
Follow-up assessment of medication-treated dysthymia
16
ELSEVIER Prq. h’euro_Psychophmmacol. &Bid. Psychiat. 1996. Vol. 20. pp. 427-442 Copyright C’ 1996 Elsevier Science Inc. All rights reserved PII SO278-5846(!36)00007-3 0278 - 5646/96 $32.00 FOLLOW-UP ASSESSMENT OF MEDICATION-TREATED DYSTHYMIA DAVID J. HELLERSTEIN ls4 LISA WALLNER SAMSTAG’, MARC CANTILLON3, MARTIN MAURER’.‘, JESSE ROS’ENTHALzs4, PHILIP YANOWITCH3,4, ARNOLD WINSTON3,4 ‘Psychiatric Outpatient Services and *Mood Disorders Research Unit, 3Beth Israel Medical Center, New York, N.Y., U.S.A. 4Department of Psychiatry, Albert Einstein College of Medicine, Bronx, N.Y., U.S.A. (Final form, February, 1996) Hellerstein, David J., Lisa Wallner Samstag, Marc Cantillon, Martin Maurer, Jesse Rosenthal, Philip Yanowitch and Arnold Winston: Follow-Up Assessment of Medication- Treated Dysthymia. Prog. Neuro-Psychopharmacol. & Biol. Psychiat. 1996, 20 1. The objective was to assess long-term efficacy of antidepressant medications in dysthymia. 2. In a naturalistic study, patients with DSMIII-R dysthymia who had participated in previous antidepressant trials with fluoxetine and trazodone were evaluated at a mean of 40.0 weeks of follow-up to assess whether medication response persisted over time. A multivariate analysis was performed for patients on vs. off medicatioin. Relapse rates (with relapse defined as HDRS score > 13) were also compared for these two groups. 3. Of 40 patients, the 24 still on medication showed significantly lower scores on most rating scales (HDRS, Cornell Dysthymia Rating Scale, and CGI, but not on the SCL- 58) than the heterogeneous group of 16 patients not taking medication. Relapse was low (17.4%) among patients remaining on medication. 4. These preliminary findings suggest that dysthymia patients who remain on medication maintain improvement over time. Kaywords: chronic depression, clinical trial, dysthymia, fluoxetine, medication treatment . Abbrevlatlons: Clinical Global Impressions (CGI), Cornell Dysthymia Rating Scale (CDRS), Diagnostic and Statistical Manual, III Edition, Revised (DSM-III-R), Hamilton Depression Rating Scale (HDRS), Hopkins Symptom Checklist (58 item) (SCL-581, Monamine Oxidase Inhibitor antidepressants (MAOIs), Structured Clinical Interview for DSM-III-R, Patient Version (SCID-PI, Selective Serotonin Reuptake Inhibitor antidepressants (SSRls), Tricycfic Antidepressants (TCAs). 427
-
Upload
longisland -
Category
Documents
-
view
2 -
download
0
Transcript of Follow-up assessment of medication-treated dysthymia

ELSEVIER
Prq. h’euro_Psychophmmacol. &Bid. Psychiat. 1996. Vol. 20. pp. 427-442 Copyright C’ 1996 Elsevier Science Inc.
All rights reserved
PII SO278-5846(!36)00007-3 0278 - 5646/96 $32.00
FOLLOW-UP ASSESSMENT OF MEDICATION-TREATED DYSTHYMIA
DAVID J. HELLERSTEIN ls4 LISA WALLNER SAMSTAG’, MARC CANTILLON3, MARTIN MAURER’.‘, JESSE ROS’ENTHALzs4, PHILIP YANOWITCH3,4, ARNOLD WINSTON3,4
‘Psychiatric Outpatient Services and *Mood Disorders Research Unit, 3Beth Israel Medical Center, New York, N.Y., U.S.A.
4Department of Psychiatry, Albert Einstein College of Medicine, Bronx, N.Y., U.S.A.
(Final form, February, 1996)
Hellerstein, David J., Lisa Wallner Samstag, Marc Cantillon, Martin Maurer, Jesse Rosenthal, Philip Yanowitch and Arnold Winston: Follow-Up Assessment of Medication- Treated Dysthymia. Prog. Neuro-Psychopharmacol. & Biol. Psychiat. 1996, 20
1. The objective was to assess long-term efficacy of antidepressant medications in dysthymia.
2. In a naturalistic study, patients with DSMIII-R dysthymia who had participated in previous antidepressant trials with fluoxetine and trazodone were evaluated at a mean of 40.0 weeks of follow-up to assess whether medication response persisted over time. A multivariate analysis was performed for patients on vs. off medicatioin. Relapse rates (with relapse defined as HDRS score > 13) were also compared for these two groups.
3. Of 40 patients, the 24 still on medication showed significantly lower scores on most rating scales (HDRS, Cornell Dysthymia Rating Scale, and CGI, but not on the SCL- 58) than the heterogeneous group of 16 patients not taking medication. Relapse was low (17.4%) among patients remaining on medication.
4. These preliminary findings suggest that dysthymia patients who remain on medication maintain improvement over time.
Kaywords: chronic depression, clinical trial, dysthymia, fluoxetine, medication treatment
. Abbrevlatlons: Clinical Global Impressions (CGI), Cornell Dysthymia Rating Scale (CDRS), Diagnostic and Statistical Manual, III Edition, Revised (DSM-III-R), Hamilton Depression Rating Scale (HDRS), Hopkins Symptom Checklist (58 item) (SCL-581, Monamine Oxidase Inhibitor antidepressants (MAOIs), Structured Clinical Interview for DSM-III-R, Patient Version (SCID-PI, Selective Serotonin Reuptake Inhibitor antidepressants (SSRls), Tricycfic Antidepressants (TCAs).
427
428 D.J. Hellerstein et cd.
Dysthymia (American Psychiatric Association, 1987) or chronic depression, is a
psychiatric disorder affecting about 3% of the population. Recent studies have clarified
the phenomenology of dysthymia (Keller et al., 1991; Keller et al., 19951, and indicate
that dysthymics suffer significant medical and psychiatric comorbidity (Markowitz,
19931, with increased utilization of health services (Howland, 1993) and significant
psychosocial dysfunction (Friedman, 1993).
Medication studies demonstrate that dysthymia and other chronic depressive
disorders often respond to acute trials with medications, including TCAs (Kocsis et al.,
1988) and MAOls (Quitkin et al., 1989). Our studies have demonstrated positive
results with SSRls. In our recent 8-week double-blind study of fluoxetine vs. placebo
(Hellerstein et al., 19931, 62.5% of fluoxetine subjects (IO/161 were responders [with
response defined by a 50% or greater decrease in Hamilton-Depression Rating Scale
(HDRS) score (Hamilton, 1960) and a score of 1 or 2 “very much improved” or “much
improved” on the Clinical Global Impressions Scale (CGI) (Guy, 197611, compared to
only 18.8% (3/16) of placebo subjects. These findings confirmed the results of our
earlier open-label studies of fluoxetine vs. trazodone (Rosenthal et al., 1992; Hellerstein
et al., 19941, in which 61.3% of dysthymic patients completing 3-month medication
trials responded to fluoxetine (14/23 subjects; 60.9%) or trazodone (5/8 subjects;
62.5%).
However, few studies have assessed continued efficacy of antidepressant treatment
in dysthymia. While there is some evidence (Keller et al., 1983) for poor results with
naturalistically-treated chronic depression, other studies suggest that patients receiving
adequate antidepressant trials have good outcome, and that initial medication response
may be maintained over long periods of time (Howland, 1991; Harrison et al., 1986).
Patients who are initially medication responsive may have particularly good outcome.
In imipramine-treated patients, Kocsis et al. (1991) found 89% percent of initial
imipramine responders met the criteria for recovery at follow-up of one to five years,
compared with 31% of nonresponders and noncompleters.
Given the paucity of systematic follow-up studies, even preliminary naturalistic
Follow up assessment of medication-treated dysthymia 429
studies can shed light on the question whether dysthymic symptoms are improved after
longterm medication treatment. The authors report results from a naturalistic follow-up
of patients from their prior efficacy studies. Our hypothesis is that dysthymics taking
antidepressant medications will continue to have relief of depressive symptoms at
follow-up, while patients who have discontinued medication will tend to relapse.
Participants in previous dysthymia studies (Hellerstein et al., 1993; Rosenthal et al.,
1992; Hellerstein et al., 1994) at Beth Israel Medical Center’s Mood Disorders Research
Unit were contacted for follow-up assessment. Subjects had been enrolled in the
original studies by the following procedure:
After providing informed consent, a semistructured clinical interview was conducted,
and prospective subjects were systematically questioned using the Structured Clinical
Interview for DSM-III-R, Patient Version (SCID-P) (Spitzer et al., 1988) mood disorder
section. Subjects between the age of 21 and 65 were included if their diagnosis of
dysthymia was what DSM-III-R terms primary, that is, not related to a pre-existing,
chronic, nonmood Axis I or Axis Ill disorder. The SCID-P sections on major depression
and dysthymia were used to ensure that subjects met diagnostic criteria for dysthymia.
Exclusion criteria for the original studies were as follows: Axis I conditions such as
DSM-III-R psychoactive substance use disorders (within the past six months), panic
disorder, schizophrenia, anorexia or bulimia; a history of mania or hypomania; severe
stress, whether acute or chronic (a score of 4 or greater on DSM-III-R’s Axis IV); a
history of suicide attempts and self-mutilation; significant medical illness; and use of
any psychotropic medication within one month prior to the study. For a more detailed
description of the original studies’ inclusion criteria, the reader is directed to those
respective papers (Hellerstein et al., 1993; Rosenthal et al., 1992; Hellerstein et al.,
1994).
A total of 50 patients, of a possible 63 who had completed treatment protocols, were

430 D.J. Hellerstein et al
reached either by telephone or mail, and 40 patients (63.5% of the total sample) agreed
to a follow-up assessment. Patients provided informed consent for participation in a
follow-up study. The 40 subjects who made up the study sample of the present
research consisted of 35 who had met criteria for a DSM-III-R diagnosis of dysthymia
(American Psychiatric Association, 1987), without concurrent major depression, and
five who had met criteria for double depression (Keller et al., 1983). Patients had been
randomly assigned to either fluoxetine, trazodone, or placebo in the original studies.
The study sample of 40 patients was comprised of 21 (52%) women and 19 (48%)
men, with a mean age of 38.OA9.4 years. The mean number of weeks from the time
patients completed the treatment protocol to the date of the follow-up assessment was
40.0&29.1. Most patients were currently employed (85% of the sample); 27 (68%)
were single, 10 (25%) were married, and one (2%) was divorced (information regarding
marital status was unavailable for two patients). Thirty-two (80%) patients had
completed a college degree, with 14 (35%) having also completed a graduate degree.
The 40 patients agreeing to follow-up interviews were compared with the 23 who could
not be contacted or who declined reassessment, using chi-square (with exact p values
where sample sizes are small) or t-test analyses; they did not differ significantly on any
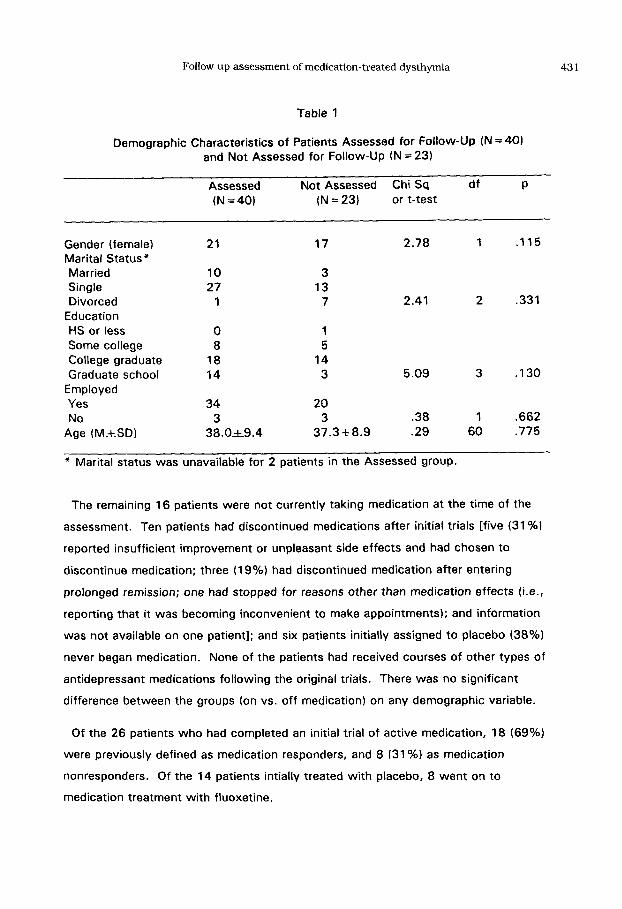
of the demographic variables (Table 1).
At the time of the follow-up assessment, 24 (60%) patients were taking medication
(23 (58%) taking fluoxetine, and one (2%) taking trazodone); the mean dosage of the
subjects on fluoxetine was 30.5 mgkl8.7 mg, with a mean of 35.9L25.3 weeks of
use. One patient was taking trazodone at a dose of 150 mg/day. Blood levels for
fluoxetine and metabolites have not consistently been related to response (Kelly, et al.,
1989); in this study, levels were drawn primarily to assess compliance. The mean&SD
blood level for fluoxetine was 214.4~195.4 ng/ml and norfluoxetine was
249.3h146.5 ng/ml. Only 7 patients reported entering individual or group
psychotherapy during the follow-up period; 4 were members of the on-medication
group, and 3 were members of the off-medication group.
Follow up assessment of medication-treated dysthymia 431
Table 1
Demographic Characteristics of Patients Assessed for Follow-UP (N=W and Not Assessed for Follow-Up (N = 23)
Assessed Not Assessed Chi Sq df P (N=40) (N = 23) or t-test
Gender (female) Marital Status* Married Single Divorced
Education HS or less Some college College graduate Graduate school
Employed Yes No
Age (M.+SD)
21 17 2.78 1 .I15
10 3 27 13
1 7 2.41 2 .331
0 1 8 5
18 14 14 3 5.09 3 .I30
34 20 3 3 .38 1 .662
38.Ok9.4 37.318.9 .29 60 .775
* Marital status was unavailable for 2 patients in the Assessed group.
The remaining 16 patients were not currently taking medication at the time of the
assessment. Ten patients had discontinued medications after initial trials [five (31 %I
reported insufficient improvement or unpleasant side effects and had chosen to
discontinue medication; three (19%) had discontinued medication after entering
prolonged remission; one had stopped for reasons other than medication effects (i.e.,
reporting that it was becoming inconvenient to make appointments); and information
was not available on one patient]; and six patients initially assigned to placebo (38%)
never began medication. None of the patients had received courses of other types of
antidepressant medications following the original trials. There was no significant
difference between the groups (on vs. off medication) on any demographic variable.
Of the 26 patients who had completed an initial trial of active medication, 18 (69%)
were previously defined as medication responders, and 8 (31 %I as medication
nonresponders. Of the 14 patients intially treated with placebo, 8 went on to
medication treatment with fluoxetine.
432 D.J. Hellerstein et cd.
Subjects who provided informed consent to the follow-up assessment participated in
a structured clinical interview conducted by teams of clinicians and staff researchers.
Interviewers were blind to initial response status, but not to current medication use
(i.e, if patients were currently on or off medication). Patients completed the self-
report version of the Hopkins Symptom Checklist (SCL-58; Derogatis et al., 19741,
and were rated for current severity of depression with the 21-item Hamilton
Depression Rating Scale (HDRS; Hamilton, 1960) and the Cornell Dysthymia Rating
Scale (CDRS; Mason et al., 1993). These measures were completed in order to
assess current level of mood and general symptomatology, as well as to compare
ratings to post-treatment levels in the initial studies. Results of reliability assessment
with the HDRS and the CDRS are reported elsewhere (Hellerstein et al., 1993;
Rosenthal et al., 1992; Hellerstein et al., 1994). The interviewers provided a
Clinician’s Global Impression rating (CGI; Guy, 1976) and assessed the patient with
respect to DSM-III-R criteria for dysthymia and major depression. Fluoxetine and
norfluoxetine blood levels were also collected.
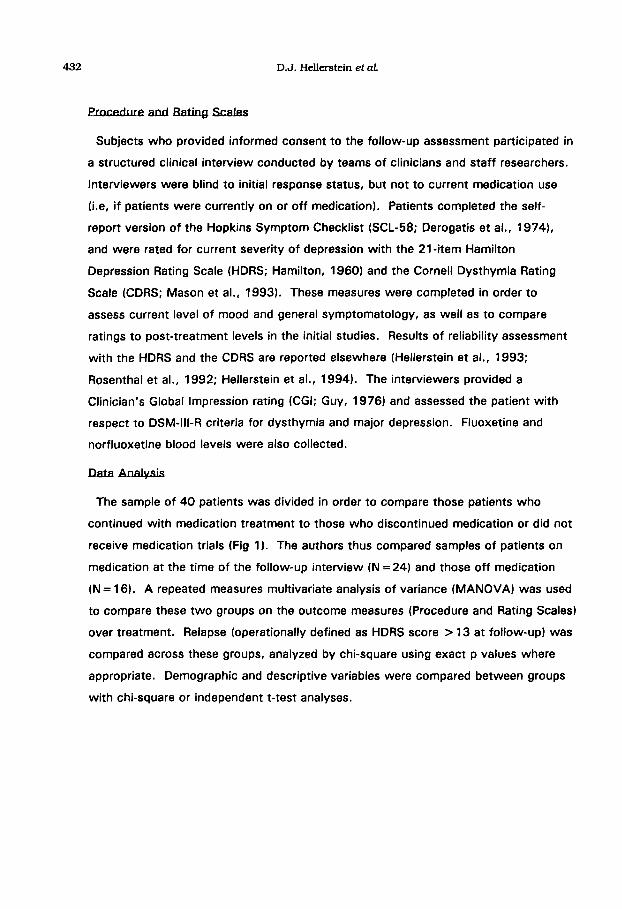
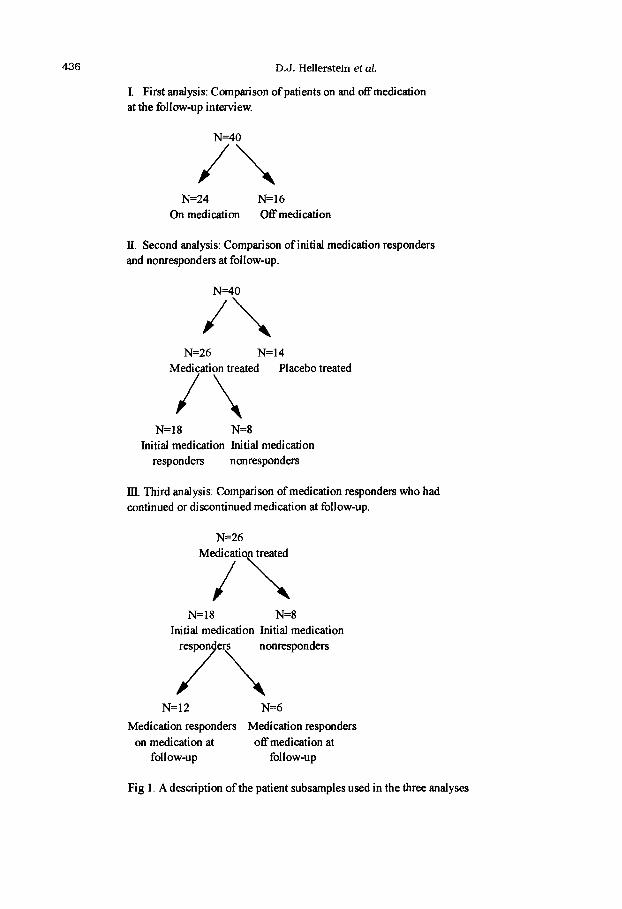
The sample of 40 patients was divided in order to compare those patients who
continued with medication treatment to those who discontinued medication or did not
receive medication trials (Fig 1 J. The authors thus compared samples of patients on
medication at the time of the follow-up interview (N = 24) and those off medication
(N = 16). A repeated measures multivariate analysis of variance (MANOVA) was used
to compare these two groups on the outcome measures (Procedure and Rating Scales)
over treatment. Relapse (operationally defined as HDRS score > 13 at follow-up) was
compared across these groups, analyzed by chi-square using exact p values where
appropriate. Demographic and descriptive variables were compared between groups
with chi-square or independent t-test analyses.

Follow up assessment of medication-treated dysthymia 433
In this naturalistic study, the duration of the follow-up period for the 24 patients
remaining on medication varied greatly (M =37.0 weeks, SD~25.7 weeks). In order
to determine whether there was any effect of treatment duration on follow-up scores,
the authors divided the sample into those patients assessed at less than 40 weeks
(N = 16) vs. those assessed at greater than 40 weeks (N = 8). Follow-up ratings were
compared using a series of t-tests. HDRS scores (lO.lk3.9 vs. 7.91L4.9; t = 1 .I 9,
df=21, NS), CDRS scores (19.OA7.2 vs. 19.9f9.4; t=.24, df=21, NS), SCL-58
scores (I .8&.32 vs. 1.9k.4; t = .38, df =21, NS) and CGI scores (2.Ok.8 vs.
1.9+1 .l; t = .35, df =21, NS) did not differ significantly between groups. Thus the
two groups were collapsed for subsequent analyses,
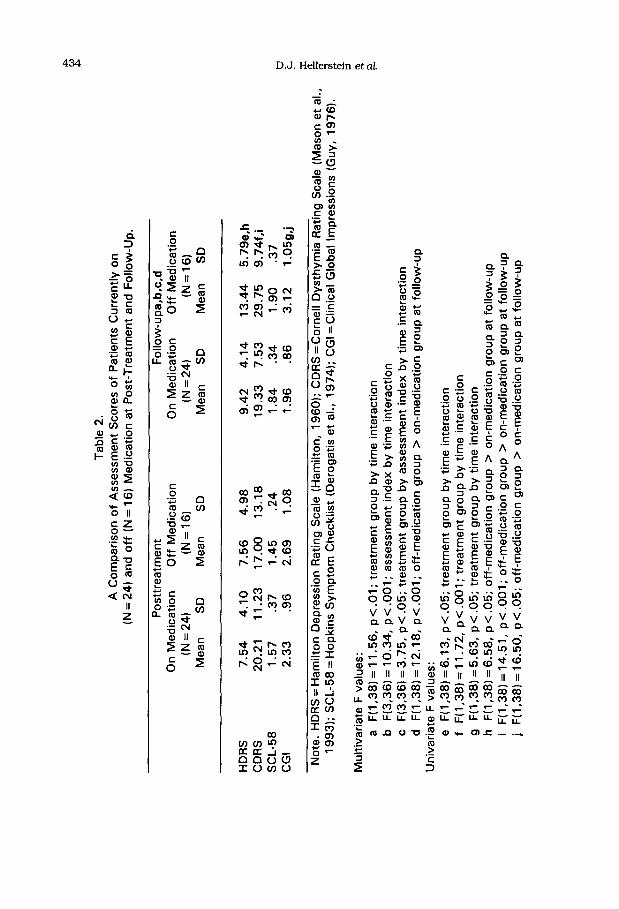
The authors compared posttreatment and follow-up assessment scores of patients
who were on or off medication at the time of the follow-up interview (Table 2). A
2X2X4 repeated measures multivariate analysis of variance (MANOVA), with the
HDRS, CDRS, SCL-58 and CGI as dependent measures, revealed a significant
interaction of these two groups from post-treatment to follow-up (F(1,38) = 11.56,
p < .Ol). A significant interaction of the different indices over time was found
(F(3,36) = 10.34, p < .OOl), as well as a three-way interaction of the assessment
indices over time between the on- and off-medication groups (F(3,36) = 3.75, p < .Od).
While there was no significant difference between these groups at posttreatment, at!
follow-up the overall scores of the group off medication were significantly higher thdn
those of the group on medication (F(1,38) = 12.18, p < .OOl). Univariate F tests
revealed a significant group by time interaction with the HDRS (F(1,38) =6.13,
p<.O5), the CDRS (F(1,38)=11.72, p<.OOl), and the CGI (F(1,38)=5.63, pC.051,
with the off-medication group evidencing significantly higher HDRS (F(1,38) = 6.58,
p<.O5), CDRS (F(1,38)= 14.51, p<.OOl), and CGI (F(1,38) =16.50, p<.OOl) scores
than the on-medication group at follow-up. The SCL-58 scores of the two groups
were not significantly different either at post-treatment or follow-up. There was no
significant difference between groups with respect to the number of weeks from
Tab
le
2.
A C
om
par
iso
n
of
Ass
essm
ent
Sco
res
of
Pat
ien
ts
Cu
rren
tly
on
(N
= 2
4)
and
off
(N
= 1
6)
Med
icat
ion
at
Po
st-T
reat
men
t an
d
Fo
llow
-Up
.
Po
sttr
eatm
ent
Fo
llow
-up
a,b
,c,d
O
n M
edic
atio
n
Off
M
edic
atio
n
On
Med
icat
ion
O
ff
Med
icat
ion
(N
= 2
4)
(N =
16)
(N
= 2
4)
(N=1
61
Mea
n
SD
M
ean
S
D
Mea
n
SD
M
ean
S
D
HD
RS
C
DR
S
SC
L-5
8 C
GI
7.54
4.
10
7.56
4.
98
9.42
4.
14
13.4
4 5.
79e.
h
20.2
1 11
.23
17.0
0 13
.18
19.3
3 7.
53
29.7
5 9.
74f.
i 1.
57
.37
1.45
.2
4 1.
84
.34
1.90
.3
7 2.
33
.96
2.69
1.
08
1.96
.8
6 3.
12
l.O5g
,j tl
t
No
te.
HD
RS
= H
amilt
on
D
epre
ssio
n
Rat
ing
S
cale
(H
amilt
on
, 19
60);
C
DR
S =
Co
rnel
l D
ysth
ymia
R
atin
g
Sca
le
(Mas
on
et
al.,
19
93);
S
CL
-58
= H
op
kin
s S
ymp
tom
C
hec
klis
t (D
ero
gat
is
et a
l.,
1974
);
CG
I =
Clin
ical
G
lob
al
Imp
ress
ion
s (G
uy,
19
76).
Mu
ltiv
aria
te
F v
alu
es:
a F
(1,3
8)
= 11
.56,
p
< .
Ol;
tr
eatm
ent
gro
up
b
y ti
me
inte
ract
ion
b
F
(3,3
6)
= 10
.34,
p
< .
OO
l; as
sess
men
t in
dex
b
y ti
me
inte
ract
ion
c
F(3
,36)
=
3.75
, p
< .0
5;
trea
tmen
t g
rou
p
by
asse
ssm
ent
ind
ex
by
tim
e in
tera
ctio
n
d
F(1
,38)
=
12.1
8,
p <
,00
1;
off
-med
icat
ion
g
rou
p
> o
n-m
edic
atio
n
gro
up
at
follo
w-u
p
Un
ivar
iate
F
val
ues
: e
F(1
,38)
=
6.13
, p
< .
05;
trea
tmen
t g
rou
p
by
tim
e in
tera
ctio
n
f F
(1.3
8)
= 11
.72,
p
C .
OO
l; tr
eatm
ent
gro
up
b
y ti
me
inte
ract
ion
g
F
(1,3
8)
= 5.
63,
p <
.05
; tr
eatm
ent
gro
up
b
y ti
me
inte
ract
ion
h
F
(1,3
8)
=6.5
8,
p<
.05;
o
ff-m
edic
atio
n
gro
up
>
on
-med
icat
ion
g
rou
p
at f
ollo
w-u
p
i F
( 1,3
8)
= 14
.51,
p
< .
OO
l ;
off
-med
icat
ion
g
rou
p
> o
n-m
edic
atio
n
gro
up
at
follo
w-u
p
j F
(1,3
8)
= 16
.50,
p
< .
05;
off
-med
icat
ion
g
rou
p
> o
n-m
edic
atio
n
gro
up
at
fo
llow
-up
Follow up assessment of medication-treated dysthymia 435
posttreatment to follow-up (N = 24:37.2&_9.0; N = 16:38.9&10.5).
The authors did an additional analysis of relapse at follow-up, between patients on
and off medication, where relapse was operationally defined as an HDRS score > 13
at follow-up. Of patients on medication at follow-up, only 4/23 (17.4K) had relapsed,
versus 7/14 (50%) of those who were off medication (3 cases deleted for missing
data). While this was a significant difference (Chi sq with Fisher’s Correction
factor =4.43, df = 1, p = .0424), this finding must be qualified by the fact that the
patients off medication were a heterogeneous sample (including medication
responders, medication nonresponders, and patients never treated with medication).
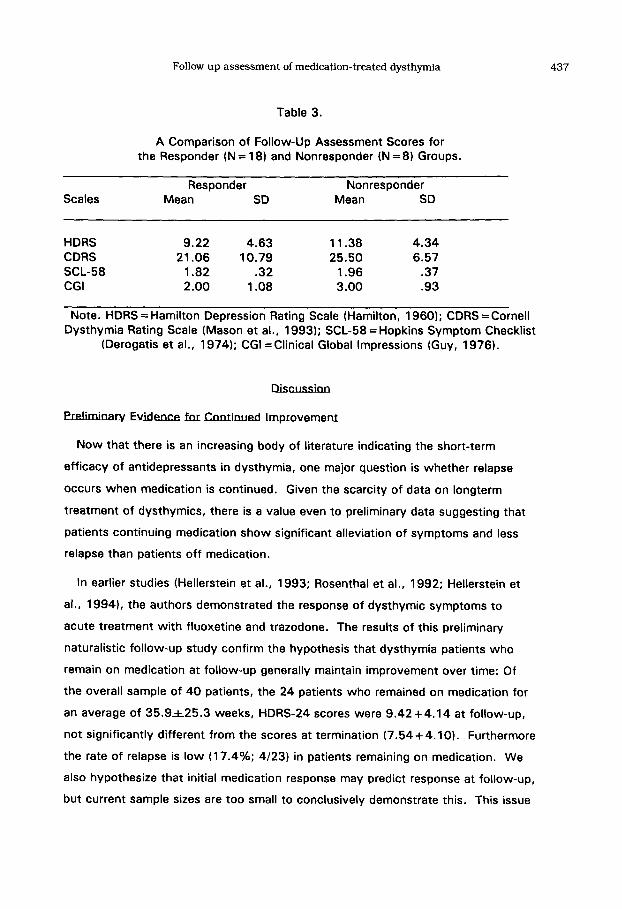
In addition to continuation of medication use, it has been suggested (Kocsis, et al.,
1991) that initial medication response may predict good long-term outcome. Of the
26 patients who had completed a medication trial (as opposed to placebo) in the
original studies, 18 were previously defined as medication responders and eight as
medication nonresponders, based on the two-dimensional criteria described earlier (Fig
I). Comparative scores for these groups on post-treatment and follow-up HDRS,
CDRS, SCL-58 and CGI are shown in Table 3. Because of the small size of these
samples, statistical analysis was not performed. The mean scores of the responder
group were lower at follow-up than those of the nonresponder group, and it is possible
that these differences would be statistically significant with a larger sample size. A
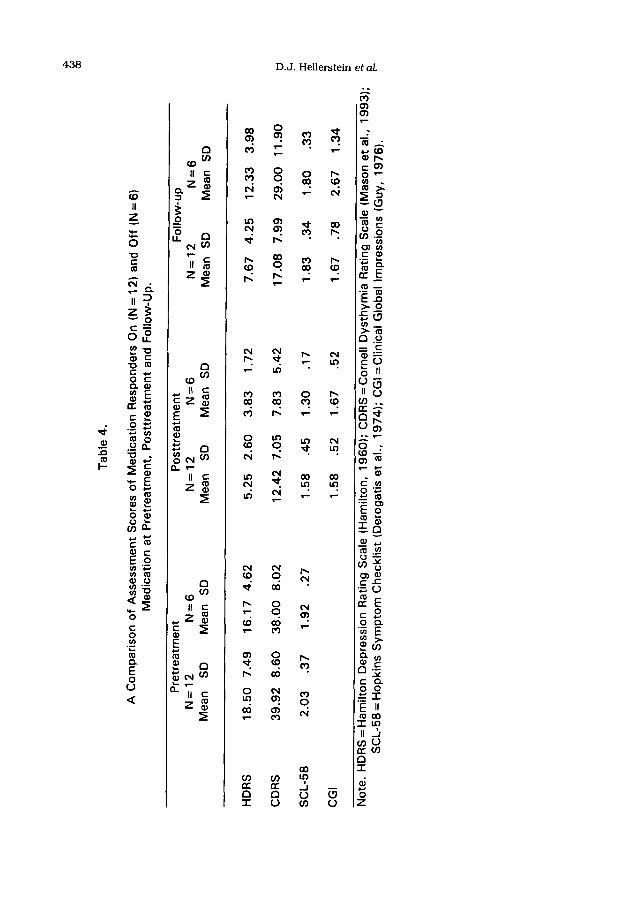
similar comparison was performed for the 26 patients who had completed a
medication trial (as opposed to placebo) in the original studies, of whom 18 were
previously defined as medication responders and eight as medication nonresponders
(Fig 1 and Table 4). Again, small sample size precludes statistical analysis, but scores
on several scales (HDRS, CDRS, CGI, but not SCL-58) suggest the possibility that
medication responders who discontinue medication may have recurrence of
symptoms, whereas patients remaining on medication may have persistent remission;
436 D.J. Hellerstein et al.
I. First analysis: Comparison of patients on and off medication at the follow-up interview.
N=40
J\
N=24 N=16 On medication Offmedication
II. Second analysis: Comparison of initial medication responders and nonresponders at follow-up.
N=40
N=26 N=14 Medication treated Placebo treated
N=18 N=8 Initial medication Initial medication
responders nonresponders
III. Third analysis: Comparison of medication responders who had continued or discontinued medication at follow-up.
N=26 Medicatio treated
/L
N=18 N=8 Initial medication Initial medication
respon ers nonresponders
/\ N=12 N=6
Medication responders Medication responders
on medication at off medication at follow-up follow-up
Fig 1. A description of the patient subsamples used in the three analyses
Follow up assessment of medication-treated dysthymia 437
Table 3.
A Comparison of Follow-Up Assessment Scores for the Responder (N = 18) and Nonresponder (N = 8) Groups.
Scales Responder Nonresponder
Mean SD Mean SD
HDRS 9.22 4.63 11.38 4.34
CDRS 21.06 10.79 25.50 6.57
SCL-58 1.82 .32 1.96 .37
CGI 2.00 1.08 3.00 .93
Note. HDRS = Hamilton Depression Rating Scale (Hamilton, 1960); CDRS = Cornell Dysthymia Rating Scale (Mason et al., 1993); SCL-58 = Hopkins Symptom Checklist
(Derogatis et al., 1974); CGI = Clinical Global Impressions (Guy, 1976).
Now that there is an increasing body of literature indicating the short-term
efficacy of antidepressants in dysthymia, one major question is whether relapse
occurs when medication is continued. Given the scarcity of data on longterm
treatment of dysthymics, there is a value even to preliminary data suggesting that
patients continuing medication show significant alleviation of symptoms and less
relapse than patients off medication.
In earlier studies (Hellerstein et al., 1993; Rosenthal et al., 1992; Hellerstein et
al., 19941, the authors demonstrated the response of dysthymic symptoms to
acute treatment with fluoxetine and trazodone. The results of this preliminary
naturalistic follow-up study confirm the hypothesis that dysthymia patients who
remain on medication at follow-up generally maintain improvement over time: Of
the overall sample of 40 patients, the 24 patients who remained on medication for
an average of 35.9A25.3 weeks, HDRS-24 scores were 9.42+4.14 at follow-up,
not significantly different from the scores at termination (7.54+4.10). Furthermore
the rate of relapse is low (17.4%; 4/23) in patients remaining on medication. We
also hypothesize that initial medication response may predict response at follow-up,
but current sample sizes are too small to conclusively demonstrate this. This issue
Tab
le
4.
A C
om
par
iso
n
of
Ass
essm
ent
Sco
res
of
Med
icat
ion
R
esp
on
der
s O
n
(N =
12)
an
d O
ff
(N =
6)
Med
icat
ion
at
Pre
trea
tmen
t,
Po
sttr
eatm
ent
and
F
ollo
w-U
p.
Pre
trea
tmen
t P
ost
trea
tmen
t N
=12
N=6
N
=12
N=6
M
ean
S
D
Mea
n
SD
M
ean
S
D
Mea
n
SD
Fo
llow
-up
N
=12
N=6
M
ean
S
D
Mea
n
SD
HD
RS
18
.50
7.49
16
.17
4.62
5.
25
2.60
3.
83
1.72
7.
67
4.25
12
.33
3.98
CD
RS
39
.92
8.60
38
.00
8.02
12
.42
7.05
7.
83
5.42
17
.08
7.99
29
.00
11.9
0 u
t
SC
L-5
8 2.
03
.37
1.92
.2
7 1.
58
.45
1.30
.1
7 1.
83
.34
1.80
.3
3 g
K
C
GI
1.58
.5
2 1.
67
.52
1.67
.7
8 2.
67
1.34
1 8 5
No
te.
HD
RS
= H
amilt
on
D
epre
ssio
n
Rat
ing
S
cale
(H
amilt
on
, 19
60);
C
DR
S =
Co
rnel
l D
ysth
ymia
R
atin
g
Sca
le
(Mas
on
et
al.,
19
93);
S
CL
-58
= H
op
kin
s S
ymp
tom
C
hec
klis
t (D
ero
gat
is
et a
l.,
1974
);
CG
I =C
linic
al
Glo
bal
Im
pre
ssio
ns
(Gu
y,
1976
).
$ r
Follow up assessment of medication-treated dysthymia 439
requires further study.
The findings in this study are in many ways similar to those of Kocsis’s
naturalistic follow-up study of 25 patients (Kocsis et al., 1991). In both studies,
patients by self-report state that their depressive symptoms average 20 or more
years in duration, and prior treatment consisted primarily of psychotherapy, and in
both studies patients continuing medication generally have persistent relief. One
significant difference is that whereas 96% (24/25) of Kocsis et al. (1988)‘s
patients suffered from “double depression, ” in our sample only 12.5% were doubly
depressed, and 87.5% (35/40) met criteria for dysthymia only. Thus our study
suggests that dysthymia uncomplicated by major depression responds on a long-
term basis to medication.
. . . LlmlmmsofIbisstuIiy
The present findings must be qualified by a number of factors. Follow-up
assessment was done cross-sectionally rather than longitudinally, and was done at
variable time intervals. Sample sizes were small and heterogeneous. The group off
medication at follow-up included patients who discontinued medications for a
variety of reasons, and some patients who never received medication, and
therefore there is no definitive evidence that discontinuation leads to relapse,
though our preliminary findings suggest that it may. Controlled discontinuation
studies are needed to assess this issue. In addition, small sample size makes it
impossible to rule out possible Type II errors, and replication is obviously required.
Patients were drawn from two studies, one with open-label and the other with
placebo-controlled design; however, differences are minimized by the continuity
both of study staff and assessment procedures between studies. In addition,
patients continuing medication also may have received therapeutic benefit from
contact with physicians, whereas patients who discontinued medication generally
ended ongoing treatment contact. The authors assessed other possibly important
factors (psychotherapy in follow-up period, variable duration of medication
treatment, and characteristics of patients agreeing to or refusing follow-up
assessment), and found no significant differences.
440 D.J. Hellerstein et al.
The lack of a significant between-group finding for the SCL-58, a patient-rated
scale, in comparison to the other (clinician-rated) inventories, raises the possibility
of rater bias. However, in the double-blind study (Hellerstein et al., 19931, the
SCL-58 also did not differ significantly between placebo and fluoxetine groups.
Studies of major depression (Greenberg, et al., 1992) also show consistently less
medication effect as assessed by patient-rated than clinician-rated scales, the
reasons for which are unclear. Additional patient-rated and observer-rated
inventories should be used in dysthymia outcome studies to clarify this issue.
Finally, there is the question of generalizability. The present sample consists of
patients with primary dysthymia, most without concurrent major depression.
Epidemiological studies (Klein et al., 1988; Markowitz 1993; Horwath et al., 1992)
suggest that about 75% of dysthymics have other comorbid medical or psychiatric
disorders, whereas our patients were screened to exclude such disorders. It is
important to determine whether similar findings apply to primary dysthymics with
comorbid disorders (e.g. anxiety disorders, etc.), and whether they apply to
patients with secondary dysthymia (e.g. dysthymia secondary to other psychiatric
or medical disorders).
The preliminary findings thus suggest that continued antidepressant treatment
leads to long-term symptom improvement in many dysthymics. Discontinuation of
medication may be associated with recurrence of symptoms. These results require
replication in prospective, controlled studies with blinded raters, and with a variety
of patient and observer-rated instruments.
This study was supported by a grant from Eli Lilly and Company.
Follow up assessment of medication-treated dysthymia 441
AMERICAN PSYCHIATRIC ASSOCIATION (1987) Diagnostic and Statistical Manual of Mental Disorders, 3rd ed, revised. Washington DC.
DEROGATIS, L.R. LIPMAN, R.S., RICKELS, K. UHLENHUTH, E.H. and COVI, L. (1974) The Hopkins Symptom Checklist (HSCL): A Self-Report Symptom Inventory. Behav Science I.9 l-l 5.
FRIEDMAN, R.A. (1993) Social Impairment in Dysthymia. Psychiat Annals 23, 632- 637.
GREENBERG, R.P., BORNSTEIN, R.F., GREENBERG, M.D. and FISHER, S. (1992) A Meta-Analysis of Antidepressant Outcome Under “Blinder” Conditions. J Consulting and Clin Psycho1 6.0, 664-669.
GUY, W. (1976) ECDEU Assessment Manual for Psychopharmacology. DHEW Pub No (ADM)76-338. Rockville, MD: National Institute of Mental Health.
HAMILTON, M. (1960) A Rating Scale for Depression. J Neurosurg Psychiat 25, 56-62.
HARRISON, W., RABKIN, J., STEWART, J.W., MCGRATH, P.J., TRICAMO, E. and QUITKIN, F. (1986) Phenelzine for Chronic Depressions: A Study of Continuation Treatment. J Clin Psychiat 42, 346-9.
HELLERSTEIN, D.J., YANOWITCH, P., ROSENTHAL, J., SAMSTAG, L.W., MAURER, M., KASCH, K., BURROWS, L., POSTER, M., CANTILLON, M. and WINSTON, A. (1993) A Randomized Double-Blind Study of Fluoxetine Versus Placebo in Treatment of Dysthymia. Am J Psychiat l5.6, 1169-l 175.
HELLERSTEIN, D.J., YANOWITCH, P., ROSENTHAL, J., HEMLOCK, C., KASCH, K., SAMSTAG, L.W. and WINSTON, A. (1994) Long-Term Treatment of Double Depression: a Preliminary Study with Serotonergic Antidepressants. Prog Neuropsychopharmacol and Biol Psychiat I.8 139-l 47.
HORWATH, E., JOHNSON, J., KLERMAN, G.L. and WEISSMAN, M. (1992) Depressive Symptoms as Relative and Attributable Risk Factors for First-Onset Major Depression. Arch Gen Psychiat 49, 817-823.
HOWLAND, R.H. (1991) Pharmacotherapy of Dysthymia: a Review. J Clin Psychopharmacol 11, 83-92.
HOWLAND, R.H. (1993) Chronic Depression. Hospital and Comm Psychiat 44, 633- 639.
KELLER, M.B., KLEIN, D.N., HIRSCHFELD, R.M.A., KOCSIS, J.H., MCCULLOUGH, J.P., MILLER, I., FIRST, M.B., HOLZER C.P.3rd, KEITNER, G.I., MARIN, D.B., and SHEA, T. (1995) Results of the DSM-IV Mood Disorders Field Trial. Am J Psychiat l!i2, 843-849.
KELLER, M.B., LAVORI, P.W., ENDICOTT, J., CORYELL, W. and KLERMAN, G.L. (1983) “Double Depression”: Two Year Follow-Up. Am J Psychiat I4.9, 689694.
KELLER, M.B. and RUSSELL, C.W. (1991) Refining the Concept of Dysthymia. Hosp and Commun Psychiat 42, 892-893.
442 D.J. Hellerstein et al.
KELLY, NW., PERRY, P.J., HOLSTAD, S.G. and GARVEY, M.J. (1989) Serum Fluoxetine and Norfluoxetine Concentrations and Antidepressant Response. Therapeutic Drug Monitoring Il, 165-I 70.
KLEIN, D.N., CLARK, D.C., DANSKY, L. and MARGOLIS, E.T. (1988) Dysthymia in the Offspring of Parents with Primary Unipolar Affective Disorder. J of Abnorm Psycho1 9.2, 265-274.
KLEIN, D.N., TAYLOR, E.B., DICKSTEIN, S. and HARDING, K. (1988) Primary Early- Onset Dysthymia: Comparison with Primary Nonbipolar Nonchronic Major Depression on Demographic, Clinical, Familial, Personality, and Socioenvironmental Characteristics and Short-Term Outcome. J of Abnorm Psycho1 92, 387-398.
KOCSIS, J.H., FRANCES, A.J., VOSS, C.B., MANN, J.J., MASON, B.J. and SWEENEY, J. (1988) lmipramine for Treatment of Chronic Depression. Arch Gen Psychiat 45, 253-257.
KOCSIS, J.H., SUTTON, B.M. and FRANCES, A.J. (1991) Long-Term Follow-Up of Chronic Depression Treated with Imipramine. J Clin Psychiat 52, 56-59.
MARKOWITZ, J.C. (1993) Comorbidity of Dysthymia. Psychiatr Annals 23, 617-
624.
MASON, B.J., KOCSIS, J.H., LEON, A.C., THOMPSON, S., FRANCES, A.J., MORGAN, R.O. and PARIDES, M.K. (1993) Measurement of Severity and Treatment Response in Dysthymia. Psychiatr Annals 23, 625-637.
QUITKIN, F.M., MCGRATH, P.J., STEWART, J.W., HARRISON, W., WAGER, S.G., NlJNES, E., RABKIN, J.G., TRICAMO, E., MARKOWITZ, J. and KLEIN, D.F. (1989) Phenelzine and lmipramine in Mood-Reactive Depressives. Arch Gen
Psychiat 46, 787-793.
ROSENTHAL, J., HEMLOCK, C., HELLERSTEIN, D.J., YANOWITCH, P., KASCH, K., SCHUPAK, C., SAMSTAG, L.W. and WINSTON, A. (1992) A Preliminary Study of Serotonergic Antidepressants in Treatment of Dysthymia. Prog Neuropsychopharmacol and Biol Psychiat IL6 933941.
SPITZER, R.L., WILLIAMS, J.B.W., GIBBON, M. and FIRST, M.D. (1988) Structured Clinical Interview for DSM-Ill-R--Patient Version (SCID-P). New York, New York State Psychiatric Institute, Biometrics Research.
Inquiries and reprint requests should be addressed to:
David J. Hellerstein, MD 212-420-2800; FAX 212-420-3936 Psychiatric Outpatient Services Beth Israel Medical Center First Avenue and 16th St. New York, NY 10003 USA




















