
Genitourinary leiomyomas
6
UROPATHOLOGY GENITOURINARY LEIOMYOMAS JOHN A. BELIS, M.D. GREGORY J. POST, M.D. STEPHEN C. ROCHMAN, M.D. D. FRANKLIN MILAM, M.D. From the Division of Urology, West Virginia University Medical Center, Morgantown, West Virginia ABSTRACT - Leiomyomas may originate from any anatomic location of smooth muscle in the genitourinary system but are uncommon neoplasms. Five unusual cases of leiomyomas arising from the renal pelvis, bladder, spermatic cord, and glans penis are presented. The leiomyoma arising from the glans penis in a three-year-old boy is the first case of a leiomyoma in that location noted in the literature. A review of leiomyomas from each genitourinary structure of origin is presented. Genitourinary leiomyomas are uncommon but may arise from any structure or organ contain- ing smooth muscle. ‘ ,’ These neoplasms often mimic malignant lesions and depending upon location can often be diagnosed only after surgi- cal removal. Leiomyomas usually involve single organs, but multiple organ involvement has been reportede3 The kidney capsule is the most common location for genitourinary leiomyomas,4 Five unusual cases of genitourinary leiomyomas are reported, including the radiographic and histologic findings. One case, that of a three- year-old white boy with a leiomyoma of the glans penis, is the first case noted in the lit- erature of a leiomyoma in that location. The re- maining 4 cases were in the renal pelvis, blad- der, and spermatic cord. Leiomyomas in these locations as well as other areas of the genitouri- and these are often small and found at autopsy. nary system are discussed. 424 FIGURE 1. Case 1. (A) Intra- venous pyelogram reveals de- layed function left kidney. (B) Left retrograde p yelogram demonstrates filling defect in renal pelvis. UROLOGY i APRIL 1979 / VOLUME XIII, NUMBER 4
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Genitourinary leiomyomas

UROPATHOLOGY
GENITOURINARY LEIOMYOMAS
JOHN A. BELIS, M.D.
GREGORY J. POST, M.D.
STEPHEN C. ROCHMAN, M.D. D. FRANKLIN MILAM, M.D.
From the Division of Urology, West Virginia University Medical Center, Morgantown, West Virginia
ABSTRACT - Leiomyomas may originate from any anatomic location of smooth muscle in the genitourinary system but are uncommon neoplasms. Five unusual cases of leiomyomas arising from the renal pelvis, bladder, spermatic cord, and glans penis are presented. The leiomyoma arising from the glans penis in a three-year-old boy is the first case of a leiomyoma in that location noted in the literature. A review of leiomyomas from each genitourinary structure of origin is presented.
Genitourinary leiomyomas are uncommon but may arise from any structure or organ contain- ing smooth muscle. ‘,’ These neoplasms often mimic malignant lesions and depending upon location can often be diagnosed only after surgi- cal removal. Leiomyomas usually involve single organs, but multiple organ involvement has been reportede3 The kidney capsule is the most common location for genitourinary leiomyomas,4
Five unusual cases of genitourinary leiomyomas are reported, including the radiographic and histologic findings. One case, that of a three- year-old white boy with a leiomyoma of the glans penis, is the first case noted in the lit- erature of a leiomyoma in that location. The re- maining 4 cases were in the renal pelvis, blad- der, and spermatic cord. Leiomyomas in these locations as well as other areas of the genitouri-
and these are often small and found at autopsy. nary system are discussed.
424
FIGURE 1. Case 1. (A) Intra- venous pyelogram reveals de- layed function left kidney. (B) Left retrograde p yelogram demonstrates filling defect in renal pelvis.
UROLOGY i APRIL 1979 / VOLUME XIII, NUMBER 4
Case Reports
Case 1
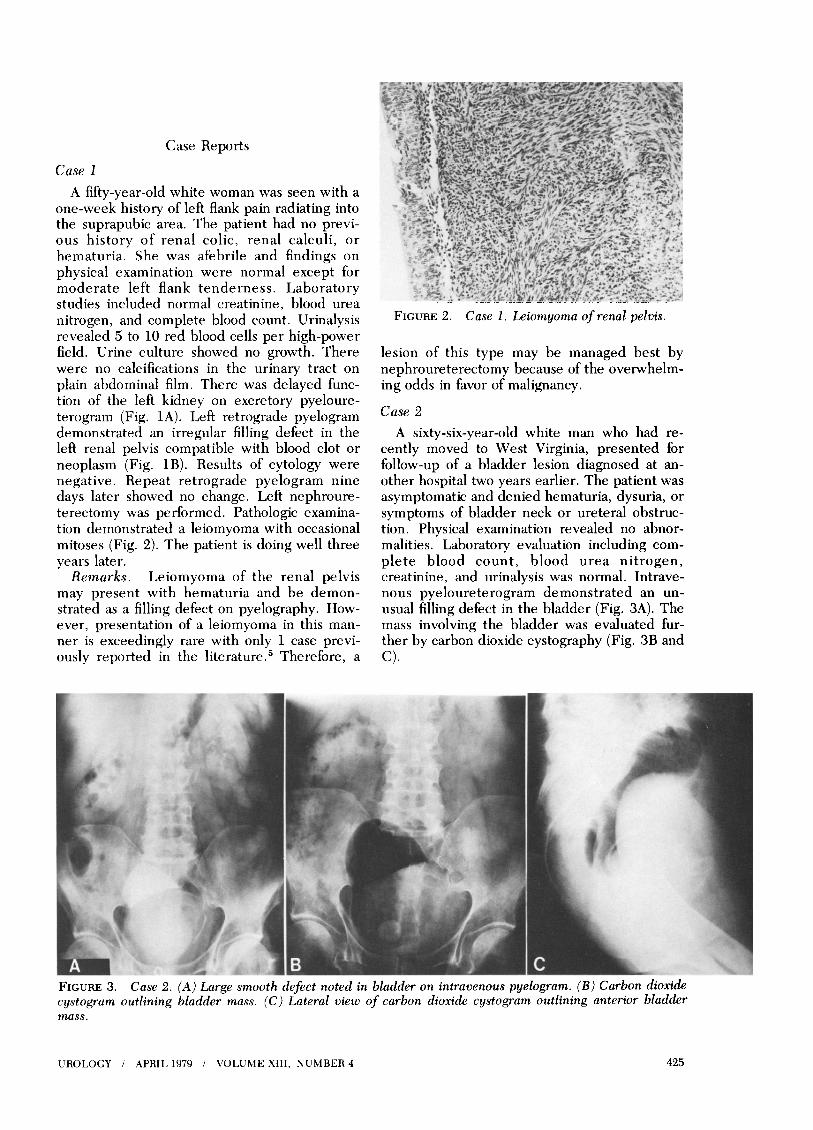
A fifty-year-old white woman was seen with a one-week history of left flank pain radiating into the suprapubic area. The patient had no previ- ous history of renal colic, renal calculi, or hematuria. She was afebrile and findings on physical examination were normal except for moderate left flank tenderness. Laboratory studies included normal creatinine, blood urea nitrogen, and complete blood count. Urinalysis revealed 5 to 10 red blood cells per high-power field. Urine culture showed no growth. There were no calcifications in the urinary tract on plain abdominal film. There was delayed func- tion of the left kidney on excretory pyeloure- terogram (Fig. 1A). Left retrograde pyelogram demonstrated an irregular filling defect in the left renal pelvis compatible with blood clot or neoplasm (Fig. 1B). Results of cytology were negative. Repeat retrograde pyelogram nine days later showed no change. Left nephroure- terectomy was performed. Pathologic examina- tion demonstrated a leiomyoma with occasional mitoses (Fig. 2). The patient is doing well three years later.
Remarks. Leiomyoma of the renal pelvis may present with hematuria and be demon- strated as a filling defect on pyelography. How- ever, presentation of a leiomyoma in this man- ner is exceedingly rare with only 1 case previ- ously reported in the literature.5 Therefore, a
FIGURE 2. Case 1. LAomyoma of renal pelvis.
lesion of this type may be managed best by nephroureterectomy because of the overwhelm- ing odds in favor of malignancy.
Case 2 A sixty-six-year-old white man who had re-
cently moved to West Virginia, presented for follow-up of a bladder lesion diagnosed at an- other hospital two years earlier. The patient was asymptomatic and denied hematuria, dysuria, or symptoms of bladder neck or ureteral obstruc- tion. Physical examination revealed no abnor- malities. Laboratory evaluation including com- plete blood count, blood urea nitrogen, creatinine, and urinalysis was normal. Intrave- nous pyeloureterogram demonstrated an un- usual filling defect in the bladder (Fig. 3A). The mass involving the bladder was evaluated fur- ther by carbon dioxide cystography (Fig. 3B and C).
FIGURE 3. Case 2. (A) Large smooth defect noted in bladder on intravenous pyelogram. (B) Carbon dioxide cystogram outlining bladder mass. (C) Lateral view of carbon dioxide cystogram outlining anterior bladder mass.
UROLOGY / APRIL1979 / VOLUMEXIII. NUMBER4 425
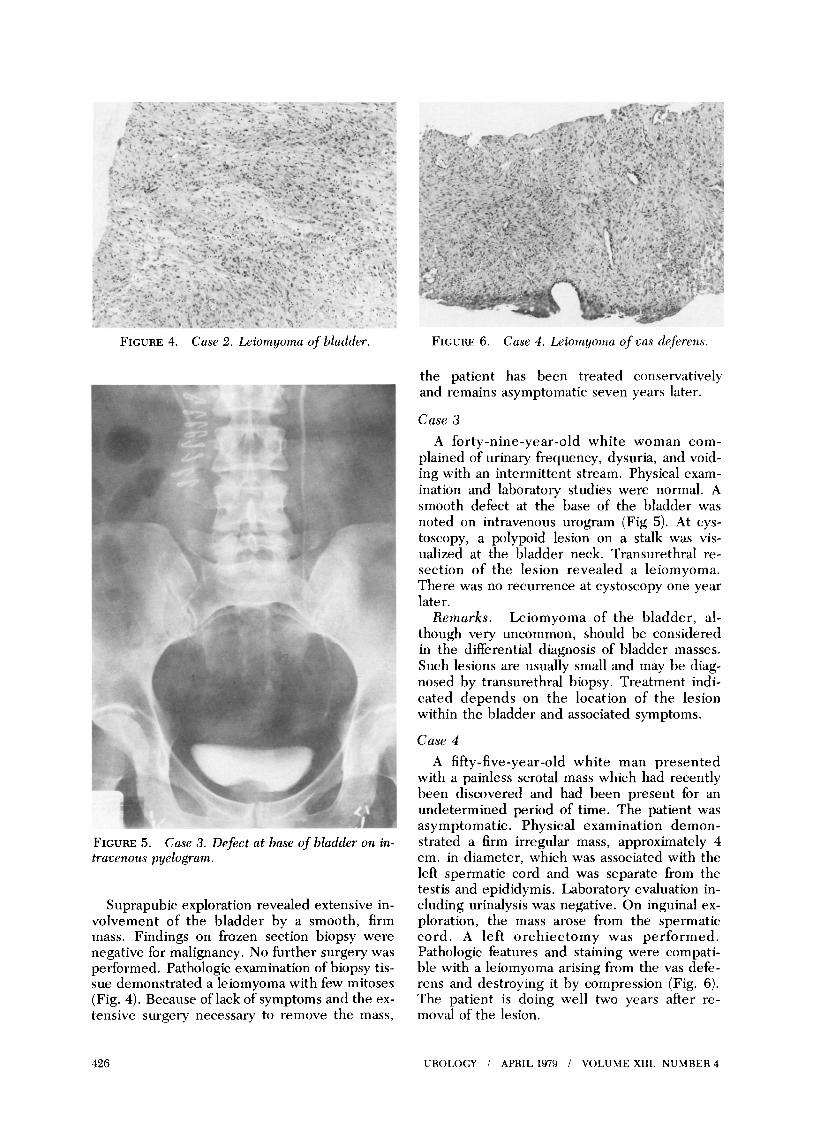
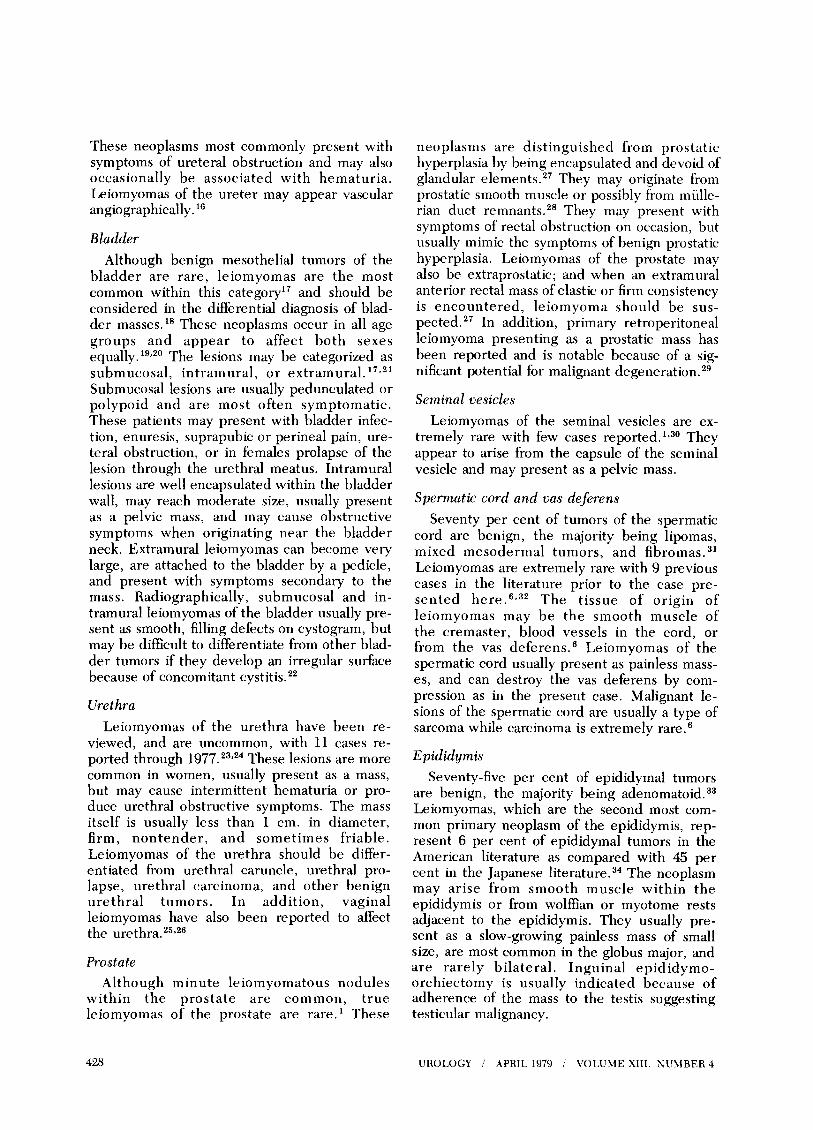
FIGURE 4. Case 2. Leiomyoma of bladder. FIGURE 6. Case 4. LAomyoma of vas deferens.
FIGURE 5. Case 3. Defect at base of bladder on in- travenous pyelogram.
Suprapubic exploration revealed extensive in- volvement of the bladder by a smooth, firm mass. Findings on frozen section biopsy were negative for malignancy. No further surgery was performed. Pathologic examination of biopsy tis- sue demonstrated a leiomyoma with few mitoses (Fig. 4). Because of lack of symptoms and the ex- tensive surgery necessary to remove the mass,
the patient has been treated conservatively and remains asymptomatic seven years later.
Case 3
A forty-nine-year-old white woman com- plained of urinary frequency, dysuria, and void- ing with an intermittent stream. Physical exam- ination and laboratory studies were normal. A smooth defect at the base of the bladder was noted on intravenous urogram (Fig 5). At cys- toscopy, a polypoid lesion on a stalk was vis- ualized at the bladder neck. Transurethral re- section of the lesion revealed a leiomyoma. There was no recurrence at cystoscopy one year later.
Remarks. Leiomyoma of the bladder, al- though very uncommon, should be considered in the differential diagnosis of bladder masses. Such lesions are usually small and may be diag- nosed by transurethral biopsy. Treatment indi- cated depends on the location of the lesion within the bladder and associated symptoms.
Case 4 A fifty-five-year-old white man presented
with a painless scrotal mass which had recently been discovered and had been present for an undetermined period of time. The patient was asymptomatic. Physical examination demon- strated a firm irregular mass, approximately 4 cm. in diameter, which was associated with the left spermatic cord and was separate from the testis and epididymis. Laboratory evaluation in- cluding urinalysis was negative. On inguinal ex- ploration, the mass arose from the spermatic cord. A left orchiectomy was performed. Pathologic features and staining were compati- ble with a leiomyoma arising from the vas defe- rens and destroying it by compression (Fig. 6). The patient is doing well two years after re- moval of the lesion.
426 UROLOGY / APRIL 1979 / VOLUME XIII. NUMBER 4

Remarks. Lesions arising from spermatic cord structures are unusual and predominantly benign. However, as many as 30 per cent of spermatic cord neoplasms are sarcomas of vari- ous types6 and inguinal orchiectomy is the pri- mary treatment.
Case 5 A three-year-old white boy presented with a
painless lesion at the base of the glans penis of four weeks’ duration. Although the youngster was asymptomatic, his mother noticed the le- sion to be gradually increasing in size.
Physical examination demonstrated a 1.5-cm., pale, firm nodule over the lateral base of the glans penis (Fig. 7). Laboratory evaluation in- cluding urinalysis and complete blood count was within normal limits. Excisional biopsy was per- formed. Pathologic examination revealed a vas- cular leiomyoma with no evidence of mitoses (Fig. 8). The youngster was doing well three months later.
Remarks. Leiomyoma of the penis is ex- tremely rare with only one previously reported case involving the penile shaft.’ This is the first case report of a leiomyoma of the glans penis. Excisional biopsy is recommended.
Comment
Kidney
Leiomyomas of renal origin have previously been reviewed in the literature.2,4*7,8 These neoplasms are of three basic types:4 (1) small subcortical lesions, which are not rare, are often multiple, and are most commonly found inci- dentally at surgery; (2) large solitary neoplasms associated with vessels9 or renal capsule; and (3) neoplasms arising within the renal pelvis.5 The small subcortical lesions often contain muscle, fibrous tissue, and fat, may be of congenital ori- gin, and possibly may not be true leiomyomas.‘” The large solitary neoplasms occur infrequently, are slow growing, most commonly present as a mass, and may reach large proportions as noted in 1 case of a 4,940-Gm. tumor.” Large solitary lesions are more common in women, may be ac- companied by occasional flank pain or discom- fort, and rarely cause hematuria. These tumors may calcify, while angiographically they show no evidence of neovascularity or tumor stain.” They occur in all age groups including in- fants.4’12 Leiomyomas of the renal pelvis are ex- ceedingly rare with only 1 case reported5 prior to the case presented here. These lesions may
FIGURE 7. Case 5. Physical appearance of leiomyoma of glans penis.
FIGURE 8. Case 5. Leiomyoma of glans penis.
be associated with hematuria and appear to mimic malignant tumors of the renal pelvis.
It should also be noted that renal leiomyomas and leiomyosarcomas have been experimentally induced in rats with the carcinogen, methyl- azoxymethanol, suggesting a possible car- cinogenic cause for these lesions.13
Ureter
Benign nonepithelial mesodermal tumors of the ureter are rare, while leiomyomas further represent a small proportion of this group.14,15
UROLOGY / APRIL1979 / VOLUMEXIII, NUMBER4 427
These neoplasms most commonly present with symptoms of ureteral obstruction and may also occasionally be associated with hematuria. Leiomyomas of the ureter may appear vascular angiographically. l6
Bladder
Although benign mesothelial tumors of the bladder are rare, leiomyomas are the most common within this category” and should be considered in the differential diagnosis of blad- der masses. la These neoplasms occur in all age groups and appear to affect both sexes equally. ig,*O The lesions may be categorized as submucosal, intramural, or extramural. “,*l Submucosal lesions are usually pedunculated or polypoid and are most often symptomatic. These patients may present with bladder infec- tion, enuresis, suprapubic or perineal pain, ure- teral obstruction, or in females prolapse of the lesion through the urethral meatus. Intramural lesions are well encapsulated within the bladder wall, may reach moderate size, usually present as a pelvic mass, and may cause obstructive symptoms when originating near the bladder neck. Extramural leiomyomas can become very large, are attached to the bladder by a pedicle, and present with symptoms secondary to the mass. Radiographically, submucosal and in- tramural leiomyomas of the bladder usually pre- sent as smooth, filling defects on cystogram, but may be difficult to differentiate from other blad- der tumors if they develop an irregular surface because of concomitant cystitis.**
Urethra
Leiomyomas of the urethra have been re- viewed, and are uncommon, with 11 cases re- ported through 1977. 23,24 These lesions are more common in women, usually present as a mass, but may cause intermittent hematuria or pro- duce urethral obstructive symptoms. The mass itself is usually less than 1 cm. in diameter, firm, nontender, and sometimes friable. Leiomyomas of the urethra should be differ- entiated from urethral caruncle, urethral pro- lapse, urethral carcinoma, and other benign urethral tumors. In addition, vaginal leiomyomas have also been reported to affect the urethra.25,26
Prostate
Although minute leiomyomatous nodules within the prostate are common, true leiomyomas of the prostate are rare.’ These
neoplasms are distinguished from prostatic hyperplasia by being encapsulated and devoid of glandular elements. *’ They may originate from prostatic smooth muscle or possibly from mulle- rian duct remnants. *’ They may present with symptoms of rectal obstruction on occasion, but usually mimic the symptoms of benign prostatic hyperplasia. Leiomyomas of the prostate may also be extraprostatic; and when an extramural anterior rectal mass of elastic or firm consistency is encountered, leiomyoma should be sus- pected. *’ In addition, primary retroperitoneal leiomyoma presenting as a prostatic mass has been reported and is notable because of a sig- nificant potential for malignant degeneration.2g
Seminal vesicles
Leiomyomas of the seminal vesicles are ex- tremely rare with few cases reported.‘s30 They appear to arise from the capsule of the seminal vesicle and may present as a pelvic mass.
Spermatic cord and vas deferens
Seventy per cent of tumors of the spermatic cord are benign, the majority being lipomas, mixed mesodermal tumors, and fibromas.31 Leiomyomas are extremely rare with 9 previous cases in the literature prior to the case pre- sented here.6*32 The tissue of origin of leiomyomas may be the smooth muscle of the cremaster, blood vessels in the cord, or from the vas deferens. Leiomyomas of the spermatic cord usually present as painless mass- es, and can destroy the vas deferens by com- pression as in the present case. Malignant le- sions of the spermatic cord are usually a type of sarcoma while carcinoma is extremely rare.6
Epididymis
Seventy-five per cent of epididymal tumors are benign, the majority being adenomatoid.33 Leiomyomas, which are the second most com- mon primary neoplasm of the epididymis, rep- resent 6 per cent of epididymal tumors in the American literature as compared with 45 per cent in the Japanese literature.34 The neoplasm may arise from smooth muscle within the epididymis or from wolffian or myotome rests adjacent to the epididymis. They usually pre- sent as a slow-growing painless mass of small size, are most common in the globus major, and are rarely bilateral. Inguinal epididymo- orchiectomy is usually indicated because of adherence of the mass to the testis suggesting testicular malignancy.
428 UROLOGY / APRIL 1979 / VOLUME XIII. NUMBER 4

Tunica albuginea
Tumors of the testicular tunics are extremely rare with an estimated 65 per cent being be- nign35 and the most common benign tumor a pure fibroma. Of these, one leiomyoma has been reported3’j along with a number of others arising from the gubernaculum testis;37 that par- ticular case occurred in a ten-year-old boy and presented as a torsion of a testicular appendage when the tumor twisted upon its stalk.36
Testis
A single report of an intratesticular leiomyoma possibly arising from contractile cells present in the tunica propria of the seminiferous tubules has been recorded.38 Since a preopera- tive histologic diagnosis is impossible, inguinal orchiectomy is indicated.
Penis
Prior to the present case of a leiomyoma of the glans penis, one other case of leiomyoma of the penis had been reported.’ That leiomyoma arose from the dorsum of the proximal penile shaft in a fifty-one-year-old man. The lesion had been noted by the patient for many years, gradually became larger, and finally interfered with coitus. The tumor was subcutaneous, freely movable, and did not invade the underlying corpora cavernosa penis.
Scrotum
Leiomyoma arising from the scrotum is ex- ceedingly rare. Most reported cases have pre- sented as a small, firm, nontender, slowly en- larging freely movable mass within the scrotum, 3g40
Morgantown, West Virginia 26506 (DR. BELIS)
ACKNOWLEDGMENT. To Shoukry L. Francis, M.D. and Harry L. Shannon, M.D. for permission to describe Cases 1 and 3.
References
1. Herbut PA: Urological Pathology, Lea and Febiger Com- pany, Philadelphia, 1952, p. 851.
2. Levitt MH, McCov RC, and Fetter BF: GIomerulonathv in medullary sponge kidneys, J. Ural. 112: 710 (1974). L ’
3. Lin 11, and Svoboda Dl: MultiDIe congenital mesenchvmal tumors, Cancer 28: 1046 (1971). - ”
I
4. Zuckerman IC, Kershner D, Laytner BD, and Hirsch1 D: Leiomyoma of the kidney, Ann. Surg. 126: 220 (1947).
5. Lit&y GM, Seidel RF, and O’Brien JE: Leiomyoma of the renal pelvis, J. Uml. 105: 171 (1971).
6. DougaIl AJ, and Wilson RR: Leiomyoma of the vas deferens, Br. J. Ural. 41: 348 (1969).
7. Coutlseller V’S, and Menville JG: Leiomyoma associated with benign cysts in a kidnev with duohcated Delves. 1. Ural. 35: 253 (1936).
8. Foster DG: Large benign renal tumors: review of literature and report of case in childhood, ibid. 76: 231 (1956).
9. Gordon MP, Kimmelstiel P, and Cabell CL: Leiomyoma of the kidney, ibid. 42: 507 (1939).
10. Fishbone G, and Davidson AJ: Leiomyoma of the renal capsule, Radiology 92: 1006 (1969).
11. Bailey OT, and Harrison JH: Large benign neoplasms: their pathology and clinical behavior, with report of five cases, J, Ural. 38: 509 (1937).
12. Addison NV, and Peach B: Smooth muscle tumors of the kidney, Br. J, Ural. 38: 382 (1966).
13. Reuber MD: leiomyomas and leiomyosarcomas of the kid- ney in 4-day-old BUF rats given methylazoxymethanol acetate in- traperitoneally, J. Natl. Cancer Inst. 56: 405 (1976).
14. Kao, VCY, Gratf PW, and Rappaport H: Leiomyoma of the ureter, Cancer 24: 535 (1969).
15. Mondschein LJ, Sutton AP, and Rothfeld SH: Leiomyoma of ureter in child: first reported case, J. Urol. 116: 516 (1976).
16. Lambeth JT, and Ranniger K: Angiographic demonstration of a benign tumor of the ureter, Radiology 91: 929 (1968).
17. Campbell EW, and Gislason GJ: Benign mesothelial tumors of the urinary bladder: review of literature and a report of a case of leiomyoma, I. Ural. 70: 733 (1953).
18..O’ConneIl K, and Edson M: Leiomyoma of bladder, Urol- ogy 6: 114 (1975).
19. Mutchler RW, and Gorder JL: Leiomyoma of the bladder in a child, Br. J. Radio]. 45: 538 (1972).
20. Katz RB, and Waldbaum RS: Benign mesothelial tumor of bladder, Urology 5: 236 (1975).
21. Thompson IM, and BaIfour J: Leiomyomatous vesicle outlet obstruction, ibid. 3: 92 (1974).
22. Williams DI, and Schistad G: Lower urinary tract tumors in children, Br. I. UroI. 36: 51 (1964).
23. Shield DE, and Weiss’ RM:’ Leiomyoma of the female ure- thra, J. Ural. 109: 436 (1973).
24. Wani NA, Bhan BL, Guru AA, and Garyali RK: Leiomyoma of female urethra, ibid. 116: 120 (1976).
25. Adducci J: Leiomyoma of the anterior vaginal wall in a sub- urethral location causing stress incontinence: report of a case, ibid. 93: 255 (1965).
26. Smith HW, and Campbell EW: Benign periurethml masses in women, ibid. 116: 451 (1976).
27. Kaufman JJ, and Bemeike RB: Leiomyoma of the prostate, ibid. 65: 297 (1951).
28. Carson RB: Leiomyoma of prostate, ibid. 64: 373 (1950). 29. Albert PS, Sinatra T, and Nagamatsu GR: Retroperitoneal
leiomyoma presenting as prostatic mass, Urology 3: 607 (1974). 30. Plaut A, and Standard S: Cystomyoma of seminal vesicles,
Ann. Surg. 119: 253 (1944). 31. Thompson GJ: Tumors of spermatic cord, epididymis, and
testicular tunics, Surg. Gynecol. Obstet. 62: 712 (1936). 32. Deluise VP, Draper JW, and Gray GF: Smooth muscle
tumors of the testicular adnexa, J. Urol. 115: 685 (1976). 33. Broth G, Bullock WK, and Morrow J: Epididymal tumors,
ibid. 100: 530 (1968). 34. Spark RP: Leiomyoma of epididymis, Arch. Pathol. 93: 18
(1972). 35. Hinman F, and Gibson TE: Tumors of the epididymis,
spermatic cord, and the testicular tunics, Arch. Surg. 8: 106 (1924).
36. Albert PS, and Mininberg DT: Leiomyoma of the tunica albuginea, J, Urol. 107: 869 (1972).
37. Thompson GJ: Tumors of the spermatic cord, epididymis, and testicular tunics. Surg. Gynecol. Obstet. 62: 712 (1936).
38. Honore LH, and Sullivan LD: Intratesticular Ieiomyoma, J. Ural. 114: 631 (1935).
39. Siegal GP, and Gaffey TA: Solitary leiomyomas arising from tunica dartos scroti, ibid. 116: 69 (1976).
40. Iloreta AT, Bekirov H, and Newman HR: Leiomyoma of scrotum, Urology 10: 48 (1977).
UROLOGY / APRIL 1979 / VOLUME XIII, NUMBER 4 429






