
Gamma knife irradition—Induced changes in the normal rat brain studied with 1H magnetic resonance...
9
1995 AUR Memorial Award Gamma Knife Irradiation-Induced Changes in the Normal Rat Brain Studied with 1H Magnetic Resonance Spectroscopy and Imaging Reed A. Omary, MD, MS 1, Stuart S. Berr, PhD 1, Toshifumi Kamiryo, MD 2, Giuseppe Lanzino, MD 2, Neal F. Kassell, MD 2, Kevin S. Lee, PhD 2, M. Beatriz Lopes, MD 3, Bruce J. Hillman, MD 1 Rationale and Objectives. The pathogenesis of brain injury following radiosurgery is poorly under- stood. To better elucidate the relationship between blood-brain barrier disruption and metabolic derange- ments, we used magnetic resonance (MR) imaging and 1H MR spectroscopy to detect early changes from focused single-fraction, high-dose irradiation injury in rat brains. Methods. Using the Leksell gamma knife, we irradi- ated the frontoparietal cortex of 11 male Wistar rats with a single dose of 120 Gy. Four weeks later, we sequentially performed water-suppressed 1H MR spec- troscopy and gadopentetate dimeglumine-enhanced Tl-weighted MR imaging. Metabolic maps were created of n-acetylaspartate (NAA), creatine and choline (Cr/ Cho), and lactate from the MR spectroscopy data set. Detection of irradiation injury among the tested modali- ties was assessed by receiver operating characteristic analysis and by quantitative signal intensity changes. Pathologic confirmation of irradiation damage was obtained in all rats. Results. Gadopentetate dimeglumine-enhanced T1- weighted MR imaging was the only imaging modality that detected statistically significant signal intensity changes (p < .05). No reproducible changes in the metabolites of interest could be detected by ]H MR spectroscopy. Conclusion. In our animal model, blood-brain bar- rier disruption was a reproducible, integral finding of single-fraction, high-dose irradiation injury. No repro- ducible metabolic derangements of ischemia or necro- sis were detected by 1H MR spectroscopy, possibly because of dose-latency effects or sensitivity issues. Key Words. Rat brain; magnetic resonance imaging; magnetic resonance spectroscopy; radiosurgery; gamma knife. ~ Dadiosurgery '' is a term introduced by Leksell [1] to ,describe the single-fraction, high-dose applica- tion of focused radiation beams to produce local tissue destruction or partial injury. Under stereotaxic guid- ance, these radiation beams are used to perform local- ized neurosurgical ablation of brain lesions or subnecrotic injury to selected malformations. There are three types of beams currently in use: charged-particle beams, the cobalt-60 source Leksell gamma knife (Elek- ta, Motala, Sweden), and conventional linear accelera- tor (linac) X-ray beams [2]. Of these three types, the gamma knife has been used the longest clinically. Since its first clinical use in 1968 [3], the gamma knife has been used to successfully treat an array of abnormali- ties in the central nervous system (CNS), including arte- riovenous malformations [4, 5], neoplasms [6], and From the Departments of 1Radiology, 2 Neurosurgery, and 3pathology, University of Virginia Health Sciences Center, Charlottesville, VA. This research was partly supported by a grant from the RadiologicalSociety of North America's Research and Education Fund (1993-1994) awarded to Reed A. Omary. Address reprint requests to R. A. Omary, MD, MS, Department of Radiology, Box 170, University of Virginia Health Sciences Center, Charlottesville, VA 22908. Received March 14, 1995, and accepted fer publication after revision August 1, 1995. Acad Radiol 1995;2:1043-1051 © 1995, Association of University Radiologists 1043
Transcript of Gamma knife irradition—Induced changes in the normal rat brain studied with 1H magnetic resonance...
1995 A U R M e m o r i a l A w a r d
Gamma Knife Irradiation-Induced Changes in the Normal Rat Brain Studied with 1H Magnetic
Resonance Spectroscopy and Imaging Reed A. Omary, MD, MS 1, Stuart S. Berr, PhD 1, Toshifumi Kamiryo, MD 2, Giuseppe Lanzino, MD 2, Neal F. Kassell, MD 2,
Kevin S. Lee, PhD 2, M. Beatriz Lopes, MD 3, Bruce J. Hillman, MD 1
Rationale and Objectives. The pathogenesis of brain injury following radiosurgery is poorly under- stood. To better elucidate the relationship between blood-brain barrier disruption and metabolic derange- ments, we used magnetic resonance (MR) imaging and 1H MR spectroscopy to detect early changes from focused single-fraction, high-dose irradiation injury in rat brains.
Methods. Using the Leksell gamma knife, we irradi- ated the frontoparietal cortex of 11 male Wistar rats with a single dose of 120 Gy. Four weeks later, we sequentially performed water-suppressed 1H MR spec- troscopy and gadopentetate dimeglumine-enhanced Tl-weighted MR imaging. Metabolic maps were created of n-acetylaspartate (NAA), creatine and choline (Cr/ Cho), and lactate from the MR spectroscopy data set. Detection of irradiation injury among the tested modali- ties was assessed by receiver operating characteristic analysis and by quantitative signal intensity changes. Pathologic confirmation of irradiation damage was obtained in all rats.
Results. Gadopentetate dimeglumine-enhanced T1- weighted MR imaging was the only imaging modality that detected statistically significant signal intensity changes (p < .05). No reproducible changes in the metabolites of interest could be detected by ]H MR spectroscopy.
Conclusion. In our animal model, blood-brain bar- rier disruption was a reproducible, integral finding of single-fraction, high-dose irradiation injury. No repro- ducible metabolic derangements of ischemia or necro- sis were detected by 1H MR spectroscopy, possibly because of dose-latency effects or sensitivity issues.
Key Words. Rat brain; magnetic resonance imaging; magnetic resonance spectroscopy; radiosurgery; gamma knife.
~ D a d i o s u r g e r y '' is a term introduced by Leksell [1] to ,describe the single-fraction, high-dose applica-
tion of focused radiation beams to produce local tissue destruction or partial injury. Under stereotaxic guid- ance, these radiation beams are used to perform local- ized neurosurgical ablation of brain lesions or subnecrotic injury to selected malformations. There are three types of beams currently in use: charged-particle beams, the cobalt-60 source Leksell gamma knife (Elek- ta, Motala, Sweden), and conventional linear accelera- tor (linac) X-ray beams [2]. Of these three types, the gamma knife has been used the longest clinically. Since its first clinical use in 1968 [3], the gamma knife has been used to successfully treat an array of abnormali- ties in the central nervous system (CNS), including arte- riovenous malformations [4, 5], neoplasms [6], and
From the Departments of 1Radiology, 2 Neurosurgery, and 3pathology, University of Virginia Health Sciences Center, Charlottesville, VA.
This research was partly supported by a grant from the Radiological Society of North America's Research and Education Fund (1993-1994) awarded to Reed A. Omary.
Address reprint requests to R. A. Omary, MD, MS, Department of Radiology, Box 170, University of Virginia Health Sciences Center, Charlottesville, VA 22908.
Received March 14, 1995, and accepted fer publication after revision August 1, 1995.
Acad Radiol 1995;2:1043-1051 © 1995, Association of University Radiologists
1043

OMARY ET AL. VOI. 2, No. 12, December 1995
refractory epilepsy [7]. Although approximately 6,000 procedures are performed annually in 37 medical cen- ters worldwide (unpublished data), the basic mecha- nism of treatment is still poorly understood.
In the most commonly accepted model of CNS radia- tion damage, there are three phases: (1) acute, occur- ring within days to 2 weeks of irradiation; (2) ear ly-
delayed, occurring weeks to months after irradiation; and (3) late-delayed, evolving months to years after irradiation [8]. Although this scheme is helpful for clas- sification, pathologic features of each stage may over-
lap based mainly on the radiation dose [9]. The results of previous studies have suggested that the pathogene- sis of ear ly-delayed irradiation injury involves a combi- nation of blood-brain barrier disruption, ischemia, and necrosis [9-15].
1H magnetic resonance (MR) spectroscopy, which allows the noninvasive in vivo measurement of metab- olite concentrations in living tissue, has shown promise
in elucidating potential disruptions in metabolic path- ways in the CNS [16, 17].
Limited data [18, 19] suggest that 1H MR spectroscopy
may detect changes in brain metabolites following irra- diation, including depressed n-acetylaspartate (NAA)/
creatine-phosphocreatine and NAA/choline-containing compound peak ratios [18], as well as elevated lipid and diminished phoshatidylcholine peaks [19]. The
detection by Yousem et al. [18] of 1H MR spectroscopy metabolite changes in two irradiated cats, despite nor- mal or equivocal histopathologic examinations, implies that proton MR spectroscopy might have the capability of detecting metabolic abnormalities before histopatho- logic changes are evident. Since the histologic appear-
ance of a cell may not adequately represent its state of functional abnormality [20], this implication has bio- logic plausibility.
On the basis of that preliminary research, we hypoth- esized that gamma knife irradiation to the normal fron- toparietal cortex of rats would produce characteristic
metabolite changes in the early-delayed radiation injury stage that we could measure by 1H MR spectroscopy:
decreased NAA, decreased creatine and choline com- pounds (Cr/Cho), and increased lactate. We hypothe- sized that these abnormalities might be reproducibly
detected with 1H MR spectroscopy before histopatho- logic evidence of ischemia and necrosis was present, and possibly before injury could be detected by con- trast-enhanced Tl-weighted MR imaging. To assess this hypothesis, and to investigate the mechanisms of
gamma knife injury, we used 1H MR spectroscopy and
both unenhanced MR imaging and gadopentetate dime- g lumine-enhanced MR imaging to detect early-delayed
irradiation injuw, using histopathology as the standard of evidence.
MATERIALS AND METHODS
Stereotaxic Device and Gamma Knife Irradiation
Eleven male Wistar rats (weight = 250-300 g) were used in our study. We received approval from our insti- tution's animal research committee and complied with the guidelines issued by the National Institutes of Health for the care and use of animals in laboratory research.
We used the stereotaxic device of Kamiryo et al. [21] to allow accurate positioning of rats for focal brain irra- diation using the Leksell gamma knife. Consisting of ear
plugs, an incisor bar, and sliding Y and Z scales, the design and use of this device have been described else- where [21]. The device also includes a brain cutting sys-
tem with a vertical moving razor blade that cuts the rat brain in the coronal plane as described in a standard rat stereotaxic atlas [22].
A stereotaxic frame with external fiducial markers [21]
also was used during MR and spectroscopic imaging to allow accurate anatomic localization of the projected site of frontoparietal irradiation. During imaging, use of the fiducial markers allowed the rapid and accurate
assessment of stereotaxic coordinates corresponding to those described in the atlas. We previously confirmed that the spatial accuracy of using the stereotaxic fl-ame's fiducial markers with MR imaging contains a max imum error of 1.2-1.4 m m [23].
We anesthetized each rat with ketamine (80 mg/kg)
and xylazine (8 mg/kg) intramuscularly prior to irradia- tion. We then sequentially placed the 11 rats into the stereotaxic device and irradiated the frontoparietal cor- tex using our 201-source cobalt-60 Leksell gamma knife. This cortical site was selected for irradiation because it represents a common location for arterio- venous malformations that are irradiated by the gamma
knife in humans. The side of irradiation (i.e., left or right) for each rat was randomized by using a random number table. The side of irradiation was known only to the neurosurgeon performing the radiosurgery and was kept secret from the observers participating in the
analysis phase of the study. The stereotaxic coordinates of irradiation (X = 5 mm, Y = 10 mm, and Z = 6.5 mm) were relative to the rat interaural line and the midline and were based on corresponding sections from the standard rat stereotaxic atlas [22].
1044

Vol. 2, No. 12, D$cember 1995 GAMMA KNIFE IRRADIATION- INDUCED CHANGES
The rats were irradiated using a 4-mm collimator
beam at a max imum central dose of 120 Gy, corre- sponding to a 60-Gy peripheral dose at the 50% isodense line. The total time of irradiation for each rat was approximately 55 min. Figure 1 portrays isodose contours overlayed on a sample coronal Tl -weighted MR image through the site of radiation.
To assess whether 1H MR spectroscopy could be
used to measure metabolic derangements prior to histo- logic evidence of such change, we selected a radiation dose and latency period at which ischemia and necrosis
were not grossly manifested on histologic examination. The 120-Gy central dose was chosen based on our
previous but still unpublished histopathologic studies demonstrating disruption of the b lood-bra in barrier, vasodilatation, capillary thickening, mild scattered foci
of necrosis and demyelination, and gliosis 4 weeks after irradiation in this same locus in the rat frontoparietal cortex. We classified this pathologic change within the
early-delayed stage of irradiation injury.
MR a n d 1H S p e c t r o s c o p i c I m a g i n g
All rats survived the stereotaxic irradiation procedure. Prior to imaging, we anesthetized each rat with ketamine (80 mg/kg) and xylazine (8 mg/kg) intramuscularly. An
intravenous catheter was then placed in the femoral vein
FIGURE 1. Coronal Tl-weighted magnetic resonance image depicting isodose contours in rat brain. "X" marks the center of irradiation, and numbers represent percentages of maximum irradiation.
of seven rats and in the tail vein of four rats. The cathe- ters, filled with heparinized saline, were then connected to a syringe filled with gadopentetate dimeglumine (Magnevist; Berlex, Wayne, NJ). After placing the rats within the stereotaxic frame, but before inserting them
into the bore of the magnet, we gave each rat a booster intramuscular anesthesia dose of ketamine (20 mg/kg) and xylazine (8 mg/kg).
MR imaging data were acquired on a spectroscopy imaging system (Varian, Palo Alto, CA) 200/400 4.7-T system fitted with high-performance gradients (maxi- m u m = 100 mT/m). A quadrature bird cage radiofre- quency coil designed and built for imaging rat brains
was used in all studies. We initially obtained T1- weighted MR images (repetition time [TR] = 650 msec, echo time [TEl = 12 msec, thickness = 4 ram, 128 × 128,
5 × 5 cm) to determine the coronal slice corresponding to the coordinates of irradiation using the fiducial marker system. This slice was sh immed to reduce mag- netic field inhomogeneities. A high-resolution T1-
weighted MR image was obtained from this slice. A water-suppressed 1H spectroscopic image was
obtained from the same spatial location as this T1- weighted MR image (2 spatial dimensions, 1 chemical
shift dimension, TR = 650 msec, TE = 136 msec, thick- ness = 4 mm, 24 × 24 × 512 zero-filled to 64 × 64 × 512, 5 cm × 5 cm × 2000 Hz, number of excitations = 2, voxel size = 1.56 × 1.56 × 4 m m 3, spectroscopic image
time = 20 min). Water suppression was performed using a series of Gaussian pulses, followed by dephas- ing gradients before each phase-encoding step [24].
Metabolic maps were created from the spectroscopic
imaging data set using software deve loped by Maudsley et al. and described in detail e lsewhere [25]. Errors attributable to residual magnetic field inhomogeneities were corrected using this software by shifting NAA res- onances to line up with one another. This correction algorithm does not correct for intravoxel inhomogene- ities or for distortions arising from eddy currents. Spec-
troscopic images were created by integrating signal intensity (SI) over the chemical shift ranges of 1.9-2.3
p p m for NAA, 2.87-357 p p m for Cr/Cho, and 1.27-0.85 p p m for lactate. This software does not differentiate be tween overlapping resonances. A high-pass-filtered Tl-weighted MR image was placed over the spectro- scopic images to help identify anatomic positions in the
spectroscopic images. After we acquired the spectroscopic imaging data set,
we injected 0.2 ml gadopentetate dimeglumine intrave- nously, without moving the rat, and then obtained
1045

OMARY ET AL. vol, 2, No. 12, December 1995
another Tl-weighted MR image. The total time for cathe- ter placement and imaging was about 2 hr for each rat.
Pathology
After the MR studies were completed, the rats were
euthanized with an intracardiac perfusion of 10% zinc formalin. We sectioned the brains using the stereotaxic device's cuffing system to include whole coronal slices from 7 to 10 m m and 10 to 13 m m (anterior to the inter- aural line). These slices were postfixed overnight in
zinc formalin and routinely processed for paraffin embedding. Our neuropathologist, w h o did not know which side was irradiated, pe r formed histologic exami- nation using hematoxylin and eosin stain. The resultant
slides were evaluated using light microscopy.
Analysis
The data were treated in two ways: reader interpreta- tion of images, as analyzed by receiver operating char- acteristic (ROC) curves, and quantitative average SI
measurements obtained from a circular area the size of the irradiating beam.
ROC analysis. Two observers w h o did not know which side was irradiated independent ly analyzed all images in a randomized batch fashion. Randomization was separate for the Tl -weighted MR images, the con-
trast-enhanced T]-weighted MR imagesl and the spec- troscopic metabolite maps. All randomization was performed using a random number table.
Observer data were collected for each rat using a 5- point graded response scale for the presence of radia- tion injury using unenhanced MR imaging, contrast-
enhanced MR imaging, and 1H MR spectroscopy meta- bolic maps for NAA, Cr/Cho, and lactate. The graded responses on individual data sheets were collected and tabulated. We used ROC curve analysis [26] to assess observer diagnostic performance in detecting radiation
injury using MR imaging and 1H MR spectroscopy metabolite maps.
Individual and pooled ROC curves for each type of Tl-weighted MR imaging (unenhanced and enhanced) and for the spectroscopic data of each metabolite (NAA, Cr/Cho, and lactate) were generated using an IBM PC-compatible computer outfitted with the INDROC program (developed by Charles Metz, Univer-
sity of Chicago, Chicago, IL). This program estimates the binormal ROC curves from ratings data using maxi- mum-likelihood estimation [27].
The areas generated underneath each ROC curve [26] were used to compare the diagnostic performance of each reader for the detection of radiation injury. In the cases in which ROC results under maximum-likel ihood estimation were degenerate, the areas underneath the
ROC curves were estimated using the trapezoidal rule [26]. Pooled ROC curves for each metabolite also were generated to provide an overall graphic representation
of the results. Because of the small sample size, we did not perform statistical comparisons of the ROC areas. Instead, we provide 95% coilfidence intervals [28] to aid the reader in determining the importance of the differ- ences in performance among the test modalities.
SI analysis. Average Sis were obtained from the pix- els contained within a circular area located at the site of irradiation and at the contralateral nonirradiated side of
the brain. The location of the circular region of interest (ROI) was determined from the fiduciat markers and the brain landmarks in the Tl-weighted MR images and was used for subsequent measurements on the T1- weighted and contrast-enhanced MR images and the
spectroscopic images. The Sis of the irradiated ROI were normalized by dividing by the corresponding SI from the nonirradiated ROI.
We assessed differences in the SI ratios for each
modality by computing the 95% confidence intervals (two-sided case) of the mean. The hypothesis that there was no difference in SI ratios for each modality was rejected at the .05 level if the 95% confidence interval
did not contain 1.0 [29].
RESULTS
Six rats were irradiated in the right cerebral hemi- sphere and five on the left. Early histologic changes were identified in all animals at the site of stereotaxic irradiation. For all rats, these abnormalities were most
prominent in the coronal brain slices located approxi- mately 10 m m anterior to the interaural line. This site of maximum injury in the frontoparietal cortex, as deter- mined by pathology, confirmed the location of the ini- tial anticipated site of irradiation. As shown by the isodose contours of Figure 1, the vast majority of the
contralateral hemisphere received far less than 10% of the central max imum irradiation dose.
The lesions consisted of extensive proliferation of small blood vessels, formed by a thin wall composed mainly of endothelial cells, consistent with capillaries. There was a moderate degree of astrocytosis. These find-
1046
Vol. 2, No. 12, December 1995 G A M M A K N I F E I R R A D I A T I O N - I N D U C E D C H A N G E S
ings were more pronounced in the cortical ribbon; how- ever, segmental involvement of the white matter also
was observed in the majority of the cases. Although areas of rank necrosis were not present, cavitation of the parenchyma, with accumulation of proteinaceous mate-
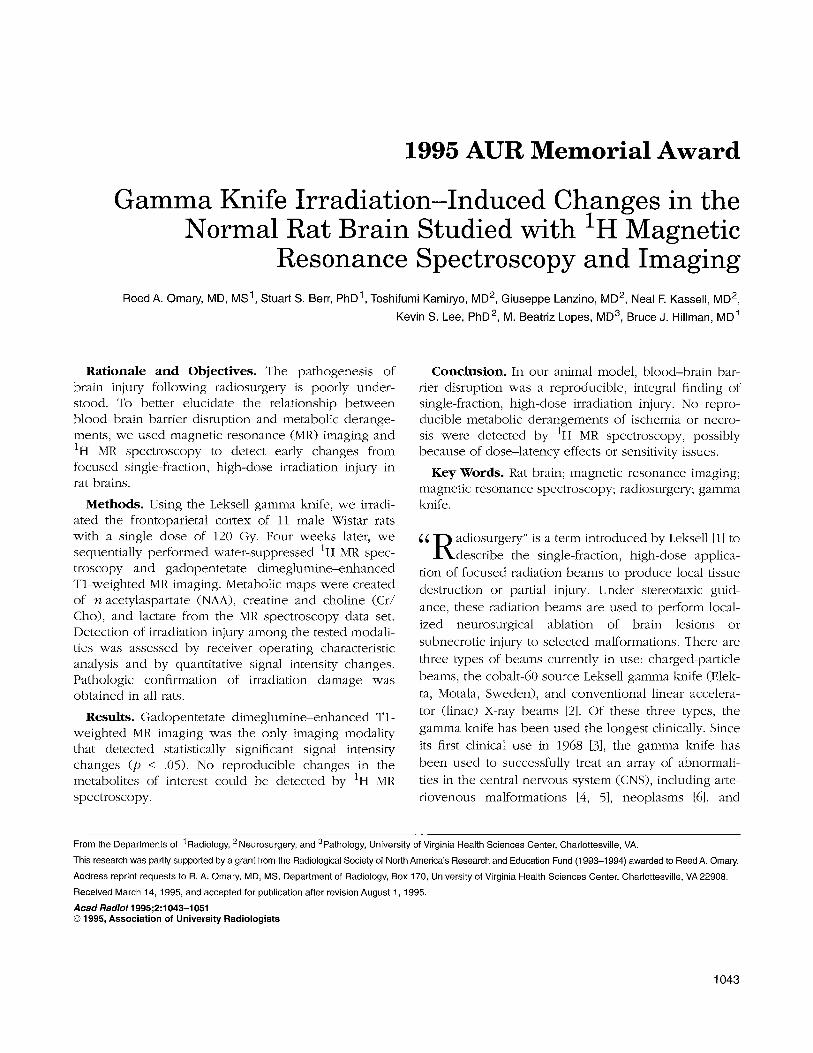
rial, was observed in five of the 11 rats. Thickening of the vessel wails and endothelial proliferation were not present. Figure 2 depicts the vascular proliferation, cystic
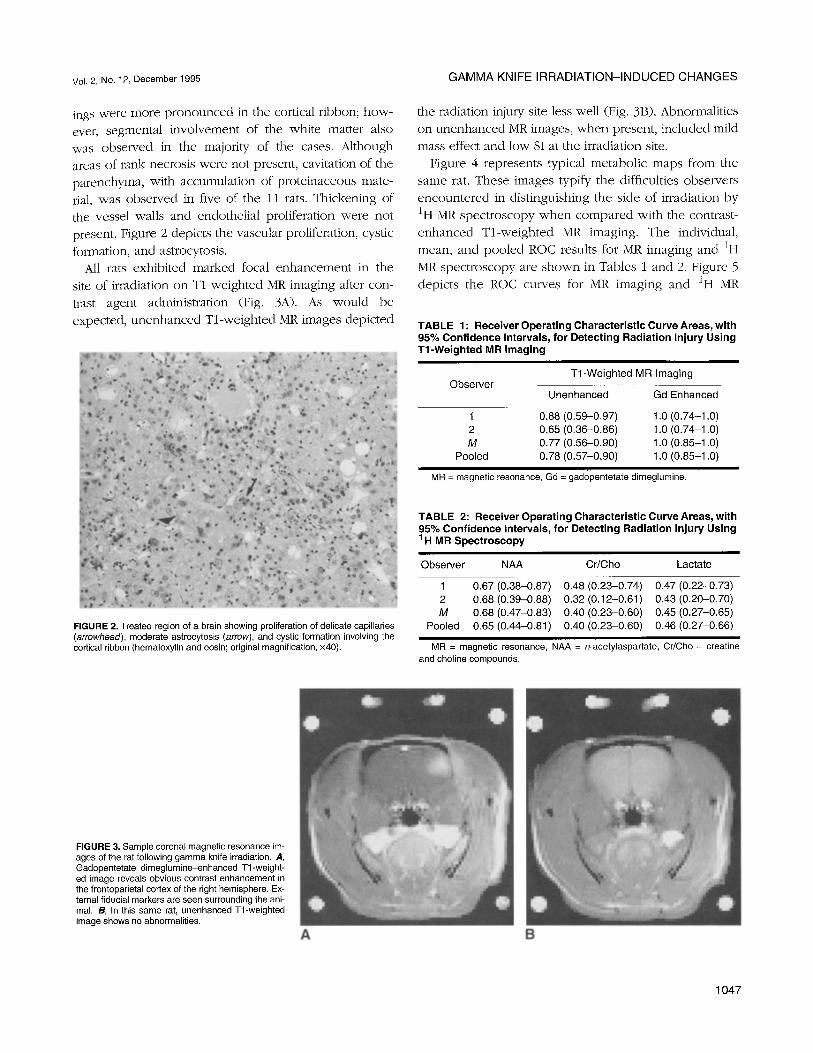
formation, and astrocytosis. All rats exhibited marked focal enhancement in the
site of irradiation on Tl-weighted MR imaging after con- trast agent administration (Fig. 3A). As would be expected, unenhanced Tl-weighted MR images depicted
the radiation injm T site less well (Fig. 3B). Abnormalities on unenhanced MR images, when present, included mild mass effect and low SI at the irradiation site.
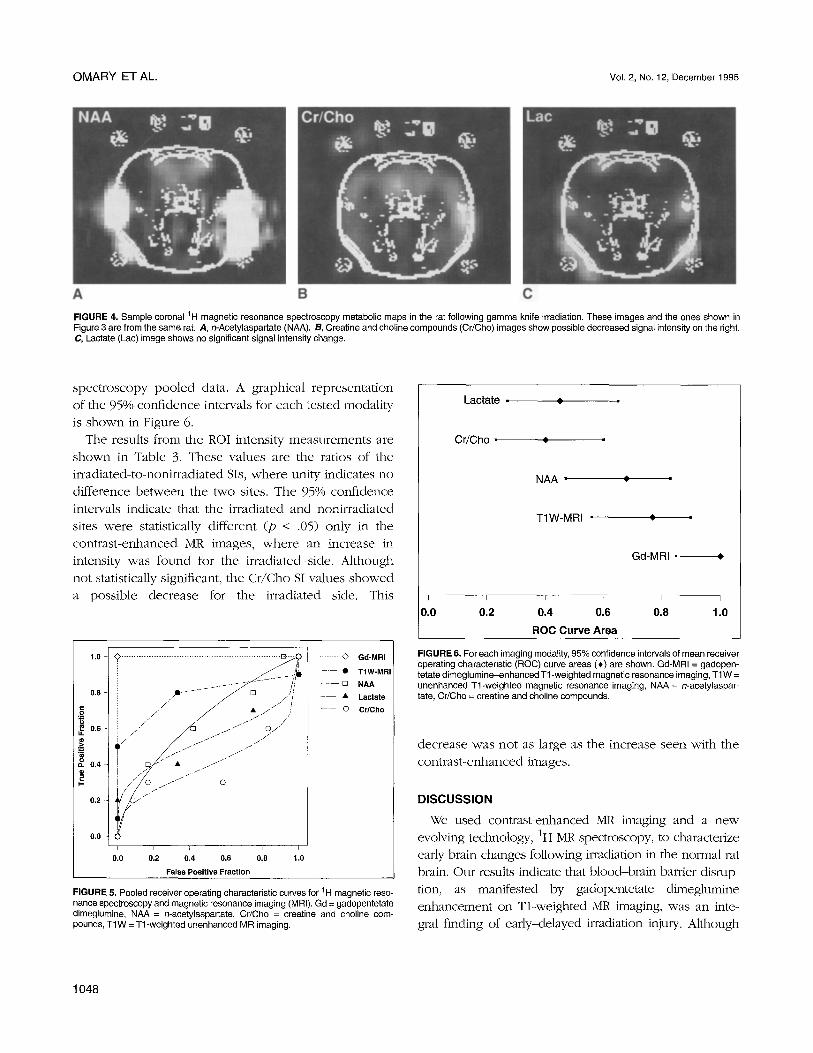
Figure 4 represents typical metabolic maps from the same rat. These images typify the difficulties observers encountered in distinguishing the side of irradiation by ~H MR spectroscopy when compared with the contrast- enhanced Tl-weighted MR imaging. The individual,
mean, and pooled ROC results for MR imaging and 1H MR spectroscopy are shown in Tables 1 and 2. Figure 5 depicts the ROC curves for MR imaging and 1H MR
TABLE 1" Receiver Operating Characteristic Curve Areas, with 95% Confidence Intervals, for Detecting Radiation Injury Using T1-Weighted MR Imaging
Observer T1-Weighted MR Imaging
Unenhanced Gd Enhanced
1 0.88 (0.59-0.97) 1.0 (0.74-1.0) 2 0.65 (0,36-0.86) 1.0 (0.74-1.0) m 0.77 (0.56-0.90) 1.0 (0.85-1.0)
Pooled 0.78 (0.57-0.90) 1.0 (0.85-1.0)
MR = magnetic resonance, Gd = gad0pentetate dimeglumine.
FIGURE 2. Treated region of a brain showing proliferation of delicate capillaries (arrowhead), moderate astrocytosis (arrow), and cystic formation involving the cortical ribbon (hematoxylin and eosin; original magnification, x40).
TABLE 2: Receiver Operating Characteristic Curve Areas, with 95% Confidence Intervals, for Detecting Radiation Injury Using 1H MR Spectroscopy
Observer NAA Cr/Cho Lactate
1 0.67 (0.38-0.87) 0.48 (0.23-0.74) 0.47 (0.22-0.73) 2 0.68 (0.39-0.88) 0.32 (0.12-0.61) 0.43 (0.20-0.70) M 0.68 (0.47-0.83) 0.40 (0.23-0.60) 0.45 (0.27-0.65)
Pooled 0.65 (0.44-0.81) 0.40 (0.23-0.60) 0.46 (0.27-0.66)
MR = magnetic resonance, NAA = n-acetylaspartate, Cr/Cho = creatine and choline compounds.
FIGURE 3. Sample coronal magnetic resonance im- ages of the rat following gamma knife irradiation. A, Gadopentetate dimeglumine-enhanced Tl-weight- ed image reveals obvious contrast enhancement in the frontopadetal cortex of the right hemisphere. Ex- ternal fiducial markers are seen surrounding the ani- mal. B, In this same rat, unenhanced Tl-weighted image shows no abnormalities.
A B
1047
O M A R Y E T AL . VoI. 2, No. 12, D e c e m b e r 1 9 9 5
A B C
FIGURE 4. Sample coronal tH magnetic resonance spectroscopy metabolic maps in the rat following gamma knife irradiation. These images and the ones shown in Figure 3 are from the same rat. A, n-Acetylaspartate (NAA). B, Creatine and choline compounds (Cr/Cho) images show possible decreased signal intensity on the right. C, Lactate (Lac) image shows no significant signal intensity change.
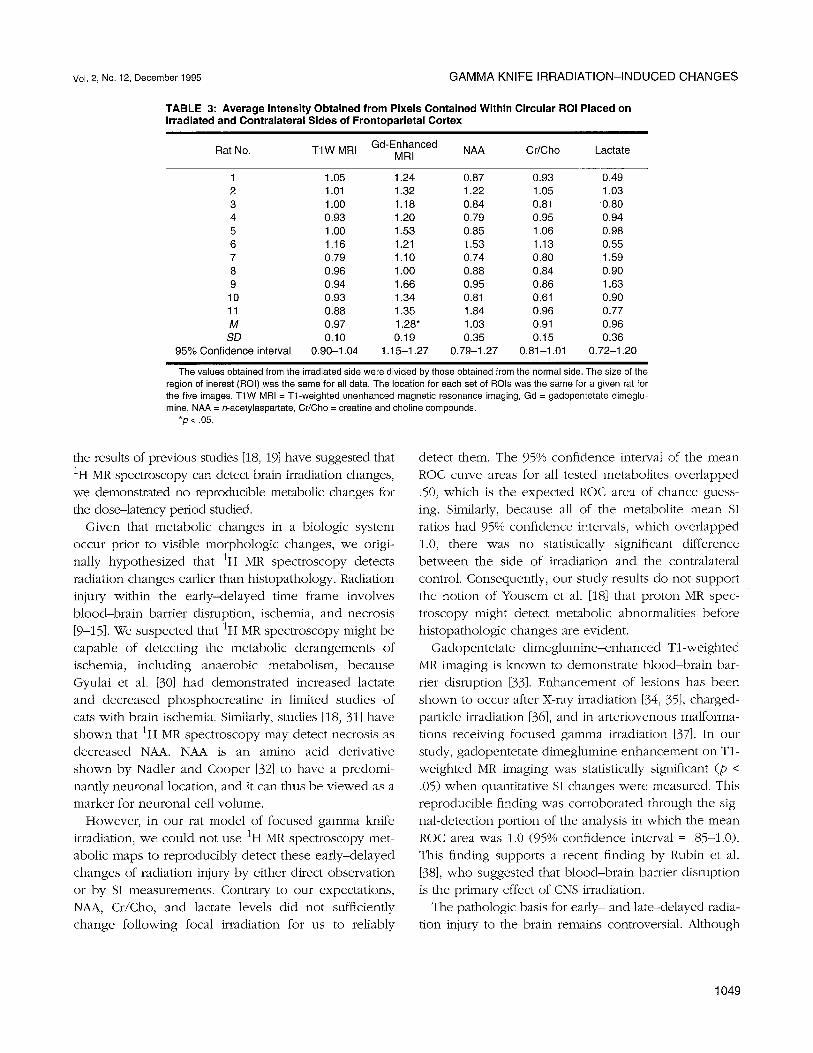
spectroscopy pooled data. A graphical representation of the 95% confidence intervals for each tested modality
is shown in Figure 6. The results from the ROI intensity measurements are
shown in Table 3. These values are the ratios of the irradiated-to-nonirradiated Sis, where unity indicates no
difference between the two sites. The 95% confidence intervals indicate that the irradiated and nonirradiated sites were statistically different (p < .05) only in the contrast-enhanced MR images, where an increase in intensity was found for the irradiated side. Although
not statistically significant, the Cr/Cho SI values showed a possible decrease for the irradiated side. This
1.0 q © . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . E l . :
0.8 -t / .
/ . - 0 , 6 q : . . / '
Ol4 q
. ......... J o .:/ • / . / J
f / / j l / O / . / / / / / 7 '
/ / / / / / / / / /
j / . / / . / O
0 . 0 q i i i i i i
0 . 0 0.2 0,4 0.6 0.8 1.0
False Posit ive F r a c t i o n
• .- O Gd-MRI
• T1W-MRI
- - [] N A A
- • L a c t a t e
--.-- o C r / C h o
FIGURE 5. Pooled receiver operating characteristic curves for 1H magnetic reso- nance spectroscopy and magnetic resonance imaging (MRI). Gd = gadopentetate dimeglumlne, NAA = n-acetylaspartate, Cr/Cho = creatine and choline com- pounds, T1W = Tl-weighted unenhanced MR imaging.
Lactate • 0
Cr /Cho = ¢
NAA •
T I W - M R I • o
Gd-MRI = ¢
I I I L I I
0.0 0,2 0.4 0.6 0.8 1.0
ROC Curve Area
FIGURE 6. For each imaging modality, 95% confidence intervals of mean receiver operating characteristic (ROC) curve areas (+) are shown. Gd-MRI = gadopen- tetate dimeglumine-enhanced Tl-weighted magnetic resonance imaging, TlW = unenhanced Tl-weighted magnetic resonance imaging, NAA = n-acetylaspar- tate, Cr/Cho = creatine and choline compounds.
decrease was not as large as the increase seen with the contrast-enhanced images.
DISCUSSION
We used contrast-enhanced MR imaging and a new evolving technology, 1H MR spectroscopy, to characterize early brain changes following irradiation in the normal rat brain. Our results indicate that blood-brain barrier disrup- tion, as manifested by gadopentetate dimeglumine enhancement on Tl-weighted MR imaging, was an inte- gral finding of early-delayed irradiation injury. Although
1 0 4 8
Vol. 2, No. 12, December 1995 G A M M A KNIFE I R R A D I A T I O N - I N D U C E D C H A N G E S
TABLE 3: Average Intensity Obtained from Pixels Contained Within Circular ROI Placed on Irradiated and Contralateral Sides of Frontoparietal Cortex
Gd-Enhanced Rat No. T1W MRI NAA Cr/Cho Lactate
MRI
1 1.05 1.24 0.87 0.93 0.49 2 1.01 1.32 1.22 1.05 1.03 3 1.00 1.18 0.84 0.81 0.80 4 0.93 1.20 0.79 0.95 0.94 5 1.00 1.53 0.85 1.06 0.98 6 1.16 1.21 1.53 1.13 0.55 7 0.79 1.10 0.74 0.80 1,59 8 0.96 1.00 0.88 0.84 0.90 9 0.94 1.66 0.95 0.86 1.63 10 0.93 1.34 0.81 0.61 0.90 11 0.88 1.35 1.84 0.96 0.77 M 0.97 1.28* 1.03 0.91 0.96 SD 0.10 0.19 0.35 0.15 0.36
95% Confidence interval 0.90-1.04 1.15-1.27 0.79-1.27 0.81-1.01 0.72-1.20
The values obtained from the irradiated side were divided by those obtained from the normal side. The size of the region of inerest (ROI) was the same for all data. The location for each set of ROIs was the same for a given rat for the five images. TlW MRI = Tl-weighted unenhanced magnetic resonance imaging, Gd = gadopentetate dimeglu- mine, NAA = n-acetylaspartate, Cr/Cho = creatine and choline compounds.
*p < .05.
the results of previous studies [18, 19] have suggested that 1H MR spectroscopy can detect brain irradiation changes, we demonstrated no reproducible metabolic changes for the dose-latency period studied.
Given that metabolic changes in a biologic system occur prior to visible morphologic changes, we origi- nally hypothesized that 1H MR spectroscopy detects radiation changes earlier than histopathology. Radiation injury within the early-delayed time frame involves blood-brain barrier disruption, ischemia, and necrosis [9-15]. We suspected that 1H MR spectroscopy might be capable of detecting the metabolic derangements of ischemia, including anaerobic metabolism, because Gyulai et al. [30] had demonstrated increased lactate and decreased phosphocreatine in limited studies of cats with brain ischemia. Similarly, studies [18, 31] have shown that 1H MR spectroscopy may detect necrosis as decreased NAA. NAA is an amino acid derivative shown by Nadler and Cooper [32] to have a predomi- nantly neuronal location, and it can thus be viewed as a marker for neuronal cell volume.
However, in our rat model of focused gamma knife irradiation, we could not use 1H MR spectroscopy met- abolic maps to reproducibly detect these early-delayed changes of radiation injury by either direct observation or by SI measurements. Contrary to our expectations, NAA, Cr/Cho, and lactate levels did not sufficiently change following focal irradiation for us to reliably
detect them. The 95% confidence interval of the mean ROC curve areas for all tested metabolites overlapped .50, which is the expected ROC area of chance guess- ing. Similarly, because all of the metabolite mean SI ratios had 95% confidence intervals, which overlapped 1.0, there was no statistically significant difference between the side of irradiation and the contralateral control. Consequently, our study results do not support the notion of Yousem et al. [18] that proton MR spec- troscopy might detect metabolic abnormalities before histopathologic changes are evident.
Gadopentetate dimeglumine-enhanced Tl-weighted MR imaging is known to demonstrate blood-brain bar- rier disruption [33]. Enhancement of lesions has been shown to occur after X-ray irradiation [34, 35], charged- particle irradiation [36], and in arteriovenous malforma- tions receiving focused gamma irradiation [37]. In our study, gadopentetate dimeglumine enhancement on T1- weighted MR imaging was statistically significant (p < .05) when quantitative SI changes were measured. This reproducible finding was corroborated through the sig- nal-detection portion of the analysis in which the mean ROC area was 1.0 (95% confidence interval = .85-1.0). This finding supports a recent finding by Rubin et al. [38], who suggested that blood-brain barrier disruption is the primary effect of CNS irradiation.
The pathologic basis for early- and late-delayed radia- tion injury to the brain remains controversial. Although
1049

O M A R Y ET AL. Vol. 2, No. 12, December 1995
numerous studies have shown that blood-brain barrier disturbances are important in the evolution of CNS radia- tion injury [10-15, 38], the relative roles that glial versus vascular damage play in the development of radiation necrosis remain to be elucidated [9]. The hypothesis that blood-brain barrier disruption produces vasogenic edema, leading to decreased regional cerebral blood flow, ischemia, and infarction, is appealing [12]; how- ever, multiple mechanisms involving some interplay between progressive oligodendrocyte and endothelial cell damage probably exists [9].
Two plausible explanations for why 1H MR spectros- copy failed to detect changes of early-delayed irradia- tion injury include dose-latency effects and sensitivity issues. The term "dose-latency effects" refers to the well-known concept that an increasing radiation dose will diminish the latency period for pathologic change [39]. Consequently, the changes that develop at one radiation dose and latency period do not necessarily occur at another dose and latency period. Optimally, we would have liked to have studied additional rats at different time points and radiation doses in order to characterize more completely the appearance of ~H MR spectroscopy-detected metabolic changes. Because of time and monetary considerations, we studied rats at only one dose and time period within the early- delayed time frame following injury. At this single radi- ation dose and latency period, histopathologic exami- nation showed no evidence of active ischemic necrosis, on which significant 1H MR spectroscopy changes may depend. Future research at different latency periods may be help elucidate this issue.
Alternatively, these pathologic mechanisms were present at the time of imaging, and our techniques were not sensitive enough to detect the metabolic changes. In hydrogen spectroscopy, the metabolites of interest are roughly 10,000 times less concentrated than the hydro- gen in water and fat [17], yielding an inherently low sig- nal-to-noise ratio. The water signal was sufficiently suppressed, but no attempt was made to suppress fat. We relied on the spatial separation of the fat from the region of irradiation. Bleedover of the fat signal could have affected some of the results. In particular, the lac- tate results were most at risk because of the close chem- ical shift proximity to fat. Increasing the spatial resolution would have helped to alleviate this problem, but our sig- nal-to-noise ratio would have suffered from the smaller voxel size. Our voxel size was selected as a compromise between higher signal-to-noise ratio and lower spatial
resolution. Perhaps furore refinements in spectroscopic imaging techniques and improvements in equipment will be necessary before these potentially subtle metabolic changes can be detected.
This study was limited by the small number of ani- mals and readers. Still, the SI changes were so dramatic following gadopentetate dimeglumine administration that statistical significance was reached easily. As for the 1H MR spectroscopy, a larger sample size would clearly increase the power of the study to detect a sta- tistical difference if one actually existed. We used 95% confidence intervals to provide the range of values that the true quantitative SI mean ratios are likely to fall within. Additionally, because this study was a con- trolled laboratory experiment in rats, the results cannot necessarily be extrapolated to humans.
In summary, statistically significant contrast enhancement on Tl-weighted MR imaging occurred following gamma knife irradiation in rats, strongly suggesting that blood-brain barrier breakdown is an integral finding of early-delayed CNS radiation damage. Metabolic disruptions of ischemia and necrosis, as measured by 1H MR spectroscopy, clearly could not be detected at this early time period.
REFERENCES
1. Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand 1951 ;102:316-319.
2. Luxton G, Petrovich Z, Jozsef G, et al. Stereotactic radiosurgery: principles and comparison of treatment methods. Neurosurgery 1993;32:241-259.
3. Leksell L. Cerebral radiosurgery: I. Gamma thalamotomy in two cases of intractable pain. Acta Chit Scand 1988;134:585-595.
4. Steiner L, Lindquist C, Adler JR, et al. Clinical outcome of radiosurgery for cerebral arteriovenous malformations. J Neurosurg 1992;77:1-8.
5. Lunsford LD, Kondziolka D, Flickinger JC, et al. Stereotactic radiosurgery for arteriovenous malformations of the brain, J Neurosurg 1991 ;75:512-524.
6. Coffey R J, Lunsford LD, Flickinger JC. The role of radiosurgery in the treatment of malignant brain tumors. Neurosurg Clin North Am 1992;3: 231-244.
7. Barcia-Salorio JL, Barcia JA, Roldan P, Hernandez G, Lopez-Gomez L. Radiosurgery of epilepsy. Acta Neurochir 1993;58[suppl]:195-197.
8. Sheline GE, Wara WM, Smith V. Therapeutic irradiation and brain injury. Int J Radiat Oncol Biol Phys 1980;6:1215-1228.
9. van der Kogel AJ. Central nervous system radiation injury in small animal models. In: Gutin PH, Leibel SA, Sheline GE, eds. Radiation injury to the nervous system. New York, Raven Press, 1991:91-111.
10. Caveness WE Pathology of radiation damage to the normal brain of the monkey. Natl Cancer Inst Monogr 1977;46:57-76.
11. Remler MP, Marcussen WH. Time course of early delayed blood-brain barrier changes in individual cats after ionizing radiation. Exp Neurol 1981 ;73:310-314.
12. Myers R, Rogers MA, Hornsey S. A reappraisal of the roles of glial and vascular elements in the development of white matter necrosis in irradi- ated rat spinal cord. Br J Cancer 1986;53[suppl. 7]:221-223.
13. Delattre JY, Rosenblum MK, Thaler HT, et al. A model of radiation myel- opathy in the rat: pathology, regional capillary permeability changes and treatment with dexamethasone. Brain 1988; 111 : 1319-1336.
14. Lo EH, Fabrikant JI. Delayed biologic reactions to stereotactic charged- particle radiosurgery in the human brain. Stereotact Funct Neurosurg 1991;56:197-212.
1050

Vol. 2, No. 12, December 1995 G A M M A K N I F E I R R A D I A T I O N - I N D U C E D C H A N G E S
15. Lo EH, DeLaPaz RL, Frankel KA, etal. MRI and PET of delayed heavy-ion radi- ation injury in the rabbit brain. Int J Radiat Onco Biol Phys 1991;20:689~396.
16. Weiner MW. The promise of magnetic resonance spectroscopy for medi- cal diagnosis. Invest Radio11988;23:253-261.
17. Bottomley PA. Human in vivo NMR spectroscopy in diagnostic medicine: clinical tool or research probe? Radiology 1989; 170:1-15.
18. Yousem DM, Lenkinski RE, Evans S, et al. Proton MR spectroscopy of experimental radiation-induced white matter injury. J Cemput Assist Tomogr 1992; 16:543-548.
19. Richards T, Budinger T. NMR imaging and spectroscopy of the mammalian cen- tral nervous system after heavy ion radiation. Radiat Res 1988; 113:79-101.
20. Hopewell JW, Wright EA. Modification of subsequent freezing damage by previous local brain irradiation. Exp Neuro11970;26:160-172.
21. Kamiryo T, Berk HW, Lee KS, et al. A stereotactic device for experimental gamma knife radiosurgery in rats: a technical note. Acta Neurochir (Wien) 1993;125:156-160.
22. Paxinos G, Watson C. The rat brain in stereotaxic coordinates (2nd ed.). San Diego, CA: Academic Press, 1986.
23. Omary RA, Berr SS, Kamirye T, et al. Stereotactic MRI-guided gamma knife irradiation to rat brain (abstr). Proc Soc Magn Reson 1994;3:1403.
24. Ogg R J, Kingsley PB, Taylor JS. WET, a T1- and Bl-insensitive water- suppression method for in vivo localized 1H NMR spectroscopy. J Magn Reson Series B 1994; 104:1-10.
25. Maudsley AA, Lin E, Meiner MW. Spectroscopic imaging display and analysis. Magn Reson Imaging 1992; 10:471-485.
26. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982;143:29-36.
27. Dorfman DD, Air E. Maximum likelihood estimation of parameters of sig- nal detection theory and determination of confidence intervals rating method data. J Math Psycho11969;6:487-496.
28. Berry CC. A tutorial on confidence intervals for proportions in diagnostic radiology. A JR 1990; 154:477-480.
29. Rosner B. Fundamentals of biostatistics (3rd ed.). Belmont, CA: Duxbury Press, 1990:219-221.
30. Gyulai L, Schnall M, McLaughlin AC, et al. Simultaneous 31p and 1H- nuclear magnetic resonance studies of hypoxia and ischemia in the cat brain. J Cereb Blood Flow Metab 1987;7:543-551.
31. Bruhn H, Frahm J, Gyngell ML, Merboldt KD, et al. Cerebral metabolism in man after acute stroke: new observations using localized proton NMR spectroscopy. Magn Reson Med 1989;9:126-131.
32. Nadler JV, Cooper JR. n-acetyl-l-aspartic acid content of human neural tumors and bovine peripheral nervous tissues. J Neurochem 1972;19:313-319.
33. Grossman RL, Joseph PM, Wolf G, et al. Experimental intracranial septic in- farction: magnetic resonance enhancement. Radiology 1985; 155:649-653.
34. Hecht-Leavitt C, Grossman RI, Curran W Jr, et al. MR of brain radiation injury: experimental studies in cats. Am J Neuroradio11987;8:427-430.
35. Lo EH, Frankel KA, Steinberg GK, et al. High dose single-fraction brain irradiation: MRI, cerebral blood flow, erectrophysiological, and histological studies. Int J Radiat Oncol Biol Phys 1991 ;22:47-55.
36. Lo EH, Frankel KA, DeLaPaz RL, et al. Cerebrovascular and metabolic pertubations in delayed heavy charged particle radiation injury. Brain Res 1989;504:168-172.
37. Yamamoto M, Jimbo M, Kobayashi M, et al. Long-term results of radiosur- gery for arterovenous malformation: neurodiagnostic imaging and histo- logical studies of angiographically confirmed nidus obliteration. Surg Neurol 1992;37:219-230.
38. Rubin P, Gash DM, Hansen JT, et al. Disruption of blood-brain barrier as the primary effect of CNS irradiation. Radiother Onco11994;31:51-60.
39. Zeman W, Curtis H J, Baker CP. Histopathologic effect of high-energy-particle micro- beams on the visual codex of the mouse brain. Radiat Res 1 g61;15:496-514.
1051




















