Fostering Internationalisation in Higher Education by Virtual ...

Men, sex and power
� Editorial – 1
� Reseach Notes – 3Does men’s involvement work?Evidence from evaluatedinterventions
� Programme Feature – 5Promoting gender equity amongyoung men. Positive experiences ofthe Yari-dosti project in India
� Special Article – 7Fostering alternative views of maleidentity among boys in LatinAmerica and the Caribbean
� Programme Feature – 9Using edutainment and socialactivities to challenge machismo inNicaragua. The example of SomosDiferentes, Somos Iguales
� Research Notes – 10Male identity, poverty andreproductive health in Namibia
� Special Article – 12Behind the bars of South Africanprisons. Gendered roles andvulnerability of male inmates toforced sex
� Special Article – 14Men who have sex with men anddisempowerment in South Asia
� Online Resources – 16
Next issue: ManagingHIV/AIDS inside NGOs
Men, sex and powerEngaging men in achieving gender equality and sexual and
reproductive health
Alan Greig
The 1994 International Conference on Population and Development (ICPD) in Cairo isstill a rallying cry for advocates of male involvement in the struggle to achieve genderequality. ICPD was the first forum in which the international community challengedmen to play their full part in the fight for gender equality. Within a year, the BeijingPlatform for Action called on men to support women’s struggle for gender equality bysharing child-care and household work equally and by taking responsibility in HIV andsexually transmitted infection (STI) prevention. A decade after the ICPD, the UnitedNations Commission on the Status of Women met in New York City to consider, for thefirst time, the role of men and boys in the achievement of gender equality.
In the past decade, these global policy commitments have been translated intomany programmes working with men on sexual health and gender equality on allcontinents. According to the United Nations Population Fund (UNFPA), condomeducation and distribution initiatives exist in virtually every country and have led tohigh levels of knowledge of male condoms among men. Clinic-based efforts havesought to engage men, either in primary health care or in specialized reproductive andsexual health clinics. Links between gender inequality, sexual vulnerability and the HIVpandemic have spurred a dramatic increase in HIV prevention efforts targeting men’ssexual behaviour.
Men making a differenceThe “Men Make a Difference” World AIDS Campaign in 2000-2001 showcasedexamples of peer education efforts with male adolescents and outreach HIV educationwith male-dominated occupational groups. There are now projects working with mento prevent perinatal transmission, supporting men to get involved in home-based
2005/2
Photo: USAID/Chris Thomas
Sexual HealthEXCHANGE
www.sexualhealthexchange.org [email protected]

2 Sexua l Hea l th Exchange 2005/2
care, and starting support groups for HIV-positive fathersto promote their own health and well-being andencourage them to support their partners and children.Fatherhood is an important theme of this work, which hasincluded campaigns and services to encourage men toparticipate in childbirth and efforts to enlist male supportfor maternal health by educating them on warning signsof maternal complications. Mass media is being used topromote positive images of men’s participation in thelives of children. A few programmes are pioneeringeducational sessions, group discussions, or supportgroups for fathers.
Violence has also become an important focus for workwith men, including intervention programmes with menwho have used violence against women as well asprevention initiatives. Such initiatives have either beenintegrated into a broader programme (as in the SteppingStones approach to addressing violence as part of its workon HIV/AIDS) or have been stand-alone efforts (as in theWhite Ribbon Campaign, a movement of men working toend violence against women in more than 30 countries).
Addressing the complex realities of men’slivesBut perhaps the most interesting work is being done withmen on what many regard as the root of the problem; thegender socialization, pressures and norms that confinemen of all ages within patterns of thinking, feeling andacting that are not only harmful to women but also tothemselves. The Men as Partners (MAP) programme inSouth Africa offers a good example of the evolution ofsuch work from gender awareness-raising with men toworking to change individual behaviours, communitynorms and government policy. The programme, togetherwith other allies, has recently secured the establishmentof a cabinet-level coordinating committee on men andgender equality within the South African government’snational gender machinery.
Working with men to transform the gender norms andstructures (economic, social and political) that maintaingender inequality marks a significant step beyond thegender-neutral approaches (targeting men in order toimprove women’s health) and gender-sensitiveapproaches (responding to men’s own sexual healthneeds and their risk-taking behaviour) that havecharacterized the targeting of men in sexual health work(see Box). This gender-transformative approach, asadvocated by Geeta Rao Gupta of the International Centerfor Research on Women among others, confronts men’scomplex relationship to power. Michael Kaufman speakseloquently of men’s contradictory experiences of power:
“Men enjoy social power,many forms of privilege,and a sense of often-unconscious entitlementby virtue of being male.But the way we have setup that world of powercauses immense pain,isolation, and alienationnot only for women, butalso for men”.1
Directions forchangeThe need to come to gripswith this contradiction isfurther deepened whenthe gender framework isbroadened to includeother structures ofinequality within which men (and women) live. Men mayhave power because of their gender but may lack powerbecause of, among others, their economic class,ethnic/racial identity, sexuality and age.
These internal contradictions suggest two importantdirections for developing work with men in terms of theirrelationship to power and privilege, namely to: 1) exploremen’s emotional lives and 2) address men’s politicalconditions. Sexual health work with men has tended tofocus on the interpersonal sphere (men’s relations withwomen as well as with other men). But these contra-dictions reveal the importance of developing more workin both the internal/emotional and institutional/politicalspheres. This framework of the three I’s (Internal,Interpersonal and Institutional) of fighting oppressionprovides a useful structure for developing such work withmen.2
Internal work: Exploring men’s emotionallivesRozan, a women’s empowerment NGO in Pakistan, haspioneered gender-based work with the police. In seekingto engage the police service to promote gender equality,Rozan provided gender education and a space for malepolice officers to talk about, and begin to heal from, theemotional harms of their masculine socialization and tosee how these harms play out in their treatment ofwomen. According to Rozan, helping men to heal mustbe accompanied by an equal emphasis on strengtheningmen’s empathy for women’s suffering from misogyny, orthe hatred of women.
Paying attention to masculinity and misogyny iscritical in developing this “internal” work with menbecause it allows for a richer understanding of thecomplexities of male socialization and men’s sexuality.
Institutional work: Addressing men’s politicalconditionsIn its anti-sexist work with young men, the ConscientisingMale Adolescents (CMA) programme in Nigeria seeks tohold its young men accountable for understandinggender oppression (in women’s and men’s lives) andworking to change it. By framing their work in terms ofwomen’s struggle for gender equality, the programmestresses young men’s role as allies to women in thisstruggle. Focusing on men’s role as an ally counters the
Involving men in HIV/AIDScare and supportPhoto: Edward Reilly/Lutheran WorldRelief, Courtesy of Photoshare
Best practice programming for the gay/MSM communityMen are targeted because they are:
� Gatekeepers, who control women’s sexual and reproductive health (SRH)
� Decision-makers, who decide on policies and budgets that affect SRHprogrammes
� Clients, who are deprived of SRH services
� Risk-takers, who pose a threat to the public health as well as themselvesin terms of HIV and STIs
� Vulnerable populations, whose human rights are denied because oftheir sexual or drug-using behaviour
� Community members, whose harmful attitudes and behaviours are theresult of the pressure to “be a man”.

3Sexua l Hea l th Exchange 2005/2
danger of reinforcing unequal power relations throughmen taking on the paternalistic role of protecting womenfrom sexism or taking over women’s leadership in aneffort to end sexism.
This emphasis on being an ally also suggests to theyoung men that the programme is not just working withthem on their individual attitudes and behaviours but thattheir personal change is part of a bigger story of socialchange. The bigger story moves them beyond the genderquestion of what it means to be a more equitable man tothe broader question of what it takes for men and womento live in more equitable societies. Answering thisquestion involves addressing the role that institutions(social, economic and political) play in creating injustice,including the gender injustice that women experience.
Building men’s political consciousness in this way iscritical to sexual health work. Such an approach makesclear that men’s violence against women is not simply
interpersonal but structural, and that efforts to end it musttackle the structures of male power in society whichreproduce and rely on such violence. A more politicizedapproach to sexual health work with men would also holdspecific institutions, such as religious authorities and thestate, accountable for trying to limit discussion ofsexuality to the realm of reproduction and “family life”.
The HIV pandemic will not be controlled by preserving thestereotype of the irresponsible male who must bepersuaded to remain faithful or use a condom “as a lastresort”. Instead, sexual health work with men (andwomen) should open up discussion of sexual pleasureand sexual diversity, within the context of rights andrelationships, and challenge the powerful interests thatare vested in maintaining the status quo. Above all,developing this political work with men would linkwomen’s struggle for their liberation to other struggles forjustice (such as economic, racial, sexual) from which mostmen stand to gain.
Alan Greig, Consultant, USA; e-mail: [email protected]
1. M. Kaufman. Men, feminism and men's contradictory experiencesof power, www.europrofem.org/02.info/22contri/2.04.en/1en.gend/02en_gen.htm.
2. A school to build a movement: Political education workshopmanual, School of Unity and Liberation, Oakland, California, USA,2000.
MMoorree iinnffoorrmmaattiioonn aabboouutt tthhee pprrooggrraammmmeess mmeennttiioonneedd iinn tthhiiss aarrttiiccllee::�� SStteeppppiinngg SSttoonneess:: wwwwww..sstteeppppiinnggssttoonneessffeeeeddbbaacckk..oorrgg�� WWhhiittee RRiibbbboonn CCaammppaaiiggnn:: wwwwww..wwhhiitteerriibbbboonn..ccaa�� MMeenn aass PPaarrttnneerrss ((MMAAPP)),, SSoouutthh AAffrriiccaa::
wwwwww..eennggeennddeerrhheeaalltthh..oorrgg//iiaa//wwwwmm�� RRoozzaann:: wwwwww..rroozzaann..oorrgg�� CCoonnsscciieennttiissiinngg MMaallee AAddoolleesscceennttss ((CCMMAA)) pprrooggrraammmmee,, NNiiggeerriiaa:: ““MMyyffaatthheerr ddiiddnn''tt tthhiinnkk tthhiiss wwaayy"" –– NNiiggeerriiaann bbooyyss ccoonntteemmppllaattee ggeennddeerr eeqquuaalliittyy,,FF.. GGiirraarrdd,, PPooppuullaattiioonn CCoouunncciill 22000033,, wwwwww..ssyynneerrggyyaaiiddss..ccoomm//ddooccuummeennttss//NNiiggeerriiaa__GGeennddeerrEEqquuaalliittyy..ppddff
Men receiving counseling on contraception offered bythe CASA programme in San Miguel de Allende, MexicoPhoto: Rick Maiman/David and Lucile Packard Foundation, Courtesy ofPhotoshare
Does men’s involvement work? Evidence fromevaluated interventionsPeter Sternberg & John Hubley
Against a backdrop of rapidly increasing HIV infection rates, widespread reports of violence againstwomen and appalling statistics on maternal and infant mortality, delegates at the 1994 InternationalConference on Population and Development (ICPD) agreed that an international effort should bemade to involve men as active participants in sexual and reproductive health promotion. A decadelater, men’s involvement still attracts criticism and invites serious questions. These questions includewhich methods are appropriate for involving men, which strategies lead men to change theirbehaviour and, importantly, what effect does men’s involvement in sexual and reproductive healthpromotion have on women? This article is a short summary of findings from 26 evaluations ofinterventions that targeted adult heterosexual men which were published until July 2003.1
ResearchNotes
There is a great deal of rhetoric about men’s involvementand particularly discussion about the meaning of men’sinvolvement in sexual and reproductive healthprogrammes. For health promoters, men’s involvementimplies that they are involved, not just as passive recipients,but as full partners in programmes designed to meet theirneeds and the needs of their families. Programmes that aimto involve men encompass a wide range of activities frompromoting condoms, addressing parenting issues toworking to change gender norms that lead to thesubordination of women and domestic violence.
Early critics of men’s involvement thought that menwould not be interested in participating and that involving
them would waste time and money. Inreality, however, a large number of menactually want to be involved because theyare genuinely interested in their ownhealth and the health and welfare of theirpartners and families.
Changing men – whichstrategies work?Evidence from many family planning services targeting menshows it is not enough just to offer a service and expect mento use it. The service must be tailored to meet their needs
Photo: WHO/P. Virot

4 Sexua l Hea l th Exchange 2005/2
and efforts need to be made to reach out to them. ManyHIV/AIDS programmes that target adult men use theirworkplace as the prime site and focus for intervention.Sectors that have used workplaces to initiate interventionsfor men include transportation, mining, the military andfisheries. Several strategies – applied at the workplace or inother settings – seem to have promising results:
Using existing non-health programmes – One way toinvolve men is to extend projects that already involvethem, such as small business or farm projects, into therealms of sexual and reproductive health. A programmein Honduras used two strategies. One involved trainingagricultural extension workers to give health educationsessions to their clients; the other extended an agri-cultural programme, the “Farm Management Plan”, intoareas of family planning through the use of a “familymanagement” booklet.
Peer education – Several studies indicate that peereducation may be an effective strategy to increasecondom use amongst men. A truck drivers’ peereducation programme in Tanzania found that reportedcondom use increased by nearly 20% in the two years ofthe maintenance phase that followed the intervention. Asimilar programme in Senegal found that sex workersreported a greater proportion of their clients usedcondoms and fewer clients offered extra money forunprotected sex after a peer education programme whichtargeted their clients – mostly truck drivers.
Cognitive behavioural interventions – Anotherstrategy that might hold some promise uses cognitivebehaviour principles. These usually involve teachingpeople to overcome barriers to behaviour change andmotivating change by using realistic incentives. A study oftrucking company workers in Kenya found increases incondom use and a decrease in the percentage of menwho had had extramarital sex as well as a decline in thenumbers of men who had had sex with a sex workerfollowing a cognitive behavioural intervention.
Involving religious leaders – Some countries havesuccessfully involved religious leaders in education onand promotion of sexual and reproductive health to men.Of particular interest are projects in Gambia andBangladesh, which involved Muslim religious leaders inprogrammes to educate men on the link between familyplanning and Islam. Both programmes resulted inincreased use of contraception amongst the men whowere involved.
Edutainment – This strategy uses entertainment toeducate men. A good example is the Zimbabwean FamilyPlanning Council's “Male Motivation Project”. The Projectused a wide variety of media: TV, radio, newspapersadvertisements, and articles as well as a television soapopera. Men exposed to the campaign were significantlymore likely to use condoms than men who had not.
Stages of change approach – Astudy involving men from rural Vietnamfound that it was useful to categorizemen according to their stage of changein order to tailor interventions topromote their involvement incontraceptive decisions. This strategyseems effective with many differenttarget groups, not just men, because itallows interventions to be targeted tomeet people’s real needs according tohow far along they are in the process ofchange.
How involving men affects womenEvidence from the literature on how men's involvementimpacts on women is rare because few studies haveexamined this question. A study of Ethiopian menexamined whether involving men in family planningdiscussions with their wives made a difference to the uptakeof modern contraception methods. A year after thediscussions, almost twice as many people that participatedin the intervention were using a modern contraceptionmethod as people in the control group. The fact that menwere participating did seem to make an important differenceto contraceptive uptake by their spouses.
In an Indian programme, men were given informationabout antenatal care services, diet, nutrition and weightgain during pregnancy as well as information aboutcontraception. Male participants in the study had a greaterknowledge of the importance of antenatal care servicesand their partners made more visits to antenatal careclinics.
The Men's Collective of Egalitarian Relationships(CORIAC) targeted violent men in Mexico City and helpedparticipants to examine their masculinity and to learn toexpress emotion in non-violent ways. A similarprogramme in Nicaragua that was based on themethodology of Popular Education (reflection/action)reported positive changes, which included moreparticipation in domestic chores, fewer incidents ofphysical and psychological violence and moreinvolvement with children.
ConclusionThe little available literature suggests that even a decadeafter the ICPD, few programmes are actually targetingmen. Men’s involvement seems a promising strategy,however, there is a real need for more work with men thatis properly evaluated and reported on. Although menmay no longer be seen as just part of the problem, as theywere in the 1980s, they have yet to be taken seriously aspart of the solution.
Many of the studies reviewed were implementedwithin the narrowly conceived framework of “malemotivation” and targeting men's pathological behaviour. Itis important to note that men's behaviours in manycountries are reinforced by cultural stereotypes, whichplace great value on concepts like physical strength,sexual prowess and machismo. Yet men are also victimsbecause they can feel that they are not “real men” unlessthey conform to these stereotypes. Thus, an effectiveprogramme to reach men must also challenge prevailingconcepts of masculinity.
We were disappointed to find that none of theprogrammes, except CORIAC and the Nicaraguan anti-violence programme, addressed issues from the point ofview of masculinity. This is a serious flaw, particularlywhen there is a realization that many problems in sexualand reproductive health have their roots in genderinequities between men and women.
Peter Sternberg, Winona State University, USA; e-mail:[email protected] & John Hubley, Leeds MetropolitanUniversity, Leeds, UK; e-mail: [email protected]
1. For reasons of space, we have not included any references. Theycan be found in the online edition available at www.sexualhealthexchange.org or in the original paper on which this article wasbased: Evaluating men’s involvement as a strategy in sexual andreproductive health promotion, Health Promotion International, Vol.19, No. 3, 2004: p. 389-396.Photo: WHO/P. Virot

Sexua l Hea l th Exchange 2005/2 5Promoting gender equity among young menPositive experiences of the Yari-dosti project in India
Ravi Verma, Julie Pulerwitz, Vaishali Sharma Mahendra, Sujata Khandekar &Gary Barker
In India, the HIV epidemic is growing, and more than five million people are estimated to be livingwith HIV and AIDS. A key factor contributing to the increasing number of people living with HIVin the country is societal norms that keep women’s status low in the home and community andfoster men’s greater control over resources and decision-making. This includes norms related tomonogamy and the number of sexual partners, as well as safer sex. There is increased awarenessof the role that inequitable gender norms play in HIV and violence risk, yet few studies haveattempted to influence these norms and measure change in both norms and risk behaviour due toan intervention. The Horizons Program, implemented by the Population Council and partners, andlocal partners CORO for Literacy (India) and Instituto PROMUNDO (Brazil), have developed andimplemented operations research in India to examine the role of gender equity and gender normsin HIV and violence risk and prevention.
The first step of this project was conducting formativeresearch in 2003, with young men in low-incomecommunities in Mumbai (formerly known as Bombay),India, on the links between gender and masculinity,sexuality, and health risk. Formative research involvedqualitative methods of data gathering employing keyinformant and in-depth interviews, mapping exercisesand focus group discussions (FGDs). Trained peer leadersfrom three low-income communities conducted a total of51 interviews with young men in the age group of 16-24years and four FGDs with community leaders and youngwomen from the same communities.
Then, intervention activities for young men weredeveloped/adapted, including a curriculum for groupeducation. In the second half of 2004, peer leaders weretrained to implement the activities, and a group of over 100young men participated in group education sessions overa 6-month period. Pre and post-test surveys wereconducted, as well as qualitative interviews andobservations, by an independent study team to determinethe feasibility and acceptability, as well as the impact of theintervention. Changes in attitudes towards gender norms –using the Gender-Equitable Men (GEM) Scale developed
by Horizons and Instituto PROMUNDO (see Box) – as wellas changes in violence and HIV risk behaviours weremeasured. A gender-equitable man was defined for thisproject as one that: 1) supports relationships based onrespect, equality and intimacy rather than sexual conquest;2) is an involved father, both financially and in terms of care-
The Gender-Equitable Men ScaleThe GEM Scale was developed by the Horizons Program, Instituto PROMUNDO, and partners in Brazil. It was testedwith a community-based sample of 749 men aged 15 to 60 in low- and middle-income neighbourhoods in Rio deJaneiro. The scale consists of a list of statements about attitudes regarding gender roles in domestic work and childcare, sexuality and sexual relationships, reproductive health and disease prevention, and intimate partner violence,as well as attitudes toward homosexuality and close relationships with other men.
In the initial testing of the GEM Scale, “traditional” attitudes were reported by some men, examples of which are: � Men are always ready to have sex� Women who carry condoms on them are “easy”� I would never have a gay friend� Changing diapers, giving the kids a bath, and feeding the kids are the mother’s responsibility� I would be outraged if my wife asked me to use a condom� A woman should tolerate violence in order to keep her family together� There are times that a woman deserves to be beaten.
By documenting and analysing responses to the statements on the GEM Scale before and after an intervention,changes in gender attitudes can be measured.
More information: J. Pulerwitz, G. Barker, M. Segundo, Promoting healthy relationships and HIV/STI prevention for youngmen: Positive findings from an intervention study in Brazil. Horizons Research Update, 2004: www.popcouncil.org/pdfs/horizons/brgndrnrmsru.pdf.
ProgrammeFeature
Yari-dosti group education for young men led by a peerleaderPhoto: CORO

6 Sexua l Hea l th Exchange 2005/2
giving; 3) takes responsibility for reproductive health anddisease prevention; and 4) opposes intimate partnerviolence.
Real men and womenDuring the formative research, young men described anasli mard (“real man” in Hindi) as someone who wasphysically attractive, dominant, aggressive, and sexuallypowerful. Controlling women and violent behaviour wereimportant parts of the definition of a real man. Young menalso thought that young women sought this type of realman. They stated that it was important to prove one’smanhood, and that proving manliness was characterisedby violence against women, risky sexual behaviour, andalcohol and drug use. According to some of the youngmen interviewed, a real man: “should be a body builder…He must have physical strength and must take a lead inphysical fights. A real man has to provide proof of hismardangi (manliness).”
The concept of an asli nari or an “ideal woman” wasalso explored. She was shy and did not respond to men’ssexual advances. These women were considered“marriageable”. In contrast, girls who did not match theseideals “deserved” (and often were subject to) sexualharassment.
Yari-dosti – Tapping alternative voicesBased on the results from the formative study, the teamdeveloped an intervention called Yari-dosti, whichmeans friendship or bonding among men. Theintervention was adapted from Program H, a group-based project working with young men that wasdeveloped and tested by Instituto PROMUNDO andpartners in Brazil.1 Both Program H and the Yari-dostiproject seek to tap into “alternative” voices of youngmen that promote more gender-equitable norms andbehaviours. During a weeklong workshop, followed bytwo months of community consultations, the teamadapted 20 group educational exercises for the Indiancontext. Among the main themes covered in theexercises were STI/HIV risk and prevention, partner,family and community violence, gender and sexuality,and the reproductive system.
These exercises were then piloted and tested with agroup of young men from low-income communities inMumbai. Selected peer leaders underwent an intensivetwo-week training programme to strengthen theirknowledge and facilitation skills. Peer leaders thenrecruited young men from the community to participatein the intervention. The 126 participants thus recruitedwere divided into four groups of 30-35 participants each.The pilot started with an intensive week of groupeducational activities, facilitated by peer leaders andgender specialists and was followed by two to three-hoursessions every week, led by peer leaders only, for aduration of six months.
Results from the interventionProcess data indicate that almost all of the young menrecruited for the project consistently participated inactivities. Also, most were greatly interested in the topicareas addressed, as it was their first opportunity todiscuss these issues with other men. Participants wereinitially most interested in factual/biological information(e.g., on the human body, sex, HIV), but over time theyfound sessions on gender-related attitudes, sexual
violence, and power dynamics between men and womenvery engaging. The peer leaders observed that theprocess of change began with denial of existing normsand their links to risk, to gradual acceptance that thesenorms existed, and that change would be worthwhile,and then to exploring ways to challenge these norms andbehaviours.
The researchers were able to collect pre-test surveysfrom 107 young men, and post-test surveys from 92young men. GEM Scale responses during pre and post-tests indicated that a significant proportion of young menmoved away from more inequitable attitudes to moreegalitarian attitudes towards gender. For example, theproportion of men who said that “it is okay for a man tohit his wife if she refuses sex with him” declined from 28%during the pre-test to 3% during the post-test. Similarly,the proportion of young men who believed that “a manshould have the final word about decisions in his home”declined from 34% to 11%. Self-reported harassment ofgirls over the last three months (referred to as “eveteasing” in India) significantly declined from 80% duringthe pre-test to 43% during the post-test. A trend towardsincreasing condom use with casual sex partners and sexworkers was observed.
The next stepsBased on the experiences generated during the pilotintervention, a large evaluation of the group educationintervention – with over 1000 young men – has begun inthe city of Mumbai and the states of Goa and UttarPradesh. In addition, a community-based “lifestyle” socialmarketing campaign, consisting of activities such as streettheatre and poster distribution, is under development.The campaign will act to reinforce the gender equitableand HIV prevention messages from the group educationsessions. With the tag line Soch sahi mard vahi (“A realman has the right attitude”), the campaign is beingdesigned and executed by young men from thecommunity.
Ravi K. Verma ([email protected]) & Vaishali SharmaMahendra ([email protected]), Horizons Program/Population Council; Julie Pulerwitz ([email protected]),Horizons Program/PATH; Sujata Khandekar ([email protected]), CORO for Literacy, India; & Gary Barker,Instituto PROMUNDO, Brazil ([email protected]).
CCoonnttaacctt ppeerrssoonn:: RRaavvii KK.. VVeerrmmaa,, PPooppuullaattiioonn CCoouunncciill IInnddiiaa,, 5533 LLooddhhiiEEssttaattee,, NNeeww DDeellhhii,, 111100000033,, IInnddiiaa;; tteell..:: ++9911--1111--224466..110099..1133,, ee--mmaaiill;;rraavviivveerrmmaa@@ppcciinnddiiaa..oorrgg
1. More information about both the Yari-dosti intervention and ProgramH: Young Men and HIV Prevention, Horizons Report, December 2004:www.popcouncil.org/horizons/newsletter/horizons(9).html.
Percentage of young men harassing girls reduced almosthalf after attending the Yari-dosti programme

Sexua l Hea l th Exchange 2005/2 7Fostering alternative views of male identity amongboys in Latin America and the CaribbeanMatilde Maddaleno, Francisca Infante, Rodrigo Aguirre, Pedro Güell &Sarah White
Young men in Latin America and the Caribbean tend to engage in high-risk behaviours such asdrug abuse, unprotected sex and violence that can have long-term consequences for themselvesand others. Approximately 50% of young men aged 17 and under are sexually active, but do notpractise safe sex. In Brazil, though 96% of adolescents know that condom use prevents HIVinfection, only 60% report using them. Twenty percent of sexually active young males in ElSalvador report condom use, while only 11% of sexually active adolescents in Nicaragua reportregularly using any type of contraception. In many countries in the region, up to one third of babiesare born to young women aged 10-19. Young people are particularly affected by the AIDSepidemic, as around half of new HIV infections occur among youth aged 15-24. Violence –especially related to drug trafficking and gang membership – is a serious problem that can lead todeath among male adolescents.1
SpecialArticle
However, males are not born with an inherent desire totake risks. Rather, they are socialized to take on masculinecharacteristics early in life, which are later reproduced inan effort to exhibit manhood. As part of an effort toaddress the threats to adolescent male health, the WorldHealth Organization (WHO)/Pan American HealthOrganization (PAHO), in collaboration with otheragencies, undertook a multi-country, qualitative study tounderstand the relationship between high-risk behavioursand the construction of male identity.2 Focus groups andinterviews were conducted with young male participantsaged 10-24 from rural and marginalized urban areas inBrazil, Costa Rica, El Salvador, Guatemala, Honduras,Jamaica, Mexico and Nicaragua. Focus groups were usedto shed light on the idealized common views of youth,while interviews were used to gather information abouttheir real behaviours.
Topics of discussion varied by age group, andincluded the meaning of manhood, development ofsexuality, sources of information, and relationships withfamily, female partners and peers. Results were compiledand from them were derived participants’ views oncharacteristics that define masculinity as well as theirideas about “mandates” (ideas, norms and rules) thatgovern actions and relationships with others.
The construction of the male identityThe central male characteristic emerging from the studywas strength through physical capacity, aggressivenessand competitiveness. The youth stated that men arestrong by nature and that this is reflected in their bodilystrength. Strength of character, they said, could beexhibited through resistance to challenges, control ofemotions and the capacity to take on responsibilities.
Mandates identified through the study tend to focuson the requirements for the transition that adolescentmales make from the home to the outside world,particularly the “street”. The street world is the domain ofviolence and other risk behaviours such as drug andalcohol abuse. It is rife with challenges and it is wherepeers meet and manhood is constructed. Participantsstated that men are of the street and women and childrenare of the family. They said that men accepted thechallenges posed by others and were therefore fighters,risk-takers and imitators of group behaviours. Theirrelations with women helped in the definition ofmasculinity. Mandates included possessing women,
subordinating them sexually, and seducing them withintent to deceive them. Men were described as the hunter,unfaithful partner and the sexual satisfier. They felt thatuse of contraception was not their responsibility. Men,they added, use any opportunity to engage in sexualintercourse.
The above descriptions provide a clear context forhigh-risk behaviours. Such behaviours serve the dualpurposes of demonstrating manhood and therebygaining acceptance and respect from peers, confirmingthe need for adolescent males to detach themselves fromtheir intimate selves, their homes and families.
Alternative viewsIn individual interviews, participants were more likely tosuggest a certain struggle to achieve these ideas ofmanhood, and “confess” gender-equitable characteristicsthat in the group they would most likely deny. Forinstance, they recognized the contradiction in upholding
There is a need to promote alternative views of maleidentity which will be beneficial to men and womenPhoto: Nel van Beelen

8 Sexua l Hea l th Exchange 2005/2
both risk behaviour and responsibilityas key masculine characteristics. It wasmentioned that an overemphasis on theworld of peers could lead one to neglectwork and family responsibilities. Thealternative view regarding relations withwomen placed a higher value onsentiment and legitimizes the emotionalaspects of masculinity. Without denyingthe role of men as conquerors,participants also suggested that it wasbest for sexual relations to occur withinthe context of a committed and lovingrelationship.
Programmes promoting action orattitudes that threaten the hegemonic
model and the process of masculinity construction arelikely to fail. However, there is a need to promotealternative views of male identity which will be beneficialto men and women. Such views, which are beingespoused by some male youth are useful in thenegotiation of daily life. Educational programmes shouldbuild upon them. Interventions targeting young malesshould take place in environments that are important foryouth, take into account their treacherous path toconstructing themselves as men, and work within thisframework with the aim of finding ways to reinforcehealthy and gender-equitable attitudes and behaviours.
The Football, Health and Gender programmeBased on the results of the study, PAHO/WHO and theJohan Cruyff Foundation developed a strategy to usesoccer to reach and educate young males. Theprogramme, entitled “Football, Health and Gender: ANew Approach to Health in Pre-Adolescent Males”, isunderway in six Latin American countries and utilizessoccer coaches to promote gender-equitable healthbehaviours and relationships among pre-adolescent boysaged 8-12. Soccer plays a role in the lives of many youngmales, and the game embodies values promoted bydominant ideas of masculinity (see Box), as well asoffering a fertile environment for enhancing alternativeviews of how to become a man.
The programme requires soccer coaches to integratehealth and gender education into soccer practice.Coaches are trained in:� Gender awareness and sensitivity to improveperceptions of masculinity� Sexual and reproductive health education, includingHIV/AIDS and prevention of unwanted pregnancy
� Conflict resolution, anger management, and life skillsdevelopment� Prevention of substance abuse through the promotionof good nutrition and well-being.
After the training, coaches conduct “soccer schools”sessions for consecutive days. The soccer schools areopen to local youth and held in public areas of low-income neighbourhoods. The project has already beenimplemented in Argentina, Brazil, Chile, Paraguay, Mexicoand Venezuela and has involved over 1000 adolescents.
The project is an example of how programmes can reachyoung men by working at the level of their daily world.The risks that concern public health officials are rarely aconcern of young people themselves. From the point ofview of boys, what is at risk is their own identity and theirtransition to manhood. The successful and healthycompletion of this transition can be a common objectiveof both health policies and the youth they target. Byunderstanding the fragile nature of masculinityconstruction and working with emerging alternativemasculinities, health officials can help adolescent malesgrow into the best men they can be.
Matilde Maddaleno, Francisca Infante, Rodrigo Aguirre, PedroGüell & Sarah White, Child and Adolescent Health departmentPAHO/WHO, Washington, USA; tel.: +1-202-974.35.23, fax:+1-202-974.36.31/3640; e-mail: [email protected], web:www.paho.org/adolescence, www.adolec.org (AdolescentVirtual Health Library)
1. Health in the Americas. Volume II. PAHO, 20022. R. Aguirre & P. Güell. Hacerse hombres: La construcción de la
masculinidad en los adolescentes y sus riesgos (“Becoming men:masculinity construction in adolescents and its risks”. PAHO, 2002(Spanish only)
Adolescence, soccer and masculinityAt present, soccer is the most popular sport with masculinity nuances. It is a masculine game par excellence. The masculinity ideal thatsoccer espouses strikes a chord with the youth. The values associated with the soccer practice are similar to those inherent in masculinity.Soccer condenses, produces and reproduces the masculinity hegemonic (superiority) model. It helps reaffirm the masculine subjectivity,the bonds between men, the exercise of paternity, the bonds with women and how tasks can be organized. Soccer connects directlywith the masculine competitive side. When playing it, one feels that it is possible to exert power on other equals.
Soccer generates much passion that can transform into fanaticism. This can be explained by soccer personalities or idols beingadmired by adolescents. The soccer player is the epitome of masculinity, recreating the idea of the superman: tough, brave,competitive, loyal to the group, successful and recognized by peers. Passion for soccer is inherited very early in life from fathers tochildren. Thus, the boy learns that soccer is a virile sport – it nurtures the masculine body and it is a measure of one’s strength.
Finally, soccer builds affection and allows expression of bonds. It triggers diverse emotions and feelings, among them joy whenmen are playing it and, especially, when they win.
Percy Fernández Dávila, PhD student of psychology at the Ramon Llull University of Barcelona

Sexua l Hea l th Exchange 2005/2 9
According to the 2004 UNAIDS report on the global AIDSepidemic, it is estimated that 0.2% of Nicaraguansbetween 15-49 years of age are infected with HIV. Thisprevalence is much lower than figures for the region as awhole and neighbouring Honduras (0.5% and 1.8%,respectively). Despite having one of the lowest HIV-infection rates in Latin America and the Caribbean, social,political, demographic and cultural factors makeprevention difficult and could lead to a rapid spread of HIV.Sexual activity begins at an early age and the effect ofmachismo on both men’s and women’s sexuality issignificant. Unprotected sex is the most common form oftransmission. This puts the future of the next adultgeneration at risk.
Cultural norms in Nicaragua encourage male sexualirresponsibility and efforts to prevent the spread ofHIV/AIDS, through the promotion of condom use and thereduction of stigma, are hampered by custodians oftradition, especially the Catholic Church. In 2003, thesesectors forced the government to withdraw a manual oncomprehensive sex education for schools. In this context,mass media becomes a useful tool to fight HIV/AIDS, andusing mass media in Nicaragua has at least two mainadvantages. Television and radio are by far the mainforms of entertainment for Nicaraguans and almost allhouseholds have them. Furthermore, men and womenseem to have equal access to them.
Mass media and social actionBetween 2002 and 2005, SDSI has taken on HIVprevention. The programme aims to increase youngpeople’s perception and personalization of risk ofinfection; encourage them to develop or adopt moreequitable gender norms and behaviours; and promote anenvironment where young people can engage inprevention actions, individually and collectively. SDSIcombines two components that complement each other:mass media and social action.1
Mass media – The strategy promotes favourableconditions at the level of public opinion and social supportto facilitate prevention and non-discrimination. More thanhalf a million young people between ages 13 and 24 inNicaragua are targeted by the mass media componentthrough the weekly drama TV series Sexto Sentido(“Sixth Sense”) and Sexto Sentido Radio, botheducational entertainment (“Edutainment”) programmes.Sexto Sentido Radio is a call-in debate programmehosted by young presenters. Sexto Sentido Television
weekly soap opera is about the daily lives of a group ofyouth, and is broadcast on the largest commercial TVstation and re-broadcast on 11 local cable channels.
Social action – Through agreements with more than80 local service providers, Puntos seeks to increaseaccess to quality SRH services for young people, andtogether with some 200 collaborating organizations, ithopes to create a more favourable environment for youngpeople to develop their own initiatives.
Challenging machismo to prevent HIVUnder the campaign slogan “We need to be able to talk”,there is an argument that machismo is a risk factor thatincreases the chances of contracting HIV. The TV seriesapproaches this issue from various angles. For example,one of the main characters becomes infected andconfronts the prejudices – including his own – aboutforms of transmission and what kinds of people get HIV. Ayoung woman living with HIV shows the difference inmen’s and women’s experiences with HIV/AIDS. Theshow also demonstrates the accumulated effects ofgender-based bias and stigma towards women,homosexuals and sex workers. The series conveys themessage that with awareness, open communication andequitable decision-making processes between men andwomen, HIV can be prevented.
Monitoring and evaluationThe current focus on HIV/AIDS responds, to a largeextent, to the needs expressed by young people in theprevious period. The evaluation of the programmeconsists of a sequential approach of quantitative andqualitative research. For the 2002-2005 HIV/AIDS project,the effects are being measured in a cohort of 4,800 youngpeople (13-24 years old) randomly selected in three citiesin Nicaragua who will be interviewed three times: for
ProgrammeFeature
Using edutainment and social activities to challengemachismo in NicaraguaThe example of Somos Diferentes, Somos Iguales
Henry Espinoza
“Somos Diferentes, Somos Iguales” (SDSI), Spanish for “We’re Different, We’re Equal”, is acommunication for social change strategy to promote the empowerment of young men andwomen and prevent HIV infection in Nicaragua. The strategy focuses on the social and culturalissues that hinder prevention of HIV by promoting the transformation of social norms towardsgreater gender equity and sexual responsibility. Furthermore, SDSI places HIV transmission in thecontext of daily life issues such as “machismo” (roughly translated as sexism or a system ofsubordination of women by men), gender-based violence, and drug and alcohol abuse, amongothers. The elements of the strategy have been developed by the Nicaraguan feminist organizationPuntos de Encuentro (“Meeting Points” or “Common Ground”) since the late 1990s, but the HIVprevention project begun in 2002 and will end in 2005.
“It is your life... Be bold!” Sexto Sentido’s affiche
baseline, for mid-term evaluation and several monthsafter the project activities end. About 200 young peoplewill be enrolled into the two qualitative measures, whichcomprise focus groups and individual interviews withyoung participants and non-participants of social actionactivities (workshop, camps, etc.). The evaluation is beingconducted by a multi-agency team comprised byHorizons/Population Council, Program for AppropriateTechnology (PATH), Centro de Investigación deDemografía y Salud (CIDS) and local consultants.
Lessons learnedThe findings of the baseline survey were not surprising:while there is good knowledge about HIV/AIDS, AIDS-related stigma is prevalent, and safer sex is not practisedvery often. There is already some evidence to suggestthat the strategy may play a helpful role to prevent HIV.Several factors can be seen as windows of opportunity fora sustainable strategy:
Questioning cultural norms – Challenging machismois a long-term process. SDSI is contributing to young menand women beginning to question, among other things,the social norms that govern their interpersonal relationsand sex lives, and which negatively affect their quality oflife.
Integrated approach – The integration of differentthemes plays an important role in the sustainability of theSDSI strategy. HIV/AIDS and machismo are linked to arange of relevant themes: drug and alcohol abuse,physical, psychological, and sexual violence againstwomen and girls, and early pregnancy, which are seriousproblems in Nicaragua.
Capitalizing on popularity – In the four years sinceSexto Sentido began national broadcasts, the series hasbecome a source of national pride, especially whenrelatives in the United States reported seeing the show onTV “up there”.2 The popularity of the TV programme andits cast has helped reduce opposition from someconservative sectors, especially at the Ministry ofEducation, since actors are allowed to go to local highschools and talk with students about topics andperspectives that are usually not allowed in the curriculum.
Collaboration – Working in an alliance providesanother opportunity to sustain the programme.Collaborating organizations have already developedsome ownership of approaches, themes and methods. Ininterviews with representatives from organizations,service providers and local media outlets with whomPuntos de Encuentro works, it was clear that SDSI is seento have supported their own organizational work on theseissues.
ChallengesThe use of the media in SDSI has helped reach a widerpublic and provide information on prevention, existingservices and the rights of people living with HIV/AIDS,including the right not to be discriminated against.Nevertheless, it is a challenge to demonstrate thatchanges in attitudes, norms and behaviours are takingplace in the target population and to disentangle theattribution of those changes to SDSI and its components.While initial cost analysis shows that the programme isvery inexpensive given its reach,3 additional analyses ofcosts in relation to impact are warranted.
Henry Espinoza, independent consultant at Puntos deEncuentro; Rotonda Güegüense 4 cuadras abajo, 1 cuadraal lago, Managua, Nicaragua; tel.: +505-268.12.27; fax:+505-266.63.05, e-mail: [email protected], web:www. puntos.org.ni
TThhee aauutthhoorr wwoouulldd lliikkee ttoo tthhaannkk AAmmyy BBaannkk aanndd IIrreellaa SSoolloorrzzaannoo ooff PPuunnttoossddee EEnnccuueennttrroo,, JJuulliiee PPuulleerrwwiittzz ooff HHoorriizzoonnss//PPooppuullaattiioonn CCoouunncciill,, aannddVVaanneessssaa KKuurrzz ffoorr tthheeiirr vvaalluuaabbllee ccoonnttrriibbuuttiioonnss..
1. An extended description of the SDSI components can be found inan article previously published in Sexual Health Exchange (2002,No. 1): www.sexualhealthexchange.org
2. Sexto Sentido has recently begun broadcasting in the USA toHispanic-Central American audiences via Centroamérica TV, asatellite cable station. It will also soon begin broadcasting onHonduran and Costa Rican TV stations.
3. Based on audience estimates, the national broadcast of SextoSentido costs US$0.04 per youth viewer per episode. The cost perviewer is less if adults and children are taken into account as well,and it is even less as the total audience increases as a result ofbroadcast in other countries and distribution of videos.
10 Sexua l Hea l th Exchange 2005/2
Male identity, poverty and reproductive health inNamibiaBritt Pinkowski Tersbøl
The link between gender-based inequalities and the spread of HIV/AIDS has been an issue inacademic debates and a focus in programme efforts for more than a decade. Women’s heightenedbiological vulnerability coupled with socio-cultural factors, have placed girls and women atparticular risk of HIV infection. As a result, HIV prevention programmes have tended to focus moreon women and girls. Unfortunately, women’s vulnerability has led to a tendency to assign theresponsibility for safer sexual practices to women, often leaving men out of prevention efforts. Byleaving out men, opportunities are missed to address more fundamental sexual and relationshipdynamics and the relational aspect of power and powerlessness.
ResearchNotes
This is a lesson that should have been learned from the earlyfamily planning programmes that targeted mainly women.In the context of gender theory and in particular within socialscience work on reproductive health and HIV/AIDS, therehas increasingly, over the past decade, been a focus on thesituations of men and constructions of masculinities in sub-
Saharan Africa. Research findings indicate that increasedsocial and cultural disempowerment of men is detrimentalto reproductive health, promotes the spread of HIV and alsohampers prevention efforts.1
One of these studies was undertaken in Namibiaamong the Kwanyamas, the largest ethnic group among

Sexua l Hea l th Exchange 2005/2 11
the Ovambo population.2 Kwanyama society hasundergone significant transitions since the advent ofChristianity and colonialism in the 19th century.Subsistence agriculture, with animal husbandry (goatsand cattle), was the economic mainstay of the ethnicgroup. Socio-economic and political changes havecaused a large of number of community members tomove to urban settings in the south. Systematicexploitation and pauperization of particularly blackpopulation groups took place during the colonial era,which only ended in 1990 when the country got itsindependence.
In this qualitative anthropological study, which wascarried out in rural and urban Namibia on heterosexualrelationships and their socio-cultural context, 61 men and62 women were interviewed. The study involvedinterviews and participant observation amongKwanyamas living in the northern rural region ofOhangwena and in the central coastal town of Walvis Bay,a town to which many Kwanyamas move from theirvillages to seek economic opportunities.
Constructions of masculinities are dynamic processesand possible models of masculinities exist and areconstantly contested as societies change and newmodels emerge. Although study informants pointed tomore than one valued type of masculinity, a general trendcan be summarised as follows: Men are supposed to bethe leaders within the family and community, and providefor members of their maternal clan, wives and children.Boys and men are expected to possess skills associatedwith agriculture and livestock production. The importanceof cattle is underlined as young boys are frequentlywithdrawn from primary schools to become herdsmen.Girls are more often allowed to continue schooling untiltheir teens when many are forced to leave due topregnancies. With only a few years of primary education,the boys are ill equipped for the future, particularlybecause economic recession has resulted in fewer jobsfor unskilled labourers.
In the urban sphere, men must demonstrate that theyare able to find and keep a job in order to invest theirearnings in their rural families and livelihoods in thenorth. Marriage is perceived as one of the life transitionsthat bestow adulthood on men. To marry, men shouldideally have work, millet fields and cattle. While marriageis significant, it is equally important to be pro-active in thesexual sphere and prove virility through engaging inmore than one sexual relationship and fathering children.
A 27-year-old respondent said having many childrenwould make him proud and that failure to have childrenwould invite ridicule. Going out at night to drink is alsoperceived by some informants as”natural” behaviour ofreal men.
Poverty and existential crisisRespondents said poverty caused them significant stressand emotional suffering as they sought for economicopportunities in vain. Poverty is mainly attributable to lackof access to fertile land, cattle, education and jobopportunities. The study supports findings of similarresearch in other sub-Saharan African countries whichconcluded that poverty and lack of prospects led toconfusion and loss of self esteem and meaning. AlthoughHIV/AIDS is perceived to be a serious problem,respondents view concerns over poverty and loss ofhope for the future as more acute.
This study suggests that health promotionprogrammes should provide men with a platform forcommunication and education that take their urgentconcerns as a starting point. Such platforms shouldaddress men’s experiences of exclusion to challenge theexisting perceptions and interpretations that men have ofthemselves and their partners. Also, men’s conduct in thesexual sphere and how it affects their partners, childrenand communities should be addressed.
One community-driven initiative in Namibia hasfocused on social relations and violence, including sexualviolence, in a disadvantaged community.3 Throughdialogue and reflection, the programme helped partici-pants to analyse the ideologies and structures thatoppress them and others, and devise strategies for action.There is a need to encourage social science research,particularly action research – such as the work done inBrazil, which include comprehensive transformationaleducation on HIV/AIDS among poor youth4 – to findapproaches that are effective in motivating andempowering men to take part in controlling HIV/AIDS,and in protecting the health and rights of women andyoung girls.
Britt Pinkowski Tersbøl, Researcher, Department of Womenand Gender Research in Medicine, Institute of Public Health,University of Copenhagen, Denmark; tel.: +45-353.272.82,fax: +45-353.277.36, e-mail: [email protected]
1. M. Silberschmidt, Disempowerment of men in rural and urban EastAfrica: Implications for male identity and sexual behaviour. WorldDevelopment, Vol. 29, No. 4, 2001, p. 657-671.
2. B.P. Tersbol, How to make sense of lover telationships – Kwanyamaculture and reproductive health. In: Namibia, Society, Sociology, V.Winterfeldt, T. Fox & P. Mufune (eds.), University of Namibia Press,Windhoek, 2002.
3. N. Kandirikirira, Deconstructingdomination: Gender disem-powerment and the legacy ofcolonialism and Apartheid inOmaheka, Namibia. In:Masculinities Matter! Men,Gender and Development, F.Cleaver (ed.), Zed Books,London, 2003.
4. V. Paiva, Gendered scripts andthe sexual scene: Promotingsexual subjects amongBrazilian teenagers. In: Framingthe sexual subject: The politicsof gender, sexuality and power.R. Parker, R. Barbosa & P.Aggleton (eds.), University ofCalifornia Press, Berkeley,2000.
For many Namibian peoples, owning cattle is of theutmost importancePhoto: Maite Rodriguez
Poverty drives people from the countryside tourban areasPhoto: Gabor Zsoldos

12 Sexua l Hea l th Exchange 2005/2
SpecialArticle
Behind the bars of South African prisonsGendered roles and vulnerability of male inmates to forced sex
Sasha Gear
In South African prisons, different kinds of sexual interactions and relationships take placebetween men. The majority of these are abusive, exploitative, and involve rape and variousdegrees of coercion. Newcomers to prison are especially vulnerable because they are unfamiliarwith the “rules” of inmate culture and are easily manipulated. Seasoned inmates regard them assources of material goods including sex, and as potential gang members. Often, a newcomeraccepts goods and services such as protection, food or cigarettes from another inmate withoutrealizing that sex will be expected from him as payment for the unknowingly created “debt”. Rapefrequently follows as a consequence.
A qualitative study by the South African Centre for theStudy of Violence and Reconciliation (CSVR) showed thatthe trickery frequently used to subordinate inmates relieson the exchange value that is attributed to sex.1 Becausesex is embedded in the prison economy, those who arepoor tend to be amongst the more vulnerable. Prisonerswho do not get visitors (an important source ofcommodities and money) are often economically needy.As one respondent put it, “money makes prison goround” and prisoners’ basic rights – food rations, blankets,beds – become embroiled in this economy.
The risks of rape are higher among those who arephysically weak, not prepared to use violence or who areperceived to have committed a “sissy crime” (often thosethat do not involve violence or weapons). Having “goodlooks” also increases the likelihood of being targeted.
However, there are no absolute prerequisites for sexualviolation. Both poverty and fear, for example, can becreated by fellow inmates to ensure anyone’scompliance.
Gendered rolesBeyond the trauma of unwanted sex, rape is understoodto demolish the victim’s manhood and turn him into a“woman”. This is linked to the way in which dominantinmate culture perceives gender to be connected tocertain sex roles: men penetrate and women arepenetrated. Rape and coercion are, as a result, used tobrutally impose a feminized identity on a portion of themale prisoner population.
“Women” are generally stigmatized as inferior andbecome the sexual property of inmates identified as“men”: prison “womanhood” usually means being theconstant target of harassment and abuse. In the words ofone young inmate: “We are all criminals in here and if Isay you are a criminal that means that I respect you. Butif you have had sex done to you, even the criminal in youis now gone and you are now a woman… There isnothing we can do for you. Some people just look andsome want to sleep with you and when you walk pastpeople, they want to touch or threaten to rape you.”
An initial rape often sees victims being taken by theperpetrators as prison “wives” or wyfies (in Afrikaans-influenced prison slang) in long-term coercive
HIV/AIDS and prisons in South AfricaThe majority of prisoners in South Africa fall into a category at high risk for HIV infection: young, uneducated, blackmen. They face problems of overcrowding, violence and poor nutrition. Very little is known about HIV prevalenceamong inmates however. Based on the assumption that HIV prevalence in South African prisons is twice that of theprevalence amongst the same age and gender in the general population, the Institute for Security Studies (ISS)estimated in 2003 that some 40% of male and female inmates were HIV infected in the year before.1 A study among271 male inmates of the Westville Medium Security Prison in Durban, KwaZulu-Natal Province, showed that 30%was infected with HIV.2
“Natural deaths” in prison, most of which are believed to be AIDS-related, are on the rapid increase. During theperiod 1995-2004 the annual death rate escalated from 1.65 per 1000 prisoners to 9.1 deaths per 1000 prisoners. In2004, 1689 deaths were considered natural and 69 were unnatural.3
The South African Department of Correctional Services has introduced a range of policies to address HIV/AIDSin prison, based on human rights principles and international guidelines, and covering issues such as confidentiality,non-discrimination, condom provision, medical treatment etc. However, due largely to chronic overcrowding andinadequate resources, these policies are at best, unevenly implemented – more often barely so.
1. K.C. Goyer. HIV/AIDS in prison. Problems, policies and potential. ISS Monograph No 79, 2003: www.iss.co.za/Pubs/Monographs/No79/Content.html.
2. J. Gow, G. Smith, K.C. Goyer & M. Colvin. The socio-economic characteristics of HIV in a South African prison. Abstract no. WePeD6529, XVInternational AIDS Conference, 2004, Bangkok.
3. Judicial Inspectorate of Prisons. Annual Report 2004/2005. Cape Town.

Sexua l Hea l th Exchange 2005/2 13relationships known as “prison marriages”. The“husband” provides material goods and consumables forhis wyfie, who is required to do domestic tasks and beconstantly sexually available to him. While suchrelationships contain differing levels of coercion andevolve differently over time, it is generally agreed that themajority of wyfies despise their positions, remaining inthem only because of fear.
Particularly oppressive notions of gender are at thecentre of much of the sex happening in prison. To benaïve, trusting, poor, and not prepared to use violence arequalities associated with inferiority and womanliness.Manliness is equated with the use of violence and theability to endure certain forms of it, deviousness, andparticipation in the prison economy (through smugglingand theft). Power lies with men. The centrality of violenceto manhood is highlighted in the typical requirement thatwyfies seeking promotion to manhood perform a specificviolent deed in order to prove worthiness of manhood.
Homophobia and alternative sexual relations A Stop Prison Rape activist once said that in Americanprisons an inmate “could be fucking his cellmate everynight, but will truthfully, as far as he is concerned deny thathe has had a homosexual experience in prison”. It is muchthe same in South African prisons where the mostcommon and sanctioned forms of sexual interaction (inmarriages and the like) tend not to be connected tonotions of homosexuality by many of the people involved.
Indeed, some other types of sexual interaction areconsidered deviant precisely because they are associatedwith homosexuality. Ushintsha ipondo – literally meaningto “exchange a pound” – is reportedly common but alsoa punishable offence according to the inmate code. It ischaracterized by consensual sex and often spoken of as“doing each other favours” (regularly, it involves peoplewho are simultaneously other prisoners wyfies). In theserelationships, neither partner is considered to beinferior/superior, and both take turns to penetrate andreceive. By doing so they are disrupting the system thatdemands that penetration is only for “men” and receivingonly for “women”, and cannot therefore be divided intogenders on the basis of a restricted sex role. This blurringof gender leads to its association with homosexuality andthe threat it poses to the sexual status quo behind bars.
Institutionalization of forced sexA potentially vast range of circumstances surround prisonsex. For instance, sex interactions contained inrelationships defined by love feelings between partnersare also reported, although less commonly. It is rape,coercion, and exploitation that have the strongest hold,and while the boundaries in prison between consent andcoercion are particularly blurred, blatantly forced sexfrequently escapes being viewed as such, but is ratherconsidered normal and acceptable. Sexual abuse isembedded within inmate culture, and is most visible inthe rules, rituals, and ranks employed by powerful prisongangs to organize sex along the destructive lines of“marriage”. At another level, such practices are alsoendorsed by the lack of attention they receive from prisonofficials.
Important to recognize however, is that the ways thatpeople outside of prison relate to each other play afundamental part in these damaging prison processes.Popular beliefs around gender, for example, are behind
the inferior way in which “prison women” are viewed, theentitlement of men to sex from them, and the powerfulperception that victims of forced sex in prison, like thoseoutside, are to blame for what has happened to them. Themyth that, “real men do not get raped” has a grip in theoutside world as well. Explanations from prisonershighlight the connections with broader society: “Wyfiesare treated just like women outside”, said one. Or, in thewords of another, “You can’t rape your wife”.
Damaging and damaged identitiesParticularly destructive notions of what it means to be aman or woman are intensified and entrenched in prison.Intolerances are fuelled, abusive and dangerousbehaviours learnt and trauma caused. Prison is likely toprovide young inmates with some of their most decisiveviews on sexuality and gender, ones on which they willbase future relationships. Further, sexual violence hassevere consequences for the spread of HIV and STIs andthe health of prisoners. Amidst high crime levels, punitivepublic attitudes prevail and the health and well-being ofinmates are not of popular concern. If the realities of lifebehind bars continue to be ignored, many men exposedto life in prison will be condemned to living out damagingand damaged identities.
But while the area is starved of the attention it sourgently requires, a sprinkling of individuals and groupshave made a vital start: like the successful committee ofinmates and staff in one KwaZulu-Natal prison that worksto manage and prevent HIV/AIDS there, or another, set upin the notorious Cape Pollsmoor prison, to supportvictims of prison rape; or the drama performances by aGauteng NGO that challenge the oppressive andgendered inmate power relations at the same time as theyraise awareness of HIV risk. The learnings andexperiences provided in initiatives like these need to beshared and drawn on to focus a broad and concertedstrategy to prevent the violence and safe-guard prisoners’health.
Sasha Gear, Researcher Centre for the Study of Violence andReconciliation; PO Box 30778, Braamfontein, South Africa,2017; tel.: +27-11-403.56.50 ext 141, fax: +27-11-339.67.85,e-mail: [email protected], web: www.csvr.org.za
1. S. Gear & K. Ngubeni. Daai ding: Sex, sexual violence and coercionin men’s prisons. Centre for the Study of Violence andReconciliation, 2002: www.csvr.org.za/papers/papsgkn.htm.
Image: International HIV/AIDS Alliance
14 Sexua l Hea l th Exchange 2005/2
Men who have sex with men and disempowerment inSouth AsiaShivananda Khan
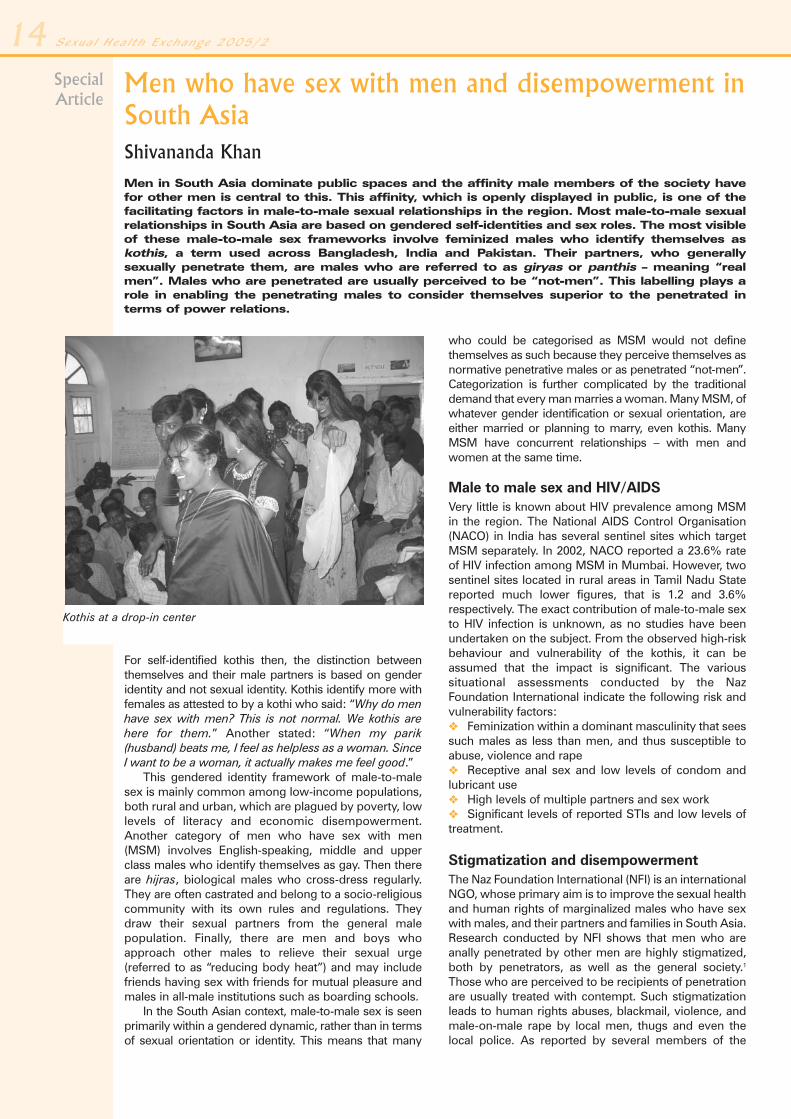
Men in South Asia dominate public spaces and the affinity male members of the society havefor other men is central to this. This affinity, which is openly displayed in public, is one of thefacilitating factors in male-to-male sexual relationships in the region. Most male-to-male sexualrelationships in South Asia are based on gendered self-identities and sex roles. The most visibleof these male-to-male sex frameworks involve feminized males who identify themselves askothis, a term used across Bangladesh, India and Pakistan. Their partners, who generallysexually penetrate them, are males who are referred to as giryas or panthis – meaning “realmen”. Males who are penetrated are usually perceived to be “not-men”. This labelling plays arole in enabling the penetrating males to consider themselves superior to the penetrated interms of power relations.
SpecialArticle
For self-identified kothis then, the distinction betweenthemselves and their male partners is based on genderidentity and not sexual identity. Kothis identify more withfemales as attested to by a kothi who said: “Why do menhave sex with men? This is not normal. We kothis arehere for them.” Another stated: “When my parik(husband) beats me, I feel as helpless as a woman. SinceI want to be a woman, it actually makes me feel good.”
This gendered identity framework of male-to-malesex is mainly common among low-income populations,both rural and urban, which are plagued by poverty, lowlevels of literacy and economic disempowerment.Another category of men who have sex with men(MSM) involves English-speaking, middle and upperclass males who identify themselves as gay. Then thereare hijras, biological males who cross-dress regularly.They are often castrated and belong to a socio-religiouscommunity with its own rules and regulations. Theydraw their sexual partners from the general malepopulation. Finally, there are men and boys whoapproach other males to relieve their sexual urge(referred to as “reducing body heat”) and may includefriends having sex with friends for mutual pleasure andmales in all-male institutions such as boarding schools.
In the South Asian context, male-to-male sex is seenprimarily within a gendered dynamic, rather than in termsof sexual orientation or identity. This means that many
who could be categorised as MSM would not definethemselves as such because they perceive themselves asnormative penetrative males or as penetrated “not-men”.Categorization is further complicated by the traditionaldemand that every man marries a woman. Many MSM, ofwhatever gender identification or sexual orientation, areeither married or planning to marry, even kothis. ManyMSM have concurrent relationships – with men andwomen at the same time.
Male to male sex and HIV/AIDSVery little is known about HIV prevalence among MSMin the region. The National AIDS Control Organisation(NACO) in India has several sentinel sites which targetMSM separately. In 2002, NACO reported a 23.6% rateof HIV infection among MSM in Mumbai. However, twosentinel sites located in rural areas in Tamil Nadu Statereported much lower figures, that is 1.2 and 3.6%respectively. The exact contribution of male-to-male sexto HIV infection is unknown, as no studies have beenundertaken on the subject. From the observed high-riskbehaviour and vulnerability of the kothis, it can beassumed that the impact is significant. The varioussituational assessments conducted by the NazFoundation International indicate the following risk andvulnerability factors:� Feminization within a dominant masculinity that seessuch males as less than men, and thus susceptible toabuse, violence and rape� Receptive anal sex and low levels of condom andlubricant use� High levels of multiple partners and sex work� Significant levels of reported STIs and low levels oftreatment.
Stigmatization and disempowermentThe Naz Foundation International (NFI) is an internationalNGO, whose primary aim is to improve the sexual healthand human rights of marginalized males who have sexwith males, and their partners and families in South Asia.Research conducted by NFI shows that men who areanally penetrated by other men are highly stigmatized,both by penetrators, as well as the general society.1
Those who are perceived to be recipients of penetrationare usually treated with contempt. Such stigmatizationleads to human rights abuses, blackmail, violence, andmale-on-male rape by local men, thugs and even thelocal police. As reported by several members of the
Kothis at a drop-in center

Sexua l Hea l th Exchange 2005/2 15Network of Indian People with Alternate Sexualitiesliving with HIV/AIDS (NIPASHA), MSM living withHIV/AIDS are stigmatized by other men who are alsoliving with HIV/AIDS because men in heterosexualrelationships deem their routes of HIV infection“normal”.
Many kothis also face harassment, sexual violenceand rape from former friends in schools and colleges,and from those in positions of trust such as relatives,neighbourhood elders and teachers. Gang rape iscommon, along with violence and abuse from sexualpartners. Such forced sex is always unsafe and oftenresults in serious physical injury such as a rupturedrectum, internal haemorrhage and even HIV infection.
One of the central issues that have arisen from NFIresearch is that often it is effeminacy (acting or lookinglike a woman) and not the factual knowledge of male-to-male sexual behaviour that leads to harassment andviolence. This effeminacy is expressed through bodylanguage, and at times, through cross-dressing, wearingmake-up and use of effeminate language. Harassmentand sexual violence result from the fact that many kothisdo not live up to the expected normative standards ofmasculine behaviour. It is this belief that leads to thenotion that those who are feminized can be exploitedand abused and that being feminized somehowweakens the person, a notion often harboured by thekothis themselves.
The disempowerment of kothis has been found tocreate significant levels of suicidal impulses and self-damage, an expression of self-hatred and despair. Thisincreases their vulnerability to STI/HIV as well asimpeding successful implementation of risk-reductionstrategies.
What needs to be doneAccepted notions around effeminacy are, therefore, oneof the major factors that lead to disempowerment andopens kothis to abuse and assault. The fact that kothisthemselves have internalized these notions so strongly,means that specific tools need to be developed for themto enable them to value their lives, enhance their self-respect and reduce their risks of contracting HIV. Thesetools would include gender-sensitivity trainingprogrammes that address differing sexualities, targetingthe judiciary and law enforcement agencies2 andeducation and vocational training programmes forkothis, to make them less economically dependent ontheir partners. Examples drawn from female sexworkers projects, such as the Sonagachi Project inCalcutta, India, indicates this could be a viable process
for enhancing self-esteem, increasing othersources of income, andmore effective riskmanagement.
Also, the legal, socio-cultural and economicimpediments to MSMsexual health inter-ventions urgently need tobe understood andaddressed. An NFI studyin Bangladesh (Againstthe odds, 2002, 2004)clearly identifies this as a
major concern. Empowering MSM to develop their ownself-help services will be central because community-based organizing is often the best approach tosustaining behaviour change. NFI has assisted in thedevelopment of 28 such community-based serviceproviders in Bangladesh, India, Nepal and Pakistan, whoare showing the way. There are several otherorganizations in the region which have arisen fromnetworks of MSM and developed as self-help providers,including Humsafar Trust in Mumbai, MANAS Bangla inCalcutta, Sahodaran in Chennai, Blue Diamond Societyin Kathmandu, and Bandhu Social Welfare Society inBangladesh. While these, and others, are providingexcellent services, in a region of 1.5 billion people thereis still a lot more that can be done, and should be done.Some of the issues that need to be addresses are:� Repeal of legislation that impedes sexual healthpromotion among MSM� Address human rights violations of MSM and reducesexual violence, harassment and abuse� Empower local networks of self-identified MSM todevelop their own services� Address the risks of unprotected anal sex in allHIV/STI education programmes for the generalpopulation� Include MSM in policy and decision-making at alllevels� Ensure that appropriate STI treatment centres areavailable, accessible and sympathetic to the needs of themany differing sub-populations of MSM.
Since 1996, NFI, along with several other MSM agenciesin the region, has been strongly advocating for change,and for ensuring that appropriate services for at-riskpopulations of MSM are available and accessible.Donors, governments and NGOs in South Asia are nowbeginning to recognize the real risks of the HIV epidemicspreading through the various MSM sub-populations,and into the general population. However, suchadvocacy needs to be maintained, strengthened, andupstreamed, so that more funds can be leveraged todevelop new services, and those most at risk can beensured equity, social justice and well-being.
Shivananda Khan, Chief Executive Naz FoundationInternational; Palingswick House, 241 King Street, LondonW6 9LP, UK; tel.: +44-20-856.301.91, fax: +44-20-874.198.41, e-mail: [email protected], web: www.nfi.net.Regional Office: 9 Gulzar Colony, New Berry Lane, Lucknow226 001, India; tel.: +91-522-220.57.81/2, fax: +91-522-220.57.83, e-mail: [email protected]
1. Resources located on the NFI website (www.nfi.net): e.g.,Situational Assessment Report for Hyderbad, 2000; NFI BriefingPaper No. 7: Social Justice, human rights and MSM; and Againstthe odds – a report on the impact of legal, socio-cultural, legislativeand socio-economic impediments to effective HIV/AIDSinterventions with males who have sex with males in Bangladesh.NFI also publishes the quarterly newsletter Pukaar on HIV/AIDS,sexual health and Asian masculinities and sexualities (availableonline).
2. NFI is currently supporting a number of its partner agencies todevelop local advocacy cells within their programmes, which takeon this sensitization role. A toolkit consisting of 6 books onimplementing an MSM sexual health project has recently beenpublished: Developing manual. Developing community-basedorganisations addressing HIV/AIDS, sexual health, welfare andhuman rights issues for males-who-have-sex-with-males, theirpartners and families, NFI, 2005. Available online.

Sexual Health Exchange is published four times per year by the Royal Tropical Institute (KIT) in the Netherlands, in collaboration with SAfAIDS (SouthernAfrica HIV and AIDS Information Dissemination Service), Zimbabwe. Financial support has been provided by the Dutch Ministry of Foreign Affairs andGTZ, Deutsche Gesellschaft für Technische Zusammenarbeit, Germany. Articles may be reproduced free of charge, provided that the source is creditedand clippings are sent to our contact address. All correspondence should be sent to: [email protected] or Sexual Health Exchange, The Editor, c/o RoyalTropical Institute, Information & Library Services; P.O. Box 95001, 1090 HA Amsterdam, the Netherlands.
Managing editor: Nel van Beelen
Executive editors: Nel van Beelen & Eliezer Wangulu (SAfAIDS)
Secretarial and administrative support: Dorothy Timmerman & Ewa Cudowska
Editorial advisers: Mabel Bianco (Argentina), Maria de Bruyn (USA), Jacques du Guerny (France), Helen Jackson (Zimbabwe), Gesa Kupfer(Germany), Lee-Nah Hsu (Thailand), Marina Mahathir (Malaysia).
Layout: Fontline Electronic Publishing (Pvt) Ltd. (Zimbabwe) Printer: Drukkerij MacDonald/SSN Nijmegen (The Netherlands)
ISSN: 1388-3046
Online Resources
�� Recent articles in Sexual Health Exchange(www.sexualhealthexchange)
- The need to scale up HIV/AIDS programmes for gay men andother MSM in Latin America and the Caribbean. S. Lewis, No.1, 2005
- Working with young men to address violence and HIV inTanzania. H. Lary et al., No. 3/4, 2004
�� Gender inequality, masculinity & violence
- Young men and the construction of masculinity in sub-Saharan Africa: Implications for HIV/AIDS, conflict andviolence. G. Barker & C. Ricardo (Instituto Promundo, Brazil).World Bank Social Development Papers No. 26, 2005 (96 p.):www.promundo.org.br/Pesquisa/Young Men SubSaharan_Web.pdf
- Special issue of Sexuality in Africa magazine on masculinity.Vol. 2, No. 1, April 2005:www.arsrc.org/downloads/sia/apr05/apr05.pdf
- Gender equality and men: Learning from practice. S. Ruxton,Oxfam Publishing, 2004 (258 p.):www.oxfam.org.uk/what_we_do/resources/geneqmen.htm,hardcopy: £13.95 ([email protected])
- Hacerse hombres (“Becoming men”, Spanish only). WHO/PAHO, 2002 (30 p.):www.paho.org/Spanish/HPP/HPF/ADOL/Hacerse%20hombres1.pdf
- Working with men and boys to promote gender equality and toend violence against boys and girls. L. Karlsson & R. Karkara,Save the Children Sweden-Denmark, Regional Programme forSouth and Central Asia, 2004 (20 p.):www.crin.org/docs/resources/publications/SC-Masculinities.doc
- HIV prevention with men: Toward gender equality and socialjustice. A. Greig, discussion paper expert group meeting on“The role of men and boys in achieving gender equality”, Brazil,October 2003 (19 p.):www.un.org/womenwatch/daw/egm/men-boys2003/EP7-Greig.pdf
- Addressing gender-based violence from the reproductivehealth/HIV sector. A literature review and analysis. A. Guedes,Poptech/IGWG, 2004 (115 p.):www.prb.org/pdf04/AddressGendrBasedViolence.pdf
�� HIV/AIDS
- The role of men in the fight against HIV/AIDS. N. Wainaina, UNDivision for the Advancement of Women/ILO/UNAIDS/UNDP,2003 (11 p.): www.un.org/womenwatch/daw/egm/men-boys2003/EP4-Wainaina.pdf
- Working with men. Special issue AIDS action, No. 48, 2000:www.aidsaction.info/aa/aa48.html
- Young men and HIV – Culture, poverty and sexual risk. T. Scalway,Panos Report No 41, Panos Institute/UNAIDS, 2001 (48 p.):www.panos.org.uk/resources/reportsection.asp?ID=1001
- Young men and HIV prevention. Horizons Report, 2004 (12 p.):www.popcouncil.org/pdfs/horizons/hrptdec04.pdf
- Working with men, responding to AIDS. Gender, sexuality andHIV – a case study collection. International HIV/AIDS Alliance,2003 (68 p.): www.eldis.org/static/DOC13895.htm
- Between men – HIV/STI prevention for men who have sex withmen. International HIV/AIDS Alliance, 2003 (64 p.):www.eldis.org/static/DOC13606.htm (English, French orSpanish)
�� Sexual and reproductive health
- Enlisting the armed forces to protect reproductive healthand rights. Lessons learned from nine countries. UNFPA,2003 (99 p.): www.unfpa.org/rh/armedforces
- It takes 2: Partnering with men in reproductive and sexualhealth. UNFPA, 2003 (59 p.):www.unfpa.org/publications/detail.cfm?ID=99&filterListType=1,hardcopy: [email protected] (Michele Chapoteau)
- Reaching men to improve reproductive health for all.Implementation guide. Interagency Gender Working Group,USAID, 2003 (142 p.): www.jhuccp.org/igwg
- Working with young men to promote sexual and reproductivehealth. K. Rivers & P. Aggleton, Safe Passages to AdulthoodProgramme, 2002 (37 p.):www.socstats.soton.ac.uk/cshr/pdf/guidelines/workingwithymen.pdf
All resources are accessible through our website:www.sexualhealthexchange.org
Copyright © 2022 FDOKUMEN