
Extracorporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is...
9
Extra-corporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is still to be learned A. Zonta a, , T. Pinelli d,e , U. Prati b , L. Roveda b , C. Ferrari a , A.M. Clerici a , C. Zonta a , G. Mazzini c , P. Dionigi a , S. Altieri d,e , S. Bortolussi d,e , P. Bruschi d , F. Fossati d,e a Department of Surgery, University of Pavia, Pavia, Italy b Oncologic Surgery, Cancer Center of Excellence Fond. ‘‘T. Campanella’’, Catanzaro, Italy c Department of Animal Biol., IGM-CNR Histochemistry and Cytometry Section, Pavia, Italy d Department of Nuclear and Theoretical Physics, University of Pavia, Pavia, Italy e National Institute of Nuclear Physics (INFN) Pavia Section, Pavia, Italy article info Keywords: Boron neutron capture therapy Liver BNCT BPA Recurrences abstract Almost eight years ago, in December 2001, we performed for the first time in the world thermal neutron irradiation on an isolated liver of a patient. The organ was affected by diffuse metastases of a colon carcinoma and had been previously loaded with a 10 B compound. In July 2003, the same procedure was applied again on a patient for the treatment of unresectable and incurable hepatic metastases of a carcinoma of the rectum. Both patients are dead at present. Now we can analyze in depth the clinical history of these patients and evaluate the effectiveness of this therapy. From this exciting experience we learned much, and we also found out about complications till then unknown, which need to be studied and addressed experimentally. Unfortunately we can base our conclusions just on the experience we had with these two patients. We could have been much more detailed and firm in our statements if the number of clinical cases was larger. The BNCT Pavia project has been suspended, but it is more than likely to resume in a short time. Good findings were many. The procedure is feasible; the original concept of complete immersion of the diseased liver in a homogeneous neutron field proved effective and winning. The tumor masses resulted completely necrotic and unknown metastases too appeared radically treated; healthy hepatic tissue was preserved from both morphological and functional points of view; no symptoms of cirrhosis appeared even four years after treatment. For the long term surviving patient, quality of life was excellent. Other findings require to be tackled in depth. The ‘‘post-irradiation syndrome’’ we observed in both patients, with identical symptoms and biochemical derangements, creates a dramatic—even though totally reversible—clinical condition, that is the probable cause of death for our second patient, suffering from cardiomyopathy, 33 days after treatment. For the first patient, recurrences were a late yet fatal complication, for which even a further surgical revision was ineffective. We offer some hypotheses about their origin and possible prevention. & 2009 Elsevier Ltd. All rights reserved. 1. Introduction About the end of nineties Pinelli and Zonta (Pinelli et al., 1996, 2001) proposed and then, in 2001, performed the first in the world extra-corporeal application of BNCT to an isolated liver, suffering from diffuse metastases. This therapeutic project had been conceived some twenty years before and elaborated in detail during several long series of experimental researches (Pinelli et al., 2002). It deals with a new concept from many points of view. For the first time an abdominal organ is treated with BNCT; an extra-corporeal irradiation is carried out; the target of thermal neutrons is the liver, which is known to be highly sensitive to radiations. Nevertheless two other features of the therapeutic proposal are noteworthy. The neutron treatment is performed using not a collimated beam, as in traditional BNCT applications, but a neutron isotropic field. Moreover, the diseased part of the organ is pre-treated, i.e. (a) deprived of all its blood content through washing and (b) made hypothermic at a temperature near 4 1C by flushing it with a B-free, chilled Wisconsin solution. This modality of neutron irradiation warrants several precious advantages, improving the specificity, selectivity and efficacy of BNCT. ARTICLE IN PRESS Contents lists available at ScienceDirect journal homepage: www.elsevier.com/locate/apradiso Applied Radiation and Isotopes 0969-8043/$ - see front matter & 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.apradiso.2009.03.087 Corresponding author. E-mail address: [email protected] (A. Zonta). Applied Radiation and Isotopes 67 (2009) S67–S75
Transcript of Extracorporeal liver BNCT for the treatment of diffuse metastases: What was learned and what is...

ARTICLE IN PRESS
Applied Radiation and Isotopes 67 (2009) S67–S75
Contents lists available at ScienceDirect
Applied Radiation and Isotopes
0969-80
doi:10.1
� Corr
E-m
journal homepage: www.elsevier.com/locate/apradiso
Extra-corporeal liver BNCT for the treatment of diffuse metastases: What waslearned and what is still to be learned
A. Zonta a,�, T. Pinelli d,e, U. Prati b, L. Roveda b, C. Ferrari a, A.M. Clerici a, C. Zonta a, G. Mazzini c,P. Dionigi a, S. Altieri d,e, S. Bortolussi d,e, P. Bruschi d, F. Fossati d,e
a Department of Surgery, University of Pavia, Pavia, Italyb Oncologic Surgery, Cancer Center of Excellence Fond. ‘‘T. Campanella’’, Catanzaro, Italyc Department of Animal Biol., IGM-CNR Histochemistry and Cytometry Section, Pavia, Italyd Department of Nuclear and Theoretical Physics, University of Pavia, Pavia, Italye National Institute of Nuclear Physics (INFN) Pavia Section, Pavia, Italy
a r t i c l e i n f o
Keywords:
Boron neutron capture therapy
Liver BNCT
BPA
Recurrences
43/$ - see front matter & 2009 Elsevier Ltd. A
016/j.apradiso.2009.03.087
esponding author.
ail address: [email protected] (A. Zonta).
a b s t r a c t
Almost eight years ago, in December 2001, we performed for the first time in the world thermal neutron
irradiation on an isolated liver of a patient. The organ was affected by diffuse metastases of a colon
carcinoma and had been previously loaded with a 10B compound. In July 2003, the same procedure was
applied again on a patient for the treatment of unresectable and incurable hepatic metastases of a
carcinoma of the rectum. Both patients are dead at present. Now we can analyze in depth the clinical
history of these patients and evaluate the effectiveness of this therapy.
From this exciting experience we learned much, and we also found out about complications till then
unknown, which need to be studied and addressed experimentally.
Unfortunately we can base our conclusions just on the experience we had with these two patients.
We could have been much more detailed and firm in our statements if the number of clinical cases was
larger. The BNCT Pavia project has been suspended, but it is more than likely to resume in a short time.
Good findings were many. The procedure is feasible; the original concept of complete immersion of
the diseased liver in a homogeneous neutron field proved effective and winning. The tumor masses
resulted completely necrotic and unknown metastases too appeared radically treated; healthy hepatic
tissue was preserved from both morphological and functional points of view; no symptoms of cirrhosis
appeared even four years after treatment. For the long term surviving patient, quality of life was
excellent.
Other findings require to be tackled in depth. The ‘‘post-irradiation syndrome’’ we observed in both
patients, with identical symptoms and biochemical derangements, creates a dramatic—even though
totally reversible—clinical condition, that is the probable cause of death for our second patient,
suffering from cardiomyopathy, 33 days after treatment. For the first patient, recurrences were a late yet
fatal complication, for which even a further surgical revision was ineffective. We offer some hypotheses
about their origin and possible prevention.
& 2009 Elsevier Ltd. All rights reserved.
1. Introduction
About the end of nineties Pinelli and Zonta (Pinelli et al., 1996,2001) proposed and then, in 2001, performed the first in the worldextra-corporeal application of BNCT to an isolated liver, sufferingfrom diffuse metastases. This therapeutic project had beenconceived some twenty years before and elaborated in detailduring several long series of experimental researches (Pinelliet al., 2002). It deals with a new concept from many points of
ll rights reserved.
view. For the first time an abdominal organ is treated with BNCT;an extra-corporeal irradiation is carried out; the target of thermalneutrons is the liver, which is known to be highly sensitive toradiations. Nevertheless two other features of the therapeuticproposal are noteworthy. The neutron treatment is performedusing not a collimated beam, as in traditional BNCT applications,but a neutron isotropic field. Moreover, the diseased part of theorgan is pre-treated, i.e. (a) deprived of all its blood contentthrough washing and (b) made hypothermic at a temperaturenear 4 1C by flushing it with a B-free, chilled Wisconsin solution.This modality of neutron irradiation warrants several preciousadvantages, improving the specificity, selectivity and efficacy ofBNCT.

ARTICLE IN PRESS
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75S68
Actually, in comparison with traditional BNCT applications, theintrinsic specificity of neutron irradiation is enhanced by avoidingthe dangerous damage to endothelial cells and lowering to aminimum the background irradiation: these results derive fromthe removal of blood content before irradiation.
Secondly in our project the selectivity of action is assuredbecause the diseased organ, after being loaded with the boroncompound, is extracted, dipped into a homogeneous neutron fieldand then reconnected. In this way any interfering effect due toirradiation of other organs or tissues is abolished.
Finally the efficacy of BNCT is exalted because not only aportion but the whole volume of the diseased organ is exposed tothe neutron flux so that the dose of the absorbed radiation is thesame in any known or unknown tumor nodule, depending merelyon boron concentration reached in its cells.
Table 1Neutron flux and g dose in air in the liver irradiation position.
Fth (cm�2 s�1) o0.2 eV 1.4�1010
Fepi 0.2 eV–0.5 MeV 3.3�107
Ffast 43.5 MeV 2.0�106
Ffast 48.2 MeV 9.4�104
2 �13
2. The radio-surgical procedure
In December 2001, after the approval of the project ascompassionate therapeutic action by the Ethics Committee ofPavia San Matteo Hospital and the Italian Ministry of Health, weperformed the first clinical application of BNCT on an isolated
Fig. 1. Vertical section of the reactor, showing the (a) core and the liver irradiation
position inside the graphite thermal column. In the enlargement (b) the bismuth
screens are visible.
human liver. In 2003 a second patient was submitted by us to thesame procedure.
According to the guidelines approved for the clinical protocol,the candidates should be of young age (o55 years), with liver-only metastases of a colon carcinoma already radically excisedand should have all vital organs in good health without seriousimpairment of liver functions.
The adopted procedure consisted basically of three phases. Theearly surgical phase includes the liver perfusion for 2 h (h) with asolution of 10boronophenylalanine (10BPA), a biopsy of metastaticand normal hepatic tissue after 1 h of perfusion and anotherbiopsy at the end of it in order to verify a favorable concentrationratio of 10B between the samples (higher than 4:1) and then thehepatectomy with contemporary starting of a veno-venous extra-corporeal circulation (inferior cava—superior caval shunt and
Dg (Gy cm ) 1.6�10
8
7
6
5
4
3
2
1
00 2 4 6 8 10 12
t (hours)
T (t)
Fig. 2. Behavior of the boron concentration ratio between tumor and normal liver
at different times after BPA infusion in a rat model.
Table 2Values of the boron concentrations and of the doses produced by a neutron fluence
cn ¼ 4�1012 cm�2 in the normal liver and in the tumor of the two treated
patients.
Boron concentration (ppm) Absorbed dose (Gy)
First patient Second patient First patient Second patient
Tumor 4772 4575 1871 1871
Liver 871 871 670.3 670.3
Tumor/liver 5.9 5.6 3 3
ARTICLE IN PRESS
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75 S69
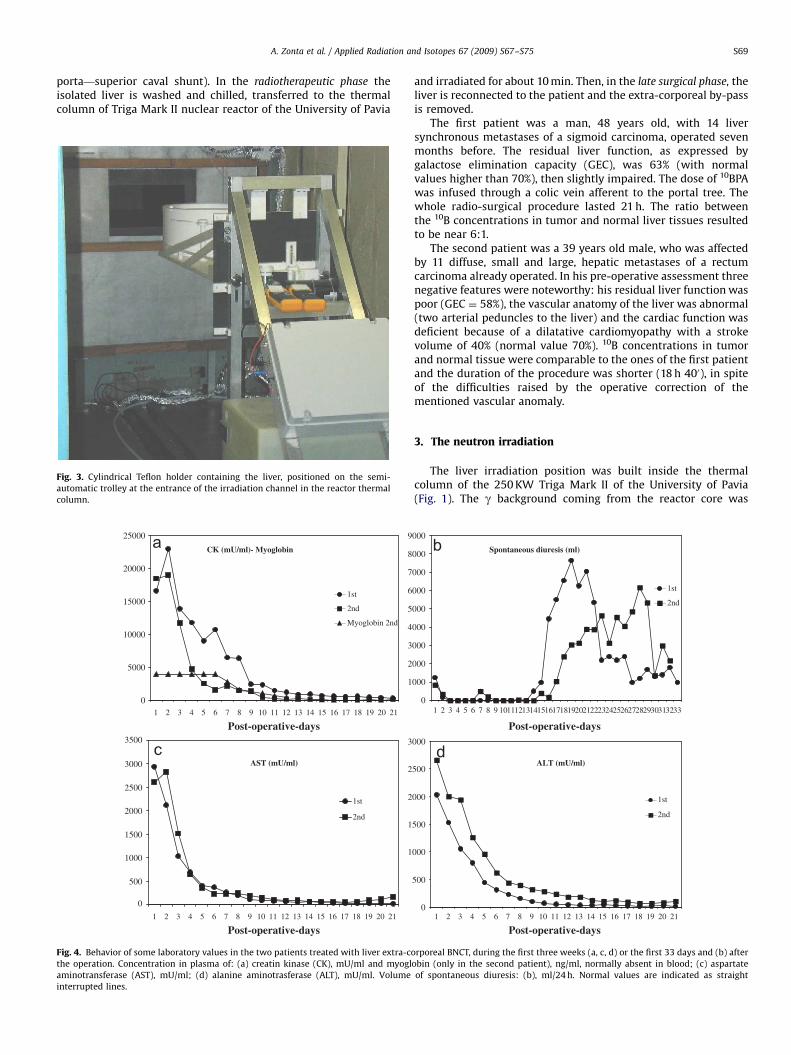
porta—superior caval shunt). In the radiotherapeutic phase theisolated liver is washed and chilled, transferred to the thermalcolumn of Triga Mark II nuclear reactor of the University of Pavia
Fig. 3. Cylindrical Teflon holder containing the liver, positioned on the semi-
automatic trolley at the entrance of the irradiation channel in the reactor thermal
column.
0
5000
10000
15000
20000
25000
1
1st
2nd
Myoglobin 2nd
CK (mU/ml)- Myoglobin
0
500
1000
1500
2000
2500
3000
3500
1st
2nd
AST (mU/ml)
1
2
3
4
5
6
7
8
9
1
1
2
2
3
Post-operative-days2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
1
Post-operative-days2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Fig. 4. Behavior of some laboratory values in the two patients treated with liver extra-co
the operation. Concentration in plasma of: (a) creatin kinase (CK), mU/ml and myogl
aminotransferase (AST), mU/ml; (d) alanine aminotrasferase (ALT), mU/ml. Volume
interrupted lines.
and irradiated for about 10 min. Then, in the late surgical phase, theliver is reconnected to the patient and the extra-corporeal by-passis removed.
The first patient was a man, 48 years old, with 14 liversynchronous metastases of a sigmoid carcinoma, operated sevenmonths before. The residual liver function, as expressed bygalactose elimination capacity (GEC), was 63% (with normalvalues higher than 70%), then slightly impaired. The dose of 10BPAwas infused through a colic vein afferent to the portal tree. Thewhole radio-surgical procedure lasted 21 h. The ratio betweenthe 10B concentrations in tumor and normal liver tissues resultedto be near 6:1.
The second patient was a 39 years old male, who was affectedby 11 diffuse, small and large, hepatic metastases of a rectumcarcinoma already operated. In his pre-operative assessment threenegative features were noteworthy: his residual liver function waspoor (GEC ¼ 58%), the vascular anatomy of the liver was abnormal(two arterial peduncles to the liver) and the cardiac function wasdeficient because of a dilatative cardiomyopathy with a strokevolume of 40% (normal value 70%). 10B concentrations in tumorand normal tissue were comparable to the ones of the first patientand the duration of the procedure was shorter (18 h 400), in spiteof the difficulties raised by the operative correction of thementioned vascular anomaly.
3. The neutron irradiation
The liver irradiation position was built inside the thermalcolumn of the 250 KW Triga Mark II of the University of Pavia(Fig. 1). The g background coming from the reactor core was
0
000
000
000
000
000
000
000
000
000
1
1st
2nd
Spontaneous diuresis (ml)
0
500
000
500
000
500
000
1st
2nd
ALT (mU/ml)
1
Post-operative-days2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Post-operative-days
2 3 4 5 6 7 8 9 101112131415161718192021222324252627282930313233
rporeal BNCT, during the first three weeks (a, c, d) or the first 33 days and (b) after
obin (only in the second patient), ng/ml, normally absent in blood; (c) aspartate
of spontaneous diuresis: (b), ml/24 h. Normal values are indicated as straight

ARTICLE IN PRESS
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75S70
lowered with two bismuth screens, whose overall thickness was20 cm. In the irradiation channel the neutron flux was measuredwith Au and Cu wires and foils and the g dose was measured byBeO TLD dosimeters. The results of in-air measurements in theliver irradiation position are listed in Table 1.
For the boron concentration in hepatic tissues a method basedon the a particles spectrometry was developed. Thin tissuesamples are irradiated in a position of the thermal column andthe a particles emitted from the reaction 10B(n, a)7Li are detected.The measurement method is described in (Chiaraviglio et al. 1989;Wittig et al., 2008). The a spectrometry was coupled to animaging technique based on neutron autoradiography in order toget precise information about the boron biodistribution inside theanalyzed samples (Altieri et al., 2008).
With these techniques, a boron pharmacokinetic study wasperformed on a rat animal model with diffuse hepatic metastasesinduced by a colon adenocarcinoma cell line (Roveda et al., 2004).Hundred rats were treated with BPA (300 mg/kg) and sacrificedafter different interval of times from the infusion. Both tumoraland healthy liver samples were frozen in liquid nitrogen forsubsequent boron concentration analysis. In Fig. 2 the ratio of theboron concentration between tumor and normal liver tissue as a
1
2
3
4
5
6
0
5
10
15
20
25
1
TNF
n
2
4
6
8
10
12
0
100
200
300
400
500
600
700
800
900
1
VEGF
n
2 3 4 5 6 7 8 9 10
2 3 4 5 6 7 8 9 10
Fig. 5. Values for some humoral mediators of clinical importance in the second pat
operation. Concentration in plasma (pg/ml) of: (a) tumor necrosis factor (TNF); (b) interl
factor (HGF). n ¼ number of sequential samples:
n Time of sampling
1 Pre-operative value before anaesthesia
2 10 min after the end of BPA intra-venous administrat
3 1 h after starting of extra-corporeal circulation (liver-
4 6 h after starting of extra-corporeal circulation (liver-
5 Liver reconnection completed
6 2 h after liver reconnection
7 4 h after liver reconnection
8 6 h after liver reconnection
9 8 h after liver reconnection
10 2nd p.o.d. (in the surgical intensive care unit)
function of the time after BPA infusion is showed. Between 2 and4 h, the ratio is higher than 5. The statistical analysis of the dataevidenced that, after 2 h from the infusion, the probability to havea ratio equal or higher than 4 is 80%.
When the boron concentrations are known in the liver (CH) andin the tumor (CT), the respective doses DH and DT produced by aneutron fluence cn ¼ 4�1012 cm�2 are calculated with therelation:
DH;TðGyÞ ¼ 3:6þ 0:32 CH;T ðppmÞ
In Table 2 the concentrations measured in liver and tumorsamples of the two patients are listed together with the dosescorresponding to a neutron fluence cn ¼ 4�1012 cm�2.
For the irradiation, the liver was located inside two Teflonbags then positioned in a circular Teflon container. A semi-automatic trolley (Fig. 3) was used to position the liver insidethe irradiation channel. Using a remote control, the cylindricalholder was rotated by 1801 halfway through the irradiationtime, in order to increase the uniformity of the thermal neutronflux distribution inside the organ (Bortolussi and Altieri,2007).
0
00
00
00
00
00
00
1
0
000
000
000
000
000
000
1
HGF
n
IL-6
n2 3 4 5 6 7 8 9 10
2 3 4 5 6 7 8 9 10
ient treated with liver extra-corporeal BNCT, during the first two days after the
eukin 6 (IL-6); (c) vascular endothelial growth factor (VEGF); (d) hepatocyte growth
H of the operation day, 1st or 2nd p.o.d.
08:25
ion 15:00
less phase) 18:00
less phase) 23:00
00:15
02:00
04:15
06:10
08:00
16:00

ARTICLE IN PRESS
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75 S71
4. The post-treatment follow-up
The first 3 weeks after BNCT were very similar in both patientsand proved the heavy impact of the procedure on their clinicalconditions. The patients, who were admitted after the operationto a surgical intensive care unit, remained in general anaesthesiawith controlled ventilation for a period of three and four weeks;then a gradual reversal of anaesthetic agents was adopted untilthe post-operative recovery. During this period the most evidentsymptoms were characterized for both patients by rabdomyolysis,with early brutal elevation of creatin kinase and myoglobin inblood (Fig. 4a), altered endothelial barrier permeability, with hugeimbibition of subcutaneous tissue, especially in the face, andmental confusion. Other signs of this complex derangement weredue to liver insufficiency with jaundice and renal failure from alikely acute tubular necrosis with transitory anuria (Fig. 4b),which required renal replacement therapy (extra-corporealhemodialysis). Laboratory tests showed an early importantincrease of the values for hepatic microsomal enzymes likeaspartate aminotransferase AST (Fig. 4c) and alanine amino-transferase ALT (Fig. 4d). These clinical and hematochemicalaberrations were present in both patients with the same temporalcadence and evolution towards recovery. We are led to believethey are expression of a post-irradiation syndrome mediated by arelease of a great amount of cytokines as an effect of cellularnecrosis (Zonta et al., 2006).
Only in the second patient we evaluated some of the mostpowerful humoral mediators of clinical interest. The determina-tions were sequential during the first 48 h after BNCT, noting thatthe first analysis is pre-operative, the second one refers to the endof BPA perfusion, the third and fourth are in the liver-less phase,the fifth to ninth are at 0, 2, 4, 6 and 8 h after liver reconnectionand the last one coincides with the 2nd p.o.d.. For tumor necrosis
Fig. 6. CT scans in the first patient treated with liver extra-corporeal BNCT. Modification
BNCT (b, d) CT scans. From (Zonta et al., 2006), mod.
factor TNF there was a late and important increment afterreconnection. For interleukin 6 IL-6 the raise was early, verymarked and persistent. Vascular endothelial growth factor VEGF,which is normally non-appreciable, showed also an importantincrement after reconnection of the irradiated liver. Hepatocyte
growth factor HGF, after a normal value in the pre-operativesample, demonstrated always supra-maximal values with a trendtowards reduction in the last samples (Fig. 5).
In the same period of time we found a similar evolution of theliver lesions in both patients, as proved by sequential CT scans ofthe abdomen. In the first patient, already at the 7th day afterBNCT, areas of tissue necrosis are present corresponding to the sitewhere tumor nodules had been documented pre-operatively. Theyare larger than the previous metastases, showing a wide damagedue to neutron irradiation and peri-focal edema (Fig. 6).
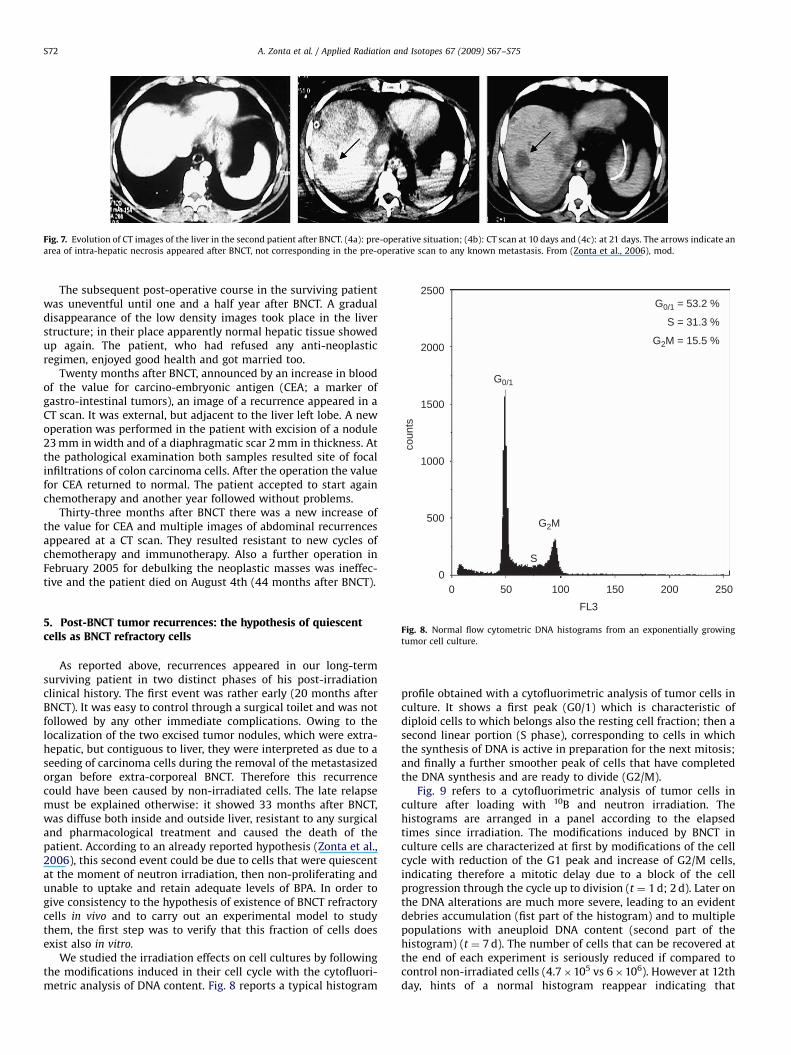
Also in the second patient the complete evolution towardsnecrosis of the tumor nodules is well documented in CT scans atthe 10th and 21st p.o.d. (Fig. 7). It is worth of mention that smallerareas of necrosis are also apparent where no tumor nodules werepre-operatively evident: we think it likely that sub-macroscopictumor foci were also damaged up to necrosis.
In the fourth week after BNCT the clinical evolution of the twopatients became different. The first one kept on improving inhealth with a progressive return to normal of all alteredlaboratory values. In particular neoplastic markers turned nega-tive and also the residual liver function became normal (73% forGEC). The patient was discharged 40 days after BNCT in a goodstate of health. The second patient was suffering from a dilatativecardiomyopathy and the clinical situation worsened towards theend of the first month: he indeed incurred subsequent circulatorycomplications consisting in a thrombosis of the hepatic artery andlater on a cardiac congestive failure, which caused his death onthe 33th p.o.d.
s of images on a cranial (3a, b) and caudal (3c, d) level in pre-BNCT (3a, c) and post-
ARTICLE IN PRESS
Fig. 7. Evolution of CT images of the liver in the second patient after BNCT. (4a): pre-operative situation; (4b): CT scan at 10 days and (4c): at 21 days. The arrows indicate an
area of intra-hepatic necrosis appeared after BNCT, not corresponding in the pre-operative scan to any known metastasis. From (Zonta et al., 2006), mod.
2500
2000
1500
1000
500
0S
G2M
G0/1
G0/1 = 53.2 %
S = 31.3 %
G2M = 15.5 %
coun
ts
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75S72
The subsequent post-operative course in the surviving patientwas uneventful until one and a half year after BNCT. A gradualdisappearance of the low density images took place in the liverstructure; in their place apparently normal hepatic tissue showedup again. The patient, who had refused any anti-neoplasticregimen, enjoyed good health and got married too.
Twenty months after BNCT, announced by an increase in bloodof the value for carcino-embryonic antigen (CEA; a marker ofgastro-intestinal tumors), an image of a recurrence appeared in aCT scan. It was external, but adjacent to the liver left lobe. A newoperation was performed in the patient with excision of a nodule23 mm in width and of a diaphragmatic scar 2 mm in thickness. Atthe pathological examination both samples resulted site of focalinfiltrations of colon carcinoma cells. After the operation the valuefor CEA returned to normal. The patient accepted to start againchemotherapy and another year followed without problems.
Thirty-three months after BNCT there was a new increase ofthe value for CEA and multiple images of abdominal recurrencesappeared at a CT scan. They resulted resistant to new cycles ofchemotherapy and immunotherapy. Also a further operation inFebruary 2005 for debulking the neoplastic masses was ineffec-tive and the patient died on August 4th (44 months after BNCT).
0 50 100 150 200 250FL3
Fig. 8. Normal flow cytometric DNA histograms from an exponentially growing
tumor cell culture.
5. Post-BNCT tumor recurrences: the hypothesis of quiescentcells as BNCT refractory cells
As reported above, recurrences appeared in our long-termsurviving patient in two distinct phases of his post-irradiationclinical history. The first event was rather early (20 months afterBNCT). It was easy to control through a surgical toilet and was notfollowed by any other immediate complications. Owing to thelocalization of the two excised tumor nodules, which were extra-hepatic, but contiguous to liver, they were interpreted as due to aseeding of carcinoma cells during the removal of the metastasizedorgan before extra-corporeal BNCT. Therefore this recurrencecould have been caused by non-irradiated cells. The late relapsemust be explained otherwise: it showed 33 months after BNCT,was diffuse both inside and outside liver, resistant to any surgicaland pharmacological treatment and caused the death of thepatient. According to an already reported hypothesis (Zonta et al.,2006), this second event could be due to cells that were quiescentat the moment of neutron irradiation, then non-proliferating andunable to uptake and retain adequate levels of BPA. In order togive consistency to the hypothesis of existence of BNCT refractorycells in vivo and to carry out an experimental model to studythem, the first step was to verify that this fraction of cells doesexist also in vitro.
We studied the irradiation effects on cell cultures by followingthe modifications induced in their cell cycle with the cytofluori-metric analysis of DNA content. Fig. 8 reports a typical histogram
profile obtained with a cytofluorimetric analysis of tumor cells inculture. It shows a first peak (G0/1) which is characteristic ofdiploid cells to which belongs also the resting cell fraction; then asecond linear portion (S phase), corresponding to cells in whichthe synthesis of DNA is active in preparation for the next mitosis;and finally a further smoother peak of cells that have completedthe DNA synthesis and are ready to divide (G2/M).
Fig. 9 refers to a cytofluorimetric analysis of tumor cells inculture after loading with 10B and neutron irradiation. Thehistograms are arranged in a panel according to the elapsedtimes since irradiation. The modifications induced by BNCT inculture cells are characterized at first by modifications of the cellcycle with reduction of the G1 peak and increase of G2/M cells,indicating therefore a mitotic delay due to a block of the cellprogression through the cycle up to division (t ¼ 1 d; 2 d). Later onthe DNA alterations are much more severe, leading to an evidentdebries accumulation (fist part of the histogram) and to multiplepopulations with aneuploid DNA content (second part of thehistogram) (t ¼ 7 d). The number of cells that can be recovered atthe end of each experiment is seriously reduced if compared tocontrol non-irradiated cells (4.7�105 vs 6�106). However at 12thday, hints of a normal histogram reappear indicating that

ARTICLE IN PRESS
500
400
300
200
100
00 50 100 150 200 250
t = 7d
coun
ts
t = 1d
400
320
240
160
80
00 50 100 150 200 250
t = 2d
t = 12d400
320
240
160
80
0
coun
ts
1 10 100 1000
FL3
3200
2560
1920
1280
640
010 100 1000
FL3
coun
tsco
unts
G0/1 = 31.5 %
G2M = 46.4 %
n = 4.7x105
G0/1 = 22.9 %
G2M = 59.7 %
n = 4x105
G0/1 = 7 %
n = 4.7 x 105
G0/1 = 61.1 %
G2M = 20.1 %
n = 1.4x106
Fig. 9. DNA content analyses performed on tumor cell line culture at subsequent times after BNCT treatment (from 1 to 21 days). The % values refer to the proportion of the
proliferating cells (G2/M) to the whole of the cells in culture. The numbers indicate the millions of cells recollected from each flask at the end of the experiment. From
(Zonta et al, 2006), mod.
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75 S73
neoplastic cells, spared by neutron irradiation, have restored anormal tumor population as evident at 20 days.
The number of these ‘‘resistant’’ cells was quantified after astandard irradiation with the plating efficiency test, whichmeasures the capability of cells to form colonies in culture. Thisvalue decreases in parallel to the increase in intra-cellularretained 10B concentration and gets to zero when this concentra-tion reaches a value of 100 ppm. Then the ‘‘resistant’’ cells are nota fixed fraction of tumor cells in a culture, but their numberdepends on the condition of irradiation, i.e. on the absorbedradiation dose (Ferrari et al., 2008).
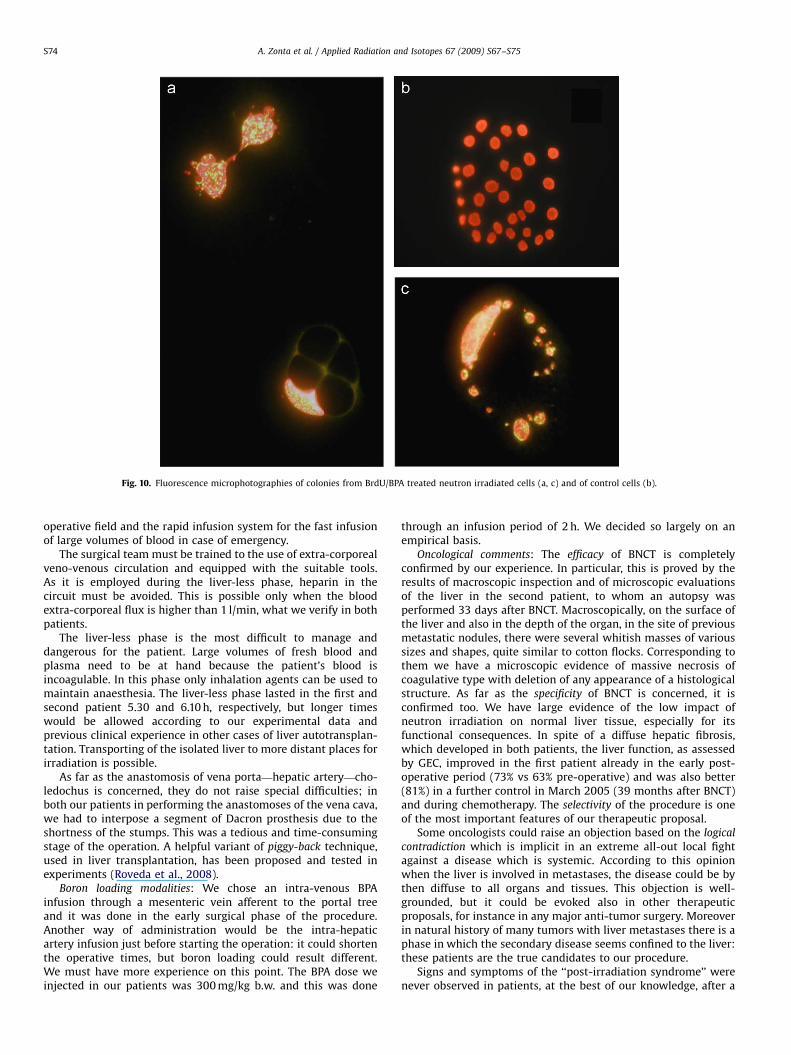
The hypothesis that ‘‘resistant cells’’ are basically ‘‘non-proliferating cells’’ was tested with a double labelling technique.It is well known that proliferating cells can be labelled with thereagent bromodeoxyuridine (BrdU), an analog of thymidine. Itspresence in cells can be revealed by an immunofluorescence testwhich tag proliferating cells. Both proliferating and non-prolifer-ating cells can be detected in culture with another reagent,propidium iodide (PI), which labels all cells. Therefore, byexposing to neutron irradiation tumor cells, previously treatedwith BPA and BrdU, in a subsequent fluorescence analysis it is
possible to distinguish damaged and undamaged cells. Theprevious ones were proliferating at the time of the BPA exposureand therefore positive to both BrdU and PI, the latter, non-proliferating, are only PI labelled. Severe cell damages are evidentin the double labelled cells (green/FITC; red/PI) (Fig. 10a, c), whileundamaged cells are only labelled by PI (red) (Fig. 10b).
6. Discussion and conclusions
About this complex clinical experience and the many problemsit raises, it is possible to argue only in reference to a few moreimportant issues.
Surgical aspects: from the surgical point of view the applicationof BNCT procedure requires a heavy and not easy operation, suchas the liver autotransplantation, but it is feasible. The length of theprocedure is largely dependent on the learning curve, as it is alsoshown by our two cases: indeed in our second case the procedurewas more than 10% shorter than in the first one.
Some special instrumentation is essential: for instance asystem for recovering and processing the blood collected in the
ARTICLE IN PRESS
Fig. 10. Fluorescence microphotographies of colonies from BrdU/BPA treated neutron irradiated cells (a, c) and of control cells (b).
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75S74
operative field and the rapid infusion system for the fast infusionof large volumes of blood in case of emergency.
The surgical team must be trained to the use of extra-corporealveno-venous circulation and equipped with the suitable tools.As it is employed during the liver-less phase, heparin in thecircuit must be avoided. This is possible only when the bloodextra-corporeal flux is higher than 1 l/min, what we verify in bothpatients.
The liver-less phase is the most difficult to manage anddangerous for the patient. Large volumes of fresh blood andplasma need to be at hand because the patient’s blood isincoagulable. In this phase only inhalation agents can be used tomaintain anaesthesia. The liver-less phase lasted in the first andsecond patient 5.30 and 6.10 h, respectively, but longer timeswould be allowed according to our experimental data andprevious clinical experience in other cases of liver autotransplan-tation. Transporting of the isolated liver to more distant places forirradiation is possible.
As far as the anastomosis of vena porta—hepatic artery—cho-ledochus is concerned, they do not raise special difficulties; inboth our patients in performing the anastomoses of the vena cava,we had to interpose a segment of Dacron prosthesis due to theshortness of the stumps. This was a tedious and time-consumingstage of the operation. A helpful variant of piggy-back technique,used in liver transplantation, has been proposed and tested inexperiments (Roveda et al., 2008).
Boron loading modalities: We chose an intra-venous BPAinfusion through a mesenteric vein afferent to the portal treeand it was done in the early surgical phase of the procedure.Another way of administration would be the intra-hepaticartery infusion just before starting the operation: it could shortenthe operative times, but boron loading could result different.We must have more experience on this point. The BPA dose weinjected in our patients was 300 mg/kg b.w. and this was done
through an infusion period of 2 h. We decided so largely on anempirical basis.
Oncological comments: The efficacy of BNCT is completelyconfirmed by our experience. In particular, this is proved by theresults of macroscopic inspection and of microscopic evaluationsof the liver in the second patient, to whom an autopsy wasperformed 33 days after BNCT. Macroscopically, on the surface ofthe liver and also in the depth of the organ, in the site of previousmetastatic nodules, there were several whitish masses of varioussizes and shapes, quite similar to cotton flocks. Corresponding tothem we have a microscopic evidence of massive necrosis ofcoagulative type with deletion of any appearance of a histologicalstructure. As far as the specificity of BNCT is concerned, it isconfirmed too. We have large evidence of the low impact ofneutron irradiation on normal liver tissue, especially for itsfunctional consequences. In spite of a diffuse hepatic fibrosis,which developed in both patients, the liver function, as assessedby GEC, improved in the first patient already in the early post-operative period (73% vs 63% pre-operative) and was also better(81%) in a further control in March 2005 (39 months after BNCT)and during chemotherapy. The selectivity of the procedure is oneof the most important features of our therapeutic proposal.
Some oncologists could raise an objection based on the logical
contradiction which is implicit in an extreme all-out local fightagainst a disease which is systemic. According to this opinionwhen the liver is involved in metastases, the disease could be bythen diffuse to all organs and tissues. This objection is well-grounded, but it could be evoked also in other therapeuticproposals, for instance in any major anti-tumor surgery. Moreoverin natural history of many tumors with liver metastases there is aphase in which the secondary disease seems confined to the liver:these patients are the true candidates to our procedure.
Signs and symptoms of the ‘‘post-irradiation syndrome’’ werenever observed in patients, at the best of our knowledge, after a

ARTICLE IN PRESS
A. Zonta et al. / Applied Radiation and Isotopes 67 (2009) S67–S75 S75
clinical BNCT application. In our cases they were likely dueto the liver itself, which was at the same time the site ofmetastases, of surgical manipulation and of neutron irradiationand were mediated by the abrupt release of large amounts ofcytokines.
We could evaluate some of them only in the second patient.We deem it difficult to decide whether their presence in blood in aso-altered concentration is cause or consequence of the compleximbalance existing in the patients. Nevertheless, the clinicalalterations observed were quite similar, in nature even if not indegree, to the ones described in some experiments after admin-istration to volunteers of some of these mediators (Michie et al.,1988).
As regards the onset of the observed alterations and theirpossible role, it seems convenient to consider separately twocritical phases covered by the cytokines subsequent evaluations:the liver-less phase and the period of time following thereconnection of the irradiated liver. Trying to interpret theirbehavior, we observe that IL-6 and HGF increases have apparentlyan aspecific meaning, because they occur even before the startingof hepatectomy and then flatten to supra-maximal values. Theaberrant levels of TNF and VEGF appear to be more directly boundto an effect of liver irradiation, because they show after the liverreconnection and behave as run out in the 2nd p.o.d.. Of coursemore clinical experiences are needed in order to clarify thisimportant aspect.
Recurrences after BNCT are a dramatic challenge. On the basisof clinical considerations and experimental results, they couldderive from cells, perhaps tumoral stem cells, which are refractoryto BNCT because lacking of adequate amounts of 10B content dueto their quiescence. Therefore efforts must be addressed to theresearch of new boronated compounds or strategies able to targetalso neoplastic stem cells.
References
Altieri, S., Bortolussi, S., Bruschi, P., Chiari, P., Fossati, F., Stella, S., Prati, U., Roveda,L., Zonta, A., Zonta, C., Ferrari, C., Clerici, A., Nano, R., Pinelli, T., 2008. Neutron
autoradiography imaging of selective boron uptake in human metastatictumours. Appl. Radiat. Isot. 66 (12), 1850–1855.
Bortolussi, S., Altieri, S., 2007. Thermal neutron irradiation field design for boronneutron capture therapy of human explanted liver. Med. Phys. 34, 4700–4705.
Chiaraviglio, D., De Grazia, F., Zonta, A., Altieri, S., Brughieri, A., Fossati, F., Pedroni,P., Pinelli, T., Perotti, A., Specchiarello, M., Perlini, G., Rief, H., 1989. Evaluationof selective boron absorption in liver tumors. Strahlenther Onkol. 165, 170–172.
Ferrari, C., Clerici, A.M., Zonta, C., Cansolino, L., Boninella, A., Altieri, S., Ballarini, F.,Bortolussi, S., Bruschi, P., Stella, S., Bakeine, J., Dionigi, P., Zonta, A., 2008. Boronneutron capture therapy of liver and lung coloncarcinoma metastases: an invitro survival study. In: Zonta, A., et al. (Eds.), Proceedings of 13th InternationalCongress on Neutron Capture Therapy, Florence. ENEA, Roma, pp. 331–336.
Michie, H.R., Manogue, K.R., Spriggs, D.R., Revhaug, A., O’Dwyer, S., Dinarello, C.A.,Cerami, A., Wolff, S.M., Wilmore, D.W., 1988. Detection of circulating tumornecrosis factor after endotoxin administration. N. Engl. J. Med. 318, 1481–1486.
Pinelli, T., Altieri, S., Fossati, F., Zonta, A., Cossard, D., Prati, U., Roveda, L., Ricevuti,G., Nano, R., 1996. Development of a method to use boron neutron capturetherapy for diffused tumors of liver (Taormina project) neutron capturetherapy for cancer. In: Mishima, Y. (Ed.), Proceedings of the Sixth InternationalSymposium, Kobe, Japan, 1994. Plenum, New York, pp. 783–794.
Pinelli, T., Altieri, S., Fossati, F., Zonta, A., Ferrari, C., Prati, U., Roveda, L., NgnitejeuTata, S., Barni, S., Chiari, P., Nano, R., Ferguson, D.M., 2001. Operative modalitiesand effects of BNCT on liver metastases of colon adenocarcinoma. Amicroscopical and ultrastructural study in the rat. Frontiers in neutron capturetherapy. In: Hawthorne, M.F., et al. (Eds.), Proceedings of the EighthInternational Symposium, Los Angeles, CA, USA, 1998. Kluwer Academic/Plenum Publishers, New York, pp. 1427–1440.
Pinelli, T., Zonta, A., Altieri, S., Barni, S., Brughieri, A., Pedroni, P., Bruschi, P., Chiari,P., Ferrari, C., Fossati, F., Nano, R., Ngnitejeu Tata, S., Prati, U., Ricevuti, G.,Roveda, L., Zonta, C., 2002. Taormina: from the first idea to the application tothe human liver. Research and development in neutron capture therapy. In:Sauerwein, W., et al. (Eds.), Proceedings of the 10th International Congress onNeutron Capture Therapy, Essen, Germany. Monduzzi, Bologna, pp. 1065–1072.
Roveda, L., Prati, U., Bakeine, J., Trotta, F., Marotta, P., Valsecchi, P., et al., 2004. Howto study boron biodistribution in liver metastases from colorectal cancer. J.Chemother. 16 (Suppl. 5), 15–18.
Roveda, L., Zonta, A., Staffieri, F., Timurian, D., DiVenere, B., Bakeine, G.J., Crovace,A., Prati, U., et al., 2008. Experimental modified orthotopic piggy-back liverautotransplantation, Appl. Radiat. Isot., this issue, doi:10.1016/j.apradi-so.2009.03.087.
Wittig, A., Michel, J., Moss, R.L., Stecher-Rasmussen, F., Arlinghaus, H.F., Bendel, P.,Mauri, P.L., Altieri, S., Hilger, R., Salvadori, P.A., Menichetti, L., Zamenhof, R.,Sauerwein, W.A.G., 2008. Boron analysis and boron imaging in biologicalmaterials for boron neutron capture therapy (BNCT). Crit. Rev. Oncol. Hematol.68, 66–90.
Zonta, A., Prati, U., Roveda, L., Ferrari, C., Zonta, C., Zonta, S., Clerici, A.M., Pinelli, T.,Fossati, F., Altieri, S., Bortolussi, S., Bruschi, P., Nano, R., Barni, S., Chiari, P.,Mazzini, G., 2006. Clinical lessons from the first applications of BNCT onunresectable liver metastases. J. Phys. Conf. Ser. 41, 484–495.




















