A Family Planning Hypothesis: Some Empirical Evidence from ...
Upload
khangminh22Category
view
3download
0
FINAL REPORT
MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
USAlD Contract No. 608-C-94-00006
Submitted: June 18, 2001 To the: Ministry of Health and
USAID/Morocco
Maroc
ii
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
FOREWORD AND ACKNOWLEDGEMENTS
This final report, submitted to the Ministry of Health and USAID/Morocco, describes the achievements of and lessons learned from the Family Planning and Maternal Child Health (FP/MCH) Phase V Project in Morocco, implemented between 1994 and 2000 under a bilateral agreemenf befween the Moroccan Ministry of Health and USAID, and with the technical assistance of John Snow, lnc. (JSI) as institutional contractor. For further defails, the reader is referred to other project documents, of which an exhaustive bibliography is provided in Annex 2.
The drafting of the final report of the FPIMCH Phase V Project, as well as the project itself, are the result of a team effort. It is in this sense therefore that the use of the word "we" in this report should be understood. First of all, I should like to thank, on behalf of the JSI team, my colleagues of the Ministry of Health (MOH) who gave body and soul to the Prpjed and, especially, Dr. Mostafa Tyane, Director of Population, who was the Project coordinator. I should also like to thank the USAlD team, under the direction of Michele Moloney-Kitts and Susan Wright, who provided technical, administrative and moral support throughout the project. Lastly, neither the implementation of the FPIMCH Phase V Project nor the drafting of this document could have been possible without the commitment and enthusiasm of the JSI team and the sub-contractors, of whom I am only the representative. Annex 4 provides a list of the main collaborators.
For the editing and formatting of this document, I wish to thank Taoufik Bakkali, Nawal Birdaha and Boutaina El Omari in Rabat, and Stacey Harrison and Emily Alfeld in Boston.
Boston, November 13, 2000
Theo Lippeveld
JSI Chief of Party of the FP/MCH phase V Project
John Snow, Inc. 3 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table of Contents
ACRONYMS .............................................................................................................. 6
INTRODUCTION ........................................................................................................ 8 Indicators of the FPIMCH Phase V Project ................................................................................. 9
Institutional Contractors and Cooperating Agencies of the Project .......................................... 10
Structure and Contents of the FPlMCH Phase Project Final Report ..................................... 10
RESULTS OF THE FPIMCH PHASE V PROJECT ................................................. 13 lntermediate Result I: Greater Access to Quality FPIMCH Services Responsive to Client Demand .................................................................................................................................... 13
A . Geographical Extension of FPIMCH Services ................................................................ 13
B . Family Planning .................................................................................................................. 15
C . Maternal Health .................... .. ......................................................................................... 26
D . Child Health ..................... .. ............................................................................................... 33
lntermediate Result II: Improved Policy Environment Supporting Expansion of FPIMCH Services ................................................................................................................................... 42
................................................................................................ A . Information and Analysis 42
B . Contraceptive Financing Phase-Over ............................................................................... 43
.................................................................................... C . Advocacy Tools and Interventions 45
lntermediate Result Ill: Reinforced Capacity to Manage FPIMCH Services with Particular Emphasis on Decentralized Approaches Responsive to Client Demand ......................... 51
.................................................................... A . Decentralized Management at Regional Level 52
......... ........................................................ B . Information. Education and Communication .. 57
........................................................................ C . Integrated Quality Management in Morocco 62
....................................................................... D . Pre-service Training and In-service Training 68 . .
E . Contraceptive Log~st~cs ..................................................................................................... 79
............................................................................................... F . Evaluation .................... .. 82
.................................................................................................. G . Health Information System 85
lntermediate Result IV: Increased Diversification of the Resource Base Supporting the Delivery of FPIMCH Services .......................................................................................... 94
...................... ........................................... A . Private Sector General Practitioners .... 94
........................................................................................... B . Contraceptive Social Marketing 99
................. RESOURCE MANAGEMENT OF THE FPlMCH PHASE V PROJECT 111
................... ..... ......................................... 1 . Planning, Follow-up and Evaluation .. ... 111
......................................................................................... 2 . Human Resource Management 112 . . .................... ................................................................. 3 . Coord~nat~onlCollaboration .. 112
4 . Project Procurement ...................... .. ............................................................................. 113
5 . Financial Management ...................................................................................................... 118
6 . Training, Study Trips, Conferences ................................................................................. 119
CONCLUSIONS AND RECOMMENDATIONS ...................................................... 120
John Snow. Inc . 4 Contract No . 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT a.
ANNEXES .............................................................................................................. 123 Annex 1: Summary of Technical Results ................................................................................ 125
Annex 2: Bibliography of FPIMCH Phase V Project Documents ........................................ 133
Annex 3: Training materials and IEC products of the FPIMCH Phase V Project ................... 144
Annex 4: The FPIMCH Phase V Project Team ...................... .. ........................................... 149
Annex 5: List of JSIIURCIJHU-CCP Consultants on the FPIMCH Phase V Project ............. 153
Annex 6: Financial Report ................................................................................................ 166
Annex 7: Summary of Participant Travel ............................................................................. 168
Annex 8: Summary of Invitational Travel ............................................................................... 173
John Snow, Inc. 5 Contract No. 608-C-00-94-00006 b

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Acronyms
ALCO BEOC C A CD A CEOC CEP CFR CHU CME CMS CNFRH
CTM D A DELM DF DHSA DlEC DIM DMP DP DPF DPRF DRC DRH DSA DSMl ECCD2 ENPS EOC EPPS
FPLM FPMD FPRC GP HIS IEC IFCS lMCl INAS IR IUD JHPIEGO
JHUlCCP JSI LTCM MCHIFP MOH MOST
Alternative Consultants Basic Emergency Obstetric Care Cooperating Agency Community Development Agents Complete Emergency Obstetric Care Community Evaluation and Planning Case Fatality Rate Centre Hospitalier Universitaire Continuing Medical Education Commercial Marketing Strategies Centre National de Formation en Reproduction Humaine. National Human Reproduction Training Center Compagnie de Transport Marocain Division de I'Approvisionnement Direction de I'Epidemiologie et de la Lutte contre les Maladies Division de la Formation Direction des HBpitaux et des Soins Ambulatoires Division de I'lnformation, Education et Communication Division de I'lnformatique et des Methodes Direction du Medicament et de la Pharmacie Directeur de la Population Division de Planification Familiale Direction de la Planification et des Ressources Fiancieres Direction de la Reglementation et du Contentieux Direction des Ressources Humaines Division des Soins Ambulatoires Division de la Sante Maternelle et Infantile Etude sur les Causes et Circonstances des Deces infanto-juveniles Enquete Nationale de Population et de Sante Emergency Obstetrical Care Enquete de Panel sur la Population ei la Sante. Survey of the Population and Health Panel Family Planning Logistics Management Family Planning Management Development Family Planning Referral Centers General Practitioner Health Information System Information, Education, and Communication lnstitut de Formation en Carrieres de Sante Integrated Management of Childhood Illnesses lnstitut National d'Administration Sanitaire Intermediate Results Intra-uterine device Johns Hopkins Program for International Education in Reproductive Health Gynecology and Obstetrics John Hopkins UniversityICenter for Communication Programs John Snow Inc. Long-Term Contraceptive Methods Maternal and Child Health and Family Planning Ministry of Health Micronutrient Operational Strategies and Technologies
John Snow. Inc. 6 Contract No. 608-C-00-94-00006

- FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
MSH MSMP MSR NHA NIP NTF NGO OMNl ONDE ONG PGP PHR PNAQ PNI Q A RH SEGMA SEE SlGL SM SMSM SOMARC URC USAID VI I VSC
Management Sciences for Health Moroccan Social Marketing Program Maternite Sans Risque National Health Accounts National Immunization Program New Transcentury Foundation Non-Governmental Organization Opportunities for Micronutrient Interventions Observatoire National des Droits de I'Enfant Organisation non Gouvernementale Private General Practitioner Partnerships for Health Reform Programme National d'Assurance Qualite Programme National d'lmmunisation Quality Assurance Reproductive Health Service d'Etat Gere de Maniere Autonome Service des Etudes et d'lnformation Sanitaire Systeme d'lnformation en Gestion Logistique Safe Motherhood Societe Marocaine des Sciences Medicales Social marketing of Contraceptives University Research Corporation United States Agency for International Development Vaccine Independence Initiative Voluntary Surgical Contraception
John Snow, Inc. 7 Contract No. 608-C-00-94-00006

1
FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
la Introduction
The FPIMCH Phase V Project - Withdrawal of USAlD Bilateral Assistance
The Family Planning and Maternal and Child Health (FPIMCH) Phase V Project in Morocco was the last phase of bilateral assistance between USAlD and the Ministry of Public Health, initiated in 1970. This association generated impressive achievements in the framework of FPlMCH services. The total fertility rate declined from 5.9 in 1979 to 3.1 in 1997. Between 1979 and 1997, the contraceptive prevalence rate increased from 19 to 59%. During the same period, infant mortality decreased from 138 to less than 50 (between 37 and 50) in 1997. The rate of institutional deliveries increased from 26% in 1987 to 46% in 1997. The complete immunization coverage of children was 87% and the use of oral rehydration salts doubled, going from 14% in 1992 to 29% in 1997. These health indicator trends clearly indicate substantial impact on the well-being of the Moroccan population.
Therefore, the design of the Phase V Project took place at an advanced stage in the development of the Moroccan public health system, allowing the project to focus on the implementation of sustainable and equitable systems, and to launch the country towards a stable and healthy future, both economically and socially.
The Ministry of Health (MOH) and USAlD were well aware that the fifth phase of USAlD bilateral assistance was the last one, and that the success of Phase V achievements would condition the nature of USAlD non-bilateral assistance in the healthlpopulation sector after 2000. Thus, after project initiation in 1994, the USAlD Mission, in collaboration with the MOH, prepared (in 1995) a Transition Plan to ensure that the Phase V Project would contribute to the highest degree to the sustainability of family planning and maternal and child health (FPIMCH) services. The Transition Plan provided the strategic framework for work plan implementation from 1997 onwards. Without changing either the Strategic Objective or the USAlD framework of health results, the focus of Project activities changed from the classical approach of FPlMCH service provision to targeted attention to service access issues that were critical to project sustainability.
Target, Objectives and Framework of FPIMCH Phase V Project Results
From the very beginning and during the entire implementation of the FPIMCH Phase V Project, the aim of the project was to improve the health of children under five and women of childbearing age. Project objectives had been determined so as to achieve these two results:
(1) Increased use of quality FPIMCH services, and (2) Sustainability of FPIMCH services.
Based on the 1996 Transition Plan, four intermediate results (IR) had been defined to achieve these results. The objective of the first intermediate result was increased use of FPIMCH services. The other three intermediate results were aimed primarily at the sustainability of FPIMCH services.
John Snow, Inc. 8 Contract No. 608-C-00-94-00006

IR 1: Greater access to quality FPIMCH services responsive to client demand; L,
IR 2: Improved policy environment supporting expansion of FPIMCH services; U
IR 3: Reinforced capacity to manage FPIMCH programs with particular emphasis on decentralized approaches responsive to client demand;
h
IR 4: Increased diversification of the resource base supporting the delivery of FPIMCH services.
ir
lndicators of the FPIMCH Phase V Project
As indicated by the contract between USAlD and JSI, it had been planned to measure Project results using two impact indicators and a series of performance indicators for each intermediate result. The changes of these indicators during the project will be discussed in detail in the technical part of the report and in Annex 1, which includes a discussion of the quality of data utilized to calculate indicators.
Impact Indicators
The total fertility rate reaches 3.0 at the end of 1999.
The infant mortality reaches 52 at the end of 1999.
lntermediate Result I
A greater number of women use effective contraceptive methods of their own choice as documented by an increase in the contraceptive prevalence rate (CPR) from 35% in 1992 to 48% by the end of 1999.
An increase in the % of couple-years protection (CYP) by long-term methods (tuba1 ligation, IUD, injectables) from 28% in 1992 to 45% in 1999.
An increase in the % of women with obstetric complications properly treated (met obstetric need) in the pilot regions, from 43% in 1997 to 61% in 1999.
= An increase in the % of sick children correctly treated in health facilities of the pilot regions, from 47% to 70% in 1999.
lntermediate Result 2
An increase in the % recurrent costs of the bilateral MOHIUSAID ~roiect financed by the Government (including contraceptive costs disbursed by the MOH) from 72% in 1997 to 83% in 1999.
An institutional environment favorable to the rapid expansion of FPIMCH services through high-level support, appropriate measures and regulations and budget support by the Government to FPIMCH services.
Intermediate Result 3
= An increase in the % of provinces reporting stock availability of 3-month contraceptive supplies each month of the year.
John Snow, Inc. 9 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
= Documented evidence that each pilot region had taken at least three FPIMCH program actions based on FPIMCH data analysis.
Intermediate Resulf 4
An increase in the % of CYP by the private sector as compared to the publiclprivate sector total from 32.3% in 1997 to 44% in 1999.
An increased number of private general practitioners (PGP) providing FP services according to MOH standards.
lnstitutional Contractors and Cooperating Agencies of the Project
In agreement with the Ministry of Health, USAlD entrusted the technical assistance contract for the implementation of the FPIMCH Phase V Project to John Snow Inc. (JSI) and their sub-contractors, Johns Hopkins UniversityICenter for Communication Programs (JHUICCP), University Research Corporation (URC), New Transcentury Foundation (NTF) and Alternative Consultants (ALCO).
Besides its major responsibility as Institutional Contractor, JSI was also in charge of coordinating the efforts of cooperating agencies (CA) within the Project, the major ones being BASICS, EVALUATION (and later MEASURE), INTRAH, JHPIEGO, Macro, MSH, OMNl (and later MOST), PHR, POLICY, SOMARC (and later CMS) and Tulane University. The scopes of responsibility of the lnstitutional Contractor, the sub-contractors and the cooperating agencies are set out in Table 1.
Structure and Contents of the FPIMCH Phase Project Final Report
The goal of the final report is to provide a comprehensive overview of the results of the FPIMCH Phase V Project in Morocco and to analyze these results in terms of targets and resources used. The report deals with the achievements during the entire project period, i.e. from June 1994 to September 2000, by the MOH, JSI and their sub-contractors and the other cooperating agencies.
The report first provides an overview of the technical aspects of the project. Its structure follows that of the project as outlined in "The implementation priorities of the USAIDIMorocco transition plan", with objectives and achievements grouped under the technical components of the four intermediate results (see Table 1). During the lifetime of the project, the grouping of activities under components and intermediate results changed several times. Table 1 therefore reflects the grouping as prevailing during the last years of the project. For example, contraceptive financing, initially part of IR 4, was treated under IR 2. Also, under the component of evaluation capacity building, only activities reinforcing the research capacity were dealt with. Activities aimed at improved utilization of FPIMCH data, which were initially also managed by Tulane Universitv, were dealt with under the Health Information Svstem comoonent. The results of each component are commented on and analyzed so as i o determine to what extent project objectives have been achieved, taking into account contextual opportunities and constraints.
John Snow, Inc. 10 Contract No. 608-C-00-94-00006

L
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT ,"..
The second part of the report is concerned with project management. It includes sections on *r
project planning, follow-up and evaluation, technical assistance staff, the financial situation, procurements, training and study trips. For further details, the reader is referred to the relevant appendices. L-r
Lastly, the conclusion discusses the contribution of the FPIMCH Phase V Project to increase use and the sustainability of FPlMCH services and suggests strategic directions to continue - the work begun.
To keep this report within a reasonable length, the reader is referred for further details to the i
annual reports and other complementary documents listed in appendix 2.
John Snow, Inc. 11 Contract No. 608-C-00-94-00006 LY

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table 1: Projecf Sfrucfure and Executive Responsibilities
John Snow, Inc. 12 Contract No. 608-C-00-94-00006

d
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Results of the FPIMCH Phase V Project
lntermediate Result I: Greater Access to Quality FPIMCH Services Responsive to Client Demand
Since the beginning of the 1970s, USAID, being the major donor in family planning, contributed greatly to the significant results achieved by the FPIMCH programs of the Ministry of Health (MOH). While the major task of the FPIMCH Phase V Project was to ensure the sustainability of these investments, the Phase V Project, through its lntermediate Result 1 (IR I), continued its contribution to the extension and quality improvement of FPIMCH services. Historically, the priority target of USAlD assistance was family planning services and later child health. The FPIMCH Phase V Project was to include support to maternal health services. Consequently, IR I had these three objectives:
(1) Ensure greater access to FPIMCH services for isolated populations and increase the available service package;
(2) Improve the quality of FPlMCH services through quality assurance techniques and better integrated delivery and supervision;
(3) Extend and increase the quality of information, education and communication (IEC) activities supporting FPIMCH services.
During the first two years of the project, a large part of the project team's efforts focused on the extension of FPlMCH services to geographically isolated populations. These activities are explained and commented on in afirg chapter.
The USAlD Transition Plan, developed in 1996, targeted interventions in each of the three FPIMCH programs. From 1997 onwards, technical assistance priority interventions were therefore: (1) long-term family planning methods; (2) maternal health and, specifically, emergency obstetric care in the Center-North region; and (3) child health and, in particular, the Integrated Management of Childhood Illnesses (IMCI).
A. Geographical Extension of FPlMCH Services
One of the MOH priority strategies since the 1980s was the extension of FPIMCH service coverage to populations living outside the geographical catchment areas of fixed health services. Indeed, although the Panel Survey on Population and Health (EPPS, 1995) showed that over 90% of all households lived less than 30 km from a health facility, international literature demonstrates that the utilization of fixed facilities by the population decreases beyond 10 km for curative care and beyond 5 km for preventive care. The conclusions of the EPPS 1995 on the FPIMCH services provided through the outreach and mobile strategy were upsetting. Household visits, launched by the VDMS program, declined from 20% in 1987 to 8% in 1992 and to 5% in 1995. The input of the mobile teams also declined from 4% in 1992 to less than 1% in 1995.
John Snow, Inc. 13 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Achievements
The MOH responded by investing in the building of 157 new health centers and the recruitment of 400 physicians and 800 nurses to serve in rural areas. The FPIMCH Phase V Project contributed to this effort with a series of activities that were implemented during the first years of the project in order to reinforce the primary health care network and, specifically, that of the mobile teams. The main achievements can be summarized as follows:
Procurement of medical and audiovisual equipment for the 157 new rural centers, 8 reference centers and 19 other health delivery structures;
Strengthening the MOH Car Pool by providing 180 Chevrolet pick-up vehicles for the transportation of mobile teams, a major batch of vehicle spare parts, two trucks to transport contraceptive products, two Cherokee Jeeps and spare parts for the 44 Cherokee Jeeps procured under past projects;
Assistance to the Car Pool and peripheral vehicle maintenance centers by creating a database for maintenance follow-up and training 180 drivers and 104 car technicians in the use and maintenance of the 180 pick-ups;
Training of some 3000 care providers of the new mobile teams through serial training in association with the Training Divisionlln-service Training Unit. A management manual for mobile teams was developed and tested, and was ready for printing and dissemination by the end of the Project.
Procurement of 180 medical equipment kits and camping equipment for the mobile teams.
Lessons learned and fufure perspectives
Project intervention in the geographical extension of FPJMCH services was a major investment, using some US$ 8 million or almost 20% of total project funding. This raises the universal dilemma of the cost-efficiency of covering geographically isolated populations and sparsely populated areas in a country like Morocco. Even though part of the investment into coverage extension was provided by external funding, recurrent costs to maintain a network of remote health centers and mobile teams in such areas are extremely high and a heavy burden on the MOH. It is difficult to keep personnel in remote health centers, and the unsatisfactory supply of medications and other supplies in such centers is one of the major causes for the poor utilization of such centers by the population.
Mobile teams seem to be a valid alternative to reach isolated populations, but the running costs of these teams are high in terms of fuel, vehicle maintenance and travel exoenses. At the end of the FPIMCH Phase Project, an ev&ation of the functioning of mobile teams is needed to document the number of services provided and their costs.
Lastly, to be more responsive to the needs of local communities and their priorities, the population should be more involved in the decision-making on the most appropriate mechanism to bring health care closer. The new pilot project on the decentralization of primary health services (Progress) will provide an opportunity for testing innovative models of FPIMCH services in remote populations. For example, to alleviate the burden of recurrent costs of mobile teams, the population could pay for the gasoline required by the mobile team to reach their community.
John Snow, Inc. 14 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
B. Family Planning
Between 1980 and 1995, the contraceptive prevalence rate in Morocco showed a spectacular increase, from about 20% to 50% for all methods, or 16.4% to 42.5% for the modern methods. Despite efforts made by the MOH since the beginning of the 1990s to offer a choice of contraceptive methods to users, the preeminence of the pill among the contraceptive methods clearly persisted at the beginning of the project. Thus, between 1992 and 1995, the proportion of IUD users increased only slightly from 8% to 9%, despite the training of over 1300 physicians and nurses in IUD insertion techniques.
At the same time, the FPIMCH Phase V Project - the last project of the bilateral assistance between USAlD and the MOH - considered a progressive transfer of the burden of contraceptive financing from USAlD to the Moroccan Government before the end of the project. In view of the withdrawal of the USAlD contribution to contraceptive financing, it therefore became necessary to develop strategies for the sustainability of FP program results. The transition plan suggested several mechanisms: (1) identify and address factors preventing the supply of FP quality services; (2) promote the decentralization of FP service structures and decision-making for these services; and (3) stimulate an increased participation of the private sector in the delivery of such services. The latter strategy will be developed in detail under Intermediate Result IV.
Objectives and Performance Indicators
The Family Planning (FP) activities of the FPIMCH Project therefore aimed at two objectives:
(1) safeguard the achievements of the family planning program through the decentralized management of FP services and improved quality of care.
(2) promote long-term contraceptive methods, i.e. the IUD, VSC, injectables and Norplant.
Two performance indicators were proposed:
A greater number of women using efficient modern contraceptive methods of their own choice as documented by an increase in the contraceptive prevalence rate (CPR) from 35% in 1992 to 48% end 1999.
An increase in the % of Couple-Years of Protection (CYP) through long-term methods (tuba1 ligations, IUDs, injectables) from 28% in 1992 to 45% in 1999.
Achievements
The following paragraphs provide a comprehensive overview of progress achieved in the implementation of family planning activities between 1994 and 2000. This implementation was coordinated by the Family Planning Division of the Population Directorate. The main partners were the IEC Division of the Population Directorate, the faculties of medicine and, specifically the National Center for Training in Human Reproduction (CNFRH). The JSI team and several expatriate and local consultants provided technical and management assistance.
This section begins with an overview of interventions aimed at a global change in the management of family planning services. Then, it presents the specific work achieved for each of the long-term contraceptive methods.
As highlighted in the introduction to this section, the strategy is to sustain FP program achievements by decentralizing program management and improving the quality of health care.
-
John Snow, Inc. 15 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The 1996 Transition Plan emphasized: "The Government of Morocco and USAID/Morocco are aware that the improvement of the health level of an increasing population, with decreasing support provided by donors and the government budget, will require decentralized leadership and a healthy management of system resources". From 1998 onwards, and with the financial and technical support from the project, a decentralized managemenf mechanism of FP/MCH programs was therefore tested in five pilot regions: Doukkala-Abda, Fez-Boulemane, Meknes-Tafiialet and Taza-Al Hoceima-Taounate.
Each of the five pilot regions had prepared a situational analysis of FPIMCH services since 1992. The general consensus was that the FP program had seen stagnation, even decline, in services in recent years, most particularly of the long-term methods. Among several project proposals to redress this situation, two projects promoting long-term contraceptive methods were chosen for Project funding. The project of the Taza-Al Hoceima-Taounate region, aimed more specifically at the extension of injectables and the involvement of local NGOs, informed and raised awareness among 200 health professionals and 300 relay agents on the use of injectables. The Doukkala-Abda project implemented a number of joint interventions between the two provinces to increase the proportion of long-term methods. Consequently, between 1998 and 1999, the percentage of LTM increased from 30.8% to 33.9% (see also RI Ill, Decentralized management at regional level).
The lack of the quality of FP services has been identified as one of the major obstacles to both the sustainability of FP program achievements and a change of the contraceptive structure in Morocco. In view of this, various interventions took place to improve the quality of FP services, in general, and the long-term methods in particular. A first initiative was the development of FP service standards.
The development of this document, undertaken with the assistance of consultants from the University of Rabat, took almost four years, from its design in 1996 to its official presentation during the MOH meeting on "The Good Management Pact" attended by all MOH directors and delegates. The length of this process can be explained by the fad that it was one of the first initiatives to develop national standards for Moroccan health services. Solving methodological problems and the achievement of a consensus through the exchange of several drafts of the document took considerable time. The next step will be the dissemination of standards to managers, care providers and trainers at all levels.
Another important step toward the improvement of the quality of FP services was the programmatic decision to integrate supervision for all contraceptive methods. An integrated supervisory form was developed in collaboration with DPFIDP managers and some provincial managers. It takes into account the FP standards that will henceforward be the unique reference for the management of FP services in Morocco.
In September 1998, a workshop took place in Marrakech on the strategies to consolidate reproductive health (RH) programs in general and the FP program specifically. This important event was attended by the major decision-makers and planners in the public and private sectors. It dealt with the following topics:
a Contraceptive financing
= Meeting unmet needs
Changing the structure of contraceptive methods
Distribution of service delivery by sector
John Snow, Inc. 16 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Recommendations on contraceptive financing are reported under IR 2 in the Section "Contraceptive Financing Phase-over". Programmatic recommendations were:
Target public actions and resources on couples with unmet needs;
Provide services and respond to demands in RH of adolescents, unmarried women, and men;
Plan, program and manage programs at the decentralized level in the framework of regionalization;
Promote RH and FP services at private provider level (see also under the introduction to IR IV).
Following this workshop, several meetings were held at the level of the Population Directorate to discuss strategies to implement these recommendations.
Strengthening the IUD Program
The qualitative evaluation of IUD services undertaken by Dr. N. Hajji in 1996 showed that the under-utilization of the IUD can, in part, be explained by a lack of information on and explanation of the chosen method by care providers. Initial efforts therefore focused on training in counseling of health professionals. In 1996, 700 care providers doing IUD insertions were trained in counseling techniques to achieve a better acceptance of this contraceptive method and promote its use.
Following this, between 1997 and 1998, a series of decentralized training sessions in IUD insertion techniques by instructors from nine regional centers allowed the training of 841 new care providers in IUD insertion. The educational support of this training was a module on contraceptive and counseling techniques, produced and finalized by the MOH.
To strengthen the existing technical setup, 650 health facilities were provided with basic equipment and 1200 IUD kits were procured and delivered to the FP units of health facilities between 1998-1999. Also, 1500 additional flashcards, part of the demonstration kit, were produced.
Still in the context of improving service quality, 5000 copies of both a laminated form and a wall-chart on infection prevention were developed, printed and disseminated.
To evaluate the impact of training at service delivery level, the percentage of early withdrawals (less than 6 months) was chosen as an indicator of IUD service quality. An evaluation protocol of early IUD withdrawal was therefore developed. The study was carried out in August 1999 on a representative sample in the five pilot regions. Out of a random sample of 854 insertions carried out in 1997 and 1998, 144 withdrawals (17%) were recorded, out which 64 were early withdrawals (7.5%). This is far lower than the 15% chosen as achievement indicator.
Expanding the Use of lnjectables
lnjectables as a long-term hormonal contraceptive method are a valid alternative to other hormonal contraceptive methods, especially in view of both the cost/duration and the ease of use. This method was introduced in Morocco in 1994 to meet an identified need for long- term hormonal contraception. Following a pilot period in 10 centers until July 1996, the
John Snow, Inc. 17 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
method was launched in 12 provinces of the Kingdom. In 1997, its use was extended to the other provinces through a pre-established action plan.
In May 1998, three evaluation meetings were held where representatives from all the provinces discussed the state of implementation of the action plan. The overall statement was that the number of sites providing injectables remained very insufficient in some regions. Moreover, data were not provided in a standard format that would allow comparative studies bebeen provinces and regions. For example, there was no standard definition of discontinuation of use. Several actions were programmed during this meeting:
Development of a standard data collection grid defining the recruitment rate, continuation rate and discontinuation rate;
Promotion and extension of injectables to other health facilities following a regional action plan that takes into account the demand, accessibility and feasibility of this extension;
The need for inter-provincial coordination to address the nomad population and reflection on a strategy adapted to nomads;
The reinforcement of counseling and management of side effects.
Based on these recommendations, a standard algorithm for the management of the side effects of injectables was developed and disseminated to the different provinces. 1800 persons were trained in prescription for and management of these side effects. A module on the use of injectables was developed by the DPF with JSI assistance and used in provincial training courses.
While the proportion of injectables in the method mix increased from 4.5% in 1998 to 5.4%. this increase is much lower than expected. As to the quality of services provided for injectables, a survey was conducted on a representative sample of users in the five pilot regions to measure the discontinuation rate after the 3'* injection. Out of 469 users having had their first injection before November 21, 1998, 159 returned for a 3rd injection, i.e. 36%. This represents a discontinuation rate of 54%, considerably higher than the 50% planned for the achievement indicator. A qualitative survey of the Souss-Massa-DrSa population showed that one of the principal causes of the under-utilization of injectables is the issue of the management of side-effects, in particular amenorrhea and metrorrhagia. Other factors are the lack of information and the influence of the women's environment. Although these results were not representative, there are reasons to believe that the situation is not much different in the other regions.
Strengthening the VSC Program
The number of interventions for voluntary surgical contraception (VSC), introduced as a contraceptive method in 1982, has gradually increased, culminating -as shown by graph 1 -in a peak in 1994 of about 9000 interventions, due to a well prepared campaign with media coverage. After 1994, there was an evident decline for three years, which has stabilized at around 4000 interventions per year since 1997.
John Snow, Inc. 18 Contract No. 608-C-00-94-00006

FnnL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Graph 1: Annual trends of VSC performances, from 1982 to 1999
This decline in performances was not concomitant with investments made both in equipment (i.e. opening new VSC units and upgrading equipment) and the training of providers and technicians to ensure equipment maintenance.
At the inception of the project in 1996, 5 training sessions in laparoscopy were organized by the CNFRH, 20 technicians were trained in the maintenance of laparoscopy equipment and 5 new VSC sites became operational. Later, in 1997 and 1998, the CNFRH organized training sessions on VSC techniques for 24 physicians, 25 operating-room nurses and 15 anesthetists, and six new VSC sites were opened in rural provinces.
In collaboration with the CNFRH and the JSI team, the DPFIDP explored the reasons underlying this major decline in VSC performances. At the end of 1997, a CNFRH team undertook some 20 survey visits to a sample of VSC sites. The results of this study, presented at a meeting in March 1998, showed that there were at least four decisive factors answerable for this decline in VSC performances: (1) the lack of communication between peripheral centers and the VSC unit; (2) the instability of gynecologists trained in laparoscopy techniques, several of whom had left for the private sector; (3) the lack of supplies; and (4) equipment maintenance problems.
Following this meeting, several decisions were made: (1) develop a data collection form on the functioning and organization of services; (2) organize meetings at regional level to study specific solutions to identified problems; and (3) organize a meeting on the maintenance of VSC equipment. This meeting took place shortly afterwards, and a new decentralized maintenance pattern was set up, under which each VSC unit would be served by a maintenance center following the pattern of administrative divisions.
As to the other issues, it was decided that the regions should take the initiative of organizing VSC meetings themselves. Unfortunately, for various reasons there was little follow-up at regional level. As mentioned above, two regions had decided to focus their actions on the improvement of FP activities and, specifically, VSC. The Doukkala-Abda region therefore sent two gynecologists to the CNFRH for training in VSC techniques. The regional Taza-Al Hoceima-Taounate project undertook a number of actions to improve the relationship between peripheral structures in charge of recruitment and the central VSC unit.
In Doukkala-Abda especially, the percentage of VSC services almost doubled, from 2.9% in 1998 to 5.6% in 1999. For the country as a whole, however, VSC services declined still more to 3,596 in 1999 (provisional data provided by the systeme SMIPF).
John Snow. Inc. 19 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Norplant Evaluation
Norplant was introduced in stages in Morocco. At the end of 1992, a first phase took the form of a feasibility study in six centers (RabatlCNFRH, RabatISouissi Maternity, Marrakech, Agadir, Casa Anfa and Casa Ain Sebaa), then a second phase with the extension to 12 additional centers. A linear evaluation study was carried out in 18 centers on 4,773 users who were observed for two years. A consultant was recruited in 1997 to analyze data and write a report.
The report of this evaluation study of Norplant Program performance was submitted for reading, after considerable delay, to DPFIDP executives in August 1998. It was presented at a meeting of all interested parties in November of the same year. Here are some of the findings of the study, but for further details the reader is referred to the report on the study:
The continuation rate was fairly high for this method: 93.4% 12 months after insertion, 80.1% after 24 months and 69.4% after 36 months of use.
= The total number of withdrawals was 931, i.e. 19.5% of all insertions.
The average length of use was 22.2 months.
= Efficiency is high: 11 pregnancies for 4773 insertions, i.e. a gross percentage of 0.2%.
= Based on the average length of use, the cost of the method is high: 45 Dirhams per month of use.
= The need of a surgical procedure for insertion and withdrawal, the clinical training required to do so, and the lack of stability of trained personnel make it is a method difficult to manage.
Despite the methodological limitations of the study, its findings were considered sufficiently reliable to make programmatic decisions. In a private meeting at the FP Division with Division staff and USAlD and JSI representatives, it was decided not to continue the Norplant program at the national level and to explore the possibility of introducing this method in the private sector by involving a number of pharmaceutical firms in Morocco.
Strengthening of FP Reference Centers
To strengthen 35 Family Planning Reference Centers (FPRC), a renewed effort was made to improve the utilization of these centers. 16 FPRCs with different profiles (university centers as support, regional centers, provincial centers) were selected. Project funded activities were: (1) refresher courses in counseling for 4 persons per center, (2) follow-up through field visits by 2 MOH staff, and (3) procurement of audiovisual and technical equipment (delivered in 1998) for the upgrading of reference centers.
A consensus meeting on the role of reference centers and actions to strengthen them was held on March 17, 1998, attended by representatives of 17 provinces. The primary role identified was the admission of FP clients referred by other health facilities. This should be achieved in close collaboration with SIAAP, the hospital and the reference center, and take into account the local environment of each region. In order to strengthen and improve the use of reference centers, the participants developed a work plan for each separate region, including a schedule for the implementation and evaluation of proposed actions. The second role identified was that of an in-service training center. In collaboration with the IFCS, the FPRC could receive probationers (stagiaires) from other health centers and dispensaries.
John Snow, Inc. 20 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Communication in the FP Program
Support to IEC in family planning in the Phase V Project focused on the consolidation and strengthening of links with the media through the organization of information days, workshops, production of audiovisual supports and collaboration with the MOH and the Ministry for Culture and Communication.
In 1996, staff of the FP Division worked with professionals of the Moroccan national radio and television (RTM) to produce a documentary on the national family planning program. This production was used in various national and international venues to make the Moroccan national FP program better known.
Conscious of the importance of communication between health personnel and the population, staff of the FP division, in collaboration with the DlEC personnel, took steps to improve the counseling skills of care providers. Three IEC support materials were developed: (1) a FP kit; (2) a FP counseling guide, and (3) a training video on counseling. The FP kit, presented as a small suitcase (for carrying by itinerants), included samples of existing contraceptive methods and a set of flash-cards on each of these methods. The kit proved good support for health professionals in their counseling work on the choice of a contraceptive method. The new counseling FP guide was developed and 500 copies were printed and then distributed to all regional trainers in FP training centers, to be used as a didactic guide. Lastly, the training video on counseling "Sahal MahaP' presented simple principles of good communication to help women and their husbands choose a FP method. Copies of the video together with samples of the kit were distributed to all the FP units throughout the country. These productions were also used in various training courses both in the public and private sectors.
In May 1997, the draft of a communication strategy to promote long-term contraceptive methods was developed. The final version of this document has never been produced. However, the major themes of this strategy were used in the planning of IECIFP activities. These themes focused on involving men increasingly in FP and encouraging discussion among the couple on the choice of a contraceptive method.
Consequently, the 1998 calendar was illustrated with men of various ages and social classes and the 1999 calendar with photos of couples. A Moroccan delegation participated in a conference on the "Participation of men in reproductive health in Francophone countries", held at Ouagadougou from March 30 to April 4,1997. The Moroccan presentation highlighted the lack of data on the knowledge and attitudes of men to FP.
To partly rectify this lack of information, 24 focus groups were held for married and single men in three regions chosen according to their contraceptive prevalence (high, medium and low) based on PAPCHILD survey results. The main purpose was to determine the understanding of, and attitudes to, family planning among males.
The final report presented by the national consultant, who had conducted the study, shows that notions linked to family planning and birth spacing had well circulated in the various strata of Moroccan society. Health, qualify of life and order are the major concepts men have in mind when speaking about FP. The most precise and global vision is, without contest, that of young bachelors. On IEC, men think that the system and its partners have opted for "privileging women" and to "addressing themselves exclusively fo them". The findings of the survey on men and FP provided an information base to enrich the scenarios of audiovisual productions supported by the project: The film "Oulad Lghial" and the radio series on FP.
- -
John Snow, Inc. 21 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
In 1999, a video film on family planning was produced by the DlEC in collaboration with the DPF, produced by Mr. Bennani. The title of this film "Oulad Lghial" touches on the negative connotation of badly spaced births. Played by renowned Moroccan actors, this film broaches the involvement of men and the couple's discussion on the strategic choice of a contraceptive method. The film was launched in the 7" Art Cinema in the presence of H.E. the Minister of Health, HE. the US Ambassador and a number of high officials. Then the film was distributed to all Moroccan provinces. In several regions of the country, the film was also presented by mobile caravans as well as screened on the buses of the CTM. To increase the audience of this film, it was also screened by the RTM on July 11, 2000 on World Population Day.
Focus group data have also been used to develop the scenarios of 15 episodes of a radio series to reinforce messages transmitted by the FP film on decision-making by the couple, the positive involvement of men in this decision and the choice of a non-constraining and appropriate method for long-term birth spacing. This radio series was produced by the DlEC studio, with the participation of well-known Moroccan actors loved by the public. Considering the usefulness and success of this series, its production is being continued with the support of UNFPA and other private sector partners.
In order to make the national family program more widely known, a kit containing files and brochures on the program was produced for the International Conference on Population and Development in Cairo in 1994. Since Reproducfive Health was the concept used for speaking about family planning as well as other priority health themes, the same kit was printed a second time for the 27Ih Maghreb Congress held in Casablanca from May18-20, 1999 on the topic of "Reproductive health and FP in the countries of the Maghreb".
Comments
After five years of activities to ensure "Greater access to quality FPlMCH services responsive to client demand" an assessment of results, based on the two performance indicators explained at the beginning of this section, is required: the contraceptive prevalence rate (CPR) and the % of CYP by long-term methods (LTM). The following paragraphs briefly discuss these results.
Concerning the CPR, the PAPCHILD survey demonstrated that the CPR for modern contraceptive methods was 49% in 1994, therefore exceeding the target of 48% set for 1999. The results are those for both the public and private sectors together such as obtained directly from interviewed households.
The data in Table 2, provided by the collection of public and private data, show a slight progress of the number of CYP during the project period, but this is almost entirely due to progress achieved by the private sector. Indeed, the share of the private sector in the total CYP increased from 27.9% in 1995 to 36.9% in 1999.
John Snow, Inc. 22 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table 2: GYP Trends 1995 - 1999
1257055 1279664 1316141 1450069 1470097 Total
Cn'
Public Sector
Source: Public sector--Systerne SMIPF, DPRFISEIS, MS Private sector- SOMARCICMS and sales by the pharmaceutical industry.
1995
351120
27.9
Private Sector
In this section, our specific aim is to evaluate public sector services using as a first performance indicator the gross utilization rate (GUR) of the public sector, or the ratio of CYP to the number of married women in the childbearing age group who use the public sector. Graph 2 shows the trend of family planning methods between 1995 and 1998. The GUR decreased slightly from 25.1% in 1995 to 24.8% in 1998 and to 23.3% in 1999. The target set for a GUR of 28% in the public sector has thus not been reached. It should not be forgotten that these figures, and especially the one for 1999, underestimate the actual situation. As explained in Appendix 1, the transition from the old system of data processing to the new systeme SMIPF caused problems in data retrieval for some provinces.
No
%
No
Graph 2: Evolution of the GUR by contraceptive method during the 1995-1999 period
1996
391064
30.6
I Years 1
905935
As to the second performance indicator, i.e. the proportion of use of long-term methods to the entire method mix in the public sector, it changed very little during the project period. From 40.6% in 1992 it decreased to 36.1% in 1997, then increased to 38.4% in 1999, therefore still a long way from the target of 48%. The pill remains the most used method and its share in the method mix, which was 57.1% in 1995, reached 59.6% in 1999. The IUD is in second position with 29.1% (32.8% in 1995). lnjectables overtook VSC to take third place. Although their position is still modest, they now represent 5.4% of the modern method mix (1.5% in 1995). As explained above, VSC decreased from 6.3% in 1995 to 3.9% in 1999.
1997
425644
32.3
%
John Snow, Inc. 23 Contract No. 608-C-00-94-00006
888600
1998
485539
33.5
72.1
1999
541781
36.9
890497
69.4
964530 928313
67.7 66.5 63.1

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
It should be noted that there are major differences in the percentage of LTM use between urban and rural areas. The 1997 PAPCHILD survey showed that LTM use in urban areas was almost twice that of rural areas. This shows once again that innovative mechanisms must be found for quality services to reach geographically isolated populations.
The percentage trend of long-term method use in the 5 pilot regions does not differ from the trends indicated by table 3.
Table 3: LTM use in the 5 pilot regions
Regions 1 %I996 ) % 1 9 9 7 1 % 1 9 9 8 1 % 1 9 s 1 % 1 I I I I
. . ~ -
Fez-Boulemane
Meknes-Tafilalet
Souss-Massa-Dr6a
Taza-Al Hoceima-Taounate
The initial % decline between 1996 and 1997 in four of the five regions was due to a decline in IUD andlor VSC use. The increase of a few points in the following years in the same regions can almost entirely be explained by an increase in the use of injectables.
45.8 1 46.7 1 48.6 1 44.7 1 50
Doukkala-Abda
Concerning the quality of FP services, a major effort was made during the project lifetime to improve the quality of IUD service delivery. Using the % of IUD withdrawals as quality indicator, a mini-survey was conducted in 1999 on a representative sample in the five pilot regions. It showed that out of a random sample of 854 IUD insertions in 1997 and 1998, there were 144 withdrawals (17%), out of which 64 (7.5%) were early withdrawals. This is by far lower than the 15% set as achievement indicator. It therefore seems that, at least in the pilot regions, the quality of IUD service delivery improved.
31.8
39,l
36,8
As to iniectables, the discontinuation rate after the 3rd iniection was chosen as aualitv
burce: Sysferne SMlPF - Repotfs of fhe FWMCH Health Information Sub-sysfem SystSme 1997-1999.
36,9
indicator. Out of 469 users who received their first injection before November 21, 1998, 156 returned for their 3'd injection, i.e. 36%. This represents a discontinuation rate of 64%, which
25,6
31,6
30,5
is considerably higheF than the 50% planned for the achievement indicator. Other studies show that the care providers themselves are often badly informed about side effects and counseling on injectables. It is evident that the lack of quality of injectable service delivery can, in part, explain why this method has not been very successful.
29,5
Lastly, there is still the issue of VSC. Continuing waiting lists show that there is demand for this contraceptive method. There is evidently a problem of supply. Several factors have been remarked upon in the complex cvcle of VSC services between the initial reauest made
28,5
35,3
35,2
by a woman, often in a distant health center, to the final laparoscopy by a gynecoiogist. It is felt that this problem could be solved by quality improvement methods to be implemented by
30,7
- . all the staff involved at the level of the region or the province.
30.6
33.9
32.7
What was the contribution of IEC activities in FP during the Phase V Project? Firstly, quality printed and audiovisual supports were produced to meet the needs for promoting FP services and specifically long-term contraceptive methods. Also, the Project contributed to the strengthening of links with the media to convey key messages and give priority to the positive actions of men in improving the discussion on FP within the couple. Moroccan television, radio, actors and artists are now among the partners of the MOH. The awareness
34
33
34
34.3
John Snow, Inc. 24 Contract No. 608-C-00-94-00076
28

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
of newspapers and magazines was raised through information days and workshops organized throughout the project. Articles on FP and FP services are now a regular feature of several Moroccan newspapers and magazines. Secondly, the Project contributed to the strengthening of the communication skills of health staff with the target population through a number of interventions and tools: training in counseling, FP kit, the Sahal Mahal video and the FP counseling guide.
Lessons learned and fufure perspectives
The contraceptive prevalence rate in Morocco, as measured by the 1997 PAPCHILD survey, was close to 60% and reached 49% for modern methods. This spectacular result should not let us forget that there has been stagnation for several years in the public sector both of FP services and the percentage of LTMs. The main lesson learned from the FPIMCH Phase V Project is that the only means to progress is through the direct management of FP programs by the regions and provinces. Indeed, it is through decentralized management that the unmet needs of geographically or economically marginal populations can be met and that appropriate solutions can be found to the operational issues of LTM services, often very specific to a region or a province.
The FPIMCH Project did some major work to identify and establish basic mechanisms for decentralized management. These mechanisms include the introduction of the quality management approach at the level of peripheral units. Pilot experiences have shown that quality management can contribute to problem solving. Is it therefore by chance that the Tanger-Tetouan region, one of the most active in implementing the quality management approach, has a LTM user rate of 62.1%, the highest in Morocco?
In the same spirit, the development and validation of national FP standards was one of the major Project contributions to the sustainability of FP program achievements. FP standards are central to the introduction of quality FP services. They will be the reference for the self- assessment of care providers, the implementation of integrated supervisory systems of primary health services, and of FP pre-service and in-service training.
To ensure the sustainability of the FP program, historically one of the best performing in the world, there is still a full agenda of interventions:
Continue with the decentralization of FP program planning and management in the context of regionalization;
Develop innovative mechanisms to increase the part of LTMs in FP services, especially in rural areas, through operational research, pilot experiences, the study of existing "good practices";
Promote LTMs by stressing the role of men and discussion among the couple, using IECIFP supports produced for this purpose, and strengthening the counseling skills of care providers;
Ensure dissemination of FP standards to care providers, supervisors and trainers;
Implement an integrated supervisory system for reproductive health, using FP standards and quality assurance methods;
Seek local solutions to the problem of VSC services by applying quality assurance methods.
John Snow, Inc. 25 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
C. Maternal Health
Following the international Safe Motherhood initiative in Nairobi, the Ministry of Health created the Pregnancy and Childbirth Surveillance Program (PSGA) in 1987. Despite major investments by the MOH, the maternal mortality rate, estimated at 332 in 1992 by ENPS-II, declined too slowly as compared to other health indicators. Efforts by the MOH and international agencies focused mainly on prenatal consultations (PNC) and traditional birth attendants (TBA). However, an increase in PNCs had no major impact on the maternal mortality rate (MMR). The screening of life-threatening pregnancies, on which prenatal programs are based, is generally of little use for the identification of women who will have complications during childbirth. Although the number of assisted childbirths has increased, this did not result in a major improvement of maternal survival. There appears also to be an issue of quality of care and the inability of medical staff and health facilities to manage correctly obstetric emergencies. This is because of a lack of competence, or because women arrive too late in the health facilities.
Consequently, during the initial implementation of maternal health activities by the Project, it became evident that the strategy needed to be changed. International studies, including those by Deborah Maine and Sereen Thaddeus, both project consultants, have shown that ensuring access to quality obstetric care may rapidly reduce maternal mortality by more than 50%. Therefore, as early as 1995, the MOH opted for a new strategy to combat maternal mortality, based on the improved supply of obstetric services throughout the country. In this context, the FPIMCH Project focused on two major interventions:
(1) Development of a national communication strategy to raise public awareness on maternal mortality issues and means to prevent it;
(2) Improvement of emergency obstetric care (EOC) through a pilot project in the Fez- Boulemane and Taza-Al Hoceima-Taounate regions.
The following paragraphs review the achievements of these two interventions and discuss their rationale in the context of the new strategy to combat the problem of maternal mortality. For further details, the reader is referred to two documents published by the Project: (1) Pilot Project in Emergency Obstetric Care in the Fez-Boulemane and Taza-Al Hoceima-Taounate regions, and (2) Communication in Safe Motherhood.
National Communication Strategy in Maternal Mortality
To increase the awareness of the population on maternal mortality, a national communication strategy was developed and implemented between 1995 and 1998 by the IEC Division, in collaboration with the MCH Division of the MOH Population Directorate, and with JHUICCP assistance.
At the beginning of 1996, a working group composed of representatives of the DlEC and the IEC advisor of the Phase V Project developed a communication strategy to reduce maternal mortality in Morocco. The principal objectives of this strategy were to raise the awareness of various audiences on the excessively high maternal mortality rate and to channel the message "obstetric complications can be treated", thereby reducing maternal deaths.
Underlying any intervention and strategy was the simple but powerful concept that "it is not necessary for a woman to die in labor". This message should resound for each target group: decision-makers who might influence the political orientation and the funding of improved services and resources; care providers whose effective response to obstetric emergencies
John Snow, Inc. 26 Contract No. 608-C-00-94-00006

could save the lives of women; women and their families who might recognize the signs of complications and immediately seek reliable medical care.
The national communication strategy was initiated concurrently with the pilot project in improvement of emergency obstetric care. Like the pilot project, it was based on the three- delays model (see section on the pilot project). From the very beginning, the communication component was an integral part of efforts made to reduce maternal mortality, with all of its overall contributions to reduce each delay. Based on these considerations, the Safe Motherhood working group developed specific objectives and strategic approaches for each of the three target audiences and used media appropriate to each of them.
Achievements
The communication strategy, which included activities in advocacy, provider motivation and education of the public, was implemented in two stages.
The firsf phase focused on raising the awareness of policy-makers on the high rate of maternal mortality in Morocco to achieve their commitment to reducing this rate. The key production for this advocacy activity was a widely disseminated video documentary, Khlat Eddar, calling for the mobilization of resources and the improvement of emergency obstetric care (EOC or SOU). Concurrently, support materials designed for health professionals urged them to take on the responsibility of preventing maternal deaths, emphasizing EOC competencies adapted to each level of the health system. The documentary and the press kit that went with it were so well received that the media coverage on maternal mortality issues increased. Dissemination of this production was also promoted through speeches made by the late King Hassan 11 in which he called for making maternal mortality a priority health issue. Support materials for care providers were mainly disseminated by the Safe Motherhood information stand, created by the IEC Division to raise awareness and facilitate the advocacy effort. This mobile stand, impressive to the eye and full of pictures, statistics and slogans, had been used in over 30 major conferences and meetings between 1996 and 1999, including major professional meetings on health that were held in Morocco.
The second phase of the communication strategy aimed at helping women and their families to recognize the signs of complications during pregnancy and birth in order to make timely decisions to look for assistance. The "enter (tain)-education" approach was proposed for this audience, with caravans presenting the play "Aide-toi, le Ciel t'aidera" in the major urban and rural areas, accompanied by messages on safe motherhood, and the video film "Bent Ettajer" was screened by the mobile teams. Dissemination of these productions by the national television and on the main interregional bus lines throughout the country increased their impact. Survey results show that the audience understood most of the messages on obstetric complications and the importance of timely and appropriate care during pregnancy and birth.
The approach and achievements of the Moroccan communication strategy to reduce maternal mortality have been shared at the international level several times: the technical meeting of the Safe Motherhood Working Group in Colombo (Sri Lanka) in October 1997; the exhibition of the World Health Organization in Geneva for the sixth anniversary of SM; the Regional Panafrican Conference on the participation of men in reproductive health in Burkina Faso in March 1998; and lastly, the workshop on the role of the media in reproductive health in Cyprus in June 1998.
Observations and lessons
The example of the Moroccan communication strategy to reduce maternal mortality can teach precious lessons to individuals working in IEC, and maternal and child health. Here
John Snow, lnc. 27 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
are some observations and lessons to be learned from the strategic approach and the achievements:
Begin early: A communication strategy should be designed when any major health initiative is being implemented and carefully coordinated with key program components. In the case of Morocco, the global approach to the reduction of maternal mortality based on the three-delays model shaped all facets of the program and fostered harmony between communication activities, supports and messages designed for each type of audience.
= Create a communication strategy: The planning and successive phases of communication interventions should be based on their affective and chronological relation with the target populations, as well as among themselves, in the appropriate context of a region or country. This is why key decision-makers should first of all be made aware of the gravity of the situation in the country and the need for change. Awareness of care providers, improvement of skills and upgrading of health facilities should precede the dissemination of messages to women and their families, stating that quality emergency care is available and should be sought as soon as the first signs of complication occur.
Lastly, it was essential for women and their families to understand that maternal deaths are preventable and not necessarily a fatality, trained providers are ready to help and the attitudes and decisions on recourse to care can help prevent fatalities.
Base the material and messages on real stories: Quantitative data and qualitative research results are essential to the development of support materials. By incorporating true stories, support materials can be further improved. Talking and listening to women and their families were important steps in the creation of key support materials: the Khlat Eddar documentary, the play "Aide-toi, le Ciel t'aidera" and the docudrama "Bent Ettajer".
Involve each audience directly to achieve changes: Interventions for each group were designed to interest the audiences, to raise their sense of responsibility and to turn them into active actors in the effort to reduce maternal deaths.
Facilitate the transformation of decision-makers info advocates: By providing decision- makers with the Khlat Eddar text and the press kits, they can more easily disseminate correct and up-to-date information on maternal mortality to other people.
Create innovative means of communication: The "enter-education" approach was used to tackle the complex and serious problems of maternal mortality by producing a theater play and a docudrama screened by mobile teams in public areas and during health related events. Another original method was the use of CTM buses as an innovative channel for the dissemination of the various support materials.
Create partnerships: A nation-wide communication effort provides a unique opportunity for creating links with people in different fields: public health, medicine, transport, media, theater, cinema, as well as among local, regional and national organizations.
Program impact evaluation: Basic research is a prerequisite to evaluating the impact of any major communication initiative. Although the findings of various IEC supports assessments, produced in the context of the Moroccan maternal mortality reduction program, show that the various target audiences understood the messages of the strategy, no basic information was collected prior to implementation. It is therefore not
28 Li John Snow, Inc. Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
possible to determine the quantitative impact of strategy interventions on the knowledge, attitudes and behaviors relevant to maternal mortality prevention.
Conclusion
The communication strategy succeeded in turning maternal mortality decrease into a priority issue on the national agenda, which resulted in a mobilization of resources to improve emergency obstetric care. Out-reach activities for using the "enter-educate" approach have helped women and their families to learn that an obstetric complication is not a fatality. With such encouraging results and the congratulations by the American First Lady, Mrs. Hillary Rodham Clinton, to the Moroccan government for their commitment to reducing maternal mortality, the Ministry of Health plans to duplicate SM activities with the support of various donors.
Emergency Obstetric Care Pilot Project
The emergency obstetric care pilot project was initiated in 1995 in the Central-North Region at a time when Morocco entered into a new policy of support to hospital maternities. Because of the regional administrative reform, the project was extended, in 1998, to the eight provinces of the two regions Fez-Boulemane and Taza-Al Hoceima-Taounate, covering a population of 3,186,651. The project was implemented by the Mother and Child Health Protection Service of the MOH and by the regional teams of the two pilot regions, assisted by JSI and international consultants.
Project Strafegy
The project relied on the three delays model (T. McCarthy and D. Maine, 1991);
A first delay in deciding whether to use emergency obstetric care; - A second delay in reaching emergency obstetric care services; and
= A third delay, after arrival at a health facility, in being provided with efficient care (the transfer between first-level services and the reference level are part of the third delay).
Experience has shown that most life-threatening obstetric complications are neither predictable nor preventable, but can be successfully treated. The project therefore proposed . . a technical package to be set up at two levels of the health system:
At the level of rural maternities and ambulatory health centers, basic emergency obsfetric care (BEOC or SOUB) included: parental administration of injectable oxytocics, antibiotics and anticonvulsants; uterine revision, assisted delivery, use of vacuum extractor, as well as reference and transport to a reference center.
At the level of hospital maternities: Comprehensive emergency obstetric care (CEOC or SOUC) included the same essential services as BEOC plus cesarean sections and blood transfusions.
The priority of the pilot project was clearly the upgrading of health services "to reduce the znd and 3rd delays" before tackling the obstacles of accessibility, lack of information on and confidence in health care quality. Actions for community mobilization or regional IEC were therefore planned beyond the implementation phase of the project.
John Snow, Inc. 29 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Objectives and Project indicators
= lncrease the availability of emergency obstetric care: at least one health facility providing complete emergency obstetric care (CEOC or SOUC) per 500,000 inhabitants; and one health facility providing basic emergency obstetric care (BEOC or SOUB) per 125,000 inhabitants;
lncrease the utilization of emergency obstetric care to achieve. a 70% coverage of the obstetric complications expected in 1999;
= Improve the quality of emergency obstetric care.
Rather than measuring maternal mortality, an indicator very costly to operationalize, the project opted for availability and process indicators that can demonstrate the short-term efficiency of the project. There were five project indicators:
The population per health facility providing CEOC and BEOC;
The proportion of assisted deliveries;
Met need for EOC, i.e. the percentage of obstetric complications treated, estimated to be 15% of expected births;
= Met need for cesarean sections, i.e. the percentage of c.s. compared to the expected number of c.s., estimated to be 5% of expected births;
The Case fatality rate (CFR) of obstetric complications in health facilities.
Pilot Project Achievemenfs
The major achievements were, in short:
On the basis of standard material and equipment lists, 7 CEOC and 45 BEOC health facilities were equipped;
33 health facilities were upgraded or repaired, including the operating room of the lbn El Khatib hospital in Fez and a training classroom at the Al Ghassani hospital (Fez JDD);
283 staff in the pilot regions received in-service training in emergency obstetric and neonatal care (SONU), including 36 trainers, 242 care providers and 4 surgeons who were trained in cesarean sections;
National normslstandards were developed for emergency obstetric and neonatal care (SONU) and a methodology to audit maternal deaths was implemented in CEOC facilities;
In IEC, a social-anthropological study based on focus groups was conducted with the participation of health care staff and an IEC plan, by region and by province, was developed.
The routine national information system has been revised, introducing new data collection tools: obstetric register and monthly activity report.
John Snow, Inc. 30 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The overall cost of the project was US$2,125,000, excluding technical assistance and recurrent costs, i.e. US$0.67 per inhabitant over 3 years. These investment costs seem reasonable and were distributed as follows:
Category I Cost in S I Percentage 1500000 71%
Trainin 300000 14% infrastructures 225000 11% Monitorin 25000
75000 3% Total
The Project was coordinated in two phases: an initial technical and centralized phase and a second more decentralized and managerial phase. Regional coordination of the emergency obstetric care pilot project, however, remained "functional" until the end of the project, which means that the creation of regional committees with specific tasks "proposed by international consultants at the beginning of the project" has never been implemented.
Results and commentary
Overall, the project could prove its efficiency through an increase in the availability of CEOC and BEOC services, met need for cesarean sections and met need for EOC. Project results are:
(1 995) (1 999) Met need in EOC (management of obstetric complications) 26% 72%
(1 996) (1 999) Met need for cesarean sections 22% 38%
IIoaR\ (1 999)
The project derives its strengths mainly from the innovative character of the three delays model. The project strategy - based on this model - relied on a simple and clear notion: the rapid and appropriate management of obstetric complications can prevent the majority of maternal deaths. This approach broached directly the bottleneck to reducing maternal mortality, i.e. the insufficient availability and utilization of obstetric services.
The following are some of the remarkable achievements of the project:
= Decentralized in-service training in basic emergency obstetric care (BEOC);
Restructuring the routine information system to include obstetric care indicators, currently adopted at national level;
Development of a quality assurance approach in obstetric services, including the definition of norms and standards for obstetric and neonatal care (SONU) and the development of a protocol to audit maternal deaths;
Strengthening the regionalization process.
The impressive results achieved by the pilot project should not prevent the researching and analyzing of the less successful aspects of the project. Indeed, such an analysis may teach us important lessons to be used when duplicating the approach in other regions of Morocco.
John Snow, Inc. 31 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Several limits of the project have been identified and are analyzed in greater detail in the synthetic report on the pilot project:
= The unplanned expansion of BEOC facilities and the issue of availability of qualified personnel and quality care it raises;
The lack of stability of gynecologists at their post in the public service and the ensuing lack of effective permanence of gynecological skills;
The lack of motivation of health personnel and the bad reception of parturients, managed too late in the course of the project;
The partial coverage by the project of delays in the treatment of obstetric complications and, specifically, the problems of transport from the home to the health service or between a basic facility and a reference facility;
The absence of specific strategies to manage postpartum and newborn complications.
Although the project emphasized emergency obstetric care as a means to improving the management of obstetric complications, institutional deliveries remain a safe means for preventing obstetric complications and speeding up their treatment. However, the percentage of institutional deliveries, although a key project indicator, has increased little between 1995 and 1999: from 22% to 27% in the Taza-Al Hoceima-Taounate region and from 37% to 42% in the Fez-Boulemane region. One of the major constraints remains the lack of availability of qualified staff in the BEOC facilities, which are the ones closest to the population. In the pilot project area, out of 29 maternity facilities only 8 were open at night. Antenatal consultations should therefore be retargeted on the basis of the three delays model and promote institutional deliveries.
Conclusions and Recommendations
The emergency obstetric care pilot project in the Fez-Boulemane and Taza-Al Hoceima- Taounate regions succeeded in improving the treatment of obstetric complications and has definitely contributed to a decrease in maternal mortality in both regions. It now remains to ensure its sustainability at local level and its reproducibility at national level. The major challenges are the consolidation, maintenance and extension of emergency obstetric services in the framework of the decentralization of health services.
For the sustainability of the project, recommendations can be summarized as follows:
(1) Ensure that supervisory and follow-up activities, as well as the renewal and maintenance of equipment, are programmed and budgeted annually;
(2) Ensure in-service training mechanisms of peripheral personnel through refresher courses andlor rotations at regionallprovincial level;
(3) Operationalize the management system of obstetric care based on standardslnorms.
The reproducibility of the emergency obstetric care approach is currently an issue of interest at both central and regional levels. In this context, and with the support of the Gates Foundation, a project to monitor emergency obstetric care has been initiated within the DP. This project will help regions to determine their EOC needs and to follow up the implementation of EOC projects. It is important that all involved in the duplication
John Snow, Inc. 32 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
understand that the approach used by this model differs, in many aspects, from prior attempts to bring maternal mortality down.
A major aspect of reproducibility will be to sustain and maintain the decentralized aspects of project planning and implementation. Another condition for success is good coordination between the central and regional levels to avoid duplication of efforts and ensure technical homogeneity.
Based on the lessons learned from the pilot project, and to increase the efficiency of the treatment of obstetric complications, a priority intervention in the implementation of new EOC projects is strengthening the level of basic emergency obstetric care. Each maternity facility should have at least two qualified birth attendants, be open day and night and have a means of transportation available - preferably through community participation - for emergency transfers to reference maternities. It is hoped that in this way women will be increasingly attracted to maternity homes; normal deliveries and minor complications could be treated closer to the community, and reference maternities could focus on their role of treating complicated cases. Also, it is recommended to organize, at local level, qualitative research studies within the communities for a better understanding of the reasons for the under- utilization of maternal health care in Morocco.
D. Child Health
In the field of child health, the Project focused on the implementation of the lMCl approach (Integrated Management of Childhood Illnesses) in the two pilot provinces (Meknes and Agadir). The Project also provided limited assistance to other interventions related to child health and, more specifically, to the National Immunization Program (PNI) and the Micro- nutrient Program.
Objectives
(1) Assist the MOH in the implementation of the lMCl approach in the two pilot provinces.
(2) Assist the MOH in the eradication of poliomyelitis,
(3) Assist the MOH in the development of a strategy to eliminate micronutrient deficiencies in Morocco.
Integrated Management of Childhood Illnesses
Owing to the efforts made by the MOH in the context of vertical programs, there was a remarkable improvement in child health as demonstrated by a decline in infant and child mortality (Table 4). However, the stagnation of the principal health indicators during the last years, an infanffchild mortality rate still over 40 per thousand, the results of the different evaluations that have shown a lack of synergy and coordination between the different programs, besides the desire to improve the quality of care, have been among the arguments that have led the MOH to adopt the lMCl approach (Integrated Management of Childhood Illnesses) in 1997.
John Snow. Inc. 33 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table 4: Mortality Trends of Children
under five in Morocco
Infant Child 1 "M","::: 1 Mortality I Mortality ' 1 Mortality I
In the initial phase, the new strategy was tested in the two provinces of Meknes El Menzeh and Agadir Ida Outanane. The extension phase in 2000 followed the evaluation of the initial experience.
General lMCl Objectives
= Reduce the mortality and morbidity of children under 5.
Promote the harmonious development of children.
Operational objectives
For the 1997-2000 period, the Ministry of Health adopted the following objectives:
Adapt the guidelines for clinical management to the national context;
Develop educational and didactic support materials required for lMCl training;
Develop the IEC support materials required for the dissemination of lMCl messages;
Implement lMCl at the level of all health facilities in the two pilot provinces: Meknes El Menzeh and Agadir Ida Outanane.
Achievements
The lMCl strategy was implemented by the MCH Division of the DP, in collaboration with the pediatrics departments of the Casablanca and Rabat faculties of medicine and the technical assistance of BASICS and JSI. The following paragraphs highlight the major achievements of the implementation of the lMCl strategy between 1997 and 2000 for each of the three IMCl components:
(1) Clinical component improving the skills of health professionals through their clinical training in the field.
(2) Service organizafion: improving the health system by revising the circuit of the ill child and of the data collection system, improving the availability of essential medications and strengthening the supervisory system.
(3) Community component improving family and community practices in lMCl by mobilizing members of the community and involving them effectively in the promotion of health.
John Snow, Inc. 34 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
I. Clinical Component
Between November 1997 and August 1998, the clinical guidelines for lMCl were adapted to the epidemiological context of the country and the didactic materials for training were finalized. Clinical training in lMCl was intended to improve the clinical skills of health personnel with the support of several algorithms which, because of priority health issues, are to guide providers in the identification of the health problem and its comprehensive management, including counseling of mothers.
Between 1998 and 2000, 347 care providers, including 64 trainers and 34 supervisors, were trained in a standard 11 to 12 day lMCl course. Most of the health professionals trained in IMCI, in both Meknes and Agadir, received two follow-up visits to collect data on the management of ill children and strengthen the providers' skills. Follow-up visits showed that the majority of the trained health professionals used the algorithms and other supports and applied the guidelines of the lMCl strategy. Also, care providers expressed their satisfaction with the quality of their training. They said that lMCl contributed to a better collaboration between physicians and nurses within health facilities and between the pediatrics unit and the outpatient structures at hospital level.
2. Sewice Organization
The second lMCl comoonent concerns the imorovement of service oraanization within a health facility. 1nterve;ltions included four components: (1) the circuiibf the child; (2) the integrated information system; (3) supplies of essential pharmaceutical products, and (4) integrated supervision.
(1) Patient flow: Based on a consensus among care providers, the patient flow for child care in all health facilities in the pilot provinces has been adapted to meet the following conditions:
- Any child under 5, whatever the motive of the visit, will be immediately directed to the MCH unit.
- MCH staff identify three different groups of children: (1) severe cases requiring immediate transfer; (2) cases requiring medical advice; and (3) benign cases that can be managed at the level of the MCH unit.
MCH personnel meet the preventive care needs of apparently healthy children and meet their curative needs even though they are not expressed.
- Taking into account the needs of the population programs services, consultations for chronic diseases and most of the preventive consultations are programmed for the . - afternoon.
(2) Integrated information system: The existing data collection system on child visits was very heavy and fragmented into priority programs. It therefore resulted in a useless overload of work for MCH staff and hampered the smooth running of clinical services. In 1998, an integrated register of child health activities was developed and the monthly report of MCH services was consolidated into a single document. Initially tested in the two pilot provinces, the new integrated system was later extended throughout the country.
(3) Essential medications: To ensure the improved availability of essential medications for the management of ill children, a list of essential medications for lMCl was developed in collaboration with the Directorate for Medications and Pharmacy and then sent to the
John Snow, lnc. 35 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
managers of the two provinces. Supplying medicines to rural health facilities is now ensured directly by the relevant delegation instead of going through the health district (circonscription sanitaire = CS). Despite these provisions, the needs for medications are not entirely met and stock-outs often occur.
(4) lnfegrated supervision: The training in supervisory visits provided an opportunity for creating a team of supervisors familiar with integrated supervisory techniques, especially the clinical component. These supervisors were, moreover, required to further develop horizontal supervision.
3. Community component
This lMCl component aimed at improving, through community participation, family and community practices relevant to the management of the child, both the healthy (immunizations and nutritional practices appropriate to the first two years of life) and the ill child (care at home and correct administration of the prescribed medications, knowledge of mothers concerning the signs of seriousness of a disease).
Several preliminary studies were conducted to achieve a better understanding of the socio- cultural context in which the lMCl was to be initiated, among others the nutritional practices mothers use with their young children, the meaning of local terminology relevant to child pathology and the perceptions of the population regarding health services.
Next, an operational research phase was implemented in the two pilot provinces. Evaluafion and Community Planning (CEP) was used with several communities on a pilot basis. This technique, the methodology of which has been developed by a BASICS team, aims at identifying, through household surveys, the practices and behaviors of mothers in lMCl by analyzing "key behaviors". The health team then "negotiates" a community action plan with the community to improve a number of behaviors considered priorities. The experiment took place at two sites in each of the pilot provinces (Meknes and Agadir) and at a site in a province where lMCl had not yet been introduced (Safi province).
On the basis of these research results, the central, provincial and local teams met with BASICS/JSI consultants during several workshops to reach a consensus on the community approach concept, the CEP methodology, the "focal" role of health in the multi-sectorial partnership and the role of relay agents in this approach. This process was documented in three successive reports collated by Prof. Jamal Eddine NAJI.
Between March and April 2000, health professionals were trained in the community approach in the lFCSs of the two pilot regions. These sessions were addressed to S IMP officials and health professionals of rural health facilities. In this context, a team including members of the MCH, the Training Division, IFCS managers and JSI consultants developed two documents: - A reference manual as a reference tool for decision-makers for information and
reflection, and for the training staff (SIMP, iFCS). This manual contains methodological forms for the trainers.
A training manual for health personnel at CS level in charge of the implementation of the community approach. Its contents present a simplified summary of the major elements of the four modules of the reference manual.
Lastly, the community development (relay) agents of the pilot communities were trained in the use of the CDA manual developed by the DlEC (see RI 3).
John Snow, Inc. 36 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Introducing IMCl in Pre-service Training
The MOH considered the introduction of lMCl in pre-service training as a priority since it helps reduce the extensive cost of training and ensure the sustainability of IMCI. Concurrently, the lMCl familiarizes students with an innovative and global approach to client management, both ill and healthy, based on the standardization of health care, and emphasizing the importance of the organizational aspects of health care and of the need to involve communities in the search for sustainable solutions. Activities introducing the lMCl concerned future physicians as well as nurses.
The strategy used to introduce lMCl in the lFCSs was based on a consensus reached during a workshop held from December 6 to 9, 1999 in collaboration with WHO and PRIMEIUSAID. Following this, several workshops were held to adapt and harmonize the teaching modules with the IMCI guidelines and to finalize the lMCl guide for teachers. lMCl will be introduced on a pilot basis in September 2000 in the Agadir and Meknes IFCSs.
An action plan to introduce the lMCl in faculties of medicine was developed following a seminar in March 2000 under the aegis of WHOIEMRO. Several preparatory activities took place during year 2000:
Creation of a follow-up committee at the level of the Casablanca and Rabat faculties of medicine.
Participation of 4 pediatrics teachers in a visit to the University of Alexandria to share experiences during March 2000.
Participation of 2 pediatrics teachers in a 5-day course organized at the University of Alexandria in July-August 2000.
Organization of a 5-day course for 11 pediatrics teachers at the level of the Casablanca Faculty of Medicine in July 2000.
Results and Commentary
To evaluate the impact of lMCl implementation in the two pilot provinces, several evaluation studies were conducted in April 2000. For the clinical component, a cross-sectional study was conducted with the assistance of a USAlD consultant. This study made it possible to compare the management of ill children in a representative sample of health facilities in the two pilot provinces (experimental group) with that of another group of ill children in a representative sample of other health facilities where lMCl had not yet been introduced (non- equivalent control group) in the Tetouan and Larache provinces. The survey involved 64 health facilities, 32 being pilot sites and 32 control sites, and made it possible to observe the management of 523 children aged between 1 week and 59 months by 116 health professionals. Two other studies of lesser scope were undertaken, an internal evaluation of the "service organization" component and a visit to observe the community component by UNICEF expert.
The principal results of the evaluation of the clinical component were:
A year after training, the quality of sick child ailment, treatment, and of the counseling to ill children were significantly better at the lMCl sites than at the non-IMCI sites for most of the measured indicators;
However, lMCl guidelines were often badly applied by trained care providers;
John Snow, Inc. 37 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
There was no significant difference between IMCl and non-IMCI sites in the satisfaction of mothers. This result could be explained by the difficulty of measuring satisfaction in general.
Evaluation of the "service organization" component showed:
= Very good availability of vaccines at lMCl sites and also at the non-IMCI sites;
Poor availability of essential medications and medico-technical materials at lMCl sites;
= Supervision and circuit of ill children better organized at lMCl sites.
Lastly, it was premature to undertake an in-depth evaluation of the community component since the experience was limited in time and space and benefited only a limited number of families. However, the preliminary results of the community component of the lMCl strategy in Morocco appear promising. Playing a "pivotal" role in the initiative of this strategy, the health professionals concerned with the community approach have provided proof of dynamism, open-mindedness to concepts outside their usual scope of thought and, finally, humility in accepting to question their own image.
Though still fragile, this "undertaking" raises major interest in faculty staff who teach community health and are in the search of "fields of implementation". Within other Directorates, fascinating experiences are being conducted in community participation. It would be useful to develop an inter-university and inter-directorate collaboration to share knowledge and achieve better dissemination and mutual enrichment.
Recommendations
Based on the results of the lMCl pilot experience, the MOH developed a number of recommendations, among which:
Planning
Improve the coordination of lMCl activities at central level through a better coordination between directorates and the grouping within the same structure of all IMCI-related programs (PLMD, PLMC, PNI, PLIRA, etc.);
Demonstrate the benefits of the lMCl strategy and advocate it at all levels of the health system and with donors and NGOs;
Develop an lMCl planning guide for regional and provincial managers, based on the WHO guidelines.
Improve the skills of health professionals
= Adapt the photo album and videocassettes and revise the "sore throat", "nutritional problems" and "other problems" boxes of the lMCl algorithm.
Explore means for introducing lMCl in the shortest possible delay, including the community approach in the pre-service training of physicians and nurses.
lmprovemenf of the Health System
Rationalize the supply and utilization of medications and equipment essential to lMCl implementation at all levels;
John Snow, Inc. 38 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
= Ensure that all lMCl medications are included in the national list of essential medications;
Train all lMCl trainers and S I M P facilitators in post-training follow-up techniques and strengthen the integrated supervisory system;
Constitute a "think-tank" committee to achieve improved adaptation of the health information system to lMCl guidelines.
Improvement of Family and Community Practices
= Define a strategy to improve family and community practices in lMCl and define the tasks of the different levels (central, regionallprovincial).
Prepare action plans for the family and community component of the lMCl at provincial level.
= Associate other experts (sociologists, anthropologists, health economists) with the evaluation of progress achieved by IMCI;
Initiate operational research at all levels and on all lMCl components, more specifically also on the means to reduce the various costs and of alternative training methods;
* The survey at health facility level should be complemented by a household survey to ascertain changes in behavior, not only at health facility level but also within the community.
Consolidation and Extension
The lMCl strategy should first be extended to the other provinces of the Agadir and Mekn6s regions; as to the extension to the other regions, the chef-lieu province of the region should necessarily be involved. - The pace of the extension will be determined by the availability of financial resources as well as by the capacity of the region toimplement this strategy.
Conclusion
The initial results of lMCl implementation in Morocco demonstrated that implementing the lMCl strategy had a positive impact on the quality of the management of ill children. Several constraints related to the organization of the health system emerged, in particular the availability of essential drugs and equipment. The community approach was conducted quasi independently of the development of other components of the lMCl strategy. It would be beneficial if the community component could be developed concurrently with clinical training and the reorganization of the health care system so as to contribute to the effectiveness, efficiency and sustainability of the lMCl strategy in Morocco.
Based on these results, extension of lMCl to the other provinces of the Kingdom was included in the 2000-2004 five-year plan. To achieve deconcentration, at present it seems appropriate to manage the strategy from the regions. The latter will themselves decide on the policy of implementing the three components of the lMCl strategy as well as the choice of "shadow zones" favorable to the community approach. An opportunity for testing this decentralized approach is provided by the Tanger-Tetouan and Souss-Massa-Dr2a regions
John Snow, Inc. 39 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
where it is planned to model the regional management of health services, with USAlD technical and financial assistance.
Other Interventions in Child Health
Especially during the first years, the Project provided technical and financial assistance to programs to control targeted childhood diseases: the program to control diarrheic diseases (PLMD); the program to control acute respiratory diseases (PLIRA); the national immunization program (PNI) and the program to control deficiency diseases (PLMC). Examples are:
Refresher training (called "combined training") in 1996-1998 of over 2000 MCH facilitators and nurses from health centers throughout the country to improve the quality of the management of child health problems in the following: diarrheic diseases, acute respiratory diseases, malnutrition, growth monitoring, vaccination coverage and, in particular, epidemiological surveillance of cases of acute flaccid paralysis. - Development and production of IEC support materials and procurement of oxygenetors for the PLlRA program.
Development and production of a guide to the integrated management of diarrheic children.
Applied research studies were done concerning persistent diarrheas and, in collaboration with the Peace Corps, of the community management of diarrheic and nutritional diseases. In particular, the PNI and the micronutrient program benefited from continued project support.
National Immunization Program (PNI)
To ensure a continuum to USAlD assistance provided by prior projects, the Project provided major support to the National Immunization Program (PNI), which is an internationally recognized example of exceptional performance, by maintaining a vaccination coverage rate of generally over 80% (the PAPCHILD survey found 87.8% in 1997). This support was provided in collaboration with JSI, BASICS and PHR. The activities outlined below have been reported in greater detail in the annual reports of the Project:
Procurement of refrigerator trucks to transport vaccines throughout the country;
Installation of a cold chain, including a generator, at the Sale warehouse;
Development, printing and general dissemination throughout the country of a vaccination guide (BASICS, 1997);
Financial support to IEC activities during National Vaccination Days, continued until 1999;
= $500,000 provided to the operating capital for vaccine procurement.
Two key reports on strategic PNI planning were produced with Project assistance: (1) Report on the condition of the cold chain by Paul lckx (BASICS, 1996), and (2) Case study on the cost and funding of vaccination activities in Morocco by Miloud Kaddar et al. (PHR, 1999). These reports are still the guidelines for MOH planners in the institutionalization and sustainability of vaccination services in Morocco.
John Snow, lnc. 40 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Two conditions subsist that threaten the sustainability of the impressive progress made in vaccination coverage during the past ten years: (1) use, until now, of a World Bank loan to finance most of the PNI recurrent costs; and (2) PNI dependence on national vaccination days (JNV) to maintain its high rate of vaccination coverage. The answers to these two problems should be sought in the sustained implementation of the decentralized management of FPIMCH services. An increased involvement of local communities in PNI organization could contribute to the sustainability of both the delivery and funding of vaccination services. The new USAlD pilot project in the Souss-Massa-Dria and Tanger- Tetouan regions aims at this target through the development of innovative mechanisms in FPIMCH service delivery with the involvement of local authorities, civil society and the communities themselves.
Micro-nutrient Program
National surveys on micronutrients, carried out by the MOH with OMNl support, showed that anemia caused by iron and Vitamin A deficiencies is a major public health issue.
The Technical Committee of malnutrition control, which groups all the cadres of the MOH and universities involved in nutritional issues, developed a global and integrated strategy against micronutrient deficiencies. This strategy included the following components:
(I) supplementation of deficient target groups, especially pregnant women and children under 5;
(2) nutritional education based on a communication and information plan, and
(3) fortification of staple foods such as flour, oil and butter.
The committee then developed an action plan of which the following activities are underway:
Training of health professionals
Design and production of IEC support materials
Development of a marketing campaign for fortified flour.
All these activities had the technical and material support of the MOSTIUSAID project (after the end of the OMNl project in 1998) and the CMS Project. I
John Snow, Inc. 41 Contract No. 608-C-00-94-00006
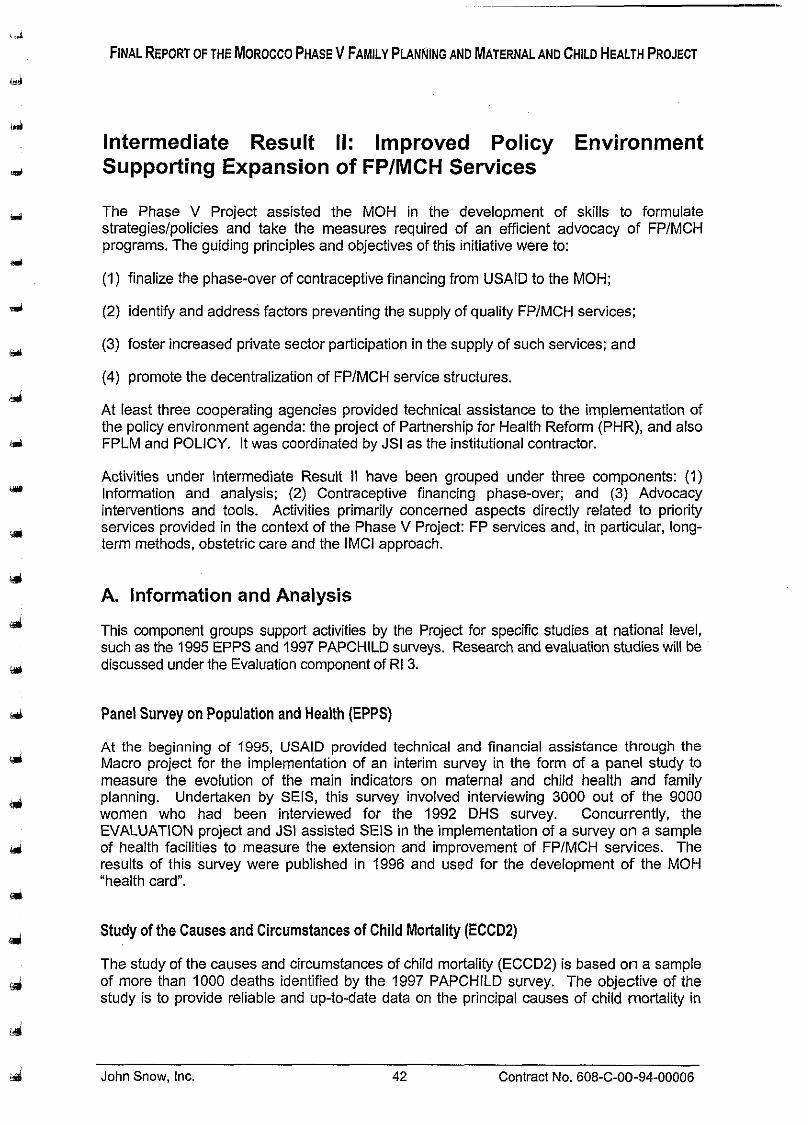
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
lntermediate Result II: Improved Policy Environment Supporting Expansion of FPIMCH Services
The Phase V Project assisted the MOH in the development of skills to formulate strategieslpolicies and take the measures required of an efficient advocacy of FPIMCH programs. The guiding principles and objectives of this initiative were to:
(1) finalize the phase-over of contraceptive financing from USAlD to the MOH;
(2) identify and address factors preventing the supply of quality FPIMCH services;
(3) foster increased private sector participation in the supply of such services; and
(4) promote the decentralization of FPIMCH service structures.
At least three cooperating agencies provided technical assistance to the implementation of the policy environment agenda: the project of Partnership for Health Reform (PHR), and also FPLM and POLICY. It was coordinated by JSI as the institutional contractor.
Activities under lntermediate Result II have been grouped under three components: (1) lnformation and analysis; (2) Contraceptive financing phase-over; and (3) Advocacy interventions and tools. Activities primarily concerned aspects directly related to priority services provided in the context of the Phase V Project: FP services and, in particular, long- term methods, obstetric care and the lMCl approach.
A. lnformation and Analysis
This component groups support activities by the Project for specific studies at national level, such as the 1995 EPPS and 1997 PAPCHILD surveys. Research and evaluation studies will be discussed under the Evaluation component of RI 3.
Panel Survey on Population and Health (EPPS)
At the beginning of 1995, USAlD provided technical and financial assistance through the Macro project for the implementation of an interim survey in the form of a panel study to measure the evolution of the main indicators on maternal and child health and family planning. Undertaken by SEIS, this survey involved interviewing 3000 out of the 9000 women who had been interviewed for the 1992 DHS survey. Concurrently, the EVALUATION project and JSI assisted SElS in the implementation of a survey on a sample of health facilities to measure the extension and improvement of FPIMCH services. The results of this survey were published in 1996 and used for the development of the MOH "health card".
Study of the Causes and Circumstances of Child Mortality (ECCD2)
The study of the causes and circumstances of child mortality (ECCD2) is based on a sample of more than 1000 deaths identified by the 1997 PAPCHILD survey. The objective of the study is to provide reliable and up-to-date data on the principal causes of child mortality in
John Snow, Inc. 42 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Morocco that could be used for the development of new strategies, in particular on the prevention of child deaths.
A team of SEE and DP staff carried out the field survey by verbal autopsy and the analysis benefited from the technical assistance of Michel Garenne, JSI consultant, who had already assisted the MOH with a similar survey in 1988. The study results were presented on July 13, 2000 during a dissemination day of the results of the EOC (Emergency Obstetric Care) and lMCl pilot projects. They revealed a spectacular decline in mortality from the target diseases of the PNI program and from diarrheic diseases. These results are important for the MOH in the development of child health related strategies, especially on the avoidability of child deaths.
6. Contraceptive Financing Phase-Over
As most contraceptive supplies to the public sector were financed by USAlD up to the beginning of the 1990s, the Moroccan Government had to develop a strategy of financial autonomy to finance contraceptive procurement. In 1999, an agreement was signed between USAlD and the MOH to achieve the phase-over to self-sufficiency of the Moroccan National Family Planning Program. This agreement specified the respective contribution of each party to contraceptive financing during the phase-over period and defined the transition strategy, i.e. the overall framework of the measures to be taken for the sustainability of the logistics management system of contraceptives distributed by the public sector.
Especially from 1997 onwards, just prior to USAlD withdrawal from public sector contraceptive financing in Morocco, a team composed of DP, DPRF and JSI staff undertook a number of activities with the technical assistance of PHR, POLICY and FPLM. The aim was for the MOH and its partners of the FPlMCH Phase V Project to undertake complementary analyses, which are essential information sources and tools for strategic decision-making.
Objectives
(1) Identify a reliable and realistic strategy for MOH autonomous procurement of public sector contraceptive supplies.
(2) Achieve consensus on the sources and modalities of supplying the pipeline after 2000.
Achievements
The following paragraphs provide an overview of the various studies and tools developed under the project. For further details, the reader is referred to the original documents listed in Annex 2.
Advocacy document (with PHR assistance): A basic document, a summary in Arabic as well as slides were produced to enable the MOH to convince the government of the need to increase the resources ear-marked for FP in general and contraceptive procurement in particular.
Synthesis of international phase-over experiences: The FPLM project produced a report, which provides an analysis of various experiences in withdrawal of USAlD funding of contraceptive procurement; this report was submitted to the Ministry of Health and USAID/Rabat in July 1998.
John Snow, Inc. 43 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Exchange visit on phase-over: The analysis of "phase-over" experiences was to facilitate the choice of a destination for the exchange visit. Due to an overload of Project activities, the tour was cancelled.
Market segmentation study: The POLICY project prepared a segmentation study of the Moroccan FP market. It included a projection exercise to assess FP service demand through 2005. According to this, in 2005 the potential FP market would be 3.4 million couples, out of which 2.7 million would use modern methods. Public sector demand should increase by 20%, while private sector demand would practically triple. This study was a major tool in informing GOM officials on market segmentation and assumptions through 2005.
Study of tax waivers: A comparative study of tax waivers in several countries was produced with PHR technical assistance.
Study of the local market: This study, undertaken in 1997 by JSI consultants, reviews the legislative framework and the local contraceptive market in Morocco.
Study of contraceptive procuremenf options for the MOH: Following the earlier study, it was necessary to update data on prices obtained by the MOH since the latter had started procuring contraceptives. This study presented three procurement options to the MOH: (1) procurement by local and international public tender; (2) a procurement agreement between the GOM and UNFPA; and (3) a mixed solution. The best solution will emerge locally when suppliers find interest in a regular supply with payment warranted by regular MOH funds.
Training in long-term contraceptive needs assessment techniques: With POLICY technical assistance, MOH staff and CERED (Center for Demographic Study and Research) researchers were trained in the usage of the Spectrum models system.
A major part of the activities planned under this component by the last Work Plan were used for the preparation and work of the "Atelier sur les Strategies de Consolidation des Programmes de Sante Reproductive, Volet Planification Familiale" in Marrakech on September 25 and 26, 1998. This workshop was attended by partners from the various sectors involved in family planning in Morocco. Participants unanimously recommended including the budget required for funding MOH contraceptive needs in the 1999-2004 five- year plan. Following the workshop, a FPLM consultant assisted the DP in calculating the amounts required each financial year, taking into account USAID, European Union and UNFPA contributions.
Study of the Financing of Reproductive and Child Health Programs: Under the aegis of the Higher Population Commission, a cost-efficiency study of reproductive health was undertaken with POLICY and PHR assistance. The study was presented to the Conference on the Financing of Reproductive and Child Health Programs, organized by the MOH Population Directorate and CERED on July 7, 2000 in Tangier. Public and private sector decision-makers, local representatives, civil society and international cooperation organizations attended the conference. The participants set themselves three major targets: reflection on a methodology to determine the costs of reproductive and child health; strengthening the partnership mechanisms between all the actors in this field, and identification of new financing mechanisms.
Results and future perspectives
The results aimed at by the contraceptive financing phase-over component have been, for the most part, successfully achieved. The Marrakech workshop and the multiple meetings
John Snow, Inc. 44 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
on the Five-Year Plan resulted in a consensus within the MOH on the sources and modalities of supply. The forecasts of pipeline supply are known and a scenario through 2004 has been prepared. The latter expects that, while the MOH will initially still be assisted by USAID, UNFPA and European Union grants, it will mobilize 100% of the resources required for contraceptive procurement from 2002 onwards.
This satisfactory result is largely due to the unrelenting advocacy efforts of the Population Directorate and its partners during the past years. One major concern that should be stressed is that the MOH vaccine and contraceptives budget is financed by a World Bank loan until 2001. It is therefore crucial to remain vigilant in the coming years so that the above scenario is effectively implemented and to continue advocacy efforts.
Concurrently, the work initiated by "post-Marrakech commissions should be pursued to reduce the costs of the public sector FP program by all possible means: through efforts decreasing taxes and customs duties, promotion of long-term contraceptive methods and increased involvement of the private sector and NGOs in FP service delivery. This strategy has recently proved successful: the Ministry of Economy and Finances approved a substantial decrease in taxes and customs duties on contraceptives.
C. Advocacy Tools and Interventions
PHR
Since 1996, the Partnership for Health Reform (PHR) project provided technical assistance to assist the Ministry of Health and USAID to achieve Intermediate Result 2: "Improved policy environment supporting expansion of family planning and maternal and child health services". PHR assistance during the past four years was made possible by the presence in Morocco of a PHR representative as well as by the programming of several interventions and short-term consultancies of PHR experts. The PHR representative ensured coordination of activities with USAID, development of a work plan as well as PHR activities (including short-term technical assistance activities) undertaken in collaboration with other cooperating agencies involved in the Phase V Bilateral Project, especially JSI and POLICY.
Objectives
FP program support and funding, especially the financing of contraceptive products (in the framework of contraceptive financing phase-over);
A better policy and legal environment for the delivery of family planning and maternal and child health services in both the public and private sectors.
Achievements
The main activities that were carried out are:
Maintain a high level of contraceptive prevalence at a time when USAID financial support to the FP program comes to en end.
- Advocacy File - PHR supported the MOH in the development of its advocacy strategy aimed at providing the necessary resources for the family planning program. At the end of the fiscal year (September 1998), a document known as "Advocacy File" was finalized. The file, designed for presentations, included several Powerpoint slides, a 20-page technical document and a short notice summarizing the constraints
John Snow, Inc. 45 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
the FP program faces. The objective of this file, prepared by PHR in collaboration with the MOH, USAID, the JSI team and the POLICY Project, was to convince policy- makers to act so as to ensure the sustainability of the FP program by providing adequate resources. SElS and the Health Economy Service (SES) updated the data of the model developed by Dr Daniel Kress. The model described FP costs and, specifically, the benefits the nation could derive from a program that provides FP with adequate resources. Policy-makers used this updated file as an argument in lobbying activities.
Reduce the substantial cost of taxes and administrative costs associated with the procurement of FP and vaccination products
- Study of taxes - PHR finalized a major study on taxes in forty-four countries. This study shows how different tax policies have been applied in these countries and how these policies were used to achieve objectives assigned to various public health programs. In a number of countries tax relief was a means for reducing the consumer price of three so-called key products (vaccines, oral rehydration salts and contraceptive products), as well as for increasing the supply of these products, but also and specifically for achieving a reduction in the budgetary requirements of ministries of health. Moroccan decision-makers were as aware of the need for tax relief on key public health products as they were aware of the benefits of such a relief to the State, suppliers and consumers. One constraint remained, however: the rationale of the Ministry of Economy and Finance which is closely linked to the volume and value of the tax base.
- Structure of costs - PHR participated in a major seminar "Atelier sur les Strategies de Consolidation des Programmes de Sante Reproductive, Volet Planlfication Familiale" in Marrakech in September 1998. The documents developed by PHR, the reviews undertaken by POLlClY on FP market segmentation as well as the JSI contribution on supply options and the impact of taxation on contraceptive procurement were the foundation of the work of the various commissions. Follow-up on this workshop was very positive since it became the working platform for reflection on and development of a five-year plan for the department. It also enabled the MOH to constitute six working commissions (financing, IEC, private sector development, involvement of gynecologists and pharmacists, diversification of methods and products). Working under the supervision of Dr Hajji, head of the FP Division, the PHR representative coordinated the post-Marrakech commissions to encourage reflection on the recommendations of the Marrakech workshop.
- Development of an advocacy strategy - the task of the financing commission was to review means for the government to reduce FP program costs (tax and customs waivers, working capital, more active private sector involvement in FP service delivery, etc.). Based on discussions within the commissions, recommendations were presented to the MOH on reducing the costs of contraceptive procurement. Joint efforts of the Population Directorate and USAID, together with PHR, JSI and POLICY technical assistance, proved successful since the budget programmed under the five-year plan covers FP needs.
Another major success achieved by the Population Directorate, i.e. the request for a tax and customs waiver presented to the Ministry of Economy and Finance, had a positive impact since taxes and customs duties on contraceptive products decreased considerably. The new tariffs to become effective presently are the following:
John Snow. Inc. 46 Contract No. 608-C-00-94-00006
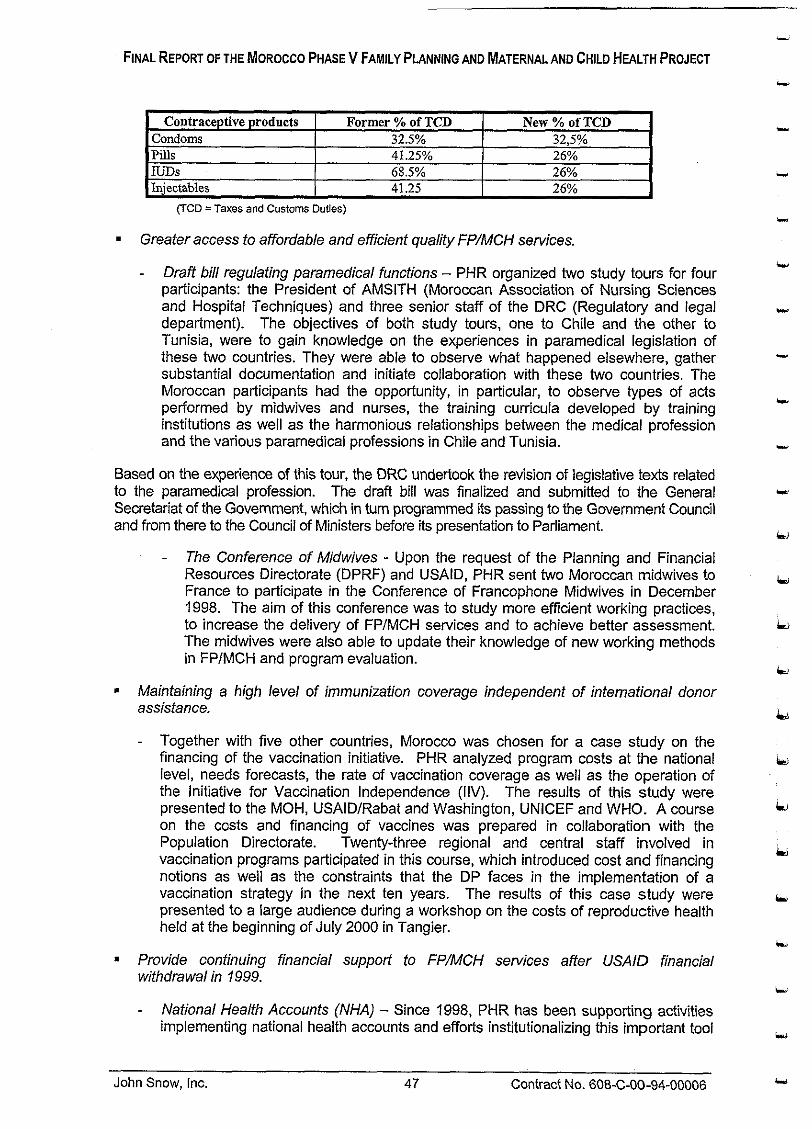
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
= Greater access to affordable and efficient quality FP/MCH services.
Contraceptive products Condoms Pills IUDs Injectables
- Draff bill regulating paramedical functions - PHR organized two study tours for four participants: the President of AMSITH (Moroccan Association of Nursing Sciences and Hospital Techniques) and three senior staff of the DRC (Regulatoly and legal department). The objectives of both study tours, one to Chile and the other to Tunisia, were to gain knowledge on the experiences in paramedical legislation of these two countries. They were able to observe what happened elsewhere, gather substantial documentation and initiate collaboration with these two countries. The Moroccan participants had the opportunity, in particular, to observe types of acts performed by midwives and nurses, the training curricula developed by training institutions as well as the harmonious relationships between the medical profession and the various paramedical professions in Chile and Tunisia.
Based on the experience of this tour, the DRC undertook the revision of legislative texts related to the paramedical profession. The draft bill was finalized and submitted to the General Secretariat of the Govemment, which in turn programmed its passing to the Govemment Council and from there to the Council of Ministers before its presentation to Parliament.
(TCO =Taxes and Customs Duties)
Former % of TCD 32.5% 41.25% 68.5% 41.25
- The Conference of Midwives - Upon the request of the Planning and Financial Resources Directorate (DPRF) and USAID, PHR sent two Moroccan midwives to France to participate in the Conference of Francophone Midwives in December 1998. The aim of this conference was to study more efficient working practices, to increase the delivery of FPJMCH services and to achieve better assessment. The midwives were also able to update their knowledge of new working methods in FPlMCH and program evaluation.
New % of TCD 32,5% 26% 26% 26%
Maintaining a high level of immunization coverage independent of international donor assistance.
Together with five other countries, Morocco was chosen for a case study on the financing of the vaccination initiative. PHR analyzed program costs at the national level, needs forecasts, the rate of vaccination coverage as well as the operation of the Initiative for Vaccination Independence (IIV). The results of this study were presented to the MOH, USAIDJRabat and Washington, UNICEF and WHO. A course on the costs and financing of vaccines was prepared in collaboration with the Population Directorate. Twenty-three regional and central staff involved in vaccination programs participated in this course, which introduced cost and financing notions as well as the constraints that the DP faces in the implementation of a vaccination strategy in the next ten years. The results of this case study were presented to a large audience during a workshop on the costs of reproductive health held at the beginning of July 2000 in Tangier.
Provide confinuing financial support to FP/MCH services affer USAID financial wifhdrawal in 1999.
- National Health Accounts (NHA) - Since 1998, PHR has been supporting activities implementing national health accounts and efforts institutionalizing this important tool
John Snow, Inc. 47 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
in understanding the Moroccan national health system. With the NHA it is possible to identify problems of resource allocation and evaluate progress toward a specific objective. The NHA also provides the MOH with reliable evaluation components that may assist senior department staff in improving the development of five-year plans. In this respect, NHA are a useful planning tool.
- Project implementation proceeded as follows: During the initial phase, the SESIDPRF team collected data on a pilot province (Settat), developed matrixes, identified missing information and prepared an action plan for data collection at the national level. To achieve this, a number of regional seminars were organized in four training centers (Marrakech, Agadir, Fez and Rabat) for all the provinces of the Kingdom between September 27 and October 8, 1999. The collected data underwent a specific process before being aggregated to obtain health accounts at the national level. The draft report presenting the results of the first national health accounts in Morocco is being finalized. It is to be noted that the Ministry of Economy and Finance, the Statistics Department of the Ministry of Plan as well as the Royal Armed Forces are associated with this project.
To achieve the implementation of NHA, PHR organized three regional workshops (Middle East and North Africa) and an international seminar in Rotterdam in which senior staff of the Ministry of Health, the Ministry of Economy and Finance and the Statistics Department participated.
- Strengthening the financial analysis skills of the MOH at regional level - In 1999 and 2000, the MOH and PHR organized a number of seminars to strengthen the financial management skills of MOH staff in the context of regionalization, by providing them with the methodological tool of financial analysis. Two of these seminars (in April 1999 and 2000 in Marrakech), also attended by Algerian and Tunisian participants, were organized with the participation of RESSMA and co- financed by WHO, the Algerian International Rotary and the USAIDIANE Regional Bureau.
Assessment of training organized by PHR shows it to be very positive, with 106 department managers trained in health economics. Among the 106 individuals were 38 delegates, 20 hospital directors, senior S I M P and health center physicians, 27 administrators/bursars and 21 PNI program animateurs, as well as matrons and cadres of the regional epidemiological observatories. REESMA (Network of Maghreb Health Economists) seminars involved 29 Moroccan, 13 Tunisian and 10 Algerian cadres. Altogether, 39 out of the country's 68 provinces benefited from training in health economics.
Constraints
Several PHR activities presume continued MOH and Government commitment to achieve progress on some decisions. It should be noted that while PHR continues providing the necessary assistance and advice, numerous final decisions depend on decision-makers outside the MOH. To illustrate this, an example can be cited: the draft bill regulating paramedical functions was prepared by the Regulatory and Legal Department (DRC) in collaboration with PHR. Progress of the file depends on decisions, within the scope of the General Secretariat of the Government, on the programming of bills passed on to Parliament for reading, and on the time required both by the first chamber and the chamber to adopt this bill. Another example is the study of the costs of vaccine financing, which revealed the risks Morocco will incur as long as the recurrent costs of the vaccination program are financed by an international loan. This study confirmed, however, that the mechanism set up by the Population Directorate currently remains
John Snow, Inc. 48 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
the best solution for financing both the National Vaccination Days (JNV) and the routine campaigns and mini-campaigns.
Achievements and future perspectives
Phase-over in family planning (see also above):
One of the remarkable results to be credited first to the Population Directorate and then to excellent collaboration of PHR with USAID, JSI and POLICY, is that the MOH succeeded in significantly increasing its budget for reproductive health by earmarking 36,500,000.00 Dh (about $ 3.7 million) under the 1999-2000 Financial Law. This budget should enable the MOH to finance all its FP activities without any other USAlD financial support as highlighted by the study undertaken by Mr. Edward Wilson (FPLM). Moreover, amounts programmed under the five-year plan should be sufficient to finance FP during the remaining four years of the five-year plan.
Reduce the substantial cost of taxes and administrative costs associated with the procurement of FP and vaccination products.
- Based on the advocacy file and the study of tax waivers conducted by PHR, the Population Directorate implemented a strategy aimed at reducing taxes and customs duties. This strategy was successful since the Ministry of Economy and Finances favorably received the MOH request.
Greater access to affordable and efficient quality FP/MCH se~vices.
- The two study tours to Chile and Tunisia, organized by PHR for four MOH senior staff, were useful to the Regulatory and Legal Department in the preparation of a draft bill regulating the paramedical professions. The terms of this bill should enable midwives and nurses to practice in private surgeries or clinics, thereby improving the access to FPIMCH services, especially in rural areas where few physicians practice. It should be noted that the legislation presently regulating paramedical functions dates from colonial times.
Maintain a high level of national vaccination coverage independent of international donor assistance.
- With the immunization study, it was possible to update all the constraints impeding the financing of the National Immunization Program in the medium and long term. A strategic plan to ensure adequate PNI funding was prepared by PHR in collaboration with the Population Directorate. A training workshop was organized and facilitated by PHR experts. In this workshop, cost and funding issues of the immunization program were broached and the vaccination strategy for the next ten years was discussed. Based on study results, USAlDlRabat agreed to provide an additional $500,000 to the vaccine working capital in view of USAlD withdrawal.
Reinforced capacity of the MOH to manage a diversified resource base.
- The MOH entrusted the National Health Accounts (NHA) project to a competent DPRF team. PHR worked in close collaboration with the Health Economy Service on the development of matrixes to be used as a base for data collection. Aware of the major efforts made, USAIDIRabat responded favorably to a request for additional funding to obtain more reliable data to be collected at the level of each province and prefecture in the country. Although the NHA enjoys the assistance of eminent international PHR experts, it is the Health Economy Service (SES), with its national
John Snow, Inc. 49 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
competence, that has been the actual artisan of the first Moroccan NHA. It should also be noted that, despite restrictions on the creation of posts in the public sector, the DPRF was able to reinforce the SES team by recruiting two senior economistsl statisticians to better progress its project of institutionalizing NHA.
This same team, in close collaboration with the RESSMA network, also guarantees the sustainability of training activities in financial management. The local WHO bureau will finance the evaluation by an independent Moroccan expert of all the training activities undertaken by PHR. Moreover, the local WHO bureau agreed in principle to participate in the funding of a third RESSMA seminar.
Other advocacy activities
To promote the new strategies and approaches in maternal and child health care, the Project contributed financially to the organization of several public health conferences:
The annual congresses of the Observatoire National des Droits de I'Enfant (ONDE): promoting the lMCl approach;
The annual congresses of the Societe Marocaine des Sciences Medicales (SMSM): promoting private sector participation in preventive FPIMCH services;
The meetings of the South-South Partnership in Population and Development enabling Morocco to share experiences in reproductive health with other countries.
John Snow, Inc. 50 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
lntermediate Result Ill: Reinforced Capacity to Manage FPIMCH Services with Particular Emphasis on Decentralized Approaches Responsive to Client Demand
Activities carried out under the FPlMCH Phase V Project to achieve the Intermediate Result Ill had a twofold objective:
1. Reinforce the capacity of the regions to plan and undertake actions in FP, Safe Motherhood and IMCI; and
2. Reinforce the capacity of MOH central and regional levels to decentralize the management of FPIMCH services in an organized and efficient fashion.
Under the first objective, and since the creation in 1997 of sixteen regions, the Project initiated a series of experiences to operationalize regionalization in the five regions, which are specified under Decentralized management at regional level.
Activities relevant to the second objective were aimed at strengthening support systems to decentralized management and the individual and institutional capacity to manage these systems at regional and provincial levels. They are summarily described under six components:
Information, education and communication (IEC)
Quality management
Pre-service and in-service training
- Contraceptive logistics
Evaluation
Health Information System (SIS)
For each of these components, activities first targeted the central level and then moved gradually to the peripheral level.
Several cooperating agencies contributed to the implementation of activities planned under the components of this intermediate result: JHUICCP as JSI sub-contractor for the IEC component; URC, JSI sub-contractor for quality management; JHPIEGO, PRIME and MSH for the pre-service and in-service training component; and Tulane University through the EVALUATION and MEASURE Projects for the evaluation and information and management systems components.
USAlD chose two indicators to measure the results of activities under this intermediate result. The evolution of these indicators and other complementary indicators during the lifetime of the Project will be discussed in greater detail under each component:
An increase in the % of provinces reporting availability of three-month contraceptive stocks each month of the year.
Documented evidence for each pilot region of at least three FPIMCH programmatic actions based on FPlMCH data analysis.
John Snow. Inc. 51 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
A. Decentralized Management at Regional Level
In 1997, Morocco legalized a model of decentralized government at regional level. Sixteen new regions were created and an elected "regional council" was to ensure devolution in each region. The creation of regional organizational structures for each department ("deconcentration") was to follow rapidly.
It is in this context that the FPIMCH Proiect team took the strateoic decision. at end 1997. to support the Ministry of Health (MOH) in Its effort to operationalize the newly created regional level within health services. The rationale was that decentralized manaaement. as facilitated by regionalization, is the best means for achieving the Project objective,-i.e. th; sustainability of FPIMCH services after the end of the bilateral cooperation agreement. The 1996 Transition Plan emphasizes that: "The Government of Morocco and USAlDlMorocco recognize that the improvement in health of a growing population, with declining support by donors and the government budget, will require decentralized leadership and healthy management of the resources of the system".
Objectives
Test decentralized management models in the five pilot regions through the implementation of projects managed by regional teams, and
= Explore multi-sectorial partnership mechanisms at regional level.
Performance indicators
In each of the five pilot regions, and based on a situational analysis, the FPIMCH action committee identified, organized and financially managed at least one FPIMCH project.
Achievements
From 1998 onwards, several decentralized management activities had been implemented with Project financial and technical support:
(1) Implementation of projects autonomously managed by regional teams in the five pilot regions: Doukkala-Abda (D-A), Fez-Boulemane (F-B), MeknBs-Tafilalet (M-T), Souss- Massa-DrSa (S-M-D) and Taza-Al Hoceima-Taounate (T-A-T). These were regions where various Phase V Project pilot activities such as Safe Motherhood , IMCI or the health information system, were being implemented.
(2) Exploration of multi-sectorial collaboration in S-M-D where USAlD was involved in several development projects.
(3) Other activities to strengthen the regional management capacity, such as inter-regional visits and training abroad.
Regional Projects
During 1998 and based on the results of the situational analysis of FPIMCH programs, each pilot region identified a regional project with well distributed issues: two projects concerning family planning, two on prenatal consultations (PNC), and one on neonatal mortality. A
John Snow, Inc. 52 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
document was developed for each project providing details on objectives, indicators, work plans and a budget. Project implementation began at the end of 1998 and evaluation at the end of 1999. The following paragraphs provide an overview of project progress in each region, achievements and a number of observations on the project management process.
Souss-Massa-Draa: Internal Audit of Early Neonatal Death
The objective of this project was to achieve a decline in early intra-hospital neonatal mortality in six hospitals of the region through the creation of internal audit committees. The project, initiated at the end of 1998, was well designed and planned and the first to start before all the other regional projects. Most of the scheduled activities were implemented in 1999. Audit committees were established in the six hospitals of the region and their members were trained in audit procedures. With the technical assistance of INAS, the project was evaluated by the regional team in October 1999. The results show that the audit of neonatal deaths had become a procedure accepted by service providers and resulted in the implementation of measures to improve the quality of neonatal care.
Confronted with the necessity of fairly specific assistance for audits, numerous resource persons were involved in this project, including a person from the DP, professors of the Rabat CHU, an INAS teacher and even a team of neonatologists from the Montreal Children's Hospital who were visiting Morocco. This contributed well to the technical level of project assistance, but concurrently required major coordination efforts and good project management. Since all the members of the project management committee were involved in other activities in the region and even at national level, it was not always possible for them to follow closely project activities. Despite this, the project went through all of the programmed stages, probably also because of the considerable involvement of resource persons.
Fez-Boulemane: Improvement of Prenatal Consultations
The Safe Motherhood pilot project implemented in this region raised the awareness of regional decision-makers on the issue of matemal mortality. In the framework of decentralized management of the maternal health program, a regional project on prenatal consultations (CPN) was therefore identified to complement the approach selected by the SM pilot project. The project revised the CPN from a new perspective: How can the CPN contribute to a program of maternal mortality reduction, although most of the potential complications of childbirth are not predictable? Taking this into account, the major project activity was the development of a CPN module focused on the IEC aspects of CPN and, in particular, key messages to convey to women on the signs of potential complications and to encourage them to give birth in an institutional setting.
An internal evaluation of the project showed that all provinces had increased both their CPN recruitment rates and their rates of institutional deliveries in 1998 and 1999. Project implementation was monitored through regular meetings of the regional management committee. The latter was composed of the delegates of the five provinces of this region, plus several other resource persons from the region. All provinces were involved in the various stages of the project, although some activities, such as technical training for which each province had developed its own training module, were conducted without much coordination between the provinces. The project had been delayed because of the absence of the principal project conceiver during the first two months of project implementation. This could have been avoided if a good management team had been involved from the very beginning. The result was that follow-up meetings took place at the same time as other regional activities.
John Snow, Inc. 53 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Meknes-Tafilalet: Improvement of CPN Quality
Development of this project was based on a case study of perinatal mortality at the Mohamed V Hospital in Meknes. Survey results questioned the quality of the PNC provided by the health facilities. Accordingly, the objective of the project was to improve the quality of pregnancy supervision to make sure that the messages targeted at women in terms of possible complications and the advantages of giving birth in an institutional environment were clear and adequately conveyed. The project also attempted to consolidate the relation between referral structures and first-level MCH facilities. In the course of the project, 132 FPlMCH nurses of the region's 5 provinces were trained.
To evaluate this project, an observation grid was used that showed that the quality of CPN service delivery distinctly improved between 1998 and 1999. Positive facts emerge from the management of this project. Implementation of activities was more or less up-to-date and conformed to the budget. All provinces were actively involved. Leadership was clearly based at Meknes and it appears that the tasks of the management committee were well distributed and respected. The regional team had shown evidence of considerable independence in the management of the PNC project, without any intervention by resource persons from outside the region. Exchanges with the Fez-Boulemane management team were fruitful.
Taza-A1 Hoceima-Taounate: Project to improve the knowledge of long-term contraceptive methods
The target of the Taza-Al Hoceima-Taounate project was to promote long-term contraceptive methods through different actions such as: (1) creating awareness in relay persons; (2) improving the quality of interpersonal communication; and (3) extending the use of injectables.
The implementation of project activities was delayed because of a lack of coordination and leadership at the regional level. Finally, the regional coordinator of Al Hoceima, i.e. the regional capital, accepted to ensure project monitoring and coordination at regional level. The project team managed to inform and raise the awareness of 200 health professionals and 300 relay agents about the use of injectables. A DPIJSI team provided technical assistance for the development of an evaluation protocol. The latter included a number of quantitative indicators to measure project impact on the FP program and other quality indicators to evaluate project impact on the process and dynamics of regionalization.
Doukkala-Abda: Promotion of Long-term Confracepfive Methods
The objective of this project was to promote long-term contraceptive methods (LTCM) by improving the treatment of clients. Bad reception had been identified as a priority issue. The regional team therefore decided to improve the conditions of reception, stressing the respect of client privacy. Other project activities were the extension of the use of injectables and training in IUD and VSC. As in the TAT region, project evaluation was implemented with the technical assistance of the DPIJSI team. It showed that between 1998 and 1999 the percentage of LTM increased from 30.8% to 33.9%.
This was the last region to have initiated its project. There was a real problem in this region as to the competence to develop projects and to coordinate between the two provinces. The regional managers requested a workshop on project development for representatives of the two provinces. This was conducted with the assistance of an INAS teacher. Besides strengthening the capability directly related to project development, this seminar resulted in the improvement of coordination and communication within the regional team. The
John Snow, Inc. 54 Contract No. 608-C-00-94-00006

Doukkala-Abda regional team proved very motivated and persevered in the search for favorable results. It may be concluded that the planning workshop played a major role in the capacity building of the regional team.
Publiclprivate Partnerships
An MOH team, assisted by the POLICY Project, reviewed the mechanisms of multi-sectorial collaboration in the S-M-D region, where USAlD was involved in several development projects. Initial activities were of an exploratory and planning nature:
ldentification of regional partners to initiate a multi-sectorial dialogue on reproductive health and family planning - ldentification of mechanisms through which the regional multi-sectorial dialogue can take place: all partners (public, private, associative) agreed that the health commission of the regional council could be used as a dialogue forum.
Design and implementation of regional health strategies require the creation of a solid partnership with various actors. Among the latter, civil society is most often the closest to the population, but also the least organized at regional level. To prepare the regional dialogue forum, a number of provincial round-tables were organized in April 2000 to identify representative organizations. The major objectives of these round-tables were to: (1) diagnose the potential available to NGOs in terms of regional approach to development in general, and to health and population in particular; (2) initiate and promote a regional dialogue among NGOs; and (3) prepare a regional debate between NGOs and the various actors. A detailed report on the results of these workshops was produced and distributed to all participants and partners in the regional dialogue.
Following these seminars, the regional council of Souss-Massa-DrSa, in collaboration with the Wilaya of the region, the provincial delegations and the lbn Zohr University/Faculty of Arts and Human Sciences, and with USAlD technical support provided through JSI and POLICY, organized a workshop on the regional dialogue on health and population in Agadir on June 6, 2000. The objectives of this workshop were:
Organize and initiate a regional dialogue between the different actors in the health sector and thepopulation in the S-M-D region
Determine a forum for the regional dialogue on health and population; and
Define the mission of this forum and the role of each of its members.
A report on this day has been drafted, printed and distributed to each of the actors at regional level.
Other activities to strengthen regional management capacity
During the last year of the project, interregional exchange visits were organized to share experiences in techniques and management. In the context of interregional coordination, visits were organized to Meknes to share information and expertise between the two regions implementing CPN projects.
Concurrently, several training activities on the decentralized management of health programs were organized. A total of twenty-five individuals from central and regional level (I 1 from the
John Snow, Inc. 55 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
pilot regions) participated in international courses, each focused on an aspect of decentralized management. Out of these twenty-five, twelve (three from the pilot regions) from regional and central level participated in the international course on "The Decentralized Management of Health Systems" held by MSH in collaboration with INAS. Seven staff members (four from the pilot regions) received international training in "Follow-up and Evaluation of Development Projects" that took place at Settat and was organized by the University of Pittsburgh. Two people (one from Fez) participated in a training course in the US organized by the University of Pittsburgh on "Project Planning and Management". Lastly, three midwives from the pilot regions and a representative of a national NGO, attended training in the Design and Planning of Reproductive Health Programs in Santa Cruz, California.
Lessons Learned
The results of the first experiences in decentralized management were discussed in two regional reflection and coordination meetings: one in Agadir in October 1999 with the public and private partners in the S-M-D region and another in Fez in April 2000 when the teams of the five regions met.
The operationalization of decentralized management has a different impact and pace from one region to another. This assertion is valid, but once the projects were underway, the differences were not so noticeable. Once the notion of region was understood, the differences were more in form than in substance. It should also be noted that the different regions appreciated exchanges among themselves either during seminars or interregional visits.
There was a lack of planning and management experience and competence at regional level. This absence no longer seems as important as it did earlier. This is perhaps due to the ex~erience aained in the manaaement of a ~roiect or ~ e r h a ~ s because a lame number " of in training courses on the management of decentralization. It should, however, be stressed that there is still need for data analysis skills.
What is the role of the central level? This year it has become increasingly evident, even for central level executives, that the central level perhaps does not have a major role in regional management. The problem is that the central level does not perceive its role very well at the regional level and that the latter has its own functions. The moment therefore has clearly come to specify the role of the central level in its relations with the regions.
The link between the decentralized management of FPIMCH programs and the various support management systems has become clearer. Information, training and quality are closely linked, with each playing a major role in the management of health projects and services in general. The regions have started integrating all of these activities and managing them instead of being managed by them.
Regionalization in the other sectors has not progressed much and links with the health sector are not always well defined. Some activities have been initiated with NGOs, but not with other ministries. One initiative going in the right direction was organized by the S I M P delegation in the context of the lMCl approach. They convened several departments to find solutions to the problems raised by the population during ECPs (see lMCl report). Also, as noted by the POLICY annual report, a tentative exploration of inter-sectorial collaboration had started in the Souss-Massa-Dria region.
The major concern of all regional teams was the lack of progress in the formalization and implementation of regional structures. Since last year, regional coordinators are nominated officially, but they have no regional budget. A major activity was the development, at regional level, of the five-year plan. This exercise was a confirmation of the official government policy in regionalization and forced the regions to think collectively.
John Snow, Inc. 56 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Conclusions and future perspectives
The result indicator of this component was achieved: "In each of the five pilot regions, and based on a situational analysis, the FPlMCH action committee identified, organized and managed financially at least one FPIMCH project". But more than this, the "field exercise" in regional management, which initially concerned only the management of FPIMCH services, was really telltale and seems to have been the catalyst for regional management in general.
It is understood that the aoal of the Ministrv of Health is to extend decentralized management throughout the country. It is therefore absolutely essential to continue research on appropriate intra- and inter-sectorial regional management structures. This had first been initiated in the S-M-D where, during the post-bilate&l period, USAlD supported a more global development approach. Then, it was initiated in the Tanger-Tetouan region, which will be part of the USAlD post-bilateral project, and finally in the Marrakech-Tensift-El Haouz region with UNFPA support and in the Eastern region with European Union support.
B. Information, Education and Communication
While the supply of quality health care may considerably contribute to an improvement in the health level of a country, the behaviors and attitudes of populations towards health play a major role and ultimately determine the use of health care services. Information, education and communication (IEC) activities play the role of positively influencing behaviors and attitudes to lead them towards health and the rational utilization of health services.
In Morocco, the importance of IEC had been recognized by the highest levels of the Ministry of Health through the national health education program "Tous pour la Sante (All for Health), which considered social mobilization a key approach. For its part, USAID, aware of the considerable contribution of IEC to the sustainability of FPIMCH services, included IEC as an integral component of the FPlMCH Phase V Project. Well-targeted and high quality IEC activities can contribute to an increased use of family and maternal health services. However, the objective of the project was not solely FPIMCH-related IEC production, but also to strengthen the MOH's capacity to produce an efficient IEC program adapted to the needs of the Moroccan populations.
JSI, the institutional contractor, subcontracted the technical assistance for the IEC component, until the end of 1998, to the Center of Communication Programs of Johns Hopkins University (CCPIJHU), recognized leader in IEC, through a resident technical advisor. During the last two years of the Project, JSI managed IEC activities directly.
The following paragraphs deal only with IEC capacity-building activities such as defined under intermediate result Ill. IEC products and messages on family planning and maternal health and their impact on the use of FPIMCH services have been presented and reviewed under intermediate result I.
Objectives and Performance Indicators
The objectives of this component were:
= lncrease the DIEC's technical capacity in the design and development of communication strategies and IEC support materials to sustain FPIMCH programs.
lncrease the IEC's human resources capacity at all levels of the health system: the DlEC team, regional and provincial management teams, service providers and community development agents.
John Snow. Inc. 57 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Three performance indicators were used:
At the end of the Project, 85% of the printed and audiovisual support materials are entirely produced by the DIEC;
80% of the IEC animateurs and FPIMCH nurses regularly use IEC support materials in their communication with the population;
At least 50% of the volunteers trained within the involved NGOs organize awareness sessions in their centers or during home visits.
Achievements
In conformity with Project objectives, activities focused on the development of two strategies: (1) the strengthening of the DlEC as an IEC design and production agency, and (2) the reinforcement of the IEC skills of health personnel.
I . Strengthening the DlEC as an IEC design and production agency
At the inception of the program, the extended project team made the strategic decision to strengthen the design and production capacity of the IEC Division of the DP. Although a major part of the audiovisual and printed productions could have been carried out by private agencies, a basic capacity in technical equipment and human resources existed already within the DIEC, and recourse to the private sector represented a substantial financial burden for the MOH. Also, another considerable advantage was that the MOH could monitor directly the quality of IEC products and messages. The long-term vision was for the DlEC to achieve the status of Service d'Etat Gere de Maniere Autonome (SEGMA, i.e. Autonomously Managed State Service) and consequently to generate its own funds for the sustainability of design and production activities for IEC support materials.
Interventions to strengthen the DlEC are described under three headings: (1) consolidate the roles and responsibilities of DlEC services; (2) strengthen design and production skills; and (3) project the image of a new dynamic and competent DIEC.
Consolidafion of roles and tasks
Activities to strengthen the DlEC were initiated in 1995 by consolidating the roles and tasks of DlEC services through a team-building seminar. This seminar was attended by all of the DlEC personnel and permitted discussion of problems of daily management and the creation of a good working relations within the two DlEC services: the design service and the production service.
Strengthening design and production skills
The Project procured equipment required for the print shop and the audiovisual studio so that the production service could meet the needs for DlEC support materials as well as the short-term needs of other DP divisions, and possibly to meet the demands of other directorates and even other ministerial departments in the long term. Priority was given to equipment that would allow reducing the very high production costs of both printed and audiovisual supports. In the lifetime of the Project, the premises of the print shop and of the audiovisual studio were reorganized and rehabilitated to maximize available space and install the programmed equipment.
John Snow. Inc. 58 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Audiovisual equipment provided by the Project permitted project-supported audiovisual productions principally for safe motherhood and family planning programs. Four videocassettes were produced: Sahel Mahel and Oulad Lghial for FP, and Khlat Eddar and Bent Ettajer for SM. These productions also facilitated on-the-job training of the audiovisual team. Members of the latter, especially the cameraman, the cutter and the officials in charge of television and radio, received appropriate practical training (sfage) in their specific fields at the prestigious INA (National Audiovisual Institute) in Paris.
Television is the MOH's favorite medium to channel and popularize health messages, since about 70% of all Moroccan households own a W set. Besides typical W spots, the DlEC produced, since 1994, a fortnightly screening of a quarter of an hour sequel of the Asseha series. In 1996, the Project provided support to the production, in association with a private agency, of 13 sequels of a series illustrating mainly family planning and safe motherhood topics. An audience survey on W broadcasts, the first of this type, was carried out by the project in 1999. This survey shows that the audience appreciates this genre since the MOH maintains its reliability for anything dealing with the health of the population. A means had, however, to be found to ensure the sustainability of this series since outside production proved very costly. This is why the Project supported the co-production of the Asseha series together with a private agency to capitalize on the technical and human resources of the DlEC studio. This last phase resulted in a decrease of costs and an improvement of the skills of the audiovisual team. This co-productive experience also allowed the confrontation between public and private sectors to highlight the bureaucratic red tape, which had been an impediment to this action, thus causing delays. At the end of the process, 12 Asseha sequels (renamed "Ma sante d'abord" or "My health comes first") had been produced and 12 others were underway and will be completed by the DlEC studio.
Besides television, radio is a regular medium used by the MOH for health education since the majority of the population has a radio, with major coverage in rural areas. The audience poll on radio programs, conducted in 1998, showed that the health messages and spots were favorably received. In order to capitalize on the investments made under the Project, the radio section of the DlEC studio now has the capacities needed to continue the production of daily radio broadcasts, aired since 1993, while seeking their improvement and diversification.
Regular meetings with television and radio professionals were an opportunity to revive the links between the MOH and radio and TV, to achieve better coverage of the efforts made to improve the health of the population. The agreement between the Ministry of Communication and the MOH, signed during the lifetime of the Project, is an expression of this reinforced relationship with the media. It was also a means of ensuring the continuity of activities while ensuring the broadcast at preferential rates of all MOH productions.
Following procurement by the project of more sophisticated material for the print-shop and the training of print-shop personnel in its use, the DlEC was able to produce a large number of printed supports and documents for the different MOH services and directorates, from design to final printing. The offset printer, paper-trimmer, engraver, CAP units (Computer Assisted Production) procured under the Project were all used for these productions. This enabled the DlEC to cut production costs by at least 50% and to collaborate with various MOH services and directorates and even other ministries.
Projecting the new DlEC image
The second phase consisted of projecting this new image as designer and producer of printed and audiovisual support materials to the various users within the MOH, other ministerial departments and civil society. A permanent exhibition was mounted on the walls of the DP in 1998. This exhibition illustrates the efforts undertaken, for some twenty years,
John Snow, Inc. 59 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
in the design and production of health education support materials. With the assistance of a consultant, a photo library on the different FPIMCH themes as well as a catalogue of IEC support materials produced during the last decade by different MOH departments were developed. The catalogue is part of a file prepared for the open-door days of the IEC Division organized on July 12, 2000 for the international population day, in the presence of H.E. the Minister of Health, H.E. the US Ambassador and the press. All of the guests took a guided visit of the audiovisual studio and the print shop and samples of the major audiovisual and printed support materials. The open-door days provided an opportunity for publicizing the division's new capacities in the design and printing of quality support materials that were achieved through investments made by the Phase V Project.
2. Strengfhening the IEC skills of health personnel
The second major strategic component focused on strengthening the skills of health staff to communicate health messages to individuals and communities throughout the country, and especially in rural areas where illiteracy, geographic isolation and a deteriorating socio- economic situation impede accessibility to health services.
A key activity was the training of health professionals from rural areas in group facilitation techniques (TGFT). In 1996, this training was piloted in three regions (Safi, Taroudant and Taza) with the assistance of CPI, a Casablanca-based agency. 100 mobile team and itinerant nurses could be trained in six sessions. From 1997 onwards, TGFT was generalized throughout the country through a training-of-trainers. With CPI assistance, 16 TGFT trainers were thus able to train 660 other mobile team and itinerant nurses. Following this, they made follow-up visits to participants to build up the contents of the training. While TGFT was aimed at general communication skills, other more specific training activities in counseling for FPIMCH services were undertaken with Project support, but having the same target of improving the IEC skills of health personnel. These training activities are reviewed under RI I.
The second activity was the creation of tools to improve the efficiency of communication and health education efforts of itinerant and mobile team nurses. The first success of this activity was the design and production of an IEC family planning kit (see under RI 1). Following a workshop organized at Benslimane in November 1996, the DIEC personnel, a number of itinerants, as well as an expert in materials creation from CCPIJHU developed two new IEC support materials adapted to work in rural areas: a flanelograph and a message-carrier. Very elaborate pre-testing and the originality of the materials used, delayed mass production of these tools until December 1998. Highly appreciated by the first 400 itinerant nurses to receive them, these tools were disseminated in the field with additional support provided by UNFPA and WHO to cover all of the itinerant and mobile team workers. A mobile team of the Ouarzazate province also presented the two supports to Mrs. Hillary Clinton during her visit to the village of Tassalmante. Copies of the flanelograph were also distributed at the occasion of the children's parliament, in a spirit of collaboration between the MOH and schools, so that health education becomes the concern of everyone and of all the sectors.
Concurrently with this effort, actions were dertaken to improve the quality of IEC sessions in fixed facilities. Designed by the DIEC, these actions included instituting thematic IEC sessions, an audio corner with cassette player and a corner with posters on the same theme. In this context, the Project supported the procurement of a set of materials (bill- boards, benches, TV sets and cassette players) to improve the organization and frequency of health education sessions. All fixed health facilities providing FPIMCH services were given the IEC support materials developed under the Project, such as the FP demonstration kit, the flanelograph and the audio and videocassettes.
- --
John Snow, Inc. 60 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
In view of the magnitude of the IEC effort, the MOH included other partners to act as relays in the information communication chain: agents from other socially oriented ministries, and especially civil society, represented by development NGOs. Being very close to the population, they are the doors opening onto the rural environment and specifically women, for whom the constraints of accessibility and illiteracy are the worst. To build a better- structured partnership with NGOs and agents from other social ministries, reflection days were organized at national and regional levels in 1999 and 2000, with the participation of at least 20 NGOs, several socially oriented ministries and a number of donors.
To achieve an efficient and lasting partnership, a training guide in communication and health education was developed with the assistance of an international consultant. This guide for "community development agents" (CDA) was then tested during training sessions with the UNFM (National Union of Moroccan Women). The final version of the CDA guide was completed with the involvement of the managers of the different FPIMCH programs, TGFT trainers as well as a number of NGOs.
The CDA guide, together with the flanelograph and the message-carrier, were presented to NGOs who had expressed a need for training and information to achieve better usage. 2000 copies of the CDA guide and 1000 copies of the flanelograph were produced to meet the training needs of these associations. Three regions (Souss-Massa-Drga, Fez-Boulemane and Tanger-Tetouan) were chosen for pilot training in the IEC kit. TGFT trainers conducted two training sessions of 20 NGOs in each of the three regions. These sessions generated positive dynamics for increased social mobilization around health. Follow-up committees representing the participating NGOs were created to achieve the sustainability of health awareness actions. The different participants prepared detailed documentation on all these activities undertaken with NGOs in the framework of the Project.
Another innovative action supported by the Phase V Project was to take advantage of the unique opportunity provided by the prenuptial visit to meet the young couple and raise their awareness on problems related to reproductive and child health. This activity was piloted in the Rabat and Benslimane provinces in the form of information and awareness-raising days for public and private general practitioners in charge of prenuptial consultations. This project was extended to 20 other provinces, the pilot regions of the Project. To accompany this project, 100,000 IEC folders were produced on reproductive health behaviors to be adopted at the beginning of married life.
Lessons learned and future perspectives
Overall, the IEC activities undertaken under the FPJMCH Phase V Project were successful because of their innovative approach and the permanent concern of the Project to institutionalize, within the MOH, and sustain the human and material resources capacities set up by the Project.
An innovative IEC approach
Particularly innovative was the "educate-entertain" strategy used for the development of several communications tools, such as videocassettes, the flanelograph and the drama on SM. Since messages on reproductive and child health are most of the time addressed to people who are not ill, the absorption by the target audience of these messages is greatly facilitated by entertaining content. Although no external evaluation was conducted, audience surveys and the great demand for these support materials suggest that this strategy has proved particularly effective, not only in influencing behaviors and attitudes to reproductive and child health, but also in increasing the demand for FPIMCH services.
John Snow, Inc. 61 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
We should like to highlight at least one very successful activity in interpersonal communication: the prenuptial consultation as an ideal communication opportunity between the young couple and the health services. Besides its impact on the behavior of the young couple and their demand for FPlMCH services, the implementation of this activity in itself has also contributed to the consolidation of links between the public and private sectors by creating a specific framework for information sharing. The MOH decided to continue with this project in prenuptial counseling to cover most provinces throughout the Kingdom.
Susfain the IEC capacity within the MOH
As to the sustainability of IEC activities within the MOH, a few comments are required on the decision to invest considerable resources in the strengthening of the DlEC as a design and production agency of IEC strategies and tools. The impressive list of IEC support materials developed during the project is certainly a positive indication of the division's improved capacity, both in physical and human resources. However, as highlighted by the final report on the experience of N screening of "My Health First" (Ma Sanfe Avant Touf), several problems remain to be solved before the DlEC can acquire autonomous status (Service d'Efaf Gere de Maniere Autonome or SEGMA), when it will be able to generate its own funds to continue activities in the design and production of IEC support materials. The major problems are related to a lack of staff, the absence of a mechanism motivating the existing staff to manage an increasing workload, and the need to adjust administrative procedures to improve the conditions of audiovisual production and printing. Solutions can come only from the highest levels of the MOH and the Ministry for Public Service. Meanwhile, the DlEC must look for new partners to achieve improved performance and profitability of these new capacities. Open-door days were an opportunity to make the public better acquainted with the DIEC, as well as an advocacy method to discuss the constraints that exist in their daily work.
Lastly, the Project made a major investment into the improvement and institutionalization of the communication and health education capacities of all the people involved in raising public awareness about health. Training in group facilitation techniques (TGFT) was highly appreciated by peripheral health teams because of its innovative and participatory methodology and useful contents. Its implementation required a major mobilization of the DlEC and regional teams. Owing to the technical collaboration of the DFC (In-service Training Division) and the regional IFCSs, it has been possible to perpetuate this activity. The MOH now has 16 regional trainers whose communication skills have been strengthened and who have become regional resource persons to pursue the effort of improving communication skills, not only of health professionals but also of relay and NGO development agents. Institutionalization of TGFT training has been confirmed now that the DF has included facilitation techniques in the pre-service training curriculum of the IFCSs.
As to the sustained development of a structured partnership between the MOH and civil society, unique dynamics have developed in three pilot regions. One of the lessons to be learned from this experience is the discrepancy of capacities of the NGOs involved as well as the degree of awareness and motivation of health professionals to promote a constructive collaboration with civil society. This is why the post-bilateral project could include in its work plan the strengthening of links between associations and health professionals and the search for new collaborative mechanisms in the two relevant regions. It would also be interesting to follow up on this activity in the Fez-Boulemane region.
C. Integrated Quality Management in Morocco
From the very beginning, the Project considered the quality of care as extremely important to achieving the health objectives for the Moroccan population. The Project defined a strategy
John Snow, Inc. 62 Contract No. 608-C-00-94-00006
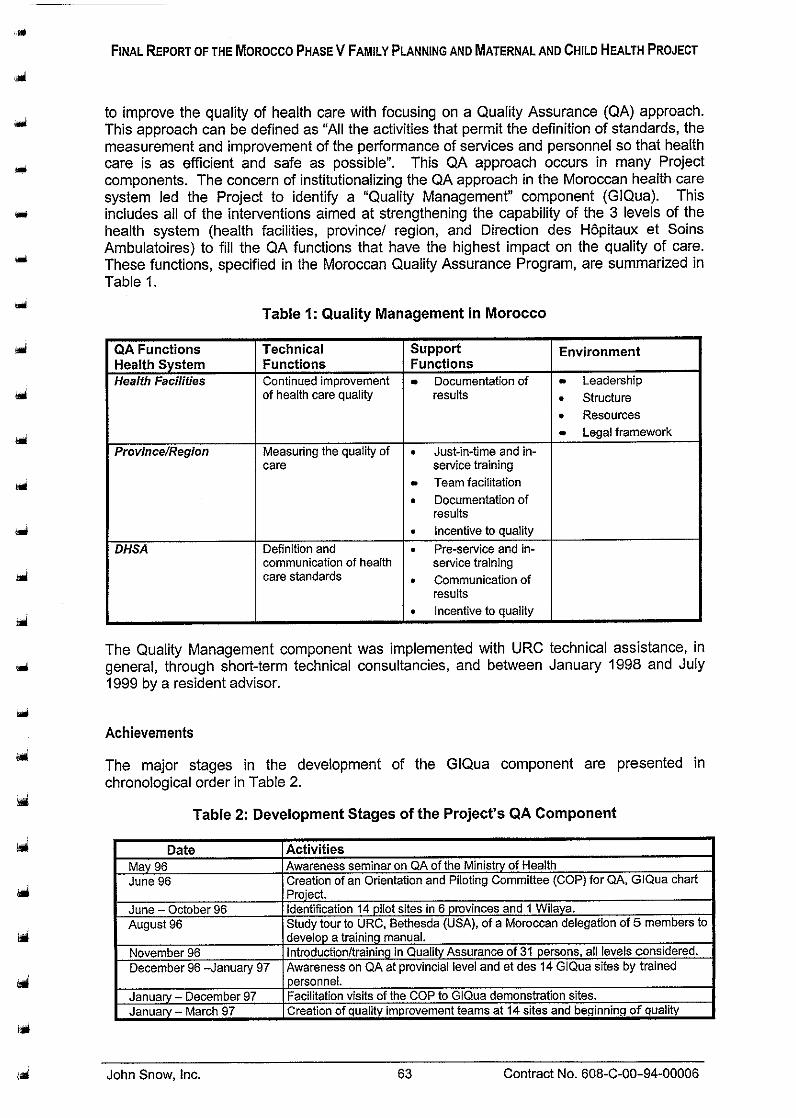
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
to improve the quality of health care with focusing on a Quality Assurance (QA) approach. This approach can be defined as "All the activities that permit the definition of standards, the measurement and improvement of the performance of services and personnel so that health care is as efficient and safe as possible". This QA approach occurs in many Project components. The concern of institutionalizing the QA approach in the Moroccan health care system led the Project to identify a "Quality Management" component (GIQua). This includes all of the interventions aimed at strengthening the capability of the 3 levels of the health system (health facilities, province1 region, and Direction des HBpitaux et Soins Ambulatoires) to fill the QA functions that have the highest impact on the quality of care. These functions, s~ecified in the Moroccan Quality Assurance Program, are summarized in . . Table 1.
Table 1: Quality Management in Morocco
QA Functions I Technical Health System I Functions Health Facilities I Continued im~rovement
of health care quality
I Province/Region Measuring the quality of
care
I DHSA Definition and
communication of health care standards
Support Functions
Documentation of results
. Just-in-time and in- service training Team facilitation . Documentation of results incentive to quality . Pre-service and in- service training . Communication of results . Incentive to aualitv
-
Environment
Leadership . Structure . Resources Legal framework
The Quality Management component was implemented with URC technical assistance, in general, through short-term technical consultancies, and between January 1998 and July 1999 by a resident advisor.
Achievements
The major stages in the development of the GlQua component are presented in chronological order in Table 2.
Table 2: Development Stages of the Project's QA Component
-
ate 1 Activities May 96 I Awareness seminar on QA of the Ministry of Health June 96 1 Creation of an Orientation and Piloting Committee (COP) for QA, GiQua chart
1 Pro,'ect. June - October 96 I Identification 14 pilot sites in 6 prov:nces and 1 Wilaya. Auqust 96 I Study tour to URC, Bethesda (USA), of a Moroccan delegation of 5 members to . I develop a training manual. November 96 I Introductionltraining in Quality Assurance of 31 persons, all levels considered. December 96 -January 97 I Awareness on QA at provincial level and et des 14 GlQua sites by trained
1 personnei. Jan~ary - December 97 ( Facilitation visits of the COP to G Qua demonstrat'on sites. Jan~ary - March 97 I Creat'on of quality improvement teams at 14 sites and beqinnnq of auality
John Snow, Inc. 63 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
. . (spain).
April 98 Development of a strategy to extend QA to 5 regions. April - May 98 Seminar to raise awareness about QA for 8 regions. April - May 98 Inter-site exchange visits for 3 representatives of each GlQua team. September-November 98 Training of the librarian of the QA resource center at INAS. October 98 Presentation of a paper at the international ISQUA conference. Budaoest
October 98 November 98
December 98 December 98 January 99
March 99
I care standards. June 99 I Initiation of an evaluation of the cost-efficiencv of GlQua teams throuah
(Hungary); participa$on of 2 Moroccans. Creation of quality improvement unit, depending on the DHSA Director. Preparation of a training program, resources and trainers for the Training workshop of regional trainers. Training in QA of 25 regional trainers. Creation of QA Resources Center at the DHSA. Sessions on QA awarenesslplanning for 5 regional management teams; choice of 25 new QA sites; beginning of 25 new teams. National consensus seminarlworkshoo national on the national QA orooram of
April 99 June 99
May 99 -June 99
- 1 operational research (activity financed by the'QA Project) June 99 I Participation of 2 Moroccans in summer course at Johns Hopkins University on
. " the MOH, 60 participants. Redefinition of the QA Program Piloting Committee. Workshop to develop a national strategy and implementation plan of QA within the MOH, 25 participants. Training of 14 teams and 7 facrlitators in the local use and follow-up of health
June 99 June 99 September 99 November 99 November-Decemoer 99
John Snow, Inc. 64 Contract No. 608-C-00-94-00006
Quality Assurance. Planning of GlQua activities for tne 99-00 extension phase. Departure of the Resident Advisor from Morocco. Beginning of the 1 year extension phase of the Project: 1999-2000. Mission to finalize the GlQua 1999-2000 work plan. Workshop to develop a g~ ide on the development of health care standards in
October-November 99 January 00 January 00
January 00 February 00 March 00
Morocco. 21 participants. Training of 30 facilitators in the local utilization of care standards. Training of 30 team leaders and 5 facilitators in facilitation techniques. Development of a regional training plan in quality assurance and planning of facilitation visits. Development of a curriculum for the QA training of the paramedical professions Workshop on the monitoring of SSP quality, 30 participants. Participation of 2 Moroccans in the EurODean Forum on the Qualitv of Care.

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
I Date 1 Activities I I MOH. June 00 I Study tour by the national QA program lo Costa Rica, 3 participants. June 00 I Data collection for operational research on the cost-effciency of GlQua teams. September 00 I First draft of the research on the cost-etficiency of teams. SeDtember 00 13 documents are being published in Morocco: 1) Tne PNAQ; 2) Le Guide I I M6thodologique de d&v.eioppement de normes de soins; 3) La Qualit6 en
Action. I These activities have been documented in mission reports by consultants and the annual performance reports of the Project, of which a complete list can be found in Annex 2. These activities resulted in the develo~ment of trainina and reference materials adapted to the
v
specific needs of Morocco.
Results
A solid structure for QA, implemented at all the levels:
Health facilities I 63 aualitv imurovement teams active . . . I Local capability of uselfollow-up of health care standards
Province/Region I 8 regions have active quality improvement teams
Central level
67 facilitatorsltrainers Plans to integrate the PNAQ in the regions Ca~acitv to monitor the auality of care . . ~O'IFCS trainers in QA National Quality Assurance Program (PNAQ) PNAQ Piloting Committee Quality Assurance Unit within the DHSA 7 facilitators Guide national d'elaboration des normes de soins QA capacity of the Training Division QA documentation center
I . Data base for team follow-up
Substantial results in the improvement in health care quality for target populations in a specific health facility, documented by measurable indicators, for example:
- Reduction of neonatal mortality from 46% to 31 %;
- Screening of contacts of tuberculosis cases increased from 33% to 100%;
- lncrease in the coverage by prenatal visits from 40% to 52%;
- Decline in the rate of children who do not receive their treatment in time from 43% to 11%;
lncrease in the satisfaction rate of patients from to 71% to 95%;
- IUD acceptance rate increased from 121month to 20lmonth;
- lncrease in the anti-tetanus vaccination coverage rate of pregnant women from 37% to 75%;
- lncrease in the participation of men in family planning from 36% to 56%;
- Achievement rate of 3 prenatal visits increased from 21.5% to 90%.
John Snow, Inc. 65 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The results of the QA activities of each of the 63 teams are reviewed in greater detail in the report of the July 2000 documentation mission (by E. Knebel, URC).
Analysis
Considering the results and the dynamics of the QA component, there is little doubt that the approach used in Morocco (continued quality improvement by problem-solving teams) is not only efficient, but can also be extended to all the health structures. The following paragraphs provide an overview of our reflection on the GlQua component, organized by strengths, weaknesses and constraints.
Strengths
Overall, QA activities in Morocco progressed well. After 4 years of effort, the approach is institutionalized at all the levels of the health system owing to the official status of the National Quality Assurance Program (PNAQ).
The last year of the Project was particularly successful since all programmed activities were completed to the satisfaction of the beneficiaries the Project was able to include two additional activities (documentation of case studies and operational research on the cost-efficiency of teams).
QA is in full expansion since increasing demand by health facilities has resulted in exceeding the initial coverage objectives.
The Ministry of Health has adopted the QA approach and now uses the PNAQ as a reference document for numerous other projects (e.g. the hospital and health sector reform supported by the World Bank and European Union).
The relationship between the MOH QA team and the URC technical assistance team is excellent and has created a congenial, productive and motivating working climate.
Weaknesses
* The absence of a QA resident expert in Morocco during the last year was an impediment since the application of methods taught or the plans developed in the workshops did not have follow-up after training.
QA activities remained somehow "disconnected" from other Project activities, especially the more clinical ones, such as the development of standards for emergency obstetric care or the introduction of the lMCl approach. QA methods could have contributed more directly to the achievement of Project objectives, which all had a quality dimension.
Collaboration among partners remained limited. During the multiple QA missions during the last year, a common debriefing session (DHSA, DP and USAID) took place only once. Consultants used as relays between the partners..
Despite the creation of a QA unit within the DHSA, the capability of the central level to provide the regions and provinces with technical support for quality of health care has remained very limited. On the one hand, human resources are inadequate, while, on the other, the leadership of non-medical personnel is not always recognized by the regionallprovincial teams.
John Snow, Inc. 66 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Localizing such a project in one central directorate incurs the risk of excluding the other directorates, which do not always feel involved. This is particularly detrimental for QA, which affects all the functions, services and programs of the health system and requires the commitment of everybody.
Constraints
As in many other fields, local leadership influenced the achievement of objectives and it was noticeable that differences in leadership between regions had an impact on the stamina and success of teams.
= The "absorptive capacity" of the Moroccan MOH has limits. Personnel constraints and the multiplicity of development projects in the health sector create a situation where the GlQua component does not get the required follow-up between two consultancy missions. Despite the obvious commitment of authorities, numerous activities suffered delays.
The team problem-solving method has internal limitations. Teams tend to select non- clinical problems and have often problems collecting and using the data. These problems are easy to overcome through close and effective coaching, which is not always available in all the regions.
Lessons learned
QA activities that were the direct responsibility of the regions were regularly reprogrammed (exchange visits, training and quality days). This raises doubts as to the capability of the regions to absorb overly ambitious programs with agendas that compete with other programs, while the regional entity is not yet functional.
Regions that benefit from entrepreneurial leadership succeed much better in QA, which requires creativity and taking risks to manage change. The "higher" levels should redefine their roles of support to the levels where health care is provided.
Hospitals and physicians are the structures and staff that most slowly adopt QA, which concords with the experiences of other countries. In an overly hierarchical society and a compartmentalized clinical world (physicians/nurses), teamwork is difficult to promote.
Despite the existence of several constraints, there is definitely a potential for the success of QA implementation in Morocco, due to a willingness to change and the open- mindedness of leaders who have accompanied the GiQua component since the beginning.
Future Perspectives and Recommendations
All of the partners of QA activities (DP, DHSA, USAID) should attend debriefing after each consultancy mission. For logistic reasons, it will be difficult to systematically associate the regions targeted by the new project, but they will probably have been debriefed on the spot.
In view of the absence of a URC resident QA expert, it is desirable for the commitment of the principal beneficiary (DHSA) to result in the identification and full-time availability of a resource person for the follow-up of QA activities.
John Snow. Inc. 67 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The development of QA capacities at central level must continue in order to institutionalize QA in Morocco. Each level has a role to play, especially in the support of directly lower levels.
It is desirable to refocus QA assistance by providing direct technical support (an expert comes to assist the regions with the implementation of quality assurance) instead of training workshops. Above all, results and learning should be privileged by achievement instead of capacity-building, which is not always expressed later. Moreover, many capacities have been built in Morocco, but it is application that raises a problem when technical assistance is discontinued.
A particular effort should be made to monitor quality to achieve the continuum of data collection by the teams, which would show that any changes made in the health care process have the expected results on the degree of adhesion to standards of care. This will promote the documentation on the progress of QA and the piloting of the program.
Lastly, the future project will benefit greatly from a "regional" approach where opportunities for quality improvement will be identified and coordinated by the region. This will avoid diluting results to a population confined to one health center, while involving the regional team more in the support of health facilities to tackle priority issues of maternal and child health
D. Pre-service Training and ln-service Training
The pre-service and in-service training activities of the FPIMCH Phase V Project were implemented with the assistance of three central USAlD projects: (1) the FPMD project managed by MSH; (2) the JHPIEGO project, and (3) the PRIME project. The JSI team was in charge of local management and coordination of activities.
MSH
The goal of FPMD technical assistance (TA) was to contribute to the programmatic, financial and organizational sustainability of the CNFRH and INAS in support of the FPIMCH goals of the Moroccan national program. The objectives of TA activities, and work performed between January 1997 and December 1999, were:
Objectives
1. Develop the capacity of the CNFRH as a sustainable organization that supports the Moroccan National Family PlanninglReproductive Health Program.
2. Support the development of a partnership between CNFRH and INAS to strengthen their institutional capacity.
3. Develop strategic linkages among the CNFRH, INAS, MSH's Management Training Program and other regional institutions.
Achievements
Develop the capacity of the CNFRH as a sustainable organization that supports the Moroccan National Family PlanningIReproductive Health Program.
John Snow, Inc. 68 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
A Sustainability Plan for the CNFRH was prepared. Development of the Plan was initiated in September 1996 when Prof. Alaoui visited Boston for two days of intensive discussions with MSH technical consultants. A draft Plan was prepared by MSH technical consultants in November 1996 in consultation with Moroccan counterparts and was submitted for review and feedback to the CNFRH, MOH, USAID, and INAS. Feedback on the Plan was obtained from all parties in February 1997 and the CNFRH Sustainability Plan was finalized in March 1997. This Sustainability Plan is included in the Final Report on "Strategic Directions for Building the Institutional Capacity of the National Training Center for Reproductive Health and the National Institute of Health Administration", prepared by Mr. Jan Hoey, Mr. Charles Stover, and Dr. James Wolff, dated March 10, 1997. The document is comprehensive, describing the roles, responsibilities, and activities of all institutions which are contributing to the sustainability of the CNFRH and INAS, e.g., MSH, USAID, JSI, other cooperating agencies, the MOH, etc.
Mr. Hoey attended, observed, and held discussions with trainers and participants during a Bday training seminar on IUD insertion conducted by the CNFRH on November 15-16. 1997. Mr. Hoey discussed training methodologies with the Course Director and 3 co- trainers, and provided feedback on his observations concerning the course and course materials.
MSH and ECS lnformatique signed a contract with MSH in October 1998 to install a financial management system at INAS and CNFRH to strengthen the financial management capacity of both institutions. ECS lnformatique has completed the development of a computerized financial management system for CNFRH and INAS as described in the contract with MSH and provided both institutions with user manuals in July 1999 and trained the staff at INAS and CNFRH in December 1999. This system helped the two institutions track the funds received from donors and other sources.
Support the development of a partnership between the CNFRH and INAS to strengthen their institutional capacities.
Through a local vendor (MTDS), two computers, three modems, and lnternet access were installed at the CNFRH and INAS in April 1997, Key staffs at these institutions were trained in lnternet technology and electronic communications. The availability of electroniccommunications greatly enhanced communications between FPMDIMSH and Moroccan counterparts between TA trips as well as among Moroccan counterparts themselves. In addition, lnternet access provides the institutions with access to innumerable international resources.
The directors and key staff of CNFRH and INAS conducted a one-day strategic planning session in November of 1997 independent of MSH. The two agencies worked on a joint collaboration strategy, formalized in a draft inter-agency agreement. They reviewed the activities in the 1998-99 work ~ l a n and olanned other initiatives that existed outside of the plan and assigned staff responsibilities for key activities. The results of the workshop were im~ortant stew toward the achievement of closer links between CNFRH and INAS. an objective suppo;ted by the FPMD activities.
MSH provided the CNFRH and INAS with simple market study methodologies to gather information to help identify additional training courses for private sector physicians. He coordinated with both JSI and SOMARC concerning the technical aspects of the market study, and gathered preliminary information through focus groups with participants at the IUD training course.
In July 1998, MSH facilitated a workshop on "Preparing Successful Proposals", which resulted in the development and submission of a proposal for a project in Mauritania under
John Snow, Inc. 69 Contract No. 608-C-00-94-00006

the South-South initiatives. This proposal was submitted to the Regional Director for the Middle East and North Africa for the Partners in Population Development Program.
MSH conducted a consultant workshop for the CNFRH and INAS in Rabat in early May 1999. With USAIDIMorocco support, and in collaboration with the Partners for Population and Development Project (Partners), a panel of distinguished guests from international donor organizations was organized and included representatives from USAIDIMorocco, WHO, UNICEF, UNFPA, World Bank and Partners. The panel discussed the utilization and demand for Francophone consultants in Morocco and the region. The three-day workshop, designed for the specific needs and objectives of CNFRH and INAS, divided its focus on addressing individual training needs, donor collaboration, and development of an organizational plan of action. This workshop provided an excellent orientation to basic consulting skills, the importance of networking and potential sources of support.
Following the consultant workshop in May 1999, MSH provided technical assistance in July and September 1999 to CNFRH and INAS to develop CNFRHllNAS internal management systems to facilitate South-to-South consulting activities. MSH worked closely with Dr. Amina Essolbi of INAS and Ms. Fedoua Hassouni of CNFRH to review their internal manaaement svstems. and D ~ O D O S ~ ~ a basic manual recornmending the - creation of a specialized unit charged with' the management of consultants. MSH develo~ed two manuals on the manaaement and coordination of consulting activities for INAS h d CNFRH in close collabo~ation with Dr. Essolbi and Mrs. ~>ssouni. The manuals were titled " Unite de Coordination des Consultations". Copies of the manuals were distributed during the Reunion de reflexion sur I'avenir du partenariat CNFRH/INAS/MSH. These manuals were designed to meet the needs of INAS and of CNFRH and will facilitate their consultant activities.
MSH conducted an internal evaluation of the MSHIFPMD program in September 1999 through a Reunion de Reflexion sur les Activites a Jour et les Implications pour Mvenir du Partenariat CNFRH/INAS/MSH 1997-1999 in Rabat. The MSH team worked with Prof. Alaoui, Prof. Fikri, Dr. Bezad and Dr. Essolbi to develop and revise the objectives and agenda for the workshop scheduled on September 27 with 17 participants including all of the critical CNFRH and INAS staff involved in the project. The overall tone and results of the meeting were very positive. MSH held extensive interviews with relevant staff from CNFRH, INAS, MSH, JSI, and USAID. The summary results of the evaluation were presented at the Reunion de Reflexion.
Develop strategic linkages among the CNFRH, INAS, MSH's Management Training Program and other regional institutions.
At the request of INAS, FPMD shipped a large supply of FPMD publications (e.g., The Family Planning Manager's Handbook, a complete set of the quarterly Family Planning Manager) for use and distribution during INAS management training courses. Moreover, FPMD procured and shipped approximately 40 books requested by INAS on a variety of management training topics, including the design and management of training courses, and training techniques.
MSH supported the participation of two INAS trainers (Dr. Jbara and Dr. Lardi) at its Boston course on "New Concepts and Techniques for Efficient Leadership" in SeptemberIOctober 1997. As lead trainers in a number of the course sessions, INAS staffs were able to practice new participatory training techniques and apply their knowledge of adult learning. They were also exposed to MSH's approach to the designlorganization, implementation and monitoring of management training courses for international participants. Dr. Jbara and Dr. Lardi also met with MSH Development
John Snow. Inc. 70 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Office staff and learned how to access information (via print and electronic mechanisms) on international foundations, how to track requests for proposals being bid or offered by international donors, and how to respond to such bids.
FPMD designed and co-facilitated (with CNFRH and INAS trainers) a three-day workshop on adult learning, training techniques, and tools for trainers of adult learners in Rabat in the spring of 1998. Participants were trainers from the CNFRH, INAS, and the Training Division (DRH) of the MSP. The workshop received a positive evaluation and plans were made to maintain the momentum and follow-up with focused training and application activities.
INAS and MSH collaborated in the planning, marketing, coordinating administration and logistics of, developing the curriculum of, conducting and evaluating the course titled "Management of Decentralized Health Systems" through hosting Mr. Abdelwahab Zayyoun to come to Boston to work with MSH staff. In collaboration with MSH's Management Training Program, INAS completed a very successful training for 27 participants from 10 Francophone countries on decentralizing health systems. Participants were sponsored by 10 different donors--WHO, GTZ, World Bank, IPPF, Save the Children, UNICEF, PAHO, DFID, and USAlD (PRISMIGuinea, ARDIHaiti, JSIIMorocco, MSHIFPMDIMorocco).
Analysis
Strengths
The Decentralization course in December 1998 provided INAS with valuable experience in managing the numerous complex aspects of international training events.
The workshop "Practical Skills for Consultants" in May 1999 received praise for providing an excellent orientation to basic consulting skills, the importance of networking and potential sources of support.
The role and objectives of the Partnership respond to the true needs of health services.
The personnel of the two institutions are very interested and excited with the idea of the Partnership.
The staff of each institution has a good level of respect for each other's skills.
There is exceptional talent among the members of the Partnership to apply to the needs of Morocco and other countries.
The Ministry of Health, as well as the other agencies, are ready to do the publicity for the Partnership as soon as their marketing plan is launched.
Lessons Learned
* To introduce new training modules into the private market, one must make a constant and coordinated effort in the technical, administrative and marketing perspectives.
To assure the applicability of the new training modules, one must have the participation of INAS for their development.
It will be important to utilize, to the maximum extent, the existing electronic networks since they are excellent marketing vehicles.
John Snow, Inc. 71 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
= The circulation to all concerned of the signed partnership agreement between CNFRH and INAS will serve as an important testimony of the confidence of the partnership in its collective future.
Constraints and future perspecfives - The legal and bureaucratic constraints on contracting and directly receiving and dispensing funds by INAS affect their ability to respond to market opportunities.
The Partnership between NTCRHIINAS, while progressing, is not yet at a stage which allows operational joint projects.
To better assure the sustainability of the CNFRHIINAS Partnership, it is recommended that they use the marketing plan as soon as possible.
JHPIEGO
Introduction
Maternal health and family planning are priority programs of the Ministry of Health (MOH). Strategies to reduce maternal mortality are developed through the management of pregnancies, childbirth and obstetric emergencies and require a health staff aware of these problems and having the skills required to confront this calamity. This requires reinforcing the skills of health personnel in safe motherhood and family planning.
Until recently, initial training in reproductive health was inadequate, especially that of physicians. To remedy the deficiency of physicians in FP and maternity, the MOH has organized numerous training and refresher courses for over 10 years. The problem had to be attacked at its very roots, i.e. proceed to an in-depth revision of the medical curricula of physician training.
In March 1996, an initial meeting took place, chaired by the Moroccan Minister of Health, in which all the managers of the Rabat and Casablanca hospital centers, and MOH and USAlD key staff participated. A committee was charged with developing a training module, preparing the trainers and identifying the needs of the health levels to be trained. In 1996, JHPIEGO, which had been working for several years in Morocco to improve access to contraceptive methods, responded to this new request for technical assistance to reinforce the reproductive health component (specifically family planning and safe motherhood) of clinical training of the curriculum of the two Moroccan medical schools.
Objective
To assist the faculties of medicine and the MOH with the introduction of family planning and safe motherhood modules in the university curriculum.
Achievements
At the end of November 1996, a consensus meeting with representatives of the MOH Population Directorate and the two Moroccan medical schools was held in Rabat to define the basis for the introduction of family planning and safe motherhood modules in the university curriculum. At the end of January and beginning of February, Dr. Robert Johnson, director general of JHPIEGO, went to Rabat, Casablanca and Marrakech to evaluate the clinical installations used by the faculties of medicine, inventory the teaching material and
John Snow, Inc. 72 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
supplies used in the two faculties and select the teachers to be charged with the training of the initial nucleus of trainers under this new curriculum.
At the end of April and beginning of May 1997, a group of 12 trainers went to Baltimore for training in the effective transmission of knowledge and skills in FPISM to students and revise the first draft of the modules to be used in the new curriculum. From June 11 to 24, 1997, Anne Pfitzer, director of programs at JHPIEGO, visited Rabat and then Agadir for the follow- up and coordination of assistance provided by her organization.
In June and July 1997, two workshops took place in Agadir for Rabat and Casablanca teachers. Over 40 of them could thus be trained in FPISM teaching. These workshops also provided an opportunity for revising the modules to be used in the curriculum.
In September 1997, the new practical training course (stage) in FPISM was initiated in four services in Rabat. To achieve this, the Phase V Project financed the upgrading and equipment of the training premises. In November 1997 and February-March 1998, JHPIEGO carried out two other consultancies to determine progress achieved since the inception of the new curriculum, ensure follow-up of recommendations made following the survey of institutional needs in February 1997 and proceed with the finalization of the FPISM modules. In June 1998, at the request of the MOH, Prof. Pierre Jean undertook a formative evaluation of the project. Lastly, in September 1998, the FPISM stage was also initiated in Casablanca and the training premises were upgraded and equipped. The training manual has been finalized, printed and distributed to 6Ihyear students.
Analysis
The findings of the evaluation of 6" year students in 1998 showed that more than two thirds and up to four fifths of the students were proficient in the sentinel tasks chosen for this assessment. Evaluation of experience and confidence in certain skills showed, however, that FP-related tasks were lower than SM-related tasks. This confirms the finding that one single student was incompetent for any SM tasks, but that 18 students (8%) were incompetent for any FP task. These findings highlight the need to address a lack of experience in FP clinical practice.
Based on these results and the evaluation of the restructuring process of FPISM stages for medical students, the following implementation strengths and weaknesses were found:
. Managemenf of implemenfafion
The consensus and discussion about services during project planning do not seem to have survived until the implementation of the new curriculum. For example, the head of the Casablanca maternity unit decided not to implement the program, without consulting either the Ministry or the other project partners. Moreover, the curriculum committee did not meet often after project inception. The consultants who frequently came to Morocco insisted, to no avail, on the importance of re-creating the curriculum committee. Lastly, the June 1998 evaluation provided an opportunity for sharing the experiences of everybody, revising the curriculum and proceeding in such a way that all students could benefit from comparable training.
Teacher training
From the beginning, the project emphasized the training of teachers of the Rabat and Casablanca maternities. A total of over fifty teachers were trained following an approach focused on the acquisition of skills, which is the standard JHPIEGO approach. These
John Snow, Inc. 73 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
teachers are now able to communicate their knowledge and skills in FPISM to students. Workshops on clinical training skills produced remarkable results. For the trained teachers, it is not a question of teaching as they did before. The student has become the focus of any training. The participatory approach has become their major modus operandi. A team member could attend one of the teaching sessions and observe some of them at work with the students. The teachers trained under this program are the best pledge for sustainability. If it has been possible to implement the project in the Rabat maternity units despite certain difficulties, this is in part due to the unanimous adhesion of the teachers trained in this new student-focused approach. It would be good if all the teachers could share this vision.
Development of didactic supporf materials
The FPlSM teaching module, that was to be used as a common basis for the standard training of students whatever service they are assigned to, met with several difficulties before, during and after its development. Draff versions were used in various ways according to the services. Several attempts were made, to get the module validated by the main interested parties. In the end, the document was finalized and validated. Other didactic support materials should be developed, i.e. the student's stage booklet and the audiovisual material. It is important to charge a small nucleus of teachers from the different services with these tasks, who will then have the responsibility of developing an initial version to be validated after utilization.
Evaluation of student skills and of 'ktage"assessments
While the new teaching method is based on the learning of clinical skills, the evaluation instruments of this learning process generally remained as they were in the former curriculum, namely a written test measuring the simple recollection of knowledge and the overall observation of students during or even only at the end of the stage. It seems, moreover, that the exam at the end of the 7'h year continues to be the same as ever, i.e. a test to measure knowledge rather than skills. Assessment appears to have been the weakness of the new curriculum. Stage assessment by students is carried out only in one service.
Availability of patients for teaching purposes
While students have sufficient opportunities for learning obstetric care, the relatively limited number of FP clients makes learning in this field more difficult as demonstrated by the evaluation. This lack is only partly compensated by the prior use of anatomic models and postpartum counseling.
Teaching materials /Documentary resources / Supplies
Teaching materials took some time reaching each of the services. Even when the materials are delivered, they are not always available to teachers. Because of the absence of teaching premises in the services, these materials are often locked away in the office of the chief of service. Teaching suffers from a quasi-total lack of documentation materials. In practically all of the services, there is no library adequately stacked with FP and SM reference manuals. Also, the teachers are often obliged to buy themselves supplies like felt pens, transparencies, etc.
Extension of the program to the seventh year
Training of students "functioning as interns" in the regional health centers eludes the authority of medical schools. Remuneration of teachers (salary supplements) seems to
John Snow, Inc. 74 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
have been one of the factors preventing implementation of the project in the 7Ih year of medical studies. It is desirable to find a way of remunerating the teachers who work on tasks beyond those normally assigned to a teacher.
JHPIEGO technical suppoii
Evaluation also demonstrated that JHPIEGO experience and expertise were essential to the planning of the new curriculum. Needs assessment tools, pedagogic training materials and anatomic models provided by JHPlEGO were already available and teachers with experience in reproductive health and in the design of stages contributed to project implementation.
Conclusions and future perspectives
Strengthening of clinical training in family planning and safe motherhood in Moroccan faculties of medicine is well underway. This can be attributed, mostly, to the commitment of the teachers trained in a pedagogic approach focused on skill acquisition. The implementation of the project with the desired result - provide 6" year students with training focused on FP and SM skills - has been demonstrated. Overall, students are well prepared for the 7" year, having the knowledge and experience of numerous skills required for their internship.
Despite sometimes unfavorable conditions and difficulties of reaching agreement at service level, both the Casablanca and Rabat faculties of medicine now use the new 6Ih year curriculum. The project, however, remains fragile. It is important to maintain the impetus and assure continued support to the program. Here are a few ideas to contribute to the sustainability of this project:
Many teachers use their new teaching skills for a variety of training situations and not only for teaching sixth year students.
Most of the interviewed teachers feel that students having completed the new FPISM sfage are much more competent than those of the two preceding years.
The Dean of the Rabat Faculty of Medicine has committed himself to the introduction of a training methodology in other "stages", beginning with the one in pediatrics.
This clinical training in reproductive health of medical students, which in the long term might result in a reduction of maternal mortality, could be a model for clinical teaching in other fields in schools of medicine in Morocco and elsewhere in the world.
PRIME
Background
In 1996, USAlDlMorocco invited PRIME to support its Population and Health Transition Plan (1996-1999) by strengthening the capacity to manage training needs within the Ministry of Health (MOH) and contributing to the strategic objective 3 for a "reinforced capacity to manage FPIMCH programs with particular emphasis on decentralized approaches responsive to client demand."
PRIME'S principal partners were the Training Division within the Directorate of Human Resources of the MOH, the MOWS nine IFCSs (Health Training and Careers Institutions) and INAS (the National Institute of Health Administration). PRIME technical assistance was
John Snow, Inc. 75 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
provided in close coordination with the bilateral project managed by JSI and the three PRIME partners: (1) INTRAH provided overall technical guidance and management; (2) Training Resources Group (TRG) assisted with strategic planning and training capacity building and (3) the American College of Nurse Midwives (ACNM) provided distance learning expertise.
At the center of PRIME'S program in Morocco was the reinvigoration of the national in- service training strategy. This national strategy introduced the concept of performance improvement to Morocco and, for the first time, strongly linked performance-based training with improved quality of services.
PRlME Goals and Objectives
The goal of PRIME'S support to Morocco was to build national capacity to manage quality FPIReproductive Health (RH) training and human resource development activities. More specifically, PRIME worked under three general project objectives:
To increase the capacity of the MOH to coordinate pre-service and in-service training programs through the development, application and evaluation of a national strategic training plan.
To strengthen the capacity of the MOH to establish, implement and evaluate decentralized pre-service and in-service training activities.
To augment the capacity of INAS to develop and apply distance learning education to in- service FP training.
Key Results by Objective
Objective 1: To increase the capacity of the MOH to coordinate pre- service and in-service training programs through the development, application, and evaluation of a national strategic training plan.
The MOH's expectations for the national training strategy were the creation of an in-service training system that responded to service delivery needs in an integrated, decentralized and coordinated fashion. The strategy would focus on the improvement of the performance of health workers and encourage health workers to be motivated and capable of contributing to improved quality of care. The strategy would outline functional coordination mechanisms as well as the roles, responsibilities and expected activities at different levels of the system (national, regional, provincial, and service delivery site).
The training strategy focuses attention on strengthening the role of the MOH training division as well as the IFCSs. The lFCSs have responsibilities for pre-service and in-service training of nurses and midwives. The vision for the MOH was the existence of strong training institutions in each of the fourteen administrative regions in the country. As part of the strategy, regional in-service trainers were to be based out of the training institutes to strengthen the institutes' ability to respond to the needs of the service delivery structures at the community level and to enhance the linkages between the pre-service and in-service functions. PRIME worked with the nine existing IFCSs.
Results
= Successfully revised, disseminated and applied a nationally sanctioned and endorsed in- service training strategy, which placed the MOH Training Division in a key leadership position. The strategy was officially launched in early 1999 and became the official MOH policy at that time.
John Snow, Inc. 76 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Improved the quality and the consistency of training activities - including performance assessments, design, facilitation and evaluation - at central and regional levels through the creation and dissemination of national training standards. The standards describe the conditions under which training is an appropriate intervention for improving service provider performance and establish minimum expectations on how to manage and conduct experiential, client-focused training.
Objective 2: To strengthen the capacity of the MOH to establish, implement and evaluate decentralized pre-service and in-service fraining activities.
Results: Pre-Sewice Training
* Nine regional IFCSs able to better prepare nurses and midwives to provide FP information and services.
Strengthened capacity of 25 pre-service tutors and preceptors to design and conduct training programs.
Developed a pre-service FP module and integrated it into the overall curriculum of nursing and midwifery schools. The module includes World Health Organization (WHO) eligibility criteria and focuses on service provider performance on the job.
Supported linkages between INAS and a Canadian university leading to an action plan for the creation of an advanced nursing diploma course.
= Facilitated the integration of lMCl (Integrated Management of Childhood Diseases) into pre-service training and education through the development of a strategy and plan and establishment of formal linkages with the WHO lMCl Unit.
Results: In-Sewice Training
A strong central MOH Training Division capable of providing leadership and facilitating the smooth functioning of a national, decentralized training system.
Produced, disseminated and applied a set of national training and supervision tools.
Created a central MOH team of eight master trainers with advanced competencies in performance needs assessment, training design, experiential learning methods, and training evaluation.
A strong network of more than seventy highly qualified regional trainers at nine training institutes with demonstrated capability of conducting responsive, performance-based FP training programs.
Strengthened regional trainers' training skills as well as their ability to interact with community service delivery structures (their "clients") and respond to their performance needs.
Gained the political support from the IFCS directors to support regional trainers, conduct outreach to service delivery structures and implement the national training strategy.
Established strong linkages between the pre-service and in-service functions within the lFCSs by strengthening collaboration and coordination among pre-service tutors and in- service trainers.
John Snow, lnc. 77 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Objective 3: To augment fhe capacity of INAS to develop and apply distance learning education to in. service FP training.
The MOH was interested in exploring distance learning because classroom-based, in- service training for service providers has long been a significant recurrent cost for the health sector in Morocco. Distance learning was considered as a way to enable the MOH to more rapidly and affordably improve the skills of a larger portion of service providers.
INAS was the lead agency responsible for implementing the distance learning program with support from the MOH Training Division and representatives of the service delivery sector. INAS, which focuses on the training of health professionals, specializing in health administration and public health administration, had previous experience in developing and managing distance learning programs for graduate level students and an interest in gaining broader experience and expertise in distance learning.
With PRIME support, INAS managed a distance learning program among 40 nurses and nurse aides in Fez and Marrakech. The four-month curriculum included FP and management modules. The program included a strong learner support system relying on tutors/facilitators to help guide learners through the curriculum.
Results
Demonstrated the effectiveness of distance learning as a means of improving primary service provider performance in FP.
Significant difference in pre and post knowledge test scores of learners, demonstrating that the changes are associated with the distance learning course.
Significant difference between learners' FP counseling skills (15.4 versus 8.5 out of a total of 16 possible points) and infection prevention skills (11.4 versus 4.6 out of a total of 12 possible points) and those of a control group.
Strengthened capacity of INAS and the MOH Training Division to design, execute and evaluate a distance learning program.
Designed, tested and used a comprehensive FP and management curriculum.
Established a multi-sectorial coordination team to design, manage and evaluate the course.
Analysis
The Moroccan experience in revising and applying a national, decentralized strategic training plan is considered a resounding success. For the first time, the strategy and standards linked the training system directly with the ultimate performance of providers at the service delivery level, thus making training more responsive to the needs of the service delivery structures, the health and ambulatory care centers that use their services. The strategy and standards were nationally validated and accepted by the institutions and individuals responsible for in-service training at all levels and are guiding all subsequent training programs and capacity building at the regional level. The MOH Training Division has taken on a prominent leadership role in the coordination of activities within and outside the MOH. Pre-service and in-service training programs are linked, with a stronger focus on pre-service training.
PRIME, as well as other institutions, have used the Moroccan experience in strengthening its national training system as a model throughout Africa and globally. The documents, processes, and outcomes of the work in Morocco have been shared in such places as Mali, Tanzania and Bangladesh. In addition, Moroccan public sector professionals involved in the in-service training program have been used as resource persons in other country contexts.
John Snow, Inc. 78 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The distance learning program was designed, implemented and evaluated by a multi-sectorial team of professionals from the key training institutions in the country. These institutions gained valuable experience and insight into the viability of distance leaming as an alternative approach to traditional classroom training. INAS and the MOH can be considered national distance learning resources for expanding the existing course and in taking a leadership role in the country in identifying other content areas and cadres of health workers where distance learning will be an appropriate approach.
Lessons learned and future perspectives
1. Regional trainers have gained valuable skills and competence. In order to maintain and expand regional trainers' skill level, motivation and expertise, they should be exposed to opportunities to continue using their skills and to interact and share experiences with other trainers. The trainers themselves recommended a number of mechanisms of continued support, including study tours among the regions, establishment of trainers' association, or creation of trainers' newsletter.
2. Distance learning is an effective learning approach for the improvement of FP service provider's performance. Distance learning approaches not only increase learner knowledge, but also can reinforce clinical skills and performance of service providers. The results of the evaluation could be used to recommend strategies for expanding and applying distance learning to other areas in Morocco, particularly for those providers who do not have access to classroom training.
3. In order to ensure sustainability of distance learning approaches, the regional training institutions should be fully implicated in the design and implementation of future distance learning programs. INAS and the MOH Training Division could both play an important role in transferring distance learning expertise to the IFCSs.
4. While training interventions can have an impact on the performance of service providers, non-training interventions are also important factors that influence performance. These non-training interventions include recruitment, hiring, deployment, incentives and promotions. The potential of these non-training interventions to improve the performance of primary providers could be further explored.
E. Contraceptive Logistics
To achieve the sustainability of family planning services, the contraceptive logistics system was a crucial element for the quality of services. The logistics system received substantial support under two agreements (Phase IV and V) signed with USAID. The target of this support was to develop the institutional capacity within the MOH to manage and procure contraceptives in an autonomous fashion. Technical support was provided in the form of collaboration between FPLM and JSI, who provided a technical advisor through August 1998.
Objectives
1. Strengthen the contraceptive logistics management system to ensure the permanent availability of contraceptive products in all of the health facilities of the country.
2. Reinforce the management capacity of personnel involved at the different levels of the "pipeline" in view of an autonomous and decentralized management (without external technical support).
John Snow, Inc. 79 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT - Performance indicators U
Adequate quantities of contraceptive products are available at all levels of the system to meet the demand of female and male users. L,
The logistics system is managed by qualified staff without external support. b
Achievements C
The contraceptive logistics system underwent major changes under the project. The former system of allocations provided by the central level, or "push system", has been replaced by a Lri
new system of orders given by the user and based on past consumption, or "pull system". This required the restructuring and strengthening of all system components:
ir
Organization and composition of MOH staff
A total of about 3500 staff has been trained in the new procedures of the logistics system C
and are able to carry out the calculations required by the ordering system. ii
The Manuel de gestion de stocks des produits contraceptifs (Manual for contraceptive stocks management) has been widely distributed and used, by trained staff as well as new untrained personnel who have only the manual to guide them. - - The training capacity has been built up through the training of provincial trainers and the dissemination to IFCSs and the FP Division of a set of documents on contraceptive u
management produced by FPLM.
The in-service training strategy in contraceptive logistics has been developed with FPLM li technical assistance as well as a training module. This module has been printed and then distributed to all lFCSs and trainers. I d
Distribution b
The same 3500 staff were trained in the new stock control procedures.
Implementation of a new distribution system resulted in a decrease of stock-outs, Li unbalanced stocks and out-of-date stocks.
The two trucks procured for the MOH central level by USAID/DIM clearly improved li
product distribution to provinces.
(ri Logistics Management Information System (SIGL)
New "Order and Delivery Form of Contraceptive Products", "Stock Form of Contraceptive *ri
Products" and "Register of Contraceptive Products" were designed, tested (and documented in the same Manuel de Gesfion de Stocks des Produits contracepfifs) and applied nationwide. iu
SIGL data are used to issue new routine and emergency orders throughout the entire new decentralized demand system at all levels of the health care system. iu
Consumption data provided by the national health information system (SNIS) are ir
regularly used for forecasting contraceptive needs.
John Snow. Inc. 80 Contract No. 608-C-00-94-00006 b"

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The systeme SMlPF application, developed with JSI technical assistance, permits the entry and analysis of data on family planning service delivery provided by SNlS at provincial level.
The software to computerize analysis at the central level of SlGL data (Order Form) was designed and implemented locally.
Storage and warehousing
The new Sale warehouse was opened (built under the Phase V Project) and equipment required for its operation has been procured.
Storage conditions at the contraceptive products warehouse in Casablanca and the new Sale warehouse are very good and, with the additional central storage capacity, will be adequate in the years to come.
Storage conditions vary at the weakest level, but almost everywhere the personnel abides by good warehousing practices (First-Out-Of-Date First-Issued, environmental protection measures).
For the stock management of the Casablanca and Rabat warehouses, a computerized application has been developed by a DP computer specialist, with the support of DIM engineers and technicians.
A regional warehouse for the storage of products and medicines was opened, on an experimental basis, in Agadir for the Souss-Massa-DrAa region. Its functioning will be tested under the new decentralization project.
National needs forecasts
Since 1999, the DPF has itself prepared the Contraceptive Procurement Tables (CPT) to calculate annual contraceptive needs forecasts using the FPLMIUSAID method.
At present, forecasts take into account stocks available at all the levels of the distribution system and are based on SNlS consumption data.
a The number of stock-outs and out-of-date products has clearly decreased following, in part, better forecasts and, in part, better stock control.
Procurement
* MOH budget, procurement and quality control procedures exist and are operational as demonstrated by several procurements made by the MOH in the transition phase.
In the context of the implementation of a condom quality control program, the necessary equipment has been procured and installed at the Laboratoire National de ContrGle des Medicaments. Four individuals, i.e. two lab technicians and two inspector-pharmacists, were trained by PATH in the use of this material.
Comments and future perspectives
Contraceptive logistics had substantial support under two grant agreements (Phases IV and V) with USAID.
John Snow, Inc. 81 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Implementation of a new ordering system placed by the user on the basis of past consumption (pull system) to replace the former system of allocations provided by the central level (push system) is an impressive result of the cooperation between the MOH, USAlD and JSI. This new system, developed in support of the MOH decentralization initiative, achieved major success by reducing stock imbalances and forestalling stock-outs and out-of-date products.
The inception of the logistics management information system (SIGL), the development of a manual and the training, in contraceptive logistics management, of 3500 staff nationwide are among the most remarkable results. With the participation of external consultants, the MOH has implemented a contraceptive needs assessment system before the central level initiates orders based on CPTs. This system ensures continued supply of the contraceptive pipeline through USAlD grants. Concurrently, increased mobilization of State funds for contraceptive procurement enabled the MOH to test procurement procedures and the local market.
In view of decentralization, a number of functions linked to products logistics of programs could be subjected to in-depth analysis. Could product storage and transportation not be organized more efficiently? Should they necessarily be assigned to the Ministry of Health? Could this type of service not be entirely or partly sub-contracted to the private sector (outsourcing) or a specialized autonomous agency?
F. Evaluation
This component aimed, in general, at strengthening the evaluation and follow-up capacity of FPIMCH programs, based on information provided both by the routine information system and surveys and research studies. It was supported by technical assistance provided by Tulane University, through the EVALUATION Project between 1992 and 1997, and through the MEASURE Project, in collaboration with the JSI team, between 1997 and 2000.
Since the implementation of the 1998-1999 Work Plan, activities aimed at the utilization of data from the routine information system have rather been relocated under the Information and Management System component. Although Tulane University (under the MEASURE Project) still technically assisted these activities, they were then directly managed by JSI.
This section therefore concerns only activities aimed at building up the operational research (OR) and evaluative capacity.
Objective
Strengthening the MOH capacity:
to identify needs in operational and evaluative research;
- to develop and implement research methods; and
to integrate research results into the design of FPIMCH programs.
Achievements
Project achievements in research capacity-building have been classified under three intervention headings: (1) evaluative research studies; (2) training in operational and evaluative research; and (3) development of action plans for operational and evaluative
John Snow, Inc. 82 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
research. The following paragraphs provide an overview of these activities. For further details, the reader is referred to annual reports and the document "Dynamics of the Moroccan FP program: Key results of evaluative research, 1992-1 997".
1 . Evaluative research studies
Between 1992 and 1997, in the context of the EVALUATION Project and in collaboration with John Snow Inc., different researchers undertook research studies evaluating the Moroccan FP program. These studies were designed to achieve better understanding of the "black box" of service delivery in Morocco and measure the impact of FP services on reproductive behavior, including contraceptive use. A list of research studies by theme is ~rovided in table 6. The orinci~al results were summarized in "Dvnamics of the Moroccan FP program: Key results of evaluative research, 1992-1997".
Table 6: Evaluative Research Topics Offer of services: . Access
- Availability of family planning services in Morocco 1992-1995 (Zaoui, El Harim and Brown).
Quality - Quality of care (Tyane, Abou-Ouakil, Brown, Bertrand. Lauro) - IUD under-utilization (Hajji, Lakssir and Brown)
Utilization of services: Levels and trends in service statistics 1992-1996 (Azelmat, Naya-Edwards, Edwards).
Contraceptive practice: - Discontinuation, change and failure of a method (Lakssir). - The effects of using MCH on future contraceptive use in Morocco (Azelmat,
Heikel, Hotchkiss, Magnani, Rous and Mroz). - The role of husbands in decision-making on contraception (Speizer). - Contraceptive intentions and future use: program impact (Magnani, Shafer
Hotchkiss, Florence). - The impact of family planning programs on reproductive behavior: results of a
panel in Morocco (Hotchkiss, Magnani, et al.). Fertility:
- The impact of family planning programs on reproductive behavior: cross- sectional facts (Hotchkiss, Magnani, et al.).
Other: - Reliability of calendar data (Stricker, Magnani, Brown). - Determinants of the utilization of maternal health services (Eckert).
Household expenditures for health care in Morocco: indications for health care reform (Zineddine, Hazim, Hotchkiss).
Besides evaluative studies, this collaboration resulted in other important "products":
An interactive data base to track FPIMCH statistics that can be consulted on personal computers and the Internet (see under IR 3lF);
A user guide to FPIMCH program data, adapted for Morocco.
John Snow, Inc. 83 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The MEASURE Project was expected to provide the MOH with technical assistance for the secondary analyses of the PAPCHILD databases that were ready for analysis in 1998. For lack of time and availability of personnel, these studies had not yet begun at close-out of the Phase V Project.
2. Training in operafional and evaluative research
The MEASURE and Phase V Projects financed a number of activities to strengthen technical capacity in evaluation. Several seminars were organized at central and peripheral levels as well as on-the-job training in all the aspects of data collection (especially for qualitative studies). In 1998, six SEIS, DP and INAS staff members were trained in survey data analysis on SPSS software; the most advanced analysis methods were brought up during this training.
The Project financed the visit of several key MOH staff to Tulane to undertake in-depth studies and topical analyses of FPIMCH programs. A total of 9 persons went to Tulane at different times and completed the following:
User guide to data and manual of FPIMCH program indicators,
Statistical analysis of FPIMH services for the 1992-1996 period,
Data analysis of the Service Availability Module completed in 1995 together with the DHS,
Study of household expenditures for health care.
Based on discussions with the DP and INAS, it was decided that the best way to help INAS institutionalize an evaluation course would be to send one of the teachers for additional training. Therefore, through the joint financing of the Phase V and MEASURE 2 Projects, Mr. Noureddine Jbaara, INAS teacher, and Mr. Taoufik Bakkali, of the JSI team, participated in a workshop on the evaluation of FPIMCH services at Chapel Hill (University of North Carolina) from May 24 to June 18, 1999. With the skills learned there, Mr. Jbaara developed a module on "Evaluation and follow-up methods for health", which will be taught by Mr. Jbaara-and Mr. Bacheikh from September 2000 onwards as part of the 6'h INAS Course in Public Health.
Lastly in 2000, together with the MEASURE project, the MOH and JSI organized a series of training workshops on qualitative research techniques for the Souss-Massa-DrAa regional team. 35 staff from the different provinces of this region practiced, in the field, the different research planning and data collection techniques to which they had been introduced, and finalized the research protocol for a qualitative study of the under-utilization of injectables. The field survey and the transcription of focus groups and in-depth interviews took place in March and April 2000. Analysis of this survey was completed by the time the training seminar-workshop on qualitative data analysis techniques took place. During this workshop, participants were trained in the use of ETHNOGRAPH software for qualitative data analysis.
The interesting results of this study, and the enthusiasm of the staff involved in this training, should encourage MOH managers to repeat this training with other regional teams.
3. Development of acfion plans for operational research and evaluafion
To better structure research studies focused on FPIMCH programs and consequently the improved usage of research results, the development of an action plan for applied research was launched end 1997. The first planned activity was a consensus meeting on FPIMCH research priorities. A MOHIINASIJSI team made a fairly complete inventory of FPIMCH studies during the past ten years. The work was entrusted to three INAS students of public
John Snow, Inc. 84 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
health under the supervision of an INAS teacher. Two students dedicated their thesis to this work, analyzing and criticizing the quantity, quality and relevance of research undertaken in the field of child health and family planning during the past decade. The third student was to tackle research on maternal health, but preferred to discontinue this work for lack of a sufficient number of publications. Unfortunately, several factors, including lack of time, resignation of a supervising professor and the difficulty of gathering a representative group of researchers and managers around a table, resulted in the consensus meeting never taking place.
Lessons learned and fufure perspectives
The collaboration between the MOH, the EVALUATION and MEASURElTulane University project and JSIIMorocco resulted in a number of activities:
Secondary analysis of EDSIMDS data to measure program access, quality and impact;
Qualitative studies focusing on the strengths and weaknesses of service delivery;
Development of an interactive computer system to promote increased data use by program managers;
Research and evaluation capacity-building through training and the professional network.
This collaboration resulted in the strengthening of capacities to design, implement and analyze evaluative research within the MOH. It also permitted the completion of a number of research studies with program implications and contributed to the development of an "evaluation culture" within the MOH divisions in charge of FPIMCH programs.
The climate of evaluative research, within the Moroccan Ministry of Health, is excellent. Without exception, managers in charge either of the FPIMCH program (DP) or researchlhealth statistics (SEIS) participated actively in this five-year collaboration, which generated research results and other "evaluation products". At present, user-friendly service statistics are available to program managers at regional and provincial level. Study results were used to re- focus program activities, as was the case for the studies on health care quality and the under- utilization of the IUD. The availability of this wealth of Moroccan data allowed the completion of studies that could not have been done elsewhere (e.g. the availability of the EDS calendar, since Morocco is the only country having conducted a panel study of the same respondents) or only in few other countries (e.g. measuring the impact of the context of FP services on contraceptive use). Also, several PSP staff had advanced training in reproductive health program evaluation, thus improving the future sustainability of these activities.
Important evaluation tasks have been completed and some people might say that it is time to move on to other issues, while a similarly convincing argument says that this 5-year collaboration has laid the foundations for the complete utilization of evaluation for further improvement of the Moroccan FPIMCH program. Morocco already is a leader in this field and could gain even greater recognition through high-quality documentation of its successes and continued efforts to identify means for increasing the efficiency of its FPIMCH program in the future.
G. Health Information System
Aware of the lack of relevant and reliable information for the planning and follow-up of FPIMCH programs, the MOH has, since 1987, worked to restructure the national routine health information system (SNIS) and particularly the FPIMCH subsystem. SEIS (Studies
John Snow, Inc. 85 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
and Health lnformation Service) was charged with this task, in collaboration with the DP, DELM and DIM.
Despite these efforts, at the inception of the Project in 1994 the maternal and child health information system was affected by four sets of problems: (1) the poor quality and incomplete nature of data produced by the routine collection system; (2) the fragmentation of data collection systems, too often vertically organized rather than by priority programs; (3) delay in the availability of information at all levels; and (4) insufficient utilization of available data for the planning, management and evaluation of services.
The FPIMCH Phase V Project planned to tackle each of these issues, emphasizing the integration of the routine health information system and information management capacity building at peripheral level.
Objectives
lmprove FPIMCH data management by integrating the data collection system and delegating management responsibilities to peripheral structures;
lmprove the utilization of data at central and peripheral levels to facilitate decision- making on the management of FPIMCH services;
Develop, within the MOH, computer technology as a tool to manage and utilize FPIMCH data.
Performance Indicators
At the end of the Project;
FPIMCH program data generated by at least 90% of the health facilities in the pilot regions will be available at regional level within no more than 4 weeks, and electronically transmitted to the central level within 1 week at most.
= In the pilot regions, at least 2 actions have been implemented for each priority program based on the analysis of regional data.
Achievements
A restructuring of the SNlS was undertaken to prepare the MOH to assume technical and financial responsibility for activities of the lnformation and Management System after withdrawal of USAlD bilateral assistance. Technical assistance was provided by the JSI team together with Tulane University, under the EVALUATION (1994-1997) and MEASURE (1 998-2000) projects.
This included two components: (1) development of the data collection, processing and utilization system; and (2) computerization of SNlS within the MOH.
Part I: Restructuring the Health Information System
Three concerns of the MOH guided the restructuring of the information system: (1) promote use of information to improve service quality; (2) integrate data collection from the different FPIMCH programs by facilitating a holistic approach to child and reproductive health; and (3)
John Snow, Inc. 86 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
introduce new programmatic focuses, such as the integrated management of childhood illnesses (IMCI) and the management of obstetric emergencies.
Restructuring activities concerned three aspects of SNIS: (1) revision of data collection supports; (2) development of a computerized FPIMCH data entry and analysis system; and (3) training of managers at regional and provincial levels in the utilization of data for decision-making.
A study was undertaken in 1998 on the quality of FPIMCH data collected in health facilities in order to identify critical weaknesses in the production and utilization process of routine data. The study was conducted by a multidisciplinary MOH team, composed of representatives of the DP, SElS and the general inspection, in collaboration with a WHO1 Geneva consultant and JSI. The study confirmed the persistence of several problems identified at the beginning of the Project, such as the lack of precision of data collection and the lack of utilization of information at local level.
1 . Revision of data collection instruments
One of the features of the FPIMCH data collection system in first-level health facilities was a multiplicity of registers, daily forms and reports, which resulted in the development of distinct data collection systems for each program. Consequently PNI, PLMD, PIRA, PNT, PSGA and FPP had each their own set of supports. Transmission procedures were also very confused. Besides the SEIS, the service centralizing information, several other parallel transmission channels conveyed data directly to the national programs. Although at the beginning of the 1990s some simplification work on data collection resulted in a listing of the principal indicators for the management of priority programs, the multitude of data collection instruments continued and was a de-motivating workload for service providers in health facilities.
In 1997, several working groups were set up to adapt the data collection supports (DCS) to the needs generated by the integration of reproductive and child health programs, and by the new programmatic approaches to emergency obstetric care and IMCI. These working groups were composed of key staff representing the relevant programs, SElS and JSI resource persons. Following a series of meetings, the following decisions were taken:
Maintain the DCSs of family planning services
Restructure DCSs linked to child health to better respond to the needs of the lMCl approach
Restructure the DCSs of obstetrical services
Simplify FPIMCH data transmission procedures by creating a monthly report in booklet form, which would contain all of the FPIMCH data of a health facility
Operational research on the decentralization of epidemiological surveillance
Child health programs: The introduction of the lMCl approach led to the principle that any child entering a MCH unit will have integrated care, taking into account all potential health issues as well as preventive care opportunities. The multiplicity of existing data collection supports was an impediment to this approach. Indeed, a survey of data collection supports for the four child health programs showed that there were 13 information supports: 5 registers, 3 daily forms and 5 monthly reports.
John Snow, Inc. 87 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
After several months of consultation between managers of the different child health programs and of SEIS, an integrated information system was developed for child health. This makes it possible to record, in one single document, all the curative and preventive care provided to any child under five. The 13 information supports used until then for child health were reduced to four:
integrated daily child health activity register
register for the national vaccination program
daily PNI activity form, and
integrated monthly child health activity report.
Maternal health program: The maternal health information system was revised to address the information needs of the new emergency obstetric care strategy. The following were revised: (1) the obstetric childbirth register which became the obstetric register; (2) the monthly obstetric activity report; and (3) the monthly pre and postnatal report.
An integrated monthly report: All of the monthly reports of the FPIMCH programs were grouped into a booklet so that they could be sent together and follow-up could be implemented.
After developing the new supports, a pre-test was done in the Agadir and Meknes provinces for the integrated child health system, and in the Taza-Al Hoceima-Taounate and Fez- Boulemane regions for the maternal health programs. The MCH personnel of the health facilities and the SlAAP staff of these provinces were trained in the use of this new system. Following field visits by SEE, MCH Division and JSI staff, the different reports were revised until a final version was produced that responded to the needs of the majority of information users at the different levels of the system.
The new DCSs were approved for generalized use throughout the country at the beginning of 1999. They were printed by the DIEC, first for the 5 pilot regions with Project funding, then for the rest of the country at the charge of the MOH and other donors. Later, cascaded training of the personnel of all the health facilities was organized in the five pilot regions. Following the issue of a circular letter by the Secretary General announcing the invalidation of the former information supports, all Moroccan provinces officially started using the new supports from January 2000 onwards.
2. Development of a computerized FP/MCH data entry and analysis system
One of the explanations for the poor use of information by peripheral managers was the centralized processing and analysis of routine data. At the same time, the central level was not able to provide feedback to the periphery within acceptable delays. Lastly, health service providers and managers limited data transmission to the central level, without much regard for quality. The trend toward decentralized management of health services during recent years opened the door to a change in the management of the health information system and prepared managers at regional and provincial levels to process and analyze data themselves.
In a first phase, it was decided to implement a computerized and interactive system that provides peripheral managers with easy access to 20 FPlMCH performance indicators. This task was given to Tulane University. The first application (SNISSTAT) was developed in DOS, based on data entered at SEIS level. This made it possible to produce tables, multiple graphs and maps for each indicator over 5 years (from 1992 to 1996) as well as for the
John Snow, Inc. 88 Contract No. 608-C-00-94-00006
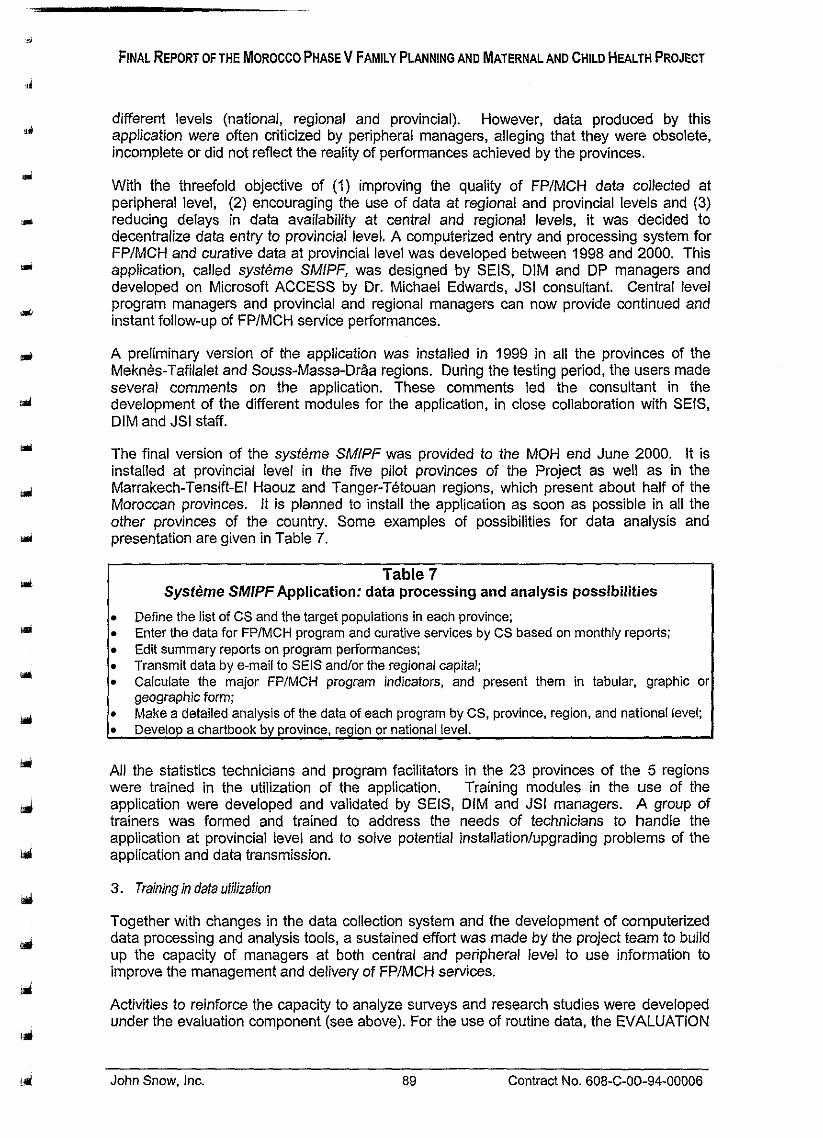
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
different levels (national, regional and provincial). However, data produced by this application were often criticized by peripheral managers, alleging that they were obsolete, incomplete or did not reflect the reality of performances achieved by the provinces.
With the threefold objective of (I) improving the quality of FPIMCH data collected at peripheral level, (2) encouraging the use of data at regional and provincial levels and (3) reducing delays in data availability at central and regional levels, it was decided to decentralize data entry to provincial level. A computerized entry and processing system for FPIMCH and curative data at provincial level was developed between 1998 and 2000. This application, called systeme SMIPF, was designed by SEIS, DIM and DP managers and developed on Microsoft ACCESS by Dr. Michael Edwards, JSI consultant. Central level program managers and provincial and regional managers can now provide continued and instant follow-up of FPlMCH service performances.
A preliminary version of the application was installed in 1999 in all the provinces of the Meknes-Tafilalet and Souss-Massa-DrAa regions. During the testing period, the users made several comments on the application. These comments led the consultant in the development of the different modules for the application, in close collaboration with SEIS, DIM and JSI staff.
The final version of the syst6me SMlPF was provided to the MOH end June 2000. It is installed at provincial level in the five pilot provinces of the Project as well as in the Marrakech-Tensift-El Haouz and Tanger-Tetouan regions, which present about half of the Moroccan provinces. It is planned to install the application as soon as possible in all the other ~rovinces of the country. Some exam~les of Dossibilities for data analvsis and prese&ation are given in Table 7.
Table 7 Sysfeme SMlPF Application: data processing and analysis possibilities
Define the list of CS and the target populations in each province; Enter the data for FPlMCH program and curative services by CS based on monthly reports; Edit summary reports on program performances; Transmit data by e-mail to SEiS and/or the regional capital; Calculate the major FP/MCH program indicators, and present them in tabular, graphic o geographic form;
s Make a detailed analysis of the data of each program by CS, province, region, and national level; Develop a chartbook by province, region or national level.
All the statistics technicians and program facilitators in the 23 provinces of the 5 regions were trained in the utilization of the application. Training modules in the use of the application were developed and validated by SEIS, DIM and JSI managers. A group of trainers was formed and trained to address the needs of technicians to handle the application at provincial level and to solve potential installationlupgrading problems of the application and data transmission.
3. Training in data utilizafion
Together with changes in the data collection system and the development of computerized data processing and analysis tools, a sustained effort was made by the project team to build up the capacity of managers at both central and peripheral level to use information to improve the management and delivery of FPIMCH services.
Activities to reinforce the capacity to analyze surveys and research studies were developed under the evaluation component (see above). For the use of routine data, the EVALUATION
John Snow. Inc. 89 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
project organized, between 1995 and 1997, several training sessions in program evaluation techniques and the use of indicators and tableaux de bord for program management at the DP and in the provinces. This training was mainly for statistics technicians and program facilitators at provincial level.
With the creation of regions and the perspective of regionalized management of health services, SEIS and DP staff, assisted by the JSI and Tulane team, organized regional seminars for provincial decision-makers (delegates and SlAAP senior physicians) on the use of FPlMCH routine data in program planning and management. These seminars took place in the Fez-Boulemane, Meknes-Tafilalet, Souss-Massa-DrAa and Doukkala-Abda regions. During each workshop, participants were asked to prepare a regional chartbook, thus practicing the techniques learned during the workshop. These chartbooks enabled health service managers to identify major problems and proceed with problem-solving actions.
A problem thus identified often required an in-depth, more qualitative investigation to find operational solutions. With Tulane University assistance, training in qualitative research was therefore organized for the Souss-Massa-Dria region (see the above evaluation component).
Lastly, in the context of the decentralization of FPIMCH services and in collaboration with DELM, the Project supported the creation of a Regional Epidemiological Observatory (ORE) in the Souss-Massa-DrAa region. Its objectives were to strengthen the provincial and regional capacity to manage epidemiological information for decision-making and action at local and regional level. Training in epidemiological surveillance of provincial managers was organized, a computerized system of early alert detection was developed together with local managers and printing of the ORE bulletin was initiated.
Part 11: Compuferizafion of SNlS within the MOH
Project investments in computer equipment and staff training were planned to strengthen the capacity of all MOH levels to manage the computerized FPIMCH system.
Before the Phase V Project, the MOH had very little computer equipment, users were not very familiar with computer technology and there were no equipment and software standards. Each department had its own software and hardware configuration, which resulted in enormous communication and data-sharing problems. In 1996, the MOH created the Computer and Methods Division (DIM) to focus and supervise all MOH computer-related activities. One of the first DIM activities was to produce a computer master plan. Consequently, Project assistance to the introduction of new computer technologies in the Ministry of Health was based on this master plan.
Procurement of computer equipment
During the Project, a variety of computer equipment was procured and distributed to different departments at central MOH level and to the provinces. Computer networks were installed at the DIM and SEIS, in the major MOH directorates especially at the DP, INAS, CNFRH and several university maternities, as well as at the level of regional capitals and the IFCSs. All provinces of the Project pilot regions were provided with computers and printers. An e-mail system and a Web site were set up for the Ministry of Health and all of the above-mentioned structures were given e-mail and lnternet access.
The last year of the Project was dedicated to using this infrastructure and its maintenance so as to meet the increasing demand of users at all levels. The MOH equipped itself in lnternet technology, and has become an lnternet provider for all MOH users at both provincial and regional level.
John Snow, Inc. 90 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table 8 summarizes the major computer equipment procurements made under the Project:
Table 8
Major computer equipment procured under the FPIMCH Phase V Project 21 servers
298 computers
164 printers
5 Datashow projectors . Cabling of networks at central level and in 12 regions . Installation of modems and Zip drives in 23 provinces
Procurement of French and Arabic business software, software for WEB page design (Frontpage and MSPublisher), database management (Magic) and data analysis (SPSS)
Training in computer technology
A considerable effort was made during the entire Project to train health staff:
= Training of DIM technicians in computer tools to prepare them to be the future trainers for the MOH;
Training of DIM key staff in network management software to meet the MOH needs;
Training of DIM technicians in management tools of the MOH Web site and e-mail system;
Training of at least 200 central-level health professionals in office automation tools, e- mail and lnternet;
Training of 100 technical officials of regional delegations (10 per delegation) in office automation and network usage;
Training o f the delegates, statistics technicians and facilitators in 30 provinces in office automation, e-mail and lnternet;
Strengths and weaknesses
A beneficial, but operationally complicated, restructuring effort of the FP/MCH information system
The restructuring of the routine FPIMCH information system has greatly contributed to the sustainability of programmatic achievements and the institutionalization of decentralized management of FPIMCH services. The integration and simplification of several data collection instruments and monthly reports will decrease the workload of service providers and help them to use a holistic approach to case management. As the systeme SMlPF application will allow provincial and regional managers to process and analyze FPIMCH data themselves, it will have a beneficial impact on the decentralized management of FPIMCH services: (1) by enabling the local level to proceed with a rapid and targeted analysis of the major performance indicators, it will increase the use of information in FPIMCH management decision-making; and (2) the improved use of data will lead managers and service providers to collect better quality data promptly. In its turn, this should result in more rapid transmission of quality data to the decision-makers of national programs.
John Snow, Inc. 91 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Such a restructuring process was not always easy and lacked coordination between the different restructurina ohases, i.e. between the oroduction and distribution of new data collection supports ( ~ c s ) , th; training program in' DCS use and the implementation of the systeme SMlPF application. For example, because of the limited number of DCSs distributed initially, some managers had decided not to use the new information supports as long as the quantity made available to them did not cover a period of at least 6 months. Others had started using these supports. As a result, the SElS received two different monthly report formats. The circulation of these two different monthly report formats also generated data entry problems with the new application. The co-existence of these two data processing systems is disrupting the national databases available to program planners and managers at national level.
At the end of the Project, the new FPIMCH information system, although conceptually very beneficial and promising, has not yet succeeded in achieving, in all of the five pilot regions, the speed of data transmission and quality required by the performance indicator. All users must realize that such a large-scale restructuring of the routine information system is very complex and can seriously perturb, at least temporarily, the smooth running of health services. The transition difficulties will continue as long as restructuring is not completed for the whole country.
Creating an information culture is a long-term behavioral intervention
The major project objective for the health information system was to improve the usage of FPIMCH data generated by the system for decision-making at all levels. Although SIS restructuring transformed the system into a more relevant, reliable and rapid information production tool, it was now time to use it. For five years, the Project therefore undertook several activities to convince the managers of programs and peripheral health services, that information can lead to action. Training organized by the Project was designed as exercises in FPIMCH data analysis to help participants identify problems and propose solutions. During the last three years of the Project, the planning and implementation of small projects in the pilot regions, based on an in-depth analysis of the regional situation of FPIMCH services, were particularly revealing for most of the participating managers, and engendered enthusiasm which might be transmitted to other managers and service providers.
However, these exercises also revealed the lack of confidence of managers in the existing routine information system, whose quality control has evaded them until now. It is difficult to change the reasoning prevailing with most managers, namely that it is useless to undertake certain actions based on information as long as they did not sufficiently control the use of resources. It is hoped that the implementation of decentralized management structures at regional level, together with that of the new decentralized data processing and analysis system, will result in a genuine "information culture".
Computerization: optimize investments
The Project made major investments in the acquisition of high-performance computer equipment and the training of managers from all levels in its use. Despite these efforts, the information tool is not yet well utilized by most MOH key staff and decision-makers, at both central and peripheral levels. In effect, few use daily the available software for planning and management tasks, and few use e-mail as a communication medium to plan meetings or to transmit data or reports. It happens ail too often that the computer sitting on the desk remains a mysterious object, a status symbol and an end in itself. Again, this is a problem of attitudes and behavior. To achieve better results, the MOH should invest in pre-service and in-service computer training of all MOH senior staff, both medical and administrative.
John Snow, Inc. 92 Contract No. 608-C-00-94-00006

Another danger threatening the computer pool is its rapid decline into dysfunction without continued maintenance of both hardware and software. The amount of equipment to be maintained has increased enormously, and the needs expressed by the different users at central and peripheral level have become so vast that they exceed the capacity of the DIM, especially when this requires going to the four corners of the country. The maintenance function of the computer pool should therefore be rapidly decentralized, if necessary by outsourcing.
Recommendations and future perspectives
On the basis of this analysis, we propose recommendations and future perspectives on the sustainability and institutionalization of the health information system as a management tool for FPIMCH services:
Rapid extension of the sysfeme SMlPFthroughout the country
The major and urgent task is to extend the new data entry and processing system to the whole country. As long as the old centralized processing system and the sysfeme SMIPF are used concurrently, production of national data will remain disturbed and reverting to the old system will remain a possibility, thus wasting all benefits of a major investment. To succeed, this operation will necessarily require the support and collaboration of all the central departments and regional and provincial decision-makers, as well as donor assistance.
Consolidate the restructured information system before undertaking any new restructuring
Many efforts are still required to assure that the FPIMCH data produced by the new information system are reliable, complete and timely. A continued supply of DCSs, and especially an integrated monthly report, must be provided. Ultimately, the regions could themselves become responsible for their production. All relevant central departments should provide continued support to the regions and provinces, both to resolve problems that might arise with the use of the systeme SMIPF and to motivate and raise the awareness of managers on the importance of information for FPIMCH service management.
Proceed with the integration and decentralization of the management of the routine health information system
It is obvious that large-scale restructuring takes place over several years. In the meantime, the process initiated to integrate and decentralize the management of the routine health information system must go on. For example, decentralizing the management of epidemiological data, undertaken on a pilot basis by the Project through the S-M-D regional epidemiological observatory, should continue and be extended throughout the country. Operational research could be carried out to identify sustainable mechanisms for integrating the management of FPIMCH and epidemiological data.
= Strengthen the capacity to use computer technology as an information management tool
As discussed above, in order to optimize Project and MOH investments in the computerization of health services management, sustainable mechanisms must be created to ensure the maintenance of the computer pool and to train health personnel in its use.
John Snow, Inc. 93 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Intermediate Result IV: Increased Diversification of the Resource Base Supporting the Delivery of FPIMCH Services
In 1994, although the private medical sector covered 60% of all curative care, it was involved only marginally in preventive care and in reproductive and child health.
With the gradual withdrawal of USAlD support to preventive care programs, the Ministry of Health was looking for innovative strategies to ease the financial burden of its programs, while ensuring the completion of its objectives. This was, in particular, the case with contraceptive products. Without private sector involvement, the MOH found it impossible to provide the population with free FP services. As Morocco was undergoing major economic development there was an increase in the demand for such services in the private sector (pharmacies). The MOH, however, continued supplying a substantial number of households who could pay for such services in the private sector. If segmentation could be achieved by attracting these households to the private sector, the MOH could redirect these resources to better serve needy populations.
To achieve sustainability of FPIMCH services, the FPIMCH Phase V Project therefore focused major efforts on private sector development through two mechanisms: (1) implementation of a public-private sector partnership in MCH and FP with the increased involvement of private general practitioners (PGP), and (2) social marketing of contraceptive products which would enable PGPs to provide affordable FP services.
A. Private Sector General Practitioners
Several governments in developing countries have started involving private practitioners in primary health care delivery. In Morocco, the initiative of private sector involvement in preventive care started at the beginning of the 1990s with the social marketing of contraceptives and oral rehydration salts. This operation concerned both the pharmaceutical industries and pharmacies.
Development of fhe private sector strategy
Under the FPIMCH Phase V Project, an initial strategy of private sector involvement was developed in 1994. Titled "Partnership for Health", this strategy proposed a partnership between the MOH and the private sector in the widest sense: physicians, pharmacists, nurses, midwives, private clinics, local communities, industry, other ministerial departments and civil society. The strategy was to develop and promote an integrated primary health care package focused principally on family planning and mother and child health.
Several factors can explain the poor progress achieved in the first two years. Among these factors are: (1) the scope of the strategy was over-ambitious insofar as the MOH was not used to work with the private sector, which covered over 30,000 local NGOs and 200 professional health associations; (2) the private medical sector is essentially concentrated in urban areas; (3) several legal restrictions prevent NGOs from providing health care, even though they are located in peri-urban areas and can provide affordable services; and (4) the proposed approach fragmented the efforts and diluted the potential impact on service delivery.
Following an evaluation conducted in 1996 by a short-term URC consultant, in collaboration with the Moroccan Society of Medical Sciences (SMSM), the model chosen for extending FPIMCH services in the private sector was the strengthening of the network of private
John Snow, Inc. 94 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
general practitioners. This choice took into account the time and financial and human resources available to the project, Interest in the network of practitioners was also due to the fact that SOMARC was developing a strategy to launch IUD social marketing and therefore needed to prepare general practitioners to confront this new demand.
Objectives
The objectives of strengthening the PGP network were to:
1. Augment the contribution of the private medical sector to affordable and quality FPIMCH services.
2. Consolidate and institutionalize the PGP network through continuing medical training (CMT) and quality assurance.
Achievements
To inventory and extend preventive services provided by PGPs, five essential activities were identified: (1) PGP training in FP; (2) improvement and follow-up of the quality of PGP services; (3) promotion of preventive care with PGPs; (4) policy environment of the PGP; and (5) research and evaluation.
PGP Training in FP
ALCO conducted a preliminary survey, which determined the interest of practitioners in preventive care, their need to upgrade their knowledge in contraceptive methods (especially injectables and Norplant as methods newly introduced on the market) and the feasibility of training, taking into account the availability of private practitioners. Another finding of this survey was the total lack of interest by PGPs in the promotion of contraceptive methods (which led to including a counseling module in their training).
To provide quality training, agreements were signed between the CNFRH, FARGO and the Lalla Myriem maternity to conduct a course on family planning methods focused on IUD insertion. From the inception of this training in 1996 through 1998, a total of 965 physicians were trained.
The implementation of this training met with certain institutional and logistic obstacles and constraints. First, new contracts had to be negotiated with the training centers on the basis of a fixed rate per trained PGP instead of a flat rate per session. While improving the efficiency of training, this delayed the signing of these contracts and sometimes also resulted in the cancellation of training sessions for lack of sufficient participants. Also, the number of health centers available for practical training decreased seriously during national vaccination campaigns.
Following an initial evaluation of this training, it appeared that a major investment had to be made in the doctor-patient relationship. A sample of 300 PGPs already trained in FP attended refresher courses in inter-personal communication. The same training was also provided for medical assistants who play an important role in the reception and admission of patients.
Qualify improvement and follow-up of PGP services
An evaluation of the private practitioner training offered under the Project confirmed the potential for success of a peer review system to assure quality in private medical surgeries.
John Snow, Inc. 95 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
To develop such a system is a long-term task, which involves developing quality standards, identifying and creating peer groups, then training them and providing them with evaluation tools and advice.
In May 1999, Prof. Andre Jacques of Quebec Medical College and Dr Ahmed Moussaoui, private gynecologist, carried out a feasibility and design study of a quality assurance model in the private medical sector through peer review. Peer review is a process where a colleague (peer) reviews the work of another colleague of the same profession. The process can be structured as an informal group learning mechanism. It differs from supervision insofar as there is no administrative relation between the peers. It is generally considered as an opportunity to improve the quality of health care through the learning process among peers.
Prof. Jacques facilitated a design workshop for 15 Casablanca-based general practitioners to initiate the quality assurance pilot project. Specific targets selected by the group were oral contraception and the intrauterine device (IUD), though not excluding other elements of family planning. A choice had to be made between several peer-review methods. Three models drew attention, depending on the target chosen for assessment: (1) structured objective clinical assessment (ECOS), where case simulation is the preferred method; (2) self- assessment facilitated by a validated self-administered questionnaire to be filled in and returned to the assessed PGP for feedback; and (3) direct observation on an anatomic model.
The steps that followed the design of the model were: (1) support and supervise the group of 15 GPs who wish to participate in the pilot project; (2) develop evaluation tools based on standardslnoms already developed for family planning; (3) validate the different tools in the field and train the evaluators and standardize them to the method; (4) apply the process to the group of 15 PGPs; (5) plan continuing medical training in accordance with identified needs; and (6) develop and implement the evaluation of the pilot project in accordance with the above criteria. All these stages were covered and project extension will be undertaken under the new private sector CMS project.
Promote prevenfive care with PGPs
A poster on the counseling stages and flash-cards on FP methods were developed and distributed to the trained physicians. Other didactic support materials in the form of excerpts from journals such as Network, Population Report and Outlook were made available to PGPs or reproduced in specialized journals. It should, however, be noted that the communication component is absent in private surgeries and the SOMARC project decided to develop it at the same time as positioning their range of Al Hilal products. In fact, CMS encountered the same problem of promoting service providers through a logo that might possibly be given media coverage, but legal restrictions on the promotion of service providers has, until now, prevented this.
Policy environment of the PGP
Although the private sector has considerable potential, it is burdened by numerous constraints: financial, fiscal, geographic distribution and purchasing power of consumers. These constraints limit its development and service supply. Within this context, an activity was planned to develop a training module in management of a private practice. Its target is to allow the private physician to improve the quality of his services and rationalize the management of office. Control of fees for services provided and fiscal charges will allow the doctor to lower his fees, particularly for preventive care services.
For this activity, the project team initiated collaboration with the Moroccan Society of Medical Science (SMSM) and recruited an external consultant to supervise the team. The "Guide d'installation du medecin" was developed by the SMSM in collaboration with the DP, DRC,
John Snow, Inc. 96 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
DELM, the Conseil National de I'Ordre des Medecins, the Conseil National de la Jeunesse et de I'Avenir (CNJA) and the Banque Populaire (initiator of the Credit to Young Promoters). Among the components covered by this manual were: marketing the services of the private practitioner; preventive programs of the MOH and potential fields of a public-private partnership; the minimum equipment kit to assure the quality of care; and the medical file and its importance for the continuity of care and health insurance. The printing and dissemination of this manual were completed in 1998.
To achieve sustainability of training efforts for private medical practitioners, a Continuing Medical Training (CMT) strategy was developed in collaboration with the SMSM. This strategy was preceded by a study conducted under 6 headings: (1) a survey of organizations conducting CMT; (2) a study of the activity programs of CMT organizations; (3) opinion survey of physicians on CMT; (4) their current sources for updating knowledge and their needs as to CMT; (5) a study of current legislation and regulations; and (6) study of CMT experiences in other countries.
A number of other activities related to the policy environment were initiated by the Project:
Assisting with the creation of the Federation of Associations of Private General Practitioners through Project collaboration with the SMSM;
Initiating the approach to standardize and reduce fees for FP services in the private sector (250 Dh for an IUD insertion, including the product and a check-up visit) and involvement of two private insurance companies for the reimbursement of medical fees; and
Organizing a national consensus conference on vaccination and design and printing of a harmonized vaccination calendar.
Research and Evaluafion
A study of the literature and documents developed by the private sector was undertaken by ALCO to prepare the strategy for the Partnership in Health project. Other studies were carried out to prepare specific initiatives of private sector development, such as a KAP study of female workers in Agadir to develop the FIPROMER strategy and a study undertaken by Mr. Claude Gingembre before initiating the development of the "Guide d'installation du MBdecin".
Three major evaluations were conducted during the implementation of the Partnership for Health. The first was on the project launching strategy itself and its results have been described at the beginning of this report. The second evaluation concerned PGP training in FP. It was conducted jointly by Prof. Pierre Jean and Prof. Moussaoui. Its results led the Project to develop an IPC module to PGP training. The third evaluation concerned the assessment of PGP training in IPC and the investigation of the PGP's interest in CMT.
Analysis of results
The evaluation results of PGP training are encouraging in terms of the involvement of PGPs and the development of their technical skills in FP. It remains nevertheless necessary to accompany this effort with in-depth work and act at the level of demand stimulation. The evaluation conducted by Professors Moussaoui and Pierre Jean showed a definite increase of FP services and, especially, in pill prescriptions, but only a weak increase in IUD insertions, which went from 0 to 1.5 per month per trained PGP. This finding can be interpreted in two ways: (1) the evaluation was carried out only a few months after training, which is a relatively short period for observing any radical change in behavior; (2) FP training of private medical practitioners and media coverage of Al Hilal products are not sufficient and a change of strategy is necessary.
- - - -
John Snow, Inc. 97 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
After several years of working with private general practitioners in the context of the Project, it has become obvious that FP services are not a major concern of a PGP because they do not generate enough income for FP. There is the issue of demand: the trained PGP is not considered by the population as being entitled to provide such services, which are of the domain of the gynecologist, or can be obtained at no cost in public centers. Finally, FP services alone are not sufficient for a physician to create a loyal clientele and to educate it in preventive care. We therefore concluded that the focus should be on the re-positioning of the PGP in general. This will be discussed further below.
The second objective of this component was the development of a model for continuing medical training. The SMSM is already a leader in this field. The December 1999 SMSM congress resulted in a general consensus between all interested parties on the need to organize structured CMT and preferably focused on improving the positioning of the general practitioner. The results of the sectorial study undertaken by the SMSM show that there is great potential for the financing of CMT by the PGPs themselves as well as by other sources.
Lessons learned and future perspectives
Future prospects for the re-positioning of the PGP remain uncertain and depend on the professional constraints of PGPs, themselves, linked to the organization of the Moroccan health system and economic and social contingencies. A preliminary study on the situation of private medicine in Morocco, conducted in December 1996 by Dr. Claude Gingembre, shows that, despite considerable progress being achieved, undeniable obstacles and constraints still impede the development of private medicine in Morocco, and specifically private general medicine. The major difficulties encountered by the private practitioner are: (1) high cost of setting up a private medical practice; (2) the absence of any supervision and orientation once the physician leaves medical school; (3) the problem of clientele linked to the poor purchasing power of the population; (4) the issue of profitability linked to over-equipment; (5) lack of post- graduate supervision and of CMT, both technical and managerial; (6) social coverage is not generalized; (7) self-medication and recourse to pharmacies without medical prescriptions; and (8) the unfair competition of "TPA" (temps plein amenage i.e. they are allowed to practice part-time in the private sector) by university professors, the medical consultations organized by CNSS clinics and other semi-public organizations, such as the Office Cherifien des Phosphates and the National Electricity Board.
Any strategy involving the private sector in preventive care priority programs cannot ignore these problems. The experience of the Partnership for Health project may be a lesson in this field. Although investment in human and material means had been modest compared to the magnitude of the problem, it remains valid that the development model - i.e. the re- positioning of the PGP - could result in an innovative approach to the solving of some structural problems of the profession. This will probably result in a better coordination between the private and public sectors and therefore in a better segmentation of the target populations. A network of family doctors must be developed that would provide an integrated service package of good quality at affordable rates to a sector of the population which until now has received these services free of charge in the public sector.
The first steps in the development of this model have been completed. Indeed, the general practitioners have now a representation at national level, namely the federation of associations of private general practitioners in Morocco. The principal mission of this federation will be the rehabilitation of the status of the private general practitioner. However, to enable the PGPs in Morocco (2,500) to become family doctors, they will at least need a structured program of continuing medical training, a quality assurance mechanism, products sold through social marketing and generation of demand through the media coverage of the product and the service provider.
John Snow, Inc. 98 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Such an undertaking was evidently beyond the scope of this project, but will remain a priority in the context of the diversification of the resource base supporting the delivery of FlMCH services to the entire Moroccan population. It is hoped that the new private sector project funded by USAID through the CMS project (Commercial Marketing Services) will be able to contribute increased support to this cause.
B. Contraceptive Social Marketing
The Moroccan Social Marketing Program (MSMP) was launched in 1998 by the Ministry of Health with USAlDlRabat support and SOMARC technical assistance. From the beginning, this project was associated with the private sector in the development and promotion of family planning. Consequently, for the project components and activities - production, distribution, advertising or promotion - the MSMP had recourse to an active partnership between producers, pharmacists and distributors.
Objectives
The objectives of the Moroccan Social Marketing Program (MSMP) were threefold:
The first objective is social, since it concerns an increase in contraceptive prevalence, which was 36% at the national level (1 987 ENPS).
. The second objective is economic: to capture affordable demand in urban and semi- urban areas by ensuring the availability of good quality and affordable contraceptive products to low-income groups.
. The third objective is financial: to ensure sustainability, it was necessary to find a self- financing mechanism both for product procurement and educational campaigns by levying a percentage on sales incomes with which a project fund could be established.
Achievements
I. Marketing of condoms (since 1989)
The objectives of this marketing strategy were:
Greater awareness of the condom as a family planning method through product valorization, improved acceptability of the product and better information on the condom as a FP method.
Introduction of Protex as a new brand sold by the private sector and targeting:
9 low and medium-income male population
P users of traditional contraceptive methods,
9 non-users of contraceptive methods.
The project used the following marketing techniques:
A communication policy and a positioning that valorizes the responsibility of men in the choice of a contraceptive method: "family Planning is also the responsibility o f men".
John Snow, Inc. 99 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
A policy promoting the product by creating a social and psychological climate favorable to the launching of a campaign: Public Relations campaigns with government policy- makers and opinion leaders, raising the awareness of prescribing doctors, pharmacists and aid-pharmacists, press campaigns, sponsoring radio and N broadcasts.
A price policy affordable to the consumer of the target market and profitable for all the distribution levels: a preferential price for wholesalers, pharmacists and as compared to the competition. The price of 6Dhs fixed for a pack of 3 Protex condoms was 43% lower than that of the leading brand on the market.
A distribution policy which ensured that the condom was distributed to all pharmacies and assured delivery to and stocking by all the most important retailers in the country.
An advertising strategy based on a positioning that valorizes the condom as a FP method by using the radio, which, for the first time in Morocco, mentioned the brand name of a condom.
A large-scale training program was targeted, for one year, at all the sales-persons in pharmacies and the pharmacists. This program, entirely managed by the National Federation of Pharmacists' Syndicates (FNSP) was able to raise the awareness of 1400 pharmacist-aids and I000 pharmacists, including training in the use of condoms and counseling customers.
The project developed in three stages: (1) in the beginning all the aspects of the product were financed by USAID, whether research, promotion or communication; (2) as soon as the project fund was set up by levying 30% on sales incomes, co-financing became possible by both the Promopham lab, importer of the product, and USAID; and (3) by the end of 1993, the project was entirely self-financed by sales incomes.
An evaluation study carried out in 1993 showed that the condom is mentioned by 92% of the sample as a contraceptive method, 60% consider it efficient in preventing pregnancy, 94% spontaneously use the word Protex for a condom and 38% of those who use Protex never used any contraceptive before. In 1994, a second positioning was achieved with the condom providing protection against STD and AIDS and, for the first time in Morocco, Protex was mentioned by unmarried people as a means for protection against STDIAIDS in radio campaigns.
2. Social marketing of oral confraceptives (from 1992 onwards)
The second phase of the Moroccan social marketing program concerned the marketing of oral contraceptives at a price that is affordable for low-income populations. The project was initiated in December 1992.
The project was justified for the following reasons:
Despite a decline in the fertility rate (from 5.9 in 1980 to 4.2 in 1992), it was still high with repercussions on population growth and it impaired maternal and child health.
= A major discrepancy subsisted between a high level of awareness of the pill (98.9%) and the prevalence rate for this method (28.2%). - Prevailing unmet needs: 24% of the women not using contraception questioned in 1992 wished to space births and 49.1% wished no more children.
John Snow, Inc. 100 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
A great number of users who had already tried the pill and discontinued it because they did not know how to use it properly.
= Information available to users is often poor and incorrect.
The need to emphasize information, education and communication campaigns through the major media to fill this void .
The following objectives resulted from this:
. Increase the contraceptive prevalence of modern methods.
Promote the social marketing of oral contraceptives and make them affordable for low and medium income populations.
Transfer part of the demand to the pharmaceutical distribution sector.
Develop education campaigns to reinforce the final adoption of the pill by users and limit the chances of discontinuation.
The development of the oral contraceptives project was achieved through an active partnership with:
The National Federation of Pharmacists' Syndicates in charge of training pharmacists and their assistants in contraceptive technology and counseling on oral contraception.
The Moroccan Association of Pharmaceutical Industries in charge of the marketing of the product, market surveys, advertising and sales monitoring. An agreement protocol was signed between PolymedicISchering (producer of Mycrogenon), WyethlMaphar (producer of Minidril) and AMlP for the contractual management of research and advertising activities outsourced to a consultancy and an advertising agency.
The companies representing Schering and Wyeth (Polymedic and Maphar) each chose one of their brands as brand for social marketing represented by the generic Kinat Al Hilal. This allowed bypassing the legal obstacles that prohibit pharmaceutical firms from publicly advertising any medication, including contraceptives. The two pill brands were marketed at the public price of 8 Dh, i.e. nearly a third less than the cheapest of equivalent pill brands.
The strategy was defined as follows:
Position Kinat Al Hilal in the field of health and family well-being.
Valorize and insist on the role of counseling, information and assistance in pharmacies.
Emphasize the accessibility of the selling price.
Distribute the two Kinat Al Hilal oral contraceptives in private sector pharmacies throughout the Kingdom.
Assure coverage of the network of pharmaceutical wholesalers.
Each laboratory has undertaken actions to launch and position the product with gynecologists, pharmaceutical wholesalers and pharmacies.
Promote Kinat Al Hilal, underscoring the qualities of this product: innocuity, safety, affordability and presence in pharmacies
John Snow, Inc. 101 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Inform physicians and gynecologists about the targets of the program and raise their awareness of the problems of poor use and discontinuation of the pill.
When the product was launched, the two laboratories mobilized their sales forces. Schering assigned their marketing team to pharmacies to place Kinat Al Hilal stickers and to the wholesalers with blocks of information leaflets to be given to each user purchasing the pill. Maphar was in charge of distributing the information poster on oral contraception to all pharmacies throughout the country.
Several educational materials were produced and promotional and awareness actions were undertaken:
Information leaflet on how to use the pill properly.
. Question/Answer poster on oral contraception to be posted in pharmacies.
. Kinat Al Hilal stickers for all pharmacies.
. Mystery Shopper competition organized in December 1993: a mystery client talks exclusively to assistant pharmacists asking for oral contraception. To be qualified the assistant had to suggest Kinat Al Hilal and be able to answer all the questions asked by the client on its use.
. Production for TV programs for the medical channel, special TV channel for physicians with 3 weekly airings.
. Publication of articles on oral contraception and FP in the specialized press.
. The objectives of the advertising campaign were to increase awareness of the product with the MSMP logo so as to achieve, through information, improved awareness and use of the pill, and to highlight the service and availability of the network for counseling and information and ultimately overcome the factors causing discontinuation. Several advertising spots were produced for this campaign.
A major research program was undertaken to sanction the decisions on the marketing creation and strategy with the target population.
A training program was organized for 1200 pharmacist- aids and 1000 pharmacists in one- day training workshops for groups of 10 to 15 participants. The program was regionalized and organized by pharmacists. With SOMARC assistance, the FNSP trained a nucleus of 40 trainer-pharmacists from all the regions, who adapted the educational material and supervised the participants.
First-year sales forecasts almost doubled. Based on an estimation of 600,000 cycles in the first year to reach 2.2 million cycles in 1995, this was largely exceeded since 1.148.052 had been sold by the end of the first year.
Moreover, observation of the oral contraceptives market shows that the PMMS had generated new demand since the other pill brands also profited by the communication campaign. Their sales increased substantially. Kinat Al Hilal did not replace existing demand.
The financing mechanism of the project followed the same logic to result in project self- financing. From the very beginning, a project fund had been created by levying 10% of product sales in order to finance the advertising, promotion and follow-up and evaluation
John Snow, Inc. 102 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
actions of the project. Since December 1996, the Kinat Al Hilal project has been entirely self-financed from sales incomes and no longer supported by USAID.
3. Marketing of long-term methods
In 1995, the third phase of the program was initiated for the marketing of long-term methods. The overall objective was:
To diversify the contraceptive method mix by introducing new methods fo respond to the unmet needs of women and couples who wish to plan their families.
The specific objectives of the project were:
. To attract new acceptors to long-term methods.
. To meet the MOH objective of strengthening the role of the private sector in FP.
. To make long-term affordable methods available to low-income couples.
The project extended the partnership initiated under the preceding two projects by strengthening the Advisory Council, from then on, composed of representatives of the MOH, USAID, the directors of producing firms, SOMARC, FNSP, the Conseil National de I'Ordre des M6decins and of Ordre des Pharmaciens, the Confederation of Syndicats des Medecins Prives, the Royal Gynecological Society and the Moroccan Society for Contraception and Fertility. The Council's role was to orient PMMS activities and validate strategic decisions.
Taking into account the specificities of long-term methods (LTM) and the constraints the project expected following the LTM public sector experience, a specific strategy based on an excellent knowledge of the environment was to be initiated. A research plan was prepared to identify constraints.
Qualitative studies showed that the user-related constraints were:
= Quality of the service provided;
For the IUD, the image of the method;
= For injectables, unfamiliarity with the method;
= Price and accessibility of private sector services.
Whereas constraints identified for service provider were:
PGP lack of mastery of and skills for IUD insertion; Availability of the IUD in the pharmaceutical distribution network; Resistance to injectables considered as a method for the "insane" and the "poor"
Based on these assumptions, a large-scale survey was undertaken on 603 women aged 18- 40, users and non-users, and 570 health professionals (gynecologists, private and public general practitioners and pharmacists). Survey findings may be summarized as follows:
= Women have very poor knowledge of injectables: hardly 4.3% mentioned them spontaneously as a contraceptive method.
John Snow, Inc. 103 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
For the IUD, knowledge of the method reaches 73%' 28% of the women cannot see any usefulness in it, 65% mention extra-uterine pregnancies, bleeding and pain as drawbacks and 50% do not foresee using it.
As to health professionals, 53% of the private gynecologists and 40% of the general practitioners are totally opposed to injectables: 41% of all the physicians consider it as a method for the mentally retarded and 59% are opposed to this method because of its side-effects.
= For the IUD, 94% of the physicians consider it as an efficient method, 91% prescribe it and 70% (mostly all gynecologists) insert it.
Private sector general practitioners asked for training in contraceptive technology and especially in IUD insertion to improve skills.
The PMMS marketing strategy for long-term methods was based on the following elements:
For the target population:
Valorize injectables as an efficient and safe contraceptive method;
Valorize injectables as the ideal contraceptive for breast-feeding mothers;
Valorize injectables as a discreet contraceptive method;
Valorize the service, the counseling available from private prescribing doctors and pharmacists.
For private service providers:
Promote injectables in collaboration with the Syndicate of private physicians and the scientific societies to overcome the resistance of physicians and pharmacists to injectables;
Strengthen the technical competency of the medical sector and train physicians.
The JSI team of the FPlMCH Phase V Project was charged with the training in IUD insertion of some 1,000 private physicians. Concurrently, under a training program in 1996-1997, 600 pharmacists and 150 general practitioners and gynecologists were trained in injectables.
Following this, a consensus conference was held on the introduction of injectables in the private sector with representatives of the scientific societies, the Ordres des mkdecins and pharmaciens, syndicates of doctors and pharmacists, the Rabat and Casablanca faculties of medicine and the MOH.
A1 Hilal program
Launching the Hoqnat Al Hilal injectable contraceptive and the Lawlab Al Hilal Intrauterine Device (IUD) resulted in the creation of the Al Hilal contraceptive product line, identified by the generic Al Hilal logo that, through mass media advertising, gradually superceded the specific Kinat Al Hilal logo. Consequently, and to emphasize the identity synergy, the program itself was renamed Al Hilal program with the objective of conveying the concept of affordable quality family planning throughout the public sector.
John Snow, Inc. 104 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Kinaf A1 Hilal
Although self-sufficient, the Kinat Al Hilal project was maintained in the realm of a program providing technical assistance to the Wyeth-Maphar and Schering-Aventis partners for oral contraceptive advertising campaigns financed by sales returns. A new marketing plan, aimed at positioning Kinat A1 Hilal as a method for starting contraceptive life and addressing the young married urban and rural woman who wants to delay the arrival of her first child, allowed the development of new mass media supports to replace the former 1992 advertising spots. The CMS re-initiated discussions with its partners in order to renew the preceding protocols of agreement and maintain Kinat in the marketing line of the Al Hilal product range.
Hoqnaf A1 Hilal
Hoqnat A1 Hilal is the injectable contraceptive Depo-Provera produced by Pharmacia & Upjohn. Following an agreement with the SOMARC project and its partners, the MOH and USAID, its price was fixed at 34.40 Dh a dose, including the disposable syringe. Since the laboratory had undertaken the distribution and promotional efforts with the medical profession, the project undertook the following marketing activities, with the support of and technical validation by the Ministry of Health:
Training physicians and pharmacists in injectable contraceptive technology (see above).
Didactic information guides for the target population as well as information leaflets, technical forms on injectables for doctors were produced and distributed.
When the method was launched in 1997 and during the first months of 1998, pan-Arabic spots produced by SOMARC for several Arab countries and adapted to the Moroccan dialect were widely disseminated. A maintenance campaign took place in 1999.
Display units with Arabic and French leaflets were distributed to pharmacies to be displayed on counters as counseling supports.
= The brochure "Management of the side-effects of injectables" was produced and distributed by medical representatives to general praditioners and gynecologists. It was so successful with service providers that Pharmacia & Upjohn reproduced it at their own cost.
Didactic and promotional inserts were published in specialized journals (Cahiers du Medecin, Caducee, Espdrance Medicale, Sages-femmes, Remedes).
= The project has recently developed a didactic and promotional brochure on Hoqnat A1 Hilal bases on the Ministry of Health FP Norms and Standards targeted at private sector generalists and gynecologists.
Lawlab A l Hilal
Lawlab Al Hilal is the Cooper T 380 IUD produced by Pregna Ltd. And imported by Reacting S.A. with packaging developed directly by Pregna. Its unit price is 50 Dh for the doctor (which may be reduced by 25% in case of multiple purchase) and its price to the consumer is 60 Dh in order to avoid internal competition of distribution circuits.
With the extensive training program of the Phase V Project, through which over 1,000 general practitioners were trained, the program was able to increase the population of potential prescribers. The JSI and SOMARC projects had collaborated in a joint mailing
John Snow, Inc. 105 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
action that included information on IUD training and an information leaflet on the availability of Lawlab Al Hilal to optimize service delivery.
To launch the product, SOMARC had produced Moroccan mass media supports on Lawlab Al Hilal. Three TV spots were developed based on a creative brief that emphasized the notion of time and tranquility provided by this method. Each spot represents a woman with a particular life style (a housewife with three children who wants to limit births, a young mother with a little daughter who wishes to defer and an active women, mother of two children, who had already experienced birth spacing with Lawlab Al Hilal).
The campaign to launch the product took place during the first half of 1998 since the product had been available since November 1997. In December 1997, Reacting's sales force was trained in sales techniques and interpersonal communication with the physician.
The first awareness poster for waiting rooms was developed and produced. In 1999, Question-Answer posters in French and Arabic focusing on the evolution of attitudes were developed and produced for waiting rooms.
To mitigate the deficiencies inherent to a limited insertion practice, especially of general practitioners, the project developed, with MOH support, an illustrated poster on IUD insertion techniques for doctors' consultation rooms
Didactic and promotional inserts were published in specialized journals (Cahiers du Medecin, Caducee, Esperance Medicale, Sages-femmes, Remedes).
The project also worked in close collaboration with the distributor to open the road to pharmaceutical wholesalers and institutionalize Lawlab distribution in pharmacies.
A third means of distribution, i.e, sales by catalogue, has been developed by Centrambdic, distributor specialized in the sales of medical equipment and consumables.
A1 Hilal contraceptive choice
With the availability of three Al Hilal methods, the program started promoting the concept "Choix contraceptif A1 Hilal' that allows each woman to choose the method best adapted to her in the available range. A TV and radio spot "Al Hilal Family" was produced to convey the concept of a well-informed choice based on the doctor's advice.
Strengths, weaknesses and future perspectives
When activities endorsed by SOMARC started again, the CMS project continued with its social marketing activities for long-term methods while initiating a large-scale research activity (qualitative and quantitative KAP surveys) whose objective for social marketing was to determine the market situation - including consumers and providers - for injectables and the IUD. The next step will be to develop adequate marketing plans to achieve increased use of these methods and sustain their positioning on the private contraceptive market.
The project has, however, undertaken initial analyses with the following results:
Hoqnat Al Hilal
When this injectable contraceptive was launched, it was a completely new method both for prescribers and patients. For the latter, Hoqnat Al Hilal had the advantage of a novelty as is
John Snow, inc. 106 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
demonstrated by sales figures after the launching campaign. Moreover, the close correlation between advertising airings and an increase in sales shows that the impact of mass media advertising is limited to prompting women to test the method.
Sales trends demonstrate discontinuation rates after one use, which had basically been a "novelty test". Indeed, ill tolerated side-effects and, especially, the lack of preparation of medical service providers and the fact that prescription is not accompanied by counseling means that the discontinuation rate is high.
The following challenges were identified:
Decrease the discontinuation rate for this method
Continue generating new users
Increase the size of its market niche.
Opportunities
There is still an advocacy effort to be done with service providers, starting with gynecologists as opinion leaders in contraceptive service delivery.
Information/training of physicians must be further developed.
A proportion of the service providers who prescribe it (to be evaluated) and who could be the advocates.
Market segmentation and positioning of the product are not yet clearly established (confusion because of concurrent efforts for the IUD and the ever-present pill).
Injectable contraceptives face the same obstacles in all the countries where it exists; take advantage of lessons learned and innovative follow-up strategies.
Based on this analysis, the project set mileposts for the following strategies:
Supply Strategy
Assess the attitudes and practices prevailing among opinion leaders of the gynecological community.
Formally identify information needs and obstacles to prescription: (1) baseline survey of LTMs; (2) evaluation of SOMARC training; and (3) small-scale qualitative survey (to be considered).
= Define a strategy and an action plan in view of a positive change of behavior of the prescriber favorable to the method.
Use peer advocacy through spokesmen convinced about the method.
Demand Strategy
KAP evaluation (baseline survey) and identification of obstacles.
Definition of a marketing plan establishing the productlmarket adequation and including the positioning of the "marketing niche" based on the concept of "alternative method responsive to specific prescription contexts to be developed (postpartum/breast-feeding,
John Snow. Inc. 107 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
estrogen intolerance, constraining discipline with the pill, etc.) and similar positioning with prescribers.
Analyze the experiences of culturally similar countries (Muslim context) such as Jordan and Pakistan; review implemented strategies and what can be transposed to the Moroccan context.
Lawlab Al Hilal
For the marketing plan prior to the launching of Lawlab Al Hilal, the priority "prescriber" target were the PGPs trained by the Phase V Project. These physicians had received a set of 5 free IUDs after their training. When they were visited by Reacting, it appeared that most of them still had IUDs in stock and that insertions were not frequent, whence their refusal to stock more. It is therefore true that until now the trained PGPs have a marginal role in IUD service delivery.
However, gynecologists and private clinics were from the start the biggest clients. IUD insertions in the private sector are mainly done by doctors who found in Lawlab Al Hilal an opportunity to increase the profitability of their medical act. Indeed, Lawlab Al Hilal costs them only 50 Dh, but they maintain the fees for this consultation at about 600 Dh on average.
After discussions and reviews with Reacting, the following points emerged:
The pipeline is full and sales are at a standstill and even decline because stock depletion is slow at the level of both service providers and pharmacies.
Although service providers are in favor of the method, they come up against patients' fears related to negative and lively rumors.
Although the private PGP is trained, he does not insert a sufficient number and, little by little, loses what he learned in training. Consequently, and since he is increasingly less at ease, he tends to shift clients to the pill, which is much more manageable.
In the big towns on the Kenitra-Al Jadida axis (including Casablanca and Rabat), the IUD act in the private sector takes place at the gynecologist's. It will take a lot of time and perseverance for women to start asking the PGP for this service.
Everywhere else in the country, PGPs are more likely to provide this service because of the scarcity of specialists.
Challenges
* Position the PGP as a FP service provider, including IUD insertions.
Find incentives for gynecologists to reduce their fees.
Create pharmacy-physician reference systems to support stock turnover in pharmacies.
Physicians are in favor of the method. Consequently, they are already halfway to promoting it with their clientele.
John Snow, Inc. 108 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The CMS strategy of positioning the PGP as the "family doctor", including FP services, should help with the development of these services.
Work on the enhancement of the private practitioner via the "Doctor-Citizen" concept through media coverage presenting him as a partner of national programs.
Midwives are a non-negligible population of service providers and could play a major role in a "non-competitive" area with gynecologists and PGPs.
IUD users are wholly satisfied with the method and very rarely change methods once they get used to the IUD.
Supply Strategy
Arrange the country into geographical areas:
Area with major presence of gynecologists Area with major presence of PGPs Area marked by absence of medical care providers and presence of midwives
Determine specific area-related intervention strategies to optimize the interventions of the different types of service providers.
Position the private GP as FP service provider in the framework of the "Family Doctor" strategy and promote his capacities as provider of such services (find concrete means).
Uphold the development of Lawlab Al Hilal distribution circuits.
Demand Strategy
* Define a strategy to combat rumors:
Develop a "Peer Advocacy" strategy through convinced users. Organize televised round-tables involving opinion leaders of the medical world and civil society on the health of women. Study the possibility of setting up a free Al Hilal information line.
Resume the advertising campaign (product notoriety to be kept up).
Organize a brainstorming session with all the partners to define "bridges" between the trained private GP and his potential clientele (Example: itemize the idea of making the GP more proactive and more "vendor" of his services and develop other ideas of a potential, more direct promotion.)
At present, the contribution of the MSMP is undeniable in view of the increasing contribution of private actors in the National Family Planning Program. The A1 Hilal program has indeed been a pioneer in mass media communication on contraceptive methods sold on the private market. Since Protex, the condom is no longer a taboo and the market is open to other brands competing at the level of accessibility and affordability. With Kinat Al Hilal the oral contraceptives market has been diversified and is growing. These two products have reached a level of self-sufficiency and their promotion has been - since 1993 for Protex and since 1996 for Kinat Al Hilal -financed by the laboratories themselves. Lastly, the Program has also essentially been a forum for dialogue and a fruitful collaboration between public and private sectors, professional organizations, scientific societies and medical boards.
John Snow, Inc. 109 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
On the other hand, as much as the traditional "product" approach has been efficient and easy for Protex and Kinat Al Hilal, insofar as these methods are "self-consumed", so did it show its limits in the case of Hoqnat and Lawlab because of the unavoidable aspect of medical services with which they are linked and therefore the need to add an extra link in the user chain: the service at the service provider's. The example of Hoqnat Al Hilal illustrates the obstacles that arise when the medical profession is not sufficiently aware of a method and when opinion leaders are not sufficiently involved. Also, on the basis of the lessons learned from prior social marketing projects, CMS assigned itself the task of "re-conquering" service providers before making an effort to generate demand so, as a first step, to overcome the physician's opposition, making him more proactive in the contraceptive choice of his patient.
The accessibility of the population to affordable quality FP services in the private sector remains a major problem impeding the development of the use of injectables and IUDs by
' private practitioners. Consequently, the central strategy of the CMS project will be to act on the mobilization of private service providers around a FP project, included in a more global family health project and relying on the critical concepts of the quality and affordability of services.
To achieve this, components of the institutional, economic and technical environment become priorities in the identification of obstacles to the expansion of private medical practice and the accessibility for the population to reproductive health care through the private sector, and in the definition of actions that would help surmount them.
Lastly, the effort to raise the awareness of the population: information on how the methods work, supply sources, combating rumors, developing product notoriety (quality, accessibility, affordability) and communication on the availability of services in both the public and private sectors, must be a sustained. A continuous effort must be made so as to perpetuate - even anchor - the achievements of ten years of contraceptive social marketing.
John Snow, Inc. 110 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Resource Management of the FPIMCH Phase V Project
What were the resources used to achieve the results of the FPIMCH Phase V Project? Resources are presented under six headings: (1) planning, follow-up and evaluation; (2) human resource management, (3) coordination/collaboration; (4) procurement and maintenance; (5) financial management; and (6) training, study trips and conferences.
1. Planning, Follow-up and Evaluation
Project Management Structures
Project management was achieved through two structures:
(1) The Project Committee of Directors: this committee was co-chaired by H.E. the Minister of Health and the Director of USAlD and all MOH directors were members, as were the USAlD health team and the Director of the JSI Project. It met twice a year.
(2) The Project Management Unit (PMU): chaired by the Director of Population, its regular members were key staff of the Population Directorate, the health team of USAID/Morocco and the JSI team. Key staffs from other Directorates and USAID cooperating agencies were invited according to the agenda. The PMU met every two weeks.
Project Planning
Throughout the project, a participatory planning process was followed, thus granting a steady consensus on oroiect imolementation modalities between the Ministw of Health. USAID. JSI and the other cooperating agencies. This process was structured through the project committee of Directors and the PMU. The PMU coordinated the preparation of work plans. The Committee of Directors revised and approved work plans.
An initial Work Plan was developed in 1994 and updated in 1995 and 1996. In 1996, in collaboration with a USAlDNVashington team, USAlDlMorocco prepared a Transition Plan to ensure the continuum between the bilateral project that was to end in 1999 and the period of post-bilateral technical assistance. Since this transition plan partly modified the conceptual framework of the Project, the JSI team prepared a document titled "Priorities for the Implementation of the Transition Plan", which proposed the restructuring of project activities. The final version of this document was approved by all the partners in January 1997 and was the basis for the I997 Work Plan.
One of the changes in project management from 1997 onwards was the increased role of JSI in the coordination of technical activities with other cooperating agencies. This contributed substantially to the rationalization of the planning and implementation of project activities. For example, JSI provided administrative support to the local activities of these agencies in accordance with a pre-established budget.
End 1997, the 1998-1999 Work Plan was prepared to program activities through to the end of the Project. While implementing the Work Plan, it became clear that some strategically
John Snow, Inc. 111 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
important activities for the post-bilateral project would not be completed by June 30, 1999, the end of the 1998-1999 Work Plan. Consequently, after consulting with the MOH, USAlD decided to extend the project by one year through September 30, 2000. The extension work plan programmed a series of activities in accordance with the needs of the post-bilateral project.
Lastly, during the last year of the Project, the JSI team prepared the project's close-out plan. This plan, listing a number of activities to be implemented following a schedule, was submitted to USAlD in December 1999.
Project Follow-up and Evaluation
Follow-up of project implementation was ensured through the Committee of Directors and, especially, through regular twice-weekly meetings of the PMU. To this effect, Work Plans, quarterly and annual Project reports and the Project procedures manual were used as reference documents. This manual described all management procedures for the project. It was drafted by JSI in agreement with the MOH and USAlD and was distributed, following PMU validation, to all persons concerned.
There was no overall project evaluation, internal nor external, but several project components were evaluated separately during the Project, either by the project team itself or by external evaluators. The results of these evaluations have been communicated under their respective components.
2. Human Resource Management
The composition of the JSI team followed the volume and nature of Project activities. Thus, from a relatively small team of about ten in the beginning, it grew to 21 at the end of 1997, including 5 expatriate advisors, 6 local technical staff and 10 administrative staff. In 1999, toward the end of project activities, first the number of expatriate advisors was reduced to one, and then, in 2000, the number of local staff was reduced in accordance with decreasing needs. Except for a difficult period between the departure of the first project director and the arrival of the second, the internal cohesion of the JSI team was the backbone of the project throughout its lifetime.
For short-term technical assistance, JSI organized 125 consultancies, URC 30 and JHUICCP 14. Over 100 other consultancies took place through either USAlD directly or the cooperating agencies. Administrative support from the United States was generally provided by a minimum of 2 JSIIBoston staff, as well as by one person from URC and JHUICCP. Appendix 4 lists resident staff in Rabat and support staff in Boston, while Appendix 5 provides a list of JSI - URC - JHUICPP consultants.
Achievement of FPIMCH Phase V Project sustainability objectives depended largely on the coordination and collaboration between the different Project partners: the MOH (both central services and delegations), other government departments, USAID, its contractors and cooperating agencies, other donors, the private sector, civil society and the press.
Concerning the collaboration between the JSI team and the Ministry of Health, this report has many times emphasized the importance of the joint implementation of activities, which had been the rule throughout the project. This collaboration was made easier because of the exceptional stability of MOH key staff since the beginning of the Project. The JSI team also facilitated the
John Snow, Inc. 112 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
coordination and collaboration between central level staff and regional and provincial level staff. Despite this, as already underlined in other sections of this report, the lack of definition of the functions of the center vs. the periphery is an impediment to the current regionalization process.
In 1997, as mentioned in the introduction, USAlD entrusted JSI with the responsibility of coordinating all USAID-funded health activities in Morocco. This decision, taken at a moment when an increasing number of cooperating agencies made project implementation increasingly complex, has largely contributed to the coordination between the MOH, USAlD and other cooperating agencies during the last years of the Project.
The FPIMCH Phase V Project team maintained a close collaboration with other externally funded projects. Among them were projects funded by UNFPA, the European Union, UNICEF, GTZ, the World Bank and Belgian and Spanish cooperation.
Also, in the framework of the sustainability of FPlMCH services, privileged relationships were developed between the Project team and organizations of the private sector and civil society. Without being exhaustive, we should mention the Societe Marocaine des Sciences Medicales (SMSM), the Conseil National de I'Ordre des Medecins (CNOM), the Syndicafs des Medecins et Pharmaciens, the Observatoire National des Droits de I'Enfant (ONDE), the National Union of Moroccan Women (UNFM), the Moroccan Society for Solidarity and Development (AMSED), the Moroccan Family Planning Association (AMPF), etc.
Lastly, in order to promote FPIMCH services, the Project team maintained permanent contacts with the audiovisual and written press through radio and television broadcasts, press conferences and publications in journals such as Sage-femme, the SMSM review and Caducee (the journal of pharmacists).
4. Project Procurement
Procurement was a major component of the FPIMCH Phase V Project, not only because of the allocated budget ($15,063,000 or over 37% of the total budget), but also because of its contribution to the Project objective of implementing quality FPIMCH services.
In the following paragraphs, we discuss not only the procurement process, but also, in the framework of sustaining project achievements, the efforts and perspectives of utilization and maintenance of the equipment provided.
Procurement
Major features of FPIMCH Phase V Project procurement were the huge quantities of items, the great number of structures to be equipped and the complexity of procurement procedures. Table 9 provides a summary overview
John Snow, Inc. 113 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Table 9: Procurement by FPIMCH Phase V Project
Category
Vehicles
Medical equipment
Computer equipment
IEC equipment
Other
TOTAL
Major Items
180 Chevrolet pick-ups 3 Cherokee jeeps 4 Trucks 1 Chevrolet sedan Basic equipment for 157 health centers, 8
reference centers and 19 other structures Equipment for 6001 UD centers Basic equipment for 180 mobile teams 1200 IUD kits Equipment for 6 EOC facilities and 46 BEOC
facilities Cabling networks at central level and in 12
regions 21 servers 298 computers 164 printers 5 datashow projectors Audiovisual material: SO video tape recorders 58 N sets 4V studio equipment
Print-shop equipment : I flacheuse 1 offset press Heidelberg I drum scanner
Office equipment: 30 photocopiers, O-H projectors, screens.
desks, etc, Laboratory equipment:: Zondom quality control equipment Materiel for the Sale warehouse:: ! fork-lift trucks, 6 transpalets, generator, cold
room
Amount % (of procuremen
budget)
Procurement Procedures
Equipment procurement procedures are complex because they take into account a number of regulations enforced by USAlD and the Moroccan Government. Thus typically, between the moment of deciding to purchase an item and its actual delivery to the user, the following steps are necessary:
. Needs identification: consensus between the MOH, USAlD and JSI
. Procurement request presented by the MOH
Development of specifications by the MOH, assisted by JSI and/or consultants
Validation of final lists by MOHIUSAID
John Snow, Inc. 1 14 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
. Identification of procurement options:.
Local procurement: procedures lighter as compared to: Procurement in the United States
. Submitting specifications to JSI/Boston and/or Washington
. Preparing the tender document (Invitation for BID-IFB)
Publication Preparing replies to suppliers Opening of bids
Analysis of bids and recommendations
. Final approval of bids by MOHlUSAlD
Award and placing of orders
. Reception of orders
Packing /Assembly of kits
. Transportation (either by sea or air)
. Arrival and customs clearing
. Delivery and distribution to the MOH
Procurement Process
The procurement process occured in two phases: (1) through New Transcentury Foundation (NTF), JSI sub-contractor, and (2) directly by JSI. During the first two years, all procurements initiated from the United States were completed by NFT. From 1997 onwards, to have more direct control over the complex procurement procedures and all resulting delays, JSI recruited Hamady Tall, a procurement specialist. JSI used Geologistics (formerly Matrix) as its transport company. Most of the equipment for the provinces and health centers was warehoused by Geologistics before being sent to the port or airport.
Commentary
Taking into account the volume of procurements, the Ministry of Health was, overall, satisfied with all the equipment procured under the Project. The major constraint and cause of frustration, for the MOH, USAlD and JSI, was the considerable delay for procurements made in the US. This was not surprising bearing in mind the number of steps required by the procurement procedures and the great number of partners involved. Below are a few comments on the steps that were the major causes for delays.
Delay in finalization of specifications
Fairly long at the beginning, it was reduced when procurement was directly done by JSI, thus eliminating an intermediary and making communication between JSI and the buyer a lot easier.
John Snow, Inc. 115 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Delay in kit assembly
Kit assembly of equipment for the provinces and health facilities contributed to delays in the delivery of equipment, since it was an additional stage in the procurement cycle. This kit assembly did, however, prove extremely useful to ensure that the material was indeed routed to the planned recipient. Codification of the parcels made it easier to identify them and distribute them directly to the provinces. It would have been preferable if, for major procurements made for health facilities, a central MOH staff member wuld have assisted with the kit assembly to make sure that the material conformed to the one ordered. It is difficult for decision-makers to rectify errors in orders once the material is delivered to a distant health facility.
Delays in customs clearance
One of the major delays was caused by customs clearance. The Moroccan customs clearance system is very complicated. It includes the following stages:
Sending transport documents to JSI/Morocco to begin the clearance operation
Preparing the grant certificate in which ail the information on arrival (number of packages, nature of the equipment, port of arrival) is mentioned and which then is sent to USAlD for signature.
Transmission of the customs clearance file in Morocco to the Service de Gestion des Sfocks (SGS) of the Central Pharmacy, who will pay the costs for container rental and storage.
Retrieval of containers and transport to the MOH warehouse.
It is for this reason that the customs clearance unit of the Ministry of Health must continue its advocacy with the Direction des Douanes et Administration des IrnpBfs (customs and inland revenue) to facilitate the customs clearance process. The SGS (stock management service) must provide strict and daily follow-up of customs clearance files so as to reduce storage delays since storage costs are at the charge of the MOH. These costs can grow quickly in case of delays due to late payment charges.
Delays in distribufion
Lastly, some of the delays occurred at the level of heavy and bulky equipment distribution. This equipment required the use of forklift trucks, transpalets and trucks, which were generally not easily available at provincial level, as was the case for equipment procured for the Safe Motherhood project. To avoid delays at the level of the provinces, it was necessary for the latter to own their material and manual means of handling. It is therefore useful to appeal to the local authorities that own the necessary resources to make them available to the delegations when the need arises.
Utilization and Maintenance
In order to achieve the sustainability of project achievements, the major objective of the considerable investments made by the project into equipment and materials should not be forgotten, namely the long-term utilization of this equipment and material to improve the quality of FPIMCH services. In effect, at least three actions were required: (1) inventory the equipment and its condition; (2) assure its correct utilization; and (3) ensure its maintenance. These three actions are discussed below.
John Snow, Inc. 1 16 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Inventory
All of the procured equipment was inventoried as it arrived. An inventory report of all the items procured as well as the computerized database were transmitted to the Ministry of Health. The database, which will be assigned to one of the MOH specialized services, could be the point of departure for following up on the condition of equipment and be added to as other equipment items are procured. The database, which had been developed on the basis of Project procurements, could be used for formulating specifications for other orders under the government budget or by other donors. This had been the case for an order of obstetrical equipment for the Safe Motherhood project financed by the European Union and UNFPA.
Utilization
During the lifetime of the Project, several activities were undertaken to ensure the correct utilization of equipment procured under the Project. As most of these activities have been discussed under their respective components, we mention only the following:
Training of service providers in IU insertion
. Training of service providers and technicians in the utilization of obstetric equipment
. Computer training of users at different levels of the MOH
Training of users in print-shop equipment
. Training of users in condom quality control equipment
. Training of vehicle drivers
Follow-up visits made during the physical inventory showed that most of the Project equipment was being used correctly. It is obvious that a sustained effort will be required after project close-out to ensure satisfactory utilization of this equipment, taking into account, in particular, frequent transfers of staff.
Maintenance
Equipment is probably the most vulnerable aspect of the sustainability of project procurements. Under the bilateral agreement between the Ministry of Health and USAID, the maintenance of the procured material is at the charge of the MOH. As a result, budget constraints and bureaucratic procedures have prevented and will threaten the smooth running of a maintenance system within the MOH.
This is the case, in particular, for computers, printers and office equipment (photocopiers), in view of the great number of breakdowns of such items. Instead of entrusting maintenance to one MOH unit or contracting maintenance to a central level, we consider it more efficient for each department and regionlprovince to have its own maintenance contract.
For sophisticated medical equipment, it is desirable to train the personnel in charge in order to avoid breakdowns caused by bad handling. The Fez experience in obstetric equipment showed that such training can be organized at regional level by regional biomedical engineers assisted by a representative of the equipment suppliers.
John Snow, Inc. 117 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
The last problem is that of the delay in repairs of car breakdowns. Cars often remain immobilized for a period of two months to a year until spare parts are available at the Central Warehouse. Better communication and coordination between the Car Pool Division and the provinces are necessary to repair mobile team vehicles.
A field trip by a team of Car Pool mechanics to the Northern provinces produced positive results insofar as some vehicles could be repaired on the spot and others were taken to Rabat. It would be sensible to organize other field missions to provide better assistance to the provinces.
5. Financial Management
The JSI contract began in May 1994 with a total budget of $38,501,858 for an initial duration of 5 years. The project first obtained a 3-month extension through September 30,1999 and then obtained a second extension through September 30, 2000 with additional funds totaling $1,519,044.
The total amount of the JSI contract was therefore $40,020,902, out of which $26,145,210 or 65.3% was allocated to programmatic activities with the Ministry of Health and $13,875,692 or 34.67% for JSI administrative expenditures. Out of the total budget, JSI allocated $10,900,000 to its 3 international sub-contractors: Johns Hopkins University (JHU) close to $4 million to carry out the project's IEC activities; University Research Corporation (URC) close to $1 million for quality assurance activities; and New Transcentury Foundation (NTF) $5.9 million for project procurements.
As of September 30, 2000, total project expenditure was $39,379,109. However, including accrued expenditures the total project expenditure is expected to reach the total budget of $40,020,902 allocated to JSI. Throughout the project, expenditure evolving to reach a maximum of $7.8 million a year, or 19.65% of the total budget (see graph below). There was, however, a major increase in expenditure during 1995 because of the procurement of pick- up trucks for over $4 million.
Graph 3 JSI Phase V Project Annual Expenses
-Real
- * - Committed
94 95 96 97 98 99 00
Years
John Snow, Inc. 118 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
As of September 30, 2000 program expenditure totaled some $26 million, i.e. 66% of total expenditure. The majority of this expenditure (57%) was for US or local procurements. Administrative costs of the project reached almost $13.5 or 34% of overall expenditure. This distribution of expenditure reflects the budget structure and demonstrates that administrative costs developed to a great degree in relation to program activities.
The provisional financial standing as of September 30, 2000 is included in Annex 6.
6. Training, Study Trips, Conferences
Training in Morocco concerned thousands of Ministry of Health employees, personnel of other social departments and NGOs and community-association relay agents. For further details, the reader is referred to the relevant sections in and the lists appended to the annual reports.
As to training abroad, the Phase V Project financed the participation of 63 Moroccan health managers in short-tern training courses, 35 in study tours and 75 in international conferences. Detailed lists can be found in Appendices 7 and 8.
John Snow, Inc. 119 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Conclusions and Recommendations
The FPIMCH Phase V Project was the last of a series of bilateral projects between USAlD and the Moroccan Ministry of Health to improve the health of children under five and women of the reproductive age group. The project aimed at two results: (1) increased utilization of quality MCHIFP services; and (2) sustainability of MCHlFP services.
As to the increased utilization of quality MCHlFP services, the Project has contributed substantially through several mechanisms:
(1) the pilot implementation of innovating interventions aimed at the improved quality of MCHIPF services, such as emergency obstetric care and the integrated management of childhood illnesses;
(2) the geographical extension of MCHIFP services by strengthening the mobile teams, through which an improved accessibility to MCHlFP services could be achieved, especially in isolated areas;
(3) the increased participation of private medical practitioners in preventive MCHIFP service delivery; and
(4) interventions to strengthen management support systems, such as quality assurance, training, contraceptive logistics and the health information system, which, owing to the efficiency and quality of services provided, should increase the utilization of MCHIFP services by the population.
Has the Project contributed to the sustainability of MCHIFP services in Morocco? Or, to put the question more specifically: will the functioning of MCHIFP services after the Project remain at least at the same level as during the Project period, without the resources made available by the Project? Ideally, the answer to this question should be solicited again in three-year's time, just as for the study of the sustainability of USAlD projects conducted at the end of the 80s by Thomas Bossert' and his team. These researchers had identified at least five characteristics of a project as predictors of the sustainability of the activities of a health project: (1) project efficiency, i.e. a project which reached its assigned objectives and is therefore considered as efficient; (2) integration of project activities into existing administrative structures (or its institutionalization); (3) funding of project activities, ideally by the government budget of the receiving country or through cost-recovery mechanisms; (4) the project includes a major component of training activities; and (5) a participatory planning process between donor and receiving country.
Comparing these characteristics with the results of FPIMCH Phase V Project presented in this report, we feel that this project could be classified with those having a strong chance of sustainability:
(1) Project efficiency. Health facilities offer a range of MCHIFP services whose efficiency has been demonstrated by the continued improvement of indicators relevant to the health of children and women of reproductive age. It is hoped that project activities to reinforce emergency obstetric care will also have a long-term impact on maternal mortality, which remains a priority problem to be resolved.
'Thomas J. Bossert, 1990. Can they go along with us? Sustainability of donor-supported health projects in Central America and Africa. Soc. Sci. med. Vol 30, No 9, pp 1015-1023.
John Snow. Inc. 120 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
(2) Integration of MCH/FP services into existing strucfures. Phase V Project activities have particularly contributed to the integration of MCHlF services into the organization of health services. The lMCl approach aims at changing management of childhood illnesses through vertical programs into comprehensive and holistic management of the child. Above all, the decentralized management of MCHIFP services, initiated under the Project, perfectly matches the efforts undertaken by the government to devolve and deconcentrate planning and management of administrative and social services to the newly created regions.
(3) Financing MCH/FP services. One of the most impressive results of the Phase V Project, after that of Vaccine Independence Initiative (VII), was for the Moroccan government to take over contraceptive financing, thus resulting in quasi total financial autonomy of the recurrent costs of MCHlFP services.
(4) Project training activities. As outlined in the preceding pages, the Phase V Project has considerably invested in the strengthening of the individual capacity of human resources in both the public and private health sectors: through in-service as well as pre-service training and more specifically the in-service training of physicians, often very resistant to any reform effort.
(5) Participatory planning. Lastly, this project, as the preceding ones, resulted from an entirely consultative and participatory consultation process between the Ministry of Health and USAID, aiming at sustainable mechanisms for quality MCHlFP service delivery.
To these characteristics favorable to sustainability should be added the relative economic and institutional stability prevailing in Morocco now and during the past 20 years, which is an additional asset to the sustainability of MCHIFP services in Morocco. Indeed, the analysis made by Bossert and his team revealed the importance of contextual factors to health project sustainability: a minimum economic and institutional stability is required for project impact to prevail over time.
To maximize the effect of this favorable climate on the sustainability of health services in Morocco, we should like to finish this report with a few caveats and recommendations:
Improve the qualify of MCH/FP services, especially in rural areas. Several studies conducted under the Project demonstrated that the poor utilization of MCHlFP services by rural populations can, in part, be explained by the lack of quality of the services provided and even more simply by poor inter-personal communication between care providers and the population. A special effort should therefore be made to strengthen the skills of health workers at this level, among others through in-service training and quality assurance techniques.
Stimulate communify participation. Another means of restoring the confidence of the population in health services is to stimulate community participation in the planning and organization of health services. As demonstrated by the Phase V Project, the MOH will greatly benefit from a solid partnership with civil society.
Ensure financial autonomy. Morocco should further reduce its dependence on donors in the financing of primary health services, especially for the recurrent costs of drugs, vaccines and contraceptive products. The most obvious mechanism, already operational and confirmed by the 2000-2004 five-year plan, consists of the allocation of funds from the central budget, but this mechanism has well-known limits. In the years to come, innovative mechanisms should be researched to generate additional resources at the local level.
John Snow, Inc. 121 Contract No. 608-C-00-94-00006 w

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
* Regionalize health services. Lastly, the improvement of service quality, as well as of community participation and cost recovery, can be more easily achieved in the context of a decentralized health system. Efforts to regionalize health services should therefore be continued. It should, however, be remembered that decentralization is not a Danacea. It will onlv have a favorable impact on the accessibilitv of aualitv sustainable MCHIFP services, i i the management structures at regional and provincial ievels have a solid financial basis, an adeauate administrative ca~acitv, and are conducive to motivate the health service p&sonnel'in assuming their responsidilities.
John Snow, Inc. 122 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
ANNEXES
John Snow, Inc. 123 Contract No. 608-C-00-94-00006

Annex I: Summary of Technical Results
John Snow, Inc. 124 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 1 : Summary of Technical Results
Evolution of several FPIMCH Indicators over the Duration of the FPIMCH Phase V Project (1 995 - 1999)
In the following tables, we present the evolution of four key indicators to the health of children and women of reproductive age over the course of the FPIMCH Phase V project:
Vaccination Coverage Rates
Gross Contraceptive Utilization Rates
Prenatal Consultation Rates
r Assisted Delivery Rates
The data originate form the MOH application "Systeme SMIPF" managed by the SEIS. This application contains data collected from monthly reports originating in all of the provinces. It is possible that the quality of a portion of the data was compromised due to multiple changes in the data collection system and the creation of new provinces over the course of the last five years.
I Vaccination Coverage Rates
Oued Eddahab - Lagouira
DAKHLA
Regional total
Laayoune - Boujdour - Sakia Lhamra
BOUJDOUR
LAAYOUNE
Regional total
Guelmim - Smara
ASSA ZAG
ES-SMARA
GUELMiM
TAN TAN
TATA
Regional total
Souss - Massa - Dria
AGADiR IDA OUTANANE
CHTOUKA AIT BAHA
INEZGANE AIT MELLOUL
OUARZAZATE
TAROUDANT
TiZNlT
ZAGORA
Regional total
Gross Contraceptive Utilization Rates
John Snow, Inc. 125 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
El Gharb Chrarda Beni Hssein
KENITRA
SlDl KACEM
Reaional total
Chaouia Ourdigha
BEN SLIMANE
KHOURIBGA
SETTAT
Regional total
Marrakech-Tensifl- El Haouz
MARR. MENARA
MARR. S.Y.B.A.
CHICHAOUA
MARR. HAOUZ
EL KELAA
ESSAOUIRA
MARR. MEDiNA
Regional total
Oriental
OUJDA ANGAD
BERKANE TAOURIRTE
JERADA
FlGUlG
NADOR
TAOURIRT
Regional total
Grand Casablanca
CASA ANFA
CASA AL FDA
C. H. M. AIN SEBAA
CASA AIN CHOK H.H.
C. S. BERNOUSSI ZNATA
CASA B. MSiK S.O.
MOHAMMADiA
Regional total
RabatSale-Zemmour-Zair
WEAT
SALE
SKHIRAT TEMARA
KHEMISSET
Regional total
Doukkala - Abda
EL JADIDA
SAFl
Regional total
Tadla - Aziiai
AziLAL
BEN1 MELLAL
Regional total
- ccina - 1996 - 82.3
76.9
80.1 - 68.4
81.7
73.6
75.0 - 109.2
91.8
48.8
62.2
81.3
79.0
110.4
79.4 - 92.9
89.6
75.8
56.6
75.2
81.2 - 60.6
81.3
72.5
71.4
91.9
98.0
81.3
79.6 - 87.5
141.1
90.0
77.3
101.1 - 60.1
79.9
68.3 - 42.9
80.1
66.2 -
- Gros - 1995 - 33.3
24.5
29.8 - 23.0
33.2
34.1
32.2 - 37.9
24.8
18.3
26.3
28.1
28.0
28.8
27.9 - 32.0
44.3 29.7
24.3
24.1
26.9 - 17.9
28.0
32.0
17.7
29.5
24.1
25.3
24.3 - 13.3
35.5
25.5
27.2
21.7 - 26.1
21.3
23.9 - 23.6
42.2
35.7 -
- ptive - 1997 - 25.9
21.5
24.2 - 25.3
30.0
25.4
26.6 - 30.3
23.6
15.8
22.4
35.2
25.5
28.5
27.1 - 39.9
25.0
24.7
25.3
19.6
26.6 - 16.3
22.9
26.7
14.7
21.8
21.3
18.7
20.3 - 15.4
32.1
17.5
25.4
23.6 - 9.3
14.6
14.7 - 14.9
14.9
14.9 -
- lizatic - 1998 - 27.9
28.3
28.1 - 30.2
30.8
27.7
28.9
33.1
38.7
16.9
25.1
37.2
37.4
35.6
32.3 - 45.1
23.8 27.5
25.7
20.8
24.0
28.1 - 16.0
22.5
27.0
15.6
24.4
24.0
24.3
21.6 - 16.0
23.7
20.6
32.2
23.1 - 23.0
21.8
22.4 - 26.5
37.6
33.7 - John Snow, Inc. 126 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
bleknes - Tafilalet
MEKNES EL MENZEH
MEKNES ISMAILIA
EL HAJEB
ERRACHlDlA 89.9
i FRANE
KHENiFRA
Regional total
Fez - Boulemane
FES JDlD D.D.
FES MEDlNA
FES 2. MY. YAAKOUB
BOULEMANE
SEFROU
Regional total
Taza - Al Hoceima - Taounate
AL HOCEiMA
TAOUNATE
TAZA
Regional total
ranger - Tetouan
TETOUAN
LARACHE
CHEFCHAOUEN
FAHS BEN1 MAKADA
TANGER - ASSiLAH
Regional total 100.0
TOTAL 86.6
source: FPIMCH Program, Ministry of Health
I Coveraoe Rates I Gross Contra ceptive Utilizatio
C) : The province was not in existence during the year in question.
John Snow, Inc. 127 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
I 199:
Oued Eddahab - Lagouira I DAKHLA 1 82.6
Regional total ( 82.6
Laayoune - Boujdour- Sakia Lhamra ( BOUJDOUR
LAAYOUNE
Regional total
Guelmim - Smara
ASSA ZAG
ES-SMARA
GUELMIM
TAN TAN
TATA
Reaional total
Souss - Massa - Dr2a
AGADIR IDA OUTANANE
CHTOUKA AiT BAHA
INEZGANE AIT MELLOUL
OUARUVATE
TAROUDANT
TlZNlT ZAGORA
Regional total 42.7
El Gharb Chrarda Beni Hssein I KENITRA 32.3
SlDl KACEM I 27.8
Regional total 30.4
Chaouia Ourdigha I BEN SLIMANE
KHOURIBGA
SETTAT
Regional total
Marrakech-Tensifl- El Haouz
MARR. MENARA
MARR. S.Y.B.A.
CHICHAOUA
MARR. HAOUZ
EL KELAA
ESSAOUIRA
MARR. MEDINA
Regional total 42.7
Jriental I OUJDA ANGAD BERKANE TAOURIRTE JERADA FiGUlG NADOR TAOURIRT
Regional total 35.6
- 1 Deliv -
199i - 190.E
190.6 - 137.1
110.2
114.2
- 'Rate - 199E -
200.4
200.4 - 120.3
106.5
108.6 - 45.4
86.5
70.7
132.8
19.7
61.8 - 100.8
25.2
94.4
39.1
65.0 55.1
14.3
60.2
62.0
39.1
52.6 - 21.1
96.9
62.9
65.9 - 234.0
2.0
16.7
16.5
51.8
51.6
0.0
60.2 - 102.4 88.4 17.1
37.7 67.2
32.6
68.3 - John Snow, Inc. 128 Contract No. 608-C-00-94-00006

.i
ill
7 t U
"#4
',a
6d
md
d
ul
Ed
m
d
d
sr)
ta
d
d
d
d
d
d
d
tll
ul
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Grand Casablanca CASA ANFA
CASA AL FlDA C. H. M. AIN SEBAA CASA AIN CHOK H.H.
C. S. BERNOUSSI ZNATA CASA B. MSlK S.O. MOHAMMADIA
Regional total 36.5
RabatSale-Zemmour-Zalr I RABAT SALE SKHIRAT TEMARA KHEMiSSET
Regional total
Doukkala - Abda EL JADIDA
SAFl Regional total
Tadla - Azilal
AZlLAL BENl MELLAL
Regional total 34.5
MeknBs - Tafilalet I MEKNES EL MENZEH
MEKNES iSMAlLlA EL HAJEB ERRACHlDlA IFRANE KHENIFRA
Regional total 43.7
Fez - Boulemane I FES JDlD D.D. FES MEDINA
FES 2. MY. YAAKOUB BOULEMANE SEFROU
Regional tofai 32.3
Taza - Al Hoceima - Taounate I AL HOCEIMA
TAOUNATE TAZA
Regional total 21.3
Tanger - Tetouan I TETOUAN LARACHE CHEFCHAOUEN FAHS BENl MAKADA TANGER - ASSILAH
Regional total 1 24.4
TOTAL 1 35.8
- ,n Ra' - 199t - 13.9
31.2 33.2
29.9 38.8 47.4
45.2 33.4 - 42.9 48.5 47.6 33.9 42.7 - 23.8 33.7 27.9 - 30.1 43.9 38.7 - 53.6
68.8 40.9 31.6
43.2 35.2 42.4 - 32.9 39.1
32.8 39.2 24.9 34.0 - 15.7 25.9 27.4 24.3
30.4 27.4 22.7
3.5 21.4 23.4 - 36.9 -
~ e K e r y Rates
=FP
Source: (SNISSTAT) - SEISIDPRF, Ministry of Health (') :The province was part of TANGER -ASSiLAH prior to 1998
John Snow, Inc. 129 Contract No. 608-C-00-94-00006

Evolution of Met Need for Obstetrical Complications 0 In the regions of Fez-Boulemane and Taza-Al Hoceima-Taounate from1 996 to 1999 5 % -I I rn
5 a 0 0 0 0 TI I z m < 2' F <
F Z 5 Z G) * Z w s 3 rn 7J Z
i=- * Z w
9

Evolution of Caesarean Section Rates
In the regions of Fez-Boulemane and Taza-Al Hoceima-Taounate from 1996 to 1999
Provinces Births Expected Caesarians Expected (5%) Actual Cesareans Performed
1996 1997 1998 1999 1996 1997 1998 19991 1996 1997 1998 1999
I I I Nb % Nb % Nb % Nb %
Fez 1 23631 1 21840 1 22479 1 22618 1 1182 1 1092 1 1124 1 1131 1 582 1 49 1 819 ( 75 1 725 1 65 1 736 1 65
Sefrou 7107 5228 5271 5220 255 261 264 261 0 0 26 10 70 27 39 15
Boulemane 1 5338 1 3941 / 3988 1 3995 1 267 1 197 1 199 1 ZOO 1 o 1 29 1 15 1 331 17
TofalRegion 36076 31009 31738 31833 1804 1550 1587 1592 582 32 845 55 824 52 808 51 I
Taza 22522 17400 17592 17525 1126 870 880 876 145 13 247 28 240 27 245 28
Al Hoceima 12255 10421 10552 10560 613 521 528 528 295 48 335 64 444 84 403 76
Taounate 21738 15504 15625 16016 1087 775 781 801 0 0 0 0 0 0 0 0
TotalRegion 56515 43325 43773 44101 2826 2166 2189 2205 440 16 582 27 684 31 648 30 2
1 Total 1 92591 1 74334 1 75511 1 75934 1 4630 1 3717 1 3776 1 3797 1 1022 1 22 1 1427 1 38 1 1508 1 40 1 1456 1 38

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 2: Bibliography of FPIMCH Phase V
Project Documents
d
d
d
d
d
eJ
ul
ui
d John Snow, Inc. 132 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 2: Bibliography of FPIMCH Phase V Project Documents
Contract Reports
Start-up Action Plan (May - December 1994). Annual Action Plan (1 995). Annual Action Plan (1 996). Priority Actions of the USAID/Morocco Transition Plan (January 1997). Action Plan (1997). Action Plan (1 998Il999). Revised Action Plan (1 998 - 1999). Extension Action Plan (1 999/2000). Annual Progress Report (1 994). Annual Progress Report (1 995). Annual Progress Report (1 996). Annual Progress Report (1 997). Annual Progress Report (1 998). Annual Progress Report (1 999). Annual Progress Report (2000). Quarterly Progress Report (January - Mars 1995). Quarterly Progress Report (April - June 1995). Quarterly Progress Report (July - September 1995). Quarterly Progress Report (January - March1996). Quarterly Progress Report (April - June 1996). Quarterly Progress Report (July - September 1996). Quarterly Progress Report (January - March 1997). Quarterly Progress Report (April -June 1997). Quarterly Progress Report (October - December 1997). Quarterly Progress Report (January - March 1998). Quarterly Progress Report (April - June 1998). Quarterly Progress Report (October 1 - December 31, 1998). Quarterly Progress Report (January 1 -March 31, 1999). Quarterly Progress Report (April 1 - June 30, 1999). Quarterly Progress Report (October 1 - December 31, 1999). Quarterly Progress Report (January 1 - March 31,2000). Material and lnventory Report (1 996). Material and lnventory Report (1 997). Material and lnventory Report (1 998). Material and lnventory Report (1999). Material and lnventory Final Report (2000).
John Snow, Inc. 133 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Consultant Reports
Baron, DanielleIJHU. Technical Assistance Report Workshop to Develop Visual Aid for Itinerant Nurses. November, 1996.
Bero, CinddylJSI. Review of JSl/Morocco's Computer Network. April, 1995.
Bezad, Rachid. Consultancy Report of January I to June 30, 2000.
Boucar, MainalURC. Appui a I'atelier de formation des animateurs de provinces en techniques de facilitation, au Maroc. March, 2000.
Bouchet, Bruno and Boucar, MainalURC. Consultancy Report ofApril 14 to 25, 2000.
Bouchet, BrunolURC and Gagne, SoniaISIPDT. Consultancy Report of May 24 to June 4, 1999.
Bouchet, BrunoIURC. Consultancy Report of October 31 to November 5, 1999.
Bouchet, BrunoIURC. Consulfancy Report of February 9 to 22, 2000.
Bouchet, BrunolURC; Boucar, MainalURC; Martin, Jules; and Gagne, SoniaISIPDT. Consultancy Report. March, 1999.
Brown, LisannelEvaluation Project. Plan the 1995 Service Availability Module. May, 1995.
Collin, SylvieISIPDT. Formation aux habiletes d'aide et de communication du personnel accoucheur. September, 1999.
De Malvinsky, JeanIJHU. Strategic IEC/PF. May, 1997.
de Metz, Nicolas. Mission de courte duree relative a la phase de retrait (Phase-over) de I'assistance de I'USAID pour la fournifure de produits contraceptifs au programme national de planification familiale. July, 1997.
Debay, MarkIJHU. Evaluafion des besoins en equipement pour la maternite sans risque. May, 1995.
Debay, MarWJHU. Finaliser la liste d'equipement pour la maternite sans risque. December, 1995.
Eddine Naji, Jarnal. PCIMELAC Phase de finalisation du modele d'application. September, 1999.
Eddine Naji, Jarnal. Consultancy Reporf of October 20 to November 30, 1999.
Edwards, MichaelITulane University. Consultancy Report of June 4 to July 17, 1997 on Management lnformation System.
Edwards, MichaelIJSI. Activity Report (at New Orleans) (August- December, 1997).
Edwards, MichaeVJSI. Activify Report (at New Orleans) (February-May, 1998) on Management lnformation System. May, 1998.
Edwards, MichaellJSI. Consultancy Report of December 11, 1997 to January 11, 1998.
John Snow, Inc. 134 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Edwards, MichaellJSI. Consultancy Report of May 14 fo July 23, 1998 on Management lnformafion System.
Edwards, MichaelIJSI. Consulfancy Report of December 15, 1998 to January 9, 1999 on Managemenf lnformation System.
Edwards, MichaellJSI. Consultancy Report of June I to 30, 1999 on Management lnformation System.
Edwards, MichaelIJSI. Consulfancy Report of May 15 to June 2 2000 on Managemenf lnformafion System.
Edwards, MichaelIJSI. Consulfancy Reporf of December 19 to January 14,2000,
Edwards, MichaelIJSI. Consultancy Report of February 14 to March 11, 2000 on Management Information System.
Escoffier, Claire. La Composanfe Communaufaire de la Strategie de la Prise en Charge Infegree des Maladies de I'Enfant--Phase Pilofe: April f998-Jyly, 2000.
Forsythe, B.lJHU/CCP. Finance et administration de CCP. March, 1995.
Fort, Cathy/URC. Developpement des activifes du secteur prive. April, 1995.
Fort, CathyIURC. Strategie - Secteur Prive (revision a la lumiere du plan de transition) (September - October, 1996).
Fort, CathyiURC. Developpement des activites du secfeurprive. June, 1995.
Fort, CathyIURC. Developpement des activites du secteurprive. September, 1995.
Forthney, Judith. Panel of Experts Report. May, 1995.
Garenne, MichellCEPED. Efudier Ies possibilites de realisations d'une seconde enqu6te sUr les causes et les circonstances des deces des enfants au Maroc. May, 1995.
Garenne, MichellCEPED. 2eme Enqu6fe sur les Causes et les Circonstances des Deces des Enfants au Maroc-Visite de preparation. June, 1997.
Garenne, MichelICEPED. 2eme Enquete sur les Causes ef les Circonstances des Deces des enfants au Maroc-Analyse des donnees. February, 1999.
Gingembre, Claude. Conception du Guide Prafique pour le Medecin qui s'insfalle au Maroc en Liberal. June, 1997.
Gingembre, Claude/JSI. Evaluation sommaire de la capacife en gesfion des medecins prives. December, 1996.
Goodsmith, LareenIJHUlCCP. Evaluation des besoins audio visuels. March, 1995.
Goodsmith, LaurenlJHUICCP. Assistance technique pourproducfion video. August, 1995.
Goodsmith, LaurenlJHUICCP. Technical Assistance Report TV Episodes/Maternal Morfalify Video/General IEC Issues (September - October, 1996).
John Snow, Inc. 135 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Goodsmith, LaurenIJHUlCCP. Technical Assistance Report: Planning for TV Episodes and Maternal Mortality Video. June, 1996.
Jabre, BouchralJHUICCP. Creativity Workshop for Radio Announcers. June, 1995.
Jabre, BouchraIJSI. Assistance technique pour un plan de mise en oeuvre IEC. January, 1995.
Jacques, Andre (Independent). Evaluation par les pairs des medecins generalistes du secteurprive en Planificafion Familiale au Maroc. August, 2000.
Jacques, Andre et Moussaoui, Ahmedllndependents. Evaluation par les pairs des medecins generalistes de pratique privee en Planificafion Familiale au Maroc. June, 2000.
Karki, MahamaneIURC. Appui a I'atelier de formation sur I'elaboration des standards et le suivi de la qualite. November, 1999.
Karki, MahamanelURC. Appui a Yelaboration de la strategic nationale #integration de I'assurance qualite dans le cursus des instituts de formation aux carri6res de sante (IFCS) au Maroc. March, 2000.
Karki, MahamanelURC. Appui technique pour Y6laboration du materiel pedagogique d'assurance qualite pour les instituts de formation aux carrieres de sanfe (IFCS) au Maroc. April, 2000.
Karki, MahamaneIURC. Consultancy Report ofApril 19 to May 9,2000.
Karki, MahamanelURC. Consultancy Report of April 24 to May 11, 1999.
Kerzner, JeffIJSI. Consultancy Report of September 17 to October 1, 1999.
Klein, Susan F. et Tall, HamadyIJSI. Mission Report of November 15 to 28, 1997.
Knebel, ElisaIURC. Consultancy Report of May 31 to June 17, 2000.
Lippeveld, TheolJSI. Mission Report - NCIH Conference June 26 to 29, 7998.
Maine, DeborahIColumbia University. Assistance technique pour le d6veloppement d'une approche regionale maternite sans risque. November, 1995.
Maine, DeborahlColumbia University. Consultation initiale pour le developpement d'un programme matemite sans risque. February, 1995.
Maine, Deborah/Columbia University. Consulfancy Report of June 4 to 5, 1998.
Mattar, Paul/JHU/CCP. Creativity Workshop for Radio Announcers. June, 1995.
Moore, RichardlJSI. JSI Management Review. September, 1995.
Morin, Eric. Documentation du Projet Pilofe Maternite sans Risque. October, 1999.
Morin, Eric. Documentation du Projet Pilote Maternife sans Risque. March, 2000.
Murphy, Gael et Winter, LaurielURC. Atelier de demarrage du projet Gestion lnt6grale de la Qualite (GIQua). May, 1996.
John Snow, Inc. 136 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Murphy, GaellURC. Assistance technique en Assurance Qualife et Secteur Prive. January, 1996.
Olivola, MayeIJSI. Accomplissemenfs majeurs July - September, 1995.
Olivola, MayelJSI. Acfivifes desfinees a informer le secfeurprive. August, 1995.
Olivola, MayelJSI. Collaboration avec les professionnels de la sanfe. June, 1995.
Olivola, MayeIJSI. Efude sur la Mottalife Infantile. April, 1995,
Olivola, MayeIJSI. Evaluation Biosel (SRO) situation et besoin. June, 1995.
Olivola, MayelJSI. Final Peace Corps Repott on Community Liaison: Recommendation for the Development ofApplied Research in Morocco (May - June 1996).
Olivola, MayelJSI. Training of Community Development Agents (January - February, 1996).
Olivola, MayeIJSI. Training of social agents. May, 1995.
Olivola, MayeIJSI. Formation des pharmaciens ef medecins (PSI, Prive). June, 1995.
Olivola, MayeIJSI. Hypotaminose A Projet d'explorafion. June, 1995.
Olivola, MayelJSI. Programme de lutte contre les maladies diarrheiques. January, 1995.
Olivola, MayelJSI. Recommandation pour la mise en oeuvre de la PClME au Maroc (July - December, 1996).
Olivola, MayelJSI. Recommandation pour les activifes integrees de SMI/CDD. November, 1995.
Orzeszyna, StanislawlOMS, Geneva. Consultancy Report ofApril 20 to May 2, 1998.
Oubnichou, MohamedIJSI. Etude des Opfions d'Approvisionnement du Ministere de la Sante Publique en Produifs de Contraception (April - May, 1996).
Plopper, Susan. Formation des formafeurs en counseling PF. October, 1995.
Radi, Sasdia. Les maladies de I'enfant au Maroc: Representations pratiques et recours therapeutiques. October, 1999.
Renaud, Pierre. Formation de groupe de travail pour la division de I'education sanitaire. May, 1995.
Renaud, PierrelJHUICCP. Deuxieme seminaire atelier sur I'appreciafion sysfematique de la Qualife (APSQ) a Taounafe.
Safar, Jean-Fran~oislURC. Consulfancy Repott of November 15 to December 11, 1999. December 1999.
Steele, GaryIFPLM. Assistance technique liee a la formafion en gesfion de la logistique des confraceptifs au MS. August, 1998.
Thaddeus, SereenIJHU. Consulfancy Repott of October 31 to November 11, 1998.
John Snow, Inc. 137 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Vansintejan, Gilberte. Emergency Obstetrical Cares Cenfre - Nord Region. March 15, 1997.
Vansintejan, GiIbertelJSI. Formation ef assistance technique en mafernite sans risque province de Fes (second cycle de formafion SOU). June, 1996.
Vansintejan, GilbertelJSI. Maternife sans risque ef planificafion familiale. January, 1996.
Vansintejan, GilberteIJSI. Privafe Sector and Safe Motherhood (province of Agadir). September, 1996.
Vansintejan, GilberteIJSI. Soins obstetricaux d'urgence Region Centre-Nord ( ler cycle de formafion SOU) Actualisation des centres de reference (March - May, 1996).
Vekemans, MarcellJSI. Promouvoir I'ensemble des aspects medicaux du plan d'action. January, 1995.
Veldhyzen Van Zanten, TisnalURC. Consultancy Report of December 9 to 17, 1998. December, 1998.
Walter, George et De Malvinsky, Jean. Formation de Formafeurs Cours Avances 2eme Cycle. March, 1997.
Walters, GeorgellHP, WCPH. Plan sfrafegique pour un centre pedagogique. March, 1995.
Walters, GeorgesIlHP-WCPH. Mobil Team Training Curriculum Developmenf. October, 1995.
Wickham, AnnIJSI. Administrafive Support September, 1995.
Wilson, EdwardlFPLM. MOPH Computer Network Competitive Bid. March, 1995.
Wilson, EdwardlFPLM. Preparation des CPT 1996. November, 1995.
Wilson, EdwardtFPLM. Consultancy Report ofAugust 24 fo Sepfember 3, 1998.
Wilson, Norma and Murphy, GaelIURC. Consulfancy Report ofApril 28 fo May 30, 1997.
Wilson, Norma et Veldhuzen Van Zanten, TisnalURC. Formation en Gesfion de la Qualife. November, 1996.
Wilson, NormalURC. Assurance de la qualite dans les sewices de SMI ef PF au sein du MSP, Maroc. September, 1997.
Wilson, NormaIURC. Consultancy Report of January 6 fo 17, 1997.
Wilson, NormalURC. Consultancy Report. July, 1997.
Zimicki, Susan. Consulfancy Reporf of July 21 fo 30, 1997.
John Snow. Inc. 138 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Thematic Documents and Studies
ALCO. Diagnostique C.A.P. aupres des ouvrieres des conserveries. October, 1996.
ALCO. Document de Strategie de sensibilisation des ouvrieres de la FIPROMER August, 1997.
Aouad, M. El. Amelioration des seances d'education sanitaire au niveau peripherique May, 1998.
Brown, Lisanne; Tyane, Mostafa; Bertrand, Jane; Lauro, Don; Abou Ouakil, Mohamed; et de Maria, Lisa. Quality of Care in Family Planning Services in Morocco (Studies In Family Planning). June, 1995.
Cakir, VolcanlPOLICY. Etude de segmentation du marche de planification familiale au Maroc. September, 1998.
de Metz, NicolasIJSI. Options d'Achat des Produits Contraceptifs par le Ministere de la Sante. August, 1998.
DHS. Resultats Preliminaires de I'Enquete Nationale sur la Population et la Sante. June, 1995.
Dialmy, Abdessamad. La gestion socioculturelle de la complication obstetricale (Rapport par province / Rapport de synthese) February, 1999.
Dialmy, Abdessamad. L'identite masculine et sante reproducfive au Maroc. September, 2000.
Duclos, Philippe et Landry, Monique. Conference de Consensus sur la Vaccination. January 6 to 17,1997.
El Aouad, MohamedNHU. Etude Pre-test des Supports d'lEC destines aux lnfirmiers Itinerants. April, 1997.
Errih, Mohamed; Bezad, Rachid; et Bakkali, TaoufiklJSI. Evaluation des Performances du Programme Norplant. August, 1998.
Frantz, Todd. Diagnostic de la situation d'hygiene. April, 1996.
Goodburn, Elisabeth Anne. Evaluation de la Formation Continue en Soins Obstetricaux d'Urgences de Base (SOUB). May, 1998.
Goodburn, Elisabeth; Maine, Deborah; Columbia University. Evaluation du projet pilote Maternite sans risque. August, 1999.
Hart, CarolynIFPLM. Questions cruciales relatives au transfert du financement des contraceptifs au Maroc. August, 1998.
Ibaaquil, Larbi. Rapport de synthese, mobilisation autour de la sante (MS/DP/ONG/Departements ministeriels, organismes d'application au developpement). April, 1999.
John Snow, Inc. 139 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Jacques, Andre et Moussaoui, Ahmed. Conception d'un projet pilote d'evaluation par les pairs des medecins generalistes du secteur prive en planification familiale au Maroc. July, 1999.
Jean, Pierre et Quist, CharlesIJHPIEGO. Evaluation du Projet de Renforcement de la Formation Clinique en PF et MSR dans les Facultes de Medecine Marocaines de Rabat et Casablanca. June, 1998.
JSI. Algorithme de Prise en Charge des Effets Secondaires des lnjectables. 1997.
JSI. Document de Recueil des Recherches Recenfes concernant la SMI et la PF. 1997.
Kampman, Katy. Manual of Annotated Bibliography of Documents in MCH/FP in Morocco. 1994.
Krasovec, KathyIPHR. Etude sur les Exonerations des articles de sante publique September, 1998.
Krasovec, KathylPHR. Un investissement strategique: la planification familiale au Maroc. July, 1998.
Kress, Daniel H./PHR. Note technique: Mefhodologie et Explication des Estimations de I'lmpact Demographique et Financier du Programme Marocain de PF, January, 1998.
Laasri, Malika; Bezad, Rachid; Tyane, Mostapha; et Lippeveld, Theo How to Sell Family Planning to the Private Sector: papier presente a la conference NCIH a Washington en juin 1998. June, 1998.
Lauro, DonIJSI, Morocco. From Indicator to Program Performance: a Field Pers~ective from Morocco. A Paper Presented at 1995~~o~u la f i on Association of ~mer ica. April, 1995.
Lhaloui, Zohra; de Metz, Nicolas; et Ouchrif, Brahim 1998 Contraceptive Procurement Tables (CPT's). May, 1998.
Lippeveld, Theo et Reier, SuzanneIJSI. Decentralisation des services de sank? au Maroc. September, 1998.
LMS Conseil. Etude #Audience Radio. June, 1998.
Maine, DeborahlColumbia University. Presentation de la mafernite sans risque au congres des droits de I'enfant a Kenifra. May, 1995.
Mernissi, Fatima. Distribution a base communautaire utilisant les ONG rurales (etude de faisabilitb). August, 1996.
Ministere de la Sante du Maroc (avec I'assistance technique de Bezzad, Rachid; Kharbach, Aicha; Moussaoui, Ahmed; El Fehri, Haddou Sennane). Les standards des methodes de planification familiale au Maroc. September, 1999.
Ministere de la Sante du Maroc (avec I'assistance technique de Elisa Knebel). La Qualite en Action au Maroc. September, 2000.
Ministere de la Sante du Maroc (avec I'assistance technique de Eric Morin et Theo Lippeveld). Document de synthese "Maternite sans risque". September, 2000.
John Snow, Inc. 140 Contract No. 608-C-00-94-00006
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Ministere de la Sante du Maroc (avec I'assistance technique de EVALUATIONIJSI). Guide d'Utilisation des Donnees des Programmes SMIIPF. 1997.
Ministere de la Sante du Maroc (avec I'assistance technique de JHUICCP). La Communication dans la Maternite Sans Risque. September, 2000.
Ministere de la Sante du Maroc (avec I'assistance technique de Michel Garenne). Deuxieme enquete sur les causes et les circonstances des deces des enfants au Maroc (ECCD-11). June, 1999.
Ministere de la Sante du Maroc (avec I'assistance technique de PAPCHILD). Enquefe Nationale Sur la Sanfe de la Mere ef de I'Enfant (ENSME) 1997.
Ministere de la Sante du Maroc (avec I'assistance technique de Rachid Bezad et Ahmed Moussaoui). Les standards SONU. July, 2000.
Ministere de la Sante du Maroc (avec I'assistance technique de Stan Orzeszyna). Etude de la qualite de donnees SMI/PF. September, 2000.
Ministere de la Sante du Maroc (avec I'assistance technique de URC). Programme National d'Assurance Qualite. September, 2000.
Ministere de la Sante du Maroc. Carnet de sante. April, 2000.
Ministere de la Sante du Maroc. Compte Rendu du Deroulement de la Formation Combinee en Soins de I'Enfant. May, 1997.
Ministere de la Sante du Maroc. Etude regionale sur la carence en Vitamine A. September, 1999.
Ministere de la Sante du Maroc. Evaluation Projet CJM. July, 1998.
Ministere de la Sante du Maroc. Rappott de la reunion du 9-10 Juin 99 sur la r.ionalisation. August, 1999.
Naji, Jamal Eddine. Precis surla PClMEpar approche communautaire. July, 1999.
Obermeyer, Carla. Projet de recherche sur la sante reproductive. June, 1999.
Olivola, MayeIJSI. Consultation Epid6miologie du CDC: Document recapitulafif. December, 1994.
Olivola, MayeIJSI. Programme de lufte contre les maladies diarrheiques: Document recapitulatif. December, 1994.
Oubnichou, MohamedIJSI. Etude des Options d'Approvisionnement du Ministere de la Sante Publique en Produits de Contraception. January, 1998.
Societe Marocaine des Sciences Medicales. Etude sur la formation medicale continue. July, 2000.
Steele, GaryIFPLM. Perennisafion du systeme de logistique des contraceptifs par le biais de la formation en cours d'emploi. May, 'l999.
John Snow, Inc. 141 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Volontaires du Corps de la PaixlJSIIUSAIDIMS. Etude Exploratoire Des Compodements Affectant I'Etat Nutritionnel Des Enfanfs Dans Les Zones Rurales du Maroc. September, 1997.
Wilson, Edward. Estimation des besoins contraceptifs 1999- 2000. May, 1999.
Wilson, NormatURC et I'equipe de la DHSA Evaluation Interne du Projet GlQua. August, 1998.
Wilson, NormaIURC. Assurance de la Qualife dans les services SMIVPF au sein du MSP, Maroc. September, 1997.
John Snow, Inc. 142 Contract No. 608-C-00-94-00006 +,

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 3: Training and IEC Materials Produced
by the FPIMCH Phase V Project
John Snow, Inc. 143 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 3: Training materials and IEC products of the FPIMCH Phase V Project
?raining Manuals
Contraceptive Stock Management Manual (update) Basic Manual of Complete Quality Management (GIQua)
Long Term Methods of Contraception Counseling Module lniectables Module Logistics System Sustainability Plan Poster on Counseling Steps introduction of an IEC strategic plan for the promotion of Long term contraceptive methods Draft report of the first training session of UNFM managers
Report on the progression of training sessions for private doctors in FP
Training Manual for Private Sector Medical Generalists (draft)
~. I
I~rainer's Guide for data entry of FPIMCH treatment ISEISIDIMIJS~ I I ~ o r i i 99
AuthorIOrganization
DPIPNPF URC
Khalil Amrani JSI JSI
Guide to Vaccination Training Manual in Reproductive Health for 8" year students (draft)
Date
1997 1997
1997 1997 1997 - -
Richard OwendGary Steele DP Mahassine lraki
MSP
CNFRHlLalla Myriem
CNFRHIJSI
May 1997 March 1997 1997
22-25 July 1997
March-Sept 1997
August 1998
MSIBASICSIJSI CHU-RabatIJHPIEGO
and results
User's Guide for data entry of FPIMCH treatment and results
User's Guide of the national sub-system of FPIMCH medical information and treatments
Training of Trainers Guide (techniques in animation and adult pedagogy) Quality Improvement Module for presentations using communication techniques (facilitator module)
Quality Improvement Module for presentations using communication techniques (participant module)
Training Guide in assistance and communication skills for delivery personnel
September 1998 August 1998
Training Manuals in Contraceptive Logistics
Training Manual in PClME (for IFCS) Quality Assurance Training Manual (for IFCS)
lntegrated Care Coverage of Childhood Illnesses I Community Participation
Basic documentation for the trainer's use
lntegrated Care Coverage of Childhood Illnesses I Community Participation
SEISIDIMIJSI
SEISIJSIIDP
Health Consultant
Health Consultant
Health Consultant
ConsultantKIPlJSI
I I
April 99
June 99
May 99
July 99
June 99
September 99
DPFIDP (AT Gary Steele)
DFIDRH et DSMllDP DFIDRH et DSMilDP (AT Mahamane Karki)
DSMllDP (AT Jamal Eddine Naji and Claire Escoffler)
Training Manual for health personnel
infertility file "Life Skills Manual for Midwives" and English translation
John Snow, Inc. 144 Contract No. 608-C-00-94-00006
September 00
May 00 May 00
August 00
Methodological guide to elaboration, adaptation, and follow-up of care references
DSMIIDP (AT Jamal Eddine Naji and Claire Escoffier)
CNFRH (AT MSH) ACNM Translation bv JSI
August 00
September 00 March 1996
DHSA (AT Jean Franpis Safar) September 2000

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Type
6 radio spots (presented, not finalized)
Audio Visual Subject
1997 Video Khlat Eddar. Arabic version
Video of the theater piece
Pregnancy
Long term FP methods
I I I
Reducing Maternal Mortality is a
should not be considered
not a normal development of pregnancy
Audience
Maternal Mortality
Maternal Mortality
Scenario for the Docudrama
Objective I Key message
Married men and women of reproductive age
Decision Makers
General Public
Maternal Mortality
Video Docudrama "Bent Ettajer" (Daughter of the Merchant)
I Film "Ouled Lghial" FP, approaching General Public Discussion by the FP Is a decision an1 births couple about FP and a choice of the
birth couple
Convey LT Methods as convenient
Awareness of the intensity of the problem
Awareness
Scenario for FP film
1999
Long term methods are the opportune choice
General Public
Maternal Mortality, Obstetrical Comolications
Recognize Complications of
Responsibility of the man; FP (Long term contraceptive methods)
Radio series
2000
General Public
-~ ~ ~
Production of 12 segments of "My Health Comes First"
Documentary on the DP
Theater
I Help yourself and Heaven will Maternal Mortality General Public Awareness Maternal mortality help you should not be
considered
General Public
RH, FP, hygiene, etc.
1996 Scenario for a play of an hour
1997
John Snow, Inc. 145 Contract No. 608-C-00-94-00006
Recognize Complications of Preonancv
Health priorities (FP, RH, breastieeding)
Presentation of the DP and its divisions
Maternal mortality should not be considered -
Discussion by the couple about FP
General Public
Maternal Mortality
inevitable FP, a decision, a choice ...
General Public
Health personnel, journalists, lenders
Awareness of RH and FP as important issues for discussion within couples and families
General Public
---
RH and FP are the responsibility of the couple
Awareness around health priorities
Presentation of the DP and particularly the DlEC and its new capacities
Various
Awareness Maternal mortality should not be considered inevitable

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Subject Audience Objective I Key message
I I NO matter where yo1

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Type Subject Audience Objective Key message Printed Material 1997 Poster The Stages of FP Private sector Recall Counseling ensure
Counseling medical generalists an informed choic~ Production 1999 Message board Reproductive Health Mobile health Information, Various on FP, chil
workers and Motivation health, maternal ar community agents family health
Feltboard Reproductive Health Mobile teams and Information, Various on FP, chi1 community agents Motivation health, maternal ar
family healh Television 1997 Airings of Assehha Long term methods General Public Informatbn, Various (LT methoc
of FP Motivation are not permanent) Airings of Assehha Complications of General Public Information, Pregnancy is
pregnancy Motivation natural, but there a1
1998 risks
lAirings of Assehha (pregnancy and Birthl~eneral Public (information, \various Motivation
Training 1996 Counseling module Long term FP Beneficiaries Counseling
methods 1997 Group Animation Techniques Group animation IEC Trainers Training Group Animation Techniques Group animation Nurses and mobile Training (participant notebook) teams 1998
I i I Guiae to Group Animation (Group animation ,Bene!cianes. Information and Knowledge, inreresi Techniques (French version) techniq~es partlclpants in the ao~renticnshio action . .
sessions Community Agent's Health Public health and Community agents Information and Community agents Education Guide primary care Training can spread
knowledge of maternai health
Finalization of the Counseling FP Counseling FP Trainers Recall Counseling ensure. Guide an informed choice Conception 1998 Message board Reproductive Health Mobile health Information, Various - FP, child
workers and Motivation health, maternal an community agents family health
Feltboard Reprodudwe Health Mobile teams and Information, Various - FP, child community agents Motivation health, maternal an
family health Posters 1999 Infection Prevention FP Beneficiaries of information Infection prevention
heaith services 2000 Global Health Council Conference (June 2000)
Community Diagnostic

FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 4: The FPIMCH Phase V Project Team
- ~ ~ ~ - ~ p
John Snow, Inc. 148 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
d Annex 4: The FPIMCH Phase V Project Team
Principal Collaborators of the MOH Team
Note: Given the high number of collaborators within the MOH, the following list includes only directors and chiefs of participating directorates and units.
Direction de la Population (DP)
Dr. Mostafa Tyane, Directeur de la Population et Coordinateur du Projet PFISMI Phase V Dr. Abdelouahab Zerrari, Chef de Division de la Sante Maternelle et Infantile Dr. Hamid Chekli, Chef de Service de la Protection de la Sant6 de I'Enfant, DSMI Dr. Ali Ben Salah, Chef de Service de la Protection de la Sante de la Mere, DSMI Dr. Mohamed Braikat, Chef du Programme National d'lmmunisation, DSMI Dr. Najia Hajji, Chef de Division de la Planification Familiale Dr. Wafia Lantry, Chef de Service de la Planification Familiale, DPF Dr. Mohamed Abouakil, Chef de Service de la Coordination Intersectorielle, DPF Mr. Brahim Ouchrif, administrateur principal, DPF Dr. Amina Balafrej, ex-Chef de Division IEC Mr. El Amouri Bouazza, Chef de Service de la Production, DlEC Mr. Mohamed Madi, Chef de Service de Conception, DlEC Mr. Mohamed Fennane, Chef de I'Unite Audiovisuelle. DlEC Mr. Brahim Boumzough, Chef de I'Unite de I'lmprimerie, DlEC Mr. Mohamed Jouai, Chef de Service Administratif, DP Mme Naima Seksane, Responsable Unite d'lnformation et de Documentation
Direction de la Planification et des Ressources Financieres (DPRF)
Mr. Mohamed Laaziri, Directeur Mr. Zine-Eddine El Idriss, Chef de Service de I'Economie Sanitaire Mr. Mustapha Azelmat, Chef de Service des Etudes et de I'lnformation Sanitaire Mr. Mustafa Ben Abla, Chef de Division de la Cooperation.
Direction de I'EpidBmiologie et de la Lutte contre les Maladies (DELM)
Dr. Jaouad Mahjour, Directeur Dr. Ahmed Zidouh, Chef de service de la Surveillance Epidemiologique
Direction de la Reglementation et du Contentieux
Mme Khadua Meshak, Directeur
Direction des HBpitaux et des Soins Ambulatoires
Dr. Saida Jrondi Choujaa, Directeur Dr. Katr-Ennada Darkaoui, Chef de Division des Soins Ambulatoires
Direction des Ressources Humaines
Mr. Mohamed Sairi, Directeur Mr. lsmael Achaati, Chef de Division de la Formation Dr. Mohamed ~ a a r i Jabiri, Chef de Service de la Formation Continue Mr. Ahmed Agyo, Chef de Service de la Formation de Base John Snow, Inc. 149 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Division de I'lnformatique et des Mbthodes (DIM)
Mr. Slimane Hajra, Chef de Division
Inspection Generale
Dr. My Mustapha lsrnaili Alaoui, lnspecteur General
lnstitut National &Administration Sanitaire (INAS)
Prof. Ben Brahim Fikhri, Directeur
Centre Nationale de Formation en Reproduction Humaine (CNFRH)
Prof. My Tahar Alaoui, Directeur
Coordinateurs regionaux (regions pilotes)
Dr. Ahmed Bendali, region FBs-Boulemane Dr. Farouk Fasla, region Souss-Massa-DrAa Dr. Abdelouahab Cherradi, region Doukkala-Abda Dr. Ahmed Cherrat, region Mekn6s-Tafilalet Dr. Abdelmajid El Yassern, region Taza-A1 Hoceima-Taounate
HPN Team USAlDlMorocco
Mme Ursula Nadolny (until 1996) Mr. William Jansen, Chief (until 1997) Mme Nancy Nolan (until 1998) Dr. Amina Essolbi (until 1998) Mme Zohra Lhaloui Mme Helene Rippey Mme Michele Moloney-Kitts, Chief (1997-2000) Mme Susan Wright
Principal Collaborators of Cooperating Agencies
BASICS: Mr. Jonathan Ross EVALUATION (MEASURE): Dr. Jane Bertrand FPMD: Mr. Jan Hoey JHPIEGO: Mme Anne Pfitzer Macro: Dr. Mohamed Ayad MOST: Mr. Shawn Baker PHR: Mr. Moharned Oubnichou POLICY: Dr. Volcan Cakir PRIME: Mr. Pape Gaye SOMARC (CMS): Mme Houda Bel Haj
JSI Resident and Support Team
JSVMaroc
Redouane Abdelmoumen, Clinical Advisor - JSIIMaroc (August 1997 - July 2000). Mohamed Ait Mansour, Driver and MaillFile Clerk - JSIIMaroc (November 1996 - July 2000). Taoufik Bakkali, Monitoring & Evaluation Manager - JSllMaroc (June 1995 - September
2000). Youssef Barka, Driver and MaillFile Clerk - JSllMaroc (January 1998 -July 2000). Youssef Belabdia, ComputerIMIS Assistant - JSIIMaroc (June 1995 - July 2000).
John Snow, Inc. 150 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Geb Berry, MIS Manager - JSIIMaroc (August 1992 - December 1995). Rachid Bezad, lntermittent Clinical Advisor - JSllMaroc (January 1997 - September 2000). Khadva Bouhlal, Activity Support - JSIIMaroc (December 1994 - July 2000). Fatiha Bouricha, Administrative Assistant - JSIIMaroc (October 1998 - June 2000). Nicolas de Metz, Logistic Advisor - JSIIMaroc (September 1997 - September 1998). Hind El Attar, Procurement Manager - JSIIMaroc (August 1997 -August 2000). Boutaina El Omari. IEC Manaaer - JSIIMaroc (October 1996 - Julv 2000). Latifa Fihri, ~dministrat ivel~c~ount in~ ~ssistant - JSllMaroc (~une 1994'- February 1997). Cathy Fort, lntermittent Private Sector Specialist - JSllMaroc (June 1994 - NA). ~oumia Guennoun, Accounting ~ssistant - JSIIMaroc ( ~ e ~ t e m b e r 1997 - sep<ember 1999). Peter Halpert, Logistics Specialist - JSIIMaroc (June 1994 - June 1997). Nabila Karhat, Administrative Assistant - JSllMaroc (March 1997 - March 1999). Younes Laaboudi, Driver and MaillFile Clerk - JSIIMaroc (August 1995 - December 1997). Malika Laasri, Private Sector Program Manager - JSllMaroc (June 1994 -July 2000). Don Lauro, Chief of Party - JSllMaroc (May 1994 - 1996). Theo Lippeveld, Chief of Party - JSIIMaroc (May 1997 - September 2000). Ahmed Loukili, Procurement Specialist - JSIIMaroc (June 1994 - December 1997). Mounia Msefer, Financial Manager - JSllMaroc (September 1994 - July 2000). Birdaha Nawal, Office ManagerIAdministrative Assistant - JSIIMaroc (March 1997 -
September 2000). Ken Olivola, Management Specialist - JSllMaroc (May 1994 - August 1997). Souad Rahibe, Activity Support - JSIIMaroc (July 1997 -July 2000). Suzanne Reier, Management Advisor - JSIIMaroc (November 1997 - July 1999). Mustapha Says, Administrative Assistant - JSllMaroc (January 1995 - March 1997). Marcel Vekemans, lntermittent Clinical Advisor - JSllMaroc (May 1994 - February 1995; July
1996 - June 1997).
Emily Alfeld, Program Manager - JSIIBoston (June 2000 - September 2000). Jennie Coates, Prooram Associate - JSllBoston (May 1994 - May 1997). Jeff Kerzner, program Manager - JSIIBoston ( ~ u i ~ 1999 - ~ u ~ u s t 2000). Susan Klein, Senior Advisor - JSIIBoston (June 1997 -June 1999). Richard Moore, Senior Advisor - JSllBoston (May 1994 - May 1997). Roger Swartz, Senior Advisor - JSllBoston (July 1999 - August 2000). Ann Wickham, Program Manager - JSIIBoston (May 1994 - May 1997). Florencia Zulberti, Program Associate - JSllBoston (June 1997 - December 1999).
JHU/CCP
Sereen Thaddeus, IEC Advisor - JHUICCPIMaroc (June 1994 -June 1998).
URC/Rabat ef Washington
Bruno Bouchet, Senior Advisor - URCNVashington (January 1998 - September 2000). Norma Wilson, Quality Assurance Advisor - URCIMaroc (January 1998 -July 1999).
John Snow, Inc. 151 Contract No. 608-C-00-94-00006

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 5: List of Consultants on the FPIMCH
Phase V Project
John Snow. Inc. 152 Contract No. 608-C-00-94-00006

& O L E L -
L & $ @ - 9 . $ & & & % . r e @ 0 re & L
Annex 5: List of JSllURClJHUCCP Consultants on the FPIMCH Phase V Project


Name of Consultant
Lauren Goodsmith Cathy Fort Gilberte Vansintejan Rita Leavell
Maggie Huff- Rousselle
Norma Wilson Tisna Veldhuyzen Van Zanten
Claude Gingembre
Richard Moore
Claude Gingembre
Mohamed El Aouad
Norma Wilson
Gilberte Vansintejan George Walter
Jean de Malvinsky
Organization
JHU URC JSI Independent
Independent
URC URC
'Hicham Taoussi Rahhali Gael Murphy
Norma Wilson
Independent
JSI
Independent
ENAlRabat
URC
JSI lnt'l Health Program
Westem Consortium
Mahassine lraki
7
Arrival Date (daylmonthlyear)
26/08/96 16/09/96 01/09/96 13/10/96
0811 0196
26/10/96 2611 0196
Consultant local URC
URC
18/11/96
03/12/96
02/12/96
01/06/97
01/06/97
22/02/97 1 0/02/97
10/02/97
Consultant local
Departure Date (daylmonthlyear)
31/10/96 0311 0196 08/09/96 2611 0196
2011 2/96
16/11/96 16/11/96
01 103197 28/04/97
28/04/97
2511 1/96
1211 2/96
0711 2/96
31/03/97
17/06/97
15/03/97 21/03/97
21/03/97
04/04/97
Objective of the Visi t
Safe Motherhood Private sector strategy planning Safe Motherhood Discussion I Evaluation of MIS management capacity Strategic planning for Phase V (decide on the priorities of the transition plan to be operationalized)
Quality management training Quality management training
31/07/97 1 0/05/97
10/05/97
Financial Source
JHU URC JSI JSI
JSI
URC URC
Conduct a brief evaluation of the management needs of medical generalists in the private sector
Follow-up project visit (replacing the chief of party, contract amendment, other management problems)
Follow-up visit for evaluation of the management needs of medical generalists in the private sector
Conduct a pretest of the audio visual material (Flannel board and message board)
Review the progress made at the provincial level in the implementation of Project GlQua at the model sites and assist with 1997 planning
Safe Motherhood Conduct a 4-week advanced training of trainers course Conduct a 4-week advanced training of trainers
06/06/97
JSI
JSI
JSI
JSI
JSI JSI
JSI course Conceive ideas for printed cartoon messages Develop a technical assistance plan for quality management start-up
Develop a technical assistance plan for quality
JHU URC
URC . . management start-up
Develop a structure for the IEC strategy that will promote Long-term contraceptive methods
JSI

Imaternalmortality'in Morocco I
Arrival Date (daylmonthlyear)
17/04/97
05/05/97 05/05/97 04/05/97
12/05/97
12/05/97
Departure Date (daylmonthlyear)
23/05/97
17/05/97 17/05/97 25/05/97
26/05/97
15/06/97
Name of Consultant
Khalil Amrani
Gary Steele Richard Owens Paul Matar
Jean De Maivinsky
Bouchra Bahiji
Michael Edwards ulane
Michel Garenne
Claude Gingembre
Norma Wilson
Mohamed Errih
Nicolas de Metz
Susan Zimicky
Susan Klein
Norma Wilson
Organization
Consultant local
FPLM FPLM Johns Hopkins University
Western Consortium
Objective of the Visit
Prepare a synthesis of principle results taken from the qualitative studies for presentation on the development of the IEC strategy for May 19-23
Evaluate contraceptive logistics and Project start-up Evaluate contraceptive logistics and Project start-up Begin filming a docudrama highlighting the avoidable causes of the majority of maternal deaths
Conduct a meeting for the deveiopment of a national FPIiEC strategy
Confirm the interviews, contacts and collection of testimonies to finalize the script and the texts necessaw for the ~roduction of the docudrama on
07/06/97
CEPED
C2G Consultants
URC
Consultant local
ARCH
JSI
URC
Financial Source
JSI
JSI JSI JHU
JHU
JSI
19/07/97
09/06/97
21/06/97
19/06/97
07/07/97
10/07/97
21/07/97
20/08/97
26/08/97
Develop the program "Tableaux de Bord" and a basis for results
20/06/97
28/06/97
12/07/97
09/05/97
25/07/97
30/07/97
30/08/97
15/09/97
JSI
Work on a training technique for survey personnel of the MSP in order to develop an interview format
Participate in the development of a manual on the management of medicine stores for generalists practicing in the private sector Follow-up of training done for facilitators and team leaders in the 14 model sites
Evaluate and analyze Norplant utilization in order to determine the role of this contraceptive method in the national family planning strategy
Assist in the preparation of the meeting with the Committee Director and plan the meeting of Oct 30 regarding the "Phase-over" Plan the research component of the 1997 action plan Meet USAID and MOH representatives and review the administrative system with JSI staff
Develop the next steps for the GlQua project and plan the internal evaluation
JSI
JSI
JSI
JSI
JSI
JSI
JSI
JSi
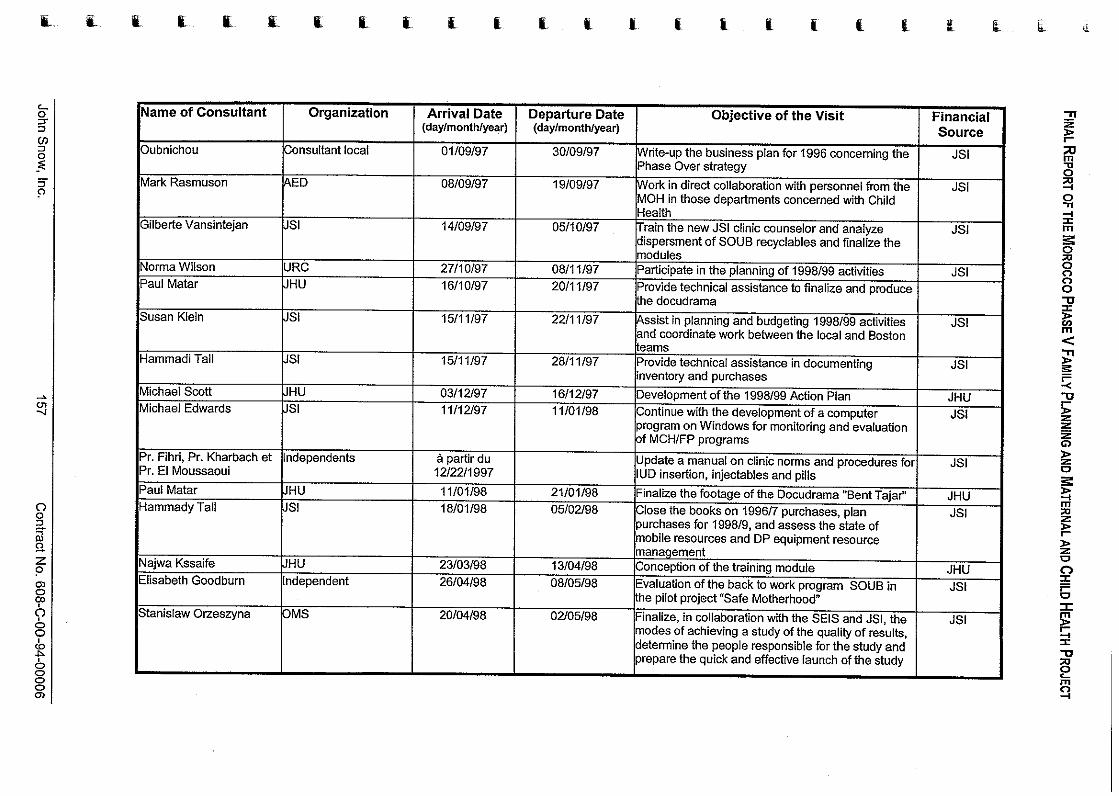
Name of Consultant Organization
I Gilberte Vansintejan SI
Norma Wilson URC Paul Matar JHU
I Susan Klein SI
I Hammadi Tall SI
Michael Scott JHU Michael Edwards JSI
Pr. El Moussaoui
Paul Matar Hammady Tall
Stanislaw Olzeszyna I
Arrival Date (daylmonthlyear)
01/09/97
08/09/97
14/09/97
Departure Date (daylmonthlyear)
I lmodules
30/09/97
19/09/97
0511 0197
2711 0197
khe docudrama
Objective of the Visit
0811 1/97 /Participate in the planning of 1998199 activities JSI
1511 1/97
1511 1/97
03/12/97 11/12/97
I purchases for 199819, and assess theitate of mobile resources and DP equipment resource
Financial Source
Write-up the business plan for 1996 concerning the Phase Over strategy
Work in direct collaboration with personnel from the MOH in those departments concerned with Child Health Train the new JSI clinic counselor and analyze dispersment of SOUB recyclables and finalize the
JSI
JSI
JSI
16/10/97
22/11/97 ssist in planning and budgeting 1998199 activities nd coordinate work between the local and Boston
2811 1/97
1611 2/97 11/01/98
a partir du 12/22/1997
11/01/98 18/01/98
modes of achieving a study of the quality of results. determine the people responsible for the study and prepare the quick and effective launch of the study
2011 1/97 1Prov:de technical assistance to finalize and oroduce I
JSI
Update a manual on clinic norms and procedures for IUD insertion, injectables and pills
Finalize the footage of the Docudrama "Bent Tajar" Close the books on 1996i7 ourchases. olan
21/01/98 05/02/98
23/03/98 26/04/98
20/04/98
teams Provide technical assistance in documenting inventory and purchases
Development of the 1998199 Action Plan Continue with the development of a computer program on Windows for monitoring and evaluation of MCHIFP programs
JSI
JHU .Is!
JSI
JHU JSI
13/04/98 08/05/98
02/05/98
management Conception of the training module Evaluation of the back to work program SOU0 in the pilot project "Safe Motherhood"
Finalize, in collaboration with the SElS and JSI. the
JHU JSI
.IS1

Name of Consultant
Gary Steele
Michael Edwards
Arrival Date (daylmonthlyear)
Organization
Carolyn Hart
Deborah Maine
Michael Edwards
Edward Wilson
Pierre Jean
A. Moussaoui
Nezha Mouane
Sereen Thaddeus
Michel Garenne
Susan Klein
FPLM
JSi
Departure Date (daylmonthlyear)
FPLM
Columbia University
JSI
FPLM
Independent
Independent
Independent
JHU
CEPED
JSI
04/05/98
14/05/98
Objective of the Visit
0 1/04/98
04/06/98
01/08/98
24/08/98
18/09/98
18/09/98
28/08/98
31/10/98
06/12/98
0711 2/98
Financial 'II Source g
16/05/98
23/07/98
01/06/98
05/06/98
11/01/99
03/09/98
01/10/98
01/10/98
0911 0198
Il/T1/98
18/12/98
19/12/98
Develop, in collaboration with a technical team, a strategy for ongoing trainings
Finalize the program for data entry of FPIMCH program results at the peripheral level, and test its utility at the regional and provincial levels
Present an analysis of the Phase Over experiences of those countries which have already gone through such transitions after the retreat of USAlD
Assist in the preparation of the pilot project's. Obstetrical Emergency Care, evaluation planned for the end of 1998
Continue with the development of a decentralized FPIMCH information system that would allow for results management at the regional and provincial levels Lend support to the development of a computer application to manage stocks at the central depot level Evaluate the FP training program for private practice medical generalists and the program's impact on the utilization of FP methods across the private sector
Collaborate w~th Dr Pierre Jean in the evaluation of the FP training program for private sector medical generalists and the program's impact on the utilization of FP methods across the private sector
Support the PClME participants and evaluate the training tools
Pmvide technical assistance and follow-up for IEC activities
Assist in coding mortalities and in preparing an analysis of the results of this study
Participate in the planning process and budgeting activities for 1999 activities and solve administrative and financial questions relative to project close-out
JSI
JSI
r
z? 2 2 %
JSI
JSI
JSI
JSi
- JSI
- JSI
JSI
JHU
JSI
JSI
.. -I I rn b 0 w 2 o 0 -0 I z rn < 2' S 5 F Z
Z z o 5 0
E 3 rn E r= 5 0
Z 0
6
E r; I -0 w 2 z 4

anten
Name of Consultant Organization
Gary Steeie I Michael Edwards JSI
Stanislaw Orzeszyna OMS
Sylvie Coiiin
I B. Bouchet IURC
SiPDT
I isna Veldhuyzen URC
M. Boukar Jules Martin Sonia Gag&
URC
SlPDT
I
Arr ival Date :day/rnonthlyear)
0911 2/98
Claire Escoffier
Larbi lbaaquii
01/02/99
22/02/99 (134 days)
07/03/99
04/03/99
Independent
independent
(daylrnonthlyear)
ontent for the program svnthesis meetina to be he1 . - - ]in Feb 1999
11/01/99 Continue the development of a decentralized FPIMCH information svstem to Dermit results /management at the regional and provincial levels I
10/02/99 Organize a workshop, with the assistance of a echnical team, in order to devei00 a new strateqv or decentraiized training in logist& managem&t o E ontraceptives
I 13/02/99 Finalize, in collaboration with the SElS and JSI, the
nalysis of survey results and the wording of the - study report
30/07/99 Prepare, organize and evaluate the training of midwives and labor and delivery nurses in care giving and proper communication skills in the context of birthing
15/03/99 Coordinate the technical activities and facilitate the national pre-seminar and seminar-workshop on quality assurance
15/03/99 Coordinate the technical activities and facilitate the national pre-seminar and seminar-workshop on uality assurance
I
15/03/99 Facilitate planning and preparation sessions of the national pre-seminar and seminar-workshop on quality assurance
31/07/99 Finalize the methodological tools of the EPC and establish a link with the technical component of the PClME
14/04/99 Facilitate and animate the meeting with the NGOs ir a neutral manner to maximize ideas and basis for collaboration
Financial Source
URC
JSi
JSI
JSI
JSI
URC
URC
URC URC URC
JSI
JSI

ame of Consultant
ahamane Karki
imed Moussaoui
Jsan Klein
idre Jacques
imed Moussaoui
imei Eddine Naji
ichel Garenne
arla Obermeyer
lward Wilson
uno Bouchet
Organization
ndependent
EPED
PLM
Arrival Date [daylmonthlyear)
24/04/99
Mail99
01/05/99
Departure Date (daylmonthlyear)
I I I
04/05/99
JuilleU99
08/05/99
08/05/99
07/05/99
10/05/99
he research project on reproductive health including he medical and anthrouoloaical asuects as rewired
Objective of the Visi t
16/06/99
17/05/99
Financial Source
Prepare the training workshop plan, technical content, and resource material for participants during the workshop in Fes
Collaborate in the development of Obstetrical and Neo-natal Emergency Care Standards
Participate in preparing the project extension proposal and solve administrative and financial questions
14/05/99 ssist the Family Planning Project of Morocco in the onceution of a Deer review uilot test for urivate
20/05/99
15/07/99
URC
JSI
JSI
JSI
22/05/99
23/05/99
17/05/99
24/05/99
secto;family planning services
Collaborate with Dr Andre Jacques in the conception of a pilot test for peer review of private sector FP services
Finalize the methodological tools of the EPC and establish a link with the technical component of the D P l h d F
JSI
JSI
, .,,,.,- Prepare in conjunction with the SEE and the DP the analysis report of survey results on the causes and circumstances of infant mortality
Examine the state of advancement and planning for
29/05/99
04/06/99
JSI
JSI
by the MOH, the F N U ~ , and USA~D
Establish contraceptive orders for the FP program in the form of an actual forecast for 1999-2003 and evaluate the progress in developing the application for central stock depot management against the time table established by the preceding mission
Organize and prepare the awareness seminar; write- up, with the pilot committee, the major themes of a national plan to operationalize a Quality Assurance Program; and prepare the activities of the 7199-6/00
JSI
URC

Elisabeth Goodburn Independent Deborah Maine IColumbia Universitv
ael Edwards DSI
Saidia Radi
Jeff Kerzner
Michael Edwards
I hmed Moussaoui Independent
independent
JSI
JSI
Sylvie Collin
Eric Morin Independent
SlPDT
Arrival Date (daylmonthlyear)
24/05/99
. . information system allowing for FPIMCH
ata management at the regional and provincial
31/05/99 01/06/99 01/06/99
Departure Date (daylmonthlyear)
27/05/99
12/06/99 08/06/99 31/07/99
I /levels I
Objective o f the Visi t
Collaborate with Bruno Bouchet in organizing and animating the seminar on quality management awareness
16/06/99
17/09/99
system; continue develop:ng the modules for raph~c and geographic analysis of the FPIMCH
Financial Source
JSI
Evaluate the Pilot Project "Safe Motherhood" Evaluate the Pilot Project "Safe Motherhood" Continue with the deveiooment of a decentralized
03/08/99 \Conduct a study permitting the understanding of the I JSI
I . .
lmanagement issues
JSI JSI JSI
01/10/99
26/09/99
1 lof birthing I 01/04/99 31/12/99 IEditing of a final SONU document based on the .IS1
15/09/99
01/09/99
22/02/99 (20 days)
rational, underlying trendsof practice and inchidual behavior and communities relative to child health
Familiarize himself with the FPIMCH Phase V project and assist the chief of party with
06/1 1/99
JSI
31/12/99
01/11/99
31/12/99
(20 days)
0411 0199
Reinforce the start-up of the module on survey results for the FPIMCH program at all levels of the
JSI
. . . system Finalize the methodological tools of the EPC and establish the link with the technical components of PClME Propose a system of archiving and classifying photos and existing slides held by the DIEC, and create a model for cataloging the supports developed over the last 10 years
Prepare, organize, and evaluate the training of midwives and laborldelivery nurses in proper assistance and communication skills in the context
1511 0199
JSI
JSI
JSI
cornmints and suggestions of committee members who validated its content
Assist the MOH in the production of an analytical document on the experience of those involved in the obstetrical emergencies management pilot
JSi
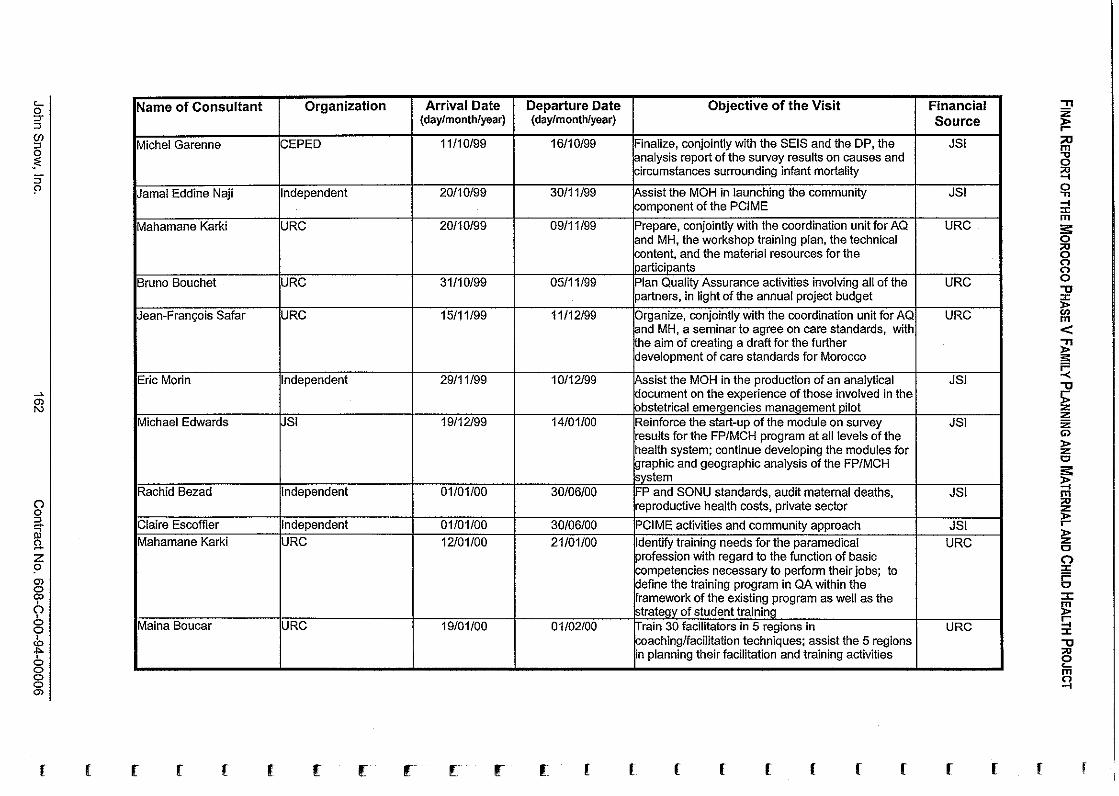
Name of Consultant
Michel Garenne
Jamai Eddine Naji
Mahamane Karki
Arrival Date (daylmonthlyear)
Organization
I
CEPED
Independent
URC
lparticipants
Jean-Fran~ois Safar
Eric Morin
Michael Edwards
Departure Date (daylmonthlyear)
I I I bystem I
I I I ]strategy of student training - I Maina Boucar ~URC 19/01/00 01/02/00 hrain 30 facilitators in 5 reaions in U RC
11/10/99
20/10/99
20/10/99
URC
Independent
JSi
Claire Escoffier Mahamane Karki
I oaching/facilitation techni&es; assist the 5 regions planning their facilitation and training activities
Objective of the Visit
B ~ n o Bouchet
Rachid Bezad
Financial Source
1611 0199
3011 1/99
0911 1/99
3111 0199 URC
1511 1/99
2911 1/99
19/12/99
independent 01/01/00
Independent URC
Finalize, conjointly with the SElS and the DP, the analysis report of the survey results on causes and circumstances surrounding infant mortality
Assist the MOH in launching the community component of the PCiME
Prepare, conjointly with the coordination unit for AQ and MH, the workshop training plan, the technical content, and the material resources for the
0511 1/99
11/12/99
1 0/12/99
14/01/00
30/06/00
01/01/00 12/01/00
JSI
JSI
URC
Plan Quality Assurance activities involving all of the partners. in light of the annual Droiect budget - . . - Organize, conjointly with the coordination unit for AQ and MH, a seminar to agree on care standards, with the aim of creating a drafl for the further development of care standards for Morocco
Assist the MOH in the production of an analytical document on the experience of those involved in the obstetrical emergencies management pilot Reinforce the start-up of the module on suwey results for the FPIMCH program at all levels of the heaith system: continue developing the modules for graphic and geographic analysis of the FPIMCH
FP and SONU standards, audit maternal deaths, reproductive health costs, private sector
30/06/00 21/01/00
URC
URC
JSI
JSI
JSI
PClME activities and community approach Identify training needs for the paramedical profession with regard to the function of basic competencies necessary to perform their jobs; to define the training program in QA within the framework of the existing program as well as the
JSI URC

Name of Consultant
Bruno Bouchet
Michael Edwards
Organization
Andre Jacques
Ahmed Moussaoui
/program and help plan the realizatioiof these roles I Bruno Bouchet IURC I 12/04/00 1 25/04/00 lHelp regional teams define their roles in the I URC
URC
JSI
Mahamane Karki
Rachid Filali Moknassi
Maina Boucar
Arrival Date (daylmonthlyear)
Independent
Independent
09/02/00
14/02/00
URC
Independent
URC
Mahamane Karki
Jeff Kerzner
Departure Date (daylmonthlyear)
26/02/00
27/02/00
20/02/00
1 1 /03/00
01/03/00
04/03/00
14/04/00
URC
JSI
Objective of the Visit
07/03/00
06/03/00
Financial Source
Organize a training workshop in quality care monitoring and help conceive a regionai quality monitoring system taking into account the specifics of each region
Reinforce the start-up of the module on survey results for the FPIMCH program at ail levels of the health system; continue developing the modules for Qraphic and geographic analysis of the FPlMCH
28/03/00
05/03/00
25/04/00
19/04/00
20/04/00
URC
JSI
system Develop evaluation tools based on norms and standards prepared by pilot FP projects
Assist Dr. Andre Jacques in developing evaluation tools based on norms and standards prepared by pilot FP projects
JSI
JSI
Develop/identify manuals for QA training and develop the training manuals for the trainer and the student
Assist private sector physicians in the creation of a federation of private sector associations of medical generalists
Help regional teams define their roles in the execution of QAfunctions identified by the national
09/05/00
12/05/00
URC
JSI
URC
execution of QA functions identified by the national program and help plan the realization of these roles
Train future national trainers in understanding and using previously developed training material and assist the trainers in accomplishing their first training of paramedical personnel in QA
Assist the JSI team of Rabat in various project activities like exchanging a maximum amount of information on the state of project implementation
URC
JSI

system: reinforce a n i develop technical apacities of SElS and DIM frameworks to deal with
application.
Financial Source
Andre Jacques
Michael Edwards
Departure Date (daylmonthlyear)
Arrival Date (daylmonthlyear)
Name of Consultant
Independent
JSI
M. Akhchichen
Objective of the Visit Organization
lrec&nmendations
~ ~
06/05/00
15/05/00
Independent
Elisa Knebel
Brahim Hafidi
Roger Swartz
Alyssa Karp
JSI
16/05/00
02/06/00
22/05/00 (10 days)
M. Akhchichen
URC
Independent
JSI
JSI
22/5/00 (36 davs)
Independent
Follow-up with the evaluation pilot project by pairs of private sector physicians in family planning
Reinforce the start-up of the module on survey results for the FPIMCH Droclram at all levels of the
0711 0100
0711 0100 Evaluate the unfolding and hold-ups of the MGP rainina worksho~s in inter~ersonal communication . .
31/05/00
02/06/00 (5 days) 09/06/00
17/09/00
JSI
JSI
Moderate and facilitate the national conference on the financing of reproductive and child health aroarams to maximize ideas and make
17/06/00
08/06/00
01/07/00
29/09/00
JSI
- Document quality improvement activities by the local teams and recommend a model of documentation of quality improvement activities in Morocco Facilitate and animate the forum of regional dialogue in order to maximize ideas and recommendations
Assist the JSVRabat team in managing all program and administrative project activities during Mr. Llppeveld's absence and manage activities relative to project closeout
Assist the chief of party of the JSi Rabat team in multiple close-out activities
URC
JSI
JSI
JSI

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 6: Financial Report of
the FPIMCH Phase V Project
John Snow, Inc. 165 Contract No. 608-C-00-94-00006
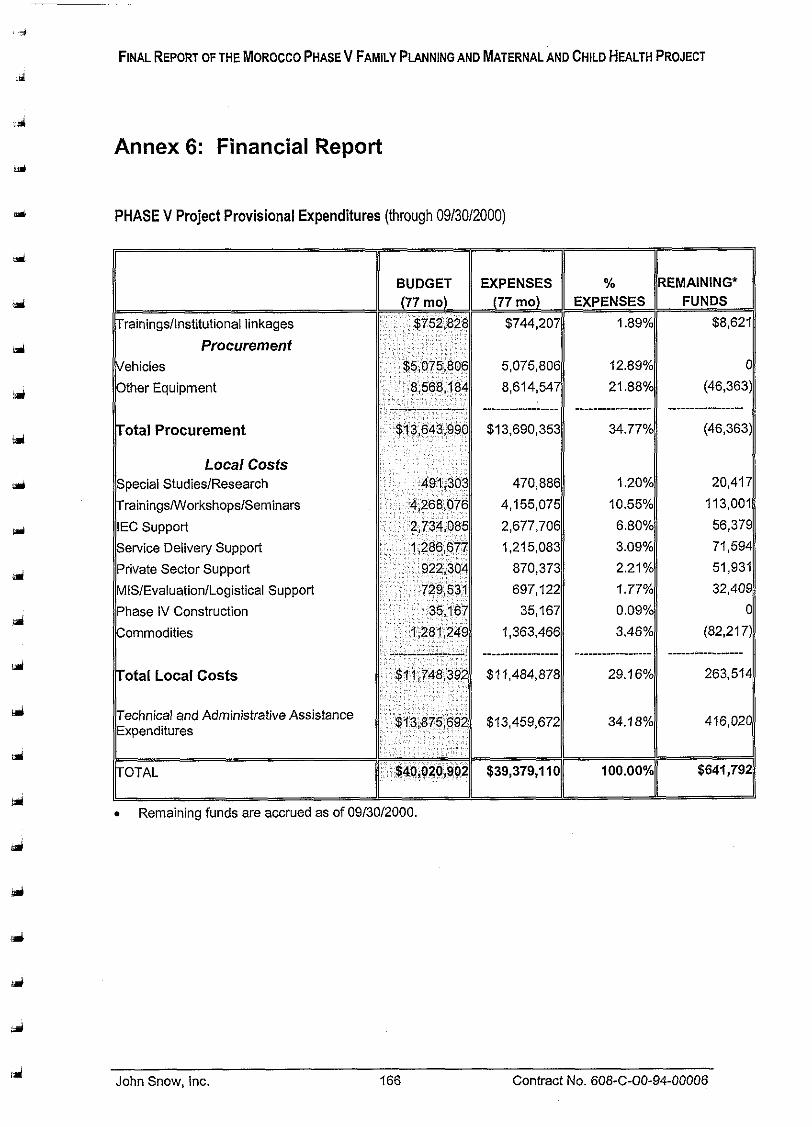
FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 6: Financial Report
PHASE V Project Provisional Expenditures (through 09/3012000)
Procurement
otal Procurement
Local Costs
rainingsNVorkshopslSeminars
otal Local Costs
Remaining funds are accrued as of 09/30/2000.
John Snow, Inc. 166 Contract No. 608-C-00-94-00006

FINAL REPORT OFTHE MOROCCO PHASEV FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 7: Summary of Participant Travel
John Snow, Inc. 167 Contract No. 608-C-00-94-00006

Annex 7: Summary of Participant Travel
List of Participants Financed through JSI for "Participant Travel" May 1994-September 2000
barticioant Name I MIF I Province I Depart I Return I Purpose of Visit I Destination ~ H t e Dater
Belkheiri M 04/06/94 12/08/97 Participer B un cours sur I'Bconomie et la gesfion Boston (USA) des ressources dans les programmes de sante
Driss Bacheikh M Rabat 31/08/94 03/09/94 Partici~er une formation des formateurs Santa Cruz (USA)
. . kpeciaux
M ssister a un seminaire-atelier inter-pays consacre Cairo (Egypt) la sante aenesiaue Dour la reduction de la
lmortalite iaterneile ' I Fouad Bouchareb I M I Fez !29/03/97 104104197 /Assister a un seminaire-atelier inter-pays consacre I Cairo (Egypt) I I I I I k3 la sante aenBsiaue oour la reduction de la I - . .
mortaiite maternelle Fouad Hamadi M Rabat 23104197 27104197 Participer au Forum EuropBen sur I'Amelioration de Paris (France)
la Qualit6 dans les Soins de Sante Mustapha Essolbi M Rabat 23104197 27/04/97 Participer au Forum Europeen sur I'Amelioration de Pans (France)
la Qualite dans les Soins de Sante Ahmed Cherrat M Meknes 23/04/97 27/04/97 Participer au Forum Europeen sur I'Amelioration de Paris (France)
la Quaiit6 dans les Soins de Sante

Participant Name I MIF
Slimane Hajra * l ~ r i s s Bacheikh I M
bdelwahab Zerrari * Fatima Dehbi I F
I Khalid Slaitane M
bdelhaq M'Ghari
Rachid Khadraoui
M'Barek El Ouidali
hmed Fadili
Driss Bacheikh M I
. Achahboune M I
Farouk Fasla M I
oussef N'has M I
hmed Mountacer I M
Province I De~ar t I Return I Pur~ose of Visit I ate I Dater I
Rabat 123104197 127104197 lparticiper au Forum Europeen sur I'Amelioration d, I I Ila Qualit6 dans les Soins de Sante
Rabat k3/04/97 127104197 1Parlic:per au Forum E u ~ o D & ~ sur I.Amelioration dl la ~ua l i t e dans les soins be Sante
Rabat 09/05/97 24/05/97 Assister au Tours de Formation Clinique de la Prise en Charge lntegrbe de I'Enfant Malade"
Rabat 27/2/98 8/3/98 Assister a un cours deformation sur la rise en 1 lcharge integree des maladies de l'enfant
Rabat 127/2/98 18/3/98 bssister a un cours de formation sur la prise en I I lcharge integree des maladies de I'enfant
Rabat 12712198 18/3/98 hssister a un cours de formation sur la rise en
Destination
Paris (France)
Paris (France)
Lusaka (Zambia)
Madagascar
Madagascar
Madagascar
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Murcia (Spain)
Pittsburgh (USA)
Pittsburgh (USA)
Pittsburgh (USA)

(participant Name ( MIF ( Province ( Depart I Return I Purpose of Visit Destination Date Dater
Salaheddine Bennani M Sale 8/6/98 3/7/98 Assister a un cours sur les methodes de Pittsburgh (USA) management moderne
Abdelhak Zerouaii M Rabat 21/6/98 31/6/98 Assister a la formation sur les Routers ClSCO Quebec City (Canada) Slimane Haira M Rabat 2017198 01/7/98 Assister au cours sur la mise en oeuvre et la Boston (USA)
management des projets de developpement Lahcen Amal M Tiznit 8/9/98 2/10/98 Assister au cours sur la planification et le Pittsburgh (USA)
management des projets de developpement M'Hammed El Azzouni M Errachidia 8/9/98 211 0198 Assister au cours sur la planification et le Pittsburah (USA) - . .
management des projets de developpement Brahim Ouchrif M Rabat 21/9/98 911 0198 Assister 2 ia formation sur la logistique en PF Arlington (USA) Zakia Ayaou F AI Hoceima 07/03/99 25/03/99 Assister a la formation intemationale sur le suivi et Settat (Maroc)
I'8valuation des projets de developpement Habib Cherrat M AI Hoceima 07/03/99 ,25103199 ,4ssister a la formation intemationale sur le suivi et Settat (Maroc)
I I 1 I ll'6valuation des projets de developpement I bdelhak Benielloun 1 M 1 Safi b7/03/99 !25/03/99 kssister a la formation internationale sur ie suivi et I Settat (Maroc) . - ,
IUvaluation des projets de developpement Soumaya Belhamdounia F Safi 07/03/99 25/03/99 Assister a la formation internationale sur le suivi et Settat (Maroc)
I'evaluation des projets de developpement Amina Azami idrissi F Settat 37/03/99 25/03/99 Assister a la formation intemationaie sur le suivi et Settat (Maroc)
\ - --, I'evaluation des projets de developpement
Mohamed ifleh M Settat 37/03/99 25/03/99 Assister a la formation internationale sur le suivi et Settat (Maroc) I'evaluation des projets de developpement
Hamid Elachhab M Settat 07/03/99 25/03/99 Assister 3 la formation intemationale sur le suivi et Settat (Maroc) II'evaluation des projets de developpement
mina Lamghari, LMPE 1 F 1 Rabat 124105199 118/06/99 IParticiper a I'atelier sur I'elaboration et gestion des ( Santa Cruz (USA)
I -
I I I I ]programmes de sante reproductive I

Participant Name
Fadila El Kihel, MS
hmed Cherrat, MS I" El Laarbi Rjimati, MS I----
bdelhouahid Karimi ? bdelmajid Bouazza
Mohamed Fennane I------ Mustapha Lalaoui
hmed Cherrat P------ Katre-Ennada Darkaoui I---- Salah Oulioul I Noureddine Ben Jbara, 1:
MIF I Province I Deoart I Return I Puroose of Visit I Destination 1 ~ i t e I Dater I
F 1 Rabat /24/05/99 118/06/99 l~art ic i~er a I'atelier sur I'elaboration et gestion des 1 Santa Cruz (USA)
I I I lprogrammes de sante reproductive I M I Meknes 11 1/07/99 115/07/99 (Presenter I'experience marocaine Damascus (Syria)
F
F
Rabat
Rabat
Ireunion inter-pays sur la PCIME
F M M
1 I~ommunication" I M I Rabat (Aoril 2000 horil2000 IParticioer a I'atelier "Advances in Familv Health I Fataa (Lebanon)
24/05/99
24/05/99
Damascus (Syria)
M
M
M
Rabat Rabat F&s
18/06/99
18/06/99
11/07/99 Rabat
Rabat
Rabat
I~ommunication"
13/09/99 13/09/99 22/3/00
. .
I I I ISantg I
programmes de sante reproductive Participer a I'atelier sur Elaboration et gestion des programmes de sante reproductive Participer a I'atelier sur I'elaboration et gestion des
15/07/99
22/3/00
April 2000
M I Rabat 108/05/00 k7/05/00 l~articiper a la formation "Mehodes &Evaluation de I Montreal (Canada)
I~ualite I
l~ual i te -
M I Rabat k4/05/99 118/06/99 IParticiper a un atelier sur I'evaluation des services I Chapel Hill (USA)
Santa Cruz (USA)
Santa Cruz (USA)
Prt5senterI'exp6riencemarocaine PCIME/Aooroche Communautaire a I'atelier sur
24/09/99 24/09/99 33/26/00
Costa Rica; Egypt M
-
03/26/00
April 2000
Costa Rica; Egypt
I'6laborat& et gestion des programmes a la reunion inter-pays sur la PCIME Participer au cours "Le comedien et la radio" Participer au cours "Le comedien et la radio" Participer au "Forum Europeen sur I'Amelioration
Meknes
F
Costa Rica; Egypt M
Paris (France) Paris (France)
Amsterdam (Holland) de la dualite dans les Soins de SantC Participer au "Forum Europeen sur I'Amelioration de la Qualite dans les Soins de SantC Participer a I'atelier "Advances in Family Health
18/06/00 0/06/00 Partager I'experience marocaine dans la mise en euvre du Programme National d'Assurance
18/06/00 Rabat
Amsterdam (Holland)
Fatqa (Lebanon)
30/06/00 artager I'experience marocaine dans la mise en euvre du Proaramme National &Assurance
Rabat 18/06/00 30/06/00 artager I'experience marocaine dans la mise en euvre du Proaramme National &Assurance

FINAL REPORT OF THE MOROCCO PHASE V FAMILY PLANNING AND MATERNAL AND CHILD HEALTH PROJECT
Annex 8: Summary of Invitational Travel
John Snow, Inc. 172 Contract No. 608-C-00-94-00006

Annex 8: Summary of Invitational Travel
List of Participants Financed through JSI for "Invitational Travel" May 1994September 2000
Participant Name MIF Province
bdeslam Drissi Rabat
Rabat
M'Hammed Al Jem Rabat
I Abdellylah Lakssir M Rabat
I I
Khadija Rachouk I F I Rabat Karima El Harim F Rabat
I I Slimane Hajra M Rabat
Depart Date
01/08/94 01/08/94 01/08/94 05/08/94
Return Dater
13/09/94
13/09/94
13/09/94
30108194 09/11/94
03/08/94 03/08/94 03/08/94 13/09/94
I I I
Purpose of Visit
et le ~ e v e l o ~ ~ e m e n t
Participer a la conference internationale sur la Population et le Developpement
Participer a la confdrence internationale sur la Population et ie Developpement
Participer a la conference internationale sur la Population et le D6veloppement
Participer a un sgminaire sur I'lslam et la PF Travailler conjointement avec le personnel de I'universite de Tulane sur le developpement et le renforcement des ~apacites d'Bvaluation
10/10/94
0611 1/94 01/01/95
Destination
Participer a un atelier Participer a un atelier Participer a un atelier Partici~er a la conference internationale sur la Pooulation ~ -,. ,
Cairo (Egypt)
Cairo (Egypt)
Cairo (Egypt)
Niamey (Niger) New Orleans (USA)
01/01/95
Jakarta (Indonesia) Jakarta (Indonesia) Jakarta (Indonesia)
Cairo (Eavotl
0911 1/94 ravailler conjointement avec le personnel de I'universite de Tulane sur le d6velo~~ement et le renforcement des
1911 1/94 28/02/95
I I I
New 0r.eans (USA)
28/02/95
14/01/95
. . capacites d'evaluation
Participer a atelier de communication avancee Developper avec le MSP la capacite institustionnelle pour I'utilisation et I'evaiuation des donnees de programme
Tunis (Tunisia) New Orleans (USA)
Developper avec le MSP la capacite institustionnelle pour .'utilisat;on et I'evaluation des donnees de programme
30/01/95
New Orleans (USA)
Identifier ies specifications pour I'achat de materiel et I'installation d'un reseau informatique a la DPES
Washington; Boston (USA)

Participant Name
I l l les responsabies de Transcentuj Matrix et autres qui ~euvent assister dans les achats futurs I
Sabah Benjelloun
Ahmed Hajji
I I I I I. I Mustapha Mahfoudi M I Rabat ( 22/10/95 (27110195 (Participer B la 5iBme rencontre du CVI Consultative Group( Sao Paula (Brazil)
MIF
F
M
Province
Fatima El Kadioui
Jaafar Heikel
l ~ a j a e Ei Aouad I ! I I I I 1 F I Rabat 106/12/95 117/12/95 [Partici~era la IXieme Conference internationale sur le I Karnoala (Uaanda)
Rabat
Rabat
I I I I - - -
I
. . - ~ ~ I D A et les MST
dellatif Lfarakh I M 1 Rabat 1 11112195 (16112195 Jparticiper au S h e colioque de I'association maghrebine 1 Tunis (Tunisia)
Depart Date
F
M
Baba Filali
I I I I I. . . I bdellilah Yaakoubd M Rabat 11/12/95 16/12/95 Participer au 9eme colloque de I'association maghrbbine Tunis (Tunisia)
pour I'btude de la population
22/01/95
14/05/95
Return Dater
Rabat
Rabat
M
24/01/95
22/05/95
Purpose of Visit
1511 1/95
06/12/95
Rabat
Destination
Participer a la seconde conference internationale sur les methodes d'evaiuation dietetiques
Visiter plusieurs institutions americaines telles que la National Library of Medicine, Library of Congress et JHU
Boston (USA)
Washington; Baltimore (USA)
2311 1/95
17/12/95
06/12/95
Participer a la 44ieme rencontre annuelle de la Societe Americaine de MBdecine Tropicale
Participer a la IXieme Conference Internationale sur le SlDA et les MST
17/12/95
San Antonio
Kampala (Uganda)
Participer a la IXieme Conference Internationale sur ie SlDA et ies MST
Kampala (Uganda)

Participant Name I hmed Bendali I*
Mina Abakrouch
El Arbi Rjimati I------ iza Lyaghfouri
mina Saad k-- Rokia Belahsen I
mina Balafrej k---- bdelwahab Zerrari 7 awad Mahjour P oussef Chami 7 aafar Heikel r hmed Zidouh F------
Rachid Bezad I
MIF Province Depart Return Purpose of Visit Destination Date Dater
I - -.-
I M Fes 11/12/95 16/12/95 Participer au 9eme colloque de I'association maghrbbine Tunis (Tunisia)
Dour I'etude de la population 1 ).
F I Rabat 1 11/12/95 116/12/95 IPartici~er au 9eme colloque de I'association maghrbbine I 4
Tunis (Tunisia) (pour I'itude de la population
M I Rabat 1 16/03/96 125/03/96 Pssister a la conference internationale sur la vitamine A I Guatemala City I I I
F I Rabat 1 16/03/96 125103196 bssister a la conference internationale sur la vitamine A 1 1 Guatemala City
I F Rabat 16/03/96 25/03/96 sister a la conference internationale sur la vitamine A Guatemala City
I I I I I F Rabat 1 16/03/96 )25/03/96 p t e r a la conference internationale sur la vitamine A 1 Guatemala City
Guatemala City I I I I I
F Rabat 16/03/96 25/03/96 ssister a la conference internationale sur la vitamine A Guatemala City
I I I I I F I Rabat 1 15/06/96 122106196 IParticioer a Conference sur la prevention de la morialite I Accra (Ghana)
lmaternelle
M I Rabat 1 15/06/96 122106196 IParticiper a Conference sur la prevention de la mortalit6 1 Accra (Ghana) lmaternelle
F I Rabat 1 15/06/96 122/06/96 IPartici~er a Conference sur la prevention de la mortalit6 I Accra (Ghana) lmaternelle
M Rabat 05/07/96 12/07/96 Participer a Xieme Conference Internationale sur le SlDA Vancouver (Canada)
i I I I I M Rabat 05/07/96 13/07/96 Participer a Xieme Confbrence Internationale sur ie SlDA Vancouver (Canada)
I I i I I M Rabat 05/07/96 13/07/96 Participer 2 Xieme Conference Internationale sur le SlDA Vancouver (Canada)
I I I I I
M 1 Rabat 1 05/07/96 1 13/07/96 IParticiper a Xieme Conference lnternationale sur le SlDA I Vancouver (Canada)
F 05/07/96 13/07/96 [Participer a Xieme Conference Internationale sur le SlDA Vancouver (Canada)
I I I I M Rabat 05/07/96 13/07/96 Participer a Xieme Conference Internationale sur le SlDA Vancouver (Canada)

art icipant Name
bdelKarim Zalim
abria Lahgui
a'ila Hakkou
atima Akka
ouria Bellalij
lajia Hajji
doharned Abou Ouakil
)r Mekkaoui
louallou Abdelmajid
'rovince
Rabat
Rabat
Rabat
Rabat
Rabat
Rabat
Rabat
Rabat
Fes
- Depart Date -
11 103197
- )1/03/97
- 31/03/97
- 01/03/97
- D1/03/97
- 12/05/97
- 30/3/98
- 3013198
- 1/5/98
procedures de tests, normes de qualite, les procedures de ests, normes de aualite, les prodedes industriels de It '
Destination
Seattle (USA)
Return Dater
14/03/97
14/03/97
14/03/97
14/03/97
14/03/97
Purpose of Visi t
Acquerir une opinion complete sur les diverses procedures de tests, normes de qualite, les procedures de tests, normes de qualite, ies procedes industriels de fabrication des preseivatifs et les parametres dans le cadre juridique
Acquerir une opinion complete sur les diverses procedures detests, normes de qualite, les procedures de tests, normes de qualite, les procedes industriels de fabrication des preseivatifs et ies parametres dans le cadre juridique
Acquerir une opinion complete sur les diverses procedures detests, normes de qualite, ies procedures de tests, normes de qualite, les procedes industriels de fabrication des preservatifs et ies parametres dans ie cadre juridique
Acquerir une opinion complete sur ies diverses procedures de tests, normes de qualite, les procedures de tests, normes de quaiite, les procedes industrieis de fabrication des preseivatifs et les parametres dans le cadre juridique
p.cqu6rir une opinion complete sur les diverses
16/05/97
3/4/98
Seattle (USA)
Seattle (USA)
Seattle (USA)
Seattle (USA)
$e domaine de la Sante de la Reproduction"
fabrication des preservatifs et les parametres dans le cadre juridique
Definir et finaliser avec JHPIEGO et I'USAID les prochaines etapes de I'activite Revision du Cursus Universitaire
Assister a la Conference "Participation des Hommes dans
3/4/98 ssister a la Conference "Participation des Hommes dans le dornaine de la Sante de la Reproduction" I
Baltimore (USA)
Ouagadougou (Burkina Fasc
Ouagadougou (Burkina Fasc
SanBa, Yemen 8/5/98 Presenter I'experience du projet pilote MSR a la reunion internationaie organisbe par EMROIOMS



3 z ?= R v o 2 g -I I rn
5 w 0 0 0 o -0 I > V) rn < 7 s 7 ? z z Z
Destination
Dakar (Senegal)
Washington (USA)
Cairo (Egypt) Washington (USA)
Washington (USA)
Washington (USA)
Washington (USA)
Cairo (Egypt)
Cairo (Egypt)
Purpose of Visit
Revoir le protocol nouvellement developpe de I'evaluation PClME Participer a la reunion international sur la Sante de la Mere Participer a la reunion des partenaires Sud-Sud Participer a la Conference annuelle de Global Health Council Participer a la Conference annuelle de Global Health Council
Participer a la Conference annuelle de Global Health Council
Participer a la Conference annuelle de Global Health Council
Participer a la reunion du comite executif du partenariat Sud-Sud
Participer a la reunion du comitb executif du partenariat Sud-Sud
Return Dater
03/09/00
04/05/00
03/06/00 16/06/00
16/06/00
16/06/00
16/06/00
31/06/00
31/08/00
Depart Date
03/04/00
02/05/00
27/05/00 13/06/00
13/06/00
13/06/00
13/06/00
26/06/00
26/08/00
Province
Rabat
Rabat
Rabat Rabat
Sefrou
Rabat
Agadir
Rabat
Rabat
Participant Name
Ajcha Lamrani
Ali Bensalah
Ben Abla Mustapha Abdelwahab Zerrari
Youssef Riouch
Hamid Chekli
Fatima Guenar
Ben Abla Mustapha
Mohamed Abou Ouakil
MIF
F
M
M M
M
M
F
M
M
Copyright © 2022 FDOKUMEN