
A Qualitative Study On the Needs of Caregivers of Inpatients With Schizophrenia in India
15
E CAMDEN SCHIZOPH A QUALITATIVE STUDY ON THE NEEDS OF CAREGIVERS OF INPATIENTS WITH SCHIZOPHRENIA IN INDIA A. JAGANNATHAN, J. THIRTHALLI, A. HAMZA, V.R. HARIPRASAD, H.R. NAGENDRA & B.N. GANGADHAR ABSTRACT Aim: To explore the needs of caregivers of inpatients with schizophrenia in India. Material: Thirty caregivers of inpatients with schizophrenia participated in five focus group discussions (FGD), where the needs of the caregivers were discussed. The FGDs were recorded, transcribed and similar needs were grouped and ranked according to their order of importance. Discussion: The main needs that emerged were regarding: managing the behaviour of patients; managing social-vocational problems of patients; health issues of caregivers; education about schizophrenia; rehabilitation; and managing sexual and marital problems of patients. Conclusion: This study has identified additional needs of caregivers from those found in other studies. Key words: needs, caregivers, schizophrenia, focus group discussion, qualitative analysis INTRODUCTION The importance of the role of family caregivers in the treatment of a person with mental illness cannot be overemphasized. Family caregivers provide considerable support to their ill relatives even while they experience significant burden (Leff, 1994). In a survey conducted by Consumer Health Sciences (CHS) and the National Mental Health Association (NMHA), one third of the 1,328 family caregivers surveyed said that the emotional and behavioural symptoms of the illness caused them extreme hardship and was a constant source of anxiety (Consumer Health Sciences, 2008). Caregivers who are in ‘high contact’ with the patient in their daily life often face the highest burden (Winefield & Harvey, 1994). Family coping strategies accounted for a substantial proportion of the variance observed in objective and subjective burden respectively among caregivers of persons with schizophrenia (Magliano et al., 1998). This highlights the fact that studying the needs of family caregivers of patients with severe mental disorders is important from a public health perspective. In India, the majority of the people with schizophrenia stay with their families (Thara et al., 1998; Murthy, 2006). There have been no systematic scientific Indian studies to assess the needs of caregivers; however, several different opinions have been expressed. Some of the needs opined are the need for awareness about the nature and outcome of mental illnesses in the community, International Journal of Social Psychiatry. © The Author(s), 2011. Reprints and permissions: http://www.sagepub.co.uk/journalsPermissions.navVol 57(2): 180–194 DOI: 10.1177/0020764009347334
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of A Qualitative Study On the Needs of Caregivers of Inpatients With Schizophrenia in India

180 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)E CAMDEN SCHIZOPH
AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERSOFINPATIENTSWITHSCHIZOPHRENIAININDIA
A.JAGANNATHAN,J.THIRTHALLI,A.HAMZA,V.R.HARIPRASAD, H.R.NAGENDRA&B.N.GANGADHAR
ABSTRACT
Aim: To explore the needs of caregivers of inpatients with schizophrenia in India.Material: Thirty caregivers of inpatients with schizophrenia participated in five focus group discussions (FGD), where the needs of the caregivers were discussed. The FGDs were recorded, transcribed and similar needs were grouped and ranked according to their order of importance. Discussion: The main needs that emerged were regarding: managing the behaviour of patients; managing social-vocational problems of patients; health issues of caregivers; education about schizophrenia; rehabilitation; and managing sexual and marital problems of patients. Conclusion: This study has identified additional needs of caregivers from those found in other studies.
Key words: needs, caregivers, schizophrenia, focus group discussion, qualitative analysis
INTRODUCTION
Theimportanceoftheroleoffamilycaregiversinthetreatmentofapersonwithmentalillnesscannotbeoveremphasized.Familycaregiversprovideconsiderablesupport totheir illrelativesevenwhiletheyexperiencesignificantburden(Leff,1994).InasurveyconductedbyConsumerHealthSciences(CHS)andtheNationalMentalHealthAssociation(NMHA),onethirdofthe1,328familycaregiverssurveyedsaidthattheemotionalandbehaviouralsymptomsoftheillnesscausedthemextremehardshipandwasaconstantsourceofanxiety(ConsumerHealthSciences,2008).Caregiverswhoarein‘highcontact’withthepatientintheirdailylifeoftenfacethehighestburden(Winefield&Harvey,1994).Familycopingstrategiesaccountedforasubstantialproportionofthevarianceobservedinobjectiveandsubjectiveburdenrespectivelyamongcaregiversofpersonswithschizophrenia(Maglianoet al.,1998).Thishighlightsthefactthatstudyingtheneedsoffamilycaregiversofpatientswithseverementaldisordersisimportantfromapublichealthperspective.
InIndia,themajorityofthepeoplewithschizophreniastaywiththeirfamilies(Tharaet al.,1998;Murthy,2006).TherehavebeennosystematicscientificIndianstudiestoassesstheneedsofcaregivers;however,severaldifferentopinionshavebeenexpressed.Someoftheneedsopinedaretheneedforawarenessaboutthenatureandoutcomeofmentalillnessesinthecommunity,
InternationalJournalofSocialPsychiatry.©TheAuthor(s),2011.Reprintsandpermissions:http://www.sagepub.co.uk/journalsPermissions.navVol57(2):180–194DOI:10.1177/0020764009347334
JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 181
theneedforprimarypsychiatricandotherprofessionaltreatment,andpsychosocialrehabilitation(Goswami,2006;Janardhan,2006).Caregiversofinpatientsreportexperiencingasignificantlyhigherburdenthancaregiversofoutpatients.Unmetneedsofthepatientshavealsobeenfoundtobesignificantlyrelatedtocaregiverburden(Clearyet al.,2005).Meetingtheseneedswouldhelptoenhancetheleveloffunctioningofthepatient(Solomon&Draine,1994)andtodecreasetheemotionalproblemsoffamilymembers(Johnson,1994).
Familymembersofapatientwithchronicschizophreniahavemultipleneeds.Themajorcon-cernsandsupportneedsofindividualswhoassumethisstressfulroleincludeobtainingsupport,reducingriskstotheirownwell-being,andpromotingthewell-beingofthementallyill(Chafetz&Barnes,1989).Theyoftenexpresstheneedformoresupportandcomplainofnothavingenoughopportunities to relieve the burden imposed on them (Angermeyer et al., 2000). Educationalneedsincludegaininginformationaboutearlywarningsignsoftheillnessandrelapse,theeffectsofmedicationandwaysofcopingwiththepatient’sbizarreandassaultivebehaviour(Chien&Norman,2003).Oftenfamilymemberslivingwithillpersonsarelessawareofthepsychiatricnatureoftheillness(Padmavathiet al.,1998).Thusitisnecessarytounderstandtheneedsoffamiliesofpersonswithmentalillnessandtodevelopspecificinterventionstomeettheminordertohelpreducecaregiverburden(Clearyet al.,2006;Murthy,2006).
ThepresentstudywasconductedinordertoassesstheneedsofthecaregiversofschizophrenicpatientsinIndia.Indiaspendsamere0.83%ofitstotalhealthbudgetonmentalhealthcomparedtoEnglandandWaleswhichspends13.8%(WHO,2001);thus,theextenttowhichtheneedsofcaregiverswillbemetinIndiaislikelytobedifferent.Furthermore,giventhedifferencesinthesocio-culturalmilieu,theresultsofthestudiesdoneinotherculturesmaynotberelevantinanIndiancontext.
Further, studiesusing scales to assess caregiverneedshave the limitationof forcing the re-spondentstoanswerfromalist.Forinstance,studieseitherfocusonspecificneedssuchasedu-cationalneeds(Chien&Norman,2003)orongroupsofneedssuchascounsellingandsupportservices,educationandfinancialentitlements(Wancataet al.,2006;Barrowcloughet al.,1998).Weusedaqualitativeapproachtoassesstheneedsofcaregiversforseveralreasons:(a)thisapproachisusefulintappingabroaderrangeofneedsthatarespecifictothecontextinwhichitisused;(b)studyingtheneedsofcaregiversinvolvesprobingofsensitive,emotionalandpersonalthemesofneeds,whichismoresuitedtoaqualitativeapproach(Hidayet al.,2002;Padget,1998);and(c) qualitative studies are especially helpful when one intends to generate impressions and todevelopassessmentscales,programmesorservices(Stewartet al.,2007).
METHOD
SampleThe participants were 30 caregivers of inpatients with schizophrenia at the National InstituteofMentalHealthandNeuroSciences(NIMHANS)inBangalore,India–atertiarycarecentre.NIMHANShasa900-bedteachinghospitalwithtrainingandresearchfacilitiesinpsychiatryandotherneurosciences.InApril2008,caregiversofallinpatientswithschizophreniawerescreened.Intotal,59patientswithadiagnosisofschizophreniawereadmittedtothehospitalduringthisperiod.CaregiversofpatientswithadiagnosisofschizophreniawereincludedinthestudyiftheyweretocontinuetoprovidecareforthemfollowingdischargeandiftheyspokeKannada,Tamil,EnglishorHindi.Caregiverswithpsychiatricorneurologicaldisordersandthosecaringforanother

182 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
relativewithpsychiatricillnesswereexcluded.Thirtyeightcaregiverswhofulfilledtheseinclusionandexclusioncriteriawereapproached.Of these38caregivers,30consented toparticipate inthestudy.Theseincludedfamiliesfromdifferentsocioeconomicbackgrounds,differentstatesofIndiaandfromdifferentcarerroles.The30caregivers thusrecruitedparticipatedinfivefocusgroupdiscussions(FGDs),withapproximatelysixcaregiversparticipatingineachoftheFGDs.ThesociodemographicdataofthecaregiverswhoparticipatedintheFGDsandaprofileoftheirillrelativeswerecompiled(Table1).
Focus group discussion Fromtherangeofqualitativeresearchmethodsavailable,theFGDmethodwasselected(vis-à-visindividualinterviews),asitislesstime-consuming,economicalandhasthebenefitsofgroupprocesses(Stewartet al.,2007).ThediscussionsfollowedtherecommendationsofStewartet al.(2007)–theyinvolvedsixtoeightindividualswhodiscussedtheresearchquestion‘Whataretheneedsoffamilycaregiversofinpatientswithschizophrenia?’forapproximately1.5–2.5hours.TheFGDwasconductedunderthedirectionofamoderator(AJ/HVR)whopromotedinteractionsandensuredthatthediscussionsremainedfocusedonthetopicofinterest.
ScriptA standardized script for conducting the FGD was developed on the basis of the aims of thestudy,literaturereviewanddiscussionwithfourexperiencedfocusgroupresearchers.Thescriptfollowedasemi-structuredformatusingopen-endedquestionsinaface-to-face‘conversational’styleratherthanaformalquestion/answerformat.(Thescriptisavailablefromtheauthorsonrequest.)Althoughthegroupdiscussionscriptwasflexibleinnature,somedirectionwasgivenwhenthefocuswaslostandprobeswereusedwhennecessary.Thescriptincludeddiscussionaboutthefeltneedsofthecaregiversincaringfortheirrelativewithschizophrenia,andthegroupingandrankingofsimilarneedsaccordingtotheirorderofimportance.
ProcedureThestudywasreviewedandapprovedbytheInstitute’sethicscommittee.Writteninformedconsentofthefamilycaregiverswasobtainedtoparticipateinthestudyandasociodemographicsheetelicitinginformationontheirage,occupation,monthlyincome,maritalstatus,patientvariablesandfamilyconstellationwascompleted.EachFGDwasvideo-recordedandwasfacilitatedbytheresearcher(psychiatricsocialworker)andaco-facilitator.Theresearcherfacilitatedthegroupprocessandtheco-facilitatorhelpedinrecordingtheobservationsofthegroupsession(audio/videoandbytakingdownnotes).
TheFGDinvolvedtheresearcheraskingthecaregiverstolisttheirneeds(Appendix),groupthelistofneedsintomainthemes,operationallydefinethethemesandranktheminorderofimportance.Asthemethodologyoffreelistingofneedswasused,alltheneedsexpressedbythecaregiverswerenoted.AcrossallfiveFGDs,theneedsofcaregiverswerefoundtobelargelycomparable.Thus,noneedsweredeletedfromthelistandallneedswereaccommodatedintoeitheroneofthecategories/themes.Incaseofdifferencesofopinionwithinthegroupaboutthegroupingandrankingofsimilarneeds,furtherdiscussionandcross-clarification(iteration)wasconductedamongthememberswhodifferedintheiropiniontillaconsensuswasreached.Ingroupswhereconsensuscouldnotbereached,thethemesweregivensimilarranking(e.g.inFGD-2,thethemesofhealthofcaregivers,rehabilitationoptionsandmanagingsocial/behaviouralproblemsofpatientsweregivensimilarranking).

JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 183
Tabl
e 1
Soci
odem
ogra
phic
dat
a of
car
egiv
ers
and
pati
ents
Car
egiv
ers
(n =
30)
Pat
ient
s (n
= 2
9)**
Var
iabl
en
(%)
mea
n (S
D)
Var
iabl
en
(%)
mea
n (S
D)
Var
iabl
en
(%)
mea
n (S
D)
Age
of t
he c
areg
iver
(ye
ars)
*
50.6
(13
.4)
Edu
cati
on
(yea
rs)*
10
.2(
6.4)
Age
of p
atie
nt (
year
s)*
31
(
8.7)
Gen
der
m
ale
fe
mal
e
13
(43.
3)
17
(56
.7)
Mar
ital
sta
tus
si
ngle
m
arri
ed
wid
owed
3
(10)
25
(8
3.3)
2
(6.7
)
Gen
der
m
ale
fe
mal
e
17
(58
.6)
12
(
41.4
)
Rel
igio
n
Hin
du
Chr
istia
n
27
(90
)
3(
10)
Fam
ily
type
nu
clea
rfa
mily
jo
intf
amily
23
(7
6.7)
7
(23
.3)
Edu
cati
on in
yea
rs*
11
.38
(4.
9)
Eco
nom
ic s
tatu
s
low
m
iddl
e
high
13
(
43.3
)
6(
20)
11
(
36.7
)
Rel
atio
nshi
p w
ith
the
pati
ent
pa
rent
si
blin
g
othe
rre
latio
ns
spou
se
21
(7
0)
4(
13.3
)
3(
10)
2
(6.
7)
Dur
atio
n of
the
illn
ess*
10
3.60
(59
.5)
Occ
upat
ion
un
empl
oyed
da
ily-w
age
labo
urer
pr
ofes
sion
al
hous
ewif
e
retir
ed
stud
ent
1
(3.
3)
8(
26.7
)
4(
13.3
)
8(
26.7
)
8(2
6.7)
1
(3.
3)
Com
orbi
d ph
ysic
al il
lnes
s
nil
di
abet
esm
ellit
us
hype
rten
sion
ot
hers
20
(6
6.7)
3
(10
)
4(
13.3
)
3(
10)
Type
of s
chiz
ophr
enia
pa
rano
id
hebe
phre
nic
ca
tato
nic
un
diff
eren
tiate
d
schi
zoaf
fect
ive
19
(6
5.5)
2
(6.9
)
1(3
.4)
5
(17.
2)
2(6
.9)
*Mea
n(S
D),
**
Two
care
give
rsr
epre
sent
edo
nep
atie
ntin
one
of
the
FGD
s.
184 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
Data analysis Thefirstlevelofdataanalysiswasdoneduringeachofthefocusgroupsessions.Theresearchermadealistofneedsduringthediscussion.Thegroup(caregivers)thendividedtheseneedsintothemesandsub-themesandrankedthemaccordingtotheirimportance.Followingthetechniqueofiteration,thegroupwentoverthesethemesandrankingsseveraltimesbeforefinalizingthem.IneachFGDthemostimportanttheme(basedongroupingandrankingatleveloneandtwoofdatamaking)wasgiventhehighestscore(equaltothenumberofthemeslisted)andtheleastimportantthemewasgiventheascoreof1.IftwoormorethemesweredeemedashavingequalimportanceduringtheFGD,thensuchthemesweregivensimilarscores.IfathemewasnotrepresentedinaparticularFGD,itwasgivenascoreof0inthatFGD.
EachFGDwastranscribedandfurtherdatamakingandanalysiswasconductedbytheresearcher(secondlevelofdatamaking).Basedonthefirstlevelofdatamaking,theresearcherreviewedthelistingofthemesandwherevertwoorthreethemesseemedtorepresentacommontheme,theyweregroupedunderanappropriatetheme.Thethemethusgeneratedwasgivenascorebyaveragingthescoresfromthefirstlevelofdatamaking.Forexample,inFGD-5,outofthesixthemesidentifiedbythecaregivers,themesof‘educationalneeds’(score=6)and‘informationonmanagementofsideeffectsofmedicines’(score=4)weregroupedbytheresearcherasonemainthemeof‘educationneeds’andgivenascoreof5.
Theresearcherthencheckedtheremainingtextforleftoverlistsofneedsandputthemunderthemostappropriatetheme.ThescoresforeachthemeacrossthefiveFGDsweretotalled.Thefinalrankingofthethemescorrespondedtothesetotals;thethemewithhighesttotalscorewasrankedasthemostimportantneed(Table2).
TheneedsundereachthemeacrossthefiveFGDswerelisted.Afinallistofthemesandneedsunder each theme was tabulated for analysis.As the sample size in each FGD was small, nocomputer-assistedsoftwarepackagewasusedforthedataanalysis.Computersoftwarewouldhavebeenappropriateif30individualinterviewshadbeenconductedinsteadofsixgroups.
Duringtheentirestudyperiod,theillrelativecontinuedtoreceivetheroutinetreatmentprescribedbythedoctorsatNIMHANS.ThetreatingdoctorswereconsultedandtheirapprovaltoconducttheFGDwasobtained.
RESULTS
ThemainneedsthatemergedfromtheanalysisoftheFGDsaredescribedinTable2.
I: Managing illness behaviourTheareasinwhichthecaregiversneededhelptomanagetheillnessbehaviouroftheirrelativewere:managingtheirnon-compliancewithmedication;uncooperativebehaviour;aggressiveanddemandingbehaviour;dealingwiththeirillnesssymptoms(hallucinations/delusions,wandering,insomnia, spending behaviour, reduced food intake); increased substance use; handling theirunpredictablebehaviour;lackofinterestinself-care;concentrationproblems;andlackofdailyroutine.Thefollowingquotesofthecaregiversdepicttheproblemstheyfacedinmanagingtheillnessbehaviouroftheirrelative.
‘Evenwhenthefamilymembersadviseorrequest,mybrothersays,“NoIamnotthepatient;youhaveaproblem,sowhyshouldItakethemedication?”’(MrS.M.(47years),FGD-2)
JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 185
‘Ifsomebodyvisitsus,andwearetalking,mydaughterfeelsasifwearetalkingabouther.Whatevertopicwetalkabout,shetellsthatwearetalkingabouther.NextwhenIgiveherfood,shesuspectsthatIhavemixedpoisonorfaecesinthefood.’(MrsJ.(36years),FGD-3)
‘Suddenlymydaughtergetsangry,veryangrytoanextentthatshedoesnotgetpacifieduntilandunlessshehurtssomeone,evenifitweremysonormyself.’(MrsJ.(36years),FGD-3)
‘Mydaughterdoesnotdoanything.Ihavetodoeverythingforher…fromcombingherhair,washingherclothes.Ihavetoscrubandbatheheralso.’(MrsJ.(36years),FGD-3)
II: Managing social-vocational problems Caregiversdiscussedvariousareaswheretheyneededprofessionalhelpinmanagingthesocial-vocational problems of their ill relative.These were: dealing with patient’s lack of interest insocialization/notgoingoutofthehouse;relationshipproblems;uninhibitedbehaviour;anddifficultyininitiatingandmaintainingactivities/job.Thefollowingquotesofthecaregiversthrowlightonthesocial-vocationalproblems.
‘Mysonisalwaysinthehome.Henevergoesout.Hedoesnotmixevenwithourrelativesorworkers…hefindsitdifficulttogetoutoftheroom.’(MrsB.M.(60years),FGD-2)
‘Mysoncomesoutofthebathroomattimeswithoutwearinghisclothes.Evenwhenwetellhim,hedoesnotlisten.Itbecomesverydifficultifthereareguestsathome.’(MrM.S.(45years),FGD-3)
‘Iwouldwantmysontogotoajob.Hehasforgottenaboutgoingforthejobcompletely.Hedoesnothaveamindtogoforajob.(MrM.R.(65years),FGD-4)
Mysonhaschangedsevencompanies.Innocompanyhehasworkedformorethantwotothreedays…Hegetsajobeasily.Fourappointmentsareinhand.Butafterjoining,hecannotmaintainthejob.’(MrR.(68years),FGD-4)
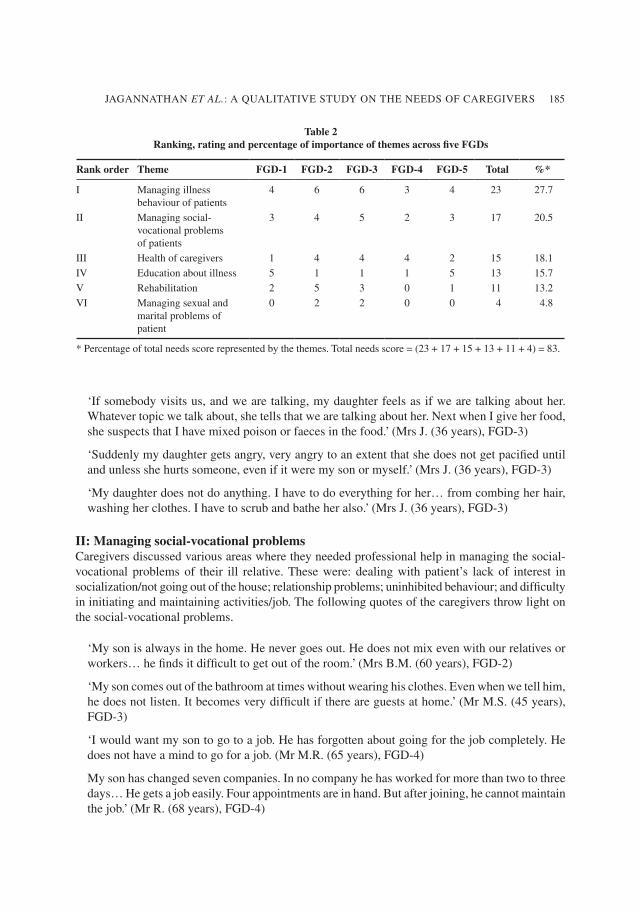
Table 2 Ranking, rating and percentage of importance of themes across five FGDs
Rank order Theme FGD-1 FGD-2 FGD-3 FGD-4 FGD-5 Total %*
I Managingillnessbehaviourofpatients
4 6 6 3 4 23 27.7
II Managingsocial-vocationalproblemsofpatients
3 4 5 2 3 17 20.5
III Healthofcaregivers 1 4 4 4 2 15 18.1
IV Educationaboutillness 5 1 1 1 5 13 15.7
V Rehabilitation 2 5 3 0 1 11 13.2
VI Managingsexualandmaritalproblemsofpatient
0 2 2 0 0 4 4.8
*Percentageoftotalneedsscorerepresentedbythethemes.Totalneedsscore=(23+17+15+13+11+4)=83.
186 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
III: Health needs of caregiversCaregivershadanumberofhealthneeds.Theyrequiredhelpin:managingtheiremotions(anger,depression, fear); handling their stress; taking decisions; dealing with lack of social support;reducedpersonallife;andbalancingworkandpatientcare.Thefollowingquotesofthecaregiversexemplifytheirhealthneeds.
‘Iamalwaysworriedaboutthepossibilityofsucheventshappeningathome[violentoutburstofthepatient].Sowecontinuouslysufferfromtensionandsadness.’(MrM.S.(45years),FGD-3)
‘Nofacility,noneighbours,norelativesorfriendscametohelpuswhenthepatientwasviolent.Wewerehelplessanddidnotknowwhattodo.[MrC.R.isoverwhelmedandstartscrying.]EvenifIcalledfortheambulanceatourplace,theydonotcome.Thuswestartgettingnegativefeelingslikeanger.Weneedtoknowhowtocontrolthesefeelings.’(MrC.R.(25years),FGD-2)
‘Forthepast10years[sincemybrother’sillnessstarted],theconceptofmypersonallifeiscompletelyzero.IamnowadjustedtothislifeandIstoppedmystudies.Inowtakecareofmybrotherfull-timeasmyparentsareaged.’(MrS.(33years),FGD-4)
IV: EducationEducationneedsofthecaregiversincluded:educationabouttheillness;informationonmedication/sideeffects/emergencymedicine(sedatives);informationonavailableconcessions/benefitsofferedbythegovernment;andinformationonhowtodealwithstigma.Thefollowingquotesdepictthecaregiverneedsforeducation.
‘Themedicineshavesomanysideeffects.Thedoctordoesnottellusthatthismedicinewillgivesideeffects.’(MrI.K.(60years),FGD-1)
‘Ineventof thepatientbecomingveryviolent andnot responding tous, if there is anypillwhichcanbegiventohimatthattimeandifhesleeps…[anothergroupmembercontinues]…one liquid…ifbyaddinga fewdrops in food,hewillbeok,wecan thenbringhim to thehospital.Butwedon’tknowwhattogiveandwhatnottogive[pill].Weneededucationonthat.’(MrS.M.(47years)andMrsB.M.(60years),FGD-2)
‘Forthepatientandcaregiversweshouldknowabouttheconcessionsavailablefromthegov-ernment.Forotherpeople[ofotherdisorders]theygetreimbursedfortheirtreatment.Wearenotgettinganymoneyfromanywhereandwehavetospendalotofmoney.’(MrsB.M.(60years),FGD-2)
‘Thereisalotofstigmaaboutthisillness…alotofmisconceptionsaboutmentallyillpatients.Theydonotunderstandwhattypeofillnessthisis,whatistheproblem.Soeducatingsocietyisimportant.’(MrC.R.(25years),FGD-2)
V: Rehabilitation
Allcaregiverscitedtheserehabilitationneeds:knowingaboutfinancialandrehabilitationoptions;localsupportgroupsandhelplineservices;office/workbenefitsforcaregivers;andlocalreferralsystems.Thefollowingquotesdepicttherehabilitationneedsofthecaregivers.
JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 187
‘Psychiatricpatientshaveveryfewrehabilitationoptions…patientswhoarewell…around70%ofthem,ifsomesmalljobscanbeprovidedforthem…smallencouragementcanbegiventothembythegovernment,itwouldbehelpful.’(MrI.K.(60years),FGD-1)
‘Developmentoflocalsupportgroupsincity/hometownslikepalliativecaregroupsforcancerpatientswillbeagreatrelieftoallpeople,whereverweare.’(MrsM.(52years),FGD-2)
‘Atleastinmedicalcolleges,connectedwiththisissueahelplinecanbeopened.Thegovernmentcandothis.’(MrsB.M.(60years),FGD-2)
‘Ifwearegovernmentemployees,atanytime,wedonotgetleaveandwecangettransferred.EvenwhenItriedtoconvincemysuperiorsthatIhadtotakecareofthreementallyillpersonsat home [officers] theydidnot listen.Theyprocessed my transfer order.So if certain rulesandregulations togive leave tousasacaregiverofapatientaremade, itwouldbeuseful.’(MrC.R.(25years),FGD-2)
‘Asmallcentreshouldbemadeavailable[developed]inourstate,inanyofthecitiesorinanyplaceinthestate–withonedoctor.IfpatientdoesnotwanttocometoNIMAHNS,wedonotknowwheretotakehim.Ineverycrisissituationwecannotcomeoverhere[toNIMHANS].Thereneedstobealocalreferralsystem.’(MrsB.M.(60years),FGD-2)
VI: Managing the sexual and marital problems of patientsCaregiversofpersonswithmentalillnessfacedanumberofproblemsrelatedtothesexualandmaritalissuesofthepatient.Theyneededhelpindealingwithissuessuchas:whethertogetthepatientmarried;problemsingettingpatientmarried;problemsinmaintainingthepatient’smarriagepost-illness(separation/divorceissues);andproblemsofthepatientrelatedtosexualactivities/maritaldiscord.Thefollowingquotesofcaregiversexemplifysomeoftheabovethemes.
‘Wehaveseenafewgirlsformyson’smarriage.Butallthepartieswegotosee,somebodyinourvillagewouldhavealreadytoldthemthatheisnotmentallywellandthealliancewouldberejected.’(MrsB.M.(60years),FGD-2)
‘Mybrotherismarriedbuthiswifedoesnotstaywithhim.Hehasachildandhiswifehasputthechildinahostel.Thisisbecausefrom1999heisgettingtreatmentfromNIMHANSandhewasnotcured.Afterhegoesbackhome,withinafewdaysthesymptomsrelapse.Sohiswife’sfatherandmotherhaveadvisedhernottogobacktoherhusband.Wedonotknowhowtodealwiththissituation.’(MrS.M.(47years),FGD-2)
DISCUSSION
Theneedsofthecaregiversareextensiveandvaryacrosscultures.Anin-depthassessmentandanalysis is of paramount importance in order to develop programmes to cater to the needs ofcaregiversinaculturalcontext.ThepresentstudyexploredtheneedsofcaregiversofinpatientswithschizophreniainIndia.ThethreemainneedsthatemergedfromtheanalysisoftheFGDs,
188 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
were (in order of importance) help in: (1) managing the illness behaviour of the patients;(2) managing social-vocational problems of patients; and (3) health needs of the caregivers.Somepublishedstudieshavefocusedonspecificneedssuchasrehabilitationand/oreducation(Chien&Norman,2003;Winefield&Harvey,1994).Mostotherstudieshaveusedastandardizedneedsquestionnairetoassesscaregiverneeds.TheCamberwellAssessmentofNeed(CAN),oneofthemostwidelyused,ismoreoftenusedwithpersonswhoareincontactwithmentalhealthservicesandarereceivinginpatient,outpatientorday-patientcare(Phelanet al.,1995).TheCarer’sNeedsAssessment(CNA)andtheRelativesCardinalNeedsAssessment(RCNS),ontheotherhand,focusoncaregivers’educational,financial,socialandinterpersonal,professionalsupportandhealthneeds(Wancataet al.,2006;Barrowcloughet al.,1998).
Assessingtheneedsthroughthemethodofaquestionnairecouldlimittherangeofexpressionoftheneedsofcaregivers.Thequalitativeassessmentmethodusedinthisstudyhasbeenusefulinfindingin-depthrequirementsofcaregiversineachneedarea–anadditionalcomprehensiveresult,differentfromthatofotherstudies.Forexample,under‘healthneeds’variouscaregivers’requirementswerecoveredsuchastheneedtomanagestressandemotions,theneedtomaintainbalancebetweencaregivingandpersonallife/workandtheneedtoknowhowtotakedecisionsinstressfulsituations.
Theresultsofthecurrentstudycouldalsobeinterpretedintermsofthesample–howneedsofcaregiversofinpatients(whohadrecentlybecomeillorwhoseillnesshadexacerbated)coulddifferfromthoseofcaregiversofoutpatients(Clearyet al.,2006).Thecaregiverswhoparticipatedinthisstudyweremorepatient-focusedratherthancarer-focused.Thisreflectsnotjustthealtruisticpreoccupationsoffocusgroupparticipants,butalsothefactthatallthesecaregiversweretakingcareofpatientswhowerecurrentlysymptomaticandrequiredimmediatehospitalizationfortheirsymptomcontrol.Managing the symptomsof thepatientswas always consideredas themostimportantpriority.Thereweredifferencesinopinionbetweencaregiversinsomegroupsaboutwhetherrehabilitation,educationortheirhealthneedswasthenextimportantneed.Thehomogeneityofthesample(allcaregiversofinpatientswithschizophrenia)couldbeareasonforallthecaregivershavingsimilarprioritiesintakingcareoftheirpatient.
Furtherculturalfactors,suchasstrongfamilysystems,couldhaveabearingontheresultsofthestudy.InIndiathepatientisalwaysaccompaniedbythefamilymember(whoisthecaregiver)ascomparedtoothercountrieswherecaregiversarenotnecessarilyfamilymembers(Tharaet al.,1998;Leff,1994).
ThesociodemographicprofileofthecaregiversinthisstudyisconsistentwiththatofearlierstudiesonIndiancaregiversofpersonswithschizophrenia(Srinivasan,2006;Murthy,2007). Allcaregiverswerefamilymembers.Mostofthemwereparents,especiallymotherswhohadalowerincomeandwereintolateadulthoodoroldage.Itmayalsobenotedthattheproportionofpatientslivinginnuclearfamiliesinthisstudy(76.7%)iscomparabletothatofthegeneralpopulationofIndia(70.4%;OfficeoftheRegistrarGeneralandCensusCommissioner,India,2001).
Caregiversinthestudyreportedthattheirprimaryneedwashelpinmanagingthesymptomsofthepatient.Duetolackofknowledge,fearandstigmaassociatedwithmentalillness,caregiversoftenfoundthemselvesatalossastohowtodothis(Gandonet al.,2008).Dealingwiththesocial-vocationalproblemsofthepatient(secondneed),wasanotherareaofconcernforthecaregivers.Someexpressedmoreconcernabout‘negative’symptomsofschizophrenia(e.g.socialwithdrawal)
JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 189
thanaboutpositiveones(e.g.hallucinations)(Northet al.,1998).Furthercaregiversseemedtounderstandthattheyhadtotakecareoftheirownhealth(thirdneed)inordertobettercareforthepatient.
Apartfromtheabovethreemainneeds,caregiversalsoperceivedtheneedforeducation(fourthneed)asimportant,asitwouldhelpreducestigmainsocietyaboutmentalillness(Murthy,2006).Caregiversrequiredinformationnotonlyabouttheillness,butalsoaboutmedication/sideeffects/emergency medication (sedatives) and about the available concessions/benefits offered by thegovernment(Clearyet al.,2005;Chien&Norman,2003).TheconceptofstigmawasdiscussedbythecaregiverswhoparticipatedinFGD-2inthecontextof‘educatingthesocietytominimizethestigmainsociety’.Thus,theissuewasconsideredunderthecategoryofeducationasthefocuswasoneducatingsociety–clearingmisconceptions,noteradicatingstigma.Rehabilitation(fifthneed)wasexpressedasimportantbythecaregivers;asmostofthecaregiversstayedinnuclearfamilies, they requiredhelp in the formoffinancialand legalconcessions,office/work-relatedbenefitsforcaregivers,rehabilitationcentres/daycarenearhome,helplineservicesandlocalsupportgroups.Apartfromtheavailabilityoftheseservices,theyalsoneededinformationaboutthemandhelpinaccessingtheseservices(Clearyet al.,2005).Thesixthneedwassexualandmaritalprob-lemsandknowinghowtodealwiththem.ThiswasasignificantneedintheIndiancontextasmarriageandprocreationareconsidered tobe important stages in the Indian family lifecycle(Madan,1987).Caregiverswanted toknowwhether toget theirpatientmarried; thestigmaofgettingthepatientmarriedwithamentalillness;andhowtodealwithdifficultiespost-marriagelikerelapseofsymptomsandmaritaldiscord.
Inacountrywherethereareveryfewpsychiatrists,thefocusoftreatmentismoreonsymptomcure.EveninatertiarymultidisciplinarycentrelikeNIMHANS,thefocusisoftenonneedsotherthanthehealthneedsofthecaregivers.Estimatesshowthat50%ofpatientsapproachNIMHANSasaprimarycarecentre(Kareet al.,2008).Thismakesitdifficulttodealwithalltheneedsofthepatientsandcaregivers.Needslikerehabilitation,educationandsexualconcernsofthepatientcanbemanagedathospitallevel.However,thehealthneedsofcaregiversthatareequallyimportantareoftennottakenaspartofthepatients’treatmentprocessatthehospital.Asitsaim,thisstudywillattempttodevelopastructuredinterventionprogrammebasedontheholisticcoverageofalltheneedsofthefamilycaregivers.
Certainmethodologicalissuesofthisstudyneedtobementioned.ThemethodofFGDhascertaininherentlimitationssuchasthegroupmembers’responsesarenotindependentofoneanother,whichrestrictsthegeneralizabilityoftheresults(Stewartet al.,2007).Someofthememberswerehesitanttotalkinagroupsituation–especiallywhensharingsensitiveissues.Caregiversmayhaveexpressedotherneedsiftheyhadbeeninterviewedindividually.Individualinterviewscouldthushaveaddedconsiderablestrengthtotheresultsofthestudy.Anyinterpretationoftheresultsneedstobedonekeepinginmindtheexclusionofcarerswhowerenotcomfortablewithagroupsituation.Further,theresultsobtainedfromtheFGDmayhavebeenbiasedbyaverydominantoropinionatedmember.Futurestudiescouldexaminethevalidityofthehierarchyofneedsbypresentingthefindingsofthisstudytoanotherfocusgroupofcarers.
To counter some of these methodological limitations, informed consent of the members toparticipateinafocusgroupwastakenbeforethestartoftheFGD.Thosememberswhowerenotcomfortablewithtalkinginagroupsituationwerenotchosenforthestudy.Further,themoderatorbiaswasminimizedbyaskingthegroupmembersthemselvestolistandranktheneedswithoutconsultingthemoderator.

190 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
All family caregivers who attended the FGDs emphatically stated that they required helpin managing all their needs and expressed their willingness to participate in any training thataddressedthis.
CONCLUSIONS
ThisstudyisoneofthefirstscientificallyresearchedqualitativeneedsassessmentstudiesofthecaregiversofinpatientswithschizophreniainIndia.Further,thisstudygivesanholisticviewoftheneedsofcaregiverswiththelistofthemesandsub-themesthatneedtobeconsideredforanyfutureaction.Itputssignificantemphasisonhealthneedsofthecaregivers(thirdimportanttheme),whichhasoftenbeenignoredinotherinterventions.Itmustbenotedthateachpatientmayhavemorethanonecaregiverandhelpofanykindtomanagetheirhealthneedsmayhavepublichealthsignificance.
Finally,thesefindingsarehighlyindicativeandfuturestudiescouldtesttheresultsinalargerquantitativesampletoreconfirmthevalidity,reliabilityandgeneralizabilityoftheresults.Ifvalidated,itwouldenablethedevelopmentofanyprogrammedevelopedforIndianfamilycaregiversbasedontheneedsassessment.Asanoutcomeofthisstudy,theresearchersplantodevelopapsychosocialandyogaprogrammeforfamilycaregiversofinpatientswithschizophreniainIndia.
ACKNOWLEDGEMENTS
TheresearcherswouldliketothankDrShekharP.Seshadri,DrPrabhaS.Chandra,DrJayashreeRamakrishnanandDrK.Subbakrishnafortheirvaluableinput,whichhelpedinthedevelopmentofthefocusgroupscript.
REFERENCES
Angermeyer,M.C.,DiazRuizdeZarate,J.&Matschinger,H.(2000)Informationandsupportneedsofthefamilyofpsychiatricpatients.Gesundheitswesen,62(10),483–486.
Barrowclough, C., Marshall, M., Lockwood,A., Quinn, J. & Sellwood,W. (1998)Assessing relatives’ needsfor psychosocial interventions in schizophrenia:A relatives’ versionofCardinalNeedsSchedule (RCNS).Psychological Medicine,28,531–542.
Chafetz,L.&Barnes,L.(1989)Issuesinpsychiatriccaregiving.Archives Psychiatric Nursing,3(2),61–68.Chien,W.T.&Norman, I. (2003)Educationalneedsof familiescaring forChinesepatientswithschizophrenia.
Journal of Advanced Nursing,44(5),490–498.Cleary,M.,Freeman,A.,Hunt,G.E.&Walter,G.(2005)Whatpatientsandcarerswanttoknow:Anexploration
of informationandresourceneeds inadultmentalhealthservices. Australian and New Zealand Journal of Psychiatry,39,507–513.
Cleary,M.,Freeman,A.,Hunt,G.E.&Walter,G.(2006)Patientandcarerperceptionsofneedandassociationswithcaregivingburdeninanintegratedadultmentalhealthservice.Social Psychiatry and Psychiatric Epidemiology, 41,208–214.
ConsumerHealthSciences(2008)National Health and Wellness Survey 2008.Princeton:ConsumerHealthSciences.www.chsinternational.com

JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 191
Gandon,P.,Jenaro,C.&Lemos,S.(2008)Primarycaregiversofschizophreniaoutpatients:Burdenandpredictorfactors.Psychiatry Research,158,335–343.
Goswami,M.(2006)Fromafamilycaregivertoacaregiveratthecommunitylevel–‘AshadeepModel’.InMental Health by the People(ed.R.S.Murthy).Bangalore:People’sActionforMentalHealth(PAMH).
Hiday,V.A.,Swartz,M.S.,Swanson,J.W.,Borum,R.,Wagner,H.R.&D’Cruz,P.(2002)Familiesinsociety.Journal of Contemporary Human Services,83,416–430.
Janardhan(2006)Communitymentalhealthanddevelopmentmodelevolvedthroughconsultingpeoplewithmentalillness. In Mental Health by the People (ed. R.S. Murthy). Bangalore: People’sAction for Mental Health(PAMH).
Johnson,D.L.(1994)Currentissuesinfamilyresearch:Cantheburdenofmentalillnessberelieved?InHelping Families Cope with the Mental Illness (eds.H.P.Lefley&M.Wasow),pp309–328.Newark,NJ:HarwoodAcademy.
Kare, M.,Thirthalli, J.,Varghese, R.S., Ross, D., Reddy, K.S., Jagannathan,A.,Venkatasubramanian, G. &Gangadhar,B.N.(2008)Reducingthedelayintreatmentofpsychosis.Wheredoweintervene?Astudyoffirst-contactpatientsinNIMHANS.BestPosterAwardattheRichmondFellowshipAsia-PacificConference2008onRehabilitationAcrossCultures. Bangalore:NIMHANS.
Leff, J. (1994)Working with families of schizophrenic patients. British Journal of Psychiatry, 164 (Supp 23),71–76.
Madan,G.R.(1987)Indian Sociology. Revised Fourth Edition.NewDelhi:AlliedPublishersPrivateLtd.Magliano,J.,Fadden,G.,Economou,M.,Held,T.&Xavier,M.(1998)Burdenonthefamiliesofpatientswith
schizophrenia: Results of the BIOMED 1 Study. Social Psychiatry and Psychiatric Epidemiology, 33(9),112–223.
Murthy,R.S.(2006)Mental Health by the People.Bangalore:People’sActionforMentalHealth(PAMH).Murthy, R.S. (2007) Family and Mental Healthcare in India. Bangalore: People’sAction for Mental Health
(PAMH).North,C.S.,Pollio,D.E.,Sachar,B.,Hong,B.&Isenberg,K.(1998)Thefamilyascaregiver:Agrouppsychoeducation
modelforschizophrenia.American Journal of Orthopsychiatry,68(1),39–46.OfficeoftheRegistrarGeneralandCensusCommissioner,India(2001)Census of India 2001.NewDelhi:Officeof
theRegistrarGeneralandCensusCommissioner,India.Padget,D.K. (1998)Qualitative Methods in Social Work Research: Challenges and Rewards.NewDelhi:Sage
Publications.Padmavathi,R.,Rajkumar,S.&Srinivasa,T.N.(1998)Schizophrenicpatientswhowerenevertreated–Astudyin
anIndianurbancommunity.Psychological Medicine,28,1113–1117.Phelan,M.,Slade,M.,Thornicroft,G.,Dunn,G.,Holloway,F.,Wykes,T.,Strathdee,G.,Loftus,L.,McCrone,P.&
Hayward,P.(1995)TheCamberwellAssessmentofNeed:Thevalidityandreliabilityofaninstrumenttoassesstheneedsofpeoplewithseverementalillness.British Journal of Psychiatry,167,589–595.
Solomon,P.&Draine,J.(1994)Examination of Adoptive Coping Among Individuals with a Seriously Mentally Ill Relative.Unpublishedpaper.Philadelphia:HanermanUniversity,DepartmentofPsychiatryandMentalHealthScience.
Srinivasan,N.(2006)Togetherwerise–KshemaFamilyPower.InMental Health by the People(ed.R.S.Murthy).Bangalore:People’sActionforMentalHealth(PAMH).
Stewart,D.W.,Shamdasani,P.N.&Rook,D.W.(2007)Focus Groups – Theory and Practice. Second Edition.Applied Social Research Methods Series, Vol 20.NewDelhi:SagePublications.
Thara,R.,Padmavathi,R.,Kumar,S.&Srinivasan,L.(1998)BurdenAssessmentSchedule:Instrumenttoassessburdenoncaregiversofchronicallymentallyill.Indian Journal of Psychiatry,40,21–29.
Wancata,J.,Krautgartner,M.,Berner,J.,Scumaci,S.,Freidl,M.,Alexandrowicz,R.&Rittamannsberger,H.(2006)The ‘Carers’ needsAssessment for Schizophrenia’. Social Psychiatry and Psychiatric Epidemiology, 41,221–229.
Winefield,H.R.&Harvey,E.J.(1994)Needsoffamilycaregiversinchronicschizophrenia.Schizophrenia Bulletin, 20(3),557–566.
WorldHealthOrganization(2001)Atlas: Country Profiles on Mental Health Resources 2001.Geneva:WorldHealthOrganization.
192 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
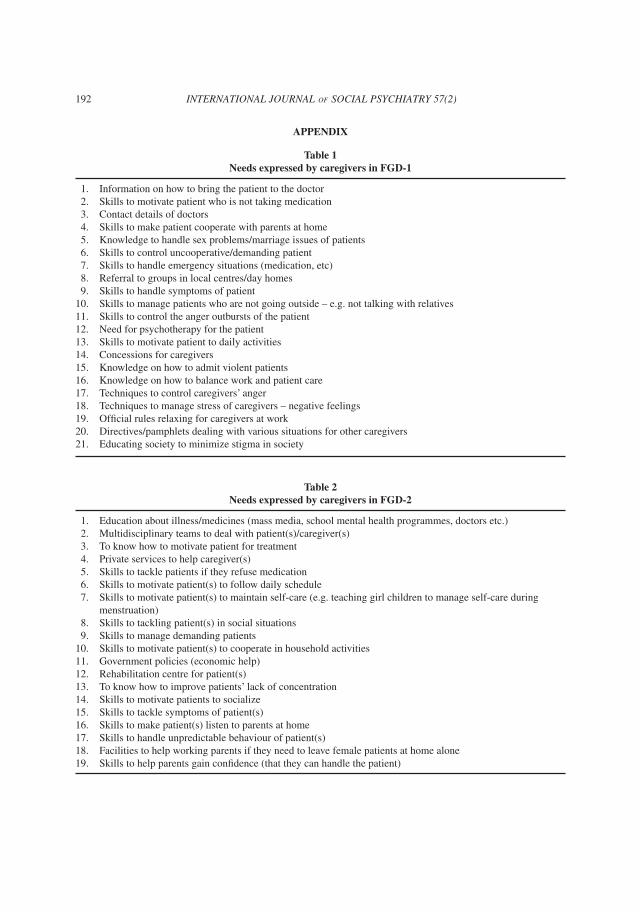
APPENDIX
Table 1 Needs expressed by caregivers in FGD-1
1. Informationonhowtobringthepatienttothedoctor 2. Skillstomotivatepatientwhoisnottakingmedication 3. Contactdetailsofdoctors 4. Skillstomakepatientcooperatewithparentsathome 5. Knowledgetohandlesexproblems/marriageissuesofpatients 6. Skillstocontroluncooperative/demandingpatient 7. Skillstohandleemergencysituations(medication,etc) 8. Referraltogroupsinlocalcentres/dayhomes 9. Skillstohandlesymptomsofpatient10. Skillstomanagepatientswhoarenotgoingoutside–e.g.nottalkingwithrelatives11. Skillstocontroltheangeroutburstsofthepatient12. Needforpsychotherapyforthepatient13. Skillstomotivatepatienttodailyactivities14. Concessionsforcaregivers15. Knowledgeonhowtoadmitviolentpatients16. Knowledgeonhowtobalanceworkandpatientcare17. Techniquestocontrolcaregivers’anger18. Techniquestomanagestressofcaregivers–negativefeelings19. Officialrulesrelaxingforcaregiversatwork20. Directives/pamphletsdealingwithvarioussituationsforothercaregivers21. Educatingsocietytominimizestigmainsociety
Table 2 Needs expressed by caregivers in FGD-2
1. Educationaboutillness/medicines(massmedia,schoolmentalhealthprogrammes,doctorsetc.) 2. Multidisciplinaryteamstodealwithpatient(s)/caregiver(s) 3. Toknowhowtomotivatepatientfortreatment 4. Privateservicestohelpcaregiver(s) 5. Skillstotacklepatientsiftheyrefusemedication 6. Skillstomotivatepatient(s)tofollowdailyschedule 7. Skillstomotivatepatient(s)tomaintainself-care(e.g.teachinggirlchildrentomanageself-careduring
menstruation) 8. Skillstotacklingpatient(s)insocialsituations 9. Skillstomanagedemandingpatients10. Skillstomotivatepatient(s)tocooperateinhouseholdactivities11. Governmentpolicies(economichelp)12. Rehabilitationcentreforpatient(s)13. Toknowhowtoimprovepatients’lackofconcentration14. Skillstomotivatepatientstosocialize15. Skillstotacklesymptomsofpatient(s)16. Skillstomakepatient(s)listentoparentsathome17. Skillstohandleunpredictablebehaviourofpatient(s)18. Facilitiestohelpworkingparentsiftheyneedtoleavefemalepatientsathomealone19. Skillstohelpparentsgainconfidence(thattheycanhandlethepatient)
JAGANNATHANET AL.:AQUALITATIVESTUDYONTHENEEDSOFCAREGIVERS 193
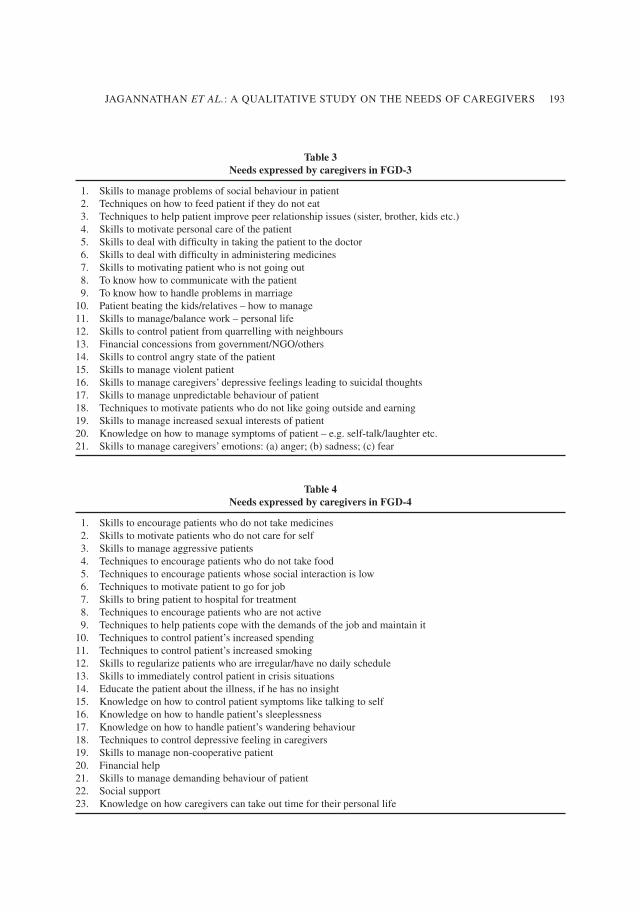
Table 3 Needs expressed by caregivers in FGD-3
1. Skillstomanageproblemsofsocialbehaviourinpatient 2. Techniquesonhowtofeedpatientiftheydonoteat 3. Techniquestohelppatientimprovepeerrelationshipissues(sister,brother,kidsetc.) 4. Skillstomotivatepersonalcareofthepatient 5. Skillstodealwithdifficultyintakingthepatienttothedoctor 6. Skillstodealwithdifficultyinadministeringmedicines 7. Skillstomotivatingpatientwhoisnotgoingout 8. Toknowhowtocommunicatewiththepatient 9. Toknowhowtohandleproblemsinmarriage10. Patientbeatingthekids/relatives–howtomanage11. Skillstomanage/balancework–personallife12. Skillstocontrolpatientfromquarrellingwithneighbours13. Financialconcessionsfromgovernment/NGO/others14. Skillstocontrolangrystateofthepatient15. Skillstomanageviolentpatient16. Skillstomanagecaregivers’depressivefeelingsleadingtosuicidalthoughts17. Skillstomanageunpredictablebehaviourofpatient18. Techniquestomotivatepatientswhodonotlikegoingoutsideandearning19. Skillstomanageincreasedsexualinterestsofpatient20. Knowledgeonhowtomanagesymptomsofpatient–e.g.self-talk/laughteretc.21. Skillstomanagecaregivers’emotions:(a)anger;(b)sadness;(c)fear
Table 4 Needs expressed by caregivers in FGD-4
1. Skillstoencouragepatientswhodonottakemedicines 2. Skillstomotivatepatientswhodonotcareforself 3. Skillstomanageaggressivepatients 4. Techniquestoencouragepatientswhodonottakefood 5. Techniquestoencouragepatientswhosesocialinteractionislow 6. Techniquestomotivatepatienttogoforjob 7. Skillstobringpatienttohospitalfortreatment 8. Techniquestoencouragepatientswhoarenotactive 9. Techniquestohelppatientscopewiththedemandsofthejobandmaintainit10. Techniquestocontrolpatient’sincreasedspending11. Techniquestocontrolpatient’sincreasedsmoking12. Skillstoregularizepatientswhoareirregular/havenodailyschedule13. Skillstoimmediatelycontrolpatientincrisissituations14. Educatethepatientabouttheillness,ifhehasnoinsight15. Knowledgeonhowtocontrolpatientsymptomsliketalkingtoself16. Knowledgeonhowtohandlepatient’ssleeplessness17. Knowledgeonhowtohandlepatient’swanderingbehaviour18. Techniquestocontroldepressivefeelingincaregivers19. Skillstomanagenon-cooperativepatient20. Financialhelp21. Skillstomanagedemandingbehaviourofpatient22. Socialsupport23. Knowledgeonhowcaregiverscantakeouttimefortheirpersonallife
194 INTERNATIONAL JOURNAL OF SOCIAL PSYCHIATRY 57(2)
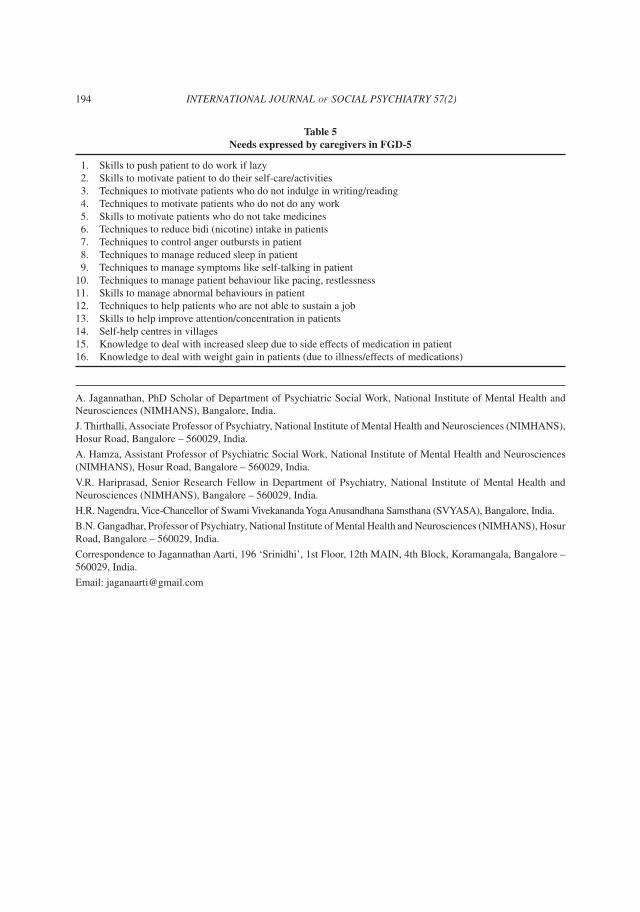
Table 5 Needs expressed by caregivers in FGD-5
1. Skillstopushpatienttodoworkiflazy 2. Skillstomotivatepatienttodotheirself-care/activities 3. Techniquestomotivatepatientswhodonotindulgeinwriting/reading 4. Techniquestomotivatepatientswhodonotdoanywork 5. Skillstomotivatepatientswhodonottakemedicines 6. Techniquestoreducebidi(nicotine)intakeinpatients 7. Techniquestocontrolangeroutburstsinpatient 8. Techniquestomanagereducedsleepinpatient 9. Techniquestomanagesymptomslikeself-talkinginpatient10. Techniquestomanagepatientbehaviourlikepacing,restlessness11. Skillstomanageabnormalbehavioursinpatient12. Techniquestohelppatientswhoarenotabletosustainajob13. Skillstohelpimproveattention/concentrationinpatients14. Self-helpcentresinvillages15. Knowledgetodealwithincreasedsleepduetosideeffectsofmedicationinpatient16. Knowledgetodealwithweightgaininpatients(duetoillness/effectsofmedications)
A.Jagannathan,PhDScholarofDepartmentofPsychiatricSocialWork,NationalInstituteofMentalHealthandNeurosciences(NIMHANS),Bangalore,India.
J.Thirthalli,AssociateProfessorofPsychiatry,NationalInstituteofMentalHealthandNeurosciences(NIMHANS),HosurRoad,Bangalore–560029,India.
A.Hamza,AssistantProfessorofPsychiatricSocialWork,NationalInstituteofMentalHealthandNeurosciences(NIMHANS),HosurRoad,Bangalore–560029,India.
V.R. Hariprasad, Senior Research Fellow in Department of Psychiatry, National Institute of Mental Health andNeurosciences(NIMHANS),Bangalore–560029,India.
H.R.Nagendra,Vice-ChancellorofSwamiVivekanandaYogaAnusandhanaSamsthana(SVYASA),Bangalore,India.
B.N.Gangadhar,ProfessorofPsychiatry,NationalInstituteofMentalHealthandNeurosciences(NIMHANS),HosurRoad,Bangalore–560029,India.
CorrespondencetoJagannathanAarti,196‘Srinidhi’,1stFloor,12thMAIN,4thBlock,Koramangala,Bangalore–560029,India.
Email:[email protected]



















