Genetics and mathematics: Evidence from Prader-Willi syndrome
7
Neuropsychologia 46 (2008) 206–212 Genetics and mathematics: Evidence from Prader-Willi syndrome Carlo Semenza a,b,∗ , Riccardo Pignatti b , Laura Bertella b,c , Francesca Ceriani b , Ileana Mori b,d , Enrico Molinari b,e , Daniela Giardino f , Francesca Malvestiti f , Graziano Grugni b a Department of Psychology, University of Trieste, Italy b Istituto Auxologico Italiano, Ospedale S. Giuseppe, Piancavallo di Verbania, Italy c Clinica Hildebrand, Brissago, TI, Switzerland d Dipartimento di Scienze della Persona, University of Bergamo, Italy e Catholic University of Sacred Heart, Milano, Italy f Istituto Auxologico Italiano, Laboratorio di Citogenetica Medica e Genetica Molecolare, Milano Received 7 February 2007; received in revised form 23 July 2007; accepted 26 July 2007 Available online 2 August 2007 Abstract Mathematical abilities were tested in people with Prader-Willi syndrome (PWS), using a series of basic mathematical tasks for which normative data are available. The difference between the deletion and the disomy variants of this condition was explored. While a wide phenotypic variation was found, some basic findings emerge clearly. As expected from previous literature, deletion and disomy participants were found to differ in their degree of impairment, with disomy being overall the most spared condition. However, the tasks selectively spared in the disomy condition are not necessarily the easiest ones and those that discriminate less the PWS group from controls. It rather seems that disomy patients are spared, with respect to deletion, in tasks entailing transcoding and comparison of numbers in the Arabic code. Overall a particular difficulty was detected in reliably performing parity judgments. This task has been shown to be very frequently spared after a brain injury, even in severe aphasic conditions. The most interesting result is the sparing in analog number scale, whereby PWS seem, overall, to outperform controls. This finding may help in understanding previously reported, surprising results about cognitive skills in PWS. Elevated performances in PWS may result from life-long hyper-reliance on one visuo-spatial system in presence of underdevelopment of the other. © 2007 Elsevier Ltd. All rights reserved. Keywords: Prader-Willi syndrome; Genetic disorders; Numbers; Calculation; Visuo-spatial system 1. Introduction Prader-Willi syndrome (PWS) is a genetically based disor- der characterized by muscular hypotonia, hyperphagia, obesity, hypogonadism, short stature, maladaptive behavior and men- tal retardation. PWS affects males and females equally and is caused by the paternal deletion within 15q11–q13 (70–75% of cases), maternal uniparental disomy of chromosome 15 (UPD15) (20–25%), or by a defect in the imprinting centre (2%) (Butler & Thompson, 2000). It has a prevalence estimated at ∗ Corresponding author. E-mail address: [email protected] (C. Semenza). about 1:8000–1:16,000 live births (Burd, Vesely, Martsolf, & Korbeshian, 1990; Whittington et al., 2001). On average symp- tom severity seems to be dampening in UPD cases with respect to deletion cases (Dykens, Cassidy, & King, 1999). All PWS patients suffer some degree of intellectual impair- ment. Language milestones are usually delayed. Cognitive abnormalities become evident as the child reaches school age. Most subjects fall in the mildly mentally retarded range (mean IQ: 60–70), with approximately 40% having borderline retarda- tion or low normal intelligence and about 20% having moderate retardation (Cassidy, 1997; Molinari, 2002). Regardless of measured IQ, most PWS children have multi- ple severe learning disabilities, and their academic performance is poor for their mental abilities (Curfs, Wiegers, Sommers, 0028-3932/$ – see front matter © 2007 Elsevier Ltd. All rights reserved. doi:10.1016/j.neuropsychologia.2007.07.017
-
Upload
auxologico -
Category
Documents
-
view
1 -
download
0
Transcript of Genetics and mathematics: Evidence from Prader-Willi syndrome

A
dw
ott
atp©
K
1
dhtco((
0d
Neuropsychologia 46 (2008) 206–212
Genetics and mathematics: Evidence from Prader-Willi syndrome
Carlo Semenza a,b,∗, Riccardo Pignatti b, Laura Bertella b,c, Francesca Ceriani b,Ileana Mori b,d, Enrico Molinari b,e, Daniela Giardino f,
Francesca Malvestiti f, Graziano Grugni b
a Department of Psychology, University of Trieste, Italyb Istituto Auxologico Italiano, Ospedale S. Giuseppe,
Piancavallo di Verbania, Italyc Clinica Hildebrand, Brissago, TI, Switzerland
d Dipartimento di Scienze della Persona, University of Bergamo, Italye Catholic University of Sacred Heart, Milano, Italy
f Istituto Auxologico Italiano, Laboratorio di Citogenetica Medica eGenetica Molecolare, Milano
Received 7 February 2007; received in revised form 23 July 2007; accepted 26 July 2007Available online 2 August 2007
bstract
Mathematical abilities were tested in people with Prader-Willi syndrome (PWS), using a series of basic mathematical tasks for which normativeata are available. The difference between the deletion and the disomy variants of this condition was explored. While a wide phenotypic variationas found, some basic findings emerge clearly.As expected from previous literature, deletion and disomy participants were found to differ in their degree of impairment, with disomy being
verall the most spared condition. However, the tasks selectively spared in the disomy condition are not necessarily the easiest ones and thosehat discriminate less the PWS group from controls. It rather seems that disomy patients are spared, with respect to deletion, in tasks entailingranscoding and comparison of numbers in the Arabic code.
Overall a particular difficulty was detected in reliably performing parity judgments. This task has been shown to be very frequently spared afterbrain injury, even in severe aphasic conditions. The most interesting result is the sparing in analog number scale, whereby PWS seem, overall,
o outperform controls. This finding may help in understanding previously reported, surprising results about cognitive skills in PWS. Elevatederformances in PWS may result from life-long hyper-reliance on one visuo-spatial system in presence of underdevelopment of the other.
2007 Elsevier Ltd. All rights reserved.
isuo-
aKtt
ma
eywords: Prader-Willi syndrome; Genetic disorders; Numbers; Calculation; V
. Introduction
Prader-Willi syndrome (PWS) is a genetically based disor-er characterized by muscular hypotonia, hyperphagia, obesity,ypogonadism, short stature, maladaptive behavior and men-al retardation. PWS affects males and females equally and isaused by the paternal deletion within 15q11–q13 (70–75%
f cases), maternal uniparental disomy of chromosome 15UPD15) (20–25%), or by a defect in the imprinting centre (2%)Butler & Thompson, 2000). It has a prevalence estimated at∗ Corresponding author.E-mail address: [email protected] (C. Semenza).
MItr
pi
028-3932/$ – see front matter © 2007 Elsevier Ltd. All rights reserved.oi:10.1016/j.neuropsychologia.2007.07.017
spatial system
bout 1:8000–1:16,000 live births (Burd, Vesely, Martsolf, &orbeshian, 1990; Whittington et al., 2001). On average symp-
om severity seems to be dampening in UPD cases with respecto deletion cases (Dykens, Cassidy, & King, 1999).
All PWS patients suffer some degree of intellectual impair-ent. Language milestones are usually delayed. Cognitive
bnormalities become evident as the child reaches school age.ost subjects fall in the mildly mentally retarded range (mean
Q: 60–70), with approximately 40% having borderline retarda-ion or low normal intelligence and about 20% having moderate
etardation (Cassidy, 1997; Molinari, 2002).Regardless of measured IQ, most PWS children have multi-le severe learning disabilities, and their academic performances poor for their mental abilities (Curfs, Wiegers, Sommers,

sycho
BFDupPnp(at
ssp1tMeoomhmce
rmswmTaitomwt
Pcsanbammi
tmfts
eevAmotPptiai(ttmttfp
ptrctpaosd
2
2tiIaWt
Ctasittpc(
1
C. Semenza et al. / Neurop
orghgraef, & Fryns, 1991; Curfs, Hoondert, van Lieshout, &ryns, 1995; Dykens, Hodapp, Walsh, & Nash, 1992). State andykens (2000) showed a distinctive, although not necessarilynique, profile of cognitive strengths and weaknesses of PWSatients compared to controls with mental retardation. SomeWS patients have relative strengths in spatial–perceptual orga-ization and visual processing and, as a group, they score on aar with normal subjects on word searches: a surprising findingDykens, 2002) is that, overall, children with PWS outperformge-matched normal peers with jigsaw puzzles, placing morehan twice as many pieces as the typically developing group.
Weaknesses have been noted in sequential processing andhort-term memory tasks, including visual, motor, and auditoryhort-term memory; academically, reading/decoding and com-rehension may exceed arithmetic skills (Holm, 1981; Masheim,981). Indeed, disproportionate difficulties with mathematicalasks have been systematically reported (Sulzbacher, Wong,
cKeen, Glock, & MacDonald, 1981). Until very recently, how-ver, this finding was only anecdotally portrayed in the majorityf available studies and was mostly based on the administrationf rather generic tasks which could only broadly tap mathe-atical abilities. The first and only systematic investigation
as been so far reported by Bertella et al. (2005) where theain components of mathematical cognition were separately
onsidered in the context of a complete neuropsychologicalxamination.
Bertella et al. (2005) study could indeed confirm previouseports: PWS patients show a systematically worse perfor-ance in arithmetic tests than in tasks tapping other cognitive
kills. This finding first emerged in the administration of WAIS,hereby the lowest graded scores were found on the arith-etic subtest (only Digit Span was disturbed almost as much).he WAIS arithmetic subtest was also found disproportion-tely disturbed in PWS with respect to a group of IQ-matchedntellectually disabled subjects: thus a low IQ could not behe only explanation for the PWS group’s selective impairmentf mathematical abilities. The disproportionate impairment inathematical skills became however more evident when patientsere administered a wide battery of specific neuropsychological
asks (Spinnler & Tognoni, 1987).Bertella et al. (2005) then provided, on a lesser number of
WS patients, a systematic assessment of a number of more spe-ific mathematical tasks: dots counting, knowledge of countingequences, parity judgements, comparison of Arabic numeralsnd written verbal numerals, reading and writing of Arabicumerals, transcoding from written verbal numerals to Ara-ic numerals and vice versa, recognition and comprehension ofrithmetical signs, retrieval of arithmetical facts, verification ofultiplication facts, mental multi-digit calculation and writtenulti-digit calculation. None of these tasks resulted unaffected
n PWS.The case by case analysis seemed to reveal a wide pheno-
ypic variation: PWS does not necessarily affect all specific
athematical functions, since ceiling or close to ceiling per-ormance was shown by at least one subject in every singleask. However, what could be a specific pattern of deficiteemed to emerge. Number transcoding difficulties were found
6Irrm
logia 46 (2008) 206–212 207
specially in cases where a syntactic frame has to be gen-rated in order to produce Arabic numbers starting from aerbal numeral: as a result syntactic errors tended to prevail.nother specific weakness was found in multiplication facts:ore specifically PWS subjects tended to miss considering one
f the two operands and hence proceed in multiplying one ofhe operands by a different number (operand errors). FinallyWS patients also appeared to perform poorly using calculationrocedures. An analysis of their errors did not reveal consis-ent and systematic “bugs” or faulty strategies. It rather showednconsistent and unsystematic errors, reflecting no strategies,ll sub-procedures being occasionally correct. Thus, accord-ng to the criteria expressed by Semenza, Miceli, and Girelli1997), their deficit seems to lie in a monitoring defect ratherhan in a distorted or missing knowledge of procedures. A spa-ial component to the deficit could not be safely excluded, since
isalignment of numbers in their appropriate columns and spa-ial number inversion were observed. The study, possibly due tohe limited number of subjects, could not detect any reliable dif-erence between the two PWS groups, the deletion and the UPDatients.
Overall Bertella’s et al. (2005) findings suggest how someortions of chromosome pair 15 may play a pivotal role inhe genetic transmission of capacities that can be potentiallyecruited for mathematical tasks. However, Bertella’s et al. studyonstituted only a preliminary, though systematic, exploration,hat cannot by any means be considered a exhaustive one. Theresent investigation is meant to further explore mathematicalbilities in PWS by using a much more complete testing batteryn a larger number of participants. One important aim of thetudy is to assess the difference for the first time between theeletion and the UPD conditions.
. Subjects and methods
Twenty-three adult PWS patients (10 males and 13 females), aged9.61 ± 6.53, range 19–44, were included in the study. Most of them belongedo a group of PWS people that have been followed up and extensively stud-ed for at least 3 years at the Ospedale S. Giuseppe, Piancavallo di Verbania,taly, a section of the Istituto Auxologico Italiano. The entire study protocol waspproved by the ad hoc Ethical Committee of the Istituto Auxologico Italiano.
ritten informed consent was obtained by the parents and, where applicable,he patients.
All patients showed the typical PWS clinical phenotype (Holm et al., 1993).ytogenetic analysis was performed in all participants: 15 of them had intersti-
ial deletion of the proximal long arm of chromosome 15 (del15q11–q13); it waslso possible to determine that three subjects had a type 1 (i.e. large as opposed tomall) deletion; uniparental maternal disomy for chromosome 15 (UPD15) wasnstead found in eight individuals. All participants were living with their families:his is customary in Italy for PWS who are not affected by additional incapaci-ating pathological conditions. Years of education received were 9.04 ± 1.72: 16articipants had completed lower secondary school (8 years) with special edu-ational support and seven participants had attended higher secondary school10–13 years).
IQ was measured in each participant via the WAIS-R (Wechsler,981) battery with the following results: whole group: mean verbal IQ
0.26 ± 15.21, range 45–117, performance IQ 67.22 ± 10.57, range 46–84, totalQ 59.70 ± 11.68, range 45–99; deletion group: mean verbal IQ 56.87 ± 8.30,ange 45–78, performance IQ 66.27 ± 12.54, range 46–84, total 57.33 ± 9.01,ange 45–76; UPD group: mean verbal IQ 66.63 ± 22.78, range 52–117, perfor-ance IQ 69.00 ± 5.58, range 57–75, total 64.13 ± 15.22, range 54–99.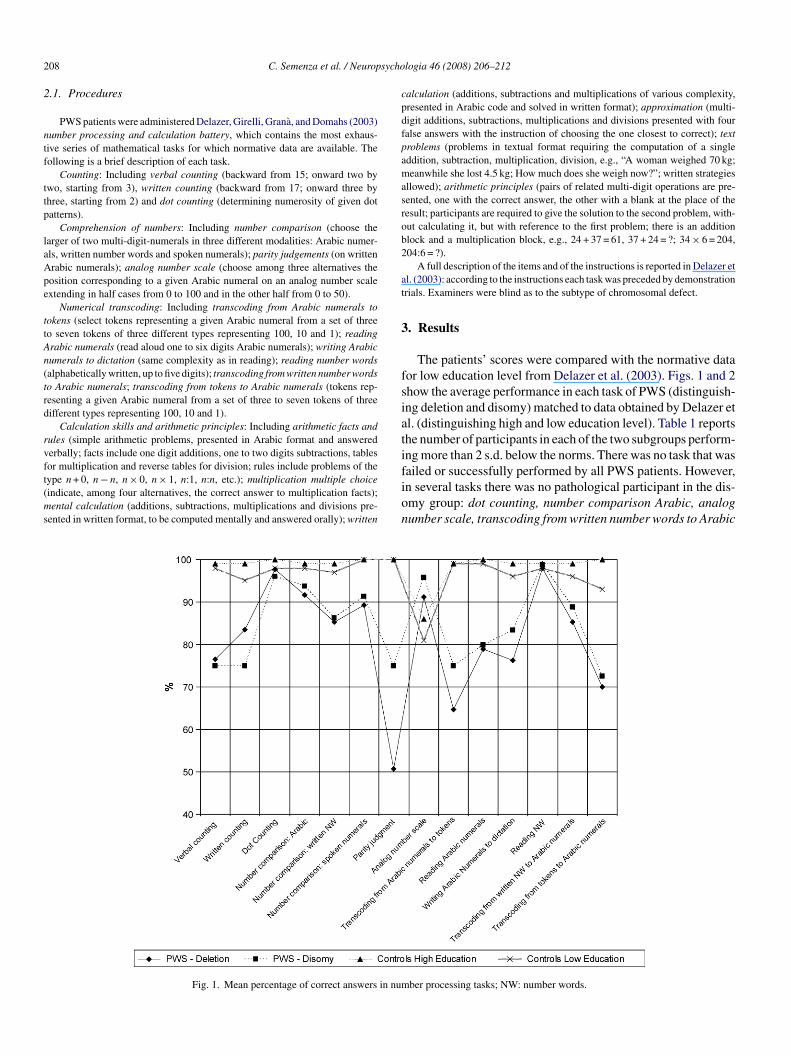
2 sycho
2
ntf
ttp
laApe
ttAn(trd
rvft(ms
cpdfpamasrob2
at
3
fsiati
08 C. Semenza et al. / Neurop
.1. Procedures
PWS patients were administered Delazer, Girelli, Grana, and Domahs (2003)umber processing and calculation battery, which contains the most exhaus-ive series of mathematical tasks for which normative data are available. Theollowing is a brief description of each task.
Counting: Including verbal counting (backward from 15; onward two bywo, starting from 3), written counting (backward from 17; onward three byhree, starting from 2) and dot counting (determining numerosity of given dotatterns).
Comprehension of numbers: Including number comparison (choose thearger of two multi-digit-numerals in three different modalities: Arabic numer-ls, written number words and spoken numerals); parity judgements (on writtenrabic numerals); analog number scale (choose among three alternatives theosition corresponding to a given Arabic numeral on an analog number scalextending in half cases from 0 to 100 and in the other half from 0 to 50).
Numerical transcoding: Including transcoding from Arabic numerals tookens (select tokens representing a given Arabic numeral from a set of threeo seven tokens of three different types representing 100, 10 and 1); readingrabic numerals (read aloud one to six digits Arabic numerals); writing Arabicumerals to dictation (same complexity as in reading); reading number wordsalphabetically written, up to five digits); transcoding from written number wordso Arabic numerals; transcoding from tokens to Arabic numerals (tokens rep-esenting a given Arabic numeral from a set of three to seven tokens of threeifferent types representing 100, 10 and 1).
Calculation skills and arithmetic principles: Including arithmetic facts andules (simple arithmetic problems, presented in Arabic format and answerederbally; facts include one digit additions, one to two digits subtractions, tables
or multiplication and reverse tables for division; rules include problems of theype n + 0, n − n, n × 0, n × 1, n:1, n:n, etc.); multiplication multiple choiceindicate, among four alternatives, the correct answer to multiplication facts);ental calculation (additions, subtractions, multiplications and divisions pre-ented in written format, to be computed mentally and answered orally); written
fion
Fig. 1. Mean percentage of correct answers in num
logia 46 (2008) 206–212
alculation (additions, subtractions and multiplications of various complexity,resented in Arabic code and solved in written format); approximation (multi-igit additions, subtractions, multiplications and divisions presented with fouralse answers with the instruction of choosing the one closest to correct); textroblems (problems in textual format requiring the computation of a singleddition, subtraction, multiplication, division, e.g., “A woman weighed 70 kg;eanwhile she lost 4.5 kg; How much does she weigh now?”; written strategies
llowed); arithmetic principles (pairs of related multi-digit operations are pre-ented, one with the correct answer, the other with a blank at the place of theesult; participants are required to give the solution to the second problem, with-ut calculating it, but with reference to the first problem; there is an additionlock and a multiplication block, e.g., 24 + 37 = 61, 37 + 24 = ?; 34 × 6 = 204,04:6 = ?).
A full description of the items and of the instructions is reported in Delazer etl. (2003): according to the instructions each task was preceded by demonstrationrials. Examiners were blind as to the subtype of chromosomal defect.
. Results
The patients’ scores were compared with the normative dataor low education level from Delazer et al. (2003). Figs. 1 and 2how the average performance in each task of PWS (distinguish-ng deletion and disomy) matched to data obtained by Delazer etl. (distinguishing high and low education level). Table 1 reportshe number of participants in each of the two subgroups perform-ng more than 2 s.d. below the norms. There was no task that was
ailed or successfully performed by all PWS patients. However,n several tasks there was no pathological participant in the dis-my group: dot counting, number comparison Arabic, analogumber scale, transcoding from written number words to Arabicber processing tasks; NW: number words.

C. Semenza et al. / Neuropsychologia 46 (2008) 206–212 209
Fa
ntTewfnifaAwm
pinAm
tDsL
Table 1Number of PWS subjects, with disomy or deletion, who performed under twoz-scores from normative data
Subtests Disomy(n = 8)
Deletion(n = 15)
Verbal counting 3 6Written counting 4 5Dot counting 1 1Number comparison: Arabic 1 4Number comparison: written NW 4 7Number comparison: spoken numerals 4 8Parity judgement 5 11Analog number scale 0 1Transcoding from Arabic numerals to tokens 3 9Reading Arabic numerals 5 10Writing Arabic numerals to dictation 5 8Reading NW 1 2Transcoding from written NW to Arabic numerals 2 5Transcoding from tokens to Arabic numerals 2 5Addition facts 2 7Addition rules 0 2Subtraction facts 3 2Subtraction rules 1 7Multiplication facts 7 9Multiplication rules 0 3Division facts 6 8Division rules 2 7Multiplication multiple choice 5 7Mental additions 2 7Mental subtractions 3 9Mental multiplications 5 8Mental divisions 6 11Written additions 2 3Written subtractions 3 7Written multiplications 5 6Approximations 5 11Text problems 4 8AA
dwstsfrbwtbtpo&c(
ig. 2. Mean percentage of correct answers in tasks of calculation skills andrithmetic principles.
umerals, transcoding from tokens to Arabic numerals, addi-ion facts, addition rules, multiplication rules, mental additions.
tests for independent samples were performed separately forach task and revealed that PWS participants scored significantlyorse than normals, at least at the p < .002 level (one-tailed Bon-
erroni correction applied), in each task but for dot counting,umber comparison Arabic, reading number words, transcod-ng from written number words to Arabic numerals, transcodingrom tokens to Arabic numerals, addition facts, addition rulesnd written addition, where no significant difference was found.
remarkable exception concerned the analog number scale,here PWS participants performed significantly better than nor-als (p < .007).Further analyses contrasted the two PWS groups. Deletion
articipants performed significantly worse than disomy partic-pants in number comparison Arabic, transcoding from Arabicumerals to tokens, transcoding from written number words torabic numerals, transcoding from tokens to Arabic numerals,ental addition (t tests, p < .05 or less).In order to identify which tasks better distinguished between
he PWS group and the low education normed sample fromelazer’s et al. (2003) study, a stepwise discriminant analy-
is (Table 2) was performed yielding significant results (Wilks’ambda (34) = 0.261, p < .0001). Parity judgement was the most
ots
rithmetic principles: addition 4 9rithmetic principles: multiplication 4 9
iscriminating task, being the most demanding task for PWSith respect to normals; by contrast, analog number scale
howed the opposite trend, with PWS patients performing betterhan normals. Finally, reading number words and dot countingeemed to be the less discriminative tasks, due to their greatacility for both the PWS and the normal sample. Classificationesults, after cross-validation of squared Mahalanobis distanceased on observations, yielded two participant groups, one ofhich was composed only of PWS participants (n = 16) and
he other was composed by normal participants plus the sevenest PWS performers (five belonging to the deletion type plushe two disomy persons with the highest IQ). These same 16atients individually showed significant differences (p < .0001r less) compared to normals when the TVARDIFF (Garthwaite
Crawford, 2004) procedure was applied to each of them inomparison to the normal sample contrasting parity judgementthe task PWS performed worse) and analog number scale.
Finally, two hierarchical cluster analyses were performed in
rder to study, respectively, the pattern of similarities amongasks and among PWS patients. In both analyses, data were clas-ified employing the average linkage agglomeration rule and the
210 C. Semenza et al. / Neuropsychologia 46 (2008) 206–212
Table 2Discriminant analysis: pooled within-groups correlations between discriminat-ing variables and standardized canonical discriminant functions
Task Function
Parity judgment .671Reading Arabic numerals .551Division facts .537Multiplication facts .536Number comparison: spoken numerals .470Transcoding from Arabic numerals to tokens .447Multiplication multiple choice .395Writing Arabic numerals to dictation .370Number comparison: written NW .367Arithmetic principles: multiplication .346Arithmetic principles: addition .345Mental divisions .345Approximations .342Verbal counting .319Text problems .318Addition facts .272Transcoding from tokens to Arabic numerals .271Mental multiplications .262Written multiplications .256Mental subtractions .253Transcoding from written NW to Arabic numerals .238Subtraction facts .227Mental additions .221Number comparison: Arabic numerals .209Written subtractions .208Division rules .194Written counting .188Addition rules .167Multiplication rules .159Subtraction rules .142Analog number scale −.134Written additions .083Dot counting .026R
T
sfiaevpAiftiAonAnfamgu
Table 3Cluster membership of tasks
Task Clusters
Verbal counting 1Written counting 1Dot counting 1Number comparison: Arabic 1Number comparison: written NW 1Number comparison: spoken numerals 1Parity judgment 2Analog number scale 1Transcoding from Arabic numerals to tokens 3Reading Arabic numerals 1Writing Arabic numerals to dictation 1Reading NW 1Transcoding from written NW to Arabic numerals 1Transcoding from tokens to Arabic numerals 3Addition facts 1Addition rules 1Subtraction facts 1Subtraction rules 1Multiplication facts 3Multiplication rules 3Division facts 3Division rules 3Multiplication multiple choice 3Mental additions 3Mental subtractions 3Mental multiplications 3Mental divisions 4Written additions 1Written subtractions 3Written multiplications 3Approximations 4Text problems 3AA
gtlaaigedbsit
4
nidegree of general cognitive impairment. Such findings are indeed
eading NW .008
asks ordered by absolute size of correlation within function.
quared euclidean distance as similiarity/distance method. Therst cluster analysis was carried out on the percentage of correctnswers in each task from all PWS patients. Four groups of tasksmerged (Table 3). A first group (cluster 1 in the table) includederbal counting, written counting, dot counting, number com-arison, analog number scale, reading Arabic numerals, writingrabic numerals to dictation, reading number words, transcod-
ng from written number words to Arabic numerals, additionacts, addition rules, subtraction facts, subtraction rules and writ-en addition. Most number manipulation tasks appear to clustern this group as well as some of the easiest calculation tasks.
second group (cluster 2) was constituted by parity judgementnly. As reported above this was the most difficult and discrimi-ating task. A third group (cluster 3) included transcoding fromrabic numerals to tokens, transcoding from tokens to Arabicumerals, multiplication facts and multiplication rules, divisionacts and division rules, multiplication multiple choice, mentalddition, subtraction and multiplication, written subtraction and
ultiplication, text problems and Arithmetic principles. Thisroup includes most calculation tasks as well as number manip-lation tasks whereby tokens are involved. Finally, a fourth
nwd
rithmetic principles: addition 3rithmetic principles: multiplication 3
roup (cluster 4) included mental division and approximation,wo tasks of about the same discriminating value, possibly theess familiar ones in education. A second cluster analysis wasimed at looking for subgroups of persons within the PWS. Thenalysis was carried out on the percentage of correct answersn each task from each individual PWS participant. Three sub-roups emerged from this analysis (Table 4). The first subgroupncompassed eight subjects, including four deletion and fourisomy patients. The two disomy patients with the highest ver-al IQ, belonged to the second subgroup that encompassed theix PWS patients that could not be distinguished from normalsn the discriminant analysis. The third subgroup encompassedhe remaining six participants.
. Discussion
This investigation confirms the existence of a wide phe-otypic variation in performing math tasks within PWS. Thempairment in math ability is only marginally related to the
ot surprising and are in line with Bertella’s et al. (2005) data andhat is shown for cognitive functions in most chromosomic syn-romes. Which are, however, very seldom investigated (and this

C. Semenza et al. / Neuropsycho
Table 4Details of screening variables, genetics, IQ scores and cluster membership fromPWS patients
PatientId.
Age Genetics VerbalIQ
PerformanceIQ
TotalIQ
Cluster
1 26 Disomy 72 74 71 12 24 Disomy 78 57 64 23 36 Deletion 48 48 45 14 35 Disomy 54 67 57 15 31 Deletion 54 51 48 36 20 Disomy 49 71 54 17 32 Deletion 67 64 62 28 23 Deletion 52 55 47 39 32 Deletion 57 71 59 1
10 29 Deletion 57 72 61 311 25 Deletion 59 84 66 212 19 Deletion 62 70 61 213 25 Deletion 54 84 63 114 34 Deletion 78 76 76 215 29 Disomy 54 71 57 116 24 Deletion 57 82 64 317 35 Deletion 46 59 48 318 34 Deletion 59 66 58 219 31 Deletion 58 66 57 120 29 Deletion 45 46 45 321 22 Disomy 57 69 57 322 42 Disomy 52 68 54 32
i(SsamoiadmecIasnttcaal
tcitrd
bid
sffcast
sticDcatltpvietoitpoeaPlsmalahjq
atu(S(tcing with jigsaw puzzles. On the whole, these abilities, Dykens
3 44 Disomy 117 75 99 2
s particularly true for math abilities) in such detailed fashionsee, however, Paterson, Girelli, Butterworth, & Karmiloff-mith, 2006, where much less complex math functions weretudied, with respect to the present investigation, in Turner’snd William’s syndromes). It would be extremely interesting toatch math performance for conditions like, indeed, Turner’s
r William’s syndromes on exactly the same tasks administeredn the present study. However, in such conditions, the IQ is, onverage, higher than in PWS, and a direct comparison amongifferent chromosomic conditions hard to make (IQ is insteaduch lower in Down syndrome, another group of potential inter-
st). For this reason, in the present investigation the strategy washosen to match the patients’ performance to available norms.ndeed the most interesting results in this study are the elevatedbility and the peculiar hardship found in PWS people for somepecific tasks that are known to be, respectively, not so easy andot so hard for other low IQ populations. Not every result ofhe present study, however, lends itself to an easy interpreta-ion. More extended investigations are thus needed in order tolarify the role of chromosome 15 in supporting abilities thatre recruited for math performance. This notwithstanding, therere a few clear and interesting results, worth discussing at someength.
In mathematics, deletion and disomy patients seem to differ inheir degree of impairment, whereby disomy is the most sparedondition. However, it seems that the tasks selectively sparedn the disomy condition are not necessarily the easiest ones and
hose that discriminate less the PWS group from controls. Itather seems that disomy patients are spared, with respect toeletion, in tasks entailing transcoding and comparison of num-(sd
logia 46 (2008) 206–212 211
ers in the Arabic code, a finding that did not emerge clearlyn Bertella’s et al. (2005) study. Given the limited number ofisomy participants this finding needs replication.
Another finding that did not emerge so clearly in previoustudies is the particular difficulty that PWS have in reliably per-orming parity judgments. This task has been shown to be veryrequently spared after a brain injury, even in severe aphasiconditions (Semenza et al., 2006). There is no refined theorybout this task and the fact that it may impose particular hard-hips on a specific pathological population may encourage betterheoretical shaping and further empirical investigations.
Probably the most interesting result of the present study is theparing of the PWS group in analog number scale: indeed, in thisask, PWS seem to outperform controls. This finding may helpn understanding previously reported, surprising results aboutognitive skills in PWS. In fact, a relatively recent study ofykens (2002), already mentioned in the introduction, empiri-
ally demonstrated what was for long time rumored: PWS havespecial talent for jigsaw puzzles and indeed they outperform
heir normal peers in such task. Dykens (2002) goes at greatength in considering possible reasons for explaining why men-ally retarded people like PWS could show above the averageerformance in jigsaw puzzles as well as in other tasks implyingisuo-spatial skills. She could not exclude those critical factorsn determining PWS performance in her study could be previousxposure to puzzles and practice with them. Also, PWS seemedo show a special attraction to puzzles, and indeed enjoymentf puzzles was the strongest predictor of puzzle performancen the study. However, while these considerations must induceo caution in interpreting the surprisingly good performance inuzzles, as Dykens (2002) quite rightly argues, “even if pleasurer practice with puzzles contributes to puzzle proficiency, thesexplanations beg at least the question of why children with PWSre attracted to jigsaw puzzles to begin with”. The finding thatWS outperform controls in analog number scale makes it less
ikely that above average performance with some visuo-spatialkills in PWS exclusively results from practice, particular enjoy-ent or obsessive concern. In fact, the Analog number scale task
dministered in this study simply requires referring a particu-ar numerosity measure, expressed with an Arabic number, tovisually presented analog scale. This task is very unlikely toave been the object of particular previous practice, and, unlikeigsaw puzzles, does not seem to have a particularly entertaininguality.
The analog number scale task rather relies on visuo-spatialnd possibly attentional abilities. This task requires at least thewo following steps: (a) to spatially elaborate the numerical val-es, building a mental image map, i.e. a “mental number line”Dehaene, Bossini, & Giraux, 1993; Di Luca, Grana, Semenza,eron, & Pesenti, 2006), subject to attentional exploration, andb) to map this mental image to the spatial array provided withhe task. Mapping spatially mental images to a given spatialonfiguration constitutes, indeed, a critical component in deal-
2002) hints, may pertain more closely to processing and repre-entation of static rather than dynamic information, sustained inifferent brain structures and hence dissociable by brain injury

2 sycho
odst(tpmdaseisTet
A
dasgC
R
B
B
B
C
C
C
C
D
D
D
D
D
D
G
H
H
M
M
M
P
R
S
S
S
S
S
W
Wsione italiana. Firenze: Organizzazioni Speciali.
12 C. Semenza et al. / Neurop
r unequally distributed brain maturation failure. Recent evi-ence (Castelli, Glaser, & Butterworth, 2006) seems indeed touggest how the general magnitude evaluation system believedo be neurologically implemented in the inferior parietal lobeWalsh, 2003) may be further divided into subsystems reflectinghe architectonic differentiation of the cortex lining the inferiorarietal sulcus. The specific anomalies caused by the chromoso-al defect in PWS brain are still largely unknown. Indeed, to this
ay, systematic neuroimaging investigations of this syndromere missing. It is possible that a peculiar pattern of damage andparing concerns the parietal structures sustaining magnitudevaluation. What are emerging as being elevated performancesn PWS may result from life-long hyper-reliance on one visuo-patial system in presence of underdevelopment of the other.his hypothesis remains highly speculative and calls for furthermpirical research as well as sharpening of existing theories andask analyses.
cknowledgements
We are grateful to Margarete Delazer for providing the fullata base for her normal controls on the Number Processingnd Calculation Battery and to Klaus Willmes for advice on thetatistical treatment. This research was supported in part by arant from the Italian Ministry of Education and from a Marieurie Network Grant (NUMBRA) to the first author.
eferences
ertella, L., Girelli, L., Grugni, G., Marchi, S., Molinari, E., & Semenza, C.(2005). Mathematical skills in Prader-Willi syndrome. Journal of IntellectualDisability Research, 49(2), 159–169.
urd, L., Vesely, B., Martsolf, J., & Korbeshian, J. (1990). Prevalence studyof Prader-Willi syndrome in North Dakota. American Journal of MedicalGenetics, 37(1), 97–99.
utler, M., & Thompson, T. (2000). Prader-Willi syndrome: Clinical and genet-ical findings. The Endocrinologist, 10, 3–16.
assidy, S. B. (1997). Prader-Willi syndrome. Journal of Medical Genetics,34(11), 917–923.
astelli, F., Glaser, D. E., & Butterworth, B. (2006). Discrete and analoguequantity processing in the parietal lobe: A functional MRI study. Proceedingsof the National Academy of Science, 103(12), 4693–4698.
urfs, L. M., Wiegers, A. M., Sommers, J. R., Borghgraef, M., & Fryns, J. P.(1991). Strengths and weakness in the cognitive profile of youngsters withPrader-Willi syndrome. Clinical Genetics, 40(6), 430–434.
urfs, L. M., Hoondert, G., van Lieshout, V. C. F. M., & Fryns, J. P. (1995).Personality profiles of youngsters with Prader-Willi syndrome and young-sters attending regular schools. Journal of Intellectual Disability Research,39(3), 241–248.
ehaene, S., Bossini, S., & Giraux, P. (1993). The mental representation of par-
ity and number magnitude. Journal of Experimental Psychology: General,122(3), 371–396.elazer, M., Girelli, L., Grana, A., & Domahs, F. (2003). Number processingand calculation—normative data from healthy adults. The Clinical Neuropsy-chologist, 17(3), 331–350.
W
logia 46 (2008) 206–212
i Luca, S., Grana, A., Semenza, C., Seron, X., & Pesenti, M. (2006). Finger-digit compatibility in Arabic numeral processing. Quarterly Journal ofExperimental Psychology, 59(9), 1648–1663.
ykens, E. M. (2002). Are jigsaw puzzle skills ‘spared’ in persons withPrader-Willi syndrome? Journal of Child Psychology and Psychiatry, 43(3),343–352.
ykens, E. M., Cassidy, S. B., & King, B. H. (1999). Maladaptive behaviordifferences in Prader-Willi syndrome due to paternal deletion versus mater-nal uniparental disomy. American Journal of Mental Retardation, 104(1),67–77.
ykens, E. M., Hodapp, R. M., Walsh, K., & Nash, L. J. (1992). Profiles, cor-relates, and trajectories of intelligence in Prader-Willi syndrome. Journal ofthe American Academy of Child and Adolescent Psychiatry, 31(6), 1125–1130.
arthwaite, P. H., & Crawford, J. R. (2004). The distribution of the differencebetween two t-variates. Biometrika, 91, 987–994.
olm, V. (1981). The diagnosis of Prader-Willi syndrome. In V. Holm, S.Sulzbacher, & P. Pipes (Eds.), Prader-Willi syndrome (pp. 24–40). Balti-more: University Park Press.
olm, V. A., Cassidy, S. B., Butler, M. G., Hanchett, J. M., Greenswag, L. R.,Whitman, B. Y., et al. (1993). Prader-Willi syndrome: Consensus diagnosticcriteria. Pediatrics, 91(2), 398–401.
asheim, P. (1981). Psychological data and course in psychotherapy of threemildly retarded adolescents with Prader-Willi syndrome. Child PsychiatryQuarterly, 14, 59–63.
olinari, E. (2002). Clinica psicologica in sindromi rare. Aspetti genetici eriabilitativi. Torino: Bollati Boringhieri.
olko, N., Cachia, A., Riviere, D., Mangin, J. F., Bruandet, M., Le Bihan,D., et al. (2003). Functional and structural alterations of the intraparietalsulcus in a development dyscalculia of genetic origin. Neuron, 40(4), 847–858.
aterson, S. J., Girelli, L., Butterworth, B., & Karmiloff-Smith, A. (2006). Arenumerical impairments syndrome specific? Evidence from Williams syn-drome and Down’s syndrome. Journal of Child Psychology and Psychiatry,47(2), 190–204.
oof, E., Stone, W., MacLean, W., Feurer, I. D., Thompson, T., & Butler, M. G.(2000). Intellectual characteristics of Prader-Willi syndrome: Comparison ofgenetic subtypes. Journal of Intellectual Disability Research, 44(1), 25–30.
emenza, C., Delazer, M., Bertella, L., Grana, A., Mori, I., Conti, F., et al. (2006).Is math lateralised on the same side as language? right hemisphere aphasiaand mathematical abilities. Neuroscience Letters, 406(3), 285–288.
emenza, C., Miceli, L., & Girelli, L. (1997). A deficit for arithmetical proce-dures: Lack of knowledge or lack of monitoring? Cortex, 33(3), 483–498.
pinnler, H., & Tognoni, G. (1987). Standardizzazione e taratura italiana di testneuropsicologici. The Italian Journal of Neurological Sciences, 8(Supple-mento 6), 1–118.
tate, M. W., & Dykens, E. M. (2000). Genetics of childhood disorders: XV.Prader-Willi syndrome: Genes, brain and behavior. Journal of the AmericanAcademy of Child and Adolescent Psychiatry, 39(6), 797–800.
ulzbacher, S., Wong, B., McKeen, J., Glock, J., & MacDonald, B. (1981).Long term therapeutic effects of a three month intensive growth group. TheJournal of Clinical Psychiatry, 42(4), 148–153.
alsh, V. (2003). A theory of magnitude: Common control metrics of time,space and quantity. Trends in Cognitive Sciences, 7(11), 483–488.
echsler, D. (1981). Wechsler adult intelligence scale revised (WAIS-R); ver-
hittington, J. E., Holland, A. J., Webb, T., Butler, J., Clarke, D., & Boer, H.(2001). Population prevalence and estimated birth incidence and mortal-ity rate for people with Prader-Willi syndrome in one UK Health Region.Journal of Medical Genetics, 38(11), 792–798.