
Gender, Health and Initiation of Breastfeeding
22
This article was downloaded by: [Lucía Colodro-Conde] On: 25 February 2015, At: 05:39 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Click for updates Women & Health Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wwah20 Gender, Health, and Initiation of Breastfeeding Lucía Colodro-Conde PhD ab , Rosa M. Limiñana-Gras PhD a , M. Pilar Sánchez-López PhD c & Juan R. Ordoñana PhD ab a University of Murcia (Regional Campus of International Excellence ‘Campus Mare Nostrum’), Murcia, Spain b IMIB-Arrixaca, Murcia, Spain c Complutense University of Madrid, Madrid, Spain Accepted author version posted online: 18 Nov 2014.Published online: 06 Feb 2015. To cite this article: Lucía Colodro-Conde PhD, Rosa M. Limiñana-Gras PhD, M. Pilar Sánchez-López PhD & Juan R. Ordoñana PhD (2015) Gender, Health, and Initiation of Breastfeeding, Women & Health, 55:1, 22-41, DOI: 10.1080/03630242.2014.972015 To link to this article: http://dx.doi.org/10.1080/03630242.2014.972015 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Transcript of Gender, Health and Initiation of Breastfeeding
This article was downloaded by: [Lucía Colodro-Conde]On: 25 February 2015, At: 05:39Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Click for updates
Women & HealthPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/wwah20
Gender, Health, and Initiation ofBreastfeedingLucía Colodro-Conde PhDab, Rosa M. Limiñana-Gras PhDa, M. PilarSánchez-López PhDc & Juan R. Ordoñana PhDab
a University of Murcia (Regional Campus of International Excellence‘Campus Mare Nostrum’), Murcia, Spainb IMIB-Arrixaca, Murcia, Spainc Complutense University of Madrid, Madrid, SpainAccepted author version posted online: 18 Nov 2014.Publishedonline: 06 Feb 2015.
To cite this article: Lucía Colodro-Conde PhD, Rosa M. Limiñana-Gras PhD, M. Pilar Sánchez-LópezPhD & Juan R. Ordoñana PhD (2015) Gender, Health, and Initiation of Breastfeeding, Women & Health,55:1, 22-41, DOI: 10.1080/03630242.2014.972015
To link to this article: http://dx.doi.org/10.1080/03630242.2014.972015
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
Women & Health, 55:22–41, 2015Copyright © Taylor & Francis Group, LLCISSN: 0363-0242 print/1541-0331 onlineDOI: 10.1080/03630242.2014.972015
Gender, Health, and Initiation of Breastfeeding
LUCÍA COLODRO-CONDE, PhDUniversity of Murcia (Regional Campus of International Excellence ‘Campus Mare Nostrum’),
and IMIB-Arrixaca, Murcia, Spain
ROSA M. LIMIÑANA-GRAS, PhDUniversity of Murcia (Regional Campus of International Excellence ‘Campus Mare Nostrum’),
Murcia, Spain
M. PILAR SÁNCHEZ-LÓPEZ, PhDComplutense University of Madrid, Madrid, Spain
JUAN R. ORDOÑANA, PhDUniversity of Murcia (Regional Campus of International Excellence ‘Campus Mare Nostrum’),
and IMIB-Arrixaca, Murcia, Spain
The aim of this study was to explore the associations of health, gen-der, and motherhood with the decisions about breastfeeding. Thesample consisted of 265 pregnant women (mean age: 32.34, SD:4.01 years) who were recruited in healthcare centers and hospi-tals in southeast Spain between 2010 and 2011. Mental health wasmeasured by the 12-Item General Health Questionnaire and gen-der by the Conformity to Feminine Norms Inventory. Women in oursample showed a higher conformity to gender norms than womensurveyed in the adaptation of the inventory to the Spanish popula-tion (t = 11.25, p < 0.001, effect estimate (Cohen’s d) = 0.59). Afteradjustment for covariates, women who exclusively breastfed did notdiffer significantly in their conformity to gender norms from thosewho used partial breastfeeding or bottle feeding. Although good,our expectant mothers had worse mental health than the womenaged 15–44 years in the Spanish National Health Survey (t = 2.96,p < 0.001, d = 0.26). Those who partially breastfed had signifi-cantly better mental health values. Gender norms were modulatorsin a model of factors related to initiation of breastfeeding. This
Received July 8, 2013; revised March 7, 2014; accepted March 13, 2014.Address correspondence to Lucía Colodro-Conde, PhD, University of Murcia (Regional
Campus of International Excellence ‘Campus Mare Nostrum’), 30100 Murcia, Spain. E-mail:[email protected]
22
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

Gender, Health, and Breastfeeding 23
study provides information about health and social constructionof gender norms.
KEYWORDS breastfeeding, health, gender
INTRODUCTION
Substantial evidence suggests that breastfeeding has significant biopsychoso-cial benefits for women, babies, and society as a whole (WHO 2003). Hence,breastfeeding has been considered a health behavior (Kong and Lee 2004).Public health programs have been very focused on increasing breastfeed-ing rates, but multidisciplinary research is recommended to identify effectiveways promote it (WHO 2003).
Feminist analyses of breastfeeding as a key public health issue havebeen scarce (Blum 1999; Boblel 2001; Carter 1995; Gordon 1989; Wall 2001).In some contexts, infant feeding has been medicalized and commercialized,while women’s capacity to breastfeed has been undermined (Smith 2008),and some earlier works (Blum 1993; Carter 1995) have concluded that notonly bottle feeding but breastfeeding as well have become medicalized (Wall2001). Certain educational breastfeeding materials focus on the unique, inti-mate, and embodied connection between mother and child and the benefitsand technical advice, but forget the mother who has legitimate needs andwants (Wall 2001) and tend to unify the discourse without taking into accountsituational or contextual issues (Esteban 2003). The outcome has been thatlittle is known about the effects of the current social and sanitary contextson the well-being and health of women when they have children. In aneffort to understand the decision making of women regarding the way offeeding children, a substantial amount of literature has aimed to describe thesocio-demographic predictors of the initiation and duration of breastfeeding(Callen and Pinelli 2004) and structural factors, such as working conditionsand those circumstances related to the women’s partners and family, thesocial milieu where they live, and their health interventions (Barona-Vilar,Escribá-Agüir, and Ferrero-Gandía 2009; Earle 2002; Ekström, Wiström, andNisse 2003; Swanson and Power 2005). Nonetheless, recent studies havereported the implication of certain psychosocial factors in exclusive breast-feeding duration (de Jager et al. 2013; O’Brien, Buikstra, and Hegney 2008).
Some studies have highlighted the importance of roles and identity gen-der in processes related to motherhood and adherence to breastfeeding.Motherhood has sometimes been conceptualized as feminine identity as anadult (Woollett and Phoenix 1991) and women’s gender identity has beenfound to be reinforced by mothering (Arendell 2000). Moreover, it has beenobserved that parents (especially, first-time parents) become more traditionalin their gender-role attitudes and behavior following the birth of a child and
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

24 L. Colodro-Conde et al.
that women change more than men (Katz-Wise, Priess, and Hyde 2010).The study conducted by Hernández and Callahan (2008) identified threefactors determining high endorsement for breastfeeding: to fulfill genderroles, to prevent health risks, and because of external encouragement; littleendorsement was given for the physiological advantages for babies, pleasantsensations, and preference factors.
Other works have proposed the use of the concept of social gendernorm to make sexual roles operative (Mahalik 2000; Mahalik et al. 2003,2005). Here, gender has been defined as a concept constructed on sexualrole, as a consequence of a developmental process by which social expec-tations and norms are internalized (Limiñana-Gras, Corbalán-Berná, andSánchez-López 2010), so gender, together with biological, temperamental,personal, socioeconomic, and environmental differences, shapes the healthrisk and promotion factors in women and men (Limiñana-Gras 2006).
We attempted to explore the relationships among the conformity to gen-der roles, specific health outcomes, and breastfeeding. We focused on thefirst month of maternity, when the adaptation process to the new situationis crucial, and on exclusive breastfeeding, as WHO (2001) recommends. Ourmain objective was to describe the connection between health and gender,by means of measuring the conformity to feminine gender norms in expec-tant mothers, and its relationship with motherhood and breastfeeding. Theworking hypotheses we proposed were based on previous studies, reportedabove, about the associations among motherhood, breastfeeding, femininity,and gender roles and attitudes (Arendell 2000; Katz-Wise, Priess, and Hyde2010; Hernández and Callahan 2008; Woollett & Phoenix 1991), and the rel-evance of gender as a health risk and promotion factor (Limiñana-Gras 2006;Sánchez-López, Cuéllar-Flores, and Dresch 2012):
1. The conformity to feminine gender norms in the selected sample ofexpectant mothers would be higher than the conformity in the refer-ence population. Additionally, the conformity to feminine gender normsof women who exclusively breastfed one month after childbirth wouldbe higher than conformity in the reference population and also higher incomparison with those in our sample who used partial breastfeeding orbottle feeding.
2. Expectant mothers would have at least the same level of physical andpsychological well-being as non-pregnant women of their age.
3. Breastfeeding would be a multifactorial experience in which demo-graphic, clinic, and health variables played a part. The association of thesefactors with the probability of breastfeeding would be modulated by theconformity to gender norms.
To summarize, our research aimed to help to understand therelationships among health, initiation of breastfeeding, and the modulationby gender in expectant mothers.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

Gender, Health, and Breastfeeding 25
MATERIALS AND METHODS
Participants
Fifteen primary care health centers (42% of the total existing centers in thearea) and two hospitals were contacted and agreed to participate in thestudy. A field researcher set one date to visit each of the health centers(67.9%) and two different dates to visit each of the hospitals and, withthe support of a midwife working in each center, all women who wereattending childbirth preparation or being assisted for monitoring of preg-nancy on the arranged day/s, were explained the purpose and proceduresof this study and asked to participate in it. Women who were in the thirdtrimester of pregnancy were recruited, and the only inclusion criteria were tobe a Spanish-speaking person, willing to complete the questionnaires, andanswer a follow-up phone interview one month after delivery. The responserate ranged from 40 to 80%, being higher in the samples from hospitals.Women with babies with severe complications in the postpartum periodwere excluded from the analyses (8.16%).
A total of 289 women were recruited for the study, but not all of themcould be contacted for the follow-up or were not eligible. Hence, the sam-ple consisted of 265 pregnant women (91.7%) who were assisted for theirlabor in the Murcia and Almería Health Services (Southeast of Spain), during2010 and 2011. To accomplish the aims of our study, they were compared toa national Spanish reference population in their conformity to gender norms,mental health, and self-perceived health.
For the conformity to gender norms, the reference population consistedof the women surveyed for the Spanish adaptation of this questionnaire(Sánchez-López et al. 2009), in which the International Test Commission’s(2000) international guidelines for the adaptation of tests were followed.Women were enrolled for this survey from college campuses throughclassroom recruitment. Then, snowball sampling was used, such that exist-ing study participants recruited more participants among their colleagues,friends, and acquaintances into the sample. Each student was asked to bringtwo questionnaires completed by two adult women with certain demo-graphic characteristics regarding age, educational level, and work activity,achieving Mahalik et al.’s (2005) recommendation about the need to includewomen with diverse demographic characteristics to obtain a good theoreticaland clinical perspective in the adaptation. The total sample of the Spanishadaptation for this questionnaire consisted of 780 women. According to theauthors, the participation rate was 87.86% of the eligible sample participation(Sánchez-López et al. 2009). For mental health and self-perceived health,the reference population consisted of women aged 15 to 44 years fromthe Spanish National Health Survey conducted by the National Institute ofStatistics in a partnership agreement with the Ministry of Public Health, SocialServices and Equality in Spain. Its main objective was to obtain data on the
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

26 L. Colodro-Conde et al.
state of health and determinant factors from the citizens’ viewpoint. Samplingwas stratified in three phases. The first stage units were the census sections,and the second ones were the main family dwellings, with all the habitualresidences included. Within each selected household, an adult (over the ageof 15 years) was selected to complete the individual Adult Questionnaire bymeans of a random procedure assigning equal probability to all adults in thehousehold. The data collection was by computer-assisted personal interview.A sample of approximately 24,000 dwellings distributed in 2,000 census tractswas selected, and the overall participation rate was 71.19%. Regarding theadult women expected to answer the Adult Questionnaire, 72.67% partici-pated (the rest of them refused, were absent, or unable to answer). Amongwomen under 40 years old, 72.54% collaborated with the Spanish NationalHealth Survey (INE, 2012: http://www.ine.es/).
Measurement Instruments
We used four questionnaires, three of them at the time of recruitment andthe last one in a telephone interview after delivery:
The first questionnaire was designed for this study, collecting basic demo-graphic, clinical, breastfeeding, and health related data. Items were basedon common epidemiological surveys (e.g., Spanish National Health Survey2011/2012).
The 12-Item General Health Questionnaire (GHQ-12; Goldberg andWilliams 1988; Spanish adaptation by Sánchez-López and Dresch 2008)was used to measure mental health, as it was for the Spanish NationalHealth Survey (Ministerio de Sanidad, Servicios Sociales e Igualdad (MSSSI)2012). This is an extensively used screening instrument that detects tem-porary alterations of normal psychological functioning and, to a lesserextent, stable disorders; it also includes stress-related alterations of adap-tive behavior (Sánchez-López et al. 2008). GHQ-12 items were rated byrespondents on a 4-point Likert scale, stating whether they had recentlyexperienced a particular symptom or behavior. The first two of theseanswers were categorized as no psychological distress and the two remain-ing answers as psychological distress. The GHQ-12 gives a total scoreranging from 0 to 12. In the Spanish population of women (Sánchez-Lópezand Dresch 2008), Cronbach’s alpha was 0.75.
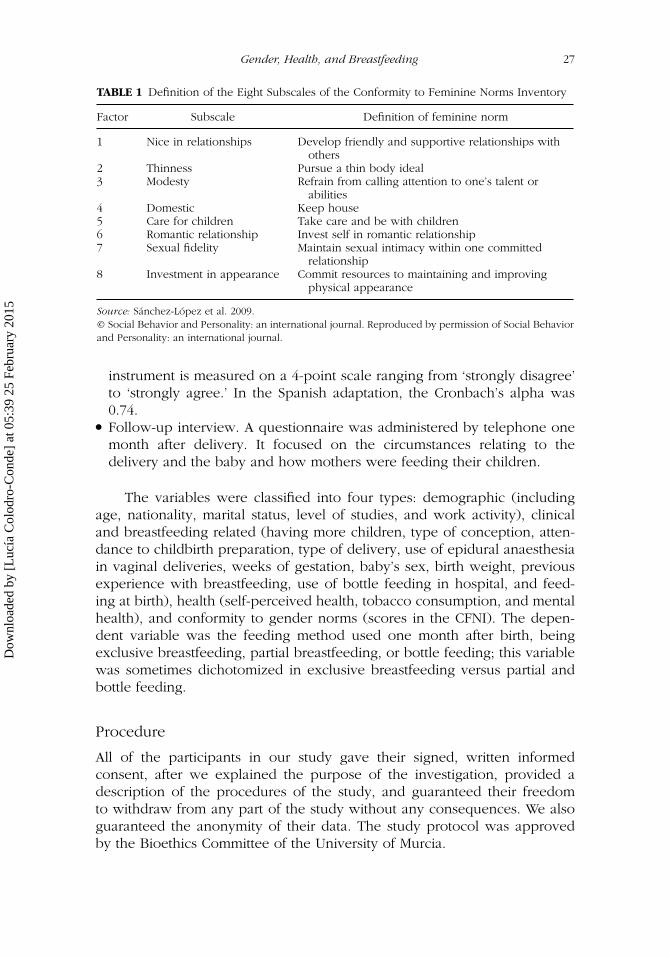
Gender was measured by means of the Conformity to Feminine NormsInventory (CFNI; Mahalik et al. 2005; Spanish adaptation by Sánchez-Lópezet al. 2009). This questionnaire has 84 items that evaluate the degreeof conformity to a series of feminine norms (Table 1). The statementswere designed to measure various attitudes, beliefs, and behaviors asso-ciated with feminine gender roles, both traditional and untraditional. The
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
Gender, Health, and Breastfeeding 27
TABLE 1 Definition of the Eight Subscales of the Conformity to Feminine Norms Inventory
Factor Subscale Definition of feminine norm
1 Nice in relationships Develop friendly and supportive relationships withothers
2 Thinness Pursue a thin body ideal3 Modesty Refrain from calling attention to one’s talent or
abilities4 Domestic Keep house5 Care for children Take care and be with children6 Romantic relationship Invest self in romantic relationship7 Sexual fidelity Maintain sexual intimacy within one committed
relationship8 Investment in appearance Commit resources to maintaining and improving
physical appearance
Source: Sánchez-López et al. 2009.© Social Behavior and Personality: an international journal. Reproduced by permission of Social Behaviorand Personality: an international journal.
instrument is measured on a 4-point scale ranging from ‘strongly disagree’to ‘strongly agree.’ In the Spanish adaptation, the Cronbach’s alpha was0.74.
Follow-up interview. A questionnaire was administered by telephone onemonth after delivery. It focused on the circumstances relating to thedelivery and the baby and how mothers were feeding their children.
The variables were classified into four types: demographic (includingage, nationality, marital status, level of studies, and work activity), clinicaland breastfeeding related (having more children, type of conception, atten-dance to childbirth preparation, type of delivery, use of epidural anaesthesiain vaginal deliveries, weeks of gestation, baby’s sex, birth weight, previousexperience with breastfeeding, use of bottle feeding in hospital, and feed-ing at birth), health (self-perceived health, tobacco consumption, and mentalhealth), and conformity to gender norms (scores in the CFNI). The depen-dent variable was the feeding method used one month after birth, beingexclusive breastfeeding, partial breastfeeding, or bottle feeding; this variablewas sometimes dichotomized in exclusive breastfeeding versus partial andbottle feeding.
Procedure
All of the participants in our study gave their signed, written informedconsent, after we explained the purpose of the investigation, provided adescription of the procedures of the study, and guaranteed their freedomto withdraw from any part of the study without any consequences. We alsoguaranteed the anonymity of their data. The study protocol was approvedby the Bioethics Committee of the University of Murcia.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

28 L. Colodro-Conde et al.
Data Analyses
Descriptive and analytical unadjusted statistical procedures includedPearson’s correlation coefficient, Chi Square test, contingent coefficient,Student t and ANOVA, which were applied to explore the variables andthe relationships among them.
Measures of conformity to feminine gender norms were compared tothe reference Spanish population by means of Student t and Cohen’s d,calculated based on sample size (Hedges’ Adjustment) to control the differ-ences in the sample size. A hierarchical cluster analysis was conducted usingWard’s method with Euclidean distances, based on a principal componentsanalysis with Varimax rotation (KMO = .67), to define the groups of womenwith extreme clusters. Finally, a multiple logistic regression was performedto calculate the relations of certain variables to exclusive breastfeeding.A full regression model was used, including the 5 demographic variables,the 11 clinical and breastfeeding related variables, and the 3 health-relatedvariables, and retaining those independent variables that reached statisticalsignificance (p < 0.05) in relation to exclusive breastfeeding, by means ofa backward stepwise procedure (stepwise regression). This model showedan adequate fit according to Hosmer and Lemeshow test (χ2 (7) = 1.33,p = 0.99). The interaction between breastfeeding initiation and cluster wasexamined. All of the analyses were conducted with SPSS v.19.
RESULTS
Women in our sample were Spanish (92.3%) or from a Spanish-speakingcountry. Mean age was 32.34 years (SD = 4.01), ranging from 21 to 44 years.Most of them were married (n = 224, 84.5%) and 75.5% (n = 200) wereworking. Concerning educational level, 47.5% (n = 126) had college degrees,41.5% (n = 109) had completed secondary school, and 10.2% (n = 27) hadcompleted primary school. The reference population used to study thedegree of conformity to gender norms consisted of 780 Spanish womenbetween 18 and 59 years of age (mean = 31.39 years, SD = 10.93), amongwhom 63.9% were working. Most of them (75.5%) had college degrees,and they lived in different regions in Spain. Consequently, the range ofages of women in our sample was smaller than in the reference popula-tion. More women in our sample were working, and the percentage witha college degree was lower; also, they lived in the Southeast of Spain,while the reference population resided in different regions in our country.In the analysis of the scores in the GHQ-12 and self-perceived health, thereference population consisted of women aged 15 to 44 years who were sur-veyed in the Spanish National Health Survey, which was more similar to oursample.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

Gender, Health, and Breastfeeding 29
One hundred and sixty women (60.4%) reported using exclusivebreastfeeding one month after delivery; 51 (20.4%) were using formula milk,and the remaining 54 (19.2%) were feeding their babies with both methods.
Gender, Health, and Breastfeeding
The reliability of the CFNI indicated that the internal consistency of theinstrument was acceptable (α = 0.84), being similar to that of the Spanishadaptation. Women in our sample had a significantly higher total score inthe CFNI than the adult Spanish women reference population (t = 11.25,p < 0.001, d = 0.59). Specifically, they showed higher conformity withsix of the eight scales: Thinness, Domestic, Care for children, Involvementin romantic relationships, Sexual fidelity, and Investment in appearance.Cohen’s d ranged from 0.22 to 0.64. (Table 2).
In unadjusted analyses, the total score obtained in the CFNI in womenwho established exclusive breastfeeding was significantly higher than the ref-erence population (t = 7.83, p < 0.001, d = 0.55), but the norms did not dif-fer significantly from those who used partial breastfeeding or bottle feeding.
Regarding their perceived health during last year, 83.4% of womenreported that it had been good or very good; this is similar to the perceivedhealth of the Spanish reference population (p = 0.73). The self-perceivedhealth status was not related to the method of infant feeding one monthafter delivery.
In unadjusted evaluations, the mean score in the GHQ-12 during preg-nancy was 2.50 (SD = 2.56), meaning good mental health, according to
TABLE 2 Means and Standard Deviations of the CFNI Scales in the Sample of ExpectantMothers and in the Reference Population, Difference of Means
Expectant-mothers
(N = 261)Mean (SD)b
Women Spanishpopulationa
(N = 780)Mean (SD) t Effect size (d)
1. Nice in relationships 35.96 (5.10) 36.15 (6.30) −.612. Thinness 16.36 (5.27) 15.18 (5.44) 3.61∗∗∗ 0.223. Modesty 13.41 (3.01) 13.16 (3.38) 1.324. Domestic 18.48 (3.14) 16.05 (4.01) 12.51∗∗∗ 0.645. Care for children 24.65 (5.64) 21.84 (6.57) 8.05∗∗∗ 0.446. Romantic
relationship14.87 (2.94) 13.72 (3.48) 6.31∗∗∗ 0.34
7. Sexual fidelity 18.89 (4.72) 16.03 (5.45) 9.78∗∗∗ 0.548. Investment in
appearance12.18 (3.23) 11.09 (3.40) 5.45∗∗∗ 0.32
Total 154.79 (16.62) 143.22 (20.51) 11.25∗∗∗ 0.59
aData from Sánchez-López et al. (2009).bRange of scores of the scales was from 3 to 50. Range of total score was from 111 to 199.∗∗∗p < .001.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
30 L. Colodro-Conde et al.
Goldberg et al. (1997). However, compared with the Spanish reference pop-ulation, the women in our study sample had significantly worse unadjustedmental health (t = 7.44, p < 0.001), the best mental health being for thosewho partially or exclusively breastfed and the worse for those who bottlefed (F = 3.65, p < 0.05).
Breastfeeding as a Multifactorial Experience: The Modulationof Gender
In our sample, the only demographic, clinical, and breastfeeding-related vari-ables showing a relation to exclusive breastfeeding one month after deliverywere: not working (c = 0.12; p < 0.05), vaginal delivery (77.4% versus 65.4%;c = 0.13; p < 0.05). Additionally, in unadjusted analyses, more women usingexclusive breastfeeding had attended childbirth preparation (84.6% versus72.8%; c = 0.14; p < 0.05), had previous experience in breastfeeding (34.6%versus 22.1%; c = 0.13; p < 0.05), had been breastfed as an infant (78.44%versus 64%; c = 0.13; p < 0.05), not having received epidural anaesthesia ifthey had had a vaginal delivery (92.5% versus 79.5%; c = 0.17; p < 0.05) andhad not experienced bottle feeding at the hospital1 (79.4% versus 36.8%;c = 0.38; p < 0.001).
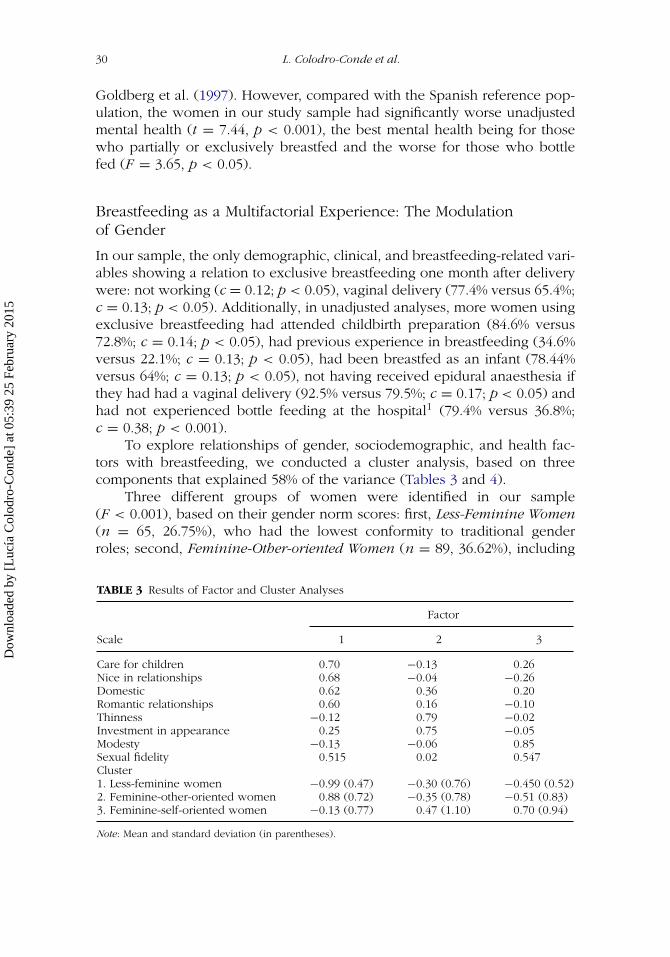
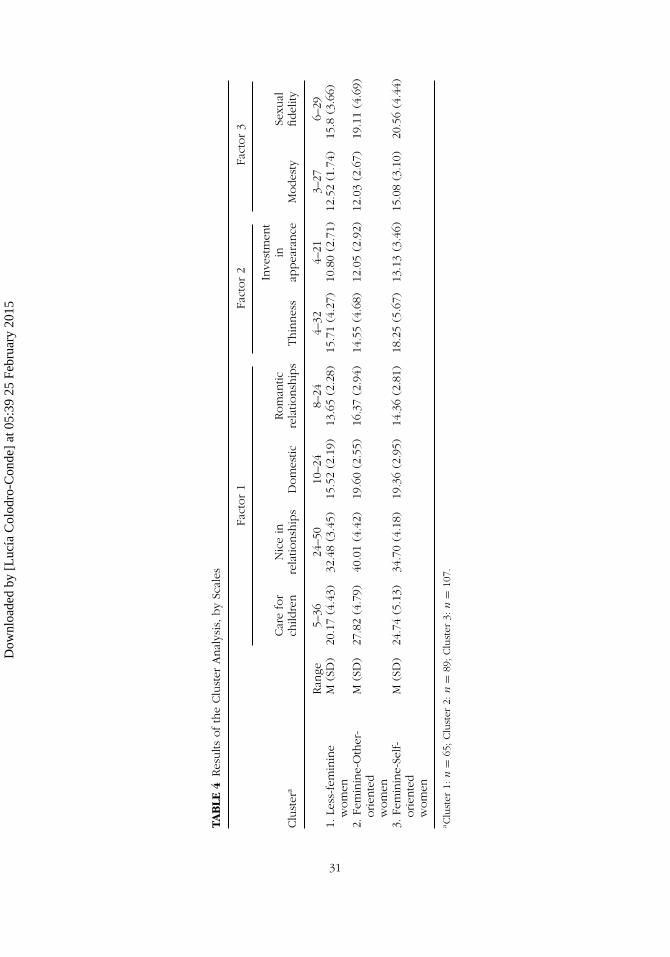
To explore relationships of gender, sociodemographic, and health fac-tors with breastfeeding, we conducted a cluster analysis, based on threecomponents that explained 58% of the variance (Tables 3 and 4).
Three different groups of women were identified in our sample(F < 0.001), based on their gender norm scores: first, Less-Feminine Women(n = 65, 26.75%), who had the lowest conformity to traditional genderroles; second, Feminine-Other-oriented Women (n = 89, 36.62%), including
TABLE 3 Results of Factor and Cluster Analyses
Factor
Scale 1 2 3
Care for children 0.70 −0.13 0.26Nice in relationships 0.68 −0.04 −0.26Domestic 0.62 0.36 0.20Romantic relationships 0.60 0.16 −0.10Thinness −0.12 0.79 −0.02Investment in appearance 0.25 0.75 −0.05Modesty −0.13 −0.06 0.85Sexual fidelity 0.515 0.02 0.547Cluster1. Less-feminine women −0.99 (0.47) −0.30 (0.76) −0.450 (0.52)2. Feminine-other-oriented women 0.88 (0.72) −0.35 (0.78) −0.51 (0.83)3. Feminine-self-oriented women −0.13 (0.77) 0.47 (1.10) 0.70 (0.94)
Note: Mean and standard deviation (in parentheses).
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
TAB
LE4
Res
ults
ofth
eClu
ster
Anal
ysis
,by
Scal
es
Fact
or
1Fa
ctor
2Fa
ctor
3
Clu
ster
aCar
efo
rch
ildre
nN
ice
inre
latio
nsh
ips
Dom
estic
Rom
antic
rela
tionsh
ips
Thin
nes
s
Inve
stm
ent
inap
pea
rance
Modes
tySe
xual
fidel
ity
Ran
ge5–
3624
–50
10–2
48–
244–
324–
213–
276–
291.
Less
-fem
inin
ew
om
enM
(SD
)20
.17
(4.4
3)32
.48
(3.4
5)15
.52
(2.1
9)13
.65
(2.2
8)15
.71
(4.2
7)10
.80
(2.7
1)12
.52
(1.7
4)15
.8(3
.66)
2.Fe
min
ine-
Oth
er-
orien
ted
wom
en
M(S
D)
27.8
2(4
.79)
40.0
1(4
.42)
19.6
0(2
.55)
16.3
7(2
.94)
14.5
5(4
.68)
12.0
5(2
.92)
12.0
3(2
.67)
19.1
1(4
.69)
3.Fe
min
ine-
Self-
orien
ted
wom
en
M(S
D)
24.7
4(5
.13)
34.7
0(4
.18)
19.3
6(2
.95)
14.3
6(2
.81)
18.2
5(5
.67)
13.1
3(3
.46)
15.0
8(3
.10)
20.5
6(4
.44)
aClu
ster
1:n
=65
;Clu
ster
2:n
=89
;Clu
ster
3:n
=10
7.
31
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

32 L. Colodro-Conde et al.
women who were very focused on relationships or on care; and last,Feminine-Self-oriented Women (n = 107, 44.03%) who agreed with theimportance of being thin and having a better physical appearance and didnot usually like to show their talent.
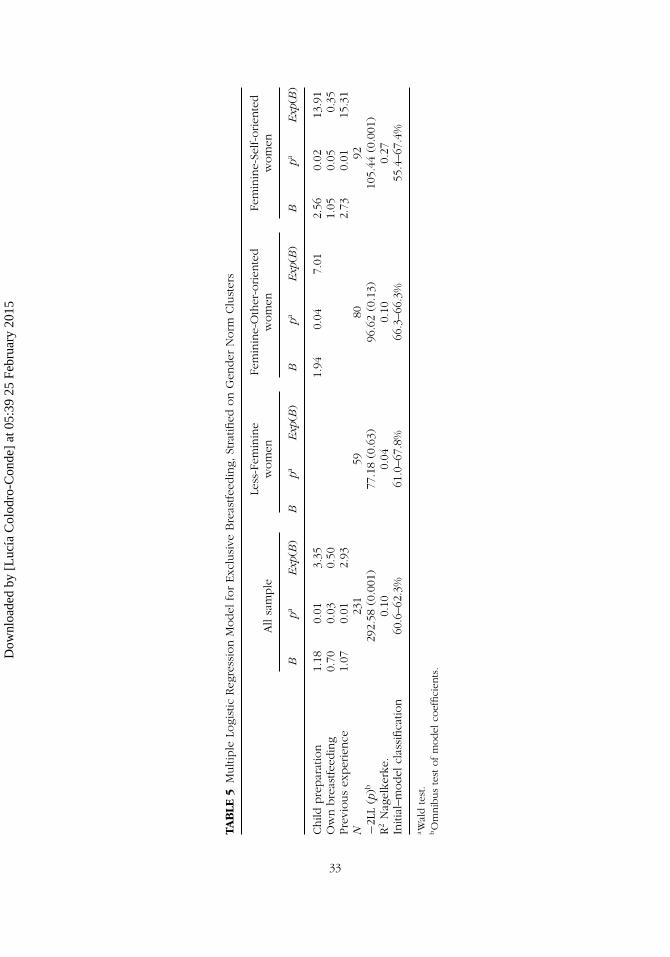
The conformity to gender norms showed modulation in a model webuilt to analyze factors related to the initiation of exclusive breastfeeding(Table 5). In this multivariable model, we controlled for the three gendernorm clusters, that is, the three groups of women previously identifiedaccording to their different conformity to feminine norms. We observed thatthe variables most related to the probability of breastfeeding exclusively inthe whole sample were: having attended at childbirth preparation, believingthat they had been breastfed, and having previous experience breastfeeding.However, these variables not always were significantly related to theprobability to establishing exclusive breastfeeding when we consideredwomen’s conformity to gender norms—the gender norm cluster—that is,none of these three variables included in the model were significantlyrelated to the probability of initiating exclusive breastfeeding for women inthe groups called either Less-Feminine Women or Feminine-Other-orientedWomen. However, these three variables were related to a higher probabilityof initiation of exclusive breastfeeding for the Feminine-Self-oriented Womengroup, and this relation was even stronger than the one found in the wholesample. Consequently, Feminine-Self-oriented Women had a higher proba-bility of exclusively breastfeeding if they had attended childbirth preparation(OR = 13.91, CI 95%: 1.55, 107.23), if they had been breastfed (OR = 0.35,CI 95%: 0.12, 1.0) and if they had experience in breastfeeding (OR = 15.31,CI 95%: 1.80, 130.22). Thus, from this multiple logistic regression model,the relation of some variables with the probability to breastfeed exclusivelydiffered when conformity to gender norms of the expectant mothers wastaken into account.
DISCUSSION
The objective of this study was to explore the relationships among con-formity to feminine norms, some health variables, and the processes ofmotherhood and the method selected to feed infants one month after deliv-ery. Our main aim was to understand better the psychology of women tofacilitate the design of health interventions oriented to their well-being inrelation to their reproductive lives.
Gender, Health, and Breastfeeding
Our former hypothesis stated, first, that conformity to feminine gender normsin our sample of expectant mothers would be higher than the conformity
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
TAB
LE5
Multi
ple
Logi
stic
Reg
ress
ion
Model
for
Exc
lusi
veB
reas
tfee
din
g,St
ratifi
edon
Gen
der
Norm
Clu
ster
s
All
sam
ple
Less
-Fem
inin
ew
om
enFe
min
ine-
Oth
er-o
rien
ted
wom
enFe
min
ine-
Self-o
rien
ted
wom
en
Bpa
Exp
(B)
Bpa
Exp
(B)
Bpa
Exp
(B)
Bpa
Exp
(B)
Child
pre
par
atio
n1.
180.
013.
351.
940.
047.
012.
560.
0213
.91
Ow
nbre
astfee
din
g0.
700.
030.
501.
050.
050.
35Pre
vious
exper
ience
1.07
0.01
2.93
2.73
0.01
15.3
1N
231
5980
92−2
LL(p
)b29
2.58
(0.0
01)
77.1
8(0
.63)
96.6
2(0
.13)
105.
44(0
.001
)R
2N
agel
kerk
e.0.
100.
040.
100.
27In
itial
–model
clas
sifica
tion
60.6
–62.
3%61
.0–6
7.8%
66.3
–66.
3%55
.4–6
7.4%
aW
ald
test
.bO
mnib
us
test
ofm
odel
coef
fici
ents
.
33
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

34 L. Colodro-Conde et al.
found in the reference population; that conformity of those women whoestablished exclusive breastfeeding would be higher than conformity in thereference population; and that conformity of women who were breastfeedingexclusively would be also higher than those in our sample who used partialbreastfeeding and bottle feeding. This hypothesis was partially confirmed.Indeed, the conformity to feminine norms was higher for the whole sampleof expectant mothers than the Spanish reference population. This is coherentwith the conclusions of such authors as Woollett and Phoenix (1991) andArendell (2000), that being a mother reinforced feminine identity. It alsoagrees with the conclusion of previous studies about the more traditionalgender-role attitudes and behavior in new mothers (Katz-Wise, Priess, andHyde 2010). On the other hand, women who exclusively breastfed afterone month had higher conformity to feminine norms than the referencepopulation. However, this group of women did not have higher conformityto feminine norms than those who partially breastfed or bottle fed. Therefore,we could state that these women had specific gender behavioral patterns,more similar to the feminine gender stereotypes that were related to theexperience of motherhood, but not to the decision about breastfeeding.
Our second hypothesis stated that women in this sample would have atleast the same health levels as women of their age. As expected, perceivedself-status of expectant mothers in our sample, regardless of the methodof feeding children they used later, was the same as women of the sameage group of the general Spanish population. The mental health of ourstudy sample was also good, but it was significantly worse than the mentalhealth of the reference population, according to the results of the NationalHealth Survey (MSSSI 2012). It is possible that, during pregnancy, theirpsychological well-being worsened and that this situation was reversedover time. Regarding the relationship between mental health and themethod of feeding infants, we found that women with the best mentalhealth combined both breast and bottle feeding, or exclusively breastfed,followed by those who bottle fed. This is consistent with several studiesthat have found a relationship between anxiety, stress, and/or postpartumdepression and an early abandonment of breastfeeding (Cooke, Schmied,and Sheehan 2007; Paricio et al. 1999; Tarkka, Paunonen, and Laippala 1999)and between depression during pregnancy and decreased breastfeedinginitiation (Grigoriadis et al. 2013).
Breastfeeding as a Multifactorial Experience: The Modulationof Gender
The review of demographic variables revealed ‘work status’ as the mostrelevant in relation to the initiation of breastfeeding. Those who wereunemployed were more likely to establish exclusive breastfeeding. This isconsistent with some studies that have found a relationship between return
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

Gender, Health, and Breastfeeding 35
to work and the initiation and duration of breastfeeding (Calnen 2010): ini-tiation rates are not significantly related to employment status, but they arewhen women return to work shortly after delivery (6 weeks of delivery); andbreastfeeding duration is significantly longer for nonworking than for work-ing mothers. Other variables that have consistently appeared to be associatedwith initiation of breastfeeding (de Jager et al. 2013)—maternal age, socio-economic status, level of education, and marital status—were not relatedto this outcome in our sample, possibly because our sample did not haveenough variability regarding these variables. Also, if breastfeeding is becom-ing the norm, variables such as level of education lose relevance; in fact, atrend seems to be appearing in Spain such that women with less educationare increasing their rates of breastfeeding faster than women with greatereducation, and it is possible that the differences will become insignificant(MSC 2006). Apart from that, not all of the factors related to breastfeedingare constant within and between societies and they may vary over the years(Colodro-Conde et al. 2011).
Regarding the clinical and breastfeeding variables, having attendedchildbirth preparation, having had a vaginal delivery, and not having usedepidural anesthesia (in the case of vaginal deliveries) were variables relatedto a higher probability to breastfeed. Women who had previous experiencebreastfeeding, those who had not used bottle feeding at the hospital, andthose women who thought that they were breastfed as an infant, were alsomore likely to breastfeed exclusively than those who had not. Similar resultshave been reported before regarding education and support for breastfeed-ing as an integral part of childbirth education classes (Lu et al. 2003), vaginaldelivery versus cesarean section (Barriuso et al. 2000; Estévez et al. 2002), useof epidural anesthesia (Baumgarder et al. 2003; Gubler et al. 2012), previousexperience in breastfeeding (Romero et al. 2004), use of supplemental for-mula in the nursery (Baumgarder et al. 2003), and breastfed women (Wagneret al. 2006).
Our analyses revealed three defined groups according to the conformityto gender norms and a differential relation of some variables to breastfeed-ing according to the different conformity to gender norms detected in oursample. Feminine-Self-oriented Women had the lowest, although not signifi-cant, probability to breastfeed. This probability was increased when they hadattended childbirth preparation, when they were breastfed as an infant, andwhen they had previous experience with breastfeeding. For those womenwho had a clearly feminine and self-oriented social construction of gen-der, the differential relation of these clinical variables to breastfeeding wasstronger than for other groups. This differential relation may have been dueto the positive image of breastfeeding associated with these experiences,which could have facilitated the initiation of breastfeeding, especially inthis group—women having high conformity to gender norms related to thestereotypes of female beauty and appearance.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

36 L. Colodro-Conde et al.
Practical Implications
The findings of this study have some practical implications. Esteban (2000,2003) highlighted that in the expert’s discourse, breastfeeding is limited tothose aspects related to feeding and the baby’s well-being and that breast-feeding is a fundamental area of socialization. Esteban (2000) also statedthat breastfeeding was suffering a process of renaturalization, meaning thatthe emotional dimension was highlighted at the expense of its reproductivework value and, consequently, at the expense of the social and symbolicacknowledgment. Therefore, interventions should increase the value of thereproductive work and have in mind the individuality and integral well-beingof each woman, in addition to focusing on the baby and on the emotionaldimension. Also, a useful framework for a feminist promotion of breastfeed-ing is the one proposed by Smith (2008): she attempted to explore the valuesthat women bring to their decision-making about how to allocate their time,money, energy, and bodies in meeting their needs as individuals, work-ers, and mothers to, finally, repossess breastfeeding. Ecofeminism, similarly,defends breastfeeding that favors recovery of perception and sensibility, inboth the physical body and the psychosomatic areas, so the experience ofbreastfeeding might facilitate a release and reconciliation of women withtheir bodies (Blázquez 2004).
Limitations
The present study had some limitations that should be taken into consider-ation. The main one was the relatively low number of participants, whichcould have resulted in insufficient power to detect some meaningful dif-ferences as statistically significant. In addition, the method of selection ofsample, which was not representative but a convenience sample, could belinked to the low variability that we found in certain demographic variablesand could limit the generalizability of the findings. Finally, part of our samplewas recruited at the beginning of the third trimester of pregnancy and oth-ers at the end, and the psychological processes are different at these stages(Langer 1965).
CONCLUSIONS
In conclusion, women involved in processes of motherhood have a moresimilar behavioral pattern to the feminine gender stereotypes, but they didnot show a differential pattern of conformity to feminine norms accordingto the initiation of any method for feeding infants. Their perceived healthwas the same as that of the reference population and, although their men-tal health was good, it was worse than the general population of women;the best mental health was found in those who breastfed, both partially and
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
Gender, Health, and Breastfeeding 37
exclusively. Finally, the association between some clinical and breastfeedingvariables with the decisions regarding breastfeeding, seemed to be moder-ated by the conformity to traditional norms of femininity, so that gender maybe a small moderator in breastfeeding behaviors.
Our results point out that those women with a clearly feminine andoriented to others social construction of gender and who agreed withaffectivity-related norms, were more likely to breastfeed, although adher-ence to gender norms was not significantly related to breastfeeding. Thesocial construction of gender, its development throughout life, and its conse-quences in the configuration of the feminine identity should be definitivelyexplored further (Esteban 2003).
Women’s decisions regarding maternity, birth control, and nursing havechanged throughout recent decades. This has not occurred in an isolatedcontext, but in a changeable milieu in which social context, norms, andhealth interventions have been modified. Some of the most evident resultsare the modification in both men’s and women’s roles at work and in fam-ily and personal lives. Now more than ever, as Blázquez (2004) stated,breastfeeding should become a right and an act of well-being and health.
ACKNOWLEDGMENTS
We are grateful to the women for their participation in this study. We wouldalso like to thank all of the midwives and healthcare professionals who madepossible the data collection.
FUNDING
The authors disclosed receipt of the financial support for the research,authorship, and/or publication of this article: Lucía Colodro-Conde wassupported by a fellowship provided by the Séneca Foundation—RegionalAgency for Science and Technology, Murcia, Spain (12431/FPI/09).
NOTE
1. Due to different hospital procedures, not all women answered this question. This lastcomparison is based on a reduced n = 180.
REFERENCES
Arendell, T. 2000. Conceiving and investigating motherhood: The decade’s scholar-ship. J Marriage Fam 62:1192–207. doi:10.1111/j.1741-3737.2000.01192.x
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
38 L. Colodro-Conde et al.
Barona-Vilar, C., V. Escribá-Agüir, and R. Ferrero-Gandía. 2009. A qualitativeapproach to social support and breast-feeding decisions. Midwifery 25:187–94.doi:10.1016/j.midw.2007.01.013
Barriuso, L., F. Sánchez-Valverde, C. Romero, and J. C. Vitoria. 2000. Pautas hospi-talarias respecto a la lactancia materna en el centro-norte de España [Hospitalguidelines regarding breastfeeding in the North-Central Spain]. Anales Españolesde Pediatría 52:225–31.
Baumgarder, D. J., P. Muehl, M. Fischer, and B. Pribbenow. 2003. Effect of laborepidural anesthesia on breast-feeding of healthy full-term newborns deliveredvaginally. J Am Board Fam Prac 16:7–13.
Blázquez, M. J. 2004. Ecofeminismo y lactancia [Ecofeminism and breastfeeding].In Libro de Actas del III Congreso Nacional de Lactancia Materna. Santander:Asociación Española de Pediatría.
Blum, L. 1993. Mothers, babies and breastfeeding in late capitalist America: Theshifting contexts of feminist theory. Feminist Studies 19:290–311.
Blum, L. M. 1999. At the breast: Ideologies of breastfeeding and motherhood in thecontemporary United States. Boston, MA: Beacon.
Boblel, C. 2001. Bounded liberation: A focused study of La Leche LeagueInternational. Gender Soc 15:130–51.
Callen, V., and V. Pinelli. 2004. Incidence and duration of breastfeeding for terminfants in Canada, United States, Europe, and Australia: A literature review.Birth 31:4.
Calnen, G. 2010. The impact of maternity leave on breastfeeding rates. BreastfeedingMed 5:233–34. doi:10.1089/bfm.2010.0064
Carter, P. 1995. Feminism, breasts and breastfeeding. New York, NY: St. MartinsPress.
Colodro-Conde, L., J. F. Sánchez-Romera, M. J. Tornero-Gómez, F. Pérez-Riquelme,M. Polo-Tomás, and J. R. Ordoñana. 2011. Relationship between level of edu-cation and breastfeeding duration depends on social context: Breastfeedingtrends over a 40-year period in Spain. J Human Lactation 27:272–78.doi:10.1177/0890334411403929
Cooke, M., V. Schmied, and A. Sheehan. 2007. An exploration of the relation-ship between postnatal distress and maternal role attainment, breast feedingproblems and breast feeding cessation in Australia. Midwifery 23:66–76.doi:10.1016/j.midw.2005.12.003
de Jager, E., H. Skouteris, J. Broadbent, L. Amir, and K. Mellor. 2013. Psychosocialcorrelates of exclusive breastfeeding: A systematic review. Midwifery 29:506–18.doi:10.1016/j.midw.2012.04.009
Earle, S. 2002. Factors affecting the initiation of breastfeeding: Implications forbreastfeeding promotion. Health Promot Int 17:205–14.
Ekström, A., A. M. Wiström, and E. Nisse. 2003. Breastfeeding support from part-ners and grandmothers: Perceptions of Swedish women. Birth 30:261–66.doi:10.1046/j.1523-536X.2003.00256.x
Esteban, M. L. 2000. La maternidad como cultura [Motherhood and culture]. InMedicina y cultura. Estudios entre la antropología y la medicina [Medicine andculture. Studies between anthropology and medicine], ed. E. Perdiguero and J.Comelles, 207–26. Barcelona: Bellaterra.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015
Gender, Health, and Breastfeeding 39
Esteban, M. L. 2003. Cuidado y salud: Costes en la salud de las mujeres y ben-eficios sociales. [Care and health: Costs and benefits in women’s health andsocial benefits]. In Congreso Internacional Sare 2003. Cuidar cuesta: Costes ybeneficios del cuidado, 63–84. Gasteiz: EMAKUNDE/Instituto Vasco de la Mujer.
Estévez, M. D., D. Martell, R. Medina, E. García, and P. Saavedra. 2002. Factoresrelacionados con el abandono de la lactancia materna [Factors related to theabandonment of maternal lactation]. Medicina Fetal Y Neonatología 56:144–50.
Goldberg, D., and P. Williams. 1988. A user’s guide to the General HealthQuestionnaire. Windsor: NFER-Nelson.
Goldberg, D. P., R. Gater, N. Sartorius, T. B. Ustun, M. Piccinelli, O. Gureje, and C.Rutter. 1997. The validity of two versions of the GHQ in the WHO study ofmental illness in general health care. Psychol Med 27:191–97.
Gordon, J. 1989. Choosing” to breastfeed: Some feminist questions. Resourc FeministRes 18:10–12.
Grigoriadis, S., E. H. VonderPorten, L. Mamisashvili, G. Tomlinson, C.-L. Dennis,G. Koren, et al. 2013. The impact of maternal depression during pregnancyon perinatal outcomes: A systematic review and meta-analysis. J Clin Psych74:e321–41. 10.4088/JCP.12r07968
Gubler, T., F. Krähenmann, M. Roos, R. Zimmermann, and N. Ochsenbein-Kölble.2012. Determinants of successful breastfeeding initiation in healthy term sin-gletons: A Swiss university hospital observational study. J Perinatal Med41:331–39.
Hernández, P. T., and S. Callahan. 2008. Attributions of breastfeeding determi-nants in a French population. Birth Iss Perinatal Care 35:303–12. doi:10.1111/j.1523-536X.2008.00257.x
Instituto Nacional de Estadística (INE). 2012. National health survey 2011–2012.http://www.ine.es/ (accessed October 2013).
International Test Commission (ITC). 2000. International guidelines for test use.www.intestcom.org/itc_projects.htm
Katz-Wise, S. L., H. A. Priess, and J. S. Hyde. 2010. Gender-role attitudes and behavioracross the transition to parenthood. Dev Psychol 46:18–28. doi:10.1037/a0017820
Kong, S. K. F., and D. T. F. Lee. 2004. Factors influencing decision to breastfeed. JAdv Nurs 46:369–79. doi:10.1111/j.1365-2648.2004.03003.x
Langer, M. 1965. Maternidad y sexo. Estudio psicoanalítico y psicosomático[Maternity and sex. Psychoanalytic and psychosomatic study]. Buenos Aires:Paidós.
Limiñana-Gras, R. M. 2006. Personalidad y adaptación psicológica parental a la dis-capacidad [Parental personality and psychological adjustment to disability]. PhDthesis, University of Murcia, Murcia, Spain.
Limiñana-Gras, R. M., F. J. Corbalán-Berná, and M. P. Sánchez-López. 2010. Is cre-ativity a modulating variable of the relationship between health and gender?In School and health 21st century. Health education: International experiences,ed. E. Rehulka, 221–32. Brno, Czech Republic: Masarykova univerzita.
Lu, M. C., J. Prentice, S. M. Yu, M. Inkelas, L. O. Lange, and N. Halfon. 2003.Childbirth education classes: Sociodemographic disparities in attendance andthe association of attendance with breastfeeding initiation. Matern Child HealthJ 7:87–93. doi:10.1023/A:1023812826136
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

40 L. Colodro-Conde et al.
Mahalik, J. R. 2000. A model of masculine gender role conformity. SymposiumMasculine gender role conformity: Examining theory, research, and prac-tice. 108th Annual Convention of the American Psychological Association,Washington, DC.
Mahalik, J. R., B. Locke, L. Ludlow, M. Diemer, R. P. J. Scott, M. Gottfried, and G.Freitas. 2003. Development of the conformity to masculine norms inventory.Psychol Men Masculin 4:3–25. doi:10.1037/1524-9220.4.1.3
Mahalik, J. R., E. B. Morray, A. Coonerty-Femiano, L. H. Ludlow, S. M. Slattery, andA. Smiler. 2005. Development of the conformity to feminine norms inventory.Sex Roles 52:417–35. doi:10.1007/s11199-005-3709-7
Ministerio de Sanidad y Consumo (MSC). 2006. Encuesta Nacional de Salud, 2006[National health survey, 2006]. http://www.msc.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm (accessed May 2012).
Ministerio de Sanidad, Servicios Sociales e Igualdad (MSSSI). 2012. Encuesta Nacionalde Salud de España 2011/2012 [National health survey, 2011/2012]. http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2011.htm (accessed March 2013).
O’Brien, M., E. Buikstra, and D. Hegney. 2008. The influence of psychological factorson breastfeeding duration. J Adv Nurs 63:397–408. doi:10.1111/j.1365-2648.2008.04722.x
Paricio, J. M., L. Santos, A. Fernández, E. Martí, A. Bernal, M. Ferriol, et al.1999. Lactancia materna: Conocimientos; actitudes y ambigüedad sociocultural[Breastfeeding: knowledge, attitudes and cultural ambiguity]. Atención Primaria24:337–42.
Romero, M. E., S. Algaba, M. J. Albar, E. Núñez, C. Calerom, and I. M.Pérez. 2004. Influencia de las prácticas hospitalarias en el inicio y el man-tenimiento de la lactancia materna [Influence of hospital practices in theinitiation and maintenance of breastfeeding]. Enfermería Clínica 14:194–202.doi:10.1016/S1130-8621(04)73885-1
Sánchez-López, M. P., I. Cuéllar-Flores, and V. Dresch. 2012. The impact of genderroles on health. Women Health 52:182–96. doi:10.1080/03630242.2011.652352
Sánchez-López, M. P., I. Cuéllar-Flores, V. Dresch, and M. Aparicio-Garciá. 2009.Conformity to feminine gender norms in the Spanish population. Soc BehavPersonality 37:1171–85. 10.2224/sbp.2009.37.9.1171
Sánchez-López, M. P., and V. Dresch. 2008. The 12-Item General HealthQuestionnaire (GHQ-12): Reliability, external validity and factor structure inthe Spanish population. Psicothema 20:839–43.
Sánchez-López, M. P., J. J. López-García, V. Dresch, and J. Corbalán. 2008.Sociodemographic, psychological and health-related factors associated withpoor mental health in Spanish women and men in midlife. Women Health48:445–65. doi:10.1080/03630240802575096
Smith, P. 2008. “Is it just so my right?” Women repossessing breastfeeding. IntBreastfeeding J 3:12. doi:10.1186/1746-4358-3-12
Swanson, V., and K. Power. 2005. Initiation and continuation of breastfeeding:Theory of planned behaviour. J Adv Nur 50:272–82. doi:10.1111/j.1365-2648.2005.03390.x
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015

Gender, Health, and Breastfeeding 41
Tarkka, M. P., M. Paunonen, and P. Laippala. 1999. Factors related to successfulbreast feeding by first-time mothers when the child is 3 months old. J Adv Nurs29:113–18.
Wagner, C. L., M. T. Wagner, M. Ebeling, K. G. Chatman, M. Cohen, and T. C. Hulsey.2006. The role of personality and other factors in a mother’s decision to initiatebreastfeeding. J Human Lactation 22:16–26.
Wall, G. 2001. Moral constructions of motherhood in breastfeeding discourse. GenderSoc 15:592–610. doi:10.1177/089124301015004006
Woollett, A., and A. Phoenix. 1991. Psychological views of mothering. InMotherhood, meanings, practices and ideologies, ed. A. Phoenix, A. Woollett,and E. Lloyd, 28–46. London: Sage.
World Health Organization. 2001. The optimal duration of exclusive breastfeeding.Note for the Press No 7 . Geneva: World Health Organization.
World Health Organization. 2003. Global strategy for infant and young child feeding.Geneva: World Health Organization.
Dow
nloa
ded
by [
Luc
ía C
olod
ro-C
onde
] at
05:
39 2
5 Fe
brua
ry 2
015




















