Guidelines to Obstetrical Examination and Appropriate ...
37
305 Guidelines to Obstetrical Examination and Appropriate Measurements Equipment Documentation First-Trimester Ultrasound Second- and Third-Trimester Ultrasound Ultrasound examinations are performed by sonog- raphers and sonologists with varied experience levels and with equipment of different specifications and image quality. An attempt to standardize all ultrasound studies began in 1985 when the American College of Radiology (ACR) and the American Institute of Ultra- sound in Medicine (AIUM) approved the concept of examination guidelines. They created similar but sepa- rate antepartum obstetrical ultrasound guidelines. The American College of Obstetricians and Gynecologists (ACOG) was involved in this initial discussion but chose to create an obstetrical ultrasound technical note rather than a guideline. This document was twice updated by the ACR and by the AIUM as a standard. Most recently, in 2003, an updated collaborative antepartum obstetrical ultrasound document, renamed as a practice guideline, was created by a combined effort of the ACR, AIUM, and ACOG. This most recent collaborative guidelines is described below. Although it is not possible for ultrasound to identify all in utero problems, many significant abnormalities can be detected with a systematic approach. A uniform evaluation is therefore necessary when a pregnant woman needs an ultrasound examination, regardless of clinical history, because most women pregnant with an abnormal fetus will have no predisposing risk factors. Some examiners originally suggested that the obstet- rical ultrasound examination could be divided into two levels of study. Proposed in 1977 in conjunction with maternal serum α-fetoprotein (MSAFP) screening pro- grams, a level 1 sonogram would be performed to detect obstetrical problems, unrelated to structural abnormali- ties, that could elevate MSAFP levels: most commonly inaccurate menstrual dates but also associated with multiple gestations and fetal demise. Maternal weight can also elevate these levels. If the MSAFP levels are still ele- vated, in a woman with a living intrauterine pregnancy of appropriate dates, a level 2 sonogram would then be per- formed to look for fetal anomalies, including open (not skin covered) fetal defects most commonly related to the neural axis and to the abdominal wall. Because it is easier to do a level 1 than a level 2 study, some practitioners interpreted this approach to mean that it might be acceptable to have a level 1 study performed by an exam- iner with less expertise and equipment; a level 2 study would need more operator experience and better equip- ment. To make matters more confusing, some practi- tioners dealing with complex cases declared themselves “level 3” examiners, a designation with no adequate def- inition. The concept of levels has therefore not been uni- formly applied and has consequently lost its validity. A high level of expertise is needed for all ultrasound obstet- rical examinations, and it is therefore recommended that this terminology be discarded. The anteparteum obstetrical ultrasound guideline defines four classifications of examinations: first- trimester, standard second- or third-trimester, limited (to answer a specific question) and specialized (a more detailed anatomic examination). This practice guideline also specifies clinical indications to perform an obstet- rical ultrasound. The guideline also defines or references other guidelines that detail expected parameters for physicians performing and interpreting diagnostic examinations, documentation of findings, equipment specifications, and fetal safety. Quality control and improvement, infection control, and patient education concerns are also referenced. Of these, the equipment and fetal safety, documentation, the first-trimester, and the standard second- and third-trimester examinations are discussed below. Direct quotes from the guideline will be shown in bolded type. CHAPTER 12
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Guidelines to Obstetrical Examination and Appropriate ...

305
Guidelines toObstetricalExamination andAppropriateMeasurements
EquipmentDocumentationFirst-Trimester UltrasoundSecond- and Third-Trimester Ultrasound
Ultrasound examinations are performed by sonog-raphers and sonologists with varied experience levelsand with equipment of different specifications andimage quality. An attempt to standardize all ultrasoundstudies began in 1985 when the American College ofRadiology (ACR) and the American Institute of Ultra-sound in Medicine (AIUM) approved the concept ofexamination guidelines. They created similar but sepa-rate antepartum obstetrical ultrasound guidelines. TheAmerican College of Obstetricians and Gynecologists(ACOG) was involved in this initial discussion but choseto create an obstetrical ultrasound technical note ratherthan a guideline. This document was twice updated bythe ACR and by the AIUM as a standard. Most recently,in 2003, an updated collaborative antepartum obstetricalultrasound document, renamed as a practice guideline,was created by a combined effort of the ACR, AIUM, andACOG. This most recent collaborative guidelines isdescribed below.
Although it is not possible for ultrasound to identifyall in utero problems, many significant abnormalities can be detected with a systematic approach. A uniformevaluation is therefore necessary when a pregnantwoman needs an ultrasound examination, regardless ofclinical history, because most women pregnant with anabnormal fetus will have no predisposing risk factors.
Some examiners originally suggested that the obstet-rical ultrasound examination could be divided into twolevels of study. Proposed in 1977 in conjunction withmaternal serum α-fetoprotein (MSAFP) screening pro-grams, a level 1 sonogram would be performed to detectobstetrical problems, unrelated to structural abnormali-ties, that could elevate MSAFP levels: most commonly
inaccurate menstrual dates but also associated withmultiple gestations and fetal demise. Maternal weight canalso elevate these levels. If the MSAFP levels are still ele-vated, in a woman with a living intrauterine pregnancy ofappropriate dates, a level 2 sonogram would then be per-formed to look for fetal anomalies, including open (notskin covered) fetal defects most commonly related to theneural axis and to the abdominal wall. Because it is easierto do a level 1 than a level 2 study, some practitionersinterpreted this approach to mean that it might beacceptable to have a level 1 study performed by an exam-iner with less expertise and equipment; a level 2 studywould need more operator experience and better equip-ment. To make matters more confusing, some practi-tioners dealing with complex cases declared themselves“level 3” examiners, a designation with no adequate def-inition. The concept of levels has therefore not been uni-formly applied and has consequently lost its validity. Ahigh level of expertise is needed for all ultrasound obstet-rical examinations, and it is therefore recommended thatthis terminology be discarded.
The anteparteum obstetrical ultrasound guidelinedefines four classifications of examinations: first-trimester, standard second- or third-trimester, limited (toanswer a specific question) and specialized (a moredetailed anatomic examination). This practice guidelinealso specifies clinical indications to perform an obstet-rical ultrasound. The guideline also defines or referencesother guidelines that detail expected parameters forphysicians performing and interpreting diagnosticexaminations, documentation of findings, equipmentspecifications, and fetal safety. Quality control andimprovement, infection control, and patient educationconcerns are also referenced. Of these, the equipmentand fetal safety, documentation, the first-trimester, andthe standard second- and third-trimester examinations arediscussed below. Direct quotes from the guideline willbe shown in bolded type.
CHAPTER12

306 ULTRASOUND: THE REQUISITES
A B
C DFigure 12-1 Measurement of crown-rump length at various stages of gestation. Crown-rumplength is measured from the top of the embryo’s head (crown) to the bottom of its torso (rump)(cursors). The yolk sac (arrows) should not be included in the measurement. A, Crown-rumplength of 2.2 mm corresponds to gestational age of 5.7 weeks. B, Crown-rump length of 5.5 mmcorresponds to gestational age of 6.3 weeks. C, Crown-rump length of 13.2 mm corresponds togestational age of 7.5 weeks. D, Crown-rump length of 38.7 mm corresponds to gestational age of 10.8 weeks.
EQUIPMENT
Ultrasound studies should be performed with real-time scanners by the transabdominal (TA) or trans-vaginal (TV) approach, or both. A transducer ofappropriate frequency (≥ 3 MHz for TA examination or≥ 5 MHz for TV studies) should be used. The choice offrequency is a tradeoff between beam penetration(better at lower frequencies) and resolution (better athigher frequencies). In general, the highest frequencythat still affords adequate penetration should beselected. The lowest ultrasound exposure settings
should also be used to gain necessary diagnostic infor-mation. This has been called the ALARA principle, whichmeans “as low as reasonably achievable.”
DOCUMENTATION
Adequate documentation is essential for ensuringappropriate patient care. A permanent record of theultrasound images is needed, including measurementsand anatomic findings. Images should be labeled withthe examination date, patient’s name, and/or identifica-tion number. Image orientation, if important, should be

Guidelines to obstetrical Examination and Appropriate Measurements 307
labeled. A written report of the ultrasound findingsshould be prepared and included in the patient’s medicalrecord.
FIRST-TRIMESTER ULTRASOUND
Imaging Parameters
Overall Comment
Scanning in the first trimester may be per-formed either transabdominally or transvaginally.If a transabdominal examination is not definitive,a transvaginal scan or transperineal scan shouldbe performed whenever possible.a. The uterus should be evaluated for the pres-
ence of a gestational sac. If a gestation sac isseen, its location should be documented. Thegestational sac should be evaluated for thepresence or absence of a yolk sac or embryo,and the crown-rump length should berecorded, when possible.
Comment: The crown-rump length is a moreaccurate indicator of gestational (menstrual) agethan is mean gestational sac diameter. However,the mean gestational sac diameter should berecorded when an embryo is not identified.
Caution should be used in making the pre-sumptive diagnosis of a gestational sac in theabsence of definite embryo or yolk sac. Withoutthese findings an intrauterine fluid collectioncould represent a pseudogestational sac associatedwith an ectopic pregancy.
In an obstetrical ultrasound examination, the termsgestational age, embryonic age or fetal age, and men-strual age are used synonymously, all originating fromthe first day of onset of the woman’s last normalmenstrual period. The embryo is typically identified by6 weeks, and the yolk sac is usually seen approximatelyone-half week earlier. Both are occasionally imaged evenearlier by the TV approach. The embryonic or crown-rump length (CRL) is the primary measurement forestablishing gestational age during the first trimester,with a precision of ±5 to 7 days. The CRL is measured inthe sagittal scan plane from the top of the embryo’s head(crown) to the bottom of its torso (rump) (Fig. 12-1).The yolk sac and extremities should not be included inthe CRL measurement (Table 12-1). The gestational saccan routinely be identified by 5 weeks’ gestation andwith TV scanning is occasionally seen earlier. The meangestational sac diameter or mean sac diameter (MSD) iscalculated by averaging three orthogonal measurementsof the gestational sac. These measurements of sac di-ameter are obtained from the inner-to-inner edge of the
Table 12-1 Predicted Menstrual Age from CRLMeasurements from 5.7 to 12 Weeks
*Range is the 95% confidence interval ±8% of the predicted age rounded tofarthest 0.1. Only 5.7 to 12.0 weeks are reported.From Hadlock FP, Shah YP, Kanon DJ, et al: Fetal crown-rump length: Reevaluation of relation to menstrual age (5-18 weeks) with high-resolutionreal-time US. Radiology 182:501-505, 1992.

hyperechoic rim, thereby including the fluid in the ges-tational sac but not the wall of the sac (Fig. 12-2). Likethe CRL, the MSD can be used to estimate gestational agewith a precision of ±5 to 7 days (Table 12-2), but theprimary value of the gestational sac as an age predictoris in the time period before the embryo is visualized,usually between 5 and 6 weeks. Once the embryo can beseen, the CRL, and not the MSD, should be used to assigngestational age. The MSD has not been as extensivelystudied as the CRL, and there are substantial discrepan-cies in the MSDs reported in different studies. Forexample, at 5 weeks, the mean gestational sac sizesreported in the literature range from 2 to 10 mm.Although this may seem a large range, the gestational sacnormally grows about 1 mm a day, so that even an 8-mmdifference is equivalent to only 1 week.
308 ULTRASOUND: THE REQUISITES
A
BFigure 12-2 Transvaginal scans showing measurement ofmean sac diameter. A and B, The mean sac diameter is measuredby obtaining three orthogonal diameters of the gestational sacwith calipers positioned on the inner edge of the hyperechoicrim. In this case, the average of the three diameters (7.9 mm, 5.7mm, and 11.9 mm) calculates to a mean sac diameter of 8.2 mm,consistent with a gestational age of 5.7 weeks.
A note of caution is needed in diagnosing a normalintrauterine pregnancy when only a gestational sacwithout a yolk sac or embryo is identified. On occasion apseudogestational sac (fluid within the endometrial canalseen in the setting of an ectopic pregnancy) may exhibitan appearance similar to that of a normal gestational sac.b. Presence or absence of cardiac activity should
be reported.Embryonic life can be detected by the real-time or
color Doppler observation of heart activity. Heartmotion should be evident in all embryos with a CRL ofat least 5 mm using TV ultrasound (equivalent to anembryonic age of 6.2 weeks) (see Table 12-1) and usuallyis seen earlier. Heart rate can also be evaluated: at 5 to 6weeks it should be at least 100 beats per minute, risingto between 140 and 160 beats per minute by 8 weeks.
Table 12-2 Mean Diameter of Gestational Sac andCorresponding Estimates of GestationalAge*
Gestational Age (wk)Mean Sac 95% Prediction Interval
Diameter (mm) Mean (Rounded to Farthest 0.1)
2 5.0 4.5-5.53 5.1 4.6-5.64 5.2 4.7-5.75 5.4 4.8-5.96 5.5 5.0-6.07 5.6 5.1-6.18 5.7 5.2-6.39 5.9 5.4-6.4
10 6.0 5.5-6.511 6.1 5.6-6.612 6.2 5.7-6.813 6.4 5.9-6.914 6.5 6.0-7.015 6.6 6.1-7.116 6.7 6.2-7.317 6.9 6.4-7.418 7.0 6.5-7.519 7.1 6.6-7.620 7.3 6.7-7.821 7.4 6.9-7.922 7.5 7.0-8.023 7.6 7.1-8.124 7.8 7.2-8.325 7.9 7.4-8.426 8.0 7.5-8.527 8.1 7.6-8.728 8.3 7.7-8.829 8.4 7.9-8.930 8.5 8.0-9.0
*The mean gestational age was calculated from a regression equation.Adapted from Daya S, Woods S, Ward S, et al: Early pregnancy assessmentwith transvaginal ultrasound scanning. Can Med Assoc J 144:441-445, 1991.

Guidelines to obstetrical Examination and Appropriate Measurements 309
There is a lower limit of normal for the heart rate: less than 90 beats per minute at 5 to 6 weeks and less than 120 beats per minute by 8 weeks. There is noestablished upper limit of concern for heart rate. If therate needs documentation, an M-mode recording can be performed. Pulsed Doppler sonography should beavoided in the first trimester because of its increasedpower.c. Fetal number should be reported.
Multiple gestations can be accurately determined by acareful analysis of the number of embryos and thenumber of gestational sacs. Overestimations of fetalnumber may occur if fluid in the endometrial cavity, asubchorionic hematoma, or the normal separation of the
amnion and chorion is misinterpreted as a gestationalsac. Underestimations may also occur, particularly ifthere are more than two closely situated gestational sacson transabdominal images. In these cases TV scanningwill often be of diagnostic value.d. Evaluation of the uterus, adnexal structures,
and cul-de-sac should be performed.The size and location of fibroids (Fig. 12-3) need to be
noted and monitored, because they tend to enlarge duringpregnancy. In the first trimester, fibroids occasionallycause gestational sac malposition and miscarriage.
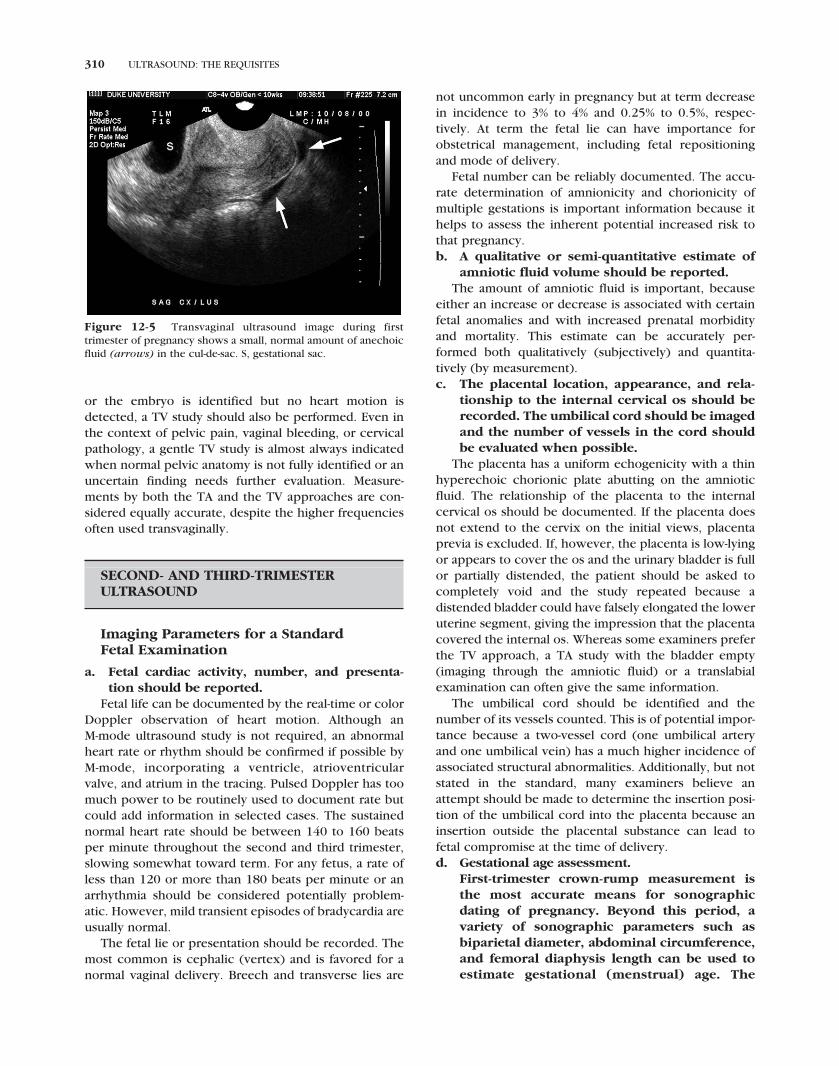
The most common adnexal mass, the corpus lutealcyst, is usually less than 3 cm in diameter and typicallyresolves by the mid-second trimester (Fig. 12-4). Theamount and echogenicity of cul-de-sac fluid, if present,should be noted. In a normal first-trimester pregnancy,only a small amount of anechoic fluid should be present(Fig. 12-5). Noncystic adnexal and cul-de-sac massesshould be evaluated for echogenicity and size. Surgicalremoval usually in the second trimester, if needed, isrelated to the mass’s size, position, and characteristicsthat would suggest malignancy (by physical examina-tion, ultrasound, and occasionally MRI).
In the first trimester, the initial ultrasound examina-tion can be performed transabdominally or transvagi-nally. TA ultrasound allows a more comprehensiveoverview of the uterus and adnexa, but TV ultrasoundprovides superior resolution and detail. If TA ultrasoundis done first and all normal landmarks are identified,including the gestational sac, the embryo with heartmotion, and the ovaries, further evaluation with TVultrasound is not required. If, however, the gestationalsac is not identified, the sac is seen without an embryo,
Figure 12-3 Fibroids in first-trimester pregnancy. Transverseendovaginal image of uterus shows two small fibroids (arrows) atsame level as gestational sac (S).
A BFigure 12-4 Examples of corpus luteal cysts during first trimester of pregnancy. A, Axial trans-vaginal image reveals small corpus luteal cyst (arrow) in right ovary, immediately posterior to theuterus. B, Longitudinal transabdominal image reveals moderate-sized corpus luteal cyst (arrow) in anovary immediately superior to the uterus. S, gestational sac in uterus.
310 ULTRASOUND: THE REQUISITES
Figure 12-5 Transvaginal ultrasound image during firsttrimester of pregnancy shows a small, normal amount of anechoicfluid (arrows) in the cul-de-sac. S, gestational sac.
or the embryo is identified but no heart motion isdetected, a TV study should also be performed. Even inthe context of pelvic pain, vaginal bleeding, or cervicalpathology, a gentle TV study is almost always indicatedwhen normal pelvic anatomy is not fully identified or anuncertain finding needs further evaluation. Measure-ments by both the TA and the TV approaches are con-sidered equally accurate, despite the higher frequenciesoften used transvaginally.
SECOND- AND THIRD-TRIMESTERULTRASOUND
Imaging Parameters for a Standard Fetal Examination
a. Fetal cardiac activity, number, and presenta-tion should be reported.
Fetal life can be documented by the real-time or colorDoppler observation of heart motion. Although an M-mode ultrasound study is not required, an abnormalheart rate or rhythm should be confirmed if possible byM-mode, incorporating a ventricle, atrioventricularvalve, and atrium in the tracing. Pulsed Doppler has toomuch power to be routinely used to document rate butcould add information in selected cases. The sustainednormal heart rate should be between 140 to 160 beatsper minute throughout the second and third trimester,slowing somewhat toward term. For any fetus, a rate ofless than 120 or more than 180 beats per minute or anarrhythmia should be considered potentially problem-atic. However, mild transient episodes of bradycardia areusually normal.
The fetal lie or presentation should be recorded. Themost common is cephalic (vertex) and is favored for anormal vaginal delivery. Breech and transverse lies are
not uncommon early in pregnancy but at term decreasein incidence to 3% to 4% and 0.25% to 0.5%, respec-tively. At term the fetal lie can have importance forobstetrical management, including fetal repositioningand mode of delivery.
Fetal number can be reliably documented. The accu-rate determination of amnionicity and chorionicity ofmultiple gestations is important information because ithelps to assess the inherent potential increased risk tothat pregnancy.b. A qualitative or semi-quantitative estimate of
amniotic fluid volume should be reported.The amount of amniotic fluid is important, because
either an increase or decrease is associated with certainfetal anomalies and with increased prenatal morbidityand mortality. This estimate can be accurately per-formed both qualitatively (subjectively) and quantita-tively (by measurement).c. The placental location, appearance, and rela-
tionship to the internal cervical os should berecorded. The umbilical cord should be imagedand the number of vessels in the cord shouldbe evaluated when possible.
The placenta has a uniform echogenicity with a thinhyperechoic chorionic plate abutting on the amnioticfluid. The relationship of the placenta to the internalcervical os should be documented. If the placenta doesnot extend to the cervix on the initial views, placentaprevia is excluded. If, however, the placenta is low-lyingor appears to cover the os and the urinary bladder is fullor partially distended, the patient should be asked tocompletely void and the study repeated because adistended bladder could have falsely elongated the loweruterine segment, giving the impression that the placentacovered the internal os. Whereas some examiners preferthe TV approach, a TA study with the bladder empty(imaging through the amniotic fluid) or a translabialexamination can often give the same information.
The umbilical cord should be identified and thenumber of its vessels counted. This is of potential impor-tance because a two-vessel cord (one umbilical arteryand one umbilical vein) has a much higher incidence ofassociated structural abnormalities. Additionally, but notstated in the standard, many examiners believe anattempt should be made to determine the insertion posi-tion of the umbilical cord into the placenta because aninsertion outside the placental substance can lead tofetal compromise at the time of delivery.d. Gestational age assessment.
First-trimester crown-rump measurement isthe most accurate means for sonographicdating of pregnancy. Beyond this period, avariety of sonographic parameters such asbiparietal diameter, abdominal circumference,and femoral diaphysis length can be used toestimate gestational (menstrual) age. The

Guidelines to obstetrical Examination and Appropriate Measurements 311
variability of gestational (menstrual) age esti-mations, however, increases with advancingpregnancy. Significant discrepancies betweengestational (menstrual) age and fetal measure-ments may suggest the possibility of fetalgrowth abnormality, intrauterine growthrestriction, or macrosomia.
While the crown-rump length (CRL) is an excellentmethod of establishing gestational age, there is ampleevidence in the literature to suggest that the head meas-urements up to 20 weeks have very good precision,almost equivalent to the CRL, with the femur length con-siderably less precise (Table 12-3). By the third trimester,while no parameter offers adequate accuracy, the femurlength measurement is slightly more precise than thehead measurements.
The abdominal measurements are far less precise inboth the second and third trimesters and should not beused to establish gestational age (see Table 12-3).Instead, abdominal measurements should be used, alongwith the head and femur length measurements, to ana-lyze fetal proportionality and growth.i. Biparietal diameter is measured at a standard
level of the thalami and cavum septi pellucidi.The cerebellar hemispheres should not bevisible in this scanning plane. The measure-ment is taken from the outer edge of the prox-imal skull to the inner edge of the distal skull.Comment: The head shape may be flattened(dolichocephalic) or rounded (brachycephalic)as a normal variant. Under these circumstances,certain variants of normal fetal head develop-ment may make measurement of the headcircumference more reliable than biparietaldiameter for estimating gestational (men-strual) age.
ii. Head circumference is measured at the samelevel as the biparietal diameter, around theouter perimeter of the calvarium. The meas-urement is not affected by head shape.
iii. Femur diaphysis length can be reliably usedafter 14th week of gestational (menstrual) age.
The long axis of the femur shaft is most accu-rately measured with the beam of insonationbeing perpendicular to the shaft, excluding thedistal femoral epiphysis.
iv. Abdominal circumference should be deter-mined at the skin line on a true transverse viewat the level of the junction of the umbilical vein,portal sinus, and fetal stomach when visible.Comment: Abdominal circumference meas-urement is used with other parameters toestimate fetal weight and may allow detec-tion of intrauterine growth restriction and macrosomia.
The biparietal diameter (BPD) is measured from theleading edge to the leading edge of the temporoparietalbones (Fig. 12-6) and the corresponding gestational ageis determined using a standard BPD table (Table 12-4).
The accuracy of the BPD is dependent on a normalhead shape. If the fetal head is unusually rounded(brachycephalic) or elongated (dolichocephalic), theBPD measurement will overestimate or underestimategestational age, respectively. To correct this potentialinaccuracy, a second linear measurement is obtained fromthe same image as the BPD, the fronto-occipital diameter(FOD). Using both measurements, a cephalic index (CI) iscalculated by the following formula (Fig. 12-7):
CI = (BPD + FOD) × 2/100.
The mean CI is 78.3 with a normal range of 70 to 86at 2 standard deviations (SD). For the purposes of thiscorrection, both the BPD and FOD should ideally beobtained from outer edge to outer edge. In actuality theBPD is usually not remeasured but is kept as an outer-to-inner-edge measurement.
Figure 12-6 Measurement of the biparietal diameter (BPD).The BPD is measured at the level of the thalami (T) or midbrain,from the leading edge to the leading edge (outer to inner) of the calvarium (cursors). In this example, the measured BPD of 65.3 mm corresponds to a gestational age of 25.6 weeks.
Table 12-3 Gestational Age Interval (Weeks)
From Benson CB, Doubilet PM: Sonographic prediction of gestational age:Accuracy of second- and third-trimester fetal measurements. AJR Am JRoentgenol 157:1275-1277, 1991.
312 ULTRASOUND: THE REQUISITES
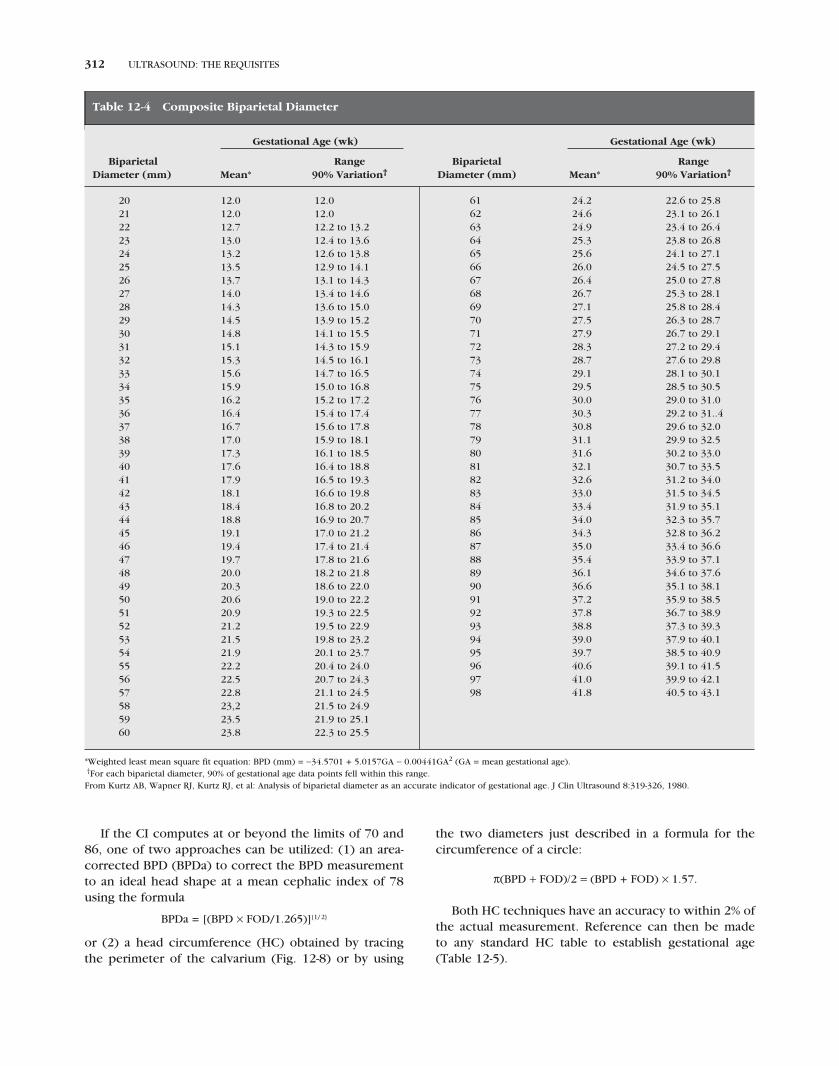
If the CI computes at or beyond the limits of 70 and86, one of two approaches can be utilized: (1) an area-corrected BPD (BPDa) to correct the BPD measurementto an ideal head shape at a mean cephalic index of 78using the formula
BPDa = [(BPD × FOD/1.265)]{1/ 2}
or (2) a head circumference (HC) obtained by tracingthe perimeter of the calvarium (Fig. 12-8) or by using
the two diameters just described in a formula for thecircumference of a circle:
π(BPD + FOD)/2 = (BPD + FOD) × 1.57.
Both HC techniques have an accuracy to within 2% ofthe actual measurement. Reference can then be made to any standard HC table to establish gestational age(Table 12-5).
Table 12-4 Composite Biparietal Diameter
Gestational Age (wk) Gestational Age (wk)
Biparietal Range Biparietal RangeDiameter (mm) Mean* 90% Variation† Diameter (mm) Mean* 90% Variation†
20 12.0 12.021 12.0 12.022 12.7 12.2 to 13.223 13.0 12.4 to 13.624 13.2 12.6 to 13.825 13.5 12.9 to 14.126 13.7 13.1 to 14.327 14.0 13.4 to 14.628 14.3 13.6 to 15.029 14.5 13.9 to 15.230 14.8 14.1 to 15.531 15.1 14.3 to 15.932 15.3 14.5 to 16.133 15.6 14.7 to 16.534 15.9 15.0 to 16.835 16.2 15.2 to 17.236 16.4 15.4 to 17.437 16.7 15.6 to 17.838 17.0 15.9 to 18.139 17.3 16.1 to 18.540 17.6 16.4 to 18.841 17.9 16.5 to 19.342 18.1 16.6 to 19.843 18.4 16.8 to 20.244 18.8 16.9 to 20.745 19.1 17.0 to 21.246 19.4 17.4 to 21.447 19.7 17.8 to 21.648 20.0 18.2 to 21.849 20.3 18.6 to 22.050 20.6 19.0 to 22.251 20.9 19.3 to 22.552 21.2 19.5 to 22.953 21.5 19.8 to 23.254 21.9 20.1 to 23.755 22.2 20.4 to 24.056 22.5 20.7 to 24.357 22.8 21.1 to 24.558 23,2 21.5 to 24.959 23.5 21.9 to 25.160 23.8 22.3 to 25.5
61 24.2 22.6 to 25.862 24.6 23.1 to 26.163 24.9 23.4 to 26.464 25.3 23.8 to 26.865 25.6 24.1 to 27.166 26.0 24.5 to 27.567 26.4 25.0 to 27.868 26.7 25.3 to 28.169 27.1 25.8 to 28.470 27.5 26.3 to 28.771 27.9 26.7 to 29.172 28.3 27.2 to 29.473 28.7 27.6 to 29.874 29.1 28.1 to 30.175 29.5 28.5 to 30.576 30.0 29.0 to 31.077 30.3 29.2 to 31..478 30.8 29.6 to 32.079 31.1 29.9 to 32.580 31.6 30.2 to 33.081 32.1 30.7 to 33.582 32.6 31.2 to 34.083 33.0 31.5 to 34.584 33.4 31.9 to 35.185 34.0 32.3 to 35.786 34.3 32.8 to 36.287 35.0 33.4 to 36.688 35.4 33.9 to 37.189 36.1 34.6 to 37.690 36.6 35.1 to 38.191 37.2 35.9 to 38.592 37.8 36.7 to 38.993 38.8 37.3 to 39.394 39.0 37.9 to 40.195 39.7 38.5 to 40.996 40.6 39.1 to 41.597 41.0 39.9 to 42.198 41.8 40.5 to 43.1
*Weighted least mean square fit equation: BPD (mm) = −34.5701 + 5.0157GA − 0.00441GA2 (GA = mean gestational age).†For each biparietal diameter, 90% of gestational age data points fell within this range.From Kurtz AB, Wapner RJ, Kurtz RJ, et al: Analysis of biparietal diameter as an accurate indicator of gestational age. J Clin Ultrasound 8:319-326, 1980.

Guidelines to obstetrical Examination and Appropriate Measurements 313
The BPDa and HC measurements in the secondtrimester (up to 20 and perhaps up to 24 weeks) have aprecision of ±1.2 weeks (see Table 12-3), close to that ofthe first-trimester CRL. By the third trimester, particularlyafter 26 weeks, the precision of the head measurementsdecreases to ±3.3 weeks and after 32 weeks it decreasesto ±3.8 weeks.
Femur length is used in conjunction with the headmeasurement to establish gestational age. The femoraldiaphysis length (FL) is a linear structure and is meas-ured along its ossified shaft (diaphysis) from one end to
Figure 12-7 Measurement of fronto-occipital diameter (FOD)and calculation of cephalic index. The FOD is measured on thesame image as the BPD (cursors labeled 1) by positioning caliperson the outer edge of the frontal and occipital bones in the midline(cursors labeled 2). The cephalic index (CI) is then calculated fromthe formula: CI = (BPD/FOD) × 100. In this example, the CI of 70.7is normal (normal range = 70 to 86).
Figure 12-8 Measurement of head circumference (HC). TheHC is measured by tracing the perimeter of the calvarium (dottedline), along the outer surface of the calvarium in an axial scanplane at the same level used to measure BPD. In this example, themeasured head circumference of 285.6 mm corresponds to agestational age of 31.4 weeks.
Table 12-5 Head Circumference Measurement
From Hadlock FP, Deter RL, Harrist RB, Park SK: Fetal head circumference:Relation to menstrual age. AJR Am J Roentgenol 138:649-653, 1982.

314 ULTRASOUND: THE REQUISITES
A BFigure 12-10 Comparison of configuration and length of femur in near and far field. A, Femurclosest to the transducer. Surface of this femur (cursors) appears straight because the lateral surfaceof the femur is imaged. B, Femur farthest from the transducer. Surface of this femur appears to becurved (cursors, arrows) because the medial surface of this femur is measured. Despite this, thefemur lengths obtained from both femurs are identical (32.3 mm). They correspond to a gestationalage of 19.7 weeks.
the other, disregarding the epiphyseal cartilages(Fig. 12-9). The normal diaphysis has a straight lateraland curved medial border. If measured medially, astraight measurement is still obtained disregarding thecurvature (Fig. 12-10). The FL is considered slightly moreprecise in the third trimester (see Table 12-3) and can beused to assign gestational age by itself (Table 12-6) whenthe BPD and HC are considered unreliable for technical
or pathologic reasons. Another use of the FL is to analyzeits proportionality to the head, which can detect skeletaldysplasias and growth disturbances (Table 12-7).Whereas the guideline recommends identification andmeasurement of one femur, with the assumption thatthe other would also be normal, an attempt to identifyand measure the other femur is suggested if the first FLis either too long or short when compared with the BPD.
If more than one study is performed, it is critical thatthe gestational age not be reestablished on each subse-quent examination, particularly in the third trimester.Instead, the current fetal age is the initial fetal age (estab-lished on the first examination) plus the number of weeksthat have elapsed. For example, if a fetus with an initialCRL equivalent to 7 weeks’ gestation is restudied 20weeks later, the gestational age is 27 weeks (7 weeks + 20weeks = 27 weeks), regardless of the new fetal measure-ments. A mean gestational age is always given. A rangearound this mean is sometimes also reported because itgives an assessment of the range of gestational ages likelyto correspond to the fetus’ actual gestational age.
The fetal abdomen is measured axially at the level ofthe fetal liver, just below the heart, using the landmarkof the umbilical portion of the left portal vein at itsjunction with the portal sinus and right portal vein(Fig. 12-11). This left portal vein should be imagedentirely within the liver and equidistant from the sides ofthe abdomen. The abdominal circumference (AC) can bedetermined either by tracing the perimeter of theabdomen or by averaging two orthogonal abdominaldiameters (ADs) and calculating AC from the equation
Figure 12-9 Measurement of femur length (FL). The femurlength is measured by positioning calipers on the edge of the prox-imal and distal segments of the diaphysis (cursors). When possible,the femur should be oriented approximately perpendicular to theultrasound beam. The epiphyseal cartilages (E) should not beincluded in the measurement. In this example, the femur length of55.3 mm corresponds to a gestational age of 25.9 weeks.

Guidelines to obstetrical Examination and Appropriate Measurements 315
for the circumference of a circle. The ADs should bemeasured from the outer edge to outer edge of the softtissues (Fig. 12-12).
Abdominal measurements should not be used toestimate gestational age because they are not as accurateas head and femur measurements for establishing gesta-tional age. Their primary value is instead in the calcula-tion of estimated fetal weight (EFW) and in thedetermination of normal proportionality with the headso that growth disturbances can be identified by thehead-to-abdominal circumference ratio (Table 12-8).Alternatively, the proportionality of the BPD to the ADcan be evaluated (Table 12-9). With either method thehead is normally larger than the body in the second andearly third trimesters, with reversal by term.
A ratio of the FL to the AC has also been proposed.The cut-off ratios separating a normal from a possiblelarge or small abdomen (potential macrosomia andgrowth restriction) have not been found precise. Theratio is therefore not recommended because too muchoverlap exists for clinical utility.e. Fetal weight estimation. Fetal weight can be
estimated by obtaining measurements such asthe biparietal diameter, head circumference,abdominal circumference, and femoral diaph-ysis length. Results from various predictionmodels can be compared to fetal weight per-centiles from published monograms.
The fetal weight tables are derived from head, body,and femur measurements (Tables 12-10 and 12-11). Their
Table 12-6 Gestational Age (GA) Prediction Based on Femur Length (FL) Measurements
Predicted GA (wk) Predicted GA (wk)
FL (mm) Mean 2 SD Range* FL (mm) Mean 2 SD Range*
10 13.7 12.5 to 14.911 13.9 12.7 to 15.112 14.2 13.0 to 15.413 14.4 13.2 to 15.614 14.6 13.4 to 15.815 14.9 13.7 to 16.116 15.1 13.9 to 16.317 15.4 14.2 to 16.618 15.6 14.4 to 16.819 15.9 14.7 to 17.120 16.2 15.0 to 17.421 16.4 15.2 to 17.622 16.7 15.5 to 17.923 17.0 15.8 to 18.224 17.3 16.1 to 18.525 17.6 16.4 to 18.826 17.9 16.7 to 19.127 18.2 17.0 to 19.428 18.5 17.3 to 19.729 18.8 17.6 to 20.030 19.1 17.9 to 20.331 19.4 18.2 to 20.632 19.7 18.5 to 20.933 20.1 18.2 to 22.034 20.4 18.5 to 22.335 20.7 18.8 to 22.636 21.1 19.2 to 23.037 21.4 19.5 to 23.338 21.8 19.9 to 23.739 22.2 20.3 to 24.140 22.5 20.6 to 24.441 22.9 21.0 to 24.842 23.3 21.4 to 25.243 23.7 21.8 to 25.644 24.1 22.2 to 26.0
45 24.5 22.6 to 26.446 24.9 23.0 to 26.847 25.3 23.4 to 27.248 25.7 23.8 to 27.649 26.2 23.5 to 28.950 26.6 23.9 to 29.351 27.0 24.3 to 29.752 27.5 24.8 to 30.253 28.0 25.3 to 30.754 28.4 25.7 to 31.155 28.9 26.2 to 31.656 29.4 26.7 to 32.157 29.9 27.2 to 32.658 30.4 27.7 to 33.159 30.9 28.2 to 33.660 31.4 28.7 to 34.161 31.9 29.2 to 34.662 32.5 28.5 to 36.563 33.0 29.0 to 37.064 33.6 29.6 to 37.665 34.1 30.1 to 38.166 34.7 30.7 to 38.767 35.3 31.3 to 39.368 35.9 31.9 to 39.969 36.5 32.5 to 40.570 37.1 33.1 to 41.171 37.7 33.7 to 41.772 38.3 35.1 to 41.573 39.0 35.8 to 42.274 39.6 36.4 to 42.875 40.3 37.1 to 43.576 40.9 37.7 to 44.177 41.6 38.4 to 44.878 42.0 38.8 to 45.2
*2 SD = 2 standard deviations.Adapted from Doubilet PM, Benson CB: Improved prediction of gestational age in the late third trimester. J Ultrasound Med 12:647-653, 1993.

316 ULTRASOUND: THE REQUISITES
Figure 12-11 Measurement of abdominal circumference (AC).The abdominal circumference is measured on an axial image of thefetal abdomen at the level of the liver, preferably at the confluenceof the left (black arrow) and right (white arrow) portal veins,which assume a C-shaped configuration. The AC should be meas-ured along the outer edge of the soft tissues of the abdomen(dotted line).
Table 12-7 Fetal Long Bone Measurements TrueMean and Range from 5th to 95thPercentile (mm) (2 SD)
Biparietal Diameter Femur Humerus
Gesta-tional True True TrueAge (wk) Mean 2 SD Mean 2 SD Mean 2 SD
13 23 20-26 11 9-13 10 8-1214 27 24-30 13 11-15 12 10-1415 30 29-31 15 13-17 14 12-16
16 33 31-35 19 16-22 17 15-1917 37 34-40 22 19-25 20 16-2418 42 37-47 25 22-28 23 20-2619 44 40-48 28 25-31 26 23-2920 47 43-51 31 28-34 29 26-32
21 50 45-55 35 31-39 32 28-3622 55 50-60 36 33-39 33 30-3623 58 53-63 40 36-44 37 34-4024 61 56-66 42 39-45 38 34-4225 64 59-69 46 43-49 42 38-46
26 68 63-73 48 44-52 43 40-4627 70 67-73 49 46-52 45 43-4728 73 68-78 53 48-58 47 43-5129 76 71-81 53 48-58 48 44-5230 77 71-83 56 53-59 50 45-55
31 82 75-89 60 54-66 53 49-5732 85 79-91 61 55-68 54 50-5833 86 82-90 64 59-69 56 51-6134 89 84-94 66 60-72 58 53-6335 89 82-96 67 61-73 59 53-65
36 91 84-98 70 63-77 60 54-6637 93 84-102 72 68-76 61 57-6538 95 89-101 74 68-80 64 61-6739 95 89-101 76 68-84 65 59-7140 99 92-107 77 73-81 66 62-70
41 97 91-103 77 73-81 66 62-7042 100 95-105 78 71-83 68 61-75
From Merz E, Kim-Kern M, Pehl S: Ultrasonic mensuration of fetal limb bones inthe second and third trimesters. J Clin Ultrasound 15: 175–183, 1987.
Figure 12-12 Measurement of abdominal diameters (AD). Analternative to directly measuring the abdominal circumference(AC) is to measure two orthogonal abdominal diameters andcalculate the AC from the equation for the circumference of acircle. Abdominal diameters are measured at the same level as theAC from the outer edge to the outer edge of the soft tissues (cur-sors). Black arrow, left portal vein; white arrow, right portal vein.
utility is limited by a sizable variation around the meanweight, at least ±17% to 20% for a table using two pa-rameters and ±15% for a table using three parameters.Nevertheless, the mean weight can be of value indetermining if the fetus is appropriate in size providedthat the fetal age is known from an earlier first- orsecond-trimester study, when age determination is moreprecise. Then the calculated weight can be comparedwith the expected weight of a fetus for that age (Table12-12). For example, if in Table 12-10, the BPD and AC are70 and 350 mm, respectively, a weight of 2368 g isobtained. If the fetal age is known to be 35 weeks from aprior ultrasound study, Table 12-12 shows that at 35
weeks a weight of 2368 g is between the 25th and 50thpercentile, which is normal. If the weight falls below the10th percentile the fetus is considered small for gesta-tional age, and if it is above the 90th percentile the fetusis considered large for gestational age.
The guideline recommends that on all follow-upstudies the interval growth should be assessed. For this,

Guidelines to obstetrical Examination and Appropriate Measurements 317
longitudinal growth data should be applied when pos-sible. Most measurement tables use cross-sectional data,which was collected by evaluating multiple fetuses onlyonce. Cross-sectional data permit accurate estimations ofgestational age but are not optimal for analysis of intervalgrowth. For evaluation of interval growth, longitudinalgrowth studies are preferred. Longitudinal growth tablesevaluate multiple fetuses multiple times, comparing indi-vidual and population growth. Although the mean num-bers are approximately the same from cross-sectionaland longitudinal studies, the ranges are very different.
There are three main approaches to interval growthanalysis. The least precise compares the gestational agescorresponding to fetal measurements from two exami-nations, sometimes utilizing different gestational agetables. This approach can be used at any time during thepregnancy and is the method most commonly used toassess interval growth between the first and the secondtrimesters. For example, if the initial ultrasound haddetected an embryo of 10 mm, equivalent to mean ges-tational age of 7.1 weeks (see Table 12-1), 10 weeks laterwhen a second study is performed the assigned gesta-tional age would be 17.1 weeks. If on that second studythe BPD measures 36 mm, equivalent to a mean age of16.4 weeks (see Table 12-4), the measured gestationalage by BPD (16.4 weeks) would be within 1 week of theassigned gestational age (17.1 weeks), and it would beassumed that there is likely no problem with head
growth. As discrepancies approach or exceed 2 weeks,however, the possibility of a growth disturbance wouldbe raised.
A second method of evaluating interval growth con-sists of plotting fetal measurements on a graph, whichdisplays a measurement parameter such as EFW or ACon one axis and gestational age on the other axis. Linesdelineating the mean and predetermined percentile orstandard deviation levels for the parameter are superim-posed on the graph to facilitate assessment of whetherfetal size is appropriate for gestational age and whetherinterval growth has been appropriate. A variation of thismethod uses a table or computer program to report thepercentile or standard deviation level of a parameter forthe fetus’ assigned gestational age. If there is marked
Table 12-8 Head to Abdomen Circumference Ratio Table
Ratio of Head Circumference/Abdominal Circumference
Gestational Age Range from(wk) Mean 5th to 95th Percentile
13-14 1.23 1.14-1.3115-16 1.22 1.05-1.3917-18 1.18 1.07-1.2919-20 1.18 1.09-1.3921-22 1.15 1.06-1.2523-24 1.13 1.05-1.2125-26 1.13 1.04-1.2227-28 1.13 1.05-1.2129-30 1.10 0.99-1.21.31-32 1.07 0.96-1.1733-34 1.04 0.96-1.1135-36 1.02 0.93-1.1137-38 0.98 0.92-1.0539-40 0.97 0.87-1.0641-42 0.96 0.93-1.00
From Campbell S, Thoms A: Ultrasound measurement of the fetal head toabdomen circumference in the assessment of growth retardation. Br J ObstetGynaecol 84:165-174, 1977.
Table 12-9 Abdominal Diameter MeasurementTable
Average Abdominal Diameter (mm)
PredictedMean Range from
Gestational Biparietal Predicted 5th to 95th Age (wk) Diameter (mm) Mean Percentile
13 25.6 22.7 18.2-27.214 28.5 26.4 21.7-31.115 31.5 30.1 25.3-34.916 34.6 33.7 28.6-38.817 37.7 37.3 32.0-42.718 40.9 40.9 35.4-46.519 44.1 44.5 38.7-50.320 47.4 48.0 41.9-54.021 50.6 51.4 45.2-57.722 53.9 54.9 48.3-61.523 57.1 58.3 51.4-65.224 60.4 61.7 54.5-68.925 63.5 65.0 57.5-72.626 66.6 68.4 60.5-76.227 70.0 71.7 63.4-79.928 72.6 74.9 66.3-83.629 75.4 78.2 69.1-87.230 78.1 81.4 71.9-90.931 80.7 84.6 74.6-94.532 83.1 87.7 77.2-98.233 85.4 90.8 79.8-101.834 87.5 93.9 82.4-105.535 89.4 97.0 84.8-109.236 91.1 100.1 87.3-112.937 92.6 103.1 89.5-116.538 93.8 106.1 91.9-120.339 94.8 109.0 94.1-124.040 95.5 112.0 96.2-127.8
From Eriksen PS, Sechor NJ, Weis-Bentzon M: Normal growth of the fetalbiparietal diameter and the abdominal diameter in a longitudinal study: Anevaluation of the two parameters in predicting fetal weight. Acta ObstetGynecol Scand 64: 65-70, 1985.

Table 12-10 Estimated Fetal Weight (g) Based on Biparietal Diameter (BPD) and Abdominal Circumference (AC)*
AC (mm)
BPD (mm) 155 160 165 170 175 180 185 190 195 200 205 210 215
31 224 234 244 255 267 279 291 304 318 332 346 362 37832 231 241 251 263 274 286 299 312 326 340 355 371 38833 237 248 259 270 282 294 307 321 335 349 365 381 39734 244 255 266 278 290 302 316 329 344 359 374 391 40835 251 262 274 285 298 311 324 338 353 368 384 401 41836 259 270 281 294 306 319 333 347 362 378 394 411 42937 266 278 290 302 315 328 342 357 372 388 404 422 44038 274 286 298 310 324 337 352 366 382 398 415 432 45139 282 294 306 319 333 347 361 376 392 409 426 444 46240 290 303 315 328 342 356 371 386 403 419 437 455 47441 299 311 324 338 352 366 381 397 413 430 448 467 48642 308 320 333 347 361 376 392 408 424 442 460 479 49843 317 330 343 357 371 387 402 419 436 453 472 491 51144 326 339 353 367 382 397 413 430 447 465 484 504 52445 335 349 363 377 393 408 425 442 459 478 497 517 53846 345 359 373 386 404 420 436 454 472 490 510 530 55147 355 369 384 399 415 431 448 466 484 503 524 544 56548 366 380 395 410 426 443 460 478 497 517 537 558 58049 376 391 406 422 438 455 473 491 510 530 551 572 59450 387 402 418 434 451 468 486 505 524 544 565 587 61051 399 414 430 446 463 481 499 518 538 559 580 602 62552 410 426 442 459 476 494 513 532 552 573 595 618 64153 422 438 455 472 489 508 527 547 567 589 611 634 65754 435 451 468 485 503 522 541 561 582 604 627 650 67455 447 464 481 499 517 536 556 577 598 620 643 667 69156 461 477 495 513 532 551 571 592 614 636 660 684 70957 474 491 509 527 547 566 587 608 630 653 677 701 72758 488 505 524 542 562 582 603 625 647 670 695 719 74559 502 520 539 558 578 598 619 642 664 688 713 738 76460 517 535 554 573 594 615 636 659 682 706 731 757 78461 532 550 570 590 610 632 654 677 700 725 750 777 80462 547 566 586 606 627 649 672 695 719 744 770 797 82463 563 583 603 624 645 667 690 714 738 764 790 817 84564 580 600 620 641 663 686 709 733 758 784 811 838 86765 597 617 638 659 682 705 728 753 778 805 832 860 88966 614 635 656 678 701 724 748 773 799 826 853 882 91167 632 653 675 697 720 744 769 794 820 848 876 905 93568 651 672 694 717 740 765 790 816 842 870 898 928 95869 670 691 714 737 761 786 811 838 865 893 922 952 98370 689 711 734 758 782 807 833 860 888 916 946 976 100871 709 732 755 779 804 830 856 883 912 941 971 1002 103372 730 763 777 801 827 853 880 907 936 965 996 1027 106073 751 775 799 824 850 876 904 932 961 991 1022 1054 108774 773 797 822 847 874 901 928 957 987 1017 1049 1081 111475 796 820 845 871 898 925 954 983 1013 1044 1076 1109 114376 819 844 870 896 923 951 960 1009 1040 1072 1104 1137 117277 843 868 894 921 949 977 1007 1037 1068 1100 1133 1187 120278 868 894 920 947 975 1004 1034 1065 1096 1129 1162 1197 123279 893 919 946 974 1003 1032 1062 1094 1126 1159 1193 1228 126480 919 946 973 1002 1031 1061 1091 1123 1156 1189 1224 1259 129681 946 973 1001 1030 1060 1090 1121 1153 1187 1221 1256 1292 132982 974 1001 1030 1059 1089 1120 1152 1185 1218 1253 1288 1325 136383 1002 1030 1059 1089 1120 1151 1183 1217 1251 1286 1322 1359 139784 1032 1060 1090 1120 1151 1163 1216 1249 1284 1320 1356 1394 143385 1062 1091 1121 1151 1183 1216 1249 1283 1318 1355 1392 1430 146986 1093 1122 1153 1184 1216 1249 1283 1318 1354 1390 1428 1467 150787 1125 1155 1186 1218 1250 1284 1318 1353 1390 1427 1465 1505 154588 1157 1188 1220 1252 1285 1319 1354 1390 1427 1465 1504 1543 158489 1191 1222 1254 1287 1321 1356 1391 1428 1465 1503 1543 1583 162590 1226 1258 1290 1324 1358 1393 1429 1456 1504 1543 1583 1624 166691 1262 1294 1327 1361 1396 1432 1468 1506 1544 1584 1624 1666 170892 1299 1332 1365 1400 1435 1471 1508 1546 1586 1626 1667 1709 175293 1337 1370 1404 1439 1475 1512 1550 1588 1628 1668 1710 1753 179694 1376 1410 1444 1480 1516 1554 1592 1631 1671 1712 1755 1798 184295 1416 1450 1486 1522 1559 1597 1635 1675 1716 1758 1800 1844 188996 1457 1492 1528 1565 1602 1641 1680 1720 1762 1804 1847 1892 193797 1500 1535 1572 1609 1547 1686 1726 1767 1809 1852 1895 1940 198698 1544 1580 1617 1654 1693 1733 1773 1815 1857 1900 1945 1990 203799 1589 1625 1663 1701 1740 1781 1822 1864 1907 1951 1996 2042 2089
100 1635 1672 1710 1749 1789 1830 1871 1914 1958 2002 2048 2094 2142
*Estimated fetal weights: Log (birth weight) = −1.7492 + 0.166 (BPD) + 0.046 (AC) −0.00264 (AC × BPD).From Shepard MJ, Richards VA, Berkowitz RL, et al: An evaluation of two equations for predicting fetal weight by ultrasound. Am J Obstet Gynecol 147:47-54, 1982.
318

Table 12-10—Cont’d
AC (mm)
BPD (mm) 220 225 230 235 240 245 250 255 260 265 270 275 280
31 395 412 431 450 470 491 513 536 559 584 610 638 66632 405 423 441 461 481 502 525 548 572 597 624 651 68033 415 433 452 472 493 514 537 560 585 611 638 666 69334 425 444 463 483 504 526 549 573 598 624 652 680 71035 436 455 475 495 517 539 562 587 612 638 666 695 72536 447 466 486 507 529 552 575 600 626 653 681 710 74037 458 478 498 519 542 565 589 614 640 667 696 725 75638 470 490 510 532 554 578 602 628 654 682 711 741 77239 482 502 523 545 568 592 616 642 669 697 727 757 78940 494 514 536 558 581 606 631 657 684 713 743 773 80641 506 527 549 572 595 620 645 672 700 729 759 790 82842 519 540 562 585 609 634 660 688 716 745 776 807 84143 532 554 576 600 624 649 676 703 732 762 793 825 85944 545 567 590 614 639 665 692 719 749 779 810 843 87745 559 581 605 629 654 680 708 736 765 796 828 861 89646 573 596 620 644 670 696 724 753 783 814 846 880 91547 588 611 635 660 686 713 741 770 801 832 865 899 93448 602 626 650 676 702 730 758 788 819 851 884 919 95449 617 641 666 692 719 747 776 806 837 870 903 938 97550 633 657 683 709 736 765 794 824 856 889 923 959 99651 649 674 699 726 754 783 812 843 876 909 944 980 101752 665 690 717 744 772 801 831 863 895 929 964 1001 103953 682 708 734 762 790 820 851 883 916 950 986 1023 106154 699 725 752 780 809 839 870 903 936 971 1007 1045 108455 717 743 771 799 828 859 891 924 958 993 1030 1068 110756 735 762 789 818 848 879 911 945 979 1015 1052 1091 113157 753 780 809 838 869 900 933 966 1001 1038 1075 1114 115558 772 800 829 858 889 921 954 989 1024 1061 1099 1139 118059 792 820 849 879 911 943 977 1011 1047 1085 1123 1163 120560 811 840 870 900 932 965 999 1035 1071 1109 1148 1189 123161 832 861 891 922 955 988 1023 1058 1095 1134 1173 1214 125762 853 882 913 945 977 1011 1046 1083 1120 1159 1199 1241 128463 874 904 935 967 1001 1035 1071 1107 1145 1185 1226 1268 131164 896 927 958 991 1025 1059 1096 1133 1171 1211 1253 1295 133965 919 950 982 1015 1049 1084 1121 1159 1198 1238 1280 1323 136866 942 973 1006 1039 1074 1110 1147 1185 1225 1266 1308 1352 139767 965 997 1030 1065 1100 1136 1174 1213 1253 1294 1337 1381 142768 990 1022 1056 1090 1126 1163 1201 1241 1281 1323 1367 1411 145869 1015 1048 1082 1117 1153 1190 1229 1269 1310 1353 1397 1442 148970 1040 1074 1108 1144 1181 1219 1258 1298 1340 1383 1427 1473 152171 1066 1100 1135 1171 1209 1247 1287 1328 1370 1414 1459 1505 155372 1093 1128 1163 1200 1238 1277 1317 1358 1401 1445 1491 1538 158673 1121 1156 1192 1229 1267 1307 1348 1390 1433 1478 1524 1571 162074 1149 1184 1221 1259 1297 1338 1379 1421 1465 1511 1557 1605 165575 1178 1214 1251 1289 1328 1369 1411 1454 1499 1544 1592 1640 169076 1207 1244 1281 1320 1360 1401 1444 1487 1533 1579 1627 1676 172777 1238 1275 1313 1352 1393 1434 1477 1522 1567 1614 1663 1712 176478 1269 1306 1345 1385 1426 1468 1512 1557 1603 1650 1699 1749 180179 1301 1339 1378 1418 1460 1503 1547 1592 1639 1687 1737 1787 184080 1333 1372 1412 1453 1495 1538 1583 1629 1676 1725 1775 1826 187981 1367 1406 1446 1488 1531 1575 1620 1666 1714 1763 1814 1866 191982 1401 1441 1482 1524 1567 1612 1657 1704 1753 1803 1854 1906 196083 1436 1477 1518 1561 1605 1650 1696 1744 1793 1843 1895 1948 200284 1473 1513 1555 1599 1643 1689 1735 1784 1833 1884 1936 1990 204585 1510 1551 1594 1637 1682 1728 1776 1825 1875 1926 1979 2033 208986 1548 1589 1633 1677 1722 1769 1817 1866 1917 1969 2022 2077 213487 1586 1629 1673 1717 1764 1811 1859 1909 1960 2013 2067 2122 217988 1626 1669 1714 1759 1806 1854 1903 1953 2005 2058 2113 2169 222689 1667 1711 1756 1802 1849 1897 1947 1998 2050 2104 2159 2216 227490 1709 1753 1799 1845 1893 1942 1992 2044 2097 2151 2207 2264 232291 1752 1797 1843 1890 1938 1988 2039 2091 2144 2199 2255 2313 237292 1796 1841 1888 1936 1984 2035 2086 2139 2193 2248 2305 2363 242393 1841 1887 1934 1982 2032 2083 2135 2188 2242 2298 2356 2414 247594 1887 1934 1982 2030 2080 2132 2184 2238 2293 2350 2407 2467 252795 1935 1982 2030 2080 2130 2182 2235 2289 2345 2402 2460 2520 258296 1984 2031 2080 2130 2181 2233 2287 2342 2398 2456 2515 2575 263797 2033 2082 2131 2181 2233 2286 2340 2396 2452 2510 2570 2631 269398 2085 2133 2183 2234 2286 2340 2395 2451 2508 2567 2627 2688 275199 2137 2186 2237 2288 2341 2395 2450 2507 2565 2624 2684 2746 2810
100 2191 2241 2292 2344 2397 2452 2507 2564 2623 2682 2743 2806 2870
319
Continued

Table 12-10 Estimated Fetal Weight (g) Based on Biparietal Diameter (BPD) and Abdominal Circumference (AC)*—Cont’d
AC (mm)
BPD (mm) 285 290 295 300 305 310 315 320 325 330 335 340 345
31 696 726 759 793 828 865 903 943 985 1029 1075 1123 117332 710 742 774 809 844 882 921 961 1004 1048 1094 1143 119333 725 757 790 825 861 899 938 979 1022 1067 1114 1163 121434 740 773 806 841 878 916 956 998 1041 1087 1134 1183 123535 756 789 823 858 896 934 975 1017 1061 1107 1154 1204 125635 772 805 840 876 913 953 993 1036 1080 1127 1175 1226 127837 788 822 857 893 931 971 1012 1056 1101 1147 1196 1247 130038 805 839 874 911 950 990 1032 1076 1121 1168 1218 1269 132339 822 856 892 930 969 1009 1052 1096 1142 1190 1240 1292 134640 839 874 911 949 988 1029 1072 1117 1163 1212 1262 1315 136941 857 892 929 968 1008 1049 1093 1138 1185 1234 1285 1338 139342 875 911 948 987 1028 1070 1114 1159 1207 1256 1308 1361 141743 893 930 968 1007 1048 1091 1135 1181 1229 1279 1331 1385 144244 912 949 987 1027 1069 1112 1157 1204 1252 1303 1355 1410 146745 932 969 1008 1048 1090 1134 1179 1226 1275 1326 1380 1435 149246 951 989 1028 1069 1112 1156 1202 1249 1299 1351 1404 1406 151847 971 1010 1049 1091 1134 1178 1225 1273 1323 1375 1430 1486 154548 992 1031 1071 1113 1156 1201 1248 1297 1348 1401 1455 1512 157149 1013 1052 1093 1135 1179 1225 1272 1322 1373 1426 1482 1539 159950 1034 1074 1115 1158 1203 1249 1297 1347 1399 1452 1508 1566 162651 1056 1096 1138 1181 1226 1273 1322 1372 1425 1479 1535 1594 165552 1078 1119 1161 1205 1251 1298 1347 1398 1451 1506 1563 1622 168353 1101 1142 1185 1229 1276 1323 1373 1425 1478 1533 1591 1651 171354 1124 1166 1209 1254 1301 1349 1399 1452 1506 1562 1620 1680 174255 1148 1190 1234 1279 1327 1376 1426 1479 1534 1590 1649 1710 177356 1172 1215 1259 1305 1353 1402 1454 1507 1562 1619 1678 1740 180357 1197 1240 1285 1332 1380 1430 1482 1535 1591 1649 1709 1770 183558 1222 1266 1311 1358 1407 1458 1510 1564 1621 1679 1739 1802 186659 1248 1292 1338 1386 1435 1486 1539 1594 1651 1710 1770 1834 189960 1274 1319 1366 1414 1464 1515 1569 1624 1682 1741 1802 1866 193261 1301 1346 1393 1442 1493 1545 1599 1655 1713 1773 1835 1899 196562 1328 1374 1422 1471 1522 1575 1630 1686 1745 1805 1868 1932 199963 1356 1403 1451 1501 1552 1606 1661 1718 1777 1838 1901 1967 203464 1385 1432 1481 1531 1583 1637 1693 1751 1810 1872 1935 2001 206965 1414 1462 1511 1562 1615 1669 1725 1784 1844 1906 1970 2037 210566 1444 1492 1542 1594 1647 1702 1759 1817 1878 1941 2006 2073 214267 1474 1523 1574 1626 1679 1735 1792 1852 1913 1976 2042 2109 217968 1505 1555 1606 1658 1713 1769 1827 1887 1949 2012 2078 2147 221769 1537 1587 1639 1692 1747 1803 1862 1922 1985 2049 2116 2184 225570 1570 1620 1672 1726 1781 1839 1898 1959 2022 2087 2154 2223 229571 1603 1654 1706 1761 1817 1875 1934 1996 2059 2125 2193 2262 233472 1636 1688 1741 1796 1853 1911 1971 2044 2098 2164 2232 2302 237573 1671 1723 1777 1832 1890 1948 2009 2072 2137 2203 2272 2343 241674 1706 1759 1813 1869 1927 1987 2048 2111 2176 2244 2313 2384 245875 1742 1795 1850 1907 1965 2025 2087 2151 2217 2265 2354 2426 250176 1779 1833 1888 1945 2004 2065 2127 2192 2258 2326 2397 2469 254477 1816 1871 1927 1985 2044 2105 2168 2233 2300 2369 2440 2513 258876 1855 1910 1966 2025 2085 2146 2210 2275 2343 2412 2484 2557 263379 1894 1949 2006 2065 2126 2188 2252 2318 2386 2456 2528 2603 267980 1934 1990 2048 2107 2168 2231 2296 2362 2431 2501 2574 2649 272581 1975 2031 2089 2149 2211 2275 2340 2407 2476 2547 2620 2695 277382 2016 2073 2132 2193 2255 2319 2385 2462 2522 2594 2667 2743 282183 2059 2116 2176 2237 2300 2364 2431 2499 2569 2641 2715 2791 287084 2102 2160 2220 2282 2345 2410 2477 2546 2617 2689 2764 2841 292085 2146 2205 2266 2328 2392 2457 2525 2594 2665 2739 2814 2891 297086 2192 2251 2312 2375 2439 2505 2573 2643 2715 2789 2864 2942 302287 2238 2298 2359 2423 2488 2554 2623 2693 2765 2840 2916 2994 307488 2285 2346 2408 2472 2537 2604 2673 2744 2817 2892 2968 3047 312889 2333 2394 2457 2521 2587 2655 2725 2796 2869 2944 3021 3101 318290 2382 2444 2507 2572 2639 2707 2777 2849 2923 2998 3076 3155 323791 2433 2495 2559 2624 2691 2760 2830 2903 2977 3053 3131 3211 329392 2484 2547 2611 2677 2744 2814 2885 2958 3032 3109 3187 3268 335093 2536 2599 2664 2731 2799 2869 2940 3014 3089 3166 3245 3326 340994 2590 2853 2719 2786 2854 2925 2997 3070 3146 3224 3303 3384 348895 2644 2709 2774 2842 2911 2982 3054 3129 3205 3283 3362 3444 352896 2700 2765 2831 2899 2969 3040 3113 3188 3264 3343 3423 3505 358997 2757 2822 2889 2958 3028 3099 3173 3248 3325 3404 3484 3567 365198 2815 2881 2948 3017 3088 3160 3234 3309 3387 3466 3547 3630 371599 2874 2941 3009 3078 3149 3222 3296 3372 3450 3529 3611 3694 3779
100 2935 3002 3070 3140 3211 3285 3359 3436 3514 3594 3676 3759 3845
*Estimated fetal weights: Log (birth weight) = −1.7492 + 0.166 (BPD) + 0.046 (AC) −0.00264 (AC × BPD).From Shepard MJ, Richards VA, Berkowitz RL, et al: An evaluation of two equations for predicting fetal weight by ultrasound, Am J Obstet Gynaecol 147:47-54, 1982.

Table 12-10—Cont’d
AC (mm)
BPD (mm) 350 355 360 365 370 375 380 385 390 395 400
31 1225 1279 1336 1396 1458 1523 1591 1661 1735 1812 189332 1246 1301 1258 1418 1481 1546 1615 1686 1761 1838 192033 1267 1323 1381 1441 1504 1570 1639 1711 1786 1865 194634 1289 1345 1403 1464 1528 1595 1664 1737 1812 1891 197335 1311 1367 1426 1488 1552 1619 1689 1762 1839 1918 200136 1333 1390 1450 1512 1577 1645 1715 1789 1865 1945 202937 1356 1413 1474 1536 1602 1670 1741 1815 1893 1973 205738 1379 1437 1498 1561 1627 1696 1768 1842 1920 2001 208639 1402 1461 1523 1586 1653 1722 1794 1870 1948 2030 211540 1426 1486 1548 1612 1679 1749 1822 1898 1977 2059 214541 1451 1511 1573 1638 1706 1776 1849 1926 2005 2088 217442 1475 1536 1599 1664 1733 1804 1878 1954 2035 2118 220543 1500 1562 1625 1691 1760 1832 1906 1984 2064 2148 223644 1526 1588 1652 1718 1788 1860 1935 2013 2094 2179 226745 1552 1614 1679 1746 1816 1889 1964 2043 2125 2210 229846 1579 1641 1706 1774 1845 1918 1994 2073 2156 2241 233047 1605 1669 1734 1803 1874 1948 2024 2104 2167 2273 236348 1633 1697 1763 1832 1904 1976 2055 2136 2219 2306 239849 1661 1725 1792 1861 1934 2009 2086 2187 2251 2339 242950 1689 1754 1821 1891 1964 2040 2118 2200 2284 2372 246351 1718 1783 1851 1922 1995 2071 2150 2232 2317 2406 249852 1747 1813 1882 1953 2027 2103 2183 2266 2351 2440 253253 1777 1843 1913 1984 2059 2136 2216 2299 2386 2475 256854 1807 1874 1944 2016 2091 2169 2250 2333 2420 2510 260455 1838 1906 1976 2049 2124 2203 2284 2368 2456 2546 264056 1869 1938 2008 2082 2158 2237 2319 2403 2491 2582 267757 1901 1970 2041 2115 2192 2272 2354 2439 2528 2619 271458 1934 2003 2075 2150 2227 2307 2390 2475 2564 2657 275259 1966 2037 2109 2184 2262 2342 2426 2512 2602 2694 279060 2000 2071 2144 2219 2298 2379 2463 2550 2640 2733 282961 2034 2105 2179 2255 2334 2416 2500 2588 2678 2772’ 286962 2069 2140 2215 2291 2371 2453 2538 2626 2717 2811 290963 2104 2176 2251 2328 2408 2491 2577 2665 2757 2851 294964 2140 2213 2288 2366 2446 2530 2616 2705 2797 2892 299165 2176 2250 2328 2404 2485 2569 2656 2745 2838 2933 303266 2213 2287 2364 2443 2524 2609 2696 2786 2879 2975 307567 2251 2326 2403 2482 2564 2649 2737 2827 2921 3018 311768 2290 2365 2442 2522 2605 2690 2778 2869 2964 3061 316169 2329 2404 2482 2563 2646 2732 2821 2912 3007 3104 320570 2368 2444 2523 2604 2688 2774 2863 2955 3050 3149 325071 2409 2485 2564 2846 2730 2817 2907 2999 3095 3193 329572 2450 2527 2607 2689 2773 2861 2951 3044 3140 3239 334173 2491 2569 2649 2732 2817 2905 2996 3089 3186 3285 338674 2534 2612 2693 2776 2862 2950 3041 3135 3232 3332 343575 2577 2656 2737 2821 2907 2996 3088 3182 3279 3380 348376 2621 2700 2782 2866 2953 3042 3134 3229 3327 3428 353177 2666 2746 2828 2912 3000 3090 3128 3277 3376 3477 358178 2711 2792 2874 2959 3047 3137 3230 3326 3425 3526 363179 2757 2838 2921 3007 3095 3186 3279 3376 3475 3576 368180 2804 2886 2969 3056 3144 3235 3329 3426 3525 3627 373381 2852 2934 3018 3105 3194 3286 3380 3477 3577 3679 378582 2901 2983 3068 3155 3244 3336 3431 3529 3629 3732 383883 2950 3033 3118 3206 3296 3388 3483 3581 3682 3785 389184 3001 3084 3169 3257 3348 3441 3536 3634 3735 3839 394585 3052 3135 3221 3310 3401 3494 3590 3688 3790 3894 400086 3104 3188 3274 3363 3454 3548 3644 3743 3845 3949 405687 3157 3241 3328 3417 3509 3603 3700 3799 3901 4005 411388 3210 3295 3383 3472 3565 3659 3756 3855 3958 4063 417089 3265 3351 3438 3528 3621 3716 3813 3913 4015 4120 422890 3321 3407 3495 3585 3678 3773 3871 3971 4074 4179 428791 3377 3464 3552 3643 3736 3832 3930 4030 4133 4239 434792 3435 3522 3611 3702 3795 3891 3989 4090 4193 4299 440893 3494 3581 3670 3761 3855 3951 4050 4151 4254 4361 446994 3553 3641 3738 3822 3916 4013 4111 4213 4316 4423 453295 3614 3701 3791 3884 3978 4075 4174 4275 4379 4486 459596 3675 3763 3854 3946 4041 4138 4237 4339 4443 4550 465997 3738 3826 3917 4010 4105 4202 4302 4404 4508 4615 472498 3802 3890 3981 4074 4170 4267 4367 4469 4573 4680 479099 3866 3956 4047 4140 4236 4333 4433 4536 4640 4747 4857
100 3932 4022 4113 4207 4303 4400 4501 4603 4708 4815 4924
321

322 ULTRASOUND: THE REQUISITES
Table 12-11 Estimated Fetal Weight (g) Based on Abdominal Circumference and Femur Length*
*Based on regression model: Log10 body weight = 1.3598 + 0.051 (abdominal circumference) + 0.1844 (femur length) − 0.0037 (abdominal circumference × femur length).From Hadlock FP, et al: Sonographic estimation of fetal weight. Radiology 150:535-540, 1984.

Guidelines to obstetrical Examination and Appropriate Measurements 323
Table 12-11—Cont’d

change in this percentile level between studies, agrowth disorder is considered. This approach is cur-rently the most widely used for assessing fetal size andgrowth, but it has the disadvantage that it uses dataestablished from cross-sectional rather than longitudinalstudies.
A method of assessing interval growth that is moreprecise and has the advantage that it uses longitudinaldata has been developed and can be used to evaluategrowth of the fetal head, abdomen, and femur in thesecond and third trimesters (Table 12-13). Because thisconcept may be new to the reader, a detailed discussionand examples follow.
As background, measurement errors cause an inac-curacy of at least 1 mm per study, and this inaccuracydoubles to 2 mm when two studies are compared. As thenumber of weeks between studies increases, the meas-urement error decreases in significance. The error islargest when the number of weeks between studies isless than 3 weeks (20% to 30% error) and smallest whenthere are more than 10 weeks between studies (only 7%to 10% error). Interval growth tables were thereforedeveloped at 4, 6, 8, and greater than or equal to 10 weeksto mathematically correct for this error (see Tables12-13A to D). The mean measurement numbers in all the
tables remain constant, with narrower ranges as thenumber of weeks between studies increases.
Analysis of interval growth is based on the followingprinciples. The growth of a normal fetus is faster in theearly second trimester and decreases until term. Eachfetal parameter has a predictable linear or curvilineargrowth pattern. The fetus that grows between the 10thand 90th percentile is almost always normal and haslittle chance of growth disturbance. The fetus withgrowth below the 10th percentile or the fetus that isinitially above and then drops below the 10th percentileis at risk for growth retardation. Conversely, the fetusthat grows above the 90th percentile or is initially belowand then rises above the 90th percentile is at risk formacrosomia.
Interval growth can be analyzed when there are twofetal studies. The initial and repeat measurements of thehead, abdomen, and femur and the time intervalbetween the studies are then known. The rate of changeof the measurement parameters is equal to millimeters of growth from the first to the second study divided bythe number of interval weeks, or mm/week of growth.This growth rate is then evaluated at the mean fetal age between the two studies. The growth table to beused depends on the number of weeks between studies
324 ULTRASOUND: THE REQUISITES
Table 12-12 Neonatal Weight Table (Male and Female Subjects Combined)
*Age to the nearest week.From Doubilet PM, Benson CB, Nadel AS, Ringer SA: Improved birth weight table for neonates developed from gestations dated by early sonography.J Ultrasound Med 16:241-249, 1997.

Guidelines to obstetrical Examination and Appropriate Measurements 325
Table 12-13B Interval Growth Table: 6 Weeks
The mean growth rates and confidence limits calculated from the regression equations are given at each mean gestational age.From Nazarian LN, Halpern EJ, Kirtz AB, et al: Normal interval fetal growth rates based on obstetrical ultrasound measurements. J Ultrasound Med 14, 1995.
Table 12-13A Interval Growth Table (mm/wk): 4 Weeks
The mean growth rates and confidence limits calculated from the regression equations are given at each mean gestational age.From Nazarian LN, Halpern EJ, Kirtz AB, et al: Normal interval fetal growth rates based on obstetrical ultrasound measurements. J Ultrasound Med 14, 1995.

326 ULTRASOUND: THE REQUISITES
Table 12-13D Interval Growth Table: ≥10 Weeks
The mean growth rates and confidence limits calculated from the regression equations are given at each mean gestational age.From Nazarian LN, Halpern EJ, Kirtz AB, et al: Normal interval fetal growth rates based on obstetrical ultrasound measurements. J Ultrasound Med 14, 1995.
Table 12-13C Interval Growth Table: 8 Weeks
The mean growth rates and confidence limits calculated from the regression equations are given at each mean gestational age.From Nazarian LN, Halpern EJ, Kirtz AB, et al: Normal interval fetal growth rates based on obstetrical ultrasound measurements. J Ultrasound Med 14, 1995.

Guidelines to obstetrical Examination and Appropriate Measurements 327
(i.e., 4, 6, 8, or ≥10 weeks). Odd week intervals shouldbe rounded up to the next even number (e.g., for 3weeks, use the 4-week table). If a clinician wants aninterval growth study at less than 3 weeks (particularlyin the late third trimester), it should be discouragedbecause of potentially significant measurement errors.
Two examples of this ultrasound growth analysis areshown. Only the BPD and the AD will be described,although the AC and FL growth are also available (seeAppendix I).
In multiple gestations, more commonly twins, gesta-tional age analysis is similar to that of singleton pregnan-cies and use of the same measurement tables isrecommended. In the second and early third trimester,normal growth and weight is the same as in singletongestations. After that, while these parameters tend toslow down toward the lower 10th percentile, theyshould not be below the 10th percentile if growth isnormal. Because singleton tables are based on manymore numbers than multiple gestation tables, it isrecommended that the same singleton tables be used.f. Maternal anatomy—evaluation of the uterus
and adnexal structures should be performed.There should be a careful search for fibroids and
adnexal masses. During the second and early thirdtrimester the length and shape of the cervix should beassessed because shortening of the cervix and/oropening of the internal cervical os are important signs ofincompetent cervix and preterm labor.g. Fetal anatomic survey. Fetal anatomy, as
described in this document, may adequately beassessed by ultrasound after approximately 18weeks’ gestational (menstrual) age. It may bepossible to document normal structures beforethis time, although some structures can bedifficult to visualize due to fetal size, position,movement, abdominal scars, and increasedmaternal wall thickness.
The following areas of assessment represent theessential elements of a standard examination of fetalanatomy: head (cerebellum, choroid plexus, cisternamagna, lateral cerebral ventricles, midline falx, cavumsepti pellucidi), heart (four-chamber view of the heartincluding its position within the thorax), spine (cervical,thoracic, lumbar, and sacral), abdomen (stomach, kid-neys, urinary bladder, and the umbilical cord insertionsite into the anterior abdominal wall), extremities (thelegs and arms: presence or absence of the legs andarms), and the umbilical cord vessel number. Fetalgender may be obtained when medically indicated.
Whereas these anatomic areas are more completelydiscussed in the respective chapters, a brief discussionof each anatomic area follows.
In the head, the atria of the lateral ventricles areimaged by tilting the transducer slightly caudad from the
standard axial view. The atrial measurement is easilyreproducible and essentially constant from 14 to 38weeks’ gestation. The generally accepted upper limit ofnormal is 10 mm. In addition, the hyperechoic choroidplexus normally fills at least 60% and more often up to90% of each atrium.
Imaging of the posterior fossa in the axial plane iden-tifies the cerebellum and cisterna magna by tilting thetransducer slightly more posteriorly toward the occiput.The cerebellum has a bilobed shape with the midlinehyperechoic vermis and larger hypoechoic hemispheres.An axial measurement of the cerebellum can beobtained and compared with the BPD. The normal cis-terna magna is always identified as an anechoic spaceposterior to the vermis and has a normal size range of 2 to 10 mm.
A four-chamber view of the heart is obtained in axialprojection. The heart is normally on the left side withthe apex pointing toward the left anterior chest wall atan approximately 45-degree angle. The chamber closestto the chest wall is the right ventricle. A four-chamberview can identify both ventricles and their interven-tricular septa, both atria and their intervening foraminaovalia, and the atrioventricular valves. From 18 weeks toterm, a satisfactory view can be obtained in 95% offetuses. Although the current standard for the obstetricultrasound examination only requires the four-chamberview of the heart, some observers believe that it shouldinclude additional cardiac views and, in particular,images of the ventricular outflow tracts.
Careful analysis of the spine is important to detectneural tube defects. Of the three ossification centers ateach vertebral level, the two posterior centers form theneural arches. These arches and the overlying posteriorsoft tissues are almost always affected by neural defectsso that a complete examination requires visualization ofall vertebral levels, particularly the lumbosacral region.This can best be accomplished by axial images. Ifsuboptimal, midline sagittal images can visualize the softtissues and coronal images can visualize the posteriorossification centers.
The fetal stomach is an anechoic structure in the leftupper quadrant. It should routinely be identified by16 weeks. When the stomach is not seen, particularlyafter 19 weeks with scanning performed for up to60 minutes, the fetus is likely to be abnormal. Whenmarked oligohydramnios is present, however, the fetusmay have no amniotic fluid to fill its stomach.
The kidneys can be identified in their paraspinal loca-tion on an axial view just below the level of the liver.The kidneys may be recognized as early as 12 weeks andby 17 weeks may be seen in almost all normal fetuses. Inthe second trimester, it may be difficult to distinguishthe kidneys from the surrounding perinephric tissues;after 26 weeks, the perinephric fat and renal sinus

328 ULTRASOUND: THE REQUISITES
become more hyperechoic and the relatively hypo-echoic renal parenchyma is identified more easily. Thenormal renal sinus is often separated by an anechoicspace, corresponding to pyelectasis. Minimal pyelectasisis considered a normal finding. If the subjective impres-sion of the examiner is that there is more than a minimalamount of pyelectasis, the anteroposterior dimension ofthe renal pelvis should be measured on an axial image.The thresholds reported in the literature for this meas-urement vary. In the second and early third trimester,pyelectasis can be considered a normal finding if themeasurement is less than 4 to 5 mm. Later in the thirdtrimester typically 7 mm (and occasionally up to 10 mm)is considered the upper limit of normal. If caliectasis orureterectasis is imaged, however, the collecting systemdilatation should be considered abnormal regardless ofthe measurement of the renal pelvis.
The urinary bladder is a round or ovoid anechoicstructure in the pelvis. If the normal bladder is not ini-tially identified in the second or third trimester, it willalmost always appear if sequential scans are performedat 10- to 15-minute intervals for up to 1 hour. A dis-tended or an absent bladder needs further evaluation,including a careful analysis of the fetal kidneys and theamniotic fluid.
Finally, the insertion site of the umbilical cord intothe fetal abdominal wall is an important landmark inthe evaluation for a ventral abdominal wall defect. Theremainder of the anterior abdominal wall should alsobe carefully scanned to ensure that no defects arepresent.
SUGGESTED READINGS
ACR Practice Guidelines for the Performance of AntepartumObstetrical Ultrasound 2003. Reston, VA, ACR Standards (Res. 19, effective 10/1/03).
Allen LD: A practical approach to fetal heart scanning. SeminPerinatol 24:324, 2000.
American Institute of Ultrasound in Medicine: Guidelines forthe Performance of the Antepartum Obstetrical UltrasoundExamination. J Ultrasound Med 15:185, 1996.
Barboza JM, et al: Prenatal diagnosis of congenital cardiacanomalies: A practical approach using two basic views.Radiographics 22:1125, 2002.
Benson CB, Doubilet PM: Sonographic prediction of gesta-tional age: Accuracy of second- and third-trimester fetal meas-urements. AJR Am J Roentgenol 157:1275, 1991.
Bowie JD, et al: The changing sonographic appearance of fetal kidneys during pregnancy. J Ultrasound Med 2:505, 1983.
Bromley B, et al: Fetal echocardiography: Accuracy andlimitations in a population at high and low risk for heartdefects. Am J Obstet Gynecol 166:1473, 1992.
Brown DL, et al: Sonography of the fetal heart: Normal variantsand pitfalls. AJR Am J Roentgenol 160:1251, 1993.
Budorick NE, et al: Ossification of the fetal spine. Radiology181:561, 1991.
Budorick NE, Pretorius DH, Nelson TR: Sonography of the fetalspine: Technique, imaging, findings, and clinical implications.AJR Am J Roentgenol 16:421, 1995.
Campbell BA: Utilizing sonography to follow fetal growth.Obstet Gynecol Clin North Am 25:750, 1998.
Cardoza JD, Goldstein BB, Filly RA: Exclusion of fetal ventricu-lomegaly with a single measurement: The width of the lateralventricular atrium. Radiology 169:711, 1988.
Chitty LS, Altman DG: Charts of fetal size: Limb bones. BJOG109:919, 2002.
Clautice-Engle T, Pretorius DH, Budorick NE: Significance ofnonvisualization of the fetal urinary bladder. J Ultrasound Med10:615, 1991.
Copel JA, et al: Fetal echocardiographic screening for congen-ital heart disease: The importance of the four-chamber view.Am J Obstet Gynecol 157:648, 1987.
Corteville JE, Gray DL, Crane JP: Congenital hydronephrosis:Correlation of fetal ultrasonographic findings with infant out-come. Am J Obstet Gynecol 165:384, 1991.
Doubilet PM, Greenes RA: Improved prediction of gestationalage from fetal head measurements. AJR Am J Roentgenol142:797, 1984.
Farrell TA, et al: Fetal lateral ventricles: Reassessment of normalvalues for atrial diameter at US. Radiology 193:409, 1994.
Filly RA: Level 1, level 2, level 3 obstetric sonography: I’ll seeyour level and raise you one. Radiology 172:312, 1989.
Frates MC: Sonography of the normal fetal heart: A practicalapproach. AJR Am J Roentgenol 173:1363, 1999.
Goldstein RB, Filly RA: Sonographic estimation of amnioticfluid volume: Subjective assessment versus pocket measure-ments. J Ultrasound Med 7:363, 1988.
Gotoh H, Masuzaki H, Fukuda H, et al: Detection and assess-ment of pyelectasis in the fetus: Relationship to postnatal renalfunction. Obstet Gynecol 92:226, 1998.
Grumbach K, et al: Twin and singleton growth patterns com-pared using ultrasound. Radiology 158:237, 1986.
Hadlock FP, et al: Estimating fetal age: Effect of head shape onBPD. AJR Am J Roentgenol 137:83, 1981.
Hadlock FP, et al: Fetal abdominal circumference as a predictorof menstrual age. AJR Am J Roentgenol 139:369, 1982.
Heiserman J, Filly RA, Goldstein RB: Effect of measurementerrors on sonographic evaluation of ventriculomegaly. J Ultra-sound Med 10:121, 1991.
Hertzberg BS, et al: Diagnosis of placenta previa during thethird trimester: Role of transperineal sonography. AJR Am JRoentgenol 159:83, 1992.
Hertzberg BS, et al: Sonographic evaluation of fetal CNS:Technical and interpretive pitfalls. AJR Am J Roentgenol 172:253, 1999.

Hilpert PL, Hall BE, Kurtz AB: The atria of the fetal lateralventricles: A prospective study of normal size and choroidsplexus filling. AJR Am J Roentgenol 164:731, 1995.
Kurtz AB, et al: Twin pregnancies: Accuracy of first-trimesterabdominal US in predicting chorionicity and amnionicity. Radiology 185:759, 1992.
Levi CS, et al: Endovaginal US: Demonstration of cardiacactivity in embryos of less than 5.0 mm in crown-rump length.Radiology 176:71, 1990.
Mahony BS, Filly RA, Callen PW: Amnionicity and chorionicityin twin pregnancies: Prediction using ultrasound. Radiology155:205, 1985.
McGahan JP: Sonography of the fetal heart: Findings on thefour-chamber view. AJR Am J Roentgenol 156:547, 1991.
McKenna KM, Goldstein RB, Stringer MD: Small or absent fetal stomach: Prognostic significance. Radiology 197:729,1995.
Millener PB, Anderson NG, Chisholm RJ: Prognostic signifi-cance of nonvisualization of the fetal stomach by sonography.AJR Am J Roentgenol 160:827, 1993.
Monteagudo A, et al: Early and simple determination ofchorionic and amniotic type in multifetal gestations in the firstfourteen weeks by high-frequency transvaginal ultrasonog-raphy. Am J Obstet Gynecol 170:824, 1994.
Pennell RG, et al: Prospective comparison of vaginal andabdominal sonography in normal early pregnancy. J UltrasoundMed 10:63, 1991.
Perez CG, Goldstein RB: Sonographic borderlands in the fetalabdomen. Semin Ultrasound CT MR 19:336, 1998.
Persutte WH, Hussey M, Chyu J, et al: Striking findingsconcerning the variability in the measurement of the fetal renalcollecting system. Ultrasound Obstet Gynecol 15:186, 2000.
Persutte WH, Klyle M, Lenke RR, et al: Mild pyelectasis ascer-tained with prenatal sonography is pediatrically significant.Ultrasound Obstet Gynecol 10:12, 1997.
Pilu G, Reece EA, Goldstein I, et al: Sonographic evaluation ofthe normal developmental anatomy of the fetal cerebralventricles: II. The atria. Obstet Gynecol 783:250, 1989.
Pretorius DH, et al: Sonographic evaluation of the fetalstomach: Significance of non-visualization. AJR Am JRoentgenol 151:987, 1988.
Scardo JA, et al: Prospective determination of chorionicity,amnionicity, and zygosity in twin gestations. Am J ObstetGynecol 173:1376, 1995.
Seeds JW: Borderline genitourinary tract abnormalities. SeminUltrasound CT MR 19:347, 1998.
Wilcox DT, Chitty LS: Non-visualization of the fetal bladder:Aetiology and management. Prenat Diagn 21:977, 2001.
Guidelines to obstetrical Examination and Appropriate Measurements 329
Appendix I
Example 1: The first study is performed at 20 weeks’gestation, and the second study is done at 30 weeks’gestation. The mean fetal age is 25 weeks’ gestation.There are 10 weeks between studies so Table 12-13D(interval growth = 10 weeks) is used. At 20 weeks thebiparietal diameter (BPD) and abdominal diameter (AD)measurements are both 45 mm. At 30 weeks, the BPDand AD measurements have increased to 79 mm and 81mm, respectively. The interval growth rate for the BPD is79 mm − 45 mm/10 weeks = 3.4 mm/week. The intervalgrowth rate for the AD is 81 mm − 45 mm/10 weeks =3.6 mm/week. Table 12-13D shows that, at a mean of 25 weeks, both parameters are growing normally,between the 10th and the 90th percentiles.
Example 2: The first study is performed at 32 weeks’gestation, and the second study is done at 36 weeks’gestation. The mean gestational age is 34 weeks. Thereare 4 weeks between studies, and Table 12-13A (intervalgrowth of 4 weeks) is used. The BPD and AD at32 weeks are 81 mm and 79 mm, respectively, and at36 weeks have increased to 89 mm and 84 mm, respec-tively. The interval growth rate for the BPD is 89 mm −81 mm/4 weeks = 2.0 mm/week, equivalent to growthbetween the 50th and 90th percentiles. The intervalgrowth rate for the AD is 84 mm − 79 mm/4 weeks =1.25 mm/week, a growth below the 10th percentile. Theabdomen is growing too slowly, relative to the BPD, andthe fetus is at risk for asymmetric growth restriction.
Fetal Growth and Well-Being
330
Intrauterine Growth RestrictionUltrasound
Fetal Structures and Measurements
Amniotic Fluid
The Placenta
Other Fetal Parameters
Umbilical Artery Doppler Velocity Waveform Analysis
Biophysical Profile
Summary of IUGR
MacrosomiaFor Key Features summary see p. 340
Improved equipment and increased ultrasoundsophistication have permitted the examiner to gobeyond a routine evaluation of the fetal structure. Par-ticularly in the third trimester, fetal function and meas-urements, separately or in combination with the clinicalfindings, have been used to analyze fetal well-being.These findings have helped in the prediction of fetusesthat are either too small or too large, allowing increasedaccuracy in the detection of the compromised fetus and,in some cases, in the timing of delivery.
INTRAUTERINE GROWTH RESTRICTION
Intrauterine growth restriction (IUGR) is a complexproblem not always detected in utero. By definition, achild with a low birth weight is deemed small for gesta-tional age (SGA). There are two main types of SGAinfants: the constitutionally small infant is small butotherwise normal, whereas the infant with IUGR ispathologically smaller than its expected gestational age.
The overall incidence of growth restriction varies indifferent studies but is usually between 3% and 10% of allbirths. On average, 1 in every 20 infants (5%) is growthrestricted, approaching 1 in 10 infants (10%) in certainhigh-risk groups. Most studies use a weight cutoff for
SGA infants of less than the lower 10th percentile. Thespecificity of detection of IUGR infants increases witheven lower weights, at the lower 5th and 2.5th per-centile, for example.
Two characteristics, age and weight (size), areneeded to evaluate infants and also fetuses for growthrestriction. In utero, the weight of the fetus for its gesta-tional age can predict size appropriateness. Unfortu-nately, in utero determination of age and weight are notprecise. By using 2 standard deviations (2 SD or 95%) ina large group of women, an optimal menstrual historycan only predict fetal age to within ±2.5 weeks. Withuncertain dates, this precision decreases to ±4 weeks ormore. Using ultrasound, the first-trimester crown-rumplength and second-trimester head measurements areaccurate to ±1 to 1.2 weeks with the third-trimester pre-cision decreased to ± 3 to 4 weeks. Fetal weight is evenless precise, with an accuracy of at best ±15% whenthree parameter tables (head, abdomen, and femur) areused. A 3000-g fetus for example would have a weightrange of 900 g, from 2550 to 3450 g.
To further complicate this analysis, there are twotypes of growth restriction and numerous risk factorsthat can be separated into maternal, fetal, and placental,with some overlap. The maternal risk factors range froma young maternal age to chronic hypoxia and includesystemic hypertension, collagen vascular diseases,insulin-dependent diabetes, smoking, and certain drugs(including alcohol and cocaine). Fetal risk factorsinclude a previously growth-restricted fetus, structuralabnormalities, chromosomal abnormalities, and in uteroinfections such as the TORCH viruses of toxoplasmosis,rubella, cytomegalovirus, and herpes simplex. Placentalproblems include infarction, abnormal umbilical cordinsertion, placenta previa, and abruption. Premature pla-cental aging (dysmaturity), vascular problems (anticar-diolipin antibodies and hypercoagulable states), andplacental tumors also adversely affect the fetus.
CHAPTER13

Although not fully understood, women with persistentlyelevated α-fetoprotein levels (without structural fetalcauses) suggest increased placental permeability andhave a higher incidence of growth-restricted fetuses laterin the pregnancy.
Abnormally low growth stems from two distinctmechanisms: fetal malnutrition and diminished cellulargrowth. These manifest themselves as the two types ofIUGR: asymmetric and symmetric. There is significantoverlap between the asymmetric and symmetric formsof IUGR. Asymmetric IUGR (malnutrition) constitutesthe majority (up to 90%) of the cases. It is uncommonlydetected earlier than the third trimester. Placental andmaternal problems predominate, with the fetus receivinga less-than-adequate blood supply and nourishment.Because asymmetric IUGR is a form of starvation, thereis an initial loss of subcutaneous tissue and liverglycogen stores, and thus a decrease in abdominal size.Head and femur measurements (part of the fetalskeleton) are also affected, but to a lesser extent. Asstarvation persists, however, the entire fetus becomesequally affected. The fetus then assumes a “symmetric”appearance that signifies severe growth restriction.
Asymmetric IUGR creates chronic stress on the fetusand is not infrequently accompanied by oligohydram-nios (Fig. 13-1). The differentiation in the third trimesterbetween this severe form of asymmetric growth and thetruly symmetric growth restriction (described in thenext paragraph) must often rely on history and, ifpresent, on the finding of decreased amniotic fluid.Because asymmetric IUGR is a late onset in uteroproblem, not affecting organ development, the prog-nosis depends on the severity of the perinatal and
Fetal Growth and Well-Being 331
immediate neonatal problems. If successfully treated,this type of child will experience normal development.
The symmetric type of IUGR (diminished cellulargrowth) comprises the remaining cases of pathologicIUGR. It occurs early in pregnancy, usually in the firsttrimester, as a result of an insult to the fetus or itsmother. Chromosomal abnormalities, drug toxicities,and in utero infections are among the causes of this formof IUGR. The fetus is stunted. The head and body (andfemur) are equally affected, and the fetus is symmetri-cally small. The volume of amniotic fluid is usuallynormal. Because it occurs early, it can adversely affectorgan development, particularly in the central nervoussystem, and thus manifest as slow development afterbirth.
Ultrasound
Fetal Structures and MeasurementsBecause fetal anomalies either may be the cause of or
be associated with growth restriction, the fetus shouldbe carefully evaluated to determine structural normalcy.Even when the fetus appears grossly normal, however,chromosomal anomalies and/or in utero infections maystill adversely affect fetal growth and development.Measurement of fetal parts, in particular the head, body, and femur, are therefore important on both thefirst and on any follow-up examination. Amniotic fluid,occasional Doppler evaluation, and, very infrequently,placental appearance may be of value. Additionally,there are internal fetal structures that will be discussedthat have been suggested, but not as yet proven, to beuseful in the diagnosis of IUGR.
A BFigure 13-1 Oligohydramnios associated with IUGR. A, Axial image of lower abdomen of a 29-week fetus shows severe oligohydramnios. B, bladder; arrow, spine. B, Abdominal circumfer-ence measurement on same fetus as in A. Value of 21.8 cm is less than the 2.5th percentile for 29weeks (see Table 13-1). Likewise, the estimated fetal weight of 716 g is less than the 10th percentile.

332 ULTRASOUND: THE REQUISITES
All standard ultrasound measurements are performedaccording to the antepartum obstetric ultrasound stan-dard (see Chapter 12). The gestational age is ideallyestablished within the first 20 to 24 weeks by either afirst-trimester crown-rump length or second-trimesterhead and femur length measurement (see Tables 12-1, 12-3, and 12-4). If follow-up examinations are per-formed, the fetal age is the initial ultrasound age plus thenumber of intervening weeks. The fetal body measure-ment (usually obtained as a circumference rather than anaverage diameter) is of value in the determination offetal size and growth. Its use in the weight formulas hasbeen well established.
The overall ultrasound detection rate for IUGR is 70%.Asymmetric growth restriction is more commonlydetected. When combined with the clinical assessmentof a fetus into low and high risk for IUGR, ultrasound canbe used to accomplish different tasks: to suggest that alow-risk fetus is smaller than expected, to confirm that afetus at high risk is too small, to find out if the ultrasoundfindings are compatible with the clinical impression of a small fetus, and to monitor the pregnancy when thediagnosis of a small fetus is made.
The accuracy of ultrasound in detecting IUGR isdifferent in these different circumstances. A small fetalabdomen detected during an examination performedsolely to establish fetal age is less likely to be caused byIUGR than a small fetal abdomen found in a woman withhypertension. In a “screening” group, there is a largerproportion of constitutionally small fetuses and conse-quently higher false-positive and lower positive pre-dictive values for diagnosing IUGR than in a group ofhigher-risk women. If only abnormal fetal measurementsare found, suggesting a small fetus, it is more prudent to initially call the fetus SGA rather than IUGR and torequest a follow-up study.
The calculated fetal weight uses a combination ofmeasurements of the head, body, and femur (see Tables12-10 and 12-11). Similarly, the abdominal circumfer-ence (AC) can help predict if there is a small fetal body (Table 13-1). Percentile tables are available for both,using the lower 10th percentile as the cut-off limit toseparate normal for gestational age fetuses from SGAfetuses. To make this determination, however, a com-parison of the calculated fetal weight (or the AC) to the anticipated fetal weight (or the AC) for the assignedfetal age is needed (see Table 12-12). This expected ageis ideally established earlier in the pregnancy; in a late-registrant woman the fetal age may be uncertain. Andwhen uncertain, the calculated weight (or AC) is oflimited value.
For example, if the fetal biparietal diameter and ACare 80 and 340 mm, respectively, the fetal weight wouldbe 2649 g (Table 12-10). If the fetal age is known to be36 weeks from an earlier study, this weight would
be normal, between the 50th and 75th percentiles (see Table 12-12). However, if the fetal age were uncer-tain and believed to be as advanced as 39 weeks, thissame weight would be below the 10th percentile, and a SGA fetus with possible growth restriction would bemore likely.
A comparison of the fetal head and body can predictthe presence of asymmetric IUGR if fetal age is known.Because the abdomen is initially affected more severelythan either the head or femur, a ratio of its head-to-abdominal circumferences has a high degree of sensi-tivity. A table of the circumference ratios from 13 to 42weeks’ gestation shows the head to be normally largerthan the abdomen in the second trimester (ratio of >1),with reversal near term (ratio of <1) (see Table 12-8).Because the ratio is not constant but changes with ges-tational age, precise gestational age is important. Thisratio can create uncertainty if the age is not known in alate registrant woman. A comparison of the BPD to theaverage body diameter yields comparable resultswithout its dependence on gestational age (see Table 12-9). Both methods suggest that a normal proportion ofthe head to abdomen likely diagnoses a normal fetusexcept in the situations of advanced malnutrition (star-vation) in which the head and body are both adverselyaffected. In symmetric IUGR all fetal parts are affectedequally, and this comparison is not of diagnostic value.
Ratios of other fetal parameters have not shownpredictive advantages in asymmetric IUGR but never-theless deserve mentioning. The initially promisingfemur length-to-abdominal circumference ratio is an age-independent ratio from 22 weeks to term. Although thisratio is elevated in asymmetric IUGR (small body) anddecreased in macrosomia (large body), subsequentstudies have shown poor sensitivities and poor positivepredictive value for both conditions. In symmetric IUGRthis ratio is not of diagnostic value. The head to femurratio may have value in certain skeletal disproportionsbut does not appear to be of diagnostic value in eithersymmetric or asymmetric IUGR. Although some casereports have suggested that the femur may be shorterthan normal in asymmetric IUGR, this has not beenborne out in larger studies.
Normal growth of the fetal parameters (head, body,and femur) is usually linear or mildly curvilinear, faster in the second trimester, and then progressively sloweruntil term. In asymmetric IUGR the fetus typically growsnormally into the third trimester, with decreased growth(which can be marked) in the third trimester. In sym-metric IUGR the fetus grows slowly from the time of theinitial early insult. Regardless of the types of IUGR, thesmall fetus with IUGR grows slower than a normal fetusof similar size.
Interval change in fetal weight or abdominal size canbe evaluated and even plotted on a graph. Interval

be analyzed either qualitatively (subjectively) or quanti-tatively (by measurement). When the results of meas-urement techniques are compared with the findingsfrom the subjective analysis of amniotic fluid, the sub-jective impression is as accurate as the objective (quan-titative) approach, with excellent intraobserver andinterobserver agreement.
Nevertheless, quantitative analysis can at times behelpful. Although different measurement techniques havebeen proposed, the most widely used in a singleton preg-nancy is a four-quadrant analysis called the amniotic fluidindex (AFI). Taking the largest anteroposterior (AP) fluidpocket in each quadrant (either in a sagittal or axialprojection), the four measurements are totaled (Fig. 13-2).There is a lack of consensus regarding the optimal tech-nique for measuring the AFI. Some groups only includefluid pockets that are free of fetal parts or umbilical cord,whereas others use fluid pockets that contain umbilicalcord or an extremity, provided the pocket is predomi-nantly fluid filled. Although there are week-to-week fluc-tuations, the AFI is usually normal when between 7 and25 cm (Table 13-2). The AFI should be performed withthe patient supine, and each measurement should beobtained strictly perpendicular even if a larger pocket offluid can be imaged in an oblique scan plane.
Fetal Growth and Well-Being 333
growth of fetal parameters is, however, the best methodfor identifying both types of growth restriction. A dis-cussion and examples of this approach using the head(biparietal diameter), abdominal (diameter and circum-ference), and femur length measurements were given inChapter 12 and its Appendix 1 using Table 12-13.
It is anticipated that normal fetal growth should beabove the 10th percentile. Although 10% of normalfetuses will grow slower (SGA fetuses), so will almost all fetuses with IUGR. It is also expected that mostfetuses will maintain predetermined growth percentilesthroughout fetal life so that a fetus growing at the 10thor 50th percentile early in pregnancy, for example, willtypically remain at a similar percentile until term. Usingthis, four types of growth patterns have been described.Growth consistently above the 10th percentile andgrowth spurts from below to above the 10th percentileshould be considered normal. Continued slow growth(below the 10th percentile) or a growth slowdown, par-ticularly if from above to below the 10th percentile islikely to be abnormal.
Amniotic FluidThe uterine cavity should be scanned to determine
the amount of amniotic fluid. Amniotic fluid volume can
Table 13-1 Fetal Abdominal Circumference (mm)
Percentile
Weeks of Gestation 2.5 5 10 25 50 75 80 95 97.5
18 98 103 109 119 131 142 145 159 16419 111 116 123 133 144 156 159 172 17820 121 126 133 143 154 166 169 182 18821 137 142 148 159 170 181 184 198 20322 147 152 158 169 180 191 194 208 21323 160 165 171 182 193 204 207 221 22624 172 177 183 194 205 216 219 233 23825 180 185 191 202 213 224 227 241 24626 188 193 199 210 221 232 235 249 25427 204 209 215 226 237 248 251 265 27028 220 225 231 242 253 264 267 281 28629 236 241 247 258 269 280 283 297 30230 241 246 252 263 274 285 288 302 30731 247 252 258 269 280 291 294 308 31332 254 259 265 276 287 298 301 315 32033 257 262 268 279 290 301 304 318 32334 268 273 279 290 301 312 315 329 33435 289 294 300 311 322 333 336 350 35536 300 305 311 322 333 344 347 361 36637 311 316 322 333 344 355 358 372 37738 324 329 335 346 357 368 371 385 39039 326 331 337 348 359 370 373 387 39240 328 333 339 350 361 372 375 389 39441 338 343 349 360 371 382 385 399 404
From Tamura RK, Sabbagha RE: Percentile ranks of fetal sonar abdominal circumference measurements. Am J Obstet Gynecol 138:475, 1980.

334 ULTRASOUND: THE REQUISITES
The subjective analysis of the amniotic fluid volume isof particular importance in borderline high and lowfluid. In these cases, especially when there is a discrep-ancy between the subjective analysis and the AFI, it is recommended that the subjective determination befavored. If, for example, the AFI calculates in the lownormal range but subjectively the fluid appearsdecreased in volume, the examiner should considerfavoring the subjective interpretation and diagnosingoligohydramnios.
The PlacentaAsymmetric IUGR is caused by a placenta that does
not supply adequate blood and nutrition to the fetus.Although there are no absolute criteria for identifying a
dysfunctioning placenta, three placental properties havebeen analyzed: its thickness and its echogenicity(discussed in Chapter 20) and Doppler waveforms of theumbilical artery (described later in this chapter).
As the placenta ages, it begins to thin and in the thirdtrimester may calcify. These changes are variable, but in approximately 15% of cases the calcifications extendcompletely through the substance of the placenta, com-pletely outlining the cotyledons (see Fig. 20-5D). Theseare termed grade 3 changes and should not occur before34 weeks. Although data from prospective studies arenot available, a composite of data from case reports has shown that the incidence of asymmetric IUGRapproaches 50% in fetuses younger than 34 weeks’gestation with grade 3 changes. Conclusive work on
A B
C DFigure 13-2 Amniotic fluid index (AFI). The depth of the largest amniotic fluid pocket in theright upper (A), right lower (B), left upper (C), and left lower (D) quadrants has been measuredwith electronic calipers (cursors). The sum of the corresponding four values, 11.1 cm, is a normalAFI for the fetus’ gestational age of 36 weeks.
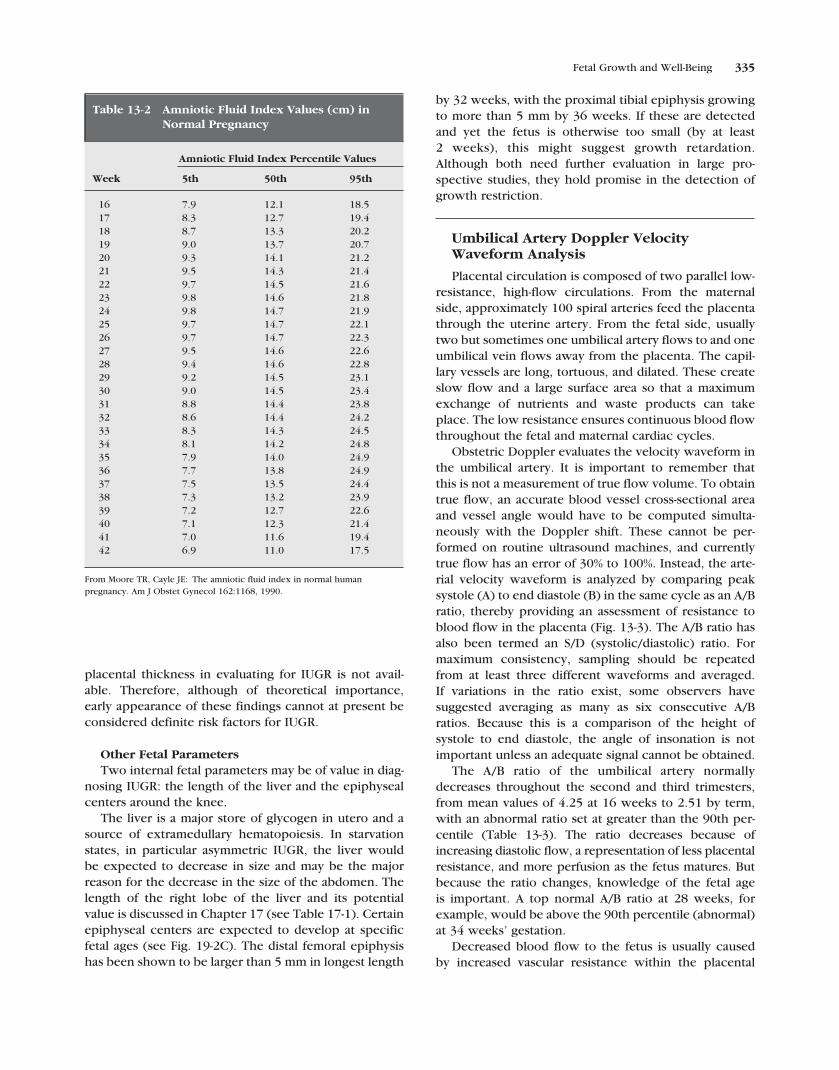
Fetal Growth and Well-Being 335
placental thickness in evaluating for IUGR is not avail-able. Therefore, although of theoretical importance,early appearance of these findings cannot at present beconsidered definite risk factors for IUGR.
Other Fetal ParametersTwo internal fetal parameters may be of value in diag-
nosing IUGR: the length of the liver and the epiphysealcenters around the knee.
The liver is a major store of glycogen in utero and asource of extramedullary hematopoiesis. In starvationstates, in particular asymmetric IUGR, the liver would be expected to decrease in size and may be the majorreason for the decrease in the size of the abdomen. Thelength of the right lobe of the liver and its potential value is discussed in Chapter 17 (see Table 17-1). Certainepiphyseal centers are expected to develop at specificfetal ages (see Fig. 19-2C). The distal femoral epiphysishas been shown to be larger than 5 mm in longest length
by 32 weeks, with the proximal tibial epiphysis growingto more than 5 mm by 36 weeks. If these are detectedand yet the fetus is otherwise too small (by at least 2 weeks), this might suggest growth retardation.Although both need further evaluation in large pro-spective studies, they hold promise in the detection ofgrowth restriction.
Umbilical Artery Doppler VelocityWaveform Analysis
Placental circulation is composed of two parallel low-resistance, high-flow circulations. From the maternalside, approximately 100 spiral arteries feed the placentathrough the uterine artery. From the fetal side, usuallytwo but sometimes one umbilical artery flows to and oneumbilical vein flows away from the placenta. The capil-lary vessels are long, tortuous, and dilated. These createslow flow and a large surface area so that a maximumexchange of nutrients and waste products can takeplace. The low resistance ensures continuous blood flowthroughout the fetal and maternal cardiac cycles.
Obstetric Doppler evaluates the velocity waveform inthe umbilical artery. It is important to remember thatthis is not a measurement of true flow volume. To obtaintrue flow, an accurate blood vessel cross-sectional areaand vessel angle would have to be computed simulta-neously with the Doppler shift. These cannot be per-formed on routine ultrasound machines, and currentlytrue flow has an error of 30% to 100%. Instead, the arte-rial velocity waveform is analyzed by comparing peaksystole (A) to end diastole (B) in the same cycle as an A/Bratio, thereby providing an assessment of resistance toblood flow in the placenta (Fig. 13-3). The A/B ratio hasalso been termed an S/D (systolic/diastolic) ratio. Formaximum consistency, sampling should be repeatedfrom at least three different waveforms and averaged. If variations in the ratio exist, some observers havesuggested averaging as many as six consecutive A/Bratios. Because this is a comparison of the height ofsystole to end diastole, the angle of insonation is notimportant unless an adequate signal cannot be obtained.
The A/B ratio of the umbilical artery normallydecreases throughout the second and third trimesters,from mean values of 4.25 at 16 weeks to 2.51 by term,with an abnormal ratio set at greater than the 90th per-centile (Table 13-3). The ratio decreases because ofincreasing diastolic flow, a representation of less placentalresistance, and more perfusion as the fetus matures. Butbecause the ratio changes, knowledge of the fetal age is important. A top normal A/B ratio at 28 weeks, forexample, would be above the 90th percentile (abnormal)at 34 weeks’ gestation.
Decreased blood flow to the fetus is usually caused by increased vascular resistance within the placental
Table 13-2 Amniotic Fluid Index Values (cm) inNormal Pregnancy
Amniotic Fluid Index Percentile Values
Week 5th 50th 95th
16 7.9 12.1 18.517 8.3 12.7 19.418 8.7 13.3 20.219 9.0 13.7 20.720 9.3 14.1 21.221 9.5 14.3 21.422 9.7 14.5 21.623 9.8 14.6 21.824 9.8 14.7 21.925 9.7 14.7 22.126 9.7 14.7 22.327 9.5 14.6 22.628 9.4 14.6 22.829 9.2 14.5 23.130 9.0 14.5 23.431 8.8 14.4 23.832 8.6 14.4 24.233 8.3 14.3 24.534 8.1 14.2 24.835 7.9 14.0 24.936 7.7 13.8 24.937 7.5 13.5 24.438 7.3 13.2 23.939 7.2 12.7 22.640 7.1 12.3 21.441 7.0 11.6 19.442 6.9 11.0 17.5
From Moore TR, Cayle JE: The amniotic fluid index in normal humanpregnancy. Am J Obstet Gynecol 162:1168, 1990.

336 ULTRASOUND: THE REQUISITES
vascular bed, in the vessels supplying the placenta, orfrom the fetus. Less commonly, it stems from maternalcardiovascular problems. As the resistance increases in any of these conditions, the diastolic componentdecreases initially toward the baseline value (see Fig. 13-3B). This elevates the A/B ratio above the 90thpercentile. As the resistance further increases, end dias-tole can become nonexistent (see Fig. 13-3C) and evenreverse (see Fig. 13-3D) in more severe cases. Further
increase in resistance can cause the systolic componentto become blunted and decreased in height.
An abnormal Doppler ratio indicates an underlyingproblem that is adversely affecting fetal circulation. Anormal Doppler ratio is more difficult to interpret. Ifthere are clinical and/or other ultrasound findings ofIUGR, then a normal ratio tells the examiner little. Itmight be that the fetus will not exhibit an abnormalsignal (not all fetuses with IUGR have abnormal ratios)
A B
C DFigure 13-3 Umbilical artery Doppler imaging. Examples of normal and abnormal umbilicalartery Doppler waveforms. A, Normal waveform. Spectral Doppler tracing obtained from umbilicalartery in the mid cord at 36 weeks shows a normal waveform with good diastolic flow. The A/B ratioof .52/.20 is 2.6, which is normal for 36 weeks (see Table 13-3). Short arrow, peak systole; longarrow, end diastole. B, Decreased diastolic flow. Umbilical artery spectral Doppler tracing at 31 weeks shows decreased diastolic flow resulting in a markedly elevated A/B ratio of 7.6 (see Table13.3). The fetus also was small for gestational age. Electronic calipers (cursors) indicate peak systoleand end diastole. C, Absent diastolic flow. Spectral Doppler tracing from umbilical artery at 29 weeks shows a markedly abnormal waveform, with no diastolic flow. D, Reversed diastolic flow.Spectral Doppler waveform from umbilical artery of a 26-week fetus with severe growth restrictionis markedly abnormal, with reversed diastolic flow (arrows).

Fetal Growth and Well-Being 337
or that the fetus is not as yet severely affected. A differ-entiation of these two possibilities may be very difficultor impossible.
Furthermore, when an abnormal signal is detectedthat suggests fetal compromise, can the abnormal ratiobe equated with the extent of that compromise (distressor demise)? The answer to this question is at presentunfortunately “no.” Although the abnormal Dopplersignal, particularly when other variables such as fetalbiometric measurements are abnormal, elevates thefetus to an increased risk level, there is no definitivecorrelation with the extent of the fetal compromise. Inmost pregnancies, if diastolic flow is still seen, closeobservation without intervention is considered the cor-rect approach unless the fetus is mature enough to bedelivered. Absent or reversed diastolic flow is of moreconcern and is often an indicator of severe fetal com-promise, but even these markedly abnormal spectralwaveform patterns sometimes improve on follow-upexaminations. As a general rule, however, the earlier anabnormal ratio is detected, the worse the prognosis.
It is not recommended that all fetuses have a routineDoppler examination, even in the third trimester. Umbil-ical artery Doppler should be considered an adjunctivetest and the indications for performing Doppler ultra-sound should be limited to the selected cases that arelikely to have IUGR and more specifically to those likelyto be malnourished (asymmetric IUGR).
More recently there has been an attempt to directlyanalyze the fetus’ internal circulation (the descendingthoracic aorta or kidneys) and cranial circulation (thecarotid or middle cerebral arteries (Fig. 13-4). By con-vention this is usually performed with another Doppler
index, the pulsatility index (PI), which is a ratio of peaksystole minus end diastole divided by the area under thecurve of one waveform. In fetuses with asymmetricIUGR, there is evidence that blood flow to the head willinitially remain stable at the expense of blood flow to theremainder of the body. As the fetus further fails, how-ever, the cerebral PI will rise as the diastolic componentof the waveform elevates. This indicates that the fetushas now lost its ability to autoregulate its blood flow andhas increasing distress. Although this analysis added tothe umbilical artery Doppler is being used more often insuspected fetal compromise, its clinical significance andits predictive value in fetal distress have not beenworked out. At present, at most institutions, the A/Bratio of the umbilical artery is performed first, and if it isnormal, the Doppler examination is stopped. Only whenthe ratio is abnormal, or when there are additional clin-ical or ultrasound concerns for an abnormal fetus, is thecerebral PI performed.
Biophysical Profile
Perinatal mortality is of clinical concern in the latethird trimester. Deaths in premature deliveries are to alarge extent caused by the prematurity itself (46%). Interm deliveries, deaths are usually secondary to grossfetal anomalies (57%). In both settings, however, 17% ofperinatal mortality (one out of every six fetuses) iscaused by hypoxia. Can hypoxia be detected?
The biophysical profile (BPP) is an extensivelystudied in utero evaluation that can help in the predic-tion and management of fetuses with hypoxia. Five testsare combined in the BPP: four are of the fetus (assessingacute hypoxia) evaluating cardiac function, breathing,
Table 13-3 Umbilical Artery Peak Systolic–to–End-Diastolic Ratio
From Fogarty P, et al: Continuous wave Doppler flow velocity waveforms from the umbilical artery in normal pregnancy. J Perinat Med 18:51, 1990.
Figure 13-4 Middle cerebral artery Doppler imaging. Axialcolor Doppler image of fetal head at 26 weeks shows the right andleft middle cerebral arteries (arrows). A spectral tracing has beenobtained from the middle cerebral artery.

338 ULTRASOUND: THE REQUISITES
gross body movement, and overall tone, and one is ofthe amniotic fluid (assessing chronic hypoxia). Of these,the heart rate study (the nonstress test [NST]) uses anexternal monitor to analyze passive normal episodes ofcardiac accelerations whereas the other four (breathing,gross body movements, tone, and amniotic fluid) areevaluated by ultrasound.
The BPP uses a binomial grading system, with eachvariable assigned a 2 if that characteristic is present(normal) or 0 if absent (abnormal), for a maximum scoreof 10 and a minimum score of 0. The four fetal charac-teristics develop from different central nervous systemcenters. During embryogenesis the earliest developingcenter involves fetal tone, followed by development ofthe areas associated with fetal movement, then fetalbreathing movements, and lastly fetal heart rate.Hypoxia appears to affect these centers in reverse order.Therefore, it is possible to evaluate the degree of acutehypoxia by observing how many fetal characteristics are involved. These centers, and in particular the cardiaccenter, are not fully developed until 26 to 28 weeks’gestation so that the BPP is a third-trimester evaluation.
A normal fetus goes through sleep-wake cycles lasting20 to 40 minutes. An important assumption of the BPP isthat a fetus cannot be spontaneously awakened. When itis asleep, the normal fetus will resemble a compromised(hypoxic) fetus. However, the sleeping fetus will even-tually awaken and start to move, whereas the compro-mised fetus will not. The BPP is scheduled to last 30 minutes. During that time the examiner is looking forfour parameters. If the fetus is normally responsive thestudy can be completed within 10 minutes. If the fetusis not moving, however, it is necessary to continuouslyobserve the fetus for the full 30 minutes. If stillunresponsive, the fetus is probably compromised.
Definitions have been given to each of the variables.Since the initial studies, only the definition of gross bodymovements has remained unchanged; the definitions ofthe other four have been modified, and this is describedby Finberg and coworkers. It has been suggested thatfetal tone too closely mirrors gross body movements andthat fine body movements such as those of the handsshould be used instead. Another group has suggestedgiving the fetus a “partial credit” of 1 (instead of 2) forany response that is somewhere between a full responseand no response. Still others have recommended usingthe contraction stimulation test, an active cardiac testrequiring nipple stimulation or the administration ofoxytocin, either in addition to or instead of the NST.Lastly, evaluation of the amniotic fluid has undergonechanges from a single pocket measurement, with mostexaminers now using the AFI.
These variations notwithstanding, there is a highdegree of correlation between the BPP and perinatalmorbidity (fetal distress) and mortality (fetal demise).
Fetal distress has a linear relationship to the BPP: there isalmost no likelihood of fetal distress (<3%) associatedwith a BPP of 10, with this likelihood increasing steadilyto 100% with a BPP of 0. A score of 0 or 2, meaning thatevery characteristic is abnormal or that only one charac-teristic is normal, is highly associated with impendingdemise. For a BPP score of 8 or 10, the negative predic-tive accuracy for a normal live outcome within 1 weekof the test is 99.224%. Certain groups of high-riskmothers, particularly insulin-dependent diabetics, mayneed to be reexamined more than once a week. Themeaning of the intervening scores of 4 to 7, unfortu-nately, has not been resolved.
It would be tempting to assume that all growth-restricted fetuses should have their BPP assessed. How-ever, a number of fetuses with IUGR are not hypoxic anda number of hypoxic fetuses are not growth restricted.Therefore, although there is overlap in the characteris-tics of both, and many IUGR fetuses may be studied withthe BPP, these two groups should not be considered the same.
A full BPP may not be needed in most cases, becausethe cardiac portion (NST), representing acute hypoxia,and the amniotic fluid assessment, representing chronichypoxia, may be representative of the entire BPP. Inparticular, when comparing the BPP against the NST, thepositive predictive value for an abnormal BPP score is much greater than that for an abnormal NST result(56.6% vs. 13.1%), but the negative predictive value fora normal BPP score is virtually identical to a normal NSTresult (98.8% vs. 98.0%). As a result, it may be reasonableto perform the NST first and obtain a BPP only when theNST result is abnormal.
There is a distinct difference between the indicationsfor a full ultrasound obstetrical antenatal examinationand a BPP. The ultrasound examination is performed anytime in pregnancy to establish fetal age and to evaluatefor anomalies and amniotic fluid; the BPP is performedto evaluate fetal function in the late second trimester andthird trimester.
Summary Of IUGR
When the gestational age is known, weight andabdominal circumference are helpful predictors of SGAfetuses with the lower 10th percentile picked as the cut-off. The lower the weight or abdominal circumference,the greater likelihood that IUGR is present. When thegestational age is not known or uncertain, the onlyconsistently useful characteristic for the analysis ofsymmetric growth restriction is slow interval growth.Multiple additional characteristics are potentially avail-able for determining asymmetric growth retardation: anabnormal head-to-body proportion, slow interval growth,decreased volume of amniotic fluid, and abnormal

Fetal Growth and Well-Being 339
Doppler velocity waveforms. Each case of asymmetricIUGR differs in its presentation and in its abnormalcharacteristics.
The BPP is a valuable test for predicting both normal(nonhypoxic) fetuses and impending fetal demise.However, there is need for uniform definitions of thecharacteristics and the scoring system needs to bestandardized.
MACROSOMIA
The terms large for gestational age (LGA) andmacrosomia are often used interchangeably to describea newborn above the 90th percentile by weight or onewho weighs more than either 4000 or 4500 g. However,if strictly defined, the terms are not synonymous. LGAfetuses are symmetrically large with fat distributedevenly over the entire body. In contradistinction, macro-somic fetuses are asymmetrically enlarged with fatdistributed more to the shoulders and body, so macro-somic fetuses are at greatest risk for shoulder dystociaduring vaginal delivery; that is, the head can be delivered
without difficulty but the shoulders may impact. Ifexcessive traction on the neck is required to disengagethe shoulders, injury to the newborn, most commonlyErb’s palsy (neurologic damage to the brachial plexus),can result. At times, despite the use of all aggressiveobstetrical maneuvers, the results of delivery may bedisastrous. Macrosomia is commonly associated withmaternal gestational diabetes and mild insulin-dependentdiabetes (Fig. 13-5).
Estimated fetal weight alone cannot predict the dis-proportionality of the shoulders and body and thereforedoes not optimally predict the potential for shoulderdystocia. In addition, because there is a minimum of a15% error in the calculation of the fetal weight, the fetuswould have to have a mean weight of at least 4600 g toconfidently predict a weight of more than 4000 g.
There have been attempts to measure the head, thehead-to-body ratio, and shoulder length (from the neck tothe edge of the shoulder) for the prediction of dystocia.This work is incomplete and has not been consistent in predicting potential problems at time of delivery. Atpresent, therefore, macrosomia can only be inferred fromthe estimated fetal weight and clinical suspicion.
A BFigure 13-5 Macrosomia associated with gestational diabetes. A, AC measurement of 34.9 cm inthis 34-week pregnancy complicated by gestational diabetes is above the 97.5th percentile for ges-tational age (see Table 13-1). The EFW was at the 99th percentile. B, Axial image of abdomen ofsame fetus obtained at the level of the kidneys (K) shows polyhydramnios, also due to gestationaldiabetes. F, amniotic fluid.

340 ULTRASOUND: THE REQUISITES
Key Features
Neonates with small birth weights, usually defined asbelow the 10th percentile, are considered small forgestational age (SGA). These SGA children can beeither constitutionally small or growth restricted.
Intrauterine growth restriction (IUGR) varies inincidence. On average, it affects 5% of the generalpopulation. In a high-risk population, this rate canrise to 10% of fetuses.
There are two types of IUGR: diminished cellular growthleading to a symmetrically small fetus (usually occur-ring in the first or early second trimester) and fetalmalnutrition leading to an asymmetrically small fetus(usually occurring in the third trimester). If themalnutrition is extreme, however, the asymmetricfetus may appear symmetric.
If an accurate fetal age is known, either from an earlyultrasound examination or accurate menstrual dates,or both, then the measured abdominal circumferenceand calculated fetal weight can be used to determineif the fetal size and weight are appropriate.
When an accurate age is not known, additional lesssensitive and less specific characteristics for identi-fying IUGR are needed. They are interval growth, thehead-to-body ratio, the amniotic fluid volume, andthe Doppler velocity waveform. Of these, onlyinterval growth can be used to assess both types ofIUGR.
Structural anomalies may be either the cause of or asso-ciated with IUGR.
The ability of ultrasound to detect IUGR is different indifferent clinical risk groups. A slightly small fetus ora fetus growing at the lower 10th percentile is oftenless of a clinical concern if the woman is in a low-risk rather than in a high-risk group.
The volume of amniotic fluid can be evaluated eithersubjectively by scanning the entire uterine content orby a four-quadrant measurement (the amniotic fluidindex [AFI]). Subjective analysis is as accurate as theAFI and is of particular value in borderline cases.
Doppler evaluation makes use of a ratio of peak systoleand end diastole from the arterial waveform in theumbilical artery. With decreasing diastole (highervascular resistance), the ratio increases and the fetusis then at greater risk for circulatory problems. Morerecently, the fetal cerebral circulation has beenstudied but no specific conclusions as to its predic-tive accuracy have yet been made.
It is not recommended that Doppler sonography beperformed in all pregnancies. When there is asuggestion of a compromised fetus, however, theumbilical artery Doppler study is performed. Only if the study is abnormal does the fetal cerebralcirculation need to be studied.
The biophysical profile (BPP) can predict perinatalmortality by detecting in utero hypoxia (17% of allfetuses).
The BPP consists of five tests, four fetal for identifyingacute hypoxia and one of the amniotic fluid foridentifying chronic hypoxia. Each characteristic israted as 2 if normal and 0 if absent, for a total scoreof from 0 to 10.
The fetus with a BPP score of 7 or more can be consid-ered “safe” in most cases for up to a week but is atrisk for impending demise if the score is less than 4.Intervening numbers indicate risk but usually not thedanger of sudden demise.
The two most sensitive BPP tests are the cardiac test for acute hypoxia (the nonstress test [NST]) andamniotic fluid assessment for chronic hypoxia.
The terms large for gestational age (LGA) and macro-somia have been used interchangeably. There arethree definitions: a weight exceeding 4000 g, a weightexceeding 4500 g, or ultrasound findings that suggestthat the fetus is larger than the 90th percentile.
There are no problems with a macrosomic fetus inutero. At delivery, particularly if asymmetrically largewith fat distributed more in the shoulders and body,the fetus is at risk for shoulder dystocia.

Fetal Growth and Well-Being 341
SUGGESTED READINGS
Baschat AA, Harman CR: Antenatal assessment of the growthrestricted fetus. Curr Opin Obstet Gynecol 13:161, 2001.
Benson CB, et al: Intrauterine growth retardation: Diagnosisbased on multiple parameters: A prospective study. Radiology177:499, 1990.
Campbell BA: Utilizing sonography to follow fetal growth.Obstet Gynecol Clin North Am 25:750, 1998.
Craigo SD: The role of ultrasound in the diagnosis and man-agement of intrauterine growth retardation. Semin Perinatol18:292, 1994.
Doubilet PM, Benson CB: Sonographic evaluation ofintrauterine growth retardation. AJR Am J Roentgenol 164:709,1995.
Finberg HJ, et al: The biophysical profile: A literature reviewand reassessment of its usefulness in the evaluation of fetalwell-being. J Ultrasound Med 9:583, 1990.
Fong KW, Ohlsson A, Hannah ME, et al: Prediction of perinataloutcome in fetuses suspected to have intrauterine growthrestriction: Doppler US study of fetal cerebral, renal, andumbilical arteries. Radiology 213:681, 1999.
Galan HL, Ferrazzi E, Hobbins JC: Intrauterine growth restric-tion (IUGR): Biometric and Doppler assessment. Prenat Diagn22:331, 2002.
Goldstein RB, Filly RA: Sonographic estimation of amnioticfluid volume: Subjective assessment versus pocket measure-ments. J Ultrasound Med 7:363, 1988.
Hershkovitz R, Kingdom JC, Geary M, et al: Fetal cerebralblood flow redistribution in late gestation: Identification ofcompromise in small fetuses with normal umbilical arteryDoppler. Ultrasound Obstet Gynecol 15:209, 2000.
Landon MB: Prenatal diagnosis of macrosomia in pregnancycomplicated by diabetes mellitus. J Matern Fetal Med 9:52,2000.
Manning FA: Fetal biophysical profile. Obstet Gynecol ClinNorth Am 26:557, 1999.
Manning FA, Platt LD, Sipos L: Antepartum fetal evaluation:Development of a fetal biophysical profile. Am J ObstetGynecol 136:787, 1980.
Marsal K: Intrauterine growth restriction. Curr Opin ObstetGynecol 14:127, 2002.
Pollack RN, Divon MY: Intrauterine growth retardation andetiology. Clin Obstet Gynecol 35:99, 1992.
Resnick R: Intrauterine growth restriction. Obstet Gynecol99:490, 2002.
Rochelson B, et al: The significance of absent end-diastolicvelocity in umbilical artery velocity waveforms. Am J ObstetGynecol 156:1213, 1987.
Rochelson BL, et al: The clinical significance of Doppler umbil-ical artery velocimetry in the small for gestational age fetus. AmJ Obstet Gynecol 156:1223, 1987.
Sacks DA, Chen W: Estimating fetal weight in the managementof macrosomia. Obstet Gynecol Surv 55:229, 2000.
Sholl JS, et al: Intrauterine growth retardation risk detection forfetuses of unknown gestational age. Am J Obstet Gynecol144:709, 1982.
Trudinger BJ, et al: Fetal umbilical artery velocity waveformsand subsequent neonatal outcome. Br J Obstet Gynaecol98:378, 1991.
Vintzileos AM, et al: The fetal biophysical profile and itspredictive value. Obstet Gynecol 62:271, 1983.