Brainstem circuitry of tracheal–bronchial cough: c- fos study in anesthetized cats

M. Ding et al. (eds.), Innovation and Marketing in the Pharmaceutical Industry, International Series in Quantitative Marketing 20, DOI 10.1007/978-1-4614-7801-0_17, © Springer Science+Business Media New York 2014
Abstract Governmental health agencies frequently issue warnings about new health hazards (e.g., smoking and excessive drinking). This chapter discusses fac-tors affecting adherence to governmental warnings against the use of household products previously perceived safe. To be effective, a health warning must reach its intended audience and bring about behavior modification. This is challenging because, in order to modify behavior, the warning message must counteract and overpower the effect of habitual safe experience. Indeed the questions of how peo-ple perceive such warnings, whether they adhere to them, and what promotes or prevents adherence are central in marketing practice and research.
In this chapter, we review the psychological decision-making literature on trust of the source issuing the warning and safe experience with the risk-causing agent. Next we touch on basic requirements of awareness and understanding of the message. We then review the marketing literature on message design, focusing on factors practical for widespread implementation (i.e., vividness of message, one-sided vs. two-sided messages, regulatory fit). Next, based on behavioral decision research, we discuss how to counteract cognitive and emotional consumer biases that may reduce adher-ence. Finally, as a case in point, we evaluate adherence to the 2008 United States Food and Drug Administration (FDA) warning against administration of over-the-counter cough and cold medication (OTC-CCM) in children under age 2. We describe the results of three studies that examine whether parents had heard about OTC-CCM warnings and whether they intended to adhere to them. We conclude with recom-mendations for optimizing the design and dissemination of similar warnings.
Chapter 17Factors Affecting Adherence to Governmental Health Warnings and the Case of Over-the- Counter Cough and Cold Medications (OTC- CCM) in Children Under Two
Talya Miron-Shatz, Glen M. Doniger, and Yaniv Hanoch
T. Miron-Shatz (*) Center for Medical Decision Making, Ono Academic College, Kiryat Ono, Israele-mail: [email protected]
G.M. Doniger • Y. Hanoch Department of Psychology, University of Plymouth, Plymouth, UKe-mail: [email protected]; [email protected]
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28

Governmental health agencies must frequently warn citizens about newly discov-ered health hazards (e.g., smoking and excessive drinking). This chapter discusses factors affecting adherence to governmental warnings against the use of household products previously perceived to be safe. To be effective a health warning must first reach its intended audience. In addition, the message must also successfully con-vince its intended audience to change its behavior. This is a challenging exercise in marketing, because in order to successfully convince consumers to modify behavior, the warning message must counteract and overpower the effect of habitual safe experience. Thus the questions of how people perceive such warnings, whether they adhere to them, and what promotes or prevents adherence are central factors to mar-keting practice and research.
This chapter is structured as follows: we begin by examining the psychological decision-making literature on such factors as trust of the source issuing the warning and safe experience with the risk-causing agent. Next we touch on basic require-ments of awareness and understanding of the message. We proceed to review the marketing literature on message design (Keller and Lehmann 2008),1 focusing on factors practical for widespread implementation, including vividness of message, one-sided vs. two-sided messages, and regulatory fit. Next, based on behavioral decision research (Ratner et al. 2008), we discuss natural cognitive and emotional consumer biases that may reduce adherence and how they may be counteracted. See Fig. 17.1 for an outline of the factors reviewed. To illustrate various factors, we
Fig. 17.1 Factors influencing adherence to health warnings
1 For an exhaustive treatment of the topic, we refer the interested reader to the meta-analysis of 60 studies and 22,500 participants by Keller and Lehmann (2008), showing that message tactics have a significant impact upon intention to adhere to health-related recommendations.
T. Miron-Shatz et al.
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49

include four sample warnings (Samples A through D). We go on to evaluate the specific case of the 2008 United States Food and Drug Administration (FDA) warning against administration of over-the-counter cough and cold medication (OTC-CCM) to children under age 2 (FDA 2008). The FDA warning serves as a prime illustrative case and nicely captures many of the issues relevant to health warning effectiveness identified by earlier literature. We describe the results of three studies, two conducted in the USA and one in the UK, that examine whether parents had heard about OTC-CCM warnings and whether they intended to adhere to them. Finally, we make recommendations for optimizing the design and dissemination of similar warnings in light of the literature reviewed.
17.1 Factors Influencing Adherence to Health Warnings
17.1.1 Trust of the Source Issuing the Warning
Trust of the individual or institution issuing a health warning has been shown a key aspect of health-related decision making (O’Neill 2002; Mechanic 2004; Hanoch et al. 2010). Even if a warning with the appropriate content reaches and is under-stood by its target audience, recipients may still not know what to believe if com-municators are perceived to have a vested interest (Morgan et al. 2002; Jackson et al. 2004). Mechanic (2004) suggests trust in large organizations is equivalent to trust in government and business, which tends to be low. Walls et al. (2004) cite various studies indicating that trust falls as the level of abstraction of the institution goes up (e.g., “government scientists” or “local authorities” vs. “department of health”). Similarly, Brown and Calnan (2010) suggest that trust is low for broad systems/institutions, in part, because they are faceless to consumers. In contrast, patients seem to trust doctors over health care institutions, possibly due to their personal relationship (Mechanic 2004) and direct interaction (Brown 2009). In the UK, for example, parents’ decisions not to vaccinate against measles, mumps, and rubella (MMR) despite assurances and campaigns to the contrary by the UK gov-ernment stemmed largely from lack of trust in messages about the safety of these vaccines (Casiday 2007; Casiday et al. 2006; Hobson-West 2007). Similar issues have been studied in the context of genetic technology (Barnett et al. 2007), and there is a growing literature on trust as important to the link between risk perception and decision making (Williams and Noyes 2007).
17.1.2 (Safe) Experience with the Risk-Causing Agent
A growing body of literature has shown that people rarely incorporate information about negative rare events into their decision-making process (Barron and Erev 2003; Erev and Barron 2005; Fox and Hadar 2006; Hertwig et al. 2004; Kahneman
[AU1]
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
50
51
52
53
54
55
56
57
58
59
60
61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85

and Tversky 1979; Li et al. 2009). That is, given positive experience with a product, people tend to underestimate the likelihood that a negative rare event will occur (Brown and Calnan 2010). When information about a rare event comes externally from a description, as from a warning, people tend to overweigh the rare event in their decisions (Barron and Erev 2003; Li et al. 2009). In other words, people behave as if the rare event is more likely to occur than its objective probability. Conversely, when people learn from their own experiences, they tend to underweigh rare events, behaving as though the event is less likely to occur than its objective probability (Barron and Erev 2003; Erev and Barron 2005; Fox and Hadar 2006; Hertwig et al. 2004; Li et al. 2009).
In practice, people gain information from both external descriptions and personal experience. In deciding whether to adhere to a given warning, people who have previously used the risk-causing agent are subject to potentially conflicting influ-ences from the warning and past experience. Others, possessing little or no experi-ence with the risk-causing agent, are presumably more reliant upon the warning. Research has shown that inertia tends to guide the risk-taking behavior of people who have had safe experiences with the risk-causing agent, such that they continue their exposure to the agent despite new information about associated dangers (Barron et al. 2008).
Unlike trust in the source issuing the warning and experience with the risk- causing agent, the following factors pertain to the message itself rather than factors external to it.
17.1.3 Basic Requirements: Awareness and Understanding of the Warning
Though self-evident, for a warning to be effective, its target audience must be aware of the warning and receive sufficient warning-related information. To accomplish this, the target audience must be exposed to the message, preferably through mul-tiple channels. Moreover, the target audience must have a clear understanding of the warning content. Related to message clarity is message vividness, one of the several message characteristics identified in the marketing literature as a promoter of adher-ence and suitable for widespread implementation.
17.1.4 Vividness of the Warning
Tailoring health messages to target a broad audience (e.g., all US parents of children under 2) is not trivial. Should warning messages be phrased in scientific terminol-ogy, or should regulators couch the warning in descriptive narrative underscoring the risks associated with the relevant product? Marketers have dealt with this
T. Miron-Shatz et al.
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121

question in the context of vividness—the degree to which a message incorporates imagery that makes the message come to life. Block and Keller (1997) examined vividness in the context of health communications related to sexually transmitted diseases and skin cancer. They found a preference for vivid over non-vivid material, but only when participants believed they could follow the recommendations in the message (high self-efficacy). Another moderator of the effectiveness of vivid vs. pallid messages is congruence between the vivid elements and the theme of the message (Smith and Shaffer 2000). Vivid information led to greater recall, as long as the language was congruent with the message (e.g., describing a smoker as “gasp-ing desperately for air,” p. 777). Noncongruent vivid information, on the other hand, impaired recall of the message (e.g., “the nonsmoker’s lung capacity is so powerful that the individual has the ability to inflate a balloon the size of a cow. The smoker, on the other hand, can only inflate a balloon the meager size of a golf ball,” p. 778). In another study, Lemal and Van den Bulck (2010) compared narrative messages, deemed to be more vivid, and nonnarrative messages containing the same informa-tion with a control non-message condition. Four weeks later, participants exposed to the narrative message were 2–4 times more likely to have engaged in health promot-ing actions, compared to participants in the control group. In contrast, participants exposed to the nonnarrative condition only differed from that of the control group in that they sought out more information about skin cancer. Avis and colleagues (2004) found that more women who viewed a videotape promoting mammography had a mammogram in the preceding year as compared to a group who had received a pamphlet, but this effect was not significant after controlling for baseline screening rates in both groups (75 % reported a mammogram in previous year; 90 % in previ-ous 2 years). Still, this increase was higher than for many other interventions. Further, the video group showed several longitudinal effects, whereby they became more likely to report feeling control over getting a mammogram (self-efficacy), and the percent of women who believed they had control increased over time. Also, the video group became more likely to report feeling that mammograms are beneficial and assuring. These longitudinal effects are particularly relevant in the context of the FDA warning, which was issued only once though parents are expected to adhere indefinitely. Finally, Keller and Block (1997) demonstrated the importance of resource allocation, indicating that irrespective of the vividness of the message, maximum persuasiveness will be achieved when there is a match between the resources allocated to the message (presumably high for OTC-CCM given the risk of life-threatening side effects) and those associated with the message. Thus, in addition to considering the vividness of the message, government agencies may need to determine how to achieve this resource match.
As they use large, vivid pictures to illustrate the benefits vs. harms of adherence vs. non-adherence, Sample Warnings A and B epitomize the use of vividness in communicating the intended health message. Sample Warning D also uses images, but they are less prominent and do not depict the consequences associated with adherence or non-adherence (i.e., quitting or continuing to smoke). Still, the images encourage the recipient to adopt the desired behavior of getting help.
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165

17.1.5 One-Sided vs. Two-Sided Arguments
Should a message be one-sided, or, even when making a specific claim, should a message contain arguments to the contrary? Would such a two-sided approach be more persuasive, or would it dilute the effectiveness of the message? Rucker et al. (2008) suggest that two-sided messages are more persuasive than one-sided ones. Their account is based on attitude certainty. Rucker et al. (2008) propose that consumers value not only the content of their attitudes but also how they came to form them, so that if attitudes were formed using deliberation and weighing of evidence, rather than mere adoption of a message, consumers would have greater confidence in them. In other words, under-standing how you came to have an attitude is a moderator of your certainty in it. Rucker et al. (2008) hypothesized further that making the presence of a two-sided frame salient to consumers (i.e., understanding the pros and cons and awareness that both were con-sidered by others) may lead them to believe that their attitudes are based on greater knowledge and increase certainty. This is especially the case if the negatives are present but appear inconsequential as consumers may assume that there must be few remaining unknown negative attributes and can be confident in their positive evaluation of the mes-sage position. On the other hand if negatives are absent, consumers may feel they are missing information and will therefore be less certain of the attitude formed. The authors substantiated this premise in a series of experiments, showing that two-sided messages resulted in greater attitude certainty, although the effect was mitigated by knowledge, such that attitude certainty was increased by negative information only in participants of low self-reported knowledge. This finding is consistent with the idea introduced above that experience with a product may render consumers more immune to warning mes-sages. Finally, Rucker et al. (2008) linked two-sided messages with behavior (Experiment 5), showing that individuals receiving the two- sided frame reported a greater willingness to purchase the product than those receiving the one-sided frame. Attitudes were also more predictive of behavioral intentions following a two-sided frame. As this study was run in the context of products associated with predominantly positive information, fur-ther research is needed to evaluate whether two-sided messages would also facilitate behavior and increase attitude certainty when the information on the product or service is mainly negative.
The messages conveyed by Sample Warnings A, C, and D are one-sided. However, Sample Warning B alludes to the positive consequences of non-adherence by referring to the “buzz” and playing on the phrase “takes your breath away” typi-cally associated with a positive experience.
17.1.6 Achieving Regulatory Fit: Preventive or Promotional Focus
Described by researchers as a “loss” or “gain” frame, most health messages may be phrased as preventive and cautionary (e.g., “unless you eat carrots, you may lose your eyesight”) or prophylactic and promotional (e.g., “eat carrots to preserve good eyesight”).
T. Miron-Shatz et al.
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205

This has been examined in the context of people’s regulatory focus (whether preventive or promotional) and their appraisal of response efficacy (i.e., will the behavior result in the desired outcome) or self-efficacy (i.e., can I undertake the behavior). It has been shown that a preventive regulatory focus fits better with response efficacy and a promotion regulatory focus fits better with self-efficacy, and that regulatory focus may determine the weights for response and self-efficacy (Keller 2006). Critically, regulatory focus–efficacy fit has been shown to increase the desired behavior. Thus health messages phrased in the “loss” frame and appeal-ing to response efficacy may lead to higher intentions to comply in individuals with a prevention regulatory focus, and those phrased in the “gain” frame and appealing to self-efficacy lead to better compliance individuals with a promotion regulatory focus (Keller 2006). In support, Zhao and Pechmann (2007) found that antismoking advertisements were most persuasive when the viewer’s regulatory focus, the mes-sage’s regulatory focus, and the message frame were compatible. As expected, for promotion-focused adolescents, a promotion-focused positively (“gain”) framed message was most effective at persuading them not to smoke, but for prevention- focused adolescents a prevention-focused negatively (“loss”) framed message was most effective. As previous research demonstrated that adolescents do not respond well to disease-related consequences (Hastings and MacFadyen 2002; Pechman et al. 2003), both prevention and promotion messages in the Zhao and Pechmann (2007) study focused exclusively on social consequences.
For examples of promotion-focused positively (“gain”) framed messages, see Sample Warnings A and D. For examples of prevention-focused negatively (“loss”) framed messages, see Sample Warnings B and C.
17.1.7 “Nudging” vs. Coercing
Thus far we have dealt with how warnings and alerts should be constructed to opti-mize receptiveness and efficacy. Ratner et al. (2008) raise the important issue of the legitimacy of limiting consumer freedom by disseminating messages that encourage specific actions (e.g., smoking cessation). They remind us that once health mes-sages intended to increase personal and public welfare are released to the public, the consumer is free to choose adherence or non-adherence. Thus an intervention that guides consumers to be better off without restricting their choices may be necessary to assist them in making better, unbiased decisions (Thaler and Sunstein 2003). Indeed in their book entitled Nudge: Improving decisions about health, wealth, and happiness, Thaler and Sunstein (2009) elaborate on this “libertarian paternalistic” approach—creating a choice architecture that gently “nudges” citizens, patients, or consumers in the desired direction. This approach has been applied in a variety of contexts, including organ donation (Johnson and Goldstein 2003), where a default policy of organ donation (with an opt-out option) enhances personal and societal welfare by increasing prevalence of organ donation, relative to a default policy of no organ donation (with an opt-in option). Thus increased adherence to a health
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
206
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246

warning may be obtained if the message is worded in a manner that “nudges” rather than coerces the recipient to adhere.
Sample Warning A exemplifies “nudging” rather than coercion in that it is worded to increase the recipient’s awareness of the safer option and its conse-quences without explicitly instructing the recipient to choose it. Sample Warning B is a bit more coercive, but still makes it clear that the choice is ultimately up to the recipient (i.e., “think twice”). Sample Warnings C and D are more coercive, clearly instructing the recipient to adopt the desired healthier behaviors (e.g., avoid water contact and call Quitline).
17.1.8 Excessive Deliberation
Ratner et al. (2008) discuss several natural cognitive and emotional biases that may be counteracted to assist consumers in making better medical decisions. For exam-ple, consumers who deliberate excessively tend to focus too much on less relevant criteria (Wilson and Schooler 1991), become more emotionally attached to the options (Carmon et al. 2003), and experience lower post-decision satisfaction (Dijksterhuis et al. 2006).
All of the sample warnings included in the chapter involve some degree of delib-eration represented by the textual portion of the warning poster. However, for highly vivid warnings like Sample Warnings A and B, deliberation is clearly secondary to the immediate impact of an emotionally charged image. Sample Warning C relies most upon deliberation, as it consists almost exclusively of text outlining the logical arguments in favor of adherence to the warning. Sample Warning D also relies upon deliberation in providing the recipient with a brief summary of the scientific evi-dence in favor of adherence; images are also included but (unlike Sample Warnings A and B) do not illustrate the risks of non-adherence or the benefits of adherence.
17.1.9 The “Present Bias”
Ratner et al. (2008) also review findings that people often weigh the here and now disproportionately (referred to as “the present bias”) (O’Donoghue and Rabin 1999) and appear overconfident about how they will act differently in the future (“I can stop smoking later if I want to”) (Soman 1998; Zauberman 2003; Zauberman and Lynch 2005). In the context of the FDA warning, “the present bias” may be evident as a tendency to administer the medication to the child, thereby achieving immedi-ate improvement in the child’s symptoms and discomfort despite the risk of poten-tial harmful side effects. “The present bias” may be counteracted by suggesting alternative means of relieving children’s cough and pain, and reducing their fever. Such alternative natural remedies may include honey and a humidifier to alleviate cough, and mild temperature baths to reduce fever.
T. Miron-Shatz et al.
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283

17.2 An Illustrative Case: The FDA Warning Against Over-the- Counter Cough and Cold Medication in Children Under Age 2
17.2.1 The FDA Warning: Background
The FDA is responsible for ensuring public health and safety, and, like similar agencies around the world, it does so “by assuring the safety, efficacy and security of human and veterinary drugs, biological products, medical devices, food supply, cosmetics, and products that emit radiation” (FDA 2010). While government organi-zations like the FDA are obligated to provide citizens with guidelines and warnings about possible health risks, citizens are often free to reject these recommendations. As part of its broad mission, the FDA often issues warnings about various consumer products (food, food supplements, makeup, and medications). On June 6, 2011, for example, it issued five recall, market withdrawal, and safety alerts on nonmedical products, including a Bratz makeup kit (FDA 2011a) and Kashi frozen pizzas (FDA 2011b). Given the wide range of products that may be recalled or pose a risk to con-sumers, FDA warnings are intended to reach a diverse range of audiences. This underscores the importance of creating messages that are persuasive and can con-vince citizens to modify behaviors previously considered risk-free.
Serious adverse events from OTC-CCM are relatively rare: while an estimated 95 million packages are sold each year (Brown 2008), approximately 1,500–1,600 children under 2 were admitted to emergency rooms for OTC-CCM-related issues between 2004 and 2005 (Centers for Disease Control and Prevention (CDC) 2007; Schaefer et al. 2008). In 2007, the FDA completed a review indicating that between 1969 and the fall of 2006 there were a total of 54 reported child deaths from decongestants and 69 from antihistamines, most involving children under 2 (Akhayan- Toysekani et al. 2007). Nonetheless, based on these safety data and the paucity of studies demonstrating effi-cacy in children under 2, the FDA strongly recommended “that OTC cough and cold products should not be used to treat infants and children less than 2 years of age because serious and potentially life-threatening side effects can occur from such use” (FDA 2008). In 2008, the Medicines and Healthcare Products Regulatory Agency (MHRA) of the UK issued similar guidelines discouraging use of OTC-CCM in children under 6. Given the ubiquity of OTC-CCM use (i.e., millions of bottles sold each year; Brown 2008), the FDA and MHRA recommendations attracted much media attention. Having generated substantial public interest and associated surveys and research, these warn-ings are prime candidates for examining issues related to adherence.
Were the FDA and MHRA warnings successful? For example, did they reach their intended audience (i.e., parents of children under 2), and did the recommenda-tions actually precipitate a change in behavior? Having surveyed some recommen-dations from the marketing and behavioral decision-making literature on how to construct an effective warning, we now move on to describe the actual FDA warning. The original FDA press release (FDA 2008) was based on the FDA’s review of data and discussion at a joint meeting of the Nonprescription Drugs and Pediatric
[AU3]
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325

Advisory Committees on October 18 and 19, 2007. It addressed parents and caregivers, “recommending that OTC cough and cold products should not be used to treat infants and children less than 2 years of age because serious and potentially life-threatening side effects can occur from such use.” It went on to specify what medications categories (e.g., decongestants) were subsumed under the recommen-dation. The stated reasoning of the FDA against use of the medication was twofold. First, the FDA described the perils of using the medication: “There are a wide vari-ety of rare, serious adverse events reported with cough and cold products. They include death, convulsions, rapid heart rates, and decreased levels of conscious-ness.” Then, the FDA quoted a statement by Charles Ganely, M.D., director of the FDA’s Office of Nonprescription Products, as follows: “The FDA strongly recom-mends to parents and caregivers that OTC cough and cold medicines not be used for children younger than 2. These medicines, which treat symptoms and not the under-lying condition, have not been shown to be safe or effective in children under 2.” The release then went on to indicate that use of the medication in children ages 2–11 will be determined at a later stage and offered advice for safe usage; for example: “only use measuring spoons or cups that come with the medicine or those made specially for measuring drugs.” Finally, the FDA recommended that “anyone with questions contact a physician, pharmacist or other health care professional to dis-cuss how to treat a child with a cough or cold.”
17.2.2 Did the Comply with Recommendations from the Marketing Literature?
The press release used to disseminate the FDA warning, as it appears on the agency’s website, is not written in a vivid, narrative style (though its coverage in the popular press may have been more vivid). Further, the message is conveyed in a paternalistic tone, compelling, rather than nudging, parents to avoid administering OTC-CCM to their children under 2. Based on the marketing literature reviewed above, it may be more effective for the FDA to disseminate descriptions of vivid case studies illustrating the detrimental effects of OTC-CCM, thereby exploiting the affect heuristic (Slovic et al. 2002) and targeting the experiential rather than the rational system (Epstein 1994; Loewenstein et al. 2001; Slovic et al. 2004). We also note that the recommendation included two reasons for withholding administration of the medication—that it is neither safe nor effective. The implicit equal weighting of these consequences may actually have been suboptimal because parents appear to place more weight on safety (i.e., side effects) than efficacy (e.g., fever reduction) (see findings described below from participants in the Miron-Shatz et al. 2010 study). Further, Zhao and Pechmann’s (2007) work also suggests that for a message to be effective, it must be pretested for attributes that resonate well with the target audience (e.g., social vs. health conse-quences for adolescents). Finally, the warning did not include suggestions for alterna-tive means of relieving children’s pain and cough, or for reducing fever, potentially important for minimizing “the present bias” (see above).
[AU2]
T. Miron-Shatz et al.
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366

17.2.3 Were the FDA and MHRA Warnings Effective? Experimental Evidence
Shortly after the FDA warning become public, we (Hanoch et al. 2010) surveyed US parents’ awareness of the new guidelines about OTC cough and cold medication use, their trust in the FDA, and their intention to stop or continue using the medication. We were also interested in parents’ general knowledge, perception, and behavior with regard to OTC-CCM. Overall, 377 parents of children under 6 responded to our online survey, the majority of whom (280) were female.
Of all 330 respondents without missing data, our results showed, first, that 93 (or about 30 %) had not heard about the FDA warning. Next we examined whether parents with children less than 2 years old were more likely to have heard of the FDA warning compared to parents of children over 2 years of age. Among parents of children under 2, 142 of 189 (about 75 %) had heard of the FDA warning. In comparison, 95 of 141 (about 67 %) parents with children over the age of 2 had heard of the FDA warning. Although, as part of the target audience, parents of chil-dren under 2 were more likely to be aware of the new FDA guidelines, over 25 % of them had not heard of the FDA warning.
Our results were consistent with those of a National Public Radio/Kaiser Family Foundation/Harvard School of Public Health (2007, henceforth “NPR”) study that surveyed a representative sample of US parents by telephone. In the NPR study, 32 % of parents indicated that they had heard either nothing at all or not much about the FDA warning. The NPR survey also inquired regarding whether parents under-stood the warning. They found that over a third (37 %) of parents indicated confu-sion about the warning. Thus not only was a substantial minority of parents unaware of the new recommendations, but among those who had heard of the warning, a similar percentage was unclear on how to interpret the recommendations.
Next, we examined parents’ intentions regarding further use of OTC-CCM. Of the parents who had heard the warning, about a third (46, 32.4 %) indicated that they would continue using it and a similar number of parents (43, 30.3 %) were unsure what they would do. The remaining parents (53, 37.3 %) indicated that they would adhere to the warning.
Finally, we explored the relationship between parents’ trust in the FDA and their intention to continue administrating OTC-CCM to their children. In our sample, close to 50 % of parents with children under 2 reported not trusting the FDA recom-mendations or were unsure whether to trust them. In accordance with our prediction and the literature cited above, we found that parents who expressed the least trust in the FDA recommendations were also more likely to continue using OTC-CCM. It should be noted that although the NPR (2007) study did not examine the relation-ship between adherence to the FDA recommendations and trust, it did find that as many as 71 % of parents reported trusting their child’s doctors while only 29 % reported trusting the FDA.
Our results thus highlighted the need to effectively communicate health warnings to the general public by ensuring that they actually reach their intended audience.
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409

In addition, our data highlight the role of trust in determining intention to adhere to governmental health warnings. Therefore, in keeping with the requirements outlined above for effective health communication, the FDA must both step up its efforts to reach target audiences and to do so convincingly. The challenges of creat-ing effective health communications faced by the FDA may be unique to the USA and not representative of those relevant to similar health organizations in other countries. Indeed low trust of the FDA may be attributable to its recent approval and subsequent removal of another drug for chronic pain (Harris 2005) or low public satisfaction with healthcare reform (Taylor-Gooby 2006; Taylor-Gooby and Bromley 2003). Warnings about OTC-CCM usage are a prime case study for com-paring similar warnings across countries.
The UK and USA differ with respect to their health care coverage (Laugesen and Rice 2002) and access to health care professionals, which may also affect trust in governmental health organizations. As such, in our second study (Himmelstein et al. 2011), we administered a similar survey to over 900 UK parents. This time we asked whether they had heard about the MHRA warning issued (following the FDA recommendations) in March 2008 (MHRA 2008a). Similar to our US findings, over a third (343, 36.5 %) of UK parents reported that they had not heard about the MHRA warning. Of the parents who had heard of the warning and who had given OTC-CCM to their children (349), over half (54.4 %) indicated that they did not trust the MHRA or were unsure whether to trust them. Of the 382 parents who responded to our question about adherence to the MHRA warning, over 60 % (239) indicated that they would continue giving their children OTC-CCM. Furthermore, as with the US sample, we found a positive correlation between trust and adherence. Thus, UK parents exhibited similar tendencies to those expressed by their US coun-terparts. Not only did a sizeable minority not hear about the MHRA warning, but those who had heard the warning did not seem to place a great deal of trust in it, nor were they likely to stop giving OTC-CCM to their children.
On the basis of our two studies (Hanoch et al. 2010; Himmelstein et al. 2011) reviewed thus far, it appears that both the FDA and MHRA have had difficulty reaching their target audience and changing behavior. As above, one of the chal-lenges facing the FDA and MHRA is the potential impact of varying levels of previ-ous experience with OTC-CCM. Parents who have had extensive experience with OTC-CCM might therefore be more likely to ignore the FDA recommendation. Our third study (Miron-Shatz et al. 2010) examined the effect of parental experience on adherence to the FDA OTC-CCM warning.
By measuring adherence in parents with older children—who presumably have more experience with colds and use of OTC-CCM in children under 2—and those without older children, we were able to test the following hypothesis: behavioral inertia due to safe experience with OTC-CCM would reduce adherence to the FDA warning. In our study (Miron-Shatz et al. 2010), we surveyed 218 parents of chil-dren age 2 or younger who had heard of the FDA warning. Next, to examine the impact of experience, we divided participants into two groups: experienced parents (with older children in addition to a child age 2 or younger) and inexperienced par-ents (with only a child age 2 or younger).
T. Miron-Shatz et al.
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454

In line with previous literature and our prediction that experienced parents’ decisions would be based upon behavioral inertia (Brown 2008) motivated by a his-tory of safe experiences with OTC-CCM, experienced parents (with older children in addition to a child age 2 or younger) were far less likely to adhere to the FDA warning relative to parents with only a child 2 or younger. That is, previous parental experience with OTC-CCM was a significant predictor of adherence, such that inexperienced (vs. experienced) parents were almost 3 times more likely to adhere to the FDA warning. In contrast, we found no significant differences on any of the other measures (i.e., amount of warning information received, prevalence of side effects, trust in the FDA, frequency of child’s coughs and colds). Thus, the difference in adherence rate between experienced and inexperienced parents could not be attributed to any of these factors. However, amount of information did have a differential impact upon adherence within the experience groups. Among inexperienced parents, amount of information did not affect adherence rate. In contrast, among the experienced group, adherence to the FDA warning was higher in parents who had received more information. Thus only among experienced parents did amount of information received impact their decision regarding whether to continue administering OTC-CCM to their children. Taken together, these findings indicate that future FDA communication efforts should target households with many young children, as experienced parents are least adherent and yet most receptive to additional information.
As above, trust of the government agency issuing the warning and prior safe experience with the product appear to be key determinants of adherence. Indeed in both the USA and the UK, adherence to warnings against administering OTC-CCM to young children appears related to these variables. With regard to trust, it is star-tling that approximately half of parents in a US study (Hanoch et al. 2010) and a UK study (Himmelstein et al. 2011) did not trust the warning or were unsure what to believe. Regarding experience, as with other medications (Barron et al. 2008), pre-vious safe experience with OTC-CCM in children over the age of 2 seems related to poorer adherence (Miron-Shatz et al. 2010). Based upon the marketing literature previously reviewed, we propose alternative phrasing and targeting of future warn-ings to help counter the barriers of low trust and safe past experience. We propose promising directions for further research in applying marketing principles to the design of pharmaceutical warnings and examining their impact on behavior and, subsequently, health outcomes.
17.2.4 Recommendations for Further Improving Warning Effectiveness
In this section we propose several directions for improving the effectiveness of pub-lic announcements of governmental warnings, such as the one against OTC-CCM in young children. These directions are based on our findings, as well as the marketing literature surveyed above.
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494

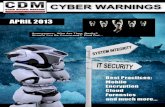
First, we propose ways to increase awareness for the warning. Drug packages, especially in the case of OTC medication, are highly visible to the consumer. In addition to direct-to-physician dissemination of the warning, if the FDA were to mandate printing the warning on the packaging (similar to Sample Warning D), it would reach every potential consumer prior to the decision to purchase and possibly at home prior to the decision to administer the medication (if the medication is stored in its original packaging). This may be more practical than depending on a pediatrician, patients’ most trusted source of information (Mechanic 2004; Brown 2009; Fig. 17.2), to convey the warning, especially in the context of over-the- counter products not necessitating a doctor’s visit prior to purchase. We (Miron-Shatz et al. 2010) found that approximately half (55 %) of parents trust warnings on packaging at least somewhat, with experienced parents slightly more likely to trust the warn-ings. (Average trust ratings of participants in the Miron-Shatz et al. (2010) study for various sources of trust are shown in Fig. 17.2, separately for experienced and inex-perienced parents.) Packaging has been used effectively for warnings in other con-texts, including smoking (Kees et al. 2006; see Sample Warning D). Similarly, to warn smokers of the associated health risks, in 2003, the World Health Organization (WHO) adopted the Framework Convention on Tobacco Control requiring that health warning information cover at least 30 % of the principal display areas on tobacco packaging (WHO 2003, Article 11). Thus, warnings such as those of the FDA and MHRA may be more effective if printed on the medication package rather than by public announcement (but see Lokker et al. 2009).
Further, regarding awareness to the warning, the FDA warning was issued in 2008 and not repeated since (though the agency recently announced removal from the market of many unapproved prescription drugs with the same ingredients as OTC-CCM; FDA 2011c). Similarly, the MHRA did not repeat its 2008 warning (though the agency extended the warning to children under 6 in 2009; MHRA 2009). Parents who initially heard these warnings may have forgotten them, and new parents may be completely unaware of the warnings. Incorporating agency warnings into drug packaging may also serve to keep them prominent in consumers’ minds. In fact, MHRA has indicated that it is working with industry to incorporate its warning into product labeling (MHRA 2009).
Second, in spite of Ratner et al.’s (2008) recommendation to minimize excessive deliberation in processing health and other public welfare messages, the FDA rec-ommendation mentioned both safety and efficacy as reasons for discontinuing OTC-CCM use. We examined the importance of various factors in parents’ delibera-tions regarding whether to administer OTC-CCM (for participants in the Miron- Shatz et al. 2010 study). Side effects were deemed “very important” by 53.6 % of the respondents. By comparison, a smaller proportion of respondents indicated that the following attributes were “very important”: reduce child’s fever, relieve child’s pain, and relieve child’s cough (40.5 %, 27.7 %, and 26.7 %, respectively). The greater parental emphasis on safety over efficiency is consistent with a more preven-tive regulatory focus and suggests that parents may have exhibited better adherence to the FDA and MHRA warnings had they been phrased in a “loss” or prevention frame appealing to response efficacy (Keller 2006), particularly prevalence of side
T. Miron-Shatz et al.
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539

effects. This way, excessive deliberation is minimized and there is a better fit with parents’ focus on prevention of side effects relative to promotion of efficacy. Pretesting for the specific attributes that resonate best may be warranted.
Third, we suggest rephrasing the warning for greater vividness, ensuring congruence between the imagery and the message, and repeating the message over time (or incorporating in packaging). Our fourth recommendation is to construct a
1
2
3
4
Pediat
rician
Pharm
acist
Nation
al org
aniza
tions
of pe
diatric
ians
The FDA
Medici
ne pa
ckag
es
Family
and f
riend
s
Advert
isemen
ts
Ave
rage
Tru
st R
atin
gExperienced ParentsInexperienced Parents
Fig. 17.2 Average parental trust of information sources by experience. “How much do you trust each of the following sources to provide you with accurate information about the safety and effectiveness of over-the-counter medicines for your children?” Experienced parents (N = 142) had older children in addition to a child age 2 or younger. Inexperienced parents (N = 76) had only a child age 2 or younger. Trust Scale: 1 = Not At All; 2 = A Little; 3 = Somewhat; 4 = A Lot. Sample warnings, Sample Warning A: A poster from the “Road Crew” organization of Wisconsin intended to reduce drunk driving by offering alternative transportation services between bars and homes in older luxury vehicles. “Road Crew” is funded by the National Highway Traffic Safety Administration, the Wisconsin Department of Transportation, and Miller Brewing. See: http://www.roadcrewonline.org/ and http://nudges.wordpress.com/how-do-you-keep-drunk-drivers-off-the- road-give-em-a-ride-home-in-a-limo/ (both accessed September 27, 2011). Sample Warning B: A poster from the FDA aimed at reducing misuse of prescrip-tion pain relievers among young people. Downloaded from: http://www.flickr.com/photos/fdapho-tos/5323869799/in/set- 72157625747043384 (accessed September 27, 2011). Sample Warning C: A warning sign from the North Coast Regional Water Quality Control Board in California about water safety issues due to toxic algae in the Klamath River. Downloaded from: http://www.klamathriver.org/images/Algae-warning-sign.jpg (accessed September 27, 2011). Sample Warning D: A cigarette pack-age warning label from the Australian Department of Health and Ageing outlining the benefits of smok-ing cessation and promoting a help line for those who wish to quit. Downloaded from: http://www.docstoc.com/docs/32770535/Quitting-will-improve-your-health (accessed September 27, 2011)
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
540
541
542
543
544
545

two-sided warning, as such messages have been shown more persuasive, augmenting recipients’ sense of choice and certainty. We also suggest incorporating alternative safe approaches (e.g., natural remedies) to counteract “the present bias.” Finally, future studies should evaluate consumer resource allocation to a warning message so that resources associated with the message can be matched to it for enhanced effectiveness.
We believe that by implementing these suggestions gleaned from the marketing literature and our own research, governmental health agencies can increase the effi-cacy of their health warnings, resulting in significantly greater adherence and reduc-ing the prevalence of adverse consequences in the general public associated with non-adherence.
References
Akhayan-Toysekani G, Chang YJ, Ahmed SR (United States Food and Drug Administration (FDA), Division of Drug Risk Evaluation) (2007) Postmarketing safety review of serious adverse events in children less than 6 years of age associated with the use of cough and cold medications. http://www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4323b1-02-FDA.pdf. Accessed 28 June 2011
Avis NE, Smith KW, Link CL, Goldman MB (2004) Increasing mammography screening among women over age 50 with a videotape intervention. Prev Med 39(3):498–506
Barnett J, Cooper H, Senior V (2007) Belief in public efficacy, trust, and attitude toward modern genetic science. Risk Anal 27(4):921–933
Barron G, Erev I (2003) Small feedback-based decisions and their limited correspondence to description-based decisions. J Behav Decis Mak 16(3):215–233
Barron G, Yechiam E (2009) The coexistence of overestimation and underweighting of rare events and the contingent recency effect. Judgm Decis Mak 4(6):447–460
Barron G, Leider S, Stack J (2008) The effect of safe experience on a warnings’ impact: sex, drugs, and rock-n-roll. Organ Behav Hum Decis Process 106(2):125–142
Block LG, Keller PA (1997) Effects of self-efficacy and vividness on the persuasiveness of health communications. J Consum Psychol 6(1):31–54
Brown D (2008) Curbing cough syrup for kids: FDA weighs limits on use of remedies. The Washington Post (October 7), HE01. http://www.washingtonpost.com/wp-dyn/content/arti cle/2008/10/03/AR2008100303245_pf.html. Accessed 28 June 2011
Brown PR (2009) The phenomenology of trust: a Schutzian analysis of the social construction of knowledge by gynaeoncology patients. Health Risk Soc 11(5):391–407
Brown P, Calnan M (2010) Braving a faceless new world? Conceptualizing trust in the pharmaceu-tical industry and its products. Health (London) 16(1):57–75
Camilleri AR, Newell BR (2009) The role of representation in experience-based choice. Judgm Decis Mak 4(7):518–529
Carmon Z, Wertenbroch K, Zeelenberg M (2003) Option attachment: when deliberating makes choosing feel like losing. J Consum Res 30(1):15–29
Casiday RE (2007) Children’s health and the social theory of risk: insights from the British mea-sles, mumps, and rubella (MMR) controversy. Soc Sci Med 65(5):1059–1070
Casiday R, Cresswell T, Wilson D, Panter-Brick C (2006) A survey of UK parental attitudes to the MMR vaccine and trust in medical authority. Vaccine 24(2):177–184
Centers for Disease Control and Prevention (CDC) (2007) Infant deaths associated with cough and cold medications—two states, 2005. MMWR. Morbidity and Mortality Weekly Report 56(1): 1–4. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5601a1.htm. Accessed 28 June 2011
[AU4]
T. Miron-Shatz et al.
546
547
548
549
550
551
552
553
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573
574
575
576
577
578
579
580
581
582
583
584
585
586
587
588
589
590
591
592

Dijksterhuis A, Bos MW, Nordgren LF, van Baaren RB (2006) On making the right choice: the deliberation-without-attention effect. Science 311(5763):1005–1007
Epstein S (1994) Integration of the cognitive and the psychodynamic unconscious. Am Psychol 49(8):709–724
Erev I, Barron G (2005) On adaptation, maximization, and reinforcement learning cognitive strate-gies. Psychol Rev 112(4):912–931
Fox CR, Hadar L (2006) ‘Decisions from experience’ = sampling error + prospect theory: recon-sidering Hertwig, Barron, Weber & Erev (2004). Judgm Decis Mak 1(2):159–161
Hadar L, Fox CR (2009) Information asymmetry in decision from description versus decision from experience. Judgm Decis Mak 4(4):317–325
Hanoch Y, Gummerum M, Miron-Shatz T, Himmelstein M (2010) Parents’ decision following the Food and Drug Administration recommendation: the case of over-the-counter cough and cold medication. Child Care Health Dev 36(6):795–804
Harris, Gardiner (2005) F.D.A. Official admits ‘lapses’ on Vioxx. The New York Times (March 5). http://www.nytimes.com/2005/03/02/politics/02fda.html. Accessed 28 June 2011
Hastings G, MacFadyen L (2002) The limitations of fear messages. Tob Control 11(11):73–75Hertwig R, Barron G, Weber EU, Erev I (2004) Decisions from experience and the effect of rare
events in risky choice. Psychol Sci 15(8):534–539Himmelstein M, Miron-Shatz T, Hanoch Y, Gummerman M (2011) Over-the-counter cough and
cold medicines for children: parental usage, perception and trust in governmental health orga-nizations. Health Risk Soc 13:451–4685
Hobson-West P (2007) ‘Trusting blindly can be the biggest risk of all’: organized resistance to childhood vaccination in the UK. Sociol Health Illn 29(2):198–215
Jackson L, Putnam W, Twohig P, Burge F, Nicol K, Cox J (2004) What has trust got to do with it? Cardiac risk reduction and family physicians’ discussions of evidence-based recommenda-tions. Health Risk Soc 6(3):239–255
Johnson EJ, Goldstein D (2003) Do defaults save lives? Science 302(5649):1338–1339Kahneman D, Tversky A (1979) Prospect theory: an analysis of decision under risk. Econometrica
47(2):263–291Kees J, Scot Burton J, Andrews C, Kozup J (2006) Tests of graphic visuals and cigarette package
warning combinations: implications for the framework convention on tobacco control. J Publ Pol Market 25(2):212–223
Keller PA (2006) Regulatory focus and efficacy of health messages. J Consum Res 33(1):109–114Keller PA, Block LG (1997) Vividness effects: a resource-matching perspective. J Consum Res
24(3):295–304Keller PA, Lehmann DR (2008) Designing effective health communications: a meta-analysis.
J Publ Pol Market 27(2):117–130Laugesen MJ, Rice T (2002) Appendix: overview of the health service systems in ten developed
countries. In: Rice T (ed) The economics of health reconsidered, 2nd edn. Health Administration Press, Chicago, pp 275–305
Lemal M, Van den Bulck J (2010) Testing the effectiveness of a skin cancer narrative in promoting positive health behavior: a pilot study. Prev Med 51(2):178–181
Li SYW, Rakow T, Newell BR (2009) Personal experience in doctor and patient decision making: from psychology to medicine. J Eval Clin Pract 15(6):993–995
Loewenstein GF, Weber EU, Hsee CK, Welch N (2001) Risk as feelings. Psychol Bull 127(2):267–286
Lokker N, Sanders L, Perrin EM, Kumar D, Finkle J, Franco V, Choi L, Johnston PE, Rothman RL (2009) Parental misinterpretations of over-the-counter pediatric cough and cold medication labels. Pediatrics 123(6):1464–1471
Mechanic D (2004) In my chosen doctor I trust: and that trust transfers from doctors to organiza-tions. Br Med J 329(7480):1418–1419
Medicines and Healthcare Products Regulatory Agency (MHRA) (2008a) Press release: updated advice—over-the-counter cough and cold medicines for young children. http://www.mhra.gov.uk/NewsCentre/Pressreleases/CON014446. Accessed June 28, 2011
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
593
594
595
596
597
598
599
600
601
602
603
604
605
606
607
608
609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624
625
626
627
628
629
630
631
632
633
634
635
636
637
638
639
640
641
642
643
644
645
646

Medicines and Healthcare Products Regulatory Agency (MHRA) (2008b) Overview—risk: benefit of OTC cough and cold medicines in children. http://www.mhra.gov.uk/home/groups/pl-p/documents/websiteresources/CON041374.pdf. Accessed 28 June 2011
Medicines and Healthcare Products Regulatory Agency (MHRA) (2009) Press release: better medicines for children’s coughs and colds. http://www.mhra.gov.uk/NewsCentre/Pressreleases/CON038902. Accessed 28 June 2011
Miron-Shatz T, Barron G, Hanoch Y, Gummerman M, Doniger GM (2010) To give or not to give: parental experience and adherence to the food and drug administration warning about over-the- counter cough and cold medicine usage. Judgm Decis Mak 5(6):428–436
Morgan MG, Fischhoff B, Bostrom A, Atman CJ (2002) Risk communication: a mental models approach. Cambridge University Press, New York
National Public Radio/Kaiser Family Foundation/Harvard School of Public Health (2007) Children’s OTC cold medicines: the public, and parents weigh in. http://www.kff.org/kaiser-polls/pomr121307pkg.cfm. Accessed 28 June 2011
O’Donoghue T, Rabin M (1999) Doing it now or later. Am Econ Rev 89(1):103–124O’Neill O (2002) A question of trust: the BBC Reith lectures 2002. Cambridge University Press,
CambridgePechman C, Zhao G, Goldberg ME, Reibling ET (2003) What to convey in antismoking advertise-
ments for adolescents: the use of protection motivation theory to identify effective message themes. J Market 67(2):1–18
Ratner RK, Soman D, Zauberman G, Ariely D, Carmon Z, Keller PA, Kyu Kim B, Lin F, Malkoc S, Small DA, Wertenbroch K (2008) How behavioral decision research can enhance consumer welfare: from freedom of choice to paternalistic intervention. Market Lett 19(3–4):383–397
Rucker DD, Petty RE, Brinol P (2008) What’s in a frame anyway?: A meta-cognitive analysis of the impact of one versus two-sided message framing on attitude certainty. J Consum Psychol 18(2):137–149
Schaefer MK, Shehab N, Cohen AL, Budnitz DS (2008) Adverse events from cough and cold medications in children. Pediatrics 121(4):783–787
Slovic P, Finucane M, Peters E, MacGregor DG (2002) The affect heuristic. In: Gilovich T, Griffin D, Kahnemann D (eds) Heuristics and biases: the psychology of intuitive judgment. Cambridge University Press, New York, pp 397–420
Slovic P, Finucane ML, Peters E, MacGregor DG (2004) Risk as analysis and risk as feelings: some thoughts about affect, reason, risk, and rationality. Risk Anal 24(2):311–322
Smith SM, Shaffer DR (2000) Vividness can undermine or enhance message processing: the mod-erating role of vividness congruency. Pers Soc Psychol Bull 26(7):769–779
Soman D (1998) The illusion of delayed incentives: evaluating future effort-money transactions. J Market Res 35(4):427–437
Taylor-Gooby P (2006) Trust, risk and health care reform. Health Risk Soc 8(2):97–103Taylor-Gooby CH, Bromley C (2003) Querulous citizens: welfare knowledge and the limits to
welfare reform. Soc Pol Admin 37(1):1–20Thaler RH, Sunstein CR (2003) Behavioral economics, public policy, and paternalism: libertarian
paternalism. Am Econ Rev 93(2):175–179Thaler RH, Sunstein CR (2009) Nudge: improving decisions about health, wealth, and happiness.
Penguin, LondonUnited States Food and Drug Administration (FDA) (2008) FDA releases recommendations
regarding use of over-the-counter cough and cold products: products should not be used in children under 2 years of age; evaluation continues in older populations. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2008/ucm116839.htm. Accessed 28 June 2011
United States Food and Drug Administration (FDA) (2010) About FDA: what we do http://www.fda.gov/aboutfda/whatwedo/default.htm. Accessed 28 June 2011
United States Food and Drug Administration (FDA) (2011a) MGA recalls item #504788 Bratz makeup design sketch book because of possible health risk. http://www.fda.gov/Safety/Recalls/ucm258088.htm. Accessed 28 June 2011
T. Miron-Shatz et al.
647
648
649
650
651
652
653
654
655
656
657
658
659
660
661
662
663
664
665
666
667
668
669
670
671
672
673
674
675
676
677
678
679
680
681
682
683
684
685
686
687
688
689
690
691
692
693
694
695
696
697
698
699

United States Food and Drug Administration (FDA) (2011b) Kashi recalls select frozen pizzas because they may contain plastic fragments. http://www.fda.gov/Safety/Recalls/ucm258012.htm. Accessed 28 June 2011
United States Food and Drug Administration (FDA) (2011c) FDA intends to remove unapproved drugs from market. http://www.fda.gov/downloads/ForConsumers/ConsumerUpdates/ucm245228.pdf. Accessed 28 June 2011
Walls J, Pidgeon N, Weyman A, Horlick-Jones T (2004) Critical trust: understanding lay percep-tions of health and safety risk regulation. Health Risk Soc 6(2):133–150
Williams DJ, Noyes JM (2007) How does our perception of risk influence decision-making? Implications for the design of risk information. Theor Issues Ergon Sci 8(1):1–35
Wilson TD, Schooler JW (1991) Thinking too much: introspection can reduce the quality of pref-erence and decisions. J Pers Soc Psychol 60(2):181–192
World Health Organization (WHO) (2003) WHO framework convention on tobacco control http://whqlibdoc.who.int/publications/2003/9241591013.pdf. Accessed 28 June 2011
Zauberman G (2003) The intertemporal dynamics of consumer lock-in. J Consum Res 30(3):405–419
Zauberman G, Lynch JG Jr (2005) Resource slack and propensity to discount delayed investments of time versus money. J Exp Psychol Gen 134(1):23–37
Zhao G, Pechmann C (2007) The impact of regulatory focus on adolescents’ response to antismok-ing advertising campaigns. J Market Res 44(4):671–687
17 Factors Affecting Adherence to Governmental Health Warnings and the Case…
700
701
702
703
704
705
706
707
708
709
710
711
712
713
714
715
716
717
718
719

Author QueriesChapter No.: 17 0001997877
Queries Details Required Author’s Response
AU1 Please check whether the head levels are set appropriately.
AU2 Please check the heading “Did the Comply … Marketing Literature?” for clarity.
AU3 Please check if the edit made in the sentence “On June … (FDA 2011b).” is appropriate.
AU4 Following references: Barron and Yechiam (2009); Camilleri and Newell (2009); Hadar and Fox (2009); MHRA (2008b) are not cited in text. Please cite.
Copyright © 2022 FDOKUMEN