Naturalised epistemology, reciprocal containment and metaphysical realism
Upload
westenglandCategory
view
0download
0
AUTHOR QUERY FORM
Journal title: JEA
Article Number: 373104
Dear Author/Editor,
Greetings, and thank you for publishing with SAGE. Your article has been copyedited, and we have a few queries for you. Please respond to these queries when you submit your changes to the Production Editor.
Thank you for your time and effort.
Please assist us by clarifying the following queries:
No Query
1 PLEASE PROVIDE TWO TO FIVE KEYWORDS FOR THE ARTICLE.
2 PLEASE CONFIRM WHETHER THE GIVEN CONFLICT OF INTEREST STATEMENT IS ACCURATE AND CORRECT.
3 PLEASE CONFIRM WHETHER THE GIVEN FUNDING DISCLOSURES STATEMENT IS ACCURATE AND CORRECT.
4 PLEASE INDICATE WHERE SHOULD ATTIE & BROOKS-GUNN, 1995, APPEAR, OR ALLOW US TO DELETE THE REFERENCE.

Journal of Early AdolescenceXX(X) 1 –15
© The Author(s) 2010Reprints and permission:
sagepub.com/journalsPermissions.navDOI: 10.1177/0272431610373104
http://jea.sagepub.com
Family Meal Frequency and Alcohol and Tobacco Use in Adolescence: Testing Reciprocal Effects
James White1 and Emma Halliwell2
Abstract
This longitudinal study tested the direction of associations between family meals and alcohol and tobacco consumption during early adolescence. We examined family meal frequency, family connectedness, alcohol (binge drinking, drunkenness), and tobacco consumption (past year, daily frequency) in 671 adolescents (51% women; mean age, Wave 1 = 14.05 years). Structural equation modeling (SEM) was employed to estimate the associations between meal frequency and increases in alcohol and tobacco consumption, and alcohol and tobacco consumption on increases in meal frequency over a year, while adjusting for family connectedness, social class, and age. Family meals were associated with reductions in alcohol and tobacco consumption in girls but not boys. Alcohol consumption was also associated with reductions in the frequency of meals among girls, but not
1Cardiff University, Cardiff, UK1University of the West of England, Bristol, UK
Corresponding Author:James White, Department of Primary Care and Public Health, School of Medicine, Cardiff University, 4th Floor Neuadd Meirionnydd, Heath Park, Cardiff, CF14 4YS, United KingdomEmail: [email protected]

2 Journal of Early Adolescence XX(X)
boys. Results supported the assertion that family meals protect some girls from substance abuse but suggest meals may have little impact on existing users.
Keywords
[AQ: 1]
Adolescence is typically the period when risky behaviors, including alcohol, tobacco, substance abuse, and unsafe sexual practices are initiated (Fergusson & Lynskey, 1996; Johnston & Bachman, 1999). As the onset of heavy alco-hol use (e.g., binge drinking) and tobacco use (e.g., daily smoking) in early adolescence have been closely linked to dependency in adulthood (Chassin, Pitts, & Prost, 2002; Grant & Dawson, 1997), research has attempted to iden-tify factors that delay or prevent these behaviors. Among these contributory factors, numerous studies have examined the family environment, as a source of both risk and protective factors. Parent–child communication, family con-flict, support, and parenting style have all been found to have an impact on adolescent health and health behaviors (Kingon & O’Sullivan, 2001; Repetti, Taylor, & Seeman, 2002; Resnick et al., 1997). A recent research focus has been on the impact of family meals in reducing substance abuse during early adolescence (Eisenberg, Neumark-Sztainer, Fulkerson, & Story, 2008; Franko, Thompson, Affenito, Barton, & Striegel-Moore, 2008).
The frequency of family meals has been inversely associated with alcohol and tobacco use in cross-sectional studies (Fulkerson et al., 2006) and longi-tudinal research with adolescent girls (Eisenberg et al., 2008; Franko et al., 2008), even after controlling for sociodemographic variables and family con-nectedness. As family connectedness (the perceived emotional closeness to parents) is a well-known protective factor for risk behaviors in adolescence (Kingon & O’Sullivan, 2001; Resnick et al., 1997), these studies suggest family meal frequency is not acting as a proxy for closeness with parents. However, there is a lack of understanding on the mechanisms that might explain how family meals affect adolescent health.
Eisenberg, Olson, Neumark-Sztainer, Story, and Bearinger (2004) sug-gested regular family meals might increase family connectedness or provide an opportunity for parents to discuss high-risk behaviors and model coping strategies. These effects have been supported by studies showing family meals protect against health risk behaviors by increasing family cohesion (Franko et al., 2008) and are associated with developmental assets (e.g., enhancing decision making and social skills; Fulkerson et al., 2006). How-ever, existing research has yet to investigate the possibility that adolescents

White and Halliwell 3
who start to use alcohol and tobacco may actively avoid family meals to con-tinue these behaviors.
A series of theorists have argued that problem behaviors (e.g., antisocial behaviors) and problematic family relationships emerge in childhood and adolescence within transactional system (Dishion, Nelson, & Bullock, 2004; Patterson, Reid, & Dishion, 1998). The issue of the direction of effects between adolescent health and the quality of family relationships has specifi-cally been addressed in other studies. For instance, Byley, Archibald, Graber, and Brooks-Gunn (2000) found adolescent girls who perceived their family relationships to be of low quality were more likely to increase their use of harmful dieting behaviors. However, other studies investigating bidirectional relationships have found harmful dieting behaviors in girls were a stronger predictor of reductions in the quality of family relationships than the reverse effect (Archibald, Linver, Graber, & Brooks-Gunn, 2002). In the context of early adolescence, where family relationships are still a dominant influence, bidirectional effects may exist between family relationship and substance abuse. For example, adolescents who start to smoke or drink alcohol may intentionally avoid family meals and communicate less frequently with par-ents to avoid detection and censure for these behaviors. Similarly, adolescents who start to smoke but live with parents who have expressed antismoking attitudes may avoid interactions. Thus, the experimentation and intensifica-tion of alcohol or tobacco use common to early adolescence (Johnston & Bachman, 1999) may bring about an incremental reduction in meal frequency. Bidirectional relationships also offer viable explanations. Meal frequency may delay experimentation, but once alcohol and tobacco use is initiated adolescents may reduce their frequency of attending meals. It is important to rule out the possibility of reverse causality to determine whether interventions that aim to increase the frequency of family meals would influence adolescent substance abuse.
To date, most studies investigating family mealtimes have used a cross-sectional design (Eisenberg et al., 2004; Fulkerson et al., 2006), and those using a longitudinal design (Eisenberg et al., 2008) have not examined the possibil-ity of reverse causal relationships, whereby alcohol and tobacco use reduce the frequency of family meals and family connectedness over time. Moreover, past research has used measures of yearly alcohol and tobacco consumption (Eisenberg et al., 2004) rather than heavy alcohol (e.g., binge drinking, severe drunkenness) and tobacco use (e.g., daily smoking), which have been more closely linked to dependency in adulthood (Chassin et al., 2002; Grant & Dawson, 1997). These represent substantial gaps in the literature on the influence of the family meals on adolescent substance abuse.

4 Journal of Early Adolescence XX(X)
Accordingly, the primary aim of the present study was to investigate the degree to which family meals were associated with changes in alcohol and tobacco use over time in a nonclinical sample of early adolescents. In order to establish the temporal ordering of effects of family meals on alcohol and tobacco use, we employed a longitudinal design. This enabled us to test hypotheses that frequent family meals reduce the consumption of alcohol and tobacco as well as the possibility that alcohol and tobacco consumption reduce the frequency of family meals and levels of family connectedness. Utilizing structural equation modeling, the longitudinal associations between family meals and changes in alcohol and tobacco use, and the influence of alcohol and tobacco use on changes in meal frequency, were simultaneously investigated. This model adjusted for established risk factors for alcohol and tobacco use (Resnick et al., 1997; Scal, Ireland, & Borowsky, 2003) and fac-tors that might affect family meal frequency during adolescence (e.g., age, socioeconomic status, and family connectedness).
MethodThe sample included 332 male (49%) and 339 (51%) female adolescents surveyed at two time points one year apart (age at follow-up: M = 14.26, SD = 1.11, range 12.15-16.53 years; 77.5% aged 11-14). Study protocols and materials were approved by the university departmental ethics review board prior to initiation. Students completed measures in a large school hall on single desks supervised by researchers and teachers.
As the study focused on early adolescence, all students in Grades 7, 9, and 10 of a school based in an urban city of the United Kingdom were invited to participate. Passive parental consent (96.4%) and student assent (98.8%) was received from the majority of potential participants. At Wave 1, 984 students (Grades 7, 9 and 10), of which 495 (50%) were boys and 489 (50%) were girls completed surveys during the 2005-2006 school year. Out of the origi-nal Wave 1 cohort of students, 290 (29%) were lost by Wave 2. The remain-ing 684 participants, representing 71% of the Wave 1 cohort, completed the survey.
Complete longitudinal data were available for 671 participants, represent-ing 68% of the Wave 1 cohort. Compared to the Wave 1 cohort, the follow-up sample were younger, of lower socioeconomic status, and had more frequent family meals (all p’s <.05).
This final follow-up sample was primarily made up of participants who were White and socioeconomically diverse. Nearly half (45.3%) of participants’ par-ents (or guardians) worked in higher or lower managerial professions, 21% were in semiroutine or routine occupations, and 10.7% had never worked or
White and Halliwell 5
were unemployed. The ethnic backgrounds of participants were as follows: 93% were White, 4.7% mixed race, 1% Asian, 0.7% Black, and 0.7% identi-fied themselves as from another ethnic origin.
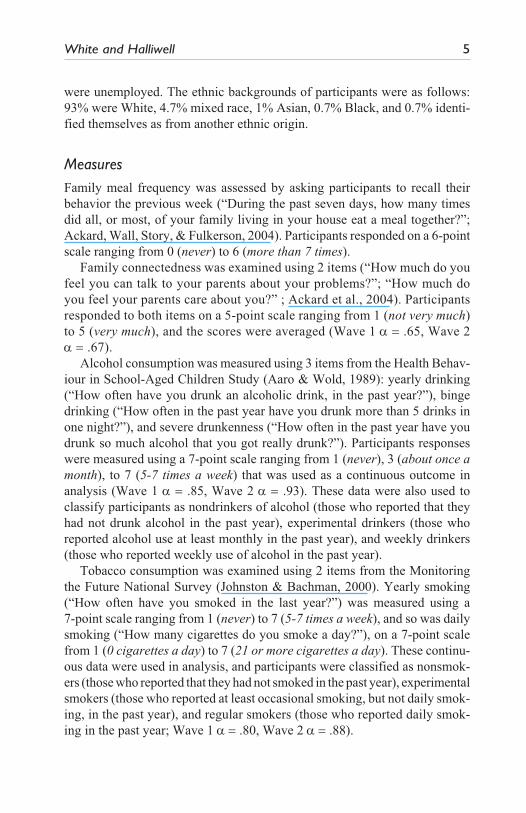
MeasuresFamily meal frequency was assessed by asking participants to recall their behavior the previous week (“During the past seven days, how many times did all, or most, of your family living in your house eat a meal together?”; Ackard, Wall, Story, & Fulkerson, 2004). Participants responded on a 6-point scale ranging from 0 (never) to 6 (more than 7 times).
Family connectedness was examined using 2 items (“How much do you feel you can talk to your parents about your problems?”; “How much do you feel your parents care about you?” ; Ackard et al., 2004). Participants responded to both items on a 5-point scale ranging from 1 (not very much) to 5 (very much), and the scores were averaged (Wave 1 a = .65, Wave 2 a = .67).
Alcohol consumption was measured using 3 items from the Health Behav-iour in School-Aged Children Study (Aaro & Wold, 1989): yearly drinking (“How often have you drunk an alcoholic drink, in the past year?”), binge drinking (“How often in the past year have you drunk more than 5 drinks in one night?”), and severe drunkenness (“How often in the past year have you drunk so much alcohol that you got really drunk?”). Participants responses were measured using a 7-point scale ranging from 1 (never), 3 (about once a month), to 7 (5-7 times a week) that was used as a continuous outcome in analysis (Wave 1 a = .85, Wave 2 a = .93). These data were also used to classify participants as nondrinkers of alcohol (those who reported that they had not drunk alcohol in the past year), experimental drinkers (those who reported alcohol use at least monthly in the past year), and weekly drinkers (those who reported weekly use of alcohol in the past year).
Tobacco consumption was examined using 2 items from the Monitoring the Future National Survey (Johnston & Bachman, 2000). Yearly smoking (“How often have you smoked in the last year?”) was measured using a 7-point scale ranging from 1 (never) to 7 (5-7 times a week), and so was daily smoking (“How many cigarettes do you smoke a day?”), on a 7-point scale from 1 (0 cigarettes a day) to 7 (21 or more cigarettes a day). These continu-ous data were used in analysis, and participants were classified as nonsmok-ers (those who reported that they had not smoked in the past year), exp erimental smokers (those who reported at least occasional smoking, but not daily smok-ing, in the past year), and regular smokers (those who reported daily smok-ing in the past year; Wave 1 a = .80, Wave 2 a = .88).

6 Journal of Early Adolescence XX(X)
Research has verified that self-reports on smoking from adolescents show high level of agreement with biological measures (e.g., carbon monoxide from expired air; Wills & Cleary, 1997). In fact, self-reports of alcohol and tobacco use from nonclinical populations of adolescents have been found to provide some of the valid (Winters, Stinchfield, Henly, & Schwartz, 1991) and reliable (Brener, Collins, Kann, Warren, & Williams, 1995) measures of these behaviors.
Socioeconomic status was assessed by four questions, including the fol-lowing two: (1) “Does your father have a job?,” and “If you have circled Yes, please write where he works and what he does”; these items were repeated for mothers. Responses were assigned to a socioeconomic status using the National Statistics Socioeconomic Classification method (NS-SEC 1990; Rose & Pevalin, 2003) with parental occupational title and employment status. The eight categories were higher managerial, lower managerial, intermediate occupations, small employers/account workers, lower supervisory/technical workers, semiroutine, routine, and never worked/long-term unemployed. Ethnicity was assessed with 1 item, “What is your ethnic group?,” with the following response options, White, Asian, Black, mixed race, and Other.
Data AnalysisStructural equation modeling (SEM; using EQS version 6.1; Bentler, 2005) was used to estimate the impact of family meals at Wave 1 on the changes in a latent alcohol use variable (measures: yearly alcohol consumption, binge drinking, episodes of severe drunkenness) and a latent tobacco consumption variable (measures: yearly, daily consumption), and alcohol and tobacco consumption at Wave 1 on changes in family meal frequency over a year. Although tobacco consumption was estimated using two rather than three observed variables, a number of studies suggest this approach is valid in mod-eling self-report data (Anderson & Gerbing, 1988; Kline, 2005). All relationships were adjusted in both directions for the influence of age, socioeconomic status, and family connectedness.
The following sequence of analysis was undertaken (Bentler, 2005). First, the psychometric properties of the measures of alcohol and tobacco con-sumption (i.e. the measurement model) in the whole sample were examined. Next, gender differences were examined in the measurement and hypothesized causal relationships between boys and girls, by applying equality constraints to all model parameters (i.e. factor loadings, hypothesized causal pathways). Third, all nonsignificant pathways and variables were identified and models respecified. All predictors and outcomes were modeled as continuous variables.
White and Halliwell 7
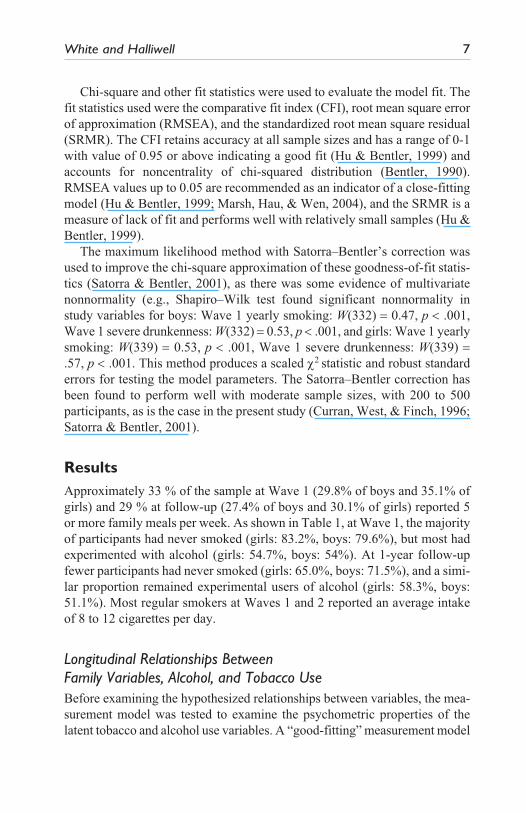
Chi-square and other fit statistics were used to evaluate the model fit. The fit statistics used were the comparative fit index (CFI), root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). The CFI retains accuracy at all sample sizes and has a range of 0-1 with value of 0.95 or above indicating a good fit (Hu & Bentler, 1999) and accounts for noncentrality of chi-squared distribution (Bentler, 1990). RMSEA values up to 0.05 are recommended as an indicator of a close-fitting model (Hu & Bentler, 1999; Marsh, Hau, & Wen, 2004), and the SRMR is a measure of lack of fit and performs well with relatively small samples (Hu & Bentler, 1999).
The maximum likelihood method with Satorra–Bentler’s correction was used to improve the chi-square approximation of these goodness-of-fit statis-tics (Satorra & Bentler, 2001), as there was some evidence of multivariate nonnormality (e.g., Shapiro–Wilk test found significant nonnormality in study variables for boys: Wave 1 yearly smoking: W(332) = 0.47, p < .001, Wave 1 severe drunkenness: W(332) = 0.53, p < .001, and girls: Wave 1 yearly smoking: W(339) = 0.53, p < .001, Wave 1 severe drunkenness: W(339) = .57, p < .001. This method produces a scaled c2 statistic and robust standard errors for testing the model parameters. The Satorra–Bentler correction has been found to perform well with moderate sample sizes, with 200 to 500 participants, as is the case in the present study (Curran, West, & Finch, 1996; Satorra & Bentler, 2001).
ResultsApproximately 33 % of the sample at Wave 1 (29.8% of boys and 35.1% of girls) and 29 % at follow-up (27.4% of boys and 30.1% of girls) reported 5 or more family meals per week. As shown in Table 1, at Wave 1, the majority of participants had never smoked (girls: 83.2%, boys: 79.6%), but most had experimented with alcohol (girls: 54.7%, boys: 54%). At 1-year follow-up fewer participants had never smoked (girls: 65.0%, boys: 71.5%), and a simi-lar proportion remained experimental users of alcohol (girls: 58.3%, boys: 51.1%). Most regular smokers at Waves 1 and 2 reported an average intake of 8 to 12 cigarettes per day.
Longitudinal Relationships Between Family Variables, Alcohol, and Tobacco UseBefore examining the hypothesized relationships between variables, the mea-surement model was tested to examine the psychometric properties of the latent tobacco and alcohol use variables. A “good-fitting” measurement model

8
Tab
le 1
. Fam
ily V
aria
bles
and
Cla
ssifi
catio
n of
Lev
el o
f Alc
ohol
and
Tob
acco
Use
Wav
e 1
Wav
e 2
Boys
(n
= 33
2)G
irls
(n
= 33
9)Bo
ys (
n =
332)
Gir
ls (
n =
339)
Cha
ract
eris
tics
n%
MSD
Min
Max
n%
MSD
Min
Max
n%
MSD
Min
Max
n%
MSD
Min
Max
Wee
kly
freq
uenc
y
of m
eals
Nev
er 4
212
.7—
——
— 4
112
.1—
——
— 4
714
.2—
——
— 6
017
.7—
——
—1
2 tim
es 8
726
.2—
——
— 9
026
.5—
——
— 9
127
.4—
——
—10
129
.8—
——
—3
4 tim
es10
431
.3—
——
— 8
926
.3—
——
—10
331
.0—
——
— 7
622
.4—
——
—5
or m
ore
times
99
29.8
——
——
119
35.1
——
——
91
27.4
——
——
102
30.1
——
——
Fam
ily c
onne
cted
ness
3.7
1.0
1.0
5.0
3.8
1.0
1.0
5.0
3.6
1.1
1.0
5.0
1.0
3.5
1.2
1.0
5.0
Alc
ohol
cl
assi
ficat
ion
Nev
er10
932
.8—
——
—14
141
.6—
——
— 9
227
.0—
——
— 8
725
.8—
——
—
Expe
rim
enta
l17
954
.0—
——
—18
554
.7—
——
—17
351
.1—
——
—19
858
.3—
——
—
Reg
ular
44
13.1
——
——
13
3.7
——
——
73
21.9
——
——
54
16.0
——
——
Smok
ing
clas
sific
atio
nN
ever
264
79.6
——
——
282
83.2
——
——
238
71.5
——
——
220
65.0
——
——
Expe
rim
enta
l 5
316
.1—
——
— 3
4 9
.9—
——
— 4
814
.6—
——
— 8
123
.9—
——
—
Reg
ular
15
4.4
——
——
23
6.8
——
——
46
13.9
——
——
38
11.0
——
——

White and Halliwell 9
in this context is defined by checking fit indices against specific threshold values (Hu & Bentler, 1999; Marsh et al., 2004). These values are used to evaluate the quality of measurement of the alcohol and tobacco latent vari-ables. The fit of the data for the combined sample to the measurement model was good, S-B c2(21) = 55.36, p < .001, CFI = 0.98, RMSEA = 0.05, 90% confidence interval (CI) RMSEA = 0.03-0.07, SRMR = 0.03. The measure-ment model also provided a good fit to the data from boys, S-B c2 (21) = 29.90, p = .09, CFI = 0.99, RMSEA = 0.04, 90% CI RMSEA < 0.01-0.06, SRMR = 0.03, and girls, S-B c2 (21) =27.80, p = .15, CFI = 1.00, RMSEA= 0.03, 90% CI RMSEA < 0.01-0.06, SRMR = 0.04.
Next, equality constraints were applied across boys and girls measure-ment models to examine gender differences in the measurement and stability of alcohol and tobacco use. The frequency of daily smoking factor loading (c2 = 6.89, p = .009) and the pathway representing the stability of smoking (c2 = 5.80, p = .016) were stronger in boys. Due to these differences in the measurement and stability of alcohol and tobacco use, equality constraints were applied to the hypothesized longitudinal relationships across boys and girls data. The effect of family connectedness on changes in smoking (c2 = 6.20, p = .013), and meal frequency on changes in smoking (c2 = 3.81, p = .04), were stronger in girls than boys. Combining these results with evidence from previous studies that have also found family meals have a nonsignifi-cant effect in boys (Eisenberg et al., 2004, 2008), models of hypothesized causal relationships were respecified separately in boys and girls.
For boys, all hypothesized causal paths between family meals, family con-nectedness, and alcohol and tobacco use were nonsignificant (all p’s > .05). Boys data did not fit the hypothesized longitudinal model, even after remov-ing nonsignificant relationships, S-B c2 (80) = 255.39, p < .001, CFI = 0.83, RMSEA = 0.08, 90% CI RMSEA = 0.07-0.09, SRMR = 0.05.
The fit of the longitudinal model to girls data was also poor, S-B c2 (80) = 177.44, p < .001, CFI = 0.96, RMSEA = 0.06, 90% CI RMSEA = 0.05-0.07, SRMR = 0.06. Respecification involved dropping the following nonsignifi-cant variables and paths: social class variable (as it had a nonsignificant effect on all variables), the relationships between family connectedness (Wave 1) with family meals (Wave 2) and tobacco use (Wave 2), and tobacco use (Wave 1) with meal frequency (Wave 2). After respecification, the fit of final model to girls data was very good, S-B c2 (59) = 59.35, p = .46, CFI = 1.00, RMSEA < 0.01, 90% CI RMSEA ≤ 0.01-0.03, SRMR = 0.04.
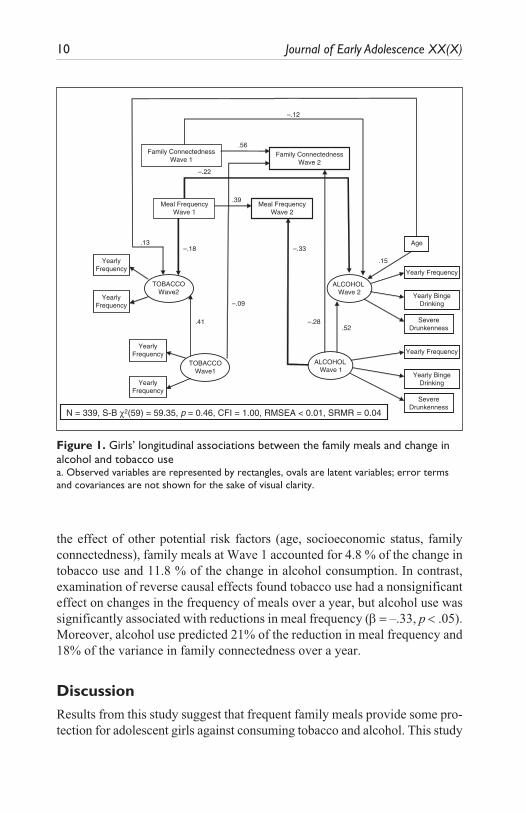
Within the final model fitted to girls’ data, family meals were associated with a significant reduction in the frequency of alcohol (b = –.22, p < .05) and tobacco use (b = –.18, p <.05) in girls over the past year. After adjusting for
10 Journal of Early Adolescence XX(X)
the effect of other potential risk factors (age, socioeconomic status, family connectedness), family meals at Wave 1 accounted for 4.8 % of the change in tobacco use and 11.8 % of the change in alcohol consumption. In contrast, examination of reverse causal effects found tobacco use had a nonsignificant effect on changes in the frequency of meals over a year, but alcohol use was significantly associated with reductions in meal frequency (b = –.33, p < .05). Moreover, alcohol use predicted 21% of the reduction in meal frequency and 18% of the variance in family connectedness over a year.
DiscussionResults from this study suggest that frequent family meals provide some pro-tection for adolescent girls against consuming tobacco and alcohol. This study
TOBACCOWave1
TOBACCOWave2
ALCOHOLWave 1
ALCOHOLWave 2
Yearly Frequency
SevereDrunkenness
Yearly BingeDrinking
YearlyFrequency
YearlyFrequency
YearlyFrequency
YearlyFrequency
Meal FrequencyWave 1
Family ConnectednessWave 1
Family ConnectednessWave 2
Meal FrequencyWave 2
Yearly Frequency
SevereDrunkenness
Yearly BingeDrinking
Age
.56
.39
.13
.15
–.12
–.22
.41.52
–.18 –.33
–.28
–.09
N = 339, S-B χ2(59) = 59.35, p = 0.46, CFI = 1.00, RMSEA < 0.01, SRMR = 0.04
Figure 1. Girls’ longitudinal associations between the family meals and change in alcohol and tobacco usea. Observed variables are represented by rectangles, ovals are latent variables; error terms and covariances are not shown for the sake of visual clarity.

White and Halliwell 11
adds to the small number of longitudinal studies that have found family meals reduce the subsequent risk for substance use in girls but not boys (Eisenberg et al., 2008; Franko et al., 2008). Although measures were not available to explore reasons behind this difference in the current study, adolescent girls have been found to have higher levels of interpersonal connectedness (Helgeson, 1994) and emotional disclosure with parents than do boys (Papini, Farmer, Clark, Micka, & Barnett, 1990). These gender differences have been found to explain girls being more sensitive to family conflict than are boys (Davies & Lindsay, 2004), suggesting that girls may also be more sensitive to the support offered during family meals. In line with this assertion, a recent cross-sectional study found girls, but not boys, who thought meal-times had a positive atmosphere were less likely to smoke or drink alcohol (White & Halliwell, in press). Future prospective studies with a wider array of family variables are needed to identify specific reasons for these sex differences.
More important, the present study addresses a gap in the literature by showing that alcohol consumption had an impact on reductions in the fre-quency of family meals. This study’s findings suggest a number of pro-cesses may underpin these relationships. First, family meals provide a forum for parents to talk about substance abuse, communicate their values, and enhance perceptions of family cohesion closely linked to reductions in substance abuse (Franko et al., 2008). Second, simply having adolescents at home for meals increases parental monitoring, which decades of research has found delays the initiation of substance use (Cleveland, Gibbons, Gerrard, Pomery, & Brody, 2005; Li, Stanton, & Feigelman, 2000). Con-versely, once alcohol use has started, girls may avoid family meals to avoid parental monitoring, and thus, to potential censure for alcohol consump-tion. As the majority of girls at Wave 1 (58.4 %) and 1-year follow-up (74 %) were experimental or regular consumers of alcohol, the preventative role of meals in delaying alcohol consumption may have had limited impact. This interpretation is strengthened by the rapid decreases in meal frequency (5% reduction in eating 5 or more meals a week with their family) seen during the follow-up period.
Replicating the findings of previous longitudinal research into the fam-ily meals (Eisenberg et al., 2008), the effect of family meals on alcohol and tobacco was independent of family connectedness, which can contrib-ute to levels of substance abuse during adolescence (Resnick et al., 1997; Scal et al., 2003) and, potentially, to the frequency of family meals. More important, the impact of alcohol use on changes in meal frequency was also independent of the effect of family connectedness, age, and social class. Thus, the changes in alcohol, tobacco use, and meal frequency were
12 Journal of Early Adolescence XX(X)
not dependent on whether young people reported having a good relation-ship with their parents.
Several limitations of the current study need to be taken into account when interpreting the findings. First, there was evidence of selective attrition: Partici-pants included in the longitudinal analysis were younger, of lower socioeco-nomic status, and had more frequent family meals. This pattern of attrition may be problematic if follow-up participants were also different on other unmeasured family variables, which might affect substance abuse, such as meal priority and atmosphere (White & Halliwell, in press). Second, the results described here could be attributable to time spent with family versus with friends, and behaviors that may reduce the frequency of family meals (e.g., sexual activity, media use) were not assessed. Third, although adolescent reports of alcohol and tobacco use have been found to have high test–retest validity (Winters et al., 1991), measures of meal frequency have not been validated against a more objective criterion. For instance, it is possible that “all, or most, of your family living in your house” ate a meal together, but the respondent did not attend. Similarly, the use of only 2 items as a measure of family connectedness may have led to poor estimates of actual levels of connectedness between parents and adolescents. Future longitu-dinal studies with a wider array of family variables are needed to identify specific causal mechanisms and provide a basis for interventions.
In summary, this study adds to the growing longitudinal literature that has found the family meal frequency is associated with reductions in alcohol and tobacco use (Eisenberg et al., 2008; Franko et al., 2008). However, it does also suggest that family meals may have a limited impact on alcohol and tobacco use in adolescent girls once these behaviors have been initiated. These results highlight the importance of considering bidirectional relationships when exam-ining associations between family relationships and health behaviors during early adolescence.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.[AQ: 2]
Funding
This research was funded by the University of the West of England.[AQ: 3]
References
Aaro, L., & Wold, B. (1989). Health behaviour in school-aged children (HBSC), a WHO cross-national survey: Research protocol for the 1989-90 study. Bergen, Norway: Research Centre for Health Promotion, University of Bergen.
White and Halliwell 13
Ackard, D. M., Wall, M., Story, M., & Fulkerson, J. A. (2004). Are family meal pat-terns associated with disordered eating behaviors among adolescents? Journal of Adolescent Health, 35, 350-359.
Anderson, J. C., & Gerbing, D. W. (1988). Structural equation modeling in practice: A review and recommended two-step approach. Psychological Bulletin, 103, 411-423.
Archibald, A. B., Linver, M. R., Graber, J. A., & Brooks-Gunn, J. (2002). Parent-adolescent relationships and girls’ unhealthy eating: Testing reciprocal effects. Journal of Research on Adolescence, 12, 451-461.
Attie, I., & Brooks-Gunn, J. (1995). The development of eating regulation across the life span. Developmental Psychopathology, 2, 332-368.[AQ: 4]
Bentler, P. M. (1990). Comparative fit indexes in structural models. Psychological Bulletin, 107, 238-246.
Bentler, P. M. (2005). EQS structural equations program manual. Encino, CA. Mul-tivariate Software.
Brener, N. D., Collins, J. L., Kann, L., Warren, C. W., & Williams, B. I. (1995). Reli-ability of the Youth Risk Behavior Survey Questionnaire. American Journal of Epidemiology, 141, 575-580.
Byely, L., Archibald, A. B., Graber, J., & Brooks-Gunn, J. (2000). A prospective study of familial and social influences on girls’ body image and dieting. Interna-tional Journal of Eating Disorders, 28, 155-164.
Chassin, L., Pitts, S. C., & Prost, J. (2002). Binge drinking trajectories from ado-lescence to emerging adulthood in a high-risk sample: Predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology, 70(1), 67-78.
Cleveland, M. J., Gibbons, F. X., Gerrard, M., Pomery, E. A., & Brody, G. H. (2005). The impact of parenting on risk cognitions and risk behavior: A study of media-tion and moderation in a panel of African American adolescents. Child Develop-ment, 76, 900-916.
Curran, P. J., West, S. G., & Finch, J. F. (1996). The robustness of test statistics to nonnormality and specification error in confirmatory factor analysis. Psychologi-cal Methods, 1(1), 16-29.
Davies, P. T., & Lindsay, L. L. (2004). Interparental conflict and adolescent adjust-ment: Why does gender moderate early adolescent vulnerability? Journal of Fam-ily Psychology, 18, 160-170.
Dishion, T. J., Nelson, S. E., & Bullock, B. M. (2004). Premature adolescent auton-omy: Parent disengagement and deviant peer process in the amplification of prob-lem behaviour. Journal of Adolescence, 27, 515-530.
Eisenberg, M. E., Neumark-Sztainer, D., Fulkerson, J. A., & Story, M. (2008). Family meals and substance use: Is there a long-term protective association? Journal of Adolescent Health, 43, 151-156.

14 Journal of Early Adolescence XX(X)
Eisenberg, M. E., Olson, R. E., Neumark-Sztainer, D., Story, M., & Bearinger, L. H. (2004). Correlations between family meals and psychosocial well-being among adolescents. Archives of Pediatrics and Adolescent Medicine, 158, 792-796.
Fergusson, D. M., & Lynskey, M. T. (1996). Alcohol misuse and adolescent sexual behaviors and risk taking. Pediatrics, 98(1), 91-96.
Franko, D. L., Thompson, D., Affenito, S. G., Barton, B. A., & Striegel-Moore, R. H. (2008). What mediates the relationship between family meals and adolescent health issues. Health Psychology, 27, 109-117.
Fulkerson, J. A., Story, M., Mellin, A., Leffert, N., Neumark-Sztainer, D., & French, S. A. (2006). Family dinner meal frequency and adolescent develop-ment: Relationships with developmental assets and high-risk behaviors. Journal of Adolescent Health, 39, 337-345.
Grant, B. F., & Dawson, D. A. (1997). Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: Results from the national longitudi-nal alcohol epidemiologic survey. Journal of Substance Abuse, 9, 103-110.
Helgeson, V. S. (1994). Relation of agency and communion to well-being: Evidence and potential explanations. Psychological Bulletin, 116, 412-412.
Hu, L., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance struc-ture analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1-55.
Johnston, L. D., & Bachman, J. G. (1999). National survey results on drug use from the Monitoring the Future Study, 1975-1998. Vol. II: College students and young adults. Washington, DC: U.S. Government Printing Office.
Johnston, L. D., & Bachman, J. G. (2000). Monitoring the Future National Survey results on drug use, 1975-1999. Vol. I: Secondary School Students. Washington, DC: U.S. Government Printing Office.
Kingon, Y. S., & O’Sullivan, A. L. (2001). The family as a protective asset in adoles-cent development. Journal of Holistic Nursing, 19(2), 102-121.
Kline, R. B. (2005). Principles and practice of structural equation modeling. New York: Guilford.
Li, X., Stanton, B., & Feigelman, S. (2000). Impact of perceived parental monitoring on adolescent risk behavior over 4 years. Journal of Adolescent Health, 27, 49-56.
Marsh, H. W., Hau, K. T., & Wen, Z. (2004). In search of golden rules: Comment on hypothesis-testing approaches to setting cutoff values for fit indexes and dangers in overgeneralizing Hu and Bentler’s (1999) findings. Structural Equation Model-ing, 11, 320-341.
Papini, D. R., Farmer, F. F., Clark, S. M., Micka, J. C., & Barnett, J. K. (1990). Early adolescent age and gender differences in patterns of emotional self-disclosure to parents and friends. Adolescence, 25, 959-976.

White and Halliwell 15
Patterson, G. R., Reid, J. B., & Dishion, T. J. (1998). Antisocial boys. In Human emo-tions: A reader (pp. 330-336). Cambridge, MA: Blackwell.
Repetti, R. L., Taylor, S. E., & Seeman, T. E. (2002). Risky families: Family social environments and the mental and physical health of offspring. Psychological Bul-letin, 128, 330-366.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., et al. (1997). Protecting adolescents from harm. Findings from the National Longi-tudinal Study on Adolescent Health. JAMA: The Journal of the American Medical Association, 278, 823-832.
Rose, D., & Pevalin, D. J. (2003). A researcher’s guide to the national statistics socio-economic classification. Thousand Oaks, CA: Sage.
Satorra, A., & Bentler, P. M. (2001). A scaled difference chi-square test statistic for moment structure analysis. Psychometrika, 66(4), 507-514.
Scal, P., Ireland, M., & Borowsky, I. W. (2003). Smoking among American adoles-cents: A risk and protective factor analysis. Journal of Community Health, 28(2), 79-97.
White, J., & Halliwell, E. (in press). Alcohol and tobacco use during adolescence: The importance of the family mealtime environment. Journal of Health Psychology.
Wills, T. A., & Cleary, S. D. (1997). The validity of self-reports of smoking: Analyses by race/ethnicity in a school sample of urban adolescents. American Journal of Public Health, 87(1), 56.
Winters, K. C., Stinchfield, R. D., Henly, G. A., & Schwartz, R. H. (1991). Valid-ity of adolescent self-report of alcohol and other drug involvement. International Journal of the Addictions, 25, 1379-1395.
Bios
James White (PhD) is a research associate in social epidemiology at the Cardiff Uni-versity. His research concentrates on understanding risk factors for the development of alcohol and tobacco use and the prevention of these behaviors in adolescence.
Emma Halliwell (DPhil) is a senior lecturer in psychology at the University of the West of England. Her research interests include understanding risk factors for adoles-cent health.
All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.
Copyright © 2022 FDOKUMEN