Guidance for research-practice partnerships (R-PPs) and collaborative research
12
Guidance for research-practice partnerships (R-PPs) and collaborative research John Ovretveit, Susanne Hempel, Jennifer L. Magnabosco, Brian S. Mittman, Lisa V. Rubenstein and David A. Ganz (Affiliations at end of article) Abstract Purpose – The purpose of this paper is to provide evidence based guidance to researchers and practice personnel about forming and carrying out effective research partnerships. Design/methodology/approach – A review of the literature, interviews and discussions with colleagues in both research and practice roles, and a review of the authors’ personal experiences as researchers in partnership research. Findings – Partnership research is, in some respects, a distinct “approach” to research, but there are many different versions. An analysis of research publications and of their research experience led the authors to develop a framework for planning and assessing the partnership research process, which includes defining expected outcomes for the partners, their roles, and steps in the research process. Practical implications – This review and analysis provides guidance that may reduce commonly-reported misunderstandings and help to plan more successful partnerships and projects. It also identifies future research which is needed to define more precisely the questions and purposes for which partnership research is most appropriate, and methods and designs for specific types of partnership research. Originality/value – As more research moves towards increased participation of practitioners and patients in the research process, more precise and differentiated understanding of the different partnership approaches is required, and when each is most suitable. This article describes research approaches that have the potential to reduce “the research-practice gap”. It gives evidence- and experience-based guidance for choosing and establishing a partnership research process, so as to improve partnership relationship-building and more actionable research. Keywords Knowledge sharing, Action research, Evidence-based practice, Research methods, Implementation, Research methodology Paper type General review The current issue and full text archive of this journal is available at www.emeraldinsight.com/1477-7266.htm The authors would like to thank Roberta Shanman, Lopamudra Das, Jodi Lui, and Tanja Perry for assistance with the literature review, and Deborah Delevan for editorial assistance. The authors would also like to thank John Midolo for provision of information on QUERI partnered research evaluation centers, and Amy Kilbourne for her comments on a prior version of this manuscript. This project was funded by the US Department of Veterans Affairs, Veterans Health Administration Quality Enhancement Research Initiative through core funding to the Center for Implementation Practice and Research Support (Project # TRA 08-379). Additional support for investigator time and visiting professorship was provided from the Medical Management Center, Karolinska Institutet, Stockholm, and by a Career Development Award to David Ganz from the US Department of Veterans Affairs, Health Services Research and Development (HSR&D) Service (Project #VA CD2 08-012-1). Research- practice partnerships 115 Journal of Health Organization and Management Vol. 28 No. 1, 2014 pp. 115-126 q Emerald Group Publishing Limited 1477-7266 DOI 10.1108/JHOM-08-2013-0164
Transcript of Guidance for research-practice partnerships (R-PPs) and collaborative research

Guidance for research-practicepartnerships (R-PPs) andcollaborative research
John Ovretveit, Susanne Hempel, Jennifer L. Magnabosco,Brian S. Mittman, Lisa V. Rubenstein and David A. Ganz
(Affiliations at end of article)
Abstract
Purpose – The purpose of this paper is to provide evidence based guidance to researchers andpractice personnel about forming and carrying out effective research partnerships.
Design/methodology/approach – A review of the literature, interviews and discussions withcolleagues in both research and practice roles, and a review of the authors’ personal experiences asresearchers in partnership research.
Findings – Partnership research is, in some respects, a distinct “approach” to research, but there aremany different versions. An analysis of research publications and of their research experience led theauthors to develop a framework for planning and assessing the partnership research process, whichincludes defining expected outcomes for the partners, their roles, and steps in the research process.
Practical implications – This review and analysis provides guidance that may reducecommonly-reported misunderstandings and help to plan more successful partnerships and projects.It also identifies future research which is needed to define more precisely the questions and purposesfor which partnership research is most appropriate, and methods and designs for specific types ofpartnership research.
Originality/value – As more research moves towards increased participation of practitioners andpatients in the research process, more precise and differentiated understanding of the differentpartnership approaches is required, and when each is most suitable. This article describes researchapproaches that have the potential to reduce “the research-practice gap”. It gives evidence- andexperience-based guidance for choosing and establishing a partnership research process, so as toimprove partnership relationship-building and more actionable research.
Keywords Knowledge sharing, Action research, Evidence-based practice, Research methods,Implementation, Research methodology
Paper type General review
The current issue and full text archive of this journal is available at
www.emeraldinsight.com/1477-7266.htm
The authors would like to thank Roberta Shanman, Lopamudra Das, Jodi Lui, and Tanja Perryfor assistance with the literature review, and Deborah Delevan for editorial assistance. Theauthors would also like to thank John Midolo for provision of information on QUERI partneredresearch evaluation centers, and Amy Kilbourne for her comments on a prior version of thismanuscript.This project was funded by the US Department of Veterans Affairs, Veterans HealthAdministration Quality Enhancement Research Initiative through core funding to the Center forImplementation Practice and Research Support (Project # TRA 08-379). Additional support forinvestigator time and visiting professorship was provided from the Medical Management Center,Karolinska Institutet, Stockholm, and by a Career Development Award to David Ganz from theUS Department of Veterans Affairs, Health Services Research and Development (HSR&D)Service (Project #VA CD2 08-012-1).
Research-practice
partnerships
115
Journal of Health Organization andManagement
Vol. 28 No. 1, 2014pp. 115-126
q Emerald Group Publishing Limited1477-7266
DOI 10.1108/JHOM-08-2013-0164

IntroductionIt often takes many years for treatments and management interventions that have beenfound to be more effective to be widely implemented. Interest about, and research into“closing the gap between research and practice” has grown over the last fifteen years.There are a number of explanations for the gap. Research and researchers aresometimes criticized as being “too distant” from real practice in health services (Kesslerand Glasgow, 2011; van de Ven and Johnson, 2006). Some practitioners say that thefindings of research do not give useful guides to action (Campbell et al., 2009). For theirpart, researchers point to the apparent disinterest of some practitioners in the findingsof research, and to the work pressures that make it difficult for practitioners to givetime to changing their practice. Sometimes, researchers also note an unwillingness orinability of practitioners to think through what a particular piece of research mightmean for practice in their setting.
Whether, when or how researchers should help practitioners interpret research inorder to improve care is a question increasingly asked. The view that “research in, andwith, practice” might be a more effective way to make better use of researchers andresearch in implementing or adapting research in practice settings (Green and Ottoson,2004), has been gathering weight with research funders and government agencies.Some have called for a greater emphasis on “rapid cycle learning” and “fast cycleresearch” involving closer research-practice collaborations (Gold et al., 2011).Initiatives such as the USA NIH translational research program (National Instituteof Health, 2007) have aimed to respond to this call for improvements in closing theresearch-practice gap. Partnerships between researchers and practitioners have beenestablished with the aim of producing “more relevant” or “more actionable” research(Department of Health, 2007). Another aim of such partnerships has been to enable theimplementation of research (Bosworth et al., 2010).
The purpose of this article is to give an overview of different approaches to“research-practice partnerships” (R-PPs) and to give research-informed guidance forestablishing and developing such partnerships. We define partnered research as “anactivity where researchers and practitioners work together, with different roles, to useresearch both to solve practical problems and to contribute to science”. Throughoutthis article, the term “practitioner” is used to refer to clinicians and managers alike.
The perspective on partnerships given here is based on a synthesis of the literaturecoupled with our own experience conducting “partnered research”, and also oninterviews with individuals in both research and operations roles who have beeninvolved in such partnerships within the US Veterans Health Administration (VA) andin one UK University and National Health Service (NHS) collaborative researchprogram (Øvretveit et al., 2010). More details on one set of partnership research in theVA can be found at VA Health Services Research and Development (2013b). In 2008,the UK NHS started nine “Collaborations for Leadership in Applied Health Researchand Care” (CLAHRCs) between University health research centers and NHSservice-providing organizations and local communities. The aim is to “stimulateinnovation and best practice across local health communities using two-waycollaborative learning and delivery pathways” in order to link researchers withresearch users who include policymakers, managers, front-line clinical professionals,patients and community representatives (“local health community”). More details aregiven by Baker et al. (2009), Rycroft-Malone et al. (2011) and Øvretveit et al. (2010).
JHOM28,1
116

With this background, our conceptualization of partnerships emphasizesrelationships between researchers and practitioners for clinical research and clinicalimprovement, rather than for policy or population public health practice.
Findings from the overview of the literature about research-practicepartnershipsOur review of the literature identified many different “approaches” to partnershipresearch, which overlap both in concept and application. Broad categories of R-PPsdescribed in the literature include:
. Community based participatory research (CBPR): defined in one paper as“conducting research by equitably partnering researchers and those directlyaffected by and knowledgeable of the local circumstances that impact health”(Horowitz et al., 2009).
. Practice-based research networks (PBRN): defined as “a group of clinicians,practices, or institutions that are devoted primarily to the delivery of patient careand are affiliated with each other in order to investigate questions related tocommunity-based practice” (Kutner et al., 2005).
. Practice-based quality improvement research (PBQIR): research by practitionersor academic researchers on changes to clinical practice or organization, where theresearcher works with practitioners to collect data and sometimes to report datato enable improvement.
. Action research (specifically for improving healthcare): defined as “a period ofinquiry, which describes, interprets and explains social situations whileexecuting a change intervention aimed at improvement and involvement”(Waterman et al., 2001).
. Specially-created health services research-practice partnerships involvinguniversities/academic medical centers: examples are the UK University-NHSCLAHRCs (e.g. Baker et al., 2009) or a US academic medical center communitypartnership (Yaggy et al., 2006). These are broad-based “umbrellas” for a rangeof research-practitioner studies and have tended to be university-driven andvehicles for research-into-practice “translational research”.
Our review found information lacking about many practical aspects of partnershipsincluding the nature and level of participation of practitioners in different stages ofprojects, and this made it difficult to assess whether the partnership was in name onlyor more substantive. In exploring how to define key features of a partnership approach,we assessed a range of studies which did give details. Table I gives a sample of studiesshowing the different ways that R-PPs can be established and run. We built on thisreview, our interviews and our varied experience as researchers in the UK, the USA,Europe and Australia to define criteria which differentiate more substantialpartnership research and a framework to specify a particular type of partnership(Figure 1). We return to this after noting other observations from the literature review.
A second finding from our overview is that investigators showed significantlydifferent understandings of “research” and of the role of practitioners with respect toresearch. At least three conceptions of research could be identified in the literature:research as knowledge generation, as existing evidence, and research as referring to
Research-practice
partnerships
117

Stu
dy
Ty
pe
Hea
lth
care
syst
em/c
onte
xt
Cli
nic
alar
eaP
artn
ersh
ipop
erat
ion
aliz
atio
nL
esso
ns
lear
ned
DeV
oeetal.
(201
2)P
ract
ice-
bas
edre
sear
chn
etw
ork
(PB
RN
)
AH
RQ
fun
ded
PB
RN
toco
mp
lem
ent
aco
mm
un
ity
hea
lth
coll
abor
ativ
eof
safe
tyn
etor
gan
izat
ion
sca
lled
OC
HIN
and
isb
ased
inth
eW
este
rnst
ates
ofU
SA
Pri
mar
yca
reO
CH
INis
aco
llab
orat
ive,
mem
ber
-bas
edor
gan
izat
ion
offe
der
ally
qu
alifi
edh
ealt
hce
nte
rsan
dsi
mil
aren
titi
esth
atp
rov
ides
ap
rim
ary
hea
lth
care
“saf
ety
net
”to
vu
lner
able
pop
ula
tion
s.U
sin
ga
coll
abor
ativ
ele
arn
ing
org
aniz
atio
nm
odel
,OC
HIN
faci
lita
tes
its
mem
ber
s’ad
opti
onof
hea
lth
info
rmat
ion
tech
nol
ogy
toim
pro
ve
pat
ien
tca
req
ual
ity
.T
oth
isen
d,
OC
HIN
mai
nta
ins
one
elec
tron
ich
ealt
hre
cord
(EH
R)
wit
ha
sin
gle
mas
ter
pat
ien
tin
dex
lin
ked
acro
ssal
lcl
inic
site
s.O
CH
INis
reco
gn
ized
by
the
Hea
lth
Res
ourc
esan
dS
erv
ices
Ad
min
istr
atio
nas
ah
ealt
hce
nte
r-co
ntr
olle
dn
etw
ork
and
now
has
mor
eth
an62
mem
ber
org
aniz
atio
ns
and
over
200
clin
ics
Str
ateg
icfa
ctor
sim
por
tan
tto
the
succ
ess
ofa
PB
RN
:(1
)sh
ared
vis
ion
and
com
mit
men
tto
au
niq
ue
pat
ien
tp
opu
lati
on;
(2)
stro
ng
lead
ersh
ip,
men
tors
hip
,co
llab
orat
ion
;(3
)cr
eati
ve
app
roac
hes
toen
gag
ing
bu
sycl
inic
ian
s/b
rid
gin
gth
ew
orld
sof
acad
emia
and
pra
ctic
e;(4
)h
arn
essi
ng
elec
tron
ich
ealt
hre
cord
dat
a,n
avig
atin
gd
ata
pro
tect
ion
,sh
arin
g,
own
ersh
ipN
agy
kal
di
etal.
(200
6)P
ract
ice
faci
lita
tors
Ok
lah
oma
Ph
ysi
cian
sR
esou
rce/
Res
earc
hN
etw
ork
,C
olor
ado
Res
earc
hN
etw
ork
,O
reg
onR
ura
lP
ract
ice-
Bas
edR
esea
rch
Net
wor
k;
Un
iver
sity
atB
uff
alo
Fam
ily
Med
icin
eR
esea
rch
Inst
itu
tean
dU
pst
ate
New
Yor
kP
ract
ice-
bas
edR
esea
rch
Net
wor
k
All
Pra
ctic
efa
cili
tato
rsp
arti
cip
ate
mos
tof
ten
inex
tern
ally
fun
ded
rese
arch
pro
ject
s;cl
inic
ian
sm
ayh
ave
anac
tiv
ero
lein
the
pla
nn
ing
and
the
com
ple
tion
ofth
ese
pro
ject
sb
ut
the
acti
vit
ies
are
dri
ven
mos
tly
by
the
stu
dy
pro
toco
ls;
faci
lita
tors
act
asre
sear
chas
sist
ants
,d
evel
opre
lati
onsh
ips,
assi
stcl
inic
ian
sin
loca
lre
sear
chan
dQ
Ip
roje
cts
init
iate
db
yth
ep
ract
ices
,h
elp
wit
has
sess
men
tof
the
pra
ctic
e’s
nee
ds
and
pot
enti
alto
imp
lem
ent
inte
rven
tion
s,an
dty
pic
ally
inte
ract
wit
ha
“ch
amp
ion
”p
hy
sici
anor
pra
ctic
ele
ader
asw
ell
ask
eyp
erso
nn
elto
ensu
reco
mm
un
icat
ion
Pra
ctic
efa
cili
tato
rsca
nb
ea
par
ticu
larl
yu
sefu
lre
sou
rce
En
gel
ke
and
Mar
shb
urn
(200
6)
Nu
rsin
gse
rvic
ean
dre
sear
ch
Eas
tC
arol
ina
Un
iver
sity
Sch
ool
ofN
urs
ing
,P
itt
Cou
ntr
yM
emor
ial
Hos
pit
al
Hos
pit
al,
nu
rsin
gC
olla
bor
ativ
ere
sear
chb
ased
onco
mm
itm
ent
tote
amw
ork
,re
cip
roci
ty,
and
mu
tual
ben
efit;
rese
arch
inte
rest
sn
eed
tob
eal
ign
ed;
two
mec
han
ism
sto
fost
erco
llab
orat
ion
:co
llab
orat
ive
rese
arch
day
(on
ed
ay)
and
coll
abor
ativ
ere
sear
chaw
ard
($1,
000)
Com
mit
men
tto
pro
vid
efu
nd
ing
and
sup
por
tas
wel
las
the
wil
lin
gn
ess
ofth
ep
artn
ers
toev
alu
ate
and
rev
ise
the
pro
gra
mh
ave
bee
ncr
itic
al
(continued
)
Table I.Examples ofresearch-practicepartnership“arrangements”
JHOM28,1
118

Stu
dy
Ty
pe
Hea
lth
care
syst
em/c
onte
xt
Cli
nic
alar
eaP
artn
ersh
ipop
erat
ion
aliz
atio
nL
esso
ns
lear
ned
Hel
met
al.
(201
0)H
ealt
hco
llab
orat
ion
Un
iver
sity
ofH
awai
’iR
ura
lH
ealt
hC
olla
bor
atio
n(U
HR
HC
)M
enta
lh
ealt
h,
psy
chia
tric
serv
ices
Est
abli
shed
toin
crea
seru
ral
acce
ssto
beh
avio
ral
hea
lth
serv
ices
,p
rim
aril
yv
iate
le-p
sych
iatr
yth
rou
gh
par
tner
ship
sw
ith
com
mu
nit
yh
ealt
hcl
inic
s.D
irec
tp
atie
nt
care
isp
rov
ided
eith
erfa
ceto
face
orv
iav
ideo
tele
con
fere
nci
ng
.U
HR
HC
use
sa
serv
ice-
lear
nin
gap
pro
ach
tow
ork
forc
ed
evel
opm
ent,
wh
ich
allo
ws
un
iver
siti
esto
con
trib
ute
toim
pro
ved
pu
bli
ch
ealt
hth
rou
gh
stru
ctu
red
trai
nee
exp
erie
nce
sin
com
mu
nit
yse
ttin
gs
such
asfe
der
ally
qu
alifi
edh
ealt
han
dco
mm
un
ity
hea
lth
cen
ters
Com
mu
nit
yen
gag
emen
tw
ascr
itic
alto
cult
ivat
ing
refe
rral
sou
rces
;in
teg
rate
dra
ther
than
coll
ocat
edtr
ain
ing
and
serv
ice
del
iver
ysh
ould
be
init
iate
d;
eth
no-
cult
ura
lan
dd
iag
nos
tic
div
ersi
tysh
ould
be
ato
pp
rior
ity
;th
ere
are
crit
ical
con
sid
erat
ion
sfo
rre
sear
chet
hic
sw
hen
acad
emic
inst
itu
tion
sp
artn
erw
ith
ind
igen
ous
com
mu
nit
ies
Gre
ene
etal.
(201
2)G
rou
ph
ealt
hR
apid
Lea
rnin
gH
ealt
hS
yst
em(R
LH
S)
All
Th
eR
apid
Lea
rnin
gH
ealt
hS
yst
emle
ver
ages
rece
nt
dev
elop
men
tsin
hea
lth
info
rmat
ion
tech
nol
ogy
and
ag
row
ing
hea
lth
dat
ain
fras
tru
ctu
reto
acce
ssan
dap
ply
evid
ence
inre
alti
me,
wh
ile
sim
ult
aneo
usl
yd
raw
ing
kn
owle
dg
efr
omre
al-w
orld
care
-del
iver
yp
roce
sses
top
rom
ote
inn
ovat
ion
and
hea
lth
syst
emch
ang
eon
the
bas
isof
rig
orou
sre
sear
ch.
Imp
lem
enti
ng
the
RL
HS
syst
emin
vol
ves
six
step
s:(1
)in
tern
al/e
xte
rnal
scan
toid
enti
fyp
rob
lem
san
dso
luti
ons;
(2)
des
ign
ing
evid
ence
bas
edca
rean
dev
alu
atio
n;
(3)
imp
lem
enti
ng
the
pla
nin
pil
otan
dco
ntr
olse
ttin
g;
(4)
eval
uat
ing
wh
atw
ork
sor
doe
sn
otw
ork
;(5
)ad
just
ing
evid
ence
toin
flu
ence
con
tin
ual
imp
rov
emen
t;an
d(6
)d
isse
min
atio
nof
resu
lts
toim
pro
ve
care
for
ever
yon
e.M
odel
pro
mot
esb
idir
ecti
onal
dis
cov
ery
and
anop
enm
ind
atth
esy
stem
lev
el,r
esu
ltin
gin
wil
lin
gn
ess
tom
ake
chan
ges
onth
eb
asis
ofev
iden
ceth
atis
bot
hsc
ien
tifi
call
yso
un
dan
dp
ract
ice-
bas
ed
Hal
lmar
ks
ofth
eR
LH
Sar
eth
ev
ital
par
tner
ship
bet
wee
nre
sear
chan
dcl
inic
alop
erat
ion
san
da
shar
edco
mm
itm
ent
tole
ver
age
scie
nti
fic
kn
owle
dg
ean
dev
alu
atio
nfo
rra
pid
,p
oin
t-of
-car
eim
pro
vem
ents
(continued
)
Table I.
Research-practice
partnerships
119

Stu
dy
Ty
pe
Hea
lth
care
syst
em/c
onte
xt
Cli
nic
alar
eaP
artn
ersh
ipop
erat
ion
aliz
atio
nL
esso
ns
lear
ned
Sch
illi
ng
etal.
(201
1)K
aise
rP
erm
anen
teK
aise
rP
erm
anen
te(K
P)
Per
form
ance
Imp
rov
emen
tS
yst
em’s
Lea
rnin
gO
rgan
izat
ion
All
Six
“bu
ild
ing
blo
cks”
wer
eid
enti
fied
toen
able
KP
tom
ake
the
tran
siti
onto
bec
omin
ga
lear
nin
gor
gan
izat
ion
:(1
)re
al-t
ime
shar
ing
ofm
ean
ing
ful
per
form
ance
dat
a;(2
)fo
rmal
trai
nin
gin
pro
ble
m-s
olv
ing
met
hod
olog
y;
(3)
wor
kfo
rce
eng
agem
ent
and
info
rmal
kn
owle
dg
esh
arin
g;
(4)
lead
ersh
ipst
ruct
ure
s,b
elie
fs,
and
beh
avio
rs;
(5)
inte
rnal
and
exte
rnal
ben
chm
ark
ing
;an
d(6
)te
chn
ical
kn
owle
dg
esh
arin
g
Cre
atin
ga
lear
nin
gor
gan
izat
ion
req
uir
eda
com
bin
atio
nof
top
-d
own
and
bot
tom
-u
pst
rate
gie
s.T
he
dem
and
for
real
-tim
em
ean
ing
ful
per
form
ance
dat
aca
nco
nfl
ict
wit
hp
rior
itiz
edch
ang
esto
hea
lth
info
rmat
ion
syst
ems.
Itis
anon
goi
ng
chal
len
ge
tote
ach
per
form
ance
imp
rov
emen
t,ch
ang
em
anag
emen
t,in
nov
atio
n,
and
pro
ject
man
agem
ent
toal
lm
anag
ers
and
staf
fw
ith
out
con
sum
ing
too
mu
chtr
ain
ing
tim
e.C
hal
len
ges
wit
hw
ork
forc
een
gag
emen
tin
clu
de
low
init
ial
use
ofto
ols
inte
nd
edto
dis
sem
inat
ein
form
atio
nth
rou
gh
vir
tual
soci
aln
etw
ork
ing
Sol
ber
g(2
006)
Hea
lth
Par
tner
sM
edic
alg
rou
ps
inM
inn
esot
aw
ho
wer
eal
sop
art
ofth
eM
inn
esot
aC
omm
un
ity
Mea
sure
men
tp
ub
lic
rep
orti
ng
init
iati
ve
Men
tal
hea
lth
/p
rim
ary
care
Des
crib
esse
ven
fact
ors
affe
ctin
gre
cru
itm
ent
ofm
edic
alp
ract
ices
inim
ple
men
tati
onre
sear
ch:
(1)
rela
tion
ship
ofth
ere
cru
iter
wit
hth
elo
cal
med
ical
com
mu
nit
y;
(2)
rep
uta
tion
ofth
ere
cru
iter
sw
ith
inth
em
edic
alre
sear
ch/Q
Ico
mm
un
ity
;3)
req
uir
emen
tsfo
rre
sear
chp
arti
cip
atio
nth
atd
on
otim
pos
eto
ob
urd
enon
bu
syp
hy
sici
ans
inth
eg
rou
p;
4)re
war
ds
(not
alw
ays
fin
anci
al)
and
reco
gn
itio
nfo
rti
me
inv
este
db
yth
ep
arti
cip
ants
;5)
reci
pro
city
;6)
reso
luti
onto
kee
ptr
yin
gu
nti
ly
oure
ach
the
rig
ht
per
son
tog
etth
ejo
bd
one;
and
(7)
resp
ect
ofth
ere
cru
iter
for
the
par
tici
pan
t’s
con
trib
uti
on,
con
stra
ints
,an
dti
me
Wh
ile
all
stu
die
sw
ill
not
hav
eal
lof
thes
efa
ctor
sin
such
goo
dal
ign
men
t,at
ten
tion
toth
emm
ayb
eim
por
tan
tto
oth
eref
fort
sto
add
toou
rk
now
led
ge
ofim
ple
men
tati
onsc
ien
ce
Table I.
JHOM28,1
120

researchers, i.e. professionals for whom the main job description is to conduct research(van de Ven and Johnson, 2006).
Similarly, reports describe the role of practitioners in the partnership in differentways. Practitioners can be research “clients”, can facilitate research, or can do both. Inour research in the VA, we are perhaps most familiar with practitioners as“customers”, who seek to use expertise from researchers to improve practice. In someinstances, the partnership with practitioners was primarily established to facilitateresearch, for example by establishing data agreements, patient confidentiality
Figure 1.Guide for defining roles
and tasks in partnershipresearch projects
Research-practice
partnerships
121

arrangements, or working together to build an information technology platform tofacilitate data collection (McDonald and Viehbeck, 2007).
Overall, the literature characterized R-PPs mostly in terms of the objectives,function, or the main activities of the partnership (King et al., 2008; Mendel et al., 2009;Mold and Peterson, 2005). R-PPs have also been characterized in terms of theproductivity of the partnerships as regards products, tools or deliverables, such aspublications or grants (King et al., 2008; Gold and Taylor, 2007), or in terms of impact.For many, a dual objective is to contribute to both resolving practical problems andproducing generalizable knowledge. However, there are different conceptions of how toassess the effectiveness and impact of the partnership, and these include lastingchange (Waterman et al., 2001), measurable change in clinical practice (processmeasures, cost savings or other organizational impacts, or improvements in patients’health), or the degree of spread (Gold and Taylor, 2007).
Defining “R-PPs”Drawing on our literature review, interviews and discussions, we propose the followingcriteria to differentiate R-PPs from other ways of conducting research:
. researchers contribute to actions taken by practitioners or community membersacting on or at one or more levels of a health system;
. studies are intended to produce quickly and directly actionable findings, but alsoto be published in peer-reviewed scientific journals;
. studies involve both researchers and practitioners in defining the researchquestions and interpreting the findings;
. studies involve a “significant” amount of time or other contributions (such as adata gathering system) from both researchers and practitioners; and
. a formulated description of the partnership approach has been published, withaims and methods, and there are published empirical studies showing theapproach as applied (i.e. not just a conceptual description of a possible approachwithout examples).
A guide that we developed to help future partnership researchers and practitionersdefine roles at different stages of the project is given in Figure 1. The goal of this guideis to increase the likelihood of those interested creating a substantive R-PP rather thanthe superficial “involvement” that characterizes many collaborations. The guide hasnot been formally validated as a tool; it is intended to stimulate discussion amongresearchers and practitioners before undertaking a project, so that the parties morefully understand what is involved and agree upon roles at different stages of theventure. We are not presenting recommendations about where a partnership should beplaced on this matrix, as there is insufficient evidence for this and because it may welldepend on the purpose of the partnership and its objectives. Another guide we founduseful is CACSH (2013).
Implications for research-practice partnership programsAs regards VA research or UK CLAHRCs, our overview of the literature did not reveal apartnership typology that adequately characterized or categorized the research we hadreviewed or which was useful for the future. In the VA, several partnership approacheshave been, or are being, used, including PBRNs (Frayne et al., 2013), practice-based quality
JHOM28,1
122
improvement research (Rubenstein et al., 2010), and action research. Similarly, there are arange of collaborative research approaches used in UK CLAHRCs and elsewhere.
Within the VA setting, and as part of an evaluation of the VA Quality EnhancementResearch Initiative (QUERI), we are currently assessing the degree to which fundedQUERI projects include “partnered work”. Based on the significant conceptual overlap inthe various partnership approaches above, our strategy for completing this evaluationwill be less concept-driven and more empirical, focusing on characterizing theindividuals or organizational entities involved in the partnership, the partnershipactivities that were proposed compared to what happened, and the various outputs fromthe partnership. This approach may be suitable for reviewing or evaluating or otherpartnerships, such as the UK CLAHRCs and/or for planning their future development.
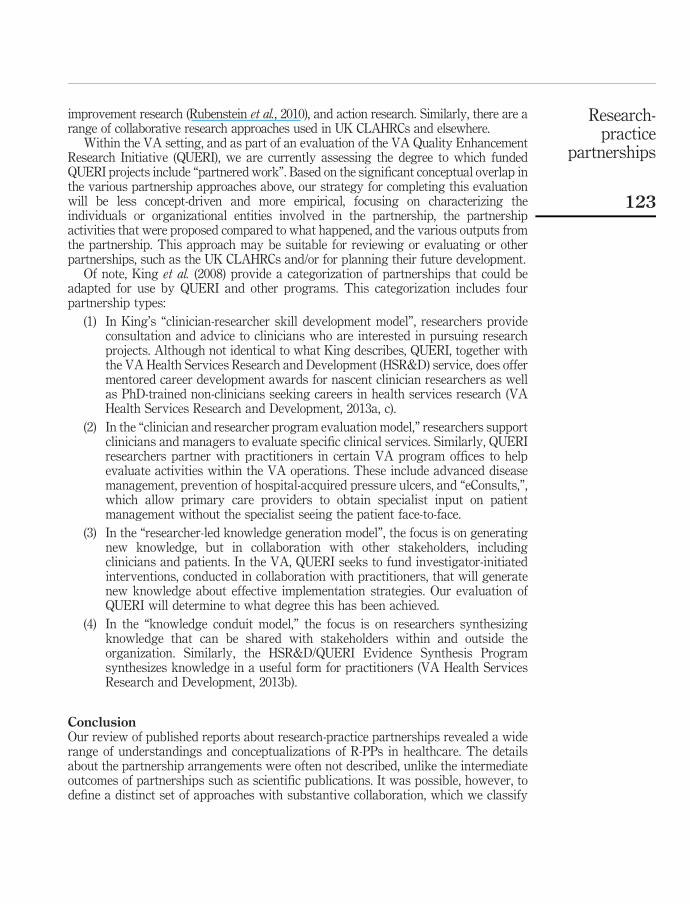
Of note, King et al. (2008) provide a categorization of partnerships that could beadapted for use by QUERI and other programs. This categorization includes fourpartnership types:
(1) In King’s “clinician-researcher skill development model”, researchers provideconsultation and advice to clinicians who are interested in pursuing researchprojects. Although not identical to what King describes, QUERI, together withthe VA Health Services Research and Development (HSR&D) service, does offermentored career development awards for nascent clinician researchers as wellas PhD-trained non-clinicians seeking careers in health services research (VAHealth Services Research and Development, 2013a, c).
(2) In the “clinician and researcher program evaluation model,” researchers supportclinicians and managers to evaluate specific clinical services. Similarly, QUERIresearchers partner with practitioners in certain VA program offices to helpevaluate activities within the VA operations. These include advanced diseasemanagement, prevention of hospital-acquired pressure ulcers, and “eConsults,”,which allow primary care providers to obtain specialist input on patientmanagement without the specialist seeing the patient face-to-face.
(3) In the “researcher-led knowledge generation model”, the focus is on generatingnew knowledge, but in collaboration with other stakeholders, includingclinicians and patients. In the VA, QUERI seeks to fund investigator-initiatedinterventions, conducted in collaboration with practitioners, that will generatenew knowledge about effective implementation strategies. Our evaluation ofQUERI will determine to what degree this has been achieved.
(4) In the “knowledge conduit model,” the focus is on researchers synthesizingknowledge that can be shared with stakeholders within and outside theorganization. Similarly, the HSR&D/QUERI Evidence Synthesis Programsynthesizes knowledge in a useful form for practitioners (VA Health ServicesResearch and Development, 2013b).
ConclusionOur review of published reports about research-practice partnerships revealed a widerange of understandings and conceptualizations of R-PPs in healthcare. The detailsabout the partnership arrangements were often not described, unlike the intermediateoutcomes of partnerships such as scientific publications. It was possible, however, todefine a distinct set of approaches with substantive collaboration, which we classify
Research-practice
partnerships
123

here as R-PPs and for which we define criteria so as to distinguish them from manythat are only partnerships in name but not in substance.
We found the King et al. (2008) categorization a useful starting point for definingdifferent approaches, but this categorization did not describe a number of partnershipsreported in research, or which we had observed or experienced in the VA and UKCLAHRCs. To characterize these, we find the guide which we developed and presentedin Figure 1 more useful. We offer this guide for others to try when describing to othersa particular type of partnership being used, or when choosing an approach. or to helpto see how the partnership might be developed and to develop one type into anothertype of partnership.
Ultimately, the impact of the partnership should be assessed, but the mostappropriate approach to measurement remains to be shown. An important question forfuture research is for which objectives R-PPs are more effective than “conventionalresearch” for producing actionable research, or for enabling research to be applied inpractice for improvement.
References
Baker, R., Robertson, N., Rogers, S., Davies, M., Brunskill, N., Khunti, K., Steiner, M., Williams, M.and Sinfield, P. (2009), “The National Institute of Health Research (NIHR) Collaboration forLeadership in Applied Health Research and Care (CLAHRC) for Leicestershire,Northamptonshire and Rutland (LNR): a programme protocol”, Implementation Science,Vol. 4, p. 72.
Berwick, D. (1998), “Developing and testing changes in delivery of care”, Annals of InternalMedicine, Vol. 128 No. 8, pp. 651-656.
Bosworth, H.B., Almirall, D., Weiner, B.J., Maciejewski, M., Kaufman, M.A., Powers, B.J., Oddone,E.Z., Lee, S.Y., Damush, T.M., Smith, V., Olsen, M.K., Anderson, D., Roumie, C.L., Rakley,S., Del Monte, P.S., Bowen, M.E., Kravetz, J.D. and Jackson, G.L. (2010), “Theimplementation of a translational study involving a primary care based behavioralprogram to improve blood pressure control: the HTN-IMPROVE study protocol (01295)”,Implementation Science, Vol. 5, p. 54.
CACSH (2013), “Partnership self assessment tool”, Center for the Advancement of CollaborativeStrategies in Health, available at: www.lmgforhealth.org/node/190 (accessed 6 August2013).
Campbell, D., Redman, S., Jorm, L., Cooke, M., Zwi, A. and Rychetnik, L. (2009), “Increasing theuse of evidence in health policy: practice and views of policy makers and researchers”,Australia and New Zealand Health Policy, Vol. 6, p. 21.
Department of Health (2007), Report of the High Level Group on Clinical Effectiveness chaired byProfessor Sir John Tooke, Department of Health, London.
DeVoe, J.E., Likumahuwa, S., Eiff, M.P., Nelson, C.A., Carroll, J.E., Hill, C.N., Gold, R. andKullberg, P.A. (2012), “Lessons learned and challenges ahead: report from the OCHINSafety Net West practice-based research network (PBRN)”, Journal of the American Boardof Family Medicine, Vol. 25 No. 5, pp. 560-564.
Engelke, M.K. and Marshburn, D.M. (2006), “Collaborative strategies to enhance research andevidence-based practice”, Journal of Nursing Administration, Vol. 36 No. 3, pp. 131-135.
Frayne, S.M., Carney, D.V., Bastian, L., Bean-Mayberry, B., Sadler, A., Klap, R., Phibbs, C.S.,Kimerling, R., Vogt, D., Yee, E.F., Lin, J.Y. and Yano, E.M. (2013), “The VA Women’sHealth Practice-Based Research Network: amplifying women veterans’ voices in VAresearch”, Journal of General Internal Medicine, Vol. 28, Supplement 2, pp. 504-509.
JHOM28,1
124

Gold, M. and Taylor, E.F. (2007), “Moving research into practice: lessons from the US Agency forHealthcare Research and Quality’s IDSRN program”, Implementation Science, Vol. 2, p. 9.
Gold, M., Helms, D. and Guterman, S. (2011), Identifying, Monitoring, and Assessing PromisingInnovations: Using Evaluation to Support Rapid-Cycle Change, Issue Brief, TheCommonwealth Fund, Washington, DC.
Green, L.W. and Ottoson, J.M. (2004), “From efficacy to effectiveness to community and back:evidence-based practice vs practice-based evidence”, From Clinical Trials to Community:The Science of Translating Diabetes and Obesity Research, National Institutes of Health,Bethesda, MD.
Greene, S.M., Reid, R.J. and Larson, E.B. (2012), “Implementing the learning health system: fromconcept to action”, Annals of Internal Medicine, Vol. 157 No. 3, pp. 207-210.
Helm, S., Koyanagi, C., Else, I., Horton, M. and Fukuda, M. (2010), “Public-academic partnerships:the University of Hawai’i Rural Health Collaboration: partnerships to provide adulttelepsychiatry services”, Psychiatric Services, Vol. 61 No. 10, pp. 961-963.
Horowitz, C.R., Robinson, M. and Seifer, S. (2009), “Community-based participatory researchfrom the margin to the mainstream: are researchers prepared?”, Circulation, Vol. 119 No. 19,pp. 2633-2642.
Kessler, R. and Glasgow, R.E. (2011), “A proposal to speed translation of healthcare research intopractice: dramatic change is needed”, American Journal of Preventive Medicine, Vol. 40No. 6, pp. 637-644.
King, G., Currie, M., Smith, L., Servais, M. and McDougall, J. (2008), “A framework of operatingmodels for interdisciplinary research programs in clinical service organizations”,Evaluation and Program Planning, Vol. 31 No. 2, pp. 160-173.
Kutner, J.S., Main, D.S., Westfall, J.M. and Pace, W. (2005), “The practice-based research networkas a model for end-of-life care research: challenges and opportunities”, Cancer Control,Vol. 12 No. 3, pp. 186-195.
McDonald, P.W. and Viehbeck, S. (2007), “From evidence-based practice making topractice-based evidence making: creating communities of (research) and practice”,Health Promotion Practice, Vol. 8 No. 2, pp. 140-144.
Mendel, P., Damberg, C.L., Sorbero, M.E., Varda, D.M. and Farley, D.O. (2009), “The growth ofpartnerships to support patient safety practice adoption”, Health Services Research, Vol. 44No. 2 Part 2, pp. 717-738.
Mold, J.W. and Peterson, K.A. (2005), “Primary care practice-based research networks: workingat the interface between research and quality improvement”, Annals of Family Medicine,Vol. 3, Supplement 1, pp. S12-S20.
Nagykaldi, Z., Mold, J.W., Robinson, A., Niebauer, L. and Ford, A. (2006), “Practice facilitatorsand practice-based research networks”, Journal of the American Board of Family Medicine,Vol. 19 No. 5, pp. 506-510.
National Institute of Health (2007), “Re-engineering the clinical research enterprise: translationalresearch”, available at: http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp (accessed June 4, 2013).
Øvretveit, J., Lomas, J., Davies, H. and Powell, A. (2010), Evaluation of the LNR CLAHRC: Report tothe Management Board, Department of Health Sciences, University of Leicester, Leicester.
Rubenstein, L.V., Chaney, E.F., Ober, S., Felker, B., Sherman, S.E., Lanto, A. and Vivell, S. (2010),“Using evidence-based quality improvement methods for translating depression collaborativecare research into practice”, Families, Systems, & Health, Vol. 28 No. 2, pp. 91-113.
Research-practice
partnerships
125

Rycroft-Malone, J., Wilkinson, J., Burton, C., Andrews, G., Ariss, S., Baker, R., Dopson, S.,Graham, I., Harvey, G., Martin, G., McCormack, B., Staniszewska, S. and Thompson, C.(2011), “Implementing health research through academic and clinical partnerships: arealistic evaluation of the Collaborations for Leadership in Applied Health Research andCare (CLAHRC)”, Implementation Science, Vol. 6 No. 1, p. 74, available at: www.implementationscience.com/content/6/1/74
Schilling, L., Dearing, J.W., Staley, P., Harvey, P., Fahey, L. and Kuruppu, F. (2011), “KaiserPermanente’s performance improvement system. Part 4: creating a learning organization”,Joint Commission Journal on Quality and Patient Safety, Vol. 37 No. 12, pp. 532-543.
Solberg, L.I. (2006), “Recruiting medical groups for research: relationships, reputation, requirements,rewards, reciprocity, resolution, and respect”, Implementation Science, Vol. 1, p. 25.
VA Health Services Research and Development (2013a), “Career Development Program”,available at: www.hsrd.research.va.gov/cdp/ (accessed August 5, 2013).
VA Health Services Research and Development (2013b), “Evidence-based Synthesis Program”,available at: www.hsrd.research.va.gov/publications/esp/ (accessed August 5, 2013).
VA Health Services Research and Development (2013c), “QUERI factsheets”, available at: www.hsrd.research.va.gov/publications/queri_factsheets/#.Uk0Y-mRgboE (accessed October 3, 2013).
van de Ven, A.H. and Johnson, P.E. (2006), “Knowledge for theory and practice”, Academy ofManagement Review, Vol. 31, pp. 802-821.
Waterman, H., Tillen, D., Dickson, R. and de Koning, K. (2001), “Action research: a systematicreview and guidance for assessment”, Health Technology Assessment, Vol. 5 No. 23.
Yaggy, S.D., Michener, J.L., Yaggy, D., Champagne, M.T., Silberberg, M., Lyn, M., Johnson, F.and Yarnall, K.S. (2006), “Just for Us: an academic medical center-community partnershipto maintain the health of a frail low-income senior population”, Gerontologist, Vol. 46 No. 2,pp. 271-276.
Author affiliationsJohn Ovretveit is at the Medical Management Center (MMC), Karolinska Institutet, Stockholm,Sweden.
Susanne Hempel is at the RAND Corporation, Santa Monica, California, USA.Jennifer L. Magnabosco is at the VA QUERI California Mental Health Services Authority, Los
Angeles, California, USA and Yo San University of Traditional Chinese Medicine, Los Angeles,California, USA.
Brian S. Mittman is at the VA Greater Los Angeles Healthcare System, Los Angeles,California, USA, VA QUERI Center for Implementation Practice and Research Support,Sepulveda, California, USA, and Kaiser Permanente Southern California Department of Researchand Evaluation, Oakland, California, USA.
Lisa V. Rubenstein and David A. Ganz are at the VA Greater Los Angeles Healthcare System,Los Angeles, California, USA, VA QUERI Center for Implementation Practice and ResearchSupport, Sepulveda, California, USA, David Geffen School of Medicine, University of CaliforniaLos Angeles, California, Los Angeles, USA and RAND Corporation, Santa Monica, California,USA.
Corresponding authorJohn Ovretveit can be contacted at: [email protected]
JHOM28,1
126
To purchase reprints of this article please e-mail: [email protected] visit our web site for further details: www.emeraldinsight.com/reprints