how to set option code/ tatacara mengisi kod option - npcdn.net

Care Management Journals • Volume 5, Number 2 • Summer 2004 73
© 2004 Springer Publishing Company
Changes in health services and care needs have created highdemand for case management of in-home services. To addressthis challenge, several models of case management have beenused. Evaluations to date suggest that clients need differentapproaches for different circumstances at different times tooptimize cost-effectiveness. Accordingly, one Canadian homecare program adopted flexible client-driven case management,engaging clients as partners in flexibly selecting either an inte-grated team, consumer-managed or brokerage model of casemanagement in keeping with their preferences and abilities.Using an exploratory, multimeasure quasi-experimental design,a generic model of program evaluation, and both quantitativeand qualitative methods, researchers identified challenges inimplementing this intervention, policy impediments the clientscharacteristically in each of the three case management models,and client, provider, and caregiver outcomes of flexible, client-driven care. While further longitudinal investigation is needed,findings suggest several important considerations for thoseinterested in this option for care management. Alternative casemanagement models do attract different client groups, andhaving a choice does not alter care costs or outcomes. Flexibleclient-driven case management may be experienced positivelyby case managers and other providers.
Keywords: case management models; home care delivery; serviceapproaches
Flexible Client-DrivenIn-Home CaseManagement: An Option to Consider
Carol L. McWilliam, MScN, EdD Moira Stewart, PhDEvelyn Vingilis, PhDJeffrey Hoch, PhDCatherine Ward-Griffin, PhDAllan Donner, PhDGina Browne, PhDPeter Coyte, PhDKaren Anderson, MSc
Restructuring of hospitals, social services, and mental healthservices, increasingly complex technology, escalating acu-ity of care and an aging population have increased the vol-
ume and complexity of case management for in-home healthservices in recent years. As service demand exceeds resources,home care case managers carry caseloads far in excess of recom-mended standards (Kane, Pendrod, & Kivnick, 1994; Shapiro,1995). To address this challenge, several approaches to case man-agement have been used: the brokerage model, with a designatedcase manager impartially determining needs and arranging, coor-dinating and monitoring contracted services (Ontario Ministry ofHealth, 1992; Zawadski & Eng, 1988); the integrated teamapproach, with case management facilitated by the professionalprovider team, one of whom has designated leadership responsi-bilities (New Brunswick Ministry of Health, 1991); a consumer-managed model, with clients or informal caregivers assessed asappropriate for self-managed care selecting and coordinating theresources needed (Alberta Ministry of Health, 1993; CanadianHome Care Association, 1995; Manitoba Ministry of Health,1994). Limited evaluations indicate that these three models maywork well for different clients under different circumstances andat different times, with different costs and benefits (Bly & Kissick,1994; Campbell et al., 1997; Dalby, Williams, & Hadnott, 1996;Jennings, 1994; Peruselli, Paci, Franceschi, Legori, & Mannucci,1997; Van Minnen, Hoogduin, & Broekman, 1997).
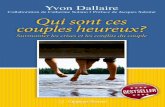
With due regard for this realization, one Ontario home careprogram has converted its service delivery to a flexible client-driven approach (Figure 1), in which the case manager respondsflexibly to clients as partners in determining their involvement intheir own care management, in accordance with their own prefer-ences and abilities. The case management strategy is accordinglyadjusted to permit the client and/or their informal caregiver to befully directive (consumer-managed model), to engage in his/hercase management with his/her team of in-home service providers(integrated team model) or to opt to have a case manager directall care (brokerage model). The opportunity to choose the modelachieves client empowerment, equitably mobilizing the client’spersonal knowledge, abilities, and right to be involved (Clarke,1989). The approach thus facilitates client-centered, client-empowering care, and direction of case management expertisetoward clients who most need it.
The purpose of this study was to evaluate the comparativecosts and outcomes of this flexible client-driven service deliveryapproach to case management. Evaluators hypothesized that thisapproach would achieve among clients, greater participation indecision making, greater health-promoting effort, and greater sat-isfaction with care with no increase in care costs; among providers(including case managers), greater empowerment, health-promotingeffort, job satisfaction, and motivation, as well as a more positiveperspective on job characteristics; and among informal caregivers,a more positive experience of empowerment, choice, worker char-acteristics, and satisfaction with care, with no change in caregiverburden.
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 73

McWilliam et al.
74
LITERATURE REVIEW
Research evidence to inform the theory and practice of case man-agement is limited. Evaluations of care management innovationshave as yet achieved ambiguous results (Bergman & Béland,2000; Gagnon, Schein, McVey, & Bergeron, 1999; Weissert &Hendrick, 1994). To date, evaluations have documented theimpact of case management on the care of specific client groups,including people with mental disorders (D’Ercole, Struening,Curtis, Milman, & Morris, 1997; Goering, Wasylenki, Farkas,Lancee, & Ballantyne, 1988; Gray, Marshall, Lockwood, &Morris, 1997), school-aged clients (Tiezzi, Lipshutz, Wrobleski,
Darton, Johnson, Stone, & Traske, 1991b; Goaring et al., 1988;Jones, 1995; Marshall, Lockwood, & Gath, 1995; Swindle,Weyant, & Mar, 1994; Weissert, 1998); the integrated teammodel (Zawadski & Eng, 1988; Zimmer, Eggert, & Chiverton,1990); or the consumer-managed model (Alberta Ministry ofHealth, 1993; Manitoba Ministry of Health, 1994; SaskatchewanHealth, 1996; Seltzer, Ivry, & Litchfield, 1987), identifying thestrengths and limitations of each. Findings underscore the bene-fits of provider knowledge, expertise, and authority in care man-agement for clients who are particularly dependent, frail, and inneed of complex care (Bigelow & Young, 1991; Challis et al.,1991a, 1991b; Jones, 1995; Goering et al., 1998), and converse-ly, the benefits of optimizing client and caregiver knowledge, abil-ities, and rights (Alberta Ministry of Health, 1993; CanadianHome Care Association, 1995; Manitoba Ministry of Health,1994) where feasible. The disadvantages of imposing too much(Geron & Chassler, 1994; Jackson, 1994; McWilliam, Brown,Carmichael, & Lehman, 1994; Weissert, 1998) or too little(Geron & Chassler, 1994; Jackson, 1994; McWilliam, 1992;McWilliam et al., 1994; Seltzer, Ivry, & Litchfield, 1987) providerknowledge, expertise, and authority in the care management rela-tionship have also been documented. However, investigations todate do not indicate what would happen if all three major casemanagement models were made available in accordance withclients’ preferences and abilities.
Limited evaluations of consumer-managed models (AlbertaMinistry of Health, 1993; Canadian Home Care Association,1995; Manitoba Ministry of Health, 1994), and of client-centered assessment processes (Saskatchewan Health, 1996) have
. . . comparing results to thoseattained using the traditionalbrokerage approach in another
home care program . . .
Figure 1. A model of flexible client-driven care management.
Case Manager schedules & monitors services
Team leader works with client &providers to monitor & adjust care plan
Case Manager monitors & adjusts careplan with input from client & providers
Client still needs case
management
Client no longerneeds case
management
Client still needs case
management
Client no longerneeds case
management
Client needsincrease
Client needs stable
INFORMED CLIENT CHOICE
INTEGRATED TEAM
Professional primary caregiver with most client contact
intiates team efforts
BROKERAGE
Informed client or informal caregiver selects & schedules
services needed
CONSUMER-MANAGED
Re-assess & revise to Brokerage orIntegrated Team model as needed
Client and/or informal caregiver monitors & adjusts care plan
Vaughan, & McCarthy, 1997), high-risk perinatal clients(Gonzalez-Calvo, Jackson, Hansford, Woodman, & Remington,1997), and long-term care client sectors (Weissert, 1988). Theseinvestigations have examined case management strategies alignedto the brokerage model (Bigelow & Young, 1991; Braun & Rose,1994; Challis, Darton, Johnson, Stone, & Traske, 1991a; Challis,
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 74

identified the client’s potential for involvement. Evidence fromresearch (Auton, 1995; Cahill, 1996; Carnaby, 1997; Davies, Laker,& Ellis, 1997; Gilmore, 1991; Hurst, 1996; Jirsch, 1993; Jones,Dougherty, & Martin, 1997; Kane, Caplan, Urv-Wong, Freeman,Aroskar, & Finch, 1997; Lathrop, Seufert, MacDonald, & Martin,1991; Tidikis & Strasen, 1994) and observation of case managerswho intuitively implement a more client-driven partneringapproach to creating, implementing, and evaluating the service plan(Rose, 1992a, 1992b) suggests that more cost-effective service deliv-ery may result. While recent investigations of client-centered hospi-tal care strategies have produced mixed results (Jones et al., 1997;Snyder & Lathrop, 1995; Twyman & Libbus, 1994) the evidencesuggests that such strategies are cost-justified, and increase qualityand service levels (Snyder & Lathrop, 1995). Exploratory researchon the experience of transition from hospital to home (McWilliam,1992; McWilliam et al., 1994) has uncovered client disempower-ment and dependence fostered by care management approaches.Results (McWilliam et al., 1999) of a randomized controlled trial totest the efficacy of a client-centered, client-driven approach to caremanagement with frail chronically ill seniors receiving in-home careindicated that this approach achieved greater independence ( p =.0008), perceived ability to manage one’s own health ( p = .0014),and quality of life ( p = .0006), and lessened information needs ( p= .0035) immediately postintervention (22 weeks), with patternspersisting at the 1-year follow-up. Findings also indicated cost sav-ings, as individuals in the intervention used few services and spentfewer days in hospital (McWilliam et al., 1999).
METHODS
Study Design
An exploratory, multimeasure quasi-experimental evaluation design(Cook & Campbell, 1979; Greene, Caracelli, & Graham, 1989)was used to evaluate the costs and outcomes of the approach prein-tervention and postintervention, comparing results to thoseattained using the traditional brokerage approach in another homecare program of similar size, case mix groupings, operating budget,and policy jurisdiction. Having a comparator program permittedidentification of seasonal and cyclical trends created by interveningvariables like policy changes, professional practice trends, and hos-pital downsizing, and any additional confounding variables requir-ing control. To systematically assess the conceptualization,implementation processes, costs, and impact of the intervention(Thompson, 1992), a generic model of program evaluation(Vingilis & Pedersen, 2001) was applied to identify indirect as wellas direct influences on program outcomes. Both quantitative andqualitative methods were employed to evaluate overlapping, but dif-ferent facets of program implementation (Cook & Campbell,1979; Greene et al., 1989; Posavac & Carey, 1997).
Study Sample
Providers and clients within the two organizations were random-ly selected, while caregivers constituted a convenience sampleidentified by the randomly selected clients. Consistent with the
nature of the intervention, only clients who were in receipt ofchronic in-home care (a minimum of 3 months of continuousservice) were included. The client sample was comprised of fourhomogeneous subsamples representing the most prevalent chron-ic care needs, including: three groups of clients over 65 years withthe primary diagnoses of arthritis, cardiovascular disease, or respi-ratory disease, and one group of adults aged 18 to 64 years withfunctional limitations from multiple sclerosis, paralysis, and othermedical problems classified as disabling. Clients who were cogni-tively impaired (a score of 20 or less on the Folstein Mini-MentalState Examination) (Folstein, Folstein, & McHugh, 1975) or pal-
Flexible Client-Driven Case Management
75
Providers . . . were, on average, 45 years of age and had
10.4 years of experience, 59.6%having worked six or more years
in home care.
TABLE 1. Summary of Sample Size Targets
Planned Obtained
Sample/ Study Follow- StudyYear Total Baseline Up Total
Clients 1,152 2,304 974 809 1,783Caregivers 288 576 249 303 552Providers 288 576 291 288 579
liative were excluded from the study. Consistent with exploratoryprogram evaluation, the sample size was premised on the maxi-mum number of participants feasible, as determined by the proj-ect budget and the availability of clients, caregivers, and providers(Table 1).
Data Collection
Except in instances in which frail clients requested the researchassistant to administer the questionnaire, data were acquired byquarterly anonymously returned mailed questionnaires using theDillman method (Hoddinott & Bass, 1986) of reminders to pro-mote return. In addition to demographics, the client survey meas-ured: (a) functional status, a variable requiring control, using aself-administered adaptation of the Functional IndependenceMeasure (FIM) (McDowell & Newell, 1996) to assess physicaland cognitive disability; (b) the total cost of health service utiliza-tion, using the self-report Health and Social Service Utilization
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 75

McWilliam et al.
76
Questionnaire (Browne, Arpin, Corey, Fitch, & Gafni, 1990;Browne et al., 1992) that permits the application of unit costs (in2001 dollars) to the self-reported units of service, including visitsto professionals, emergency room visits, hospitalizations, diagnos-tic services, home care, out-of-pocket expenditures for aids,devices, medications, travel, and parking, and indirect costs asso-ciated with absence from work or other activities; (c) the 8-itemversion of the Service Evaluation Questionnaire (Nguyen,Attkinsson, & Stegner, 1983), measuring client satisfaction withservices; (d) a Health-Promoting Effort scale (McWilliam,Stewart, Brown, Desai, & Coderre, 1996), comprised of 39 100-mm visual linear analogues measuring the individual’s attention tohis/her own health, self-efficacy for managing life and health,experience of relationship-building, and partnering with providersin managing life and health as a resource for everyday living; and(e) Beisecker and Beisecker’s 10-item Locus of Authority inDecision Making (Beisecker, 1988), to assess the client’s partneringin health care decision making.
The provider survey included: the Work and Life AttitudesSurvey (subscales 2, 4, and 5), capturing intrinsic motivation, per-ceived job characteristics that might give rise to job satisfaction,and job satisfaction, an overall satisfaction comprised of bothintrinsic and extrinsic factors (Warr, Cook, & Wall, 1979); fourLikert scales measuring perceived effectiveness in care goal attain-ment; Spreitzer’s (1995) Empowerment Questionnaire, measuringpersonal empowerment; and the Provider’s Health PromotingEffort Scale (McWilliam et al., 1996, 1999), comprised of 35100-mm visual linear analogue scales measuring providers’ con-scious attention to the client’s health as a resource for everyday liv-ing and encouragement of client participation. The questionnairefor caregivers included: the 14-item abbreviated version of theMontgomery Burden Scale (Hooyman, Gonyea, & Montgomery,1985, adapted by Chappell, Havens, Hollander, Miller, &
imately 30 clients, informal caregivers, and providers in the inter-vention home care program (McCracken, 1988; Morse, 1991)during the implementation of the intervention were used toobtain a descriptive evaluation of the process.
Data Analysis
Quantitative evaluation included a measurement of the “neteffects” or impact of the intervention on clients, providers, andcaregivers, quantitatively controlling or qualitatively account-ing for the influence of other processes and events that mighthave affected outcomes (Rossi & Freeman, 1993). With dueconsideration of preliminary descriptive statistics, logarithmictransformations and adjustments, as appropriate, were under-taken to control for potential confounders. Using the trans-formed and/or adjusted outcomes, analyses of variance wereperformed, using the approach (i.e., intervention versus com-parator brokerage approach to care management), the assess-ment period (preinervention vs. postintervention), and theinteraction effect (Approach ¥ Assessment) to determine theimpact of the intervention on each of the variables. For theintervention to be effective, a change between assessments thatdiffered between programs was expected. Thus, a significantp value for the interaction effect would indicate that the inter-vention had an impact for that variable.
RESULTS
Survey data were obtained from baseline samples of 974 clients(58% participation rate); 249 caregivers (62% participationrate), and 291 providers (59% participation rate) and follow-upsamples of 809 (31%), 303 (49%), and 288 (36%) respectively.Table 3 presents client demographics. Participants did not differdemographically from nonparticipants, with the exception ofclients in the follow-up sample, who differed significantly fromnonparticipants in as much as they were predominantly morefemale (71% vs. 65%) and older (mean age = 72.9 years vs. 71 years).
Providers (9.1% = case managers; 29.7% = nurses; 53.7% =personal support workers; 7.5% = therapists or social workers)were, on average, 45 years of age and had 10.4 years of experience,59.6% having worked six or more years in home care. Caregiversaveraged 61 years of age and were predominantly female (71.4%),married (80.1%), and English speaking (69.2%). Overall, 22.3%of caregivers had university degrees and 39.8% were currentlyemployed full time.
The Implementation System
The intervention organization’s Education and Quality Assurancestaff conducted an evidence-based (McWilliam, Stewart, Desai,Wade, & Galajda, 2000; McWilliam, Diehl-Jones, Jutai &Tadrissi, 2000) 16-hour, 4-session training and reinforcementprogram on flexible client-driven care, offering this program 22times over 2 years, beginning 3 months prior to the initial imple-mentation of the intervention, through to 3 months prior to the
. . . case management options doserve different client groups
differently . . .
McWilliam, 2004) to measure caregiver burden; a modified ver-sion of the Spreitzer’s (1995) Empowerment Questionnaireadapted to measure caregivers’ psychological empowerment; and18 items measuring caregiver experience of choice of by whom,what, and when services were provided, assessment of workercharacteristics, and satisfaction with needs met, services received,and overall effectiveness in promoting the care recipient’s inde-pendence (Chappell et al., 2004) (Table 2). Field notes, documentreview, and in-depth interviews of a purposeful sample of approx-
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 76

Flexible Client-Driven Case Management
77
TABLE 2. Validation of Instruments Selected for Key Variables
Cronbach’s Alphas
Instrument Scale Previously Published Current Study
Client Functional independence 0.93–0.95 0.89Quality of life 0.78 0.66Satisfaction with services 0.87 0.81Health-promoting effort 0.82 0.88Partnering in decision making 0.73 0.86
Provider Job satisfaction 0.82–0.91 0.87Job motivation — 0.60Job characteristics — 0.84Empowerment 0.85 0.83Health-promoting effort — 0.86Perceived effectiveness in care goal attainment — 0.79
Caregiver Caregiver burden 0.79–0.91 0.89Dementia behavior disturbance — 0.80Empowerment — 0.91Satisfaction with care 0.79–0.87 0.87Satisfaction with choice — 0.87Satisfaction with worker characteristics — 0.87
TABLE 3. Demographic Characteristics of Clients Sampled in Intervention and Comparator Organizations
Assessment
I (%) C (%)Variable Value Labels (n = 906) (n = 886) Missing p Value
Gender Male 29.59 29.2 40 .856Female 70.41 70.8
Marital status Married 19.46 13.74 706 .018Widowed 37.56 44.04Other 42.98 42.22
Education Public school 21.03 30.91 143 <.001Secondary 50.66 48.52Post secondary 21.86 16.13Other 6.45 4.43
First language English 88.99 82.71 120 <.001French 0.59 4.72Other 10.41 12.58
Income < $20,000 54.85 55.05 871 .617$20,000–$39,000 31.09 32.93> $39,000 14.06 12.02
Living arrangements Family/friends 52.87 47.84 147 .041Alone 47.13 52.16
Sum of chronic problems 1–3 chronic problems 74.64 71.52 134 .1514–8 chronic problems 25.36 28.48
Accommodation Own home 43.64 58.24 132 <.001Other 56.36 41.76
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 77

McWilliam et al.
78
final follow-up data collection. A total of 349 providers (43% fulltime and 57% part time employees) attended, including 90 casemanagers (25.8%), 89 professional providers (25.5%), 91 para-professionals (26.1%), 49 support staff (14.0%), and 30 manage-rial staff (8.6%). Attendees constituted 30% of all staff. Policiesand procedures outlining case management roles, client assess-ment and in-home record keeping, and client brochures outliningthe approach were also provided. Periodic media releases informedthe public, and organizational newsletters afforded providers,clients, and caregivers regular reminders and updates.
Overall, the implementation of the intervention progressedslowly. By the end of the 1-year follow-up data collection period,with an organization caseload of 6,125 clients, client participationin flexible client-driven care was at 43.9%, with 506 (8.3%) hav-ing elected to be in the consumer-managed model, 466 (7.6%) inthe integrated team model, and an estimated 1,717 (28%), in thebrokerage model. The remaining 56.1% of clients remained in thebrokerage model as the intervention had not yet been initiatedwith them.
Endogenous Mediating Variables
Several significant unanticipated system changes impeded theintervention. One month into the implementation, governmentfunding was reduced, forcing reductions in services to clients. Inmonths 6 to 8, legislation mandating more centralized manage-ment and resource control was introduced and finalized. Homecare program Chief Executive Officers were replaced with gov-ernment-appointed, limited-term Acting Executive Directors,and community-elected board members were replaced with gov-ernment appointees. In the 10th month, the government intro-duced a standardized case management assessment protocolnecessitating staff training. Case managers, providers, andclients alike redirected their attention to these changes(McWilliam & Ward-Griffin, in press) and key leaders responsi-ble for championing the intervention left the organization.
Client Outcomes
The implementation of flexible client-driven care did not resultin client outcomes that differed significantly from those achievedwith a brokerage approach to all in-home case management(Table 4). Table 5 portrays the distribution of sampled clients (n= 417) in the intervention organization after implementation offlexible client-driven care. Consistent with a sample that was75% seniors, seniors were predominant in all three models ofcase management. However, odds ratios indicated that clients inthe consumer managed model were 2.8 times more likely to beadults with disabilities, while clients in the integrated teammodel were 3 times more likely to be seniors. Overall, the bro-kerage model of case management retained just under 75% of theintervention organization’s clients, with clients in that model 1.5times more likely to be seniors. As one would expect, the demo-graphics of seniors differed significantly from adults with disabil-ities, the former being predominantly female, widowed, withoutpostsecondary education, in lower income brackets, living with
family or friends, and suffering from four or more chronic med-ical problems (Table 6).
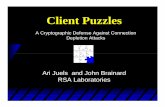
Figure 2 portrays the client mix across the three case man-agement models. Seniors clearly tended to remain in the broker-age model of case management (76.8%), with those choosing analternative model equally likely to choose the integrated or con-sumer-managed model. In contrast, 31.7% of adults with dis-abilities chose alternatives to the usual brokerage model of caremanagement, primarily (27.6%) the consumer-managed model.Comparisons of these client subgroups in the three optional casemanagement models offered in the flexible client-driven careintervention identified no significant differences (Table 7).Reflective of the difference in client mix in the three models,clients in the integrated team model tended to be older thanthose in the other two models, and clients in the consumer-managed model tended to be much younger (Table 8). Bothseniors and adults with disabilities in the integrated team modelhad the lowest satisfaction with services. Seniors in the con-sumer-managed model reported greater health-promoting effortand partnering in decision making than seniors in other casemanagement models. Costs of total health services utilizationvaried widely among clients in each model, particularly amongadults with disabilities. A review of the medical conditions andproblems of adults with disabilities indicated considerable vari-ation in degree of impediments to independent living, withthose in the integrated team model more apt to have extensivefunctional limitations attributable to advanced debilitating dis-ease, while those in the consumer-managed model were manag-ing more independently, despite more static physical disabilities(e.g., paraplegia).
Provider Outcomes
Providers in the intervention organization did not experience worksignificantly differently from those in the comparator organizationproviding service using only brokerage case management (Table 9).Differences in providers’ job satisfaction ( p = .07) and perceivedjob characteristics ( p = .07) approached significance, suggestingthat providers in the intervention organization may have experi-enced the implementation of flexible-client-driven care positively.Normalized data for providers in both the intervention and com-parator home care programs (Table 10) indicated positive changesbetween the premeasurements and postmeasurements for Health-Promoting Effort and Job Characteristics for both groups, withlarger gains in the intervention group. Job motivation dropped inboth groups, more in the comparator organization. Job satisfactionwas essentially unchanged in the intervention home care programbut dropped for providers in the comparator home care program.
Caregiver Outcomes
The outcomes for caregivers in the intervention home care pro-gram (Table 11) differed significantly only with regard to caregiv-er burden, with those in the intervention organization reportinggreater burden ( p value = .00012). Figure 3 portrays the increased
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 78

burden of caregivers in the intervention home care program overtime as compared to those in the comparator organization. Ananalysis of variance to test for a difference in the burden scores ofcaregivers of clients in the three case management models revealedno significant differences ( p value = .0158). Thus, the fact that thecaregiver burden scores for those in the intervention home careprogram had increased in the postassessment could not be attrib-uted to selection of case management models.
DISCUSSION
The generalizability of evaluative findings of organization-wide interventions is limited by the unavoidable nonrandomallocation of organizations to such endeavors. The results ofthis study are further limited by the low rates of return fromthe follow-up samples, as well as by the inability to measure the
impact of endogeneous variables such as mandated service reduc-tions, loss of leaders who championed the intervention, staffturnover, and consequent incomplete implementation of theintervention. Inasmuch as a policy context of economic constraintand centralized control also philosophically conflicts with theintervention’s empowering partnering approach to care manage-ment, the inconclusive results are not surprising. Further longitu-dinal investigation is needed.
Nevertheless, this evaluation of organization-wide implemen-tation of a flexible client-driven approach to case management ofin-home services illustrates what can be achieved in just 2 years,despite the policy context. Study findings suggest several impor-tant considerations for those interested in exploring this optionfor case management. Clients in the intervention home care pro-gram did not cost more and experienced outcomes similar tothose of the comparator group. Subanalyses of clients in the three
Flexible Client-Driven Case Management
79
TABLE 4. ANCOVA Comparing Client Outcomes for the Intervention Versus Comparator Organization’s Care Management Approach
Adjusteda
Outcome Source F Statistic p Value
Costs of total health services Utilizationb
Satisfaction with servicesc
Health-promoting effort
Partnering in decision makingd
aCosts of Total Health Services Utilization and Satisfaction with Care have been adjusted for risk levels and number of health prob-lems/chronic conditions. Health-promoting effort and Partnering in Decision-Making are adjusted for the same two covariates as well asliving arrangements. bLog transformation required to satisfy equality of variance. cSquare transformation required to satisfy equality ofvariance.dFifth power transformation required to satisfy equality of variance.
TABLE 5. Distribution of Respondents by Group: Adults With Disabilities (AD) Versus Seniors
Percentage of Respondents Odds Ratios
Model Seniors AD Seniors AD
Consumer managed (n = 65) 11.91% 27.55% 0.36 2.81Integrated team (n = 40) 11.29% 4.08% 2.99 0.34 Brokerage (n = 312) 76.80% 68.37% 1.53 0.65
Approach F1,1041 = 0.950 .329Assessment F1,1041 = 6.500 .011Approach ¥ Assessment F1,1041 = 0.010 .909Error (3.399)Approach F1,980 = 0.110 .735Assessment F1,980 = 85.940 <.001Approach ¥ Assessment F1,980 = 0.060 .808Error (145419.300)Approach F1,845 = 3.090 .079Assessment F1,845 = 0.030 .860Approach ¥ Assessment F1,845 = 0.520 .471Error (134.033)Approach F1,952 = 0.400 .527Assessment F1,952 = 24.230 <.001Approach ¥ Assessment F1,952 = 0.780 .377Error (6.685E13)
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 79

McWilliam et al.
80
TABLE 6. Characteristics of Clients: Seniors/Adults With Disabilities (AD)
Seniors/Adults With Disabilities
Seniors (%) AD (%)Variable Value Labels (n = 1,372) (n = 420) Missing p Value
Gender Male 26.87 37.62 40 <.001Female 73.13 62.38
Marital status Married 11.23 35.74 706 <.001Widowed 43.25 31.33Other 45.52 32.93
Education Public school 31.45 8.14 143 <.001Secondary 50.88 45.55Post secondary 12.74 39.19Other 4.94 7.12
First language English 83.72 92.89 120 <.001French 3.05 1.27Other 13.22 5.84
Income < $20,000 58.14 44.8 871 <.001$20,000–$39,000 33.43 27.15> $39,000 8.43 28.05
Living arrangements Family/friends 55.34 34.03 147 <.001Alone 44.66 65.97
Sum of chronic problems 1–3 chronic problems 66.64 94.75 134 <.0014–8 chronic problems 33.36 5.25
Accommodation Own home 49.69 54.66 132 .087Other 50.31 45.34
74.8% 76.8%
68.4%
74.8% 76.8%
68.4%
15.6%11.9%
27.6%
Total SampleSeniors >= 65 yearsAdults with Disabilities, 18–64 years
Brokerage Model Integrated Team Model Consumer Managed Model
100%
80%
60%
40%
20%
0%
Figure 2. Flexible client-driven care: Client mix in models of case management.
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 80

models of case management suggest that client health care costsand outcomes in these three options are potentially similar.Significant differences in the demographic attributes of clients inthe two alternatives to the brokerage model suggest that these casemanagement options do serve different client groups differently,with the integrated team model more aligned to senior clientswith relatively stable supportive care requirements, and the con-sumer-managed model more aligned to the needs of adults withdisabilities, despite high needs for service.
Compared to previous research that suggested approximately40% of home care clients might appropriately select either theintegrated team or consumer-managed models as alternatives tobrokerage case management (McWilliam et al., 2000), the clientsin the intervention home care program were less inclined to haveexperienced such a change. Given the implementation constraints,this may have been due to clients’ lack of opportunity to partner inchoosing their case management approach. Alternatively, althoughreported demographics and morbidity levels of client samples were
Flexible Client-Driven Case Management
81
TABLE 8. Descriptive Statistics Elaborating the Attributes of Client Groups in Each of Three Optional Models of CaseManagement Offered Within the Intervention Organization
Brokerage Integrated Team Consumer(N = 312) (N = 40) (N = 65)
Descriptor Group M SD M SD M SD p Value
Age Seniors 80.6 7.27 82.8 8.22 80.1 7.18 0.188AD 50.2 12.43 44.8 16.13 44.3 13.92 0.375
Assessed need for support Seniors 2.5 0.70 2.5 0.75 2.7 0.80 0.183AD 3.4 1.14 3.7 1.53 3.5 1.07 0.814
Functional independence Seniors 57.0 23.02 51.4 24.96 55.0 24.90 0.751AD 60.7 15.19 65.5 4.20 60.2 10.61 0.561
Cost of total health services utilization Seniors 3,241.5 4,545.91 3,063.9 4,934.64 3,805.7 4,742.04 0.525
AD 4,185.2 5,031.98 15,118.4 21,513.41 4,956.6 6,983.24 0.903Satisfaction with services Seniors 32.9 6.66 29.8 6.79 32.9 7.28 0.050
AD 32.1 6.06 27.3 4.19 33.6 5.58 0.586Health-promoting effort Seniors 59.8 11.75 59.8 12.23 66.1 11.72 0.049
AD 62.0 11.29 55.8 18.11 60.9 8.15 0.725Partnering in decision making Seniors 22.5 5.87 19.3 6.79 23.8 5.25 0.014
AD 24.8 4.35 24.7 2.21 24.3 4.94 0.6876
TABLE 7. ANCOVA Comparing Outcomes for Seniors Versus Adults With Disabilities by Case Management Model Selected inthe Intervention Organization
Adjusteda
Outcome Source F Statistic p Value
Costs of total health services Utilizationb
Satisfaction with servicesc
Health-promoting effort
aCosts of Total Health Services Utilization and Satisfaction with Care have been adjusted for risk levels and number of health prob-lems/chronic conditions. Health-promoting effort is adjusted for the same two covariates as well as living arrangements. bLog transfor-mation required to satisfy equality of variance. cSquare transformation required to satisfy equality of variance.
Group F1,1041 = 143 .233Model F2,329 = 0.13 .879Group ¥ Model F2,329 = 0.30 .738Error (4.086)Group F1,299 = 0.63 .428Model F2, 299 = 1.63 .197Group ¥ Model F2, 299 = 0.11 .899Error (1.591E5)Group F1,254 = 1.14 .286Model F2,254 = 2.12 .123Group ¥ Model F2,254 = 1.75 .176Error (129.97)
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 81

McWilliam et al.
82
similar, overall client functional levels and health status in thestudy reported herein may have differed from those of the previousstudy (McWilliam et al., 2000), altering the comparative appro-priateness of participation in alternative case management models.As well, the intervening service reduction policy may have under-mined clients’ trust in an approach that fostered greater involve-ment in their own care management.
The outcomes experienced by providers involved in the flexi-ble client-driven approach to case management merit considera-tion. Despite their similar exposure to government-imposedreductions and changes, quite likely factors contributing todeclines in job motivation and satisfaction in both organizations,
providers (including case managers) in the intervention organiza-tion viewed their job characteristics more positively after the inter-vention was implemented than did those in the comparatororganization. Given the challenges of recruitment and retention ofin-home service providers, these trends support further effort toimplement and test flexible client-driven care management.
The experience of increased caregiver burden in the interven-tion home care program raises the concern that affording clients an
TABLE 10. Percent Change Comparisons Between Providersin the Intervention and Comparator Home Care Programs
% Change From Baseline Absolute
Outcome Intervention Comparator DifferenceJob satisfaction -0.40% -2.85% 2.45%Job motivation -8.83% -11.08% 2.25%Job characteristics 5.17% 1.28% 3.89%Empowerment 1.60% 1.79% 0.18%Health-promoting effort 3.84% 2.63% 1.20%
TABLE 9. ANCOVA Comparing Provider Outcomes for the Intervention Versus Comparator Organization’s Care Management Approach
Adjusteda
Outcome Source F Statistic p Value
Job satisfactionb
Job motivationb
Job characteristicsb
Empowerment
Health-promoting effortc
aAdjusted for professional versus para-professional and employment status (i.e., full time vs. part time). bLog transformation required tosatisfy equality of variance. cCubic power transformation required to satisfy equality of variance.
Approach F1,553 = 2.12 0.146Assessment F1,553 = 3.59 0.059Approach ¥ Assessment F1,553 = 3.40 0.066Error (0.010)Approach F1,553 = 0.17 0.683Assessment F1,553 = 119.75 <.001Approach ¥ Assessment F1,553 = 1.18 0.277Error (0.012)Approach F1,552 = 2.14 0.144Assessment F1,552 = 4.96 0.026Approach ¥ Assessment F1,552 = 3.35 0.067Error (0.025)Approach F1,553 = 7.95 0.005Assessment F1,553 = 1.52 0.219Approach ¥ Assessment F1,553 = 0.09 0.767Error (42.389)Approach F1,552 = 1.41 0.236Assessment F1,552 = 1.55 0.213Approach ¥ Assessment F1,552 = 0.63 0.428Error (1.203E10)
InterventionComparator
PRE
Mea
n C
are
Bur
den
Scor
e
POST
31.5
35.1
32.2
33.8
36
35
34
33
32
31
30
29
Figure 3. Change in caregiver burden in the intervention versuscomparator organization from baseline to follow-up.
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 82

opportunity to become more engaged as partners in their caremanagement might create more burden for caregivers. However,inasmuch as caregivers of clients who chose the integrated team orconsumer-managed models of case management experienced nogreater burden than those caring for clients in the brokeragemodel, this concern is somewhat allayed. Nevertheless, furtherinvestigation is needed before firm conclusions can be drawn.
Overall, study findings afford leaders in the field of home carecase management some degree of assurance that they may pro-ceed to employ and test alternative approaches to care manage-ment without dire consequences, despite challenging policycontexts. However, findings also make apparent that both chang-ing care management, a function that fulfills a broad mandatewithin health services delivery, and achieving statistically signifi-cant outcomes takes time. Clearly, sustained leadership effort toensure educational preparation for and implementation of suchinterventions is essential. Greater success may be achieved ifimplementation systems were more integrated into everyday serv-ice delivery processes, hence, less prone to curtailment by majorpolicy changes. For instance, transformative educationalapproaches (Ackerman-Anderson & Anderson, 2001; Lindstrom,2003; Mezirow, 1991, 1999) that engage all involved in develop-ing and mastering the new approach as a part of ongoing dailypractice may expedite implementation, and consequently, theattainment of the anticipated outcomes.
The need for more extensive longitudinal evaluation studiesis readily apparent. The comparative cost-effectiveness of thethree models of case management particularly merits furtherinvestigation. As contextual mediating variables like major poli-cy changes are uncontrollable and inevitable, use of a compre-hensive program evaluation model and comparator groups inthe same policy context is essential in continuing evaluativeresearch of this nature.
CONCLUSIONS
Case management is essential for achieving cost-effective, well-coordinated, integrated in-home service delivery. Yet to date, therehas been little research to inform evidence-based evolution of mod-els for case management. Tests of case management interventionsthat optimize the potential of the limited human resources avail-able for in-home care management particularly have been over-looked in past research agendas. This evaluative research studyprovides foundational information for further development of casemanagement. Study findings suggest that flexible-client-drivencare does not increase resource consumption or undermine careoutcomes. Furthermore, the integrated team and consumer-man-aged case management models may appropriately serve differentclient groups. Despite challenging policy contexts, case manage-ment leaders may draw upon this study to more confidently
Flexible Client-Driven Case Management
83
TABLE 11. ANOVA Comparing Caregiver Outcomes for the Intervention Versus Comparator Organization’s Care Management Approach
Adjusteda
Outcome Source F Statistic p Value
Caregiver burdena
Empowerment
Satisfaction with care score
Satisfaction with choice
Satisfaction with worker characteristics
aAdjusted for dementia behavior disturbance score.
Approach F1,363 = 0.63 .4271Assessment F1,363 = 0.00 .9981Approach ¥ Assessment F1,363 = 10.6 .0012Error (72.193)Approach F1,372 = 0.310 .580Assessment F1,372 = 0.000 .950Approach ¥ Assessment F1,372 = 1.100 .295Error (78.894)Approach F1,368 = 0.060 .815Assessment F1,368 = 0.480 .490Approach ¥ Assessment F1,368 = 0.070 .795Error (48.076)Approach F1,361 = 0.530 .469Assessment F1,361 = 0.630 .427Approach ¥ Assessment F1,361 = 0.110 .740Error (4.551)Approach F1,361 = 0.060 .802Assessment F1,361 = 0.030 .856Approach ¥ Assessment F1,361 = 0.010 .929Error (23.476)
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 83

McWilliam et al.
84
explore options for case management. As the findings of this studysuggest, if cost-effective health care reform is to transpire, furtherlongitudinal implementation and investigation of alternativeapproaches to case management may help to achieve this aim.
REFERENCES
Ackerman-Anderson, L., & Anderson, D. (2001). Awake at the wheel:Moving beyond change management to conscious change leader-ship. OD Practitioner, 33(3) 40–48.
Alberta Ministry of Health. (1993). Self-managed care pilot project.Technical report. Alberta, Canada: Author.
Auton, G. M. (1995). The role of total quality management in patient-centered restructuring [Review]. Journal of the Society for HealthSystems, 5(1), 63–71.
Beisecker. A. (1988). Aging and the desire for information and input inmedical decisions: Patient consumerism in medical encounters.The Gerontologist, 28(3), 330–335.
Bergman, H., & Béland, F. (2000). Evaluating innovation in the care ofCanada’s frail elderly population. Canadian Medical AssociationJournal, 162(4), 511–512.
Bigelow, D. A., & Young, D. J. (1991). Effectiveness of a case manage-ment program. Community Mental Health Journal, 27(2), 115–123.
Bly, J. L., & Kissick, P. (1994). Hospice care for patients living alone:Results of a demonstration program. Hospice Journal, 9(4), 9–20.
Braun, K. L., & Rose, C. L. (1994). Testing the impact of a case man-agement program on caregiver appraisal. Journal of GerontologicalSocial Work, 21(3/4), 51–69.
Browne, G., Arpin, K., Corey, P., Fitch, M., & Gafni, A. (1990).Individual correlates of health services utilization and the cost ofpoor adjustment of chronic illness. Medical Care, 28(1), 43–58.
Browne, G., Gafni, A., Arpin, K., Corey, P, & Finch, M. (1992). Healthand social service utilization: Paper 92–12, Working paper series.Hamilton, Canada: McMaster University, Faculties of Health andSocial Sicences, Health System-Linked Research Unit.
Cahill, J. (1996). Patient participation: A concept analysis. Journal ofAdvanced Nursing, 24, 561–571.
Campbell, A. J., Robertson, M. C., Gardner, M. M., Norton, R. N.,Tilyard, M. W., & Buchner, D. M. (1997). Randomized controlledtrial of a general practice programme of home based exercise to pre-vent falls in elderly women. British Medical Journal, 315(7115),1065–1069.
Canadian Home Care Association. (1995, Spring). At home: Officialnewsletter of the Canadian Home Care Association. Ottawa: Author.
Carnaby, S. (1997). “What do you think?”: A qualitative approach toevaluating individual planning services. Journal of IntellectualDisability Research, 41(3), 225–231.
Challis, D., Darton, R., Johnson, L., Stone, M., & Traske, K. (1991a).An evaluation of an alternative to long-stay hospital care for frailelderly patients: 1. The model of care. Age and Aging, 20, 236–244.
Challis, D., Darton, R., Johnson, L., Stone, M., & Traske, K. (1991b).An evaluation of an alternative to long-stay hospital care for frailelderly patients: 2. Costs and effectiveness. Age and Aging, 20,245–253.
Chappell, N., Havens, B., Hollander, M., Muller, J., & McWilliam, C.(2004). Home care: A cost-effective alternative to residential serv-ices. The Gerontologist, 44(3), 389–400.
Clarke, P. (1989). The philosophical foundation of empowerment:Implications for geriatric health care programs and practice.Journal of Aging and Health, 1, 267–285.
Cook, T., & Campbell, D. (1979). Quasi experimentation design andanalysis issues for field settings. Boston: Houghton Mifflin.
Dalby, D. M., Williams, J. I., & Hodnott, E. (1996). Postpartum safetyand satisfaction following early discharge. Canadian Journal ofPublic Health, Revue Canadienne, 87(2), 90–94.
Davies, S., Laker, S., & Ellis, L. (1997). Promoting autonomy and inde-pendence for older people within nursing practice: A literaturereview. Journal of Advanced Nursing, 26, 408–417.
D'Ercole, A., Struening, E., Curtis, J. L., Millman, E. J., & Morris, A.(1997). Effects of diagnosis, demographic characteristics, and casemanagement on rehospitalization. Psychiatric Services, 48(5),682–688.
Folstein, M., Folstein, S., & McHugh, P. (1975). Mini-mental state: Apractical guide for grading the cognitive state of patients for the cli-nician. Journal of Psychiatric Research, 12, 189–198.
Gagnon, A. L, Schein, C., McVey, L., & Bergeron, H. (1999).Randomized controlled trial of nurse care management of frail olderpeople. Journal of the American Geriatrics Society, 47, 1118–1124.
Geron, S., & Chassler, L. (1994). Guidelines for case management practiceacross the long-term care continuum. Bristol, CT: ConnecticutCommunity Care.
Gilmore, T. N. (1991). Leadership transitions and the impact on patientcare [Review]. Journal of the Society for Health Systems, 2(3), 59–72.
Goering, P. N., Wasylenki, D. A., Farkas, M., Lancee, W. J., &Ballantyne, R. (1988). What difference does case managementmake? Hospital and Community Psychiatry, 39(3), 272–276.
Gonzalez-Calvo, J., Jackson, J., Hansford, C., Woodman, C., &Remington, N. S. (1997). Nursing case management and its role inperinatal risk reduction: Development, implementation, and eval-uation of a culturally competent model for African Americanwomen. Public Health Nursing, 14(4), 190–206.
Gray, A. M., Marshall, M., Lockwood, A., & Morris, J. (1997). Problemsin conducting economic evaluations alongside clinical trials.Lessons from a study of case management for people with mentaldisorders. British Journal of Psychiatry, 170, 47–52.
Greene, J., Caracelli, V., & Graham, W. (1989). Toward a conceptualframework for mixed-method evaluation designs. EducationalEvaluation and Policy Analysis, 11(3), 255–274.
Hoddinott, S., & Bass, M. (1986, November). The Dillman Total DesignSurvey Method: A sure-fire way to get high survey return rates.Canadian Family Physican, 32, 2366–2368.
Hooyman, N., Gonyea, J., & Montgomery, R. (1985). The impact of in-home services termination on family caregivers. The Gerontologist,25(2), 141–145.
Hurst, K. (1996). The managerial and clinical implications of patient-focused care. Journal of Management in Medicine, 10(3), 59–77.
Jackson, M. E. (1994). Rationing case management: Six case studies.Report prepared for the Department of Health and HumanServices Office of the Assistant Secretary for Planning andEvaluation. Washington, DC: US Department of Health andHuman Services.
Jennings, P. (1994). Learning through experience: An evaluation of hos-pital at home. Journal of Advanced Nursing, 19(5), 905–911.
Jirsch, D. (1993). Patient-focused care: The systemic implications ofchange [Review]. Healthcare Management Forum, 6(4), 27–32.
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 84

Jones, A. (1995). An analysis of case management—The efficient utilityof human resources, but to what end. Journal of NursingManagement, 3, 143–149.
Jones, R. A., Dougherty, M., & Martin, S. (1997). Program evaluation ofa unit re-engineered for patient-focused care. Holistic NursingPractice, 11(3), 31–46.
Kane, R. A., Caplan, A. L., Urv-Wong, E., Freeman, I. C., Aroskar, M.A., & Finch, M. (1997). Everyday matters in the lives of nursinghome residents: Wish for and perception of choice and control.Journal of the American Geriatrics Society, 45, 1086–1093.
Kane, R., Penrod, J., & Kivnick, H. (1994). Case managers discussethics: Dilemmas of an emerging occupation in long-term care inthe United States. Journal of Case Management, 3(1), 3–11.
Lathrop, J. P., Seufert, G. E., MacDonald, R. J., & Martin, S. B. (1991).The patient-focused hospital: A patient care concept. Journal of theSociety for Health Systems, 3(2), 33–50.
Lindstrom, R. R. (2003). Evidence-based decision making in healthcare:Exploring the issues through the lens of complex, adaptive systemstheory. Healthcare Papers, 3(3), 29–35.
Manitoba Ministry of Health. (1994). Impact on self-managed care par-ticipants [Technical Report]. Manitoba, Canada: Author.
Marshall, M., Lockwood, A., & Gath, D. (1995). Social services casemanagement for long-term mental disorders: A randomized con-trolled trial. Lancet, 345, 409–412.
McCracken, G. (1988). The long interview: Qualitative research methodsseries 13. Newbury Park, CA: Sage.
McDowell, I., & Newell, C. (1996). Measuring health: A guide to ratingscales and questionnaires (2nd ed.). New York: Oxford UniversityPress.
McWilliam, C. L. (1992). From hospital to home: Elderly patients dis-charge experiences. Family Medicine, 24(6), 256–267.
McWilliam, C. L., Diehl-Jones, W., Jutai, J., & Tadrissi, S. (2000). Caredelivery approaches and seniors’ independence: A systematic reviewand synthesis of the literature. Canadian Journal on Aging,19(Suppl. 1), 101–124.
McWilliam, C., Stewart, M., Desai, K., Wade, T., & Galajda, J. (2000).Case management. Health Care Management Forum, 13(3), 37–44.
McWilliam, C. L., Brown, J. B., Carmichael, J. L., & Lehman, J. M.(1994). A new perspective on threatened autonomy in elderly per-sons: The disempowering process. Social Science & Medicine, 38(2),327–338.
McWilliam, C. L., Stewart, M., Brown, J. B., Desai, K., & Coderre, P.(1996). Creating health with chronic illness. Advances in NursingScience, 18(3), 1–15.
McWilliam, C. L., Stewart, M., Brown, J. B., McNair, S., Donner, A.,Desai, K., et al. (1999). Home-based health promotion for chron-ically ill older persons: Results of a randomized controlled trial of acritical reflection approach. Health Promotion International, 14(1),27–41.
McWilliam, C., & Ward-Griffin, C. (in press). Implementing organiza-tional change in health and social services. Journal ofOrganizational Change Management.
Mezirow, J. (1991). Transformative dimensions of adult learning. SanFrancisco: Jossey-Bass.
Mezirow, J. (1999). Transformation theory: Postmodern issues. RetrievedDecember 16, 2002, from http://www.edst.educ.ubc.ca.aerc/1999/abl999.htm
Morse, T. (Ed). (1991). Qualitative nursing research: A contemporary dia-logue. Newbury Park, CA: Sage.
New Brunswick Ministry of Health. (1991). The New Brunswick Extra-Mural Hospital: A response to the future. Fredericton, NewBrunswick, Canada: Author.
Nguyen, T. D., Attkinsson, C. C., & Stegner, B. L. (1983). Assessment ofpatient satisfaction: Development and refinement of a service evalu-ation questionnaire. Evaluation and Program Planning, 6, 299–314.
Ontario Ministry of Health. (1992, December 21). Debriefing note of theOntario Ministry of Health and the Ontario Home Care ProgramsAssociation meeting. Toronto, Canada: Author.
Peruselli, C., Paci, E., Franceschi, P., Legori, T., & Mannucci, R. (1997).Outcome evaluation in a home palliative care service. Journal ofPain & Symptoms Management, 13(3), 158–165.
Posavac, E., & Carey, R. (1997). Program evaluation methods & case stud-ies (5th ed.). Upper Saddle River, NJ: Prentice Hall.
Rose, S. M. (Ed.). (1992a). Case management and social work practice.New York: Longman.
Rose, S. M. (1992b). Empowering case management clients. AgingInternational, 19(3), 1–4.
Rossi, P., & Freeman, J. (1993). Evaluation research: Socialization pro-grams (5th ed.). Newbury Park, CA: Sage.
Saskatchewan Health. (1996). Final report: Saskatchewan CaseManagement Pilot Project. Regina, Canada: Author.
Seltzer, M. M., Ivry, J., & Litchfield, L. C. (1987). Family members ascase managers: Partnership between the formal and informal sup-port networks. The Gerontologist, 27(6), 722–728.
Shapiro, E. (1995). Case management in long-term care: Exploring itsstatus, trends, and issues. Journal of Case Management, 4(2), 43–47.
Snyder, G. H., & Lathrop, J. P. (1995). Cost reduction using patient-focused care concepts. Managed Care Quarterly, 3(2), 43–51.
Spreitzer, G. (1995). An empirical test of a comprehensive model ofinterpersonal empowerment in the workplace. American Journal ofPsychology, 23(5), 601–629.
Swindle, D. N., Weyant, J. L., & Mar, P. S. (1994). Nurse case manage-ment: Collaboration beyond the hospital walls. Journal of CaseManagement, 3(2), 51–55.
Thompson, J. (1992). Program evaluation within a health promotionframework. Canadian Journal of Public Health, 83(Suppl. 1),S67–S71.
Tidikis, F., & Strasen, L. (1994). Patient-focused care units improve serv-ice and financial outcomes. Healthcare Financial Management,48(9), 38–40, 42, 44.
Tiezzi, L., Lipshutz, J., Wrobleski, M., Vaughan, R. D., & McCarthy, J.F. (1997). Pregnancy prevention among urban adolescents youngerthan 15: Results of the In Your Face program. Family PlanningPerspectives, 29(4), 173–176.
Twyman, D. M., & Libbus, M. K. (1994). Case-management of AIDSclients as a predictor of total in-patient hospital days. Public HealthNursing, 11(6), 406–411.
Van Minnen, A., Hoogduin, C. A., & Broekman, T. G. (1997). Hospitalvs. outreach treatment of patients with mental retardation and psy-chiatric disorders: A controlled study. Acta PsychiatricaScandinavica, 95(6), 515–522.
Vingilis, E., & Pederson, L. (2001). Using the right tools to answer theright questions: The importance of evaluative research techniquesfor health services evaluation research in the 21st century. TheCanadian Journal of Program Evaluation, 16(2), 1–26.
Flexible Client-Driven Case Management
85
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 85

McWilliam et al.
86
Warr, P., Cook, J., & Wall, T. (1979). Scales for the measurement of somework attitudes and aspects of psychological well-being. Journal ofOccupational Psychology, 52, 129–148.
Weissert, W. J. (1988). The National Channeling Demonstration: Whatwe knew, know now, and still need to know. Health ServicesResearch, 23(1), 176–187.
Weissert, W. G., & Hedrick, S. C. (1994). Lessons learned from researchon effects of community-based long-term care. Journal of theAmerican Geriatrics Society, 42, 348–353.
Zawadski, R. T., & Eng, C. (1988). Case management in capitated long-term care. Health Care Financing Review, Annual Supplement,10(12), 75–81. HFCA Publ. No. 03275.
Zimmer, J. G., Eggert, G. M., & Chiverton, P. (1990). Individual versusteam case management in optimizing community care for chroni-cally ill patients with dementia. Journal of Aging and Health, 2(3),357–372.
Carol McWilliam, MScN, EdD, Professor of Nursing, Universityof Western Ontario (UWO), has focused on collaborative inter-disciplinary research in home care and the management of in-home care. Moira Stewart, PhD, Professor and Director, Centrefor Studies in Family Medicine, UWO, is a Canadian ResearchChair, whose research has focused on client-centered practice.Evelyn Vingilis, PhD, Professor and Director, Population andCommunity Health Unit, UWO, is a psychologist whose researchhas focused on evaluation of numerous population and commu-nity health programs and initiatives. Jeffrey Hoch, PhD, AssistantProfessor, UWO, is a health economist focused on the evaluationof health services delivery. Catherine Ward-Griffin, PhD,Associate Professor, Nursing, UWO, has focused on research ofrelationships between and among providers, clients and informalcaregivers involved in community-based care. Allan Donner,PhD, Professor, UWO, is an internationally renowned biostatisti-cian. Gina Browne, PhD, Professor and Director, System-LinkedResearch Unit, McMaster University, has focused on research andevaluation of community-based programs and health services.Peter Coyte, PhD, Professor and Director, Home Care EvaluationResearch Unit, is a health economist and Canadian ResearchChair focused on the evaluation of in-home health services deliv-ery. Karen Anderson, MSc, Research Assistant, is a PhD studentat the Ivey School of Business, the University of Western Ontario.
Acknowledgments. This study was funded by the CanadianInstitutes of Health Research. The findings and conclusions con-tained in this article are those of the authors. No official endorse-ment by CIHR is intended, nor should it be inferred.
Offprints. Requests for offprints should be directed to:Carol L. McWilliam, MScN, EdDFaculty of Health SciencesUniversity of Western OntarioLondon, ON, Canada N6A 5C1E-mail: [email protected]
CMJ5(2)_02_mcwilliam.qxd 4/20/05 12:40 PM Page 86

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
Copyright © 2022 FDOKUMEN