility of the health professional.
Completed when due
The Health Action Plan is reviewed regularly to ensure that time frames are not missed. Depending on the Health Action, a review could be needed every week until the action is complete.
Appointment Checklist
The Appointment Checklist is a non-mandatory tool which provides guidance to the person and support worker when making health appointments.
It is designed to present the person’s information to the health professional in a clear and coordinated way. The health professional can then make informed decisions on how to best meet the person’s health and wellbeing needs.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Note
Indicators of ill health in the Annual Health Summary can also be used throughout the year as a guide, when identifying changes to the person's health and wellbeing, for recording in the Health Learning Log.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Different ways
The GP or treating doctor may choose to record information in:
• A written report; • A Medicare Chronic Disease Management Plan, such as a GP Management Plan or Team Care Arrangement; • A template developed by a peak agency, NSW Ministry of Health and the Department of Health and Ageing; • An existing ADHC support plan, such as:
o Hospital Support Plan; o Nutrition and Swallowing Risk Checklist; o Mealtime Management Plan; o Epilepsy Management Plan; o Behaviour Support Plan; o Enteral Nutrition Plan; o My Oral Health Plan; o Physical Activity Checklist and Plan.
Good to Great e-Learning Module

Health Planning Procedures
Review and update
Reviewing the plan is essential for:
• Monitoring and recording changes to the person's health; • Highlighting any health patterns of concern; • Reviewing the status of any aids or equipment that the person uses; • Keeping track of the completion of recommendations and actions prescribed by the person's GP and any
other health professional; • Prompting support workers to record new information about the person and their health and wellbeing.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Accommodation support service
• Group home; • Large Residential Centre; • Specialist Supported Living.
Usual GP
Medicare defines the person's usual GP as:
'The GP (or a GP in the same practice) who has provided the majority of services to the patient in the past 12 months and / or is likely to provide the majority of services in the following 12 months.'
Note
For all other ADHC accommodation support services, such as in-home support, you must provide information to the person on their entitlement to have an annual health assessment conducted by their usual GP under Medicare.
Good to Great e-Learning Module

Health Planning Procedures
Five Medicare health assessments
The health assessments available to people with intellectual disability under Medicare are:
Medicare health assessment type
Length of assessment Medicare item no.
Brief 701 max. 30 min
Standard 703 30 - 45 min
Long 705 45 - 60 min
Prolonged 707 min. 60 min
Aboriginal and Torres Strait Islander People 715 Not specified
Note
The health assessment can be claimed by the GP once every twelve months. You should book the annual health assessment appointment as soon as possible after the twelve months has elapsed.
Other health assessment tools may be used by the GP, including:
• Comprehensive Health Assessment Program (CHAP); • New England Medicare Local health assessment tool.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
https://www1.health.gov.au/internet/main/publishing.nsf/Content/mbsprimarycare-factsheet-chronicdisease.htm
Good to Great e-Learning Module

Health Planning Procedures
Allied health professional
A referral to an allied health services such as a physiotherapist or occupational therapist can assist a person whose physical health and mobility deteriorates by providing advice on equipment, home modifications and manual handling.
Speak to a line manager about making a referral to an ADHC allied health professional or by contacting mainstream support services such as Independent Living Centres for advice on products and equipment to manage daily life
Note
Regardless of the age of the person, it is good practice to have discussions with the person and their family about the person’s preferences for end of life care, rather than waiting for the person to be terminally ill and unable to be involved in the discussions.
Refer to the End of Life Care Planning Guidelines in the Health and Wellbeing Policy and Practice Manual, Volume 2 for further information.
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
Maximising Health & WB 4 Children & Young People in - https://intranet.facs.nsw.gov.au/about-facs/divisions/disabilty-services
Young people
While all people under 18 years of age are regarded under the law as children, young people are given special consideration by the NSW Civil and Administrative Tribunal (NCAT) Guardianship Division. A young person can provide their own consent on a range of matters, or they can be assigned a Public Advocate by NCAT if they need a legally appointed decision maker (refer to the Decision Making and Consent Policy and Guidelines).
Note 1
Under Medicare, children aged at least three years and less than five years of age are entitled to a one-off Healthy Kids Check health assessment, provided they have received or are receiving their four year old immunisation.
Medicare’s Child Dental Benefits Schedule (CDBS) enables access to basic dental services for children two to 17 years of age.
Good to Great e-Learning Module

Health Planning Procedures
Note 2
Medicare also funds a number of initiatives for children with disability and their families to assist with assessment, diagnosis, and provision of early intervention services for eligible disabilities. For instance:
1. A one-off assessment by a specialist or GP for early diagnosis and treatment of a range of conditions; and 2. The Better Start for Children with Disability and Helping Children with Autism programmes to assist children
under the age of six years and their families with accessing early intervention services.
Refer to Australian Government Department of Social Services for eligibility requirements, payment thresholds and information on the transition of these services to the National Disability Insurance Scheme.
Good to Great e-Learning Module

Health Planning Procedures
Move your cursor over each of the steps and the icon for more information.
Step 1: Review the current health assessment
Review actions and recommendations made by the GP from the last annual health assessment.
The 'What is Working / Not Working' person-centred tool is useful in assessing the effectiveness of health care actions and why previous actions were not achieved / completed, or did not appear to make a difference.
Any actions that have not been completed over the previous year are noted and discussed further with others (see Step 6) and the GP at the person's health assessment.
Step 2: Review the Health Promotion Register
Review the person's Health Promotion Register, located in Part B of the My Health and Wellbeing Plan.
Any fields that are out of date or 'unknown' are noted and discussed with the GP during the appointment. The GP will recommend actions to take.
Medicare's health assessment criteria outline a number of items to prompt a review of health promotion activities. For instance, hearing and vision health, men's and women's health, and physical activity.
Good to Great e-Learning Module

Health Planning Procedures
Step 3: Review the person's health data sheets
The information contained in the person's health data sheets is collated so that they can be discussed with the GP at the health assessment appointment.
The person's current height and weight is measured either before the appointment, if they need to access specialised equipment, or by the GP during the health appointment.
Step 4: Review existing support plans
Support plans (documented in the Support Plan Register, located in Part C of the My Health and Wellbeing Plan) for the person are reviewed and updated in preparation for the annual health assessment and can include the following plans / checklist:
• Epilepsy Management; • Enteral Nutrition;
• Nutrition and Swallowing; • Behaviour Support;
• Mealtime Management; • Oral Health.
• Physical Activity Checklist and Plan;
You must follow the review cycle and requirements in the procedures / guidelines relating to each support plan. Any changes that are made to existing plans must be discussed with other support workers and the GP / dentist at the health appointment.
Step 5: Complete an Annual Health Summary OR Part A of the CHAP tool
The Annual Health Summary must be completed prior to the person's annual health assessment.
It is important that each body system in the Annual Health Summary is reviewed as some indicators of illness may be common to more than one body system (for example, the skeletal, muscular or digestive systems).
The Annual Health Summary is completed by the person and support workers. If the person has difficulty with communication or chooses not to participate then it will need to be completed by those who know the person well.
Step 6: Discuss the information with others
Use the 'Four + One Questions' tool to review and understand the health actions that were completed and any lessons learnt. This will assist with future health planning.
Information sharing can occur individually with a line manager, or in a group setting, such as a team meeting. Team meetings are a useful environment for support workers to share different experiences and understanding of the person's health and wellbeing with other members of the team.
Additional information about the person's health that is identified during discussion with others, is recorded in the Annual Health Summary and discussed with the GP.
Good to Great e-Learning Module

Health Planning Procedures
Additional support
If the person has a chronic health condition, the line manager can place a referral for additional support from an ADHC Clinical Nurse.
The ADHC Clinical Nurse may also be able to provide additional support to the person and support worker by speaking to the GP about the person's complex health support requirements at the annual health assessment appointment.
Step 7: Make an appointment with the person's GP and dentist
The Appointment Checklist is a non-mandatory tool to guide actions when making the health assessment appointment.
The person and the GP may decide that a number of appointments are needed for the health assessment. For instance, the person may have two preliminary consultations to gather information, followed by a third longer appointment to undertake the Medicare Prolonged health assessment.
Dentist
An appointment with a public or private dentist for the person's annual dental review is made at this stage if possible.
If the person attended a Public Oral Health Service Referral Centre within the last year, an appointment may have been made for the next annual dental review. Look in the person's My Oral Health Plan for a record of the appointment or call the Public Oral Health Service Referral Centre and confirm if an appointment was made.
If the person usually attends a private dentist, make an appointment as soon as possible.
Step 8: Attend the appointment
The person must attend the health assessment appointment. The GP cannot perform a comprehensive health assessment if the person is absent. If the person is physically unable to attend, request that the health assessment appointment occurs at the person's home at a time suitable to the person.
Remind the GP that:
• The purpose of the appointment is for an annual health assessment, and that it is a long or prolonged consultation;
• A copy of the health assessment containing a written record of the recommended treatment and actions will be required.
Provide the GP with the ‘People with intellectual disability - Information for GPs during health assessments’ Factsheet (Other Resources). Inform the GP that a copy of the health assessment containing a written record of the recommended treatment and actions will be required.
Good to Great e-Learning Module

Health Planning Procedures
Step 9: Use the Health Assessment Criteria
The Health Assessment Criteria tool lists the minimum Medicare criteria to be covered in the annual health assessment. It is not mandatory to use this tool however it can help to support the person's involvement during the assessment.
Use the Health Assessment Criteria to guide discussions with the GP about the person's health and wellbeing concerns, as these contain the health areas that should be covered under Medicare during a health assessment for a person with intellectual disability.
Regardless of what health assessment template the GP decides to use, it is the responsibility of the attending support worker to ensure that at least all the criteria outlined by Medicare are discussed during the appointment. If the GP is using the CHAP tool or the assessment tool developed by the New England Medicare Local, all sections in those tools need to be addressed.
Step 10: Discuss the person's current health issues
In this step, the information collected in steps 1 to 6 should be provided to the GP. This is:
• Information collected in the Annual Health Summary (or Part A of the CHAP tool). Any body system that has been checked must be discussed with the GP and noted in the far right column of the form;
• Outcome of actions completed / not completed from the last health assessment and previous health appointments;
• The person's My Health and Wellbeing Plan; • Other relevant health professional reports that the GP may not have received; • Medication Chart, Record and Profile.
Step 11: Discuss the person's chronic health conditions
If the person has a chronic health condition or disease, now is the time to discuss the need for additional support. This will depend on how complex the person's health and wellbeing needs are and is determined by the GP or other health specialist.
If the GP indicates that the person's chronic disease or long-term health condition is not being effectively managed, they may decide that a Medicare Chronic Disease Management Plan is required. If the GP decides to manage the person's complex health care with multi-disciplinary specialised health support, the GP can refer the person to:
• A specialist health professional; • A state-wide Specialised Intellectual Disability Health Service (SDS); • An allied health professional to manage particular chronic conditions; • A pharmacist to review the person’s medications under Medicare item 900, Domiciliary Medication
Management Review (otherwise known as the Home Medicines Review).
Step 12: Obtain a copy of the health assessment
By the end of the consultation, it should be clear to you and the person what actions need to be taken.
Good to Great e-Learning Module

Health Planning Procedures
The GP must provide an easy to read and understandable, written copy of the health assessment for use by non-clinical staff to support the person in managing their health. Read the copy with the GP before leaving the appointment to ensure you understand what has been recorded and any prescribed recommendations.
You may also need to prompt the GP to:
• Prescribe new and ongoing medication prescriptions; • Prepare a referral to a Specialised Intellectual Disability Health Service, where required; • Prepare a referral to any other health professional, e.g. Public Oral Health Service; • Provide written endorsement of reviewed and updated support plans; • Record changes to prescribed medication in the:
o Medication Chart / Webster-pak Signing Sheet; o Medication Record.
Step 13: Actions after the appointment
Update the Health Action Plan to keep track of the completion of health actions prescribed by the GP.
If the Appointment Checklist tool was used to prepare for the health assessment, with the person work through Checklist 3 of the Appointment Checklist, ‘After the appointment’ and complete each of the actions listed in the Health Action Plan.
Consent
If the person is unable to or does not want to participate in a discussion about their health, or any other step of the health assessment, others who know the person well will need to be engaged in the process. For example, the line manager, other members of the team and if the person is unable to consent, the person responsible.
If personal information is to be discussed with others, permission should first be obtained from the person to maintain their right to privacy and confidentiality.
The person's consent is required for the health assessment. If the person is not able to provide consent, consent from the person responsible is not required unless the person is objecting or a minor treatment is to be performed at the time of the assessment (for example, a blood test).
Referral
If the person has not attended a Public Oral Health Service Referral Centre before and is eligible for the service, a referral will be required. The referral should be discussed and obtained from the person's GP at the time of the health assessment appointment.
If the GP or health professional decides that a Chronic Disease Management Plan is needed, make another appointment with the GP or health professional at the end of the consultation.
Good to Great e-Learning Module

Health Planning Procedures
Changes
Any changes to the health assessment document must be made by the GP. At no stage should support workers transcribe or rewrite any written information provided by the GP; this is the responsibility of the GP.
This also relates to other health appointments the person attends during the course of the year.
Medication
The person may have a reaction to new medication and it is important that the person and support worker ask the GP:
• What the person may experience as a result of a change in medication regime; • How long to monitor the person for signs of a reaction; • When to seek medical advice if a reaction does occur.
Good to Great e-Learning Module

Health Planning Procedures
Note
If the person does not have teeth, the GP assesses the condition of the person's gums and mouth at the time of the health assessment.
If the GP thinks it is needed, they will make a referral to dental health services. Refer to the Health Planning Procedures, Other Resources for further information about the Public Oral Health Service including the NSW Oral Health Fee for Service Scheme and Special Care Dentistry Services.
Good to Great e-Learning Module

Health Planning Procedures
Note
Before leaving a dental appointment book the next dental review. Record the appointment date in the person’s My Oral Health Plan.
The Team Leader must sign and date that they have reviewed the outcome and recommendations made by the health professional at the dental review.
Good to Great e-Learning Module

Health Planning Procedures
NSW Health https://www.health.nsw.gov.au/oralhealth/pages/default.aspx
Public Oral Health Service
The eligibility requirements for an adult to receive free Public Oral Health Service are available on the NSW Health website.
Local Health Districts can be contacted for oral health information, and contact details are on the NSW Health website.
Special Care Dentistry Service
Special Care Dentistry Service:
Special Care Dentistry Service is for people who are not suitable for routine dental care at a Public Oral Health Service. If the person has not previously accessed a Referral Centre, a referral will need to be completed by a medical or dental practitioner.
Prior to the initial appointment, information about the person's communication and support needs may be provided to the Referral Centre to facilitate the appointment. The initial dental appointment may be an assessment of the person's dental health, and decisions about treatment (if needed).
Good to Great e-Learning Module

Health Planning Procedures
Following the dental appointment, and before leaving the Referral Centre, book the next dental appointment. Record the appointment date in the person's My Oral Health Plan.
Private dentist
The person may choose to visit a private dentist instead of the free Public Oral Health Service. Accessing a private dentist will depend on the person's:
• Physical abilities; • Urgent need of dental care; • Financial capacity or private health insurance with dental care extras.
The person may also be eligible to receive a Public Oral Health Service through a private dentist registered under the NSW Oral Health Fee for Service Scheme (OHFFSS).
Further information relating to oral health and hygiene is provided in the Nutrition and Swallowing Guidelines of the Health and Wellbeing Policy and Practice Manual, Volume 1 and the Chronic Disease Guidelines in the Health and Wellbeing Policy and Practice Manual, Volume 2.
Note
Special Care Dentistry Services are provided in NSW at three Referral Centres:
• Sydney Dental Hospital (SDH) in Surry Hills (central Sydney); • Westmead Centre for Oral Health (WCOH) (near Parramatta); • The Children's Hospital Westmead, Dental Department.
Any offer of an appointment from a Referral Centre must be acknowledged for the referral to remain valid. If the person has difficulty attending the appointment on the day, it is essential that the Referral Centre is contacted so that alternate arrangements can be made.
Consent
The person or person responsible must normally consent to any dental treatment, including a referral.
For consent requirements in particular situations (for example, there is no person responsible or the person is objecting to treatment), seek advice from the Guardianship Division of the NSW Civil and Administrative Tribunal (NCAT).
Good to Great e-Learning Module

Health Planning Procedures
Maximising Health & Wellbeing for Children & Young People in Out-of-home-Placements https://intranet.facs.nsw.gov.au/about-facs/divisions/disabilty-services
Good to Great e-Learning Module

Health Planning Procedures
Good to Great e-Learning Module

Health Planning Procedures
QUIZ
Good to Great e-Learning Module

Health Planning Procedures
Q1: The Health Planning Procedures provide clear guidelines for which of the following aspects of health support?
Answer 1 Planning and documentation. Answer 2 Implementation and review. Answer 3 All of the above.
Correct answer: All of the above. Q2: What are the requirements for developing and reviewing a person’s My Health and Wellbeing Plan?
Answer 1 Support workers complete the Annual Health Summary or Part A of the CHAP Tool each year prior to the annual health assessment. Answer 2 The My Health and Wellbeing Plan must be reviewed quarterly. Answer 3 The My Health and Wellbeing Plan must be reviewed whenever there is a change in the person's health status. Answer 4 All of the above.
Correct answer: All of the above. Q3: Respecting a person with disability’s right to choose from a range of health services means that we may not seek to influence their or their family’s choices as a result of our own health care beliefs. True or false?
Answer 1 True. Answer 2 False.
Correct answer: True. Q4: Respecting a person with disability’s right to privacy, confidentiality and dignity means that we may NOT discuss their health issues in which of the following circumstances?
Answer 1 With other staff members, except those who need to know.Answer 2 In front of the person with a disability if they are not included in the discussion. Answer 3 Without the person’s consent or in public. Answer 4 All of the above.
Good to Great e-Learning Module

Health Planning Procedures
Correct answer: All of the above. Q5: How can we support and encourage people with disability to make informed decisions and exercise choices to the extent of their ability?
Answer 1 Foster an environment which assists people with disability to make healthy choices. Answer 2 Encourage people with disability to plan a healthy lifestyle and routine. Answer 3 Encourage people with disability to incorporate a high standard of personal hygiene, healthy eating, regular sleep and regular exercise into their routine. Answer 4 All of the above.
Correct answer: All of the above. Q6: What steps can we take to ensure the early detection of health risks?
Answer 1 Schedule an annual health assessment with a General Practitioner. Answer 2 Conduct quarterly reviews of the person’s My Health and Wellbeing Plan and support plans. Answer 3 Provide immediate assistance and access to medical care when a person appears ill or in pain, or if there is an observable change in the person’s health or wellbeing. Answer 4 All of the above.
Correct answer: All of the above. Q7: We must provide health support to people with disability in a manner that preserves their dignity, confidentiality, privacy and safety. True or false?
Answer 1 True. Answer 2 False.
Correct answer: True Q8: Which of the following is a way to fulfill our duty of care while providing support to people with a disability?
Answer 1 Convey accurate information and daily observations of the person’s health to the treating medical practitioner. Answer 2 Promptly follow up on health actions and recommendations prescribed by health professionals. Answer 3 Assist people with a disability to plan their lifestyle and routine to include a high level of personal hygiene, healthy eating with regular sleep and exercise patterns. Answer 4 All of the above.
Good to Great e-Learning Module

Health Planning Procedures
Correct answer: All of the above. Q9: True or False: Every person with a disability living in an accommodation support service should be supported to meaningfully participate in the development of their My Health and Wellbeing Plan.
Answer 1 True. Answer 2 False.
Correct answer: True. Q10: Decisions relating to the person with disability’s health do not need to consider their cultural and linguistic background, as only their health matters. True or False?
Answer 1 True. Answer 2 False.
Correct answer: False. Q11: In providing support to Aboriginal and Torres Strait Islander people with disability, you should take care to do which of the following?
Answer 1 Ensure you have met their cultural leader(s). Answer 2 Gather information about their cultural background, including any specific traditions and customs from the person, their family or other significant people in their community. Answer 3 Ask them if they currently access any Aboriginal Health Services.
Correct answer: Gather information about their cultural background, including any specific traditions and customs from the person, their family or other significant people in their community. Q12: The treating doctor or dental practitioner is responsible for determining if the person is capable of understanding the general nature and effect of treatment and whether they are able to give valid consent. True or False?
Answer 1 True. Answer 2 False.
Correct answer: True. Q13: It is not required to document consent for regular health care reviews and visits to the doctor or dentist. True or False?
Answer 1
Good to Great e-Learning Module

Health Planning Procedures
True. Answer 2 False.
Correct answer: False. Q14: Consent is required from the person or their person responsible or guardian for emergency medical treatment. True or False?
Answer 1 True. Answer 2 False.
Correct answer: False. Q15: Who can provide support workers with guidance on who can be the person responsible for giving or withholding consent when it is required?
Answer 1 The person.Answer 2 The Person Responsible. Answer 3 The General Practitioner. Answer 4 The Guardianship Division of the NSW Civil and Administrative Tribunal.
Correct answer: The Guardianship Division of the NSW Civil and Administrative Tribunal. Q16: All people with disability in accommodation services must have a My Health and Wellbeing Plan and an annual health assessment conducted by their general practitioner. True or False?
Answer 1 True. Answer 2 False.
Correct answer: True Q17: Which of the following tools are required to be used in the annual health assessment?
Answer 1 The Annual Health Summary or Part A of the CHAP (Comprehensive Health Assessment Program) tool. Answer 2 Health Promotion Register. Answer 3 My Oral Health Plan. Answer 4 All of the above.
Good to Great e-Learning Module

Health Planning Procedures
Correct answer: All of the above. Q18: What is the primary source of health information given to the general practitioner at the annual health assessment to inform the person’s health and wellbeing needs for the coming year?
Answer 1 The Health Care Procedures Register. Answer 2 The Comprehensive Health Assessment Program (CHAP).
Correct answer: The Comprehensive Health Assessment Program (CHAP). Q19: Part A of the CHAP Tool or the Annual Health Summary must be completed by a support worker who knows the person well prior to the annual health assessment, while Part B of the CHAP Tool or the Medicare health assessment is completed by the General Practitioner during the annual health assessment. True or False?
Answer 1 True. Answer 2 False.
Correct answer: True. Q20: A person who accesses an ADHC operated centre-based respite service requires an up to date Respite Care Profile, and may choose to supplement it with components of the Plan. True or False?
Answer 1 True. Answer 2 False.
Correct answer: True.
Good to Great e-Learning Module

Health Planning Procedures
ATTACHMENTS
1. Abuse and Neglect Policy 2. Abuse and Neglect Prevention Guidelines 3. Abuse and Neglect Procedures 4. ADHC Health and Wellbeing Policy 5. Annual health summary 6. Appointment checklist 7. Bowel care guidelines 8. Bowel chart 9. CHAP 10. Chronic Disease Guidelines 11. Decision Making and Consent Guidelines 12. Decision Making and Consent Policy 13. Flowchart 14. GP Fact Sheet 15. Health action plan 16. Health and Wellbeing Plan 17. Health appointment sheet 18. Health learning log19. Health planning procedures 20. Health Promotion Guidelines 21. Health promotion register 22. Information for DSW 23. Medicare Health Assessment 24. Menstruation chart 25. My oral health plan26. Other Resources 27. PART A_My Health and Wellbeing Plan 28. PART B_My Health and Wellbeing Plan 29. PART C_My Health and Wellbeing Plan 30. PART D_My Health and Wellbeing Plan 31. Person Responsible FlowChart 32. Sexuality and Relationship Guidelines 33. Strategies 34. Support plan register 35. Support workers fact sheet36. Team meeting37. Weight chart
Good to Great e-Learning Module

Abuse and Neglect Policy
Document name
Policy
Version number
Approval date
Policy manual
Approved by
Summary
Replaces document
Authoring unit
Applies to
Review date
Abuse and Neglect Policy
Abuse and Neglect
1.0
January 2016
Safeguarding Policy and Practice Manual
Deputy Secretary, ADHC
The Abuse and Neglect Policy provides information and guiding principles to support paid and unpaid workers of ADHC operated and funded non-government disability support services, with the means to prevent, identify and respond to abuse and neglect when it occurs or is suspected.
Abuse and Neglect Policy and Procedures 2014
Contemporary Residential Options Directorate
People who are being supported in ADHC operated and ADHC funded non-government disability support services.
2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment Amendment notes date
V1.0 January 2016 The Policy is one of three documents (Policy, Procedures, and Prevention Guidelines) that replaces the Abuse and Neglect Policy and Procedures December 2014.
Abuse and Neglect Policy, V1.0, January 2016 2

Table of contents
Table of contents ...........................................................................................3
1 Purpose of policy ..................................................................................4
1.1 Purpose...........................................................................................4
1.2 Background.....................................................................................4
2 Scope and application ..........................................................................4
2.1 ADHC operated services.................................................................4
2.2 ADHC funded non-government services.........................................5
2.3 Types of abuse and neglect ............................................................5
3 Principles ...............................................................................................6
3.1 Person centred approaches ............................................................6
3.2 Identifying abuse and neglect .........................................................6
3.3 Prevention.......................................................................................7
3.4 Early intervention ............................................................................8
3.5 Reporting abuse and neglect ..........................................................8
3.6 Responding to a report of abuse or neglect ....................................8
3.7 Responding to abuse and neglect of a person with disability by a member of staff or by another person with disability....................................9
3.8 Privacy and confidentiality...............................................................9
3.9 Resolution .......................................................................................9
4 Identifying abuse and neglect ..............................................................9
5 Patterns of abuse and neglect ...........................................................10
6 Incidents of abuse and neglect reportable to the NSW Ombudsman.................................................................................................22
7 Critical incidents involving children and young people reportable to the Children’s Guardian ..........................................................................23
8 Policy links...........................................................................................24
9 Legislative context ..............................................................................25
10 Definitions............................................................................................26
11 Policy and Practice Unit contact details............................................33
Abuse and Neglect Policy, V1.0 January 2016 3

1 Purpose of policy
1.1 Purpose
The purpose of the Abuse and Neglect Policy (the Policy) is to set the context for providing an environment free of abuse and neglect and provide a set of principles for minimising the risk of abuse and neglect.
1.2 Background
The United Nations’ Convention on the Rights of Persons with Disabilities1 (the UN Convention) states that a person with disability has the right to liberty, security and freedom from abuse and neglect, and where these rights have been violated, to have equal recognition by law and access to justice.
The Policy is consistent with the objects and principles of the Disability Inclusion Act 2014, and is based on the principles of legal and human rights found in the NSW Disability Service Standards.
The Policy includes principles recognising the needs of particular groups, such as Aboriginal and Torres Strait Islander people, people from culturally and linguistically diverse (CALD) backgrounds and women and children with disability.
The Policy aims to deliver culturally sensitive information about how to safeguard people from abuse and neglect and, that supports Aboriginal and Torres Strait Islander people and people from CALD communities.
2 Scope and application
The Policy should be read in conjunction with the Abuse and Neglect Procedures and Prevention Guidelines which have been developed to support a structured, consistent and transparent approach to safeguarding people from abuse and neglect.
The Policy, Procedures and Prevention Guidelines provide paid and unpaid workers of Family and Community Services NSW (FACS), Ageing, Disability and Home Care (ADHC) operated and funded non-government disability support services with the means to identify abuse and neglect, and to respond quickly and appropriately to allegations of abuse and neglect.
2.1 ADHC operated services
1 Convention Rights of People with Disability, United Nations 2006 http://www.un.org/disabilities/convention/conventionfull.shtml
Abuse and Neglect Policy, V1.0 January 2016 4

The following ADHC operated services have designated reporting lines in accordance with the organisation’s structure that must be adhered to following an allegation of abuse and neglect:
Accommodation support services (in-home support, group homes and
large residential centres)
Specialist Supported Living
Flexible and centre based respite services
Community Support Teams
For reporting abuse and neglect to external agencies and services such as the NSW Police and Ambulance services, please refer to the Abuse and Neglect Procedures (2015).
2.2 ADHC funded non-government services
People who are being supported in ADHC funded non-government disability support services are required in accordance with the Standards in Action (2012) to have reporting procedures in place that include:
Standard 1: Rights: Each person receives a service that promotes and respects their legal and human rights and enables them to exercise choice like everyone else in the community.
Standard 4: Feedback and complaints: When a person wants to make a complaint, the service provider will make sure the person’s views are respected, that they are informed as the complaint is dealt with and have the opportunity to be involved in the resolution process.
Standard 6: Service Management: Service providers are well managed and have strong and effective governance to deliver positive outcomes for people they support.
2.3 Types of abuse and neglect
Abuse and neglect is used throughout the Policy to describe behaviour or actions that cause harm, whether physical, emotional or financial, to a person with disability. The types of abuse and neglect referred to in this Policy are defined below in Section 5 - Table 2, however they are not limited to these. Definitions, examples and signs of abuse and neglect are also provided.
Abuse as it is used throughout this Policy refers to sexual assault, physical, emotional, financial and systems abuse, domestic violence, unauthorised use of restraints and restrictive practices, and neglect. When abuse and neglect occurs in the person’s home by other residents, professionals, paid and unpaid carers, family members and friends, it is accepted practice to define violence within any of these relationships and living situations as domestic violence.
Abuse and Neglect Policy, V1.0 January 2016 5

3 Principles
The following principles apply to ADHC operated and funded non-government disability support services.
ADHC funded non-government disability support services must ensure that the intent of the Principles is reflected in their operational procedures.
ADHC acknowledges that prevention is the best protection from abuse and neglect. Service providers have a duty of care to implement prevention strategies that include suitable recruitment screening processes and protocols for identifying the risk indicators for abuse and neglect. Refer to FACS Probity in Employment for FACS Funded Disability Service Providers 2015.
ADHC is committed to implementing the Zero Tolerance Framework (the Framework) outlined by National Disability Services. The Framework provides specific strategies for service providers to improve prevention, early intervention and responses to abuse, neglect and violence experienced by people with disability2. For further information about the Framework see the Abuse and Neglect Prevention Guidelines.
3.1 Person centred approaches
People with disability remain at the centre of prevention and responses to abuse and neglect. A person centred approach involves:
Providing positive support for people to exercise choice and control over their
lives, by facilitating and maintaining relationships and connection to
communities.
Listening and learning to understand the way people communicate, including
their communication preferences and wishes.
Keeping people informed about what is going to happen before taking action
and throughout any response to abuse and neglect.
Ensuring that people with high support needs and/or communication difficulty
are well supported to enable detection and prevention of abuse and neglect.
Providing information in a format that supports the person (for example, plain
English, Communication Pictographs (COMPIC), photos, picture cards, audio
hearing), and as relevant, their family and friends, to identify and report abuse
or neglect.
Ensuring appropriate physical, emotional and psychological support is
available to and easily accessible by a person following an allegation or report
of abuse or neglect.
3.2 Identifying abuse and neglect
2 NDS Zero Tolerance Framework: http://www.nds.org.au/projects/article/194
Abuse and Neglect Policy, V1.0 January 2016 6

Paid and unpaid workers supporting people with disability understand the types, behaviours and actions that constitute abuse and neglect (Section 4). Refer to the NSW Ombudsman’s information sheet, Guide for Services: Reportable incidents in disability supported group accommodation.
Paid and unpaid workers supporting with people with disability can recognise signs that may indicate abuse and neglect (Section 6).
Service providers recognise that people with challenging behaviour, and people who have difficulty communicating, can be at greater risk of abuse and neglect.
Service providers take measures to ensure people with disability, and their family and carers and employees are not victimised or harassed in any way for making an allegation.
Service providers ensure that procedural fairness in decision making is fair and reasonable. Refer to the NSW Ombudsman Fact Sheet for information on the principles of procedural fairness and decision making for Public Sector agencies3.
3.3 Prevention
Prevention strategies should provide for the employment of skilled staff who respect the rights of people with disability, who are aware of current policies and legislation pertaining to abuse and neglect, and who will support people and their families or guardians to access complaint mechanisms and raise any concerns they have about services.
The Disability Inclusion Act 2014 requires Family and Community Services (FACS) and FACS funded non-government disability support service providers to perform certain checks at the recruitment stage when employing or appointing a person to work with people with disability. These include the:
National Criminal History Record Check for “relevant workers” employed by FACS to provide disability supports and services directly to people with
disability in a way that involves face to face or physical contact.
Working with Children Check for any paid and unpaid workers in any roles
working with or in the vicinity of children or young people, (anyone aged under
18 years of age) in accordance with the Child Protection (Working with
Children) Act 2012 (the Act) and the Child Protection (Working with Children)
Regulation 2013.
Refer to Disability Inclusion Act 2014 FACS Fact Sheet 4 and the FACS Working with Children Policy 2015 for further information.
Also see the ADHC Abuse and Neglect Prevention Guidelines.
3 http://www.ombo.nsw.gov.au/__data/assets/pdf_file/0017/3707/FS_PSA_14_Natural_justice_Procedural_fairness.pdf
Abuse and Neglect Policy, V1.0 January 2016 7

Paid and unpaid staff
Service providers take reasonable steps to ensure that all paid and unpaid workers understand and perform their roles in preventing abuse and neglect of a person with disability by another person.
People with disability
Service providers take reasonable steps to ensure that all people with disability understand what constitutes abuse and neglect, how to protect themselves, how to make a report of abuse or neglect, and to know their rights if they are abused or neglected.
3.4 Early intervention
Service providers implement protocols that minimise the risk of abuse and neglect to the people they support.
3.5 Reporting abuse and neglect
Procedures for reporting abuse and neglect, or suspected abuse or neglect, and the responsibilities of all parties, are clearly articulated.
All paid and unpaid workers are aware of their duty of care to report allegations of abuse in accordance with the service provider’s documented procedures.
Services promote a positive complaints culture that welcomes feedback, and responds promptly to concerns from people, families, friends and carers.
The culture of the organisation or service encourages and supports any person who has witnessed abuse or neglect of a person or persons, or suspects that abuse or neglect has occurred.
Barriers to the disclosure of abuse and neglect are identified and removed, and people who report abuse or neglect are free from retribution. It is an offence to disadvantage a person who reports an incident of abuse and neglect or complains about the provision of services.
3.6 Responding to a report of abuse or neglect
Response is prompt, appropriate and in accordance with clearly documented procedures.
Where necessary the response includes a report to the NSW Police, and the provision of medical care, including transfer to hospital by an ambulance, and referral to a Sexual Assault Service, if the assault is of a sexual nature.
When the victim is unable to give consent, the family, guardian or other support person is notified of the incident as soon as possible.
If it is appropriate and the victim has given consent, the family, guardian or other support person is informed of the allegation of abuse or neglect as soon as possible after the report is made.
The safety of alleged victims is maintained throughout the investigation.
Abuse and Neglect Policy, V1.0 January 2016 8

All parties are encouraged and assisted to access appropriate supports following an allegation of abuse or neglect.
Refer to the ADHC Abuse and Neglect Procedures and FACS Incident Reporting and Management Policy and Guidelines for people accessing Ageing and Disability Direct Services 2014 for direction on responding and reporting when abuse and neglect occurs or is suspected.
3.7 Responding to abuse and neglect of a person with disability by a member of staff or by another person with disability
All incidents and allegations of abuse and neglect are documented and reported to a manager – refer to the ADHC Abuse and Neglect Procedures and FACS Incident Reporting and Management Policy and Guidelines for people accessing Ageing and Disability Direct Services November 2014.
All reasonable steps are taken to ensure that all people are protected from further harm.
The rights of the alleged offender and responsibilities of the employer are adhered to in accordance with the appropriate legislation.
3.8 Privacy and confidentiality
Access to records is restricted to those who are directly involved in reporting and responding to the incident or allegation to ensure that a person’s right to privacy is upheld.
A designated person is appointed to be the sole contact for the person, family, guardian or other support person, when providing information about the incident or allegation and subsequent investigations.
3.9 Resolution
Service providers will address the nature and impact of the incident or allegation from a person’s perspective. This will help to determine whether the person has experienced abuse or neglect, a breach of rights and trauma as a separate and equal consideration.
4 Identifying abuse and neglect
Observed abuse and neglect
Staff of accommodation support services, or any other service accessed by people with disability, are most likely to observe incidents of abuse or neglect towards people.
Reported abuse and neglect
Abuse and Neglect Policy, V1.0 January 2016 9

Abuse and neglect may be reported directly to staff by the victim or by another person with disability who has observed the incident or multiple incidents. A support worker or any other person, may observe that abuse or neglect of a person or persons, and report it to an appropriate person such as a line manager.
Suspected abuse and neglect
A disability worker or any other person may detect unusual behaviors or events that could be indicators of abuse or neglect of a person with disability. Another carer, a family member or a guardian who knows a person well and has reason to suspect that the person is being abused or neglected should inform a manager or in the case where that particular manager is suspected, another manager. Any other person who is not necessarily familiar with the person but suspects an abusive or neglectful situation, should also report a suspicion to a manager who knows or is involved in the person’s circle of friends.
5 Patterns of abuse and neglect
A pattern of abuse and neglect occurs where there is repeated physical abuse or ill treatment and/or harassment of a person with disability by another person.
The types of patterns that abuse and neglect occur are provided in the table below.
Table 1: Patterns of abuse and neglect
Type Definition and examples
Long term abuse Abuse that occurs over a period of time. E.g. Can occur in the context of family or other ongoing living arrangement.
Serial abusing Perpetrator seeks out vulnerable individuals, and abuses several persons according to a pattern. E.g. Sexual abuse usually falls into this pattern, as do some forms of financial abuse.
Opportunistic abuse
Where a person takes advantage of an opportunity or exploiting opportunities and situations in general, especially in a devious or unprincipled way. E.g. Because a person has access to another person’s bank account, and they take their money.
Opportunistic abuse is also referred to as situational abuse.
Neglect A person’s needs are neglected because those around him or her are unable to provide care or there is a lack of services or inappropriate services. This includes failure to provide access to key services such as health care, dentistry or prosthesis. E.g. a staff member does not respond to a person communicating they are not feeling well and need to see a doctor.
Abuse and Neglect Policy, V1.0 January 2016 10

Type Definition and examples
Institutional abuse The features are poor care standards, lack of positive responses to complex needs, rigid routines, inadequate staffing and insufficient knowledge within the service/s. E.g. not rostering enough staff on shift to meet the needs of the people requiring support.
Unacceptable ‘treatments’ or programs
Punishment such as withholding of food and drink, seclusion, unnecessary or unauthorised use of control or restraint or over-medication or the unlawful administration of prescribed medications are unacceptable treatments. E.g. giving a person more medication then they have been prescribed.
Failure of agencies
Agencies are responsible for ensuring that staff receive appropriate guidance on antidiscrimination practice and cultural sensitivity. E.g. not providing staff with training on anti-discrimination and/or cultural sensitivity.
Misappropriation Use of the person’s money by others, fraud or intimidation. E.g. staff using a person’s money to buy something for themselves.
Abuse and Neglect Policy, V1.0 January 2016 11

Table 2: Types of abuse4
Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
Physical Any non-accidental physical injury Roughly handling a person while Inconsistent and vague or unlikely abuse or injuries to a child or adult by
any other person. This includes but is not limited to inflicting pain of any sort, and causing harm or injuries or causing bruises, fractures, burns, electric shock or any unpleasant sensation.
providing supports such as personal care or transfers.
Hitting, smacking, biting, kicking, pulling limbs, hair or ears, striking with closed or open hand or with an implement of any kind.
Dragging, carrying or pushing people who do not want to be moved unless involuntary relocation is part of a behaviour management plan or emergency response.
Unauthorised physical restraint.
Threats of violence.
Leaving someone on the toilet too long or not taking them to the toilet when they need it.
Bathing in water too hot or too
explanation for injury
Unexplained injuries:
- broken bones, fractures,
sprains, bruises, burns, bite
marks, scratches or welts in
various stages of healing
Other bruising and marks may suggest the shape of the object that caused it
Avoidance or fearful of a particular person or staff member or over compliance to staff
Frequent and overall drowsiness
Out of character aggression
4 These formal definitions of abuse and neglect – National Disability Abuse and Neglect Hotline http://www.disabilityhotline.net.au/what-is-abuse-and-neglect/formal-definitions-of-abuse-and-neglect/
Abuse and Neglect Policy, V1.0 January 2016 12

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
cold.
Inappropriate administration of alcohol or other drugs.
Inappropriate kinds of discipline including withholding food or removing essential equipment.
Unauthorised Restraining or isolating an adult Physical restraint – prolonged use Broken or unmaintained aids or restraints and for reasons other than medical on any part of a person’s body to equipment that restricts a person’s restricted necessity or the absence of a less restrict their free movement. movement e.g. uncharged battery practices restrictive alternative to prevent
self-harm.
This may include the use of chemical, physical, mechanical, psycho- social and seclusion as a means or the denial of basic human rights or choices such as
Chemical restraint – inappropriate use of medication to control a person’s behaviour.
Mechanical restraint – the inappropriate use of a device to restrict the free movement of a
on a wheel chair.
Overdose of medication.
Locks on outside of bedroom doors.
Locks on food pantry and refrigerators without Restrictive
religious freedom, freedom of association, access to property or resources or freedom of movement. These practices are not considered abuse if they are applied under a Restricted Practice Authorisation and a Behaviour Support Plan (refer to Behaviour Support Policy).
person.
Psycho-social restraint – the use of verbal communications and/or threats of social or material punishment which elicit fear and restrain a person’s behaviour.
Seclusion – involves confinement in a room or area, in which an exit is prevented: or where a person
Practice Authorisation.
Abuse and Neglect Policy, V1.0 January 2016 13

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
believes they cannot or should not leave a room without permission.
Sexual Any sexual contact between an Anal or vaginal intercourse without
Direct or indirect disclosure. assault/abuse adult and child under 16 years of
age or any sexual activity with an adult who is unable to understand, has not given consent, is threatened, coerced or forced to engage in sexual behaviour.
Sexual assault is any unwanted sexual act or behaviour which is threatening, violent, forced or coercive and to which a person has not given consent or was not able to give consent, including sex with a person in a position of care or authority.
consent.
Fingers or object inserted into vagina or anus without consent.
Cunnilingus or fellatio without consent.
Masturbation of another person without consent.
Indecent exposure.
Masturbation by a person in the presence of the victim.
Voyeurism.
Displaying pornographic photography or literature.
Sexually explicit comments, inappropriate conversations of a sexual nature.
Bruises, pain, bleeding including redness and swelling around breasts and genitalia.
Torn, stained or bloody under clothing, or bedding.
Repeating the word or sign e.g. ‘bad’, ’dirty’.
Presence of sexually transmitted disease.
Pregnancy.
Sudden changes in behaviour or temperament, e.g. depression, anxiety attacks (crying, sweating, trembling, withdrawal, agitations, anger, violence, absconding, seeking comfort and security).
Sleep disturbances and refusing to go to bed, going to bed fully clothed.
Refusing to shower or constant
Abuse and Neglect Policy, V1.0 January 2016 14

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
showering.
Psychological Verbal assaults, threats of Treating people in ways that deny Depression, withdrawal, crying. or emotional maltreatment, harassment, them of their dignity.
Secretive and trying to hide abuse and humiliation or intimidation or
Humiliating a person for losing information and personal verbal abuse failure to interact with a person or
failure to acknowledge that person’s presence. This may include the use of chemical or physical means or the denial of basic human rights or choices such as religious freedom, freedom of association, access to property or resources or freedom
control of their bladder or bowel or about other private matters.
Denying cultural or religious needs such as serving pork to Jewish or Muslim persons.
Not allowing a person to express themselves out of fear of retaliation.
belongings.
Speech disorders.
Weight gain or loss.
Feelings of worthlessness about life and self; extreme low self-esteem self-abuse or self destructive behaviour.
of movement. Discouraging personalisation of rooms or clothing.
Limiting social freedom available to people.
Criticising, teasing, belittling, insulting, rejecting, ignoring and isolating a person.
Making a person beg for help.
Shouting orders to people.
Verbal taunts, humiliation,
Extreme attention seeking behaviour and other behavioural disorders (e.g. disruptiveness, aggressiveness, bullying).
Excessive compliance.
Abuse and Neglect Policy, V1.0 January 2016 15

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
intimidation and insults (bullying).
Removing aids or equipment (such as wheelchair or communication device).
Domestic Domestic violence is a range of Any form of abuse that occurs in a Depression, withdrawal, crying. violence abusive behaviours perpetrated in
the victim’s home by someone who is well-known to them.
person’s home including:
- Physical abuse
- Sexual abuse
- Sexual assault
- Restricted practice and
restraints
- Psychological or emotional
abuse and verbal abuse
- Financial abuse
- Systems abuse
- Legal or civil abuse
- Neglect
- Wilful deprivation
- Passive neglect
- Emotional neglect
Feelings of worthlessness about life and self; extreme low self-esteem self-abuse or self destructive behaviour.
Extreme attention seeking behaviour and other behavioural disorders (e.g. disruptiveness, aggressiveness, bullying).
Excessive compliance.
Financial abuse
The improper use of another person’s assets or the use or withholding of another person’s
Denying a person access to or control over their money when they have a demonstrated
Sudden decrease in bank balances.
No financial records or incomplete
Abuse and Neglect Policy, V1.0 January 2016 16

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
resources. capacity to manage their own finances.
Denying a person access to information about their personal finances.
Taking a person’s money or other property without their consent (which is likely to be a criminal offence).
Forcing changes to wills or other legal documents. Having cheques or credit card payments forged, or using a person’s personal banking cards without their authorisation.
Using a person’s belongings for personal use.
The improper use of another person’s assets or the use or withholding of another person’s resources.
records kept of expenditure and purchases.
Person controlling finances does not have legal authority.
Sudden changes in banking practices.
Sudden changes in wills or other financial documents.
Unexplained disappearance of money or valuable possessions.
Person has insufficient money to meet budgetary needs.
Person is persistently denied outings and activities due to lack of funds.
Borrowing, begging, stealing money or food.
Systems Failure to recognise, provide or Service providers arriving late or Over or under use of medication. abuse (also attempt to provide adequate or leaving early (without agreement).
Over or under use of restrictive includes wilful appropriate services, including
Relevant policies and procedures practices. deprivation) services that are appropriate to
Abuse and Neglect Policy, V1.0 January 2016 17

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
the person’s age, gender, culture, are not implemented. Lack of staff to provide necessary needs or preferences.
People are denied the option to make decisions affecting their lives.
Unacceptable staff attitudes have become normalised.
Lack of policy awareness and inadequate staff training and education.
Service or social isolation.
Not identifying and reporting abuse and neglect.
A person with disability is dependent on one person or service for all support.
Not providing people with disability access to a telephone, internet or significant others or a way to independently leave the house.
Failure to provide adequate or appropriate services.
support.
Provision of care by a staff person with whom the person feels uncomfortable or unsafe.
Ignoring a person when they ask for help.
Intentionally making a person wait for help.
Neglecting to recharge the battery of a person’s wheelchair.
Providing physical care in a way that is unnecessarily rough or careless.
Refusing to provide help unless the person agrees to lend money.
Purposely unplugging or turning off or not maintaining adaptive equipment.
Legal or civil abuse
Denial of access to justice or legal systems that is available to other
Denial of access to justice or legal systems that is available to other
Abuse and Neglect Policy, V1.0 January 2016 18

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
citizens. citizens.
Denial of access to protection.
No legal support or representation with known reports of abuse.
Neglect Neglect is a failure to provide the necessities of care, aid or guidance to dependent adults or children by those responsible for their care
Failure to provide the following:
- supervision for long periods of
time when the risk of
foreseeable harm or injury to
the person requiring care is
high
- adequate nutrition, clothing or
personal hygiene
- clean clothing
- appropriate health care or
medical treatment
- safe environment
- social interaction and
engagement
Denying or withhold food or drink for example, because a person has not completed a task
Hurrying or rushing assistance
Inappropriate or inadequate shelter or accommodation
Hunger and/or weight loss
Requesting, begging, scavenging or stealing food
Constant fatigue, listlessness or falling asleep
Direct or indirect disclosure
Extreme longing for company
Poor hygiene
Inappropriate or inadequate clothing for climatic conditions
Unattended physical problems or medical needs
Social isolation
Loss of social and communication skills
Abuse and Neglect Policy, V1.0 January 2016 19

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
with eating or drinking to fit in with staff timetables rather than the person’s need
Withdrawal or denial of privileges planned outing or personal items that are not designated and planned behaviour management strategies
Displaying inappropriate or excessive self-comforting behaviours
Physical neglect
Failure to provide adequate food, shelter, clothing, protection, supervision, medical and/or dental care, or to place persons at undue risk through unsafe environments or practices.
Not supporting the person to maintain hygiene.
Not providing adequate medical or dental care.
Unmaintained house.
Failing to report hazards.
Not completing annual comprehensive health, risk and swallowing assessments.
Improper sleeping, cooking, bathing arrangements.
Unclean and unsanitary living conditions.
Poor grooming – overgrown finger and toe nails, unclean hair, unshaven, unbathed, wearing dirty or damaged clothing.
Smelling of urine or faeces.
Emotional The failure to support and Ignoring a person. No social or recreation activities. neglect encourage, protect and provide
stimulation needed for the social, intellectual and emotional growth or well being of an adult or child.
Forced isolation.
Depriving a person of their right to express their cultural identity, their sexuality or other desires.
No day time or work activities.
No family contact.
No means of communication.
Abuse and Neglect Policy, V1.0 January 2016 20

Types of abuse
Description Examples of abuse Behavioural indicators and physical signs that abuse may be occurring
Not using a communication device to enable expression of needs or other communication.
Passive A caregiver’s failure to provide or Denial of dental or medical care, Not using equipment and neglect withholding of the necessities of
life, including food, clothing and shelter or medical care.
therapeutic devices or other physical assistance.
Failure to provide proper food – lack of fresh fruit and vegetables.
therapeutic devices as prescribed by a health professional for a person with a disability for example; no lap strap fixed when transporting a person in a wheel chair; inadequate pressure care, not positioning a person properly etc.
Very hungry or thirsty.
Inadequate supply of fresh food.
Unattended medical and dental issues.
Unclean and unsanitary living conditions.
Ripped or torn clothing.
Not enough warm clothing.
Abuse and Neglect Policy, V1.0 January 2016 21

6 Incidents of abuse and neglect reportable to the NSW Ombudsman
Reportable incidents of abuse and neglect in disability accommodation, flexible or centre based respite, or any service that provides direct care to people must be reported to the NSW Ombudsman under the Disability Inclusion Act 2014.
Under Part 3C Protection of People with Disability of the Ombudsman Act 1974 (NSW) all incidents of abuse or neglect of people with disability, living in supported group accommodations (including centre-based respite) that are operated or funded by FACS under Part 5 of the Act, are reported to the NSW Ombudsman.
Each service has a responsibility to report incidents to the NSW Ombudsman. The disability reportable incidents scheme is allegations-based which means that it is the nature of the alleged conduct (and not the finding of any inquiries) that will decide whether or not an incident is notifiable.
There are four categories of ‘reportable incidents’ reported to the NSW Ombudsman. Any of the following involving a person with disability living in supported group accommodation
1. Employee to person with disability incident
2. Client to client incidents
3. Contravention of an apprehended violence order taken out to protect the
person with disability
4. Unexplained serious injury to a person with disability.
The ADHC Reportable Incidents team is responsible for supporting ADHC operated services to report and review the remaining reportable incidents categories. Managers are required to provide the ADHC Reportable Incident team with all documentation relevant to the reportable incident and the clients involved within five business days of the incidents occurring for further information refer to Abuse and Neglect Procedures 2015, section 2.6.
The Professional Conduct Ethics and Performance unit retains responsibility for employee to client incidents they coordinate the processes to be followed dealing with allegations of staff misconduct for further information refer to FACS Incident Reporting and Management Policy and Guidelines for people accessing Ageing and Disability Direct Services 2014.
For a description of the four categories, refer to the NSW Ombudsman Guide for Services: Reportable incidents in disability supported group accommodation in Other Resources5 or Section 9 of this document.
Reportable incidents are reported in accordance with the FACS Incident Reporting and Management Policy and Guidelines for people accessing Ageing
5 NSW Ombudsman https://www.ombo.nsw.gov.au/news-and-publications/publications/fact-sheets/community-and-disability-services/guide-for-services-reportable-incidents-in-disability-supported-group-accommodation
Abuse and Neglect Policy, V1.0 January 2016 22

and Disability Direct Services November 20146 and the Disability Inclusion Act 2014.
7 Critical incidents involving children and young people reportable to the Children’s Guardian
Under Schedule 3 of the Children and Young Persons (Care and Protection) Regulation 2012, all designated agencies accredited to arrange for the provision of statutory out-of-home care in NSW, are required to notify the Children’s Guardian, in writing, of any allegation of sexual misconduct or serious physical assault towards a child or young person in out-of-home care, committed by a child-related worker.
The term sexual misconduct includes sexual offences. These offences include:
Indecent assault
Sexual assault
Aggravated sexual assault
Sexual intercourse and attempted sexual intercourse
Possession / dissemination / production of child pornography or child
abuse material
Using children to produce pornography
Grooming or procuring children under the age of 16 years for unlawful
sexual activity
Deemed non-consensual sexual activity on the basis of special care
relationships.
There are three categories of sexual misconduct in addition to the sexual offences listed above. These include:
Crossing professional boundaries
Sexually explicated comments and other overtly sexual behaviour
Grooming behaviour
A physical assault is considered serious where:
It results in the child being injured, beyond a type of injury like a minor
scratch, bruise or graze; or
It had the potential to result in a serious injury; or
The injury suffered may be minor, but the assault is associated with
aggravating circumstances.
6 http://dadhc-intranet.nsw.gov.au/documents/policies/FACS-Incident-Reporting-and-Management-Policy-ADDS.pdf
Abuse and Neglect Policy, V1.0 January 2016 23

The Office of the Children’s Guardian has developed resources for employers to assist in understanding what the above constitutes. ‘Information for reporting bodies – reporting certain misconduct involving children’ is a useful resource for all designated agencies and is published on the Office of the Children’s Guardian website7.
The Office of the Children’s Guardian will maintain a record of these allegations. This information will be taken into account as part of ongoing assessments of a designated agency as part of continued accreditation to arrange for the provision of statutory out-of-home care in NSW.
The requirement to notify allegations of sexual misconduct does not preclude an agency for their responsibility to report to the Office of the Children’s Guardian, following an investigation, of any finding that sexual misconduct or serious physical assault occurred.
A form is available for these notifications and is located at the link http://www.kidsguardian.nsw.gov.au/out-of-home-care/statutory-out-of-home-care/fact-sheets and in the Abuse and Neglect Other Resources.
8 Policy links
ADHC Behaviour Support Policy May 2012
ADHC Child Protection: Responding to Allegations Against Employees: Policy and Procedures May 2010
Child Protection Guidelines: What ADHC staff need to know about child protection May 2014
Child Protection Fact Sheet: Child protection laws: What ADHC staff should know, Oct 2013
NSW Mandatory Reporter Guide: Keeping Them Safe - A share to child well being, December 2014
Code of Ethical Conduct, September 2013
Criminal Records Check
Decision Making and Consent Policy and Procedures
Engagement of Agency Staff, September 2007
FACS Aboriginal Strategy 2013-2015
FACS Aboriginal Cultural Inclusion Framework 2015-2018
FACS Community Complaints Policy for Ageing and Disability Direct Services, September 2014
FACS Community Complaints Guidelines for Ageing and Disability Direct Service, September 2014
FACS Cultural Diversity Framework 2014 – 2017
7 http://www.kidsguardian.nsw.gov.au/
Abuse and Neglect Policy, V1.0 January 2016 24

FACS Incident Reporting and Management Policy for people accessing Ageing and Disability Direct Services November 2014
FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services November 2014
FACS Probity in Employment for FACS funded disability service providers (2015)
FACS Statement of Commitment
FACS Working with Children Policy 2015
Fraud and Corruption Prevention Policy, May 2012 and Prevention Plan May 2012
Resolution of Workplace Grievances Policy April 2005
Risk and Safety Policy 2015
Service Charter of Standards for Aboriginal Clients
Sexuality and Relationship Guidelines 2015
Standards in action – Practice requirements and guidelines for services funded under the Disability Service Act 1993, edition June 2012 (repealed December 2014).
Addendum Guide Services Working With Children and Young People, January 2014
Working with Children Check
FACS Public Interest Disclosures Internal Reporting Policy, November 2013 and Procedures for managing Public Interest Disclosures
9 Legislative context
Carers Regulation 2010 NSW
Children and Young Persons (Care and Protection) Act 1998
Children and Young Persons (Care and Protection) Regulation 2012, Schedule 3
Child Protection (Working with Children) Act 2012
Child Protection (Offenders Regulation Registration) Act 2000
Community Services (Complaints, Reviews and Monitoring) Act 1993 (CRAMA)
Crimes (Domestic and Personal Violence) Act 2007 and Amendment Act 2008 No: 119
Criminal Procedures Act 1986
Criminals Record Act 1991
Disability Inclusion Act 2014
Government Information (Public Access) Act 2009 (GIPA Act)
Guardianship Act 1987
Abuse and Neglect Policy, V1.0 January 2016 25

Independent Commission Against Corruption Act 1988
Law Enforcement (Powers and Responsibilities) Act 2002
Mental Health (Criminal Procedure) Act, 1990
NSW Crimes Act 1900 and Section 316
NSW Crimes (Forensic Procedures) Act 2000
Ombudsman Act 1974 (NSW) Part 3C Reportable Incidents
Privacy and Personal Information Protection Act, 1998
The Home Care Service Act, 1988
The Public Interests Disclosure Act 1994 (NSW)
Victims Rights and Support Act 2013
10 Definitions
Table 3: List of terms, keywords and/or abbreviations used throughout this document. Many are adapted from definitions in the Ombudsman’s Guide for services: Reportable incidents in disability supported group accommodation8.
Term Definition
Advocate A person who promotes supports and represents the rights and interests of another person. An advocate is often involved in acting, speaking or responding on behalf of another person for people with disability who are supported in ADHC operated or funded non-government disability support services.
Ageing, Disability and Home Care (ADHC) services
Services provided directly by NSW Family and Community Services to people who are ageing and/or with disability. These include accommodation, flexible and centre-based respite, day program services or other services where ADHC staff provide direct care to a person with disability.
Allegation A claim or assertion that someone has done something illegal or wrong, often one made without proof.
Apprehended violence order
The term Apprehended Violence Order (AVO) has the same meaning as in the Crimes (Domestic and Personal Violence) Act 2007.
An AVO is a protection order that is made by a court, to provide a person at risk of experiencing violence by another person, with legal protection from the person who is threatening violence.
Assault Assault, as described in the Crimes Act 1900, is against
8 NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group accommodation. December
2014
Abuse and Neglect Policy, V1.0 January 2016 26

Term Definition
the law. For the purpose of this policy assault is any unwanted physical contact, or attempt or threatened attempt to cause physical contact or bodily harm that puts the victim in fear of such harm or contact.
The NSW Ombudsman defines assault in relation to the reportable incident scheme as an act by which a person intentionally inflicts unjustified use of physical force against a person with disability. An assault can also occur if a person causes a person with disability to reasonably fear that unjustified force will be used against them. Even if a person who inflicts, or causes the fear of, physical harm does not intend to inflict the harm or cause the fear, they may still have committed an assault if they acted recklessly (i.e. the person ought to have known that their actions would cause physical harm or the fear of such harm)9 .
Crimes of A failure to act where there is a duty to act. E.g. where a omission disability support worker has a duty to feed and care for
someone and they do not provide food to the person or other care which results in harm to that person for which the worker could then be charged with a criminal offence.
Deemed sexual offences
Includes carer and exploitation offences under section 66F the Crimes Act 1900 (NSW). Irrespective of the consent of a person, the Crimes Act 1900 prohibits sexual intercourse in the following circumstances:
Between a person with a cognitive impairment and a
person who is responsible for the care of that person
(the ‘carer’s offence’ s.66 F(2)), and
Between a person with a cognitive impairment and any
other person who has the intention of taking advantage
of that person’s cognitive impairment (the ‘exploitation
offence’ s.66 F(3)).
Note also that consent by a person with a cognitive impairment to indecent assault or act of indecency by a carer or person intending to take advantage of a person with a cognitive impairment is not a defence. s.66F (6).
Domestic Domestic violence is a range of abusive behaviours violence perpetrated in the victim’s home by someone who is well-
known to them. People with intellectual disability live in a wide range of domestic situations such as institutions, hostels and group homes where they have daily
9 = NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group accommodation. December 2014
Abuse and Neglect Policy, V1.0 January 2016 27

Term Definition
relationships with other residents, professionals, paid and unpaid carers, family members and friends who all could be potential perpetrators of domestic violence. It is accepted practice to define violence within any of these relationships and living situations as domestic violence.
Duty of care The requirement a disability service has to take reasonable care to avoid foreseeable harm to a person with disability.
Grooming behaviour10
The Ombudsman Guidelines say that behaviour should only be seen as ‘grooming’ behaviour where there is evidence of a pattern of conduct that is consistent with grooming the alleged victim for sexual activity and therefore is no other reasonable explanation for that pattern. The types of behaviour that may lead to such a conclusion include (but are not limited to):
persuading a person with disability or group of people
with disability that they have a ‘special ‘ relationship by: - Inappropriately giving gifts
- Inappropriately showing special favours to them but
not to others, or
- Asking the person to keep the relationship to
themselves.
‘Testing boundaries’, for example by:
- Undressing in front of a person with disability
- Encouraging inappropriate physical contact (even
when it is not overtly sexual), or
- ‘Accidental’ intimate touching. Extending a relationship with a person outside of their
usual reason for contact (except where it may be
appropriate – for example, where there is an existing
friendship with the person’s family, or as part of regular
social interactions in the community)
- Inappropriate personal communication (including emails, telephone calls, texts, messaging, social media and web forums) that inappropriately explores sexual feelings or intimate personal feelings with a person with disability.
Anyone (including staff) requesting that a person with disability keep any aspect of the relationship secret, would generally increase the likelihood that grooming is occurring.
10 Adapted from: NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group accommodation. December 2014
Abuse and Neglect Policy, V1.0 January 2016 28

Term Definition
Guardian11 A guardian is a person appointed to make legally valid decisions on behalf of a person with disability who is unable to make decisions on their own or without support. In NSW this occurs under the Guardianship Act 1987.
Refer to this link Public Guardian
A substitute decision-maker with authority to make personal or lifestyle decisions about the person under guardianship. A guardian is appointed for a specified period of time and is given specific functions (e.g. able to make decisions about where the person lives, or services and medical treatment the person receives). A guardian may be appointed who is a family member or friend provided the criteria set out in the legislation are satisfied. Otherwise, the Guardianship Tribunal will appoint the Public Guardian. A guardian must be 18 years and over.
See also Decision Making and Consent Policy and related resources.
Incident An incident is an event resulting in, or having the potential for, injury, ill health, damage or other loss.
Natural supports Natural supports are relationships that occur in everyday life. They include family, friends and other trusted people, neighbours, acquaintances, and people with shared interests. Natural supports enhance a sense of security and quality of life for people.
Part 3C reportable incident
Part 3C of the Ombudsman Act 1974 (NSW) requires that ‘reportable incidents’ are notified to the NSW Ombudsman. Reportable incidents are:
1. An incident involving any of the following in connection
with an employee (including agency staff, volunteers
and contractors) of FACS or a funded provider and a
person with disability living in supported group
accommodation:
i) any sexual offence committed against, with or in the
presence of the person with disability
ii) sexual misconduct committed against, with or in the
presence of the person with disability, including
grooming the person for sexual activity.
iii) an assault of the person with disability (not including
the use of physical force that, in all the
circumstances, is trivial or negligible, but only if the
matter is to be investigated under workplace
11 http://www.publicguardian.justice.nsw.gov.au/publicguardian/pg_guardianship/pg_whatisguard.html
Abuse and Neglect Policy, V1.0 January 2016 29

Term Definition
employment procedures)
iv) an offence under Part 4AA of the Crimes Act 1900
(fraud and similar offences) committed against the
person with disability
v) ill-treatment or neglect of the person with disability,
or
2. An incident involving an assault of a person with
disability living in supported group accommodation by
another person with disability living in the same
supported group accommodation that:
i) is a sexual offence, or
ii) causes serious injury, including, for example, a
fracture, burns, deep cuts, extensive bruising or
concussion, or
iii) involves the use of a weapon, or
iv) is part of a pattern of abuse of the person with
disability by the other person, or
3. An incident occurring in supported group
accommodation and involving a contravention of an
apprehended violence order made for the protection of
a person with disability, regardless of whether the order
is contravened by an employee of FACS or a funded
provider, a person with disability living in the supported
group accommodation or another person, or
4. An incident involving an unexplained serious injury to a
person with disability living in supported group
accommodation.
Pattern of abuse Repeated physical abuse or ill treatment and/or harassment of a person with disability by another person.
Abusive conduct includes the following, alone or in combination:
Abuse of a sexual or non-sexual nature
Physical force or inappropriate physical contact
Threats of physical force or threats of inappropriate
physical conduct
Conduct that causes physical harm or emotional
distress to the victim.
Person Someone who has the authority to consent to treatment for responsible an adult who is unable to give a valid consent to their own
medical or dental treatment. Sometimes, a person is unable to make the decision or does not understand what the treatment is about or its effects. In these cases, the
Abuse and Neglect Policy, V1.0 January 2016 30

Term Definition
person responsible can give substitute consent on behalf of the other person.
Reportable12
allegation An allegation against a person of a reportable incident or an allegation of behaviour that may involve a reportable incident.
Reportable conviction
A conviction (within the meaning of the Criminal Records Act 1991) of an offence involving a reportable incident under Part 3C of the Ombudsman Act 1974 (NSW).
Sexual13
misconduct Sexual misconduct includes a broad range of sexualised behavior with or towards people with disability in supported group accommodation.
Sexual misconduct involving people with disability includes (but not limited too) the following:
Sexualised behavior with or towards a person
Inappropriate conversations of a sexual nature
Inappropriate comments relating to sexual acts
Unwarranted and inappropriate touching of a person
Personal correspondence and communication
Inappropriate exposure of people to sexual behaviours
of others and/or
Watching people undress in circumstances where
supervision is not required and it is clearly
inappropriate.
Sexual offence14 The term ‘sexual offence’ encompasses all criminal offences involving a sexual element that are committed against, with, or in the presence of a person.
These offences include (but are not limited too):
Sexual assault – this is a broad term describing all
sexual offences. Sexual assault includes the specific
offence when a person has sexual intercourse with
another person without their consent. Sexual assault
also includes when a person is forced, coerced or
tricked into sexual acts against their will or without their
consent.
Aggravated sexual assault – involves sexual
12 NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group accommodation. December 2014
13 NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group accommodation. December 2014
Adapted from NSW Ombudsman Guide for Services: Reportable Incidents in disability supported group
accommodation. December 2014
Abuse and Neglect Policy, V1.0 January 2016
14
31

Term Definition
intercourse with another person without their consent in
circumstances of aggravation. Circumstances of
aggravation can include the offender seriously injuring
or threatening to seriously injure the person, breaking
into a home to commit the offence, or the victim having
a serious physical disability or cognitive impairment.
Indecent assault – involves touching (or threatening to
touch) a person’s body in a sexual manner without the
consent of the other person. For example, it can include
unwanted touching of a person’s breast, bottom or
genitals.
Deemed sexual offences – see “Deemed sexual
offences” above.
Support network People with disability accessing ADHC operated and funded non-government services have different types of support networks. People have families who are closely involved in their lives or may be reliant on legally appointed guardians to make particular decisions for them. Other people with disability are represented by advocacy services and for some people these advocates are their only support network.
Support person In the context of this policy a person with a disability who is either a victim or offender of an act of abuse or neglect, may be required to talk to the police, a sexual assault worker or representative of a legal or victim’s service, and will need support at these times. Under the Law Enforcement (Powers and Responsibilities) Regulation 2005 - a vulnerable person as defined in regulation 24 (person with disability) is entitled to have a support person present when a person is being interviewed by police (regulation 27).
The support person does not have the same function as the ‘person responsible’ and will not make decisions for the person with disability. However, it is someone who is a guardian or any other person who is responsible for the person or a relative or friend who has the consent of the detained person to be their support person. A support person’s role during an investigation procedure is to assist and support the person, observe whether or not the interview is being conducted fairly and to identify any communication problems with the person.
Abuse and Neglect Policy, V1.0 January 2016 32

11 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
Abuse and Neglect Policy, V1.0 January 2016 33

Abuse and Neglect Prevention Guidelines
Document name
Policy
Version number
Approval date
Policy manual
Approved by
Summary
Replaces document
Authoring unit
Applies to
Review date
Abuse and Neglect Prevention Guidelines
Abuse and Neglect
1.0
January 2016
Safeguarding Policy and Practice Manual
Deputy Secretary, ADHC
The Abuse and Neglect Prevention Guidelines provide paid and unpaid workers of ADHC operated and funded non-government disability support services, with information and resources to prevent abuse and neglect from occurring and strategies to intervene early when abuse or neglect is suspected.
New Prevention Guidelines
Contemporary Residential Options
People who are being supported in ADHC operated and funded non-government disability support services.
2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 The Prevention Guidelines are one of three documents (Policy, Procedures, and Prevention Guidelines) that replace the Abuse and Neglect Policy and Procedures December 2014.
Abuse and Neglect Prevention Guidelines, V1.0, January 2016 2

Table of contents
1 Purpose ..................................................................................................4
2 Zero Tolerance Framework...................................................................4
2.1 Understanding abuse and neglect ..................................................5
2.2 Primary prevention: Practices and safeguards................................8
2.3 Targeted prevention: Vulnerable groups .......................................13
2.4 Secondary prevention: Responding to abuse and neglect ............18
2.5 Tertiary prevention: Systemic issues.............................................20
3 Policy and Practice Unit contact details............................................22
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 3

1 Purpose
The Abuse and Neglect Prevention Guidelines (the Prevention Guidelines) is a guide for paid and unpaid workers of ADHC operated and funded non-government disability support services. It provides information and resources to prevent abuse and neglect from occurring and strategies for early intervention when abuse or neglect is suspected.
The types and definitions of abuse and neglect are outlined in the Abuse and Neglect Policy. Response procedures to abuse and neglect are discussed in the Abuse and Neglect Procedures. It is important to read the Guidelines in conjunction with the Policy and Procedures.
2 Zero Tolerance Framework
The Prevention Guidelines are written in the context of the National Disability Services (NDS) Zero Tolerance Framework (the Framework) which aims to provide disability services with practical support, tools and resources to improve prevention, early intervention and responses to abuse and neglect1.
The Framework has five layers (Diagram 1). In each of the following sections, each layer is discussed and good practice guidelines provided which are relevant to the support provided by ADHC operated and funded non-government disability support services.
Diagram 1: The Zero Tolerance Framework
Understanding abuse and Understanding types of abuse, neglect and neglect violence; prevalence and risk factors
Primary Prevention Promoting practices and safeguards which
prevent abuse and neglect
Targeted Prevention Identifying and addressing risk factors and
vulnerable groups
Secondary Prevention Responding to incidents and allegations of
abuse and neglect
Tertiary Prevention Identifying and addressing underlying
causes and systemic issues
1 NDS Zero Tolerance Framework
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 4

2.1 Understanding abuse and neglect
Knowing the types of abuse, neglect, and risk factors is important in preventing abuse and neglect. A clear understanding of the person’s rights, what constitutes abuse and neglect and how to respond, by the person and their support network, will greatly reduce the person’s exposure to abuse and neglect.
2.1.1 Incidents of abuse and neglect and risk factors
Abuse and neglect involves a person or a group of people exercising power and control over another. Abuse and neglect can occur as an isolated incident or be ongoing over a period of time. It can be intentional or unintentional, subtle involving coercion and deceit, or it can be explosive and violent.
In comparison to the general population, people with disability are more likely to experience abuse and neglect2. The abuse and neglect is more likely to be severe in impact, to involve multiple incidents, to be sustained over a long period of time and to involve multiple perpetrators3.
There are additional risk factors for people with disability that are not present in the general population. For instance, people with disability are more likely to experience abuse and neglect due to:
the unique environments where people live, work and socialise such as group homes, hostels, institutions, boarding houses, day programs and sheltered workshops
a dependency on others to meet physical and intimate support needs
an inability to express to others that abuse and neglect is occurring due to cognitive, communication and/or sensory impairment
being dependent on one person or service to provide all supports
being isolated from family, advocacy and community connections
having limited community participation due to transport costs and the availability of appropriate transport facilities.
People with disability are more likely to experience abuse and neglect by someone they know, either a family member, paid support worker or another person with disability4. The potential sources of abuse and neglect are provided in the following table.
2 Violence against women with disabilities – An overview of the literature. Women with Disabilities Australia. 3 Abuse Prevention Strategies in Specialist Disability Services. Commonwealth Department of Family and Community Services. 4 Learning from Complaints – Occasional Paper No.1 Safeguarding People’s Rights to be Free from Abuse – Key considerations for preventing and responding to alleged staff to client abuse in disability services, Disability Services Commission Victoria.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 5

Table 1: Potential sources of abuse and neglect
Direct support staff Have the greatest opportunity because they have extended periods of one to one contact with the person, are the providers of many of the necessities of life and assist with intimate activities such as bathing and hygiene. They may also have access to the person’s money.
Other support workers Have regular opportunities for unsupervised contact with people with disability and their property. They may also have access to the person’s money.
Management decisions
Management decision can intentionally and unintentionally restrict a person’s access to services, freedom of movement and expression, choice and control over matters of daily living.
Other people with disability
Are in regular and close contact with people with disability, some of whom may have diminished responsibility due to their own disability.
Visitors Have opportunities to spend time with individuals and build relationships based on trust that can later be violated.
Family Can spend extended periods of time with the person on their own, or away from staff and other people with disability, and may have unlimited access to finances and property.
Guardians, financial managers or trustees
Are in a position to make lifestyle and health related decisions about the person and can approve the use of the person’s finances.
Other Service providers
May have regular contact with the person away from carers and family and are in positions of trust.
Strangers Whenever the person is unsupervised or away from their usual environment they may be at risk of abuse and neglect from strangers.
2.1.2 Recognising warning signs
Support workers and management play an important role in protecting a person with disability from further harm by recognising the indicators of abuse and neglect and responding to them. The presence of one or more indicators does not mean that abuse and neglect has occurred but does require support workers to be vigilant on the person’s behalf.
Indicators of abuse and neglect are not always obvious, and while the person or others may suspect that abuse and neglect has occurred there might not be any evidence to confirm the suspicion. Indicators are variable, and people
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 6

who are familiar and have a strong positive relationship with the person, are best placed to recognise behavioural changes that may suggest abuse and neglect is occurring (refer to section 6 of the Abuse and Neglect Policy for behavioural indicators and physical signs of abuse and neglect).
2.1.3 Good practice guidelines
Understanding abuse and neglect
Understanding types of abuse, neglect and violence; prevalence and risk factors
Educate the person, their families and support workers on the right of the person to live a life free from harm as outlined in the Disability Inclusion Act 2014, the UN Convention of the Rights of Persons with Disabilities and ADHC’s Standards in Action.
Provide people with disability with information and access to resources in a format suitable to their communication style.
Use the Lifestyle Planning tools: What Am I Communicating To You, Communication Profile and Communication Chart to facilitate this.
Discuss the person’s relationships at the annual Lifestyle Planning meeting. Discuss with the person if they would like to extend their social and support network.
Use Lifestyle Planning tools to facilitate this such as the Relationship Map, History Map, Matching Tool and Presence to Contribution.
Provide resources and training to the person on what a healthy relationship looks like. Read and discuss the Sexuality and Relationship Guidelines with the person and their family.
Engage the person with services provided by Family Planning NSW (see Other Resources).
Ensure the person has a current My Safety Plan5 which addresses risk factors relating to abuse and neglect.
Provide copies of fact sheets, complaints processes and the National
Disability Abuse Hotline number (1800 880 052) to people and their
families on an annual basis.
Provide training to support workers and managers on abuse and neglect so that they have the information and skills to respond quickly when risk factors are identified and abuse and neglect is suspected.
Include abuse and neglect as a standard agenda item at team meetings to discuss, identify and respond to risk factors. Refer to Table 2 of the Abuse and Neglect Policy for the types, behavioural indicators and physical signs of abuse and neglect. Use the information in this table to prompt and facilitate discussion at team meetings.
Engage with marginalised groups such Aboriginal and Torres Strait Islanders, culturally and linguistically diverse groups, women’s and lesbian,
5 Refer to the ADHC Risk and Safety Policy and Procedures 2015
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 7
Understanding abuse and neglect
Understanding types of abuse, neglect and violence; prevalence and risk factors
gay, bisexual, transsexual, intersex or queer (LGBTIQ) groups to gain a better understanding of local needs and priorities and to help facilitate access to culturally appropriate resources and services.
If culturally appropriate resources are not available, encourage the person to access mainstream services.
2.2 Primary prevention: Practices and safeguards
Primary prevention relates to practices and safeguards which value and uphold the rights of people with disability to live a life free from harm. Primary prevention acknowledges that people who have greater control and ownership of their life are more likely to be able to maintain their own safety6. Primary prevention requires a multi-layered approach which takes into account the person, organisational structure and community perceptions of disability and abuse and neglect.
2.2.1 Community safeguards and practices
At the community level, primary prevention involves promoting at every opportunity the valued status of people with disability and their right to be active members of the community. This may involve addressing community attitudes which reinforce abuse and negative stereotypes of disability.
Practices at the community level include facilitating meaningful community connections to prevent isolation, engaging and involving the person’s family, fostering fulfilling relationships and natural supports, and ensuring access to advocacy when the person has no family or is unable to advocate for themselves.
For people living in institutions or group accommodation, external statutory bodies such as the NSW Ombudsman and Community Visitor program play a vital role in monitoring the quality of services and safeguarding the interests of people with disability7.
2.2.2 Organisational culture and practices
Embedding person centred approaches into organisational policy and practice is a fundamental safeguard to preventing abuse and neglect. Person centred approaches mean putting the person at the centre of all decision making and discussion. These approaches also promote positive attitudes and relationships between the person, their family and support staff.
6 NDS Zero Tolerance Framework 7 Learning from Complaints – Occasional Paper No.1 Safeguarding People’s Rights to be Free from Abuse – Key considerations for preventing and responding to alleged staff to client abuse in disability services, Disability Services Commission Victoria.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 8

The protection of people and prevention of harm will be enhanced by an organisational culture that provides the person with opportunities to express their needs and preferences. A healthy organisational culture also actively supports the person and staff to raise concerns about service delivery without fear of reprisal.
Effective prevention strategies include recruitment screening processes to protect people from exposure to individuals who have a history of harming vulnerable people. By adequately screening new recruits, organisations can maximise their chances of employing suitable individuals to work with people with disability from the start.
The Disability Inclusion Act 2014 requires Family and Community Services (FACS) and FACS funded non-government disability support service providers to perform certain checks when employing or appointing a person to work with people with disability. These include the:
National Criminal Record Check for “relevant workers” employed by FACS to provide disability supports and services directly to people with disability in a way that involves face to face or physical contact8
Working with Children Check for new and existing paid and unpaid workers engaged in child-related work in accordance with the Child Protection (Working with Children) Act 2012 and the Child Protection (Working with Children) Regulation 2013.
Refer to Disability Inclusion Act 2014 FACS Fact Sheet 49 and the FACS Working with Children Check Policy 2015 for further information.
Provide clear expectations of staff behaviour towards people with disability during orientation sessions. This can aid in the prevention of abuse and neglect by increasing support workers’ ability to recognise early signs of abuse and neglect, and to respond accordingly. Position descriptions which clearly outline the expectations of professional behaviour are crucial, as is regular training to reinforce appropriate behaviour and how to respond when abuse and neglect is suspected.
2.2.3 Empowering the person
At the individual level, primary prevention empowers the person to self-protect and communicate to others when abuse and neglect has occurred. Strategies include activities which develop the person’s self confidence, positive self image and assertive communication skills.
Understanding and addressing the barriers to people reporting abuse and neglect are important in identifying the practice and safeguards needed to prevent abuse. Barriers to reporting abuse and neglect are provided in Table 2.
8 FACS Employment Screening Policy 9 http://www.adhc.nsw.gov.au/about_us/legislation_agreements_partnerships/nsw_disability_inclusion_act
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 9

Table 2: Barriers to reporting abuse and neglect 10
Limited education and The person may have limited access to education training opportunities and training opportunities to understand their
rights, recognise abuse and neglect when it occurs and respond accordingly.
Isolation The person may have limited social and support networks which prevents opportunities to discuss and disclose abuse and neglect to others.
Fear The person may not report abuse and neglect as there is a fear of reprisal. The victim may fear further violence if they disclose the abuse and neglect to others including threats involving the safety of loved ones.
The person may have a reputation with authorities like the NSW Police and fear they will not be believed if they report the abuse and neglect.
The victim may fear the consequence of reporting the abuse and neglect. For instance the victim may depend on or have a perceived dependence on the perpetrator, and fear the loss of support.
The victim may fear the shame and embarrassment the abuse and neglect creates on the reputation of the family.
Person’s history The person’s history and circumstances will influence whether the person is at risk of becoming a victim or a perpetrator of abuse and neglect. For instance the person may have experienced abuse and neglect as a child and therefore have a distorted view of a safe and healthy relationship.
Reports of abuse and neglect may have been discounted when the person disclosed abuse and neglect to others in the past.
Language and The victim may rely on augmented or alternative communication communication strategies which unintentionally
limit the person’s vocabulary to describe and report abuse and neglect when it occurs. For instance key words such as ‘genitals’, ‘rape’ or ‘assault’ may be absent from the person’s vocabulary.
Views of disability and The person may have a lack of basic knowledge sexuality about sexuality and therefore not know what is or
may be assault.
People with disability are often believed to be
10 Responding to young people disclosing sexual assault: A resource for schools. ACSSA Wrap No.6
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 10

asexual or childlike and therefore sexuality is not openly discussed.
Discussion about sex may be discouraged in some environments such as the family home or group accommodation. This means the person may not have the opportunity to talk about what is happening to them.
Access to mainstream supports
Mainstream supports may not cater for a person with disability. For instance women’s refuges may not have staff trained to support a person with disability.
Victim’s services may only be available to women and not suitable or accessible to men who are victims of abuse and neglect.
2.2.4 Good practice guidelines
Primary Prevention Promoting practices and safeguards which
prevent abuse and neglect
Embed person centred approaches in to organisational policy and practices which are informed by national and international best practice.
Promote community inclusion and social participation. This includes promoting the valued status of people with disability at every level of the organisation and within the wider community.
Foster an organisational culture from the top down which supports respectful attitudes and relationships between staff, the person and their family.
Ensure recruitment practices are in line with requirements of the Disability Inclusion Act 2014.
During the recruitment process, focus on the values, attitudes and personal attributes of applicants to ensure they are in line with organisational values and person centred approaches to service delivery11 .
Implement clear internal feedback mechanisms which provide the person and their family with opportunities to communicate what is and isn’t working. This includes formal mechanisms such as complaints policies and procedures and informal mechanisms such as regular family meetings with frontline managers.
Ensure external safeguards are in place to oversee the quality of services by engaging with the Community Visitor, advocates and the NSW Ombudsman.
Inform the person and their family that they can request a visit from a
11 Learning from Complaints – Occasional Paper No.1 Safeguarding People’s Rights to be Free from Abuse – Key considerations for preventing and responding to alleged staff to client abuse in disability services, Disability Services Commission Victoria.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 11

Primary Prevention Promoting practices and safeguards which
prevent abuse and neglect
Community Visitor.
Address the barriers that prevent the person and support staff from identifying and reporting abuse and neglect (see Table 2).
Educate the person, their families and support workers on the right of the person to live a life free from harm as outlined in the Disability Inclusion Act 2014, the UN Convention of the Rights of Persons with Disabilities and the Standards of Action.
Always provide information to the person in a format suitable to their communication style.
Ensure the person has a meaningful Lifestyle Plan in place which addresses social participation and how they can achieve genuine connection with the community.
Use Lifestyle Planning tools to facilitate this such as the Relationship Map, Important To/For, Presence to Contribution, Working/Not Working.
Where possible, give the person the opportunity to control their services and decide who they want in their network of support.
Provide information and clear pathways to access resources which promote healthy relationships and the expression of the person’s sexuality.
Read and discuss the Sexuality and Relationship Guidelines with the person.
Engage the person with services provided by Family Planning NSW (see Other Resources).
Value and support the informal relationships in a person’s life as people are more likely to be safe when they are surrounded by enduring and genuine relationships with those who love and care for them.
Provide information and resources which develop the person’s ability to self protect. Follow through with skill development by regularly practicing self protection skills with the person.
Use the ‘Looking After Me’ Resource kit to educate people with disability about healthy relationships (refer to Other Resources).
Ensure staff read and understand key internal safeguarding policies such as the FACS Code of Ethical Conduct, Client Finances Policy and Procedures 2010 and the Fraud and Corruption Prevention Policy 2010.
Facilitate annual training for staff and managers on rights based legislation, policies, procedures and issues associated with abuse and neglect of people with disability such as, how to recognise abuse and neglect and respond.
Provide monthly staff supervision which promotes reflective practice, skill development and continuous improvement of services.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 12

2.3 Targeted prevention: Vulnerable groups
Targeted prevention involves the use of strategies to target groups within the community at greater risk of being the victims of abuse and neglect including:
People with disability
Women
Children
Aboriginal and Torres Strait Islanders
People from cultural and linguistically diverse backgrounds.
People with a sensory impairment are at greater risk of abuse and neglect as their ability to communicate may be limited or not understood by others. The person may not have the language to describe and report the abuse and neglect. When communication support strategies are absent or not understood by others, the person may communicate with their behaviour.
Behaviours of concern (previously referred to as challenging behaviour) as a form of communication can result from the person’s inability to be understood. People who display behaviours of concern are at risk of abuse and neglect as responses to manage the behavior may be unlawful, unethical and prohibited (prohibited practices12). The use of prohibited practices can be due to poor organisational culture, inadequate staffing levels and supervision of staff, the absence of staff training, poor attitudes towards the person and poor understanding of the disability13. Refer to the Behaviour Support Policy and Practice Manuals 2012 for details on the appropriate provision of behavior support.
The physical and sexual abuse and neglect of women with disabilities occurs in similar situations to all women. That is, they are most likely to be assaulted by someone they know, it is most likely to be a man, and will occur in a familiar and private place14.
Refer to section 2.1.1 for risk factors that expose people with disability to greater levels of abuse and neglect.
Domestic violence is often thought to occur between a person and an intimate partner however it also includes the abuse and neglect of a person by another resident(s), professional, paid or unpaid worker, family or friend in domestic situations such as institutions, hostels and group homes15.
Women and children are the main victims of domestic and family violence. Significantly, Aboriginal and Torres Strait Islander women are subjected to
12 Practices such as physical and chemical restraint, aversive strategies, denied access to basic needs and supports 13 Evidence-based guidelines to reduce the need for restrictive practices in the disability sector. The Australian Psychological Society 14 Understanding Violence Facts and Figures. Our Watch ltd. 15 Domestic violence fact sheet. Women’s Health NSW
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 13

16family violence at a rate six times higher than that of non-Aboriginal women . The prevalence of domestic violence in the community is thought to be much greater as most incidents of abuse and neglect are not reported17.
Social disadvantage plays a significant part in increasing the risk of abuse and neglect amongst vulnerable groups in the community. Some of the reasons for this are provided in Table 3.
Table 3: Risk factors of vulnerable groups
Gender inequality Women are the main victims of violence. The reason for this is complex and involves a power imbalance between males and females which is reinforced by political, cultural, social and economic systems18 . Significantly, it is estimated that 90% of women with disability have been subjected to sexual abuse19 .
Sexuality The types of domestic and family violence for people who identify as lesbian, gay, bisexual, transsexual, intersex or queer (LGBTIQ) is similar to that of the heterosexual community. The rate at which it occurs however is unclear. This is partly due to traditional views that abuse and neglect occurs only within heterosexual relationships and a lack of acknowledgement, understanding and response by government20 .
Historical events and Historical events and experiences which stem from cultural experiences government policy and practice has created
significant disadvantage for certain groups in the community. For instance assimilation policies such as the forced removed of Aboriginal children from their families have led to significant social disadvantage of Aboriginal communities. Aboriginal people have lower socio-economic outcomes, high rates of homelessness, significantly poorer health outcomes, and are over-represented in the criminal justice, welfare and child protection systems21 .
Migrants who have fled their country due to war and persecution bring with them experiences of trauma. This can impact on parents providing children with appropriate care and consequently an
16 Women in NSW 2013 Safety and justice snapshot. Fact sheet July 2013. Family and Community Services 17 Women in NSW 2014 report. Chapter 6 Safety and justice. Family and Community Services 18 Domestic violence fact sheet. Women’s Health NSW 19 ‘Double the Odds’ – Domestic Violence and Women with Disabilities. Women with Disabilities Australia. 20 Groups and communities at risk of domestic and family violence: A review and evaluation. Australian Institute of Family Studies 21 Working with Aboriginal Communities. A Practice Guide. NSW Department of Community Services
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 14

over representation of culturally and linguistically diverse groups in the child protection system22 .
Customs and beliefs Customs and beliefs amongst certain cultures can perpetuate the abuse and neglect of women and children. For instance forced marriage, child brides and genital mutilation of children for cultural and religious reasons.
Geographic isolation Women from remote, rural and regional locations are at greater risk of violence as the involvement and responsiveness of NSW Police, access to health services, legal resources, women’s refuges and vacancies in alternate supported accommodation23 is limited, or in some cases, may be non-existent24 .
Childhood trauma Children and young people are particularly vulnerable to abuse and neglect, especially those with disability. Children or young people with disability may be dependent on people other than parents for support, which can increase their vulnerability to abuse and neglect. This situation is worsened when they are unable to communicate that abuse or neglect is occurring, either verbally or through their behaviour.
Abuse and neglect can have long term damaging effects on children and young people. An example is domestic and family violence, as it affects emotional, social and physical development, and life outcomes in adulthood. Domestic violence in the home is a strong indicator that other types of abuse and neglect are also occurring25 .
Children who have experienced and/or witnessed domestic family violence are also at risk of becoming perpetuators in intimate relationships later on in life26 .
22 Culturally appropriate service provision for culturally and linguistically diverse children and families in the New South Wales child protection system. NSW Department of Community Services
http://www.adhc.nsw.gov.au/__data/assets/file/0019/228043/Allocation_of_Places_in_Supported_Accommodation_P olicy_and_Procedures_Dec2011.pdf 24 Groups and communities at risk of domestic and family violence: A review and evaluation. Australian Institute of Family Studies 25 An assault on our future: The impact of violence on young people and their relationships. White Ribbon Foundation. 26 ASCA Response to: Consultation Paper on the Establishment of the Royal Commission into Institutional Responses to Child Sexual Abuse. Adults Surviving Child Abuse.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015
23
15

2.3.1 Good practice guidelines
Targeted Prevention Identifying and addressing risk factors and
vulnerable groups
Assist people with disability to build and exercise their capacities to prevent, identify, and manage violence, abuse and neglect through training, education and skill development. For instance use the ‘Looking After Me’ Resource kit to educate people with disability on domestic violence and healthy relationships (refer to Other Resources).
Assess the person’s capacity to make decisions and provide consent. Discuss the Decision Making and Consent Policy with the person and their support network and identify situations where alternate decision makers are required.
Use the Department of Justice Capacity Toolkit to assess the person's capacity to make decisions (see Other Resources).
There may be situations were a professional is needed to assess the person’s capacity, rather than support staff. For instance, if the person exhibits sexual behaviours of concern and / or a person’s capacity to consent is in doubt. Support from a behaviour specialist should be sought immediately. Refer to the Sexuality and Relationship Guidelines in the Lifestyle Planning Policy and Practice Manual for further information.
Ensure the specific support needs of the person are assessed and clearly understood and followed by staff to prevent abuse or neglect. For instance if a person’s health and wellbeing plan is not implemented by staff, this can be viewed as systems abuse and neglect.
Facilitate access to specialist support services if the person has complex health and wellbeing needs so that tailored support strategies can be developed.
For people with complex communication needs, ensure they have a current communication assessment and augmentative and alternate communication strategies, and supports in place. If required this includes the development and implementation of a comprehensive behaviour support plan by an appropriate clinician (refer to ADHC Behaviour Support Policy and Practice Manuals).
A Behaviour Support Plan should include person-centre approaches which build on the strengths and skills of the person.
If a Restricted Practice is prescribed to manage the person’s behaviour, ensure it is closely monitored to safeguard against potential abuse and neglect. The Restricted Practice should also be replaced with a less restrictive strategy as soon as possible27 (refer to ADHC Behaviour Support Policy and Practice Manual).
Seek to understand the reasons for the person’s behaviour especially if it is unusual for the person. Behaviours of concern may indicate that
27 ADHC Behaviour Support Policy and Practice Manual Part 1: Policy and Practice
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 16

Targeted Prevention Identifying and addressing risk factors and
vulnerable groups
something out of the ordinary is happening to the person including abuse and neglect.
Provide appropriate training and education to staff and managers who support people with complex communication needs such as:
- Inclusive Communication and Behaviour Support (ICABS)
- Professional Assault Response Training
- Non-Violent Crisis Intervention training
- Positive Behavioural Support
- Disability specific education
- Cultural awareness and competency training
- Sexuality and relationships training
Ensure the person has a current My Safety Plan28 in place which addresses risk factors relating to abuse and neglect.
Encourage staff, the person and their family to access and utilise communication resource libraries set up in some FACS District offices.
Support women to access services offered at local Women’s Health Centres. Services include preventative health care, community education and development, advocacy and empowerment.
For women experiencing domestic and family violence, support the person to access gender sensitive specialist services and support groups which target different socio-economic, educational and cultural groups29
Support individuals identifying as lesbian, gay, bisexual, transgender, intersex or queer (LGBTIQ) to access support services specialising in the needs of this group.
Ensure that staff who support children are trained and have a clear understanding of Mandatory Reporter Guidelines and how to promptly respond to suspected abuse and neglect of children. Refer to the FACS Child Protection Guidelines: What ADHC staff need to know about child protection, May 2014.
Engage with marginalised groups to gain a better understanding of local needs and priorities and to help facilitate access to appropriate resources.
Gain an understanding of the history, experiences and customs of the person and their community especially if they are Aboriginal or have migrated from another country.
An insight in to a person’s background can help inform what strategies are needed to support the person appropriately.
Refer to the Abuse and Neglect Procedures for important information on Aboriginal cultural considerations and culturally and linguistically diverse
28 Refer to the ADHC Risk and Safety Policy and Procedures 2015 29 Domestic violence fact sheet. Women’s Health NSW
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 17

Targeted Prevention Identifying and addressing risk factors and
vulnerable groups
groups.
Engage the use of interpreters and translators where they are needed for people of CALD backgrounds.
2.4 Secondary prevention: Responding to abuse and neglect
2.4.1 Response procedures
Refer to the Abuse and Neglect Procedures for direction in responding to allegations and incidents of abuse and neglect.
The FACS Incident Reporting and Management Policy for people accessing Ageing and Disability Direct Services 2014 assists staff with decision making about how to report, manage and respond to incidents. The FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 2014 provide the process for reporting and managing incidents.
Refer to the Abuse and Neglect Other Resources section for useful contacts, complaints and victims’ support information.
2.4.2 Supporting the person
How and when an allegation or incident of abuse and neglect is responded to will influence the person’s welfare, pursuit of justice and recovery from abuse and neglect. Person centred organisations look at the broader impact of the incident on the person, not at whether the allegation or incident can be substantiated or tested in a court of law30. Acknowledging and addressing the impact on the person will influence their ability to recover from the incident.
Due to the prevalence of abuse and neglect of people with disability, people accessing accommodation supports are more likely to have experienced abuse and neglect at some point in their life (see section 2.1.1). The disclosure of abuse and neglect can occur immediately after the incident or it may take months, years or even decades to disclose.
Disclosing abuse and neglect can take considerable courage by the survivor and trust in the recipient of the information. The response the survivor receives can have a significant impact on recovery. It is crucial that the response is respectful, empathetic, validates the person’s experience and prevents re-traumatisation31.
30 Learning from Complaints – Occasional Paper No.1 Safeguarding People’s Rights to be Free from Abuse – Key considerations for preventing and responding to alleged staff to client abuse in disability services, Disability Services Commission Victoria.
31 ASCA Response to: Consultation Paper on the Establishment of the Royal Commission into Institutional Responses to Child Sexual Abuse. Adults Surviving Child Abuse.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 18

Allowing the person to talk about the abuse and neglect is an essential part of recovery. Hearing the person’s story however can trigger strong emotions for the person receiving the information. The listener will therefore need to balance the needs of the victim with their own health and wellbeing.
Staff must also be mindful that any information about the incident, that is disclosed by the victim and/or alleged offender, may interfere with preliminary investigations. For instance, staff must not ask the person leading questions relating to the incident or continue to ask questions once information relating to an allegation is clear. This is the role of NSW Police and the appropriate support services.
2.4.3 Good practice guidelines
Secondary Prevention Responding to incidents and allegations of
abuse and neglect
Ensure staff read and are familiar with response procedures outlined in:
- Abuse and Neglect Procedures
- FACS Incident Reporting and Management Policy and Guidelines for people accessing Ageing and Disability Direct Services 2014
Where an allegation is against a paid worker, stop contact between that
worker and the person with disability until the allegation has been fully
resolved. Even where an allegation has not been proven, future contact
between the worker and person concerned is avoided.
Take each allegation seriously. Support the person by32
1. Validating the person’s experience and acknowledging the impact of the allegation and/or incident on the person, their family and significant others.
2. Listening intently until the person has been ‘heard’. Address any concerns they may have along the way. Keep emotions in check as strong reactions can prevent the person ‘opening up’ about the incident.
3. Identifying what is important to and for the person to inform what future actions are required. Don’t provide advice unless it is asked for.
4. Involving the person as much as they can and want to be involved.
5. Keeping the person and their family or guardian fully informed of the progress of an investigation including what and why particular decisions were made. Provide information in a format the person can understand.
6. Apologising to the person and their family where appropriate.
Arrange immediate access to appropriate counselling or support if the
32 How should you respond when someone you love tells you they were abused as a child? Adults Surviving Child Abuse.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 19

Secondary Prevention Responding to incidents and allegations of
abuse and neglect
person wishes this.
Take a case management response to allegations and incidents of abuse and neglect to facilitate a coordinated cross agency approach.
Encourage staff to seek support and counselling through the Employee Assistance Program on 1300 687 327.
Analyse the incident and response measures and promptly make changes to policy and practices where needed.
Ensure records relating to the incident are kept. Records should include actions and decisions that are accurate, factual and objective.
Maintain the person’s dignity and right to privacy and confidentiality by following approved records management procedures. For instance, securely store all records relating to a sensitive and confidential incident in TRIM, ensuring appropriate access restrictions (refer to the Records Management Procedures for Supported Accommodation Services 2015).
2.5 Tertiary prevention: Systemic issues
Organisations need to be informed on the risks and prevalence of abuse and neglect. Tertiary prevention is aimed at the culture of a service and systemic issues which increase the risk of abuse and neglect occurring.
Practices and strategies in tertiary prevention focus on the recording, analysis and monitoring of data. This aids in identifying areas where continuous improvement in service delivery can occur. It includes identifying systemic weaknesses and failures such as the absence of formal procedures, and the presence of informal practices which sustain abuse and neglect33.
34:Services can fail to protect people with disability in the following ways
services do not inform and guide staff on how to protect people from abuse and neglect
services are not aware of what constitutes abuse and neglect and certain behaviours and/or incidents are considered normal, for example the use of unauthorised restrictive practices
staff are not aware of policy and procedures and do not have the skills to identify, report and support people with disability who are experiencing abuse and neglect
services have unstable workforce for example high staff turnover, stress and high use of agency or casual staff
33 ASCA Response to: Consultation Paper on the Establishment of the Royal Commission into Institutional Responses to Child Sexual Abuse. Adults Surviving Child Abuse.
34 Abuse Prevention Strategies in Specialist Disability Services. Commonwealth Department of Family and Community Services.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 20

complaints and incidents are not viewed as opportunities to learn and improve service delivery
partnerships with statuary bodies and external support services are not pursued, resulting in organisations working in isolation.
2.5.1 Good practice guidelines
Tertiary Prevention Identifying and addressing underlying
causes and systemic issues
Have clear policies and procedures for recognising and responding to allegations. Ensure policies and practices are informed by national and international best practice legislation.
Create an organisational culture that promotes and supports disclosure and allegations are always taken seriously, and responded to promptly.
Identify and address underlying causes and systemic issues that can lead to abuse or neglect.
Promote community attitudes that support peoples’ rights to live a life free from abuse and neglect.
Ensure services are accessible to the person and meet individual needs.
Provide meaningful and accessible sexuality and rights-based education to people at risk. Engage the person with services provided by Family Planning NSW (see Other Resources).
Support access to advocacy which is tailored to the person’s communication needs.
Provide support and referral to the person to access appropriate counselling and support services including specialist sexual assault services in the case of sexual abuse. Refer to Other Resources for contact details.
Provide support workers and managers with regular training in responding to incidents of abuse and neglect, duty of care, bystander accountability and access to resources.
Learn from incidents for continuous quality improvement. Be open to feedback from external agencies to improve on service delivery.
Provide clear pathways for people and their families to make complaints about services. This includes internal and external pathways.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 21

3 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
Abuse and Neglect Prevention Guidelines, V1.0, November 2015 22

Abuse and Neglect Procedures
Document name Abuse and Neglect Procedures
Policy Abuse and Neglect
Version number 1.0
Approval date January 2016
Policy manual Safeguarding Policy and Practice Manual
Approved by Deputy Secretary, ADHC
Summary The Abuse and Neglect Procedures aim to provide
paid or unpaid workers of ADHC operated and
funded non-government disability support services,
with the means to respond quickly and appropriately
to allegations of abuse and neglect.
Replaces document Abuse and Neglect Policy and Procedures 2014
Authoring unit Contemporary Residential Options
Applies to People who are being supported in ADHC operated and funded non-government disability support services.
Review date 2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment Amendment notes date
V1.0 January 2016 The Procedures are one of three documents (Policy, Procedures, and Prevention Guidelines) that replaces the Abuse and Neglect Policy and Procedures December 2014.
Abuse and Neglect Procedures, V1.0, January 2016 2

Table of contents
1 Response procedures for ADHC operated services ......................4
1.1 Receiving a report of abuse or neglect................................................4
1.2 Abuse and neglect of a child or young person ....................................4
2 Immediate response..........................................................................5
2.1 Contact emergency services – dial 000 ..............................................5
2.2 Immediate response flowchart ............................................................7
3 Roles and responsibilities................................................................8
3.1 Support worker....................................................................................8
3.2 Line manager ......................................................................................9
3.3 District ...............................................................................................11
3.4 FACS Executive ................................................................................12
3.5 ADHC Reportable Incidents Team ....................................................12
3.6 Professional Conduct Ethics and Performance Unit (PCEP).............13
4 Person centred support..................................................................14
4.1 Support for the victim of abuse and neglect ......................................14
4.2 Support for an alleged offender with disability...................................15
4.3 Support for Aboriginal and Torres Strait Islanders ............................15
4.4 Support for people from Culturally and Linguistically Diverse (CALD) backgrounds ................................................................................................16
4.5 Support for women with a disability ...................................................16
4.6 Support for children and young people .............................................16
4.7 Support for staff.................................................................................17
5 Privacy and confidentiality.............................................................17
6 Record keeping ...............................................................................18
7 Managing risk ..................................................................................18
8 Policy and Practice Unit contact details .......................................19
Abuse and Neglect Procedures, V1.0, January 2016 3

1 Response procedures for ADHC operated services
The types and definitions of abuse and neglect are outlined in the Abuse and Neglect Policy (the Policy). These Procedures should be read in conjunction with the Policy as the types and definitions of abuse and neglect inform the response to be taken.
Sources, risk factors, early intervention and prevention strategies for abuse and neglect are discussed in the Abuse and Neglect Prevention Guidelines.
The Abuse and Neglect Procedures (the Procedures) provides paid and unpaid workers of ADHC operated and funded non-government disability support services, who have contact with adults and children with disability, with the means to respond quickly and appropriately to allegations of abuse (including neglect).
The Procedures are mandatory for paid workers of ADHC operated disability support services. ADHC funded non-government disability support services may adopt or adapt the Procedures to meet the organisation’s needs.
1.1 Receiving a report of abuse or neglect
Some people with disability can be vulnerable and susceptible to abuse and neglect by others. Abuse may be perpetrated by a member of staff, another person with disability, family, friends or strangers.
A report of abuse may be received from:
A person with disability using any communication method.
Another person with disability, member of staff or any other person, who may witness abuse of the person and make a report or
Staff, a family member or others who know the person well upon observing one or more indicators of abuse, suspects that a person or people with disability have been or are being abused or neglected.
1.2 Abuse and neglect of a child or young person
The Child Protection Guidelines: What ADHC staff need to know about child protection, May 2014 describes the circumstances and procedures that staff must be aware of in relation to the abuse or neglect of children (0-15 years) and young people (16-17 years).
Abuse and Neglect Procedures, V1.0, January 2016 4

The Mandatory Reporters Guide (MRG)1 assists frontline mandatory reporters to determine whether a report is to be made to the Child Protection Helpline.
2 Immediate response
When abuse and neglect is identified or disclosed, the immediate response is to protect the person and others from further harm. The following procedures must be followed when abuse of any sort towards a person is known or suspected. Refer the flowchart below (section 2.2) for immediate response procedures to a report of abuse and neglect.
Failure to act immediately on knowledge of abuse and neglect, or identified risks to the welfare and safety of a person, is a breach of duty of care. Failure to act can lead to disciplinary action, and the involvement of external authorities such as the NSW Police or NSW Ombudsman.
It is paramount that the person’s dignity is upheld prior to and during an investigation of an allegation or suspicion of abuse and neglect.
2.1 Contact emergency services – dial 000
2.1.1 Ambulance
If the person sustains an injury as the result of an assault, the NSW Ambulance Service is called on 000 which can be dialled from any fixed or mobile phone, pay phones and certain Voice over Internet Protocol (VoIP) services. Call 106 for the text-based emergency relay service for people who have a hearing or speech impairment.
If the person is injured apply first aid until the Ambulance arrives.
2.1.2 NSW Police
Sexual and physical assaults of a person are serious offences and must be reported to the NSW Police. When a person has been assaulted or is in immediate danger of an assault the NSW Police must be called on 000.
A report of domestic violence that doesn’t involve a sexual or physical assault must be reported to a manager as soon as possible. For instance, reporting to a manager abuse by neglect, the use of unauthorised restricted practices, emotional, financial and systems abuse. Depending on the circumstances however, it may be appropriate to report abuse other than sexual or physical assault to the NSW Police as well as a manager.
If in doubt about whether the abuse needs to be reported to the NSW Police, contact FACS Legal ([email protected] or 9716 2307) or the NSW Police for advice. For non urgent matters, contact the Police Assistance line on 131 444.
1 Mandatory Reporters Guide http://www.keepthemsafe.nsw.gov.au/reporting_concerns/mandatory_reporter_guide
Abuse and Neglect Procedures, V1.0, January 2016 5

2.1.3 Contact with the NSW Police
A person with disability may come in contact with the NSW Police as a witness, victim or suspect. When dealing with the Police, refer to the Criminal Justice Resources Manual 20092 for direction:
With providing information to the NSW Police.
When supporting an alleged offender with disability.
When a staff member is a witness to an allegation of abuse and neglect.
When forensic procedures are required.
2.1.4 Protecting evidence for NSW Police
Staff or line managers at the scene must use their best endeavours to ensure that any evidence the NSW Police may require in their investigation is not disturbed.
Evidence may be lost if a victim of sexual assault bathes soon after the assault. Try and delay bathing until the NSW Police arrive if the victim is not distressed by the delay.
If possible, preserve the victim’s clothing as evidence following an assault of any type.
If possible, isolate the area where the incident occurred and do not allow anyone to enter the area until the NSW Police arrive.
Apart from ascertaining their physical condition and state of mind, avoid questioning the person and others about the incident to reduce contamination of their recall and confusion about the events.
2 ADHC Criminal Justice Resource Manual http://dadhc-intranet.nsw.gov.au/documents/client_services/office_of_senior_practitioner/criminal_justice_services_policy_and_re source_manual/CJRM_Final_June_09.pdf
Abuse and Neglect Procedures, V1.0, January 2016 6

2.2 Immediate response flowchart
Sexual and/or physical abuse
Financial abuseNeglect Systems abuse
An allegation of abuse and/or neglect received
(observed, reported, suspected)
IMMEDIATE RESPONSEØ Ensure the person and others are safe from
further harmØ Contact emergency services on 000 for an
ambulance if anyone is injured and PoliceØ Mandatory reporters must make a report of
abuse and neglect of a child or young person IMMEDIATELY to the Child Protection Helpline on 133 627 (24hrs/7days)
Provide a verbal report immediately to the line manager, on-call and/or senior manager
Contact the local Sexual Assault Service for advice concerning
sexual assaults
Protect evidence for PoliceInform the person,
guardian or administrator of the person’s finances.
Otherwise notify the Guardianship Tribunal
Identify source and circumstances of neglect and / or emotional abuse
Confirm use of restricted practice has approval by the Restricted Practice Authorisation Panel
If the practice is unathorised, refer to a manager for immediate action
Follow reporting protocols outlined in FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services
Provide report to PCEP for all staff related matters i.e. alleged offender is staff and/or line manager
Inform the person’s family if consent has been provided
Inform the person and / or family where
applicable
Abuse and Neglect Procedures, V1.0, January 2016 7

3 Roles and responsibilities
3.1 Support worker
Staff or line managers at the scene must ensure that the person (the victim) is protected from any further harm or contact with the person who caused the harm (the alleged offender).
Staff who are present at the time of an assault should take appropriate measures to maintain their own safety, and that of others.
Staff or line managers at the scene must contact the NSW Police immediately if a person has been physically or sexually assaulted or dies as the result of an assault. Inform the Police that the person, whether the victim or alleged offender, is to be treated as a ‘vulnerable person’ as per the Law Enforcement (Power and Responsibilities) Regulation 2005. The Police are obliged to arrange a support person to be present prior to an interview taking place3 .
Staff or line managers at the scene must also contact the local Sexual Assault Service if a person has been sexually assaulted (see Other Resources for a list and contact details of Sexual Assault Services in your area).
Staff or line managers at the scene must notify the doctor or ambulance if the person and others are injured.
Mandatory reporters (frontline staff) must follow the NSW Mandatory Reporter Guide4 if they suspect a child or young person is at risk of significant harm from abuse or neglect.
Mandatory reporters must make a report of abuse and neglect of a child or young person immediately to the Child Protection Helpline (the Helpline) on 133 627 (24 hours/7 days).
Non mandatory reporters, including the general public, make a report to the Helpline on 132 111 if they are concerned that the child or young person is at risk of serious harm (ROSH)5 6.
Contacting the Helpline initiates the process of assessing whether statutory child protection is required.
If it is witnessed or suspected that a member of staff has abused a person or a group of people, the line manager or ‘on call’ line manager must be informed immediately.
If it is suspected that the line manager is involved in the abuse the matter must be reported immediately to the next level manager.
If a manager is not available, a report can be made directly to FACS Professional Conduct, Ethics and Performance Unit7 (PCEP) on:
3 clause 24 of Law Enforcement (Power and Responsibilities) Regulation 2005
4 Mandatory Reporters Guide http://www.keepthemsafe.nsw.gov.au/reporting_concerns/mandatory_reporter_guide
5 A child or young person is at risk of significant harm if the circumstances that are causing concern for the safety, welfare or wellbeing of the child or young person are present to a significant extent Keep Them Safe – Making a child protection report fact sheet.
6 http://dadhc-intranet.nsw.gov.au/client_services/community_access/keep_them_safe_a_shared_approach_to_child_wellbeing
Abuse and Neglect Procedures, V1.0, January 2016 8

- (02) 9716 2073
- (02) 9716 2700
- secure email [email protected]
- TTY 1800 555 630 and/or [email protected] (for people with a sensory impairment)
Reports of abuse and neglect can also be made to the National Disability Abuse and Neglect Hotline on 1800 880 052. The Hotline provides guidance to callers on ways of dealing with reports of abuse or neglect through referral, information and support. It is not a crisis service. Anyone can contact the Hotline including the person with disability, family, friends, carers, advocated and staff from government and non-government service providers.
When one person with disability is the suspected or known source of abuse towards another, staff must ensure that the rights of both people are observed during the response and reporting processes.
The line manager refers reports of historical abuse to the NSW Police by calling the Police Assistance Line on 131 444. Give the person the option of counselling, and provide support if accessing support services, as talking about past incidents may be traumatic for the person.
Staff of ADHC operated services are required to comply with the ADHC reporting processes if they suspect irregularities in the management of the person’s finances, and report them to the line manager for immediate attention.
Staff must follow the incident reporting requirements of the FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 2014.
Any decisions made in relation to managing the incident must be fully documented for future reference, along with the reason for the decision and the name and contact details of the person making the decision (see section 5).
3.2 Line manager
The line manager should ensure that all emergency procedures have been followed and the appropriate emergency services have been called.
Where management believes that a member of staff is the source of abuse of a person the matter must be referred to the NSW Police.
A member of staff who is suspected of abusing a person with disability must not be permitted to have any unsupervised contact with the person, and may be immediately transferred to alternative duties following the allegation and until the matter is resolved.
7 PCEP: http://dadhc-intranet.nsw.gov.au/corporate_services/pcep
Abuse and Neglect Procedures, V1.0, January 2016 9

Any cases of suspected abuse and neglect by a member of staff must be reported to PCEP.
If a manager believes that an incident of abuse or assault between two people with disability has occurred, the matter must be referred to the NSW Police. The manager must inform the Police that the victim and alleged offender with disability should be treated as a ‘vulnerable person’ .
It is the role of the line manager to follow up with any reports of abuse and neglect made to the NSW Police to ensure the matter is progressing and the rights of the person are upheld.
The line manager must ensure that the wishes of the victim and the alleged offender are followed in relation to advising family, guardian or other support person about the incident, where they are capable of making this known. When the victim or the alleged offender lacks capacity to make their wishes known, the line manager reports the incident to the appropriate person as soon as possible and within 12 hours of the incident occurring.
The line manager facilitates access to appropriate support for the victim and the alleged offender, their families and staff, and ensures they have information about available services (see Other Resources).
When there is an allegation of financial abuse, the manager must notify the person, family, guardian or the administrator of the person’s finances. The matter may be reported to the NSW Police.
The line manager must follow the incident reporting requirements of the FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 2014.
The line manager must complete a Notification Form to the Children’s Guardian8 for any allegation of sexual misconduct or serious physical assault towards a child or young person in out-of-home care, attach this to the incident report surrounding the allegation for endorsement.
A report of the death of a person with disability is provided in accordance with the Death Procedures in the Health and Wellbeing Policy and Practice Manual, Volume 2.
The line manager is responsible for ensuring that documentation of the incident is completed and all communication kept private (see Section 4).
The line manager encourages support workers to keep their own notes in relation to the allegation or suspicion of abuse and neglect.
The line manager is responsible for ensuring reports are forwarded to the appropriate levels of management.
As far as possible, the line manager will ensure a support worker reporting an allegation of abuse is safe from retribution.
8 http://www.kidsguardian.nsw.gov.au/ArticleDocuments/453/Notification_allegation_sexual_misconduct-physical_assault.docx.aspx
Abuse and Neglect Procedures, V1.0, January 2016 10

As far as possible, the line manager will ensure the principles of procedural fairness are applied when a decision is being made9.
The line manager encourages and provides information to staff who would benefit from informal and formal debriefing services through the Employee Assistance Program.
3.3 District
3.3.1 Each District:
Is responsible for adopting a protocol for making referrals to the NSW Police and for managing the referral process locally
Will follow the incident reporting requirements of the FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 2014
Will report the death of a person with disability in accordance with the Death Procedures in the Health and Wellbeing Policy and Practice Manual, Volume 2
Will report incidents of abuse and neglect by a member of staff to PCEP
Will endorse and forward to the FACS Executive, a completed Notification Form to the Children’s Guardian10 for any allegation of sexual misconduct or serious physical assault towards a child or young person in out-of-home care.
Will conduct an investigation into incidents of abuse and neglect and inform relevant areas of FACS about the outcome of the investigation, including lessons learnt
Is responsible for recording the incident of abuse and neglect on the Client Information System (CIS) and/or SAP-HR Workplace Safety
Will ensure criminal record and reference checks are completed every four years for paid and unpaid workers who have contact with adults and children receiving direct support services through ADHC
Will ensure paid and unpaid workers have a Working with Children Check prior to working with children or young people under the age of 18
Will ensure frontline staff and managers are familiar with policies and procedures relevant to Abuse and Neglect
Is responsible for regular qualitative reviews of support systems, and for ensuring mandatory support documentation is implemented for people receiving direct support services through ADHC.
9 Refer to the NSW Ombudsman’s Fact Sheet on Natural Justice/Procedural Fairness for Public Sector Agencies http://www.ombo.nsw.gov.au/__data/assets/pdf_file/0017/3707/FS_PSA_14_Natural_justice_Procedural_fairness.pdf
10 http://www.kidsguardian.nsw.gov.au/ArticleDocuments/453/Notification_allegation_sexual_misconduct-physical_assault.docx.aspx
Abuse and Neglect Procedures, V1.0, January 2016 11

3.4 FACS and ADHC Executive
The ADHC Deputy Secretary and Northern Cluster Deputy Secretary will follow the incident reporting requirements of the FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 2014.
The Secretary or head of funded services must notify the NSW Ombudsman of a Part 3C reportable incident11 as soon as is practicable and no later than 30 days of becoming aware of a reportable incident.
The Secretary or head of funded services must notify the NSW Ombudsman of the outcome of investigations including relevant and appropriate risk management actions.
The Secretary of FACS is required to notify the Children’s Guardian when the agency receives and allegation of sexual misconduct or serious physical assault towards a child or young person in out-of-home care, committed by a child-related worker (inclusive of employees, authorised cares, adult household members and board members)12.
3.5 ADHC Reportable Incidents Team
There are four types of reportable incidents which must be reported to the NSW Ombudsman (refer to Section 6 of the Abuse and Neglect Policy):
Employee-to-client incidents of sexual assault, sexual misconduct, assault, fraud, ill-treatment or neglect,
Client-to-client incidents of sexual and physical assault (causing serious injury or involving the use of a weapon), or that form a pattern of abuse,
Contravention of an Apprehended Violence Order (AVO) taken out to protect a person with disability,
Serious, unexplained injury of a person with disability.
Whilst PCEP retains responsibility for employee to client incidents, the Reportable Incidents Team is responsible for supporting FACS operated accommodation support services to report and review the remaining reportable incidents categories. Managers must complete a Category 1 – Incident Executive Briefing within 24 hours if an incident is assessed as being reportable to the NSW Ombudsman. The Category 1 is to be forwarded concurrently to Strategic Change and the ADHC Reportable Incidents team:
11 An incident that must be reported to the NSW Ombudsman under Part 3C of the Ombudsman Act 1974. Refer to the NSW Ombudsman’s Guide for services: Reportable incidents in disability supported group accommodation for types and definitions of Part 3C reportable incidents (Other Resources)
12 http://www.kidsguardian.nsw.gov.au/ArticleDocuments/542/FactSheet6PrincipalOfficers.pdf.aspx?Embed=Y
Abuse and Neglect Procedures, V1.0, January 2016 12

Managers are required to provide the ADHC Reportable Incident team with all documentation relevant to the reportable incident and the person(s) involved within five business days of the incident occurring.
3.6 Professional Conduct Ethics and Performance Unit (PCEP)
PCEP will offer advice and assistance to Districts in the investigation and management of suspected abuse by staff, alleged misconduct and significant performance management matters.
Staff can report a matter to PCEP by:
1. Telephone on (02) 9716 2073, 2. fax on (02) 9716 2700 3. completing a PCEP notification form and either emailing
[email protected], faxing or mailing the form to:
Professional Conduct Ethics and Performance Unit Department of Family and Community Services 4-6 Cavill Avenue Ashfield NSW 2131 DX 21212 ASHFIELD
For people who are deaf, or have a hearing impairment or speech impairment, TTY 1800 555 630 or email [email protected]
Abuse and Neglect Procedures, V1.0, January 2016 13

4 Person centred support
4.1 Support for the victim of abuse and neglect
The line manager appoints a primary contact person to communicate with the victim and family, guardian or other support person, to ensure that information relating to the incident is provided through one coordinated source.
Information provided to a person with disability, guardian or other support person, about legal rights, options and support services, must be provided in a format that suits their individual communication needs. The line manager must ensure a support person is available who knows the victim’s communication requirements.
Staff must ensure that the victim is adequately supported by an independent person, who could be a relative, friend, advocacy service or legal practitioner.
When the victim is unable to make decisions about any aspect of the incident, a family member or guardian must be present to make decisions on the victim’s behalf. Where this relates to medical treatment or forensic examination consent must be provided by a person responsible in accordance with the Guardianship Act 1987.
The victim and family, guardian or other support person should be assisted to access any debriefing, counselling, legal or other support services if that is their wish.
Victims of abuse and their families or guardians should be referred to Victims Services and Support13 on 1800 633 063 and be advised of their rights and the support services that are available to them (see Other Resources).
Managers will facilitate access for victims of violent crimes and their families who may be eligible to apply for counselling with the Approved Counselling Service provided by Victims Services and Support.
The victim, family, guardian or other support person will have the choice of pursuing the matter through the legal system and must be supported to access the services and advice they require. The Abuse and Neglect Other Resources contains a list of organisations that provide legal advice and services.
Where the person is vulnerable, and unable to manage their personal finances, this may be done informally by the family, guardian or other support person. In the absence of a suitable informal financial manager, application is made to the NSW Civil & Administrative Tribunal (NCAT) to appoint a formal financial manager.
13 http://www.victimsservices.justice.nsw.gov.au/Pages/vss/Hidden/VS_specificneeds1.aspx
Abuse and Neglect Procedures, V1.0, January 2016 14

4.2 Support for an alleged offender with disability
Information provided to a person with disability, guardian or other support person about legal rights, options and support services, must be provided in a format that is understandable to the person. This includes having a support person available who understands the alleged offender’s communication requirements.
Staff must ensure that the alleged offender is adequately supported by an independent person, who could be a relative, friend, advocacy service or legal practitioner.
When the alleged offender is unable to make decisions about any aspect of the incident, a family member or guardian must be present to make decisions on the alleged offender’s behalf. Where this relates to medical treatment or forensic examination consent must be provided by a person responsible in accordance with the Guardianship Act 1987.
4.3 Support for Aboriginal and Torres Strait Islanders
Be aware that sexual assault is not uncommon in Aboriginal communities, and it has an impact on individuals in the community. A high degree of sensitivity is required to support the person and family with a history of sexual assault.
Certain issues are personal and sensitive, and are only for discussion with the appropriate family member. The person, family or carers should be consulted to learn what matters are sensitive, and which family member or carer to speak to about the matter. The information is recorded in the person’s records. Certain types of abuse, for example sexual abuse, may only be discussed within gender groups.
Shame can be a barrier to people accessing services. People face other barriers such as location of services, issues of confidentiality, and willingness to access health services to discuss these matters, especially in small remote communities.
Determine if the person and family would prefer an Aboriginal identified worker, or service, to communicate with the identified family spokesperson. It may be in breach of cultural protocol for a non-Aboriginal person to approach the spokesperson.
Learn what services the person or family want to use, as they may prefer to use services operated by Aboriginal providers.
Understanding cultural sensitivity includes understanding the person’s individual history, experiences and choices. For example, a person who identifies as one of the Stolen Generation has experienced trauma as a child and possibly sexual abuse. If this is the case, supporters should contact the Aboriginal Health Service for advice, and offer a referral to a counsellor if the person is interested.
Abuse and Neglect Procedures, V1.0, January 2016 15

4.4 Support for people from Culturally and Linguistically Diverse (CALD) backgrounds
The person and family or carer’s cultural and religious beliefs about abuse and neglect should be established. Demonstrate respect and sensitivity to the person’s culture by considering:
the person and the family or carer’s views about abuse and neglect
the role of spiritual and religious beliefs about abuse and neglect
how the person and the family or carer communicate, for instance, through an interpreter
the person’s own role in problem solving and decision making.
4.5 Support for women with a disability
Ensure access to services specifically for women, including women’s health and counseling supports14, is available if this is the person’s preference (see Other Resources).
Ensure support networks are chosen by the person (enabling the person to choose female or male supporters).
Involve and encourage contribution of natural supports15 where the person wants this. People who are isolated from the community and have limited natural supports are at greater risk of abuse and exploitation.
Ensure access to information and supports about reproductive health and sexuality, intimate relationships and self-protective strategies is available. Refer to the Sexuality and Relationship Guidelines in the Lifestyle Policy and Practice Manual.
4.6 Support for children and young people
Services must take reasonable care to protect children and young people from risks of harm that can and should be foreseen. All staff are to make a report to the Child Protection Helpline on 132 111 if they suspect a child or young person is at risk of significant harm (see section 1.2).
The types, use and consent for Restricted Practices for children and young people differs to the requirements required for adults. For instance certain restricted practices are prohibited for children and young people including seclusion, any form of corporal punishment, any punishment that takes the form of immobilisation, force-feeding or depriving of food, any punishment
14 Women’s Health and Counselling Services http://www.whnsw.asn.au/PDFs/WHNSW_Brochure.pdf
15 Natural supports are relationships that occur in everyday life. They include family, friends and other trusted people, neighbours, acquaintances, and people with shared interests. Natural supports enhance a sense of security and quality of life for people. Refer to ‘Mapping Natural Supports’ http://www.ndis.gov.au/sites/default/files/documents/mapping_natural_supports_full_report.docx
Abuse and Neglect Procedures, V1.0, January 2016 16

that is intended to humiliate or frighten the person. Refer to the Behaviour Support Policy for further information.
Vulnerable children, young people and families at risk of statutory child protection intervention can be referred for support services through Keep Them Safe Family Referral Services16.
Staff working with children must read and understand their obligations and responsibilities in protecting children from abuse and neglect as outlined in the FACS Child Protection Guidelines: What ADHC staff need to know about child protection
4.7 Support for staff
The line manager must ensure all staff under their responsibility are provided with training on the Abuse and Neglect Policy, Procedures and Prevention Guidelines and any resources that inform and support the Abuse and Neglect Procedures.
Individual counselling or group debriefing may be beneficial, and gives support workers the opportunity to talk about how they feel immediately after the event and over time. Staff should be offered a debriefing session within 24 hours of the incident occurring17.
Debriefing can be done by managers as an informal discussion with the team in a supportive, safe and accepting environment, or by formal debriefing with a skilled counsellor.
In ADHC operated services, formal debriefing or individual counselling is available for individuals and teams through the Employee Assistance Program (1300 687 327). This is a free service provided by registered psychologists.
Refer to the Death Procedures in the Health and Wellbeing Manual Volume 2 for advice and support if the person has died.
5 Privacy and confidentiality
All staff members who are in contact with the victim or the alleged offender will maintain confidentiality of information relating to the incident.
Confidentiality must be maintained when making a report to external agencies. Failure to do so could prejudice any subsequent investigation and cause unnecessary hurt or embarrassment to individuals.
16 Keep Them Safe http://www.kidsfamilies.health.nsw.gov.au/current-work/programs/programs-and-initiatives/keep-them-safe/
17 Refer to the Fact Sheet: Requesting and approving EAP on-site serious incident counselling support
Abuse and Neglect Procedures, V1.0, January 2016 17

6 Record keeping
Comprehensive and accurate documentation is to be maintained in the interests of all parties to ensure accountability and transparency in decision-making.
Records are maintained to comply with the standards published under the authority of the State Records Act 1998 that also requires records of disciplinary proceedings in relation to employees to be retained indefinitely.
Sensitive and confidential records must be stored securely in TRIM and only accessed by persons with a legitimate reason for viewing the documents. Refer to the Records Management Procedures for Supported Accommodation Services 2015 for further information.
Refer to the FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services 201418. It provides direction on reporting and managing incidents, in particular, the seven step incident management process to guide decision making and action.
A detailed written report should be completed as soon as possible to ensure it is an accurate record of the incident. The report should include:
the nature and extent of the incident and an Incident Reporting Category
a description of the incident completed as soon after the event as possible and being an exact record of the events
additional reports written by other witnesses or persons present at the time the incident occurred
the name and contact details of all those involved, particularly in relation to decisions that are made as a result of the incident
the response provided to the person making the allegation
the date and signature of the person making the report
ongoing actions required to resolve the matter and
the outcome, although, depending on the nature of the incident an outcome may be delayed.
7 Managing risk
The line manager and staff must assess the risk of further incidents and update any risk management plans pertaining to the event and the people involved.
18 Refer to FACS Incident Reporting and Management Guidelines for people accessing Ageing and Disability Direct Services for a guide to incident reporting categories.
Abuse and Neglect Procedures, V1.0, January 2016 18

The line manager and staff must review the My Safety Plan19 of any person with disability involved in the incident to assess and manage the risk of further incidents of abuse. Refer to the Risk and Safety Policy, Procedures and Guidelines for identifying and managing risk.
Refer to the Abuse and Neglect Prevention Guidelines for information around early intervention and prevention of abuse and neglect.
8 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
19 ADHC Risk and Safety Policy, Procedures and Guidelines
Abuse and Neglect Procedures, V1.0, January 2016 19

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
This form can be used instead of Part A of the CHAP tool. Before the person attends the annual health assessment with the GP, complete the form with the person, to record health information for the 12 months since the last assessment.
Date of last health assessment Today’s date:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Sensory -Vision
Visible changes to the eye e.g. cloudy
Person hesitates when walking
Unsteady on feet and/or falling
Vision test not performed in last 5 years
Sensory -Hearing
Person not responding when addressed
Muscular-skeletal
Holding a part of their body
Swollen, painful or tender joints
Swollen, painful or tender muscles
Stiffness
Redness
Difficulty holding and lifting items
Unsteady on feet and/or falling
Cardio Person communicates pain in chest, back, jaw, arm or shoulder
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
vascular Rapid heart beat
Swollen ankles
Shortness of breath
Blue skin (fingers/lips/toes)
Respiratory Uncommon cough
Short of breath
Wheezing
Coughing up blood and/or stuff?
Temperature/fever
Bluish tinge around mouth and finger tips
Snoring at night
Restless at night
Urinary Urinary incontinence
Increased frequency of urinating
Blood
Person communicates pain when urinating
Smell
Digestive Weight loss
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Weight gain
Pressure areas
Risks identified from the Nutrition and Swallowing Risk Checklist
Regurgitate or vomit
Reflux
Diarrhoea
Constipation
Black bowel motions
Increased flatulence
Faecal incontinence
Person communicates abdominal pain
Person communicates pain after eating
Increase or decrease in thirst
Increase or decrease in hunger
Lacking energy
Nervous Fainting
system Unsteady on feet and/or falling
Weakness in limbs
Person communicates strange feelings of skin such as tingling
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Changes in epilepsy (seizure frequency; intensity; type)
Reproductive - Changes to menstruation (heavier/lighter) women’s Mid-cycle bleeds health Person communicates painful periods
Abnormal vaginal discharge
Vaginal irritation
Menopausal symptoms e.g. hot flushes
Behavioural changes
Pap smear not completed in last 2 years
Mammogram not completed in last 2 years for women over 50
Reproductive - Discharge from penis men’s health Scarring
Sores
Changes in shape of penis and/or testes
Integumentary Rashes
– skin, hair, Itchiness nails Flaky skin
Pressure areas
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Dryness
Redness
Oral health Person communicates pain i.e. holding their jaw, refusing food (mouth, teeth Changes in gum condition (bleeding, colour) and gums) Missing teeth
Loose teeth
Changes to smell of breath
Decay of teeth
Changes in behaviour
Mental health Low mood
(psychiatric (Appears depressed, withdrawn, sad, tearful, irritable) and High mood behavioural)
(Extreme excitement, hyperactivity, inappropriate laughing, giggling)
Irritable mood
(Short fuse, verbal and physical aggression, frustration)
Loss of interest and/or pleasure
(Refusing or needing more encouragement or prompting than usual to participate in routine activities, no longer engaged in previously enjoyed activities)
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Anxiety
(More or less sleep, change in waking and sleeping routines, disturbed sleep, eating more or less, gaining and losing weight)
Other behaviours
(Spending more time alone, interacting less with others, loss of skills, no longer completing tasks, self-injurious behaviour, dis-inhibited behaviour, increased activity levels such as pacing, rocking, rearranging furniture, walking)
Changes in Person smokes lifestyle Person consumes alcohol
Physical activity (changes in activity type, changes in motivation, changes in stamina)
Change in sleep pattern
Change in domestic abilities
Change in self-care abilities
Other
Other
Other
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Notes to discuss with the GP at the health assessment appointment
People involved in completing the Annual Health Summary
Name Position /
relationship
Date involved Name Position /
relationship
Date involved
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

1
Appointment checklist My name:
Make the appointment
Make the appointment action Notes Guidelines
Refer to Supporting Me at a Health Appointment My Health and Wellbeing Plan (Part A)
Inform me of why I need this appointment Use the NSW CID Healthier Lives Fact Sheets ‘Some signs of sickness’ and ‘Me and my doctor’
Ask who is the best person to support me at the appointment?
Identify who has the most knowledge and experience of me and who I am most comfortable with
What time of day suits me best? Base this on my daily routine, my home routine, best person/support worker availability
Who is my person responsible?
Do I need my person responsible to attend to provide consent?
Yes No If I have a person responsible, they will need to attend the appointment to provide consent for medical or dental treatment
Do I want my person responsible to attend? Yes No Whether I want my person responsible with me at the appointment
Are they available to attend? Yes No
Locate my details and relevant documents in preparation
My Health and Wellbeing Plan; Unit Diary; Medication folder
Call my health professional
If I can’t make the call, identify yourself to the receptionist
Inform the receptionist of the purpose of the appointment
Negotiate a date and time
Record the date and time of the appointment
Support me to make the phone call
Who you are; where you are from; why you are calling. e.g. check-up; medication review; follow-up appointment
A time suitable to both me and the health professional – I may require a long consultation if it is for my annual health assessment
In the Unit Diary
Inform others of the appointment Use the Communication Book for staff; inform my person responsible
Health Planning, Tools and templates, V1.3, June 2016 1

2
Appointment checklist My name:
Prepare for the appointment
Prepare for the appointment action Notes Guidelines
Is My Health and Wellbeing Plan current and up to date?
The My Health and Wellbeing Plan must be current and up to date
Do I need a blood test before the appointment?
Only if prescribed
Refer to Supporting Me at a Health Appointment if I have issues with blood tests. A pathologist can visit my home if I prefer
Do I need to take an appointment card or referral letter to the appointment?
Is my referral letter up to date?
The GP or specialist may have issued a referral to bring to the next appointment
Referrals are written for a set period of time. Ask the GP practice if the referral is current
Do I need my Medicare card? If it is a new health professional
Do I need my health care/pension card?
Do I need money for the appointment? In case the doctor does not bulk bill
Print out a blank Health Appointment Sheet In case the health professional wants to use the template to record the person’s information
®Take medication folder and Webster-pak To review and update medications
Take my One-page Profile and Communication Profile To demonstrate how best to communicate with me
For the annual health assessment prepare as above and also take:
Notes Guidelines
A completed Annual Health Summary This is essential information for a health assessment
Part 1 of the CHAP tool (if required) Only use if the GP uses the CHAP tool
A copy of the Health Assessment Criteria This will help guide the person and support person through the appointment
The current support plans for any of my health conditions e.g. Epilepsy Management Plan; Nutrition and Swallowing Risk Checklist; My Oral Health Plan, Mealtime Management Plan
‘Fact Sheet – People with intellectual disability – information for General Practitioners’
For the GP to understand the role of support workers in ADHC
Health Planning, Tools and templates, V1.3, June 2016 2

3
Appointment checklist My name:
After the appointment
After the appointment actions Notes Guidelines
Go to the chemist if my medications have changed and provide the chemist with new / changed script(s)
To ensure changes to my medication are updated by the pharmacist when prescribed by my treating doctor
®Get Webster-pak repacked. Take to the pharmacy
Ask the chemist to print out a new medication profile ®
When the new Webster-pak is being filled
Print out a CMI sheet for new medication Consumer Medication Information
Update the information in My Health and Wellbeing Plan
Attach doctor’s instructions to the My Health and Wellbeing Plan. DO NOT TRANSCRIBE DOCTOR’S INSTRUCTIONS
Inform my person responsible of the appointment outcome
If not present at the appointment
Inform other staff of the appointment outcome and actions to be taken
Use the Communication Book and daily notes and give feedback at the team meeting
Make a review appointment with my health professional If advised by my health professional
Make appointments with other health professionals For instance, if a referral was written for me or if a blood test was ordered for me
Record all future appointments In the Unit Diary and Communication Book
Do I need a referral to a clinical nurse consultant? For example, if I have a complex health condition and need advice, or help with coordinating my care
Add agenda item to the next team meeting Discuss the details of the appointment and prescribed actions.
Do I understand the advice given to me by the health professional?
Use the NSW CID Easy Health Fact Sheets – After visiting the doctor
Has the health professional provided advice or recommendations in a written format?
Under Medicare the doctor is required to record the health assessment findings and recommendations. The person or support worker requests a copy of the doctor’s record
Update the Health Action Plan
Record anything new in Supporting Me at a Health Appointment
Refer to the person-centred thinking tool Learning Log in Lifestyle Planning Policy and Practice Manual
Update the person’s Communication Profile / Chart
and the Part A of the My Health and Wellbeing Plan Supporting Me at a Health Appointment
Health Planning, Tools and templates, V1.3, June 2016 3

Bowel Care Guidelines
Bowel Care Guidelines
Health and Wellbeing Policy
1.1
January 2016
Health and Wellbeing Policy and Practice Manual Volume 1
Deputy Secretary, ADHC
A guide for carers who do not have a formal background in health care to support a person to have a healthy bowel. The guidelines contain information about signs and symptoms that indicate when bowel health is compromised and requires intervention by a health professional.
New guidelines
Contemporary Residential Options Directorate
People who are supported in ADHC operated accommodation support services
2017
Document name
Policy
Version number
Approval date
Policy manual
Approved by
Summary
Replaces document
Authoring unit
Applies to
Review date

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 November 2014 Bowel Care Guidelines V1.0
V1.1 January 2016 Amended to incorporate feedback
Bowel Care Guidelines, V1.1, January 2016 2

Acknowledgement
Good practice advice for the Bowel Care Guidelines was provided by the following panel of specialists in bowel care and treatment.
Jann Capizzi
Clinical Nurse Consultant
Dysphagia Nutrition/Developmental Disability
Westmead Hospital
Rachel Gangemi
CNC Dysphagia and Nutrition
Gastroenterology
The Children’s Hospital at Westmead
Rohini Maharaj
Dietitian
ADHC Metro Residences
Department of Family & Community Services, NSW
Doug Taupin
Staff Specialist Gastroenterologist
Gastroenterology and Hepatology Unit
The Canberra Hospital
The panel was supported by ADHC clinical specialists.
Monika Kaatzke-McDonald
Acting Director, Policy and Practice Team
Clinical Innovation and Governance
Ageing, Disability and Home Care
Department of Family and Community Services
Karen Alexanderson
Practice Leader, Nursing and Health Care
Clinical Innovation and Governance
Ageing, Disability and Home Care
Department of Family and Community Services
Bowel Care Guidelines, V1.1, January 2016 3

Table of contents
1 Bowel Care Guidelines ......................................................................... 5
1.1 Introduction..................................................................................... 5
1.2 Bowel health................................................................................... 5
1.3 Bowel dysfunction........................................................................... 6
1.4 Resources .................................................................................... 11
2 Policy and Practice Unit contact details ........................................... 11
Bowel Care Guidelines, V1.1, January 2016 4

1 Bowel Care Guidelines
1.1 Introduction
The Bowel Care Guidelines are an additional resource to support the ADHC Health Planning Procedures.
The Health Planning Procedures (the Procedures) embody the principles of legal and human rights found in the New South Wales Disability Service Standards (the Standards), the commitment to deliver culturally responsive services to Aboriginal people under the Aboriginal Policy Statement (the Statement), and the person centred guiding principles of the ADHC Health and Wellbeing Policy.
The Bowel Care Guidelines are provided for carers who support people to manage their health and wellbeing, and in particular their bowel health. The Guidelines are for use by carers who do not have a formal background in health care, but who support people to make decisions about bowel health under the guidance of their ‘usual’ General Practitioner (GP)1 and other health specialists.
In the context of these Guidelines the carer is the ‘primary carer’ and is a support worker, but may also be a family member or other informal support person, and is not a nurse.
Refer to the Health Planning Procedures for guidance on providing culturally sensitive support for managing bowel health with Aboriginal and Torres Strait Islander people.
1.2 Bowel health
Although it is common to have a bowel motion each day, there is no such thing as a ‘normal’ bowel habit. How often it happens is different for everyone, but most people have a pattern that is ‘usual’ for them.
Bowel health is directly related to good nutrition, and together they are essential for the overall health and wellbeing of the person. Bowel health can be adversely affected by many aspects of daily life, including:
a diet lacking in fibre
insufficient fluid intake
disruption to regular diet or routine
delaying bowel actions due to pain e.g. from haemorrhoids
some medications
1 Medicare defines the person’s ‘usual’ GP as: ‘The GP (or a GP in the same practice) who has provided the majority of
services to the patient in the past 12 months, and/or is likely to provide the majority of services in the following 12 months’.
Bowel Care Guidelines, V1.1, January 2016 5

recent illness or hospitalisation
low activity levels and reduced mobility, and
reduced physical and emotional wellbeing.
People with disability are at risk of having a bowel that does not function properly (bowel dysfunction) for any or all of the reasons described above. Some conditions make people with disability more vulnerable to bowel problems due to physical immobility, neurological injury or muscle weakness, for example, Down Syndrome, Rett Syndrome and Cerebral Palsy.
Having a healthy bowel is essential to good quality of life for all people, but is a subject that people are often unwilling to discuss. For this reason it is important for carers to know the usual bowel habits of the person they support, and to recognise when something is wrong.
When a person is experiencing problems with bowel function carers should understand:
the issues that affect bowel function, especially for the person they support
signs and symptoms of bowel problems
why they need to document bowel patterns to detect changes, and
the importance of involving health professionals to assess the causes of bowel dysfunction, especially for people with complex health conditions.
1.3 Bowel dysfunction
1.3.1 What is it?
Bowel dysfunction is described as difficulty passing faeces (sometimes called stools), or keeping faeces contained in the bowel, or passing faeces that is not considered to be ‘normal’2 in consistency.
Bowel dysfunction is classified under three headings:
constipation and poor bowel emptying
diarrhoea
faecal incontinence
Constipation causes discomfort and affects quality of life. It is described as difficulty or pain when passing faeces, or passing faeces infrequently.
Poor bowel emptying occurs for various reasons and causes constipation.
Diarrhoea is loose watery faeces and is usually frequent.
2 See the attached Bristol Stool Chart for descriptions of different types of faeces
Bowel Care Guidelines, V1.1, January 2016 6

Faecal incontinence is uncontrolled passing of faeces and creates social or hygiene problems for the person. The person may not always be aware that it is happening.
1.3.2 Signs and symptoms
There are a number of signs of constipation including:
straining or pain when trying to pass faeces
lumpy or hard faeces
feeling that the rectum is not completely empty
having fewer than three bowel motions per week
passing liquid stools (overflow) but having symptoms of constipation
behaviour that is unusual for the person.
Diarrhoea can be observed by a carer but is difficult to identify if the person uses the toilet and does not report it. It may be associated with stomach bloating and pain, and be accompanied by vomiting.
Signs of faecal incontinence include the person’s inability to get to the toilet in time, and repeated occasions of soiled clothing.
Other signs of bowel dysfunction may be reported by the person or observed by a carer.
Any of the following signs require immediate referral to the GP or local hospital:
vomiting blood or faecal matter
diarrhoea and/or vomiting that is more than a one-off event
bleeding from the bowel
fresh (red) or old (black) blood in faeces – see note below
unusual pain before, during or after a bowel action.
NOTE Black faeces occur when a person is taking iron supplements. Take care not to confuse it with old blood in faeces which is also black.
NOTE An outbreak of diarrhoea must be reported to the NSW Ministry of Health, Public Health Unit. An outbreak occurs when diarrhoea affects two or more people in the house or unit, even when the cause is unknown. Follow this link to your nearest Public Health Unit http://www.health.nsw.gov.au/Infectious/Pages/phus.aspx
1.3.3 Causes and risks
Constipation can be caused by disorders affecting digestion and bowel function, psychological or neurological conditions, or a bowel that is not necessarily diseased, but does not function as well as it should. Constipation may be associated with low mobility, inadequate diet, slow movement of faeces through the bowel, or abnormality of the muscles involved in emptying the bowel (pelvic floor muscles).
Bowel Care Guidelines, V1.1, January 2016 7

Diarrhoea can be acute and short lived, for example with food poisoning or a bowel infection, and may be spread to other people. It can be chronic as a result of inflammatory bowel disease, irritable bowel syndrome and coeliac disease. Diarrhoea may also be caused by food allergies, medications, radiation therapy, overuse of laxatives and diabetes.
Faecal incontinence can be caused by poor muscle control, or muscle damage after surgery or child birth, infection or inflammation of the bowel, irritable bowel syndrome, or stress from haemorrhoids or other conditions involving the rectum or sphincter muscle. It may also be developmental.
Nerve damage or disease caused by spinal chord injury, multiple sclerosis or spina bifida can result in faecal incontinence, as can lifestyle and environment factors. Some examples include poor toilet facilities, diet, and lack of independence to move around or manage clothing. A person with dementia may suffer loss of memory and skills, and experience incontinence.
1.3.4 Monitoring and supporting bowel health
Carers are not required to diagnose health problems. However, they are required to monitor and report regularly on the health and wellbeing of the people they support, including their bowel health.
What you can do to support the person to have a healthy bowel:
1. Learn about the person’s usual bowel habit so you can identify when there is a change. A Bowel Chart and the Bristol Stool Chart are included among the Health Planning tools for recording bowel habits. These can also help you to know when medical intervention is required.
2. Use the Bowel Chart to record when the person has a bowel motion and the Bristol Stool Chart to describe what the motion looks like.
3. When the Bowel Chart shows that the person’s bowel habit has changed (refer to signs and symptoms for commonly observed changes) record it in the person’s Health Learning Log (My Health and Wellbeing Plan Part B).
4. As much as is possible, talk to the person about the observed change in bowel habit in case there has been some variation in the person’s circumstances that might explain the change, for example, new medication, different diet or recent illness.
5. Report the change to a line manager or GP and agree on a plan of action.
6. Review Part B of the person’s My Health and Wellbeing Plan for any previous occasions of changed bowel habits and what action was taken.
7. If there is an ongoing concern (see the previous page for signs that require immediate referral to the GP or hospital), make an appointment with the person’s GP, as soon as possible, for an assessment of the observed changes.
8. The carer who is most familiar with the person, and this particular health issue, should accompany the person to the GP appointment.
Bowel Care Guidelines, V1.1, January 2016 8

9. Take the person’s Bowel Chart, Medication Chart and My Health and Wellbeing Plan to the GP appointment.
10. Following a diagnosis and recommendations by the GP, continue to monitor the person’s bowel habit.
11. If the GP has developed a bowel care plan, follow it and record what happens in the Bowel Chart.
12. Take the person back to the GP if there has not been a change within the timeframe recorded in the bowel care plan.
1.3.5 Health professionals
The carer supports the person to communicate bowel problems to the GP for diagnosis and treatment. The GP may not diagnose bowel dysfunction during the person’s annual health assessment unless the person or carer report changes in bowel habits to the GP at the time.
If the person needs a bowel care plan, the GP develops one with the person and carer. Before leaving the surgery the person and carer should be certain that they understand how to implement the bowel care plan.
IMPORTANT Confirm with the GP what should happen following implementation of the bowel care plan, and how long it should take for the problem to be resolved.
Depending on the diagnosis, the GP may refer the person to another health professional such as a gastroenterologist or a dietitian. If the person’s bowel dysfunction is chronic or complex, the GP has access to Medicare items for referring the person to a multidisciplinary team for management. Refer to the Chronic Disease Guidelines3 for information about GP Management Plans.
A health professional may also prescribe bowel retraining after illness or surgery. The person could require special equipment prescribed by an occupational therapist for seating in the best position to empty the bowel.
The person may need a nutrition review by a dietitian to establish the right amount of fibre and fluid for continuing bowel health.
A person with faecal incontinence may experience skin problems from exposure to faecal fluids and constant cleaning, and require a skin care assessment by a specialist.
There are many treatments for bowel dysfunction, and health professionals will prescribe different treatments depending on the diagnosis, their preferred approach, and other elements of the person’s health and wellbeing.
1.3.6 Treatment
Some treatments are administered by a health professional, either a gastroenterologist, GP or a nurse specialist. Other treatments can be administered by the person or carer.
3 ADHC Health and Wellbeing Policy and Practice Manual, Volume 2.
Bowel Care Guidelines, V1.1, January 2016 9

Treatments that are safely administered by a person or carer, are taken either by mouth (orally) or inserted into the rectum. The method of administration, the dose and frequency is prescribed by the health professional.
Carers should request information and support from the health professional if they are to implement prescribed treatments.
Some examples of common treatments that can be safely administered by carers are:
Oral - laxatives Action Comments
Lactulose, Duphulac, Actilax
Increase water content in stools to make them more bulky and softer
Used for adults.
Small doses of Lactulose and Duphalac are used in children with mild constipation.
Movicol, Increases water content in stools to make them more bulky and softer
Used for adults and children with chronic or more severe constipation that requires a daily medication.
Metamucil, Benefiber Adds fibre to stools to make them more bulky
Dissolve in fluids for easier administration
Senna, Osmolax Stimulates peristalsis in the bowel
Senna: Long term use should be avoided due to adverse effect on bowel motility
Coloxyl Softens hard stools Safe for long term use
Rectal - treatments
Glycerol Stimulant suppository Works well and is low risk
Microlax Enema to soften stools Low risk
Due to the intrusive nature and possibility of injury associated with rectal enemas, it is not recommended that carers, as defined in these Guidelines, administer enemas other than Microlax.
Microlax enemas are suitable for children less than three years old and, as such, present minimal risk of injury to children or adults during administration.
Consumer Medication Information is available for all medications, and carers should read it before administering Microlax and any other bowel medication.
Bowel Care Guidelines, V1.1, January 2016 10

1.4 Resources
1. Management of lower bowel dysfunction, including DRE and DRF. Royal
College of Nursing, 2012
2. Help patients win the constipation battle. Best practice in the prevention and
treatment of constipation in adults under 65 years. Dept Health and Ageing and
Griffith University, Sept 2003
3. The bowel management package. Hunter New England NSW Health, 2006
4. Management of constipation in older adults. Best Practice Vol 12 Issue 7, 2008
5. Impact. Bowel care for the older patient, 2010
6. Constipation. Fact Sheets. Westmead Children’s Hospital
2 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version. Following any subsequent reviews and approval this document will be uploaded to the internet and/or intranet and all previous versions removed.
Bowel Care Guidelines, V1.1, January 2016 11

Part C1: My support plans: Bowel chart My name:
Date of birth
CIS number TRIM number
Amount and code Code Amount Code
Smear Sm Large – 1 cup or more L
Small – ¼ cup S Unobserved Un
Moderate – ½ cup M
Bristol Stool Chart (Heaton, K W & Lewis, S J 1997, 'Stool form scale as a useful guide to intestinal transit time'. Scandinavian Journal of Gastroenterology, vol.32, no.9, pp.920 – 924)
Type 1 Type 2 Type 3 Type 4 Type 5 Type 6 Type 7
Separate hard lumps like nuts (hard to pass)
Sausage-shaped but
lumpy
Like a sausage but
with cracks on its surface
Like a sausage or snake,
smooth and soft
Soft blobs with clear-cut edges (passed easily)
Fluffy pieces with ragged edges, a
mushy stool
Watery, no solid pieces.
Entirely liquid
Record the person’s bowel movements on each shift, if required, including bowels not open (BNO), in the Bowel Chart below. If there are any changes to the person’s usual bowel pattern it must be reported immediately to the person’s GP for action.
Health Planning, Tools and templates, V1.3, June 2016 1

Part C: My support plans: Bowel chart My name:
Date Day
(A shift)
Evening
(B shift)
Night
(C shift)
Type 1-7 Bristol Stool Chart
Amount Other observations Person completing entry
e.g.1.8.15 Nil Nil Yes 3 S Nil P. Evans
Record the person’s bowel movements on each shift, if required, including bowels not open (BNO), in the Bowel Chart. If there are any changes to the person’s usual bowel pattern it must be reported immediately to the person’s GP for action.
Health Planning, Tools and templates, V1.3, June 2016 2

Comprehensive Health Assessment Program (CHAP) 2015
Version 15
Queensland Centre for Intellectual and Developmental Disability

Comprehensive Health Assessment Program (CHAP) 2015
PERSON (with intellectual disability)
FAMILY MEMBER / SUPPORT STAFF
GENERAL PRACTITIONER
STEPS TO FOLLOW:
1. Person, family member and/or support staff is to fill in the first part of this book for
the person. It is OK to get information from records, family members and staff.
2. Make a long appointment for the person with his/her usual GP.
3. Take this book to the appointment with the GP.
4. If the clinic has a Practice Nurse, then speak with them about completing this
assessment as s/he may be able to assist.
5. The GP will look through the first part of this book, and fill in the second part while
examining the person.
6. It is important that the Action Plan is filled in at the end of the consultation. One
copy of the Action Plan is to be kept with the person’s personal record.
7. Medicare supports this assessment. Ask the GP.
People with intellectual disability generally have poor health and their health-care is generally of a
low standard. The CHAP was designed to improve the interaction between GP and patient with
intellectual disability through dedicated health history taking by the carer or person and guidelines
for the GP around commonly missed health issues for this population. Use of the CHAP can
improve the health of a person with intellectual disability. Several randomised controlled trials and
observational studies have demonstrated its beneficial effect through the detection of new disease
enhanced health screening and promotion. Find more health information on our website
http://www.qcidd.com.au/
For further information, please see our contact details below. © 2015 The University of Queensland,
Brisbane, Australia - Not to be reproduced in any form without the expressed written permission of the Queensland
Centre for Intellectual and Developmental Disability, the School of Medicine, The University of Queensland - Contact
QCIDD on 61-7-31632412 or [email protected] - This information is updated on an annual basis in line with current
evidence and national and international guidelines.
1

Comprehensive Health Assessment Program (CHAP) 2015
Please tick in the boxes below if the person has experienced any of the following signs and symptoms in the last year. If you are unsure or don’t know the answer, please tick the “unsure/don’t know” box.
To make an accurate medical assessment of the person's health, the doctor needs to know about these signs and symptoms.
1). BREATHING SYSTEM YES NO Unsure/
don't know
Does the person cough? Does the person cough up blood? Does the person cough up stuff/mucous/sputum? Does the person get short of breath? Does the person wheeze?
2). HEART SYSTEM
Does the person have chest pain?
Does the person’s heart “race”/beat quickly?
Do the person’s ankles swell?
Does the person get short of breath while lying in bed?
Does the person get blue skin (e.g. fingers/lips/toes)?
YES
NO Unsure/
don't know
3). MUSCLES & JOINTS YES NO Unsure/
don't know
Does the person have joint pain or back pain? Does the person have muscle pain?
2

Comprehensive Health Assessment Program (CHAP) 2015
4). STOMACH & BOWEL SYSTEM
Has the person lost weight?
Does the person have trouble swallowing?
Does the person regurgitate/vomit?
Does the person get “heart burn”?
Does the person have diarrhoea?
Does the person have black bowel motions?
Does the person get constipated?
Does the person lose control of bowel movements?
Does the person have abdominal/stomach pain?
YES
NO Unsure/
don't know
5). URINARY SYSTEM YES NO Unsure
don't know
Does the person have pain when passing urine? Does the person have blood in the urine? Does the person lose control passing urine/incontinence? Does the person urinate a lot/more than usual?
6). NERVOUS SYSTEM YES
(Please note that epileptic episodes are not included here)
Does the person faint? Does the person get unsteady when walking? Do the person's arms or legs become weak? Does the person have tingling or strange feelings
in the skin?
NO Unsure/
don't know
7). PAIN PERCEPTION
What is the person’s perception of pain?..................................................................
How does the person communicate pain?.................................................................
…………………………………………………………………………………………………………………..
3

____________________________________________________________
______ ___________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
8). MEDICATIONS
It is important for the doctor to know ALL medication.
List the medication/s prescribed by any doctor.
Name How often and how much is taken?
List medications bought “over the counter” without a script, including alternative health remedies.
Name How often and how much is taken?
9). SLEEP - Are there any problems with sleep? YES NO Unsure
YES
10). ALLERGIES Please list any medications the person is allergic to:
4

_______________________________________________________________________
_______________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
11). CAUSE OF INTELLECTUAL DISABILITY YES NO Unsure/
don't know
Is the cause of intellectual disability known?
If YES Please state cause:
12). EPILEPSY YES NO Unsure/
don't know
During the person’s life, has he or she had epileptic seizures/ fits?
If NO Please go to Question 13
If YES Please list the type and number of seizures during the last year.
Type of Seizures Number Usual duration
Which doctor treats the epileptic seizures/fits?
GP
Neurologist
Other:
When did this doctor last review the person’s epilepsy?
(month and year if known) ___/___/_____
Since this review, have the seizures:
Become worse
(Please tick one)
_______________
Unknown (Please tick one)
Remained the same Improved
5

______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
13). HUMAN RELATIONS YES NO Unsure/
don't know
Has the person ever been sexually active? Has the person ever been abused? (sexual, physical or psychological)
Comments:____________________________________________________________
FOR MEN, PLEASE GO TO QUESTION 15:
14). WOMEN'S HEALTH YES NO Unsure/
don't know
Does the woman have menstrual periods? Does the woman use Depo Provera? Does the woman use Implanon? Does the woman take the oral contraceptive pill?
What is the name of the pill: ______________________________________
Date of last period ___/___/_____ N/A
YES NO Unsure/
don't know
Does the woman have any of the following:
Pre-Menstrual Syndrome? Mid-cycle bleeds? Painful periods? Abnormal vaginal discharge? Vaginal irritation (eg. thrush)? Menopausal symptoms (e.g. hot flushes)?
6

__________________________________________________________________________
_______________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
WOMEN'S HEALTH (cont'd)
Women with intellectual disability have the same reason for needing a Pap Smear test as women in the general population. A test every two years is recommended for women (between 18 and 70 years) who have ever been sexually active.
YES NO Unsure/
don't know
Has the person had a Pap smear? If YES When was the last test: ___/___/___
If NO Does the person need a Pap smear?
If a Pap smear is needed but has not happened, please indicate why:
Distress Pap smear planned Desensitisation/preparation planned Desensitisation/preparation in progress Other:
A mammogram should be arranged every 2 years for women over 50 years of age, or women with a family history of breast cancer.
YES NO Unsure/
don't know
Are the woman's breasts checked by a GP?
Has the woman ever had a mammogram? If YES When was the last mammogram? ___/___/_____
If a mammogram is needed but has not happened, please indicate why:
Distress Mammogram planned Desensitisation/preparation planned Desensitisation/preparation in progress Other:
FOR WOMEN, PLEASE GO TO QUESTION 16 ON THE NEXT PAGE
7

_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
_______________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
15). MEN'S HEALTH YES NO Unsure/
don't know
Does he have any abnormality or discharge from his penis? Does he have undescended testes?
16). PROBLEM BEHAVIOURS YES NO Unsure/
don't know
Does the person have any problem behaviours?
If YES Please describe the behaviours and any help the person receives for these
behaviours:
17). MENTAL HEALTH YES NO Unsure/
don't know
Does the person have a psychiatric illness? If YES Please describe the psychiatric illness and any help the person receives for the psychiatric illness:
8

________________________________________________________________
________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
18). VISION YES NO Unsure/
don't know
Does the person have a known problem with vision? If YES Please describe the problem:
If NO YES NO Unsure/
don't know
Do you suspect the person may have a problem with vision? Has the person ever been prescribed glasses? Does the person usually wear the glasses? When was the last vision test?
(month and year if known) __/_____ Unknown Never
Who performed this test?
Eye doctor / ophthalmologist Optometrist GP Test while at school Unknown
Result of last vision test:
Normal Unknown
Abnormality found Please describe:
9

_________________________________________________________________________
_________________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
19). HEARING YES NO Unsure/
don't know
Does the person have a problem with hearing?
If YES Please describe the problem:
If NO YES NO Unsure/
don't know
Do you suspect the person has a hearing problem?
When was the person’s last hearing test?
(month and year if known) ___/_____ Unknown Never
Who performed this test?
Audiologist GP
Other: __________________________________
Result of last hearing test:
Normal Unknown
YES NO Unsure/
don't know
Has the person been prescribed a hearing aid?
Does the person usually wear the hearing aid?
10

Comprehensive Health Assessment Program (CHAP) 2015
20). HEALTH PROMOTION & SCREENING
a). Dental: Date of last review: ___/___/_____
b). Blood pressure: Date of last check: ___/___/_____
c). Cigarettes smoked (per day):
d). Alcohol (Standard drinks per week):
Unknown
Unknown
e). Thyroid function test (TFT): If the person has Down syndrome, when was the most recent test?
Date: ___/___/_____ Unknown
f). Vitamin D test: Date of last review: ___/___/_____ Unknown
Vitamin D deficiency appears to be quite common in people with intellect
g). Bowel cancer test: Date of test: ___/___/_____
ual disability.
Unknown Current guidelines recommend that men and women aged over 50 years should complete a bowel cancer screening test known as a Faecal Occult Blood Test every two years. People may also need a bowel cancer assessment if they have a family history of bowel cancer, a personal history of bowel disease or symptoms of bowel cancer such as bleeding from bowel, changes in regular bowel habits, cramping or abdominal pain, or feelings of general weakness, tiredness and breathlessness.
h). Diabetes test: Date of test: ___/___/_____ Unknown
21). ACTIVITY & LIFESTYLE (Inactivity and poor diet can lead to significant health problems and depression)
a) Have there been any mobility changes over time? Yes No
b) Has there been any decline in the person’s abilities? Yes No
c) Does the person have sufficient exercise? Yes No
d) Does the person have any diet problems or abnormal eating behaviours?
Yes No e) How could the person’s diet be improved?
11

Comprehensive Health Assessment Program (CHAP) 2015
22). IMMUNISATIONS YES NO Unsure/don't know
a). Tetanus/Diptheria/Pertussis
If YES Date of most recent immunisation: ___/___/_____
If NO Reason why: ______________________________
b). Hepatitis A (If required- check with the GP)
If YES Date of most recent immunisation: ___/___/____
If NO Reason why: __________________________
c). Hepatitis B (If required- check with the GP)
If YES Date of most recent immunisation: ___/___/____
If NO Reason why: __________________________
d). Influenza (If required- check with the GP)
If YES Date of most recent immunisation: ___/___/_____
If NO Reason why: ______________________________
e). Pneumococcus (If required - check with the GP)
If YES Date of most recent immunisation: ___/___/_____
If NO Reason why: ______________________________
f). Measles, Mumps and Rubella (Check with the GP)
If YES Date of most recent immunisation: ___/___/_____
If NO Reason why: ______________________________
g). Cervical Cancer – for women (Check with the GP)
If YES Date of most recent immunisation: ___/___/_____
If NO Reason why: ______________________________
12

________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
23). PERSON'S MEDICAL HISTORY
Please list any information about the person’s health history, which has not been recorded in this booklet. Consider medical problems, surgery/operations, gynaecological, obstetric and psychiatric conditions:
24). FAMILY MEDICAL HISTORY
Has anyone in the person's family (blood relation) had any of the following conditions?
YES NO Unsure/
don't know
Diabetes Psychiatric Disorders Heart Disease Epilepsy Breast Cancer Intellectual Disability Bowel cancer
25). SUMMARY OF HEALTH CONCERNS
List the concerns that you have about the person’s health.
Remember: If the clinic has a Practice Nurse, then speak with them about completing this assessment as
s/he may be able to assist. This will make the consultation with the GP easier.
13

Comprehensive Health Assessment Program (CHAP) 2015
For the GENERAL PRACTITIONER
Thank you for reviewing this person's health care
Date of visit ___/___/_____
A. Please review the history provided in the First section.
B. The following list shows commonly neglected areas of health in this population:
cause of intellectual disability hearing and vision impairment +/- unrecognised pathology
incomplete immunisation schedules
health screens - BP, skin, breast, Pap smear
obesity / malnutrition
over-use and inadequate review of tranquillisers/anti-convulsants
unrecognised constipation
unrecognised reflux oesophagitis / H.pylori infection / dysphagia
psychiatric assessment / management
epilepsy assessment / management
unrecognised pain or infections
poor dental care
unrecognised osteoporosis
undescended testes/ hypogonadism
Vitamin D deficiency
information about menstrual management
information about human relations.
The Medicare Benefits Schedule items for Health Assessments provided for people with an intellectual disability are 701 (brief), 703 (standard), 705 (long) or 707 (prolonged). The Chronic Disease Care Management items are GP Management Plan (item 721), Team Care Arrangements (item 723).
Please perform a COMPREHENSIVE REVIEW of your patient’s health: -Full physical examination
Screening areas often neglected Urine analysis
Other tests you feel are indicated Please record your findings on the following pages
*The last page of this book has syndrome specific information for you to keep
Use of the CHAP can improve the health of a person with intellectual disability. Several randomised
controlled trials and observational studies have demonstrated its beneficial effect through the
detection of new disease, enhanced health screening and promotion. Contact QCIDD on 61-7-31632412
or [email protected] This information is updated on an annual basis in line with current evidence and national and
international guidelines. Find more useful information about intellectual and developmental disabilities on our
website http://www.qcidd.com.au/
14

Comprehensive Health Assessment Program (CHAP) 2015
1). Height: ___ cm Weight: __ kg Blood Pressure: ____ mmHg Pulse Rate____
If the person has a weight / blood pressure problem, please specify action taken: -
Weight control: _________________________________________________________
Hypertension: _________________________________________________________
Is waist measurement necessary?
2). Systems Check
Please perform a complete comprehensive physical examination
NEW FINDINGS
CARDIOVASCULAR
RESPIRATORY
MUSCULO-SKELETAL
RENAL / UROGENITAL
ENDOCRINE
GASTROINTESTINAL
NERVOUS
PSYCHIATRIC/ BEHAVIOURAL
SKIN
3). Mental Health – People with intellectual disability have very high rates of mental ill health which is often unrecognised.
Is there any evidence of an underlying psychiatric disorder?
GP-1
15

______________________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
4). Epilepsy (if present)
Has the person’s seizure control been reviewed? Yes No
Has a referral been considered? Yes No
5). Vision test (A special “Reading Card” is on the back of this book to aid testing)
Has the person’s vision been tested? Yes No
Test result: Both eyes___________ R)_________ L)___________
Unable to test
Uncertain If abnormal, unable to test or uncertain, consider referral.
6). Hearing test (Appropriate hearing test: Whisper test both sides at 0.6 metre & tympanometry)
Has an otoscopy been performed? Yes No
Test result: R)_________ L)___________
Unable to test
Uncertain If abnormal, unable to test or uncertain, consider referral.
7). Aetiology - If there is no definitive diagnosis:
FIRST Recommend testing for karyotype and Fragile X, a urinary and plasma metabolic screen
THEN Recommend a CGH Microarray (In some situations, this may not be covered by Medicare)
AND Recommend the person is referred to a genetics clinic every five years
8). Sleep – Does the person have sleep apnoea or sleep problems? Yes No
9). Women's Health
Was a breast examination undertaken? Yes No
Was a Pap smear test taken/organised for the future? Yes No
10). Men's Health
Was the person checked for undescended testicles? Yes No
Does this person need prostate screening? Yes No
11). Sexual and reproductive health Recommend a review of their reproductive health, sexual activity and sexual development
GP-2
16

______________________________________________________________________________
______________________________________________________________________________
Comprehensive Health Assessment Program (CHAP) 2015
12). Abuse Check for signs of physical, psychological or sexual abuse
13). Dental Health
Has the person been reviewed by a dentist in the last six months?
Is there obvious dental pathology?
Yes
Yes
No
No
14). Dysphagia or gastro-oesophageal disease (especially for people with cerebral palsy)
Has the person been assessed? Yes No
15). Bowel and bladder function
Does the person experience incontinence?
Does the person have chronic constipation?
Has the person had a test for bowel cancer?
Yes
Yes
Yes
No
No
No
16). Activity and Lifestyle (Inactivity and poor diet can lead to significant health problems and depression)
Have there been any mobility changes over time? Yes No
Has there been any functional decline over time? Yes No
Does the person have sufficient exercise? Yes No
Does the person have any diet problems/abnormal eating behaviours? Yes No
Is a referral needed for any of these? Yes No
17). Health Promotion and Screening
Blood Glucose tested? Yes No
Lipid Screen tested? Yes No
Thyroid function tested? (especially in people with Down syndrome) Yes No
Colorectal cancer assessment? (Same risk factors as general population)Yes No
Osteoporosis risk assessed? Yes No
Vitamin D deficiency, poor diet, lack of exercise, hypogonadism and medication issues all appear to be common in some people with intellectual disability.
GP-3 17

Comprehensive Health Assessment Program (CHAP) 2015
18). Immunisations - Are the following immunisations indicated?
Tetanus, diphtheria & pertussis (dTpa)
Hepatitis A
Hepatitis B
Influenza
Pneumococcus
Measles, Mumps & Rubella
HPV cervical cancer
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Influenza and Pneumococcus may be indicated for people with Down syndrome and others at risk of infectious disease. For more details, please refer to The Australian Immunisation Handbook.
http://www.immunise.health.gov.au/
19). Medication Review (including prescription and non-prescription medications)
Have the person’s medications been reviewed? Yes No
Communication of indications, side effects and interactions Yes No
If possible, would you please assist the carer or support worker to complete the "ACTION PLAN" on the following page? A copy of the "ACTION PLAN" can be given to the person and their care provider. This book needs to be returned to the care provider who came to this consultation.
Thank you for your comprehensive health review of this person. Your efforts are part of improving the poor health status of Australians with intellectual disability.
Based on this, you can make a further appointment to do the formal management plan.
The Medicare Benefits Schedule items for Health Assessments provided for people with an intellectual disability are 701 (brief), 703 (standard), 705 (long) or 707 (prolonged).
The Chronic Disease Care Management items are GP Management Plan (item 721), Team Care Arrangements (item 723).
GP-4
18

Comprehensive Health Assessment Program (CHAP) 2015
Name of Person: Address:
ACTION PLAN
Problem(s) Identified Action(s) to be Taken
MEDICATION CHANGES (Name of medication, how often, how much OR
whether to cease)
Action(s) by, Arranged by:
By when (Date) Actions completed & date
Comments or notes about the consultation:
Details of CASE CONFERENCE (including other professionals involved):
Completed by: (please print): Signature:
19

Comprehensive Health Assessment Program (CHAP) 2015
Name of Person: Address:
ACTION PLAN
Problem(s) Identified Action(s) to be Taken
MEDICATION CHANGES (Name of medication, how often, how much OR whether to cease)
Action(s) by, Arranged by:
By when (Date)
Comments or notes about the consultation:
Details of CASE CONFERENCE (including other professionals involved):
Completed by: (please print): Signature:
20

Comprehensive Health Assessment Program (CHAP) 2015
SYNDROME SPECIFIC LIST FOR GENERAL PRACTITIONERS
SYSTEM CEREBRAL PALSY DOWN SYNDROME PRADER-WILLI 1:500 1:700 1:25,000
AUDIOVISUAL Visual: Increased risk of cicatricial retinopathy of prematurity, cortical visual impairment, strabismus Hearing: Sensorineural hearing
Visual most common - Refractive errors (myopia, hyperopia, astigmatism), Strabismus, Nystagmus Hearing: Otitis media affects 50 to 70 % DS children Annual assessments recommended
Strabismus
Myopia
ENDOCRINE Thyroid dysfunction & diabetes (both hypo or hyperthyroidism) – Hypo is more common - Annual TFT recommended Growth, short statue, obesity
Hypothalamic & pituitary dysfunction Growth hormone deficiency Adrenal insufficiency Hypothyroidism, Type 2 Diabetes, Hypogonadism, Delayed puberty
PSYCHIATRIC/ Depression Depression Hyperphagia PSYCHOLOGICAL
Neurodevelopmental disorder or intellectual disability
Alzheimer’s type dementia (Clinical onset uncommon before 40 years) Intellectual disability
Impulse control difficulties Self-injury
C.N.S. Epilepsy Epilepsy
(Usually clonic/tonic)
CARDIOVASCULAR Congenital Heart Defects (Common - in 40 to 50%)
ADDITIONAL Genito-urinary problems Incontinence, Constipation Dental problems Recurrent aspiration Oesophagitis, Reflux +/-bleeding/anaemia Swallowing/eating difficulties - Speech disorders affect 40-50% Abnormal function of oropharyngeal muscles Orthopaedic disorders Osteopenia Pulmonary disease (caused by reflux & aspiration) Growth failure
Blood dyscrasias Childhood leukaemia – AML, ALL Sleep apnoea Increased risk of infections Coeliac disease Urological abnormalities Skin disorders Gastrointestinal abnormalities
Infantile failure to thrive, then hyperphagia and severe obesity High tolerance to pain Decreased ability to vomit Sleep apnoea Osteoporosis Undescended testes Dental Abnormalities Hypertension Gastroesophageal reflux Orthopaedic problems (scoliosis)
INHERITANCE 75% prenatal causes 8-10% perinatal asphyxia
Most cases are sporadic; 4% due to translocation involving chromosome 21 or rarely, parental mosaicism
Atypical. Most cases are sporadic.
21

Comprehensive Health Assessment Program (CHAP) 2015
SYNDROME SPECIFIC LIST FOR GENERAL PRACTITIONERS
NEUROFIBRO MATOSIS RETT NOONAN TUBEROUS SCLEROSIS Type 1 - 1:3,000
SYSTEM 1:10,000 FEMALES <1:10,000 1:6,000-17,000 Type 2 - 1:30,000
AUDIOVISUAL Refractory errors Strabismus, refractive errors
Vision/hearing impairments
Retinal tumours Eye rhabdomyomatas
Hearing impairment (Glioma affecting auditory nerve) Optic gliomas
ENDOCRINE Various endocrine abnormalities
PSYCHIATRIC/ PSYCHOLOGICAL
Severe intellectual disability Mild intellectual disability Variable intellectual capacity Sleep problems Hyperactivity Aggressive behaviour Autism spectrum disorder
Variable intellectual capacity Increased risk of attention deficit disorders
C.N.S. Epilepsy Vasomotor instability
Epilepsy Cerebral astrocytomas
Epilepsy
Variable clinical phenomena depending on site of the tumours Epilepsy
CARDIOVASCULAR Prolonged QT interval Pulmonary Valvular Stenosis
ASD, VSD, PDA Rhabdomyomatas Hypertension
Rarely structural cardiac complications Increase in blood pressure with age
MUSCULAR/ SKELETAL
Osteopenia Fractures Scoliosis Gate abnormality
Scoliosis Talipes equinovarus Pectus carinatum/ excavatum
Bone Rhabdomyomata
Skeletal abnormalities esp. Kyphoscoliosis
ADDITIONAL Hyperventilation Apnoea Reflux Feeding difficulties Growth failure Partial or complete loss of acquired spoken language Partial or complete loss of purposeful hand skills Impaired sleep pattern
Abnormal clotting factors, Platelet dysfunction Undescended testes, Deficient spermatogenesis Lymphoedenoma Hepatosplenomegaly Cubitus valgus, Hand abnormalities Characteristic facial features Short stature (80%)
Kidney & lung hamartomata Polycystic kidneys Liver Rhabdomyomata Dental abnormalities Skin lesions Subependymal nodules
Variable clinical phenomena depends on neurofibroma location Tumours susceptible to malignant change Cafe au lait spots Axillary and inguinal freckling Usually back pain & headaches Phaeochromocytoma & renal artery stenosis rare
INHERITANCE Usually sporadic. X linked.
Autosomal dominant, may be sporadic
Autosomal dominant Autosomal dominant
22

Comprehensive Health Assessment Program (CHAP) 2015
SYNDROME SPECIFIC LIST FOR GENERAL PRACTITIONERS
FRAGILE X PHENYLKETONURIA ANGELMANN SYNDROME WILLIAMS SYSTEM 1:4,000 to 7,000 1 1:13,500-1:19,000 1:10,000-52,000 <1:20,000
AUDIOVISUAL Visual Impairment – Multifactorial, Strabismus
Hearing Impairment - Recurrent ear infections
Glaucoma Strabismus is possible
Hyperacusis Strabismus
ENDOCRINE Diabetes Hypercalcaemia Hypothyroidism
PSYCHIATRIC/ PSYCHOLOGICAL
Attention deficit/ hyperactivity Variable intellectual capacity Disabled in social functioning Anxiety & Autism Spectrum Disorders
Variable intellectual capacity Phobic anxiety Disabled in social functioning
Easily excitable Hyperactive
Variable intellectual capacity Attention deficit problems in childhood
C.N.S. Epilepsy (Usually clonic/tonic, complex partial)
Epilepsy Hyperactivity Tremor & pyramidal tract signs Extrapyramidal syndromes
Severe developmental delay Epilepsy
Perceptual & motor function reduced
CARDIOVASCULAR Aortic dilatation, Mitral Valve prolapse (related to connective tissue dysplasia
Cardiac abnormalities Hypertension, CVAs Chronic hemiparesis
MUSCULAR/ SKELETAL
Herniae (CT related) Abnormalities of speech & language Avoidant behaviour Delayed language development Obesity & hyperphagia
Eczema Low phenylalanine diet provides considerable benefit Excessive sadness, fear & anxiety; sense of isolation & poor self-image Osteopenia
Joint contractures & scoliosis (in adults)
Joint contractures Scoliosis Hypotonia
ADDITIONAL X linked
Autosomal recessive Speech impairment, Movement & balance disorder; Characteristic EEG changes; Gastrointestinal problems; Orthopaedic problems; Sleep problems; Obesity; Microcephaly
Renal abnormalities Short stature Characteristic facial features (elfin) Gastrointestinal problems
INHERITANCE Variety of genetic mechanisms on Chromosome 15
Microdeletion on chromosome 7
Adapted from an original unpublished version by Michael Kerr and Glyn Jones
1 Permutation prevalence - 1 in 130-250 females; 1 in 250-810 males http://www.irdrjournal.com/files/IRDR_2014Vol3No4_pp100_182.pdf 23

Comprehensive Health Assessment Program (CHAP) 2015
A
V T
U
X O
H
24

Chronic Disease Guidelines
Document name Chronic Disease Guidelines
Policy Health and Wellbeing Policy
Version number 1.0
Approval date January 2016
Policy manual Health and Wellbeing Policy and Practice Manual Volume 2
Approved by Deputy Secretary, ADHC
Summary The Chronic Disease Guidelines provide support workers with information and guidance to understand chronic health conditions that are commonly diagnosed in people with disability. The Guidelines help support workers to recognise when the person they support is unwell, and to know when the person needs to see the GP.
Replaces document Health Care Policy and Procedures, 2012 and Attachments 1 - 13
Authoring unit Contemporary Residential Options Directorate
Applies to People who are being supported in ADHC operated accommodation support services.
Review date 2017

1.1
Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version
Each subsequent revision of the final document increases by 0.1, for example version 1.2, Version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 Chronic Disease Guidelines V1.0
Chronic Disease Guidelines, V1.0, January 2016 2

Table of contents 1 Introduction............................................................................................4
1.1 Chronic disease ..............................................................................4
1.2 Examples of chronic disease ..........................................................4
1.3 Risks associated with chronic disease............................................5
1.4 Importance of managing chronic disease........................................5
1.5 Self-managed chronic disease........................................................5
1.6 Roles and responsibilities in chronic disease support .....................6
2 Specific chronic diseases ...................................................................10
2.1 Arthritis..........................................................................................10
2.2 Asthma..........................................................................................11
2.3 Cancer ..........................................................................................14
2.4 Cardiovascular disease.................................................................16
2.5 Chronic Obstructive Pulmonary Disease (COPD).........................18
2.6 Dementia.......................................................................................20
2.7 Dental and oral disease ................................................................22
2.8 Depression and anxiety ................................................................25
2.9 Diabetes .......................................................................................27
2.10 Gastro Oesophageal Reflux Disease (GORD)..............................29
2.11 Osteoporosis.................................................................................31
3 Policy and Practice Unit contact details ............................................33
Chronic Disease Guidelines, V1.0, January 2016 3

1 Introduction
The ADHC Chronic Disease Guidelines (the Guidelines) embody the principles of legal and human rights found in the New South Wales Disability Service Standards (the Standards), the commitment to deliver culturally responsive services to Aboriginal people under the Aboriginal Policy Statement (the Statement) and the person centred guiding principles of the ADHC Health and Wellbeing Policy.
The Guidelines are provided to support people with disability to exercise their rights and entitlements under the Standards and Statement. The Guidelines describe how ADHC supports people to recognise chronic disease, to know the risks associated with chronic disease and to understand the importance of managing chronic disease under the guidance of their ‘usual’ General Practitioner (GP)1 and other health specialists.
Chronic disease is associated with symptoms that can cause a person to feel unwell or to be limited in performing daily activities. People with chronic disease require specific health care to lessen the impact of symptoms on their lives.
1.1 Chronic disease
A chronic disease is one that has been (or is likely to be) present for at least six months. It often has more than one cause, is long term, causes some form of disability and is rarely cured completely. People with disability are more likely to have a chronic disease, and to have it occur earlier, than people without disability2.
1.2 Examples of chronic disease
Chronic diseases that occur commonly in all people are asthma and other lung diseases, cancer, diabetes, heart disease and diseases of bones and joints. There are many others.
Chronic diseases that frequently affect people with disability are diabetes, heart disease, high blood pressure, gastro-intestinal conditions, mental illness, tooth and gum disease and lung diseases.
1 Medicare defines the person’s ‘usual’ GP as: ‘The GP (or a GP in the same practice) who has provided the majority of services to the patient in the past 12 months, and/or is likely to provide the majority of services in the following 12 months’.
2 Disability and health inequalities in Australia www.vichealth.vic.gov.au
Chronic Disease Guidelines, V1.0, January 2016 4

1.3 Risks associated with chronic disease
Lifestyle and behaviours that are known to cause and worsen chronic disease are:
tobacco smoking
diets high in fat and sugar and; low in fruit and vegetables
insufficient physical activity and
excessive alcohol consumption.
People with disability are more often represented in ‘at risk’ groups for acquiring a chronic disease for example by, being overweight, having unhealthy eating habits, being smokers and engaging less in physical activity.
For guidance on supporting a person to manage these risks refer to the Nutrition and Swallowing Guidelines and Health Promotion Guidelines in the Health and Wellbeing Policy and Practice Manual Volume 1.
1.4 Importance of managing chronic disease
When chronic disease is not managed, people can experience mental, emotional and physical ill health, pain, unplanned encounters with the health system and hospital admissions, disability and premature death.
Even with good management, a person may die from a chronic disease or from complications relating to the disease. A diagnosis of chronic disease can act as a ‘clinical trigger’ for a person or carer to think about planning for future support (end of life care planning). Planning allows the person and others to explore how they want to live with the disease, as it progresses, and as the person approaches the end stage of the illness.
For more information refer to the End of Life Care Planning Guidelines in the Health and Wellbeing Policy and Practice Manual, Volume 1.
1.5 Self-managed chronic disease3
Self management of chronic disease is an approach used in the mainstream health system. It has been shown that people who are supported to actively participate in managing their chronic disease have better health outcomes. Symptoms of their disease are reduced, progress of the disease is slowed, fewer emergency hospital visits and shorter stays in hospital are required, and visits to GP and other health professionals are less frequent. Where possible, people are encouraged to follow this approach to achieve an improved health outcome.
3 The Flinders Program TM http://www.flinders.edu.au/medicine/sites/fhbhru/self-management.cfm
Chronic Disease Guidelines, V1.0, January 2016 5

1.6 Roles and responsibilities in chronic disease support
It is important to understand the roles of those who are involved in supporting a person with chronic disease. The three main participants are the person, the carer and the GP.
1.6.1 The person
As much as possible, carers support the person to ‘self manage’ all areas of health and wellbeing, and particularly chronic disease.
The person can be supported to self manage chronic disease by being helped to understand as much as possible about the disease. This can be done in various ways:
explain the symptoms of the disease and how the GP plans to manage them
recruit a nurse or other health professional to talk to the person about the disease if carers are not able to do it
arrange with the person to attend a support group for the disease
support the person to avoid the ‘risks’ associated with the disease, for example, discuss and prepare healthy meals with someone whose disease is made worse by being overweight
explain the negative effects on the person’s life of continuing to take risks that make the disease worse
support the person during health checks and assist the health professional to communicate using a method the person understands
if the GP has provided a management plan, help the person to understand and follow it.
Aboriginal people have significantly poorer health outcomes than other Australians, and late diagnosis of disease means that many Aboriginal people enter the chronic phase of a disease before it is diagnosed.
In addition to the health support described above, the Aboriginal person can be well supported if culturally sensitive and person centred approaches are employed. The person can be supported to engage with the disability and health service systems in the following ways:
use the person’s communication profile to learn the best way of communicating information about the disease and its management
understand the person’s history and experiences, and difficult relationships, especially with hospitals
ask how the whole of life view (life-death-life) affects health care management and the person’s acceptance of a chronic disease
Chronic Disease Guidelines, V1.0, January 2016 6

ask how and where the Aboriginal person would prefer to receive services
record the name of the proper contact person to discuss health issues and provide consent
determine which health issues or practices are sensitive or taboo and who to refer to if they are
confirm whether the person or family would prefer to work with the health system through an Aboriginal Liaison Officer
ensure that the person and family understand the health service options and how they can access them.
1.6.2 The carer
In the context of these Guidelines the carer is the ‘primary carer’ and is often a support worker or nurse, but it may also be a family member or other support person.
As well as supporting the person to understand the disease, the carer can learn about its progress and symptoms and be able to recognise when the person is unwell.
Most common diseases have a national or state-based association, for example the Heart Foundation. The association’s website contains basic information about the disease and its management, and the person’s GP can provide more if it is needed.
Information about staying well and preventing certain diseases is provided in the Health Promotion Guidelines and Nutrition and Swallowing Guidelines of the Health and Wellbeing Policy and Practice Manual, Volume 1 that is located in each accommodation support unit.
A carer who is familiar with, and understands the person’s health, should accompany the person to the GP appointment.
If the GP has provided a management plan for the person’s disease, carers should understand and be able to explain and support the person to follow the plan. If the person does not agree to any part of the plan, the carer supports the person to understand the consequences of this decision, and how to achieve the best possible health outcomes.
A carer is not required to diagnose the person’s condition. However, in the course of monitoring the person’s overall health, and recording health related events in the Health and Wellbeing Log, the carer should be aware of changes that indicate the person is unwell, and be able to communicate them to the GP.
1.6.3 The GP
The doctor who manages the person’s chronic disease from ‘day-to-day’ is the person’s ‘usual’ GP. Medicare recognises the ‘usual’ GP as the doctor
Chronic Disease Guidelines, V1.0, January 2016 7

who has provided the majority of care over the last 12 months or will be providing it over the next 12 months.
Medicare supports chronic disease management with a range of Medicare items that the GP can use to identify, treat and manage chronic disease.
The GP conducts the person’s annual health assessment and provides other medical support during the year, as the person requires it. At any time the GP may decide that the person needs a management plan for chronic disease.
The GP can develop a GP Management Plan for chronic disease under Medicare (item 721) once a year. The GP assesses the person, agrees on management goals with the person and carer, identifies actions to be taken by the person, prescribes treatments and services, and enters the information in a GP Management Plan. A date for reviewing the Plan is recorded at the same time, and the GP can claim a review of the Plan under Medicare every three months.
Under the terms of Medicare, the GP is required to explain to the person and carer how the GP Management Plan is developed, and to record the person’s agreement to having the Plan. The GP must also offer the person and carer a copy of the Plan.
If the GP decides that the chronic disease requires treatment from other health professionals, a Medicare Team Care Arrangement (item 723) is used to coordinate services from a multidisciplinary team. The team must consist of at least three health or care providers, one of whom is the GP. The GP also has access to a range of Medicare item numbers for referring a person to individual allied health services (items 10950-10970).
The GP coordinates the Team Care Arrangement by collaborating with the other providers, developing a plan of treatment and service goals for all the providers, getting agreement from the person for actions contained in the treatment plan, and securing dates to review the Team Care Arrangement.
As with the GP Management Plan, the GP explains to the person and carer how the Team Care Arrangement is developed, identifies the contributing providers and their services, and gets agreement from the person to have the Team Care Arrangement. The GP must also offer the person and carer a copy of the Team Care Arrangement.
Summary of roles and responsibilities
Person report illness, pain and discomfort to carer
attend GP’s appointments with carer
agrees to management goals and actions in the GP Management Plan
Carer observe changes in the person’s health and wellbeing
record and report changes in health and wellbeing
Chronic Disease Guidelines, V1.0, January 2016 8

make appointments with the GP or other health professionals
accompany the person to the GP’s appointment
support the GP to understand the person’s communication style
understand the actions required by the person in the GP Management Plan
support the person to follow the Plan
GP identify and diagnose symptoms
develop a management plan or other disease management strategy
OR
refer the person to a specialist
explain and document the plan, and the actions required, to the person and carer
provide a copy of the plan to the person and carer
book in a review of the plan for a future date
Chronic Disease Guidelines, V1.0, January 2016 9

2 Specific chronic diseases
2.1 Arthritis4
What is it? Arthritis is the term used for more than 100 medical conditions that affect muscles, bones and joints (the musculoskeletal system). Common arthritic conditions are osteoarthritis, rheumatoid arthritis and gout.
Signs and symptoms Common symptoms of arthritis are pain, swelling, redness, deformation, weakness and loss of dexterity, often affecting joints.
Causes and risks The causes depend on the type of arthritis and can be wear and tear, related to lifestyle (inactivity and diet), the result of injury or auto-immune disease.
Treatment and management Most types of arthritis cannot be cured, but treatments can manage the symptoms. Early diagnosis is important for effective treatment, and can prevent damage to the joints.
Symptoms of arthritis are managed by following the GP Management Plan if the GP has provided one. The Plan could include prescription of medication to manage the inflammation and pain, an exercise program and other methods of maintaining mobility and managing symptoms.
If the person is following the Plan and any of the symptoms reappear or worsen, the person should consult the GP for a review of the Plan and to receive a general health check.
If the person does not have a GP Management Plan, and has pain or weakness in the joints and muscles, the GP should be consulted for an assessment of the symptoms.
Health professionals The person’s GP is the first contact for arthritis and other health concerns. The GP will provide treatment and information.
If the person does not have a clear diagnosis of arthritis the GP may make a referral to a rheumatology specialist. The specialist diagnoses and treats the condition. The person may need further referral to an orthopaedic specialist for diagnosis and surgical treatment, or for other management options.
A range of allied health professionals are available to provide support for people with arthritis. If the GP decides to use a Team Care Arrangement to manage the person’s arthritis, the person may be eligible to claim five allied health services per year from Medicare.
More information: Arthritis Australia www.arthritisaustralia.com.au
4 Sourced from Arthritis Australia www.arthritisaustralia.com.au
Chronic Disease Guidelines, V1.0, January 2016 10

2.2 Asthma5
What is it? Asthma is a disease of the tubes that carry air in and out of the lungs. Many people with asthma have allergies such as hay fever.
Asthma can be made worse by smoking tobacco or being overweight.
When a person is diagnosed with asthma it is important to have regular check-ups with the GP. The person and the GP can then manage the condition together.
Signs and symptoms Asthma causes wheezing, breathlessness and chest tightness due to widespread narrowing of the airways6. A person with asthma does not always have all the symptoms. The symptoms are often worse at night, in the early morning or during exercise.
Causes and risks While the underlying causes of asthma are not clear, people have different triggers for an asthma attack. The most common triggers are:
respiratory infections (such as the common cold)
exercise
cold weather and changes in weather
breathing cigarette smoke and other irritants
house dust mites, pollen, moulds and animal fur
work-related triggers (such as wood dust, chemicals, metal salts)
some food additives
some medicines (such as aspirin, some blood pressure drugs).
Treatment and management An asthma attack can come on gradually (with a cold) or quickly (from inhaling a trigger such as pollen). If symptoms are getting worse refer to the person’s Asthma Management Plan or consult the GP. An asthma attack can become life-threatening if not treated properly, even in someone whose asthma is usually mild or well controlled
If symptoms get worse quickly call an ambulance.
5 Sourced from the National Asthma Council Australia www.nationalasthma.org.au
6 Australian Institute of Health and Welfare http://www.aihw.gov.au/what-is-asthma/
Chronic Disease Guidelines, V1.0, January 2016 11

The person with asthma is well when:
there is no night-time wheezing, coughing or chest tightness
there is occasional wheezing, coughing or chest tightness during the day
the person needs reliever medication only occasionally or before exercise
the person can do usual activities without getting asthma symptoms
Maintain the current management regime
The person with asthma is not well when:
there is night-time wheezing, coughing or chest tightness
there are morning asthma symptoms when the person wakes up
the person needs to take reliever medication more than usual e.g. more than 3 times per week
asthma is interfering with the person’s usual activities.
Refer to the person’s Management Plan or see the doctor for a review of asthma management
The person with asthma is having an asthma attack when:
there is increasing wheezing, cough, chest tightness or shortness of breath
the person is waking often at night with asthma symptoms
the person needs to use the reliever medication again within 3 hours.
Refer to the person’s Management Plan for instructions
The person with asthma is an emergency when:
the symptoms get worse very quickly
there is severe shortness of breath
the person can’t speak comfortably or lips look blue
reliever medication gives little or no relief.
Call the ambulance on 000 and say
THIS IS AN ASTHMA EMERGENCY
Chronic Disease Guidelines, V1.0, January 2016 12

Health professionals The GP plays a central role in asthma management by assessing and reviewing the person’s condition, prescribing medication, providing education and managing acute attacks. The GP Management Plan contains comprehensive information about the person’s asthma and its management. It includes actions to help the person and carer to understand when symptoms of asthma are worsening and how they should respond.
More information:
National Asthma Council Australia: www.nationalasthma.org.au
Australian Institute of Health and Welfare: http://www.aihw.gov.au/what-is-asthma/
Chronic Disease Guidelines, V1.0, January 2016 13

2.3 Cancer7
What is it? Cancer refers to around 100 different diseases caused by uncontrolled growth of the body’s cells. Cancer can be benign (generally not dangerous although it can be) or malignant.
Signs and symptoms Detection of cancer relies partly on observation of changes in the look and feel of a person’s body, and of changes in regular body functions. Support workers have a role in supporting people to recognise when any of these changes occur, and in referring the person to the GP for further investigation.
Changes that could indicate the presence of cancer are:
changes in the shape or colour of breasts or nipples
a lump in the neck, armpit or anywhere else in the body
sores or ulcers that don't heal
cough or hoarseness that won't go away or coughing up blood
blood in a bowel motion
new moles or skin spots, or ones that have changed
unusual vaginal discharge or bleeding
unexplained weight loss.
Causes and risks Some cancers share common risks, for example, being older, female (e.g. breast cancer) or male (e.g. prostate cancer), overweight or a smoker, but the cause of many cancers is unknown.
Carers can support people to avoid some of the risks by helping protect their skin from excessive exposure to the sun, and encouraging them to eat healthy foods and including vegetables and fruit in their diets, not smoke, and have regular cancer screening checks.
Treatment and management Treatments vary depending on the type of cancer, as well as the benefits and risks of treatments. Treatments include surgery, radiotherapy, chemotherapy, hormone therapy, and complementary and alternative therapies.
The most common cancers in Australia are skin, prostate, bowel, breast, melanoma and lung cancer. Treatment of cancer can be more effective if it is found early (early detection). Screening a person for cancer is one way of detecting the disease early.
7 Sourced from the Cancer Council Australia http://www.cancer.org.au/about-cancer/early-detection/general-advice.html
Chronic Disease Guidelines, V1.0, January 2016 14

Australia has population screening programs for cancer of the breast, cervix, bowel and prostate, that are available free of charge to eligible individuals. These cancers were chosen for screening programs because they are more common in the population than other cancers (bowel, breast and prostate cancer), and can be easily detected at an early stage (all four). A person who has a screening test may not have any symptoms at the time of screening.
As people with disability access screening services less frequently than the rest of the population, it is the carer’s role to remind the person and the GP when a regular screening test is due. Difficulty accessing screening facilities and poor understanding of health issues are among the reasons for the less frequent use of screening services by people with disability.
For more information on the detection and prevention of cancers that occur in particular parts of the body refer to the Health Promotion Guidelines contained in the Health and Wellbeing Policy and Practice Manual.
Health professionals The GP is likely to be the first contact for a person who has symptoms that could indicate the presence of cancer. Initially, the GP’s role is early diagnosis and referral to specialist services. The GP has a continuing role in follow-up after diagnosis and treatment, detection of a recurrence, and support for patients to survive cancer. The GP may develop a GP Management Plan if it is the best way of managing the person’s illness following diagnosis and treatment of cancer.
Chronic Disease Guidelines, V1.0, January 2016 15

2.4 Cardiovascular disease8
What is it? Cardiovascular disease is a common term for all conditions and diseases that affect the heart and blood vessels. Common cardiovascular diseases are:
coronary heart disease
deep vein thrombosis
high blood pressure
heart failure
stroke
angina.
Signs and symptoms Pain is associated with angina, deep vein thrombosis and heart attack. Other cardiovascular conditions e.g. high blood pressure, are often only detected during a health check.
Heart attack is a common cause of death from heart disease and it is important to recognise when a person is showing any of the following symptoms of heart attack:
pain, pressure, heaviness or tightness in the chest, shoulder/s, neck, arm/s, jaw or back
nausea
dizziness
cold sweat
shortness of breath.
If a person experiences any or all of these symptoms call 000 (or 112 on a mobile if 000 does not work) for an ambulance. The sooner the ambulance attends, the less long term damage is done to the heart muscle.
Causes and risks People who are most at risk of heart disease are:
older
overweight
inactive
smokers
socially isolated, depressed and lack social support
8 From Heart Foundation http://heartfoundation.org.au/your-heart/heart-conditions
Chronic Disease Guidelines, V1.0, January 2016 16

or have
heart defects from birth
a family history of heart disease
high blood pressure
high cholesterol
diabetes.
Treatment and management Following emergency treatment, the person’s GP and carers can support a person to recover, and to achieve a good long term health outcome. Diabetics can be supported to manage blood glucose, keep within the normal range, and follow the doctor’s advice. A person, who has a heart disease, can be supported and encouraged to make practical lifestyle changes that reduce the chance of another heart attack. For example, attendance at a cardiac rehabilitation program is known to help the person resume a productive life and function more efficiently following a heart attack.
For more information on how a person with cardiovascular disease can be supported to stay well through physical activity and healthy eating, refer to the Health Promotion Guidelines and Nutrition and Swallowing Guidelines contained in the Health and Wellbeing Policy and Practice Manual.
Health professionals The GP measures the person’s blood pressure and performs general checks of heart function at the annual health assessment. If any abnormalities are detected, the GP prescribes treatments and, depending on the severity of the condition, may draw up a GP Management Plan or refer the person to a heart or vascular specialist.
Chronic Disease Guidelines, V1.0, January 2016 17

2.5 Chronic Obstructive Pulmonary Disease (COPD)9
What is it? COPD describes long term lung conditions that cause shortness of breath, including chronic bronchitis and emphysema. Many people with COPD have a combination of emphysema, chronic bronchitis and asthma.
Signs and symptoms COPD gets worse over time with increased shortness of breath, coughing and lung secretions.
Causes and risks People at risk of COPD are smokers or ex-smokers, those experiencing long term exposure to irritants in their environment including second hand smoke, those with genetic predisposition and females.
People with cerebral palsy can develop COPD due to aspiration of food and fluids, repeated lung infections or gastro-oesophageal reflux disease (see section 2.5.1 below).
Treatment and management Supporting the person to manage the disease is the best way to improve lung function and relieve some of the symptoms.
People can be supported to manage COPD in various ways:
stop smoking or avoid inhaling second hand smoke and other irritants
seek help from health professionals
understand and take GP prescribed medications
join a COPD exercise program
vaccinate against flu, pneumococcal and other infectious diseases
seek treatment for a chest infection quickly
join a support group.
Health professionals The GP may decide that the best way to manage the person’s COPD is with a GP Management Plan or Team Care Arrangement. The person and carer follow the actions recommended in the plans to work with the doctor and other health professionals in keeping track of the person’s health, and progress of the disease.
Carers can help the person to understand the management plan and support the person to follow the recommended actions. The doctor is consulted if the person is:
having trouble following the management plan
coughing more than usual
more breathless or tired than usual
otherwise obviously unwell.
9 The Australian Lung Foundation http://lungfoundation.com.au/patient-support/copd/
Chronic Disease Guidelines, V1.0, January 2016 18

2.5.1 Cerebral Palsy and respiratory problems10
What is it? Cerebral palsy is the term for a number of disorders that affect a person’s ability to move. It is a permanent life-long condition, but generally does not worsen over time. It is caused by damage to the developing brain either during pregnancy or shortly after birth.11
It is common for people with cerebral palsy, especially severe forms, to experience respiratory complications. People with cerebral palsy are often less able to cough properly and clear material from their breathing passages.
Signs and symptoms People with cerebral palsy, especially those who are not able to communicate, can have trouble expressing their discomfort, and respiratory problems can go undetected for a long time.
Some common signs of respiratory problems in people with cerebral palsy include:
recurrent chest infections
persistent cough
noisy breathing
breathing faster than normal, or difficulty breathing
bluish or greyish colour of lips or fingernails
Causes and risks Lower mobility, reduced muscle function and structural deformity can all contribute to the risk of respiratory complications. They can cause:
frequent aspiration of food and fluids
dysphagia
gastro – oesophageal reflux
poor cough and airway clearance
respiratory muscle weakness
obstructive sleep apnoea
Treatment and management Follow the treatment and management for COPD and pay additional attention to 24 hour positioning, mealtime management, oral hygiene, saliva and bowel management.
Health professionals Consult with occupational therapists, speech pathologists, physiotherapists, dentists, dental hygienists and dietitians for management of the specific needs of people with cerebral palsy.
10 MyChild http://cerebralpalsy.org/about-cerebral-palsy/conditions/respiratory/
11 Cerebral palsy alliance https://www.cerebralpalsy.org.au/what-is-cerebral-palsy/
Chronic Disease Guidelines, V1.0, January 2016 19

2.6 Dementia12
What is it? Dementia is a general term for loss of memory and other mental abilities that is severe enough to interfere with daily life. It is caused by physical changes in the brain and is often associated with ageing. There are a number of different types of dementia and the two most common forms are Alzheimer’s Disease and Vascular Dementia.
Symptoms of dementia are also found in people with Parkinson’s Disease, Huntington’s Disease, Creutzfeldt-Jakob Disease (mad cow disease) and Wernicke-Korsakoff Syndrome (a thiamine deficiency mostly caused by alcohol misuse).
Early onset of dementia is seen in some syndromes associated with intellectual disability, for example, Down Syndrome.
Signs and symptoms People with dementia may have problems with:
short-term memory
keeping track of everyday items (purse or keys)
paying bills
planning and preparing meals
remembering appointments
travelling in unfamiliar areas.
or show signs of:
apathy and depression
impaired judgement
disorientation and confusion
behaviour changes
difficulty speaking and swallowing
difficulty with mobility.
Changes in the brain that cause these symptoms are mostly permanent and get worse over time. Some conditions or lifestyle factors can cause thinking and memory problems, for example depression, medication, alcohol, thyroid, and vitamin deficiency. Thinking and memory problems can often be improved if the condition is treated.
Causes and risks Dementia is caused by damage to brain cells which prevents the cells having normal communication with each other. The body
12 Alzheimer’s Association http://www.alz.org/dementia/types-of-dementia.asp
Chronic Disease Guidelines, V1.0, January 2016 20

functions that are affected by dementia will depend on the part of the brain that contains damaged cells.
Treatment and management Treatment depends on the cause, and many types of dementia have no cure or treatment, for example, Alzheimer’s Disease. However, there are drug treatments that can temporarily improve symptoms.
A medical assessment will identify symptoms that are caused by medications or other health conditions, for example, infection or pain, and hearing or vision problems, and adjustments may be made to reduce the symptoms.
Other treatments can help reduce the behavioural responses that often accompany dementia. They include minimising the amount of change that occurs in the person’s life, for example, changes in the familiar environment or changes of familiar care givers.
Other non-medical approaches include:
monitor personal comfort
avoid arguing about facts
redirect the person’s attention
allow adequate rest between activities
explore a range of solutions
not taking the person’s behaviour personally.
Health professionals The GP is likely to be the health professional to first diagnose dementia based on the person’s medical history, physical examination, laboratory tests, and the characteristic changes in memory and day-to-day function associated with each type of dementia.
GPs can usually make a firm diagnosis of dementia from the range of tests they perform. But it is harder to be sure of the exact type of dementia because the symptoms and brain changes of different dementias can overlap. In some cases the GP may diagnose dementia but not the type. If this occurs the person may need to see a specialist such as a neurologist or psychiatrist.
Chronic Disease Guidelines, V1.0, January 2016 21

2.7 Dental and oral disease
What is it? Dental and oral disease affects any part of the mouth, teeth and gums. The two main forms are tooth decay13 and gum disease14. Oral cancer15 can occur on the lips, tongue, gums, mouth and throat.
Tooth decay is a result of plaque build-up on teeth that allows bacteria to collect and convert sugars into acids and cause cavities to develop.
Gum disease is a result of plaque that builds up on teeth near the gum line. If left untreated teeth and bone are affected and teeth can be lost.
Signs and symptoms Tooth decay is usually detected during dental examination or by pain when chewing food.
Signs of gum disease are bleeding, redness and swelling of the gums. At a more advanced stage, bad breath, bad taste in the mouth and loose teeth are additional signs of gum disease.
Symptoms of oral cancer vary and include:
a visible mass or lump that may or may not be painful
an ulcer that won’t heal
a persistent blood blister
bleeding from the mass or ulcer
loss of sensation anywhere in the mouth
trouble swallowing
impaired tongue mobility
difficulty moving the jaw
speech changes, such as slurring or lack of clarity
loose teeth and/or sore gums
altered taste
swollen lymph glands.
Causes and risks Tooth decay and gum disease are caused by a build up of plaque on teeth as a result of poor tooth brushing routines and frequent snacking on sugary foods.
13 https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/teeth
14 https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/gum-disease
15 https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/mouth-cancer
Chronic Disease Guidelines, V1.0, January 2016 22

The exact cause of oral cancer is unknown although tobacco use is thought to be a significant factor in most cases. Risks associated with oral cancer include:
tobacco use
regular and heavy alcohol consumption
advancing age
sun exposure
poor diet
poor oral hygiene and gum disease
habitual chewing of the lips or cheeks
irritants, such as breathing in smoky, or constantly polluted, atmospheres
leukoplakia (light-coloured patches of atypical cells inside the mouth)
herpes simplex infection (cold sores)
human papilloma virus infection (warts)
family history of cancer (genetic makeup).
Treatment and management Following treatment for cavities and plaque removal, ongoing oral and dental care is often performed by the person or carer. The dentist or oral hygienist can provide instruction on a tooth and gum cleaning routine that maintains good oral health.
General tips for good oral and dental health are to:
have regular dental checks
clean teeth at least twice a day after meals
use fluoride toothpaste
have a wide variety of nutritious foods
limit intake of sugary foods and snacks – especially between meals
drink plenty of tap water – especially if fluoridated.
Treatment of oral cancer depends on the size, type and location and whether it has spread and includes surgery, radiotherapy and chemotherapy. Ongoing monitoring is maintained to check for recurrence of oral cancer. Speech therapy or dietary advice may be required in addition to regular medical follow-up. Clinical psychologists, social workers and counsellors can also help people come to terms with the post-operative changes to their lives and appearance.
Tooth decay and gum disease are common problems for people with disability. Good oral hygiene requires constant monitoring and is aided by
Chronic Disease Guidelines, V1.0, January 2016 23

using an Oral Health Plan. Refer to the Nutrition and Swallowing Guidelines and Health Planning Procedures for best practice in oral health and hygiene.
Health professionals The GP may be the first to detect the presence of tooth decay or gum disease during an annual health assessment and should refer the person to a dentist or oral health professional for diagnosis and treatment.
The GP is also likely to detect symptoms of oral cancer during a routine examination and would refer the person to a specialist for tests to determine the cause. Specialists provide treatment and management of oral cancer.
The GP has a continuing role in follow-up after diagnosis and treatment for detection of a recurrence and support for patients to survive cancer. The GP may develop a GP Management Plan if it is the best way of managing the person’s illness following diagnosis and treatment of oral cancer.
Chronic Disease Guidelines, V1.0, January 2016 24

2.8 Depression and anxiety16 17
What is it? Depression is a serious and common illness. It refers to a feeling of being ‘down’ that can arise when things in life don’t seem to be going well, or sometimes, for no reason at all.
A Generalised Anxiety Disorder can develop over time and is associated with excessive worrying following a stressful event, or sometimes, for no reason at all. Other forms of anxiety disorder include:
Panic Disorder
Post Traumatic Stress Disorder
Obsessive Compulsive Disorder
Phobia.
Websites provide specific information about different forms of anxiety disorder.
Signs and symptoms Depression is associated with certain behaviours:
moodiness that is out of character
increased irritability and frustration
finding it hard to take minor personal criticisms
spending less time with friends and family
loss of interest in food, sex, exercise or other pleasurable activities
being awake throughout the night
increased alcohol and drug use
staying home from work or school
increased physical health complaints like fatigue or pain
being reckless or taking unnecessary risks (e.g. driving fast or dangerously)
slowing down of thoughts and actions.
Anxiety disorders are associated with:
persistent, excessive or unrealistic worries (generalised anxiety disorder)
compulsions and obsessions which can't be controlled (obsessive compulsive disorder)
intense excessive worry about social situations (social anxiety disorder)
panic attacks (panic disorder)
16 The Black Dog Institute http://www.blackdoginstitute.org.au/public/depression/depressionexplained/index.cfm
17 beyondblue http://www.beyondblue.org.au/index.aspx?link_id=89
Chronic Disease Guidelines, V1.0, January 2016 25

an intense, irrational fear of everyday objects and situations (phobia).
Causes and risks Depression can be caused by a mix of personal factors and recent events.
Personal factors include:
past bad experiences
personality (worrier, perfectionist, shy, low self-esteem)
high anxiety
changes in the brain (brain injury, stroke)
inherited tendency
illness or medical treatment (thyroid, cancer, infection, chronic pain).
Recent events include:
family or interpersonal conflict
recent losses and disappointments
poor working conditions
drugs and alcohol
medical illness or treatment (thyroid, cancer, infection, chronic pain).
Treatment and management The person’s GP can treat depression or anxiety if the condition is at an early stage and not severe, or may choose to refer the person to a specialist. Other treatment options include hospitalisation, and a range of therapies that can help the person to recover from an acute episode and prevent it recurring.
Health professionals The GP has access to a number of Medicare items to treat a person with a mental illness. The GP assesses the person and develops a GP Mental Health Treatment Plan (items 2700, 2701, 2715, 2717) which includes access to psychologists. The GP provides ongoing management at an extended consultation under Medicare (item 2713).
The GP refers the person to a psychiatrist if the person’s depression is severe, is complicated by medical problems, the person is likely to self-harm or requires intensive treatments or monitoring.
Similarly a person with anxiety may require referral to a psychiatrist if:
the anxiety is severe
it lasts a long time or comes back
the person is likely to self-harm
the person has failed to respond to treatment, or
the GP doesn’t feel sufficiently skilled to treat the person effectively.
Chronic Disease Guidelines, V1.0, January 2016 26

2.9 Diabetes 18
What is it? Diabetes occurs when the body produces insufficient insulin to undertake the normal body process of converting the glucose we eat in food, into energy. There are various forms of Diabetes, and Types 1 and 2 are the most common. In Type 1 the pancreas stops making insulin altogether, and in Type 2 it makes insufficient amounts.
Signs and symptoms Type 1 and 2 Diabetes have many of the same symptoms:
excessive thirst
increased urine output
tiredness and lethargy
always hungry
slow healing cuts
itching, skin infections
blurred vision
unexplained weight loss (Type 1)
gradual weight gain (Type 2)
mood swings
headaches
dizziness
leg cramps.
Causes and risks Type 1 Diabetes is an auto-immune disease. Its cause is unknown but it does have a strong family link.
Type 2 Diabetes has no single cause but risks are well known:
family history
age
being overweight
high blood pressure
Aboriginal or Torres Strait Islander background
18 Diabetes Australia http://www.diabetesaustralia.com.au/
Chronic Disease Guidelines, V1.0, January 2016 27

having given birth to a child over 4.5 kg (9 lbs), or gestational diabetes during pregnancy
some medications
some auto-immune diseases.
Type 2 Diabetes is a result of environmental and genetic factors and is more common than Type 1. The chance of developing Type 2 is greatly increased by association with any of the risks above.
Treatment and management Treatment of Type 1 Diabetes requires insulin by injection up to four times a day. It is life threatening if not treated.
Type 2 Diabetes is managed initially by healthy eating and regular physical activity. Eventually medication is needed in the form of tablets or insulin.
Type 1 Diabetes is not curable or preventable. Type 2 Diabetes may be prevented in many cases by following a healthy lifestyle of:
maintaining a healthy weight
regular physical activity
making healthy food choices
managing blood pressure
managing cholesterol levels
not smoking.
For more information on managing Diabetes with healthy eating refer to the Nutrition and Swallowing Guidelines.
Health professionals People with Type 1 Diabetes are generally referred to a specialist by the GP or hospital.
People with Type 2 Diabetes may have a GP Management Plan and Team Care Arrangement. The plan is developed by the GP to manage acute symptoms, blood sugar levels and other risk areas e.g. vision and wound healing, existing complications of Diabetes and prevention activities.
Under a Team Care Arrangement the person with Diabetes may access a Diabetes educator, dietitian, endocrinologist, ophthalmologist, physiotherapist or podiatrist for ongoing support to maintain a healthy lifestyle and prevent or manage complications of Diabetes.
Chronic Disease Guidelines, V1.0, January 2016 28

2.10 Gastro Oesophageal Reflux Disease (GORD)19
What is it? GORD is described as frequent heartburn and occurs when the stomach contents wash back up into the oesophagus (reflux) and damage the lining.
Signs and symptoms GORD causes a range of mild to extreme symptoms, the most common and well known being heartburn. This is a burning sensation in the stomach or lower chest that rises into the throat. Other symptoms include:
regurgitation causing a sour acid taste in the mouth
difficult or painful swallowing
nausea
excessive burping
chest pain
bad breath
chronic cough.
A person who is unable to verbally communicate symptoms of GORD may display the following symptoms:
distress after eating
apparent discomfort when eating
stops eating or refuses food
gags while eating
excessive saliva and dribbling
hiccups that won’t stop
night cough.
Causes and risks Symptoms of GORD usually appear after eating, and can be brought on by lying down or bending over. People who receive enteral feeding are prone to GORD and some medications can aggravate it.
Being overweight, smoking and drinking alcohol, are also among the risks for experiencing GORD.
Acid refluxing to the throat can cause pain in the throat or changes in the person’s voice, and if acid regularly reaches the mouth, it can dissolve tooth enamel.
19 http://www.mydr.com.au/gastrointestinal-health/gastro-oesophageal-reflux-disease
Chronic Disease Guidelines, V1.0, January 2016 29

Some people with GORD regurgitate acid into the lungs (aspiration) causing them to wheeze or cough. This can lead to aspiration pneumonia and cause serious health issues. It is a common condition in people with disability who have swallowing and other gut problems.
Treatment and management Avoiding foods or drink that make the symptoms of GORD worse, for example, alcohol, coffee, spicy or fatty foods, large meals and cigarettes, is a good start.
Aspirin and non-steroidal anti-inflammatory drugs may increase symptoms of GORD and should be discussed with the doctor who prescribed the medications, or where not prescribed, before using aspirin.
Milder symptoms can be managed with over-the-counter medications like antacids, but it is preferable to seek advice from the GP who is best placed to diagnose and treat GORD.
Treatment may start with medication, and be followed by tests if there is no relief from symptoms. Tests include an endoscopy, which allows the doctor to view the lining of the oesophagus and stomach for damage.
Oesophageal pH monitoring can be applied to test the gut’s acidity, and is useful for diagnosing a cough that could be caused by GORD. Surgery may be considered if medication does not provide relief from symptoms.
Health professionals The GP and a gastroenterologist are responsible for treating the symptoms of GORD.
A team of allied health professionals may be required to support the management of symptoms:
an occupational therapist for advice on correct positioning during and after meals to avoid reflux
a speech pathologist to develop a Mealtime Management Plan for a person with eating and swallowing problems
a dietitian to provide advice on foods that are suitable for a person with GORD and/or to develop an Enteral Nutrition Plan.
Chronic Disease Guidelines, V1.0, January 2016 30

2.11 Osteoporosis20
What is it? Osteoporosis refers to bones that have become weak because of calcium loss. It is not normally associated with pain and illness but, because bones become fragile and less dense, they break easily. Most commonly, breaks are in the spine, hip and wrist, and occur after a minor fall or knock.
Women are three times more likely to have osteoporosis than men.
Signs and symptoms There are usually no signs or symptoms of osteoporosis until a bone breaks.
In older people a loss of height can be a sign of osteoporosis, resulting in compression of the bones of the spine which can be painful and cause stooping21. This can increase the risk of falling and lead to difficulty with digestion and breathing.
Hip fractures require hospitalisation and surgery, and recovery can be painful and prolonged. They may also result in permanent loss of mobility.
Causes and risks There are a number of factors that can put a person at risk of osteoporosis:
family history of osteoporosis (mother, sister or grandmother) or fractures at older age
insufficient calcium in the diet
low vitamin D levels
cigarette smoking
alcohol intake of more than two standard drinks per day
caffeine intake of more than three cups of tea, coffee or equivalent per day
lack of physical activity
entering menopause before the age of 45
loss of menstrual period (and reduced oestrogen) e.g. following excessive dieting and exercise
long-term use of medications such as corticosteroids for rheumatoid arthritis and asthma.
Some health conditions can increase the risk of osteoporosis, for example:
thyroid disease or an overactive thyroid gland
20 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Osteoporosis
21 http://www.bonehealthforlife.org.au/about-osteoporosis/implications
Chronic Disease Guidelines, V1.0, January 2016 31

rheumatoid arthritis
chronic liver and kidney disease
conditions that affect the body’s ability to absorb nutrients, such as Crohn’s disease, coeliac disease and other inflammatory bowel conditions.
Treatment and management Men and women can take steps to develop and maintain bone density and prevent osteoporosis by:
having a healthy and varied diet with plenty of fresh fruit, vegetables and whole grains
eating calcium rich foods e.g. dairy food, canned sardines, white or kidney beans, sweet potato, green leafy vegetable, almonds, brazil nuts, pistachio nuts and hard tofu
getting enough Vitamin D (10 – 20 minutes of sun exposure each day, before 11am and after 3pm)
avoiding or stopping smoking
drinking less alcohol (no more than 2 drinks per day)
drinking less tea and coffee (no more than 2 cups per day)
doing regular weight-bearing and muscle strengthening activities e.g. walking, dancing, using weights.
People who are diagnosed with osteoporosis can be treated to reduce bone loss and reduce the risk of fractures with medication. While minor falls or even coughing can result in a fracture at any age, older people are at particular risk of falling, and could benefit from having a falls prevention assessment.
The best management of osteoporosis is to develop strong bones early in life, eat well, be active and avoid the known risks where possible.
For more information on managing Osteoporosis with healthy eating refer to the Nutrition and Swallowing Guidelines.
Health professionals People may be diagnosed with osteoporosis in a variety of ways:
the GP orders a bone density scan for women entering menopause
scanning a person on long term corticosteroids
during treatment for a fracture following a minor fall or knock.
The GP or a specialist (endocrinologist or rheumatologist) will diagnose osteoporosis, and recommend treatments to reduce its progression and to prevent bone fractures.
Chronic Disease Guidelines, V1.0, January 2016 32

3 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version. Following any subsequent reviews and approval this document will be uploaded to the internet and/or intranet and all previous versions removed.
Chronic Disease Guidelines, V1.0, January 2016 33

Decision Making and Consent Guidelines
Document name Decision Making and Consent Guidelines
Policy Decision Making and Consent Policy
Version number 1.0
Approval date January 2016
Policy manual Lifestyle Policy and Practice Manual
Approved by Deputy Secretary ADHC, FACS
Summary The Decision Making and Consent Guidelines affirms the rights of people to make decisions that affect them and to receive support when they want or need it to make decisions.
Replaces document New Guidelines
Authoring unit Contemporary Residential Options Directorate
Applies to People who are being supported in ADHC operated and ADHC funded non-government disability support services.
Review date 2017

Version control The first and final version of a document is Version 1.0.
The subsequent final version of the first revision of a document becomes Version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 New Guidelines
Decision Making and Consent Guidelines, V1.0, January 2016 2

Table of contents
1 Guidelines ........................................................................................... 4 2 Capacity............................................................................................... 4 3 Decision making ................................................................................. 5 4 Consent ............................................................................................... 9 5 Making decisions about services.................................................... 10 6 Information and privacy ................................................................... 10 7 Medical and dental treatment in accommodation support services
............................................................................................................ 11 8 Behaviour support............................................................................ 13 9 Consent and sexual relationships................................................... 13 10 Marriage and living in a de facto relationship................................ 14 11 Financial management in accommodation support services....... 14 12 Consent to inform family if a person is abused, assaulted or
neglected........................................................................................... 16 13 Forensic procedures ........................................................................ 16 14 Legally Appointed Decision Makers ............................................... 18 15 Definitions ......................................................................................... 19 16 Policy and Practice Unit Contact Details........................................ 26
Decision Making and Consent Guidelines, V1.0, January 2016 3

1 Guidelines The Guidelines refer to supporting people with disability to exercise their rights and entitlements to make decisions and choices about things that affect them in a range of situations.
The Guidelines are for use in Family and Community Services (FACS), Ageing, Disability and Home Care (ADHC), operated disability support services, and can be referenced by other agencies and providers.
These Guidelines introduce a number of aspects of decision making, capacity and consent. They also examine ways of supporting people to make their own decisions, when consent is required, how to support people to provide informed consent, and when input from a legally appointed decision maker is needed.
Decision making and consent is a key component of Lifestyle Planning. The associated Lifestyle Planning Guidelines and Person-Centred Thinking tools in the Lifestyle Policy and Practice Manual are useful references for supporting decision making and consent.
2 Capacity
2.1 Definition of capacity
Under the law people are presumed, in the first instance, to have the capacity to make their own decisions. The Capacity Toolkit 1 (the Toolkit) defines capacity as the ability ‘to make decisions about things that affect daily life’. The Toolkit states that:
Generally, when a person has capacity to make a particular decision they can:
• understand the facts and choices involved
• weigh up the consequences, and
• communicate the decision.
Some people may need support to exercise their capacity to make decisions that affect them, and to increase their decision making skills and confidence.
Capacity is unique to each individual and situation, and should not be assessed simply on the basis of a type of disability or a one-off assessment. A person has capacity to consent if she or he is able to understand the general
1 Department of Justice, Capacity Toolkit: http://www.diversityservices.justice.nsw.gov.au/divserv/ds_capacity_tool.html
Decision Making and Consent Guidelines, V1.0, January 2016 4

nature and effect of a particular decision or action, and can communicate an intention to consent (or refuse consent) to the decision or action.
2.2 Factors that influence a person’s capacity Capacity can be affected by a range of things including health, mood, time of day, setting, and relationship with the person seeking consent. The person may not have previously had opportunities to make decisions, or express their preferences in a way that others understand.
A person’s decision making skills, confidence and capacity can be enhanced by improving communication systems, supporting the person to understand the decision making process, and providing opportunities to practice making decisions.
2.3 Tools to support decision making capacity Using the person’s Communication Profile, Decision Making Profile and Agreement, Communication Expressive and Receptive Profiles and other tools and templates from the Lifestyle Policy and Practice manual (Tools and templates)2 will provide information to support the person and optimise their decision making capacity.
When a person has been unable to make a decision even with support, a legally appointed guardian with the specific decision making function will be required to make particular decisions.
The Capacity Toolkit (see Other Resources) is a resource that can be referred to whenever there are questions about a person’s capacity to make decisions, particularly about those with life changing consequences.
3 Decision making In their dealings with the people they support, service providers and their workers have a role in ensuring that the rights of people with disability to make decisions that affect their lives are upheld.
People make decisions every day about matters of varying importance. Those decisions that have serious consequences for the person require consent, for example, finances, receiving services, information and privacy, medical and dental treatment, risk management, behaviour support and relationships. Other decisions about what to wear, watch on television or eat for lunch, still require
2 Lifestyle Planning Tools: http://www.adhc.nsw.gov.au/publications/policies/policies_a-z/?result_237652_result_page=L
Decision Making and Consent Guidelines, V1.0, January 2016 5

the person’s agreement, but this can be obtained through a less formal process.
The way we approach different decisions may depend on a range of factors including how we make decisions (our decision making style), the significance of a decision, perception of consequences and our emotional state at the time of facing a decision. We may put more thought or effort into a critical decision, or we may act on impulse. Either way, decision making is a skill that is learnt and the outcomes of decisions can help people grow, improve decision making, and increase their capacity to participate in community life.
3.1 Supported decision making
People and their interests are at the centre of supported decision making in keeping with their rights under the United Nations Convention on the Rights of Persons with Disabilities (the UN Convention) and the Disability Inclusion Act, 2014 (NSW) (the Act).
Supported decision making is a relationship between a person with disability (the decision maker) and the person they choose to assist them with a particular decision (the supporter). A person may have more than one supporter, depending on the type of decision and how they prefer to be supported.
Some people may want additional support for decisions. They might ask for assistance, or need an offer of assistance if they appear to be having difficulty making a decision. This support can include practical help to find and access information, explore options, and consider consequences.
People with disability can experience barriers to decision making including communication (giving and receiving information), understanding information, other people’s perceptions of their ability to make decisions, and equal access to information in a format the person understands. Supported decision making can help to overcome these barriers.
The Supported Decision Making Framework3 provides person-centred resources to support and build the capacity of people to make decisions in their own lives, and help to determine who provides consent when it is required (see Other Resources). Refer to these resources for information about the different roles and steps in supported decision making.
3.2 Why support people with their decision making The decisions we make shape the life we lead and who we are as people. When we make decisions for ourselves, we feel more in control and we make
3 ‘My life, my decision – A handbook for decision makers’; ‘Supported Decision Making – A handbook for supporters’; ‘Supported Decision Making – A handbook for facilitators’.
Decision Making and Consent Guidelines, V1.0, January 2016 6

choices that are meaningful to us. When people with disability need support to make decisions, and they receive it, they have the opportunity to experience the same sense of control and meaning for themselves.
3.3 Dignity of risk People have a right to make decisions that affect their own lives that others may believe are risky or unwise. These decisions can provide opportunities for new experiences and to learn from positive outcomes and mistakes. Supported decision making upholds the person’s views and decisions, and this is particularly important where there is disagreement about the person’s decision among a person’s support network.
Where support workers or managers are concerned about the risks associated with a decision, the focus is on understanding and accepting or managing the risks, not changing the person’s decision. The Risk and Safety Policy and Procedures (Health and Wellbeing Policy and Practice Manual Volume 3) provide guidance about supporting people to make decisions that involve risk.
3.4 Vested interest and conflicts of interest A person involved in the supported decision making process may have a vested interest, that is, a personal or private reason for wanting something to be done or to happen. This may include a conflict of interest, that is, they may gain some advantage, or avoid some disadvantage, from a particular decision.
Vested or conflicts of interest can occur throughout the decision making process, from identifying a decision to acting on it. Conflicts of interest can occur between a person and the supporters they choose, such as a family member or friend, if the outcome of the decision is likely to have an impact (positive or negative) on the supporter.
Conflicts of interest may also occur between the person and support workers. A person’s goal might be in conflict with a support worker’s values and beliefs, or create additional duties for the support worker. As the person’s values and interests are primary, a support worker must put their own values and interests aside and not influence the person in their decision making.
Refer to the Supported Decision Making resources for information on identifying and managing conflicts of interest (Other resources).
3.5 Supporter and facilitator roles in supported decision making
In supported decision making, the person chooses who they want to support them or to facilitate supported decision making. People should be encouraged to seek support from natural supporters, such as family and friends, where it is appropriate.
Decision Making and Consent Guidelines, V1.0, January 2016 7

Some people won’t have natural supports in their life, or sometimes the matter requiring a decision will result in disagreement with their other supporters. For example a person may not wish to discuss intimate relationships or drinking alcohol with their parents, who would usually support them with decision making. Similarly the person may want their parents to be supporters but because the decision involves some risk, wants a facilitator to help keep the decision making on track.
Sometimes the person may choose a support worker to be their supporter or facilitator. Being a supporter or facilitator is different to being a support worker. Where a person chooses a support worker as their supporter or facilitator, these differences should be discussed with the person to make sure the roles do not become confused. The support worker can also help the person to identify other possible supports for future decisions.
There is no requirement for support workers to take on the role of supporter or facilitator. Support workers should speak with their line manager if they have any questions or concerns about being involved in supported decision making especially if the person has asked the support worker to be a supporter or facilitator.
Refer to the Supported Decision Making resources (Other Resources) for information about the roles of supporter and facilitator.
3.6 Critical decisions Critical decisions have significant immediate and long term consequences, and may therefore require more information and consideration for the person to make an informed choice. These include decisions in relation to where to live and with whom, medication and health, education and employment, and major financial decisions.
When making a critical decision the person should have the support required from trusted family or friends, and/or other supporters of their choice, to be fully informed and supported. The person may also want or need information and advice from specialists about health, financial or legal matters.
Workers involved in supporting the person must document the process to demonstrate how any decisions were reached.
3.7 Documenting decisions
Recording decisions and the decision making process will depend on the issue and the service provided. For instance, household routines, day programs and recreational activities are documented as part of Lifestyle Planning. Lifestyle Plan goals are recorded in the person’s Action Plan. Decisions about health, such as treatments or therapy services, are documented in the My Health and Wellbeing Plan.
Decision Making and Consent Guidelines, V1.0, January 2016 8

Good records assist in understanding how decisions were made by the person for future reference, and can also act as a reflection of what worked or didn’t work. These documents are legal records of how a duty of care is met during the provision of support to the person.
The Lifestyle Planning resources include a number of Person Centred Thinking tools that can be used for documenting decisions, such as the Decision Making Agreement, Important to/for and the Learning Log.
See also the Records Management Procedures for Accommodation Support Services 2015.
4 Consent Consent in this policy refers to the permission given by a person or legally appointed guardian concerning services, finances, relationships, medical and dental treatment, behaviour support and forensic procedures. For consent to be valid it must be voluntary, informed, specific and current. Consent by legally appointed decision makers can only be given on matters for which they have been authorised to give consent. More information about this can be found in section 14 of these Guidelines – Legally Appointed Decision Makers.
4.1 Voluntary consent A person must be free to exercise genuine choice about whether to give or withhold consent. This means they haven’t been pressured or coerced into make a decision, and they have all the information they need in a format they understand. Voluntary consent requires that the person is not affected by medications, other drugs or alcohol when making the decision.
4.2 Informed consent A person’s capacity to make decisions will vary depending on the type of decision or its complexity, or how the person is feeling on the day. The way information is provided to a person will also affect his or her capacity to make decisions. Choices must be offered in a way that the person understands, for example by using images or signing.
If it is required, support must be provided for the person to communicate their consent. A current Decision Making Profile (see Lifestyle Policy and Practice Manual, Tools and templates) will assist in documenting and communicating the person’s preferred decision making style and the support they need.
4.3 Specific consent
Consent must be sought for matters separately and for each occasion that it is relevant. For example, if a person requires medical treatment, the health
Decision Making and Consent Guidelines, V1.0, January 2016 9

practitioner will need to obtain consent each time they provide treatment such as prescribing medication, ordering tests or performing a procedure.
4.4 Current consent Consent must be established each time it is required. It cannot be assumed to remain the same indefinitely, or as the person’s circumstances change. People and guardians are entitled to change their minds and revoke consent at a later time.
5 Making decisions about services People will face many choices about the services that are available to them. When faced with a range of options, they may require support to decide and consent to the service, and provider of their choice. People may not want to receive all their formal supports from specialist disability services, and this should be reflected in the person’s Lifestyle Plan.
Genuine choices about support can only be made when people have had the opportunity to experience and consider a range of options. Person Centred Thinking tools (see Lifestyle Planning Policy, Tools and templates) can be used to explore the person’s interests and goals. From here, the person can develop an Action Plan to assist with decision making about the supports that will help to achieve some of their goals.
6 Information and privacy People have a right to privacy and to make informed choices about what information is collected about them and how this is used. The Privacy and Personal Information Protection Act 1998 (NSW) and the Health Records and Information Privacy Act 2002 (NSW) regulate the practices of FACS funded non-government disability support services when collecting, storing, using and disclosing person and health information. These laws have privacy principles that tell us:
• what information we can collect and how we can collect it.
• how we store and protect personal and health information.
• how people can find out what information we hold about them and if it is correct.
• how we can use and disclose information including special protection for health and other sensitive information.
• how people can complain about breaches of their privacy.
Decision Making and Consent Guidelines, V1.0, January 2016 10

The ADHC Privacy Management Plan4 provides guidance to workers on how to ensure appropriate management of information, and protecting the privacy of people they support.
7 Medical and dental treatment in accommodation support services
People should be encouraged and supported to choose their health care providers. People may have particular preferences about where they receive treatment, such as a health service or other professional of a particular gender or from a particular cultural background. The person’s preferences are documented in their My Health and Wellbeing Plan.
People must be supported to provide consent to treatment wherever possible. Support workers will assist to enable communication between people they support and treating practitioners. The person’s Communication Profile is used to record and share the best way to support the person, so they can receive and give information that is understood.
The ADHC Health Planning Procedures and Guidelines (in the Health and Wellbeing Policy and Practice Manual Volume 1) also provide information about supporting people when they access medical and health services. The NSW Council for Intellectual Disability has easy read fact sheets about health, mental health, surgery and mental health5.
From the age of 14 years a person can give consent to medical treatment, provided the doctor or health professional has determined they have capacity6. Where the person is unable to give consent, a parent can provide consent for a child up to 16 years of age.
If the person is 16 years or over, and does not understand the issue and the treatment, the NSW Guardianship Act 1987 determines who can give consent (see 7.1 Person responsible, below).
7.1 Person responsible Where a person is 16 years or over, and it has been determined that the person does not have the capacity to provide consent for medical or dental treatment, a ‘person responsible’ can give or withhold consent. The term ‘person responsible’ is defined in the Guardianship Act 1987 (see Definitions
4 https://www.adhc.nsw.gov.au/__data/assets/file/0004/234580/Privacy_Management_Plan_Jan2013.pdf
5 NSW Council for Intellectual Disability http://www.nswcid.org.au/health/ee-health-pages/easy-fact-sheets.html
6 Young people and the law: http://www.lawstuff.org.au/nsw_law/topics/medical
Decision Making and Consent Guidelines, V1.0, January 2016 11

table in Section 15). More information is available from the NSW Civil and Administrative Tribunal (NCAT) factsheet7.
The ‘person responsible’ has authority to consent on behalf of a person who is incapable of providing consent to only Minor and Major medical and dental treatment (the NCAT website has details of Minor and Major treatments8).
The doctor or dentist has responsibility to assess a person’s capacity to consent to medical or dental treatment, and to obtain consent before the treatment is performed or medication is administered. The support worker may assist the doctor or dentist by providing information about the person that can help the practitioner in making his or her assessment. If the person is unable to make a decision about receiving treatment, the support worker may assist the practitioner by providing contact details of the ‘person responsible’, or the legally appointed guardian with the medical or dental consent function.
Alternatively, the support worker may arrange for the ‘person responsible’ to attend medical or dental appointments or to be available to discuss the decision about treatment with the practitioner.
Consent is not required for the following:
• Non-intrusive examinations for the purpose of making a diagnosis.
• First Aid.
• Urgent treatment to save life or alleviate pain or distress.
Notwithstanding any of the above, the support worker will keep the ‘person responsible’ informed about appointments or examinations and any health issues facing the person.
If the person does not have a ‘person responsible’ or a guardian, then an application should be made by the doctor or dentist to the NCAT Guardianship Division for consent to treat the person using the Guardianship Division’s application form (see Tools and templates). Consent must be obtained before the treatment is given.
If a person is objecting to either Minor or Major treatment, a ‘person responsible’ cannot override a person’s objections. A guardian may be appointed with the authority to override the person’s objection if:
The person lacks understanding of what the treatment involves, and why it is being proposed; and
The treatment is clearly in the best interests of the person.
7 NCAT Person responsible factsheet: http://www.ncat.nsw.gov.au/Pages/guardianship/publications_resources/gd_fact_sheets.aspx
8 http://www.ncat.nsw.gov.au/Pages/guardianship/guardianship.aspx
Decision Making and Consent Guidelines, V1.0, January 2016 12

Requests for consent to treatment that override a person’s objections must be in writing to the NCAT. The consent to such treatment must also be in writing.
The NSW Council for Intellectual Disability has easy read Medical and Dental Treatment Fact sheets and Checklists9.
8 Behaviour support The ADHC Behaviour Support Policy (March 2012) outlines the requirements for consent for general behaviour support strategies10.
The Behaviour Support Policy also outlines additional mandatory authorisation and consent requirements for the use of Restricted Practices11.
All staff should familiarise themselves with the requirements of this policy, accessible through the following link:
http://www.adhc.nsw.gov.au/publications/policies/policies_a-z/?result_237652_result_page=B
See Other Resources for links to online ELMO e-learning modules for Restrictive Practices and Positive Behaviour Support.
9 Consent and sexual relationships A person has the legal right to consent to a sexual relationship if both partners are of legal age (legal age of consent is 16 years for both males and females whether heterosexual or homosexual), providing that the person has given free and informed consent.
Consent, as it relates to a person with disability consenting to a sexual relationship, is the permission or agreement given by the person to the relationship, as long as both partners are of legal age. To give valid consent the person must understand what they are physically consenting to, for example, petting, kissing or penetration.
The person must also understand the sexual nature of the touching, as opposed to non-sexual touching associated with washing or receiving medical treatment. Additionally, the consent given by the person must be given freely and the person must understand and be able to exercise the right to refuse a sexual relationship.
9 NSW Council for Intellectual Disability: http://www.nswcid.org.au/
10 Behaviour Support Policy (March 2012), Section 2.6. 11 Behaviour Support Policy (March 2012), Section 3
Decision Making and Consent Guidelines, V1.0, January 2016 13

A sexual relationship is a crime under Section 66F of the Crimes Act 1900 (NSW) if:
• the other person is a disability worker supervising the person; and/or
• the other person intends to take advantage of or sexually exploit the person, and knows the person has an intellectual disability.
It is the responsibility of support workers to inform and educate people they work with, who wish to engage in a sexual relationship, if support is needed.
Guidance on these issues is provided in the Sexuality and Relationships Guidelines (in the Lifestyle Planning manual) or on the Family Planning NSW website http://www.fpnsw.org.au or by telephoning the Family Planning health line on 1300 658 886.
10 Marriage and living in a de facto relationship
Consent, as it relates to a person with disability agreeing to marry or live in a de facto relationship, is the permission or agreement given by the person to the relationship.
A person has the right to consent to marry if the nature and effect of the marriage ceremony is understood and the members of the couple are aged 18 years or over, provided that the person has given free and informed consent. The Marriage Act 196112 states that a marriage is void where a ‘party was mentally incapable of understanding the nature and effect of the marriage ceremony’.
For consent to be valid, the person must understand what she or he is consenting to, for example, living with another person, having a sexual relationship with that person, and being financially interdependent.
It is the responsibility of a person legally authorised to perform a marriage ceremony (such as a Civil Celebrant or Ministers of recognised religious denominations) to determine whether a person has capacity to give consent to marry.
11 Financial management in accommodation support services
Under Article 12 of the UN Convention, ‘all appropriate and effective measures must be taken to ensure the equal right of persons with disabilities to own or
12 Marriage Act 1961 (Commonwealth): http://www.comlaw.gov.au/Details/C2013C00164
Decision Making and Consent Guidelines, V1.0, January 2016 14

inherit property, to control their own financial affairs and to have equal access to bank loans, mortgages and other forms of financial credit, and …ensure that persons with disabilities are not arbitrarily deprived of their property”.
People who can manage their own finances are encouraged to do so, with input from natural supports if required. Principle 3 of the Disability Inclusion Act 2014 (NSW) supports this by stating that “people with disability have the right to participate in and contribute to social and economic life and should be supported to develop and enhance their skills and experience”.
People should also have access to independent advice about major financial matters such as inheritances, trust funds and making a will.
Consent is required where a person needs support from someone else to manage or handle their finances. In situations where the person has an appointed Financial Manager they should still be involved as much as possible in their finances within their capacity, and have access to supports to enable this.
Annual budgets are prepared by the support worker or appointed Financial Manager, with the person and family (if the person wishes) as part of Lifestyle Planning. The budget contains information on planned and unplanned expenditures for people who are being supported to manage their own finances.
An application to the New South Wales Civil and Administrative Tribunal (NCAT) Guardianship Division for financial management is made when:
• supported decision making does not provide sufficient safeguarding of the person’s financial interests, and/or
• there is an ongoing conflict of interest with a family member which cannot be informally resolved, and/or
• where there is no family member to informally support a person to manage their finances and assets, and/or
• there are substantial assets, such that the person would benefit from legal financial management, and/or
• the person is at risk of exploitation
• AND all attempts at supported decision making and managing identified risks have not resolved the need for formal support regarding financial matters.
If the case manager or support worker believes that any of these factors exist they should refer the matter to their line manager. The relevant line manager or more senior manager should make an application to the NCAT Guardianship Division to appoint a financial manager.
Decision Making and Consent Guidelines, V1.0, January 2016 15

12 Consent to inform family if a person is abused, assaulted or neglected
Family members should be informed about any incident of abuse of a person as long as the person can and does consent to them being so informed. In this case the person must have the capacity to give or withhold consent as described in these Guidelines under sections 2 (Capacity) and 4 (Consent).
The person, or their legally appointed guardian who has been appointed for the purposes of decision making, can refuse consent to their family being informed of an incident of abuse. Consideration is given to the potential impact on the person who has been abused, and any investigation, before a decision is made.
A decision not to inform the family does not preclude ADHC’s abuse, neglect and incident reporting protocols within ADHC operated accommodation support services. Workers are still required to follow the reporting requirements outlined in the ADHC Abuse and Neglect Procedures; the Incident Reporting and Management Guidelines for Ageing and Disability Direct Services, and other relevant policies, procedures and guidelines.
ADHC funded non-government disability support services should follow their own abuse, neglect and reporting protocols.
13 Forensic procedures Where it is suspected that a crime has been committed, police will investigate. Their investigation can include forensic procedures13, which involve the collection of certain types of physical evidence.
13 Crimes (Forensic Procedures) Act 2009
‘Forensic procedure’ means:
a) an intimate forensic procedure, or
b) a non-intimate forensic procedure,
but does not include
c) repealed
d) any intrusion into a person’s body cavities except the mouth, or
e) the taking of any sample for the sole purpose of establishing the identity of the person from whom the sample is taken
Note: Paragraph (e) makes it clear that the Act only applies to samples taken for forensic purposes and not to samples taken purely to establish the identity of a person.
For the definition of the terms ‘intimate forensic procedure’ and ‘non-intimate forensic procedure’ please refer to Section 15 of these Guideline.
Decision Making and Consent Guidelines, V1.0, January 2016 16

13.1 For suspects If NSW Police is investigating a crime and wish a person who is a suspect in the investigation to submit to a ‘forensic procedure’ (as defined by the Crimes (Forensic Procedures) Act), only a Magistrate or an authorised officer can provide consent when the individual is an ‘incapable person’. ‘Incapable person’ is defined in Section 3 of the Crimes (Forensic Procedures) Act, 2000, to mean an adult who is:
• incapable of understanding the general nature and effect of a forensic procedure, or
• incapable of indicating whether he or she consents or does not consent to a forensic procedure being carried out.
NSW Police is to be alerted to the fact that a person may be an ‘incapable person’ under the Crimes (Forensic Procedures) Act if the person is detained by NSW Police or asked to attend the police station for the purposes of undergoing a forensic procedure.
ADHC staff cannot provide consent for a forensic procedure to be performed on a person who is a suspect in the investigation of a crime.
Any person with intellectual disability is entitled to access specific legal supports. Free specialist legal advice and representation is available through the Intellectual Disability Rights Service (see Other Resources). Where a person comes into contact with police as a suspect or victim in a crime, ADHC staff should contact the Intellectual Disability Rights Service for advice on how to proceed.
13.2 For victims When a person is a victim of a crime and the NSW Police wish the person to submit to a ‘forensic procedure’, the person or a legally appointed guardian with the appropriate forensic consent function, will give or withhold consent to undergo the procedure. It should be noted that a victim may withdraw or give consent at any time. For example a victim may initially decline to participate in a forensic procedure and then later give consent.
It is important that an appropriately trained person (for example a psychologist or counselor) discusses the nature of the forensic procedure and collection of evidence with the person, so that she or he can make an informed choice. The person may choose to have a trusted family member, friend or other supporter with them during such discussions. The person’s Communication Profile may be used to help the person understand what is being proposed.
Decision Making and Consent Guidelines, V1.0, January 2016 17

14 Legally Appointed Decision Makers People are provided with appropriate and adequate support to make their own decisions. Where the person has not been able to reach a decision even with support, a legally appointed guardian may be required. In these circumstances, an application is made to the NCAT Guardianship Division to request the appointment of a guardian or financial manager for the person under the Guardianship Act, 198714.
Guardians are appointed to make decisions in certain areas of a person’s life outlined in the guardianship order, and are generally only appointed for a limited time. Decisions can be about accommodation, services, medical and dental treatment and contact with others. Financial managers are appointed to make decisions about finances and assets.
The formal appointment of a guardian or financial manager is made as a last resort. In the first instance the NCAT will seek to appoint a family member or significant other in the person’s life, with oversight and support from the Public Guardian. If no one suitable is available, the Public Guardian or Public Trustee is appointed.
A person who has a legally appointed guardian with a specific function, or a financial manager, is to be represented by that person whenever a decision is required. A legally appointed guardian with a specific function may only decide for a person on the function defined by the Guardianship Order.
If support workers are unclear about the need to refer to a legally appointed guardian for a decision, they should check the person’s file for details of the guardian’s function and contact the guardian to discuss. If there is no legally appointed guardian, support workers should contact the NCAT Guardianship Division for advice about applying for the appointment of a guardian.
If workers are concerned that the support given with decisions by the family or a guardian are not in the person’s best interests, they should refer the matter to a line manager who will assess the need for a review by the NCAT Guardianship Division.
14 NCAT application forms and factsheets: http://www.ncat.nsw.gov.au/Pages/guardianship/guardianship.aspx
Decision Making and Consent Guidelines, V1.0, January 2016 18

15 Definitions There are some key words which are important for support workers to understand in the context of decision making and consent.
Abuse All forms of maltreatment of adults with disability and violation of their individual rights. ‘Abuse’ refers to sexual assault, physical, emotional, financial and systemic abuse, domestic violence, constraints and restrictive practices, and to neglect.
Refer to the ADHC Abuse and Neglect Policy and Procedures and Guidelines.
The policy and procedures concerning the abuse of children and young people are contained in the document: Child Protection Guidelines; What ADHC staff need to know about child protection, 201415
Adult A person who is 18 years or older is considered to be an adult.
For the purpose of making a guardianship order, or for giving medical or dental consents, the NSW Civil and Administrative Tribunal (NCAT) Guardianship Division regards anyone aged 16 years or over as an adult.
Authorised officer Defined in the Crimes (Forensic Procedures) Act 2000 as:
• Magistrate or Children’s Magistrate; or
• Registrar of a Local Court; or
• An employee of the New South Wales Attorney General’s Department authorised by the New South Wales Attorney General as an authorised officer for the purposes of this Act either personally or as the holder of a specified title.
Carers Family members, parents, partners, significant others, friends or neighbours who provide care on an unpaid basis. These are sometimes described as ‘those within the person’s circle of support’.
15 http://www.adhc.nsw.gov.au/__data/assets/file/0019/232732/ADHC_Child_Protection_Guidelines.pdf
Decision Making and Consent Guidelines, V1.0, January 2016 19

Case Manager In ADHC, case managers work with the person and the person’s family to identify the person’s strengths and needs, and to design an individually tailored plan of support. The case manager then negotiates, coordinates and monitors the delivery of support based on the plan.
Child A person who is under 16 years of age.
Parents and guardians of people under 16 years have the right to make decisions for them but the child should be involved in decisions that affect them, in an age-appropriate way. For exceptions, refer to Section 2 (Capacity) of these Guidelines
Consent Consent refers to the permission given by a person. For consent to be valid it must be voluntary, informed, specific and current. A person must be free to exercise genuine choice about whether to give or withhold consent. Consent must be given without coercion or threat and with sufficient time to understand the request and, if appropriate, take advice.
Consent must be established each time it is required. A person who has given consent to a specific matter may change her or his mind and subsequently revoke consent.
In certain circumstances, consent may also be provided by a legally appointed guardian on behalf of the person. Consent for medical or dental treatment may be given by a person responsible.
Critical Decision These decisions relate to vital or essential issues in a person’s life such as particular medical and dental treatments, certain behaviour support and intervention practices, legal issues, accommodation choices or service delivery decisions. They are decisions which have potentially long term or serious impacts on the person’s life including health, lifestyle and financial outcomes.
Family In the context of this policy ‘family’ refers to any person who is a relative or friend having a close and continuing relationship with a person, and who has a personal interest in the welfare of the person.
Financial Manager Financial managers with the authority to make decisions about the finances of a person who lacks capacity to make such decisions are appointed by the NSW Civil and
Decision Making and Consent Guidelines, V1.0, January 2016 20

Administrative Tribunal (NCAT) Guardianship Division, the Supreme Court or a Magistrate.
If a person is found to be incapable of managing her or his finances the preference is for a family member to be appointed to manage the person’s finances, with oversight from the NSW Trustee and Guardian. As a last resort, the NSW Trustee and Guardian is appointed to provide financial management services directly to a person, where there is no other person available.
Forensic These are intrusive procedures requiring consent from the Procedures16 - person (if the person is a victim of crime and is capable of Intimate providing it) or a legally appointed guardian with the
appropriate function, or an order from a Magistrate or authorised officer (if the person is a suspect in a crime) including:
17• an external examination of a person’s private parts, ,
• the carrying out on a person of an other-administered buccal swab,
• the taking from a person of a sample of the person’s blood,
• the taking from a person of a sample of the person’s pubic hair,
• the taking from a person of a sample of any matter, by swab or washing, from the person’s private parts,
• the taking from a person of a sample of any matter, by vacuum suction, scraping or lifting by tape, from the person’s private parts,
• the taking from a person of a dental impression,
• the taking of a photograph of the person’s private parts,
• the taking from a person of an impression or cast of a wound from the person’s private parts.
Forensic Procedures –
These are less intrusive procedures requiring consent from the person (if the person is a victim of crime and is capable of providing it) or a legally appointed guardian with the
16 Taken from Part 1, section 3 of the Crimes (Forensic Procedures) Act 2000 No 59
17 "Private parts" means a person’s genital area, anal area or buttocks, and, in the case of a female or transgender person who identifies as a female, includes the person’s breasts.
Decision Making and Consent Guidelines, V1.0, January 2016 21

Non- Intimate appropriate function, or an order from a Magistrate or authorised officer (if the person is a suspect in a crime) including:
• an external examination of a part of a person’s body, other than the person’s private parts, that requires touching of the body or removal of clothing.
• the carrying out on a person of a self-administered buccal swab.
• the taking from a person of a sample of the person’s hair, other than pubic hair.
• the taking from a person of a sample (such as a nail clipping) of the person’s nails or of matter from under the person’s nails.
• the taking from a person of a sample of any matter, by swab or washing, from any external part of the person’s body, other than the person’s private parts.
• the taking from a person of a sample of any matter, by vacuum suction, scraping or lifting by tape, from any external part of the person’s body, other than the person’s private parts.
• the taking from a person of the person’s hand print, finger print, foot print or toe print.
• the taking of a photograph of a part of a person’s body, other than the person’s private parts.
• the taking from a person of an impression or cast of a wound from a part of the person’s body, other than the person’s private parts.
• the taking of measurement of a person’s body or any part of a person’s body (other than the person’s private parts) whether or not involving the marking of the person’s body.
Guardian18 • Guardians are appointed by the NCAT Guardianship Division or the Supreme Court to make one or more decisions on behalf of another person about matters relating to health and lifestyle.
18 Office of the Public Guardian fact sheets: http://www.publicguardian.justice.nsw.gov.au/Pages/publicguardian/pg_publications/pg_factsheets/pg_factsheets.aspx
Decision Making and Consent Guidelines, V1.0, January 2016 22

Guardianship Order
• Where there is a need to assist the person who lacks capacity to make lifestyle or health decisions, the NCAT Guardianship Division will appoint a private individual (sometimes known as a ‘private guardian’) to be the guardian wherever possible.
• When there is no available, willing or suitable private individual, the Public Guardian will be appointed as the guardian of last resort. The guardianship order authorises the guardian to exercise a specific decision making function that is time limited. Private guardians and the Public Guardian have the equal authority to act according to a Guardianship Order.
• An enduring guardian is another form of guardianship appointment and is chosen by an individual to make lifestyle and health care decisions should the individual lose capacity to make her or his own decisions at some time in the future. The appointment is not time limited and is only reviewed by the Guardianship Tribunal on request. Individuals cannot choose the Public Guardian as an enduring guardian.
The NSW Civil and Administrative Tribunal (NCAT) Guardianship Division can appoint a guardian with specified functions detailed in a written order. Functions determined under such an order can include but are not limited to:
• Accommodation - to decide where a person should live. Sometimes the Guardian can also authorise others, including members of the NSW Police Service and/or the NSW Ambulance Services to take the person from their present location to accommodation consented to by the guardian, keep the person at that accommodation and bring the person back to that accommodation if they leave.
• Health care - to decide what health services a person should receive.
• Medical and Dental treatment - to provide or withhold consent to medical and dental treatment, including the use of medication as part of a Behaviour Support Plan.
• Services - to authorise others to provide personal services to the person, and decide which agencies should provide services.
• Restrictive practices - to decide about the use of restrictive practices, usually in the context of behaviour
Decision Making and Consent Guidelines, V1.0, January 2016 23

intervention and support.
• Access - to decide who should have access to a person and under what conditions.
• Advocacy - to advocate on behalf of a person (this is only occasionally a function in itself, but is implicit in other functions).
• Legal services - to make decisions about legal services for the person, such as arranging for legal advice to be given and other supports.
• Forensic – is required when a medical examination is purely for the gathering of evidence. There are two aspects to this function - consent to gather the evidence and, consent to release the evidence.
Guardians are appointed with a specific function and for the period of time specified in the order. The order is reviewed near the end of that period, at which time the NCAT Guardianship Division will decide to continue, vary or dismiss the order. There may be more than one guardian for a person, each with a different function, or there may be joint guardians with the same function.
Manager or Senior Manager
The designated manager of an individual service, including a large residential centre, or the next line manager in the organisation’s structure.
Natural supports Natural supports are relationships that occur in everyday life. They include family, friends and other trusted people, neighbours, acquaintances, and people with shared interests. Natural supports enhance a sense of security and quality of life for people.
New South Wales When the Civil and Administrative Tribunal Act 2013 came Civil and into force on 1 January 2014, it established the New South Administrative Wales Civil and Administrative Tribunal (NCAT). The Tribunal (NCAT) Guardianship Division of NCAT exercises jurisdiction set out Guardianship in the Guardianship Act 1987. Division One of its functions is to determine applications for
guardianship and financial management orders. It can appoint a guardian for a person aged 16 years or over who is incapable of making health, finance or lifestyle decisions independently. It will not usually appoint a guardian for day to day lifestyle decisions if informal decision making is working well and there is no need for a formal guardianship
Decision Making and Consent Guidelines, V1.0, January 2016 24

order.
The Guardianship Division also provides or withholds consent for people to receive medical or dental treatment in certain circumstances (see the ‘NCAT Guardianship Division Information for Applicants, Application for consent to medical and dental treatment’ in Tools and templates).
Lifestyle Plan A Lifestyle Plan is developed with the person and others who are important in the person’s life. It belongs to the person and tells others about the person’s lifestyle priorities and goals, and focuses on the person’s strengths.
Person The person with disability who receives ADHC operated or ADHC funded non-government disability support services.
Person Responsible A person responsible is not necessarily the person’s next of kin.
The Guardianship Act 1987 has a hierarchy of people who can be the person responsible. They are:
1. A guardian (including an enduring guardian) who has the function of consenting to medical and dental treatments.
If no-one as specified in item 1:
2. A spouse or de facto spouse or partner where there is a close, continuing relationship.
If no-one as specified in item 1 and 2:
3. A carer who provides or arranges for domestic support on a regular basis and is unpaid. The Carer Allowance is not considered payment in this context. If the person is in residential care (i.e. receiving accommodation supports and not living with family or a carer), then the carer before the person went into residential care.
If no-one as specified in item 1, 2 and 3:
4. A close personal friend or close relative where there is both a close personal relationship, frequent personal contact and a personal interest in the patient's welfare, on an unpaid basis. The person next in the hierarchy may become the person responsible if:
• a person responsible declines in writing to exercise the function, or
• a medical practitioner or other qualified person certifies in writing that the person responsible is not
Decision Making and Consent Guidelines, V1.0, January 2016 25

capable of carrying out their functions 19 .
Support Worker A paid supporter who is the person’s primary contact. The support worker is responsible for supporting the person to participate in daily activities, stay healthy and safe, and to pursue the goals and aspirations identified in the person’s Lifestyle Plan.
Young Person A person who is 16 or 17 years old.
For the purpose of making a guardianship order, or for giving medical or dental consents, the NSW Civil and Administrative Tribunal (NCAT) Guardianship Division regards anyone aged 16 years or over as an adult.
16 Policy and Practice Unit contact details You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
19 Taken from NCAT Person responsible fact sheet: http://www.ncat.nsw.gov.au/Pages/guardianship/publications_resources/gd_fact_sheets.aspx
Decision Making and Consent Guidelines, V1.0, January 2016 26

Decision Making and Consent Policy
Document name Decision Making and Consent Policy
Policy Decision Making and Consent Policy
Version number 1.0
Approval date January 2016
Policy manual Lifestyle Policy and Practice Manual
Approved by Deputy Secretary ADHC, FACS
Summary The Decision Making and Consent Policy affirms the rights of people to make decisions that affect them and to receive support when they want it to make decisions. A set of Guiding Principles provides a framework for decision making in the context of capacity and consent.
Replaces document Decision Making and Consent Policy and Procedures 2011
Authoring unit Contemporary Residential Options Directorate
Applies to People who are being supported in ADHC operated and funded non-government disability support services.
Review date 2017

Version control The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 Replaces Decision Making and Consent Policy 2011
Decision Making and Consent Policy, V1.0, January 2016 2

Table of contents
1 Decision Making and Consent Policy ....................................................4
1.1 Background ..................................................................................4
1.2 Purpose........................................................................................4
1.3 Guiding Principles ........................................................................5
1.4 Application of the Principles .........................................................6
2 Legislation .............................................................................................6
3 Aboriginal and Torres Strait Islander people .........................................7
4 Cultural and Linguistic Diversity ............................................................7
5 Women..................................................................................................8
6 Children and young people ...................................................................8
7 Policy and Practice Unit Contact Details .............................................10
Decision Making and Consent Policy, V1.0, January 2016 3

1 Decision Making and Consent Policy
1.1 Background
The ADHC Decision Making and Consent Policy (the Policy) and associated resources are based on the principles of human rights found in the United Nations Convention on the Rights of Persons with Disabilities (the UN Convention)1, the Disability Inclusion Act 2014 (NSW), (the Act) and the New South Wales Disability Service Standards (the Standards).
Decision Making is contained in Article 12 of the UN Convention, which states that “parties shall recognise that persons with disabilities enjoy legal capacity2 on an equal basis with others in all aspects of life” and “parties shall take appropriate measures to provide access by persons with disabilities to the support they may require in exercising their legal capacity”.
The Policy is also based on the commitment to deliver culturally responsive services to Aboriginal and Torres Strait Islander people under the Aboriginal Policy Statement (the Statement), as well as people from culturally and linguistically diverse backgrounds, women and children, as recognised in the Act.3
1.2 Purpose The Policy principles are a requirement in Family and Community Services (FACS), Ageing, Disability and Home Care (ADHC), operated and ADHC funded non-government disability support services. The Policy provides a framework for supporting people with disability to exercise their rights to self determination as defined in the Act and the UN Convention.
The Policy highlights the person centred approach to supporting people to make decisions that affect them, and to give informed consent. The Policy recognises the vital role of family and others, and legally appointed decision makers, in ensuring the rights of the person with disability are protected.
Decision making and consent issues addressed in the Policy apply to people who need and want support to make decisions in all areas of their lives, who are 16 years and older, and reside in or access ADHC operated and ADHC funded non-government disability support services.
1 United Nations Convention on the Rights of Persons with Disabilities 2006, ratified in 2008: http://www.un.org/disabilities/convention/conventionfull.shtml 2 Legal capacity means a person’s authority under law to engage in a particular undertaking or maintain a particular status. 3 The Disability Inclusion Act 2014 recognises that people from Aboriginal and Torres Strait Islander and Culturally and Linguistically Diverse backgrounds as well as Women and Children require particular consideration in the design and delivery of disability services.
Decision Making and Consent Policy, V1.0, January 2016 4

The Guidelines are a requirement for ADHC operated disability support services to follow when they are applying the Principles of the Policy. ADHC funded non-government disability support services may adopt the Guidelines, or develop their own.
1.3 Guiding Principles 1. People have the right to make decisions about things that affect their lives.
2. People are presumed to have the capacity to make their own decisions and give consent when it is required, unless there is evidence otherwise.
3. People are supported to make informed decisions when their consent is required.
4. Consent is obtained from the person, or a legally appointed guardian, for life decisions such as accommodation, medical and dental treatment, forensic procedures, and behaviour support.
5. Consent for financial matters is obtained from the person, or a legally appointed financial manager or person appointed under a Power of Attorney.
6. People are supported to identify opportunities to make decisions about their own lives and to build their decision making confidence and skills.
7. When support to make decisions is wanted or needed by the person, it is provided in ways preferred by the person and by a supporter of their choice.
8. Support with decision making respects the person’s cultural, religious and other beliefs.
9. If the person wants to be supported by natural supporters, such as family and friends, this is encouraged and facilitated.
10. Support is provided in ways that uphold the person’s right to self determination, privacy, and freedom from abuse and neglect.
11. Decision making and self determination are not limited by the interests, beliefs or values of those providing the decision making support.
12. The amount or type of support required by people to make decisions will depend on the specific decision or the situation.
13. People are supported to make decisions that affect their own lives even if other people don’t agree with them, or regard the decisions as risky.
14. People are supported to access opportunities for meaningful participation and active inclusion in their community where they want this.
15. Information is provided in formats that everyone can understand, and enables the person, their supporters and other relevant people, such as legally appointed guardians, to communicate effectively with each other.
Decision Making and Consent Policy, V1.0, January 2016 5

1.4 Application of the Principles The Guiding Principles of the Policy are the basic mandatory requirements for ADHC operated and ADHC funded non-government disability support services to follow when supporting people in their decision making and when seeking consent.
Refer to the decision making and consent flowchart when determining the person’s decision making and consent requirements (Tool and templates).
2 Legislation The Decision Making and Consent Policy (The Policy) is consistent with the objects and principles of the Disability Inclusion Act 2014 (NSW), (the Act). The objects and principles of the Act require service providers to acknowledge and uphold the rights of people with disability to participate in social, civic and economic life in their community.
In particular:
Object in Section 3(c) of the Act is “to enable people with disability to exercise choice and control in the pursuit of their goals and the planning and delivery of their supports and services”.
Principle in Section 4(5) of the Act states “People with disability have the same rights as other members of the community to make decisions that affect their lives (including decisions involving risk) to the full extent of their capacity to do so and to be supported in making those decisions if they want or require support”.
Principle Section 4(9) of the Act states “People with disability have the right to access information in a way that is appropriate for their disability and cultural background and enables them to make informed choices”.
The Policy embodies the objects and principles of the Act by obligating and enabling services to support people in making decisions about the things that affect their lives.
The Policy’s Guiding Principles recognise the role of legally appointed decision makers under the Guardianship Act 1987 (NSW), and the Decision Making and Consent guidelines provide more information on this topic.
Decision Making and Consent Policy, V1.0, January 2016 6

3 Aboriginal and Torres Strait Islander people
The Act provides that Aboriginal and Torres Strait Islander people with disability are to be provided with services that recognise their particular needs4.
To make a difference, services need to be culturally competent, responsive and sensitive to the needs of Aboriginal and Torres Strait Islander people. The Aboriginal Policy Statement underpins ADHC’s strategic direction for Aboriginal Torres Strait Islander people5.
The Aboriginal Cultural Inclusion Framework provides a mode of accountability for monitoring programs and services to ensure real improvements are delivered to older Aboriginal Torres Strait Islander people, Aboriginal Torres Strait Islander people with disability, their families, carers and communities6.
Aboriginal Torres Strait Islander people have higher rates of disability and support needs compared to non-Aboriginal people and access relatively fewer services. For many Aboriginal Torres Strait Islander people this is compounded by broad socio-economic disadvantage and geographical isolation.
This information guides staff with an opportunity to provide supports and services that are culturally competent, responsive and sensitive for Aboriginal Torres Strait Islander people, their families and carers. If an Aboriginal Torres Strait Islander person who receives accommodation services requires decision making support, they have the right to receive it.
See Other Resources for more information on working with people from Aboriginal and Torres Strait Islander communities.
4 Cultural and Linguistic Diversity The Act provides that services and supports are to be provided to people with disability of a Culturally and Linguistically Diverse background in a way that addresses the barriers that may be created due to cultural, language and other differences7.
The behaviour of the person and their family, attitudes, preferences and decisions about decision making and consent, are influenced by culture and religious practices.
4 See Section 5(2) of the Disability Inclusion Act 2014
5 Aboriginal Policy Statement: http://www.adhc.nsw.gov.au/publications/aboriginal
6 Aboriginal Inclusion Framework: http://www.adhc.nsw.gov.au/publications/aboriginal 7 See Section 5(3) of the Disability Inclusion Act 2014
Decision Making and Consent Policy, V1.0, January 2016 7

A person’s cultural and religious preferences for supported decision making should be determined early in support planning. Demonstrate respect and cultural sensitivity by considering:
• The person and the family’s perspective on decision making and consent.
• The person and the family’s perspective on alternate decision making and advocacy.
• The role of spiritual and religious beliefs and practices in decision making.
• How the person and their family communicate, for instance, through an interpreter.
• The person’s own role in the process of problem solving and decision making.
5 Women The Act recognises that “women with disability may face multiple disadvantages and are potentially more vulnerable to risk of abuse or exploitation”8.
In supporting women with decision making and seeking consent, respect is shown by:
• Ensuring supporters are chosen by the person such as allowing the person to choose female or male supporters.
• Involving and encouraging contribution by natural supports where the person wants this (natural supports are a protective factor in preventing abuse and exploitation).
• Ensuring access to information and supports regarding reproductive health and sexuality that enable informed decision making and consent about general health and wellbeing, intimate relationships and self-protective strategies.
6 Children and young people In the context of the Policy, a child is any person under 16 years of age and a young person is anyone 16 years or older and under the age of 18 years9.
8 See Section 5(4)(a) of the Disability Inclusion Act 2014 9 Children and Young Persons (Care and Protection) Act 1998: www.legislation.nsw.gov.au/fullhtml/inforce/act+157+1998+FIRST+0+N
Decision Making and Consent Policy, V1.0, January 2016 8

Children and young people have a right to be involved in decisions that affect them in ways appropriate to their age and stage of development under the UN Convention on the Rights of the Child10.
Even very young children can make choices and communicate their feelings, ideas and wishes in numerous ways before they are able to communicate through spoken or written language. Children should be involved in decisions that affect them, in an age appropriate way. This provides opportunities for children to develop decision making skills and confidence to prepare them for adulthood, and allows parents and guardians to see them as decision makers.
Parents and guardians of people under 16 years have the right to make certain decisions for them. Parents or legal guardians also have a role in decision making concerning their children because they have primary responsibility for children’s upbringing and development.
The Standards in Action Manual11 provide guidance for workers to support decision making in a child and family centred way, recognising the important roles and responsibilities of parents of children and young people, and the shift to a person centred approach to decision making as children develop and mature.
The Disability Inclusion Act 2014 requires service providers to consider the particular needs of children and young people with disability so that supports and services are provided in a way that:
• Recognises the child or young person’s right to live a life with full and active participation in family, cultural and social life, with dignity and conditions that promote self-reliance.
• Recognises that children and young people are more vulnerable to the risk of abuse and exploitation.
• Respects the views of the child or young person (with respect to their age and maturity)12.
Support with decision making will be provided to children and young people, and their families, within these frameworks.
While all people under 18 years of age are regarded under the law as children, young people are given special consideration by the NSW Civil and Administrative Tribunal (NCAT) Guardianship Division. A young person can provide their own consent on a range of matters, or they can be assigned a Public Advocate by NCAT if they need a legally appointed decision maker (see Decision Making and Consent flowchart, Tools and templates).
10 United Nations Convention on the Rights of the Child: http://www.unicef.org.au/Discover/What-we-do/Convention-on-the-Rights-of-the-Child.aspx
11 ADHC Standards in Action: www.adhc.nsw.gov.au/sp/quality/standards_in_action 12 See Section 5(5) of the Disability Inclusion Act 2014
Decision Making and Consent Policy, V1.0, January 2016 9

The Guidelines also provide further information about young people and consent, in the relevant sections. See Other Resources for further information about young people and the law.
7 Policy and Practice Unit Contact Details You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
Decision Making and Consent Policy, V1.0, January 2016 10

Flow chart: The escalation strategy for unsatisfactory health appointments

Fact sheet January 2016
People with intellectual disability - information for General Practitioners during health assessments
ADHC disability support workers facilitate communication between the GP and the person
The majority of ADHC support workers are not nurses Disability support workers cannot give consent on behalf of the people
they support ADHC policy requires the person with disability to have an annual health
assessment
Role of ADHC staff The primary role of disability support workers is to support people with disability to be as fully engaged in their own lives as possible. Consent for treatment People who cannot make decisions independently receive informal decision making support from the family or a person responsible OR have a legally appointed guardian to make decisions. Annual health assessment The ADHC Health and Wellbeing Policy requires disability support workers to arrange an annual health assessment with the usual GP of the person they support. Disability support workers will book one or more long or prolonged appointments for the assessment under Medicare item numbers 705 or 707. Disability support workers will bring the following documents to the appointment: - Comprehensive Health Assessment Program (CHAP) Part 1 completed
OR an equivalent health summary - Medication records and blister packs - Test results and screening reports - Epilepsy Management Plan if relevant - Other condition specific plans for review GP support Disability support workers rely on the GP for advice and information about the person’s ongoing day to day health support needs and management of chronic disease. Please support them by providing clear written information and instructions suitable for a team of non-clinical staff to follow.
www.adhc.nsw.gov.au

Part B3 – Information about my health: Health action plan My name:
Health action Date and name of health professional who prescribed the action
(information provided on the Health report)
Who is responsible for completing the action
Date due
Date completed
Progress Team leader signature and date
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Health and Wellbeing Policy
Document name Health and Wellbeing Policy
Policy Health and Wellbeing Policy
Version number 1.1
Approval date January 2016
Policy manual Health and Wellbeing Policy and Practice Manual, Volume 1
Approved by Deputy Secretary, ADHC
Summary The Health and Wellbeing Policy consolidates all health related resources, including health planning, nutrition and swallowing, medication, health promotion, chronic disease, epilepsy, and end of life care planning, under one framework.
Specific guidelines and procedures for each health area are contained in the Health and Wellbeing Policy and Practice Manuals for use by support workers when implementing the resources.
Replaces document Health Care Policy and Procedures, 2012 and Attachments 1 - 13
Authoring unit Contemporary Residential Options Directorate
Applies to People who are being supported in ADHC operated and funded accommodation support services.
Review date 2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment Amendment notes date
V1.0 November Replaces Health Care Policy, April 2012 2014
V1.1 January 2016 Amended to incorporate feedback
Health and Wellbeing Policy, V1.1, January 2016 2

Table of contents
1 Health and Wellbeing Policy ................................................................ 4
1.1 Background .................................................................................... 4
1.2 Purpose .......................................................................................... 4
2 Person centred guiding principles ...................................................... 5
2.1 Person at the centre ....................................................................... 5
2.2 Considering culture......................................................................... 5
2.3 One health plan .............................................................................. 5
2.4 Health assessment ......................................................................... 5
2.5 Regular review................................................................................ 5
2.6 Communication............................................................................... 5
2.7 Inclusion of others .......................................................................... 6
2.8 Service access ............................................................................... 6
2.9 Continuity of care............................................................................ 6
2.10 Access to skilled supports .............................................................. 6
2.11 Nutrition .......................................................................................... 6
2.12 Medication ...................................................................................... 7
2.13 Chronic disease.............................................................................. 7
2.14 Epilepsy.......................................................................................... 7
2.15 End of life care planning and death ................................................ 8
3 Application of principles ...................................................................... 8
4 Legislation............................................................................................. 8
5 Aboriginal and Torres Strait Islander people ..................................... 9
6 Cultural and linguistic diversity........................................................... 9
7 Policy and Practice Unit contact details ........................................... 10
Health and Wellbeing Policy, V1.1, January 2016 3

1 Health and Wellbeing Policy
1.1 Background
The Health and Wellbeing Policy (the Policy) embodies the principles of legal and human rights found in the New South Wales Disability Service Standards (the Standards), and the commitment to deliver culturally responsive services to Aboriginal and Torres Strait Islander people under the Aboriginal Policy Statement (the Statement).
The Policy defines how people with disability and their families exercise their rights and entitlements, under the Standards and Statement, to make informed decisions about health services, including health promotion opportunities, treatments, therapy and rehabilitation.
The Policy presents a basis for planning, to achieve the best possible health and wellbeing outcomes for all people with disability in ADHC operated and funded accommodation support services.
The Policy highlights the importance of identifying symptoms of illness and changes in health status early, and of communicating and recording health information. The Policy recognises that establishing clear pathways for referral is fundamental to achieving the best possible health and wellbeing outcomes, and requires the development of key partnerships between the person, family, carers and health professionals.
Establishment of these partnerships is articulated in the National Disability Strategy NSW Implementation Plan 2012-2014. Partnerships with health providers in the mainstream health system are key elements of the NSW Ministry of Health’s response to the Service Framework to Improve Health Care of People with Intellectual Disabilities and Future Directions for Health in NSW.
1.2 Purpose
The Policy applies to ADHC operated and funded accommodation support services, and aims to streamline the health and wellbeing support system. Under the Policy framework the existing ADHC health, nutrition, medication, epilepsy, palliative care and death policy principles, are assembled to reflect the health and wellbeing support continuum for people with short and long term health conditions.
A Policy and Practice Manual, founded on evidence-based best practice, accompanies the Policy, and includes procedures, guidelines, tools, templates, and other resources. The purpose of the Manual is to streamline the Policy framework by reducing the duplication and recording of health and wellbeing information that has previously been imposed by the separation of health related policies.
The procedures are a requirement for ADHC operated accommodation support services to follow when they are applying the principles of the Policy. ADHC
Health and Wellbeing Policy, V1.1, January 2016 4

funded non-government accommodation support services may adopt the procedures, or develop their own.
Tools and templates are provided as aids for gathering and recording information, and other resources support health planning and other policy activities.
2 Person centred guiding principles
Health, nutrition, chronic disease, medication, epilepsy, end of life care planning and death.
2.1 Person at the centre
1. The person is central to health planning and is supported to understand health related discussions and to make healthy lifestyle decisions.
2.2 Considering culture
2. Health planning and management takes culture and religion into account as they relate to health and wellbeing.
2.3 One health plan
3. Every person has one health plan which incorporates all health and wellbeing assessments, reports, plans and recommendations.
2.4 Health assessment
4. Every person has an annual health assessment, conducted by a medical practitioner, which informs the health plan.
5. Health planning advice is provided by the medical practitioner during the annual health assessment with input from other health and wellbeing practitioners.
6. Health planning includes at least an annual dental and oral health check, conducted by a health professional, which informs the health plan.
2.5 Regular review
7. Health and related plans are reviewed every three months with the person and support workers, and with input from the family, others important to the person and other health and wellbeing practitioners where it is required.
2.6 Communication
8. The person is encouraged to self-advocate, and is supported to communicate health needs and treatment preferences to health care professionals.
Health and Wellbeing Policy, V1.1, January 2016 5

9. Health care professionals are supported to understand the person’s health and wellbeing needs, and given the means to communicate health information in a way the person understands.
2.7 Inclusion of others
10. In accordance with the person’s wishes, health planning and support is provided wherever it is required by the family, person responsible or guardian, health professionals and support workers.
2.8 Service access
11. Every person is supported to access mainstream health services of their choice, as well as disability specific specialist health services where they are needed.
2.9 Continuity of care
12. Relationships are established with health care professionals and providers to promote continuity of care and to enhance mutual understanding of people’s health care preferences and needs.
2.10 Access to skilled supports
13. Each person receives services that optimise their health, wellbeing and quality of life.
14. Services are delivered by a range of support workers and health professionals who have, or will acquire, the necessary skills.
2.11 Nutrition
15. Every person has access to good quality and nutritious food, and is supported to enjoy long-term health and wellbeing.
16. Each person has an annual assessment to identify risks associated with nutrition and swallowing.
17. Risks identified in the assessment are addressed using mealtime management plans developed by a qualified health professional.
18. Any person who requires a special diet has it prescribed by a qualified health professional.
19. Mealtime management plans and diets are reviewed regularly as part of health planning.
20. Food preferences and mealtime support are documented in a nutrition profile and reviewed as part of health planning.
21. Nutritional support is provided in the context of a person’s health needs, culture, religion and personal preferences, and includes family and other people important to the person.
Health and Wellbeing Policy, V1.1, January 2016 6

22. Each person is encouraged and supported to engage in good nutritional practices through participation in social and physical activities that promote good eating and a healthy lifestyle, and include regular exercise.
23. Support is provided to access mainstream nutrition promotion strategies to reduce the risk of developing some common chronic health conditions.
2.12 Medication
24. Medical needs are determined by a treating practitioner, and prescribed medications are administered according to the practitioner’s orders.
25. Medication reviews are conducted during regular health assessments and include medications prescribed by other health providers.
26. Predicted risks and benefits of prescribed medication are explained to the person in a way that meets her or his communication needs.
27. A record of prescription and non-prescription medications is documented in a medication chart by the treating practitioner or is supplied by the pharmacist using medication management software.
28. Suitably skilled workers are available to support people with disability to administer their own medications independently, or to manage and administer medications and maintain accurate and current medication records.
29. Processes are in place to ensure that all medications are administered safely, and stored securely.
30. Systems exist for auditing medication supplies, and for recording and managing any irregularities in medication supply, administration and consumption.
2.13 Chronic disease
31. Annual health assessments identify and monitor long term physical and mental illness.
32. Referrals are made to appropriate mainstream chronic disease management programs or specialist disability services.
33. People are supported to access mainstream or disability-specific specialist disease management programs as appropriate.
2.14 Epilepsy
34. The person with epilepsy is supported to access quality health care and to have full involvement in decision making and exercising choice about support and treatment.
35. Each person with epilepsy has a plan that records the type of epilepsy, seizure description, treatments, management and risks associated with the condition, and is reviewed during regular health assessments.
36. Each person with epilepsy is supported by workers who are appropriately trained and skilled in seizure response and management.
37. Management of chronic health conditions such as epilepsy requires regular auditing of environmental and other risks to the person with epilepsy, and identification of triggers that can prompt a seizure.
Health and Wellbeing Policy, V1.1, January 2016 7

38. A person with epilepsy with ongoing seizures is supported to understand how ‘duty of care’ is considered before ‘dignity of risk’ around activities involving water.
39. Attempts to reduce risk for the person with epilepsy should avoid compromising other aspects of safety and dignity, or impairing quality of life, as much as possible.
40. Monitoring and supervision of the person with epilepsy is as discreet as possible, minimising disturbance to the person, and promoting the person’s health and safety.
2.15 End of life care planning and death
41. Planning for the person’s health and wellbeing support needs towards the end of life is a positive process that represents the person’s values, beliefs and choices, and guides future decision making if the person is unable to communicate a preference.
42. Each person who has a life-threatening illness is supported to plan for the treatment or illness management that reflects their own end of life support wishes.
43. The support plan is reviewed regularly to align with changes in the person’s care and support needs for the duration of the illness.
44. The person’s wishes about advance care planning, end of life support, death and post-death, are recorded in the health plan and followed, with the involvement of the family, person responsible or guardian.
3 Application of principles
The Policy’s person centred guiding principles are the basic mandatory requirements for ADHC operated and funded accommodation support services when planning with people to achieve good health and wellbeing.
4 Legislation
The Policy is consistent with the objects and principles of the Disability Inclusion Act 2014 (the Act). The objects and principles of the Act require the State and community to support people with disability to exercise their rights, choice and control in pursuing their goals, to promote their independence and social and economic inclusion, and to realise their physical, social, sexual, reproductive, emotional and intellectual capacities. The Policy embodies the objects and principles of the Act by supporting people to be actively involved in achieving the best possible health and wellbeing outcomes throughout their lives.
The Policy’s person centred guiding principles align with the principles of the United Nations Convention on the Rights of Persons with Disabilities (ratified by Australia in 2008) relating to health and wellbeing outcomes.
Health and Wellbeing Policy, V1.1, January 2016 8

5 Aboriginal and Torres Strait Islander people
Cultural sensitivity is fundamental in a person centered approach to health and wellbeing, and without it, health and wellbeing outcomes of Aboriginal and Torres Strait Islander people are compromised.
The traditional Aboriginal perspective of health is holistic, and encompasses land, environment, physical body, community, relationships and law. Health is connected to the social, emotional, and cultural wellbeing of the whole community, and the sense of being indigenous1.
In addition to the person centred health principles featured in the Policy, the following culturally sensitive matters should be considered when supporting Aboriginal or Torres Strait Islander people to manage their health and wellbeing:
recognising the person’s culture is a way of acknowledging and valuing the person’s identity
acknowledge the history of difficult relationships with government services
recognise family, kinship and friend relationships and the person’s connection to community and the land
determine who in the family or community should be approached for decisions and consent about health support and treatment
ask how and where the person would prefer to receive services
confirm whether the person or family would prefer to work with the health system through an Aboriginal Liaison Officer
determine which health issues or practices are sensitive or taboo and who to refer to if they are.
6 Cultural and linguistic diversity
People bring their values, beliefs and experiences with them when they relocate to another country. The person and family’s behaviour, attitude, preferences and decisions about health and wellbeing, are influenced by culture and religious practices.
A person’s cultural and religious preferences for health and wellbeing should be ascertained early in support planning. Demonstrate respect and sensitivity by considering:
the person and the family’s perspective on health and illness
the person and the family’s perspective on health management and treatment
1 Health Facts _Info Net – Health Status 2012
Health and Wellbeing Policy, V1.1, January 2016 9

the person and the family’s views about Western health care practices and their use of alternative traditional practices
the role of spiritual and religious beliefs and practices in health care
how the person and the family communicate, for instance, through an interpreter
the person’s own role in the process of problem solving and decision making.
7 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the ADHC intranet to confirm that you are reviewing the most recent version. Following any subsequent reviews and approval this policy will be uploaded to the internet and/or intranet and all previous versions removed.
Health and Wellbeing Policy, V1.1, January 2016 10

Health appointment sheet
Person / support worker to complete
My name
CIS number TRIM number
I like to be called
Date I was born I am Female
Male
Who I am visiting People supporting me at this appointment
Date & time of appointment
Location
Name of person responsible
(if applicable)1
Issues to discuss at the appointment
(ensure all issues recorded in the Health Learning Log are included)
Line manager review (e.g. team leader)
Signature and date
1 Refer to NCAT for a description of the person responsible. The health professional is responsible for gaining consent for any medical and dental intervention.
Health Planning, Tools and templates, V1.3, June 2016 1

Health appointment sheet
Diagnosis, treatment advice, recommendations, actions required
To be completed by the treating doctor / health professional
Diagnosis of illness
Prescribed treatment
Referral to other health professional No Yes
Potential side effect of treatment / medication
Observations for support workers to monitor any side effects of treatment
Has the person’s medication chart been updated or new medication prescribed?
No Yes
If Yes, ensure the person’s medication record is updated and includes any medications which have been ceased.
Health professional name
Speciality
Date
Signature
Health Planning, Tools and templates, V1.3, June 2016 2

Part B1 – Information about my health: Health learning log My name:
Date and time of event
What did the person do (what, where, when, how long, who was there)?
Date reviewed by health professional
Actions updated in the Health Action Plan (Y / N / NA)
Person recording this information
Line manager signature and date
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Health Planning Procedures
Document name Health Planning Procedures
Policy Health and Wellbeing Policy
Version number 1.3
Approval date January 2016
Policy manual Health & Wellbeing Policy and Practice Manual, Volume 1
Approved by Deputy Secretary, ADHC
Summary The Health Planning Procedures describe how the person and support workers, plan, document, implement and review the person’s health and wellbeing needs in consultation with health professionals, and the person responsible or guardian.
Replaces document New procedures
Authoring unit Contemporary Residential Options Directorate
Applies to People who are being supported in ADHC operated and funded non-government accommodation support services.
Review date 2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 November 2014 Replaces procedures outlined in the Health Care Policy and Procedures, 2012
V 1.1 January 2015 Amended to incorporate feedback
V 1.2 January 2016 Amended to incorporate feedback from consultation
V 1.3 June 2016 Amended to incorporate feedback from Districts
Health Planning Procedures, V1.3, June 2016 2

Table of contents
1 Health Planning Procedures ................................................................ 4
1.1 Background .................................................................................... 4
1.2 Application of the Procedures......................................................... 4
1.3 Person centred health planning...................................................... 4
2 Roles and responsibilities.................................................................... 7
2.1 Support workers ............................................................................. 7
2.2 Decision making support and consent............................................ 8
2.3 The person responsible and consent.............................................. 8
2.4 Escalation strategy ......................................................................... 9
3 My Health and Wellbeing Plan ........................................................... 13
3.1 One comprehensive health plan ................................................... 13
3.2 Application of the My Health and Wellbeing Plan ......................... 13
3.3 Part A – Information about me...................................................... 14
3.4 Part B – Information about my health ........................................... 17
3.5 Part C – My support plans ............................................................ 23
3.6 Part D – Review record ................................................................ 25
4 Annual health assessment................................................................. 27
4.1 Health assessment and tools ....................................................... 27
4.2 Medicare’s Chronic Disease Management Program .................... 28
4.3 Aged care ..................................................................................... 29
4.4 Women ......................................................................................... 30
4.5 Children ........................................................................................ 30
4.6 Procedures for preparing and attending an annual health assessment appointment.................................................................................. 31
5 Oral health ........................................................................................... 39
5.1 Annual dental review .................................................................... 39
5.2 My Oral Health Plan ..................................................................... 40
6 Index of tools and templates.............................................................. 41
7 Policy and Practice Unit contact details ........................................... 42
Health Planning Procedures, V1.3, June 2016 3

1 Health Planning Procedures
1.1 Background
The ADHC Health Planning Procedures (the Procedures) embody the principles of legal and human rights found in the New South Wales Disability Service Standards (the Standards), the commitment to deliver culturally responsive services to Aboriginal and Torres Strait people under the Aboriginal Policy Statement (the Statement), and the person centred guiding principles of the ADHC Health and Wellbeing Policy.
The Procedures are a guide for supporting people with disability to exercise their rights and entitlements under the Standards and Statement. The Procedures describe how ADHC supports people to make health related decisions, and to direct their own health planning and management, under the guidance of their ‘usual’ General Practitioner (GP)1 and other health specialists.
1.2 Application of the Procedures
The Procedures are a requirement for ADHC operated accommodation support services to follow when they are applying the Guiding Principles of the Health and Wellbeing Policy. ADHC funded non-government accommodation support services may adopt the Procedures, or develop their own.
1.3 Person centred health planning
This section relates to the Health and Wellbeing Policy Guiding Principles 1, 2, 7, 8, 9, 10.
Various tools and templates accompany the Procedures to assist the person, and support workers with health planning. In addition to health planning tools and templates, a range of person centred thinking tools are also suggested.
The blue boxes in the right hand margin refer to a specific health Tools and planning tool or template that can be used. Templates
A gold box in the right hand side margin refers to a specific person Person centred thinking tool. Person centred thinking tools are part of the centred
Lifestyle Planning Policy and Practice Manual. thinking tool
Person centred thinking tools support the person to lead and direct their own health planning. The tools can be used to identify:
when the person’s health support needs change
1 Medicare defines the person’s ‘usual’ GP as: ‘The GP (or a GP in the same practice) who has provided the majority of services to the patient in the past 12 months, and/or is likely to provide the majority of services in the following 12 months’.
Health Planning Procedures, V1.3, June 2016 4

how a decline in the person’s general health and wellbeing can affect their independence
the person’s preferred treatment and health support
how particular treatments can affect the person’s lifestyle and wellbeing
issues relating to family, social interactions, psychological or emotional wellbeing, or spiritual needs.
When using each tool and completing each step, it is important to involve the person as much as possible. Engaging with the person will assist:
the person by giving them the opportunity to discuss their health and wellbeing goals, and what is important to them
support workers to advocate for the person and gather information in a coordinated way
health professionals to better understand the person
with communication between support workers and significant others
in determining what actions are needed and who is responsible.
1.3.1 Aboriginal and Torres Strait Islander people
Aboriginal and Torres Strait Islander people have significantly poorer health outcomes than other Australians. The traditional Aboriginal and Torres Strait Islander perspective of health is holistic, and encompasses land, environment, physical body, community, relationships and law. Health is connected to the social, emotional, and cultural wellbeing of the whole community, and the sense of being indigenous2.
An Aboriginal or Torres Strait Islander person can be well supported if culturally sensitive and person centred approaches are employed during health planning in the following ways:
use the person’s communication profile to learn the best way of communicating information about the disease and its management
understand the person’s history and experiences, and difficult relationships, especially with hospitals
ask how the whole-of-life view (life-death-life) affects health planning and management
ask how and where the Aboriginal and Torres Strait Islander person would prefer to receive services
record the name of the proper contact person to discuss health issues and provide consent
2 Health Facts _Info Net – Health Status 2012
Health Planning Procedures, V1.3, June 2016 5

determine which health issues or practices are sensitive or taboo and who to refer to if they are
confirm whether the person or family would prefer to work with the health system through an Aboriginal Liaison Officer
ensure that the person and family understand the health service options and how they can access them.
1.3.2 Culturally and linguistically diverse (CALD) people
The person and family or carer’s cultural and religious beliefs about health and wellbeing should be established. Demonstrate respect and sensitivity to the person’s culture by considering:
the person and the family or carer’s views about health and wellbeing
the role of spiritual and religious beliefs in health and wellbeing
how the person and the family or carer communicate, for instance, through an interpreter
the person’s own role in problem solving and decision making
access to culturally appropriate health services.
Health Planning Procedures, V1.3, June 2016 6

2 Roles and responsibilities
This section relates to the Health and Wellbeing Policy Guiding Principles 11, 12, 13, 14.
2.1 Support workers
Support workers and health professionals play an important role in supporting a person to be healthy and well, however their roles and responsibilities are very different.
Support workers are not expected to diagnose or prescribe treatment for the person. The role of all support workers is to observe and monitor the person’s health and wellbeing on a day to day basis. The health professional diagnoses, prescribes, applies and coordinates treatment for health issues. The role of support workers in health planning is to support the person to follow the prescriber’s recommendations to maintain good health.
Two factsheets have been developed, one for support workers and one for the GP. The factsheet for GPs informs them about the roles and responsibilities of support workers. This knowledge can help a GP to tailor health advice and prescribed health actions. The factsheet for support workers informs them of the GP’s role in health planning (see ‘Other resources’).
2.1.1 Health advocacy3
Support workers often need to promote and uphold the rights and interests of the people they support. This is called advocacy.
The role of support workers is to advocate for the person during a health appointment by helping the person to communicate their health concerns to the GP, and to ensure that the GP provides written advice about managing the health concern.
In the context of health planning with the person, health advocacy includes:
1. Support, by providing health information, encouragement and skill development to empower the person to self-advocate.
2. Assistance, by prompting the person to communicate their health needs and issues with health professionals. For instance, supporting the person during the health assessment to communicate what health treatment advice is working or not working for them.
3. Representing the person, by speaking up when the person’s rights are violated and they are unable to do so for themselves. For instance, if the health professional does not engage with or provide adequate advice and support to the person during a health assessment appointment.
3 Advocacy role adapted from Victorian Advocacy League for Individuals with Disability (VALID)
Health Planning Procedures, V1.3, June 2016 7

Note: Representing the person does not include making health decisions for the person. This is the role of the person responsible4.
The following diagram is based on the person centred thinking tool the Donut. The donut outlines the various roles and responsibilities for supporting the person during the health planning process.
The centre of the donut, ‘core responsibility’, outlines key Donut responsibilities of support workers in maintaining a person’s health
and wellbeing.
The middle section of the donut ‘use judgement and creativity’ contains a network for the support worker to access to help solve problems and provide direction, and when to refer matters of concern to line managers.
The outer circle of the donut ‘not the support workers paid responsibility’ outlines the role and responsibility of senior managers and others involved in health planning.
2.2 Decision making support and consent
People should be encouraged and supported to make decisions about who provides their medical and dental treatment. When people have the capacity to consent to receiving treatment, including changes to medications, they must be supported to do so.
See Decision Making and Consent Policy in the Lifestyle Planning Policy and Practice Manual for more information about capacity and consent.
2.3 The person responsible and consent
The treating doctor or dental practitioner is responsible for determining if the person is capable of understanding the general nature and effect of treatment and whether they are able to give valid consent. If not, and consent is required, it is given by the person responsible. The role of the person responsible is only relevant to giving or withholding consent for dental or medical treatments.
The NSW Civil and Administrative Tribunal (NCAT), Guardianship Division, provides guidance on who can be the person responsible for giving or withholding consent5.
4 NCAT Person responsible factsheet: http://www.ncat.nsw.gov.au/Documents/gd_factsheet_person_responsible.pdf
5 NCAT Consent to medical and dental treatment fact sheet http://www.ncat.nsw.gov.au/Documents/gd_factsheet_consent_to_medical_or_dental_treatment.pdf
Health Planning Procedures, V1.3, June 2016 8

Diagram 1: Roles and responsibilities in health planning
Records changes to the person’s health status
Facilitates appointments
Communicates with families
Helps the person with
health planning
Informs the team of changes to the person’s health
needs
Monitors the person’s health on a daily basis
Seeks support from the line
manager in all aspects of health
planning
Collaborates with relevant parties when concerns with
health planning escalate to line managers
Works with others on issues
relating to a person’s complex
health needs
Works to approved good
practice standards in health planning
Works as a team during the
health planning process
Seeks support from line managers when issues with a health professional
occurTranscribes and
provides a written record of
prescribed health treatments and
advice (GP)
Provides health services for all
people residing in NSW
(NSW Health)
Accesses training and support for
specific health planning issues
Actively engages during
supervision to work through
issues
Provides advice and support to
GPs(Primary Health
Networks)
Promotes the adoption of
good practice standards
(senior manager)
Designs and improves systems and
practices with the District
(senior manager)
Assists in the monitoring and
reviewing systems e.g. CIRT
Establishes local networks between
NSW Health and ADHC
(District leads)
Not the support worker’s
paid responsibility
Support worker – Core responsibility
Support worker –Use judgement and creativity
Supports the person to
communicate and to self-advocate
Acts as the ‘person
responsible’ and provides consent
Consults with families and
guardians around a person’s
health needs
Assists health professionals
to better understand the
person
Interprets and diagnoses a
person’s health issue(GP)
Applies and coordinates
medical treatment for the person
(GP)
Promptly follows up on health actions and recommendations
prescribed by health professionals
Establishes capacity and seeks consent (doctor /
dentist)
2.4 Escalation strategy
If the outcome of a health appointment with a health professional is not satisfactory, the support worker will need to either approach the health professional or refer the matter to a line manager for further action.
At an unsatisfactory appointment the health professional may:
refuse to provide recommendations in writing
refuse to provide a copy of an annual health assessment
not act on concerns raised about the person’s health and wellbeing.
If the person, person responsible or support worker are not satisfied with the outcome of the health appointment, and have not been able to raise their concerns
Health Planning Procedures, V1.3, June 2016 9

directly with the health professional during a consultation, the matter must be referred to the line manager for further action.
It is the line manager’s responsibility to escalate the matter by:
discussing the concerns directly with the health professional
informing a senior manager of the issue
making a referral to an ADHC Clinical Nurse for advice and support with approaching the health professional.
If the above strategies do not provide a satisfactory response from the health professional, the person has the option of looking for another who will provide a service that suits the person better.
Health Planning Procedures, V1.3, June 2016 10
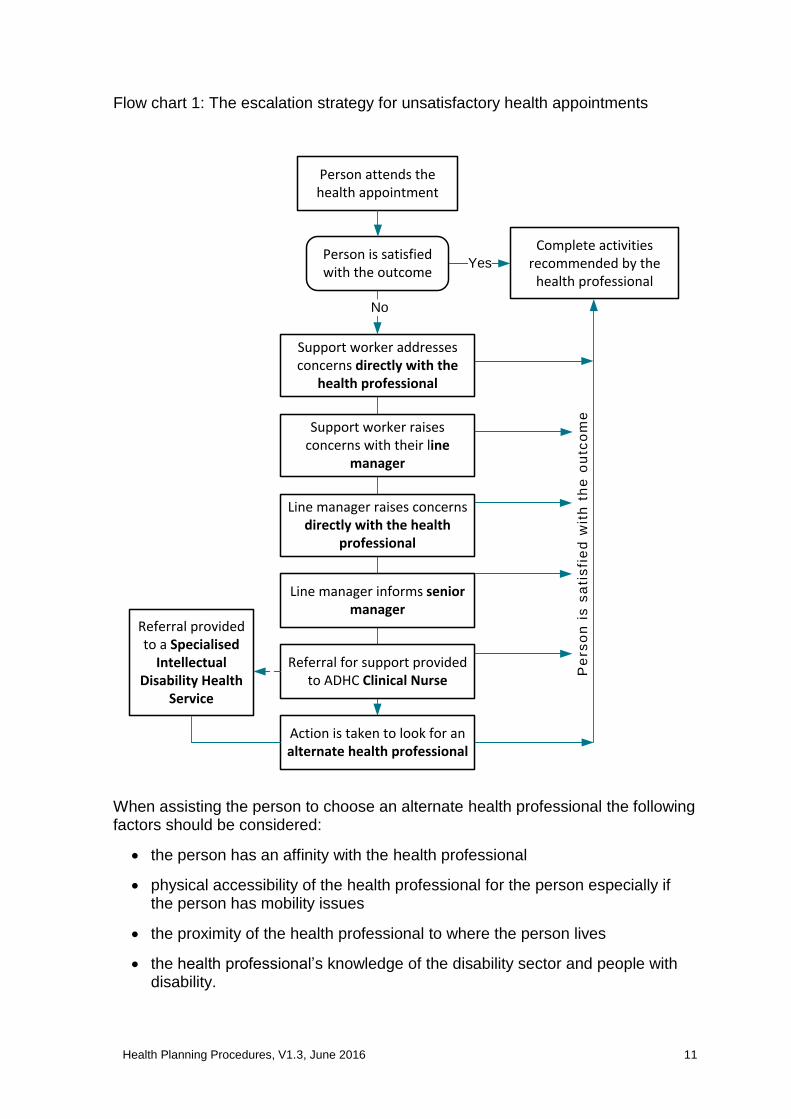
Flow chart 1: The escalation strategy for unsatisfactory health appointments
No
Yes
Support worker addresses concerns directly with the
health professional
Support worker raises concerns with their line
manager
Line manager raises concerns directly with the health
professional
Line manager informs senior manager
Referral provided to a Specialised
Intellectual Disability Health
Service
Action is taken to look for an alternate health professional
Person attends the health appointment
Person is satisfied with the outcome
Complete activities recommended by the
health professional
Referral for support provided to ADHC Clinical Nurse
Pe
rso
n i
s s
ati
sfi
ed
wit
h t
he
ou
tco
me
When assisting the person to choose an alternate health professional the following factors should be considered:
the person has an affinity with the health professional
physical accessibility of the health professional for the person especially if the person has mobility issues
the proximity of the health professional to where the person lives
the health professional’s knowledge of the disability sector and people with disability.
Health Planning Procedures, V1.3, June 2016 11

2.4.1 Specialist disability services
If the person is unwell or has complex health needs, action must be taken promptly. The person has the option of being seen by a Specialised Intellectual Disability Health Service for assessment.
A Specialised Intellectual Disability Health Service can provide a responsive course of action and provide advice and training in the area of disability to health professionals such as the person’s GP.
Some Specialised Intellectual Disability Health Services will require a referral from a medical practitioner. Demand for specialist services may mean that the person is placed on a waiting list. If the person is put on a waiting list, the person and support worker need to seek advice from the person’s GP or another GP on how to manage the person’s health needs in the meantime.
Health Planning Procedures, V1.3, June 2016 12

3 My Health and Wellbeing Plan
This section relates to the Health and Wellbeing Policy Guiding Principle 3.
3.1 One comprehensive health plan My Health and
Wellbeing The comprehensive health plan used in ADHC operated Plan accommodation support services is the My Health and Wellbeing Plan.
One comprehensive health plan integrates all current personal health, wellbeing and support needs, and health records for the person.
Benefits of an integrated health plan include:
a format which assists and encourages the person to lead and direct their own health planning
a document which is used everyday to record observations and changes in the person’s health status
a comprehensive document which can be taken to health appointments
an easy source of information about the person for support workers and health professionals
a medical and social history of the person to help inform future health and wellbeing decisions
less repetition of information in different documents.
3.2 Application of the My Health and Wellbeing Plan
It is mandatory for ADHC operated group homes to have a My Health and Wellbeing Plan (the Plan) in place for every person.
Large Residential Centres and Specialist Supported Living can adapt the Plan by adding any additional documentation needed to meet the complex needs of the people they support, and the requirements of nurses’ professional registration.
A person who accesses an ADHC operated centre-based respite service requires an up to date Respite Care Profile, and may choose to supplement it with components of the Plan.
A person accessing other ADHC operated accommodation support, in-home or drop-in support services may choose to have a Plan or use components of the Plan to capture their health and wellbeing needs.
The person’s Plan is a living document which is used on a daily basis by the person and support workers.
The Plan should not be ‘filed away’ as this will discourage the person and support workers from using it. When not in use, the Plan should sit in a location where it is private and safe from damage or loss, but is physically accessible to the person,
Health Planning Procedures, V1.3, June 2016 13

support workers and others involved in supporting the person’s health and wellbeing.
The Plan template is provided in the ‘Tools and templates’ section of the Health Planning Procedures as either a complete template incorporating Parts A to D. Alternatively the sections within each Part are also provided to assist in the ongoing review and recording of health and wellbeing information.
3.3 Part A – Information about me
Part A of the person’s My Health and Wellbeing Plan contains all of the person’s health and wellbeing details. It is developed from the person’s perspective.
There are eleven sections to Part A as outlined in Image 1.
Image 1: My Health and Wellbeing Plan: Part A – Information about me
Decision making agreement
11
Decision making profile
10
Sensitive information
9
My history
8
Immunisation record
7
Supporting me at a health appointment
6
Communicating my health needs
5
My support team
4
My health professionals
3
Medical alerts and allergies
2
My personal details
1
Part A is completed by the person and support workers who know the person well. In situations where the person is unable to provide personal details, the information is sourced from the person’s records and from other people who know the person (Table 1 following).
Health Planning Procedures, V1.3, June 2016 14

Knowing the person well includes having a good relationship with the person, understanding the person’s communication style and being an advocate for the person as necessary (see section 2.1.1).
If there are details about the person in Part A that are unknown, it is important to record this in the relevant section and to leave no fields blank. For instance if it is unclear if the person has received a Hepatitis B Immunisation injection, then record ‘unknown’ in the person’s My Immunisation record
Record. This information can be discussed further with the person’s GP.
Information in Part A is only recorded once, and if any changes to the person’s details occur they are updated at the time or as part of a quarterly review cycle (see section 3.6 Part D – Review record).
Table 1: Sources of information about the person
Source Further information
The person and the person’s family
When requesting information from families, support workers are to be sensitive and respectful, especially if the person has an experience of trauma.
Remember to be mindful of these sensitivities when asking questions about the person’s medical and family history.
People who have known the person for a long time
Friends and advocates
Long term support workers
Support workers who currently or have previously supported the person
The Client Information System (CIS)
Discuss with your line manager about recording information on CIS.
Information about the person from files
People who have been with ADHC for some time, and who have received support from ADHC clinicians (psychologists, speech pathologists, occupational therapists, physiotherapists), may have a hard-copy file containing personal information.
Discuss with your line manager about accessing information from these files.
eHealth6 eHealth is a record system which stores a person’s health information online. The person has control
6 http://www.ehealth.gov.au/internet/ehealth/publishing.nsf/content/home
Health Planning Procedures, V1.3, June 2016 15

Source Further information
over what information is stored and who has access to it.
An authorised representative can be appointed if the person does not have the capacity to apply for and manage their eHealth record.
Archived information Past documents relating to the person are stored in the Government Records Repository. If information is missing about the person it may be contained in archived records.
Discuss with your line manager about whether it is necessary to access archived information.
The My History section is based on the Lifestyle Planning person centred thinking tool, History Map. It records significant events in the person’s life which may impact on their health and wellbeing such as medical diagnoses, family medical history of relevance to the person and social history. The information in this section can be recorded in a table or as a diagram.
The Sensitive Information section alerts the reader to whether the person has experienced a traumatic event in the past and provides a record of situations and/or actions to be avoided to prevent the person recalling the event. It is not necessary to record the details of the traumatic event. If there is more than one event, add extra pages. A referral can also be made to an ADHC Behaviour Support Team for support.
When completing the My History and Sensitive Information sections, care must be taken to preserve the person’s and their family’s right to privacy and confidentiality. It is good practice to check with the person’s family before recording personal information, as the information may be private and confidential.
My History
History Map
Sensitive Information
Health Planning Procedures, V1.3, June 2016 16

3.4 Part B – Information about my health
Part B of the My Health and Wellbeing Plan contains information on the person’s current health status.
There are six sections to Part B as outlined in Image 2.
Image 2: My Health and Wellbeing Plan: Part B – Information about my health
Annual health assessment report or Part B CHAP tool
Annual Health Summary or Part A CHAP tool
5
Health Promotion Register
4
Health Action Plan
3
z
Health reports
2
Health Learning Log
1
6
Part B allows support workers to record and store information about the person’s health and wellbeing.
All support workers who provide support to the person are responsible for keeping this section current and up to date. This includes permanent, temporary, casual and agency support workers.
3.4.1 Health Learning Log
The Health Learning Log is a tool used every day to record any Health
observed or communicated changes in the person’s health. Learning
LogRecording health information in one place helps health professionals to understand what is happening for the person over time, and to identify indicators and patterns of ill health. It avoids the need to rely on one person’s understanding or memory of the person’s health issues.
The Health Learning Log also supports holistic health care as health professionals are made aware of treatments and prescriptions by other professionals.
Health Planning Procedures, V1.3, June 2016 17

It is the responsibility of all support workers to record changes in the person’s health status in the Health Learning Log. This includes permanent, temporary, casual and agency support workers.
To determine whether a change in the person’s health status has occurred, refer to:
the person directly
how the person communicates their health needs as outlined in Part A of the My Health and Wellbeing Plan
other support workers on shift or at other services the person may have attended recently such as a day program or work place
recent written records such as the person’s daily notes/shift report, the Communication Book, and completed incident reports.
Observations of the person’s health status are recorded in the Health Learning Log and changes promptly provided to a health professional for interpretation and action.
Any actions arising from a health consultation should be recorded in a health report prepared by the health professional (see section 3.4.2 – Health Reports). The action and follow-up from the health report is then communicated to other support workers:
verbally during shift handover (if possible)
by noting the information on the Individual Shift Report (for ADHC operated group homes)
in the Communication Book
in the diary if time frames and appointments are involved
at the next team meeting
in the Health Action Plan (see section 3.4.3).
Observations on what worked and didn’t work at the appointment can also be recorded in the person’s Health Learning Log. This information is then used to update the Supporting Me at a Health Appointment section of the My Health and Wellbeing Plan (see section 3.3 Part A – Information about me).
Support workers record the person’s detailed health and wellbeing information in the person’s Health Learning Log.
For example, if the person fell over and sprained their ankle:
1. Apply first aid and seek medical attention.
2. Complete an incident report7 outlining the situation, how it occurred, follow up action and any recommendations to prevent reoccurrence.
7 CIS incident form
Health Planning Procedures, V1.3, June 2016 18

3. Make observations of the injury and record these in the Health Learning Log.
4. Refer the reader to where detailed information has been recorded by entering this information in the person’s daily notes/shift report. For example, ‘Danny tripped on a rock and sprained his ankle when walking to the corner store. Danny went to see Dr Mathews. Refer to the Incident Report, Health Learning Log, GP’s health report and Health Action Plan for detailed information and further actions required’.
5. Make references to any additional support requirements in the Urgent Matter Alert on the Individual Shift Report.
6. Update any new information in the person’s Communication Profile and Health Action Plan.
A reference to the incident can be made in the daily notes and Individual Shift Report.
3.4.2 Health reports
The Health Reports section contains all advice and health information recorded during a health appointment or consultation with the person’s health professional.
When the person requires medical attention or has a scheduled health appointment, the support worker must ask the GP or treating doctor to provide a written record of the issue, treatments and any actions that are to be taken.
A written record provided by the health professional will eliminate the risk of support workers transcribing and misinterpreting information.
Support workers are not responsible for recording the advice and recommendations provided by the health professional in any format.
A written record from the health professional can be hand written or typed and should outline:
when the consultation occurred
who conducted the consultation
the reason for the consultation
any diagnoses that are made
written instructions of prescribed treatment
further actions and recommendations.
The health professional can record information on their own template or in the Health Appointment Sheet template. It is not Health
Appointment mandatory for support workers or the GP to use this tool. Give the Sheet
GP the option of using this tool by providing a copy at the beginning of the consultation.
If the health professional provides a hand written report, the support worker attending the appointment needs to go through it with the health professional to
Health Planning Procedures, V1.3, June 2016 19

understand it and ensure that it is legible and clear enough for other support workers to read.
The written record provided by the health professional is filed in the Health Reports section by date, with the most recent health report at the top.
3.4.3 Health Action Plan
The Health Action Plan is a tool to assist the person and support workers to keep track of the completion of actions prescribed by a Health
health professional. Action Plan
The Health Action Plan is not intended to be used to transcribe and record health information from a health professional. This is solely the responsibility of the health professional (see section 2 – Roles and responsibilities).
The Health Action Plan assigns responsibility, to complete or monitor the completion of actions, to a support worker within a set time.
Each action should have a time frame for completion. When an action is completed, the line manager initials and dates the entry to indicate that they have reviewed the completed action. This will ensure that heath actions are monitored and completed when due.
For instance, after the person’s annual appointment with the neurologist, actions may be recorded as shown in the example of a Health Action Plan below:
Action Date and name of health professional prescribing the action
Who is responsible for completing the action
Date due Progress Date complete
Team leader signature and date
(information provided on the Health report)
Get pharmacist to 1.7.15, Dr Elmo Peters 2.7.15 Complete 2.7.15 A.Smith repack Webster-pak® Sommerville 16.7.15 with new medication
Book blood test to check Tegretol levels
1.7.15, Dr Sommerville
Cindy Jones 15.7.15 Complete 14.7.15 A.Smith 16.7.15
Get person responsible to sign Epilepsy Management Plan
Not applicable Cindy Jones 2.7.15 Forms sent to Alan Hines. Waiting for return
In progress
by post
The Health Action Plan is reviewed regularly to ensure that time frames are not missed. Depending on the health action, a review could be needed every week until the action is complete.
The Appointment Checklist is a non-mandatory tool which provides guidance to the person and support worker when making health appointments.
Health Planning Procedures, V1.3, June 2016 20

Appointment Checklist
It is designed to present the person’s information to the health professional in a clear and coordinated way. The health professional can then make informed decisions on how to best meet the person’s health and wellbeing needs.
Where possible, a support worker, who knows the person and the person’s medical history, attends the health appointment. With the person’s consent, a family member, or someone else who knows the person well, may also attend the appointment.
Store completed Appointment Checklists behind the Health Action Plan to keep track of items recorded and review it quarterly or sooner if required.
3.4.4 Health Promotion Register
Health promotion activities are often a neglected area for people with disability. The Health Promotion Register outlines what healthy living and health screening activities have been implemented and / or need to be completed with the person. It is essential that this section is completed to help the person monitor their health on an ongoing basis.
If there are details about the person’s health in this section that are unknown, it is important to record this in the relevant section and to leave no fields blank.
For instance, if it is unclear if the person has received a vision check, record ‘unknown’ in the relevant field in the Health Promotion Register. This information is then discussed with the person’s GP who will document any referrals or prescribed treatments during the annual health assessment.
It is good practice for people to have a completed Physical Activity Checklist and Plan. This tool assesses the person’s level of physical activity and provides a record of actions to improve the person’s fitness (see ‘Tools and templates’). Any plan developed should be discussed first with the person’s GP at the annual health assessment appointment or an allied health professional such as a physiotherapist or exercise physiologist.
Refer to the Health Promotion Guidelines in the ADHC Health and Wellbeing
Policy and Practice Manual, Volume 2 for further information on health promotion and physical activity ideas for the person.
3.4.5 Annual Health Summary or Part A of the CHAP tool
The Annual Health Summary tool summarises the person’s health information gathered over the year. The summary is used to inform the annual health assessment with the person’s GP.
The Annual Health Summary is divided into body systems, for example, sensory, muscular-skeletal, respiratory and cardiovascular. Each section outlines symptoms that may occur if there is a problem in that body system.
Health Promotion Register
Physical Activity
Checklist and Plan
Annual Health
Summary
Health Planning Procedures, V1.3, June 2016 21

It is the responsibility of support workers to record the health issue that is communicated by the person or observed by support workers, not to interpret what it means. It is the role of the GP to determine what each health indicator may mean and recommend any action that is required.
If the GP prefers to use the CHAP tool, the support worker completes the first section of the CHAP tool instead of the Annual
CHAP tool Health Summary and stores the completed document in this section.
3.4.6 Medicare health assessment or Part B of the CHAP tool
This section contains the most recent annual health assessment report completed by the person’s usual GP.
The health assessment is the primary source of health information in which the GP directs the person and support workers on what health and wellbeing actions are needed. It is used to assess the person’s health status by:
gathering information about the person’s current and long-term health and wellbeing
identifying health risks
recording diagnoses
recording health information and advice
recording actions and treatment regimes to manage current and long term health conditions
recording changes to medication
recording preventative health care actions
placing the responsibility of health planning with the health professional
providing a financial incentive to the GP with its completion.
Health Planning Procedures, V1.3, June 2016 22

3.5 Part C – My support plans
A support plan outlines treatment and support information to help manage a person’s health condition. Depending on the health condition and the plan itself, a support plan may be prepared by the person and support worker, or the treating doctor.
There are three sections to Part C as outlined in Image 3.
Image 3: My Health and Wellbeing Plan: Part C – Health data and support plans
Support plan
Support plan
Health report
Support Plan Register
2
Health data
1
3.5.1 Health data
The Health Data section contains data sheets used to record information requested by the person’s GP or health professional, to monitor an issue and better understand what is happening with the person’s health.
It is the responsibility of all support workers to maintain the person’s Weight
health data. This includes permanent, temporary, casual and agency Chart
support workers.
This includes health data which may or may not have a support plan for a health condition such as a Weight Chart.
Each person requires a Weight Chart. It is mandatory for support workers to accurately record the person’s weight at least monthly and height at least annually in the Weight Chart.
Menstruation
It is recommended good practice to maintain a Menstruation Chart Chart
where relevant for the person, however it is not mandatory (see ‘Tools and templates’).
Health Planning Procedures, V1.3, June 2016 23

Bowel Chart
People with disability frequently require health support to maintain a healthy bowel. It is good practice to record a person’s bowel action as a way of monitoring activity and detecting change from bowel habits that are normal for the person. Refer to the Bowel Care Guidelines in this Manual for information on how to monitor and support bowel health, the causes and risks of bowel dysfunction, and treatments. Use the Bowel Chart (see ‘Tools and templates’) to record bowel activity.
3.5.2 Support Plan Register
The Support Plan Register records the person’s diagnosed health conditions and support plans. It is a mandatory tool that must be completed as it records the support plans prescribed for the person by a health professional.
Support Plan
Register
3.5.3 Support plans
Support plans are located in this section, behind the Support Plan Register unless support workers need to access them at certain places and times. For example, if a person is prescribed a Mealtime Management Plan, it may be kept in the kitchen for easy access when meals are being prepared and served.
The GP or treating doctor may choose to record support plan information and treatment recommendations in different ways.
For example:
a written report
a Medicare Chronic Disease Management Plan such as a GP Management Plan or Team Care Arrangement (see section 4 – Annual health assessment)
a template developed by another health agency, such as the NSW Ministry of Health or the Australian Government Department of Health, e.g. Asthma Action Plan
an existing ADHC support plan.
If the person’s GP or health professional has developed a treatment or management plan for a health condition, the support worker supporting the person at the appointment must establish with the health professional when the plan is due for review and what outcomes should be expected from following the plan.
For further information relating to specific health areas, refer to the procedures
and guidelines for each area (in the Health and Wellbeing Policy and Practice Manual, Volumes 1 and 2).
Health Planning Procedures, V1.3, June 2016 24

3.6 Part D – Review record
There are two sections to Part D as outlined in Image 4.
Image 4: My Health and Wellbeing Plan: Part D – Review record
People who have read and understood the plan
2
Review record
1
The person’s My Health and Wellbeing Plan is reviewed and updated every three months or sooner if the person’s health needs change.
Reviewing the My Health and Wellbeing Plan is essential for:
monitoring and recording changes to the person’s health
highlighting any health patterns of concern
reviewing the status of any aids or equipment that the person uses
keeping track of the completion of recommendations and actions prescribed by the person’s GP and any other health professional
prompting support workers to record new information about the person and their health and wellbeing.
When reviewing the My Health and Wellbeing Plan, the person must remain the focus of the review. It is good practice to meet with the person first when reviewing the My Health and Wellbeing Plan. After meeting with the person, the support worker consults with the rest of the team to discuss changes to the person’s health, and the My Health and Wellbeing Plan.
There are many opportunities for the My Health and Wellbeing Plan to be reviewed with other support workers on a regular basis.
Reviews occur during:
Monthly supervision
Monthly supervision involves a formal discussion between each support worker and their line manager. Supervision includes a discussion about the person’s
Health Planning Procedures, V1.3, June 2016 25

health and wellbeing needs and concerns, and actions the support worker is responsible for completing.
Every team meeting
Team The person’s health and wellbeing is a standard agenda item which is Meeting discussed at every team meeting. A sample Team Meeting Agenda is Agenda
provided to facilitate discussion between the line manager and support workers at each team meeting (see ‘Tools and templates’).
Keeping the There are several Lifestyle Planning tools that are also of use, in Plan Alive particular, Keeping the Plan Alive, Working / Not Working and Four
+ One Questions. These tools help to maintain the focus of the review on the needs and wants of the person.
Working / Not working A designated support worker must also communicate to other relevant
parties if any changes to the My Health and Wellbeing Plan occur as a result of a review. This includes the person responsible and the
Four + One person’s place of work or day program. Consent must first be obtained Questions from the person or family about what information is to be disclosed and
to whom.
If any concerns or issues are raised during discussion with the person and other support staff, or if there is health information that needs clarification, consult with the person’s GP or other relevant health professional.
Record any changes that have been made to My Health and Wellbeing Review Plan on the Review Record template. If there are no changes, record record
‘no changes’.
The line manager endorses the review and any changes made to the Plan by signing in the right hand column.
Date of review
Changes made Initials of support workers completing the review
Line manager signature and date
17.11.15 Information provided in first draft of plan LB, MR, MK Annie James
17.11.15
15.12.15 Added information to Part A Health professionals
Updated information in Medication Support Plan
New annual health assessment added to Part B
LB, MR, MK, PC Annie James
15.12.15
1.2.15 No changes LB, PC, MK, LM Annie James
1.2.15
Part D also provides a record of the support workers who have read, understood and signed the My Health and Wellbeing Plan. Each support worker who supports the person must sign this section. This includes newly inducted staff, casuals and agency workers.
People who have read and understood the
plan
Support workers who have difficulty understanding any aspect of the person’s My Health and Wellbeing Plan must clarify the issue with the relevant line manager.
Health Planning Procedures, V1.3, June 2016 26

4 Annual health assessment
This section relates to the Health and Wellbeing Policy Guiding Principles 4, 5, 6, 11, 31, 32 and 33.
Each person living in an ADHC operated or funded accommodation support service (Group Home, Large Residential Centre and Specialist Supported Living) must have a health assessment completed every year. The responsible professional for completing the annual health assessment is the person’s usual GP.
For all other ADHC accommodation support services, such as in-home support, support workers provide information to the person they support about their entitlement to have an annual health assessment conducted by their usual GP under Medicare.
4.1 Health assessment and tools
There are five Medicare health assessment items that the GP can use to assess the health and wellbeing needs of a person with intellectual disability (Table 2).
Each Medicare health assessment has a separate Medicare item number depending on the length of the assessment (see Medicare Health Assessment Factsheet in ‘Other Resources’).
Table 2: Medicare items
Medicare item Item number
Length of assessment
Frequency of service
Medicare health assessment
Brief 701 Not more than 30 minutes
Every 12 months Standard 703
Between 30 and 45 minutes
Long 705 Between 45 and 60 minutes
Prolonged 707 At least 60 minutes
Aboriginal and Torres Strait Islander people
715 Not specified Every 9 months
Chronic Disease Management Program
GP Management Plan 721
Not specified
Every 12 months
Team Care Arrangement 723 Every 12 months
Domiciliary Medication Management Review
900 Every 12 months
Health Planning Procedures, V1.3, June 2016 27

Medicare item Item number
Length of assessment
Frequency of service
Mental Health Treatment Plan
2700, 2701 2715, 2717
Every 12 months
Individual Allied Health Services
10950-10970
Maximum of five allied health services in a calendar year
A long or prolonged consultation is recommended (item 705 and 707) as this allows adequate time for the GP to discuss any health and wellbeing concerns with the person, and how these can be managed.
The person and the GP may decide that a number of appointments are needed for the health assessment. For instance, the person may have two preliminary consultations with the GP to gather information, followed by a third prolonged appointment to undertake the Medicare health assessment.
As well as the Medicare Health Assessment tool, other health assessment tools have been developed for the disability sector. These assessment tools are based on the content of the Medicare Health Assessment tool. Examples are the Comprehensive Health Assessment Program (CHAP), and the assessment tool developed by the New England Division of General Practice. Whichever tool the GP uses, it must meet the minimum criteria outlined by Medicare.
In ADHC operated or funded accommodation support services, the annual health assessment appointment should be booked as soon as possible after the twelve months has elapsed (or 9 months if the person is Aboriginal or a Torres Strait Islander and the GP uses Medicare item 715).
Templates for the Medicare health assessments are available in the ‘Tools and templates’ and ‘Other Resources’ sections of the Health Planning Procedures.
4.2 Medicare’s Chronic Disease Management Program
If the person has two or more chronic conditions and / or a terminal illness, the GP can manage their health needs under Medicare’s Chronic Disease Management Program. The chronic disease Medicare items are additional to the Medicare health assessment items.
Under the Chronic Disease Management Program a range of support plans are available to assist the GP in coordinating the person’s health care needs (Table 2).
Information on the Chronic Disease Management Program is available through the Australian Government Department of Health website8.
8 Medicare Chronic Disease Management Program
Health Planning Procedures, V1.3, June 2016 28

Chronic disease Medicare items and the Chronic Disease Guidelines contain
information about specific health conditions. These are contained in the Health and Wellbeing Policy and Practice Manual, Volume 2.
4.3 Aged care
Due to improvements in medical and social developments, people with disability are living longer. People with disability have the same aged related health concerns as the rest of the population however age related conditions may develop sooner9. Because of this, it is necessary for people who are ageing to access mainstream and specialist health supports to manage age-related health conditions.
Complex health needs are managed by the person’s GP through:
the Chronic Disease Management Program (section 4.2 above)
referral to a health professional such as a Geriatrician who specialises in the health care of older people
referral to an allied health professional to provide advice and support on daily living activities
by referring the person to a Specialised Intellectual Disability Health Service (see section 2.4.1).
A referral to allied health services such as a physiotherapist or occupational therapist can assist a person whose physical health and mobility deteriorates by providing advice on equipment, home modifications and manual handling. Speak to a line manager about making a referral to an ADHC allied health professional or by contacting mainstream support services such as Independent Living Centres for advice on products and equipment to manage daily life10.
If the person is 65 years or older and there is concern the person’s accommodation setting does not provide the right support, discuss the options with the person or family. The person’s needs may be met better in a specialist accommodation support service or aged care facility. With the person or family’s consent, a referral can be made to the Aged Care Assessment Team (ACAT) who will assess eligibility for aged care services11 with the person and family. The support worker can also discuss this option with a line manager.
Regardless of the age of the person, it is good practice to have discussions with the person and their family about the person’s preferences for end of life care, rather than waiting for the person to be terminally ill and unable to be involved in the discussions. Refer to the End of Life Care Planning Guidelines in the Health and Wellbeing Policy and Practice Manual, Volume 2 for further information.
9 http://www.nswcid.org.au/health/se-health-pages/specialised-intellectual-disability-health-services.html
10 http://ilcaustralia.org.au/products/search/advanced?major_code_id=5&minor_code_id=1254&q=
11 http://www.myagedcare.gov.au/aged-care-homes/considering-aged-care-home
Health Planning Procedures, V1.3, June 2016 29

4.4 Women
The Disability Inclusion Act 2014 recognises that “women with disability may face multiple disadvantages and are potentially more vulnerable to risk of abuse or exploitation”12.
In supporting women with health planning:
involve and encourage contribution by natural supports where the person wants this (natural supports are a protective factor in preventing abuse and exploitation)
ensure supporters are chosen by the person such as allowing the person to choose female or male supporters
ensure access to mainstream health services such as Women’s Health Centres and Family Planning NSW for information and support with health promotion activities, reproductive health and sexuality
ensure that information supports informed decision making and consent about general health and wellbeing, intimate relationships and self-protective strategies.
Refer to the Health Promotion Guidelines, Decision Making and Consent
Policy and Guidelines and the Sexuality and Relationship Guidelines.
4.5 Children
The Disability Inclusion Act 2014 requires service providers to consider the particular needs of children and young people with disability13 so that supports and services are provided in a way that:
recognises the child or young person’s right to live a life with full and active participation in activities which promote their health and wellbeing
recognises that children and young people are more vulnerable to the risk of abuse and exploitation
respects the views of the child or young person (with respect to their age and maturity)14.
While all people under 18 years of age are regarded under the law as children, young people are given special consideration by the NSW Civil and Administrative Tribunal (NCAT) Guardianship Division. A young person can provide their own consent on a range of matters, or they can be assigned a public advocate by
12 See Section 5(4)(a) of the Disability Inclusion Act 2014
13 A child is any person 0-15 years of age and a young person is anyone 16-17 years of age. Children and Young Persons (Care and Protection) Act 1998
14 See Section 5(5) of the Disability Inclusion Act 2014
Health Planning Procedures, V1.3, June 2016 30

NCAT if they need a legally appointed decision maker (refer to the Decision Making and Consent Policy and Guidelines).
The Maximising Health and Wellbeing for Children and Young People in Out-of-Home Placements Policy and Procedures provides guidance to support workers of ADHC operated and funded non-government accommodation support services on supporting and maximising the health, and meeting the medical and dental needs of children and young people with disability living in out-of-home placements. Refer to the policy and procedures to support a child or young person with disability with health planning.
Medicare’s Child Dental Benefits Schedule (CDBS) enables access to basic dental services for children two to 17 years of age (refer to the NSW Ministry of Health for a list of services and eligibility requirements15).
Medicare also funds a number of initiatives for children with disability and their families to assist with assessment, diagnosis, and provision of early intervention services for eligible disabilities. For instance:
a one-off assessment by a specialist or GP for early diagnosis and treatment of a range of conditions
the Better Start for Children with Disability and Helping Children with Autism programmes to assist children under the age of six years and their families with accessing early intervention services.
Refer to Australian Government Department of Social Services for eligibility requirements, payment thresholds and information on the transition of these services to the National Disability Insurance Scheme16.
4.6 Procedures for preparing and attending an annual health assessment appointment
The annual health assessment is a document used by the person and support workers throughout the year.
The information contained in the annual health assessment usually includes diagnoses, health information and advice, record of changes to medication and treatment regimes to manage certain health conditions (see section 4.2 – Medicare’s Chronic Disease Management Program).
As support workers will often support and advocate for the person during the health assessment, it is good practice to prepare the information to be discussed with the GP before the appointment.
Each step involved with preparing for the health assessment appointment can be completed over a series of meetings between the person and support workers who
15 Child Dental Benefits Schedule
16 https://www.dss.gov.au/our-responsibilities/disability-and-carers/program-services/for-people-with-disability
Health Planning Procedures, V1.3, June 2016 31

know the person well. If the person consents, this can involve the family or person responsible. Refer to the steps below when preparing for and attending the annual health assessment appointment.
STEP 1: Review the current health assessment
This step involves reviewing actions and recommendations made by the GP from the last annual health assessment.
The person centred tool Working / Not Working is a useful tool to Working / assess the effectiveness of health care actions and why previous
not working actions were not achieved or completed, or did not appear to make a difference.
Any actions that have not been completed over the previous year are noted and discussed further with the person and others (see Step 6) and the GP at the person’s health assessment appointment (see Steps 8 – 12).
STEP 2: Review the Health Promotion Register
Medicare’s health assessment criteria outline a number of items to prompt a review of health promotion activities. For instance, hearing and vision health, men’s and women’s health and physical activity.
This step involves reviewing the person’s Health Promotion Register, located in Part B of the My Health and Wellbeing Plan (see section 3.4.4 – Health Promotion Register).
Any fields that are out of date or ‘unknown’ are noted and discussed with the GP during the appointment. The GP recommends what actions are to be taken.
It is good practice to complete a Physical Activity Checklist and Physical Activity Plan with the person at this stage. The plan can then be discussed with the GP at the health assessment appointment. The GP may refer the person on to an allied health professional such as a physiotherapist or exercise physiologist.
STEP 3: Review the person’s health data sheets
In this step, the information contained in the person’s health data sheets is collated so that they can be discussed with the GP at the appointment (see section 3.5.1 – Health data).
The person’s current height and weight is measured either before the appointment if they need to access specialised equipment or by the GP during the health assessment appointment.
STEP 4: Review existing support plans
The Support Plan Register located in Part C of the My Health and Wellbeing Plan records mandatory checklists and support plans, and support plans prescribed for the person by a health professional (see section 3.5 Part C – My support plans).
Support plans for the person are reviewed and updated in preparation for the person’s annual health assessment.
Health Planning Procedures, V1.3, June 2016 32

They can include but are not confined to the person’s:
My Oral Health Plan
Behaviour support plans
My Eating and Drinking Profile OR Mealtime Management Plan OR Enteral Nutrition Plan
Nutrition and Swallowing Risk Checklist
Epilepsy Management Plan
End of life care support plans.
Follow the review cycle and requirements in the procedures or guidelines relating to each support plan, and to section 3.6 of these Health Planning Procedures.
Any changes that are made to existing support plans are discussed with others (Step 6) and the GP at the health assessment appointment (Steps 8 – 12).
Changes to the person’s My Oral Health Plan should be made by the GP during the health assessment or by the person’s dentist at the person’s annual dental review (see section 5 – Dental health).
STEP 5: Complete an Annual Health Summary or Part A of the CHAP tool
The Annual Health Summary or Part A of the CHAP tool must be Annual completed prior to the person’s annual health assessment. Health
Summary It is important that each body system in the Annual Health Summary is reviewed as some indicators of illness may be common to more than one body system for example, the skeletal, muscular or digestive systems.
If the GP prefers to use the CHAP tool, the support worker completes the first section of the CHAP tool instead of the Annual Health Summary.
The Annual Health Summary or Part A of the CHAP tool is completed by the person and support workers. If the person has difficulty with communication or chooses not to participate then it will need to be completed by support workers who know the person well.
After the Annual Health Summary or Part A of the CHAP tool is completed, review the information collected with the person, person responsible and, with the person’s consent, others who know the person well. Record the people who were involved in completing the Annual Health Summary or CHAP.
STEP 6: Discuss the information with others
A useful person centred thinking tool for this step is the Four + One Four + One Questions. The tool guides the person and support workers with Questions future health planning by reviewing and understanding the health
actions that have been completed and any lessons that were learnt.
If the person is unable to or does not want to participate in a discussion about their health, others who know the person well need to be engaged in the process. They
Health Planning Procedures, V1.3, June 2016 33

will most likely include the line manager, other members of the team and, if the person is unable to consent, the person responsible.
If personal information is to be discussed with others, permission should first be obtained from the person if possible, to maintain the person’s right to privacy and confidentiality.
Support workers often know a lot of important information about the person’s health and wellbeing. Information sharing can occur in several ways, either individually with a line manager during monthly supervision, or in a group setting such as a team meeting. The team meeting is a useful environment for support workers to share different experiences and understanding of the person’s health and wellbeing with other members of the team.
If the person has a chronic health condition, the line manager can place a referral for additional support from an ADHC Clinical Nurse. The ADHC Clinical Nurse may also be able to provide additional support to the person and support worker by speaking to the GP about the person’s complex health support requirements at the annual health assessment appointment.
Any additional information about the person’s health that is identified during discussion with others is recorded in the Annual Health Summary or Part A of the CHAP tool and discussed with the person’s GP.
The person’s consent is required for the health assessment17. If the person is not able to provide consent, consent from the person responsible is not required unless the person is objecting or, a minor treatment is to be performed at the time of the assessment, for example, a blood test. In this case, the GP must obtain consent for the treatment from the person, or person responsible.
STEP 7: Make an appointment with the person’s GP and dentist
Use the Appointment Checklist tool to guide actions when making the health assessment appointment.
An appointment with a public or private dentist for the person’s annual dental review is made at this stage if possible.
If the person attended a Public Oral Health Service Referral Centre within the last year an appointment may have been made for the next annual dental review. Look in the person’s records such as the My Oral Health Plan or call the Public Oral Health Service Referral Centre and confirm if an appointment was made (see ‘Other resources’). If not, make an appointment as soon as possible.
The person may also be eligible to receive a Public Oral Health Service through a private dentist registered under the NSW Oral Health Fee for Service Scheme (OHFFSS). Refer to the NSW Ministry of Health18 or the ‘Other resources’ section of these Procedures.
17 NSW Civil and Administrative Tribunal (NCAT) Fact Sheet – Consent to medical and dental treatment http://www.ncat.nsw.gov.au/Documents/gd_factsheet_consent_to_medical_or_dental_treatment.pdf
18 OHFFSS
Health Planning Procedures, V1.3, June 2016 34

STEP 8: Attend the appointment
The person must attend the health assessment appointment. The GP cannot perform a comprehensive health assessment if the person is absent.
If the person is physically unable to attend the appointment, request that the health assessment appointment occurs at the person’s home at a time suitable to the person.
Remind the GP that the purpose of the appointment is for an annual health assessment, and that it is a long or prolonged consultation.
Provide the GP with the ‘People with intellectual disability - Information for GPs during health assessments’ Fact Sheet (‘Other Resources’).
Inform the GP that a copy of the health assessment containing a written record of the recommended treatment and actions will be required.
STEP 9: Use the Health Assessment Criteria
The Health Assessment Criteria tool lists the Medicare criteria. It is Health
not a mandatory tool, and is designed for support workers to help them Assessment Criteria involve the person during the appointment, and to guide the discussion
with the GP about the person’s health and wellbeing concerns.
Regardless of what health assessment template the GP decides to use (e.g. Medicare health assessment or CHAP tool), it is the responsibility of the attending support worker to ensure that all the criteria outlined by Medicare are discussed during the appointment.
If the GP is using the CHAP tool or the assessment tool developed by the New England Division of General Practice (see section 4.1), all sections in those tools need to be addressed.
STEP 10: Discuss the person’s current health issues
Provide the information collected during Steps 1 through to 6 to the GP for their consideration.
That is:
the information collected in the Annual Health Summary or Part A of the CHAP tool. Any body system that has been checked in the Annual Health Summary must be discussed with the GP during the health assessment appointment and noted in the far right hand column of the form,
the outcome of actions completed or not completed from the last health assessment and previous health appointments,
the person’s My Health and Wellbeing Plan. In particular the person’s:
− history
− immunisation status including missing vaccination records
− Health Learning Log
− health data
Health Planning Procedures, V1.3, June 2016 35

− previous treatment plans
− Health Promotion Register (including the Physical Activity Checklist and Plan)
− reviewed and updated support plans
− other relevant health professional reports that the GP may not have received.
medication chart, medication record and medication profile.
If the person has not attended a Public Oral Health Service before and is eligible for the service, a referral will be required. The referral should be discussed and obtained from the person’s GP at the time of the health assessment appointment.
STEP 11: Discuss the person’s chronic health conditions
If the person has a chronic health condition or disease, now is the time to discuss the need for additional support from Medicare’s Chronic Disease Management Program (see Section 4.2). This will depend on how complex the person’s health and wellbeing needs are and is determined by the person’s GP or other health specialist.
If the GP indicates that the person’s chronic disease or long-term health condition is not being effectively managed, the GP may decide that a Medicare Chronic Disease Management Plan is required in addition to the Medicare annual health assessment.
If the GP decides to manage the person’s complex health care with multi-disciplinary specialised health support, the GP can refer the person to:
a specialist health professional who the GP liaises with directly
a Specialised Intellectual Disability Health Service (SDS) who will coordinate treatment arrangements (see section 2.4.1)
an allied health professional to manage particular chronic conditions such as, dysphagia or mental illness
a pharmacist to review the person’s medications under Medicare item 900, Domiciliary Medication Management Review (otherwise known as the Home Medicines Review).
If the GP or health professional decides that a Chronic Disease Management Plan is needed, make another appointment with the GP or health professional at the end of the consultation (see section 4.2).
Refer to the Chronic Disease Guidelines for more information relating to the
support worker’s role in supporting a person with a chronic disease.
STEP 12: Obtain a copy of the health assessment
By the end of the consultation the GP should have outlined how the person’s health needs will be coordinated and managed. It should be clear to the person and support worker what actions they need to take after the appointment.
Health Planning Procedures, V1.3, June 2016 36

The GP is required to provide a copy of the Medicare health assessment at the end of the appointment. Support workers may need to ask the GP to print out a copy for the person.
It is important to tell the GP that the information in the health assessment needs to be easy to read and understand, as it will be used by non-clinical staff to support the person to manage their health.
Before leaving the consultation, go through the health assessment with the GP to ensure that you understand what has been recorded and what recommendations have been prescribed. If there is any action that is not clear, you must seek clarification from the GP before the end of the consultation.
Any changes to the health assessment document must be made by the GP. At no stage should support workers transcribe or rewrite any written information provided by the GP in the health assessment document. This is the responsibility of the GP. This also relates to other health appointments the person attends during the course of the year.
In addition to the health assessment report, the person and support worker may need to prompt the GP to:
prescribe new and ongoing medication prescriptions for the person
prepare a referral to a Specialised Intellectual Disability Health Service where required (see section 2.4.1)
prepare a referral to any other health professional such as a Public Oral Health Service or allied health professional
provide written endorsement of reviewed and updated support plans. For example an epilepsy management plan, oral health plan, asthma management plan, allergy management plan, skin care plan, bowel management plan
record changes to prescribed medication in the:
− medication chart/ Webster-pak® Signing Sheet,
− My Medication Record (refer to the Medication Procedures).
The person may have a reaction to new medication and it is important that the person and support worker ask the GP:
what the person may experience as a result of a change in medication regime
how long to monitor the person for sign of a reaction
when to seek medical advice if a reaction does occur.
STEP 13: Actions after the appointment
Update the Health Action Plan to keep track of the completion of health actions prescribed by the GP.
Health Planning Procedures, V1.3, June 2016 37

If the Appointment Checklist tool was used to prepare for the health assessment, with the person work through Checklist 3 of the Appointment Checklist, ‘After the appointment’ and complete each of the actions listed in the Health Action Plan.
Health Planning Procedures, V1.3, June 2016 38

5 Oral health
This section relates to the Health and Wellbeing Policy Guiding Principles 6, 11, 12, 13, 14.
5.1 Annual dental review
Every person living in an ADHC operated or funded accommodation support service requires an annual dental review. It is best practice for the annual dental review to be completed around the time of the person’s annual health assessment.
Dental health is one of the criteria listed in the Medicare health assessment item. During the health assessment appointment, the person’s dental and oral health is reviewed by the GP. If the person does not have teeth, the GP assesses the condition of the person’s gums and mouth at the time of the health assessment.
If the GP thinks it is needed, a referral is made to dental health services in the following circumstances:
1. The person has not previously accessed and is eligible for free Public Oral Health Services including the NSW Oral Health Fee For Service Scheme (OHFFSS)19
2. The person is not suited for routine dental care at a Public Oral Health Service and has not previously accessed and is eligible for Special Care Dentistry Services20
3. The GP has difficulty assessing the condition of the person’s teeth and mouth. For instance the person may be reluctant to open his or her mouth at the time of the health assessment.
If the person is unable to consent to the referral, a person responsible is required to provide consent. If there is no person responsible or the person is objecting to treatment, seek advice from the NSW Civil and Administrative Tribunal (NCAT) (previously the Guardianship Tribunal)21.
The person may choose to visit a private dentist instead of the free Public Oral Health Service. Accessing a private dentist will depend on the person’s:
physical abilities
urgent need of dental care
financial capacity or private health insurance with dental care extras.
Prior to a dental appointment, information about the person’s communication and support needs may be provided to the dentist to facilitate the appointment.
19 OHFFSS
20 Oral Health Specialist Referral Protocols PD2011_071
21 NSW Civil and Administrative Tribunal (NCAT)
Health Planning Procedures, V1.3, June 2016 39

Refer to Information on accessing free Public Oral Health Services including
Specialist Dentistry is provided on the NSW Health website and the Health Planning Procedures, ‘Other resources’.
5.2 My Oral Health Plan
Each person living in an ADHC operated or funded accommodation support service (group home, Large Residential Centre and Specialist Supported Living) must have a current oral health plan. The oral health plan used in ADHC operated accommodation support services is the My Oral Health Plan.
There are four parts to the My Oral Health Plan. The first part records information on the support the person needs to maintain adequate oral health and hygiene. This information is recorded by the person and/or a support person who knows the person well.
My Oral Health Plan
The second and third parts of the My Oral Health Plan is a record of the prescribed oral health routine and the outcome of the oral health review recommended by the dentist or the person’s GP, including future actions. Changes to the person’s My Oral Health Plan are made by the GP during the health assessment if the person does not have teeth or by the person’s dentist at the person’s annual dental review.
The fourth part of the My Oral Health Plan provides evidence that the plan has been completed and endorsed by a health professional. The line manager (e.g. Team Leader) must also sign and date that they have reviewed the outcome and recommendations made by the health professional at the dental review.
Before leaving a dental appointment book the next dental review. Record the appointment date in the person’s My Oral Health Plan.
Further information relating to oral health and hygiene is provided in the
Nutrition and Swallowing Guidelines of the Health and Wellbeing Policy and Practice Manual, Volume 1 and the Chronic Disease Guidelines in the Health and Wellbeing Policy and Practice Manual, Volume 2.
Health Planning Procedures, V1.3, June 2016 40

6 Index of tools and templates
Annual Health Summary ...............................................................21, 22, 33, 34, 36
Appointment Checklist.........................................................................20, 21, 35, 38
Bowel Chart.......................................................................................................... 24
CHAP tool................................................................................22, 28, 33, 34, 35, 36
Chronic Disease Medicare Items.............................................................. 24, 28, 36
Donut...................................................................................................................... 8
Health Action Plan...............................................................................18, 19, 20, 38
Health Appointment Sheet ................................................................................... 19
Health Assessment Criteria .................................................................................. 35
Health Learning Log ............................................................................17, 18, 19, 36
Health Promotion Register ....................................................................... 21, 32, 36
Health Reports ..................................................................................................... 19
Immunisation Record ........................................................................................... 15
Menstruation Chart............................................................................................... 23
My Health and Wellbeing Plan ......................................................13, 14, 18, 25, 26
My History ............................................................................................................ 16
My Oral Health Plan ....................................................................................... 33, 40
People who have read and understood the plan .................................................. 26
Physical Activity Checklist and Plan ............................................................... 21, 36
Review record .......................................................................................... 15, 25, 26
Sensitive Information............................................................................................ 16
Support Plan Register .................................................................................... 24, 33
Support Plans....................................................................................................... 24
Supporting Me at a Health Appointment............................................................... 18
Team Meeting Agenda ......................................................................................... 26
Weight Chart ........................................................................................................ 23
Health Planning Procedures, V1.3, June 2016 41

7 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the ADHC intranet to confirm that you are reviewing the most recent version. Following any subsequent reviews and approval this document will be uploaded to the internet and/or intranet and all previous versions removed.
Health Planning Procedures, V1.3, June 2016 42
Health Promotion Guidelines
Document name Health Promotion Guidelines
Version number 1.0
Approval date January 2016
Policy manual Health and Wellbeing Policy and Practice Manual Volume
2
Approved by Deputy Secretary, ADHC
Summary The Health Promotion Guidelines provide information on
healthy living and disease prevention strategies which
aim to support the person to improve health outcomes.
Replaces document Health Care Policy and Procedures, 2012, Appendix C
Authoring unit Contemporary Residential Options Directorate
Applies to People with disability, their families and others who are
part of the person’s support network. All support workers
who support the health and wellbeing of people with a
disability.
Review date 2017

Version control
The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 Guidelines replace the health promotion information outlined in the Health Care Policy and Procedures, Appendix C
Health Promotion Guidelines, V1.0, January 2016 2

Table of contents
1 Health and wellbeing .............................................................................4
1.1 Health promotion.............................................................................6
1.2 Health promotion guidelines............................................................6
2 Healthy living .........................................................................................8
2.1 Physical activity ..............................................................................8
2.2 Oral health and hygiene ................................................................12
2.3 Sleeping well .................................................................................14
2.4 Food and nutrition .........................................................................17
2.5 Bladder and bowel health..............................................................18
2.6 Foot care .....................................................................................22
2.7 Alternate / complementary therapies ............................................28
2.8 Personal care and hygiene ...........................................................31
2.9 Healthy ageing ..........................................................................35
2.10 Mental fitness ...............................................................................39
2.11 Confidence and self-esteem..........................................................42
3 Screening activities: Preventing disease, premature death and disability ...............................................................................................45
3.1 Immunisation ..............................................................................45
3.2 Eye health ..................................................................................48
3.3 Hearing health .............................................................................52
3.4 Smoking ......................................................................................55
3.5 Drugs and alcohol .........................................................................59
3.6 Breast cancer prevention and screening .......................................62
3.7 Cervical cancer prevention and screening ....................................64
3.8 Prostate cancer prevention and screening ....................................66
3.9 Testicular cancer prevention and screening..................................68
3.10 Skin cancer prevention and screening .........................................70
3.11 Bowel cancer prevention and screening........................................72
3.12 Thyroid functioning ......................................................................74
4 Policy and Practice Unit contact details ............................................77
Health Promotion Guidelines, V1.0, January 2016 3

1 Health and wellbeing
The ADHC Health Promotion Guidelines (the Guidelines) embody the principles of legal and human rights found in the New South Wales Disability Service Standards (the Standards), the commitment to deliver culturally responsive services to Aboriginal and Torres Strait Islander people under the Aboriginal Policy Statement (the Statement) and the person centred guiding principles of the ADHC Health and Wellbeing Policy.
The Guidelines support people to exercise their rights and entitlements under the Standards and the Statement. The Guidelines provide information on healthy living, and strategies to prevent disease and improve health outcomes under the guidance of the person’s ‘usual’ General Practitioner (GP)1 and other health specialists.
The Health Promotion Guidelines are applicable to ADHC operated and funded non-government accommodation support services including group homes, large residential centres, specialist supported living and other types of accommodation where people are being supported with their health and wellbeing
Health is the inter-relation of a person’s physical, mental, emotional and spiritual wellbeing as outlined in the diagram below. This means that if one aspect of wellbeing changes, other aspects will also be influenced.
Wellbeing
emotional
physical mental
spiritual
= Health
1 Medicare defines the person’s ‘usual’ GP as: ‘The GP (or a GP in the same practice) who has provided the majority of
services to the patient in the past 12 months, and/or is likely to provide the majority of services in the following 12 months’
Health Promotion Guidelines, V1.0, January 2016 4

How people feel about themselves and their life will have a significant influence on their ability to move towards and maintain good health2 .
Good health is a resource that a person uses every day. Without good health, a person struggles to engage fully in every day life. This is the case for many people with disability who often have poor health3.
People with disability have poor health for various reasons including:
the prevalence of disability-related chronic health conditions,
poor access to health care and health promotion initiatives,
poor health education and opportunities for education,
lack of understanding of disability and health-related conditions4 by health professionals.
Aboriginal and Torres Strait Islander people with poor health may also struggle to participate fully in every day life. When providing health promotion support to Aboriginal and Torres Strait Islander people, that is culturally appropriate and empowering, the following impacts are to be considered:
communicate with the person and family in a way that is understood; if the person has a communication profile use it to learn the best way of communicating,
acknowledge the history of trauma and loss that Aboriginal and Torres Strait Islander people have experienced since settlement,
understand their experiences and difficult relationships with government services, especially hospitals,
enquire about the proper contact person for discussing issues of health promotion in general,
ask who the Aboriginal and Torres Strait Islander person would prefer to have as a contact or support person,
determine how the issue of health promotion is viewed in the person’s community,
confirm whether the person or family would prefer to work through an Aboriginal Liaison Officer,
ensure that the person and family understand the support options that are available in the areas of health promotion, and how they can access them.
2 Better Health Channel
3 Health of Australians with disability: health status and risk factors
4 National Disability Strategy:
http://www.fahcsia.gov.au/sites/default/files/documents/05_2012/national_disability_strategy_2010_2020.pdf
Health Promotion Guidelines, V1.0, January 2016 5

1.1 Health promotion
Health promotion activities enable the person to move towards their full health potential by empowering the person to take control of their health5.
Early prevention through health promotion activities is vital to increasing the person’s wellbeing and health outcomes and to preventing certain conditions from emerging.
1.2 Health promotion guidelines
The Health Promotion Guidelines provide information on activities which promote good health. Information is presented in two sections:
1. Healthy living activities. This section provides health literacy information aimed at empowering the person to modify their behaviour and make informed lifestyle decisions which promote good health. For instance, understanding how smoking damages health and where to seek help to stop smoking.
2. Screening activities aimed at preventing disease, disability and premature death from occurring. For instance, undergoing bowel cancer screening from 60 years of age, or earlier if there is a family history of bowel cancer.
The hand symbol refers to further information found in other sections of these
guidelines and / or other Procedures and Guidelines covered under the Health and Wellbeing Policy.
1.2.1 Health Planning and Health Promotion
Health promotion activities are part of the person’s health planning. The My History section of the person’s My Health and Wellbeing Plan is completed as far as possible to include all health and disability diagnoses and family medical histories where appropriate. This will help the General Practitioner (GP) and other health professionals to identify, plan and manage health issues which are existing and / or which may emerge at a later stage.
During the person’s annual health assessment, health promotion activities are discussed with the GP and a plan of action is developed which:
provides advice and recommendations
outlines a plan of healthy living activities (e.g. completing a Physical Activity Checklist and Physical Activity Plan located in the Tools and templates section of the Health Planning Procedures.
5 http://www.who.int/healthpromotion/Milestones_Health_Promotion_05022010.pdf
Health Promotion Guidelines, V1.0, January 2016 6

contains referrals for health screening if applicable to the person.
Health promotion activities are recorded in the person’s Health Promotion Register in Part B of the My Health and Wellbeing Plan. Support plans developed by a health professional are kept in Part C of the My Health and Wellbeing Plan.
Health Promotion Guidelines, V1.0, January 2016 7

2 Healthy living
6 7 82.1 Physical activity
Physical activity is ‘any bodily movement produced by the muscles attached to the skeleton that requires energy expenditure and produces progressive health benefits’. It includes everyday activities like walking to the shop, gardening, and organised activities, such as weight training and exercise classes.
Compared to the general population, many people with disability do not get enough exercise.
Physical activity can improve a person’s health and wellbeing and is an important part of a healthy lifestyle. Activities such as walking, swimming, dancing and cycling are all good forms of exercise and promote social interaction.
2.1.1 Benefits
The benefits of regular physical activity include:
Prevention of heart disease, stroke and high blood pressure
Reduction in the risk of developing Type 2 Diabetes
Management of digestive function including constipation
Reduction of pressure sores and muscle contracture
Improved respiratory function
Prevention of some cancers
Increased energy levels and decreased body fat
Building and maintaining healthy bones, muscles and joints
Reduced risk of injury
Promotion of psychological wellbeing
Improved mood and concentration
Increased participation and inclusion
Improved sleep.
6 http://www.health.gov.au/internet/main/publishing.nsf/Content/phy-activity
7 http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines
8 AIHW 2010, Health of Australians with disability: health status and risk factors. AIHW bulletin no. 83. Cat. no. AUS 132.
Canberra: AIHW.
Health Promotion Guidelines, V1.0, January 2016 8

2.1.2 Good practice guidelines
When to seek medical attention:
Check with the person’s GP before any exercise program is implemented, as some types of physical activities may not be appropriate, or may be detrimental, to the person’s health.
This is essential if the person has an existing health condition or is older.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Discuss the person’s physical activity with the GP at the time of the health assessment.
Make a plan Complete a Physical Activity Checklist and Physical Activity Plan (see Health Planning Procedures, Tools and templates) with the person as part of the annual health review or simply structure daily physical activity with the person in their weekly routine.
Record a visual reminder of when physical activity has been scheduled for the person and support workers.
Daily health promotion activities
Identify enjoyable activities
Make it fun. Try to find something the person enjoys and then build it into their weekly routine. The more enjoyable the activity, the more likely the person will do it again.
NSW children aged 7 to 13 years of age and above a health weight, can enrol in the free Go4Fun healthy lifestyle program that focuses on eating habits, confidence and fitness9 .
The activity does not have to involve a formal exercise program such as going to the gym or an aerobics class. It can be walking to the local shops or to work, going dancing or working in the garden.
Explore with the person what activities they have tried in the past and whether they would like to try them again.
Encourage the person to be
Support the person to engage in domestic chores such as hanging out the washing; putting out the garbage bins; doing
9 https://go4fun.com.au/
Health Promotion Guidelines, V1.0, January 2016 9

Daily health promotion activities
as active as possible throughout the day
their own washing; gardening; walking to the corner store for groceries.
Think of physical activity as an opportunity not an inconvenience. For instance, assist the person to make a habit of walking instead of using the shared vehicle. Also park away from a destination and walk with the person the rest of the way.
People with limited or no active muscular control can benefit from support with passive movement.
Set a goal and Encourage the person to choose something they like doing to track progress build up their fitness.
If the person is doing more physical activity as part of a plan to lose weight, schedule a monthly weigh-in and celebrate weight loss as a win.
For adults, aim for at least 30 minutes of moderate intensity physical activity10 every day if possible.
If 30 minutes of physical activity is too much at first, break it up into three 10 minutes sessions per day.
The national recommendation11 for children and young people is at least 60 minutes of moderate to vigorous intensity physical exercise every day.
Factor in costs The person’s budget will determine the activities they do. If the person does not have much money to spare, help them to pick something within their budget.
Look for cost effective alternatives by hiring an exercise video from the local library or purchasing a video gaming device that has games requiring physical activity.
Make it social Combine physical activity with a social activity. For instance, the person could meet a friend at a park to go for a walk followed by a picnic.
Joining a club or sport event is also a great way to meet new people and engage with the general community12 . For example, sports clubs, council recreation centres; ten-pin bowling clubs; local gyms; swimming pools, community centres and neighbourhood houses.
Support staff should take the time to check community notice boards at libraries, local shopping centres, and social
10 Moderate intensity physical activity will cause a slight, but noticeable, increase in breathing and heart rate and may cause
light sweating in some people. 11
http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines#apa512 12
Office of Sport (Sport and Recreation) https://sportandrecreation.nsw.gov.au/findaclub/disability
Health Promotion Guidelines, V1.0, January 2016 10

Daily health promotion activities
networking sites as they can offer a range of opportunities.
Enquire whether there are any recreational groups which cater for people with disability in the local area, for example, Riding for the Disabled and Sail Ability. The person’s preferences and availability of opportunities will determine the choices made.
Get help from If the person has complex health issues or has mobility others issues, consult and refer to other health professionals for
advice.
Access to exercise physiologists and physiotherapists is available to a person who has ongoing health conditions. Costs associated with accessing allied health professionals can be subsidised through Medicare’s Chronic Disease Management Program13 . Talk to the person’s GP about these options.
13 http://www.health.gov.au/internet/main/publishing.nsf/Content/mbsprimarycare-chronicdiseasemanagement
Health Promotion Guidelines, V1.0, January 2016 11

2.2 Oral health and hygiene14
Good oral and dental health is not just about having an attractive smile. A clean, comfortable mouth is essential for good physical health and quality of life.
Poor oral health and hygiene can lead to dental and gum disease. Oral health issues can also have a significant impact on the person’s self-esteem and sense of wellbeing as it can affect the way a person looks and feels and their ability to undertake activities of every day life.
People with disability are more likely to have substantial oral health problems than the general population.
2.2.1 Good practice guidelines
When to seek medical attention:
If there is a change in the person’s oral health needs, speak to the person’s GP and / or book an appointment with the dentist.
The person should also visit a dentist if they have any of the following:
A toothache
Bleeding gums
Facial swelling
Bad breath
Dental trauma such as a loose or dislodged tooth.
For information on oral and dental disease, refer to the Chronic Disease
Guidelines in the Health and Wellbeing Policy and Practice Manual Volume 2
Annual health promotion activities
Annual oral health check
Every person is required to have an annual oral health check performed by a GP or dentist.
Planning for an annual oral health check is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
If the person does not have teeth, the person’s GP is to
14 Oral health and Victorians with an intellectual disability 2013
https://www2.health.vic.gov.au/about/publications/researchandreports/oral-health-and-victorians-with-an-intellectual-disability-2013
Health Promotion Guidelines, V1.0, January 2016 12

Annual health promotion activities
check the condition of the person’s mouth and gums at the annual health assessment.
Oral Health Plan
Every person is required to have an updated Oral Health Plan which is endorsed by a GP or dentist.
An Oral Health Plan outlines what support the person needs to maintain good oral health care and hygiene.
Daily health promotion activities
Oral health and hygiene
For information on oral and dental hygiene and care, refer to
the Nutrition and Swallowing Guidelines.
Health Promotion Guidelines, V1.0, January 2016 13

2.3 Sleeping well15
2.3.1 Why is sleep important?
Sleep is essential for good health. It refreshes the mind and repairs the body. Lack of sleep causes fatigue, poor concentration and memory, moodiness, impaired judgement and reaction time, and poor physical coordination.
The concept of ‘a good sleep’ differs widely from person to person. While many adults need around eight hours, some people only need five to function well. Other people like to sleep for 10 hours or more. What seems like insomnia to one person might be considered a good sleep by another. While there is no one ideal amount of sleep, adults typically require approximately eight hours per day.
2.3.2 Causes and risks factors for sleep disorders
Respiratory conditions which inhibit breathing
Snoring and obstructive sleep apnoea (temporary cessation of breathing, especially during sleep)16
A person with Down Syndrome can be susceptible to obstructive sleep apnoea
Dysphagia
Stress, anxiety or depression
Obesity
Untreated pain
Pre-bedtime distractions such as TV and the internet
Age and dementia
Drinks containing caffeine
Some medications
Alcohol
Smoking
15 https://www.sleepoz.org.au/sleep-disorder-fact-sheets
16 http://www.oxforddictionaries.com/definition/english/apnoea
Health Promotion Guidelines, V1.0, January 2016 14

2.3.3 Good practice guidelines
When to seek medical attention:
If the person has tried the tips in the daily activities section below and still has trouble sleeping.
If the person can’t get to sleep regularly, wakes in the middle of the night unusually.
If the person snores or stops breathing during sleep
If the person feels excessively tired often during the day despite getting a reasonable night’s sleep.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
If the person has poor sleeping habits, support the person to discuss this with their GP at the time of the health assessment. The GP may refer the person to a specialist sleep centre if they think there is a problem.
Daily health promotion activities
Sleep routine Discourage the person from taking naps during the day, or try to limit the nap to 15 minutes.
When it is time for bed, darken the room by drawing blinds and switching off bright lights.
Before going to bed, encourage the person not to engage in activities that excite or mentally stimulate them such as exercise, TV or the internet.
Encourage the person to go to bed at the same time each night and wake up at the same time each morning.
Encourage the person to practice relaxation techniques before going to bed such as listening to relaxing music or reading a book.
Remember that it is not the role of support workers to force the person to go to bed to sleep if the person is resistant. Be flexible to the person’s needs and lifestyle.
Ensure the person takes medications as prescribed and at the time outlined by the treating GP.
Continence of the person
If the person wakes up to go to the toilet, consider encouraging them to restrict fluid intake after their evening meal.
If the person is incontinent at night, consult the person’s GP about a referral to a Continence Nurse.
A Continence Nurse can provide advice on times for good toileting practice and what aids to use to keep the person dry and comfortable during the night.
Health Promotion Guidelines, V1.0, January 2016 15

Daily health promotion activities
Physical Physical activity is important for good physical health and activity mental wellbeing.
Establish a regular exercise program, preferably early in the day.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet Encourage the person to avoid drinks that contain caffeine such as energy drinks, chocolate, tea or coffee, especially close to bedtime.
Avoid a heavy meal or spicy food late at night. Obesity, allergies and hay fever can cause or aggravate
snoring which disturbs sleep.
Avoid smoking Smoking can aggravate snoring. Quitting smoking eliminates the stimulant effects of nicotine
which contribute to sleep loss.
Refer to the Smoking section (3.4) for information on quitting.
Health Promotion Guidelines, V1.0, January 2016 16

2.4 Food and nutrition
Refer to Nutrition and Swallowing Guidelines in the Health and Wellbeing
Policy and Practice Manual Volume 2 for good practice information on food and nutrition.
Health Promotion Guidelines, V1.0, January 2016 17

2.5 Bladder and bowel health17
Incontinence can have a major impact on quality of life. It affects both men and women, regardless of age or background. Incontinence can be treated, managed and in many cases cured.
Incontinence is the accidental or involuntary loss of urine from the bladder (urinary incontinence) or faeces or wind from the bowel (faecal or bowel incontinence).
2.5.1 Causes and risk factors
Weakened pelvic floor muscles,
health conditions and diseases such as Irritable Bowel Syndrome (IBS), Inflammatory Bowel Disease (IBD), respiratory conditions, diabetes, dementia (see Chronic Disease Guidelines in in the Health and Wellbeing Policy and Practice Manual Volume 2),
constipation or severe diarrhoea,
pregnancy (both pre- and post-natal women),
younger women who have had children,
menopause and old age,
obesity,
urinary tract infections,
certain types of surgery,
reduced mobility preventing a person from getting to or using the toilet,
neurological and musculoskeletal conditions such as multiple sclerosis and arthritis,
some medications.
17 http://www.continence.org.au/
Health Promotion Guidelines, V1.0, January 2016 18

2.5.2 Good practice guidelines
Seek medical attention if the person:
Has trouble emptying their bladder
Rushes to use the toilet often
Is anxious that they might lose control of their bladder or bowel
Wakes up twice or more during the night to go to the toilet regularly
Sometimes leaks:
- before they get to the toilet
- when lifting something heavy or coughing
- exercising or playing sport
- changing from a seated or lying position to a standing position
Sometimes soils their underwear
Strains to empty their bowel
Plans their daily routine around where the nearest toilet is.
For information on having a healthy bowel refer to the Bowel Care
Guidelines in Health and Wellbeing Policy and Practice Manual Volume 1.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
The GP assesses urinary tract and bowel functioning at the annual health assessment.
The GP may refer the person on to a continence specialist for assessment and advice.
Daily health promotion activities
Drink well Encourage the person to drink plenty of water. This equals about 2.6lt for adult males and 2.1lt for adult females18 per day, unless advised otherwise by the person’s GP.
Evenly spread fluid consumption throughout the day and avoid drinks immediately before going to bed
Cut down on alcohol, soft drinks, and caffeinated drinks Increase water intake during high temperatures and
18 Australian Dietary Guidelines Section 2.6.1
Health Promotion Guidelines, V1.0, January 2016 19

Daily health promotion activities
increased physical activity.
A healthy diet Eat plenty of fibre to improve bowel function and help avoid constipation.
A high fibre diet requires plenty of fluid and should be used under medical supervision when urinary incontinence is also a problem.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information
Physical Physical activity is important for good physical health and activity mental wellbeing.
Exercise is important for regular bowel movement. Pelvic floor muscles control the tone of bladder and bowel
muscles. Weakened pelvic floor muscles can be strengthened with specific exercises. Consult the person’s GP for a referral to a physiotherapist as required.
Refer to the Physical Activity section (2.1) for more
information.
Practice good Go to the toilet when the urge to open their bowels occurs. habits Get into the correct sitting position on the toilet. The person
should sit on the toilet leaning forward, with elbows on knees and feet supported on a footstool.
Bulge out the tummy, relax the back passage and let go (do not to hold the breath or strain). When finished encourage the person to firmly draw up the back passage.
Avoid going to the toilet 'just in case' and only go when needed.
Get help from When incontinence occurs seek help to prevent it worsening others and affecting the person’s lifestyle.
Refer the issue on to a Continence Nurse advisor or ADHC Clinical Nurse who can provide advice on recommended aids to use to keep the person dry and comfortable during the day and night.
Seek help from the person’s GP for a referral to a physiotherapist or an exercise physiologist to design an exercise program which strengthens the pelvic floor muscles.
Plan outings Download the National Public Toilet Map19 to find where the closest toilets are to where you are going.
Be prepared and take a change of clothes and additional continence aids in case of an accident.
Avoid smoking Chronic coughing associated with smoking can weaken the
19 https://toiletmap.gov.au/
Health Promotion Guidelines, V1.0, January 2016 20

Daily health promotion activities
muscles of the pelvic floor and lead to bladder and bowel control problems.
Get financial Continence aids can be costly. The Continence Aids help Payment Scheme (CAPS) is an Australian Government
Scheme that provides a payment to assist eligible people who have permanent and severe incontinence to meet some of the cost of their continence products.
A person with a Pensioner Concession Card who has frequent and uncontrollable loss of urine or faeces caused by an eligible20 condition is entitled to the CAPS.
A person residing in an ADHC operated group home; Large Residential Centre (LRC’s) and Specialist Supported Living (SSL) service may be entitled to financial assistance to support the cost of continence aids through the Aids and Equipment in Supported Accommodation (AESA).
Refer to the AESA Guidelines (in Health and Wellbeing
Policy and Practice Manual Volume 2) for more information.
20 http://www.humanservices.gov.au/customer/services/medicare/continence-aids-payment-scheme
Health Promotion Guidelines, V1.0, January 2016 21

21 22 232.6 Foot care
Good foot health is important for everyone. Prevention of problems and daily maintenance are the foundation of healthy feet.
Problems with feet can be an indicator that the person has a serious underlying health condition such as diabetes, arthritis or nerve disorders (refer to the Chronic Disease Guidelines in this Manual for more information about some of these conditions). Other factors that can affect feet include poor circulation, disease, being overweight, smoking, getting older, inadequate nail care and wearing shoes that don’t fit properly.
Good foot care should be a habit that is practiced every day. This includes regularly checking the person’s toes and toenails including in-between their toes and the top and bottom of each foot. When checking the condition of feet, look for redness, swelling, blisters and sores, scratches, waterlogged skin, cuts and cracks in the skin and bruising.
Take note of symptoms which may indicate the following conditions and consult the person’s GP.
2.6.1 Causes and risk factors
Condition Description
Smelly feet Caused by excessive perspiration and an overgrowth of fungi and/or bacteria.
Fungal infections
Fungal infections generally begin between the toes and can spread onto your foot if left untreated (e.g. Athlete’s foot or Tinea pedis). Athlete’s foot appears as patches of soft, white, cracked skin, sometimes with red areas visible between toes. It may cause itching, burning or stinging and can have an unpleasant odour and make walking painful.
Fungal nail infections
Also known as Tinea unguium are often caused by the spread of Athlete’s foot but can occur on its own. Toenails will look thick and discoloured (white or yellowish) and/or be brittle or crumbly in parts. These infections are more difficult to treat as the entire nail must grow out.
Warts Warts are skin growths caused by viruses. Planter warts (Verrucae) often appear on the soles of feet and are often painful. They can spread if not treated. Planter warts may occur in clusters and appear as a round area of thickened skin, with an uneven or
21 www.podiatry.asn.au
22 http://epodiatry.com/diabetic-foot.htm
23 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Diabetes_and_feet
Health Promotion Guidelines, V1.0, January 2016 22

Condition Description
slightly lumpy surface. They may look white or grey and have small, black dots on them.
Corns and calluses
Corns and calluses are areas of hard, thickened skin caused by pressure when the bony parts of feet rub against shoes. Corns are smaller than calluses and develop on non weight-bearing parts of the foot (e.g. on tops or sides of toes). They have a hard centre and can be very painful. Calluses are flatter and less painful than corns and can be found on the soles of feet (e.g. on the heel or ball of the foot).
Dry skin Dry skin can cause itching, burning feet and cracks in the skin appear. Cracked heels are common in summer when people wear sandals, thongs or go barefoot and the skin on the feet dries out.
Bunions Bunions are swollen and tender joints that can develop at the base of the big toes. Bunions can be hereditary and also caused by shoes that are too small or have pointed toes.
Ingrown toenails
Ingrown toenails are caused by a piece of the nail piercing the skin. This can happen when toenails are not cut straight across resulting in the corner of the nail becoming embedded in the skin.
Neuromas Neuromas are the result of a build-up of tissue around an inflamed nerve in the foot. They may cause tingling, numbness or pain in the ball of your foot and toes. This may cause the person to lose their balance.
Hammertoe Hammertoe is caused by a shortening of the tendons that control toe movements. The toe joint grows and pulls the toe back. Over time, the joint gets bigger and stiffens as it rubs against shoes. This can affect a person’s balance.
Spurs Spurs are bony bumps that grow on bones of the feet. They are caused by stress on the feet. Standing for long periods of time, wearing badly fitting shoes or being overweight can make spurs worse. Spurs are sometimes painful.
Swollen feet Standing for long periods may cause feet to swell. If feet and ankles stay swollen after elevating the legs, it may be a sign of a health problem.
Health Promotion Guidelines, V1.0, January 2016 23

2.6.2 Good practice guidelines
When to seek medical attention:
Indicators that the person’s feet require attention from the GP include:
wounds on feet are not healing
ankles are swollen
red lines or ‘tracking’ on the feet or legs can be indicators of infection
pain, throbbing or heat in feet and legs
changes to skin and toenails e.g. ingrown or discoloured toenails, corns, skin rashes
foot injury
recurrent trips and falls
problems with getting the person’s shoes to fit
Maintain good hygiene
Maintenance of hygienic shower and bath facilities through regular cleaning is extremely important in preventing further foot care issues in a shared household.
Diabetes
Foot care is particularly important if the person has diabetes. The feet of a person with diabetes are affected by:
Reduced blood flow to the feet, which makes cuts and abrasions slower to heal.
Damaged nerves in the feet, which means the person can experience numbness and be less able to feel minor cuts or blisters on the feet.
People with diabetes should:
Check feet daily for signs of poor condition and developing problems.
Seek medical advice and treatment immediately from their GP and/or podiatrist if feet become red and swollen or if an existing injury does not appear to be healing.
Have toenails trimmed and maintained by a qualified health professional such as a podiatrist or foot nurse.
Have at least an annual foot check-up with their GP and/or podiatrist to examine their feet for any evidence of nerve damage or poor circulation.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information on Diabetes.
Health Promotion Guidelines, V1.0, January 2016 24

Annual health promotion activities
Annual health Planning for an annual health assessment is outlined in the assessment Health Planning Procedures in Health and Wellbeing Policy
and Practice Manual Volume 1. During the person’s annual health assessment, foot health
should be checked by the person’s GP. If issues are identified at the time of the health assessment,
the GP must indicate what health actions need to occur throughout the year.
Chronic If the person has a chronic health condition such as Diabetes, Disease the GP can also refer the person to a podiatrist for advice and
treatment under Medicare’s Chronic Disease Management Program
Refer to the Chronic Disease Guidelines in Health and
Wellbeing Policy and Practice Manual Volume 2 for more information.
Diabetes See above under ‘When to seek medical attention’.
Daily health promotion activities
Daily foot care Have the person practice good foot care daily by checking feet regularly to look for changes in condition.
Wash feet daily and dry well between the toes. Use a clean towel for feet so that infections are not spread to other areas of the body.
Keep feet clean, warm and dry. Apply cream to dry feet (especially cracked heels).
Dust feet with powder to keep them dry and remove excess powder from between toes.
Maintain good blood circulation to the feet. Do this by elevating feet when sitting or lying down; stretching and walking frequently; gentle foot massage and taking a warm foot bath.
Avoid exposing feet to cold temperatures. Change socks daily and wear natural fibres such as cotton
and wool instead of synthetic fibres.
Avoid injury to the feet
Avoid barefoot walking. Properly fitted footwear protects feet. A shoe with a firm sole
and soft upper is best for daily activities. The person should keep toenails trimmed. Recommended
practice is to trim toenails straight across and use an emery board to smooth nails using downward strokes. Do not cut down into the nail corners; this could result in ingrown toenails. Nails should never be cut down to the flesh.
If the person has Diabetes, a health professional such as a podiatrist or a foot care nurse is the only person who should cut toenails.
The temperature of bath water should be checked with the
Health Promotion Guidelines, V1.0, January 2016 25

Daily health promotion activities
elbow before the person steps into the bath (i.e. lukewarm water not hot water) and a mild soap should be used, preferably one that contains moisturiser, or use a moisturiser separately.
Encourage the person not to sit for long periods of time (especially with legs crossed).
Avoid smoking as it decreases blood supply and increases the chance of swelling and other circulatory problems.
Encourage the person not to place their feet too close to heaters and heating pads (e.g. hot water bottles) as this may cause burns.
Infection Fungi thrive in warm and moist environments. Tinea is control spread by direct contact and wet floors.
Plantar warts are spread via wet floors, such as changing rooms, showers and baths.
Encourage the person to consider wearing thongs in communal showers to prevent the spread of fungal infections and viruses such as plantar warts and Tinea.
Ensure communal shower/bath areas are thoroughly cleaned between uses.
Refer to the ADHC Infection Control Policy24 on the ADHC
Intranet for more information.
A healthy diet A good diet is important for healthy living. Refer to the Nutrition and Swallowing Guidelines (in Health and Wellbeing Policy and Practice Manual Volume 1) for more information.
Being overweight has a negative impact on the way the foot and lower limb functions during walking, running and other physical activities.
Excess weight in older people impairs their mobility, participation in social activities and can reduce quality of life.
Physical Exercise regularly. Walking is considered good for the feet as activity well as for general health, provided good fitting shoes and
socks are used. Foot powder can be used to minimize sweating, but does not
replace regular washing and drying.
Refer to the Physical Activity information in Section 2.1 for
more information.
Shopping for Always have both feet measured for length and width (note
http://dadhc-
intranet.nsw.gov.au/documents/working_at_dadhc/ohs/risk_management/infection_control/infection_control_policy.pdf
Health Promotion Guidelines, V1.0, January 2016
24
26

Daily health promotion activities
new shoes most people have one foot slightly bigger than the other) The shoes should fit the natural shape of the foot especially
around the toes. The top of the shoe should allow toes to move freely and not
be squashed from the top or the sides. Shoes should fit comfortably around the heel and not be too
loose or too tight.
Health Promotion Guidelines, V1.0, January 2016 27

2.7 Alternate / complementary therapies 25
Complementary therapies include herbal medicine, traditional Chinese medicine, acupuncture, homeopathy, naturopathy, iridology, aromatherapy, Reiki, meditation and relaxation techniques, as well as dietary therapies, herbs, and vitamins and minerals and many others.
If you are unsure about the use of any alternate or complementary therapy, consult the person’s GP, or your line manager for guidance.
2.7.1 Are they safe?
Complementary medicines listed on the Australian Register of Therapeutic Goods (ARTG) are those that have been evaluated as safe for use. If you are unsure about any particular product, you (or ask your line manager to if you don’t have computer access) can search the register at: http://www.tga.gov.au/australian-register-therapeutic-goods
There is no legal requirement for a person to have formal qualifications or training to identify as a complementary therapist. If therapists belong to professional associations (such as the Australian Association of Acupuncturists) they will usually have a minimum level of training as specified by the association.
Consult the person’s GP or health practitioner before using any complementary medicines.
25 http://www.nhmrc.gov.au/health-topics/complementary-medicines
Health Promotion Guidelines, V1.0, January 2016 28

2.7.2 Good practice guidelines
When to seek medical attention:
If the person experiences any adverse reaction from taking complementary medicine or receiving therapy, refer to a health professional as soon as possible.
Prescriptions are not necessary for many herbal remedies. Herbal remedies can be purchased in supermarkets or health food stores, which mean that people can self-medicate without consulting a health professional.
Complementary medicines can interact with prescribed medications and a GP is to be consulted before the person takes any additional medicines that are not prescribed (see Medication Procedures in Health and Wellbeing Policy and Practice Manual Volume 2).
Do not stop any medications in exchange for a complementary medicine without first consulting with the person’s GP.
Complementary medicines also need to be dispensed for administration under the same conditions as regular medication.
If the GP indicates that he/she has concerns about the recommended treatment, this must be documented and provided to the person, and the person responsible or guardian. This information will inform the decision to proceed, or not, with the complementary therapy.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1. Discuss complementary therapies and medicines the person is using with their GP at the time of the health assessment.
Daily health promotion activities
Duty of care Complementary therapies, including medicines, should not be suggested or promoted to the person by support workers. However, the person is supported to consider them if they wish, and in consultation with the person’s GP.
Use a therapist who is a member of a professional association
A complementary therapist who is a member of a professional association should be consulted.
Ensure that complementary therapists can provide as much information about the treatment they prescribe as would be expected from a GP.
Complementary medicines and other therapies should only be used as directed. In the event of unexpected results or side effects, the therapist or GP should be notified at once.
Information about a complementary therapy is to be provided in writing by the therapist and given to the person. This includes recommendations involving the
Health Promotion Guidelines, V1.0, January 2016 29

Daily health promotion activities
administration of therapeutic substances or changes to the person’s diet or lifestyle. That is: 1. Details about the contents of the substance and its
administration or the nature of the diet or lifestyle change; 2. The goal of the treatment and desired outcome; 3. Any possible side effects, potential interactions with
complementary substance and prescribed or over the counter medicines that the person is taking;
4. The date for review of the treatment; 5. The proposed duration of the treatment.
This information is then provided to the person’s GP to advise if there are known interactions with the person’s existing medication, or if there are known risks associated with the treatment.
Health Promotion Guidelines, V1.0, January 2016 30

26 272.8 Personal care and hygiene
2.8.1 What is personal care?
Personal care includes activities of daily living which are intimate and sensitive to the person, such as:
bathing, showering, sponge bath
toileting and continence support
shaving and hair care
dressing and undressing
menstrual management.
Good personal care is provided in a way that promotes the person’s privacy, dignity and independence.
That is:
Privacy – freedom from observation, intrusion and unwanted attention.
Dignity – treating a person with honour, respect and worthiness.
Independence – supporting a person to be as independent as possible in their decision making.
26 Home Care Service of NSW Personal Care Manual
27 Guidelines for the Provision of Personal Care in ADHC Supported Accommodation Options and Respite Centres
Health Promotion Guidelines, V1.0, January 2016 31

2.8.2 Good practice guidelines
When to seek medical attention:
The person should visit their GP if the following symptoms occur:
any rash or blister on the body
any unusual injuries, cuts or bruises
wounds that are not healing
swelling of body parts
any hardness or lumps in the body
unusual moles or pigmentation
excessive loss of hair
change in menstruation patterns
change in toileting patterns.
Annual health promotion activities
Establish a routine
A Personal Care Plan outlines the person’s care needs, preferences and daily routine. Recording a person’s routine is important as it provides a consistent approach to support, and is respectful of the person’s preference.
The person-centred thinking tool ‘Routines and Rituals’ (See Lifestyle Planning resources) helps to establish morning and evening routines which outline what personal care is required, what is important to the person, and how best to support the person.
If the person has complex care needs, refer to a Clinical Nurse for assistance in developing a Personal Care Plan.
If the person has health conditions such as skin allergies consult with the person’s GP for advice on suitable products to use.
Annual review of personal care
A Personal Care Plan is reviewed as part of the person’s annual Health Planning.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Personal care appropriate to the person
Providing personal care appropriate to the person involves: Understanding what care tasks a person can and cannot do
independently, and providing support that matches individual needs.
Encouraging the person to maintain their existing skill level and match the level of physical contact with the appropriate level of support.
Health Promotion Guidelines, V1.0, January 2016 32

Daily health promotion activities
Understanding a person’s cultural and religious background, preferences and sensitivities and where possible, accommodating cultural and religious expectations.
Matching the needs of the person appropriate to their life stage. For instance, the needs of adolescents will differ greatly from the needs of the frail aged.
Communication Understand how the person communicates and if appropriate, use communication aids.
Be clear with the person and explain what you are going to do before you start.
Give the person time to attend to personal care. Don’t rush. Ensure that communication preferences during personal
care are included in the person’s communication profile.
Create a Matching the person’s preferences can make personal care supportive a positive experience. For instance, the person may feel environment more comfortable dressing and undressing in a room free
from distractions and interruptions such as their bedroom. The person may prefer to be assisted by a male or female
support worker. Use comfortable seating and relaxing music if it helps the
person to stay calm and relaxed.
Choice and Support the person to choose preferred personal care products personal and equipment such as soaps, hair shampoo and conditioner, preferences skin moisturisers, the colour and print of their towel, face
washers and bathrobe.
Washing hands Encourage and model appropriate hand cleaning techniques and infection after the person has been to the toilet. control
Refer to the Infection Control Policy28 on the ADHC
Intranet for more information on infection control practices such as hand washing.
Toileting and Where required, physically support the person to change continence aids menstruation and continence aids at regular intervals
throughout the day. This will help to prevent discomfort, rashes and infections from occurring.
Refer to the Bladder and Bowel section (2.5).
Hair cuts A visit to the hairdresser can be pleasurable and an important social interaction for a person.
Encourage the person to choose how they would like their
http://dadhc-
intranet.nsw.gov.au/documents/working_at_dadhc/ohs/risk_management/infection_control/infection_control_policy.pdf
Health Promotion Guidelines, V1.0, January 2016
28
33

Daily health promotion activities
hair styled and / or consult with the person’s family and/or friends for advice.
Trimming finger Support the person to trim their nails safely. nails / toe nails Any discoloration, ingrown or broken nails should be noted
and discussed with a health care professional. If the person has a health condition such as Diabetes, a
referral to a podiatrist is needed.
Refer to the Foot Care section (2.7).
Shaving Support the person to shave and groom themselves according to their likes and dislikes.
Electric or safety razors are preferred as it reduces the risk of cutting the person’s skin.
Every person must have their own razor or shaver to prevent the spread of infection.
Aids, equipment and environmental modifications
An occupational therapist (OT) supports a person to participate in the activities of everyday life.
Refer to the person’s GP for a referral to an OT for recommendations on aids, equipment and environmental modifications if the person has difficulty attending to personal care.
Refer to the AESA Guidelines in Health and Wellbeing
Policy and Practice Manual Volume 2 for information on obtaining financial assistance to purchase mobility aids and equipment.
Manual handling If the person requires physical support to perform personal requirements care, a Manual Handling Support Plan29 located on the
ADHC Intranet in the Working at ADHC, WHS page30 must be developed.
A Manual Handling Support Plan outlines how to handle the person in a safe and dignified way. Consult the person’s GP and an occupational therapist or physiotherapist where required.
Mealtimes If a person has difficulty keeping food in their mouth during a meal, a clothing protector is recommended.
After the meal, remove the clothing protector, change soiled clothing and support the person to clean and wash their face. This will ensure that the person’s dignity and personal hygiene is maintained at all times.
29 http://dadhc-
intranet.nsw.gov.au/documents/working_at_dadhc/ohs/risk_management/manual_handling/Manual _Handling_Policy_March_2010_V3.pdf 30
http://dadhc-intranet.nsw.gov.au/working/ohs
Health Promotion Guidelines, V1.0, January 2016 34

31 32 33 34 352.9 Healthy ageing
Healthy ageing refers to the activities and behaviours a person undertakes to increase physical, emotional and mental health and reduce the risk of illness and disease. Healthy activities and behaviours are important at all life stages.
Some groups of people with disability are more susceptible to premature ageing and the impact associated with the ageing process more severe.
Lack of physical activity is a significant contributor to physical decline and ageing. Without regular exercise, a person over the age of 50 years (or sometimes younger) can experience a range of health problems including:
reduced bone strength
reduced muscle mass, strength and physical endurance
reduced coordination and balance
reduced joint flexibility and mobility
increased body fat levels
increased blood pressure
increased susceptibility to mood disorders, such as anxiety and depression
increased risk of illness such as cardiovascular disease and stroke.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information on age related illnesses such as arthritis, osteoporosis, and dementia.
31 www.myagedcare.gov.au
32http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Healthy_ageing_stay_physically_active
33 http://www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines
34 http://whqlibdoc.who.int/publications/2011/9789240685215_eng.pdf?ua=1
35 http://www.nhmrc.gov.au/health-topics/alcohol-guidelines
Health Promotion Guidelines, V1.0, January 2016 35

2.9.1 Good practice guidelines
When to seek medical attention:
If there is a change in the person’s physical, mental and emotional health, support the person to consult their GP. The GP may refer the person on to an allied health professional for advice.
If the person appears unsteady on their feet or has had a fall, consult the person’s GP.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Essential screening activities
There are several health screening activities aimed at preventing the onset of serious illnesses and disease.
Refer to the Screening Activities section (3).
Advance care An Advance Care Plan outlines the person’s wishes and planning preferences for care at the end of their life.
A discussion on advance care arrangements with the person, their family and others, who know the person well, can occur at any stage of the person’s life regardless of age and health status.
Refer to the End of Life Care Planning Guidelines in
Health and Wellbeing Policy and Practice Manual Volume 2 for more information.
Daily health promotion activities
Physical Exercise to increase muscle and bone fitness can reduce the activity risk of disability and disease and increase recovery from
illness.
Exercise can help an older person to maintain independence.
Exercise improves physical health and boosts cognitive abilities such as memory and logic.
Refer to the Physical Activity section (2.1) for more
information.
Falls Falling over is not an inevitable part of ageing. It is however a prevention major cause of injury for older people.
Unsteadiness and falling over may indicate the person has an underlying health issue. For instance, a person’s unsteadiness on their feet could be due to inappropriate foot care, changes in a person’s eye sight, medications and
Health Promotion Guidelines, V1.0, January 2016 36

Daily health promotion activities
vitamin deficiencies.
A healthy diet A diet with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for information on good nutrition.
Mental health Depression is not a normal part of ageing.
and fitness Refer to the Chronic Disease Guidelines in Health and
Wellbeing Policy and Practice Manual Volume 2 for information on mental illness such as depression and anxiety.
Refer to the Mental Fitness section (2.11) for information on
how to maintain and improve mental fitness.
Stay involved Social interaction and meeting new people are important as a person ages. Retiring from work or a day program can result in a dramatic decrease in daily social interaction with others.
Activities such as enrolling in an adult education course, taking up a hobby, joining a social group or volunteering can keep the person involved in the community.
Refer to the Lifestyle Planning Guidelines in the Lifestyle
Policy and Practice Manual
Sexual health Sexual health and relationships are important to the health and wellbeing of all people regardless of age and disability.
Refer to the Sexuality and Relationships Guidelines in the
Lifestyle Planning Policy and Practice Manual for further information.
Avoid smoking Smoking at any age increases the risk of many diseases and illnesses.
Refer to the Smoking section (3.4) for information on quitting.
Limit alcohol Alcohol is the most widely used social drug in Australia with
intake excessive long term use associated with liver disease, pancreatitis, diabetes, epilepsy, and some cancers.
Alcohol is high in calories, and best consumed in moderation and under the advice of a doctor if the person needs to keep their weight under control.
For healthy men and women, no more than two standard drinks on any day is recommended to reduce the harm associated with alcohol related injury and illness.
Independence If the person has mobility or independence issues, refer to the
aids person’s GP for a referral to an allied health professional such as an Occupational Therapist or Physiotherapist for advice.
Refer to the AESA Guidelines in Health and Wellbeing
Policy and Practice Manual Volume 2 for information on obtaining financial assistance to purchase mobility aids and
Health Promotion Guidelines, V1.0, January 2016 37

Daily health promotion activities
equipment.
Seek help from others
Chronic illnesses such as arthritis, osteoporosis and advanced cardiovascular disease can limit a person’s choice of physical activity.
Consult a health professional such as the GP or exercise physiotherapist to devise an exercise program that is healthy, safe and specific to the needs of the person.
Refer to the Chronic Disease Guidelines in Health and
Wellbeing Policy and Practice Manual Volume 2 for further information.
Health Promotion Guidelines, V1.0, January 2016 38

2.10 Mental fitness36 37
As with other parts of the body, the health and function of the brain is supported when it is stimulated and exercised. Lifestyle factors, not age, play a large part in the decline of a person’s mental ability and functioning.
Other factors which contribute to a decline in brain functioning include:
Health conditions such as dementia, depression, anxiety and conditions which affect cardiovascular health
Lifestyle choices including a lack of regular physical exercise, poor diet, smoking and excessive alcohol consumption
Certain medications or combination of medications.
2.10.1 Good practice guidelines
When to seek medical attention:
When there are changes to the person’s physical condition, mood and behaviour.
For information on depression and anxiety refer to the Chronic Disease
Guidelines in the Health and Wellbeing Policy and Practice Manual Volume 2
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Lifestyle Planning
During the annual Lifestyle Planning meeting or review, discuss activities which can be incorporated into the person’s weekly routine to increase mental fitness.
Refer to the Lifestyle Planning Guidelines in the Lifestyle
Policy and Practice Manual.
36 https://www.betterhealth.vic.gov.au/health/healthyliving/healthy-ageing-stay-mentally-active
37 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/self_esteem
Health Promotion Guidelines, V1.0, January 2016 39

Daily health promotion activities
Physical Exercise improves physical health and boosts cognitive exercise abilities such as memory and logic.
Physical exercise delivers oxygen to the brain. This can help to improve physical health, memory, reasoning abilities and reaction times.
Refer the Physical Activity section (2.1).
Read Support the person to keep an active interest in the world through reading.
If the person is unable to read, investigate to the use of audio books or set time aside to read to them.
A healthy diet A diet containing foods from all five food groups, especially wholegrain cereals, leafy greens, dairy foods and vitamin B is essential to brain health.
Refer to the Nutrition and Swallowing Guidelines (in Health
and Wellbeing Policy and Practice Manual Volume 1) for information on good nutrition.
Challenge Activities which mentally challenge the person are important intellect and for brain health. For example play games or offer puzzles memory which make the person think through their moves or answer
questions. See also: Engage in stimulating conversations (below)
Take time to Excessive stress can be harmful to the brain. relax Encourage the person to schedule regular periods of
relaxation into their week. This could include walking along the beach, in a park, listening to relaxing music or watching a favourite DVD.
Take up a new Learning something new stimulates the brain and promotes hobby or brain health. volunteer Hobbies such as woodwork and sewing or activities like
skipping can help the person improve their spatial awareness and reaction time.
Investigate whether there are any local groups such as ‘Men’s Sheds38’ or hobby groups the person could be supported to join.
Engage in Communicate with the person the way they understand. stimulating Develop and use communication aids such as story books and conversations chat books, picture cards, and objects that stimulate
conversation and communication with the person. Ensure all successful communication strategies are included
in the person’s communication profile.
38 http://www.mensheds.org.au/mens-health
Health Promotion Guidelines, V1.0, January 2016 40

Daily health promotion activities
Encourage the person to talk to friends and family about a wide range of topics. This helps them to use their brain to explore, examine and enquire.
Take time to ‘be’ with the person. This can be as simple as discussing what has happened during the day. For instance, asking the person what was the best thing that happened today and what they are looking forward to tomorrow.
The person-centred thinking tool, ‘History Map’, can be used to stimulate the person’s brain by prompting the person to remember past events and experiences.
Health Promotion Guidelines, V1.0, January 2016 41

2.11 Confidence and self-esteem39
Self confidence is the belief and trust a person has in their ability. A self confident person has greater control in achieving what they plan for their lives.
Self esteem is about a person liking themselves and is not conceit or boastfulness. A person with high self-esteem values themselves. This can lead to the person having more self confidence.
People can lack confidence every now and again, but a person with low self esteem feels unhappy and lacks confidence most of the time. Low self-esteem can be associated with depression.
Lack of confidence and self-esteem can negatively impact a person’s wellbeing and is linked to poor health and stress, heart disease and anti-social behaviour.
Some people with disability may have confidence and self esteem issues because they feel they are not in control of the decisions which affect them or that they don’t have influence over their lives. See the Decision Making and Consent Policy (in the Lifestyle Policy and Practice Manual) for guidance on how to support people in making their own decisions.
2.11.1 Why is self-esteem important?
Self-esteem is important as it:
gives the person a sense of pride and contentment
allows the person to feel that they have a place in the world
gives the person courage to try new things
fosters independence
gives the person the willingness to try something again even if they failed the first time
helps a person to feel that they can develop their own skills and contribute to their community
helps the person to establish boundaries in their relationships with other people.
39 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/self_esteem
Health Promotion Guidelines, V1.0, January 2016 42

2.11.2 Characteristics of low confidence and poor self-esteem
The following characteristics may indicate the person has low confidence and poor self-esteem. The person:
is extremely critical of himself or herself
does not acknowledge their own positive qualities or achievements
blame themselves when things go wrong
describe themselves using negative words such as unlovable and stupid
finds it hard to believe and accept compliments
is socially anxious or shy
neglects self care
lacks assertiveness and experiences difficulties with communication
engages in self harming behaviours such as drug and alcohol abuse.
2.11.3 Good practice guidelines
When to seek medical attention:
If there is a change in the person’s mood and behaviour
If the person engages in self harming behaviours
The GP can refer the person to an appropriate therapist for treatment if they are diagnosed with mental health issues such as anxiety and depression.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information on anxiety and depression.
Annual health promotion activities
Annual health assessment
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
NOTE: The following Person Centred Thinking Tools referred to below are found in the Lifestyle Policy and Practice Manual.
Focus on positive aspects of the person’s life
Person-centred thinking tools can be used to gain an understanding of how the person feels and to highlight their positive attributes. For instance:
- Gifts and strengths - Good day, bad day - History map - Important to/for
Health Promotion Guidelines, V1.0, January 2016 43

Daily health promotion activities
Work together Encourage the person to seek out positive people and to be open to new experiences. Use the person-centred thinking tools:
- Hopes and dreams - Presence to contribution - Relationship map - Hopes and fears - Dreaming
Self Help the person to practice self acceptance and not compare acceptance themselves to others. Use the person-centred thinking tools:
- Reputations - One page profile - Gifts and Strengths
Assertiveness Promote assertive behaviour by providing the person with opportunities to communicate opinions, beliefs, needs, and wants to others. Use the person-centred thinking tools:
- Decision making - Communication profile and communication charts
Engage in the community
Encourage friendships and the person’s involvement in their local community.
Celebrate achievements
Celebrate the person’s achievements and successes and give the person praise.
Actively listen to the person
Take the time to sit, listen and communicate with the person about what is happening for them. Do this on a regular basis.
Physical Encourage the person to engage in regular exercise. Physical activity exercise increases the natural 'feel good chemicals' in the brain
and helps to relieve stress.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information on good nutrition and health.
Health Promotion Guidelines, V1.0, January 2016 44

3 Screening activities: Preventing disease, premature death and disability
40 41 42 433.1 Immunisation
3.1.1 What is immunisation?
Immunisation is when a person has become immune to an infectious disease as a result of receiving a vaccine. When a person receives a vaccine they are exposed to a small dose of the disease. This triggers the body’s natural defence mechanism, the immune system, to respond to the disease as it normally would but without the symptoms.
If the person is later exposed to the disease, the immune system will respond in a way that prevents the person from developing the disease.
Immunisation not only protects the person but also protects the community by reducing the spread of infectious disease to others.
3.1.2 The Immunise Australia Program
The Immunise Australia Program is a combined Government initiative to increase immunisation rates across Australia. The National Immunisation Program (NIP) is funded under the Immunise Australia Program to provide vaccines to address the spread of 16 preventable diseases.
3.1.3 Immunisation schedules
The National Immunisation Program Schedule provides advice on the immunisation schedules for:
Child program – Birth to 4 years of age
School programs – 10 to 17 years of age
Immunisation for special groups – 6 months to 65 years of age and over.
40Immunisation Australia Program. http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/about-the-
program 41
https://www.betterhealth.vic.gov.au/health/healthyliving/immunisation-childhood 42
National Immunisation Program Schedule. http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/national-immunisation-program-schedule 43
Australian Immunisation Handbook (edition 10). http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/Handbook10-home
Health Promotion Guidelines, V1.0, January 2016 45

Immunisations for all people with disability, including adults, should follow the current National Immunisation Program Schedule (refer to Other Resources) unless advised otherwise by the person’s GP.
3.1.4 Vaccination for those at increased risk of infection
Certain medical conditions may increase the risk of infectious diseases even if the immune system is functioning properly. People with these medical conditions should be supported to understand their health risks and to receive the appropriate vaccination if they choose to do so.
3.1.5 Good practice guidelines
When to seek medical attention:
Adverse reactions:
If the person requires a vaccination, ask the GP about what signs and symptoms indicate the person is having an adverse reaction to the vaccination.
Keep a close eye on the person after the vaccination and address any concerns with the GP immediately.
Annual health promotion activities
Annual health assessment
If the person’s immunisation record is incomplete or unknown, bring this to the attention of the person’s GP at the time of the health assessment.
The GP is responsible for deciding which vaccinations are necessary and appropriate for the person.
Essential immunisation activities
Immunisation schedules for children, young people and adults with intellectual disability should follow National Immunisation Program Schedule (refer to Other Resources).
Hepatitis A immunisation is recommended for all people with intellectual disability
Hepatitis B immunisation is recommended for all people in residential or non-residential facilities
An annual Influenza vaccination is recommended for all people especially those with asthma, chronic lung disease, congenital heart disease, diabetes and Down Syndrome. The Influenza vaccination should occur before the onset of the flu season, between March and May.
Overseas travel
Vaccinations may be required if the person is planning to travel overseas. This should be discussed in advance at the time of the Lifestyle Planning meeting and with the person’s GP.
Health Promotion Guidelines, V1.0, January 2016 46

Daily health promotion activities
Infection control
Effective hand washing is an important component to Infection Control.
Frequent hand washing prevents the spread of illnesses such as Influenza, Hepatitis A and gastrointestinal infections.
Refer to the Infection Control Policy on the ADHC Intranet
for advice.
Health Promotion Guidelines, V1.0, January 2016 47

44 45 46 473.2 Eye health
People can have many different problems with their eyes or vision (sight). Some problems are temporary and treatable, whereas other problems are permanent.
A permanent vision problem is called ‘vision impairment’. Vision impairment can affect a person’s movement, communication and social interactions.
There are different degrees of vision impairment from mild loss to total blindness. Blindness and degenerative conditions are not curable.
3.2.1 Causes and associations
Certain genetic disorders such as Down Syndrome have a higher incidence of visual problems
maternal infections experienced during pregnancy (e.g. rubella, cytomegalovirus, venereal diseases, toxoplasmosis)
complications at birth and complications associated with extreme prematurity
consequences of disease (e.g. diabetes, glaucoma, trachoma, tumours)
trauma
poisoning
medications.
3.2.2 Treatment
Vision impairment can be corrected by wearing glasses or contact lenses or through medical treatment such as the surgical removal of cataracts.
3.2.3 Good practice guidelines
When to seek medical attention:
The person should consult the GP if they:
44 Health care in people with intellectual disability: http://www.cds.med.usyd.edu.au/cdsresearch/publications-and-
presentations/cat_view/50-health-publications 45
Health guidelines for adults with an intellectual disability: http://www.intellectualdisability.info/how-to../health-guidelines-for-adults-with-an-intellectual-disability 46
Guide Dogs: http://guidedogs.com.au/education-and-resources/helping-people-with-impaired-vision/how-to-guide-a-person 47
Vision Australia: http://www.visionaustralia.org/living-with-low-vision/family-friends-and-carers/communicating-effectively-with-people-who-are-blind-or-vision-impaired
Health Promotion Guidelines, V1.0, January 2016 48

have any change in their vision
have frequent headaches
have sore eyes
have an avoidance to light
have visible changes to the eye e.g. cloudiness of the lens of the eye
hesitate before walking, are unsteady on their feet or fall over
have not had a vision test in the last 5 years.
Annual health promotion activities
Annual health assessment
A person’s eye health should be tested annually as part of the person’s annual health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
At the health assessment appointment ensure: - the person’s vision has been reviewed - a referral is made by the GP for the person to have an
eye test if required.
Essential screening activities
The recommended guidelines around eye health assessment and review include:
- Routine screening for age-related vision loss conducted by a ophthalmologist or optometrist (if possible) every 5 years from the age of 45 years
- For people with existing vision / eye problems, more frequent reviews may be necessary.
- For people with Down Syndrome, an extra assessment at 30 years is required as ocular disorders are common for this population.
Daily health promotion activities
Communication guidelines
Refer to the person’s Communication Profile / Chart to understand how the person communicates with others.
Communicate with the person by: - Identifying yourself and others when you enter the room,
and indicate your purpose - Letting the person know when you leave the room - Not raising your voice or slowing your speech unless this
has been identified as an appropriate way to communicate with the person
- Using everyday language such as ‘look’ and ‘see’ - Addressing the person directly and not excluding them in
conversation - Never assuming the person with vision impairment needs
or wants your help. Ask the person if they want help and in what form i.e. verbal promoting, physical guidance.
- Being familiar with appropriate guiding techniques when
Health Promotion Guidelines, V1.0, January 2016 49

Daily health promotion activities
assisting the person in the community. Refer to Guide 48Dogs ‘How to guide a person ’ also located in Other
Resources for more information.
Aids and equipment
Support the person to obtain, use and maintain optical aids such as glasses in accordance with the prescribing health professional’s instructions.
Refer the Occupational therapists and physiotherapists can assess the person to an person’s functional mobility and provide advice on aids, allied health equipment and mobility. professional Support workers can make an internal referral for a service
or if the person has a chronic condition obtain a referral from the GP for allied health services through Medicare’s Chronic Disease Management Program.
Access specialist services
Guide Dogs and Vision Australia offer a range of services to a person who has vision impairment.
Guide Dogs can assess the person’s vision and functional mobility, recommend aids and provide orientation, mobility and low vision services where required.
Refer the person to Guide Dogs: - If you have concerns about the person’s vision - If the person exhibits a loss of confidence - If the person has recently moved - For free training for the person, family and support
workers.
Risk assess the Ensure environmental risks to the person associated with environment vision impairments are identified, eliminated and / or
controlled. For example: - ensure there is adequate lighting along walkways - ensure there are handrails on stairs - place furniture in a way that does not obstruct walkways.
In ADHC operated accommodation support services, annual audits are conducted to assess risk in the environment. These audits include the
Continuous Improvement Review Tool and the Group Home/Residence Workplace Safety & Security
Inspection Checklist.
Assist with A person with vision impairment may need to learn social social skills skills for use during conversation with others.
A person with vision impairment may not interact with their peers much, and may not initiate social contact due to reduced eye contact and movement.
Assist the person when communicating with others (if
48 http://www.guidedogs.com.au/education-and-resources/helping-people-with-impaired-vision/how-to-guide-a-person
Health Promotion Guidelines, V1.0, January 2016 50

Daily health promotion activities
appropriate). For instance, inform the person if they miss out on body language and gestures and are not aware when others are looking, smiling or waving at them.
Include in the person’s communication profile what assistance the person needs when communicating with others.
Health Promotion Guidelines, V1.0, January 2016 51

49 50 513.3 Hearing health
Hearing loss occurs either at birth or shortly after (congenital) or later on during childhood, adolescence and adulthood (acquired). Hearing loss is common in people with intellectual disability.
Hearing loss is classified as mild, moderate, moderate to severe, severe or profound. Once a person’s hearing has been damaged it will not come back.
Hearing loss can affect a person in many ways. For instance, hearing loss can limit the person’s ability to learn, join in and understand conversations or obtain a job. This can lead to frustration, a lack of self-esteem and confidence, and feelings of isolation. Hearing loss can also make it difficult for the person to hear important warning sounds in the environment like smoke alarms, sirens and approaching traffic.
There may be no obvious signs of hearing loss and existing symptoms may be misinterpreted. That is, a person with hearing loss may be accused of ‘selective listening’, dementia or rudeness.
3.3.1 Treatment of hearing loss
The treatment for hearing loss will depend on the cause and the severity of the impairment.
A hearing aid will increase hearing however it does not return a person’s hearing back to what it was before.
A cochlear implant allows a modified form of hearing. It is sometimes called a bionic ear because it uses technology to allow the person to hear and is designed to stimulate the surviving nerve cells in the inner ear
3.3.2 Good practice guidelines
When to seek medical attention:
Refer to the person’s GP if they complain of or display the following symptoms. The person:
Does not understand what is being said when it is noisy
Mistakes words
Appears not to understand the conversation
49 Health guidelines for adults with an intellectual disability:
http://www.intellectualdisability.info/how-to../health-guidelines-for-adults-with-an-intellectual-disability 50
Australian Hearing: http://www.hearing.com.au 51
Health care in people with intellectual disability: http://www.cds.med.usyd.edu.au/cdsresearch/publications-and-presentations/cat_view/50-health-publications
Health Promotion Guidelines, V1.0, January 2016 52

May think other people are mumbling
Needs to turn the television or radio up very loud
Does not respond when addressed
Complains of or indicates pain around the ear area or head
Has visible changes to the ear area e.g. discharge from the ear, redness
Has not had a hearing test in the last 5 years.
Annual health promotion activities
Annual health assessment
A person’s hearing should be tested annually as part of the person’s annual health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
At the health assessment appointment ensure: - the GP reviews the person’s hearing - the GP provides a referral to an audiologist for a hearing
assessment if it is indicated.
Essential screening activities
The recommended guidelines around hearing health assessment and review include: - Routine screening for age-related hearing loss of all adults
by an audiologist every 5 years from the age of 45 years (if possible)
- Screening of the hearing function of adults with Down Syndrome every 3 years throughout life as people with Down Syndrome are at high risk of age-related hearing loss.
Daily health promotion activities
Prevention Encourage the person to: Listen to music on MP3 players and stereos at a volume
where they can hear you speaking at arm’s length Limit the amount of time they are exposed to very loud
noise. For example, take time out periodically from noisy environments e.g. where there is loud music, construction noise or many people.
Fit ear plugs and ear muffs properly and wear them when exposed to industrial noise and loud machinery.
Communication Refer to the person’s Communication profile / chart to understand how the person communicates with others. When communicating with a person with hearing loss52:
52 Australian Hearing:
http://www.hearing.com.au/ViewPage.action?siteNodeId=33&languageId=1&contentId=-1
Health Promotion Guidelines, V1.0, January 2016 53

Daily health promotion activities
- Choose a quiet location and reduce background noise by turning off radios and television.
- Gain the person’s attention before beginning a conversation. - Be sure that light is not shining in the person’s eyes - Sit face to face and at the same eye level. This allows the
listener to use visual cues he or she may need to help understand what is being said.
- Speak to the person normally and don’t shout. - If the person has difficulty understanding what is being said,
try saying it another way.
Aids and equipment
When the brain and hearing nerves are deprived of sound they weaken. If the person has partial hearing a hearing aid may be prescribed to help prevent further weakening of hearing nerves.
Use auditory aids in accordance with the prescribing health practitioner’s instructions.
Assist the person to maintain hearing aids by keeping them clean as per practitioner instructions.
Be aware that the person may have difficulty understanding speech even with a hearing aid.
Be aware that hearing aids are sensitive to mechanical noise e.g. lawnmowers, kettles, other appliances, so the person may not be able to hear voices when they are being used.
Refer the person to an allied health professional
Health professionals such as audiologists and speech pathologists can assess the person’s communication needs and provide advice on communication strategies, aids and equipment.
Support workers can make an internal referral for an allied health service or, if the person has a chronic condition, obtain a referral from the GP for allied health services through Medicare’s Chronic Disease Management Program.
Access available services
Australian Hearing provides a number of services which are free to pension card holders. Australian Hearing services include: - hearing assessment - selecting and fitting hearing devices - regular hearing checks to monitor changes in hearing levels - training to the person, family and support workers to improve
listening and communication skills.
Health Promotion Guidelines, V1.0, January 2016 54

53 543.4 Smoking
Smoking is the leading cause of preventable death in Australia.
The burning of each cigarette releases more than 7000 harmful chemicals in to the body including nicotine, tar, hydrogen cyanide, carbon monoxide, free radicals, radioactive compounds, acetone, methanol and ammonia. These chemicals enter the blood stream when a person inhales tobacco smoke.
Nicotine is the chemical in tobacco smoke which causes a person to become addicted to smoking. The amount of nicotine the person requires depends on how much tobacco smoke the person inhales to make them feel normal.
When a person becomes addicted to nicotine they are compelled to ‘top up’ nicotine levels by continuing to smoke. When a person doesn’t ‘top up’ nicotine levels they experience uncomfortable and stressful withdrawal symptoms.
If a person quitting smoking shows significant behaviour changes that are of concern, contact the person’s GP and/or the local ADHC Behaviour Intervention Team.
Passive smoking occurs when non-smokers are exposed to second hand smoke. Exposure to second hand smoke increases the non-smokers risk of disease and death.
3.4.1 Risk factors
Inhaling the chemicals associated with burning tobacco harms every organ in the body. People who continue to smoke have a higher rate of disease than non-smokers. Diseases include:
cancer (lung, mouth, nose, voice box, tongue, nasal sinus, oesophagus, throat, pancreas, bone marrow, kidney, cervix, ovary, urethra, liver, bladder, bowel and stomach)
respiratory and lung disease (emphysema, chronic obstructive pulmonary disease (COPD), chronic bronchitis)
heart and blood vessel disease (coronary artery disease, heart disease, heart attack and stroke)
ulcers of the digestive system
osteoporosis and hip fracture.
53 Better Health Channel: http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Smoking_effects_on_your_body
54 iCanQuit: http://www.icanquit.com.au/health/reasons-to-quit/fitness
Health Promotion Guidelines, V1.0, January 2016 55

Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 on diseases associated with smoking (cancer, COPD, heart disease).
3.4.2 Good practice guidelines
When to seek medical attention:
Encourage and support the person to quit smoking at every opportunity and seek help and treatment advice from the GP for medication, nicotine replacement therapy and counseling.
If the person does quit smoking consult the person’s GP as the chemicals in cigarettes can change the way some medications work. Look out for common withdrawal symptoms and address these issues with the person’s GP.
Withdrawal symptoms include:
mood changes e.g. anger, irritability, frustration
mental health issues such as depression and anxiety
difficulty concentrating, restlessness and dizziness
sleep disturbances and disorders such as insomnia, vivid dreams
coughing
appetite changes
constipation
decreased heart rate.
If the person continues to smoke, be aware of signs and symptoms which may indicate the onset of a chronic health condition and consult the GP immediately.
Health Promotion Guidelines, V1.0, January 2016 56

Annual health promotion activities
Annual health assessment
Encourage the person to discuss their smoking habits with their GP at the annual health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Get informed Australian and State government health initiatives such as iCanQuit and Quitnow target people who smoke. These initiatives provide a lot of useful information to support people to quit smoking.
Get started Identify triggers which make the person crave a cigarette including alcohol, being around other smokers, stress, and caffeine drinks (e.g. coffee, tea, energy drinks).
Make a plan A plan to quit smoking: - Identifies the most appropriate method to quit such as
nicotine replacement therapy or a prescribed medication - Lists known triggers for the person - Identifies strategies to keep the person on track - Outlines how the person will change smoking related
routines with a beneficial activities such as going for a walk at morning tea time
- Identifies the person’s support networks. 55
Download the Quit because your can booklet to help with planning.
Seek guidance from the person’s GP or the local ADHC Behaviour Intervention team if you are concerned about any behavioural issues that may arise from nicotine withdrawal.
Celebrate wins Cigarettes are expensive to buy. By giving up smoking, the person will save a considerable amount of money. Encourage the person to either save the money they would otherwise spend on smoking or plan an activity such as a holiday to motivate the person to stay on track.
If the person has a setback, support and encourage the person to get back on track.
Celebrate each day the person stays on track.
Refer the Health professionals such as a psychologist can help the person to an person devise strategies to quit smoking. allied health Support workers can make an internal referral for service or if professional the person has a chronic condition obtain a referral from the
55 http://www.quit.org.au/downloads/resource/general-brochures/quit-because-you-can.pdf
Health Promotion Guidelines, V1.0, January 2016 57

Daily health promotion activities
person’s GP for allied health services through Medicare’s Chronic Disease Management Program.
Physical Physical exercise increases the natural 'feel good chemicals' exercise in the brain and can act as a distraction from smoking.
The body can start repairing itself from the moment the person stops smoking. Physical exercise can help in the repair process.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet A diet with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Designated Smoking in the workplace is not permitted (including Group smoking areas homes and agency vehicles) with the exception of designated
smoking areas (refer to ADHC’s Smoke free workplace policy)56
Smoking is not permitted in covered areas (verandas and pergolas) that are commonly used
Support workers should never smoke in front of a person who has an addiction to smoking as it reinforces the behaviour.
A person who smokes should be encouraged to do so through controls which include not smoking in the house, not smoking near other people and disposing of their waste.
Dispose of cigarette butts responsibly such as in a public bin or a locked cigarette butt container. Disposing of cigarette butts on the ground, beach or from a car window is littering. Littering incurs a fine.
Designated smoking areas must be clearly signposted and not located in an area commonly used by other people, or where it will not contaminate other parts of the house and workplace,
Designated smoking areas must have appropriate bins provided for rubbish disposal, be maintained at all times and all cigarette butts disposed of in rubbish bins provided.
56 http://dadhc-
intranet.nsw.gov.au/documents/working_at_dadhc/ohs/risk_management/smoke_free_workplace/smoke_free_environment _policy.pdf
Health Promotion Guidelines, V1.0, January 2016 58

57 583.5 Drugs and alcohol
A drug is any substance which is taken into the body and affects the way the body works. Medicines, vitamin supplements, caffeine, tobacco, inhalants, alcohol, cannabis, heroin and steroids are all drugs.
The legal status of drugs depends on certain factors. For example alcohol is a legal drug but it is illegal to sell it to people under the age of 18 years.
3.5.1 Main drug groups and their effects
This information sheet refers to drugs and alcohol that affect the central nervous system.
Drugs are often grouped according to the effect they have on the central nervous system.
There are three main drug groups:
1. Depressants: Alcohol, minor tranquilisers, inhalants (glue, petrol and spray paint), codeine such as Panadeine, opiates such as methadone, cannabis (marijuana, hashish, hashish oil) and narcotics such as heroin.
Depressants slow down the person’s heart rate, breathing, central nervous system and the messages being sent to and from the brain.
2. Stimulants: Nicotine (cigarettes), caffeine (coffee, cola, chocolate, slimming tablets, some energy drinks), pseudoephedrine (found in some cough and cold medicines), cocaine, non-prescription amphetamines, methamphetamines (ice, base and speed), and ecstasy.
Simulants speed up the central nervous system and the messages going to and from the brain. They increase the heart rate, body temperature and blood pressure.
3. Hallucinogens: Hallucinogens include LSD, magic mushrooms, mescaline, ecstasy and marijuana (in strong doses).
Hallucinogens affect perception. People who take hallucinogens see or hear things in a distorted way. The senses become confused, especially time, sound and colour. The effects of hallucinogens vary greatly and are not easy to predict.
57 http://watershed.org.au/drug-information.html
http://www.drugabuse.gov/publications/drugfacts/understanding-drug-abuse-addiction 58
http://www.nhmrc.gov.au/health-topics/alcohol-guidelines
Health Promotion Guidelines, V1.0, January 2016 59

3.5.2 How do drugs affect people?
The effects of a drug will vary from person to person and depend on:
The individual: including mood, size, weight, gender, personality and health status.
The drug: the amount taken, the strength, how it is used (smoked, eaten, or injected) and whether the person has taken other drugs at the same time.
The environment: whether the person is with trusted friends, alone, in a social setting or at home.
The possible harm associated with taking drugs include:
Harm to the body, especially the liver and kidneys
Harm to family relationships, friendships and community inclusion
Harm to lifestyle factors such as employment, education and accommodation
Harm associated with breaking the law
Mental illness
Instability in the home
Intoxication which causes impaired judgment and taking risks the person normally would not take.
3.5.3 Signs and symptoms
It can be difficult to tell if someone is using drugs. There are no physical or emotional changes that are specific to drug use. A person behaving in an unusual way over a long period of time may be involved in drug use.
Some warning signs include:
the person lacking energy
changes in the person’s eating patterns
extreme mood swings and explosive outbursts
the person staying out all night
the person experiencing trouble at day programs, their place of work or school
a sudden and frequent change of friends
an unexplained need for money or having a lot of money
valuable items going missing
the person experiencing trouble with police.
Health Promotion Guidelines, V1.0, January 2016 60

If you suspect a person is using illegal drugs refer to your line manager for advice.
3.5.4 Good practice guidelines
When to seek medical attention:
If the person admits to a drug problem and wants help, consult the person’s GP for advice and support. The GP may refer the person on to a counsellor or drug and alcohol clinic for treatment.
Annual health promotion activities
Annual health assessment
Encourage the person to discuss their smoking, alcohol consumption and drug use with their GP at the annual health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Get the facts Talk to the person. If they admit to taking drugs, find out which drug is being taken and how often.
The person may have been experimenting with the drug and has since stopped using it.
Choose the right moment to discuss the person’s drug use, not when they are intoxicated or under the influence of the drug.
Seek help If you become aware of the person taking drugs, document the person’s behaviour and discuss it with your line manager
The line manager can escalate the issue to a senior manager or relevant level of district management for advice.
Advice can also be sought from the Behaviour Intervention Team and the Clinical Innovation and Governance unit.
Advice can also be obtained from the state-wide Australian Drug Information Network counselling and referral service on 1800 888 236.
Health Promotion Guidelines, V1.0, January 2016 61

3.6 Breast cancer prevention and screening59
Breast cancer is the most common cancer in women. In NSW, 1 in 9 women will develop breast cancer by the age of 85.
3.6.1 Risk Factors
Family history of breast cancer
Never having children and never breastfeeding.
Increasing age. Over 65% of women diagnosed with breast cancer are over 65 years of age.
Being female. Only about 1% of breast cancer occurs in males.
Early onset of menstruation and late onset of menopause.
Being overweight, especially after menopause.
Drinking excessive amounts of alcohol.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information about cancer, treatment and the responsibilities of the person, support workers and health professionals.
3.6.2 Good practice guidelines
When to seek medical attention:
Pain in the breast is an uncommon symptom of breast cancer.
Contact the GP immediately if the person displays the following symptoms:
A lump or feeling of lumpiness, or thickness, somewhere in the breast or armpit
Abnormal discharge from the nipple
A nipple that becomes inverted
Dimples in the breast
A change in the shape, feel or colour of the skin of the breast.
59 Preventative Women’s Health Care for Women with Disabilities:
http://www.csp.nsw.gov.au/information-and-resources-for-health-professionals/publications/preventative-womens-health-care
Health Promotion Guidelines, V1.0, January 2016 62

Annual health promotion activities
Essential screening activities
The recommended guidelines for women with intellectual disabilities are the same for the general population. This includes:
- A mammogram (x-ray) every two years for women 60between 50 and 69 years of age .
- If the person has a family history of breast cancer, mammograms may be performed at an earlier age.
- The GP may order an ultrasound in addition to a mammogram in some circumstances.
Annual health Breast cancer screening is discussed with the person’s GP at assessment the time of the health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Self-care Encourage the person to talk to their GP or Practice Nurse about how to examine their breasts correctly and how often.
Physical activity
Physical activity is important for all people to enjoy good physical health and mental wellbeing. Physical activity can also help to prevent a range of health issues, including some cancers.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet A diet with plenty of fresh fruit and vegetables and wholegrain cereals, may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Avoid smoking Smoking is a known risk factor for developing cancer and other significant health conditions.
Refer to the Smoking section (3.4) for information on quitting.
60 Breast Screen NSW: http://www.bsnsw.org.au/
Health Promotion Guidelines, V1.0, January 2016 63

3.7 Cervical cancer prevention and screening
Cervical cancer is the abnormal growth of cells in the cervix (neck of the uterus) of a woman. Most women who develop advanced cervical cancer have either never had a Papanicolaou test (Pap Smear test) or did not have them on a regular basis.
If diagnosed early, cervical cancer is one of the most treatable of cancers. Early detection therefore increases the likelihood of successful treatment.
3.7.1 Risk factors
If the person has been sexually active throughout their lifetime
Increasing age
The person is exposed to the Human Papilloma Virus (HPV or wart virus)
The person smokes
The person is obese
The person has a family history of cervical cancer.
Refer to the Chronic Disease Guidelines (Health and Wellbeing Policy and
Practice Manual Volume 2) for information about cancer, cancer treatment and the responsibilities of the person, support workers and health professionals.
3.7.2 Good practice guidelines
When to seek medical attention:
Symptoms and signs are uncommon in the early stages.
Contact the GP immediately if the person displays the following symptoms:
unexpected bleeding
unusual vaginal discharge
leg and lower back pain
vaginal bleeding after menopause.
Health Promotion Guidelines, V1.0, January 2016 64

Annual health promotion activities
Immunisation A vaccine is now available for girls and young women who have never had sex.
The vaccination does not prevent all cervical cancers so regular Pap Smear Tests are needed every two years.
Essential screening activities
The recommended guidelines for women with intellectual disabilities are the same for the general population. This includes61:
- Between the ages of 18 and 70 a Pap Smear Test is done every 2 years, if the woman has ever been sexually active.
The risks and benefits of a Pap Smear Test are discussed with the person’s GP and the person responsible. Sedation may be required if there is difficulty with the person receiving a Pap Smear Test.
Annual health assessment
Cervical cancer screening is discussed with the person’s GP at the time of the health assessment.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Physical activity
Physical activity is important for all people to enjoy good physical health and mental wellbeing. Physical activity can also help to prevent a range of health issues, including some cancers.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet A diet with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Avoid smoking Smoking is a known risk factor for developing cancer and other significant health conditions.
Refer to the Smoking section (3.4) for information on quitting.
61 Preventative Women’s Health Care for Women with Disabilities:
http://www.csp.nsw.gov.au/information-and-resources-for-health-professionals/publications/preventative-womens-health-care
Health Promotion Guidelines, V1.0, January 2016 65

3.8 Prostate cancer prevention and screening62
The prostate is a small gland situated just below the bladder in men. It wraps around the urethra, the tube that carries urine from the bladder to the tip of the penis.
A normal prostate is the size of a golf ball.
Prostate cancer is an abnormal growth in the prostate gland. It is the second most common cancer in Australian men, after skin cancer.
3.8.1 Risk factors
Increasing age. Prostate cancer is less common in men under 50 years of age, most common in men over 65 years.
Family history of prostate cancer, breast or ovarian cancer.
It has been discovered that the BRCA2 gene (gene that causes breast 63cancer) can also cause prostate cancer .
A diet high in animal fat and low in fresh fruit and vegetables.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information about cancer, treatment and the responsibilities of the person, support workers and health professionals.
3.8.2 Good practice guidelines
When to seek medical attention:
There may be no symptoms in the early stages of prostate cancer.
Contact the GP immediately if the person displays the following symptoms:
passing urine more frequently than usual, especially at night
pain when passing urine
blood in the urine
difficulty starting the flow
trouble emptying the bladder
enlargement of the prostate gland
62 https://www.canteen.org.au/about-cancer/cancer-types/prostate-cancer/
63 http://www.prostate.org.au/awareness/
Health Promotion Guidelines, V1.0, January 2016 66

change in shape or texture of the prostate gland
lower back and pelvic pain.
Annual health promotion activities
Screening activities
There is no national screening program for prostate cancer. If prostate cancer is suspected or the person has a family history of prostate cancer, the following medical treatments may be prescribed by the treating doctor:
- A Digital Rectal Examination (DRE) may be performed by a GP if the presence of prostate cancer is suspected.
- The GP may also prescribe a PSA (prostate-specific antigen) blood test to assist in diagnosing the disorder.
Annual health assessment
Prostate cancer screening is discussed with the person’s GP at the time of the health assessment or sooner if symptoms occur.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Physical Physical activity is important for all people to enjoy good physical activity health and mental wellbeing. Physical activity can also help to
prevent a range of health issues, including some cancers.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet Obesity is a known risk factor for cancer and many other health conditions.
A diet low in animal fats with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Avoid smoking Smoking is a known risk factor for developing cancer and other significant health conditions.
Refer to the Smoking section (3.4) for information on quitting.
Health Promotion Guidelines, V1.0, January 2016 67

3.9 Testicular cancer prevention and screening64
The testicles (testes) are two small, oval-shaped organs located behind the penis in a skin sack called the scrotum. They are part of the male reproductive system. Sperm and sex hormones are made by the testicles.
Testicular cancer is not common. Early diagnosis and treatment can cure most cases of testicular cancer.
3.9.1 Risk factors
Testicular cancer is more likely in men aged between 25- 44 years
Certain racial and social groups
Having testicles that have not moved down (descended) into the scrotum (which is common in people with intellectual disability)
A rare complication of mumps known as Orchitis
Family history of testicular cancer.
Refer to the Chronic Disease Guidelines in Health and Wellbeing Policy and
Practice Manual Volume 2 for information about cancer, treatment and the responsibilities of the person, support workers and health professionals.
3.9.2 Good practice guidelines
When to seek medical attention:
Contact the GP immediately if the person displays or communicates the following symptoms:
A swelling or lump in the testicle, usually painless
A feeling of heaviness in the scrotum
Persistent ache in the lower abdomen or the affected testicle.
Annual health promotion activities
Essential screening activities
There is no national screening program for testicular cancer. If testicular cancer is suspected or the person has a family
history of testicular cancer, the following medical treatments may be prescribed by the treating doctor:
64 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Testicular_cancer
Health Promotion Guidelines, V1.0, January 2016 68

Annual health promotion activities
- A testicular examination at the annual health assessment or more often if indicated by the risk factors.
- A scrotal ultrasound.
Annual health assessment
Testicular cancer screening is discussed with the person’s GP at the time of the health assessment or sooner if symptoms occur.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Self-care A training plan can be developed by a suitably trained health professional should the person be able to, and choose to, conduct regular self-examinations for testicular cancer.
Physical activity
Physical activity is important for all people to enjoy good physical health and mental wellbeing. Physical activity can also help to prevent a range of health issues, including some cancers.
Refer to the Physical Activity section (2.1) for more
information.
A healthy diet A diet with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Avoid smoking Smoking is a known risk factor for developing cancer and other significant health conditions.
Refer to the Smoking section (3.4) for information on quitting.
Health Promotion Guidelines, V1.0, January 2016 69

65 663.10 Skin cancer prevention and screening
Skin cancer is caused by rays from the sun called ultraviolet radiation (UVR). UVR cannot be seen and is present even on cloudy days. UVR is strongest in the middle of the day. Staying in the shade will not offer complete protection as UVR can be reflected.
In Australia sun exposure accounts for 95% to 99% of skin cancer. Most skin cancers can be cured if they are found early enough. A balanced approach to sun exposure is required as total protection from sunlight can result in low Vitamin D levels. Low Vitamin D levels can result in a person developing fragile bones and other health problems. Check with the person’s GP if you are concerned about Vitamin D deficiency.
3.10.1 Risk factors
Regular exposure to the sun
Increased age
People with fair skin and who get sunburnt easily
People who have a lot of moles or freckles
People with sun spots (solar keratoses)
A family history of skin cancer.
Refer to the Chronic Disease Guidelines in the Health and Wellbeing Policy
and Practice Manual Volume 2 for information about cancer, treatment and the responsibilities of the person, support workers and health professionals.
3.10.2 Good practice guidelines
When to seek medical attention:
Contact the GP immediately if the person displays the following symptoms:
small lumps that are red, pale or pearly in colour
new spots, freckles or moles changing in colour, thickness or shape over a period of weeks to months (especially those dark brown to black, red or blue-black in colour)
Any crusty non-healing sore.
65 Cancer Council: http://www.cancer.org.au/about-cancer/types-of-cancer/skin-cancer.html
66 Health guidelines for adults with an intellectual disability:
http://www.intellectualdisability.info/how-to../health-guidelines-for-adults-with-an-intellectual-disability
Health Promotion Guidelines, V1.0, January 2016 70

Annual health promotion activities
Essential screening activities
The GP checks the person’s skin for signs of skin cancer during the annual health assessment or refers the person on to a specialist clinic for assessment.
Annual health assessment
Skin cancer screening is discussed with the person’s GP at the time of the health assessment or sooner if symptoms occur.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Self care If the person is able, encourage them to do regular whole body self checks of their skin (including the soles of the feet) for symptoms or early warning signs.
Check the Support workers should be observant of any changes to the person’s skin person’s skin when providing personal care.
Support workers have a responsibility to record any signs of skin cancer and report them to the person’s GP immediately.
Inform the person
Support workers must provide the person with information and support to maximise the person’s understanding of risks associated with harmful exposure to the sun.
Prevention -Sun Smart Guidelines67
Support workers have a duty of care to protect the person from the risk of sunburn by assisting and encouraging the person to take the following precautions:
- Slip on some sun-protective clothing – that covers as much skin as possible
- Slop on broad spectrum, water resistant SPF30+ sunscreen. Apply liberally 20 minutes before the person goes outdoors and every two hours afterwards.
- Slap on a hat – broad brim or legionnaire style to protect their face, head, neck and ears.
- Seek shade – and if possible minimise time the person spends in the sun between 11 am and 3 pm (daylight saving time), 10 am and 2 pm (Eastern Standard Time).
- Slide on sunglasses that meet Australian Standards.
Plan the day Long trips in a vehicle still require protection from the sun well (UVR) if the windows are down.
Where possible, plan outings outside of the middle of the day when UVR is least intense.
67 http://www.sunsmart.com.au/sun_protection
Health Promotion Guidelines, V1.0, January 2016 71

3.11 Bowel cancer prevention and screening68
Bowel cancer (also known as colorectal cancer) is the second most common cancer in NSW. Bowel cancer most commonly occurs in the colon or rectum.
The colon and rectum are known as the large bowel. The large bowel is commonly affected by bowel cancer.
Bowel cancer is more common in older people.
3.11.1 Risk factors
Increasing age - being aged 50 years and over.
Having bowel polyps or previous bowel cancer.
Having had ulcerative colitis or Crohn’s Disease (together these conditions are known as Inflammatory Bowel Disease).
Having a family history of bowel cancer or polyps.
Having a family history of other cancers.
Being overweight or obese.
Refer to other policies in the Chronic Disease Guidelines in Health and
Wellbeing Policy and Practice Manual Volume 2 for information about cancer, treatment and the responsibilities of the person, support workers and health professionals, and the Bowel Care Guidelines in Health and Wellbeing Policy and Practice Manual Volume 1 for information about maintaining a healthy bowel.
3.11.2 Good practice guidelines
When to seek medical attention:
Contact the GP immediately if the person displays the following symptoms:
In the early stages of bowel cancer there may be no symptoms
Blood in the person’s bowel motion or in the toilet bowl
Changes in the person’s bowel habits e.g. diarrhoea, constipation, or feeling that they have not gone completely
Cramping or bloating in the stomach.
68 https://www.bowelcanceraustralia.org/national-bowel-cancer-screening-program
Health Promotion Guidelines, V1.0, January 2016 72

Annual health promotion activities
Essential The National Bowel Cancer Screening Program69 offers free screening bowel screening for people aged 60 years and 70 years of activities age. Eligible people will be sent a letter of invitation to
participate in the program. A faecal occult blood test (FOBT) tests for blood in the
faeces may be prescribed by the GP every 2 years for people over 50 years of age.
If there is a family history of bowel cancer, the GP may recommend a colonoscopy every 5 years.
Annual health Bowel cancer screening is discussed with the person’s GP at assessment the time of the health assessment or sooner if symptoms
occur. Planning for an annual health assessment is outlined in the
Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Know the person’s medical history
Where possible, obtain information about the person’s family medical history to identify whether the person is at risk.
Physical Physical activity is important for all people to enjoy good physical activity health and mental wellbeing. Physical activity can also help to
prevent a range of health issues, including some cancers.
Refer to the Physical Activity section (2.1) for more
information.
Good nutrition Obesity is a known risk factor for cancer and many other health conditions.
A diet with plenty of fresh fruit and vegetables and wholegrain cereals may help to protect against a number of cancers and health problems.
Refer to the Nutrition and Swallowing Guidelines in Health
and Wellbeing Policy and Practice Manual Volume 1 for more information.
Avoid smoking Smoking is a known risk factor for developing cancer and other significant health conditions.
Refer to the Smoking section (3.4) for information on quitting.
69 http://www.cancerscreening.gov.au/internet/screening/publishing.nsf/Content/bowel-screening-1
Health Promotion Guidelines, V1.0, January 2016 73

70 71 723.12 Thyroid functioning
The thyroid is a gland located in the front of the neck, just below the larynx (Adam’s apple). The thyroid gland produces hormones which affect every cell in the body and is particularly important for normal growth and energy usage.
Disorders of the thyroid gland occur when it becomes underactive (Hypothyroidism) or overactive (Hyperthyroidism). Hypothyroidism can be easily treated with oral medication.
3.12.1 Risk factors
A family history of thyroid disease
Presence of goitre or nodules on the thyroid. Goitre is an enlargement of the thyroid gland that appears as a swelling at the front of the neck.
History of thyroiditis
Other autoimmune disorders such as Hashimoto’s disease and Grave’s disease
Partial or total removal of the thyroid
Down Syndrome
Turner Syndrome
Some medications e.g. Lithium
Being female
Aged over 50 years.
70 Health guidelines for adults with an intellectual disability
http://www.intellectualdisability.info/how-to../health-guidelines-for-adults-with-an-intellectual-disability 71
Better Health Channel https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/thyroid-hypothyroidism 72
Better Health Channel https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/thyroid-hyperthyroidism
Health Promotion Guidelines, V1.0, January 2016 74

3.12.2 Good practice guidelines
When to seek medical attention:
Contact the GP immediately if the person displays the following symptoms:
Hypothyroidism:
Unexplained weight gain
Constipation
Fatigue or exhaustion
Hair loss
Dry skin
Puffy face, hands, and feet
Aching muscle
Depression
Heavier periods
More sensitive to cold
Behavioural or mood changes.
Hyperthyroidism:
Unexplained weight loss
Always feel hot, flushed and sweaty
Frequent bowel motions or diarrhoea
Irritability
Nervousness, agitation and anxiety
Lack of periods in women
Accelerated heart rate or heart palpitations
Muscle weakness
Dry eyes
Protrusion of the eyes
Increased desire to eat
A swelling in the front of the neck.
Annual health promotion activities
Essential screening activities
The recommended guidelines include: - An annual thyroid function test for people with Down
Syndrome, Turner Syndrome or a previous history of thyroid disease.
- A thyroid function test every 3 to 5 years for all other people with disability.
Health Promotion Guidelines, V1.0, January 2016 75

Annual health promotion activities
Annual health assessment
Thyroid function screening is discussed with the person’s GP at the time of the health assessment or sooner if symptoms occur.
Planning for an annual health assessment is outlined in the Health Planning Procedures in Health and Wellbeing Policy and Practice Manual Volume 1.
Daily health promotion activities
Limit stress Stress, both physical and emotional, is known to affect the responsiveness of the immune system.
Autoimmune conditions appear to have an association between stress and the onset of autoimmune conditions such as Graves' disease in susceptible people.
Medication review
Certain medications such as iodine and lithium can affect the thyroid.
Thyroid function tests and medication reviews prescribed by the GP are therefore required as part of the person’s annual health check.
Iodine Iodine deficiency in a person’s diet can lead to Hypothyroidism as it can prevent the thyroid gland from producing hormones.
In Hyperthyroidism, too much iodine can trigger autoimmune conditions such as Graves' disease in susceptible people.
Iodine is found in dairy products, seafood, kelp, eggs, bread, some vegetables and iodised salt.
Health Promotion Guidelines, V1.0, January 2016 76

4 Policy and Practice Unit contact details
You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version of the Policy. Following any subsequent reviews and approval this policy will be uploaded to the internet/and/or intranet and all previous versions removed.
Health Promotion Guidelines, V1.0, January 2016 77

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity1
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Y / N / NA
Date of last review
Has the person had a vision check
Has the person had a hearing check
Does the person engage in daily physical activity?
Does the person smoke cigarettes?
Does the person drink alcohol?
Does the person take illegal drugs?
WOMEN’S reproductive health2
Does the person have Menstruation issues
Cervical screen – Pap smear test
Breast examination
1 Refer to the Health Promotion Guidelines for information on health screening activities 2 Preventative women’s health care for women with disabilities
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity1
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Y / N / NA
Date of last review
Mammogram
Sexual health issues
Menopause
MEN’S reproductive health
Prostate check
Testicular check
Sexual health issues
OTHER
Bowel cancer check
Skin cancer check
Thyroid function check
RECURRING HEALTH ISSUES Do I have recurring health issues Yes No
Name of recurring health issue e.g. urinary tract infections, fungal infections, piles
Source of information
Name of health professional issue discussed with
Date discussed
Was a plan developed Yes / No / NA
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Fact sheet January 2016
Information for disability support workers: about the GP
At the annual health assessment the GP will:
Explain Ask Collect Assess
the purpose and benefits of the assessment for the person’s consent to do the assessment personal and health information the person’s overall health and wellbeing - including physical, psychological, social - need for preventive health care - need for health education
Review Order
results of tests and screening procedures tests and procedures if needed
Discuss Recommend
- for example, blood tests or screening for cancer findings from assessment treatments and services
Provide - for example, allied health or medical specialist advice and information
Write Share
- for example, health preventive or promotion activity a health report a copy of the health report with the person and carer
During Chronic Disease management (CDM) planning the GP will:
Explain steps for developing a CDM plan to the person and carer Ask the person for consent to develop a CDM plan Develop a GP Management Plan Coordinate a Team Care Arrangement OR Contribute to a multidisciplinary care plan Describe disease and care needs Discuss health goals and get agreement from the person Design health actions with the person and carer Recommend treatment and services Arrange services Provide advice and information to the person and carer Book a review date
www.adhc.nsw.gov.au

Medicare Health Assessments (MBS Items 701-707 and 715) Medicare health assessments provided by general practitioners (GPs) may be delivered using Medicare items 701 to 707 (the general, time-tiered health assessment items) and 715 (the Aboriginal and Torres Strait Islander Health Assessment).
The health assessments are generally made up of the following elements:
information collection, including taking a patient history and undertaking or arranging examinations and investigations as required;
making an overall assessment of the patient;
recommending appropriate interventions;
providing advice and information to the patient;
keeping a record of the health assessment, and offering the patient a written report about the health assessment, with recommendations about matters covered by the health assessment; and
offering the patient’s carer (if any, and if the GP considers it appropriate and the patient agrees) a copy of the report or extracts of the report relevant to the carer.
Practice nurses and Aboriginal and Torres Strait Islander health practitioners may assist GPs in performing a health assessment, in accordance with accepted medical practice and under the supervision of the GP. This may include activities associated with:
information collection, including gathering of patient information for the medical practitioner and the taking and recording of routine measurements; and
providing patients with information about recommended interventions at the direction of the GP.
All other components of the health assessment must include personal attendance by the GP.
The time needed to undertake the aspects above of the health assessment by the practice nurse or Aboriginal and Torres Strait Islander health practitioner may be added to the time taken by the GP to complete the assessment.
It is important to note that the GP must have appropriate involvement and overall responsibility for the service, with the practice nurse or Aboriginal and Torres Strait Islander health practitioner assisting in accordance with accepted medical practice.
However, the time spent by the GP and the practice nurse or Aboriginal and Torres Strait Islander health practitioner in undertaking the health assessment is only one consideration in determining the most appropriate Medicare health assessment item to use. In deciding which item is most appropriate, the GP should consider the time spent with the patient, the level of complexity of the patient’s presentation and health needs and any assistance provided by a practice nurse or Aboriginal and Torres Strait Islander health practitioner.
The specific requirements of the health assessments are set out in the Health Insurance (General Medical Services Table) Regulation 2014, which is available on-line at ComLaw. The item descriptors and explanatory notes for the items are available at MBS Online. Medical practitioners undertaking the health assessments should familiarise themselves with the requirements set out in these documents.
Last updated: 26/08/2014
Medicare Benefits Schedule Fact Sheet: Medicare Health Assessments (MBS Items 701-707 and 715) Page 1 of 1
MBS Online

Part C1: My support plans: Menstruation chart
My name Year
CIS number TRIM number
Record M for each day I menstruate.
Date Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
Health Planning, Tools and templates, V1.3, June 2016 1

Insert my photo
My Health and Wellbeing Plan
My name:
Health Planning, Tools and templates, V1.3, June 2016 1

Part A1 – Information about me: My personal details My name:
I like to be called When I was born
Where I live
I am Female
Male
My phone number My pension number
CIS number TRIM number
My Medicare number My private health insurance details
eHealth record Yes
No
My blood group
Health Planning, Tools and templates, V1.3, June 2016 2

Part A1 – Information about me: My personal details My name:
My religion
My language and culture
Sight issues Hearing issues
Mobility Aids and equipment
Distinguishing features
Communication
Health Planning, Tools and templates, V1.3, June 2016 3

Part A2 – Information about me: Medical alerts and allergies My name:
Do I have any medical alerts and / or allergies? No Yes
If yes:
Medications: Refer to:
- Medication Chart / Webster-pak® signing sheet
Allergies: Refer to:
- Part C2 – My support plans: Support plan register and / or
- Medication Chart / Webster-pak® signing sheet
Other:
Other:
Health Planning, Tools and templates, V1.3, June 2016 4

Part A3 – Information about me: My health professionals My name:
The health professionals who support me with my health and wellbeing:
Who Phone Address Type of health professional
How the health professional supports me
e.g. Dr Adams 02 9999 9999 67 Sixth St Wollongong 2000
Neurologist Annual review of epilepsy and Epilepsy Management Plan
Health Planning, Tools and templates, V1.3, June 2016 5

Part A4 – Information about me: My support team My name:
The people who support me each day with my health and wellbeing
Who Phone Address Relationship How they support me
e.g. Janice Winters
02 9999 9999
0499 999 999
19 Winters Ave Roselee
Sister Janice supports me at my medical and dental appointments
Health Planning, Tools and templates, V1.3, June 2016 6

Part A5 – Information about me: Communicating my health needs My name:
What healthy and well looks like for me
What sick, anxious or confused looks like for me
How I communicate pain
How best to support me to communicate
Health Planning, Tools and templates, V1.3, June 2016 7

Part A6 – Information about me: Supporting me at a health appointment My name:
If there is more than one situation, add more pages
I need support from staff Yes No
I need support with
Situation where I need extra support
How best to support me
Health Planning, Tools and templates, V1.3, June 2016 8

Part A7 – Information about me: My immunisation record My name:
This is a record of the known immunisations and vaccinations I have had during my life time.
If staff are unsure of the date, it is important to record ‘unknown’ and discuss this with my GP.
Vaccination Date last given Source of information and date information received1
Tetanus
Diphtheria
Hepatitis A
Hepatitis B
Polio (Poliomyelitis)
Pneumococcal
Influenza (annual)
Measles, Mumps, Rubella (MMR)
1 Source can include medical history report, annual health assessment, GP, specialist, family, staff etc.
Health Planning, Tools and templates, V1.3, June 2016 9

Part A8 – Information about me: My history My name:
What2 When Source of information3
Other information
2 Please check with my family about recording personal information in this section as the information may be private and confidential. 3 Include significant events in my life which may impact on my health and wellbeing. It can include medical diagnoses, family medical history of relevance to me and my social history.
Health Planning, Tools and templates, V1.3, June 2016 10

Part A9 – Information about me: Sensitive information My name:
I have experienced trauma in the past§
Triggers
Record situations/actions that make me recall/relive my past trauma/experience
Support
I have a support plan that shows how to avoid reminding me of the situations/actions
Yes No
Yes No If No** , record below how I need to be supported to prevent triggering trauma:
§ Please check with my family about recording personal information in this section as the information may be private and confidential. It is not necessary to record the details of the traumatic event. If there is more than one event, add extra pages. ** A referral for support can be made to an ADHC Behaviour Support Team.
Health Planning, Tools and templates, V1.3, June 2016 11

Part A10 – Information about me: Decision making profile My name:
I need to be involved in making decisions about how I need and want support. This profile shows how you can best support me to make my own choices and decisions.
How I like my information
How to present a choice to me
How to help me understand
The best times for me to make a decision
When it is not a good time for me to make a decision
Health Planning, Tools and templates, V1.3, June 2016 12

Part A11 – Information about me: My decision making agreement My name:
If I am unable to make a decision or give consent, the people who can do so on my behalf are below:
Health and wellbeing decision Who will make the final decision if I am unable to?
Their relationship to me
Medical
Dental
► The treating doctor is responsible for determining if I am able to consent to medical or dental
procedures.
► At no time can support workers consent for me or be my person responsible.
Refer to the Decision Making Flowchart provided in the Decision Making and Consent ‘Tools and templates’ section of the Lifestyle Planning Policy and Practice Manual, when determining who supports me to make decisions and the NSW Civil and Administrative Tribunal (NCAT) Person Responsible Fact Sheet for who can be my person responsible ††
†† NSW Civil and Administrative Tribunal (NCAT)
Health Planning, Tools and templates, V1.3, June 2016 13

Part B1 – Information about my health: Health learning log My name:
Date and time of event
What did the person do
(what, where, when, how long, who was there)?
Date reviewed by health professional
Actions updated in the Health Action Plan
(Y / N / NA)
Person recording this information
Line manager signature and date
Health Planning, Tools and templates, V1.3, June 2016 14

Part B2 – Information about my health: Health reports My name:
Health Planning, Tools and templates, V1.3, June 2016 15

Part B3 – Information about my health: Health action plan My name:
Health action Date and name of health professional who prescribed the action
(information provided on the Health report)
Who is responsible for completing the action
Date due
Date completed
Progress Team leader signature and date
Health Planning, Tools and templates, V1.3, June 2016 16

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity7
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Yes / No / NA
Date of last review
Has the person had a vision check
Has the person had a hearing check
Does the person engage in daily physical activity?
Does the person smoke cigarettes?
Does the person drink alcohol?
Does the person take illegal drugs?
WOMEN’S reproductive health8
Does the person have menstruation issues
Cervical screen – Pap smear test
Breast examination
7 Refer to the Health Promotion Guidelines for information on health screening activities 8 Preventative women’s health care for women with disabilities
Health Planning, Tools and templates, V1.3, June 2016 17

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity7
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Yes / No / NA
Date of last review
Mammogram
Sexual health issues
Menopause
MEN’S reproductive health
Prostate check
Testicular check
Sexual health issues
OTHER
Bowel cancer check
Skin cancer check
Thyroid function check
RECURRING HEALTH ISSUES Do I have recurring health issues Yes No
Name of recurring health issue e.g. urinary tract infections, fungal infections, piles
Source of information
Name of health professional issue discussed with
Date discussed
Was a plan developed Yes / No / NA
Health Planning, Tools and templates, V1.3, June 2016 18

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
This form can be used instead of Part A of the CHAP tool. Before the person attends the annual health assessment with the GP, complete the form with the person, to record health information for the 12 months since the last assessment.
Date of last health assessment Today’s date:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Sensory -Vision
Visible changes to the eye e.g. cloudy
Person hesitates when walking
Unsteady on feet and/or falling
Vision test not performed in last 5 years
Sensory -Hearing
Person not responding when addressed
Muscular-skeletal
Holding a part of their body
Swollen, painful or tender joints
Swollen, painful or tender muscles
Stiffness
Redness
Difficulty holding and lifting items
Unsteady on feet and/or falling
Cardio
vascular
Person communicates pain in chest, back, jaw, arm or shoulder
Rapid heart beat
Swollen ankles
Health Planning, Tools and templates, V1.3, June 2016 19

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Health issue communicated by the person or observed by staff Discussed with the Double click or tick the box if the indicator applies to the person. Body system GP at the annual
health assessment
Shortness of breath
Blue skin (fingers/lips/toes)
Respiratory
If more than 1 indicator is listed, tick the indicator that applies to the person
Uncommon cough
Short of breath
Wheezing
Coughing up blood and/or stuff?
Temperature/fever
Bluish tinge around mouth and finger tips
Snoring at night
Restless at night
Urinary Urinary incontinence
Increased frequency of urinating
Blood
Person communicates pain when urinating
Smell
Digestive Weight loss
Weight gain
Pressure areas
Risks identified from the Nutrition and Swallowing Risk Checklist
Regurgitate or vomit
Reflux
Health Planning, Tools and templates, V1.3, June 2016 20

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Health issue communicated by the person or observed by staff Discussed with the Double click or tick the box if the indicator applies to the person. Body system GP at the annual
health assessment
Diarrhoea
Constipation
Black bowel motions
Increased flatulence
Faecal incontinence
Person communicates abdominal pain
Person communicates pain after eating
Increase or decrease in thirst
Increase or decrease in hunger
Lacking energy
Nervous
If more than 1 indicator is listed, tick the indicator that applies to the person
Fainting system Unsteady on feet and/or falling
Weakness in limbs
Person communicates strange feelings of skin such as tingling
Changes in epilepsy (seizure frequency; intensity; type)
Reproductive - Changes to menstruation (heavier/lighter) women’s Mid-cycle bleeds health Person communicates painful periods
Abnormal vaginal discharge
Vaginal irritation
Menopausal symptoms e.g. hot flushes
Health Planning, Tools and templates, V1.3, June 2016 21

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Health issue communicated by the person or observed by staff Discussed with the Double click or tick the box if the indicator applies to the person. Body system GP at the annual
health assessment
Behavioural changes
Pap smear not completed in last 2 years
Mammogram not completed in last 2 years for women over 50
Reproductive -
If more than 1 indicator is listed, tick the indicator that applies to the person
Discharge from penis men’s health Scarring
Sores
Changes in shape of penis and/or testes
Integumentary Rashes – skin, hair, Itchiness nails Flaky skin
Pressure areas
Dryness
Redness
Oral health Person communicates pain i.e. holding their jaw, refusing food (mouth, teeth Changes in gum condition (bleeding, colour) and gums) Missing teeth
Loose teeth
Changes to smell of breath
Decay of teeth
Changes in behaviour
Health Planning, Tools and templates, V1.3, June 2016 22

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Mental health Low mood (psychiatric (Appears depressed, withdrawn, sad, tearful, irritable) and High mood behavioural)
(Extreme excitement, hyperactivity, inappropriate laughing, giggling)
Irritable mood
(Short fuse, verbal and physical aggression, frustration)
Loss of interest and/or pleasure
(Refusing or needing more encouragement or prompting than usual to participate in routine activities, no longer engaged in previously enjoyed activities)
Anxiety
(More or less sleep, change in waking and sleeping routines, disturbed sleep, eating more or less, gaining and losing weight)
Other behaviours
(Spending more time alone, interacting less with others, loss of skills, no longer completing tasks, self-injurious behaviour, dis-inhibited behaviour, increased activity levels such as pacing, rocking, rearranging furniture, walking)
Changes in lifestyle
Person smokes
Person consumes alcohol
Physical activity (changes in activity type, changes in motivation, changes in
Health Planning, Tools and templates, V1.3, June 2016 23

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Health issue communicated by the person or observed by staff Discussed with the Double click or tick the box if the indicator applies to the person. Body system GP at the annual
health assessment
stamina)
Change in sleep pattern
Change in domestic abilities
Change in self-care abilities
Other
Other
Other
If more than 1 indicator is listed, tick the indicator that applies to the person
Notes to discuss with the GP at the health assessment appointment
Health Planning, Tools and templates, V1.3, June 2016 24

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
People involved in completing the Annual Health Summary
Name Position /
relationship
Date involved Name Position /
relationship
Date involved
Health Planning, Tools and templates, V1.3, June 2016 25

Part B6 – Information about my health: Annual health assessment or Part B of the CHAP tool
My name:
Health Planning, Tools and templates, V1.3, June 2016 26

Part C1 – My support plans: Health data My name:
Health Planning, Tools and templates, V1.3, June 2016 27

Part C2 – My support plans: Support plan register My name:
Name of support plan Date
developed
Quarterly review dates Location of support plan Q1 Q2 Q3 Q4
Hospital Support Plan – Part 1
Mandatory
Nutrition and Swallowing Risk Checklist
Mandatory
My Oral Health Plan
Mandatory
Health Planning, Tools and templates, V1.3, June 2016 28

Part C3 – My support plans: Support plans My name:
Health Planning, Tools and templates, V1.3, June 2016 29

Part D1 – Review record: Review record My name:
Date plan developed:
Date of review
Changes made Initial of support workers completing the review and date
Line manager signature and date
Health Planning, Tools and templates, V1.3, June 2016 30

Part D2 – Review record: People who have read and understood this plan My name:
I was involved in the development of this plan on (date)
My signature
I reviewed this plan on (dates)
Support workers and line manager:
I have read and understood the My Health and Wellbeing Plan and am able to implement it in accordance with the Health Planning Procedures:
Name Position Signature Date Name Position Signature Date
Health Planning, Tools and templates, V1.3, June 2016 31

My oral health plan My name:
Insert photo
CIS number
TRIM number
Person responsible
My support Completed by the person and support worker
Do I have my natural teeth? Yes
No If no, do I have dentures?
Yes
No
What support do I need with my oral health?
None
Some help
I need full support
Verbal prompting
Physical help
Other:
_________________
The place I prefer to have my teeth / mouth cleaned is:
What is best way to communicate with me about my oral health needs?
What special oral hygiene requirements do I have, if any, e.g. how do I use mouthwash or floss my teeth?
My routine Completed by the GP and / or dentist
I need my teeth / mouth cleaned (number of times per day and when):
Tools I need to use:
Toothbrush
Soft and regular
Electric
Modified toothbrush
Suction
Mouth swab
Toothpaste I don’t use toothpaste I use toothpaste
Recommended product:
Mouthwash
I don’t use mouthwash I use mouthwash
When / how do I use it?
Recommended product:
Health Planning, Tools and templates, V1.3, June 2016 1

My oral health plan My name:
Floss
Yes No
When / how do I use it?
Recommended product:
Dentures
Yes No
Scrub with a brush Soak overnight
Recommended product:
I take medication that causes dry mouth Yes No
Dry mouth product
Yes No
When do I use it?
How do I use it?
Recommended product:
Other information
My annual review Completed by the GP and / or dentist
Date of the last oral health review by my GP or dentist
Outcome of the oral health review (health professional to record or attach report)
Date of the next oral health review
Plan endorsement
Name of professional (dentist / GP)
Signature of professional
Date
Line manager signature and date
Health Planning, Tools and templates, V1.3, June 2016 2

Other resources
Health Planning
1. Link to ELMO e-learning module
2. Australia’s National Oral Health Plan 2015-2024: Healthy Mouths, Healthy Lives
3. Aboriginal resources
4. Link to Medicare items
5. NSW Council for Intellectual Disability
6. Women
7. Children
8. Oral Health Services
9. Medicare health assessment fact sheet
10. Fact sheet for General Practitioners
11. Fact sheet for disability support workers
Health Planning, Other resources, V1.3, June 2016 1

1 Link to ELMO e-learning module for Health Planning
Good to Great Live Portal
URL: http://www.elearn.com.au/adhc/goodtogreat
Username: adhc
Password: goodtogreat
2 Australia’s National Oral Health Plan 2015-2024: Healthy Mouths, Healthy Lives
Council Of Australian Governments (COAG) Health Council
http://www.coaghealthcouncil.gov.au/Publications/Reports/ArtMID/514/ArticleID/81 /Australias-National-Oral-Health-Plan-2015-2024
3 Aboriginal resources
Aboriginal Indigenous Health InfoNet
http://www.healthinfonet.ecu.edu.au/key-resources/organisations
Aboriginal Health and Medical Research Council of NSW
http://www.ahmrc.org.au/index.php?option=com_content&view=article&id=2&Itemi d=2
First Peoples Disability Network (Australia)
http://fpdn.org.au/
Conflict resolution
http://www.cjc.nsw.gov.au/agdbasev7wr/cjc/documents/pdf/cjc pamphlet - blewin -jan 2012.pdf Guidelines
Aboriginal Home Care
http://www.adhc.nsw.gov.au/individuals/help_at_home/aboriginal_home_care
Aboriginal staff and positions
Refer to District Disability Directors for information on the location of Aboriginal staff and positions available in your District. You can also search the ADHC intranet by typing in Aboriginal and seeing what positions and roles are available within ADHC Aboriginal Service Delivery and Development Directorate (ASDD)
3 Link to Medicare items
Health assessments
Medicare health assessment for people with an intellectual disability – MBS items 701,703,707
Health Planning, Other resources, V1.3, June 2016 2

Medicare health assessment for Aboriginal and Torres Strait Islander people aged 15 to 54 – MBS item 715
Medicare health assessment for Aboriginal and Torres Strait Islander people aged 55+ – MBS item 715
4 NSW Council for Intellectual Disability
Health Information Fact Sheets
http://www.nswcid.org.au/
Specialist Disability Services
http://www.nswcid.org.au/images/pdf/health_fact_sheets/21_Fact%20Sheet.pdf
5 Women
Women’s Health NSW
http://whnsw.asn.au/womens-health-centers-nsw/
Family Planning NSW
http://www.fpnsw.org.au/
6 Children
ADHC Maximising Health and Wellbeing for Children and Young People in Out-of-Home Placements Policy
http://dadhc-intranet.nsw.gov.au/documents/client_services/community_access/MaximisingHea lthandWellbeingforCandYPPolicy.pdf
Child Dental Benefits Schedule
http://www.health.gov.au/internet/main/publishing.nsf/Content/childdental
Early Intervention Services
https://www.dss.gov.au/our-responsibilities/disability-and-carers/program-services/for-people-with-disability/early-intervention-services-for-children-with-disability
7 Oral Health Services
Public Oral Health Service
The eligibility requirements for an adult to receive free Public Oral Health Service are available on the NSW Ministry of Health website
http://www0.health.nsw.gov.au/policies/pd/2009/pdf/PD2009_074.pdf
Health Planning, Other resources, V1.3, June 2016 3

Local Health Districts can be contacted for oral health information, and contact details are on the NSW Ministry of Health website
http://www.health.nsw.gov.au/oralhealth/Pages/contacts.aspx
NSW Oral Health Fee For Service Scheme (OHFFSS)
The OHFFSS provides and alternative way for people eligible for public oral health care to receive dental treatment by a private practitioner who is registered with the OHFFSS. Services includes emergency care, general dental care and dentures. Information on the OHFFSS is available at:
http://www.health.nsw.gov.au/oralhealth/Pages/nsw-oral-health-fee-for-service-scheme.aspx
Special Care Dentistry Service
People who are not suitable for routine dental care at a Public Oral Health Service are entitled to Special Care Dentistry Services. Special Care Dentistry Services are provided in NSW at three Referral Centres:
Sydney Dental Hospital (SDH) in Surry Hills (central Sydney)
Westmead Centre for Oral Health (WCOH) (near Parramatta)
The Children’s Hospital Westmead, Dental Department
If the person has not previously accessed a Referral Centre, the person will need a referral completed by a medical or dental practitioner. Refer to the flowchart below and the NSW Ministry of Health website for information on the referral process
http://www0.health.nsw.gov.au/policies/pd/2011/pdf/PD2011_071.pdf
Health Planning, Other resources, V1.3, June 2016 4

Flow chart: The Special Care Dentistry Referral Centre referral process1
Person requires specialist dental
attention/review
Annual health
assessment
Person’s dental
condition deteriorates
GP
Private dentist
Referral prepared
Referral sent to Referral Centre
Referring practitioner advised of:
§ the outcome of the consultation/s
and proposed course of care or
reasons why specialist service is
not proceeding
§ How best to manage the person
whilst waiting for a general
anaesthesia (if required)
Person and referring practitioner
advised of any wait listing
Person is contacted with an offer of a
consultation appointment
Person is prioritised according to
need
Referral reviewed according NSW
Ministry of Health policy
Referral acknowledged in a timely
manner and person’s details logged
GP/
Dentist
GP/
Dentist
Refe
rra
l C
entr
e
Communicate
the person’s
communication
and support
needs to the
Referral Centre
Fam
ily, frie
nd
s o
r
care
rs
1 Oral Health Specialist Referral Protocols PD2011_071
Health Planning, Other resources, V1.3, June 2016 5

My Health and Wellbeing Plan
My name:
Health Planning, Tools and templates, V1.3, June 2016
Insert my photo

Part A1 – Information about me: My personal details My name:
I like to be called When I was born
Where I live
I am Female
Male
My phone number My pension number
CIS number TRIM number
My Medicare number Private health
Insurance details
eHealth record Yes
No
Blood group
Health Planning, Tools and templates, V1.3, June 2016

Part A1 – Information about me: My personal details My name:
Religion
Language and culture
Sight issues Hearing issues
Mobility Aids and equipment
Distinguishing features
Communication
Health Planning, Tools and templates, V1.3, June 2016

Part A2 – Information about me: Medical alerts and allergies My name:
Do I have any medical alerts and / or allergies? No Yes
If yes:
Medications: Refer to:
- Medication Chart / Webster-pak® signing sheet
Allergies: Refer to:
- Part C – My support plans: Support Plan Register and / or
- Medication Chart / Webster-pak® signing sheet
Other:
Other:
Health Planning, Tools and templates, V1.3, June 2016

Part A3 – Information about me: My health professionals My name:
The health professionals who support me with my health and wellbeing:
Who Phone Address Type of doctor
How the person supports me
e.g. Dr Adams 02 9999 9999 67 Sixth St Wollongong 2000
Neurologist Annual review of epilepsy and Epilepsy Management Plan
Health Planning, Tools and templates, V1.3, June 2016

Part A4 – Information about me: My support team My name:
The people who support me each day with my health and wellbeing
Who Phone Address Relationship How they support me
e.g. Janice Winters
02 9999 9999
0499 999 999
19 Winters Ave Roselee
Sister Janice supports me at my medical and dental appointments
Health Planning, Tools and templates, V1.3, June 2016

Part A5 – Information about me: Communicating my health needs My name:
What healthy and well looks like for me
What sick, anxious or confused looks like for me
How I communicate pain
How best to support me to communicate
Health Planning, Tools and templates, V1.3, June 2016

Part A6 – Information about me: Supporting me at a health appointment My name:
If there is more than one situation, add more pages
I need support from staff Yes / No
I need support with
Situation where I need extra support
How best to support me
Health Planning, Tools and templates, V1.3, June 2016

Part A7 – Information about me: My immunisation record My name:
This is a record of the known immunisations and vaccinations I have had during my life time.
If staff are unsure of the date, it is important to record ‘unknown’ and discuss this with my GP.
Vaccination Date last given Source of information and date information received1
Tetanus
Diphtheria
Hepatitis A
Hepatitis B
Polio (Poliomyelitis)
Pneumococcal
Influenza (annual)
Measles, Mumps, Rubella (MMR)
1 Source can include medical history report, annual health assessment, GP, specialist, family, staff etc.
Health Planning, Tools and templates, V1.3, June 2016

Part A8 – Information about me: My history My name:
What2 When Source of information3
Other information
2 Please check with my family about recording personal information in this section as the information may be private and confidential. 3 Include significant events in my life which may impact on my health and wellbeing. It can include medical diagnoses, family medical history of relevance to me and my social history.
Health Planning, Tools and templates, V1.3, June 2016

Part A9 – Information about me: Sensitive information My name:
I have experienced trauma in the past§
Triggers
Record situations/actions that make me recall/relive my past trauma/experience
Support
I have a support plan that shows how to avoid reminding me of the situations/actions
Yes No
Yes No If No** , record below how I need to be supported to prevent triggering trauma:
§ Please check with my family about recording personal information in this section as the information may be private and confidential.
It is not necessary to record the details of the traumatic event. If there is more than one event, add extra pages ** A referral for support can be made to an ADHC Behaviour Support Team
Health Planning, Tools and templates, V1.3, June 2016

Part A10 – Information about me: Decision making profile My name:
I need to be involved in making decisions about how I need and want support. This profile shows how you can best support me to make my own choices and decisions.
How I like my information
How to present a choice to me
How to help me understand
The best times for me to make a decision
When it is not a good time for me to make a decision
Health Planning, Tools and templates, V1.3, June 2016

Part A11 – Information about me: My decision making agreement My name:
If I am unable to make a decision or give consent, the people who can do so on my behalf are below:
Health and wellbeing decision Who will make the final decision if I am unable to?
Their relationship to me
Medical
Dental
► The treating doctor is responsible for determining if I am able to consent to medical or dental
procedures.
► At no time can support workers consent for me or be my person responsible.
Refer to the Decision Making and Consent policy flowchart provided in the Decision Making and Consent Tools and templates section of the Lifestyle Planning Policy and Practice Manual, when determining who supports me to make decisions and the NSW Civil and Administrative Tribunal (NCAT) Person Responsible Fact Sheet for who can be my person responsible 6
6 NSW Civil and Administrative Tribunal (NCAT)
Health Planning, Tools and templates, V1.3, June 2016

Part B1 – Information about my health: Health learning log My name:
Date and time of event
What did the person do
(what, where, when, how long, who was there)?
Date reviewed by health professional
Actions updated in the Health Action Plan
(Y / N / NA)
Person recording this information
Line manager signature and date
Health Planning, Tools and templates, V1.3, June 2016

Part B2 – Information about my health: Health reports My name:
Health Planning, Tools and templates, V1.3, June 2016

Part B3 – Information about my health: Health action plan My name:
Health action Date and name of health professional who prescribed the action
(information provided on the Health report)
Who is responsible for completing the action
Date due
Date completed
Progress Team leader signature and date
Health Planning, Tools and templates, V1.3, June 2016

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity1
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Y / N / NA
Date of last review
Has the person had a vision check
Has the person had a hearing check
Does the person engage in daily physical activity?
Does the person smoke cigarettes?
Does the person drink alcohol?
Does the person take illegal drugs?
WOMEN’S reproductive health2
Does the person have Menstruation issues
Cervical screen – Pap smear test
Breast examination
1 Refer to the Health Promotion Guidelines for information on health screening activities 2 Preventative women’s health care for women with disabilities
Health Planning, Tools and templates, V1.3, June 2016

Part B4 – Information about my health: Health promotion register My name:
Healthy living and health screening activity1
Yes / No / NA
Date last discussed with health professional
Name of health professional
Was a plan developed Y / N / NA
Date of last review
Mammogram
Sexual health issues
Menopause
MEN’S reproductive health
Prostate check
Testicular check
Sexual health issues
OTHER
Bowel cancer check
Skin cancer check
Thyroid function check
RECURRING HEALTH ISSUES Do I have recurring health issues Yes No
Name of recurring health issue e.g. urinary tract infections, fungal infections, piles
Source of information
Name of health professional issue discussed with
Date discussed
Was a plan developed Yes / No / NA
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
This form can be used instead of Part A of the CHAP tool. Before the person attends the annual health assessment with the GP, complete the form with the person, to record health information for the 12 months since the last assessment.
Date of last health assessment Today’s date:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Sensory -Vision
Visible changes to the eye e.g. cloudy
Person hesitates when walking
Unsteady on feet and/or falling
Vision test not performed in last 5 years
Sensory -Hearing
Person not responding when addressed
Muscular-skeletal
Holding a part of their body
Swollen, painful or tender joints
Swollen, painful or tender muscles
Stiffness
Redness
Difficulty holding and lifting items
Unsteady on feet and/or falling
Cardio
vascular
Person communicates pain in chest, back, jaw, arm or shoulder
Rapid heart beat
Swollen ankles
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Shortness of breath
Blue skin (fingers/lips/toes)
Respiratory Uncommon cough
Short of breath
Wheezing
Coughing up blood and/or stuff?
Temperature/fever
Bluish tinge around mouth and finger tips
Snoring at night
Restless at night
Urinary Urinary incontinence
Increased frequency of urinating
Blood
Person communicates pain when urinating
Smell
Digestive Weight loss
Weight gain
Pressure areas
Risks identified from the Nutrition and Swallowing Risk Checklist
Regurgitate or vomit
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Reflux
Diarrhoea
Constipation
Black bowel motions
Increased flatulence
Faecal incontinence
Person communicates abdominal pain
Person communicates pain after eating
Increase or decrease in thirst
Increase or decrease in hunger
Lacking energy
Nervous Fainting system Unsteady on feet and/or falling
Weakness in limbs
Person communicates strange feelings of skin such as tingling
Changes in epilepsy (seizure frequency; intensity; type)
Reproductive - Changes to menstruation (heavier/lighter) women’s Mid-cycle bleeds health Person communicates painful periods
Abnormal vaginal discharge
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Vaginal irritation
Menopausal symptoms e.g. hot flushes
Behavioural changes
Pap smear not completed in last 2 years
Mammogram not completed in last 2 years for women over 50
Reproductive - Discharge from penis men’s health Scarring
Sores
Changes in shape of penis and/or testes
Integumentary Rashes – skin, hair, Itchiness nails Flaky skin
Pressure areas
Dryness
Redness
Oral health Person communicates pain i.e. holding their jaw, refusing food (mouth, teeth Changes in gum condition (bleeding, colour) and gums) Missing teeth
Loose teeth
Changes to smell of breath
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Decay of teeth
Changes in behaviour
Mental health Low mood (psychiatric (Appears depressed, withdrawn, sad, tearful, irritable) and High mood behavioural)
(Extreme excitement, hyperactivity, inappropriate laughing, giggling)
Irritable mood
(Short fuse, verbal and physical aggression, frustration)
Loss of interest and/or pleasure
(Refusing or needing more encouragement or prompting than usual to participate in routine activities, no longer engaged in previously enjoyed activities)
Anxiety
(More or less sleep, change in waking and sleeping routines, disturbed sleep, eating more or less, gaining and losing weight)
Other behaviours
(Spending more time alone, interacting less with others, loss of skills, no longer completing tasks, self-injurious behaviour, dis-inhibited behaviour, increased activity levels such as pacing, rocking, rearranging furniture, walking)
Health Planning, Tools and templates, V1.3, June 2016

Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
Body system
Health issue communicated by the person or observed by staff
Double click or tick the box if the indicator applies to the person.
If more than 1 indicator is listed, tick the indicator that applies to the person
Discussed with the GP at the annual
health assessment
Changes in lifestyle
Person smokes
Person consumes alcohol
Physical activity (changes in activity type, changes in motivation, changes in stamina)
Change in sleep pattern
Change in domestic abilities
Change in self-care abilities
Other
Other
Other
Notes to discuss with the GP at the health assessment appointment
Health Planning, Tools and templates, V1.3, June 2016
Part B5 – Information about my health: Annual health summary or Part A of the CHAP tool
My name:
People involved in completing the Annual Health Summary
Name Position /
relationship
Date involved Name Position /
relationship
Date involved
Health Planning, Tools and templates, V1.3, June 2016

Part B6 – Information about my health: Annual health assessment or Part B of the CHAP tool
My name:
Health Planning, Tools and templates, V1.3, June 2016

Part C1 – My support plans: Health data My name:
Health Planning, Tools and templates, V1.3, June 2016

Part C2 – My support plans: Support plan register My name:
Name of support plan Date developed Quarterly review dates Location of support plan
Q1 Q2 Q3 Q4
Hospital Support Plan – Part 1
Mandatory
Nutrition and Swallowing Risk Checklist
Mandatory
My Oral Health Plan
Mandatory
Health Planning, Tools and templates, V1.3, June 2016

Part C3 – My support plans: Support plans My name:
Health Planning, Tools and templates, V1.3, June 2016

Part D1 – Review record: Review record My name:
Date plan developed:
Date of review
Changes made Initial of support workers completing the review and date
Line manager signature and date
Health Planning, Tools and templates, V1.3, June 2016

Part D2 – Review record: People who have read and understood this plan My name:
I was involved in the development of this plan on (date):
My signature
I reviewed this plan on (dates):
Support workers and line manager:
I have read and understood the My Health and Wellbeing Plan and am able to implement it in accordance with the Health Planning Procedures:
Name Position Signature Date Name Position Signature Date
Health Planning, Tools and templates, V1.3, June 2016


Sexuality and Relationship Guidelines
Document name Sexuality and Relationship Guidelines
Policy Lifestyle Planning Policy
Version number 1.0
Approval date January 2016
Policy manual Lifestyle Policy and Practice Manual
Approved by Deputy Secretary, ADHC
Summary The Sexuality and Relationship Guidelines are written for any person who is supporting a person with disability to explore and express their sexuality. The Guidelines are intended to provide direction about the roles and responsibilities of all supporters to enhance opportunities for people while exercising their duty of care to avoid harm. The Guidelines focus particularly on the importance of providing access to information and education to people, and decreasing their vulnerability to abuse and exploitation.
Replaces document Sexuality and Human Relationships Policy and Procedures 1996, amended 2010
Authoring unit Contemporary Residential Options Directorate
Applies to All people who are being supported in New South Wales disability services.
Review date 2017

Version control The first and final version of a document is version 1.0.
The subsequent final version of the first revision of a document becomes version 1.1.
Each subsequent revision of the final document increases by 0.1, for example version 1.2, version 1.3 etc.
Revision history
Version Amendment date Amendment notes
V1.0 January 2016 Replaces Sexuality and Human Relationships Policy and Procedures 1996, amended 2010
Sexuality and Relationship Guidelines, V1.0, January 2016 2

Table of contents 1 Sexuality and relationship guidelines................................................. 4
1.1 Context ........................................................................................... 4 1.2 Scope ............................................................................................. 4 1.3 Rights based principles .................................................................. 4 1.4 Sexuality......................................................................................... 5 1.5 Education........................................................................................ 5 1.6 Reproductive and sexual health ..................................................... 9 1.7 Advocacy...................................................................................... 10 1.8 Supported decision making and consent...................................... 10 1.9 Duty of care and dignity of risk ..................................................... 13 1.10 Having the conversation ............................................................... 13 1.11 Culture.......................................................................................... 16 1.12 Opportunity................................................................................... 18 1.13 Lifestyle Planning ......................................................................... 20 1.14 Sexual behaviours of concern ...................................................... 22 1.15 NSW Ombudsman reportable incidents ....................................... 29
2 Definitions ........................................................................................... 31 3 Policy and Practice Unit contact details ........................................... 33
Sexuality and Relationship Guidelines, V1.0, January 2016 3

1 Sexuality and relationship guidelines
1.1 Context
The United Nations’ Convention on the Rights of Persons with Disabilities (the Convention) operates on the principle of respect for the individual’s dignity and autonomy by promoting the individual’s freedom to make choices, to be an independent and effective participant in society, and to enjoy equality of opportunity.
What the Convention is saying is that a person with disability has the right to make choices about all aspects of life and that others are to respect that right. The Sexuality and Relationship Guidelines (the Guidelines) are founded on this principle.
The Guidelines are consistent with the objects and principles of the Disability Inclusion Act 2014 which state that people with disability have the right to realise their physical, social, sexual, reproductive, emotional and intellectual capacities, and the right to respect for their cultural or linguistic diversity, age, gender, sexual orientation and religious beliefs.
The Guidelines embody the principles of legal and human rights found in the New South Wales Disability Service Standards. Other person centred guiding principles are contained in the ADHC Lifestyle Planning Policy.
The Guidelines aim to deliver culturally sensitive information about sexuality that supports Aboriginal and Torres Strait Islander people and people from culturally and linguistically diverse (CALD) communities.
1.2 Scope These Guidelines are for reference by all people supporting people with disability. They are particularly relevant in environments where people can have limited opportunity to meet people outside their disability service, and may include accommodation support environments, Transition to Work and Day Programs. However, the rights based principles are relevant in any disability support environment.
1.3 Rights based principles
The following rights based principles are protected by the law and are consistent with the objects and principles of the Disability Inclusion Act 2014.
1. People with disability are supported to express and explore their sexuality across their lifespan.
2. People are supported to understand their rights, to exercise them to enjoy sexual experiences, and to have their privacy and dignity respected.
Sexuality and Relationship Guidelines, V1.0, January 2016 4

3. People are provided with information and education in a way that supports them to form their own values and beliefs about sexuality.
4. Sexual expression is acknowledged as a normal part of development, and people are supported to develop healthy self-esteem and self-respect.
5. People have the right to make decisions about their own bodies, and live free of exploitation and sexual harassment.
6. People are supported to exercise their rights to form relationships of their choosing, to marry or live as a family, and to have children.
7. People have information that is accessible and understandable to them when they are making decisions about forming sexual relationships.
8. People are supported to identify and address risks to their health and safety, such as unsafe sex or sexual exploitation and abuse.
9. Access to sexual and reproductive health services, and population health and screening programs, is available to all people.
10. Information about reproduction, contraception and parenting is accessible to people who want it and is in a format they understand.
1.4 Sexuality Sexuality is part of a person’s identity and develops throughout life. It encompasses sex, gender identities and roles, sexual orientation, eroticism, pleasure, intimacy and reproduction.
It is natural for people at every stage of life to express and explore their sexuality through their behaviour. Sexual exploration is a process of learning what is normal for the person, and what feels good and right for them. Where sexual exploration is balanced with interest in other aspects of life, it is normal and healthy.
Sexuality is not just about behaviour, and is experienced and expressed in thoughts, fantasies, attitudes, values, practices, roles and relationships. It is influenced by personal matters such as physical and psychological characteristics, and social and economic circumstances. It is affected by environment and community factors such as political, religious and cultural beliefs, and legal and historical considerations (WHO, 2006).
1.5 Education Education is essential to understand how to apply the rights based principles, and provide supports for people to develop healthy relationships and understand gender and sexual identity.
Lack of adequate education regarding sex, sexuality and relationships, and the lack of opportunity for sexual expression, can make people vulnerable to exploitation and to not having their sexual needs and rights met. It can also lead to people engaging in behaviours of concern (see section 1.14 for examples).
Sexuality and Relationship Guidelines, V1.0, January 2016 5

1.5.1 Sexuality and relationship education for people who support people with disability
The rights based principles underpinning these Guidelines, and their associated legislation, require that people are supported and informed to make decisions and understand their rights. Workers who support people in a service environment1
such as accommodation support, Transition to Work or Day Programs, have a role to inform and educate people about their rights in relation to sexuality and relationships. A skilled workforce is needed to achieve this, and requires the full support of service providers to offer opportunities for the professional development of their workers in the area of sexuality and developing relationships.
People with or without disability do not always understand that people with disability are able to have fulfilling sex lives. Negative myths and stereotypes about ‘disability and sexuality’ contribute to the lack of sexuality education provided to people with disability.
The values and attitudes of others influence the amount and type of information provided to people to explore and express their sexuality. People have different experiences that affect their views about sexuality and that make them their own. Education helps supporters to explore their own values, beliefs and sensitivities about sexuality and relationships, which can impact on their ability to effectively support others. People have the right to be informed and supported to develop their own views and beliefs about sexuality without influence.
In a service environment supporters must be able to:
• assist people to understand sex and relationships, and help them to address their reproductive and sexual health needs
• understand their responsibilities to the person and the limitations and boundaries related to their role
• identify what sexual behaviours are legal and illegal, and to fulfill their obligations to support the person and respond appropriately.
Education provides understanding of the behaviours associated with sexual development that are typical of an age group. Depending on a person’s level of intellectual disability, typical behaviours may occur at different ages, and should be understood by those who are supporting people to express their sexuality2.
A behaviour or sexuality specialist will not be available every time a matter about sexuality arises. Family Planning NSW3 runs regular courses on sexuality for
1 A service environment is any place where a person with disability is receiving paid support
2 Johnson, T. C. Helping Children with Sexual Behaviour Problems, 2007 3 http://www.fpnsw.org.au/education
Sexuality and Relationship Guidelines, V1.0, January 2016 6

service providers, support workers and health professionals to build their skills in providing education and support to people with disability.
1.5.2 Sexuality and relationship education for people with disability
Some people with disability may require education from a person or organisation specialising in sexuality and relationships, others will learn from those in their support network, including paid workers, or they may choose to be educated about their sexuality independently. Family Planning NSW Talkline4 can provide referral to services and professionals who provide sexuality education and support.
Education usually starts in the school system and informs people about sexual development, describing the changes in emotion and body that occur as the person matures, and demonstrates as normal the behaviours associated with those changes. The basic concepts of sexuality education are about private and public behaviours and places, safety, consent and pleasure5.
An important aspect of education for people who are exploring their sexuality is to learn protective behaviours, so they can avoid unintended pregnancy and disease, and recognise and report exploitative and abusive treatment. While supporting the person to stay safe, it is equally important for education to focus on how the person can enjoy healthy relationships and make decisions for their own body.
Information about sexuality will only be useful if communication methods are used that the person understands. Supporters should explore what communication methods suit the person and could be pictures, images or videos. In a service environment the person should have a communication profile which will provide a guide to the person’s preferred method for receiving information.
1.5.3 Respecting diversity
Education informs people that they have a gender identity, that is, they identify as being a man, a woman or transgender. People can have different gender identities and should be supported to understand that it is possible and acceptable to identify as being the opposite gender to the sex they were born.
Education also informs people that they have a sexual identity which is about how they identify and feel about themselves, in relation to their sexual orientation and who they are attracted to.
People can have different sexual orientations and should be supported to understand that it is possible and acceptable to be attracted to the opposite sex, the same sex or both.
4 http://www.fpnsw.org.au/talkline
5 McDonagh, A., Barrett, J. and Ryan, L. (2000). Design and Deliver: Developing training programs in sexuality, sexual health and intellectual disability. Sydney, FPA Health (now Family Planning NSW)
Sexuality and Relationship Guidelines, V1.0, January 2016 7

1.5.4 Responsibility and the law
It is important for people to know that they have rights and responsibilities, and how to exercise them when expressing their sexuality. They should also understand that some sexual behaviour is against the law. Some of those laws apply to their behaviour, and some to other people’s behaviour towards them.
One of the laws that adults must learn early is that they have to give their consent to participate in sexual activity with another person. If a person engages in sexual activity with another person without their consent, it is sexual assault, and is a crime that is reportable to the New South Wales Police. Victims of sexual assault can receive services including free counseling and financial assistance from Victims services and support (see Other resources).
People can break the law in other ways. For example, a person who has a sexually transmissible infection and does not inform a sexual partner, and has unprotected sex, could be prosecuted for causing grievous bodily harm with intent to another person6 (see Section 1.8 for other examples of illegal sexual activity).
1.5.5 Sexuality education for children and young people with disability
A well rounded sexuality education starts when the person is a child and continues through adulthood. The primary source of knowledge, values and emotional support to children and young people is most often the family.
Some people receive education about sexuality from their parents, especially to understand how they value their sexuality, and what behaviours are acceptable in society.
The NSW Department of Education is responsible for school curricula that include concepts to support healthy sexuality and relationships.
Working in partnership with parents will help to support a child’s positive and healthy sexual development. Parents can benefit from opportunities to learn about and discuss their child’s sexuality and relationships and supporters should enable this to occur where possible. Family Planning NSW conducts Parent Forums7 and has a range of books for loan and purchase to assist parents in understanding their children’s sexual development.
Information and support should be provided to children and young people to promote their health, and their understanding of the need to self-protect.
6 section 33 of the Crimes Act 1900
7 http://www.fpnsw.org.au/parentforums
Sexuality and Relationship Guidelines, V1.0, January 2016 8

1.6 Reproductive and sexual health
People require access to information and education from health professionals on a range of health issues, for example sexually transmissible infections, cervical and breast cancer screening, prostate cancer screening and testicular examination. Parents and carers of children with disability can attend free forums provided by Family Planning NSW8 on sexuality and disability, puberty and sexual health.
For information about maintaining good health see the Health Promotion Guidelines in the Health and Wellbeing Policy & Practice Manual, Volume 2.
People who are considering parenthood may seek or require advice about health issues relating to conception, pregnancy and birth. Depending on the circumstances, genetic counselling may be an important part of the decision to become parents, and should be available to those who want or need it.
Family Planning NSW has resources that people can use to inform themselves or others9.
1.6.1 Contraception and safe sex
It is preferable for both sexual partners to take responsibility for safe sex including prevention of sexually transmissible infections and unintended pregnancies. Where contraception is being used, the person’s choice, and its relevance to the person’s lifestyle are key deciding factors in its prescription and administration.
If contraception is being used for menstrual management, training strategies to assist the person to manage menstruation independently should be thoroughly explored before a decision is made to recommend long term contraceptive medication. If a person is prescribed a long acting injectable hormonal substance to avoid unintended pregnancy, for menstrual regulation, or as a treatment aimed at eliminating menstruation, the person or person responsible must consent to its use.
Most forms of contraception require a visit to a doctor or family planning clinic, and support is provided as needed for the person to communicate their wishes to the health practitioner. The health practitioner should also advise the person of side-effects of any medication, and if there is a need to monitor and review its use.
Even when using contraceptives, condoms need to be used as protection against most sexually transmissible infections. Condom use can be encouraged in service environments by making them freely available to people, and locating them where they can be accessed in private. Family Planning NSW provides resources that
8 http://www.fpnsw.org.au/parentforums 9 http://www.fpnsw.org.au/index_factsheets.html
Sexuality and Relationship Guidelines, V1.0, January 2016 9

show how condoms are applied and when they are used, and supporters can obtain easy English resources about safe sex and condom use free of charge10.
1.7 Advocacy While it is important to be educated about sexuality, it is equally important for people to develop self-advocacy skills. This includes understanding that they have rights and know how to exercise them.
People can be supported to develop the confidence to speak on their own behalf when expressing their sexuality. This might include saying yes or no to sex or a relationship, use of contraception, continuing a sexual relationship or thinking about becoming a parent.
Due to the personal nature of sexuality and its expression, when a person needs advocacy support it is best provided by someone who is known by the person, and can be trusted not to impose their own values and judgements on the person.
It is possible that the person may seek support from someone who is uncomfortable talking about sex, or who has beliefs that conflict with the person’s expression of their sexuality. If supporters find themselves in this situation, they have a responsibility to avoid infringing the person’s right to free sexual expression. In a service environment, a supporter should advise a line manager if they feel uncomfortable so that another trusted supporter can continue the conversation with the person.
1.8 Supported decision making and consent11
Supported decision making is based on principles in the United Nations Convention12 and the NSW Disability Inclusion Act 2014 that confirm the rights of people with disability to have choices and make decisions about things that affect them and to receive support to do so.
Supported decision making recognises the right of people to take reasonable risks in their lives the same as any other person in the community. It includes removing the barriers that can prevent people with disability from making decisions.
Informed consent means that the person understands what they are consenting to, and is able to make informed decisions. Supporters have a role to create opportunities that increase a person’s decision making skills and confidence. This can be done by improving communication systems, supporting the person to
10 http://www.fpnsw.org.au/266843_6.html
11 http://www.fpnsw.org.au/supportingdecisionmaking 12 UN Convention on the Rights of Persons with Disabilities
Sexuality and Relationship Guidelines, V1.0, January 2016 10

understand the decision making process, and providing opportunities to practice making decisions.
People have the legal right to consent to having sexual relations in NSW if they:
• are 16 years of age (for males and females, and whether heterosexual or homosexual), and
• have the capacity to give consent (i.e. do not have a cognitive impairment that makes a person incapable of giving consent), and
• have given free and informed consent (e.g. not coerced, or tricked into giving consent).
Anyone providing support to a person with cognitive impairment has a duty of care (Section 1.9) to ensure that the person with cognitive impairment:
• has the capacity to give consent to sexual activity
• has freely consented to sexual activity with another person
• understands what that consent means for them and the other person.
There are many other situations where the person’s consent is required, for example:
• using a contraceptive and the method
• having a pap test
• choosing whether to have a date with a person.
The Capacity Toolkit13 has a section on capacity assessment principles which may be helpful at this stage. If supporters are in any doubt about the person’s capacity to make decisions about, or consent to, having sexual relations or any other aspect of sexuality, they have a responsibility to refer the person to an appropriate specialist, for example a behavior specialist or psychologist.
Note that it is a crime under Section 66F of the Crimes Act 1900 for a person responsible for the care of a person with cognitive impairment to have sexual relations with the person who has cognitive impairment. A person responsible for the care of a person with cognitive impairment includes a:
• disability support worker,
• volunteer providing care,
• health professional providing care,
• person providing care in the form of education,
• person providing home care, or
13 Capacity Toolkit http://www.justice.nsw.gov.au/diversityservices/Pages/divserv/ds_capacity_tool/ds_capacity_tool.aspx
Sexuality and Relationship Guidelines, V1.0, January 2016 11

• person supervising a person with cognitive impairment.
It is also a crime for any person (even if not providing care) to have sexual relations with a person with cognitive impairment where the person intends to take advantage of or sexually exploit the person with cognitive impairment.
Refer to Section 1.14 for responding to sexual behaviours of concern and mandatory reporting requirements.
It is important for people to understand that consent to sexual relations (whether short or long term) only applies at a point in time and either person in the relationship can change their mind and withdraw their consent to sexual relations.
Supporters should explore the person’s understanding of what it means to form or have a sexual relationship. Specifically that the person:
• is entering the relationship freely, that is, without being coerced or threatened
• understands what they are physically consenting to, for example, petting, kissing or penetration
• knows it is possible to change their minds at any time, and
• has the supports required to make an informed decision.
The person must understand that there are risks and responsibilities associated with being sexually active. For example, contracting a sexually transmissible infection is one risk that can affect the person’s reproductive health in the future, and that of any sexual partners. The “Sex, Safe and Fun” book from Family Planning NSW14 will help supporters to have these conversations.
A person who cannot consent to a test for HIV or any sexually transmissible disease, and is aged 16 years or over, cannot be tested without the consent of a person responsible or the NCAT Guardianship Division.
While a person may not fully understand all the issues, it does not mean that they cannot consent and must be fully supported to make decisions about exploring their sexuality (see Section 1.6 Reproductive and sexual health)15.
For more information on supported decision making and consent see ADHC Decision Making and Consent Policy and Guidelines in the Lifestyle Policy and Practice Manual.
14 Safe Sex and Fun http://www.fpnsw.org.au/266843_6.html 15 Supporting decision making http://www.fpnsw.org.au/supportingdecisionmaking
Sexuality and Relationship Guidelines, V1.0, January 2016 12

1.9 Duty of care and dignity of risk Duty of care is the obligation to take reasonable care to avoid injury to a person when it could be reasonably foreseen that the person could be harmed by another person’s actions, or failure to act. Refer to the ADHC Risk and Safety Policy, Procedures and Guidelines in the Safeguarding Manual.
In a service environment, supporters have a duty of care to provide access to education and information, support the person’s access to health and other relevant services, and create opportunities for the person to develop relationships. Absence of this support can lead to negative consequences for the person, such as being vulnerable to abuse and exploitation and making uninformed choices and decisions.
While these Guidelines promote the enhancement of people’s opportunities to explore and express their sexuality, duty of care is required to avoid putting the person at risk of harm.
When supporters of a person who is exploring her or his sexuality identify a potential risk to that person or others, they should not only consider how to protect the person from harm, but also the person’s right to make choices and take reasonable risks in life.
Duty of care is balanced with dignity of risk. This means that people are to be supported to take reasonable risks that are based on an informed supported decision making process that is fully documented. Refer to the Risk and Safety Procedures in the Safeguarding Manual, Section 2.1.4 for information about balancing Dignity of Risk with Duty of Care and documenting the outcomes.
1.10 Having the conversation Don’t wait until there is a problem before actively supporting a person to develop an understanding of sexuality and relationships.
Before getting started ask yourself the questions from the ‘Decision making checklist’ in the Other Resources section of these Guidelines.
1.10.1 Getting started
First, learn about the person’s communication method and preference for receiving information. In accommodation support services, if the person’s communication style has not been identified during Lifestyle Planning, it should be done before starting the conversation.
If the subject of sexuality and relationships does not come up naturally in conversation with the person, supporters should ensure that the person is comfortable to have it raised as a topic for discussion.
If supporters cannot talk about sexuality with the person because it is in conflict with their own values and beliefs, or their personal experiences, they should advise a line manager that they are unable to have the conversation. Supporters must be able to exercise their rights in this regard without fear of retribution.
Sexuality and Relationship Guidelines, V1.0, January 2016 13

The following points may help to get the conversation started:
• Ask the person if they would like someone else to be present, and share the responsibility for having the conversation.
• Take the opportunity to talk about sexuality when it comes up in everyday conversation, for example, if relationships are a topic in the person’s favourite television show.
• Before starting the conversation, be sure that the person is interested to talk and wants to learn more about their sexuality.
• If the first conversation doesn’t get very far, and the person shows an interest in talking about their sexuality, take opportunities to continue at another time.
• Listen to the person and learn where there are gaps in the person’s knowledge of sexuality and use that information to steer the conversation.
• Learn how the person wants to express themselves sexually and be open and supportive of the options for the person to be opposite sex, same sex or both sex attracted.
Use other sources of information that are relevant to the person’s interest and that are easily understood by the person (see Other resources).
Some people may not received even basic information about sexuality when they were growing up, and as a result, may not show any interest in having a conversation about it. In this case supporters will need to be proactive in raising the subject and if needed, can access basic training to get started16.
The person’s knowledge of sexuality will determine where the conversation to increase their understanding starts. It could begin with discussions about the difference between the sexual nature of touching and how it makes the person feel, as opposed to non-sexual touching associated with washing or receiving medical treatment.
Issues such as sexual and reproductive health rights can be discussed when the person expresses an interest in knowing more about these matters, or when the conversation has progressed naturally to this stage.
In any conversation around sexuality, the person may benefit from having access to visual resources to assist their understanding. For example, photos or a video of the birth process if the conversation is about pregnancy, or a model of the reproductive system if the conversation is about menstruation. This conversation must include contraception and the responsibilities of parenthood, and any resources that help to clarify the concepts should be used (see Other resources).
16 Family Planning NSW training http://www.fpnsw.org.au/education
Sexuality and Relationship Guidelines, V1.0, January 2016 14

If the conversation is a response to behaviour, learn the reason for the behaviour first. The danger of responding to the behaviour is that this becomes the focus rather than the person’s needs. In this case the rights of the person can be overlooked.
For example, a young woman is asking men she does not know to be her boyfriend. Supporters respond by teaching her not to approach strangers because of ‘stranger danger’. The supporters, although well meaning, are not supporting her to form relationships. While it is important to alert the woman to the potential danger from strangers, supporters should also be supporting her to learn how to meet people, and build her skills in making friends and dating, and educating her about positive, healthy relationships.
1.10.2 Challenging topics
Conversations about sexuality may raise some unexpected issues that are difficult to discuss. It is important to approach the topic of sexuality carefully as many people with intellectual disability have experienced some form of sexual abuse. There is a risk of re-traumatising people if they are not ready and feeling safe to have this discussion.
The discussion can be difficult for other reasons because some people with disability may never have been allowed to discuss sexuality, or were told that sexuality wasn’t important for them.
In a service environment, if issues arise during conversations about previous sexual abuse or trauma, supporters may be legally required to make a report. The supporter must advise the person that it might not be legally possible to maintain the confidentiality of their conversation and that a line manager may need to be informed.
If the sexual abuse or trauma involves a child or young person, under Part 3A of the Ombudsman’s Act 1974, the matter must be reported to a responsible person. It will also come under the mandatory reporting requirements17 (Section 1.14).
The supporter must decide whether to end the conversation and seek advice from a line manager. This must be done in a respectful way that acknowledges what has been said, explains why the conversation should not continue and what will happen next. The line manager should also determine what support the person wants or needs, for example, referral to a specialist in abuse or trauma.
The matter may be a reportable incident to the NSW Ombudsman under Part 3C of the Ombudsman Act 1974. If a person indicates to an employee of a FACS operated or funded group accommodation support service that they are aware of, or have been involved in a reportable incident (see 1.15 for more information about reportable incidents and the Ombudsman’s role), the employee reports the
17 http://www.keepthemsafe.nsw.gov.au/reporting_concerns/mandatory_reporter_guide
Sexuality and Relationship Guidelines, V1.0, January 2016 15

matter to a line manager. The line manager will follow the protocol for reporting the incident to the Ombudsman18.
In a service environment, if the person indicates an intention to engage in behaviours of concern, the supporter advises the person of the consequences of the behavior and makes a report to the line manager. Refer to 1.14 for responding to sexual behaviours of concern.
For information about responding to sexual exploitation and abuse refer to the ADHC Abuse and Neglect Policy, Procedures and Guidelines in the Safeguarding Manual.
1.11 Culture Sexual expression may be viewed differently within cultural groups. Before starting conversations about sexuality, supporters and others should first learn what topics and behaviours are sensitive for discussion in other cultures.
1.11.1 Aboriginal and Torres Strait Islander people
Sensitivity to cultural norms is important in discussions about sexuality and relationships with Aboriginal and Torres Strait Islander people. While the person’s right to make decisions about their own life must be upheld, the following culturally sensitive matters are fundamental for consideration when supporting Aboriginal or Torres Strait Islander people to explore and express their sexuality:
• recognise that acknowledging the person’s culture is a way of acknowledging and valuing the person’s identity
• acknowledge the history of difficult relationships between governments and Aboriginal people
• recognise family, kinship and friend relationships and the person’s connection to community and the land
• determine who in the family or community should be approached for discussions about sexuality and relationships
• ask the person or family if they wish to choose who would provide sexual health services, Aboriginal or mainstream providers.
Sexual issues are personal and sensitive and discussion with some people is taboo. The person and family or carers should be consulted to learn what sexual matters are sensitive. Identify the family member or carer to speak to about matters of sexuality and relationships, and record the information in the person’s records.
18 http://www.ombo.nsw.gov.au/__data/assets/pdf_file/0014/20534/Guide-for-services-Reportable-incidents-in-disability-supported-group-accommodation.pdf
Sexuality and Relationship Guidelines, V1.0, January 2016 16

Understanding cultural sensitivity includes understanding the person’s individual history, experiences and choices. For example, a person who identifies as one of the Stolen Generation has experienced trauma, which may include sexual abuse, as a child. If this is the case, supporters should contact the Aboriginal Health Service19 for advice, and possibly a referral to a counsellor if the person wants this. A high degree of sensitivity is required to support the person and family with a history of sexual abuse.
Sexual health can be a private matter and is often discussed within gender groups. Shame can be a barrier to people accessing health services and being tested for sexually transmissible infections. People face other barriers such as location of services and issues of confidentiality, especially in small remote communities, and willingness to access health services to discuss sexual health matters20.
1.11.2 Cultural and Linguistic Diversity
People may still retain their values, beliefs and experiences, even when they no longer live in the culture where they learned them. The person and family’s behaviour, attitudes, preferences and decisions about sexuality and relationships, are influenced by culture and religious practices.
The person and family or carer’s21 cultural and religious beliefs about sexuality and relationships should be understood before starting a conversation with the person about exploring and expressing their sexuality.
Demonstrate respect and sensitivity to their culture by considering:
• the person and the family or carer’s perspective on sexuality and relationships
• the person and the family or carer’s views about Western sexuality and relationship practices
• the role of spiritual and religious beliefs and practices in sexual development
• how the person and the family or carer communicate, for instance, through an interpreter
• the person’s own role in problem solving and decision making.
It is important to acknowledge that some people may choose to adopt practices, values and attitudes that are different from those of their parents or family. Supporters need to be aware of this and provide support according to the person’s wishes.
19 https://www.iwsml.org.au/services-and-support/services-aboriginal
20 http://www.curriculumsupport.education.nsw.gov.au/sexual_health/inclusive/atsi.htm 21 Carer is any paid or unpaid person supporting a person with disability
Sexuality and Relationship Guidelines, V1.0, January 2016 17

1.12 Opportunity22
People living in accommodation support environments sometimes need support to form friendships both within and outside their home. Forming friendships requires positive action, both to find friends, and to retain them. People accessing other support environments such as, Transition to Work and Day Programs, will have more opportunities to form friendships and learn social skills outside the home, but may still require support.
Finding friends can be harder for people who need support to undertake activities of daily living or who have mobility and communication difficulties. They require thoughtful and sensitive support to overcome barriers to developing social networks.
A sexual relationship is one of a number of relationships that a person can have. All types of relationships help in the development of social skills, and those of a non-sexual nature help the person to engage with others and participate in recreational activities, while building personal skills.
Skill building could include:
• increasing lifestyle opportunities to form relationships that are equal and balanced for both people
• building capacity to recognise and interpret non-verbal cues and unwanted behaviour, and to give or withhold consent based on an understanding of the behaviour
• providing opportunities to make choices and communicating these choices in a variety of life areas, including who they want to spend time with
• learning conversation and communication styles, for example, taking turns, being part of a group conversation, maintaining comfortable physical distance between people and acceptable touching of other people.
Society and the media can perpetuate a view of the way people should look, which people with disability may not always feel they can match23. These feelings can contribute to people lacking the confidence to look outside their home for friendship, resulting in social contacts that are limited to their family, housemates or paid carers. Supporters can boost the person’s confidence by helping them with grooming, and dressing appropriately for their age and particular social events.
A lack of information and understanding about forming friendships and sexual relationships can inhibit people in developing social and sexual networks. This may be compounded by supporters not understanding the person’s relationship or sexuality interest and needs.
22 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Intellectual_disability_and_sexuality 23 http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Intellectual_disability_and_sexuality
Sexuality and Relationship Guidelines, V1.0, January 2016 18

People living in accommodation support services require consideration of their privacy to make phone calls or have space for sexual activity, to receive information, and be supported to access items such as condoms and lubrication.
In order to meet the sexual needs of people, accommodation support services should promote opportunities for sexual activity to happen. A person may wish to spend time in the privacy of their room with a sexual partner, or invite someone home who may become a sexual partner.
If a person wants a sexual partner to stay overnight the decision is made with the agreement of the other members of the household. While the individual person’s needs are to be considered, they must be balanced with the rights and safety of others in the home. In a shared living situation there are privacy and safety issues that have to be considered by and for all the residents.
House rules may be required that everyone agrees on, to ensure the person has privacy, and that other residents are able to go about their preferred activities without feeling uncomfortable or unsafe. If everyone agrees to the house rules there should be no surprises, and opportunities for spontaneous or planned sexual activity can occur around other household activities.
1.12.1 Sex workers
A person’s choice and right to use a sex worker is to be respected and treated with confidentiality. Any costs incurred when using services provided by the sex industry are met by the person using the services.
Engaging a sex worker is one of a range of available options to satisfy the sexual needs of a person, but should not be the first strategy for meeting a person’s need for intimacy. Nor is it an appropriate strategy to satisfy a person’s identified need for developing friendships.
Decriminalisation of the sex industry in New South Wales has contributed to improved access to sex workers for people with disability, while supporting the rights of sex workers. As a result there are ways for people to access the sex industry without feeling discrimination or shame.
In a service environment, supporters have an active, legal and legitimate role to support people to access a sex worker. This may include contacting an organisation for information about sex workers, or driving the person to see the sex worker. Touching Base Inc24 is one organisation that people with disability can contact for access to information about sex services and providers (see Other resources). Procedures for accessing sex services through Touching Base Inc can be purchased through the website, or viewed at the Family Planning NSW library.
24 http://www.touchingbase.org/clients/referral-list
Sexuality and Relationship Guidelines, V1.0, January 2016 19

1.12.2 Sex aids
In a service environment people cannot expect supporters to provide physical assistance with masturbation and sexual positioning. Visual aids and resources25
are available from recognised organisations, and supporters may assist people to contact suppliers for advice if they want more information (See Other resources).
Occupational therapists are also a possible source of advice and information about positioning to use sex aids and equipment for people with limited mobility. Alternatively supporters can contact the Independent Living Centre NSW26 for access to clinicians who work in this area, or to make enquiries about adaptive equipment.
If the person agrees, and privacy can be assured, the person’s support needs for sexual activities may be documented in their My Health and Wellbeing Plan or Lifestyle Plan.
1.13 Lifestyle Planning A person accessing accommodation support services is encouraged to participate in Lifestyle Planning (refer to the Lifestyle Policy and Practice Manual). In other service environments some sort of person centred planning usually occurs. This is when conversations about the person’s wishes and desires occur, and supporters can use this opportunity to start the conversation about sexuality and relationships.
Successful Lifestyle Planning depends in large part on growing the person’s networks, and is the perfect time for supporting the person to develop relationships outside the paid care environment. Lifestyle Planning conversations are a chance to discuss the different types of relationships that the person can have with others, and can naturally lead into the topics of sexuality and intimate relationships.
At all times the person’s privacy must be considered and the timing of these conversations is important. For example, a young adult may not want to talk about sensuality or sexual interests at a meeting that includes a parent.
Support workers and the person decide together about the information that is documented in the Lifestyle Plan, remembering that the person may share it with others. Equally, anyone supporting a person to explore their sexuality must consider the sensitive nature of some of the personal information to which they have access.
The Person Centred Thinking tools, the Learning Log and Working/Not Working tool (all in the Lifestyle Policy and Practice Manual), may be useful for recording the person’s response to conversations about sexuality or experiences when meeting potential sexual partners.
25 http://www.dhrn.ca/files/sexualhealthmanual_lowres_2010_0208.pdf 26 https://www.ilcnsw.asn.au/home/what_we_do/what_we_do
Sexuality and Relationship Guidelines, V1.0, January 2016 20

The Learning Log is a record of what was tried, what happened and who was involved. It provides a reference for future conversations or when supporting the person to meet sexual partners. The Learning Log should only be used if the person agrees to the information being recorded in writing, and if it can be kept somewhere private.
The Learning Log and the person’s recall are helpful when using the Working/Not Working tool to explore how planned actions from Lifestyle Planning have contributed to achieving the person’s goals. Actions that are working can be built on and those that are not working are reviewed and refined.
The number of people who “need to know” about the person’s sexuality and relationships, are likely to be very few. Needing to know can be thought of from the point of view of people in the general community, including a support person, who would or would not want others to know the details of their sexual interests.
Sexuality and Relationship Guidelines, V1.0, January 2016 21

1.14 Sexual behaviours of concern
“Sexual behaviours of concern are those that are deemed inappropriate as a result of the nature of the behaviour or the setting in which they occur. These behaviours may be self directed or directed at others, including targeting or fixating on others. Where others are involved the contact may be unwanted or non-consensual.
These behaviours occur on a continuum from minor behaviours up to and including sexual assault. In addition, the behaviour may interfere with normal activity or be harmful or distressing to self or others.” (Lockart et al, 2009)27
Not all sexual behaviour is a concern and not all sexual behaviours will require referral for specialist assessment and intervention. The challenge is to decide if there is a reason to be concerned. This requires a good understanding of the behaviour and the context in which it occurs, including the presence or absence of consent, equality and coercion.
Tools such as Traffic Lights28 (Family Planning Queensland, 2006 - see below) can assist supporters in this task. While all behaviours will require some form of attention and response, the level and kind of response will vary.
Children and young people
When sexual abuse is suspected supporters should consult the Online Mandatory Reporter’s Guide then contact the Child Protection Helpline on 13 3627 if significant risk of harm (see Section 1.16) is indicated.
The ADHC Child Protection Guidelines are clear about the responsibility of staff in reporting risk to children and young people:
‘The Children and Young Persons (Care and Protection) Act 1998 defines certain classes of people who work with children and their managers as mandatory reporters, who have a statutory obligation to report children who are at risk of significant harm (ROSH) to Community Services’.
Under Schedule 3 of the Children and Young Persons (Care and Protection) Regulation 2012, all designated agencies accredited to arrange for the provision of statutory out-of-home care in NSW, are required to notify the Children’s Guardian, in writing, of any allegation of sexual misconduct or serious physical assault towards a child or young person in out-of-home care, committed by a child-related worker.
In certain circumstances, when a child or young person is displaying problematic sexual behaviours towards another person, it may be a criminal act. After ensuring the safety of the ‘victim’, supporters should seek guidance from the NSW Police.
27 Lockart, K., Guerin, S., Shanahan, S., & Coyle, K. (2009). Defining “Sexualized Challenging Behaviour” in Adults with Intellectual Disabilities. Journal of Policy and Practice in Intellectual Disabilities, 6 (4), 293-301
28 Family Planning Queensland, 2006 Sexualised Behaviour in Children and Adolescents: The Traffic Lights Model www.fpq.com.au
Sexuality and Relationship Guidelines, V1.0, January 2016 22

1.14.1 Questions & Appropriate Responses & Support for People Displaying Sexual Behaviour
GREEN LIGHT =
Sexual behaviours that are characterised as spontaneous, curious, light-hearted, easily distracted, experimental and are displayed amongst equals in age, size and ability levels. These behaviours are considered to be a healthy part of development
Example Behaviours / Responses for Green Light for children:
1. Does the child express increased curiosity about gender differences and questions about babies?
Yes No
The child should be provided with positive feedback and information to support ongoing development of healthy sexuality
The child should be given opportunities for positive feedback and information to support ongoing development of healthy sexuality
2. Does the child demonstrate an increased need for privacy?
Yes No
The child should be provided with positive feedback and information to support ongoing development of healthy sexuality
The child should be provided with positive feedback and information to support ongoing development of healthy sexuality
Example Behaviours / Responses for Green Light for young people / adults:
3. Does the young person or adult show an interest in non violent / non coercive erotica?
Yes No
The young person or adult should be provided with positive feedback and information to support ongoing development of healthy sexuality
The young person or adult should be given opportunities for positive feedback and information to support ongoing development of healthy sexuality
Sexuality and Relationship Guidelines, V1.0, January 2016 23

4. Does the young person or adult engage in sexual activity including hugging, kissing, holding hands, foreplay and mutual masturbation with a person / people of similar ages and abilities?
Yes No
The young person or adult should be provided with positive feedback and information to support ongoing development of healthy sexuality
The young person or adult should be given opportunities for positive feedback and information to support ongoing development of healthy sexuality
ORANGE LIGHT =
Sexual behaviours which are persistent or frequent, or represent inequality in age and/or developmental abilities
Example Behaviours / Responses for Orange Light for children:
1. Does the child ask persistent or frequent questions about sexual activity despite them being answered already?
Yes No
Report to your line Manager
Consider referral for behaviour support to assist in developing monitoring procedures
A response is not indicated at this time
2. Does the child demonstrate pseudo maturity, including inappropriate knowledge and discussion of sexuality?
Yes No
Report to your line Manager
Consider referral for behaviour support to assist in developing monitoring procedures
A response is not indicated at this time
Sexuality and Relationship Guidelines, V1.0, January 2016 24

Report to your line Manager
Consider referral for behaviour support to assist in developing monitoring procedures
A response is not indicated at this time
Example Behaviours / Responses for Orange Light for young people / adults:
3. Is the young person or adult preoccupied with pornography?
Yes No
4. Does the young person or adult give false gender, age, sexuality details online in an adult chat room?
Yes No
Report to your line Manager
Consider referral for behaviour support to assist in developing monitoring procedures
A response is not indicated at this time
Sexuality and Relationship Guidelines, V1.0, January 2016 25

RED LIGHT =
Sexual behaviours which are excessive, secretive, compulsive, coercive or degrading
Example Behaviours / Responses for Red Light for children:
1. Does the child engage in persistent masturbation, particularly in front of others?
Yes No
2. Does this child coerce others, including younger or less able children into sexual activity?
Yes No
Report to your line Manager via an incident report
Consider referral for behaviour support
A response is not indicated at this time
Report to your line Manager via an A response is not indicated at this incident report time
Complete the Mandatory Reporting Guide (MRG)
Consider referral for behaviour support
Sexuality and Relationship Guidelines, V1.0, January 2016 26

Example Behaviours / Responses for Red Light for young people / adults:
Does the young person or adult attempt to force others to show their genitals?
Yes No
3. Does the young person or adult have sexual contact with animals?
Yes No
Ensure immediate physical safety of A response is not indicated at this others time
Report to your line Manager via an incident report
Where a minor (under 16 years) is involved complete the MRG
Report to Police
Consider referral for behaviour support
Ensure physical safety of animals A response is not indicated at this immediately time
Report to your line Manager via an incident report
Report to Police
Consider referral for behaviour support
Consider referral for forensic risk assessment
Sexuality and Relationship Guidelines, V1.0, January 2016 27

1.14.2 Response to behaviours of concern
In the first instance, it is essential that safety measures are put in place. These interim strategies should aim to reduce the risk of harm occurring. For example, they may be as simple as increasing levels of supervision and support until more comprehensive assessment and intervention can be undertaken. A behaviour clinician should be consulted to provide advice about a suitable response.
Any known or suspected sexual offence by or against the person must be reported. This includes, accessing illegal content e.g. child pornography, sexual intercourse with another person without their consent, touching or threatening to touch another person without their consent, sexual exploitation of a person with cognitive impairment where the perpetrator is responsible for that person, and/or has the intention of taking advantage of that person’s cognitive impairment.
If a criminal offence is suspected, it is reported to the NSW Police who will determine if a crime has been committed. Refer to the Criminal Justice Resource Manual29 (ADHC intranet) for information about dealing with the Police. Refer to the ADHC Abuse and Neglect Policy, Procedures and Guidelines30 for information about preventing, identifying, responding to and reporting sexual abuse.
Certain incidents may also be reportable to the NSW Ombudsman (see Section 1.15)
If behaviours of concern are occurring between adults with disability, they both require support. Support includes an assessment of the circumstances, and the capacity of both individuals to participate freely. Where the circumstances or the person’s capacity are in any doubt, an opinion from a behavior specialist or other relevant specialist is sought without delay.
Referrals for additional support should be made when the behaviour places the person or others at risk of harm, or when it limits the person’s access to the community. Referrals can be made to a sexual health service, psychologist, behaviour support practitioner or counsellor. This professional will assess the situation to help better understand the person’s behaviour which will inform the choice of intervention and support to be provided.
1.14.3 Protective measures
The background of a person who has a history of sexual behaviours of concern must be recorded and known to relevant supporters. This will reduce the danger of placing the person and others at risk of harm, or of contact with the criminal justice
29 http://dadhc-intranet.nsw.gov.au/documents/client_services/office_of_senior_practitioner/criminal_justice_services_policy_and_resource _manual/CJRM_Final_June_09.pdf 30http://www.adhc.nsw.gov.au/__data/assets/file/0020/228062/Abuse_and_Neglect_Policy_and_procedures.pdf
Sexuality and Relationship Guidelines, V1.0, January 2016 28

system. These historical records are held under the legal privacy and confidentiality requirements of any support agency.
When documenting behaviours of concern, avoid applying labels and personal opinions to people that may follow them around, and cause others to respond to them inappropriately.
The ADHC Justice Services Policy and Criminal Justice Resource Manual provide guidance for support workers about how to support someone who may come into contact with the criminal justice system, for example if the person is accused of sexual assault. Support workers and managers should be aware of the contents of these documents and receive training in their roles to implement them.
1.15 NSW Ombudsman reportable incidents
Under the Disability Inclusion Act 2014 which commenced on 3 December 2014, the Ombudsman is to be notified of any reportable incidents that involve people with disability living in FACS operated or funded supported group accommodation (including respite care)31.
Part 3C of the Ombudsman Act 1974 establishes the Disability Reportable Incidents Scheme (the Scheme) which places reporting obligations on disability services.
Reportable incidents include:
• any sexual offence, sexual misconduct, assault, fraud, ill-treatment or neglect in connection with an employee of FACS or a funded provider, and a person with disability living in supported group accommodation
• an assault of a person with disability living in supported group accommodation by another person with disability living in the same accommodation that is a sexual offence, causes serious injury, involves the use of a weapon, or is part of a pattern of abuse
• an incident occurring in supported group accommodation and involving a contravention of an apprehended violence order made for the protection of a person with disability
• an unexplained serious injury to a person with disability living in supported group accommodation.
The purpose of the Scheme is to improve the systems of accommodation support and respite services in managing and reporting incidents, and thereby improve the safety and welfare of people with disability.
Disability reportable incidents: http://www.ombo.nsw.gov.au/what-we-do/our-work/community-and-disability-services/part-3c-reportable-incidents
Sexuality and Relationship Guidelines, V1.0, January 2016
31
29

More details about the reporting requirements for staff can be found on ADHC’s intranet (http://intranet.facs.nsw.gov.au/reforms/disability-inclusion-act-2014-dia/reportable-incidents-part-3c). The Ombudsman’s website32 also has more details about the Scheme.
32 http://www.ombo.nsw.gov.au/
Sexuality and Relationship Guidelines, V1.0, January 2016 30

2 Definitions Behaviours of concern
Includes behaviours that are considered to be appropriate in some contexts but not others, and behaviours that would not be considered appropriate in any circumstances.
Factors affecting the considerations include the nature of the behaviour, the setting in which it occurs, the impact or potential impact on the person displaying the behaviour, and the recipient/s of the behaviour.
Capacity The ability to make decisions about things that affect the person’s daily life.
Child Refers to a person under the age of 16 years as defined in the Children and Young Person’s (Care and Protection) Act (1998)
Consent Consent refers to the permission given by a person. For consent to be valid it must be voluntary, informed, specific and current. A person must be free to exercise genuine choice about whether to give or withhold consent. Consent must be given without coercion or threat and with sufficient time to understand the request and, if appropriate, take advice.
Consent must be established each time it is required. A person who has given consent to a specific matter may change her or his mind and subsequently revoke consent.
In certain circumstances, consent may also be provided by a legally appointed guardian on behalf of the person. Consent for medical or dental treatment may be given by a person responsible.
For more information on consent see ADHC Decision Making and Consent Policy and Guidelines in the Lifestyle Policy and Practice Manual.
Eroticism Anything that is designed to arouse sexual desire or excitement.
Gender identity
Being female, male or transgender.
Intimacy Intimacy is about being close to another person. It involves being able to share the whole range of feelings and experiences we have as human beings - pain and sadness, as well as happiness and love.
http://www.relationships.org.au/relationship-advice/faqs/what-is-intimacy-and-why-is-it-so-important
Legislated Consistent with the objects and principles of the Disability Inclusion
Sexuality and Relationship Guidelines, V1.0, January 2016 31

Rights Act 2014.
Mandatory reporter
Staff who work with children and young people are legally required to report when they reasonably suspect risk of significant harm (ROSH) to children or young people (see ‘Risk of Significant Harm’, below)..
Managers, including both paid employees and volunteers, who supervise direct services are also mandated to report and can report on behalf of the staff they supervise.
Non coercive erotica
Anything that is used to arouse sexual desire or excitement between people with their mutual consent.
Pseudo-maturity
In the context of these Guidelines pseudo-maturity refers to children who speak about sex or behave in sexual ways that would usually be seen in an adult.
Relationship A relationship is when people know each other. There are different types of relationships including work mates, family, friends, support workers and casual acquaintances.
http://www.fpnsw.org.au/factsheet_09_relationships.pdf
Reportable incident
An incident which occurs in FACS operated or funded non-government supported group accommodation which must be reported to the NSW Ombudsman under Part 3C of the Ombudsman Act 1974 (see section 1.15)
Risk of significant harm (ROSH)
In the context of the Sexuality and Relationship Guidelines a child or young person is at risk of significant harm if current concerns exist for the safety, welfare and wellbeing of the child or young person because of the presence, to a significant extent, (of one or more) of the following circumstances:
the child or young person has been, or is at risk of being, physically or sexually abused or ill-treated.
Note: ‘Physical or sexual abuse may include an assault and can exist despite the fact that consent has been given’.
[Children and Young Persons (Care and Protection) Act, 1998]
Sexual identity
How a person identifies and feels about their sexual orientation.
Sexual orientation
Attraction to the opposite sex, the same sex or both.
Sexuality Sexuality is a central aspect of being human. Throughout life it encompasses sex, gender identities and roles, sexual orientation,
Sexuality and Relationship Guidelines, V1.0, January 2016 32

eroticism, pleasure, intimacy and reproduction. Sexuality is experienced and expressed in thoughts, fantasies, desires, beliefs, attitudes, values, behaviours, practices, roles and relationships. While sexuality can include all of these dimensions, not all of them are always experienced or expressed.
Sexuality is influenced by the interaction of biological, psychological, social, economic, political, cultural, legal, historical, religious and spiritual factors. http://www.who.int/reproductivehealth/topics/sexual_health/sh_defin itions/en/
Supporter Any individual, paid or unpaid, who supports a person to explore and express their sexuality.
Transgender Some people present themselves differently to their biological sex. Those who look like boys when they were born but grow up feeling like they are a girl, present themselves as a girl, and vice versa. These people call themselves transgender.
Young person
Refers to a person who is aged 16 or 17 years as defined in the Children and Young Person’s (Care and Protection) Act (1998).
3 Policy and Practice Unit contact details You can get advice and support about this Policy from the Policy and Practice Unit, Contemporary Residential Options Directorate.
Policy and Practice, Service Improvement
Contemporary Residential Options Directorate
ADHC
If you are reviewing a printed version of this document, please refer to the Intranet to confirm that you are reviewing the most recent version. Following any subsequent reviews and approval this document will be uploaded to the internet and/or intranet and all previous versions removed.
Sexuality and Relationship Guidelines, V1.0, January 2016 33


Part C2 – My support plans: Support plan register My name:
Name of support plan Date developed Quarterly review dates Location of support plan
Q1 Q2 Q3 Q4
Hospital Support Plan – Part 1
Mandatory
Nutrition and Swallowing Risk Checklist
Mandatory
My Oral Health Plan
Mandatory
My Health and Wellbeing Plan, Health Planning Procedures, Tools and Templates, V1.3, June 2016

Fact sheet January 2016
Information for disability support workers: about the GP
At the annual health assessment the GP will:
Explain Ask Collect Assess
the purpose and benefits of the assessment for the person’s consent to do the assessment personal and health information the person’s overall health and wellbeing - including physical, psychological, social - need for preventive health care - need for health education
Review Order
results of tests and screening procedures tests and procedures if needed
Discuss Recommend
- for example, blood tests or screening for cancer findings from assessment treatments and services
Provide - for example, allied health or medical specialist advice and information
Write Share
- for example, health preventive or promotion activity a health report a copy of the health report with the person and carer
During Chronic Disease management (CDM) planning the GP will:
Explain steps for developing a CDM plan to the person and carer Ask the person for consent to develop a CDM plan Develop a GP Management Plan Coordinate a Team Care Arrangement OR Contribute to a multidisciplinary care plan Describe disease and care needs Discuss health goals and get agreement from the person Design health actions with the person and carer Recommend treatment and services Arrange services Provide advice and information to the person and carer Book a review date
www.adhc.nsw.gov.au

Team meeting agenda
Unit name Date of meeting
Chair Minute taker
Staff present
Specific agenda item for discussion at this meeting Staff member
Item Time guide
Good news story from the unit 5 mins
Review of actions from last meeting 5 mins
Health Planning, Tools and templates, V1.3, June 2016 1

Team meeting agenda
Item Time guide
Health and wellbeing issues
Health Learning Log entries since last team meeting
- Discuss observations
Health Action Plan
- Actions completed / not completed
Health data
- Weight increases / decreases
- Other data recorded
Health reports
- Recent professional reports from health appointments
Nutrition and swallowing
Staff observations
Support plans
What is working / not working
Risk and safety
Changes to each person’s My Safety Plan since the last meeting
What is working/not working?
10 mins
(each person)
Lifestyle planning
Review of planning activities
Person’s finances
- Weekly budget
- Tracking of person’s annual budget
10 mins
(each person)
Home meetings and activity planning
Discuss the outcomes from home meetings held weekly with the people you support i.e. upcoming activities, outings, meal planning, other issues.
10 mins
Family / day program / work place communication 15 mins
Review of incident reports
What worked / didn’t work
10 mins
Health Planning, Tools and templates, V1.3, June 2016 2

Team meeting agenda
Item Time guide
Lessons learnt
Recommendations and actions
Policy discussion
Discussion of a policy area. Relate it to the unit and people you support
10 mins
NSW Ombudsman’s Preventing deaths of people with disabilities in care Fact Sheets1
Read and discuss one or all of the 5 fact sheets in relation to the people you support.
10 mins
CIRT
Review CIRT results from last review
Review CIRT action / improvement plan
10 mins
Work health and safety (WHS)
Staff incidents
Hazards
Discuss the units emergency and evacuation plans, profiles and monthly fire drills. Update information in plans and profiles and inform line manager (e.g. Coordinator,A&R) of any issues.
10 mins
Unit finances
Unit budget
Petty cash issues
Unit credit cards
10 mins
Staff management
Roster consultation
Staff duties
Filling vacant shifts
Casual / agency usage
New support worker inductions
Orientation of new staff to emergency and evacuation plans.
20 mins
1 http://www.ombo.nsw.gov.au/news-and-publications/publications/fact-sheets/community-and-disability-services/preventing-deaths-of-people-with-disabilities-in-care-information-for-staff-of-disability-services
Health Planning, Tools and templates, V1.3, June 2016 3

Team meeting agenda
Item Time guide
Staff training
Training opportunities
Feedback from staff who recently attended training events
10 mins
Planning for next meeting
Nominate policy to discuss for next meeting
Confirm minute taker / chair for next meeting
Guest speaker
Other
5 mins
Review of meeting
Have all agenda items been discussed
Did the meeting run well
What can be improved upon
5 mins
Other
Health Planning, Tools and templates, V1.3, June 2016 4

Team meeting agenda
Schedule of team meeting roles:
Month Chair Minute taker Reviewer of
meeting
January
February
March
April
May
June
July
August
September
October
November
December
Health Planning, Tools and templates, V1.3, June 2016 5

Part C1: My support plans: Weight chart
My name Year
CIS number TRIM number
Weigh the person each month and at the same time if possible e.g. in the morning before breakfast1
Weigh the person without shoes
If the person needs to be weighed more frequently than each month, insert additional rows.
If there has been an unplanned change in weight since the last record, review the Nutrition and Swallowing Risk Checklist.
Month Date Height (cms) Weight (kgs) BMI
Weight difference from last weight record
January
February
March
April
May
June
July
August
September
October
November
December
1 Refer to the Nutrition and Swallowing Guidelines for information on how to accurately measure the person’s height and weight
Health Planning, Tools and templates, V1.3, June 2016 1
Copyright © 2022 FDOKUMEN




















