
Gut Infections: Etiopathogenetic and Clinical Remarks
73
Gut Infections: Etiopathogenetic and Clinical Remarks Daniele Dionisio HIV-Related Inflammatory Conditions Other than Opportunistic Infections HIV-Related Enteropathy In approximately 30% of human immunodeficiency virus (HIV)-infected diarrheic patients, no oppor- tunistic infections can be detected [1]. These cases are often labeled as HIV enteropathy or HIV colitis and may be associated with a series of functional and histopathological gut alterations that include villous atrophy, abnormal lipid accumulation, enterocyte cytoplasmic vacuolation, crypt epithelial cell apopto- sis, lamina propria inflammation, impaired gastric acid, and intrinsic factor secretion, malabsorption, and dysfunctions in intestinal immunoglobulin pro- duction [1,2]. Moreover, in 30%-70% of all patients, HIV was found within lymphocytes and macro phages in intestinal lymphoid tissue [1,3-5]. In addition, HIV was isolated from enterocytes and colonic cells, as well as from enterochromaffin cells in small-bowel mucosa and in colonic ulcers or in areas of colonic inflammation [3,6]. Together with the enhanced expression of func- tional HIV-l co receptors in normal intestinal mucosa [7], these findings indicate that the gastrointestinal (GI) tract is a major reservoir of HIV and a site of intensive HIV replication [8, 9]. Overall, these find- ings lead to the hypothesis that most cases of HIV enteropathy are due to HIV, although there is uncer- tainty whether HIV produces mucosal damage direct- ly or by induction of immunological disturbances. Based on established knowledge of a direct relation- ship between the intestinal immune system and intes- tinal structure and function, it is conceivable that most so-called HIV enteropathy cases may result from HIV -induced regional immunological impairment [1]. It is now well established that in humans infected with HIV, a very early, marked, and more pronounced decrease of CD4+ T cells occurs in the gut mucosa in comparison to the peripheral blood [10, 11]. This might lead to a breakdown of the mucosal immune barrier and also to mucosal atrophy or enterocyte dys- function, according to the established role of CD4+ T cells present in the normal lamina propria in the maintenance of the mucosal architecture [12]. Indeed, atrophy with epithelial hypoproliferation, dysmatura- tion of enterocytes, and markedly decreased brush- border enzyme activity have been documented in late- phase HIV infection [11]. These findings are more pro- nounced in patients without secondary gut infections and with detectable P24 antigen in the lamina propria than in HIV-infected patients without detectable P24 [13]. Concurrently, increased numbers of activated CD8+ cells may be detected in the intestinal mucosa in late-stage HIV disease. This condition may lead to vil- lous atrophy by production of proinflammatory cytokines, probably acting through activation of mes- enchymal cells and production of matrix metallopro- teinases [14-16]. Recently, gpl20-induced activation of Bob/GPRI5, an HIV coreceptor abundantly expressed on the basolateral surface of intestinal epithelium, has been proposed as an additional cause of HIV enteropathy, as supported by the inhibition of such effects with anti-Bob neutralizing antibodies [17]. Taken together, these findings suggest that, regard- less of the presence of enteric pathogens, increased absorption ofluminal antigens with secondary inflam- matory response is expected to result from impaired barrier function of the mucosa. This may account for sometimes precocious diarrhea, malabsorption, and some, if not all, of the other disturbances and histopathological alterations in this setting, as men- tioned above. The documented effectiveness of combi- nation antiretroviral therapy on symptoms, on reduc- ing mucosal HIV RNA levels and contents of apoptot- ic cells, and on increasing mucosal CD4+ lymphocyte numbers further supports the causative role of HIV in producing intestinal dysfunction [18,19]. Idiopathic Esophageal Ulcers Chronic ulcers of unknown etiology, either single or multiple, seen on clinical and histological evaluation in the mid to distal esophagus have been found posi- tive for HIV [20]. Using in situ hybridization and immunoperoxidase staining, HIV-l RNA and P24 were demonstrated in lymphocytes and macrophages D. Dionisio (ed.), Textbook-Atlas of Intestinal Infections in AIDS © Springer-Verlag Italia, Milano 2003
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Gut Infections: Etiopathogenetic and Clinical Remarks

Gut Infections: Etiopathogenetic and Clinical Remarks Daniele Dionisio
HIV-Related Inflammatory Conditions Other than Opportunistic Infections
HIV-Related Enteropathy
In approximately 30% of human immunodeficiency virus (HIV)-infected diarrheic patients, no opportunistic infections can be detected [1]. These cases are often labeled as HIV enteropathy or HIV colitis and may be associated with a series of functional and histopathological gut alterations that include villous atrophy, abnormal lipid accumulation, enterocyte cytoplasmic vacuolation, crypt epithelial cell apoptosis, lamina propria inflammation, impaired gastric acid, and intrinsic factor secretion, malabsorption, and dysfunctions in intestinal immunoglobulin production [1,2]. Moreover, in 30%-70% of all patients, HIV was found within lymphocytes and macro phages in intestinal lymphoid tissue [1,3-5]. In addition, HIV was isolated from enterocytes and colonic cells, as well as from enterochromaffin cells in small-bowel mucosa and in colonic ulcers or in areas of colonic inflammation [3,6].
Together with the enhanced expression of functional HIV-l co receptors in normal intestinal mucosa [7], these findings indicate that the gastrointestinal (GI) tract is a major reservoir of HIV and a site of intensive HIV replication [8, 9]. Overall, these findings lead to the hypothesis that most cases of HIV enteropathy are due to HIV, although there is uncertainty whether HIV produces mucosal damage directly or by induction of immunological disturbances. Based on established knowledge of a direct relationship between the intestinal immune system and intestinal structure and function, it is conceivable that most so-called HIV enteropathy cases may result from HIV -induced regional immunological impairment [1]. It is now well established that in humans infected with HIV, a very early, marked, and more pronounced decrease of CD4+ T cells occurs in the gut mucosa in comparison to the peripheral blood [10, 11]. This might lead to a breakdown of the mucosal immune barrier and also to mucosal atrophy or enterocyte dysfunction, according to the established role of CD4+ T
cells present in the normal lamina propria in the maintenance of the mucosal architecture [12]. Indeed, atrophy with epithelial hypoproliferation, dysmaturation of enterocytes, and markedly decreased brushborder enzyme activity have been documented in latephase HIV infection [11]. These findings are more pronounced in patients without secondary gut infections and with detectable P24 antigen in the lamina propria than in HIV-infected patients without detectable P24 [13]. Concurrently, increased numbers of activated CD8+ cells may be detected in the intestinal mucosa in late-stage HIV disease. This condition may lead to villous atrophy by production of proinflammatory cytokines, probably acting through activation of mesenchymal cells and production of matrix metalloproteinases [14-16]. Recently, gpl20-induced activation of Bob/GPRI5, an HIV coreceptor abundantly expressed on the basolateral surface of intestinal epithelium, has been proposed as an additional cause of HIV enteropathy, as supported by the inhibition of such effects with anti-Bob neutralizing antibodies [17].
Taken together, these findings suggest that, regardless of the presence of enteric pathogens, increased absorption ofluminal antigens with secondary inflammatory response is expected to result from impaired barrier function of the mucosa. This may account for sometimes precocious diarrhea, malabsorption, and some, if not all, of the other disturbances and histopathological alterations in this setting, as mentioned above. The documented effectiveness of combination antiretroviral therapy on symptoms, on reducing mucosal HIV RNA levels and contents of apoptotic cells, and on increasing mucosal CD4+ lymphocyte numbers further supports the causative role of HIV in producing intestinal dysfunction [18,19].
Idiopathic Esophageal Ulcers
Chronic ulcers of unknown etiology, either single or multiple, seen on clinical and histological evaluation in the mid to distal esophagus have been found positive for HIV [20]. Using in situ hybridization and immunoperoxidase staining, HIV-l RNA and P24 were demonstrated in lymphocytes and macrophages
D. Dionisio (ed.), Textbook-Atlas of Intestinal Infections in AIDS© Springer-Verlag Italia, Milano 2003

138 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
present in the lamina propria at the ulcer bases [20]. Symptoms include odynophagia and substernal or back pain; relief with antacids is poor. Based on these findings, a causative role of HIV itself in producing esophageal ulcers was postulated, although general agreement is lacking due to the difficulty of ruling out the responsibility of coexisting pathogens [22, 23]. This is not the case in esophageal ulcers presenting with odynophagia during HIV seroconversion, which endoscopically appear as randomly located, 3-to Is-mm-wide round or oval ulcers [21]. Indeed, HIV, but not cytomegalovirus or herpes simplex virus (HSV), was found in these ulcers which resolve spontaneously within 2 weeks.
Lymphoid Hyperplasia
Nodular lymphoid hyperplasia affecting the entire gut is often associated with common variable hypogammaglobulinemia [20], but it has also been described in acquired immunodeficiency syndrome (AIDS) [S, 20] . Lymphoid hyperplasia limited to the terminal ileum was responsible for intussusception in one patient in this setting [20] (Fig. 1).
Opportunistic Infections
For many years, intestinal infections caused by opportunistic organisms have represented a major
problem in immunocompromised patients with AIDS. In western countries, a decreased incidence of parasitic intestinal infections has been registered over the last years, mainly as a result of immunological reconstitution in patients receiving highly active antiretroviral therapy (HAART) [24]. Nevertheless, even in the HAART era, diarrhea is still an occurring symptom in HIV-infected people [2S, 26] and 2.8% of IS,OOO patients hospitalized with a diarrheal illness in New York City in 1998 harbored intestinal pathogens [27]. On the contrary, in geographical areas where treatment is not available, such as in developing countries, these infections still playa major role in morbidity and mortality of AIDS patients [28, 29]. The antiparasitic effect ofHAART is indirect and not always associated with eradication, as relapsing intestinal parasitoses in patients with decreased CD4 cell counts following virological HAART failure or discontinuation of treatment are commonly reported [30,31].
Once the symptoms of chronic diarrhea and weight loss in severely immunodeficient AIDS patients have been recognized, diagnosis of single or mixed infections by Cryptosporidium, micro sporidia, Giardia, nontuberculous mycobacteria, cytomegalovirus, or other conventional agents often follows. These microorganisms, however, are not the only pathogens that may infect the intestinal tract of AIDS patients. Indeed, more and more infections are being reported from animal pathogens not previously described in humans or from unrecognized agents both in animals
Fig. 1. Nodular lymphoid hyperplasia of the terminal ileum

Table 1. AIDS-related intestinal pathogens'
Commonly found Cytomegalovirus Herpes simplex virus Epstein-Barr virus Candida spp. Mycobacterium avium-intracellulare Mycobacterium genavense Cryptosporidium Microsporidia Giardia lamblia Leishmania infantum Enteroadherent bacteria Penicillium marneffeib
Less commonly found Adenoviruses Picobirnaviruses Papillomavirus Cryptococcus neoformans Pneumocystis carinii Mycobacterium tuberculosis Mycobacterium kansasii Cyc/ospora cayetanensis Isospora belli Blastocystis hominis Entamoeba histolytica Salmonella spp. Campylobacter spp. Shigella spp. Chlamydia trachoma tis Enteroadherent spirochetes Strongyloides stercoralis Histoplasma capsulatumb
Rarely found Astroviruses Coronaviruses Rotaviruses Norwalk virus Human herpes virus 8 Toxoplasma gondii Bartonella spp. Nocardia spp.
'Mixed infections increasingly recognized in late-stage immunodeficiency (CD4 cell count below lOo/mm'). bEndemic countries.
and in humans [32-35]. They often combine with conventional pathogens, so their role may be difficult to establish. In addition, old pathogens such as toxoplasma, leishmania, or Pneumocystis may selectively cause gut involvement in patients with AIDS [20].
One or more enteric pathogens, including viruses, bacteria, protozoa, and fungi, have been demonstrated in 44%-68% of patients with AIDS who had concomitant GI symptoms [20] (Table 1). The most common pathogens are mycobacteria, cytomegalovirus (CMV), Cryptosporidium, and micro sporidia organisms [20]. The diagnosis of these infections must be
Gut Infections: Etiopathogenetic and Clinical Remarks 139
based on a combination of stool culture, examination of stool for ova and parasites, and multiple endoscopic biopsies for light microscopy and, possibly, transmission electron microscopy [32-34].
With such a combined approach, mixed rather than single infections are expected to be found in patients with high-grade immunodeficiency [35]. This is important not only to explain treatment failures but also because elimination of drug-susceptible pathogens may lead to clinical recovery or even to the disappearance of an untreatable microbial agent [32].
Viral Infections
Viral infections of the GI tract are common in patients with HIV. Although CMV is the most common viral pathogen [20], other viruses such as herpes simplex virus (HSV), adenoviruses, Epstein-Barr virus (EBV), and a variety of other species, including astroviruses, caliciviruses, picobirnaviruses, small round-structured viruses, and rotaviruses, have been implicated in HIV -related intestinal injury. Apart from CMV and HSV, there is no known specific treatment for these infections.
Infection with Herpes Simplex Virus
Infection with HSV in the HIV -infected host results from reactivation of latent virus, usually when CD4+ cells decrease below 50 mm' [20,36]. Herpes simplex virus types 1 and 2 (HSV -1, HSV -2) are both implicated in infection of the GI tract. GI infection with HSV most commonly presents as esophagitis but also may cause proctocolitis and severe anal ulceration, especially in patients with AIDS [3,20] (Figs. 2-4). Double infection, with HSV at the edge and CMV in the
Fig. 2. Herpetic esophagitis: fragile mucosa with confluent irregularly outlined ulcerations. (Courtesy of Dr. A. Macor)

140 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 3. Herpetic esophagitis: a crater-like ulceration resulting from a broken vesicle. (Courtesy of Dr. A. Macor)
Fig. 4. Herpetic perianal ulceration. (Courtesy of Dr. A. Macor)
base of anal ulcers, has been reported [37]. This would be no surprise given that HSV and CMV are the most frequently encountered pathogens in the esophagus and anorectum in the HIV setting [20,38].
Symptoms of dysphagia, odynophagia, chest pain, vomiting, nausea, fever, diarrhea, anorectal pain, and tenesmus, sometimes with sacral root symptoms such as dysuria, constipation, and leg pain, may arise in various combinations from these localizations [39, 40]. Asymptomatic infections may occur and asymptomatic perianal shedding, most often due to HSV-2, is common in patients with AIDS, even in the absence of perianal HSV lesions [41, 42]. Likewise, perirectal HSV -2 reactivation in HIV -infected men is almost always subclinical [43]. Endoscopic findings vary from vesicles to erosions and round 1- to 3-mmwide ulcers, which may coalesce to form larger ulcerations. Radiographic findings are not specific. Diagnosis can be reached by viral culture and light microscopic examination of brushings and biopsy specimens. These must be taken from the margins of ulcers because HSV is present in the squamous mucosa only [44]. Multinucleate cells with inclusions in ground-glass-appearing nuclei are characteristic features. Immunohistochemistry, in situ hybridization, and type-specific PCR-based assays may improve diagnostic sensitivity [45]. Digestive tract HSV infection may be complicated with perforation, bleeding, strictures, hiccups, superinfection on mucosal necrosis, tracheoesophageal fistula, and extraintestinal dissemination [46-50]. Ulcerative infection with HSV -2 may be resistant to acyclovir, but retains its susceptibility to other inhibitors of viral DNA polymerase, such as foscarnet and vidarabine [20,51].
Infection with Cytomegalovirus
Infection with CMV is the most common serious opportunistic infection in HIV -positive patients with a CD4 cell count below 100/mm3 and usually represents reactivation of latent virus [20]. Especially in children with AIDS, CMV intestinal manifestations carry high morbidity and mortality rates [52]. In the AIDS setting, infection with CMV can involve any part of the GI tract, although the colon is most frequently affected and esophageal disease is more common than gastroduodenal disease [20]. This condition is frequently overlooked, as the reported incidence of GI involvement varies widely (4.4%-52%) [20]. The need for endoscopy and biopsy to reach diagnosis partly explains these discrepancies [32,35]. CMV -induced vasculitis leading to thrombosis, occlusion, and ischemia has been proposed as a pathogenetic mechanism for clinical disease [53]. Symptoms of GI disease caused by CMV depend largely on the location and severity of the infection. Most patients affected by colitis complain of fever, watery or bloody diarrhea, either intermittent or

Fig. 5. Pre-pyloric CMV ulcerations in the gastric antrum (Courtesy of Dr. A. Macor)
continuous, with abdominal cramps, rebound tenderness, tenesmus, and loss of weight [54]. Symptomatic CMV esophagitis is almost always associated with odynophagia or epigastric pain. On the other hand, CMV inclusion bodies have occasionally been detected in asymptomatic patients, while in symptomatic ones symptoms may not arise from an actual infection with CMV but from a coexisting infection, commonly esophageal candidiasis [20], cryptosporidiosis [55], or gut bacterial infection [20]. In the esophagus, CMV preferentially affects the middle or distal third section and accounts for 45% of all ulcers seen during endoscopy [25]. Ulcers greater than 1 cm but less than 2 cm in size are commonly observed and they may be multiple in 58% of cases [56]. Mucosal friability, erythema, and occasionally pseudo tumoral masses have been described [20]. Co infection with Candida was found in up to 20% of patients presenting with esophagitis and conjunction with lymphoma has been reported [57, 58]. Gastric involvement may be present at endoscopic examination, with thickened and edematous mucosal folds, erosions, and ulcerations, and usually is associated with entire GI tract involvement [20] (Fig. 5). CMV duodenal localization may result in severe GI bleeding and dyspepsia, while diffuse mucosal involvement of the duodenum and jejunum may lead to malabsorption. Endoscopically, CMV colitis may present with normal-appearing mucosa, but more commonly, ulcerations varying from punctate superficial erosions to deep ulcers and granular, friable masses are seen [20] (Figs. 6-8). The endoscopic appearance can mimic inflammatory bowel disease [54] and severe cases may manifest as necrotizing colitis frequently
Gut Infections: Etiopathogenetic and Clinical Remarks 141
Fig. 6. CMV ulcerative colitis. (Courtesy of Dr. E. Torelli)
Fig. 7. CMV ulcerative colitis. (Courtesy of Dr. E. Torelli)
Fig. 8. Double CMV -Strongyloides stercoralis colitis: irregularly shaped confluent ulcerations. (Courtesy of Dr. A. Macor)
progressing to perforation [3]. Hemorrhage, sometimes massive and life-threatening, obstruction, and toxic megacolon have been reported [20,59,60]. Colitis from CMV usually is patchy and predominantly

142 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 9. CMV ulceration at the ileocecal valve. (Courtesy of Dr. A. Macor)
affects the cecum and right colon [201 (Fig. 9). Pseudomembranous colitis caused by CMV in patients with AIDS may also occur [611. Liver and biliary tree involvement by CMV, leading to hepatitis, acalculous cholecystitis, and sclerosing cholangitis, sometimes with ampullary stenosis, have been reported in one-third of patients with AIDS, and coinfections, particularly with Cryptosporidium, are frequently observed [62, 631.
Rare GI manifestations of CMV infection include isolated jejunal ulcers that may perforate, perianal ulcers, ileocecal obstruction resulting from a large inflammatory mass, and appendicitis [20,641.
To aid diagnosis, multiple biopsy specimens from the center of the ulcers should be taken. Since CMV may be present in normal-appearing mucosa, random biopsy samples from noninflamed surfaces are mandatory. Histopathological examination may reveal cell enlargement, with basophilic intranuclear inclusions on hematoxylin-eosin (H&E) stains, surrounded by a clear halo resulting in the so-called owl's eye appearance. Smaller cytoplasmic inclusions can also be found [651. CMV particles inside all these inclusions can be documented by electron microscopy (Fig. 10). Enhancement of biopsy sensitivity can be achieved by using in situ hybridization or immunohistochemical staining (Fig. 11). This approach provided better definition of some recently reported cases of CMV enterocolitis in pediatric AIDS patients presenting with minimal focal mucosal ulceration but with extensive leiomyolysis of the muscularis propria [661.
Drug therapy with intravenous (Lv.) ganciclovir for a 2- to 3-week induction period is usually highly effective in achieving clinical remission. If not, switching to Lv. foscarnet is recommended. Patients harboring CMV strains resistant to either drug may respond to a combination treatment with both drugs concurrently [671.
Fig. 10. CMV bodies within a colonic enterocyte. rEM, XIO,OOO
Fig.". CMV antigen detection. Immunofluorescence, XlOO.
(Courtesy of Dr. R. Rossetti)
Enteroviruses
Picobirnaviruses
Picobirnaviruses are small, bisegmented, doublestranded RNA viruses that have been associated with diarrhea in vertebrate animals and, more recently, in 9%-14 % of HIV -infected patients with prolonged viral shedding and chronic diarrhea [68, 691. Other

studies, however, failed to associate fecal detection of picobirnaviruses with diarrhea or to determine them as the primary pathogens [70,71]. Therefore, the role of picobirnavirus in producing diarrhea still needs to be defined.
Adenoviruses
Adenovirus intestinal infections, either of the small or large bowel, are reported in 7%-26% of HIV -positive patients with diarrhea and the isolates are almost always subgenus D serotypes [72-74]. Most patients are co infected with other enteropathogens and onehalf of adenovirus infections remain asymptomatic; consequently, the pathogenetic role of adenoviruses is difficult to assess [75]. Further difficulties arise from their detection in both inflamed and normalappearing bowel mucosa [76]. In the past, subgenus F adenoviruses (serotypes 40 and 41) were never found in HIV-positive patients. Recently, a chronic intestinal infection due to type 40 adenovirus lasting
Fig. 12. Adenovirus particles within the nucleus of a duodenal enterocyte. rEM, x5,oOO. (From [77] with permission)
Gut Infections: Etiopathogenetic and Clinical Remarks 143
13 months in a patient with AIDS was documented by an electron microscopy study of duodenal biopsy samples and by stool examination with ELISA monoclonal antibodies to adenovirus group antigen and types 40 and 41 [77] (Figs. 12-14). These findings sug-
Fig. 13. Detail of Fig. 12. Virions show an ordered crystalline array. TEM, X12,OOO
Fig. 14. Duodenal adenovirus infection: mucosal hypotrophy with a lymphocytic-plasmocytic infiltrate are visible. Enlarged nuclei are seen focally within the enterocytes (arrows). Giemsa, x40. (From [77] with permission)

144 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
gest that subgenus F adenoviruses may be important pathogens in immunocompromised patients, although they are probably underestimated.
Rotaviruses
In HIV -infected African children, rotavirus-associated diarrhea was reported as no more common or more severe than in HIV-negative children [78]. More recently, however, the low level of CD4+ cell counts, rather than the HIV-1-RNA concentration, was reported as predictive of death in HIV-positive children co infected with rotavirus [79]. Rotavirus was associated with diarrhea in 13% of HIV-infected adults with otherwise unexplained diarrhea in Germany [80]. Diarrhea was prolonged, accompanied by abdominal cramping, and did not show the seasonal variations typical of infantile rotavirus infection. Other studies in the HIV setting did not confirm a major enteropathogenetic role for these viruses, though increased viral shedding was weakly associated with immunodeficiency [69,70,81-83]. These studies also failed to support a major role for other enteric viruses such as astrovirus, Norwalk virus, and coronavirus. Additional reports, however, while failing to document any prominent role of rotavirus in HIV-related diarrhea, found astrovirus, coronavirus, as well as calicivirus and small round-structured viruses to be significantly associated with diarrhea in this setting [68, 84].
Overall, although available data support a causal role of enteroviruses in producing diarrhea in patients with HIV, their major role, mainly due to the high frequency of coinfections, is still questionable. Because of coinfections, indeed, the detection of stool viruses was reported to reduce the rate of unexplained diarrhea by an average of only 5% [84].
Other Viral Infections
Varicella-zoster Virus
Esophagitis resulting from infection with varicellazoster virus has been described in the setting of HIV [20, 22]. The virus was detected in the muscularis propria and myenteric plexuses of the colon in a patient with herpes zoster and small bowel pseudoobstruction (Ogilvie's syndrome) [85].
Papillomavirus
Anal condylomata acuminata resulting from infection with various subtypes of human papillomavirus
are usually present either on the perianal skin or in the rectal mucosa transgressing the dentate line [40]. A high recurrence rate in HIV-infected patients is expected. Normal-appearing but histologically altered mucosa in human papillomavirus infection has been documented [40] and the risk of progression to intraepithelial neoplasia was assessed as depending directly on the magnitude of depletion in cellular immunity [86, 87]. Esophageal ulcerations associated with papillomavirus in the setting of AIDS have been documented [88] and concurrent infection with human papillomavirus and EBV was found by in situ hybridization in esophageal ulcers of several patients [89]. Enhanced PCR detection of EBV and human papillomavirus from the anal mucosa in HIVseropositive homosexual men has been reported [42]. In this series, EBV was not related to alterations in cytology or to poor levels of CD4+ cell count.
HHV-8
Human herpesvirus 8 (HHV-8), a newly described gamma herpesvirus that is the agent of Kaposi's sarcoma, has been detected in rectal samples with and without inflammatory changes in HIV-infected men [90]. Furthermore, association of HHV-8 with primary lymphoma of the bowel in the setting of advanced HIV-related immunodeficiency has been described and symptoms included diarrhea and intestinal obstruction [91]. More recently, evidence suggesting a direct role of HHV -8 as an etiological agent of diarrhea has been provided [92].
BVDVirus
Involvement of bovine viral diarrhea (BVD) virus, a pestivirus of animals associated with diarrhea, immunosuppression, and synergy with other pathogens, as a concurrent agent of HIV-related diarrhea was hypothesized on the basis of the increased seroprevalence of anti-BVD virus antibodies documented in HIV -seropositive Zambian patients with chronic diarrhea [93]. The significance of BVD virus in the setting of HIV and its interactions with other opportunistic agents in humans, however, remains to be defined.
Bacterial Infections
HIV -related bacterial infections of the GI tract fall into three main categories: (1) infections resulting from overgrowth of normal gut flora; (2) infections that can affect immunocompetent hosts as well, such

as salmonellosis, shigellosis, campylobacteriosis, and infections with Clostridium difficile organisms; and (3) infections caused by opportunistic pathogens that almost exclusively affect immunocompromised individuals such as the Mycobacterium avium complex.
Small-Bowel Bacterial Overgrowth
The role played by overgrowth of resident flora in digestive symptoms of HIV-infected patients is still controversial [941. Failure of mechanisms controlling bacterial growth such as low pH, gastric emptying, small-intestine motility, and local immunity has been reported in advanced HIV -related immunodeficiency [951. Consequently, bacterial overgrowth leading to diarrhea, malabsorption, and weight loss is expected to occur in this setting. Pseudomembranous necrotizing jejunitis associated with Klebsiella pneumoniae in the duodenal fluid, Serratia marcescens cholecystitis, and protein-losing enteropathy have been described in children with AIDS and small-intestine bacterial overgrowth [96, 971. Staphylococcus aureus liver abscesses following small-bowel biopsy in an adult AIDS patient with significant Staphylococcus aureus overgrowth in his small bowel have also been reported [981. In addition, two studies applying sterile gastric and duodenal sampling to HIV-infected patients found a strong association between diminished gastric acid secretion and gastric and/or duodenal bacterial overgrowth, which was asymptomatic and of oropharyngeal type in one of these studies, thus suggesting a descending colonization route [95,991. Furthermore, the role of HIV -related autonomic denervation and impaired gut mucosa immunity in small-bowel bacterial colonization was suggested by other studies [100-102].
Enterobacteria
Enterobacteria, including Salmonella, Shigella, and Campylobacter species, represent significant pathogens in people infected with HIV, sometimes as agents of the so-called gay bowel syndrome. Salmonella and Campylobacter organisms are commonly associated with advanced immunodeficiency, while Shigella is frequently diagnosed in the early stages of HIV [1031. The presentation and course of these infections include severe febrile diarrhea, commonly with nausea, bloating, cramping, and tenesmus. Association with Reiter's syndrome (Fig. 15), toxic megacolon, or pseudomembranous colitis was reported [31. Impairment of both humoral immune response and intracellular macrophage killing sec-
Gut Infections: Etiopathogenetic and Clinical Remarks 145
Fig. 15. Balanitis circinata erosiva as part of Reiter's syndrome in a patient with severe Shigella infection
ondary to failure of T-cell function may result in persistent, possibly asymptomatic, intestinal infection or in life-threatening recurrent septicemia, sometimes with negative stool cultures [3,1031. Diagnosis is achieved by stool examination, which may additionally disclose blood, mucus, and fecal leukocytes. As enteric infections with these agents in the setting of HIV are more likely to produce invasive disease, prompt treatment just after detection of Gram-negative bacteria at stool work-up is recommended. To this aim, ciprofloxacin or the newer quinolones are considered drugs of choice because of their effectiveness against all of the considered enteric bacterial pathogens. Due to the high relapse rate, long-term antibiotic suppressive treatment following the acute episode is advisable (at least 6 months in salmonellosis) [1041. Recent findings from a nonrandomized study in the setting of salmonellosis suggested, however, that secondary prophylaxis with ciprofloxacin might be shortened, as discontinuation of ciprofloxacin 1 month after starting with concurrent HAART did not lead to bacteremic recurrence [105].

146 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Salmonellosis
In western countries, salmonellosis resulting from infection with non-typhoid Salmonella (more often S. typhimurium) is 20 times more common in persons with AIDS (about 2%) than in the general population [106]. Relapsing infection has been reported commonly in patients with low CD4 T-lymphocyte counts, in those with an initial septicemic illness, and in those not treated with ciprofloxacin [103]. Administration of cotrimoxazole as prophylaxis against Pneumocystis carinii infection was found to prevent development of salmonellosis [103]. In endemic countries, association of active schistosomiasis with Salmonella bacteremia in patients with acquired immunodeficiency syndrome should be kept in mind [107] (Fig. 16-19).
(ampylobaderiosis
In Los Angeles County, a 1% Campylobacter infection rate (c. jejuni and, of lesser extent, C. coli, and C. fetus) was reported in AIDS patients during 1983-1987 [106]. AIDS patients have a 39-fold increase in incidence of infection with Campylobacter organisms and are more prone to protracted diarrhea, persistent or recurrent Campylobacter infection, and bacteremia than the general population [106]. Acalculous cholecystitis may complicate Campylobacter bacteremia [108]. In AIDS patients, fatal bacteremia in the absence of enteric disease, and with negative stool cultures, has been described, as well as asymptomatic infections detected on routinely performed stool cultures [109, 110]. Campylobacter co infection with other intestinal pathogens was found in up to 42% of patients [m]. Prolonged diarrhea with persistent or relapsing Campylobacter in
Fig. 16. Egg of Schistosoma mansoni with a pronounced lateral spine. Formalin, x40. (Courtesy of Dr. A. Orsi)
feces despite appropriate therapy frequently reveals in vivo selection of resistant, sometimes multiresistant, isolates to quinolones, macrolides, and tetracyclines [m, 112]. This was the case of HIV-infected patients with relapsing bacteremia due to quinolone-
Fig. 17. Egg of Schistosoma mansoni inside the rectal mucosa. Grocott, X230. (Courtesy of Prof. S. Di Lollo)
..
Fig. 18. Rectum: endoluminal Schistosoma mansoni egg evidencing the lateral spine. Grocott, original X230. (Courtesy of Prof. S. Di Lollo)

Fig. 19. Chicamba lake bordering Mozambique and Zimbabwe (central Africa): an endemic area for Schistosoma infection
Fig. 20. Campylobacter organisms. Gram, Xl,OOO. (Courtesy of Dr. P. Pecile)
resistant C. fetus [113J. Because of the prevalence of antibiotic resistance, in vitro susceptibility testing should guide antimicrobial therapy [lllJ. Diagnosis of HIV -related Campylobacter infection relies on isolation procedures in stool (Fig. 20) or blood sampIes. The yield of culture from colonic tissue in HIV diarrheic patients is low (about 10%), although some cases of C. jejuni-coli infections detected by culture of ileal or colonic tissue had negative stool cultures and showed a normal-appearing mucosa at colonoscopy [114, 115J. Diagnostic problems are further complicated by the fact that endoscopic lesions mimicking Crohn's disease can be observed in immunodeficient patients with Campylobacter intestinal infection [116, 117J.
Shigellosis
Increased morbidity from Shigella infections among people with HIV has been documented [103J. Shigel-
Gut Infections: Etiopathogenetic and Clinical Remarks 147
la organisms (S. flexnerii, S. dysenteriae, S. sonnei, S. boydii) have been isolated by stool culture in 5% of diarrheic patients with AIDS in developed countries, and Shigella appears to be the most frequent cause of HIV -associated bloody diarrhea in Zimbabwe [20, 118J. Identification of S. boydii in colonic malacoplakia from an HIV-infected patient has been reported [119J. AIDS-associated shigellosis can potentially be fatal [20 J.
Clostridium difficile Infection
Colitis resulting from infection with C. difficile commonly affects individuals with various types of immunosuppression, including those with HIV, in whom C. difficile enterotoxin was found in up to 58.8% of diarrheic patients [20,27, 120J. The presentation and course of C. difficile infection in these patients are no different than in controls [121J. Either oral vancomycin or, preferably, metronidazole are successful drugs for C. difficile colitis also in HIVinfected patients. Recurrence (as relapse in 64%, reinfection in 32%, and relapse plus reinfection in 4%) occurs in up to 25% of patients after antibiotic discontinuation and requires new treatment [3, 122J.
Bacillary Angiomatosis
This infection, caused by two species of the genus Bartonella (B. henselae or B. quintana), is a vascular proliferative disease that occurs mainly in late-stage AIDS. Vascular skin lesions, fever, anemia, lung infiltrates, pleural effusions, polypoid endobronchial lesions, as well as isolated bacteremia are commonly reported [123, 124J. GI involvement includes bacillary peliosis hepatis, abdominal adenopathy, ascites, esophageal polyps, colonic localization, or intraabdominal masses associated with GI hemorrhage [123-126J. Bacillary angiomatosis is a treatable disease which usually responds to macrolides, doxicycline, or fluoroquinolones. It should be included in the differential diagnosis of AIDS-related GI manifestations such as infections or Kaposi's sarcoma lesions.
Enteroadherent Bacteria
Bacterial enteropathy, possibly due to enteroadherent Escherichia coli, was recently found in colonic biopsy specimens from almost 20% of AIDS patients with idiopathic chronic diarrhea (Figs. 21-26) and four distinct patterns of bacterial interaction with the epithelium were documented: (1) bacteria with pedestal-like

148 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 21. Bacterial enteropathy: rows of bacteria on the surface epithelium. Methylene blue, azure II, basic fuchsin, X960. (Courtesy of Prof. I.M. Orenstein)
Fig. 23. Bacterial enteropathy: rows of bacteria attached to the epithelium. Toluidine blue, x640. (Courtesy of Prof. I.M. Orenstein)
attachments, which adhere to and efface the brush border, leading to a loss of microvilli (Figs. 27, 28); (2) vertically oriented bacteria intercalated with microvilli; (3) bacteria loosely associated with the brush border; (4) prominent neutrophil infiltration and long rods invading damaged, frequently shedding entero-
Fig. 22. Bacterial enteropathy: bacteria in rows and clusters. Methylene blue, azure II, basic fuchsin, x640. (Courtesy of Prof. I.M. Orenstein)
Fig. 24. Bacterial enteropathy: bacteria on the epithelium and free in the lumen. Gram stain, x640. (Courtesy of Prof. I.M. Orenstein)
cytes [127, 128). Each pattern was associated with a cytopathic effect of the involved epithelium and the bacteria were most abundant in the right colon and were not found in the proximal small bowel. More recently, similar interactive patterns between Hep-2 cells and Escherichia coli isolates from symptomatic

Fig. 25. Bacterial enteropathy: bacterial aggregates are visible in the lumen. H&E, X640. (Courtesy of Prof. J.M. Orenstein)
Fig. 27. Bacterial enteropathy: adhering and effacing bacteria, some with pedestal-like attachment. TEM, x5,700. (Courtesy of Prof. J.M. Orenstein)
AIDS patients were reported in an in vitro study [1291. However, despite similarities to the patterns of known pathogenic strains [1301, none of these isolates hybridized with standard probes for enteropathogenic, enteroaggregative, diffusely adherent, enterotoxigenic, and enteroinvasive E. coli strains. This raised the possibility that such organisms would be atypical enteropathogenic E. coli strains.
Gut Infections: Etiopathogenetic and Clinical Remarks 149
Fig. 26. Mucosal biopsy of terminal ileum of Zambian patient with AIDS and chronic diarrhea. Numerous basophilic rods are strongly attached to surface epithelium. H&E, Xl,OOO. (From [133] with permission). (Courtesy of Prof. H.L. Du Pont)
Fig. 28. Bacterial enteropathy: adhering and effacing bacteria. TEM, x26,000. (Courtesy of Prof. J.M. Orenstein)
Although general agreement is lacking, the findings reported above suggest a causative role for potentially diarrheogenic E. coli organisms in HIVrelated chronic diarrhea [131]. Accordingly, enteropathogenic E. coli has been isolated from infants with diarrhea born to HlV-infected mothers in Zaire, and enteroadherent E. coli strains were suspected to be responsible for 60% of cases of diarrhea in patients with AIDS in Zambia [132, 1331. In addition, Hep-2 cell-adherent E. coli strains were detected more often in HIV-infected patients with diarrhea than in HlV-negative patients with diarrhea [1331.
Spirochetosis
Enteroadherent spirochetes, although seen in normal, healthy subjects, are more commonly found in

150 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 29. Intestinal spirochetosis: fuzzy coat on the epithelium surface. H&E, x640. (Courtesy of Prof. J.M. Orenstein)
Fig. 30. Intestinal spirochetosis: fuzzy coat on the epithelium surface. Methylene blue, azure II, basic fuchsin, x640. (Courtesy of Prof. J.M. Orenstein)
colorectal biopsies from homosexual HIV-positive men, in whom they correlate well with coinfection with protozoans, syphilis, or gonorrhea [134]. In this setting, intestinal spirochetosis demonstrates potential clinical significance; its incidence reached 53.7% in one study [135]. Intestinal spirochetosis appears histologically on H&E or basic fuchsin as a 3-6-J.lm basophilic fuzzy coat on the surface of the epithelium (Figs. 29,30), consisting of dense aggregates of spirochetes adherent to and oriented perpendicular to the epithelial plasma membranes [136]. However, the basophilic fringe is not specific and spirochetosis may be only focal, so that it is often inapparent or overlooked [1371 . Electron microscopy, periodic acidSchiff, Warthin Starry, Steiner silver stains, and immunostains may be needed to facilitate diagnosis of intestinal spirochetosis and differentiate it from mucus. In their ultrastructure, spirochetes show sev-
Fig. 31. Intestinal spirochetosis. rEM, x43,OOO. (Courtesy of Prof. J.M. Orenstein)
eral convolutions, cone-shaped cell terminations, and measure up to 18 /lm in length and about 0.2 /lm in width [136,138] (Fig. 31). Extension of spirochetosis into the Lieberkiihn crypts, invasion of the colonic mucosa, and a conspicuous macrophage inflammatory infiltrate in the underlying lamina propria have been described [136]. Treatment with metronidazole or mebendazole improves symptoms in most cases [138- 140].
Chlamydia trachomatis
Chlamydial proctitis is a common finding in homosexual HIV-positive men [40,141,142] (Figs. 32, 33). Depending on the serotype, lymphogranuloma or non-lymphogranuloma venereum proctitis can develop approximately 10 days after anoreceptive intercourse. In the first case, nodular-ulcerated neoplastic-like lesions, frequently confined to the first 10 cm of the anal margin, appear. They possibly lead to fistula-forming strictures and this complication may require fecal diversion or excision. In the second case, proctitis without ulceration is seen together with fever, tenesmus, and local pain. Coinfection
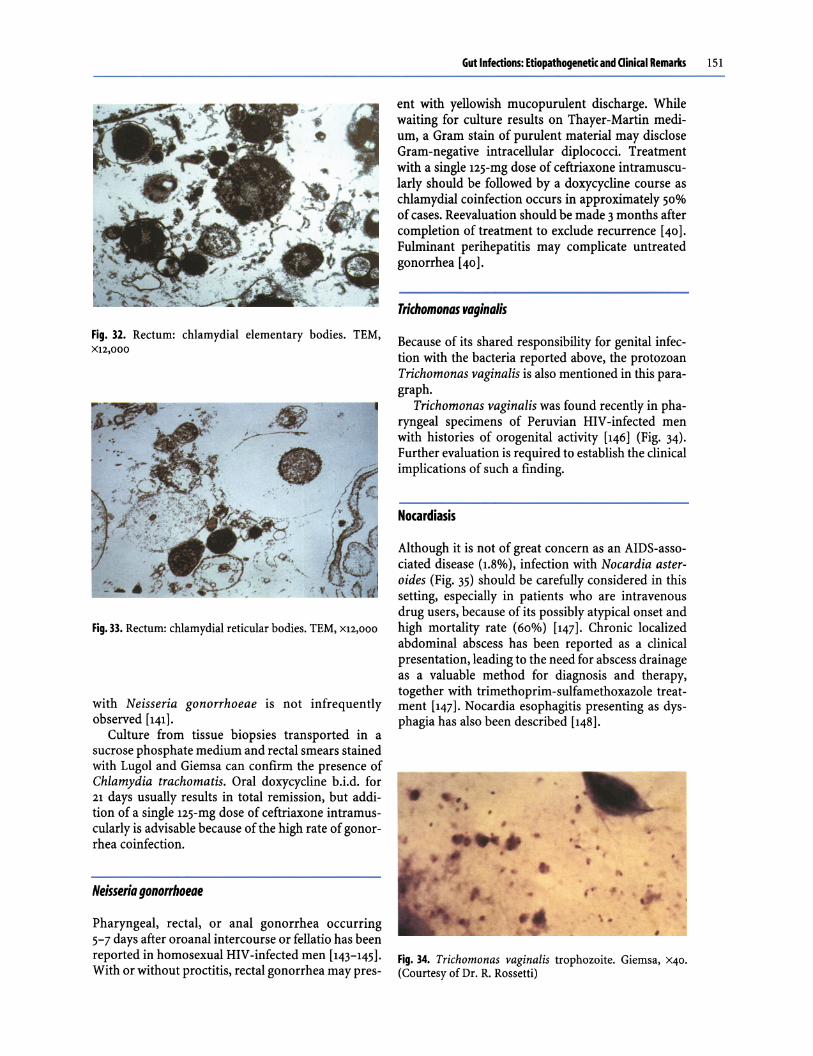
Fig. 32. Rectum: chlamydial elementary bodies. TEM, X12,OOO
Fig. 33. Rectum: chlamydial reticular bodies. TEM, X12,OOO
with Neisseria gonorrhoeae is not infrequently observed [1411.
Culture from tissue biopsies transported in a sucrose phosphate medium and rectal smears stained with Lugol and Giemsa can confirm the presence of Chlamydia trachoma tis. Oral doxycycline b.i.d. for 21 days usually results in total remission, but addition of a single 125-mg dose of ceftriaxone intramuscularly is advisable because of the high rate of gonorrhea co infection.
Neisseria gonorrhoeae
Pharyngeal, rectal, or anal gonorrhea occurring 5-7 days after oroanal intercourse or fellatio has been reported in homosexual HIV-infected men [143-1451. With or without proctitis, rectal gonorrhea may pres-
Gut Infections: Etiopathogenetic and Clinical Remarks 151
ent with yellowish mucopurulent discharge. While waiting for culture results on Thayer-Martin medium, a Gram stain of purulent material may disclose Gram-negative intracellular diplococci. Treatment with a single 125-mg dose of ceftriaxone intramuscularly should be followed by a doxycycline course as chlamydial coinfection occurs in approximately 50% of cases. Reevaluation should be made 3 months after completion of treatment to exclude recurrence [401. Fulminant perihepatitis may complicate untreated gonorrhea [401.
Trichomonas vagina/is
Because of its shared responsibility for genital infection with the bacteria reported above, the protozoan Trichomonas vaginalis is also mentioned in this paragraph.
Trichomonas vaginalis was found recently in pharyngeal specimens of Peruvian HIV-infected men with histories of orogenital activity [1461 (Fig. 34). Further evaluation is required to establish the clinical implications of such a finding.
Nocardiasis
Although it is not of great concern as an AIDS-associated disease (1.8%), infection with Nocardia asteroides (Fig. 35) should be carefully considered in this setting, especially in patients who are intravenous drug users, because of its possibly atypical onset and high mortality rate (60%) [1471. Chronic localized abdominal abscess has been reported as a clinical presentation, leading to the need for abscess drainage as a valuable method for diagnosis and therapy, together with trimethoprim-sulfamethoxazole treatment [1471. Nocardia esophagitis presenting as dysphagia has also been described [1481.
Fig. 34. Trichomonas vaginalis trophozoite. Giemsa, X40.
(Courtesy of Dr. R. Rossetti)

152 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 35. Nocardia colonies: blood agar, sabouraud agar, Lowenstein Jensen. (Courtesy of Dr. R. Rossetti)
Actinomyces
In patients with AIDS, superinfection with actinomyces (Fig. 36) has been documented in esophageal ulcers produced by other microorganisms [149,150 J.
Mycobacterial Infections
HIV-related GI mycobacterial infections include those caused by M. tuberculosis, M. avium complex (MAC), and other atypical mycobacteria.
Tuberculosis
Although tuberculosis is common in AIDS patients, with extrapulmonary tuberculosis occurring in 60%-70%, intestinal localization is unusual and only occurs in 3%-5% of patients, slightly more frequent-
Fig. 36. Actinomyces colonies. Gram, XIOO. (Courtesy of Dr. R. Rossetti)
ly than in the non-HIV population (2%) [20J. This reflects the difficulties in diagnosis, which is often delayed because of the absence of typical signs and symptoms and the poor reliability of current methods. Due to these limitations, diagnosis of GI tuberculosis is often only made after established complications, such as acute hemorrhage or perforation. Likewise, in cases of jejunal tuberculosis, a misdiagnosis of Crohn's disease is possible if specific PCR and cultures of small-bowel biopsy specimens yield falsenegative results [151J.
Esophageal and, more frequently, small intestinal and colonic tuberculosis have been described [152J. Esophageal tuberculosis may develop as a direct extension of pulmonary or mediastinal lymph node tuberculosis or as a dissemination of infection. In some cases, transmucosal invasion from swallowed mycobacteria occurs and transmural inflammation of the esophagus can result in radiographic and endoscopic findings, for example ulcers, fistulas (tracheoesophageal, esophagoesophageal, broncoesophageal), and thickened surface folds [20, 153J. Symptoms related to single esophageal or combined esophageal and pulmonary involvement may be present. They commonly include malaise, cough, weight loss, and fever.
Intestinal tuberculosis most frequently affects the small bowel, the ileocecal area, and the ascending colon, possibly with complications such as obstruction, perforation (either single or multiple), and fistulas, which may include choledochoenteric fistulas [154-156J. Tuberculosis of the appendix, sometimes presenting as an abscess, has been documented [157J. In contrast to the typically diffuse distribution of MAC infection, intestinal involvement from M. tuberculosis is usually segmental and may occur early in HIV infection with unimpaired CD4 T-cell count and function. Colonoscopic findings such as nodules, nodules with ulcerations, ulcerations alone, nodules with strictures, and polypoidal masses are commonly observed and granulomas with tuberculous characteristics are found on histopathology [158J. The clinical presentation and course may include fever, cramping abdominal pain, anemia, vomiting, chronic diarrhea, and weight loss [159J.
Remission of symptoms and recovery of HIVrelated intestinal tuberculosis is rapidly achieved with classic antituberculous drug regimens.
Infection with Mycobaderium avium Complex
Disseminated MAC infection is the most common opportunistic disease among patients with AIDS in western countries, although it is probably underdiagnosed. Only 10%-24% occurrence was reported in in

vivo studies [20], while at least 66% occurrence was documented at autopsy [160]. Infection occurs when CD4+ cell counts decline below lOo/mm', and either the respiratory or the GI tract are recognized entry portals [161-163]. M. avium enters intestinal epithelial cells through the apical membrane and then it is phagocytosed by the lamina propria macrophages [164,165]. Survival into macrophages lets it be transported to the abdominal lymph nodes through lymphatic drainage and subsequently disseminated through the bloodstream. MAC rarely is a direct cause of death, although death can result from MACrelated wasting or superinfection [165]. Duodenal co infection of MAC and visceral leishmaniasis, also in the same lesion, has been reported [166, 167]. Fever, weight loss, night sweats, malabsorption, diarrhea, abdominal pain, wasting, anemia, liver and
Gut Infections: Etiopathogenetic and Clinical Remarks 153
Fig. 37. MAC infection: abdominal polylymphadenopathy. (From [338] with permission)
spleen enlargement, intra-abdominal lymphadenopailiy (Fig. 37), and raised serum alkaline phosphatase are the most common features of infection with MAC [161]. Other manifestations include obstructive jaundice (arising from involvement of peripancreatic/portahepatis lymph nodes), intestinal obstruction secondary to lymphadenopathy, intussusception, as well as terminal ileitis resembling Crohn's disease, and fistula or chronic gastric ulcer formation [3,160,168]. All intestinal tracts, including the biliary tract, may be involved, although the small bowel is involved in the majority of cases [62, 65] (Fig. 38). Endoscopically, a coarsely granular and edematous mucosa with abnormal folds and with a widespread but patchy whiteness alternating with erythematous areas are the most common, although not always present, features [169-171] (Fig. 39). His-

154 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 38. MAC infection: diffusely enlarged small bowel
Fig. 40. MAC infection: acid-fast positive infiltration diffusely involving the duodenum lamina propria. ZiehlNeelsen, XlOO. (Courtesy of Prof. S. Di Lollo)
tological examination confirms expansion of intestinal villi due to infiltration of the lamina propria by histiocytes filled with acid-fast rod-shaped bacilli (Figs. 40-45). Although confirmation by culture of biopsy samples, blood, or other normally sterile body sites is required, the histological findings of MAC infection are so characteristic that a presumptive diagnosis can be suggested on biopsy. Because many weeks are necessary for culture results, treatment should begin just after collecting biological samples. Initially, it should consist at least of clarithromycin or azithromycin plus ethambutol; in appropriate cases, additional agents such as rifampin or rifabutin, ciprofloxacin, or amikacin in combinations of three to four agents can be added [3, 172, 173]. To produce remission of symptoms, 2-8 weeks or more are required. To avoid relapse, lifelong maintenance treatment with clarithromycin, azithromycin, or rifabutin is advisable.
Fig. 39. MAC infection: a coarsely granular duodenal mucosa. (Courtesy of Dr. A. Macor)
Fig. 41. MAC infection: duodenal villi infiltrated by acid-fast histiocytes. Ziehl-Neelsen, X300. (Courtesy of Dr. A. Macor)
Fig. 42. MAC infection: histiocytes fllled with rod-shaped bacilli in duodenal lamina propria. Semi-thin. Toluidine blue, Xl,OOO. (From [339] with permission)

Fig. 43. MAC infection. Duodenum: rod-shaped bacilli filling the histiocyte cytoplasm. rEM, X12,000. From [339] with permission)
I Fig. 45. MAC infection. Duodenum: a rod-shaped bacillus. rEM, X32,000. (From [339] with permission)
Infection with Mycobacterium kansas;;
The paucity of documented infections with M. kansasii in patients who test positive for HIV (less than 1.0%) is remarkable [1741. Infections with these organisms usually occur late in the course of HIV infection, when extreme immunodeficiency is estab-
Gut Infections: Etiopathogenetic and Clinical Remarks 155
Fig. 44. MAC infection. Duodenum: detail of Fig. 43. rEM, XlS,OOO. (From [340] with permission)
lished [1741. M. kansasii infection mainly presents as a pulmonary disease, although cases of bloodstreamdisseminated disease with isolation of the organism also (or exclusively) from nonpulmonary sources such as pleura, skin, bone marrow, kidney, liver, lymph node, bowel, and appendix are common [174-1761. The frequent isolation of this agent from stool suggests that the GI tract is a significant source of disseminated infection [1771. Intestinal involvement in AIDS patients may present with major symptoms, including high-grade fever, severe diarrhea, cramping abdominal pain, and acute bowel dilatation (Fig. 46), and symptoms of life-threatening systemic disease usually coexist. Thickening of the bowel wall can be documented at ultrasound or radiographic examination (Fig. 47). Disseminated coinfection with M. avium complex and M. kansasii in a patient with AIDS and liver abscess has been observed [1751. Due to its potential lethality, infection with M. kansasii in HIV -positive patients should be aggressively treated for at least 18 months, with 15 months of culture negativity [1781. Combination therapy should include isoniazid, rifampin, and ethambutol. Rifampin must be substituted by either rifabutin or clarithromycin in HlV -positive patients taking protease inhibitors [1781. Sulfamethoxazole and pyridoxine should be added to

1 S6 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 46. M. kansasii infection: bowel dilatation. (Courtesy of Dr. F. Leoncini)
the drug regimen if resistance to rifampin or progression of infection is observed.
Infection with Mycobacterium genavense
M. genavense is a recognized agent of disseminated infection in severely immunocompromised patients with AIDS (CD4+ cell count below so/mm') [1791. M. genavense infection probably begins in the GI tract
Fig. 47. M. kansasii infection. rAC: thickening of duodenum wall
after mouth contamination from water sources [180-182]. It was suggested that this species causes more than 10% of disseminated nontuberculous mycobacterial infections in patients with AIDS [183]. Unique to the syndrome of M. genavense infection is the tropism for the small bowel, spleen, liver, and lymph nodes, with a relative sparing of the lungs, myocardium, and kidney [184]. Owing to the lethality of untreated infection, early diagnosis is mandatory. Clinically, M. genavense infection can be suspect-

ed in the presence of high-level pyrexia, diarrhea, weight loss, abdominal pain, and mental derangement, and suspicion is strengthened if abdominal lymphadenopathy, thickening of the small-bowel wall, splenomegaly, and hepatomegaly are revealed by CT scan or ultrasound examination [185, 186]. Sclerosing cholangitis may also occur [187]. The clinical pattern resembles that of a generalized infection with M. avium-intracellulare. However, abdominal pain is more frequently seen in patients infected with M. genavense than in patients infected with MAC, and stool specimens from patients infected with M. genavense are more often smear-positive than those from patients with MAC.
M. genavense is a slow-growing mycobacterium whose isolation and identification requires acidic liquid media and molecular biological techniques, whereas MAC can be easily cultured on solid media [188]. Double infection with MAC and M. genavense has been reported [189]. Although fine nodularities with a velvety thickened appearance have been described at endoscopy on the mucosa of the proximal small bowel, the range of endoscopic findings in patients with disseminated M. genavense infection is extremely variable, from normal to deeply altered mucosa [190, 191]. Biopsy specimens from infected organs may reveal extensive infiltration with foamy histiocytes containing acid-fast bacilli and ill-formed granulomas [184,190].
Available data suggest that M. genavense is sensitive to rifamycins, newer fluoroquinolones, macrolides, clofazimine, and amikacin, whereas it is resistant to isoniazid [179, 183, 192-194].
Infection with Mycobacterium gordonae
These mycobacteria, widely distributed in the environment, are a rare cause of GI disease in patients with AIDS. Gastric and small-intestine involvement with unusually large numbers of intracellular and extracellular bacteria have been described [20].
Infection with Mycobaderium fortuitum
Isolation of M. jortuitum from abscesses and fistulas in an HIV-infected man complaining of anorectal disease has been reported [38].
Fungal Infections
Candidiasis
In patients with AIDS, Candida infection is the most frequent cause of esophagitis, being diagnosed in
Gut Infections: Etiopathogenetic and Clinical Remarks 157
Fig. 48. Candida esophagitis. (Courtesy of Dr. A. Macor)
Fig. 49. Severe Candida esophagitis: exudation-free mucosa shows erosions. (Courtesy of Dr. A. Macor)
42%-79% of cases, and it may also occur in acute HIV infection [21]. Co infection with CMV occurs frequently (21%), but in most patients symptoms of dysphagia or odynophagia vanish with antifungal treatment alone [58]. Creamy yellowish white peeling plaques with erythematous mucosa are the endoscopic findings and underlying erosions, only occasionally bleeding, are disclosed after plaque removal (Figs. 48, 49). Definite identification of C. albicans, the species most frequently isolated, can be made by culture and cytological or histological examination of brushings or biopsy samples, which can reveal the typical budding yeast cells, with hyphae and pseudohyphae (Fig. so). The pathogenesis of esophageal candidiasis was thought to begin with normal oral flora being replaced with a less complex flora, then to progress to involve the oropharynx if CD4+ cells further decrease (mean 179/mml), and finally to involve the esophagus when the CD4+ cell count decreases even further (mean 129/mml) [195].
C. albicans infection is usually responsive to azole

158 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 50. Candida: blastospores and pseudomycelia. Gram, X300
antifungal agents. Azole-resistant candidiasis is often sustained by C. glabrata, C. tropicalis, and C. krusei. Candida was found in large-bowel biopsy samples from an HIV-infected patient with watery diarrhea, cramping, and abdominal pain, and a report of fatal necrotizing candida enterocolitis in AIDS is available [196,197]. Notwithstanding, the significance of Candida as a cause of diarrhea is still unclear because it has also been found in stool or colonic tissue cultures in cases without diarrhea and without endoscopic abnormalities [198].
Histoplasmosis
Reactivation oflatent histoplasmosis with dissemination to lymphatic tissue, rather than primary infection, is quite common in highly immunodeficient patients with AIDS living in or returning from endemic areas (mainly central United States) [3, 199-201]. In these areas, disseminated disease develops in approximately 5% of patients with AIDS [20, 202]. Gut involvement, possibly affecting any segment, has been reported in up to 75% of patients with disseminated histoplasmosis [3]. Localization to the terminal ileum and colon is a frequent finding (Fig. 51), but also localizations to the mouth, esophagus, stomach, small bowel, anus, and liver have been described [3, 201-205] (Figs. 52, 53). At endoscopy, patchy erythematous mucosa, elevated plaques, ulcers, pseudo polyps or pseudo tumoral masses, and skip areas can be seen on the surface of either smallbowel or colonic mucosa [204]. In addition, multiple small, umbilicated, round submucosal nodules, with erosions, erythema, and friability of the surrounding mucosa have been described at endoscopy in the involved esophagus [206]. Advanced infection can result in often ulcerated strictures leading to obstruc-
Fig. 51. Colonic histoplasmosis. X-ray: pseudotumoral mass in the left colon. (From [341] with permission). (Courtesy of Prof. J. Wheat)
Fig. 52. Histoplasmosis: tongue ulceration. (From [341] with permission). (Courtesy of Prof. J. Wheat)
Fig. 53. Histoplasmosis: hemorrhagic and erosive gingivitis. (Courtesy of Prof. J. Wheat)

Fig. 54. Histoplasmosis. X-ray: esophageal stricture. (From [341] with permission). (Courtesy of Prof. J. Wheat)
Fig. 56. Esophageal histoplasmosis. X-ray: dilatation, parietal thickening, and an ulcerated pseudo tumoral mass are seen. (From [341] with permission). (Courtesy of Prof. J. Wheat)
Gut Infections: Etiopathogenetic and Clinical Remarks 159
Fig. 55. Histoplasmosis. X-ray: esophageal fistula. (From [341] with permission). (Courtesy of Prof. J. Wheat)
tion and, possibly, perforation and bleeding [201, 207] (Figs. 54-56). Circumferential thickening of the gut wall and local lymphadenopathy can be observed by CT scan, and apple-core pseudo tumoral lesions have been described in the affected colon [3]. Symptoms may be absent, but, depending on the location of infection, a variety of symptoms can occur, including fever, weight loss, abdominal or retrosternal pain, odynophagia, diarrhea or constipation, tenesmus, and intestinal bleeding, sometimes with abnormal liver function test values [3, 199]. Detection of histoplasma yeast-like morphologies within lamina propria macrophages in examined Giemsa-stained biopsy specimens is crucial because culture can take several weeks [20]. Recently, utilization of monoclonal antibodies in the detection methods of histoplasma antigen has added new tools for a reliable diagnostic power [200, 208]. Amphotericin B or, alternatively, itraconazole are recommended drugs for attacking, and often lifelong maintenance therapy of, disseminated histoplasmosis in patients with AIDS. More recently, liposomal amphotericin B rather than itraconazole was suggested for initial treatment of AIDSrelated disseminated histoplasmosis based on the more rapid clearance of fungemia obtained in a trial

160 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
comparing both drugs [209]. In the cases of no response to medical approach, surgical treatment can be provided to prevent the major complications of advanced intestinal histoplasmosis such as obstruction, bleeding, or perforation.
(ryptococcosis
Cryptococcus neoformans is a capsulated yeast occasionally found in intestinal biopsy specimens from patients with AIDS. Cryptococcal GI disease was detected at autopsy in 33% of cases of disseminated cryptococcosis, including patients receiving corticosteroid therapy as well as patients with AIDS or hematological malignancies [20]. The esophagus and colon were most frequently involved, while the stomach and terminal ileum were only rarely involved. Duodenal cryptococcosis as well as chronic cryptococcal rectal abscess with anal fistula as part of disseminated neurological and bony fungal disease have been described [210, 211]. Neutrophilic infiltrate, illdefined granulomas, low-grade or no inflammation at all can be observed in enteric biopsy specimens from patients with intestinal cryptococcosis [212]. H&E stain reveals cryptococci as basophilic ovalshaped yeasts which vary in size and are surrounded by a clear mucinous capsule (Fig. 57). This can be quite thin and stains with PAS and mucicarmine [65]. Standard amphotericin B or fluconazole regimens useful for meningeal localization can be used to treat intestinal cryptococcosis.
Pneumocystosis
Extrapulmonary infection with Pneumocystis carinii was identified in 1.6%-2.5% of persons with AIDS
... ~. .... , 'I •• .. •
I ,e' '6)
:. eE> .~":
• ~ ~ ~'1
e tl "
. ,$ • • efID -AI
• • ~ E> e • . '"
~ rI' E)
e ' • • • .e •
, Fig. 57. Cryptococcus neoformans. Ink test. (Courtesy of Dr. A.Orsi)
[20, 213]. Approximately half of all patients with extrapulmonary pneumocystosis had used aerosolized pentamidine, which does not prevent extrapulmonary spread [20]. This usually occurs late during the course ofHIV infection and almost always in patients with a CD4+ cell count less than 50/mm'. GI pneumocystosis develops after hematogenous or lymphatic dissemination from the lungs or after reactivation of latent gut infection that was seeded previously [214]. Swallowed organisms from the lungs could represent an alternative mechanism for gut infection [214] (Figs. 58-61). Gut involvement is increasingly frequently diagnosed antemortem at endoscopic biopsy, usually after an episode of P. carinii pneumonia but sometimes even in its absence. Intestinal pneumocystosis may involve any segment of the digestive tract and both single or multiple localizations to the esophagus, stomach, duodenum, jejunum, ileum, appendix, colon, liver, pancreas, peritoneum, and abdominal lymph nodes have been reported [214-220]. Endoscopy can reveal diffuse exudate with focal superficial ulceration or partially ulcerated plaque-like tumor masses [214, 217]. Sonographic evidence of peritoneal fluid collection or hepatosplenic lesions, suggesting lymphoma or tuberculosis, have also been reported [216]. Granular eosinophilic aggregates with a honeycombed or foamy appearance on Papanicolaou-stained biopsy specimens strongly suggest P. carinii etiology and silver stain may reveal the typical parasite cysts [216]. As far as peritoneal pneumocystosis is concerned, cytological examination of the ascitic fluid may obviate the need for organ biopsy [219]. Clinical manifestations of intestinal pneumocystosis range from asymptomatic to dysphagia, fever, weight loss, abdominal pain, increasing abdominal girth, diarrhea, or intestinal hemorrhage. Recent reports of acute intestinal obstruction and small intestine perforation as a consequence of bowel infection by P. carinii further substantiate some of the above-mentioned symptoms [221-223]. Extrapulmonary infection with P. carinii often resolves with standard antipneumocystis therapy [20].
Penicilliosis marneffei
Penicillium marneffei, a dimorphic fungus of the genus Penicillium, can infect both healthy and immunocompromised individuals residing in or traveling to areas where the organism is endemic. These include southeast Asia, southern China, and Hong Kong [224]. P. marneffei has been isolated from several species of bamboo rats in endemic areas [225]. However, although it seems likely that inhalation may be the route leading to infection in humans, the natu-

Gut Infections: Etiopathogenetic and Clinical Remarks 161
AL
Fig. 58a,b. a Young trophozoite or vegetative form of rat-derived Pneumocystis attached to the alveolar epithelium. Trophozoites are mononuclear cells that represent usually more than 95% of parasite population in infected lungs. They are characterized by an electron-dense thin cell wall that facilitates its identification in ultrathin sections. b Trophozoite of mousederived Pneumocystis showing abundant cross-sectioned thin fIlopodia (asterisk). Filopodia are cytoplasmic tubular expansions that play probably a role in the attachment of parasites to the lung epithelium. They are abundan~ in vegetative forms and much less numerous in pre cystic or cystic stages. Alveolar lumen (AL); nucleus (N). Electron mIcrographs: Bar = 0.5 11m. (Courtesy of Prof. E. Dei Cas and Prof. E.M. Aliouat)
ral reservoir of P. marneffei is yet unknown [225,226]. The majority of cases have been reported in patients with advanced HIV infection (CD4+ cell count less than 50/mm3) and penicilliosis marneffei ranks as the third most common opportunistic infection in HIVpositive patients in Thailand [225, 227]. In these patients, disseminated infection most commonly occurs with fever (99%), anemia (78%), pronounced weight loss (76%), generalized lymphadenopathy (58%), liver enlargement (51%), and papular molluscum contagiosum-like lesions of the skin (71%) [224, 225, 228] (Fig. 62). GI symptoms, secondary to Penicillium involvement from the oral cavity to the colon, are relatively common in patients with disseminated disease and include anorexia, dysphagia, abdominal pain, bloody stool, and diarrhea (23.2%-31% of HIVinfected patients) [227, 229]. Acute mesenteric lymphadenitis can be one of the unusual manifestations of P. marneffei infection, and should be considered in HIV-infected patients presenting with prolonged fever and abdominal pain [230]. Endoscopic findings consist in multiple solitary and swallow ulcers in the colon, erosions at the gastric antrum, and bleeding tumor of the main duodenal papilla [224]. Oral P. marneffei lesions present as shiny papules, erosions, or shallow ulcers covered with whitish yellow necrot-
ic slough, which may be seen on the oropharynx, tongue, palate, gingiva, and labial mucosa [226] (Figs. 63, 64). Histopathological examination and/or culture from biopsy tissue specimens, blood, and bone marrow aspirates usually provide diagnosis. Curiously, only a few reports with positive stool cultures for P. marneffei are currently available [224]. Infiltration with lymphocytes and histiocytes distended with yeasts is often disclosed at histopathological examination. Differentiation from H. capsula tum is based on P. marneffei-distinguishing features such as the evidence of a central septation, elongated sausageshaped yeast forms by Gomori-methenamine silver stain, and the lack of buds attached by a narrow neck [224]. Serological tests may provide presumptive diagnosis, but are more useful when surveillance studies on the prevalence and latency of the infection are concerned [226].
Although disseminated Penicillium marneffei is a treatable disease, it may be fatal if diagnosis and treatment are delayed; the reported mortality rate for untreated HIV-positive patients was 75% [231]. Itraconazole and ketoconazole are drugs of choice for mild to moderately severe disease, whereas i.v. amphotericin B is required for seriously involved patients [226].
162 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
a
b
d
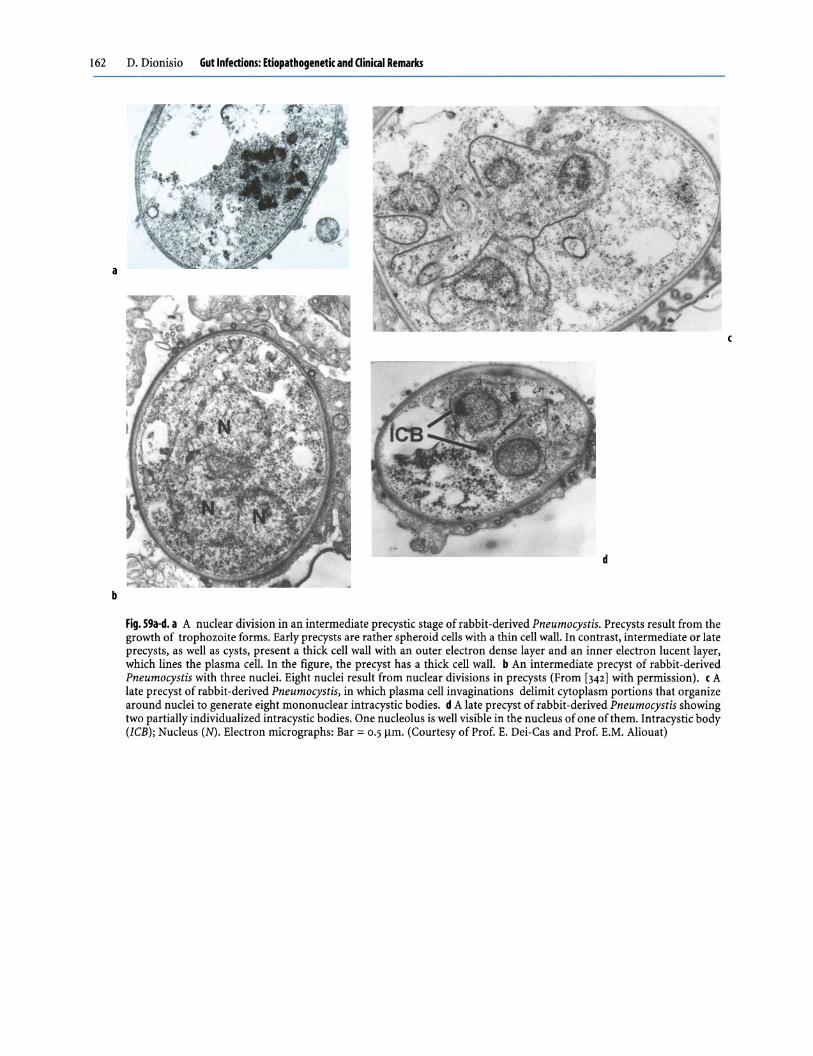
Fig. 59a-d. a A nuclear division in an intermediate precystic stage of rabbit -derived Pneumocystis. Precysts result from the growth of trophozoite forms. Early precysts are rather spheroid cells with a thin cell wall. In contrast, intermediate or late precysts, as well as cysts, present a thick cell wall with an outer electron dense layer and an inner electron lucent layer, which lines the plasma cell. In the figure, the precyst has a thick cell wall. b An intermediate precyst of rabbit-derived Pneumocystis with three nuclei. Eight nuclei result from nuclear divisions in precysts (From [342] with permission). c A late precyst of rabbit -derived Pneumocystis, in which plasma cell invaginations delimit cytoplasm portions that organize around nuclei to generate eight mononuclear intracystic bodies. d A late precyst of rabbit -derived Pneumocystis showing two partially individualized intracystic bodies. One nucleolus is well visible in the nucleus of one of them. Intracystic body (ICB); Nucleus (N). Electron micrographs: Bar = o.Sl1m. (Courtesy of Prof. E. Dei-Cas and Prof. E.M. Aliouat)

Fig.60. A mature cyst of rabbit -derived Pneumocystis where three cross-sectioned intracystic bodies are well visible. An arrowhead shows the thick cell wall. According to the most accepted hypothesis about Pneumocystis life cycle, intracystic bodies are able to leave the cyst, probably through a preformed pore, to become trophozoites. These forms are able to attach to type 1 epithelial alveolar cells evolving into early precysts. (From [342] with permission). Electron micrograph: Bar = 0.5 ~m
Fig. 62. Skin lesions presenting as generalized erythematous papules on the forearm in a 27-year-old heterosexual Thai man with disseminated penicilliosis marneffei. (From [226] with permission) (Courtesy of Dr. W. Nittayananta)
Gut Infections: Etiopathogenetic and Clinical Remarks 163
~~. I Trophozoite
&t1y precyst
ute precyst
Fig. 61. Hypothetical life cycle of Pneumocystis: parasites are represented as observed in the lung using transmission electron microscopy. Ameboid, thin-walled mononuclear vegetative trophozoites evolve into thin-walled precysts and then into thick-walled intermediate, late precystic and cystic stages. Multiple nuclear division leads to the formation of eight intracystic bodies. These forms are able to leave the cyst and to attach specifically to type-l epithelial alveolar cells. (Courtesy of Prof. E. Dei-Cas and Prof. E.M. Aliouat)
Fig. 63. Oral penicilliosis presenting as shiny papules on the soft palate in a 29-year-old heterosexual Thai woman with AIDS. (From [343] with permission). (Courtesy of Dr. W. Nittayananta)

164 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 64. Oral penicilliosis appearing as a shallow painful ulcer on the lateral border of the tongue in the same patient as in Fig. 62. (From [226] with permission) (Courtesy of Dr. W. Nittayananta)
Based on the high recurrence rate, maintenance treatment following clinical remission is recommended [226].
Mucormycosis, Aspergillosis, and Torulopsis glabrata Infections
Mucormycosis
Esophageal, gastric, and small-bowel mucormycosis, usually as part of disseminated disease, has occasionally been reported in patients infected with HIV [232-234]. Indeed, mucormycosis rarely occurs in this setting and almost exclusively in extremely immunodeficient AIDS patients, especially if transient neutropenia was registered within 4 months before clinical onset.
Aspergillosis
Aspergillus has been uncommonly reported as a cause of refractory esophagitis in patients with AIDS [235].
Torulopsis Infection
Torulopsis glabrata esophagitis with ulcerations has occasionally been observed in this setting [236].
Protozoal Infections
Protozoal infections of the GI tract are the most common cause of AIDS-related infectious diarrhea, with
cryptosporidia and micro sporidia being the most commonly identified protozoa.
Cryptosporidiosis
Originally described in a variety of animal species, cryptosporidia were first discovered in 1976 to cause enterocolitis in humans, both in immunocompetent and immunocompromised individuals [20]. Only Cryptosporidium parvum has been related to human disease, even though recent molecular studies indicate that immunocompromised individuals are susceptible to a wide range of Cryptosporidium species and genotypes, including C. meleagridis and C. felis [237-239]. Although also involved in biliary disease, hepatitis, pancreatitis, arthritis, and possibly respiratory tract infections, Cryptosporidium organisms are primarily responsible for watery diarrhea [20, 237]. A mean infective dose of 132 oocysts has been proven to be adequate in producing infection in healthy volunteers [237]. Diarrhea is self-limited in immunocompetent individuals or in those whose CD4 cell counts are higher than 200/mm\ but may be severe, sometimes cholera-like, and unremitting or relapsing in severely immunodeficient patients (CD4 cell counts below lOo/mm'). In these cases, chronic infection can lead to dehydration, malnutrition, malabsorption, wasting, and frequently death [240]. Biliary cryptosporidiosis is more frequent in patients with CD4 cell counts below so/mm' and commonly presents with right upper quadrant pain, nausea, fever, and vomiting. Diarrhea may be absent and laboratory findings include elevated serum alkaline phosphatase and bilirubin levels, with only scant elevation of liver transaminase levels. Coinfection with cytomegalovirus or microsporidia has frequently been found in biliary cryptosporidiosis [237,241].
Some cases of pneumatosis cystoides intestinalis in AIDS-associated cryptosporidiosis have been reported, suggesting a pathogenetic role for the parasite [242,243]. Despite long-term excretion of Cryptosporidium oocysts in infected people after clinical resolution [237], recent results suggest that isolation of adult patients with cryptosporidial diarrhea is not necessary to prevent roommate-to-roommate transmission [244]. Cryptosporidiosis occurs in 3%-11% of patients with AIDS in all risk groups, but is most frequent in men who have sex with males, thus related to the gay bowel syndrome [20,240]. Other AIDSdefining illnesses precede the onset of cryptosporidiosis in 85% of cases [20]. All segments of the GI tract may be involved, but the small bowel is the main target organ followed by the colon [20] (Fig. 65). Esophageal cryptosporidiosis, with parasites attached to the squamous mucosa and the lumi-

Fig. 65. Cryptosporidium duodenitis: the mucosa appears as hyperemic and fragile. (Courtesy of Dr. A. Macor)
Fig. 67. Cryptosporidium hemorrhagic gastritis: antral mucosa with erosions and hyperemia. (Courtesy of Dr. A. Macor)
nal borders of submucosal glands and ducts, has been described both in adults and in children with AIDS [20]. Gastric cryptosporidiosis, possiblyinducing partial gastric outlet obstruction, is quite common and may present with hemorrhagic erosions [245, 246] (Figs. 66-68). Intestinal co infection by C. parvum and Cyclospora species or cytomegalovirus is not rarely documented [55,247].
Diagnosis of cryptosporidiosis is made by identification of the organisms in either duodenal aspirates, stool, or tissue samples (Figs. 69-71). The organisms can be clearly observed on Giemsa or H&E-stained sections as rows or clusters of spherical structures 2-4 11m in diameter attached to the microvillous border of the epithelial cells (Fig. 72). In the small intestine, tips and lateral aspects of villi show the greatest numbers of organisms, whereas in the colon an equal involvement of crypts and surface epithelium appears. Infection begins with ingestion of the oocysts (see end of chapter, Cryptosporidium life cycle). Excystation of the oocysts within the small intestine leads to the release of sporozoites that enter epithelial
Gut Infections: Etiopathogenetic and Clinical Remarks 165
Fig. 66. Cryptosporidium hemorrhagic gastritis: antral mucosa shows erosions and hyperemia. (Courtesy of Dr. A. Macor)
Fig. 68. Cryptosporidium gastritis: hyperemia and erosions are present in the gastric angulus. (Courtesy of Dr. A. Macor)
Fig. 69. Cryptosporidium oocysts. Kinyoun, XI00. (Courtesy of Dr. A. Orsi)
gut cells and develop into trophozoites (Figs. 7J, 74). Trophozoite location is intracellular beneath the host cell membrane, although it is extracytoplasmic. The intracellular location is not obvious by light microscopy; only electron microscopy demonstrates

166 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 70. Cryptosporidium oocysts, some releasing their four sporozoites. Kinyoun, XlOO. (Courtesy of Dr. A. Orsi)
Fig. 72. Gastric biopsy sample: rows of Cryptosporidia on the epithelium surface. Giemsa, X40. (Courtesy of Dr. A. Macor)
the thin rim of epithelial cytoplasm surrounding the organisms [20] (Fig. 73).
Following asexual multiplication, trophozoites form merozoites (Figs. 73, 75), which in turn invade more host cells and initiate (certain types) sexual multiplication until development of female stages and male microgametes. Fertilization produces the oocyst, which either is excreted (environmentally resistant thick-walled oocyst) or (20%) leads to the release of sporozoites in situ to repeat the cycle (thinwalled oocyst: autoinfective life cycle) [248].
C. parvum can be regarded as a minimally invasive mucosal pathogen, since it invades the surface cells lining the intestinal tract, but does not invade deeper layers. In spite of this, infection can present with pronounced watery diarrhea and marked mucosal inflammation [2491. Postulated pathogenetic factors including a secretory state mediated by enterotoxin production in the proximal small bowel have not been confirmed [250]. Based on the evidence that infections extensively involving both the small and large
Fig. 71. Cryptosporidium oocysts. Immunofluorescence. (Courtesy of Dr. R. Rossetti)
Fig. 73. Duodenal cryptosporidiosis: an early trophozoite, a female stage, and a type II meront with four merozoites (right to left). TEM, x6,00o. (Courtesy of Prof. L. Ibba Manneschi)
bowel produce the most severe disease, it was further hypothesized that Cryptosporidium diarrhea might be caused by malabsorption from a reduced absorptive surface [3,251]. Nevertheless, no correlations between histological intensity of cryptosporidiosis and clinical

Fig. 74. Duodenal cryptosporidiosis: developing trophozoites adhering to microvillus-free areas are seen. SEM, X7,000. (Courtesy of Prof. L. Ibba Manneschi)
Fig. 75. Duodenal cryptosporidiosis: a meront with bananashaped merozoites and a stage evidencing the feeder organelle at its attachment base are shown. SEM, X7,000.
(Courtesy of Prof. L. Ibba Manneschi)
severity have been found so far [2521. In addition, in vitro results indicate that gut cryptosporidiosis may induce epithelial barrier disruption with marked changes in permeability to macromolecules [31. Finally, recent evidence suggests that epithelial apoptosis
Gut Infections: Etiopathogenetic and Clinical Remarks 167
mediated by cytotoxic host T cells might playa role in the development of colonic lesions in AIDS-related cryptosporidiosis [2531. Specific drug therapy for this parasitosis is not yet available. Paromomycin is only transiently effective on symptoms and general agreement is lacking about the therapeutic potential of azithromycin and nitazoxanide [254a, 254b, 254C, 2551. Increasing evidence suggests, however, that combination antiretroviral therapy may be curative [30, 31, 2561.
Cyclosporiasis
Cyclospora cayetanensis is a coccidian parasite initially reported in residents in or travelers from developing countries, particularly Nepal and Peru [257,2581. Indigenous Cyclospora infections from patients with no travel history have also been described in many countries [20, 2591. The reported cases also include immunocompromised patients with AIDS [20, 248, 260], in whom co infection with other pathogens is sometimes present [2471. Humans are the only proven reservoir of infection, for which contaminated water (even chlorinated) and food are the main transmission vehicles [20, 2571. Unlike Cryptosporidium, oocysts of C. cayetanensis are not infectious when passed, as they require a period of about 2 weeks for sporulation. Susceptible humans are infected by ingesting sporulated oocysts. The infectious dose, even though unknown, is presumably low [2571. Studies in developing countries such as Peru and Haiti have demonstrated the high frequency of asymptomatic excretion [20,2581. In these countries, frequent exposure may predispose to asymptomatic infection in children and absence of infection in adults [2541. After an incubation period of approximately 17 days, diarrhea occurs accompanied by cramping, abdominal pain, nausea, vomiting, fatigue, and occasionally fever [248, 2581. Diarrhea alternating with constipation has commonly been reported and biliary disease has been described [248, 2611. Diarrhea can be prolonged and appears to be more severe than that experienced with Cryptosporidium. In general, infection is self-limited in otherwise healthy adults but in the immunocompromised it may result in chronic diarrhea if untreated. In AIDS patients, infection tends to last up to 4 months [20,2481. While both Cyclospora and Cryptosporidium can be visualized in feces with acid-fast stains, Cyclospora oocysts are not consistently acid fast and are slightly larger (8-10 /lm compared with 3-5 /lm) (Fig. 76). Cyclospora can also be identified in fecal samples by autofluorescence at 330-380 nm under ultraviolet microscopy [201. Infection does not cause gross intestinal abnormalities, as is revealed during endoscopy. However, jejunal biop-

168 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
•
Fig. 77. Numerous Cyc/ospora merozoites within a schizont lying in the enterocyte cytoplasm close to the villous surface. Electron micrograph: original magnification x3,OOO. (Courtesy of Dr. B.A. Connor)
Fig. 76. Oocysts of Cyclospora cayetanensis. Modified Ziehl-Neelsen (left); phase contrast (right), XIOO.
(Courtesy of Dr. P.L. Garavelli)
sies revealed shortening and widening of the intestinal villi due to diffuse edema and mixed inflammatory cell infIltrate [258]. In addition, infIltration of intestinal epithelium by lymphocytes and reactive hyperemia with dilatation and congestion of villous capillaries have been observed [258]. The parasite most likely completes its life cycle within one host as both sexual and asexual forms within parasitophorous vacuoles have been documented in biopsies examined by light and transmission electron microscopy [258]
Fig. 78. Mature Cyclospora merozoites within a vacuole inside the enterocyte cytoplasm. There is evidence of the apical complex. Electron micrograph: original magnification X12,OOO. (Courtesy of Dr. B.A. Connor)

a
Gut Infections: Etiopathogenetic and Clinical Remarks 169
b
Fig. 79a, b. Mature Cyclospora merozoites in intestinal tissue sample. a Longitudinal section: ribosomes, micronemes and rhoptries are seen. b Cross section. Electron micrograph: original magnification X12,OOO. (Courtesy of Dr. B.A. Connor)
(Figs. 77-79) (see end of chapter, Cyclospora life cycle). Trimethoprim-sulfamethoxazole has provided rapid improvement in the clinical symptoms and cleared Cyclospora after 10 days of treatment. AIDSassociated cases require chronic suppression with daily trimethoprim-sulfamethoxazole [240]. The effectiveness of ciprofloxacin in the attack and suppressive treatment of cyclosporiasis has recently been reported [262].
Blastocystosis
Blastocystis hominis, a taxonomically established nocyst-forming protozoan inhabitant of the human bowel (Fig. 80-82) (see end of chapter, Blastocystis hominis life cycle), has increasingly been recognized as a potential cause of diarrhea, possibly relapsing and frequently associated with nausea, fever, eosinophilia, tenesmus, and abdominal pain, both in the immunocompetent and immunodeficient host [263-266] (Fig. 83). Fecal carriage of B. hominis among homosexual men and late-stage patients with
AIDS may be as high as 46% [267]. However, inclusion of this agent among the diarrheogenic agents in HIV -infected patients is still controversial because several studies failed to establish a causal relationship between the detection of B. hominis and intestinal symptoms [267,268]. Indeed, association of this protozoan with other concurrently isolated diarrhea-
BLASTOCYST.S HOMINI5
Vacuolar Amoebic Granular
o 10 l O '1---..... ' ---I' ~ m .
Fig. 80. Blastocystis hominis morphologies

170 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 82. Blastocystis hominis vacuolated form. Trichrome, XIOO. (Courtesy of Dr. P.L. Garavelli)
causing agents and spontaneous resolution of symptoms, or even asymptomatic infections, were found in most patients [267,2681. The protein and antigenic heterogeneity of B. hominis isolates and the existence of demes with different pathogenic implications could help to explain the conflicting results on the diarrheogenic potential of this microorganism [2691. Treatment should be limited to patients with persistent symptoms in the presence of a large number fecal B. hominis (at least 5/40 x field; Fig. 84) found in the absence of other pathogens and after exhaustive screening, including endoscopic evaluation and examination of multiple specimens. Metronidazole and, more recently, rifaximin have been reported as effective in relieving the symptoms and clearing the parasite in HIV -1-infected patients [270, 2711.
Fig. 81. Blastocystis hominis vacuolated forms. Giemsa, MIF, China Ink, phase contrast, respectively (left to right), XIOO. (Courtesy of Dr. P.L. Garavelli)
Fig. 83. Blastocystosis-associated hyperemia of the colonic mucosa. (Courtesy of Dr. P.L. Garavelli)
Fig. 84. Blastocystis hominis vacuolated forms. Phase contrast, X40. (Courtesy of Dr. P.L. Garavelli)

Fig. 85. Giardia cyst: the four nuclei, the parabasal bodies, and the cyst wall are evident
Fig. 86. Giardia cyst. Trichrome, XIOO. (Courtesy of Dr. A. Orsi)
Giardiasis
Although not considered as a major cause of enteritis, the flagellate protozoan Giardia lamblia is associated with diarrhea in HIV -infected patients, frequently as an agent of the gay bowel syndrome mainly in the advanced stage of disease [272,2731. Ingestion of cysts (Figs. 85, 86) in contaminated food or drinking water
Gut Infections: Etiopathogenetic and Clinical Remarks 171
Fig. 87. Giardia trophozoite: there is evidence of the two nuclei, the central axostyle, and the flagella
Fig. 88. Giardia trophozoite. XIOO. (Courtesy of Dr. A. Orsi)
and oroanal contacts in homosexual populations are common ways of transmission [2741. In the gastric acid pH, the trophozoites excyst, attach to small-bowel mucosa, and multiply by binary division (Figs. 87-90) (see end of chapter, Giardia life cycle). Cysts develop in the colon [2481. After 1-2 weeks of incubation, clinical symptoms may vary from asymptomatic to cramping abdominal gaseous discomfort or mild, sometimes severe, watery diarrhea with weight loss.

172 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 89. Giardia trophozoite within the intestinal lumen. TEM, X5,OOO. (Courtesy of Prof. L. Ibba Manneschi)
Fig. 91. Giardia cyst. Formalin, XIOO. (Courtesy of Dr. A. Orsi)
Endoscopically, the small-bowel mucosa appears as normal or as slightly erythematous [651 and pearshaped trophozoites adjacent to the epithelial surface or free in the lumen are commonly seen on histological examination. Diagnosis is made by detection of cysts and trophozoites in fresh stool (Figs. 91, 92). Enterotest or duodenal aspiration may help diagnosis as parasite excretion in feces can be sporadic. Enzyme immunoassays, direct fluorescent-antibody methods with monoclonal antibodies, and peR methods on fecal specimens may contribute to refining the diagnosis [248,2751. Biliary giardiasis which does not respond to high-dose i.v. metronidazole has been reported
Fig. 90. Giardia trophozoite attaching to the enterocyte surface. The lamellar structure of the adhesive disk and a flagellar remnant are shown. TEM, X32,OOO. (Courtesy of Prof. L. Ibba Manneschi)
.-
•
Fig. 92. Giardia trophozoite. Formalin, x40. (Courtesy of Dr. A.Orsi)
[2761. Although underestimated, coinfection is common and association with Enterocytozoon bieneusi has been documented [34, 2771. Also, asymptomatic patients should be offered treatment, and quinacrine, metronidazole, tinidazole, ornidazole, albendazole, furazolidone, as well as paromomycin are the most commonly employed drugs. Recently, the effectiveness of nitazoxanide has been suggested, also in metronidazole and albendazole-resistant giardiasis in AIDS patients [256,2781. Relapse may occur [2741.
Amebiasis
Homosexual men infected with HIV show a high prevalence of infection with Entamoeba histolytica, most frequently as asymptomatic carriers of nonpathogenic zymodemes (Entamoeba dispar) [2791. Invasive amebiasis, as amebic liver abscess (Figs. 93-96) and possibly fulminant colitis sustained by pathogenic zymodemes, may also occur in this setting and fre-

Fig. 93. rAe: amebic liver abscess. (From [343] with permission)
Gut Infections: Etiopathogenetic and Clinical Remarks 173
Fig. 94. Sonography: amebic liver abscess. (From [343] with permission)

174 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 95. X-ray: amebic liver abscess. Raised right diaphragm. (From [344] with permission)
Fig. 96. X-ray: amebic liver abscess. The same patient as Fig. 95: lateral
quently coexists with other enteric pathogens [280-282]. Notably, amebic liver abscess and colitis can be presentations for HIV infection in the Far East [282]. Through the orofecal or oroanal route, ingested cysts reach the neutral or slightly alkaline small-bowel environment where developing trophozoites excyst. In the large intestine, both mature trophozoites (Fig. 97) and one-, two-, and four-nucleated infective cysts are present [248) (Fig. 98) (see end of chapter, Entamoeba histolyca life cycle). The incubation period commonly ranges from 1-4 months, after which symptoms including fever, abdominal pain, and grossly bloody diarrhea may arise. Complications such as toxic mega-
Fig. 97. Amebic trophozoite. Trichrome, XIOO. (Courtesy of Dr. A. Orsi)
Fig. 98. Two-nucleated amebic cyst. Formalin, x40. (Courtesy of Dr. A. Orsi)
colon, strictures, and perforation are described [3]. At endoscopy, nonspecific colitis or pseudomembranecovered ulcerations surrounded by inflamed or hemorrhagic mucosa can be seen throughout the colon. Diagnosis lies on stool and wet mount examination that shows motile trophozoites containing ingested erythrocytes. DNA-based assays and enzyme immunoassays with monoclonal antibodies to distinguish pathogenic and nonpathogenic strains directly from stool samples are also available [248]. Metronidazole, tinidazole, or ornidazole are choice drugs for invasive disease, whereas paromomycin, or iodoquinol are luminally active agents, which may be sufficient for treating asymptomatic passing cyst patients. Indications for the last drugs, however, also include invasive disease, for which they are employed as prosecution therapy to eliminate endoluminal cysts, which are resistant to metronidazole.

Fig. 99. Microsporidian spore with evidence of the coiled polar tube
Microsporidiosis
Microsporidia are obligate spore-forming protozoan parasites whose life cycle begins with ingestion (or possibly inhalation) of spores by a susceptible host. Fecal-oral transmission, through sexual and waterborne routes, is well recognized [283, 2841. Of micro sporidia that infect humans, Enterocytozoon bieneusi and Encephalitozoon intestinalis (formerly Septata intestinalis) are the most common. In severely immunodeficient patients with AIDS (CD4 counts less than 100/mm'), they cause chronic watery diarrhea with weight loss and wasting as a result of small intestinal injury and malabsorption [285,2861. Association of microsporidiosis with lactase, alkaline phosphatase, and alpha-glucosidase deficiency, in the presence of reduced villus height and surface, crypt hyperplasia, and decreased xylose absorption are reported [287, 2881. Occurrence of infection with E. intestinalis accounts for about 10% of the frequency of Enterocytozoon infection, but mixed infections can occur [289-291]. No seasonal variation in the prevalence of infection has been documented [292]. The pathogenesis of intestinal disease is related to the excess death of infected enterocytes as a result of possibly different mechanisms of cell invasion. In the small bowel, depending on pH or changes in ionic concentrations, E. bieneusi spores extrude a coiled polar tube through which the sporoplasm is injected
Gut Infections: Etiopathogenetic and Clinical Remarks 175
Fig. 100. E. bieneusi spore. There is a dense nucleus, a polaroplast (arrow), an electron-lucent vacuole, and a double row of coils of the polar tube. TEM, X5,960. (From [3101 with permission)
Fig. 101. Uninucleated early proliferative plasmodial stage of E. bieneusi closely approximated to the cup-shaped host nucleus. Host mitochondria border the parasite plasmalemma. The plasmodial cytoplasm has no mitochondria and contains only ribosomes. A nuclear plaque (arrow) is visible on the nuclear envelope, indicating starting of nuclear division. TEM, X21,OOO. (Courtesy of Prof. L. Ibba Manneschi)

176 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 102. Early proliferative plasmodial stage of E. bieneusi: multiple membrane-outlined elongated nuclei and electron-lucent inclusions (arrow) are seen. TEM, X20,OOO. (Courtesy of Prof. 1. Ibba Manneschi)
Fig. 104. Developing proliferative plasmodial stage of E. bieneusi: electron-lucent inclusions and elongatedroundish nuclei are present. TEM, X21,OOO. (Courtesy of Prof. 1. Ibba Manneschi)
within surface enterocytes (Figs. 99, 100) (see end of chapter, Microsporidia life cycle). The sporoplasm undergoes merogony, giving rise to proliferative plasmodial stages (Figs. 101-104), which multiply forming sporogonial plasmodia (Figs. 105-110). Sporoblasts resulting from division of sporogonial plasmodia (Fig. 111) directly transform into environmentally resistant spores, which accumulate in the enterocyte cytoplasm, leading to cell rupture and release of spores infecting other nearby cells or spreading to the external environment [248, 293]. A different, or possibly additional mechanism of cell entry by actin-mediated phagocytosis, consistent with in vitro evidence after infection of the human
Fig. 103. Proliferative plasmodial stage of E. bieneusi: there are multiple nuclei with relatively dispersed chromatin. The parasite is limited by a unit membrane in direct contact with the host cell cytoplasm. TEM, X19,ooo. (Courtesy of Prof. 1. Ibba Manneschi)
Fig. 105. Early sporogonial plasmodium of E. bieneusi: electron-dense disks (precursors of the polar tube) can be seen in stacks, together with an electron-lucent inclusion and multiple not densely stained membrane-outlined nuclei
enterocyte-like cell line Caco-2, was recently suggested for E. intestinalis [294]. E. intestinalis differs from E. bieneusi in its electron microscopic appearance and life cycle, as it is located within a septated, honeycombed intracellular vacuole with a single-row polar tubule coil structure of spores as its most distinctive features (Fig. 112).

Fig. 106. Early sporogonial plasmodium of E. bieneusi: there are roundish more densely stained nuclei and several electron-dense discs. TEM, X20,OOO. (Courtesy of Prof. L. Ibba Manneschi)
Fig. 108. E. bieneusi sporogoniaI plasmodium: it is fIlled with electron-dense disks, some in stacks, some fused into arcs (arrow). Round dense nuclei are present. TEM, x18,ooo. (Courtesy of Prof. L. Ibba Manneschi)
Electron microscopy of E. bieneusi can reveal various developmental stages lying in direct contact with the cytoplasm of a single enterocyte. Host cell mitochondria frequently are located beneath the parasite membrane (Figs. WI, 102). The enterocyte nucleus may be indented (Fig. 101). Spores exhibit one nucleus, up to eight coils of polar tube, and a thin endospore (Figs. 113, 114). Clusters of up to 22 spores may be seen in the enterocyte apical cytoplasm (Fig. 115). Spores may be mistaken for prominent api-
Gut Infections: Etiopathogenetic and Clinical Remarks 177
Fig. 107. E. bieneusi sporogonial plasmodium: disks of varying electron density, some in stacks, are present together with dense chromatin nuclei. TEM, x18,ooo. (Courtesy of Prof. L. Ibba Manneschi)
Fig. 109. E. bieneusi spores near a sporogonial plasmodium filled with elongated electron-dense disks and several nuclei. TEM, XIO,OOO. (Courtesy of Prof. L. Ibba Manneschi)
callysosomes. Initially it was thought that diagnosis could only be made with electron microscopy (Fig. 116), but now GI microsporidiosis diagnosis is commonly made by light microscopy spore detection in stool with Weber's modified trichrome stain or optical brightening agents such as UVITEX 2B and calcofluor white M2R [2951 (Figs. 117-120). The mature spores of E. intestinalis measure 2.0Xl.2 11m and are larger than those of E. bieneusi. Species identification is easily obtained using appropriate

178 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 110. E. bieneusi late sporogonial plasmodium: fused electron-dense disks are seen in coiled, stacked, and cross sectional profiles. Electron-lucent inclusions are seen in cross section. Membrane outlined nuclei present with uniformly arranged chromatin. rEM, x9,OOO. (From [3101 with permission)
Fig. 112. Encephalitozoon intestinalis: the fibrillar matrix between spores gives the vacuole a septated honeycombed appearance. Mature spores, immature spores, and proliferative forms are present. rEM, x7,000. (Courtesy of Dr. R. Weber)
primers with PCR, either in feces or biopsy samples, as well as by in situ hybridization in biopsy specimens or by immunofluorescence antibody testing in stool samples [285,290,291,296-298]. Four types of
Fig. 111. Sporoblast of E. bieneusi: a dense nucleus, an anchoring disk with associated polaroplast membranes (arrow), and some polar tube coils are seen. rEM, Xll,170.
(From [3101 wiili permission)
Fig. 113. E. bieneusi spore. A dense nucleus, an electronlucent vacuole, and some coils of the polar tube are visible. Beyond the external sporoplasm membrane is the thick electron-lucent endospore layer and the outer electrondense exospore coat. rEM, X60,000
E. bieneusi strains have been found by PCR-restriction fragment length polymorphism (PCR-RFLP) analysis in the stool of patients with intestinal microsporidiosis, and type 1 strain was the most

Fig. 114. E. bieneusi spore with evidence of the polaroplast (arrow) and the electron-lucent vacuole. TEM, x53,OOO
Gut Infections: Etiopathogenetic and Clinical Remarks 179
Fig. 115. Cluster of microsporidian spores in the apical enterocyte cytoplasm. Semi-thin section. Toluidine blue, Xl,OOO. (Courtesy of Prof. S. Di Lollo)
Fig. 117. Stool sample: normal microsporidian spore with the typical pinkish red belt-like strip. Modified trichrome,
.. x795. (Courtesy of Dr. A. Orsi)
Fig. 116. Stool sample: E. bieneusi spore evidencing coils of the polar tube. TEM, X62,OOO. (Courtesy of Dr. T. Van Gool)
commonly found [299]. On the contrary, only one genetic lineage was found among human isolates of E. intestinaZis, suggesting a clonal distribution of this agent in HIV-infected patients [300]. These results may be useful for epidemiological investigations looking for possible animal sources. However, although E. bieneusi has been identified in nonhuman primates, pigs, dogs, and a cat, and E. intestinaZis in dogs, pigs, cows, goats, and donkeys, no correlation of these strains with the common human lineages has been reported yet [301]. The prevalence of
Fig. 118. Normal microsporidian spore showing the central belt-like strip. Modified trichrome, X795. (Courtesy of Dr. A.Orsi)
microsporidiosis in patients with AIDS and chronic diarrhea ranges between 7% and 51% [302,303], but even patients without symptoms may harbor the organisms [259]. Microsporidiosis resulting from

180 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 119. Stool sample: microsporidian spores. Uvitex 2B, Xl,OOO. (Courtesy of Dr. r. Van Gool)
Fig. 121. E. bieneusi sporogonial plasmodium (after treatment). Nuclei are deformed with disarrangement of chromatin and disruption of nuclear membrane. Electrondense disks are extremely disorganized and pale. rEM, Xll,OOO. (From [309] with permission)
enterocyte infection with E. bieneusi affects almost exclusively the small intestine, while E. intestinalis may also involve the large bowel, infecting fibroblasts, macro phages, and endothelial cells of the lamina propria, from which it disseminates to distant targets such as the urinary and respiratory tract epithelium, the gallbladder, and the nasal epithelium [289]. Multiorgan E. bieneusi microsporidiosis involving the respiratory or the biliary tract has been reported [304,305]. Microsporidiosis in AIDS patients can be quantified by counting spores in stool and in smallbowel biopsy, because a strict correlation, varying greatly from patient to patient, exists between fecal
Fig. 120. Stool sample: microsporidian spores. Uvitex 2B, Xl,OOO. (Courtesy of Dr. A. Orsi)
Fig. 122. E. bieneusi sporogonial plasmodium (after treatment). Nuclei are deformed with disarrangement of chromatin and disruption of nuclear membranes. Electrondense disks do not fuse into arcs and appear disorganized; some are disrupted and pale. rEM, x6,460. (From [310] with permission)
spore contents and duodenal biopsy spore counts [306]. Therapeutic options are still limited. Albendazole can be curative in E. intestinalis infection [307], although albendazole failure has occasionally been reported [308]. No established treatment for E. bieneusi is currently available [254]. Recently, however, limited experience has suggested that combined treatment with furazolidone and albendazole may be effective against E. bieneusi, as correlations between persistent clinical remission and persistent decrease in parasite load both in tissue and in stool, along with morphological changes in the protozoan, have been documented [309, 310] (Figs. 121-125). Moreover,

Fig. 123. Mature spores of E. bieneusi (after treatment). Osmiophilic spores are present, some containing a very enlarged vacuole. TEM, X9,800. (From [310] with permission)
Fig.12S. Microsporidian spores (stool specimen after treatment). Many spores are evident, almost all showing a pronounced red stained clot instead of the typical pinkish red belt-like strip. Modified trichrome, x795. (From [310] with permission)
treatment with fumagillin has promise as an effective oral treatment for E. bieneusi infection, although side effects still limit its suitability for clinical use [311, 312]. Increasing evidence suggests that, in countries where it is available, successful antiretroviral therapy can effectively cure AIDS-related microsporidiosis [30,31,256].
Isosporiasis
Isospora belli is a coccidian protozoan parasite which causes self-limited enteritis in immunocompetent patients but results in chronic and sometimes lifethreatening diarrhea in a number of settings of immunosuppression, including AIDS [20, 313]. Isosporiasis is a common complication of AIDS in
Gut Infections: Etiopathogenetic and Clinical Remarks 181
Fig. 124. Mature spores of E. bieneusi (after treatment). Very electron-dense spores are seen. One spore is broken (arrow). TEM, x6,380. (From [310] with permission)
Fig. 126. Isospora belli trophozoite within a parasitophorous vacuole in a duodenal enterocyte. There is evidence of the large nucleus with nucleolus. Electron-dense and electronlucent granules are seen. TEM, X28,80o. (From [345] with permission)
developing countries, ranging from 10% to 20% in Haitian, Brazilian, Indian, and African patients [20], while it is rare in industrialized countries (0.2%) [3, 313-315]. Infection occurs via the fecal-oral route. After ingestion, sporulated oocysts release sporozoites that penetrate mucosal epithelial cells of the distal duodenum and proximal jejunum where they develop into trophozoites lying within vacuoles in the enterocyte cytoplasm [316] (Figs. 126, 127) (see

182 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 127. Detail of Fig. 126: evidence of the two-layer pellicle contouring the parasite
Fig. 129. Transverse sectioning of a merozoite of Isospora belli within a parasitophorous vacuole in a duodenal enterocyte. Micronemes, electron-dense and -lucent granules, and the two-layer pellicle surrounding the parasite are seen. TEM, X22,4oo. (From [345] with permission)
end of chapter, Isospora belli life cycle). After both sexual and asexual stages of development (Figs. 128-131), the resulting immature, asporulated oocysts are passed in the feces (Figs. 132, 133). Outside
Fig. 128. Isospora belli merozoite showing the anterior conoid with micronemes (M), nucleus (N), and cytoplasmic granules presumed to contain polysaccharide (P). (From [345] with permission)
the body, infective mature oocysts (20-33 /lm x 10-9 /lm) develop within 2-3 days (Figs. 134, 135). Approximately 1 week after oocyst ingestion, symptoms arise, including profuse, nonbloody watery diarrhea, abdominal cramping, weight loss, and, rarely, low-grade fever. In patients with AIDS,' persistent diarrhea with dehydration and malabsorption is a common finding and presentation as hemorrhagic colitis can occur [3, 248, 313]. Atypical features include reactive arthritis, acalculous cholecystitis, and disseminated extraintestinal disease. Spread to mesenteric and tracheobronchial lymph nodes and the large intestine has been described [20]. The infection can be diagnosed by light microscopy oocyst identification in the stool or in duodenal secretions taken by endoscopy or string test. Collection of multiple stool samples is mandatory because few parasites are intermittently shed in feces. Light and electron microscopy examination of small intestinal biopsies demonstrates a variety of intravacuolar developmental stages, usually in epithelial cells but

Fig. 130. Duodenal enterocyte: Isospora belli macrogametocyte within a cytoplasm parasitophorous vacuole. The central nucleus with nucleolus and pale granular nucleoplasm and the numerous electron-lucent granules are visible. TEM, Xll,360. (From [345] with permission)
Fig. 132. Isospora belli immature oocyst. Kinyoun, XlOO. (Courtesy of Dr. A. Orsi)
rarely also extracellularly and in lamina propria histiocytes [316]. The infection produces mucosal atrophy and tissue and systemic low-grade eosinophilia. Stools may contain Charcot-Leyden crystals. Pathogenesis of isosporiasis, although not clearly defined
Gut Infections: Etiopathogenetic and Clinical Remarks 183
Fig. 131. Duodenal biopsy sample. Developing stages of Isospora belli (left to right); a macrogametocyte, a merozoite, and a trophozoite. TEM, x4,8oo. (From [345] with permission)
"
" . • oJ .. ;
Fig. 133. Isospora belli immature oocyst. Formalin, x40. (Courtesy of Dr. a. Orsi)
yet, has been related to mechanical cell damage secondary to parasite invasion, cell-mediated inflammation, or toxic release from mast cells [313]. Trimethoprim-sulfamethoxazole is the drug of choice for isosporiasis. Because of a 50% chance of recurrence

IB4 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
•
,
Fig. 134. Isospora belli oocyst with one sporocyst. Formalin, x40. (Courtesy of Dr. A. Orsi)
Fig. 136. Duodenal leishmaniasis: a hyperemic mucosa is seen. (Courtesy of Dr. A. Macor)
within 6-B weeks of discontinuing treatment, lifelong suppressive therapy is required in the setting of AIDS. In patients intolerant to trimethoprim-sulfamethoxazole, limited experience suggests that pyrimethamine alone or treatments with diclazuril or with a combination of albendazole and ornidazole might be effective as well [313].
Leishmaniasis
Leishmania-HIV coinfection is frequently reported, L. infantum being the most common species found [317, 31B]. Infection is most frequent in immunosuppressed patients with CD4 cell counts below 200/mm3 and in parenteral drug addicts. Leishmania intestinal involvement presents with atypical symptoms for visceral leishmaniasis and may appear as the first manifestation of infection or as a relapse in significantly immunodepressed patients, suggesting an opportunistic behavior. Esophageal, gastric, duo de-
Fig. 135. Mature Isospora belli oocyst with two sporocysts. Formalin, x40. (Courtesy of Dr. A. Orsi)
Fig. 137. Leishmania promastigote. May-Grunwald Giemsa, XIOO. (Courtesy of Dr. A. Orsi)
nal, rectal, and anal locations of leishmaniasis have been described [20, 319-324] (Fig. 136)(see end of chapter, Leishmania life cycle). Duodenal co infection with Leishmania and Mycobacterium avium-intracellulare may occur [166-167]. Symptoms of intestinalleishmaniasis include diarrhea, dysphagia and/or odynophagia, abdominal or epigastric pain, as well as gastrointestinal hemorrhage and rectal discomfort [322]. Parasite demonstration in biopsy samples, directly or by culture, is diagnostic (Figs. 137-139). Gut infection by Leishmania should be included in the differential diagnosis of digestive symptoms when a previous history of leishmaniasis or a trip to an endemic area in immunocompromised patients is recalled. Treatment with liposomal amphotericin B

a
b
Fig. 138a, b. a Leishmania amastigotes. May-Grunwald Giemsa, XlOO. (Courtesy of Dr. A. Orsi) b Duodenal gut biopsy from an HIV positive patient. Leishmania amastigotes in macrophages. Electron micrograph: X4,OOO. (Courtesy of Prof. S. Croft)
may be effective but, due to the high relapse rate, secondary prophylaxis is advisable [254].
Toxoplasmosis
Toxoplasma gondii infection of the GI tract, pancreas, and liver has rarely been reported in patients with
Gut Infections: Etiopathogenetic and Clinical Remarks 185
Fig. 139. Leishmania amastigotes. May-Grunwald Giemsa, XIOO. (Courtesy of Dr. A. Orsi)
Fig. 140. Toxoplasma gondii tachyzoite. May-Grunwald Giemsa, XIOO. (Courtesy of Dr. A. Orsi)
AIDS [325]. Overall, antemortem diagnosis of extracerebral toxoplasmosis has been achieved in less than 1% of patients in this setting, while 6.1% GI involvement has been reported at autopsy [326, 327]. Indeed, toxoplasmic GI involvement is often silent and this would explain why it is so rarely diagnosed antemortem. AIDS-related GI toxoplasmosis must be interpreted as a reactivated illness (Fig. 140), which frequently coexists with other opportunistic infections and may involve the entire GI tract or only one segment [20,325] (see end of chapter, Toxoplasma gondii life cycle). Involvement of the stomach and colon is more common than that of the esophagus and small intestine [328-330]. Hepatic, pancreatic, and peritoneal involvement have also been reported [325, 331]. Due to the inadequacy of serology and possibly negative results from stool examination [330], diagnosis of AIDS-related intestinal toxoplasmosis depends on examination of biopsy samples taken at endoscopy as

186 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 141. Filariform larva of Strongyloides stercoralis. Formalin, X40. (Courtesy of Dr. R. Rossetti)
Fig. 143. Duodenal biopsy sample. S. stercora lis newly hatched larvae within vacuole. A linear profIle surrounds all larvae. Semi-thin section; bar, 30 mil. (From [333] with permission)
well as from n.ormal-appearing areas. Indeed, endoscopic findings may show an apparently normal endoluminal surface, or reveal a broad range of alterations which include thickened gastric folds, purplish and umbilicated diffuse lesions of the stomach, ubiquitous single or multiple ulcerations, and duodenal friable mucosa with whitish exudates [325,326]. Intracellular toxoplasma trophozoites and pseudocysts can be seen at histopathology in epithelial and stromal cells, while acute and/or chronic inflammatory changes are present in the lamina propria [328]. Toxoplasma organisms demonstrated in liver biopsies usually are associated with hepatocytolysis and mild portal and lobular changes, with or without granulomatous hepatitis
Fig. 142. Parthenogenic female of Strongyloides stercoralis within the intestinal mucosa. Semi-thin section. Toluidine blue, Xl,OOO. (Courtesy of Prof. L. Ibba Manneschi)
[325]. Abdominal CT scans may reveal thickening of the gastric wall, while narrowing of gastric antrum may be disclosed by upper gastrointestinal radiography [328]. Depending on the location and severity of digestive tract involvement, clinical presentation may include fever, abdominal pain, vomiting, anorexia, and watery diarrhea, possibly with occult blood in feces, and moderately increased transaminase levels. If diagnosed early, intestinal toxoplasmosis can be favorably treated with the same drug regimens used for cerebral location [325,328].
Strongyloidiasis
Strongyloides stercoralis is a worldwide parasitic nematode which is endemic in many developing countries but also in some parts of Europe, the southeastern United States, and Puerto Rico [332]. Infection occurs when free-living third-stage (filariform) larvae penetrate the skin, pass through the circulation to the lungs, enter the airways, and are then swallowed (Fig. 141). In the small intestinal mucosa, third-stage larvae develop into parthenogenic females, which deposit eggs that then release first-stage larvae [332, 333] (Figs. 142-145). These are passed to the environment and can be seen during stool examination (Figs. 146, 147) (see end of chapter, Strongyloides stercoraUs life cycle). The spectrum of GI features includes abdominal pain, anorexia, nausea, vomiting, and diarrhea. The clinical pattern relates to the thickening and congestion of mucosal lining of the small and large bowel, and to the frequent mucosal ulceration. Steatorrhea, malabsorption, protein-losing enteropathy, and paralytic ileus are commonly seen

Fig. 144. Duodenal biopsy sample. Release into the gut lumen of two larvae of S. stercoralis lying within a broken vacuole. Thin membrane (t); thick membrane (T). TEM; bar, 3 m,.!. (From [333] with permission)
Fig. 146. Rhabditoid larva of S. stercora/is. Formalin, x40. (Courtesy of Dr. A. Orsi)
Fig. 147. Rhabditoid larva of S. stercora/is: detail of the anterior end. Formalin, XlOO. (Courtesy of Dr. R. Rossetti)
Gut Infections: Etiopathogenetic and Clinical Remarks 187
T
Fig. 145. Duodenal biopsy sample. S. stercoralis newly hatched larvae within vacuole. Thin membrane (t); thick membrane (n fuzzy coat (F). TEM; bar, 2 mil. (From [333] with permission)
in GI strongyloidiasis. Radiographic findings include duodenal edema with irregular mucosal folds, ulcerations, and strictures. Eosinophilia is a common finding as is elevation of levels of nonspecific and specific IgE. Autoinfection also occurs, whereas rhabditiform larvae change into filariform larvae while they are within the gut lumen and then penetrate the intestinal wall or perianal region. If the host's immune response (particularly T cell function) is suppressed, this cycle may accelerate, leading to disseminated strongyloidiasis with lung involvement (hyperinfection syndrome). CorticQsteroid therapy appears to be the common denominator in these cases [201. Despite the prevalence of parasitosis in areas where HIV infection is epidemic, Strongyloides hyperinfection is rarely reported in patients with immunosuppression secondary to HIV. Indeed, this syndrome mainly occurs in immunocompromised patients also having little or no ability to mount a complete eosinophilic response. Consequently, despite the association of skin lesions, pulmonary infiltrates, abdominal pain, and diarrhea with eosinophilia strongly suggests the possibility of strongyloidiasis, the eosinophil count may not be elevated [332,3341. As an important feature of the hyperinfection syndrome, gut flora may invade host tissues through damaged intestinal

188 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Fig. 148. Duodenal biopsy sample. Unidentified parasite morphology. rEM, X16,ooo. (From [337] with permission)
Fig. 150. Detail of Fig. 148. Cluster of ten electron-dense irregular inclusions (A); non-membrane-outlined nucleus (B)
epithelium or through penetration of infective larvae from the gut lumen. The resulting recurrent bacteremia, frequently due to Escherichia coli and Klebsiella species, may be a direct cause of death. Diagnosis of strongyloidiasis depends on the detection of parasites in stool and in histological samples from affected tissues, although the parasites may not be found in stool despite a high intestinal load. Prompt treatment, alternatively with thiabendazole, albendazole, or ivermectin, can be effective also in extremely immunodeficient patients [335,336].
Unidentified Parasite Morphologies
The submicroscopic morphology of an unknown parasite lying within a duodenal enterocyte of a patient with AIDS has recently been described [337]. The parasite seemed to be in contact with the host
Fig. 149. Detail of Fig. 148. Large, contoured circular organelle containing a cerebroid mass (A); mitochondriallike structure (B)
Fig. 151. Poorly defined intravacuolar parasite morphology within the cytoplasm of a duodenal enterocyte. rEM, XlO,OOO
cell cytoplasm and was oval shaped measuring 2.8X2.3 ~m. It had a single outer membrane surrounding a central hyperchromic nucleus that was not outlined by membrane, profiles of endoplasmic reticulum, free ribosomes, polysaccharide-like granules, a mitochondrial-like structure, a large, circular double-contoured organelle with a cerebroid content, a smaller circular structure, and a cluster of ten irregular electron-dense inclusions (Figs. 148-150). A further poorly defined intravacuolar morphology displaying tubular-like structures was present within an adjacent enterocyte (Figs. 151, 152).
This microorganism did not conform to either classified or emergent parasites and it did not appear to be an immature form of any known parasite. Nevertheless, it resembled a protozoan and its inclusion in the coccidian subclass was assumed on the basis of the similarity with some stages of conventional coccidian protozoa.

Fig. 152. Detail of Fig. 151. Tubular-like structures (A)
References
1. Veazey RS, Lackner AA (1998) The gastrointestinal tract and the pathogenesis of AIDS. AIDS 12 [SuppljA:S35-S42
2. Lake-Bakaar G, Elsakr M, Hagag N, et al (1996) Changes in parietal cell structure and function in HIV disease. Dig Dis Sci 41:1398-1408
3. Lew EA, Poles MA, Dieterich DT (1997) Diarrheal diseases associated with HIV infection. Gastroenterol Clin North Am 26:259-290
4. Brodie SJ (2000) Nonlymphoid reservoirs of HIV replication in children with chronic-progressive disease. L Leukoc Bioi 68:351-359
5. Lewin-Smith M, Wahl SM, Orenstein JM (1999) Human immunodeficiency virus-rich multinucleated giant cells in the colon: a case report with transmission electron microscopy, immunohistochemistry, and in situ hybridization. Mod PathoI12:75-81
6. Lu SS (1997) Pathophysiology ofHIV-associated diarrhea. Gastroenterol Clin North Am 26:175-189
7. Anton PA, Elliott J, Poles MA, et al (2000) Enhanced levels of functional HIV-1 co-receptors on human mucosal T cells demonstrated using intestinal biopsy tissue. AIDS 14:1761-1765
8. Kotler DP, Reka S, Borcich A, Cronin WJ (1991) Detection, localization, and quantitation of HIV -associated antigens in intestinal biopsies from patients with HIV. Am J PathoI139:823-830
9. Schmidt W, Fackler OT, Schafer M, et al (1998) Similar proviral load but increased HIV-1 P24 in the intestinal mucosa compared to the peripheral blood in HIVinfected patients. Ann N Y Acad Sci 859:276-279
10. Clayton F, Snow G, Reka S, Kotler DP (1997) Selective depletion of rectal lamina propria rather than lymphoid aggregate CD4 lymphocytesin HIV infection. Clin Exp ImmunoI107:288-292
11. Zeitz M, Ullrich R, Schneider T, et al (1998) HIV/SIV enteropathy. Ann N Y Acad Sci 859: 139-148
12. Reka S, Kotler DP (1998) Correlation of intestinal structure and function in HIV infection. Gastrointest Endosc Clin North Am 8:841-856
Gut Infections: Etiopathogenetic and Clinical Remarks 189
13. Ullrich R, Heise W, Bergs C, et al (1992) Effects of zidovudine treatment on the small intestinal mucosa in patients infected with HIV. Gastroenterology 102:1483-1492
14. Stockmann M, Schmitz H, Fromm M, et al (1998) The mechanism of diarrhea in HIV is based on an impaired epithelial barrier function that could be induced by a specific cytokine pattern. Ann N Y Acad Sci 859:267-270
15. Olsson J, Poles M, Spetz AL, et al (2000) Human immunodeficiency virus type 1 infection is associated with significant mucosal inflammation characterized by increased expression of CCR5, CXCR4, and betachemokines. J Infect Dis 182:1625-1635
16. Pender SL, Tickle SP, Docherty AJ, et al (1997) A major role for matrix metalloproteinases in T cell injury in the gut. J ImmunoI158:I582-1590
17. Clayton F, Kotler DP, Kuwada SK, et al (2001) Gp120-induced Bob/GPR15 activation: a possible cause of human immunodeficiency virus enteropathy. Am J PathoI159:1933-1939
18. Kotler DP (1999) Characterization of intestinal disease associated with human immunodeficiency virus infection and response to antiretroviral therapy. J Infect Dis 179 [SUPpI3j:S454-S456
19. Talal AH, Monard S,Vesanen M, et al (2001) Virologic and immunologic effect of antiretroviral therapy on HIV-1 in gut-associated lymphoid tissue. J Acquir Immune Defic Syndr 26:1-7
20. Rotterdam H, Tsang P (1994) Gastrointestinal disease in the immunocompromised patient. Hum Pathol 25:1123-1140
21. Noyer CM, Simon D (1997) Oral and esophageal disorders. Gastroenterol Clin North Am 26:241-257
22. Smith PD, Eisner MS, Manischewitz JF, et al (1993) Esophageal disease in AIDS is associated with pathologic processes rather than mucosal human immunodeficiency virus type 1. J Infect Dis 167:547-552
23. Wilcox CM, Zaki SR, Coffield LM, et al (1995) Evaluation of idiopathic esophageal ulceration for human immunodeficiency virus. Mod Pathol 8:568-572
24. Monkemuller KE, Call SA, Lazenby AJ, Wilcox CM (2000) Declining prevalence of opportunistic gastrointestinal disease in the era of combination antiretroviral therapy. Am J Gastroenterol 95:457-462
25. Knox T A, Spiegelman D, Skinner SC, Gorbach S (2000) Diarrhea and abnormalities of gastrointestinal function in a cohort of men and women with HIV infection. Am J GastroenteroI95:3482-3489
26. Wanke CA, Silva M, Knox TA, et al (2000) Weight loss and wasting remain common complications in individuals infected with human immunodeficiency virus in the era of highly active antiretroviral therapy. Clin Infect Dis 31:803-805
27. Anastasi JK, Capili B (2000) HIV and diarrhea in the era of HAART: 1998 New York State hospitalizations. Am J Infect Control 28:262-266
28. Mwachari C, Batchelor BI, Paul J, et al (1998) Chronic diarrhoea among HIV -infected adult patients in Nairobi, Kenya. J Infect 37:48-53
29. Katabira ET (1999) Epidemiology and management of diarrheal disease in HIV-infected patients. Int J Infect Dis 3:164-167

190 D. Dionisio Gut Infections: Etiopathogeneticand Clinical Remarks
30. Maggi P, Larocca AM, Quarto M, et al (2000) Effect of antiretroviral therapy on cryptosporidiosis and microsporidiosis in patients infected with human immunodeficiency virus type 1. Eur J Clin Microbiol Infect Dis 19:213-217
31. Miao YM, Awad-EI-Kariem FM, Franzen C, et al (2000) Eradication of cryptosporidia and micro sporidia following successful antiretroviral therapy. J Acquir Immune Defic Syndr 25:124-129
32. Blanshard C, Francis N, Gazzard BG (1996) Investigation of chronic diarrhoea in acquired immunodeficiency syndrome. A prospective study of 155 patients. Gut 39:824-832
33. Orenstein JM, Dieterich DT (2001) The histopathology of 103 consecutive colonoscopy biopsies from 82 symptomatic patients with acquired immunodeficiency syndrome: original and look-back diagnoses. Arch Pathol Lab Med 125:1042-1046
34. Dionisio D, di Lollo S, Ibba Manneschi L, et al (1997) Morphological injury of the intestinal mucosa and infection in patients with AIDS. Ital J Gastroenterol Hepatol 29:25-39
35. Weber R, Ledergerber B, Zbinden R, et al (1999) Enteric infections and diarrhea in human immunodeficiency virus-infected persons: prospective community-based cohort study. Swiss HIV Cohort Study. Arch Intern Med 159:1473-1480
36. Corey L, Spear PG (1986) Infections with herpes simplex viruses (2). N Engl J Med 314:749-757
37. Fraile G, Rodriguez-Garcia JL, Espana A, et al (1991) Anogenital ulcer caused by cytomegalovirus and herpes simplex virus in AIDS. Rev Clin Esp 188:325-326
38. Goldberg GS, Orkin BA, Smith LE (1994) Microbiology of human immunodeficiency virus anorectal disease. Dis Colon Rectum 37:439-443
39. Genereau T, Lortholary 0, Bouchaud 0, et al (1996) Herpes simplex esophagitis in patients with AIDS: report of 34 cases. Clin Infect Dis 22:926-931
40. Pare AA, Gottesman L (1997) Anorectal diseases. Gastroenterol Clin North Am 26:367-376
41. Pannuti CS, Cristina M, Finck DS, et al (1997) Asymptomatic perianal shedding of herpes simplex virus in patients with acquired immunodeficiency syndrome. Arch Dermato113p80-183
42. Lowhagen GB, Bergbrant 1M, Bergstrom T, et al (1999) PCR detection of Epstein-Barr virus, herpes simplex virus and human papillomavirus from the anal mucosa in HIV -seropositive and HIV -seronegative homosexual men. Int J STD AIDS 10:615-618
43. Schacker T, Zeh J, Hu HL, et al (1998) Frequency of symptomatic and asymptomatic herpes simplex virus type 2 reactivations among human immunodeficiency virus-infected men. J Infect Dis 178:1616-1622
44. McBane RD, Gross JB Jr. (1991) Herpes esophagitis: clinical syndrome, endoscopic appearance, and diagnosis in 23 patients. Gastrointest Endosc 37:600-603
45. Do Nascimento MC, Sumita LM, de Souza VA, Pannuti CS (1998) Detection and direct typing of herpes simplex virus in perianal ulcers of patients with AIDS by PCR. J Clin Microbiol 36:848-849
46. Wilcox CM (1999) Esophageal strictures complicating ulcerative esophagitis in patients with AIDS. Am J Gastroenterol 94:339-343
47. Rattner HM, Cooper DJ, Zaman MB (1985) Severe bleeding from herpes esophagitis. Am J Gastroenterol 80:523-525
48. Cronstedt JL, Bouchama A, Hainau B, et al (1992) Spontaneous esophageal perforation in herpes simplex esophagitis. Am J GastroenteroI87:124-127
49. Cirillo NW, Lyon DT, Schuller AM (1993)Tracheoesophageal fistula complicating herpes esophagitis in AIDS. Am J Gastroenterol 88:587-589
50. Cain JS, Amend W (1993) Herpetic esophagitis causing intractable hiccups. Ann Intern Med 119:249
51. Stellbrink HJ, Albrecht H, Loning T, Greten H (1991) Herpes simplex virus type 2 ulcers resistant to acyclovir in an AIDS patient - successful treatment with foscarnet. Klin W ochenschr 69:274-278
52. Kahn E (1997) Gastrointestinal manifestations in pediatric AIDS. Pediatr Pathol Lab Med 17:171-208
53. Gallant J, Moore RD, Richman DD, et al (1992) Incidence and natural history of cytomegalovirus disease in patients with advanced human immunodeficiency virus disease treated with zidovudine. J Infect Dis 166:1223-1227
54. Wilcox CM, Chalasani N, Lazenby A, et al (1998) Cytomegalovirus colitis in acquired immunodeficiency syndrome: a clinical and endoscopic study. Gastrointest Endosc 48:39-43
55. Viriyavejakul P, Rojanasunan P, Viriyavejakul A, et al (1999) Cytomegalovirus and Cryptosporidium infections in AIDS: a necropsy study. Southeast Asian J Trop Med Public Health 30:257-258
56. Wilcox CM, Straub RF, Schwartz DA (1994) Prospective endoscopic characterization of cytomegalovirus esophagitis in AIDS. Gastrointest Endosc 40:481-484
57. Laine L, Bonacini M, Sattler F, et al (1992) Cytomegalovirus and Candida esophagitis in patients with AIDS. J AIDS 5:605-609
58. Dieterich DT, Wilcox CM (1996) Diagnosis and treatment of esophageal diseases associated with HIV infection. Am J Gastroenterol 91:2265-2269
59. Chalasani N, Wilcox CM (1998) Etiology and outcome of lower gastrointestinal bleeding in patients with AIDS. Am J GastroenteroI93:175-178
60. Lai IR, Chen KM, Shun CT, Chen MY (1996) Cytomegalovirus enteritis causing massive bleeding in a patient with AIDS. Hepatogastroenterology 43:987-991
61. Olofinlade 0, Chiang C (2001) Cytomegalovirus infection as a cause of pseudomembrane colitis: a report of four cases. J Clin GastroenteroI32:82-84
62. Goldin RD, Hunt J (1993) Biliary tract pathology in patients with AIDS. J Clin PathoI46:691-693
63. French AL, Beaudet LM, Benator DA, et al (1995) Cholecystectomy in patients with AIDS: clinicopathologic correlations in 107 cases. Clin Infect Dis 21:852-858
64. Nico MM, Cymbalista NC, Hurtado YC, Borges LH (2000) Perianal cytomegalovirus ulcer in an HIVinfected patient: case report and review of literature. J DermatoI27:99-105
65. Clayton F, Clayton CH (1997) Gastrointestinal pathology in HIV-infected patients. Gastroenterol Clin North Am 26:191-239
66. Smith VV, Williams AJ, Novelli V, Malone M (2000)

Extensive enteric leiomyolysis due to cytomegalovirus enterocolitis in vertically acquired human immunodeficiency virus infection in infants. Pediatr Dev Pathol 3:591-596
67. Dieterich DT, Poles MA, Lew E, et al (1993) Concurrent use of ganciclovir and foscarnet to treat cytomegalovirus infection in AIDS patients. J Infect Dis 167:1184-1188
68. Grohmann GS, Glass RI, Pereira HG, et al (1993) Enteric viruses and diarrhea in HIV-infected patients. N Eng! J Med 329:14-20
69. Giordano MO, Martinez LC, Rinaldi D, et al (1999) Diarrhea and enteric emerging viruses in HIV -infected patients. AIDS Res Hum Retroviruses 15=1427-1432
70. Gonzalez GG, Pujol FH, Liprandi F, et al (1998) Prevalence of enteric viruses in human immunodeficiency virus seropositive patients in Venezuela. J Med Virol 55:288-292
71. Rosen BI, Fang ZY, Glass RI, Monroe SS (2000) Cloning of human picobirnavirus genomic segments and development of an RT-PCR detection assay. Virology 277:316-329
72. Durepaire N, Ranger-Rogez S, Gandji JA, et al (1995) Enteric prevalence of adenovirus in human immunodeficiency virus seropositive patients. J Med Virol 45:56-60
73. Yi ES, Powell HC (1994) Adenovirus infection of the duodenum in an AIDS patient: an ultrastructural study. Ultrastruct PathoI18:549-551
74. Maddox A, Francis N, Moss J, et al (1992) Adenovirus infection of the large bowel in HIV -positive patients. J Clin Pathol 45:684-688
75. Khoo SH, Bailey AS, de Jong JC, Mandai BK (1995) Adenovirus infections in human immuno-deficiency virus-positive patients: clinical features and molecular epidemiology. J Infect Dis 172:629-637
76. Janoff EN, Orenstein JM, Manischewitz JF, et al (1991) Adenovirus colitis in the acquired immunodeficiency syndrome. Gastroenterology 100:976-979
77. Dionisio D, Arista S, Vizzi E, et al (1997) Chronic intestinal infection due to subgenus F-type 40 adenovirus in a patient with AIDS. Scand J Infect Dis 29:305-307
78. Oshitani H, Kasolo FC, Mpabalwani M, et a1 (1994) Association of rotavirus and human immunodeficiency virus infection in children hospitalized with acute diarrhea, Lusaka, Zambia. J Infect Dis 169:897-900
79. Jere C, Cunliffe NA, Hoffman IF, et al (2001) Plasma HIV burden in Malawian children co-infected with rotavirus. AIDS 15:1439-1442
80. Albrecht H, Stellbrink HJ, Fenske S, et al (1993) Rotavirus antigen detection in patients with HIV infection and diarrhea. Scand J Gastroenterol 28:307-310
81. Thea DM, Glass R, Grohmann GS, et al (1993) Prevalence of enteric viruses among hospital patients with AIDS in Kinshasa, Zaire. Trans R Soc Trop Med Hyg 87:263-266
82. Liste MB, Natera I, Suarez JA, et al (2000) Enteric virus infections and diarrhea in healthy and human immunodeficiency virus-infected children. J Clin MicrobioI38:2873-2877
83. Cegielski JP, Msengi AE, Miller SE (1994) Enteric viruses associated with HIV infection in Tanzanian
Gut Infections: Etiopathogenetic and Clinical Remarks 191
children with chronic diarrhea. Pediatr AIDS HIV Infect 5:296-299
84. Schmidt W, Schneider T, Heise W, et al (1996) Stool viruses, coinfections, and diarrhea in HIV -infected patients. Berlin Diarrhea/Wasting Syndrome Study Group. J Acquir Immune Defic Syndr Hum Retrovirol 13:33-38
85. Pui JC, Furth EE, Minda J, Montone KT (2001) Demonstration of varicella-zoster virus infection in the muscularis propria and myenteric plexi of the colon in an HIV-positive patient with herpes zoster and small-bowel pseudo-obstruction (Ogilvie's syndrome). Am J GastroenteroI96:1627-1630
86. Metcalf AM, Dean T (1995) Risk of dysplasia in anal condyloma. Surgery 118:724-726
87. Citchlow CW, Surawicz CM, Holmes KK, et al (1995) Prospective study of high-grade anal squamous intraepithelial neoplasia in a cohort of homosexual men: influence of HIV infection, immunosuppression and human papillomavirus infection. AIDS 9:1255-1262
88. Schechter M, Pannain VLN, de Oliveira A V (1991) Papovavirus-associated esophageal ulceration in a patient with AIDS. AIDS 5:238-239
89. Kitchen VS, Helbert M, Francis ND, et al (1990) Epstein-Barr virus associated oesophageal ulcers in AIDS. Gut 31:1223-1225
90. Thomas JA, Brookes LA, McGown I, et al (1996) HHV8 DNA in normal gastrointestinal mucosa from HIV seropositive people. Lancet 347:1337-1339
91. DePond W, Said JW, Tasaka T, et al (1997) Kaposi's Sarcoma-associated Herpesvirus and human Herpesvirus 8 (KSHVIHHV8)-associated lymphoma of the bowel. Am J Surg PathoI2I:719-724
92. Wang QJ, Jenkins FJ, Jacobson LP, et al (2001) Primary human herpesvirus 8 infection generates a broadly specific CD8 (+) T-cell response to viral lytic cycle proteins. Blood 97:2366-2373
93. Giangaspero M, Vacirca G, Morgan D, et al (1993) Anti-bovine viral diarrhoea virus antibodies in adult Zambian patients infected with the human immunodeficiency virus. Int J STD AIDS 4:300-302
94. Wilcox CM, Waites KB, Smith PD (1999) No relationship between gastric pH, small bowel bacterial colonisation, and diarrhoea in HIV-l infected patients. Gut 44:101-105
95. Chave JP, Thorens J, Frohlich F, et al (1994) Gastric and duodenal bacterial colonization in HIV-infected patients without gastrointestinal symptoms. Am J Gastroenterol 89:2168-2171
96. McLoughlin LC, Nord KS, Joshi VV, et al (1987) Severe gastrointestinal involvement in children with the acquired immunodeficiency syndrome. J Pediatr Gastroenterol Nutr 6:517-524
97. Jain A, Reif S, O'Neil K, et al (1992) Small intestinal bacterial overgrowth and protein-losing enteropathy in an infant with AIDS. J Pediatr Gastroenterol Nutr 15:452-454
98. Gunnarsson G, Friedman LS, Wanke C (1994) Liver abscesses due to Staphylococcus aureus in a patient with AIDS who underwent small bowel biopsy: case report and review. Clin Infect Dis 18:802-804
99. Beiitsos PC, Greenson JK, Yardley JH, et al (1992)

192 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Association of gastric hypoacidity with opportunistic 116. Green ES, Parker NE, Gellert AR, Beck ER (1984) enteric infections in patients with AIDS. J Infect Dis Campylobacter infection mimicking Crohn's disease 166:277-284 in an immunodeficient patient. BMJ 289:159-160
100. Batman PA, Miller ARO, Sedgwick PM, et al (1991) 117· Bernard E, Roger PM, Carles D, et al (1989) Diarrhea Autonomic denervation in jejunal mucosa of homo- and Campylobacter infections in patients infected sexual men infected with HIV. AIDS 5:1247-1252 with the human immunodeficiency virus. J Infect Dis
101. Budhraja M, Levendoglu H, Kocka F, et al (1987) Duo- 159:143-144 denal mucosal T cell subpopulation and bacterial cul- 118. Gwavava C, Chihota VN, Gangaidzo IT, Gumbo T tures in acquired immune deficiency syndrome. Am J (2001) Dysentery in patients infected with human Gastroenterol 82:427-431 immunodeficiency virus in Zimbabwe: an emerging
102. Ellakany S, Whiteside TL, Schade RR, Van Thiel DH role for Schistosoma mansoni and Escherichia coli (1987) Analysis of intestinal lymphocyte subpopula- 0157? Ann Trop Med ParasitoI95:509-13 tions in patients with acquired immunodeficiency 119· Raguin G, Nemeth J, WassefM, et al (1999) Identifica-syndrome (AIDS) and AIDS-related complex. Am J tion of Shigella boydii in colonic malacoplakia by uni-Clin PathoI87:356-364 versal bacterial16S ribosomal DNA-based amplifica-
103· Nelson MR, Shanson DC, Hawkins DA, Gazzard BG tion in a human immunodeficiency virus-infected (1992) Salmonella, Campylobacter and Shigella in patient. Clin Infect Dis 28:142-143 HIV -seropositive patients. AIDS 6:1495-1498 120. Wongwanich S, Ramsiri S, Kusum M, Warachit P
104· Kovacs JA, Masur H (2000) Prophylaxis against (2000) Clostridium difficile infections in HIV -positive opportunistic infections in patients with human patients. Southeast Asian J Trop Med Public Health immunodeficiency virus infection. N Engl J Med 31:537-539 342:1416-1429 121. Lu SS, Schwartz JM, Simon DM, Brandt LJ (1994)
105· Hung CC, Hsieh SM, Hsiao CF, et al (2001) Risk of Clostridium difficile-associated diarrhea in patients recurrent non-typhoid Salmonella bacteraemia after with HIV positivity and AIDS: a prospective con-early discontinuation of ciprofloxacin as secondary trolled study. Am J GastroenteroI89:1226-1229 prophylaxis in AIDS patients in the era of highly active 122. Alonso R, Gros S, Pelaez T, et al (2001) Molecular antiretroviral therapy. AIDS 15:645-655 analysis of relapse vs re-infection in HIV-positive
106. Sorvillo FJ, Lieb LE, Waterman SH (1991) Incidence of patients suffering from recurrent Clostridium difficile campylobacteriosis among patients with AIDS in Los associated diarrhoea. J Hosp Infect 48:86-92 Angeles county. J Acquir Immune Defic Syndr 123· Chang AD, Drachenberg CI, James SP (1996) Bacillary 4:598-602 angiomatosis associated with extensive esophageal
107· Lambertucci JR, Rayes AA, Gerspacher-Lara R (1998) polyposis: a new mucocutaneous manifestation of Salmonella-So mansoni association in patients with acquired immunodeficiency disease (AIDS). Am J acquired immunodeficiency syndrome. Rev Inst Med Gastroenterol 91:2220-2223 Trop Sao Paulo 40:233-235 124· Koehler JE, Cederberg L (1995) Intra-abdominal mass
108. Wheeler AP, Gregg CR (1986) Campylobacter bac- associated with gastrointestinal hemorrhage: a new teremia, cholecystitis, and the acquired immunodefi- manifestation of bacillary angiomatosis. Gastroen-ciency syndrome. Ann Intern Med 105:804 terology 109:2011-2014
109· Manfredi R, Nanetti A, Ferri M, Chiodo F (1999) Fatal 125· Moore EH, Russell LA, Klein JS, et al (1995) Bacillary Campylobacter jejuni bacteraemia in patients with angiomatosis in patients with AIDS: multiorgan imag-AIDS. J Med MicrobioI48:601-603 ing findings. Radiology 197:67-72
110. Lortholary 0, Guillevin L (1989) Campylobacteriose 126. Huh YB, Rose S, Schoen RE, et al (1996) Colonic bacil-asymptomatique au cours de l'infection par Ie VIH. lary angiomatosis. Ann Intern Med 124:735-737 Ann Med Interne (Paris) 140:742-743 127· Kotler DP, Giang TT, Thiim M, et al (1995) Chronic
111. Molina J, Cas in I, Hausfater P, et al (1995) Campy- bacterial enteropathy in patients with AIDS. J Infect lobacter infections in HIV-infected patients: clinical Dis 171:552-558 and bacteriological features. AIDS 9:881-885 128. Orenstein JM, Kotler DP (1995) Diarrheogenic bacter-
112. Tee W, Mijch A, Wright E, Yung A (1995) Emergence ial enteritis in acquired immune deficiency syndrome: of multidrug resistance in Campylobacter jejuni iso- a light and electron microscopy study of 52 cases. Hum lates from three patients infected with human immun- PathoI26:481-492 odeficiency virus. Clin Infect Dis 21:634-638 129. Polotsky Y, Nataro JP, Kotler D, et al (1997) HEp-2 cell
113· Meier PA, Dooley DP, Jorgensen JH, et al (1998) Devel- adherence patterns, serotyping, and DNA analysis of opment of quinolone-resistant Campylobacter fetus Escherichia coli isolates from eight patients with AIDS bacteremia in human immunodeficiency virus-infect- and chronic diarrhea. J Clin MicrobioI35:1952-1958 ed patients. J Infect Dis 177:951-954 130. Rii JR, Guccion JG, Gilbert CL (1996) Enteroadherent
114· Beaugerie L, Salauze B, Bure A, et al (1996) Results of eaeA-positive Escherichia coli associated with chronic culture from colonoscopically obtained specimens for AIDS-related diarrhea. Ann Intern Med 125:523 bacteria and fungi in HIV-infected patients with diar- 131. Sehultsz C, Snijders F, Dankert J (1996) No evidence rhea. Gastrointest Endose 44:663-666 for a role of enteroadherent Escherichia coli in diar-
115· Perlman DM, Ampel NM, Schifman RB, et al (1988) rhea in human immunodeficiency virus-infected Persistent Campylobacter jejuni infections in patients patients. J Infect Dis 174:246 infected with human immunodeficiency virus (HIV). 132. Pavia AT, Long EG, Ryder RW, et al (1992) Diarrhea Ann Intern Med 108:540-546 among African children born to human immunodefi-

ciency virus I-infected mothers: clinical, microbiologic and epidemiologic features. Pediatr Infect Dis 11:996-1003
133. Mathewson JJ, Jiang ZD, Zumla A, et al (1995) HEp-2 cell-adherent Escherichia coli in patients with human immunodeficiency virus-associated diarrhea. J Infect Dis 171:1636-1639
134. Law CL, Grierson JM, Stevens SM (1994) Rectal spirochaetosis in homosexual men: the association with sexual practices, HIV infection and enteric flora. Genitourin Med 70:6-29
135. Trivett-Moore NL, Gilbert GL, Law CL, et al (1998) Isolation of Serpulina pilosicoli from rectal biopsy specimens showing evidence of intestinal spirochetosis. J Clin MicrobioI36:261-265
136. Guccion JG, Benator DA, Zeller J, et al (1995) Intestinal spirochetosis and acquired immunodeficiency syndrome: ultrastructural studies of two cases. Ultrastruct PathoI19:15-22
137. Wu ML, Cortina G (2001) Special studies help diagnose intestinal spirochetosis in HIV -positive patients. Am J Clin Pathol115:613-617
138. Kasbohrer A, Gelderblom HR, Arasteh K, et al (1990) Intestinal spirochetosis in HIV infection: prevalence, isolation and morphology of spirochetes. Dtsch Med Wochenschr 115=1499-1506
139. Burns DG, Hayes MM (1985) Rectal spirochaetosis: symptomatic response to metronidazole and mebendazole. S Afr Med J 68:335-336
140. Peghini PL, Guccion JG, Sharma A (2000) Improvement of chronic diarrhea after treatment for intestinal spirochetosis. Dig Dis Sci 45:1006-1010
141. Mora M, Rivas A, Dib J (1989) Chlamydial proctitis in homosexual men. GEN 43:295-297
142. Laughon BE, Druckman DA, Vernon A, et al (1988) Prevalence of enteric pathogens in homosexual men with and without acquired immunodeficiency syndrome. Gastroenterology 94:984-993
143. Murray AB, Greenhouse PR, Nelson WL, et al (1991) Coincident acquisition of Neisseria gonorrhoeae and HIV from fellatio. Lancet 338:830
144. Donovan B, Bodsworth NJ, Rohrsheim R, et al (2001) Characteristics of homosexually-active men with gonorrhoea during an epidemic in Sydney, Australia. Int J STD AIDS 12:437-443
145. McMillan A, Young H, Moyes A (2000) Rectal gonorrhoea in homosexual men: source of infection. Int J STD AIDS 11:284-287
146. Press N, Chavez VM, Ticona E, et al (2001) Screening for sexually transmitted diseases in human immunodeficiency virus-positive patients in Peru reveals an absence of Chlamydia trachomatis and identifies Trichomonas vaginalis in pharyngeal specimens. Clin Infect Dis 32:808-814
147. Marquez-Diaz F, Soto-Ramirez LE, Sifuentes-Osornio J (1998) Nocardiasis in patients with HIV infection. AIDS Patient Care STDS 12:825-832
148. Kim J, Minamoto GY, Grieco MH (1991) Nocardial infection as a complication of AIDS: report of six cases and review. Rev Infec Dis 13:624-629
149. Poles M, Lew E, Dieterich D (1994) Actinomyces superinfection of esophageal ulcers in an AIDS patient. Am J GastroenteroI89:1569-1572
Gut Infections: Etiopathogenetic and Clinical Remarks 193
150. Spencer GM, Poach D, Skucas J (1993) Actinomyces of the esophagus in a patient with AIDS: findings on barium esophograms. Am J RoentgenoI16l:795-796
151. Artru P, Lavergne-Slove A, Joly F, et al (1999) Isolated jejunal tuberculosis mimicking Crohn disease. Diagnosis by push video-enteroscopy. Gastroenterol Clin Bioi 23:1086-1089
152. Nzarubara GR (1998) Gastro-intestinal tuberculosis: an emerging diagnostic dilemma. East Afr Med J 75:124-126
153. Allen CM, Craze J, Grundy A (1991) Tuberculous broncho-oesophageal fistula in the acquired immunodeficiency syndrome. Clin Radiol 43:60-62
154. Horvath KD, Whelan RL (1998) Intestinal tuberculosis: return of an old disease. Am J Gastroenterol 93:692-696
155. Deb T, Singh TY, Singh NB, et al (1998) Multiple tubercular ulcer perforation of ileum in an AIDS patient: case report. J Commun Dis 30:175-178
156. Desta TT, Man KM, Bouvier D, Leung JW (1998) Choledoco-enteric fistula due to Mycobacterium tuberculosis in a patient with acquired immunodeficiency syndrome. Gastrointest Endosc 48:623-626
157. Pintor E, Velasco M, Piret MV, et al (1997) Tuberculous abscess simulating complicated acute appendicitis in a patient with HIV infection. Enferm Infecc Microbiol Clin 15:497-498
158. Das HS, Rathi P, Sawant P, et al (2000) Colonic tuberculosis: colonoscopic appearance and clinico-pathologic analysis. J Assoc Physicians India 48:708-710
159. Antinori S, Galimberti L, Parente F (2001) Intestinal tuberculosis as a cause of chronic diarrhoea among patients with human immunodeficiency virus infection: report of two cases. Dig Liver Dis 33:63-67
160. Hawkins CCM, Gold JWM, Whembey E, et al (1986) Mycobacterium complex infections in patients with the acquired immunodeficiency syndrome. Ann Intern Med 105:1184-1188
161. Benson CA (1994) Disease due to Mycobacterium avium complex in patients with AIDS: epidemiology and clinical syndrome. Clin Infect Dis 18 [Suppl 3] :S218-S222
162. Mazurek GH, Chin DP, Hartman S, et al (1997) Genetic similarity among Mycobacterium avium isolates from blood, stool, and sputum of persons with AIDS. J Infect Dis 176:976-983
163. Bermudez LE, Wagner D, Sosnowska D (2000) Mechanisms of Mycobacterium avium pathogenesis. Arch Immunol Ther Exp (Warsz) 48:521-527
164. Sangari FJ, Goodman J, Bermudez LE (2000) Mycobacterium avium enters intestinal epithelial cells through the apical membrane, but not by the basolateral surface, activates small GTPase Rho and, once within epithelial cells, expresses an invasive phenotype. Cell MicrobioI2:561-568
165. Horsburgh CR Jr (1999) The pathophysiology of disseminated Mycobacterium avium complex disease in AIDS. J Infect Dis 179 [SuppI3]:S461-S465
166. Velasco M, Flores L, Guijarro-Rojas M, Roca V (1998) Simultaneous intestinal leishmaniasis and mycobacterial involvement in a patient with acquired immune deficiency syndrome. J Clin Gastroenterol 27:271-273
167. Wang J, Vaniey C, Miyamoto E, et al (1999) Coinfec-

194 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
tion of visceral leishmaniasis and Mycobacterium in a patient with acquired immunodeficiency syndrome. Arch Pathol Lab Med 123:835-837
168. Pursner M, Haller JO, Berdon WE (2000) Imaging features of Mycobacterium avium-intracellulare complex (MAC) in children with AIDS. Pediatr Radiol 30:426-429
169. Klatt EC (1987) Pathology of Mycobacterium aviumintracellulare infection in acquired immunodeficiency syndrome. Hum PathoI18:709-714
170. Kooijman CD, Poen H (1984) Whipple-like disease in AIDS. Histopathology 8:705-708
171. Cappell MS, Philogene C (1995) The endoscopic appearance of severe intestinal Mycobacterium avium complex infection as a coarsely granular mucosa due to massive infiltration and expansion of intestinal villi without mucosal exudation. J Clin Gastroenterol 21:323-326
172. BensonCA (1994) Treatment of disseminated disease due to the Mycobacterium avium complex in patients with AIDS. Clin Infect Dis 18 [SuppI3j:S237-S242
173. Woods GL(1994) Disease due to the Mycobacterium avium mmplex in patients infected with human immunodeficiency virus: diagnosis and susceptibility testing. Clin Infect Dis 18 [SuppI3j:S227-S232
174. Carpenter JL, Parks JM (1991) Mycobacterium kansasii infections in patients positive for human immunodeficiency virus. Rev Infect Dis 13=789-796
175. Massenkeil G, Opravil M, Salfinger M, et al (1992) Disseminated coinfection with Mycobacterium avium complex and Mycobacterium kansasii in a patient with AIDS and liver abscess. Clin Infect Dis 14:618-619
176. Enani MA, Frayha HH, Halim MA (1998) An appendiceal abscess due to Mycobacterium kansasii in a child with AIDS. Clin Infect Dis 27:891-892
177. Klein JL, Corbett EL, Slade PM, et al (1998) Mycobacterium kansasii and human immunodeficiency virus co-infection in London. J Infect 37:252-259
178. Wallace RJ Ir, Cook JL, Glassroth J, et al (1997) Diagnosis and treatment of disease caused by nontuberculous mycobacteria. American Thoracic Society Statement. Am J Respir Crit Care Med 156[Supplj:Sl-S25
179. Bottger EC, Hirschel B, Coyle MB (1993) Mycobacterium genavense sp. nov. Int I Syst BacterioI43:841-843
180. Portaels F, Realini L, Bauwens L, et al (1996) Mycobacteriosis caused by Mycobacterium genavense in birds kept in a zoo: 11-year survey. J Clin MicrobioI34:319-323
181. Hillebrand-Haverkort ME, Kolk AH, Kox LF, et al (1999) Generalized mycobacterium genavense infection in HIV -infected patients: detection of the mycobacterium in hospital tap water. Scand J Infect Dis 31:63-68
182. Kuijper EJ, de Witte M, Verhagen DW, et al (1998) Mycobacterium genavense infection in 2 HIV seropositive patients in Amsterdam. Ned Tijdschr Geneeskd 142:970-972
183. Pechere M, Opravil M, Wald A, et al (1995) Clinical and epidemiologic features of infection with Mycobacterium genavense. Arch Intern Med 155:400-404
184. Maschek H, Georgii A, Schmidt RE, et al (1994) Mycobacterium genavense: autopsy findings in three patients. Am J Clin PathoI101:95-99
185. Bottger Ee, Teske A, Kirschner P, et al (1992) Dissem-
ina ted Mycobacterium genavense infection in patients with AIDS. Lancet 340:76-80
186. Monill JM, Franquet T, Sambeat MA, et al (2001) Mycobacterium genavense infection in AIDS: imaging findings in eight patients. Eur Radiol11:193-196
187. Albrecht H, Rusch-Gerdes S, Stellbrink HJ, et al (1997) Disseminated Mycobacterium genavense infection as a cause of pseudo-Whipple's disease and sclerosing cholangitis. Clin Infect Dis 25:742-743
188. Thomsen YO, Dragsted UB, Bauer J, et al (1999) Disseminated infection with Mycobacterium genavense: a challenge to physicians and mycobacteriologists. J Clin MicrobioI37:3901-3905
189. Tortoli E, Simonetti MT, Dionisio D, et al (1995) Mycobacterium genavense and Mycobacterium avium mixed infection in an AIDS patient. Clin Microbiol NewsI17:175-176
190. Koehler M, Chak A, Setrakian S, Sivak MV Jr (1996) Endoscopic appearance of Mycobacterium genavense: case report and review of the literature. Gastrointest Endosc 44:331-333
191. Dumonceau JM (1997) Endoscopic appearance of Mycobacterium genavense. Gastrointest Endosc 45:334
192. Nadal D, CaduffR, Kraft R, et al (1993) Invasive infection with Mycobacterium genavense in three children with the acquired immunodeficiency syndrome. Eur J Clin Microbiol Infect Dis 12:37-43
193. Tortoli E, Simonetti T, Dionisio D, Meli M (1994) Cultural studies on two isolates of Mycobacterium genavense from patients with AIDS. Diagn Microbiol Infect Dis 18:7-12
194. Tortoli E, Brunello F, Cagni E, et al (1998) Mycobacterium genavense in AIDS patients, report of 24 cases in Italy and review of the literature. Eur J Epidemiol 14:219-224
195. Lopez-Dupla M, Sanz PM, Garcia VP, et al (1992) Clinical, endoscopic, immunologic, and therapeutic aspects of oropharyngeal and esophageal candidiasis in HIV-infected patients: a survey of 114 cases. Am J GastroenteroI89:1771-1776
196. Iayagopal S, Cervia JS (1992) Colitis due to Candida albicans in a patient with AIDS. Clin Infect Dis 15:555
197. Balthazar EJ, Stern J (1994) Necrotizing Candida enterocolitis in AIDS: CT features. I Comput Assist Tomogr 18:298-300
198. Levine J, Dykoski RK, Janoff EN (1995) Candida-associated diarrhea: a syndrome in search of credibility. Clin Infect Dis 21:881-886
199. Fredricks DN, Rojanasthien N, Jacobson MA (1997) Aids-related disseminated histoplasmosis in San Francisco, California. West J Med 167:315-321
200. Wheat J (1997) Histoplasmosis. Experience during outbreaks in Indianapolis and review of the literature. Medicine (Baltimore) 76:339-354
201. Gumbs MA, Girishkumar H, Yousuf A, et al (2000) Histoplasmosis of the small bowel in patients with AIDS. Postgrad Med I 76:367-369
202. Winburn GB, Yeh KA (1999) Severe anal ulceration secondary to Histoplasma capsulatum in a patient with HIV disease. Am Surg 65:321-322
203. Warnakulasuriya KA, Harrison JD, Johnson NW, et al (1997) Localised oral histoplasmosis lesions associated

with HIV infection. J Oral Pathol 26:294-296 204. Boulard F, Cnudde F, Teron-Aboud B, et al (1994)
Digestive histoplasmosis in a patient with AIDS from Guadeloupe. Ann Gastroenterol Hepatol (Paris) 30:97-100
205. Piratvisuth T, Siripaitoon P, Sriplug H, Ovartlarnporn B (1999) Findings and benefit of liver biopsies in 46 patients infected with human immunodeficiency virus. J Gastroenterol HepatoI14:146-149
206. Forsmark CE, Wilcox CM, Darragh TM, Cello JP (1990) Disseminated histoplasmosis in AIDS: an unusual case of esophageal involvement and gastrointestinal bleeding. Gastrointest Endosc 36:604-605
207. Flannery MT, Chapman V, Cruz-Gonzales I, et al (2000) Ileal perforation secondary to histoplasmosis in AIDS. Am J Med Sci 320:406-407
208. Hamilton AJ (1998) Serodiagnosis of histoplasmosis, paracoccidioidomycosis and penicilliosis marneffei: current status and future trends. Med Mycol 36:351-364
209. Wheat LJ, Cloud G, Johnson PC, et al (2001) Clearance of fungal burden during treatment of disseminated histoplasmosis with liposomal amphotericin B versus itraconazole. Antimicrob Agents Chemother 45:2354-2357
210. Michiels JF, Saint Paul MC, Hofman P, et al (1992) Histopathologic features of opportunistic infections of the small intestine in acquired immunodeficiency syndrome. Ann PathoI12:165-173
211. Van Calck M, Motte S, Rickaert F, et al (1988) Cryptococcal anal ulceration in a patient with AIDS. Am J Gastroenterol 83:1306-1308
212. White MH, Armstrong D (1994) Cryptococcosis. Infect Dis Clin North Am 8:383-398
213. Witt K, Nielsen TN, Junge J (1991) Dissemination of Pneumocystis carinii in patients with AIDS. Scand J Infect Dis 23:691-695
214. Carter TR, Cooper PH, Petri WA Jr, et al (1988) Pneumocystis carinii infection of the small intestine in a patient with Acquired Immune Deficiency Syndrome. Am J Clin Pathol 89:679-683
215. Matsuda S, Urata Y, Shiota T, et al (1989) Disseminated infection of Pneumocystis carinii in a patient with the acquired immunodeficiency syndrome. Virchows Arch A Pathol Anat Histopathol 414:523-527
216. Abati A, Opitz L, Brones C, et al (1992) Cytology of extra pulmonary Pneumocystis carinii infection in the Acquired Immunodeficiency Syndrome. Acta Cytol 36:440-444
217. Grimes MM, LaPook JD, Bar MH, et al (1987) Disseminated Pneumocystis carinii infection in a patient with Acquired Immunodeficiency Syndrome. Hum Pathol 18:307-308
218. Sachs JR, Greenfield SM, Sohn M, Turner JL (1991) Disseminated Pneumocystis carinii infection with hepatic involvement in a patient with the acquired immune deficiency syndrome. Am J Gastroenterol 86:82-85
219. Mathews WC, Bozzette SA, Harrity S, et al (1992) Pneumocystis carinii peritonitis. Antemortem confirmation of disseminated pneumocystosis by cytologic examination of body fluids. Arch Intern Med 152:867-869
Gut Infections: Etiopathogenetic and Clinical Remarks 195
220. Ramos-Soriano AG, Saavedra JM, Wu TC, et al (1996) Enteric pathogens associated with gastrointestinal dysfunction in children with HIV infection. Mol Cell Probes 10:67-73
221. Olcoz Gonni JL, Moran Blanco A, Bahamonde Carrasco A, et al (1998) Intestinal obstruction and necrotizing thyroiditis secondary to Pneumocystis carinii infection in a seropositive hemophiliac patient seropositive for human immunodeficiency virus. Gastroenterol HepatoI21:13-15
222. BierhoffE, Tran A, Pakos E, et al (1996) Perforation of the small intestine in a patient with disseminated Pneumocystis carinii infection in AIDS. Gen Diagn PathoI141:255-260
223. Kinchen K, Kinchen TH, Inglesby T Jr (1998) Pneumocystis carinii infection of the small intestine. J N atl Med Assoc 90:625-627
224. Chow-In K, Chien-Ching H, Mao-Yuan C, et al (1999) Endoscopic diagnosis of intestinal penicilliosis marneffei: report of three cases and review of the literature. Gastrointest Endosc 50:111-114
225. Sirisanthana T (2001) Penicillium marneffei infection in patients with AIDS. Emerg Infect Dis 7 [SuPpI3J:s6l
226. Nittayananta W (1999) Penicilliosis marneffei: another AIDS-defining illness in Southeast Asia. Oral Dis 5:286-293
227. Supparatpinyo K, Khamwan C, Baosoung V, et al (1994) Disseminated Penicillium marneffei infection in southeast Asia. Lancet 344:110-113
228. Borradori L, Schmit JC, Stetzkowski M, et al (1994) Penicilliosis marneffei infection in AIDS. J Am Acad Dermatol 31:843-846
229. Duong TA (1996) Infection due to Penicillium marneffei, an emerging pathogen: review of 155 reported cases. Clin Infect Dis 23:125-130
230. Ukarapol N, Sirisanthana V, Wongsawasdi L (1998) Penicillium marneffei mesenteric lymphadenitis in human immunodeficiency virus-infected children. J Med Assoc Thai 81:637-640
231. Supparatpinyo K, Nelson KE, Merz WG, et al (1993) Response to antifungal therapy by human immunodeficiency virus infected patients with disseminated Penicillium marneffei infections and in vitro susceptibilities of isolates from clinical specimens. Antimicrob Agents Chemother 37:2407-2411
232. Brullet E, Andreu X, Elias J, et al (1993) Gastric mucormycosis in a patient with acquired immunodeficiency syndrome. Gastrointest Endosc 39:106-107
233. Lagorce Pages C, Fabre A, Bruneel F, et al (2000) Disseminated mucormycosis in AIDS. Ann Pathol 20:343-345
234. Nagy-Agren SE, Chu P, Smith GJ, et al (1995) Zygomycosis (mucormycosis) and HIV infection: report of three cases and review. J Acquir Immune Defic Syndr Hum RetroviroI1O:441-449
235. Bluhm CS, Backerstaff CA, Holt S (1990) Refractory esophageal candidiasis in acquired immune deficiency syndrome (AIDS). Am J GastroenteroI85:479-480
236. Tom W, Aaron JS (1987) Esophageal ulcers caused by Torulopsis glabrata in a patient with acquired immune deficiency syndrome. Am J Gastroenterol 82:766-768
237. Montero JA, Sinnott JT, Holt DA, Lloyd C (2001) Bil-

196 D. Dionisio Gut Infections: Etiopathogeneticand Clinical Remarks
iary cryptosporidiosis: current concepts. Infect Med 18:305-311
238. Morgan U, Weber R, Xiao L, et al (2000) Molecular characterization of Cryptosporidium isolates obtained from human immunodeficiency virus-infected individuals living in Switzerland, Kenya, and the United States. I Clin MicrobioI38:1180-1183
239. Pieniazek NI, Bornay-Llinares FI, Slemenda SB, et al (1999 ) New cryptosporidium genotypes in HIV -infected persons. Emerg Infect Dis 5:444-449
240. Okhuysen PC, White AC Ir (1999) Parasitic infections of the intestines. Curr Opin Infect Dis 12:467-472
241. Blumberg RS, Kelsey P, Peppone T, et al (1984) Cytomegalovirus and cryptosporidium-associated acalculous gangrenous cholecystitis. Am I Med 76:m8-1123
242. Hemet AM, Pokieser P, Ketenbach I, et al (1998) Pneumatosis intestinalis in AIDS-associated chronic intestinal cryptosporidiosis: a benign course in a severelooking disease. Eur Radiol 8:1499
243. Samson VE, Brown WR (1996) Pneumatosis cystoides intestinalis in AIDS-associated cryptosporidiosis. More than an incidental finding? I Clin Gastroenterol 22:311-312
244. Bruce BB, Blass MA, Blumberg HM, et al (2000) Risk of Cryptosporidium parvum transmission between hospital roommates. Clin Infect I Dis 31:947-950
245. Rossi P, Rivasi F, Codeluppi M, et al (1998) Gastric involvement in AIDS-associated cryptosporidiosis. Gut 43:476-477
246. Moon A, Spivak W, Brandt LI (1999) Cryptosporidiurn-induced gastric obstruction in a child with congenital HIV infection: case report and review of the literature. I Pediatr Gastroenterol Nutr 28:108-111
247. Scaglia M, Gatti S, Bassi P, et al (1994) Intestinal coinfection by Cyclospora sp. and Cryptosporidium parvum: first report in an AIDS patient. Parasite 1:387-390
248. Marshall MM, Naumovitz D, Ortega Y, Sterling CR (1997) Waterborne protozoan pathogens. Clin MicrobioI Rev 10:67-85
249. Laurent F, McCole D, Eckmann L, KagnoffMF (1999) Pathogenesis of Cryptosporidium parvum infection. Microbes Infect 1:141-148
250. Kelly P, Thillainayagam AV, Smithson I, et al (1996) Iejunal water and electrolyte transport in human cryptosporidiosis. Dig Dis Sci 41:2095-2099
251. Lumadue lA, Manabe YC, Moore RD, et al (1998) A clinicopathologic analysis of AIDS-related cryptosporidiosis. AIDS 12:2459-2466
252. Manabe YC, Clark DP, Moore RD, et al (1998) Cryptosporidiosis in patients with AIDS: correlates of disease and survival. Clin Infect Dis 27:536-542
253. Reijasse D, Patey-Mariaud de Serre N, Canioni D, et al (2001) Cytotoxic T cells in AIDS colonic cryptosporidiosis. I Clin Pathol 54:298-303
254a. Derouin F, Gangneux IP (1998) Changing patterns of disease and treatment of opportunistic parasitic infections in patients with AIDS. Curr Opin Infect Dis 11:711-716
254b.Dionisio D (2002) Cryptosporidiosis in HIV-infected patients. I Postgrad Med 48(3):215-216
254c. Kadappu KK, Nagaraja MV, Rao PV, Shastry BA
(2002) Azithromycin as treatment for Cryptosporidiosis in human immunodeficiency virus disease. I Postgrad Med 48(3}:179-181
255. Doumbo 0, Rossignol IF, Pichard E, et al (1997) Nitazoxanide in the treatment of cryptosporidial diarrhea and other intestinal parasitic infections associated with acquired immunodeficiency syndrome in tropical Africa. Am I Trop Med Hyg 56:637-639
256. Carr A, Marriot D, Field A, et al (1998) Treatment of HIV -I-associated microsporidiosis and cryptosporidiosis with combination antiretroviral therapy. Lancet 351:256-261
257. Sterling CR, Ortega YR (1999) Cyclospora: an enigma worth unraveling. Emerg Infect Dis 5:48-53
258. Ortega YR, Nagle R, Gilman RH, et al (1997) Pathologic and clinical findings in patients with cyclosporiasis and a description of intracellular parasite life-cycle stages. I Infect Dis 176:1584-1589
259. Cegielski IP, Ortega YR, McKee S, et al (1999) Cryptosporidium, Enterocytozoon, and Cyclospora infections in pediatric and adult patients with diarrhea in Tanzania. Clin Infect Dis 28:314-321
260. Deodhar L, Maniar IK, Saple DG (2000) Cyclospora infection in acquired immunodeficiency syndrome. I Assoc Physicians India 48:404-406
261. Sifuentes-Osornio I, Porras-Cortes G, Bendall RP, et al (1995) Cyclospora cayetanensis infection in patients with and without AIDS: biliary disease as another clinical manifestation. Clin Infect Dis 21:1092-1097
262. Verdier RI, Fitzgerald DW, Johnson WD Jr, Pape JW (2000) Trimethoprim-sulfamethoxazole compared with ciprofloxacin for treatment and prophylaxis of Isospora belli and Cyclospora cayetanensis infection in HIV-infected patients. A randomized, controlled trial. Ann Intern Med 132:885-888
263. Zierdt CH (1991) Blastocystis hominis - past and future. Clin Microbiol Rev 4:61-77
264. Telalbasic S, Pikula ZP, Kapidzic M (1991) Blastocystis hominis may be a potential cause of intestinal disease. Scand J Infect Dis 23=389-390
265. Brites C, Barberino MG, Bastos MA, et al (1997) Blastocystis hominis as a potential cause of diarrhea in AIDS patients: a report of six cases in Bahia, Brazil. Braz I Infect Dis 1:91-94
266. Garavelli PL, Scaglione L, Bicocchi R, Libanore M (1990) Blastocystosis: a new disease in the acquired immunodeficiency syndrome? Int J STD AIDS 1:134-135
267. Albrecht H, Stellbrink HI, Koperski K, Greten H (1995) Blastocystis hominis in human immunodeficiency virus-related diarrhea. Scand J Gastroenterol 30:909-914
268. Udkow MP, Markell EK (1993) Blastocystis hominis: prevalence in asymptomatic versus symptomatic hosts. I Infect Dis 168:242-244
269. Lanuza MD, Carbajal lA, Villar J, et al (1999) Solubleprotein and antigenic heterogeneity in axenic Blastocystis hominis isolates: pathogenic implications. Parasitol Res 85:93-97
270. Wilson KW, Winget D, Wilks S (1990) Blastocystis hominis infection: signs and symptoms in patients at Wilford Hall Medical Center. Mil Med 155:394-396
271. Amenta M, Dalle Nogare ER, Colomba C, et al (1999)

Intestinal protozoa in HIV-infected patients: effect of rifaximin in Cryptosporidium parvum and Blastocystis hominis infections. J Chemother 11:391-395
272. Esfandiari A, Swartz J, Teklehaimanot S (1997) Clustering of giardiasis among AIDS patients in Los Angeles county. Cell Mol BioI (Noisy-Ie-Grand) 43:lO77-1083
273. Angarano G, Maggi P, Di Bari MA, et al (1997) Giardiasis in HIV: a possible role in patients with severe immune deficiency. Eur J Epidemio113:485-487
274. Moolosart P (1999) Giardia lamblia in AIDS patients with diarrhea. J Med Assoc Thai 82:654-659
275. Mathis A, Deplazes P, Kohler P, Eckert J (1996) PCR for detection and characterization of parasites (Leishmania, Echinococcus, Microsporidia, Giardia). Schweiz Arch Tierheilkd 138:133-138
276. Aronson NE, Cheney C, Rholl V, et al (2001) Biliary giardiasis in a patient with human immunodeficiency virus. J Clin Gastroentero133:167-170
277. Hewan-Lowe K, Furlong B, Sims M, Schwartz DA (1997) Coinfection with Giardia lamblia and Enterocytozoon bieneusi in a patient with acquired immunodeficiency syndrome and chronic diarrhea. Arch Pathol Lab Med 121:417-422
278. Abboud P, Lemee V, Gargala G, et al (2001) Successful treatment of metronidazole- and albendazole-resistant giardiasis with nitazoxanide in a patient with acquired immunodeficiency syndrome. Clin Infect Dis 32:1792-1794
279. Allason-Jones E, Mindel A, Sargeaunt P, Katz D (1988) Outcome of untreated infection with Entamoeba histolytica in homosexual men with and without HIV antibody. BMJ 10:654-657
280. Fatkenheuer G, Arnold G, Steffen HM, et al (1997) Invasive amoebiasis in two patients with AIDS and cytomegalovirus colitis. J Clin Microbio135:2168-2169
281. Hung CC, Chen PJ, Hsieh SM (1999) Invasive amoebiasis: an emerging parasitic disease in patients infected with HIV in an area endemic for amoebic infection. AIDS 13:2421-2428
282. Liu CJ, Hung CC, Chen MY, et al (2001) Amebic liver abscess and human immunodeficiency virus infection. A report of three cases. J Clin Gastroentero133:64-68
283. Hutin YJ, Sombardier MN, Liguory 0, et al (1998) Risk factors for intestinal microsporidiosis in patients with human immunodeficiency virus infection: a case-control study. J Infect Dis 178:904-907
284. Cotte L, Rabodonirina M, Chapuis F, et al (1999) Waterborne outbreak of intestinal microsporidiosis in persons with and without human immunodeficiency virus infection. J Infect Dis 180:2003-2008
285. Ferreira FM, Bezerra L, Santos MB, et al (2001) Intestinal microsporidiosis: a current infection in HIVseropositive patients in Portugal. Microbes Infect P015-1019
286. Kotler DP, Orenstein JM (1998) Clinical syndromes associated with microsporidiosis. Adv Parasitol 40:321-349
287. Schmidt W, Schneider T, Heise W, et al (1997) Mucosal abnormalities in microsporidiosis. AIDS 11:1589-1594
288. Kotler DP, Giang TT, Thiim M, et al (1995) Chronic bacterial enteropathy in patients with AIDS. J Infect Dis 171:552-558
Gut Infections: Etiopathogenetic and Clinical Remarks 197
289. Schwartz DA, Sobottka I, Leitch GJ, et al (1996) Pathology of microsporidiosis. Emerging parasitic infections in patients with acquired immunodeficiency syndrome. Arch Pathol Lab Med 120:173-188
290. Moura H, Sodre FC, Bornay-Llinares FJ, et al (1999) Detection by an immunofluorescence test of Encephalitozoon intestinalis spores in routinely formalin-fixed stool samples stored at room temperature. J Clin Microbio137:2317-2322
291. Muller A, Stellermann K, Hartmann P, et al (1999) A powerful DNA extraction method and PCR for detection of microsporidia in clinical stool specimens. Clin Diagn Lab Immunol 6:243-246
292. Conteas CN, Berlin OG, Lariviere MJ, et al (1998) Examination of the prevalence and seasonal variation of intestinal microsporidiosis in the stools of persons with chronic diarrhea and human immunodeficiency virus infection. Am J Trop Med Hyg 58:559-561
293. Cali A, Owen RL (1990) Intracellular development of Enterocytozoon, a unique microsporidian found in the intestine of AIDS patients. J Protozooo137:145-155
294. Foucault C, Drancourt M (2000) Actin mediates Encephalitozoon intestinalis entry into the human enterocyte-like cell line, CaCO-2. Microb Pathog 28:51-58
295. Ignatius R, Henschel S, Liesenfeld 0, et al (1997) Comparative evaluation of Modified Trichrome and Uvitex 2B stains for detection of low numbers of microsporidial spores in stool specimens. J Clin Microbio135:2266-2269
296. Accoceberry I, Thellier M, Desportes-Livage I, et al (1999) Production of monoclonal antibodies directed against the microsporidium Enterocytozoon bieneusi. J Clin Microbio137:4107-4112
297. Velasquez IN, Carnevale S, Labbe JH, et al (1999) In situ hybridization: a molecular approach for the diagnosis of the microsporidian parasite Enterocytozoon bieneusi. Hum Patho130:54-58
298. Gainzarain JC, Canut A, Lozano M, et al (1998) Detection of Enterocytozoon bieneusi in two human immunodeficiency virus-negative patients with chronic diarrhea by polymerase chain reaction in duodenal biopsy specimens and review. Clin Infect Dis 27:394-398
299. Liguory 0, David F, Sarfati C, et al (1998) Determination of types of Enterocytozoon bieneusi strains isolated from patients with intestinal microsporidiosis. J Clin Microbio136:1882-1885
300. Liguory 0, Fournier S, Sarfati C, et al (2000) Genetic homology among thirteen Encephalitozoon intestinalis isolates obtained from human immunodeficiency virus-infected patients with intestinal microsporidiosis. J Clin Microbio138:2389-2391
301. Curry A (1999) Human microsporidial infection and possible animal sources. Curr Opin Infect Dis 12:473-480
302. Sobottka I, Schwartz DA, Schottelius J, et al (1998) Prevalence and clinical significance of intestinal microsporidiosis in human immunodeficiency virusinfected patients with and without diarrhea in Germany: a prospective coprodiagnostic study. Clin Infect Dis 26:475-480
303. Gumbo T, Sarbah S, Gangaidzo IT, et al (1999) Intesti-

198 D. Dionisio Gut Infections: Etiopathogeneticand Clinical Remarks
nal parasites in patients with diarrhea and human immunodeficiency virus infection in Zimbabwe. AIDS 13:819-821
304. Georges E, Rabaud C, Amiel C, et al (1998) Enterocytozoon bieneusi multiorgan microsporidiosis in a HIV -infected patient. J Infect 36:223-225
305. Pol S, Romana C, Richard S, et al (1992) Enterocytozoon bieneusi infection in acquired immunodeficiency syndrome-related sclerosing cholangitis. Gastroenterology 102:1778-1781
306. Goodgame R, Stager C, Marcantel B, et al (1999) Intensity of infection in AIDS-related intestinal microsporidiosis. J Infect Dis 180:929-932
307. Molina JM, Chastang C, Goguel J, et al (1998) Albendazole for treatment and prophylaxis of microsporidiosis due to Encephalitozoon intestinalis in patients with AIDS: a randomized double-blind controlled trial. J Infect Dis 177:1373-1377
308. Kucerova-Pospisilova Z, Stankova M, Ditrich 0 (1999) Encephalitozoon intestinale infection in an AIDS patient - a case report. Cent Eur J Public Health 7:43-46
309. Dionisio D, Ibba Manneschi L, Di Lollo S, et al (1997) Enterocytozoon bieneusi in AIDS: symptomatic relief and parasite changes after furazolidone. J Clin Pathol 50:472-476
310. Dionisio D, Ibba Manneschi L, Di Lollo S, et al (1998) Persistent damage to Enterocytozoon bieneusi, with persistent symptomatic relief, after combined furazolidone and albendazole in AIDS patients. J Clin Pathol 51:731-736
311. Molina JM, Goguel J, Sarfati C, et al (2000) Trial of oral fumagillin for the treatment of intestinal microsporidiosis in patients with HIV infection. ANRS 054 Study Group. Agence Nationale de Recherche sur Ie SIDA. AIDS 14:1341-1348
312. Conte as CN, Berlin OG, Ash LR, Pruthi JS (2000) Therapy for human gastrointestinal microsporidiosis. Am J Trop Med Hyg 63:121-127
313. Keystone JS, Kozarsky P (2000) Isospora belli, Sarcocystis species, Blastocystis hominis, and Cyclospora. In: Mandell GL, Bennett JE, Dolin R (eds) Principles and practice of infectious diseases, 5th edn. Churchill Livingstone, Philadelphia, pp 2915-2920
314. Prasad KN, Nag VL, Dhole TN, Ayyagari A (2000) Identification of enteric pathogens in HIV -positive patients with diarrhoea in northern India. J Health Popul Nutr 18:23-26
315. Wiwanitkit V (2001) Intestinal parasitic infections in Thai HIV-infected patients with different immunity status. BMC Gastroenteroll:3
316. Trier JS, Moxey P, Schimmel EM, Robles E (1974) Chronic intestinal coccidiosis in man: intestinal morphology and response to treatment. Gastroenterology 66:923-935
317. Laguna F, Adrados M, Alvar J, et al (1997) Visceral leishmaniasis in patients infected with the human immunodeficiency virus. Eur J Clin Microbiol Infect Dis 16:898-903
318. Rosenthal E, Marty P, Ie Fichoux Y, Cassuto JP (2000) Clinical manifestations of visceral leishmaniasis associated with HIV infection: a retrospective study of 91 French cases. Ann Trop Med Parasitol 94:37-42
319. Datry A, Similowski T, Jais P, et al (1990) AIDS-associated leishmaniasis: an unusual gastro-duodenal presentation. Transact R Soc Trop Med Hyg 84:239-240
320. Alonso MJ, Munoz E, Picazo A, et al (1997) Duodenal leishmaniasis diagnosed by biopsy in two HIV-positive patients. Pathol Res Pract 193:43-47
321. Jablonowski H, Szelenyi H, Borchard F, et al (1994) Visceral leishmaniasis with gastrointestinal involvement in a 30-year-old HIV -infected patient. Z GastroenteroI32:405-407
322. Laguna F, Garcia-Samaniego J, Soriano V, et al (1994) Gastrointestinal leishmaniasis in human immunodeficiency virus-infected patients: report of five cases and review. Clin Infect Dis 19:48-53
323. Albrecht H, Sobottka I, Emminger C, et al (1996) Visceralleishmaniasis emerging as an important opportunistic infection in HIV -infected persons living in areas nonendemic for Leishmania donovani. Arch Pathol Lab Med 120:189-198
324. Villanueva JL, Torre-Cisneros J, Jurado R, et al (1994) Leishmania esophagitis in an AIDS patient: an unusual form of visceral leishmaniasis. Am J Gastroenterol 89:273-275
325. Bonacini M, Kanel G, Alamy M (1996) Duodenal and hepatic toxoplasmosis in a patient with HIV infection: review of the literature. Am J Gastroenterol 91:1838-1840
326. Bertoli F, Espino M, Arosemena JR 5th, et al (1995) A spectrum in the pathology of toxoplasmosis in patients with acquired immunodeficiency syndrome. Arch Pathol Lab Med 119:214-224
327. Jautzke G, Sell M, Thalmann U, et al (1993) Extracerebral toxoplasmosis in AIDS. Histological and immunohistological findings based on 80 autopsy cases. Pathol Res Pract 189:428-436
328. Kofman E, Khorsandi A, Sarlin J, Adhami K (1996) Gastric toxoplasmosis: case report and review of the literature. Am J GastroenteroI91:2436-2438
329. Alpert L, Miller M, Alpert E, et al (1996) Gastric toxoplasmosis in acquired immunodeficiency syndrome: antemortem diagnosis with histopathologic characterization. Gastroenterology 110:258-264
330. Pauwels A, Meyohas MC, Eliaszewicz M, et al (1992) Toxoplasma colitis in the acquired immunodeficiency syndrome. Am J GastroenteroI87:518-519
331. Israelski DM, Skowron G, Leventhal JP, et al (1988) Toxoplasma peritonitis in a patient with acquired immunodeficiency syndrome. Arch Intern Med 148:1655-1657
332. Mahmoud AAF (1996) Strongyloidiasis. Clin Infect Dis 23:949-953
333. Dionisio D, Ibba Manneschi L, di Lollo S, et al (2000) Strongyloides stercoralis: ultrastructural study of newly hatched larvae within human duodenal mucosa. J Clin PathoI53:110-116
334. Gompels MM, Todd J, Peters BS, et al (1991) Disseminated strongyloidiasis in AIDS: uncommon but important. AIDS 5:329-332
335. Gann PH, Neva FA, Gam AA (1994) A randomized trial of single- and two-dose ivermectin versus thiabendazole for treatment of strongyloidiasis. J Infect Dis 169:1076-1079
336. Lindo JF, Conway DJ, Atkins NS, et al (1994) Prospec-

tive evaluation of enzyme-linked immunosorbent assay and immunoblot methods for the diagnosis of endemic Strongyloides stercoralis infection. Am J Trop Med Hyg 51:175-179
337. Dionisio D, Meli M, Sterrantino G, et al (1996) Unidentified parasite from duodenum of a patient with AIDS. AIDS 10:107-108
338. Dionisio D, Tortoli E, Simonetti MT, et al (1994) Intestinal mycobacterial infections in AIDS: clinical aspects and therapeutical options for Mycobacterium avium, Mycobacterium kansasii, and Mycobacterium genavense. Recenti Prog Med 85: 526-536
339. Dionisio D, Di Lollo S, Milo D, et al (1990) Whipplelike disease by atypical mycobacteria in AIDS: a clinical and electronmicroscopical study of two cases. Recenti Prog Med 81:571-575
340. Dionisio D, Di Lollo S, Orsi A, et al (1991) The intes-
Gut Infections: Etiopathogenetic and Clinical Remarks 199
tinal microbial pathology in AIDS. A case-record. Recenti Prog Med 82:140-147
341. Wheat J (2000) Histoplasmosis. In Diamond RD Ed. Atlas of Fungal Infections. Current Medicine Inc. Philadelphia, USA
342. Palluault F, Dei-Cas E, Siomianny C, Soulez B, Camus D (1990) Golgi complex and Iysosomes in rabbitderived Pneumocystis carinii. Bioi Cell 70:73-82
343. Nittayananta W, Chungpanich S (1997) Oral lesions in a group of Thai people with AIDS. Oral Dis 3 (suppl. 1):41-45
344. Dionisio D, Marucelli F, Mazzotta D, et al (1990) The amebic liver abscess: two imported cases. Recenti Prog Med 81:493-498
345. Dionisio D, Santucci M, Comin CE, et al (1992) Isosporiasis and sarcocystosis. The current status. Recenti Prog Med 83:719-725

200 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
\ r f 2
1
0-G "3
'= ." en

fP ~ t
Gut Infections: Etiopathogenetic and Clinical Remarks
1 ~
\
\ " - ... . ~:::....
~ r= ..,.
"" ;r: ~ .. ,.-..
0 .~ -' :!i
~j I.l> "" ;:; :2 ;; <:> ---' a=
=-::>. W
~ <J .....l q: ;.
It;
"""
201
.J ~
~ ~
~

202 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
_ 8 V/LVollIR
at . 'Rn",m
fECfH-ORitL TRAtVSK\S~W"
EtJV\RO~\l.EtJTftL em) TfttWI ftT{(JN
Diu "1 FIHtON
--... (~r"")

1) Ingestion 01 cysts.
( Person to person spread: schools, day-care centers, residential institutions, intimate oral-anal contact.
Ingestion of food and water contaminated.
Gut Infections: Etiopathogenetic and Clinical Remarks 203
Giardia intestinalis life cycle
2) Excystation in the proximal small intestine: tropholOites in the crypts within the duodenum.
3) Parasites multiply by binary lission.
4) Cysts lormation takes place as the organisms move down through the
colon.
5) Fecal emission of cysts and trophozoites ,
Adherence 01 trophozoite to the epitelium of duodenum with the ventral surface, (the ·sucking disc"),
Contamination of food and water.
Dog
Axonemes
U l lA lli W'7'7' _ _ nuclei
eII ...... ~::.. Median bodies
Mature cyst average size: 11-141lm in length,
"'Jm '0 wi"}.
6) Cysts can survive in moist cool conditions, and in water and lood.
Beaver
Many wild and domestic animals carry the parasite, and act as a reservoir of inleclion, by elimination 01 cysts.
Domestic cat
- IL!f--il----'::.. Nuclei
Trophozoite (ventral surface): Average length: 10-20 11m

204 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks
Entamoeba histolytica life cycle
2) Excystation in the small bowel
Schematic representation of ileocecal junction and large bowel (colon. sigma and rectum).
3) Encystment in the large bowel.
Immature trophozoites
Diffusion per contiguity to lungs and sub-diaphragm
Liver abscesses.
Ulcers extending through the mucosa and muscolaris mucosae Into the submucosa.
Diffusion via the blood stream
\ to lungs and brain.
6) Diffusion to extraintestinal localizations. \
4) Fecal elimination of infective cysts with 2-3-4 nuclei.
Uving trophozoite (invasive) . average size 20-60 11m
.. .. ~
Bacteria and debris in vacuoles.
Fecal elimination 01 trophozoites (which degenerate within minutes).
~

(jut Infections: Etiopathogenetic and Clinical Remarks 205
•

206 D. Dionisio Gut Infections: Etiopathogenetic and Clinical Remarks

Gut Infections: Etiopathogenetic and Clinical Remarks 207
In humans and other susceptible mammals, leishmanias are lound In cells 01 reticuloendothelial origin as intracellular amastigotes.
Leishmania donovanilinfantum life cycle
Wild canines Dogs 1) The Invertebrate vectors
(female phlebotomine sandflles) ingest amastigoles during a blood meal on an infected mammalian reservoir.
Klnetoplasts _ .....:!,L-- , ..
Promastigotes Average length: 12j.lm
2) In the sandfly gut amastlgotes convert to promastigotes which multiply by longitudinal fission and migrate to the hypostome (proboscis).
4) IAmastigoles multiply by binary fission , within the phagosomal vacuoles of the phagocytic cells.
5) IPhagocytic cells are destroyed. and the parasites are phagocytized by olher " reticuloendothelial cells. ., .".:'::
Viscerat leishmaniasis (Kala azarl: TIssue macrophages parasitized by leishmania donovanilinfantum organisms enter the blood stream and are carried to reticuloendothelial centers (where the amastigote stages rapidly multiply): lymph nodes; liver; spleen; bone marrow; lymphatic tissue of small bowel.
liver: Increase of size and number of kuppfer cells with amastigotes.
Mononucleated cells with amastlgotes In the submucosa of the small intestine,with necrosis and mucosae damage: common pattem in HIV positive patient.
3) Promastigotes are released during the next blood meal by the sandfly. In the phagocytic cells promastlgotes convert to amastigotes
Amastigotes 1-5 J,lm long 1-2 J,lm wide
Cutaneous leishmaniasis: multiplication of the parasites in the histiocytes with destruction of the papule along with necrosis of the epidermis.
Bone marrow: mononuclear cells filled with amastigotes.
Spleen: lymphoid follicles are replaced by parasitized mononuclear cells.

208 D. Dionisio Gut Infections' Etio , pathogenetic and (I' , Inlcal Remarks

4) Larvae migrate via resplralOry tree to the trachea and pharynK, and are swallowed.
3) Through right sections of heart larvae migrate to the lungs where they break out 01 the pulmonary capillaries into the alveoli.
2) Larvae are carried via the cutaneus blood vessels.
1) Skin penetration of the filariform larvae from the fecally contamined soil.
Filariform larvae (average lenglh: 630 ~m and width: 16 ~m) may remain viable in soil or water for several days.
Gut Infections: Etiopathogenetic and Clinical Remarks 209
Strongyloides stercoralis life cycle
7) The rhabditiform larvae bore through the epitelium to the intestinal lumen
Larva in lung tissue.
5) Larvae undergo a final moult in the duodenum and upper jejunum
and pass out of the intestinal tract.
\
to become adult females which live in the mucosa and reproduce by parthenogenesis.
6) Eggs hatch in the intestinal mucosa
Autoinlection cycle: Rhabditiform larvae that are in the intestine develop into the filariform larvae while passing through the bowel. and can reinfect the host: by invading the intestinal mucosa. travelling via the portal system to the lungs: after being passed out in the feces, by reaching the perianal or perineal skin.
8) Larvae are passed out onto the soil in the feces.
1 0) The rhabditiform larvae (in temperate climate) can metamorphose into the filariform infectious forms third stage filariform larva)
9) tn presence of proper conditions of warmth and moisture in the soil larvae moult twice and differentiate into free 1M" _, (I_I" ",d ~I" 1.\
~2 ~I!!!!!:=:~I 11 ) After copulation female worms
12) Larvae derivating from hatched eggs can molt 10 form filariform larvae
deposite embryonated eggs in the soil which hatch and may repeat the cycle .




















