From the Flight Deck to the Operating Room: An Initial Pilot Study of the Feasibility and Potential...
9
2007 APDS SPRING MEETING From the Flight Deck to the Operating Room: An Initial Pilot Study of the Feasibility and Potential Impact of True Interdisciplinary Team Training using High-Fidelity Simulation John Paige, MD,* Valeriy Kozmenko, MD, † Barbara Morgan, MD, † D. Shannon Howell, BA, ‡ Sheila Chauvin, MEd, ‡ Charles Hilton, MD, ‡ Isidore Cohn, Jr, MD,* and J. Patrick O’Leary, MD* *Department of Surgery, † Department of Anesthesia, and ‡ Office of Medical Education, Louisiana State University Health Sciences Center, New Orleans, Louisiana BACKGROUND: The operating room is a dynamic environ- ment in which proper teamwork is essential. After piloting a simulation-based interdisciplinary operative team training program, we examined the impact of these sessions on the participants. METHODS: Three interdisciplinary operating room teams participated in the training model. Each team of 3 or 4 mem- bers completed the training in a virtual minimally invasive op- erating room using a standardized operative scenario. Upon completion of the training, participants completed a voluntary and anonymous training effectiveness questionnaire. RESULTS: All 10 participants completed the training evalua- tion questionnaires. Across the 3 teams, all participants felt that the training was worthwhile and would participate again. Eight participants said that the session would change their practices in the operating room. All participants felt that the session was effective in promoting team communication skills and crisis- related teamwork. Nine of the 10 felt that the training model was effective in recognizing operating room errors. CONCLUSIONS: Implementing true interdisciplinary team training with a high-fidelity simulation can be accomplished effectively. Team training has the potential for facilitating pos- itive behavioral changes in operating room personnel that are important for adaptive team function in a crisis situation. (J Surg 64:369-377. Published by Elsevier Inc. on behalf of the Association of Program Directors in Surgery.) KEY WORDS: interdisciplinary team training, operating room, simulation, human factors, error reduction, patient safety COMPETENCY: Patient Care, Systems Based Practice BACKGROUND The operating room is a high-risk environment requiring close coordination among all team members. In such a dynamic set- ting, lapses in team function can negatively impact patient care. Reliable teamwork, therefore, is paramount. Important charac- teristics of a highly reliable team include the ability to adapt to changes within the work environment, to maintain open and flexible communication, and to anticipate the needs of each member of the team. 1 These characteristics allow team coordi- nation in high-stress, high-workload situations and facilitate adaptive responses that produce superior performance. 1 Unfortunately, operating room teams often fail to perform in an ideal manner. Although these teams comprise well-trained individuals with expertise in their particular field, the interac- tion between members is frequently problematic. Trained ob- servers in 1 study 2 found that the teamwork between surgeons and anesthesiologists in the operating room was poor to mini- mal up to 50% of the time. In contrast, poor team interaction occurred approximately 15% of the time between pilots on the flight deck. 2 The self-assessment of teamwork also reveals major problems in the operating room as 86% of consultant anesthe- siologists rated teamwork between themselves and their peers very high, whereas only 36% of this group gave similar marks when comparing teamwork between themselves and surgeons. 3 In an effort to address this lack of teamwork within the health-care system, the Institute of Medicine (IOM) included the recommendation of creating interdisciplinary team training programs in To Err is Human: Building a Safer Healthcare Sys- tem. 4 In 2003, the IOM again stressed the importance of team- work in healthcare by listing the ability to work in interdisci- plinary teams as 1 of its 5 core competencies for all health professionals. 5 Spurred by the IOM recommendations, the Joint Commission on Accreditation of Healthcare Organiza- tions (JCAHO) has included team training as part of its sug- Correspondence: Inquiries to John Paige, MD, 503 Bolivar Street, Room 508, New Orleans, LA 70112, fax: (504) 568-4633; e-mail: [email protected] Journal of Surgical Education • Published by Elsevier Inc. on behalf of the 1931-7204/07/$30.00 Association of Program Directors in Surgery doi:10.1016/j.jsurg.2007.03.009 369
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of From the Flight Deck to the Operating Room: An Initial Pilot Study of the Feasibility and Potential...

2
FAPT
JS
*U
Bmspp
Mpbeca
Rttpterw
CteiiSA
Kr
C
CL
J
007 APDS SPRING MEETING
rom the Flight Deck to the Operating Room:n Initial Pilot Study of the Feasibility andotential Impact of True Interdisciplinaryeam Training using High-Fidelity Simulation
ohn Paige, MD,* Valeriy Kozmenko, MD,† Barbara Morgan, MD,† D. Shannon Howell, BA,‡heila Chauvin, MEd,‡ Charles Hilton, MD,‡ Isidore Cohn, Jr, MD,* and J. Patrick O’Leary, MD*
Department of Surgery, †Department of Anesthesia, and ‡Office of Medical Education, Louisiana State
niversity Health Sciences Center, New Orleans, LouisianaB
TctRtcflmna
aitsamoflpsvw
htptwppJ
ACKGROUND: The operating room is a dynamic environ-ent in which proper teamwork is essential. After piloting a
imulation-based interdisciplinary operative team trainingrogram, we examined the impact of these sessions on thearticipants.
ETHODS: Three interdisciplinary operating room teamsarticipated in the training model. Each team of 3 or 4 mem-ers completed the training in a virtual minimally invasive op-rating room using a standardized operative scenario. Uponompletion of the training, participants completed a voluntarynd anonymous training effectiveness questionnaire.
ESULTS: All 10 participants completed the training evalua-ion questionnaires. Across the 3 teams, all participants felt thathe training was worthwhile and would participate again. Eightarticipants said that the session would change their practices inhe operating room. All participants felt that the session wasffective in promoting team communication skills and crisis-elated teamwork. Nine of the 10 felt that the training modelas effective in recognizing operating room errors.
ONCLUSIONS: Implementing true interdisciplinary teamraining with a high-fidelity simulation can be accomplishedffectively. Team training has the potential for facilitating pos-tive behavioral changes in operating room personnel that aremportant for adaptive team function in a crisis situation. (Jurg 64:369-377. Published by Elsevier Inc. on behalf of thessociation of Program Directors in Surgery.)
EY WORDS: interdisciplinary team training, operatingoom, simulation, human factors, error reduction, patient safety
OMPETENCY: Patient Care, Systems Based Practice
torrespondence: Inquiries to John Paige, MD, 503 Bolivar Street, Room 508, New Orleans,A 70112, fax: (504) 568-4633; e-mail: [email protected]
ournal of Surgical Education • Published by Elsevier Inc. on behalf ofAssociation of Program Directors in Su
ACKGROUND
he operating room is a high-risk environment requiring closeoordination among all team members. In such a dynamic set-ing, lapses in team function can negatively impact patient care.eliable teamwork, therefore, is paramount. Important charac-
eristics of a highly reliable team include the ability to adapt tohanges within the work environment, to maintain open andexible communication, and to anticipate the needs of eachember of the team.1 These characteristics allow team coordi-
ation in high-stress, high-workload situations and facilitatedaptive responses that produce superior performance.1
Unfortunately, operating room teams often fail to perform inn ideal manner. Although these teams comprise well-trainedndividuals with expertise in their particular field, the interac-ion between members is frequently problematic. Trained ob-ervers in 1 study2 found that the teamwork between surgeonsnd anesthesiologists in the operating room was poor to mini-al up to 50% of the time. In contrast, poor team interaction
ccurred approximately 15% of the time between pilots on theight deck.2 The self-assessment of teamwork also reveals majorroblems in the operating room as 86% of consultant anesthe-iologists rated teamwork between themselves and their peersery high, whereas only 36% of this group gave similar markshen comparing teamwork between themselves and surgeons.3
In an effort to address this lack of teamwork within theealth-care system, the Institute of Medicine (IOM) includedhe recommendation of creating interdisciplinary team trainingrograms in To Err is Human: Building a Safer Healthcare Sys-em.4 In 2003, the IOM again stressed the importance of team-ork in healthcare by listing the ability to work in interdisci-linary teams as 1 of its 5 core competencies for all healthrofessionals.5 Spurred by the IOM recommendations, theoint Commission on Accreditation of Healthcare Organiza-
ions (JCAHO) has included team training as part of its sug-the 1931-7204/07/$30.00rgery doi:10.1016/j.jsurg.2007.03.009
369

gte
otfspcpK
ffeospawp
M
T
A(McavsApT
fao
orcMtaotcuew“
ttbopAscntlliaoidrp
T
ThtctbtwwgUfptF
M
3
ested comprehensive patient safety curriculum for institu-ions.6 In fact, it has pushed for Congressional action to helpmphasize greater focus on interdisciplinary team education.7
Although the health-care profession has taken significant stepsver the last decade in developing high-fidelity, simulation-basedraining of operating room professionals, most work thus far hasocused on training particular crews within the operating room,uch as anesthesiologists8,9 or surgical trainees.10,11 Interdisci-linary training has received little attention. One notable ex-eption is the Team Oriented Medical Simulator (TOMS)rogram developed in the 1990s at the University of Baselantonsspital in collaboration with the University of Texas.12,13
A simulation-based interdisciplinary team training programor the operating room was developed by the authors, whichocuses on the behavioral competencies associated with highlyffective teams. Two primary hypotheses guided this work: (1)perating room team member participants would perceive theimulated scenarios as authentic and worthwhile; (2) partici-ants would perceive the interdisciplinary simulation trainings effective methods for enhancing communication and team-ork during an operating room crisis. The training model wasiloted in the summer of 2005.
ETHODS
raining Setting
ll scenarios took place within a Virtual Operating RoomVOR) developed for team training at the Isidore Cohn, Jr.,
D Learning Center in the School of Medicine. The spaceonsisted of a modern minimally invasive surgery (MIS) oper-ting room suite containing boom technology and flat-paneliewing monitors (Fig. 1). This suite was developed in partner-hip with Stryker Communications (Flower Mound, Texas).n affiliated workstation housed a main router, touch-screenanel control, digital capture device, and voice control system.he router allowed for transmission of audio and video material
iIGURE 1. The VOR is a modern minimally invasive surgical suite with aETI Human Patient Simulator (HPS) and Simbionix LapMentor machine.
70 Journal of Surgical
rom the suite to a viewing/control room adjacent to the suitend to outside locations, which included remote classrooms orperating rooms with appropriate technology.
The simulation equipment consisted of a full-scale computer-perated mannequin (Medical Education Technologies Incorpo-ated [METI], Sarasota, Florida) as well as a virtual reality chole-ystectomy machine (Simbionix Ltd, Lod, Israel) (Fig. 1). The
ETI mannequin simulates human physiologic responseso treatment interventions, medications, and anestheticgents. A bar-code system allows for manual administrationf “medications” during sessions. The mannequin connectso an anesthetic machine within the simulation suite that isapable of interpreting the gas composition during the sim-lated intubation. The virtual reality machine allows an op-rator to perform a cholecystectomy from start to finishithout prompting. This type of experience is described as
free training.”A novel quad screen system was developed to support simul-
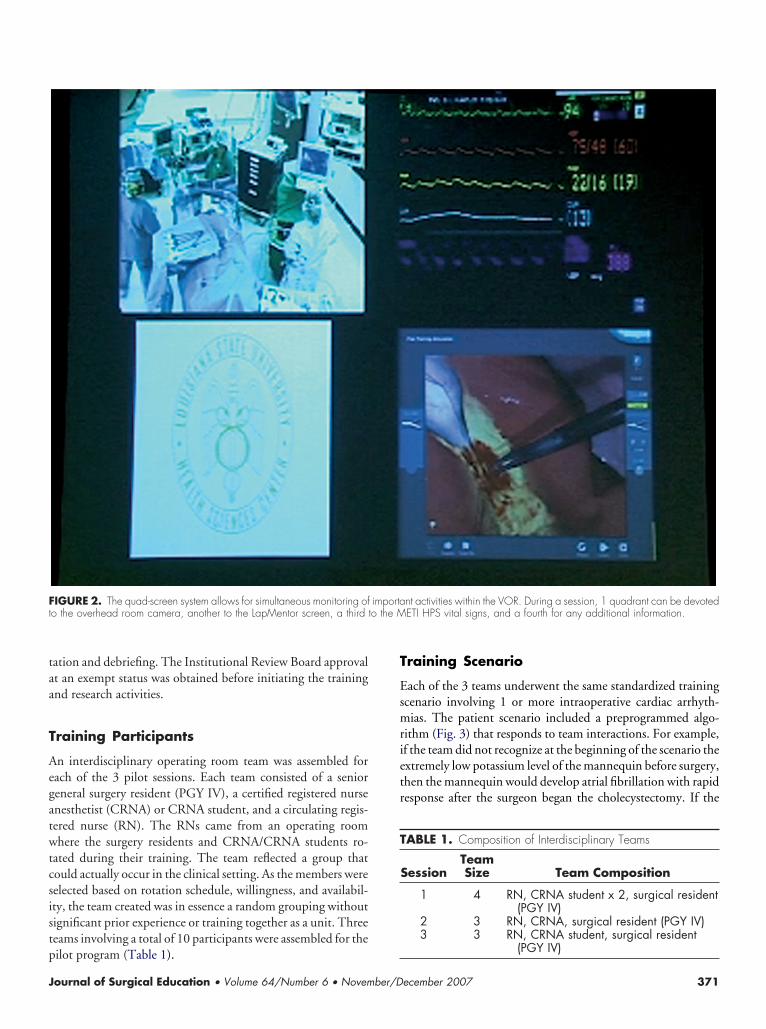
aneous monitoring and recording of important activity withinhe suite (Fig. 2). For example, 1 section of the quad screen cane used by participants to track team member interaction via anverhead room camera, whereas another section can be used byarticipants to track the progress of the virtual cholecystectomy.third screen can be used by participants to monitor the vital
igns of the mannequin during the scenario, and a fourth screenan be devoted to any additional monitoring or informationeeded for the session. Interchangeability between screens ofhe quad system allows for customization to fit the teaching,earning, and assessment needs of the training session. An in-ight camera housed within the handle of the overhead operat-ng room light can also be used by the participants for viewingctivity in the suite, especially in relation to a closer view of theperative field. The recording of multiple, simultaneous viewss particularly useful for enhancing the after-action debriefingiscussions, facilitating professional reflection and critique, andeinforcing teaching points with direct observation of specificerformance.
raining Format
raining sessions occurred in the morning and lasted up to 3ours, depending on the length of time spent working throughhe scenario and completing the video-facilitated debriefing dis-ussion. Upon arrival, team members were briefly oriented tohe VOR and how it functioned. After orientation, team mem-ers were assembled together and had the goals and objectives ofhe training explained. The background for the patient case thatas the focus of the training scenario was reviewed in a way thatas authentic to the operating room setting, and the team wasiven the patient chart to review before starting the scenario.pon completion of the scenario, the team engaged in a video-
acilitated debriefing discussion guided by the trainer. Threeeople were required to run the training session: a programmero oversee mannequin function, a person to assist with record-
ng the session, and a trainer/facilitator who helped with orien-Education • Volume 64/Number 6 • November/December 2007
taa
T
Aegatwtcsistp
T
Esmrietr
Ft to the M
T
J
ation and debriefing. The Institutional Review Board approvalt an exempt status was obtained before initiating the trainingnd research activities.
raining Participants
n interdisciplinary operating room team was assembled forach of the 3 pilot sessions. Each team consisted of a senioreneral surgery resident (PGY IV), a certified registered nursenesthetist (CRNA) or CRNA student, and a circulating regis-ered nurse (RN). The RNs came from an operating roomhere the surgery residents and CRNA/CRNA students ro-
ated during their training. The team reflected a group thatould actually occur in the clinical setting. As the members wereelected based on rotation schedule, willingness, and availabil-ty, the team created was in essence a random grouping withoutignificant prior experience or training together as a unit. Threeeams involving a total of 10 participants were assembled for the
IGURE 2. The quad-screen system allows for simultaneous monitoring ofo the overhead room camera, another to the LapMentor screen, a third
ilot program (Table 1).
ournal of Surgical Education • Volume 64/Number 6 • November/D
raining Scenario
ach of the 3 teams underwent the same standardized trainingcenario involving 1 or more intraoperative cardiac arrhyth-ias. The patient scenario included a preprogrammed algo-
ithm (Fig. 3) that responds to team interactions. For example,f the team did not recognize at the beginning of the scenario thextremely low potassium level of the mannequin before surgery,hen the mannequin would develop atrial fibrillation with rapidesponse after the surgeon began the cholecystectomy. If the
nt activities within the VOR. During a session, 1 quadrant can be devotedETI HPS vital signs, and a fourth for any additional information.
ABLE 1. Composition of Interdisciplinary Teams
SessionTeamSize Team Composition
1 4 RN, CRNA student x 2, surgical resident(PGY IV)
2 3 RN, CRNA, surgical resident (PGY IV)3 3 RN, CRNA student, surgical resident
importa
(PGY IV)
ecember 2007 371

ttcpmcs
owr
ftbo
wTcsd
F physiolom sinus rh
3
eam did not properly diagnose or treat the atrial fibrillation,hen the arrhythmia would deteriorate into ventricular tachy-ardia. However, if the operating room team recognized the lowotassium level and initiated adequate treatment, then theannequin would not develop atrial fibrillation during the pro-
edure. Thus, while the patient case remained the same, thecenario became dynamic and unique to the team in training.
The other aspect of the training session included specificpportunities for every operating room team to engage in team-ork competencies. Each patient case included a specific set of
IGURE 3. The patented software interface supports the development ofyocardial infarction, PEA � pulseless electrical activity, NSR � normal
esponses, regardless of the intraoperative scenario that un- p
72 Journal of Surgical
olded. For example, the mannequin in the patient case used byhe participants for the pilot training sessions always developedradycardia with the creation of pneumoperitoneum, regardlessf the actions of the team.
The effectiveness of teamwork during the training scenarioas assessed based on process and patient outcome measures.he actions of the team were judged on features of communi-
ation, coordination, situational awareness, and adaptive re-ponse, as well as on a set of patient outcomes. A checklist waseveloped as part of the patient scenario that reflected expected
gically complex scenarios involving the mannequin. BL � baseline, MI �ythm, K � potassium, VTach � ventricular tachycardia, J � joules.
atient outcomes and appropriate clinical actions for the intra-
Education • Volume 64/Number 6 • November/December 2007

owpiotaoido
T
EanufsattTsds
afostw5Eaarecettis
R
Tisrad
C3dyiToi
tfosaigw
tsgpawiseiogieRCpimtfdr
C
Ttfhrcloit
J
perative event encountered in the training. Specific actionsere identified as necessary or “critical” for successful teamerformance in addressing the patient problem (Fig. 3). Onemportant critical performance indicator comprising patientutcome measures of the training included administering po-assium intravenously to treat the low preoperative value. Thisction avoided further arrhythmias during the scenario. An-ther important critical performance indicator involved releas-ng the pneumoperitoneum to resolve completely the bradycar-ia. Treating the bradycardia with pharmacologic agents wouldnly partially resolve it.
raining Debriefing and Questionnaire
ach team participated in a debriefing activity immediatelyfter their completion of the scenario. An important compo-ent included observation of their video-taped performancesing the quad-screen recording system. Guided by the trainer/acilitator, the team used the videos to identify and discusspecific performances regarding teamwork, communication,nd situational awareness. The debriefing activity was designedo provide only formative assessment and feedback to the par-icipants regarding team behavioral skills in crisis situations.he assessment checklist was used by the trainer/facilitator
olely as a guide for enhancing reflective practice and learninguring the debriefing activity and not to implement a scoringystem for evaluating the performance of the team.
After completion of the debriefing activity, participants weresked to complete a voluntary and anonymous questionnaireocusing on the effectiveness of the training session. Threepen-ended questions solicited both yes/no and narrative re-ponses regarding overall satisfaction with, and perceptions of,raining effectiveness for specific elements. Another 3 itemsere included about specific attributes of teamwork and used a-point Likert-type response scale (A � Not effective at all to� Very effective) (Fig. 4). Questionnaire data were collated
nd analyzed after completion of all pilot sessions to assurenonymity of responses. The mean scores for the Likert-typeesponses were determined by assigning numerical values toach response (A � 1, B � 2, C � 3, D � 4, E � 5). Frequencyounts of positive (yes)/negative (no) responses of the 3 open-nded questions were determined. Results were used to assesshe feasibility and effectiveness of the training model based onhe perceptions of trainees of the pilot training sessions, interestn ongoing interdisciplinary operating room team training, anduggestions for future refinement.
ESULTS
he response rate for the questionnaire across the 3 pilot train-ng sessions was 100% (total n � 10). The average age of theenior surgical residents was 31.3 years, with a female-to-maleatio of 1:2. They had an average of 5 years of experience overallnd within the institution. One surgical resident reported un-
ergoing prior team training. The average age of the CRNA/ dournal of Surgical Education • Volume 64/Number 6 • November/D
RNA students was 30.5 years. The female-to-male ratio was:1 (1 team had 2 CRNA students). The CRNA/CRNA stu-ents had an average of 6 years of experience overall and 1.5ears within the institution. One CRNA reported participatingn prior team training. The average age of the RNs was 58 years.he female-to-male ratio was 2:1. Overall, they had an averagef 23.7 years of experience and 10 years of experience at thenstitution. Two RNs reported having had prior team training.
The frequency counts of the affirmative and negative answerso the open-ended questions revealed that all 10 participantsound the training session worthwhile and would attend an-ther session. Eight out of 10 participants said that the trainingession would change the way they practiced within the oper-ting room. One RN did not think that the session wouldnfluence how this RN practiced. One CRNA student did notive an affirmative or negative response to whether the trainingould influence how this student practiced.Mean scores for items targeting the perceived effectiveness by
he participants of the training session were examined. Ashown in Table 2, item mean scores for the total respondentroup were 4.5 for improving communication and 4.7 for im-roving teamwork, and 4.4 for recognizing errors in the oper-ting room. In fact, every participant thought that the sessionsere effective (rating � 4) to very effective (rating � 5) for
mproving teamwork and communication. Nine of the 10 re-pondents felt that the training model was effective (4) to veryffective (5) for recognizing problems and errors in the operat-ng room, and the remaining response was neutral (CRNA, 3n the 5-point scale). As shown in Table 2, disciplinary sub-roup scores were consistent with the total group scores. Thetem mean scores for each discipline support the training asffective in all 3 of the above domains. Item mean scores for theNs were overall the highest for all 3 domains. The view ofRNA/CRNA students of the effectiveness of the session inromoting teamwork was the highest ratings mean score acrosstems and disciplinary subgroups. In fact, the teamwork do-
ain had the highest average score for each subgroup and theotal group. Error recognition had the lowest item mean scoreor general surgery residents and CRNA/CRNA students. Ad-itionally, it was the lowest item mean score for the total groupesponses.
OMMENTS
his pilot study focused on the receptivity of the participants torue interdisciplinary operating room team training and theeasibility of conducting ongoing training in an academicealth center environment. As with any study, limitations to theesearch design are important considerations in drawing con-lusions and suggest implications for future directions. Severalimitations should be considered. First, the pilot study consistedf only 3 iterations of implementing the training model andnvolved only 10 participants (ie, 3 to 4 individuals per trainingeam). Second, the research design was descriptive, based on
ata from a post-session participant questionnaire to obtainecember 2007 373

fntttii
oaopat
uestion
T
PPF*
3
ormative feedback from participants about training effective-ess and supplemented by direct faculty observation and post-raining session debriefings. Consequently, the descriptive na-ure of the research design, the small number of iterations andraining participants, and training implementation at only 1nstitution precludes drawing definitive conclusions or general-zing to other settings.
Que
Items were included to obtain participant
gender, age, profession, overall and local
institution), prior team training experienc
Open-ended questions included the follow
• Was today’s session worthwhile?
• Will it change your practice?
• Would you attend this session aga
Items requiring responses to a 5-point Lik
E/5=Very effective)
Please rate the effectiveness of
• Promoting team communi
• Promoting teamwork in a
• Recognizing and addressin
FIGURE 4. Q
ABLE 2. Interdisciplinary Team Training Effectiveness
Training EffectivenessOverall M
Score
romotes team communication 4.5romotes teamwork in crises 4.7acilitates recognition of problems and errors 4.4
Includes CRNA students.74 Journal of Surgical
Evaluation of training effectiveness was based on the resultsf the participant questionnaire data that reflected perceptionsnd self-reported learning and intention to change behaviornly—not evidence of actual learning, behavior change, or im-act resulting from the training. The goal of this pilot was tossess participant receptiveness and overall feasibility of theraining model and not to try to assess actual behavioral change.
naire Content
cteristics for the following categories:
rience (years in training, years at
ype scale A/1=Not effective at all to
session in
skills
ors and problems in the operating room
naire content.
RN MeanScore
CRNA* MeanScore
Resident MeanScore
4.7 4.5 4.34.7 4.8 4.74.7 4.3 4.3
stion
chara
expe
e
ing
in?
ert-t
the
cation
crisis
g err
ean
Education • Volume 64/Number 6 • November/December 2007

Ab
cetssdwutm
atsmotdtinowetttatadat
wiridppuuow
iwscdt
ooont
wtfdcmoeue
topToaop
adsawttMtUdc
tdinliSUt
fetpe
J
ccepting these limitations, several conclusions can be madeased on this model and other teamwork simulation reports.This operating room team training model was designed spe-
ifically to enhance interdisciplinary team interactions. The op-rating room is a dynamic, complex environment that bringsogether an interdisciplinary team of professionals who musteamlessly coordinate their expertise and activities to provideafe, effective care to the patient. This group of experts oftenoes not act like a team.2 Each member has a clear picture ofhat s/he does but does not approach his/her tasks with a clearnderstanding of what each of the others will do or may needo do.14 The members do not have a shared image or “mentalodel” of how the team should work and interact.14
A shared mental model is necessary for team members tonticipate, adapt, and respond effectively to each other and tohe situation (ie, adaptive response) in the dynamic and high-tress situation of the operating room.1 The lack of a sharedental model among team members is reflected in a survey of
perating room teams in which members rated the degree ofeamwork among disciplines.2 Whereas 73% of surgical resi-ents and 64% of attending surgeons reported high levels ofeamwork with other attending surgeons, only 39% of attend-ng anesthesiologists, 28% of surgical nurses, 25% of anesthesiaurses, and 10% of anesthesia residents reported similar levelsf teamwork with surgeons. A similar disconnect was presenthen comparing teamwork between disciplines within the op-
rating room. Sixty-two percent of the surgical staff rated theeamwork with the anesthesia staff highly, but only 41% ofhe anesthesia staff held the same view toward teamwork withhe surgical staff. Such disparity suggests a failure among oper-ting room members to create a common understanding of howhe team members, individually and collectively, should inter-ct and work together effectively. The lack of a common un-erstanding impacts the effectiveness of team communicationnd the awareness of members of the unfolding situationhroughout an operative procedure.
Another factor that seems to contribute to ineffective team-ork is related to the concept of a shared mental model and
nvolves a lack of professional role clarity among operatingoom team members. Results based on focus group interviewsnvolving 52 operating room team members revealed a strikingissonance between how surgeons and nurses define their ownrofessional roles in the operating room versus how each disci-line would define the role of the other.15 This finding is attrib-ted to a lack of interdisciplinary training resulting in a poornderstanding of the culture, skills, and roles across the variousperating room disciplines and reinforces the “silo” effectithin team members.Ineffective communication is a third factor commonly cited
n the literature as leading to a breakdown in team functioningithin the operating room. In a follow-up study, 48 general
urgical and vascular procedures were observed and communi-ation events were categorized.16 Of 421 events deemed proce-urally relevant, 129 (30.6%) were classified as a communica-
ion failure. These failures were grouped into 4 categories: iournal of Surgical Education • Volume 64/Number 6 • November/D
ccasion, content, purpose, and audience. Importantly, 36.4%f the communication failures had an apparent negative impactn the system function within the operating room. Of theseegative impacts, the top 3 were inefficiency (17.8%), teamension (12.3%), and delay (7.7%).
The lack of teamwork within the operating room createshat James Reason called a latent condition within the team for
he commission of errors.17 These team-based errors fall intoour main categories: procedural errors, communication errors,ecision errors, and intentional noncompliance errors.18 Ac-ording to the University of Texas Threat and Error Manage-ent Model (TEMM), a team error can result in 1 of 3 distinct
utcomes.18 The most benign outcome is one in which therror is inconsequential. Alternately, an error can result in anndesired state or condition. Finally, it can lead to anotherrror, which becomes part of an error chain.
Improving teamwork within the operating room has the po-ential for enhancing patient safety. A team training session forperating room personnel at 1 institution significantly im-roved communication for anesthesiologists and surgeons.19
he improved communication, coupled with the introductionf a preoperative briefing protocol, increased the rate of on-timedministration of prophylactic antibiotics and applicationf sequential compression stockings for deep vein thrombosisrophylaxis.Because of the similarities in team dynamics, breakdowns,
nd organizational cultures, the operating room and flighteck possess strong parallels.20 The success of high-fidelityimulation-based team training within the flight deck hasttracted the attention of health-care professionals workingithin the operating room. Anesthesia was the first discipline
o adapt crew resource management (CRM) principles. Anes-hesia Crisis Resource Management is their training module.8,9
ore recently, surgeons have begun using high-fidelity simula-ion and CRM principles. At the Imperial College in London,nited Kingdom, a realistic mock operating room has beeneveloped to evaluate the responses of surgical trainees torises.10,11
Unfortunately, CRM is effective at teaching and evaluatinghe behavioral skills of professionals within a discipline, but itoes not provide appropriate focus on interdisciplinary team
nteractions. Also, CRM does not provide sufficient opportu-ities to engage in realistic scenarios followed by cycles of de-
iberate and focused reflection, feedback, and practice related tomproving how an operating room team can function as a unit.uch clinical team training has never been described in thenited States, and the world literature contains only 1 descrip-
ion of a now-defunct program (TOMS).12,13
High-fidelity simulation-based training has been expandedrom a discipline-specific, crew-based experience to a new gen-ration of team training that reflects interdisciplinary interac-ions in an actual operating room. The highly consistent andositive results of the initial pilot study involving the experi-nces of 3 teams with the new training model provides convinc-
ng evidence of both receptivity to and feasibility of team train-ecember 2007 375

iartaCcaotpatinteirv
pttiretdbbaar
tsltdindsiea
R
1
1
1
1
1
1
3
ng. Participants viewed the training context and the scenarioss authentic and the training activities as valuable. The pilotesults demonstrated that simulation-based operating roomeam training is effective without the addition of embeddedctors that has been typical of previous training models usingRM simulation-based approaches. The use of actual interdis-
iplinary teams in a highly authentic simulation environmentllowed participants to enhance their understanding of the rolef each other and improve their abilities to communicate effec-ively with team members of other disciplines. Feedback fromarticipants revealed that such training can be accomplished in“safe” environment where members can use deliberate prac-
ice and feedback to hone important teamwork competencies,ncluding the use of a shared mental model, situational aware-ess, anticipatory and adaptive response, effective communica-ion, and leadership. The goal was not to define outcome-basedvidence of actual behavior change but to examine the receptiv-ty of health professionals to the simulation model. Evaluationesults revealed positive attitudes and suggest it is perceived asaluable by the participants.
These results suggest that this training model could be incor-orated into the educational mission for in-training and con-inuing education programs and could be accomplished effec-ively. Therefore, as the program is refined, opportunities tontegrate training sessions into appropriate curricula will beesearched. The training activities and patient scenarios will bexpanded to develop a comprehensive, interdisciplinary teamraining curriculum. A specific area of current study includesevelopment of a competency-based assessment system foroth the operating room team21 and the individual team mem-ers22-24 that can be used in both simulated and real-life oper-ting room settings. The importance of evaluating changes inctual learning, behavior, and outcomes is all recognized. Theseesearch goals must be integrated into future investigations.
In conclusion, results of this pilot study support the recep-ivity to and the feasibility of implementing a high-fidelityimulation-based interdisciplinary team training program at aarge academic health sciences center. Participants involved inhis pilot program found it worthwhile. Additionally, they in-icated that it is effective in promoting teamwork in a crisis,
mproving communication among team members, and recog-izing errors in the operating room. The results support con-ucting additional research and development into high-fidelityimulation-based interdisciplinary operating room team train-ng to examine the extent to which this innovative approach cannhance behavioral skills that are important for effective oper-ting room teamwork in high workload environments.
EFERENCES
1. Entin EE, Serfaty D. Adaptive team coordination. Hum
Factors. 1999;41:312-325.76 Journal of Surgical
2. Sexton JB, Thomas EJ, Helmreich RL. Error, stress, andteamwork in medicine and aviation: cross sectional sur-veys. BMJ. 2000;320:745-749.
3. Flin R, Fletcher G, McGeorge P. Anaesthetists’ attitudesto teamwork and safety. Anaesthesia. 2003;58:233-242.
4. Kohn LT, Corrigan J, Donaldson MS, eds. To Err is Hu-man: Building a Safer Health System. Washington, DC:National Academies Press; 2000.
5. Greiner AC, Knebel E, eds. Health Professions Education:A Bridge to Quality. Washington, DC: National Acade-mies Press; 2003.
6. Joint Commission on Accreditation of Healthcare Orga-nizations. Sample outline for a patient safety plan. Avail-able at: http://www.jointcommission.org/PatientSafety/pt_safety_plan.htm. Accessed April 14, 2006.
7. “Patient Safety: Instilling Hospitals with a Culture ofContinuous Improvement.” Testimony of DennisO’Leary, M.D. President, Joint Commission on Accredi-tation of Healthcare Organizations. Before the SenateCommittee on Governmental Affairs. Available at: http://www.jointcommission.org/NewsRoom/OnCapitolHill/testimony_061104.htm. Accessed April 14, 2006.
8. Holzman RS, Cooper JB, Gaba DM, et al. Anesthesiacrisis resource management: real-life simulation trainingin operating room crises. J Clin Anesth. 1995;7:675-687.
9. Gaba DM, Howard SK, Fish KJ, et al. Simulation-basedtraining in anesthesia crisis resource management(ACRM): a decade of experience. Simul Gaming. 2001;32:175-193.
0. Aggarwal R, Undre S, Moorthy K, et al. The simulatedoperating theatre: comprehensive training for surgicalteams. Qual Saf Health Care. 2004;13:27-32.
1. Moorthy K, Munz Y, Adams S, et al. A human factorsanalysis of technical and team skills among surgical train-ees during procedural simulations in a simulated operat-ing theatre. Ann Surg. 2005;242:631-639.
2. Musson DM, Helmreich RL. Team training and resourcemanagement in health care: current issues and future di-rections. Harvard Health Policy Rev. 2004;5:25-35.
3. Betzenderfer D. Anesthesia Patient Safety Foundation.Available at: http://www.apsf.org/resource_center/newsletter/1996/spring/apsfled_betzen.html. AccessedApril 14, 2006.
4. Undre S, Sevdalis N, Healey AN, et al. Teamwork in theoperating room: cohesion or confusion? J Eval Clin Pract.2006;12:182-189.
5. Lingard L, Reznick R, DeVito I, Espin S. Forming pro-
fessional identities on the health care team: discursive con-Education • Volume 64/Number 6 • November/December 2007

1
1
1
1
2
2
2
2
2
J
structions of the ‘other’ in the operating room. Med Educ.2002;36:728-734.
6. Lingard L, Espin S, Whyte S, et al. Communication fail-ures in the operating room: an observational classificationof recurrent types and effects. Qual Saf Health Care. 2004;13:330-334.
7. Reason J. Human error: models and management. BMJ.2000;320:768-770.
8. Grote G, Helmreich RL, Sträter O, et al. Setting the stage:characteristics of organizations, teams and tasks influenc-ing team processes. In: Dietrich R, Childress TM, eds.Group Interaction in High Risk Environments. Aldershot,UK: Ashgate Publishing Limited; 2004:111-139.
9. Awad SS, Fagan SP, Bellows C, et al. Bridging the com-munication gap in the operating room with medical team
training. Am J Surg. 2005;190:770-774.ournal of Surgical Education • Volume 64/Number 6 • November/D
0. Helmreich RL, Merritt AC. Culture at work in aviationand medicine: national, organizational, and professional in-fluences. Aldershot, UK: Ashgate Publishing Limited;1998.
1. Healy AN, Undre S, Vincent CA. Developing observa-tional measures of performance in surgical teams. Qual SafHealth Care. 2004;13:33-40.
2. Yule S, Flin R, Paterson-Brown S, Maran N. Non-technical skills for surgeons in the operating room: areview of the literature. Surgery. 2006;139:140-149.
3. Fletcher GC, McGeorge P, Flin RH, et al. The role ofnon-technical skills in anaesthesia: a review of current lit-erature. Br J Anaesth. 2002;88:418-429.
4. Fletcher G, Flin R, McGeorge P, et al. Rating non-technical skills: developing a behavioural marker sys-tem for use in anaesthesia. Cogn Tech Work. 2004;6:
165-171.ecember 2007 377