Exceeding the Benchmark: Nursing Sensitive Indicators
29
Oncology Nursing Society 42nd Annual Congress May 4–7, 2017 • Denver, CO 1 Clinical Practice David Rice, PhD, RN, NP Director, Professional Practice and Education City of Hope National Medical Center [email protected] Key Session Takeaways 1. YOU impact the care quality and safety of oncology patients in measurable ways. 2. YOU impact the care quality and safety of oncology patients in ways that can’t be measured. 3. YOU impact the care quality and safety of oncology patients in immeasurable ways. Be compassionate. Be self, patient, and population aware. Be data driven. __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ __________________________________________ Exceeding the Benchmark Nursing Sensitive Indicators David Rice, PhD, RN, NP Director, Professional Practice and Education City of Hope National Medical Center Disclosures I have no financial disclosures. David Rice, PhD, RN, NP Director, Professional Practice and Education City of Hope National Medical Center Exceeding the Benchmark: Nursing Sensitive Indicators
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Exceeding the Benchmark: Nursing Sensitive Indicators

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 1Clinical Practice
David Rice, PhD, RN, NPDirector, Professional Practice and EducationCity of Hope National Medical [email protected]
Key Session Takeaways1. YOU impact the care quality and safety of oncology
patients in measurable ways.2. YOU impact the care quality and safety of oncology
patients in ways that can’t be measured.3. YOU impact the care quality and safety of oncology
patients in immeasurable ways.
Be compassionate. Be self, patient, and population aware. Be data driven.
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Exceeding the BenchmarkNursing Sensitive Indicators
David Rice, PhD, RN, NPDirector, Professional Practice and Education
City of Hope National Medical Center
Disclosures
I have no financial disclosures.
David Rice, PhD, RN, NPDirector, Professional Practice and Education
City of Hope National Medical Center
Exceeding the Benchmark: Nursing Sensitive Indicators
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO2 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Exceeding the BenchmarkNursing Sensitive Indicators
David Rice, PhD, RN, NPDirector, Professional Practice and Education
City of Hope National Medical Center
Takeaways• YOU impact the care quality and safety of
oncology patients in measurable ways• YOU impact the care quality and safety of
oncology patients in ways that can’t be measured
• YOU impact the care quality and safety of oncology patients in immeasurable ways– Be compassionate– Be self, patient, and population aware– Be data driven
Objectives
• Define benchmark• Understand nurses’ key role in delivering safe, quality
cancer care• Understand how quality, financial, resource utilization
data impact care delivery• Appreciate transparency in healthcare• Appreciate underserved populations and nurses’
impact on providing equitable cancer care access• Take the message from the Extravasation Benchmark
measure that RNs help to set benchmarks
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 3Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
ANA Nursing’s Social Policy Statement (2010)
Four Essential Components of Nursing Practice
• Attention to the full range of the human experience
• Integration of objective and subjective phenomena
• Application of scientific knowledge• Provision of care that reinforces nursing’s intent
Improving performance• Continually identifying, understanding, and
adapting outstanding practices and processes found inside and outside the organization– Company– Public sector or private organization– University / college (e.g. nursing curricula)– Healthcare– Government
Benchmarking
What is a Benchmark?
Standard, or a set of standards, used as a point of reference for evaluating performance or level of quality. Benchmarks may be drawn from a firm's own experience, from the experience of other firms in the industry, or from legal requirements such as environmental regulations.
http://www.businessdictionary.com/definition/benchmark.html

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO4 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Quality – Why Quality Indicators• Quality “the degree to which health services for individuals
and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.” (Lohr, 1990)
• To “use data to monitor the outcomes of care processes and use improvement methods to design and test changes to continuously improve the quality and safety of health care systems.” (Cronenwett et al., 2007)
• Why Nurse Sensitive Quality Indicators? "Because nursing absorbs at least 50% of most hospitals’ expense budgets, and nursing also bears the continual risk of being targeted as a potential source of cost savings in response to economic and market pressures." (Le, 2014)
Agency for Healthcare Research and Quality (AHRQ)Six domains of Health Care Quality
• Safe– Avoiding harm to patients from the care that is intended to help them
• Effective– Providing services based on scientific knowledge to all who could benefit
and refraining from providing services to those not likely to benefit (avoiding underuse and misuse, respectively).
• Patient-centered– Providing care that is respectful of and responsive to individual patient
preferences, needs, and values and ensuring that patient values guide all clinical decisions.
• Timely– Reducing waits and sometimes harmful delays for both those who receive
and those who give care• Efficient
– Avoiding waste, including waste of equipment, supplies, ideas, and energy• Equitable
– Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status.
https://www.ahrq.gov/professionals/quality-patient-safety/talkingquality/create/sixdomains.html
Public facing web pages - Transparencywww.csqi.on.ca
http://www.cancercenter.com/lung-cancer/statistics/tab/lung-cancer-NSCLC-survival-statistics/
https://moffitt.org/for-healthcare-providers/outcomes/rectal-cancer/
https://moffitt.org/for-healthcare-providers/outcomes/patient-satisfaction/

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 5Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
EQUALITY VS EQUITY
Used with permission from Liz Margolies, Executive Director, National LGBT Cancer Network
History

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO6 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
W. Edwards Deming
• Father of Total Quality Management (TQM), Continuous Quality Improvement (CQI), Performance Improvement (PI)
• Focus on statistics, systems, decreasing variation– 14 points for management
• Cease dependence on inspection to achieve quality• Institute a vigorous program of education and self-
improvement for everyone• Put everyone in the company to work accomplishing the
transformation
Ways nurses use data to deliver quality, safe care and improve performance
• Improve clinical pathways– Standardization (reduce variation)– Bundles – evidence-based – improve outcomes
• TJC National Patient Safety Goals• LEAN efforts
– Maximize value for customers and minimize waste• Root cause analysis
– Review event for underlying causes• Failure Mode Effects Analysis (FMEA)
– Improve the quality, reliability, and safety of a process
Avedis Donabedian, MD, MPH• University of Michigan
– Evaluating the quality of medical care (1966)– Models for organizing the delivery of health services
and criteria for evaluating them (1972)– The Quality of Care: How Can it be Assessed? (1988)
STRUCTURE PROCESS OUTCOMES
“Ultimately, the secret of quality is love. ….. If you have love, you can then work backward to monitor and improve the system.”

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 7Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Don Berwick, MD, MPP• Management of healthcare systems
– Scientific methods– Evidence-based medicine– Comparative effectiveness research
• President and CEO of Institute for Healthcare Improvement (IHI)– Independent not-for-profit to lead improvement of
healthcare by building the will to change, cultivating promising concepts for improving patient care, and helping healthcare system put ideas into action
• 2010 – President Obama appointed Berwick to service as the administrator of CMS.
“20-30% of health spending is ‘waste’ with no benefit to patients, because of overtreatment, failure to coordinate care, administrative complexity and fraud, and that part of this problem was because of CMS regulations.” "Health Official Takes Parting Shot at 'Waste'" Robert Pear, The New York Times, December 3, 2011
Seminal Institute of Medicine Reports
• To Err is Human (2000)• Crossing the Quality Chasm (2001)• Building a Better Delivery System: A New
Engineering / Health Care Partnership (2005)• The Future of Nursing (2010)• Delivering High Quality Cancer Care – A System in
Crisis (2013)• Assessing Progress on the Institute of Medicine
Report The Future of Nursing (2015)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO8 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Visible / Public Identities
AgeSex
Gender expressionPhysical appearance
RaceClass
Health / ability
Invisible Identities
Ethnicity / national originGender Identity
PoliticsReligion
Relationship statusEmployment status
Personal habitsCommunication style
Educational backgroundWork experience
Socioeconomic status
The National Institutes of Health (NIH) defines diversity as “the range of human differences, including but not limited to race, ethnicity, gender, sexual orientation, age, social class, physical ability or attributes, religious or ethical value system, national origin, and political beliefs.”

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 9Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Underserved PopulationsCancer Access Healthcare Disparities

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO10 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Underserved PopulationsCancer Access Healthcare Disparities

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 11Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Impact of Sexual Orientation and Gender Identity on Cancer Care
• Of the nearly 10 million lesbian, gay, bisexual, and transgender people in the United States– Tobacco use higher– Alcohol use 3X higher– Risk of sexually transmitted disease higher– Eating disorders / obesity– Elevated risk depression, anxiety, psychological distress,
suicidality– Higher cancer risks and lower cancer screening rates– Increased challenges in survivorship
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
POVERTY AND ITS IMPACT ON LGBT HEALTH
• 1/3 of LGBT people are uninsured– 34% of gay men – 31% of lesbians– 29% of bisexual people
• 2/3 of the uninsured had been without coverage for more than 2 years
• Nearly 40% of uninsured respondents carry medical debt
• 44% of the insured put off medical care because they couldn’t afford it

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO12 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
The highest-, lowest-ranked states for health carehttps://www.advisory.com/daily-briefing/2017/03/06/state-health-
rankings?WT.mc_id=Email|DailyBriefing+Headline|DBA|DB|2017Mar06|SurveyDB2017Mar06||||&elq_cid=1515155&x_id=003C000001gGXtJIAW
• Access to care (33%)– Six metrics, including health insurance enrollment,
adult and child wellness visits, and health care affordability
• Health care quality (33%)– Three metrics: Medicare quality, CMS nursing home
citations, and hospital readmission rates• Public health (33%)
– Six metrics, including infant mortality, overall mortality, smoking, suicide, and obesity rates
The highest-, lowest-ranked states for health carehttps://www.advisory.com/daily-briefing/2017/03/06/state-health-
rankings?WT.mc_id=Email|DailyBriefing+Headline|DBA|DB|2017Mar06|SurveyDB2017Mar06||||&elq_cid=1515155&x_id=003C000001gGXtJIAW
1. Hawaii 2. Massachusetts3. Minnesota4. New Hampshire5. Iowa6. Vermont7. Rhode Island8. New Jersey9. Washington10. California
41. Indiana42. Tennessee 43. Wyoming44. Kentucky45. Louisiana46. West Virginia47. Alabama48. Oklahoma49. Mississippi 50. Arkansas

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 13Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Information and Communications Systems:The Backbone of the Health Care Delivery System
• True?– EMRs – Help? Hinder? Hope?
• Financial systems versus clinical systems?
– Event reports• 50 – 70% of errors / events have some element of
communication failure– Handover– Transitions in care– Quality peer review
IN 1928, MAY AYRES BURGESS was commissioned and completed A Study of the Economics of Nursing Conducted by the Committee on the Grading of Nursing Schools. According to patients interviewed by Burgess, “the better the nursing, the less the ordinary patient thinks about it” (p. 203). Burgess pointed out the nurse moves the patient toward recovery in many ways imperceptible to the patient. Today, health care economic choices are made based on hard data yet nursing’s value remains imperceptible. Nursing struggles in communicating its value in a measureable way.
Rising health care costs and limited health care resources have created a call for data that documents the true value of nursing and these data are critical “to assure adequate investment in the nursing profession” (Rutherford, 2008, p. 347). Nursing is a costly yet essential resource and it is essential nursing leaders embrace those measures that chronicle its value.
Rutherford, Nursing Economics 2012
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Caring done well … Kristen Swanson
Theory of Caring and Healing “Doing for”

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO14 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Rutherford, 2012
Nursing care quality processes• Directly or indirectly influence patient outcomes
– Nursing Sensitive Indicators• CLABSI – Central Line Associated Blood Stream Infection• HAPI – Hospital Acquired Pressure Injury• Injury falls / falls prevalence• Use of Restraints• CAUTI – Catheter Associated Urinary Tract Infection• VAE – Ventilator Associated Events• Sepsis prevention and management• Pain management• Preventable hospital readmission• Vesicant Chemotherapy Extravasation
Ways to Display Data(Keep it simple – RN should be able to look at the
graphic and interpret the data easily)• Tools
– Bar graph– Histogram– Pareto diagram– Scatter charts– Run charts / control charts– Flowcharts– Cause and effect diagrams
– Pie charts– Gaussian curve
charts– PERT charts– Gant charts– Breakeven charts– Likert scales– Fishbone diagram
(“Ishikawa” diagram)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 15Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Hospital Acquired Infections (HAIs)http://www.shea-online.org/priority-topics/compendium-of-strategies-to-prevent-hais
Medical Error
• The $17.1 Billion Problem: The Annual Cost of Measurable Medical Errors (in 2008) (Bos et al. 2011)– 10 types of errors accounts for more than 2/3 total costs– Leading error pressure ulcers, followed by post-op
infections– 6th on the list – infection due to central venous catheter
• Institute of Medicine (2000) estimates– 1.5 million patients harmed by medication errors annually– Increased hospital costs of $3.5 billion annually 2nd to
medication error complications• At least 25% are preventable
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
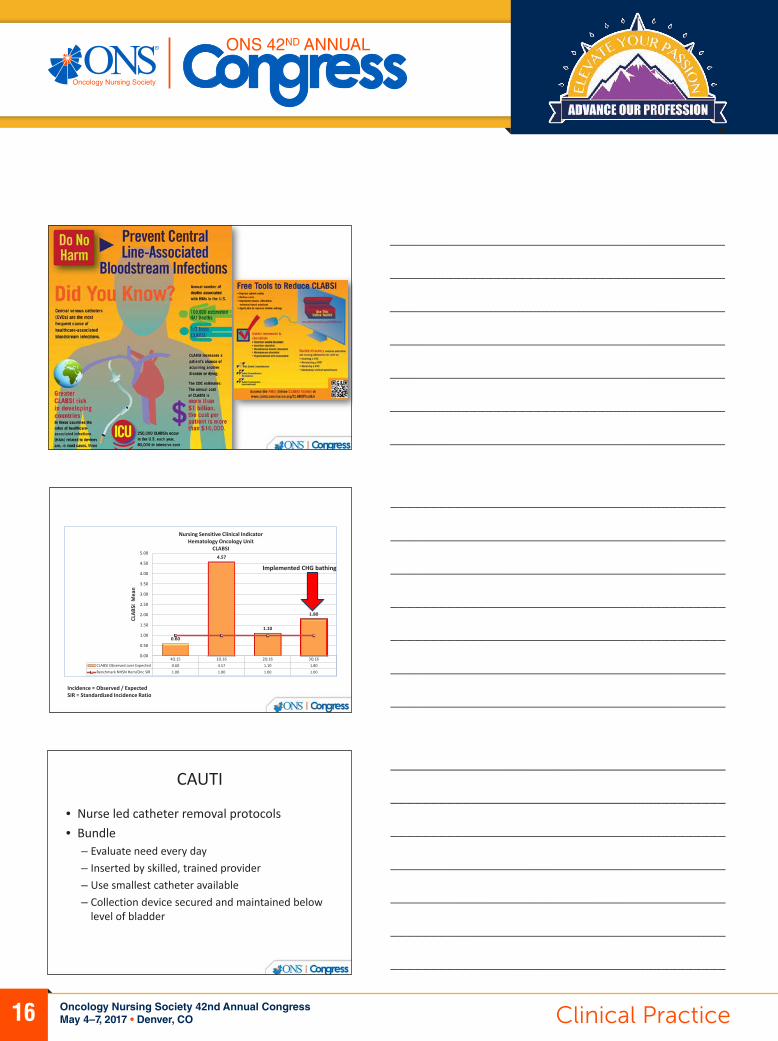
CLABSI – TJC Toolkit
https://www.jointcommission.org/topics/clabsi_toolkit.aspx
Annual education about CVADsBundles (insertion, maintenance, surveillance)2-person dressing changes (practitioner /
observer)CVAD dressing change validationAre you patients / families doing dressing
changes at home?
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO16 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
4Q 15 1Q 16 2Q 16 3Q 16CLABSI Observed over Expected 0.60 4.57 1.10 1.80Benchmark NHSN Hem/Onc SIR 1.00 1.00 1.00 1.00
0.60
4.57
1.10
1.80
0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
CLAB
SI M
ean
Nursing Sensitive Clinical IndicatorHematology Oncology Unit
CLABSI
Incidence = Observed / ExpectedSIR = Standardized Incidence Ratio
Implemented CHG bathing
CAUTI
• Nurse led catheter removal protocols• Bundle
– Evaluate need every day– Inserted by skilled, trained provider– Use smallest catheter available– Collection device secured and maintained below
level of bladder

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 17Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
4Q 15 1Q 16 2Q 16 3Q 16CAUTI rate (per 1,000 catheter days) 1.12 1.06 2.22 1.00Benchmark NDNQI Teaching Hospital Mean 1.46 1.27 1.26 1.37
1.12 1.06
2.22
1.00
0.00
0.50
1.00
1.50
2.00
2.50
CAU
TI M
ean
Nursing Sensitive Clinical IndicatorGeriatric Oncology Care Unit
CAUTI
Injury Falls
• Patients with a diagnosis of cancer are already at risk– Particularly with inpatient admission
• Risk scales (e.g. Morse, Hendrich II, etc.) not particularly sensitive but help to define risk elements
• Multiple interventions – can’t be studied separately
• Tai chi positive intervention in community dwelling elders
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
A Model of Care Delivery to Reduce Falls in a Major Cancer Center
Nancy E. Kline, PhD, RN, CPNP, FAAN; Bridgette Thom, MS; Wayne Quashie, MPH, RN; Patricia Brosnan, MPH, RN; Mary Dowling, MSN, RN
1. History of falls2. Help transferring (bed to chair; to commode; or
complete transfer)3. Sensory deficits (visual / auditory impairment
affecting mobility or peripheral neuropathy)4. Motor deficits (gait imbalance, R or L side
weakness, lower extremity weakness)5. Psychotropics (e.g., sleep medications, hypnotics,
sedatives, anxiolytics) or anticonvulsants

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO18 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
4Q 15 1Q 16 2Q 16 3Q 16 FALLS w/Injury rate (per 1,000 patient days) 0.15 0.16 0.13 0.22Benchmark NDNQI Teaching Hospital Mean 0.20 0.18 0.19 0.20
0.150.16
0.13
0.22
0.00
0.05
0.10
0.15
0.20
0.25
Falls
w/I
njur
y M
ean
Nursing Sensitive Clinical IndicatorMedical Surgical Oncology Unit
Falls with Injury
HAPI
• Patients with a diagnosis of cancer are already at risk• Frequency of Braden score
– Interrater reliability• Focus interventions on relevant subscale of Braden• RN staging of pressure injury
– Wound Treatment Associate (WTA®) program - WOCN• Turn and position – ambulate – early mobility• Caution with layers of linens and transfer devices on
bed• Specialty surfaces
4Q 15 1Q 16 2Q 16 3Q 16HAPU prevalence ≥ Stage 2 10% 6.25% 4.20% 3.00%Benchmark NDNQI Teaching Hospital (%) 4.46% 4.35% 4.30% 4%
10%
6.25%
4.20%
3.00%
0%
2%
4%
6%
8%
10%
12%
14%
% P
ts w
ith H
APU
≥ S
tage
2
Nursing Sensitive Clinical IndicatorOncology Progressive Care Unit
HAPU ≥ Stage 2

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 19Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Pain Management
• “Pain is whatever the experiencing person says it is, existing whenever the experiencing person say it does.” (McCaffery & Beebe)
• Pivotal and critical role of RN in cancer pain management– Assessment / Intervention / Reassessment– Educate, inform, validate, advocate
• Education / support may prevent avoidable readmission for pain
• Press Ganey perception of pain metric– Some pain will not be preventable (e.g. Grade III mucositis)
– so RN management and validation is critical
4Q 15 1Q 16 2Q 16 3Q 16Perception of Pain Mgmt Mean Score 94.00 95.00 96.77 97.01Press Ganey Benmark Mean 95.23 95.33 96.02 95.82
94.00
95.00
96.7797.01
92.00
92.50
93.00
93.50
94.00
94.50
95.00
95.50
96.00
96.50
97.00
97.50
Perc
ep o
f Pai
n M
gmt
Mea
n
Press Ganey ResultsSurgical Oncology
Perception of Pain Management
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
End of life metrics
• RN comfort level in caring for the dying patient– Measure of education such as End of Life Nursing
Education Consortium (ELNEC) training– Risk of provider burnout (“trauma”)
• Chemotherapy given within 14 days of death• Hospice referral utilization• Supportive Care Medicine utilization

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO20 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
• Acknowledge Suffering: We should acknowledge that our patients are suffering and show them that we understand.
• Body Language Matters: Non-verbal communication skills are as important as the words we use.
• Anxiety is Suffering: Anxiety and uncertainty are negative outcomes that must be addressed.
• Coordinate Care: We should show patients that their care is coordinated and continuous, and that “we” are always there for them.
• Caring Transcends Diagnosis: Real caring goes beyond delivery of medical interventions to the patient.
• Autonomy Reduces Suffering: Autonomy helps preserve dignity for patients.
Federal, “Watch dog,” and Professional Organizations
• HCAHPS –– Hospital Consumer Assessment of Healthcare Providers
and Systems survey is the first national, standardized, publicly reported survey of patients’ perspectives of hospital care
– Jointly developed 2002 by CMS (Centers for Medicare and Medicaid Services) and AHRQ (Agency for Healthcare Research and Quality)
• Both CMS and AHRQ are federal agencies in the Department of Health and Human Services
• Cancer care CAHPS
CAHPS Cancer Care Survey Measures
• Getting timely appointments, care, and information• How well the cancer care team communicates with patients• Cancer care team’s use of information to coordinate patient care• Helpful, Courteous, and Respective Office Staff• Cancer care team supports patients in managing the effects of their
cancer and treatment• Cancer care team is available to provide information when needed• Involvement of family members and friends• Availability of Interpreters• Patients’ ratings of cancer care team / overall cancer care

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 21Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Federal, “Watch dog,” and Professional Organizations
• TJC– National Patient Safety Goals– ORYX Performance Reporting Requirements
• AMI - Primary Percutaneous Coronary Intervention (PCI) Received Within 90 Minutes of Hospital Arrival
• Median Time from ED Arrival to ED Departure for Admitted ED Patients
• Influenza Immunization • Tobacco screening
Federal, “Watch dog,” and Professional Organizations
• Hospital Compare www.medicare.gov/hospitalcompare/search.html
• Leapfrog http://www.leapfroggroup.org/compare-hospitals
• Oncology Nursing Society• ASCO - American Society of Clinical Oncology
– ASCO - ONS – e.g. joint guidelines (standard for chemotherapy 2016 update)
– ASCO QOPI –Quality Oncology Practice Initiative– NCI – ASCO Teams Special Series – Journal of Oncology Practice
Vol. 12(11) November 2016• NQF National Quality Forum
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Federal, “Watch dog,” and Professional Organizations
• C3NSI– Cancer Centers Consortium Nursing-Sensitive Indicators
• C4QI– Comprehensive Cancer Centers for Quality
Initiatives
• C3IC– Comprehensive Cancer Centers Infection Control

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO22 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
American Society of Clinical OncologyQOPI Quality Oncology Practice Initiative
Databases
• Vizient (formerly UHC) database• NDNQI – National Database of Nursing Quality
Indicators (now merged with Press-Ganey)• Press Ganey• ONS The Oncology Quality Clinical Data
Registry (in collaboration with CECity) https://www.ons.org/practice-resources/qualified-clinical-data-registry

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 23Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Vesicant Chemotherapy Extravasation
Establishing a National Benchmark
Cancer Center Consortium Nursing Sensitive Indicators
Cancer Centers Consortium Nursing Sensitive Indicators
Formed in 2010 to establish oncology-specific, ambulatory nurse sensitive metrics 19 centers have participated in the consortium 11 centers contributed data to the IRB approved study
Vesicant Chemotherapy AdministrationNo benchmark in the literature
“For the purposes of quality assurance, a tolerable frequency of chemotherapy extravasation should be significantly less than 1% of drug administration.” (Morris, Holland 2000)
Siteman Cancer Center* City of Hope Dana Farber Cancer Institute
Duke Cancer Institute Fox Chase Cancer Center*
Dartmouth Hitchcock Norris Cotton Cancer
Center
Ohio State University The James Cancer
Center*
Karmanos Cancer Center M D Anderson Cancer Center
Moffitt Cancer Center
Roswell Park Cancer Institute*
Memorial Sloan Kettering Cancer Center*
Seattle Cancer Care Alliance*
University of Iowa Holden Cancer Center*
University of Virginia*
Sylvester Cancer Center Vanderbilt University Ingram Cancer Center*
Yale New Haven Hospital Smilow Cancer Center*
Emory HealthcareWinship Cancer Center*
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
• Extravasation: The inadvertent administration of a vesicant solution or medication into surrounding tissue – Tissue damage can progress from local pain and erythema to
sloughing, desquamation, ulceration and necrosis
• Incidence– Peripheral IV 0.07% to 7.0%– Central Vascular Access Device 0.01% to 4.7%
• Infiltration refers to fluids inadvertently leading out of the veins and into the tissues (such as IV fluid, IV medications, blood component products)
Extravasation
Jackson-Rose, DelMonte, Katania, et al. (2015)Ener et al. (2004)
Coyle (2014) Schulmeister (2010)
Payne, Savarese (2010)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO24 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Damage potential / Classifications Vesicant Irritant Irritant with vesicant potential
Actual and suspected treated as events
Reported on 17 quarters of data between 2011 -2015
Continue to collect and report data under IRB
Centers use for ambulatory quality indicator
C3NSI (Cancer CenterConsortium Nursing Sensitive Indicators) Consensus for Extravasation Project (Jackson-Rose, Del Monte, Catania, et al 2015)1
Vesicant agents:DactinomycinDaunorubicinDoxorubicinEpirubicinIdarubicinMechlorethamineMitomycinVinblastineVincristineVinorelbine
Irritants / Irritants with Vesicant Potentialagents:
Albumin-bound paclitaxelBortezomibCarmustineCisplatinDocetaxelEtoposideGemcitabineLiposomal doxorubicinMelphalanMitoxantroneOxaliplatinPaclitaxelStreptozocin
Chemotherapy andBiotherapy Guidelines and Recommendations for Practice (Polovich, Olsen & LeFebvre, 2014)2
Vesicant agents:Albumin-bound PaclitaxelDactinomycinDaunorubicinDocetaxelDoxorubicinEpirubicinIdarubicinMechlorethamineMitomycinMitoxantronePaclitaxelVinblastineVincristineVinorelbine
Irritants / Irritants with Vesicant Potentialagents:
BleomycinCarboplatinCarmustineDacarbazineEtoposideFloxuridineGemcitabineIfosfamideLiposomal daunorubicinLiposomal doxorubicinOxaliplatinStreptozocinTopotecan
1 Used with permission by David Rice, 20162 Polovich, Lefebvre, & Olsen (2014)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 25Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Category DosesAdministered
ExtravasationsCentral Venous
Access Device IV
Extravasations Peripheral IV
TotalExtravasations
ExtravasationRate
(95% CI)
Vesicants 123,993 11 79 90 0.07% (0.07%, 0.08%)
Irritants and Irritants with Vesicant Potential
615,819 19 564 583 0.09% (0.09%, 0.10%)
Totals 739,812 30 643 673 0.09% (0.09%, 0.09%)
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO26 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 27Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO28 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Observations• Significantly higher incidence of peripheral IV extravasations
compared to CVAD• Taxanes• Large volume drugs / long infusion times / movement during
infusion• Evaluation of drugs which irritate but don’t actually cause
tissue damage when extravasation occurs (e.g. gemcitabine)• Administration order of Cisplatin and Fosaprepitant (Emend
injection for delayed nausea)• Subgroup reviewed patient / family education from centers
and made a recommendation for standard• Manuscript – accepted for publication in CJON August 2017
Benchmarks – In Conclusion
• Nurses in all practice settings play key roles in designing, delivering, evaluating, managing safe, effective quality cancer care
• Nurses use data, measurement techniques, benchmarking, and analysis in their everyday practice
• The combination of nursing ethos, expert practice, application of data, interprofessional teamwork, and use of information technology, results in improved patient outcomes.
References and Resources

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 29Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
References and Resources