
Strategies to improve dietary, fluid, dialysis or medication ...
Upload
khangminh22Category
view
0download
0
Using Education to Improve Medication Adherence in Hypertension
Submitted by
Chinyere Oghide
A Direct Practice Improvement Project Presented in Partial Fulfillment
of the Requirements for the Degree
Doctor of Nursing Practice
Grand Canyon University
Phoenix, Arizona
February 18, 2021

© by Chinyere Oghide, 2021
All rights reserved.

GRAND CANYON UNIVERSITY
Using Education to Improve Medication Adherence in Hypertension
by
Chinyere Oghide
has been approved
February 18, 2021
APPROVED:
JoAnna Cartwright, PhD, APRN, NNP-BC, DPI Project Chairperson
Maurene Schneider, MSN, RN, DPI Project Committee Member
ACCEPTED AND SIGNED:
__________
Lisa G. Smith, PhD, RN, CNE
Dean and Professor, College of Nursing and Health Care Professions
_________________________________________
Date
2/19/2021

Abstract
Antihypertensive medication non-adherence is a common problem in healthcare.
Currently, the project site has no program to increase medication adherence (MA) in their
hypertensive patients. Therefore, the purpose of this quantitative, quasi-experimental
quality improvement project was to determine if the implementation of the Million Hearts
program impacted the adherence to antihypertensive medication among adult patients,
with known hypertension (HTN) in a primary care clinic setting in New York, over a four
week period. Orem’s self-care theory and Ajzen’s theory of planned behavior were the
project’s theoretical foundation. Data on MA was measured using the Hill-Bone
Medication Adherence Scale HB-MAS scale in hypertensive adults aged 18 years and
older (n = 15) at baseline and at four weeks. A two-tailed paired sample t-test showed
that there was a clinical and statistically significant improvement in patients MA (M =
35.6; SD = 1.55; p = 0.00). The results of the Million Hearts program may increase MA
adherence in this population of patients. Based on the results, it is recommended that the
project is sustained at the site, blood pressure measurements are trended over a year to
determine if the increased MA improves the blood pressure measurements.
Keywords: HTN, medication adherence, Hill-Bone Medication Adherence Scale,
theory of planned behavior, Ajzen, Orem, self-care theory, American Heart Association,
Million Hearts.

Dedication
This project is dedicated to my parents, Eze Omeudo Peter and Lolo Beatrice
Oduoza, of happy memory, who believed in education as the best route to success. My
father’s statement of encouragement was always “Forward ever, backward never.” and
believed in my successful capabilities. Both of you have gone ahead of me to God, but
are evergreen on earth and your influence has made possible my DNP educational
journey.

Acknowledgments
First and foremost, my gratitude goes to my Almighty God who, in his infinite
mercy and goodness, inspired me to begin and to complete this project. Though the DNP
journey initially appeared distant, I am exceptionally grateful to all those who contributed
to making it a pleasant journey.
My wholehearted gratitude goes to my committee chairperson, Dr. JoAnna
Cartwright who consistently guided and encouraged me during my project. I extend my
sincere gratitude to my content expert, Maurene Schneider, who was always there for me
and very supportive at my project site. I would like to thank Dr. Stephanie Hills for her
encouragement from the foundation to the end of my DNP journey. I also like to thank all
my instructors for their dedication.
Very many thanks to my project site primary care nurses, Mary, Felicia, and
Lena, for their contribution to my project. I extend my profound gratitude to Anne
Wilburn for constant encouragement and forever being pleasant throughout the journey.
Finally, I thank my family – my dear husband, Godwin, my darling daughter,
Esosa, and my darling son, Nosa, for keeping me company during my sleepless nights,
and helping my computer illiteracy. I extend my gratitude to my six brothers and three
sisters for their daily prayers. To my parents, I say ‘Adieu’ as they rest in perfect peace
with God.

Table of Contents
Chapter 1: Introduction to the Project ..................................................................................1
Background of the Project ...............................................................................................2
Problem Statement ...........................................................................................................4
Purpose of the Project ......................................................................................................5
Clinical Question .............................................................................................................6
Advancing Scientific Knowledge ....................................................................................7
Significance of the Project ...............................................................................................9
Rationale for Methodology ............................................................................................10
Nature of the Project Design ..........................................................................................11
Definition of Terms .......................................................................................................13
Assumptions, Limitations, Delimitations ......................................................................14
Summary and Organization of the Remainder of the Project ........................................16
Chapter 2: Literature Review .............................................................................................18
Theoretical Framework ..................................................................................................22
The theory of planned behavior (TPB) ......................................................................22
Orem’s self-care theory. .............................................................................................24
Review of the Literature ................................................................................................25
Medication non-adherence .........................................................................................26
Uncontrolled HTN .....................................................................................................37
Strategies for medication adherence (MA) ................................................................48
Summary ........................................................................................................................58
Chapter 3: Methodology ....................................................................................................61

Statement of the Problem ...............................................................................................62
Clinical Question ...........................................................................................................63
Project Methodology ......................................................................................................65
Project Design ................................................................................................................66
Population and Sample Selection ..................................................................................67
Instrumentation and Sources of Data .............................................................................69
Hill-Bone Medication Adherence Scale (HB-MAS) .................................................69
Self-Measured Blood Pressure (SMBP) ....................................................................70
Electronic Health Records (EHRs) ............................................................................70
Validity ..........................................................................................................................71
Reliability .......................................................................................................................72
Data Collection Procedures ...........................................................................................73
Data Analysis Procedures ..............................................................................................74
Potential Bias and Mitigation ........................................................................................76
Ethical Consideration .....................................................................................................77
Limitations .....................................................................................................................78
Summary ........................................................................................................................79
Chapter 4: Data Analysis and Results ................................................................................81
Descriptive Data ............................................................................................................82
Data Analysis Procedures ..............................................................................................85
Results ............................................................................................................................86
Summary ........................................................................................................................90
Chapter 5: Summary, Conclusions, and Recommendations ..............................................92
Summary of the Project .................................................................................................93
Summary of Findings and Conclusion...........................................................................94
Implications ...................................................................................................................96
Theoretical implication ..............................................................................................96
Practical implications .................................................................................................97
Future implications ....................................................................................................97
Recommendations ..........................................................................................................98
Recommendations for future projects ........................................................................98
Recommendations for future practice ........................................................................99
References ........................................................................................................................101
Appendix A ......................................................................................................................126
Grand Canyon University Institutional Review Board Outcome Letter ......................126
Appendix B ......................................................................................................................127
Hill-Bone Medication Adherence Scale (HB-MAS) ...................................................127
Appendix C ......................................................................................................................128
Permission to Use Hill Bone Scale (HB-MAS) ...........................................................128
Appendix D ......................................................................................................................129
Center for Disease Control and Prevention Million Hearts Tools ...............................129
Appendix E ......................................................................................................................132
Permission to Use Center of Disease Control and Prevention Million Hearts Tools ..132

List of Tables
Table 1. Demographics of Project Sample ....................................................................... 83
Table 2. Total scores of MA Data as measured with HB-MAS Tool ............................... 84
Table 3. Blood Pressure Comparison................................................................................ 85
Table 4. Pre/Post-Intervention Comparison ...................................................................... 89

List of Figures
Figure 1. Bar Graph displaying the mean scores as measured by HB-MAS. ................... 88
Figure 2. Pre and post blood pressure comparison using the mean BPs........................... 89

1
Chapter 1: Introduction to the Project
Medication non-adherence is not taking medications as ordered by their primary
care provider (Galozy, Nowaczyk, Sant, Ohlsson, & Lingman, 2020). Non-adherence to
medicines is a significant health problem, especially for patients with chronic diseases
requiring multiple medications (Smith et al., 2017).
Currently, the project site has over 50% of their patients that are noncompliant
with their hypertensive treatment. Nurses at the project site identified the obstacles of
adherence to antihypertensive medications as a public health problem, which led to this
project's development. The complexity of hypertensive medication adherence is directly
related to the patients' knowledge, perception, and refills from the pharmacy (Galozy et
al., 2020). Patients' medication non-adherence in hypertension (HTN) can decrease but
requires thorough assessment and cooperation between the care provider and patients
(Nafradi, Galimbertti, Nakamoto, & Schultz, 2016). Non-adherence to antihypertensive
medications is a significant public health problem, causing annual deaths of about 9.4
million worldwide (Nielsen, Shrestha, Neupane, & Kallestrup, 2017). Effective treatment
for non-adherence depends on the patient's willingness to assess and understand the
conditions that prevent adherence.
Hypertension is a significant precursor of heart and kidney diseases, causing
about two-thirds of the world's mortalities and claiming about 7.1 million deaths annually
(Nikparvar et al., 2019). Hence, hypertensive patients need to understand their disease
process and agree to the definition of medication adherence. Patients need to take their
medications as recommended by health care professionals and take an active part in their
treatment plan for HTN and their providers (Turcu-Stiolica, Subtirelu, Meca, & Bogdan,

2
2019). Non-adherence to antihypertensive medication is a general problem among adults,
but it is more prevalent among elderly patients (Al-Ruthia et al., 2017). This age group is
more likely to have comorbidities and be on multiple medications, which predispose
them to medication non-adherence.
Chapter 1 will present the background of the project, describing the problem,
purpose, and clinical questions which directed it. Then, how the project advanced
scientific knowledge and its significance will be described. The rationale for the
methodology and design will be discussed. The chapter will end with a discussion of key
terms, assumptions, limitations, and delimitations.
Background of the Project
The primary care clinic for the quality improvement project is an adult care clinic.
Seventy-five percent of the clinic patients have a diagnosis of HTN, and most of them are
non-adherent to their HTN medications. HTN is a public health disease worldwide
(Nielsen et al., 2017). According to the guidelines of the American Heart Association
([AHA] 2017), HTN is any blood pressure (BP) that is equal to or greater than 130/80.
The estimate was that by the year 2025, 29.2% of adults in the world would have HTN
(Veisani, Jenabi, Nematollahi, Delpisheh, & Khazaei, 2019). Eghbali-Babadi, Khosravi,
Feizi, and Sarrafzadegan (2017) predict that there will be 1.56 billion people with HTN in
2025. HTN is a chronic disease, but can be controlled to prevent cardiovascular disease
and death's adverse effects, which is crucial, considering the 10.4 million deaths globally
in 2017 (Wang et al., 2020). Though antihypertensive medication can control HTN, poor
adherence to the drug has a negative outcome and could pose an economic burden to
society (Abbas et al., 2020). Non-adherence or poor adherence to hypertension

3
medication is a global problem and varied in prevalence. For instance, as noted in the
literature, a non-adherence of 86.7% and 12.7%, respectively, were discovered in two
outpatient clinics in Brazil. (Magnabosco et al., 2015). The statistics show that non-
adherence to antihypertensive medication can vary in different parts of New York, such
as urban areas. In the study of Li et al. (2019) about prevalence in New York City, the
researchers found non-adherence of 36% among 18 to 44 years of age, 11.8% among 45
to 64 years of age, 4.7% among 65 years old and above. The project site calculation
estimates that about 68% of the population with HTN have non-adherence to their
antihypertensive medication.
The estimated prevalence of medication non-adherence in older adults worldwide
is about 50% of hypertensive patients (Mahmoodi et al., 2019). Studies have shown that
there is an increase in mortality with uncontrolled HTN when there is non-adherence
(Bansal, Rajput & Mathur, 2019). This is exemplified by Carvalho and Santos (2020)
who found that 50% of hypertensive patients had controlled BP secondary to adherence
to their medications and influence from other non-pharmacological factors.
The DPI project attempts to improve medication adherence among hypertensive
primary care patients. Healthcare professionals are available to help the patients maintain
normal BPs by prescribing appropriate medications and scheduling office visits, but
many of the patients do not keep their appointments. Factors affecting their non-
adherence include forgetfulness, which may or may not be intentional, background
knowledge of HTN, other complications, costs, medication side effects, and general
attitude towards treatments (Abbas et al., 2020).

4
The project site facility makes reasonable accommodation for all patients to
maintain health, such as home-based primary care (HBPC), a community-based outreach
center (CBOC), and home telehealth. The primary care providers (PCP) can evaluate the
BP readings from electronic health records (EHRs) and adjust the BP medications
accordingly. However, gaps in knowledge still exist despite these opportunities. Hence
this evidence-based DPI project attempts to close the gap with education on the
relationship between HTN and medication adherence.
Problem Statement
It was unknown if or to what degree the implementation of the Million Hearts
education program impacted adherence to antihypertensive medication as measured by
the Hill-Bone Medication Adherence Scale (HB-MAS) when compared to current
practice among adult patients 18 years and older with known hypertension in rural New
York state. Medication non-adherence occurs at any age, but it is more prevalent in the
elderly population due to mental status and other age-related factors (Mahmoodi et al.,
2019). Though the exact cause of antihypertensive medication non-adherence is
unknown, research has identified knowledge deficit and forgetfulness as the leading
proponents (Abbas et al., 2020). The current clinic practice of mentioning taking all
medications as prescribed during an office visit has not improved adherence. In this
project, nurses target non-adherence to antihypertensive medication, using the Million
Hearts educational intervention to address the knowledge gap. The goal is for the patients
to know the adverse effects and the resultant associated comorbidities and take their BP
medications, subsequently preventing cardiovascular diseases (CVD) complications such
as stroke, heart failure, and renal insufficiency.

5
Hypertensive patients are selected from the population as they come for their
routine clinic appointments with the PCPs. Though the population's age criterion was 18
years and above, the project patients were older adults between 46 and 97. The principal
investigator (PI) supplied the education tool from the Million Hearts program (see
Appendix D), instructed the nurses, and the nurses taught the patients using the teaching
tool. The HB-MAS questionnaire measured the project's evidence by pre- and post-
interventions and was used once every week, for four weeks, to evaluate the patients'
medication adherence.
Purpose of the Project
The purpose of this quantitative, quasi-experimental project was to determine if or
to what degree the implementation of the Million Hearts education program could impact
the adherence to antihypertensive medication as measured by HB-MAS, when compared
to current practice among adult patients 18 years and older with known hypertension, in a
primary care clinic setting in New York over four weeks. This DPI project aimed to
determine if education could impact medication adherence to hypertensive patients. The
strategies were to empower patients to proper self-care; check their BP; help them
understand that HTN is the most significant risk factor for CVD, that adverse effects
could be prevented if patients' HTN was controlled; and be aware that prescribed
antihypertensive medications could control HTN if the patients took them as prescribed.
This evidence-based project was expected to improve patients' medication adherence
(MA).
The project's independent variable was the Million Hearts education, and the
dependent variable included the patient outcome of the medication adherence as

6
measured by the HB-MAS. This instrument measured weekly MA by self-report of the
patients. The second dependent variable was the patients' self-measured BP at home
using their BP kit. The nurse also took the patients' BPs at the office at pre-intervention,
and post-intervention. Although the length of the project would not show a substantial
change in blood pressure, the primary investigator (PI) included the blood pressure
measurements to look at the trends and relationship to medication adherence as
additional, but not primary, data. The BP readings were not for measuring medication
adherence. The clinic nurses for the project were instructed on using the tools and were
comfortable monitoring the patients every week. Each patient would receive a weekly
telephone call from the nurses to assess their MA's progress using the patients' responses
from the HB-HBP questionnaire.
The project contributed to evidence-based practice (EBP) in nursing because
nurses are very involved in their healthcare. When new policies and procedures are
written, the implementation is carried out by the bedside nurses. According to Karaman
and Akyolcu (2019), nurses spend more time with patients and their relatives who are
incredibly, if not critically, ill. In this DPI project, the PI instructed the nurses about the
Million Hearts education using a power-point presentation, and the nurses taught the
same information to the patients. The EBP could become a policy at the facility after this
project. Consequently, it will be applied to solve other healthcare problems.
Clinical Question
The following clinical question guided the DPI project:
Q. To what degree does the implementation of the Million Hearts education
impact the adherence to antihypertensive medication as measured by HB-MAS,

7
when compared to current practice among adult patients 18 years and older with
known hypertension in a primary care clinic setting in upstate New York over
four weeks?
This DPI was a quantitative project with a quasi-experimental design, using the
HB-MAS questionnaire to evaluate the outcome. The goal of the development was to
improve antihypertensive medication adherence using an education program. Hence, the
fulfillment of the project outcome expectation is that the patients, after receiving the
intervention, would benefit from taking their medications as prescribed compared to
before the intervention. The data from the baseline questionnaire for each person would
be compared to the post-intervention questionnaires' data at the end of the four weeks of
intervention to evaluate adherence. The outcome was expected to be positive to support
the problem statement of impacting adherence to BP medication. The pre- and post-BP
would also be checked. The PI included blood pressure measurement only as an
additional, not a primary data, to look at the trends and relationship to medication
adherence. The length of the project would not show a substantial change in blood
pressure.
Advancing Scientific Knowledge
Nursing science is vital to patient care, since its focus is on individualized care
through patient and family-centered care to achieve a maximum quality outcome (Grady,
2017). According to the National Institute of Health (NIH, 2017), individualized care is a
better approach to the patient's general welfare, because care delivery is planned between
the providers and the patient. Adherence to antihypertensive medications is significant in
health care and to the patient's general interest, which, if untreated in this case, can result

8
in uncontrolled HTN. This public health problem can be prevented or reduced with
adherence to BP prescribed medications. Following nursing science, the clinic nurses in
this project will actively engage the patients in their care plan to understand the
importance of controlled BP. The DPI project can fill the gap created by antihypertensive
non-adherence with a resultant malignant HTN.
Applying nurses' scientific knowledge, holistic care comprising all aspects of life
such as social, educational, biological, and environmental, and how these factors affect
health, will be considered in the project. Education to the patients, using the Million
Hearts program as in this DPI project, will make the patients informed in their self-care.
The provision of technological equipment, such as a blood pressure monitoring kit, also
fosters patient and family-centered care by applying nursing science (Grady, 2017).
According to Grady (2017), nursing science's goal is to improve quality of life by
individualizing patients' care needs. Future interventions that could improve the patients'
MA and subsequent BP control would be a referral to a home telehealth program. These
technologies, such as smartphone apps and computers, are linked to the health care
providers for ease of BP monitoring and medication adherence (McKoy et al., 2015).
The theory used to provide the foundation for this DPI project is the theory of
planned behavior (TPB) developed by Icek Ajzen in 1985, from a descriptive qualitative
study. This theory explains the relevance of the intentions of doing things and the
consideration of how important things are to a person (Hartley, Hoch, & Cramer, 2018).
In the case of medication adherence, frequent, friendly monitoring would eventually
foster the relevance of doing it without monitoring or further education.

9
Another theory that was applied to the foundation of this DPI project was Orem's
self-care theory, which described the association between a person and the environment
(Orem, 2001). Blood pressure is one of the chronic diseases and can be monitored and
controlled by health care providers with the patients' cooperation. In this project, the
nurses used the Million Hearts program to educate the patients and HB-MAS to monitor
their medication adherence.
Registered professional nurses were conscious of their capabilities and
management of non-adherence to antihypertensive medication and the effects of blood
pressure. Nurses applied their expertise to effectively manage such chronic conditions as
summarized by Orem’s self-care theory. Hence, the reasoning of improving medication
adherence with telephone calls is supported with the scientific knowledge background.
Significance of the Project
Using the implementation of Million Hearts education program to improve blood
pressure medication adherence fits into current health maintenance technologies. HTN
has no warning signs and can be silent, unrecognized, and untreated for many years until
it becomes an emergency (Achhab, Nazek, Maalej, Alami, & Nejjari, 2019). Considering
non-adherence to antihypertensive medication is one of the significant causes of strokes,
heart attacks, kidney failure, and death, as described by Pawloski et al. (2016). An
aggressive regimen, team based-approach to improve MA, is required in the control of
HTN.
This DPI project was important because the patients would benefit from the
intervention as evidenced by the HB-MAS data. Yazdanpanah, Saleh Moghadam,
Mazlom, Ali Beigloo, and Mohajer (2019) strongly recommended medication adherence

10
to prevent uncontrolled HTN. The potential practical application from this project was
the patients would take an active part in their care by monitoring their BP and taking their
medications as prescribed. The PI included blood pressure measurement only as an
additional, not a primary data, to look at the trends and relationship to medication
adherence. The length of the project would not show a substantial change in blood
pressure.
Rationale for Methodology
The methodology for the project was quantitative. The quantitative method was
the best for the project because the data collection was measurable and quantifiable. It
had to be numerically measurable for statistical analysis of data (Ali & Bhaskar, 2016).
The significant measurable variable for this project was the number of times the patient
took the BP medication as prescribed during the four weeks of the intervention to
improve medication adherence. The HB-MAS was the pre- and post-questionnaire to
evaluate the patients' medication adherence. Weekly data of the patients' medication
adherence was obtained over the phone using the same HB-MAS questionnaire. Logs of
the patients' data were compared to evaluate adherence to their antihypertensive
medication. There was also a comparison between the pre- and post-BP. Although the
project's length would not show a substantial change in blood pressure, the blood
pressure measurements were included to look at the trends and relationship to medication
adherence as additional, but not primary, data.
The quantitative methodology was the best approach to this project because the
dependent and independent variables needed quantifying accurate comparison. The use of
numbers, tables, and ratios were significant in the accuracy of the interpretations of an

11
EBP project's findings. The research identified quantitative methodology as a stable, in-
depth analysis in confirming a study (Bolondi, Branchetti, & Giberti, 2018). A qualitative
method is not appropriate for this evidence-based DPI project because qualitative
methods explore occurrences more. They use structured interviews or reviews of case
records. According to Van den Berg and Struwig (2017), a qualitative approach is
appropriate for explaining theories' events and development. The theories for this project,
Orem's self-care theory, and the theory of Planned Behavior, have already been
developed.
Nature of the Project Design
This DPI project applied a quasi-experimental design which required a pre-
intervention questionnaire and a post-intervention questionnaire using the HB-MAS.
Blood pressure was checked before the intervention and post-intervention. Blood
pressure measurements were included only as an additional, not primary data, to look at
the trends and relationship to medication adherence. The length of the project would not
show a substantial change in blood pressure. Nurses at the project site were instructed
using a PowerPoint presentation based on the Million Hearts education tool. Then the
nurses taught the patients using the same Million Hearts education as the intervention.
The pre-intervention screening of the patients using HB-MAS was done to
evaluate their baseline medication adherence. The intervention required individualized
teaching at the PCP's office. The teaching information was consistent with the Million
Hearts education program on HTN and the importance of medication adherence. Pre-
intervention BP was also checked for the purpose of monitoring the trends. The nurses'
weekly telephone calls to the patients were to obtain data regarding their medication

12
adherence for the week. Each patient would respond numerically to each of the nine
questions following the HB-MAS questionnaire. After four weeks of the intervention, the
post-intervention questionnaire provides numerical data for comparison with the baseline
medication adherence. The patients' BP checked at post-intervention was included by the
PI only as an additional, not a primary data, to look at the trends and relationship to
medication adherence. The length of the project (four weeks) would not show a
substantial change in blood pressure.
A quasi-experimental design was the best design for this DPI project because it
would address the PICOT question more appropriately than any other method. The
system is consistent with the quasi-experimental design described by Bloomfield and
Fisher (2019), because there could be a causal-comparative relationship between the
dependent and independent variables. It addressed the extent that implementing the
Million Hearts education program would impact the adherence to antihypertensive
medication. The HB-MAS questionnaire was used to obtain data for the patients'
medication adherence. A cross-sectional study design is not appropriate for this DPI
project because this design is more of an observational study of outcomes (Bangdiwala,
2018). Though a questionnaire can be used in collecting the data like a quasi-
experimental design, the analysis of a cross-sectional design does not establish a causal
relationship for comparison.
The steps taken for the data collection were as follows: (a) recruit the sample of
hypertensive patients who were non-adherent to antihypertensive medication as
determined by the HB-MAS, (b) obtain baseline numerical data from the samples, (c)
have the nurses teach the patients using the Million Hearts education materials, (d) check

13
baseline blood pressures, (e) establish weekly phone calls from the nurse, and (f) obtain
post-intervention medication adherence data, and post-intervention BP check. Although
the project's length is too short for showing a substantial change in blood pressure, the PI
included the blood pressure measurements to look at the trends and relationship to
medication adherence as additional, but not primary data.
Definition of Terms
The following terms were used in this project:
Cardiovascular disease (CVD). Cardiovascular disease is the general name for
heart diseases such as stroke and heart attack. Their main cause is uncontrolled high
blood pressure (high BP), but this can be prevented or controlled by taking any
medication ordered by the provider (Pioli et al., 2018).
Hypertension (HTN). Hypertension is a condition when blood pressure (BP) is
higher than the set normal limits of 130/80, where 130 is the systolic blood pressure
(SBP), and 80 is the diastolic blood pressure (DBP). Any SBP greater than 130 or DBP
greater than 80, is referred to as HTN (Ihm et al., 2019). It is a silent killer and has no
warning signs until it becomes a medical emergency (Achhab et al., 2019).
Medication adherence (MA). Medication adherence in HTN is a public health
problem that affects all ages but especially the elderly population. MA is taking
medications as prescribed by the clinician (Galozy et al., 2020).
Million Hearts. Million Hearts is an extensive advertisement that the American
Heart Association (AHA) uses to teach and encourage people to prevent heart diseases.
The aim is to prevent one million heart attacks, kidney diseases, strokes, and death within
five years. The aim is medication adherence (CDC, 2015).

14
Hills-Bone medication adherence scale (HB-MAS). HB-MAS is a scale with
nine questions used in testing the medication taking of the patients concerning the
patients' MA. It has one to four numerical responses designed by The Hill Bone Scales
Team (Kim, Hill, Bone, & Levine, 2000). According to Johns Hopkins University School
of Nursing (2020), Hill-Bone Medication Adherence Scale (HB-MAS), a nine-item scale,
is specifically designed originally for measuring compliance with the treatment of HTN.
The scale can measure medication adherence in other chronic conditions, such as diabetes
and chronic obstructive pulmonary disease. The university recommends the use of the
Hill-Bone scale at every health care visit for improved patients' outcomes.
Non-adherence in HTN. Non-adherence in HTN is not doing what is supposed
to be done to prevent hypertension. Non-adherence to antihypertensive medication can
predispose to CVD, stroke, heart failure, and kidney failure, and these have increased
mortality due to uncontrolled HTN. Non-adherence to BP medication is a significant
cause of uncontrolled HTN (Abbas et al., 2020).
Assumptions, Limitations, Delimitations
It was assumed the patients would present to the outpatient clinic whenever they
were scheduled to come. It was also assumed the patients would show up at their
appointments and be interested in taking their medications as prescribed, but tend not to
take, probably because they forget or do not know the importance. If so, there would be
no HTN medication non-adherence, which is currently a significant medical problem
(Smith et al., 2017). It was assumed all the patients would remember to check their BP as
needed. However, forgetfulness and not knowing the importance of BP treatment are
among the significant reasons for patients' medication non-adherence (Abbas et al.,

15
2020). There was an assumption that after receiving education every adult is aware of the
complications of uncontrolled HTN, and prescribed pharmacological management is not
the only regimen for the control of HTN and prevention of CVD (Mahmoodi et al.,
2019).
The project was designed for adult patients from 18 years of age and above, but
HTN is more prevalent among older adults (Al-Ruthia et al., 2017). Hence, this project's
general population was 46 to 97 years old, though the proposed age group was 18 years
and above. Another limitation was the small sample size of 15 patients. This population
was too small to show statistical significance or reach generalizable findings. Though
there were many uncontrolled hypertensive patients among the population, only 15
consented to participate in the project. Being a DPI project, every uncontrolled
hypertensive patient should be accepted to participate. Large samples produce more
accuracy with a low margin of error, because a large data reveals every detail with high
statistical significance (Khalilzadeh & Tasci, 2017).
Though HTN has no warning sign, CVD's warning sign, such as stroke, is HTN
(Barua et al., 2019). The project facility provided extensive care for the patients'
convenience and obtained the maximum quality outcome of care. The patients could
utilize the resources closest to their homes, such as community-based outreach centers
(CBOC), for frequent checks of their BPs. They could also be enrolled in home-based
primary care (HBPC) if unable to go to the CBOC or be registered in-home telehealth to
monitor the BP closely. The DPI project aimed to close the existing gap using education.
Hence, having care locations at proximity makes it easier to check BPs and adjust
antihypertensive medications.
16
Empowerment could enable patients' self-care and to monitor their BP. Not all
patients want to monitor their BP, despite being provided with a BP kit. However, the
nurses provided individualized teaching of appropriate BP testing for accurate results.
This activity might have made the patients feel more responsible for their care, with
subsequent adherence to antihypertensive medication.
Summary and Organization of the Remainder of the Project
Research defined medication adherence in various ways, but the definitions
explain that medication should be taken as prescribed by a health care professional
(Galozy et al., 2020). The researchers reported that HTN, a chronic disease, requires
pharmacological intervention for older adults' control with other associated health
problems. Medication non-adherence has been found in all age groups, but research
determined it was more prevalent with older adults (Smith et al., 2017). Hypertension
was found to be the most significant risk factor for CVD and death from its complications
(Wang et al., 2020). Antihypertensive medications have been shown to control HTN, but
non-adherence to the medications, as reported by Bansal, Rajput, and Mathur (2019), was
found to be a significant cause for uncontrolled HTN.
This evidence-based project attempted to improve MA by enabling the control of
HTN and preventing CVD and its associated public health costs and death. The patients
were taught about HTN, related factors, and the importance of taking antihypertensive
medications using the Million Hearts education program. The period of the intervention
was four weeks. The pre- and post-interventions were numerically measured with be the
HB-MAS questionnaire. The HB-MAS was the tool used for obtaining the MA data. The

17
evaluation of the data from the HB-MAS for pre- and post-intervention, and weekly
during the intervention period of four weeks; were compared to give the MA outcome.
Nursing science is vital in obtaining a maximum quality outcome of care (Grady,
2017), and it was applied in this project. The theory of planned behavior (Ajzen, 1985)
and Orem's self-care theory (2001) were also applicable because, after completing the
DPI project, the patients are expected to continue taking their BP medications as
prescribed without any further intervention after the project period. The methodology and
design for this DPI project was a quantitative, quasi-experimental design from which
numerical data were obtained and compared for accuracy of the project interpretations
(Bolondi et al., 2018).
The next section is Chapter 2 of the project, which provides a literature review of
about 50 related articles. The chapter will involve analyzing and synthesizing the articles,
identifying the themes, subthemes, and identifying at least one quantitative methodology.
In Chapter 3, the project's methodology, which builds off the literature, will be described
in detail. Chapter 4 will provide the results of data collection and analysis. Chapter 5 will
provide and interpretation of the results.

18
Chapter 2: Literature Review
As defined by Pan, Lei, Hu, and Li (2020), medication adherence (MA) is the
taking of medications as prescribed. Furthermore, if taken as prescribed, antihypertensive
medication produces positive BP control (Pan et al., 2020). Medication non-adherence is
defined as a situation where medication is not taken as prescribed even if the reason is
that it is forgotten (Malek, Heath & Green, 2017). Typically, clinicians provide advice
and information regarding prescribed medications, and patients are expected to follow
accordingly. Medication non-adherence is a significant public health problem, especially
for hypertensive patients, affecting 20% to 50% of the patients (Nafradi, Galimberti,
Nakamoto, & Schultz, 2016).
Hypertension is the precursor of heart and kidney diseases and causes about two-
thirds of the world's mortalities and 7.1 million deaths annually (Nikparvar et al., 2019).
The Centers for Disease Control and Prevention (CDC) in 2017 reported an estimated
death of 472,000 people from HTN in the US, and this approximates 1,300 deaths per
day. Approximately 108 million people in the United States have HTN, and only 24% of
them have controlled BP (CDC, 2017).
The lists of the items to improve medication adherence (MA) among the patients
(who will be further discussed in the literature review) are divided into three themes and
nine subthemes. The themes are medication non-adherence, uncontrolled HTN, and
strategies for medication adherence. The subthemes are (a) patients-providers
communication of non-adherence, (b) barriers to MA, (c) factors affecting MA, (d)
factors associated with uncontrolled HTN, (e) patient-clinician communications about

19
HTN, (f) disparities in HTN, (g) patient education, (h) facilitators, and (i) outpatient
monitoring.
Many factors determine non-adherence to medication, such as patients, provider
relationships, and medications (Acosta et al., 2015). Patients' involvement and
communication with health care professionals are significant aspects of medication
adherence, including behavioral factors and knowledge (Nafradi et al., 2016). Costa et al.
(2015) recommended improvement methods to reduce risk factors to the patients and
described them as behavioral, self-management, educational, and reminder interventions.
The literature review to improve adherence to antihypertensive medications requires an
outline approach that focuses on the patients' role, the healthcare providers, and
medicines.
Multiple studies linked uncontrolled HTN to medication non-adherence and
describe the relationship as a significant public health problem that affects all aspects of
health (Ruppar et al., 2015). Ruppar et al.'s systematic review of the clinical practice
guidelines (2015) includes the declaration of the World Health Organization (WHO) in
its 2003 report on non-adherence to medications as affecting mainly people with chronic
conditions, leading to higher risks for treatment failure and increased healthcare
utilization and associated hospitalization (Ruppar et al., 2015; WHO, 2003).
As described by the US Institute of Medicine, clinical practice guidelines enable
maximum outcome patient care as cited by Ruppar et al. (2015), which are developed
from the existing knowledge to improve medication adherence. The purpose of this
quantitative, quasi-experimental project was to determine if or to what degree the
implementation of the Million Hearts education program could impact the adherence to
20
antihypertensive medication as measured by HB-MAS, when compared with current
practice among adult patients 18 years and older with known hypertension, in a primary
care clinic setting in New York over four weeks.
The existing gap in the literature of medication non-adherence could be filled by
the DPI project using education as an intervention. The clinic nurses always check the
patients' vital signs whenever the patients go for their clinicians' appointments, and the
patients are notified of the status of their BP, which is a way of monitoring their BP. This
evidence-based project added to the current knowledge level to improve medication
adherence. The gap of non-adherence to antihypertensive medication was determined for
multiple reasons, including the patients' knowledge deficit, and the project's educational
interventions can fill it. Nafradi et al. (2017) promoted treatment adherence and positive
outcome of care, considering the patient takes an active part in their prescribed
treatments. The DPI filled the gap by teaching the patients the importance of taking their
BP medications as prescribed and included behavior and lifestyle modifications. The
endpoint was the patients' positive health outcome, as measured by the HB-MAS.
According to the American College of Cardiology (ACC) and American Heart
Association (AHA) guidelines for HTN in 2017, HTN is any BP equal to or above 130/80
where 130 mmHg is the systolic BP, and 80 mmHg is the diastolic BP (CDC, 2020).
Antihypertensive medications control HTN, but non-adherence to HTN medication is a
significant cause of uncontrolled HTN (Pan et al., 2020). According to Barua, Faruque,
Banik, and Ali (2019), HTN is the most common and significant cause of cardiovascular
disease (CVD) in the world. Being non-infectious and silent, HTN can remain dormant
for many years until it causes harm (Achhab et al., 2019).
21
Environmental and genetic factors predispose an individual to HTN as discovered
by Zilbermint, Hannah-Shmouni, and Stratakis (2019). The researchers found HTN to be
more prevalent among African Americans than any other ethnic group, and it is
significant due to genetics, which explains the familial relationship. Other indicators that
predict the existence of HTN include socioeconomic status (SES), gender, age, obesity,
and lifestyle (Neufcourt, Deguen, Bayat, Zins, & Grimaud, 2020). Historically, people
with low SES have poor control of HTN due to knowledge deficit, low level of
education, and low income. Neufcourt et al. (2020) further explained HTN as being more
prevalent among men than women.
Non-adherence to hypertension medication has many associated factors, but
according to Etebari, Pezeshki, and Fakour (2019), non-adherence has no prior history.
The event is created by the patients who did not take their medications as prescribed, and
they end up with uncontrolled HTN. One factor determining non-adherence to HTN
medication is the patient's low treatment motivation, which explains the patients' lack of
interest in their health condition. Bansal et al. (2019) ascribed this low motivation to a
lack of education about HTN. SES of the patients, their attitudes towards treatment, and
beliefs about medications are contributory determinants to HTN medication non-
adherence (Abbas et al., 2020). Mahmoodi et al. (2019) discussed the high economic
costs affecting the affordability of the long-term use of HTN medications. Etebari et al.
(2019) reported therapeutic control of HTN as the adherence to the medicines and all
other recommendations from the clinician. HTN is a chronic disease, so it requires long-
term treatment to sustain HTN control. The DPI project will be designed to enable the
patients suffering from HTN to take an active part in the management of their HTN. The

22
care will involve the education of the patients, including knowledge about behavior and
lifestyle modifications.
The rest of this chapter will present the results of the literature review. It will
begin with a discussion of the theoretical framework. Then, the literature will be
discussed according to themes and subthemes. The themes were medication non-
adherence, uncontrolled hypertension, and medication adherence strategies. The
subthemes were: patient and provider communication, barriers to medication adherence,
the factors affecting medication adherence, associated factors, patient-clinician
communication, disparity in hypertension, patient education, facilitators, and outpatient
monitoring for sustainability.
Theoretical Framework
The theoretical framework explains the model from which the evidence based
project is constructed. Two theories were applied in this project. The selected theories
were: the theory of planned behavior and Orem’s self-care theory. The theories supply a
background explanation to the transmission of the project by the participating nurses.
The theory of planned behavior (TPB). The theory used to provide the
foundation for this practice project is the theory of planned behavior (TPB). Theory of
planned behavior was developed through a descriptive qualitative study to analyze five
physical education teachers' beliefs about their students with disabilities (Ajzen, 1985).
The disabled students were Japanese and were integrated into a class with regular
students. Demographic data were collected by questionnaires and used open-ended
questions. The teachers applied structured face-to-face interviews after validation and
translation of the tool from English to Japanese. The data were statistically analyzed. The

23
students' disabilities influenced the teachers' beliefs, and their views were higher with
severe disabilities, though it was a difficult task (Sato & Hodge, 2009). Overall, the study
had a positive outcome.
The literature discussed various modes of behavior and found a specific aspect of
an individual's behavior could be predicted correctly (Ajzen, 1985); thus, TPB resulted.
TPB explained the relevance of the intentions of doing things and how important it is to
the person (Hartley et al., 2018). In medication adherence, frequent friendly reminders to
take medications as prescribed will eventually foster patients' relevance of taking their
antihypertensive medications without being reminded. Blood pressure (BP), one of the
chronic diseases, can be monitored and controlled by the health care providers with the
cooperation of the patients. HTN is a chronic condition without a complete cure. In this
case, self-care provides an opportunity for monitoring the patients' association. People's
appropriate treatment, if applied as prescribed, yields the expected results.
The theory of planned behavior is related to the DPI project in many ways,
starting from the theory's purpose, which evaluated the teachers' beliefs about teaching
disabled students. There was a concern for them since they were in the same class with
regular students without disabilities. They should have equal opportunity in education
without discrimination. The teachers modified their beliefs even though it was not easy to
accommodate the students with their chronic disabilities to reduce disparity. Similarly,
the DPI project has identified medication non-adherence in HTN and will address it to
enable the patients to achieve a positive outcome of care.
The theory of planned behavior applied in the teaching tool was to help
hypertensive patients to understand their chronic disease and was the best way to achieve

24
a quality patient outcome. Being knowledgeable about the predictive factor of HTN and
how to keep it controlled was significant, and TPB predicted the factors. Emphasis was
placed on the use of medications and, more significantly, on medication adherence
(Etebari et al., 2019). Other non-pharmacological therapies, such as exercise and lifestyle
modifications, diet, and weight reduction, are adjunct therapy to medications. Gao et al.
(2020) applied the TPB in predicting exercise for diabetic patients (a chronic disease, like
HTN), and it was successful. Since the treatment outcome was predicted using TPB (Gao
et al., 2020), the DPI project's education intervention outcome predicted a positive result.
The researchers applied TPB in the evaluation of clinical errors in a hospital, and
225 nurses were involved in the study about reporting clinical errors. Findings were
consistent with the positive behavioral effect on the nurses' clinical errors with a p-value
of less than 0.05 (Seyedin, Ravaghi & Nikmaram, 2016). Jeong and Kim (2016) studied
knowledge and belief about hand hygiene among 208 nursing students and found 68.1%
correct response. The evaluation's focus was based on the TPB; the study concluded with
positive behavioral beliefs influenced by hand hygiene compliance (Jeong & Kim, 2016).
Orem’s self-care theory. Orem's self-care theory (2001) is another theory which
relates the patient and its environment, especially the nursing care. According to Whelan
(1984), this nursing intervention was crucial in supporting the patients' health. Analyzing
Orem's self-care model, the patient needs the nurses' intervention to sustain life and
maintain health (Whelan, 1984). Orem's self-care theory applies to the DPI project
because patients try to take care of themselves, and nurses were expected to intervene in
the patients' area of deficits.

25
Applying Orem's self-care theory, the nurses would determine the patients'
deficiencies in adherence to antihypertensive medication using the HB-MAS. Then the
nurses applied the intervention with Million Hearts education to remove the patients'
deficits. The nurses followed-up with the patients, using weekly telephone calls to obtain
the data on the number of times the patients took, or did not take, the antihypertensive
medications. Following Orem's theory, the nurses would continue helping the patients
until they arrive at their highest medication adherence level. Hosseinzadeh et al. (2019)
studied the dietary salt consumption of 250 hypertensive patients and applied Orem's
self-care theory. The study was based on the patients' capability and deficiency of self-
care, while the nurses used education for the intervention, with a resultant patients'
reduction of dietary salt consumption (Hosseinzadeh et al., 2019).
Review of the Literature
The literature review was divided into three major themes: medication non-
adherence, uncontrolled hypertension, and medication adherence (MA) strategies. Each
theme was further divided into subthemes, and they were discussed in the review of the
literature. Search engines used in collecting the literature were the Cumulative Index of
Nursing and Allied Health Literature (CINAHL), Cochrane, and Google Scholar. Search
terms used were HTN, medication adherence, heart health education, HB-MAS, and
peer-reviewed articles. More than 85% of the literature sources were published in the last
five years. MA will be examined in line with HTN. The aim is to synthesize HTN, what
constitutes uncontrolled HTN, and how medication non-adherence is related to
uncontrolled HTN. The next part examines the strategies, including the interventions and
pharmacological methods, to control HTN and sustain adherence to antihypertensive

26
medications. This DPI project used Million Hearts education to teach the patients about
their disease and its relationship with MA.
Medication non-adherence. The first theme of the DPI project is medication
non-adherence. The literature will define and review MA with particular reference to
HTN medications. Non-adherence to medications is prevalent in people with chronic
diseases, especially cardiovascular disease, and is associated with an increased risk of
hospitalization and mortality (Mekonnen & Gelayee, 2020). In chronic conditions,
patients tend to be on many medications for their symptoms, which also affects MA
(Walsh, Bennett, Wallace, & Cahir, 2020). Patients might not have full knowledge of all
the medicines prescribed to them. Meckonnen and Gelayee (2020) found the patients'
understanding of their medications, such as the purpose, dosage, and side effects, can
influence their MA.
First Kilic and Dag (2020) presented descriptive cross-sectional research on the
relationship between health literacy and medication adherence among patients with HTN
and related this to chronic diseases. HTN is a chronic disease, and low health literacy
affects the control of HTN (Firat Kilic & Dag, 2020). HTN is the leading cause of
cardiovascular disease, and older adults are more likely to experience medication non-
adherence (Etebari, Pezeshki, & Fakour, 2019). Besides, Firat Kilic and Dag (2020)
described other effects to prevent MA, especially the health knowledge deficit of the
clinician's medications. The question was whether there is a relationship between health
literacy and MA in HTN. A descriptive cross-sectional study comprised of 101 adult
people suffering from HTN who attended outpatient clinics were studied using Adult
Health Literacy Scale (AHLS) with 23 items (First et al., 2020). These authors found that

27
patients with low numbers of years for their diseases had higher AHLS, and poor AHLS
was associated with HTN and subsequent medication non-adherence. In this study, 57.4%
of the population had HTN for about ten years. The study identified the use of one center
for the research as a limitation. For future studies, the researchers recommended a more
prominent center for a larger population.
Khayyat et al. (2019) presented their research of the association between MA and
quality of life (QOL) among patients with HTN and diabetes (DM). Chronic conditions,
such as HTN and DM, are health conditions and can challenge QOL and subsequent MA
(Khayyat et al., 2019). The researchers studied 300 adult patients with chronic conditions
of HTN and DM. A cross-sectional study from five primary care clinics was selected, and
Morisky Medication Adherence Scale (MMAS-8) and World Health Organization
Quality of Life -BREF (WHOQOL-BREF) questionnaires were applied for data
collection. The study was conducted in line with this DPI project because it would also
use a questionnaire. Khayyat et al. (2019) concluded that females had lower QOL and
poor MA than males, and patients with low education experienced poor MA, considering
their covariates of physical, psychological, social, and environmental factors. There was
no mention of the actual numbers of males or females. The study's limitation was the
questionnaires were self-reported, which could have reduced the survey's accuracy.
Wahyuni et al. (2019) studied adherence to antihypertensive medication among
80 patients in primary care located in Medan city. These researchers defined HTN as a
significant health problem for senior citizens. Antihypertensive medication is the
treatment of choice for controlling HTN in this age group, but it is ineffective without
adherence to the prescribed medications (Wahyuni et al., 2019). The study's purpose was

28
to show the relationship between the knowledge of HTN, attitude towards treatment, and
effective communication of medication adherence by the clinicians. Wahyuni et al.
(2019) used a cross-sectional analytic methodology and studied 80 randomly selected
hypertensive patients on antihypertensive medication. Data collection was by
questionnaire. The research findings showed 76.3% had insufficient knowledge of MA,
73.8% had negative attitudes toward MA, while 56.3% were adherent to antihypertensive
medication due to good communication with clinicians (Wahyuni et al., 2019).
Non-adherence to antihypertensive medication was studied by Nielsen, Shrestha,
Neupane, and Kallestrip (2017), and the aim was to review the relationship between
medication adherence, antihypertensive drugs, and income status. The methodology was
a review of articles using the Meta-analysis of Observational Studies in Epidemiology
Guideline (MOOSE). The research covered 22 low- and middle- income countries such
as South Asia, Arab, and sub-Saharan countries (Nielsen et al., 2017). The researchers
found that non-adherence was worse in low-income countries, which Nielsen et al. (2017)
attributed the non-adherence to lack of health care resources and affordability, which led
to poor quality of life in the population. The researchers also identified the limitation of
the search process, which did not cover non-English speaking countries. There was
minimum selection bias by including the population from a structured community setting
with MA. Another limitation is the varying sample sizes, two of which were large, which
impacted the result (Nielsen et al., 2017).
In synthesis for medication non-adherence, the literature reviewed showed
medication non-adherence is a public health problem, especially in HTN. The adverse
effects of non-adherence to antihypertensive medications led to stroke and other

29
cardiovascular diseases. Hence, patients need to be very involved in their care. While
Nielsen et al. (2017) attributed low income and affordability to the cause of non-
adherence to antihypertensive medication, knowledge deficit of the patients and poor
knowledge of the dosage, side effects, and purpose of their medications also influence
their medication adherence (Wahyuni et al., 2019; Meckonnen & Gelayee, 2020). Only
about 158 (39.3%) of the population were adherent to antihypertensive medications, had
good knowledge of medications, and were associated with higher adherence (Meckonnen
& Gelayee, 2020).
Patient and provider communication of non-adherence. The first subtheme for
medication non-adherence is patient and provider communication. HTN is a chronic
disease, requiring interaction between the patient and the health provider to incorporate
diet and lifestyle modifications such as physical activity and stress control (Ruiz-
Fernandez, Marcos-Jorquera, Gilart-Iglesias, Vives-Boix, & Ramirez-Navarro, 2017).
Patients' attitudes towards the disease and understanding the relationship with the
medications play a significant role in MA. Ruiz-Fernandez et al. (2017) presented their
research on the empowerment of patients with HTN. The researchers described that many
patients tend to forget to take their BP medication, and some deny their diagnosis of
HTN. Patients' poor understanding of HTN leads to ineffective treatment and subsequent
health care costs (Ruiz-Fernandez et al., 2017).
The study of Zullig et al. (2015) described the patient's communication with the
provider regarding questions during office visits and explored medication adherence
status in terms of the patient's race. A cross-sectional analysis of the patients was
conducted. The study's purpose included the improvement of post-myocardial infarction
30
management of risk factors of cardiovascular disease (Zullig et al., 2015). The
researchers found that of the 298 (74%) patients who had all their questions answered by
their provider, 183 were adherent to their medications, while 115 patients were non-
adherent to their medications. Both groups admitted that their provider answered all their
questions. Results on racial communication were not completely clarified based on some
differences in adherence and would require further evaluation (Zullig et al., 2015).
Nafradi et al. (2016), in their quantitative study on intentional and unintentional
medication non-adherence in HTN, provided an example of the importance of effective
communication between patients and their healthcare providers to improve medication
adherence in HTN. Non-adherence to antihypertensive medication, whether intentional or
unintentional, is a significant public health problem and predisposes patients to
uncontrolled HTN (Nafradi et al., 2016). This study aimed to determine the patients'
motives for their non-adherence to antihypertensive medication. The researchers studied
109 patients who were on one or more medicines for their HTN. A cross-sectional design
and quantitative method were used in analyzing the patients' characteristics for 13
months, such as their concept of medication adherence and following their providers'
advice. A face-to-face questionnaire was used to obtain demographic data. The research
applied functional health literacy measurement and statistical analysis. The researchers
found medication non-adherence among patients who had less belief in their providers
and concluded that health care providers' communication of patients' concerns regarding
their medication is significant in their patients' adherence to antihypertensive medication
(Nafradi et al., 2016).
31
The study of Schoenthaler et al. (2016) explored MA in Blacks with HTN and
addressed the prediction variables, such as patient-provider communication. Historically,
complications of HTN arising from uncontrolled HTN, which mainly results from non-
adherence to treatment, is significantly higher among blacks than whites (Nguyen-Huynh,
Young, Alexeeff, Hatfield, & Sidney, 2019). The researchers studied the MA of 815
black patients with uncontrolled HTN over 12 months with HTN education interventions,
home BP monitoring, and monthly counseling on lifestyle (Schoenthaler et al., 2016).
The purpose of the counseling was to evaluate the multilevel intervention to improve
HTN among blacks by involving the patient-provider interactions. As perceived by the
patients and the providers' encouragement to the patients, the providers' communication
quality was assessed at baseline, at six months, and at 12 months using the Likert-type
scale. The study's findings showed that self-efficacy is associated with the quality of
patient-provider communication and improvement in MA (Schoenthaler et al., 2016).
In synthesis, while MA has many foci, patients' role of active involvement can
reduce non-adherence. With a poor understanding of HTN, patients will not pay much
attention to remembering to take their antihypertensive medication. Effective
communication between the patients and their healthcare providers can enhance the
patients' understanding and enable them to take responsibility for their care. This led to
183 patients' adherence to antihypertensive medications when all their questions were
addressed, and they had a better rapport with their PCPs (Zullig et al., 2015). Nafradi et
al. (2016) agreed with the importance of effective communication between the patients
and their healthcare providers to improve medication adherence in HTN.

32
Barriers to MA. The second subtheme to medication non-adherence is the MA
barrier that focuses on anything or condition preventing effective treatment to HTN to
achieve MA, including pregnancy (Webster et al., 2018). Lack of financial support for
the patient is a barrier to medication adherence because the patient might not be able to
afford their medication (Mamaghani, Hasanpoor, Maghsoodi, & Soleimani, 2020).
Mamghani et al. (2020) also reported that living in rural areas can be a barrier, since the
patients cannot quickly get their medications, considering accessibility to their PCPs and
their nearest pharmacy. Data were expressed in percentages only. Using a cross-sectional
design, Mamaghani et al. (2020) studied 238 hypertensive patients in five different areas.
Data analysis with SPSS, showing 18% of the patients had low MA, 43.6% had medium
MA, and 38.2% had good MA.
Najimi, Mostafavi, Sharifirad, and Golshiri (2018) studied the barriers to MA in
patients with HTN using a qualitative method to identify the obstacles. Considering that
pharmacotherapy is one of the best and most common means of controlling HTN to
prevent its risks of coronary artery disease (CAD) (by 20% to 30%, and stroke by 35% to
40%), this study aimed to identify and prevent any barriers to MA (Najimi et al., 2018).
Semi-structured interviews were used to collect the purposive sampling of 60
hypertensive patients from the clinic. Najimi et al. (2018) concluded that the patients'
lifestyle, forgetting to take their antihypertensive medications, and lack of advice from
the healthcare professionals were significant barriers to non-adherence to drugs. The
results were put into codes, not numbers. The researchers identified the patients' low
socioeconomic status and the method of selection of the participants as limitations to the
study, and the identified barriers as prospective research materials to improve MA.

33
Another study for identifying a barrier to MA was the qualitative exploration of
perception towards antihypertensive medication. Tan, Hassali, Neoh, and Saleem (2017)
purposively recruited and studied 17 hypertensive patients and their perception of
medication quality using semi-structured interviews with a phenomenological approach.
Realizing the poor adherence to antihypertensive medications, which would lead to poor
quality outcomes of care and increased costs with associated products and increased
utilization of resources, the study evolved in order to remove the barriers (Tan et al.,
2017). The study resulted in the development of positive investigations to overcome
barriers to antihypertensive medication adherence. The researchers concluded that poor
antihypertensive medication adherence was a misconception of the medication side
effects and lack of knowledge. A structured questionnaire was identified as a limitation to
the method of data collection. Multiple languages were involved, and the researchers also
classified the participants' low socioeconomic status as limitations (Tan et al., 2017).
In a study of adherence to treatment among hypertensive patients,
Balasubramanian, Nair, Rakesh, and Leelamoni (2018) recruited 189 rural area
hypertensive patients. According to Balasubramanian et al. (2018), poor or non-
adherence to antihypertensive medication is a significant barrier to HTN control. The
study's purpose was to assess barriers by evaluating the adherence in India's rural area. A
cross-sectional study with a semi-structured questionnaire data collection was used to
study 189 hypertensive patients in Kerala. MA was assessed with MMAS-4 with 46% of
high MA, 41.3% of medium MA, and 12.7% of low MA. The findings from the study
showed poor MA to their antihypertensive medication. This is a barrier to HTN control,
and poor knowledge increases the risks of HTN; further, associated medication non-

34
adherence is a result of uncontrolled HTN (Balasubramanian et al., 2018). The
recommendation for the poor MA in the study is a comprehensive strategy for improving
antihypertensive medication. The only limitation reported by the researchers is the use of
the MMAS-4 scale with an un-validated language.
In synthesis, the articles discussed the identification and prevention of barriers to
MA. Identifying those usual ways of life is one aspect, but seeing them as barriers and
preventing or changing them could be challenging to patients because the patients may
not recognize them as barriers. Though identifying the barriers was from the patients'
perspectives, Tan et al. (2017) considered developing positive strategies as better options
to focus on the obstacles. Poor or non-adherence to antihypertensive medications is a
barrier to HTN control (Balasubramanian et al., 2018). Barriers to MA present in
different forms, but the endpoint is uncontrolled HTN. With barriers removed,
medication would be taken as prescribed, and HTN would be controlled.
Factors affecting medication adherence. The third subtheme for medication non-
adherence is the factors affecting MA. In a prior study, researchers identified HTN as a
public health problem that could be controlled with antihypertensive medication, and
non-adherence to the drugs led to uncontrolled HTN (Gebremichael, Berhe, &
Zemichael, 2019). Age and lack of awareness can contribute to MA, and older adults are
more affected by medication non-adherence (Jin, Kim, & Rhie, 2020). This is due to their
age-related conditions, such as the number of medications they are prescribed, dosing
frequency, understanding of the pharmacy's instructions, and the patients' satisfaction (Jin
et al., 2020).

35
Zhang et al. (2020) studied 1,916 community-managed randomly selected patients
with known HTN. A self-designed questionnaire was applied for a period of four months
for face-to-face demographic data collection. The findings of the research showed
comorbidities were associated with non-adherence to antihypertensive medications. In
contrast, the community-managed patients had reduced non-adherence, and the non-
adherence was directly related to uncontrolled HTN (Zhang et al., 2020). The researchers
reported the limitations of not having a control group for better comparison and identified
this as an opportunity for future study.
Another study links non-adherence to HTN by Mugwano et al. (2016). The
sample of the study drawn from stroke patients with HTN was evaluated. A cross-
sectional study was used in 112 patients who were over 60 years of age. Stroke, which is
a result of uncontrolled HTN, was noted to have claimed the lives of approximately 5.5
million people worldwide in 2001, out of about 15 million people had a stroke (Mugwano
et al., 2016). The research concluded that poor adherence to antihypertensive medication
is a significant problem, and lack of adequate knowledge has worsened the situation. Out
of the 112 participants, 78 (70%) had ischemic stroke secondary to lack of knowledge
(Mugwano et al., 2016).
Another factor related to non-adherence in antihypertensive medication is the
patients' knowledge towards medication, such as forgetfulness, socioeconomic status, and
general attitude towards drugs (Chetoui et al., 2016). Chetoui et al. (2016) studied CVD
patients. The purpose was to evaluate adherence to antihypertensive medications and
identify the cause of non-adherence among those patients aged 65 years old and above. In
a prior study, only 24% of the patients reached BP goal; but other findings of their study

36
revealed 93% of the sample had non-adherence to their antihypertensive medications, out
of which 44% was secondary to forgetting to take their medications, some stopped taking
the antihypertensive altogether, 15% found the medications too expensive (Chetoui et al.,
2016). These researchers concluded that adherence to antihypertensive drugs was poor
and identified the need for patient-healthcare provider communication to enhance
medication adherence (Chetoui et al., 2016). This was the gap which the DPI project was
aiming to close.
Pawloski et al. (2016) tried to identify patients' reasons for non-adherence to their
antihypertensive medications. Knowing of non-adherence in HTN is the precursor to
uncontrolled HTN, which predisposes to stroke, CVD, and renal failure. The researchers
studied the medication adherence of 240 patients in Minneapolis who were on home BP
telemonitoring. The study aimed to determine if home BP telemonitoring and HTN
medication management by pharmacists could improve medication adherence. The
pharmacy interventions consisted of the patients' medication inventories and prescription
refill history. Medication adherence was calculated at the beginning of the study and after
the twelve months of the intervention. The research findings did not show significant
improvement in antihypertensive medication adherence; there was maintenance of high
MA including at pre-intervention, and the researchers had no numerical data because
there was no significant difference between the pre-intervention and the post-intervention
(Pawloski et al. (2016).
In the synthesis of factors affecting MA, the article on community-managed
patients identified comorbidities as significant for non-adherence to antihypertensive
medication (Zhang et al., 2020). It is also noted that not every patient with a co-morbid

37
condition is non-adherent to their medications, but the literature did not signify the actual
number. One factor with comorbidity is that multiple medications are required to control
the other symptoms for other diseases. While these present as barriers to MA, there is a
correlation between non-adherence and medication affecting factors, but community
management of the patients improved MA (Zhang et al., 2020).
In summary, the researchers' commonality in this theme is the effect of non-
adherence to antihypertensive medications. While Carvalho and Santo (2020) considered
non-adherence to antihypertensive medications as being more prevalent in
underprivileged countries, Firat Kilic and Dag (2020) agreed and attributed it to their low
health literacy. All of the articles linked uncontrolled HTN to non-adherence to their
antihypertensive medications. Many patients, especially the older population, have
increased medication non-adherence (Khayyat et al. 2019). The researchers agree that
older people are on multiple medications due to their chronic conditions and poor life
quality. These, in addition to inadequate knowledge, influence medication non-
adherence.
Uncontrolled HTN. The second theme for this DPI project is uncontrolled
hypertension. HTN is a major risk factor for CVD, and the literature identified CVD
causes one in four deaths annually among all races in the United States and has claimed
about 200 billion dollars each year (Napiekowski & Prado, 2020). According to the ACC
and AHA guidelines, normal BP is a systolic BP (SBP) of equal to or less 120 mmHg and
diastolic BP (DBP) equal to or less than 80 mmHg. It is elevated if the SBP is up to 129
mmHg or DBP of 80 mmHg (Napiekowski & Prado, 2020). Any SBP of 130 mmHg or
greater or DBP of 80 or greater is regarded as HTN as amended parameters from 2017 by

38
ACC and AHA, to institute early treatment for HTN to prevent the complications of a
stroke, CVD, renal disease, and mortality (Napiekowski & Prado, 2020; ACC & AHA,
2017). SBP, which is greater than 180 mmHg or DBP greater than 120 mmHg, is
hypertensive urgency because target organ damage is eminent, thus meaning it is now
uncontrolled HTN and should be prevented (Napiekowski & Prado, 2020).
Associated factors. The first subtheme of uncontrolled HTN is the associated
factors. A challenging aspect of BP's treatment is uncontrolled HTN, considering the
related risks to CVD and target organs (Ghazali et al., 2020). Poorly controlled HTN still
exists despite many preventive measures, and lack of control is worse in the presence of
other comorbidities such as diabetes (Almalki et al., 2020). Obesity, behavioral factors
such as diet, physical activity, and other health conditions are associated with
uncontrolled HTN (Masilela, Pearce, Ongole, Adeniyi, & Benjeddou, 2020).
Ghazali et al. (2020) studied one of the factors to understand HTN and determine
the prevalence of uncontrolled HTN among patients who attended three primary care
clinics in a district in Malaysia. The study was comprised of 460 patients. A cross-
sectional method and structured modified questionnaires were used for data collection.
The patients' BP was based on the AHA definition of equal to or greater than 130/80
mmHg for HTN. In the study of 460 hypertensive patients, 249 of them, representing
54.1%, had controlled BP, while 211 patients, which represented 45.9% of the
population, showed a significantly high prevalence of uncontrolled HTN (Ghazali et al.,
2020). The researchers concluded other factors, such as diabetes, obesity, and the male
gender, were in combination with non-adherence to antihypertensive medications and
worsened the uncontrolled HTN.

39
In cross-sectional research by Tesfaye et al. (2020) at a teaching hospital, the
researchers studied 345 hypertensive patients for about four weeks, using a systematic
sampling technique. Data were collected with a face-to-face structured questionnaire and
chart review. The study aimed to determine the prevalence of uncontrolled HTN.
Analysis of the course was through the Statistical Package for the Social Sciences
(SPSS). Uncontrolled HTN was found in 52.7% of the patients, and these had significant
associated factors of knowledge deficit, cigarette smoking habit, alcohol consumption,
and obesity. The most significant predictor of uncontrolled HTN was the lack of
knowledge of hypertensive related complications (Tesfaye et al., 2020). There is a gap
created by these conditions, which fits into the DPI project. The limitation identified by
the researchers was concerning the self-reporting of the participants' lifestyle.
Nguyen-Huynh et al. (2019) did a pragmatic randomized controlled trial to
improve blood pressure control among blacks with persistent HTN. It was referred to as
the Shake Rattle and Roll (SRR) method. The purpose of the study was to determine
whether diet and lifestyle change, including enhanced monitoring, could improve HTN
among blacks over a 12-month period. The research sample was divided into three
groups: the control group who received the usual care (UC) from their primary care
provider (PCP), the enhanced monitoring patients who received their usual HTN
medication plus BP check visits, and the third group who received the enhanced
monitoring including telephone calls. The population comprised 31 to 34 PCPs, and three
groups of patients. One group consisted of 1,129, patients, the second group was 349
people, and the third group was 286 patients. The researchers reported positive results
among the patients who participated in blood pressure monitoring, but the other patients

40
remained in uncontrolled HTN because they did not partake in routine BP monitoring. In
this study, the researchers identified a possible bias in selecting the sample, and related it
to no consent required from the control group (Nguyen-Huynh et al., 2019).
Saradamma, Kottarath, Saleem, Jaya, and Thaj (2019) conducted a cross-sectional
study of 300 patients aged 18 years and above. The researchers were concerned about
persistent uncontrolled HTN despite the patients' intake of their antihypertensive
medications. The aim of the study was to determine the prevalence of uncontrolled HTN
and identify any associated contributory risk factors. The literature reviewed that HTN is
a non-communicable disease with high morbidity and mortality, and such diseases are
responsible for 60% of all deaths (Saradamma et al., 2019). Data were obtained by a
structured questionnaire on lifestyle, diet, and stress levels. Findings from the research
showed 68.3% uncontrolled HTN despite antihypertensive treatments. The findings were
associated with a sedentary lifestyle, alcoholism, psychological stress, comorbidities such
as diabetes, and family history of HTN (Saradamma et al., 2019). The researchers did not
specifically mention their study limitations but had recommendations of lifestyle
modifications and close monitoring of BP by healthcare providers.
Woodhama, Taneepanichskul, Somrongthong, and Auamkul (2018) identified
another associated factor in medication adherence among elderly hypertensive patients.
The objective was to assess antihypertensive medication adherence. The researchers
studied 408 hypertensive patients, aged 60 to 79 years old, selected by random sampling.
Data collection was by structured questionnaire, and the medication adherence was by
pill count. The research findings showed 86.8% of the patients had poor adherence to
their antihypertensive medications. With the addition of a family member as a caretaker,

41
which is also the associated factor, adherence to their antihypertensive medication
improved about eight times higher than their normal rate (Woodhama et al., 2018).
Hence, family involvement in elderly patients' care is significant in adherence to their
antihypertensive medications.
While lack of understanding of HTN is a factor in uncontrolled HTN, it is
supported by the study, which showed only 249 (54.1%) of controlled BP, while 211
(45.9%) had uncontrolled HTN (Ghazali et al., 2020). In another study, uncontrolled BP
is a little more than 50% of the population; 52.7% of the patients in the article have
uncontrolled HTN, including associated factors (Tesfaye et al., 2020). HTN was
uncontrolled for personal reasons, but they were all similar, such as lifestyle, lack of
knowledge, and other risk factors (Saradamma et al., 2019; Nguyen-Huynh et al., 2019).
Patient-clinician communication. The second subtheme for uncontrolled HTN is
the patient and clinician communication, which focused on improving HTN control and
fostering MA. Provider-patient communication intervention includes any factor which
prevents patients from adhering to their medications and other BP control regimen. By so
doing, the patients can discuss any problem that could hinder medication adherence.
Many strategies can improve adherence to antihypertensive medications when the
provider engages a face-to-face discussion about the medicines (Millions Hearts/CDC,
2016).
Robbins, Butler, and Schoenthaler (2019) addressed patient education and
counseling, especially in HTN care. The researchers identified some signs of burnout,
such as low job satisfaction, depressive look, and stress among participants. They
remarked that 25% to 65% of healthcare workers experience burnout (Robbins et al.,

42
2019). This research aimed to examine the relationship between provider burnout and
patient-provider communication and outcome of care in HTN. A cross-sectional method
was used, and the participants were 26 primary care providers (PCPs) and 80
hypertensive patients, about 61 years old. Care visits were recorded, followed by the
providers' surveys. The research findings supported the objective that provider burnout
could impact HTN with the decreased quality outcome (Robbins et al., 2018). The
limitation is the method of sampling of the participants, as reported by the researchers.
In a study by Tavakoly Sany et al. (2018), a randomized controlled method to
study the effect on HTN outcome was used. Hypertension is a worldwide public health
problem with an increased risk of stroke, heart disease, mortality, and morbidity
(Tavakoly Sany et al., 2018). The aim of the research was to improve HTN outcomes
using educational communications skills training among patients and their healthcare
providers. The study consisted of 35 healthcare providers and 240 hypertensive patients
for 12 months. The pre/post-intervention analysis showed a significant improvement in
their communication skills, antihypertensive medication adherence, and subsequent HTN
outcomes. Poor communication skills predispose the patients to uncontrolled HTN
because of a lack of trust and understanding of their health care providers. The
researchers concluded that the health care providers' communication skills training
improved patient-provider communication skills (Tavakoly Sany et al., 2018).
Another patient-clinician communication affecting the control of HTN is the
approach to understanding the medication dialogue in patients and provider relationships
(Schoenthaler, Basile, West, & Kalet, 2018). The study aimed to describe the
communication between the PCPs and their hypertensive patients regarding their

43
medications. Effective communication between the patient and the PCP is significant in
the accurate understanding of the patient's health condition and appropriate rapport,
supporting the quality outcome of care (Schoenthaler et al., 2018). The research by these
authors was a qualitative observational study from three ambulatory care settings. The
samples were 29 providers and 94 hypertensive patients, and their conversations were
audiotaped. The study result provided a clearer understanding of the patients' other
concerns, such as non-adherence to medications and interactive communication between
them and the provider. Similarly, non-effective patient-provider contact could produce an
adverse patient outcome, which results in uncontrolled HTN secondary to medication
non-adherence (Schoenthaler et al., 2018). The limitations were the use of low-income
patients, one-time patient-provider communication, and audiotapes for data collection.
Ibe and colleagues (2017) discussed their qualitative analysis, examined
community health workers' (CHW) intervention on 140 low-socioeconomic hypertensive
patients. This study aimed to investigate the effect of CHW communication on low-
income HTN patients. The randomized controlled method used coaching times by the
CHWs during the patients' office visit communication. The study's findings sought a
positive answer to the CHWs' communication activation intervention (Ibe et al., 2017).
The researchers recommended more research on CHWs intervention.
Another study on patient-clinician communication was by Brenk-Franz et al.
(2017). The aim of the study was to determine the relationship between adult attachment
and self-management and evaluate the effect of the patient-provider relationship. From
the literature review, self-management is vital in patients with chronic diseases, of which
HTN is one (Brenk-Franz et al., 2017). This study sampled 209 patients aged 50 years to

44
85 years with chronic diseases of HTN, diabetes, and other chronic diseases. The adult
attachment was measured with a self-rating questionnaire, while the resources and self-
management were measured with a self-management questionnaire. The Patient Reaction
Assessment (PRA) was used in calculating the patient-provider relationship as perceived
by the patient, and a seven-point Likert scale was applied for the data. Following
statistical analysis, the research findings showed high communication of the patients with
their healthcare providers about their illness and treatment, a developed rapport between
physicians and patients, physicians receiving patients' questions, and better self-
management for the quality outcome of care (Brenk-Franz et al., 2017). This is consistent
with the care of HTN, which is a chronic disease and can be controlled with effective
communication with the PCP when they explain medication side effects and self-
management, which, if unattended, will predispose to uncontrolled HTN.
In synthesizing the patient-clinician communication subtheme, it was noted that in
communicating necessary educational materials and counseling patients, the healthcare
provider attempts to encourage the patients to normal HTN. However, the providers'
burnout is a common problem, but there has to be a cause (Robbins et al., 2019).
According to Robbins et al. (2018), providers' poor communication can be due to
burnout. In the presence of frustration, which leads to burnout, effective HTN, or MA
information could be limited (Robbins et al., 2018). Though patient-clinician
communication is meant to improve education for positive outcomes, Tavakoyl Sany et
al. (2018) reviewed that poor communication predisposes uncontrolled HTN and lack of
trust.
45
Disparities in HTN. The third subtheme for uncontrolled HTN is a disparity in
HTN, and it can affect HTN control. Al Kibria (2019) identified discrepancies in HTN
following the 2017 guidelines of the ACC/AHA. The researcher found the disparity in the
prevalence, treatment, and control of HTN among races, advancing age, genders, body
weights, and socioeconomic statuses. There is also disparity among populations with
specific diseases such as diabetes (Al Kibria, 2019). Despite the necessity of medication
adherence to prevent uncontrolled HTN, other conditions and disparities affect the care
and sustainability of controlled HTN (Cooper et al., 2020). Cooper et al. (2020) identified
a program that would reduce HTN care disparities by improving patients' lifestyles,
considering that reducing inequalities in HTN care would provide equal opportunities for
receiving comparable treatments to control HTN.
Similarly, the study of Song et al. (2019) explored the prevalence of risk factors
of HTN among the elderly with particular reference to China. It addressed the disparity in
their urban-rural area. According to the researchers, 27.8% of Chinese adults have HTN,
and they identified as being higher among men than women in both urban and rural areas.
The sample population comprised a stratified selection of hypertensive patients whose
data were extracted from the China Health and Retirement Longitudinal Study
(CHARLS) of 2015 (Song et al., 2019). In the study, the researchers interviewed 21,097
patients and analyzed 1,776 people for the survey, including a questionnaire about their
lifestyle, demographics and checking their BPs. The research findings were consistent
with the high prevalence of HTN among the elderly in China, which also appeared about
the same prevalence in urban and rural patients but associated with different risk factors
such as diabetes (Song et al., 2019). The disparity gap created with regards to the lifestyle

46
and risk factors can be implemented into the interventions for obesity and stress-related
health problems to improve HTN in elderly patients.
Another aspect of disparity that affects HTN care is socioeconomic status. East et
al.'s (2020) study is an example of the importance of reducing differences to prevent or
plan intervention for HTN. The purpose of the article, childhood socioeconomic hardship,
was to explain how the effects of early adversity can result in adverse health problems,
such as HTN (East et al., 2020). The samples were children from low-socioeconomic
families who were obese, which resulted in a large selection of 1,039 people. The
researchers used a questionnaire to obtain more data from older children in the study on
family conflict, financial strain, anxiety, and depression. The research findings showed
higher stress levels related to the family's socioeconomic hardship and disputes as they
were growing up. These were associated with the development of HTN in early life. East
et al. (2020) further explained that children of low socioeconomic families suffer HTN in
their early adulthood; 11% had elevated BP, while 15% had HTN. Considering these risk
factors, interventions to prevent or reduce the socioeconomic disparity will impact
control of HTN (East et al., 2020).
Though uncontrolled HTN is a universal problem, ethnic disparities are
significant among hypertensive patients; and Prendergast et al. (2018), in the literature,
reviewed that uncontrolled HTN is more prevalent among Hispanics and Blacks at 52.6%
and 51.5%, respectively. Prendergast et al. (2018) developed a randomized clinical trial
to discover how to decrease disparities among these populations. Since patients from
high-risk people, minorities, and had low socioeconomic status use the emergency
department as their primary care clinics, especially as most of them have no health
47
insurance and have uncontrolled HTN, a HTN Emergency Department Intervention
Aimed at Decreasing Disparities (AHEAD2) trial was developed. AHEAD2 aimed to
control patients' BP to prevent complications of CVD and then refer the patients for a
focused HTN treatment. Being an emergency department (ED), there was no particular
number of recruitment. However, the annual number of patients was about 46,000, out of
which 80% were adults. The study showed a positive quality outcome of reduced
disparities due to providing intensified care with subsequent HTN control. (Prendergast et
al., 2018).
In synthesis, while disparities exist in many aspects of healthcare, the article on
China and HTN discussed disparity and other associated risk factors. According to Song
et al. (2019), HTN is higher among men than women in rural areas; the prevalence of
HTN is higher among the elderly population. The trend is most likely due to the patients'
age-related comorbidities, lifestyles, and socioeconomic factors.
In summary, uncontrolled HTN is broadly the result of non-adherence to
antihypertensive medication. According to this literature on disparity, many factors such
as patients' lifestyle, diet, obesity, and stress lead to uncontrolled HTN, causing high
morbidity and mortality (Saradamma et al., 2019). The researchers, Saradamma et al
(2019) identified a mortality of 60% of all deaths associated with uncontrolled HTN. The
significant contributor to uncontrolled HTN is non-adherence to antihypertensive
medication. An associated factor such as family member as a caretaker for the elderly
hypertensive patient improves medication adherence at a rate of about eight times higher
than normal (Woodhama et al., 2018).
48
A lack of education on HTN and its associative factors account for a substantial
part of the disease and the HTN improvement with patient-provider relationship (Brenk-
Franz et al., 2017; Schoenthaler et al., 2018). Communication between the patient and the
provider makes a lot of difference in their BP control. For instance, a face-to-face
discussion about the medicines improves the adherence to antihypertensive medications
(Million Hearts/CDC, 2016). With effective communication, the patient develops a
rapport and trust with the healthcare provider, leading to the patient’s acceptance of the
clinician’s advice. Poor communication could lead to distrust and non-adherence to
antihypertensive medications. The disparity is another problem affecting the control of
HTN but identified the improvement of patients’ disparities, such as lifestyles, as
contributory to hypertensive care (Song et al., 2019; Cooper et al., 2020).
Strategies for medication adherence (MA). The third theme for this DPI project
is the MA strategies, which focus on the various ways to achieve and sustain MA. The
subthemes are (a) patient education, (b) facilitators, and (c) sustainability. MA is the
capacity of taking the medications as prescribed by the healthcare provider for a health
condition (Bou Serhal et al., 2018). Though many factors such as cost, proximity to care,
and SES affect adherence to antihypertensive medications, forgetting to take the
medicines is more common among elderly patients (Abbas et al., 2020). With time, HTN
becomes uncontrolled. Non-adherence to antihypertensive medication can be decreased,
but it requires the cooperation of patients and healthcare providers (Nafradi et al., 2016).
This has led to the development of strategies to maintain MA in HTN. The patient
education strategy will improve knowledge of HTN, the effect of antihypertensive
medication, and lead facilitators to remind the patients to take their medications as

49
prescribed and increase outpatient monitoring to ensure the sustainability of MA to
prevent a relapse of uncontrolled HTN.
Patient education. The first subtheme for strategies to MA is patient education.
Patients' knowledge deficit is a problem because they need to understand the concept of
HTN, the effect of medications in controlling HTN, and the importance of continued
sustainability MA for a maximum quality outcome. Miranda et al. (2019) discussed the
cost-related medication underuse (CRMU), which patients need to understand, and made
recommendations to the problem. As a stepwise process, the problem was diagnosed, and
the solution was a collaborative effort between the patient, the health care provider, and
the patients' pharmacy. Patients in CRMU do not take their medications as prescribed,
skipping some days to make it last longer and substituting another less expensive
medicine for the antihypertensive medications despite their regular prescription (Miranda
et al., 2019). Considering the high cost of hospitalization and CVD treatment, these
researchers recommended the treatment strategy to improve MA to be education and
medication available to the patients through pharmacists.
Delavar, Pashaeypoor, and Negarandeh (2020) performed a randomized
controlled trial to evaluate the patients and determine if self-management education could
improve MA and impact BP control. Participants included 118 uncontrolled hypertensive
older adults with inadequate health knowledge were surveyed using the Morisky
Medication Adherence Scale (MMAS-8). Their MA and BP were assessed. The
intervention focused on the educational materials about HTN, its risk factors,
complications, and antihypertensive medications. The study results showed after the

50
intervention, the rate of medication adherence improved and were statistically significant,
with a p-value of less than 0.05 among the intervention groups (Delavar et al., 2020).
Ampofo, Khan, and Ibitoye (2020) did a systematic search that examined prior
studies to determine if educational interventions could improve MA among hypertensive
patients. The investigation used reliable databases such as CINHAL and PUBMED, and
they followed the Cochrane guidelines for systematic reviews (Ampofo et al., 2020). Per
Cochrane guidelines, the review was reported according to the Preferred Reporting Items
for Systematic Review and Meta-analysis (PRISMA). The period of data collection was
from 1999 to 2019. The review findings were consistent with some improvement to
health literacy and adherence to antihypertensive medications following the educational
intervention. However, an additional frequent verbal educational intervention could
increase MA's improvement among hypertensive patients (Ampofo et al., 2020).
In a cross-sectional study by Pan et al. (2020), the research aimed to assess the
patients' knowledge of HTN and MA. The study's purpose was to determine if post-
hospital discharged patients have experience of HTN and its risk factors associated with
MA among HTN and stroke patients. There were 440 patients surveyed after their
discharge from the tertiary hospital. Data collection was by telephone interviews and
medical records. The research findings showed that only 35.23% of the patients had
adherence to their antihypertensive medication. The researchers concluded that
hypertensive stroke patients' MA was poor; their knowledge of HTN was below standard
and recommended more strategies to improve the experience, which could subsequently
impact MA.

51
Another study to support strategies to MA by Cheema, Sutcliffe, Weickert, and
Singer (2018) was a randomized control trial conducted for five months. The study's
purpose was to determine if structured written and verbal education would improve
patients' knowledge of HTN and improve BP control. The study included 64 adult
patients, and the assessment was with a questionnaire at intervals of two weeks, four
weeks, and six weeks. The intervention was the structured written and verbal education
on HTN delivered by the community pharmacists. The research results showed an initial
decrease in systolic BP during the four-week follow-up visit and did not sustain any
further reduction during the 26 weeks follow up visit. Knowledge about HTN and its side
effects improved initially and maintained even at 26 weeks’ visit. In conclusion, this
randomized controlled study by Cheema et al. (2018) showed the intervention improved
the patients' knowledge about HTN but did not improve the patients' BP.
The research article by Escortell-Mayor et al. (2020) was a pragmatic cluster-
randomized study of 411 uncontrolled hypertensive patients recruited from 22 primary
care centers. Multilevel logistic regression was used for the analysis of the data. The
study's purpose was to determine if a strategy for communicating cardiovascular risk
factors to patients could impact their BP control over 12 months. The patients had no
prior knowledge of cardiovascular risks. Following the intervention period, the research
findings showed the BP of the intervention participants improved.
In synthesizing patient education, the cost-related medication underuse (CRMU)
is apparent, affecting patients and public health but could be remedied with knowledge
(Mirander et al., 2019). Patients with CRMU lack the understanding that antihypertensive
medication cannot be taken as needed because HTN is a chronic disease, and medications

52
should be taken as prescribed to control BP and sustain MA regardless of cost properly.
Delavar et al. (2020) agreed to the importance of educating the patients to decrease BP,
manage HTN, and improve MA. Most literature on education-based interventions
enhanced knowledge of the patients' BP and medication, resulting in HTN control and
medication adherence sustainability.
Facilitators. The second subtheme to MA strategies is facilitators. These
strategies support the MA. Reminder tools, such as cell phones, reminder cards,
pillboxes, and direct supervision, facilitate MA. Dillon, McDowell, Smith, Gallaher, and
Cousins (2019) surveyed and analyzed 258 online responses. The study aimed to
determine if adherence intervention from the pharmacist could facilitate adherence to
antihypertensive medications. The research survey found that pharmacy interventions
facilitated the patients' adherence to their antihypertensive medications.
Researchers identified that medication reminders and refill reminders, including
implementation of education to increase the patients' knowledge about HTN, can impact
BP control (Abbas et al., 2020). Evidence structured telephone technology for setting
alarms is a telephone reminder tool, and Morrissey, Casey, Glynn, Walsh, and Molloy
(2020) studied smartphone application for improving MA in HTN. The researchers used
an exploratory study of 24 patients with HTN, aged 50 years to 85 years old, and
explored their smartphone apps' perspectives. The smart phone apps reminded the
patients to take their BP medications and to check their BP too (Morrissey et al., 2020).
The purpose of the study was to explore the patient's smartphones using their smartphone
apps. The research found that many of the patients felt more comfortable using the apps
in monitoring their BP and felt concerned about the use of the apps for their medications

53
(Morrissey et al., 2020). These researchers reported a limitation of using very few
samples for the study. Large samples produce more accuracy with a low margin of error
because a large sample study is highly statistically significant (Khalilzadeh & Tasci,
2017).
Cimmaruta et al. (2018) performed a literature review of prior studies that
described the poly-pill strategy for blood pressure and medication adherence. The
researchers used principal observational and clinical trial data to evaluate MA in HTN in
the association of CVD risk factors. The literature review showed the poly-pill method, in
all circumstances, increased adherence to antihypertensive medication and CVD. Poly-
pill is safe and positively affects HTN and co-morbidities (Cimmaruta et al., 2018).
Abel, Jayner, Cornelius (2020) performed a qualitative descriptive design in the
study of 20 black women. The aim of the study was to describe the women's reported
self-care strategies for consistent antihypertensive MA and determine their lifestyle. The
audiotape was used for data collection, and the Hill-Bone Compliance Scale for high BP
(HB-MAS) was used for screening for inclusion criteria. The research results were not
clearly stated, but the researchers predicted adherence to their participants'
antihypertensive medications based on their self-care management strategies. This study
is recommended for further research (Abel et al., 2020).
Another facilitator to remind patients about their medications was proposed in
Maslakpak and Safaie's (2016) study. The study was comprised of 123 hypertensive
patients at a clinical education center. This study was a randomized controlled clinical
trial, and the aim was to compare the antihypertensive MA between short message
service (SMS) and reminder cards. The intervention consisted of weekly six text

54
messages for three months, while the other group of patients received training on how to
use the reminder cards. The patients' MA was tested with the Hill-Bone Medication
Adherence Scale. The research findings showed both interventions with SMS, and
reminder cards were consistent with the promotion of MA among the patients
(Maslakpak & Safaie, 2016).
In synthesis, some articles are in agreement that medication reminders are
effective strategies for MA. The choice of the reminder is dependent upon the need of the
patients. Abba et al. (2020) suggested using multiple reminders, including some
education implementation, to increase knowledge of HTN and improve MA. According
to Morrissey et al. (2020), smartphone applications are medication reminders but seem to
complicate some patients. The participants in their study used the applications mainly for
monitoring their BPs and not for their medications because they were not comfortable
using them (Morrissey et al., 2020).
Outpatient monitoring for sustainability. The third subtheme of strategies to MA
is outpatient monitoring for sustainability. In one study, patients were considered to be
adherent to their medications if they took 80% or more of their prescribed medication
days (Nguyen-Huynk et al., 2019). Outpatient assessment and monitoring of
antihypertensive MA can impact sustainability and prevent HTN treatment resistance
(Eskas et al., 2016). Eskas et al. (2016) identified direct and indirect methods of
monitoring antihypertensive medications. Self-reporting and pill count were regarded as
indirect methods, while witnessed intake and serum or urine sample analysis were direct
methods of monitoring MA (Eskas et al., 2016).

55
One of the supporting strategies to MA is sustainability to prevent treatment
resistance. McGillicuddy et al. (2015) contracted 18 patients in a retrospective analysis to
determine MA's sustainability and controlled BP using their medical records. The
monitoring was at three months, six months, and 12 months intervals for BP and
medication taking. The research results showed a reduction in BP of the patients. The
study results also provided an example of the sustainability of MA in HTN. The authors
concluded that the interventions had a sustainable impact on MA and BP. After 12
months of the study, their BP remained controlled.
Shen et al. (2017) randomly enrolled 266 and 288 patients for intervention and
control groups, respectively, from the disease surveillance system. The study was
registered through the Chinese Clinical Trial Register. The study aimed to evaluate and
determine if family member-based supervision could impact BP control and sustain MA
over 12 months. The interventions were education on HTN and its risk factors,
supervision on the patients' MA, checking of their BP, and reminders to seek clinicians'
help with BP changes. The education tool was the use of short messages service (SMS) to
give health information. Data collection was by questionnaire and statistically analyzed at
six months and 12 months. The results showed a significant decrease in BP for the
intervention group during the six-month follow-up visit but not at the 12 months visit
(Shen et al., 2017). The researchers further reported at follow up visits that 32 patients of
the control had HTN complications, including six deaths, while 26 of the intervention
group developed complications. In conclusion, family member-based supervision could
impact HTN control and sustainable MA if there is consistent supervision.

56
Conn, Ruppar, Chase, Enriquez, and Cooper (2015) performed a systematic
review and meta-analysis to synthesize MA with a focus on interventions for sustaining
MA in HTN. The sample and other data were coded, which was what they used for
measuring. Data search employed a reliable database following PRISMA guidelines.
There were 112 treatments which were compared with the control group outcome. The
interventions comprised the factors that enhance adherence, including the patients'
feedback, using pillboxes, and self-monitoring their BPs (Conn et al., 2015). Analysis of
the intervention compared to the control showed significant medication adherence
outcomes, especially over a long period among hypertensive patients.
Persell et al. (2018) enrolled 300 uncontrolled hypertensive patients in the
randomized controlled trial to determine if a mobile phone-based hypertension personal
control program (HPCP) is more effective than home BP monitoring alone in the control
of HTN. This HPCP study was associated with individualized support for the patients. It
also encouraged healthy life changes that promote HTN self-management (Persell et al.,
2018). Pre-intervention data was obtained, and at six months, there was a follow-up visit,
including data on adherence to antihypertensive medications. According to Persell et al.
(2018), HPCP is an artificial intelligence that is automated in a smartphone. It also gives
behavioral therapy, is set for medication reminders, and much more. This study provided
an example of the significance of using a telephone when combined with other
interventions that control HTN, improve quality care, and sustain adherence to
antihypertensive medications, especially as the device has medication reminders.
Sustainability is a significant concept in monitoring the patient, especially after a
stable BP is reached. McGillicuddy et al. (2015) agreed that patients should control their

57
HTN, though intermittent monitoring can identify sustainability. Without occasional
monitoring of the BPs, long-term control of HTN cannot be ascertained. While
interventions such as education on HTN and supervision can enhance the patients' MA,
checking BP every three to six months can further enhance sustainability if it remains
stable. In one study, direct monitoring, involving education and family supervision,
resulted in improved BP within the first six months, but BP became uncontrolled during
the 12-month visit (Shen et al., 2017). The ultimate result was six deaths and the
development of comorbidities due to a lack of sustainability of MA. While the literature
reviewed that family members' education and supervision enhanced MA and HTN
control sustainability, Persell et al. (2018) added HPCP, artificial intelligence in a
smartphone, is beneficial for sustainability. HPCP can be set for medication reminders to
promote MA and BP control.
In summary, and according to the literature review, there are three strategies to
support MA: patient education, facilitators, and outpatient monitoring. Each section
contributes much knowledge to the control of BP and the sustainability of
antihypertensive MA. Education provides patients with knowledge of HTN, risk factors,
complications, and the need to control HTN. Though many factors such as cost,
proximity to care, and SES affect adherence to antihypertensive medications, forgetting
to take the medicines is more common among elderly patients (Abbas et al., 2020).
Miranda et al. (2019) discussed the cost-related medication underuse. Patients do not take
their medications as prescribed, skipping some days to make it last longer and
substituting another less expensive medicine for the antihypertensive medications. In

58
their study, these researchers found uncontrolled HTN among these low-income people
due to affordability and proximity to the pharmacy.
Though education and reminders provide adequate control of HTN (Million
Hearts/CDC, 2016) and maintaining MA, sustainability remains a significant factor
without which patients' conditions become refractory to treatment (Shen et al., 2017). The
study of the educational intervention focused on the materials about HTN, its risk factors,
complications, and antihypertensive medications, showed that after the intervention, the
rate of medication adherence improved and were statistically significant, with a p-value
of less than 0.05 among the intervention groups (Delavar et al., 2020).
Facilitators give the patients a better understanding of the need to take all
medications as prescribed, and there are multiple reminder tools. The study of Dillon et
al. (2019) discussed the positive effects of pharmacy involvement in medication
adherence and found that pharmacy interventions facilitated the patients' adherence to
their antihypertensive medications. Medications and pharmacy refills were readily
available to the patients. Other facilitators reminded patients about their drugs and
improved compliance. The research findings showed that text messages and reminder
cards were consistent with promoting MA among the patients (Maslakpak & Safaie,
2016).
Summary
This chapter discussed the theoretical foundations of the DPI project and provided
a detailed review of the literature related to HTN and MA among hypertensive patients.
The theory undergirding this project was Azjen's TPB, which emphasizes how
perceptions and beliefs can be modified to address and enact changes and remove

59
disparities. This theory was crucial to this project as the focus was on changing the
attitude and behavior of hypertensive patients to medication adherence to lead to more
positive health outcomes. Orem’s (2001) self-care theory related the patient and its
environment. In this project, the nurses applied this theory and determined the patients'
deficiencies in adherence to antihypertensive medication using the HB-MAS. Then the
nurses applied the intervention with Million Hearts education to remove the patients'
deficits to achieve medication adherence.
Non-adherence to antihypertensive medication is a significant problem in the
management of HTN. Non-compliance with medicines is the basis for this DPI project.
Similarly, a poor understanding of HTN is a substantial part of non-adherence to
medications, making the patient-provider relationship an essential and significant
contributor to MA (Schoenthaler et al., 2018). With effective communication, patients
can ask questions, learn, and increase their knowledge of their medications' expected side
effects and importance (Million Hearts/CDC, 2016). Many of the articles discussed
patients forgetting to take their medication as prescribed. Socioeconomic status and
attitude towards medicines are associated with non-adherence to antihypertensive drugs,
leading to uncontrolled HTN (Chetoui et al., 2016).
This DPI project held the teaching of the patients in high priority, considering the
importance of knowledge. Instruction on the Million Hearts education program website
would benefit the patients. Just as the literature reviewed the details of the contents of the
educational materials which the researchers used successfully in the articles, the Million
Hearts programs are very detailed and easy-to-follow.

60
Another primary concept in the literature was patient and provider
communications. This relationship applied to the population in this project. Nurses were
instructed on the education materials, and the nurses then taught the patients. The nurses
had frequent communication with the population, thereby applying patient-centered care.
The patients took an active part in their care by measuring their BPs and reported them to
the nurses. In addition to the education, the patients received a weekly phone call, which
acted as reminders to take their medications as prescribed, and to foster their MA, which
was the central theme of the project. The HB-MAS was the tool for measuring their MA
and obtaining the weekly data.
Chapter 3 will provide a detailed description of the project's methodology and
elaborates on some topics from Chapters 1 and 2. Chapter 4 will present the results of the
project that were obtained using the methodology in Chapter 3. Chapter 5 will provide
the implication of the results as well as recommendations for future practice.

61
Chapter 3: Methodology
Adherence to antihypertensive medication is the goal of the management of
hypertension (HTN) (CDC, 2020). Any systolic blood pressure (SBP) equal to or greater
than 130 mmHg or diastolic blood pressure (DBP) greater than 80 mmHg is regarded as
HTN (CDC, 2020). The focus of this project was to determine the effect of education on
maintaining adherence to antihypertensive medication. The literature described HTN as a
silent disease because a hypertensive patient is often asymptomatic (Achhab et al., 2019).
Routinely monitoring blood pressure could alert to worsening BP readings. As a chronic
disease, HTN control requires long-term continuous treatment. Therapeutic control of
HTN is the adherence of the patient to antihypertensive regimens such as medications,
diet, exercise, and weight management (Etebari et al., 2019). This project involved
educating the patients on adherence to their antihypertensive medicines and the
importance of monitoring their blood pressure.
The purpose of this quantitative, quasi-experimental project was to determine if or
to what degree the implementation of the Million Hearts education program could impact
the adherence to antihypertensive medication as measured by HB-MAS when compared
to current practice among adult patients 18 years and older with known hypertension in a
primary care clinic setting in New York over four weeks. The educational intervention
was implementing the Million Hearts education program (see Appendices D, E, and F).
The nurses educated the patients about HTN, its side effects, complications,
antihypertensive medications, and adherence to their medications. The MA measuring
tool, HB-MAS (see Appendix B), made up of nine Likert questions (Kim et al., 2000),
was introduced for four weeks. These questions tested the patients' antihypertensive

62
medication adherence on a scale of one through four. The pre- and post-intervention and
weekly responses to the questionnaire provided the patients' MA level at those times. The
patients used Self-monitored blood pressure (SMBP) at home (CDC, 2013). Comparing
the pre-intervention with the post-intervention results determined the project's purpose,
which was the level of medication adherence.
This chapter will present the methodology and design of the project. It includes a
discussion of the problem and clinical question which guided the DPI design and
purpose. The population sample and instrumentation will be described. Then, after
presenting the reliability and validity of the instrument, the data collection and analysis
procedures will be described in-depth. The chapter will end with a discussion of bias
mitigation, ethical considerations, and project limitations.
Statement of the Problem
It was unknown if or to what degree the implementation of the Million Hearts
education program impacted adherence to antihypertensive medication as measured by
the Hill-Bone Medication Adherence Scale (HB-MAS), when compared to current
practice among adult patients 18 years and older with known hypertension in rural New
York state. The problem that was to be addressed was the patients' non-adherence to their
antihypertensive medication. The gap was filled to help the patients to take their
antihypertensive medicines as prescribed.
Though there were many reasons behind medication non-adherence, the Million
Hearts education program (2016) educated the patients on how to control their BP by
taking the antihypertensive medication. At the end of the intervention, it was expected
that the Million Hearts education program would solve the problem of non-adherence,

63
and the patients would consistently take their antihypertensive medications as prescribed
by their healthcare clinicians.
Clinical Question
The DPI project was guided by the following clinical question:
Q. To what degree does the implementation of the Million Hearts education
impact the adherence to antihypertensive medication, as measured by HB-MAS
when compared to current practice among adult patients 18 years and older with
known hypertension, in a primary care clinic setting in upstate New York over
four weeks?
The DPI project used a quantitative method. The primary tool for the evaluation
of the intervention was the HB-MAS questionnaire. The HB-MAS questionnaire was
applied for the following assessments in sequence: (a) the pre-intervention questionnaire
evaluated the patients' baseline adherence to their antihypertensive medications, (b) the
weekly assessment questionnaire assessed the patients' progress of medication adherence,
and (c) the post-intervention questionnaire evaluated the patients' medication adherence
at the end of the fourth week of the project.
The independent variable in the DPI project was the Million Hearts education
program. This variable was the intervention for the project. The Million Hearts education
program contained the material for teaching the patients about HTN as a chronic disease;
complications of HTN, medications for control of HTN, and the importance of
medication adherence (see Appendix D). The project had two dependent variables. The
significant variable was the HB-MAS questionnaire, and it was used to obtain medication
adherence data at baseline, every week, and at the end of the fourth week. The purpose of

64
the HB-MAS questionnaire was to measure the patients' medication adherence as
compared to the current practice of no education program in the primary care clinic
setting in upstate New York. Million Hearts/CDC (2016) is an educational program that
covered the information on HTN, association with heart disease, risk factors such as
tobacco use, cholesterol, and other risk factors and complications such as stroke and
kidney disease. The teaching included the possible side effects of medications and the
importance of taking antihypertensive medicines to prevent risk factors and
complications. There was a discussion on the best time to take drugs. Daily medications
were easier remembered if taken in the morning or in the morning and evening if the
dosing was twice daily. If no contraindications, the medications can be taken with
breakfast if daily dosing or breakfast and dinner if twice-daily dosing. The Million Hearts
education program has validity. The AHA instituted a campaign strategy for preventing
one million heart attacks, kidney disease, stroke, and death by the year 2022. Ciemins et
al. (2018) used the Million Hearts tool to study 8.92 million patients and predicted HTN
in the United States. In evaluating the Million Hearts plan to control HTN in the United
States there was positive progress towards meeting the goal (Patel et al., 2014).
The second dependent variable was blood pressure measurements using the
SMBP monitoring tool (CDC, 2013). Although the project's length would not show a
substantial change in blood pressure, the primary investigator (PI) included the blood
pressure measurements to look at the trends and relationship to medication adherence as
additional but not primary data. The dependent variable was the HB-MAS, which is made
up of nine questions. The responses are on a Likert scale of 1 to 4, and the level of
measurement is ordinal.

65
Project Methodology
The methodology for this project was quantitative. Medication adherence was
assessed at baseline, every week, and at the end of the four weeks after intervention. The
tool for assessing medication adherence was a self-reported scale, developed by Hill-
Bone called HB-MAS, which asked patients to respond to numerical answers from 1 to 4.
The quantitative method was the best for the project because the data collection was
measurable and quantifiable. It had to be numerically measurable to enable a statistical
analysis of data (Ali & Bhaskar, 2016).
This methodology was reproducible. The significant measurable variable for this
project was the number of times the patient took the BP medication as prescribed during
the four weeks of the intervention to improve medication adherence. The number of times
the antihypertensive medication was taken during the intervention period was compared
to the number of times the medication was taken before the intervention to evaluate
adherence. The comparison was among the HB-MAS questionnaire results to assess their
medication adherence. The use of numbers, tables, and ratios were significant in
assessing the findings' interpretations in this quantitative DPI project.
An alternative methodology that could have been used for this proposed project
was the qualitative method. However, it was not appropriate for this evidence-based DPI
project because the qualitative approach is more of an exploration of occurrence. It uses
interviews or reviews of case records. According to Van den Berg and Struwig (2017),
the qualitative method is appropriate for explaining the events and development of
theories. Therefore, it was not appropriate for this project.

66
Project Design
The design for this DPI project was the quasi-experimental design. This design
for evaluating the effect of the intervention required pre- and post-intervention. The
intervention was the Million Hearts education. The principal investigator instructed the
nurses on the education (about HTN, complications of uncontrolled HTN,
pharmacological and non-pharmacological interventions for the control of HTN, and
medication adherence) and how to use the HB-MAS. The intervention, the Million Hearts
education program, was taught to the patients by the nurses. The nurses measured the
patients' BP at pre-intervention to determine the baseline BP and post-intervention. The
PI included blood pressure measurement only as an additional, not a primary data, to look
at the trends and relationship to medication adherence. The length of the project would
not show a substantial change in blood pressure. The patients received a weekly
telephone call from the nurse to obtain the number of times each patient did or did not
take the antihypertensive medication, using the same HB-MAS questionnaire. At the end
of the four weeks, the post-intervention numerical data were obtained with the HB-MAS.
A statistical comparison of all the data determined the status of adherence to
antihypertensive medication.
The quasi-experimental design aligned with the quantitative methodology through
the relationship with the variables. There was a causal-comparative relationship between
the dependent variable and the independent variable (Bloomfield & Fisher, 2019). The
measurement of the patients' independent variable influenced the dependent variable. In
this project, the HB-MAS data result (dependent variable) was influenced by the Million
Hearts education program (independent variable). A quasi-experimental design was the

67
best design for this DPI project because it addressed the clinical question more
appropriately than other methods. The HB-MAS questionnaire was used in obtaining data
for the patients' medication adherence. This tool was used for the pre- and post-
intervention (Million Hearts education). The quasi-experimental design was in the form
of pre/post-intervention. The pre-intervention tested the patient's adherence to
antihypertensive medication before the implementation of the Million Hearts education
program. The post-intervention was a measure of implementing the education compared
to current practice without education implementation.
Population and Sample Selection
This section discussed the setting, the population, and the project sample. The
project site was located at the facility outpatient clinic in a town in New York. The site
was an internal medicine clinic, and patients usually had scheduled appointments to come
in to see their primary care providers. Though some patients do walk-in, most of these
patients come for blood pressure checks with the nurse or medication refills. Walk-in
meant the patients do not need to have an appointment; instead, they came to the
provider's office for a quick service such as a blood pressure check or refill of
medications. They may or may not see the PCP while at the clinic, depending on the
reason for the visit.
The participants were adult patients 18 years and older who attended the primary
care clinic at the hospital facility. The clinic had about 1,200 patients, and about 900 of
them had HTN. The project population was recruited from the 900 patients depending on
meeting the inclusion criteria. The patients lived independently in the community, were
capable of self-care, and were mentally intact. There were four primary care clinic

68
registered nurses for this population, and they worked with the principal investigator for
this project.
Though the clinic has about 900 hypertensive patients, not all of them had
uncontrolled HTN or non-adherent to antihypertensive medication. The project
population was recruited from the uncontrolled hypertensive patients based on their
persistent high BP data in the EHRs. The final sample recruitment for the project was
patients with non-adherence to their antihypertensive medications and who were willing
to partake in the project. Information from EHRs showing the prescription and refill
history of the medicine, aided the recruiting of non-adherence to medications. These
patients were recruited when they presented to the clinic for their regular appointments.
One of the significant aspects of participation in a study is informed consent. It
assures a full understanding of the study's participants, and it is entirely voluntary
(Mallia, 2018). According to Mallia (2018), the process of informed consent requires the
following: (a) information, which refers to full verbal explanation of the reason and
content of the project; (b) understanding, which requires the participant comprehend the
information clearly; (c) voluntariness, which assumes there is no coercion or pressure and
the participants can withdraw at any point of the project without consequences; (d)
competence, which shows the participants' capacity to make a decision; and (e) consent,
which is the actual signing of the written information which was already explained
verbally. However, the patients did not need to provide a signed authorization to
participate because this is a quality improvement (DPI) project, not a study or research.

69
They signed the HIPAA waiver to enable the extraction of their data from the EHRs.
The inclusion criteria were diagnosis of HTN, must be 18 years of age or above,
speak and understand English, not adherent to antihypertensive medication (a scale of
fewer than three shows non-adherence as per HB-MAS), and registered nurses were
included to work with the patients. The exclusion criteria were patients without diagnosis
of HTN, less than 18 years of age, did not speak and understand English, adherent to
antihypertensive medication (a scale of three or greater showed adherence as per HB-
MAS), non-registered nurses.
The sample size calculation was based on the confidence level of 95%,
confidence interval of 5, the population of 30, and the sample size needed defaults to 28
(Creative Research Systems, n.d.). The confidence interval calculation required the
confidence level of 95%, a sample size of 28, a population of 30, a percentage of 50, and
it gave a confidence interval of 4.86 (Creative Research Systems, n.d.).
Instrumentation and Sources of Data
The instruments for the data collection were (a) The Hill-Bone Medication
Adherence Scale which was the primary dependent variable; (b) the Self-Measured Blood
Pressure (SMBP), which was another dependent variable for monitoring trends in BP;
and (c) the Electronic Health Records from the facility records.
Hill-Bone Medication Adherence Scale (HB-MAS). Hill-Bone medication
adherence scale (see Appendix B) was used for screening how adherent the patients were
to their antihypertensive medication. The nine simple questions with the four Likert
ratings were on a scale of 1-4 (one = all the time, two = most of the time, three = some of
70
the time, four = none of the time). The HB-MAS was applied at baseline, weekly, and the
end of the four weeks.
HB-MAS scale was developed for the management of medication non-adherence
in HTN, which the developers said could not be achieved without understanding and
compliance with HTN treatment (Kim et al., 2000). These researchers reported that
compliance was linked to the patients' behavior towards salt intake, keeping their PCPs'
appointments, and taking their medications as prescribed. Kim et al. (2000) found self-
report of compliance to medications was simple, economical, and provided instant
feedback. The validity and reliability of the HB-MAS was tested and were supported
(Kim et al., 2000). According to Cheong, Tong, and Sazlina (2015), HB-MAS had
validity and reliability, as evidenced by the testing in America, Africa, and Turkey.
Self-Measured Blood Pressure (SMBP). SMBP was a tool that patients could
use to monitor their blood pressure at home. The participants checked their blood
pressure weekly, and they reported the result to their nurse when they received their
weekly evaluation call. The data from the SMBP was not for this project because the
project time was not long enough to show a significant difference in blood pressure.
Every hypertensive patient was issued a BP kit for monitoring their BP at home.
Electronic Health Records (EHRs). Patients' demographics and pre-intervention
records of medication adherence and hypertension were obtained from the EHRs.
Electronic Health Records have protected health information because they are parts of the
health care delivery that provide the pertinent history of the patients' events (Verma et al.,
2020). The EHRs retrieved such data as the patient's full name, date of birth, social
security number, allergies, diagnoses, current medications, and other historical data.

71
Validity
Validity describes the usability of the instrument. It is the extent to which the data
measured what it was meant to measure. This measurement was supposed to be
consistent as expected. It is necessary to establish the reliability and validity of data or
intervention used in the research to give users confidence (Kilgus et al., (2019). The
researchers reported that if the validity of a data or research design is established, it
means the information is correct.
The HB-MAS scale for evaluation of medication adherence has validity.
Maslakpak and Safaie (2016); Chaetziefstratiou, Giakoumidakis, Fotos, Baltopoulos, and
Brokalaki (2019); and Etebari et al. (2019) used HB-MAS in their research of
antihypertensive medication adherence and more knowledge of HTN. The study of
Etebari et al. (2019) used the HB-MAS compliance scale for evaluating the commitment
to their antihypertensive treatment and had a statistically significant p-value of less than
0.018 (p < 0.018) for medication, a p-value of less than 0.01 (p < 0.01) for dietary, and p-
value of less than 0.01 (p < 0.01) for keeping their PCPs' appointments. In this project,
the HB-MAS questionnaire measured the patients' adherence to antihypertensive
medications, and that was what it was supposed to measure.
Electronic Health Records (EHRs) are valid and reliable because they have been
electronically stored, used, updated multiple times, and they are secured, protected health
information. Whenever patients went to their PCP's office visits, the EHRs were updated
with the patient. The principal investigator had no intention of developing a scale for this
project; instead, the PI used already existing, tested, and approved instruments that have
been discussed for the project.

72
The SMBP was the tool for the patients to use in measuring their blood pressure
at their homes (CDC, 2013). Every hypertensive patient was routinely issued a BP kit.
The CDC (2013) provided validity for SMBP. It was recommended by the CDC (2013)
in support of the Million Hearts program for monitoring HTN, which could cause
complications. However, the SMBP was not used for data tracking in this DPI project.
The PI included blood pressure measurement only as an additional, not a primary data,
just to look at the trends and relationship to medication adherence because the length of
the project would not show a substantial change in the blood pressure.
Reliability
Reliability refers to the trustworthiness of the instrument. The HB-MAS is a
reliable tool because many researchers have used it many times, and it was adapted into
other languages. Chatziefstratiou et al. (2019), in their study about medication adherence
in HTN, tested the reliability of HB-MAS in comparison to Morisky Medication
Adherence Scale (MMAS) and A-14 Scale. HB-MAS had an alpha coefficient of 0.76,
while MMAS was 0.64, and the A-14 scale had 0.91, and the researchers concluded that
these scales were reliable (Chatziefstratiou et al.; 2019). The researchers also showed the
validity and reliability of the HB-MAS in their study. HB-HBP was meant to measure the
baseline medication adherence, weekly medication adherence to obtain the number of
times the patients took the antihypertensive medication and the medication adherence
information for the week, and post-intervention medication adherence. In the project, the
HB-MAS questionnaire was capable of obtaining an accurate report of how often patients
took their medications, which was a sign of their reliability to take their medications even
after the community project independently. In assessing the reliability and validity for

73
HB-MAS Cronbach's alpha at 0.8, the p-value for the systolic BP (SBP) was less than
0.01 (p < 0.01), and the p-value for the diastolic BP (DBP) was less than 0.01 (p < 0.01)
(Song et al., 2011). Validation of the internal consistency of the HB-MAS for eight items
resulted in a p-value of 0.02 (p = 0.02) for SBP and DBP, respectively (Denguir,
Yakdhane, Gamra, & Zaabouti, 2019).
Data Collection Procedures
Before actual data collection, the primary investigator ascertained that all written
approvals and permissions were in place. Written consent was obtained from the
Institutional Review Board (IRB) of the project site and GCU (see Appendix A). Since
the project data had patients' personal and health information, confidentiality and ethical
considerations were upheld. The data collection was a face-to-face encounter with the
population. The lead nurse and the assisting clinic registered nurses were notified. Before
the first day of the project intervention, the principal investigator instructed the registered
nurses about HTN, its complications, antihypertensive medications, side effects, and the
importance of medication adherence, using the powerpoint presentation adapted from the
Million Hearts education program. The PI also instructed the nurses on how to use the
HB-MAS questionnaire for the project.
The steps taken for the data collection were:
Step 1: Recruited the sample from the primary care clinic, met the inclusion
criteria and consented to participate in the project.
Step 2: The nurses obtained the pre-intervention data using the Hill-Bone
medication adherence scale to get the baseline and antihypertensive medication
adherence data and documented the scores.

74
Step 3: The nurses taught the patients what the PI instructed them during the
powerpoint presentation adapted from the Million Hearts education materials. The
teaching lasted for about 10 to 15 minutes, depending on each patient's possible concerns.
The nurses also ensured each patient knew how to use their BP kit appropriately.
Step 4: The nurse checked baseline blood pressure at the initiation of the
intervention.
Step 5: Each patient received a weekly phone call from the nurse to assess
medication adherence progress. The Hill-Bone was used by the nurse to obtain data
during the weekly telephone calls.
Step 6: At the end of the four weeks of the intervention, the patients were asked
to come for an office visit for a final BP check, and the Hill-Bone questionnaire was
administered for the last time.
Data Analysis Procedures
After the collection of data, the analysis was the next stage of the project. The
analysis was also a step-by-step procedure. The key elements of this section included the
data, the dependent and independent variables, and the statistical analysis. As a
quantitative method, numerical data were obtained for each variable. These were raw
data, and they were sorted, separated, and processed as follows:
1. A table of columns was drawn for arranging the data.
2. The weekly scores for each of the nine questions of the HB-MAS for each of
the participants were arranged in tables of columns.

75
3. The corresponding period (weeks 1-4) was arranged on the same table. The
pre-intervention scores from the dependent variable (HB-MAS) for all the project
samples were organized in a column.
4. The weekly telephone data scores from the HB-MAS scores were put on the
same column.
5. The post-intervention scores from the HB-MAS for all the samples were
organized on the same table of columns.
6. The blood pressure from pre-intervention and post-intervention were arranged
on a separate table for comparison of BPs.
The PI included blood pressure measurement only as an additional, not a primary
data, to look at the trends and relationship to medication adherence. The length of the
project would not show a substantial change in blood pressure.
This organized data, now a database, was further organized on a Microsoft
spreadsheet for analysis. Descriptive statistics were applied using Statistical Package for
Social Sciences (SPSS) for analysis using the paired t-test. Finally, there was a
comparison of the variables to arrive at the outcome of the project. The threshold of p-
values analyzed the confidence interval. This test was chosen for more reliability,
validity, and applicability. These gave the project its repeatability status. Researchers set
a p-value of 0.05 as the cut-off value for significance (Mishra et al., 2019). P-value of
0.05 or less is statistically significant.
The primary investigator used descriptive statistics to explain the relationship
between the data and the variables. The PI also used inferential statistics for answering
the PICOT question. The comparison showed the difference between the data from the

76
dependent variable (HB-MAS) and the data from after applying the independent variable
(Million Hearts education program) to show the effect of educational intervention on
medication adherence. The pre- and post-intervention blood pressure data were compared
using a graph to show any trend in the blood pressure reading and not for comparison to
show medication adherence. Blood pressure measurements were included only as an
additional, not a primary data, to look at the trends and relationship to medication
adherence. The length of the project would not show a substantial change in blood
pressure.
Potential Bias and Mitigation
Potential bias for this project would evaluate the internal validity, which could
affect the project's results. It could be from the collection of the data, obtaining the
sample population, or data analysis. The bias may or may not be purposeful. The primary
investigator anticipated a bias in this project from the sampling of the population as both
sexes were not equally represented. Though the number of hypertensive patients at the
project site was large, only about 33% of current patients at the clinic were females. The
tendency was to equalize the males and the females even if the males had worse BPs that
met the project BP inclusion criteria. It could have affected the results' reliability because
this would not have been an accurate representation of the actual sample. According to
Showalter and Mullet (2017), selection bias is a threat to validity.
Another possible potential bias was during data collection in using the
questionnaires. The data was based on unsupervised responses of the sample. It was
expected that the answers were accurate, but there was a probability for the responses to
be skewed, which would impact the internal validity of the results. Evaluating and

77
knowing the risks of bias could enable avoidance of bias and provide positive outcomes
(Faggion, 2015).
Ethical Consideration
Electronic health records (EHRs) are protected health information. All patients'
data, clinical or demographic, such as names, date of birth, social security number, birth
sex, or any other information which identified the patient, constitutes protected health
information (Dehghan et al., 2017). EHRs provide valuable and trusted information that
could be shared with other healthcare agencies. The EHRs prevent duplication of
expensive tests such as CAT scans. Considering EHRs in ethics, the sharing of the
patients' information was strictly handled for the care of the patients (Sulmasy, Lopez, &
Horwitch, 2017). However, since data had to be collected for the project, respect for the
participants was very relevant. There are protocols to be followed to enable access for
data collection. The principal investigator recognized and obtained all participants' data
following the facility's IRB. Though there were more males than females in the clinic,
this project experienced an unequal ratio of 20% of females who met the recruitment
criteria.
Another essential aspect maintained during the EHR data collection was that the
Health Insurance Portability and Accountability Act (HIPAA) had to be strictly
maintained at all times. Following the Belmont Report of 1979, it was ethical to apply the
principles of respect, justice, and beneficence to studies since humans are involved
(Friesen, Kearns, Redman, & Caplan, 2017). Respect was not only for the person but also
for the person's documents for analysis. Informed consent was a significant aspect of the
ethical principles of respect for the population. The sample's privacy was respected

78
accordingly while all information, including the risks about the project, was explained to
them. Following the Belmont Report's ethical principles, the persons were freed from
coercion, harm, and any threat, should the person refuse to partake in the project. The
IRB determined this is a quality improvement project and not research. Informed consent
would have been obtained after a full explanation of the process of the project if this was
research. The IRB determination declared this a quality improvement project, not a study.
Patients were notified that there would be no associated punishment or liabilities should
any patient decide to leave or not participate in the project.
Demographic data were already available in the electronic health records and they
are protected health information. Every data from the project was handled with utmost
privacy and not shared with anybody outside the principal investigator and the nurses.
Electronic data are stored with a password access according to the facility’s protocol for a
maximum of three years. When no longer required, the data will be permanently deleted
from the system.
Limitations
A limitation is a situation that affects the project, yet the project investigator has
no control over it (Theofanidis & Fountouki, 2018). According to Theofanidis and
Fountouki (2018), there are limitations and delimitations in every study regarding the
design, data, and other relationships. Theofanidis and Fountouki (2018) associated
delimitations as challenges that could have been better addressed.
The most outstanding limitation in this project was related to the small size. A
project with a large size likely produces better results compared to a small size, with a
narrow margin of error. The primary investigator defined the age range of the sample

79
patients as 18 years and above. This project's available age group ranged between 46 and
97 years, which did not represent the general population.
The Hill-Bone questionnaire is a valid, simple, and inexpensive tool. The
responses from the patients were supposed to be reliable. However, the responses were
based on the patients' words. Even if the project used a pill count, it was still the same
patients' response, which had to be accepted. The patients will take their BPs weekly and
report to the nurse. Though the BP readings are not strictly for analysis, there could be
skewed blood pressure data since the patients have to do it at home. Another limitation of
blood pressure was that certain factors affect blood pressure, such as diet, exercise,
medication side effects, and other barriers that could have affected BP control differently.
Summary
In summary, Chapter 3 covered the methodology and preparation for the practical
aspect of the project. The purpose of the project was defined, the problem of medication
adherence in HTN was identified, and the clinical question to address the medication
adherence was discussed. This quantitative project used the HB-MAS questionnaire to
evaluate medication adherence in adults. The intervention to assess for a change was the
Million Hearts education program (see Appendices D, E, and F). The project was a quasi-
experimental design that used a pre/post intervention and finally drew the outcome by
comparing the difference.
The population and sampling were done during regular office visits. Inclusion
criteria were hypertensive patients with non-adherence to antihypertensive medication.
The sample size was small at 15 as per the participants' inclusion criteria and consent.
The project site is a primary care facility in a town in upstate New York. The process of

80
recruitment of the sample had already been discussed. The data collection procedure was
simple but in a stepwise manner to prevent skewing the results. The intervention lasted
for four weeks, and weekly numerical data was obtained from the patients. The final
comparison of the variables in the clinical question was calculated using SPSS for
statistical results. The independent variable (Million Hearts education program)
influenced the dependent variable (medication adherence) measured by HB-MAS.
Chapter 4 will present the results of data collection and analysis. Results will be
presented in narrative and graphic form. Chapter 5, then, will provide the interpretation of
the results. It will also include the implications of the project and recommendations for
the future.

81
Chapter 4: Data Analysis and Results
It was not known if or to what degree the implementation of the Million Hearts
education program impacted the adherence to antihypertensive medication as measured
by HB-MAS, when compared to current practice among adult patients 18 years and older
with known hypertension, over four weeks. The methodology for this project was
quantitative. Medication adherence was assessed at baseline and every week for the four
weeks of the intervention. Measurable and quantifiable data to determine medication
adherence was extracted with HB-MAS, which asked patients to respond to numerical
answers from one to four (1-4). Any data less than three, showed non-adherence to
antihypertensive medication. Data of three or more than three was regarded as medication
adherence.
The clinical question was: To what degree did the implementation of the Million
Hearts education impact the adherence to antihypertensive medication as measured by
HB-MAS, when compared to current practice among adult patients 18 years and older
with known hypertension in a primary care clinic setting in upstate New York, over four
weeks? Applying the Million Hearts education to the sample was what made the
difference in the data. Demographic data were obtained from the patients' electronic
medical records. The patients' medication adherence data was obtained from the patients'
responses using the weekly questionnaire from HB-MAS.
Chapter 4 explains the process of analyzing the data at the end of the four-week
intervention period. First, the descriptive data will be presented. Then, the data analysis
procedures will be further described. It will end with a presentation and summary of the
results of data analysis.

82
Descriptive Data
The project site was located in an outpatient primary care clinic in upstate New
York. It was an adult internal medicine clinic, and the patients had appointments to see
their primary care providers (PCPs). The adult patients' population's age was 18 years and
above. However, the sample's age for the project varied between 46 and 97 years,
because uncontrolled HTN and non-adherence to antihypertensive medication were found
among these people. The sample size was 15, out of which 20% were females, while 80%
were males. The patients all had the primary education of a high school diploma. No
control group was required for the project.
The patients' data collection started after obtaining Grand Canyon University
(GCU) Institution Review Board (IRB) approval and the project site IRB approval. The
project site approval was granted on June 29, 2020. The project site approved the project
to take place at the facility on September 18, 2020. GCU IRB approved the
implementation of the project on September 22, 2020 (see Appendix A). Following the
final approval from the GCU IRB, the implementation phase of data extraction started on
September 23, 2020, and the estimated date of project completion was November 4,
2020. After approximately six weeks of the project implementation, including instructing
the nurses, recruiting the samples, and obtaining the data, the project came to completion.
Numerical data were obtained from the pre- and post-intervention using the HB-
MAS questionnaire. The sample's blood pressures were obtained on the first day of the
intervention and the last day. The various data were de-identified, arranged in tables, and
secured in a Microsoft Excel database by the primary investigator. The data were stored
on the project site. Descriptive statistics were applied. Table 1 described the demographic

83
data from the sample: the youngest was 46 years, and the oldest was 97 years of age. The
proposed number of patients who met the inclusion criteria for the project was 28, but 15
patients out of these consented to partake in the project. Table 2 describes the sample and
their associated pre-intervention data, showing the baseline medication adherence,
weekly data, and post-intervention data.
Table 1
Demographics of Project Sample
Demographics n %
Age 40 – 50 2 13.5%
51 – 60 4 26.7%
61 – 70 5 33.3%
71 – 80 1 6.7%
81 – 90 1 6.7%
91 – 100 2 13.5%
Gender Male 12 80.0%
Female 3 20.0%
Ethnicity Caucasian 5 33.3%
African-American 10 66.7%
Note: n = number of patients; % = percentages.
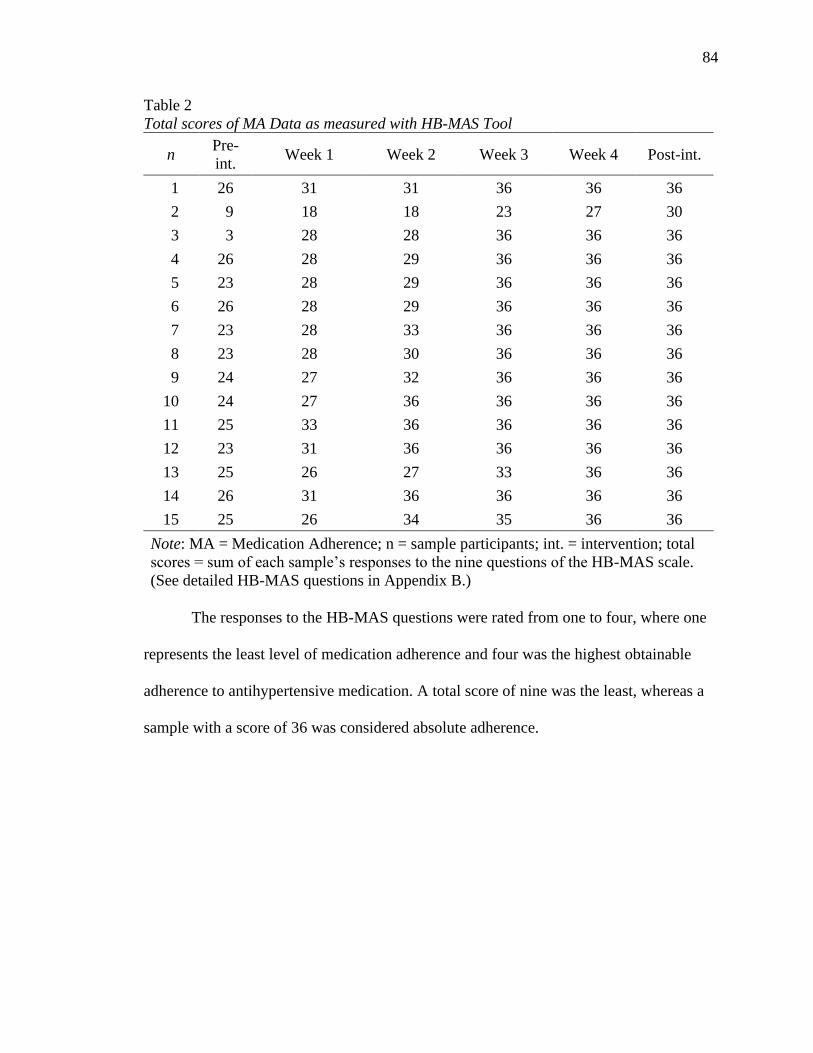
84
Table 2
Total scores of MA Data as measured with HB-MAS Tool
n Pre-
int. Week 1 Week 2 Week 3 Week 4 Post-int.
1 26 31 31 36 36 36
2 9 18 18 23 27 30
3 3 28 28 36 36 36
4 26 28 29 36 36 36
5 23 28 29 36 36 36
6 26 28 29 36 36 36
7 23 28 33 36 36 36
8 23 28 30 36 36 36
9 24 27 32 36 36 36
10 24 27 36 36 36 36
11 25 33 36 36 36 36
12 23 31 36 36 36 36
13 25 26 27 33 36 36
14 26 31 36 36 36 36
15 25 26 34 35 36 36
Note: MA = Medication Adherence; n = sample participants; int. = intervention; total
scores = sum of each sample’s responses to the nine questions of the HB-MAS scale.
(See detailed HB-MAS questions in Appendix B.)
The responses to the HB-MAS questions were rated from one to four, where one
represents the least level of medication adherence and four was the highest obtainable
adherence to antihypertensive medication. A total score of nine was the least, whereas a
sample with a score of 36 was considered absolute adherence.

85
Table 3
Blood Pressure Comparison
n Pre-intervention Post-Intervention
1 142/65 129/80
2 175/109 170/99
3 158/98 147/89
4 163/110 156/96
5 162/71 148/76
6 164/84 132/70
7 164/82 148/84
8 172/87 122/64
9 194/88 135/82
10 167/77 145/77
11 170/88 160/78
12 166/88 137/67
13 145/90 130/76
14 160/80 129/79
15 182/103 146/91
Note: n = samples.
The sample's pre-intervention blood pressure was checked at the initiation of the
project's intervention phase to understand the baseline status. Post-intervention blood
pressure was also checked. Although the length of the project would not show a
substantial change in blood pressure, the primary investigator included the blood pressure
measurements to look at the trends and relationship to medication adherence as
additional, but not primary data. The sample (n) numbers in Table 2 were the same
samples as in Table 3 for a better comparison of the relationships.
Data Analysis Procedures
The results of the descriptive were quantitatively and statistically analyzed using
the IBM SPSS version 27. The analysis process entailed an explanation of the clinical
question concerning the described data obtained from the project. The clinical question
was: To what degree did the implementation of the Million Hearts education impact the
adherence to antihypertensive medication as measured by HB-MAS, when compared to

86
current practice among adult patients 18 years and older with known hypertension in a
primary care clinic setting in upstate New York, over four weeks?
Demographic data from the EMRs for each of the 15 participating patients
included the various age ranges, gender, and ethnicity. They were analyzed using the
description of the data in Table 1 with particular reference to the percentages to show
their relationships.
The next analysis was the pre-intervention data, showing the baseline data. The
tool used for measuring the medication adherence data was the HB-MAS. The number of
times that the patients did and did not take the antihypertensive medication due to the
nine reasons in the HB-MAS was numerical. The intervention was the Million Hearts
education program. The education was the teaching by the nurses to the patients about
MA concerning uncontrolled HTN. The pre-intervention data represented the current
practice, as stated in the clinical question, and it was obtained prior to education. The pre-
intervention data were analyzed to evaluate the level of fundamental adherence to
antihypertensive medication. The next significant data was the post-intervention data
obtained at the end of the four weeks was analyzed and subjected to inferential statistics
to compare the patients' medication adherence at the end of the four weeks. Analysis of
the weekly data was compared to the pre-/post data to establish a relationship.
Results
The clinical question was:
Q. To what degree did the implementation of the Million Hearts education impact
the adherence to antihypertensive medication as measured by HB-MAS, when
compared to current practice among adult patients 18 years and older with known

87
hypertension in a primary care clinic setting in upstate New York, over four
weeks?
Following the implementation of the HB-MAS tool, the medication adherence
data at baseline, before the Million Hearts education, was obtained. Weekly data, after
the education intervention, was obtained. The patients' medication adherence outcomes
were derived from data analysis (pre- and post-intervention and weekly responses).
Statistical comparison of all the data answered the clinical question. The relationship
between the data was expressed and explained with the mean, standard deviation, and p-
values.
The next analysis was the pre-intervention data, showing the baseline data. The
tool used for measuring the medication adherence data was the HB-MAS. The number of
times that the patients did and did not take the antihypertensive medication due to the
nine reasons in the HB-MAS was numerical. The intervention was the Million Hearts
education program. The education was the teaching by the nurses to the patients about
MA concerning uncontrolled HTN. The pre-intervention data represented the current
practice, as stated in the clinical question, and it was obtained prior to education. The pre-
intervention data were analyzed to evaluate the level of fundamental adherence to
antihypertensive medication. The next significant data was the post-intervention data
obtained at the end of the four weeks which was analyzed and subjected to inferential
statistics to compare the patients' medication adherence at the end of the four weeks.
Analysis of the weekly data was compared to the pre- and post-intervention data to
establish a relationship (see Figure 1).

88
Figure 1. Bar Graph displaying the mean scores as measured by HB-MAS.
The next step was explaining all the data about the Million Hearts education and
medication adherence. The data were tabulated on table forms. The 15 sample
participants took part in the DPI project. Numerical responses to the nine-item HB-MAS
questionnaire were inferentially statistically analyzed while comparing a stepwise
explanation of the pre-intervention scores through the four weeks duration to the post-
intervention. A 2-tailed sample t-test revealed that the HB-MAS scores at one week of
the intervention showed medication adherence (MA) improvement of 19.1% and a p-
value of zero (p = 0.00). In week two, the overall responses displayed MA improvement
of 10.9% higher than week one and a p-value of zero (p = 0.00). The MA improved to
12.7% in week three more than week two, and the p-value was zero (p = 0.00). The
relationship of weeks three, four, and post-intervention was about the same, hence giving
similar scores compared to week two. This was evidenced by the similar high p-value of
0.12 (p = 0.12) in week three, and 0.33 (p = 0.33) in week four (see Table 4). Weeks
three, four, and post-intervention were very close to perfect scores of 36. Pre- and post-
intervention scores had a distinguished relationship, with an outstanding score of 52.1%
MA improvement higher than the pre-intervention (baseline) and a p-value of zero (p =

89
0.00). The results were further supported by the mean and the standard deviation, as seen
in Table 4.
Table 4
Pre/Post-Intervention Comparison
n M SD
Pre-int. 15 23.4 1.08
Week 1 15 27.9 3.40
Week 2 15 30.9 1.24
Week 3 15 34.9 3.38
Week 4 15 35.4 2.32
Post-int. 15 35.6 1.55
Note: n = number of samples; int = intervention; M = mean; SD = standard deviation.
Paired t-test scores from SPSS version 27.
The comparison of the baseline data to the post-intervention showed the effect of
the Million Hearts education. The BP readings at pre/post-intervention were statistically
analyzed with IBM SPSS Version 27, using a 2-tailed paired sample t-test. Blood
pressure was not significant in this project. Blood pressure measurements were included
only as an additional, not a primary data, to look at the trends and relationship to
medication adherence. The length of the project would not show a substantial change in
blood pressure (see Figure 2).
Figure 2. Pre and post blood pressure comparison using the mean BPs.

90
Summary
The clinical question for the project was: To what degree did the implementation
of the Million Hearts education impact the adherence to antihypertensive medication as
measured by HB-MAS, when compared to current practice among adult patients 18 years
and older with known hypertension in a primary care clinic setting in upstate New York,
over four weeks? The outcome of the intervention showed improved adherence to
antihypertensive medication. The pre-intervention data among the 15 patients showed
non-adherence, as evidenced by the HB-MAS score of less than three in each of the nine
questions, with a mean of 23.4 and a standard deviation of 4.17, compared to the post-
intervention. Million Hearts education improved adherence to antihypertensive
medication within the first three weeks of intervention and had a sustained adherence
effect from the third week to post-intervention. Maximum compliance, as measured by
the HB-MAS, was 36, which represented the sum of the nine responses of the scale from
each patient. Weeks three, four, and post-intervention means of 34.9, 35.4, and 35.6
respectively, were close to 36 compared to 23.4, the pre-intervention score.
The 52.1% medication adherence at post-intervention higher than pre-intervention
answered the clinical question. The result supported a p-value of zero (p = 0.00), which is
very statistically significant. Researchers set a p-value of 0.05 as the cut-off value for
significance (Mishra et al., 2019). Hence, a p-value of 0.05 or less is statistically
significant, with a low margin of error. The significance is that the Million Hearts
education improved adherence to antihypertensive medication, and the PICOT question
was answered. The DPI project had statistical significance and clinical significance,
which was the change the participants experienced from their education. The patients

91
changed from their habit of medication non-adherence to taking their medications as
prescribed.
The pre- and post-intervention data were statistically analyzed using IBM SPSS
Version 27, followed by interpretation of the analysis. The investigations were
statistically significant, with a resultant p-value of zero (p = 0.00). Researchers set a p-
value of 0.05 as the cut-off value for significance (Mishra et al., 2019). Hence the Million
Hearts education had a positive effect on improving the patients' adherence to their
antihypertensive medication. The improved blood pressures seemed to correspond with
the high scores from HB-MAS. Although the length of the project would not show a
substantial change in blood pressure, the primary investigator included the blood pressure
measurements to look at the trends and relationship to medication adherence as
additional, but not primary data.
Chapter 5 will provide a summary of the total project. It will include the
conclusions that can be made from the findings. Additionally, the implications of the
results for theory, practice, and the future will be discussed. The project will end with
recommendations for future projects and practice.

92
Chapter 5: Summary, Conclusions, and Recommendations
Non-adherence to antihypertensive medication was always a significant public
health problem, caused annual deaths of about 9.4 million worldwide (Nielsen et al.,
2017). The purpose of this quantitative, quasi-experimental project was to determine if or
to what degree the implementation of the Million Hearts education program could impact
the adherence to antihypertensive medication as measured by HB-MAS, when compared
to current practice among adult patients 18 years and older with known hypertension in a
primary care clinic setting in New York over four weeks. According to the guidelines of
the American Heart Association ([AHA] 2017), HTN is any blood pressure (BP) that is
equal to or greater than 130/80. It is estimated that by the year 2025, 29.2% of adults
would have HTN in the world (Veisani et al., 2019).
Hypertension is a significant precursor of heart and kidney diseases, causing
about two-thirds of the world's mortalities and claiming about 7.1 million deaths annually
(Nikparvar et al., 2019). There was increased mortality with uncontrolled HTN due to
patients not taking their antihypertensive medications as prescribed (Bansal et al., 2019).
Currently, about 900 of the patients at the project site have HTN, and 68% of them were
uncontrolled.
The main aim of this DPI project was to improve adherence to antihypertensive
medication. By so doing, BP would be controlled, and the complications of a stroke,
CAD, renal failure, and fatality caused by poorly controlled HTN would be reduced.
Medication non-adherence was a threat to healthcare at this project site, and other
interventions failed. Million Hearts education was a program designed by CDC/AHA
(2013) to prevent five million heart attacks by 2022. This program was the intervention
93
for this project. The purpose was to teach the patients more about HTN, the adverse
effects of the complications of HTN, and the importance of antihypertensive medication.
Being a DPI project, the PI instructed the clinic nurses, and the nurses taught the patients.
According to Karaman and Akyolcu (2019), nurses spend more time with patients
and their relatives. Hence, the project participating nurses impacted the patients and
improved their medication adherence with the education program's input. The tool for
measuring the effectiveness of the intervention was the HB-MAS on a Likert scale of 1-4.
The analysis of the data was by IBM SPSS version 27, using the 2-tailed paired sample t-
test.
This chapter will provide a summary of the project. It will then present the
conclusions that can be made based on the results of data analysis. The implications of
the findings for theory, practice, and the future will be discussed. Finally,
recommendations will be made for future projects and practice.
Summary of the Project
The project was about non-adherence to antihypertensive medication. Primary
care providers and nurses had tried to improve the patients' adherence to the medicines,
but non-adherence persisted. Methods that were previously tried without success included
pharmacy involvement for an automatic refill of medication, talking with patients, and
reminding them to take their medications as prescribed. Hence, the focus for
implementing the DPI project lay in the clinical question:
Q. To what degree did the implementation of the Million Hearts education impact
the adherence to antihypertensive medication as measured by HB-MAS, when
compared to current practice among adult patients 18 years and older with known

94
hypertension in a primary care clinic setting in upstate New York, over four
weeks?
The project site is a primary care outpatient clinic with 1,200 patients, out of
which about 900 of them had HTN. A sample size of 15 was recruited from the
population, based on the inclusion criteria of diagnosis of HTN, non-adherence to HTN
medication, and consent to partake in the project. The purpose of the Million Hearts
education was to enable the patients to take their medications as prescribed by their PCP.
The nurses measured the sample's medication adherence data using the HB-MAS tool at
pre-intervention, weekly for four weeks, and at post-intervention. Blood pressure,
estimated at pre- and post-intervention, described the trend. Although the length of the
project would not show a substantial change in blood pressure, the primary investigator
included the blood pressure measurements to look at the trends and relationship to
medication adherence as additional, but not primary data. All the data were statistically
analyzed using SPSS version 27, and the findings were significant, with a p-value of zero
(p = 0.00).
Summary of Findings and Conclusion
Severe comorbidities of uncontrolled HTN include heart and kidney diseases
(Nikparvar et al., 2019). Although medicines lower blood pressures, consistency in
following the prescription guidelines reflect the control of HTN. Hypertension is a
complex public health disease worldwide (Nielsen et al., 2017), and the nursing
profession tries to improve the patient outcome. Though antihypertensive medications
control HTN, non-adherence has a negative outcome (Abbas et al., 2020). Despite the
nurses' efforts, the project site's high percentage of non-adherence to antihypertensive

95
medication created a gap, which the direct practice improvement project was trying to
fill. The education tool to improve the patients' medication adherence controlled HTN
among the clinic patients. The findings in this project were consistent with the clinical
question: To what degree did the implementation of the Million Hearts education impact
the adherence to antihypertensive medication as measured by HB-MAS, compared to
current practice among adult patients 18 years and older with known hypertension in a
primary care clinic setting in upstate New York, over four weeks?
A paired t-test showed significant medication adherence improvement at the post-
intervention data of p-value of zero (p = 0.00), and 52.1% higher than the pre-
intervention data. A determination of adherence improvement progressed from the first
week of intervention through the project's four weeks. The Million Hearts education
intervention, which was the independent variable, made a statistically significant
difference in adherence to antihypertensive medication. Patients’ adherence to their
antihypertensive medication improved following the intervention.
Blood pressure measurements were included to look at the trends and relationship
to medication adherence. The length of the project would not show a substantial change
in blood pressure. The mean post-intervention systolic blood pressure, 142.27, showed a
decrease of 23 from the pre-intervention systolic blood pressure. Similarly, the trend
between the pre- and post-intervention diastolic mean blood pressures showed a little
difference between them. A determination of a significant change in blood pressure may
be seen over a more extended intervention period.
In conclusion, based on the p-value of zero (p= 0.00), the clinical question was
positively answered. The Million Hearts education improved medication adherence in

96
HTN. The project sample of size of 15 was small, thus creating a high margin of error.
However, the project still had a clinical significance, which was that the patients took
their antihypertensive medications as prescribed, and might sustain the practice even after
this project. This quality improvement project closed the clinical practice gap and
contributed to the nursing knowledge body, as evidenced by the nurses' role in this
project.
Implications
The implications in this project were divided into theoretical implications,
practical implications, and future aspects. The conduction of this project was due to non-
compliance to antihypertensive medication. Facility nurses’ expertise and knowledge
recognized the lack of patients’ understanding of the importance of maintaining normal
blood pressure in relation to medication adherence.
Theoretical implication. The main theoretical framework for this project was the
self-care theory written by Dorothea Orem in 2001. The theorist described the role of
nurses in the care of patients. In the project, hypertensive patients lacked the capability of
taking care of themselves in adhering to their medications. Consequently, the clinic
nurses stepped in to address their non-adherence using the Million Hearts education and
measured the outcome with HB-MAS. Antihypertensive medicines control HTN, but
non-adherence to HTN medication is a significant cause of uncontrolled HTN (Pan et al.,
2020). This evidence-based project recognized the importance taking medications as
prescribed and used Million Hearts education to implement the information in the
patients and there was improvement of health. This theory will be advanced if there is
sustainability of adherence to antihypertensive medication.

97
Another applicable framework was the theory of Planned Behavior (TPB),
developed by Icek Ajzen in 1985. In this DPI of medication adherence, the nurses'
weekly close monitoring eventually fostered the patients' relevance taking the
medications without monitoring or further education.
Practical implications. The project had limitations and biases. The project was
designed to accommodate all adult patients, 18 years, and older. However, this project's
available population was mainly the older adult patients, the youngest was 46 years, and
the oldest was 97 years of age. HTN is more prevalent among older adults (Al-Ruthia et
al., 2017). Another implication was the project timeline. The four-week time period for
the project's implementation was very short, considering the extended length of time for
recruiting the sample from the population. A further limitation was the participants'
geographical locations. They were outpatients in rural areas, and the nurses had to wait
for an opportunity for the patients to come in for PCP's office appointment visit. Another
practical implication was the small sample size, causing a bias, and creating a significant
error margin. However, the PI and the nurses investigated concisely with minimum error
and a zero p-value (p = 0.00). Inability to select the sample from the population within a
few days of one another predisposed the project to the selection bias.
Future implications. Nurses and their expert nursing skills, including their
decision-making capacity, can save the patients' lives by preventing stroke and other
complications of uncontrolled HTN. Nurses can utilize an evidence-based scope of
practice, such as the Million Hearts education program and weekly phone calls to the
patients to promote their medication adherence to HTN and other diseases.

98
Data and findings could have been affected by bias due to the short duration of
the project. Therefore, an appropriate future implication would be to take at least ten
weeks to implement the project. The more extended period would provide enough time
for recruitment, more data extraction, and final analysis. Conducting the project in an
urban clinic was a considerable future implication. The current project, which was
conducted in the rural area, encountered the difficulty of having enough participants, both
nurses, and patients. With the few available registered nurses and their regular work
duties, the nurses were initially reluctant to participate in the project. Hence, a larger
facility in an urban area should be considered.
Recommendations
The DPI was a quantitative project, and the recommendations for future projects
and practice follow. Nurses are autonomous in decision making about nursing practice
and capable of recognizing health changes in their patients. Future recommendations for
the project and practice for other ways of improvement will be discussed.
Recommendations for future projects. Nurses should be empowered to
determine the patients' chronic conditions such as HTN. Nurses spend 24 hours with
patients, and they are the patients' advocates of care. Hence, they work with the patients
from the acute condition to their chronic state of health. Another recommendation was to
establish follow up projects with the same participants. The pitfall to this would be the
deterioration some of the patients could encounter in a chronic condition such as HTN,
which could prevent the patients from completing the project. Since attitude to
medication adherence varies from time to time depending on the individuals, a similar
scheme should be conducted over a period of three to six months to compare results.

99
The provision of transportation for participating patients is also recommended.
Other patients of this project site facility receive federal government funding for
transportation to healthcare appointments. This federal benefit should be extended to
project participants who visit the healthcare facility for the DPI project to encourage
participation. Though this project's main goal was to establish and improve medication
adherence in HTN, a recommendation was to expand the project to HTN control and BP
monitoring. The current project monitored only a trend of BP. The reason was the
timeline of the project implementation. Four weeks of intervention were very insufficient
for a statistically significant BP difference to impact control of BP. Thus, about 12 weeks'
intervention period was recommended. Hence, details of factors associated with the
control of HTN would be analyzed. Such factors include, but are not limited to,
medication regimen, health belief, social support, and socio-demographic characteristics.
Home telehealth monitoring BP and medication adherence in replacement for weekly
telephone calls to the patients could achieve the desired therapeutic effect.
Recommendations for future practice. Change of facility and participants were
recommended. This would produce a comparison with the current project. Thus, the
general support of the facility authorities would be involved. This recommendation can
turn into a facility project so that participating nurses should be freed from other duties
during the project implementation. The method can enable more dedication and
subsequent accuracy of data collection. The nurses complained of a lack of enough time
to combine regularly assigned duties and project assignments.
For future practice, the project's modification is to monitor two dependent
variables of medication adherence and its corresponding BP in one project, using the

100
same intervention of the Million Hearts education program. The Hill-Bone scale would
be used to measure the two dependent variables. A further recommendation is that the
project implementation will last for a minimum of 10 weeks, where there will be a
statistical comparison between the dependent and independent variables will also be
defined. This will show how and to what degree adherence to antihypertensive
medication can decrease and control BP.
Another recommendation for future practice is to monitor for project
sustainability. The reason for monitoring is to evaluate the continual success of the
quality improvement project. As evidence-based, there should be a repeat of data
collection of BP and medication adherence post-intervention, at three months, six
months, and 12 months. The statistical comparison will explain sustainability. The goal
of the DPI project is to engage the patients in their care. Finally, they will follow the self-
care model of Dorothea Orem without supervision. The quasi-experimental design for
this project did not define patients' active involvement. Future project is suggested for
reconstruction, to provide more light to the patients' activities.

101
References
Abbas, H., Kurdi, M., Vries, F. de, Onzenoort, H. A. van, Driessen, J. H., Watfa, M., &
Karam, R. (2020). Factors associated with antihypertensive medication non-
adherence: A cross-sectional study among Lebanese hypertensive adults. Patient
Preference & Adherence, 14, 663–673. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S238751
Abbas, H., Kurdi, M., Watfa, M., & Karam, R. (2020). Adherence to treatment and
evaluation of disease and therapy knowledge in Lebanese hypertensive patients.
Patient Preference and Adherence. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S142453
Abel, W. M., Joyner, J. S., Cornelius, J. B., & Greer, D. B. (2020). Self-care management
strategies used by black women who self-report consistent adherence to
antihypertensive medication. Patient Preference and Adherence. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S138162
Achhab, Y. E., Nazek, L., Maalej, M., Alami, M., & Nejjari, C. (2019). Prevalence,
control and risk factors related to hypertension among Moroccan adults: A
multicentre study. Eastern Mediteranean Health Journal, 25(7), 447–453.
https://doi-org.lopes.idm.oclc.org/10.26719/emhj.18.057
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhi &
J. Beckmann (Eds.), Action control: From cognition to behavior (pp. 1139).
Heidelberg: Springer.

102
Ali, Z., & Bhaskar, S. B. (2016). Basic statistical tools in research and data analysis.
Indian Journal of Anaesthesia, 60(9), 54–61. https://doi-
org.lopes.idm.oclc.org/10.4103/0019-5049.190623
Almalki, Z. S., Albassam, A. A., Alhejji, N. S., Alotaibi, B. S., Al-Oqayli, L. A., &
Ahmed, N. J. (2020). Prevalence, risk factors, and management of uncontrolled
hypertension among patients with diabetes: A hospital-based cross-sectional
study. Primary Care Diabetes. https://doi-
org.lopes.idm.oclc.org/10.1016/j.pcd.2020.02.004
Al Kibria, G. M. (2019). Racial/ethnic disparities in prevalence, treatment, and control of
hypertension among US adults following application of the 2017 American
College of Cardiology/American Heart Association guideline. Preventive
Medicine Reports, 14. https://doi-
org.lopes.idm.oclc.org/10.1016/j.pmedr.2019.100850
Al-Ruthia, Y. S., Hong, S. H., Graff, C., Kocak, M., Solomon, D., & Nolly, R. (2017).
Examining the relationship between antihypertensive medication satisfaction and
adherence in older patients. Research in Social & Administrative Pharmacy,
13(3), 602–613. https://doi-
org.lopes.idm.oclc.org/10.1016/j.sapharm.2016.06.013
American Heart Association (n.d.). Medication adherence. Retrieved from
https://millionhearts.hhs.gov/tools-protocols/medication-adherence.html

103
Ampofo, A. G., Khan, E., & Ibitoye, M. B. (2020). Understanding the role of educational
interventions on medication adherence in hypertension: A systematic review and
meta-analysis. Heart & Lung: The Journal of Critical Care. https://doi-
org.lopes.idm.oclc.org/10.1016/j.hrtlng.2020.02.039
Balasubramanian, A., Nair, S. S., Rakesh, P. S., & Leelamoni, K. (2018). Adherence to
treatment among hypertensives of rural Kerala, India. Journal of Family Medicine
and Primary Care, 7(1), 64–69. https://doi-
org.lopes.idm.oclc.org/10.4103/jfmpc.jfmpc_423_16
Bangdiwala, S. I. (2018). Basic epidemiology research designs I: Cross-sectional design.
International Journal of Injury Control and Safety Promotion, 26(1), 124–126.
https://doi-org.lopes.idm.oclc.org/10.1080/17457300.2018.1556415
Bansal, K., Rajput, S., & Mathur, V. S. (2019). Exploring reasons for medication non-
adherence in hypertension patients. International Journal of Pharmacy & Life
Sciences, 10(6), 16.
Barua, L., Faruque, M., Banik, P. C., & Ali, A., (2019). Agreement between 2017
ACC/AHA hypertension clinical practice guidelines and seventh report of the
joint national committee guidelines to estimate prevalence of postmenopausal
hypertension in a rural area of Bangladesh A cross sectional study. Medicina, 7,
315. https://doi-org.lopes.idm.oclc.org/10.3390/medicina55070315
Bergerum, C., Thor, J., Josefsson, K., & Wolmesjö, M. (2019). How might patient
involvement in healthcare quality improvement efforts work – a realist literature
review. Health Expectations, 22(5), 952–964. https://doi-
org.lopes.idm.oclc.org/10.1111/hex.12900

104
Bloomfield, J., & Fisher, M. J. (2019). Quantitative research design. Journal of the
Australian Rehabilitation Nurses’ Association, 22(2), 27–30. https://doi-
org.lopes.idm.oclc.org/10.33235/jarna.22.2.27-30
Bolondi, G., Branchetti, L., & Giberti, C. (2018). A quantitative methodology for
analyzing the impact of the formulation of a mathematical item on students
learning assessment. Studies in Educational Evaluation, 58, 37–50. https://doi-
org.lopes.idm.oclc.org/10.1016/j.stueduc.2018.05.002
Bou Serhal, R., Salameh, P., Wakim, N., Issa, C., Kassem, B., Abou Jaoude, L., & Saleh,
N. (2018). A new Lebanese medication adherence scale: Validation in Lebanese
hypertensive adults. International Journal of Hypertension, 1–7. https://doi-
org.lopes.idm.oclc.org/10.1155/2018/3934296
Brenk-Franz, K., Straub, B., Tiesler, F., Fleischhauer, C., Schneider, N., & Gensichen, J.
(2017). Patient-provider relationship as mediator between adult attachment and
self-management in primary care patients with multiple chronic conditions.
Journal of Psychosomatic Research. https://doi-
org.lopes.idm.oclc.org/10.1016/j.jpsychores.2017.04.007
Carvalho, A. S., & Santos, P. (2020). Medication adherence in patients with arterial
hypertension: The relationship with healthcare systems’ organizational factors.
Patient Preference and Adherence. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S216091

105
Centers for Disease Control and Prevention. (2019). Hypertension cascade: Hypertension
prevalence, treatment and control estimates among US adults aged 18 years and
older applying the criteria from the American College of Cardiology and
American Heart Association’s 2017 hypertension guideline – NHANES 2013–
2016. Atlanta, GA: US Department of Health and Human Services.
Centers for Disease Control and Prevention. (2013) Self-measured blood pressure
monitoring: action steps for public health practitioners. Atlanta, GA: Centers for
Disease Control and Prevention, US Dept of Health and Human Services.
Chatziefstratiou, A., Giakoumidakis, K., Fotos, N. V., Baltopoulos, G., & Brokalaki, H.
(2019). Scales for assessing medication adherence in patients with hypertension.
British Journal of Nursing, 28(21), 1388–1392. https://doi-
org.lopes.idm.oclc.org/10.12968/bjon.2019.28.21.1388
Cheema, E., Sutcliffe, P., Weickert, M. O., & Singer, D. R. J. (2018). A randomized
controlled trial of the impact of structured written and verbal advice by
community pharmacists on improving hypertension education and control in
patients with high blood pressure. European Journal of Clinical Pharmacology,
74(11), 1391–1395. https://doi-org.lopes.idm.oclc.org/10.1007/s00228-018-2519-
0
Cheong, A. T., Tong, S. F., & Sazlina, S. G. (2015). Validity and reliability of the Malay
version of the Hill-Bone compliance to high blood pressure therapy scale for use
in primary healthcare settings in Malasia: A cross-sectional study. Malaysian
Family Physician, 10(2), 36–44.

106
Chetoui, A., Mzoughi, K., Zairi, I., Hassine, E. B. G., Daamar, H. B., Baccouche, M., …
Kraiem, S. (2016). Factors associated with medication non-adherence in
hypertensive patients. Archives of Cardiovascular Diseases Supplements, 8(3),
245.
Ciemins, E. L., Ritchey, M. D., Joshi, V. V., Loustalot, F., Hannan, J., & Cuddeback, J.
K. (2018). Application of a tool to identify undiagnosed hypertension – United
States, 2016. Morbidity and Mortality Weekly Report, 67(29), 798–802.
https://doi-org.lopes.idm.oclc.org/10.15585/mmwr.mm6729a2
Cimmaruta, D., Lombardi, N., Borghi, C., Rosano, G., Rossi, F., & Mugelli, A. (2018).
Polypill, hypertension and medication adherence: The solution strategy?
International Journal of Cardiology, 252, 181–186. https://doi-
org.lopes.idm.oclc.org/10.1016/j.ijcard.2017.11.075
Conn, V. S., Ruppar, T. M., Chase, J.-A. D., Enriquez, M., & Cooper, P. S. (2015).
Interventions to improve medication adherence in hypertensive patients:
Systematic review and meta-analysis. Current Hypertension Reports, 12, 1.
https://doi-org.lopes.idm.oclc.org/10.1007/s11906-015-0606-5
Cooper, K. D. (2020). Prevention and treatment of device-related hospital-acquired
pressure injuries. American Journal of Critical Care, 29(2), 150–154. https://doi-
org.lopes.idm.oclc.org/10.4037/ajcc2020167

107
Cooper, L. A., Marsteller, J. A., Carson, K. A., Dietz, K. B., Boonyasai, R. T., Alvarez,
C., … Wang, N.-Y. (2020). The RICH LIFE Project: A cluster randomized
pragmatic trial comparing the effectiveness of health system only vs. health
system plus a collaborative/stepped care intervention to reduce hypertension
disparities. American Heart Journal, 226, 94–113. https://doi-
org.lopes.idm.oclc.org/10.1016/j.ahj.2020.05.001
Costa, E., Giardini, A., Savin, M., Menditto, E., Lehane, E. A., Laosa, O., Pecorelli, S.,
Monaco, A., & Marengoni, A. (2015). Interventional tools to improve medication
adherence: Review of literature: Patient Preference and Adherence, 2015, 1303–
1314.
Creative Research Systems. (n.d.). Sample size calculator. Retrieved from
https://www.surveysystem.com/sscalc.htm
Dehghan, A., Kovacevic, A., Karystianis, G., Keane, J. A., & Nenadic, G. (2017).
Learning to identify protected health information by integrating knowledge- and
data-driven algorithms: A case study on psychiatric evaluation notes. Journal of
Biomedical Informatics, 75(Supplement), S28–S33. https://doi-
org.lopes.idm.oclc.org/10.1016/j.jbi.2017.06.005
Delavar, F., Pashaeypoor, S., & Negarandeh, R. (2020). The effects of self-management
education tailored to health literacy on medication adherence and blood pressure
control among elderly people with primary hypertension: A randomized
controlled trial. Patient Education and Counseling, 103(2), 336–342. https://doi-
org.lopes.idm.oclc.org/10.1016/j.pec.2019.08.028

108
Dillon, P., McDowell, R., Smith, S. M., Gallagher, P., & Cousins, G. (2019).
Determinants of intentions to monitor antihypertensive medication adherence in
Irish community pharmacy: A factorial survey. BMC Family Practice, 20(1),
N.PAG. https://doi-org.lopes.idm.oclc.org/10.1186/s12875-019-1016-6
East, P., Doom, J., Delker, E., Blanco, E., Burrows, R., Correa-Burrows, P., … Gahagan,
S. (2020). Childhood socioeconomic hardship, family conflict, and young adult
hypertension: The Santiago longitudinal study. Social Science & Medicine, 253,
N.PAG. https://doi-org.lopes.idm.oclc.org/10.1016/j.socscimed.2020.112962
Eghbali-Babadi, M., Khosravi, A., Feizi, A., & Sarrafzadegan, N. (2017). Design and
implementation of a combined observational and interventional study: Trends of
prevalence, awareness, treatment and control hypertension and the effect of
expanded chronic care model on control, treatment and self-care. ARYA
Atherosclerosis, 13(5), 211–220.
Escortell-Mayor, E., del Cura-González, I., Ojeda-Ruiz, E., Sanz-Cuesta, T., Rodríguez-
Salceda, I., García-Soltero, J., Sanz-Velasco, C. (2020). A primary healthcare
information intervention for communicating cardiovascular risk to patients with
poorly controlled hypertension: The Education and Coronary Risk Evaluation
(educore) study – a pragmatic, cluster-randomized trial. PLoS ONE, 15(1), 1–17.
https://doi-org.lopes.idm.oclc.org/10.1371/journal.pone.0226398
Eskås, P. A., Heimark, S., Eek Mariampillai, J., Larstorp, A. C. K., Fadl Elmula, F. E.
M., & Høieggen, A. (2016). Adherence to medication and drug monitoring in
apparent treatment-resistant hypertension. Blood Pressure, 25(4), 199–205.
https://doi-org.lopes.idm.oclc.org/10.3109/08037051.2015.1121706

109
Etebari, F., Pezeshki, M. Z., & Fakour, S. (2019). Factors related to the non-adherence of
medication and nonpharmacological recommendations in high blood pressure
patients. Journal of Cardiovascular & Thoracic Research, 11(1), 28–34.
https://doi-org.lopes.idm.oclc.org/10.15171/jcvtr.2019.05
Faggion, J. C. M. (2015). Evaluating the risk of bias of a study. The Journal of Evidence-
Based Dental Practice, 15(4), 164–170. https://doi-
org.lopes.idm.oclc.org/10.1016/j.jebdp.2015.09.002
Firat Kilic, H., & Dag, S. (2020). The relationship between health literacy and medication
adherence in a hypertensive patient population. International Journal of Caring
Sciences, 13(1), 101–107.
Friesen, P., Kearns, L., Redman, B., & Caplan, A. L. (2017). Rethinking the Belmont
Report? American Journal of Bioethics, 17(7), 15–21. https://doi-
org.lopes.idm.oclc.org/10.1080/15265161.2017.1329482
Galozy, A., Nowaczyk, S., Sant, A. A., Ohlsson, M., & Lingman, M. (2020). Pitfalls of
medication adherence approximation through EHR and pharmacy records:
Definitions, data and computation. International Journal of Medical
Informatics, 136. https://doi-
org.lopes.idm.oclc.org/10.1016/j.ijmedinf.2020.104092
Gao, M., Chen, X., Sun, X., Wang, F., Fan, L., & Sun, X. (2020). Predicting stage of
exercise among patients with type 2 diabetes: A test of the extended theory of
Planned Behavior. Patient Preference & Adherence, 14, 277–285. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S236813

110
Gebremichael, G. B., Berhe, K. K., & Zemichael, T. M. (2019). Uncontrolled
hypertension and associated factors among adult hypertensive patients in Ayder
comprehensive specialized hospital, Tigray, Ethiopian 2018. BMC
Cardiovascular Disorders, 1. https://doi-org.lopes.idm.oclc.org/10.1186/s12872-
019-1091-6
Ghazali, R., Lukman, K. A., Naing, D. K. S., Kadir, F., Jeffree, M. S., Robinson, F.,
…Mathew. (2020). Factors associated with uncontrolled hypertension among
hypertensive patients reported from different primary health clinics in Tuaran,
Sabah, Malaysia: A cross sectional study. Turkiye Klinikleri Journal of Medical
Sciences, 40(1), 52–58. https://doi-org.lopes.idm.oclc.org/10.5336/medsci.2019-
66559
Grady, P. A. (2017). Investigating the determinants of health: The role of nursing science.
Nursing Outlook, 5, 489. https://doi-
org.lopes.idm.oclc.org/10.1016/j.outlook.2017.04.010
Hartley, E. M., Hoch, M. C., & Cramer, R. J. (2018). Health belief model and theory of
planned behavior: A theoretical approach for enhancing lower extremity injury
prevention program participation. International Journal of Athletic Therapy &
Training, 23(1), 16–20. https://doi-org.lopes.idm.oclc.org/10.1123/ijatt.2017-0016
Hosseinzadeh, M., Mahdavi, N., Valizadeh, S., Fooladi, M., Rahmani, F., Ghanouni, F.,
& Aghajari, P. (2019). Self-care behavior and self-care agency in lowering salt
consumption in hypertensive older patients based on orem’s self-care theory.
Social Health and Behavior, 3.
111
Ibe, C., Bowie, J., Roter, D., Carson, K. A., Lee, B., Monroe, D., & Cooper, L. A. (2017).
Intensity of exposure to a patient activation intervention and patient engagement
in medical visit communication. Patient Education and Counseling, 100(7),
1258–1267. https://doi-org.lopes.idm.oclc.org/10.1016/j.pec.2016.12.016
Ihm, S.-H., Bakris, G., Sakuma, I., Sohn, I. S., & Koh, K. K. (2019). Controversies in the
2017 ACC/AHA hypertension guidelines: Who can be eligible for treatments
under the new guidelines? – an Asian perspective. Circulation Journal, 83(3),
504–510. https://doi-org.lopes.idm.oclc.org/10.1253/circj.CJ-18-1293
Jankowska-Polańska, B., Uchmanowicz, I., Dudek, K., & Mazur, G. (2016). Relationship
between patients’ knowledge and medication adherence among patients with
hypertension. Patient Preference & Adherence, 10, 2437–2447. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S117269
Jeong, S. Y., & Kim, K. M. (2016). Influencing factors on hand hygiene behavior of
nursing students based on theory of planned behavior: A descriptive survey study.
Nurse Education Today, 36, 159–164. https://doi-
org.lopes.idm.oclc.org/10.1016/j.nedt.2015.09.014
Jin, H., Kim, Y., & Rhie, S. J. (2020). Factors affecting medication adherence in elderly
people. Patient Preference and Adherence, 2117. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S118121
Karaman, A., & Akyolcu, N. (2019). Role of intensive care nurses on guiding patients’
families/relatives to organ donation. Pakistan Journal of Medical Sciences, 35(4),
1115–1121. https://doi-org.lopes.idm.oclc.org/10.12669/pjms.35.4.1285

112
Khalilzadeh, J., & Tasci, A. D. A. (2017). Large sample size, significance level, and the
effect size: Solutions to perils of using big data for academic research. Tourism
Management, 89. https://doi-
org.lopes.idm.oclc.org/10.1016/j.tourman.2017.03.026
Khayyat, S. M., Mohamed, M. M. A., Khayyat, S. M. S., Hyat Alhazmi, R. S., Korani,
M. F., Allugmani, E. B., … Abdul Hadi, M. (2019). Association between
medication adherence and quality of life of patients with diabetes and
hypertension attending primary care clinics: A cross-sectional survey. Quality of
Life Research, 28(4), 1053–1061. https://doi-
org.lopes.idm.oclc.org/10.1007/s11136-018-2060-8
Kilgus, S. P., von der Embse, N. P., Eklund, K., Izumi, J., Peet, C., Meyer, L., & Taylor,
C. N. (2019). Reliability, validity, and accuracy of the intervention selection
profile – function: A brief functional assessment tool. School Psychology.
https://doi-org.lopes.idm.oclc.org/10.1037
Kim, M. T., Hill, M. N., Bone, L. R., Levine, D. M. (2000). Development and testing of
the Hill-Bone compliance to high blood pressure therapy scale. Progress in
Cardiovascular Nursing, 15(3), 90-96. Retrieved from
https://www.ncbi.nlm.nih.gov/pubmed/10951950
Li, Y., Jasani, F., Su, D., Zhang, D., Shi, L., Yi, S. S., & Pagán, J. A. (2019). Decoding
nonadherence to hypertensive medication in New York City: a population
segmentation approach. Journal of Primary Care & Community Health, 10.
https://doi-org.lopes.idm.oclc.org/10.1177/2150132719829311

113
Luckhaupt, S. E., & Calvert, G. M. (2014). Prevalence of coronary heart disease or stroke
among workers aged < 55 years – United States, 2008-2012. Morbidity and
Mortality Weekly Report, 63(30), 645–649.
Magnabosco, P., Teraoka, E. C., de Oliveira, E. M., Felipe, E. A., Freitas, D., & Marchi-
Alves, L. M. (2015). Comparative analysis of non-adherence to medication
treatment for systemic arterial hypertension in urban and rural populations.
Revista Latino-American de Enfermagem, 23(1), 20–27. https://doi-
org.lopes.idm.oclc.org/10.1590/0104-1169.0144.2520
Mahmoodi, H., Nahand, F. J., Shaghaghi, A., Shooshtari, S., Jafarabadi, M. A., &
Allahverdipour, H. (2019). Gender based cognitive determinants of medication
adherence in older adults with chronic conditions. Patient Preference &
Adherence, 13, 1733–1744. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S219193
Malek, N., Heath, C. A., & Greene, J. (2017). A review of medication adherence in
people with epilepsy. Acta Neurologica Scandinavica, 135(5), 507–515.
https://doi-org.lopes.idm.oclc.org/10.1111/ane.12703
Mallia, P. (2018). WASP (write a scientific paper): Informed consent in research. Early
Human Development, 124, 54–57. https://doi-
org.lopes.idm.oclc.org/10.1016/j.earlhumdev.2018.04.025
Mamaghani, E. A., Hasanpoor, E., Maghsoodi, E., & Soleimani, F. (2020). Barriers to
medication adherence among hypertensive patients in deprived rural areas.
Ethiopian Journal of Health Sciences, 30(1), 85–94. https://doi-
org.lopes.idm.oclc.org/10.4314/ejhs.v30i1.11

114
Masilela, C., Pearce, B., Ongole, J. B., Adeniyi, O. L., & Benjeddou, M. (2020). Cross-
sectional study of prevalence and determinants of uncontrolled hypertension
among South African adult residents of Mkhondo municipality. BMC Public
Health, 20(1), 1–10. https://doi-org.lopes.idm.oclc.org/10.1186/s12889-020-
09174-7
Maslakpak, M. H., & Safaie, M. (2016). A Comparison between the effectiveness of
short message service and reminder cards regarding medication adherence in
patients with hypertension: A randomized controlled clinical trial. International
Journal of Community Based Nursing and Midwifery, 4(3), 209–218.
McGillicuddy, J. W., Taber, D. J., Mueller, M., Patel, S., Baliga, P. K., Chavin, K. D., …
Treiber, F. A. (2015). Sustainability of improvements in medication adherence
through a mobile health intervention. Progress in Transplantation, 25(3), 217–
223. https://doi-org.lopes.idm.oclc.org/10.7182/pit2015975
McKoy, J., Fitzner, K., Margetts, M., Heckinger, E., Specker, J., Roth, L., … Moss, G.
(2015). Are telehealth technologies for hypertension care and self-management
effective or simply risky and costly? Population Health Management, 18(3), 192–
202. https://doi-org.lopes.idm.oclc.org/10.1089/pop.2014.0073
Mekonnen, G. B., & Gelayee, D. A. (2020). Low medication knowledge and adherence
to oral chronic medications among patients attending community pharmacies: A
cross-sectional study in a low-income country. BioMed Research International,
1–9. https://doi-org.lopes.idm.oclc.org/10.1155/2020/4392058
115
Miranda, A. C., Serag-Bolos, E. S., & Cooper, J. B. (2019). Cost-related medication
underuse: Strategies to improve medication adherence at care transitions.
American Journal of Health-System Pharmacy, 76(8), 560–565. https://doi-
org.lopes.idm.oclc.org/10.1093/ajhp/zxz010
Mishra, P., Singh, U., Pandey, C., Mishra, P., & Pandey, G. (2019). Application of
student’s t-test, analysis of variance, and covariance. Annals of Cardiac
Anaesthesia, 4.
Morrissey, E. C., Casey, M., Glynn, L. G., Walsh, J. C., & Molloy, G. J. (2020).
Smartphone apps for improving medication adherence in hypertension: Patients’
perspectives. Patient Preference and Adherence, 813. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S145647
Morrissey, E. C., Durand, H., Nieuwlaat, R., Navarro, T., Haynes, R. B., Walsh, J. C., &
Molloy, G. J. (2016). Effectiveness and content analysis of interventions to
enhance medication adherence in hypertension: A systematic review and meta-
analysis protocol. Systematic Reviews, 5, 1.
Mugwano, I., Kaddumukasa, M., Mugenyi, L., Kayima, J., Ddumba, E., Sajatovic, M.,
Sila, C., DeGeorgia, M., & Katabira, E. (2016). Poor drug adherence and lack of
awareness of hypertension among hypertensive stroke patients in Kampala,
Uganda: A cross sectional study. BMC Research Notes, 9, 1–8. https://doi-
org.lopes.idm.oclc.org/10.1186/s13104-015-1830-4

116
Náfrádi, L., Galimberti, E., Nakamoto, K., & Schulz, P. J. (2016). Intentional and
unintentional medication non-adherence in hypertension: The role of health
literacy, empowerment and medication beliefs. Journal of Public Health
Research, 5(3), 111–115. https://doi-
org.lopes.idm.oclc.org/10.4081/jphr.2016.762
Náfrádi, L., Nakamoto, K., & Schulz, P. J. (2017). Is patient empowerment the key to
promote adherence? A systematic review of the relationship between self-
efficacy, health locus of control and medication adherence. PLoS ONE, 12(10), 1–
23. https://doi-org.lopes.idm.oclc.org/10.1371/journal.pone.0186458
Najimi, A., Mostafavi, F., Sharifirad, G., & Golshiri, P. (2018). Barriers to medication
adherence in patients with hypertension: A qualitative study. Journal of
Education and Health Promotion, 7, 24. https://doi-
org.lopes.idm.oclc.org/10.4103/jehp.jehp_65_16
Napierkowski, D., & Prado, K. B. (2020). Hypertension: A discussion of the guidelines.
Women’s Healthcare: A Clinical Journal for NPs, 8(3), 36–40.
National Institutes of Health. (2017). The all of us research program. Retrieved from
https://allofus-nih-gov.lopes.idm.oclc.org
Neufcourt, L., Deguen, S., Bayat, S., Zins, M., & Grimaud, O. (2020). Gender differences
in the association between socioeconomic status and hypertension in France: A
cross-sectional analysis of the CONSTANCES cohort. PLoS ONE, 4. https://doi-
org.lopes.idm.oclc.org/10.1371/journal.pone.0231878

117
Nguyen-Huynh, M. N., Young, J. D., Alexeeff, S., Hatfield, M. K., & Sidney, S. (2019).
Shake rattle & roll – design and rationale for a pragmatic trial to improve blood
pressure control among blacks with persistent hypertension. Contemporary
Clinical Trials, 76, 85–92. https://doi-
org.lopes.idm.oclc.org/10.1016/j.cct.2018.11.012
Nielsen, J. O., Shrestha, A. D., Neupane, D., & Kallestrup, P. (2017). Non-adherence to
anti-hypertensive medication in low- and middle-income countries: A systematic
review and meta-analysis of 92443 subjects. Journal of Human Hypertension, 1.
https://doi-org.lopes.idm.oclc.org/10.1038/jhh.2016.31
Nikparvar, M., Farshidi, H., Madani, A., Ezatirad, R., Azad, M., Eftekhaari, T. E., …
Kassem, H. H. (2019). Prevalence, awareness, treatment, and control of
hypertension in Hormozgan Province, Iran. International Cardiovascular
Research Journal, 13(3), 91–95.
Orem, D. E. (2001). Nursing: Concepts of practice. Savannah, Georgia: Mosby.
Pan, J., Lei, T., Hu, B., & Li, Q. (2020). Post-discharge evaluation of medication
adherence and knowledge of hypertension among hypertensive stroke patients in
northwestern China. Patient Preference and Adherence. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S147605
Patel, M. M., Datu, B., Roman, D., Barton, M. B., Ritchey M. D., Wall, H. K., &
Loustalot, F. (2014). Progress of health plans toward meeting the Million Hearts
clinical target for high blood pressure control – United States, 2010-
2012. Morbidity and Mortality Weekly Report, 63(6), 127.
118
Pawloski, P. A., Asche, S. E., Trower, N. K., Bergdall, A. R., Dehmer, S. P., Maciosek,
M. V., … Margolis, K. L. (2016). A substudy evaluating treatment intensification
on medication adherence among hypertensive patients receiving home blood
pressure telemonitoring and pharmacist management. Journal of Clinical
Pharmacy & Therapeutics, 41(5), 493.
Persell, S. D., Karmali, K. N., Stein, N., Li, J., Peprah, Y. A., Lipiszko, D., … Sato, H.
(2018). Design of a randomized controlled trial comparing a mobile phone-based
hypertension health coaching application to home blood pressure monitoring
alone: The smart hypertension control study. Contemporary Clinical Trials, 73,
92–97. https://doi-org.lopes.idm.oclc.org/10.1016/j.cct.2018.08.013
Pioli, M.R., Ritter, A.M.V., de Faria, A.P., & Modolo, R. (2018). White coat syndrome
and its variations: Differences and clinical impact. Integrated Blood Pressure
Control, 11, 73–79.
Prendergast, H. M., Del Rios, M., Petzel-Gimbar, R., Garside, D., Heinert, S., Escobar-
Schulz, S., … Daviglus, M. (2018). A hypertension emergency department
intervention aimed at decreasing disparities: Design of a randomized clinical
trial. Contemporary Clinical Trials. https://doi-
org.lopes.idm.oclc.org/10.1016/j.cct.2017.11.009
Ritchey, M., Chang, A., Powers, C., Loustalot, F., Schieb, L., Ketchum, M., Durthaler, J.
& Hong, Y. (2016). Vital signs: Disparities in antihypertensive medication
nonadherence among Medicare Part D beneficiaries – Unites States, 2014.
Morbidity and Mortality Weekly Report, 65(36), 967-976. Retrieved from
https://www.cdc.gov/mmwr/volumes/65/wr/pdfs/mm6536e1.pdf

119
Robbins, R., Butler, M., & Schoenthaler, A. (2019). Provider burnout and patient-
provider communication in the context of hypertension care. Patient Education
and Counseling, 102(8), 1452–1459. https://doi-
org.lopes.idm.oclc.org/10.1016/j.pec.2019.03.014
Ruiz-Fernández, D., Marcos-Jorquera, D., Gilart-Iglesias, V., Vives-Boix, V., &
Ramírez-Navarro, J. (2017). Empowerment of patients with hypertension through
BPM, IoT and remote sensing. Sensors, 17(10), 2273. https://doi-
org.lopes.idm.oclc.org/10.3390/s17102273
Ruppar, T. M., Dobbels, F., Lewek, P., Matyjaszczyk, M., Siebens, K., & De Geest, S.
M. (2015). Systematic review of clinical practice guidelines for the improvement
of medication adherence. International Journal of Behavioral Medicine, 22(6),
699–708. https://doi-org.lopes.idm.oclc.org/10.1007/s12529-015-9479-x
Saradamma, J. C. N., Kottarath, A. T., Saleem, A., Jaya, A. T., & Thaj, A. (2019). Risk
factors associated with uncontrolled hypertension among treated adults residing in
an urban area of Kerala – a cross sectional study. Journal of Evidence Based
Medicine and Healthcare, 6(10), 751–756. https://doi-
org.lopes.idm.oclc.org/10.18410/jebmh/2019/156
Sato, T., & Hodge, S. R. (2009). Japanese physical educators’ beliefs on teaching
students with disabilities at urban high schools. Asia Pacific Journal of
Education, 29(2), 159–177.

120
Schoenthaler, A., Basile, M., West, T. V., & Kalet, A. (2018). It takes two to tango: a
dyadic approach to understanding the medication dialogue in patient-provider
relationships. Patient Education & Counseling, 101(8), 1500–1505. https://doi-
org.lopes.idm.oclc.org/10.1016/j.pec.2018.02.009
Schoenthaler, A., Butler, M., Chaplin, W., Tobin, J., Ogedegbe, G., & Schoenthaler, A.
M. (2016). Predictors of changes in medication adherence in blacks with
hypertension: Moving beyond cross-sectional data. Annals of Behavioral
Medicine, 50(5), 642–652. https://doi-org.lopes.idm.oclc.org/10.1007/s12160-
016-9791-y
Scholte, M., van Dulmen, S. A., Neeleman-Van der Steen, C. W. M., van der Wees, P. J.,
Nijhuis-van der Sanden, M. W. G., & Braspenning, J. (2016). Data extraction
from electronic health records (EHRs) for quality measurement of the physical
therapy process: Comparison between EHR data and survey data. BMC Medical
Informatics & Decision Making, 16, 1–11. https://doi-
org.lopes.idm.oclc.org/10.1186/s12911-016-0382-4
Seyedin, S. H., Ravaghi, H., & Nikmaram, M. (2016). Applying the theory of planned
behavior to evaluate the clinical errors reported by nurses in general hospitals
affiliated to Alborz University of Medical Sciences in Karaj in 2015.19(64), 56–
64.
Shen, Y., Peng, X., Wang, M., Zheng, X., Xu, G., Lu, L., … Wang, J. (2017). Family
member-based supervision of patients with hypertension: A cluster randomized
trial in rural China. Journal of Human Hypertension, 1. https://doi-
org.lopes.idm.oclc.org/10.1038/jhh.2016.8

121
Showalter, D. A., & Mullet, L. B. (2017). Sniffing out the secret poison: selection bias in
educational research. Mid-Western Educational Researcher, 29(3), 207–234.
Smith, D., Lovell, J., Weller, C., Kennedy, B., Winbolt, M., Young, C., & Ibrahim, J.
(2017). A systematic review of medication non-adherence in persons with
dementia or cognitive impairment. PLOS ONE, 12(2). https://doi-
org.lopes.idm.oclc.org/10.1371/journal.pone.0170651
Song, H., Feng, D., Wang, R., Yang, J., Li, Y., Gao, J., … Feng, Z. (2019). The urban-
rural disparity in the prevalence and risk factors of hypertension among the
elderly in China-a cross-sectional study. PeerJ. https://doi-
org.lopes.idm.oclc.org/10.7717/peerj.8015
Song, Y., Han, H.-R., Song, H.-J., Nam, S., Nguyen, T., & Kim, M. T. (2011).
Psychometric evaluation of Hill-Bone medication adherence subscale. Asia
Nursing Research, 5(3), 183–188. https://doi-
org.lopes.idm.oclc.org/10.1016/j.anr.2011.09.007
Sonğur, C., Özer, Ö., Gün, Ç., & Top, M. (2018). Patient safety culture, evidence-based
practice and performance in nursing. Systemic Practice & Action Research, 31(4),
359–374. https://doi-org.lopes.idm.oclc.org/10.1007/s11213-017-9430-y
Sulmasy, L. S., López, A. M., & Horwitch, C. A. (2017). Ethical implications of the
electronic health record: In the service of the patient. Journal of General Internal
Medicine, 32(8), 935–939. https://doi-org.lopes.idm.oclc.org/10.1007/s11606-
017-4030-1

122
Tan, C. S., Hassali, M. A., Neoh, C. F., & Saleem, F. (2017). A qualitative exploration of
hypertensive patients’ perception towards quality use of medication and
hypertension management at the community level. Pharmacy Practice, 15(4), 1–
11. https://doi-org.lopes.idm.oclc.org/10.18549/PharmPract.2017.04.1074
Tavakoly Sany, S. B., Peyman, N., Behzhad, F., Esmaeily, H., Taghipoor, A., & Ferns,
G. (2018). Health providers’ communication skills training affects hypertension
outcomes. Medical Teacher, 40(2), 154–163. https://doi-
org.lopes.idm.oclc.org/10.1080/0142159X.2017.1395002
Tesfaye, B., Haile, D., Lake, B., Belachew, T., Tesfaye, T., & Abera, H. (2020).
Uncontrolled hypertension and associated factors among adult hypertensive
patients on follow-up at Jimma University Teaching and Specialized Hospital:
Cross-sectional study. Research Reports in Clinical Cardiology, 21. https://doi-
org.lopes.idm.oclc.org/10.2147/RRCC.S132126
The Johns Hopkins University School of Nursing. (2020). Retrieved from
https://nursing.jhu.edu/faculty_research/research/projects/hill-bone/hill-bone-
scales.html
Theofanidis, D., & Fountouki, A. (2018). Limitations and delimitations in the research
process. Perioperative Nursing, 7(3), 155–163. https://doi-
org.lopes.idm.oclc.org/10.5281/zenodo.2552022
Turcu-Stiolica, A., Subtirelu, M. S., Meca, A. D., & Bogdan, M. (2019). The importance
of medication adherence assessment for hypertensive patients. Romanian Journal
of Medical and Dental Education, 8(11), 18–24.

123
Van den Berg, A., & Struwig, M. (2017). Guidelines for researchers using an adapted
consensual qualitative research approach in management research. Electronic
Journal of Business Research Methods, 15(2), 109–119.
Veisani, Y., Jenabi, E., Nematollahi, S., Delpisheh, A., & Khazaei, S. (2019). The role of
socio-economic inequality in the prevalence of hypertension in adults. Journal of
Cardiovascular & Thoracic Research, 11(2), 116–120. https://doi-
org.lopes.idm.oclc.org/10.15171/jcvtr.2019.20
Verma, V., Ivanov, A., Benn, F., Rathi, A., Tran, N., Afzal, A., … John F Heitner, J. F.
(2020). Analyses of electronic health records utilization in a large community
hospital. PLoS ONE, 15(7), e0233004. https://doi-
org.lopes.idm.oclc.org/10.1371/journal.pone.0233004
Walsh, C. A., Bennett, K. E., Wallace, E., & Cahir, C. (2020). Identifying adherence
patterns across multiple medications and their association with health outcomes in
older community-dwelling adults with multimorbidity. Value in Health, 23(8),
1063–1071. https://doi-org.lopes.idm.oclc.org/10.1016/j.jval.2020.03.016
Wahyuni, A. S., Mukhtar, Z., Pakpahan, D. J. R., Guhtama, M. A., Diansyah, R.,
Situmorang, N. Z. & Wahyuniar, L. (2019). Adherence to consuming medication
for hypertension patients at primary health care in Medan City. Open Access
Macedonian Journal of Medical Sciences, 7(20). https://doi-
org.lopes.idm.oclc.org/10.3889/oamjms.2019.683
Wang, Z., Luo, Y., Yang, S., Zuo, M., Pei, R., He, J., Deng, Y., Zhou, M., Zhao, L., Guo,
H., & Zou, K. (2020). Death burden of high systolic blood pressure in Sichuan
Southwest China 1990-2030. BMC Public Health, 20(1), 1.

124
Webster, L., Reed, K., Seed, P., Burns, A., Gupta, P., Patel, P., Wiesender, C., Nelson-
Piercy, C., Myers, J., & Chappell, L. (2018). 230. Quantifying adherence to
antihypertensive medication for chronic hypertension during pregnancy.
Pregnancy Hypertension. https://doi-
org.lopes.idm.oclc.org/10.1016/j.preghy.2018.08.312
Whelan, E.G. (1984). Analysis and application of Dorothea Orem’s self-care practice
model. Journal of Nursing Education, 23(8), 342–345. https://doi-
org.lopes.idm.oclc.org/10.3928/0148-4834-19841001-07
Woodhama, N., Taneepanichskul, S., Somrongthong, R., Auamkul, N. (2018).
Medication adherence and associated factors among elderly hypertension patients
with uncontrolled blood pressure in rural area, Northeast Thailand. Journal of
Health Research, 32(6), 449–58. doi:10.1108/JHR-11-2018-
085/full/pdf?title=medication-adherence-and-associated-factors-among-elderly-
hypertension-patients-with-uncontrolled-blood-pressure-in-rural-area-northeast-
thailand.
Yazdanpanah, Y., Saleh Moghadam, A. R., Mazlom, S. R., Ali Beigloo, R. H., &
Mohajer, S. (2019). Effect of an educational program based on health belief
model on medication adherence in elderly patients with hypertension. Journal of
Evidence-Based Care, 9(1), 52–62. https://doi-
org.lopes.idm.oclc.org/10.22038/ebcj.2019.35215.1895

125
Yusupov, E., Krishnamachari, B., Rand, S., Abdalla, M., & Zwibel, H. (2019). Quality of
hypertension care: An improvement initiative in two outpatient health care
centers. Journal of Evaluation in Clinical Practice, 25(3), 463–468. https://doi-
org.lopes.idm.oclc.org/10.1111/jep.13067
Zhang, Y., Li, X., Mao, L., Zhang, M., Li, K., Zheng, Y., … Jing, M. (2020). Factors
affecting medication adherence in community-managed patients with
hypertension based on the principal component analysis: Evidence from Xinjiang,
China. Patient Preference and Adherence, 803. https://doi-
org.lopes.idm.oclc.org/10.2147/PPA.S158662
Zilbermint, M., Hannah-Shmouni, F., & Stratakis, C. A. (2019). Genetics of hypertension
in African Americans and others of African descent. International Journal of
Molecular Sciences, 20(5). https://doi-
org.lopes.idm.oclc.org/10.3390/ijms20051081
Zullig, L. L., Shaw, R. J., Shah, B. R., Peterson, E. D., Lindquist, J. H., Crowley, M. J.,
… Bosworth, H. B. (2015). Patient–provider communication, self-reported
medication adherence, and race in a post-myocardial infarction population.
Patient Preference and Adherence, 2015, 311–318.

126
Appendix A
Grand Canyon University Institutional Review Board Outcome Letter

127
Appendix B
Hill-Bone Medication Adherence Scale (HB-MAS)

128
Appendix C
Permission to Use Hill Bone Scale (HB-MAS)
Please consider this message as permission to use the Hill-Bone Scale(s).*
Click the link below to access articles regarding scoring, validation and the original scales.
We request that you cite the scale using the references provided in the link. We appreciate
you sharing the findings of your project with us.
Link: https://nursing.jhu.edu/faculty_research/research/projects/hill-bone/hill-bone-scales-
confirmation.html
Please don't hesitate to reach out to us at [email protected] if you have any follow-
up questions.
Best,
The Hill-Bone Scales team
* Note: Please do not share these documents with anyone else outside your project. We ask
that anyone who wishes to use the scale should submit a formal request using the link
provided for proper authorization.
Survey Powered By Qualtrics

129
Appendix D
Center for Disease Control and Prevention Million Hearts Tools

130

131
132
Appendix E
Permission to Use Center of Disease Control and Prevention Million Hearts Tools
Permission
Inbox x
Chin
yere
Oghi
de
May 24, 2020, 11:40
PM (4 days ago)
Permission to Use Tools: This is to request for permission to use the information on education on h
your company's website.
Million Hearts (CDC)
May 26, 2020, 2:18 PM
(2 days ago)
to me
Hello Chinyere,
Thank you for your interest in Million Hearts®.
You are free to use this content as you deem fit. All of our published online content is within
public domain and is available for use.
If you have any other questions, do not hesitate to reach out.
Thank you,
The Million Hearts® Team
Copyright © 2022 FDOKUMEN




















