
Headache © 2012 American Headache Society View and Perspective Migraine: Possible Role of...
21
View and Perspective Migraine: Possible Role of Shear-Induced Platelet Aggregation With Serotonin ReleasePiet Borgdorff, PhD; Geert Jan Tangelder, MD, PhD Background.—Migraine patients are at an increased risk for stroke, as well as other thromboembolic events. This warrants further study of the role of platelets in a proportion of migraine patients. Objective.—To extend the “platelet hypothesis” using literature data and observations made in a rat model of shear stress-induced platelet aggregation. Such aggregation causes release of serotonin, leading to vasoconstriction during sufficiently strong aggregation and to long-lasting vasodilation when aggregation diminishes. This vasodilation also depends on nitric oxide and prostaglandin formation. Results.—A role for platelet aggregation in a number of migraineurs is indicated by reports of an increased platelet activity during attacks and favorable effects of antiplatelet medication. We hypothesize that in those patients, a migraine attack with or without aura may both be caused by a rise in platelet-released plasma serotonin, albeit at different concentration. At high concentrations, serotonin may cause vasoconstriction and, consequently, the neuronal signs of aura, whereas at low concentra- tions, it may already stimulate perivascular pain fibers and cause vasodilation via local formation of nitric oxide, prostaglandins, and neuropeptides. Platelet aggregation may be unilaterally evoked by elevated shear stress in a stenotic cervico-cranial artery, by reversible vasoconstriction or by other cardiovascular abnormality, eg, a symptomatic patent foramen ovale. This most likely occurs when a migraine trigger has further enhanced platelet aggregability; literature shows that many triggers either stimulate platelets directly or reduce endogenous platelet antagonists like prostacyclin. Conclusion.—New strategies for migraine medication and risk reduction of stroke are suggested. Key words: migraine, platelet aggregation, shear stress, clopidogrel, serotonin, hypothesis Abbreviations: ADP adenosine diphosphate, cAMP cyclic adenosine monophosphate, COX-2 cyclooxygenase-2, CSD cortical spreading depression, 5-HT 5-hydroxytryptamine (serotonin), LDL low-density lipoprotein, L-NMA NG-methyl-L-arginine, MRI magnetic resonance imaging, NO nitric oxide, NSAID non-steroidal anti- inflammatory drug, PFO patent foramen ovale, PGI 2 prostacyclin, vWf von Willebrand factor. (Headache 2012;••:••-••) Migraine attacks occur episodically and are char- acterized by a mostly unilateral long-lasting throb- bing headache (hours to days), often accompanied by nausea and photophobia or phonophobia. They can be triggered by a variety of internal or external factors, such as female hormone levels, stress, foods, or weather conditions. 1 The syndrome affects about 18% of women and 6% of men. In 20-30% of migraineurs, the attack starts with an aura lasting 20 to 30 minutes (scintillating scotoma, fortifications). The aura phase is attended by oligemia and vasoconstriction in the From the Institute for Cardiovascular Research, VU University Medical Center, Amsterdam, The Netherlands. Address all correspondence to P. Borgdorff, Laboratory for Physiology, VUMC, Van der Boechorststraat 7, 1081 BT Amsterdam, The Netherlands, email: [email protected] Accepted for publication March 21, 2012. Conflict of Interest: The authors report no conflict of interest. There was no financial support other than from our university. ISSN 0017-8748 doi: 10.1111/j.1526-4610.2012.02162.x Published by Wiley Periodicals, Inc. Headache © 2012 American Headache Society 1
Transcript of Headache © 2012 American Headache Society View and Perspective Migraine: Possible Role of...

View and Perspective
Migraine: Possible Role of Shear-Induced Platelet AggregationWith Serotonin Releasehead_2162 1..21
Piet Borgdorff, PhD; Geert Jan Tangelder, MD, PhD
Background.—Migraine patients are at an increased risk for stroke, as well as other thromboembolic events. This warrantsfurther study of the role of platelets in a proportion of migraine patients.
Objective.—To extend the “platelet hypothesis” using literature data and observations made in a rat model of shearstress-induced platelet aggregation. Such aggregation causes release of serotonin, leading to vasoconstriction during sufficientlystrong aggregation and to long-lasting vasodilation when aggregation diminishes. This vasodilation also depends on nitric oxideand prostaglandin formation.
Results.—A role for platelet aggregation in a number of migraineurs is indicated by reports of an increased platelet activityduring attacks and favorable effects of antiplatelet medication. We hypothesize that in those patients, a migraine attack with orwithout aura may both be caused by a rise in platelet-released plasma serotonin, albeit at different concentration. At highconcentrations, serotonin may cause vasoconstriction and, consequently, the neuronal signs of aura, whereas at low concentra-tions, it may already stimulate perivascular pain fibers and cause vasodilation via local formation of nitric oxide, prostaglandins,and neuropeptides. Platelet aggregation may be unilaterally evoked by elevated shear stress in a stenotic cervico-cranial artery,by reversible vasoconstriction or by other cardiovascular abnormality, eg, a symptomatic patent foramen ovale. This most likelyoccurs when a migraine trigger has further enhanced platelet aggregability; literature shows that many triggers either stimulateplatelets directly or reduce endogenous platelet antagonists like prostacyclin.
Conclusion.—New strategies for migraine medication and risk reduction of stroke are suggested.
Key words: migraine, platelet aggregation, shear stress, clopidogrel, serotonin, hypothesis
Abbreviations: ADP adenosine diphosphate, cAMP cyclic adenosine monophosphate, COX-2 cyclooxygenase-2, CSD corticalspreading depression, 5-HT 5-hydroxytryptamine (serotonin), LDL low-density lipoprotein, L-NMANG-methyl-L-arginine, MRI magnetic resonance imaging, NO nitric oxide, NSAID non-steroidal anti-inflammatory drug, PFO patent foramen ovale, PGI2 prostacyclin, vWf von Willebrand factor.
(Headache 2012;••:••-••)
Migraine attacks occur episodically and are char-acterized by a mostly unilateral long-lasting throb-bing headache (hours to days), often accompanied bynausea and photophobia or phonophobia. They can
be triggered by a variety of internal or externalfactors, such as female hormone levels, stress, foods, orweather conditions.1 The syndrome affects about 18%of women and 6% of men. In 20-30% of migraineurs,the attack starts with an aura lasting 20 to 30 minutes(scintillating scotoma, fortifications). The aura phaseis attended by oligemia and vasoconstriction in theFrom the Institute for Cardiovascular Research, VU University
Medical Center, Amsterdam, The Netherlands.
Address all correspondence to P. Borgdorff, Laboratory forPhysiology, VUMC, Van der Boechorststraat 7, 1081 BTAmsterdam, The Netherlands, email: [email protected]
Accepted for publication March 21, 2012.
Conflict of Interest: The authors report no conflict of interest.
There was no financial support other than from our university.
ISSN 0017-8748doi: 10.1111/j.1526-4610.2012.02162.xPublished by Wiley Periodicals, Inc.
Headache© 2012 American Headache Society
1

occipital regions, while during the headache phase,vasodilation may occur. At present, the prevailinghypothesis is that aura signs and the concomitantvasoconstriction are caused by a spreading depres-sion of cortical activity (CSD). The headache phase,however, has so far not been explained by CSD.Another aspect is that migraine is an established riskfactor for stroke and subclinical ischemic brainlesions, especially in patients with aura or frequentattacks (>1/month) (for review, see2). Stroke maycause CSDs,3 but the reverse has not been reported.Because in migraine-related stroke, both hypoperfu-sion and thromboembolism seem to be causallyinvolved,4 better understanding of the possible con-tribution of blood platelets in migraine might be ofvalue for treatment and preventive measures in atleast a subgroup of patients.
In this paper, we present an extension of theplatelet hypothesis of Hanington,5 integrating datafrom previously published literature with observa-tions made in a rat model of shear stress-inducedplatelet aggregation.6-9 Our hypothesis suggests thatin a number of patients, especially those with hyper-aggregable platelets, the neural and vascular symp-toms of migraine are independently initiated byserotonin (5-hydroxytryptamine, 5-HT) releasedfrom aggregating platelets.Aggregation might be elic-ited by increased shear stress at sites of vessel abnor-malities, especially when in these patients a migrainetrigger has further enhanced platelet aggregability,for example via reduction in circulating plateletantagonists like prostacyclin (PGI2).10,11
INCREASED PLATELET ACTIVITYIN MIGRAINE
Activation and aggregation of platelets may bestarted by several factors (eg, shear stress) whichincrease platelet intracellular calcium levels. Thisleads to a release of 5-HT and adenosine diphos-phate (ADP) from platelet-dense granules andvarious proteins from a-granules. ADP and 5-HTreinforce aggregation, and this is supported by pro-duction of thromboxane (thromboxane A2, TXA2)and platelet-activating factor. Aggregation that istoo strong is controlled by a variety of factors
including the intraplatelet formation of nitric oxide(NO) and by adenosine, the breakdown product ofADP.
In a number of migraine patients, increased invivo platelet activity, as indicated by the parametersmentioned in Table 1, has been found during and, toa lesser degree, between attacks. Activation seemsmore marked in migraine with aura than in migrainewithout aura.12
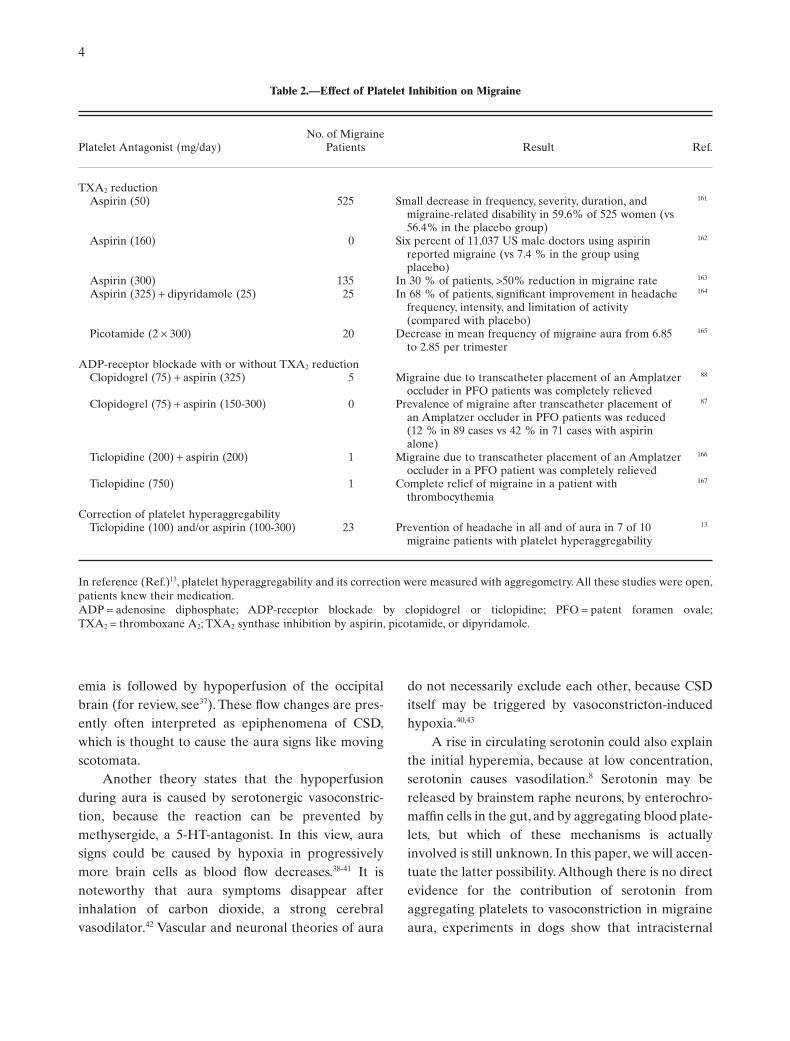
A role for platelet aggregation in the pathogen-esis of migraine is further suggested by studiesshowing diminished prevalence or relief of migraineduring inhibition of platelet aggregation (Table 2).Note the substantial effect of measured correctionof platelet hyperaggregability in 23 consecutivepatients.13 Regarding ADP-receptor blockade withor without TXA2 reduction in patent foramen ovale(PFO) patients, it is known that closure of PFO mayrelieve migraine, but placement of an Amplatzeroccluder (AGA Medical Corporation, Plymouth,MN, USA) may also start or aggravate migraine in anumber of patients. We suppose that in thesepatients, platelets are activated by increased bloodshear stress as a consequence of incomplete closureor by blood–material contact. Successful studieswith high-dose aspirin (500-1300 mg/day)14-16 arenot mentioned in the table because in these doses,aspirin might reduce migraine pain by its analgesicaction as well.
POSSIBLE ROLE OF PLATELET-RELEASED SEROTONIN IN MIGRAINEHEADACHE
Blood serotonin is almost exclusively containedin platelets, with only a small active amount freelydissolved in plasma. It is likely that during the reduc-tions of intraplatelet serotonin, observed in bothcommon and classical migraine attacks,17-19 freeplasma serotonin will have risen to active levels.However, because circulating serotonin is rapidlycleared by endothelial cells, mainly in the lungs,20
measurement of changes in its concentration is diffi-cult. Nevertheless, a causative role for platelet-released 5-HT in a certain number of migraine casesis indicated by the fact that migraine may be induced
2

by reserpine, chlorophenylpiperazine, and fenflu-ramine, agents that cause release of 5-HT.21,22 Further-more, migraine can be relieved by 5-HT-receptorantagonists like pizotifen.
Serotonin is an important regulator of pain sen-sation.23 Via vasa-vasorum, blood-borne 5-HT mayreach and activate perivascular pain fibers aroundextracranial arteries (intracranial arteries lack vasavasorum24) and cause sterile inflammation withplasma protein extravasation and edema.25 In addi-tion, serotonin sensitizes the 5-HT3 and 5-HT2A recep-tors on C-fibers in the densely innervated wall of pialand intracerebral arteries.23 The painful action ofserotonin is probably accompanied, and amplified orprolonged, by local formation of pain mediators likeNO, PGI2, and neuropeptides. During spontaneousmigraine, the levels of these substances in internaljugular-vein blood are elevated.26 In addition, head-ache may be induced by NO donors,27 or by PGI2,28
while it may be relieved by NO inhibitors,29 and bysuppression of prostaglandin formation with aid of
cyclooxygenase-2 (COX-2) inhibitors.30 Local vascu-lar31 and/or neural 32expressions of inducible NO syn-thase likely accounts for the often delayed and long-lasting effect of NO.
Serotonin exerts not only algesic but also analge-sic effects, depending on the receptor subtype and siteof action.23 Intravenous injection of 2 to 7.5 mg ofserotonin may even ease spontaneous or reserpine-induced migrainous headache.33 Sumatriptan, one ofthe most successful anti-migraine medicines, relievesmigraine pain probably not by its vasoconstrictiveeffect, but by blocking pain transmission via 5-HT1B/1D
receptors on trigeminal nerve endings.34 Sumatriptanalso scavenges superoxide, hydroxyl, and NOradicals,35 and blocks dural (neurogenic) plasmaextravasation.36
VASCULAR REACTIONS DURING THEAURA PHASE
Studies on regional cerebral blood flow duringaura have shown that an initial short-lasting hyper-
Table 1.—Studies Suggesting Increased Platelet Activity During or Between Migraine Attacks
Units During Attack Between Attacks In Controls Ref.
Serotonin (5-HT) inside platelets % ª70 (289) ª100 (289) 100 (9) 17
5-HT granules/100 platelets 48 (33) 469 (63) 448 (20) 18
ng/109 platelets 315 (14) 440 (14) 759 (14) 19
Plasma levels of a-granule proteinsb-TG ng/mL 84 (6) 39 (8) 31 (35) 91
ng/mL 128 (16) 69 (11) 61 (13) 150
ng/mL — 72 (33) 35 (19) 12
ng/mL — 151 (16) 80 (26) 151
Platelet factor 4 ng/mL — 22 (33) 6 (19) 12
ng/mL — 78 (16) 38 (26) 151
vWf antigen U/dL 130 (17) 72 (17) 72 (25) 89
% of normal — 126 (63) 106 (35) 152
P-selectin Arbitrary units — 1.41 (72) 1.29 (72) 153
PAF Not mentioned 886 (5) 565 (5) — 154
11-dehydro-thromboxane B2 pg/mL — 148 (29) 96 (27) 155
NO metabolites inside platelets nM/108 platelets 10.7 (47) 9.1 (28) 8.5 (28) 156
fM/min/mg protein 33.6 (25) 18.7 (25) 7.3 (30) 157
Circulating aggregated platelets % of all platelets — 22 (73) 5 (90) 158
23 (26) 6 (20) 159
32 (20) 10 (20) 160
Circulating platelet–leukocyte aggregates % of all platelets — 5.7 (72) 3.9 (72) 153
Mean values (number of subjects in parentheses). Patients were not diet restricted. Reference (Ref.)17 is a review of 12 studies. Ofnote: vWf, P-selectin, and PAF are not platelet specific but may also originate from endothelium or granulocytes.b-TG = b-thromboglobuline; NO = nitric oxide; PAF = platelet-activating factor; vWf = von Willebrand factor; — = not studied.
Headache 3
emia is followed by hypoperfusion of the occipitalbrain (for review, see37). These flow changes are pres-ently often interpreted as epiphenomena of CSD,which is thought to cause the aura signs like movingscotomata.
Another theory states that the hypoperfusionduring aura is caused by serotonergic vasoconstric-tion, because the reaction can be prevented bymethysergide, a 5-HT-antagonist. In this view, aurasigns could be caused by hypoxia in progressivelymore brain cells as blood flow decreases.38-41 It isnoteworthy that aura symptoms disappear afterinhalation of carbon dioxide, a strong cerebralvasodilator.42 Vascular and neuronal theories of aura
do not necessarily exclude each other, because CSDitself may be triggered by vasoconstricton-inducedhypoxia.40,43
A rise in circulating serotonin could also explainthe initial hyperemia, because at low concentration,serotonin causes vasodilation.8 Serotonin may bereleased by brainstem raphe neurons, by enterochro-maffin cells in the gut, and by aggregating blood plate-lets, but which of these mechanisms is actuallyinvolved is still unknown. In this paper, we will accen-tuate the latter possibility. Although there is no directevidence for the contribution of serotonin fromaggregating platelets to vasoconstriction in migraineaura, experiments in dogs show that intracisternal
Table 2.—Effect of Platelet Inhibition on Migraine
Platelet Antagonist (mg/day)No. of Migraine
Patients Result Ref.
TXA2 reductionAspirin (50) 525 Small decrease in frequency, severity, duration, and
migraine-related disability in 59.6% of 525 women (vs56.4% in the placebo group)
161
Aspirin (160) 0 Six percent of 11,037 US male doctors using aspirinreported migraine (vs 7.4 % in the group usingplacebo)
162
Aspirin (300) 135 In 30 % of patients, >50% reduction in migraine rate 163
Aspirin (325) + dipyridamole (25) 25 In 68 % of patients, significant improvement in headachefrequency, intensity, and limitation of activity(compared with placebo)
164
Picotamide (2 ¥ 300) 20 Decrease in mean frequency of migraine aura from 6.85to 2.85 per trimester
165
ADP-receptor blockade with or without TXA2 reductionClopidogrel (75) + aspirin (325) 5 Migraine due to transcatheter placement of an Amplatzer
occluder in PFO patients was completely relieved
88
Clopidogrel (75) + aspirin (150-300) 0 Prevalence of migraine after transcatheter placement ofan Amplatzer occluder in PFO patients was reduced(12 % in 89 cases vs 42 % in 71 cases with aspirinalone)
87
Ticlopidine (200) + aspirin (200) 1 Migraine due to transcatheter placement of an Amplatzeroccluder in a PFO patient was completely relieved
166
Ticlopidine (750) 1 Complete relief of migraine in a patient withthrombocythemia
167
Correction of platelet hyperaggregabilityTiclopidine (100) and/or aspirin (100-300) 23 Prevention of headache in all and of aura in 7 of 10
migraine patients with platelet hyperaggregability
13
In reference (Ref.)13, platelet hyperaggregability and its correction were measured with aggregometry. All these studies were open,patients knew their medication.ADP = adenosine diphosphate; ADP-receptor blockade by clopidogrel or ticlopidine; PFO = patent foramen ovale;TXA2 = thromboxane A2; TXA2 synthase inhibition by aspirin, picotamide, or dipyridamole.
4

injection of platelet-rich plasma induces acute cere-bral vasospasm.44
VASCULAR REACTIONS DURING THEHEADACHE PHASE
Dilation of large and smaller cranial arteries hasconsistently been noted during the headache phase ofa spontaneous migraine attack (Table 3). Absence ofvasodilation in a study with nitroglycerin-evokedheadache45 may probably be ascribed to less sensitivemeasurement.46
Less equivocal results have been found forregional cerebral blood flow. Studies in whichmigraine was a consequence of intracarotid injec-tion of Xenon-133 showed hyperemia in nearlyall studied patients,47-52 while no hyperemia wasobserved in red wine-induced migraine.53 Duringspontaneous migraine, an increase, no change, oreven a decrease in cerebral blood flow was observed(Table 4). Methodological differences might beinvolved. Newer methods aim to localize flow abnor-malities more precisely in deeper brain layers. Inpositron emission tomography studies, for example,blood flow in large blood vessel regions is, to thisend, often removed from the analyzed areas of inter-est.54 It is therefore conceivable that such measure-ments are more sensitive to flow changes in thecerebral microcirculation and less sensitive to
changes in large and smaller arteries. As a conse-quence, absence of hyperemia in some studies withregional cerebral blood flow measurement does notexclude a possible dilation of large arteries in super-ficial brain structures, as is indicated by the data inTable 3. This contention would imply that migrain-ous vasodilation does not occur, or is less prominent,in cerebral microcirculation of deeper brain layers,but is confined to large extracranial and intracranialvessels.
Although the large cerebral arteries are pain sen-sitive,55 migraine does not seem to be caused byvasodilation itself. For example, no migraine pain isfelt when vasodilation is elicited by vasoactive intes-tinal peptide56 (ie, a NO-independent vasodilator).Moreover, hyperemia is not time locked to ictal painduring spontaneous migraine,51,57 and the throbbingof the headache is not phase locked to the arterialpulse.58 Both pain and hyperemia during the head-ache phase are more likely caused independently by acommon factor. Circulating serotonin is a good can-didate, because it is a pain mediator and, in low con-centration, a vasodilator. Absence of pain sensationduring the aura phase, in which serotonin concentra-tion is supposed to be high, might be due to thehypoxic suppression of neuronal activity; thereafterpain might be felt as soon as cerebral hypoxia hasdiminished to a level that enables pain sensation.
Table 3.—Large Cranial Artery Diameter and Flow in the Headache Phase of Migraine
Method Change No. of Patients Ref. Year
Spontaneous attacksDiameter of
Temporal artery and conjunctival vessels Visual ↑ Common bedside observation 55 1955MCA and PCA MRA ↑ 1 168 2008MCA Doppler + SPECT ↑ 7 169 1991
Frontotemporal cutaneous blood flow Tissue clearance of NaCl ↑ 18 24,170 1964Red ear syndrome in children Visual ↑ In 7 of 8 171 2002
↑ In 40 of 172 172 2011Evoked by CGRP
MMA and MCA MRA circumference ↑ 15 46 2010Evoked by NTG
MMA and MCA MRA diameter = 20 45 2008
CGRP = calcitonin gene-related peptide; MCA = middle cerebral artery; MMA = middle meningeal artery; MRA = magnetic reso-nance angiography; NTG = nitroglycerin; PCA = posterior cerebral artery; SPECT = single photon emission computed tomography.
Headache 5

SIMILARITY BETWEEN VASCULARREACTIONS IN MIGRAINE AND THOSEELICITED BY SHEAR-INDUCEDPLATELET AGGREGATION INA RAT MODEL
The earlier 2 sections of this report on vascularreactions indicate that during migraine with aura, atriphasic reaction may occur: an initial short-lastingvasodilation, followed by a longer-lasting (20 minutesto some hours) vasoconstriction, and – in a number ofpatients – a subsequent long-lasting (hours to days)dilation of superficial cranial arteries. In commonmigraine, that is without aura, only vasodilation willoccur. It must be noted that within an animal model,such a triphasic vascular reaction can be evoked byplatelet aggregation, initiated by shear stress.
To study vascular effects due to platelet aggrega-tion in vivo, it is of crucial importance to avoid the useof platelet agonists that are vasoactive by themselves.In previous work on pentobarbital-anesthetizedrats, we have elicited platelet aggregation with aid ofelevated shear stress in a carotid-to-femoral extracor-
poreal loop of polyvinylchloride (PVC) tubing.8
Shear-induced platelet aggregation may occur at sitesof accelerated flow, as for example in patients withsevere internal carotid artery stenosis.59 It is agonistindependent and mediated by conformational changeof large multimers of plasma von Willebrand factor(vWf). When changing from a globular state into anextended chain,vWf presents itsA1 domain that bindsto platelet glycoprotein Ib receptors.60,61 This bindingtriggers intraplatelet calcium mobilization with sub-sequent release of dense body constituents (ADP,serotonin) and aggregation. In our rat experiments,compression of the extracorporeal tubing causedplatelet aggregation and dilation of the femoral bedthat were both prevented by blocking the binding ofvWf to the platelet glycoprotein Ib receptors withaurintricarboxylic acid.6 More intense platelet aggre-gation, induced with aid of a roller pump on the tubing,elicited a triphasic vascular reaction as depicted inFigure 1:an initial vasodilation followed by temporaryvasoconstriction and a long-lasting (hours) vasodila-tion. Of note, measurement of free hemoglobin in
Table 4.—Regional Cerebral Blood Flow in the Headache Phase of Spontaneous Migraine
MethodDirection of Change
(in Number of Patients)No. of Studied
PatientsType of
Migraine Ref. Year
Xenon-133 inhalation ↓ followed by ↑ (10) 10 MA 173 1971↑ (12) 13 MA+MWA 174 1978↑ (29) 42 MA+MWA 175 1986
SPECT ↑ (7) 7 MA 176 1988↓ (13) followed by ↑ (6) 25 MA 51 1990= (12) 12 MWA 57 1984↓ (8) = (3) 11 MA 57 1984
MRIPerfusion weighted ↑ (1) 1 MA 168 2008
= (mean of 14) 14 MWA 177 1999Arterial spin-labeled ↑ (1) 1 MWA 178 2010
↑ (3) 3 MA 179 2008PET
15C-O2 inhalation ↑ (mean of 9) 9 MWA 180 1995H2
15O iv injection ↑ (mean of 5) 5 MA+MWA 181 2005H2
15O iv injection ↓ (1) 1 MWA 182 1994H2
15O iv injection ↓ (5) 7 MWA 183† 2008H2
15O iv injection ↓ (8) ↑ (1) 9 MWA 54‡ 1998
†Hypoperfusion was bilateral in patients with unilateral headache.‡Large blood vessel regions excluded.iv = intravenous; MA = migraine with aura; MRI = magnetic resonance imaging; MWA = migraine without aura; PET = positronemission tomography; SPECT = single photon emission computed tomography.
6
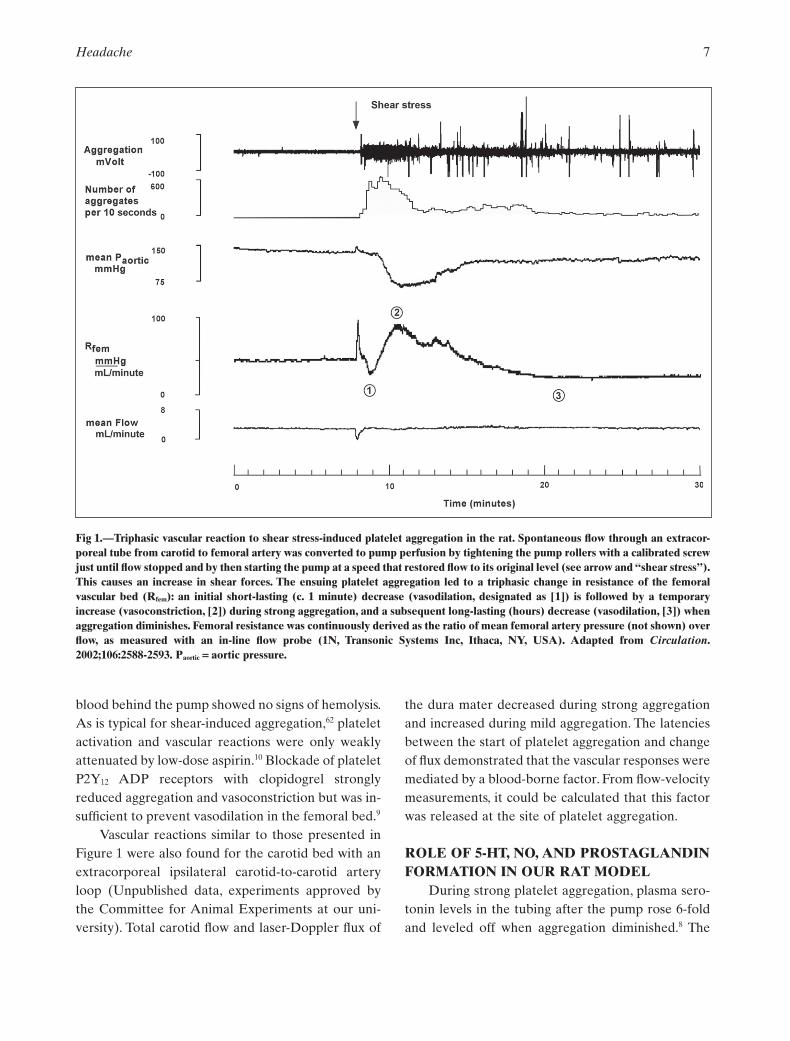
blood behind the pump showed no signs of hemolysis.As is typical for shear-induced aggregation,62 plateletactivation and vascular reactions were only weaklyattenuated by low-dose aspirin.10 Blockade of plateletP2Y12 ADP receptors with clopidogrel stronglyreduced aggregation and vasoconstriction but was in-sufficient to prevent vasodilation in the femoral bed.9
Vascular reactions similar to those presented inFigure 1 were also found for the carotid bed with anextracorporeal ipsilateral carotid-to-carotid arteryloop (Unpublished data, experiments approved bythe Committee for Animal Experiments at our uni-versity). Total carotid flow and laser-Doppler flux of
the dura mater decreased during strong aggregationand increased during mild aggregation. The latenciesbetween the start of platelet aggregation and changeof flux demonstrated that the vascular responses weremediated by a blood-borne factor. From flow-velocitymeasurements, it could be calculated that this factorwas released at the site of platelet aggregation.
ROLE OF 5-HT, NO, AND PROSTAGLANDINFORMATION IN OUR RAT MODEL
During strong platelet aggregation, plasma sero-tonin levels in the tubing after the pump rose 6-foldand leveled off when aggregation diminished.8 The
Fig 1.—Triphasic vascular reaction to shear stress-induced platelet aggregation in the rat. Spontaneous flow through an extracor-poreal tube from carotid to femoral artery was converted to pump perfusion by tightening the pump rollers with a calibrated screwjust until flow stopped and by then starting the pump at a speed that restored flow to its original level (see arrow and “shear stress”).This causes an increase in shear forces. The ensuing platelet aggregation led to a triphasic change in resistance of the femoralvascular bed (Rfem): an initial short-lasting (c. 1 minute) decrease (vasodilation, designated as [1]) is followed by a temporaryincrease (vasoconstriction, [2]) during strong aggregation, and a subsequent long-lasting (hours) decrease (vasodilation, [3]) whenaggregation diminishes. Femoral resistance was continuously derived as the ratio of mean femoral artery pressure (not shown) overflow, as measured with an in-line flow probe (1N, Transonic Systems Inc, Ithaca, NY, USA). Adapted from Circulation.2002;106:2588-2593. Paortic = aortic pressure.
Headache 7

vasoconstriction was prevented and the vasodila-tion reduced by blockade of 5-HT2-receptors withritanserin or pizotifen and could be mimicked by infu-sion of a high, respectively low dose of serotonin intothe extracorporeal tubing. These results are in linewith what is known about the vasoactive effects ofserotonin: in high dose, it causes vasoconstriction bystimulating 5-HT2A receptors on smooth muscle andperivascular nerve endings44 (or 5-HT1db receptors inthe cranial vasculature of man63), while in lower con-centration, it mainly stimulates endothelial 5-HT2B
receptors which cause vasodilation by local release ofNO.64 and prostaglandins.65 The vasodilation in ourexperiments could indeed also be reduced by sup-pression of prostaglandin formation with aid of pare-coxib,10 and completely be prevented, or evenreversed, by inhibiting the production of NO with aidof NG-methyl-L-arginine (L-NMA).8 The fact thatthe long-lasting vasodilation could, after more than 2hours, be reversed by NO blockade indicates that thevasodilation, initiated by serotonin, was sustained bycontinuously enhanced production of NO.
Figure 1 additionally shows that strong plateletaggregation was accompanied by a marked decline inmean aortic pressure. This decline was prevented byclopidogrel9 or L-NMA8 and reminds to the diastolic
hypotension (pressure below 60 mmHg) observed ina number of patients during migraine attacks.66 It isconceivable that the hypotension in migraine contrib-utes to, or may be part of, the autonomic dysfunctionthat causes nausea and emesis. Such dysfunctionmight result from increased plasma levels of seroto-nin that stimulate 5-HT3 receptors on the parasympa-thetic nuclei in the area postrema, located outside theblood–brain barrier.An increase of vagal motor activ-ity will, on its turn, stimulate release of serotonin fromenterochromaffin cells, further exciting vagal activityin a positive serotonergic–parasympathetic feedbackloop.67
ANALOGIES BETWEEN EVENTS INMIGRAINE AND HEMODYNAMICCHANGES CAUSED BY SHEAR-INDUCEDPLATELET AGGREGATION IN RATS
These analogies are summarized in Table 5. Theysuggest that in a certain number of migraine attacks,platelet aggregation induced by shear stress or othermeans, with concomitant release of serotonin, mayplay a role. The headache phase and aura are, in thisview, not independent phenomena but caused byvarying intensities of the same event, ie, a rise in freeplasma serotonin concentration. The longer duration
Table 5.—Analogies Between Human Migraine and Hemodynamic Changes Caused by Shear-Induced Platelet Aggregationin Rats
Human Migraine Shear Stress in Rats
Circulating platelet aggregates Increased IncreasedPlasma levels of 5-HT Likely increased IncreasedTriphasic vascular reaction Short hyperemia, followed by
oligemia in aura and long-lastingvasodilation in pain phase
Short-lasting dilation, followed by longerlasting constriction and long-lastingdilation
5-HT2B-receptor blockade with pizotifen Prophylaxis Reduces long-lasting vasodilationPlasma von Willebrand factor Increased Blocking its platelet receptor prevents
aggregation and vascular effectsPlatelet ADP P2Y12-receptor blockade May prevent migraine Prevents aggregation, vasoconstriction, and
systemic hypotensionLow-dose aspirin Only weak attenuation Only weak attenuation of aggregation and
vascular effectsNO inhibition Relieve Prevention or reversion of vasodilationCOX-2 (prostaglandin) inhibition Relieve Attenuates vasodilationAortic pressure Decrease Decrease
COX-2 = cyclooxygenase-2; 5-HT = serotonin; NO = nitric oxide.
8

of vasoconstriction in human migraine aura, com-pared with that in our rats, might be explained by alonger duration of sufficient serotonin release, due toa larger amount of circulating platelets.
POSSIBLE SITES OF ELEVATED SHEARSTRESS IN MIGRAINE
Head-Neck Region.—Blood shear stress might beelevated at a stenosis or at other sites of vessel abnor-malities with increased blood flow velocities. Both theinternal carotid and vertebral arteries are tortuous andhave to pass a small foramen in entering the skull.Common sites of stenosis in man are the origin andintracranial part of the vertebral artery and the inter-nal carotid artery at the bifurcation.68 In addition, in apopulation-based study on 150 healthy volunteers ahigh prevalence (58%) of incomplete posterior circleof Willis has been found.69 The relevance of such ananatomical characteristic for migraine might be that atemporal obstruction of contralateral carotid flow (eg,in the case of head rotation70) may lead to increasedflow velocity and shear stress both in the underdevel-oped branch of the circle of Willis and in the narrowedcarotid artery.71 Migraine has indeed repeatedly beenassociated with stenoses or dissection of the ipsilateralinternal carotid or vertebral artery, and also withreversible cerebral arterial vasoconstriction, and withcerebral arteriovenous malformations (Table 6). Alsounderdevelopment of collaterals in the circle of Willis
seems to be more prevalent in migraine than in con-trols,72 be it that the prevalence in controls was unex-pectly low (18%) in that study.
As known from the localization of speech func-tion by intracarotid injection of sodium amytal,carotid and vertebral blood flow are mainly directedto the ipsilateral hemisphere. Hence, a local increaseof shear stress at a vascular abnormality as a source ofmigraine would comply with the unilaterality of mostattacks.
Complete recovery from severe migraine hasbeen reported after thromboend arterectomy in apatient with carotid artery stenosis,73 and afterobliteration of an arteriovenous malformation.74-76
Because vessels may be narrowed by local muscularspasms or by unnatural body position, involvementof vessel stenosis in migraine is also suggestedby favorable consequences of 2 months chiropracticspinal therapy (>90% attack reduction in 22% andsignificant improvement in 49% of 83 patients).77
It may, furthermore, explain why migraine patients,in contrast to patients with tension-type headachewho massage their scalp, often try to relieve theirpain by changing their posture,78 as if they attemptto reduce the degree of vascular stenosis or shearstress.
Thoracic Region.—Evidence for an increasedprevalence of migraine with aura in patients withsymptomatic PFO, or other pulmonary or cardial
Table 6.—Studies in Which Migraine Might Have Been Caused by Elevated Blood Shear Stress in Head-Neck Region
Possible Site of Increased Shear Stress Prevalence Ref.
Internal carotid artery stenosis In 7 of 15 ischemic migraine attacks 184
In 16 case reports of migraine 73,185-187
Internal carotid artery spasm In 4 case reports of migraine 188,189
Middle cerebral artery narrowing In 37% of 62 migrainous children 190
Middle cerebral artery spasm In 6.5% of 62 migrainous children 190
Incomplete circle of Willis In 49% of 47 migraineurs (vs 18% in controls) 72
Vertebral artery hypoplasia In 36% of 59 and in 28% of 92 migraineurs 191,192
Cerebral arteriovenous malformation (AVM) Migraine in 47% of 51, 19% of 36, and 31% of 48patients with AVM
76,193,194
Case report of migraine in patient with AVM 74
Cervical artery dissection (CAD) In 8 case reports of migraine 195-198
Migraine in 34% of 62 CAD patients 199
Odds ratio for migraine: 2.06 and 3.6 200,201
Headache 9

shunts, is circumstantial.79-81 Migraine complaints in apatient with aortic coarctation were abolished byballoon dilatation.82
PFO.—This remnant of fetal anatomy is a slit-like interatrial shunt, which is present in approxi-mately 25 % of the adult population. Interestingly,migraine is associated with PFO when PFO is symp-tomatic,79,80 ie, in the presence of recurrent cryptoge-nic stroke or transient ischemic attacks, but hardly ornot at all with asymptomatic PFO.83,84 In the first case,shear-induced platelet aggregation may occur withinthe shunt, especially during Valsalva maneuvers (eg,straining during defecation). Closure of PFO mayreduce migraine.79,85 This was significant even in theMigraine Intervention With STARFlex Technologytrial, after correction for 2 outliers.86 A temporaryenhancement of migraine after PFO closure couldpoint to increased local shear stress as a result ofincomplete closure. This possibility is supported bythe fact that migraine in such patients was betterreduced by clopidogrel than by aspirin.87,88 From invitro studies, it is known that shear-induced plateletaggregation and thrombus formation are inhibited byclopidogrel, but not by aspirin.62 An explanationmight be that at high shear stress, aggregationdepends more on release of vWf from a-granules,which is not inhibited by aspirin, than on formation ofTXA2.10,11
POSSIBLE INITIATION OF MIGRAINEATTACKS BY TRIGGERS THAT ENHANCEPLATELET AGGREGABILITY
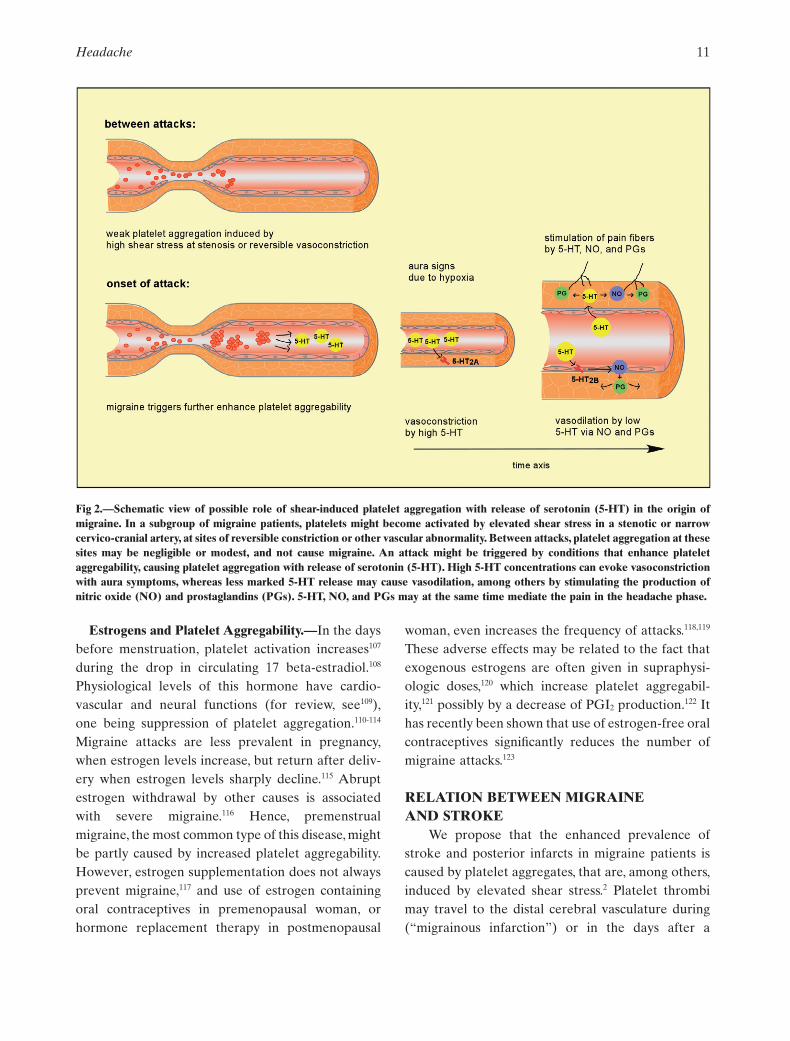
Although a number of migraine patients showincreased platelet aggregabilty,13,89-94 and their plate-lets may even continuously be activated (Table 1),aggregation might frequently be too weak to causesufficient release of platelet serotonin for a migraineattack. Because many migraine triggers are known fortheir ability to potently enhance platelet aggregability(Table 7), we propose that a proportion of migraineattacks might be triggered by a temporary furtherincrease of platelet aggregation, as depicted sche-matically in Figure 2.A further enhancement of plate-let aggregability during attacks has indeed beendocumented in several studies.90-93
The migraine triggers in Table 7 may have adirect stimulating effect on platelets or may increaseplatelet aggregability by decreasing the level of cir-culating endogenous PGI2, which is a plateletantagonist (see later). Triggers like emotional orphysical stress, or awakening in the morning, areexamples of the first; they stimulate platelet activityby a rise in plasma catecholamine levels.95,96 Estro-gens and their platelet effects will be dealt withlater. Other triggers, like, eg, alcohol and nitrites, notmentioned in Table 7, might cause migraine by directrelease of serotonin from platelets97 or by release ofNO from vascular endothelium.
PGI2 and Platelet Aggregability.—In migrainepatients, lowered levels of plasma PGI2 have beenfound.98-100 This endogenous platelet antagonist ismainly produced by endothelial COX-2. PGI2
reduces intracellular free calcium levels via stimula-tion of platelet adenylate cyclase which elevates cyclicadenosine monophosphate.101 We have recently dem-onstrated that the circulating level of PGI2 in healthymale volunteers is sufficiently high to control plateletaggregability in basal conditions, and that its reduc-tion by COX-2 inhibitors enhances platelet aggrega-bility.11 The endothelial production and half-life ofPGI2 can be temporarily suppressed by exogenousestrogens (see later), smoking,102 several foods,103
exercise,104 infections,105 low-density lipoproteins(LDL),100,106 and non-steroidal anti-inflammatorydrugs that inhibit COX-2.
Table 7.—Migraine Provoking Triggers That Increase PlateletAggregability
Estrogens:Fall in premenstrual levels;110,202,203 oral anticonceptives;204,205
hormonal replacement therapy121
Catecholamines:Emotional and physical stress;206,207 awakening in themorning;95 cold weather;208 low blood sugar; and fasting209
Additives in food and beverages:Salt;210,211 saturated fatty acids;210 glutamate (tasteenhancer);212 tyramine (preservative)213
Numbers in the table refer to references indicating increasedplatelet aggregability. For enumeration of migraine triggers, seereference.1
10
Estrogens and Platelet Aggregability.—In the daysbefore menstruation, platelet activation increases107
during the drop in circulating 17 beta-estradiol.108
Physiological levels of this hormone have cardio-vascular and neural functions (for review, see109),one being suppression of platelet aggregation.110-114
Migraine attacks are less prevalent in pregnancy,when estrogen levels increase, but return after deliv-ery when estrogen levels sharply decline.115 Abruptestrogen withdrawal by other causes is associatedwith severe migraine.116 Hence, premenstrualmigraine, the most common type of this disease, mightbe partly caused by increased platelet aggregability.However, estrogen supplementation does not alwaysprevent migraine,117 and use of estrogen containingoral contraceptives in premenopausal woman, orhormone replacement therapy in postmenopausal
woman, even increases the frequency of attacks.118,119
These adverse effects may be related to the fact thatexogenous estrogens are often given in supraphysi-ologic doses,120 which increase platelet aggregabil-ity,121 possibly by a decrease of PGI2 production.122 Ithas recently been shown that use of estrogen-free oralcontraceptives significantly reduces the number ofmigraine attacks.123
RELATION BETWEEN MIGRAINEAND STROKE
We propose that the enhanced prevalence ofstroke and posterior infarcts in migraine patients iscaused by platelet aggregates, that are, among others,induced by elevated shear stress.2 Platelet thrombimay travel to the distal cerebral vasculature during(“migrainous infarction”) or in the days after a
Fig 2.—Schematic view of possible role of shear-induced platelet aggregation with release of serotonin (5-HT) in the origin ofmigraine. In a subgroup of migraine patients, platelets might become activated by elevated shear stress in a stenotic or narrowcervico-cranial artery, at sites of reversible constriction or other vascular abnormality. Between attacks, platelet aggregation at thesesites may be negligible or modest, and not cause migraine. An attack might be triggered by conditions that enhance plateletaggregability, causing platelet aggregation with release of serotonin (5-HT). High 5-HT concentrations can evoke vasoconstrictionwith aura symptoms, whereas less marked 5-HT release may cause vasodilation, among others by stimulating the production ofnitric oxide (NO) and prostaglandins (PGs). 5-HT, NO, and PGs may at the same time mediate the pain in the headache phase.
Headache 11

migraine attack. Because platelet activation is par-ticularly strong in migraineurs with aura,12,124 the riskfor stroke will be highest in these migraine patients.
Migraine has also been linked to myocardial in-farction and other ischemic vascular disorders.125
Remarkably, both the prevalence of migraine andrisk for myocardial infarction are lower in Japanesepopulations compared with the Western popula-tions.126,127 A genetic susceptibility has been foundfor both migraine and vascular disorders, suggestingcommon pathogenic mechanisms.128 In the lipidprofile of migraineurs, increased levels of LDL arefound.129 LDL shortens the half-life of PGI2,106
thereby increasing platelet aggregability. Migrainepatients therefore seem to be at a general throm-botic risk.
PROPHYLACTIC ACTION OF CALCIUMAND b-BLOCKERS
The favorable anti-migraine effect of most b-blockers and calcium antagonists is not well under-stood.130 Because some of them are hydrophilic anddo not cross the blood–brain barrier,131,132 a directeffect on central neural mechanisms seems unlikely.Many b-blockers decrease platelet aggregability (pro-pranolol,133 metoprolol,134 pindolol,134 practolol,135
esmolol,136 carvedilol,137 alprenolol,138 atenolol133),probably by increased PGI2 formation in the arterialwall.135 Also, the prophylactic effect of calciumantagonists might be associated with their well-known antiplatelet effect.139 The same may hold forangiotensin-converting enzyme inhibitors,140 ribofla-vin,141 dark chocolate,142 and goshuyuto, a famous tra-ditional Oriental migraine medicine.143
IMPLICATIONS OF THEPLATELET-SEROTONIN-RELEASEHYPOTHESIS FOR MIGRAINE THERAPY
Although the percentage of migraine patientsthat show increased platelet aggregability has notbeen determined in a population-based study,several investigations suggest that this percentagemay be noteworthy.13,89-94 In 1 study on 23 consecu-tive patients with severe migraine, hyperaggregabil-ity was demonstrated in all of them.13 To testmigraine patients on hyperaggregability, several
devices are available.144 Platelet sensitivity toincreased shear stress may best be measured bythe Platelet Function Analyzer (PFA 100, DadeBehring, Newark, DE, USA), which aspirates cit-rated whole blood over an ADP-coated surface. Toget information about platelet aggregability in vivo,it is important to perform the tests immediatelyafter (venous) blood collection.11 A promisingeasy method to measure shear-induced aggregationwithin 90 seconds using non-anticoagulated bloodfrom a finger stick has recently been proposed.145
We suggest that in patients with hyperaggregabil-ity, attacks might be prevented by inhibiting shearstress-induced platelet aggregation. This could mostspecifically be accomplished by blockade of vWfbinding to platelet glycoprotein 1b receptors. A can-didate may be the recently developed ARC1779 thatinhibits this binding, while it gives less increase inbleeding than conventional antiplatelet agents. In arandomized trial on 36 patients, it markedly reducedcerebral embolization after carotid endarterec-tomy.146 Alternatively, shear-induced platelet aggrega-tion in humans could be suppressed by in vivoinhibition of fibrinogen binding to GPIIB/IIIA recep-tors,147 or by clopidogrel, which blocks platelet ADPP2Y12 receptors.145 A favorable effect of clopidogrel inpreventing migraine has already been mentioned insome studies (Table 2), and its efficacy is presentlytested in 2 randomized, placebo-controlled trials(“CANOA” study at Laval University, Quebec,Canada, and “Clopidogrel as prophylactic treatmentfor migraine “study by J. Chambers, London). Aneven more practical solution might be the use ofticagrelor, which, in contrast to clopidogrel, whichrequires hepatic conversion, is a direct-acting revers-ible inhibitor of platelet ADP P2Y12 receptors,148
enabling a patient to take such medication at theonset, or prodrome, of a migraine attack.
Patients in which migraine is successfully pre-vented or aborted by agents that inhibit shear-induced platelet aggregation could be successivelyscanned for the presence of a cardial or pulmonaryshunt, a stenosis or dissection of a cervico-cranialartery, or reversible cerebral arterial constriction.149
Proper treatment of these anomalies will also reducetheir important risk for cerebral stroke.
12

CONCLUSIONOur extension of the platelet hypothesis of
migraine, as depicted schematically in Figure 2, sug-gests that in a number of patients, a migraine attackwith or without aura may be caused by the sameevent, but at different intensity, namely a rise inplasma serotonin which is released from aggregatingplatelets. Aggregation may be initiated by elevatedshear stress in a stenotic cervico-cranial artery or atsites of reversible vasoconstriction or other cardio-vascular abnormality, especially when platelet aggre-gability is temporarily enhanced by a migrainetrigger. A clinical implication of the present theory isthe testing of migraineurs for increased plateletaggregability and treating them with one of therecently developed short-acting inhibitors of shear-induced platelet aggregation. Patients respondingfavorably could be scanned for cardiovascularanomalies in the thorax-head region, treatment ofwhich will reduce their risk for cerebral stroke.
REFERENCES
1. Kelman L. The triggers or precipitants of the acutemigraine attack. Cephalalgia. 2007;27:394-402.
2. Spector JT, Kahn SR, Jones MR, Jayakumar M,Dalal D, Nazarian S. Migraine headache andischemic stroke risk: An updated meta-analysis.Am J Med. 2010;123:612-624.
3. Dohmen C, Sakowitz OW, Fabricius M, et al.Spreading depolarizations occur in humanischemic stroke with high incidence. Ann Neurol.2008;63:720-728.
4. Kruit MC, Launer LJ, Ferrari MD, van BuchemMA. Infarcts in the posterior circulation territoryin migraine.The population-based MRI CAMERAstudy. Brain. 2005;128:2068-2077.
5. Hanington E. Migraine. A platelet hypothesis. Bio-medicine. 1979;30:65-66.
6. Borgdorff P, Kok WE, Vis MA, van den Bos GC.Vasodilation by shear-induced platelet aggregationin extracorporeal circuits. Am J Physiol. 1994;266:H891-H897.
7. Borgdorff P, van Den Berg RH, Vis MA, van denBos GC, Tangelder GJ. Pump-induced plateletaggregation in albumin-coated extracorporealsystems. J Thorac Cardiovasc Surg. 1999;118:946-952.
8. Borgdorff P, Fekkes D, Tangelder GJ. Hypotensioncaused by extracorporeal circulation: Serotoninfrom pump-activated platelets triggers nitric oxiderelease. Circulation. 2002;106:2588-2593.
9. Borgdorff P, Tangelder GJ. Pump-induced plateletaggregation with subsequent hypotension: Itsmechanism and prevention with clopidogrel. JThorac Cardiovasc Surg. 2006;131:813-821.
10. Borgdorff P, Tangelder GJ, Paulus WJ.Cyclooxygenase-2 inhibitors enhance shear stress-induced platelet aggregation. J Am Coll Cardiol.2006;48:817-823.
11. Borgdorff P, Handoko ML, Wong YY, TangelderGJ. COX-2 inhibition by use of rofecoxib or highdose aspirin enhances ADP-induced platelet aggre-gation in fresh blood. Open Cardiovasc Med J.2010;4:198-205.
12. D’Andrea G, Toldo M, Cananzi A, Ferro-Milone F.Study of platelet activation in migraine: Control bylow doses of aspirin. Stroke. 1984;15:271-275.
13. Fujita S. Effects of correcting platelet hyper-aggregability on prevention of migraine with auramanifested by scintillating scotoma and onmigraine outcome using the MIDAS scale. Head-ache Care. 2006;3:65-72.
14. Peto R, Gray R, Collins R, et al. Randomised trialof prophylactic daily aspirin in British maledoctors. Br Med J (Clin Res Ed). 1988;296:313-316.
15. Kirthi V, Derry S, Moore RA, McQuay HJ. Aspirinwith or without an antiemetic for acute migraineheadaches in adults. Cochrane Database Syst Rev.2010;(14):CD008041.
16. Lampl C, Voelker M, Diener HC. Efficacy andsafety of 1000 mg effervescent aspirin: Individualpatient data meta-analysis of three trials inmigraine headache and migraine accompanyingsymptoms. J Neurol. 2007;254:705-712.
17. Ferrari MD, Saxena PR. On serotonin andmigraine: A clinical and pharmacological review.Cephalalgia. 1993;13:151-165.
18. Izzati-Zade KF. The role of serotonin in the patho-genesis and clinical presentations of migraineattacks. Neurosci Behav Physiol. 2008;38:501-505.
19. Evers S, Quibeldey F, Grotemeyer KH, Suhr B,Husstedt IW. Dynamic changes of cognitivehabituation and serotonin metabolism during themigraine interval. Cephalalgia. 1999;19:485-491.
Headache 13

20. Davis RB, Wang Y. Rapid pulmonary removal of5-hydroxytryptamine in the intact dog. Proc SocExp Biol Med. 1965;118:797-800.
21. Lance JW. 5-Hydroxytryptamine and its role inmigraine. Eur Neurol. 1991;31:279-281.
22. Panconesi A, Sicuteri R. Headache induced byserotonergic agonists – a key to the interpretationof migraine pathogenesis? Cephalalgia. 1997;17:3-14.
23. Sommer C. Serotonin in pain and analgesia:Actions in the periphery. Mol Neurobiol. 2004;30:117-125.
24. Clower BR, Sullivan DM, Smith RR. Intracranialvessels lack vasa vasorum. J Neurosurg. 1984;61:44-48.
25. Koo JW, Balaban CD. Serotonin-inducedplasma extravasation in the murine inner ear:Possible mechanism of migraine-associatedinner ear dysfunction. Cephalalgia. 2006;26:1310-1319.
26. Sarchielli P, Alberti A, Codini M, Floridi A, GallaiV. Nitric oxide metabolites, prostaglandins andtrigeminal vasoactive peptides in internal jugularvein blood during spontaneous migraine attacks.Cephalalgia. 2000;20:907-918.
27. Christiansen I, Thomsen LL, Daugaard D, UlrichV, Olesen J. Glyceryl trinitrate induces attacks ofmigraine without aura in sufferers of migraine withaura. Cephalalgia. 1999;19:660-667.
28. Wienecke T, Olesen J, Ashina M. ProstaglandinI(2) (epoprostenol) triggers migraine-like attacksin migraineurs. Cephalalgia. 2010;30:179-190.
29. Lassen LH, Ashina M, Christiansen I, et al. Nitricoxide synthase inhibition: A new principle in thetreatment of migraine attacks. Cephalalgia. 1998;18:27-32.
30. Jakubowski M, Levy D, Goor-Aryeh I, Collins B,Bajwa Z, Burstein R. Terminating migraine withallodynia and ongoing central sensitization usingparenteral administration of COX1/COX2 inhibi-tors. Headache. 2005;45:850-861.
31. Reuter U, Bolay H, Jansen-Olesen I, et al. Delayedinflammation in rat meninges: Implications formigraine pathophysiology. Brain. 2001;124:2490-2502.
32. Akerman S, Williamson DJ, Kaube H, Goadsby PJ.Nitric oxide synthase inhibitors can antagonizeneurogenic and calcitonin gene-related peptideinduced dilation of dural meningeal vessels. Br JPharmacol. 2002;137:62-68.
33. Anthony M, Hinterberger H, Lance JW. Plasmaserotonin in migraine and stress. Arch Neurol.1967;16:544-552.
34. Moskowitz MA. Neurogenic versus vascularmechanisms of sumatriptan and ergot alkaloids inmigraine. Trends Pharmacol Sci. 1992;13:307-311.
35. Ikeda Y, Jimbo H, Shimazu M, Satoh K. Sumatrip-tan scavenges superoxide, hydroxyl, and nitricoxide radicals: In vitro electron spin resonancestudy. Headache. 2002;42:888-892.
36. Buzzi MG, Moskowitz MA. The pathophysiologyof migraine: Year 2005. J Headache Pain. 2005;6:105-111.
37. Tfelt-Hansen PC. History of migraine with auraand cortical spreading depression from 1941 andonwards. Cephalalgia. 2010;30:780-792.
38. Skyhoj OT. Migraine with and without aura: Thesame disease due to cerebral vasospasm of differ-ent intensity. A hypothesis based on CBF studiesduring migraine. Headache. 1990;30:269-272.
39. Skyhoj OT, Friberg L, Lassen NA. Ischemia may bethe primary cause of the neurologic deficits inclassic migraine. Arch Neurol. 1987;44:156-161.
40. Amery WK. Brain hypoxia: The turning-point inthe genesis of the migraine attack? Cephalalgia.1982;2:83-109.
41. Leao AAP. Further observations on the spreadingdepression of activity in the cerebral cortex. J Neu-rophysiol. 1947;10:409-414.
42. Marcussen RM, Wolff HG. Effects of carbondioxide-oxygen mixtures given during prehead-ache phase of the migraine attack; further analysisof the pain mechanisms in headache. Arch NeurolPsychiatry. 1950;63:42-51.
43. Nozari A, Dilekoz E, Sukhotinsky I, et al. Micro-emboli may link spreading depression, migraineaura, and patent foramen ovale. Ann Neurol.2010;67:221-229.
44. Satoh S, Suzuki Y, Harada T, et al. The role ofplatelets in the development of cerebral vaso-spasm. Brain Res Bull. 1991;27:663-668.
45. Schoonman GG, van der GJ, Kortmann C, van derGeest RJ, Terwindt GM, Ferrari MD. Migraineheadache is not associated with cerebral ormeningeal vasodilatation – A 3T magnetic reso-nance angiography study. Brain. 2008;131:2192-2200.
46. Asghar MS, Hansen AE, Amin FM, et al. Evidencefor a vascular factor in migraine. Ann Neurol. 2011;69:635-645.
14

47. Norris JW, Hachinski VC, Cooper PW. Changes incerebral blood flow during a migraine attack. BrMed J. 1975;3:676-677.
48. Skinhoj E. Hemodynamic studies within the brainduring migraine. Arch Neurol. 1973;29:95-98.
49. Skinhoj E, Paulson OB. Regional blood flow ininternal carotid distribution during migraineattack. Br Med J. 1969;3:569-570.
50. Hachinski VC, Olesen J, Norris JW, Larsen B,Enevoldsen E, Lassen NA. Cerebral hemodynam-ics in migraine. Can J Neurol Sci. 1977;4:245-249.
51. Olesen J, Friberg L, Olsen TS, et al. Timing andtopography of cerebral blood flow, aura, and head-ache during migraine attacks. Ann Neurol. 1990;28:791-798.
52. Mathew NT, Hrastnik F, Meyer JS. Regional cere-bral blood flow in the diagnosis of vascular head-ache. Headache. 1976;15:252-260.
53. Olesen J, Tfelt-Hansen P, Henriksen L, Larsen B.The common migraine attack may not be initiatedby cerebral ischaemia. Lancet. 1981;2:438-440.
54. Bednarczyk EM, Remler B, Weikart C, NelsonAD, Reed RC. Global cerebral blood flow, bloodvolume, and oxygen metabolism in patients withmigraine headache. Neurology. 1998;50:1736-1740.
55. Wolff HG. Headache mechanisms. Int ArchAllergy. 1955;7:210-278.
56. Rahmann A, Wienecke T, Hansen JM, FahrenkrugJ, Olesen J, Ashina M. Vasoactive intestinal peptidecauses marked cephalic vasodilation, but does notinduce migraine. Cephalalgia. 2008;28:226-236.
57. Lauritzen M,Olesen J.Regional cerebral blood flowduring migraine attacks by Xenon-133 inhalationand emission tomography. Brain. 1984;107:447-461.
58. Ahn AH. On the temporal relationship betweenthrobbing migraine pain and arterial pulse. Head-ache. 2010;50:1507-1510.
59. Yip HK, Lu CH, Yang CH, et al. Levels and valueof platelet activity in patients with severe internalcarotid artery stenosis. Neurology. 2006;66:804-808.
60. Siedlecki CA, Lestini BJ, Kottke-Marchant KK,Eppell SJ, Wilson DL, Marchant RE. Shear-dependent changes in the three-dimensional struc-ture of human von Willebrand factor. Blood.1996;88:2939-2950.
61. McCrary JK, Nolasco LH, Hellums JD, Kroll MH,Turner NA, Moake JL. Direct demonstration ofradiolabeled von Willebrand factor binding to
platelet glycoprotein Ib and IIb-IIIa in the presenceof shear stress. Ann Biomed Eng. 1995;23:787-793.
62. Barstad RM, Orvim U, Hamers MJ, TjonnfjordGE, Brosstad FR, Sakariassen KS. Reduced effectof aspirin on thrombus formation at high shear anddisturbed laminar blood flow. Thromb Haemost.1996;75:827-832.
63. Cohen Z, Bonvento G, Lacombe P, Hamel E. Sero-tonin in the regulation of brain microcirculation.Prog Neurobiol. 1996;50:335-362.
64. Fozard JR. The 5-hydroxytryptamine-nitric oxideconnection: The key link in the initiation ofmigraine? Arch Int Pharmacodyn Ther. 1995;329:111-119.
65. Blackshear JL, Orlandi C, Hollenberg NK. Seroto-nin and the renal blood supply: Role of prostaglan-dins and the 5HT-2 receptor. Kidney Int. 1986;30:304-310.
66. Secil Y, Unde C, Beckmann YY, Bozkaya YT,Ozerkan F, Basoglu M. Blood pressure changes inmigraine patients before, during and after migraineattacks. Pain Pract. 2010;10:222-227.
67. Lechin F, Van Der Dijs B, Lechin AE. Circulatingserotonin, catecholamines, and central nervoussystem circuitry related to some cardiorespiratory,vascular, and hematological disorders. J Appl Res.2005;5:605-621.
68. Lee RM. Morphology of cerebral arteries. Pharma-col Ther. 1995;66:149-173.
69. Krabbe-Hartkamp MJ, van der GJ, de Leeuw FE,et al. Circle of Willis: Morphologic variation onthree-dimensional time-of-flight MR angiograms.Radiology. 1998;207:103-111.
70. Glor FP, Ariff B, Hughes AD, et al. Influence ofhead position on carotid hemodynamics in youngadults. Am J Physiol Heart Circ Physiol. 2004;287:H1670-H1681.
71. Lal BK, Beach KW, Sumner DS. Intracranial collat-eralization determines hemodynamic forces forcarotid plaque disruption. J Vasc Surg. 2011;54:1461-1471.
72. Bugnicourt JM, Garcia PY, Peltier J, Bonnaire B,Picard C, Godefroy O. Incomplete posterior circleof Willis: A risk factor for migraine? Headache.2009;49:879-886.
73. Klingebiel R, Friedman A, Shelef I, Dreier JP.Clearance of a status aurae migraenalis in responseto thrombendarterectomy in a patient with highgrade internal carotid artery stenosis. J NeurolNeurosurg Psychiatry. 2008;79:89-90.
Headache 15
74. Troost BT, Mark LE, Maroon JC. Resolution ofclassic migraine after removal of an occipital lobeAVM. Ann Neurol. 1979;5:199-201.
75. Kurita H, Shin M, Kirino T. Resolution of migrainewith aura caused by an occipital arteriovenous mal-formation. Arch Neurol. 2000;57:1219-1220.
76. Kurita H, Ueki K, Shin M, et al. Headaches inpatients with radiosurgically treated occipital arte-riovenous malformations. J Neurosurg. 2000;93:224-228.
77. Tuchin PJ, Pollard H, Bonello R. A randomizedcontrolled trial of chiropractic spinal manipulativetherapy for migraine. J Manipulative Physiol Ther.2000;23:91-95.
78. Martins IP, Parreira E. Behavioral response toheadache: A comparison between migraine andtension-type headache. Headache. 2001;41:546-553.
79. Schwedt TJ, Demaerschalk BM, Dodick DW.Patent foramen ovale and migraine: A quantitativesystematic review. Cephalalgia. 2008;28:531-540.
80. Domitrz I, Mieszkowski J, Kaminska A. Relation-ship between migraine and patent foramen ovale:A study of 121 patients with migraine. Headache.2007;47:1311-1318.
81. Post MC, van Gent MW, Plokker HW, et al. Pul-monary arteriovenous malformations associatedwith migraine with aura. Eur Respir J. 2009;34:882-887.
82. Shahar E, Borenstein A, Filk D. Severe migraineassociated with coarctation of aorta: Completerecovery following balloon dilation. J Child Neurol.2000;15:826-827.
83. Rundek T, Elkind MS, Di Tullio MR, et al. Patentforamen ovale and migraine: A cross-sectionalstudy from the Northern Manhattan Study(NOMAS). Circulation. 2008;118:1419-1424.
84. Garg P, Servoss SJ, Wu JC, et al. Lack of associa-tion between migraine headache and patentforamen ovale. Results of a case-control study. Cir-culation. 2010;121:1406-1412.
85. Schwerzmann M, Wiher S, Nedeltchev K, et al. Per-cutaneous closure of patent foramen ovale reducesthe frequency of migraine attacks. Neurology.2004;62:1399-1401.
86. Dowson A, Mullen MJ, Peatfield R, et al. MigraineIntervention With STARFlex Technology (MIST)trial: A prospective, multicenter, double-blind,sham-controlled trial to evaluate the effectivenessof patent foramen ovale closure with STARFlex
septal repair implant to resolve refractory migraineheadache. Circulation. 2008;117:1397-1404.
87. Wilmshurst PT, Nightingale S, Walsh KP, MorrisonWL. Clopidogrel reduces migraine with aura aftertranscatheter closure of persistent foramen ovaleand atrial septal defects. Heart. 2005;91:1173-1175.
88. Sharifi M, Dehghani M, Mehdipour M, Al-BustamiO, Emrani F, Burks J. Intense migraines secondaryto percutaneous closure of atrial septal defects. JInterv Cardiol. 2005;18:181-183.
89. Cesar JM, Garcia-Avello A, Vecino AM, Sastre JL,Alvarez-Cermeno JC. Increased levels of plasmavon Willebrand factor in migraine crisis. ActaNeurol Scand. 1995;91:412-413.
90. Couch JR, Hassanein RS. Platelet aggregability inmigraine. Neurology. 1977;27:843-848.
91. Lechner H, Ott E, Fazekas F, Pilger E. Evidence ofenhanced platelet aggregation and platelet sensitiv-ity in migraine patients. Cephalalgia. 1985;5(Suppl.2):89-91.
92. Kovacs K, Herman F, Filep J, Jelencsik I, Magyar K,Csanda E. Platelet aggregation of migraineursduring and between attacks. Cephalalgia. 1990;10:161-165.
93. Kruglak L, Nathan I, Korczyn AD, Zolotov Z,Berginer V, Dvilansky A. Platelet aggregability,disaggregability and serotonin uptake in migraine.Cephalalgia. 1984;4:221-225.
94. Hanington E, Jones RJ, Amess JA, Wachowicz B.Migraine: A platelet disorder. Lancet. 1981;2:720-723.
95. Hsu LK, Crisp AH, Kalucy RS, et al. Early morningmigraine. Nocturnal plasma levels of catechola-mines, tryptophan, glucose, and free fatty acids andsleep encephalographs. Lancet. 1977;1:447-451.
96. Tofler GH, Brezinski D, Schafer AI, et al. Concur-rent morning increase in platelet aggregability andthe risk of myocardial infarction and suddencardiac death. N Engl J Med. 1987;316:1514-1518.
97. Pattichis K, Louca LL, Jarman J, Sandler M, GloverV. 5-hydroxytryptamine release from platelets bydifferent red wines: Implications for migraine. EurJ Pharmacol. 1995;292:173-177.
98. Mezei Z, Kis B, Gecse A, et al. Platelet arachido-nate cascade of migraineurs in the interictal phase.Platelets. 2000;11:222-225.
99. Puig-Parellada P, Planas JM, Gimenez J, et al.Plasma and saliva levels of PGI2 and TXA2 in theheadache-free period of classical migraine patients.
16
The effects of nicardipine. Headache. 1991;31:156-158.
100. Hedman C, Winther K, Knudsen JB. Platelet func-tion in classic migraine during attack-free periods.Acta Neurol Scand. 1988;78:271-277.
101. den Dekker E, Gorter G, Heemskerk JW, Akker-man JW. Development of platelet inhibition bycAMP during megakaryocytopoiesis. J Biol Chem.2002;277:29321-29329.
102. Inoue T, Hayashi M, Uchida T, Takayanagi K,Hayashi T, Morooka S. Significance of plateletaggregability immediately after blood samplingand effect of cigarette smoking. Platelets. 2001;12:415-418.
103. Schramm DD, Wang JF, Holt RR, et al. Chocolateprocyanidins decrease the leukotriene-prostacyclinratio in humans and human aortic endothelial cells.Am J Clin Nutr. 2001;73:36-40.
104. Zoladz JA, Majerczak J, Duda K, Chlopicki S.Exercise-induced prostacyclin release positivelycorrelates with VO(2max) in young healthy men.Physiol Res. 2009;58:229-238.
105. Pirich C, Efthimiou Y, O’Grady J, Zielinski C, Sin-zinger H. Apolipoprotein A and biological half-lifeof prostaglandin I2 in HIV-1 infection. ThrombRes. 1996;81:213-218.
106. Pirich C, Efthimiou Y, O’Grady J, Sinzinger H.Hyperalphalipoproteinemia and prostaglandin I2stability. Thromb Res. 1997;88:41-49.
107. Toth B, Nikolajek K, Rank A, et al. Gender-specificand menstrual cycle dependent differences incirculating microparticles. Platelets. 2007;18:515-521.
108. Silberstein SD. Sex hormones and headache. RevNeurol (Paris). 2000;156(Suppl. 4):4S30-4S41.
109. Gaglia MA Jr, Waksman R. Overview of the 2010food and drug administration cardiovascular andrenal drugs advisory committee meeting regardingticagrelor. Circulation. 2011;123:451-456.
110. Boudoulas KD, Cooke GE, Roos CM, Bray PF,Goldschmidt-Clermont PJ. The PlA polymorphismof glycoprotein IIIa functions as a modifier for theeffect of estrogen on platelet aggregation. ArchPathol Lab Med. 2001;125:112-115.
111. Roberts JM, Goldfien RD, Tsuchiya AM, GoldfienA, Insel PA. Estrogen treatment decreases alpha-adrenergic binding sites on rabbit platelets. Endo-crinology. 1979;104:722-728.
112. Hayashi T, Yamada K, Esaki T, et al. Estrogenincreases endothelial nitric oxide by a receptor-
mediated system. Biochem Biophys Res Commun.1995;214:847-855.
113. Nakano Y, Oshima T, Matsuura H, Kajiyama G,Kambe M. Effect of 17beta-estradiol on inhibitionof platelet aggregation in vitro is mediated by anincrease in NO synthesis. Arterioscler Thromb VascBiol. 1998;18:961-967.
114. Sobrino A, Oviedo PJ, Novella S, et al. Estradiolselectively stimulates endothelial prostacyclin pro-duction through estrogen receptor-{alpha}. J MolEndocrinol. 2010;44:237-246.
115. Granella F, Sances G, Zanferrari C, Costa A, Mar-tignoni E, Manzoni GC. Migraine without aura andreproductive life events: A clinical epidemiologicalstudy in 1300 women. Headache. 1993;33:385-389.
116. Amir BY, Yaacov B, Guy B, Gad P, Itzhak W, GalI. Headaches in women undergoing in vitro fertili-zation and embryo-transfer treatment. Headache.2005;45:215-219.
117. Brandes JL. The influence of estrogen on migraine:A systematic review. JAMA. 2006;295:1824-1830.
118. Aegidius K, Zwart JA, Hagen K, Schei B, StovnerLJ. Oral contraceptives and increased headacheprevalence: The Head-HUNT Study. Neurology.2006;66:349-353.
119. Aegidius KL, Zwart JA, Hagen K, Schei B, StovnerLJ. Hormone replacement therapy and headacheprevalence in postmenopausal women. The Head-HUNT study. Eur J Neurol. 2007;14:73-78.
120. Norris LA, Bonnar J. Effect of oestrogen dose onwhole blood platelet activation in women takingnew low dose oral contraceptives. ThrombHaemost. 1994;72:926-930.
121. Thijs A, Van Baal WM, Van Der Mooren MJ, et al.Effects of hormone replacement therapy on bloodplatelets. Eur J Clin Invest. 2002;32:613-618.
122. Ylikorkala O, Puolakka J, Viinikka L. Oestrogencontaining oral contraceptives decrease prostacy-clin production. Lancet. 1981;1:42.
123. Nappi RE, Sances G, Allais G, et al. Effects ofan estrogen-free, desogestrel-containing oral con-traceptive in women with migraine with aura: Aprospective diary-based pilot study. Contraception.2011;83:223-228.
124. Ribeiro CA, Cotrim MD, Morgadinho MT, RamosMI, Santos ES, de Macedo TR. Migraine, serumserotonin and platelet 5-HT2 receptors. Cephalal-gia. 1990;10:213-219.
125. Wingerchuk DM, Spencer B, Dodick DW, Demaer-schalk BM. Migraine with aura is a risk factor for
Headache 17
cardiovascular and cerebrovascular disease:A criti-cally appraised topic. Neurologist. 2007;13:231-233.
126. Sakai F, Igarashi H. Prevalence of migraine inJapan: A nationwide survey. Cephalalgia. 1997;17:15-22.
127. Fukiyama K, Kimura Y, Wakugami K, Muratani H.Incidence and long-term prognosis of initial strokeand acute myocardial infarction in Okinawa, Japan.Hypertens Res. 2000;23:127-135.
128. Lanzi G, Termine C, Rossi M, et al. Are vasculardisorders more prevalent in the relatives of chil-dren and adolescents with migraine? Cephalalgia.2003;23:887-891.
129. Scher AI, Terwindt GM, Picavet HS, VerschurenWM, Ferrari MD, Launer LJ. Cardiovascular riskfactors and migraine: The GEM population-basedstudy. Neurology. 2005;64:614-620.
130. Andersson KE, Vinge E. Beta-adrenoceptor block-ers and calcium antagonists in the prophylaxis andtreatment of migraine. Drugs. 1990;39:355-373.
131. Neil-Dwyer G, Bartlett J, McAinsh J, CruickshankJM. Beta-adrenoceptor blockers and the blood-brian barrier. Br J Clin Pharmacol. 1981;11:549-553.
132. Edvinsson L, Johansson BB, Larsson B, MacKenzieET, Skarby T, Young AR. Calcium antagonists:Effects on cerebral blood flow and blood-brainbarrier permeability in the rat. Br J Pharmacol.1983;79:141-148.
133. Punda A, Polic S, Rumboldt Z, Bagatin J, MarkovicV, Lukin A. Effects of atenolol and propranolol onplatelet aggregation in moderate essential hyper-tension: Randomized crossover trial. Croat Med J.2005;46:219-224.
134. Winther K, Trap-Jensen J. Effects of three beta-blockers with different pharmacodynamic proper-ties on platelet aggregation and platelet and plasmacyclic AMP. Eur J Clin Pharmacol. 1988;35:17-20.
135. Brandt R, Seppala E, Nowak J, Vapaatalo H. Effectof propranolol, practolol and atenolol on humanplatelet thromboxane formation and plasma levelsof prostaglandins 6-keto-F1 alpha and E2. Prosta-glandins Leukot Med. 1984;16:191-203.
136. Roth E, Matos G, Guarnieri C, Papp B, Varga J.Influence of the beta-blocker therapy on neutro-phil superoxide generation and platelet aggrega-tion in experimental myocardial ischemia andreflow. Acta Physiol Hung. 1995;83:163-170.
137. Petrikova M, Jancinova V, Nosal R, Majekova M,Danihelova E. Antiplatelet activity of carvedilol in
comparison to propranolol. Platelets. 2002;13:479-485.
138. Jurgensen HJ, Dalsgaard-Nielsen J, Kjoller E,Gormsen J. Effect of long-term beta-blockade withalprenolol on platelet function and fibrinolyticactivity in patients with coronary heart disease. EurJ Clin Pharmacol. 1981;20:245-250.
139. Jones CR, Pasanisi F, Elliott HL, Reid JL. Effectsof verapamil and nisoldipine on human platelets: Invivo and in vitro studies. Br J Clin Pharmacol.1985;20:191-196.
140. Okrucka A, Pechan J, Kratochvilova H. Effects ofthe angiotensin-converting enzyme (ACE) inhibi-tor perindopril on endothelial and platelet func-tions in essential hypertension. Platelets. 1998;9:63-67.
141. Endo Y, Mamiya S, Miura AB. Effects ofriboflavin-2′, 3′, 4′, 5′-tetrabutyrate on platelet func-tion and plasma lipids. Jpn J Med. 1985;24:13-18.
142. Innes AJ, Kennedy G, McLaren M, Bancroft AJ,Belch JJ. Dark chocolate inhibits platelet aggrega-tion in healthy volunteers. Platelets. 2003;14:325-327.
143. Hibino T, Yuzurihara M, Terawaki K, Kanno H,Kase Y, Takeda A. Goshuyuto, a traditional Japa-nese medicine for migraine, inhibits platelet aggre-gation in guinea-pig whole blood. J Pharmacol Sci.2008;108:89-94.
144. Pakala R, Waksman R. Currently availablemethods for platelet function analysis: Advantagesand disadvantages. Cardiovasc Revasc Med. 2011;12:312-322.
145. Johnson GJ, Sharda AV, Rao GH, Ereth MH,Laxson DD, Owen WG. Measurement of shear-activated platelet aggregate formation in non-anticoagulated blood: Utility in detection ofclopidogrel-aspirin-induced platelet dysfunction.Clin Appl Thromb Hemost. 2012;18:140-149.
146. Markus HS, McCollum C, Imray C, Goulder MA,Gilbert J, King A. The von Willebrand inhibitorARC1779 reduces cerebral embolization aftercarotid endarterectomy: A randomized trial.Stroke. 2011;42:2149-2153.
147. Konstantopoulos K, Kamat SG, Schafer AI, et al.Shear-induced platelet aggregation is inhibited byin vivo infusion of an anti-glycoprotein IIb/IIIaantibody fragment, c7E3 Fab, in patients under-going coronary angioplasty. Circulation. 1995;91:1427-1431.
18
148. Gurbel PA, Bliden KP, Butler K, et al. Randomizeddouble-blind assessment of the ONSET andOFFSET of the antiplatelet effects of ticagrelorversus clopidogrel in patients with stable coronaryartery disease: The ONSET/OFFSET study. Circu-lation. 2009;120:2577-2585.
149. Cloud GC, Markus HS. Diagnosis and manage-ment of vertebral artery stenosis. QJM. 2003;96:27-54.
150. Gawel M, Burkitt M, Rose FC. The platelet releasereaction during migraine attacks. Headache.1979;19:323-327.
151. Takeshima T, Shimomura T, Takahashi K. Plateletactivation in muscle contraction headache andmigraine. Cephalalgia. 1987;7:239-243.
152. Tietjen GE, Al Qasmi MM, Athanas K, Dafer RM,Khuder SA. Increased von Willebrand factor inmigraine. Neurology. 2001;57:334-336.
153. Zeller JA, Frahm K, Baron R, Stingele R, DeuschlG. Platelet-leukocyte interaction and platelet acti-vation in migraine: A link to ischemic stroke?J Neurol Neurosurg Psychiatry. 2004;75:984-987.
154. Sarchielli P, Alberti A, Coppola F, et al. Platelet-activating factor (PAF) in internal jugular venousblood of migraine without aura patients assessedduring migraine attacks. Cephalalgia. 2004;24:623-630.
155. Kitano A, Shimomura T, Takeshima T, TakahashiK. Increased 11-dehydrothromboxane B2 inmigraine: Platelet hyperfunction in patients withmigraine during headache-free period. Headache.1994;34:515-518.
156. Shimomura T, Murakami F, Kotani K, Ikawa S,Kono S. Platelet nitric oxide metabolites inmigraine. Cephalalgia. 1999;19:218-222.
157. Gallai V, Floridi A, Mazzotta G, et al. L-arginine/nitric oxide pathway activation in platelets ofmigraine patients with and without aura. ActaNeurol Scand. 1996;94:151-160.
158. Buttinelli C, Lazzaro MP, Lenzi GL, Paolucci S,Prencipe M. Correlation between migraine andcirculating platelet aggregates. Cephalalgia. 1985;5(Suppl. 2):87-88.
159. Deshmukh SV, Meyer JS, Mouche RJ. Platelet dys-function in migraine: Effect of self-medication withaspirin. Thromb Haemost. 1976;36:319-324.
160. Carrieri P, Sorge F, Orefice G, De Feo S. Plateletfunction in childhood migraine. Cephalalgia. 1985;5(Suppl. 2):99-101.
161. Bensenor IM, Cook NR, Lee IM, Chown MJ,Hennekens CH, Buring JE. Low-dose aspirinfor migraine prophylaxis in women. Cephalalgia.2001;21:175-183.
162. Buring JE, Peto R, Hennekens CH. Low-doseaspirin for migraine prophylaxis. JAMA. 1990;264:1711-1713.
163. Diener HC, Hartung E, Chrubasik J, et al. A com-parative study of oral acetylsalicyclic acid andmetoprolol for the prophylactic treatment ofmigraine. A randomized, controlled, double-blind,parallel group phase III study. Cephalalgia. 2001;21:120-128.
164. Masel BE, Chesson AL, Peters BH, Levin HS,Alperin JB. Platelet antagonists in migraine pro-phylaxis. A clinical trial using aspirin and dipy-ridamole. Headache. 1980;20:13-18.
165. Allais G, D’Andrea G, Airola G, De Lorenzo C,Mana O, Benedetto C. Picotamide in migraineaura prevention: A pilot study. Neurol Sci. 2004;25(Suppl. 3):S267-S269.
166. Tomita H, Hatakeyama K, Soda W, Kobayashi T.Efficacy of ticlopidine for preventing migraineafter transcatheter closure of atrial septal defectwith Amplatzer septal occluder: A case report. JCardiol. 2007;49:357-360.
167. Bousser MG, Conard J, Lecrubier C, Bousser J.[Migraine or transient ischemic attacks in a patientwith essential thrombocythaemia. Treatment withticlopidine (author’s transl)]. Ann Med Interne(Paris). 1980;131:87-90.
168. Hsu DA, Stafstrom CE, Rowley HA, Kiff JE, DulliDA. Hemiplegic migraine: Hyperperfusion andabortive therapy with intravenous verapamil. BrainDev. 2008;30:86-90.
169. Friberg L, Olesen J, Iversen HK, Sperling B.Migraine pain associated with middle cerebralartery dilatation: Reversal by sumatriptan. Lancet.1991;338:13-17.
170. Elkind AH, Friedman AP, Grossman J. Cutaneousblood flow in vascular headaches of the migrainetype. Neurology. 1964;14:24-30.
171. Raieli V, Monastero R, Santangelo G, Eliseo GL,Eliseo M, Camarda R. Red ear syndrome andmigraine: Report of eight cases. Headache. 2002;42:147-151.
172. Raieli V, Compagno A, Brighina F, et al.Prevalence of red ear syndrome in juvenileprimary headaches. Cephalalgia. 2011;31:597-602.
Headache 19
173. O’Brien MD. Cerebral blood changes in migraine.Headache. 1971;10:139-143.
174. Sakai F, Meyer JS. Regional cerebral hemodynam-ics during migraine and cluster headaches mea-sured by the 133Xe inhalation method. Headache.1978;18:122-132.
175. Meyer JS, Zetusky W, Jonsdottir M, Mortel K.Cephalic hyperemia during migraine headaches. Aprospective study. Headache. 1986;26:388-397.
176. Andersen AR, Friberg L, Olsen TS, Olesen J.Delayed hyperemia following hypoperfusion inclassic migraine. Single photon emission computedtomographic demonstration. Arch Neurol. 1988;45:154-159.
177. Sanchez DR, Bakker D, Wu O, et al. Perfusionweighted imaging during migraine: Spontaneousvisual aura and headache. Cephalalgia. 1999;19:701-707.
178. Kato Y, Araki N, Matsuda H, Ito Y, Suzuki C.Arterial spin-labeled MRI study of migraineattacks treated with rizatriptan. J Headache Pain.2010;11:255-258.
179. Pollock JM, Deibler AR, Burdette JH, et al.Migraine associated cerebral hyperperfusion witharterial spin-labeled MR imaging. AJNR Am JNeuroradiol. 2008;29:1494-1497.
180. Weiller C, May A, Limmroth V, et al. Brain stemactivation in spontaneous human migraine attacks.Nat Med. 1995;1:658-660.
181. Afridi SK, Giffin NJ, Kaube H, et al. A positronemission tomographic study in spontaneousmigraine. Arch Neurol. 2005;62:1270-1275.
182. Woods RP, Iacoboni M, Mazziotta JC. Brief report:Bilateral spreading cerebral hypoperfusion duringspontaneous migraine headache. N Engl J Med.1994;331:1689-1692.
183. Denuelle M, Fabre N, Payoux P, Chollet F, GeraudG. Posterior cerebral hypoperfusion in migrainewithout aura. Cephalalgia. 2008;28:856-862.
184. Olesen J, Friberg L, Olsen TS, et al. Ischaemia-induced (symptomatic) migraine attacks may bemore frequent than migraine-induced ischaemicinsults. Brain. 1993;116:187-202.
185. Solomon S, Lipton RB, Harris PY. Arterial stenosisin migraine: Spasm or arteriopathy? Headache.1990;30:52-61.
186. Micieli G, Bosone D, Tassorelli C, Zappoli F, Cas-tellano AE, Nappi G. Internal carotid occlusionassociated with migraine syndrome:A case study ofa 22-year-old female. Funct Neurol. 1996;11:45-51.
187. Masuzawa T, Shinoda S, Furuse M, Nakahara N,Abe F, Sato F. Cerebral angiographic changes onserial examination of a patient with migraine. Neu-roradiology. 1983;24:277-281.
188. Cole AJ, Aube M. Migraine with vasospasm anddelayed intracerebral hemorrhage. Arch Neurol.1990;47:53-56.
189. Iu PP, Lam HS. Migrainous spasm simulatingcarotid dissection: A pitfall in MR arteriographicfindings. AJNR Am J Neuroradiol. 2001;22:1550-1552.
190. Boasso LE, Fischer AQ. Cerebral vasospasm inchildhood migraine during the intermigrainousperiod. J Neuroimaging. 2004;14:158-161.
191. Lovrencic-Huzjan A, Demarin V, Rundek T,Vukovic V. Role of vertebral artery hypo-plasia in migraine. Cephalalgia. 1998;18:684-686.
192. Chuang YM, Hwang YC, Lin CP, Liu CY. Towarda further elucidation: Role of vertebral arteryhypoplasia in migraine with aura. Eur Neurol.2008;59:148-151.
193. Monteiro JM, Rosas MJ, Correia AP, Vaz AR.Migraine and intracranial vascular malformations.Headache. 1993;33:563-565.
194. Waltimo O, Hokkanen E, Pirskanen R. Intracranialarteriovenous malformations and headache. Head-ache. 1975;15:133-135.
195. Ramadan NM, Tietjen GE, Levine SR, Welch KM.Scintillating scotomata associated with internalcarotid artery dissection: Report of three cases.Neurology. 1991;41:1084-1087.
196. Silverman IE, Wityk RJ. Transient migraine-likesymptoms with internal carotid artery dissection.Clin Neurol Neurosurg. 1998;100:116-120.
197. Buttinelli C, Spalloni A, Fieschi C, Rasura M.Migraine and arterial dissection in a young woman.Neurol Sci. 2001;22:275-278.
198. Duyff RF, Snijders CJ, Vanneste JA. Spontaneousbilateral internal carotid artery dissection andmigraine: A potential diagnostic delay. Headache.1997;37:109-112.
199. d’Anglejan CJ, Ribeiro V, Mas JL, Bousser MG,Laplane D. Dissection of the extracranial internalcarotid artery. 62 cases. Presse Med. 1990;19:661-667.
200. Rist PM, Diener HC, Kurth T, Schurks M.Migraine, migraine aura, and cervical artery dissec-tion: A systematic review and meta-analysis. Ceph-alalgia. 2011;31:886-896.
20
201. Rubinstein SM, Peerdeman SM, van Tulder MW,Riphagen I, Haldeman S. A systematic reviewof the risk factors for cervical artery dissection.Stroke. 2005;36:1575-1580.
202. Rosenblum WI, El Sabban F, Allen AD, NelsonGH, Bhatnagar AS, Choi SC. Effects of estradiolon platelet aggregation in cerebral microvessels ofmice. Stroke. 1985;16:980-984.
203. Sasaki T, Ohno Y, Otsuka K, Suzawa T, Suzuki H,Saruta T. Oestrogen attenuates the increases inblood pressure and platelet aggregation in ovariec-tomized and salt-loaded Dahl salt-sensitive rats. JHypertens. 2000;18:911-917.
204. Huch KM, Elam MB, Chesney CM. Oral contra-ceptive steroid induced platelet coagulant hyperac-tivity: Dissociation of in vivo and in vitro effects.Thromb Res. 1987;48:41-50.
205. Rosenblum WI, El Sabban F, Nelson GH. One dayof estradiol treatment enhances platelet aggrega-tion at the site of microvascular injury withoutaltering aggregation ex vivo. Life Sci. 1988;42:123-128.
206. Naesh O, Haedersdal C, Hindberg I, Trap-Jensen J.Platelet activation in mental stress. Clin Physiol.1993;13:299-307.
207. Wallen NH, Held C, Rehnqvist N, Hjemdahl P.Effects of mental and physical stress on plateletfunction in patients with stable angina pectoris andhealthy controls. Eur Heart J. 1997;18:807-815.
208. Kawahara J, Sano H, Fukuzaki H, Saito K,Hirouchi H. Acute effects of exposure to cold onblood pressure, platelet function and sympatheticnervous activity in humans. Am J Hypertens.1989;2:724-726.
209. Hutton RA, Mikhailidis D, Dormandy KM, Gins-burg J. Platelet aggregation studies during transienthypoglycaemia: A potential method for evaluatingplatelet function. J Clin Pathol. 1979;32:434-438.
210. Dechavanne M. Influence of diet and life habits onplatelet functions. Rev Prat. 1989;39:2223-2227.
211. Nara Y, Kihara M, Nabika T, Mano M, Horie R,Yamori Y. Dietary effect on platelet aggregation inmen with and without a family history of essentialhypertension. Hypertension. 1984;6:339-343.
212. Morrell CN, Sun H, Ikeda M, et al. Glutamatemediates platelet activation through the AMPAreceptor. J Exp Med. 2008;205:575-584.
213. Grosser K, Oelkers R, Hummel T, et al. Olfac-tory and trigeminal event-related potentials inmigraine. Cephalalgia. 2000;20:621-631.
Headache 21




















