
Family Caregivers' Future Planning for Younger and Older Adults With Serious Mental Illness (SMI)
22
http://jag.sagepub.com/ Journal of Applied Gerontology http://jag.sagepub.com/content/27/4/466 The online version of this article can be found at: DOI: 10.1177/0733464808315290 2008 2008 27: 466 originally published online 23 May Journal of Applied Gerontology Whitney L. Mills Elizabeth A. Corsentino, Victor Molinari, Amber M. Gum, Lori A. Roscoe and With Serious Mental Illness (SMI) Family Caregivers' Future Planning for Younger and Older Adults Published by: http://www.sagepublications.com On behalf of: Southern Gerontological Society can be found at: Journal of Applied Gerontology Additional services and information for http://jag.sagepub.com/cgi/alerts Email Alerts: http://jag.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://jag.sagepub.com/content/27/4/466.refs.html Citations: at FLORIDA STATE UNIV LIBRARY on August 15, 2012 jag.sagepub.com Downloaded from
Transcript of Family Caregivers' Future Planning for Younger and Older Adults With Serious Mental Illness (SMI)

http://jag.sagepub.com/Journal of Applied Gerontology
http://jag.sagepub.com/content/27/4/466The online version of this article can be found at:
DOI: 10.1177/0733464808315290
2008 2008 27: 466 originally published online 23 MayJournal of Applied GerontologyWhitney L. Mills
Elizabeth A. Corsentino, Victor Molinari, Amber M. Gum, Lori A. Roscoe andWith Serious Mental Illness (SMI)
Family Caregivers' Future Planning for Younger and Older Adults
Published by:
http://www.sagepublications.com
On behalf of:
Southern Gerontological Society
can be found at:Journal of Applied GerontologyAdditional services and information for
http://jag.sagepub.com/cgi/alertsEmail Alerts:
http://jag.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jag.sagepub.com/content/27/4/466.refs.htmlCitations:
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

What is This?
- May 23, 2008 OnlineFirst Version of Record
- Jul 18, 2008Version of Record >>
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Journal of AppliedGerontology
Volume 27 Number 4August 2008 466-485© 2008 The Southern
Gerontological Society10.1177/0733464808315290
http://jag.sagepub.comhosted at
http://online.sagepub.com
466
Manuscript received: June 21, 2007; final revision received: December 3, 2007; accepted:December 3, 2007.Authors’Note: This study was conducted as part of the primary author’s undergraduate honors the-sis. It was funded by a small grant from the University of South Florida Office of UndergraduateResearch.
Family Caregivers’ FuturePlanning for Younger andOlder Adults With SeriousMental Illness (SMI)Elizabeth A. CorsentinoFlorida State University, TallahasseeVictor MolinariAmber M. GumLori A. RoscoeWhitney L. MillsUniversity of South Florida, Tampa
This study examines plans for future caregiving made by family members ofyounger (n = 59) and older adults (n = 16) with serious mental illness (SMI).An online survey was advertised through a newsletter of the National Allianceon Mental Illness. Qualitative analyses yielded four areas of caregiver concern:health of the care recipient over time, ability of caregivers to sustain support,social support available for the care recipient, and financial burden of care.Despite these concerns, few caregivers reported completed plans for futurecaregiving. One fourth of the caregivers had made no plans, nor had they dis-cussed future caregiving with others. Although most would prefer other relativesto assume care in the event they could not sustain support, these expectationsmay not be communicated openly. Generating discussion on this pertinenttopic has implications for the aging society regarding how best to care forthose with SMI and their caregivers.
Keywords: caregiving; serious mental illness; older adults
Serious mental illness, or SMI (i.e., longstanding psychiatric problemsincluding schizophrenia, major affective disorder, and bipolar disorder),
significantly interferes with day-to-day functioning. Individuals with SMI have
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Corsentino et al. / Family Caregivers’ Future Planning 467
historically received support and supervision by others from both formaland informal avenues of care. Following World War II, growing concern overthe deplorable conditions of large, undersupervised psychiatric hospitalsproduced a shift in the primary responsibility for the care of older adultswith SMI to the community. As this policy of deinstitutionalization gainedstrength in the 1960s, family caregivers frequently assumed supportivefunctions for older adults with SMI because of the scarcity of community-based housing alternatives and mental health services (Cook, Cohler,Pickett, & Beeler, 1997; Lefley, 1996). As a consequence of this abrupt shift,“the patient’s relatives [were catapulted] into a caregiving role for whichthey [were] untrained and unprepared and from which they [had] been sys-tematically excluded in the past” (Lefley, 1996, p. 19). Consequently, thismovement compelled researchers to confront the impact of deinstitutional-ization not only on patients with SMI but also on their family members whowere now expected to assume the role of “caregiver” (Rose, 1996).
Decades after these changes in patterns of care occurred, however, limitedresearch and public policy attention have been devoted to family caregiversof persons with SMI across the life course. In particular, little attention hasbeen paid to the challenges of caring for aging relatives with SMI, eventhough changes in the care recipient’s physical health and social environmentover time could seriously affect the caregiver’s ability to provide care.
The purpose of the present study was to examine the experiences of infor-mal caregivers of persons with SMI, focusing on the challenges encounteredby caregivers as relatives with SMI age. Specifically, caregivers’ level ofplanning for the future was considered. Given the importance of caregivers tothe effectiveness of care in the community, it is vital that the challengesinvolved in caregiving for persons with SMI as they age are understood.There is evidence to suggest, for instance, that patients with schizophreniawho live with informal caregivers are less likely to be hospitalized during theprevious year compared to those without informal caregivers, perhapsbecause of the community support that they receive (Tucker, Barker, &Gregoire, 1998). If a caregiver is unable to sustain support over time, an agingrelative with SMI may be prematurely transferred to a setting less suited tohis or her individual needs. Nursing homes, for instance, with the primarymission of caring for physically frail elders, are often ill equipped to handlethe unique needs of older adults with SMI because of the lack of psychiatrictraining for most nursing home staff (Molinari et al., in press).
Although there is a dearth of literature addressing the experiences,needs, and challenges associated with caring for older adults with SMI,studies have documented the typical family caregiving experiences of
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from
persons with SMI (Biegel & Schulz, 1999). One study reported thatspouses of patients with mental illness were at high risk for developing adepressive disorder (Wittmund, Wilms, Mory, & Angermeyer, 2002). Anotherstudy found that parents of outpatients with schizophrenia were significantlyless satisfied with their overall quality of life compared to a randomlyselected reference group (Foldemo, Gullberg, Ek, & Bogren, 2005). In addi-tion, caregivers’ physical health problems can be exacerbated by the stressof caregiving (Lefley, 1996). Given the taxing nature of caregiving, as evi-denced by these studies, it may be difficult for caregivers to sustain care asloved ones with SMI age. Therefore, examining caregivers’ future planningis an important topic of investigation.
Aging Parental Caregivers of Persons With SMI
Insights into the experiences and future planning of caregivers for olderadults with SMI may be found by an examination of the research literaturetargeting older caregivers of persons with SMI. Although these terms aresometimes used interchangeably, they pose different research questions;older adults with SMI are frequently supported by younger caregivers, andolder caregivers care for people of a variety of ages, not just older adults.Some research has found that caregiving brings gratification and well-beingto aging parents (Bulger, Wandersman, & Goldman, 1993; Webb et al.,1998), but results are mixed as to whether caregiving improves or becomesmore distressing as caregivers age.
Cross-sectional studies have documented feelings of burden and care-giver anxiety about planning for the future of relatives with mental illness(Cohler, Pickett, & Cook, 1991; Cook et al., 1997; Cook, Lefley, Pickett, &Cohler, 1994; Doornbos, 1997; Hatfield & Lefley, 2000; Lefley & Hatfield,1999; Rose, Mallinson, & Gerson, 2006). Cook et al. (1994) reported thatolder parents were troubled by feelings of ongoing responsibility in areasof finance, shelter, and ultimate obligation for the well-being of adultchildren, whereas younger parents were distressed by feeling more out ofcontrol or unable to manage their offspring’s behavior. In addition, onestudy reported that only 18% of older caregivers (n = 210) had completedplans for the future care of their relatives with psychiatric disabilities, cit-ing barriers including intense anxiety and lack of knowledge about how toplan, relative’s resistance to making changes, and limited appropriate hous-ing in the service system (Hatfield & Lefley, 2000). Results from a mixedmethods study of caregivers of persons with mental illness suggested thatthe greatest extent of burden for most families was worry about the future
468 Journal of Applied Gerontology
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

(Rose et al., 2006). Specifically, aging parents worried about who wouldassume their caregiving role and how the patient would manage withouttheir financial and emotional support. In another study, caregivers of youngadults with mental illness, the majority of whom were parents, were con-cerned about the future of their child after their death and who would takeon the responsibility of caring (Doornbos, 1997).
As individuals with SMI grow older within the community, dependence onan aging parent can have serious consequences if the parent dies, includinghousing disruptions and potentially traumatic transitions to other care envi-ronments (Lefley & Hatfield, 1999). Loss of a parental caregiver may“evoke an intense emotional reaction that, without proper support, may leadto decompensation and rehospitalization” (Hatfield & Lefley, 2005, p. 336).Because mothers are usually responsible for maintaining support networks,siblings often have less contact with their brothers and sisters with SMIafter their mother is deceased (Beeler, Rosenthal, & Cohler, 1999). Manysiblings anticipate becoming involved in the future care of their brothersand sisters with mental illness, but they are more likely to provide socialand emotional support than more intensive forms of instrumental support(e.g., housing, monitoring medication, or helping with household chores;Hatfield & Lefley, 2005). If siblings are unable to oversee care in the com-munity, more assistance may be required from community resources.
Comparative studies of aging mothers of adult children with mental illnessand mental retardation, both of whom face lifelong caregiving responsibil-ities, also provide insights into the unique aspects of caregiving for personswith SMI. In one study, mothers of children with SMI were more likely touse emotion-focused coping strategies than were mothers of children withmental retardation, which predicted greater maternal depression (Seltzer,Greenberg, & Krauss, 1995) and, in another study, led to declining levels ofwell-being (Kim, Greenberg, Seltzer, & Krauss, 2003). In addition, mothersof persons with SMI feel more burdened, are more likely to report depressivesymptoms, feel more pessimism about their child’s future, and report smallersupport networks than caregivers of persons with mental retardation (Greenberg,Seltzer, Krauss, & Kim, 1997). These studies have suggested that caregivingfor persons with psychiatric disabilities may in some ways be more trou-bling than caring for persons with mental disabilities. Therefore, althoughboth groups are composed of aging caregivers, something other than beingan “aging caregiver” is responsible for differences in caregiving experi-ences. The care recipient’s psychopathology appears to be an important com-ponent of the equation when looking at how caregiving changes over time.
Corsentino et al. / Family Caregivers’ Future Planning 469
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from
Impact of Aging in Older Adults With SMI
It is reasonable to expect variations in the demands made on caregiversover time because persons with mental illness often have poorer health thando others in their age group (Hatfield & Lefley, 2000). Health, education, andlifestyle choices may make patients with schizophrenia more vulnerable torisk factors that exacerbate these physical changes (Harvey, 2005). Long-term psychiatric patients are less likely to perform self-care or health promo-tion activities compared to nonpsychiatric populations and are at risk forpremature morbidity and mortality primarily because of overeating andsmoking (Holmberg & Kane, 1999). Given the increases in the health-relatedneeds of older persons with SMI, it is not certain “whether patient’s networkscan provide adequate material assistance, a problem that can worsen asmembers of their social networks also grow old” (Cohen, 2003, p. 157).
On the other hand, the burnout theory states that as persons with schiz-ophrenia age, the severity of their psychotic symptoms, such as hallucina-tions and delusions, are reduced. The florid positive symptoms are replacedby negative symptoms, including reductions in cognitive activity, motoractivity, and social motivation (Harvey, 2005). This theory suggests that ifthe severity of symptoms lessens overtime, the strains of family caregivingdecrease as loved ones with SMI age (Cohler et al., 1991). However, morerecent data have suggested that there is considerable heterogeneity in symp-toms, course, and outcomes with age, that there is still substantial sympto-matology in late life, and that negative symptoms do not necessarilyincrease with age (Harvey, 2005). Therefore, it appears that the strain inproviding care as persons with SMI age may not in fact decline and may, insome areas of care, increase. Planning for these changes may be critical forcaregivers to sustain support over the long term.
Value of Caregiver Support
Caring for adults with SMI is an intensive activity. According to onecontent analysis, care consists of five major processes: monitoring, manag-ing the illness, maintaining the home, supporting and encouraging, andsocializing. Yet despite the many hats caregivers are expected to wear, care-givers report deficiencies in services explicitly designed to assist caregivers(Doornbos, 2002), a problem that may be exacerbated as loved ones ageand new challenges are inevitably confronted. There are 44.4 millionpeople in the United States who serve as unpaid caregivers to adult familymembers or friends with various disabilities, contributing up to $275 billion
470 Journal of Applied Gerontology
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Corsentino et al. / Family Caregivers’ Future Planning 471
each year in services (National Alliance for Caregiving and AARP, 2004).Without their support, the government, health care institutions, and agen-cies would be responsible for assuming the economic burden associatedwith providing this care. Given the intensity and duration of support care-givers of persons with SMI are expected to provide, addressing the uniquechallenges and responsibilities that these caregivers must face as loved onesage is crucial in meeting their needs for services over the long term.
Family is, after all, an important component of the lives of persons withSMI, particularly as they age. Contrary to previously held assumptions,older outpatients with schizophrenia within the community are not estrangedfrom families, and their social networks predominantly consist of kin(Cohen & Kochanowicz, 1989; Meeks & Hammond, 2001; Semple et al.,1997). Because relatively few older patients with SMI, particularly schizo-phrenia, ever marry or have children (Semple et al., 1997), it is difficult formany older adults with SMI to continue to reside in the community whenthey sustain age-associated impairments or are left without the assistance oftheir unpaid caregivers; many must relocate to formal care settings such asnursing homes. It has been suggested that individuals in formal care set-tings may be at a higher risk for having decreased family contact as theyage (Beeler et al., 1999). Furthermore, nursing homes may not be the ideallocation for adults with SMI because the “striking absence of mental healthprofessionals . . . suggests that they are, at best, ill equipped” to meet theneeds of older adults with SMI (Meeks et al., 1990, p. 163). These issuesmust be examined so that caregivers can receive the proper support and per-haps forestall placement of their relatives into an institutional setting.
The purpose of the present study was to examine the experiences of infor-mal caregivers of persons with SMI, focusing on caregivers’ perceptions ofchallenges encountered as relatives with SMI age, primarily using qualitativemethods. Planning for the future needs of care recipients with SMI wasemphasized because, as noted previously, few older caregivers have completedplans for the future care of relatives with psychiatric disabilities (Beeleret al., 1999).
Method
Participants
Participants consisted of family caregivers of persons with SMI who wererecruited through a brief announcement in the winter 2007 issue of The
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

472 Journal of Applied Gerontology
Advocate, a newsletter sent quarterly to 60,000 members of the NationalAlliance on Mental Illness (NAMI). NAMI is the nation’s largest grassrootsmental health organization “dedicated to improving the lives of persons livingwith serious mental illness and their families” through promoting advocacy,research, support, and education (NAMI, 2005). Members of NAMI whoreceived the newsletter included consumers diagnosed with SMI, familymembers of persons with SMI, professionals or providers, and friends of per-sons with SMI. However, participation was restricted to family caregivers.They were asked to participate in a brief, 15-minute online survey about theircaregiving experiences and how they perceived it had changed or wouldchange over time. The advertisement contained a link to an online surveyavailable at www.surveymonkey.com, and, to increase response rates, contactinformation was also provided for participants who preferred to receive apaper copy of the survey in the mail. A university-based institutional reviewboard approved these recruitment techniques. Participants did not receivecompensation for their participation.
Measures
The survey instrument was developed by the primary author (E.C.) andwas reviewed by a licensed psychologist (V.M.). Participants were asked toprovide demographic information about themselves and the care recipient.In addition, one item was used to assess how stressful care was in the past3 months, where 1 = very stressful and 4 = not stressful at all. Caregiverswere also asked about what they considered the most stressful part of care-giving from a list of options such as communication difficulties, medicationmanagement, financial responsibilities of care, future planning, and carerecipient’s behavioral problems. For another item, they indicated their cur-rent stage of residential planning for the future residence of their loved onein the event that they were no longer able to provide care, with the options“No discussions have occurred yet,” “Some discussions have occurred, butthey were not serious,” “Serious discussions have occurred,” “Some planshave been made, but they are not definite,” and “Definite plans are made.”This item was adapted from a study assessing the predictors of the stage ofresidential planning among aging families of adults with SMI (Smith,2004), which originated in research concerning older mothers of adultswith mental retardation (Smith, Tobin, & Fullmer, 1995). Caregivers werealso asked where they would least and most prefer their loved one to live inthe event they could no longer provide care.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Corsentino et al. / Family Caregivers’ Future Planning 473
Caregivers of persons 55 and older and caregivers of persons youngerthan 55 then received similar sets of questions regarding their caregivingexperiences. Caregivers of persons 55 and older were asked to rate “Howhas caregiving changed as your loved one has aged?” whereas caregivers ofpersons younger than 55 were asked to rate “How do you envision caregivingto change when your loved one is 55 or older?” on a 5-point Likert-type scaleof 1 (a lot easier), 3 (about the same), and 5 (a lot harder).
Caregivers of persons 55 and older were given two open-ended questionsregarding what became easier and what became more difficult as their lovedone with SMI aged. Caregivers of persons younger than 55 were asked similaropen-ended questions regarding what they foresaw would become easier or moredifficult as their loved one aged. Participants provided written or typedresponses to these questions.
Analyses
Statistical software, SPSS for Windows Version 14.0, was used to computefrequencies and descriptive statistics. The qualitative responses wereentered into the ATLAS.ti Version 5.0 program, where the process of devel-oping preliminary themes was facilitated by use of the software. Tworesearchers independently developed preliminary sets of codes then subse-quently met to determine the extent to which their codes and interpretationswere in agreement and to reach a consensus on the themes represented inthe caregivers’ responses. The individual responses and preliminary themeswere also shared with other members of the research team to evaluatewhether the themes appropriately reflected the corresponding responses.The analytic techniques were similar to those used in prior research pub-lished in a peer-reviewed journal (Doornbos, 1997).
Results
Of the 56 online survey respondents, five had incomplete data and wereexcluded from the data analyses, leaving 51 respondents. A total of 41 hardcopies of the survey were requested, and 24 were returned completed.Overall, a total of 75 responses were analyzed, 59 for caregivers foryounger adults with SMI and 16 for caregivers for older adults with SMI.
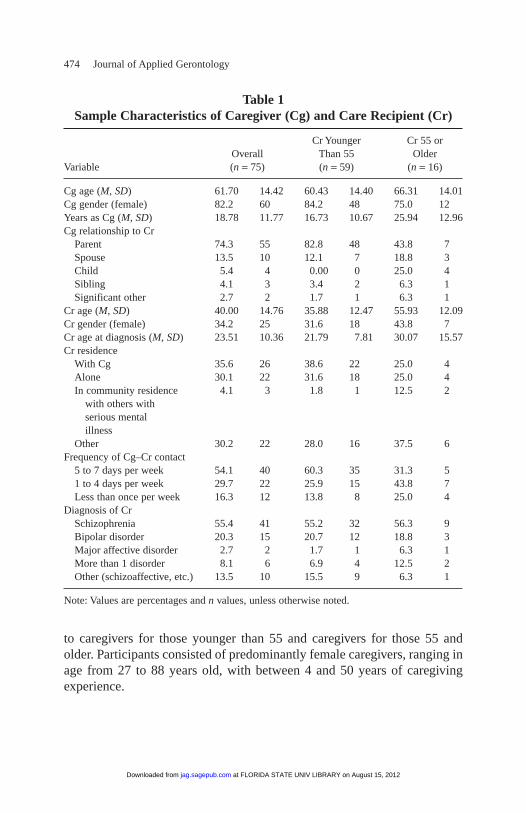
Table 1 describes the demographic information for both the caregiversand care recipients. It displays the overall findings and the findings specific
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from
474 Journal of Applied Gerontology
to caregivers for those younger than 55 and caregivers for those 55 andolder. Participants consisted of predominantly female caregivers, ranging inage from 27 to 88 years old, with between 4 and 50 years of caregivingexperience.
Table 1Sample Characteristics of Caregiver (Cg) and Care Recipient (Cr)
Cr Younger Cr 55 or Overall Than 55 Older
Variable (n = 75) (n = 59) (n = 16)
Cg age (M, SD) 61.70 14.42 60.43 14.40 66.31 14.01Cg gender (female) 82.2 60 84.2 48 75.0 12Years as Cg (M, SD) 18.78 11.77 16.73 10.67 25.94 12.96Cg relationship to Cr
Parent 74.3 55 82.8 48 43.8 7Spouse 13.5 10 12.1 7 18.8 3Child 5.4 4 0.00 0 25.0 4Sibling 4.1 3 3.4 2 6.3 1Significant other 2.7 2 1.7 1 6.3 1
Cr age (M, SD) 40.00 14.76 35.88 12.47 55.93 12.09Cr gender (female) 34.2 25 31.6 18 43.8 7Cr age at diagnosis (M, SD) 23.51 10.36 21.79 7.81 30.07 15.57Cr residence
With Cg 35.6 26 38.6 22 25.0 4Alone 30.1 22 31.6 18 25.0 4In community residence 4.1 3 1.8 1 12.5 2
with others withserious mentalillness
Other 30.2 22 28.0 16 37.5 6Frequency of Cg–Cr contact
5 to 7 days per week 54.1 40 60.3 35 31.3 51 to 4 days per week 29.7 22 25.9 15 43.8 7Less than once per week 16.3 12 13.8 8 25.0 4
Diagnosis of CrSchizophrenia 55.4 41 55.2 32 56.3 9Bipolar disorder 20.3 15 20.7 12 18.8 3Major affective disorder 2.7 2 1.7 1 6.3 1More than 1 disorder 8.1 6 6.9 4 12.5 2Other (schizoaffective, etc.) 13.5 10 15.5 9 6.3 1
Note: Values are percentages and n values, unless otherwise noted.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from
Corsentino et al. / Family Caregivers’ Future Planning 475
Quantitative Responses
Results from the quantitative responses provided by caregivers are pre-sented in Table 2. When asked how stressful care was in the past 3 months,69.5% of caregivers considered caregiving to be “somewhat stressful” or“very stressful.” The most frequent reasons for this stress were communi-cation difficulties (22.5%), their loved one’s behavioral problems (18.3%),and planning for the future (16.9%).
Furthermore, when asked to indicate their current stage of planning forthe future residence of their loved one in the event that they were no longerable to provide care, 62.0% of caregivers indicated that they had made noplans, and few (13.9%) had made definitive plans. In addition, 25.0% ofcaregivers had no plans for the future and had never discussed planningwith others.
Caregivers would most prefer loved ones to live with another familymember (31.9%), a community residence with others with SMI (26.4%), oralone (23.6%) if they could no longer provide care. They would least preferthem to live in an institutional setting (33.8%), alone (28.2%), or in a nursinghome or assisted living facility (15.5%). Nearly equal percentages preferredthat their relative live alone as those who did not prefer this option.
Responses among caregivers for persons younger than 55 were mixedregarding their perceptions of how caregiving would change as loved onesaged. Some thought that their experience would be about the same as theirloved ones aged (39.3%), whereas others believed that it would become moredifficult (39.3%), and still others believed it would become easier (21.5%).Among caregivers of persons older than 55, the majority (75.0%) thoughtcaregiving had become more difficult as their loved one aged. Others (18.8%)thought caregiving was about the same as their loved one aged, and only onecaregiver (6.3%) thought caregiving had become easier over time.
Qualitative Responses: Caregiver Concerns
Overall, responses from caregivers of older and younger adults with SMIwere extremely similar and were therefore collapsed within the same themestructure. Their concerns regarding caregiving for aging loved ones withSMI were organized into four major themes: (a) the care recipient’s healthwould continue to deteriorate over time, making caregiving more difficult,(b) the caregiver’s own health and ability to sustain support would be com-promised, (c) the care recipient would be at risk for diminished social sup-port with age, and (d) the financial burden of caregiving over time wouldtake a toll (see Table 3).
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

476 Journal of Applied Gerontology
Age-related changes of care recipients. Qualitative responses indicatedthat one of the major concerns expressed by caregivers of younger andolder adults with SMI was that the declining physical health of their loved
Table 2Caregiver Responses
Stress from caregiving in past 3 months (n = 72)Very stressful 41.7Somewhat stressful 27.8A little stressful 22.2Not stressful at all 8.3
Most stressful part of caregiving (n = 71)Communicating with care recipient 22.5Behavior problems 18.3Planning for the future 16.9Psychotic thinking 9.9Other 32.4
Level of planning for the future (n = 72)No discussions or plans 25.0Discussions, no plans 37.5Some plans 23.6Definite plans 13.9
Where caregivers would most prefer loved one to live if they couldno longer provide care (n = 72)With another family member 31.9Community residence with other with serious mental illness 26.4Alone 23.6Other 18.1
Where caregivers would least prefer loved one to live if they could nolonger provide care (n = 71)Institutional setting 33.8Alone 28.2Nursing home, ALF 15.5Other 22.5
How caregivers of persons younger than 55 perceived caregiving wouldchange as loved ones with serious mental illness age (n = 56)
Harder 39.3About the same 39.3Easier 21.5
How caregivers of persons 55 and older believed caregiving hadchanged as loved ones with serious mental illness had aged (n = 16)
Harder 75.0About the same 18.8Easier 6.3
Note: ALF = assisted living facility. Values are percentages.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Corsentino et al. / Family Caregivers’ Future Planning 477
ones with age would pose new obstacles. Responses were provided by 64caregivers of persons younger than 55 and 10 caregivers of persons 55 andolder. According to 26.6% of caregivers of persons with SMI, the physicalaging and health-related changes of their loved ones with SMI had made orwould likely make caregiving more burdensome. Caregivers pointed out thatphysical and medical issues may occur because of aging and genetics but thatthis would be “doubly hard” for a person with mental illness. For instance,side effects could occur from interactions with antipsychotic medications andmedications for physical conditions. One caregiver, whose son had not yetreached 55, was already concerned about his poor physical health:
[The care recipient’s] physical condition is now causing some problems. He’soverweight, he’s losing his teeth. He won’t listen to good advice. He smokesconstantly and doesn’t exercise. His father died at age 56 of severe heart dis-ease. No wonder I worry.
Another caregiver reiterated, “[Our 48-year-old son] . . . will require morerather than less assistance [over time] because of the likelihood of graduallyfailing health as he ages.” This was confirmed by caregivers of older adultswith SMI. One caregiver stated that “everything” had become more difficultas their loved one had aged, including “dealing with her moods, her behaviour,her finances, her health, her reasoning, her forgetfulness and aging, herinability to cope with anything.” Another caregiver explained that dealingwith medical problems, surgeries, and appointments was an aspect of care-giving that had become increasingly difficult.
Caregiver health or ability to sustain care. Many caregivers (25%) fore-saw their own health declining in the future and wondered who would carefor their loved ones as their deteriorating health or even death prevented
Table 3Qualitative Results: Caregiver Concerns
Concern Percentage of Caregivers
Care recipient’s health over time 26.6Caregiver’s health over time 25.0Diminished social support for care recipient over time 14.1Increased financial burden over time 12.5
Note: n = 64.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

them from providing care. The most difficult aspect of care over time,according to one respondent, would be “planning for the future, after I amgone. His sister . . . would help if she’d be consulted.” It is uncertainfrom this statement whether his sister had yet been approached aboutassuming this additional responsibility. Another caregiver felt a “deepgrief” about the loved one with SMI being alone. This collective sentimentwas summed up by a caregiver who stated, “I will be too old—or dead—toadequately meet [the care recipient’s] needs.”
Diminishing social support. Caregivers (14.1%) feared that their lovedones would have diminished social support as they age. For instance, onerespondent felt that “the ability to work or continue hobbies . . . havebeen essential to his wellness. Fewer friends, neighbors who have under-stood, accepted and helped him [will] be around, resulting in extreme lone-liness.” Members of the care recipients’ social networks, includingcaregivers, may be less able to provide interaction as they also age or passaway, and hence social contact may be more difficult to obtain.
Financial responsibility. The continued financial responsibility of care-giving troubled respondents (12.5%). One caregiver worried about havingto assume “supplemental work to help out . . . and still trying to makeends meet as far as paying for medicines, food, rent, utilities as prices con-tinue to increase.” Lack of financial stability would be a “serious hardship”;another caregiver worried that he may never be able to retire.
Qualitative Responses: Improvement in Care in the Future
Qualitative responses were obtained from caregivers of older adults withSMI regarding what aspects of caregiving had improved with age. Nearlyhalf of these caregivers (42.9%) responded that nothing had improved astheir loved ones aged. Others (28.6%) stated that age and frailty had slowedtheir loved ones down physically, therefore alleviating some of the burdenof caregiving (see Table 4).
Among caregivers of younger adults with SMI, four distinct themes inresponses were observed: (a) that over time the care recipient wouldbecome better adjusted to the routine of his or her illness and hence becomemore accepting of its permanent position in his or her life, (b) that nothingwould improve over time, (c) that symptoms would diminish with age, and(d) that factors extrinsic to the caregiver or care recipient would produceimprovements in care (see Table 5).
478 Journal of Applied Gerontology
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Corsentino et al. / Family Caregivers’ Future Planning 479
Fifteen caregivers of younger adults with SMI (27.8%) believed thattheir loved ones would become more stable over time. They used wordssuch as care recipients’ “acceptance” of their illness, “settling down” overtime, and becoming accustomed to “routine” to express how the course of timewould make care easier and things more “stable.” One caregiver envisionedthat as her loved one aged and her acceptance of her illness increased, “hercompliance with treatment will also increase so that she will become morestable for longer periods of time.”
Some (18.5%) caregivers of younger adults with SMI envisioned that noth-ing would improve over time. Their responses were typically one word inlength, “nothing.” Other caregivers (11.1%) envisioned that caregiving wouldonly become easier if factors extrinsic to the caregiver or care recipient wouldproduce improvements in care. Specifically, care would improve if there wereadvances in medication or even a cure for SMI. As one caregiver explained,“Hopefully medications and assistance will improve with time, I pray for thethird generation of medication to be a cure. I envision a more comprehensive
Table 4Qualitative Results: Responses of Caregivers of Persons 55 and Olderto a Question: “What Has Improved as Your Loved One Has Aged?”
Perceptions of Area of Improvement Percentage of Caregivers
Nothing has improved as loved one has aged 42.9Frailty and age have slowed loved one down 28.6
Note: n = 7.
Table 5Qualitative Results: Responses of Caregivers of PersonsYounger Than 55 to a Question: “What Do You Envision
Will Improve as Your Loved One Ages?”
PercentagePerceptions of Areas for Potential Improvement of Caregivers
Adjustment to or acceptance of illness by care recipient over time 27.8Nothing would improve as loved one aged 18.5Factors extrinsic to caregiver or care recipient would improve caregiving 11.1Symptoms would diminish with age 7.4
Note: n = 52.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

480 Journal of Applied Gerontology
approach to mental illness.” Last, one caregiver stated, “I’m hoping for a curethat would make both of our lives easier. . . . If a cure isn’t coming soon myonly relief [from the burden of caregiving] will be my death.”
Some (7.4%) caregivers of younger adults with SMI believed that theirloved ones’ symptoms would decrease with age: “I read that as people withthis disease get older they get a little better” or “Literature says [the carerecipient’s] symptoms will be less as he ages, so I envision he will be hap-pier, less angry, less psychotic, and therefore I will have less stress and lesssleepless nights.”
Discussion
The purpose of the present study was to examine the experiences of infor-mal caregivers of persons with SMI, focusing on caregivers’ perceptions ofchallenges encountered as relatives with SMI age. This is an important areathat has not been adequately addressed in the research literature to date.Caregivers of persons with SMI are generally experiencing high levels ofstress. Although there was considerable heterogeneity in caregiver responses,overall, for both caregivers of younger and older adults with SMI, the contentof their concerns and fears was quite similar. One of the main concerns fortheir loved ones as they aged was that they would have increasing medicalproblems in addition to their psychiatric conditions. Another frequent issuecaregivers faced was their own physical health. In reading the caregivers’responses, one is struck by their urgent need for assistance and resources inthe foreseeable future, as they anticipate new, less understood obstacles tocome. For some caregivers, these open-ended questions may have beentheir first invitation to address their concerns for the future. These concernswere encapsulated in the response of a caregiver whose experience couldonly be described as horribly “stressful, demanding, debilitating, etc., etc. Ifear for the future, [the care recipient’s] as well as mine—I do not knowhow to get adequate help.”
As nearly three fourths of the respondents were parents, it is likely thatmost of them (a) have provided care over the course of many years, if notthe care recipient’s entire lifetime, (b) are simultaneously dealing with theirown aging, and (c) may be outlived by the care recipient. The oldest care-giver to complete the survey was 88 years old. It is an “on going caregivingexperience that I expect to have for the rest of my life,” one caregiver stated,“I do not feel bad about that. I wish for him that it was not so.”
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Another particularly striking finding was that many caregivers appearedunprepared for the future in the event that they were no longer able to providecare. As previously mentioned, most of the caregivers were aging parents,many of whom expressed concern over their loved one outliving them.Nonetheless, many caregivers had never planned for the future or had dis-cussions about it with others. Concern for the future care of their loved onesis consistent with previous literature regarding aging parents of persons withSMI (Cohler et al., 1991; Cook et al., 1994; Cook et al., 1997; Doornbos,1997; Hatfield & Lefley, 2000; Lefley & Hatfield, 1999; Rose et al., 2006).Although most caregivers reported that they would prefer their loved ones tolive with other family members in the event that they were unable to sustainsupport, they rarely reported open communication with these familymembers regarding these wishes. It is likely that the current needs of the carerecipient, which require immediate attention, take precedence over planningfor the future. With the rapid aging of our society, it is imminently necessaryto provide caregivers with information about how to plan for the future andto motivate and to provide opportunities for them to do so. Future researchshould examine how to increase discussions among caregivers and otherfamily members regarding planning for their relatives’ future needs.
Despite their merits, the results of this study should be interpreted withconsiderable caution. Because a convenience sample was used, the findingsmay not generalize to the entire population of caregivers for relatives withSMI. The response rate in general was quite low but could not be exactlydetermined because there is no record of the number of caregivers whoreceived and/or read the NAMI newsletter. In addition, only 16 of the respon-dents were caring for individuals 55 years of age and older, thus preventinguse of comparative statistical tests. One possible reason for the low responserate among caregivers for older adults with SMI is that, given that these care-givers are likely older adults themselves, they may not have access to or becomfortable using computers and may be hesitant to complete computer-based surveys. Those completing a hard copy of the survey appeared to bemuch older on average than those completing the survey online (72 vs. 56years old, respectively). Although we attempted to address this issue bymaking paper copies of the survey available, the “digital divide” may beimplicated in the low response rate among caregivers of older adults.
Furthermore, this study is limited because the caregivers receiving TheAdvocate and volunteering to participate in this study may be distinctly dif-ferent from those caregivers who received the newsletter and chose not toparticipate. In addition, all of the caregivers were members of NAMI, anadvocacy organization for those with SMI and their families. Caregivers
Corsentino et al. / Family Caregivers’ Future Planning 481
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

who do not belong to NAMI may attribute greater stigma to mental illnessor may have contrasting experiences from those reported here. In addition,the overwhelming majority of respondents were Caucasian, making it dif-ficult to determine whether results are applicable to minority caregivers.Caregiver stress was measured using only one item, and there are more in-depth, standardized ways of measuring family burden. Because this was across-sectional study, the experiences of caregivers for younger adults werecompared to the experiences of their older counterparts rather than trackingcaregivers over time. Future research may consider exploring how the expe-riences of caregivers change over time using a longitudinal design. Theresearch literature would benefit from a mixed-methods study employingwell-validated measures to observe changes in caregiving as persons withSMI age.
Another limitation is that the survey was an ad hoc survey developed forthe purposes of this particular study. Although the questions were informedby our literature review and therefore exhibit face validity, no data werecollected regarding its psychometric properties. The qualitative analysesprovide rich information about the respondents’ experiences but may bespecific to the current sample.
Although access to computer resources may have systematically affectedthe types of caregivers who participated in this study, efforts were made toensure that all caregivers who wanted to were able to participate. This wasachieved by offering to mail a hardcopy of the survey with a self-addressed,stamped envelope to the caregivers if they could not access the online version.
Additional research should explore ways to increase discussions withSMI family members about the future. Most caregivers would prefer theirloved ones to live with other family members in the event that they wereunable to sustain support, yet they infrequently have open communicationwith these family members regarding their wishes. Lack of planning for thefuture care needs of their loved ones may lead to emergency hospitalizationor the inappropriate placement of their loved one in a more restrictive envi-ronment when the caregiver is no longer able to provide care. As previouslystated, caregivers report deficiencies in services explicitly designed forcaregivers (Doornbos, 2002). If there were enhanced resources for care-givers to utilize during current crises, they might have more energy todevote to planning for the future.
Moreover, because caregiving is expected to last over the course of manyyears, professionals and practitioners should take an active role early on inhelping caregivers prepare for the future. The Planned Lifetime AssistanceNetwork (PLAN) is one organization available in some states through
482 Journal of Applied Gerontology
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

NAMI that is designed to provide future care planning services. Highlyrated outcomes associated with PLAN include reducing family stress, giv-ing parents peace of mind, enabling parents to concentrate on retirementneeds, and helping families to be better informed about mental health issues(Obloy & Hutcheson, 2002). More widespread availability and awarenessof services to assist in planning for the future and helping older consumerscope with life changes because of aging will be necessary, particularly withthe “graying of the deinstitutionalized population” (Lefley & Hatfield,1999, p. 374).
Research exploring the experiences of family caregivers as loved ones withSMI age is, as one caregiver stated, “critical.” In particular, consideration ofcaregiver planning for the future is timely, and this study should provide impe-tus for further work in this area. As our society ages, so too will the popula-tion of individuals with SMI and their family caregivers. Investigating theunique barriers to care for adults with SMI over the lifetime is essential forfamily members to receive the support they require and deserve at each stageof the caregiver process.
References
Beeler, J., Rosenthal, A., & Cohler, B. (1999). Patterns of family caregiving and support providedto older psychiatric patients in long-term care. Psychiatric Services, 50(9), 1222-1224.
Biegel, D. E., & Schulz, R. (1999). Caregiving and caregiver interventions in aging and mentalillness. Family Relations, 48, 345-354.
Bulger, M. W., Wandersman, A., & Goldman, C. R. (1993). Burdens and gratifications of caregiving:Appraisal of parental care of adults with schizophrenia. American Journal of Orthopsychiatry,63(2), 255-265.
Cohen, C. I. (2003). Social vicissitudes of schizophrenia in later life. In C. I. Cohen (Ed.),Schizophrenia into later life: Treatment, research, and policy (pp. 155-159). Arlington,VA: American Psychiatric Publishing.
Cohen, C. I., & Kochanowicz, N. (1989). Schizophrenia and social network patterns: A surveyof black inner-city outpatients. Community Mental Health Journal, 25(3), 197-207.
Cohler, B. J., Pickett, S. A., & Cook, J. A. (1991). The psychiatric patient grows older: Issuesin family care. In E. Light & B. D. Lebowitz (Eds.), The elderly with chronic mental illness(pp. 82-110). New York: Springer.
Cook, J. A., Cohler, B. J., Pickett, S. A., & Beeler, J. A. (1997). Life-course and severe mentalillness: Implications for caregiving within the family of later life. Family Relations, 46,427-436.
Cook, J. A., Lefley, H. P., Pickett, S. A., & Cohler, B. J. (1994). Age and family burden amongparents of offspring with severe mental illness. American Journal of Orthopsychiatry,64(3), 435-447.
Doornbos, M. M. (1997). The problems and coping methods of caregivers of young adultswith mental illness. Journal of Psychosocial Nursing, 35(9), 22-26.
Corsentino et al. / Family Caregivers’ Future Planning 483
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

484 Journal of Applied Gerontology
Doornbos, M. M. (2002). Family caregivers and the mental health system: Reality and dreams.Archives of Psychiatric Nursing, 14(1), 39-46.
Foldemo, A., Gullberg, M., Ek, A., & Bogren, L. (2005). Quality of life and burden in parentsof outpatients with schizophrenia. Social Psychiatry and Psychiatric Epidemiology, 40(2),133-138.
Greenberg, J. S., Seltzer, M. M., Krauss, M. W., & Kim, H. W. (1997). The differential effects ofsocial support on the well-being of aging mothers of adults with mental illness and mentalretardation. Family Relations, 46, 383-394.
Harvey, P. D. (2005). Schizophrenia in late life: Aging effects on symptoms and course of illness.Washington, DC: American Psychological Association.
Hatfield, A. B., & Lefley, H. P. (2000). Helping elderly caregivers plan for the future care ofa relative with mental illness. Psychiatric Rehabilitation Journal, 24(2), 103-107.
Hatfield, A. B., & Lefley, H. P. (2005). Future involvement of siblings in the lives of personswith mental illness. Community Mental Health Journal, 41(3), 327-338.
Holmberg, S. K., & Kane, C. (1999). Health and self-care practices of persons with schizo-phrenia. Psychiatric Services, 50(6), 827-829.
Kim, H. W., Greenberg, J. S., Seltzer, M. M., & Krauss, M. W. (2003). The role of coping inmaintaining the psychological well-being of mothers of adults with intellectual disabilityand mental illness. Journal of Intellectual Disability Research, 47(4), 313-327.
Lefley, H. P. (1996). Family caregiving in mental illness. Thousand Oaks, CA: Sage.Lefley, H. P., & Hatfield, A. B. (1999). Helping parental caregivers and mental health consumers
cope with parental aging and loss. Psychiatric Services, 50(3), 369-375.Meeks, S., Carstensen, L. L., Stafford, P. B., Brenner, L. L., Weathers, F., Welch, R., et al. (1990).
Mental health needs of the chronically mentally ill elderly. Psychology and Aging, 5(2), 163-171.Meeks, S., & Hammond, C. T. (2001). Social network characteristics among older outpatients
with long-term mental illness. Journal of Mental Health and Aging, 7(4), 445-464.Molinari, V., Merritt, S., Mills, W., Chiriboga, D., Conboy, A., Hyer, K., et al. (in press). Serious
mental illness in Florida nursing homes: Interviews with stakeholders. Gerontology andGeriatrics Education.
National Alliance for Caregiving and AARP. (2004). Caregiving in the U.S. Westport, CT:MetLife Mature Market Institute.
National Alliance on Mental Illness. (2005). About advocate. Retrieved November 12, 2006,from http://www.nami.org/ADVTemplate.cfm?Section=About_Advocate
Obloy, C., & Hutcheson, S. (2002). Planned Lifetime Assistance Network: A new servicesmodel with promising results. Psychiatric Rehabilitation Journal, 25(4), 409-412.
Rose, L. E. (1996). Families of psychiatric patients: A critical review and future researchdirections. Archives of Psychiatric Nursing, 10(2), 67-76.
Rose, L. E., Mallinson, R. K., & Gerson, L. D. (2006). Mastery, burden, and areas of concernamong family caregivers of mentally ill persons. Archives of Psychiatric Nursing, 20(1), 41-51.
Seltzer, M. M., Greenberg, J. S., & Krauss, M. W. (1995). A comparison of coping strategiesof aging mothers of adults with mental illness and mental retardation. Psychology andAging, 10(1), 64-75.
Semple, S. J., Patterson, T. L., Shaw, W. S., Grant, I., Moscona, S., Koch, W., et al. (1997). Thesocial networks of older schizophrenia patients. International Psychogeriatrics, 9(1), 81-94.
Smith, G. C. (2004). Predictors of the stage of residential planning among aging families ofadults with severe mental illness. Psychiatric Services, 55(7), 804-810.
Smith, G. C., Tobin, S. S., & Fullmer, E. M. (1995). Elderly mothers caring at home for offspringwith mental retardation: A model of permanency planning. American Journal of MentalRetardation, 99, 487-499.
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from

Tucker, C., Barker, A., & Gregoire, A. (1998). Living with schizophrenia: Caring for a person witha severe mental illness. Social Psychiatry and Psychiatric Epidemiology, 33(7), 305-309.
Webb, C., Pfeiffer, M., Mueser, K. T., Gladis, M., Mensch, E., DeGirolamo, J., et al. (1998).Burden and well-being of caregivers for the severely mentally ill: The role of coping styleand social support. Schizophrenia Research, 34(3), 169-180.
Wittmund, B., Wilms, H. U., Mory, C., & Angermeyer, M. C. (2002). Depressive disorders inspouses of mentally ill patients. Social Psychiatry and Psychiatric Epidemiology, 37(4),177-182.
Elizabeth A. Corsentino is a doctoral student in the Clinical Psychology Program at Florida StateUniversity and a recipient of a McKnight Doctoral Fellowship. Her research interests include thefuture planning behaviors of caregivers for older adults with serious mental illness and the genetic,psychological, and social factors that influence cognitive decline among the elderly.
Victor Molinari, PhD, ABPP (Clin), is a professor in the Department of Aging and Mentalhealth of the Florida Mental Health Institute at the University of South Florida. His majorresearch interests include mental health outcomes research in long-term care, serious mentalillness in older adults, reminiscence therapy, and personality disorder in older adults.
Amber M. Gum is an assistant professor in the Department of Aging and Mental Health atthe University of South Florida. Her research focuses on older adults’ utilization of behavioralhealth sciences and integration of brief psychosocial interventions for older adults into com-munity settings.
Lori A. Roscoe is an assistant professor in the Department of Communication at the Universityof South Florida and is also the associate director of the Center for Hospice, Palliative Care, andEnd-of-Life Studies at USF. Her research examines end-of-life decision making.
Whitney L. Mills is a PhD student in the School of Aging Studies at the University of SouthFlorida. Her research focuses on personality and various aspects of long-term care.
Corsentino et al. / Family Caregivers’ Future Planning 485
at FLORIDA STATE UNIV LIBRARY on August 15, 2012jag.sagepub.comDownloaded from




















