
Females with Fabry disease frequently have major organ involvement: Lessons from the Fabry Registry
17
Females with Fabry disease frequently have major organ involvement: Lessons from the Fabry Registry William R. Wilcox a,b, * , Joa ˜o Paulo Oliveira c , Robert J. Hopkin d , Alberto Ortiz e , Maryam Banikazemi f , Ulla Feldt-Rasmussen g , Katherine Sims h , Stephen Waldek i , Gregory M. Pastores f , Philip Lee j , Christine M. Eng k , Laszlo Marodi l , Kevin E. Stanford m , Frank Breunig n , Christoph Wanner o , David G. Warnock p , Roberta M. Lemay q , Dominique P. Germain r,s a Medical Genetics Institute, Cedars-Sinai Medical Center, 8700 Beverly Blvd. SSB, Los Angeles, CA 90048, USA b Department of Pediatrics, UCLA School of Medicine, Los Angeles, CA, USA c Medical Genetics, Hospital Sa ˜o Joa ˜o, Porto, Portugal d Cincinnati Children’s Hospital, Cincinnati, OH, USA e Fundacio ´ n Jime ´nez Dı ´az, Madrid, Spain f New York University, New York, NY, USA g Department of Medical Endocrinology, Rigshospitalet, University of Copenhagen, Denmark h Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA i Hope Hospital, Salford, Manchester, United Kingdom j National Hospital for Neurology & Neurosurgery, London, United Kingdom k Department of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX, USA l Department of Infectious and Pediatric Immunology, Medical and Health Science Centre, University of Debrecen, Debrecen, Hungary m Department of Psychiatry, University of Cincinnati College of Medicine, Cincinnati, OH, USA n Department of Medicine, Division of Nephrology, University Hospital, Wu ¨ rzburg, Germany o University Hospital, Department of Medicine, Wu ¨ rzburg, Germany p University of Alabama at Birmingham, Birmingham, AL, USA q Biomedical Operations, Genzyme Corporation, USA r Centre de re ´fe ´rence de la maladie de Fabry et des maladies he ´re ´ditaires du tissu conjonctif. Assistance Publique – Ho ˆpitaux de Paris, Paris, France s University of Versailles - St Quentin en Yvelines, France Received 29 August 2007; received in revised form 24 September 2007; accepted 24 September 2007 Available online 26 November 2007 Abstract Fabry disease (FD) is an X-linked lysosomal storage disease caused by alpha-galactosidase A deficiency. The Fabry Registry is a global clinical effort to collect longitudinal data on FD. In the past, most ‘‘carrier’’ females were usually thought to be clinically unaffected. A sys- tematic effort has been made to enroll all FD females, regardless of symptomology. Of the 1077 enrolled females in the Registry, 69.4% had symptoms and signs of FD. The median age at symptom onset among females was 13 years, and even though 84.1% had a positive family history, the diagnosis was not made until a median age of 31 years. Twenty percent experienced major cerebrovascular, cardiac, or renal events, at a median age of 46 years. Among adult females with estimated glomerular filtration rate (eGFR) data (N = 638), 62.5% had an eGFR <90 ml/min/1.73m 2 and 19.0% had eGFR <60 ml/min/1.73 m 2 . Proteinuria P300 mg/day was present in 39.0% of females, and 22.2% had >1 gram/day. Quality of life (QoL), as measured by the SF-36 Ò survey, was impaired at a later age than in males, but both genders experience significantly impaired QoL from the third decade of life onward. Thus, females with FD have a significant risk for major organ involvement and decreased QoL. Females should be regularly monitored for signs and symptoms of FD, and considered for enzyme replacement therapy. 1096-7192/$ - see front matter Ó 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.ymgme.2007.09.013 * Corresponding author. Address: Medical Genetics Institute, Cedars-Sinai Medical Center, 8700 Beverly Blvd. SSB, Los Angeles, CA 90048, USA. Fax: +1 310 423 0620. E-mail address: [email protected] (W.R. Wilcox). www.elsevier.com/locate/ymgme Available online at www.sciencedirect.com Molecular Genetics and Metabolism 93 (2008) 112–128
Transcript of Females with Fabry disease frequently have major organ involvement: Lessons from the Fabry Registry

Available online at www.sciencedirect.com
www.elsevier.com/locate/ymgme
Molecular Genetics and Metabolism 93 (2008) 112–128
Females with Fabry disease frequently have major organinvolvement: Lessons from the Fabry Registry
William R. Wilcox a,b,*, Joao Paulo Oliveira c, Robert J. Hopkin d, Alberto Ortiz e,Maryam Banikazemi f, Ulla Feldt-Rasmussen g, Katherine Sims h, Stephen Waldek i,
Gregory M. Pastores f, Philip Lee j, Christine M. Eng k, Laszlo Marodi l,Kevin E. Stanford m, Frank Breunig n, Christoph Wanner o, David G. Warnock p,
Roberta M. Lemay q, Dominique P. Germain r,s
a Medical Genetics Institute, Cedars-Sinai Medical Center, 8700 Beverly Blvd. SSB, Los Angeles, CA 90048, USAb Department of Pediatrics, UCLA School of Medicine, Los Angeles, CA, USA
c Medical Genetics, Hospital Sao Joao, Porto, Portugald Cincinnati Children’s Hospital, Cincinnati, OH, USA
e Fundacion Jimenez Dıaz, Madrid, Spainf New York University, New York, NY, USA
g Department of Medical Endocrinology, Rigshospitalet, University of Copenhagen, Denmarkh Massachusetts General Hospital and Harvard Medical School, Boston, MA, USA
i Hope Hospital, Salford, Manchester, United Kingdomj National Hospital for Neurology & Neurosurgery, London, United Kingdom
k Department of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX, USAl Department of Infectious and Pediatric Immunology, Medical and Health Science Centre, University of Debrecen, Debrecen, Hungary
m Department of Psychiatry, University of Cincinnati College of Medicine, Cincinnati, OH, USAn Department of Medicine, Division of Nephrology, University Hospital, Wurzburg, Germany
o University Hospital, Department of Medicine, Wurzburg, Germanyp University of Alabama at Birmingham, Birmingham, AL, USA
q Biomedical Operations, Genzyme Corporation, USAr Centre de reference de la maladie de Fabry et des maladies hereditaires du tissu conjonctif. Assistance Publique – Hopitaux de Paris, Paris, France
s University of Versailles - St Quentin en Yvelines, France
Received 29 August 2007; received in revised form 24 September 2007; accepted 24 September 2007Available online 26 November 2007
Abstract
Fabry disease (FD) is an X-linked lysosomal storage disease caused by alpha-galactosidase A deficiency. The Fabry Registry is a globalclinical effort to collect longitudinal data on FD. In the past, most ‘‘carrier’’ females were usually thought to be clinically unaffected. A sys-tematic effort has been made to enroll all FD females, regardless of symptomology. Of the 1077 enrolled females in the Registry, 69.4% hadsymptoms and signs of FD. The median age at symptom onset among females was 13 years, and even though 84.1% had a positive familyhistory, the diagnosis was not made until a median age of 31 years. Twenty percent experienced major cerebrovascular, cardiac, or renalevents, at a median age of 46 years. Among adult females with estimated glomerular filtration rate (eGFR) data (N = 638), 62.5% hadan eGFR <90 ml/min/1.73m2 and 19.0% had eGFR <60 ml/min/1.73 m2. Proteinuria P300 mg/day was present in 39.0% of females,and 22.2% had >1 gram/day. Quality of life (QoL), as measured by the SF-36� survey, was impaired at a later age than in males, but bothgenders experience significantly impaired QoL from the third decade of life onward. Thus, females with FD have a significant risk for majororgan involvement and decreased QoL. Females should be regularly monitored for signs and symptoms of FD, and considered for enzymereplacement therapy.
1096-7192/$ - see front matter � 2007 Elsevier Inc. All rights reserved.
doi:10.1016/j.ymgme.2007.09.013
* Corresponding author. Address: Medical Genetics Institute, Cedars-Sinai Medical Center, 8700 Beverly Blvd. SSB, Los Angeles, CA 90048, USA. Fax:+1 310 423 0620.
E-mail address: [email protected] (W.R. Wilcox).

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 113
� 2007 Elsevier Inc. All rights reserved.
Keywords: Fabry disease; Heterozygote; Alpha-galactosidase A; Enzyme replacement; Chronic kidney disease; Proteinuria; Cardiomyopathy; Stroke;Quality of life; SF-36
Introduction
Fabry disease (FD, OMIM #301500) is an X-linkedinborn error of metabolism characterized by decreased orabsent activity of the lysosomal hydrolase a-galactosidaseA (aGAL, E.C. 3.2.1.22), due to mutations in the gene thatencodes the aGAL protein (GLA) [1,2]. Patients with thisdisorder are unable to effectively degrade membrane glyco-sphingolipids containing a terminal a-glycosidic galactose,especially globotriaosylceramide (GL-3), which conse-quently accumulates in various tissues. Deposition ofGL-3 increases the risk for characteristic acroparesthesiasof the hands and feet, angiokeratoma, strokes, hearing loss,myocardial microvascular ischemia and infarctions,arrhythmias, hypertrophic cardiomyopathy, valvular insuf-ficiency, gastrointestinal symptoms, hypohidrosis, temper-ature and exercise intolerance, dysregulation of vasculartone and autonomic functions, obstructive lung disease,and chronic kidney disease leading to kidney failure [3–14].
FD causes significant morbidity and mortality inaffected males. Acroparesthesias, fatigue, and gastrointesti-nal symptoms reduce emotional well being and productiv-ity. Among males, proteinuria and progressive kidneydisease are evident in the second to fifth decades of life[7]. Death occurs typically in the late fifth to early sixth dec-ade from kidney failure, strokes and cardiac events [15].
As recently as 2001, most FD females were thought tobe asymptomatic throughout a normal life span or todevelop only minor manifestations of the disease [2]. How-ever, several studies have since reported that heterozygousfemales do develop substantial symptoms of FD and are atrisk of premature death [16–20].
Enzyme replacement therapy (ERT) with recombinanthuman a-galactosidase A (r-haGAL) has been developedto treat FD [21,22]. Multiple studies have demonstratedthat biweekly intravenous infusions of r-haGAL effectivelyreduce plasma and tissue GL-3 accumulation [22,23],improve anhidrosis [24], peripheral nerve function [25], pul-monary gas exchange [26], gastrointestinal symptoms [27],acroparesthesias [21], and can stabilize kidney function[28–30]. Although relatively few women were included inthese trials, ERT also appears to benefit females [31].
With an estimated incidence of 1:40,000 in males [2,32],FD is considered to be an ‘‘ultra-orphan’’ disease. How-ever, screening studies have shown an incidence of 0.1–1% among male dialysis patients [33–36], 3–5% of ‘‘idio-pathic’’ hypertrophic cardiomyopathy cases [37–39], and4.9% of male (2.4% of female) patients with cryptogenicstrokes [40]. Late onset forms with significant residualenzyme activity may be particularly common, up to1:4600 in one study [41].
Like other rare diseases, it has been difficult todevelop a clear understanding of the natural progressionof FD due to the paucity of longitudinal clinical infor-mation, particularly on heterozygous females. The FabryOutcomes Survey (FOS), a European registry of Fabrypatients, reported symptoms and manifestations in morethan 300 females [19]. The Fabry Registry (http://www.fabryregistry.com), created in 2001, has now col-lected detailed data on 1077 female patients with FD.We analyzed the data in the Fabry Registry to comparethe age at symptom onset and at diagnosis, and the inci-dence of clinical events among male and female patients(i.e. prior to treatment with ERT).
Methods
Data analysis and statistics
The Fabry Registry is an ongoing, observational database thattracks the natural history and outcomes of patients with FD. AllFD patients are eligible to enroll in the Fabry Registry, regardlessof symptoms or whether or not they are receiving ERT. Patient andphysician participation is voluntary. All patients provided informedconsent and may decline to participate or withdraw consent at anytime. Treating physicians determine the actual frequency of assess-ments according to a patient’s individualized need for medical careand routine follow-up. However, there is a recommended schedule ofclinical assessments for patients with FD (available at http://www.fabryregistry.com).
All data collected by the Fabry Registry are entered into a databasethrough a set of standardized case report forms. All of the data used inthese analyses are natural history data (i.e., prior to any treatment withERT). Data analyses were performed using the SAS statistical softwaresystem version 8 [42] and summarized using descriptive statistics. Statis-tical comparisons between data from male versus female patients weremade for certain key parameters, as indicated in the text. Given thesporadic nature of data reported to the Fabry Registry (i.e., differentpatients had clinical assessments at widely varying ages and time inter-vals), statistical comparison of these gender differences must be inter-preted with caution. The 2-sample median test was used to comparethe median age of Fabry symptom onset, median age at first stroke,and median age at first cardiac event between males and females. The2-sample t-test for unequal variances was used to compare the meanage of neurologic pain onset and age at first reported left ventricularhypertrophy (LVH) between males and females. The Cochran-Mantel-Haenszel test was used to compare the percentage of males versusfemales with at least 1 event (cerebrovascular, cardiac, or renal),abdominal pain, diarrhea, and first symptom onset of neurologic pain.The Kaplan–Meier estimator (also known as the Product Limit Estima-tor) was used to estimate the time from birth to specific renal, cardiac,or stroke events with recorded dates through the final available naturalhistory date in the Registry for each patient. Kaplan–Meier curves werecalculated for time to any event for both males and females.
The Fabry Registry is owned and administered by Genzyme Corpo-ration as part of their post-marketing regulatory commitments. Thereare currently 3 independent advisory boards that include physiciansfrom a variety of specialties worldwide. The authors of this study rep-resent a subset of the members of those 3 boards.

114 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
Pain assessments
Pain was measured with the Brief Pain Inventory (BPI) survey, whichcontains questions relating to pain and degree of interference with dailyliving, and is the standard instrument of pain assessment for FD and otherchronic illnesses [21,43–45]. Answers range from 0 (no pain or interferencewith activity) to 10 (most severe pain and interference with activity).
Quality of life
Quality of life (QoL) was measured by the SF-36� health-related QoLsurvey [46]. This survey is a 36-item questionnaire that measures apatient’s subjective estimation of QoL and is divided into 8 subcomponentscores: physical functioning (PF), role physical (RP), bodily pain (BP),general health (GH), vitality (VT), social functioning (SF), role emotional(RE), and mental health (MH). The SF-36� instrument is a validated, reli-able measure of QoL and has been used for patients with FD as well asother chronic diseases such as asthma, renal failure, and autoimmune dis-ease [47–52]. The first 3 subscales are primarily related to physical health
Table 1Demographics and disease characteristics in all Fabry Registry patients
Parameter
Total number of patients enrolled in Fabry Registry current age (years) n
MM
EthnicityWhite n
Black n
Hispanic n
Asian n
Other n
Not stated n
Family members diagnosed with FabryYes n
No n
Age at first Fabry symptoms (years) n
MM
Age category (years)0–<10 n
P10–<20 n
P20–<30 n
P30–<40 n
P40–<50 n
P50 n
Age at Fabry diagnosis (years) n
MM
Age category (years)0–<10 n
P10–<20 n
P20–<30 n
P30–<40 n
P40–<50 n
P50 n
Relationship between diagnosis and symptom onsetSymptom onset before diagnosis n
Diagnosis before symptom onset n
Time from symptom onset to diagnosis (years) n
MM
and function, the middle 2 subscales combine physical and mental health,and the last 3 primarily relate to mental and emotional well-being. Thescores for all subscales are on a 100-point scale with a higher score indicat-ing better QoL.
Scores on the SF-36� QoL measures were compared to appropriateage- and gender-adjusted United States population norms [46] using sam-ple means and 95% confidence intervals calculated using the t-distributionfor the correct number of degrees of freedom. Group scores were deter-mined to be statistically significant versus norms if their 95% confidenceintervals did not contain the population means for the given score.
Cerebrovascular, cardiovascular, and renal manifestations and
clinical events
Cerebrovascular disease was assessed by evaluating the prevalence oftransient ischemic attacks (TIAs), and of hemorrhagic and ischemicstrokes. Cerebrovascular clinical events were defined as stroke. Cardiovas-cular disease was assessed by evaluating the prevalence of cardiovascularevents including myocardial infarction, significant cardiac procedures
Number of male patients Number of female patients
1159 1077ean (SD) 37.3 (14.9) 40.5 (17.4)edian (range) 38.0 (1.0, 82) 42.0 (0.0, 86)
(%) 871 (75.2) 830 (77.1)(%) 20 (1.7) 13 (1.2)(%) 82 (7.1) 69 (6.4)(%) 37 (3.2) 13 (1.2)(%) 46 (4.0) 26 (2.4)(%) 103 (8.9) 126 (11.7)
(%) 888 (76.6) 906 (84.1)(%) 126 (10.9) 32 (3.0)
890 581ean (SD) 13.5 (12.1) 19.9 (15.7)edian (range) 9.0 (0.0, 70) 13.0 (0.0, 77)
(%) 470 (40.6) 176 (16.3)(%) 258 (22.3) 191 (17.7)(%) 56 (4.8) 78 (7.2)(%) 50 (4.3) 52 (4.8)(%) 37 (3.2) 37 (3.4)(%) 19 (1.6) 47 (4.4)
1123 1018ean (SD) 26.3 (15.5) 32.1 (17.6)edian (range) 24.0 (0.0, 81) 31.0 (0.0, 80)
(%) 168 (14.5) 106 (9.8)(%) 277 (23.9) 170 (15.8)(%) 220 (19.0) 196 (18.2)(%) 214 (18.5) 182 (16.9)(%) 153 (13.2) 181 (16.8)(%) 91 (7.9) 183 (17.0)
(%) 778 (67.1) 473 (43.9)(%) 105 (9.1) 82 (7.6)
778 473ean (SD) 14.2 (13.0) 15.7 (14.8)edian (range) 11.0 (0.0, 57.4) 11.4 (0.0, 65.0)

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 115
(such as pacemaker placement, bypass, stent placement, valve replace-ment, transplantation, etc.), arrhythmia, angina pectoris, congestive heartfailure, and LVH. Kidney disease was assessed by the serum creatininelevel and the degree of proteinuria measured in a 24-hr urine collection.The Modification of Diet in Renal Disease (MDRD) simplified equation[53] was used to estimate glomerular filtration rate (eGFR) from serumcreatinine levels [54]. Renal clinical events were defined as dialysis, kidneytransplantation, P2 eGFR values <60 ml/min/1.73 m2 that are P90 daysapart, or a P 50% increase in serum creatinine levels.
Results
Patients demographics and onset of signs and symptoms
As of January 5, 2007, a total of 2236 patients wereenrolled in the Fabry Registry, predominantly from
0
10
20
30
40
50
60
Mea
n A
ge (Y
ears
)
Males n (mean age) 627 (10.4) 37 (16.4) 94 (12.7)
Females n (mean age) 338 (14.2) 31 (31.2) 92 (20.8)
Neuro Pain Cerebro Ophthal
0
10
20
30
40
50
60
70
b
a
Perc
enta
ge o
f Pat
ient
s
Males n (%) 716 (63.3) 54 (4.8) 114 (10.1
Females n (%) 457 (43.3) 44 (4.2) 132 (12.5
Neuro Pain Cerebro Ophthal
Fig. 1. Characterization of presenting Fabry symptoms by organ systemcerebrovascular; ophthal, ophthalmological; Cardio, cardiovascular; gastro, gasfemale patients (black bars) reporting presenting symptoms within each organfemale patients who presented with each symptom and, in parentheses, the cowhich males and females reported symptoms. Error bars represent standard dfemale patients with age data available for each presenting symptom and, in paNote that the mean age at cerebrovascular symptom onset among males (16.4 ymales, which typically occur during the fourth decade of life, among patients what onset of symptoms, is based on patient recall, and must therefore be interp
North America and Europe. Among these, 1077 patients(48.2%) were female; most patients were white and hada positive family history of FD. Demographic data formale and female patients enrolled in the Fabry Registryare summarized in Table 1. Since it is more likely thatsymptomatic females would be preferentially enrolledin the Registry, participating physicians were specificallyasked to enroll all female patients with FD in theirpractice, regardless of symptom status. All of the signs,symptoms, and events reported in these analyses arenatural history data (i.e., prior to any treatment withERT).
Not surprisingly, male patients experience a higher fre-quency of symptoms at an earlier age than females. Amongall patients in the Fabry Registry, the median age at onset
113 (21.6) 172 (10.8) 153 (23.2) 290 (12.2)
82 (33.4) 92 (18.7) 87 (30.9) 91 (19.5)
Cardio Gastro Renal Derm
) 145 (12.8) 209 (18.5) 196 (17.3) 359 (31.7)
) 106 (10.0) 126 (11.9) 112 (10.6) 118 (11.2)
Cardio Gastro Renal Derm
in Fabry Registry patients. Neuro pain, neuropathic pain; cerebro,trointestinal; Derm, dermatological. (a) Percentage of male (grey bars) and
system. The data table below the graph shows the number of male andrresponding percentage of the total number of patients. (b) Mean age ateviation. The data table below the graph shows the number of male andrentheses, the corresponding mean age at which symptoms were reported.ears) is not consistent with the reported occurrence of strokes and TIAs ino experience these events (see Table 3). Registry data pertaining to the age
reted with caution.

116 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
of symptoms in females was 13.0 years, compared to 9.0years in males (Table 1, p < 0.0001). Since the age at symp-tom onset is primarily based on patient recall, the ages ofonset are typically later than what has been reported inprospective studies of children [55–58]. In both males andfemales, the median age at diagnosis was much later thanthe age at onset of symptoms, with males being diagnosedat a median age of 24.0 years and females at 31.0 years. Themedian time between the onset of first symptoms and diag-nosis was similar between genders, 11.0 years in males and11.4 years in females. Thus, on average, female patientsexperienced symptoms and received a diagnosis substan-tially later than male patients. Only 82 females (7.6%)and 105 males (9.1%) were reported to have been diagnosedprior to symptom onset, largely due to screening of familymembers of an index patient.
To evaluate the presentation of FD, patients for whomERT status was unknown (1.8% of all patients enrolled)were excluded from the analyses, to ensure that clinicalevents occurred prior to initiation of ERT. This population(with known ERT status) included 1055 females and 1132males. A summary of Fabry symptom onset in male andfemale patients is provided in Fig. 1. The symptom mostfrequently reported at enrollment was pain, for both malesand females. Neurologic pain was reported in 43.3% offemale patients (n = 457) with onset at a mean age of14.2 ± 11.8 years compared to 63.3% of males (n = 716)at a mean age of 10.4 ± 7.8 years (p < 0.0001).
Ophthalmologic and skin findings are also among theinitial signs of FD. Ophthalmologic findings werereported as presenting symptoms in 12.5% (n = 132)and 10.1% (n = 114) of female and male patients, respec-tively. Skin symptoms were a more common presentingsymptom in males (31.7%, n = 359) than in females
Table 2Mean SF-36 scores in male and female Fabry Registry patients of various age
Female Fabry Registry patients
Age category (years) 18–<25 25–<35 35–<45 45–<55Number of patients n = 44 n = 71 n = 99 n = 82
Physical function (PF) 87.6 81.6* 76.6* 69.9*
Role Physical (RP) 79.0 69.4* 63.1* 56.7*
Body pain (BP) 70.8* 69.0* 66.0* 63.0*
General health (GH) 61.6* 59.0* 56.9* 51.2*
Vitality (VT) 54.4 52.0* 44.7* 46.2*
Social functioning (SF) 76.4 78.5 72.6* 70.3*
Role emotional (RE) 77.3 71.8* 66.7* 67.5*
Mental health (MH) 70.3 69.7 65.4* 63.8*
Number of the 8 subscales in whichpatients exhibited mean scoresbelow mean US norms
2/8 6/8 8/8 8/8
Data shown represent mean SF-36 scores among the total number of Fabry Rdata. Each patient appears once (in only one age group) for each score summawas used to compare SF-36 data from the international male and female Faindividual subscales of the SF-36 [46].
* p < 0.05 lower than age- and gender-matched US norm data.# p < 0.05 higher than age- and gender-matched US norm data.
(11.2%, n = 118). However, when clinical follow-upassessments were combined with enrollment medical his-tory data, angiokeratomas were reported by 17.7% ofmales (n = 200) and 17.8% of females (n = 188). Amongfemale patients both ophthalmologic and skin findingswere reported considerably later in life than neurologicpain, at an average of 20.8 ± 14.6 and 19.5 ± 14.3 years,respectively. A limitation of this data is that ophthalmo-logic (including slit lamp) and careful dermatologicexaminations were not performed or recorded for manypatients.
Initial symptoms that were gastrointestinal in naturewere reported by 209 males (18.5%) and 126 females(11.9%), with an average age of onset of 10.8 ± 9.6 yearsin males and 18.7 ± 13.4 years in females. However,when data from clinical follow-up assessments were com-bined with enrollment medical history data, a higher per-centage of female patients reported abdominal pain anddiarrhea, as compared to males. Among females withknown ERT status, 226 (21.4%) reported abdominal painand 199 (18.9%) reported diarrhea; whereas abdominalpain and diarrhea were reported by 152 (13.4%) and135 (11.9%) male patients (p < 0.0001 for both abdomi-nal pain and diarrhea).
The first findings indicating vital organ involvement infemale patients were noted at the following frequenciesand ages: kidney in 10.6% (mean age 30.9 ± 16.5 years,n = 87), cardiovascular in 10.0% (mean age 33.4 ± 19.4years. n = 106,) and cerebrovascular in 4.2% (mean age31.2 ± 18.6 years, n = 44). The percentages of male andfemale patients with abnormal findings by organ systemand the mean ages at onset are summarized in Fig. 1. Aconsiderable percentage of females clearly experiencemajor complications of FD.
s, as compared to US age- and gender-specific norms
Male Fabry Registry patients
55–<65 P 65 18–<25 25–<35 35–<45 45–<55 55–<65 P 65n = 50 n = 22 n = 43 n = 50 n = 52 n = 35 n = 5 n = 564.0* 46.1* 75.9* 76.0* 64.3* 63.9* 57.0 50.070.5 45.5 50.0* 59.0* 46.2* 47.1* 60.0 35.065.8 56.5 55.9* 57.6* 57.0* 60.1* 64.6 90.8#
50.5* 52.0 47.5* 47.9* 42.8* 41.3* 41.4 48.850.7* 40.9* 52.1* 49.2* 40.7* 45.6* 37.0 52.080.5 69.3 73.0* 70.3* 66.3* 71.1* 67.5 72.584.0 65.2 69.0 74.7 57.1* 63.8* 73.3 66.775.4 67.3* 70.8 70.8 63.9* 70.0 73.6 72.0
3/8 3/8 6/8 6/8 8/8 7/8 0/8 0/8
egistry patients P18 years of age with known ERT status and with SF-36ry, based on their age at the last available assessment. A one-sample z-testbry Registry cohorts to US gender-specific and age-specific norms within

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 117
Laboratory diagnosis
aGAL gene mutations were reported for 788 males(69.6%) and 806 females (76.4%). There were no significantdifferences in the frequency of specific mutations betweenmales and females. The most common mutation wasR227X, which was reported in 50 patients (2.3%).
While mutational analysis is the gold standard for diag-nosing FD in females, leukocyte aGAL enzymatic activityassays were also frequently used for diagnosis. Only 43 of349 females (12.3%) had leukocyte aGAL activity withinthe normal range, compared to 2 of 432 males (0.5%). Incontrast, analysis of aGAL enzymatic activity withinplasma was a much less reliable diagnostic indicator; 106of 158 females (67.1%) had values within the normal rangecompared to 15 of 219 males (6.8%).
0
10
20
30
40
50
60
70
80
90
100
18-<24 25-<34 35-<44 45-<54 55-<64 >65Age in Years
SF36
Sco
re
Fabry Registry Females
Physical FunctionRole PhysicalBody PainGeneral Health
VitalitySocial FunctioningRole EmotionalMental Health
0
10
20
30
40
50
60
70
80
90
100
18-<24 25-<34 35-<44 45-<54 55-<64 >65Age in Years
SF36
Sco
re
US Female Norms
a b
c d
Physical FunctionRole PhysicalBody PainGeneral Health
VitalitySocial FunctioningRole EmotionalMental Health
Fig. 2. Cross-sectional mean SF-36� subscale scores among Fabry Registry pranges from 0 to 100, with a higher score indicating better QoL. Each patient apage at the last available assessment. (a) Mean SF-36� scores for each subscale aas indicated. The numbers of patients within each age category (n) ranged fromshown from 190 male patients within 6 age categories. The numbers of patientsMean SF-36� scores for each subscale are shown from age-matched females in(n) ranged from 102 to 413 [46]. (d) Mean SF-36� scores for each subscale are sof patients in each age category (n) ranged from 71 to 293 [46].
Quality of life and pain
SF-36� questionnaire data were available on 368 femaleand 190 male patients P18 years of age. SF-36� data wereanalyzed by comparing the mean scores of males andfemales in the Fabry Registry with age- and gender-matched norms for the general U.S. population across 6age categories, as shown in Table 2. Compared to the gen-eral population, both females and males with FD showedconsistently impaired QoL within the PF, BP, GH, andVT subscales; mean scores were significantly below normalin 4 or more of the 6 age categories evaluated in each gen-der. The greatest differences between males and femaleswith FD within specific subscales were observed for theSF and MH subscales. Females scored higher than malesin the SF subscale, reporting mean SF-36� scores within
0
10
20
30
40
50
60
70
80
90
100
18-<24 25-<34 35-<44 45-<54 55-<64 >65Age in Years
SF36
Sco
re
Fabry Registry Males
0
10
20
30
40
50
60
70
80
90
100
18-<24 25-<34 35-<44 45-<54 55-<64 >65Age in Years
SF36
Sco
re
US Male Norms
Physical FunctionRole PhysicalBody PainGeneral Health
VitalitySocial FunctioningRole EmotionalMental Health
Physical FunctionRole PhysicalBody PainGeneral Health
VitalitySocial FunctioningRole EmotionalMental Health
atients and United States norms, stratified by gender and age. The scalepears once (in only one age group) for each score summary, based on theirre shown from 368 female Fabry Registry patients within 6 age categories,22 to 99, as shown in Table 2. (b) Mean SF-36� scores for each subscale arewithin each age category (n) ranged from 5 to 52, as shown in Table 2. (c)the general US population. The numbers of patients in each age category
hown from age-matched males in the general US population. The numbers

118 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
the normal range in all age categories except ages 35–<45and 45–<55 years, whereas males reported mean SF-36�
scores significantly below normal in 4 of the 6 age catego-ries (at all ages except 55–<64 and P65 years, where thenumbers of male patients are small). In contrast, malesscored higher than females in the MH subscale, reportingmean SF-36� scores within the normal range in all age cat-egories except age 35–<45 years, whereas females reportedmean SF-36� scores significantly below normal in 3 of the 6age categories (at ages 35–<45, 45–<55 years 55–<65 andP65 years, where the numbers of patients are small).
There appear to be gender differences in the age at whichQoL scores begin to decline in patients with FD. The meanscores of male Fabry Registry patients ages 18–<25 yearswere significantly lower than US male norms on 6 of the8 subscales of the SF-36� survey. In contrast, the meanscores of female patients ages 18–<25 were within the nor-mal range in all but 2 subscales (BP and GH). Both maleand female Fabry Registry patients reported the lowestmean QoL scores between the ages of 35–<55, with meanscores that were below US norms on at least 7 of the 8 sub-scales within these age categories. Compared to the below-normal scores reported between the ages of 35–55, QoLwas generally better among males and females at ages55–<65 and age P65, in terms of the number of subscalesin which mean scores fell within the normal range. How-ever, females clearly continued to exhibit impaired QoL
0
2
4
6
8
10
Mea
n Sc
ore
Males 12-20 yrs 3.2 (N=27)
Males >20-40 yrs 3.8 (N=101)
Males >40 yrs 3.1 (N=61)
Females 12-20 yrs 1.5 (N=39)
Females >20-40 yrs 2.7 (N=156)
Females >40 yrs 3.4 (N=193)
Worst Pain in the Las
Males FemNo Pain
WorstPain
Fig. 3. Mean BPI scores in males and female patients of various ages in therepresenting standard deviation. The mean BPI score and number of patients inappears once (in only one age group) for each score summary, based on their
at ages 55–<65 and age P65, particularly among the PFand VT subscales.
Mean SF-36� scores are depicted graphically inFig. 2. Although this is cross-sectional data (i.e., differ-ent patients are represented in each age group), it canbe seen that female Fabry Registry patients generallyexhibit higher mean SF-36� scores at younger ages,but lower mean scores are reported with increasedage (Fig. 2a). In contrast, male patients reported lowermean scores at younger ages across all subscales andtheir mean scores were more stable with increasingage (Fig. 2b). For comparison, normative data forfemales and males in the US general population aredepicted in Fig. 2c and d, respectively. Both malesand females among the general population exhibit fairlysteady SF-36� scores up to ages 45–<55 years. Thereaf-ter, SF-36� scores decline with aging in the normalpopulation, though mean scores in most subscalesremain substantially higher than those exhibited bypatients with FD.
Pain assessment data, derived from the Brief Pain Index(BPI) for both female and male patients are shown inFig. 3. Within the youngest age category (P12 to P20years), female patients reported less pain (i.e., lower meanBPI scores) than male patients. However, with increasingage, female patients tended to report increasing ‘‘worstpain’’ symptoms, whereas worst pain BPI scores generally
3.1 (N=27)
3.0 (N=101)
2.5 (N=60)
2.4 (N=39)
2.5 (N=154)
2.7 (N=192)
t 24 hrs
ales
Average Pain
Males Females
Fabry Registry. Data are expressed as mean BPI scores with error barseach group (N) are shown in the data table below the graph. Each patientage at the last available assessment.

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 119
remained stable with age among male patients. No statisti-cally significant differences were observed between malesand females in either ‘‘worst pain’’ or ‘‘average pain’’across any of the age groups.
SymptomOnsetN=890
DiagnosisN=1123
1stEventN=333
N
0
10
20
30
40
50
60
70
Med
ian
Age
(Yea
rs)
Ma
SymptomOnsetN=581
DiagnosisN=1018
1stEventN=199
0
10
20
30
40
50
60
70
Med
ian
Age
(Yea
rs)
Fem
a
b
Fig. 4. Median age at symptom onset, diagnosis, first clinical event, and start ofmale (a) and female patients (b) for whom appropriate data were available. Eac25th–75th percentiles; and the end of each vertical line represents the minimmyocardial infarction, angina pectoris, congestive heart failure, or a significanincluded dialysis, kidney transplantation, or P2 eGFR values <60 that are P90of symptom onset and diagnosis were not available for all patients.
Clinical events
Twenty percent of the females in the Fabry Registryreported to have suffered at least 1 cerebrovascular, cardio-
1stRenalEvent=160
1stCardiacEventN=218
1stCerebroEventN=76
1st ERTN=923
les
1stRenalEventN=46
1stCardiacEventN=147
1stCerebroEventN=44
1stERT
N=357
ales
ERT. All data shown are prior to the start of ERT (i.e., natural history) inh black line with a dot represents the median; the grey boxes encompass the
um and maximum values. Cardiac events were defined as arrhythmia,t cardiac procedure. Cerebrovascular events included stroke. Renal events
days apart or a P 50% increase in serum creatinine levels. Note that dates
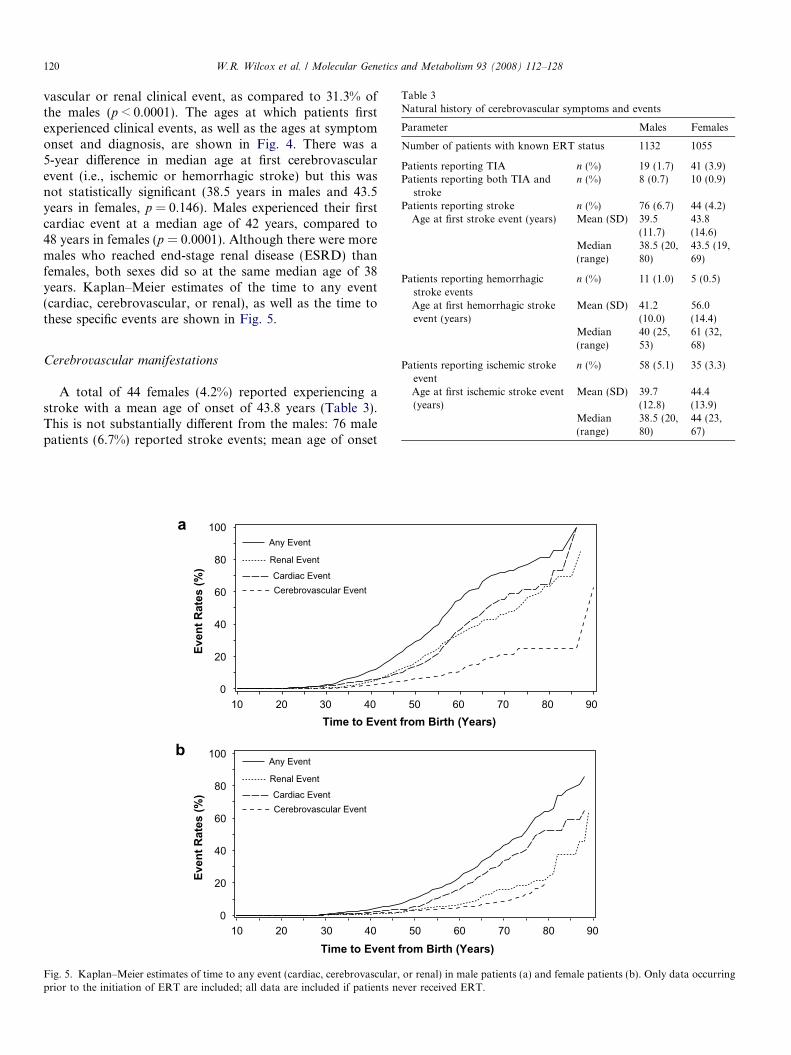
Table 3Natural history of cerebrovascular symptoms and events
Parameter Males Females
Number of patients with known ERT status 1132 1055
Patients reporting TIA n (%) 19 (1.7) 41 (3.9)Patients reporting both TIA and
stroken (%) 8 (0.7) 10 (0.9)
Patients reporting stroke n (%) 76 (6.7) 44 (4.2)Age at first stroke event (years) Mean (SD) 39.5
(11.7)43.8(14.6)
Median(range)
38.5 (20,80)
43.5 (19,69)
Patients reporting hemorrhagicstroke events
n (%) 11 (1.0) 5 (0.5)
Age at first hemorrhagic strokeevent (years)
Mean (SD) 41.2(10.0)
56.0(14.4)
120 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
vascular or renal clinical event, as compared to 31.3% ofthe males (p < 0.0001). The ages at which patients firstexperienced clinical events, as well as the ages at symptomonset and diagnosis, are shown in Fig. 4. There was a5-year difference in median age at first cerebrovascularevent (i.e., ischemic or hemorrhagic stroke) but this wasnot statistically significant (38.5 years in males and 43.5years in females, p = 0.146). Males experienced their firstcardiac event at a median age of 42 years, compared to48 years in females (p = 0.0001). Although there were moremales who reached end-stage renal disease (ESRD) thanfemales, both sexes did so at the same median age of 38years. Kaplan–Meier estimates of the time to any event(cardiac, cerebrovascular, or renal), as well as the time tothese specific events are shown in Fig. 5.
Median(range)
40 (25,53)
61 (32,68)
Patients reporting ischemic strokeevent
n (%) 58 (5.1) 35 (3.3)
Age at first ischemic stroke event(years)
Mean (SD) 39.7(12.8)
44.4(13.9)
Median(range)
38.5 (20,80)
44 (23,67)
Cerebrovascular manifestations
A total of 44 females (4.2%) reported experiencing astroke with a mean age of onset of 43.8 years (Table 3).This is not substantially different from the males: 76 malepatients (6.7%) reported stroke events; mean age of onset
Even
t Rat
es (%
)
0
20
40
60
80
100
Time to Event from Birth (Years)10 20 30 40 50 60 70 80 90
Even
t Rat
es (%
)
0
20
40
60
80
100
Time to Event from Birth (Years)10 20 30 40 50 60 70 80 90
Any Event
Renal Event
Cardiac EventCerebrovascular Event
Any Event
Renal Event
Cardiac EventCerebrovascular Event
b
a
Fig. 5. Kaplan–Meier estimates of time to any event (cardiac, cerebrovascular, or renal) in male patients (a) and female patients (b). Only data occurringprior to the initiation of ERT are included; all data are included if patients never received ERT.

Table 4Natural history of cardiovascular symptoms and events
Males Females
Number of patients with known ERT status 1132 1055
Number of patients with any cardiovascular events 218 (19.3) 147 (13.9)
Patients reporting myocardial infarction n (%) 27 (2.4) 18 (1.7)Age at first myocardial infarction (years) Mean (SD) 44.6 (11.6) 56.2 (8.8)
Median (range) 46.0 (19, 76) 55.0 (41, 74)
Patients reporting significant cardiac procedure n (%) 87 (7.7) 50 (4.7)Age at first significant cardiac procedure (years) Mean (SD) 45.0 (12.4) 53.9 (10.0)
Patients reporting an arrhythmia n (%) 128 (11.3) 75 (7.1)Age at first arrhythmia (years) Mean (SD) 38.4 (11.9) 46.4 (12.7)
Median (range) 40.5 (7, 64) 47.0 (19, 74)
Patients reporting angina n (%) 38 (3.4) 45 (4.3)Age when angina was first reported (years) Mean (SD) 41.1 (9.4) 47.3 (11.5)
Median (range) 43.0 (16, 56) 45.0 (21, 71)
Patients reporting congestive heart failure n (%) 43 (3.8) 31 (2.9)Age when congestive heart failure first reported (years) Mean (SD) 41.4 (11.9) 51.2 (11.5)
Median (range) 45.0 (11, 68) 54.0 (21, 78)
Patients reporting left ventricular hypertrophy (LVH) by echocardiogram n (%) 245 (21.6) 192 (18.2)Age when LVH first reported (years) Mean (SD) 41.6 (10.9) 49.8 (12.4)
Median (range) 42 (15, 80) 51 (0, 78)
Estimated ejection fraction in patients ever reporting LVH (%) n 173 138Mean (SD) 62.0 (10.0) 64.4 (9.2)Median (range) 62.5 (26, 80) 65.0 (22, 80)
W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 121
was 39.5 years (Table 3). TIAs occurred in 3.9% of females(n = 41) and 1.7% of males (n = 19).
Cardiovascular manifestations
Cardiovascular involvement was exhibited by females atapproximately the same rate as in males, albeit at a some-what older age (Table 4). For example, LVH was detectedin 18.2% of females at an average age of 49.81 ± 12.4 years,compared to 21.6% of male patients at a mean age of41.6 ± 10.9 years (p < 0.0001). Among patients withLVH, the ejection fraction was generally normal (Table 4).
Table 5Natural history of proteinuria (mg/24 h), Glomerular filtration rate, and rena
Total number of adult patients with proteinuria data and known ERT statusWorst proteinuria ever observed [n (%)] <300 mg/24 h
300–1000 mg>1–3.5 g/24 h>3.5 g/24 h
Total number of adult patients with GFR data and known ERT statusWorst CKD stage ever observed [n (%)] Stage 1 (P90
Stage 2 (P60Stage 3 (P30Stage 4/5 (<3
Total number of patients with ESRD (dialysis or transplant) and Known ERAge at dialysis or transplant (years) Mean (SD)
MedianRange
Renal manifestations
Many female patients exhibited significant kidneyinvolvement as manifested by proteinuria and reducedeGFR (Table 5, Fig. 6). Data on 24-hr proteinuria wereavailable for 354 male and 346 female patients. Among thesepatients, 135 females (39.0%) exhibited proteinuriaP300 mg/day, including 26 patients (7.5%) with proteinuria>3.5 g/d. eGFR data were available for 616 male and 638female patients. Nineteen percent of the female patients(121/638) exhibited eGFR values <60 mL/min/1.73m2;among these, 93 (14.6%) had chronic kidney disease
l events
Males Females
354 346128 (36.2) 211 (61.0)
/24 h 79 (22.3) 58 (16.8)115 (32.5) 51 (14.7)32 (9.0) 26 (7.5)
616 638ml/min/1.73m2) 228 (37.0) 239 (37.5)–<90) 181 (29.4) 278 (43.6)–<60) 100 (16.2) 93 (14.6)0) 107 (17.4) 28 (4.4)
T Status, n (%) 156 (13.8) 23 (2.2)38.2 (9.8) 39.2 (13.0)38.0 38.014, 79 17, 77

0
10
20
30
40
50
60
70
Mea
n A
ge (Y
ears
)Pe
rcen
tage
of P
atie
nts
Males Mean Age (years) 41.5 41.1 38.8 43.9 43.0 38.2
Females Mean Age (years) 43.6 43.7 41.3 51.8 45.8 39.2
Highest Protein:0.3-1 g/24h
Highest Protein:>1-3.5 g/24h
Highest Protein:>3.5 g/24h
eGFR <60 >50% Increasein Serum
Creatinine
Dialysis orTransplant
b
a
Males (%) 22.3 32.5 9.0 7.2 4.5 13.8
Females (%) 16.8 14.7 7.5 5.2 0.9 2.2
Highest Protein:0.3-1 g/24h
Highest Protein:>1-3.5 g/24h
Highest Protein:>3.5 g/24h
eGFR <60 >50% Increasein Serum
Creatinine
Dialysis orTransplant
0
10
20
30
40
Fig. 6. Characterization of renal manifestations in Fabry Registry patients. (a) Percentage of male and female patients reporting various renalcharacteristics. Data are expressed as a percentage of the number of all male and female patients with a known ERT status. (b) Mean age at which malesand females reported these renal characteristics. Data are expressed as mean age in years and error bars represent standard deviation. Proteinuria andeGFR data are shown for patients P18 years of age at the time of the analysis; serum creatinine and dialysis/transplant data are shown for all patients.
122 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
(CKD) stage 3 and 28 patients (4.4%) had CKD stages 4/5(eGFR < 30 ml/min/1.73 m2). Among the 1055 females withknown ERT status, 23 (2.2%) had reached ESRD, requiringdialysis or transplantation at a mean age of 39.2 years (range17–77 years). A higher proportion of males (13.8%) hadreached ESRD at a similar mean age, 38.2 years (range14–79 years). Compared to males, a lower percentage offemale patients exhibited renal manifestations across all cat-egories, as shown in Fig. 6a. However, among females whodid exhibit renal manifestations, the mean age at which thesewere reported was similar or only slightly higher than whatwas reported for male patients, as shown in Fig. 6b.
When these cross-sectional renal data are examined byage, eGFR declines significantly with age in both malesand females, although eGFR varies greatly between indi-viduals at a given age, particularly for males (Fig. 7). Nota-bly, many younger individuals have elevated eGFR,
suggesting hyperfiltration, a sign of impaired regulationof renal function. Proteinuria, however, shows no particu-lar association with age: significant proteinuria may bepresent at any age (Fig. 8).
Treatment with ERT in males and females
Females in the Fabry Registry are treated with ERT farless frequently than males. Among patients with knownERT status, 81.9% of the males have been treated withERT compared to just 33.8% of females. The lower fre-quency of treatment does not appear to be justified basedon major organ involvement. For example, 208 of 245 malepatients with LVH (84.9%) have received ERT compared to102 of 192 female patients (53.1%). Similarly, 276 of 315 ofmale patients with stage 3 or greater CKD are on ERT(87.6%), compared to 85 of 182 of female patients (46.7%).

Estim
ated
GFR
(mL/
min
/1.7
3m2 )
0
50
100
150
200
250
Age (Years)10 20 30 40 50 60 70 80 90
Estim
ated
GFR
(mL/
min
/1.7
3m2 )
0
50
100
150
200
250
Age (Years)10 20 30 40 50 60 70 80 90
b
a
Fig. 7. Distribution of eGFR by age in adult Fabry Registry patients. (a) Males. (b) Females. Only data occurring prior to the initiation of ERT areincluded; all data are included if patients never received ERT. Serum creatinine readings in the range 0.4–25 mg/dL are used in the calculation of eGFR,per the MDRD Equation for patients P18 years of age at the time of the serum creatinine value. The most recent eGFR data are displayed. Note that thedata shown are cross-sectional (i.e., data from different patients are shown at different ages). The vertical lines indicate median age and horizontal linesindicate median eGFR value. All patients P18 years of age who had eGFR data available are included in this dataset.
W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 123
Discussion
The Fabry Registry provides information on a large,international cohort of patients with FD. In this study,we found that female ‘carriers’ frequently suffer from pain,gastrointestinal symptoms, and major organ systeminvolvement as well as a substantially reduced QoL.Although the size and ascertainment of previously reportedstudies are different, the results of this natural history studyare remarkably similar to other studies [16–20].
Presenting symptoms of FD
Similar to males, many females first experienced symp-toms of neurologic pain and gastrointestinal dysfunctionduring their pediatric years, but the diagnosis of FD wasusually delayed for more than a decade (Fig. 1, Table 1).While some males present initially with major cerebrovas-
cular, cardiovascular, or renal events, these problems alsoappear to be common in females, in whom there is morevariability in disease expression.
Laboratory diagnosis of FD in females
For females with affected family members, detection ofthe familial mutation, when known, is the most efficientstrategy for diagnosis. For females suspected of having FDbased on symptomatology or findings on a tissue biopsybut without a positive family history, mutation detectionby sequence analysis is often required for a definitive labora-tory diagnosis. However, in our cohort, leukocyte aGALactivity was diagnostic in over 90% of patients (88% amongfemales and 99% among males). Thus, analysis of leukocyteenzyme activity, perhaps in conjunction with urinary GL-3measurement [58], may be an efficient way to screen femalessuspected of having the disease.

Prot
einu
ria (m
g/24
hr)
1
10
100
1000
10000
100000
Age (Years)10 20 30 40 50 60 70 80 90
Prot
einu
ria (m
g/24
hr)
1
10
100
1000
10000
100000
Age (Years)10 20 30 40 50 60 70 80 90
b
a
Fig. 8. Relationship between proteinuria and age in adult Fabry Registry patients. (a) Males. (b) Females. Only data occurring prior to the initiation ofERT are included; all data are included if patients never received ERT. The most recent proteinuria value between 0.01 and 15 g/24 h available for patientsP18 years of age are displayed. The vertical lines indicate median ages and horizontal lines indicate median proteinuria values.
124 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
Quality of life
In general, the QoL data presented here are similar toreports in previous studies of patients with FD, i.e., thesepatients consistently report experiencing decreased healthrelated QoL as compared to the general population[20,31,47–49]. However, previous studies have not includedQoL data for such a large number of patients, nor were SF-36� data stratified by age and gender. Between the ages of18–<25 years, males with FD exhibited significantly lowerQoL than the general US male population while femalepatients between the ages of 18–<25 years exhibited QoLscores within the normal range in all but 2 of the 8 sub-scales. However, QoL dramatically worsened amongfemales age 25–<35 years. Both genders exhibited signifi-cantly lower scores than the general US populationbetween the ages of 35–<55 years. There are very few malesover the age of 55 years in the Fabry Registry who have not
received ERT; males who have survived P55 years withoutbeing on ERT, may have milder disease (that is, ‘clinicalvariants’ associated with residual enzyme activity).
Pain
Similar to males, peripheral neuropathic pain (acropar-esthesia) is a common presenting symptom for females(43.3%), usually appearing first in the pediatric age group(Fig. 1). In general, the level of pain appears to be stableduring aging (Fig. 3), although individual patients mayhave persistent pain, diminishing pain with age, or onsetof pain later in life.
Cerebrovascular
Strokes, almost exclusively of the ischemic type ratherthan hemorrhagic, occurred in 4.2% of the females in the

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 125
Registry at a median age of 43.5 years. This was about 5years later in occurrence than in males, although this differ-ence was not statistically significant. The frequency ofischemic strokes and TIAs (3.9%) supports the prophylac-tic use of antiplatelet agents as has been previously recom-mended [4].
Cardiovascular
Cardiac involvement was the most common seriousmanifestation of FD among the females in our cohort.LVH and major cardiac events occurred nearly 10 yearslater in life among females than in males. Because the ejec-tion fraction is preserved, in the absence of a myocardialinfarction, angina, or arrhythmia, patients can have clini-cally silent but progressive cardiac disease for many years[59,60]. Consequently, regular monitoring by ECG andechocardiography and evaluation of palpitations, as rec-ommended [4], is prudent.
Gastrointestinal
Gastrointestinal symptoms are very common amongmales and females, although the age of onset is later amongfemales. The higher prevalence of irritable bowel syn-drome, which has similar symptoms to FD, among females[61] may explain the higher frequency of abdominal painand diarrhea reported by females with FD. In childrenand young adults, recurrent abdominal cramps and diar-rhea are the second most common presenting symptomsof FD [57].
Renal
While ESRD is less common in females with FD than inmales, when it develops, it does so at approximately thesame age (median of 38 years) for both male and femalepatients. Many females exhibit substantial levels of pro-teinuria, an independent risk factor for progression of renaldisease in FD [30]. Proteinuria may partly explain whyStage 3 or greater CKD is frequent in females.
Study limitations
There are several limitations of this study. Even withreduced male reproductive fitness, there should be morefemales with FD in the Registry than males, which is cur-rently not the case. Although there is an on-going effortto enroll all patients regardless of overt findings andsymptomatology, it is likely that preferential enrollmentof more affected individuals exists, resulting in artificiallyhigh frequency of symptoms and signs among individualsenrolled in the Registry. Conversely, less severe symptomsand signs (ophthalmologic, dermatologic, and gastrointes-tinal) tend to be under-reported compared to major organinvolvement, leading to lower than expected frequenciesfor these types of problems. Consequently, while this large
cohort cannot be used to give precise estimates of the riskof major organ involvement in an individual femalepatient, the large numbers of significantly affected femalesin this and other reports [16–20] should finally put to restthe misconception that females are rarely affected withFD. Finally, for analysis of QoL data, we have assumedthat the U.S. normative data are applicable to all FabryRegistry patients. Although several studies have demon-strated the validity of SF-36� translations in variousEuropean countries [62–64], the U.S. normative datamay not be applicable to all countries represented byFabry Registry patients.
Unanswered questions
Why are females so significantly affected by FD, andwhy do they appear to have greater phenotypic variationthan males? Some explanation surely lies in the individualpattern of X-inactivation in each female. However, inanother X-linked storage disease, mucopolysaccharidosistype II (MPS II), females are rarely ever affected becauseof cross-correction of cells with storage by functionalenzyme secreted by cells in which the non-mutant gene isactive. The relative abundance of substrates cannot explainthe difference between FD and MPS II, as GL-3 is a minorsubstrate that accumulates relatively slowly in aGAL-defi-cient cells, compared with heparin and dermatan sulfateturnover in MPS II [2,65]. In FD, the amount of aGALenzyme secreted by normal cells and taken up by deficientcells is apparently not sufficient to correct the abnormalcells. Either the amount of active enzyme secreted is insuf-ficient or the secreted enzyme is not adequately taken up bythe abnormal cells. Sixty-seven percent of females havenormal plasma aGAL levels, yet many of these femalesexhibit significant organ involvement. Regardless, withthe pharmacologic levels of enzyme achieved with ERT,there is clearance of the accumulated GL-3 from the vascu-lar endothelium of patients with FD [22,23,28].
Recommendations
Females should be followed clinically and evaluatedcomprehensively to monitor for disease burden and pro-gression. Treatment with ERT and other adjunctive ther-apies should be initiated for significant symptomatologyor evidence of major organ involvement [4]. Althoughnot the subject of this work, it has been our experiencethat females respond to ERT as well as males, with rela-tively few ever experiencing infusion reactions. However,even among the treatment centers participating in theFabry Registry, females remain undiagnosed, incom-pletely monitored, and/or under-treated. Only 53.1% ofthe females with LVH and 46.7% of the females withstage 3 or greater CKD are on ERT. We hope that thiswork will inspire FD females to seek evaluation andtreatment and for their physicians to treat themappropriately.

126 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
Disclosure
The authors (WRW, JPO, RJH, AO, MB, UF-R, KS,SW, GMP, PL, CME, LM, FB, CW, DGW, DPG) aremembers of the Board of Advisors of the Fabry Registry,and are compensated for these services by Genzyme Cor-poration. They are also paid consultants for Genzyme onmatters relating to Fabry disease and have received speak-ing fees and research grants from Genzyme related toFabry disease. RML is an employee of the GenzymeCorporation.
Acknowledgments
The authors gratefully acknowledge the participation of191 physicians in 37 countries around the world who con-tribute data to the Registry, their clinic staff, and especiallythe patients. We thank Dana Beitner-Johnson for assis-tance with the technical writing. WRW is supported by aWinnick Family Clinical Development Scholar Award,AO by Programa de Intensificacion de la Actividad Inves-tigadora (ISCIII/Agencia ‘‘Laın Entralgo’’ Comunidad deMadrid).
References
[1] R.O. Brady, A.E. Gal, R.M. Bradley, E. Martensson, A.L. Warshaw,L. Laster, Enzymatic defect in Fabry’s disease: ceramide trihexosidasedeficiency, New Eng. J. Med. 276 (1967) 1163–1167.
[2] R.J. Desnick, Y.A. Ioannou, C.M. Eng, a-Galactosidase A deficiency:Fabry disease, in: C.R. Scriver, A.L. Beaudet, W.S. Sly, D. Valle(Eds.), The Metabolic and Molecular Bases of Inherited Disease,eighth ed., McGraw Hill, New York, 2001, pp. 3733–3774.
[3] R.J. Desnick, R. Brady, J. Barranger, A.J. Collins, D.P. Germain, M.Goldman, G. Grabowski, S. Packman, W.R. Wilcox, Fabry disease,an under-recognized multisystemic disorder: expert recommendationsfor diagnosis, management, and enzyme replacement therapy, Ann.Intern. Med. 138 (2003) 338–346.
[4] C.M. Eng, D.P. Germain, M. Banikazemi, D.G. Warnock, C.Wanner, R.J. Hopkin, J. Bultas, P. Lee, K. Sims, S.E. Brodie,G.M. Pastores, J.M. Strotmann, W.R. Wilcox, Fabry disease:guidelines for the evaluation and management of multi-organ systeminvolvement, Genet. Med. 8 (2006) 539–548.
[5] A. Mehta, L. Ginsberg, FOS Investigators, Natural history of thecerebrovascular complications of Fabry disease, Acta Paediatr.Suppl. 94 (2005) 24–27.
[6] J.S. Shah, P.M. Elliott, Fabry disease and the heart: an overview ofthe natural history and the effect of enzyme replacement therapy,Acta Paediatr. Suppl. 94 (2005) 11–14.
[7] M.H. Branton, R. Schiffmann, S.G. Sabnis, G.J. Murray, J.M. Quirk,G. Altarescu, L. Goldfarb, R.O. Brady, J.E. Balow, H.A. Austin III,J.B. Kopp, Natural history of Fabry renal disease: influence of alpha-galactosidase A activity and genetic mutations on clinical course,Medicine (Baltimore) 81 (2002) 122–138.
[8] R. Schiffmann, L.J. Scott, Pathophysiology and assessment ofneuropathic pain in Fabry disease, Acta Paediatr. Suppl. 91 (2002)48–52.
[9] M. Dutsch, H. Marthol, B. Stemper, M. Brys, T. Haendl, M.J. Hilz,Small fiber dysfunction predominates in Fabry neuropathy, J. Clin.Neurophysiol. 19 (2002) 575–586.
[10] B. Stemper, M.J. Hilz, Postischemic cutaneous hyperperfusion in thepresence of forearm hypoperfusion suggests sympathetic vasomotordysfunction in Fabry disease, J. Neurol. 250 (2003) 970–976.
[11] D.M. Rosenberg, V.J. Ferrans, J.D. Fulmer, B.R. Line, J.A.Barranger, R.O. Brady, R.G. Crystal, Chronic airflow obstructionin Fabry’s disease, Am. J. Med. 68 (1980) 898–905.
[12] L.K. Brown, A. Miller, A. Bhuptani, M.F. Sloane, M.I. Zimmer-man, G. Schilero, C.M. Eng, R.J. Desnick, Pulmonary involvementin Fabry disease, Am. J. Respir. Crit. Care Med. 155 (1997) 1004–1010.
[13] G. Bierer, N. Kamangar, D. Balfe, W.R. Wilcox, Z. Mosenifar,Cardiopulmonary exercise testing in Fabry disease, Respiration 72(2005) 504–511.
[14] A. Mehta, R. Ricci, U. Widmer, F. Dehout, A. Garcia de Lorenzo, C.Kampmann, A. Linhart, G. Sunder-Plassmann, M. Ries, M. Beck,Fabry disease defined: baseline clinical manifestations of 366 patientsin the Fabry Outcome Survey, Eur. J. Clin. Invest. 34 (2004) 236–242.
[15] K.D. MacDermot, A. Holmes, A.H. Miners, Anderson-Fabrydisease: clinical manifestations and impact of disease in a cohort of98 hemizygous males, J. Med. Genet. 38 (2001) 750–760.
[16] K.D. MacDermot, A. Holmes, A.H. Miners, Anderson-Fabrydisease: clinical manifestations and impact of disease in a cohort of60 obligate carrier females, J. Med. Genet. 38 (2001) 769–775.
[17] C. Whybra, C. Kampmann, I. Willers, J. Davies, B. Winchester, J.Kriegsmann, K. Bruhl, A. Gal, S. Bunge, M. Beck, Anderson-Fabrydisease: clinical manifestations of disease in female heterozygotes, J.Inherit. Metab. Dis. 24 (2001) 715–724.
[18] S. Gupta, M. Ries, S. Kotsopoulos, R. Schiffmann, The relationshipof vascular glycolipid storage to clinical manifestations of Fabrydisease: a cross-sectional study of a large cohort of clinically affectedheterozygous women, Medicine (Baltimore) 84 (2005) 261–268.
[19] P. Deegan, A.F. Baehner, M.A. Barba Romero, D.A. Hughes, C.Kampmann, M. Beck, European FOS Investigators, Natural historyof Fabry disease in females in the Fabry Outcome Survey, J. Med.Genet. 43 (2006) 347–352.
[20] R.Y. Wang, A. Lelis, J. Mirocha, W.R. Wilcox, Heterozygous Fabrywomen are not just ‘‘carriers,’’ but have a significant burden ofdisease and impaired quality of life, Genet. Med. 9 (2007) 34–45.
[21] R. Schiffmann, J.B. Kopp, H.A. Austin 3rd, S. Sabnis, D.F. Moore,T. Weibel, J.E. Balow, R.O. Brady, Enzyme replacement therapy inFabry disease: a randomized controlled trial, JAMA 285 (2001) 2743–2749.
[22] C.M. Eng, M. Banikazemi, R.E. Gordon, M. Goldman, R. Phelps, L.Kim, A. Gass, J. Winston, S. Dikman, J.T. Fallon, S. Brodie, C.B.Stacy, D. Mehta, R. Parsons, K. Norton, M. O’Callaghan, R.J.Desnick, A phase 1/2 clinical trial of enzyme replacement in Fabrydisease: pharmacokinetic, substrate clearance, and safety studies, Am.J. Hum. Genet. 68 (2001) 711–722.
[23] C.M. Eng, N. Guffon, W.R. Wilcox, D.P. Germain, P. Lee, S.Waldek, L. Caplan, G.E. Linthorst, R.J. Desnick, InternationalCollaborative Fabry Disease Study Group, Safety and efficacy ofrecombinant human alpha-galactosidase A-replacement therapy inFabry’s disease, N. Eng. J. Med. 345 (2001) 9–16.
[24] R. Schiffmann, M.K. Floeter, J.M. Dambrosia, S. Gupta, D.F.Moore, Y. Sharabi, R.K. Khurana, R.O. Brady, Enzyme replacementtherapy improves peripheral nerve and sweat function in Fabrydisease, Muscle Nerve 28 (2003) 703–710.
[25] M.J. Hilz, M. Brys, H. Marthol, B. Stemper, M. Dutsch,Enzyme replacement therapy improves function of C-, Adelta-,and Abeta-nerve fibers in Fabry neuropathy, Neurology 62 (2004)1066–1072.
[26] G. Bierer, D. Balfe, W.R. Wilcox, Z. Mosenifar, Improvement inserial cardiopulmonary testing following enzyme replacement therapyin Fabry disease, J. Inherit. Metab. Dis. 29 (2006) 479–572.
[27] F. Dehout, D. Roland, S. treille de Granseigne, B. Guillaume, L. VanMaldergem, Relief of gastrointestinal symptoms under enzymereplacement therapy [corrected] in patients with Fabry disease, J.Inherit. Metab. Dis. 27 (2004) 499–505.
[28] D.P. Germain, S. Waldek, M. Banikazemi, D.A. Bushinsky, J.Charrow, R.J. Desnick, P. Lee, T. Loew, A.C. Vedder, R. Abichan-dani, W.R. Wilcox, N. Guffon, Sustained, long-term renal stabiliza-

W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128 127
tion after 54 months of agalsidase beta therapy in patients with Fabrydisease, J. Am. Soc. Nephrol. 18 (2007) 1547–1557.
[29] W.R. Wilcox, M. Banikazemi, N. Guffon, S. Waldek, P. Lee, G.E.Linthorst, R.J. Desnick, D.P. Germain, International Fabry DiseaseStudy Group, Long-term safety and efficacy of enzyme replacementtherapy for Fabry disease, Am. J. Hum. Genet. 75 (2004) 65–74.
[30] M. Banikazemi, J. Bultas, S. Waldek, W.R. Wilcox, C.B. Whitley, M.MacDonald, R. Finkel, S. Packman, D.G. Bichet, D.G. Warnock,R.J. Desnick, Fabry Disease Clinical Trial Study Group, Agalsidase-beta therapy for advanced Fabry disease, Ann. Intern. Med. 146(2007) 77–86.
[31] F. Baehner, C. Kampmann, C. Whybra, E. Miebach, C.M. Wiethoff,M. Beck, Enzyme replacement therapy in heterozygous females withFabry disease: results of a phase IIIB study, J. Inherit. Metab. Dis. 26(2003) 617–627.
[32] P.J. Meikle, J.J. Hopwood, A.E. Clague, W.F. Carey, Prevalence oflysosomal storage disorders, JAMA 281 (1999) 249–254.
[33] M. Tanaka, T. Ohashi, M. Kobayashi, Y. Eto, N. Miyamura, K.Nishida, E. Araki, K. Itoh, K. Matsushita, M. Hara, K. Kuwahara,T. Nakano, N. Yasumoto, H. Nonoguchi, K. Tomita, Identificationof Fabry’s disease by the screening of alpha-galactosidase A activityin male and female hemodialysis patients, Clin. Nephrol. 64 (2005)281–287.
[34] S. Nakao, C. Lodama, T. Takenaka, A. Tanaka, Y. Yasumoto, A.Yoshida, T. Kanzaki, A.L.D. Enriquez, C.M. Eng, H. Tanaka, C.Tei, R.J. Desnick, Fabry disease: detection of undiagnosed hemod-ialysis patients and identification of a ‘‘renal variant’’ phenotype,Kidney Int. 64 (2003) 801–807.
[35] M. Merta, J. Reiterova, J. Ledvinova, H. Poup?tova, R. Dobrovolny,R. Rysava, D. Maixnerova, J. Blutas, J. Motan, J. Slivkova, D.Sobotova, J. Smrzova, V. Tesar, A nationwide blood spot screeningstudy for Fabry disease in the Czech Republic haemodialysis patientpopulation, Nephrol. Dial. Transplant. 22 (2007) 179–186.
[36] P. Kotanko, R. Kramar, D. Kevrnja, E. Paschke, T. Voigtlander, M.Auinger, K. Demmelbauer, M. Lorenz, A-C. Hauser, H-J. Kofler, K.Lhotta, U. Neyer, W. Pronai, M. Wallner, C. Wieser, M. Wiesholzer,H. Zodl, M. Fodinger, G. Sunder-Plassmann, Results of a nationwidescreening for Anderson-Fabry disease among dialysis patients, J. Am.Soc. Nephrol. 15 (2004) 1323–1329.
[37] S. Nakao, T. Takenaka, M. Maeda, C. Kodama, A. Tanaka, M.Tahara, A. Yoshida, M. Kuriyama, H. Hayashibe, H. Sakuraba, H.Tanaka, An atypical variant of Fabry’s disease in men with leftventricular hypertrophy, New Engl. J. Med. 333 (1995) 288–293.
[38] B. Sachdev, P.M. Elliott, Isolated cardiac manifestations in Fabrydisease: the UK experience, Acta Paediatr. Suppl. 439 (2002) 28–30.
[39] B. Sachdev, T. Takenaka, H. Teraguchi, C. Tei, P. Lee, W.J.McKenna, P.M. Elliott, Prevalence of Anderson-Fabry disease inmale patients with late onset hypertrophic cardiomyopathy, Circula-tion 105 (2002) 1407–1411.
[40] A. Rolfs, T. Bottcher, M. Zschiesche, P. Morris, B. Winchester, P.Bauer, U. Walter, E. Mix, M. Lohr, K. Harzer, U. Strauss, J. Pahnke,A. Grossmann, R. Benecke, Prevalence of Fabry disease in patientswith cryptogenic stroke: a prospective study, Lancet 366 (2005)1794–1796.
[41] M. Spada, S. Pagliardini, M. Yasuda, T. Tukel, G. Thiagarajan, H.Sakuraba, A. Ponzone, R.J. Desnick, High incidence of later-onsetFabry disease revealed by newborn screening, Am. J. Hum. Genet. 79(2006) 31–40.
[42] SAS Institute Inc. SAS Procedures Guide, Version 8. SAS InstituteInc., Cary, NC. 1999.
[43] C.S. Cleeland, Pain assessment: the advantages of using pain scales inlysosomal storage diseases, Acta Paediatr. Suppl. 91 (2002) 43–47.
[44] M. Beck, R. Ricci, U. Widmer, F. Dehout, A.G. de Lorenzo, C.Kampmann, A. Linhart, G. Sunder-Plassmann, G. Houge, U.Ramaswami, A. Gal, A. Mehta, Fabry disease: overall effects ofagalsidase alfa treatment, Eur. J. Clin. Invest. 34 (2004) 838–844.
[45] B. Hoffmann, A. Garcia de Lorenzo, A. Mehta, M. Beck, U. Widmer,R. Ricci, FOS European Investigators. Effects of enzyme replacement
therapy on pain and health related quality of life in patients withFabry disease: data from FOS (Fabry Outcome Survey), J. Med.Genet. 42 (2005) 247–252.
[46] J.E. Ware, K.K. Snow, M. Kosinski, B. Gandek, SF-36� HealthSurvey Manual and Interpretation Guide, New England MedicalCenter, The Health Institute, Boston, MA, 1993.
[47] K.F. Gold, G.M. Pastores, M.F. Botteman, J.M. Yeh, S. Sweeney,W. Aliski, C.L. Pashos, Quality of life of patients with Fabry disease,Quality Life Res. 11 (2002) 317–327.
[48] N.J. Street, M.S. Yi, L.A. Bailey, R.J. Hopkin, Comparison ofhealth-related quality of life between heterozygotes women withFabry disease, a healthy control population, and patients with otherchronic disease, Genet. Med. 8 (2006) 346–353.
[49] A.H. Miners, A. Holmes, L. Sherr, C. Jenkinson, K.D. MacDermot,Assessment of health-related quality-of-life in males with AndersonFabry disease before therapeutic intervention, Quality Life Res. 11(2002) 127–133.
[50] S.R. Erickson, R.D. Christian Jr., D.M. Kirking, L.J. Halman,Relationship between patient and disease characteristics, and health-related quality of life in adults with asthma, Respir. Med. 96 (2002)450–460.
[51] E.G. Lowrie, R.B. Curtin, N. LePain, D. Schatell, Medical outcomesstudy short form-36: a consistent and powerful predictor of morbidityand mortality in dialysis patients, Am. J. Kidney Dis. 41 (2003)1286–1292.
[52] M. Jolly, How does quality of life of patients with systemic lupuserythematosis compare with that of other common chronic illnesses?J. Rheumatol. 32 (2005) 1706–1708.
[53] A.S. Levey, J.P. Bosch, A more accurate method to estimateglomerular filtration rate from serum creatinine: A new predictiveequation, Ann. Int. Med. 130 (1999) 461–470.
[54] L.A. Stevens, J. Coresh, T. Greene, A.S. Levey, Assessing kidneyfunction—measured and estimated glomerular filtration rate, N.Engl. J. Med. 354 (2006) 2473–2483.
[55] M. Ries, U. Ramaswami, R. Parini, B. Lindblad, C. Whybra, I.Willers, A. Gal, M. Beck, The early clinical phenotype of Fabrydisease: a study on 35 European children and adolescents, Eur. J.Pediatr. 162 (2003) 767–772.
[56] U. Ramaswami, C. Whybra, R. Parini, G. Pintos-Morell, A. Mehta,G. Sunder-Plassmann, U. Widmer, M. Beck, FOS European Inves-tigators. Clinical manifestations of Fabry disease in children: datafrom the Fabry Outcome Survey, Acta Paediatr. 95 (2006) 86–92.
[57] M. Ries, S. Gupta, D.F. Moore, V. Sachdev, J.M. Quirk, G.J.Murray, D.R. Rosing, C. Robinson, E. Schaefer, A. Gal, J.M.Dambrosia, S.C. Garman, R.O. Brady, R. Schiffmann, PediatricFabry disease, Pediatrics 115 (2005) 344–355.
[58] T. Kitagawa, N. Ishige, K. Suzuki, M. Owada, T. Ohashi, M.Kobayashi, Y. Eto, A. Tanaka, K. Mills, B. Winchester, J. Keutzer,Non-invasive screening method for Fabry disease by measuringglobotriaosylceramide in whole urine samples using tandem massspectrometry, Mol. Genet. Metab. 85 (2005) 196–202.
[59] C. Kampmann, C.M. Wiethoff, A. Perrot, M. Beck, R. Dietz, K.J.Osterziel, The heart in Anderson Fabry disease, Z. Kardiol. 91 (2002)786–795.
[60] C. Kampmann, F. Baehner, C. Whybra, C. Martin, C.M. Wiethoff,M. Ries, A. Gal, M. Beck, Cardiac manifestations of Anderson-Fabrydisease in heterozygous females, J. Am. Coll. Cardiol. 40 (2002)1668–1674.
[61] L. Chang, B.B. Toner, S. Fukudo, E. Guthrie, G.R. Locke, N.J.Norton, A.D. Sperber, Gender, age, society, culture, and the patient’sperspective in the functional gastrointestinal disorders, Gastroenter-ology 130 (2006) 1435–1446.
[62] B. Gandek, J.E. Ware Jr., Methods for validating and normingtranslations of health status questionnaires: The IQOLA Projectapproach, J. Clin. Epidemiol. 51 (1998) 953–959.
[63] A.K. Wagner, B. Gandek, N.K. Aaronson, C. Acquadro, J. Alonso,G. Apolone, M. Bullinger, J. Bjorner, S. Fukuhara, S. Kaasa, A.Leplege, M. Sullivan, S. Wood-Dauphinee, J.E. Ware Jr., Cross-

128 W.R. Wilcox et al. / Molecular Genetics and Metabolism 93 (2008) 112–128
cultural comparisons of the content of SF-36 translations across 10countries: results from the IQOLA Project. International Quality ofLife Assessment, J. Clin. Epidemiol. 51 (1998) 903–912.
[64] J.E. Ware Jr., M. Kosinski, B. Gandek, N.K. Aaronson, G. Apolone,P. Bech, J. Brazier, M. Bullinger, S. Kaasa, A. Leplege, L. Prieto, M.Sullivan, The factor structure of the SF-36 health survey in 10
countries: results from the IQOLA Project, J. Clin. Epidemiol. 51(1998) 1159–1165.
[65] E.F. Neufeld, J. Muenzer, The mucopolysaccharidoses, in: C.R.Scriver, A.L. Beaudet, W.S. Sly, D. Valle (Eds.), The Metabolic andMolecular Bases of Inherited Disease, eighth ed., McGraw Hill, NewYork, 2001, pp. 3421–3452.




















