Breastfeeding: Global practices, challenges, maternal and infant health outcomes
Upload
independentCategory
view
0download
0
Breast-feeding training for health professionalsand resultant institutional changesM.F. Westphal,1 J.A.C. Taddei,2 S.I. Venancio,3 & C.M. Bogus4
Assessed is a breast-feeding training course that was attended by health professionals at the SantosLactation Center (SLC), Santos, Sao Paulo, Brazil, as well as its impact on the implementation ofbreast-feeding programmes in maternity hospitals. Eight maternity hospitals were studied - four wererandomly allocated to the experimental group and sent three health professionals to attend an 18-daycourse at SLC; the remaining four institutions constituted the control group. The compliance of all eighthospitals with WHO/UNICEF's "Ten steps for successful breast-feeding" was determined using scoresobtained before and 6 months after the training course. Institutions in the experimental group had animproved score, but those in the control group did not.
The SLC training course was efficient since it enabled the participants to promote breast-feedingpractices. However, in order to succeed in implementing breast-feeding programmes, health profession-als require also to develop skills to apply the knowledge they acquire in the course, as well as toinvolve the whole maternity unit team in the activities.
IntroductionBreast-feeding promotion is a basic strategy forcontrolling infant mortality and morbidity. Based ondata from an evaluative study, Rodrigues-Garcia &Schaefer stated that an increase in the length ofbreast-feeding might save 1 million infant lives indeveloping countries (1).
Other studies demonstrate that compared withexclusively breast-fed infants, non-breast-fed infantshave a mean relative risk of morbidity from diar-rhoea of 3.5-4.9 during the first 6 months of life (2,3). In Brazil, Victora et al. showed that the risk ofdying from diarrhoea was 25 times greater during thefirst 6 months of life among infants who were notbreast-fed (4). In Peru similar results were foundwhen the effects of breast-feeding on the frequencyof diarrhoea were evaluated (5).
Despite such evidence, the incidence and dura-tion of breast-feeding have been decreasing, espe-cially in Latin American countries (1). Efforts arenow being made to modify this tendency.
I Associate Professor, School of Public Health; and Researcher,Epidemiological and Nutritional Research Center (NUPENS),University of Sao Paulo, Av. Dr. Arnaldo 715, 01246-904, SaoPaulo-SP, Brazil. Requests for reprints should be sent to thisauthor.2 Associate Professor, Paulista School of Medicine, Federal Uni-versity of Sao Paulo, Sao Paulo, Brazil.3 Paediatrician, Guilherme Alvaro Hospital; and Researcher,ACA Project, NUPENS, University of Sao Paulo, Brazil.4 Public Health Educator, Sao Paulo State Health Department;and Researcher, ACA Project, Sao Paulo, Brazil.
Reprint No. 5620
In Brazil, the national breast-feeding programmewas set up in 1981. Its activities include the creationof labour laws to allow working mothers to breast-feed their babies, implementation of mechanisms tocontrol breast-milk substitutes sold in the market,diffusion of breast-feeding promotion messagesthrough the media, in-service training for health pro-fessionals, use of educational material, and establish-ment of mothers' self-help groups.
In 1987, the programme was evaluated in SaoPaulo (6) and Recife (7), where the average length ofexclusive breast-feeding was found to be 43-67 daysand 14-32 days, respectively. Also, health profes-sionals were found to have increased their under-standing about the theoretical basis for breast-feeding, although they were not able to solve practi-cal breast-feeding problems. These findings indicatethat better training programmes on breast-feeding areneeded for health staff, especially those involved inmaternal and child health care, paying particularattention to the practical aspects.a
In 1989, WHO supported the establishment of acentre for breast-feeding training in Brazil to enablehealth teams to promote breast-feeding activities.WHO's interest in supporting such programmes ismainly based on studies that have shown the impactbreast-feeding can have on infant morbidity andmortality caused by diarrhoea (8).
When the centre was set up a Brazilian healthteam consisting of a paediatrician, an obstetrician,
a Rea MF, Toma TS. [Assessment of a national programme ofincentives for breast-feeding: the practice of professionals].Unpublished, Sao Paulo, 1988 (in Portuguese).
Bulletin of the World Health Organization, 1995, 73 (4): 461-468 © World Health Organization 1995 461

M.F. Westphal et al.
and a nurse were sent for training to the WellstartCenter, San Diego, CA, USA (9). Since completingtraining, the team has been operating at a public hos-pital (Guilherme Alvaro Hospital) in Santos, SaoPaulo. The hospital is linked to Santos MedicalSciences College, where breast-feeding promotionactivities have been carried out for 18 years. Theseactivities include the participation of paediatriciansin antenatal care, encouragement of breast-feeding indelivery rooms, the practice of rooming-in, a special-ized outpatient clinic for the promotion of breast-feeding, as well as training activities for medicalstudents. Recently the hospital has received the"Baby-friendly hospital" award from UNICEF.The Center for Health Professionals Training,Santos Lactation Center (SLC), is also based at thishospital.
Training courses have been offered at the SLCsince 1990 and feedback from the 120 health profes-sionals who have attended them suggest that theyhave introduced changes in the routine in their insti-tutions leading to an increase in the length of timemothers breast-feed their children.
In view of the need to carry out a systematicevaluation of the training centre and its impact onbreast-feeding promotion, we carried out a studythat, inter alia, had the following objectives:
- to identify the positive and negative characteris-tics of the various topics covered in the SLCcourse and hence improve its effectiveness; and
- to quantify and qualify the structural changes thathad occurred in institutions whose staff hadattended the training course, by comparing themwith similar institutions that had not beenexposed to it.
Theoretical framework
The "ten steps for successful breast-feeding" recom-mended by WHO/UNICEF (1) (Table 1) were usedto assess the contents and results of the breast-feeding promotion programmes. This approach wasused because the "ten steps" have been widely adop-ted and UNICEF has identified them as a strategy forimplementing programmes for the promotion ofbreast-feeding (12)
The evaluation of institutional changes resultingfrom the participation of staff in the SLC course wascarried out using the domain theory (10). Kouzes &Mico's theory of institutional domains states thatinstitutions consist of the following distinct domains:the policy, management, and service domains, eachof which operates according to different principles,success measures, structural arrangements, and workmodes (or technologies). The simultaneous existence
Table 1: Ten steps for successful breast-feedingStepnumber Step
1 Have a written breast-feeding policy that is routinelycommunicated to all health staff.
2 Train all health care staff in skills necessary to imple-ment this policy.
3 Inform all pregnant women about the benefits and man-agement of breast-feeding.
4 Help mothers initiate breast-feeding within half an hourof birth.
5 Show mothers how to breast-feed and how to maintainlactation even if they should be separated from theirinfant.
6 Give newborn infants no food or drink other than breastmilk unless medically indicated.
7 Practise rooming-in - allow mothers and infants toremain together 24 hours a day.
8 Encourage breast-feeding on demand.9 Do not give artificial teats or pacifiers to breast-feeding
infants.10 Foster the establishment of breast-feeding support
groups and refer mothers to them upon discharge fromhospital or clinic.
of the three domains within an institution, with theirdifferent and often disharmonious interests, causesconflicts, since each one aims at the legitimation ofits own standards, producing dissonant and contra-dictory interactions.
Based on this framework, we devised an opera-tional model to evaluate the influence of the policy,management and service domains on the impact ofthe SLC course on the implementation of routines toenhance breast-feeding.
MethodologyThe effects of the health professionals' training ontheir institutions, as well as on the average length oftime infants born there were breast-fed, were asses-sed in eight health institutions, group-paired, andassigned at random to either the experimental group(exposed to the SLC course) or the control group.
In order to achieve comparability, the eightinstitutions satisfied the following criteria: they werepublic or philanthropic; they were located near thecity of Sao Paulo (within 100 km); they had not pre-viously been exposed to a similar course; they hadprofessional staff available to attend the course on afull-time basis for a 3-week period; and they had atleast two births per day in their maternity facilities.
The course was evaluated, inter alia, in order tocontrol for the intermediate (institutional) and final
WHO Bulletin OMS. Vol 73 1995462

Breast-feeding training for health professionals
results. The methodology used to assess the courseand the institutional changes that followed are dis-cussed below.
Evaluation of the SLC course
Participant observation was used to become familiarwith and to evaluate the teaching-learning processemployed to train the teams that had been randomlyassigned to the experimental group (13). Two re-searchers monitored and participated in all the activ-ities, alongside the teams of three professionals, onefrom each of the four institutions in the experi-mental group.
In order to systematize the analysis of the teach-ing-learning process, each unit of the course wasassessed separately by the researchers and by each ofthe participants, according to the following aspects:contents; sequence of activities; use of audiovisualresources; teaching performance; bibliographic mate-rial; work-load; classroom performance; students'participation; evaluation technique; and adequacy ofthe methodology in relation to the proposed goals.Each item was rated as very bad, bad, sufficient,good or very good.
The course content was evaluated by applyingWHO/UNICEF's recommendations for successfulbreast-feeding (11).
Two aspects were taken into account in evaluat-ing the participants final results: improvements intrainees' knowledge (determined using pre- and post-course tests); and changes in their attitudes towardsbreast-feeding (determined using group dynamics)carried out at the beginning and at the end of thetraining.
Evaluation of institutional changes
Institutional changes were evaluated by comparingthe situation before exposure to the course with thatobserved 6 months after it had been completed. Forthis purpose, the participating institutions - both theexperimental and control - were visited twice, oneach occasion over a 2-day period, the objectives ofwhich are discussed below.
Institutional evaluation questionnaire. This instru-ment is based on the Wellstart's questionnaire, and isdesigned to collect data that demonstrate whetherinstitutions comply with the ten steps for successfulbreast-feeding (11). Basically it consists of conduct-ing interviews with professionals in the health teamwho hold managerial positions or who have directcontact with mothers and newborns; interviewingwomen who have just delivered; observing the vari-ous maternity areas (rooming-in, nursery, delivery-
room, and antenatal clinic); and interviewing preg-nant women at the antenatal clinic.b
Individual interviews. Individual interviews wereheld 6 months after the SLC course with directors incharge of the process of decision-making policies inthe participating institutions; with administrativemanagers in charge of financial and humanresources' allocation for attaining the above-men-tioned decisions; and with professionals in charge ofantenatal, rooming-in, nursery and outpatient areas.The interviews, which were tape-recorded and thentranscribed, followed previously established guide-lines and contained either open-ended or yes/noquestions, and were designed to facilitate a detailedqualitative analysis of the data collected (3).
Focus-group sessions. Structured discussions with6-15 persons, directed by a moderator were held 6months after the course with the staff involved in theinstitution's routine activities (14). The discussionswere tape-recorded and analysed later. Our mainconcem was to identify how the professionals per-ceived the breast-feeding promotion activities. Atotal of 16 focus-group sessions were held, two ineach of the institutions participating in the study; ineach case one session was held with the front-linepersonnel, and the other with graduate-level profes-sional staff who were involved in the care of thenewbom.
Analysis of the data
Institutional questionnaire data. Data gatheredthrough application of the institutional question-naires were analysed in two ways, as describedbelow.
First, a qualitative analysis was made based onstructured observations derived from the researcher'snotes made after each visit. The notes were used togenerate a chart showing an individual institution'scompliance with each one of the "ten steps", takinginto account a greater (5) or lesser (0) adherence tothe required pattem.
Second, a quantitative analysis was carried out,based on the total score (the "ten-step score"). Thisscore was obtained from the variables in the institu-tional questionnaire, grouped according to each oneof the ten steps. A weighting was assigned to eachvariable, depending on the degree of reliability of thesource of information. For example, for the analysis
b Venanclo Si. ACA project: operational and impact evaluationof a breast-feeding promotion course for health professionals.(Institutional Report No. 1). Sao Paulo, NUPENS/WHO,unpublished document, 1992.
WHO Bulletin OMS. Vol 73 1995 463
M.F. Westphal et al.
of information on breast-feeding (step 5), mother'sreports were given a greater weighting than thoseof the staff. In contrast, to check whether newbornswere receiving food other than mother's milk (step6), a greater weighting was attached to observationsmade in the nurseries than to mothers' reports. Thetotal score permitted a comparison of the situationbefore and 6 months after the course.C
In order to identify the factors that might beinfluencing the implementation of the expected insti-tutional changes, we analysed qualitatively individu-al interviews and those with the focus groups, bothtape-recorded and transcribed.
The influence of the policy and managementdomains on the impact of the SLC course wasassessed using the tape-recorded and transcribedinterviews held individually with general, clinic,and/or administrative directors of the experimentaland control institutions. Evaluation of the servicedomain was carried out using data gathered fromindividual interviews with the health professionalsresponsible for the various maternity areas, andthrough focus-group interviews with graduate profes-sionals and auxiliary personnel.
Because of the great amount of data gathered forthe service domain, we compared the various institu-tions using a comprehensive thematic analysis of theperceptions of the graduates and auxiliary staff aboutthe following:
the incentive to breast-feed in antenatal care;the incentive to breast-feed in delivery care;the incentive to breast-feed in nursery areas;the incentive to breast-feed in rooming-in areas;the incentive to breast-feed in outpatient clinics;human resources' influence, both positive andnegative;the acceptance of the activities developed, expec-tations related to breast-feeding duration, and thereasons for weaning; andwhether there was a written breast-feeding pro-gramme.
ResultsCourse evaluationStructure and organization of the course. Thecourse consisted of 45 units that covered theoreticaland practical aspects of breast-feeding over a 133-
c Venancio Si. ACA project: operational and impact evaluationof a breast-feeding promotion course for health professionals.(Institutional Report No. 2). Sao Paulo, NUPENS/WHO, unpub-lished document, 1992.
hour period (14 days, full-time schedule). A total of66% of this time consisted of lectures, with the re-mainder being spent on practical activities, realiza-tion of these practices, visits to services that promotebreast-feeding, and video-cassette sessions. The ma-jority of the instructors (57%) were SLC profession-al staff, with the remainder being invited from otherinstitutions. The group of trainees consisted of sevenphysicians (6 paediatricians and one obstetrician)and five nurses.
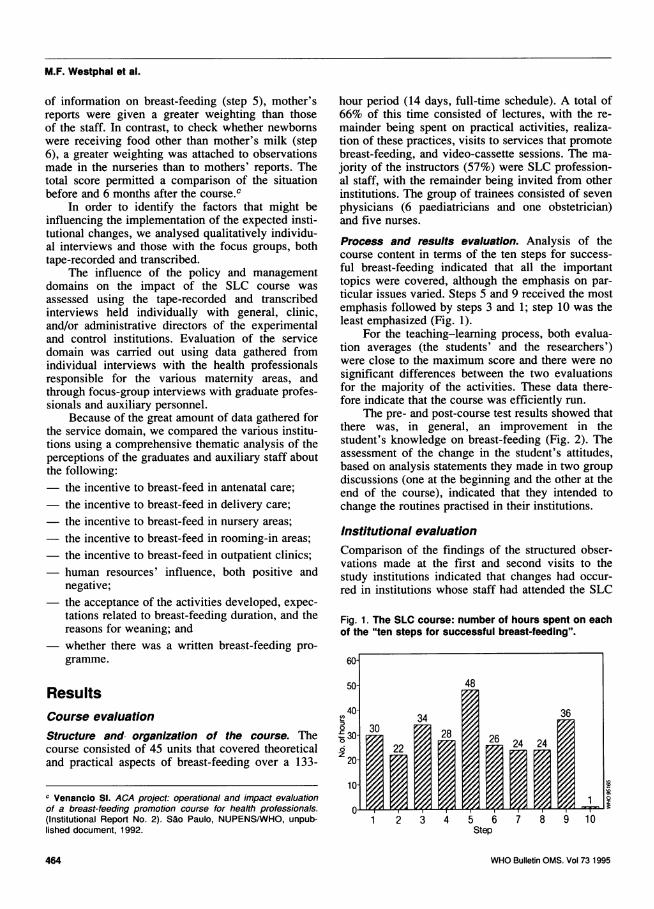
Process and results evaluation. Analysis of thecourse content in terms of the ten steps for success-ful breast-feeding indicated that all the importanttopics were covered, although the emphasis on par-ticular issues varied. Steps 5 and 9 received the mostemphasis followed by steps 3 and 1; step 10 was theleast emphasized (Fig. 1).
For the teaching-learning process, both evalua-tion averages (the students' and the researchers')were close to the maximum score and there were nosignificant differences between the two evaluationsfor the majority of the activities. These data there-fore indicate that the course was efficiently run.
The pre- and post-course test results showed thatthere was, in general, an improvement in thestudent's knowledge on breast-feeding (Fig. 2). Theassessment of the change in the student's attitudes,based on analysis statements they made in two groupdiscussions (one at the beginning and the other at theend of the course), indicated that they intended tochange the routines practised in their institutions.
Institutional evaluationComparison of the findings of the structured obser-vations made at the first and second visits to thestudy institutions indicated that changes had occur-red in institutions whose staff had attended the SLC
Fig. 1. The SLC course: number of hours spent on eachof the "ten steps for successful breast-feeding".
60-
50- 48
40- 34 360 3030 28 26 24 246 22z 20-
10-
011 2 3 4 5 6 7 8 9 10
Step
464 WHO Bulletin OMS. Vol 731995

Breast-feeding training for health professionals
Fig. 2. Evaluation of the SLC course according to thenumber of correct answers given by students In pre-and post-course tests (average number of correct ans-wers: pre-course: 20.27 ± 7.41; post-course: 26.92 ± 2.10).
c Pre-course35 U Post-course
252- 891 11z
Student
course. Changes were noted particularly in relationto steps 2 and 10. No such changes were observedfor the institutions in the control group (Fig. 3).
Institutions in the exposed group had a higherranking in the ten-step score test than those in thecontrol group, with the teaching institutions achiev-ing the best results (Fig. 4).
In general, lack of cohesion between the policy,management and service domains was a feature ofall the institutions studied.
In the service domain the possibilities for changewere limited by inter-personal conflicts, which wereaggravated by the relative autonomy of the healthprofessionals in carrying out their functions. Thischaracteristic was observed chiefly in exposed insti-
Fig. 4. Institutional changes in the study hospitals,according to their score In the "ten steps for success-ful breast-feeding" (Exp. = exposed institution; Cont. =control institution).
3 Exp. S Cont. 6 Exp. 8 Cont. 9 Exp. 11 Cont. 10 Exp. 4 CPair 1 Pair 2 Pair 3 Pair 4
tutions, where the changes introduced were imple-mented to a greater or lesser degree, and was moreevident among graduate-level professionals.
The great majority of the frontline personnelworking in all the institutions that were studiedlacked information about how to receive trainingon breast-feeding. The professional health staffexpressed a desire to improve their technical qualifi-cations in order to enable them to perform routine
Fig. 3. Institutional changes in the study hospitals, according to structured observations(exposed group = Institutions 3, 6, 9, and 10; control group = institutions 4, 5, 8, and 11):* = first evaluation visit; * = 2nd evaluation visit.
Institution
Stepa 10 04 09 11 03 05 06 08
1 * * * t
2 ** ** **+ **
3 **
4 ** *** *
5 *4 *4 *** 0* 0 0 *4t 0*
6 ***t* *0*000* t0** 0 *4 0* 00
7 *0*0* *0*0* *00* *0* *0* 0* *0
8 *** ****+ *0* *0* *0* 0* *0*
9 **** *0*0 *4* 0* 0* 0* 0*
10 ** *0* **** 0*§ *** ** **
a See Table 1 for details of steps.
WHO Bulletin OMS. Vol 73 1995 465

M.F. Westphal et al.
activities, including dealing with the mothers ofnewborns.
It was the unanimous opinion in the experimen-tal institutions that it is easier to implement newbreast-feeding incentive activities (e.g., the creationof outpatient clinics for promotion of breast-feeding)than to promote changes in previously establishedroutines (e.g., breast-feeding in the delivery-room,the non-maintenance of the breast-feeding of normalnewborns in the nursery, the non-provision of foodother than mother's milk to newborns, and the non-use of artificial teats).
Our findings indicate that there were some diffi-culties experienced by the health professionals whohad attended the SLC course in gaining support fortheir proposed changes. These difficulties may havearisen because the professionals concerned hadinsufficient authority, they had to perform adminis-trative tasks that limited the time needed to prepareand develop training courses, they lacked the supportnecessary for such initiatives, or they had encoun-tered obstacles in obtaining the necessary financialand human resources.
All the health professionals stressed the impor-tance of promoting breast-feeding during antenatalcare; none the less, few hospitals provided such care.The lack of antenatal care in all institutions and/orthe lack of commitment to counsel mothers on thebenefits of breast-feeding and to teach breast-feedingpractice are major factors that hinder the promotionof such feeding.
Discussion and conclusionsThe course implemented at SLC has, in general, thesame structure, organization, and content as that runby the Wellstart Center in San Diego (15). However,the selection of participants who attend the SLCcourse differs from that run by the Wellstart Center,in that they do not necessarily work in teaching insti-tutions. Although we consider that this differencedoes not hinder the implementation of breast-feedingpromotion programmes in health service institutions,it is probably easier for teaching institutions to attainthe goals proposed by the SLC course.
Choosing the right people to participate in thetraining course is important. The absence of obstetri-cians and the participation of health professionalswho had a heavy workload, and consequently werenot able to devote themselves to implementing thetopics covered in the course, limited the attainmentof the desired institutional changes.
Since the total scores attained by the institutionsin the exposed group showed that they had had somedifficulty in implementing programmes for the pro-motion of breast-feeding, we believe that the SLC
course should, in future, stress the importance ofinitiating feasible projects that can be realized withinthe prevailing conditions in each institution (16).
Although the health teams found it difficult todevote 3 weeks to attend the training course, thisperiod is required to develop all the aspects relatedto breast-feeding and to allow changes to occur intrainees' attitudes towards breast-feeding (17).
The application of pre- and post-course tests togauge improvements in trainees' knowledge hasbeen used by other training courses for the promo-tion of breast-feeding (17); this reinforces the ad-equacy of the instrument to assess the results of theSLC course.
Armstrong stresses the importance of followingup trainee teams (17). Therefore, the SLC couldcarry out a systematic evaluation of the institutionsthat send staff to attend its course in order to guaran-tee the implementation of breast-feeding promotionprogrammes.
Since the exposed institutions had introducedchanges that encouraged breast-feeding, but had notfully attained all the "ten steps", we searched forhypotheses to explain our findings. For this purpose,individual interviews and focus-group sessions wereanalysed using the framework proposed by Kouzes& Mico (10). In this way, we identified that the lackof cohesion between the various institutionaldomains can hinder the implementation of breast-feeding promotion programmes. According to Stok-amer, the absence of an institutional policy of actionand administrative support makes the success of suchprogrammes almost impossible (18).
Our data indicated that the service domainplayed a determinant role in governing the feasibilityor not of the breast-feeding programme. Since boththe policy and the management domains could haveeither positive or negative influences on the pro-gramme, it would appear that the policy domain,whose function is to define institutional guidelines,carries greater weight in programme implementation.
Implementation of the breast-feeding program-me was not influenced directly by the administrativesector, but was indirectly - through its distributionpolicies, including human resources. The impor-tance of a good salary for the health professionalsinvolved in activities related to breast-feeding andthe availability of resources for training courses,publications, and research have been emphasized byArmstrong (17).
The internal lack of cohesion in the servicedomain could, on its own, make the implementationof any programme impossible. In the study, the diffi-culties experienced with the graduate-level profes-sionals, especially the physicians, could have arisenbecause of their academic training, which empha-
WHO Bulletin OMS. Vol 73 1995466

Breast-feeding training for health professionals
sized treatment rather than prevention. In this sense,the physicians placed a low emphasis on events suchas birth and breast-feeding (19).
The presence of only one obstetrician among thegroup of professionals in the institutions exposed tothe training course reinforces the notion that littleattention was paid to breast-feeding by obstetricians.Many studies indicate that breast-feeding receiveslittle attention in antenatal care (19, 20). Therefore,in the exposed institutions that we studied there wasno institutional policy that gave priority to thebreast-feeding programme and allocated human andphysical resources to it. Also, many of the profes-sionals who participated in the SLC course did nothold any decision-making power and consequentlycould not increase the number of professionalsengaged in the breast-feeding programme. Thesevarious factors illustrate the lack of cohesion amongthe different domains, which do not favour adoptionof innovations and changes in working routines.
Steps ought to be taken to change the content ofthe courses taken by health professionals during theiracademic training, especially to sensitize obstetri-cians to breast-feeding and make them more recep-tive to its promotion.
The auxiliary health personnel were the mosthomogeneous group and also the most receptive toimplementing the breast-feeding programme; how-ever, in the study institutions they were not involvedat the planning level or prepared to accept new atti-tudes and functions. Instead, they were merely as-signed responsibilities to perform tasks related to theprogramme. Greater emphasis should be placed ontraining the auxiliary personnel; studies have demon-strated the favourable impact of such training onhospital policies and rules, leading to an increase inthe prevalence of exclusive breast-feeding (16).
The creation of outpatient clinics in the exposedinstitutions to promote breast-feeding probably arosebecause of the emphasis given by SLC to this activ-ity. We consider this to have been a positive stepsince the postnatal care services tend to approachbreast-feeding inadequately. One of the advantagesof this new activity is that it can be developed by asingle professional, and does not require the involve-ment of the whole team.
On the other hand, some difficulties were clearlyexperienced by the institutions in changing some ofthe maternity routines, such as providing a newbornwith water and tea, no breast-feeding in the delivery-room, and observing the newborn in the nursery for6 hours after birth. This could have arisen becausethese routines are widely used (1_49)d and because
d See footnote a, p. 461.
changes in routine presuppose the involvement of allthe health professionals in contact with mothers andnewboms.
The negligence showed by the exposed institu-tions in failing to establish written breast-feedingprogrammes and in fostering breast-feeding supportgroups within the community could be a culturalproblem. Though all the exposed institutions haveoutpatient clinics for follow-up, there is difficulty inmeeting the demand, which is also true for the ante-natal care.
These findings indicate that breast-feeding pro-motion programmes should be extended to the com-munity as a whole. Another point to be considered iswhether the second evaluation of the exposed institu-tions should have been carried out a longer periodafter the first, since the health professionals mighthave displayed some resistance to implementing newroutines favouring breast-feeding.
In summary, it can be concluded that the SLCcourse has been very efficient in providing technicalknow-how on breast-feeding; however, it couldbenefit from introducing more topics on strategiesfor implementing breast-feeding programmes, includ-ing a critical analysis of the institutional changesrequired and the need for better cohesion among theinstitutional domains.
Health departments, as well as the federal, stateand municipal governments in Brazil should contrib-ute their political support to help health institutionsachieve better results from training courses, by pro-viding hospitals with favourable operational condi-tions, particularly those to do with health personnel,bearing in mind the fundamental role that such indi-viduals play in implementing programmes.
AcknowledgementsWe are deeply indebted to the WHO Diarrhoeal DiseaseControl Programme for supporting the project (GrantNo. 91064). We also acknowledge the cooperation of theSantos Lactation Center, and the hospital directors andthe health professionals of the eight participating hospi-tals, who contributed to the success of the project.
ResumeFormation des professionnels de sant6en matiere d'allaitement maternel etmodifications des pratiques au niveaudes maternit6sCette etude 6value un cours de formation enmatiere d'allaitement maternel dispens6 aux pro-fessionnels de sant6 par le Santos Lactation Cen-
WHO Bulletin OMS. Vol 73 1995 467

M.F. Westphal et al.
ter (SLC), Santos, Sao Paulo, Br6sil, et son impactsur la mise en ceuvre des programmes d'a-laitement au sein dans les maternit6s. Ces pro-grammes sont bas6s sur les "Dix conditions pourle succes de l'allaitement maternel" recomman-dees par l'OMS et l'UNICEF. Huit maternit6s ontparticip6 a l'6tude: chacune des quatre maternit6sincluses par tirage au sort dans le groupe exp6ri-mental a envoy6 3 professionnels de sante auSLC pour y suivre un cours de 18 jours, et lesquatre autres ont servi de groupe t6moin. L'6tudeavait pour objectif d'6valuer le respect des "dixconditions" pr6cit6es avant et 6 mois apres lecours, en utilisant une 6chelle de notation. Les6tablissements du groupe exp6rimental ont enre-gistr6 une augmentation de leur note, contraire-ment aux 6tablissements du groupe temoin. Desentretiens et des reunions par petits groupes ontegalement eu lieu avec les professionnels desant6 de 1'ensemble des maternit6s participant al'etude. Les r6sultats ont ete analyses selon lath6orie des domaines institutionnels de Kouzes &Mico, qui a permis d'identifier les difficult6s ren-contr6es dans la promotion des changements enmatiere de pratiques hospitalieres. II a 6t6 concluque le cours 6tait efficient en ce qu'il permettaitaux professionnels de sant6 d'etre capables depromouvoir les pratiques d'allaitement maternel.Toutefois, pour r6ussir a r6ellement mettre enceuvre des programmes d'allaitement maternel, ilsdevront egalement d6velopper leurs competencespour pouvoir mettre en pratique les connaissancesacquises pendant le cours et faire participer 1'en-semble du personnel de la maternit6 aux activit6s.
References1. Rodriguez-Garcia R, Schaefer LA. [Promotion of
breast-feeding and the participation of nursing per-sonnel]. Boletin de la Oficina Sanitaria Panamerica-na, 1991, 111: 1-15 (in Spanish).
2. Feachem RG, Koblinsky MA. Interventions for thecontrol of diarrhoeal diseases among young chil-dren: promotion of breast-feeding. Bulletin of theWorld Health Organization, 1984, 62: 271-291.
3. Feachem RG. Preventing diarrhoea: What are thepolicy options? Health policy and planning, 1986, 1:109-117.
4. Victora CG, Vaughan JP, Lombardi C. Evidencefor protection by breast-feeding against infantdeaths from infectious diseases in Brazil. Lancet,1987, 2: 319-321.
5. Brown KH et al. Effect of continued oral feeding onclinical and nutritional outcomes of acute diarrhoeain children. Journal of pediatrics, 1988, 112:191-200.
6. Rea MF, Berqu6 ES. Impact of the Brazilian nation-al breast-feeding programme on mothers in GreaterSao Paulo. Bulletin of the World Health Organiza-tion, 1990, 68: 365-371.
7. Rea MF. The Brazilian national breast-feeding pro-gram: a success story. International journal of gyne-cology and obstetrics, 1990, 31 (suppl. 1): 79-82.
8. Hogan R, Martines J. Breast-feeding as an inter-vention within diarrheal diseases control programs:WHO/CDD activities. International journal of gyne-cology and obstetrics, 1990, 31 (suppl. 1): 1 1 5-119.
9. Wellstart: the San Diego Lactation Program.Statement of corporate capabilities. San Diego, CA,Wellstart: the San Diego Lactation Program, 1990.
10. Kouzes JM, Mico PR. Domain theory: an introduc-tion to organizational behavior in human serviceorganizations. Journal of applied behavioural sci-ence, 1979, 15: 449-469.
11. Nakajima H, Grant JP. Appendix 3: Protecting, pro-moting and supporting breast-feeding: the specialrole of maternity services; a joint WHO/UNICEFstatement. International journal of gynecology andobstetrics, 1990, 31(suppl. 1): 171-183.
12. Ellis DJ. Supporting breast-feeding: How to imple-ment agency change. NAACOGS clinical issues,1992, 3: 560-564.
13. Scrimshaw SCM, Hurtado E. Rapid assessmentprocedures for nutrition and primary health care.United Nations University, Tokyo; UNICEF/UnitedNations Children's Fund; Latin American Center,UCLA, CA, 1987.
14. Ramirez AG, Shepperd J. The use of focus groupsin health research. Scandinavian journal of primaryhealth care, supplement, 1988, 1: 81-90.
15. Nailor A. Professional education and training fortrainers. International journal of gynecology andobstetrics, 1990, 31 (suppl. 1): 25-27.
16. Rodriguez-Garcia R, Shaffer L, Yunes J. Lactationeducation for health professionals. Washington, DC,Pan American Health Organization, 1990.
17. Armstrong HC. Breast-feeding promotion: training ofmid-level and outreach health workers. Internation-al journal of gynecology and obstetrics, 1990,31(suppl. 1): 91-103.
18. Stokamer CL. Breast-feeding promotion efforts: whysome do not work. International journal of gynecol-ogy, 1990, 31(suppl. 1): 61-65.
19. Ellis DJ. The impact of agency policies and proto-cols on breastfeeding. NAACOGS clinical issues,1992, 3: 553-559.
20. Breast-feeding promotion in maternity care services:hospital programs as a catalyst to policy change.International journal of gynecology and obstetrics,1990, 31(suppl. 1): 43-45.
468 WHO Bulletin OMS. Vol 73 1995
Copyright © 2022 FDOKUMEN