Health for Life (H4L) Project - PDF Server
89
Health for Life (H4L) Project Annual Report July 1, 2014, to June 30, 2015 August 11, 2015 This publication was produced for review by the United States Agency for International Development. It was prepared by RTI International.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Health for Life (H4L) Project - PDF Server

Health for Life (H4L) Project Annual Report
July 1, 2014, to June 30, 2015
August 11, 2015
This publication was produced for review by the United States Agency for International Development. It was prepared by RTI International.

Health for Life (H4L) Project Annual Report
August 11, 2015
Contract AID-367-C-13-00001
Prepared for
COR
Office of Health and Family Planning
USAID/Nepal
P.O. Box No. 295
U.S. Embassy, Maharajgunj
Kathmandu, Nepal
Prepared by
RTI International 3040 Cornwallis Road
Post Office Box 12194 Research Triangle Park, NC 27709-2194
RTI International is one of the world's leading research institutes, dedicated to improving the human condition by turning knowledge into practice. Our staff of more than 3,700 provides research and technical services to governments and businesses in more than 75 countries in the areas of health and pharmaceuticals, education and training, surveys and statistics, advanced technology, international development, economic and social policy, energy and the environment, and laboratory testing and chemical analysis.
RTI International is a trade name of Research Triangle Institute.
The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.
Contents
List of Figures....................................................................................................................................................vi
List of Tables ....................................................................................................................................................vii
Abbreviations ..................................................................................................................................................viii
Background.........................................................................................................................................................1
A. Comparison of actual accomplishments against intended outcomes for the period in the Annual Work Plan, Capacity Building Plan, and Monitoring and Evaluation Plan .................................1
Accomplishments and intended outcomes for the period ......................................................................1
Objective 1: Improve health systems governance of district offices and sub-district level facilities............................................................................................................................................................2
1.1 Provide TA to D(P)HOs to revitalize HFOMCs and to help develop VDC health plans that are incorporated in the district AWPB ensuring appropriate budget allocations ...................................................................................................................................................2
1.2 Assist D(P)HOs, DDCs and VDCs to improve performance of 141 HFOMCs based on local context (using set criteria) primarily focusing on most disadvantaged VDCs...........................................................................................................................................................4
1.3 Provide TA to D(P)HOs and MoHP leadership to institutionalize best practices among HFOMCs and/or other civil society organizations that effectively respond to the needs of M/DAG and hard-to-reach populations to increase access, especially in most disadvantaged VDCs.......................................................................................................................5
1.4 Provide TA to MoHP, MoFALD and other stakeholders to expand local health governance strengthening activities to all 14 program districts and track progress against defined objectives and share with EDPs Forum and at the JAR..........................................6
Objective 2: Develop and implement national evidence-based policy ..................................................7
2.1 Strengthen HMIS ................................................................................................................................7
2.2 Strengthen NHRC ..............................................................................................................................8
2.3 M&E and research ............................................................................................................................13
Objective 3: Strengthen national-level stewardship of the health sector.............................................14
3.1 Collaborate with other health sector partners and assist MoHP to formulate NHSP III in a manner that is evidence-based, strategic and participatory.....................................14
3.2 Provide TA to the MoHP to link the new NHSP to the AWPB process ................................14
Objective 4: Institutionalize nationwide system for quality improvement..........................................15
4.1 Activate and maintain district QAWC Meetings in all H4L districts based on existing QA policies/guidelines to improve QI practices in HFs....................................................15
4.2 Provide TA to improve QI practices in FP/MNCH at HFs in the 140 most disadvantaged VDCs ...............................................................................................................................15
4.3 Maintain National Quality Assurance Coordination Mechanism ..............................................16
4.4 Implement revised National facility-based QI system.................................................................18
Objective 5: Improve capacity of district and local level health workers and community volunteers to deliver high quality FP/MNCH and nutrition services .................................................21
H4L— Annual Report iii

5.1 Provide TA to Divisions and Centers (FHD, CHD, NHTC, NHEICC) during revisions of strategies/guidelines/training materials for HWs and FCHVs on FP/MNCH...............................................................................................................................................23
5.2 Provide TA to develop Multi-Year Strategic Plan of Action for the Family Planning Program in coordination with other stakeholders .............................................................25
5.3 Provide support to D/PHOs in strengthening existing MSC, CB-IMCI and CB-NCP program in selected districts ........................................................................................................25
5.4 Provide TA to D(P)HOs to increase utilization of long-acting FP methods in birthing centers in H4L districts............................................................................................................30
5.5 Provide TA to FHD and D(P)HOs to improve CEONC referral system in Dang district (based on national safe motherhood and neonatal referral guidelines)..............................33
5.6 Provide TA to CTEVT to revise ANM curriculum (Pre- and Post-SLC) to incorporate SBA skills.............................................................................................................................34
5.7 Provide TA to ANM schools to improve quality of pre-service education in ANM schools.......................................................................................................................................................34
Objective 6: Improve knowledge, behavior, and use of health services among target .....................36
6.1 National-Level Activities..................................................................................................................36
6.2 District-Level Activities....................................................................................................................38
6.3 Provide TA to NHTC and RHDs for developing trainers to institutionalize GESI in MOHP system.....................................................................................................................................42
Objective 7: Strengthen capacity of USAID’s contractor for a logistical support activity ...............43
GESI..............................................................................................................................................................44
GESI activities at district level...............................................................................................................44
GESI integration in district training .....................................................................................................44
GESI Coordination group for USAID Partners ................................................................................45
H4L Staff composition ...........................................................................................................................45
B. Major challenges and constraints faced during the performance period that resulted in delays of achievement of outcomes, if applicable .......................................................................................45
1.1 Provide TA to D(P)HOs to revitalize HFOMCs and to help develop VDC health plans that are incorporated in the district AWPB ensuring appropriate budget allocations .................................................................................................................................................45
1.2 Assist D(P)HOs, DDCs and VDCs to improve performance of 140 HFOMCs based on local context (using set criteria) primarily focusing on most disadvantaged VDCs.........................................................................................................................................................45
1.4 Provide TA to MoHP, MoFALD and other stakeholders to expand local health governance strengthening activities to all 14 program districts and track progress against defined objectives and share with EDPs Forum and at the JAR........................................45
C. Highlights of the internship program as described in Section C.2.8.1................................................47
D. Cumulative quantitative monitoring and evaluation data, including information on progress towards targets and explanations of any issues related to data quality.....................................48
Contract Deliverables..................................................................................................................................48
Capacity Building Benchmarks ..................................................................................................................53
H4L— Annual Report iv

PMP and PPR Indicators............................................................................................................................58
E. Information on the status of finances, including expenditure data based on the budget and accruals, as well as, when appropriate, analysis and explanation of cost overruns or high unit cost ....................................................................................................................................................69
F. Information on management issues, including administrative problems, or problems with beneficiary groups, or implementing partners and what steps or actions were taken to manage these and lessons learned for future ...............................................................................................70
G. Anticipated future problems, delays, or conditions that may adversely impact implementation of the project and what measures are in place to deal with these................................70
Local Health Governance...........................................................................................................................70
Evidence-based Policy ................................................................................................................................70
National Stewardship ..................................................................................................................................70
Quality Improvement..................................................................................................................................70
LAFP and SBA Coaching ...........................................................................................................................70
ANM Pre-service Education......................................................................................................................71
H. Information on security issues, especially as these affect program integrity and safety of beneficiary groups and implementing partner .............................................................................................71
I. Other information, such as new opportunities for program expansion, lessons-learned and success stories, and prospects for the following year’s performance ...............................................71
Annexes .............................................................................................................................................................72
Annex 1 District QAWG Meetings ..........................................................................................................72
Annex 2 Assessment of health services reviews based on Public Health Analytics Techniques....................................................................................................................................................75
Annex 3 Internship Report from Mohd Irfan in Banke ........................................................................77
H4L— Annual Report v

List of Figures
Figure 1.1 Clinical staff positions filled in H4L project districts compared to total sanctioned positions, June 2015....................................................................................................................................................................... 4 Figure 1.2 HFOMC functionality and performance as of June 2015.................................................................. 4 Figure 1.3 Institutional deliveries in selected VDCs in H4L districts ................................................................. 5
Figure 2.1 Composition of pregnant women by caste/ethnicity against the population proportion in H4L
Figure 2.3 Percent of women that delivered at health facility and percent of women that had 1st PNC
Figure 2.4 ANC and PNC service utilization for women that delivered by caste/ethnicity in 39 sentinel
Figure 2.5 Four ANC visits by caste/ethnicity relative to Brahmin/Chhetri in 39 sentinel sites in H4L
Figure 2.6 PNC service utilization among postpartum women by caste/ethnicity in 39 sentinel sites in
Figure 2.7 FP Methods among postpartum women currently using FP methods at sentinel sites (as of
Figure 4.5 QI Follow up: Comparisons of Infection Prevention and Health Care Waste Management,
Figure 4.6 Compliance with FP counseling standards in Dang (2014/15) 4.4.2 Provide TA to MD/DOHS
Figure 5.3 Percentage of respondents demonstrating 80 percent or higher competence in specific
Figure 5.4 Percentage of respondents demonstrating 80 percent or higher competence in specific skill
Figure 6.2 Number of individuals that interacted with the mobile platform by region, Sep 2014 to May
Figure 6.3 Interactions with the mobile platform by menu option, Sep 2014 to May 2015.......................... 37
Figure 6.5 Percent of health workers who performed all required actions during FP counselling in H4L
Figure 1.4 Three-year trend of CPR in selected priority VDCs in H4L districts .............................................. 5
districts (as of June 30, 2015) ..................................................................................................................................... 9 Figure 2.2 Percent of women that had four ANC visits among those that delivered (live births) in 39 sentinel sites (as of June 30, 2015) (n=577)........................................................................................................... 10
within 24 hours among live births in 39 sentinel sites in H4L districts (as of June 30, 2015) (n=577)....... 10
sites in H4L districts (as of June 30, 2015) ............................................................................................................ 11
districts (as of June 30, 2015) ................................................................................................................................... 11
H4L districts (as of June 30, 2015).......................................................................................................................... 12
June 30, 2015) (n=63) ............................................................................................................................................... 13 Figure: 4.1 Number of QAWCs by district ........................................................................................................... 15 Figure 4.2 IP and HCWM Practices ....................................................................................................................... 16 Figure 4.3 Selected Components of the Safe Motherhood Program assessed by Districts........................... 19 Figure 4.4 Assessment of Growth Monitoring by Prioritized VDCs of Rolpa (2014/15) ............................ 20
Dang (2014/15).......................................................................................................................................................... 20
to print national QI guidelines, tools and forms................................................................................................... 21 Figure 5.1 QI Assessment of FP Training Sites.................................................................................................... 24 Figure 5.2 Birthing centers in H4L districts offering LAFP ............................................................................... 31
knowledge areas, 2015............................................................................................................................................... 35
areas, 2014 ................................................................................................................................................................... 35 Figure 6.1 SMS sent by Users and to Users, by region, Sep 2014 to May 2015 .............................................. 36
2015.............................................................................................................................................................................. 37
Figure 6.4 Percentage of total expected mothers’ group meetings .................................................................... 39
project districts ........................................................................................................................................................... 39 Figure 8.1 H4L Staff composition by ethnicity..................................................................................................... 45 Figure 8.2 H4L Staff composition by gender........................................................................................................ 45
H4L— Annual Report vi

List of Tables
Table 1.1 Summary of HFOMC Functionality compared to September 2013 Baseline................................. 3
Table 2.3 Status of women that received PNC check-ups among women from sentinel sites that had
Table 5.5 Home deliveries in which women used Misoprostol by district (Calculated against expected
Table 1.2 Summary of Performance of HFOMCs compared to Sep 2013 Baseline ........................................ 3 Table 2.1 H4L's technical support to district and ilaka-level annual and trimester review meetings, 2014-15 .................................................................................................................................................................................... 7 Table 2.2 Pregnant women tracked using mobile technology in H4L districts, as of June 30, 2015 ............. 9
completed the 90-day postpartum period.............................................................................................................. 12 Table 4.2 QAI TWG meeting.................................................................................................................................. 17 Table 4.3 Health Facility QI Teams........................................................................................................................ 19 Table 5.1 CB-IMNCI Program technical support visit by H4L staff (Jul 2014 - Jun 2015).......................... 26 Table 5.2 Participants trained on CB-IMNCI, by district ................................................................................... 27 Table 5.3 H4L support for printing and distribution of CB-IMNCI materials ............................................... 27 Table 5.4 Monitoring of CB-IMNCI...................................................................................................................... 28
pregnancy) ................................................................................................................................................................... 28 Table 5.6 Summary of district TA to MSC program at HFs and VDCs .......................................................... 29 Table 5.7 Birthing Centers (BCs) with Long Acting FP (LAFP) in H4L districts .......................................... 30 Table 5.8 CPR and LAFP Contribution (H4L districts), HMIS ........................................................................ 31 Table 5.9 H4L support to outreach clinics ............................................................................................................ 32 Table 5.10 US abortion and FP compliance monitoring (H4L districts).......................................................... 33 Table 5.11: ANM Schools action plan.................................................................................................................... 36 Figure 6.6 Percent of adolescents who know the legal age of marriage............................................................ 40 Performance Management Plan (PMP) Report, July 2014-June 2015 .............................................................. 58
H4L— Annual Report vii

Abbreviations
AFN Antenna Foundation Nepal AHW Auxiliary Health Worker ANC antenatal care ANM Auxiliary Nurse Midwife ARI acute respiratory infection ASRH adolescent sexual and reproductive health AWPB annual work plan and budget AYFS adolescent and youth friendly services BC birthing center BCC Behavior Change Communication BEOC basic emergency obstetric care/center BEONC basic emergency obstetric and neonatal care/center BP blood pressure BPP birth preparedness package CAG Content Advisory Group CAP Community Action Promoter CAP/R Community Action Promoter/Researcher CB-IMCI community-based integrated management of childhood illness CB-IMNCI community-based, integrated management of newborn & childhood illnesses CB-NCP community-based newborn care package CBO community-based organization CBS Central Bureau of Statistics CEONC comprehensive emergency obstetric and neonatal care CF Collaborative Framework CH child health CHD Child Health Division CIP Costed Implementation Plan CNCP Chlorhexidine Navi Care Program COFP/C comprehensive family planning and counselling COIA Commission on Information and Accountability COP Chief of Party CPR contraceptive prevalence rate CTEVT Council for Technical Education and Vocational Training CYP couple-years of protection D(P)HO District (Public) Health Office DAG disadvantaged group DDC District Development Committee DEO District Education Office DHGSTF District Health Governance Strengthening Task Force DHIS District Health Information System DHO District Health Office DoHS Department of Health Services DPC District Program Coordinator DPMAS District Poverty Monitoring and Analysis System DQA data quality assessment DRPM District Review and Planning Meeting DSA daily subsistence allowance EBD evidence-based design Eco-region Ecological Region EDCD Epidemiology and Disease Control Division EDP external development partner EHA essential hygiene actions ENA essential nutrition actions EPSEM Equal Probability of Selection Method
H4L— Annual Report viii

ESG Evidence Support Group FCHV Female Community Health Volunteer FEP follow-up and enhancement program FHD Family Health Division FP family planning FY fiscal year GBV gender-based violence GESI gender equality and social inclusion GFA GFA Consulting Group GIS geographic information system GiZ German Federal Enterprise for International Cooperation GON Government of Nepal H4L Health for Life HA Health Assistant HC3 Health Community Capacity Collaborative HCWM health care waste management HET Health Education Technician HF health facility HFOMC Health Facility Operation and Management Committees HFRS health facility readiness survey HISPIX health information system performance index HLD high-level disinfection HMIS health management information system HP Health Post HR human resources HTSP healthy timing and spacing of pregnancy HW health worker ICF ICF International ICP informed choice poster IEC information, education and communications IFPSC Institutionalized Family Planning Service Centers INGO international nongovernmental organization IP infection prevention IPCC interpersonal communication and counseling IRHDTC Integrated Rural Health Development Training Center IUCD intrauterine contraceptive device JAR Joint Annual Review KAP knowledge, attitudes and practices KMC Kangaroo mother care L&D labor and delivery LAFPM long-acting family planning methods LC Learning Circle LDO Local Development Office LGCDP Local Governance and Community Development Program LHGS local health governance system LHGSP Local Health Governance Strengthening Program LLN LifeLine Nepal LMIS logistics management information system M&E monitoring and evaluation M/DAG marginalized/disadvantaged group MCHW Maternal and Child Health Worker MD Management Division MDG millennium development goal MICS multiple indicator cluster survey Miso Misoprostol MNCH maternal, newborn, and child health
H4L— Annual Report ix

MNCHN maternal, newborn, and child health and nutrition MNH maternal and newborn health MoFALD Ministry of Federal Affairs and Local Development MoHP Ministry of Health and Population MOLD Ministry of Local Development (now MoFALD) MRS medical recording software MSC Matri Surakshya Chhaki, i.e., misoprostol MTOT master training of trainers MWDR Mid-Western Development Region MWRA married women of reproductive age MWRHD Mid-Western Regional Health Directorate NBC newborn care NCASC National Centre for AIDS and STD Control NCell national cell service provider NCP newborn care package NDHS Nepal Demographic and Health Survey NFCC Nepal Fertility Care Center NFHP Nepal Family Health Program NGO non-governmental organization NHEICC National Health Education, Information and Communication Center NHRC Nepal Health Research Council NHRN Nepal Health Research Network NHSP Nepal Health Sector Program NHTC National Health Training Center NPC National Planning Commission NPHL National Public Health Laboratory NSI Nick Simon Institute NSV non-scalpel vasectomy OCP oral contraceptive pills OPD out-patient department ORC outreach clinic ORS oral rehydration salts PDT Project Development Team PHA public health analytics PHAMED Public Health Administration, Monitoring and Evaluation Division PHAT public health analytic techniques PHC primary health care PHCC Primary Health Care Center PHCRD Primary Health Care Revitalization Division PHD Population Health and Development PHI public health informatics PHO Public Health Office PMP Performance Management Plan PMTCT prevention of mother-to-child transmission PNC postnatal care PPFP post-partum family planning PPH post-partum hemorrhage PPICD Policy, Planning and International Cooperation Division PPIUCD postpartum intra-uterine contraceptive device PPR Performance Progress Report PSC Public Service Commission QA quality assurance QACG Quality Assurance Coordination Group QAITWG Quality Assurance and Improvement Technical Working Group QAWC Quality Assurance Working Committee QAWG Quality Assurance Working Group
H4L— Annual Report x
QI quality improvement QIT Quality Improvement Team QITAC Quality Improvement Technical Advisory Committee RH reproductive health RHCC Reproductive Health Coordination Committee RHD Regional Health Directorate RHTC Regional Health Training Center RMNCH reproductive maternal, newborn and child health RTI Research Triangle Institute SAR semi-annual report SBA Skilled Birth Attendant SHP Sub Health Post SIR Strategic Information and Research SLC School Leaving Certificate SMP Safe Motherhood Program SNL Saving Newborn Lives SPSS Statistical Package for Social Sciences (data analysis software) SRH sexual and reproductive health STS service tracking survey TA technical assistance TOCAT technical and organizational capacity assessment tool TOR terms of reference ToT training of trainers TT tetanus toxoid TWG Technical Working Group TWG-HIM Thematic Working Group – Health Information Management UNFPA United Nations Fund for Population Activities USAID United States Agency for International Development USG United States Government VASP value-added service provider VDC Village Development Committee VHSAP village health situation analysis profile VHW Village Health Worker VSC voluntary sterilization camp WASH water, sanitation and hygiene WCDO Women and Children Development Office WDR Western Development Region WHO World Health Organization
H4L— Annual Report xi
Background
Health for Life (H4L) is an $18.2 million, five-year project (December 2012–November 2017) that is funded by the U.S. Agency for International Development (USAID) and implemented by RTI International. It works in coordination with the Government of Nepal’s Ministry of Health and Population (MoHP) to support the roll out and testing of national-level policies, guidelines, and programs. In addition to the national focus, H4L works in 14 districts in the mid-western and western regions to support implementation and identification of best practices. H4L collaborates with a wide range of stakeholders, including academic and research institutions, pre-service training centers, media partners and civil society.
The primary goal of H4L is to strengthen the Government of Nepal’s capacity to plan, manage, and deliver high-quality and equitable family planning, maternal, newborn, and child health services (FP/MNCH). H4L interventions directly address key health system constraints in the following areas: local health systems governance, data for decision making and evidence-based policy development, human resources, quality improvement systems, and knowledge and behavior change.
H4L’s objectives are to
Improve health system governance of district health offices and sub-district level facilities
Support development and implementation of national evidence-based policy
Strengthen national stewardship of the health sector
Institutionalize nationwide system for quality improvement
Improve the capacity of district and local health workers and community volunteers to deliver high-quality FP/MNCH and nutrition services
Improve knowledge, behavior, and use of health services among adolescents and marginalized groups
Strengthen the capacity of USAID’s contractor, LifeLine, to manage a logistical support activity.
This annual report covers the period July 1, 2014, to June 30, 2015. It documents activities conducted during the project’s second year. Following H4L’s seven objectives, it describes key achievements, analyzes progress and challenges to date, budget and expenditures, and other information.
A. Comparison of actual accomplishments against intended outcomes for the period in the Annual Work Plan, Capacity Building Plan, and Monitoring and Evaluation Plan
Accomplishments and intended outcomes for the period
During the past year H4L continued to make more HFOMCs functional and to improve the performance of HFOMCs as measured by better access to and availability of quality services, especially to M/DAG populations in high-priority VDCs. In a few of these high-priority VDCs where H4L has concentrated its technical assistance, there is some preliminary evidence that utilization of services, such as institutional delivery and family planning, are increasing. Implementation Guidelines for the Collaborative Framework for Local Health Governance were finalized and government staff were oriented to the Framework and Guidelines nationwide.
Tracking pregnant women in H4L’s 141 high-priority is showing some promise. 2,401 pregnant women, or 32% of the expected number of pregnant women, were registered and tracked in the 39 sentinel sites in which CAP/Rs are using mobile technology, 577 of them delivered and 182 completed their 90-day postpartum period as of the fiscal year’s end. The registered women by caste/ethnicity were more or less proportionate to their estimated populations as well. Results show considerable variation between districts and some persistent underutilization of ANC, delivery services and PNC by M/DAG groups.
With support from H4L, NHRC is now equipped to greatly expand its knowledge management capabilities following installation of new computer equipment and a network. H4L also supported the
H4L—Annual Report 1

recent recruitment of a consultant to provide NHRC the necessary technical assistance to help build their knowledge management system and further develop their web-portal.
Drafting of NHSP III was completed during the past year with considerable TA from H4L in advising, drafting and decision-making. It was approved by the Program Development Team and Steering Committee, reviewed by the High-Level Committee chaired by the Minister and will be forwarded to the Cabinet for approval shortly. The subsequent Implementation Plan has been delayed following the earthquake. The Public Financial Management Advisor supported by H4L has made some progress guiding USAID-funded government-to-government (G2G) assistance. At the beginning of the new fiscal year he will be traveling to districts with the Comptroller and senior staff to follow-up audits conducted earlier.
The new QI system has been piloted as originally planned in Dang, Jumla and Surkhet and expanded to H4L’s 10 high-priority VDCs in the other 11 project districts. Implementation will expand to all VDCs of the 3 districts as planned, as well as to the other four demonstration districts. QI activities led by government national, district and health facility committees, working groups and teams have led to numerous activities improving the quality of health care.
The revised ANM curriculum, which includes an SBA core competencies component, was approved earlier than expected on July 9, 2014. However, H4L’s assessment of student and teacher knowledge and skills at ANM training sites found teachers also lacking in necessary knowledge and skills. In the coming fiscal year H4L will help develop supplementary learning materials, improve teaching techniques and coach faculty.
In the past year H4L supported D(P)HOs in all 14 project districts to increase access to family planning services in districts. We invested heavily in increasing the number of birthing centers that provide LAFP—implants and IUCDs. A majority of the 445 birthing centers now offer at least one of the 2 methods and about a third offer both methods.
NHEICC’s mHealth initiative, with technical assistance from H4L, reached 181,577 adolescents and youth with ASRH messages and information. Whereas, Radio Bahas improved the capacity of local radio program producers to create quality content, promote health as mainstream news, improve services and filling of vacant positions at health facilities, and provided opportunities to service seekers to interact directly with service providers at public hearings.
Leadership and management training is helping LifeLine Nepal address weaknesses cited by the TOCAT baseline. Starting immediately in the next fiscal year, H4L will support a financial management firm to provide strategic financial analysis and management assistance to LifeLine, as well as continue other training and coaching as necessary.
Objective 1: Improve health systems governance of district offices and sub-district level facilities
1.1 Provide TA to D(P)HOs to revitalize HFOMCs and to help develop VDC health plans that are incorporated in the district AWPB ensuring appropriate budget allocations
H4L’s technical assistance to the District (Public) Health Offices (D(P)HOs) during the year led to a series of revitalization workshops for 57 Health Facility Operations and Management Committees (HFOMCs) and training of 773 HFOMC officials in their roles and responsibilities, including GESI and disaster preparedness. An additional 42 HFOMCs were revitalized by other development partners in H4L project districts with H4L providing technical assistance, for a total of 99 HFOMCs revitalized out of a target of 100.
The H4L team, along with D(P)HO supervisors, mentored HFOMC members and assessed their functionality and performance. A total of 131 HFOMCs were re-formed by D(P)HOs during the reporting period in H4L districts, meaning that vacant positions were filled, and those committees that had not replaced members after their three-year tenure, as stipulated in the GoN guidelines, were dissolved and reconstituted.
To enhance leadership and effectiveness of the HFOMCs, H4L staff contributed to 45 meetings with VDC Secretaries and solidified the practice of inviting VDC-level social mobilizers from the Local
H4L—Annual Report 2

Governance and Community Development Program (LGCDP) for their input on health-related issues,
strengthening collaboration and cooperation between the two in H4L’s high-priority VDCs.
Functionality and Performance of HFOMCs
Table 1.1 Summary of HFOMC Functionality compared to September 2013 BaselineH4L HFOMC Functionality Criteria Sep 13 Jul 13- Jul 14-Jun
Baseline Jun 14 15
HFOMCs formed according 30 % 89 % 84 % to guidelines/directives
HFOMCs meet on regular basis 16 % 79 % 92 % (at least quarterly)
Meeting scheduled, agenda 61 % 78 % 95 % distributed in advance and minutes documented
Participation of women and 74 % 87 % 93 % Dalit members in meeting
Health facilities with the provision N/A 99 % 99 % of health services during regular hours (10:00 hrs.-15:00 hrs.)
% of HFOMCs meeting all criteria 16 % 78 % 84%
There are now more functional and better performing HFOMCs in project districts. Assessments conducted by H4L and/or D(P)HO teams suggest that about 84 percent of HFOMCs are now fully functional (524 out of 627) in H4L project districts, assuming that HFOMCs initially assessed as
functional in earlier reporting periods remained so. Surkhet, Rolpa, Banke, Dailekh, Salyan, Pyuthan,
Bardiya and Dang have a greater proportion of functional HFOMCs than Kapilvastu, Rukum, Jajarkot, Kalikot, Jumla and Arghakhanchi. A summary of HFOMC functionality and performance shows the accumulation from June 2014 to
Table 1.2 Summary of Performance of HFOMCs compared to Sep 2013 Baseline Performance Measurement Criteria Sep 2013
Baseline Jul 13-Jun 14
Jul 14-Jun 15
Provision of expanded health services
9 % 65 % 83 %
Upgraded quality of services 25 % 55 % 82 %
Additional resource mobilization 58 % 79 % 96 %
Active involvement of Dalit and women members
13 % 51 % 78 %
Social /public Audit conducted 30 % 25 % 32 %
Prepared annual health plan 36 % 79 % 97 %
Clinical staff positions filled 80 % 73 % 91.%
% meeting all criteria 9 % 25 % 32 %
June 2015, as presented in tables 1.1 and 1.2. An additional 58 HFOMCs became fully functional during the reporting period, an increase of 12.4 percent.
With technical assistance from H4L, D(P)HOs conducted 198 social audits, 43 for the first time in selected VDCs in all 14 project districts. Additionally, H4L worked with D(P)HOs in Banke, Kapilvastu,
Dailekh and Rukum to conduct follow-up social audits in 40 VDCs.
607 HFOMCs received a total of NPR 100,960,509 ($1,062,742) from MoFALD block grants and local resources through local bodies and communities during this reporting period. These resources funded the health plans prepared by HFOMCs as part of the VDC annual plans.
H4L—Annual Report 3
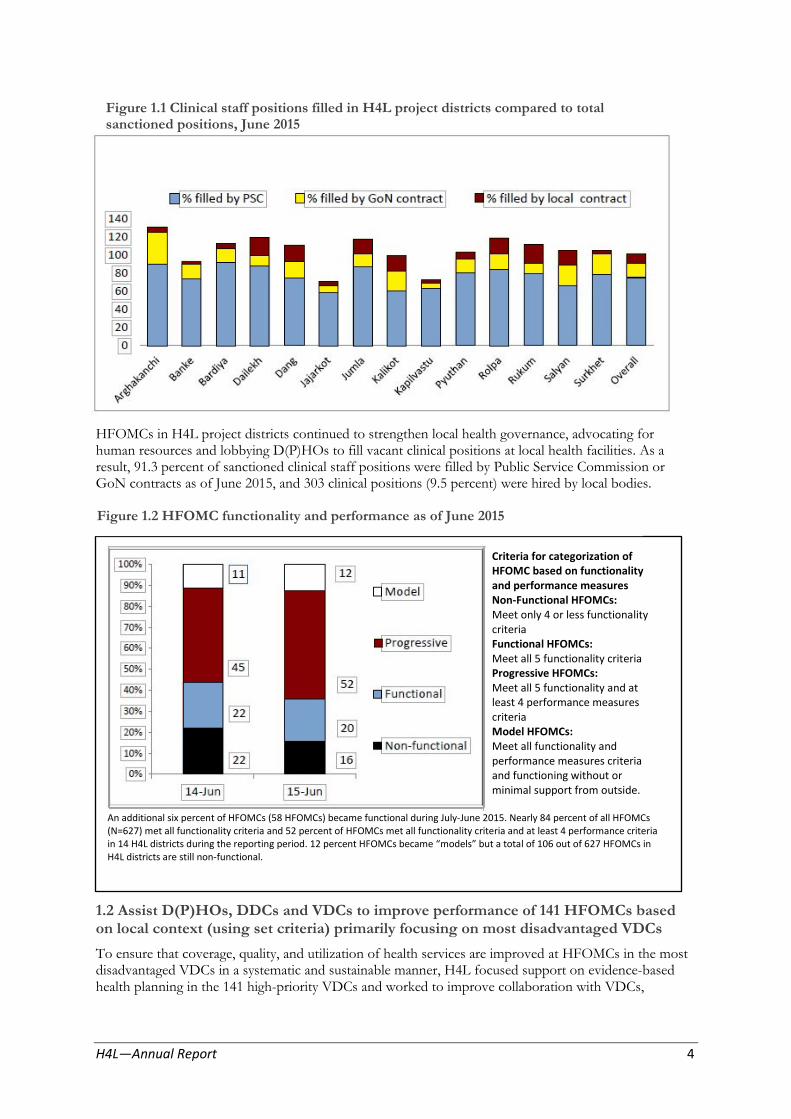
Figure 1.1 Clinical staff positions filled in H4L project districts compared to total sanctioned positions, June 2015
HFOMCs in H4L project districts continued to strengthen local health governance, advocating for human resources and lobbying D(P)HOs to fill vacant clinical positions at local health facilities. As a result, 91.3 percent of sanctioned clinical staff positions were filled by Public Service Commission or GoN contracts as of June 2015, and 303 clinical positions (9.5 percent) were hired by local bodies.
Criteria for categorization of HFOMC based on functionality and performance measures Non-Functional HFOMCs: Meet only 4 or less functionality criteria Functional HFOMCs: Meet all 5 functionality criteria Progressive HFOMCs: Meet all 5 functionality and at least 4 performance measures criteria Model HFOMCs: Meet all functionality and performance measures criteria and functioning without or minimal support from outside.
An additional six percent of HFOMCs (58 HFOMCs) became functional during July-June 2015. Nearly 84 percent of all HFOMCs (N=627) met all functionality criteria and 52 percent of HFOMCs met all functionality criteria and at least 4 performance criteria in 14 H4L districts during the reporting period. 12 percent HFOMCs became “models” but a total of 106 out of 627 HFOMCs in H4L districts are still non-functional.
Figure 1.2 HFOMC functionality and performance as of June 2015
1.2 Assist D(P)HOs, DDCs and VDCs to improve performance of 141 HFOMCs based on local context (using set criteria) primarily focusing on most disadvantaged VDCs
To ensure that coverage, quality, and utilization of health services are improved at HFOMCs in the most disadvantaged VDCs in a systematic and sustainable manner, H4L focused support on evidence-based health planning in the 141 high-priority VDCs and worked to improve collaboration with VDCs,
H4L—Annual Report 4
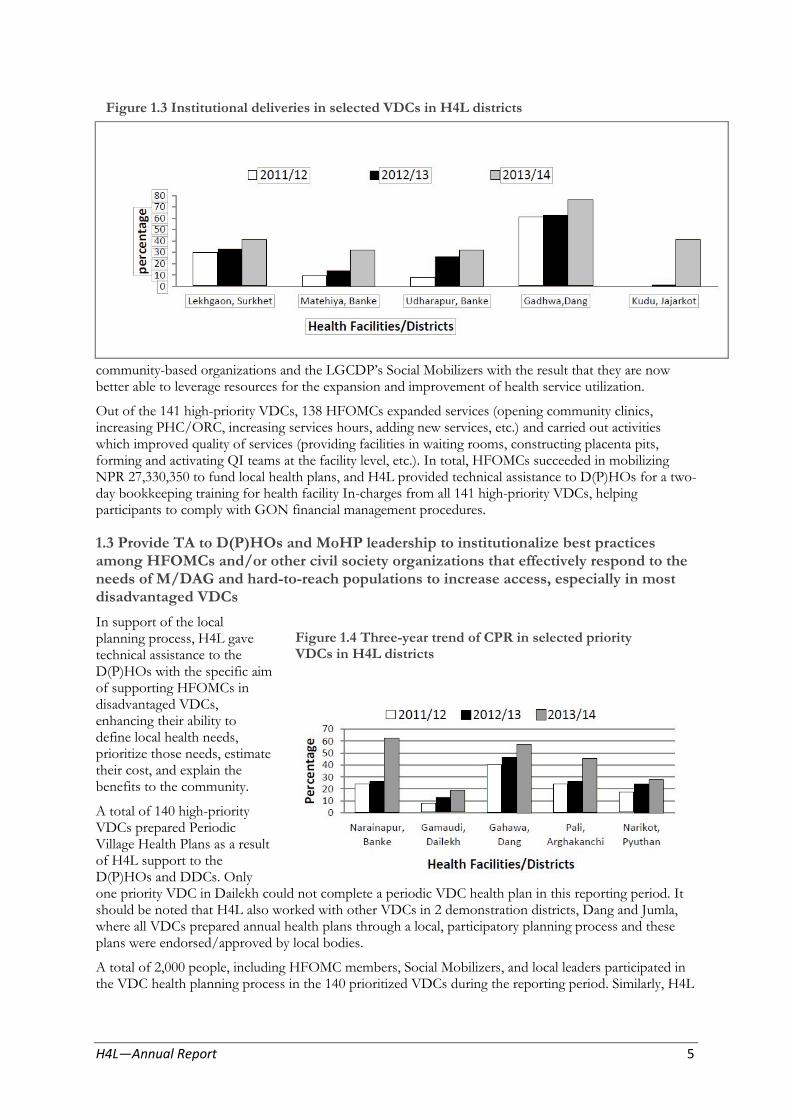
Figure 1.3 Institutional deliveries in selected VDCs in H4L districts
community-based organizations and the LGCDP’s Social Mobilizers with the result that they are now better able to leverage resources for the expansion and improvement of health service utilization.
Out of the 141 high-priority VDCs, 138 HFOMCs expanded services (opening community clinics, increasing PHC/ORC, increasing services hours, adding new services, etc.) and carried out activities which improved quality of services (providing facilities in waiting rooms, constructing placenta pits, forming and activating QI teams at the facility level, etc.). In total, HFOMCs succeeded in mobilizing NPR 27,330,350 to fund local health plans, and H4L provided technical assistance to D(P)HOs for a two-day bookkeeping training for health facility In-charges from all 141 high-priority VDCs, helping participants to comply with GON financial management procedures.
1.3 Provide TA to D(P)HOs and MoHP leadership to institutionalize best practices among HFOMCs and/or other civil society organizations that effectively respond to the needs of M/DAG and hard-to-reach populations to increase access, especially in most disadvantaged VDCs
In support of the local planning process, H4L gave technical assistance to the D(P)HOs with the specific aim of supporting HFOMCs in disadvantaged VDCs, enhancing their ability to define local health needs, prioritize those needs, estimate their cost, and explain the benefits to the community.
A total of 140 high-priority VDCs prepared Periodic Village Health Plans as a result of H4L support to the D(P)HOs and DDCs. Only one priority VDC in Dailekh could not complete a periodic VDC health plan in this reporting period. It should be noted that H4L also worked with other VDCs in 2 demonstration districts, Dang and Jumla, where all VDCs prepared annual health plans through a local, participatory planning process and these plans were endorsed/approved by local bodies.
A total of 2,000 people, including HFOMC members, Social Mobilizers, and local leaders participated in the VDC health planning process in the 140 prioritized VDCs during the reporting period. Similarly, H4L
Figure 1.4 Three-year trend of CPR in selected priority VDCs in H4L districts
H4L—Annual Report 5

support allowed D(P)HOs and DDCs to train 232 people, including VDC Secretaries and Health Facility In-charges on how to prepare annual VDC health plans in Dang and Jumla.
As a result of evidence-based local health planning in H4L districts, the capacity of HFOMCs and demand generation interventions at high-priority VDCs has improved FP/MNCH service coverage in some VDCs (Figures 1.3 and 1.4), and disparities in services utilization—particularly by Dalits and Muslims—have decreased significantly. However, disparities in service utilization by wards are still significant because some wards are more remote and/or have higher concentrations of M/DAGs. In response, HFOMCs are targeting those wards to increase access to services through PHCs/ORCs and satellite clinics.
1.4 Provide TA to MoHP, MoFALD and other stakeholders to expand local health governance strengthening activities to all 14 program districts and track progress against defined objectives and share with EDPs Forum and at the JAR
Collaborative Framework Implementation Guidelines
H4L provided technical assistance to the MoHP and MoFALD to implement the provisions of the Collaborative Framework. A draft of the Implementation Guidelines was shared with all MoHP and DoHS directors, MoFALD senior officials, the NPC and other ministries through a series of Technical Coordination Team meetings. Based on their input, the guidelines were finalized and approved by the ministries. Also during this period, H4L supported the MoHP in finalizing, printing, and disseminating the guidelines to every VDC and health facility. The Implementation Guidelines were also shared with concerned ministries, external development partners, academic and research institutions and local stakeholders.
Nationwide Orientation on Implementation Guidelines
H4L provided technical assistance and support for the MoHP/DoHS and MoFALD-led orientation on CF Implementation Guidelines during the Annual Regional Review meetings. Additionally, H4L supported the D(P)HOs and DDCs in all 14 H4L project districts to organize similar orientations at the VDC level. In total, 250 MoHP officials, 216 MoFALD officials, 564 district level officials and 2,108 VDC officials attended the orientation sessions.
Technical Assistance and Support to CF Demonstration Districts
H4L worked with both ministries to identify criteria and prepare formulas for the distribution of flexible health grants. These grants, worth NPR 50 million, are a new feature within the Management Division’s budget and are allocated to VDCs to plan and implement local health interventions.
As requested by the MoHP and MoFALD, H4L and partners oriented 125 DDCs, D(P)HOs and other district officials in the six demonstration districts where flexible health grants have been provided. H4L worked in Chitwan, Dang, Jumla and Kaski, while Kailali and Jhapa were supported by GIZ and Netherlands Leprosy Relief during orientation and VDC level health planning.
H4L provided technical assistance to D(P)HOs of four demonstration districts (Kaski, Chitwan, Dang and Jumla) during the VDC health planning process to utilize flexible health grants covering all VDCs in these districts.
A District Health Governance Strengthening Task Force (DHGSTF), as provisioned in the Collaborative Framework, has been formed in all 14 H4L districts and four additional demonstration districts. H4L district teams provided technical assistance for regular meetings of these task forces in the 14 districts. A total of 35 DHGSTF meetings were held during the reporting period. It was witnessed that DHGSTF members in demonstration districts engaged in monitoring of VDC health plans and review of progress.
H4L—Annual Report 6
Objective 2: Develop and implement national evidence-based policy
2.1 Strengthen HMIS
2.1.1 and 2.1.2 Support HMIS in customizing and rolling out DHIS-2
Although all DHIS-2 user training (85 persons trained at four events) was completed in the last reporting period, DHIS-2 has not yet been rolled out. The Management Division has yet to make a decision regarding the roll-out.
2.1.3 Strengthen evidence-based reviews and plans at the national and regional review meetings, incorporate GESI analysis and provide TA to 14 districts; and add a day to achieve it
H4L assisted the HMIS section to finalize the template for district and regional annual review meetings. Progress on H4L’s technical support to the national and regional review meetings was covered in the semi-annual report of Jul-Dec 2014.
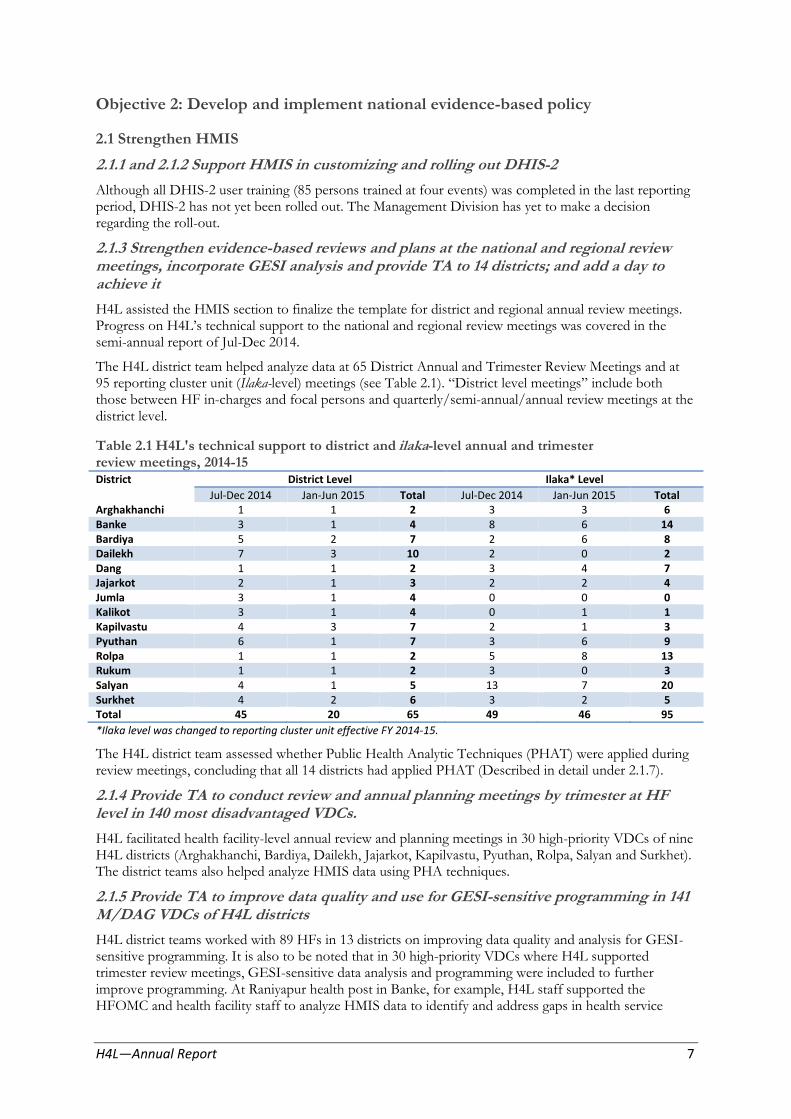
The H4L district team helped analyze data at 65 District Annual and Trimester Review Meetings and at 95 reporting cluster unit (Ilaka-level) meetings (see Table 2.1). “District level meetings” include both those between HF in-charges and focal persons and quarterly/semi-annual/annual review meetings at the district level.
Table 2.1 H4L's technical support to district and ilaka-level annual and trimester review meetings, 2014-15 District District Level Ilaka* Level
Jul-Dec 2014 Jan-Jun 2015 Total Jul-Dec 2014 Jan-Jun 2015 Total Arghakhanchi 1 1 2 3 3 6 Banke 3 1 4 8 6 14 Bardiya 5 2 7 2 6 8 Dailekh 7 3 10 2 0 2 Dang 1 1 2 3 4 7 Jajarkot 2 1 3 2 2 4 Jumla 3 1 4 0 0 0 Kalikot 3 1 4 0 1 1 Kapilvastu 4 3 7 2 1 3 Pyuthan 6 1 7 3 6 9 Rolpa 1 1 2 5 8 13 Rukum 1 1 2 3 0 3 Salyan 4 1 5 13 7 20 Surkhet 4 2 6 3 2 5 Total 45 20 65 49 46 95
*Ilaka level was changed to reporting cluster unit effective FY 2014-15.
The H4L district team assessed whether Public Health Analytic Techniques (PHAT) were applied during review meetings, concluding that all 14 districts had applied PHAT (Described in detail under 2.1.7).
2.1.4 Provide TA to conduct review and annual planning meetings by trimester at HF level in 140 most disadvantaged VDCs.
H4L facilitated health facility-level annual review and planning meetings in 30 high-priority VDCs of nine H4L districts (Arghakhanchi, Bardiya, Dailekh, Jajarkot, Kapilvastu, Pyuthan, Rolpa, Salyan and Surkhet). The district teams also helped analyze HMIS data using PHA techniques.
2.1.5 Provide TA to improve data quality and use for GESI-sensitive programming in 141 M/DAG VDCs of H4L districts
H4L district teams worked with 89 HFs in 13 districts on improving data quality and analysis for GESI-sensitive programming. It is also to be noted that in 30 high-priority VDCs where H4L supported trimester review meetings, GESI-sensitive data analysis and programming were included to further improve programming. At Raniyapur health post in Banke, for example, H4L staff supported the HFOMC and health facility staff to analyze HMIS data to identify and address gaps in health service
H4L—Annual Report 7

utilization. This resulted in an action plan addressing quality and coverage of care and it decided that additional PHC/ORC were necessary in other wards within the VDC.
2.1.6 Provide TA for NHSP-III development in the HIM thematic group and ESG
H4L’s Strategic Information and Research Advisor remained a member of the NHSP-III Thematic Group Health Information Management (TG-HIM) and the Evidence Support Group (ESG). Details of H4L’s support were included in the Jul-Dec 2014 semi-annual report.
2.1.7 Provide TA to the MD/HMIS to apply PHA in the remaining H4L districts (7 districts) and other districts based on requests from the MD/HMIS
H4L, in collaboration with the HMIS Section, developed a PHAT review checklist and used it to assess the use of PHAT at district review meetings. Based on the assessment, six of 14 districts were designated “model” districts (Banke, Bardiya, Dailekh, Kapilvastu, Rukum, and Surkhet), five as “progressive” (Arghakhanchi, Dang, Jajarkot, Pyuthan and Rolpa) and three districts as acceptable (Jumla, Kalikot and Salyan) (See PHAT review checklist in Annex 2).
2.1.8 Follow-up and update PHA techniques in the districts (7 districts) to develop village health profiles in the M/DAG VDCs where applied in 2013/14
Following PHAT training in seven districts, H4L emphasized developing village health situation analysis reports in the high-priority VDCs of each district, resulting in the preparation of 141 reports (Described in detail under 1.3).
2.2 Strengthen NHRC
2.2.1 Provide TA to strengthen NHRC’s research network and knowledge management capacity
H4L and the NHRC signed an MoU on July 17, 2014 to strengthen the capacity of NHRC to manage health research information and to coordinate research in the health sector to guide policy and program development in health. A Health Research Expert candidate has been selected and is expected to start working by August 2015.
A needs assessment was carried out by H4L and an NHRC IT Specialist, and a procurement plan was approved by USAID to support NHRC by providing computer equipment, including a server, backup system, 11 desktop PCs and a LAN network.
2.2.2 Provide TA to carry out field activities at H4L sentinel sites and document to strengthen health policies and programs
In June-July of 2014, H4L initiated activities at the sentinel sites, including subcontracting the Population and Health Development (PHD) Group to add 27 sentinel health facilities to the 2013 baseline survey. Major findings from the Health Facility Assessment of Sentinel VDC Health Facilities were reported in the Jul-Dec 2014 Semi-Annual Report.
In March 2015, Community Action Promoters/Researchers from 39 sentinel sites were hired by HFOMCs as a cost-share with H4L, trained and provided with a mobile phone for tracking of pregnant women to ensure FP/MNCH service utilization. As of June 30, 2,401 pregnant women were registered and tracked (Table 2.2); 577 of them delivered and 182 of them completed their 90-day postpartum period. 32.3 percent of the expected pregnant women at the 39 sentinel sites were registered and tracked (ranging from 16.1 percent in Rukum to 50.8 percent in Kapilvastu).
H4L—Annual Report 8

Table 2.2 Pregnant women tracked using mobile technology in H4L districts, as of June 30, 2015 District
Arghakhanchi
# of sentinel sites
2
# of expected pregnant
women in sentinel sites
250
# of pregnant
women registered
97
% of pregnant women
registered*
38.8
# of women that
delivered**
27
# of deliveries that completed
90-day postpartum
2
Banke 3 604 266 44.0 35 4
Bardiya 3 1,008 206 20.4 34 7
Dailekh 3 569 124 21.8 14 1
Dang 3 886 333 37.6 69 18
Jajarkot 2 352 87 24.7 14 2
Jumla 3 354 132 37.3 50 18
Kalikot 2 419 100 23.9 25 4
Kapilvastu 3 459 233 50.8 104 52
Pyuthan 3 432 192 44.4 46 25
Rolpa 3 431 158 36.7 34 6
Rukum 3 564 91 16.1 10 1
Salyan 3 484 130 26.9 21 4
Surkhet 3 626 252 40.3 94 38
Total 39 7,438 2,401 32.3 577 182
Note: * is against # of expected pregnant women in sentinel site. ** Live births to correspond with population-based survey (DHS and MICS).
Of the registered pregnant women, 34% were Brahmin/Chhetri followed by Janajati (25%) and Dalit (21%) (Figure 2.1) corresponding to the caste/ethnic composition recorded in the 2011 Census, with a slightly higher instance of Dalit and Muslim women registered.
Figure 2.1 Composition of pregnant women by caste/ethnicity against the population proportion in H4L districts (as of June 30, 2015)
Among registered women that delivered, 72.3% completed all four ANC visits, of which 62.4% did so according to protocol, see Figure 2.2.
H4L—Annual Report 9

Figure 2.2 Percent of women that had four ANC visits among those that delivered (live births) in 39 sentinel sites (as of June 30, 2015) (n=577)
81.6% of the 577 registered women that gave birth delivered at health institutions, ranging from 57% in Jajarkot to 100% in Bardiya (Figure 2.3). First PNC check-ups within 24 hours averaged 83.5%, ranging from 64.3% in Jajarkot to 97.9% in Surkhet.
Figure 2.3 Percent of women that delivered at health facility and percent of women that had 1st PNC within 24 hours among live births in 39 sentinel sites in H4L districts (as of June 30, 2015) (n=577)
Although a proportionally higher percentage of Dalit women are registered through the mobile-based tracking system, disparity in ANC and PNC service utilization remains a challenge. Dalit, Madhesi and Muslim women had less service utilization than Janajatis and Brahmins/Chhetris in all three major services, particularly in completing all four ANC visits (Figures 2.4 and 2.6).
H4L—Annual Report 10
28.6
38.0
48.1
52.4
56.0
60.0
60.6
60.9
61.8
65.7
66.7
76.5
78.6
79.8
62.4
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0
Jajarkot
JumlaArghakhachi
SalyanKalikotRukum
Kapilvastu
PyuthanRolpa
BankeDang
BardiyaDailekhSurkhet
Total
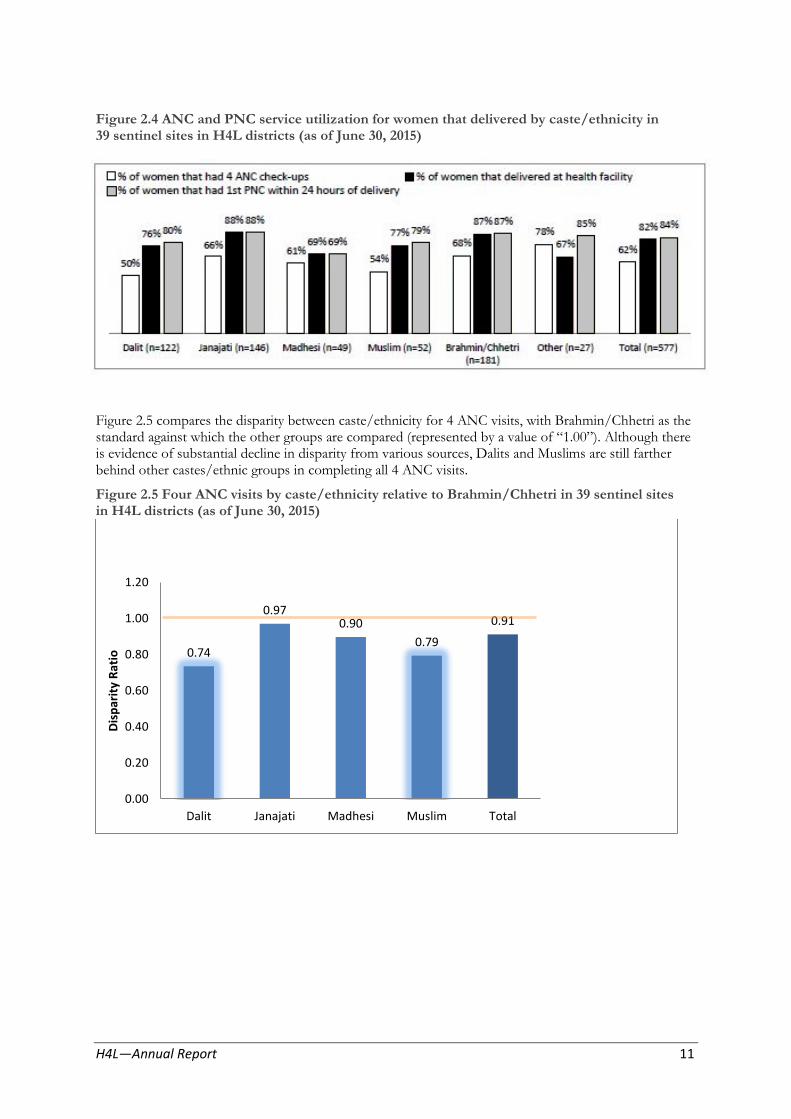
Figure 2.4 ANC and PNC service utilization for women that delivered by caste/ethnicity in 39 sentinel sites in H4L districts (as of June 30, 2015)
Figure 2.5 compares the disparity between caste/ethnicity for 4 ANC visits, with Brahmin/Chhetri as the standard against which the other groups are compared (represented by a value of “1.00”). Although there is evidence of substantial decline in disparity from various sources, Dalits and Muslims are still farther behind other castes/ethnic groups in completing all 4 ANC visits.
Figure 2.5 Four ANC visits by caste/ethnicity relative to Brahmin/Chhetri in 39 sentinel sites in H4L districts (as of June 30, 2015)
Dis
par
ity
Rat
io
1.20
0.97 1.00 0.910.90
0.79 0.80
0.60
0.40
0.20
0.00
0.74
Dalit Janajati Madhesi Muslim Total
H4L—Annual Report 11

Figure 2.6 PNC service utilization among postpartum women by caste/ethnicity in 39 sentinel sites in H4L districts (as of June 30, 2015)
Due to the very limited number of women that completed 90 days of the postpartum period to date (n=182), PNC check-ups and family planning status are analyzed only in the aggregate and not by district. Analysis reveals that 27.5% of postpartum women received PNC on the third day, 39.6% on the seventh day, and 58.8% on 42nd day after delivery, among those who completed the 90 days of the postpartum period (Table 2.3). Eight in ten (81%) of postpartum women received at least one FP counseling session during their 90-day postpartum period, ranging from 55% among Madhesi women to 100% among ‘Other’ caste women. Furthermore, slightly less than half (43%) of postpartum women that received at least one FP counseling session during the 90-day postpartum period decided to use some form of FP (Figure 2.7).
Table 2.3 Status of women that received PNC check-ups among women from sentinel sites that had completed the 90-day postpartum period FP counseling and decision to use FP methods among postpartum women
Dalit (n=48)
Janajati (n=47)
Madhesi (n=20)
Muslim (n=22)
Brahmin/ Chhetri (n=36)
Other (n=9)
Total (n=182)
Percent of women received FP 64.6% 63.8% 45.0% 63.6% 75.0% 88.9% 65.4% counseling during 1st PNC within 24 hours
Percent of women received FP 16.7% 29.8% 10.0% 13.6% 50.0% 55.6% 27.5% counseling during PNC on 3rd day
Percent of women received FP 31.3% 53.2% 20.0% 22.7% 50.0% 55.6% 39.6% counseling during PNC on 7th day
Percent of women received FP 58.3% 55.3% 40.0% 59.1% 69.4% 77.8% 58.8% counseling during PNC on 42nd day
Percent of women received at least 79.2% 85.1% 55.0% 72.7% 91.7% 100.0 81.3% one FP counseling during postpartum period
Percent of women who decided to 47.4% 42.5% 27.3% 50.0% 36.4% 60.0% 43.2% use any FP method (among women who received at least one FP counseling during postpartum period)
%
H4L—Annual Report 12

Figure 2.7 FP Methods among postpartum women currently using FP methods at sentinel sites (as of June 30, 2015) (n=63)
Other method Pills 3% 2%
Lactational
Female
IUCD Sterlization 8%
Condom male amenorrhea 19%
method 3%
2%
Implants 9%
Injectable depo 54%
2.2.3 Prepare technical and policy briefs based on findings from sentinel sites and inform district, regional and national stakeholders
Preliminary results from mobile tracking of pregnant women at sentinel VDCs have been submitted to USAID and are expected to appear in upcoming USAID publications.
2.2.4 Organize sensitizing workshop for USAID partners, research firms on NHRC ethical clearance process
Following initial discussions with the NHRC, a date was fixed for late April 2015 for the workshop. Following the earthquake April 25, NHRC suggested meeting later next Nepali fiscal year. The workshop is now scheduled for August 6-7, 2015.
2.3 M&E and research
2.3.1 Prepare H4L project technical briefs/reports on a periodic basis
H4L conforms to USAID Nepal’s communications and publications and, to date, H4L has submitted numerous updates for USAID Nepal’s Weekly Newsletter, articles for the USAID Nepal Quarterly Newsletter and social media.
2.3.2 Implement supplementary monitoring system in sentinel VDCs
Following recruitment and training of CAP/Rs at 39 sentinel sites, supplementary data collection tools that include tracking of key HMIS indicators related to ANC, delivery, FP, and childhood immunization by caste/ethnicity were designed and are operational at 39 sentinel sites. In addition, a barrier checklist was designed to collect some of the qualitative aspects of barriers that hindered service utilization by pregnant women from marginalized communities.
2.3.3 Standardize H4L’s district recording and reporting
H4L revised its M&E plan in response to a lack of HMIS data, inconsistencies and errors in data during implementation in the last reporting period and the additional indicators required by USAID. These changes are reflected in the recording and reporting tools, and the district teams were oriented on these tools during H4L’s annual review meeting in July–August 2014. Furthermore, H4L aligned the logistics related indicator (under Objective 7) with the H4L Logistics’ M&E plan. The revised M&E plan is currently awaiting formal approval.
H4L—Annual Report 13
H4L also emphasized conducting monthly HF readiness assessments during visits. H4L introduced these tools in March 2014 with a resulting increase in visits by the H4L district team; a total of 392 and 147 HF readiness assessments were carried out in the high-priority VDCs and other VDCs, respectively (including both new and repeat visits). Similarly, 777 and 235 FCHVs readiness assessments were conducted in high-priority VDCs and other VDCs, respectively and 315 and 93 client exit interviews were carried out in high-priority VDCs and other VDCs, respectively (data not shown here).
2.3.4 Assess comprehensiveness of MoHP’s information system (HISPIX)
Not planned for this period.
2.3.5 Assess district reviews conducted in accordance with PHA performance index
Detail of this activity is covered under 2.1.7.
2.3.6 Finalize Rapid Assessment of M&E and Data Demand and Use report among D(P)HOs officials and use findings for capacity building
The MD, with technical support from H4L, conducted a rapid assessment of knowledge and skills on data analysis and use among district health statisticians. Summary of findings were presented in the SAR Jul-Dec 2014.
Objective 3: Strengthen national-level stewardship of the health sector
3.1 Collaborate with other health sector partners and assist MoHP to formulate NHSP III in a manner that is evidence-based, strategic and participatory
In collaboration with NHSSP and other partners, H4L assisted the MoHP in preparing the final draft of the NHSP-III, together with the M&E Framework. The final draft was endorsed by the Program Development Team (PDT) on July 15, 2015. The Steering Committee (Chaired by the Secretary) and High-Level Committee (Chaired by the Minister) met July 19 to review and recommend revisions before forwarding to the Cabinet for final approval.
H4L’s involvement in the NHSP-III drafting process included contributions to sections on health systems and policy, local health governance and decentralized planning and budgeting, e-Health and information systems, service delivery, quality, sector reform and the M&E framework. These sections were reviewed, with the help of an international expert hired by H4L, at a series of meetings held by the PDT, thematic groups and Sounding Boards.
3.2 Provide TA to the MoHP to link the new NHSP to the AWPB process
Once the NHSP-III Strategic document and M&E Framework (draft) are approved by the Cabinet, the NHSP-III implementation plan will be prepared and linked with the AWPB process. Due to the April 25 earthquake, preparation of the Implementation Plan has been delayed. The H4L senior team will continue collaborating with the NHSSP and other health sector partners on this topic.
Public financial management
H4L has supported the MoHP by placing a Public Financial Management Advisor (PFMA) at the DoHS Comptroller’s Office to guide USAID-funded government-to-government (G2G) assistance and to support the implementation of capacity development activities aimed at strengthening the public financial management and procurement operations of the MoHP.
With support from the PFMA, the DoHS was able to complete:
Timely submission of Reimbursement Claims to USAID on a trimestral basis
Planning and preparation of Regional Financial Workshops for accounting staff of all 75 districts under DoHS.
Progress reporting of USAID’s G2G-supported Redbook activities and budgets from all respective Divisions/Centers and provide to USAID on a quarterly basis
Preparation of management comments to the audit observations and follow-up for corrective measures as recommended by auditors
H4L—Annual Report 14
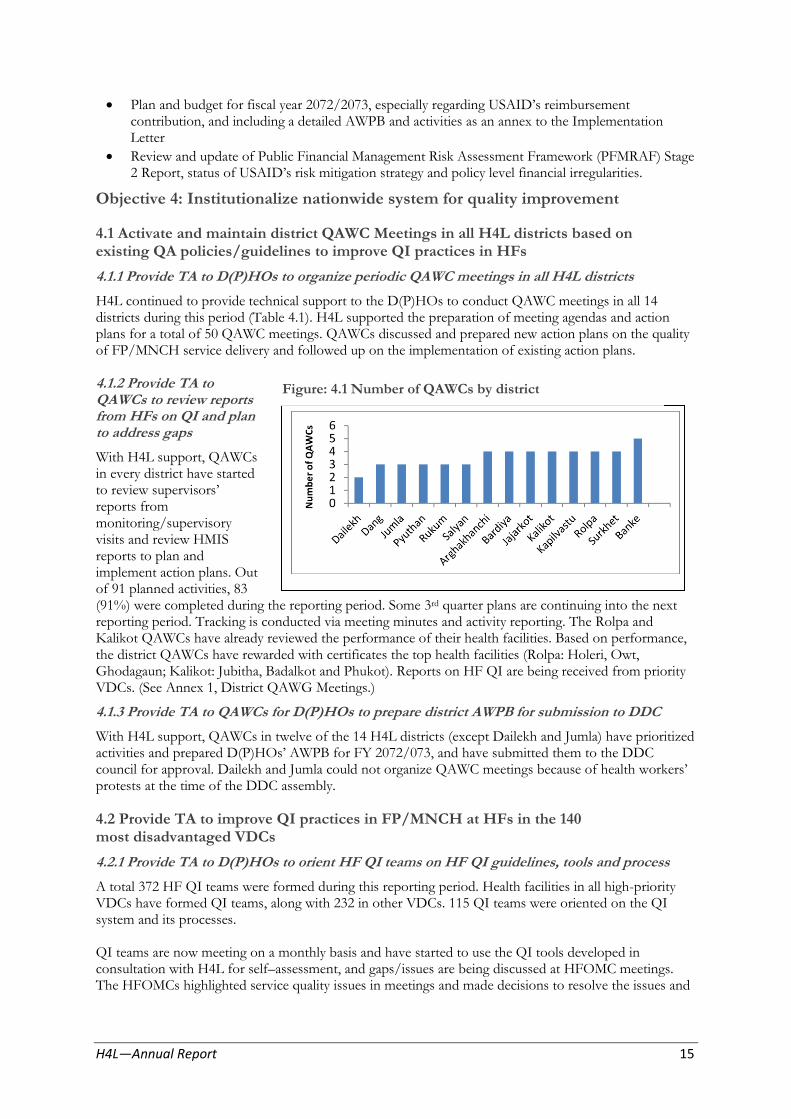
Figure: 4.1 Number of QAWCs by district
Plan and budget for fiscal year 2072/2073, especially regarding USAID’s reimbursementcontribution, and including a detailed AWPB and activities as an annex to the Implementation Letter
Review and update of Public Financial Management Risk Assessment Framework (PFMRAF) Stage 2 Report, status of USAID’s risk mitigation strategy and policy level financial irregularities.
Objective 4: Institutionalize nationwide system for quality improvement
4.1 Activate and maintain district QAWC Meetings in all H4L districts based on existing QA policies/guidelines to improve QI practices in HFs
4.1.1 Provide TA to D(P)HOs to organize periodic QAWC meetings in all H4L districts
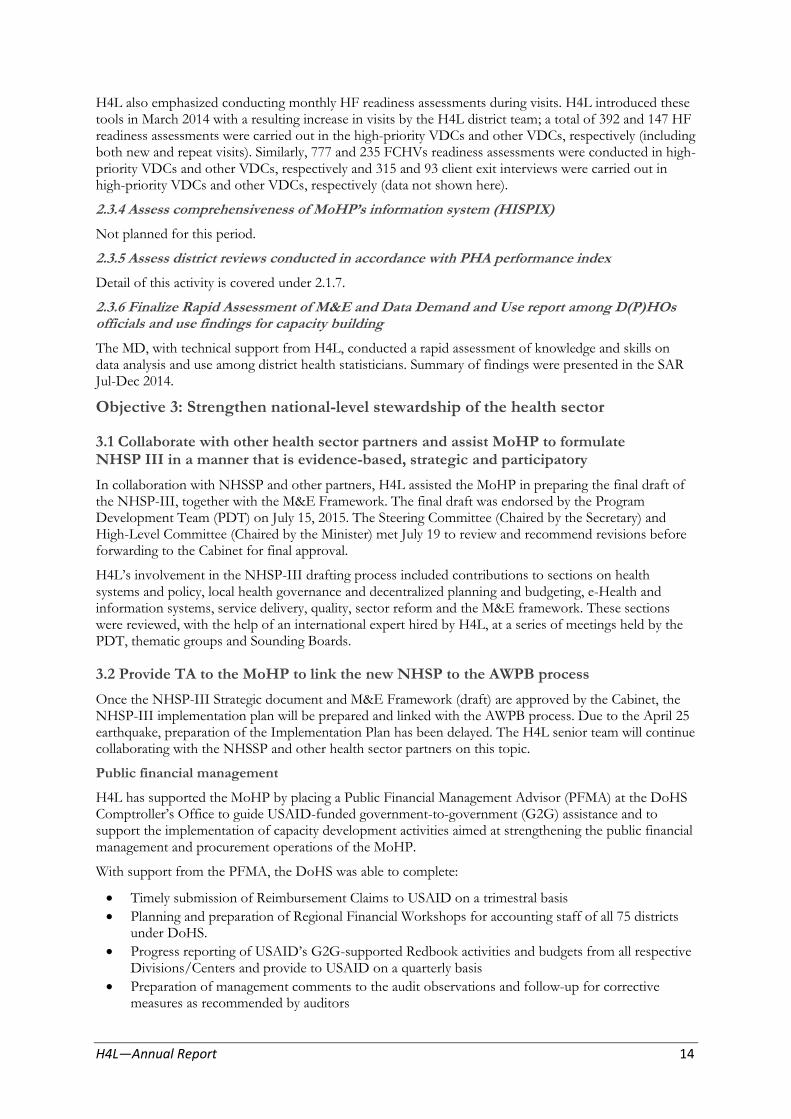
H4L continued to provide technical support to the D(P)HOs to conduct QAWC meetings in all 14 districts during this period (Table 4.1). H4L supported the preparation of meeting agendas and action plans for a total of 50 QAWC meetings. QAWCs discussed and prepared new action plans on the quality of FP/MNCH service delivery and followed up on the implementation of existing action plans.
4.1.2 Provide TA to QAWCs to review reports from HFs on QI and plan to address gaps
With H4L support, QAWCs in every district have started to review supervisors’ reports from monitoring/supervisory visits and review HMIS reports to plan and implement action plans. Out of 91 planned activities, 83 (91%) were completed during the reporting period. Some 3rd quarter plans are continuing into the next reporting period. Tracking is conducted via meeting minutes and activity reporting. The Rolpa and Kalikot QAWCs have already reviewed the performance of their health facilities. Based on performance, the district QAWCs have rewarded with certificates the top health facilities (Rolpa: Holeri, Owt, Ghodagaun; Kalikot: Jubitha, Badalkot and Phukot). Reports on HF QI are being received from priority VDCs. (See Annex 1, District QAWG Meetings.)
4.1.3 Provide TA to QAWCs for D(P)HOs to prepare district AWPB for submission to DDC
With H4L support, QAWCs in twelve of the 14 H4L districts (except Dailekh and Jumla) have prioritized activities and prepared D(P)HOs’ AWPB for FY 2072/073, and have submitted them to the DDC council for approval. Dailekh and Jumla could not organize QAWC meetings because of health workers’ protests at the time of the DDC assembly.
4.2 Provide TA to improve QI practices in FP/MNCH at HFs in the 140 most disadvantaged VDCs
4.2.1 Provide TA to D(P)HOs to orient HF QI teams on HF QI guidelines, tools and process
A total 372 HF QI teams were formed during this reporting period. Health facilities in all high-priority VDCs have formed QI teams, along with 232 in other VDCs. 115 QI teams were oriented on the QI system and its processes.
QI teams are now meeting on a monthly basis and have started to use the QI tools developed in consultation with H4L for self–assessment, and gaps/issues are being discussed at HFOMC meetings. The HFOMCs highlighted service quality issues in meetings and made decisions to resolve the issues and
H4L—Annual Report 15

reported to the districts. QI Teams are now able to report the issues and gaps to HFOMCs and D(P)HOs.
4.2.2 Provide TA to HF QI Teams to monitor HF readiness, QI practices and address gaps at HFs
H4L staff made 493 visits to HFs and worked with HF QI teams to monitor HF readiness, QI practices and address gaps. H4L staff coordinated with D(P)HOs and HFOMCs as well as other partners to manage IP, waste disposal and construction of placenta pits. H4L staff also coordinated with D(P)HOs, district stores and concerned focal persons to ensure a regular supply of necessary materials and logistics to the health facility (e.g., autoclaves, buckets, puncture-proof containers, dustbins and chlorine). As indicated by the HF readiness assessment there is a need to focus on supplying IP and QI guidelines and masks (see Figure 4.2).
4.2.3 Provide TA to HF QI Teams to prepare and submit QI reports to district DQAWC/D(P)HOs
115 HF QI teams are now able to prepare and submit QI reports to the district with technical assistance from H4L. 75% of HFs reported during this reporting period.
4.2.4 H4L will establish an eHealth system to upload health facility data by mobile device and aggregated at the district level for analysis.
Not yet done.
Figure 4.2 IP and HCWM Practices
0.360.41 0.42
0.78 0.8 0.81
0.93 0.940.97 0.98
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
HF levelguidelines for
standardprecautions
(n=267)
HF QI guidelinein examinationroom (n=269)
Masks (n=268) Latex gloves(n=268)
Sterilizationequipment
(n=267)
Disinfectant(Chlorine)(n=267)
Gloves (n=268) Puncture proofcontainer and
burning pit(n=266)
Soap or handdisinfectant
(alcohol +glycerin)(n=268)
Single use-standard
disposablesyringes(n=268)
Availability of items - standard precautions for prevention of infections on the day of visit, H4L districts (July 014-June 2015)
4.3 Maintain National Quality Assurance Coordination Mechanism
4.3.1 Provide TA to MD/DOHS at periodic meetings to make functional the QI Technical Advisory Committee
H4L continues to provide TA to the MD to functionalize the QI TAC Committee. The second QI TAC met on April 19, 2015, with support from H4L.
H4L—Annual Report 16

4.3.2 Provide TA to QI TAC to review progress in improving QoC and to develop appropriate interventions
The QI TAC met with support from H4L to discuss the management of information, and agreed to finalize the QA Implementation Guidelines once they have reviewed field experiences. They expect to endorse the guidelines in August 2015.
The QI TAC also agreed to a phased scale-up of the HF QI system in other districts, engage partners, and continue scale-up of the hospital QI process. It was also decided to discuss the details of information management during the next QAI TWG meeting and to update the guidelines.
4.3.3 Provide TA to MD/QA section at periodic meetings to make functional the QAI Technical Working Group
Quality Assurance and Improvement Technical Working Group (QAI TWG)
The QAI TWG has met nine times since its formation, including three times this year. It focused on finalizing the National QI system and implementing the QI system at HFs and the districts. The key decisions and results from the three meetings held during this reporting period are summarized in Table 4.2.
Table 4.2 QAI TWG meeting
Date QAI TWG Key discussions and decisions
August 26, 2014 Seventh Meeting Revise hospital assessment tool and expand quality domain for hospital QI, including management, OPD, emergency, lab, X-ray in the future.
January 13, 2015 Eighth Meeting
(Previous members
from different
Divisions were
transferred and new
members have joined)
Oriented new members on QA Policy, situation analysis, existing guidelines and gaps and initiatives taken to address, structure of QA TAC, QAI TWG, district QAWC, HF QI team and Hospital QI committee roles and responsibilities
Update on progress made to date regarding HF QI system – QI process, tools and reporting system and implementation in Dang and Jumla
Progress made by Taplejung and Hetauda hospitals on (HQ IP)
/Planning Section, MD discussed hospital strengthening program and grant that MD has for this AWPB; guidelines need to be developed for budget and facilitation support required for hospital board/QI committee on proper use of grant/resources
March 2, 2015 Ninth meeting Orientation to remaining new members on QA Policy, situation analysis, existing guidelines and gaps and initiatives taken to address
rom NHT� presented NHT�’s efforts on maintaining quality in the FP training sites using QI Tools and findings of two FP training sites, ICTC, Nepalgunj and WRH (Pokhara)
Finalize tools and guidelines in Nepali.
4.3.4 Provide TA to the QAI TWG to implement national QI in accordance with guidelines to strengthen the quality improvement system and monitor in 2 districts per region
Together with other partners, H4L is continuing to assist the QAI TWG with implementing the national QI system. Although the QAI TWG at first decided to implement it in two districts per region, they later decided to implement it in the same six demonstration districts as the Collaborative Framework pilot. Though district-level orientation was conducted, implementation in these districts was delayed, except in Dang and Jumla. In Dang and Jumla, the HF QI system has been implemented in all high-priority and in an additional 4 and 2 HFs, respectively.
4.3.5 Provide TA to QAI TWG to organize meetings to review progress and revise guidelines and other tools
H4L, together with partners, continued its support to the QAI TWG and oriented three people to look after QA activities. However, staffing changes resulted in fewer QAI TWG meetings than expected and were also the cause of several delays.
H4L—Annual Report 17

QI Assessment: Action Planning with HFOMCs
4.3.6 Provide TA to QAI TWG to finalize national guidelines and tools, translate into Nepali based on field experience
The QA Section at MD reviewed and finalized national guidelines and tools in Nepali in September with H4L support. H4L also provided TA to the QA and HMIS Sections to develop a reporting system along with AWPB program guidelines. A separate meeting with the HMIS Section and partners was held to further refine the reporting system, which includes reporting from health facilities and hospitals to district QAWCs and from D(P)HOs to the MD’s QA Section.
4.3.7 Provide TA to QAI TWG to strengthen district QAWCs to steer quality of services
As a QAI TWG member, H4L is supporting district QAWCs in all 14 H4L districts to steer the quality of services. All 14 district QAWCs have regular quarterly meetings where quality-related issues and challenges from different HFs are discussed and resolved. As a result, 12 QAWCs reviewed the AWPB before submitting to the DDC.
4.3.8 Provide TA to QAI TWG to inform QI TAC and stakeholders periodically
H4L provided TA to the QAI TWG to update the QI TAC (April 19, 2015 meeting) and also to inform stakeholders in a child health review meeting (CHD), Reproductive Health Sub-Cluster meeting for post-disaster response (May 20), FP trainers’ review meeting (March 29), and the IP material workshop (May 27) (NHTC).
4.4 Implement revised National facility-based QI system
4.4.1 Provide TA to QAWCs D(P)HO to implement facility-based QI system in the 14 selected districts
H4L is supporting implementation of the facility-based QI system in all 14 H4L districts, starting in 115 high-priority VDCs, and seven additional VDCs in Dang and Jumla. As a result, service providers have started assessing the quality of FP/MNCH services using the QI tools. Compliance with standards varies based on the technical area and between health facilities.
H4L—Annual Report 18

Figure 4.3 Select Components of the Safe Motherhood Program assessed by Districts
Table 4.3 Health Facility QI Teams
District
Jul 2014-Jun 2015
High-priority VDC Other VDC* No. of QI Teams
Oriented Total
Arghakhanchi Banke Bardiya Dailekh Dang Jajarkot Jumla Kalikot Kapilvastu Pyuthan Rolpa Rukum Salyan Surkhet Total
10 10 10 10 10 10 10 10 10 10 10 10 10 10
140
7 26 21 13 25 23
2 19
2 25 31 11 21
6 232
9 10 10
0 14 10
7 0
10 10 10
5 10 10
115
17 36 31 23 35 33 12 29 12 35 41 21 31 16
372
Health Facility Based QI
The HF QI system was successfully implemented in all high-priority VDCs in the H4L project districts with the exception of Dailekh and Kalikot. In Dang, Jumla and Surkhet, H4L will continue to work with the D(P)HOs to implement throughout the district. Due to the unavailability of HWs in Arghakhanchi, implementation in Simalpani VDC was not completed, but will be implemented soon.
An assessment of the QI tools was done for sub-components of each of the technical areas of FP/MNCH. Because availability of services and cases vary, and for other reasons, there is variation among health facilities.
The assessment looked at compliance with standards, where a rate of 80 percent compliance or more is considered ‘high quality’ services, but there is considerable variation among health facilities by technical area. Figure 4.4 shows compliance with standards for growth monitoring at 10 HFs in prioritized VDCs, for example, where only four HFs out of ten (Kotgaun, Dubidanda, Sulichaur and Khumel) were more than 80 percent compliant.
H4L—Annual Report 19

Follow up of Quality Improvement
The most important element of the HF QI system is addressing the gaps identified during the assessment, so in order to monitor improvements in quality of care, follow-up QI assessments were conducted. Examples of improvement may be seen in figures 4.5 and 4.6.
Figure 4.4 Assessment of Growth Monitoring by Prioritized VDCs of Rolpa (2014/15)
0102030405060708090
100
Pe
rce
nta
ge
Figure 4.5 QI Follow up: Comparisons of Infection Prevention and Health Care Waste Management, Dang (2014/15)
H4L—Annual Report 20

Figure 4.6 Compliance with FP counseling standards in Dang (2014/15)
4.4.2 Provide TA to MD/DOHS to print national QI guidelines, tools and forms H4L supported MD in photocopying the draft National QA Guidelines, the FP/MNCH tools and the reporting HF-to-District QAWC reporting forms. These materials were distributed to all H4L district QAWCs and to the health facilities of the high-priority VDCs of every H4L district. They will be printed professionally after finalization and approval.
4.4.3 Provide TA to MD, together with RHD, to orient all 75 D(P)HOs on national HF QI system at regional level
The implementation of the HF QI system in the six demonstration districts was delayed. As a result, national orientation was not carried out, but is expected to take place in the coming year, although the strategy must be reexamined.
4.4.4 HF data are uploaded by a mobile device and aggregated at the district level for analysis
Not conducted. See explanation in Section B.
Objective 5: Improve capacity of district and local level health workers and community volunteers to deliver high quality FP/MNCH and nutrition services
H4L contributed to several FPSC, SMSC, and ASRH meetings. See highlights from topics discussed in the following text box.
H4L assisted FHD in preparation of the NHSP-III strategy and implementation plan for family planning, ASRH and men’s health. H4L helped align the Costed-Implementation Plan for FP with NHSP-III.
As a member of the TAG, H4L assisted FHD in the design, pre-testing and finalization of the Decision Making Tools (DMT) and Medical Eligibility Criteria (MEC) wheel for family planning.
H4L made significant technical contributions to designing, developing and finalizing the CB-IMNCI package (HF-level modules, chart booklet and facilitator guide, and FCHV-level flip chart and management guidelines), which was endorsed by the MoHP (Oct 2014) and focuses on skill development of HWs and shorter trainings to help lower cost and health worker absenteeism at the HFs, and for FCHVs to adjust to their new role.
H4L—Annual Report 21

Additionally, H4L helped CHD and NHTC in revising the Neonatal Care Package for 1, 2, 3 level care. H4L provided technical input for primary- and secondary-level care hospitals. The package is currently in the process of being developed.
H4L contributed to formulating World Pneumonia Day celebrations, the CB-IMNCI management module, and institutionalization of IMNCI training and video development.
H4L also helped draft the NHSP III strategy and
celebration, DMPA specifications, improving implementation plan for newborn and child care (NBC LAFP services, LAPM strategy, Depo uniject, Care). Key issues included CB-IMNCI program HC3 overview, post-abortion FP service
FPSC meeting– established FP Day
implementation, maintenance, coordination with guidelines, pre-departure orientation to medical colleges and paramedical and nursing schools migrants, FP services from private sector, to incorporate the IMNCI curricula into their neonatal IUCD services by HA assessments, Panchthar and child health content, as well as the role of the Depo incident, as well as NHSP-III
private sector in NBC Care. H4L also addressed Implementation Plan for FP, AWPB for FP,
establishing newborn corners at birthing centers, and SIFPO/USAID project. stabilization units in district hospitals,
H4L supported FHD in FP logistic forecasting institutionalization of training through NHTC/RHTC, workshop in Dhulikhel (March 18-19, 2015) incorporation of newborn messages in SBA packages, organized by LMD. All required commodities as well as NB services at the community level. and other materials identified and quantified for family planning services through The H4L team supported CB-IMNCI a logistic LMD/RMS to the districts for FY 2072/73. forecasting workshop held in Dhulikhel, in which all
the required materials were identified and quantified for SMSC meeting–addressed remote MNH
initial training activities. The H4L team also helped pilot, integration of IMCI and NCP, CHD in identifying and quantifying drugs, equipment, community midwives, criteria for private
sector to provide Aama Surakchha Program, and logistics through the LMD/RMS for FY 2072/73.
findings of pelvic organ prolapse study, SM H4L organized and contributed to a one-day workshop
Policy 2014, Maternal and Perinatal Death for the NHTC, December 1, 2014, during which
Surveillance and Response Guidelines, Birth NHTC identified needs, key approaches and plans for Defects Surveillance, Prevention and Control a) FP training package revision/update; b) self-paced Plan, specification for Nyano Jhola, as well as
NHSP III IP for maternal health program, NSV and IUCD packages; c) FP training video AWPB for SM. development; and d) post-VSC recanalization training.
From March 29 to April 2, 2015 these materials were ASRH meeting–development of ASRH reviewed and revised with input from key experts from
training manual, ASRH strategy, orientation to FP training partners and FP training sites.
district ASRH program, QI and certification for AFS (adolescent-friendly services), H4L assisted the NHTC to update the knowledge of menstrual hygiene and response to post- trainers from all FP training sites on the national quality disaster (earthquake) AFS. improvement system, including QI at FP training sites
and family planning utilization in Nepal, and to update the Costed Implementation Plan (CIP) on family planning that were useful for package revision. H4L presented the key findings of the Birthing Center Assessment with the Training Working Group on September 15, 2014 and announced the approval of the revised ANM curriculum. We also provided input as a TAG member on the ASRH training package development during both the TAG meetings and workshop (October 28-29).
H4L supported the technical working group to develop the post disaster (earthquake) promotional health education communication strategy in partnership with NHEICC, UNICEF, WHO, Suaahara and HC3, and provided TA to NHIECC to develop their FP communications strategy (supported by the HC3 project). During this workshop (August 2014), H4L made a presentation on family planning focusing on youth. H4L also helped the NHIECC devise an FP media campaign (SMART FAMILY).
Additional support to CHD and FHD for Post-disaster (earth quake) response
H4L supported the CHD to finalize HW training materials pertaining to CB-IMNCI and nutrition for post-disaster situations and drafted a package that includes key messages on ANC, PNC, MSC, delivery and PPFP. H4L facilitated, together with other partners, an orientation for 42 HWs hired by I/NGOs that were expected to support the GoN HWs in emergency situations in their respective working areas.
H4L—Annual Report 22

H4L also provided TA at RH Sub-Cluster meetings for post-disaster response organized by FHD, particularly in developing a rapid assessment of sexual and reproductive health in post-disaster (earthquake) situations, health facility (or camp) readiness, FP/MH and ASRH key messages in post disaster situations, revision of the RH kit, etc.
5.1 Provide TA to Divisions and Centers (FHD, CHD, NHTC, NHEICC) during revisions of strategies/guidelines/training materials for HWs and FCHVs on FP/MNCH
5.1.1 Provide TA to FHD on FP advocacy at central level and in H4L districts
As a part of FP advocacy, H4L assisted FHD in organizing a FP Celebration Day on September 18, 2014 in Kathmandu and assisted D(P)HOs in nine H4L districts in which 161 implants and 26 IUCDs were inserted at satellite clinics, demonstrating that women will use long-term family planning methods if trained staff and services are conveniently available.
H4L also contributed to an “advocacy and message development workshop’ (June 25-26) organized by the Health Policy Project to develop messages.
5.1.2 Provide TA to FHD to develop and print advocacy materials
The project supported the development of advocacy materials and the printing of 5,000 family planning brochures, which were distributed nationwide last September. Additional printings will be done after HPP develops the messages and the CIP, and NHSP-III is fully implemented next year.
5.1.3 Provide TA to FHD during review and planning meetings of FP/RH activities
Together with other partners, H4L assisted FHD conduct the National Reproductive Health Review and Planning Workshop (February 8-9, 2015). Our TA focused mostly on family planning, safe motherhood (MSC, CEONC referral), newborn care, and ASRH. In addition, H4L provided the TA regarding the QI system, which includes quality of services pertaining to FP/MNH, strengthening of CEONC referral services, mHealth, etc.
5.1.4 Provide TA to build FP training capacity using alternative approach (self-paced) for NSV
H4L helped NHTC meet with experts to finalize the enrollment process, guidelines and course outline for the alternative approach. H4L also provided orientation and discussed this process with a trainer from the Pokhara FP training site and received feedback. H4L helped draft the necessary tippani (approval) process. However, NHTC could not move forward with the approval process, but is planning to implement the training next year.
5.1.5 Provide TA to NHTC to build FP training capacity using alternative approaches (self-paced and coaching) for IUCD
H4L supported the NHTC in drafting self-paced training modules for IUCD and received feedback from trainers and experts during a workshop conducted March 29-April 2. After finalizing early next fiscal year, NHTC has plans to start IUCD training using the approach, particularly in H4L project districts.
5.1.6 Provide TA to NHTC to establish QI system at FP training sites
To facilitate training and to improve IP and HCWM practices at HFs and hospitals, H4L helped NHTC conduct two workshops (April 13 and May 26-27) to revise and update infection prevention training materials.
In addition to updating the package, H4L assisted in developing the “on-site/whole site” approach to strengthening IP and HCWM practices. H4L has already drafted a course outline and field tested the approach during IP
training (June 3-5, 2015) in Dailekh, where participants used a check list (QI tools) to assess IP/HCWM practices at the district hospital. An action plan for improvements was made and shared with the hospital
H4L—Annual Report 23

QI committee. This hands-on approach helped participants focus on skills they most needed to improve, and showed that this approach is not only feasible and enjoyed by participants, but is helpful in bringing immediate change to the health facility while improving the skills of the participants.
H4L also oriented the hospital QI Committee on the national QI system and, at the request of NHTC, oriented the Suaahara/Jhpiego consultant on the on-site/whole-site approach for NHTC’s IP/HCWM
training in Sulukhumbu.
H4L provided technical assistance to NHTC to initiate the QI system at FP training sites. So far H4L has introduced QI tools at four FP training sites (ICTC-Nepalgunj, WRTC-Pokhara, FPAN-central, MSI-Valley). The orientation on QI tools was completed at the Maternity Hospital and a follow-up visit is planned in July 2015. A summary of compliance rates from the QI assessment is given in Figure 5.1.
5.1.7 Provide TA to CHD to conduct MTOT on revised CB-IMNCI package
At the request of CHD, H4L facilitated the TOT at RHTC Surkhet (March 27–April 2) instead of the MTOT at central level. All together 25 participants (16 male, 9 female) were trained from Jumla, Jajarkot, Surkhet and Humla, including SBAs from regional hospitals and the RHTC. H4L also supported supervision of the TOT by officials from the CHD led by the IMCI Section Chief, and by officials from the RHD.
Good training management, adequate practice with anatomical models and hands-on
Participants learning ENC using an anatomical model (MTOT) training at Surkhet’s Regional Hospital using experienced
facilitators from H4L resulted in high-quality training at the regional level that was greatly appreciated by GoN officials. In addition to conducting the TOT, H4L assisted the CHD in laying the foundation for developing the RHTC and Surkhet Regional Hospital as a clinical training site for future IMNCI training.
5.1.8 Provide TA to CHD during review and planning meetings for child health programs
Together with other partners, H4L supported CHD during their National Review, Reflection and Planning Workshop (February 16-18) and in the preparation of the AWPB for CB-IMNCI for FY 2072/73, which emphasizes better program implementation modality and institutionalization of CB-IMNCI training.
H4L—Annual Report 24

5.1.9 Provide TA to Regional Health Directorates of Mid-Western and Western region to review FP program in low CPR districts, to identify issues, and to develop plans that address the issues
H4L provided TA to the RHDs to review the CPR. The following key activities needed for scale-up in low-CPR districts were identified:
Sufficient supply of modern FP methods at HFs (condoms, pills, injectable, implants, IUCDs) and at community level (condoms and pills); identify low-supply HFs and communities, draft a supply plan and a target population needs-based supply plan
Intensive orientation for FCHVs and mothers’ group members Intensive orientation or awareness activities for eligible couples Encouragement to use long-acting FP methods Intensive auditing (monitoring & supervision) of activities Commitments from HFs and districts; provision of rewards for HFs Awareness programs through local media Assurance of reliable recording and reporting systems in HFs and communities Inclusion of private HF reports; improvement of HMIS reporting status of private HFs Maintaining accuracy of FP-related data and validation.
5.2 Provide TA to develop Multi-Year Strategic Plan of Action for the Family Planning Program in coordination with other stakeholders
H4L helped the FHD to review and develop the Costed Implementation Plan 2015-2020 for family planning as a member of the TWG (August 6 and 26). H4L was also a contributor to the validation workshop on August 8, 2014. The CIP M&E plan was also been developed and implementation is expected next year.
5.3 Provide support to D/PHOs in strengthening existing MSC, CB-IMCI and CB-NCP program in selected districts
5.3.1 Provide maintenance support (coaching, monitoring and reporting) to D(P)HOs for community-based Integrated Maternal, Neonatal and Childhood Illnesses (CB-IMNCI) and MSC intervention districts
Provided CB-IMNCI maintenance support to D(P)HOs in all 14 districts. During this reporting period H4L contributed to 20 semi-annual/trimestral review meetings and to 46 Ilaka/reporting cluster meetings. The most common problems discussed with HF in-charges were classification of nutritional status, and discrepancies between reporting and recoding.
H4L supported D(P)HOs to build capacity of health workers and volunteers. H4L staff made a total of 520 HF visits, coaching 719 HWs and 783 FCHVs on CB-IMNCI. Over 300 visits were made with D(P)HO staff last year.
During HF visits H4L district staff assessed HWs’ knowledge of CB-IMNCI technical content, examination skills for neonates and sick <5 children in the OPD, examined the IMNCI register for proper recording, observed whether mothers were properly counseled according to the age of the child for food and fluid, and for when to return for follow-up.
Staff also observed the FCHV, PHC-/ORC- and HF-level reports and provided immediate feedback to improve quality of services. During these visits, new chart booklets and job aids were provided to the HFs and FCHVs. Key issues identified and brought to the D(P)HOs attention included drug supply, equipment and staffing.
Most of the H4L districts have a reasonable number of newly hired staff (yet to be trained on IMNCI), so H4L provided coaching on all aspects of CB-IMNCI over a considerable time.
FCHVs’ knowledge of the three home rules to treat diarrhea increased from 88 percent (n=352) in Jul-Dec 2014 to 93 percent (n=988) according to the FCHV readiness assessment, albeit not representative of the 14 districts.
H4L—Annual Report 25

Table 5.1 CB-IMNCI Program technical support visit by H4L staff (Jul 2014 - Jun 2015)
Visited HF HW Coached FCHV Coached Joint Visit with D(P)HO staff
District Jul -
Dec
.14
Jan
-Ju
n'1
5
Tota
l
Jul-
Dec
.14
Jan
–Ju
n
'15
Tota
l
Jul –
Dec
.14
Jan
-Ju
n '5
Tota
l
Jul-
Dec
.14
Jan
-Ju
n 1
5
Tota
l
Kapilvastu 36 25 61 37 25 62 40 17 57 15 11 26
Arghakhanchi 12 5 17 23 8 31 14 7 21 1 7 8
Pyuthan 18 18 36 19 17 36 15 13 28 12 12 24
Rolpa 18 22 40 28 21 49 88 27 115 15 23 38
Rukum 9 19 28 10 13 23 8 10 18 5 8 13
Salyan 25 29 54 40 68 108 42 56 98 15 10 25
Dang 19 26 45 20 54 74 42 31 73 12 4 16
Banke 22 27 49 25 43 68 50 63 113 6 16 22
Bardiya 15 28 43 18 28 46 57 30 87 6 18 24
Surkhet 18 13 31 66 11 77 34 12 46 6 9 15
Dailekh 26 4 30 25 5 30 14 9 23 20 6 26
Jajarkot 15 28 43 11 32 43 14 25 39 11 32 43
Jumla 7 13 20 11 14 25 13 15 28 1 5 6
Kalikot 11 12 23 33 14 47 24 13 37 4 14 18
Total 251 269 520 366 353 719 455 328 783 129 175 304
H4L district teams provided MSC maintenance support to the D(P)HO teams to plan and organize district and Ilaka-level review meetings, and supported the D(P)HOs in reviewing MSC program activities by coaching health workers and FCHVs, conducting monitoring visits to health facilities and communities, and assisting with reporting. See more details in Table 5.6 below and section 5.3.10.
5.3.2 Provide TA to D(P)HOs and HF to improve service utilization in 140 most disadvantaged VDC in H4L districts.
H4L supported the analysis of service utilization, particularly MNCH, among different castes in 88 high-priority VDCs between July 2014 and January 2015. The purpose was to build capacity to use service data for decision-making and planning to improve service utilization. Preliminary findings (when compared with VDC population estimates), indicate variation in service utilization: in some VDCs service utilization among M/DAGs is low whereas in others it is not. Services utilization patterns among different castes/ethnicities were presented to the HF staff, HFOMCs, FCHVs and CAP/Rs in these VDCs, providing guidance in improving utilization of MNCH services. Detailed data compilation and analysis is in process.
H4L—Annual Report 26

5.3.3 Provide TA to D(P)HOs to carry out CB-IMNCI training to new FCHVs in H4L districts
Based on information collected from the 14 H4L districts, H4L found that 1,972 FCHVs needed training on CB-IMNCI. H4L supported CHD and D(P)HOs to carry out CB-IMNCI training for only 377 FCHVs from 25 high-priority VDCs by providing facilitation and materials.
Table 5.2 Participants trained on CB-IMNCI, by district
District No. of HWs Trained Funding source Batch M F Total
Surkhet 7 84 55 139 GoN Redbook
Jajarkot 2 39 5 44 ADRA Rukum 4 61 25 86 GoN Redbook Kalikot 5 65 43 108 UNICEF Total 18 249 128 377
5.3.4 Provide TA to D(P)HOs to carry out CB-IMNCI care training to new health workers in H4L districts
H4L collected information from all 14 H4L districts on health workers that needed to be trained in CB-IMNCI and found that there were 714 health workers that needed training. H4L provided TA to the CHD (along with partners) to facilitate CB-IMNCI training of 377 health workers and provided printed materials, anatomic models, equipment and instruments. Sessions were held in hospitals to provide clinical practice.
HMIS data (July 2014–May 2015) show that nearly 5,100 newborns received antibiotic treatment for infection in the 14 H4L districts. Similarly, about 317,500 children were treated for diarrhea, 187,000 children under five with suspected pneumonia received antibiotic treatment, and 43,500 newborns received postnatal check-ups within 48 hours of delivery.
5.3.5 Provide TA to D(P)HOs for additional support to review CB-IMNCI program in 14 H4L districts (add one day to review meeting)
Following approval of the CB-IMNCI package, CHD decided to focus first on implementing the new package. This new package includes a review of the CB-IMNCI program in the districts and H4L provided support to four H4L districts (Jajarkot, Surkhet, Kalikot and Rukum).
H4L continued to provide technical support at the ilaka level (HMIS monthly report collection cluster) meeting in 88 ilakas during this reporting period. H4L provided technical support during this meeting to clarify issues related to GoN revisions of the HMIS reporting forms.
5.3.6 Provide support to CHD for CB-IMNCI Table 5.3 H4L support for printing and related material printing for 14 H4L districts distribution of CB-IMNCI materials
H4L supported the CHD in printing and supplying SN Item No (pc)
various CB-IMNCI training materials as 1 CB-IMNCI Chart booklets 1,500 summarized in Table 5.3.
2 Facilitator Guides 210
3 Participant Handbooks 3,0005.3.7 Provide TA to D(P)HOs to monitor and periodically report on CB-IMNCI program 4 FCHV flipcharts 2,465
5 FCHV Job-aids 3,500H4L assisted D(P)HOs in reviewing HMIS data 6 Photograph sets 470during periodic meetings and monitor the CB-
IMNCI program and report. Table 5.4 summarizes 7 Flex charts (19 types) 95
the key problems brought to the attention of the D(P)HOs.
Participants practicing with a live newborn in
Jajarkot hospital
H4L—Annual Report 27
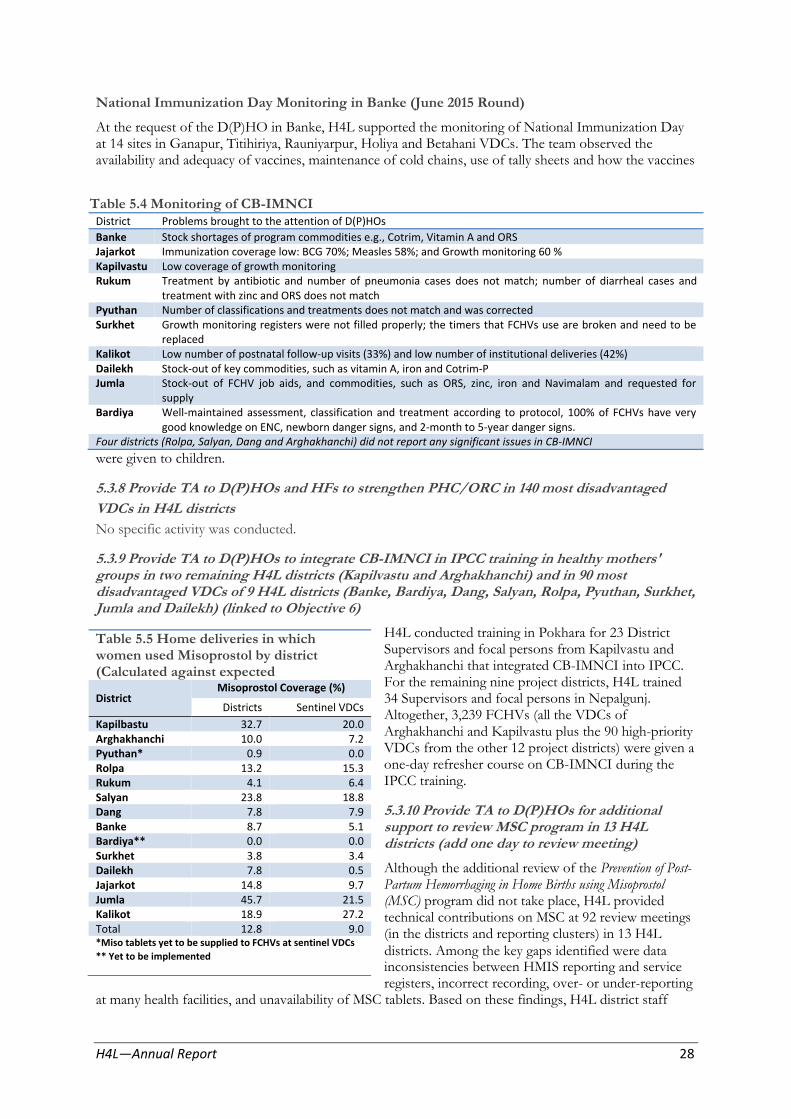
pregnancy)
National Immunization Day Monitoring in Banke (June 2015 Round)
At the request of the D(P)HO in Banke, H4L supported the monitoring of National Immunization Day at 14 sites in Ganapur, Titihiriya, Rauniyarpur, Holiya and Betahani VDCs. The team observed the availability and adequacy of vaccines, maintenance of cold chains, use of tally sheets and how the vaccines
Table 5.4 Monitoring of CB-IMNCI District Problems brought to the attention of D(P)HOs
Banke Stock shortages of program commodities e.g., Cotrim, Vitamin A and ORS Jajarkot Immunization coverage low: BCG 70%; Measles 58%; and Growth monitoring 60 % Kapilvastu Low coverage of growth monitoring Rukum Treatment by antibiotic and number of pneumonia cases does not match; number of diarrheal cases and
treatment with zinc and ORS does not match Pyuthan Number of classifications and treatments does not match and was corrected Surkhet Growth monitoring registers were not filled properly; the timers that FCHVs use are broken and need to be
replaced Kalikot Low number of postnatal follow-up visits (33%) and low number of institutional deliveries (42%) Dailekh Stock-out of key commodities, such as vitamin A, iron and Cotrim-P Jumla Stock-out of FCHV job aids, and commodities, such as ORS, zinc, iron and Navimalam and requested for
supply Bardiya Well-maintained assessment, classification and treatment according to protocol, 100% of FCHVs have very
good knowledge on ENC, newborn danger signs, and 2-month to 5-year danger signs. Four districts (Rolpa, Salyan, Dang and Arghakhanchi) did not report any significant issues in CB-IMNCI
were given to children.
5.3.8 Provide TA to D(P)HOs and HFs to strengthen PHC/ORC in 140 most disadvantaged
VDCs in H4L districts
No specific activity was conducted.
5.3.9 Provide TA to D(P)HOs to integrate CB-IMNCI in IPCC training in healthy mothers' groups in two remaining H4L districts (Kapilvastu and Arghakhanchi) and in 90 most disadvantaged VDCs of 9 H4L districts (Banke, Bardiya, Dang, Salyan, Rolpa, Pyuthan, Surkhet, Jumla and Dailekh) (linked to Objective 6)
H4L conducted training in Pokhara for 23 District Table 5.5 Home deliveries in which Supervisors and focal persons from Kapilvastu and women used Misoprostol by district Arghakhanchi that integrated CB-IMNCI into IPCC. (Calculated against expected For the remaining nine project districts, H4L trained Misoprostol Coverage (%)
District 34 Supervisors and focal persons in Nepalgunj. Districts Sentinel VDCs
Kapilbastu 32.7 Arghakhanchi 10.0 Pyuthan* 0.9 Rolpa 13.2 Rukum 4.1 Salyan 23.8 Dang 7.8 Banke 8.7 Bardiya** 0.0 Surkhet 3.8 Dailekh 7.8 Jajarkot 14.8 Jumla 45.7 Kalikot 18.9 Total 12.8
Altogether, 3,239 FCHVs (all the VDCs of 20.0
Arghakhanchi and Kapilvastu plus the 90 high-priority 7.2
VDCs from the other 12 project districts) were given a 0.0 one-day refresher course on CB-IMNCI during the 15.3
6.4 IPCC training. 18.8
7.9 5.3.10 Provide TA to D(P)HOs for additional 5.1 support to review MSC program in 13 H4L 0.0 districts (add one day to review meeting) 3.4 0.5 Although the additional review of the Prevention of Post-9.7 Partum Hemorrhaging in Home Births using Misoprostol
21.5 (MSC) program did not take place, H4L provided 27.2 technical contributions on MSC at 92 review meetings
9.0 (in the districts and reporting clusters) in 13 H4L *Miso tablets yet to be supplied to FCHVs at sentinel VDCs
districts. Among the key gaps identified were data ** Yet to be implemented inconsistencies between HMIS reporting and service registers, incorrect recording, over- or under-reporting
at many health facilities, and unavailability of MSC tablets. Based on these findings, H4L district staff
H4L—Annual Report 28
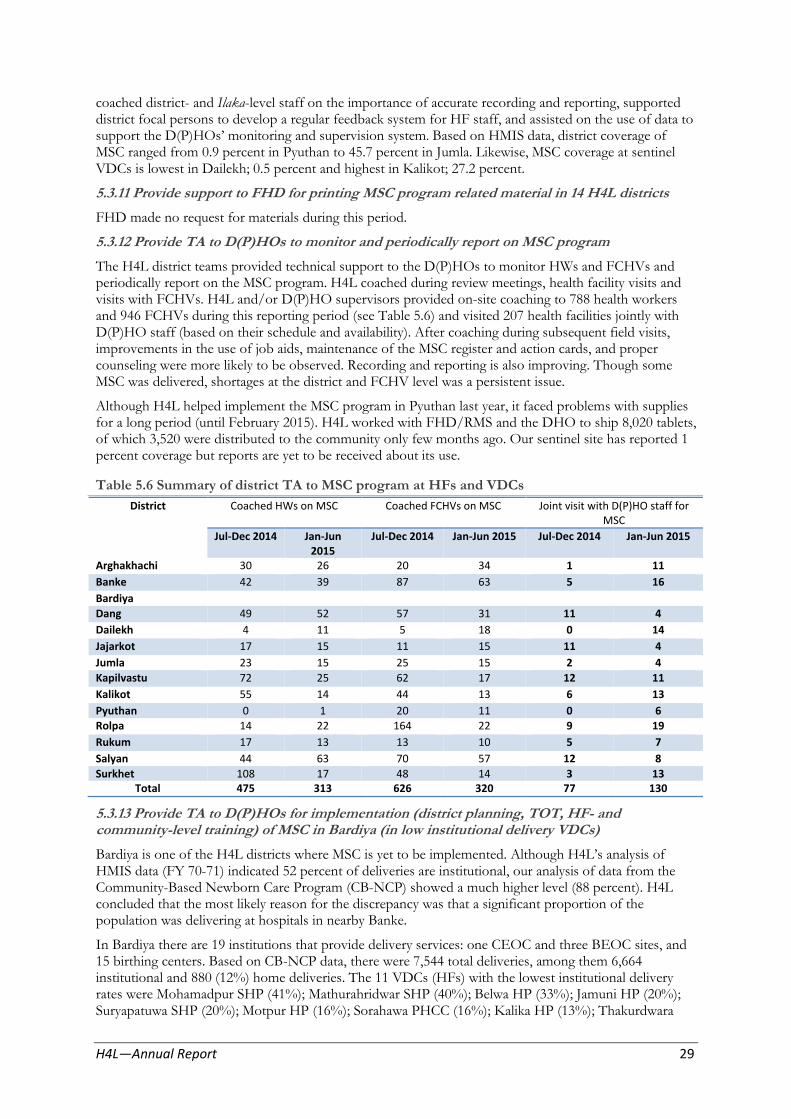
coached district- and Ilaka-level staff on the importance of accurate recording and reporting, supported district focal persons to develop a regular feedback system for HF staff, and assisted on the use of data to support the D(P)HOs’ monitoring and supervision system. Based on HMIS data, district coverage of MSC ranged from 0.9 percent in Pyuthan to 45.7 percent in Jumla. Likewise, MSC coverage at sentinel VDCs is lowest in Dailekh; 0.5 percent and highest in Kalikot; 27.2 percent.
5.3.11 Provide support to FHD for printing MSC program related material in 14 H4L districts
FHD made no request for materials during this period.
5.3.12 Provide TA to D(P)HOs to monitor and periodically report on MSC program
The H4L district teams provided technical support to the D(P)HOs to monitor HWs and FCHVs and periodically report on the MSC program. H4L coached during review meetings, health facility visits and visits with FCHVs. H4L and/or D(P)HO supervisors provided on-site coaching to 788 health workers and 946 FCHVs during this reporting period (see Table 5.6) and visited 207 health facilities jointly with D(P)HO staff (based on their schedule and availability). After coaching during subsequent field visits, improvements in the use of job aids, maintenance of the MSC register and action cards, and proper counseling were more likely to be observed. Recording and reporting is also improving. Though some MSC was delivered, shortages at the district and FCHV level was a persistent issue.
Although H4L helped implement the MSC program in Pyuthan last year, it faced problems with supplies for a long period (until February 2015). H4L worked with FHD/RMS and the DHO to ship 8,020 tablets, of which 3,520 were distributed to the community only few months ago. Our sentinel site has reported 1 percent coverage but reports are yet to be received about its use.
Table 5.6 Summary of district TA to MSC program at HFs and VDCs
District Coached HWs on MSC Coached FCHVs on MSC Joint visit with D(P)HO staff for MSC
Jul-Dec 2014 Jan-Jun Jul-Dec 2014 Jan-Jun 2015 Jul-Dec 2014 Jan-Jun 2015 2015
Arghakhachi 30 26 20 34 1 11
Banke 42 39 87 63 5 16
Bardiya
Dang 49 52 57 31 11 4
Dailekh 4 11 5 18 0 14
Jajarkot 17 15 11 15 11 4
Jumla 23 15 25 15 2 4
Kapilvastu 72 25 62 17 12 11
Kalikot 55 14 44 13 6 13
Pyuthan 0 1 20 11 0 6
Rolpa 14 22 164 22 9 19
Rukum 17 13 13 10 5 7
Salyan 44 63 70 57 12 8
Surkhet 108 17 48 14 3 13 Total 475 313 626 320 77 130
5.3.13 Provide TA to D(P)HOs for implementation (district planning, TOT, HF- and community-level training) of MSC in Bardiya (in low institutional delivery VDCs)
Bardiya is one of the H4L districts where MSC is yet to be implemented. Although H4L’s analysis of HMIS data (FY 70-71) indicated 52 percent of deliveries are institutional, our analysis of data from the Community-Based Newborn Care Program (CB-NCP) showed a much higher level (88 percent). H4L concluded that the most likely reason for the discrepancy was that a significant proportion of the population was delivering at hospitals in nearby Banke.
In Bardiya there are 19 institutions that provide delivery services: one CEOC and three BEOC sites, and 15 birthing centers. Based on CB-NCP data, there were 7,544 total deliveries, among them 6,664 institutional and 880 (12%) home deliveries. The 11 VDCs (HFs) with the lowest institutional delivery rates were Mohamadpur SHP (41%); Mathurahridwar SHP (40%); Belwa HP (33%); Jamuni HP (20%); Suryapatuwa SHP (20%); Motpur HP (16%); Sorahawa PHCC (16%); Kalika HP (13%); Thakurdwara
H4L—Annual Report 29

HP (13%); Deudakala HP (12%); and Manau SHP (11%). In the upcoming fiscal year, H4L will help the D(P)HO implement the MSC program.
5.3.14 Provide TA to FHD and D(P)HOs in H4L districts to identify key areas for improvement
based on findings from QOC assessment at birthing centers
H4L published Results from Assessing Birthing Centers in Nepal in July 2014 and discussed key areas for improvement with FHD, NHTC, CHD, and partner organizations.
A meeting with MNH partners was organized January 16, 2015 to review the findings of the assessment and to make programmatic recommendations in the areas of 1) ANC; 2) intra-partum and newborn care; and 3) knowledge, practices and training among health workers. Key recommendations were:
Strengthen quality of care (e.g., AMTSL and partograph use), re-invigorate BPP, and provide on-
site coaching (after training)
Revise the SM guidelines
Provide the necessary equipment, instruments and diagnostic supplies (e.g., Hb, urine albumin)
Where to locate birthing centers
Update SBA curriculum to include newborn care (and WHO recommendations)
Improve quality of pre-service education for ANMs.
These findings and recommendations were useful while developing the SM AWPB, newborn AWPB, NHSP III (newborn care and safe motherhood), and logistics forecasting.
5.4 Provide TA to D(P)HOs to increase utilization of long-acting FP methods in birthing centers in H4L districts
5.4.1 Provide technical support to D(P)HOs to coach providers at birthing centers on long-acting family planning services (including IUCD and implants) in H4L districts and coordinate with NHTC for training
H4L supported D(P)HOs in all 14 project districts in various ways to increase access for family planning services in districts. H4L supported D(P)HO to first identify and select birthing centers for expansion of LAFP sites.
Table 5.7 Birthing Centers (BCs) with Long Acting FP (LAFP) in H4L districts
Number of Birthing Centers BCs with IUCDs only
BCs with implants
only
BCs having both implants
and IUCDs
BCs without any LAFP
District
June total 2014
Added Jul-Dec
2014
Added Jun-Dec
2014
Added Jan-Jun
2015
June total 2015
Jun-Dec
2014
Jan-Jun
2015
Jun-Dec
2014
Jan-Jun
2015
Jun-Dec
2014
Jan- Jun 2015
Jun- Dec
2014
as of Jun
2015
Arghakhanchi 14 1 15 0 15 2 2 0 0 12 13 1 0 Banke 31 1 32 0 32 0 1 5 2 16 24 11 5 Bardiya 18 2 20 0 20 3 7 0 0 12 13 5 0 Dailekh 52 2 54 0 54 9 1 5 5 4 5 36 43 Dang 36 0 36 0 36 8 8 3 8 12 17 13 3 Jajarkot 16 0 16 8 24 0 9 3 0 6 11 7 4 Jumla 13 5 18 0 18 1 3 1 2 1 2 15 11 Kalikot 25 1 26 1 27 0 0 9 8 3 7 14 12 Kapilvastu 13 -1 12 2 14 2 3 0 5 3 5 7 1 Pyuthan 31 5 36 5 41 0 0 11 17 5 7 20 17 Rolpa 45 5 50 1 51 4 11 3 4 12 19 31 17 Rukum 21 1 22 0 22 0 2 4 2 4 10 14 8 Salyan 38 1 39 0 39 1 5 4 8 6 8 28 18 Surkhet 40 12 52 0 52 6 3 1 1 10 18 35 30
Total 393 35 428 17 445 36 55 49 62 106 159 237 169
H4L—Annual Report 30

Figure 5.2 Birthing centers in H4L
H4L coached D(P)HO staff in all 14 districts in analyzing FP services, including LAFP, and helped identify birthing centers where long-acting family planning (LAFP) services could be strengthened. The number of birthing centers in H4L districts increased from 393 in the last reporting period to 445 during this period. Of these birthing centers, 62 percent (276) now offer at least one LAFP method (55 centers provide IUCDs, 62 centers implants and 159 provide both), while 38 percent (169) still do not.
districts offering LAFP
In the 141 high-priority VDCs there are 110 birthing centers, of which 58 provide both IUCDs and implants, 25 provide only IUCDs and 18 provide only implants. Out of 31 health facilities in high-priority VDCs without birthing centers, only one provides both LAFP methods and 22 offer implants only. There are nine health facilities with birthing centers, and eight health facilities without birthing centers which offer no LAFP services.
In the past year H4L assisted D(P)HOs to establish/re-establish 50 LAFP sites by coaching staff over 2 days at each. H4L established/re-established LAFP services at a total of 127 health facilities by also improving the supply of equipment and commodities at other sites. Of these 127 health facilities, 97 have birthing centers. H4L provided TA at 49 sites providing IUCD services, 61 sites inserting implants, and 17 sites providing both services. In total, H4L coordinated and supported the supply of about 2,000 implants and 4,700 IUCDs to health facilities.
From HMIS data collected, the CPR in the 14 H4L districts stands at 40.3 percent; 3.1 percent from IUCD and 4.5 percent from Implant. And CPR of LAFP ranges from 2.7 percent in Rukum to 12.7 percent in Rolpa.
Table 5.8 CPR and LAFP Contribution (H4L Identification of FP Training Needs
districts), HMIS
District CPR for modern
methods CPR of LAFP
among MWRAs among MWRA IUCDs
% Implants
%
Kapilvastu 27.8 0.9 2.7
Arghakhanchi 25.8 1.3 3.1
Pyuthan 35.7 1.3 3.3
Rolpa 38.9 1.9 10.3
Rukum 24.9 0.5 1.8 Salyan 37.7 3.4 5.4 Dang 51.8 6.5 5.0
Banke 44.7 3.5 3.9
Bardiya 56.0 6.2 4.5
Surkhet 53.3 3.4 4.4
Dailekh 38.2 3.0 7.6
Jajarkot 34.4 1.1 5.4
Jumla 16.6 0.6 2.2
Kalikot 31.1 0.9 3.3
Total 40.3 3.1 4.5
H4L provided TA to the D(P)HOs to identify health workers that needed coaching on LAFP and training on different types of FP methods. This information was, in turn, provided to NHTC so that it could enroll health workers in training. In the H4L districts, 231 health workers were identified for training: 71 for IUCD insertion, 92 for implant insertion, 65 for COFP services,
and 3 for NSV. H4L is continuing to work with the D(P)HOs to make requests to the FHD and NHTC for training. So far, based on information available from the NHTC, 18 service providers (from four districts) were trained on COFP/C, 21 (from six districts) on IUCD insertion, 66 (from
eight districts) on implant insertion, and four (from four districts) on NSV. The final number of trained service providers is yet to be received from the D(P)HOs/RHTC/NHTC.
VSC and LAFP Outreach Clinics
Apart from directly coaching service providers, H4L provided technical assistance to organize pre-VSC interaction programs in 62 high-priority VDCs between December 2014 and May 2015 to raise awareness of family planning as a means to a better quality of life. During these pre-VSC interaction programs, dharmagurus, maulanas, dhami-jhakri (traditional leaders) and social workers participated actively.
H4L—Annual Report 31
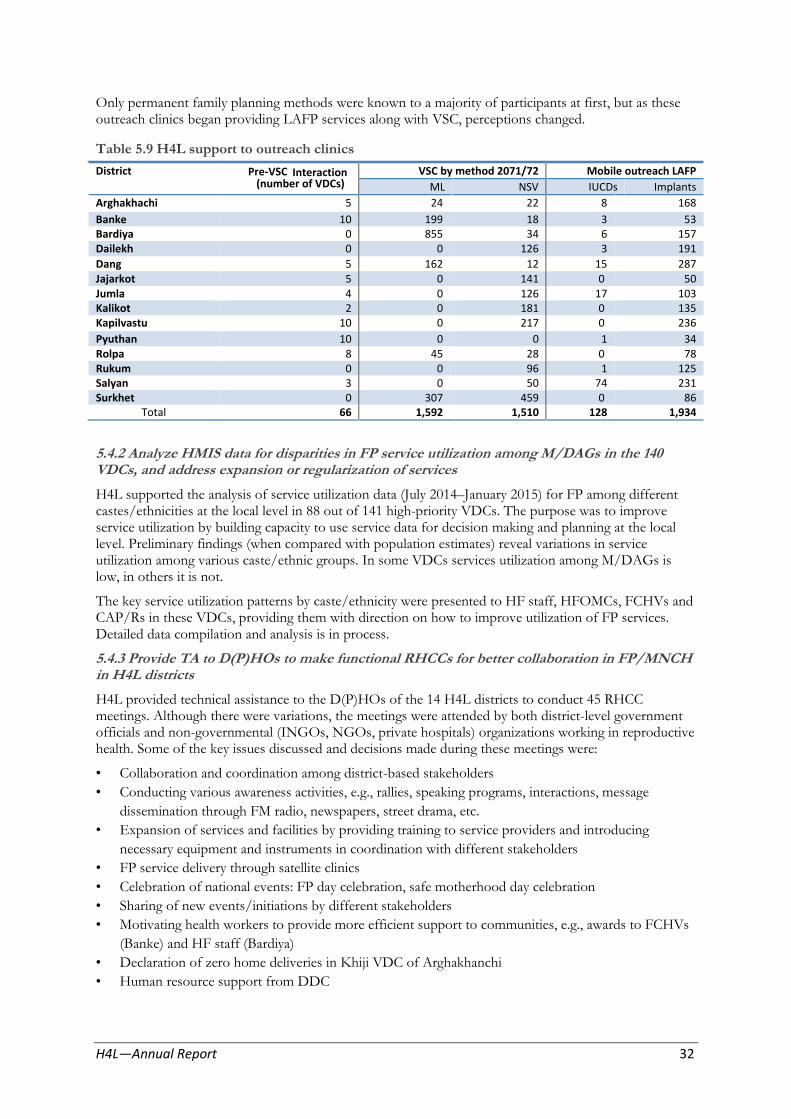
Only permanent family planning methods were known to a majority of participants at first, but as these outreach clinics began providing LAFP services along with VSC, perceptions changed.
Table 5.9 H4L support to outreach clinics
District Pre-VSC Interaction (number of VDCs)
VSC by method 2071/72 Mobile outreach LAFP
ML NSV IUCDs Implants
Arghakhachi 5 24 22 8 168
Banke 10 199 18 3 53 Bardiya 0 855 34 6 157 Dailekh 0 0 126 3 191
Dang 5 162 12 15 287 Jajarkot 5 0 141 0 50 Jumla 4 0 126 17 103 Kalikot 2 0 181 0 135 Kapilvastu 10 0 217 0 236
Pyuthan 10 0 0 1 34 Rolpa 8 45 28 0 78 Rukum 0 0 96 1 125 Salyan 3 0 50 74 231 Surkhet 0 307 459 0 86
Total 66 1,592 1,510 128 1,934
5.4.2 Analyze HMIS data for disparities in FP service utilization among M/DAGs in the 140 VDCs, and address expansion or regularization of services
H4L supported the analysis of service utilization data (July 2014–January 2015) for FP among different castes/ethnicities at the local level in 88 out of 141 high-priority VDCs. The purpose was to improve service utilization by building capacity to use service data for decision making and planning at the local level. Preliminary findings (when compared with population estimates) reveal variations in service utilization among various caste/ethnic groups. In some VDCs services utilization among M/DAGs is low, in others it is not.
The key service utilization patterns by caste/ethnicity were presented to HF staff, HFOMCs, FCHVs and CAP/Rs in these VDCs, providing them with direction on how to improve utilization of FP services. Detailed data compilation and analysis is in process.
5.4.3 Provide TA to D(P)HOs to make functional RHCCs for better collaboration in FP/MNCH in H4L districts
H4L provided technical assistance to the D(P)HOs of the 14 H4L districts to conduct 45 RHCC meetings. Although there were variations, the meetings were attended by both district-level government officials and non-governmental (INGOs, NGOs, private hospitals) organizations working in reproductive health. Some of the key issues discussed and decisions made during these meetings were:
• Collaboration and coordination among district-based stakeholders
• Conducting various awareness activities, e.g., rallies, speaking programs, interactions, message
dissemination through FM radio, newspapers, street drama, etc.
• Expansion of services and facilities by providing training to service providers and introducing
necessary equipment and instruments in coordination with different stakeholders
• FP service delivery through satellite clinics
• Celebration of national events: FP day celebration, safe motherhood day celebration
• Sharing of new events/initiations by different stakeholders
• Motivating health workers to provide more efficient support to communities, e.g., awards to FCHVs
(Banke) and HF staff (Bardiya)
• Declaration of zero home deliveries in Khiji VDC of Arghakhanchi
• Human resource support from DDC
H4L—Annual Report 32

• Expansion of birthing centers and improvement of quality of service delivery in existing health
facilities
• Quality improvement of birthing centers by maintaining HCWM and placenta pits
• Identification and planning for VSC and satellite clinics in low-CPR VDCs with M/DAGs
• Regularization of monitoring visits and on-site coaching.
5.4.4 Monitor US abortion and FP requirement compliance plan, reprint and distribute informed choice poster in H4L districts as necessary
Table 5.10 US abortion and FP compliance FP Compliance monitoring (H4L districts)
H4L has continued monitoring US Districts Number of HF monitored for Total abortion and FP regulations in H4L FP compliance districts, as per the H4L compliance
Jul.-Dec. Jan. -Jun. plan. During FY 2014/15, 192 HFs 2014 2015 were monitored and all the HFs Arghakhanchi 11 7 18 visited were found to be compliant. Banke 4 7 11 In addition, 384 government and Bardiya 0 6 6
stakeholder staff were oriented on Dailekh 6 3 9 Dang 5 1 6FP compliance during various Jajarkot 13 12 25events. Jumla 9 8 17
Of the 280 HFs that H4L staff Kapilvastu 8 10 18
visited and conducted readiness Kalikot 11 4 15 Pyuthan 5 5 10assessments at, the ICP was Rolpa 8 12 20displayed properly in 264 HFs (94
percent). 34 HFs were given Rukum 1 2 3 Salyan 6 5 11replacement posters, and all HFs Surkhet 19 4 23were sensitized to proper display. Total 106 86 192
ICP properly displayed (as HF readiness assessment)
14 22
19
12
21
24
17
18
17
22
24
21
16 17
264
5.5 Provide TA to FHD and D(P)HOs to improve CEONC referral system in Dang district (based on national safe motherhood and neonatal referral guidelines)
5.5.1 Support D(P)HOs to convene district-level workshops/meetings (orientation, gap identification and planning)
H4L continued to provide technical support to the D(P)HOs to initiate CEONC referral mechanisms in Dang. During this reporting period support was provided through the following activities:
Mapping health services of Dang; provision of general information, availability of 24-hour
delivery services, emergency transportation, blood transfusion facilities, availability of emergency
funds, referral sites and referral practices
A one-day orientation (February 26, 2015) for D(P)HO supervisors on the national referral
system guidelines for maternal and newborn health was conducted, and an implementation plan
for the CEONC referral system was drafted.
5.5.2 Support DDCs to organize stakeholders' meetings to develop mechanisms and generate
support
Not done this fiscal year; planned for early July, 2015.
5.5.3 Support D(P)HOs and FHD to develop and print protocols, job aids and forms
Not completed because the national referral guidelines are in the process of being approved.
5.5.4 Provide support to D(P)HOs to implement referral system at district level
Not done this fiscal year.
H4L—Annual Report 33

5.5.5 Provide TA to RHCC to engage in monitoring of referral mechanism
Not done this fiscal year.
5.5.6 Provide TA to D(P)HOs to disseminate lessons learned for scale-up
Because of delays in implementation, this activity was not be completed.
5.6 Provide TA to CTEVT to revise ANM curriculum (Pre- and Post-SLC) to incorporate SBA skills
5.6.1 Provide TA to CTEVT to orient all 45 ANM schools on revised curriculum
With technical support from H4L, the Center for Technical Education and Vocational Training (CTEVT) updated/revised the ANM curriculum last year. It was approved on July 9, 2014 by the CTEVT board and introduced this academic year to improve competency in core SBA skills of ANM graduates.
With support from H4L, CTEVT organized a two-day orientation for 85 ANM instructors (mainly teaching midwifery) on the revised ANM curriculum from all 44 ANM schools (one school has stopped its ANM program) in four locations (Itahari, Hetauda, Kathmandu and Nepalgunj) in September 2014. During the orientation, we also identified gaps in the existing ANM curriculum
based on SBA core skills, oriented on the revised structure and content of the new ANM curriculum and reviewed how to transfer knowledge and skills regarding use of the partograph, essential newborn care and resuscitation, and Kangaroo Mother Care.
5.6.2 Provide TA to 6 ANM schools (Banke, Dang, Kapilvastu, Jumla, Dolakha and Doti) to introduce revised curriculum
The revised curriculum was introduced in the following six ANM schools:
Kapilvastu Technical Institute -Vanaganga, Kapilvastu
Karnali Technical School, Jumla
Rapti Health Institute– Dang, Ghorahi
Sushma Koirala Memorial Trust –Nepalgunj, Banke
Jiri Technical School, Dolakha
Seti Technical School, Doti
5.6.3 Provide TA to CTEVT to develop supplementary teaching materials.
H4L has identified key technical areas in FP/MNCH with schools during curriculum orientation and stakeholder meetings, which would be helpful to teachers and/or students, including knowledge and skills assessments (QI Tools), checklists and job aids. Supplementary materials will be developed accordingly.
5.7 Provide TA to ANM schools to improve quality of pre-service education in ANM schools.
5.7.1 Conduct in-depth assessment of 6 ANM schools in H4L districts
H4L assessed the competencies of outgoing graduates and instructors in six selected ANM schools as a baseline before the revised ANM curriculum was introduced. In-depth assessments Practicing using a resuscitation bag and mask on a newborn
H4L—Annual Report 34
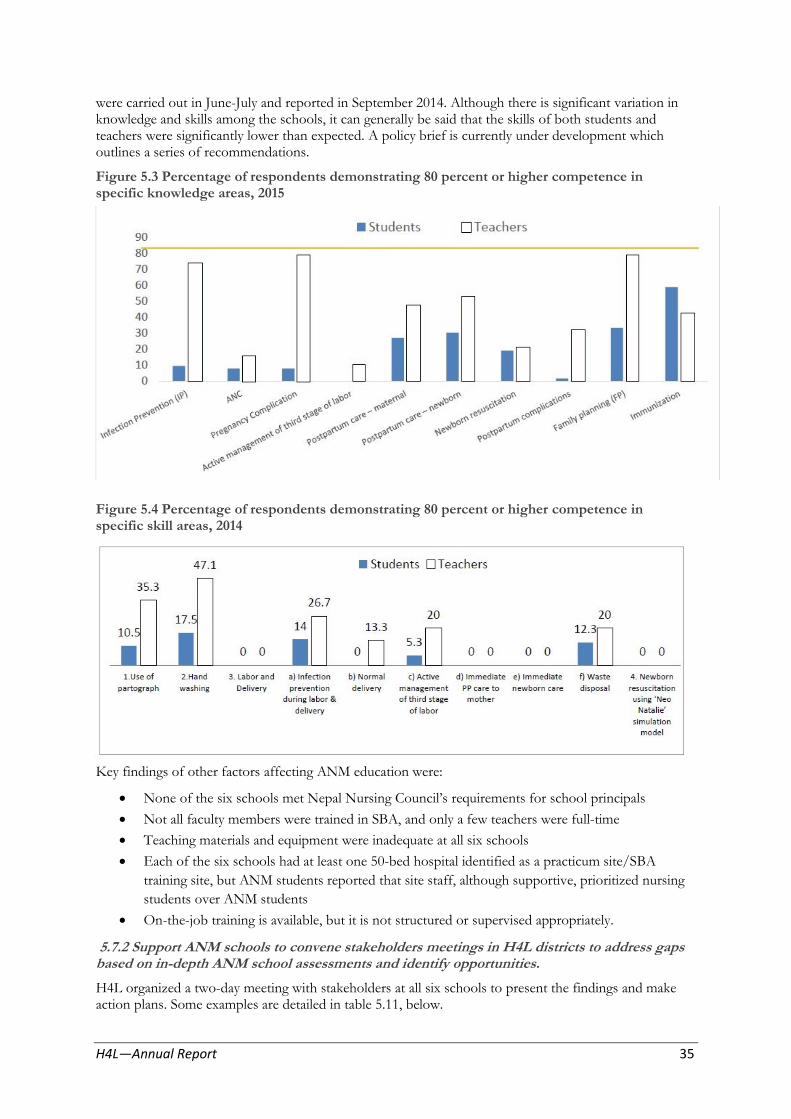
were carried out in June-July and reported in September 2014. Although there is significant variation in knowledge and skills among the schools, it can generally be said that the skills of both students and teachers were significantly lower than expected. A policy brief is currently under development which outlines a series of recommendations.
Figure 5.3 Percentage of respondents demonstrating 80 percent or higher competence in specific knowledge areas, 2015
Figure 5.4 Percentage of respondents demonstrating 80 percent or higher competence in specific skill areas, 2014
Key findings of other factors affecting ANM education were:
None of the six schools met Nepal Nursing Council’s requirements for school principals
Not all faculty members were trained in SBA, and only a few teachers were full-time
Teaching materials and equipment were inadequate at all six schools
Each of the six schools had at least one 50-bed hospital identified as a practicum site/SBA
training site, but ANM students reported that site staff, although supportive, prioritized nursing
students over ANM students
On-the-job training is available, but it is not structured or supervised appropriately.
5.7.2 Support ANM schools to convene stakeholders meetings in H4L districts to address gaps based on in-depth ANM school assessments and identify opportunities.
H4L organized a two-day meeting with stakeholders at all six schools to present the findings and make action plans. Some examples are detailed in table 5.11, below.
H4L—Annual Report 35

lab
5.7.3. Strengthen 6 ANM schools by improving teaching and learning techniques (CTS, SBA skills, upgrade classroom and skill labs)
Table 5.11: ANM Schools action plan ANM School
Karnali Technical School, Jumla
Kapilvastu Technical Institute, Kapilvastu Jiri Technical School, Jiri
Rapti Health Institute, Dang
Seti Technical School, Doti
Gaps Identified Poor scoring of students and teachers in normal delivery
Very poor scoring in NB resuscitation , students as well as teachers Poor scoring on Labor & Delivery
Poor score in infection prevention
Low skill level in labor and Delivery-
students
Possible causes
Skill lab is not well equipped Teachers are not allowed in labor room at practicum site to update their skills because they are not SBA trained
Inadequate practical exposure in skills labs and practicum sites in accordance with practicum hours
School does not have IP guideline
No practice in the skill lab No job-aid and checklist to practice
correctly
Not enough exposure to cases
Solution
Coordinate with partner agencies for equipment and model
Need to focus on practical exposure in skill labs and practicum sites using checklist and setting duty roaster of related teachers
Coordination with Jiri Hospital for delivery case exposure
Coordinate with D(P)HO for IP
Coordinate with H4L
The in-depth assessment found that to strengthen ANM schools, teaching and learning techniques must be improved. ANM instructors from these schools were identified for training, as were necessary upgrades to classrooms, skill labs and equipment.
5.7.4. Orient faculty members of 6 ANM schools to teach additional SBA core competencies, not currently in ANM curriculum (supplementary teaching)
Not yet done.
Objective 6: Improve knowledge, behavior, and use of health services among target
6.1 National-Level Activities
6.1.1 Continue rolling out interactive SMS package/apps targeting adolescent population group (mHealth) Figure 6.1 SMS sent by Users and to Users, by
The M4ASRH interactive package under region, Sep 2014 to May 2015
the mHealth initiative was very successful, reaching 181,577 adolescents and youth (September 18, 2014 to May 31, 2015). The total number of SMS received from users was 2,683,250 and the total number of messages sent back to users from the server was 4,932,664 (NTC 3,286,586, NCell 1,646,078). Because not all numbers can be traced to a specific region, there is a particularly high percentage of messages from unidentified regions. Each user received an average of 15.4 key messages with information on adolescent sexual and reproductive health. Of the four options available to users of the interactive
H4L—Annual Report 36
Teachers need SBA training, with NHTC for training
Inadequate teaching/learning equipment, such as Model
Teachers have poor knowledge and skills in IP
guidelines
Practice IP in demonstration skill lab according to checklist
Practice enough in skill lab/Repeated use of practicum skill lab
Coordinate with hospital and maternity ward sister and practice enough in the skill lab
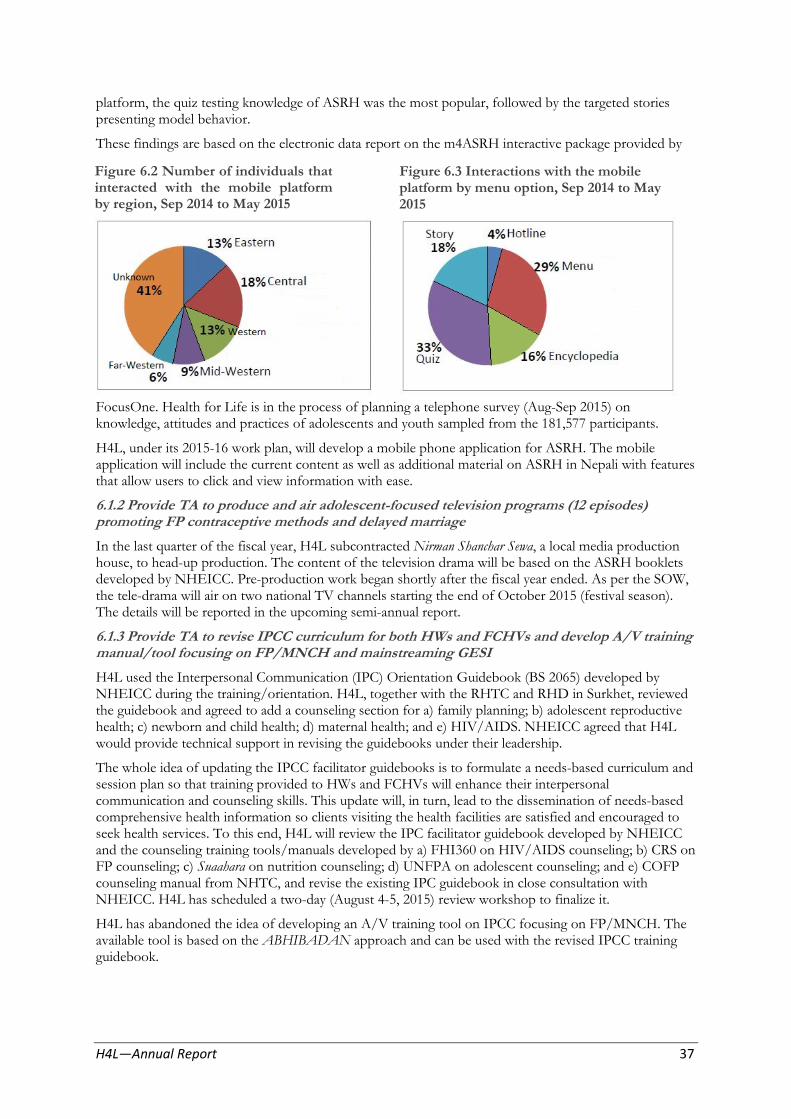
platform, the quiz testing knowledge of ASRH was the most popular, followed by the targeted stories presenting model behavior.
These findings are based on the electronic data report on the m4ASRH interactive package provided by
Figure 6.2 Number of individuals that interacted with the mobile platform by region, Sep 2014 to May 2015
Figure 6.3 Interactions with the mobile platform by menu option, Sep 2014 to May 2015
FocusOne. Health for Life is in the process of planning a telephone survey (Aug-Sep 2015) on knowledge, attitudes and practices of adolescents and youth sampled from the 181,577 participants.
H4L, under its 2015-16 work plan, will develop a mobile phone application for ASRH. The mobile application will include the current content as well as additional material on ASRH in Nepali with features that allow users to click and view information with ease.
6.1.2 Provide TA to produce and air adolescent-focused television programs (12 episodes) promoting FP contraceptive methods and delayed marriage
In the last quarter of the fiscal year, H4L subcontracted Nirman Shanchar Sewa, a local media production house, to head-up production. The content of the television drama will be based on the ASRH booklets developed by NHEICC. Pre-production work began shortly after the fiscal year ended. As per the SOW, the tele-drama will air on two national TV channels starting the end of October 2015 (festival season). The details will be reported in the upcoming semi-annual report.
6.1.3 Provide TA to revise IPCC curriculum for both HWs and FCHVs and develop A/V training manual/tool focusing on FP/MNCH and mainstreaming GESI
H4L used the Interpersonal Communication (IPC) Orientation Guidebook (BS 2065) developed by NHEICC during the training/orientation. H4L, together with the RHTC and RHD in Surkhet, reviewed the guidebook and agreed to add a counseling section for a) family planning; b) adolescent reproductive health; c) newborn and child health; d) maternal health; and e) HIV/AIDS. NHEICC agreed that H4L would provide technical support in revising the guidebooks under their leadership.
The whole idea of updating the IPCC facilitator guidebooks is to formulate a needs-based curriculum and session plan so that training provided to HWs and FCHVs will enhance their interpersonal communication and counseling skills. This update will, in turn, lead to the dissemination of needs-based comprehensive health information so clients visiting the health facilities are satisfied and encouraged to seek health services. To this end, H4L will review the IPC facilitator guidebook developed by NHEICC and the counseling training tools/manuals developed by a) FHI360 on HIV/AIDS counseling; b) CRS on FP counseling; c) Suaahara on nutrition counseling; d) UNFPA on adolescent counseling; and e) COFP counseling manual from NHTC, and revise the existing IPC guidebook in close consultation with NHEICC. H4L has scheduled a two-day (August 4-5, 2015) review workshop to finalize it.
H4L has abandoned the idea of developing an A/V training tool on IPCC focusing on FP/MNCH. The available tool is based on the ABHIBADAN approach and can be used with the revised IPCC training guidebook.
H4L—Annual Report 37
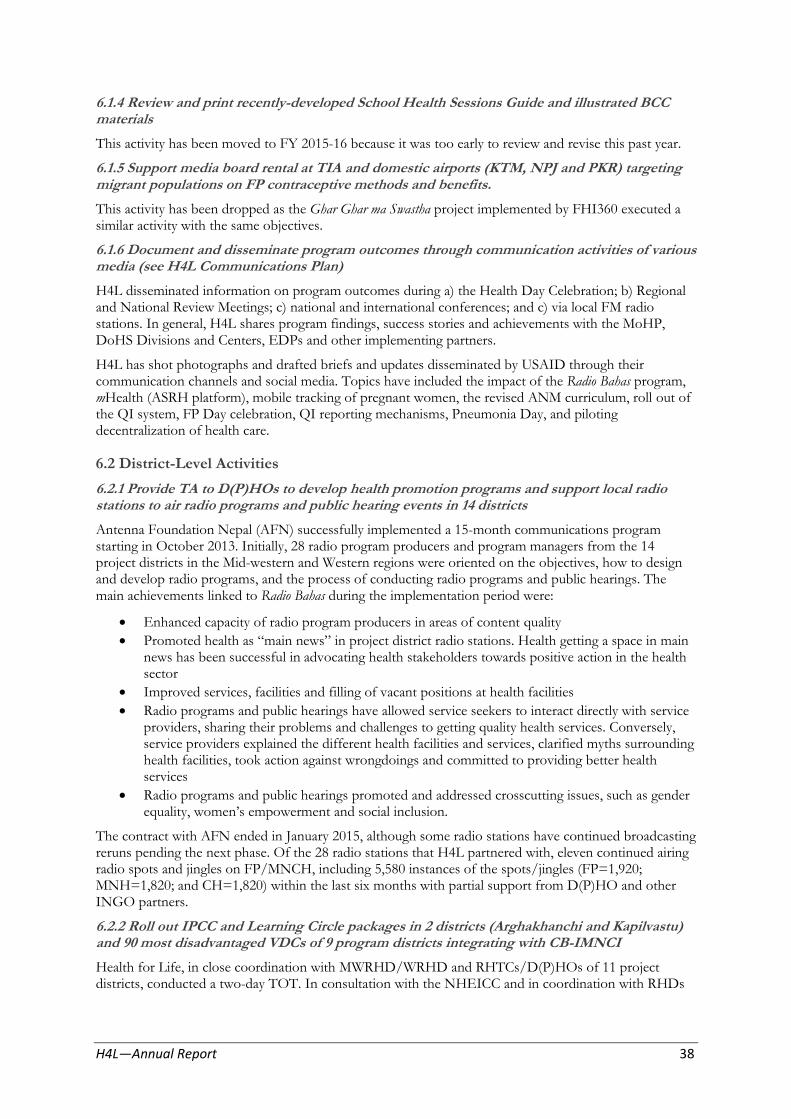
6.1.4 Review and print recently-developed School Health Sessions Guide and illustrated BCC materials
This activity has been moved to FY 2015-16 because it was too early to review and revise this past year.
6.1.5 Support media board rental at TIA and domestic airports (KTM, NPJ and PKR) targeting migrant populations on FP contraceptive methods and benefits.
This activity has been dropped as the Ghar Ghar ma Swastha project implemented by FHI360 executed a similar activity with the same objectives.
6.1.6 Document and disseminate program outcomes through communication activities of various media (see H4L Communications Plan)
H4L disseminated information on program outcomes during a) the Health Day Celebration; b) Regional and National Review Meetings; c) national and international conferences; and c) via local FM radio stations. In general, H4L shares program findings, success stories and achievements with the MoHP, DoHS Divisions and Centers, EDPs and other implementing partners.
H4L has shot photographs and drafted briefs and updates disseminated by USAID through their communication channels and social media. Topics have included the impact of the Radio Bahas program, mHealth (ASRH platform), mobile tracking of pregnant women, the revised ANM curriculum, roll out of the QI system, FP Day celebration, QI reporting mechanisms, Pneumonia Day, and piloting decentralization of health care.
6.2 District-Level Activities
6.2.1 Provide TA to D(P)HOs to develop health promotion programs and support local radio stations to air radio programs and public hearing events in 14 districts
Antenna Foundation Nepal (AFN) successfully implemented a 15-month communications program starting in October 2013. Initially, 28 radio program producers and program managers from the 14 project districts in the Mid-western and Western regions were oriented on the objectives, how to design and develop radio programs, and the process of conducting radio programs and public hearings. The main achievements linked to Radio Bahas during the implementation period were:
Enhanced capacity of radio program producers in areas of content quality
Promoted health as “main news” in project district radio stations. Health getting a space in main news has been successful in advocating health stakeholders towards positive action in the health sector
Improved services, facilities and filling of vacant positions at health facilities
Radio programs and public hearings have allowed service seekers to interact directly with service providers, sharing their problems and challenges to getting quality health services. Conversely, service providers explained the different health facilities and services, clarified myths surrounding health facilities, took action against wrongdoings and committed to providing better health services
Radio programs and public hearings promoted and addressed crosscutting issues, such as gender equality, women’s empowerment and social inclusion.
The contract with AFN ended in January 2015, although some radio stations have continued broadcasting reruns pending the next phase. Of the 28 radio stations that H4L partnered with, eleven continued airing radio spots and jingles on FP/MNCH, including 5,580 instances of the spots/jingles (FP=1,920; MNH=1,820; and CH=1,820) within the last six months with partial support from D(P)HO and other INGO partners.
6.2.2 Roll out IPCC and Learning Circle packages in 2 districts (Arghakhanchi and Kapilvastu) and 90 most disadvantaged VDCs of 9 program districts integrating with CB-IMNCI
Health for Life, in close coordination with MWRHD/WRHD and RHTCs/D(P)HOs of 11 project districts, conducted a two-day TOT. In consultation with the NHEICC and in coordination with RHDs
H4L—Annual Report 38
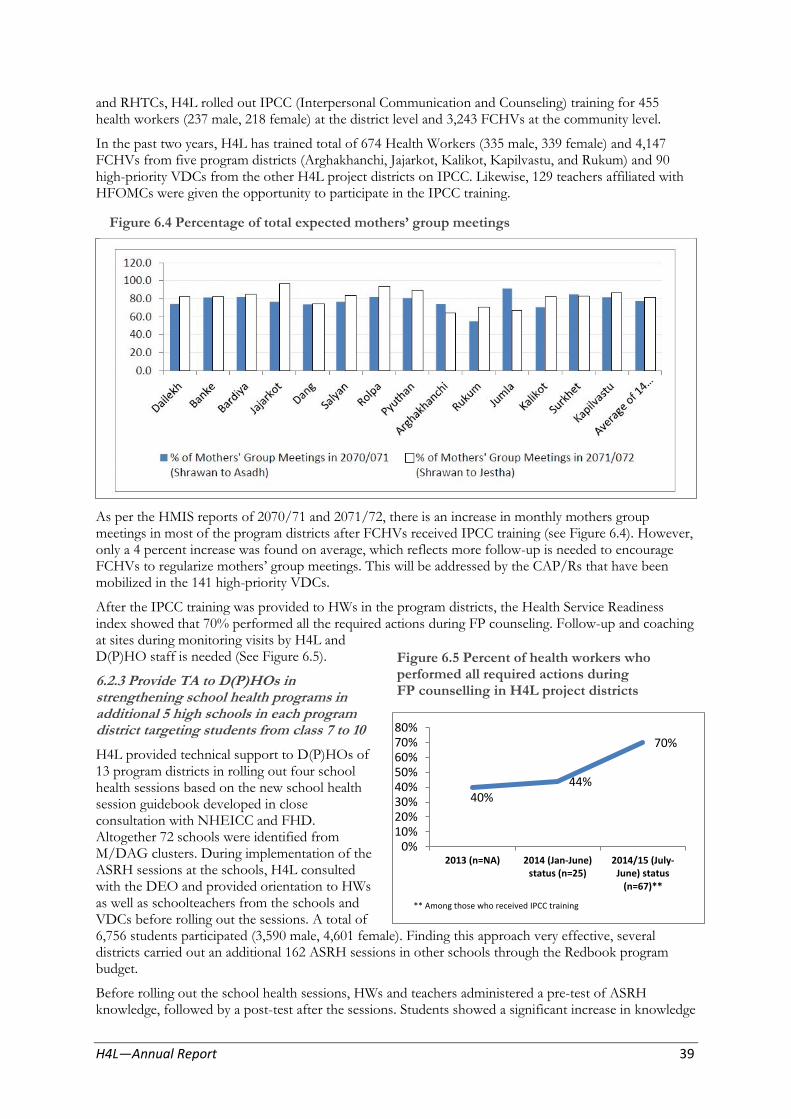
and RHTCs, H4L rolled out IPCC (Interpersonal Communication and Counseling) training for 455 health workers (237 male, 218 female) at the district level and 3,243 FCHVs at the community level.
In the past two years, H4L has trained total of 674 Health Workers (335 male, 339 female) and 4,147 FCHVs from five program districts (Arghakhanchi, Jajarkot, Kalikot, Kapilvastu, and Rukum) and 90 high-priority VDCs from the other H4L project districts on IPCC. Likewise, 129 teachers affiliated with HFOMCs were given the opportunity to participate in the IPCC training.
Figure 6.4 Percentage of total expected mothers’ group meetings
As per the HMIS reports of 2070/71 and 2071/72, there is an increase in monthly mothers group meetings in most of the program districts after FCHVs received IPCC training (see Figure 6.4). However, only a 4 percent increase was found on average, which reflects more follow-up is needed to encourage FCHVs to regularize mothers’ group meetings. This will be addressed by the CAP/Rs that have been mobilized in the 141 high-priority VDCs.
After the IPCC training was provided to HWs in the program districts, the Health Service Readiness index showed that 70% performed all the required actions during FP counseling. Follow-up and coaching at sites during monitoring visits by H4L and D(P)HO staff is needed (See Figure 6.5).
6.2.3 Provide TA to D(P)HOs in strengthening school health programs in additional 5 high schools in each program
Figure 6.5 Percent of health workers who performed all required actions during FP counselling in H4L project districts
district targeting students from class 7 to 10 80% 70%
H4L provided technical support to D(P)HOs of 60% 13 program districts in rolling out four school 50% health sessions based on the new school health 40%
session guidebook developed in close 30% 40%
consultation with NHEICC and FHD. 20%
Altogether 72 schools were identified from 10%
M/DAG clusters. During implementation of the 0%
2013 (n=NA) 2014 (Jan-June) 2014/15 (July-ASRH sessions at the schools, H4L consulted status (n=25) June) status
with the DEO and provided orientation to HWs (n=67)**
as well as schoolteachers from the schools and ** Among those who received IPCC training
VDCs before rolling out the sessions. A total of 6,756 students participated (3,590 male, 4,601 female). Finding this approach very effective, several districts carried out an additional 162 ASRH sessions in other schools through the Redbook program budget.
Before rolling out the school health sessions, HWs and teachers administered a pre-test of ASRH knowledge, followed by a post-test after the sessions. Students showed a significant increase in knowledge
44%
70%
H4L—Annual Report 39
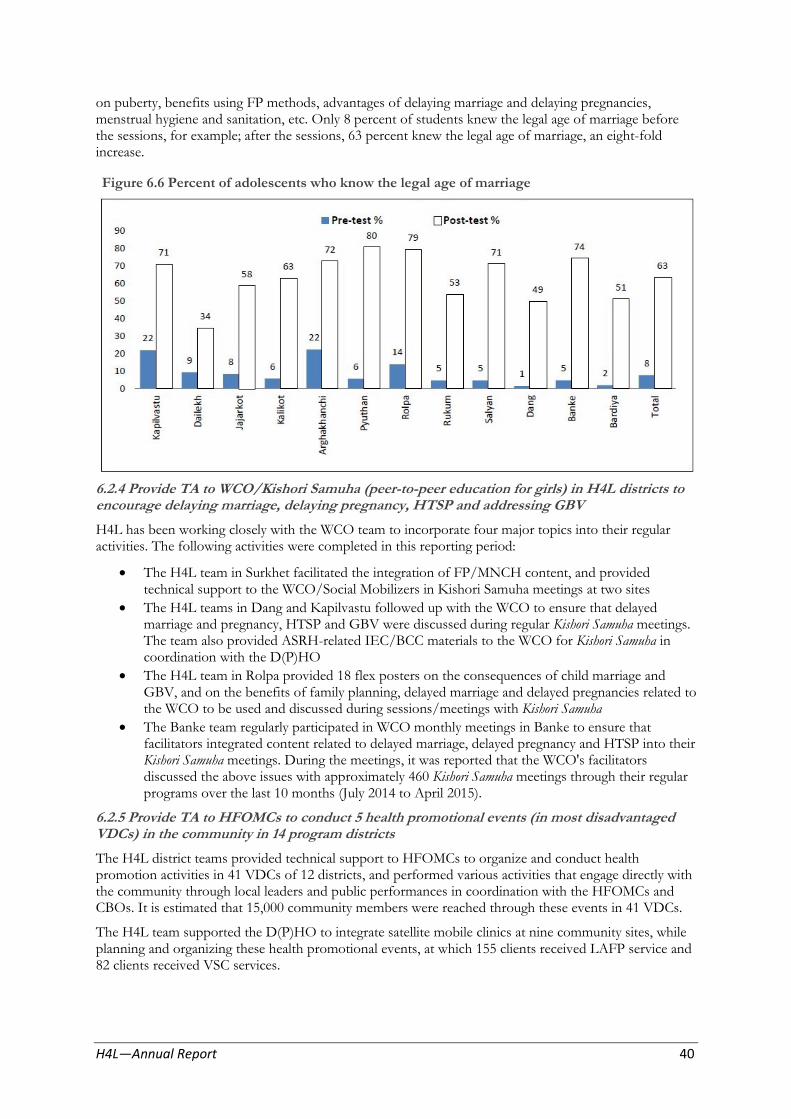
on puberty, benefits using FP methods, advantages of delaying marriage and delaying pregnancies, menstrual hygiene and sanitation, etc. Only 8 percent of students knew the legal age of marriage before the sessions, for example; after the sessions, 63 percent knew the legal age of marriage, an eight-fold increase.
Figure 6.6 Percent of adolescents who know the legal age of marriage
6.2.4 Provide TA to WCO/Kishori Samuha (peer-to-peer education for girls) in H4L districts to encourage delaying marriage, delaying pregnancy, HTSP and addressing GBV
H4L has been working closely with the WCO team to incorporate four major topics into their regular activities. The following activities were completed in this reporting period:
The H4L team in Surkhet facilitated the integration of FP/MNCH content, and provided technical support to the WCO/Social Mobilizers in Kishori Samuha meetings at two sites
The H4L teams in Dang and Kapilvastu followed up with the WCO to ensure that delayed marriage and pregnancy, HTSP and GBV were discussed during regular Kishori Samuha meetings. The team also provided ASRH-related IEC/BCC materials to the WCO for Kishori Samuha in coordination with the D(P)HO
The H4L team in Rolpa provided 18 flex posters on the consequences of child marriage and GBV, and on the benefits of family planning, delayed marriage and delayed pregnancies related to the WCO to be used and discussed during sessions/meetings with Kishori Samuha
The Banke team regularly participated in WCO monthly meetings in Banke to ensure that facilitators integrated content related to delayed marriage, delayed pregnancy and HTSP into their Kishori Samuha meetings. During the meetings, it was reported that the WCO's facilitators discussed the above issues with approximately 460 Kishori Samuha meetings through their regular programs over the last 10 months (July 2014 to April 2015).
6.2.5 Provide TA to HFOMCs to conduct 5 health promotional events (in most disadvantaged VDCs) in the community in 14 program districts
The H4L district teams provided technical support to HFOMCs to organize and conduct health promotion activities in 41 VDCs of 12 districts, and performed various activities that engage directly with the community through local leaders and public performances in coordination with the HFOMCs and CBOs. It is estimated that 15,000 community members were reached through these events in 41 VDCs.
The H4L team supported the D(P)HO to integrate satellite mobile clinics at nine community sites, while planning and organizing these health promotional events, at which 155 clients received LAFP service and 82 clients received VSC services.
H4L—Annual Report 40
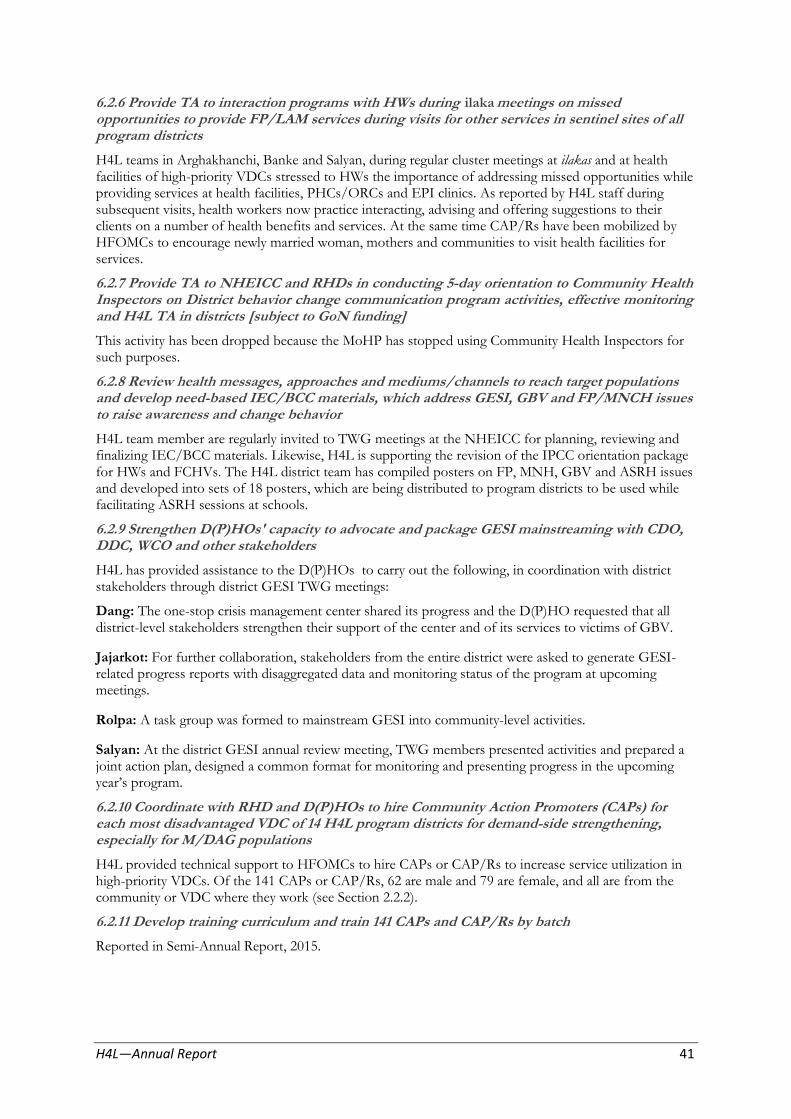
6.2.6 Provide TA to interaction programs with HWs during ilaka meetings on missed opportunities to provide FP/LAM services during visits for other services in sentinel sites of all program districts
H4L teams in Arghakhanchi, Banke and Salyan, during regular cluster meetings at ilakas and at health facilities of high-priority VDCs stressed to HWs the importance of addressing missed opportunities while providing services at health facilities, PHCs/ORCs and EPI clinics. As reported by H4L staff during subsequent visits, health workers now practice interacting, advising and offering suggestions to their clients on a number of health benefits and services. At the same time CAP/Rs have been mobilized by HFOMCs to encourage newly married woman, mothers and communities to visit health facilities for services.
6.2.7 Provide TA to NHEICC and RHDs in conducting 5-day orientation to Community Health Inspectors on District behavior change communication program activities, effective monitoring and H4L TA in districts [subject to GoN funding]
This activity has been dropped because the MoHP has stopped using Community Health Inspectors for such purposes.
6.2.8 Review health messages, approaches and mediums/channels to reach target populations and develop need-based IEC/BCC materials, which address GESI, GBV and FP/MNCH issues to raise awareness and change behavior
H4L team member are regularly invited to TWG meetings at the NHEICC for planning, reviewing and finalizing IEC/BCC materials. Likewise, H4L is supporting the revision of the IPCC orientation package for HWs and FCHVs. The H4L district team has compiled posters on FP, MNH, GBV and ASRH issues and developed into sets of 18 posters, which are being distributed to program districts to be used while facilitating ASRH sessions at schools.
6.2.9 Strengthen D(P)HOs' capacity to advocate and package GESI mainstreaming with CDO, DDC, WCO and other stakeholders
H4L has provided assistance to the D(P)HOs to carry out the following, in coordination with district stakeholders through district GESI TWG meetings:
Dang: The one-stop crisis management center shared its progress and the D(P)HO requested that all district-level stakeholders strengthen their support of the center and of its services to victims of GBV.
Jajarkot: For further collaboration, stakeholders from the entire district were asked to generate GESI-related progress reports with disaggregated data and monitoring status of the program at upcoming meetings.
Rolpa: A task group was formed to mainstream GESI into community-level activities.
Salyan: At the district GESI annual review meeting, TWG members presented activities and prepared a joint action plan, designed a common format for monitoring and presenting progress in the upcoming year’s program.
6.2.10 Coordinate with RHD and D(P)HOs to hire Community Action Promoters (CAPs) for each most disadvantaged VDC of 14 H4L program districts for demand-side strengthening, especially for M/DAG populations
H4L provided technical support to HFOMCs to hire CAPs or CAP/Rs to increase service utilization in high-priority VDCs. Of the 141 CAPs or CAP/Rs, 62 are male and 79 are female, and all are from the community or VDC where they work (see Section 2.2.2).
6.2.11 Develop training curriculum and train 141 CAPs and CAP/Rs by batch
Reported in Semi-Annual Report, 2015.
H4L—Annual Report 41

6.2.12 Provide TA to D(P)HOs to develop BCC intervention plans and include district-based stakeholders based on recently developed and approved district health communication strategies
H4L provided technical assistance to D(P)HOs in 13 districts to develop their three-year “District Health Communication Strategy 2014-16.” Other partners, such as GIZ, UNFPA and IPAS are using the strategies for their BCC program planning. Based on the documents, H4L assisted three districts in formulating their “Annual BCC Intervention Plan.” The districts that are implementing BCC programs according to their Annual BCC Intervention Plan are Kalikot, Dailekh and Rolpa.
6.3 Provide TA to NHTC and RHDs for developing trainers to institutionalize GESI in MOHP system
6.3.1 Provide TA to NHTC to conduct training needs assessments and develop a GESI TOT manual; provide TA for advanced Training of Trainers to reach Divisions and Centers staff
H4L supported the Population Division and NHTC to train 16 participants from among NHTC/RHTC, RHD, D(P)HO and MoHP trainers and officials to become a resource pool for GESI training. This activity was carried out in collaboration with the NHSSP and UNFPA.
H4L supported the Population Division in designing and developing a GESI training manual in collaboration with the NHSSP as part of developing in-house capacity to mainstream GESI in the health system, which was subsequently used in the aforementioned GESI training.
GESI master trainers sequentially organized training for HF In-charges, D(P)HO supervisors/focal persons, staff nurses and medical personnel from hospitals in the following five regions:
Far-west region: 212 health workers trained in Accham, Bajura and Bajhang.
Mid-west region: 170 participants were trained in Dang, Pyuthan and Kalikot.
Western region: 266 participants were trained in Rupandehi, Kaski, Nawalparasi and Mustang.
Central region: 216 participants were trained in Kathmandu and Sarlahi. Due to the earthquake, training could not take place in Dhading.
Eastern region: 245 participants were trained on GESI tools and methodologies in Sunsari, Saptari and in Moran.
6.3.2 Provide TA to Population Division to assess GESI focal persons' annual review and orient new focal persons on GESI in MoHP Departments and Divisions and Centers
The Population Division did not carry out this activity. H4L did, however, finalize TA related to the orientation of the GESI focal persons and GESI TWG for Divisions and Centers.
6.3.3 Provide TA to make functional GESI focal persons in Divisions, Centers and RHDs, and roll out MoHP GESI operational and GESI institutional structure guidelines
See 6.3.2.
6.3.4 Provide TA to make functional district GESI TWGs in all H4L districts based on MoHP GESI Operational and GESI institutional structure guideline
H4L supported D(P)HOs to regularize the GESI TWG’s meetings in eleven districts. Key issues discussed and decisions made during these meetings are detailed below.
Banke
Organized a program at the HF level to analyze service coverage and utilization by ward and caste/ethnicity for the FP/MNCH program, focusing on M/DAG populations, and to include GESI-responsive planning with the HFOMCs and FCHVs to address gaps in all 10 high-priority VDCs
Organized an LAFP outreach clinic for IUCD and implant services at HPs in Holiya, Bankatti, and Ganapur to provide services to eligible clients in response to data analysis and unavailability of regular LAFP services
Organized an integrated health camp in Kalaphata to provide essential health services to M/DAG.
H4L—Annual Report 42
Dang
DDC to organize a GESI Planning workshop among district-level stakeholders
Conduct an analysis of health service coverage status and plan activities on the basis of gaps identified.
Jumla
HPs in Bumramadichour, Godemahadev and Guthichour were selected for satellite camps
District stakeholders were oriented on OCMC program status and will use disaggregated data to ensure utilization by M/DAG.
Kapilvastu
A new GESI focal person was appointed for the regularization of GESI TWG meetings and to support making the district health program GESI-responsive, per MoHP GESI Guidelines
Discussed service utilization in the 10 high-priority VDCs by caste/ethnicity and the expansion of birthing centers at HPs in Jaynagar, Labani and Thuniya.
Rukum
H4L provided support to reform and orient the new GESI team.
GESI programming will be included at the beginning of every D(P)HO program, especially on training and orientation.
Surkhet
During the GESI TWG meeting on March 12 and July 10, 2015, the insensitive behavior of service providers towards clients, especially M/DAG, was addressed. TWG members recommended that H4L organize a GESI orientation for doctors and staff nurses in the district. The attendees also agreed to organize training for school teachers on making sanitary pads and to ask them to orient school children on menstrual hygiene. For this proposal, support will be requested from GIZ and UNICEF.
Objective 7: Strengthen capacity of USAID’s contractor for a logistical support activity
One of the key priorities identified in the LLN strategic plan of 2014 was leadership, management and staff development. In response, LifeLine Nepal’s board members and H4L Logistics’ senior project staff attended Management Dimensions for Effective Leadership from March 2–6, 2015. H4L Core and Envision staff also benefitted from the training.
The following suggested actions for LLN were made, based on what is most relevant and feasible in their context:
Institute a self-led lunchtime learning group (“The LLN Learning Hub”) that comes together once a month to exchange and discuss brief articles and tools relevant to LLN staff.
Encourage staff to take MOOCs (Massive Open Online Courses). Individuals or groups attending a MOOC should be asked to produce a one-page report at the end of the course, summarizing what s/he learned and make recommendations to LLN based on his/her new knowledge and skills.
Encourage all staff to create a professional development plan, with two to three goals per year and learning activities towards those goals.
H4L—Annual Report 43

Another session of “Management Dimensions for Effective Leadership” was delayed due to the earthquake. H4L Core will follow-up and reschedule within the next annual work plan period.
LLN has identified financial analysis and management, contract management, and business development as priorities for their organizational capacity development. H4L (Core) is in the process of selecting an audit firm (through a competitive bidding process) to subcontract to provide financial analysis and management support to LLN.
H4L (Core) team has been continuously coordinating with LLN to link to national-level partners on logistics-related issues and to report to USAID.
GESI
GESI activities at district level
In Arghakhanchi, Banke, Dang, Jumla, Kalikot, Kapilvastu, Rukum, Salyan and Surkhet, H4L supported the analysis of service utilization data by caste/ethnicity and presented the findings to HF In-charges, HFOMC members and the VDC assembly. H4L also assisted with the review and presentation of HMIS data at the trimester review meetings, and supported the micro-planning process.
As a result of the GESI TWG data analysis and decision-making to address service utilization gaps among M/DAG, the following specific activities were carried out with H4L TA:
Banke
NPR 50,000 in Udharapur and NPR 25,000 in Ganapur were allocated to organize the following awareness-raising activities in M/DAG communities:
Health camps (uterine prolaspe and RH services), especially for females, in both VDCs
Community interaction on domestic voilence in Udharapur (NRS 65,000 allocated)
Orientation on RH, focusing on M/DAG adolescents in both VDCs.
At Raniyapur HP, HFOMC members, FCHVs and HF staff developed an action plan on the basis of service utilization data and agreed to conduct additional PHC/ORC in wards 1 and 3 beginning in July 2015 (Sharawan 2072).
Bardiya
LAFP mobile clinics were implemented in Mahajidiya tole of Gulariya municipality-13; Chepang tole of Belwa VDC; Bhalu phata of Bhimmapur VDC; Lamki Phata of Dhadhawar VDC; and Khur khure of Baniyabhar VDC targeting M/DAG communities.
GESI integration in district training
Surkhet
H4L provided technical support to integrate GESI into two different orientation programs organized by the D(P)HO focusing on safe motherhood and FP, and to orient nursing staff from 10 HFs on GESI and FP counselling.
Pyuthan
H4L led sessions in which GESI was integrated into the orientation of 25 ANMs participating in a population program of the Management Division by the D(P)HO.
Jajarkot
In joint collaboration with the District Women and Child Development Office, GESI sessions for 59 female participants (chairpersons or secretaries of women cooperatives) were conducted. The sessions focused on reproductive health and GESI. Participants were asked to disseminate key health messages to their own communities, particularly focusing on M/DAG.
H4L—Annual Report 44

GESI Coordination group for USAID Partners
The GESI coordination group for USAID partners (Suaahara, Sajhedari, Hariyo Ban, KISAN, Saath-Saath, PAHAL, SABAL and H4L) held routine meetings. H4L provided comments on “Key AdvocacyMessages to the Gender Task Force” regarding post-disaster risk assessments and relief assistance, and also commented on “Key Indicators for Post-Earthquake Rehabilitation and Post-Disaster Planning”from a GESI perspective.
H4L Staff composition
H4L has met its goal of having at least 1/3 women and minorities on its staff.
Figure 8.2 H4L Staff composition by gender Figure 8.1 H4L Staff composition by ethnicity
B. Major challenges and constraints faced during the performance period that resulted in delays of achievement of outcomes, if applicable
1.1 Provide TA to D(P)HOs to revitalize HFOMCs and to help develop VDC health plans that are incorporated in the district AWPB ensuring appropriate budget allocations
Basic training in Arghakhanchi at 2 HFOMCs could not be completed as planned due to delays in recruiting H4L staff for a vacant position, and due to miscommunication between D(P)HO and H4L staff.
1.2 Assist D(P)HOs, DDCs and VDCs to improve performance of 140 HFOMCs based on local context (using set criteria) primarily focusing on most disadvantaged VDCsSome VDC periodic health planning activities could not be carried out as planned due to monsoon floods in Banke, Bardiya, Surkhet and Dang during first three months of this reporting period. District health teams were heavily engaged in providing emergency health and relief services to flood-affected populations. Health planning activities were completed during the 2nd half of the reporting period, but 13 VDC periodic plans could not be endorsed by VDC councils. It is expected that they will be endorsed next year.
1.4 Provide TA to MoHP, MoFALD and other stakeholders to expand local health governance strengthening activities to all 14 program districts and track progress against defined objectives and share with EDPs Forum and at the JAR
Some activities related to Local Health Governance were delayed by about a month, particularly in the six demonstration districts, due to the absence of the Local Development Officers (at DDCs) as most of them were on leave whilst preparing for the competitive examination given by the Public Service Commission as part of their career advancement. It was further hampered by the unexpected strike by health service providers. The intended technical assistance and support could not be provided to four of the demonstration districts due to delays in contract modification.
H4L—Annual Report 45
2.1.1 and 2.1.2 Support to HMIS in customizing and rolling out DHIS-2
There were some outstanding issues developing DHIS-2, including using the Nepali calendar for reporting, and issues related to data entry and report generation, which are being looked into by the University of Oslo and HISP India. As these issues were unresolved until the end of November 2014, the MD decided to continue with the existing HMIS software with some modification as an interim arrangement. The MoHP needs to make a decision regarding rolling out of the DHIS-2.
2.1.4 Provide TA to conduct review and annual planning meetings by trimester at HF level in 140 most disadvantaged VDCs
As mentioned, HMIS data entry was delayed as the DHIS-2 software was not ready. This created a lack of access to health service related data at the district level even though paper-based HMIS reporting was in place. Furthermore, transfer of the statistics assistants in most of the H4L districts and cancellation of the Computer Operator post delayed HMIS data entry in the existing HMIS software.
Additionally, flooding in four districts (Banke, Bardiya, Surkhet and Dang) during first three months of the fiscal year, and an epidemic of swine flu in Jajarkot between March and April 2015, which also affected Surkhet, Kalikot, Jumla and Rukum, caused delays in the planned activities. Later, it was proposed that activities under 2.1.4 and 2.1.5 be merged. However, as it was already in the last quarter of the year, it was envisaged that this activity be postponed in the remaining VDCs as it would not contribute to improved planning and programming since the plan for the next fiscal year was already completed and awaiting approval.
2.1.5 Provide TA to improve data quality and use for GESI-sensitive programming in 140 MDAG VDCs of H4L districts
As in 2.1.4.
2.2.4 Organize sensitizing workshop for USAID partners, research firms on NHRC ethical clearance process
A date was fixed for late April 2015 following discussions with the NHRC. The NHRC became heavily engaged in coordinating relief work in earthquake-affected districts and was not available until May. Later on, the NHRC proposed organizing the workshop next Nepali fiscal year as they were busy in wrapping up the remaining activities before the fiscal year close-out. It was conducted August 6-7.
4.2.4 H4L will establish an eHealth system to upload HF data by mobile device and aggregated at the district level for analysis
The lack of computers at the HFs made it impossible to implement the eHealth system, but there will be
further exploration on how this could be done.
4.3 Maintain National Quality Assurance Coordination Mechanism
Due to frequent changes and vacancies of the In-charge position of the QA section, there have been
significant delays in organizing meetings to review progress, steer the QAI TWG to strengthen district
QAWCs and to inform QI TAC and stakeholders periodically.
In addition, there were changes in the QA focal person at several departments such as the CHD, FHD,
NHTC and PHCRD which also added to delays.
4.4.4 HF data are uploaded by a mobile device and aggregated at the district level for analysis
As in 4.2.4.
5.1. 4 and 5.1.5 Provide TA to build FP Training Capacity using alternative approach
Delays in changing the FP training focal person and Director meant that the NHTC could not move ahead with the approval process for NSV self-paced training. Similarly there was delay in finalizing the IUCD package along with the self-paced module. These activities have been planned for the coming year.
H4L—Annual Report 46
5.3.1 Provide maintenance support (coaching, monitoring and reporting) to D(P)HOs for community-based Integrated Maternal, Neonatal and Childhood Illnesses (CB-IMNCI) and MSC intervention districts
CB-IMNCI
After finalization and approval of the CB-IMNCI package, the CHD decided to take a “whole district” approach, but our TA was not designed in such a manner. H4L, however, was able to facilitate and monitor quality of training during TOT at the regional and district level.
MSC Program
Although the supply of MSC resumed in several districts, Pyuthan received its supply very late in the fiscal year (February 2015) and then started supplying to communities in March 2015. There are still challenges in supplying it to the community level so that it can be given to pregnant women.
C. Highlights of the internship program as described in Section C.2.8.1
With an aim of building the professional capacity of women and marginalized groups in the project districts, two interns - in Banke and in Rukum - completed internships during which they had opportunities to learn and gain practical programmatic, managerial and technical experience and are now ready to assume greater decision-making roles in their communities and professional lives.
describes his experiences working with the H4L district staff in the area of local health governance in Appendix 3.
H4L—Annual Report 47
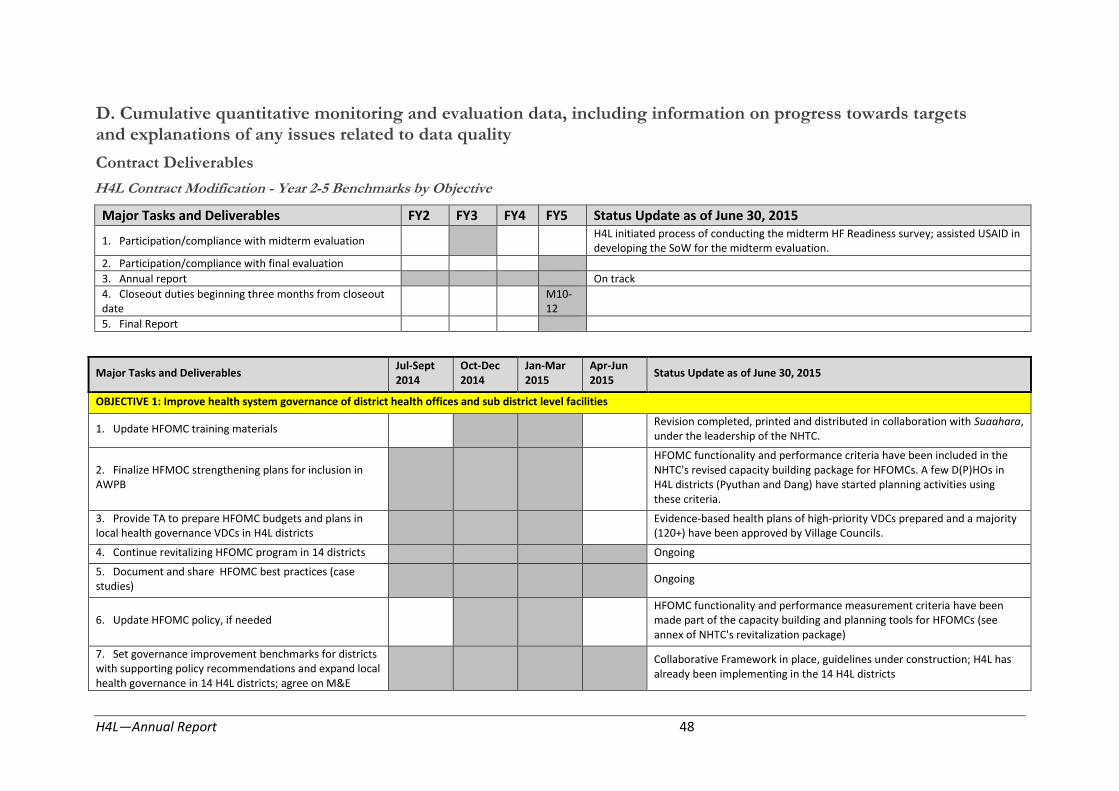
D. Cumulative quantitative monitoring and evaluation data, including information on progress towards targets and explanations of any issues related to data quality
Contract Deliverables
H4L Contract Modification - Year 2-5 Benchmarks by Objective
Major Tasks and Deliverables FY2 FY3 FY4 FY5 Status Update as of June 30, 2015
1. Participation/compliance with midterm evaluation H4L initiated process of conducting the midterm HF Readiness survey; assisted USAID in developing the SoW for the midterm evaluation.
2. Participation/compliance with final evaluation
3. Annual report On track
4. Closeout duties beginning three months from closeout date
M10-12
5. Final Report
Major Tasks and Deliverables Jul-Sept 2014
Oct-Dec 2014
Jan-Mar 2015
Apr-Jun 2015
Status Update as of June 30, 2015
OBJECTIVE 1: Improve health system governance of district health offices and sub district level facilities
1. Update HFOMC training materials Revision completed, printed and distributed in collaboration with Suaahara, under the leadership of the NHTC.
2. Finalize HFMOC strengthening plans for inclusion in AWPB
HFOMC functionality and performance criteria have been included in the NHTC's revised capacity building package for HFOMCs. A few D(P)HOs in H4L districts (Pyuthan and Dang) have started planning activities using these criteria.
3. Provide TA to prepare HFOMC budgets and plans in local health governance VDCs in H4L districts
Evidence-based health plans of high-priority VDCs prepared and a majority (120+) have been approved by Village Councils.
4. Continue revitalizing HFOMC program in 14 districts Ongoing
5. Document and share HFOMC best practices (case studies)
Ongoing
6. Update HFOMC policy, if needed HFOMC functionality and performance measurement criteria have been made part of the capacity building and planning tools for HFOMCs (see annex of NHTC's revitalization package)
7. Set governance improvement benchmarks for districts with supporting policy recommendations and expand local health governance in 14 H4L districts; agree on M&E
Collaborative Framework in place, guidelines under construction; H4L has already been implementing in the 14 H4L districts
H4L—Annual Report 48
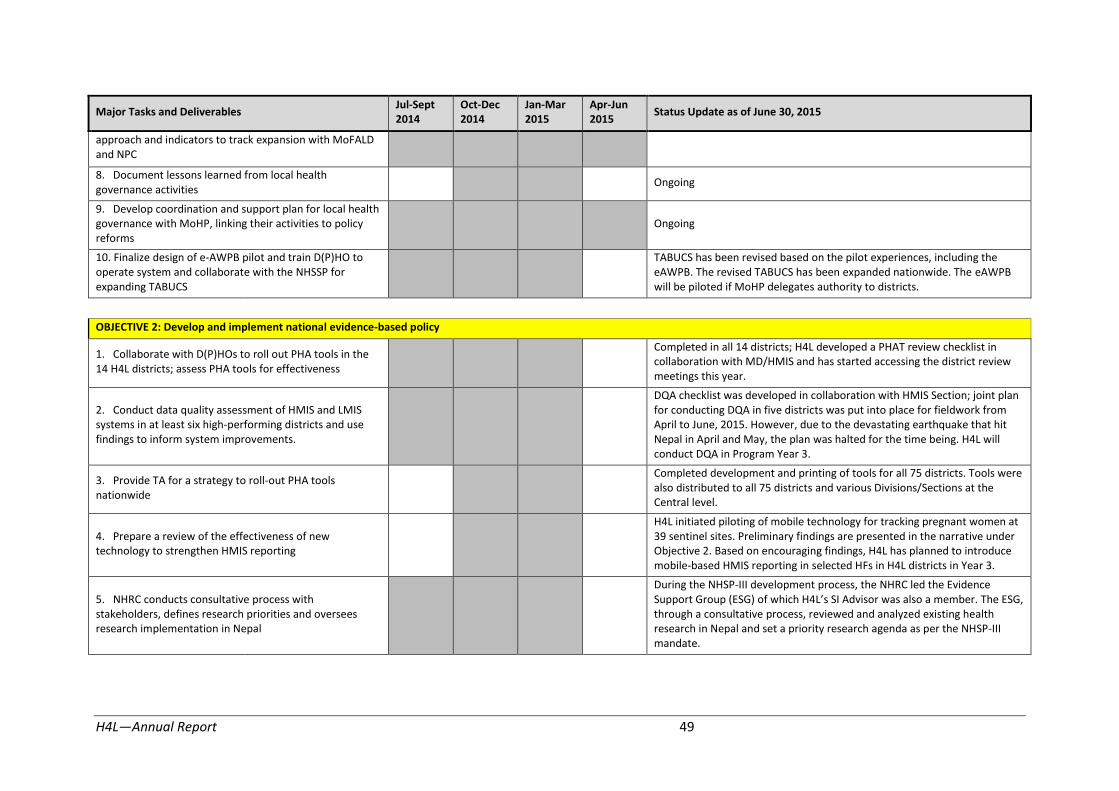
Major Tasks and Deliverables Jul-Sept 2014
Oct-Dec 2014
Jan-Mar 2015
Apr-Jun 2015
Status Update as of June 30, 2015
approach and indicators to track expansion with MoFALD and NPC
8. Document lessons learned from local health governance activities
Ongoing
9. Develop coordination and support plan for local health governance with MoHP, linking their activities to policy reforms
Ongoing
10. Finalize design of e-AWPB pilot and train D(P)HO to operate system and collaborate with the NHSSP for expanding TABUCS
TABUCS has been revised based on the pilot experiences, including the eAWPB. The revised TABUCS has been expanded nationwide. The eAWPB will be piloted if MoHP delegates authority to districts.
OBJECTIVE 2: Develop and implement national evidence-based policy
1. Collaborate with D(P)HOs to roll out PHA tools in the 14 H4L districts; assess PHA tools for effectiveness
Completed in all 14 districts; H4L developed a PHAT review checklist in collaboration with MD/HMIS and has started accessing the district review meetings this year.
2. Conduct data quality assessment of HMIS and LMIS systems in at least six high-performing districts and use findings to inform system improvements.
DQA checklist was developed in collaboration with HMIS Section; joint plan for conducting DQA in five districts was put into place for fieldwork from April to June, 2015. However, due to the devastating earthquake that hit Nepal in April and May, the plan was halted for the time being. H4L will conduct DQA in Program Year 3.
3. Provide TA for a strategy to roll-out PHA tools nationwide
Completed development and printing of tools for all 75 districts. Tools were also distributed to all 75 districts and various Divisions/Sections at the Central level.
4. Prepare a review of the effectiveness of new technology to strengthen HMIS reporting
H4L initiated piloting of mobile technology for tracking pregnant women at 39 sentinel sites. Preliminary findings are presented in the narrative under Objective 2. Based on encouraging findings, H4L has planned to introduce mobile-based HMIS reporting in selected HFs in H4L districts in Year 3.
5. NHRC conducts consultative process with stakeholders, defines research priorities and oversees research implementation in Nepal
During the NHSP-III development process, the NHRC led the Evidence Support Group (ESG) of which H4L’s SI !dvisor was also a member. The ESG, through a consultative process, reviewed and analyzed existing health research in Nepal and set a priority research agenda as per the NHSP-III mandate.
H4L—Annual Report 49

Major Tasks and Deliverables Jul-Sept 2014
Oct-Dec 2014
Jan-Mar 2015
Apr-Jun 2015
Status Update as of June 30, 2015
OBJECTIVE 3: Strengthen national level stewardship of the health sector
1. NHSP- III, which responds to and incorporates evidence-based policy, drafted
H4L supported and provided national and international TA to the MoHP to draft the NHSP-III since its inception; the draft has been approved by the Steering Committee and High-level Committee.
2. For MoHP, review partnership options with private sector, test/assess PPPs at district level (for example, a PPP between new eHealth initiatives and private developers)
H4L pursued an agreement with a vendor to carry out the mHealth program under the leadership of the NHEICC. GiZ and UNFPA participated in this intervention. After six rounds of negotiations, with USAID engagement, H4L was unable to solidify a PPP with NCell. NTC encourage using a value-added service provider. H4L planned further activities to design and test small PPP schemes in Dang (FY 2015-16)
3. Provide TA to MoHP to initiate preparation of the Third Long-Term Health Plan
Based on discussions with MoHP and as per their request, H4L provided TA to provide and prepare for a new health policy that includes components of the Third Long-Term Plan Health Plan. It is likely the GoN with not draft a Third Long-Term Health Plan.
OBJECTIVE 4: Institutionalize nationwide system for quality improvement
1. Roll out the QA system in 14 districts On track; implementation has started in all 14 districts
2. Nationwide QA system, implementation plan and benchmarks established
On track; guidelines, QI tools and a reporting system have been developed and are being field tested
OBJECTIVE 5: Improve capacity of district and local level health workers and community volunteers to deliver high-quality FP/MNCH and nutrition services
1. ANM curriculum revised ANM curriculum has been revised and approved by the CTEVT board, July 2014.
2. Roll out the ANM curriculum and training methodology in select schools in H4L core districts
The revised ANM curriculum has been introduced in all 44 ANM schools nationwide for the 2014 academic year. Orientation on the revised curriculum was given to all schools.
3. Draft the strategy for roll-out of the ANM curriculum nationwide
Will be done based on what is learned from the implementation at 6 ANM schools
4. Provide TA to the FHD/CHD-organized and led working group meetings to refocus FCHV responsibilities and update training materials
Once the results of the FCHV survey are out (expected in the near future), H4L will hold meetings to discuss the role of FCHVs. CB-IMNCI has already been integrated and the current package defines the FCHVs’ role as health promoters.
5. Providing support to the FHD, update family planning Ongoing. H4L contributed in CIP for FP and NHSP-III and its implementation
H4L—Annual Report 50
Major Tasks and Deliverables Jul-Sept 2014
Oct-Dec 2014
Jan-Mar 2015
Apr-Jun 2015
Status Update as of June 30, 2015
policies and guidelines as needed plan. PPFP strategy development is one aspect which has been identified for support to the FHD
6. Convene national meeting to discuss role of FCHVs in community continuum of care
Based on the results of the FCHV survey it is expected that FHD will initiate national level discussions. H4L is poised to support the FHD with technical assistance once the decision is made to convene these meetings.
7. IEC materials, counseling, services and training rolled-out in 14 districts for FP/MNCH/N and ENA+
On track
8. Assist the D(P)HO and QAWGs in local health governance VDCs to assess infection prevention and health care waste management practices (using standards) at health facilities, address gaps and mobilize resources based on action plans (part of HF QI system)
As a part of HF QI system, HFs are being assessed in high-priority VDCs (115 out 141) for IP/HCWM. It is ongoing in the demonstration districts.
9. FCHV refresher training on CB-IMCI rolled out in all 14 H4L districts
Ongoing. The CB-IMNCI package has been integrated and H4L has already supported phase-one implementation in four districts.
OBJECTIVE 6: Improve knowledge, behavior, and use of health services among target population
H4L, under the leadership of the NHEICC, designed and executed the
1. Innovative approaches using technology and traditional methods of information sharing implemented to reach marginalized, hard-to-reach groups (migrant families, adolescents, etc.)
m4ASRH SMS interactive package as part of its mHealth initiative. From Sept. 18, 2014 to May 31, 2015 more than 181,000 adolescent and youth received 4.9 million SMS text messages on ASRH issues. Likewise, H4L supported HFOMCs in the 141 high-priority VDCs to mobilize CAP/Rs to reach hard-to-reach groups and create service utilization demand-raising events and activities.
2. District communication strategies/plans rolled out with H4L TA in 14 districts; successes documented and presented to MoHP/DOHS and national stakeholders
D(P)HOs of 13 H4L district drafted, printed and disseminated District Health Communication Strategy documents; four of those districts developed annual IEC/BCC program implementation plans. The documents are also being used by GIZ, UNFPA and IPAS to design their BCC programs.
3. Conduct or use existing formative and barrier analyses to determine causes of non-use of FP methods, especially GESI-based constraints, and begin to develop district-specific plans to bridge gaps
H4L has periodically analyzed GESI-based constraints and non-use of health services including FP in 10 high-priority VDCs from service readiness monitoring data and has emphasized reaching M/DAGs through tailored IEC/BCC programs at the village, community and cluster level in consultation with the D(P)HO.
4. Finalize rapid assessment of opportunities to introduce H4L provided TA to the NHEICC in drafting the School Health Session Plan
H4L—Annual Report 51

Major Tasks and Deliverables Jul-Sept 2014
Oct-Dec 2014
Jan-Mar 2015
Apr-Jun 2015
Status Update as of June 30, 2015
mHealth technologies to reach remote areas with messages and information on service availability
and Guide and rolled out sessions in 72 schools this FY reaching more than 6000 school-age adolescents and youth. The adolescents and youth were encouraged to visit AYFS for services. The guidebook is being used by other agencies (GIZ, UNFPA and IPAS) in their program districts as well. During the school health program, promotion of the m4ASRH SMS interactive package was conducted, as well. H4L also worked closely with the DWCO to incorporate FP, HTSP and GBV agenda into discussions at Kishori Samuha.
5. Support FHD and NHEICC to review criteria for AYFS (if needed) and to develop training plan for peer-to-peer and school health approaches that strengthen/expand knowledge on delayed marriage and access to FP
6. Use data from District Rapid Assessments, the HF readiness survey and secondary data reviews to identify missed opportunities for LAPM, immunization, newborn care, MSC and nutrition services and to improve counseling skills and health messaging.
H4L team, through the HFOMCs, mobilized CAP/Rs to work closely with FCHVs (mothers groups) and user groups in high-priority VDCs and to bridge gaps between the community and health facilities for effective service delivery and utilization. The H4L district team also participated and raised the issue of missed opportunities during cluster (ilaka) meetings at HFs.
H4L, under the leadership of the NHEICC and with support of the RHTCs,
7. Develop plan to strengthen community-based, peer-led education (learning circles) for CB-IMCI and CB-NCP in five districts.
rolled out IPCC/LC trainings to 675 HWs and 4147 FCHVs emphasizing proper counseling for potential clients and individuals to increase FP, MNCH and ASRH services in all 14 districts. The H4L team also worked closely with the WCO to incorporate FP, HTSP and GBV into discussions at Kishori Samuha.
H4L—Annual Report 52

Capacity Building Benchmarks
Objective 1: Improve health systems governance of district health offices and sub-district level facilities
Key Component Year-2 Benchmark
(July 2014-June 2015)
Status (as of June 30, 2015) Remarks
HFOMC Performance 1. Revitalized and functioning HFOMCs are meeting some or all of the 6 performance criteria, thereby demonstrating a more active role in the local health sector, in the community, especially among M/DAGs, and in bolstering the health facility
Measurement: HFOMC performance criteria are applied to HFOMCs at 39 sentinel sites; HFOMCs in other high-priority VDCs, and HFOMCs in other VDCs were also visited
As a result of technical assistance and support provided to D(P)HOs in all 14 H4L districts, nearly 84 percent of HFOMCs met all functionality criteria and 52 percent met all functionality criteria and at least four performance criteria at the time evaluated. 12 percent of HFOM�s achieved “model” status.
New HFOMC Revitalization Package. Early attention will focus on revitalization of HFOMCs and later on demonstrating performance at HFs. Benchmarks in later years will focus on achieving all performance criteria.
Districts implement new 2. LGCDP grants to VDCs include resources allocated for Periodic and Annual VDC health plans were developed Benchmarks in later years will focus on HFOMC MoHP/MoFALD local governance HFOMCs based on selected health indicators and in 140 VDCs; 127 such plans were endorsed by VDC performance and health facility readiness, policy in VDCs to strengthen targets, as well as requests based on other local Councils during this reporting period. A significant quality of care, and performance. HFOMCs and health facilities evidence and support from D(P)HOs
Measurement: HFOMC fund allocation reviews at 39 sentinel sites, reviews at other high-priority VDCs, and in other VDCs visited
amount of resources were allocated by local bodies for increasing access to and utilization of services by M/DAG in all high-priority VDCs. A total of NPR. 10,09,60,509 in local resources was mobilized through local bodies and communities during this reporting period to fund VDC health plans, including hiring clinical staff in birthing centers, improving quality of care, opening new PHCs/ORCs, conducting FP satellite clinics etc.
H4L—Annual Report 53

Objective 2: Develop evidence-based health policy
Key Component Year-2 Benchmark Status (as of June 30, 2015) Remarks
3. D(P)HO reviews reflect evidence-based analysis of All 14 D(P)HOs organized and implemented trainings on Benchmarks in later years will focus on Analytical capacity of District (Public) Health Offices trimestral HMIS reports and other sources,
including health facility readiness assessments
PHA techniques. They have started using the PHAT manual to analyze data from HMIS and other sources.
expansion, data quality and annual district and regional reviews, including interpretation and
and complete reports from H4L’s 39 sentinel sites
representing the most impoverished VDCs to
prioritize programs and activities
Measurement: District HMIS reports, Health Facility Readiness Assessments, and other sentinel site reports incorporated at District and Regional Review and Planning meetings
The PHAT review template was developed in collaboration with HMIS/MD and used in all 14 districts to assess the district annual and trimestral review meetings. Based on the assessment, six districts have achieved “model” status, and five have achieved “progressive.”
actions.
4. The NHRC initiates partnership with H4L to H4L and NHRC signed an MOU on July 17, 2014 Benchmarks for the NHRC in later years will NHRC collaborative research network and knowledge management
expand NHR�’s knowledge management capacity,
strengthen its coordination of a research network
in Nepal’s health sector, and strengthen its
stipulating a scope of work for expanding NHR�’s knowledge management capacity. Based on this MOU, H4L supported the NHRC with computer equipment
focus on an expanded knowledge management role that supports the AWPB
capacity to impact health policies and programs
Measurement: Agreement reached between NHRC and H4L, and NHRC absorbs TA, develops a clearinghouse and web portal, establishes research network and leads network coordination meetings
(one server, 11 desktop computers and a 40-point LAN). A consultant has also been recruited for knowledge management and web portal development and has been approved.
Objective 3: Strengthen national level stewardship of the health sector
Key Component Year-2 Benchmark Status (as of June 30, 2015) Remarks
MoHP policy making 5. The MoHP manages the NHSP-III development process in cooperation with partners and completes the 3
rd health sector
program with the concurrence of the EDPs, as scheduled
Measurement: Adherence to the process outlined in the Year-1 Benchmark is reviewed as is agreement on the final document by all parties
H4L supported and provided national and international TA to the MoHP to draft the NHSP-III since its inception; the draft has been approved by the PDT, Steering Committee and High-level Committee.
Benchmarks in later years will focus on evidence-based policy making
H4L—Annual Report 54

Objective 4: Institutionalize nationwide system for quality improvement
Key Components Year-2 Benchmark Status (as of June 30, 2015) Remarks
QA/QI system 6. MD can finalize QI guidelines/tools based on findings from implementation in selected districts in all five regions for scale-up
Measurement: QI guidelines and tools finalized, 75 D(P)HOs oriented, and guidelines in use
Together with partners, H4L is continuously assisting the QAI TWG to implement the national QI system. Although the QAI TWG at first decided to implement the national QI system in two districts per region, it was later decided to implement the HF QI system in the same six demonstration districts as the CF pilot.
Delays in implementing H4L activities in the demonstration districts resulted in delays in implementing the QA/QI system.
District level orientation has been completed in all 14 H4L districts. In Dang, Jumla and Surkhet, the HF QI system has been implemented in 14, 12 and 10 HFs, respectively.
As per the decision made during the QI TAC meeting, guidelines will be finalized based on learning from Dang and Jumla.
Change in the QA focal person also caused delays.
Benchmarks in later years will focus on: use of the HF Readiness Assessments and on the MD’s updates to the QI guidelines/tools for the QI system, and on testing implementing and scaling up the new QI system in the districts
Objective 5: Improve capacity of district and local health workers and community volunteers to deliver quality family planning, maternal, newborn and child health, and nutrition services
Key Components Year-2 Benchmark Status (as of June 30, 2015) Remarks
Family Planning 7. D(P)HOs can expand birthing centers to provide long-acting FP methods to high-priority VDCs and address missed opportunities
Measurement: Number of additional birthing centers providing long-acting FP supported by D(P)HO
In the 141 high-priority VDCs there are 110 birthing centers, of which 58 offer both LAFP methods, 25 offer IUCDs only and 18 offer implants only. Nine HFs with birthing centers and 8 HFs without delivery services do not offer any LAFP services.
The number of birthing centers in H4L districts has increased from 393 in the last reporting period to 445 in this period, of which 62% (276) now offer at least one LAFP method.
Benchmarks in later years will focus on expanding LAFP, especially to M/DAGs.
H4L—Annual Report 55

ANM school strengthening 8. Four ANM schools introduce the revised curriculum and implement actions to address gaps in their training methodology, including an enabling environment based on revised curriculum
Measurement: Number of ANM schools who have introduced the revised curriculum
With technical support from H4L, the Center for Technical Education and Vocational Training (CTEVT) updated/revised the ANM curriculum last year and approved it on July 9, 2014. It was introduced starting in the 2014 academic year at four ANM schools in H4L districts, two CTVT-run ANM schools, as well as an additional 39 privately-run ANM schools nationwide.
Benchmarks in later years will focus on the capacity to implement the revised curriculum and evaluate student competency.
Objective 6: Improve knowledge, behavior and use of health services among target population
Key Components Year-2 Benchmark Status (as of June 30, 2015) Remarks
Awareness through Mass Media 9. D(P)HOs will support 28 FM radio stations to air health messages throughout the year
Measurement: Radio spots aired per day throughout the year by the FM radio stations
D(P)HOs in eight H4L districts are supporting 11 Local FM radio stations to air at least one radio spot on FP/MNCH per day. So far around 5,580 PSAs have been aired (FP=1,920; MNH=1,820; CH=1,820).
Benchmarks in later years will focus on D(P)HOs partnering with local FM radio stations to develop radio programs/PSAs on health topics and issues based on evidence and needs of the district.
District communication strategies and annual intervention plans
10. D(P)HOs are able to design and execute at least one community-based communication intervention to reach M/DAGs
Measurement: Number of interventions executed and recorded at the D(P)HO
Based on the district annual IEC/BCC intervention plan, 82 events (health quizzes at schools, street dramas, health promotion exhibitions, health song competitions and sasu-buhari interaction programs) in 41 VDCs in 13 districts were carried out.
Benchmarks in later years will focus on D(P)HOs developing their annual communication plans and implement programs in hard-to-reach clusters, targeting M/DAGs.
mHealth for ASRH 11. NHEICC can subcontract a value-added service provider to push at least five text messages
Measurement: Record of subcontract to VASP and record of text messages from VASP
NHEICC called for tenders twice to partner with telecom operators/VASPs to implement SMS text messages under the mHealth program but both were cancelled.
Benchmarks in later years will focus on NHEICC partnerships with telephone operators or VASPs to push at least five SMS text messages on important health issues.
H4L—Annual Report 56
Objective 7: Strengthen capacity of US!ID’s contractor for logistical support activity
Key Components Year-2 Benchmark Status (as of June 30, 2015) Remarks
Organizational development for LLN
12. LLN responds to training by establishing and documenting appropriate protocols and procedures to strengthen their management
Measurement: Review of documentation
One of the key priorities identified in the LLN strategic plan of 2014 was leadership, management and staff development. Following up on that priority, the course Management Dimensions for Effective Leadership was delivered (March 2 – 6, 2015) to participants from LifeLine Nepal’s board members and H4L Logistics’ senior project staff that have supervisory roles. Other partner and Envision staff also benefitted from the training.
LLN has identified finance and administration, contract management and business development as priorities for their organizational capacity development. H4L (Core) is in the process of selecting an audit firm (through a competitive bidding process) to subcontract support to LLN in these areas. LLN also requested H4L (Core) to provide them with some basic office furniture and equipment. H4L (Core) included these in the procurement plan for next year.
Benchmarks in later years will focus on whether management systems are developed and operating.
H4L—Annual Report 57
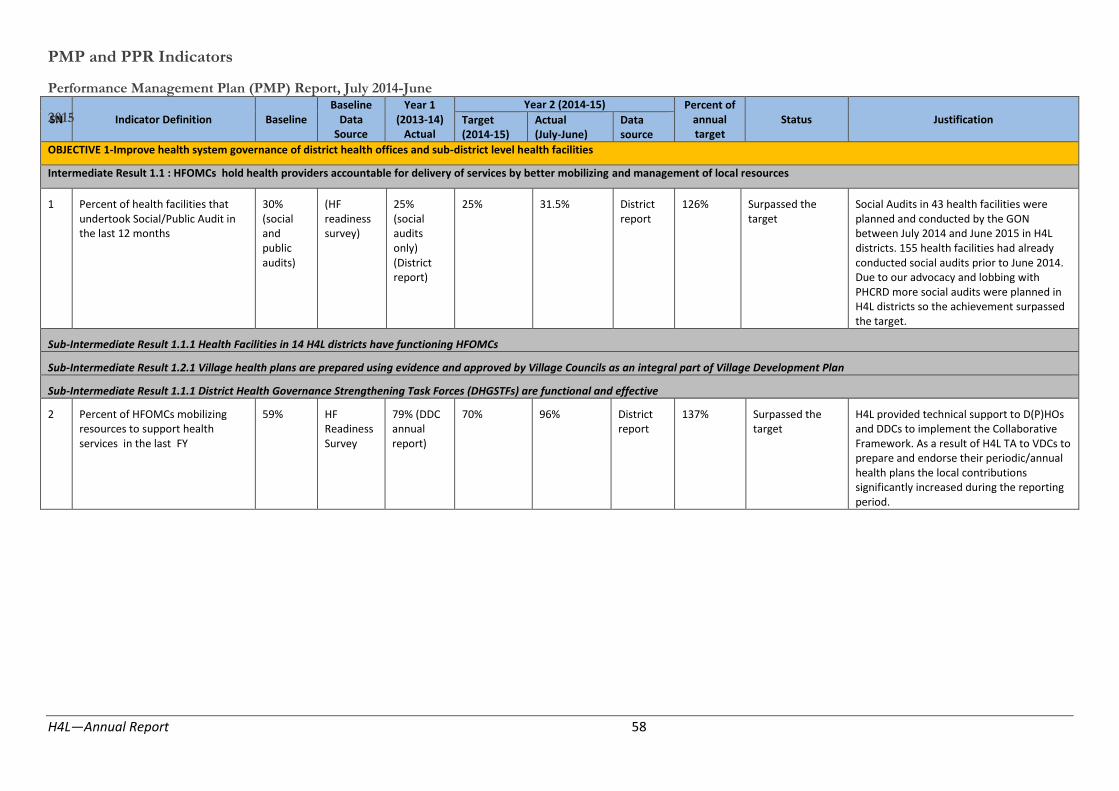
PMP and PPR Indicators
Performance Management Plan (PMP) Report, July 2014-June
SN2015 Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
OBJECTIVE 1-Improve health system governance of district health offices and sub-district level health facilities
Intermediate Result 1.1 : HFOMCs hold health providers accountable for delivery of services by better mobilizing and management of local resources
1 Percent of health facilities that undertook Social/Public Audit in the last 12 months
30% (social and public audits)
(HF readiness survey)
25% (social audits only) (District report)
25% 31.5% District report
126% Surpassed the target
Social Audits in 43 health facilities were planned and conducted by the GON between July 2014 and June 2015 in H4L districts. 155 health facilities had already conducted social audits prior to June 2014. Due to our advocacy and lobbing with PHCRD more social audits were planned in H4L districts so the achievement surpassed the target.
Sub-Intermediate Result 1.1.1 Health Facilities in 14 H4L districts have functioning HFOMCs
Sub-Intermediate Result 1.2.1 Village health plans are prepared using evidence and approved by Village Councils as an integral part of Village Development Plan
Sub-Intermediate Result 1.1.1 District Health Governance Strengthening Task Forces (DHGSTFs) are functional and effective
2 Percent of HFOMCs mobilizing resources to support health services in the last FY
59% HF Readiness Survey
79% (DDC annual report)
70% 96% District report
137% Surpassed the target
H4L provided technical support to D(P)HOs and DDCs to implement the Collaborative Framework. As a result of H4L TA to VDCs to prepare and endorse their periodic/annual health plans the local contributions significantly increased during the reporting period.
H4L—Annual Report 58
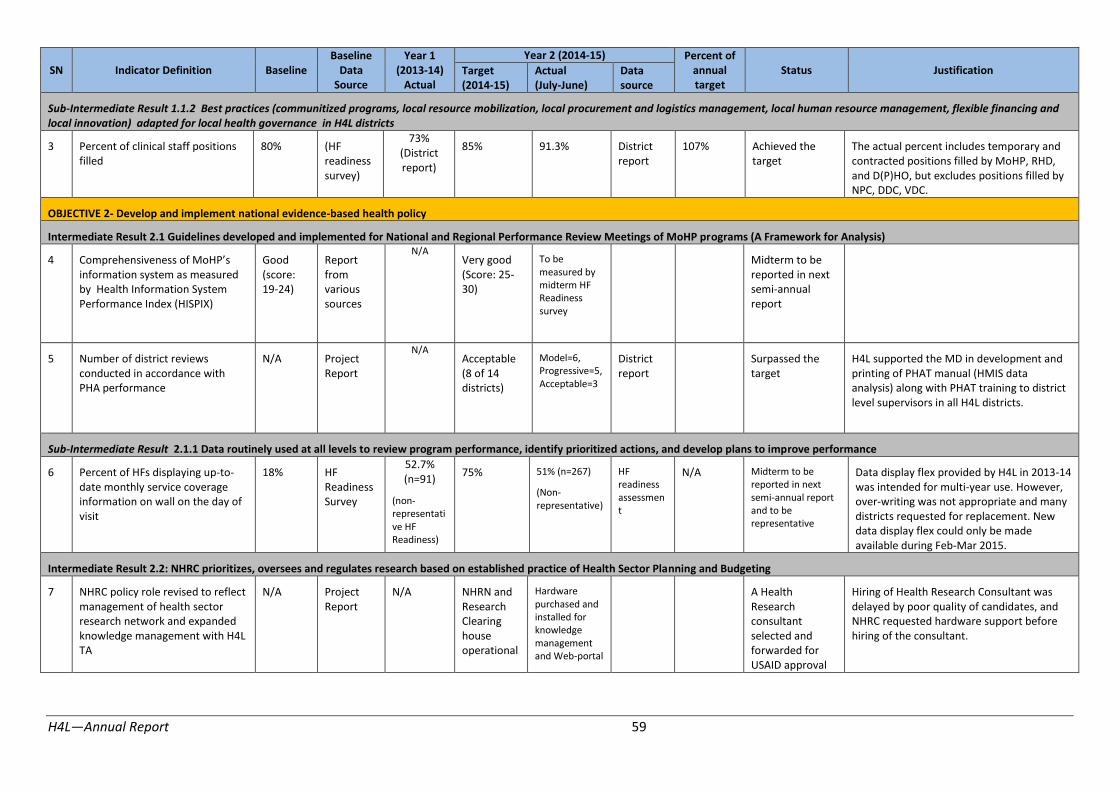
SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
Sub-Intermediate Result 1.1.2 Best practices (communitized programs, local resource mobilization, local procurement and logistics management, local human resource management, flexible financing and local innovation) adapted for local health governance in H4L districts
3 Percent of clinical staff positions filled
80% (HF readiness survey)
73% (District report)
85% 91.3% District report
107% Achieved the target
The actual percent includes temporary and contracted positions filled by MoHP, RHD, and D(P)HO, but excludes positions filled by NPC, DDC, VDC.
OBJECTIVE 2- Develop and implement national evidence-based health policy
Intermediate Result 2.1 Guidelines developed and implemented for National and Regional Performance Review Meetings of MoHP programs (A Framework for Analysis)
4 �omprehensiveness of MoHP’s information system as measured by Health Information System Performance Index (HISPIX)
Good (score: 19-24)
Report from various sources
N/A Very good (Score: 25-30)
To be measured by midterm HF Readiness survey
Midterm to be reported in next semi-annual report
5 Number of district reviews conducted in accordance with PHA performance
N/A Project Report
N/A Acceptable (8 of 14 districts)
Model=6, Progressive=5, Acceptable=3
District report
Surpassed the target
H4L supported the MD in development and printing of PHAT manual (HMIS data analysis) along with PHAT training to district level supervisors in all H4L districts.
Sub-Intermediate Result 2.1.1 Data routinely used at all levels to review program performance, identify prioritized actions, and develop plans to improve performance
6 Percent of HFs displaying up-to-date monthly service coverage information on wall on the day of visit
18% HF Readiness Survey
52.7% (n=91)
(non-representati ve HF Readiness)
75% 51% (n=267)
(Non-representative)
HF readiness assessmen t
N/A Midterm to be reported in next semi-annual report and to be representative
Data display flex provided by H4L in 2013-14 was intended for multi-year use. However, over-writing was not appropriate and many districts requested for replacement. New data display flex could only be made available during Feb-Mar 2015.
Intermediate Result 2.2: NHRC prioritizes, oversees and regulates research based on established practice of Health Sector Planning and Budgeting
7 NHRC policy role revised to reflect management of health sector research network and expanded knowledge management with H4L TA
N/A Project Report
N/A NHRN and Research Clearing house operational
Hardware purchased and installed for knowledge management and Web-portal
A Health Research consultant selected and forwarded for USAID approval
Hiring of Health Research Consultant was delayed by poor quality of candidates, and NHRC requested hardware support before hiring of the consultant.
H4L—Annual Report 59

SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
OBJECTIVE 3-Strengthen national level stewardship of the health sector
Intermediate Result 3;1 MoHP’s next Health Sector Strategy, Third Long Term Health Sector Plan (2018-2038) and Comprehensive Health Sector Plan (2016-2021) developed in collaboration with EDPs and TA programs
8 Health Sector Strategy, Third Long-Term Plan, and NHSP III:2016-2021 developed with H4L’s T!
N/A Project Report
N/A MoHP leads consultati ve process
NHSP III approved by Steering Committee
MoHP and partners jointly prepared Health Sector Strategy and NHSP-III. Likely that MoHP will not prepare Third Long-term Plan. NHSP-III draft has been endorsed by the Steering Committee and High Level Committee. To be sent to the Cabinet for final approval.
Intermediate Result 3.2 State Non-State Partnerships are identified in H4L districts documented and shared for MOHP scale up
9 NHEICC and/or DPHOs establish partnerships with Telecom and/or FM Radio to develop and implement mHealth and/or radio BCC activities
N/A Project Report
N/A List of partnership s formed
NHEICC did not partner with Telecom.
11 local FM radio station of 8 districts continue to air PSAs on health issues with partial funding from D(P)HO.
Continuing NHEICC called for tenders twice to partner with telecom operators to implement mHealth programs but both were cancelled.
OBJECTIVE 4-Institutionalize nationwide system for quality improvement
Intermediate Result 4.1 Consensus built on National QI system and piloted in in H4L districts for MoHP scale up
10 Number of district QAWG that carry out action plan in the last reporting period (by trimester)
0/14 QAWG minutes
9
(District report)
14 13 District report, QAWC meeting minutes
93% Target not achieved
All 14 districts except Dailekh had meetings and action plans carried out. 27 actions were planned and completed during the last reporting period (2
nd Trimester).
H4L—Annual Report 60

SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
Intermediate Result 4.2 D(P)HO rolls out facility-based QI system in all H4L districts
11 General Service Readiness Index of health facility
41% (HF readiness survey)
N/A 60% 49% (n=209), non-representative
HF readiness
N/A Midterm to be reported in next semi-annual report and to be representative
Total score obtained by IP and Basic Amenities is 15% and 28%, respectively. Unavailability of small items, such as Mask, led to low scores. Mechanism for HFOMC, D(P)HO and DDC to ensure achievement not established.
OBJECTIVE 5- Improve capacity of district and local health workers and community volunteers to deliver quality family planning, maternal, newborn and child health, and nutrition services
Intermediate Result 5.1 Community level health innovations and programs delivering MNCHN/FP services scaled-up and maintained
12 Percent of deliveries conducted by skilled birth attendant (doctor, nurse or ANM)
42% DHS 46% (HMIS data accessed on 9 Oct. 2014)
60% 54.7% HMIS1
91% Target not achieved
13 Percent of newborns receiving postnatal health check-up within 24 hours of birth (New indicator effective from 2014-15)
50% HMIS 2013 N/A 53% 60% HMIS 113% Surpassed the
target - PNC visits are increasing as institutional deliveries increase.
- PNC visits in Kapilvastu are relatively high because they are about double of that of institutional delivery.
Sub-Intermediate Result 5.1.1 D/PHO managed/implemented Matri Surakshya Chakki program in Bardiya district and CB-IMNCI program in H4L districts
14 Number of districts implementing a community-based integrated management of newborn and childhood illness (CB-IMNCI) package (New indicator effective from 2014-15)
0 N/A
H4L support for MTOT on revised package
4 Program report
N/A Although H4L did not sponsor the full package, it supported GON and partners to plan and train CB-IMNCI in 4 districts (Surkhet, Rukum, Jajarkot, and Kalikot).
1 HMIS data is for 11 months period – Shravan (July 15) to Jestha (June 15).
H4L—Annual Report 61
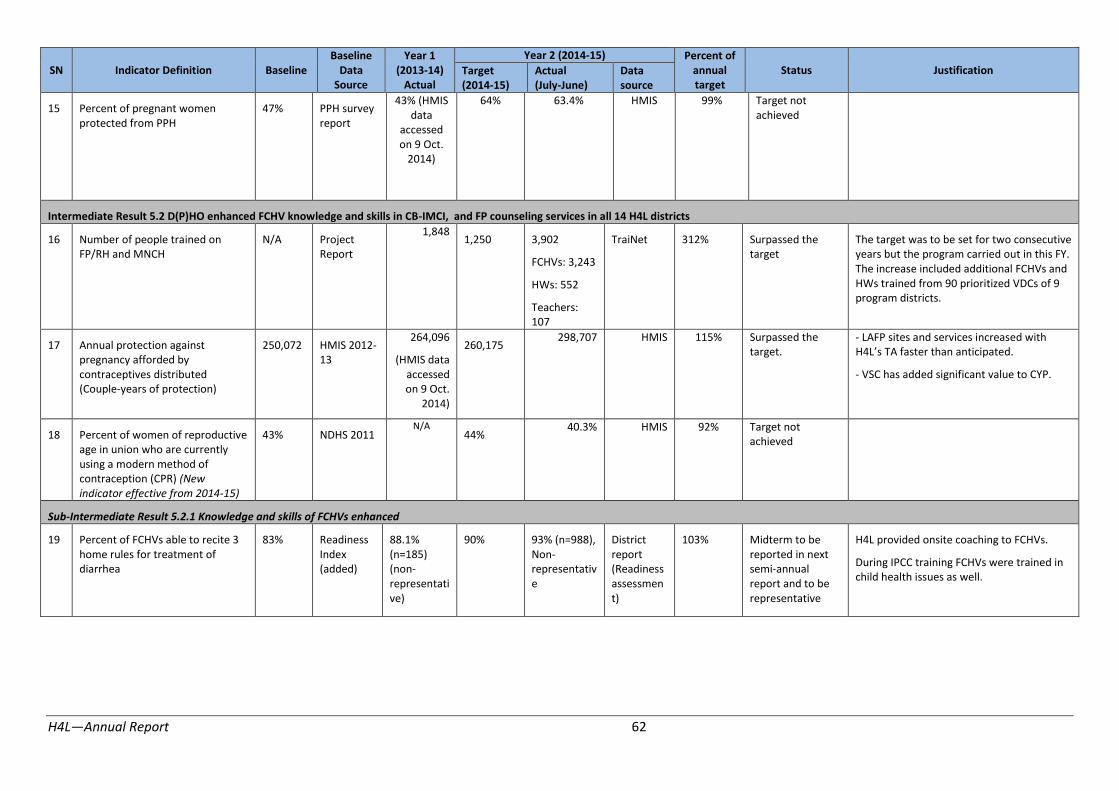
SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
15 Percent of pregnant women protected from PPH
47% PPH survey report
43% (HMIS data
accessed on 9 Oct.
2014)
64% 63.4% HMIS 99% Target not achieved
Intermediate Result 5.2 D(P)HO enhanced FCHV knowledge and skills in CB-IMCI, and FP counseling services in all 14 H4L districts
16 Number of people trained on FP/RH and MNCH
N/A Project Report
1,848 1,250 3,902
FCHVs: 3,243
HWs: 552
Teachers: 107
TraiNet 312% Surpassed the target
The target was to be set for two consecutive years but the program carried out in this FY. The increase included additional FCHVs and HWs trained from 90 prioritized VDCs of 9 program districts.
17 Annual protection against pregnancy afforded by contraceptives distributed (Couple-years of protection)
250,072 HMIS 2012-13
264,096
(HMIS data accessed on 9 Oct.
2014)
260,175 298,707 HMIS 115% Surpassed the
target. - LAFP sites and services increased with H4L’s T! faster than anticipated.
- VSC has added significant value to CYP.
18 Percent of women of reproductive age in union who are currently using a modern method of contraception (CPR) (New indicator effective from 2014-15)
43% NDHS 2011 N/A
44% 40.3% HMIS 92% Target not
achieved
Sub-Intermediate Result 5.2.1 Knowledge and skills of FCHVs enhanced
19 Percent of FCHVs able to recite 3 home rules for treatment of diarrhea
83% Readiness Index (added)
88.1% (n=185) (non-representati ve)
90% 93% (n=988), Non-representativ e
District report (Readiness assessmen t)
103% Midterm to be reported in next semi-annual report and to be representative
H4L provided onsite coaching to FCHVs.
During IPCC training FCHVs were trained in child health issues as well.
H4L—Annual Report 62

SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
Sub-Intermediate Result 5.2.1 Knowledge and skills of health workers enhanced
20 Percent of health workers who performed all of the six actions during counseling
40% Readiness Index (added)
44% (n=25) (non-representa tive)
60% 70% (n=67), Non-representative
District report (Readiness assessment)
117% Midterm to be reported in next semi-annual report and to be representative
As above H4L provided IPCC and FP coaching onsite and offsite.
N is small and is non-representative.
Intermediate Result 5.3 ANM pre-service training improved in 4 ANM schools of H4L districts
21 Percent of ANM with high level of proficiency in core SBA skills
Knowled ge: 17.5% scored 65% and above
Skills: 0% scored 65% and above
ANM Assessme nt Report
N/A N/A N/A N/A N/A Further discussion is needed (based on programmatic inputs)
OBJECTIVE 6-Improve knowledge, behavior and use of health services among target populations
Intermediate Result 6.1 Demand and utilization for MNCHN/FP services increased among M/DAG and Adolescents/Youths
22 Percent of Dalit women who delivered at HF (Revised indicator effective from 2014-15)
26.4% NDHS 2011 further analysis
N/A 28% 43.6% HMIS 156%
2 Surpassed the target
H4L introduced to HFOMCs CAPs and CAP/Rs to track pregnant women in high-priority VDCs. To date, about half of expected pregnant women are registered in 39 sentinel sites. Analysis suggests increase in equitable use of services. We await reports from other high priority VDCs.
2 Target population is derived by applying the proportion of Dalit calculated from Census 2011 data to the target population given from HMIS for 2014/15.
H4L—Annual Report 63

SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
Sub-Intermediate Result 6.1.2 GBV and early marriage are mitigated in 10 districts
23 Percent of adolescents and youth that know the legal age of marriage for men and women
10% Rapid assessment in schools by D(P)HO staff (GESI focal person)
Not available
>90% 63% School health pre and post-test
70% Target not achieved
Results to date suggest that students, especially younger students, are not retaining lessons learnt regarding legal age of marriage and reproductive health. In certain communities teaching in Nepali is less effective than in local language. Significant variation between districts reported.
Intermediate Result 6.2 Missed opportunities reduced at service delivery points to provide education and counseling on healthy behaviors for MNCHN/FP
24 Percent of post-partum women receiving counseling on comprehensive FP services
58% Readiness Index/ (Client Exit Interview)
62.9% (n=27)
Non-represent ative
70% 63%
(n=128), Non-representative
HF Readiness assessmen t
90% Midterm to be reported in next semi-annual report and to be representative
Actual percent show modest improvement but falls short of the target. IPCC skills of HWs were enhanced after training when observed during practice.
H4L—Annual Report 64

SN Indicator Definition Baseline Baseline
Data Source
Year 1 (2013-14)
Actual
Year 2 (2014-15) Percent of annual target
Status Justification Target (2014-15)
Actual (July-June)
Data source
O�JE�TIVE 7: Strengthen capacity of US!ID’s contractor for a logistical support activity
Intermediate Result 7.1 Strengthened logistics system3
25 a
Percent of USG assisted service delivery points (SDPs) that experience a stock out at any time during the reporting period of a contraceptive method (Condom, oral pills, Injectable) that the SDP is expected to provide
13% LMIS 19%
(all quarters as reported by
H4L Logistics in Dec.2014)
11% 15% LMIS from LLN (data up to 3
rd
quarter)
73% Target not achieved
Stock outs ranged from 3% of facilities in Bardiya to 50% of facilities in Jumla.
6% of HFs reported stock outs of Depo-provera while 7% reported the stock out of condoms or pills.
LMD has had delays in procurement leading to shortages and stock outs of supplies, such as condoms, pills, and injectables.
25 b
Percent of USG assisted service delivery points (SDPs) that experience a stock out at any time during the reporting period (implant, IUCD) that the SDP is expected to provide
N/A N/A N/A
N/A IUCDs 33%, Implants 57%
LMIS, LLN N/A N/A
26 Percent of USG assisted service delivery points (SDPs) that experience a stock out at any time during the defined reporting period of specific tracer drugs that the SDP is expected to provide
52% LMIS 45%
(all quarters as reported by
H4L Logistics in Dec.2014)
45% 38% LMIS from LLN (data up to 3
rd
quarter)
118% Target surpassed Data incomplete; target may need to be changed
27 Percent of service delivery points (PHCCs, HPs and SHPs) that submitted LMIS reports on time in last quarter
88% LMIS 87%
(all quarters as reported by H4L Logistics in
90% 94% LMIS, LLN 104% Target achieved
3 LMIS related indicators are aligned with H4L Logistics’ M&E Plan as agreed among US!ID, H4L Logistics and H4L Core.
H4L—Annual Report 65

SN Indicator Definition Baseline Baseline
Data Year 1
(2013-14)
Year 2 (2014-15) Percent of annual Status Justification Target Actual Data
Source Actual (2014-15) (July-June) source target Dec.2014)
Intermediate Result 7.2 Enhanced organization capacity of Lifeline Nepal
28 Performance of H4L-Logistics partner-Lifeline Nepal rated by
2 TOCAT Assessment
N/A Expected to report
Due to delays in some capacity building activities as spelled out in the strategic plan
Technical and Organization Capacity Assessment Tool
midterm in 2015/16
of LLN, Midterm TOCAT has been scheduled in the next FY (2015-16) work plan.
(TOCAT)
Project Performance Report (PPR), July 2014 - June 2015
Data
Year 1 (2013-
14)
Year 2 (2014-15)
Data
Percent of annual Year 2 Actual
SN Indicator Definition Baseline Source Actual (2014-15) (July-June) source target Status Justification
1 Number of newborn infants receiving antibiotic treatment
Target surpassed
- Dang and Bardiya districts have unusually high numbers reported.
for infection through USG-supported programs 4,742
HMIS 2012/13 4,864 5,080 8,760 HMIS 172% -Potential for misdiagnosis
2 Number of women giving birth who received
Target surpassed
- Institutional delivery is increasing faster than expected.
uterotonics in the third stage of labor through USG-
- MSC is more available in some districts.
supported programs
50,290 HMIS
2012/13 60,942 59,919 76,523 HMIS 128% - Use of trained health workers during home delivery increasing.
3 Number of cases of child Target achieved diarrhea treated in USG- HMIS assisted program 347,896 2012/13 375,557 376,284 384,991 HMIS 102%
H4L—Annual Report 66

SN Indicator Definition Baseline Data Source
Year 1 (2013-
14)
Actual
Year 2 (2014-15)
Data source
Percent of annual target Status Justification
Year 2 (2014-15)
Actual (July-June)
4 Number of children under five years of age with suspected pneumonia receiving antibiotics by trained facility or community health workers in USG-assisted programs 248,425
HMIS 2012/13 232,280 273,889 221,291 HMIS 81%
Target not achieved
- FCHVs stopped providing antibiotics to treat pneumonia due to policy change in last fiscal year.
- Stock out or shortage of antibiotics (Cotrim-P) (14% stock out up to 3
rd quarter; 9 districts had from 10% to 35% stock
out of Cotrim-P).
5 Number of babies who received postnatal care within two days of childbirth in USG-supported programs 53,033
HMIS 2012/13 63,727 61,548 61,379 HMIS 99.7%
Target not achieved
6 Couple Years Protection in USG supported programs (in thousands) (H4L districts)
250 (HMIS
2012/13) HMIS
2012/13 264,096 260,175 298,707 HMIS 115%
Target surpassed
- L!FP sites and services increased with H4L’s T! faster than anticipated.
- VSC has added significant value to CYP.
7 Couple Years Protection in USG supported programs (in thousands) (National) 1,730
HMIS 2012/13 1,541 1,747 1,666 HMIS 95%
Target not achieved.
8 Percent of USG-assisted service delivery sites providing family planning (FP) counseling and/or services 100%
HMIS 2012/13 100% 100% 100%
HMIS
100%
Target achieved
9 Number of people trained in FP/RH through USG supported programs
N/A N/A
1,224 1,250 3,902
TraiNet July-June 312%
Surpassed the target
The target was to be set for two consecutive years but the program carried out in this FY. The increase included additional FCHVs and HWs trained from 90 prioritized VDCs of 9 program districts.
Male 184 100 389 389%
Female 1,040 1,150 3,513 305%
10 Number of people trained in Health System Strengthening through USG supported programs (Custom PPR)
N/A N/A
2,074 1,550 2,878
TraiNet July-June 186%
Surpassed the target
Periodic/annual VDC health planning emerged from implementation of the Collaborative Framework that was not planned earlier. After implementing the CF, the activity resulted in training 2,122 persons in VDC planning.
Male: 1,369 1,085 1,884 174%
H4L—Annual Report 67

Data
Year 1 (2013-
14)
Year 2 (2014-15)
Data
Percent of annual Year 2 Actual
SN Indicator Definition Baseline Source Actual (2014-15) (July-June) source target Status Justification
Female: 705 465 994 214%
11 Percent of USG-supported primary health care (PHC) facilities that submitted
Target achieved
routine reports (HMIS) on time (Custom PPR) 97%
HMIS 2012/13 99.8% 98% 99.7% HMIS 102%
12 Percent of women that had Target not four ANC check-ups as per protocol in USG-supported
achieved
programs NA NA N/A 53% 50.6% HMIS 95%
13 Percent of women from marginalized groups that
Target surpassed
H4L introduced to HFOMCs CAPs and CAP/Rs to track pregnant women in high-priority VDCs. To date, about half
delivered in health facility 29% NDHS
of expected pregnant women are registered in 39 sentinel sites. Analysis suggests increase in equitable use of services.
National 2011 N/A 34% 38.3% HMIS 113% We await reports from other high priority VDCs.
H4L—Annual Report 68

E. Information on the status of finances, including expenditure data based on the budget and accruals, as well as, when appropriate, analysis and explanation of cost overruns or high unit cost
H4L—Annual Report 69
F. Information on management issues, including administrative problems, or problems with beneficiary groups, or implementing partners and what steps or actions were taken to manage these and lessons learned for future
As last year, we occasionally receive complaints from the government regarding DSA paid by H4L. In particular this past year, complaints regarding the “facilitator’s” DSA have been more frequent. In addition, travel allowance for FCHVs has sometimes emerged as an issue.
G. Anticipated future problems, delays, or conditions that may adversely impact implementation of the project and what measures are in place to deal with these
Local Health Governance
Efforts and resources committed to enhance the capacity of the Health Facility Operation and Management Committees (HFOMCs) are jeopardized in the long run if the positions of elected officials of local bodies remain vacant. In the short run, local elections would cause disruption in the districts. Furthermore, many VDC Secretaries and Health facility In-charges who are also Chairpersons and Member Secretaries of HFOMCs were transferred out, and new replacements are not able to provide adequate support due to the new roles given to them. Federalism is also an uncertainty that may impact implementation.
Frequent transfer of government staff, particularly D(P)HOs and Local Development Officers remained a challenge in all 14 H4L districts. After the transfer of D(P)HOs and LDOs that were already oriented on H4L strategies and approaches, it was difficult for H4L district teams to get the necessary support from newly-placed D(P)HOs and LDOs in most project districts.
Due to the April 25 earthquake, there is a possibility of budget cuts in unaffected districts since the GoN is under pressure to allocate more funds in earthquake districts for reconstruction. There is a possibility that the volume of flexible health grants to demonstration districts will be reduced.
Evidence-based Policy
Due to delays in the development/customization of the DHIS-2, officials from the MD are not in favor of rolling out of DHIS-2. Hence, it is likely that implementation of the DHIS-2 may be further delayed unless there is a strong push from the ministry. H4L has planned activities related to piloting mobile technology for HMIS reporting, but there might be some delays as this is a new area for MoHP. Frequent turnover of H4L M&E staff as well as among members of the district teams has also jeopardized technical support areas related to this Objective.
National Stewardship
No problems, delays or conditions anticipated.
Quality Improvement
H4L still anticipate that there will be a delay in filling staff in-charge of the QA section at MD. However, we will work closely with the assigned staff to move QI activities forward.
Because of delay in implementation in HF QI system in Dang, Jumla and Surkhet, we expect delay in finalization of QI guideline. In coordination with respective D(P)HOs, H4L plan to complete the process soon (including using consultant) and collect and document learning as soon as possible and update guidelines accordingly.
LAFP and SBA Coaching
We anticipate difficulty mobilizing trainers to coach health workers at HFs because district staff are unavailable for training/coaching in SBA, LAFP and CEONC skills. H4L plans to prepare a list of
H4L—Annual Report 70

potential GoN staff within the region and consultants that can provide such support and recruit them as appropriate.
ANM Pre-service Education
H4L expects some problems in strengthening schools by building the capacity of faculty members considering the poor knowledge and skills of faculty and students, as well as the shortcomings of the facilities’ environmental factors. H4L will define what technical assistance can be provided in this regard to selected schools and continue a dialogue with stakeholders and partners so that schools are supported. H4L also plans to recruit dedicated staff to oversee ANM pre-service education activities.
H. Information on security issues, especially as these affect program integrity and safety of beneficiary groups and implementing partner
There are no security issues to report.
I. Other information, such as new opportunities for program expansion, lessons-learned and success stories, and prospects for the following year’s performance
H4L anticipates a modification from USAID to expand to 10 earthquake-affected districts.
H4L—Annual Report 71

Annexes
Annex 1 District QAWG Meetings
Districts Dates of meeting Key planned activities Implementation status
Arghakhanchi 4 meetings
Oct 31, 2014,
Feb. 23, April 16, Jun 30, 2015
1. Followed up for HF-level QI team formation and functionality in high priority VDCs
2. Maintained incinerator and placenta pit in district hospital
3. QI orientation in high-priority VDCs 4. Prepared and submitted next year proposed
activities in DDC council 5. Expand HF QI system to other VDCs 6. IP training to hospital staff
1. Completed
2. Completed
3. Completed 4. Completed
5. Ongoing
6. Ongoing
Banke 5 meetings
Sep 9, Dec 23, 2014
Jan 7, Feb. 15, May 26, 2015
1. Construct placenta pit in 4 birthing centers, Puraini, Belbhar, Ganapur and Manikapur, with support of Plan and Save the Children
2. Provide solar power set to Khajura PHC with support from Save the Children
3. Send circular to remaining HFs to form HF QI team and send information to D(P)HO
4. Orientation to QI team for implementation of HF QI system in prioritized 10 HFs
5. Provide gas cylinder and stove, mask, utility gloves, etc. to the birthing centers to improve IP practice
6. Orientation to HF QI team on QI process and self -assessment tools
7. Prepare evidence-based AWPB for FY 2072/073 and submit to DDC council for approval
8. Install new hand pump in Betahani, Bankatti and Holiya in coordination with HFOMC, DDC or local NGOs to improve IP practice and quality of health services
9. Conduct social audit in 10 high-priority VDCs 10. Conduct integrated monitoring visits to some HFs to
improve quality of health services
1. Placenta pit construction completed in Puraini and Manikapur, and ongoing in Belbhar and Ganapur
2. Installed solar power in Khajura PHC
3. Completed 4. Completed 5. Completed
6. Completed Orientation to HF QI team in 10 high-priority VDC
7. Evidence-based AWPB prepared and submitted in DDC planning meeting
8. Hand pump installed in Betahani and Bankatti and in Holiya is in process
9. Completed 10. Ongoing
Bardiya 4 meetings
Jul 10, Dec. 23, 2014
Mar 1, May 31, 2015
1. Form and activate HF QI team in all VDCs 2. Reform QI team in remaining HFs and provide
orientation to QI team in each HF 3. Orientation to district supervisor on revised
guideline, tools and its process 4. Prepare AWPB for FY 2072/073 and submit to DDC
council for approval 5. Supply 12 Gas cylinders and 19 boiling pots to HFs as
need based
1. Formed HF QI team and functional in 30 HFs
2. Completed 3. Completed
4. Completed
5. 12 Gas cylinder and 19 boiling pots purchased under the DHO fund
Dailekh 2 meetings
Sep 22, 2014
Mar 15, 2015
1. Start conducting integrated monitoring and supervision by D(P)HO program focal person
2. Clean D(P)HO premises in participation with D(P)HO/hospital staff
3. Orientation to district supervisors on revised guideline tools and its process
4. Orientation to HF QI team on implementation of self- assessment tools
1. Integrated monitoring and supervision in HF is started
2. A hospital premise is cleaned every Friday
3. Completed
4. Completed in 10 high-priority VDC
Dang 3 meetings
Sep 10, 2014
Jan. 10, May 17, 2015
1. Provide feedback to HFs according to HMIS report 2. Discuss and make plan of action based on gaps
identified by readiness tools 3. Present HF QI assessment findings and support to HF
from D(P)HO 4. Prepare evidence-based AWPB for FY 2072/073 to
submit to DDC 5. Prepare annual monitoring and supervision plan 6. Conduct planning meeting for approval 7. Scale-up HF QI system in other VDCs
1. Feedback to HFs based on HMIS provided
2. Prepared action plan to address the gaps
3. Completed
4. Submitted
5. Completed
6. Ongoing
7. Ongoing
H4L—Annual Report 72
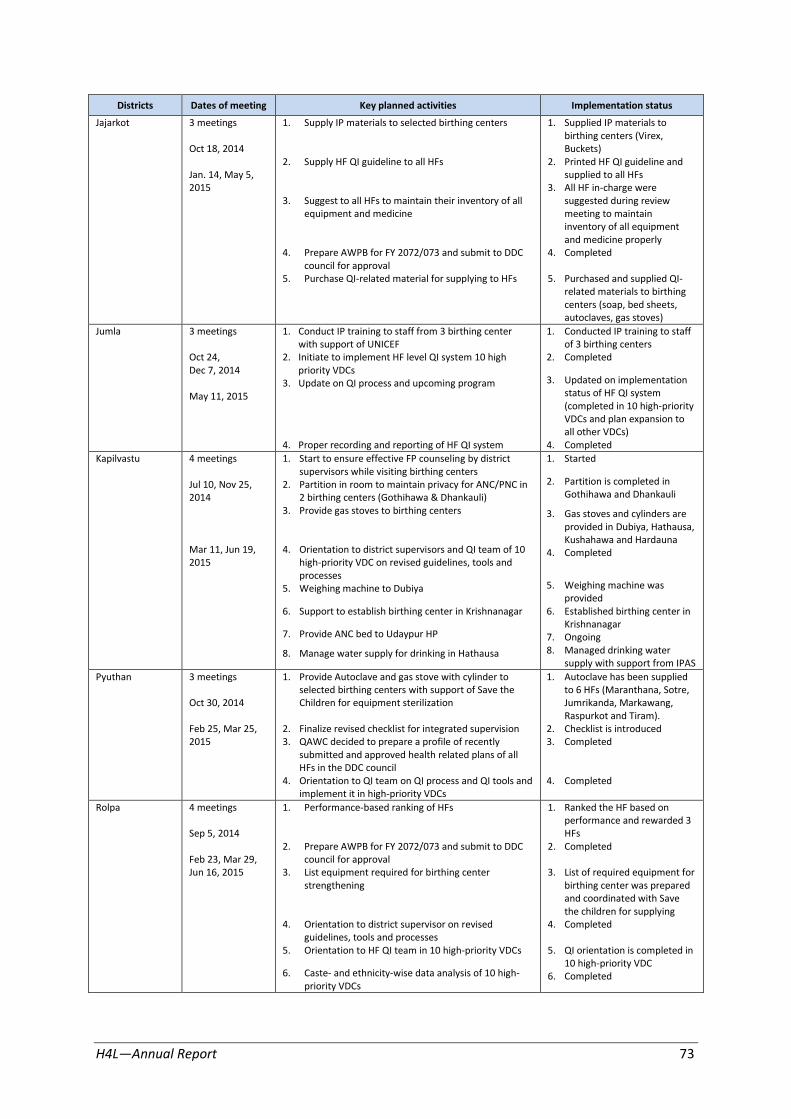
Districts Dates of meeting Key planned activities Implementation status
Jajarkot 3 meetings 1. Supply IP materials to selected birthing centers 1. Supplied IP materials to birthing centers (Virex,
Oct 18, 2014 2. Supply HF QI guideline to all HFs
Buckets) 2. Printed HF QI guideline and
Jan. 14, May 5, supplied to all HFs 2015
3. Suggest to all HFs to maintain their inventory of all equipment and medicine
4. Prepare AWPB for FY 2072/073 and submit to DDC council for approval
5. Purchase QI-related material for supplying to HFs
3. All HF in-charge were suggested during review meeting to maintain inventory of all equipment and medicine properly
4. Completed
5. Purchased and supplied QI-related materials to birthing centers (soap, bed sheets, autoclaves, gas stoves)
Jumla 3 meetings 1. Conduct IP training to staff from 3 birthing center with support of UNICEF
1. Conducted IP training to staff of 3 birthing centers
Oct 24, 2. Initiate to implement HF level QI system 10 high 2. Completed Dec 7, 2014 priority VDCs
3. Update on QI process and upcoming program 3. Updated on implementation
May 11, 2015
4. Proper recording and reporting of HF QI system
status of HF QI system (completed in 10 high-priority VDCs and plan expansion to all other VDCs)
4. Completed
Kapilvastu 4 meetings 1. Start to ensure effective FP counseling by district supervisors while visiting birthing centers
1. Started
Jul 10, Nov 25, 2. Partition in room to maintain privacy for ANC/PNC in 2. Partition is completed in
2014 2 birthing centers (Gothihawa & Dhankauli) 3. Provide gas stoves to birthing centers
Gothihawa and Dhankauli
3. Gas stoves and cylinders are provided in Dubiya, Hathausa, Kushahawa and Hardauna
Mar 11, Jun 19, 4. Orientation to district supervisors and QI team of 10 4. Completed 2015 high-priority VDC on revised guidelines, tools and
processes 5. Weighing machine to Dubiya
6. Support to establish birthing center in Krishnanagar
7. Provide ANC bed to Udaypur HP
8. Manage water supply for drinking in Hathausa
5. Weighing machine was provided
6. Established birthing center in Krishnanagar
7. Ongoing 8. Managed drinking water
supply with support from IPAS
Pyuthan 3 meetings 1. Provide Autoclave and gas stove with cylinder to selected birthing centers with support of Save the
1. Autoclave has been supplied to 6 HFs (Maranthana, Sotre,
Oct 30, 2014 Children for equipment sterilization Jumrikanda, Markawang, Raspurkot and Tiram).
Feb 25, Mar 25, 2. Finalize revised checklist for integrated supervision 2. Checklist is introduced 2015 3. QAWC decided to prepare a profile of recently
submitted and approved health related plans of all HFs in the DDC council
4. Orientation to QI team on QI process and QI tools and implement it in high-priority VDCs
3. Completed
4. Completed
Rolpa 4 meetings
Sep 5, 2014
Feb 23, Mar 29, Jun 16, 2015
1. Performance-based ranking of HFs
2. Prepare AWPB for FY 2072/073 and submit to DDC council for approval
3. List equipment required for birthing center strengthening
4. Orientation to district supervisor on revised guidelines, tools and processes
5. Orientation to HF QI team in 10 high-priority VDCs
6. Caste- and ethnicity-wise data analysis of 10 high-priority VDCs
1. Ranked the HF based on performance and rewarded 3 HFs
2. Completed
3. List of required equipment for birthing center was prepared and coordinated with Save the children for supplying
4. Completed
5. QI orientation is completed in 10 high-priority VDC
6. Completed
H4L—Annual Report 73
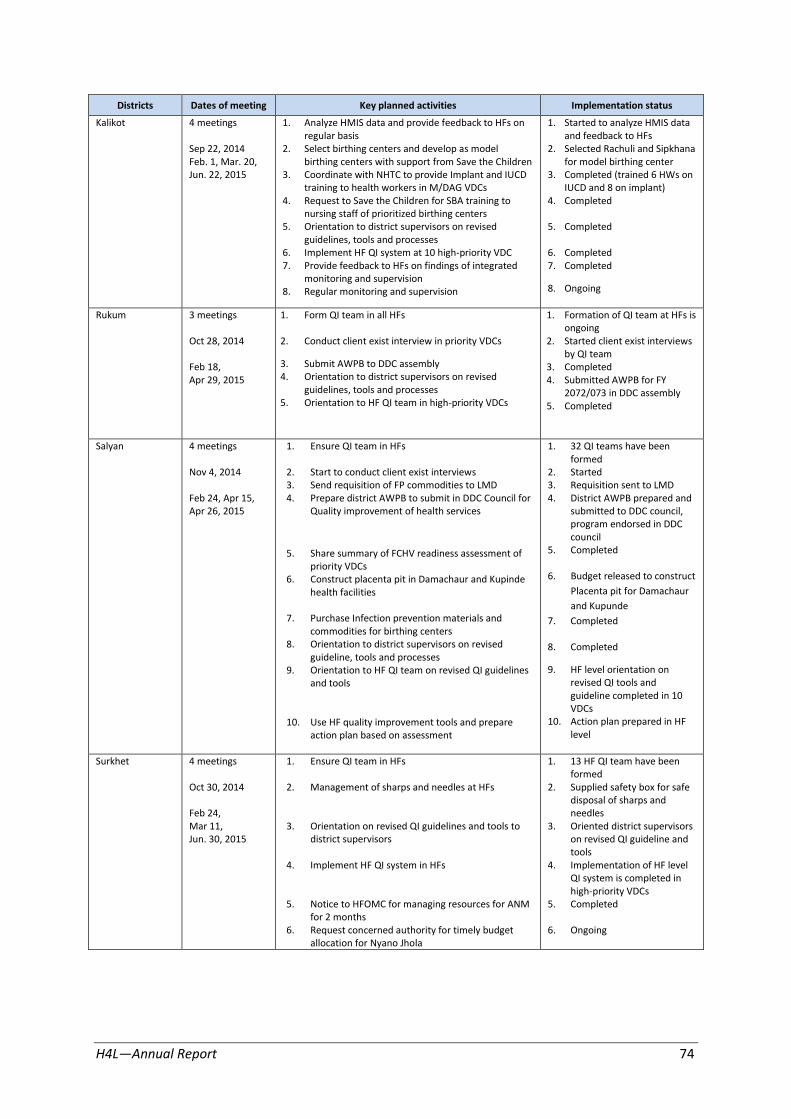
Districts Dates of meeting Key planned activities Implementation status
Kalikot 4 meetings 1. Analyze HMIS data and provide feedback to HFs on regular basis
1. Started to analyze HMIS data and feedback to HFs
Sep 22, 2014 2. Select birthing centers and develop as model 2. Selected Rachuli and Sipkhana Feb. 1, Mar. 20, birthing centers with support from Save the Children for model birthing center Jun. 22, 2015 3. Coordinate with NHTC to provide Implant and IUCD
training to health workers in M/DAG VDCs 4. Request to Save the Children for SBA training to
nursing staff of prioritized birthing centers 5. Orientation to district supervisors on revised
guidelines, tools and processes 6. Implement HF QI system at 10 high-priority VDC 7. Provide feedback to HFs on findings of integrated
monitoring and supervision 8. Regular monitoring and supervision
3. Completed (trained 6 HWs on IUCD and 8 on implant)
4. Completed
5. Completed
6. Completed 7. Completed
8. Ongoing
Rukum 3 meetings
Oct 28, 2014
Feb 18, Apr 29, 2015
1. Form QI team in all HFs
2. Conduct client exist interview in priority VDCs
3. Submit AWPB to DDC assembly 4. Orientation to district supervisors on revised
guidelines, tools and processes 5. Orientation to HF QI team in high-priority VDCs
1. Formation of QI team at HFs is ongoing
2. Started client exist interviews by QI team
3. Completed 4. Submitted AWPB for FY
2072/073 in DDC assembly 5. Completed
Salyan 4 meetings
Nov 4, 2014
Feb 24, Apr 15, Apr 26, 2015
1. Ensure QI team in HFs
2. Start to conduct client exist interviews 3. Send requisition of FP commodities to LMD 4. Prepare district AWPB to submit in DDC Council for
Quality improvement of health services
5. Share summary of FCHV readiness assessment of priority VDCs
6. Construct placenta pit in Damachaur and Kupinde health facilities
7. Purchase Infection prevention materials and commodities for birthing centers
8. Orientation to district supervisors on revised guideline, tools and processes
9. Orientation to HF QI team on revised QI guidelines and tools
10. Use HF quality improvement tools and prepare action plan based on assessment
1. 32 QI teams have been formed
2. Started 3. Requisition sent to LMD 4. District AWPB prepared and
submitted to DDC council, program endorsed in DDC council
5. Completed
6. Budget released to construct
Placenta pit for Damachaur
and Kupunde
7. Completed
8. Completed
9. HF level orientation on revised QI tools and guideline completed in 10 VDCs
10. Action plan prepared in HF level
Surkhet 4 meetings 1. Ensure QI team in HFs 1. 13 HF QI team have been formed
Oct 30, 2014 2. Management of sharps and needles at HFs 2. Supplied safety box for safe disposal of sharps and
Feb 24, needles Mar 11, 3. Orientation on revised QI guidelines and tools to 3. Oriented district supervisors Jun. 30, 2015 district supervisors
4. Implement HF QI system in HFs
5. Notice to HFOMC for managing resources for ANM for 2 months
6. Request concerned authority for timely budget allocation for Nyano Jhola
on revised QI guideline and tools
4. Implementation of HF level QI system is completed in high-priority VDCs
5. Completed
6. Ongoing
H4L—Annual Report 74

Annex 2 Assessment of health services reviews based on Public Health Analytics Techniques
Level: District/Region Name (of District, Region): Date:
Assessment carried out by: Position:
Interacted with (Name): Position:
Monitoring/Review meeting: 1st trimester 2nd trimester Annual Review Others: ……
SN Assessment Areas/Specific Questions
Response
Remarks Yes (2)
No (0)
Partial (1)
Preparation phase
1. Review meeting format is available
2. Review meeting format is used for the review meeting (followed the Time frame , Duration and Participants specified by the guideline)
3. Relevant review technical team/committee was formed for the meeting
4. Review technical team/committee performed as per the mandate/criteria
5. All public sector health facilities including hospital submitted their complete HMIS reports
6. All public sector health facilities including hospital submitted their HMIS reports on time
7. All private and NGO sector providers submitted their complete HMIS reports
8. All private and NGO sector providers submitted their HMIS reports on time
9. All program focal persons involved in data analysis, interpretation and review preparation
10. Disaggregated data (by sex, caste/ethnicity) was presented as per HMIS guideline (11 indicators)
11. Data/achievements were compared with national/regional averages and interpreted during the meeting
12. Trend analysis were performed and discussed in the review meeting
13.
Variability analysis were performed and discussed in the review meeting? (Any of: Variability by HF /inter program variability/intra-program variability)
14. Data was analyzed and presented using a variety of approaches (mixture of table, charts, diagrams, etc.)
15. Meeting participants discussed on the data presented during the meeting and interpreted the data
Meeting conduction
16. Action plan from the last review meeting followed up during this review meeting
17. Findings and recommendations from social audit and other public forums presented and discussed
18. Meeting conducted in line with the given agenda
19. Local interventions/approaches and lessons learnt (if any) were shared and discussed in the meeting
20.
Contribution of Health Facility Operation and Management Committee were presented and discussed during the review meeting (e.g. resource mobilized by HFOMCs)
21. Contribution of local bodies were presented and discussed during the review meeting
Post meeting phase
H4L—Annual Report 75

22. Feedback were provided to HFs based on the findings
23. Recommendations were provided to region based on the findings
24. An action plan was developed from the review meeting
25. Action plan was shared in relevant forums (specify in remarks)
26. Best performing health facilities were acknowledged/awarded
27. Best performing districts were acknowledged/awarded
28. Gaps identified from review meetings were incorporated in the District health sector strategic periodic plan
29. Annual Work Plan and Budget (AWPB) prepared in line with District health sector strategic periodic plan
30. Review meeting findings were shared in different meetings (e.g. QAWC, DACC, DOTS committee, etc.) Specify names in remarks
Please ask and record the main reasons/factors that hindered the process in the following areas:
Assessment Areas Reasons/Factors that hindered the process
Recommendations
Preparation phase [Please explain]
Meeting conduction [Please explain]
Post meeting phase [Please explain]
Category and Score:
23 <23 Scores Unsatisfactory
35 23-35 Scores Acceptable
46 36-46 Scores Progressive
47 >46 Model
H4L—Annual Report 76

Annex 3 Internship Report from in Banke
The Best Experience of My Life
Introduction
many areas. I was particularly interested in local health governance, because if governance is functional, capable and accountable then other parts of the system will automatically perform better, and so I joined H4L with expectation of learning
Figure 8.1 H4L Staff composition by ethnicityoject in Banke
district from June 2014 to May 2015.
As a youth, trying to find a job in Nepal is not easy, even if you have a graduate degree. This is particularly true for those who come from traditionally marginalized groups, like the Madhesi and Muslim communities. I was lucky for the opportunity to join Health for Life (H4L) as an Intern, where I have acquired some of the most valuable experiences in my life, improving my skills in
more about this topic and applying it to my future professional life. I was happy to find an encouraging work environment with support from my colleagues in the district, as well as from the regional central teams.
What I Did with H4L
This internship was an opportunity for me to get real, hands-on experience of how local governance takes place, and how best to approach strengthening that process. I was able to work in the field, traveling to various Village Development Committees (VDCs) and health facilities, where I assisted in coaching Health Facility Operation and Management Committee (HFOMC) members, preparing VDC periodic health plans, supporting HFOMCs in mobilizing resources and implementing elements of the Collaborative Framework on the ground. I also was present for the local social audit process, seeing first-hand what issues and barriers existed, and worked with the local community to resolve issues through the participation of different social groups and the HFOMC. Lastly, I took part in the Radio Bahas program which empowers local communities by giving them a forum to voice their concerns about local health care issues.
What I Learned
Before this opportunity I was a newcomer to the development sector, so there was a lot to learn. For example, I thought that VDCs were just there to certify citizenship, and that health facilities existed only to give immunizations and first aid. Through this internship, I got to know exactly how local governance takes place down to the community level, including the planning process, the composition and roles of the HFOMCs, how the Ward Citizen Forum operates and how to best coordinate with them and mobilize them.
Other skills that I acquired include using an evidence-based approach, and how to collect that evidence and identify the best solutions to a community problem. The importance of
H4L—Annual Report 77
transparency and accountability also became clear as a result of helping with the social audit process.
I believe the coaching techniques and how to facilitate meetings with local forums like the HFOMCs, FCHVs and mother's groups will be particularly useful in my future work. These committees are supposed to be inclusive, composed of local people taking responsibility for their own development, which in turn depends on their own leadership skills. �ut in the past, they have mostly been concerned with distribution of resources and don’t really talk about other community concerns. Instead of addressing health issues, they give priority to things like roads and infrastructure. What was particularly frustrating is that they were not concerned about the dozens of maternal deaths that take place every year, mostly within the Madhesi and Muslim communities.
My Expectations for the Future
My year with H4L has been very influential. I have a greater understanding of local health governance, as well as knowledge of how to effectively work with local organizations. My understanding of local health needs and how those can best be identified and addressed using local mechanisms has grown tremendously over the past few months. My leadership and organizational skills have improved, and I now feel confident working independently, facilitating meetings, mobilizing the community and coordinating trainings and planning processes.
Almost as important as the skills I gained are the relationships that I have built. My colleagues at H4L have become good friends, and I expect their professional support will be invaluable in the future. It has truly been a pleasure to work with the team.
My intention is to put the skills I have gained through this internship to greater use in the community. I am particularly keen to work with HFOMCs on improving functionality as the Collaborative Framework gets implemented nationally.
June 2015
H4L—Annual Report 78