Global Tobacco Control Diffusion: The Case of the Framework Convention on Tobacco Control
7
Global Tobacco Control Diffusion: The Case of the Framework Convention on Tobacco Control Heather L. Wipfli, PhD, Kayo Fujimoto, PhD, and Thomas W. Valente, PhD Although the risks of tobacco smoking have been known for decades, the pandemic of tobacco use continues. There are now an estimated 1.3 billion smokers worldwide, along with millions more who use various oral to- bacco products. 1 Tobacco is the leading cause of preventable death worldwide, resulting in about 6 million deaths per year. 2 Despite great progress in tobacco control, primarily in North America and Western Europe, the number of tobacco-attributable deaths is projected to grow substantially during this century, especially in low- and middle-income countries. In 1999, in recognition of the shift and growth in tobacco consumption and the po- tential for an enormous future burden of death and disease, the World Health Organization (WHO) member states initiated formal negoti- ations on an international treaty aimed at reducing this global threat. The Intergovern- mental Negotiating Body (INB), which was charged with negotiating the text of the treaty, held 6 formal negotiating sessions in Geneva between 2000 and 2003. Over 170 states sent at least 1 delegate to 1 of the INB sessions. Scientific experts and representatives of advo- cacy networks also attended the negotiations, where they held seminars on technical aspects of the convention and distributed information to delegates. GLOBALink, an online network internationally recognized for facilitating com- munication between tobacco control advo- cates, was one such network. 3 In addition to the INB sessions, countless regional negotiating sessions and technical conferences were con- vened during the period. In May 2003, the 56th World Health Assembly unanimously adopted the WHO Framework Convention on Tobacco Control (FCTC). 4 The key provisions include a compre- hensive ban on tobacco advertising, promotion, and sponsorship; a ban on misleading descriptors intended to convince smokers that certain prod- ucts are safer than ‘‘standard’’ cigarettes (for example, the term lights in Marlboro Lights); and a mandate to place rotating warnings that cover at least 30% of tobacco packaging. The FCTC also encourages countries to implement smoke- free workplace laws, address tobacco smuggling, and increase tobacco taxes. The FCTC entered into force on February 27, 2005, 90 days after the 40th member state ratified the treaty. Fur- ther ratifications or its legal equivalent (accep- tance or approval) continued over the next 4 years. As of May 2009, 168 countries were party to the treaty. The institutionalization of tobacco control within the WHO and the subsequent ratification of the FCTC by nearly all WHO member states provides an opportunity to analyze the system and network dynamics that facilitate global tobacco control diffusion. Diffusion refers to the process by which an innovation is communi- cated through certain channels over time among members of a social system. 5 The premise, which has been confirmed by empirical research, is that new ideas and practices spread through inter- personal contacts largely consisting of interper- sonal communication. 5,6 Other researchers have investigated specifically how social networks provide the channels through which new ideas and practices, such as the FCTC, are spread. 5–7 Given studies of diffusion in other contexts, we hypothesized that the global diffusion of the FCTC has been partly driven by interpersonal communication and networking developed throughout the negotiation of the FCTC and facilitated through existing global tobacco control networks. In other words, we hypoth- esized that the extent of a country’s participa- tion in the FCTC negotiations and its citizens’ involvement in international tobacco control networks would be associated with early or late FCTC ratification. However, we also expected the predictability of these social network variables to be im- pacted to some extent by the structural and Objectives. We analyzed demographic and social network variables associated with the timing of ratification of the Framework Convention on Tobacco Control (FCTC). Methods. We compiled a 2-mode data set that recorded country participation in FCTC negotiations, as well as the number of individuals per country per year who joined an online tobacco control network. We used logistic regression analysis of these 2 data sets along with geographic location to determine whether exposure to prior FCTC adoptions was associated with a country’s likelihood of adoption. Results. In the logistic regression analysis, higher income and more non- governmental organizations (NGOs) involved in the Framework Convention Alliance (a network dedicated to the FCTC) were associated with being among the earliest adopters (for income, adjusted odds ratio [AOR] = 2.41; 95% confi- dence interval [CI] = 1.55; for NGOs, AOR = 1.66; 95% CI = 1.26, 2.17) or among early adopters (for income, AOR = 1.42; 95% CI = 1.09, 1.84; for NGOs, AOR = 1.23; 95% CI = 1.03, 1.45). Network exposure and event history analysis showed that in addition to income, the likelihood of adoption increased with increasing affiliation exposure to FCTC adopters through GLOBALink (an online network facilitating communication between tobacco control advocates). Conclusions. Public health programs should include a plan for creating opportunities for network interaction; otherwise, adoption and diffusion will be delayed and the investments in public health policy greatly diminished. (Am J Public Health. 2010;100:1260–1266. doi:10.2105/AJPH.2009.167833) RESEARCH AND PRACTICE 1260 | Research and Practice | Peer Reviewed | Wipfli et al. American Journal of Public Health | July 2010, Vol 100, No. 7
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Global Tobacco Control Diffusion: The Case of the Framework Convention on Tobacco Control

Global Tobacco Control Diffusion: The Case of theFramework Convention on Tobacco ControlHeather L. Wipfli, PhD, Kayo Fujimoto, PhD, and Thomas W. Valente, PhD
Although the risks of tobacco smoking havebeen known for decades, the pandemic oftobacco use continues. There are now anestimated 1.3 billion smokers worldwide, alongwith millions more who use various oral to-bacco products.1 Tobacco is the leading causeof preventable death worldwide, resulting inabout 6 million deaths per year.2 Despite greatprogress in tobacco control, primarily in NorthAmerica and Western Europe, the number oftobacco-attributable deaths is projected to growsubstantially during this century, especially inlow- and middle-income countries.
In 1999, in recognition of the shift andgrowth in tobacco consumption and the po-tential for an enormous future burden of deathand disease, the World Health Organization(WHO) member states initiated formal negoti-ations on an international treaty aimed atreducing this global threat. The Intergovern-mental Negotiating Body (INB), which wascharged with negotiating the text of the treaty,held 6 formal negotiating sessions in Genevabetween 2000 and 2003. Over 170 states sentat least 1 delegate to 1 of the INB sessions.Scientific experts and representatives of advo-cacy networks also attended the negotiations,where they held seminars on technical aspectsof the convention and distributed informationto delegates. GLOBALink, an online networkinternationally recognized for facilitating com-munication between tobacco control advo-cates, was one such network.3 In addition tothe INB sessions, countless regional negotiatingsessions and technical conferences were con-vened during the period.
In May 2003, the 56th World HealthAssembly unanimously adopted the WHOFramework Convention on Tobacco Control(FCTC).4 The key provisions include a compre-hensive ban on tobacco advertising, promotion,and sponsorship; a ban on misleading descriptorsintended to convince smokers that certain prod-ucts are safer than ‘‘standard’’ cigarettes (forexample, the term lights in Marlboro Lights); and
a mandate to place rotating warnings that coverat least 30% of tobacco packaging. The FCTCalso encourages countries to implement smoke-free workplace laws, address tobacco smuggling,and increase tobacco taxes. The FCTC enteredinto force on February 27, 2005, 90 days afterthe 40th member state ratified the treaty. Fur-ther ratifications or its legal equivalent (accep-tance or approval) continued over the next4 years. As of May 2009, 168 countries wereparty to the treaty.
The institutionalization of tobacco controlwithin the WHO and the subsequent ratificationof the FCTC by nearly all WHO member statesprovides an opportunity to analyze the systemand network dynamics that facilitate globaltobacco control diffusion. Diffusion refers to theprocess by which an innovation is communi-cated through certain channels over time amongmembers of a social system.5 The premise, whichhas been confirmed by empirical research, is that
new ideas and practices spread through inter-personal contacts largely consisting of interper-sonal communication.5,6 Other researchers haveinvestigated specifically how social networksprovide the channels through which new ideasand practices, such as the FCTC, are spread.5–7
Given studies of diffusion in other contexts,we hypothesized that the global diffusion of theFCTC has been partly driven by interpersonalcommunication and networking developedthroughout the negotiation of the FCTC andfacilitated through existing global tobaccocontrol networks. In other words, we hypoth-esized that the extent of a country’s participa-tion in the FCTC negotiations and its citizens’involvement in international tobacco controlnetworks would be associated with early or lateFCTC ratification.
However, we also expected the predictabilityof these social network variables to be im-pacted to some extent by the structural and
Objectives. We analyzed demographic and social network variables associated
with the timing of ratification of the Framework Convention on Tobacco Control
(FCTC).
Methods. We compiled a 2-mode data set that recorded country participation
in FCTC negotiations, as well as the number of individuals per country per year
who joined an online tobacco control network. We used logistic regression
analysis of these 2 data sets along with geographic location to determine
whether exposure to prior FCTC adoptions was associated with a country’s
likelihood of adoption.
Results. In the logistic regression analysis, higher income and more non-
governmental organizations (NGOs) involved in the Framework Convention
Alliance (a network dedicated to the FCTC) were associated with being among
the earliest adopters (for income, adjusted odds ratio [AOR]=2.41; 95% confi-
dence interval [CI]=1.55; for NGOs, AOR=1.66; 95% CI=1.26, 2.17) or among
early adopters (for income, AOR=1.42; 95% CI=1.09, 1.84; for NGOs, AOR=1.23;
95% CI=1.03, 1.45). Network exposure and event history analysis showed that in
addition to income, the likelihood of adoption increased with increasing
affiliation exposure to FCTC adopters through GLOBALink (an online network
facilitating communication between tobacco control advocates).
Conclusions. Public health programs should include a plan for creating
opportunities for network interaction; otherwise, adoption and diffusion will
be delayed and the investments in public health policy greatly diminished. (Am J
Public Health. 2010;100:1260–1266. doi:10.2105/AJPH.2009.167833)
RESEARCH AND PRACTICE
1260 | Research and Practice | Peer Reviewed | Wipfli et al. American Journal of Public Health | July 2010, Vol 100, No. 7
demographic aspects of states (e.g., location,population, income level, degree of politicalfreedom, tobacco prevalence, and tobaccoproduction). For example, a country with a highsmoking prevalence may perceive tobaccocontrol as more important and ratify soonerthan a country with low prevalence. Con-versely, a tobacco-producing and exportingcountry may view tobacco control as a threat toits financial success and resist ratification. Herewe analyzed the structural, demographic, andsocial network variables that led individualcountries to ratify the FCTC when they didand made a first attempt at specifying thedriving forces behind global tobacco controldiffusion.
METHODS
The timing of the adoption of the FCTC wasmeasured as the day the country ratified theFCTC recoded to the month (coding adoptionof the FCTC monthly made the data manage-able). The ratification dates are available on theWHO’s Tobacco Free Initiative Web site.8 Inaddition, 2 dummy variables were created toindicate the earliest adopters (first 30 ratified,15.5%) and the early adopters (first 95 ratified,49.2%). The decision to divide the countries bythe first 16% and first 50% was based on pastdiffusion research that categorized adopters onthe basis of time of adoption. According toRogers, early adopters are the first16% and earlymajority are the first half.5 Several structuralcharacteristics of the countries were obtained,including population,9 gross national income,9
degree of political freedom,10 tobacco production(in tons),11 and current male and female smokingprevalence.12
Data Collection
Country participation in the negotiations wasmeasured by the number of delegates sent toeach INB session published in the official list ofparticipants. These are publicly available onthe WHO Governing Bodies Web site.13 In-creases in interaction between domestic andinternational advocates for tobacco controlwere measured through the number of newGLOBALink members per country per year bet-ween 1993 and 2006 and the number of non-governmental organizations (NGOs) per countryparticipating in the Framework Convention
Alliance, a network dedicated to the FCTCin 2009. GLOBALink staff provided theGLOBALink annual membership database toH.L.W. in 2007. The specific dates for individ-ual GLOBALink memberships were not avail-able and were undoubtedly scattered throughoutthe year. Consequently, memberships wereupdated as of December for each year. Frame-work Convention Alliance membership wasrecorded from the Framework Convention Alli-ance Web site in February 2009. Missing datawere recoded to the mean. The number ofcountries for which we imputed missing valueswas19 for gross national income, 70 for tobaccoproduction, 31 for current male smoking preva-lence, and 27 for current female smokingprevalence. Missing data analyses showed thatthe countries with any missing data (95 of 193)did not have differential adoption dates (oddsratio [OR]=1.00; P=.73), but had a lower levelof log-scaled population (OR=0.83; P<.001),had a lower level of log-scaled tobacco pro-duction (OR=0.76; P<.05), and had a lowerlevel of NGOs participating in the FrameworkConvention Alliance (OR=0.67; P<.001).
Analysis Plan
To determine the factors associated withratification of the FCTC, 4 regression modelswere estimated: (1) an ordinary least squaredregression on time of ratification (reversed), (2)a logistic regression on being an earliest rat-ifier (first 15.5%), (3) a logistic regression onbeing an early ratifier (first 49.2%), and (4) anevent-history model using logistic regressionfor the likelihood of adoption at each month. Inthe 3 logistic regressions (models 2–4), thenumeric value representing the number ofdelegates participating in each INB per countryand new members in GLOBALink per countryper year were included.
The 3 network diffusion terms calculated inthe event-history model (model 4) were: (1)distance, (2) INB participation, and (3)GLOBALink membership. Reverse distancesbetween country capitals were calculated, andthis weight matrix was used to estimate conti-guity effects. Affiliation matrices of the INBand GLOBALink data for each country weretransposed and postmultiplied to generate ad-jacency matrices.14–16 Each element in the ad-jacency matrix represented the number of peoplefrom any 2 countries that jointly attended an INB
session or enrolled in GLOBALink. These coaf-filiation matrices were used to generate vectorsof affiliation network exposures that measure thelevel of exposure to prior ratifiers for eachcountry. These matrices constitute the networkwithin which the network diffusion analyseswere conducted.7 The matrix and time of ratifi-cation variable were used to construct the 3network exposure terms that were time varying(as each network partner adopted FCTC, itincreased the focal country’s exposure). Time-constant variables, the country characteristics,were also included in the analyses.7
The model tested in the event-history model(model 4) is based on country (i) and time (t):15
ð1Þ log itðpit Þ ¼ logPrðyit ¼ 1Þ
1� Prðyit ¼ 1Þ ¼ a
1Xk
j ¼1
bjXji 1XL
l ¼1
ql ½xil �yt ;
where yit is the binary indicator of FCTCratification for country i (i=1, .., N) at time t, a isthe intercept, bj is the parameter estimate forvectors of j (j=1, . . . ,k) characteristics (Xji) ofcountry i, and ql is the parameter estimate forthe time-varying network exposure variables[xil]yt. The xil network weight matrices aredefined as one of the following xi matrices onthe basis of distance (l=1), INB participation(l=2), or GLOBALink (l=3). Note that in thisequation, xil was constant over time for thefirst 2, but varied over time for GLOBALink.To estimate this equation, the generalizedestimating equation was used with an autore-gressive correlation structure with single lagand logit link function.17 Network figures werecreated with the software program Netdraw.18
RESULTS
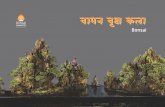
Characteristics of the countries and themean and median date of FCTC ratificationglobally and by region are shown in Table 1.The first country to ratify the FCTC was Nor-way in June 2003 followed by Fiji in Novem-ber 2003. FCTC ratification continued tospread (Figure 1) between countries over thenext 6 years until ultimately only 33 of 193countries (16.9%) resisted ratification of theFCTC (including the United States) during thetime period. The mean and median dates ofratification for all ratifying countries were
RESEARCH AND PRACTICE
July 2010, Vol 100, No. 7 | American Journal of Public Health Wipfli et al. | Peer Reviewed | Research and Practice | 1261

March 2006 and November 2005, respec-tively (approximately 2.5 years after the lastINB session). Populous and less populouscountries ratified the FCTC at approximatelythe same rate.
The ratifying countries were nearly evenlysplit among the 4 income categories. Over 77%of the ratifying countries were consideredpolitically free or partially free with an overallsmoking prevalence of 23.7% (the smokingrate among men was considerably higher,34.8%, than that among women, 13.1%). Thenumber of delegates sent to the first INBsession (October 2000) ranged from 0 to 13and averaged 2.62. By the final INB session(February 2003), the number of delegatesranged from 0 to 26 and averaged 3.59. Theaverage number of new GLOBALink membersper country varied by year and generallyincreased, although not monotonically. By theend of 2006, membership in GLOBALink bycountry ranged from 0 to 1602, with a mean of31.8. Countries in the Western Pacific andSoutheast Asia had the earliest ratificationtimes (25.2 months and 26.5 months, respec-tively), whereas Africa and the Americas werelater (44.0 months and 46.8 months, respec-tively; Table 1).
The results of the 4 models are presented inTable 2. The initial ordinary least squaredregression on reversed time of ratification (tomeasure innovativeness) indicated that higherincome level (B=0.26; P<.01) and NGOmembership in the Framework ConventionAlliance (B=0.27; P<.05) were the only vari-ables associated with earlier adoption of theFCTC. The earliest (first 15.5%) and early (first49.2%) adoption models using logistic regres-sion analyses showed that income was againassociated with being among the earliestadopters (adjusted odds ratio [AOR]=2.41;95% confidence interval [CI]=1.55, 3.74) oramong the early adopters (AOR=1.42; 95%CI=1.09, 1.84), as well as NGO membershipin the Framework Convention Alliance (forearliest adopters, AOR=1.66; 95% CI=1.26,2.17; for early adopters, AOR=1.23; 95%CI=1.03, 1.45).
The event-history model included the net-work exposure terms and was an eventhistory analysis using the generalized esti-mating equation in which each case in thedata set (N=6833 [34 ·193] average months
TABLE 1—Characteristics of the Countries and the Mean and Median Date of Ratification of
the Framework Convention on Tobacco Control (FCTC)
Value
Date FCTC ratified
Mean month (mean no. months until adoption globally) March 2006 (35.4)
Median month (median no. months until adoption globally) November 2005 (31.0)
Mean no. of months until adoption (from May 2003)
Africa 44.0
Americas 46.8
Eastern Mediterranean 41.0
Europe 39.8
Southeast Asia 26.5
Western Pacific 25.2
Population size, no. (range) 29 121 813 (81 000–1 300 000 000)
Income, %
Low income 26.50
Lower middle income 27.50
Upper middle income 20.60
High income 25.40
Democracy, %
Partially free 30.80
Free 46.70
Tobacco production, tons (range) 54 406 (30–2 685 743)
Smoking prevalence, %
Total 23.70
Male 34.80
Female 13.10
No. tobacco NGOs, mean (range) 1.57 (1–28)
No. participants in INB, mean (range)
October 18, 2000 2.62 (0–13)
May 5, 2001 2.83 (0–18)
November 25, 2001 3.09 (0–23)
March 23, 2002 2.97 (0–26)
October 21, 2002 3.30 (0–21)
February 26, 2003 3.58 (0–20)
No. new GLOBALink members, mean (range)
1993 0.26 (0–8)
1994 0.08 (0–4)
1995 0.05 (0–3)
1996 0.28 (0–19)
1997 1.85 (0–147)
1998 1.80 (0–102)
1999 1.02 (0–24)
2000 3.03 (0–176)
2001 2.82 (0–125)
2002 3.78 (0–219)
2003 4.54 (0–255)
2004 3.69 (0–250)
2005 4.35 (0–268)
2006 4.09 (0–199)
Note. INB = Intergovernmental Negotiating Body; NGO = nongovernmental organization.
RESEARCH AND PRACTICE
1262 | Research and Practice | Peer Reviewed | Wipfli et al. American Journal of Public Health | July 2010, Vol 100, No. 7

until adoption by total countries) representeda country-year up to and including the year ofratification. Robust variance estimates werecomputed at the country level. Countrycharacteristics represented time-constantvariables and exposures were time-varyingbased on the ratification behavior of the
countries’ coaffiliations. The analysis in-cluded the 33 never-ratified countries withtime of ratification coded as the 72nd month.It is customary in diffusion research to recodethe nonadopters as the last time of adoptionprovided the number of cases is not exces-sive. We repeated the analysis excluding
nonratifying countries with no change in theresults.
The results showed that exposure based ongeography was positive but not statisticallysignificant (AOR=1.51; 95% CI=0.33, 6.88).Exposure based on INB participation waspositive but not statistically significant(AOR=2.11; 95% CI=0.40, 11.06). Exposurebased on increasing GLOBALink membershipwas positive and statistically significant(AOR=2.92; 95% CI=1.25, 6.78). Thedummy variables for region indicated that theWestern Pacific and Southeast Asia regionshad earlier ratification dates (AOR=4.77;95% CI=2.08, 10.92) than did Africa(AOR=4.02; 95% CI=1.14, 14.13) andno other regions were statistically significantlydifferent from Africa. The AOR of 2.92 forthe GLOBALink effect indicated that a countrywas nearly 3 times as likely to ratify theFCTC once their exposure to other ratifiersvia membership in GLOBALink reached100%.
Note. The y-axis represents the cumulative percentage of countries that have ratified the Framework Convention on Tobacco
Control.
FIGURE 1—Global diffusion of the Framework Convention on Tobacco Control.
TABLE 2—Regression Results for Adoption of the Framework Convention on Tobacco Control (FCTC)
OLS Regression,
No. or B
Logistic Regression
Earliest Adoption,
No. or AOR (95% CI)
Logistic Regression
Early Adoption,
No. or AOR (95% CI)
Event History Analysis
Including Exposure,
No. or AOR (95% CI)
Total 193 193 193 6833
Log of population –0.12 0.92 (0.78, 1.08) 0.93 (0.83, 1.04) 0.89 (0.79, 1.01)
Log of income 0.26** 2.41*** (1.55, 3.74) 1.42** (1.09, 1.84) 1.17 (0.98, 1.41)
Democracy, partially free –0.05 0.81 (0.24, 2.71) 0.70 (0.30, 1.63) 1.02 (0.65, 1.60)
Democracy, free –0.08 0.78 (0.26, 2.35) 0.70 (0.31, 1.57) 0.87 (0.55, 1.37)
Tobacco production (in tons) 0.00 0.94 (0.76, 1.17) 1.04 (0.90, 1.21) 0.97 (0.89, 1.05)
Smoking prevalence, male 0.14 1.02 (0.98, 1.06) 1.03 (1.00, 1.06) 1.00 (0.98, 1.02)
Smoking prevalence, female 0.03 0.98 (0.93, 1.03) 1.00 (0.97, 1.04) 1.01 (0.98, 1.03)
No. NGOs in FCA 0.27* 1.66*** (1.26, 2.17) 1.23* (1.03, 1.45) 1.00 (0.93, 1.08)
Region (Africa ref)
Americas 1.09 (0.46, 2.58)
Eastern Mediterranean 1.67 (0.48, 5.82)
Europe 1.19 (0.40, 3.55)
Southeast Asia 4.02* (1.14, 14.13)
Western Pacific 4.77*** (2.08, 10.92)
No. new GLOBALink members –0.23 0.97 (0.95, 1.00) 1.00 (0.99,1.00) 1.05 (0.96, 1.15)
Exposure based on INB 2.11 (0.40, 11.06)
Exposure based on GLOBALink 2.92* (1.25, 6.78)
Exposure based on geography 1.51 (0.33, 6.88)
Note. AOR = adjusted odds ratio; CI = confidence interval; FCA = Framework Convention Alliance; INB = Intergovernmental Negotiating Body; NGO = nongovernmental organization; OLS = ordinary leastsquared.*P < .05; **P < .01; ***P < .001, by the 2-tailed test.
RESEARCH AND PRACTICE
July 2010, Vol 100, No. 7 | American Journal of Public Health Wipfli et al. | Peer Reviewed | Research and Practice | 1263

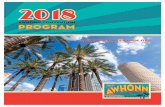
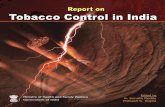
To illustrate these diffusion effects, wegraphed the network of GLOBALink affilia-tions for the earliest ratifying countries inFigure 2. This network was densely connectedwith few isolates (Naru, San Marino, andSeychelles). The core of the network containedcountries from all over the globe but alsoclearly showed considerable coaffiliation onGLOBALink membership, which permittedcommunication about tobacco control. Bycontrast, the network of the 33 countries whohave not yet ratified the FCTC are shown inFigure 3. In this network, 18 of the countrieswere isolates, indicating that they had noparticipants in GLOBALink.
These analyses indicate that wealthier coun-tries were more likely to ratify the FCTC earlierthan were poorer countries, and ratification
dates differed by geographic region. The onlyother factor that influenced adoption behaviorwas increasing membership in GLOBALink.Countries were more likely to ratify the FCTCafter more of their citizens joined GLOBALinkand as numbers of GLOBALink members fromratifying countries grew.
DISCUSSION
We analyzed the demographic and socialnetwork variables that led countries to ratifythe FCTC at the time that they did. Wecompiled a 2-mode data set that recordedcountry participation in the negotiation of theFCTC. We also recorded the number of in-dividuals by country who joined GLOBALink,an interactive online network created to
support tobacco control advocacy. These 2data sets, along with physical location (latitudeand longitude), were used to determine whetherexposure to FCTC-related information andprior FCTC adoptions was associated with acountry’s likelihood of ratification.
The initial diffusion of FCTC ratificationwas not particularly rapid. The first year con-sisted of a few scattered countries, none par-ticularly populous, ratifying the FCTC. Theevidence shows that contiguity was not a majorfactor in these early ratifications. Thus, theevidence does not indicate that countries thatratified early served as role models to whichother countries could readily point as motiva-tions for FCTC ratification. The initial delay inratification may have been a result of the factthat ratification required the completion of
Note. Figure created using Netdraw.18 For example, Norway and India had at least 1 member (although not necessarily the same individual) who subscribed to GLOBALink for at least 9 years from
1993 to 2005. Conversely, Jordan and Palau only had 1 member during the same period. There were 5 outlying countries. Thicker lines indicate stronger links on GLOBALink.
FIGURE 2—Network of the 30 countries that were the earliest to adopt the Framework Convention on Tobacco Control (first 15.5% of all
countries), with links indicating the magnitude of comembership on GLOBALink.
RESEARCH AND PRACTICE
1264 | Research and Practice | Peer Reviewed | Wipfli et al. American Journal of Public Health | July 2010, Vol 100, No. 7

domestic policy processes. Given competingpriorities and legislative schedules, it maysimply have been impossible for some coun-tries to ratify any quicker than they did. Therewas an increase in the rate of adoption in years2 through 4, after which it leveled off. Inretrospect, we can see that the FCTC is amongthe quickest treaties to enter into force, andhas become among the most widely ratifiedtreaties in existence.
Most country attribute variables did nothave a significant effect on time of ratification.One exception was the region in which a coun-try was located. Southeast Asia and the West-ern Pacific ratified the FCTC earlier than didcountries in the Americas and Africa. Partici-pation in the INB was not associated with earlyratification of the FCTC nor was an increase in
the number of delegates sent by a country.Being part of the negotiation process did notaccelerate ratification once the FCTC wascompleted.
Besides income level, network membership—as measured by both NGO participation in theFramework Convention Alliance and increas-ing membership in GLOBALink—was the onlysignificant predictor of early ratification. In-creasing membership in GLOBALink, a net-work in which information and experiencesrelated to the FCTC ratification were shared,was also associated with ratification once thediffusion process got under way. The graphiccomparison of network interactions presentedin Figures 2 and 3 clearly illustrates thedifference between countries that ratified earlyand those that ratified late in regard to
membership in GLOBALink. The core of thenetwork among nonratifying countries consistsof the United States, Switzerland, Argentina,and Indonesia, all of whom may have reasonsother than lack of awareness or informationabout the treaty for postponing ratification ofthe FCTC. Generally speaking, most countriesthat have not ratified are outside the flow ofinformation and influence (as characterized byGLOBALink membership) that may otherwiseenable them to ratify the FCTC. This is aninteresting finding because it points to thecritical role that international informationsharing may have on domestic policy processesand suggests that investment in such networksmay provide a cost-effective method for sup-porting the spread of international publichealth norms in other areas.
Note. Figure created using Netdraw.18 There were 18 outlying countries. Thicker lines indicate stronger links on GLOBALink.
FIGURE 3—Network of the 33 countries that did not adopt the Framework Convention on Tobacco Control, with links indicating the magnitude of
comembership on GLOBALink.
RESEARCH AND PRACTICE
July 2010, Vol 100, No. 7 | American Journal of Public Health Wipfli et al. | Peer Reviewed | Research and Practice | 1265

Limitations
Our study had several potential weaknesses.Social, political, and cultural characteristics ofstates are not easy to quantify and there arealways challenges in selecting appropriate var-iables. There is always the possibility that other,and perhaps better, variables could have beenused to represent the determinants of ratifica-tion. For a number of countries, information onthe variables selected was unavailable, includ-ing a lack of GLOBALink data after 2006. Theanalysis also ignored the strength of tobaccocontrol legislation in countries and whether itchanged during the period. The goal of thisanalysis, however, was simply to providegreater information to identify possible deter-minants of FCTC diffusion. Future work isneeded to improve on the empirical model andto strengthen its explanatory power.
The role of system modeling in globaltobacco control must also be weighed, as is thecase with all large-scale systems modelingefforts, against qualitative information avail-able about the process globally and withinspecific countries.19 Historical context and po-litical realities within countries cannot ade-quately be captured in such a macrostudy. Infuture studies, contextual information could beused to a greater extent to add depth and balanceto the analysis; this would provide a morecomplete picture of the role that the FCTCprocess and international tobacco control net-works have had in diffusing international tobaccocontrol norms to domestic policy.
Conclusions
This study has implications for the futurestudy of the diffusion of innovations and publichealth. Historically, it has been prohibitivelychallenging to conduct large-scale studies inwhich social network and time of innovationadoption data are available. Generally, this isbecause the time span for diffusion is long anddata collection at multiple time points becomesprohibitively expensive.5,20 The public avail-ability of the FCTC documentation and ratifica-tion dates, global databases, including the WHOReport on the Global Tobacco Epidemic9 andthe Tobacco Atlas,12 and the existence of tobaccocontrol networks, including GLOBALink and theFramework Convention Alliance, provide anincredibly rich source of data for this and futurediffusion studies.
The initiation of the FCTC process marked thefirst time that the WHO member states enactedthe organization’s power under article 19 of itsconstitution to negotiate and sign a bindingtreaty aimed at protecting and promoting publichealth. It also represented the first time that themember states cooperated worldwide in a col-lective response to prevent chronic disease.Considerable time and effort have been investedin the negotiation, ratification, and domesticimplementation of the FCTC. The evidencepresented here suggests that the speed of FCTCratification was dependent on forums in whichinvested individuals within past and potentialratifying countries could exchange information,learn about experiences, and gain reassuranceabout the consequences of action. Future publichealth programs should thus be accompanied bya plan for creating opportunities for this inter-action; otherwise, diffusion of internationallypromoted programs and policies will be delayedand the return on investments diminished. j
About the AuthorsAll authors are with the Department of Preventive Medicine,University of Southern California, Los Angeles. Heather L.Wipfli is also with the Institute for Global Health, Univer-sity of Southern California, Los Angeles. Kayo Fujimotoand Thomas W. Valente are also with the Institute forHealth Promotion and Disease Prevention Research, Uni-versity of Southern California, Los Angeles.
Correspondence should be sent to Heather L. Wipfli,PhD, Department of Preventive Medicine, Keck School ofMedicine, USC Institute for Global Health, University ofSouthern California, 1441 Eastlake Avenue, Room4425A, Los Angeles, CA 90033 (e-mail: [email protected]). Reprints can be ordered at http://www.ajph.org byclicking the ‘‘Reprints/Eprints’’ link.
This article was accepted July 5, 2009.
ContributorsH. L. Wipfli originated the study and assembled thedata. K. Fujimoto conducted network computations andanalyses. T. W. Valente originated the study and theanalysis plan. All authors interpreted findings andcontributed to the writing of the article.
AcknowledgmentsSupport for this study was provided through an AdvancingScholarship in the Humanities and Social Sciences grant toH.L. Wipfli from the University of Southern California.
Human Participant ProtectionNo protocol approval was necessary because data wereobtained from secondary sources.
References1. Guindon GE, Boisclair D. Past, Current and FutureTrends in Tobacco Use. Washington, DC: World Bank;
2003. Health, Nutrition and Population (HNP) DiscussionPaper. Economics of Tobacco Control paper no. 6.
2. World Health Organization. World Health Report—Reducing Risks, Promoting Healthy Life. Geneva, Switzer-land: World Health Organization; 2002.
3. GLOBALink Tobacco Control, The InternationalTobacco Control Community. Available at: http://www.globalink.org. Accessed March 24, 2010.
4. WHO Framework Convention on Tobacco Control.Geneva, Switzerland: World Health Organization; 2003.
5. Rogers EM. Diffusion of Innovations. 5th ed. NewYork, NY: The Free Press; 2003.
6. Valente TW. Network Models of the Diffusion ofInnovations. Cresskill, NJ: Hampton Press; 1995.
7. Valente TW. Models and methods for innovationdiffusion. In: Carrington PJ, Scott J, Wasserman S, eds.Models and Methods in Social Network Analysis. Cam-bridge, United Kingdom: Cambridge University Press;2005.
8. World Health Organization. Tobacco Free InitiativeWeb site. Available at: http://www.who.int/tobacco.Accessed April 22, 2010.
9. WHO Report on the Global Tobacco Epidemic, 2008:the MPOWER package. Geneva: World Health Organi-zation; 2008.
10. Freedom in the World 2009. Washington, DC:Freedom House Inc; 2009.
11. Food and Agricultural Organization. Tobacco LeafProduction. Available at http://faostat.fao.org. AccessedFebruary 2009.
12. Shafey O, Eriksen M, Ross H, Mackay J. The TobaccoAtlas. Atlanta, GA: American Cancer Society, WorldLung Foundation; 2009. Available at: http://www.tobaccoatlas.org. Accessed April 22, 2010.
13. World Health Organization. Framework Conventionon Tobacco Control Web site. Available at: http://www.who.int/gb/fctc. Accessed April 22, 2010.
14. Breiger RL. Duality of persons and groups. SocForces. 1974;53(2):181–190.
15. Borgatti SP, Everett MG. Network analysis of2-mode data. Soc Networks. 1997;19(3):243–269.
16. Wasserman S, Faust K. Social Networks Analysis:Methods and Applications. Cambridge, United Kingdom:Cambridge University Press; 1994.
17. Zeger SL, Liang KY. Longitudinal data analysis fordiscrete and continuous outcomes. Biometrics. 1986;42(1):121–130.
18. Borgatti SP. Netdraw. Lexington, KY: AnalyticTechnologies; 2005.
19. National Cancer Institute. Greater Than the Sum:Systems Thinking in Tobacco Control. Tobacco ControlMonograph no. 18. Bethesda, MD: US Dept of Health andHuman Services, National Institutes of Health, NationalCancer Institute; 2007. NIH publication no. 06-6085.
20. Valente TW, Rogers EM. The origins and develop-ment of the diffusion of innovations paradigm as anexample of scientific growth. Sci Commun. 1995;16(3):242–273.
RESEARCH AND PRACTICE
1266 | Research and Practice | Peer Reviewed | Wipfli et al. American Journal of Public Health | July 2010, Vol 100, No. 7