Longitudinal Stability of the CBCL-Juvenile Bipolar Disorder Phenotype: A Study in Dutch Twins
Upload
independentCategory
view
8download
0
Original Article
Functional outcome in bipolar disorder: therole of clinical and cognitive factors
Bipolar disorder has traditionally been associatedwith a better outcome than schizophrenia becauseof a presumed absence of cognitive impairmentand seemingly normal functioning between epi-sodes (1). Thus, generally little attention has beengiven to psychosocial outcomes in patients with
bipolar disorder (2). However, in contrast to earlystudies (1–3), recent studies point to a significantdegree of psychosocial dysfunction even whenpatients are euthymic (4–10). Functioning is acomplex concept since it involves the capacity towork, study, live independently and engage inrecreation and romantic life (2). Functional recov-ery has been described as the ability to achieve thelevel of functioning prior to the most recentepisode (6). A 2-year follow-up study on hospital-ized patients with a first manic episode with
Martinez-Aran A, Vieta E, Torrent C, Sanchez-Moreno J, Goikolea JM,Salamero M, Malhi GS, Gonzalez-Pinto A, Daban C, Alvarez-Grandi S,Fountoulakis K, Kaprinis G, Tabares-Seisdedos R, Ayuso-Mateos JL.Functional outcome in bipolar disorder: the role of clinical and cognitivefactors.Bipolar Disord 2007: 9: 103–113. ª Blackwell Munksgaard, 2007
Introduction: Few studies have examined the clinical,neuropsychological and pharmacological factors involved in thefunctional outcome of bipolar disorder despite the gap between clinicaland functional recovery.
Methods: A sample of 77 euthymic bipolar patients were included inthe study. Using an a priori definition of low versus good functionaloutcome, based on the psychosocial items of the Global Assessment ofFunctioning (GAF, DSM-IV), and taking also into account theiroccupational adaptation, the patients were divided into two groups:good or low occupational functioning. Patients with high (n ¼ 46) andlow (n ¼ 31) functioning were compared on several clinical,neuropsychological and pharmacological variables and the two patientgroups were contrasted with healthy controls (n ¼ 35) on cognitiveperformance.
Results: High- and low-functioning groups did not differ with respectto clinical variables. However, bipolar patients in general showed poorercognitive performance than healthy controls. This was most evident inlow-functioning patients and in particular on verbal memory andexecutive function measures.
Conclusions: Low-functioning patients were cognitively more impairedthan highly functioning patients on verbal recall and executive functions.The variable that best predicted psychosocial functioning in bipolarpatients was verbal memory.
A Martinez-Arana, E Vietaa, CTorrenta, J Sanchez-Morenoa,b, JMGoikoleaa, M Salameroa, GS Malhic,A Gonzalez-Pintod, C Dabana, SAlvarez-Grandia, K Fountoulakise, GKaprinise, R Tabares-Seisdedosf
and JL Ayuso-Mateosb
aInstitute of Neurosciences, University Hospital
Clinic of Barcelona, IDIBAPS, Barcelona,bDepartment of Psychiatry, Universidad Autonoma
de Madrid and Hospital Universitario de la
Princesa, Madrid, Spain, cNorthern Clinical School,
University of Sydney and Mood Disorders Unit,
Black Dog Institute, Sydney, Australia,dDepartment of Psychiatry, Santiago Apostol
Hospital, Osakidetza Mental Health System, Vitoria,
Spain, eThird Department of Psychiatry, Division of
Neurosciences, Faculty of Medicine, Aristotle
University of Thessaloniki, Thessaloniki, Greece,fTeaching Unit of Psychiatry and Psychological
Medicine, Department of Medicine, University of
Valencia, Valencia, Spain
Key words: bipolar disorder – cognitive
impairment – functional outcome – occupational
adaptation – psychosocial functioning – verbal
memory
Received 11 January 2005, revised and accepted
for publication 2 February 2006
Corresponding author: Eduard Vieta, MD, PhD,
Institute of Neurosciences, University Hospital
Clinic of Barcelona, Villarroel 170, 08036
Barcelona, Spain.
Fax: +34 93 2275477;
e-mail: [email protected]
The authors of this paper do not have any commercial associations
that might pose a conflict of interest in connection with this manu-
script.
Bipolar Disorders 2007: 9: 103–113Copyright ª Blackwell Munksgaard 2007
BIPOLAR DISORDERS
103

psychotic symptoms found that most patients(97%) achieved syndromal recovery at 24-monthfollow-up, whereas only 37% achieved functionalrecovery (6). These findings suggest that there is agap between clinical and functional outcome inbipolar disorder, which emerges at the very outsetof the illness. Hence, bipolar disorder can nega-tively impact the individual, reducing health-relat-ed quality of life and functioning, includingemployment and work productivity.The complex nature of bipolar illness may com-
plicate the measurement of impairment (11); how-ever, several factors have been associated with poorfunctional outcome, such as comorbid substanceabuse (12), the side-effects of medication (2), priorhistory of psychotic symptoms (5, 6), low premorbidfunctioning (13) persistent subsyndromal fluctua-tions (14–17), the number of prior episodes (5, 18),prior admissions (19, 20), younger age of onset (6)and persistent cognitive dysfunction (5, 15, 16, 21–24). However, the factors associated with functionaloutcome vary between studies and have been diffi-cult to replicate because of varied approaches andthe use of differing instruments to assess functionaloutcome. In this regard, cognitive function has notbeen routinely examined in the studies of psychoso-cial outcome in patients with bipolar disorderbecause clinical variables have been thought toimpact function more than cognition (25).The main aim of the present study was to
identify factors, among clinical, neuropsychologi-cal and pharmacological variables, which could beassociated with the functional outcome of bipolarpatients. Our hypothesis was that cognitive impair-ment, and especially verbal memory dysfunctions,would predict the low psychosocial functioning inpatients and do so better than clinical variables.This hypothesis was based on previous findingsfrom the scarce literature investigating the rela-tionship between cognition and functioning. Sev-eral authors found a correlation between verballearning and memory measures and functioning inbipolar patients (15, 16, 21–23).In contrast to previous research (15, 16), the
current study is directly focused on the psychoso-cial outcome of bipolar patients as the primaryobjective, involves a larger sample of euthymicbipolar patients that form part of a longitudinalstudy on clinical course, neuropsychologicalfunctioning and functional outcome within ourBarcelona Bipolar Disorders Program.
Methods
Patients participating in this study were enrolled atthe Bipolar Disorders Program of the University
Hospital Clinic of Barcelona. All patients metDSM-IV criteria for bipolar I or II disorder andwere euthymic. The clinical state of the patientswas determined by a psychiatrist responsible forthe follow-up of bipolar patients in the BipolarDisorders Program using DSM-IV criteria, and theStructured Clinical Interview for DiagnosticSymptoms (SCID, DSM-IV), the Spanish versionof the Hamilton Depression Rating Scale (HDRS,17-item) (26, 27) and the Young Mania RatingScale (YMRS) (28, 29). Euthymia was defined asYMRS £ 6 and HDRS £ 8, during monthly visitsover a 6-month period. After screening for inclu-sion, 77 bipolar patients and 35 healthy controlswere enrolled. The reasons for not entering thestudy were history of head injury or LOC, neuro-logical illness, substance dependence (in the lastyear), mental retardation, significant medical ill-ness, electroconvulsive therapy in the last year andsubsyndromal fluctuations. A total of 112 wereincluded initially, but 31 met one or more than oneexclusion criteria and were not admitted into thepresent study. The most common exclusion crite-rion was the presence of persistent subsyndromalsymptoms along the prior 6 months, and 22patients were excluded for this reason. Therefore,81 bipolar patients met the criteria for remission;of these 77 gave written informed consent toparticipate in the study after procedures had beenfully explained. On the contrary, in 92% ofpatients, medication was kept constant in theweeks before testing. Thirty-five healthy compar-ison subjects without psychiatric or neurologichistory were also recruited via advertisement andfrom a known pool of normal volunteers. Controlswere screened for Axis I psychiatric disorders usingthe SCID (DSM-IV), and it was ensured that nonehad first-degree relatives with bipolar disorder.With respect to the control group, six subjectscould not enter the study (two because of historyof head injury and four because of anxietydisorders). All subjects gave written informedconsent to participate in the study after theprocedures had been fully explained. Ethicalapproval for the study was granted by the EthicsCommittee.
Clinical and psychosocial assessment
Clinical variables were collected as part of theBipolar Disorders Program protocol of the Hospi-tal Clinic of Barcelona. The clinical variablesincluded in this study were the number and typeof episodes, duration of the illness (chronicity),age at onset of the illness, number of hospitaliza-tions, suicide attempts, family history of affective
Martinez-Aran et al.
104

disorders, history of psychotic symptoms, anddiagnostic type I or II.Overall functioning status was assessed using the
Global Assessment of Functioning scale (GAF,DSM-IV). The original GAF instructions call forrating symptoms or functioning. Since many othermeasures of mood symptoms were obtained as partof the evaluation, the rater was instructed to usethe GAF to measure psychosocial functioning inthe month prior to rating, as reported in previousstudies (16, 30), because it was expected that after6 months of sustained clinical remission, the func-tional recovery would be at the best point to beassessed.Second, occupational adaptation, as an addi-
tional measure of functional outcome, was estab-lished as �good occupational adaptation� whenpatients were working at a good or acceptablelevel of functioning. �Low occupational adapta-tion� was determined as not working at all orshowing moderate or severe difficulties in theirjob. This measure references the last 3 years priorto evaluation, a span of time significant enough tonot be influenced by the potential impact of longepisodes. This information was provided by thepatient himself and confirmed by a first-degreerelative or partner. For example, if the patient wasworking but showed difficulties completing evensimple tasks, the patient was classified as havinglow occupational adaptation, whereas if thepatient worked more than 75% of the time andshowed only mild work impairment, then thepatient was classified as having good occupationalfunctioning. This additional measure was usefulfor confirmation of findings and took part of thestructured interview of the protocol (15). Theclinical interview, including psychosocial function-ing, was conducted by a trained psychiatrist, andthe neuropsychological evaluation was carried outby a trained neuropsychologist, blind to theresults of the clinical and psychosocial assess-ments.The patient group was divided into two groups
with respect to psychosocial functioning asassessed through the GAF. A score of 60 was apriori considered as cut-off to distinguish patientswith good and low psychosocial functioning. Asper DSM-IV, a score higher or equal to 60represents some mild difficulty in social, occupa-tional or academic activities or satisfactory activ-ity. However, in general, the patient works quitewell and has significant interpersonal relationships.Scores below 60 indicate moderate to severeimpairment in functioning. The use of this cut-offwas previously recommended by earlier studiesthat used this cut-off to consider poor functioning
in severe psychiatric disorders, such as schizophre-nia (31–33).
Neuropsychological assessment
An extensive review of previous literature on thisissue guided the choice of neuropsychological testsused in the present study. In order to enhancereplication, only tests frequently documented bythe neuropsychological literature were employed(34, 35). The neuropsychological battery of tests isfully described elsewhere (16).
• Estimated premorbid IQ: Vocabulary subtest(Wechsler Adult Intelligence Scale) (36).
• Frontal executive functions: Wisconsin CardSorting Test (WCST) (37); Stroop Colour-WordInterference test (SCWT) (38); FAS (ControlledOral Word Association Test) (39). Attention/con-centration and mental tracking: Digit subtest(Wechsler Adult Intelligence Scale) (36); TrailMaking Test (TMT) (40).
• Verbal learning and memory: California VerbalLearning Test (CVLT) (41).
Statistical analyses
The three groups [patients with good psychosocialfunctioning (GAF ‡ 60), patients with low psycho-social functioning (GAF < 60) and healthycontrols] were compared on clinical and socio-demographic variables using ANOVA and chi-square test, as appropriate. Scatterplots wereperformed in order to confirm the appropriatenessof the a priori selected cut-off point of the GAF.MANOVA analysis was performed to show theoverall differences in neuropsychological testsbetween groups. Since multiple dependent varia-bles were used, a prior protective MANCOVAanalysis was performed with estimated premorbidintelligence as covariate and group as a mainfactor. Residual subsyndromal depressive symp-toms, as assessed using the HDRS, were thought tohave a confounding effect. When controlling forlow levels of symptoms in affected patients, theresults did not significantly vary; hence, thisvariable was not included as a covariate. Sinceneuropsychological tests are naturally correlated,this procedure was considered better thanBonferroni inequality correction that wouldincrease type II error. Group differences weretested using one-way ANOVA, followed by Tukeypost hoc comparison procedure, when significantmain effects were present. Homogeneity ofvariance was tested with Levene statistics.
Functional outcome in bipolar disorder
105
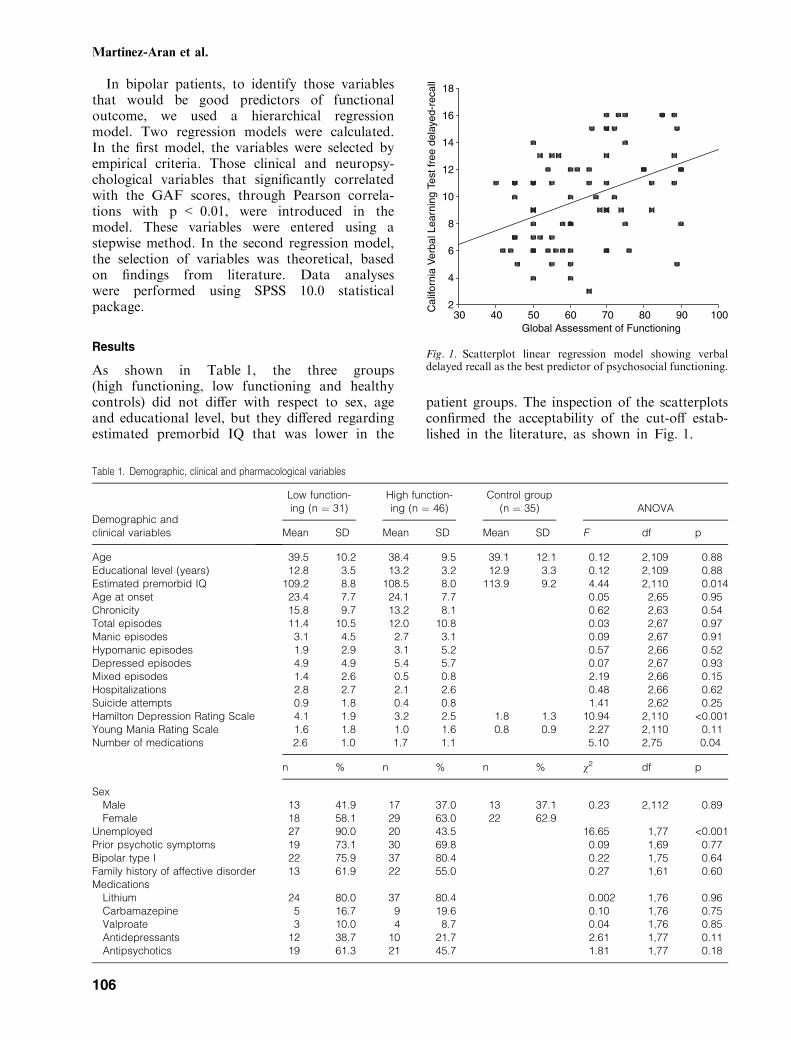
In bipolar patients, to identify those variablesthat would be good predictors of functionaloutcome, we used a hierarchical regressionmodel. Two regression models were calculated.In the first model, the variables were selected byempirical criteria. Those clinical and neuropsy-chological variables that significantly correlatedwith the GAF scores, through Pearson correla-tions with p < 0.01, were introduced in themodel. These variables were entered using astepwise method. In the second regression model,the selection of variables was theoretical, basedon findings from literature. Data analyseswere performed using SPSS 10.0 statisticalpackage.
Results
As shown in Table 1, the three groups(high functioning, low functioning and healthycontrols) did not differ with respect to sex, ageand educational level, but they differed regardingestimated premorbid IQ that was lower in the
patient groups. The inspection of the scatterplotsconfirmed the acceptability of the cut-off estab-lished in the literature, as shown in Fig. 1.
Table 1. Demographic, clinical and pharmacological variables
Demographic andclinical variables
Low function-ing (n ¼ 31)
High function-ing (n ¼ 46)
Control group(n ¼ 35) ANOVA
Mean SD Mean SD Mean SD F df p
Age 39.5 10.2 38.4 9.5 39.1 12.1 0.12 2,109 0.88Educational level (years) 12.8 3.5 13.2 3.2 12.9 3.3 0.12 2,109 0.88Estimated premorbid IQ 109.2 8.8 108.5 8.0 113.9 9.2 4.44 2,110 0.014Age at onset 23.4 7.7 24.1 7.7 0.05 2,65 0.95Chronicity 15.8 9.7 13.2 8.1 0.62 2,63 0.54Total episodes 11.4 10.5 12.0 10.8 0.03 2,67 0.97Manic episodes 3.1 4.5 2.7 3.1 0.09 2,67 0.91Hypomanic episodes 1.9 2.9 3.1 5.2 0.57 2,66 0.52Depressed episodes 4.9 4.9 5.4 5.7 0.07 2,67 0.93Mixed episodes 1.4 2.6 0.5 0.8 2.19 2,66 0.15Hospitalizations 2.8 2.7 2.1 2.6 0.48 2,66 0.62Suicide attempts 0.9 1.8 0.4 0.8 1.41 2,62 0.25Hamilton Depression Rating Scale 4.1 1.9 3.2 2.5 1.8 1.3 10.94 2,110 <0.001Young Mania Rating Scale 1.6 1.8 1.0 1.6 0.8 0.9 2.27 2,110 0.11Number of medications 2.6 1.0 1.7 1.1 5.10 2,75 0.04
n % n % n % v2 df p
SexMale 13 41.9 17 37.0 13 37.1 0.23 2,112 0.89Female 18 58.1 29 63.0 22 62.9
Unemployed 27 90.0 20 43.5 16.65 1,77 <0.001Prior psychotic symptoms 19 73.1 30 69.8 0.09 1,69 0.77Bipolar type I 22 75.9 37 80.4 0.22 1,75 0.64Family history of affective disorder 13 61.9 22 55.0 0.27 1,61 0.60Medications
Lithium 24 80.0 37 80.4 0.002 1,76 0.96Carbamazepine 5 16.7 9 19.6 0.10 1,76 0.75Valproate 3 10.0 4 8.7 0.04 1,76 0.85Antidepressants 12 38.7 10 21.7 2.61 1,77 0.11Antipsychotics 19 61.3 21 45.7 1.81 1,77 0.18
Global Assessment of Functioning10090807060504030
Cal
iforn
ia V
erba
l Lea
rnin
g Te
st fr
ee d
elay
ed-r
ecal
l
18
16
14
12
10
8
6
4
2
Fig. 1. Scatterplot linear regression model showing verbaldelayed recall as the best predictor of psychosocial functioning.
Martinez-Aran et al.
106

In regards to clinical variables, we did not findstatistical differences between patients with highand low functioning, as shown in Table 1. Thepatient groups statistically differed from thecontrol group in HDRS scores. No significantdifferences were found with respect to medicationregimens (lithium, carbamazepine, valproate, anti-depressants and antipsychotics) between thepatient groups, as shown in Table 1. Only twopatients were drug-free. Most patients (31/40) werereceiving atypical antipsychotics, and no differ-ences were observed between groups (v2 ¼ 0.94;p ¼ 0.33). Nevertheless, those patients with poorerpsychosocial functioning were treated with a highernumber of medications compared with patientswith better functioning (Table 1).With regard to neuropsychological variables,
results are shown in Table 2. MANCOVA yieldedPillai’s F ¼ 2.073, df ¼ 30,182, p ¼ 0.002 for themain effect, indicating that there were overalldifferences in neuropsychological performancebetween groups.For 12 of 15 comparisons, the differences
reached statistical significance (p < 0.05). In gen-eral, the two patient groups performed poorly onmost neuropsychological measures as comparedwith healthy controls especially in those measures
related to semantic verbal fluency (animal naming),verbal learning and memory (CVLT learning taskand cued short and delayed recall) and attentionand working memory (trail A and Digits task).Moreover, patients with lower psychosocial func-tioning showed even more impaired performanceon CVLT free short and long delay recall andrecognition task as well as on the Stroop inter-ference and trail B scores.Effect sizes are also shown in Table 2 (Cohen’s d
values). The values obtained indicate that effectsizes were, in general, medium or large (42). Largereffect sizes were observed for the low functioninggroup when compared with controls. Two regres-sion models were calculated, the former selectingthe variables following empirical criteria and thelatter theoretically.Pearson correlations were also used in order to
establish which clinical and neuropsychologicalvariables correlated with psychosocial functioning,as measured using the GAF. The variables thatwere found to correlate with psychosocial outcomewere HDRS scores (R ¼ 0.29; p ¼ 0.009), numberof medications (R ¼ )0.33; p ¼ 0.004), trail B(R ¼ )0.30; p ¼ 0.007), FAS (R ¼ 0.27; p ¼0.02) and all CVLT measures: learning task(R ¼ 0.37; p ¼ 0.001), free short recall (R ¼ 0.31;
Table 2. Neuropsychological performance in bipolar patients with high and low psychosocial functioning
A. Lowfunctioning
B. Highfunctioning
C. Controlgroup MANCOVA
Tukey posthoc tests
Cohen’s d
Mean SD Mean SD Mean SD F(2, 108) p A/C B/C A/B
Frontal executive function
WCSTCategories 5.0 1.6 5.2 1.5 5.5 1.3 0.20 0.82 0.34 0.21 0.12Perseverative errors 16.2 14.8 14.3 11.4 8.7 6.8 2.14 0.12 0.65 0.60 0.14
SCWTInterference )0.4 6.9 1.6 6.3 4.7 7.0 4.73 0.011 A<C 0.74 0.46 0.30
Attention/concentration and mental tracking
Subtest digits (WAIS)Digits forward 5.5 1.4 5.5 1.2 6.5 1.3 4.07 0.020 A, B<C 0.74 0.80 0.0Digits backward 3.9 1.1 4.1 0.9 5.0 1.2 5.53 0.005 A, B<C 0.95 0.94 0.20
TMTTrail A 46.9 20.1 42.4 14.8 30.2 11.6 7.11 0.001 A, B<C 1.02 0.91 0.25Trail B 125.8 68.5 92.4 48.1 74.6 37.1 6.47 0.002 A<C 0.93 0.41 0.56
Verbal fluency
FAS 34.2 10.9 36.1 10.3 39.6 11.9 0.81 0.45 0.47 0.31 0.17Animal naming 17.7 3.2 18.1 4.3 22.1 6.1 5.61 0.005 A, B<C 0.90 0.76 0.11
Verbal learning and memory
CVLTList A (total) 42.1 8.6 48.6 12.4 53.5 9.6 7.17 0.001 A, B<C 1.25 0.44 0.61Free short recall 8.2 3.4 10.2 3.5 11.3 3.3 5.09 0.008 A<C 0.92 0.32 0.58Cued short recall 9.9 2.8 11.2 2.8 12.7 2.3 6.65 0.002 A, B<C 1.09 0.59 0.46Free delayed recall 8.6 2.9 10.8 3.5 12.5 3.0 9.82 <0.001 A<B, C 1.32 0.52 0.68Cued delayed recall 9.8 2.9 11.3 3.1 13.0 2.6 8.06 0.001 A, B<C 1.16 0.59 0.50Recognition 13.4 2.2 14.2 2.2 15.0 1.3 4.42 0.014 A<C 0.88 0.44 0.36
CVLT ¼ California Verbal Learning Test; SCWT ¼ Stroop Colour-Word Interference Test; TMT ¼ Trail Making Test; WCST ¼ WisconsinCard Sorting Test; FAS ¼ Controlled Oral Word Association Test; WAIS ¼ Weschler Adult Intelligence Scale.
Functional outcome in bipolar disorder
107

p ¼ 0.006), cued short recall (R ¼ 0.31; p ¼ 0.006),free delayed recall (R ¼ 0.40; p < 0.001), cueddelayed recall (R ¼ 0.36; p ¼ 0.001) and recogni-tion hits (R ¼ 0.27; p ¼ 0.02). No correlationswere found between psychosocial outcome and age,chronicity, age of onset, number of hospitalizationsor suicide attempts and number or type of episodes.Therefore, those variables that correlated withpsychosocial outcome (p < 0.01), as mentionedabove, were introduced in the linear regressionmodel using stepwise method. Taking into accountthe potential impact of subsyndromal symptoms onfunctioning, this variable was included at a firstblock as well as the number of medications that alsosignificantly correlated with the GAF scores. Oncethe effect of these variables was controlled, at asecond block, neuropsychological measures thatcorrelated with the GAF scores were included. Thevariables that better predicted psychosocial func-tioning in euthymic bipolar patients were CVLTfree delayed recall (t ¼ 3.51, b ¼ 0.365, df ¼ 73,p ¼ 0.001) and the number of medications (t ¼)2.51, b ¼ )0.261, df ¼ 73, p ¼ 0.014). Overall,the model reached significance (F ¼ 11.29, df ¼2,73, p < 0.001), with an adjusted r2 ¼ 0.22. Ver-bal recall was the strongest independent predictorof psychosocial functioning, explaining 16% ofvariance (p < 0.001). Rerunning of the regressionmodel included clinical variables reported in theliterature as potential predictors of functionaloutcome, specifically, subclinical symptoms,chronicity, number of episodes and number ofhospitalizations, which were included in a firstblock, and the cognitive variables were introducedin a second block. Since the number of medicationsonly accounted for the 4% of the variance, it wastaken out of the model. The variable that bestpredicted functioning was verbal delayed recall(t ¼ 4.21, b ¼ 0.484, df ¼ 60, p < 0.001), whichaccounted for the 21% of the variance of psycho-social functioning. The other factors did not enterthe model. An interesting finding was that very lowlevels of depressive symptoms only accounted forthe 7% of the variance (t ¼ )1.34, b ¼ )0.154,df ¼ 60, p ¼ 0.19). This model accounted for the28% of the variance of psychosocial functioning(F ¼ 12.59, df ¼ 2,60, p < 0.001).Occupational adaptation, our secondary meas-
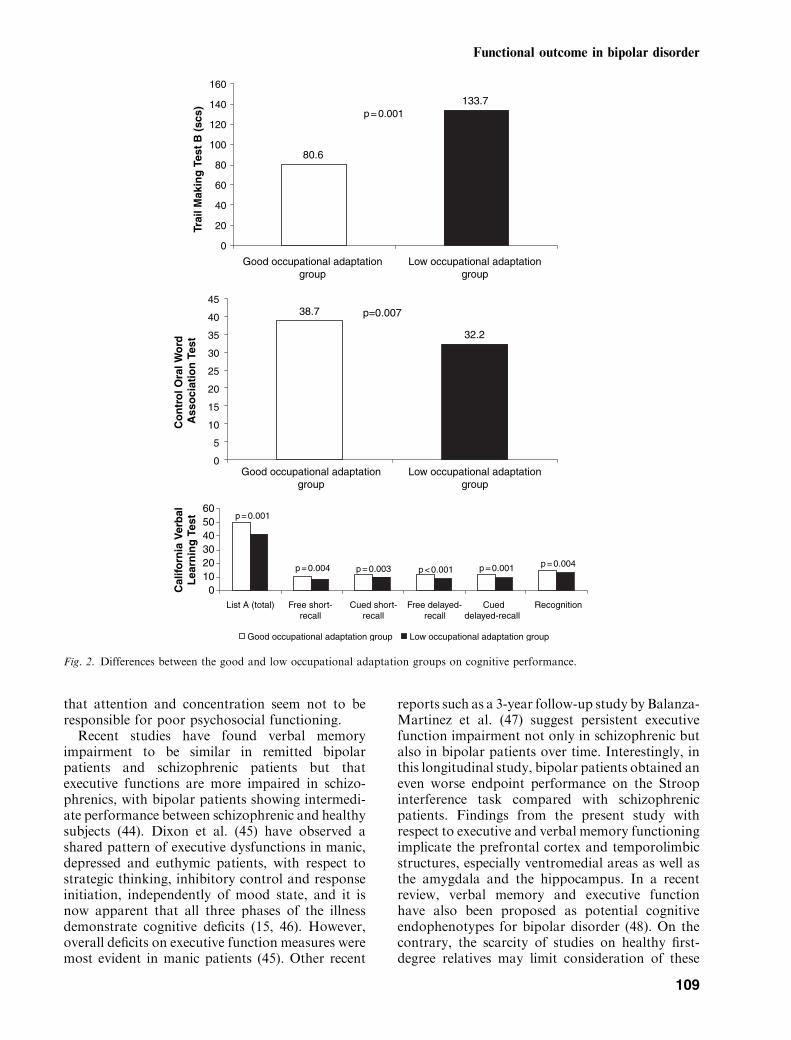
ure of functional outcome, was analysed amongthe patient groups. Neuropsychological perfor-mance between patients showing good and lowoccupational adaptation was analysed by usingANOVA. Results were confirmed when patientswith good and low occupational functioning werecompared (Fig. 2). Better neuropsychological per-formance was found in the �good occupational
adaptation� group compared with the �low occupa-tional adaptation� group, showing similar resultsthan those obtained using the GAF.
Discussion
The association of cognitive factors and psychosocialoutcomes
The present study reports that euthymic bipolarpatients with high functioning do not differ fromthose with low functioning with respect to clinicalvariables. However, they differ in terms of medi-cation (low functioning patients received highernumber of medications) and cognitive function(low-functioning patients performed worse onverbal memory and executive function measures).Euthymic bipolar patients performed poorer on
new learning as well as on recall than the compar-ison group. Both groups obtained poorer perfor-mance on attentional measures and semanticverbal fluency. Moreover, patients with low func-tioning were most impaired on measures related toinhibitory control (Stroop interference task) andworking memory (trail B), which are associatedwith frontal executive functions. Low functioningpatients showed worse performance on CVLT freedelayed recall and recognition measures comparedwith highly functioning and control groups. Thesefindings suggest that those patients with lowerpsychosocial functioning showed more generalizedverbal memory deficits, even in simpler tasks,indicating difficulties in encoding and retrieval ofverbal information. Verbal memory impairmenthas been suggested as a good predictor of workimpairment in euthymic bipolar patients (15, 16).In the present study, the verbal recovery of
information was the variable that best predictedthe psychosocial outcome of euthymic bipolarpatients. Difficulty remembering long-term infor-mation may represent a serious problem forbipolar patients in their occupational functioningas well as in their interpersonal relationships. Ingeneral, patients complain about having difficultyin remembering names and conversations both inthe distant past and more recently. These resultswere confirmed using the GAF scores as the mainmeasure as well as the occupational adaptation ofpatients during the last 3 years prior to inclusion inthe present study. Other neuropsychological vari-ables that seemed to correlate with psychosocialfunctioning, such as verbal fluency and trail B,have been reported as a predictor of outcome (24,43), but only verbal memory appeared in linearregression analysis. Probably one of the majorfindings that come out of the regression model is
Martinez-Aran et al.
108
that attention and concentration seem not to beresponsible for poor psychosocial functioning.Recent studies have found verbal memory
impairment to be similar in remitted bipolarpatients and schizophrenic patients but thatexecutive functions are more impaired in schizo-phrenics, with bipolar patients showing intermedi-ate performance between schizophrenic and healthysubjects (44). Dixon et al. (45) have observed ashared pattern of executive dysfunctions in manic,depressed and euthymic patients, with respect tostrategic thinking, inhibitory control and responseinitiation, independently of mood state, and it isnow apparent that all three phases of the illnessdemonstrate cognitive deficits (15, 46). However,overall deficits on executive function measures weremost evident in manic patients (45). Other recent
reports such as a 3-year follow-up study by Balanza-Martinez et al. (47) suggest persistent executivefunction impairment not only in schizophrenic butalso in bipolar patients over time. Interestingly, inthis longitudinal study, bipolar patients obtained aneven worse endpoint performance on the Stroopinterference task compared with schizophrenicpatients. Findings from the present study withrespect to executive and verbal memory functioningimplicate the prefrontal cortex and temporolimbicstructures, especially ventromedial areas as well asthe amygdala and the hippocampus. In a recentreview, verbal memory and executive functionhave also been proposed as potential cognitiveendophenotypes for bipolar disorder (48). On thecontrary, the scarcity of studies on healthy first-degree relatives may limit consideration of these
133.7
80.6
0
20
40
60
80
100
120
140
160
Good occupational adaptationgroup
Low occupational adaptationgroup
Good occupational adaptationgroup
Low occupational adaptationgroup
Trai
l Mak
ing
Tes
t B
(sc
s) p = 0.001
38.7
32.2
0
5
10
15
20
25
30
35
40
45
Co
ntr
ol O
ral W
ord
A
sso
ciat
ion
Tes
t
p=0.007
Cal
iforn
ia V
erb
alL
earn
ing
Tes
t
0102030405060
List A (total) Free short-recall
Cued short-recall
Free delayed-recall
Cueddelayed-recall
Recognition
Good occupational adaptation group Low occupational adaptation group
p = 0.004
p = 0.001
p = 0.003 p < 0.001 p = 0.001 p = 0.004
Fig. 2. Differences between the good and low occupational adaptation groups on cognitive performance.
Functional outcome in bipolar disorder
109

cognitive domains as endophenotypes, althoughdelayed verbal recall impairment has been re-ported in healthy first-degree relatives of bipolarprobands (49).Regarding other research on functional outcome
of bipolar disorder, in a study comparing bipolar Iand schizophrenic stable outpatients found thatbipolar patients did differ from schizophrenic onlyin 5 of 41 measures related to social functioning,quality of life and cognitive dysfunctions (23).Nevertheless, Ferrier et al. (50) did not finddifferences between patients with good and pooroutcome with regard to neurocognitive function-ing, probably because of their own definition ofoutcome, based on the clinical course of the illness.
The association of clinical factors with psychosocialoutcomes and cognition
Clinical variables that had been found to influencepsychosocial outcome in bipolar disorder in otherstudies, such as the number of episodes, age ofonset or duration of the illness, did not correlatewith GAF scores. Subclinical symptoms and espe-cially low levels of subdepressive symptoms werealso controlled in the present study. The patientshad very low levels of depressive and manicsymptoms. When results were covaried for HDRSscores, the findings did not substantially change.The only neuropsychological variable in which thepatient groups did not differ from healthy controlswas the Stroop Interference score and recognitionhits from the CVLT, as found in a previous study(16). It is likely that low levels of subclinicalsymptoms may influence some aspects of executivefunctions, such as inhibitory control and recogni-tion memory which is more impaired when en-coding processing fails. On the contrary, significantcorrelations were found between HDRS and GAFscores, as observed in previous studies (15, 16, 51).However, when this variable was introduced in thelinear regression analysis, it failed to enter in theequation. Subsyndromal depressive symptoms mayinterfere with functioning and quality of life (17).However, although inter-episode symptoms maycontribute to poor outcome (52), functional out-come is not appreciably better in studies in whichpatients have very low levels of residual sympto-matology (6, 19, 53). Some studies have suggested arelationship between cognitive impairment andpsychosocial functioning (15, 16, 22, 24) andtherefore after controlling the effects of clinicaland subclinical symptoms in our study, verbalmemory impairment was still found to influencesocial and occupational functioning in bipolarpatients (15).
Other clinical variables, such as the history ofpsychotic symptoms, did not influence psychoso-cial outcome in our bipolar sample and suchdiscrepancies have been found in other studies,for instance, with respect to the impact of psy-chotic symptoms on outcome (8, 10, 19, 50, 54).
The association of medication with psychosocial outcomesand cognition
No significant differences on neuropsychologicalperformance were found between patients takinglithium, antidepressants or antipsychotics com-pared with patients who did not take thosemedications.An unexpected finding was the influence of the
number of drugs on psychosocial outcome. Inprevious reports, this variable has been found tohave a negative impact on cognitive complaints ineuthymic bipolar patients (55). In the present studythe more medications the patients received, thegreater the psychosocial functioning impairment.Interestingly, some studies of bipolar patients onlithium monotherapy compared with patients onlithium plus other medications showed betteroccupational functioning in the former group,indicating that the former group may differ clin-ically from those requiring multiple psychotropicmedications (56). In this longitudinal open-labelstudy comparing lithium, neuroleptic, and lithium-neuroleptic therapies, significant differences werefound among monotherapy treated, combinationtherapy treated and untreated bipolar patients inoverall functioning. The lowest impairment wasfound among those on lithium monotherapy,followed by untreated individuals, those on neu-roleptic monotherapy and those on combinationtherapy. The impact of treatment on functionaloutcome has been widely reviewed in Dean et al.(11). It is still unclear whether the number ofmedications per se had a direct impact on outcomeor whether the impaired patients received a highernumber of drugs in an attempt to improve theircondition. That is, we do not really know thedirectionality cause–effect between the number ofmedications and the functional outcome, andprobably patients with low functional outcomewere more likely to be prescribed a larger numberof drugs. A longitudinal study would help to clarifythis important issue.Our study also highlights the limitations of
current treatment strategies regarding their capacityto improve the functioning and reduce the disabilityof bipolar patients. As much as 44% of a sample ofeuthymic patients followed up at a specializedprogram for bipolar disorders had a poor or low
Martinez-Aran et al.
110

functional outcome based on the psychosocial itemsof the GAF. This poor functioning, even in treatedeuthymic patients, is one of the main factors thatexplains why bipolar disorders have been rankedseventh amongst the worldwide causes of non-fataldisease burden, as measured in disability-adjustedlife years (DALYs) (57). Moreover, it is consistentwith recent studies that highlight the modest impactof available interventions on the functional out-comes of a large proportion of bipolar disorders(58), and call for a research agenda that specificallyaddresses these issues.
Limitations
The main limitation of the present study is thepartly artificial separation of the patients into twogroups based on a cut-off GAF score. However, itis probably useful to distinguish patients with no ormild impairment (highly functioning group) onpsychosocial outcome from those patients withsevere or moderate impairment (low functioninggroup). In order to avoid this limitation, a multipleregression analysis was performed including theGAF scores as a continuum variable to confirmresults found through MANCOVA. A longitudinalfollow-up may provide more information aboutthe progression or lack of progression of cognitivedysfunctions and their impact on psychosocialfunctioning. Probably, further longitudinal studiesshould include more specific instruments to assessthe functional outcome of bipolar patients. The useof measures related to the emotional processing ofinformation would probably be more associatedwith the functional outcome than basic cognitivemeasures, such as attention, memory or executivefunctions (55). Another relevant issue is the differ-ences between patients and controls with respect tomedication that could partly explain the differenceson neuropsychological performance. However,although cognitive dysfunctions may be related tothe effects of medication, they do not seem to be aprimary effect of pharmacological treatment.
Conclusions
The present findings suggest that cognitive factorsmay contribute to psychosocial outcome in bipolardisorder. Cognitive dysfunctions were found notonly in low-functioning patients but also inpatients with good psychosocial functioning. How-ever, cognitive impairments are most evident inlow-functioning patients. Differences relative tocognitive dysfunctions between high- and low-functioning patients seem to be independent ofillness severity. Verbal memory dysfunction seems
to be a good predictor of psychosocial outcome ineuthymic bipolar patients.Until recently, cognitive impairment has been
underestimated in bipolar patients, and our studyamongst others suggests that it should be consid-ered more widely with respect to the long-termmanagement of bipolar disorder. This may meansimplifying pharmacological treatment and select-ing combination therapies suitable for long-termprophylaxis, taking into account tolerability, sideeffects and interactions. The current treatments forbipolar patients have limitations regarding func-tional recovery. Therefore, psychosocial interven-tions, such as psychoeducation, family interventionand cognitive rehabilitation (15, 16, 59) should beimplemented. It is clear that clinical trials arenecessary to establish the efficacy of the differentpsychological interventions as adjunctives to phar-macological treatment in the improvement of theillness course, cognitive dysfunctions and psycho-social outcome in bipolar disorder.
Acknowledgements
This study was supported in part by grants from the SpanishMinistry of Health, Instituto de Salud Carlos III, Red deInvestigacion en Enfermedades Mentales REM-TAP andFIS no P1050206, Fundacio Marato de TV3 (2510/01), andthe Stanley Medical Research Institute, Bethesda, MD, USA.We also thank the Biostatistical Department of the HospitalClinic (Erika Sierra and Llorenc Quinto) for statistical support.
References
1. Kraepelin E. Manic-Depressive Insanity. New York: ArnoPress, 1976 (translated by Barclay RM, edited by RobertsonGM; originally published in 1921).
2. Zarate CA Jr, Tohen M, Land M, Cavanagh S. Functionalimpairment and cognition in bipolar disorder. Psychiatr Q2000; 71: 309–329.
3. Rennie TAC. Long-term outcome of major psychoses. AmJ Psychiatry 1942; 98: 801–814.
4. Tsuang MT, Dempsey GM. Long-term outcome ofmajor psychoses. II. Schizoaffective disorder com-pared with schizophrenia, affective disorders, and asurgical control group. Arch Gen Psychiatry 1979; 36:1302–1304.
5. Tohen M, Waternaux CM, Tsuang MT. Outcome inmania. A 4-year prospective follow-up of 75 patientsutilizing survival analysis. Arch Gen Psychiatry 1990; 47:1106–1111.
6. Tohen M, Hennen J, Zarate CM Jr et al. Two-yearsyndromal and functional recovery in 219 cases of first-episode major affective disorder with psychotic features.Am J Psychiatry 2000; 157: 220–228.
7. Carlson GA, Kotin J, Davenport YB, Adland M. Follow-up of 53 bipolar manic-depressive patients. Br J Psychiatry1974; 124: 134–139.
8. Goldberg JF, Harrow M, Grossman LS. Course andoutcome in bipolar affective disorder: a longitudinalfollow-up study. Am J Psychiatry 1995; 152: 379–384.
Functional outcome in bipolar disorder
111

9. Strakowski SM, Keck PE Jr, McElroy SL et al. Twelve-month outcome after a first hospitalization for affectivepsychosis. Arch Gen Psychiatry 1998; 55: 49–55.
10. Keck PE Jr, McElroy SL, Strakowski SM et al. 12-monthoutcome of patients with bipolar disorder followinghospitalization for a manic or mixed episode. Am JPsychiatry 1998; 155: 646–652.
11. Dean BB, Gerner D, Gerner RH. A systematic reviewevaluating health-related quality of life, work impairment,and healthcare costs and utilization in bipolar disorder.Curr Med Res Opin 2004; 20: 139–154.
12. Tohen M, Greenfield SF, Weiss RD, Zarate CA Jr, VaggeLM. The effect of comorbid substance use disorders on thecourse of bipolar disorder: a review. Harv Rev Psychiatry1998; 6: 133–141.
13. Cannon M, Jones P, Gilvarry C et al. Premorbid socialfunctioning in schizophrenia and bipolar disorder: similar-ities and differences. Am J Psychiatry 1997; 154: 1544–1550.
14. Gitlin MJ, Swendsen J, Heller TL, Hammen C. Relapseand impairment in bipolar disorder. Am J Psychiatry 1995;152: 1635–1640.
15. Martinez-Aran A, Vieta E, Reinares M et al. Cognitivefunction across manic or hypomanic, depressed, andeuthymic states in bipolar disorder. Am J Psychiatry2004; 161: 262–270.
16. Martinez-Aran A, Vieta E, Colom F et al. Cognitiveimpairment in euthymic bipolar patients: implications forclinical and functional outcome. Bipolar Disord 2004;6: 224–232.
17. Marangell LB. The importance of subsyndromal symp-toms in bipolar disorder. J Clin Psychiatry 2004; 65 (Suppl.10): 24–27.
18. MacQueen GM, Young LT, Robb JC, Marriott M, CookeRG, Joffe RT. Effect of number of episodes on wellbeingand functioning of patients with bipolar disorder. ActaPsychiatr Scand 2000; 101: 374–381.
19. Dion GL, Tohen M, Anthony WA, Waternaux CS.Symptoms and functioning of patients with bipolar disor-der six months after hospitalization. Hosp CommunityPsychiatry 1988; 39: 652–657.
20. O’Connell RA, Mayo JA, Flatow L, Cuthbertson B,O’Brien BE. Outcome of bipolar disorder on long-termtreatment with lithium. Br J Psychiatry 1991; 159: 123–129.
21. Atre-Vaidya N, Taylor MA, Seidenberg M, Reed R,Perrine A, Glick-Oberwise F. Cognitive deficits, psycho-pathology, and psychosocial functioning in bipolar mooddisorder. Neuropsychiatry Neuropsychol Behav Neurol1998; 11: 120–126.
22. Zubieta JK, Huguelet P, O’Neil RL, Giordani BJ. Cogni-tive function in euthymic bipolar I disorder. Psychiatry Res2001; 102: 9–20.
23. Dickerson FB, Sommerville J, Origoni AE, Ringel NB,Parente F. Outpatients with schizophrenia and bipolar Idisorder: do they differ in their cognitive and socialfunctioning? Psychiatry Res 2001; 102: 21–27.
24. Martinez-Aran A, Vieta E, Colom F et al. Neuropsycho-logical performance in depressed and euthymic bipolarpatients. Neuropsychobiology 2002; 46 (Suppl. 1): 16–21.
25. Goldberg TE, Gold JM, Greenberg R et al. Contrastsbetween patients with affective disorders and patients withschizophrenia on a neuropsychological test battery. Am JPsychiatry 1993; 150: 1355–1362.
26. Hamilton M. A rating scale for depression. J NeurolNeurosurg Psychiatry 1960; 23: 56–62.
27. Ramos-Brieva JA, Cordero-Villafafila A. A new validationof the Hamilton rating scale for depression. J Psychiatr Res1988; 22: 21–28.
28. Young RC, Biggs JT, Ziegler VE, Meyer DA. A ratingscale for mania: reliability, validity and sensitivity. Br JPsychiatry 1978; 133: 429–435.
29. Colom F, Vieta E, Martinez-Aran A et al. Spanish versionof a scale for the assessment of mania: validity andreliability of the Young Mania Rating Scale. Med Clin(Barc) 2002; 119: 366–371.
30. Altshuler LL, Gitlin MJ, Mintz J, Leight KL, Frye MA.Subsyndromal depression is associated with functionalimpairment in patients with bipolar disorder. J ClinPsychiatry 2002; 63: 807–811.
31. Liberman RP, Kopelowicz A. Recovery from schizophre-nia: a concept in search of research. Psychiatr Serv 2005;56: 735–742.
32. Kessler RC, Barker PR, Colpe LJ et al. Screening forserious mental illness in the general population. Arch GenPsychiatry 2003; 60: 184–189.
33. Whitehorn D, Kopala LC. Neuromotor dysfunction inearly psychosis. Ann Clin Psychiatry 2002; 14: 113–121.
34. Lezak MD. Neuropsychological Assessment, 3rd edn. NewYork: Oxford University Press, 1995.
35. Spreen O, Strauss E. A Compendium of Neuropsycholog-ical Tests. Administration, Norms Commentary, 2nd edn.New York: Oxford University Press, 1998.
36. Weschler D. Weschler Adult Intelligence Scale. Cleveland,OH: The Psychological Corporation, 1955.
37. Heaton RK. Wisconsin Card Sorting Test Manual.Odessa, FL: Psychological Assessment Resources, 1981.
38. Golden CJ. Stroop Colour and Word Test. Chicago:Stoelting, 1978.
39. Benton AL, Hamsher K. Multilingual Aphasia Examina-tion. Iowa City: University of Iowa, 1976.
40. Reitan RM. Validity of the Trail Making Test as aindication of organic brain damage. Percept Mot Skills1958; 8: 271–276.
41. Delis DC, Kramer JH, Kaplan E, Ober B. CaliforniaVerbal Learning Test. New York: Psychological Corpora-tion, 1987.
42. Cohen J. Statistical Power Analysis for the BehaviouralScience, 2nd edn. Hillsdale, NJ: Lawrence Erlbaum Asso-ciates, 1988.
43. Martinez-Aran A, Penades R, Vieta E et al. Executivefunction in patients with remitted bipolar disorder andschizophrenia and its relationship with functional out-come. Psychother Psychosom 2002; 71: 39–46.
44. Altshuler LL, Ventura J, van Gorp WG, Green MF,ThebergeDC,Mintz J. Neurocognitive function in clinicallystable men with bipolar I disorder or schizophrenia andnormal control subjects. Biol Psychiatry 2004; 56: 560–569.
45. Dixon T, Kravariti E, Frith C, Murray RM, McGuire PK.Effect of symptoms on executive function in bipolar illness.Psychol Med 2004; 34: 811–821.
46. Malhi GS, Ivanovski B, Szekeres V, Olley A. Bipolardisorder: it’s all in your mind? The neuropsychologicalprofile of a biological disorder. Can J Psychiatry 2004; 49:813–819.
47. Balanza-Martinez V, Tabares-Seisdedos R, Selva-Vera Get al. Persistent cognitive dysfunctions in bipolar I disorderand schizophrenic patients: a 3-year follow-up study.Psychother Psychosom 2005; 74: 113–119.
48. Glahn DC, Bearden CE, Niendam TA, Escamilla MA. Thefeasibility of neuropsychological endophenotypes in thesearch for genes associated with bipolar affective disorder.Bipolar Disord 2004; 6: 171–182.
49. Keri S, Kelemen O, Benedek G, Janka Z. Different traitmarkers for schizophrenia and bipolar disorder: a neuro-cognitive approach. Psychol Med 2001; 31: 915–922.
Martinez-Aran et al.
112

50. Ferrier IN, Stanton BR, Kelly TP, Scott J. Neuropsycho-logical function in euthymic patients with bipolar disorder.Br J Psychiatry 1999; 175: 246–251.
51. Coryell W, Turvey C, Endicott J et al. Bipolar I affectivedisorder: predictors of outcome after 15 years. J AffectDisord 1998; 50: 109–116.
52. MacQueen GM, Young LT, Joffe RT. A review ofpsychosocial outcome in patients with bipolar disorder.Acta Psychiatr Scand 2001; 103: 163–170.
53. MacQueen GM, Young LT, Robb JC, Cooke RG, JoffeRT. Levels of functioning and well-being in recoveredpsychotic versus nonpsychotic mania. J Affect Disord1997; 46: 69–72.
54. Harrow M, Goldberg JF, Grossman LS, Meltzer HY.Outcome in manic disorders. A naturalistic follow-upstudy. Arch Gen Psychiatry 1990; 47: 665–671.
55. Martinez-Aran A, Vieta E, Colom F et al. Do cognitivecomplaints in euthymic bipolar patients reflect objective
cognitive impairment? Psychother Psychosom 2005;74: 295–302.
56. Goldberg JF, Harrow M, Leon AC. Lithium treatment ofbipolar affective disorders under naturalistic followupconditions. Psychopharmacol Bull 1996; 32: 47–54.
57. World Health Organization. The World Health Report2001; Mental Health: New Understanding, New Hope.Geneva: WHO ed., 2001.
58. Chisholm D, Sanderson K, Ayuso-Mateos JL, Saxena S.Reducing the global burden of depression: population-levelanalysis of intervention cost-effectiveness in 14 worldregions. Br J Psychiatry 2004; 184: 393–403.
59. Vieta E, Colom F. Psychological interventions in bipolardisorder: from wishful thinking to an evidence-basedapproach. Acta Psychiatr Scand Suppl 2004; 34–38.
Functional outcome in bipolar disorder
113

Copyright © 2022 FDOKUMEN