Frost J, Anderson R, Argyle C, et al 12013 A pilot randomised controlled trial of a preconsultation...
10
doi: 10.1136/bmjopen-2013-003396 2013 3: BMJ Open Julia Frost, Rob Anderson, Catherine Argyle, et al. outcomes of diabetes outpatients (DIAT) improve the care quality and clinical preconsultation web-based intervention to A pilot randomised controlled trial of a http://bmjopen.bmj.com/content/3/7/e003396.full.html Updated information and services can be found at: These include: References http://bmjopen.bmj.com/content/3/7/e003396.full.html#ref-list-1 This article cites 42 articles, 9 of which can be accessed free at: Open Access non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/ terms, provided the original work is properly cited and the use is work non-commercially, and license their derivative works on different license, which permits others to distribute, remix, adapt, build upon this Creative Commons Attribution Non Commercial (CC BY-NC 3.0) This is an Open Access article distributed in accordance with the service Email alerting the box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in Collections Topic (86 articles) Patient-centred medicine (296 articles) Health services research (76 articles) Diabetes and Endocrinology Articles on similar topics can be found in the following collections Notes http://group.bmj.com/group/rights-licensing/permissions To request permissions go to: http://journals.bmj.com/cgi/reprintform To order reprints go to: http://group.bmj.com/subscribe/ To subscribe to BMJ go to: group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.com Downloaded from
Transcript of Frost J, Anderson R, Argyle C, et al 12013 A pilot randomised controlled trial of a preconsultation...

doi: 10.1136/bmjopen-2013-003396 2013 3: BMJ Open
Julia Frost, Rob Anderson, Catherine Argyle, et al. outcomes of diabetes outpatients (DIAT)improve the care quality and clinicalpreconsultation web-based intervention to A pilot randomised controlled trial of a
http://bmjopen.bmj.com/content/3/7/e003396.full.htmlUpdated information and services can be found at:
These include:
References http://bmjopen.bmj.com/content/3/7/e003396.full.html#ref-list-1
This article cites 42 articles, 9 of which can be accessed free at:
Open Access
non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/terms, provided the original work is properly cited and the use iswork non-commercially, and license their derivative works on different license, which permits others to distribute, remix, adapt, build upon thisCreative Commons Attribution Non Commercial (CC BY-NC 3.0) This is an Open Access article distributed in accordance with the
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(86 articles)Patient-centred medicine � (296 articles)Health services research �
(76 articles)Diabetes and Endocrinology � Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from

A pilot randomised controlled trial of apreconsultation web-based interventionto improve the care quality and clinicaloutcomes of diabetes outpatients (DIAT)
Julia Frost,1 Rob Anderson,2 Catherine Argyle,3 Mark Daly,3
Faith Harris-Golesworthy,4 Jim Harris,4 Andy Gibson,1 Wendy Ingram,5
Jon Pinkney,6 Obioha C Ukoumunne,1 Bijay Vaidya,7 Jane Vickery,5 Nicky Britten1
To cite: Frost J, Anderson R,Argyle C, et al. A pilotrandomised controlled trial ofa preconsultation web-basedintervention to improve thecare quality and clinicaloutcomes of diabetesoutpatients (DIAT). BMJ Open2013;3:e003396.doi:10.1136/bmjopen-2013-003396
▸ Prepublication history forthis paper is available online.To view these files pleasevisit the journal online(http://dx.doi.org/10.1136/bmjopen-2013-003396).
Received 12 June 2013Accepted 20 June 2013
For numbered affiliations seeend of article.
Correspondence toDr Julia Frost;[email protected]
ABSTRACTIntroduction: Diabetes is a chronic conditionassociated with many long-term complications. Peoplewith diabetes need to actively manage their condition,which can be complex. In consultations with healthcareprofessionals, patients receive advice about theirdiabetes but do not always discuss things whichconcern them, perhaps because of the perceivedlimited time or embarrassment. We want to test a‘preconsultation’ intervention in which the patient issupported by a healthcare assistant to complete a web-based intervention aimed at producing an agenda tohelp them identify important areas for discussion inthe consultation. Use of this agenda may enable thepatient to play a more active role in that consultationand consequently become more confident, and hencemore successful, in managing their condition.Methods and analysis: In this pilot randomisedcontrolled trial, 120 people with diabetes will berandomised with equal allocation to receive theintervention or usual clinical care. The primary outcomeis reduction in glycosylated haemoglobin(HbA1c).Secondary outcomes are patient-reportedcommunication, enablement, self-care activity, diabetes-dependent quality of life, empowerment, satisfaction,health-related quality of life and resource use. The aimof the pilot study was to estimate parameters to informthe design of the definitive trial. Follow-up onquantitative outcomes will be at 3 and 6 months.A nested qualitative study will collect data on thepatients’ experiences of producing an agenda. Resourceuse data and medication use will also be collected via areview of medical records for a sample of participants.Ethics and dissemination: Approval was granted bythe NHS Research Ethics Committee North West—Preston (13/NW/0123). Dissemination will includepublication of quantitative and qualitative findings, andexperience of public involvement in peer-reviewedjournals. Results will also be disseminated to trialparticipants via workshops led by lay coapplicants.Trial Registration: ISRCTN75070242.
ARTICLE SUMMARY
Article focus▪ This paper describes a protocol for a pilot
randomised controlled trial of a preconsultationweb-based intervention to enable patients withdiabetes to produce their own agenda for a con-sultation with their diabetologist.
Key messages▪ A preconsultation intervention in which the
patient is supported by a healthcare sssistant tocomplete a web-based intervention will facilitatethe production of ‘their agenda’ to help themidentify important areas for discussion in theconsultation.
▪ Combining trial as well as qualitative researchmethods ensures that the ‘active ingredients’ ofthe intervention are identified and explored,which will enable estimate parameters to informthe design of a definitive trial.
▪ Involving patients as collaborators ensures thatthis research deals explicitly with patients’ infor-mation needs, thus increasing the probability ofthe DIAT intervention being taken up in practice.
Strengths and limitations of this study▪ This study addresses areas identified as requir-
ing more research in the 2013 Cochrane reviewof computer-based diabetes self-managementinterventions for adults with type 2 diabetes,which identified that interventions may have asmall effect on blood glucose, but no benefits tocognitive, behavioural or emotional outcomes.The intervention is grounded in real-worldpatient experience, and pragmatically designed tobe scaled up for a definitive trial and use in prac-tice, but a potential limitation is that thefollow-up period may not be long enough todemonstrate a reduction in glycosylatedhaemoglobin.
Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396 1
Open Access Protocol
group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on September 25, 2013 - Published by bmjopen.bmj.comDownloaded from

INTRODUCTIONDiabetes will affect an estimated 439 million people glo-bally by 2030, with an estimated 2.5 million in the UK.1
Diabetes is a chronic disease, associated with a numberof serious complications, and the costs of treating aperson with diabetes rise by 60–90% as vascular pro-blems progress.2 Up to 80% of the National HealthService’s (NHS) £9.8 billion annual UK expenditure ondiabetes is spent on treating complications.3
Diabetes is largely monitored and managed by patientsthemselves.4 Self-management is complex, involving,among other things, self-monitoring, behaviouralchange, medication management and a rigorous lifestyleregimen. Advice from professionals is vital to self-management, improving patients’ ability to cope withtheir illness. Effective consultations are associated withempowerment, positive behaviour change and improveddiabetes outcomes.5–9 However, consultations with diabe-tologists are infrequent and patients often do not takefull advantage of their time with their clinician.10 Theymay feel embarrassed, rushed or simply have forgottensome of the urgent problems they encountered sincetheir previous consultation. Patients with types 1 and 2diabetes attending two diabetes centres in England per-ceived that they were not commonly questioned aboutsensitive aspects of their condition, such as erectile dys-function and gastroparesis.11 A UK service evaluationidentified that health professionals, including diabetolo-gists, felt competent in identifying patients’ psychologicalissues but less knowledgeable and skilled in handlingthem.12 Thus, methods to improve the quality of consul-tations in terms of the ability of the patient to discussissues that concern them, understand information andremember and follow advice are consistently sought.A systematic review found that the most common
methods used to improve the quality of consultations arequestion checklists and patient coaching delivered imme-diately before consultations, and that information-seeking behaviour and patient satisfaction were mostimproved by combining coaching with written material.13
Greenfield et al’s14 study, using a review of medicalrecords, a treatment algorithm and a behavioural changestrategy, improved patient participation in the consult-ation and glycaemic control. A recent systematic review ofcomputer-based diabetes self-management interventionsfor adults with type 2 diabetes identified 16 randomisedcontrolled trials, but was unable to distinguish betweenthose that were set in primary care, outpatients or com-munity settings.15 The reviewers concluded that diabetesself-management interventions may have a small effecton blood glucose, with mobile ‘phone-based interven-tions having a greater impact than computer-based inter-ventions, and no evidence of benefits to cognitive,behavioural or emotional outcomes’. In conclusion, theywere unable to discern the active ingredients or optimal‘dose’ of the interventions.A relatively inexpensive intervention has been devel-
oped by Cegala et al, evolving from an instruction
booklet, to booklet plus coaching, to a web-based train-ing module (http://patcom.jcomm.ohio-state.edu/).Cegala et al16 identified that effective communicationinvolves patients: presenting detailed information abouthow they are feeling; asking questions if desired informa-tion is not provided; checking understanding of informa-tion that is given to them and expressing any concernsabout the recommended treatment. This ‘PACE’ systemhas shown promise in oncology,17 has an outcomemeasure for communication18 and can easily be tailoredfor use by people with diabetes.The intervention has been designed to facilitate the
articulation of patients’ often unvoiced agendas16 18–25
which arise from their continual efforts to manage theirconditions.26 27 Discussion of these agendas enablespatients to manage their condition more effectively,7 28–30
which includes better adherence.31 32
The PACE intervention has been modified specificallyfor diabetes (as PACE-diabetes or PACE-D) by the DIATProject Team. PACE-D is a web-based tool, designed tobe completed by a patient before a clinic appointment.In this study, the appointment is with a consultantdiabetologist.A trained healthcare assistant (HCA) will facilitate the
use of the PACE-D tool, with the aim of assisting patientsto identify the things that they wish to discuss with thediabetologist (ie, their ‘agenda’) in the clinical consult-ation. The intervention takes approximately 20 min tocomplete, and consists of a series of open and closedquestions, prompts and a list of possible concerns thatpeople with diabetes have identified (eg, ‘increasedthirst’ or ‘depression’). On completion, a conciseagenda will automatically be produced, which thepatient will take into their consultation with a diabetolo-gist, and which may be used subsequently (ie, in discus-sions with the general practitioner (GP) or practicenurse, and to guide self-management).PACE-D aims to enable patients to identify their
agenda for discussion with the diabetologist, improvingcommunication and empowering patients to be moreproactive at managing their diabetes, potentially leadingto improved clinical and quality-of-life outcomes. Theintervention appears to be a simple and relatively inex-pensive tool but requires a rigorous test of its efficacyand cost-effectiveness. Piloting the PACE-D interventionand agenda with people with diabetes could provideimprovements in communication, blood glucose man-agement, enablement, self-care, medication use andquality of life, with little impact on cost or clinic time.We will measure enablement and patient perceptions ofthe effectiveness of the consultation, which are per-ceived as crucial to effective diabetes control.28
The aim of this pilot study was to obtain the necessaryinformation for the planning of a future definitive trialto assess the clinical and cost-effectiveness of a preclinicintervention specifically for diabetes.The primary objective of this pilot study was to test the
feasibility of running a randomised controlled trial of a
2 Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396
Open Access

preconsultation web-based intervention to improve thecare quality and clinical outcomes of people withdiabetes.The secondary objectives were to determine:
▸ The likely success of recruitment strategies.▸ The acceptability of the research plan to proposed
participants and allowance for the estimation of likelyparticipation and attrition rates.
▸ The data that will be useful for estimating therequired sample size for a full trial.
▸ The training requirements of those clinic staff taskedwith implementing the intervention.
▸ Resource use, for example, the use of staff, requiredto provide the intervention and usual care.
▸ A preliminary estimate of the cost of the intervention.▸ The validity and responsiveness of quality-of-life
outcome measures in the patient group (includinggeneric preference-based measures).
▸ The practicality and accuracy of using alternativemethods of data collection for service and resourceuse (ie, patient report/review of medical records).
Patient and public involvementPatient and public involvement (PPI) is fundamental to allaspects of this research. The research question was gener-ated from a research prioritisation exercise, undertaken bythe National Institute for Health Research (NIHR)Collaboration for Leadership in Applied Health Researchand Care in the South West Peninsula (PenCLAHRC) withactive involvement from the Peninsula Patient and PublicInvolvement Group (PenPIG).People with diabetes identified the research topic and
suggested that outpatient clinic appointments are pres-sured times, where health professionals can overlookissues that are worrying patients or where patients canfeel inhibited from voicing their concerns. The sametopic was identified by a diabetes specialist nurse (DSN)at a comparable professional workshop.A project team was convened and a scoping exercise
undertaken to assess what is known about the problem,and members of PenPIG discussed the existing researchand perceptions of current and desired future clinicconsultations. Two members of PenPIG who have dia-betes joined the research team as coapplicants on thisproposal. They also have representative roles within thelocal Diabetes Research Network and Devon DiabetesService Strategy Implementation Group. Supported by adesignated PPI Research Fellow, these two coapplicantshave cowritten the study documentation and will assist inthe analysis of the data and the dissemination of theresearch results to lay and professional audiences. Theyare members of the project management team and willassist in training HCAs.If the findings of the pilot indicate feasibility, there
will be patient and public coapplicants on the full trialproposal, which will be submitted to an appropriatesource of funding. Members of the public involved inthis pilot will be paid travel expenses and receive a
payment in recognition of their contribution to theresearch.
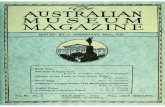
METHODSTrial designThe pilot trial is a pragmatic pilot randomised con-trolled trial. The outcomes were chosen and the inter-vention designed during the development phase of thestudy (see Discussion section; figure 1).
Participants and study settingThe pilot trial will recruit 120 patients attending diabetesoutpatient clinics at two hospitals in Devon, south-westEngland, which treat people from urban and rural set-tings. In 2010/2011, these two diabetes centres under-took approximately 9000 new appointments and 12 000follow-up appointments. People with a range of diabetescomplications and comorbidities will be included in thepilot, and the experiences gained will inform the inclu-sion and exclusion criteria of the larger trial. Althoughthe intervention might potentially have benefit for allconsultations (including those in primary care), thebenefit is likely to be greater in secondary care where typ-ically more issues and problems are discussed. Eligiblepatients are adults with type 1 or 2 diabetes mellitus whoare due to attend outpatient appointments with a diabe-tologist. Participants are aged 18 or over and have basicspoken or written English (to complete outcome mea-sures). Women with pre-existing or gestational diabetesand people receiving insulin pump therapy are excluded.
Recruitment of patientsThe study sample comprises people with diabetes whoare due to attend a general diabetes clinic appointmentat the Macleod Diabetes and Endocrine Centre at theRoyal Devon and Exeter Hospital, Exeter, or the MedicalOutpatients Department at Derriford Hospital,Plymouth. Potential participants will be identified fromthe clinic lists of participating consultant diabetologistsby a research nurse at each location. Patients who expressan interest in participating in the trial will be sent aninformation sheet. A research nurse will telephone eachpotential participant after a minimum of 1 week, discussany questions that the patient may have and establish ifthey are willing to participate. The nurse will then send aconsent form and baseline questionnaires to those willingto take part. Following receipt of informed writtenconsent and the completed baseline questionnaires, par-ticipants will be randomised to receive either the inter-vention or usual care (control), as detailed below.
InterventionIn a 20 min session immediately preceding the clinicappointment, a trained HCA will help the patient tocomplete the PACE-D tool (the aim being for thepatient to identify and produce their own agenda for
Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396 3
Open Access

the consultation). After the intervention, the patient willproceed to the clinical consultation, in which theprinted output from the PACE-D intervention will act asan agenda for the consultation. Owing to the nature ofthe intervention and the production of an agenda, itwill not be possible to blind health professionals orpatients to trial allocation. With consent, 10 participantsacross the two sites will be audio-recorded as they usethe PACE-D tool, for qualitative analysis.
ControlThis comprises clinical care normally given by the diabe-tologist in outpatient clinics.
OutcomesPrimary outcome measureThe primary outcome measure is glycosylated haemoglo-bin (HbA1c),33 a measure of glycaemic control. HbA1c
levels will be measured within 4 weeks of each assess-ment (ie, at baseline, 3 and 6 months), and will be retro-spectively obtained from participants’ medical records.
Secondary outcome measuresSecondary outcome measures (patient self-reportedrating scales) will be measured at all three time points.The rating scales will be sent to all participants withinstructions for completion and a prepaid return enve-lope. In addition, participants will be asked to documenttheir current medication at each time point, as well asthe number and type of contacts with primary and sec-ondary care practitioners during the study. Those in thetreatment arm will also be asked at 6 months about theirexperience of using the PACE-D tool and the utility ofproducing ‘their agenda’.Patient self-reported outcome measures:
Figure 1 DIAT trial schedule.
4 Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396
Open Access

Audit of Diabetes-Dependent Quality of Life-19 (ADDQoL):Developed to measure an individual’s perception ofthe impact of diabetes on their quality of life,34 thistool has 2 overview items and 19 individual domains(eg, working life, holidays, physical appearance, etc).For each domain, the respondent reports the impact ofdiabetes on their quality of life (on a 5-point scale,scored from −3 to 1 with higher scores indicating agreater impact) and the importance of the domain (ona 4-point scale score from 0 to 3 with higher scoresindicating greater importance). The quality-of-lifescore for each domain is calculated by taking theproduct of the impact and importance scores withscores ranging from –9 (maximum negative impact ofdiabetes) to +3 (maximum positive impact of dia-betes). The average weighted impact score is calculatedas the mean across the domain scores. The PatientReport of Outcomes Measure Group, Oxford35 recom-mends the use of ADDQoL as their preferred diabetes-specific measure.Client services receipt inventory: Originally developed forcollecting cost-related information for people withmental health problems over a given period (usuallythe past 6 or 12 months),36 this is a long-establishedand widely adapted questionnaire. It collects retro-spective information about the interviewee’s use ofhealth and social care services, home and employmentsituation, as well as income and benefits. We will pilota simplified version of this questionnaire, tailored fordiabetes and capturing resource use over a 3-monthperiod, for intended use in the main trial.Diabetes empowerment scale-short form (DES): This scalewas developed in the USA to measure diabetes-relatedpsychosocial self-efficacy.37 38 This eight-item scale,derived from a behaviour change model, employs afive-point Likert scale (strongly disagree (1) to stronglyagree (5)). An overall score for DES is calculated bytaking the mean of the item scores.Diabetes self-care activity measure: This 11-item instru-ment is a self-reported questionnaire of diabetes self-management which includes five aspects (activities) ofthe diabetes regimen.39 40 Questions for general diet(two items), specific diet (two items), exercise (twoitems), blood glucose testing (two items) and footcare (two items) use an eight-point Likert scale (from0 to 7) to record the number of days in the past weekthat the activity was undertaken. The overall score foreach activity is calculated as the mean of the twoitems. Smoking (during the past 7 days) is recorded asyes or no, with smokers additionally reporting thenumber of cigarettes smoked on an average day.Diabetes treatment satisfaction questionnaire—status (status,DTSQ(S)) and change versions: DTSQ(S) was developedto measure patient satisfaction with diabetes treat-ment.41 42 DTSQ(S) consists of six items to assess treat-ment satisfaction and two items to capture patientperceived hypoglycaemia/hyperglycaemia. The DTSQ(S) items are scored on a Likert scale from 0 to 6 (0=very
dissatisfied, 6=very satisfied). A total score is created as thesum of scores across the treatment satisfaction items(possible score from 0 to 36). In response to concernsabout ceiling effects, where high baseline scores providelittle opportunity to register change at follow-up,the authors produced the DTSQ ‘change’ version(DTSQ(C)), which contains the same items, but askspatients to consider their satisfaction with current treat-ment compared with their previous treatment.43 DTSQ(C) items are scored on a scale from −3 to 3 (−3=less sat-isfied now, 3=more satisfied now, with a midpoint of 0reflecting no change). The total score is again calcu-lated by summing the scores on the treatment satisfac-tion items, with the range of possible values from −18 to18. Both versions will be used in order to capture initialperceptions and any change at follow-up.EuroQoL (EQ-5D-5 L): The original EQ-5D is a genericmeasure for valuing and describing health. It defineshealth in terms of: mobility, self-care, usual activities,pain/discomfort and anxiety/depression and uses athree-point Likert scale (no problem, some problem,extreme problem44). EQ-5D health states, defined by theEQ-5D descriptive system, may be converted into asingle summary index by applying a formula thatessentially attaches values (also called weights) to eachof the levels in each dimension. The Patient Report ofOutcomes Measure Group, Oxford35 recommends theuse of EQ5D as their preferred generic measure incombination with a disease-specific instrument.However, this instrument has also been found to sufferfrom ceiling effects, and a five-level version has beendeveloped (EQ-5D-5 L), which uses a five-point Likertscale (no problem, slight problem, moderate problem, severeproblem, extreme problem) and has demonstratedincreased reliability and sensitivity.45
Patient enablement instrument (PEI): Developed tomeasure patient enablement after a consultation witha physician, PEI contains six items with a four-pointLikert scale: not applicable/same or less (0); better/more(1); much better/much more (2).46 The total score is thesum of scores across the items (possible range ofscores is 0 to a maximum score of 12). Haughneyet al47 have subsequently modified the opening state-ment to capture perspectives on treatment specifically,and this version will be used.Patient report of communication: Developed to measurecommunication in conjunction with the PACE tool,this instrument comprises 11 questions about per-ceived communication, with two items for each of thefour PACE skills, two additional items for the patient’sability to state their preferences and a global itemabout the consultation.18 It uses a 5-point Likert scalethat captures aspects of doctor–patient communica-tion as never (1), not very often (2), sometimes (3), usually(4) and always (5). Mean scores will be calculated foreach PACE skill and across all 11 items. This instru-ment has been shown to be reliable in patients withcancer and those undergoing surgery.18
Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396 5
Open Access

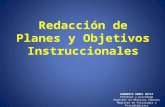
Participant timelineA brief explanation of the participant’s timeline isshown in (figure 2).
Sample sizeAs this is a pilot study, comparison of the outcomesbetween the trial arms is not a major objective and thestudy is not powered to do this. We aim to recruit 120patients, 60 at each site. At least six clinic ‘sessions’ (ie,the period of time in which a clinic is held within theoutpatient department, usually in the morning or after-noon, when 8–15 patients are seen by their consultant)at each site will be required.An objective of the pilot study is to estimate the SD for
continuous outcomes to be used in the definitive trial asthis will facilitate the sample size calculation for thatstudy. We anticipate that at least half of the participants(ie, 60) will provide the follow-up data at 6 months. Sixtypatients are sufficient to estimate an SD to within 22%
of its true value based on the upper bound of the95% CI.The study will also estimate the percentage of eligible
participants that participate and the percentage of parti-cipants that are successfully followed up. If the true per-centage of participants that provide follow-up data at6 months is 50%, this study will be able to estimate thiswith a margin of error of ±13%, based on a 95% CI,assuming that participants from a given clinic session areno more likely to drop out than those from anothersession.
RandomisationAn independent statistician based at the PeninsulaClinical Trials Unit (PenCTU) will generate the random-isation list, using computer-generated random numbers.Randomisation will be stratified by clinic session.Randomisation will be achieved by means of an auto-
mated web-based system created by a PenCTU data pro-grammer in conjunction with the independentstatistician and accessed by a separate member of thePenCTU staff on receipt of the completed consent form.Consenting participants will be allocated with equalprobability to receive PACE-D or usual clinical care,using randomly permuted blocks of varying size to gen-erate the allocation sequence and achieve balance in thenumbers of participants allocated to each group.Following randomisation, PenCTU will notify partici-
pants by standard letter about the arrival time for theirclinic appointment. Those in the intervention arm willbe notified that they are required to arrive 30 min early,while those in the control arm will be notified that theyare not required to arrive early.
Statistical methodsThe main aim of this pilot study was to estimate para-meters that will ultimately inform the design of the maintrial. The participation rate will be calculated as the per-centage of eligible participants that are randomised,with 95% CIs. The loss to follow-up rate will be reportedat 3 and 6 months with 95% CIs. SD will be reportedwith 95% CIs for the primary outcome. Other para-meters to be reported include mean duration of theclinic conversation in each trial arm.In ancillary analyses, baseline characteristics will be
reported using percentages for categorical data, andmeans and SDs (or medians and IQRs) for quantitativedata. The trial arms will be compared at 3 and 6 monthsusing the t test for quantitative outcomes and the χ² testfor binary outcomes. Linear and logistic regression,respectively, will be used to adjust comparisons for base-line scores on the outcome. There will be no interimanalyses, and neither will stopping rules be applied.Missing data will not be imputed.
Qualitative methodsTen intervention sessions will be audio-recorded withthe participants’ consent, in order to explore howFigure 2 Flow of participants.
6 Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396
Open Access

participants utilise the PACE-D intervention and theamount of assistance that they require from HCA inorder to complete their agenda form.In addition, approximately 30 clinical consultations
across both trial arms and study sites will be audio-recorded, with the consent of both the participants andtheir diabetologist. Maximum variance sampling will beused so that any impact of variables of interest (ie,patient age, clinician grade or clinic site) can beexplored.Recording consultations is crucial to understanding
the mechanism that underlies the impact of the produc-tion of an agenda on the clinical consultation, and itssubsequent utilisation in practice, when compared withusual care. Hence, we will report on the fidelity of theintervention, content of the consultation, context forthe use of the agenda and any impact on theconsultation.Semistructured interviews will also be conducted with
a sample of 30 participants across trial arms andresearch sites, after participation in the trial has beencompleted and in order to examine aspects of interven-tion and participants’ experiences of diabetes consulta-tions in more depth.48 With the participants’ consent,these interviews will be audio-recorded and will explore:participants’ experience of diabetes and clinical consul-tations; raising concerns with health professionals inprimary and secondary care; participants’ experience ofeither usual care or intervention and trial participation.For the semistructured interviews, participants in both
trial arms will be purposefully sampled to include thosewith type 1 or 2 diabetes, new and existing patients, andpeople with different ages/genders/socioeconomicbackgrounds and, where possible, different comorbid-ities, following a maximum variation sampling strategy.49
It is necessary to include interviews with participants inthe usual care arm of the trial to explore how patientsnormally voice their agendas during diabetes consulta-tions, and with what consequences. The interviews willtake place after the final follow-up at 6 months, to avoidany influence of the interview on these measures.Interviews will be conducted at a location that is con-venient to the participant.A topic guide will be used, which has been developed
with involvement from the PPI coapplicants, to ensurethat the primary issues are covered, while allowing flexi-bility for new issues to emerge from each interview.Interviews will be digitally recorded, fully transcribedand anonymised to protect confidentiality.In addition to the interviews with participants,
approximately 10 interviews with health professionals(eg, HCAs, research nurses and diabetologists) involvedin the study at each research site will be conducted nearthe end of the trial. They will explore the professionals’views about the intervention and issues around imple-mentation. A flexible topic guide will be employed andthese interviews will explore: professionals’ experienceof diabetes and clinical consultations; addressing
patients’ concerns in secondary care; professionals’experience of usual care and the intervention and trialparticipation.The audio-recordings from the consultations and
interviews will be transcribed and read in detail by teammembers who are experienced in qualitative researchmethods and a list of common themes and conceptsdrawn up.26 Data collection and analysis will be literativeand ongoing, with the coding frame refined as newthemes and categories are identified from subsequentinterviews.50 The qualitative data will be managed usingNvivo software.
Cost-effectiveness methodsAn economic evaluation will not be conducted as part ofthis pilot study. However, data will be collected to informthe design of the economic evaluation alongside theplanned definitive trial, by: comprehensively estimatingthe range of care resource use and cost impacts relatedto the intervention (ie, potential costs of implementa-tion using HCA or research nurses or DSNs or othermodes of delivery) and its expected outcomes; refiningand justifying the choices of outcome measures forhealth-related quality of life and testing the practicalityand validity of methods for collecting patient-reportedresource/service use; and providing some preliminaryestimates of different parameters and their variances.
DisseminationDissemination of the results and projected outputs willbe appropriate to that of a pilot study, and the keyoutput will be an application to an appropriate funderfor a definitive trial of the intervention. As the researchquestion was generated through the PPI Group, andservice users are integral to the research team, theresults of the study will be of particular interest to thosewho use diabetic services. The PPI coapplicants withother members of the research team will disseminatethe results of this pilot to the trial participants, via twoworkshops, which will be conducted at neutral locationstowards the end of the study.The results from the pilot will be more widely dissemi-
nated in order to share our experiences and to generateenthusiasm for the future definitive trial. We will informpeople with diabetes through articles in lay health maga-zines, electronic forums and presentations. We willinform clinicians and health-service managers throughsubmissions to appropriate journals and presentations atsuitable conferences.Results from the future definitive trial would be disse-
minated widely through a variety of media, includingpeer-reviewed journal articles and conference presenta-tions, with an emphasis on reaching NHS policymakersand commissioners, health professionals and serviceusers.
Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396 7
Open Access

DISCUSSIONDuring the development phase of the research, threekey methodological aspects were discussed.The research team has purposely chosen to trial the
PACE-D (intervention) in secondary care—a decisionwhich was much debated during the study developmentphase. Discussions included people with diabetes (bothtypes 1 and 2, including those who have experience ofconsultations with diabetologists in the hospital out-patient setting), GPs, diabetologists, DSNs, practicenurses and lay and professional members of theDiabetes Research Network and Primary Care Network.Following these lengthy discussions, a decision was madeto sample new and existing patients attending clinicappointments with six diabetologists at two different hos-pitals, as it is believed that these people may have a par-ticular set of concerns. If the intervention is successfulin this population, we may consider undertaking futureresearch with the intervention in primary care settings,where patients may have a different set of concerns.The potential for contamination between the trial
arms resulting from the use of individual patient ran-domisation was debated by the research team, and anumber of alternative randomisation strategies were con-sidered, including cluster randomisation of clinics, con-sultants or sites. The research team reached a consensusthat contamination is unlikely in this context, given thatthe active ingredient of the intervention is use of thePACE-D tool, and therefore decided to use individualrandomisation.People with diabetes identified the research topic and
requested that the intervention (PACE-D) should befacilitated by a DSN. However, while the study was beingdesigned and discussions with local NHS partners wereundertaken, it was apparent that DSNs are increasinglytime pressured. A pragmatic decision was thereforemade by the research team, including lay representa-tives, that the trial intervention should be facilitated by anumber of HCAs routinely present at general outpatientdiabetes clinics, and who will be trained in study proce-dures by a DSN coapplicant. It is thought that this willprovide a valid insight into how the intervention wouldwork in a future trial and in the ‘real world’ clinicalsetting.
CONCLUSIONPeople with diabetes need to actively monitor andmanage their condition; however, they are not alwaysable to discuss things which concern them at clinicalconsultations with their diabetologist. Guidelines in theUK emphasise the importance of more actively involvingpeople with diabetes in the consultation process andongoing management of their condition. The DIATstudy aims to inform best practice in this area by evaluat-ing an intervention to assist patients to produce anagenda for their consultation. We think that this mayenable patients to play a more active role in that
consultation and subsequently make them moreenabled, and hence successful at managing theircondition.
Author affiliations1Institute for Health Services Research, University of Exeter Medical School,Exeter, UK2PenTAG, Institute for Health Services Research, University of Exeter MedicalSchool, Exeter, UK3Macleod Diabetes and Endocrine Centre, Royal Devon and Exeter FoundationTrust, Exeter, UK4Peninsula Public Involvement Group (PenPIG), National Institute for HealthResearch (NIHR) Collaboration for Leadership in Applied Health Research andCare (CLAHRC) for the South West Peninsula5Peninsula Clinical Trials Unit, Plymouth University Peninsula Schools ofMedicine and Dentistry, Plymouth, UK6Plymouth University and Peninsula Schools of Medicine and Dentistry,Derriford Hospital, Plymouth Hospitals NHS Trust7Department of Diabetes & Endocrinology, Royal Devon and Exeter Hospital,University of Exeter Medical School, Exeter, UK
Acknowledgements The authors would like to thank the study sponsor:Royal Devon and Exeter NHS Foundation Trust. They are grateful to DonaldCegala (Emeritus Professor of Communication and Family Medicine, OhioState University) for supporting their use and modification of the PACEintervention.
Collaborators FH-G and JH, Peninsula Public Involvement Group (PenPIG),National Institute for Health Research (NIHR) Collaboration for Leadership inApplied Health Research and Care (CLAHRC) for the South West Peninsula.
Contributors NB, CA, FH-G, JH, AG, OCU, BV, MD, JP and JF conceived theoriginal study and developed the protocol with WI and JV. JF led the writingof the first draft of the manuscript, with contributions from RA, CA, MD, AG,WI, JP, OCU, BV, JV and NB. All authors contributed to the editing andredrafting.
Funding This research is funded by the National Institute for Health Research(NIHR) under its Research for Patient Benefit (RfPB) Programme (GrantReference Number PB-PG-0711-25087).
Competing interests AG is funded by the National Institute for HealthResearch (NIHR) Collaboration for Leadership in Applied Health Research andCare (CLAHRC) for the South West Peninsula. OCU is partially supported bythe National Institute for Health Research (NIHR) Collaboration for Leadershipin Applied Health Research and Care (CLAHRC) for the South West Peninsula.NB is partially supported by the National Institute for Health Research (NIHR)Collaboration for Leadership in Applied Health Research and Care (CLAHRC)for the South West Peninsula.
Ethics approval The study was approved by the NHS Research EthicsCommittee North West—Preston (13/NW/0123).
Provenance and peer review The research question was generated from aresearch prioritisation exercise, undertaken as part of the PeninsulaCollaboration for Leadership in Applied Health Research and Care (CLAHRC)Patient and Public Involvement Group (PenPIG); internally peer reviewed.
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license,which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, providedthe original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
REFERENCES1. Shaw J, Sicree R, Zimmet P. Global estimates of the prevalence of
diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87:4–14.2. Dancer S, Courtney M. Improving diabetes outcomes: framing
research into the chronic care model. J Am Acad Nurse Pract2010;22:580–5.
8 Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396
Open Access

3. Hex N, Bartlett C, Wright D, et al. Estimating the current and futurecosts of Type 1 and Type 2 diabetes in the UK, including directhealth costs and indirect societal and productivity costs. DiabeticMed 2012;29:855–62.
4. Anderson R, Funnell M. Patient empowerment: reflections on thechallenge of fostering the adoption of a new paradigm. Patient EducCouns 2005;57:153–7.
5. Piette J, Schillinger D, Potter M, et al. Dimensions of patient-providercommunication and diabetes self-care in an ethnically diversepopulation. J Gen Intern Med 2003;18:624–33.
6. Van Dam H, van der Horst F, van den Borne B, et al.Patient-provider interaction in diabetes care: effects on patientself-care and outcomes: a systematic review. Patient Educ Couns2003;51:17–28.
7. Williams G, McGregor H, Zeldman A, et al. Promoting glycaemiccontrol through diabetes self-management: evaluating a patientactivation intervention. Patient Educ Couns 2005;56:28–34.
8. Sturt J, Taylor H, Doherty A, et al. A psychological approach toproviding self-management education for people with type 2diabetes: the Diabetes Manual. BMC Fam Pract 2006;7:70.
9. Rose V, Harris M, Ho M, et al. A better model of diabetesself-management? Interactions between GP communication andpatient self-efficacy in self-monitoring of blood glucose. Patient EducCouns 2009;77:260–5.
10. Keers J, Links T, Bouma J, et al. Do diabetologists recogniseself-management problems in patients? Diabetes Res Clin Pract2004;66:157–61.
11. Grant P, Lipscomb D. How often do we ask about erectiledysfunction in the diabetes review clinic? Acta Diabetol2009;46:285–90.
12. Mosely K, Aslam A, Speight J. Overcoming barriers to diabetescare: perceived communication issues of healthcare professionalsattending a pilot diabetes UK training programme. Diabetes Res ClinPract 2010;87:e11–14.
13. Kinnersley P, Edwards A, Hood K, et al. Interventions beforeconsultations for helping patients address their information needs(review). Cochrane Database Syst Rev 2007;(3):CD004565.
14. Greenfield S, Kaplan S, Ware J, et al. Patients’ participation inmedical care: effects on blood sugar control and quality of life indiabetes. J Gen Intern Med 1988;3:448–57.
15. Pal K, Eastwood SV, Michie S, et al. Computer-based diabetesself-management interventions for adults with type 2 diabetesmellitus. Cochrane Database Syst Rev 2013;(3):CD008776.
16. Cegala D, Post D, McClure L. The effects of patient communicationskills training on the discourse of elderly patients during a primarycare interview. J Am Geriatr Soc 2001;49:1505–11.
17. Fleisher L, Buzaglo J, Collins M, et al. Using health communicationbest practices to develop a web-based provider–patientcommunication aid: the CONNECT study. Patient Educ Couns2008;71:378–87.
18. Bylund C, D’Agostino T, Ho E, et al. Improving clinicalcommunication through concordance based patient education.Commun Educ 2010;59:294–311.
19. Greenfield S, Cretin S, Worthman L, et al. Comparison of a criteriamap to a criteria list in quality-of-care assessment for patients withchest pain: the relation of each to outcome. Med Care1981;19:255–72.
20. Greenfield S, Kaplan S, Ware J. Expanding patient involvementin care: effects on patient outcomes. Ann Intern Med 1985;102:520–8.
21. Kravitz R. Patients’ expectations for medical care: an expandedformulation based on review of the literature. Med Care Res Rev1996;53:3–27.
22. Cegala D, McClure L, Marinelli T, et al. The effects ofcommunication training on patients: participation during medicalinterviews. Patient Educ Couns 2000a;41:209–22.
23. Cegala D, Marinelli T, Post D. The effects of patient communicationskills training on compliance. Arch Fam Med 2000b;9:57–64.
24. Curtin R, Sitter D, Schatell D, et al. Self-management, knowledge,and functioning and well-being of patients on hemodialysis. NephrolNurs J 2004;31:378–86.
25. Sleath B, Chewning B, Svarstad B, et al. Patient expression ofcomplaints and adherence problems with medications during chronicdisease medical visits. J Soc Adm Pharm 2000;17:71–80.
26. Barry C, Bradley C, Britten N, et al. Patients’ unvoiced agendasin general practice consultations: qualitative study. BMJ2000;320:1246–50.
27. Hamilton W, Russell D, Stabb C, et al. The effect of patient self-completion agenda forms on prescribing and adherence in generalpractice: a randomised controlled trial. Fam Pract 2007;24:77–83.
28. Funnell M, Anderson R. Empowerment and self-management ofdiabetes. Clin Diabetes 2004;22:123–7.
29. Williams G, Freedman Z, Deci E. Testing a self-determination theoryprocess model for promoting glycaemic control through diabetesself-management. Health Psychol 2004;23:58–66.
30. Williams G, Lynch M, Glasgow R. Computer-assisted interventionimproves patient-centred diabetes care by increasing autonomysupport. Health Psychol 2007;26:728–34.
31. Roter DL. Patient participation in patient-provider interaction: theeffects of patient question-asking on the quality of interaction,satisfaction, and compliance. Health Educ Monogr 1977;5:281–315.
32. Rose V, Harris M, Ho M, et al. A better model of diabetesself-management? Interactions between GP communication andpatient self-efficacy in self-monitoring of blood glucose. Patient EducCouns 2009;77:260–5.
33. Perry RC, Shankar RR, Fineberg N, et al. HbA1c measurementimproves the detection of type 2 diabetes in high-risk individuals withnon-diagnostic levels of fasting plasma glucose: the Early DiabetesIntervention Program (EDIP). Diabetes Care 2001;24:465–71.
34. Bradley C, Todd C, Gorton T, et al. The development of anindividualized questionnaire measure of perceived impact ondiabetes and quality of life. Qual Life Res 1999;8:79–91.
35. Gibbons E, Fitzpatrick R. Patient Reported Outcome MeasuresGroup. A structured review of patient reported outcome measures forpeople with diabetes: an update 2009. http://phi.uhce.ox.ac.uk/pdf/Diabetes_2009FINAL.pdf (accessed 20 May 2013).
36. Beecham J, Knapp M. Costing psychiatric interventions. In:Thornicroft G.ed. Measuring mental health needs. 2nd edn. London:Gaskell, 2001: 200–24.
37. Anderson R, Fitzgerald T, Funnell M, et al. The diabetesempowerment scale: a measure of psychosocial self-efficacy.Diabetes Care 2000;23:739–43.
38. Anderson R, Fitzgerald J, Gruppen L, et al. The diabetesempowerment scale-short form (DES-SF). Diabetes Care2003;26:1641–2.
39. Toobert D, Glasgow R. Assessing diabetes self-management: thesummary of diabetes self-care activities questionnaire. In: Bradley C.ed. Handbook of psychology and diabetes: a guide to psychologicalmeasurement in diabetes research and practice. Switzerland:Harwood Academic, 1994: 351–75.
40. Toobert D, Hampson S, Glasgow R. The summary of diabetesself-care activities measure: results from 7 studies and a revisedscale. Diabetes Care 2000;23:943–50.
41. Bradley C, Lewis KS. Measures of psychological well-being andtreatment satisfaction developed from the responses of people withtablet-treated diabetes. Diabetic Med 1990;7:445–51.
42. Bradley C. Diabetes treatment satisfaction questionnaire. In:Bradley C.ed. Handbook of psychology and diabetes: a guide topsychological measurement in diabetes research and practice.Switzerland: Harwood Academic, 1994: 111–32.
43. Bradley C. The Diabetes treatment satisfaction questionnaire(DTSQ): change version for use alongside status version providesappropriate solution where ceiling effects occur. Diabetes Care2007;22:530–2.
44. Brooks R. EuroQol: the current state of play. Health Policy1996;37:53–72.
45. Herdman M, Gudex C, Lloyd A, et al. Badia X development andpreliminary testing of the new five level version of EQ-5D(EQ-5D-5 L). Qual Life Res 2011;20:1727–36.
46. Howie J, Heaney D, Maxwell M, et al. A comparison of a PatientEnablement Instrument (PEI) against two established satisfactionscales as an outcome measure of primary care consultations. FamPract 1998;15:165–71.
47. Haughney J, Cotton P, Rosen J-P, et al. The use of a modification ofthe patient enablement instrument in asthma. Prim Care Respir J2007;16:89–92.
48. Frost J, Shaw A, Montgomery M, et al. Women’s views on the use ofdecision aids for decision making about the method of deliveryfollowing a previous caesarean section: qualitative interview study.Br J Obstet Gynaecol 2009;116:896–905.
49. Patton MQ. Qualitative research and evaluation methods. 3rd edn.London: Sage, 2002.
50. Mays N, Pope C. Qualitative research in health care. London: BMJBooks, 1996.
Frost J, Anderson R, Argyle C, et al. BMJ Open 2013;3:e003396. doi:10.1136/bmjopen-2013-003396 9
Open Access