
Focused ultrasound-mediated drug delivery to pancreatic cancer in a mouse model
11
RESEARCH Open Access Focused ultrasound-mediated drug delivery to pancreatic cancer in a mouse model Natalya Rapoport 1* , Allison Payne 2 , Christopher Dillon 1 , Jill Shea 3 , Courtney Scaife 3 and Roohi Gupta 1,4 Abstract Background: Many aspects of the mechanisms involved in ultrasound-mediated therapy remain obscure. In particular, the relative roles of drug and ultrasound, the effect of the time of ultrasound application, and the effect of tissue heating are not yet clear. The current study was undertaken with the goal to clarify these aspects of the ultrasound-mediated drug delivery mechanism. Methods: Focused ultrasound-mediated drug delivery was performed under magnetic resonance imaging guidance (MRgFUS) in a pancreatic ductal adenocarcinoma (PDA) model grown subcutaneously in nu/nu mice. Paclitaxel (PTX) was used as a chemotherapeutic agent because it manifests high potency in the treatment of gemcitabine-resistant PDA. Poly(ethylene oxide)-co-poly(D,L-lactide) block copolymer stabilized perfluoro-15-crown- 5-ether nanoemulsions were used as drug carriers. MRgFUS was applied at sub-ablative pressure levels in both continuous wave and pulsed modes, and only a fraction of the tumor was treated. Results: Positive treatment effects and even complete tumor resolution were achieved by treating the tumor with MRgFUS after injection of nanodroplet encapsulated drug. The MRgFUS treatment enhanced the action of the drug presumably through enhanced tumor perfusion and blood vessel and cell membrane permeability that increased the drug supply to tumor cells. The effect of the pulsed MRgFUS treatment with PTX-loaded nanodroplets was clearly smaller than that of continuous wave MRgFUS treatment, supposedly due to significantly lower temperature increase as measured with MR thermometry and decreased extravasation. The time of the MRgFUS application after drug injection also proved to be an important factor with the best results observed when ultrasound was applied at least 6 h after the injection of drug-loaded nanodroplets. Some collateral damage was observed with particular ultrasound protocols supposedly associated with enhanced inflammation. Conclusion: This presented data suggest that there exists an optimal range of ultrasound application parameters and drug injection time. Decreased tumor growth, or complete resolution, was achieved with continuous wave ultrasound pressures below or equal to 3.1 MPa and drug injection times of at least 6 h prior to treatment. Increased acoustic pressure or ultrasound application before or shortly after drug injection gave increased tumor growth when compared to other protocols. Keywords: Ultrasound-mediated drug delivery, Perfluorocarbon nanoemulsions, MRgFUS, Pancreatic cancer * Correspondence: [email protected] 1 Department of Bioengineering, University of Utah, 36 S. Wasatch Dr., Room 3100, Salt Lake City, UT 84112, USA Full list of author information is available at the end of the article © 2013 Rapoport et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 http://www.jtultrasound.com/content/1/1/11
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Focused ultrasound-mediated drug delivery to pancreatic cancer in a mouse model

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11http://www.jtultrasound.com/content/1/1/11
RESEARCH Open Access
Focused ultrasound-mediated drug delivery topancreatic cancer in a mouse modelNatalya Rapoport1*, Allison Payne2, Christopher Dillon1, Jill Shea3, Courtney Scaife3 and Roohi Gupta1,4
Abstract
Background: Many aspects of the mechanisms involved in ultrasound-mediated therapy remain obscure. Inparticular, the relative roles of drug and ultrasound, the effect of the time of ultrasound application, and the effectof tissue heating are not yet clear. The current study was undertaken with the goal to clarify these aspects of theultrasound-mediated drug delivery mechanism.
Methods: Focused ultrasound-mediated drug delivery was performed under magnetic resonance imagingguidance (MRgFUS) in a pancreatic ductal adenocarcinoma (PDA) model grown subcutaneously in nu/nu mice.Paclitaxel (PTX) was used as a chemotherapeutic agent because it manifests high potency in the treatment ofgemcitabine-resistant PDA. Poly(ethylene oxide)-co-poly(D,L-lactide) block copolymer stabilized perfluoro-15-crown-5-ether nanoemulsions were used as drug carriers. MRgFUS was applied at sub-ablative pressure levels in bothcontinuous wave and pulsed modes, and only a fraction of the tumor was treated.
Results: Positive treatment effects and even complete tumor resolution were achieved by treating the tumor withMRgFUS after injection of nanodroplet encapsulated drug. The MRgFUS treatment enhanced the action of the drugpresumably through enhanced tumor perfusion and blood vessel and cell membrane permeability that increasedthe drug supply to tumor cells. The effect of the pulsed MRgFUS treatment with PTX-loaded nanodroplets wasclearly smaller than that of continuous wave MRgFUS treatment, supposedly due to significantly lower temperatureincrease as measured with MR thermometry and decreased extravasation. The time of the MRgFUS application afterdrug injection also proved to be an important factor with the best results observed when ultrasound was appliedat least 6 h after the injection of drug-loaded nanodroplets. Some collateral damage was observed with particularultrasound protocols supposedly associated with enhanced inflammation.
Conclusion: This presented data suggest that there exists an optimal range of ultrasound application parametersand drug injection time. Decreased tumor growth, or complete resolution, was achieved with continuous waveultrasound pressures below or equal to 3.1 MPa and drug injection times of at least 6 h prior to treatment.Increased acoustic pressure or ultrasound application before or shortly after drug injection gave increased tumorgrowth when compared to other protocols.
Keywords: Ultrasound-mediated drug delivery, Perfluorocarbon nanoemulsions, MRgFUS, Pancreatic cancer
* Correspondence: [email protected] of Bioengineering, University of Utah, 36 S. Wasatch Dr., Room3100, Salt Lake City, UT 84112, USAFull list of author information is available at the end of the article
© 2013 Rapoport et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 2 of 11http://www.jtultrasound.com/content/1/1/11
IntroductionChemotherapy remains the treatment of choice for manytypes of cancer. During the last decade, progress innanotechnology has enabled tumor-targeted delivery ofanticancer drugs, which simultaneously decreased sideeffects and increased drug concentration in tumor tissue.However, the dream of a ‘magic bullet’ that would exclu-sively target the tumor remains elusive. In pursuit of thisgoal, a number of groups have been directing their ef-forts to increase the degree of drug tumor-targetingusing ultrasound-mediated drug delivery. In this ap-proach, drug delivery with nanoparticles is combinedwith tumor-directed ultrasound that affects both thedrug carrier and tumor tissue. The use of ultrasoundtriggers drug release from the nanoparticle carrier andincreases drug and carrier extravasation and depositionin tumor cells.Focused ultrasound (FUS) has a number of advantages
when compared with other physical methods used intumor therapy: it can penetrate deep into the body, canbe focused in a region with a diameter of approximately1 mm, can be carefully controlled, and is completelynon-invasive. FUS has both thermal (local heating of tis-sue to hyperthermia or ablative temperatures) and non-thermal mechanisms (i.e., cavitation and radiation force).These mechanisms are expected to work synergisticallyto trigger drug release from the carrier, increase extrava-sation and internalization of carrier and drug, and in-crease drug diffusion in tumor tissue, which ultimatelyresults in an enhanced treatment outcome.Development of real-time imaging methods such as
magnetic resonance imaging (MRI) or ultrasound imagingallows precise spatiotemporal control of FUS-mediateddrug delivery. Imaging assists in the identification of thetarget, guidance of ultrasound action, and evaluation oftherapeutic efficacy. Moreover, real-time temperaturemeasurements during treatment using MRI thermometryprovide data that can be used in a feedback controller toenable greater control of the energy delivery [1,2].Bioeffects of ultrasound in drug delivery may be en-
hanced by the application of microbubbles, which havebeen widely used as ultrasound contrast agents. Thisnovel application of microbubbles is associated with en-hanced cavitation [3-13]; microbubbles have been suc-cessfully used for opening blood/brain and blood/retinalbarriers [7,9,14,15] or enhancing thrombus dissolution[16-18]. However, the size of microbubbles (usually 2 to10 microns) precludes their extravasation into the tumortissue.We have developed drug-loaded perfluorocarbon
nanoemulsions that serve as nanoscale microbubble pre-cursors [19-24]. Due to their size (200 to 300 nm, i.e., atleast the order of magnitude is smaller than microbubbles),nanodroplets can extravasate into the tumor tissue. Under
the action of tumor-directed ultrasound, perfluorocarbondroplets convert into microbubbles [25-28]. Droplet-to-bubble conversion results in a release of an encapsulateddrug [21,23,29-33]. Using paclitaxel-loaded perfluoro-carbon nanoemulsions, successful therapy of breast, ovar-ian, and pancreatic cancer has been achieved in preclinicalstudies using animal models; in these studies, unfocusedultrasound was blindly applied to the tumor region [21,22].Despite these successes, many aspects of the mecha-
nisms involved in ultrasound-mediated therapy remainobscure. In particular, the relative roles of drug andultrasound applications, the effect of the time of ultra-sound application, and the effect of tissue heating arenot yet clear. The current study was undertaken withthe goal to clarify these aspects of the FUS-mediateddrug delivery mechanism. A pancreatic ductal adeno-carcinoma (PDA) model grown subcutaneously in nu/numice was used as a tumor model.PDA is the fourth leading cause of death from can-
cer in the USA, and novel approaches to PDA therapyare urgently needed. Poor PDA response to conven-tional chemotherapy is at least partly accounted for bypoor tumor vascularization and high content ofstroma that precludes effective drug delivery and diffu-sion throughout tumor volume [34-44]. Since FUS-mediated drug delivery enhances drug extravasationand diffusion, this treatment modality is expected tohave significant impact on the development of effect-ive PDA therapy.In this study, FUS-mediated drug delivery was performed
under MRI guidance. Paclitaxel (PTX) was used as a che-motherapeutic agent because it manifested high potency inthe treatment of gemcitabine-resistant PDA [45]. Poly(ethylene oxide)-co-poly(D,L-lactide) (PEG-PDLA) blockcopolymer stabilized perfluoro-15-crown-5-ether (PFCE)nanoemulsions or their mixtures with polymeric micelleswere used as drug carriers [21,31,33]. As manifested by theappearance of harmonic frequencies in the fast Fouriertransform emission spectra, PFCE nanodroplets wereconverted into microbubbles under ultrasound irradiationand underwent stable cavitation in both liquid emulsionsand gel matrices [32]. Droplet-to-bubble conversion pro-ceeded presumably via the evolution of dissolved oxygeninto a separate phase [21].The objective of this study is to better understand the
advantages and limitations of the FUS-mediated drugdelivery application to PDA therapy.
Materials and methodsDrugPTX was used as a chemotherapeutic agent because ithas manifested high potency in the treatment ofgemcitabine-resistant PDA [45]. PTX was obtained fromLC Laboratories (Woburn, MA, USA).
Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 3 of 11http://www.jtultrasound.com/content/1/1/11
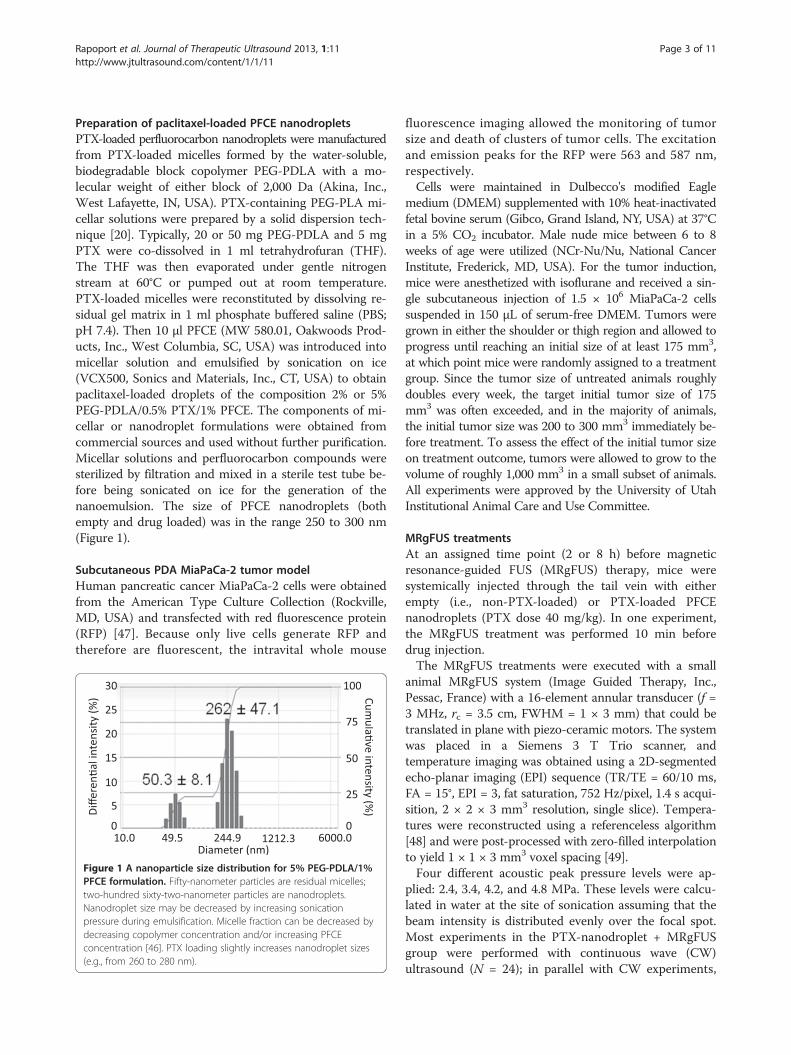
Preparation of paclitaxel-loaded PFCE nanodropletsPTX-loaded perfluorocarbon nanodroplets were manufacturedfrom PTX-loaded micelles formed by the water-soluble,biodegradable block copolymer PEG-PDLA with a mo-lecular weight of either block of 2,000 Da (Akina, Inc.,West Lafayette, IN, USA). PTX-containing PEG-PLA mi-cellar solutions were prepared by a solid dispersion tech-nique [20]. Typically, 20 or 50 mg PEG-PDLA and 5 mgPTX were co-dissolved in 1 ml tetrahydrofuran (THF).The THF was then evaporated under gentle nitrogenstream at 60°C or pumped out at room temperature.PTX-loaded micelles were reconstituted by dissolving re-sidual gel matrix in 1 ml phosphate buffered saline (PBS;pH 7.4). Then 10 μl PFCE (MW 580.01, Oakwoods Prod-ucts, Inc., West Columbia, SC, USA) was introduced intomicellar solution and emulsified by sonication on ice(VCX500, Sonics and Materials, Inc., CT, USA) to obtainpaclitaxel-loaded droplets of the composition 2% or 5%PEG-PDLA/0.5% PTX/1% PFCE. The components of mi-cellar or nanodroplet formulations were obtained fromcommercial sources and used without further purification.Micellar solutions and perfluorocarbon compounds weresterilized by filtration and mixed in a sterile test tube be-fore being sonicated on ice for the generation of thenanoemulsion. The size of PFCE nanodroplets (bothempty and drug loaded) was in the range 250 to 300 nm(Figure 1).
Subcutaneous PDA MiaPaCa-2 tumor modelHuman pancreatic cancer MiaPaCa-2 cells were obtainedfrom the American Type Culture Collection (Rockville,MD, USA) and transfected with red fluorescence protein(RFP) [47]. Because only live cells generate RFP andtherefore are fluorescent, the intravital whole mouse
Figure 1 A nanoparticle size distribution for 5% PEG-PDLA/1%PFCE formulation. Fifty-nanometer particles are residual micelles;two-hundred sixty-two-nanometer particles are nanodroplets.Nanodroplet size may be decreased by increasing sonicationpressure during emulsification. Micelle fraction can be decreased bydecreasing copolymer concentration and/or increasing PFCEconcentration [46]. PTX loading slightly increases nanodroplet sizes(e.g., from 260 to 280 nm).
fluorescence imaging allowed the monitoring of tumorsize and death of clusters of tumor cells. The excitationand emission peaks for the RFP were 563 and 587 nm,respectively.Cells were maintained in Dulbecco's modified Eagle
medium (DMEM) supplemented with 10% heat-inactivatedfetal bovine serum (Gibco, Grand Island, NY, USA) at 37°Cin a 5% CO2 incubator. Male nude mice between 6 to 8weeks of age were utilized (NCr-Nu/Nu, National CancerInstitute, Frederick, MD, USA). For the tumor induction,mice were anesthetized with isoflurane and received a sin-gle subcutaneous injection of 1.5 × 106 MiaPaCa-2 cellssuspended in 150 μL of serum-free DMEM. Tumors weregrown in either the shoulder or thigh region and allowed toprogress until reaching an initial size of at least 175 mm3,at which point mice were randomly assigned to a treatmentgroup. Since the tumor size of untreated animals roughlydoubles every week, the target initial tumor size of 175mm3 was often exceeded, and in the majority of animals,the initial tumor size was 200 to 300 mm3 immediately be-fore treatment. To assess the effect of the initial tumor sizeon treatment outcome, tumors were allowed to grow to thevolume of roughly 1,000 mm3 in a small subset of animals.All experiments were approved by the University of UtahInstitutional Animal Care and Use Committee.
MRgFUS treatmentsAt an assigned time point (2 or 8 h) before magneticresonance-guided FUS (MRgFUS) therapy, mice weresystemically injected through the tail vein with eitherempty (i.e., non-PTX-loaded) or PTX-loaded PFCEnanodroplets (PTX dose 40 mg/kg). In one experiment,the MRgFUS treatment was performed 10 min beforedrug injection.The MRgFUS treatments were executed with a small
animal MRgFUS system (Image Guided Therapy, Inc.,Pessac, France) with a 16-element annular transducer (f =3 MHz, rc = 3.5 cm, FWHM = 1 × 3 mm) that could betranslated in plane with piezo-ceramic motors. The systemwas placed in a Siemens 3 T Trio scanner, andtemperature imaging was obtained using a 2D-segmentedecho-planar imaging (EPI) sequence (TR/TE = 60/10 ms,FA = 15°, EPI = 3, fat saturation, 752 Hz/pixel, 1.4 s acqui-sition, 2 × 2 × 3 mm3 resolution, single slice). Tempera-tures were reconstructed using a referenceless algorithm[48] and were post-processed with zero-filled interpolationto yield 1 × 1 × 3 mm3 voxel spacing [49].Four different acoustic peak pressure levels were ap-
plied: 2.4, 3.4, 4.2, and 4.8 MPa. These levels were calcu-lated in water at the site of sonication assuming that thebeam intensity is distributed evenly over the focal spot.Most experiments in the PTX-nanodroplet + MRgFUSgroup were performed with continuous wave (CW)ultrasound (N = 24); in parallel with CW experiments,

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 4 of 11http://www.jtultrasound.com/content/1/1/11
some experiments were performed with pulsed ultra-sound (N = 4), with pressure levels matching those ofCW counterparts.Treatments were conducted using the following proto-
col: the free-breathing anesthetized mouse (ketamine100mg/kg, xylazine 20 mg/kg) was placed on the agarholder such that the tumor protruded through the holeas shown schematically in Figure 2A. In order to ensurean adequate acoustic window, the animal was always po-sitioned with the tumor directly above the ultrasoundtransducer. An axial image of a mouse on the MRgFUSdevice placed in the magnet is shown in Figure 2B. Thetransducer and agar holder are shown. The mouse isflanked by warm-water-filled tubes to help regulate itsbody temperature during the treatment.The tumor was localized with high-resolution sagittal
and axial images. Temperatures were monitored in asingle coronal slice placed at the focal plane of the trans-ducer. Three beam path patterns, two spiral patternsand one grid pattern, were used in these experiments(Figure 3). Transducer speed was 1 and 2.5 mm/s in the5-mm- and 8-mm-diameter spiral patterns, respectively,and 0.1 mm/s in the grid pattern.
Monitoring treatment outcomeTime lines of tumor growth or regression were docu-mented using three complimentary monitoring tech-niques: tumor size measurements with a caliper,tumor fluorescence imaging, and photography. Allthree techniques produced similar results. Fluores-cence imaging allowed the monitoring of both tumorgrowth/regression and cell death in the tumor tissue(see below).Tumor volume was calculated using the following
equation:
V ¼ L�W 2� �
=2 ð1Þ
where L is the tumor length and W is the tumor width.
tumor membrane
transducer
agar holder
degassed H20
imaging plane
A
Figure 2 Schematic representation and axial image of mouse on smapositioning on the small animal MRgFUS device; (B) An axial image of mouand agar holder. The white arrow indicates the tumor (initial size 455 mm3
The end point corresponded to the tumor, reachingabout 2 cm in diameter; the time to reach this point wastaken as a life span.
Animal groupsThe treatment groups and number of animals used in thestudy are listed in Table 1. Experimental parameters in-cluded PTX-loaded nanodroplets vs. empty nanodroplets,applied MRgFUS pressure, and time of ultrasoundapplication.
Statistical treatmentThe statistical significance of the differences betweenthe pairs of groups were calculated using the two-tailed,two-sample equal variance t test; the differences wereconsidered statistically significant for p < 0.05.
ResultsEffect of the combined treatment with PTX-loadednanodroplets and MRgFUS on tumor growth/regressionand mouse life spanTwo different scenarios of the tumor response to treatmentwere observed: the first involved a complete tumor reso-lution without recurrence. This was observed in four miceafter a single treatment with PTX-loaded nanodroplets andCW MRgFUS at an acoustic peak pressure of 2.4 or 3.4MPa for either a spiral or grid beam trajectory. An exampleof a complete tumor resolution with both photograph andfluorescence images is presented in Figure 4.The spiral steering patterns were executed with a much
faster velocity than that of the grid pattern. This faster vel-ocity in conjunction with the short MR acquisition time(approximately 1 s) led to unreliable temperature measure-ments from phase changes throughout the image causedby transducer motion. Grid steering patterns providedmore robust temperature imaging during the treatment.An example of the temperature rise obtained with a gridsteering pattern is presented in Figure 5. The tumor wastreated with PTX-loaded nanodroplets and CW MRgFUSdelivered for 350 s at 3.4 MPa. Panel (A) shows the axialimage of a mouse on the MRgHIFU device. The
transducer
agar holder
B
ll-animal MRgFUS device. (A) Schematic representation of the mousese 59 on the small animal MRgFUS device with labeled transducer).

Figure 3 Spiral and grid ultrasound beam patterns used in the study. Transducer speed was 1 and 2.5 mm/s in the (A) 5-mm- and(B) 8-mm-diameter spiral patterns, respectively, and 0.1 mm/s in the (C) grid pattern.
Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 5 of 11http://www.jtultrasound.com/content/1/1/11
transducer and agar holder are also shown. Panel (B)shows a coronal image through the tumor and the re-gion of interest for the maximum temperature projec-tion is shown in panel (C), in which the trajectoryboundaries are indicated by the overlayed rectangle. The
Table 1 Treatment parameters for all animals used in the stu
N Treatment group MRgHIFU
Trajectory Acousticpressure (MPa)
7 Negative control (no injection,no MRgFUS)
N/A N/A
7 PTX-nanodroplets + NoMRgFUS
1 No injection + MRgFUS Spiral 3.4
1 4.2
4 Grid 3.4
4 4.2
3 Empty nanodroplets + NoMRgFUS
N/A N/A
1 Empty nanodroplets + MRgFUS Spiral 3.4
2 4.2
1 4.8
4 Grid 3.4
4 PTX-nanodroplets + MRgFUS Grid 3.4
1 2.4
4 Spiral 3.4
4 2.4
1 4.2
1 4.8
5 Grid 3.4
2 4.8
2 4.2
1 Grid 3.4
1 Grid 4.2
1 Spiral 3.4
1 Spiral 4.8aMean values plus/minus standard deviations are presented; bMice that died withinhigher than 4.2 MPa) were excluded from the life span calculation; cSurvivors (N = 2
trajectory path is shown in panel (D) with voxel locationsfor the temperature response as a function of time plottedin panel (E). The mean temperature change (including allvoxels that achieved a temperature rise of >5°C) in thetreatment region is presented in panel (F).
dy
parameters Time betweeninjection andMRgFUS (h)
Life span(weeks)aDuty cycle (%),
pulse lengthTotal sonication
time (s)
N/A N/A N/A 3.5 ± 0.5
7.0 ± 0.8
100 240 4.8 ± 2.3
60
325 ± 29
300
N/A N/A 6 to 8 3.5 ± 0.5
100 60 6 to 8 3.5 ± 2.1b
60
240
313 ± 25
100 300 1 to 2 7.0 ± 1.0
100 153 ± 54 6 to 8 10.3 ± 1.6c
100 130 ± 50
100 60
100 60
100 300
100 300
100 300
50 (50 ms) 300 6.0 ± 1.4
50 (50 ms) 300
50 (100 ms) 300
50 (50 ms) 300
several days after the treatment (observed for the MRgFUS pressure of orfor the grid trajectory) were excluded from the life span calculation.

Figure 4 Mouse photographs and whole-body fluorescence images before and after combined PTX-loaded nanodroplet and MRgFUStreatment. Photographs (A, C) and whole-body fluorescence images (B, D) of a mouse before (A, B) and after (C, D) combined treatment withPTX-loaded nanodroplets and MRgFUS. The dashed circles in (B,D) indicate the tumor location. Treatment parameters: MRgFUS was applied 8 hafter drug injection; spiral beam pattern (5-mm diameter) shown in Figure 3A; FUS at 3.1 MPa; sonication time of 3 min. The tumor did not recurduring a 5-month observation. The former location of the tumor is still slightly visible in D, indicated by the dashed white circle.
Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 6 of 11http://www.jtultrasound.com/content/1/1/11
The initial tumor was small (V0 = 164 mm3); after thetreatment, the tumor regressed quickly and there was notumor visible to eye or by RFP imaging. However, tumorregrowth started 6 weeks after the treatment. The recur-rent tumor responded to a second treatment (nine injec-tions of PTX-loaded nanodroplets without MRgFUS,twice a week for 4.5 weeks) indicating that tumor cellsdid not develop drug resistance. Histological examin-ation of a tumor control showed the presence of mitoticcells and a pronounced stroma. In a recurred tumor in amouse that received the combined treatment of PTX-nanodroplets and MRgFUS, no evidence of stroma and
D
A B
E
Figure 5 Images of mouse, maximum temperature projection in timecurve. (A) Axial image of a mouse on the MRgHIFU device. The transducerwith region of interest defined. (C) Maximum temperature projection in timtrajectory boundaries. (D) MRgFUS trajectory with plotted voxel locations inresponse as a function of time for voxels indicated in (D). (F) Time curve oTotal MRgFUS time was 350 s at a pressure of 3.4 MPa.
substantial necrosis in the residual tumor areas was ob-served. The presence of significant hemosiderin deposi-tions in a treated tumor is a sign of the infarction of theinitially treated tumor that appeared completely resolvedand replaced with the scar tissue. For a different mousewith a larger initial tumor (V0 = 264 mm3) treated withthe same protocol, complete tumor resolution took alonger time (8 weeks). The tumor did not recur during a5-month observation.The cases of complete resolution of pancreatic cancer
occurred after a single pancreatic tumor treatment withPTX-loaded nanodroplets and MRgFUS. This was observed
C
F
, MRgFUS trajectory, temperature response for voxels, and timeand agar holder are shown. (B) Coronal image through the tumore within region of interest. White rectangle indicates the griddicated. One-millimeter spacing between all points. (E) Temperaturef the mean temperature rise in the treatment plane for all voxels >5°C.

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 7 of 11http://www.jtultrasound.com/content/1/1/11
in four of twenty-eight mice treated with PTX-loaded nano-droplets with various MRgFUS parameters. Survivors wereobserved at ultrasound acoustic pressures of 2.4 (N = 1) or3.4 MPa (N = 3) and did not depend on the beam steeringpattern (i.e., spiral or grid).A different tumor response scenario to the combined
PTX-loaded nanodroplet and MRgFUS treatment is il-lustrated in Figure 6 for a mouse treated with the gridpattern at 2.4 MPa. The upper panel shows a mousephotograph and fluorescent image taken 1 h before thetreatment; the lower photograph and image were taken3 weeks later. This image suggests that tumor cells werekilled in the MRgFUS-treated area but remained viablearound the treated volume causing a gradual tumorgrowth around the treated area. The growth rate of thistumor was close to that of tumors not treated withMRgFUS. Temperature data for the animal shown inFigure 6 is displayed in Figure 7; a very marginaltemperature response to MRgFUS therapy was observed.It is important to underline that the therapeutic effect
of PTX-loaded nanodroplets was also observed withoutthe MRgFUS treatment (Figure 8); however, completetumor resolution has never been achieved after a singlenanodroplet injection without MRgFUS, and the averagemouse life span after a single treatment with PTX-loaded nanodroplets without ultrasound (7 ± 0.8 weeks,N = 7) was shorter than that of mice treated withMRgFUS (10.3 ± 1.6 weeks, N = 19, grid + spiral trajec-tory, survivors were excluded from the calculation,
A B
C D
Figure 6 Mouse photographs and whole-body fluorescence images btreatment. Mouse photographs (A, C) and whole-body fluorescence imagPTX-loaded nanodroplets and MRgFUS therapy; ultrasound was applied 8 hlocation is indicated by a dashed circle in all images.
Table 1); the difference between these two groups wasstatistically significant (p < 0.05).
The role of drug in the MRgFUS-mediated tumortreatment: comparison of the effects of empty anddrug-loaded nanodropletsDramatic differences were observed in the tumor re-sponses to MRgFUS treatment with and without drug.The MRgFUS tumor treatment without any injection didnot affect tumor growth or mouse life span; any differ-ences with control were not statistically significant.Injections of empty (i.e., not PTX-loaded) nanodroplets
without MRgFUS application or with MRgFUS pressurelevels below 4.2 MPa did not exert any effect on the tumorgrowth rates or average mouse life span. Six mice weretreated with empty nanodroplets of various MRgFUS pres-sure levels from 2.4 to 4.2 MPa; their average life span was3.5 weeks, similar to the negative control; however, all micetreated with a pressure of 4.2 MPa died within 1 to 3 weeksafter the treatment. In two cases, tumor growth was notice-ably accelerated (data not shown). In contrast, the averagelife span of mice treated with PTX-loaded nanodropletsand MRgFUS was threefold longer (10.3 weeks). These dataindicate that for the combined PTX-loaded nanodroplets/MRgFUS treatment, the main therapeutic effect was causedby the drug and not by the ultrasound. Still, as follows fromFigure 8 and Table 1, MRgFUS did significantly enhancethe action of the drug for certain combinations of ultra-sound parameters.
efore and after combined PTX-loaded nanodroplet and MRgFUSes (B, D) taken before (A, B) and 3 weeks after treatment (C,D) withafter drug injection at 2.4 MPa with a grid trajectory. The tumor

Figure 9 Effect of ultrasound pressure on the tumor growthcurves in the presence of PTX-loaded nanodroplets. No MRgFUS(N = 7, diamonds); MRgFUS at 4.2 MPa (N = 3, triangles); MRgFUS at4.8 MPa (N = 2, squares).
Figure 7 Temperature response for the mouse shown in Figure 6.The temperature rise for three individual voxels indicated in thetreatment path is shown.
Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 8 of 11http://www.jtultrasound.com/content/1/1/11
Effect of the ultrasound pressureFor mice treated with PTX-loaded nanodroplets andMRgFUS, increasing ultrasound pressure above 4.2 MPaexerted a detrimental effect on the tumor growth andanimal survival (Figure 9); moreover, at a pressure levelof 4.2 MPa and especially at 4.8 MPa, grid-shaped skinburns that required special treatment were observed.The burns were resolved within 2 to 3 weeks.
Effect of the time of ultrasound applicationExperiments were performed with ultrasound applicationeither 2 (N = 5) or 6 to 8 h after the injection (N = 23). Inone experiment, ultrasound was applied 10 min before theinjection of PTX-loaded nanodroplets. No effect ofMRgFUS was observed when ultrasound was applied ei-ther before or 2 h after the nanodroplet injection; tumor
-2
0
2
4
6
8
10
12
14
16
0 50 100
no
rmal
ized
tum
or
gro
wth
time after treatment, days
Control N=3
PTX droplets no FUS N=7
PTX droplets + FUS, best results N=4
Figure 8 Tumor growth curves. Control (N = 3, squares); Tumorstreated with PTX-loaded nanodroplets without ultrasound (N = 7,triangles); Best results for tumors treated with PTX-loadednanodroplets and MRgFUS (N = 4, diamonds).
growth rates and average life span did not differ fromthose observed for PTX-loaded nanodroplets withoutMRgFUS.
Effect of pulsed ultrasoundThe experiments for pulsed and CW parameters wereperformed in parallel. The average life span of micetreated with pulsed ultrasound with various FUS param-eters (6 ± 1.4 weeks, N = 4) was significantly lower thanthat of mice treated with CW ultrasound (10.3 ± 1.6weeks, N = 19).
Effect of the initial tumor sizeThe effect of the therapy depended strongly on the ini-tial tumor size at the start of treatment. When the initialtumor size exceeded 1,000 mm3, the combined treat-ment by PTX-loaded nanodroplets and MRgFUS couldnot completely stop tumor growth; after the initial de-crease of the tumor size, tumor growth resumed in 3 to4 weeks. The average life span of animals with large ini-tial tumors was increased by the treatment (roughlyfrom 3 weeks for controls to 6 to 8 weeks for treatedanimals), but all tumors continued to grow despitethe treatment. Increasing the MRgFUS-treated vol-ume by the treatment of the two tumor planes ratherthan one plane did not exert any positive effect onthe life span of animals with large initial tumors.Moreover, tumor growth was accelerated after thetwo-plane treatment, presumably due to the increasedheating (see Discussion).
Safety issues and collateral damageSeven of the total of fifty-one animals (14%) treated withMRgFUS died within several days of the MRgFUS treat-ment. Four of seven animals died after the treatmentwith empty nanodroplets and MRgFUS at pressure levelsof 4.2 or 4.8 MPa; two animals died after the treatmentwith the same MRgFUS parameters without any injec-tion. One animal died two days after the combined

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 9 of 11http://www.jtultrasound.com/content/1/1/11
treatment with PTX-loaded nanodroplets and MRgFUSat 4.2 MPa. No animal deaths resulted from thenanodroplet treatment without MRgFUS indicating thatanimal deaths were related to the MRgFUS treatment.Presence of empty nanodroplets during MRgFUS treat-ment appeared to increase the death rate. Although theexact mechanism that led to the animal's death is un-known, it is suspected that it may be due to peritonitis.A post-treatment analysis of MR images of coronal slicesof MRgFUS treated animals suggested that the collateraldamage occurred when gas-filled intestines were locatedin the far field of the ultrasound beam (Figure 10).
DiscussionUltrasound may exert both positive and negative effectson biological tissue. Positive effects may be related to in-creased drug carrier and drug extravasation, drug releasefrom carrier, and drug internalization by tumor cells. Onthe other hand, vasodilation or vasoconstriction in re-sponse to ultrasound and cavitating microbubbles mayresult in the cellular response of surrounding tissuessuch as inflammation, edema, hemorrhage, which couldbe negative. Tissue response to ultrasound-inducedheating is multifaceted as well. In the absence of thedrug, the response to sub-ablative heating may be nega-tive due to enhanced perfusion that promotes tumorgrowth. In contrast, in the presence of the drug, en-hanced perfusion is a positive factor that promotes drugdelivery to tumor tissue; in addition, hyperthermia
Figure 10 MRI showing gas-filled intestines in the ultrasoundfar-field. This image is representative for seven mice that diedwithin several days after MRgFUS treatment. The transducer andagar holder are labeled. The long and short arrows identify thetumor and intestines, respectively.
increases vascular wall and plasma membrane perme-ability thus increasing drug internalization by tumorcells. The ultimate biological response to ultrasound pre-sumably depends on the prevalence of positive or nega-tive factors which is expected to depend on thetreatment protocol as well as biological factors.In our experiments, MRgFUS was applied at sub-
ablative pressure levels and only a fraction of thetumor was treated. For tumor therapy, this situation isunfavorable. Ultrasound treatment caused hyperther-mia (Figure 5) but did not induce coagulative necrosisof tumor tissue as manifested by the preservation ofthe tumor cell fluorescence after the MRgFUS treat-ment without the drug. At ultrasound pressure levelsused in this study, MRgFUS treatment without any in-jection did not exert statistically significant effects onthe tumor growth or animal life span. In the presenceof empty nanodroplets, the effect of MRgFUS appearedto be negative, especially at higher pressure levels (in-creased tumor growth, early animal death), whichcould be related to the droplet-to-bubble transitionand bubble cavitation that induced tissue inflamma-tion. In the presence of the drug, these negative effectsof the ultrasound treatment were suppressed. More-over, the MRgFUS treatment enhanced the action ofthe drug (Figure 8 and Table 1). This may be associ-ated with the enhanced tumor perfusion and cell per-meability caused by mild hyperthermia, which in thepresence of the drug are positive factors that increasedrug supply to tumor cells.However, increasing ultrasound pressure above a cer-
tain threshold (4.2 MPa) decreased the positive effect ofthe combined PTX-loaded nanodroplet/MRgFUS treat-ment (Figure 9). This shows that positive effects of theultrasound treatment in the presence of nanodropletscompete with negative effects in this animal model; ad-verse effects causing tissue inflammation are enhancedat higher ultrasound pressure levels. Even in the pres-ence of the drug, one animal died within a couple ofdays after the MRgFUS treatment at 4.2 MPa. However,the death rate caused by the MRgFUS treatment wasmuch higher with empty droplets.It is not immediately clear if the chemotherapeutic
drug may suppress the inflammation. One hypothesiswas suggested by Dr. Klibanov who proposed that thenanodroplet-encapsulated PTX could kill harmful mac-rophages that cause tissue inflammation (personal com-munication). This supposition remains to be explored.As suggested by the post-treatment analysis of MR im-
ages, ultrasound-induced collateral damage could resultfrom ultrasound reflection from the air-filled structures(Figure 10); possible intra-intestinal gas bubble cavita-tion in the ultrasound far field could be a peritoneum-damaging factor that results in the animal death.

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 10 of 11http://www.jtultrasound.com/content/1/1/11
In the presented experiments, no correlation was ob-served between the mean temperature in the treatedplane and the treatment outcome. More data are neededto draw a conclusion on the relative roles of thermal andmechanical modes of ultrasound action in the combinedtreatment with PTX-loaded nanodroplets and MRgFUS.The effect of the pulsed MRgFUS treatment with
PTX-loaded nanodroplets was clearly smaller than thatof CW MRgFUS treatment, which may be related to sig-nificantly lower temperature increase and/or decreasedextravasation [50].The time of the MRgFUS application proved to be an
important factor. The positive effect of the MRgFUStreatment in the presence of PTX-loaded nanodropletswas observed when MRgFUS therapy was performed 6to 8 h after the injection of drug-loaded nanodropletsbut was aborted when MRgFUS was applied before orshortly after the drug injection. This underlines the roleof the nanodroplet accumulation in the tumor volumefor the success of the treatment. The data suggest that atthe conditions studied, MRgFUS treatment did not no-ticeably enhance nanodroplet extravasation into thetumor tissue. The opposite was observed in a recentstudy where excised carotid arteries were inserted inPBS [50]. It appears reasonable to suggest that the ultra-sound susceptibility of blood vessels inserted in solidmatrices could differ from that of vessels inserted in li-quid. It might well be that enhanced extravasationin vivo requires higher ultrasound pressures than thoseused in this work. At this time, we do not have enoughdata to further explore this issue. The data presentedalso show that nanodroplet accumulation in the tumoris desirable before the ultrasound application. The tumoraccumulation of nanodroplets may take hours [21,22].The presence of nanodroplets in blood vessels of thenormal tissue in the path of the beam may scatter ultra-sound; it may also cause collateral damage induced bythe microbubble cavitation in the ultrasound far field.Since increasing the sonicated volume did not result in
a better treatment outcome for large tumors, the inabilityto completely suppress tumor growth was most probablyrelated to the insufficient concentration of drug in thetumor rather than the small sonicated tumor fraction.The data presented above suggest that there exists an
optimal range of the time of ultrasound application andultrasound pressure levels below which the treatment doesnot exert any effect and above which the effect of thetreatment is decreased. It should be emphasized that posi-tive treatment effects and even complete tumor resolutionwere achieved with only a single treatment of just a frac-tion of the pancreatic tumor. This shows the potential ofusing the combined tumor treatment with PTX-loadednanodroplets and MRgFUS for the therapy of the pancre-atic cancer, one of the most lethal cancer types.
Competing interestsThe authors declare that they have no competing interests.
Authors' contributionsNR conceived the study, designed and coordinated the project, participatedin all experiments, processed the data, and drafted the manuscript. APdesigned and ran MRgFUS experiments, participated in data processing, andedited the manuscript. CD participated in MRgFUS experiments, processedMR thermometry data, and participated in editing the manuscript. JSinoculated RFP-transfected pancreatic tumors and participated in MRgFUSexperiments. CS participated in discussions of data. RG participated in allexperiments, measured tumor sizes, took RFP images, and participated indata processing. All authors read and approved the final manuscript.
AcknowledgmentsThe NIH grant R01 EB1033 to NR is highly appreciated. The authors thankDrs. Nathan McDannold and Natalia Vykhodtseva (Brigham and Women'sHospital, Harvard Medical School) and Dr. Anna V. Shurligina (Institute ofPhysiology, Siberian Branch of the Russian Academy of Sciences) for the helpwith the histological evaluation and interpretation of histological data.
Author details1Department of Bioengineering, University of Utah, 36 S. Wasatch Dr., Room3100, Salt Lake City, UT 84112, USA. 2Department of Radiology, University ofUtah, Salt Lake City, UT 84112, USA. 3Department of Surgery, University ofUtah, Salt Lake City, UT 84112, USA. 4Current address: Department ofRadiation Oncology, Fox Chase Cancer Center, P0103, 333 Cottman Avenue,Philadelphia, PA 19111, USA.
Received: 28 December 2012 Accepted: 19 May 2013Published: 1 July 2013
References1. Salomir R, Palussiere J, Vimeux FC, de Zwart JA, Quesson B, Gauchet M,
Lelong P, Pergrale J, Grenier N, Moonen CT. Local hyperthermia with MR-guided focused ultrasound: spiral trajectory of the focal point optimizedfor temperature uniformity in the target region. J Magn Reson Imaging.2000; 12(4):571–83.
2. Salomir R, Vimeux FC, de Zwart JA, Grenier N, Moonen CT. Hyperthermiaby MR-guided focused ultrasound: accurate temperature control basedon fast MRI and a physical model of local energy deposition and heatconduction. Magn Reson Med. 2000; 43(3):342–47.
3. Holland CK, Apfel RE. Thresholds for transient cavitation produced bypulsed ultrasound in a controlled nuclei environment. J Acoust Soc Am.1990; 88(5):2059–69.
4. Klibanov AL. Microbubble contrast agents: targeted ultrasound imagingand ultrasound-assisted drug-delivery applications. Invest Radiol. 2006;41(3):354–62.
5. Klibanov AL. Preparation of targeted microbubbles: ultrasound contrastagents for molecular imaging. Med Biol Eng Comput. 2009; 47(8):875–82.
6. Klibanov AL, Shevchenko TI, Raju BI, Seip R, Chin CT. Ultrasound-triggeredrelease of materials entrapped in microbubble-liposome constructs: atool for targeted drug delivery. J Control Release. 2010; 148(1):13–7.
7. McDannold N, Arvanitis CD, Vykhodtseva N, Livingstone MS. Temporarydisruption of the blood–brain barrier by use of ultrasound andmicrobubbles: safety and efficacy evaluation in rhesus macaques.Cancer Res. 2012; 72(14):3652–63.
8. McDannold N, Vykhodtseva N, Hynynen K. Blood–brain barrier disruptioninduced by focused ultrasound and circulating preformed microbubblesappears to be characterized by the mechanical index. Ultrasound MedBiol. 2008; 34(5):834–40.
9. McDannold N, Zhang Y, Vykhodtseva N. Blood–brain barrier disruptionand vascular damage induced by ultrasound bursts combined withmicrobubbles can be influenced by choice of anesthesia protocol.Ultrasound Med Biol. 2011; 37(8):1259–70.
10. Vykhodtseva N, McDannold N, Hynynen K. Progress and problems in theapplication of focused ultrasound for blood–brain barrier disruption.Ultrasonics. 2008; 48(4):279–96.
11. Yudina A, Lepetit-Coiffe M, Moonen CT. Evaluation of the temporalwindow for drug delivery following ultrasound-mediated membranepermeability enhancement. Mol Imaging Biol. 2011; 13(2):239–49.

Rapoport et al. Journal of Therapeutic Ultrasound 2013, 1:11 Page 11 of 11http://www.jtultrasound.com/content/1/1/11
12. Frulio N, Trillaud H, Deckers R, Lepreux S, Moonen C, Quesson B. Influenceof ultrasound induced cavitation on magnetic resonance imagingcontrast in the rat liver in the presence of macromolecular contrastagent. Invest Radiol. 2010; 45(5):282–87.
13. Deckers R, Moonen CT. Ultrasound triggered, image guided, local drugdelivery. J Control Release. 2010; 148(1):25–33.
14. McDannold N, Vykhodtseva N, Raymond S, Jolesz FA, Hynynen K.MRI-guided targeted blood–brain barrier disruption with focusedultrasound: histological findings in rabbits. Ultrasound Med Biol. 2005;31(11):1527–37.
15. Hynynen K, McDannold N, Vykhodtseva N, Raymond S, Weissleder R,Jolesz FA, Sheikov N. Focal disruption of the blood–brain barrier due to260-kHz ultrasound bursts: a method for molecular imaging andtargeted drug delivery. J Neurosurg. 2006; 105(3):445–54.
16. Tiukinhoy-Laing SD, Huang S, Klegerman M, Holland CK, McPherson DD.Ultrasound-facilitated thrombolysis using tissue-plasminogenactivator-loaded echogenic liposomes. Thromb Res. 2007; 119(6):777–84.
17. Shaw GJ, Meunier JM, Huang SL, Lindsell CJ, McPherson DD, Holland CK.Ultrasound-enhanced thrombolysis with tPA-loaded echogenicliposomes. Thromb Res. 2009; 124(3):306–10.
18. Hitchcock KE, Caudell DN, Sutton JT, Klegerman ME, Vela D, Pyne-GeithmanGJ, Abruzzo T, Cyr PE, Geng YJ, McPherson DD, Holland CK.Ultrasound-enhanced delivery of targeted echogenic liposomes in anovel ex vivo mouse aorta model. J Control Release. 2010; 144(3):288–95.
19. Rapoport N, Gao Z, Kennedy A. Multifunctional nanoparticles forcombining ultrasonic tumor imaging and targeted chemotherapy.J Natl Cancer Inst. 2007; 99(14):1095–106.
20. Rapoport N, Efros AE, Christensen D, Kennedy A, Nam K-H. Microbubblegeneration in phase-shift nanoemulsions used as anticancer drugcarriers. Bub Sci Eng Tech. 2009; 1(1–2):31–9.
21. Rapoport N, Nam KH, Gupta R, Gao Z, Mohan P, Payne A, Todd N, Liu X,Kim T, Shea J, Scaife C, Parker DL, Jeong EK, Kennedy AM.Ultrasound-mediated tumor imaging and nanotherapy using drugloaded, block copolymer stabilized perfluorocarbon nanoemulsions. JControl Release. 2011; 153(1):4–15.
22. Rapoport NY, Kennedy AM, Shea JE, Scaife CL, Nam KH. Controlled andtargeted tumor chemotherapy by ultrasound-activated nanoemulsions/microbubbles. J Control Release. 2009; 138(3):268–76.
23. Gao Z, Kennedy AM, Christensen DA, Rapoport NY. Drug-loaded nano/microbubbles for combining ultrasonography and targetedchemotherapy. Ultrasonics. 2008; 48(4):260–70.
24. Nam K-H, Christensen D, Kennedy A, Rapoport N. Acoustic DropletVaporization, Cavitation, and Therapeutic Properties of Copolymer-StabilizedPerfluorocarbon Nanoemulsions. Melville: American Institute of Physics; 2009:p. 124–28.
25. Zhang M, Fabiilli ML, Haworth KJ, Fowlkes JB, Kripfgans OD, Roberts WW,Ives KA, Carson PL. Initial investigation of acoustic droplet vaporizationfor occlusion in canine kidney. Ultrasound Med Biol. 2010; 36(10):1691–703.
26. Lo AH, Kripfgans OD, Carson PL, Rothman ED, Fowlkes JB. Acoustic dropletvaporization threshold: effects of pulse duration and contrast agent.IEEE Trans Ultrason Ferroelectr Freq Control. 2007; 54(5):933–46.
27. Kripfgans OD, Fabiilli ML, Carson PL, Fowlkes JB. On the acousticvaporization of micrometer-sized droplets. J Acoust Soc Am. 2004;116(1):272–81.
28. Kripfgans OD, Fowlkes JB, Miller DL, Eldevik OP, Carson PL. Acoustic dropletvaporization for therapeutic and diagnostic applications. Ultrasound MedBiol. 2000; 26(7):1177–89.
29. Fabiilli ML, Haworth KJ, Sebastian IE, Kripfgans OD, Carson PL, Fowlkes JB.Delivery of chlorambucil using an acoustically-triggeredperfluoropentane emulsion. Ultrasound Med Biol. 2010; 36(8):1364–75.
30. Fabiilli ML, Lee JA, Kripfgans OD, Carson PL, Fowlkes JB. Delivery ofwater-soluble drugs using acoustically triggered perfluorocarbon doubleemulsions. Pharm Res. 2010; 27(12):2753–65.
31. Rapoport N. Phase-shift, stimuli-responsive perfluorocarbon nanodropletsfor drug delivery to cancer. Wiley Interdiscip Rev Nanomed Nanobiotechnol.2012; 4(5):492–510.
32. Rapoport N, Christensen DA, Kennedy AM, Nam KH. Cavitation propertiesof block copolymer stabilized phase-shift nanoemulsions used as drugcarriers. Ultrasound Med Biol. 2010; 36(3):419–29.
33. Rapoport N, Kennedy AM, Shea JE, Scaife CL, Nam KH. Ultrasonicnanotherapy of pancreatic cancer: lessons from ultrasound imaging.Mol Pharm. 2010; 7(1):22–31.
34. Mahadevan D, Von Hoff DD. Tumor-stroma interactions in pancreaticductal adenocarcinoma. Mol Cancer Ther. 2007; 6(4):1186–97.
35. Korc M. Pancreatic cancer-associated stroma production. Am J Surg. 2007;194(4 Suppl):S84–86.
36. De La OJ, Emerson LL, Goodman JL, Froebe SC, Illum BE, Curtis AB,Murtaugh LC. Notch and Kras reprogram pancreatic acinar cells to ductalintraepithelial neoplasia. Proc Natl Acad Sci U S A. 2008; 105(48):18907–12.
37. Edmonds C, Cengel KA. Tumor-Stroma interactions in pancreatic cancer:will this SPARC prove a raging fire? Cancer Biol Ther. 2008; 7(11):1816–17.
38. Pilarsky C, Ammerpohl O, Sipos B, Dahl E, Hartmann A, Wellmann A,Braunschweig T, Lohr M, Jesenofsky R, Friess H, Wente MN, Kristiansen G,Jahnke B, Denz A, Ruckert F, Schackert HK, Kloppel G, Kalthoff H, Saeger HD,Grutzmann R. Activation of Wnt signalling in stroma from pancreaticcancer identified by gene expression profiling. J Cell Mol Med. 2008;12(6B):2823–35.
39. Kim MP, Evans DB, Wang H, Abbruzzese JL, Fleming JB, Gallick GE.Generation of orthotopic and heterotopic human pancreatic cancerxenografts in immunodeficient mice. Nat Protoc. 2009; 4(11):1670–80.
40. Zischek C, Niess H, Ischenko I, Conrad C, Huss R, Jauch KW, Nelson PJ, BrunsC. Targeting tumor stroma using engineered mesenchymal stem cellsreduces the growth of pancreatic carcinoma. Ann Surg. 2009;250(5):747–53.
41. Kim MP, Gallick GE. Gemcitabine resistance in pancreatic cancer: pickingthe key players. Clin Cancer Res. 2008; 14(5):1284–85.
42. Tjomsland V, Niklasson L, Sandstrom P, Borch K, Druid H, Bratthall C,Messmer D, Larsson M, Spangeus A. The desmoplastic stroma plays anessential role in the accumulation and modulation of infiltrated immunecells in pancreatic adenocarcinoma. Clin Dev Immunol. 2011; 2011:212810.
43. Rasheed ZA, Matsui W, Maitra A. Pathology of pancreatic stroma in PDAC.In: Grippo PJ, Munshi HG, editors. Pancreatic cancer and tumormicroenvironment. Trivandrum (India): Transworld Research Network; 2012.Chapter 1.
44. Farace P, D’Ambrosio D, Merigo F, Galie M, Nanni C, Spinelli A, Fanti S,Degrassi A, Sbarbati A, Rubello D, Marzola P. Cancer-associated stromaaffects FDG uptake in experimental carcinomas. Implications forFDG-PET delineation of radiotherapy target. Eur J Nucl Med Mol Imaging.2009; 36(4):616–23.
45. Shea JE, Nam KH, Rapoport N, Scaife CL. Genexol inhibits primary tumourgrowth and metastases in gemcitabine-resistant pancreatic ductaladenocarcinoma. HPB (Oxford). 2011; 13(3):153–57.
46. Rapoport NY, Efros AL, Christensen DA, Kennedy AM, Nam KH. Microbubblegeneration in phase-shift nanoemulsions used as anticancer drugcarriers. Bub Sci Eng Tech. 2009; 1:31–9.
47. Torgenson MJ, Shea JE, Firpo MA, Dai Q, Mulvihill SJ, Scaife CL. Naturalhistory of pancreatic cancer recurrence following “curative” resection inathymic mice. J Surg Res. 2008; 149(1):57–61.
48. Rieke V, Vigen KK, Sommer FG, Daniel BL, Pauly JM, Butts K. ReferencelessPRF shift thermometry. Magn Reson Med. 2004; 51(6):1223–31.
49. Todd N, Vyas U, de Bever J, Payne A, Parker DL. The effects of spatialsampling choices on MR temperature measurements. Magn Reson Med.2011; 65(2):515–21.
50. Thakkar D, Gupta R, Monson K, Rapoport N. Effect of ultrasound on thepermeability of vascular wall to nanoemulsion. Ultrasound Med Biol.2013. in press.
doi:10.1186/2050-5736-1-11Cite this article as: Rapoport et al.: Focused ultrasound-mediated drugdelivery to pancreatic cancer in a mouse model. Journal of TherapeuticUltrasound 2013 1:11.




















