HIV testing: increasing uptake among people who may have ...
Upload
khangminh22Category
view
0download
0
Evolution and scale up of global HIV testing
service approaches: 2000-2020 by
Vincent J Wong MSc DTMPH A portfolio of research submitted in partial fulfillment
of the award of the degree of Doctor of Philosophy by Publication
Faculty of Science and Health School of Health and Care Professions
University of Portsmouth, United Kingdom
September 2021

2
Table of Contents Table of Contents ............................................................................................................................................. 2
List of Tables and Figures ................................................................................................................................. 4
Abbreviations and Acronyms ........................................................................................................................... 5
Declaration ....................................................................................................................................................... 7
Acknowledgements .......................................................................................................................................... 8
Biographical Profile / Curriculum vitae. ........................................................................................................... 9
Abstract .......................................................................................................................................................... 11
Chapter 1: Introduction ................................................................................................................................. 13
1.1 HIV Testing Services: Health Service Coverage and HTS Paradigms .................................................... 13
1.2 Research Question, Objectives, Methods, Limitations ........................................................................ 17
1.3 Application of the Framework to HIV/AIDS: 90-90-90 Goals and an Overview of 1st 90 Coverage ..... 19
1.4 Overview and Mapping of Key Select Co-authored Articles and Abstracts included in Submission .... 23
1.5 Ethics and ethical approvals related to articles ................................................................................... 24
Chapter 2: Primary Commentary: Evolution and scale up of global HIV testing service approaches: 2000-2020 ............................................................................................................................................................... 25
2.1 Key Developments and Paradigms for the Global Introduction of HIV Testing (2000-2004) ............... 25
2.1.1 The Introduction of HIV Rapid Diagnostics as a Key Technological Development ........................ 25
2.1.2 Adoption and Expansion of HIV Testing Service Minimum Standards (3C and 5C) ....................... 26
2.1.3 HIV Testing and its Role in HIV programs and response in a Prevention paradigm Mitigating the HIV Epidemic .......................................................................................................................................... 29
2.1.4 Testing coverage rates and the state of access and coverage to Anti-retroviral therapy over time ............................................................................................................................................................... 30
2.2: Expansion of HIV testing service delivery through facility and community HTS scale up. (2005-2009) ................................................................................................................................................................... 32
2.2.1 Provider Initiated Testing and Counseling in Facilities .................................................................. 32
2.2.2 Community based HTS .................................................................................................................. 33
2.2.3 Author contributions to the expansion of access and coverage in specific populations .............. 36
2.2.4 Application of Tanahashi Framework to Sub-populations ............................................................ 42
2.3 From a Prevention to a Clinical Paradigm (2010-2017) ....................................................................... 44
2.4 New HTS Pathways towards 95% Diagnosis: HIV Self Testing and Index Testing ................................ 49
2.5 Conclusions .......................................................................................................................................... 56
Chapter 3: Applicant contribution list of publications, presentations, abstracts and reports by Vincent J Wong .............................................................................................................................................................. 60
3.1 Chronological List of Core Co-authored Publications and Authorial Contribution .............................. 60
3.2 Additional Authorship Documents in Consideration of Application .................................................... 67
3.2.1 Conference abstracts and presentations, 2002-2020, chronological ............................................ 67
3.2.2 Contributions to WHO Guidelines and Frameworks, 2005-2020 .................................................. 68
3.2.3 Additional contributions: PEPFAR Guidelines and HTS Contributions .......................................... 69

3
3.3 Metrics of Impact ................................................................................................................................. 70
Chapter 4: References to Commentary ......................................................................................................... 71
Appendix 1: Co-authored Original Articles and Reviews Included in this Submission ................................... 84
Appendix 2: Selected Co-authored Conference Posters and Abstracts ......................................................... 85
Appendix 3: Research Ethics Review Checklist .............................................................................................. 86
84
397
407
4
List of Tables and Figures
Table 1: The Tanahashi health service coverage framework and HIV testing contexts ................................. 19 Table 2: WHO, 2020 and UNAIDS, 2020. Global Number on ART over Time (Adapted) ................................ 31 Table 3: Tanahashi Framework application - examples for HIV affected sub-populations and settings, and factors across elements. ................................................................................................................................ 44 Table 4: Co-authored Publications List and Authorial Contributions, Chronological ..................................... 66
Figure 1: Tanahashi health service coverage framework (adapted) .............................................................. 15 Figure 2: Select country comparison of PLHIV known status rates, 2004-06 to 2016-18; Adapted from WHO, 2010c .............................................................................................................................................................. 20 Figure 3: Adapted from UNAIDS 2020: Diagnostic, treatment and viral load suppression coverage estimates by country, absolute percentages. ................................................................................................................. 21 Figure 4: Publication Map for Vincent Wong by HIV Testing Domains and Tanahashi health access elements. ....................................................................................................................................................... 23 Figure 5: WHO HIV testing strategy for high prevalence settings (>5%), 2015 .............................................. 26 Figure 6: PEPFAR HIV Testing indicated funding (HVCT) 2006-2020. PEPFAR, 2021. ..................................... 30 Figure 7: PHIA Estimated 90-90-90 in 15-24 years (Laboratory or self-reported ARV) .................................. 39 Figure 8: UNAIDS Estimated 1st 90 estimates by sex, >15 years, select sub-Saharan African Countries ...... 40 Figure 9: PEPFAR program data on HIV positives, new on treatment and linkage proxy rates by sex, >15 years. .............................................................................................................................................................. 46 Figure 10: Zambia Treatment-adjusted Prevalence and Positivity Data, 2019. Source: WHO HTS Dashboards, 2019 .......................................................................................................................................... 47 Figure 11: HIV Self Testing demonstration, Right to Care, South Africa, 2018. ............................................. 51 Figure 12: Illustrative index testing cascades for community and facility approaches. ................................. 54

5
Abbreviations and Acronyms
AIDS acquired immune deficiency syndrome
ANC antenatal care
ART anti-retroviral therapy
ARV anti-retroviral drugs
CDC United States Centers for Disease Control and Prevention
DHS demographic and health surveys
EIA enzyme immunoassay
EMTCT elimination of mother-to-child transmission
FSW female sex worker
FY fiscal year
GF Global Fund to Fight AIDS, Tuberculosis and Malaria
HCV hepatitis C virus
HIV human immunodeficiency virus
HIVST HIV self-testing
HTS HIV testing services
KP key populations
LMIC low- and middle-income countries
MSM men who have sex with men
NGO nongovernmental organization
OPD outpatient department
PEPFAR United States President’s Emergency Plan for AIDS Relief
PHIA population HIV/AIDS impact assessment
PITC provider-initiated testing and counselling
PMTCT prevention of mother-to-child transmission
PrEP pre-exposure prophylaxis
PWID persons who inject drugs
QA quality assurance
QI quality improvement
RDT rapid diagnostic test
STI sexually transmitted infection
TB tuberculosis

6
UNAIDS Joint United Nations Programme on HIV/AIDS
USAID United States Agency for International Development
VCT HIV voluntary counselling and testing
VMMC voluntary medical male circumcision
WHO World Health Organization
7
Declaration
Whilst registered as a candidate for the above degree, I have not been registered for any other research
award. The results and conclusions embodied in this thesis are the work of the named candidate and have
not been submitted for any other academic award.
.
Vincent J Wong
September 3, 2021
8
Acknowledgements
Thanks and gratitude to:
• My mother and father for continually inspiring me in my pursuits, even after they passed away.
And thank you Mom, especially, for all of your support: you would be proud!
• My family – Margrit, Alma and Laszlo – whose unceasing support, pride and enthusiasm kept me
attending to this work.
• To each and every colleague and co-author who helped shape my expertise and provided me with
the opportunity to explore and engage in such amazing work.
• In particular, thanks to all of my HTS colleagues past and present who are pushing to mitigate the
HIV pandemic through effective testing programs.
• To Alison Cheng and Dr. Elizabeth Marum for critical feedback on early drafts.
• To Drs. Rachel Baggaley and Miriam Taegtmeyer for their early co-sponsorship and encouragement
in my application to the PhD by Publication program
• To my current employer, the U.S. Agency for International Development (USAID) and the Office of
HIV/AIDS, who have supported my work on HIV testing services since 2009 and supported my
completion of this PhD program.
• To my viva voce examination panel for critical commentary that improved the overall thesis: Dr
Aravinda Meera Guntupalli, University of Aberdeen; Prof. Sabu Padmadas, University of
Southampton; Dr Ngianga II Kandala, University of Portsmouth.
• To Prof. Saseendran Pallikadavath for his unparalleled supervision and guidance over the past year
with this thesis.

9
Biographical Profile / Curriculum vitae.
Vincent J Wong, MSc is an established public health expert and leader with over 20 years of international
experience working on HIV testing programs globally. Following being awarded a BA in Integrative Biology
at the University of California, Berkeley in 1995, he pursued work (with State of California certification) as a
Registered Veterinary Technician in emergency and critical care and surgical nursing and anesthesia. He
transitioned his career to the field of HIV/AIDS in 2000, engaged as a research biologist on an HIV
diagnostics research and development team (GAIFAR GmbH, Berlin, Germany). There he contributed to the
development of HIV rapid antibody assays and supported clinical studies in countries within Europe and
sub-Saharan Africa. This early work resulted in early rapid testing platforms that were evaluated through
internal studies in Ghana, Cote d’Ivoire, Germany, Brazil and Russia, and were central to early introduction
of HIV voluntary counseling and testing (VCT) programs.
In 2003, Vincent returned to graduate school, completing a Diploma in Tropical Medicine and Public Health
(DTMPH), and earning an MSc in International Health degree in 2005 with an overall grade of A (Excellent)
from Charité Medical School, Humboldt and Frei Universities (Berlin, Germany). His thesis was title A
descriptive study of voluntary counseling and testing and rapid HIV testing in the Accra Metro Area, Ghana.
The findings were presented at the International AIDS Conference in Toronto in 2006.
From 2005 to 2009, Vincent joined World Health Organization’s (WHO) HIV Department to work on the
development of HIV testing tools and guidelines. This led to a number of key documents that shaped HIV
testing globally, including Scaling up HIV Testing and Counseling (2005), WHO’s Provider initiated testing and
counseling guidelines (2007), Policy requirements for HIV testing and counseling of infants and young
children in health facilities (2009), and the HIV counselling package for the Asia-Pacific (2009).
In 2009, he joined the US Agency for International Development (USAID) as a Senior Technical Advisor for
HIV testing in the Office of HIV/AIDS, Division of HIV Prevention, Care and Treatment. In this role he has
provided substantial in-country and virtual technical support. He also co-chaired PEPFAR Technical
Working Groups, and participated as a member of multiple WHO guidelines committees in the
development of HIV testing normative guidance and resources. Mr. Wong has provided technical
leadership on HIV programs in generalized and concentrated epidemics at global, national and
programmatic levels, from guiding partner implementation to translating WHO policy.

10
In 2020, Vincent was promoted from Senior Technical Advisor and Team Lead to Branch Chief of the
Behavioral and Structural Interventions Branch, leading and managing the Branch and its members as a
leading global expert in his technical area, managing and coordinating large, inter-agency PEPFAR technical
groups, and as an activity manager for HIV workstreams within a WHO Grant, managing between $5-14
million per fiscal year on HIV-related normative work.
Vincent has co-authored 29 peer-reviewed publications on HIV testing services that form the basis of this
PhD by Publication. These articles represent a diverse set of studies that include randomized trials,
observational studies, systematic reviews and meta-analyses, along with critical commentaries, conference
abstracts and WHO guidelines and resources.
His RG Score currently is 28.56 (higher than 85% of all ResearchGate scores) and his h-index is 14 (this
includes over 6500 compiled reads and 966 cumulative citations)1. Additionally, he has participated on five
HTS-related WHO Guidelines Committees, co-edited two HTS-specific journal supplements, co-presented
15 conference abstracts, and participated as writer or peer reviewer for 13 additional HTS-related WHO
products. His collective published work, presented in this submission, has had an impact in the public
health field of HIV testing services across fields of research, policy and global implementation.
In the course of his professional career, he has also delivered in-person technical assistance in the area of
HIV testing services to programs in Burkina Faso, Cambodia, Cameroon, Cote d’Ivoire, Eswatini, Ethiopia,
Ghana, Jamaica, Kenya, Lesotho, Mozambique, Nigeria, South Africa, Tanzania, Uganda, Vietnam and
Zimbabwe, and many additional country programs through virtual support or regional technical meetings.
Since 2000, Vincent has brought over 21 years of technical expertise and global leadership to the HIV
response within HIV testing services. This dissertation compiles and documents this collective public health
work in its entirety for consideration in partial fulfillment of the requirement for award of the Doctor of
Philosophy by Publication degree at the University of Portsmouth, United Kingdom.
1 Source: https://www.researchgate.net/profile/Vincent_Wong9

11
Abstract The HIV pandemic has existed for forty years. In 2020, there were an estimated 37.7 million individuals
living with HIV/AIDS. HIV testing services (HTS) have been a critical intervention to the global HIV response,
increasing knowledge of serostatus among persons living with HIV/AIDS and linking them to HIV treatment
to reduce HIV-related morbidity, mortality and transmission.
This thesis integrates my 29 peer reviewed articles within a health service coverage framework, and
includes additional contributions through conference abstracts and WHO guidelines from 2000 to 2020,
along with a purposeful, non-systematic review of other relevant literature. Across studies, methods
included randomized trials, observational studies, systematic reviews and critical commentaries. Ethical
approvals are included, and broader ethical issues around programming are addressed. Throughout this
period, four phases of HIV testing expansion are described and contextualize the thesis evidence base:
1. Early phase to increase HTS access (est. 2000-2004): Introduction and expansion of rapid HIV
testing, a prevention paradigm, limited treatment availability and the establishment of WHO
minimum standards.
2. HIV testing expansion (2005-2009): Increased funding, expansion of routine testing in clinical
settings, a scale up of community approaches; expansion of treatment access
3. Clinical paradigm focus (2010-2017): Increased understanding of ‘treatment-as-prevention’ and
early treatment, introduction of 90-90-90 goals and an increased focus on a continuum of HIV care
4. New HIV testing pathways (2017-2020) Expansion of HIV self-testing and index/partner testing to
reach new sub-populations; new approaches given high rates of diagnosis in some countries.
Across the included studies and articles, HTS domains were outlined within the Tanahashi health service
coverage framework to demonstrate the utility in analyzing program effectiveness and unmet need. and
increased availability and accessibility were achieved through a number of key findings:
Accessibility and Availability
• Increasing HTS Access through expansion of PITC, ANC testing and community based HTS that
reached PLHIV earlier; critical assessments of the use of risk screening tools
• Expansion of index and partner testing and effectiveness around reaching undiagnosed sexual
partners and identifying serodiscordant couples.

12
• Expansion of HIV self-testing with identified use and awareness, and leveraging to expand
coverage for example within OPDs or for key populations. Measuring linkage and outcomes
remains a challenge area.
Acceptability
• HIV testing quality evidence assessed the degree to which lay counselors have been integrated into
national policies; factors related to misdiagnosis and misclassification in HIV testing programs; and
programmatic output shifts resulting from HTS optimization strategies that include the integration
of index approaches.
• HIV testing service delivery and linkage to care included assessments of data gaps, facilitators and
barriers to linkage to treatment following diagnosis; how IPV services may be best integrated into
standard HTS; and best practices for providing psychosocial services for children receiving a positive
result.
Addressing Contact Coverage Gaps
• Studies identified HTS gap areas in populations at risk including adult males and pediatric
populations and identified correlates of ‘never testing’ among males that included low HIV
knowledge and higher acceptance of GBV and stigma. Through program data, testing access was
shown to be higher in females than males across 20 sub-Saharan African countries, largely a result
of high ANC testing rates. Age of consent policies were identified as one barrier to testing in
pediatric populations.
Findings demonstrate contributions to key HTS elements that resulted in increases in effectiveness through
increased proportions of PLHIV knowing their serostatus and accessing anti-retroviral therapy. Across low-
and middle-income countries, knowledge of serostatus among persons living with HIV/AIDS increased to
84% in 2020, with 73% of all PLHIV were estimated to be accessing HIV treatment.
Evidence and practice from 20 years of HIV testing programming, along with health service coverage
framing can inform future directions for achieving global 95-95-95 goals. Lessons learned from successes
and challenges in HIV can inform responses to other current and future pandemics.

13
Chapter 1: Introduction
1.1 HIV Testing Services: Health Service Coverage and HTS Paradigms
Forty years ago, in 1981, the first cases of HIV were identified in New York and California (U.S. Department
of Health & Human Services, 2021). Since then, an estimated 79.3 million people have been infected with
HIV globally and 36.3 million have died (WHO, 2021a). In 2020, the estimated global cases of HIV/AIDS was
37.7 million. While 1.5 million individuals were newly infected that year, it represented a 31% reduction
from 2010 (UNAIDS, 2020a). The burden of HIV infection around the world has disproportionately
impacted low- and middle-income countries, particularly sub-Saharan Africa. The African region now
accounts for 2/3 of the total global HIV burden with 3.6% of adults living with HIV overall (WHO, 2021a).
Key populations, who are both marginalized and at increased risk based on their behaviors, are at
substantially higher risk for infection: men who have sex with men have 26 times higher relative risk to the
general population for infection; for female sex workers it is 30 times (UNAIDS, 2020c) (UNAIDS, 2020e). It
wasn’t until the late 1990’s that the international HIV response efforts began; UNAIDS for example was
established in 1996 to advocate for action and coordinate the UN agencies in the fight against HIV. Prior to
2000, much of the focus on HIV control were interventions based in primary prevention of infection and
access to anti-retroviral therapy in LMICs were limited (AVERT, 2021).
Since the early days of the HIV response, HIV testing services (HTS) have been a core component of
interventions to control the epidemic. Fundamentally, the purposes of HIV testing services have been to
determine the serostatus of an individual – primarily based on an algorithm of rapid antibody assays - and
deliver needed services to individuals based upon those results. Those found HIV-negative would be
counseled and connected to prevention interventions to reduce risk of HIV acquisition, as well as informed
about the limitations of HIV testing and the need to retest if there was a recent exposure; those found HIV-
positive would be linked to clinical services that reduced morbidity and mortality (access to HIV treatment
and regimens would also change radically over the two decades), as well as prevent onward transmission
to sexual and injecting partners and infants born to positive pregnant women.
Epidemic typologies of countries have informed overall approaches to delivering HTS. These have
traditionally been divided into:

14
• Generalized epidemics, where the HIV prevalence in the general population is greater than 5%
and/or with consistently greater than 1% HIV prevalence in pregnant women (often established
through ANC surveillance as one proxy input for modelled estimates);
• And/or concentrated epidemics, defined by prevalence rates of greater than 5% through basic
numerical proxies in at least one subpopulation and <1% among urban pregnant women
(UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance, 2000) (UNAIDS, 2016a).
Initial HTS approaches differed depending on the type of epidemics. HTS programs in generalized
epidemics sought to maximize testing coverage through both multiple community and facility approaches,
maximizing the numbers of persons tested. Concentrated epidemic settings focused testing programs on
most at-risk populations. These “key populations” (KP) were defined by those with specific risk behaviors
that put those individuals at increased risk: female sex workers (FSWs), men who have sex with men
(MSM), and people who inject drugs (PWID) (WHO, 2014). While KP populations were focal populations for
interventions in all epidemics, there are notable regional differences that inform approaches based on
concentrated and generalized epidemic criteria.
In considering the expansion of HTS in any target population, the Tanahashi framework aligns health
service goals and achievements with the key factors of availability, accessibility, contact coverage and
acceptability (Tanahashi, 1978). Applied to HIV testing services, two discrete service achievement goals
evolved over time:
• An initial HIV testing prevention paradigm that emphasized broad access to HIV testing and
counseling, and sought to maximize broad population knowledge of sero-status, mitigate
behavioral risk, and prevent mother-to-child infections;
• and an HIV testing clinical paradigm that focused on HIV case detection in populations at risk, and
linkage to anti-retroviral therapy in a care continuum to reduce morbidity, mortality and risks of
onward transmission through viral suppression.
In the early phases of the HIV response (from roughly the late 1990s and early 2000s), HIV risk reduction
counseling and HIV testing were implemented as a key prevention intervention, and in US populations had
demonstrated effectiveness at reducing rates of sexually transmitted infections and increasing reported
protective behaviors such as rates of condom use (Kamb et al., 1998). Subsequent evidence around HIV
testing paired with risk reduction counseling – then termed “Voluntary Counseling and Testing” (VCT) -

15
showed some prevention benefits in Kenya, Tanzania and Trinidad including reduced reported rates of risk
behaviors (The Voluntary HIV-1 Counseling and Testing Efficacy Study Group, 2000). As VCT began to
expand as a key early HIV prevention intervention, UNAIDS established key program tools that framed a
number of minimum standards on counseling quality and content (UNAIDS, 2000a). HTS also began to be
integrated as a minimum standard of care for prevention of mother-to-child transmission with
introduction of ART-based prevention interventions into antenatal care (WHO, 2001).
With the expansion of anti-retroviral therapy that began in the early 2000s and accelerated each year (see
Table 2 below), HIV testing framing evolved from a prevention paradigm to a clinical paradigm, connecting
diagnosis to treatment. First, from around 2007, a greater emphasis was placed on HIV case detection in
clinical settings, including improving coverage of diagnostic testing as part of clinical care in generalized
epidemics (WHO, 2007). Second, there was a critical expansion of availability and accessibility to HIV anti-
retroviral therapy and increasing numbers of individuals as WHO eligibility criteria expanded and regimens
were simplified and costs reduced (UNAIDS, 2020a). ART coverage expanded from about 590,000
individuals accessing ART in 2000, or about 2.5% of all persons living with HIV/AIDS (PLHIV) to 25.4 million,
or an estimated 67% of all PLHIV (UNAIDS, 2020a). Thirdly, the evidence around the effectiveness of ART
therapy at reducing both viral load in individuals and preventing onward transmission of HIV led to both a
prevention and clinical therapy framing of HIV testing (Cohen et al., 2011).
Again, the Tanahashi framework applied here is
reframed in the context of an HIV clinical
paradigm. The overall end goal of service
achievement changed from testing 100% of a
given sexually active population in the context of
HIV prevention, to testing those at increased risk
with an aim of virological suppression of PLHIV in
a population. The target population therefore
shifted from the intermediate objectives of
numbers of persons tested (or % ever tested as
measured in many demographic surveys), and
focused on overall populations at risk
determined by sub population, geography or Figure 1: Tanahashi health service coverage framework (adapted)

16
testing setting or modality, along with subsequent rates of diagnosis and linkage to treatment.
The core of this thesis centers on 29 peer reviewed articles published between 2006 and 2020, in addition
to conference abstracts and WHO guidelines and resources centered on increasing access to HIV testing
services to mitigate the pandemic. These articles and their findings cover a range of themes that include:
increasing the availability and accessibility of HIV testing services through facilities, communities, HIV self-
testing and index testing; they address elements of service quality, service delivery and linkage to care and
treatment as an aspect of effectiveness coverage; and they consider aspects of sub-populations such as
adult males and children who may be underserved. Together, and with other relevant literature, these
articles provide an evidence base on the progression and evolution of HIV testing services in low- and
middle-income countries that achieved an estimated 84% of PLHIV diagnosed in 2020 with 73% of PLHIV
estimated to be accessing life-saving HIV treatment.
17
1.2 Research Question, Objectives, Methods, Limitations
Within my published body of work, this thesis addresses the primary research question: How has access to
HIV testing services effectively expanded over a twenty-year period between 2000 and 2020? Additional
sub-questions include: How can this access to services be framed and evaluated within a health service
coverage framework? How have factors of availability, accessibility, acceptability, contact and
effectiveness coverage, and service program goals changed over time? In considering service goals and
effectiveness coverage, how have HIV testing service approaches changed over time? What are some of
the key lessons learned from the past twenty years of HIV testing research, policy and program
experience?
The objectives of this thesis are to provide a review of my contributions to global HIV testing programming
and coverage, and review contributing aspects of the overall expansion of HIV testing services in low- and
middle-income countries from 2000 to 2020. This period specifically covers and aligns with my professional
period of work in this area, but also parallels a period of rapid HIV testing expansion and evolution of
approaches to meet program goals. This thesis will examine key factors of global and program goals and
paradigms, provide some considerations of target populations, and increasing accessibility and availability
of HIV testing services among them. Secondarily, this thesis will utilize an overarching health service
framework to HTS and consider specific contextual elements as they relate to its discrete service goals and
frame my own key articles and publications that comprise this PhD by Publication submission.
Methodologies will include a review of both my own co-authored articles, abstracts and other works that
contributed to this expansion (Figure 4 below), along with a purposeful, non-systematic review of other
selected literature related to HIV testing programming, implementation science and global policy that will
provide an overview of the key evidence supporting and informing the objective of HTS and diagnostic
expansion as a core element of the global HIV response. HTS lessons learned from the past two decades
will be considered for the future of HIV and other potential pandemics. Additional published literature to
supplement the application’s publications will be included based on my knowledge and expertise.
As a non-systematic, purposeful review of my publications and related literature, this commentary aims to
provide a broad landscape analysis of two decades of HIV testing evidence, and programmatic and policy
impact, and is not intended to be exhaustive, systematic or meta-analytic in nature. While HTS
considerations, policies and applications can be considered global or worldwide context, the geographic
scope of my publications focuses primarily on generalized epidemics in sub-Saharan African countries
18
which bear the largest HIV burden globally and generalized populations. The time period of focus covers
my professional career, and time periods assigned within these years are approximations of program and
policy development. There may be instances of programming, policy or publications that are related and
fall outside of these years. While key populations are touched on in this commentary, they have not been
the specific focus of my published work, and are thus not a direct focus of the overall commentary.
Correlations with specific definitions of “epidemic control” are also beyond the scope of this commentary.
Finally, there is a limitation given the breadth of topics covered in this commentary on HIV testing
availability, accessibility, coverage, acceptability and the range of target populations is wide, and each area
could stand alone as a subject of in-depth systematic analyses.
19
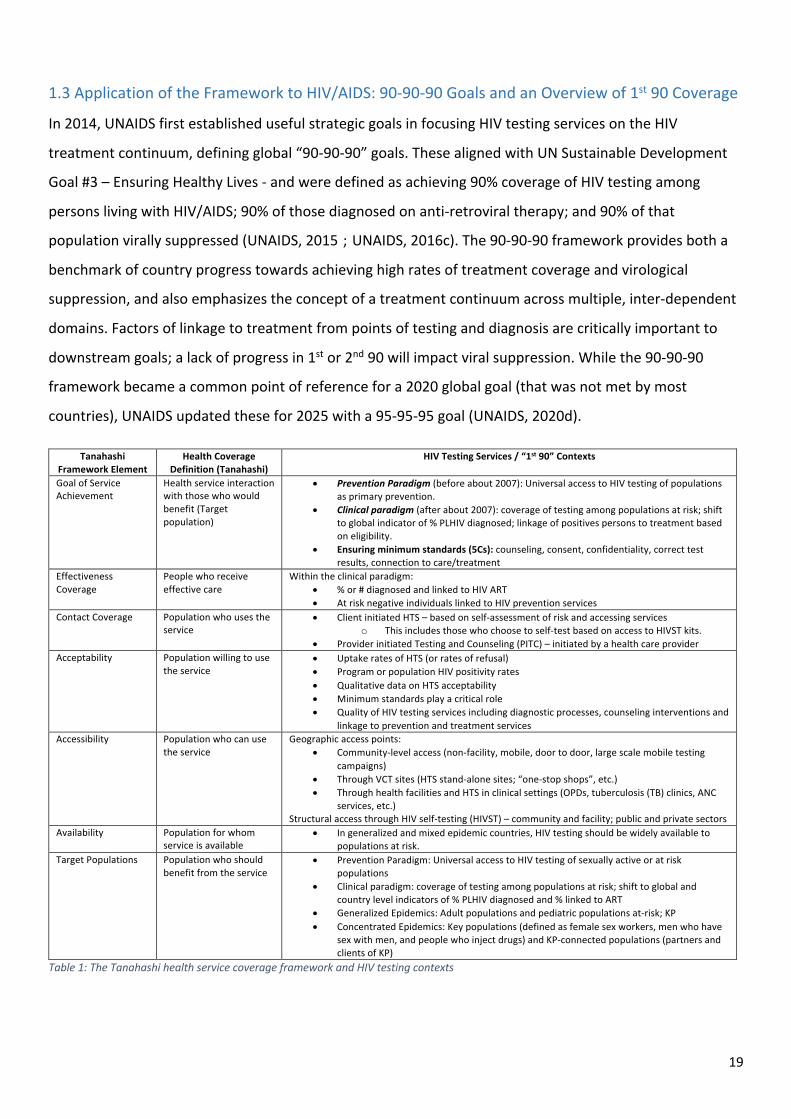
1.3 Application of the Framework to HIV/AIDS: 90-90-90 Goals and an Overview of 1st 90 Coverage
In 2014, UNAIDS first established useful strategic goals in focusing HIV testing services on the HIV
treatment continuum, defining global “90-90-90” goals. These aligned with UN Sustainable Development
Goal #3 – Ensuring Healthy Lives - and were defined as achieving 90% coverage of HIV testing among
persons living with HIV/AIDS; 90% of those diagnosed on anti-retroviral therapy; and 90% of that
population virally suppressed (UNAIDS, 2015);(UNAIDS, 2016c). The 90-90-90 framework provides both a
benchmark of country progress towards achieving high rates of treatment coverage and virological
suppression, and also emphasizes the concept of a treatment continuum across multiple, inter-dependent
domains. Factors of linkage to treatment from points of testing and diagnosis are critically important to
downstream goals; a lack of progress in 1st or 2nd 90 will impact viral suppression. While the 90-90-90
framework became a common point of reference for a 2020 global goal (that was not met by most
countries), UNAIDS updated these for 2025 with a 95-95-95 goal (UNAIDS, 2020d).
Table 1: The Tanahashi health service coverage framework and HIV testing contexts
Tanahashi Framework Element
Health Coverage Definition (Tanahashi)
HIV Testing Services / “1st 90” Contexts
Goal of Service Achievement
Health service interaction with those who would benefit (Target population)
• Prevention Paradigm (before about 2007): Universal access to HIV testing of populations as primary prevention.
• Clinical paradigm (after about 2007): coverage of testing among populations at risk; shift to global indicator of % PLHIV diagnosed; linkage of positives persons to treatment based on eligibility.
• Ensuring minimum standards (5Cs): counseling, consent, confidentiality, correct test results, connection to care/treatment
Effectiveness Coverage
People who receive effective care
Within the clinical paradigm: • % or # diagnosed and linked to HIV ART • At risk negative individuals linked to HIV prevention services
Contact Coverage Population who uses the service
• Client initiated HTS – based on self-assessment of risk and accessing services o This includes those who choose to self-test based on access to HIVST kits.
• Provider initiated Testing and Counseling (PITC) – initiated by a health care provider Acceptability Population willing to use
the service • Uptake rates of HTS (or rates of refusal) • Program or population HIV positivity rates • Qualitative data on HTS acceptability • Minimum standards play a critical role • Quality of HIV testing services including diagnostic processes, counseling interventions and
linkage to prevention and treatment services Accessibility Population who can use
the service Geographic access points:
• Community-level access (non-facility, mobile, door to door, large scale mobile testing campaigns)
• Through VCT sites (HTS stand-alone sites; “one-stop shops”, etc.) • Through health facilities and HTS in clinical settings (OPDs, tuberculosis (TB) clinics, ANC
services, etc.) Structural access through HIV self-testing (HIVST) – community and facility; public and private sectors
Availability Population for whom service is available
• In generalized and mixed epidemic countries, HIV testing should be widely available to populations at risk.
Target Populations Population who should benefit from the service
• Prevention Paradigm: Universal access to HIV testing of sexually active or at risk populations
• Clinical paradigm: coverage of testing among populations at risk; shift to global and country level indicators of % PLHIV diagnosed and % linked to ART
• Generalized Epidemics: Adult populations and pediatric populations at-risk; KP • Concentrated Epidemics: Key populations (defined as female sex workers, men who have
sex with men, and people who inject drugs) and KP-connected populations (partners and clients of KP)

20
One weakness of the goal structure given the relationships of the goal measurements is that the 90s are
not absolute measure of all PLHIV in a population across domains. In terms of coverage across the three
domains, this framework established lower baselines when the total estimated number of PLHIV is
considered: 90% rates of diagnosis among all PLHIV then corresponds to 81% treatment coverage and 72%
viral load suppression rates. Furthermore, there are additional epidemiological definitions around
epidemic control that include absolute reductions in incidence have been proposed that are
interdependent to 90-90-90 goals, but are beyond the scope of this commentary
(Galvani et al., 2018);(Ghys et al., 2018).
Survey data indicates HTS expansion and
increasing rates of diagnoses in many
generalized epidemic countries. WHO, in a
review of demographic health survey (DHS)
data, estimated in the time period 2004-2006
only an average of 16.7% of PLHIV had ever
been tested and received their results across
16 countries; the African countries of Tanzania,
Lesotho, Malawi, Uganda and Zimbabwe
averaged 19.6% (WHO, 2010c). More recent
HIV/AIDS surveys assessing 90-90-90 estimates by country in sub-Saharan Africa have demonstrated high
rates of diagnoses and treatment uptake ranging from 59% in Tanzania to 86% in Eswatini (see Figures 2
and 3) (ICAP, 2020). Further developments in refining modeling approaches have led to more accurate
estimations across countries (Marsh et al., 2019). Over a roughly 10 to 14-year span, surveys have
demonstrated marked increases in known status among persons living with HIV/AIDS. Select country
comparisons are included in Figure 2. In 2020, overall an estimated 84% of PLHIV are aware of their
serostatus (UNAIDS, 2020a) – a substantial jump from the early years of the HIV response.
Figure 2: Select country comparison of PLHIV known status rates, 2004-06 to 2016-18; Adapted from WHO, 2010c

21
Figure 3: Adapted from UNAIDS 2020: Diagnostic, treatment and viral load suppression coverage estimates by country, absolute percentages.
As we consider HIV testing availability, accessibility and contact coverage expansion, a number of
overlapping phases from the past two decades can be considered:
• Early Phase to Increase HTS Access in a prevention paradigm (from about 2000-2004): Early
expansion and adoption of HIV rapid testing, establishing global minimum standards, training of
lay counselors to expand access, establishing VCT sites for individuals to access testing
confidentially, use of mass testing campaigns and some community outreach testing; expansion
of HIV testing for prevention of mother-to-child transmission.
• An HTS expansion phase (from about 2005-2009): Increased investments (PEPFAR and Global
Fund) and increase in HTS access through additional modalities, expansion of facility-based
testing (PITC and ante-natal care testing) and community modalities including home-based HTS
• A shift to a clinical paradigm phase (from about 2010-2017): Increased targeting of existing
community and facility modalities; Increased understanding of ‘treatment-as-prevention’ and
the benefits of early treatment; introduction of 90-90-90 goals and an increased focus on a
continuum of HIV care; the importance of linkage to treatment becomes a focus; a focus on
couples testing and reaching at risk adolescents; evidence base for index and HIV self-testing
begins; HTS program positivity becomes a critical metric for program effectiveness.
Source: UNAIDS, 2020. Website: https://aidsinfo.unaids.org/

22
• New HIV testing pathways (from about 2017-2020): Expansion of new modalities to reach
undiagnosed: index testing and HIV self-testing; a renewed emphasis on linkage to prevention
for HIV negative persons; reduced positivities in clinical settings and many countries achieving
high rates of diagnosis. Newer technologies on the horizon including more blood based HIVST
kits; Ag/Ab rapid tests for detection of acute infection; and multiplex assays for detecting
diseases in addition to HIV such as syphilis.
Key aspects of this global HTS programming and policy across this time period and these phases will be
described, along with my critical contributions through the articles included.

23
1.4 Overview and Mapping of Key Select Co-authored Articles and Abstracts included in
Submission
The expansion of HTS can be aligned with a fundamental framing of health care access that is well
described by the Tanahashi framework, which addresses health interventions generally. HTS goals have
been established within the global goals of the UNAIDS’ 90-90-90 targets for HIV specifically. Here, HTS is a
core component to achieve 90% of persons living with HIV/AIDS diagnosed, and 90% receiving anti-
retroviral therapy (ART) (meaning those diagnosed have been successfully linked to treatment). My
contributions to the evidence base and literation on HIV testing services map to the health access
framework, with HTS domains tracking to availability, accessibility, acceptability, and contact coverage
(Figure 4). Notes on authorial contributions can be found in Table 3, Section 3.1.
Figure 4: Publication Map for Vincent Wong by HIV Testing Domains and Tanahashi health access elements.
Acceptability of Service Delivery Accessibility and Availability
Contact Coverage Gaps
Accessibility and Availability / Contact Coverage
Bold titles indicate first or last authorship; Authorial contributions listed in Section 3.1, Table 3. Participation in select WHO institutionally
authored products included in blue shaded boxes. See Chapter 3 for a detailed list of included publications and full citations.

24
1.5 Ethics and ethical approvals related to articles
All relevant research and studies published were undertaken in accordance with ethical standards of the
institutional and/or national research committees. Where relevant and client/patient level data was
collected, informed consent was obtained by all individual participants. Studies and their protocols have
been approved by the appropriate institutional ethics committees or review boards, in addition to the
appropriate IRBs in respective countries who have also approved the study protocols. Where required,
ethical approvals are detailed in the individual articles included in Appendix 1.
In addition to ethical approvals obtained for research included as part of this portfolio, it is worth
mentioning a number of broader ethical issues presented by HTS programming globally. Many ethical
issues can be addressed through meeting WHO’s 5C minimum standards (consent, confidentiality,
counseling, correct test results, connection to treatment), or conversely are a result of breaches in these
standards (See Section 2.1.2). Issues that require continued vigilance to ensure ethical programming can
be framed across the 5C standards and include:
• Ensuring informed consent for all forms of HIV testing. Coerced or mandatory testing does not
have a public health benefit, and WHO has continued to emphasize all HIV testing needs to remain
voluntary and consensual (WHO, 2015b). This includes all HIV self-testing as well as initiating safe
and ethical partner notification or index testing processes (see Section 2.4.2 for additional
considerations) (WHO, 2016d).
• Adequate counseling needs to be provided around all HIV testing to ensure that consent is
informed, and to ensure individuals testing – whether positive or negative - have information
sufficient to act on results to reduce HIV morbidity, mortality and transmission/acquisition (See
Section 2.1.2).
• Maintaining confidentiality of HTS processes and individual results, particularly giving the ongoing
stigma related to HIV/AIDS (See Section 2.1.2).
• HIV test kits and testing algorithms need to be established ensuring that individuals receive correct
test results, positive and negative predictive values are maximized, and risks or misclassification
are minimal (See Sections 2.1.1 and 2.1.2).
• Ensuring connection to HIV treatment and preventions services. Testing alone is insufficient to
achieve public health outcomes, and access based on results to both HIV treatment and effective
prevention needs to be ensured (See Section 2.3.1).

25
Chapter 2: Primary Commentary: Evolution and scale up of global HIV testing
service approaches: 2000-2020
2.1 Key Developments and Paradigms for the Global Introduction of HIV Testing (2000-2004)
2.1.1 The Introduction of HIV Rapid Diagnostics as a Key Technological Development
The development and introduction of rapid HIV antibody tests was a game changer in the programmatic
response to the HIV epidemic. HIV test results from lab-based assays such as enzyme immunoassays (EIAs)
and Western Blot assays used for confirmation required individuals to return one or more weeks later for a
result. In the late 1990s, an estimated 40% of cases never received their test results (Coovadia, 2000). At
early stages of development, there was clear recognition that same day results delivered substantial
benefits to the person being tested (MMWR, 1998). In 1997, WHO and UNAIDS recognized the potential
impact this simple diagnostic technology would have globally (WHO and UNAIDS, 1998). With the
translation of lab-based testing utilizing complicated assays such as EIAs and Western Blot based
diagnostics and requiring specialized expertise, to simple, rapid diagnostic test (RDT) kits in the late 1990s
and early 2000s, access to diagnostics was able to expand rapidly (WHO and UNAIDS, 1998). RDTs were
simple to perform, inexpensive, temperature-stable (requiring no cold chains) and, importantly, delivered
results on the same day or even hour (WHO and UNAIDS, 1998). In 1998, one Ugandan program provided
early evidence of high sensitivity and specificity (up to 100% in their sample) of the use of rapid tests in a
two-test algorithm and increasing the proportion of results returned (Downing et al., 1998) (Kassler et al.,
1998).
My own early work began in 2000 on research and development of HIV rapid diagnostic assays as an early
example of translating of more complex lab-based HIV testing such as EIAs into rapid HIV antigen-based
assays (Repke, Wong et al. 2002). Here, our HIV antibody rapid test (“InstantScreen®”) was developed as a
flow-through device where HIV antigens (specifically, gp120 and gp40) were blotted onto a membrane
which then captured HIV antibodies in the sample and resulted in a color signal; sensitivity and specificity
here were found to be 100% (WHO, 2002a). Most simple, rapid diagnostic tests provide a qualitative
“yes/no” result, require no cold chain, and provide results within about five minutes (WHO, 2015a). In
laboratory evaluations against characterized HIV positive and negative sera, the assay was found to have
100% sensitivity and specificity (Souza RS, 2002). By January 2002, WHO had evaluated seven simple, rapid
blood-based assays on the market and had established recommendations for minimum performance
standards at 99% sensitivity and 98% specificity. Six of these test kits were priced under $2 at that time and
performed well with sensitivities of 100% and specificities of >99% (WHO, 2002a).

26
As access to rapid diagnostic tests expanded, guidelines were also established for their use cases, with
separate algorithms recommended based on their purposes:
transfusion screening, surveillance and diagnosis (WHO and
UNAIDS, 1997);(WHO, 2004). Early on, a three-test algorithm
became the basis for the expansion of diagnostic capacity in
many low- and middle-income countries in populations and
geographies of high prevalence for both generalized and
concentrated epidemics. This required the use of a series of
different RDTs that met minimum performance standards. The
definition of algorithms for the purposes of diagnosis meant
that in populations of higher prevalence, final outcomes based
on a series of assay results would achieve higher positive
predictive values. For diagnostic purposes this was critical,
later re-affirmed in WHO guidance (WHO, 2015a). Negative results were not confirmed with additional
testing, and one substantial limitation of antibody-based diagnostics (both rapid format and lab-based
EIAs) was the risk of false negative results in the initial period following infection and prior to antibodies
being developed. The so-called “window period”, earlier defined as 4-6 weeks post infection, and more
recently with improved diagnostics established at about 3 weeks led to tailored counseling and retesting
recommendations for those with recent exposures (UNAIDS, 2000b);(Delaney et al., 2017);(WHO, 2010a).
In an era of minimal treatment access in low- and middle-income countries, rapid HIV tests became an
indispensable tool for HIV prevention and clinical programming. How and where these diagnostic tools
were deployed, and for whom HIV testing was available and accessible, became a cornerstone of the
global response to the HIV pandemic.
2.1.2 Adoption and Expansion of HIV Testing Service Minimum Standards (3C and 5C)
In parallel to the technological developments of rapid HIV diagnostic tests, WHO established minimum
standards to protect the health and rights of populations and individuals at risk and accessing HTS (WHO,
2005; WHO, 2016). Early standards were established in the United States with a focus on confidentiality,
voluntariness and risk reduction counseling, with CDC issuing a series of recommendations between 1994
and 1999 based on evidence around sero-status based counseling (CDC, 2001). Shortly thereafter, WHO
and UNAIDS established critical minimum standards in the early 2000s, supporting both the acceptability
of HIV testing and counseling services, and providing a framework that ensured that service delivery
Figure 5: WHO HIV testing strategy for high prevalence settings (>5%), 2015
27
(whether in the community or through facilities) would meet the same minimum criteria. These included
what early on became known as the “3C” standards: all testing would need to comply with informed
consent, confidentiality and counseling. These core criteria were foundational to initiating and
subsequently expanding early implementation globally.
With minimum standards established, and simple, affordable diagnostic tools available, WHO focused on
making HIV testing widely available for all through a “right to know” approach to access (WHO, 2002b)
(WHO, 2003). Recommendations here emphasized integration for HIV primary prevention, as a core
component of prevention of mother-to-child transmission, and for those with signs or symptoms of HIV.
There was a heavy emphasis on “scale up”, ensuring it was voluntary, and that post-test services were
critical. UNAIDS and WHO also made clear (in 2004 and again in 2012) that mandatory HIV testing was
counter-productive (UNAIDS and WHO, 2012).
My work on attainment of these early minimum standards were outlined in my 2005 Master’s Thesis and
subsequent IAS 2006 submission and focused on early implementation and accessibility and acceptability
in one West African country, Ghana, with an estimated HIV prevalence of 3% (Wong V, 2006). Here,
through a site level analysis, we identified a diversity of access points for HIV testing in both the public and
private sectors. Overall, there was variable application of standards around consent, confidentiality and
counseling, with only 1/3 of all sites at that time aware of normative guidelines, and the non-governmental
sector qualitatively performing better. In 2009, I conducted a policy analysis and literature review for
WHO, finding that across 147 studies there was high uptake of HIV testing services in clinical settings, a
high return rate for results (which was an early argument for moving to rapid based testing formats); and
an absence of counseling was noted only in a minority of studies reviewed (Wong & Sabin, 2010).
Additional standards were further codified by WHO in 2012 as the 5Cs – adding correct test results and
connection to care as minimum criteria (WHO, 2012c). These elements highlighted the importance on
ensuring both access and connection to anti-retroviral therapy and effective HIV prevention interventions
(such as voluntary male medical circumcision (VMMC) and pre-exposure prophylaxis (PrEP)), and quality
HIV testing – both RDTs and testing processes - that resulted in accurate results delivered to clients. All HIV
testing “should strive to provide high-quality testing services, and quality assurance mechanisms should be
in place to ensure the provision of Correct test results” and “provide Connections to prevention, Care, and
treatment services. This includes the provision of effective referrals to follow-up services as indicated,
including long-term prevention and treatment support”. As previously mentioned, WHO re-testing

28
guidelines aimed at minimizing missed diagnoses during the acute phase of infection by developing
counseling messages around retesting two weeks later if recent exposure is suspected, and in other cases
(WHO, 2010a).
My additional work around HIV testing quality was included in a number of co-authored presentations, a
systematic review and a WHO Guidelines Annex. Following reports of false diagnoses being identified in
several African countries (DRC, Burundi and Ethiopia), a focus on the quality of testing and ensuring correct
test results was at the fore (Shanks et al., 2013). In 2014, we began a systematic review of reports of false
positives or negatives in published literature. Here we identified an interquartile range of 0.4-5.2% for
false positives (30 studies provided reports on false-positive diagnostic errors), and 0-3.9% for false
negatives (28 studies provided reports on false-negative diagnostic errors) (Johnson C et al., 2014)
(Johnson C et al., 2017). In our review, almost all studies reporting false positives indicated the use of a
suboptimal testing strategies with sixteen indicating the use of a “tiebreaker” testing strategy (where a
third rapid test is used to resolve discordant results in the initial two assays), and one study reporting
misdiagnosis in Ethiopia through HIV-positive diagnosis based on a single HIV RDT. Factors contributing to
false negative errors included: Clerical and user errors, early/acute infection, presentation late in disease
stage and individuals with known HIV status on ART who sought retesting, or were retested using oral
fluid-based RDTs.
The quantitative and qualitative data reported on HIV misclassification through testing services provided
specific evidence that informed subsequent global guidelines (Johnson C, 2016). These included specific
recommendations reiterating the use of appropriate testing strategies and algorithms based on HIV
prevalence of settings and geographies, as well as the introduction of retesting for verification at clinical
sites prior to ART enrollment to ensure positive sero-status and address potential user errors in the initial
testing event (WHO, 2015b).
Ultimately, the diagnostic minimum performance criteria, testing strategies that sought to maximize
positive predictive values, and standards that informed and protected clients around testing for a highly
stigmatizing disease aimed to increase service availability and accessibility, as well as acceptability by
ensuring the quality and reach of the HIV testing services delivered.

29
2.1.3 HIV Testing and its Role in HIV programs and response in a Prevention paradigm Mitigating the HIV
Epidemic
With early introduction of HIV testing services, particularly in sub-Saharan African countries and
generalized epidemics, the intervention was established primarily within an HIV prevention paradigm.
Elements shown to be effective in high income countries such as the United States demonstrated the
potential for pairing HIV testing, knowledge of sero-status and tailored counseling to reduce exposure
through lower risk behaviors (Higgins et al., 1991);(Kamb et al., 1998). With reduced HIV risk behavior
outcomes in three countries (Trinidad, Kenya and Tanzania), intervention groups receiving both HIV testing
and counseling reported significant reductions in the key risk behavior of unprotected intercourse
compared to control groups receiving only health information (The Voluntary HIV-1 Counseling and Testing
Efficacy Study Group, 2000). This difference was more pronounced in those found to be HIV-positive.
While these outcomes were based on self-report, another early Ugandan VCT study demonstrated
significant reductions in STI infections in an intervention group (Wawer et al., 1999). Critically, the VCT
Study Group found that HIV testing and counseling interventions would be a cost effective in high
prevalence populations with a cost per HIV infection averted in Kenya and Tanzania of US$249 and $346,
respectively, and the cost per DALY saved was $12.77 and $17.78 (Sweat et al., 2000).
The finding of the potential of population level access to HIV testing and counseling to mitigate HIV
transmission translated into a number of countries with generalized epidemics initiating “know your
status” campaigns and expanding HIV counseling and testing service access under the term “Voluntary
Counseling and Testing” or VCT. Differentiated messaging based on serostatus intended to reduce risk
behaviors, connect PLHIV to care, and implement early prevention to mother-to-child transmission
(PMTCT) interventions. UNAIDS promoted these efforts in 2000 as a “relatively cost-effective intervention
in preventing HIV transmission”, and developed program tools for assessing VCT quality and effectiveness
as an HIV prevention intervention (UNAIDS, 2000b);(UNAIDS, 2000a). VCT’s early focus was on
confidentiality, prevention and risk mitigation, and limited treatment availability in a context of high levels
of stigma (Matovu & Makumbi, 2007). Broadly, VCT aimed to maximize HTS availability and knowledge of
serostatus with HIV prevention as a primary objective (Marum et al., 2008);(Holtedahl et al., 2007);(Mills &
Chong, 2006). Systematic reviews demonstrated an “increase in the odds of condom use/protected sex
among participants who received VCT compared to those who did not”, and a more pronounced and
statistically significant finding when stratified by HIV positives, with a 3.24 odds ratio compared to non-VCT
populations (Fonner et al., 2012). Other reviews found statistically significant reduced rates of unprotected
sex, but no evident impact on the number of sex partners (Denison et al., 2008). Both an abundance of

30
stand-alone VCT site, and large scale HTS campaigns served to increase availability and accessibility of HTS
for populations in many countries (McOwan et al., 2002);(M. Sharma et al., 2015);(Marum et al., 2012);
(Holtedahl et al., 2007). However, even with minimum standards, pressures to expand testing also resulted
in rights-based concerns (Human Rights Watch, 2008).
With the context of low levels of knowledge of serostatus in most low and middle-income countries in the
early 2000s (as mentioned previously and
illustrated in Fig 2), the intersection of VCT
prevention benefits, established minimum
standards and demonstrated diagnostic tools,
foundations were in place for dramatic
expansion. Note that while this thesis does not
assess overall HIV testing funding analyses, it is
worthy of mention that both the
establishment of the Global Fund (GF) and the
US President’s Emergency Plan for AIDS Relief
(PEPFAR) provided the needed funding required to scale these services. The funding for HIV testing
expanded substantially from about 2005 onwards (Macro International, 2009);(Marum et al., 2012). For
PEPFAR this resulted in about $200M per year across roughly 50 countries globally (PEPFAR, 2021c)
supporting HTS.2 Within this time frame, PEPFAR programming expanded its delivery of HIV testing from
9.4 million in FY2005 to 79.1 million tests in FY2019 and 63.3 million in FY2020 (PEPFAR, 2006);(PEPFAR,
2021a);(PEPFAR, 2020b). Global Fund also expanded its levels of HIV testing from 4.2 million tests reported
in 2005 to 133 million in FY2019 (Global Fund to Fight AIDS, 2006);(Global Fund to Fight AIDS, 2020a).
2.1.4 Testing coverage rates and the state of access and coverage to Anti-retroviral therapy over time
Between 2003 and 2006, with knowledge of serostatus among PLHIV estimated across several countries to
be 16.7% (see Figure 2), WHO showed that the total number of PLHIV diagnosed per year demonstrated
the expansion over time of the absolute numbers of persons testing positive (WHO, 2018). This overall has
driven increased contact coverage among populations to HTS Services through increases in both
2 Note these estimates are conservative analyzing budgets “tagged” for HIV Testing (e.g., budget code: HVCT) within PEPFAR programs; there are additional PEPFAR budget lines that contribute to elements of HIV testing services and are not included here. Examples include treatment (HTXS), prevention (HVOP) and PMTCT (MTCT). Assessing HTS contributions from within these budget codes is complicated given their broader purposes and beyond the scope of this thesis.
Figure 6: PEPFAR HIV Testing indicated funding (HVCT) 2006-2020. PEPFAR, 2021.
31
acceptability (based on multiple factors included increased confidentiality, rapid and accurate results, etc.)
and availability/accessibility (through increasing modalities to obtain HIV testing by different populations).
Recent UNAIDS modeling approaches (known as “Shiny 90”) confirmed increases in the proportion of
PLHIV diagnosed and on ART based on both program and surveillance data. In Cote d’Ivoire, Malawi and
Mozambique, Shiny 90 models demonstrated substantial increases in PLHIV aware of status from 2000 to
2019, reduced positivity rates over time, and a substantial proportion of positives estimated to be PLHIV
on ART retesting. (Maheu-Giroux et al., 2019).
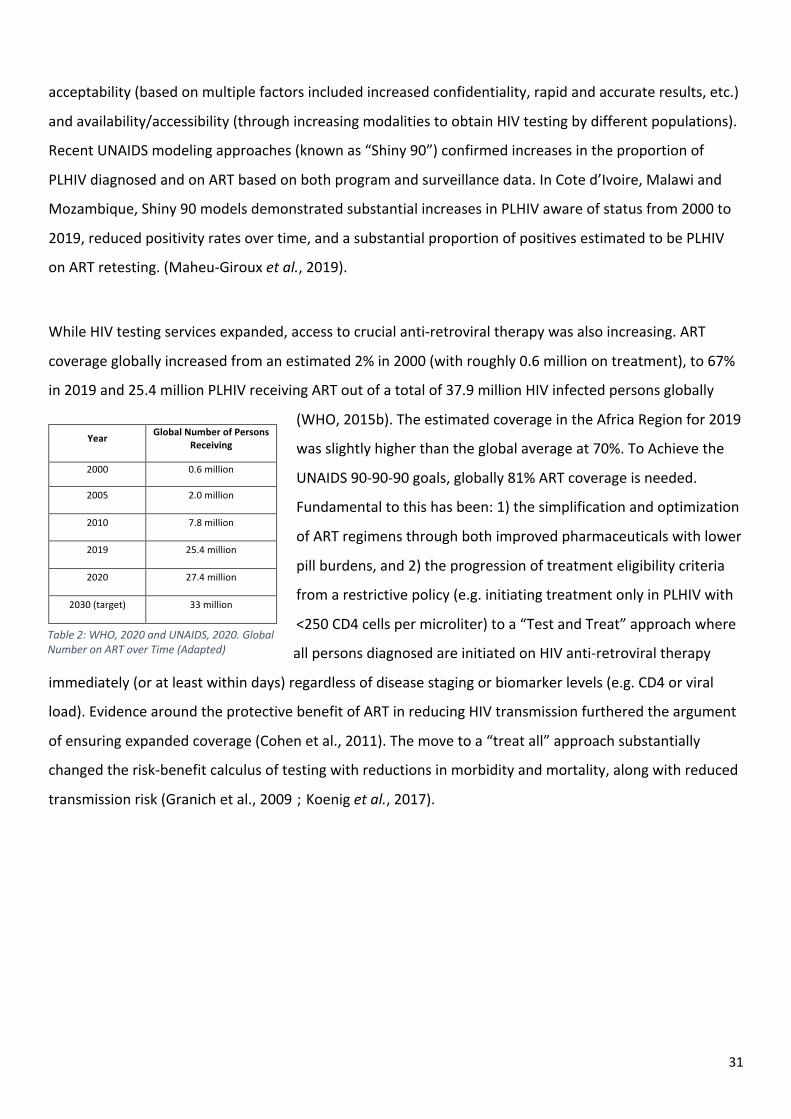
While HIV testing services expanded, access to crucial anti-retroviral therapy was also increasing. ART
coverage globally increased from an estimated 2% in 2000 (with roughly 0.6 million on treatment), to 67%
in 2019 and 25.4 million PLHIV receiving ART out of a total of 37.9 million HIV infected persons globally
(WHO, 2015b). The estimated coverage in the Africa Region for 2019
was slightly higher than the global average at 70%. To Achieve the
UNAIDS 90-90-90 goals, globally 81% ART coverage is needed.
Fundamental to this has been: 1) the simplification and optimization
of ART regimens through both improved pharmaceuticals with lower
pill burdens, and 2) the progression of treatment eligibility criteria
from a restrictive policy (e.g. initiating treatment only in PLHIV with
<250 CD4 cells per microliter) to a “Test and Treat” approach where
all persons diagnosed are initiated on HIV anti-retroviral therapy
immediately (or at least within days) regardless of disease staging or biomarker levels (e.g. CD4 or viral
load). Evidence around the protective benefit of ART in reducing HIV transmission furthered the argument
of ensuring expanded coverage (Cohen et al., 2011). The move to a “treat all” approach substantially
changed the risk-benefit calculus of testing with reductions in morbidity and mortality, along with reduced
transmission risk (Granich et al., 2009);(Koenig et al., 2017).
Table 2: WHO, 2020 and UNAIDS, 2020. Global Number on ART over Time (Adapted)
Year Global Number of Persons
Receiving
2000 0.6 million
2005 2.0 million
2010 7.8 million
2019 25.4 million
2020 27.4 million
2030 (target) 33 million
32
2.2: Expansion of HIV testing service delivery through facility and community HTS scale up. (2005-
2009)
2.2.1 Provider Initiated Testing and Counseling in Facilities
While initial efforts at HIV testing expansion in many low and middle-income countries focused on the use
of VCT and campaigns within prevention programming, and expansion within ANC/PMTCT contexts, a key
limitation was the primary method of service delivery through stand-alone sites that emphasized
confidentiality and extensive risk reduction counseling. One result of this approach was providing HIV
testing services that were largely dependent upon individual assessment of risk and decision making, and
client-initiated action to seek testing. Overall, this established some inherent limitations to accessibility;
HTS services were primarily accessible to those who decided to seek testing specifically. HIV stigma
continued to be a significant structural barrier to individuals seeking HTS (Wolfe et al., 2006).
From about 2005 to 2007, a number of countries began to expand policies focusing on HIV testing within
clinical settings. For example, the US, Botswana and Kenya all developed guidelines establishing broad
based HIV testing in clinical settings and for pregnant women through what was termed “routine HIV
testing” or “opt out” testing (NASCOP, 2006);(Weiser et al., 2006);(Branson et al., 2006). The intention was
broad based screening of clients and patients attending clinical services to maximize the numbers of
individuals tested and positive persons identified (Steen et al., 2007). In 2007, WHO provided specific
guidelines on what was termed “provider-initiated testing and counseling”, or PITC and outlined a number
of specific recommendations that aimed to expand availability beyond the existing VCT-based models
(WHO, 2006).
My work in the area of PITC introduction and its expansion covered a number of areas related to
accessibility (through uptake metrics), acceptability and policy. Our systematic reviews demonstrated that
across African country settings, studies showed PITC resulted in: high uptake and acceptability in ANC
settings with >90% rates of counseling, and identified challenges with linkage from testing to PMTCT
(Hensen B & Wong VJ, 2012); across a broader range of PITC settings, we found overall high rates of
acceptability and, by 2010, over 80% of countries had national policies on PITC (Baggaley et al., 2012); and
we compared PITC outcomes to community-based testing (see Section 2.2.2 below), where our meta-
analysis showed lower CD4 levels (i.e. later stage diagnosis) correlated with facility-based testing in five
studies, as well as higher positivity rates and no reported harms (Suthar et al., 2013). The correlation of
PITC with late diagnosis was confirmed in other studies, highlighting the challenges with reaching PLHIV at

33
earlier disease stages (Topp SM, 2014). With the expansion of programs and policies from about 2005,
facility-based testing became a major testing modality leading to increased diagnoses and has for some
years been the largest volume modality for diagnoses. For example, our recent review of 2019 PEPFAR
testing data showed that about 63% of all positives were identified through PITC modalities in sub-Saharan
African countries (Drammeh et al., 2020).
Based on early evidence of good outcomes and limited harms, WHO PITC recommendations included:
• Recommending an “opt out” approach that would maximize testing coverage in health facilities
• Simplifying pre-test counseling to pre-test information and focusing on those elements needed to
allow for informed consent.
• And establishing key criteria for different epidemic types, where HIV testing is recommended:
o For all patients irrespective of epidemic setting whose clinical presentation might result
from underlying HIV infection
o As a standard part of medical care for all patients attending health facilities in generalized
HIV epidemics
o More selectively in concentrated and low-level epidemics.
o And PITC should be accompanied by a recommended package of HIV-related prevention,
treatment, care and support services
Expansion of PITC was not without criticism, with concerns that expansion of testing through PITC could
lead to rights abuses, negative outcomes, particularly among women and girls (Csete et al., 2004; Gruskin
et al., 2008). Early systematic reviews of PITC outcome studies showed increased uptake and minimal
reports of negative outcomes (Kennedy et al., 2013). However documented challenges as PITC began
implementation included burdens on health systems and poor linkage to care (Roura et al., 2013).
2.2.2 Community based HTS
Community-based HIV testing (CBHTS) can largely be considered HIV testing that occurs outside of a health
facility. Across health service coverage metrics, community-based approaches would have the ability to
impact most of the service achievement goals. Beginning with expanded availability, accessibility,
acceptability, contact coverage, effectiveness coverage leading to an uptake in HIV treatment services
among eligible populations.

34
In 2012 and in 2015, I was part of a WHO HTS guidelines development group; we articulated frameworks
for community based HIV testing and its aims (WHO, 2012c);(WHO, 2015b). While there are a range of
different approaches, the overall aim of community-based HTS are to reduce structural and logistical
barriers to availability and accessibility coverage, and reduce potential stigma that may be associated with
accessing testing in health facilities.
Here we outlined a range of demonstrated community-based testing settings including:
• Home-based – including offering HTS door-to-door in a specific catchment area, or targeted
through community index testing services (see below).
• Outreach (for general or key populations) – this includes HTS delivered through temporary sites
established with the use of vans or tents, or within existing establishment serving target
populations (e.g., bars, brothels, entertainment venues). This includes event-based HTS approaches
and campaigns
• Workplace – targets populations within employers and/or sectors where HIV prevalence is high and
structural barriers (such as clinic opening hours) present an access barrier.
• Schools/colleges – target populations include sexually active youth with an aim to provide both
early access to treatment if needed and HIV prevention services.
The widespread availability of simple, rapid HIV tests within validated algorithms, and the use of lay testing
cadres allowed for deeper availability of HTS beyond health care settings directly within communities.
UNAIDS in 2010 emphasized a recognized limitation in facility-based approaches, stating “HIV testing and
counselling must be expanded, as most people get to know their status very late and access treatment
later, which reduces the effectiveness of treatment programmes” (UNAIDS, 2010).
A number of studies have looked at key outcomes of community-based HTS. In our published meta-
analysis, we demonstrated from published studies that community-based HTS overall reached more first-
time testers, identified PLHIV with higher CD4 levels (i.e. is correlated with earlier diagnosis), but had lower
positivity rates (Suthar et al., 2013). We inferred from these finding that community-based modalities
reached individuals who may have had less engagement with traditional health services (i.e., these HTS
modalities compensate for lower acceptability or contact coverage of traditional health services) and is
able to reach PLHIV earlier in disease stage. In one multi-country, cluster randomized trial, Sweat et al.
compared community to facility based VCT in Tanzania, Zimbabwe and Thailand. The community
intervention included mobilization activities, VCT services and community-based support post-testing.
35
Compared to facility based VCT, community VCT demonstrated statistically significant higher rates of first
time testers, higher rates of overall uptake with a mean difference of 40%; lower positivity rates, but four-
fold more cases detected in the community arms (Sweat et al., 2011). In another systematic review,
Sharma et al. looked at community HTS and its contribution to linkage to care from diagnosis (i.e. the first
two 90s), finding that different community-based modalities achieved a number outcomes of interest
relevant to effectiveness coverage: mobile testing was able to reach more males; mobile outreach to key
populations had the highest positivity rates. Overall there was higher pooled coverage rates among
community-based HTS across all modalities compared to facility-based (Monisha Sharma et al., 2015). Here
within the studies included there was overall, increased accessibility of community-based HTS, high levels
of acceptability as measured by uptake rates among those offered services, as well as increasing
availability generally.
Following the initial establishment of client-initiated VCT sites, the expansion of availability and access of
clinical testing in health facilities for patients, ANC attendees and others, the implementation of active
community outreach greatly expanded service achievement goals along with all the sub-objectives,
increasing availability through effectiveness coverage. These achievements are key to achieving the first
two of the UNAIDS’ 90-90-90 global goals.
As the programmatic evidence grew for expanding implementation of community HTS, we developed a key
framework focused for door-to-door approaches on planning, implementing and monitoring home-based
HIV testing and counseling (Taegtmeyer et al., 2012). This early community-based strategy aimed to
reduce access barriers by reaching at-risk populations in their homes (WHO, 2012b). Essential elements
were compiled based on program promising practices from Uganda, Kenya and Eswatini (then, Swaziland)
at that time, and included a number of critical areas that led to successful programming, including:
• National coordination and support
• Planning for human resources including safety and training
• Geographic mapping of households, HIV data
• Community mobilization through mass communication channels and gaining support and
endorsements of local leaders.
• HTS protocols in home settings (including quality assurance measures)
• Data collection and protection
• Follow-up and linkage to additional services

36
A further extension of a blend of community-based approaches were large-scale HIV testing campaigns
that frequently sought to reach large proportions of populations, and integrate additional health services
such as malaria and TB screenings. Early efforts documented ethical issues and rights violations due to
coercive or non-consensual testing (Human Rights Watch, 2008). In Botswana, one extended trial that ran
from 2013 to 2018 demonstrated using community-based HTS approaches to exceed 90-90-90 goals and
achieve 30% reductions in incidence (Lockman et al., 2020). Other East African studies showed high levels
of coverage achievable with incidence reductions, but control groups showed comparable reductions likely
due to increased coverage of ART (Havlir et al., 2019). While structurally such integrated approaches made
HTS services widely available, they specifically appeared to increase both acceptability and contact
coverage with close to 90% of residents accepting HTS with nearly 40% of persons positive newly
diagnosed (Chamie et al., 2016).
Broadly community-based HTS comprises multiple, non-facility approaches that increase key health service
coverage metrics: accessibility, acceptability and contact coverage, as well as overall effectiveness in ART
coverage rates. CB-HTS has been demonstrated to be an effective approach that reaches individuals earlier
in disease stages and underserved populations such as men and youth. A number of studies have shown
the contribution CBHTS can make towards achieving and even exceeding 90-90-90 goals.
2.2.3 Author contributions to the expansion of access and coverage in specific populations
HIV testing service achievement and 1st 90 coverage can be considered by sub- or target populations. The
health service coverage framework elements when viewed through specific at-risk sub populations and
their relation to 90% diagnosis rates. The scope of this commentary limits the extent of any full review of
each of these populations. My authorial contributions across a number of sub-populations serves to
highlight critical groups who need to be reached as an overarching service achievement goal of HTS across
a range of modalities.
Pregnant women and antenatal care
Access to prevention of mother-to-child transmission interventions led to the early prioritization of HIV
testing within antenatal care (ANC) settings (WHO, 2002b). In our 2012 policy review of all provider-
initiated HTS national guidelines in African countries, of the 42 out of 53 policies reviewed with a PITC
component, all had included PMTCT, with about 44% adopting policies in 2005 or 2006 (Baggaley et al.,
2012). This demonstrated an unambiguous policy shift moving towards not only testing for clinical case
management, but towards treatment for the benefit of prevention of vertical infant infection. In our

37
systematic review from 2011, ANC testing uptake expanded following the introduction of an opt-out,
provider initiated approach, with high rates of pre- and post-test counseling, but challenges at that time
with effective linkage to care and treatment, ranging from 53-77% (Hensen B & Wong VJ, 2012).
Couples HIV testing
From 2011 to 2012, I participated on a WHO Guidelines Group, developing WHO’s Guidance on couples’
HIV testing and counselling including antiretroviral therapy for treatment and prevention in serodiscordant
couples (WHO, 2012a). Couples HTS was defined as “when two or more partners are counselled, tested
and receive their results together. When couples receive their results together, there can be mutual
disclosure of HIV status, and the couple can receive appropriate support and be linked to follow-up
services”. The focus on couples testing was initially established based on good outcomes of those
accessing these services with increased uptake of PMTCT interventions. For example, one study in Nairobi
found three-fold reported higher uptake of Nevirapine and four-fold greater likelihood of condom use
(Farquhar et al., 2004). Other studies also indicated increased prevention behaviors as well as effective
pathways to increasing uptake among ANC attendees in Zambia and Rwanda with targeted promotion and
community outreach (Allen et al., 2003);(Allen et al., 2007);(Conkling et al., 2010). In the systematic review
leading to the WHO Guidelines, no statistically significant differences were found in outcomes relating to
partner violence or relationship breakup (WHO, 2012a).
Additional benefits seen with addressing HTS and couples was the identification of serodiscordancy where
one partner is HIV-positive and another HIV-negative. In 2012, compelling evidence of HIV treatment
reducing transmission rates among sexual partners was addressed in a strong recommendation with high
quality evidence (Cohen et al., 2011);(WHO, 2012a):
• “People living with HIV who are in serodiscordant couples and who are started on ART for their
own health should be advised that ART is also recommended to reduce HIV transmission to their
uninfected partner. Strong recommendation, high-quality evidence.
• Antiretroviral therapy for HIV-positive partners with >350 CD4 cells/µL in serodiscordant couples
should be offered to reduce HIV transmission to uninfected partners”
The sum of these benefits drove advocacy for couples HTS. However, there were constraints: the approach
is human resource intensive and not all want to be tested as a couple; in the Zambian and Rwandan
studies for example, only 14% and 27% returned, respectively, following promotion activities (Allen et al.,

38
2007). Notably, the WHO guidelines included a further approach which would soon be a game-changer:
partner testing, where “one partner has already been tested, and the other partner is then tested
separately and may occur with or without disclosure”.
Key Populations (MSM, FSW, PWID)
The co-authored articles submitted as part of this proposal have dealt primarily with general populations
primarily within generalized epidemics. Key populations (KP), however, comprise a main sub-population
for whom HIV testing services provides a public health benefit. WHO defines KP as “groups who, due to
specific higher-risk behaviours, are at increased risk of HIV irrespective of the epidemic type or local
context; and often have legal and social issues related to their behaviours that increase their vulnerability
to HIV”. These populations include men who have sex with men, female sex workers, and people who
inject drugs (WHO, 2016b). Transgender populations and people in prisons are also sometimes considered
key populations.
While HTS is included as a minimum standard in a package of HIV services for KP, achievement of 1st 90
goals and rates of diagnosis remain low even in 2020. UNAIDS modelling suggests across numerous
countries reporting, rates of PLHIV diagnosed among FSWs is 67.2%; MSM is 66.5%; and PWID is 61.9%
(UNAIDS, 2020b). Another multi-country bio-behavioral survey suggested even lower rates of diagnosis,
with 71% of HIV-positive KP surveyed were not previously aware of their HIV status (Herce et al., 2018).
The key role of appropriate models to maximize reach through highly acceptable community-based
approaches including one stop shops, targeted outreach, social and risk network (Wolf et al., 2018).
In my own work, contributions were made to better understanding of the role and acceptability of HIV self-
testing in West Africa (Lyons et al., 2019) as well as integration of key population HTS evidence and
considerations in WHO guidelines in which I participated (WHO, 2015b);(WHO, 2012c, 2015c);(WHO,
2016d). Each of these emphasized that critical community-based mobile and outreach HTS was essential to
KP case identification, as well as the provision of integrated services. In 2019, we expanded on existing
HTS guidelines recommending “that social network-based HIV testing approaches can be offered for key
populations as part of a package of partner services” (WHO, 2019b). Here we considered groups of
individuals linked by a common set of behaviors and mutual trust; individuals receiving testing – both HIV-
positive and -negative) would invite or link to sexual, injecting or social networks to extend voluntary HTS
to them (Stojanovski et al., 2021);(Wolf et al., 2018). A WHO commissioned systematic review found social
network testing increases diagnoses, acceptability for partner services, and that the approach was feasible
to implement and seldom led to adverse events.

39
Children, Adolescents and Young People
With less availability to HTS services generally, adolescents have been and continue to be an underserved
population with respect to
HIV testing services. In
2017, we outline some of
the major gaps in attaining
achievement of 1st 90 goals
in these younger
populations (sometimes
framed from 15-24 years)
(Wong VJ, 2017). At that
time, we cited 2013
UNICEF data that only
about 20% of HIV positive
adolescent girls knew their
status with 1/3 of new
infections occurring in 15–24-year-olds. In 2013, as part of a WHO Guidelines Development Group, we
issued specific recommendations for HTS and adolescents: Guidance for HIV testing and counselling and
care for adolescents living with HIV (WHO, 2013). Recent estimates depicted in Figure 8 show rates of
diagnoses from 45% to just over 70% in a number of sub-Saharan African countries. These surveys also
indicate “ever tested’ rates are high ranging from 69 to 87%; testing in the past 12m ranged from 24 to
57%. Both of these values suggest that accessibility and acceptability of HTS for persons 15-24 years old
are high. PEPFAR’s “DREAMS” program has been one positive example of integrating adolescent and
female-focused HIV testing in the context of a broader primary prevention package (Gourlay et al., 2019).
However, as of 2019, reviews of HIV incidence in sub-Saharan Africa in these populations remains muted
(Birdthistle et al., 2019) (Karim & Baxter, 2019).
Among younger children aged 0-9 years, UNICEF estimates 1,100,000 living with HIV globally, with 150,000
new infections yearly, with Southern and Eastern Africa being most heavily affected (UNICEF, 2020). The
majority of these infections are through vertical transmission and could be prevented through PMTCT
interventions (Mutabazi et al., 2017). However, coverage of PMTCT, while increased dramatically over the
past two decades, remains sub-optimal. UNAIDS has articulated new targets to reach 95% of pregnant
women with ART and eliminate new infections in children age 0-14 (UNAIDS, 2020e). Coverage of early
Figure 7: PHIA Estimated 90-90-90 in 15-24 years (Laboratory or self-reported ARV)
Sources: Adapted from PEPFAR COP 2022 Guidance. ICAP, 2020: Eswatini (SHIMS 2 2016), Ethiopia (EPHIA 2017), Lesotho (LePHIA 2016), Malawi (MPHIA 2015), Namibia (NAMPHIA 2017), Rwanda (RPHIA 2018), Tanzania (THIS 2016), Uganda (UPHIA 2016), Zambia (ZAMPHIA 2016), Zimbabwe (ZIMPHIA 2015)

40
infant diagnosis (which is beyond the scope of this commentary) depends on laboratory-based assays (such
as EIA or NAAT) and coverage remains low (Kufa et al., 2020).
Regarding young children and HIV testing services (non-EID), we identified early challenge areas with
respect to the policy environment. In 2006, of 20 generalized epidemic countries at that time, only 35%
had included specific guidance on HIV testing of children. Our key informant interviews on national policy
highlighted a number of challenge areas including informed consent, child counseling and stigma (Wong,
2006). These policy gaps informed our work on WHO’s Policy requirements for HIV testing and counselling
of infants and young children in health facilities (WHO, 2010b). This document provided key
recommendations on consistent application of PITC to children, addressing consent; counseling,
communication and disclosure; stigma and other critical aspects of HIV testing.
New infections among children globally reduced 24% from 2000-2008; and another 60% from 2009-2015
(UNAIDS, 2016b). An ongoing focus on pediatric testing, case finding and treatment remains critical,
particularly in those countries with slower declines. Amplifying pediatric coverage in clinical settings as
well as ensuring index testing of children of positive mothers or those with an unknown status and HIV-
positive fathers will be critical strategies to come.
Adult Males
Adult males have had less
accessibility to HIV testing
services given lower levels of
engagement with health systems
compared to females (who have
more routine access through
ANC). Therefore, achievement of
1st 90 goals in adult male
populations lags behind adult
female populations. Across a
number of sub-Saharan African
countries, UNAIDS estimates
identify a sex differential with male 1st 90 estimates ranging from 79-94% for males over 15 years, with an
average in these countries of 89% compared to 94% for females. (Fig 8). A 2021 pooled analysis of PHIA
Figure 8: UNAIDS Estimated 1st 90 estimates by sex, >15 years, select sub-Saharan African Countries Source: UNAIDS, 2020. https://aidsinfo.unaids.org
41
data from 13 countries in sub-Saharan Africa estimated 33.7% of men living with HIV/AIDS were unaware
of their serostatus – a somewhat lower figure than the UNAIDS modelled data (West et al., 2021).
Our study of Lesotho data aligned with the PHIA data, indicating that 34% of men had never been tested
compared to 15% of women (Carrasco et al., 2018). Additionally, factors such as acceptance of gender-
based violence (OR: 1.44, p < 0.001), holding discriminatory attitudes (OR: 1.50, p < 0.001), and not having
basic HIV prevention knowledge (OR: 1.53, p < 0.001) were significantly associated with never being
tested. This study highlighted the need (even in higher coverage countries) to strategically target HTS to
the adult male population, as well as integrate or connect strategies to address GBV awareness, HIV
prevention knowledge and HIV-related discrimination. Our analysis of DHS data in five additional countries
(Kenya, Malawi, Mozambique, Zambia, and Zimbabwe) identified factors associated with never having HIV
tested. Between 29.3% and 34.9% of men ages 15–49 in these countries had never tested for HIV. We
found that men who held accepting attitudes towards gender-based violence, lacked HIV knowledge, and
held stigmatizing views of HIV were more likely to report never testing for HIV (Fleming et al., 2019).
Barriers to HTS acceptability among men are substantial. For example, in Cote d’Ivoire, factors have been
described that impact decisions to test and initiate within health facilities, including interpersonal costs like
unwanted disclosure or stigma were balanced against benefits such as social support and clinical guidance
(Tibbels et al., 2019). Our Tanzania study on partner notification testing highlighted challenges to specific
approaches, finding reluctance of HIV-positive females to provide index contact information to their male
partners (relative to male-to-female index testing) (Plotkin et al., 2018). WHO HTS Guidelines reviewed
specific documented barriers to men’s access to HTS as well as acceptability including fear, stigma, feeling
healthy and the perception that health facilities are female-centric (WHO, 2015b).
Multiple HTS community and facility-based strategies will need to be leveraged to increase male diagnoses
among the final 19% undiagnosed, and support effective linkage to care. (Hensen et al., 2014);(WHO,
2021b). In our own published analysis of PEPFAR HTS programming, the while index testing had higher
positivity, the vast majority of adult male diagnoses occurred through PITC, with smaller proportions found
through VCT sites and mobile testing (Drammeh et al., 2020). To address multiple barriers, leveraging
male-friendly strategies will necessarily include effective index partner testing to female PLHIV and
targeted HIV self-testing (see Section 2.4), ongoing expansion of community-based HTS that reach men at
risk (e.g., through the workplace or geo-targeted events based on burden), optimization of PITC to ensure
integration and maximal availability coverage, and effective demand creation activities. Accessibility and

42
uptake of voluntary male medical circumcision (VMMC) also plays a role in increased access to HTS, as part
of the minimum package of services each man receives (Project SEARCH, 2013). While case detections
rates in these VMMC populations that targeted primarily HIV negative males at risk, it remains an
important intervention for normalizing HIV testing among men.
For all of the populations above, and others not mentioned here, a central programmatic concept is
providing multiple HTS options that will increase both availability and acceptability for specific groups or
individuals to increase testing contact coverage and program effectiveness. In 2018, with the International
AIDS Society, we convened a broad based technical working group to produce a framework on HTS
differentiated service delivery with the aim of advocating and strategizing around client-centric HTS
services that included consideration of a number of factors in determining program strategies (IAS, 2018):
• The specific population where HTS accessibility needs to be expanded (such as those described
above)
• Contexts including HIV prevalence, type of epidemic, % of PLHIV who know their status,
urban/rural setting
• Clinical characteristics including whether individuals are symptomatic or asymptomatic, and high
or low risk
Differentiated HTS program components that include mobilization, the testing process, and linkage to
additional services will necessarily need to be framed in the population, and where, when and how
services are delivered to be most effective.
2.2.4 Application of Tanahashi Framework to Sub-populations
In consideration of the unmet need of HIV testing services and specific sub-populations, the Tanahashi
framework can prove a useful analytic tool. In assessing strategy for health services three key questions
are addressed (Tanahashi, 1978):
1. How should HIV testing service resources be optimally allocated and services organized to
serve as many of the target population (e.g., men, partners, FSWs) as possible?
2. Are HIV testing services reaching those (e.g., men, partners, FSWs) they should serve?
3. Has HTS been effective in meeting the (sub-)population’s needs?
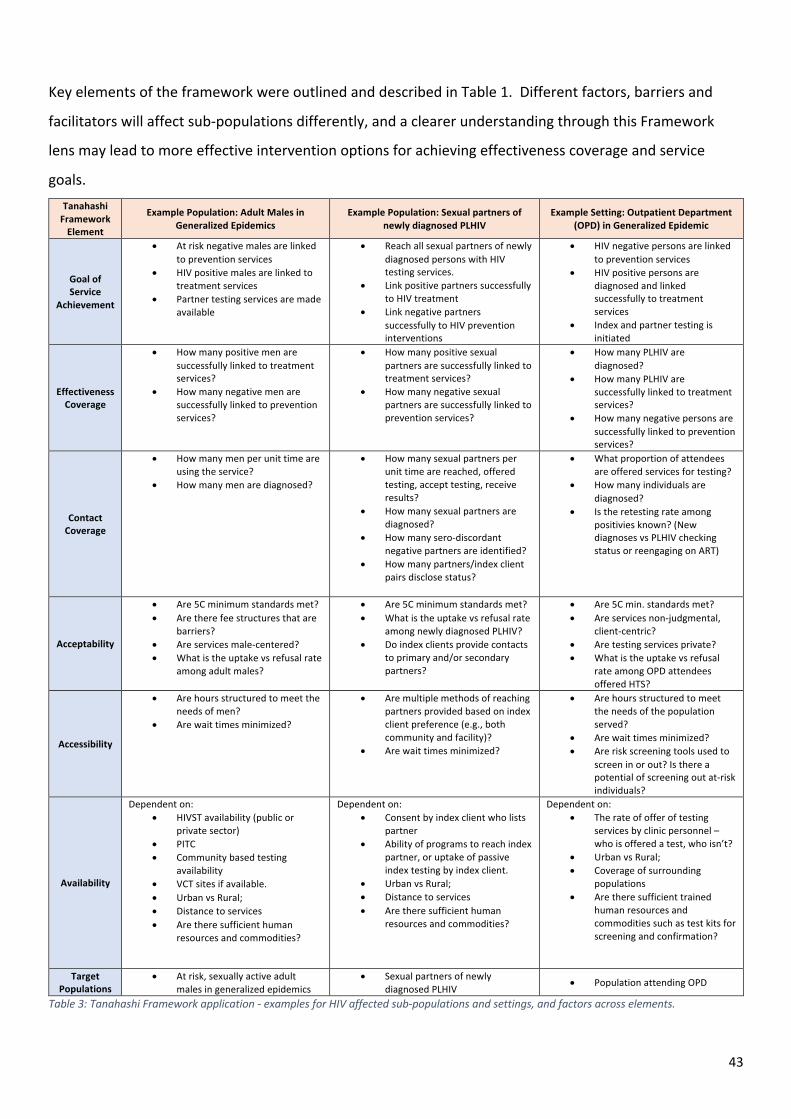
43
Key elements of the framework were outlined and described in Table 1. Different factors, barriers and
facilitators will affect sub-populations differently, and a clearer understanding through this Framework
lens may lead to more effective intervention options for achieving effectiveness coverage and service
goals. Tanahashi
Framework Element
Example Population: Adult Males in Generalized Epidemics
Example Population: Sexual partners of newly diagnosed PLHIV
Example Setting: Outpatient Department (OPD) in Generalized Epidemic
Goal of Service
Achievement
• At risk negative males are linked to prevention services
• HIV positive males are linked to treatment services
• Partner testing services are made available
• Reach all sexual partners of newly diagnosed persons with HIV testing services.
• Link positive partners successfully to HIV treatment
• Link negative partners successfully to HIV prevention interventions
• HIV negative persons are linked to prevention services
• HIV positive persons are diagnosed and linked successfully to treatment services
• Index and partner testing is initiated
Effectiveness Coverage
• How many positive men are successfully linked to treatment services?
• How many negative men are successfully linked to prevention services?
• How many positive sexual partners are successfully linked to treatment services?
• How many negative sexual partners are successfully linked to prevention services?
• How many PLHIV are diagnosed?
• How many PLHIV are successfully linked to treatment services?
• How many negative persons are successfully linked to prevention services?
Contact Coverage
• How many men per unit time are using the service?
• How many men are diagnosed?
• How many sexual partners per unit time are reached, offered testing, accept testing, receive results?
• How many sexual partners are diagnosed?
• How many sero-discordant negative partners are identified?
• How many partners/index client pairs disclose status?
• What proportion of attendees are offered services for testing?
• How many individuals are diagnosed?
• Is the retesting rate among positivies known? (New diagnoses vs PLHIV checking status or reengaging on ART)
Acceptability
• Are 5C minimum standards met? • Are there fee structures that are
barriers? • Are services male-centered? • What is the uptake vs refusal rate
among adult males?
• Are 5C minimum standards met? • What is the uptake vs refusal rate
among newly diagnosed PLHIV? • Do index clients provide contacts
to primary and/or secondary partners?
• Are 5C min. standards met? • Are services non-judgmental,
client-centric? • Are testing services private? • What is the uptake vs refusal
rate among OPD attendees offered HTS?
Accessibility
• Are hours structured to meet the needs of men?
• Are wait times minimized?
• Are multiple methods of reaching partners provided based on index client preference (e.g., both community and facility)?
• Are wait times minimized?
• Are hours structured to meet the needs of the population served?
• Are wait times minimized? • Are risk screening tools used to
screen in or out? Is there a potential of screening out at-risk individuals?
Availability
Dependent on: • HIVST availability (public or
private sector) • PITC • Community based testing
availability • VCT sites if available. • Urban vs Rural; • Distance to services • Are there sufficient human
resources and commodities?
Dependent on: • Consent by index client who lists
partner • Ability of programs to reach index
partner, or uptake of passive index testing by index client.
• Urban vs Rural; • Distance to services • Are there sufficient human
resources and commodities?
Dependent on: • The rate of offer of testing
services by clinic personnel – who is offered a test, who isn’t?
• Urban vs Rural; • Coverage of surrounding
populations • Are there sufficient trained
human resources and commodities such as test kits for screening and confirmation?
Target Populations
• At risk, sexually active adult males in generalized epidemics
• Sexual partners of newly diagnosed PLHIV
• Population attending OPD
Table 3: Tanahashi Framework application - examples for HIV affected sub-populations and settings, and factors across elements.

44
2.3 From a Prevention to a Clinical Paradigm (2010-2017)
2.3.1 Articulating a Care Continuum and the importance of linkage and program positivity in increasing
access to HIV Treatment
As HTS availability increased year-on-year globally, treatment eligibility criteria (initially based on WHO
clinical staging at time of diagnosis) shifted to be more inclusive of PLHIV at different disease stages. With
wider spread availability of point-of-care clinical laboratory assays, CD4 cell concentration levels began to
be used in place of HIV clinical staging and cutoffs were established for starting anti-retroviral therapy
(Eholie et al., 2016). From 2006-2009, WHO recommended ART initiation at CD4 levels of <350 cells/μL;
this cut-off was raised to 500 from 2009-2013 (Tymejczyk et al., 2018);(Eholie et al., 2016). In 2015, the
START Trial demonstrated benefits of starting all HIV positive persons on treatment, even those with >500
CD4 counts (Lundgren et al., 2015). WHO subsequently recommended that “ ART should be initiated
among all adults with HIV regardless of WHO clinical stage and at any CD4 cell count” (WHO, 2016c).
As the ART initiation criteria moved towards treating all HIV positive persons, in 2011, the HPTN 052 study
demonstrated the statistically significant impacts of HIV treatment on transmission with a 93% lower
transmission risk among sero-discordant partners in the early ART group (Cohen et al., 2011). A five year
follow up analysis reinforced these findings of 93% lower risk of linked partner infections compared to the
delayed ART group (Cohen et al., 2016).
The context of treatment coverage expansion among all PLHIV (both for goals of reducing morbidity and
mortality as well as reducing transmission) therefore shifted the target population from all persons in a
generalized epidemic (a universal testing approach), to persons more likely to be at risk and case
identification among undiagnosed PLHIV.
Programmatic and client-level connections from points of diagnosis to treatment became increasingly
critical in the HIV response. Since 1968, a focus on disease screening and connection to treatment has
been emphasized (Wilson & Jungner, 1968). In 2011, utilization of a clinical cascade analysis was described,
connecting HIV testing to diagnosis and uptake of treatment in sub-Saharan Africa (Rosen & Fox, 2011). At
that time, treatment eligibility criteria were CD4 based and multiple stages of the cascade were possible: 1.
CD4 testing following diagnosis; 2. Non-ART eligible and HIV care enrollment; 3. ART eligible and ART
initiated. In that systematic review, retention derived from 28 studies was estimated at 59%, 46% and 68%
for each stage, respectively. Loss was possible at interim steps and between stages and clinical cascade
retention was a critical factor for driving viral load reductions.

45
for each stage, respectively. Loss was possible at interim steps and between stages and clinical cascade
retention was a critical factor for driving viral load reductions.
Our Mozambique study identified some key issues regarding linkage to care and treatment from point of
diagnosis (Inguane et al., 2016):
• 46% of the monthly HIV testing reports expected at the district level were missing. After
adjustment for missing values, we estimated that the aggregate numbers of adults registered in
pre-ART was 75% of the number of persons tested HIV-positive in the six districts.
• In the eight health facilities, 40% of the patient charts for adults enrolled in pre-ART and 44% in ART
were missing. Of those on ART for whom charts were found, retention in treatment within 90 and
60 days prior to the study team visit was 34 and 25%, respectively. Combining these multiple data
sources, the overall estimated retention was 18% in our sample.
• Individual-level factors were identified as key influences to enrolment in HIV care and included
presence/absence of symptoms, while health facility and structural-level factors such as proximity
to health facilities, poor quality healthcare, and lack of money were perceived to be key influences
of retention.
The complexity around linkage from diagnosis to treatment identified in our work illustrated that efforts to
improve this area should address individual, health facility, and structural-level factors, and critically that
outcomes cannot be reliably assessed without improving the quality of routine health information systems.
Increasingly, attention has been paid to the non-linearity of engagement in testing, care and treatment,
where individuals engage and reengaged in testing and treatment over time (Hallett & Eaton, 2013);
(Ehrenkranz et al., 2021).
Monitoring linkage rates between diagnosis at various points of HIV testing service and HIV treatment
presented a problem. Given an absence of unique identification data related to HIV testing, this has been a
challenge. To facilitate WHO established a baseline linkage proxy indicator to focus on the importance of
treatment uptake post-diagnosis (WHO, 2012a). This was essentially defined as [total number new on
treatment/ total number of positives] in a given time period and geography. There are limitations to this
indicator which include repeat positive tests by the same individual, which may then underestimate
linkage rates.
Linkage to treatment metrics and indirect proxy indicators based on testing positivity volumes and new
treatment initiations became a critical measure of HIV program success (PEPFAR, 2020a). These data
provided a rough programmatic indicator of effectiveness when looking at positive tests compared to

46
treatment enrollment. In cases where rates were low, further programmatic attention could be paid to
improving and ensuring treatment uptake following diagnosis.
In 2015, I provided institutional authorship for a critical section of WHO’s Consolidated Guidelines on HIV
Testing Services (Chapter 3.6: Linkage to Care), highlighting promising practices supporting linkage to HIV
care and treatment (WHO, 2015b). This included a purposeful, non-systematic review of published good
practices around linkage interventions. These included integration of services, transportation vouchers,
decentralized ART provision, the use of peer navigation/expert patients, follow up text messaging and
communications, strengths-based case management and partner testing.
Within HIV programs, the target population shifted from all individuals in generalized epidemics to those
at-risk and the undiagnosed PLHIV, and the clinical paradigm became the primary focus; rates of diagnoses
within testing programs became more important. With the initial years of HIV testing introduction and
expansion, universal testing approaches and “know your status” campaigns sought to test as many
individuals as possible, along with maximizing testing coverage in key entry points such as ANC settings
(Mills & Chong, 2006);(Hensen B & Wong VJ, 2012). HIV testing program positivity rate (also sometimes
referred to as “yield”) became a critical metric in understanding program outcomes and was the simple
ratio of overall total number of confirmed positives to the total number of tests performed (WHO, 2015b).
However, HTS program positivity and overall positive volumes are two metrics that need to be considered
together to provide a broader picture of program outcomes. In Kenya for example, De Cock et al. illustrate
this issue reporting that 13 million people were tested between 7/2017 and 6/2018. In PITC settings,
125,000 positives were found at 1.2% compared to TB settings with roughly 5000 positives at 9.8%
positivity (De Cock et al., 2019). In 2019, WHO updated the HIV testing guidance and noted multiple
southern and eastern African countries had positivity rates substantially below general HIV prevalence
Figure 9: PEPFAR program data on HIV positives, new on treatment and linkage proxy rates by sex, >15 years.

47
rates, and below the 5% cutoff for defining a high prevalence setting. UNAIDS modeling across a number of
countries have also shown reductions in HIV program positivity (WHO, 2019a). Some of the positivity
reductions were considered to be a function of approaching higher rates of overall diagnoses and
corresponding decreases in treatment-adjusted prevalence. In summary, reducing positivity in the absence
of major changes to overall HTS programming reflected a challenge in case identification when most PLHIV
have been diagnosed (De Cock et al., 2019). Our
recent review of PEPFAR positivity disaggregated by
sex and modality (10/2018 to 9/2019) across 20
African countries found index testing (see below) had
the highest positivity rates for males (20.1%) and
females (24.3%); PITC had 3.9% and 2.7%,
respectively, but at substantially higher volume;
mobile testing reported average yields of 4.2% and
5.0% for males and females (Drammeh et al., 2020).
More recent efforts in clinical settings have focused
on adopting “risk screening tools” to better identify those who would benefit from HTS. These include sets
of questions assessing risk and may be used to screen in those who need testing, or screen out individuals
who may not need testing (and thereby increase positivity and program effectiveness). We conducted a
review for the WHO in 2019 and identified 29 screening tools through peer reviewed literature, and 47
from national or donor funded HTS programs (Quinn et al., 2020). While these could increase positivity,
examples of use in Eswatini, Nigeria and Tanzania showed that although positivity increased, some positive
cases were screened out. Our evaluation of risk screening tools utilized in OPDs in Malawi showed low
sensitivities compared to the standard of care (use of two basic questions on testing histories or visits
related to STIs), suggesting screening tools did not offer clear advantages (Moucheraud et al., 2021).
However, efforts at utilizing risk screening tools for children and adolescents have shown promise in some
settings, but challenges for use persist (Bandason et al., 2018);(Gill et al., 2021); (Moucheraud et al., 2018).
The future integration and effective application of HIV risk screening tools into some settings and
programs will remain a challenging area for HTS implementation.
One caveat in assessing positivity rates overall includes considerations for the volumes of non-case finding
HIV testing that is being undertaken. Much testing for adolescent girls and young women, for VMMC, and
Figure 10: Zambia Treatment-adjusted Prevalence and Positivity Data, 2019. Source: WHO HTS Dashboards, 2019

48
in the context of monitoring serostatus while on PrEP is not intended for HIV case finding, with a much
larger proportion likely to be HIV-negative. These tests are not often disaggregated from the total and may
reduce program positivities overall. To contrast case finding, considerations around monitoring “HIV
testing for prevention monitoring” has been proposed for distinguishing programming that seeks to also
ensure or document HIV negative status.
49
2.4 New HTS Pathways towards 95% Diagnosis: HIV Self Testing and Index Testing
Two more recent HTS modality strategies within global HIV programming began to be explored which
would further advance 1st 90 goals: HIV self-testing and assisted partner notification (linked to HIV testing,
which became more widely known as index testing). Both of these novel approaches increased accessibility
and to some degree availability; by extension this will expand contact and effectiveness coverage. HIV self-
testing, for example, was demonstrated through increased reach to 1st time testers along with high rates of
new diagnoses (Hatzold et al., 2019);(Katz, Wong, Medley, Johnson, et al., 2019) ;(V. Wong et al., 2019) .
2.4.1 HIV Self Testing Introduction and Expansion (2012 to Present)
HIV self-testing is a potential game-changer in achieving higher rates of diagnosis. Early interventions from
around 2010 to 2012 were documented in health care workers testing themselves for HIV as well as for
use in their sexual partners (Kalibala et al., 2014);(Kebede et al., 2013). In 2012, the United States FDA
approved the use of an HIV self-test kit based on risk benefit analysis and sensitivity meeting a 92% lower
bound threshold based on submitted performance studies in target populations (FDA, 2012). While the
approved HIV self-test kit intended for US markets was too expensive for use in LMIC programming, the
approval demonstrated proof of concept around both the approach, its public health benefit and low
documented risk. This was the first real world implementation of this type of test kit targeting populations
at risk. In an early exploratory review, we commissioned an assessment of HIV self-testing demand in
Namibia that found the use of many “grey market” kits in the private sector, and minimal to no national
policy or regulation (Nersesian P, 2013);(Rosenthal et al., 2014). In 2013, UNAIDS and WHO held a
consultation exploring the legal, ethical, gender, human rights and public health implications of HIV self-
testing scale-up (UNAIDS, 2013) (I was a delegate for USAID). While the evidence base for use in low- and
middle-income countries was limited, key benefits and risks were considered at this early stage. A primary
benefit was the increase in accessibility among populations that need HIV testing (particularly those who
are marginalized and/or in areas of high prevalence), along with autonomy, confidentiality and
convenience. Cautions or risks outlined included the potential for human error and test performance
issues, linkage to care and treatment, coercion and social harms, and (at that time) limited regulatory
controls. From this meeting, participating organizations made a commitment to prioritizing and
documenting further programmatic and policy evidence.
Evidence for an HIV self-testing use case began to build. Our analysis of HIV self-testing policies highlighted
an early disconnect between program goals of HIV self-testing expansion and national policies that in
LMIC’s were limited or non-existent at that time (Wong et al., 2014). At the time, HIV self-testing products
50
were limited, and efforts were undertaken to identify optimal product profiles focused on LMICs (Peck et
al., 2014). An early HIVST qualitative study in Malawi utilizing a clinical use oral fluid assay showed
promise with participants noting confidentiality and partner testing as key benefits (Kumwenda et al.,
2014). An initiative – The HIV Self-Testing Africa (STAR) Initiative – initiated a five-year research
partnership to build evidence on HIV self-testing in African countries, beginning with Malawi, Zambia and
Zimbabwe.3 I was guest editor of a substantial body of evidence on HIV self-testing in Africa compiled in a
journal supplement (V. Wong et al., 2019). The compiled articles provided key evidence and findings from
HIVSTAR and other studies including:
• Assessing the effective development of instructions for use (Simwinga et al., 2019), building on
evidence around “supervised” or “assisted” HIVST where additional instruction and demonstration
is provided and has resulted in better performance by users (Pai et al., 2013).
• Reaching more first-time testers (i.e. persons reporting not previously tested), adult males and
adolescents (Hatzold et al., 2019)
• HIVST interventions appear to be cost effective using a disability-adjusted life year (DALY) of <$500
when target populations were men and FSWs (Mangenah et al., 2019) (Cambiano et al., 2019)
• The effective use of HIV self-test kits in reaching partners of PLHIV and clients of FSWs through
secondary distribution (Thirumurthy et al., 2016).
Additionally, in WHO’s review of the evidence, systematic reviews found increased uptake of HIV testing at
three and six months, increased reach to MSM, and high concordance (>80%) between HIV self-testing and
testing by trained health workers using clinical rapid diagnostic tests (Figueroa et al., 2018). Based on these
findings, WHO’s Guidelines Development Group4 issued WHO Self Testing Guidelines in 2016, stating in a
strong recommendation with moderate quality evidence that HIVST “should be offered as an additional
approach to HIV testing services” (WHO, 2016d). Critically, HIVST does not provide a final diagnosis and
further confirmatory testing is required prior to diagnosis and any initiation of ART. A WHO update
strengthened these recommendations based on the cumulative evidence (including 32 randomized
controlled trials) that demonstrated: high uptake among many populations including males, women,
adolescents and key populations; proportions linking were comparable to standard HTS; comparable rates
of positivity; and limited reports of adverse events and risk compensation, most people could perform HIV
self-testing with little additional support, and acceptability remained high. The 2019 recommendation
3 Vincent Wong was a member of the HIVSTAR Project Technical Advisory Group from May 2016 to Jan 2020. 4 Vincent Wong was a member of WHO’s HIV Self Testing and Assisted Partner Notification Guidelines Group (2016 and 2019)

51
stated that HIVST “should be offered as an approach to HIV testing services” (strong recommendations,
moderate-quality evidence).
In parallel to the growing evidence and policy base, in 2017 there were additional catalytic actions and
HIVST expansion: a concurrent process led to WHO pre-
qualifying a rest-of-world version of the OraQuick® HIV Self-
test, establishing an approved commodity for use in LMIC
programming and available for procurement by donors such as
the Global Fund and PEPFAR (WHO, 2017);(PEPFAR, 2019)
(Global Fund to Fight AIDS, 2016). Further, the Bill and Melinda
Gates Foundation provided funding to reduce the unit cost of
the kit to about US$2 (V. Wong et al., 2019). In the years since
WHO guidelines were released, there has been steady
expansion. The Global Fund reported procuring 3.7M HIV self-
test kits between 2018 and 2019 (Global Fund to Fight AIDS,
2020b). PEPFAR expanded its HIVST operational targets from
2,394,163 in FY19 in 17 countries or regions to 4,791,894 in
FY21. For FY21, overall PEPFAR HIV testing targets (not including HIVST) were 42M, representing about
10% of overall testing targets (PEPFAR, 2021b).
Recent findings have further strengthened the evidence base for HIVST implementation. HIV self-testing
may play a role in increasing HTS reach to older populations (Johnson et al., 2021). Another recent
randomized trial demonstrated increased testing coverage among males and adolescents as well as
increased ART initiations over six months (though not statistically significant), but that ongoing attention is
needed to support linkage from positive HIVST results to confirmatory testing and ART initiation
(Indravudh et al., 2021).
HIVST has demonstrated impacts across diverse populations, increasing both availability and accessibility
of HIV testing to populations at risk. While results do not deliver a final diagnosis, they do provide a sero-
status upon which individuals can base subsequent health decisions and drive effectiveness coverage.
HIVST provides a cost-effective approach that affords people autonomy, privacy and confidentiality, high
levels of accuracy for screening and ease of use. As HIVST use expands globally, other disease areas are
Figure 11: HIV Self Testing demonstration, Right to Care, South Africa, 2018. Photo credit: V Wong
52
also seeing a potential for public health benefit, with recent self-testing test kits, and broader
considerations and advocacy around self-care through health interventions more broadly, with efforts now
being considered to increase access for both Hepatitis C and COVID testing (WHO, 2021c);(WHO, 2021d);
(FDA, 2020).
2.4.2 Index and Partner Testing Initiation and Expansion (2014 to Present)
HIV testing of sexual partners (and for PWID, also injecting partners) of PLHIV has been a recent and
expanding focus of HTS to more effectively reach both undiagnosed individuals as well as HIV negative
persons at higher ongoing risk of infection. These efforts sought to increase accessibility to partners and
children of PLHIV who may not have yet been diagnosed.
Various terms are employed for this approach and relate to similar interventions; these include assisted
partner notification services, contact tracing and index partner testing. The latter term appears to be
widely used as it integrates both elements of contact tracing and extending HTS to identified and located
sexual partners as well as biological children of females (and positive males with mothers of unknown
status).
Contact tracing, partner notification and index testing, while utilized in other infectious disease areas such
as TB and sexually transmitted infections, had not been part of HIV approaches largely as a result of the
focus on individual risk, and an early emphasis on consent and confidentiality. HIV couples testing (see
Section 2.2.3) was predicated on couples testing together and receiving results and undertaking mutual
disclosure mediated by an HTS counselor (Farquhar et al., 2004). While this approach had good outcomes
for those who used the service, it failed to reach secondary sexual networks, and was labor intensive since
it aimed to reach all persons testing, and not just those found positive, limiting the overall contact
coverage.
A number of early studies demonstrated both the cost effectiveness of an index testing approach
(Armbruster et al., 2011), as well as the programmatic feasibility with high rates of positivity and reach to
undiagnosed individuals in Malawi (Brown et al., 2011). Here a number of intervention options were
described that included passive referrals (clients notified their own partners), provider referrals (where a
provider notified partners) and contract referrals (where providers contacted partners after a period of
time (e.g., 7 days) who had not reported for HTS but maintained anonymity of the index client). In 2015,
we applied lessons learned from the Armbuster and Brown studies and further demonstrated
53
programmatic feasibility and good outcomes in a Tanzanian operational research study (Kahabuka et al.,
2017). Partner notification processes with HTS were implemented at three peri-urban and rural areas in
Njombe, and free choice options were provided for passive referral, provider referral or contract referral.
Outcomes included effective partner elucidation, reach and testing: 390 index clients listed 438 sexual
partners; 56.8% were successfully referred and 96% of these individuals were tested. 91.6% of index clients
opted for passive referral. The approach also affirmed that this was a high positivity approach: 62% tested
HIV positive and all reported being newly diagnosed. Our further analysis identified deeper gender
differentials in outcomes, with males being 2.2 times more likely to successfully refer partners, and
married couples 2.5 times more likely (Plotkin et al., 2018). Additional studies in Kenya and Cameroon
around 2015 also demonstrated feasibility and impact with high rates of uptake, partner reach and new
diagnoses reflected in high positivities: 50% were positive in Cameroon and 23% in the Kenyan
intervention group (Cherutich et al., 2017);(Henley et al., 2013). The Kenya study also assessed intimate
partner violence outcomes and found no differences in their study group.
In 2016, WHO issued partner notification guidelines5 based on a review of the evidence, providing a strong
recommendation based on moderate quality evidence that “voluntary assisted partner notification
services should be offered as part of a comprehensive package of testing and care offered to people with
HIV” (WHO, 2016a);(WHO, 2016d);(WHO, 2016d).
Both WHO Guidelines and PEPFAR integration of index testing into Country Operational Planning guidance
led to the acceleration of implementation. In 2019, I was editor of a journal supplement aimed at
compiling the most recent programmatic evidence for implementation – The power of partners:
experiences from implementing and scaling up HIV partner notification and index testing services (Katz,
Wong, Medley, & Baggaley(Editors), 2019). In our summary of the evidence included, we highlighted a
number of key programmatic findings (Katz, Wong, Medley, Johnson, et al., 2019):
• Implementation effectiveness: through increased positivity (and thus case detection) rates in
Central and South Asia (6-15%); Cameroon and Zimbabwe (29-52%) and Vietnam (42%) partner
notification further demonstrated good effectiveness in expanding contact coverage and reaching
the undiagnosed.
5 Vincent Wong was a member of the WHO Guidelines Development Group, 2016. https://www.who.int/hiv/pub/vct/Annex33.pdf

54
• Client, community and provider perspectives: In Partner notification: a community viewpoint
(George Ayala et al., 2019), authors emphasized the need to maintain ethical and rights-based
approaches.
• Considerations around key populations: ensuring rights-based approaches and leveraging peer-
educator delivered programs to implement index testing in these marginalized populations.
• Social harms: published evidence indicated few adverse events for non-key populations (Wamuti et
al., 2019).
• Training is a critical component: for those implementing partner notification or index testing –
from offering index services to partner elucidation to reaching and testing partners – culturally
competent training that may include behavioral skills building is essential (Han et al., 2019) (Tembo
et al., 2019).
Additionally, PEPFAR demonstrated monitoring systems that we adapted from standard HTS metrics in
2018 to allow for improved
programmatic assessment of index
testing cascades both among sexual
partners as well as pediatric index
tests (PEPFAR, 2020a). We
illustrated this in Katz et al. 2019,
which also highlighted the
importance of both facility and
community approaches as
complementary interventions that
are critical in reaching index
partners of newly diagnosed persons.
In 2020, a number of civil society organizations outlined reported social harms that had resulted from the
implementation of index testing (MPACT, 2019). An open letter to the US Department of State’s PEPFAR
Coordinator cited a number of reported adverse outcomes associated with index testing globally. These
included withholding treatment or services to coerce partner elucidation, and unauthorized and non-
consensual disclosures (AVAC, 2020), and had occurred in both key and generalized populations.
Protection of communities that were criminalized and the need to engage and sensitize health care
providers in ensuring rights-based approaches are critical (G. Ayala et al., 2019). These outcomes further
highlighted the need to ensure WHO minimum standards are met with all HIV testing services; this
Figure 12: Illustrative index testing cascades for community and facility approaches. Katz, Wong, et al. 2019

55
includes screening for risk of intimate partner violence prior to initiating partner notification (WHO,
2016d).
In FY2020, PEPFAR programming globally (including 28 country or regional programs) which now tracks
index testing for both adults and children, identified 601,992 HIV positive partners through index testing
modalities through facility- and community-based approaches (PEPFAR, 2021b). This represented about
23.6% of all positives identified through PEPFAR HTS programming that year, and illustrated the strong
program emphasis on this approach as a key new program strategy in HIV case identification increasing
contact coverage among undiagnosed PLHIV (PEPFAR, 2019). Further, PEPFAR has articulated approaches
and minimum standards to ensuring the implementation of safe and ethical index testing (PEPFAR, 2020c).
Effective and acceptable approaches to leveraging HIV self-test kits for secondary distribution to reach
partners of PLHIV has also been demonstrated and represents a further new avenue for these novel
approaches (Masters et al., 2016);(Offorjebe et al., 2020). In addition to new diagnoses, with documented
differing rates of HIV seroconversion among uninfected male and female partners, this approach serves to
identify serodiscordant couples and provide a basis for primary HIV prevention (including PrEP) and
reducing transmission risk (Colombe et al., 2019);(Odoyo et al., 2019).
56
2.5 Conclusions
The global expansion of access to HIV testing services has been critical to both increasing the proportion of
PLHIV diagnosed and the numbers of individuals receiving anti-retroviral therapy. This thesis addresses
access to HIV testing services over a twenty-year period from 2000 to 2020, centering on 29 peer-reviewed
publications, contributions to guidelines and other normative tools, and multiple conference
presentations. These HTS-focused randomized and observational studies, systematic reviews and critical
commentaries reflect substantial and meaningful contribution to the field of HIV testing services and public
health more broadly. Their findings supported critical intervention elements, effective HTS expansion, the
quality of global HTS programming, increasing rates of diagnosis and, in part, drove treatment uptake and
HIV viral suppression.
From 2000 to 2020, HIV testing services expanded substantially and included multiple strategic phases as
availability and accessibility increased through rapid tests, increased investments, and human resource
expansion through lay cadres. Target populations shifted from broad-based general and key population
efforts as a focus of primary prevention, to an increased focus on those at increased risk of infection and
ensuring clinical care to mitigate HIV impacts. Efforts to ensure widespread access to HIV testing for all
persons in generalized epidemics have given way to more recent targeted implementation and emphasis
on ensuring HIV diagnosis and linkage within the HIV clinical cascade.
This continuum of HTS approaches within the HIV pandemic can be roughly broken into four overlapping
phases:
1. Early phase to increase HTS access (est. 2000-2004): Introduction and expansion of rapid HIV test
technologies and diagnostic algorithms; leveraging of lay cadres to deliver services; a focus on
prevention paradigms that included VCT sites and ANC test; limited treatment availability; the
establishment of minimum standards and an emphasis on counseling, consent and confidentiality
(3Cs).
2. HIV testing expansion (2005-2009): Increased funding through initiatives such as PEPFAR and
Global Fund; Expansion of PITC and routine testing in clinical settings; Scale up of community
approaches; expansion of treatment access
3. Clinical paradigm focus (2010-2017): Increased understanding of ‘treatment-as-prevention’ and
the benefits of early treatment; introduction of 90-90-90 goals and an increased focus on a
continuum of HIV care; the importance of linkage to treatment; a focus on couples testing and

57
reaching at risk adolescents; evidence base for index and HIV self-testing begins; HTS program
positivity becomes a critical metric for program effectiveness.
4. New HIV testing pathways (2017-2020) Expansion of HIV self-testing and index/partner testing to
reach target populations not yet tested or tested infrequently; Many countries are now
approaching rates of 90% of PLHIV diagnosed, and the numbers of PLHIV who are virally suppressed
continue to climb.
Across this expansion, the Tanahashi Health Service Coverage framework functions as a useful tool in
analyzing HIV testing service strategies, barriers and facilitating factors. Key pragmatic questions are
addressed and include core questions that may be applied to the intervention settings more broadly, or
sub-populations more specifically: 1. How are HIV testing resources allocated to serve target populations;
2. Are HIV testing services reaching target populations; 3. Have HIV testing services been effective in
meeting population needs?
The core HTS-related studies and articles within this thesis can be framed around Tanahashi health service
stages and identified multiple key findings that advanced the field forward:
• Accessibility and Availability
o Increasing HTS Access through expansion of PITC, ANC testing and community based HTS
that reached PLHIV earlier; critical assessments of the use of risk screening tools
o Expansion of index and partner testing and effectiveness around reaching undiagnosed
sexual partners and identifying serodiscordant couples.
o Expansion of HIV self-testing with identified use and awareness, and leveraging to expand
coverage for example within OPDs or for key populations. Measuring linkage and outcomes
remains a challenge area.
• Acceptability
o HIV testing quality evidence assessed the degree to which lay counselors have been
integrated into national policies; factors related to misdiagnosis and misclassification in HIV
testing programs; and programmatic output shifts resulting from HTS optimization
strategies that include the integration of index approaches.
o HIV testing service delivery and linkage to care included assessments of data gaps,
facilitators and barriers to linkage to treatment following diagnosis; how IPV services may

58
be best integrated into standard HTS; and best practices for providing psychosocial services
for children receiving a positive result.
• Addressing Contact Coverage Gaps
o Studies identified HTS gap areas in populations at risk including adult males and pediatric
populations and identified correlates of ‘never testing’ among males that included low HIV
knowledge and higher acceptance of GBV and stigma. Through program data, testing access
was shown to be higher in females than males across 20 sub-Saharan African countries,
largely a result of high ANC testing rates. Age of consent policies were identified as one
barrier to testing in pediatric populations.
Advances in each of these health service areas has contributed towards advancing higher rates of
diagnostic coverage. Achieving UNAIDS global goals, however, will leave a significant proportion of the
PLHIV population still virally unsuppressed and some sub-populations may continue to require
programmatic focus. While HIV estimates of HIV incidence have reduced, even countries with high ART
coverage rates continue to see new HIV infections. HTS programming will continue to evolve to refocus
efforts on primary prevention among those at risk, reengagement of individuals who have dropped out of
treatment programs, ongoing case detection and index contact tracing, and leveraging of new avenues for
self-screening and care with novel HIV self-test kits and new diagnostic technologies such as multiplex
rapid assays.
The public health response to new epidemics and pandemics such as COVID-19 stand to benefit from early
lessons learned through HIV testing. Key testing areas can be one cornerstone of prevention and care
interventions including: diagnostic technology translation to simple, rapid diagnostics; leveraging self-
testing to increase availability and accessibility; aligning accurate information and counseling based on
testing results; the need for adequate training and capacitating of health care workers and extension of
testing to non-clinical cadres; and integrating monitoring and evaluation systems that can feedback into
programmatic strategies and implementation (Carrasco, Atkins, Wong, Fleming et al. 2021). (Carrasco et
al., 2021)
My collective professional work during this period has elucidated and contributed to broader accessibility
and availability of HTS, particularly to those at increased risk of HIV infection. Through my efforts from HIV
diagnostic research and development, to the design and delivery of effective HIV testing programs, the
introduction of sound public health policy based on evidence and operations research, and, most recently,
the introduction of new HTS approaches in an effort to reduce HIV diagnostic gaps, my collective work,

59
presented within this commentary along with additional critical evidence, has supported the efforts to
achieve the global goals of 95% HIV diagnosis rates among all persons living with HIV by 2030.

60
Chapter 3: Applicant contribution list of publications, presentations, abstracts and reports by Vincent J Wong 3.1 Chronological List of Core Co-authored Publications and Authorial Contribution
# List of authors (in order shown in publication) Title of the Article and URL Journal Impact
factor Vincent Wong’s authorial
contribution No. of Citations
(Source: ResearchGate, 3/22)
1 Misheck Mphande, Paula Campbell, Risa M Hoffman,
Khumbo Phiri, Mike Nyirenda, Sundeep K Gupta,
Vincent Wong, Kathryn Dovel
Barriers and Facilitators to Facility HIV Self-Testing in Outpatient Settings in Malawi: A Qualitative Study https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8638200/
BMC Public
Health.2021 Dec
2;21(1):2200. doi:
10.1186/s12889
-021-12213-6.
2.690 5%; Inputs into manuscript; editing of draft; contribution to discussion; final approval
Recent publication – no citations at time of writing
2 Corrina Moucheraud , Risa M Hoffman , Kelvin
Balakasi , Vincent Wong, Maria Sanena, Sundeep
Gupta, Kathryn Dovel
Screening Adults for HIV Testing in the Outpatient Department: An Assessment of Tool Performance in Malawi https://link.springer.com/article/10.1007/s10461-021-03404-8
AIDS Behav.
2021 Aug 11.
doi:
10.1007/s10461
-021-03404-8.
3.312 10%; Conceptualization and interpretation of findings, editing of draft; contribution to discussion; final approval
Recent publication – no citations at time of writing
3 Maria A. Carrasco, Kaitlyn Atkins, Ruth Young, Joseph
G. Rosen, Suzanne M. Grieb, Vincent J. Wong, and
Paul J. Fleming
The HIV pandemic prevention effort can inform the COVID-19 pandemic response in the United States
https://pubmed.ncbi.nlm.nih.gov/33689445/
American
Journal of Public
Health 111,
no. 4 (April 1,
2021): 564-567.
6.464 15%; Conceptualization and drafting, editing of the HIV testing section; contribution to discussion; final approval
Recent publication – no citations at time of writing
4 Bakary Drammeh; Amy Medley; Helen Dale; Anindya
K. De; Shane Diekman; Randy Yee; Tiffiany Aholou;
Arielle Lasry; Andrew Auld; Brittney Baack; Wayne
Duffus; Ebrahim Shahul; Vincent Wong; Michael
Grillo; Teeb Al-Samarrai; Shabeen Ally,; Mtemwa
Nyangulu; Rose Nyirenda; Jacobus Olivier; Thato
Chidarikire; Nompumelelo Khanyile; Alick A. Kayange;
Oscar Ernest Rwabiyago,; Upendo Kategile; Jema
Bisimba,; Rachel A. Weber; Gertrude Ncube; Onesimo
Maguwu; Ismelda Pietersen; Denis Mali; Edington
Dzinotyiweyi; Lisa Nelson; Matovu John Bosco;
Kwarisiima Dalsone; Madina Apolot; Samson
Anangwe,; Leonard K. Soo; Mary Mugambi; Andre
Sex Differences in HIV Testing — 20 PEPFAR-Supported Sub-Saharan African Countries, 2019
https://www.cdc.gov/mmwr/volumes/69/wr/mm6948a1.htm?s_cid=mm6948a1_w
MMWR Morb
Mortal Wkly
Rep; 69:1801–
1806 (2020)
13.606
10%; Conceptualization, considerations on data inclusion framing, field coordination, discussion and conclusions.
6 Citations

61
Mbayih; Placidie Mugwaneza; Samuel S. Malamba;
Arlene Phiri; Tina Chisenga; Mary Boyd; Chanie
Temesgan; Mesfin Shimelis; Teklu Weldegebreal;
Mirtie Getachew; Shirish Balachandra; Ehui Eboi;
Willibord Shasha; Nicole Doumatey; Didier Adjoua;
Chidozie Meribe; Jerry Gwamna; Pamela Gado; Ima
John-Dada; Elie Mukinda; Luc F. Kamanga Lukusa;
Lucien Kalenga; Sudhir Bunga; Victoria Achyut,; John
Mondi; Peter Loeto; Goabaone Mogomotsi; Jenny
Ledikwe; Puleng Ramphalla; Mphotleng Tlhomola;
Justine K. Mirembe; Tse Nkwoh; Laura Eno; Leonard
Bonono; Nely Honwana; Noela Chicuecue; Ana
Simbine; Inacio Malimane; Lenhle Dube; Munamato
Mirira; Phumzile Mndzebele; Alean Frawley; Yolanda
Marina Rebello Cardo; Stephanie Behel
5 Augustine T Choko, Muhammad S Jamil, Peter MacPherson, Elizabeth Corbett, Lastone Chitembo ,Heather Ingold, Elkin Bermudez Aza, Marc d’Elbee, Meghan DiCarlo, Mohammed Majam, Tanya Schewchuk, Vincent Wong, Rachel Baggaley, Cheryl Johnson
Measuring linkage to HIV treatment services following HIV self-testing in low-income settings
https://onlinelibrary.wiley.com/doi/full/10.1002/jia2.25548
Journal of the
International
AIDS Society 23(6). (2020)
5.192 10%; Co-author, conceptualization; data reviews, writing and revision, approval of the final submitted draft.
6 Citations
6 Cheryl Johnson, Melissa Neuman, Peter MacPherson, Augustine Choko, Caitlin Quinn, Vincent J. Wong, Karin Hatzold, Rose Nyrienda, Getrude Ncube, Rachel Baggaley, Fern Terris-Prestholt & Elizabeth L. Corbett
Use and awareness of and willingness to self-test for HIV: An analysis of cross-sectional population-based surveys in Malawi and Zimbabwe https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-08855-7
BMC Public Health. 20, 779 (2020)
2.690 10%; Co-author, conceptualization and study design; design of survey questions integrated into population-based surveys to allow for study; data reviews, writing and revision, approval of the final submitted draft.
9 Citations
7 Nicole Haberland, Charity Ndwiga, Katharine McCarthy, Julie Pulerwitz, Rose Kosgei, Margaret Mak’anyengo, Amelia Peltz, Vincent J. Wong & Sam Kalibala
Addressing Intimate Partner Violence and Power in Intimate Relationships in HIV Testing Services in Nairobi, Kenya
https://link.springer.com/article/10.1007/s10461-020-02801-9
AIDS and Behavior volume 24, pages 2409-20 (2020)
3.312 15%; Co-author, conceptualization and study design, data reviews, writing and revision, approval of the final submitted draft.
3 Citations
8 Tonderai Mabuto, Nolundi Mshweshwe-Pakela, Nasiphi Ntombela, Mpho Hlongwane, Vincent Wong, Salome Charalambous, Deanna Kerrigan, Christopher J Hoffmann
Is HIV Post-test Counselling Aligned with Universal Test and Treat Goals? A Qualitative Analysis of Counselling Session Content and Delivery in South Africa
https://pubmed.ncbi.nlm.nih.gov/33241450/
AIDS and Behavior 2020 Nov
3.312 10%; Co-author, conceptualization and study design, writing and revision, approval of the final submitted draft.
Recent publication – no citations at time of writing
9 Caitlin Quinn, Vincent Wong, Muhammad S. Jamil, Rachel C. Baggaley, Cheryl C. Johnson
Symptom and risk-based screening to optimize HIV testing services: a scoping review
World Health Organization. Geneva (2020)
n/a 10%; Co-author, conceptualization, writing and revision, approval of the final submitted draft.
n/a
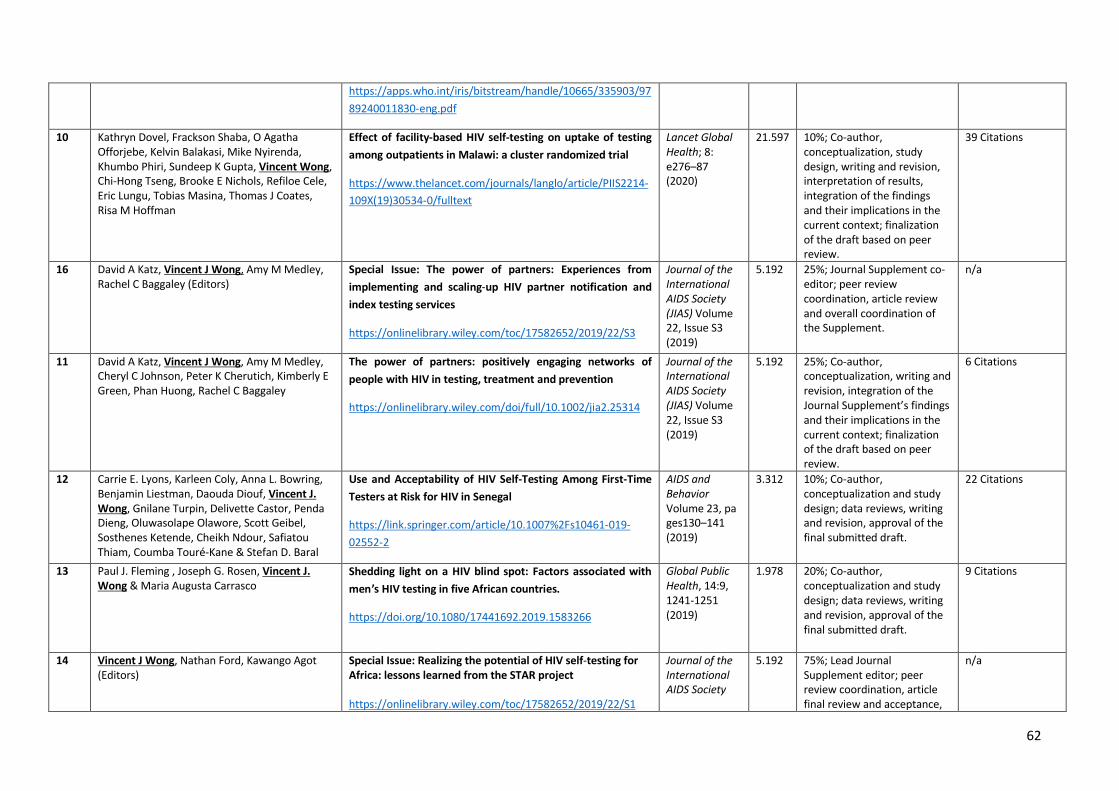
62
https://apps.who.int/iris/bitstream/handle/10665/335903/9789240011830-eng.pdf
10 Kathryn Dovel, Frackson Shaba, O Agatha Offorjebe, Kelvin Balakasi, Mike Nyirenda, Khumbo Phiri, Sundeep K Gupta, Vincent Wong, Chi-Hong Tseng, Brooke E Nichols, Refiloe Cele, Eric Lungu, Tobias Masina, Thomas J Coates, Risa M Hoffman
Effect of facility-based HIV self-testing on uptake of testing
among outpatients in Malawi: a cluster randomized trial
https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(19)30534-0/fulltext
Lancet Global
Health; 8: e276–87 (2020)
21.597 10%; Co-author, conceptualization, study design, writing and revision, interpretation of results, integration of the findings and their implications in the current context; finalization of the draft based on peer review.
39 Citations
16 David A Katz, Vincent J Wong, Amy M Medley, Rachel C Baggaley (Editors)
Special Issue: The power of partners: Experiences from
implementing and scaling-up HIV partner notification and
index testing services
https://onlinelibrary.wiley.com/toc/17582652/2019/22/S3
Journal of the
International
AIDS Society
(JIAS) Volume 22, Issue S3 (2019)
5.192 25%; Journal Supplement co-editor; peer review coordination, article review and overall coordination of the Supplement.
n/a
11 David A Katz, Vincent J Wong, Amy M Medley, Cheryl C Johnson, Peter K Cherutich, Kimberly E Green, Phan Huong, Rachel C Baggaley
The power of partners: positively engaging networks of
people with HIV in testing, treatment and prevention
https://onlinelibrary.wiley.com/doi/full/10.1002/jia2.25314
Journal of the
International
AIDS Society
(JIAS) Volume 22, Issue S3 (2019)
5.192 25%; Co-author, conceptualization, writing and revision, integration of the Journal Supplement’s findings and their implications in the current context; finalization of the draft based on peer review.
6 Citations
12 Carrie E. Lyons, Karleen Coly, Anna L. Bowring, Benjamin Liestman, Daouda Diouf, Vincent J.
Wong, Gnilane Turpin, Delivette Castor, Penda Dieng, Oluwasolape Olawore, Scott Geibel, Sosthenes Ketende, Cheikh Ndour, Safiatou Thiam, Coumba Touré-Kane & Stefan D. Baral
Use and Acceptability of HIV Self-Testing Among First-Time
Testers at Risk for HIV in Senegal
https://link.springer.com/article/10.1007%2Fs10461-019-02552-2
AIDS and
Behavior
Volume 23, pages130–141 (2019)
3.312 10%; Co-author, conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft.
22 Citations
13 Paul J. Fleming , Joseph G. Rosen, Vincent J.
Wong & Maria Augusta Carrasco Shedding light on a HIV blind spot: Factors associated with
men’s HIV testing in five African countries.
https://doi.org/10.1080/17441692.2019.1583266
Global Public
Health, 14:9, 1241-1251 (2019)
1.978 20%; Co-author, conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft.
9 Citations
14 Vincent J Wong, Nathan Ford, Kawango Agot (Editors)
Special Issue: Realizing the potential of HIV self-testing for
Africa: lessons learned from the STAR project
https://onlinelibrary.wiley.com/toc/17582652/2019/22/S1
Journal of the
International
AIDS Society
5.192 75%; Lead Journal Supplement editor; peer review coordination, article final review and acceptance,
n/a
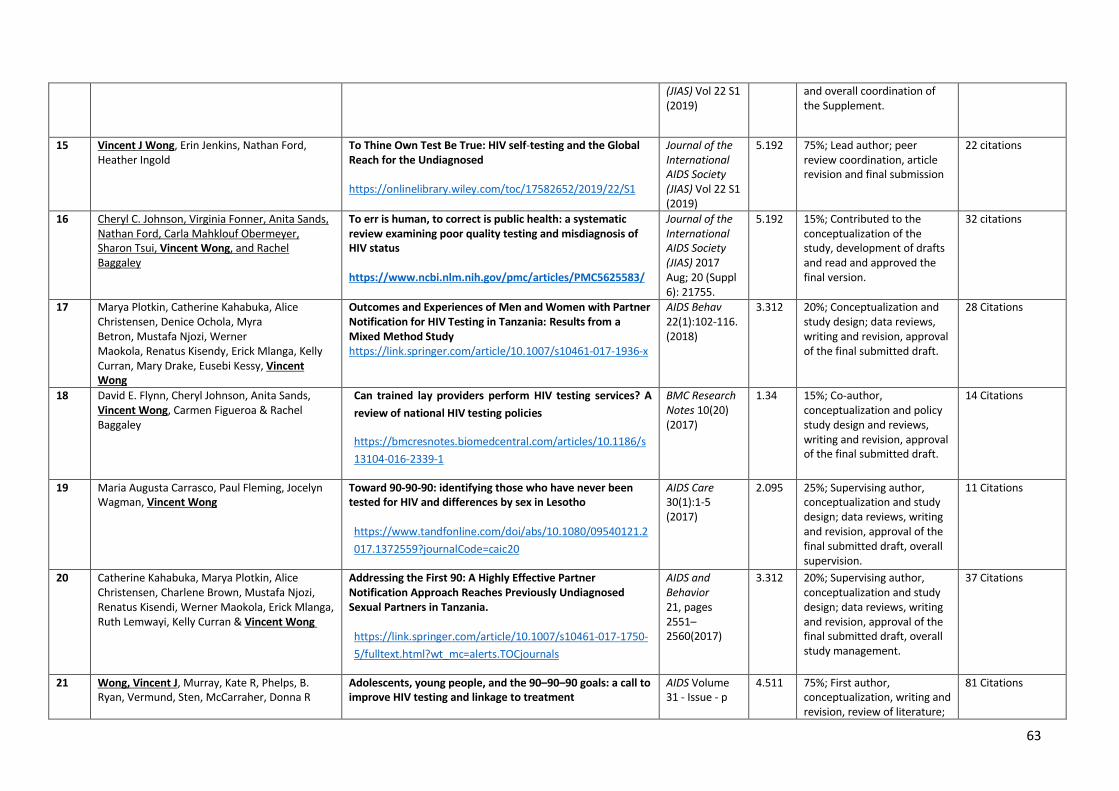
63
(JIAS) Vol 22 S1 (2019)
and overall coordination of the Supplement.
15 Vincent J Wong, Erin Jenkins, Nathan Ford, Heather Ingold
To Thine Own Test Be True: HIV self-testing and the Global
Reach for the Undiagnosed
https://onlinelibrary.wiley.com/toc/17582652/2019/22/S1
Journal of the
International
AIDS Society
(JIAS) Vol 22 S1 (2019)
5.192 75%; Lead author; peer review coordination, article revision and final submission
22 citations
16 Cheryl C. Johnson, Virginia Fonner, Anita Sands, Nathan Ford, Carla Mahklouf Obermeyer, Sharon Tsui, Vincent Wong, and Rachel Baggaley
To err is human, to correct is public health: a systematic
review examining poor quality testing and misdiagnosis of
HIV status
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5625583/
Journal of the
International
AIDS Society
(JIAS) 2017 Aug; 20 (Suppl 6): 21755.
5.192 15%; Contributed to the conceptualization of the study, development of drafts and read and approved the final version.
32 citations
17 Marya Plotkin, Catherine Kahabuka, Alice Christensen, Denice Ochola, Myra Betron, Mustafa Njozi, Werner Maokola, Renatus Kisendy, Erick Mlanga, Kelly Curran, Mary Drake, Eusebi Kessy, Vincent
Wong
Outcomes and Experiences of Men and Women with Partner
Notification for HIV Testing in Tanzania: Results from a
Mixed Method Study
https://link.springer.com/article/10.1007/s10461-017-1936-x
AIDS Behav 22(1):102-116. (2018)
3.312 20%; Conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft.
28 Citations
18 David E. Flynn, Cheryl Johnson, Anita Sands, Vincent Wong, Carmen Figueroa & Rachel Baggaley
Can trained lay providers perform HIV testing services? A
review of national HIV testing policies
https://bmcresnotes.biomedcentral.com/articles/10.1186/s13104-016-2339-1
BMC Research
Notes 10(20) (2017)
1.34 15%; Co-author, conceptualization and policy study design and reviews, writing and revision, approval of the final submitted draft.
14 Citations
19 Maria Augusta Carrasco, Paul Fleming, Jocelyn Wagman, Vincent Wong
Toward 90-90-90: identifying those who have never been
tested for HIV and differences by sex in Lesotho
https://www.tandfonline.com/doi/abs/10.1080/09540121.2017.1372559?journalCode=caic20
AIDS Care 30(1):1-5 (2017)
2.095 25%; Supervising author, conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft, overall supervision.
11 Citations
20 Catherine Kahabuka, Marya Plotkin, Alice Christensen, Charlene Brown, Mustafa Njozi, Renatus Kisendi, Werner Maokola, Erick Mlanga, Ruth Lemwayi, Kelly Curran & Vincent Wong
Addressing the First 90: A Highly Effective Partner
Notification Approach Reaches Previously Undiagnosed
Sexual Partners in Tanzania.
https://link.springer.com/article/10.1007/s10461-017-1750-5/fulltext.html?wt_mc=alerts.TOCjournals
AIDS and
Behavior
21, pages 2551–2560(2017)
3.312 20%; Supervising author, conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft, overall study management.
37 Citations
21 Wong, Vincent J, Murray, Kate R, Phelps, B. Ryan, Vermund, Sten, McCarraher, Donna R
Adolescents, young people, and the 90–90–90 goals: a call to
improve HIV testing and linkage to treatment
AIDS Volume 31 - Issue - p
4.511 75%; First author, conceptualization, writing and revision, review of literature;
81 Citations
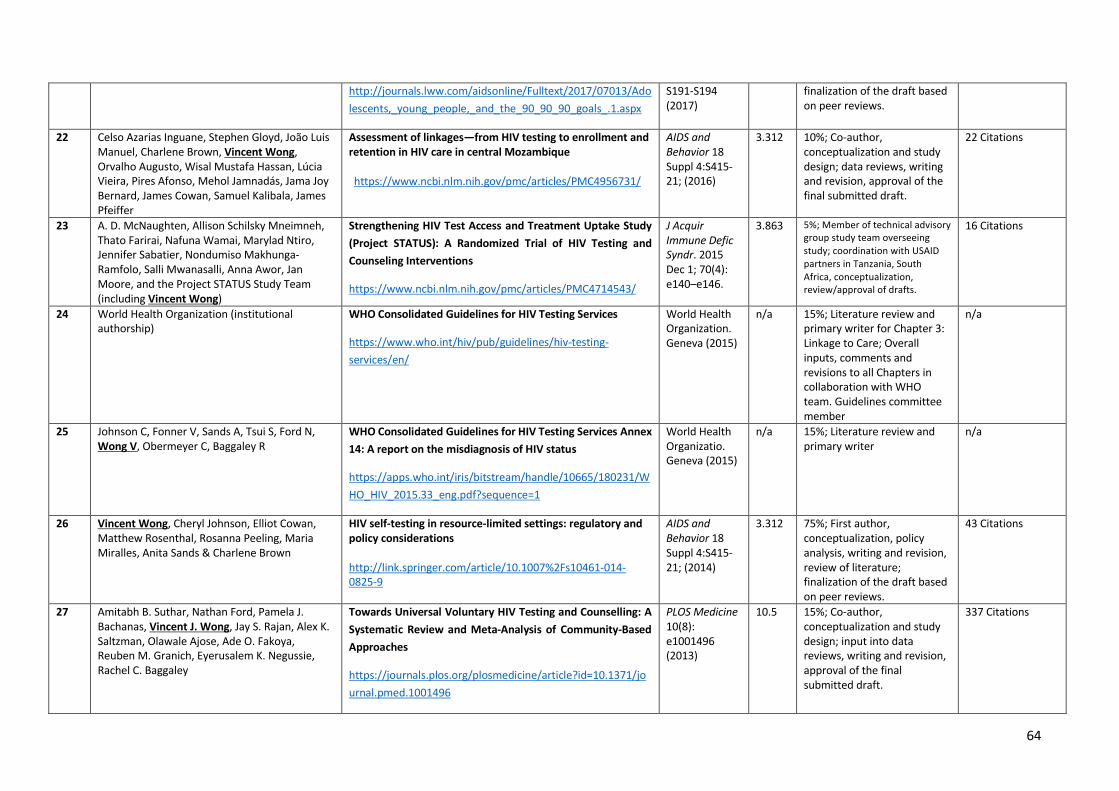
64
http://journals.lww.com/aidsonline/Fulltext/2017/07013/Adolescents,_young_people,_and_the_90_90_90_goals_.1.aspx
S191-S194 (2017)
finalization of the draft based on peer reviews.
22 Celso Azarias Inguane, Stephen Gloyd, João Luis Manuel, Charlene Brown, Vincent Wong, Orvalho Augusto, Wisal Mustafa Hassan, Lúcia Vieira, Pires Afonso, Mehol Jamnadás, Jama Joy Bernard, James Cowan, Samuel Kalibala, James Pfeiffer
Assessment of linkages—from HIV testing to enrollment and
retention in HIV care in central Mozambique
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4956731/
AIDS and
Behavior 18 Suppl 4:S415-21; (2016)
3.312 10%; Co-author, conceptualization and study design; data reviews, writing and revision, approval of the final submitted draft.
22 Citations
23 A. D. McNaughten, Allison Schilsky Mneimneh, Thato Farirai, Nafuna Wamai, Marylad Ntiro, Jennifer Sabatier, Nondumiso Makhunga-Ramfolo, Salli Mwanasalli, Anna Awor, Jan Moore, and the Project STATUS Study Team (including Vincent Wong)
Strengthening HIV Test Access and Treatment Uptake Study
(Project STATUS): A Randomized Trial of HIV Testing and
Counseling Interventions
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4714543/
J Acquir
Immune Defic
Syndr. 2015 Dec 1; 70(4): e140–e146.
3.863 5%; Member of technical advisory group study team overseeing study; coordination with USAID partners in Tanzania, South Africa, conceptualization, review/approval of drafts.
16 Citations
24 World Health Organization (institutional authorship)
WHO Consolidated Guidelines for HIV Testing Services
https://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/
World Health Organization. Geneva (2015)
n/a 15%; Literature review and primary writer for Chapter 3: Linkage to Care; Overall inputs, comments and revisions to all Chapters in collaboration with WHO team. Guidelines committee member
n/a
25 Johnson C, Fonner V, Sands A, Tsui S, Ford N, Wong V, Obermeyer C, Baggaley R
WHO Consolidated Guidelines for HIV Testing Services Annex
14: A report on the misdiagnosis of HIV status
https://apps.who.int/iris/bitstream/handle/10665/180231/WHO_HIV_2015.33_eng.pdf?sequence=1
World Health Organizatio. Geneva (2015)
n/a 15%; Literature review and primary writer
n/a
26 Vincent Wong, Cheryl Johnson, Elliot Cowan, Matthew Rosenthal, Rosanna Peeling, Maria Miralles, Anita Sands & Charlene Brown
HIV self-testing in resource-limited settings: regulatory and
policy considerations
http://link.springer.com/article/10.1007%2Fs10461-014-0825-9
AIDS and
Behavior 18 Suppl 4:S415-21; (2014)
3.312 75%; First author, conceptualization, policy analysis, writing and revision, review of literature; finalization of the draft based on peer reviews.
43 Citations
27 Amitabh B. Suthar, Nathan Ford, Pamela J. Bachanas, Vincent J. Wong, Jay S. Rajan, Alex K. Saltzman, Olawale Ajose, Ade O. Fakoya, Reuben M. Granich, Eyerusalem K. Negussie, Rachel C. Baggaley
Towards Universal Voluntary HIV Testing and Counselling: A
Systematic Review and Meta-Analysis of Community-Based
Approaches
https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1001496
PLOS Medicine 10(8): e1001496 (2013)
10.5 15%; Co-author, conceptualization and study design; input into data reviews, writing and revision, approval of the final submitted draft.
337 Citations

65
28 Rachel Baggaley, Bernadette Hensen, O Ajose, Kristina Grabbe, Vincent J Wong, Alison Schilsky, Ying R Lo, F Lule, Reuben Granich, and James Hargreaves
From caution to urgency: the evolution of HIV testing and
counselling in Africa.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3442388/
Bulletin of the
World Health
Organization
90:652–658B
(2012)
6.818 15%; Co-author, conceptualization and study design; input into data reviews, writing and revision, approval of the final submitted draft.
79 Citations
29 Bernadette Hensen, Rachel Baggaley, Vincent J.
Wong, Kristina L. Grabbe, Nathan Shaffer, Ying-Ru Jacqueline Lo, James Hargreaves
Universal voluntary HIV testing in antenatal care settings: a
review of the contribution of provider-initiated testing &
counselling
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-3156.2011.02893.x
Tropical Med
and Int
Health,;17(1):59-70. (2011)
2.308 15%; Co-author, conceptualization and study design; input into data reviews, writing and revision, approval of the final submitted draft.
95 Citations
30 Jennifer McCleary-Sills, Anjala Kanesathasan, Jonathan Brakarsh, Marnie Vujovic, Kgethi Dlamini, Eve Namisango, Rose Nasaba, Katherine Fritz, Vincent J. Wong & Sara Bowsky
Foundation for the future: meeting the psychosocial needs of
children living with HIV in South Africa and Uganda
https://www.tandfonline.com/doi/abs/10.1080/15381501.2012.749818
Journal Of
HIV/AIDS and
Social Services Vol. 12 (1) (2013)
0.284 20%; Co-author, conceptualization and study design; writing and revision, approval of the final submitted draft.
10 citations
31 Vincent Wong, Ian Macleod, Charlie Gilks, Donna Higgins & Siobhan Crowley
The lost children of universal access: issues in scaling up HIV
testing and counselling
https://www.tandfonline.com/doi/abs/10.1080/17450120600700004
Vulnerable
Children and
Youth Studies 1(1); (Apr 2006)
0.65 60%; Primary author, methodology development, data collection and analysis,
13 Citations
N/A (MSc Thesis)
Vincent J. Wong Voluntary HIV Counseling and Testing in Accra, Ghana
https://www.lap-publishing.com/catalog/details/store/fr/book/978-3-659-39586-4/voluntary-hiv-counseling-and-testing-in-accra,-ghana?search=Wong%20Ghana
LAP Publishing,
(2005; self-
published
2013)
n/a 100%; MSc Thesis; research development, primary data collection and analysis, writing and final submission. Final Grade: A (Excellent)
n/a
N/A (to be pub-lished)
Kathryn L Dovel, Kelvin Balakasi, Khumbo Phiri, Frackson Shaba, Ogechukwu Agatha Offorjebe,
Sundeep K Gupta, Vincent Wong, Eric Lungu, Brooke E Nichols, Mike Nyirenda, Tobias Masina,8 Anteneh Worku,9 Risa Hoffman
A randomized trial on index HIV self-testing for sexual
partners of ART clients in Malawi
Lancet Global
Health
(submitted March 2022)
n/a 10%; developed study protocol and materials; edited drafts; read and approved the final manuscript.
n/a
N/A (to be pub-lished)
Bakary Drammeh, Anindya K De, Emanny Sanchez, Spencer Lloyd, Amy Medley, Helen Dale, Shane Diekman, Arielle Lasry, Tiffiany Aholou, Irene Benech, Randy Yee, Avi J Hakim, Teeb Al-Samarrai, Vincent Wong, Michael Grillo et al.
The Impact of COVID-19 on HIV Testing Services and Patient
Proxy Linkage in 14 Sub-Saharan African Countries
PLOS Medicine
(Jan 2022 submitted for publication)
n/a 10% conceptualization and methodology, country coordination, inputs into final draft manuscript, final approvals for submission.
n/a

66
Table 4: Co-authored Publications List and Authorial Contributions, Chronological
N/A (to be pub-lished)
Ariana M. Traub, Amy Medley, Jessica Gross, Margo Sloan, Anouk Amzel, Megan M. Gleason, Nimasha B. Fernando, Vincent Wong, Michael P. Grillo, Hilary Wolf, Teeb Al-Samarrai, Julie Nenon, Alean Frawley, Mosarwa Segwabe, Catherine Motswere, Evelyne Baramperanye, Valery Nzima, Magdalene Mange Mayer, Lucie Dagri, Shirish Balachandra, Francois-Xavier N'siesi, Henri O. Longuma, Patricia Nyembo, Nyakallang Moyo, Sikhathele Mazibuko, Tsegaye Tilahun, Wondimu Teferi, Olbeg Desinor, MD21; Jean-Louis Reginald, Teresa Simiyu, Lennah Nyabiage, Justine Mirembe, Mamorapeli Ts’oeu, Gerald Zomba, Mtemwa Nyangulu, Argentina Wate, Jessica Greenburg Cowan, Denis Mali, Ismelda Pietersen, Dolapo Ogundehin, Dennis Onotu, Akudo Ikpeazu, Esron Niyonsaba, Jackson Bamwesigye, Hlamalani Mabasa, Gurpreet Kindra, Nicholas Baabe, Sudhir Bunga, Frederick Rwegerera, Edward Machage, Galal King'ori, Jacqueline Calnan, Esther Nazziwa, Godfrey Lingenda, Kebby Musokotwane, Ruth Bulaya-Tembo, Talent Maphosa, Meena Srivastava
Trends in Pediatric HIV Case Identification Across 22 PEPFAR-Supported Countries during the COVID-19 Pandemic, October 2019 to September 2020
MMWR (Jan 2022 submitted for publication)
n/a 5% conceptualization and methodology, inputs into final draft manuscript, final approvals for submission.
n/a

67
3.2 Additional Authorship Documents in Consideration of Application 3.2.1 Conference abstracts and presentations, 2002-2020, chronological
1. Trends in HIV testing and linkage to HIV treatment in 41 countries, 2016-2021. Conference on Retroviruses and Opportunistic Infections (CROI) 2022. Session Oral-08. Authors: Bakary Drammeh, Anindya K. De, Amy Medley, Randy Yee, Shazad Ahmed, Helen Dale, Arielle Lasry, Vincent J. Wong, Michael Grillo, Emanny Sanchez, David A. Miller, Tiffiany Aholou, Shahul Ebrahim, Stephanie Behel
2. Optimizing testing increases yield in HIV case finding in 24 countries, 2018–2019. Conference on Retroviruses and Opportunistic Infections (CROI) 2020. Session TD-05. Authors: S Ebrahim, A Lasry, R, Wayne, A Duffus, J Abellera, S Diekman, J Rurangirwa, B Drammeh, T Ahoulou, M Grillo, V Wong, S Behel
3. Correlates of condom use and procedure knowledge among men accessing voluntary medical male circumcision in Malawi, International HIV/AIDS Conference 2016, Abstract WEPEC383, Durban, South Africa. M.A. Carrasco, V. Wong, K. Ahanda, M.R. Kaufman
4. Partner notification for HIV testing services (HTS) approach in Tanzania underscores need for discordant couple package, International HIV/AIDS Conference 2016, Abstract
WEPEC214, Durban, South Africa. Authors: M. Plotkin, C. Kahabuka, R. Kisendi, A. Christensen, E. Mlanga, K. Curran, C. Brown, V. Wong
5. HIV Testing and Misdiagnosis, PEPFAR Annual Meeting, Session 7 Panel Presentation, July 18, 2016, Durban, South Africa. V Wong
6. Effective, high-yield HIV testing for partners of newly diagnosed persons in Tanzania. Abstract 16-653 Themed Discussion and Poster Presentation, Conference on Retroviruses and Opportunistic Infections (CROI), 2016, Boston MA. M Plotkin; C Kahabuka; M Amuri; M Njozi; W Maokola; E Mlanga; M Drake Curran; C Brown; V Wong
7. Are We Delivering the Wrong Results? Examining Misclassification of HIV Status and False Positive Test Results. African Society for Laboratory Medicine Conference 2014. Poster presentation, Cape Town, South Africa, Dec 1, 2014. Authors: C Johnson, V Wong, R Baggeley, A Sands. (ASLM First Place Award Best Poster)
8. Expanding HIV testing and counseling through community-based integrated family planning/HTS service delivery in Uganda. Conference on Retroviruses and Opportunistic Infections (CROI) 2014 Poster and Oral Presentations, Boston MA. Abstract 1042. A Brunie, A Cheng, P Mucheri, J Namwebya, T Petruney, B Tumwesigye, S Mercer, V Afayo, A Akol, V. Wong
9. The Costing Of HIV Testing and Counseling in Botswana: Capturing Cost and Effectiveness Data for Multiple Service Delivery Models. Dec 10, 2013. ICASA Conference, Cape
Town, South Africa. Authors: M. Stegman, W. Mosime, S. Forsythe, S. Alkenbrack, R. Lebelonyane, and V. Wong
10. Three Delays to Linkages to Care: A Systematic Review of Barriers Affecting Initial Enrollment In Care Among HIV-diagnosed Persons. Dec 2013. ICASA Conference, Cape Town, South Africa. C Johnson, C Brown, R Baggeley, V Wong.
11. Positive connections: HIV prevention among positive adolescents. International HIV/AIDS Conference, 2012, Wash DC. Book presented as poster presentation.
68
12. Out of the clinic, into the home: an assessment of PEPFAR home-based HIV testing and counseling programs in sub-Saharan Africa to inform the development of international WHO/PEPFAR support tools. International HIV/AIDS Conference, 2012, Wash DC. M. Taegtmeyer, C. Blazer, M.C. Escobar, K. Grabbe, V. Wong, R Baggeley
13. Examining reporting of quality elements in a provider-initiated HIV testing and counseling and implications for rights-based approaches: a literature review. International HIV/AIDS Conference, 2010, Vienna; Abstract no. THPE0894; July 2010. V Wong, M Sabin
14. A descriptive study of VCT implementation in the Accra Metropolitan District, Ghana. AIDS 2006 - XVI International AIDS Conference, Toronto: Abstract no. WEPE0421. V Wong.
15. Evaluation of 'InstantScreen', an ultra-rapid HIV1/2 assay based upon novel technologies for the detection of the HIV antibodies. Jul 2002. XIV International AIDS Conference Abstract: TuPeC4890 H Repke, S Nicolaus, 0 Lettau, G Vetter, V Wong
16. Evaluation of 'InstantScreen', an ultra-rapid HIV1/2 assay based upon novel technologies for the detection of the HIV antibodies [Brazil study]. Souza RS, Motta LR, Wong V, Gomez-Marin O, Mitchell C, Repke H; International Conference on AIDS. Int Conf AIDS. 2002 Jul 7-12; Abstract no. TuPeC4890.
3.2.2 Contributions to WHO Guidelines and Frameworks, 2005-2020 Official engagement as guidelines development committee member, external reviewer, writer-contributor, or WHO participating member.
2022, WHO Guidelines on COVID Self Testing (Guidelines Observer, External Review Group) (Forthcoming, 2022)
2021, UNAIDS/WHO Technical Guidance on the Use of Recency Assays for HIV Surveillance (External Reviewer) (Forthcoming, late 2022)
2021, COVID and HIV Testing Services Rapid Advice (External Reviewer) (Forthcoming, late 2021)
2021, Hepatitis C Self Testing Guidelines (External Reviewer, Guidelines Observer Status)
2019, HIV Testing Services Guidelines Update (Guidelines Committee member – Guidelines Development Group)
2016, HIV Self Testing and Partner Notification Guidelines (Guidelines Committee member)
2016, Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection, 2nd Ed. (External Reviewer: Chapter 2 - Clinical Guidelines, HIV Diagnosis)
2015, Consolidated HIV testing services guidelines (Guidelines Committee member, contributing writer – Section 3.6)
2015, Improving the quality of HIV-related point-of-care testing: ensuring the reliability and accuracy of test results (Peer reviewer, contributing writer)
2013, Guidelines on HIV testing and counseling in adolescents (Guidelines Committee member, peer reviewer)
69
2012, Service delivery approaches to HTS: a strategic framework (Concept development, Peer reviewer, contributing writer)
2012, Planning, implementing and monitoring home-based HIV testing and counseling (Concept development, peer review, writing team, final approval)
2011, Guide for monitoring and evaluating national HTS programmes (Peer reviewer, Contributing writer)
2011, Guidance on Couples HIV testing and counseling and the use of anti-retroviral therapy in sero-discordant couples. (Guidelines Committee member, writing)
2011, Retention in HIV programmes: defining the challenges and identifying solutions: meeting report (Participant, peer reviewer)
2010, A Handbook for improving HIV testing and counseling services (Conceptual development, writing, review and integration of feedback, final approval)
2010, Policy requirements for HIV testing and counseling of infants and young children in health facilities (Senior consultant, writing and development)
2009, HIV counselling package for the Asia-Pacific (Senior consultant, writing and development)
2007, Provider-initiated testing and counselling guidelines for the health sector (Senior consultant, writing and development)
2005, Scaling-up HIV testing and counselling services : a toolkit for programme managers. (Senior consultant, writing and development)
3.2.3 Additional contributions: PEPFAR Guidelines and HTS Contributions
As part of my professional duties, I provided HTS technical inputs into these US Government/PEPFAR and other HTS-related documents and working
groups from 2010-2021:
• PEPFAR Monitoring, evaluation and research indicator reference guide v2.5 (9/2020), HIV Testing indicators
o Version 2.5 Website: https://datim.zendesk.com/hc/article_attachments/360071630231/FY21_MER_2.5_Indicator_Reference_Guide.pdf
• PEPFAR Country Operational Planning (COP) Guidance Technical Considerations, HIV Testing Services Sections
o COP22 FY2023 guidance
o COP21 FY2022 guidance
o Guidance documents from 2010 – 2019: Website archive: https://web.archive.org/web/20190326225032/https://www.pepfar.gov/reports/guidance/index.htm
• PEPFAR HTS Technical Working Group Co Chair, 2010 – 2018 (ended when the TWG was dissolved)
• 2018 IAS Differentiated Service Delivery HIV Testing Framework

70
o IAS DSD Website: http://www.differentiatedservicedelivery.org/Portals/0/adam/Content/DCwLmrNFcUuLU4jWitw4-Q/File/Decision%20Framework%20HIV%20Testing%20Web%20-%20Update%20AUG19.pdf
o HTS Technical Working Group. https://www.iasociety.org/HIV-Programmes/Programmes/Differentiated-Service-Delivery/Differentiated-Care-Committees#technicalTesting
• HIVSTAR Project Technical Advisory Group, May 2016 – January 2020 (ended with the completion of HIVSTAR Phase I)
o Provided technical guidance and oversight of the HIVSTAR Project, a multi-country randomized trial of HIV self-testing in Africa.
3.3 Metrics of Impact
Vincent Wong has co-authored 29 peer-reviewed publications on HIV testing services that form the basis of this PhD by Publication. Additionally, he has
been involved in an official capacity with 17 WHO documents related to HTS, including normative guidelines, and presented on 16 poster abstracts at
multiple international HIV/AIDS conferences since 2002.
As of September 2, 2021, his RG Score is 28.57 (higher than 85% of all ResearchGate scores) and his h-index6 is 14 (this includes over 6500 compiled
reads and 969 cumulative citations from 2007 to 2022).7 8 His overall average impact factor across 29 published articles is 4.79.
These metrics indicate that his collective published work provided in this submission has had a substantial impact in the public health field of HIV testing
services and has impacted rates of diagnoses globally.
6 From ResearchGate: “The h-index is an author-level metric that measures your research output and its citation impact. It is based on a set of your most cited work and the number of citations it’s received.” 7 Source: https://www.researchgate.net/profile/Vincent-Wong-13 8 ORCID ID: https://orcid.org/0000-0001-6926-9401

Chapter 4: References to Commentary Note: Publications co-authored or contributed to by Vincent Wong which contribute to the body of work submitted for the award of PhD by Publication are included in bold. Allen, S., Karita, E., Chomba, E., Roth, D. L., Telfair, J., Zulu, I., Clark, L., Kancheya, N., Conkling, M.,
Stephenson, R., Bekan, B., Kimbrell, K., Dunham, S., Henderson, F., Sinkala, M., Carael, M., & Haworth, A. (2007). Promotion of couples' voluntary counselling and testing for HIV through influential networks in two African capital cities. BMC Public Health, 7, 349. https://doi.org/10.1186/1471-2458-7-349
Allen, S., Meinzen-Derr, J., Kautzman, M., Zulu, I., Trask, S., Fideli, U., Musonda, R., Kasolo, F., Gao, F., & Haworth, A. (2003). Sexual behavior of HIV discordant couples after HIV counseling and testing. AIDS, 17(5), 733-740. https://doi.org/10.1097/00002030-200303280-00012
Armbruster, B., Helleringer, S., Kalilani-Phiri, L., Mkandawire, J., & Kohler, H. P. (2011). Exploring the relative costs of contact tracing for increasing HIV case finding in sub-Saharan countries. J Acquir Immune Defic Syndr, 58(2), e29-36. https://doi.org/10.1097/QAI.0b013e31822a9fa8
AVAC. (2020). Open Letter to Ambassador Birx regarding Index Testing in the 2020 Country Operating Plan Guidance endorsed by 76 organizations. In A. D. Birx (Ed.).
AVERT. (2021). History of HIV & AIDS overview. Retrieved 8/23/2021 from https://www.avert.org/professionals/history-hiv-aids/overview
Ayala, G., Bahati, M., Balan, E., Chang, J., Do, T. D., Fokeerbux, N. A., Hassan, A., Kerboghossian, J., Poonkasetwatana, M., Saavedra, J., Spieldenner, A., Thomas, R. M., Tohme, J., & Walimba, J. (2019). Partner Notification: A Community Viewpoint. J Int AIDS Soc, 22 Suppl 3, e25291. https://doi.org/10.1002/jia2.25291
Ayala, G., Bahati, M., Balan, E., Chang, J., Do, T. D., Fokeerbux, N. A., Hassan, A., Kerboghossian, J., Poonkasetwatana, M., Saavedra, J., Spieldenner, A., Thomas, R. M., Tohme, J., & Walimba, J. (2019). Partner notification: a community viewpoint. J Int AIDS Soc, 22(S3), e25291. https://doi.org/10.1002/jia2.25291
Baggaley, R., Henson, B., Ajose, O., Grabbe, K., Wong, V., & Schilsky, A. (2012). From caution to urgency: the evolving response to HIV testing. Bull World Health Organ, 90, 652-658B. http://www.who.int/bulletin/volumes/90/9/11-100818/en/, accessed 08 October 2014
Bandason, T., Dauya, E., Dakshina, S., McHugh, G., Chonzi, P., Munyati, S., Weiss, H. A., Simms, V., Kranzer, K., & Ferrand, R. A. (2018). Screening tool to identify adolescents living with HIV in a community setting in Zimbabwe: A validation study. PloS one, 13(10), e0204891. https://doi.org/10.1371/journal.pone.0204891
Birdthistle, I., Tanton, C., Tomita, A., de Graaf, K., Schaffnit, S. B., Tanser, F., & Slaymaker, E. (2019). Recent levels and trends in HIV incidence rates among adolescent girls and young women in ten high-prevalence African countries: a systematic review and meta-analysis. Lancet Glob Health, 7(11), e1521-e1540. https://doi.org/10.1016/S2214-109X(19)30410-3
Branson, B. M., Handsfield, H. H., Lampe, M. A., Janssen, R. S., Taylor, A. W., Lyss, S. B., Clark, J. E., Centers for Disease, C., & Prevention. (2006). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep, 55(RR-14), 1-17; quiz CE11-14. https://www.ncbi.nlm.nih.gov/pubmed/16988643
Brown, L. B., Miller, W. C., Kamanga, G., Nyirenda, N., Mmodzi, P., Pettifor, A., Dominik, R. C., Kaufman, J. S., Mapanje, C., Martinson, F., Cohen, M. S., & Hoffman, I. F. (2011). HIV partner notification is effective and feasible in sub-Saharan Africa: opportunities for HIV treatment and prevention. J Acquir Immune Defic Syndr, 56(5), 437-442. https://doi.org/10.1097/QAI.0b013e318202bf7d (Yes)
71

Cambiano, V., Johnson, C. C., Hatzold, K., Terris-Prestholt, F., Maheswaran, H., Thirumurthy, H., Figueroa, C., Cowan, F. M., Sibanda, E. L., Ncube, G., Revill, P., Baggaley, R. C., Corbett, E. L., Phillips, A., & for Working Group on Cost Effectiveness of, H. I. V. s.-t. i. S. A. (2019). The impact and cost-effectiveness of community-based HIV self-testing in sub-Saharan Africa: a health economic and modelling analysis. J Int AIDS Soc, 22 Suppl 1, e25243. https://doi.org/10.1002/jia2.25243
Carrasco, M. A., Atkins, K., Young, R., Rosen, J. G., Grieb, S. M., Wong, V. J., & Fleming, P. J. (2021). The HIV Pandemic Prevention Efforts Can Inform the COVID-19 Pandemic Response in the United States. Am J Public Health, 111(4), 564-567. https://doi.org/10.2105/AJPH.2021.306158
Carrasco, M. A., Fleming, P., Wagman, J., & Wong, V. (2018). Toward 90-90-90: identifying those who have never been tested for HIV and differences by sex in Lesotho. AIDS Care, 30(3), 284-288. https://doi.org/10.1080/09540121.2017.1372559
CDC. (2001). Revised Guidelines for HIV Counseling, Testing, and Referral. MMWR, 50 (RR19), 1-58. https://www.cdc.gov/mmwr/preview/mmwrhtml/rr5019a1.htm
Chamie, G., Clark, T. D., Kabami, J., Kadede, K., Ssemmondo, E., Steinfeld, R., Lavoy, G., Kwarisiima, D., Sang, N., Jain, V., Thirumurthy, H., Liegler, T., Balzer, L. B., Petersen, M. L., Cohen, C. R., Bukusi, E. A., Kamya, M. R., Havlir, D. V., & Charlebois, E. D. (2016). A hybrid mobile approach for population-wide HIV testing in rural east Africa: an observational study. Lancet HIV, 3(3), e111-119. https://doi.org/10.1016/S2352-3018(15)00251-9
Cherutich, P., Golden, M. R., Wamuti, B., Richardson, B. A., Asbjornsdottir, K. H., Otieno, F. A., Ng'ang'a, A., Mutiti, P. M., Macharia, P., Sambai, B., Dunbar, M., Bukusi, D., Farquhar, C., & a, P. S. S. G. (2017). Assisted partner services for HIV in Kenya: a cluster randomised controlled trial. Lancet HIV, 4(2), e74-e82. https://doi.org/10.1016/S2352-3018(16)30214-4
Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N., Hakim, J. G., Kumwenda, J., Grinsztejn, B., Pilotto, J. H., Godbole, S. V., Chariyalertsak, S., Santos, B. R., Mayer, K. H., Hoffman, I. F., Eshleman, S. H., Piwowar-Manning, E., Cottle, L., Zhang, X. C., . . . Team, H. S. (2016). Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N Engl J Med, 375(9), 830-839. https://doi.org/10.1056/NEJMoa1600693
Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N., Hakim, J. G., Kumwenda, J., Grinsztejn, B., Pilotto, J. H. S., Godbole, S. V., Mehendale, S., Chariyalertsak, S., Santos, B. R., Mayer, K. H., Hoffman, I. F., Eshleman, S. H., Piwowar-Manning, E., Wang, L., . . . Fleming, T. R. (2011). Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med, 365(6), 493-505. https://doi.org/10.1056/NEJMoa1105243
Colombe, S., Beard, J., Mtenga, B., Lutonja, P., Mngara, J., de Dood, C. J., van Dam, G. J., Corstjens, P., Kalluvya, S., Urassa, M., Todd, J., & Downs, J. A. (2019). HIV-seroconversion among HIV-1 serodiscordant married couples in Tanzania: a cohort study. BMC Infect Dis, 19(1), 518. https://doi.org/10.1186/s12879-019-4151-8
Conkling, M., Shutes, E. L., Karita, E., Chomba, E., Tichacek, A., Sinkala, M., Vwalika, B., Iwanowski, M., & Allen, S. A. (2010). Couples' voluntary counselling and testing and nevirapine use in antenatal clinics in two African capitals: a prospective cohort study. J Int AIDS Soc, 13, 10. https://doi.org/10.1186/1758-2652-13-10
Coovadia, H. M. (2000). Access to voluntary counseling and testing for HIV in developing countries. Ann N Y Acad Sci, 918, 57-63. https://doi.org/10.1111/j.1749-6632.2000.tb05474.x
Csete, J., Schleifer, R., & Cohen, J. (2004). "Opt-out" testing for HIV in Africa: a caution. Lancet, 363(9407), 493-494. https://doi.org/10.1016/S0140-6736(04)15509-8
De Cock, K. M., Barker, J. L., Baggaley, R., & El Sadr, W. M. (2019). Where are the positives? HIV testing in sub-Saharan Africa in the era of test and treat. AIDS, 33(2), 349-352. https://doi.org/10.1097/QAD.0000000000002096
Delaney, K. P., Hanson, D. L., Masciotra, S., Ethridge, S. F., Wesolowski, L., & Owen, S. M. (2017). Time until emergence of HIV test reactivity following infection with HIV-1: implications for interpreting test
72

results and retesting after exposure. Clin Infect Dis, 64(1), 53-59. https://doi.org/10.1093/cid/ciw666
Denison, J. A., O'Reilly, K. R., Schmid, G. P., Kennedy, C. E., & Sweat, M. D. (2008). HIV voluntary counseling and testing and behavioral risk reduction in developing countries: a meta-analysis, 1990--2005. AIDS Behav, 12(3), 363-373. https://doi.org/10.1007/s10461-007-9349-x
Downing, R. G., Otten, R. A., Marum, E., Biryahwaho, B., Alwano-Edyegu, M. G., Sempala, S. D., Fridlund, C. A., Dondero, T. J., Campbell, C., & Rayfield, M. A. (1998). Optimizing the delivery of HIV counseling and testing services: the Uganda experience using rapid HIV antibody test algorithms. J Acquir Immune Defic Syndr Hum Retrovirol, 18(4), 384-388. https://doi.org/10.1097/00042560-199808010-00011
Drammeh, B., Medley, A., Dale, H., De, A. K., Diekman, S., Yee, R., Aholou, T., Lasry, A., Auld, A., Baack, B., Duffus, W., Shahul, E., Wong, V., Grillo, M., Al-Samarrai, T., Ally, S., Nyangulu, M., Mchd, Nyirenda, R., . . . Behel, S. (2020). Sex Differences in HIV Testing - 20 PEPFAR-Supported Sub-Saharan African Countries, 2019. MMWR Morb Mortal Wkly Rep, 69(48), 1801-1806. https://doi.org/10.15585/mmwr.mm6948a1
Eholie, S. P., Badje, A., Kouame, G. M., N'Takpe J, B., Moh, R., Danel, C., & Anglaret, X. (2016). Antiretroviral treatment regardless of CD4 count: the universal answer to a contextual question. AIDS Res Ther, 13, 27. https://doi.org/10.1186/s12981-016-0111-1
Ehrenkranz, P., Grimsrud, A., Holmes, C. B., Preko, P., & Rabkin, M. (2021). Expanding the Vision for Differentiated Service Delivery: A Call for More Inclusive and Truly Patient-Centered Care for People Living With HIV. J Acquir Immune Defic Syndr, 86(2), 147-152. https://doi.org/10.1097/QAI.0000000000002549
Farquhar, C., Kiarie, J. N., Richardson, B. A., Kabura, M. N., John, F. N., Nduati, R. W., Mbori-Ngacha, D. A., & John-Stewart, G. C. (2004). Antenatal couple counseling increases uptake of interventions to prevent HIV-1 transmission. J Acquir Immune Defic Syndr, 37(5), 1620-1626. https://doi.org/10.1097/00126334-200412150-00016
FDA. (2012). Summary of Safety and Effectiveness, July 3, 2012 - OraQuick (PDF - 424KB). US Food and Drug Administration. Retrieved July 7, 2021 from https://wayback.archive-it.org/7993/20190207203522/https://www.fda.gov/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/PremarketApprovalsPMAs/ucm310436.htm
FDA. (2020). Coronavirus (COVID-19) Update: FDA Authorizes First COVID-19 Test for Self-Testing at Home. Retrieved May 18, 2021 from https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-covid-19-test-self-testing-home
Figueroa, C., Johnson, C., Ford, N., Sands, A., Dalal, S., Meurant, R., Prat, I., Hatzold, K., Urassa, W., & Baggaley, R. (2018). Reliability of HIV rapid diagnostic tests for self-testing compared with testing by health-care workers: a systematic review and meta-analysis. Lancet HIV, 5(6), e277-e290. https://doi.org/10.1016/S2352-3018(18)30044-4
Fleming, P. J., Rosen, J. G., Wong, V. J., & Carrasco, M. A. (2019). Shedding light on a HIV blind spot: Factors associated with men's HIV testing in five African countries. Glob Public Health, 14(9), 1241-1251. https://doi.org/10.1080/17441692.2019.1583266
Fonner, V. A., Denison, J., Kennedy, C. E., O'Reilly, K., & Sweat, M. (2012). Voluntary counseling and testing (VCT) for changing HIV-related risk behavior in developing countries. Cochrane Database Syst Rev(9), CD001224. https://doi.org/10.1002/14651858.CD001224.pub4
Galvani, A. P., Pandey, A., Fitzpatrick, M. C., Medlock, J., & Gray, G. E. (2018). Defining control of HIV epidemics. Lancet HIV, 5(11), e667-e670. https://doi.org/10.1016/S2352-3018(18)30178-4
Ghys, P. D., Williams, B. G., Over, M., Hallett, T. B., & Godfrey-Faussett, P. (2018). Epidemiological metrics and benchmarks for a transition in the HIV epidemic. PLoS Med, 15(10), e1002678. https://doi.org/10.1371/journal.pmed.1002678
73

Gill, M. M., Jahanpour, O., van de Ven, R., Barankena, A., Urasa, P., & Antelman, G. (2021). HIV risk screening and HIV testing among orphans and vulnerable children in community settings in Tanzania: Acceptability and fidelity to lay-cadre administration of the screening tool. PloS one, 16(3), e0248751. https://doi.org/10.1371/journal.pone.0248751
Global Fund to Fight AIDS, T. a. M. (2006). Annual Report 2005. https://www.theglobalfund.org/media/1331/corporate_2005annual_report_en.pdf
Global Fund to Fight AIDS, T. a. M. (2016). Operational research note on HIV self-testing. Geneva: The Global Fund to Fight AIDS, Tuberculosis and Malaria
Global Fund to Fight AIDS, T. a. M. (2020a). Annual Report 2020. https://www.theglobalfund.org/media/10103/corporate_2020resultsreport_report_en.pdf
Global Fund to Fight AIDS, T. a. M. (2020b). Results Report 2020. https://www.theglobalfund.org/media/10103/corporate_2020resultsreport_report_en.pdf
Gourlay, A., Birdthistle, I., Mthiyane, N. T., Orindi, B. O., Muuo, S., Kwaro, D., Shahmanesh, M., Baisley, K., Ziraba, A., & Floyd, S. (2019). Awareness and uptake of layered HIV prevention programming for young women: analysis of population-based surveys in three DREAMS settings in Kenya and South Africa. BMC Public Health, 19(1), 1417. https://doi.org/10.1186/s12889-019-7766-1
Granich, R. M., Gilks, C. F., Dye, C., De Cock, K. M., & Williams, B. G. (2009). Universal voluntary HIV testing with immediate antiretroviral therapy as a strategy for elimination of HIV transmission: a mathematical model. Lancet, 373(9657), 48-57. https://doi.org/10.1016/S0140-6736(08)61697-9
Gruskin, S., Ahmed, S., & Ferguson, L. (2008). Provider-initiated HIV testing and counseling in health facilities--what does this mean for the health and human rights of pregnant women? Dev World Bioeth, 8(1), 23-32. https://doi.org/10.1111/j.1471-8847.2007.00222.x
Hallett, T. B., & Eaton, J. W. (2013). A side door into care cascade for HIV-infected patients? J Acquir Immune Defic Syndr, 63 Suppl 2, S228-232. https://doi.org/10.1097/QAI.0b013e318298721b
Han, H., Myers, S., Mboh Khan, E., Masyuko, S. J., Paredes, Z., Chimoun, F. T., Mudender, F., Wamuti, B. M., Nambu, W., Kemunto, E., Mugambi, M., Kariithi, E., Golden, M. R., Tih, P. M., Welty, T., & Farquhar, C. (2019). Assisted HIV partner services training in three sub-Saharan African countries: facilitators and barriers to sustainable approaches. J Int AIDS Soc, 22 Suppl 3, e25307. https://doi.org/10.1002/jia2.25307
Hatzold, K., Gudukeya , S., Mutseta, M., Chilongosi, R., Nalubamba, M., Nkhoma , C., Munkombwe, H., Munjoma, M., Mkandawire, P., Mabhunu, V., Smith, G., Madidi, N., Ahmed, H., Kambeu, T., Stankard, P., Johnson, C., & Corbett, E. (2019). HIV self-testing: breaking the barriers to uptake of testing among men and adolescents in sub-Saharan Africa, experiences from STAR demonstration projects in Malawi, Zambia and Zimbabwe. J Int AIDS Soc, 22(Suppl 1), e25244.
Havlir, D. V., Balzer, L. B., Charlebois, E. D., Clark, T. D., Kwarisiima, D., Ayieko, J., Kabami, J., Sang, N., Liegler, T., Chamie, G., Camlin, C. S., Jain, V., Kadede, K., Atukunda, M., Ruel, T., Shade, S. B., Ssemmondo, E., Byonanebye, D. M., Mwangwa, F., . . . Petersen, M. (2019). HIV testing and treatment with the use of a community health approach in rural africa. N Engl J Med, 381(3), 219-229. https://doi.org/10.1056/NEJMoa1809866
Henley, C., Forgwei, G., Welty, T., Golden, M., Adimora, A., Shields, R., & Muffih, P. T. (2013). Scale-up and case-finding effectiveness of an HIV partner services program in Cameroon: an innovative HIV prevention intervention for developing countries. Sex Transm Dis, 40(12), 909-914. https://doi.org/10.1097/OLQ.0000000000000032
Hensen B, B. R., & Wong VJ, G. K., Shaffer N, Lo Y, Hargreaves J. (2012). Universal voluntary HIV testing in antenatal care settings: a review of the contribution of provider-initiated testing and counselling. Trop Med Int Health, 17(1), 59-70.
Hensen, B., Taoka, S., Lewis, J. J., Weiss, H. A., & Hargreaves, J. (2014). Systematic review of strategies to increase men's HIV-testing in sub-Saharan Africa. AIDS, 28(14), 2133-2145. https://doi.org/10.1097/qad.0000000000000395
74
Herce, M. E., Miller, W. M., Bula, A., Edwards, J. K., Sapalalo, P., Lancaster, K. E., Mofolo, I., Furtado, M. L. M., & Weir, S. S. (2018). Achieving the first 90 for key populations in sub-Saharan Africa through venue-based outreach: challenges and opportunities for HIV prevention based on PLACE study findings from Malawi and Angola. J Int AIDS Soc, 21(Suppl 5), e25132. https://doi.org/10.1002/jia2.25132
Higgins, D. L., Galavotti, C., O'Reilly, K. R., Schnell, D. J., Moore, M., Rugg, D. L., & Johnson, R. (1991). Evidence for the effects of HIV antibody counseling and testing on risk behaviors. JAMA, 266(17), 2419-2429. https://www.ncbi.nlm.nih.gov/pubmed/1920748
Holtedahl, K., Salpou, D., & Bonono, L. (2007). Lessons from HIV counselling and testing campaigns. Lancet, 369(9568), 1166. https://doi.org/10.1016/S0140-6736(07)60557-1
Human Rights Watch. (2008). A testing challenge: the experience of Lesotho’s universal HIV counselling and testing campaign. https://www.hrw.org/report/2008/11/18/testing-challenge/experience-lesothos-universal-hiv-counseling-and-testing
IAS. (2018). Differentiated service delivery for HIV: a decision framework for HIV testing services. http://www.differentiatedservicedelivery.org/Guidance/Dsd-decision-frameworks
ICAP. (2020). PHIA Project. https://phia-data.icap.columbia.edu/ Indravudh, P. P., Fielding, K., Kumwenda, M. K., Nzawa, R., Chilongosi, R., Desmond, N., Nyirenda, R.,
Neuman, M., Johnson, C. C., Baggaley, R., Hatzold, K., Terris-Prestholt, F., & Corbett, E. L. (2021). Effect of community-led delivery of HIV self-testing on HIV testing and antiretroviral therapy initiation in Malawi: A cluster-randomised trial. PLoS Med, 18(5), e1003608. https://doi.org/10.1371/journal.pmed.1003608
Inguane, C. A., Gloyd, S., Manuel, J. L., Brown, C., Wong, V., Augusto, O., Hassan, W. M., Vieira, L., Afonso, P., Jamnadas, M., Bernard, J. J., Cowan, J., Kalibala, S., & Pfeiffer, J. (2016). Assessment of linkages from HIV testing to enrolment and retention in HIV care in Central Mozambique. J Int AIDS Soc, 19(5 Suppl 4), 20846. https://doi.org/10.7448/IAS.19.5.20846
Johnson C, Fonner V, Sands A, Ford N, Obermeyer C, Tsui S, Wong V, & R, B. (2017). To err is human, to correct is public health: a systematic review examining poor quality testing and misdiagnosis of HIV status. J Int AIDS Soc, 20(Suppl 6), 21755.
Johnson C, Sands A, Fonner V, Tsui S, Wong V, Obermeyer C, & R, B. (2014, 30 Nov–5 Dec). Are we delivering the wrong results?: examining misclassification of HIV status and false positive test results African Society of Laboratory Medicine, Cape Town, South Africa.
Johnson C, F. V., Sands A, Tsui S, Ford N, Wong V, Obermeyer C, Baggaley R. (2016). Annex 14: A report on the misdiagnosis of HIV status. https://www.ncbi.nlm.nih.gov/books/NBK316023/
Johnson, C., Kumwenda, M., Meghji, J., Choko, A. T., Phiri, M., Hatzold, K., Baggaley, R., Taegtmeyer, M., Terris-Prestholt, F., Desmond, N., & Corbett, E. L. (2021). 'Too old to test?': A life course approach to HIV-related risk and self-testing among midlife-older adults in Malawi. BMC Public Health, 21(1), 650. https://doi.org/10.1186/s12889-021-10573-7
Kahabuka, C., Plotkin, M., Christensen, A., Brown, C., Njozi, M., Kisendi, R., Maokola, W., Mlanga, E., Lemwayi, R., Curran, K., & Wong, V. (2017). Addressing the First 90: A Highly Effective Partner Notification Approach Reaches Previously Undiagnosed Sexual Partners in Tanzania. AIDS Behav, 21(8), 2551-2560. https://doi.org/10.1007/s10461-017-1750-5
Kalibala, S., Tun, W., Cherutich, P., Nganga, A., Oweya, E., & Oluoch, P. (2014). Factors associated with acceptability of HIV self-testing among health care workers in Kenya. AIDS Behav, 18 Suppl 4, S405-414. https://doi.org/10.1007/s10461-014-0830-z
Kamb, M. L., Fishbein, M., Douglas, J. M., Jr., Rhodes, F., Rogers, J., Bolan, G., Zenilman, J., Hoxworth, T., Malotte, C. K., Iatesta, M., Kent, C., Lentz, A., Graziano, S., Byers, R. H., & Peterman, T. A. (1998). Efficacy of risk-reduction counseling to prevent human immunodeficiency virus and sexually transmitted diseases: a randomized controlled trial. Project RESPECT Study Group. JAMA, 280(13), 1161-1167. https://doi.org/10.1001/jama.280.13.1161
75

Karim, S. S. A., & Baxter, C. (2019). HIV incidence rates in adolescent girls and young women in sub-Saharan Africa. Lancet Glob Health, 7(11), e1470-e1471. https://doi.org/10.1016/S2214-109X(19)30404-8
Kassler, W. J., Alwano-Edyegu, M. G., Marum, E., Biryahwaho, B., Kataaha, P., & Dillon, B. (1998). Rapid HIV testing with same-day results: a field trial in Uganda. Int J STD AIDS, 9(3), 134-138. https://doi.org/10.1258/0956462981921882
Katz, D. A., Wong, V., Medley, A., & Baggaley(Editors), R. (2019). The power of partners: experiences from implementing and scaling up HIV partner notification and index testing services J Int AIDS Soc, 22. https://onlinelibrary.wiley.com/toc/17582652/2019/22/S3
Katz, D. A., Wong, V. J., Medley, A. M., Johnson, C. C., Cherutich, P. K., Green, K. E., Huong, P., & Baggaley, R. C. (2019). The power of partners: positively engaging networks of people with HIV in testing, treatment and prevention. J Int AIDS Soc, 22 Suppl 3, e25314. https://doi.org/10.1002/jia2.25314
Kebede, B., Abate, T., & Mekonnen, D. (2013). HIV self-testing practices among Health Care Workers: feasibility and options for accelerating HIV testing services in Ethiopia. Pan Afr Med J, 15, 50. https://doi.org/10.11604/pamj.2013.15.50.2328
Kennedy, C. E., Fonner, V. A., Sweat, M. D., Okero, F. A., Baggaley, R., & O'Reilly, K. R. (2013). Provider-initiated HIV testing and counseling in low- and middle-income countries: a systematic review. AIDS Behav, 17(5), 1571-1590. https://doi.org/10.1007/s10461-012-0241-y
Koenig, S. P., Dorvil, N., Devieux, J. G., Hedt-Gauthier, B. L., Riviere, C., Faustin, M., Lavoile, K., Perodin, C., Apollon, A., Duverger, L., McNairy, M. L., Hennessey, K. A., Souroutzidis, A., Cremieux, P. Y., Severe, P., & Pape, J. W. (2017). Same-day HIV testing with initiation of antiretroviral therapy versus standard care for persons living with HIV: A randomized unblinded trial. PLoS Med, 14(7), e1002357. https://doi.org/10.1371/journal.pmed.1002357
Kufa, T., Mazanderani, A. H., Sherman, G. G., Mukendi, A., Murray, T., Moyo, F., Technau, K. G., & Carmona, S. (2020). Point-of-care HIV maternal viral load and early infant diagnosis testing around time of delivery at tertiary obstetric units in South Africa: a prospective study of coverage, results return and turn-around times. J Int AIDS Soc, 23(4), e25487. https://doi.org/10.1002/jia2.25487
Kumwenda, M., Munthali, A., Phiri, M., Mwale, D., Gutteberg, T., MacPherson, E., Theobald, S., Corbett, L., & Desmond, N. (2014). Factors shaping initial decision-making to self-test amongst cohabiting couples in urban Blantyre, Malawi. AIDS Behav, 18 Suppl 4, S396-404. https://doi.org/10.1007/s10461-014-0817-9
Lockman, S., Holme, M. P., Makhema, J., Bachanas, P., Moore, J., Wirth, K. E., Lebelonyane, R., & Essex, M. (2020). Implementation of Universal HIV Testing and Treatment to Reduce HIV Incidence in Botswana: the Ya Tsie Study. Curr HIV/AIDS Rep, 17(5), 478-486. https://doi.org/10.1007/s11904-020-00523-0
Lundgren, J. D., Babiker, A. G., Gordin, F., Emery, S., Grund, B., Sharma, S., Avihingsanon, A., Cooper, D. A., Fatkenheuer, G., Llibre, J. M., Molina, J. M., Munderi, P., Schechter, M., Wood, R., Klingman, K. L., Collins, S., Lane, H. C., Phillips, A. N., & Neaton, J. D. (2015). Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N Engl J Med, 373(9), 795-807. https://doi.org/10.1056/NEJMoa1506816
Lyons, C. E., Coly, K., Bowring, A. L., Liestman, B., Diouf, D., Wong, V. J., Turpin, G., Castor, D., Dieng, P., Olawore, O., Geibel, S., Ketende, S., Ndour, C., Thiam, S., Toure-Kane, C., & Baral, S. D. (2019). Use and Acceptability of HIV Self-Testing Among First-Time Testers at Risk for HIV in Senegal. AIDS Behav, 23(Suppl 2), 130-141. https://doi.org/10.1007/s10461-019-02552-2
Macro International. (2009). The five-year evaluation of the Global Fund to Fight AIDS, Tuberculosis and Malaria. https://www.theglobalfund.org/en/technical-evaluation-reference-group/evaluations/2009-five-year-evaluation/
Maheu-Giroux, M., Marsh, K., Doyle, C., Godin, A., Lanièce Delaunay, C., Johnson, L., Jahn, A., Abo, K., Mbofana, F., Boily, M., Buckeridge, D., Hankins, C., & Eaton, J. (2019). National HIV testing and
76

diagnosis coverage in sub-Saharan Africa: a new modeling tool for estimating the “first 90” from program and survey data. AIDS, 33(Suppl 3), S255. https://doi.org/10.1097/QAD.0000000000002386
Mangenah, C., Mwenge, L., Sande, L., Ahmed, N., d'Elbee, M., Chiwawa, P., Chigwenah, T., Kanema, S., Mutseta, M. N., Nalubamba, M., Chilongosi, R., Indravudh, P., Sibanda, E. L., Neuman, M., Ncube, G., Ong, J. J., Mugurungi, O., Hatzold, K., Johnson, C. C., . . . Terris-Prestholt, F. (2019). Economic cost analysis of door-to-door community-based distribution of HIV self-test kits in Malawi, Zambia and Zimbabwe. J Int AIDS Soc, 22 Suppl 1, e25255. https://doi.org/10.1002/jia2.25255
Marsh, K., Eaton, J. W., Mahy, M., Sabin, K., Autenrieth, C., Wanyeki, I., Daher, J., & Ghys, P. D. (2019). Global, regional and country-level 90-90-90 estimates for 2018: assessing progress towards the 2020 target. AIDS, 33(Suppl 3), S213. https://doi.org/10.1097/QAD.0000000000002355
Marum, E., Morgan, G., Hightower, A., Ngare, C., & Taegtmeyer, M. (2008). Using mass media campaigns to promote voluntary counseling and HIV-testing services in Kenya. AIDS, 22(15), 2019-2024. https://doi.org/10.1097/QAD.0b013e3283104066
Marum, E., Taegtmeyer, M., Parekh, B., Mugo, N., Lembariti, S., Phiri, M., Moore, J., & Cheng, A. S. (2012). "What took you so long?" The impact of PEPFAR on the expansion of HIV testing and counseling services in Africa. J Acquir Immune Defic Syndr, 60 Suppl 3, S63-69. https://doi.org/10.1097/QAI.0b013e31825f313b
Masters, S. H., Agot, K., Obonyo, B., Napierala Mavedzenge, S., Maman, S., & Thirumurthy, H. (2016). Promoting Partner Testing and Couples Testing through Secondary Distribution of HIV Self-Tests: A Randomized Clinical Trial. PLoS Med, 13(11), e1002166. https://doi.org/10.1371/journal.pmed.1002166
Matovu, J. K., & Makumbi, F. E. (2007). Expanding access to voluntary HIV counselling and testing in sub-Saharan Africa: alternative approaches for improving uptake, 2001-2007. Trop Med Int Health, 12(11), 1315-1322. https://doi.org/10.1111/j.1365-3156.2007.01923.x
McOwan, A., Gilleece, Y., Chislett, L., & Mandalia, S. (2002). Can targeted HIV testing campaigns alter health-seeking behaviour? AIDS Care, 14(3), 385-390. https://doi.org/10.1080/09540120220123766
Mills, E. J., & Chong, S. (2006). Lesotho embarks on universal HIV testing. HIV AIDS Policy Law Rev, 11(1), 27-28. https://www.ncbi.nlm.nih.gov/pubmed/16805014
MMWR. (1998). Update: HIV Counseling and Testing Using Rapid Tests -- United States, 1995. MMWR, 47(11);211-215. https://www.cdc.gov/mmwr/preview/mmwrhtml/00051718.htm
Moucheraud, C., Chasweka, D., Nyirenda, M., Schooley, A., Dovel, K., & Hoffman, R. M. (2018). Simple Screening Tool to Help Identify High-Risk Children for Targeted HIV Testing in Malawian Inpatient Wards. J Acquir Immune Defic Syndr, 79(3), 352-357. https://doi.org/10.1097/QAI.0000000000001804
Moucheraud, C., Hoffman, R. M., Balakasi, K., Wong, V., Sanena, M., Gupta, S., & Dovel, K. (2021). Screening Adults for HIV Testing in the Outpatient Department: An Assessment of Tool Performance in Malawi. AIDS Behav. https://doi.org/10.1007/s10461-021-03404-8
MPACT. (2019). COMMUNITY ADVISORY: Index Testing Could be Harmful to Your Rights and Well-Being. https://mpactglobal.org/community-advisory-index-testing-could-be-harmful-to-your-rights-and-well-being/
Mutabazi, J. C., Zarowsky, C., & Trottier, H. (2017). The impact of programs for prevention of mother-to-child transmission of HIV on health care services and systems in sub-Saharan Africa - A review. Public Health Rev, 38, 28. https://doi.org/10.1186/s40985-017-0072-5
NASCOP. (2006). National Guidelines for HIV Testing and Counselling in Kenya. Nersesian P, H. M., Cloutier S, and Chintalova-Dallas R. (2013). Assessment of Over-the-Counter HIV Rapid
Test Kits in Namibia. .
77
Odoyo, J. B., Morton, J. F., Ngure, K., O'Malley, G., Mugwanya, K. K., Irungu, E., Awuor, M., Dolla, A., Ongolly, F., Bukusi, E. A., Mugo, N. R., Baeten, J. M., & Partners Scale-Up Project, T. (2019). Integrating PrEP into HIV care clinics could improve partner testing services and reinforce mutual support among couples: provider views from a PrEP implementation project in Kenya. J Int AIDS Soc, 22 Suppl 3, e25303. https://doi.org/10.1002/jia2.25303
Offorjebe, O. A., Hoffman, R. M., Shaba, F., Balakasi, K., Davey, D. J., Nyirenda, M., & Dovel, K. (2020). Acceptability of index partner HIV self-testing among HIV-positive clients in Malawi: A mixed methods analysis. PloS one, 15(7), e0235008. https://doi.org/10.1371/journal.pone.0235008
Pai, N. P., Behlim, T., Abrahams, L., Vadnais, C., Shivkumar, S., Pillay, S., Binder, A., Deli-Houssein, R., Engel, N., Joseph, L., & Dheda, K. (2013). Will an unsupervised self-testing strategy for HIV work in health care workers of South Africa? A cross sectional pilot feasibility study. PloS one, 8(11). http://www.scopus.com/inward/record.url?eid=2-s2.0-84896708955&partnerID=40&md5=a284884ee58dc9da1259922391ec9651
Peck, R. B., Lim, J. M., van Rooyen, H., Mukoma, W., Chepuka, L., Bansil, P., Knight, L. C., Muturi, N., Chirwa, E., Lee, A. M., Wellhausen, J. D., Tulloch, O., & Taegtmeyer, M. (2014). What should the ideal HIV self-test look like? A usability study of test prototypes in unsupervised HIV self-testing in Kenya, Malawi, and South Africa. AIDS Behav, 18 Suppl 4, S422-432. https://doi.org/10.1007/s10461-014-0818-8
PEPFAR. (2006). PEPFAR 2005 annual report to congress. https://2009-2017.state.gov/s/gac/rl/60847.htm PEPFAR. (2019). PEPFAR 2019 Country Operational Plan Guidance for all PEPFAR Countries. Washington DC
Retrieved from https://www.state.gov/wp-content/uploads/2019/08/PEPFAR-Fiscal-Year-2019-Country-Operational-Plan-Guidance.pdf
PEPFAR. (2020a). Monitoring, evaluation and reporting indicator reference guide (Version 2.5). https://www.state.gov/pepfar-fiscal-year-2020-monitoring-evaluation-and-reporting-guidance/
PEPFAR. (2020b). PEPFAR 2019 Annual Report to Congress. https://www.state.gov/pepfar-reports-to-congress-archive/
PEPFAR. (2020c). PEPFAR Guidance on Implementing Safe and Ethical Index Testing Services. Washington D.C. Retrieved from https://www.pepfarsolutions.org/resourcesandtools-2/2020/7/10/pepfar-guidance-on-implementing-safe-and-ethical-index-testing-services
PEPFAR. (2021a). PEPFAR 2020 Annual Report to Congress. https://www.state.gov/pepfar-reports-to-congress-archive/
PEPFAR. (2021b). PEPFAR Panorama Spotlight. Washington DC Retrieved from https://data.pepfar.gov/programareas
PEPFAR. (2021c). Where we work. Retrieved Feb 25 from https://www.state.gov/where-we-work-pepfar/ Plotkin, M., Kahabuka, C., Christensen, A., Ochola, D., Betron, M., Njozi, M., Maokola, W., Kisendy, R.,
Mlanga, E., Curran, K., Drake, M., Kessy, E., & Wong, V. (2018). Outcomes and Experiences of Men and Women with Partner Notification for HIV Testing in Tanzania: Results from a Mixed Method Study. AIDS Behav, 22(1), 102-116. https://doi.org/10.1007/s10461-017-1936-x
Project SEARCH. (2013). Integration of provider initiated testing and counselling for HIV with voluntary medical male circumcision services. https://www.jhsph.edu/research/centers-and-institutes/research-to-prevention/publications/Integration-hiv-vmmc.pdf
Quinn, C., Wong, V., Jamil, M., Baggaley, R., & Johnson, C. (2020). Web Annex L: Symptom and risk-based screening to optimize HIV testing services: a scoping review. Geneva: World Health Organization Retrieved from https://apps.who.int/iris/bitstream/handle/10665/335903/9789240011830-eng.pdf
Rosen, S., & Fox, M. P. (2011). Retention in HIV care between testing and treatment in sub-Saharan Africa: a systematic review. PLoS Med, 8(7), e1001056. https://doi.org/10.1371/journal.pmed.1001056
78

Rosenthal, M., Pieterson, I., Johnson, C., Nersesian, P., & Hulsman, M. (2014). Assessment of Over-the-Counter HIV Rapid Test Kits in Namibia. AIDS Research and Human Retroviruses, 30. https://www.liebertpub.com/doi/abs/10.1089/aid.2014.5220b.abstract
Roura, M., Watson-Jones, D., Kahawita, T. M., Ferguson, L., & Ross, D. A. (2013). Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational implementation. AIDS, 27(4), 617-626. https://doi.org/10.1097/QAD.0b013e32835b7048
Shanks, L., Klarkowski, D., & O'Brien, D. P. (2013). False positive HIV diagnoses in resource limited settings: operational lessons learned for HIV programmes. PloS one, 8(3), e59906. https://doi.org/10.1371/journal.pone.0059906
Sharma, M., Ying, R., Tarr, G., & Barnabas, R. (2015). Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature, 528, S77. https://doi.org/10.1038/nature16044
https://www.nature.com/articles/nature16044#supplementary-information Sharma, M., Ying, R., Tarr, G., & Barnabas, R. (2015). Systematic review and meta-analysis of community
and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature, 528(7580), S77-85. https://doi.org/10.1038/nature16044
Simwinga, M., Kumwenda, M. K., Dacombe, R. J., Kayira, L., Muzumara, A., Johnson, C. C., Indravudh, P., Sibanda, E. L., Nyirenda, L., Hatzold, K., Corbett, E. L., Ayles, H., & Taegtmeyer, M. (2019). Ability to understand and correctly follow HIV self-test kit instructions for use: applying the cognitive interview technique in Malawi and Zambia. J Int AIDS Soc, 22 Suppl 1, e25253. https://doi.org/10.1002/jia2.25253
Souza RS, M. L., Wong V, Gomez-Marin O, Mitchell C, Repke H. (2002, 2002 Jul 7-12). Evaluation of 'InstantScreen', an ultra-rapid HIV1/2 assay based upon novel tecnhologies for the detection of the HIV antibodies. International Conference on AIDS, Barcelona.
Steen, T. W., Seipone, K., Gomez Fde, L., Anderson, M. G., Kejelepula, M., Keapoletswe, K., & Moffat, H. J. (2007). Two and a half years of routine HIV testing in Botswana. J Acquir Immune Defic Syndr, 44(4), 484-488. https://doi.org/10.1097/QAI.0b013e318030ffa9
Stojanovski, K., Naja-Riese, G., King, E. J., & Fuchs, J. D. (2021). A Systematic Review of the Social Network Strategy to Optimize HIV Testing in Key Populations to End the Epidemic in the United States. AIDS Behav, 25(9), 2680-2698. https://doi.org/10.1007/s10461-021-03259-z
Suthar, A. B., Ford, N., Bachanas, P. J., Wong, V. J., Rajan, J. S., Saltzman, A. K., Ajose, O., Fakoya, A. O., Granich, R. M., Negussie, E. K., & Baggaley, R. C. (2013). Towards universal voluntary HIVtesting and counselling: a systematic review and meta-analysis of community-based approaches. PLoS Med, 10(8), e1001496. https://doi.org/10.1371/journal.pmed.1001496
Sweat, M., Gregorich, S., Sangiwa, G., Furlonge, C., Balmer, D., Kamenga, C., Grinstead, O., & Coates, T. (2000). Cost-effectiveness of voluntary HIV-1 counselling and testing in reducing sexual transmission of HIV-1 in Kenya and Tanzania. Lancet, 356(9224), 113-121. https://doi.org/10.1016/S0140-6736(00)02447-8
Sweat, M., Morin, S., Celentano, D., Mulawa, M., Singh, B., Mbwambo, J., Kawichai, S., Chingono, A., Khumalo-Sakutukwa, G., Gray, G., Richter, L., Kulich, M., Sadowski, A., & Coates, T. (2011). Community-based intervention to increase HIV testing and case detection in people aged 16-32 years in Tanzania, Zimbabwe, and Thailand (NIMH Project Accept, HPTN 043): a randomised study. Lancet Infect Dis, 11, 525-532. https://doi.org/10.1016/S1473-3099(11)70060-3
Taegtmeyer, M., Blazer, C., Escobar, M., Grabbe, K., Wong, V., & Baggaley, R. (2012). Out of the clinic and into the home: development of WHO/PEPFAR home-based HIV testing and counseling support tools International HIV/AIDS Conference, Washington DC.
Tanahashi, T. (1978). Health service coverage and its evaluation. Bull World Health Organ, 56(2), 295-303. https://www.ncbi.nlm.nih.gov/pubmed/96953
79

Tembo, T. A., Kim, M. H., Simon, K. R., Ahmed, S., Beyene, T., Wetzel, E., Machika, M., Chikoti, C., Kammera, W., Chibowa, H., Nkhono, Z., Kavuta, E., Kazembe, P. N., & Rosenberg, N. E. (2019). Enhancing an HIV index case testing passive referral model through a behavioural skills-building training for healthcare providers: a pre-/post-assessment in Mangochi District, Malawi. J Int AIDS Soc, 22 Suppl 3, e25292. https://doi.org/10.1002/jia2.25292
The Voluntary HIV-1 Counseling and Testing Efficacy Study Group. (2000). Efficacy of voluntary HIV-1 counselling and testing in individuals and couples in Kenya, Tanzania, and Trinidad: a randomised trial. The Voluntary HIV-1 Counseling and Testing Efficacy Study Group. Lancet, 356(9224), 103-112. https://www.ncbi.nlm.nih.gov/pubmed/10963246
Thirumurthy, H., Masters, s., Obonyo, B., Napierala Mavedzenge, S., Maman, S., Omanga, E., & Agot, K. (2016, 18-22 July). Promoting male partner and couples HIV testing through secondary distribution HIV self-tests: a randomized trial 21st International AIDS Conference, Durban, South Africa.
Tibbels, N. J., Hendrickson, Z. M., Naugle, D. A., Dosso, A., Van Lith, L., Mallalieu, E. C., Kouadio, A. M., Kra, W., Kamara, D., Dailly-Ajavon, P., Cisse, A., Seifert-Ahanda, K., Thaddeus, S., Babalola, S., & Hoffmann, C. J. (2019). Men's perceptions of HIV care engagement at the facility- and provider-levels: Experiences in Cote d'Ivoire. PloS one, 14(3), e0211385. https://doi.org/10.1371/journal.pone.0211385
Topp SM, L. S., Chipukuma JM, Chiko MM, Matongo E, Bolton-Moore C, Reid SE,. (2014). Does provider-initiated counselling and testing (PITC) strengthen early diagnosis and treatment initiation? Results from an analysis of an urban cohort of HIV-positive patients in Lusaka, Zambia. J Int AIDS Soc, 15(2), 17352.
Tymejczyk, O., Brazier, E., Yiannoutsos, C., Wools-Kaloustian, K., Althoff, K., Crabtree-Ramirez, B., Van Nguyen, K., Zaniewski, E., Dabis, F., Sinayobye, J. D., Anderegg, N., Ford, N., Wikramanayake, R., Nash, D., & Ie, D. E. A. C. (2018). HIV treatment eligibility expansion and timely antiretroviral treatment initiation following enrollment in HIV care: A metaregression analysis of programmatic data from 22 countries. PLoS Med, 15(3), e1002534. https://doi.org/10.1371/journal.pmed.1002534
U.S. Department of Health & Human Services. (2021). A Timeline of HIV and AIDS. Retrieved 8/13/2021 from https://www.hiv.gov/hiv-basics/overview/history/hiv-and-aids-timeline
UNAIDS. (2000a). Tools for evaluating HIV voluntary counselling and testing https://www.unaids.org/en/resources/documents/2000/20000621_jc685-tools%20for%20eval_en.pdf
UNAIDS. (2000b). Voluntary Counseling and Testing (VCT) Technical Update. https://www.unaids.org/en/resources/documents/2000/20000518_jc379-vct_en.pdf
UNAIDS. (2010). Report on the global HIV/AIDS epidemic. Geneva Retrieved from https://www.unaids.org/en/resources/documents/2010/20101123_globalreport
UNAIDS. (2013). Report on the first international symposium on self-testing for HIV: the legal, ethical, gender, human rights and public health implications of self-testing scale-up. http://www.who.int/hiv/pub/vct/self_test/en/
UNAIDS. (2015). 90-90-90 - an ambitious treatment target to help end the AIDS epidemic. http://www.unaids.org/en/resources/documents/2017/90-90-90
UNAIDS. (2016a). Methods for Deriving UNAIDS Estimates. https://www.unaids.org/sites/default/files/media_asset/2016_methods-for-deriving-UNAIDS-estimates_en.pdf
UNAIDS. (2016b). On the fast track to an AIDS free generation. Geneva Retrieved from https://www.unaids.org/en/resources/documents/2016/GlobalPlan2016
UNAIDS. (2016c). The Sustainable Development Goals and the HIV response: stories of putting people at the centre. https://www.unaids.org/en/resources/documents/2017/SDGsandHIV
80

UNAIDS. (2020a). Fact Sheet - World AIDS Day 2020. https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf
UNAIDS. (2020b, Oct 26 2020). Key populations have suboptimal knowledge of their HIV status Retrieved Mar 3 2021 from https://www.unaids.org/en/resources/presscentre/featurestories/2020/october/20201026_key-populations-knowledge-hiv-status
UNAIDS. (2020c). New HIV infections increasingly among key populations. Retrieved 8/23/2021 from https://www.unaids.org/en/resources/presscentre/featurestories/2020/september/20200928_new-hiv-infections-increasingly-among-key-populations
UNAIDS. (2020d). Prevailing against pandemics by putting people at the centre. Geneva Retrieved from https://aidstargets2025.unaids.org/
UNAIDS. (2020e). Start free stay free AIDS free - 2020 report. Geneva Retrieved from https://www.unaids.org/en/resources/documents/2020/start-free-stay-free-aids-free-2020-progress-report
UNAIDS and WHO. (2012). Statement on HIV testing and counseling: WHO, UNAIDS re-affirm opposition to mandatory HIV testing. http://www.who.int/hiv/events/2012/world_aids_day/hiv_testing_counselling/en/
UNAIDS/WHO Working Group on Global HIV/AIDS and STI Surveillance. (2000). Guidelines for second generation HIV surveillance. https://www.who.int/hiv/pub/surveillance/pub3/en/
UNICEF. (2020, July 2020). Global and regional trends. Retrieved Mar 4, 2021 from https://data.unicef.org/topic/hivaids/global-regional-trends/
Wamuti, B. M., Welty, T., Nambu, W., Chimoun, F. T., Shields, R., Golden, M. R., Farquhar, C., & Muffih, P. T. (2019). Low risk of social harms in an HIV assisted partner services programme in Cameroon. J Int AIDS Soc, 22 Suppl 3, e25308. https://doi.org/10.1002/jia2.25308
Wawer, M. J., Sewankambo, N. K., Serwadda, D., Quinn, T. C., Paxton, L. A., Kiwanuka, N., Wabwire-Mangen, F., Li, C., Lutalo, T., Nalugoda, F., Gaydos, C. A., Moulton, L. H., Meehan, M. O., Ahmed, S., & Gray, R. H. (1999). Control of sexually transmitted diseases for AIDS prevention in Uganda: a randomised community trial. Rakai Project Study Group. Lancet, 353(9152), 525-535. https://doi.org/10.1016/s0140-6736(98)06439-3
Weiser, S. D., Heisler, M., Leiter, K., Percy-de Korte, F., Tlou, S., DeMonner, S., Phaladze, N., Bangsberg, D. R., & Iacopino, V. (2006). Routine HIV testing in Botswana: a population-based study on attitudes, practices, and human rights concerns. PLoS Med, 3(7), e261. https://doi.org/10.1371/journal.pmed.0030261
West, C. A., Chang, G. C., D, W. C., Bray, R., Kinchen, S., Behel, S., McCullough-Sanden, R., Low, A., Bissek, A., Shang, J. D., Ndongmo, C. B., Dokubo, E. K., Balachandra, S., Lobognon, L. R., Dube, L., Nuwagaba-Biribonwoha, H., Li, M., Pasipamire, M., Getaneh, Y., . . . A, C. V. (2021). Unawareness of HIV Infection Among Men Aged 15-59 Years in 13 Sub-Saharan African Countries: Findings From the Population-Based HIV Impact Assessments, 2015-2019. J Acquir Immune Defic Syndr, 87(Suppl 1), S97-S106. https://doi.org/10.1097/QAI.0000000000002708
WHO. (2001). Prevention of mother-to-child transmission: selection and use of Nevirapene technical notes. Retrieved from http://apps.who.int/iris/bitstream/10665/66808/1/WHO_HIV_AIDS_2001.3.pdf
WHO. (2002a). HIV assays: operational characteristics (Phase I) Report 12: simple/rapid tests, whole blood specimens. Geneva Retrieved from https://www.who.int/diagnostics_laboratory/publications/hiv_assays_rep_12.pdf
WHO. (2002b). Increasing access to HIV testing and counselling. WHO. (2003). Right to Know. https://www.who.int/hiv/pub/vct/pub34/en/ WHO. (2004). Rapid HIV tests: guidelines for use in HIV testing and counseling services in resource-
constrained settings. https://apps.who.int/iris/handle/10665/42978?show=full WHO. (2006). Guidelines on provider-initiated testing and counselling. Geneva: World Health Organization
81
WHO. (2007). Guidance on provider-initiated HIV testing and counselling in health facilities. https://www.who.int/hiv/pub/vct/pitc2007/en/
WHO. (2010a). Delivering HIV test results and messages for re-testing and counselling in adults. https://www.who.int/hiv/pub/vct/hiv_re_testing/en/
WHO. (2010b). Policy requirements for HIV testing and counselling of infants and young children in health facilities. Geneva Retrieved from https://www.who.int/hiv/pub/paediatric/testing_counselling/en/
WHO. (2010c). Towards Universal access: scaling up priority HIV/AIDS interventions in the health sector. https://www.who.int/hiv/pub/2010progressreport/report/en/
WHO. (2012a). Guidance on couples HIV testing and counselling - including antiretroviral therapy for treatment and prevention in serodiscordant couples: recommendations for a public health approach. http://www.who.int/hiv/pub/guidelines/9789241501972/en/
WHO. (2012b). Planning, implementing and monitoring home-based HIV testing and counseling. https://www.who.int/hiv/pub/vct/home_based_care/en/
WHO. (2012c). Service delivery approaches for HIV testing and counselling: a strategic framework. http://www.who.int/hiv/pub/vct/htc_framework/en/
WHO. (2013). HIV and adolescents: guidance for HIV testing and counselling and care for adolescents living with HIV: recommendations for a public health approach and considerations for policymakers and managers. https://apps.who.int/iris/handle/10665/94334
WHO. (2014). Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations. https://www.who.int/hiv/pub/guidelines/keypopulations/en/
WHO. (2015a). Annex 7: Diagnostics for HIV diagnosis. http://apps.who.int/iris/bitstream/10665/180221/1/WHO_HIV_2015.26_eng.pdf?ua=1
WHO. (2015b). Consolidated guidelines on HIV testing services. http://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/
WHO. (2015c). Consolidated strategic information guidelines for HIV in the health sector. https://www.who.int/hiv/pub/guidelines/strategic-information-guidelines/en/
WHO. (2016a). Annex 18: GRADE evidence profile comparing assisted partner notification to passive referral. https://www.who.int/hiv/pub/vct/Annex18.pdf
WHO. (2016b). Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations – 2016 update. Geneva: World Health Organization Retrieved from https://www.who.int/hiv/pub/guidelines/keypopulations-2016/en/
WHO. (2016c). Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. Geneva Retrieved from https://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/
WHO. (2016d). Guidelines on HIV self-testing and partner notification: a supplement to the consolidated guidelines on HIV testing services. https://www.who.int/hiv/pub/vct/hiv-self-testing-guidelines/en/
WHO. (2017). WHO Prequalification of In Vitro Diagnostics Public Report: OraQuick HIV Self-Test (version 2.0). https://www.who.int/diagnostics_laboratory/evaluations/pq-list/170720_final_amended_pqdx_0159_055_01_oraquick_hiv_self_test_v2.pdf?ua=1
WHO. (2018). Reaching first 90 and impact of HIV self-testing (HIVST) Presentation. In. WHO. (2019a). HIV Testing Services Dashboard: Zambia. Retrieved 4/16/2021 from
https://whohts.web.app/ZMB WHO. (2019b). WHO recommends that social network-based HIV testing approaches can be offered for key
populations as part of a package of partner services. Geneva: World Health Organization Retrieved from https://www.who.int/publications-detail/Social-network-hiv-testing-approach-for-key-populations
WHO. (2021a). HIV/AIDS global situation and trends. Retrieved 8/23/2021 from https://www.who.int/data/gho/data/themes/hiv-aids
WHO. (2021b). Improving men’s uptake of HIV testing and linkage to services. Geneva Retrieved from https://www.who.int/publications/i/item/9789240018938
82

WHO. (2021c). Recommendations and guidance on hepatitis C virus self-testing. World Health Organization. Retrieved July 15, 2021 from https://www.who.int/publications/i/item/9789240031128
WHO. (2021d). WHO consolidated guideline on self-care interventions for health. Retrieved July 15, 2021 from https://app.magicapp.org/#/guideline/Lr21gL
WHO and UNAIDS. (1997). Revised recommendations for the selection and use of HIV antibody tests. http://www.who.int/diagnostics_laboratory/publications/en/Selection_HIV_tests.pdf
WHO and UNAIDS. (1998). The importance of simple/rapid assays in HIV testing. Wkly Epidemiol Rec, 73(42), 321-326. https://www.ncbi.nlm.nih.gov/pubmed/9803168
Wilson, J. M., & Jungner, Y. G. (1968). Principles and practice of mass screening for disease. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/37650/WHO_PHP_34.pdf?sequence=17&isAllowed=y
Wolf, R. C., Bingham, T., Millett, G., & Wilcher, R. (2018). Building the evidence base to optimize the impact of key population programming across the HIV cascade. J Int AIDS Soc, 21 Suppl 5, e25146. https://doi.org/10.1002/jia2.25146
Wolfe, W. R., Weiser, S. D., Bangsberg, D. R., Thior, I., Makhema, J. M., Dickinson, D. B., Mompati, K. F., & Marlink, R. G. (2006). Effects of HIV-related stigma among an early sample of patients receiving antiretroviral therapy in Botswana. AIDS Care, 18(8), 931-933. https://doi.org/10.1080/09540120500333558
Wong V. (2006). A descriptive study of VCT implementation in the Accra Metropolitan District, Ghana International HIV/AIDS Conference, Toronto. http://www.abstract-archive.org/Abstract/Share/49937
Wong, V., Ford, N., & Agot(Editors), K. (2019). Realizing the potential of HIV self-testing for Africa: lessons learned from the STAR project. J Int AIDS Soc, 22(S1). https://www.iasociety.org/Portals/0/Files/JIAS_Vol22-S1_complete_file.pdf
Wong, V., Jenkins, E., Ford, N., & Ingold, H. (2019). To thine own test be true: HIV self-testing and the global reach for the undiagnosed. J Int AIDS Soc, 22 Suppl 1, e25256. https://doi.org/10.1002/jia2.25256
Wong, V., Johnson, C., Cowan, E., Rosenthal, M., Peeling, R., Miralles, M., Sands, A., & Brown, C. (2014). HIV self-testing in resource-limited settings: regulatory and policy considerations. AIDS Behav, 18 Suppl 4, S415-421. https://doi.org/10.1007/s10461-014-0825-9
Wong, V., & Sabin, M. (2010, July 2010). Examining reporting of quality elements in a provider-initiated HIV testing and counseling and implications for rights-based approaches International HIV/AIDS Conference, Vienna. http://www.abstract-archive.org/Abstract/Share/2884
Wong VJ, M. K., Phelps BR, Vermund SH, McCarraher DR. (2017). Adolescents, young people, and the 90-90-90 goals: a call to improve HIV testing and linkage to treatment. AIDS, 31 Suppl 3, S191-S194. https://doi.org/10.1097/QAD.0000000000001539
Wong, V. M., I.; Gilks, C.; Higgins, D.; Crowley, S. (2006). The lost children of universal access – issues in scaling-up HIV testing and counselling. Vulnerable Children and Youth Studies, 1(1), 44-55. https://doi.org/10.1080/17450120600700004
83
Appendix 1: Co-authored Original Articles and Reviews Included in this Submission
84
1
Barriers and Facilitators to Facility HIV Self-Testing in Outpatient Settings in Malawi: A Qualitative Study Misheck Mphande1*, Paula Campbell2, Risa M Hoffman2, Khumbo Phiri1, Mike Nyirenda1, Sundeep K Gupta2, Vincent Wong3, Kathryn Dovel1,2 *Corresponding author 1. Partners in Hope, Lilongwe, Malawi 2. Division of Infectious Diseases, David Geffen School of Medicine, University of California Los Angeles, CA 3. Office of HIV/AIDS, United States Agency for International Development, Washington D.C
Contact information: Mr. Misheck Mphande Partners in Hope Box 302, Lilongwe, Malawi Email: [email protected] Telephone: +265999097063
Target Journal: BMC Public Health Word limit: 3,500 Word count: 3,667 Keywords:
Accepted for publication on Aug 28, 2021 in BMC Public Health
85
2
ABSTRACT (/350)
Background: Facility HIV self-testing (HIVST) within outpatient departments can increase HIV 2 testing coverage by facilitating HIVST use in outpatient waiting spaces while clients wait for 3 routine care. Facility HIVST allows for the majority of outpatients to test with minimal health 4 care worker time requirements. However, barriers and facilitators to outpatients’ use of facility 5 HIVST are still unknown. 6
Methods: As part of a cluster randomized trial on facility HIVST in Malawi, we conducted in-7 depth interviews with 57 adult outpatients (>15 years) who were exposed to the HIVST 8 intervention and collected observational journals that documented study staff observations from 9 facility waiting spaces where HIVST was implemented. Translated and transcribed data were 10 analyzed using constant comparison analysis in Atlas.ti. 11
Results: Facility HIVST was convenient, fast, and provided autonomy to outpatients. The 12 strategy also had novel facilitators for testing, such as increased motivation to test due to seeing 13 others test, immediate support for HIVST use, and easy access to additional HIV services in the 14 health facility. Barriers to facility HIVST included fear of judgment from others and unwanted 15 status disclosure due to lack of privacy. Desired changes to the intervention included private, 16 separate spaces for kit use and interpretation and increased opportunity for disclosure and post-17 test counseling. 18
Conclusions: Facility HIVST was largely acceptable to outpatients in Malawi with novel 19 facilitators that are unique to facility HIVST in OPD waiting spaces. 20
Trial registration: The parent trial is registered with ClinicalTrials.gov, NCT03271307, and Pan 21 African Clinical Trials, PACTR201711002697316.22
86

INTRODUCTION
In 2019, there were 20.7 million people living with HIV (PLHIV) in sub-Saharan Africa (SSA) [1].
However, more than 25% of adults in the region still do not know their serostatus [2]. In Malawi, only 42%
of the adult population tested for HIV within the past 12 months [3], with 35% of men having never tested
for HIV [4, 5]. Additionally, there are an estimated 33,000 new HIV infections in Malawi per year requiring
diagnosis and treatment [6]. Facility-based provider-initiated testing and counseling (PITC) remains the
primary strategy for testing [7], although it continues to have limited reach in busy outpatient settings [8,
9].
HIV self-testing (HIVST) can improve PITC among outpatients in high-burden settings (i.e., facility
HIVST) and studies have shown that HIVST is highly acceptable [10-12]. We previously conducted a
randomized control trial (RCT) and found that facility HIVST can increase testing among adult outpatients
by 200% compared to standard PITC [2] and is cost-effective in routine settings by capitalizing on the
existing health infrastructure [13]. Although there is insufficient data on barriers and facilitators for facility
HIVST implementation, there is extensive literature community HIVST [11]. Known facilitators for
community HIVST include increased privacy, perceived autonomy and confidentiality of test results,
perceived convenience, and minimal time required to test [14-16]. These benefits are believed to largely
remove demand-side barriers to traditional testing strategies, including travel time and cost, fear of
unwanted disclosure, and long clinic wait times [15]. Reported barriers are few and include doubts or
misconceptions about the accuracy of HIVST kits and individuals’ ability to use and interpret HIVST kits
unsupervised [11, 17].
The abovementioned barriers and facilitators may differ for facility HIVST since this strategy reduces the
privacy as compared to community HIVST (testing at the facility is often done in public areas such as
waiting spaces), but may also provide immediate linkage and prevention services. Given this gap in
evidence, we analyzed qualitative data collected as part of a parent facility HIVST trial to examine adult
87
perceptions of HIVST in outpatient departments, and understand what components of facility HIVST
strategies are crucial for intervention scale-up.
METHOD
Design and Setting
Our parent cluster-randomized trial aimed to assess the impact of facility HIVST among adults attending
outpatient departments (OPD) in Malawi. Outpatient departments are the primary entry point to most
service delivery strategies in Malawi and offer a range of services from acute care for injuries and general
illness to treatment for sexually transmitted infections. The parent trial compared the impact of facility
HIVST against standard PITC and optimized PITC, whereby additional training and job aids were given
to health workers, and morning HIV testing was offered to all outpatients [13]. In the study (a full
description is published elsewhere) [13, 18], 15 facilities were cluster randomized 1:1:1 to three arms: (1)
standard PITC, (2) optimized PITC, and (3) facility HIVST whereby OraQuick ADVANCE HIV I/II self-
testing kits [19] were distributed during adult outpatient services in waiting spaces. In this paper, we
include data from the facility HIVST arm that was implemented in 5 randomly selected facilities
including a district hospital (n=1); rural hospital (n=1), non-profit hospital (n=1); and health center (n=2).
Eligibility criteria for participation in the parent study included: >15 years of age and having received
outpatient services on the day of recruitment.
Intervention
Facility HIVST included three overarching components: (1) HIVST demonstration and distribution; (2)
HIVST use and interpretation; and (3) post-test services and counseling (Fig 1). A 10-minute health talk
about the importance of HIV testing and a 15-minute demonstration on HIVST kits, followed by kit
distribution, was conducted in outpatient waiting spaces. HIVST was offered one-on-one in order to
create a true opt-out service; however, distribution was in open waiting spaces – private rooms were not
used for demonstration and distribution activities.
88
Outpatients took and used the kit in the OPD waiting space prior to receiving routine outpatient services.
HIVST users were strongly encouraged to not look at their HIVST result in the public waiting space. For
privacy in the waiting space, HIVST kits were stored in an opaque bag for processing.. Private spaces
(rooms or kiosks near the OPD) were provided for HIVST interpretation prior to receiving routine
outpatient services. Trained study staff were available to assistance with HIVST use as needed. Finally,
post-test counselling and referral to additional HIV services were available upon request – outpatients
were not asked HIVST results by study staff. Outpatient HCWs were encouraged to ask about HIVST test
results, but disclosure was not mandatory.
-- Fig 1 about here --
Data Collection
For the parent trial, exit surveys were conducted with a 5885 sample of outpatients. In the HIVST arm,
2097 surveys were completed and provided the sampling frame for our current sub-study. Two forms of
qualitative data are included in the current sub-study: in-depth interviews with outpatients (n=57) and
observation journals collected by research assistants who observed OPD waiting spaces in participating
facilities (81 typed pages from 38 observation days).
In-depth interviews
Participants in the parent trial were randomly selected for an in-depth interview using an electronic
randomization tool. Eligibility criteria for the additional in-depth interviews included: 1) >15 years of
age; 2) received outpatient services on the day of recruitment; 3) enrolled in the larger trial; and 4)
exposed to the facility HIVST intervention (defined as heard of HIVST while at the health facility that
same day). All respondents provided oral informed consent prior to data collection. All interviews were
89

conducted the same day in a private location within the health facility and all participants were given the
equivalent of $4 for their time.
A guide was developed based on existing literature [17,18] and included questions about previous
experiences with HIV testing services, experience with facility HIVST that day, barriers and facilitators to
facility HIVST, and recommendations (see Appendix A for the Interview Guide). Respondents and
interviewers were matched by gender (i.e., man interviewing a man). Interviews were conducted in the
local language (Chichewa) and lasted approximately 40 minutes.
Observational journals
Observational journals were collected by research assistants during the parent intervention. Observational
journals are a form of local ethnography [20, 21] whereby research assistants observed facility waiting
spaces where HIVST kits were distributed and used. At the end of each day, research assistants wrote
what they observed, recalling as much detail as possible about the content and context of client and client-
provider interactions. Observational journals are well suited to capture practices within a health
institution, documenting what people say and how they interact with others, which can be different from
what they report in traditional research settings [21]. While journals cannot capture all events within one
setting, they provide an important overview of common interactions and conversations within routine
settings [22].
Research assistants made observations and described the content and context of interactions within OPD
waiting spaces over 38 days (resulting in over 81 typed pages of observational journals). Researchers
were instructed to document interactions on the following topics: (1) distribution of HIVST; (2)
conversations between regarding HIVST; (3) potential or observed unwanted disclosure, including others
asking about one’s test result; and (4) discussed or observed concerns regarding facility HIVST. Two of
the five facilities were excluded from analysis due to research staff shortages and incomplete data.
90
Data Analysis
In-depth interviews and observational journals were transcribed and translated into English (if needed).
All transcripts were coded using inductive and deductive strategies [23]. The same coding techniques and
codebook were applied to both in-depth interview and observational journal data. Deductive codes were
developed based on existing literature [23], and were the basis for the original codebook. MM and PM
piloted the codebook on 5 in-depth interviews and 4 observational journals. Inductive codes were added
as needed. Co-authors reviewed codes and resolved any disagreements to make a final codebook. Two co-
authors (MM and PM) coded all transcripts using Atlas.ti [24]. Coded data were analyzed using constant
comparison methods [25]. We compared dominant and emerging themes by HIVST users and non-users
and by sex, reporting any differences.
Ethical Approval
All study activities were approved by the Institutional Review Board at University of California Los
Angeles (Protocol number 17-000109) and the National Health Sciences Review Committee in Malawi
(Protocol number 1664). All data collection efforts were carried out in accordance with relevant
guidelines and regulations.
RESULTS
We conducted in-depth interviews with 57 adult outpatients who were offered HIVST at the OPD
between Sept 12, 2017 and Feb 23, 2018. Twenty-six in-depth interview respondents were male and 31
were female. Among respondents interviewed, 46 reported using HIVST during their OPD visit (users),
while 11 respondents heard about HIVST but did not use a kit (non-users). (See Table 1)
-- Table 1 about here –
91

Among non-users, the primary reason reported for not using HIVST was having tested recently, often
within the past three months (see Table 2). Notably, only one client reported that he did not test because
he did not trust the accuracy of HIVST.
-- Table 2 about here --
Below, we present results according to each component of the facility HIVST intervention: (1) health
talk/demonstration and distribution; (2) HIVST use and interpretation; and (3) provider disclosure and
linkage to additional care (see Fig 2). We present respondent perceptions of each component, including
the most salient themes around the benefits and challenges to facility HIVST, distinguishing between
users and non-users, and men and women.
-- Fig 2 about here –
HIVST Demonstration and Distribution
Easy to Understand and Use
None of the interview respondents had ever used HIVST prior to the current intervention, however most
reported that they had enough education about how to use HIVST and that the demonstrations were clear.
All respondents could explain how to use and interpret HIVST.
I was thinking that maybe the procedure is a bit difficult because when you do things for the first
time, it seems as if it's difficult. But when we followed [directions], it is the shorter method and
easy to understand and very cheap [fast]. (Male, HIVST User, Health Center)
Motivated by Seeing Others Test
92

Over half of HIVST users explained that open, group distribution inspired them to test. The open layout
meant that anyone in the waiting space could easily see who accepted a HIVST kit. Respondents
described being “carried away” or persuaded by seeing others take HIVST kits or discussing HIVST with
others in the waiting space. Other outpatients who rapidly took up testing acted as positive reinforcement,
encouraging respondents who were initially unsure to test. More females reported having open
conversations about HIVST; however, more men viewed their conversations as crucial to their decision to
test.
What the HCWs were explaining all this year, I wasn’t taking to heart, …. [but] With the way
they explained [HIVST] I got carried away. For the first time I tested. I saw that people were
getting tested so I thought I should also do the test … they [other clients] just said, ‘Let us get
them [HIVST].’ We were just talking to each other which means they also got carried away like
I did. (Male, HIVST User, Non-Profit Facility)
Since I was also looking at my friends [outpatients] self-testing then I thought, ‘I too should test
instantly’ [right away]. (Female, HIVST User, Health Center)
Observational journals frequently documented similar stories of group distribution inspiring testing.
They [outpatients] saw other people carrying the self-test kits … A certain man [outpatient]
answered, ‘It is a new testing method.. If you are a patient and you are ready to test yourself, tell
the owners [study staff] to give you the test kits. They will teach you how to use them’ … All three
women got the kits and used them. (Observational Journal, Rural Hospital)
93
Fear of Judgement by Others
Less than a quarter of interview respondents believed group distribution lacked privacy, hindering HIVST
uptake. More men than women reported lack of privacy as a barrier to uptake. Some respondents also
reported feeling “shy” or uncomfortable receiving a kit because others would question their HIV status or
assume they were sexually promiscuous.
When I was receiving it [HIVST], many people were looking at me, and I could feel shyness on my
face. It was difficult to stay happy. But all-in-all, I tried getting the kit and used it. (Male, HIVST
User, District Hospital)
Observational journals documented two instances where clients refused HIVST because they felt
uncomfortable taking kits in waiting spaces. Study staff heard one male outpatient explain:
I cannot ask for the kit here and use it in the presence of all these people. Had it been that they are
calling us one-by-one in a private room, I could have managed to ask for the test kit. (Rural
Hospital Observational Journal 3, 14:9)
HIVST Use and Interpretation
Convenient and Fast
The majority of interview respondents reported that using HIVST while waiting for routine outpatient
services was fast and efficient when compared to routine blood-based HIV testing with PITC. Many
outpatients positively described facility HIVST as allowing them to “kill two birds with one stone.”
I felt it would be better I do both [OPD services and HIVST] at once to kill two birds with one
stone ... by the time I am going to meet the doctor I am also at the same time knowing my HIV
status with this [HIVST] kit. (Male, HIVST User, Rural Hospital)
94

When asked if he would have tested for HIV that day if HIVST was not available, one man replied:
I shouldn’t lie, I wouldn’t have gotten tested… I came because of malaria. But when I also heard
that there is something else [HIVST] and the way is not hard [to use] I just said, ‘Aah I should
rush [to test].’ (Male, HIVST User, District Hospital)
Peer support on how to use HIVST
Over half of respondents reported discussing how to use HIVST with others in the waiting space.
However, about a quarter of respondents stated that they or other outpatients had questions or needed
additional help regarding HIVST. Some respondents understood the HIVST process better than others
and would clarify kit use for others. Other respondents simply discussed the benefits of HIV testing and
encouraged each other to continue testing in the future.
The topic we [outpatients] were discussing was all about [HIVST] that it is good … in the
process of chatting the 20 minutes time [for processing] was done and we were very open people.
(Male, HIVST User, Rural Hospital)
95

Fear of Unwanted Disclosure
Despite positive experiences expressed by most respondents, nearly a quarter of interview respondents
desired more privacy for interpreting HIVST results. A handful of respondents feared other people in the
waiting space may try to look at their HIVST kit results (referred to as “peeping”), while a few others
described other outpatients either trying to look at their test result or directly asking what their HIVST
result was.
Because it was an open place, I had worries that when opening to see the results my friends will
be peeping to see. (Female, HIVST User, Rural Hospital)
Journals also recorded a handful of instances where outpatients were afraid that others would make
educated guesses or assumptions about their HIV status based on body language or facial expressions
after leaving spaces for interpretation of results. Limited available private space in clinics meant that most
facilities relied on standing booths for private spaces to interpret HIVST results. While the booths
themselves were private, located either in OPD waiting spaces against a wall so no one could see the
interpretation space or outside the waiting space, others in the waiting space could see individuals
walking to or from the interpretation booths, prompting onlookers to make assumptions about one’s HIV
status. One journal reported:
‘We [OPD clients] are chatting and smiling each other here because I know nothing about my
status. But once I read my [HIVST result], my face will change [when I leave the booth]. I can
even cry here... Those who saw me receiving the kit will automatically know that I am crying
because I have read my test results, and it will mean to them [they will assume] that I am HIV
positive.’ (Observational Journal, Non-Profit Facility)
96

Due to fear of unwanted disclosure, a quarter of outpatients interviewed recommended having private
rooms away from the OPD waiting space for HIVST interpretation, as rooms were believed to be more
private than portable interpretation booths used by the intervention.
Maybe you should have a separate room. For those who are open, [they] can get the kit there
[waiting space], and for those who are shy to do it in public, [they] can go to that room. (Female,
HIVST Non-User, Rural Hospital)
Post-Test Counseling and Services
Autonomy
HIVST users liked that they had control over whether or not to disclose their HIVST result to HCWs. The
desire to not disclose largely stemmed from a reported lack of trust in HCWs’ ability to maintain
confidentiality, while some respondents simply appreciated not having the anxiety related to waiting for
someone else to interpret their test results.
I didn’t trust those people [HCW’s]. Since they were telling you [your] results, it is possible
they could tell other people that, “Did you see the one who just went out there? Results came
out HIV positive!” It’s something so disappointing and pathetic. You can have bad ideas that
you should not do it [test] again. So I think this way [HIVST] is very good because you are the
only one who can know your results … It’s all up to you. (Female, HIVST User, Non-Profit
Facility)
Limited Opportunity to Disclose HIVST Results
While most interview respondents did not want to disclose their HIVST results to HCWs, they also said
they had no opportunity to do so during routine outpatient consultations. The vast majority of respondents
97

reported that HCWs did not ask about HIVST results, and clients did not bring it up. Respondents stated
that they felt uncomfortable initiating conversations about HIVST because clinicians seemed too busy.
I didn’t discuss with anyone … He [HCW] asked what’s wrong, I told him I am having a stomach
problem … I had it [HIVST kit] in my hands, but he didn’t ask anything. (Female, HIVST User,
Health Center)
However, only two respondents indicated that the lack of engagement by HCWs left them with
unanswered questions or concerns.
Additional Post-Test Counseling
In light of minimal disclosure to HCWs, about a quarter of HIVST users recommended additional post-
test counseling in facility HIVST. Most, however, wanted counseling without having to disclose their
own test result. Client suggestions included having follow-up group post-counseling sessions with
everyone in the outpatient waiting spaces (similar to the pre-counseling and HIVST demonstration), or
one-on-one post-counseling during the outpatient consultation whereby the provider would provide broad
post-test messaging for those who did not want to disclose. Most respondents suggested additional
information on prevention strategies and the benefits of immediate ART initiation – including treatment
as prevention –to motivate others to test.
They should explain deep [post-counseling]. People were left in suspense. They [health care
workers] should go into details, … if you see your results whether positive or negative you must
meet the doctor. (Male, HIVST User, Non-Profit Facility)
DISCUSSION
98

Facility HIVST was highly acceptable to both female and male adult outpatients in Malawi. Facility
HIVST retained some of the most important benefits of traditional HIVST identified throughout the
literature – HIVST was still seen as easy to use, convenient, required minimal time, and provided
confidential results [16], although there were some concerns about privacy of distribution and use. We
found that the group-style distribution of HIVST also resulted in additional facilitators to HIV testing
usually not associated with HIVST, such as increased motivation to test due to seeing others test, being
able to directly communicate with others about HIVST, and receiving immediate support from facility
staff.
Many respondents in our study described being motivated by seeing other people test. The visible
distribution of kits in waiting spaces helped to create a critical mass of outpatients testing, normalizing
testing behavior in this particular setting. Similar arguments have been made for HIVST in other settings
[26] and other stigmatized services that benefit from opt-out strategies [27]. However, frequent and highly
motivating health talks and HIVST demonstrations in OPD are likely required in order to create
excitement for HIVST and achieve a high coverage.
While group distribution acted as a facilitator for many respondents, it also served as a barrier for others.
For some, group distribution discouraged testing because they believed other outpatients would see them
test and judge them, making assumptions about their sexual risk behavior and HIV status. Similar
findings have been reported in other studies, noting that private testing areas are essential in order to
avoid stigma associated with taking up HIV testing [28, 29]. A handful of respondents were also
concerned that using HIVST in waiting spaces would lead to potential coercion or unwanted status
disclosure to other outpatients. Private spaces for HIVST distribution and use would mitigate these
concerns, however, infrastructure constraints remain a major concern for local health facilities and may
not be addressed without extensive investment.
99

We found that nearly half of respondents reported talking with other outpatients about how to use HIVST
and about HIV more broadly. Even with a HIVST demonstration, some outpatients were still unclear on
exactly how to use the kit and found other outpatients helpful in guiding them through the process. Other
HIVST interventions vary in levels of support provided, with some offering assisted HIVST use [30] and
others, such as secondary distribution of HIVST, offering no additional support [31]. HIVST
interventions should maximize opportunities to support correct HIVST use to ensure optimal testing. Our
study shows opportunities for support do not have to be exclusively from HCWs – other community
members who have seen HIVST demonstrations may be able and willing to provide support.
Nearly all respondents believed they had little opportunity to disclose HIVST result to HCWs in OPD
settings, largely because HCWs did not directly ask respondents about their results (disclosure was
completely opt-in) and outpatients were not comfortable initiating the conversation. As a result, HCWs
rarely offered post-test counseling, which was highly desired by respondents in the study, regardless of
their HIVST result. Other studies find that disclosure is highest when individuals believe they will receive
support from HCWs, and lowest when they expect blame and discrimination from HCWs [32]. Future
HIVST interventions should foster a welcoming environment where HCWs actively ask about HIVST
results and provide a safe space for post-test counseling.
Even though very few respondents disclosed their HIVST result to a HCW at OPD, many perceived the
ability to immediately self-initiate connection (link) to additional HIV services at that same health facility
as a major benefit to facility HIVST. Our parent trial on facility HIVST found that 79% of those who
tested HIV-positive with HIVST initiated ART within 3-months, but only 7% disclosed their HIV-
positive status to a HCW in OPD department. The vast majority went directly to the ART department
within that same facility to link themselves to HIV care [13]. The fact that many HIVST users self-
referred to the ART clinic for immediate treatment initiation may reflect a continued autonomy and
ownership over one’s own health care that is promoted through self-testing. Further, situating HIVST
100

strategies within OPD, which is on the same campus as ART services, may facilitate linkage as logistical
barriers to initiation are already overcome, since individuals are already at the facility for acute or routine
care. Other HIVST interventions within community settings report lower rates of linkage and ART
initiation [33-36]. Future HIVST interventions should consider additional strategies to further reduce gaps
to linkage to HIV treatment services.
This study has several limitations that should be noted. Facility HIVST was implemented by high-level
research assistants with secondary school education. In routine care, similar interventions would likely be
implemented by lower-level HCWs with multiple responsibilities, therefore, routine implementation may
not see the same benefits. Second, there is always risk of social desirability bias in reporting acceptability
of an intervention; however, qualitative researchers were not involved in implementation of HIVST,
potentially minimizing any social desirability bias. Third, observational journals are based on events and
conversations observed by study staff and cannot capture all events – mundane events may be particularly
missed if staff deem them unworthy of documentation. Additional limitations of observational journals
are discussed elsewhere [22]. Finally, the sample size of HIVST non-users is small, making it difficult to
draw conclusions for this specific population. Additional research should be conducted with those in need
of HIV testing but refuse HIVST.
Conclusion
Facility HIVST in OPD waiting spaces was acceptable and feasible among adult outpatients in Malawi.
Using waiting spaces for HIVST distribution and use, alongside private spaces for kit interpretation,
facilitated HIV testing for most respondents. Strategies to promote privacy throughout the HIVST
process, to improve disclosure of test results to HCWs, and to strengthen post-test counseling are
important areas for future research.
Declarations
101

Ethics approval and consent to participate
All study activities were approved by the Institutional Review Board at University of California Los
Angeles and the National Health Sciences Review Committee in Malawi. All respondents provided oral
informed consent prior to data collection.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on
reasonable request.
Competing Interests
None declared.
Author Contributions
KD and RMH conceived and designed the research. MH, KP, OO, and FS collected the data. MH, KP,
PC, and KD coded and analyzed the data. MM, PC, and KD drafted the manuscript. RMH and KP
provided substantive additions throughout the first draft and OO, FS, SG, MN and VW provided feedback
of the manuscript.
Acknowledgements
We are grateful to the numerous outpatients and HCWs who gave their time and insight throughout the
study. We are grateful to Eric Lungu, Pericles Kalande, and Kelvin Balakasi for their continued support
on study implementation, data cleaning, and data coding procedures.
102

Funding: The main trial was funded by USAID Cooperative Agreement: AID-OAA-A-15-00070. KD
receives funding from the Fogarty International Center K01-TW011484-01, UCLA CFAR grant
AI028697, CHIPTS, and the Bill and Melinda Gates Foundation (grant #001423). The views in this
publication do not necessarily reflect the views of the U.S. Agency for International Development
(USAID), the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), or the United States
Government.
Conflicts of Interest: None declared. The funders had no role in study design, data collection and
analysis, decision to publish or preparation of the manuscript.
103

REFERENCES 1. UNAIDS. Global HIV & AIDS Statistics ‑ 2020 fact sheet. 2020 October 29, 2020];
Available from: https://www.unaids.org/en/resources/fact-sheet. 2. Indravudh, P.P., A.T. Choko, and E.L. Corbett, Scaling up HIV self-testing in sub-
Saharan Africa: a review of technology, policy and evidence. Current Opinion in Infectious Diseases, 2018. 31(1): p. 14-24.
3. National Statistical Office (NSO) [Malawi] and ICF, Malawi Demographic Health Survey 2015. 2017: Zomba, Malawi, and Rockville, Maryland, USA. NSO and ICF.
4. Ministry of Health Malawi, Population-based HIV Impact Assessment (MPHIA) 2015–16: First Report, M.o. Health, Editor. 2017: Lilongwe, Malawi.
5. Hargreaves, J.R., et al., Strengthening primary HIV prevention: better use of data to improve programmes, develop strategies and evaluate progress. Journal of the International AIDS Society, 2020. 23(S3): p. e25538.
6. UNAIDS Country Overview: Malawi. [cited 2020 September 30]; Available from: https://www.unaids.org/en/regionscountries/countries/malawi.
7. De Cock, K.M., et al., Where are the positives? HIV testing in sub-Saharan Africa in the era of test and treat. AIDS, 2019. 33(2).
8. Mabuto, T., et al., HIV testing services in healthcare facilities in South Africa: a missed opportunity. Journal of the International AIDS Society, 2019. 22(10): p. e25367.
9. Roura, M., et al., Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational implementation. AIDS, 2013. 27(4): p. 617-626.
10. Ahmed, S., et al., Lost opportunities to identify and treat HIV-positive patients: results from a baseline assessment of provider-initiated HIV testing and counselling (PITC) in Malawi. Tropical Medicine & International Health, 2016. 21(4): p. 479-485.
11. Stevens, D.R., et al., A Global Review of HIV Self-testing: Themes and Implications. AIDS and Behavior, 2018. 22(2): p. 497-512.
12. Choko, A.T., et al., The uptake and accuracy of oral kits for HIV self-testing in high HIV prevalence setting: a cross-sectional feasibility study in Blantyre, Malawi. PLoS Med, 2011. 8(10): p. e1001102.
13. Dovel, K., et al., Effect of facility-based HIV self-testing on uptake of testing among outpatients in Malawi: a cluster-randomised trial. Lancet Glob Health, 2020. 8(2): p. e276-e287.
14. Nichols, B., et al., Economic evaluation of facility-based HIV self-testing among adult outpatients in Malaw. JIAS, Pending.
15. Njau, B., et al., A systematic review of qualitative evidence on factors enabling and deterring uptake of HIV self-testing in Africa. BMC Public Health, 2019. 19(1): p. 1289.
16. Peck, R.B., et al., What Should the Ideal HIV Self-Test Look Like? A Usability Study of Test Prototypes in Unsupervised HIV Self-Testing in Kenya, Malawi, and South Africa. AIDS and Behavior, 2014. 18(4): p. 422-432.
17. Musheke, M., et al., A systematic review of qualitative findings on factors enabling and deterring uptake of HIV testing in Sub-Saharan Africa. BMC Public Health, 2013. 13(1): p. 220.
18. Dovel, K., et al., Evaluating the integration of HIV self-testing into low-resource health systems: study protocol for a cluster-randomized control trial from EQUIP Innovations. Trials, 2018. 19(1): p. 498.
19. OraSure Technologies, Bethlehem, PA, USA. 20. Kaler, A., AIDS-talk in everyday life: the presence of HIV/AIDS in men's informal
conversation in Southern Malawi. Social science & medicine, 2004. 59(2): p. 285-297.
104

21. Angotti, N. and A. Kaler, The More You Learn the Less You Know?: Interpretive Ambiguity across Three Modes of Qualitative Data. Demographic Research, 2013. 28(33): p. 951.
22. Kaler, A., S.C. Watkins, and N. Angotti, Making meaning in the time of AIDS: Longitudinal narratives from the Malawi Journals Project. African Journal of AIDS Research, 2015. 14(4): p. 303-314.
23. Azungah, T., Qualitative research: deductive and inductive approaches to data analysis. Qualitative Research Journal, 2018.
24. Atlas.ti, v., Scientific Sofware Development GmbH: Berlin., 2011. 25. Glaser, B.G., The constant comparative method of qualitative analysis. Social problems,
1965. 12(4): p. 436-445. 26. Wood, B.R., C. Ballenger, and J.D. Stekler, Arguments for and against HIV self-testing.
HIV/AIDS (Auckland, N.Z.), 2014. 6: p. 117-126. 27. Young, S.D., B. Monin, and D. Owens, Opt-out testing for stigmatized diseases: a social
psychological approach to understanding the potential effect of recommendations for routine HIV testing. Health psychology : official journal of the Division of Health Psychology, American Psychological Association, 2009. 28(6): p. 675-681.
28. HIV/AIDS Fast-track: ending the AIDS epidemic by 2030. Geneva: UNAIDS. 2014. 29. Dovel, K., et al., Gendered health institutions: examining the organization of health
services and men's use of HIV testing in Malawi. J Int AIDS Soc, 2020. 23 Suppl 2: p. e25517.
30. Hector, J., et al., Acceptability and performance of a directly assisted oral HIV self-testing intervention in adolescents in rural Mozambique. PloS one, 2018. 13(4): p. e0195391-e0195391.
31. Korte, J.E., et al., HIV testing preferences among pregnant women attending antenatal care and their male partners: a discrete choice experiment in Uganda. African Journal of AIDS Research, 2019. 18(4): p. 332-340.
32. Obermeyer, C.M., P. Baijal, and E. Pegurri, Facilitating HIV disclosure across diverse settings: a review. Am J Public Health, 2011. 101(6): p. 1011-23.
33. Yeatman, S., S. Chamberlin, and K. Dovel, Women's (health) work: A population-based, cross-sectional study of gender differences in time spent seeking health care in Malawi. PLoS One, 2018. 13(12): p. e0209586.
34. Ortblad, K., et al., Direct provision versus facility collection of HIV self-tests among female sex workers in Uganda: A cluster-randomized controlled health systems trial. PLoS Med, 2017. 14(11): p. e1002458.
35. Sibanda, E., et al., Linkage to care after HIV self-testing in Zimbabwe: a cluster-randomised trial., in Conference on retroviruses and opportunistic infections. 2018: Boston, MA, USA.
36. MacPherson, P., et al., Effect of optional home initiation of HIV care following HIV self-testing on antiretroviral therapy initiation among adults in Malawi: a randomized clinical trial. Jama, 2014. 312(4): p. 372-9.
105
Vol.:(0123456789)1 3
AIDS and Behavior https://doi.org/10.1007/s10461-021-03404-8
ORIGINAL PAPER
Screening Adults for!HIV Testing in!the!Outpatient Department: An!Assessment of!Tool Performance in!Malawi
Corrina!Moucheraud1 !· Risa!M.!Ho"man2!· Kelvin!Balakasi3!· Vincent!Wong4!· Maria!Sanena3!· Sundeep!Gupta2!· Kathryn!Dovel2,3
Accepted: 24 July 2021 © The Author(s) 2021
AbstractLittle is known about screening tools for adults in high HIV burden contexts. We use exit survey data collected at outpatient departments in Malawi (n = 1038) to estimate the sensitivity, specificity, negative and positive predictive values of screen-ing tools that include questions about sexual behavior and use of health services. We compare a full tool (seven relevant questions) to a reduced tool (five questions, excluding sexual behavior measures) and to standard of care (one question, never tested for HIV or tested > 12!months ago). Suspect STI and " 3 sexual partners were associated with HIV positivity, but had weak sensitivity and specificity. The full tool (using the optimal cuto# score of " 3) would achieve 55.6% sensitivity and 84.9% specificity for HIV positivity; the reduced tool (optimal cuto# score " 2) would achieve 59.3% sensitivity and 68.5% specificity; and standard of care 77.8% sensitivity and 47.8% specificity. Screening tools for HIV testing in outpatient departments do not o#er clear advantages over standard of care.
Keywords Screening!· HIV testing!· Health systems!· Malawi
Introduction
In order to achieve control of the HIV epidemic, UNAIDS has set a series of ambitious targets striving for 95% of individuals living with HIV to know their status, 95% of those to initiate ART, and 95% of those on ART to reach viral suppression [1]. There are, however, persistent gaps in identifying people living with HIV. Approximately 11% of people living with HIV in Eastern and Southern Africa do not know their HIV status [2]. Although there has been progress in the past decade, it has been slow and variable by region [3]. Additionally, as HIV testing coverage increases
and HIV incidence declines [4], more resources are needed to diagnose each new case [5, 6].
The global community is thus seeking innovative ways to more e$ciently identify people who should be tested for HIV—including new technologies (self-testing) [7], new operational approaches to testing (e.g., index partner testing, community-based contact tracing, and social or risk network testing) [8–10], and the use of screening tools to identify those most in need of testing [11]. Clinical HIV guidelines in many African settings currently recommend testing all preg-nant women, individuals with newly-diagnosed tuberculosis, and all sexually active adults annually and whenever they seek care for a sexually transmitted infection (STI) [4]—but, risk assessment through screening may be more sensitive and/or specific than this standard of care (SOC). Screening tools have previously been developed for pediatric HIV diag-nosis in sub-Saharan Africa [12, 13], and may be a useful tool to prioritize high-risk adults for testing. If a screening tool has su$ciently high sensitivity and specificity for HIV infection, it can guide how to use limited testing resources including supplies, sta# and space.
Outpatient departments (OPDs) offer an opportunity for case finding [14] as many adults present regularly to OPDs for acute services [15, 16]. Facility-based testing also
* Corrina Moucheraud [email protected] Department of!Health Policy and!Management, Fielding
School of!Public Health, University of!California, 650 Charles E. Young Dr. S., 31-235A, Los!Angeles, CA!90095, USA
2 Division of!Infectious Diseases, David Ge#en School of!Medicine, University of!California, Los!Angeles, CA, USA
3 Partners in!Hope, Lilongwe, Malawi4 USAID Global Health Bureau, Washington, DC, USA
Content courtesy of Springer Nature, terms of use apply. Rights reserved.106

AIDS and Behavior
1 3
o!ers advantages through better linkage to ART services and cost savings compared to community-based testing [8, 17, 18]; however traditional provider-initiated-testing-and-counseling (PITC) has low coverage in OPD settings due to overcrowded and understa!ed departments [19, 20] and has traditionally demonstrated low HIV positivity rates among those tested [14]. The “yield” (positivity among those tested) of current diagnostic approaches in Africa is also declining more broadly [21]. An HIV screening tool specific to OPD settings may improve testing e"ciencies. However, under-standing sensitivity and specificity of the tool is critical, as the introduction of a new workflow in OPD will impose additional time required for patients and sta!. Therefore, assessing tool performance relative to SOC is an important first step in the decision to implement an HIV screening tool in OPD settings.
The nature of screening tool questions for crowded OPD settings also requires careful consideration. For example, questions regarding sexual risk behavior may unintentionally stigmatize certain individuals and populations. Although questions about recent sexual behavior may be predictive of HIV status [22, 23], these may not be feasible to imple-ment in busy OPD settings due to lack of private spaces to ask sensitive questions and obtain accurate responses [19, 22]. For example, during screening for STI or HIV testing in the United States, health care providers in busy emer-gency departments were routinely less likely to ask questions regarding sexual health as compared to other non-sensitive topics [22]. In order to develop more e"cient strategies for HIV testing in OPD settings, more evidence is needed about how screening tools perform with and without sensitive questions, and compared to SOC.
The goal of our study was to assess whether a screen-ing tool could increase the e"ciency of HIV testing among adults seeking care in OPD settings in Malawi, as compared to SOC. We compare the estimated performance of two ver-sions of a screening tool—one with sexual behavior ques-tions (i.e., full tool) and one without (i.e., reduced tool)—to assess the sensitivity and specificity of potential screening tools in OPD settings.
Methods
Parent Study
Data were collected during exit surveys from a large cluster-randomized trial which aimed to assess the impact of facility HIV self-testing among adult outpatients compared to PITC. Health facilities were randomized to one of three arms (five facilities per arm) using constrained randomization based on region and facility type. The intervention is described in more detail elsewhere [24, 25]. For this secondary analysis,
we used data from the HIV self-testing arm (five facilities) due to high HIV testing coverage within the arm, there-fore with su"cient numbers of outpatients tested in order to reach su"cient power for this sub-analysis. In the HIV self-testing arm, outpatients were approached in outpa-tient waiting spaces and encouraged to test for HIV if they were > 15#years of age, had never received an HIV-positive diagnosis, and had not tested HIV-negative within the last 3#months (or never tested). Facilities were equally spread across central and southern Malawi and varied in facility type: one district hospital; one mission hospital; and three large health centers.
Data Collection
A subset of outpatients at participating facilities were recruited using a systematic sampling strategy. Research sta! recruited every tenth outpatient exiting the outpatient department to complete an exit survey. Eligibility criteria were: $ 15#years of age; accessed and completed all out-patient services to be received that day. Oral consent was attained and exit surveys completed in private, quiet loca-tions at the health facility. The survey was administered by trained research sta!, who asked survey questions aloud and recorded the respondents’ answers on a tablet using data collection software. From the five HIV self-testing arm facilities, 2183 adult outpatients were approached to com-plete exit surveys about their testing experience and 2097 respondents were eligible and completed a survey (Septem-ber 2017–February 2018). This analysis includes survey data from individuals who reported testing for HIV on the day of enrollment, and reported never testing HIV-positive prior to the day of enrollment (in order to examine screening tool performance in the context of new HIV diagnoses).
Survey Tool
The exit survey tool was created based on conceptually-driven hypotheses about associations with HIV status, including: (1) sociodemographic variables; (2) previous use of HIV services and test results; (3) risky sexual behavior in the past 12#months; (4) health services received that day; and (5) use of HIV testing and result of any HIV test received that day. All surveys were completed in the local language (Chichewa) and lasted approximately 20#min on average.
Data Analysis
We used questions from the exit survey to approximate a screening tool; questions that captured factors hypothetically associated with HIV risk were included in the analysis.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.107

AIDS and Behavior
1 3
Operationalizing the!Screening Tool
We included seven variables in the full screening tool. We included suspected sexually transmitted infections (STI) (defined as attending the facility for an STI) because STIs are a known risk factor for seroconversion [26], and attend-ing the facility for malaria-like symptoms since malaise and fever have previously been associated with recent HIV seroconversion in similar settings [27]. We also included “overlooked” groups who do not have a standard entry point for HIV testing: women below the age of 25 (since women often test during pregnancy at antenatal visits), and men over the age of 24 because men almost exclusively seek care via OPD for acute needs [15, 28], therefore if they are not engaged at OPD they may not be reached. These groups are also important for the evolving HIV epidemic in the region: both men and young women have higher HIV positivity, test less often and may not be well-served by current HIV test-ing modalities [3, 29–31]. Finally, never tested for HIV or tested > 12-months ago was included as SOC. The response to each tool question was scored as a 0/1 (no/yes), and these responses were summed to create the total screening tool score.
We also dichotomized two questions with continuous response options (number of recent health visits, and number of recent sexual partners). Cut points were selected based on association with HIV status: we assessed the “inflection point” at which these items became strongly associated with HIV positivity (e.g., having two or more sexual partners was not significantly associated but having three or more sexual partners was).
Analyzing Screening Tool Performance
The analysis aimed to estimate the performance of screen-ing tools, comprised of survey questions as described above, to predict HIV positivity among outpatients testing
for HIV during routine outpatient services. We analyzed the data in two ways (1) using all relevant questions from the survey (items 1–7 in Table!1) and (2) using a reduced tool that excluded questions about number of sexual part-ners and sex outside of marriage (items 1–5 in Table!1). The SOC approach to HIV testing was captured by items 1 and 2 in Table!1.
Of the 2097 outpatients who completed a survey, 1034 were excluded from this analysis due to not testing for HIV on the day of enrollment, 11 were excluded because they had previously tested HIV-positive and 14 were excluded because they either refused to disclose the test result or reported not knowing the test result. All included respond-ents (n = 1038) had complete data for the survey questions used to calculate the screening tool score. This sample size is su"cient for assessing a tool with 40% sensitivity (with specificity up to 99%) given estimated adult HIV prevalence of 9% [32].
We used logistic regression to assess the relationship between HIV status and respondent characteristics (age and sex), response to each screening tool item, and total screening tool scores (full and reduced tool). We calcu-lated the sensitivity, specificity, negative and positive predictive values (NPV and PPV, respectively) for each screening tool item and total screening tool scores (full and reduced) using Stata v14. The optimal screening tool cuto# was identified by plotting the receiver operating characteristic curve and estimating the partial area under the curve (correcting for ties).
Ethical Review
The parent trial including the exit survey methodology and instrument received ethical approval from the Malawi National Health Sciences Review Committee and the Uni-versity of California Institutional Review Board.
Table 1 Screening tool questions
*Full (F), Reduced (R), Standard of care (S)
Question(s) Tool*
HIV testing history 1. Never been tested for HIV before Or, Tested previously for HIV but 12 + months ago
F,R,S
Medical history 2. At health facility today for suspected STI F,R,S3. At health facility today for suspected malaria F,R4. Received health services 4 + times during the last 6!months
(excluding today's visit)F,R
Demographic risk 5. “Overlooked” groups: female and < 25 Or, male and > 24 F,RBehavioral risk 6. Have had 3 + sexual partners in the past 12!months F
7. Had sex without a condom with someone besides spouse in the past 12!months
F
Content courtesy of Springer Nature, terms of use apply. Rights reserved.108

AIDS and Behavior
1 3
Results
As described above, a total of 1038 adults participated in an exit survey, used a HIV self-test kit, and had a known HIV test result so are included in this analysis. Most participants were female (n = 684, 65.9%) and the mean age was 32.2!years (SD 13.0) (Table!2). Overall, 2.6% of respondents (n = 27) tested HIV-positive. Approximately half of respondents had been tested > 12!months ago (or never tested) (n = 540, 52.0%), 44.2% were a member of an “overlooked” group (women < 25 and men > 24!years) (n = 459); and just under one-quarter reporting having " 3 sexual partners in the past year (n = 247, 23.8%). The aver-age score was 1.5 (SD 1.1) for the full screening tool (out of a maximum possible score of 7) and 1.2 (SD 0.8) for the reduced screening tool (out of a maximum possible score of 5).
HIV positivity was significantly and strongly associ-ated with screening questions (Table!2). Among those with a suspected STI, 11.1% tested HIV-positive (versus only 2.5% of those who attended OPD for other reasons); and 6.5% of people reporting > 3 sexual partners in the past 12-months were HIV-positive (versus 2.2% of people with
fewer sexual partners). In adjusted models that included covariates for age and sex, the odds of being HIV-posi-tive was approximately 2–4 times higher for all screening questions compared to respondents who answered “no” to the same question (Appendix Table!A1). HIV positivity increased with higher screening tool score (both full and reduced tool) (Appendix Table!A2).
Table!3 examines the specificity and sensitivity of each item and of the full and reduced (without sexual behavior questions) screening tools. The most sensitive items were: tested " 12!months ago or never tested (sensitivity 74.1%, 95% CI 53.7–88.9%), and being in an “overlooked” group (sensitivity 59.3%, 95% CI 38.8–77.6%). However, both had low specificity (56.2% and 48.6%, respectively). The items with highest specificity were: suspected STI (specificity 98.4%, 95% CI 97.4–99.1%); suspected malaria (specificity 92.9%, 95% CI 91.1–94.4%); and > 3 recent sexual partners (specificity 91.5%, 95% CI 89.6–93.1%)—however, these items had low sensitivity (7.4%, 14.8%, 22.2%, respectively).
For the full screening tool, examining the score as a continuous measure shows that at a cuto# of " 1, the tool specificity was 16.0% (95% CI 13.8–18.4%) and sensitiv-ity was 92.6% (95% CI 75.7–99.1%) for HIV test positiv-ity. Using a cuto# score of " 2 the specificity was 55.8%
Table 2 Characteristics of study participants
‡ Odds ratios include robust standard errors^Full tool includes: “overlooked groups,” tested " 12! months ago or never; came in for STI; " 4 recent health consultations; came in for malaria; " 3 recent sexual partners; recent condomless sex with a non-stable partner. Possible score ranges 0–7^^Reduced tool includes: “overlooked groups,” tested " 12!months ago or never; came in for STI; " 4 recent health consultations; came in for malaria. Possible score ranges 0–5^^^ Standard of care is tested " 12!months ago or never; and/or came in for STI. Possible score ranges 0–1
Overall (n = 1038) Among those HIV-negative (n = 1011)
Among those HIV-positive (n = 27)
Odds ratio‡ (95% CI) p-value
Age, mean (SD) 32.2 (13.0) 32.1 (13.1) 34.1 (11.0) 1.01 (0.99, 1.03) 0.33Gender, n (%)!Female 684 (65.9%) 667 (66.0%) 17 (63.0%) 1.14 (0.52, 2.52) 0.75!Male 354 (34.1%) 344 (34.0%) 10 (37.0%)
Screening items, n (%)!“Overlooked” groups (women 15–24, men 25 +) 459 (44.2%) 443 (43.8%) 16 (59.3%) 1.86 (0.86, 4.06) 0.12!Tested " 12!months ago or never tested 540 (52.0%) 520 (51.4%) 20 (74.1%) 2.70 (1.13, 6.44) 0.03!Came in for a suspected STI 18 (1.7%) 16 (1.6%) 2 (7.4%) 4.98 (1.08, 22.82) 0.04!" 4 recent health consultations (last 6!months) 127 (12.2%) 120 (11.9%) 7 (25.9%) 2.60 (1.08, 6.28) 0.03!Came in for suspected malaria (i.e., fever,
malaise, etc.)76 (7.3%) 72 (7.1%) 4 (14.8%) 2.27 (0.76, 6.74) 0.14
!" 3 recent sexual partners (last 12!months) 92 (8.9%) 86 (8.5%) 6 (22.2%) 3.07 (1.21, 7.82) 0.02!Recent condomless sex with a non-stable partner
(last 12!months)247 (23.8%) 235 (23.2%) 12 (44.4%) 2.64 (1.22, 5.72) 0.01
Full screen^ score, mean (SD) 1.5 (1.1) 1.5 (1.0) 2.5 (1.4) 2.11 (1.50, 2.98) < 0.001Reduced screen^^ score, mean (SD) 1.2 (0.8) 1.2 (0.8) 1.8 (1.0) 2.43 (1.50, 3.96) < 0.001Standard of care^^^ score, mean (SD) 0.5 (0.5) 0.5 (0.5) 0.8 (0.4) 3.20 (1.28, 8.00) 0.01
Content courtesy of Springer Nature, terms of use apply. Rights reserved.109
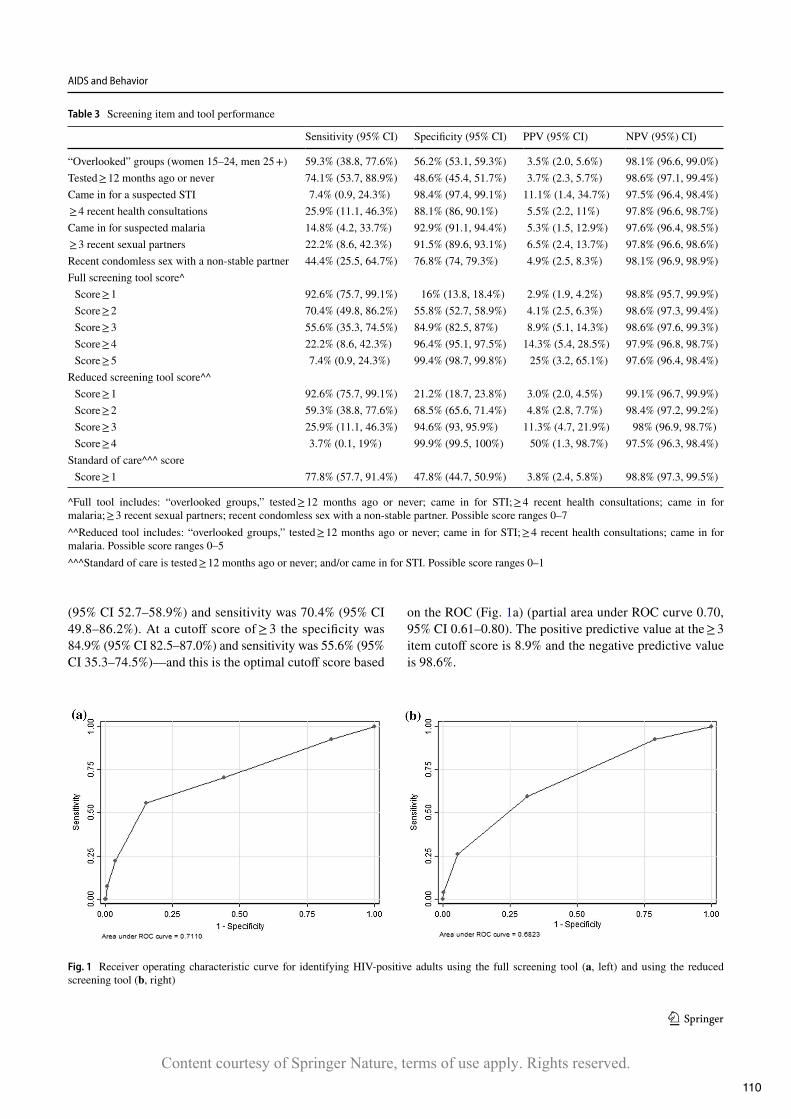
AIDS and Behavior
1 3
(95% CI 52.7–58.9%) and sensitivity was 70.4% (95% CI 49.8–86.2%). At a cuto! score of " 3 the specificity was 84.9% (95% CI 82.5–87.0%) and sensitivity was 55.6% (95% CI 35.3–74.5%)—and this is the optimal cuto! score based
on the ROC (Fig.#1a) (partial area under ROC curve 0.70, 95% CI 0.61–0.80). The positive predictive value at the " 3 item cuto! score is 8.9% and the negative predictive value is 98.6%.
Table 3 Screening item and tool performance
^Full tool includes: “overlooked groups,” tested " 12# months ago or never; came in for STI; " 4 recent health consultations; came in for malaria; " 3 recent sexual partners; recent condomless sex with a non-stable partner. Possible score ranges 0–7^^Reduced tool includes: “overlooked groups,” tested " 12#months ago or never; came in for STI; " 4 recent health consultations; came in for malaria. Possible score ranges 0–5^^^Standard of care is tested " 12#months ago or never; and/or came in for STI. Possible score ranges 0–1
Sensitivity (95% CI) Specificity (95% CI) PPV (95% CI) NPV (95%) CI)
“Overlooked” groups (women 15–24, men 25 +) 59.3% (38.8, 77.6%) 56.2% (53.1, 59.3%) 3.5% (2.0, 5.6%) 98.1% (96.6, 99.0%)Tested " 12#months ago or never 74.1% (53.7, 88.9%) 48.6% (45.4, 51.7%) 3.7% (2.3, 5.7%) 98.6% (97.1, 99.4%)Came in for a suspected STI 7.4% (0.9, 24.3%) 98.4% (97.4, 99.1%) 11.1% (1.4, 34.7%) 97.5% (96.4, 98.4%) " 4 recent health consultations 25.9% (11.1, 46.3%) 88.1% (86, 90.1%) 5.5% (2.2, 11%) 97.8% (96.6, 98.7%)Came in for suspected malaria 14.8% (4.2, 33.7%) 92.9% (91.1, 94.4%) 5.3% (1.5, 12.9%) 97.6% (96.4, 98.5%) " 3 recent sexual partners 22.2% (8.6, 42.3%) 91.5% (89.6, 93.1%) 6.5% (2.4, 13.7%) 97.8% (96.6, 98.6%)Recent condomless sex with a non-stable partner 44.4% (25.5, 64.7%) 76.8% (74, 79.3%) 4.9% (2.5, 8.3%) 98.1% (96.9, 98.9%)Full screening tool score^#Score " 1 92.6% (75.7, 99.1%) 16% (13.8, 18.4%) 2.9% (1.9, 4.2%) 98.8% (95.7, 99.9%)#Score " 2 70.4% (49.8, 86.2%) 55.8% (52.7, 58.9%) 4.1% (2.5, 6.3%) 98.6% (97.3, 99.4%)#Score " 3 55.6% (35.3, 74.5%) 84.9% (82.5, 87%) 8.9% (5.1, 14.3%) 98.6% (97.6, 99.3%)#Score " 4 22.2% (8.6, 42.3%) 96.4% (95.1, 97.5%) 14.3% (5.4, 28.5%) 97.9% (96.8, 98.7%)#Score " 5 7.4% (0.9, 24.3%) 99.4% (98.7, 99.8%) 25% (3.2, 65.1%) 97.6% (96.4, 98.4%)
Reduced screening tool score^^#Score " 1 92.6% (75.7, 99.1%) 21.2% (18.7, 23.8%) 3.0% (2.0, 4.5%) 99.1% (96.7, 99.9%)#Score " 2 59.3% (38.8, 77.6%) 68.5% (65.6, 71.4%) 4.8% (2.8, 7.7%) 98.4% (97.2, 99.2%)#Score " 3 25.9% (11.1, 46.3%) 94.6% (93, 95.9%) 11.3% (4.7, 21.9%) 98% (96.9, 98.7%)#Score " 4 3.7% (0.1, 19%) 99.9% (99.5, 100%) 50% (1.3, 98.7%) 97.5% (96.3, 98.4%)
Standard of care^^^ score#Score " 1 77.8% (57.7, 91.4%) 47.8% (44.7, 50.9%) 3.8% (2.4, 5.8%) 98.8% (97.3, 99.5%)
Fig. 1 Receiver operating characteristic curve for identifying HIV-positive adults using the full screening tool (a, left) and using the reduced screening tool (b, right)
Content courtesy of Springer Nature, terms of use apply. Rights reserved.110

AIDS and Behavior
1 3
The reduced screening tool had improved specificity when compared to the full tool at all cuto! points, but sen-sitivity was slightly lower. At a score of " 1, the specific-ity was 21.2% (95% CI 18.7–23.8%) and sensitivity was 92.6% (95% CI 75.7–99.1%) for HIV test positivity. At a score of " 2 the specificity was 68.5% (95% CI 65.6–71.4%) and sensitivity 59.3% (95% CI 38.8–77.6%), with a positive predictive value of 4.8% and a negative predictive value of 98.4%; and this is the optimal cuto! with a partial area under ROC curve of 0.64 (95% CI 0.54–0.74) (Fig.#1b).
The SOC screen—i.e., tested > 12#months ago or never, and/or presented with an STI—had a sensitivity of 77.8% (95% CI 57.7–91.4%) and a specificity of 47.8% (95% CI 44.7–50.9%). SOC screening had a positive predictive value of 3.8% (95% CI 2.4–5.8%) and a negative predictive value of 98.8% (95% CI 97.3–99.5%).
Discussion
We found that in OPD settings neither a tool with sexual behavior questions nor one excluding sexual behavior ques-tions performed better than the standard of care approach to HIV testing in Malawi, and we could not identify a set of questions that was both highly sensitive and specific. The full screening tool at an optimal score of " 3 would achieve 55.6% sensitivity and 84.9% specificity for HIV positiv-ity among adult outpatients in Malawi. The reduced tool at an optimal score of " 2 would achieve 59.3% sensitiv-ity and 68.5% specificity, while standard of care of having at least one of two questions would achieve a sensitivity of 77.8% and specificity of 47.8%. Although standard of care screening had the highest sensitivity, it also had lower specificity than either full or reduced tools at their optimal cuto! scores. Similar to other literature, newly-diagnosed HIV infection was highly correlated with having suspected STI and " 3 sexual partners in the past 12-months, [33–35], although adding these questions did not improve screening tool performance.
Our findings highlight the challenging trade-o!s in find-ing an approach that is e$cient (i.e., tool sensitivity) and still reaches the majority of unidentified individuals liv-ing with HIV (i.e., tool specificity). Given the adult HIV prevalence in Malawi (8.9%) [32], the treatment-adjusted prevalence of 1.7% [36], and the fact that less than 23% of individuals living with HIV were undiagnosed at the time of our study [37], for each 1000 adult outpatients screened, the full screening tool at an optimal score (" 3) would result in 162 people being tested for HIV, and 14 of these peo-ple would test positive; while among those not tested, there would be 12 HIV-positive people left undiagnosed. If 1000 people were screened using the reduced tool, using its opti-mal score (" 2), 322 would undergo an HIV test, among
which 15 people would be diagnosed as HIV-positive and 11 HIV-positive people would be left undiagnosed.
One aim of screening tools is to save resources by prior-itizing who gets tested. To achieve this, tools must have high sensitivity and specificity because their implementation adds burden for facility sta! who are already under significant constraints due to high patient volume and limited resources in OPD settings. Program data from other screening experi-ences among outpatients in Malawi indicate that multiple-question screening tools (with sexual behavior questions) require five to seven minutes to administer per person screened [38]. Screening tools that include questions about sexual behavior also require private space for implementa-tion, as well as patient-provider trust in order to promote open, honest responses from outpatients [22, 23].
Screening tool performance is a!ected by underlying prevalence, and there is an increased likelihood of more false positives in low-prevalence settings, which would a!ect the screening tool’s predictive values. Therefore, in contexts with controlled or near-controlled epidemics, it may be par-ticularly challenging to identify adult HIV testing screening tools with su$ciently high specificity to o!er e$ciencies over standard of care, and su$ciently high sensitivity to cap-ture most infected individuals. A recent paper analyzed the performance of a similar adult outpatient screening tool in Kenya, and found that the optimal set of questions (which included both demographic characteristics and sexual risk behavior questions) would reduce the number of people requiring testing by 75%, but would miss approximately half of HIV-positive individuals [33]. Taken together with our findings from Malawi, it is evident that screening tools are not an optimal solution for HIV testing in outpatient depart-ments. As local epidemics evolve, multi-pronged approaches will be increasingly necessary to find the relatively small number of individuals unidentified with HIV.
While screening tools for adults in OPD settings have suboptimal performance, screening tools for pediatric HIV testing in sub-Saharan African OPDs show more promise, with sensitivity of approximately 71–92% and specificity of approximately 32–88% [39]. Pediatric tools may perform better than adult tools in OPD settings because questions related to vertical transmission risk are easier to include in a screening tool, compared to HIV horizontal acquisition risk factors for adults which may encompass a range of sensitive behaviors and exposures. Additionally, the physical manifes-tations of HIV infection may be easier to detect in children than in adults, for example frequent infections and failure to thrive [40]. Even still, the highest-performing pediatric HIV screening tool identified in a recent systematic review (with sensitivity and specificity " 95%) was quite complex and may be di$cult to take to scale. The tool incorporated 17 questions that included locally-relevant risk factors for HIV status such as father’s occupation, location and health status
Content courtesy of Springer Nature, terms of use apply. Rights reserved.111

AIDS and Behavior
1 3
[39]—suggesting that deploying optimal screening tools, even for pediatrics, requires substantial resources includ-ing dedicated and trained personnel to administer lengthy questionnaires.
Without a well-performing screening tool, what strategies can increase HIV testing e!ciency in OPD settings? Facil-ity HIV self-testing can test many adults without increased personnel or the need for additional infrastructure [25]. HIV self-testing is e"ective and can provide cost savings for identifying newly-diagnosed adults in OPD as compared to standard blood-based testing [41] – but does require procure-ment and distribution of a high volume of test kits, which may be challenging in low-resource health systems. Other options might be facility-based testing “campaigns” or tar-geted time periods of concentrated testing aimed at achiev-ing high coverage with consolidated resources. Reaching the remaining unidentified individuals living with HIV will likely require an approach that combines sustained OPD test-ing with higher-yield testing strategies, such as index partner testing, leveraging social networks of high-risk populations, and providing work-based testing for men in higher-risk occupations [8–10]. Programs and policymakers should also consider whether ensuring comprehensive HIV testing using SOC in OPDs, despite increasing ine!ciencies and cost due to evolution of the HIV epidemic, is simply a necessary cost of sustaining control of a generalized epidemic.
This study has some limitations that should be noted. We performed a post-hoc analysis of a “constructed” hypotheti-cal screening tool based on questions from an exit survey collected as part of a large trial about HIV self-testing. Some key risk factors that may be predictive of HIV positivity among adults—such as region of residence, number of life-time partners, household wealth, migratory labor, and sus-pect tuberculosis [42–46]—were not included in the parent study survey tool so could not be analyzed here. There may have been selection bias into participation into the parent study (those who opted to use the HIV self-test), and there may have been response bias to the exit survey questions, especially those about sexual behavior. For example, peo-ple may have answered questions about their risk behaviors based on their HIV status, as diagnosed just prior to data collection. Additionally, the survey was asked at the con-clusion of each person’s clinical encounter, so their experi-ence at the facility that day—including learning of their HIV status for those newly diagnosed—may have a"ected their responses to survey questions. Lastly, the scoring algorithm used here is simplistic (summing dichotomous values) and does not consider the relative importance of di"erent factors or how this might a"ect overall scores, for example through a weighted average. Given the small number of HIV cases in this population and our interest in identifying a screening tool that could be easily implemented in a busy OPD setting, we pursued this less complex approach when designing the
screening tool. However, a more nuanced clinical predictive tool, that scores based on strength of association between the factor and the outcome, is worthy of further study par-ticularly in lager populations with higher underlying HIV prevalence.
Conclusions
While we found screening questions that were highly cor-related with HIV status, the screening tools (full or reduced) did not o"er compelling advantages to e!ciency or feasibil-ity beyond the SOC. These findings, in addition to the added burden and complexities of introducing an adult screening tool within limited-resource OPD settings, and the large het-erogeneity in health facility and epidemiological contexts within countries, call into question the use of screening tools for improving the e!ciency of HIV testing in OPDs. While identification of an e"ective screening tool would represent a needed step forward in fighting the HIV epidemic, this study highlights the need for rigorous evidence before introducing such an approach at scale.
Supplementary Information The online version contains supplemen-tary material available at https:// doi. org/ 10. 1007/ s10461- 021- 03404-8.
Acknowledgements We are grateful to the Partners in Hope programs team and facility sta" who gave their time and insights throughout the study. We thank Tanya Shewchuk and Naoko Doi for input on data interpretation, and Eric Lungu for continued support around data cleaning and data coding.
Author Contributions KD and RH led the parent trial. KD designed this sub-analysis. CM led this analysis, and all authors provided input on interpretation of findings. CM wrote the first draft of the paper, with significant inputs from KD. All authors provided edits and approved the final version for submission.
Funding This study was supported by the United States Agency for International Development (Cooperative Agreement AID-OAA-A-15-00070). CM receives support from Center for HIV Identifica-tion, Prevention, and Treatment (CHIPTS; NIMH Grant MH58107); and the National Center for Advancing Translational Sciences (NCATS Grant KL2TR001882). KD receives support from the Fogarty Interna-tional Center (Grant K01TW011484), and the Bill and Melinda Gates Foundation (Grant 001423). KD and RH receive support from UCLA CFAR (Grant AI028697). The views in this publication do not neces-sarily reflect the views of the U.S. Agency for International Develop-ment (USAID), the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), or the United States Government.
Declarations
Conflict of interest The authors have no relevant financial or non-fi-nancial interest to disclose.
Ethical Approval The parent trial including the exit survey methodol-ogy and instrument received ethical approval from the Malawi National
Content courtesy of Springer Nature, terms of use apply. Rights reserved.112

AIDS and Behavior
1 3
Health Sciences Review Committee and the University of California Los Angeles Institutional Review Board.
Informed Consent All participants gave oral informed consent before engaging in this study.
Open Access This article is licensed under a Creative Commons Attri-bution 4.0 International License, which permits use, sharing, adapta-tion, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http:// creat iveco mmons. org/ licen ses/ by/4. 0/.
References
1. UNAIDS Understanding Fast-Track. Accelerating action to end the AIDS epidemic by 2030. Geneva: Joint United Nations Pro-gramme on HIV/AIDS; 2015.
2. UNAIDS. AIDSInfo 2020 3. UNAIDS. Data Report 2019. Geneva. 2019. 4. WHO. Consolidated guidelines on HIV Testing Services for a
changing epidemic. Geneva: WHO; 2019. 5. Dwyer-Lindgren L, Cork MA, Sligar A, Steuben KM, Wilson KF,
Provost NR, et!al. Mapping HIV prevalence in sub-Saharan Africa between 2000 and 2017. Nature. 2019;570(7760):189–93.
6. Remme M, Siapka M, Sterck O, Ncube M, Watts C, Vassall A. Financing the HIV response in sub-Saharan Africa from domes-tic sources: moving beyond a normative approach. Soc Sci Med. 2016;169:66–76.
7. Granich R, Williams B, Montaner J, Zuniga JM. 90–90–90 and ending AIDS: necessary and feasible. Lancet. 2017;390(10092):341–3.
8. Sharma M, Ying R, Tarr G, Barnabas R. Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature. 2015;528(7580):S77–85.
9. Dave S, Peter T, Fogarty C, Karatzas N, Belinsky N, PantPai N. Which community-based HIV initiatives are e"ective in achieving UNAIDS 90–90–90 targets? A systematic review and meta-anal-ysis of evidence (2007–2018). PloS ONE. 2019;14(7):e0219826.
10. Lillie TA, Persaud NE, DiCarlo MC, Gashobotse D, Kamali DR, Cheron M, et!al. Reaching the unreached: performance of an enhanced peer outreach approach to identify new HIV cases among female sex workers and men who have sex with men in HIV programs in West and Central Africa. PloS ONE. 2019;14(4):e0213743.
11. Opito R, Nanfuka M, Mugenyi L, Etukoit MB, Mugisha K, Opendi L, et!al. A case of TASO tororo surge strategy: using double lay-ered screening to increase the rate of identification of new HIV positive clients in the community. Science. 2019;5(1):19–25.
12. Lowenthal E, Lawler K, Harari N, Moamogwe L, Masunge J, Masedi M, et!al. Validation of the pediatric symptom check-list in HIV-infected Batswana. J Child Adolesc Ment Health. 2011;23(1):17–28.
13. Odafe S, Onotu D, Fagbamigbe JO, Ene U, Rivadeneira E, Car-penter D, et!al. Increasing pediatric HIV testing positivity rates
through focused testing in high-yield points of service in health facilities—Nigeria, 2016–2017. PloS ONE. 2020;15(6):e0234717.
14. De Cock KM, Barker JL, Baggaley R, El Sadr WM. Where are the positives? HIV testing in sub-Saharan Africa in the era of test and treat. AIDS. 2019;33(2):349–52.
15. Dovel K, Balakasi K, Gupta S, Mphande M, Robson I, Kalande P, et!al.: Missing men or missed opportunity? Men’s frequent use of health services in Malawi. In: International AIDS conference; San Fransisco, CA. 2020.
16. Yeatman S, Chamberlin S, Dovel K. Women’s (health) work: a population-based, cross-sectional study of gender di"erences in time spent seeking health care in Malawi. PLoS ONE. 2018. https:// doi. org/ 10. 1371/ journ al. pone. 02095 86.
17. Sanga ES, Lerebo W, Mushi AK, Clowes P, Olomi W, Maboko L, et!al. Linkage into care among newly diagnosed HIV-positive individuals tested through outreach and facility-based HIV testing models in Mbeya, Tanzania: a prospective mixed-method cohort study. BMJ Open. 2017;7(4):e013733.
18. Maughan-Brown B, Beckett S, Kharsany AB, Cawood C, Khany-ile D, Lewis L, et!al. Poor rates of linkage to HIV care and uptake of treatment after home-based HIV testing among newly diag-nosed 15-to-49!year-old men and women in a high HIV prevalence setting in South Africa. AIDS Care. 2020. https:// doi. org/ 10. 1080/ 09540 121. 2020. 17190 25.
19. Mabuto T, Hansoti B, Charalambous S, Ho"mann C. Understand-ing the dynamics of HIV testing services in South African pri-mary care facilities: project SOAR results brief. Washington, DC: Population Council; 2018.
20. Roura M, Watson-Jones D, Kahawita TM, Ferguson L, Ross DA. Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational imple-mentation. AIDS. 2013;27(4):617–26.
21. Giguère K, Eaton JW, Marsh K, Johnson LF, Johnson CC, Ehui E, et!al. Trends in knowledge of HIV status and e#ciency of HIV testing services in sub-Saharan Africa, 2000–20: a modelling study using survey and HIV testing programme data. Lancet HIV. 2021;5:e688.
22. Niforatos JD, Nowacki AS, Cavendish J, Gripshover BM, Yax JA. Emergency provider documentation of sexual health risk factors and its association with HIV testing: a retrospective cohort study. Am J Emerg Med. 2019;37(7):1365–7.
23. Haukoos JS, Lyons MS, Lindsell CJ, Hopkins E, Bender B, Roth-man RE, et!al. Derivation and validation of the Denver Human Immunodeficiency Virus (HIV) risk score for targeted HIV screening. Am J Epidemiol. 2012;175(8):838–46.
24. Dovel K, Shaba F, Nyirenda M, O"orjebe OA, Balakasi K, Phiri K, et!al. Evaluating the integration of HIV self-testing into low-resource health systems: study protocol for a cluster-randomized control trial from EQUIP Innovations. Trials. 2018;19(1):498.
25. Dovel K, Nyirenda M, Shaba F, O"orjebe A, Balakasi K, Nichols B, et!al. Facility-based HIV self-testing for outpatients dramati-cally increases HIV testing in Malawi: a cluster randomized trial. Lancet Global Health. 2018;21:28.
26. Ward H, Rönn M. The contribution of STIs to the sexual transmis-sion of HIV. Curr Opin HIV AIDS. 2010;5(4):305.
27. Rutstein SE, Ananworanich J, Fidler S, Johnson C, Sanders EJ, Sued O, et!al. Clinical and public health implications of acute and early HIV detection and treatment: a scoping review. J Int AIDS Soc. 2017;20(1):21579.
28. Dovel K, Dworkin SL, Cornell M, Coates TJ, Yeatman S. Gen-dered health institutions: examining the organization of health services and men’s use of HIV testing in Malawi. J Int AIDS Soc. 2020;23:e25517.
29. Drammeh B, Medley A, Dale H, De AK, Diekman S, Yee R, et!al. Sex di"erences in HIV testing—20 PEPFAR-supported
Content courtesy of Springer Nature, terms of use apply. Rights reserved.113

AIDS and Behavior
1 3
sub-Saharan African Countries, 2019. Morb Mortal Wkly Rep. 2020;69(48):1801.
30. Merzouki A, Styles A, Estill J, Orel E, Baranczuk Z, Petrie K, et!al. Identifying groups of people with similar sociobehavioural characteristics in Malawi to inform HIV interventions: a latent class analysis. J Int AIDS Soc. 2020;23(9):e25615.
31. Lightfoot M, Dunbar M, Weiser SD. Reducing undiagnosed HIV infection among adolescents in sub-Saharan Africa: pro-vider-initiated and opt-out testing are not enough. PLoS Med. 2017;14(7):e1002361.
32. UNAIDS. Country Factsheet: Malawi HIV/AIDS estimates. 2019. 33. Muttai H, Guyah B, Musingila P, Achia T, Miruka F, Wanjohi
S, et!al. Development and validation of a sociodemographic and behavioral characteristics-based risk-score algorithm for targeting HIV testing among adults in Kenya. AIDS Behav. 2020. https:// doi. org/ 10. 1007/ s10461- 020- 02962-7.
34. Chen L, Jha P, Stirling B, Sgaier SK, Daid T, Kaul R, et!al. Sexual risk factors for HIV infection in early and advanced HIV epidem-ics in sub-Saharan Africa: systematic overview of 68 epidemio-logical studies. PloS ONE. 2007;2(10):e1001.
35. Rosenberg MS, Gómez-Olivé FX, Rohr JK, Houle BC, Kabudula CW, Wagner RG, et!al. Sexual behaviors and HIV status: a pop-ulation-based study among older adults in rural South Africa. J Acquir Immune Defic Syndr (1999). 2017;74(1):e9.
36. HIV Testing Services Dashboard. In: World Health Organization, editor. 2021.
37. Ministry of Health Social Welfare Tanzania, Ministry of Health Zanzibar, National Bureau of Statistics Tanzania, O"ce of Chief Government Statistician Tanzania, ICF International. Tanzania Service Provision Assessment Survey 2014–2015. Dar es Salaam, Tanzania: MoHSW/Tanzania, MoH/Tanzania, NBS/Tanzania, OCGS/Tanzania, and ICF International. 2016.
38. PEPFAR. Implementing Partners Strategic Meeting. Malawi. 2019.
39. Clemens SL, Macneal KD, Alons CL, Cohn JE. Screening algo-rithms to reduce burden of pediatric HIV testing. Pediatr Infect Dis J. 2020. https:// doi. org/ 10. 1097/ INF. 00000 00000 002715.
40. Lowenthal ED, Bakeera-Kitaka S, Marukutira T, Chapman J, Goldrath K, Ferrand RA. Perinatally acquired HIV infection in adolescents from sub-Saharan Africa: a review of emerging chal-lenges. Lancet Infect Dis. 2014;14(7):627–39.
41. Nichols B, Offorjebe OA, Cele R, Shaba F, Balakasi K, Chivwara M, et!al. Economic evaluation of facility-based HIV self-testing among adult outpatients in Malawi. J Int AIDS Soc. 2020;23:e25612.
42. Nutor JJ, Duah HO, Agbadi P, Duodu PA, Gondwe KW. Spa-tial analysis of factors associated with HIV infection in Malawi: indicators for effective prevention. BMC Public Health. 2020;20(1):1–14.
43. Nliwasa M, MacPherson P, Gupta-Wright A, Mwapasa M, Horton K, Odland JØ, et!al. High HIV and active tuberculosis preva-lence and increased mortality risk in adults with symptoms of TB: a systematic review and meta-analyses. J Int AIDS Soc. 2018;21(7):e25162.
44. Nliwasa M, MacPherson P, Mukaka M, Mdolo A, Mwapasa M, Kaswaswa K, et!al. High mortality and prevalence of HIV and tuberculosis in adults with chronic cough in Malawi: a cohort study. Int J Tuberc Lung Dis. 2016;20(2):202–10.
45. Anglewicz P, VanLandingham M, Manda-Taylor L, Kohler H-P. Migration and HIV infection in Malawi: a population-based lon-gitudinal study. AIDS (Lond, Engl). 2016;30(13):2099.
46. Camlin CS, Akullian A, Neilands TB, Getahun M, Bershteyn A, Ssali S, et!al. Gendered dimensions of population mobility asso-ciated with HIV across three epidemics in rural Eastern Africa. Health Place. 2019;57:339–51.
Publisher's Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional a"liations.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.114

1.
2.
3.
4.
5.
6.
Terms and Conditions Springer Nature journal content, brought to you courtesy of Springer Nature Customer Service Center GmbH (“Springer Nature”). Springer Nature supports a reasonable amount of sharing of research papers by authors, subscribers and authorised users (“Users”), for small-scale personal, non-commercial use provided that all copyright, trade and service marks and other proprietary notices are maintained. Byaccessing, sharing, receiving or otherwise using the Springer Nature journal content you agree to these terms of use (“Terms”). For thesepurposes, Springer Nature considers academic use (by researchers and students) to be non-commercial. These Terms are supplementary and will apply in addition to any applicable website terms and conditions, a relevant site licence or a personalsubscription. These Terms will prevail over any conflict or ambiguity with regards to the relevant terms, a site licence or a personal subscription(to the extent of the conflict or ambiguity only). For Creative Commons-licensed articles, the terms of the Creative Commons license used willapply. We collect and use personal data to provide access to the Springer Nature journal content. We may also use these personal data internally withinResearchGate and Springer Nature and as agreed share it, in an anonymised way, for purposes of tracking, analysis and reporting. We will nototherwise disclose your personal data outside the ResearchGate or the Springer Nature group of companies unless we have your permission asdetailed in the Privacy Policy. While Users may use the Springer Nature journal content for small scale, personal non-commercial use, it is important to note that Users maynot:
use such content for the purpose of providing other users with access on a regular or large scale basis or as a means to circumvent access
control;
use such content where to do so would be considered a criminal or statutory offence in any jurisdiction, or gives rise to civil liability, or is
otherwise unlawful;
falsely or misleadingly imply or suggest endorsement, approval , sponsorship, or association unless explicitly agreed to by Springer Nature in
writing;
use bots or other automated methods to access the content or redirect messages
override any security feature or exclusionary protocol; or
share the content in order to create substitute for Springer Nature products or services or a systematic database of Springer Nature journal
content. In line with the restriction against commercial use, Springer Nature does not permit the creation of a product or service that creates revenue,royalties, rent or income from our content or its inclusion as part of a paid for service or for other commercial gain. Springer Nature journalcontent cannot be used for inter-library loans and librarians may not upload Springer Nature journal content on a large scale into their, or anyother, institutional repository. These terms of use are reviewed regularly and may be amended at any time. Springer Nature is not obligated to publish any information orcontent on this website and may remove it or features or functionality at our sole discretion, at any time with or without notice. Springer Naturemay revoke this licence to you at any time and remove access to any copies of the Springer Nature journal content which have been saved. To the fullest extent permitted by law, Springer Nature makes no warranties, representations or guarantees to Users, either express or impliedwith respect to the Springer nature journal content and all parties disclaim and waive any implied warranties or warranties imposed by law,including merchantability or fitness for any particular purpose. Please note that these rights do not automatically extend to content, data or other material published by Springer Nature that may be licensedfrom third parties. If you would like to use or distribute our Springer Nature journal content to a wider audience or on a regular basis or in any other manner notexpressly permitted by these Terms, please contact Springer Nature at
115

The HIV PandemicPrevention E!orts CanInform the COVID-19Pandemic Response in theUnited StatesMaria A. Carrasco, MPP, MPH, PhD, Kaitlyn Atkins, MPH, Ruth Young, MSc,Joseph G. Rosen, MSPH, Suzanne M. Grieb, PhD, MSPH, Vincent J. Wong, MSc, andPaul J. Fleming, PhD, MPH
ABOUT THE AUTHORS
Maria A. Carrasco is with the O!ce of Population and Reproductive Health at the UnitedStates Agency for International Development (USAID), Washington, DC. Kaitlyn Atkins, RuthYoung, and Joseph G. Rosen are with the Johns Hopkins Bloomberg School of Public Health,Department of International Health, Baltimore, MD. Suzanne M. Grieb is with the JohnsHopkins School of Medicine, Center for Child and Community Health Research, Baltimore.Vincent J. Wong is with the O!ce of HIV/AIDS at USAID. Paul J. Fleming is with theDepartment of Health Behavior and Health Education, University of Michigan School ofPublic Health, Ann Arbor.Note. The views in this publication do not necessarily re"ect the views of the USAID, the USPresident’s Emergency Plan for AIDS Relief, or the US government.
Although COVID-19 is new, this is not
the !rst time that we face an in-
fectious disease pandemic. We need to
use lessons from past pandemics, like
the HIV/AIDS pandemic, to enhance
the COVID-19 response. The HIV and
COVID-19 pandemics expose gaps in the
current US health care system and
highlight the role of social determinants
of health in transmission and outcomes.
In addition, both pandemics have clear
behavioral prevention strategies (i.e.,
condom use or sexual partner reduction
for HIV and mask wearing or social
distancing for COVID-19). These are
important alone or as part of combi-
nation prevention, which adds biomed-
ical strategies such as vaccines to the
prevention toolbox. While we wait for
biomedical breakthroughs to be widely
available, an enhanced COVID-19 be-
havioral prevention response is essen-
tial. In this article, we highlight six speci!c
prevention strategies implemented in
the HIV response that could enhance
the COVID-19 response in the United
States:
1 Address rumors and
misconceptions;
2 Help people determine their
level of risk to take appropriate
precautions;
3 Implement prevention strategies
that are targeted to vulnerable
groups (i.e., key populations);
4 Develop and disseminate clear,
adaptive messages through multiple
trusted communication channels;
5 Implement widespread testing as a
powerful prevention tool; and
6 Engage behavioral scientists to help
lead our response.
ADDRESS RUMORS ANDMISCONCEPTIONS
Parmet and Paul refer to COVID-19 as
the “!rst post-truth pandemic” and point
to the barrage of false information that
has eroded trust in health leaders.1(p945)
As they point out, this is not new. Ru-
mors and misconceptions have in"u-
enced delivery of HIV interventions
throughout the HIV pandemic.2,3 Com-
munication, communitymobilization, and
formative research have been key to
address and dispel rumors and establish
trust in the HIV response3 and are more
crucial than ever in the case of the “post-
truth” COVID-19 pandemic. Skepticism
and misinformation about the COVID-19
response are ampli!ed as they spread
rapidly through social media, the Inter-
net, and high-pro!le individuals.
To address such “infodemics,” ap-
propriate and timely information should
be the foundation of prevention e#orts.4
Rumors and misconceptions should be
addressed and dispelled up front, re-
gardless of the source of misinforma-
tion, via various channels and strategies.
In the HIV response, such channels have
included peers or community mobilizers
and mass and social media, and strat-
egies have included engaging religious
and community leaders to provide ac-
curate information.
DETERMINE RISK LEVEL
The HIV response has demonstrated
that no single prevention strategy is
Editorials Carrasco et al.
AJPH
April2021,Vol111,No.4
EDITORIALS
116

universally acceptable, appropriate, and
e!ective. E!orts to prevent and control
COVID-19 should recognize that one
strategy does not "t all.5 Instead, poli-
cymakers should contextualize preven-
tion strategies in consultation with
medical, public health, and health be-
havior experts.
Prevention measures should also ac-
knowledge the spectrum of COVID-19
risk. In the HIV response, harm reduc-
tion bene"ts populations for whom
abstinence from high-risk behaviors
is infeasible.6 In the COVID-19 era,
abstaining from nonhousehold contacts
is not possible for many and may
present further risks by exacerbating
mental distress, reducing access to in-
come and essential services, or straining
social networks. It is important to create
an environment where individuals are
not stigmatized for their choices around
work and interactions.7 Harm reduction
for COVID-19 relies on health systems
and local authorities to provide high-
quality services and accurate informa-
tion. As a result, policymakers and
employers can support policies that
reduce harm in higher-risk environ-
ments (e.g., workspaces, businesses),
and individuals can make informed de-
cisions about their activities (e.g., mask
wearing).
IMPLEMENT PREVENTIONSTRATEGIES
In 2013, UNAIDS highlighted the need
for targeted interventions, recommend-
ing a shift from “know your epidemic” to
“know your local epidemics.”8 E#cient
and e!ective HIV prevention strategies
target speci"c groups, responding to
their particular characteristics, needs,
and assets.9,10 Indeed, targeted behav-
ioral interventions have successfully
addressedHIV prevention and treatment
among key populations who remain
disproportionately a!ected by HIV as a
result of behavioral factors (e.g., injection
drug use), as well as social and structural
issues that heighten their vulnerability
(e.g., criminalization, access to health
care).
Like HIV, COVID-19 has made eco-
nomic and racial disparities highly visi-
ble.11 Targeted interventions should
prioritize resource allocation based on
need and allow focused messaging,
addressing population-speci"c con-
cerns. For example, a disproportionate
number of racial and ethnic minorities
are low-wage essential workers without
"nancial safety nets and are residents
of multigenerational households, for
whom physical distancing would not be
feasible. Targeted strategies can foster
interventions addressing these speci"c
challenges while utilizing appropriate
messages, language, and imagery. For
example, community testing sites can
provide access to quick testing, letters
documenting testing date and negative
results (to provide to employers),
supplies such as masks, and informa-
tion about relevant community
resources.
Where possible, such targeted strat-
egies should be done in partnership
with a!ected communities. Throughout
the HIV response, community-led ini-
tiatives have played a key role in curbing
outbreaks. To reach vulnerable com-
munities and ensure strategies are
trusted, appropriate, and e!ective,
COVID-19 prevention e!orts should be
similarly community-led.
DISSEMINATE CLEAR,ADAPTIVE MESSAGES
Throughout the COVID-19 pandemic,
unclear messaging through multiple
channels has bred distrust and mired
uptake of interventions and innovations.
However, these same channels, when
paired with clear, adaptive messaging,
can be used to promote intervention
uptake. The global HIV/AIDS response
is no stranger to adaptive prevention
messaging: successful HIV prevention
campaigns have identi"ed and engaged
trusted information sources, from reli-
gious leaders to peers, in combination
with other outlets such as mass media.3
In the HIV response, strategies to pro-
mote uptake of interventions have
changed over time to respond to the
concerns of di!erent groups.12,13
Given the divisive nature of the news
media in the United States,1 there is
an urgent need to leverage alternative
dissemination channels for COVID-19
prevention messaging. Communication
strategies should also adapt over time to
promote more widespread intervention
adoption and keepupwith rapid changes
as we learn more about COVID-19. For
instance, health authorities initially rec-
ommended people abstain from pur-
chasing and wearing face masks, fearing
personal protective equipment short-
ages for health care workers. However,
in the face of widespread community
transmission, evidence of asymptomatic
transmission, new evidence about the
positive aspects of using face masks, and
pressure to reopen economies, health
authorities quickly adapted to the shifting
landscape and recommended face cov-
erings be donned in public places.
Unfortunately, themixedmessages and
the lack of clari"cation for the reasons for
shifting policy left many in the United
States skeptical about the importance of
wearing a mask. Adaptive communication
strategies through multiple channels
should not only promote widespread
uptake of COVID-19 interventionsbut they
should also keep pace with the dynamism
of new "ndings about the virus.14
Editorials Carrasco et al.
EDITORIALS
AJPH
April
2021
,Vol
111,
No.
4
117
IMPLEMENT WIDESPREADTESTING
HIV testing has remained at the core of
global e!orts to end theHIV pandemic.15
Although initial HIV diagnostics took
weeks to return results, the early de-
velopment of rapid antibody assays
along with algorithms that ensured
correct results allowed immediate tai-
loring of services and messaging based
on serostatus. Similar to COVID-19, an
extended asymptomatic period among
persons living with HIV meant that
identifying positive, presymptomatic in-
dividuals was critical to mitigating
transmission. Elements of HIV testing
programs, which can be drawn upon for
COVID-19 testing, include
· Widespread access to quality
rapid diagnostics, appropriate
algorithms, and immediate (or at
least same-day) results and self-
testing;
· Focusedmessaging to drive testing
demand, prioritize information for
contact tracing, and reduce on-
ward transmission from those
diagnosed;
· Services tailored to serostatus with a
focus on linkage from testing to ef-
fective prevention and treatment
interventions; and
· Use of testing volume, positivity
rate, and survey data to re"ne
programs and inform targeting by
geography, population, and access
points.
To enhance COVID-19 prevention ef-
forts, identifying those who have the
virus is similarly critical. Not only can
case identi"cation reduce transmission,
but it also can help individuals deter-
mine their level of risk and shape uptake
of preventive behaviors.
ENGAGE BEHAVIORALSCIENTISTS TO HELP LEAD
While advances in COVID-19 vaccine and
treatment research are promising,
without a stronger and more coordi-
nated prevention approach in the
United States, it is likely that many more
will su!er and die. Early prevention ef-
forts erroneously relied on best-case
scenarios, which assumed widespread
adoption of preventive behaviors. Expe-
rience, however, has shown that policy
changes are insu#cient behavior change
catalysts and that investments in be-
havioral interventions are imperative.
The HIV response, both in the United
States and abroad, is multisectoral, en-
gaging local communities, governments,
and international agencies to promote
preventive actions and uptake of novel
biomedical agents to treat and prevent
HIV. These e!orts have included dis-
semination of evidence-based HIV pre-
vention information, changing harmful
community norms, mobilizing commu-
nities, and creating choice architectures
to facilitate uptake of key prevention
approaches like HIV testing. Likewise,
urgent investments in behavioral
COVID-19 prevention are needed in
the United States to promote adoption
of prevention behaviors and address
vaccine hesitancy, and these e!orts
must be informed by behavioral
scientists.
CONCLUSIONS
COVID-19 may be new, but global pan-
demics of a novel virus are not. In the
1980s, HIV emerged as a novel virus for
which there was no treatment, vacci-
nation, or cure. The HIV prevention re-
sponse implemented by behavioral
scientists and public health experts in
the United States and abroad, in
collaboration with local communities and
leaders, provides valuable lessons from
which COVID-19 response leadership
could draw. Implementing such lessons
can help to slow the spread of COVID-19
in the United States and save lives.
CORRESPONDENCE
Correspondence should be sent to Maria A. Car-rasco, Senior Implementation Sciences TechnicalAdvisor, 05.4.1A, 500 D St SW, Washington, DC20547 (e-mail: [email protected]). Reprints canbe ordered at http://www.ajph.org by clicking the“Reprints” link.
PUBLICATION INFORMATION
Full Citation: Carrasco MA, Atkins K, Young R, RosenJG, Grieb SM, Wong VJ, Fleming PJ. The HIV pandemicprevention e!orts can inform the COVID-19 pan-demic response in the United States. Am J PublicHealth. 2021;111(4): e1–e4.
Acceptance Date: January 4, 2021.
DOI: https://doi.org/10.2105/AJPH.2021.306158
CONTRIBUTORS
All authors contributed equally to this article.
ACKNOWLEDGMENTS
We are grateful to Jason Reed for reviewing anearlier draft of this article and providing comments.
CONFLICTS OF INTEREST
There are no con$icts of interest to disclose.
REFERENCES
1. Parmet WE, Paul J. COVID-19: the "rst posttruthpandemic. Am J Public Health. 2020;110(7):945–946.https://doi.org/10.2105/AJPH.2020.305721
2. Carrasco MA, Wilkinson J, Kasdan B, Fleming P.Systematic review of barriers and facilitators tovoluntary medical male circumcision in prioritycountries and programmatic implications for serviceuptake. Glob Public Health. 2019;14(1):91–111.https://doi.org/10.1080/17441692.2018.1465108
3. Gold E, Carrasco MA, Sallet J, et al. Guide on high-impact practices to create demand for voluntarymedical male circumcision services. StrengtheningHigh-Impact Interventions for an AIDS-FreeGeneration (AIDSFree) Project. 2019. Available at:https://www.malecircumcision.org/resource/guide-high-impact-practices-create-demand-voluntary-medical-male-circumcision-services.Accessed September 8, 2020.
4. Trevisan M, Le LC, Le AV. The COVID-19 pandemic: aview from Vietnam. Am J Public Health. 2020;110(8):1152–1153. https://doi.org/10.2105/AJPH.2020.305751
5. Halperin DT. Coping with COVID-19: learning frompast pandemics to avoid pitfalls and panic. GlobHealth Sci Pract. 2020;8(2):155–165. https://doi.org/10.9745/GHSP-D-20-00189
Editorials Carrasco et al.
EDITORIALS
AJPH
April2021,Vol111,No.4
118

6. Peterson PL, Dime! LA, Tapert SF, SternM, GormanM. Harm reduction and HIV/AIDS prevention. In:Marlatt GA, ed. Harm Reduction: PragmaticStrategies for Managing High-Risk Behaviors. NewYork, NY: The Guilford Press; 1998:218–297.
7. Kutscher E, Greene RE. A harm-reduction approachto coronavirus disease 2019 (COVID-19)–safersocializing. JAMA Health Forum. 2020;1(6):e200656.https://doi.org/10.1001/jamahealthforum.2020.0656
8. Joint United Nations Programme on HIV/AIDS. TheGap Report. 2014. Available at: http://"les.unaids.org/en/media/unaids/contentassets/documents/unaidspublication/2014/UNAIDS_Gap_report_en.pdf. Accessed September 20, 2020.
9. Anderson S-J, Cherutich P, Kilonzo N, et al.Maximising the e!ect of combination HIVprevention through prioritisation of the people andplaces in greatest need: a modelling study. Lancet.2014;384(9939):249–256. https://doi.org/10.1016/S0140-6736(14)61053-9
10. Lin F, Farnham PG, Shrestha RK, Mermin J, SansomSL. Cost e!ectiveness of HIV preventioninterventions in the U.S. Am J Prev Med. 2016;50(6):699–708. https://doi.org/10.1016/j.amepre.2016.01.011
11. Oppel RA Jr, Gebelo! R, Lai KKR, Wright W, Smith M.The fullest look yet at the racial inequity ofcoronavirus. New York Times. July 5, 2020. Availableat: https://www.nytimes.com/interactive/2020/07/05/us/coronavirus-latinos-african-americans-cdc-data.html. Accessed September 7, 2020.
12. Reed JB, Patel RR, Baggaley R. Lessons from adecade of voluntary medical male circumcisionimplementation and their application to HIV pre-exposure prophylaxis scale up. Int J STD AIDS. 2018;29(14):1432–1443. https://doi.org/10.1177/0956462418787896
13. Atkins K, Yeh PT, Kennedy CE, et al. Service deliveryinterventions to increase uptake of voluntarymedical male circumcision for HIV prevention: asystematic review. PLoS One. 2020;15(1):e0227755.https://doi.org/10.1371/journal.pone.0227755
14. Stankevitz K, Schwartz K, Hoke T, et al. Reaching at-risk women for PrEP delivery: what can we learnfrom clinical trials in sub-Saharan Africa? PLoS One.2019;14(6):e0218556. https://doi.org/10.1371/journal.pone.0218556
15. World Health Organization. Consolidated Guidelineson HIV Testing Services. 2016. Available at: https://www.who.int/hiv/pub/guidelines/hiv-testing-services/en. Accessed August 30, 2020.
Editorials Carrasco et al.
EDITORIALS
AJPH
April
2021
,Vol
111,
No.
4
119
Morbidity and Mortality Weekly ReportWeekly / Vol. 69 / No. 48 December 4, 2020
Sex Differences in HIV Testing — 20 PEPFAR-Supported Sub-Saharan African Countries, 2019
Bakary Drammeh, DrPH1; Amy Medley, PhD1; Helen Dale, BVSc, MBChB1; Anindya K. De, PhD1; Shane Diekman, PhD1; Randy Yee, MSc1; Tiffiany Aholou, PhD1; Arielle Lasry, PhD1; Andrew Auld, MD2; Brittney Baack, MPH2; Wayne Duffus, MD, PhD1; Ebrahim Shahul, MD1; Vincent Wong,
MSc3; Michael Grillo, PhD4; Teeb Al-Samarrai, MD5; Shabeen Ally, PhD5; Mtemwa Nyangulu, MCHD2; Rose Nyirenda, MD6; Jacobus Olivier, PhD7; Thato Chidarikire, PhD8; Nompumelelo Khanyile, MBA9; Alick A. Kayange, MD10; Oscar Ernest Rwabiyago, MD11; Upendo Kategile, MSc12; Jema Bisimba, MPH12; Rachel A. Weber, PhD13; Gertrude Ncube, MPH14; Onesimo Maguwu, MPH15; Ismelda Pietersen, MPH16; Denis Mali, MD17;
Edington Dzinotyiweyi, MA18; Lisa Nelson, MD19; Matovu John Bosco, MPH20; Kwarisiima Dalsone, MD21; Madina Apolot, MSc19; Samson Anangwe, MSc22; Leonard K. Soo, MPH23; Mary Mugambi, MD24; Andre Mbayiha, MD25; Placidie Mugwaneza, MPH26; Samuel S. Malamba, PhD27; Arlene
Phiri, MCD28; Tina Chisenga, MD29; Mary Boyd, MD30; Chanie Temesgan, MD31; Mesfin Shimelis, MD31; Teklu Weldegebreal, MD32; Mirtie Getachew, MPH33; Shirish Balachandra, MD34; Ehui Eboi, PhD35; Willibord Shasha, MD36; Nicole Doumatey, MSc34; Didier Adjoua, MD37; Chidozie Meribe, MD38; Jerry Gwamna, MD38; Pamela Gado, MPH39; Ima John-Dada, MSc40 ; Elie Mukinda, MD41; Luc F. Kamanga Lukusa, MD42; Lucien
Kalenga, MD43; Sudhir Bunga, MD44; Victoria Achyut, MD45; John Mondi, MSc44; Peter Loeto, MSc46; Goabaone Mogomotsi, MPH47; Jenny Ledikwe, PhD48; Puleng Ramphalla, MSc49; Mphotleng Tlhomola, MSc50; Justine K. Mirembe, MBA51; Tse Nkwoh, MPH52; Laura Eno, MSc52; Leonard Bonono, MSc53; Nely Honwana, MA54; Noela Chicuecue, MD55; Ana Simbine MSc56; Inacio Malimane, MD54; Lenhle Dube, BSc57; Munamato
Mirira, MSc58; Phumzile Mndzebele, MPH59; Alean Frawley, DO60; Yolanda Marina Rebello Cardo, MSc60; Stephanie Behel, MPH1
Despite progress toward controlling the human immunode-ficiency virus (HIV) epidemic, testing gaps remain, particularly among men and young persons in sub-Saharan Africa (1). This observational study used routinely collected programmatic data from 20 African countries reported to the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) from October 2018 to September 2019 to assess HIV testing coverage and case finding among adults (defined as persons aged !15 years). Indicators included number of HIV tests conducted, number of HIV-positive test results, and percentage positivity rate. Overall, the majority of countries reported higher HIV case finding among women than among men. However, a slightly higher percentage positivity was recorded among men (4.7%) than among women (4.1%). Provider-initiated counseling and testing (PITC) in health facilities identified approximately two thirds of all new cases, but index testing had the highest percentage positivity in all countries among both sexes. Yields from voluntary counseling and testing (VCT) and mobile testing varied by sex and by country. These findings highlight the need to identify and implement the most efficient strate-gies for HIV case finding in these countries to close coverage
Continuing Education examination available at https://www.cdc.gov/mmwr/mmwr_continuingEducation.html
INSIDE1807 Multidisciplinary Community-Based Investigation
of a COVID-19 Outbreak Among Marshallese and Hispanic/Latino Communities — Benton and Washington Counties, Arkansas, March–June 2020
1812 Disproportionate Incidence of COVID-19 Infection, Hospitalizations, and Deaths Among Persons Identifying as Hispanic or Latino — Denver, Colorado March–October 2020
1817 Regional Analysis of Coccidioidomycosis Incidence — California, 2000–2018
1822 Survey of Teen Noise Exposure and E!orts to Protect Hearing at School — United States, 2020
1827 Increase in Hospital-Acquired Carbapenem-Resistant Acinetobacter baumannii Infection and Colonization in an Acute Care Hospital During a Surge in COVID-19 Admissions — New Jersey, February–July 2020
1832 Notes from the Field: Interpretation of Rapid Diagnostic Tests for Leptospirosis During a Dengue Outbreak — Yap State, Federated States of Micronesia, 2019
1838 QuickStats
U.S. Department of Health and Human ServicesCenters for Disease Control and Prevention
120

Morbidity and Mortality Weekly Report
MMWR / December 4, 2020 / Vol. 69 / No. 48 US Department of Health and Human Services/Centers for Disease Control and Prevention
The MMWR series of publications is published by the Center for Surveillance, Epidemiology, and Laboratory Services, Centers for Disease Control and Prevention (CDC), U.S. Department of Health and Human Services, Atlanta, GA 30329-4027.Suggested citation: [Author names; first three, then et al., if more than six.] [Report title]. MMWR Morb Mortal Wkly Rep 2020;69:[inclusive page numbers].
Centers for Disease Control and PreventionRobert R. Redfield, MD, Director
Anne Schuchat, MD, Principal Deputy DirectorIleana Arias, PhD, Acting Deputy Director for Public Health Science and Surveillance
Rebecca Bunnell, PhD, MEd, Director, Office of ScienceJennifer Layden, MD, PhD, Deputy Director, Office of Science
Michael F. Iademarco, MD, MPH, Director, Center for Surveillance, Epidemiology, and Laboratory Services
MMWR Editorial and Production Staff (Weekly)Charlotte K. Kent, PhD, MPH, Editor in Chief
Jacqueline Gindler, MD, EditorPaul Z. Siegel, MD, MPH, Guest Associate Editor
Mary Dott, MD, MPH, Online EditorEmilio Dirlikov, PhD, Guest Associate Online Editor
Terisa F. Rutledge, Managing Editor Douglas W. Weatherwax, Lead Technical Writer-Editor
Glenn Damon, Soumya Dunworth, PhD, Teresa M. Hood, MS, Jeffrey D. Sokolow, MA,
Technical Writer-Editors
Martha F. Boyd, Lead Visual Information SpecialistAlexander J. Gottardy, Maureen A. Leahy,
Julia C. Martinroe, Stephen R. Spriggs, Tong Yang,Visual Information Specialists
Quang M. Doan, MBA, Phyllis H. King, Terraye M. Starr, Moua Yang,
Information Technology Specialists
MMWR Editorial BoardTimothy F. Jones, MD, Chairman
Matthew L. Boulton, MD, MPHCarolyn Brooks, ScD, MA
Jay C. Butler, MD Virginia A. Caine, MD
Jonathan E. Fielding, MD, MPH, MBADavid W. Fleming, MD
Kate Galatas, MPHWilliam E. Halperin, MD, DrPH, MPH
Jewel Mullen, MD, MPH, MPAJeff Niederdeppe, PhD
Celeste Philip, MD, MPHPatricia Quinlisk, MD, MPH
Patrick L. Remington, MD, MPH Carlos Roig, MS, MA
William Schaffner, MD Nathaniel Smith, MD, MPHMorgan Bobb Swanson, BS
Ian Branam, MA, Acting Lead Health Communication Specialist
Shelton Bartley, MPH,Lowery Johnson, Amanda Ray,
Jacqueline N. Sanchez, MS,Health Communication Specialists
Will Yang, MA,Visual Information Specialist
gaps. Strategies might need to be tailored for men who remain underrepresented in the majority of HIV testing programs.
In 2014, the Joint United Nations Programme on AIDS (UNAIDS) launched its 90–90–90 strategy for ending the global HIV pandemic: 90% of all persons living with HIV/AIDS (PLHIV) know their status; of these, 90% are receiving antiretroviral treatment (ART); and of these, 90% are virally suppressed (2). PEPFAR provides guidance on reaching these targets to all its supported countries (3). PEPFAR also col-lects data on standardized indicators as part of its Monitoring, Evaluation, and Reporting system (4). These data are collected by facility and community sites and are reported quarterly by each country program.
Routine program data reported to PEPFAR from October 2018 to September 2019 from 20 sub-Saharan African coun-tries and modeling data from UNAIDS were used to identify progress toward achieving the first of the three 90–90–90 goals. These countries were selected because they collectively repre-sent the highest HIV prevalence among PEPFAR-supported countries. Indicators used included the number of HIV tests conducted among adults, the number of HIV-positive test results, and yield (or percentage positivity) defined as the number of positive test results divided by the total number of tests reported. Results for each country are presented overall and disaggregated by sex and testing strategy. Testing strategies include index testing (offering an HIV test to the partners and biologic children of PLHIV), PITC (providers recommending an HIV test as part of routine care), VCT (HIV testing at a
clinic dedicated to this purpose), and mobile testing (HIV test-ing offered at an ad hoc location in the community [e.g., van, workplace, or school]).The standard test statistic for the differ-ence in proportions between men and women was computed on the basis of pooled variance formulation. P-values <0.05 were considered statistically significant for each pairwise dif-ference and were computed under the asymptomatic normality assumption (5). PITC was used as the reference strategy for comparisons among strategies because the highest number of new HIV cases are identified by PITC in sub-Saharan Africa (1). The percentage positivity for the three other strategies (index testing, VCT, and mobile testing) was compared with PITC for each country and by sex.
From October 2018 to September 2019, PEPFAR sup-ported 60,945,355 tests that identified 2,603,560 adults with positive HIV test results (5.0% yield; Table 1). Approximately one fifth (19.9%) of all testing occurred in South Africa. More women received tests than men (women, 40,263,510; men, 20,681,845). However, yield was slightly higher among men (970,100; 4.7% yield) than among women (1,633,460; 4.1% yield). Over one half (51.6%) of all HIV-positive results among men were reported by South Africa, Tanzania, and Zambia, and approximately one third (29.2%) were reported by South Africa alone.
Across the 19 countries (excluding Malawi because of limited data), PITC identified the most PLHIV (63.2%) compared with index testing (17.4%), VCT (11.0%), and mobile test-ing (8.4%). HIV case finding among men followed a similar
121
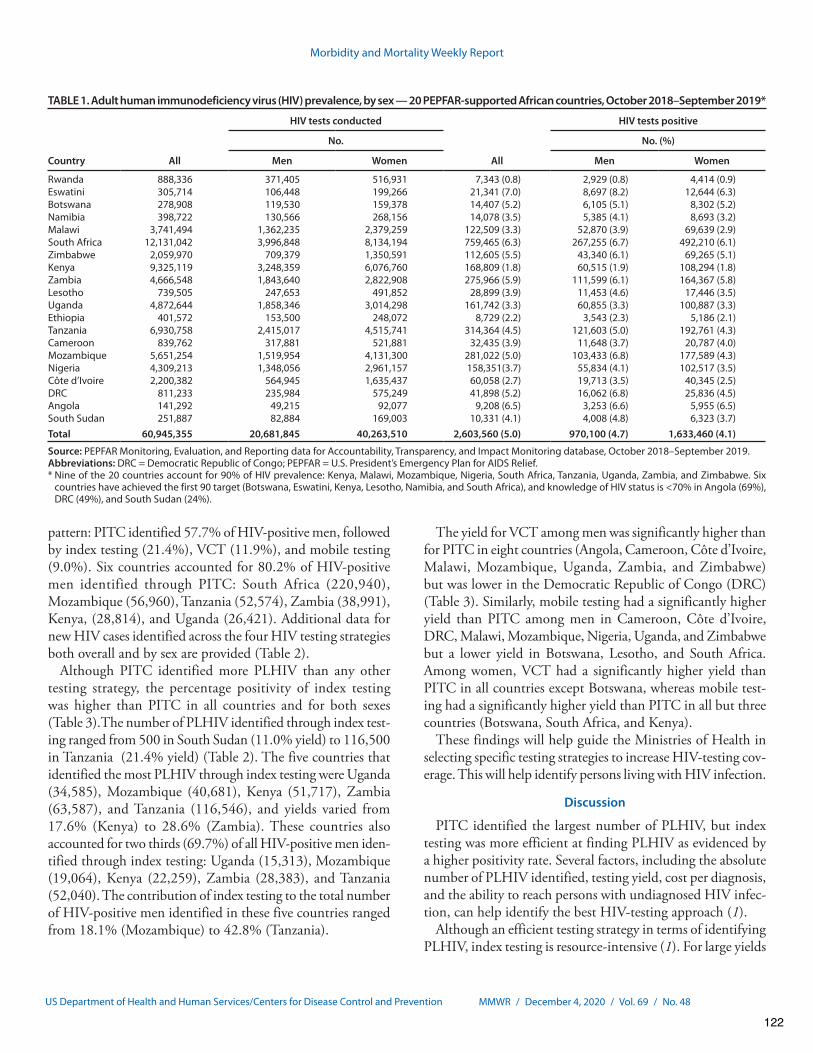
Morbidity and Mortality Weekly Report
MMWR / December 4, 2020 / Vol. 69 / No. 48 US Department of Health and Human Services/Centers for Disease Control and Prevention
TABLE 1. Adult human immunodeficiency virus (HIV) prevalence, by sex — 20 PEPFAR-supported African countries, October 2018–September 2019*
Country All
HIV tests conducted
All
HIV tests positive
No. No. (%)
Men Women Men Women
Rwanda 888,336 371,405 516,931 7,343 (0.8) 2,929 (0.8) 4,414 (0.9)Eswatini 305,714 106,448 199,266 21,341 (7.0) 8,697 (8.2) 12,644 (6.3)Botswana 278,908 119,530 159,378 14,407 (5.2) 6,105 (5.1) 8,302 (5.2)Namibia 398,722 130,566 268,156 14,078 (3.5) 5,385 (4.1) 8,693 (3.2)Malawi 3,741,494 1,362,235 2,379,259 122,509 (3.3) 52,870 (3.9) 69,639 (2.9)South Africa 12,131,042 3,996,848 8,134,194 759,465 (6.3) 267,255 (6.7) 492,210 (6.1)Zimbabwe 2,059,970 709,379 1,350,591 112,605 (5.5) 43,340 (6.1) 69,265 (5.1)Kenya 9,325,119 3,248,359 6,076,760 168,809 (1.8) 60,515 (1.9) 108,294 (1.8)Zambia 4,666,548 1,843,640 2,822,908 275,966 (5.9) 111,599 (6.1) 164,367 (5.8)Lesotho 739,505 247,653 491,852 28,899 (3.9) 11,453 (4.6) 17,446 (3.5)Uganda 4,872,644 1,858,346 3,014,298 161,742 (3.3) 60,855 (3.3) 100,887 (3.3)Ethiopia 401,572 153,500 248,072 8,729 (2.2) 3,543 (2.3) 5,186 (2.1)Tanzania 6,930,758 2,415,017 4,515,741 314,364 (4.5) 121,603 (5.0) 192,761 (4.3)Cameroon 839,762 317,881 521,881 32,435 (3.9) 11,648 (3.7) 20,787 (4.0)Mozambique 5,651,254 1,519,954 4,131,300 281,022 (5.0) 103,433 (6.8) 177,589 (4.3)Nigeria 4,309,213 1,348,056 2,961,157 158,351(3.7) 55,834 (4.1) 102,517 (3.5)Côte d’Ivoire 2,200,382 564,945 1,635,437 60,058 (2.7) 19,713 (3.5) 40,345 (2.5)DRC 811,233 235,984 575,249 41,898 (5.2) 16,062 (6.8) 25,836 (4.5)Angola 141,292 49,215 92,077 9,208 (6.5) 3,253 (6.6) 5,955 (6.5)South Sudan 251,887 82,884 169,003 10,331 (4.1) 4,008 (4.8) 6,323 (3.7)Total 60,945,355 20,681,845 40,263,510 2,603,560 (5.0) 970,100 (4.7) 1,633,460 (4.1)
Source: PEPFAR Monitoring, Evaluation, and Reporting data for Accountability, Transparency, and Impact Monitoring database, October 2018–September 2019.Abbreviations: DRC = Democratic Republic of Congo; PEPFAR = U.S. President’s Emergency Plan for AIDS Relief.* Nine of the 20 countries account for 90% of HIV prevalence: Kenya, Malawi, Mozambique, Nigeria, South Africa, Tanzania, Uganda, Zambia, and Zimbabwe. Six
countries have achieved the first 90 target (Botswana, Eswatini, Kenya, Lesotho, Namibia, and South Africa), and knowledge of HIV status is <70% in Angola (69%), DRC (49%), and South Sudan (24%).
pattern: PITC identified 57.7% of HIV-positive men, followed by index testing (21.4%), VCT (11.9%), and mobile testing (9.0%). Six countries accounted for 80.2% of HIV-positive men identified through PITC: South Africa (220,940), Mozambique (56,960), Tanzania (52,574), Zambia (38,991), Kenya, (28,814), and Uganda (26,421). Additional data for new HIV cases identified across the four HIV testing strategies both overall and by sex are provided (Table 2).
Although PITC identified more PLHIV than any other testing strategy, the percentage positivity of index testing was higher than PITC in all countries and for both sexes (Table 3).The number of PLHIV identified through index test-ing ranged from 500 in South Sudan (11.0% yield) to 116,500 in Tanzania (21.4% yield) (Table 2). The five countries that identified the most PLHIV through index testing were Uganda (34,585), Mozambique (40,681), Kenya (51,717), Zambia (63,587), and Tanzania (116,546), and yields varied from 17.6% (Kenya) to 28.6% (Zambia). These countries also accounted for two thirds (69.7%) of all HIV-positive men iden-tified through index testing: Uganda (15,313), Mozambique (19,064), Kenya (22,259), Zambia (28,383), and Tanzania (52,040). The contribution of index testing to the total number of HIV-positive men identified in these five countries ranged from 18.1% (Mozambique) to 42.8% (Tanzania).
The yield for VCT among men was significantly higher than for PITC in eight countries (Angola, Cameroon, Côte d’Ivoire, Malawi, Mozambique, Uganda, Zambia, and Zimbabwe) but was lower in the Democratic Republic of Congo (DRC) (Table 3). Similarly, mobile testing had a significantly higher yield than PITC among men in Cameroon, Côte d’Ivoire, DRC, Malawi, Mozambique, Nigeria, Uganda, and Zimbabwe but a lower yield in Botswana, Lesotho, and South Africa. Among women, VCT had a significantly higher yield than PITC in all countries except Botswana, whereas mobile test-ing had a significantly higher yield than PITC in all but three countries (Botswana, South Africa, and Kenya).
These findings will help guide the Ministries of Health in selecting specific testing strategies to increase HIV-testing cov-erage. This will help identify persons living with HIV infection.
Discussion
PITC identified the largest number of PLHIV, but index testing was more efficient at finding PLHIV as evidenced by a higher positivity rate. Several factors, including the absolute number of PLHIV identified, testing yield, cost per diagnosis, and the ability to reach persons with undiagnosed HIV infec-tion, can help identify the best HIV-testing approach (1).
Although an efficient testing strategy in terms of identifying PLHIV, index testing is resource-intensive (1). For large yields
122
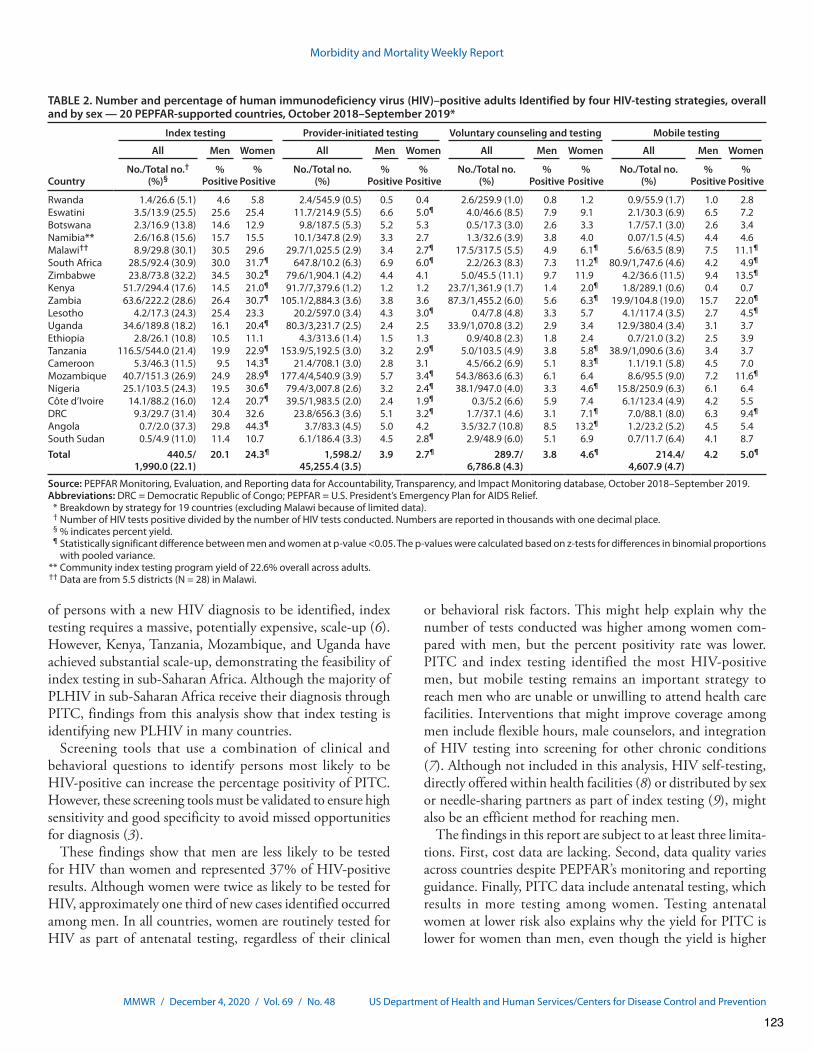
Morbidity and Mortality Weekly Report
MMWR / December 4, 2020 / Vol. 69 / No. 48 US Department of Health and Human Services/Centers for Disease Control and Prevention
TABLE 2. Number and percentage of human immunodeficiency virus (HIV)–positive adults Identified by four HIV-testing strategies, overall and by sex — 20 PEPFAR-supported countries, October 2018–September 2019*
Country
Index testing Provider-initiated testing Voluntary counseling and testing Mobile testing
All Men Women All Men Women All Men Women All Men Women
No./Total no.† (%)§
% Positive
% Positive
No./Total no. (%)
% Positive
% Positive
No./Total no. (%)
% Positive
% Positive
No./Total no. (%)
% Positive
% Positive
Rwanda 1.4/26.6 (5.1) 4.6 5.8 2.4/545.9 (0.5) 0.5 0.4 2.6/259.9 (1.0) 0.8 1.2 0.9/55.9 (1.7) 1.0 2.8Eswatini 3.5/13.9 (25.5) 25.6 25.4 11.7/214.9 (5.5) 6.6 5.0¶ 4.0/46.6 (8.5) 7.9 9.1 2.1/30.3 (6.9) 6.5 7.2Botswana 2.3/16.9 (13.8) 14.6 12.9 9.8/187.5 (5.3) 5.2 5.3 0.5/17.3 (3.0) 2.6 3.3 1.7/57.1 (3.0) 2.6 3.4Namibia** 2.6/16.8 (15.6) 15.7 15.5 10.1/347.8 (2.9) 3.3 2.7 1.3/32.6 (3.9) 3.8 4.0 0.07/1.5 (4.5) 4.4 4.6Malawi†† 8.9/29.8 (30.1) 30.5 29.6 29.7/1,025.5 (2.9) 3.4 2.7¶ 17.5/317.5 (5.5) 4.9 6.1¶ 5.6/63.5 (8.9) 7.5 11.1¶
South Africa 28.5/92.4 (30.9) 30.0 31.7¶ 647.8/10.2 (6.3) 6.9 6.0¶ 2.2/26.3 (8.3) 7.3 11.2¶ 80.9/1,747.6 (4.6) 4.2 4.9¶
Zimbabwe 23.8/73.8 (32.2) 34.5 30.2¶ 79.6/1,904.1 (4.2) 4.4 4.1 5.0/45.5 (11.1) 9.7 11.9 4.2/36.6 (11.5) 9.4 13.5¶
Kenya 51.7/294.4 (17.6) 14.5 21.0¶ 91.7/7,379.6 (1.2) 1.2 1.2 23.7/1,361.9 (1.7) 1.4 2.0¶ 1.8/289.1 (0.6) 0.4 0.7Zambia 63.6/222.2 (28.6) 26.4 30.7¶ 105.1/2,884.3 (3.6) 3.8 3.6 87.3/1,455.2 (6.0) 5.6 6.3¶ 19.9/104.8 (19.0) 15.7 22.0¶
Lesotho 4.2/17.3 (24.3) 25.4 23.3 20.2/597.0 (3.4) 4.3 3.0¶ 0.4/7.8 (4.8) 3.3 5.7 4.1/117.4 (3.5) 2.7 4.5¶
Uganda 34.6/189.8 (18.2) 16.1 20.4¶ 80.3/3,231.7 (2.5) 2.4 2.5 33.9/1,070.8 (3.2) 2.9 3.4 12.9/380.4 (3.4) 3.1 3.7Ethiopia 2.8/26.1 (10.8) 10.5 11.1 4.3/313.6 (1.4) 1.5 1.3 0.9/40.8 (2.3) 1.8 2.4 0.7/21.0 (3.2) 2.5 3.9Tanzania 116.5/544.0 (21.4) 19.9 22.9¶ 153.9/5,192.5 (3.0) 3.2 2.9¶ 5.0/103.5 (4.9) 3.8 5.8¶ 38.9/1,090.6 (3.6) 3.4 3.7Cameroon 5.3/46.3 (11.5) 9.5 14.3¶ 21.4/708.1 (3.0) 2.8 3.1 4.5/66.2 (6.9) 5.1 8.3¶ 1.1/19.1 (5.8) 4.5 7.0Mozambique 40.7/151.3 (26.9) 24.9 28.9¶ 177.4/4,540.9 (3.9) 5.7 3.4¶ 54.3/863.6 (6.3) 6.1 6.4 8.6/95.5 (9.0) 7.2 11.6¶
Nigeria 25.1/103.5 (24.3) 19.5 30.6¶ 79.4/3,007.8 (2.6) 3.2 2.4¶ 38.1/947.0 (4.0) 3.3 4.6¶ 15.8/250.9 (6.3) 6.1 6.4Côte d’Ivoire 14.1/88.2 (16.0) 12.4 20.7¶ 39.5/1,983.5 (2.0) 2.4 1.9¶ 0.3/5.2 (6.6) 5.9 7.4 6.1/123.4 (4.9) 4.2 5.5DRC 9.3/29.7 (31.4) 30.4 32.6 23.8/656.3 (3.6) 5.1 3.2¶ 1.7/37.1 (4.6) 3.1 7.1¶ 7.0/88.1 (8.0) 6.3 9.4¶
Angola 0.7/2.0 (37.3) 29.8 44.3¶ 3.7/83.3 (4.5) 5.0 4.2 3.5/32.7 (10.8) 8.5 13.2¶ 1.2/23.2 (5.2) 4.5 5.4South Sudan 0.5/4.9 (11.0) 11.4 10.7 6.1/186.4 (3.3) 4.5 2.8¶ 2.9/48.9 (6.0) 5.1 6.9 0.7/11.7 (6.4) 4.1 8.7Total 440.5/
1,990.0 (22.1)20.1 24.3¶ 1,598.2/
45,255.4 (3.5)3.9 2.7¶ 289.7/
6,786.8 (4.3)3.8 4.6¶ 214.4/
4,607.9 (4.7)4.2 5.0¶
Source: PEPFAR Monitoring, Evaluation, and Reporting data for Accountability, Transparency, and Impact Monitoring database, October 2018–September 2019. Abbreviations: DRC = Democratic Republic of Congo; PEPFAR = U.S. President’s Emergency Plan for AIDS Relief. * Breakdown by strategy for 19 countries (excluding Malawi because of limited data). † Number of HIV tests positive divided by the number of HIV tests conducted. Numbers are reported in thousands with one decimal place. § % indicates percent yield. ¶ Statistically significant difference between men and women at p-value <0.05. The p-values were calculated based on z-tests for differences in binomial proportions
with pooled variance. ** Community index testing program yield of 22.6% overall across adults. †† Data are from 5.5 districts (N = 28) in Malawi.
of persons with a new HIV diagnosis to be identified, index testing requires a massive, potentially expensive, scale-up (6). However, Kenya, Tanzania, Mozambique, and Uganda have achieved substantial scale-up, demonstrating the feasibility of index testing in sub-Saharan Africa. Although the majority of PLHIV in sub-Saharan Africa receive their diagnosis through PITC, findings from this analysis show that index testing is identifying new PLHIV in many countries.
Screening tools that use a combination of clinical and behavioral questions to identify persons most likely to be HIV-positive can increase the percentage positivity of PITC. However, these screening tools must be validated to ensure high sensitivity and good specificity to avoid missed opportunities for diagnosis (3).
These findings show that men are less likely to be tested for HIV than women and represented 37% of HIV-positive results. Although women were twice as likely to be tested for HIV, approximately one third of new cases identified occurred among men. In all countries, women are routinely tested for HIV as part of antenatal testing, regardless of their clinical
or behavioral risk factors. This might help explain why the number of tests conducted was higher among women com-pared with men, but the percent positivity rate was lower. PITC and index testing identified the most HIV-positive men, but mobile testing remains an important strategy to reach men who are unable or unwilling to attend health care facilities. Interventions that might improve coverage among men include flexible hours, male counselors, and integration of HIV testing into screening for other chronic conditions (7). Although not included in this analysis, HIV self-testing, directly offered within health facilities (8) or distributed by sex or needle-sharing partners as part of index testing (9), might also be an efficient method for reaching men.
The findings in this report are subject to at least three limita-tions. First, cost data are lacking. Second, data quality varies across countries despite PEPFAR’s monitoring and reporting guidance. Finally, PITC data include antenatal testing, which results in more testing among women. Testing antenatal women at lower risk also explains why the yield for PITC is lower for women than men, even though the yield is higher
123
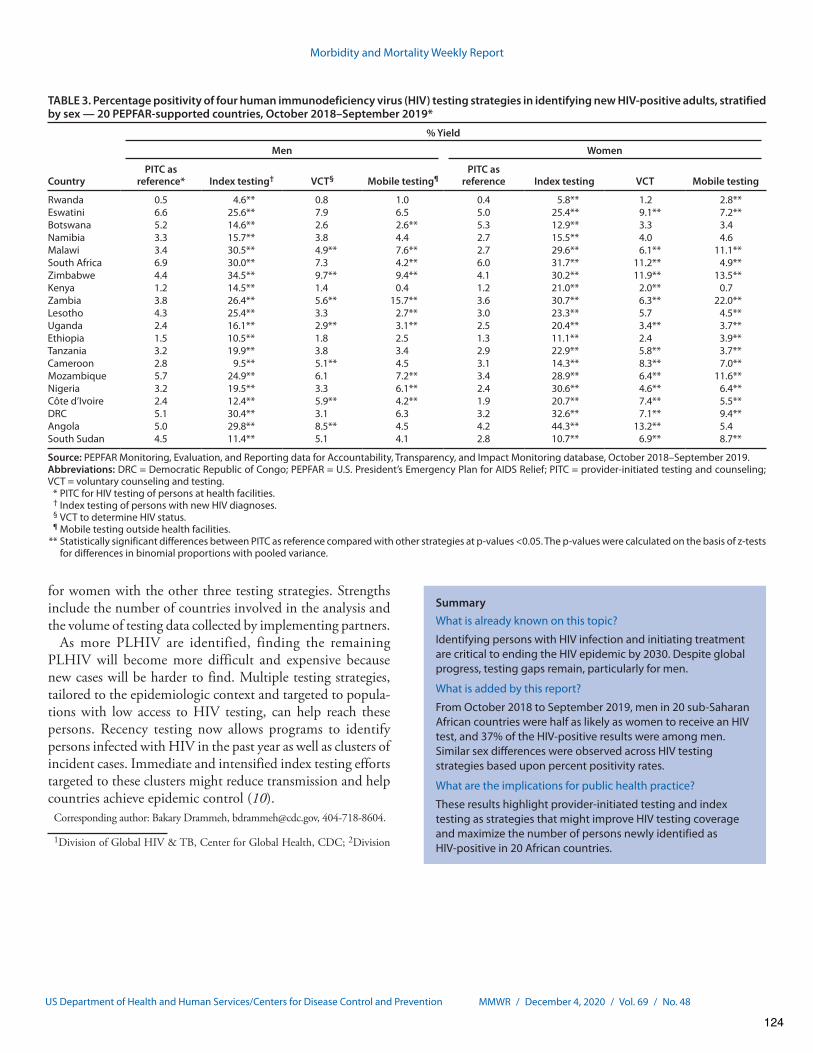
Morbidity and Mortality Weekly Report
MMWR / December 4, 2020 / Vol. 69 / No. 48 US Department of Health and Human Services/Centers for Disease Control and Prevention
TABLE 3. Percentage positivity of four human immunodeficiency virus (HIV) testing strategies in identifying new HIV-positive adults, stratified by sex — 20 PEPFAR-supported countries, October 2018–September 2019*
Country
% Yield
Men Women
PITC as reference* Index testing† VCT§ Mobile testing¶
PITC as reference Index testing VCT Mobile testing
Rwanda 0.5 4.6** 0.8 1.0 0.4 5.8** 1.2 2.8**Eswatini 6.6 25.6** 7.9 6.5 5.0 25.4** 9.1** 7.2**Botswana 5.2 14.6** 2.6 2.6** 5.3 12.9** 3.3 3.4Namibia 3.3 15.7** 3.8 4.4 2.7 15.5** 4.0 4.6Malawi 3.4 30.5** 4.9** 7.6** 2.7 29.6** 6.1** 11.1**South Africa 6.9 30.0** 7.3 4.2** 6.0 31.7** 11.2** 4.9**Zimbabwe 4.4 34.5** 9.7** 9.4** 4.1 30.2** 11.9** 13.5**Kenya 1.2 14.5** 1.4 0.4 1.2 21.0** 2.0** 0.7Zambia 3.8 26.4** 5.6** 15.7** 3.6 30.7** 6.3** 22.0**Lesotho 4.3 25.4** 3.3 2.7** 3.0 23.3** 5.7 4.5**Uganda 2.4 16.1** 2.9** 3.1** 2.5 20.4** 3.4** 3.7**Ethiopia 1.5 10.5** 1.8 2.5 1.3 11.1** 2.4 3.9**Tanzania 3.2 19.9** 3.8 3.4 2.9 22.9** 5.8** 3.7**Cameroon 2.8 9.5** 5.1** 4.5 3.1 14.3** 8.3** 7.0**Mozambique 5.7 24.9** 6.1 7.2** 3.4 28.9** 6.4** 11.6**Nigeria 3.2 19.5** 3.3 6.1** 2.4 30.6** 4.6** 6.4**Côte d’Ivoire 2.4 12.4** 5.9** 4.2** 1.9 20.7** 7.4** 5.5**DRC 5.1 30.4** 3.1 6.3 3.2 32.6** 7.1** 9.4**Angola 5.0 29.8** 8.5** 4.5 4.2 44.3** 13.2** 5.4South Sudan 4.5 11.4** 5.1 4.1 2.8 10.7** 6.9** 8.7**
Source: PEPFAR Monitoring, Evaluation, and Reporting data for Accountability, Transparency, and Impact Monitoring database, October 2018–September 2019.Abbreviations: DRC = Democratic Republic of Congo; PEPFAR = U.S. President’s Emergency Plan for AIDS Relief; PITC = provider-initiated testing and counseling; VCT = voluntary counseling and testing. * PITC for HIV testing of persons at health facilities. † Index testing of persons with new HIV diagnoses. § VCT to determine HIV status. ¶ Mobile testing outside health facilities. ** Statistically significant differences between PITC as reference compared with other strategies at p-values <0.05. The p-values were calculated on the basis of z-tests
for differences in binomial proportions with pooled variance.
for women with the other three testing strategies. Strengths include the number of countries involved in the analysis and the volume of testing data collected by implementing partners.
As more PLHIV are identified, finding the remaining PLHIV will become more difficult and expensive because new cases will be harder to find. Multiple testing strategies, tailored to the epidemiologic context and targeted to popula-tions with low access to HIV testing, can help reach these persons. Recency testing now allows programs to identify persons infected with HIV in the past year as well as clusters of incident cases. Immediate and intensified index testing efforts targeted to these clusters might reduce transmission and help countries achieve epidemic control (10).
Corresponding author: Bakary Drammeh, [email protected], 404-718-8604.
1Division of Global HIV & TB, Center for Global Health, CDC; 2Division
SummaryWhat is already known on this topic?Identifying persons with HIV infection and initiating treatment are critical to ending the HIV epidemic by 2030. Despite global progress, testing gaps remain, particularly for men.
What is added by this report?From October 2018 to September 2019, men in 20 sub-Saharan African countries were half as likely as women to receive an HIV test, and 37% of the HIV-positive results were among men. Similar sex differences were observed across HIV testing strategies based upon percent positivity rates.
What are the implications for public health practice?These results highlight provider-initiated testing and index testing as strategies that might improve HIV testing coverage and maximize the number of persons newly identified as HIV-positive in 20 African countries.
124

Morbidity and Mortality Weekly Report
MMWR / December 4, 2020 / Vol. 69 / No. 48 US Department of Health and Human Services/Centers for Disease Control and Prevention
of Global HIV & TB, Center for Global Health, CDC Malawi; 3US Agency for International Development, Office of HIV/AIDS, Washington, DC; 4US Department of Defense, HIV/AIDS Prevention Program; 5Office of the US Global AIDS Coordinator and Health Diplomacy, US Department of State; 6Ministry of Health, Malawi; 7Division of Global HIV & TB, Center for Global Health, CDC South Africa; 8HIV Prevention Programmes, National Department of Health, Ministry of Health, South Africa; 9US Agency for International Development, South Africa; 10US Department of Defense, HIV/AIDS Program, Tanzania; 11Division of Global HIV & TB, Center for Global Health, CDC Tanzania; 12US Agency for International Development, Tanzania; 13Division of Global HIV & TB, Center for Global Health, CDC Zimbabwe; 14Ministry of Health, Zimbabwe; 15US Agency for International Development, Zimbabwe; 16Division of Global HIV & TB, Center for Global Health, CDC Namibia; 17US Agency for International Development, Namibia; 18Ministry of Health and Social Services, Namibia; 19Division of Global HIV & TB, Center for Global Health, CDC Uganda; 20Ministry of Health, Uganda; 21US Agency for International Development Uganda; 22Department of Defence, Kenya; 23US Agency for International Development, Kenya; 24Ministry of Health, Kenya; 25Division of Global HIV & TB, Center for Global Health, CDC Rwanda; 26 Ministry of Health, Rwanda; 27Division of Global HIV & TB, Center for Global Health, CDC Rwanda; 28US Agency for International Development, Zambia; 29Ministry of Health, Zambia; 30Division of Global HIV & TB, Center for Global Health, CDC Zambia; 31Division of Global HIV & TB, Center for Global Health, CDC Ethiopia; 32US Agency for International Development, Ethiopia; 33Federal Ministry of Health, Ethiopia; 34Division of Global HIV & TB, Center for Global Health, CDC Côte D’Ivoire; 35Ministry of Health, Côte D’Ivoire; 36US Agency for International Development, Côte D’Ivoire; 37Department of Defense, Côte D’Ivoire; 38Division of Global HIV & TB, Center for Global Health, CDC Nigeria; 39US Agency for International Development, Nigeria; 40Federal Ministry of Health, Nigeria; 41Division of Global HIV & TB, Center for Global Health, CDC Democratic Republic of Congo; 42Ministry of Health, Democratic Republic of Congo; 43US Agency for International Development, Democratic Republic of Congo; 44Division of Global HIV & TB, Center for Global Health, CDC South Sudan; 45Ministry of Health, South Sudan; 46Division of Global HIV & TB, Center for Global Health, CDC Botswana; 47Ministry of Health, Botswana; 48International Training and Education Center, Botswana; 49Division of Global HIV & TB, Center for Global Health, CDC Lesotho; 50Ministry of Health, Lesotho; 51US Agency for International Development, Lesotho; 52Division of Global HIV & TB, Center for Global Health, CDC Cameroon; 53Ministry of Health, Cameroon; 54Division of Global HIV & TB, Center for Global Health, CDC Mozambique; 55Ministry of Health, Mozambique; 56US Agency for International Development, Mozambique; 57Ministry of Health, Eswatini; 58US Agency for International Development, Eswatini; 59Division of Global HIV & TB, Center for Global Health, CDC Eswatini; 60Division of Global HIV & TB, Center for Global Health, CDC Angola.
References 1. De Cock KM, Barker JL, Baggaley R, El Sadr WM. Where are the
positives? HIV testing in sub-Saharan Africa in the era of test and treat. AIDS 2019;33:349–52. PMID:30557162 https://doi.org/10.1097/QAD.0000000000002096
2. Joint United Nations Programme on HIV/AIDS (UNAIDS). 90–90–90: an ambitious treatment target to help end the AIDS Epidemic. Geneva, Switzerland: UNAIDS; 2014. https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf
3. US President’s Emergency Plan for AIDS Relief. PEPFAR 2020 country operational plan guidance for all PEPFAR countries. Washington, DC: US President’s Emergency Plan for AIDS Relief; 2020. https://www.state.gov/wp-content/uploads/2020/01/COP20-Guidance_Final-1-15-2020.pdf
4. US President’s Emergency Plan for AIDS Relief. Monitoring, evaluation, and reporting indicator reference guide, version 2.4. Washington, DC: US President’s Emergency Plan for AIDS Relief; 2019. https://www.state.gov/wp-content/uploads/2019/10/PEPFAR-MER-Indicator-Reference-Guide-Version-2.4-FY20.pdf
5. Siegel and Castellan. Nonparametric statistics for the behavioral sciences. 2nd ed. New York, NY: McGraw-Hill; 1988.
6. Sharma M, Smith JA, Farquhar C, et al. Assisted partner notification services are cost-effective for decreasing HIV burden in western Kenya. AIDS 2018;32:233–41. PMID:29135576
7. Sharma M, Barnabas RV, Celum C. Community-based strategies to strengthen men’s engagement in the HIV care cascade in sub-Saharan Africa. PLoS Med 2017;14:e1002262. PMID:28399122 https://doi.org/10.1371/journal.pmed.1002262
8. Dovel K, Shaba F, Offorjebe OA, et al. Effect of facility-based HIV self-testing on uptake of testing among outpatients in Malawi: a cluster-randomised trial. Lancet Glob Health 2020;8:e276–87. PMID:31981557 https://doi.org/10.1016/S2214-109X(19)30534-0
9. Choko AT, Corbett EL, Stallard N, et al. HIV self-testing alone or with additional interventions, including financial incentives, and linkage to care or prevention among male partners of antenatal care clinic attendees in Malawi: an adaptive multi-arm, multi-stage cluster randomised trial. PLoS Med 2019;16:e1002719. PMID:30601823 https://doi.org/10.1371/journal.pmed.1002719
10. Kim AA, Behel S, Northbrook S, Parekh BS. Tracking with recency assays to control the epidemic: real-time HIV surveillance and public health response. AIDS 2019;33:1527–9. PMID:31021850 https://doi.org/10.1097/QAD.0000000000002239
125

VIEWPOINT
Measuring linkage to HIV treatment services following HIVself-testing in low-income settingsAugustine T Choko1,2 , Muhammad S Jamil3,§ , Peter MacPherson1,4,5, Elizabeth Corbett1,5, Lastone Chitembo6,Heather Ingold7, Elkin Bermudez Aza8, Marc d’Elbee9, Meghan DiCarlo10, Mohammed Majam11, Tanya Shewchuk12,Vincent Wong13 , Rachel Baggaley3, Cheryl Johnson3 and on behalf of the World Health Organization HIV self-testing technical working group§Corresponding author: Muhammad S. Jamil, World Health Organization, Global HIV, Hepatitis and SITs Programmes, Ave Appia 20, Geneva, 1211, Switzerland. Tel:+41 227 913 225. ([email protected])
Keywords: HIV testing services; HIV self-testing; linkage; HIV care; monitoring and evaluation
Received 4 February 2020; Accepted 14 May 2020
Copyright © 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of International AIDS SocietyThis is an open access article under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium,provided the original work is properly cited.[Correction added on 22 July 2020, after first online publication: The author name has been corrected to Tanya Shewchuk in this version.]
Globally, HIV testing services (HTS) have been scaled upresulting in 79% of all people with HIV aware of their status in2018 [1]. However, 8.1 million people remain undiagnosed [1],many of whom are hard to reach through traditional HTSapproaches. In 2016, the World Health Organization (WHO)strongly recommended HIV self-testing (HIVST) as an HTSapproach, followed by an update in 2019 [2,3]. Since 2016, thenumber of countries with supportive HIVST policies has grownrapidly to 77 with 38 countries implementing HIVST as of July2019 [1]. HIVST has proved effective in reaching people withundiagnosed HIV and those at high ongoing risk [4-6], how-ever, many countries are yet to implement or scale up HIVST.As with any HTS, HIVST needs to provide a pathway to
appropriate HIV treatment, care and prevention services.Because no single test, including HIVST, can provide an HIV-positive diagnosis, all individuals with reactive HIVST resultsmust receive further testing by a trained provider before initi-ating antiretroviral therapy (ART) [5]. Measuring linkage toART is important to demonstrate programme effectivenessand impact, however, monitoring linkage after HIVST can bechallenging because of its private nature. We highlight keychallenges in measuring linkage to treatment and care follow-ing HIVST and suggest pragmatic approaches to addressingthese in low-income settings that routinely offer HIVST.Evidence from randomized trials shows that the proportion
of people linked to ART following HIVST is comparable to thatof standard facility-based HTS [5]. However, outside a researchor trial environment, it may be unclear whether routine pro-grammatic HIVST implementation results in similar successes.The challenges to accurately measuring linkage followingHIVST include: (i) not knowing the number of HIVST kits usedout of the number distributed, particularly when distributed in
the community or via secondary distribution to partners and/or social contacts; (ii) clients on ART using HIVST to “check”their HIV status without disclosing their HIV-positive statusand/or ART use to the provider (kit distributor); (iii) clientsusing HIVST as a prompt for “re-engaging” in care or “restart-ing” ART without disclosing their HIV-positive status and/orART use to the provider (kit distributor) [7]; (iv) clients withreactive HIVST results who are lost to follow-up; and (v) use ofpaper-based and unlinked clinic records, such as clinic registersor logbooks and the lack of case-based surveillance in manylow-income settings, leading to duplicate or missing informa-tion, an issue affecting HTS monitoring broadly.Given these challenges, measuring linkage in programmes at
the individual level following HIVST may not be feasible inmany low-income settings. Such an effort may requirerepeated follow-up with self-testers which can be resourceintensive in the absence of client information and linked elec-tronic records. Attempts by providers to ascertain the client’sHIVST results through repeated follow-up can also be per-ceived as being against client autonomy and could deterHIVST utilization in the future. Concerns about monitoringlinkage have kept several national HIV programmes from mak-ing HIVST available to clients. We believe that resource inten-sive monitoring efforts should not come in the way of makingHIVST widely available at the earliest. We give below a fewpragmatic approaches to measuring linkage to treatment ser-vices that programmes can consider and adapt depending ontheir local context.
i Monitor ART initiations at treatment centres/facilities before andduring HIVST distribution in the relevant catchment area [8,9].For example use of this approach in the HIV Self-Testing
Choko AT et al. Journal of the International AIDS Society 2020, 23:e25548http://onlinelibrary.wiley.com/doi/10.1002/jia2.25548/full | https://doi.org/10.1002/jia2.25548
126
Africa (STAR) Initiative showed a significant 27% increase inART initiations after introduction of HIVST [9]. Thisapproach will require the availability of reliable ART pro-gramme data and will be most useful for settings rapidlyscaling HIVST and seeking to achieve high coverage in speci-fic geographical settings and/or focus populations. Thesedata will give an indication of whether target populationsare being reached by HIVST kit distribution and whetherthose who are diagnosed are effectively linked to ART.However, careful interpretation is needed as increases inART initiations may not be attributable to HIVST alone, andcan be due to broader efforts to expand testing anddemand creation initiatives within the catchment area.
ii Include questions in clinic registers that can help to ascertain if thepresent clinic visit/testing was prompted by prior HIVST use. It isimportant to note that these data are subject to recall bias andsome people may not disclose prior HIVST use and/or resultsfor reasons such as stigma or to get a result from the providerwithout biases. These data also do not provide a denominatorto measure linkage following HIVST. Nonetheless, such datacan provide useful information on the proportion of ART initia-tions prompted by HIVST.
iii Population-based surveys such as demographic and health sur-veys, integrated bio-behavioural surveys and other special sur-veys provide opportunities to monitor HIVST use and linkageat the population level. These surveys are particularly usefulfor monitoring trends over time, such as awareness, use,coverage and linkage, provided appropriate questions areincluded. Because these surveys are usually repeated everythree to five years, they may not be useful for ongoing pro-gramme monitoring.
iv Digital tools, such as messaging Apps, websites, hotlines andsocial media platforms, can also be leveraged to collect HIVSTusage and linkage information. For example in South Africa, asurvey of a random sample of self-testers through mHealthplatforms such as interactive voice response and SMS wasfound feasible for estimating HIVST usage and linkage [10].
v Lastly, individual-level follow-up to confirm linkage may beconsidered in the context of small-scale demonstration pro-jects or within research studies to assess the effectivenessof linkage interventions. One example of such an approachis when women in antenatal care distribute HIVST kits totheir partners. Women can be given an invitation letter fortheir partner along with a self-test kit. The male partnersare asked to show the invitation letter when they attendclinics for HTS and women can also be interviewed at theirsecond visit [11]. The linkage among male partners afterHIVST may be an underestimate if they do not present theletter, seek testing at another clinic or already know theirHIV-status or are on ART. Individual-level follow-up toassess linkage will not be feasible in resource-limited set-tings as programmes scale up due to the extensiveresources required.
No single method would give an accurate measure of link-age following HIVST due to the limitations of each of them.However, using data and information from diverse sources,such as survey and programme data, can increase confidencein linkage estimates and minimize missing information. WHOis developing guidance for countries to monitor and evaluateHIVST, including linkage.
HIVST is an important testing approach for meeting the glo-bal goals of diagnosing 95% of all people with HIV by 2025.Effective linkage to appropriate services following HIVST isimportant. Given the privacy of HIVST, which allows auton-omy, fosters empowerment and reaches people who may nototherwise test, a resource-intensive approach to monitor link-age is neither feasible nor desirable as programmes scale upHIVST. The need to collect in-depth linkage data should notdelay the wider availability of HIVST. Programmes, donors andimplementers should consider pragmatic and innovative waysto measure linkage.
AUTHORS ’ AFF I L IAT IONS1TB/HIV Group, Malawi Liverpool Wellcome Trust Clinical Research Pro-gramme, Blantyre, Malawi; 2Department of Infectious Disease Epidemiology,London School of Hygiene and Tropical Medicine, London, United Kingdom;3Global HIV, Hepatitis and SITs Programmes, World Health Organization, Gen-eva, Switzerland; 4Department of Clinical Sciences, Liverpool School of TropicalMedicine, Liverpool, United Kingdom; 5Department of Clinical Research, LondonSchool of Hygiene and Tropical Medicine, London, United Kingdom; 6WorldHealth Organization Country Office for Zambia, Lusaka, Zambia; 7Unitaid, Gen-eva, Switzerland; 8M!edecins Sans Fronti"eres Holland, Amsterdam, Netherlands;9Department of Global Health and Development, London School of Hygiene andTropical Medicine, London, United Kingdom; 10FHI 360, Washington, DC, USA;11Wits Reproductive Health and HIV Research Institute, Johannesburg, SouthAfrica; 12Bill and Melinda Gates Foundation, Seattle, WA, USA; 13Global HealthBureau, Office of HIV/AIDS, Prevention Care and Treatment Division, UnitedStates Agency for International Development (USAID), Arlington, VA, USA
AUTHORS ’ CONTR IBUT IONS
MSJ, CJ, ATC and PM conceived the idea. ATC wrote the first draft of manu-script. MSJ, PM, EC, EC, LC, HI, EBA, MdE, MDC, MM, TS, VW, RB and CJreviewed, provided input and approved the final draft of manuscript.
COMPET ING INTERESTS
The authors declare no conflicts of interest.
ACKNOWLEDGEMENTS
WHO HIV Self-testing Technical Working Group members who are not co-au-thors: Amy Medley, Anita Sands, Asha Hedge, Christine Kisia, Elena Vovc, ElkinBermudez, Emmanuelle Bomo, Ena Oru, Euphemia Sibanda, Florence Anam,Francesca Merico, Fritz Fonkeng, Germina Mphoso, Giovanni Ravasi, Jean Njab,Jennifer Cohn, Karen Champenois, Karin Hatzold, Kimberly Green, KristinaGrabbe, Lelia Coppens, Maeve de Mello, Mark Lanigan, Morganne Ahmar,Muhammad Safdar Pasha, Naoko Ishikawa, Nay!e Bah, Olga Denisiuk, PatriciaGarcia, Peris Urassa, Philippe Girault, Simbarashe Mabaya, Sofia Furqan, ThatoChidarikire, Valdilea Veloso, Van Thi Thuy Nguyen and Wanjiru Mukoma.
FUNDING
Bill and Melinda Gates Foundation OPP1177903 and Unitaid(PO# 10140–0-600 and PO# 8477–0-600). PM is funded bythe Wellcome Trust (206575/Z/17/Z). EC is funded under aWellcome Trust Senior Research Fellowship in Clinical Science(grant number: WT091769) and by Unitaid-STAR Initiative(NCT02718274).
DISCLA IMER
The authors alone are responsible for the views expressed inthis article and they do not necessarily represent the views,decisions or policies of the institutions with which they areaffiliated including the World Health Organization, the U.S.President’s Emergency Plan for AIDS Relief, the U.S. Agencyfor International Development and the U.S. Government. The
Choko AT et al. Journal of the International AIDS Society 2020, 23:e25548http://onlinelibrary.wiley.com/doi/10.1002/jia2.25548/full | https://doi.org/10.1002/jia2.25548
127

corresponding author had final responsibility for the decisionto submit for publication.
REFERENCES
1. Joint United Nations Programme on HIV/AIDS. Global AIDS update 2019 —communities at the centre. Geneva: Joint United Nations Programme on HIV/AIDS; 2019.2. World Health Organization. Guidelines on HIV self-testing and partner notifi-cation. Supplement to consolidated guidelines on HIV testing services. Geneva:World Health Organization; 2016.3. World Health Organization. Consolidated guidelines on HIV testing servicesfor a changing epidemic. Geneva: World Health Organization; 2019.4. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al.Examining the effects of HIV self-testing compared to standard HIV testing ser-vices: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594.5. World Health Organization. WHO recommends HIV self-testing – evidenceupdate and considerations for success. Geneva: World Health Organization;2019.6. Jamil MS, Eshun-Wilson I, Witzel TC, Siegfried N, Figueroa C, Chitembo L,et al. Effectiveness of HIVST distribution models in the general population in
SSA: a systematic review. International Conference on AIDS and STIs in Africa;2-7 Dec; Kigali; 2019.7. Hallett TB, Eaton JW. A side door into care cascade for HIV-infectedpatients? J Acquir Immune Defic Syndr. 2013;63(Suppl 2):S228–32.8. MacPherson P, Lalloo DG, Webb EL, Maheswaran H, Choko AT, MakombeSD, et al. Effect of optional home initiation of HIV care following HIV self-test-ing on antiretroviral therapy initiation among adults in Malawi: a randomizedclinical trial. JAMA. 2014;312(4):372–9.9. Sibanda EL. Does community-based HIVST increase coverage of HIV testingand uptake of ART, and at what cost? Insights from randomised trials in Malawi,Zambia and Zimbabwe 22nd International AIDS Conference; 23-27 July; Ams-terdam; 2018.10. Majam M, Quaife M, Phatsoane M, Venter W. High self-reporting of HIVself-test results through an interactive voice response telephone line in innercity Johannesburg. International AIDS Society Conference; 21-24 July; MexicoCity; 2019.11. Choko AT, Fielding K, Stallard N, Maheswaran H, Lepine A, Desmond N,et al. Investigating interventions to increase uptake of HIV testing and linkageinto care or prevention for male partners of pregnant women in antenatal clin-ics in Blantyre, Malawi: study protocol for a cluster randomised trial. Trials.2017;18(1):349.
Choko AT et al. Journal of the International AIDS Society 2020, 23:e25548http://onlinelibrary.wiley.com/doi/10.1002/jia2.25548/full | https://doi.org/10.1002/jia2.25548
128
RESEARCH ARTICLE Open Access
Use and awareness of and willingness toself-test for HIV: an analysis of cross-sectional population-based surveys inMalawi and ZimbabweCheryl Johnson1,2* , Melissa Neuman3, Peter MacPherson4,5, Augustine Choko2,4, Caitlin Quinn1, Vincent J. Wong6,Karin Hatzold7, Rose Nyrienda8, Getrude Ncube9, Rachel Baggaley1, Fern Terris-Prestholt10 andElizabeth L. Corbett2,4
Abstract
Background: Many southern African countries are nearing the global goal of diagnosing 90% of people with HIVby 2020. In 2016, 84 and 86% of people with HIV knew their status in Malawi and Zimbabwe, respectively. However,gaps remain, particularly among men. We investigated awareness and use of, and willingness to self-test for HIVand explored sociodemographic associations before large-scale implementation.
Methods: We pooled responses from two of the first cross-sectional Demographic and Health Surveys to includeHIV self-testing (HIVST) questions in Malawi and Zimbabwe in 2015–16. We investigated sociodemographic factorsand sexual risk behaviours associated with previously testing for HIV, and past use, awareness of, and futurewillingness to self-test using univariable and multivariable logistic regression, adjusting for the sample design andlimiting analysis to participants with a completed questionnaire and valid HIV test result. We restricted analysis ofwillingness to self-test to Zimbabwean men, as women and Malawians were not systematically asked this question.
Results: Of 31,385 individuals, 31.2% of men had never tested compared with 16.5% of women (p < 0.001). Formen, the likelihood of having ever tested increased with age. Past use and awareness of HIVST was very low, 1.2and 12.6%, respectively. Awareness was lower among women than men (9.1% vs 15.3%, adjusted odds ratio[aOR] = 1.55; 95% confidence interval [CI]: 1.37–1.75), and at younger ages, and lower education and literacy levels.Willingness to self-test among Zimbabwean men was high (84.5%), with greater willingness associated with havingpreviously tested for HIV, being at high sexual risk (highest willingness [aOR = 3.74; 95%CI: 1.39–10.03, p < 0.009]),and being !25 years old. Wealthier men had greater awareness of HIVST than poorer men (p < 0.001). The highestwillingness to self-test (aOR = 3.74; 95%CI: 1.39–10.03, p < 0.009) was among men at high HIV-related sexual risk.
(Continued on next page)
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] HIV, Hepatitis and STI programme, World Health Organization,Geneva, Switzerland2Department of Clinical Research and Infection Disease, London School ofHygiene and Tropical Medicine, London, UKFull list of author information is available at the end of the article
Johnson et al. BMC Public Health (2020) 20:779 https://doi.org/10.1186/s12889-020-08855-7
129

(Continued from previous page)
Conclusions: In 2015–16, many Malawian and Zimbabwean men had never tested for HIV. Despite low awarenessand minimal HIVST experience, willingness to self-test was high among Zimbabwean men, especially older menwith moderate-to-high HIV-related sexual risk. These data provide a valuable baseline against which to investigatepopulation-level uptake of HIVST as programmes scale up. Programmes introducing, or planning to introduce,HIVST should consider including relevant questions in population-based surveys.
Keywords: HIV/AIDS, HIV self-test, HIV testing, Men, Sub-Saharan Africa, Population-based survey, Sexual riskbehaviour
BackgroundBoth Malawi and Zimbabwe have made tremendousprogress toward the “first 90” global target of diagnosing90% of people with HIV. In 2016, estimates showed that84% of people with HIV in Malawi and 86% inZimbabwe were aware of their status [1]. By end-2018,90% of all people with HIV had been diagnosed: 940000and 1.3 million people in Malawi and Zimbabwe, re-spectively [1]. As a result, reaching the remaining peoplewith HIV who do not know their status is becomingcostly and challenging, with national programmesreporting declining numbers of people with HIV diag-nosed through HIV testing services [2, 3]. Global andnational priorities now include defining sustainable ap-proaches that maintain these high rates of testing cover-age, while reaching individuals and groups still in needof HIV testing, prevention and treatment.Across southern Africa, men are less well served by
HIV programmes than women, less likely to have evertested [4] and more likely to develop advanced HIV dis-ease, reflecting late diagnosis and/or treatment initiation[5]. Men have fewer opportunities for HIV testing com-pared to women, as well as social–cultural, economicand systemic barriers that reduce access to and uptakeof services [6, 7].HIV self-testing (HIVST) is recommended by the
World Health Organization (WHO) [2] and is a keyintervention for reaching populations who may not testotherwise, particularly men [8]. Results from multipleevaluations show that HIVST has a high uptake, can in-crease the population coverage of HIV testing, and hashigh safety and acceptability globally [9, 10]. As of July2019, this recommendation has been taken up globally,with nearly 7 million HIVST kits procured by major do-nors, and 77 countries reporting that they have anHIVST policy, 38 of which are fully implementing self-testing [11, 12].Both Malawi and Zimbabwe were early adopters of
self-testing, with pilot studies starting between 2010 and2015 [13, 14]. These pilots were then followed by the de-velopment of national policies and initiation of large-scale implementation in mid-2015 under the STAR(Self-Test AfRica) Initiative [15]. Since then, multiple
evaluations of HIVST in each country have shown com-munity- and facility-based HIVST, as well as partner-delivered HIVST, to be feasible and effective ways ofreaching first-time testers, men, young people, as well aspartners of people with HIV [10, 16–19]. Recent math-ematical modelling suggests that HIVST can also becost-effective with appropriate targeting of men insouthern Africa among other priority groups [20, 21].As both countries move toward broader scale up of
self-testing, we used Demographic and Health Survey(DHS) data from 2015 to 16 to analyse population-levelawareness and use of, and willingness to self-test priorto large-scale implementation [22, 23]. These questionswere initially optional additions to the DHS question-naire in 2015. As such, the objective of this study was toprovide a point of comparison with future evaluationspost national scale up, as well as to inform future imple-mentation of HIVST. We assessed early implementationof HIVST questions in population-based surveys, and as-sociations with awareness and use of, and future willing-ness to, self-test.
MethodsWe obtained population-based survey data from the2015–16 Malawi and Zimbabwe DHS with standard per-missions from DHS and ICF International [22, 23].These provide data from a representative sample of men(15–54 years) and women of reproductive age (15–49years) living in Malawi and Zimbabwe, with linked la-boratory HIV test results. We limited our analysis toparticipants who had completed interviewer-administered questionnaires, provided blood specimensfor HIV testing, and had a valid result from this HIVtest.Our main outcomes of interest were self-reported
by survey respondents: ever testing for HIV, aware-ness and use of HIVST, and willingness to self-testin the future. Willingness to self-test was asked onlyin Zimbabwe, and included only in the male ques-tionnaire. The complete survey questionnaires areaccessible on the DHS website: https://dhsprogram.com/.
Johnson et al. BMC Public Health (2020) 20:779
130

Independent variablesThe choice of independent covariates was informed by theliterature on factors influencing testing for HIV and adap-tation of the simplified hierarchical framework for HIVtesting (including self-testing) among men in sub-SaharanAfrica (see Fig. 1). We also pre-specified a stratified ana-lysis by HIV testing history to explore differences inawareness and use of, and willingness to, self-test for HIV.Independent variables used in the analysis included
country (i.e. Malawi or Zimbabwe), sex (i.e. male or fe-male), household wealth (i.e. measured by standardquintiles), age (i.e. measured by five-year age bands from15 to 45 years and 45+ years), education (i.e. measuredby secondary education or lower), literacy (i.e. ability toread, or not read, a full sentence), employment (i.e. ac-tively working in the past 7 days), marital status (i.e.married or cohabiting), and HIV status reported duringthe survey (i.e. HIV-positive or HIV-negative). A three-category HIV-related sexual risk variable was definedfrom reported sexual activity (i.e. measured by sexual ac-tivity, or inactivity, in the past 4 weeks), and the follow-ing high-risk exposures in the previous 12months:multiple (i.e. !2) partners; any paid sex (asked to men);having received gifts, cash or other compensation in ex-change for sex (asked to women); and having a sexuallytransmitted infection (STI). Individuals with one ormore of these risk variables were classified as “high-risk”.The remaining respondents reporting no other risk ex-posures were classified as “moderate risk” if sexually ac-tive in the past 4 weeks and “low-risk” if reporting nosexually activity in the past 4 weeks.
Data analysisWe used Stata version 11 for analysis (College Station,Texas). We set standard country-specific sampling and
cluster weights provided by DHS using the survey (svy)commands. We excluded participants with missing datafor outcomes or independent variables from the analysis.As independent variables were all categorical, we re-
ported baseline characteristics as proportions. We se-lected variables for inclusion in multivariable models bythe putative causal framework (Fig. 1), and by investigat-ing effect modification and collinearity. Univariable andmultivariable analyses used logistic regression. We calcu-lated p-values across age, wealth and HIV-related sexualrisk using the Wald test.We investigated associations between independent and
outcome variables using univariable odds ratios (ORs)with 95% confidence intervals (CI). Before multivariableanalysis, we explored confounding and collinearity be-tween independent variables by investigating associa-tions between variables for all those with significantassociations with any given outcomes. We explored po-tential effect modification [24] using stratified analysesby sex, HIV status, previous HIV testing history andHIV-related sexual risk category.
ResultsBaseline characteristicsWe included 31,385 survey respondents reporting onHIV testing history: 14,911 and 16,474 records fromMalawi and Zimbabwe, and 14,027 and 17,358 amongmen and women, respectively (Table 1). Of these, a totalof 24,683 individuals were asked about HIVST, and 6702(21.4%, n = 31,385) not asked. An additional 15 individ-uals (0.06%, n = 24,683) asked about HIVST had missingdata related to questions on sexual activity used to de-termine HIV-related sexual risk.A total of 78.6% and 75.4% of people reported ever hav-
ing tested for HIV in Zimbabwe and Malawi, respectively
Fig. 1 Mechanisms affecting HIV testing uptake in adults (aged 15+ years) in southern Africa, by age, gender, and sexual risk behaviour
Johnson et al. BMC Public Health (2020) 20:779
131

Table 1 Baseline characteristics in Malawi and Zimbabwe, 2015–16Variablesa Ever tested
(N = 31,385)bEver self-test(N = 24,683)b
Aware self-test(N = 24,683)b
N % p-value§ N % p-value§ n % p-value§
Total population 24,148 76.9 287 1.2 3118 12.6
Country < 0.001 < 0.001 < 0.001
Malawi 11,726 75.4 141 1.0 1671 11.4
Zimbabwe 12,422 78.6 146 1.5 1447 14.5
Sex < 0.001 0.008 < 0.001
Female 14,500 83.5 103 1.0 983 9.1
Male 9648 68.8 184 1.3 2135 15.3
Residence < 0.001 < 0.001 < 0.001
Urban 7951 79.9 151 2.1 1516 21.2
Rural 16,197 75.9 136 0.8 1602 9.1
Age group (years) < 0.001 < 0.001 < 0.001
15–19 3252 44.8 30 0.5 437 7.0
20–24 4703 80.7 42 0.9 562 12.1
25–29 4337 90.3 59 1.6 580 16.0
30–34 4070 91.1 55 1.7 497 15.2
35–39 3247 89.2 42 1.5 426 15.7
40–44 2446 87.4 35 1.7 303 15.0
45+ 2093 80.8 24 1.1 313 14.7
Wealth < 0.001 < 0.001 < 0.001
Poorest 3697 76.4 18 0.5 246 6.4
Poorer 4029 75.8 38 0.9 336 7.8
Middle 4252 75.3 26 0.6 279 8.3
Rich 5594 77.6 56 0.9 669 12.2
Richest 6576 78.5 149 2.3 1488 22.8
HIV status < 0.001 0.108 0.029
HIV negative 20,646 75.0 249 1.1 2760 12.5
HIV positive 2570 90.6 38 1.5 358 10.4
Marital status < 0.001 0.005 < 0.001
Single 7595 58.9 99 0.9 1175 11.2
Married or cohabiting 16,553 89.5 188 1.3 1943 13.7
Employment < 0.001 0.033 < 0.001
Not actively working 8719 70.1 85 1.0 823 9.4
Actively working 15,429 81.4 202 1.3 2295 14.4
Education < 0.001 < 0.001 < 0.001
" Primary 10,617 74.8 70 0.6 927 7.5
! Secondary 13,531 78.7 217 1.8 2191 17.8
Literacy < 0.001 < 0.001 < 0.001
Illiterate 5211 73.5 44 0.7 488 8.0
Literate 18,937 77.9 243 1.3 2630 14.2
Sexually active < 0.001 < 0.001 < 0.001
Sexually inactive 9064 64.0 107 1.5 1225 17.7
Active in past4 weeks
15,053 87.6 180 1.5 1890 14.2
Johnson et al. BMC Public Health (2020) 20:779
132

(p < 0.001). More women compared to men (83.5% vs68.8%; p < 0.001), and more urban compared to rural resi-dents (79.9% vs 75.9%; p < 0.001) had tested previously. Alarger proportion of those never tested were 15–24 yearscompared to those who were ! 25 years (see Table 1).The proportion of people who had ever self-tested was
1.2% and similar in both countries. However, while over-all 12.6% had awareness of HIVST, it was greater inZimbabwe compared to Malawi (14.5% vs 11.4%; p <0.001) and among men compared to women (15.3% vs9.1%; p < 0.001) (Table 1). Among the respondents,those with greater awareness of self-testing were ! 30years of age (!30 years: 21.1% vs < 30 years: 9.1%; p <0.001), wealthier (richest: 22.8% vs poorest: 6.4%; p <0.001) and those with higher education levels (at leastsecondary education: 17.8% vs primary education or less:7.5%; p < 0.001) than those aged < 30 years, those whowere poorer and had lower education levels.Willingness to self-test could be assessed only among
7372 Zimbabwean men (48 men had missing data onwillingness), as only men were asked about willingnessto self-test, and this question was not included in theMalawi DHS questionnaire.Most Zimbabwean men (84.5%) were willing to self-test
(Supplementary Table S1 includes baseline characteristicsof Zimbabwean men on willingness to self-test, 2015–16).Men aged !25 years reported greater willingness to self-testthan men aged < 25 years (88.7% vs 78.8%; p < 0.001).High-risk men also reported greater willingness to self-testthan low-risk men (78.8% vs 63.5%; p < 0.001). Most menwilling to self-test had tested in the past 12months (88.5%).However, 86.4% of the men who had not tested forHIV in the previous two or more years were alsowilling to self-test.
Ever testing for HIVAge, HIV status and HIV-related sexual risk appeared tomodify effects in the multivariable analysis across anumber of variables (Table 2). Collinearity affected theresults of multivariable analysis, notably between ageand HIV-related sexual risk, marital status and HIV-related sexual risk, age and education level, and educa-tion level and literacy.On multivariable analysis, after assessing for collinearity,
being Malawian was associated with ever having tested forHIV (adjusted odds ratio [aOR] = 1.26; 95% confidenceinterval [CI]: 1.15–1.38, p < 0.001) (Table 2). However,men had substantially lower odds of having ever tested forHIV compared to women (aOR = 0.39; 95%CI: 0.36–0.42,p < 0.001). Individuals between 30 and 34 years of age hadgreater odds of ever having tested for HIV compared to15–19 year olds (aOR = 8.86; 95%CI: 7.63–10.29, p <0.001). Additional factors associated with ever havingtested for HIV included: an HIV-positive test result in thesurvey (HIV-positive vs HIV-negative: aOR = 2.11, 95%CI:1.80–2.49, p < 0.001), employment (actively working vsnot actively working: aOR = 1.16; 95%CI: 1.06–1.26, p <0.001), literacy (being literate vs being illiterate: aOR =1.63, 95%CI: 1.50–1.78, p < 0.001), and reporting moreHIV-related sexual risk behaviours (moderate vs low:aOR = 2.15; 95%CI: 1.96–2.36, p < 0.001, and high-risk vslow-risk: aOR = 1.54; CI: 1.80–2.49, p < 0.001).
Use and awareness of self-testingA complete analysis of ever self-testing is shown in sup-plementary Table S2. Table 3 provides outcomes fromthe univariable and multivariable analyses for awarenessof HIV self-testing.
Table 1 Baseline characteristics in Malawi and Zimbabwe, 2015–16 (Continued)
Variablesa Ever tested(N = 31,385)b
Ever self-test(N = 24,683)b
Aware self-test(N = 24,683)b
N % p-value§ N % p-value§ n % p-value§
HIV-related riskc < 0.001 < 0.001 < 0.001
Low risk 8457 63.5 94 0.9 1102 10.3
Moderate risk 13,092 88.7 134 1.2 1497 13.6
High risk 2570 78.8 59 2.0 516 17.2aEver tested refers to people surveyed on HIV testing history who reported that they previously tested for HIV before the survey. Overall, 31,385 people wereasked about their HIV testing history and 24,148 responded that they had tested previously. Ever self-tested refers to people surveyed on HIV self-testing whoreported that they had previously self-tested. Overall, 24,683 people were asked whether they had self-tested and 287 reported that they had self-testedpreviously. Aware of self-testing refers to people surveyed who reported that they were aware of HIV self-testing. Overall, 24,683 people were asked whether theywere aware of self-testing and 3118 reported that they were aware of self-testingbOut of 31,385 people surveyed, 31,348 were included as 37 people were missing information on sexual activity and HIV-related risk. Not all participants weresystematically surveyed on self-testing questions. Out of 31,385 people surveyed, 24,683 were asked about self-testing, resulting in a smaller sample size. Amongthese were 15 people reporting on self-testing who did not provide information on sexual activity and HIV risk. Population size asked about ever testing for HIV:31347 (HIV risk/sexual activity). Population size asked about awareness or ever self-testing for HIV: 24668 (HIV risk/sexual activity)cHIV risk as defined in this analysis includes reported sexual activity in the past four weeks, and the following high-risk exposures in the previous 12 months:multiple (i.e. !2) partners, any paid sex (asked to men), having received gifts, cash or other compensation in exchange for sex (asked to women), and having asexually transmitted infection (STI). Individuals with any “high-risk” exposures were classified as “high-risk”, with the remaining respondents classified as “low risk”if reporting no sexually activity in the past four weeks, and as “moderate risk” otherwise§ P-value based on cluster-adjusted chi-squared test
Johnson et al. BMC Public Health (2020) 20:779
133

Table 2 Univariable and multivariable associations between sociodemographic factors and ever testing for HIV in Malawi andZimbabwe, 2015–16Variables Univariable (weighted)
N = 31,375aMultivariable (weighted)N = 31,347a
OR 95% CI andp-value
aOR 95% CI andp-value
Country
Zimbabwe 1 1
Malawi 1.18 1.10–1.28 1.26 1.15–1.38
Sex
Female 1 1
Male 0.42 0.3–0.45 0.39 0.36–0.42
Age (years)
15–19 1 p < 0.001§ 1 p < 0.001§
20–24 5.40 4.87–5.98 4.37 3.91–4.87
25–29 11.89 10.48–13.48 8.24 7.18–9.46
30–34 14.19 12.38–16.27 8.86 7.63–10.29
35–39 10.42 9.01–12.05 6.41 5.47–7.50
40–44 8.44 7.27–9.80 5.30 4.50–6.25
45+ 5.16 4.50–5.91 3.72 3.20–4.34
Residence
Urban 1 1
Rural 0.83 0.76–0.90 1.00 0.88–1.14
HIV status
HIV negative 1 1
HIV positive 3.44 2.98–3.97 2.11 1.80–2.49
Marital status
Single 1 1
Married or cohabiting 6.07 5.62–6.54 b b
Wealth
Poorest 1 p < 0.003§ 1 p < 0.581§
Poor 0.94 0.84–1.05 1.02 0.89–1.16
Middle 0.91 0.81–1.01 1.09 0.96–1.25
Rich 1.04 0.93–1.16 1.05 0.91–1.20
Richest 1.09 0.97–1.23 1.11 0.94–1.31
Employment
Not actively working 1 1
Actively working 1.81 1.69–1.95 1.16 1.06–1.26
Education
" Primary 1 1
! Secondary 1.26 1.17–1.35 b b
Literacy
Illiterate 1 1
Literate 1.30 1.20–1.40 1.63 1.50–1.78
HIV-related riskc
Low risk 1 p < 0.001§ 1 p < 0.001§
Moderate risk 4.58 4.23–4.96 2.15 1.96–2.36
Johnson et al. BMC Public Health (2020) 20:779
134

In the multivariable analysis, men aged 30–34 yearshad greater odds of past self-testing use compared toyounger men (age 15–19 years) (aOR = 2.89; 95%CI:1.47–5.68, p < 0.002) (Table S2). Across wealth quin-tiles, being wealthier was also associated with previousself-testing (p < 0.001), with the wealthiest individualshaving the greatest odds of past self-testing (aOR forrichest vs poorest = 3.59; 95%CI: 1.79–7.18, p < 0.001).In the multivariable analysis, respondents in Malawi and
those from a rural setting were less likely to be aware ofHIVST compared with Zimbabweans and urban partici-pants (Table 3). However, the following variables were sig-nificantly associated with being aware of HIVST: beingmale (male vs female: aOR = 1.55; 95%CI: 1.37–1.75, p <0.001), aged 15–19 years (when compared with those aged25–29 years: aOR = 1.76; 95%CI: 1.43–2.17, p < 0.001 andaged 35–39 years: aOR = 1.69; 95%CI: 1.34–2.12, p <0.001), wealthier (wealthiest vs poorest: aOR = 3.03;95%CI: 2.46–3.73, p < 0.001), having employment (activelyworking vs not actively working: aOR = 1.25; 95%CI: 1.12–1.42, p < 0.001), being literate (literate vs illiterate: aOR =1.17; 95%CI: 1.01–1.36, p < 0.035) and having previouslytested for HIV (ever tested vs never tested: aOR = 1.89;95%CI: 1.65–2.17, p < 0.001).
Willingness to self-test among Zimbabwean menThe relationship between willingness to test and socio-economic variables (wealth and actively working) andHIV status substantially differed according to both highand low HIV-related sexual risk (Table 4): see, for ex-ample, univariable OR for HIV status and employment.Thus, we adapted our planned multivariable analysis toaccount for effect modification between HIV-related sex-ual risk categorization and socioeconomic variables. Onmultivariable analysis, men with high HIV-related sexualrisk behaviours were more likely than low-risk men toexpress willingness to self-test if they were also fromhigher socioeconomic quintiles, not working, in ruralsettings and had tested previously (interaction terms:
socioeconomic status, p = 0.066; rural residence, p =0.071; employment p = 0.003; literacy, p = 0.225; mar-ried, p = 0.401; aware of self-test, p = 0.605; previoustesting, p = 0.001; and HIV status p = 0.162).On multivariable analysis of men at high HIV-related
sexual risk, willingness to self-test increased with age(p = 0.030), with the strongest association for those aged35–39 years compared to those aged 15–19 years (aOR =4.87; 95%CI: 2.14–11.07, p < 0.001). Similarly, willingnessto self-test among men with high HIV-related sexual riskincreased in rural settings (rural vs urban: aOR = 3.56,95%CI: 1.61–7.90, p = 0.002) and with greater wealthquintiles (wealthiest vs least wealthy: aOR = 3.74, 95%CI:1.39–10.53, p = 0.009).While actively working men with high HIV-related
risk were less willing to self-test (actively working vs notactively working: aOR: 0.57, 95%CI: 0.34–0.95, p =0.030), actively working low-risk men were more willingto self-test than when not actively working (aOR 1.41;95%CI: 1.13–1.77, p = 0.003). The association with previ-ous testing and willingness to test was also more pro-nounced for low-risk men (ever tested vs never tested:aOR 1.48; 95%CI: 1.18–1.85, p < 0.001) than high-riskmen (ever tested vs never tested: aOR 1.20; 95%CI:0.76–1.90, p = 0.435), while associations with age (p =0.106) and wealth (p = 0.102) were less pronounced thanfor high-risk men (Table 4, described above).We additionally conducted a stratified analysis to in-
vestigate whether willingness to self-test varied by pastHIV-testing behaviour (i.e. previously tested or not) (seesupplementary Table S3). Patterns of willingness to self-test were similar for the 2437/7372 (33.1%) men whohad never previously tested as for those with at least onepast HIV test, with greater willingness in older men.
DiscussionThe main findings from this analysis of 2015–16 surveydata captured immediately before HIVST implementa-tion in Malawi and Zimbabwe were that awareness and
Table 2 Univariable and multivariable associations between sociodemographic factors and ever testing for HIV in Malawi andZimbabwe, 2015–16 (Continued)
Variables Univariable (weighted)N = 31,375a
Multivariable (weighted)N = 31,347a
OR 95% CI andp-value
aOR 95% CI andp-value
High risk 2.14 1.92–2.40 1.54 1.80–2.49a Both samples were weighted based on standard DHS weights; Strata = 56; PSU = 1256. Univariable draws from a total of 31,385 observations, population size31,375. Multivariable draws from a total of 31,348 observations and population size of 31,338. This excludes 37 people who did not report on sexual activity andrisk behaviours and are missing from the “HIV risk category”bRepresents variables that were not included in the multivariable analysis due to identified collinearityc HIV risk as defined in this analysis includes reported sexual activity in the past four weeks, and the following high-risk exposures in the previous 12 months:multiple (i.e. !2) partners, any paid sex (asked to men), having received gifts, cash or other compensation in exchange for sex (asked to women), and having asexually transmitted infection (STI). Individuals with any “high-risk” exposures were classified as “high-risk”, with the remaining respondents classified as “low risk”if reporting no sexually activity in the past four weeks, and as “moderate risk” otherwise§ P-value based on the Wald test. P-values for variables with more than two categories are shown
Johnson et al. BMC Public Health (2020) 20:779
135
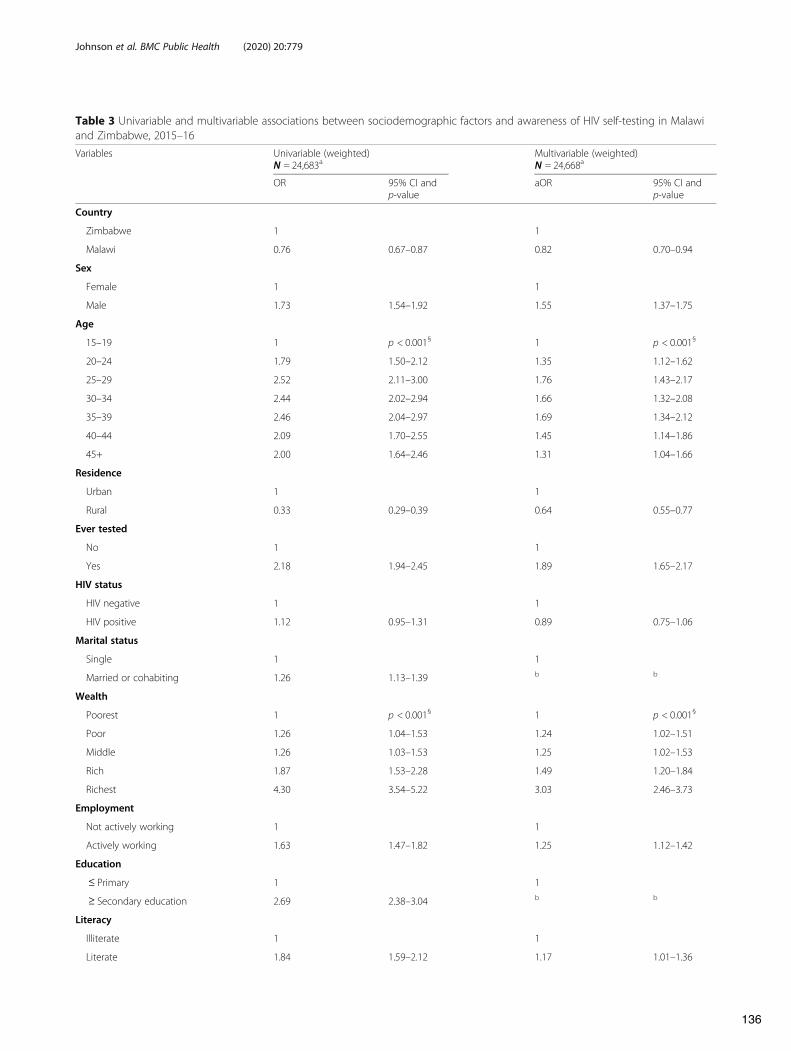
Table 3 Univariable and multivariable associations between sociodemographic factors and awareness of HIV self-testing in Malawiand Zimbabwe, 2015–16Variables Univariable (weighted)
N = 24,683aMultivariable (weighted)N = 24,668a
OR 95% CI andp-value
aOR 95% CI andp-value
Country
Zimbabwe 1 1
Malawi 0.76 0.67–0.87 0.82 0.70–0.94
Sex
Female 1 1
Male 1.73 1.54–1.92 1.55 1.37–1.75
Age
15–19 1 p < 0.001§ 1 p < 0.001§
20–24 1.79 1.50–2.12 1.35 1.12–1.62
25–29 2.52 2.11–3.00 1.76 1.43–2.17
30–34 2.44 2.02–2.94 1.66 1.32–2.08
35–39 2.46 2.04–2.97 1.69 1.34–2.12
40–44 2.09 1.70–2.55 1.45 1.14–1.86
45+ 2.00 1.64–2.46 1.31 1.04–1.66
Residence
Urban 1 1
Rural 0.33 0.29–0.39 0.64 0.55–0.77
Ever tested
No 1 1
Yes 2.18 1.94–2.45 1.89 1.65–2.17
HIV status
HIV negative 1 1
HIV positive 1.12 0.95–1.31 0.89 0.75–1.06
Marital status
Single 1 1
Married or cohabiting 1.26 1.13–1.39 b b
Wealth
Poorest 1 p < 0.001§ 1 p < 0.001§
Poor 1.26 1.04–1.53 1.24 1.02–1.51
Middle 1.26 1.03–1.53 1.25 1.02–1.53
Rich 1.87 1.53–2.28 1.49 1.20–1.84
Richest 4.30 3.54–5.22 3.03 2.46–3.73
Employment
Not actively working 1 1
Actively working 1.63 1.47–1.82 1.25 1.12–1.42
Education
" Primary 1 1
! Secondary education 2.69 2.38–3.04 b b
Literacy
Illiterate 1 1
Literate 1.84 1.59–2.12 1.17 1.01–1.36
Johnson et al. BMC Public Health (2020) 20:779
136

lifetime use of self-testing were low, with 12.6% of re-spondents being aware of self-testing and 1.2% havingever self-tested for HIV. Willingness to self-test washigh, although this question was asked only of maleZimbabweans, with 84.5% respondents reporting them-selves willing, including 30.4% of all previously untestedmen. Self-testing appeared to appeal most strongly toolder men and those with high-to-moderate HIV-relatedsexual risk. The highest willingness to self-test was inmen aged 35–39 years and those in rural settings, wherehaving never previously tested for HIV was more com-mon than in urban settings. Factors independently asso-ciated with greater awareness of HIVST included men,urban residence, and literacy; with many of these samefactors also associated with having tested for HIV atleast once in this analysis of 2015–16 data. Poorer andunemployed individuals were less likely to be aware ofself-testing.Despite significant gains and scale up of HIV test-
ing in both Malawi and Zimbabwe, men continue tobe missed [1, 2]. According to recent “first 90” esti-mates in sub-Saharan Africa, the absolute number ofmen with HIV aged !25 years are much less likely toknow their HIV-positive status than women overalland younger men [25]. As the median age of allpeople with HIV continues to increase [26], identify-ing and scaling-up strategies that appeal to older agegroups will be needed, especially older men and thoseat high risk. Greater efforts are needed to roll outevidence-based HIVST approaches to reaching men,such as through health facilities and secondary distri-bution from female partners attending antenatal carein high HIV-burden settings, or through networks ofother high-risk sexual, drug injecting or social con-tacts, including those with HIV [9, 16, 27, 28].
Considering the high willingness to self-test in high-risk men in rural areas, additional community outreachstrategies may be needed. HIVST in workplaces andthrough faith-based organizations should also be consid-ered, as early programmatic data suggest it may be par-ticularly useful for reaching older men [29]. However,more focused programmatic efforts and communicationstrategies for workplace HIVST may be needed, as incontrast to low-risk men, high-risk men who were work-ing were less willing to self-test. Further evaluation isneeded to understand the utility of HIVST through for-mal and informal workplace programmes and how wellthey can reach high-risk men. It will be important to as-sess differences in HIVST awareness, use and willingnessamong older and higher-risk men in future surveys.The importance of high willingness to self-test among
older Zimbabwean men, including those with higher riskfactors, should not be underestimated. This challengesperceptions that men may not want to test or are afraidto test for HIV and underscores the importance of pro-viding more opportunities and HIV testing options thatare acceptable to men. As reported in a recent analysisamong never tested men in sub-Saharan Africa, nearlyall those offered HIV testing in the survey accepted itand learnt their results [4].Since these surveys, HIVST, alongside conventional
testing, has been rapidly scaled up, notably so for Malawiand Zimbabwe. Between May 2015 and July 2017, theSTAR Initiative alone distributed 172,830 and 265,091HIVST kits in Malawi and Zimbabwe, respectively [10].Following publication of the WHO guidelines and WHOprequalification of four HIVST products, as well as mul-tiple large-scale implementation studies [2, 30], volumescontinue to increase annually, with latest estimates sug-gesting that between 2017 and 2020, with existing donor
Table 3 Univariable and multivariable associations between sociodemographic factors and awareness of HIV self-testing in Malawiand Zimbabwe, 2015–16 (Continued)
Variables Univariable (weighted)N = 24,683a
Multivariable (weighted)N = 24,668a
OR 95% CI andp-value
aOR 95% CI andp-value
HIV riskc
Low risk 1 p < 0.001§ 1 p < 0.518
Moderate risk 1.37 1.24–1.53 1.03 0.90–1.17
High risk 1.75 1.51–2.03 1.10 0.93–1.31a Both samples were weighted based on standard Demographic and Health Survey weights; Strata = 56; PSU = 1256. Not all participants were systematicallysurveyed on self-testing questions. Out of 31,385 people surveyed, 24,683 were asked about self-testing, resulting in a smaller sample size. Among those reportingon HIV self-testing, 15 did not provide information on sexual activity and HIV risk. Population size asked about awareness or ever self-testing for HIV: 24668 (HIVrisk), 24,668 (sexual activity)b Represents variables that were not included in the multivariable analysis due to identified collinearityc HIV risk as defined in this analysis includes reported sexual activity in the past four weeks, and the following high-risk exposures in the previous 12 months:multiple (i.e. !2) partners, any paid sex (asked to men), having received gifts, cash or other compensation in exchange for sex (asked to women), and having asexually transmitted infection (STI). Individuals with any “high-risk” exposures were classified as “high-risk”, with the remaining respondents classified as “low risk”if reporting no sexually activity in the past four weeks, and as “moderate risk” otherwise§ P-value based on the Wald test. P-values for variables with more than two categories are shown
Johnson et al. BMC Public Health (2020) 20:779
137
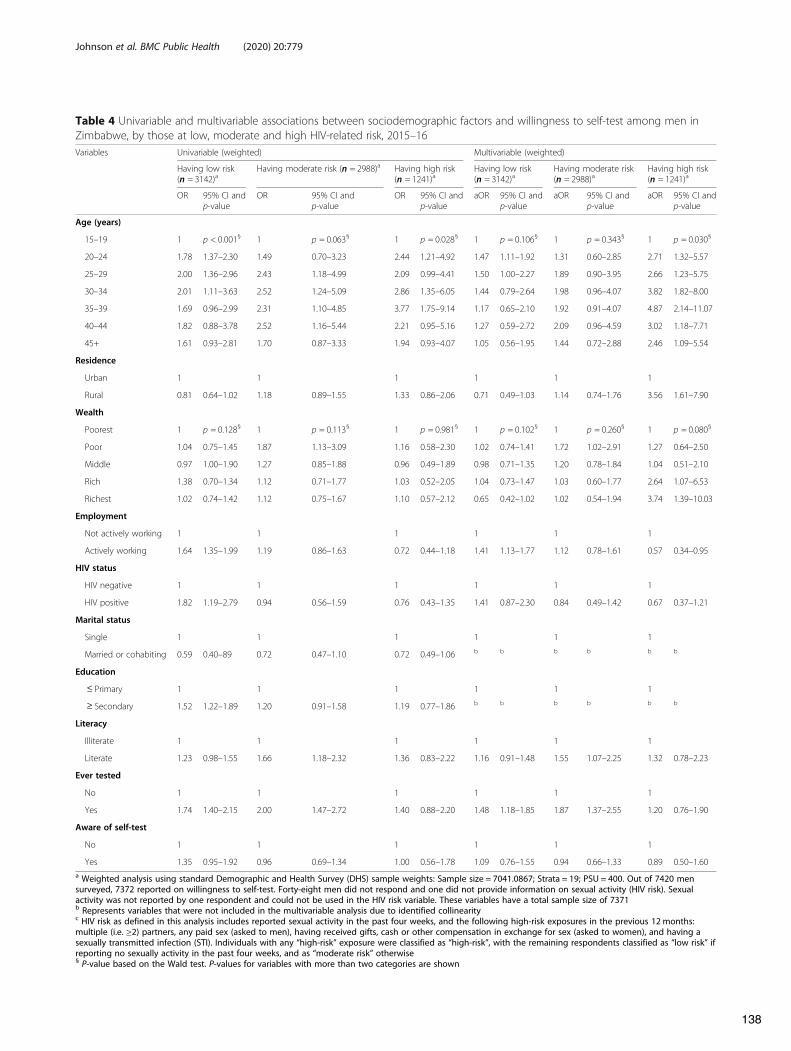
Table 4 Univariable and multivariable associations between sociodemographic factors and willingness to self-test among men inZimbabwe, by those at low, moderate and high HIV-related risk, 2015–16Variables Univariable (weighted) Multivariable (weighted)
Having low risk(n = 3142)a
Having moderate risk (n = 2988)a Having high risk(n = 1241)a
Having low risk(n = 3142)a
Having moderate risk(n = 2988)a
Having high risk(n = 1241)a
OR 95% CI andp-value
OR 95% CI andp-value
OR 95% CI andp-value
aOR 95% CI andp-value
aOR 95% CI andp-value
aOR 95% CI andp-value
Age (years)
15–19 1 p < 0.001§ 1 p = 0.063§ 1 p = 0.028§ 1 p = 0.106§ 1 p = 0.343§ 1 p = 0.030§
20–24 1.78 1.37–2.30 1.49 0.70–3.23 2.44 1.21–4.92 1.47 1.11–1.92 1.31 0.60–2.85 2.71 1.32–5.57
25–29 2.00 1.36–2.96 2.43 1.18–4.99 2.09 0.99–4.41 1.50 1.00–2.27 1.89 0.90–3.95 2.66 1.23–5.75
30–34 2.01 1.11–3.63 2.52 1.24–5.09 2.86 1.35–6.05 1.44 0.79–2.64 1.98 0.96–4.07 3.82 1.82–8.00
35–39 1.69 0.96–2.99 2.31 1.10–4.85 3.77 1.75–9.14 1.17 0.65–2.10 1.92 0.91–4.07 4.87 2.14–11.07
40–44 1.82 0.88–3.78 2.52 1.16–5.44 2.21 0.95–5.16 1.27 0.59–2.72 2.09 0.96–4.59 3.02 1.18–7.71
45+ 1.61 0.93–2.81 1.70 0.87–3.33 1.94 0.93–4.07 1.05 0.56–1.95 1.44 0.72–2.88 2.46 1.09–5.54
Residence
Urban 1 1 1 1 1 1
Rural 0.81 0.64–1.02 1.18 0.89–1.55 1.33 0.86–2.06 0.71 0.49–1.03 1.14 0.74–1.76 3.56 1.61–7.90
Wealth
Poorest 1 p = 0.128§ 1 p = 0.113§ 1 p = 0.981§ 1 p = 0.102§ 1 p = 0.260§ 1 p = 0.080§
Poor 1.04 0.75–1.45 1.87 1.13–3.09 1.16 0.58–2.30 1.02 0.74–1.41 1.72 1.02–2.91 1.27 0.64–2.50
Middle 0.97 1.00–1.90 1.27 0.85–1.88 0.96 0.49–1.89 0.98 0.71–1.35 1.20 0.78–1.84 1.04 0.51–2.10
Rich 1.38 0.70–1.34 1.12 0.71–1.77 1.03 0.52–2.05 1.04 0.73–1.47 1.03 0.60–1.77 2.64 1.07–6.53
Richest 1.02 0.74–1.42 1.12 0.75–1.67 1.10 0.57–2.12 0.65 0.42–1.02 1.02 0.54–1.94 3.74 1.39–10.03
Employment
Not actively working 1 1 1 1 1 1
Actively working 1.64 1.35–1.99 1.19 0.86–1.63 0.72 0.44–1.18 1.41 1.13–1.77 1.12 0.78–1.61 0.57 0.34–0.95
HIV status
HIV negative 1 1 1 1 1 1
HIV positive 1.82 1.19–2.79 0.94 0.56–1.59 0.76 0.43–1.35 1.41 0.87–2.30 0.84 0.49–1.42 0.67 0.37–1.21
Marital status
Single 1 1 1 1 1 1
Married or cohabiting 0.59 0.40–89 0.72 0.47–1.10 0.72 0.49–1.06 b b b b b b
Education
" Primary 1 1 1 1 1 1
! Secondary 1.52 1.22–1.89 1.20 0.91–1.58 1.19 0.77–1.86 b b b b b b
Literacy
Illiterate 1 1 1 1 1 1
Literate 1.23 0.98–1.55 1.66 1.18–2.32 1.36 0.83–2.22 1.16 0.91–1.48 1.55 1.07–2.25 1.32 0.78–2.23
Ever tested
No 1 1 1 1 1 1
Yes 1.74 1.40–2.15 2.00 1.47–2.72 1.40 0.88–2.20 1.48 1.18–1.85 1.87 1.37–2.55 1.20 0.76–1.90
Aware of self-test
No 1 1 1 1 1 1
Yes 1.35 0.95–1.92 0.96 0.69–1.34 1.00 0.56–1.78 1.09 0.76–1.55 0.94 0.66–1.33 0.89 0.50–1.60a Weighted analysis using standard Demographic and Health Survey (DHS) sample weights: Sample size = 7041.0867; Strata = 19; PSU = 400. Out of 7420 mensurveyed, 7372 reported on willingness to self-test. Forty-eight men did not respond and one did not provide information on sexual activity (HIV risk). Sexualactivity was not reported by one respondent and could not be used in the HIV risk variable. These variables have a total sample size of 7371b Represents variables that were not included in the multivariable analysis due to identified collinearityc HIV risk as defined in this analysis includes reported sexual activity in the past four weeks, and the following high-risk exposures in the previous 12 months:multiple (i.e. !2) partners, any paid sex (asked to men), having received gifts, cash or other compensation in exchange for sex (asked to women), and having asexually transmitted infection (STI). Individuals with any “high-risk” exposure were classified as “high-risk”, with the remaining respondents classified as “low risk” ifreporting no sexually activity in the past four weeks, and as “moderate risk” otherwise§ P-value based on the Wald test. P-values for variables with more than two categories are shown
Johnson et al. BMC Public Health (2020) 20:779
138

support, both countries will have procured at least 4 mil-lion self-testing kits [12].High willingness to self-test in Malawi and Zimbabwe
has also been underscored by the observed high uptakein community-based HIVST interventions. Uptake by45–75% was reported by end-line surveys between 2016and 2019 in three population-level cluster randomizedtrials in rural communities [18, 19, 31]. In 2017, a surveyfollowing community-based HIVST kit distribution inrural Zimbabwe, with or without supply-side financialincentives for post-test linkage, showed that 81.7% ofresidents were aware of self-testing and 55.8% had self-tested [18]. Two trials of community distribution ofHIVST kits in rural Malawi showed high uptake ofHIVST, with significant increase in ever testing for HIVin men and adolescents [19, 31]. Even in the standard-of-care arms, 31.5% of participants in the 2016–17 trialand 32.3% in the 2018–19 trial, respectively, were awareof HIVST [18, 19, 31].These are substantial increases compared to the low
awareness and use of self-testing in the 2015–16 DHS,and highlight the broader impact on awareness fromlarge implementation science studies, such as the STARInitiative. In 2015–16, HIVST was limited to small pilotstudies in each country, as national and internationalpolicies were still under development and there were nonationally registered or WHO-prequalified productsavailable [32].As HIVST continues to expand globally, monitoring
overall HIVST use, and awareness of and willingness totest will contribute to a better understanding of thereach and impact of HIVST. Ideally, the extent to whichsocial determinants such as urban residence, literacy andaffluence dictate awareness of HIVST will diminish withmore comprehensive distribution strategies such asthose through community outreach, health facilities, bysexual partners and in other venues such as workplacesand private sector pharmacies. Population-based surveys,like the DHS, will then provide an important source ofinformation for countries implementing HIVST, as wellas those planning to add HIVST as part of existing HIVtesting services. Together with routine programmaticdata and special studies, population-based surveys thathave included questions on HIVST can then providea meaningful baseline and point of comparison forfuture analyses and important insights for futureimplementation.Although Malawi and Zimbabwe have scaled up HIV
testing and have now achieved the first “90”, gaps remain,particularly among men. Efforts are on to reach the first“95” by 2030 – diagnosing 95% of all people with HIV –which is the new goal. As a result, strategies for diagnos-ing the shrinking number of people with HIV who do notknow their status are becoming more challenging and also
less cost-effective unless targeted toward specific popula-tions and settings with lower knowledge of status amongpeople with HIV [3]. Maintaining the high testing cover-age and knowledge of status achieved will not be inexpen-sive and HIVST is likely to play a role in sustainingservices and potentially reducing costs. Furthermore,HIVST also addresses patient costs of accessing servicesand equity concerns, which also need to be considered, es-pecially as programmes get closer to the national goals.Programmes will need to carefully evaluate how they
can both maintain essential HIV testing services in facil-ities, while also deploying highly focused and effective out-reach with limited resources. Strategies such as offeringHIVST through specific channels among priority popula-tions, or through periodic and geographically targetedcommunity outreach (such as every 5 years), may be morecost-effective and affordable as more people with HIVlearn their status and new infections decline [20].
LimitationsThis study has many strengths, such as its large samplesize and that it is one of the first to provide an assess-ment of HIVST use and awareness of, and willingnessto, self-test in two early-adopter African countries priorto wide-scale implementation. As such, it providesinsight into the progress and changes made since HIVSThas been rolled out, serving as an example for countriesmonitoring HIVST implementation and scale up. Pool-ing results, however, may have limited the ability to ana-lyse some differences between countries.As a cross-sectional survey using self-reported infor-
mation, there may be reporting bias due to social desir-ability [33]. Previous studies have highlighted challengeswith collecting self-reported data, particularly related tosexual risk behaviours and HIV testing history [34, 35].Thus, it is possible that there may be differences be-tween what people reported and their actual behaviour.Given that HIVST was relatively new during the surveys,it is possible that willingness may also change as morepeople have experience self-testing. Additionally, few re-spondents reported awareness of and past self-testing,which may introduce bias and affect the reliability of theresults. It will be important to assess awareness and useof self-testing, as well as willingness to self-test in the fu-ture, following broader implementation and scale up.Like many population-based surveys, the respondents
included were limited to women 15–49 years old andmen 15–54 years old. Efforts will be needed to considerolder populations, particularly as the median age ofpeople with HIV increases. Also, given that we includedtwo of the first countries to include questions onHIVST, there were discrepancies in implementation,such that not all those surveyed were asked about self-testing, and willingness to self-test could not be assessed
Johnson et al. BMC Public Health (2020) 20:779
139

in Malawians or Zimbabwean women. Willingness toself-test may be similar or different among women andamong Malawians, and it will be important to ensurethat their replies to these questions are included in fu-ture surveys.
ConclusionsEven in 2019, the percentage of people who had nevertested for HIV remained above target for Malawian andZimbabwean men aged !25 years [25]. Reaching thesemen will be critical to achieving the 2030 goals andmaintaining low HIV incidence. Despite low awarenessand previous use of HIVST among 2015–16 DHS re-spondents, willingness to self-test was high, especiallyamong older Zimbabwean men with high sexual risk.Reaching these groups is a priority for HIV testing, pre-vention and care services as we move towards HIV elim-ination. Social determinants – notably urban residence,paid employment, literacy and wealth – had a pro-nounced impact on awareness of HIVST in 2015–16, atime that preceded programmatic implementation.These data provide a valuable baseline against which
to investigate population-level HIVST uptake and equityas programmes scale up. Countries conductingpopulation-based surveys, especially those where HIVSTis being used or is soon to be introduced, should con-sider including questions to assess knowledge andawareness of, and willingness to self-test, with the aim ofproviding baseline data, and to better understand the po-tential impact of HIVST over time and across and withincountries.
Supplementary informationSupplementary information accompanies this paper at https://doi.org/10.1186/s12889-020-08855-7.
Additional File 1: Table S1. Baseline characteristics of men inZimbabwe reporting on willingness to self-test, 2015–16. Supplementarydata with baseline characteristics of men in Zimbabwe reporting on will-ingness to self-test
Additional File 2: Table S2. Univariable and multivariable associationsbetween sociodemographic factors and ever-self-testing for HIV in Malawiand Zimbabwe, 2015–16. Supplementary data with univariable and multi-variable associations between sociodemographic factors and ever-self-testing for HIV in Malawi and Zimbabwe
Additional File 3: Table S3. Univariable and multivariable associationsbetween sociodemographic factors and willingness to self-test amongmen in Zimbabwe, by testing history, 2015–16. Supplementary data withunivariable and multivariable associations between sociodemographicfactors and willingness to self-test among men in Zimbabwe
AbbreviationsaOR: Adjusted odds ratio; CI: Confidence internal; DHS: Demographic andhealth survey; HIV: Human immunodeficiency virus; HIVST: HIV self-testing;IRB: International review board; OR: Odds ratio; STAR: Self-testing AfRica;STI: Sexually transmitted infection; WHO: World health organization
AcknowledgementsWe thank the U.S. Agency of International Development and Noah Bartlett atDemographic Health Surveys for supporting the development of questionsand sharing data.
Authors’ contributionsCJ led the manuscript preparation, data analysis, and interpretation. ELC, MNand PM contributed to interpretation and manuscript and statistical analysis.RN, GN and CQ assisted with collecting and accessing data. AC, VW, KH, RB,FTP provided substantial input and contributed to manuscript. All authors(CJ, MN, PM, AC, CQ, VW, KH, RN, GN, RB, FTP, ELC) have read and approvedthe manuscript.
FundingThe study was funded by a Wellcome Trust Senior Research Fellowship inClinical Science to ELC (grant number: WT091769) and by Unitaid under theSTAR Initiative (NCT02718274). PM is funded by Wellcome (206575/Z/17/Z).The funder had no role in the design of the study and collection, analysis,and interpretation of data or in writing the manuscript.
Availability of data and materialsWe obtained required permissions from DHS and accessed data from theDHS website. All data and materials used in this analysis are availablethrough the DHS programme: https://dhsprogram.com/.
Ethics approval and consent to participateAll DHS and data collection procedures were approved by the ICFInstitutional Review Board (IRB), as well as in the country of research. InZimbabwe, the survey protocol and biomarker collection including HIVtesting procedures were reviewed and approved by the Medical ResearchCouncil of Zimbabwe (MRCZ), the Institutional Review Board of ICFInternational, and the Centers for Disease Control and Prevention (CDC) inAtlanta. In Malawi, the survey protocol, including biomarker collection andHIV testing procedures were reviewed and approved by the National HealthSciences Research Committee in Malawi and the ICF Institutional ReviewBoard. Participation was voluntary, and all individuals provided verbalinformed consent according to approved survey protocols. This articlefeatures a secondary analysis of publicly available DHS data which does notrequire further ethics approval. Details on ethical procedures are provided inthe annexes to DHS reports and on the DHS website: https://dhsprogram.com/What-We-Do/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm.
Consent for publicationIndividual-level data not presented. Not applicable.
Competing interestsThe authors have no competing interests. The contents in this article arethose of the authors and do not necessarily reflect the view of the WorldHealth Organization or the U.S. President’s Emergency Plan for AIDS Relief,the U.S. Agency for International Development or the U.S. Government.
Author details1Global HIV, Hepatitis and STI programme, World Health Organization,Geneva, Switzerland. 2Department of Clinical Research and Infection Disease,London School of Hygiene and Tropical Medicine, London, UK. 3Departmentof Infectious Disease Epidemiology and MRC Tropical Epidemiology Group,London School of Hygiene and Tropical Medicine, London, UK.4Malawi-Liverpool Wellcome Trust, HIV/TB Group, Blantyre, Malawi.5Department of Clinical Sciences, Liverpool School of Tropical Medicine,Liverpool, UK. 6U.S. Agency for International Development, Washington, DC,USA. 7Population Services International, Johannesburg, South Africa. 8Ministryof Health, Lilongwe, Malawi. 9Ministry of Health and Child Care, Harare,Zimbabwe. 10Department of Public Health and Policy, London School ofHygiene and Tropical Medicine, London, UK.
Received: 29 January 2020 Accepted: 5 May 2020
References1. UNAIDS. Communities at the Centre. Geneva: Joint United Nations
Programme on HIV/AIDS; 2019.
Johnson et al. BMC Public Health (2020) 20:779
140

2. WHO. Consolidated guidelines on HIV testing services. Geneva: WorldHealth Organization; 2019.
3. Phillips AN, Cambiano V, Nakagawa F, Bansi-Matharu L, Wilson D, Jani I,et al. Cost-per-diagnosis as a metric for monitoring cost-effectiveness of HIVtesting programmes in low-income settings in southern Africa: healtheconomic and modelling analysis. J Int AIDS Soc. 2019;22(7):e25325.
4. Quinn C, Kadengye DT, Johnson CC, Baggaley R, Dalal S. Who are themissing men? Characterising men who never tested for HIV frompopulation-based surveys in six sub-Saharan African countries. J Int AIDSSoc. 2019;22(10):e25398.
5. Chihana ML, Huerga H, Van Cutsem G, Ellman T, Goemaere E, Wanjala S,et al. Distribution of advanced HIV disease from three high HIV prevalencesettings in sub-Saharan Africa: a secondary analysis data from threepopulation-based cross-sectional surveys in Eshowe (South Africa), Ndhiwa(Kenya) and Chiradzulu (Malawi). Glob Health Action. 2019;12(1):1679472.
6. Hawkes S, Buse K. Gender and global health: evidence, policy, andinconvenient truths. Lancet. 2013;381(9879):1783–7.
7. Baker P, Dworkin SL, Tong S, Banks I, Shand T, Yamey G. The men's healthgap: men must be included in the global health equity agenda. Bull WorldHealth Organ. 2014;92(8):618–20.
8. Johnson CC, Kennedy C, Fonner V, Siegfried N, Figueroa C, Dalal S, et al.Examining the effects of HIV self-testing compared to standard HIV testingservices: a systematic review and meta-analysis. J Int AIDS Soc. 2017;20(1):21594.
9. Jamil M, Wilson I, Witzel C, Figueroa C, Barr-Dichiara M, Rodgers A, et al. ShouldHIV self-testing be offered as an HIV testing approach? ICASA; 2–7 December2019; Kigali, Rwanda. Abstract: THPEC104, https://www.professionalabstracts.com/icasa2019/iplanner/#/presentation/2504. Accessed 16 May 2020.
10. Hatzold K, Gudukeya S, Mutseta M, Chilongosi R, Nalubamba M, Nkhoma C,et al. HIV self-testing: breaking the barriers to uptake of testing among menand adolescents in sub-Saharan Africa, experiences from STARdemonstration projects in Malawi, Zambia and Zimbabwe. J Int AIDS Soc.2019;22(Suppl 1):e25244.
11. UNAIDS. UNAIDS laws and policies Geneva: Joint United NationsProgramme on HIV/AIDS and World Health Organization; 2019. Availablefrom: http://lawsandpolicies.unaids.org/. Accessed 2020 3 Jan.
12. WHO. WHO HIV self-testing need and demand forecast, 2019–2025. Geneva:World Health Organization; 2019.
13. Choko AT, Desmond N, Webb EL, Chavula K, Napierala-Mavedzenge S,Gaydos CA, et al. The uptake and accuracy of oral kits for HIV self-testing inhigh HIV prevalence setting: a cross-sectional feasibility study in Blantyre,Malawi. PLoS Med. 2011;8(10):e1001102.
14. Mavengere Y, Sibanda E, Hatzold K, Cowan F, Mugurungi O, Mavedzenge S.Can ‘late-read’ of self-test devices be used as a quality assurance measure?:results of a pilot HIV self-test project in Zimbabwe. 21st International AIDSconference; 18–22 July 2016; Durban, South Africa. Abstract: TUPEE636; http://programme.aids2016.org/Abstract/Abstract/4171. Accessed 16 May 2020.
15. Neuman M, Indravudh P, Chilongosi R, d'Elbée M, Desmond N, Fielding K, et al.The effectiveness and cost-effectiveness of community-based lay distributionof HIV self-tests in increasing uptake of HIV testing among adults in ruralMalawi and rural and peri-urban Zambia: protocol for STAR (self-testing forAfrica) cluster randomized evaluations. BMC Public Health. 2018;18(1):1234.
16. Choko AT, Corbett EL, Stallard N, Maheswaran H, Lepine A, Johnson CC,et al. HIV self-testing alone or with additional interventions, includingfinancial incentives, and linkage to care or prevention among male partnersof antenatal care clinic attendees in Malawi: an adaptive multi-arm, multi-stage cluster randomised trial. PLoS Med. 2019;2019(1):e1002719.
17. Choko AT, MacPherson P, Webb EL, Willey BA, Feasy H, Sambakunsi R, et al.Uptake, accuracy, safety, and linkage into care over two years of promotingannual self-testing for HIV in Blantyre, Malawi: a community-basedprospective study. PLoS Med. 2015;12(9):e1001873.
18. Sibanda E, Neuman M, Tumushime M, Hatzold K, Watadzaushe C, MutsetaM, et al. Linkage to care after HIV self-testing in Zimbabwe: a cluster-randomised trial. Conference on opportunistic infections and retroviruses;3–6 Mar 2018; Boston, USA.
19. Indravudh P, Fielding K, Kumwenda M, Nzawa R, Chilongosi R, Desmond N,et al. Community-led delivery of HIV self-testing targeting adolescents andmen in rural Malawi: a cluster-randomised trial. 10th International AIDSsociety conference; 21–24 July 2019; Mexico City, Mexico. Abstract:MOSY0105LB; http://programme.ias2019.org/Abstract/Abstract/4874.Accessed 16 May 2020.
20. Cambiano V, Johnson CC, Hatzold K, Terris-Prestholt F, Maheswaran H,Thirumurthy H, et al. The impact and cost-effectiveness of community-based HIV self-testing in sub-Saharan Africa: a health economic andmodelling analysis. J Int AIDS Soc. 2019;22(Suppl 1):e25243.
21. Johnson LF, van Rensburg C, Govathson C, Meyer-Rath G. Optimal HIVtesting strategies for South Africa: a model-based evaluation of population-level impact and cost-effectiveness. Sci Rep. 2019;9(1):12621.
22. NOS and ICF. Malawi Demographic and Health Survey 2015–16. Zomba,Malawi: National Statistical Office and ICF; 2017.
23. Zimbabwe National Statistics Agency and ICF International. ZimbabweDemographic and Health Survey 2015. Final report. Zimbabwe NationalStatistics Agency and ICF International: Rockville, Maryland, USA; 2016.
24. Corrani P, Olsen M, Pedersen L, Dekkers O, Vandenbroucke J. Effectmodification, interaction and mediation: an overview of theoretical insightsof clinical investigators. Clin Epidemiol. 2017;9:331–8.
25. Giguère K, Eaton J, Marsh K, Stannah J, Maheu-Giroux M. “First 90” estimates:where are the gaps? ICASA; 2–7 Dec 2019; Kigali, Rwanda.
26. UNAIDS. UNAIDS estimates, average age of people living with HIV. Geneva:Joint United Nations Programme on HIV/AIDS; 2019.
27. Offorjebe O, Shaba F, Balakasi K, Nyrienda M, Hoffman R, Dovel K, et al.Partner-delivered HIV self-testing increases the perceived acceptability ofindex partner testing among HIV-positive clients in Malawi. 22ndInternational AIDS Conference; 23–27 July 2018; Amsterdam, Netherlands.Abstract: WEPEE683; http://programme.aids2018.org/Abstract/Abstract/5275.Accessed 16 May 2020.
28. Dovel K, Shaba F, Offorjebe OA, Balakasi K, Nyirenda M, Phiri K, et al. Effectof facility-based HIV self-testing on uptake of testing among outpatients inMalawi: a cluster-randomised trial. Lancet Glob Health. 2020;8(2):e276–e87.
29. WHO and ILO. HIV self-testing at the workplace. Geneva: InternationalLabour Organization; World Health Organization; 2018.
30. Wong V, Jenkins E, Ford N, Ingold H. To thine own test be true: HIV self-testing and the global reach for the undiagnosed. J Int AIDS Soc. 2019;22(Suppl 1):e25256.
31. Indravudh P, Fielding K, Neuman M, Chilongosi R, Mkandawire P, Nyondo E,et al. Increasing knowledge of HIV status and demand for antiretroviraltherapy using community-based HIV self-testing in rural communities: acluster randomised trial in Malawi. 22nd International AIDS conference; 25–27 July 2018; Amsterdam, Netherlands. Abstract: THPDC0103; http://programme.aids2018.org/Abstract/Abstract/7310. Accessed 16 May 2020.
32. WHO and Unitaid. Landscape for HIV rapid diagnostic tests for HIV self-testing. Geneva: Unitaid and World Health Organization; 2015.
33. Fisher R. Social desirability bias and the validity of indirect questioning. JConsum Res. 1993;20(2):303–15.
34. Rentsch CT, Reniers G, Machemba R, Slaymaker E, Marston M, Wringe A,et al. Non-disclosure of HIV testing history in population-based surveys:implications for estimating a UNAIDS 90-90-90 target. Glob Health Action.2018;11(1):1553470.
35. Slaymaker E. A critique of international indicators of sexual risk behaviour.Sex Transm Infect. 2004;80(Suppl 2):ii13–21.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Johnson et al. BMC Public Health (2020) 20:779
141

Vol.:(0123456789)1 3
AIDS and Behavior (2020) 24:2409–2420 https://doi.org/10.1007/s10461-020-02801-9
ORIGINAL PAPER
Addressing Intimate Partner Violence and!Power in!Intimate Relationships in!HIV Testing Services in!Nairobi, Kenya
Nicole!Haberland1 !· Charity!Ndwiga2!· Katharine!McCarthy1!· Julie!Pulerwitz3!· Rose!Kosgei4!· Margaret!Mak’anyengo4!· Amelia!Peltz5!· Vincent!J.!Wong5 !· Sam!Kalibala3
Published online: 6 February 2020 © The Author(s) 2020
AbstractIntimate partner violence (IPV) undermines women’s uptake of HIV services and violates their human rights. In a two-arm randomized controlled trial we evaluated a short intervention that went a step beyond IPV screening to discuss violence and power with women receiving HIV testing services during antenatal care (ANC). The intervention included training and sup-port for HIV counselors, a take-home card for clients, and an on-site IPV counselor. One third (35%) of women (N = 688) reported experiencing IPV in the past year; 6% were living with HIV. Among women experiencing IPV, program participants were more likely to disclose violence to their counselor than women receiving standard care (32% vs. 7%, p < 0.001). At second ANC visit, intervention group women were significantly more likely to report that talking with their counselor made a positive di!erence (aOR 2.9; 95% CI 1.8, 4.4; p < 0.001) and felt more confident in how they deserved to be treated (aOR 2.7; 95% CI 1.7, 4.4; p < 0.001). Exploratory analyses of intent to use ARVs to prevent mother-to-child transmission and actions to address violence were also encouraging.
Keywords HIV testing services"· Intimate partner violence"· Power in relationships
Introduction
Meeting HIV epidemic control goals and closing gaps in the HIV testing to treatment cascade entails more than expanded testing and antiretroviral treatment (ART) provi-sion; it entails active engagement with the structural barri-ers to treatment initiation and adherence. Prominent among these structural barriers is intimate partner violence (IPV) which requires urgent attention not only in and of itself, but
also because of its impact on other health and development indicators, including those related to HIV testing services (HTS). For example, a systematic review and meta-analysis found IPV to be associated with significantly lower ART use, lower ART adherence, and lower odds of viral load suppression among women [1]. Similar results were found in a recent scoping review [2]. A study in Zambia found that women who reported experiencing IPV had signifi-cantly reduced odds of adherence to medications to prevent mother-to-child transmission, including a reduced likelihood of adherence to drugs during pregnancy, adherence to drugs postpartum, and adherence to giving the infant prophylaxis [3].
The number of women a!ected by IPV is significant. The World Health Organization (WHO) has estimated that 30% of ever-partnered women globally have experienced physi-cal and/or sexual IPV, calling IPV a public health problem of “epidemic proportions” [4]. In Nairobi, Kenya, the most recent Demographic and Health Survey (2014 DHS) found that about a third (35%) of ever-married women reported experiencing physical and/or sexual violence at the hands of their intimate partner in the past 12"months [5].
Electronic supplementary material The online version of this article (https ://doi.org/10.1007/s1046 1-020-02801 -9) contains supplementary material, which is available to authorized users.
* Nicole Haberland [email protected] Population Council, One Dag Hammarskjold Plaza,
New"York, NY"10017, USA2 Population Council, Nairobi, Kenya3 Population Council, Washington, DC, USA4 Kenyatta National Hospital, Nairobi, Kenya5 O#ce of"HIV/AIDS, United States Agency for"International
Development, Washington, DC, USA
142

AIDS and Behavior (2020) 24:2409–2420
1 3
Thus, increasingly, the recommendation is to incorpo-rate attention to IPV in HIV testing services so as to sup-port women’s dignity and rights, and so that we do not lose women experiencing violence in the testing to treat-ment cascade [6, 7]. What to do and how to do it, however, remains a question. WHO guidelines for IPV, for example, discourage universal screening, but note that routine inquiry is warranted in antental care (ANC) settings and, though further research is needed, it may also be warranted in HTS [8]. Screening and referral interventions have been found to be acceptable and welcomed by women [9, 10], though the identification of women experiencing IPV is often low when compared to estimated IPV prevalence. For example, a recent systematic review of brief screening interventions in healthcare settings found a median disclosure prevalence of 8 percent [11] and a study in Kenya found the same preva-lence in an IPV screening feasibility study [9]. Moreover, even among those women who disclose, many do not fol-low up on referrals. This has led some researchers [9–11] to recommend testing interventions that take a step beyond IPV screening and referral. Recommendations include providing basic psychosocial support for IPV and information at the time of screening, or equipping counselors to discuss gender power inequality in relationships more broadly, including IPV as a manifestation of that inequality.
These recommendations are bolstered by both theory and qualitative research. The theory of gender and power has been used in the HIV field to articulate how gender norms and power inequalities in relationships increase women’s HIV risk through multiple pathways, including norms of male toughness and acceptance of IPV perpetration, vio-lence as a way to control women and maintain male domi-nance, notions of masculinity that endorse multiple partners and condomless sex for men, and notions of femininity that value women’s compliance and placing others’ needs above their own [12–14]. IPV and inequalities in relationships are thus mutually reinforcing and both decrease women’s ability to avoid HIV risk.
Qualitative research on what women who experience violence want from health professionals suggests that what providers say, and the nature of the interaction may be more important than whether a woman discloses violence or not [15–17]. A review of qualitative studies by Feder and col-leagues found several recurring themes across 29 articles (25 studies) [15]. These themes included, for example, that women want providers to be nonjudgmental and to raise the issue of IPV in a compassionate and sensitive manner. It is important to confirm that the violence is unacceptable and not their fault. Women want to deal with the issue at their own pace and not be pressured to disclose to the provider. Learning about available resources regardless of whether they are ready to pursue them and feeling supported were other key themes. These findings suggest why interventions
where providers ask screening questions such as, “Has your partner ever hit, choked, or physically hurt you?” and rely on the woman to disclose and follow-up on a referral, tend to have low rates of IPV disclosure and referral uptake. Not only does this leave women who disclose but are not ready to pursue a referral without support, it also leaves the women who either do not yet recognize that they are being abused, or who are not yet ready to disclose, without support or knowledge about resources available.
To respond to these evidence gaps and recommendations, we rigorously tested a simple pilot intervention that aimed to take a step beyond IPV screening and discuss violence and power with all women receiving HIV testing services. Our theory of change was that if all women were engaged with this basic information during HTS they would be more likely to feel comfortable disclosing violence, would receive important first-line support regardless of whether they fol-lowed up on a referral, and even if they chose not to disclose, would receive valuable information about their rights and where to go if and when they decide to seek help. The pri-mary hypothesis was that IPV knowledge would be greater in the experimental group compared to the control group. Our secondary hypothesis was that women who received the intervention would be more likely to feel supported than women in the control group, and our exploratory hypotheses were that women in the experimental group, compared to the control group, would be more likely to do something about the violence and adhere to ART.
Methods
Setting
The study took place in Kenyatta National Hospital’s (KNH’s) ANC clinic in Nairobi, Kenya, from February 2015 to August 2015. KNH is a teaching hospital and the oldest and largest public referral hospital in the East Africa region, with KNH’s ANC clinic receiving upwards of 1000 clients per month. All ANC clients at KNH receive HTS as part of their first ANC visit of their current pregnancy. Women can choose to opt out of HIV testing. While IPV screening is supposed to be part of standard HTS counseling in the ANC clinic, it is inconsistently implemented.
Referrals for IPV are to KNH’s Gender-Based Violence Recovery Centre (GBV Centre), located within the KNH complex, about 5 min walk from the ANC clinic [18]. The GBV Centre provides comprehensive post-rape care that includes emergency care such as post-exposure prophylaxis (PEP); treatment for sexually transmitted infections (STIs); trauma counseling; and psychological support via individual counseling, support groups, and connecting women to social workers. The Centre also arranges referrals to safe houses
143

AIDS and Behavior (2020) 24:2409–2420
1 3
if the client’s home environment is unsafe, to police, and to organizations that o!er legal services.
Standard HTS Care
For HIV-negative mothers, standard HTS counseling in the ANC clinic consists of discussing a birth plan, couple coun-seling if accompanied by a partner, information on danger signs during pregnancy, importance of attending scheduled ANC visits, maternal nutrition, STI risk reduction, postpar-tum family planning, hygiene and self-care, infant feeding, and male partner engagement in ANC/childcare. Women are also supposed to be screened for IPV and referred to the GBV Centre if they are experiencing violence. Mothers with HIV, in addition to the preceding, receive counseling on CD4 counts, ART, importance of adherence, and specialized care such as mother-to-mother groups and nutrition clinics.
Intervention
The pilot intervention was implemented from March to July 2015 and included four main parts. The first component was a provider training. All providers in the ANC clinic partici-pated in a 1-day o!-site training on GBV. While providers had previous training at KNH in IPV screening and care, this training provided a refresher and an orientation to the intervention and study. The training included participatory activities—for example, myths and facts about IPV, and how relationship inequalities a!ect women’s well-being—and evidence on the impact of IPV and power inequalities in rela-tionships on HIV prevention and care. The HTS counselors also received hands-on practice conducting the intervention. The 28 HTS counselors—25 females and 3 males—included lay counselors with between 2 and 10"years of experience, and nurses with between 4 and 20"years of experience.
The second intervention component included counseling aids for providers to use during the post-test counseling ses-sion. One was a small tri-fold card with key messages and resources regarding IPV, power, and women’s health. Cards developed by Futures Without Violence [19] for clinical set-tings in the U.S. were adapted by the study team to meet the objectives of this study and setting. The cards included a panel on facts, such as prevalence of IPV in Nairobi, and that being in a relationship characterized by IPV or low power for the woman increases her risk for HIV and STIs and can harm her baby’s health. Another panel posed reflective ques-tions about the nature of the relationship—for example, is my partner’s communication honest and open? Who is mostly responsible for making decisions? Does my partner value my opinions and respect my choices? Is my partner respectful and kind to me? Relationship control and IPV were the focus of a third panel and asked about controlling behavior, physical and sexual abuse, and whether the woman
was afraid to ask about condom use or tell her partner she has an STI or HIV. A highlighted panel included messages to remember such as, “You matter. You have a right to be free from violence,” “You are not to blame if you are experienc-ing any form of abuse,” and “There are people here who can help you.” Two additional panels covered possible things that a woman could do if she is being hurt or feels powerless, and provided contact information for four places to turn to for help in Nairobi: The GBV Centre at KNH, the Women’s Rights Awareness Programme (which provides safe shelter), Nairobi Women’s Hospital Gender Violence and Recovery Centre, and Centre for Rights Education and Awareness. HTS counselors gave the card to the woman as a resource to keep or share.
Counselors used a counseling script that elaborated the main messages on the card. The script guided counselors to introduce the topic of IPV by saying something like, “We’ve begun giving this card to all our ANC clients so they know how to get help for themselves if they need it, or so they can help a friend or family member who might need it.” For the card’s relationships panel, for example, the script read, “I am talking with all my clients about their relationships. Even if you are not in a relationship now, this is still important information for the future. I want you to think about these questions… Is your partner kind to you? Does he respect you and support you? If so, that is great. That makes it easier for you to protect your health and your children’s health.” Other key messages in the script included, “Remember, you have a right to be free from violence and you deserve to be treated with respect” and “Even if you don’t need any of this sup-port now, relationships change—remember you can always come back to KNH for help.” The enhanced counseling took on average 6.5"min longer to implement than standard HTS (29"min vs. 23"min), the most common length (mode) of both enhanced and standard HTS sessions was 10"min.
Third, an IPV counselor from the GBV Centre was posted on-site in the ANC clinic to handle all IPV referrals immedi-ately, with the intent of cutting down logistical and time bar-riers women face when following-up on referrals to clinics elsewhere in the KNH complex. To further facilitate access to the IPV counselor, a volunteer peer counselor accom-panied referred women to the IPV counselor and/or GBV Centre.
Finally, HTS counselors involved in the study attended support group sessions facilitated by experienced counselor supervisors from KNH’s mental health unit. The purpose of the sessions was to o!er a space for the counselors to debrief and process vicarious trauma, and to discuss questions and strategies about how to handle di!erent situations.
144

AIDS and Behavior (2020) 24:2409–2420
1 3
Study design
A randomized controlled trial assessed indicators on the hypothesized pathway of change—i.e., whether clients were screened for IPV, whether clients disclosed IPV, whether they received a referral, and whether they fol-lowed up on a referral—and intermediate outcomes—i.e., our primary outcome: IPV knowledge; and second-ary outcome: whether clients felt supported. While the study was not designed to assess whether the interven-tion helped women address IPV or improve antiretroviral (ARV) adherence (the intervention’s longer term aims), we examined intent to adhere to ARVs to prevent mother-to-child transmission and actions taken to address IPV as exploratory outcomes.
All first-visit ANC clients during the study period (882) were approached and screened for eligibility. Out of 852 eligible women, 698 (82%) agreed to par-ticipate. Reasons given for declining to participate in the study were time concerns and competing obligations. Consenting participants were randomly assigned 1:1 to either intervention (IPV-HTS) or control (standard HTS) counseling.
To minimize bias that could be the result of counselors’ skills, experience, or personality, all counselors provided both the intervention and the standard counseling. While this increased the risk of spillover, the importance of adhering to the protocol was emphasized in training and in regular check-ins. In addition, the clients’ folders included standard HTS materials or IPV-HTS materials, depend-ing on the ANC clients’ assignment to the intervention or control group. Because IPV screening is part of standard HTS counseling, if women in standard care disclosed IPV to their HTS counselor, the counselors explained the ser-vices available, i.e., IPV counseling in the ANC clinic and the GBV Centre; and referred her based on the women’s situation and needs.
Review of clients’ ANC card and HTS forms supple-mented survey questionnaires administered to participants. Participants were interviewed immediately after receiving their ANC and HTS services, and then interviewed again approximately 1"month later at a subsequent ANC visit. The first-round interview was conducted after the inter-vention for ethical and research design reasons. Had we interviewed women before they received their HTS, and if a participant disclosed experiencing violence to the inter-viewer, the interviewer would, for ethical reasons, o!er empathy and refer the woman for IPV counseling before she even saw an IPV-HTS or standard HTS counselor. As identifying women who are experiencing violence and referring them for IPV counseling are part of the interven-tion, such support and referrals by the interviewer would have pre-empted the intervention. Thus, both women in
the intervention and control groups were interviewed post-HTS. In the post-HTS interviews, survey questions asked every participant about IPV, and if women responded that they had experienced IPV, the interviewer referred the woman for counseling. The interviewers did this regard-less of which study arm the woman was in.
Inclusion/Exclusion Criteria
Inclusion criteria were: first-time ANC client (i.e., a woman presenting for her first ANC visit of her current pregnancy) and being aged between 15 and 49"years. Exclusion criteria were having received an HIV test in the previous 6"months.
Data collection
Following their post-test HIV counseling, clients were inter-viewed by research sta! using a structured questionnaire. Surveys were translated into Swahili and scales’ internal consistency (reliability) was assessed after adaptation to the local language. Questions covered socio-demographic information, clients’ relationship status, partner character-istics, condom use, HIV testing, couples HTS, disclosure of HIV status, knowledge of partner’s status, and perceived di#culty disclosing or asking about a partner’s HIV status. Power inequalities in the relationship were assessed using the Sexual Relationship Power Scale (SRPS) (Cronbach’s $ = 0.67) [12]. As recommended, the Relationship Control and Decision-making Dominance subscales of the overall SRPS were combined and rescaled to have a final score ranging from 1 to 4, with a higher score indicating greater relationship power for the woman. Attitudes toward gender norms were measured using a South African adaptation of the GEM Scale (Cronbach’s $ = 0.80) [20, 21]. The total scale items were averaged so that the overall scale ranged from 1 to 3, with a higher score indicating greater endorse-ment of gender equitable norms.
We asked about women’s experience of emotional, physical, and sexual violence in her lifetime, in the past 12"months, and by current and other partner/s. For exam-ple, for emotional violence, women were asked whether in the past 12"months her current partner had insulted her or made her feel bad about herself; belittled or humiliated her in front of other people; did things to scare or intimidate her on purpose; or threatened to hurt her or someone she cared about. If the answer to each of these questions was ‘no,’ they were followed up with whether her current partner had ever done any of these things; whether another partner had done these things in the past 12"months, or if anyone had ever done these things. We also asked whether the woman had ever sought help for IPV. For most analyses, we operation-alized IPV as any IPV—emotional, physical, or sexual—experienced in the past 12"months. Where noted, we also
145

AIDS and Behavior (2020) 24:2409–2420
1 3
looked separately at those women who reported physical and/or sexual violence only in the past 12"months. Finally, the questionnaire also asked women about their HTS coun-seling experience, including whether she disclosed violence to the counselor and her follow-up or intent to follow-up on the referral. Information on HIV status was extracted from participants’ ANC medical charts.
A second interview was conducted with participants at a subsequent ANC visit (mean duration between inter-views was 4.4"weeks) to ascertain whether women had followed up on referrals, assess whether any beneficial e!ects were sustained, and to monitor whether she had experienced any adverse outcomes due to the intervention. We asked relevant behavioral and self-e#cacy questions, such as confidence in ability to regularly take ARVs to pre-vent maternal to child transmission, to explore whether the intervention had the potential to improve these outcomes.
Analysis
Sample size was calculated to detect a 13% point di!er-ence between study arms in IPV-related knowledge and awareness. As no prior data on these indicators existed, 57% baseline prevalence was assumed using endorsement of IPV from the DHS as a proxy variable [22]. Calcula-tions were based on the following additional assumptions: % = 0.80, $ = 0.05, 10% non-response rate, and 25% attri-tion while applying the continuity correction. The study was not powered to assess changes in subgroup analyses (e.g., among women living with or without HIV).
Statistical analysis was performed in R Studio Version 3.1 (R Studio Inc., Boston, MA), using an intent-to-treat approach. Chi-square and two-sample t-tests were used to assess whether women systematically di!ered on sociode-mographic characteristics, endorsement of gender norms, or relationship characteristics with regard to study arm or attrition status. Bivariate analyses were also used to assess cross-sectional di!erences between intervention and con-trol group participants at first and second follow-up. Pair-wise missing data were excluded from analysis. We used multivariate logistic and linear regression analysis to assess di!erences in outcomes at each follow-up time by interven-tion assignment. Di!erences were considered statistically significant at p < 0.05.
Ethical Review
The study protocol was reviewed and approved by the Popu-lation Council Institutional Review Board (New York), and the Kenyatta National Hospital/University of Nairobi Ethics
and Research Committee. Written informed consent was obtained from each respondent prior to study participation.
Trial Registration
ClinicalTrials.gov #NCT02577380.
Results
A total of 698 ANC clients attending KNH’s ANC clinic during the enrollment period met study eligibility criteria, provided written informed consent, and were randomized to intervention or control groups. Ten questionnaires had conflicting data on intervention assignment that could not be resolved and were excluded from analysis. We success-fully interviewed 535 of 688 women at a next ANC visit (78% retention). Of the women lost to follow-up, most did not return to KNH for a subsequent ANC visit because they had delivered their baby, changed clinics, or did not pursue additional ANC visits. Study arms did not di!er with respect to attrition rate. There were no significant di!erences in the types of respondents who remained in the study and those lost to follow-up in terms of age, edu-cation, marital status, HIV status, or experience of IPV.
Participant Characteristics
Women participating in the study were, on average, 29"years old (Table"1). Half (49.6%) of participants had completed some tertiary education. Four-fifths (82%) were currently married; of the remainder (data not shown) 2% were unmarried but living with a man, 9% had a regular partner but were not living together, and 6% were single. Based on HIV data in ANC client charts, 5.7% of women were living with HIV. Approximately 8% of women reported food insecurity. Women’s average scores were 2.5 on the GEM Scale (with 1 being the least and 3 being the most endorsement of equitable gender norms) and 2.5 on the SRPS (with 1 being a low power position for women and 4 being a high power position). Thirty-eight percent of women reported ever experiencing IPV.
Of the women who had ever experienced IPV, the vast majority—93% (241 out of 258)—had experienced it in the past year. Emotional IPV was reported by 29% of women; physical IPV was reported by 14% of women; and sexual violence was reported by 13% of women. One in five (21%) of women reported experiencing physical or sexual violence. The intervention and control groups do not di!er statistically on any type of reported IPV,
146

AIDS and Behavior (2020) 24:2409–2420
1 3
Table 1 Sample characteristics by study arm
a Chi-square test for categorical variables and independent t-test for continuous variables. Significance at p < 0.05b Married or living togetherc GEM scale measured on 1 to 3-point scale with higher score indicating more equitable views on gender normsd SRPS measured on 1 to 4-point scale with higher score indicating more equitable relationships
TotalN = 688 (%)
InterventionN = 337 (%)
ControlN = 351 (%)
P-valuea
Age group"15–19 1.6 1.1 2.1 0.31"20–24 16.4 16.9 15.9"25–29 34.1 35.0 33.2"30–34 29.9 31.2 28.4"35–39 15.4 12.6 18.3"40–45 2.6 3.2 2.1
Mean age (SD) 29.4 (± 5.2) 29.2 (± 5.2) 29.6 (± 5.3) 0.26Education"Primary 17.8 19.1 16.4 0.47"Secondary 32.6 33.4 31.6"College/University 49.6 47.4 51.9
Marital statusb
"No 18.1 16.6 19.7 0.32"Yes 81.9 83.4 80.3
HIV status"Negative 94.3 94.5 94.1 0.86"Positive 5.7 5.5 5.9
Food insecure"No 91.9 92.3 91.4 0.68"Yes 8.1 7.7 8.6
Gender equitable normsc Mean (SD) 2.5 (± 0.4) 2.4 (± 0.4) 2.5 (± 0.4) 0.08Sexual relationship powerd Mean (SD) 2.5 (± 0.4) 2.5 (± 0.4) 2.5 (± 0.4) 0.009Ever experienced IPV"No 62.1 59.2 65.2 0.11"Yes 37.9 40.8 34.8
IPV in past 12"months (any type)"No 65.0 61.8 68.2 0.008"Yes 35.0 38.2 31.8
Emotional IPV in past 12"months"No 70.9 68.1 73.9 0.11"Yes 29.1 31.9 26.1
Physical IPV in past 12"months"No 85.8 85.1 86.5 0.66"Yes 14.2 14.9 13.5
Sexual IPV in past 12"months"No 87.1 85.6 88.6 0.26"Yes 12.9 14.4 11.4
Physical or sexual IPV in past 12"months"No 78.7 77.3 80.2 0.40"Yes 21.3 22.7 19.8
Days between survey rounds"Mean (SD) 30.9 (± 20.4) 31.0 (± 20.4) 30.9 (± 20.5) 0.99
147
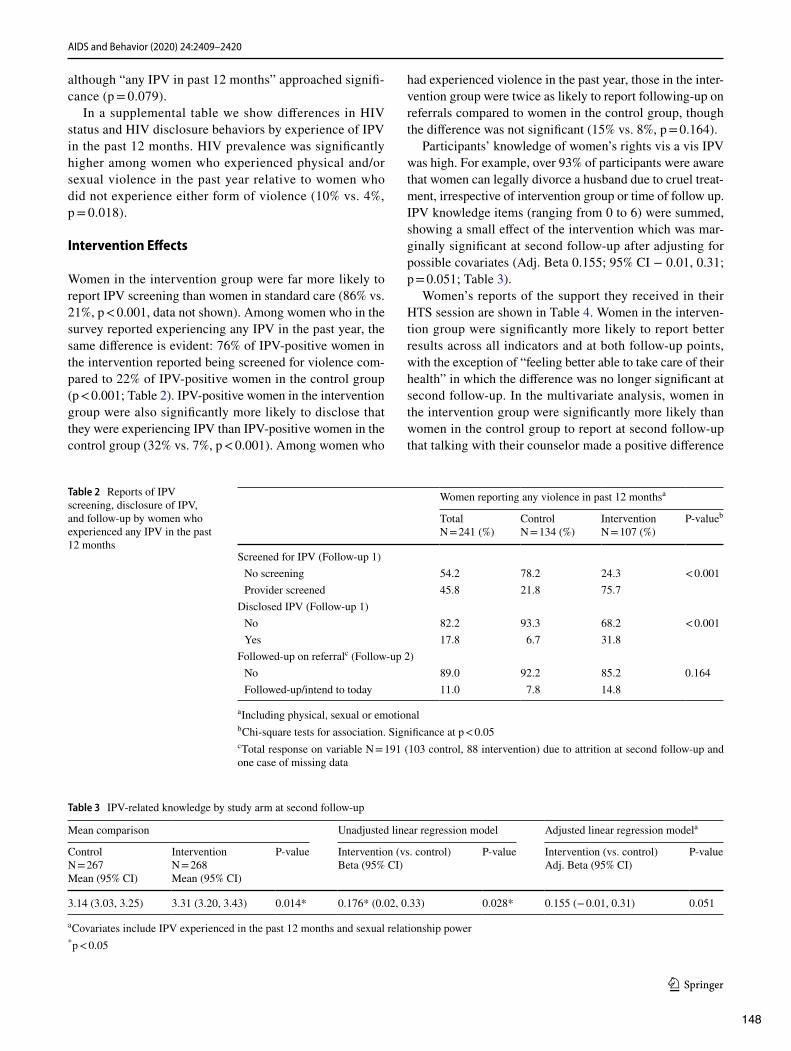
AIDS and Behavior (2020) 24:2409–2420
1 3
although “any IPV in past 12"months” approached signifi-cance (p = 0.079).
In a supplemental table we show di!erences in HIV status and HIV disclosure behaviors by experience of IPV in the past 12"months. HIV prevalence was significantly higher among women who experienced physical and/or sexual violence in the past year relative to women who did not experience either form of violence (10% vs. 4%, p = 0.018).
Intervention E!ects
Women in the intervention group were far more likely to report IPV screening than women in standard care (86% vs. 21%, p < 0.001, data not shown). Among women who in the survey reported experiencing any IPV in the past year, the same di!erence is evident: 76% of IPV-positive women in the intervention reported being screened for violence com-pared to 22% of IPV-positive women in the control group (p < 0.001; Table"2). IPV-positive women in the intervention group were also significantly more likely to disclose that they were experiencing IPV than IPV-positive women in the control group (32% vs. 7%, p < 0.001). Among women who
had experienced violence in the past year, those in the inter-vention group were twice as likely to report following-up on referrals compared to women in the control group, though the di!erence was not significant (15% vs. 8%, p = 0.164).
Participants’ knowledge of women’s rights vis a vis IPV was high. For example, over 93% of participants were aware that women can legally divorce a husband due to cruel treat-ment, irrespective of intervention group or time of follow up. IPV knowledge items (ranging from 0 to 6) were summed, showing a small e!ect of the intervention which was mar-ginally significant at second follow-up after adjusting for possible covariates (Adj. Beta 0.155; 95% CI & 0.01, 0.31; p = 0.051; Table"3).
Women’s reports of the support they received in their HTS session are shown in Table"4. Women in the interven-tion group were significantly more likely to report better results across all indicators and at both follow-up points, with the exception of “feeling better able to take care of their health” in which the di!erence was no longer significant at second follow-up. In the multivariate analysis, women in the intervention group were significantly more likely than women in the control group to report at second follow-up that talking with their counselor made a positive di!erence
Table 2 Reports of IPV screening, disclosure of IPV, and follow-up by women who experienced any IPV in the past 12"months
a Including physical, sexual or emotionalb Chi-square tests for association. Significance at p < 0.05c Total response on variable N = 191 (103 control, 88 intervention) due to attrition at second follow-up and one case of missing data
Women reporting any violence in past 12 monthsa
TotalN = 241 (%)
ControlN = 134 (%)
InterventionN = 107 (%)
P-valueb
Screened for IPV (Follow-up 1)"No screening 54.2 78.2 24.3 < 0.001"Provider screened 45.8 21.8 75.7
Disclosed IPV (Follow-up 1)"No 82.2 93.3 68.2 < 0.001"Yes 17.8 6.7 31.8
Followed-up on referralc (Follow-up 2)"No 89.0 92.2 85.2 0.164"Followed-up/intend to today 11.0 7.8 14.8
Table 3 IPV-related knowledge by study arm at second follow-up
a Covariates include IPV experienced in the past 12"months and sexual relationship power* p < 0.05
Mean comparison Unadjusted linear regression model Adjusted linear regression modela
Control N = 267Mean (95% CI)
Intervention N = 268Mean (95% CI)
P-value Intervention (vs. control)'eta (95% CI)
P-value Intervention (vs. control)Adj. 'eta (95% CI)
P-value
3.14 (3.03, 3.25) 3.31 (3.20, 3.43) 0.014* 0.176* (0.02, 0.33) 0.028* 0.155 (& 0.01, 0.31) 0.051
148

AIDS and Behavior (2020) 24:2409–2420
1 3
(aOR 2.9; 95% CI 1.8, 4.4; p < 0.001), they learned new things about a woman’s rights in her relationship (aOR 3.7; 95% CI 2.3, 6.1; p < 0.001), and felt more confident in how they deserved to be treated (aOR 2.7; 95% CI 1.7, 4.4; p < 0.001).
While our sample was not powered to detect changes among subgroups, we conducted exploratory analyses to assess whether there were di!erences among women who reported experiencing any IPV in the past 12"months (Table"5). At second follow-up, agency for asking partner to go to couples HTS tended to be higher in the intervention group than the control group (though not significantly so) (76% vs. 71%, p = 0.59), and so were: being better able to take care of one’s health/well-being (88% vs. 80%, p = 0.16), asking partner to use a condom (58% vs 49%, p = 0.31), and intending to regularly take medications to prevent mother-to-child transmission (among those women living with HIV, 62% vs. 48%, p = 0.38).
Finally, we conducted exploratory analyses of IPV-related outcomes (Table"6). Among women who had experienced any type of violence in the past year, a higher proportion in the intervention group reported taking any action to address the violence (i.e., following up on a referral, leaving a
partner, telling someone, or going somewhere for help) com-pared to control (36% vs. 26%, p = 0.09) at second follow-up. Among those women experiencing physical or sexual vio-lence in the past year, the proportion of women taking any action was also higher in the intervention group compared to the control (46% vs. 31%, p = 0.07).
Discussion
IPV is widely recognized as a pandemic that must be addressed as a problem in its own right, and because of its deleterious e!ects on health and development, including on outcomes along the HIV prevention, treatment and care con-tinuum. Because IPV may a!ect disclosure of HIV status, ability to follow-up on treatment, and the safety of women who disclose, HTS has been identified as a service deliv-ery point that can contribute to a multi-sector response to IPV, though further research is needed [8]. We tested a pilot intervention that sought to provide all ANC clients receiving HTS, regardless of whether they screened positive for IPV, with basic information and resources about IPV and power inequalities in relationships during post-test HIV counseling.
Table 4 Regression model of perceived intervention support, by study arm at first and second follow-up using logistic regression analysis
a Adjusted analyses also included sexual relationship power and experience of intimate partner violence within the past 12"monthsb Response dichotomized as ‘Yes a lot’ vs. ‘A little’, ‘A fair amount’ or ‘Not at all’c Variable not comparable between rounds and only Follow-up 2 is displayedd Response coded as ‘Better’, ‘Same’ or ‘Worse’. Note: No women responded ‘Worse’Significance at p < 0.05
Unadjusted intervention (vs. control) Adjusteda intervention (vs. control)
OR (95% CI) P-value aOR (95% CI) P-value
Talking with provider made positive di!erenceb
"Follow-up 1""Agree a lot (vs. agree somewhat or disagree) 2.83 (1.78, 4.52) < 0.001 2.76 (1.72, 4.42) < 0.001
"Follow-up 2""Agree a lot (vs. agree somewhat or disagree) 2.95(1.89, 4.60) < 0.001 2.89 (1.84, 4.41) < 0.001
Learned new things about a woman’s rights in her relationshipb
"Follow-up 2c
""Agree a lot (vs. agree somewhat or disagree) 3.79 (2.32, 6.19) < 0.001 3.72 (2.27, 6.10) < 0.001Feel better able to take care of health than before visitd"Follow-up 1""Better (vs. same) 3.83 (2.03, 7.22) < 0.001 4.00 (2.08, 7.71) < 0.001
"Follow-up 2""Better (vs. same) 1.23 (0.50, 3.03) 0.643 1.15 (0.47, 2.85) 0.754
Feel more confident in how deserve to be treatedd
"Follow-up 1""Better (vs. same) 4.96 (3.30, 7.44) < 0.001 5.03 (3.33, 7.86) < 0.001
"Follow-up 2""Better (vs. same) 2.81 (1.76, 4.49) < 0.001 2.72 (1.70, 4.36) < 0.001
149

AIDS and Behavior (2020) 24:2409–2420
1 3
Although women who received IPV/power-enhanced counseling had greater IPV knowledge compared to women in the control group, after adjusting for possible covariates the di!erence was just marginally significant at p = 0.051, possibly because of relatively high knowledge levels among all women in the study. IPV/power-enhanced counseling sig-nificantly increased the proportion of IPV-positive women who disclosed IPV to their HTS counselor compared to standard care. The proportion of women in the intervention who followed up on referrals for IPV services was double that among women in the control group, though this di!er-ence was not significant, likely because of the small sample size. The percent of women who perceived meaningful sup-port from the HTS session was significantly higher among women in the intervention than in the control group, a di!er-ence that was maintained after controlling for other variables and at second follow-up. This perception of support may be an important intermediate outcome as other studies have found that the provision of social support to women expe-riencing IPV is linked with improved physical and mental health outcomes [23, 24]. Finally, per responses to the sur-vey, recent IPV a!ected a full third of the ANC clients, yet only a third of women experiencing IPV in the intervention arm—and a much smaller percent in the control arm—dis-closed to their counselor. Thus, in many instances the HTS counselors did not know that their client was experiencing
violence. In the intervention arm, however, because coun-selors discussed IPV with all clients, women who chose not to disclose IPV to their HTS counselor still received sup-portive messages and important information about IPV and resources available in Nairobi.
While this study was not powered to assess e!ects among HIV-positive and IPV-positive subgroups on indicators related to HIV care and prevention, or IPV prevention and treatment, exploratory analyses are encouraging. Of note are the higher proportions of IPV-positive women reporting intention to regularly take ARVs to prevent mother-to-child transmission and agency to ask their partner to use a condom (not significant). Among women experiencing physical or sexual violence, the percentage of women who took some sort of action to address the violence was higher (marginally significant) in the intervention than the control group (46% vs. 31%, p = 0.07).
Based on these results, providing brief IPV/power coun-seling to all women—not just screening, and not just to those who disclose violence—may be warranted in settings such as HTS and ANC and should be tested with a larger sample and over a longer period of time in order to track outcomes such as ARV adherence and women’s experience of IPV. Counse-lors’ feedback suggests that the provider support groups are an important feature of the intervention to maintain, as are the escorts who brought women to their referral destination.
Table 5 Exploratory analysis: agency and health-promoting behaviors among women who reported experiencing IPV in the past 12"months, by study arm at second follow-up
a Including physical, sexual or emotional; all indicators initially assessed on 5-point scale: Agree a lot, Agree somewhat, Neither agree nor disagree, Disagree somewhat, Disagree a lot; then dichotomized as indicatedb Chi-square tests for association. Significance at p < 0.05c Among those women living with HIV
Women reporting any violence in past 12 monthsa
Total(%) N = 241
Control(%) N = 134
Intervention(%) N = 107
P-valueb
Could ask partner to go to couples HTC (CHTC)"Agree a lot 73.2 71.3 75.7 0.59"Agree somewhat or disagree 26.8 28.7 24.3
My partner and I have discussed going to CHTC"Agree a lot 55.2 55.7 54.7 1.00"Agree somewhat or disagree 44.8 44.3 45.3
Can take better care of my health/well-being"Agree a lot 83.9 80.2 88.2 0.16"Agree somewhat or disagree 16.1 19.8 11.8
I will regularly take medications to prevent mother-to-child transmissionc
"Agree a lot 54.5 47.8 61.9 0.38"Agree somewhat or disagree 45.5 52.2 38.1
I can ask my partner to use a condom"Agree a lot 52.8 48.8 58.3 0.31"Agree somewhat or disagree 47.2 51.2 41.7
150

AIDS and Behavior (2020) 24:2409–2420
1 3
We note several limitations and considerations. The find-ings, while encouraging, and obtained with a rigorous ran-domized design, have limited generalizability. Our study population was urban, and more highly educated than the general Kenyan population. Approximately half of study participants reported more than secondary education, com-pared to a quarter (24%) of women in Nairobi reporting this in the DHS [5]. Also, we note that KNH is an unusual hospi-tal in terms of the pre-existing awareness and infrastructure for addressing IPV. Replicating this intervention in other set-tings would entail more upfront awareness raising and likely more work to establish referral linkages. While we sought to
ensure that no spillover occurred between intervention and control groups, it is possible that some counselors, intention-ally or not, at times provided all or part of the intervention to women in the control group. This could have led to an underestimation of the e!ect of the intervention. Addition-ally, due to ethical reasons, it was not possible to conduct a baseline assessment, as women who reported IPV in the survey would warrant counseling and referral for services. It was therefore not possible to account for baseline levels of variables although randomization should have ensured equivalence between groups.
Table 6 Exploratory analysis: women’s actions since first follow-up interview among those experiencing IPV in the past 12"months, by study arm at second follow-up
a Chi-square tests for association. Significance at p < 0.05b Including physical, sexual or emotionalc Yes to any of following categories: followed up on referral, left partner, told someone, or went anywhere for help
Total (%) Control (%) Intervention (%) P-valuea
Women reporting any violence in past 12 monthsb N = 241 N = 134 N = 107"Followed up on referral""No 89.0 92.2 85.2 0.095""Yes 11.0 7.8 14.8
"Left partner""No 66.1 73.5 57.1 0.191""Yes 33.9 26.5 42.9
"Told someone""No 83.9 85.4 82.0 0.559""Yes 16.2 14.6 18.0
"Went anywhere for help""No 91.2 94.1 88.2 1.00""Yes 8.8 5.9 11.8
"Any of abovec
""No 69.1 73.8 63.6 0.088""Yes 30.9 26.2 36.4
Women experiencing physical and/or sexual violence in past 12 months
N = 145 N = 79 N = 66
"Followed up on referral""No 86.0 89.8 81.8 0.163""Yes 14.0 10.2 18.2
"Left partner""No 57.5 70.0 45.0 0.100""Yes 42.5 30.0 55.0
"Told someone""No 79.1 81.4 76.8 0.354""Yes 20.9 18.6 23.2
"Went anywhere for help""No 88.5 91.7 85.7 1.00""Yes 11.5 8.3 14.3
"Any of abovec
""No 62.3 69.5 54.6 0.073""Yes 37.7 30.5 45.5
151

AIDS and Behavior (2020) 24:2409–2420
1 3
The study illuminated some important questions for future evaluations. One is whether it would be better to ran-domize at the cluster (health facility) level as opposed to the individual level. While this would help avoid spillover, it too carries drawbacks as health facilities di!er from one another on a host of characteristics that could bias results. While randomization should take care of that to some degree, it does not always do so in practice. Second, the fact that a substantial proportion of women who did not disclose IPV to their HTS counselor but subsequently acknowledged experi-encing violence during the survey is interesting. A possible explanation is that the IPV counseling during the HTS ses-sion prepared the woman and even though she was not ready to disclose during HTS, she had a little time to process it and thus felt more comfortable disclosing IPV when asked in the interview. Indeed, data from Feder and colleagues shows that women tend to want to deal with the issue at their own pace [15]. Research to determine why this happened could provide useful insight for future research and interventions. For example, if asking women about their IPV experience multiple times facilitates disclosure, discussing IPV could be built into all of a woman’s ANC visits, not just her first ANC visit for a pregnancy.
The pilot intervention—using simple tools and counselor training and support—demonstrated some significant posi-tive intermediate e!ects, as well as encouraging exploratory results, despite adding only 6.5"min to HTS counseling time. Six and a half minutes is not a small amount of time in high-volume clinics, indeed providers at KNH expressed concern about the added time given their client load. Nonetheless, they all still viewed the intervention as worthwhile and in many HTS clinic settings such an intervention may be easily scalable. While UNAIDS reports progress towards achiev-ing the 90–90–90 treatment targets, stretching the final mile will entail enhancing clinical services to address structural factors such as IPV that hinder HIV treatment initiation and adherence. Knowing whether a woman is experiencing IPV can allow for better tailoring of the HIV counseling session to her situation—including how best to immediately start and stay on ART should she fear her partner’s reaction—but it also o!ers the opportunity to provide immediate support to her. Such immediate, “first-line” assistance for IPV includes being non-judgmental and supportive; listening carefully and empathetically; and helping her access information and legal, social, and health resources, including, if indi-cated, trauma counseling and post-exposure prophylaxis [8]. Findings from this study suggest—though the study was not powered to determine—that in addition to providing more appropriate care, there are potentially positive health and behavioral benefits to including IPV/power in HTS coun-seling. A larger study, incorporating lessons from this pilot is warranted.
Acknowledgements We would like to thank the management and sta! of Kenyatta National Hospital’s Reproductive Health and Mental Health departments, and University of Nairobi’s Obstetrics and Gyne-cology department for their technical support and participation in the study. Specifically, we thank Dr. John Ong’ech, head of OB-GYN department, Kenyatta National Hospital (KNH); Prof. Omondi Ogutu, head of OBGYN department, University of Nairobi; Nerea Ojanga, Nurse Manager OB-GYN department; Hellen Obaga, Nurse Manager Reproductive Health clinic; and Gertrude Kanyua, Nurse Manager Mental Health department for facilitating all study activities. We are also grateful to Dr. Bartilol Kigen and Dr. Annie Nganga, Reproductive and Maternal Health Services Unit, and Dr. Martin Sirengo, NAS-COP, Ministry of Health, Kenya, for their support, and strategic and policy guidance before and during the study. The management and sta! of Nairobi Women’s Hospital are also appreciated for their input in conceptualizing the intervention. We are grateful to the counselors and nurses at KNH’s antenatal care clinic, their compassion and com-mitment is an inspiration. Antony Kiema, the research coordinator, the study counselor Niceta Ireri, and our research assistants did an outstanding job—we thank them all.
Funding This study was supported by the U.S. President’s Emergency Plan for AIDS Relief and the U.S. Agency for International Develop-ment (USAID) via HIVCore, a Task Order funded by USAID under the Project SEARCH indefinite quantity contract (Contract No. AID-OAA-TO-11-00060). The contents in this article are those of the authors and do not necessarily reflect the view of the U.S. President’s Emergency Plan for AIDS Relief, the U.S. Agency for International Development or the U.S. Government.
Compliance with Ethical Standards
Conflict of interest The authors declare that they have no conflict of interest.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the insti-tutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Informed consent was obtained from all individual participants included in the study.
Open Access This article is licensed under a Creative Commons Attri-bution 4.0 International License, which permits use, sharing, adapta-tion, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creat iveco mmons .org/licen ses/by/4.0/.
References
1. Hatcher AM, Smout EM, Turan JM, Christofides N, Stöckl H. Inti-mate partner violence and engagement in HIV care and treatment
152

AIDS and Behavior (2020) 24:2409–2420
1 3
among women: a systematic review and meta-analysis. AIDS. 2015;29(16):2183–94.
2. Leddy AM, Weiss E, Yam E, Pulerwitz J. Gender-based violence and engagement in biomedical HIV prevention, care and treat-ment: a scoping review. BMC Public Health. 2019;19:897.
3. Hampanda KM. Intimate partner violence and HIV-positive wom-en’s non-adherence to antiretroviral medication for the purpose of prevention of mother-to-child transmission in Lusaka, Zambia. Soc Sci Med. 2016;153:123–30.
4. World Health Organization, Department of Reproductive Health and Research, London School of Hygiene and Tropical Medicine, South African Medical Research Council. Global and regional estimates of violence against women: prevalence and health e!ects of intimate partner violence and non-partner sexual vio-lence. Geneva: WHO; 2013. 51 p.
5. Kenya National Bureau of Statistics (KNBS), Ministry of Health, National AIDS Control Council, Kenya Medical Research Insti-tute, National Council for Population and Development, The DHS Program, ICF International. Kenya Demographic and Health Sur-vey 2014. Rockville: KNBS and ICF International; 2015. 575 p.
6. PEPFAR. The United States President’s Emergency Plan for AIDS Relief: Updated Gender Strategy. Washington (DC): PEPFAR; 2013. 52 p.
7. New York State Department of Health. Guidelines for Integrat-ing Domestic Violence Screening into HIV Counseling, Testing, Referral & Partner Notification [Internet]. Albany: NYS DOH; Revised 2013 Nov [cited 2017 Jul 31]. https ://www.healt h.ny.gov/disea ses/aids/provi ders/regul ation s/domes ticvi olenc e/guide .htm.
8. World Health Organization. Responding to intimate partner vio-lence and sexual violence against women: WHO clinical and policy guidelines. Geneva: WHO; 2013. p. 56.
9. Undie CC, Maternowska MC, Mak’anyengo M, Askew I. Is routine screening for intimate partner violence feasible in public health care settings in Kenya? J Interpers Violence. 2016;31(2):282–301.
10. Christofides N, Jewkes R. Acceptability of universal Screening for intimate partner violence in voluntary HIV testing and counseling services in South Africa and service implications. AIDS Care. 2010;22(3):279–85.
11. O’Doherty L, Hegarty K, Ramsay J, Davidson LL, Feder G, Taft A. Screening for intimate partner violence in healthcare settings. Cochrane Database Syst Rev. 2015. https ://doi.org/10.1002/14651 858.CD007 007.pub3.
12. Pulerwitz J, Gortmaker SL, DeJong W. Measuring sex-ual relationship power in HIV/STD research. Sex Roles. 2000;42(7/8):637–60.
13. Wingood GM, DiClemente RJ. Application of the theory of gender and power to examine HIV-related exposures, risk fac-tors, and e!ective interventions for women. Health Educ Behav. 2000;27(5):539–65.
14. Jewkes R, Morrell R. Gender and sexuality: emerging perspectives from the heterosexual epidemic in South Africa and implications
for HIV risk and prevention. J Int AIDS Soc. 2010;13:6. https ://doi.org/10.1186/1758-2652-13-6.
15. Feder GS, Hutson M, Ramsay J, Taket AR. Women exposed to intimate partner violence: expectations and experiences when they encounter health care professionals: a meta-analysis of qualitative studies. Arch Intern Med. 2006;166:22–37.
16. Chang JC, Cluss PA, Ranieri L, Hawker L, Buranosky R, Dado D, McNeil M, Scholle SH. Health care interventions for intimate partner violence: what women want. Women’s Health Issues. 2005;15:21–30.
17. Spangaro J, Koziol-McLain J, Rutherford A, Zwi AB. “Made me feel connected”: a qualitative comparative analysis of intimate partner violence routine screening pathways to impact. Violence Against Women. 2019. https ://doi.org/10.1177/10778 01219 83025 0.
18. Undie CC, Maternowska MC, Mak’anyengo M, Birungi H, Kees-bury J, Askew I. Routine screening for intimate partner violence in public health care settings in Kenya: an assessment of accept-ability. Nairobi, Kenya: Population Council; 2012. https ://www.popco uncil .org/uploa ds/pdfs/2012R H_APHIA II_Intim atePa rtner Viol.pdf.
19. Miller E, Decker MR, McCauley HL, Tancredi DJ, Levenson RR, Waldman J, et"al. A family planning clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception. 2011;83(3):274–80.
20. Gottert A, Barrington C, Pettifor A, McNaughton-Reyes HL, Maman S, MacPhail C, et"al. Measuring men’s gender norms and gender role conflict/stress in a high HIV-prevalence South African setting. AIDS Behav. 2016;20(8):1785–95.
21. Pulerwitz J, Barker G. Measuring attitudes toward gender norms among young men in Brazil: development and psychometric evaluation of the GEM Scale. Men Masc. 2008;10(3):322–38.
22. Kenya National Bureau of Statistics (KNBS), ICF Macro. Kenya demographic and health survey 2008–09. Calverton: KNBS and ICF Macro; 2010. 430 p.
23. Coker AL, Watkins KW, Smith PH, Brandt HM. Social support reduces the impact of partner violence on health: application of structural equation models. Prev Med. 2003;37(3):259–67.
24. Kamimura A, Parekh A, Olson LM. Health indicators, social support, and intimate partner violence among women utiliz-ing services at a community organization. Womens Health Issues. 2013;23(3):e179–e185185. https ://doi.org/10.1016/j.whi.2013.02.003.
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional a#liations.
153

Vol.:(0123456789)1 3
AIDS and Behavior https://doi.org/10.1007/s10461-020-03075-x
ORIGINAL PAPER
Is HIV Post-test Counselling Aligned with!Universal Test and!Treat Goals? A!Qualitative Analysis of!Counselling Session Content and!Delivery in!South Africa
Tonderai!Mabuto1,2 !· Nolundi!Mshweshwe-Pakela1!· Nasiphi!Ntombela1!· Mpho!Hlongwane1!· Vincent!Wong5!· Salome!Charalambous1,2!· Deanna!Kerrigan3!· Christopher!J.!Ho"mann1,4
Accepted: 29 October 2020 © Springer Science+Business Media, LLC, part of Springer Nature 2020
AbstractEarly identification of people living with HIV (PLHIV) and subsequent engagement into HIV treatment is a key to reducing HIV-related illness, HIV-related deaths, and HIV transmission through universal test and treat approaches. With the scale-up of antiretroviral therapy (ART) programmes, counselling that is provided immediately after the diagnosis of HIV (post-test counselling) is well placed to facilitate linkage to care and ART initiation. We sought to assess whether the current delivery of post-test counselling in a routine HIV programme was aligned with the goals of universal test and treat as articulated in local and international HIV testing service guidelines. We analysed transcripts of 40 post-test counselling sessions for HIV-positive clients, performed by 34 counsellors in ten public sector health facilities in the Ekurhuleni District of South Africa. We used thematic analysis to identify key aspects of counselling techniques and content provided to the client. We identified five key themes of counselling messages: (1) specific behaviour changes that are required to maintain or improve health when living with HIV, (2) the benefits of ART, (3) behaviour changes required for ART to be e!ective, (4) the need for clients to disclose their HIV status, and (5) a need for caution with ART due to a wide range of severe side e!ects. The counselling sessions were highly didactic, which limited the opportunities for clients to express concerns or counsellors to address client’s needs during the counselling session. Based on our observations, a substantial re-adjustment is needed to deliver best-practice counselling. This may include a combination of digital media-based counselling, counselling scripts, and truly client-centred counselling for a sub-set of individuals who are at risk of not linking to care, or not initiated ART within a specified period.
Keywords HIV"· South africa"· Counselling
Introduction
Early engagement in HIV care and treatment services fol-lowing HIV diagnosis is a key to reducing HIV-related ill-ness and death, reducing HIV transmission, and improving the quality of life for people living with HIV (PLHIV) [1–4]. Over the years, the World Health Organisation (WHO) has regularly revised its recommendations on when PLHIV should start antiretroviral therapy (ART). In 2015, WHO and other global and national bodies, including the government of South Africa, endorsed polices to provide ART to all peo-ple living with HIV and to reduce the time between HIV diagnosis and ART initiation [5, 6]. Despite the considerable progress in ART scale-up, the proportion of people diag-nosed with HIV who promptly engage in HIV care (com-monly referred to as ‘linkage-to-care’) remains suboptimal
* Tonderai Mabuto [email protected] Implementation Research Division, The Aurum Institute
NPC, 29 Queens Road, Parktown, Johannesburg, South"Africa
2 The University of"the"Witwatersrand School of"Public Health, Johannesburg, South"Africa
3 Department of"Sociology, American University, Washington, DC, USA
4 Department of"Medicine, Johns Hopkins University School of"Medicine, Baltimore, USA
Global Health Bureau, O#ce of"HIV/AIDS, Prevention Care and"Treatment Division, United States Agency for"International Development (USAID), Washington, USA
Content courtesy of Springer Nature, terms of use apply. Rights reserved.154

AIDS and Behavior
1 3
[7, 8]. Globally, 79% of PLHIV know their status, but only 62% of those diagnosed are receiving ART [8]. Similarly, in South Africa, a country with the largest HIV epidemic, 85% of PLHIV in 2017 were aware of their status, but only 71% of these were receiving ART [9].
The role of HIV testing services (HTS) in the HIV epi-demic response has evolved from the time of limited avail-ability of ART to the current era of universal test and treat (UTT). Early in the HIV epidemic response, HTS had an HIV prevention focus and was often delivered through vol-untary counselling and testing (VCT) sites set apart from health facilities [10, 11]. The role of VCT on HIV preven-tion was based on the premise that behaviour change com-munication provided as part of post-test counselling could lead to changes in sexual behaviours among those testing HIV-negative. Also, people with newly diagnosed HIV were encouraged to change their sexual behaviour to place their sexual partners at lower risk of HIV infection [12–14]. As a result, risk reduction counselling formed the core of HIV pre- and post-test counselling. Additionally, health messag-ing for those testing HIV-positive focused on ‘healthy eat-ing’ and ‘active lifestyles’, as approaches for maintaining health [15].
With the scale up of ART over the years, WHO has revised its guidelines to emphasise both quality and e!-ciency in HIV counselling [16, 17]. In 2007, WHO recom-mended reducing pre- and post-test counselling to essential core elements (including ART access, client-centred inter-viewing, and providing information necessary for informed consent) to allow for e"ective and narrowly targeted coun-selling [17] and shifting the delivery of testing to an opt-out approach. Subsequent recommendations included task shift-ing of testing, the option to use brief group pre-test coun-selling and “brief health information” for those who test negative. The recommendation for those who test positive is to provide “client-centred” counselling that focuses on immediate concerns. The WHO Consolidated Guidelines of HIV testing services specifically state: “All post-test coun-selling should be “client-centred”, which means avoiding formulaic messages that are the same for everyone regard-less of their personal needs and circumstances. Instead, counselling should always be responsive to and tailored to the unique situation of each individual or couple” [16]. The 2019 update specifically recommends “concise” counselling focused on the importance of ART [18]. Potential concerns with routinizing testing and stream-lined pre and post-test counselling and a focus on ART is a failure to respect patient autonomy and to adequately address potentially substantial psychosocial consequences of a new HIV diagnosis.
Similar to other health communication strategies, for post-test counselling to be e"ective, it should be responsive to and built around client personal needs and circumstances—commonly referred to as “client-centred” counselling [16,
18, 19]. Client-centred counselling techniques, such as moti-vational interviewing and strengths-based counselling, can assist a client in identifying how to align the benefits of ART to their life goals [19–21]. These techniques may be most e"ective when the counsellor demonstrates an understand-ing of how the value-cost balance influences decisions to engage in HIV care. This balance may be the critical factor for linkage-to-care and retention on ART [22, 23]. Within this balance, linkage-to-care is more likely when a person’s perceived value of medical care exceeds the costs of engag-ing in medical care; whereas, when the perceived costs of engaging in medical care exceed the anticipated value, link-age-to-care may not occur [24].
We sought to describe post-test counselling communica-tion techniques and content related to linkage-to-care and ART initiation among clinic attendees diagnosed with HIV during routine HTS in public sector health facilities in South Africa. Specifically, in this analysis, we sought to describe key aspects of counselling techniques and content provided to the client during post-test counselling sessions with HIV-positive clients.
Methods
Study Setting
This study was embedded in a larger study which sought to characterize missed opportunities and current constraints on delivering HTS in ten public sector health facilities in the Ekurhuleni District of South Africa (SA). It was con-ducted from March 2017 to August 2018. The study sites consisted of six primary health care centres (PHC), three community health care centres (CHC) and one district-level hospital. Facilities were selected in coordination with the district Department of Health to achieve geographic diver-sity. All facilities had dedicated HIV counselling and test-ing personnel (lay counsellors) and routinely provided HTS free of charge according to the South Africa National HIV counselling and Testing Guidelines [25]. Under these guide-lines, healthcare providers were encouraged to o"er HTS to a person attending healthcare facilities as a standard com-ponent of medical care. All persons diagnosed with HIV in South Africa were eligible to start antiretroviral therapy (ART), regardless of the clinical stage [26]. All counsel-lors included in this analysis had received HTS counselling training to qualify to work as counsellors. After half of the recordings were completed, we reviewed transcripts and identified areas for improvement in counselling. The study team worked with trainers to develop and provide a one-day counseling refresher training. All the counselors involved in this study received the training.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.155

AIDS and Behavior
1 3
Data Collection
For this study, we audio-recorded 160 post-test counsel-ling sessions; 48 (30%) among male clients and 112 (70%) among female clients. Of these, 40 sessions (25%) were with participants who had an HIV-positive test result (equally distributed across participating study sites). Enrollment was restricted to clients who underwent HIV testing at the selected study sites, ! 18"years of age and provided writ-ten informed consent for participation. Informed consent for participating in this activity was obtained from both the counsellor and the client. Before providing consent, both counsellors and clients were informed of the goal to improve the quality of counselling, by identifying areas of strength and potential areas amenable to improvement. In the case of counsellors, study sta# had at least two consultative meet-ings before commencing the study. The sessions were a dia-logue outlining how the transcripts would be anonymized and reassuring the counsellors that study activities were not linked to any performance management systems. The coun-sellors consented once for participation in this study (with an option of voluntary withdrawal, and re-consenting if willing to re-join). Informed consent was administered to clients before the pre-test counselling. To maximise confidentiality and encourage participation, we only collected information on the client’s sex. Counsellors who consented to participate in the study were trained on how to use the audio-recording device. None of the research sta# were present during the HIV testing encounter and post-test counselling sessions.
Data Analysis
All audio-recordings of the selected counselling sessions were translated from local languages into English and transcribed by trained sta# from the research team. Each transcript was checked by the initial transcriber against the original audio-recording for correctness. Thereafter, all transcripts were checked by the team leader who read both the transcript and the original audio recording of the counselling session. Two researchers (TM and CJH) read and summarised all transcripts to familiarise themselves with the counselling techniques applied and the content of health messages delivered during post-test counselling. All data were managed and analysed using NVivo 10™ (QSR International Pty Ltd., Melbourne, Australia, Version 10, 2012). TM and CJH collaboratively developed a preliminary coding structure of broad codes based on two frameworks. We used the South Africa National HIV counselling and Testing Guidelines, as the coding framework for counsel-ling technique and health message content provided to the client [25]. Briefly, guidelines for post-test counselling gen-erally recommended using a client-centred approach. The core components of this approach were (1) open questions,
(2) a$rmations, (3) reflections, and (4) summaries. Using the same HTS guidelines, we also explored the inclusion of core post-test counselling components; the medical mean-ing of an HIV positive result; HIV as a chronic long-term condition; the medical benefit of ART to maintain or restore health and allow living a normal life; the recommendation of ART for all HIV-positive people; the prevention benefits of ART in reducing sexual and mother-to-child (MTC) trans-mission of HIV; the importance of starting ART as soon as possible; and how disclosure to supportive family or friends can help with coping and treatment success. We also sought to distinguish between factual information, opinion, and factually incorrect statements in the coding of transcripts. In additional analyses, we applied the ‘value versus cost’ theoretical framework as the second coding structure [24]. Using this framework, we explored how the counselling con-tent and techniques may have influenced the client’s percep-tion of values and costs of engaging in HIV medical care. Both a priori coding structures were tested on a selection of transcripts and revised to ensure that they captured relevant patterns from the narratives with minimal overlap [27].
After assigning definitions to each broad code to ensure consistency in coding, TM and CJH applied the coding structure to a few transcripts, and where indicated, revised the codebook to ensure that the broad codes captured rel-evant patterns from the client narratives with minimal overlap [27, 28]. Themes were further developed from the coded text, considering code frequency, connections between codes, and consistency with the text [27]. We purposefully framed and organised the themes to provide a pragmatic lens to identify opportunities for developing strategies to improve the content and delivery of post-test counselling sessions.
Results
Study Participants
A total of 45 counsellors across the ten facilities (range 4–6 counsellors per facility) participated in the study; most were female (41/45, 91%), all were employed by the Department of Health and had worked as HIV counsellors for a median of 12"months [Interquartile range (IQR) 6"months, 2"years]. All counsellors had received training on counselling skills and on the HTS guidelines and the HIV treatment guidelines in use at the time of the study. Of the 45 counsellors, 34 (76%) conducted at least one post-test counselling session in which a client was issued with an HIV positive result. Of the 40 clients with sessions that were analysed, 13 (33%) were male, and 27 (67%) were female. Post-test counselling sessions lasted a median duration of 15"min (IQR 7–20"min).
Content courtesy of Springer Nature, terms of use apply. Rights reserved.156

AIDS and Behavior
1 3
Counselling Content
We identified five general themes related to counselling content:
• Specific behaviour changes are required to maintain or improve health when living with HIV.
• ART has potential benefits for health and preventing mother-to-child transmission (PMTCT).
• Specific behaviour changes are required for ART to be e!ective.
• The need for clients to disclose their HIV status.• Vigilance is required when starting ART due to a wide
range of potentially severe side e!ects.
There were no notable di!erences in counselling con-tent or technique by counsellor’s sex, client’s sex, clinic, or before and after the one-day refresher training; therefore, we combined results in the analysis. Table"1 contains additional participant quotes referenced in the text.
1. Specific behaviour changes “necessary” to maintain or improve health for people with HIV
Counsellors listed behaviours required to maintain or improve health when living with HIV. These behaviours focused on avoiding some foods and eating other foods, drinking eight glasses of water daily, exercising regu-larly, and getting plenty of sleep. Messages related to nutrition were uniformly directed at the need to increase vegetable consumption and to reduce or eliminate fatty foods and sometimes to eliminate spicy foods (Quotes 1.1–1.4). The stated benefits of the recommended foods and changes in diet were diverse: improving diges-tion, cleansing the gut, helping to fight infection, giv-ing energy, and avoiding weight loss. One counsellor explained these food requirements as follows:
“The important thing is changing your lifestyle. On food, you need to take lots of fruits and fresh vegetables; they will help to fight other infections in your body. You must also take brown rice, brown bread, pap and samp; they will help to give you energy. And then you must eat beans, lettuce, chicken, fish, and eggs, they will help to build your body, and they also will keep you strong. And then you must take butter, peanut butter, nuts, cooking oil and fresh milk, they will help you to stop losing weight, and they will also give you energy. You must also take yoghurt and milk they will help you with digestion. Again, you must take eight glasses of water.” - Counsellor
Some of the counsellors sought to address the poten-tial financial impact of diet changes by briefly describing lower-cost foods compatible with HIV. This was done either in response to a client question (as below) or in anticipation of such concern.
Client: “As you speak about eating the right food. If I do not have the right food, what must I do?” Counsellor: “By the right foods, I don’t mean expensive food. Cabbage from street vendors is five rands. You can eat that cabbage. Beetroot is also five rands. Carrots are also five rands. Try to have one vegetable in your plate every day and drink water, two litres a day which is about eight glasses of water.”
One of the few client questions demonstrated a poten-tial cost of diet change beyond the direct financial cost: a need to disclose HIV status to make the listed food changes promptly.
Client: “It will take some time for me to adjust from the food that I am eating to the food that I am only supposed to eat. It will take me some time.”
Counsellor: “Why is it that it will take you some time?”
Client: “I don’t know where to start with the woman that I live with. I do not know how I will start the topic. I am stressed about where I will start, although I must tell her?”
Counsellor (after the client had highlighted other concerns with disclosure): “Sometimes it is bet-ter to tell a person, find a way to tell her as early as possible. Indeed, people do not react the same way, maybe she might be scared but she will even-tually understand that it is something that you did not get currently. Again no one asks for HIV, no one wants it. The important thing is that when you have HIV you have to move on as life does not stay still. Everything must continue the way it was.”
2. The Benefits of ART In most counselling sessions, the conversations on
the value of ART were limited to general statements that living with HIV was no longer a ‘death sentence’ because of the availability of ART (Quotes 2.1–2.6). In one typical example, the counsellor explained:
“There is no grave for an HIV positive person. It is only the person who wants to die who would be killed by HIV. Yes, before the introduction of HIV
Content courtesy of Springer Nature, terms of use apply. Rights reserved.157

AIDS and Behavior
1 3
Table 1 Selected participant quotes by counselling message themes
1. Specific behaviour change “necessary” to maintain or improve health for people with HIVRequired diet changes for people living with HIV 1.1. “…And then you will have to eat healthily, don’t eat food with a lot of oil, do
not eat deep-fried food, ensure that your food has vegetables when you prepare it, make sure that you eat at least one fruit a day.”—Counsellor
1.2. “You have to eat the right food. You eat vegetables and fruits and drink water every day. You are going to stop drinking alcohol.”—Counsellor
1.3. “…The only food that we don’t eat is that which cleanses the gut. Not that you should not eat, you can eat occasionally. There are some people when they eat spinach, it cleanses the gut, and you will find them regularly eating because they love it, and whenever they eat the spinach, it cleanses their gut. And there are people when they eat pap (staple food) and milk; they cleanse the gut. You do not eat such food. You eat occasionally.”—Counsellor
1.4. “From today you need to watch what you eat. Eat vegetables, eat fruits. When I say you should eat vegetables, I am not saying you must get home and tell them that you must eat at vegetables, they said I should not eat meat or pap (sta-ple food). What I am saying is that you need to eat vegetables at least two times a week. Vegetables are nutritious so you will be helping the pill to fight o! the virus so that the body soldiers can come alive. The pill assists the body soldiers. You have to assist the pill by eating vegetables and fruits.”—Counsellor
The benefits of ART General framing of the benefits of ART towards longevity
and maintaining a high quality of life2.1. “If you are positive, know that the only thing that will keep you alive is the
ARVs only.”—Counsellor2.2. “Take a deep breath and say whatever you want to say (Silence). You know
very well that there are people who are HIV positive and they are healthy. It is not a life sentence this thing. It is not a death sentence. It is not a death sen-tence; you can live well with ARVs.”—Counsellor
2.3. “…If you take your treatment properly, you stay normal, but if you stop the treatment and default, you are going to get AIDS. When you have moved into AIDS, it is going to be di"cult. Everyone will see that you are ill, but if you take your pill properly, no one is going to see that you are ill. You can work and do anything you want.”—Counsellor
2.4. “HIV does not mean that you have to stop things that you used to do. Just live a healthy lifestyle, use condoms, take your treatment, and continue with your life. HIV does not stop anything. Your life does not stop today because you are HIV positive. Ok?”—Counsellor
2.5. “There is no grave for an HIV positive person. It is only the person who wants to die who will be killed by HIV. Before treatment was available, yes, people died of HIV, but now that there is treatment, life goes on.”—Counsellor
2.6. “I beg you, don’t harm your body. You may end up feeling stigmatised and being afraid to look at other people. I would like to see you maintain the way that you are, even when you start with treatment. Seeing you not getting sick and being able to take your treatment well. Do you want it (HIV) to knock you out with shingles, give you scars?”—Counsellor
General framing of ART benefits concerning CD4 count and viral load
2.7. “ARVs help with your CD4 count and your viral load will go down.”—Coun-sellor
2.8. “ARVs will help with bringing your CD4 count up and bringing your viral load down. Isn’t it?”—Counsellor
2.9. “The ARVs will help your CD4 count to go up and your viral load to go down. Those are the benefits of ARVs, isn’t it? And then it will also help with reinfection so that HIV does not multiply.”—Counsellor
Content courtesy of Springer Nature, terms of use apply. Rights reserved.158

AIDS and Behavior
1 3
Table 1 (continued)
Benefits of ART in pregnancy 2.10. “Now that you are positive, today you are going to start with treatment so that you can protect the baby from HIV. Also, it is possible for a mother that is HIV positive to have a baby that is HIV negative.”—Counsellor
2.11. “When you start with treatment today, it will build up your immune system to position the virus in one place so that it doesn’t multiply every day. As long you take your pills every day and at the same time and use a condom when you have sex the virus will not replicate. The immune system goes up. It becomes strong. The baby gets protected, and the baby will be alright. That means it is all in your hands to protect the baby to be alright?” – Counsellor
2.12. “Now that you are positive, today you are going to start with treatment so that you can protect the baby from HIV, and it is possible for a mother that is HIV posi-tive to have a baby that is HIV negative.”—Counsellor
3. Essential behaviour changes required for ART to be e!ectiveRequired lifestyle changes 3.1. “And when you take these pills, make sure that you don’t take alcohol so that
the pill helps you well. Make sure that you don’t take alcohol.”—Counsellor3.2. “And please, please, please, no smoking, no alcohol, no using syringes no
drinking medicine from traditional healers, please I beg you. I am not com-manding or imposing. We are advising each other.”—Counsellor)
3.3. “The medication that you are going to take is a!ected by other things. If you are drinking alcohol, it counteracts with it because alcohol is strong. It will neu-tralise the medication. Stop drinking (alcohol), stop smoking drugs, any drug, you don’t use any drug.”—Counsellor
3.4. Counsellor: You bought a packet of 20 (cigarettes), and you have five left?Client: Yes, from yesterday morningCounsellor: No bhuti (brother) you smoke too much; you need to reduce the
levels of your smoking. Do you know that the virus target where there is more damage in your body?
Scheduling when to take ART 3.5. Client: So how does it work?Counsellor: If you drink it at 8 (pm) it must be like that. You drink them only at
nightClient: Only at night?Counsellor: Yes, if you drink them at 7"pm it must be 7"pm. if it is 8"pm it must
be 8"pm. Do not change the time, because if you change the times, the medica-tion will not be able to work its work in your body. Because they help with your body soldiers to go up and your viral load to go down. Do you know viral load?
P: No3.6. “You are supposed to take them at the same time. You will choose your time.
If you choose seven, it must be seven. If you choose eight, it must be eight and what you need to know is that the pills that you are going to start taking have side e!ects.”—Counsellor
3.7. Counsellor: As long as you take your tablets at the same time; every day. Like you have said that you do not miss days as you have said, isn’t it? Every day you take the pills at the same time. When you miss your pills, what is going to happen?
Client: You are getting hurt. You are inviting illness because the virus will go upCounsellor: Yes, the virus will go high, and the CD4 count goes where?Client: Down3.8. “And then again when you are going out thinking that you will come back in
time to get your treatment and it happens that you do not come back on time, you end up getting home before or after nine. It’s better to drink it late than not to drink it at all.”—Counsellor
3.9. “When you take your medication at 8 (pm), and your sister calls you to come and visit, and maybe you return before or after 9 (pm) and your time to take your medication has passed, as soon as you get home you must still drink your medication. It is better to drink it late than not to drink it at all. Timing is criti-cal because no one is perfect, isn’t it?”—Counsellor
Content courtesy of Springer Nature, terms of use apply. Rights reserved.159

AIDS and Behavior
1 3
Table 1 (continued)
Misinformation on condoms and replication of the virus 3.10. “Viral load is the amount of virus in your body. When you take ARVs, they suppress the virus, they bring it down, and your CD4 count goes up, but only when you drink them well, and you use condoms. Because I said if you do not use condoms, the virus multiplies.”—Counsellor
3.11. “Now that you have tested you have to accept that you have this virus, and when you have sex use a condom because the more that you don’t use a con-dom, the more the virus multiply.”—Counsellor
3.12. Counsellor: For you to be protected, you need to use a condom as you also mentioned that you heard from the radio that when you are not using protection, what do you do?
Client: You multiply the… (client trying to remember)Counsellor: You increase the viral load in your body. What happens if you do not
use the protection?Client: You increase the viral load3.13. “Use a condom always when you have sex because when you don’t use a
condom while taking the pills, they are not going to work for you those pills.”—Counsellor
3.14. “Viral load is the amount of virus in your body. When you take ARVs, they suppress the virus, they bring it down, and your CD4 count goes up, but only when you drink them well and you condomise. Because I said if you do not use condoms, the virus multiplies.”—Counsellor
3.15. “And as from now on you have to use condoms no matter what because the viral load will increase instead of going down although you are taking treatment if you don’t use a condom every time you have sexual intercourse.”—Counsel-lor
4. DisclosureCounsellor prescriptions on who clients should disclose to 4.1 “There must be someone that you tell, especially at home because it will be
di!cult when you need to drink your treatment if people at home do not know. Do you know how painful it is to drink your treatment under the table [secre-tively]? You end up doing the wrong things, your family will not abandon you, instead, they will support you, they will give you love. There are friends who can do that. I am not saying you should not tell them, but I would not advise you much about friends, I prefer someone from home, someone that you trust. You know that there is a person that you know you trust, someone that you will disclose to.”—Counsellor
4.2. “When the time comes, take your treatment. There has to be somebody that you will disclose your status to, someone at home, not a friend. A friend can go gossiping about you, so someone at home. Who do you stay with at home?”—Counsellor
4.3. “And another thing is that you need to have somebody to support you. I pre-fer someone that you are living with at home. If you had a husband, I would say tell your status to your husband. But first, you need to accept and be ok. “
Less prescriptive discussions on who clients should disclose to
4.4. “And also you have to tell someone about your status, it can be your friend, any family [member] or colleague or whoever as long as you trust that person, tell them so that they support you. Do you understand?” – Counsellor
4.5. Counsellor: So, is there someone who is going to support you who are you going to tell if your results come out positive?
Client: The person I am going to tell is in PretoriaCounsellor: In Pretoria? Are the people you are going tell, your family members?Client: Yes, it is my family because they are my husband’s family. Even now,
they are the ones who were encouraging me to test
Content courtesy of Springer Nature, terms of use apply. Rights reserved.160
AIDS and Behavior
1 3
treatment, people died of HIV but now that there is treatment. Life goes on.” - Counsellor
Counsellors also sought to describe the general bio-medical benefits of ART in terms of preventing damage to the immune system and controlling the multiplication of the virus (Quotes 2.7–2.9). However, the benefits of ART in reducing the risk of HIV transmission to sexual partners (i.e. treatment as prevention) were not men-tioned in any of the post-test counselling sessions. Ben-efits of ART that went beyond maintaining health were only listed in the context of PMTCT (Quotes 2.10–2.12).
3. Essential behaviours required for ART to be e!ective Some counsellors either directly stated or strongly
implied that specific behaviours were incompatible with ART. Specific behaviour changes needed prior to ART initiation included the cessation of smoking or drinking alcohol (Quotes 3.1–3.4). The need for these changes
was generally justified as incompatibility between smoking and drinking alcohol and ART itself, rather than potential adherence considerations with alcohol or general health problems from smoking. The following quote is illustrative:
“The medication that you are going to take coun-teracts with other things. Alcohol is strong and neutralises the medication. So, stop drinking (alcohol), stop smoking drugs, any drug, you don’t use any drug.” - Counsellor
Clients were also told they should make changes to their daily routines to assure taking ART at the same time each day. While this may be a reasonable sugges-tion to help with ART adherence, the changes to routine and need for taking ART at the same time each day, were at times, presented as a necessity for ART to work rather
Table 1 (continued)
5. The inevitable and severe side e!ects of taking ART Side e!ects of ART 5.1. “And then there are other (side e!ects) that when you see them you must
come to the clinic. Side e!ects such as thrush, swollen feet, when your eyes turn yellow it means that you have a liver problem and then a headache that does not stop. You should come to the clinic and report that since I started taking treatment this is what I have been experiencing. And then if it is vomiting and feeling dizzy, these are things that will happen for a few days and they will pass because the treatment will be getting used to your body. And then let’s say you drink your pills and then you vomit, when you are done vomiting, sit down, take a deep breath and then drink water after two to three minutes try to drink another pill again…”—Counsellor
5.2 “ARVs have side e!ects. You may experience the side e!ects, or maybe you will not experience them. Also, there are those side-e!ects which when they appear, you need to come to the clinic immediately. For example, rash, eyes that turn yellow, which are an indication of a liver problem, when your feet get swol-len or a severe headache you come to the clinic since you will be on ARVs. And when you feel dizzy, that will happen for a few days, and then it will stop. And then vomiting, you will vomit and if you do, sit down, take a deep breath, and then relax, drink water then after two to three minutes, try again. Think about the time you vomited and ask yourself if it was before or after your meals. What is causing the vomiting, then you take it from there. You will know that this pill treats me well when I have eaten or when I have not eaten.”—Counsellor
5.3. “Someone will have side e!ects. I do not know how I can put it in isiZulu (local language), someone else might develop a rash after drinking them, someone else may vomit. Yet, another person might get diarrhoea after drinking the medication. It does not mean that you should stop taking medication when you see all these things happening to you. You should not say that “the pill is making me sick”. This pill works, and I am asking you to please stick to the pills.”—Counsellor
5.4. Counsellor: But it (side e!ects) is not going to happen for the rest of your life. It will be for that small period where it made your dizzy and nauseous. Maybe feel like vomiting and feeling tired, but once your body gets used to the treatment, it becomes alright
Client: I will feel like vomiting and dizzyCounsellor: Yes, for the time being when you start, but some people do not expe-
rience like that as our bodies are not the same
Content courtesy of Springer Nature, terms of use apply. Rights reserved.161

AIDS and Behavior
1 3
than just an adherence aid (Quotes 3.5–3.7). Some coun-sellors were less prescriptive and acknowledged poten-tial challenges and described some flexibility in dosing (Quote 3.8–3.9). One counsellor explained:
“And then again, if you take your treatment at 8 (pm), and you go somewhere telling yourself that you’ll come back and drink your medication, but you end up getting home after 9 (pm). As soon as you get home, you must take your medication it is better to drink it late than not to drink it at all, alright, mama.” - Counsellor.
Nearly all sessions included misinformation on ways to maintain health and a normal CD4 count. This misin-formation often occurred ahead of or in place of infor-mation on ART. The most commonly described method for maintaining health was to use condoms consistently. Condom use was presented in nearly all counselling ses-sions as essential to prevent HIV-related complications, CD4 decline, and HIV reinfection. In some sessions, condom use supplanted the health benefits of ART. A common message was that the failure to use condoms would lead to a weak immune system (CD4 count decline) and could lead to non-suppression of the HIV viral load—essentially making ART ine!ective (Quotes 3.10–3.15). For example, one counsellor explained:
“Sometimes, when you are taking pills, and you do not use a condom - it will be like doing noth-ing. The most important thing is that you must always use a condom and on the other hand you take the pills.” Counsellor
4. Disclosure In most sessions, counsellors stated the importance for
clients to disclose their HIV-positive diagnosis. How-ever, directives were mostly given without exploring any perceived value or barriers by the client in disclos-ing their status. Counsellors stated general benefits of disclosure such as the opportunities for clients to take their medication openly without hiding, clients receiving reminders on when to take treatment, and the potential for emotional or financial support.
Counsellors used di!erent approaches for their cli-ents to identify who they would disclose to. In several sessions, counsellors were prescriptive on whom they preferred their clients to disclose to. In these sessions, counsellors told clients to disclose to family members instead of acquaintances or friends—mostly to avoid gossip (Quote 4.1–4.3). In the following quote, the client’s response to the counsellor’s recommendation highlighted how the lack of dialogue and shared under-standing of the client’s preferences led to misplaced counsellor recommendations:
Counsellor: …Do you know what I prefer? I prefer someone from your family, you know your mother or your sister will not look down upon you.
Client: I hear you. Counsellor: Never, they will not let you down.
Instead, they will comfort you and support you! Client: I live with HIV positive people, I have got
friends, so I do not think it will be a problem…I have this friend of mine. We are close. She has been taking treatment for close to ten years now. She is the one who encouraged me to come to the clinic…she didn’t want to judge me, the only thing she said was…”My friend, do you see me? I am not going to judge you, I am not going to say anything because I’m not a nurse, the only advice I can give you is that you must go and test and when you have tested, come back to me”…so I think she is the person that I can disclose to. “
In other sessions (Quote 4.4–4.5) and as illustrated in the extract below, counsellors made attempts to be less prescriptive and allowed their clients to identify whom they were comfortable disclosing to:
Counsellor: One other thing that is important as we are talking about positive things, you are going to create for yourself what we call a hand of safety. With this hand, you pick 5 people that you trust and out of these 5 people that you trust you are going to pick 1 person that you trust more. Then you will tell the one that you trust the most is the only one that you are going to tell about your situ-ation because there ought to be someone that you tell but you are not forced it will all depend on you. There ought to be someone that you trust the most and tell them about your status to support because as a person living with HIV you do need a support system, you see. Who are you going to tell, that you trust? Client: My mother.
Only a few counsellors explored their client’s self-e"cacy to proceed with disclosure or identifying cli-ent-perceived barriers to disclosure. Sessions which had these discussions were notable in their high levels of client-counsellor dialogue. The quote below is a rare example of dialogue between the counsellor and patient regarding disclosure:
Client: …Even now I don’t know what I will say, because you understand I don’t know where I will say this thing comes from or what I will say to her, but at this time I will not even be pointing fingers because we have both been irresponsible. No one tried to stop the other concerning using condoms,
Content courtesy of Springer Nature, terms of use apply. Rights reserved.162

AIDS and Behavior
1 3
so she knows that I am here at the clinic today. She also knows about the sores that I have. She knows that obviously, I need to test so I’m asking whether I should tell her that the situation is like this, or do I bring her here and we test together? Counsellor: I cannot tell you what you must do…but it’s up to you to see what should be suitable for you…whether you bring her or you explain to her that you were at the clinic: So as I was encouraged that shingles are linked with HIV, I tested and I found out that I am positive. You can either sit down with her or come with her to the clinic to test with her.
5. The inevitable and severe side e!ects of taking ART ART side e!ects were generally stated either as a sub-
stantial danger or as something requiring understand-ing and vigilance from the client. (Quotes 5.1–5.2). One counsellor explained:
“Sometimes, it (ART) will make you dizzy. Some-times you will have a rash. Sometimes you will have nightmares. Sometimes it will make you vomit. You will have bad dreams, and you will end up thinking that you are bewitched only to find that it is the medication that is doing that. You might have diarrhoea but just because you are experiencing these things it does not mean that you should stop taking your treatment and say that it is making you sick. No, you must con-tinue, that thing (side e!ects) might happen for 2 or 3"months.” - Counsellor
In contrast, some of the counsellors presented more nuanced information on side e!ects and only as a pos-sibility (Quotes 5.3–5.4).
“Our pills have side effects, some of the side e!ects are rash, but they don’t do anything to other people; nothing at all. Someone else prefers to isolate themselves, someone else has nightmares when they are sleeping, others hallucinate, but these do not happen to everyone. You know that when you are drinking some pills, you feel like sleeping…these ones are the same as well. Is it not that people are di!erent, and the side e!ects are only for a certain period? You will not have them forever; you only have them when they are still getting used to your system.” - Counsellor
Counselling Techniques
The sessions were predominantly conducted as didactic information delivery characterised by lists of instructions (as
encapsulated in several quotes described thus far). Instruc-tions on “required” behaviour changes to adjust to the HIV diagnosis or for ART to be e!ective, came as blanket state-ments because the counsellors did not ask about their clients’ current behaviour concerning the recommended health and wellness changes. Notably, counsellors failed to ask clients whether they drank alcohol or smoked tobacco, nor did they discuss how the ‘stopping’ would be achieved. Further, the need for behaviour change was generally explicit and imper-ative: “The important thing is changing your lifestyle”.
After providing a series of instructions (sometimes with justifications), interaction with the client was usually lim-ited to asking for an acknowledgement of comprehension. In one session, characterised by a heavily scripted approach to education messaging, the client voiced no recollection of what the counsellor had said on the topic—to which the counsellor provided the answer (albeit misinformation) and went on to provide even more health education messages.
Counsellor: So, I said what is the cause of coughing? Coughing can be caused by…?Client: Coughing…can be caused…Counsellor: Coughing can be caused by HIV, I told you before we got your results. Or you might be cough-ing just because you sick. Which means you were not listening?Client: Yes, I was not listening…Counsellor: I said you must be coughing because you are sick of HIV and the flu will call it opportunist dis-ease…This highly didactic approach limited the opportunities
for clients to participate in the counselling sessions. Due to minimal dialogue between counsellors and clients, we did not identify notable themes on how clients appraised the value of engaging in medical care or the perceived costs associated with engagement in care. Because of failing to identify client goals, counsellors routinely provided infor-mation on PMTCT to women regardless of pregnancy status or intent. An example of describing PMTCT to one client started as follows:
Counsellor: Alright, thank you, my dear. When you want a child, you will get one.Client: I do not want a child. I have got two kids already.We identified two sessions in which counsellors had to
deal with client resistance. The first was a client who was not ready to accept their HIV diagnosis. The counsellor took a confrontational approach and did not explore the problem to obtain new perspectives that form client-cen-tred counselling. The extract below is illustrative:
Counsellor: What is wrong?
Content courtesy of Springer Nature, terms of use apply. Rights reserved.163

AIDS and Behavior
1 3
Client: (Silence) I do not know; I ask myself how it happened. (Silence) Counsellor: I will accompany to the nurse if you are willing to have your blood taken.Client: Can I please do it on some other day when I am ready.Counsellor: You see denial. Which is wrong. Which is very, very wrong.Client: (Sighs)Counsellor: What is it that you still need to under-stand love because the virus is in your body and it is continuing hunting your cells…In the second example, the client also did not believe
the HIV test results due to beliefs of non-exposure to HIV and was not willing to start ART. In this case, the coun-sellor took a more client-centred approach and tactfully promoted the potential value of ART within the client’s narrative of long-term health issues without any notable relief. Despite the counsellor’s attempts, the client still refused to start ART and his wishes were respected by the counsellor.
Counsellor: …So I am saying will you give them (ARVs) a chance and drink them like you have been drinking the others, let us see what is going on. You say you have tried but nothing has worked. It may be helpful to see whether the government medication works because on the other side, the ones that you drank have not helped. Let us see how the govern-ment ones will treat the pain, to see if it will go away or not. It will not help me if I fill in the lab form for you to go and draw blood if you will not take the ARV treatment after getting your blood results. We only open a file if you are willing to walk the journey with us, in other words, we will do as you request. We do not force anyone no, but you must think about it, imagine if your CD4 count result comes back say-ing 0 or 20? Because from what I hear, you have been struggling with this for a long time, maybe your CD4 count is very low, you need to urgently get on treatment.
Discussion
In analysing 40 post-test counselling sessions for clients who tested HIV-positive, we observed a concerning pic-ture of the content and delivery of post-test counselling in routine public sector HIV testing services in South Africa. Post-test counselling sessions were highly didactic, with counsellors seeking to instruct clients on needed life-style changes, behaviour changes, and the range of severe possible side e!ects of ART. Further, little communica-tion was focused on the benefits of ART to prevent HIV
transmission, and erroneous health education messages often supplanted the potential value of ART.
The failure to engage with client’s concerns or goals, overshadowed by the dominance of lists of instructions from the counsellors, meant that client-centred counselling did not occur. Theoretical frameworks in medical soci-ology suggest that when people experience unwanted or aversive life events, such as receiving an HIV diagnosis, they assess the potential threat of the event to what they value and the goals they desire to achieve. This is com-monly referred to as the “significance” or the “situational meaning” of the diagnosis [29, 30], and has been shown to influence whether clients seek medical care services and the timeliness in doing so [31, 32]. However, the value that clients place on ART is not always apparent when counsellors: fail to engage with client’s concerns or goals; deliver messages that contain misinformation, or supplant the value of ART. Therefore, health communication that reassures of the continued possibility to achieve life goals and non-infectivity with an undetectable viral load could be part of motivational interviewing to introduce more immediate value for asymptomatic individuals who are prone to discounting the future benefits of ART.
Listing of behaviour changes required in the setting of HIV diagnosis, including changes to diet, smoking, drink-ing alcohol, and exercise, perpetuate HIV exceptionalism and may increase client perceived costs of ART initia-tion [33, 34]. Further, prescriptive messages by counsel-lors on who clients needed to tell about their HIV status and an overemphasis of ART side-e!ects, might have also inflated client perceptions on the costs of engaging in HIV care, resulting in some clients deferring ART initiation or disengaging from care in the early months following ART initiation. This view is supported by Shippee et"al., who highlight how the imbalances between the patient workload (i.e. demands of treatment, self-care, or general life adjustments) and the capacity of patients to handle these demands, may lead to poor care engagement out-comes [35]. In light of our findings, there is an urgent need for counsellors to be trained on appropriate “fram-ing” of health education messages [36]. As South Africa moves to roll-out ART regimens containing dolutegravir, well-framed health education messages will be required to balance side-e!ects linked to the drug and its key benefits such as improved tolerability and an increased barrier to resistance [37].
Some researchers argue that some sub-Saharan Afri-can societies and cultures respond well to paternalistic approaches of healthcare service delivery, resulting in favourable care engagement outcomes [38–40]. In other instances, patients may lack the self-e#cacy to challenge propositions made by healthcare providers and disengage from care to avoid reproach if they struggle to fulfil all the
Content courtesy of Springer Nature, terms of use apply. Rights reserved.164

AIDS and Behavior
1 3
required changes. Our findings highlighted two examples where clients were vocal about their appraisal of the HIV diagnosis and counsellors responded to the clients’ non-acceptance of the HIV test result. A better grasp of moti-vational interviewing skills would help these counsellors to support these clients, including approaches to minimise defensiveness or resistance—“rolling with resistance” or “managing discord” [20].
We are unaware of any similar work using qualitative methods to describe post-test counselling among clients with a positive test result in the current UTT era. One study using a combination of direct observations and audio-recordings reported on the processes of HIV counselling and testing (e.g. description of the testing process) and the nature of the counselling (e.g. probing was used in 30% of sessions). This study also described that South African guidelines were not well adhered to in delivery of post-test counselling, but did not describe the content [41]. Several studies have used interviews conducted after HIV testing to assess quality [42, 43]. An evaluation of the quality of counselling provided by a highly trained group of HIV counsellors employed as part of a randomised trial reported excellent delivery of content and client satisfaction with intensive didactic train-ing, a four-month in-service training, and ongoing oversight [44]. That study suggests that with dedicated and intense resources, a high level of quality can be achieved.
If our sample of 34 counsellors at 10 clinics in a single district is representative of overall post-test counselling in South Africa and the region, it may be that much of counsel-ling is counter-productive to the aims of UTT and same-day initiation of ART. Although counselling is often viewed as an essential component of providing HIV testing and ini-tiating ART in low to middle-income countries, evidence to guide post-test counselling content to best support the HIV care continuum is lacking [45]. The best evidence on counselling, particularly strengths-based counselling, is from studies of longitudinal counselling sessions starting at a time after HTS [19, 46, 47].
Strengths of our study include audio-recording of actual counselling sessions with the recording starting before obtaining test results, the inclusion of a substantial number of counsellors and performing the study during routine care at public clinics. We believe that our approach has led to findings that are likely representative of the post-test coun-selling occurring in many public clinics in South Africa and possibly elsewhere in sub-Saharan Africa. Another strength is the use of specific frameworks in coding and analysing the counselling transcripts. We also note potential limitations. One is that the counsellors or clients may have changed behaviour in the presence of the digital audio-recorder. It is possible that counsellors switched from a client-centred approach to more of a didactic approach due to the presence of the audio-recorder to impress the research team with their
comprehensiveness. We believe that this is unlikely because the audio-recording started early during an HTS session, before pre-test counselling, and the recording device was placed to the side (on a cupboard) allowing for the counsel-lor and client to easily ignore the presence of the recording device by the time post-test counselling occurred. Lastly, we did not collect qualitative data from the counsellors to explore factors which influence the content delivered dur-ing post-test counselling, including the nature and specific content of training received, and their perceptions on the level of client engagement during the sessions. This an area we recommend for further research.
In conclusion, our findings should lead implementers to assess their post-test counselling delivery and to lead poli-cymakers and researchers to interrogate the current role and e!ectiveness of post-test counselling. In its current form, post-test counselling appears to undermine the anticipated benefits of ART in reducing HIV transmission and may negatively a!ect the demand for ART by those who need it. We also acknowledge that beyond the individual-level competency of counsellors, contextual factors such as the rationalisation of limited counselling rooms, the large num-ber of clinic attendees requiring HTS services, or the pres-sure of same-day ART, can predispose counsellors towards didactic and scripted approaches to accelerate the counsel-ling process [41, 48, 49].
Based on our observations, a substantial re-adjustment is required to deliver best practice counselling aligned with WHO Guidelines. It is unclear whether additional training or the quality assurance recommended in WHO Guidelines is su"cient to meet content and delivery goals. A greater readjustment may be needed to achieve the HIV care goals of post-test counselling for those testing positive. This may include digital media-based counselling provided through interactive media or counselling scripts to increase the validity of health information and assure that counsellors communicate priority messages. A highly trained cadre of professional counsellors who consistently provide best prac-tice counselling could be available to a subset of individuals who do not link to care or initiate ART within a specified period. Further studies and policy approaches are needed to characterise what works for post-test counselling and to assure quality delivery of this counselling to best support the HIV care continuum.
Funding This study was funded through Project SOAR, a five-year cooperative agreement funded by the President’s Emergency Plan for AIDS Relief and the U.S. Agency for International Development (Agreement No. AID-OAA-A-14-00060).
Content courtesy of Springer Nature, terms of use apply. Rights reserved.165

AIDS and Behavior
1 3
Compliance with Ethical Standards
Conflict of interest The authors declare that they have no conflict of interest.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the insti-tutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the University of Witwatersrand Human Research Ethics Committee (6 May 2016, Reference Number 160101).
Informed Consent Informed consent was obtained from all individual participants included in the study.
References
1. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et!al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.
2. Ho"mann CJ, Lewis JJ, Dowdy DW, Fielding KL, Grant AD, Martinson NA, et!al. Mortality associated with delays between clinic entry and ART initiation in resource-limited settings: results of a transition-state model. J Acquir Immune Defic Syndr. 2013;63(1):105–11.
3. Tanser F, Barnighausen T, Grapsa E, Zaidi J, Newell ML. High coverage of ART associated with decline in risk of HIV acquisition in rural KwaZulu-Natal South Africa. Science. 2013;339(6122):966–71.
4. Johnson LF, Mossong J, Dorrington RE, Schomaker M, Ho"mann CJ, Keiser O, et!al. Life expectancies of South African adults starting antiretroviral treatment: collaborative analysis of cohort studies. PLoS Med. 2013;10(4):e1001418.
5. World Health Organisation. Guidelines on when to start antri-retroviral therapy and pre-exposure prophylaxis for HIV2015 20 January 2019. https ://www.who.int/hiv/pub/guide lines /early relea se-arv/en/.
6. Brazier E, Maruri F, Duda SN, Tymejczyk O, Wester CW, Somi G, et!al. Implementation of “Treat-all” at adult HIV care and treat-ment sites in the Global Ie DEA Consortium: results from the Site Assessment Survey. J Int AIDS Soc. 2019;22(7):e25331.
7. Joint United Nations Programme on HIV/AIDS. Miles to go: clos-ing gaps, breaking barriers, righting injustices. Geneva: UNAIDS; 2018.
8. UNAIDS. Global AIDS update 2019—Communities at the cen-tre2019 15 January 2019. https ://www.unaid s.org/sites /defau lt/files /media _asset /2019-globa l-AIDS-updat e_en.pdf.
9. Human Sciences Research Council. The Fifth South African National HIV Prevalence, Incidence, Behaviour and Communi-cation Survey2017 15 January 2020. https ://www.hsrc.ac.za/uploa ds/pageC onten t/9234/SABSS MV_Impac t_Asses sment _Summa ry_ZA_ADS_clear ed_PDFA4 .pdf.
10. Commonwealth Regional Health Community Secretariat. HIV/AIDS voluntary counselling and testing: review of policies, pro-grammes and guidelines in east, central and southern Africa. Aru-sha: CRHCS; 2002.
11. Joint United Nations Programme on HIV/AIDS. The impact of Voluntary Counselling and Testing A global review of the benefits and challenges. Geneva: UNAIDS; 2001.
12. Weinhardt LS, Carey MP, Johnson BT, Bickham NL. E"ects of HIV counseling and testing on sexual risk behavior: a
meta-analytic review of published research, 1985–1997. Am J Public Health. 1999;89(9):1397–405.
13. Allen S, Tice J, Van de Perre P, Serufilira A, Hudes E, Nsengu-muremyi F, et!al. E"ect of serotesting with counselling on condom use and seroconversion among HIV discordant couples in Africa. BMJ. 1992;304(6842):1605–9.
14. Wenger NS, Linn LS, Epstein M, Shapiro MF. Reduction of high-risk sexual behavior among heterosexuals undergoing HIV anti-body testing: a randomized clinical trial. Am J Public Health. 1991;81(12):1580–5.
15. World Health Organization. Guidelines for counselling about HIV infection and disease1990 2 April 2020. https ://apps.who.int/iris/handl e/10665 /39619 .
16. World Health Organisation. Consolidated guidelines on HIV test-ing services2015 15 January 2019. https ://www.who.int/hiv/pub/guide lines /hiv-testi ng-servi ces/en/.
17. World Health Organization. Guidance on provider-initiated HIV testing and counselling in health facilities2007 2 April 2020. https ://www.who.int/hiv/pub/vct/pitc/en/.
18. World Health Organisation. Consolidated guidelines on HIV test-ing services for a changing epidemic2019 1 January 2020. https ://www.who.int/publi catio ns/i/item/conso lidat ed-guide lines -on-hiv-testi ng-servi ces-for-a-chang ing-epide mic.
19. Craw JA, Gardner LI, Marks G, Rapp RC, Bosshart J, Du"us WA, et!al. Brief strengths-based case management promotes entry into HIV medical care: results of the antiretroviral treatment access study-II. J Acquir Immune Defic Syndr. 2008;47:597–606.
20. Hill S, Kavookjian J. Motivational interviewing as a behavioral intervention to increase HAART adherence in patients who are HIV-positive: a systematic review of the literature. AIDS Care. 2012;24(5):583–92.
21. Dillard PK, Zuniga JA, Holstad MM. An integrative review of the e#cacy of motivational interviewing in HIV management. Patient Educ Counsel. 2017;100(4):636–46.
22. Hodgson I, Plummer ML, Konopka SN, Colvin CJ, Jonas E, Albertini J, et!al. A systematic review of individual and contex-tual factors a"ecting ART initiation, adherence, and retention for HIV-infected pregnant and postpartum women. PLoS ONE. 2014;9(11):e111421.
23. Sanga ES, Mukumbang FC, Mushi AK, Lerebo W, Zarowsky C. Understanding factors influencing linkage to HIV care in a rural setting, Mbeya, Tanzania: qualitative findings of a mixed methods study. BMC Public Health. 2019;19(1):383.
24. Ho"mann CJ, Mabuto T, McCarthy K, Maulsby C, Holtgrave DR. A framework to inform strategies to improve the HIV care continuum in low-and middle-income countries. AIDS Educ Prev. 2016a;28(4):351–64.
25. South Africa National Department of Health. National HIV Coun-selling And Testing Policy Guidelines2015 19 January 2019. https ://www.nicd.ac.za/asset s/files /HCT-Guide lines -2015.pdf.
26. South Africa National Department of Health 2019 2019 ART Clinical Guidelines for the Management of HIV in Adults Preg-nancy Adolescents, Children, Infants and Neonates.
27. Crabtree B, Miller ML. Doing qualitative research. Thousand Oaks: Sage; 1999.
28. Miles MB, Huberman MA. Qualitative data analysis: an expanded sourcebook. Thousand Oaks: Sage; 1994.
29. Klinger E. Meaning and void: Inner experience and the incentives in peoples lives. Minneapolis: University of Minnesota Press; 1977.
30. Park CL, Folkman S. Meaning in the context of stress and coping. Rev Gen Psychol. 1997;1(2):115–44.
31. Leventhal H, Diefenbach M, Leventhal EA. Illness cognition: using common sense to understand treatment adherence and a"ect cognition interactions. Cognit Ther Res. 1992;16(2):143–63.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.166

AIDS and Behavior
1 3
32. Taylor EJ. Whys and wherefores: adult patient perspectives of the meaning of cancer. Semin Oncol Nurs. 1995;11(1):32–40.
33. Ho!mann CJ, Mabuto T, McCarthy K, Maulsby C, Holtgrave DR. A framework to inform strategies to improve the HIV care continuum in low- and middle-income countries. AIDS Educ Prev. 2016b;28(4):351–64.
34. Ahmed S, Autrey J, Katz IT, Fox MP, Rosen S, Onoya D, et"al. Why do people living with HIV not initiate treatment? A system-atic review of qualitative evidence from low-and middle-income countries. Soc Sci Med. 2018;213:72–84.
35. Shippee ND, Shah ND, May CR, Mair FS, Montori VM. Cumula-tive complexity: a functional, patient-centered model of patient complexity can improve research and practice. J Clin Epidemiol. 2012;65(10):1041–51.
36. Levin IP, Schneider SL, Gaeth GJ. All frames are not created equal: a typology and critical analysis of framing e!ects. Organ Behav Hum Decis Process. 1998;76(2):149–88.
37. Phillips AN, Bansi-Matharu L, Venter F, Havlir D, Pozniak A, Kuritzkes DR, et"al. Updated assessment of risks and benefits of dolutegravir versus efavirenz in new antiretroviral treatment initiators in sub-Saharan Africa: modelling to inform treatment guidelines. Lancet HIV. 2020;7(3):e193–200.
38. Laungani P. Replacing client-centred counselling with culture- centred counselling. Couns Psychol Q. 1997;10(4):343–51.
39. Wanyenze RK, Musinguzi G, Matovu JK, Kiguli J, Nuwaha F, Mujisha G, et"al. “If you tell People that you had sex with a fellow man, it is hard to be helped and treated”: barriers and opportuni-ties for increasing access to HIV services among men who have sex with men in Uganda. PLoS ONE. 2016;11(1):e0147714.
40. Watt MH, Maman S, Earp JA, Eng E, Setel PW, Golin CE, et"al. “It’s all the time in my mind”: facilitators of adherence to antiretroviral therapy in a Tanzanian setting. Soc Sci Med. 2009;68(10):1793–800.
41. Mohlabane N, Peltzer K, Mwisingo A, Ntespe Y, Tutshana B, Van Rooyen H, et"al. Quality of HIV counselling in South Africa. J Psychol. 2015;6(1):19–31.
42. Matseke G, Peltzer K, Mohlabane N. Clients’ perceptions and satisfaction with HIV counselling and testing: a cross-sectional study in 56 HCT sites in South Africa. Afr J Primary Health Care Fam Med. 2016;8(1):1–7.
43. Meehan SA, Naidoo P, Claassens MM, Lombard C, Beyers N. Characteristics of clients who access mobile compared to clinic HIV counselling and testing services: a matched study from Cape Town South Africa. BMC Health Servic Res. 2014;14:658.
44. Bell SA, Delpech V, Raben D, Casabona J, Tsereteli N, de Wit J. HIV pre-test information, discussion or counselling? A review of guidance relevant to the WHO European Region. Int J STD AIDS. 2016;27(2):97–104.
45. Bell S, Delpech V, Casabona J, Tsereteli N, de Wit J. Delivery of HIV test results, post-test discussion and referral in health care settings: a review of guidance for European countries. HIV Med. 2015;16(10):620–7.
46. Gardner LI, Metsch LR, Anderson-Mahoney P, Loughlin AM, del Rio C, Strathdee S, et"al. E#cacy of a brief case management intervention to link recently diagnosed HIV-infected persons to care. AIDS. 2005;19(4):423–31.
47. Ho!mann CJ, Mabuto T, Ginindza S, Fielding KL, Kubeka G, Dowdy DW, et"al. Strategies to accelerate HIV care and antiretro-viral therapy initiation after HIV diagnosis: a randomized trial. J Acquir Immune Defic Syndr. 2017;75(5):540–7.
48. Ha!ejee S, Groeneveld I, Fine D, Patel R, Bowman B. An assess-ment of counselling and support services for people living with-HIV in Gauteng, South Africa: findings of a baseline study. Afr J AIDS Res. 2010;9(4):367–72.
49. Mabuto T, Hansoti B, Kerrigan D, Mshweshwe-Pakela N, Kubeka G, Charalambous S, et"al. HIV testing services in healthcare facilities in South Africa: a missed opportunity. J Int AIDS Soc. 2019;22(10):e25367.
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional a#liations.
Content courtesy of Springer Nature, terms of use apply. Rights reserved.167

Symptom and risk-based screening to optimize HIV testing services: a scoping review Caitlin Quinn1*, Vincent Wong2, Muhammad S. Jamil1, Rachel C. Baggaley1, Cheryl C. Johnson1 1Global HIV, Hepatitis and STIs Programme, World Health Organization, Geneva, Switzerland 2 U.S. Agency for International Development, Washington, DC, USA
Abstract Introduction: The cost and challenges of identifying the remaining people with HIV who do not know their status is increasing. Given constraints on programme resources and the desire for higher testing yields, many HIV programmes are using screening tools based on symptoms, testing history, demographics and other risks to inform decisions about who receives HIV testing. To better understand these tools and their potential risks and benefits, we conducted a scoping review synthesizing the contemporary literature and programmatic use of screening tools in HIV Testing Services. Methods: We searched four electronic databases and seven conferences for literature published between 1 January 2010 and 31 December 2018. Programmatic screening tools and data were also solicited from national programmes, key experts and donors. Results: Twenty-nine screening tools from peer-reviewed literature and 47 screening tools from national and donor-funded programmes were identified in the search. Twenty-five percent (n=19/76) of all tools were validated, and most validated tools were implemented in countries with low HIV prevalence (63%, n=12/19). In validated tools, the most common screening question for adults was the date of last HIV test. For children, the most common screening questions were related to symptoms, general health and family status, such as orphanhood. Screening for HTS exhibited a dose-response between increasing risk score and HIV positivity, but missed a varying proportion of people with HIV excluded in the risk screening. Conclusions: Screening tools may offer an effective way to focus HIV testing resources during a time of changing epidemics and declining resources. Benefits may be greater where HIV testing is not routinely offered (‘screening in’ people for HIV testing), such as in low prevalence settings and amongst subpopulations with low HIV prevalence, such as children and adolescents. High HIV prevalence settings need to be cautious about screening tools as they may be missing a significant proportion of people with undiagnosed HIV.
168

Introduction Globally 37.9 million people have HIV – and 8.1 million (21%) are unaware of their HIV status (1). This gap in knowledge of HIV status contributes to morbidity and mortality, and is a missed opportunity to prevent onward transmission by initiating effective antiretroviral therapy (ART). Diagnosing the remaining people with HIV through HIV testing services (HTS) and linking them to ART is a global priority. National programmes are implementing HTS in an effort to achieve the United Nations’ Fast Track Strategy for ending the HIV epidemic – starting with diagnosing 95% of people with HIV by 2030 (2). As programmes scale-up and attain, or come close to meeting, testing and treatment targets, identifying the remaining people with HIV who do not know their status is becoming challenging and costly. HIV positivity (or yield) in HTS programmes is steadily declining in many high burden settings despite increases in testing (3). Additionally, available resources for HIV fell by nearly US$ 1 billion between 2017 and 2018 (1). Optimizing declining or static resources with focused, differentiated HTS approaches is essential (4, 5). One approach proposed to further focus HTS efforts toward those in greatest need is the use of screening tools to inform decisions about who receives HIV testing. Screening tools to identify individuals who might benefit from pre-exposure prophylaxis have been shown to be accurate in identifying people with greater HIV risk and useful to help support offer of a relatively costly intervention (6-9). Less is known about the use of screening tools for HTS. To date, screening tools for HTS have been applied largely in clinical settings to screen people in or out of testing based on symptoms, testing history, risk behaviours or other demographic characteristics, with varying effects. In some programmes, the use of screening tools suggests increased positivity, but others also highlight potential for missed opportunities to identify a significant proportion of people with undiagnosed infections (10). Despite varying results and lack of systematic evaluation of many HTS screening tools, programme implementers are considering their routine use in services to increase the efficiency and cost-effectiveness of HTS efforts. Little is known about the potential negative consequences of these tools or their feasibility and acceptability to both providers and clients. To better understand the potential risks and benefits, we conducted a scoping review synthesizing the contemporary literature and programmatic use of HTS screening tools (11, 12).
Methods Search strategy We used two strategies to identify HTS screening tools: (i) searching peer-reviewed literature; and (ii) collecting screening tools used programmatically. To identify screening tools in peer-reviewed literature, we searched four electronic databases (PubMed, Embase, ScienceDirect, Web of Science) for articles published between 1 January 2010 and 31 December 2018. We also searched for scientific abstracts from five major HIV conferences (AIDS, CROI, HIVR4P, IAS, ICASA) for recent studies employing screening tools. The full search strategy and key terms searched is described in Appendix 1. Programmatic screening tools were also solicited from national HIV programmes, Ministries of Health, key experts, and implementing partners and donors, particularly the U.S. President's Emergency Plan for AIDS Relief (PEPFAR) and World Health Organization (WHO) country offices. Records from peer-reviewed literature and programmes were assessed for inclusion by a single reviewer. The reviewer assessed eligibility of peer-reviewed literature by screening titles and abstracts to remove records that were not relevant. Then, full-text articles were obtained and reviewed to make a final inclusion decision. There were no
169

geographic or language restrictions or conditions on study design. Records in languages other than English were translated using Google Translate to identify and extract relevant information. Inclusion criteria Records from peer-reviewed literature were included if they described use of a HIV screening tool and reported relevant HIV testing outcomes. Screening tools from programmes were included if they screened clients based on demographic characteristics, symptoms or indicator conditions, behavioural risk factors or HIV testing history. Outcomes Relevant outcomes of interest included sensitivity of the HIV screening tool [defined as the proportion of true positives that are correctly identified], specificity of the HIV screening tool [defined as proportion of true negatives that are correctly identified], positive predictive value (PPV), negative predictive value (NPV), and the proportion of individuals screened who tested HIV positive, initiated treatment, or tested negative and linked to prevention services, acceptability of HIV screening amongst healthcare providers and clients and feasibility of implementation. Cost or cost-effectiveness of screening for HTS was also an outcome of interest. Additionally, we were interested in recording validation methods used to assess the dependability and accuracy of screening tools to identify people living with HIV (PLHIV).
Data extraction Data were extracted from full-text peer-reviewed articles using an Excel extraction tool. From each included record, the following information was extracted and populated in the extraction tool: location, target population, sample size, study design, setting, country HIV prevalence, HTS outcomes, screening tool performance and study limitations. From all records, details and components of the screening tool were extracted, including a description of the screening questions and the number of questions asked. Operational details and processes were also collected, including who conducted the screening, the time allotted to screening or other programmatic factors and cost or cost-effectiveness of using screening tools.
Analysis and reporting The results were organised by country HIV prevalence (high prevalence �5% or low prevalence <5%), which was obtained from 2018 UNAIDS estimates on the AIDSInfo database (13). Results were also analysed by target population [children (0-9), adolescents (10-19), adults (15+), and key populations (men who have sex with men (MSM), sex workers, people who inject drugs (PWID), people in prison and transgender people)]. Screening tool characteristics and outcomes were summarized in tables.
Results Characteristics of screening tools Across the literature and programme tool search, 76 screening tools were identified in total. In the peer-reviewed literature search, 16,397 records were identified and screened. After title, abstract and full-text screening, 29 met the inclusion criteria (Figure 1) (10, 14-41). One record was published in Spanish (14) and another in Chinese (41). Forty-seven programmatic screening tools from 16 countries were identified in addition to the literature review. All included records are summarised in Appendix 2 (tools from peer-reviewed literature) and Appendix 3 (programme tools).
170
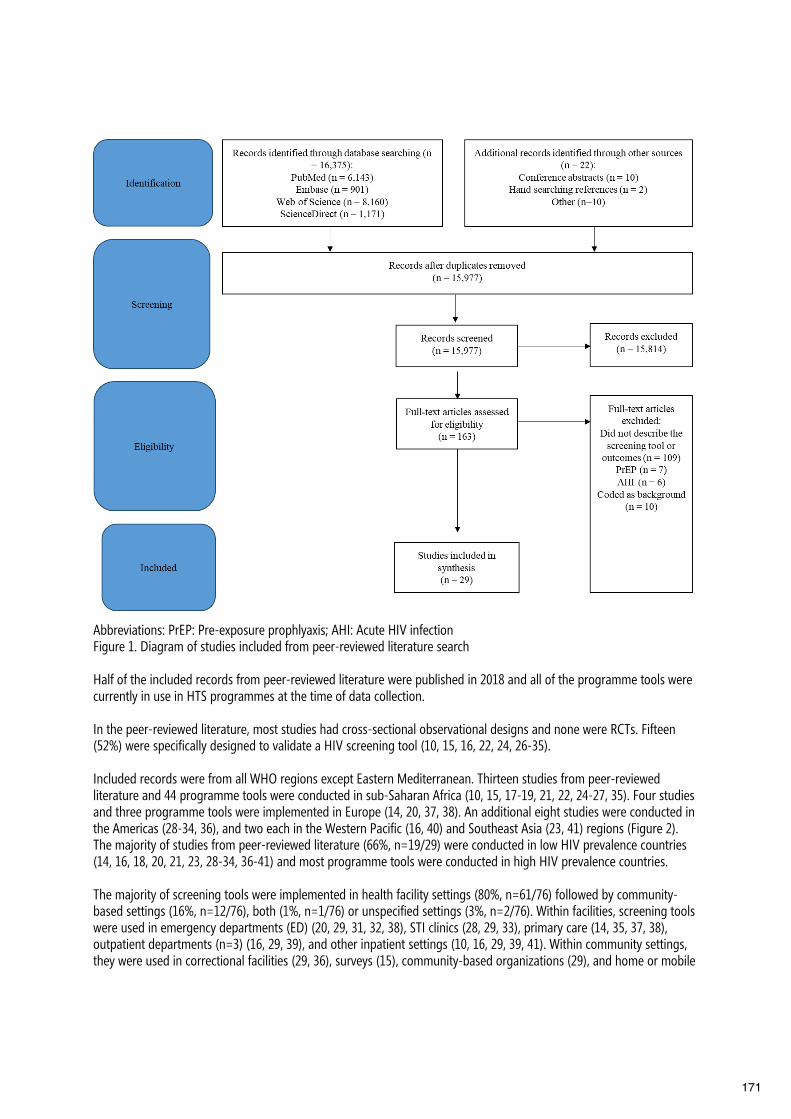
Abbreviations: PrEP: Pre-exposure prophlyaxis; AHI: Acute HIV infection Figure 1. Diagram of studies included from peer-reviewed literature search Half of the included records from peer-reviewed literature were published in 2018 and all of the programme tools were currently in use in HTS programmes at the time of data collection. In the peer-reviewed literature, most studies had cross-sectional observational designs and none were RCTs. Fifteen (52%) were specifically designed to validate a HIV screening tool (10, 15, 16, 22, 24, 26-35). Included records were from all WHO regions except Eastern Mediterranean. Thirteen studies from peer-reviewed literature and 44 programme tools were conducted in sub-Saharan Africa (10, 15, 17-19, 21, 22, 24-27, 35). Four studies and three programme tools were implemented in Europe (14, 20, 37, 38). An additional eight studies were conducted in the Americas (28-34, 36), and two each in the Western Pacific (16, 40) and Southeast Asia (23, 41) regions (Figure 2). The majority of studies from peer-reviewed literature (66%, n=19/29) were conducted in low HIV prevalence countries (14, 16, 18, 20, 21, 23, 28-34, 36-41) and most programme tools were conducted in high HIV prevalence countries. The majority of screening tools were implemented in health facility settings (80%, n=61/76) followed by community-based settings (16%, n=12/76), both (1%, n=1/76) or unspecified settings (3%, n=2/76). Within facilities, screening tools were used in emergency departments (ED) (20, 29, 31, 32, 38), STI clinics (28, 29, 33), primary care (14, 35, 37, 38), outpatient departments (n=3) (16, 29, 39), and other inpatient settings (10, 16, 29, 39, 41). Within community settings, they were used in correctional facilities (29, 36), surveys (15), community-based organizations (29), and home or mobile
171

testing sites. Screening tools were primarily implemented by a trained lay provider or health worker, with only two records reporting on use of a client self-administered tool (20, 38).
Thirty screening tools were used to screen children or adolescents (39%, 30/76), another 33 were for adults (43%, n=33/76) and nine were used for all ages (12%, n=9/76). Four tools were implemented specifically for key populations (5%, n=4/76), though many other tools for adults included questions related to key population behaviours.
Figure 2. Countries with validated and non-validated HIV screening tools identified in the literature search and program screening tool collection Development and validation of screening tools
Twenty-five percent (n=19/76) of all tools were validated (Figure 2). Most validated tools were implemented in low HIV prevalence countries (63%, n=12/19) and were identified from the peer-reviewed literature (79%, n=15/19). HTS screening tools in the published literature were validated by either internal validation, in which the authors randomly divide the dataset into a derivation and validation sample to develop and test the tool, or comprehensive internal and external validation, in which authors also tested the tool on an external sample. Tool performance was assessed by calculating the area under the receiver operating characteristic curve (AUC), sensitivity, specificity, PPV and NPV. In programmes, validation was done by retrospectively analyzing screening and testing records and calculating tool performance with sensitivity, specificity, PPV and NPV.
Screening questions to identify PLHIV
Overall, the number of questions asked on a screening tool ranged from 1 to 23, with a median of 9 questions for key populations, 8 questions for children or adolescents and 7 questions for general population adults.
Testing history or date of last HIV test was the most frequent screening question asked across validated tools for general population adults (n=11) (Appendix 4). Behavioural risk questions, such as history of injecting drugs, anal intercourse and condom usage, were more common than questions about STIs or indicator conditions associated with HIV infection, especially for validated questionnaires among key populations (n=3). Questions on demographic characteristic (gender, race/ethnicity, age) were also used. Non-validated screening tools also asked about HIV testing history, symptoms of STIs, TB or other HIV indicator conditions, and risk behaviors associated with HIV infection.
172
In validated paediatric screening tools (n=5), symptoms of HIV indicator conditions were most frequent. In general, the four characteristics from a tool developed in Zimbabwe (15, 27) were most common for identifying children for HIV testing: orphanhood, reoccurring skin problems, previous hospitalization and general poor health status. Some non-validated screening tools for children (n=7/30) addressed the child’s economic or educational situation. Although infrequent in paediatric screening tools (n=8/30), and not occurring in any of the validated tools, some screening questionnaires for children and adolescents asked about risk behaviors, such as engagement in sexual activity or experience of sexual abuse.
Some studies validated and compared individual screening questions for their predictive ability. In Malawi, the screening tool from Zimbabwe was adapted for use amongst 1-15 year olds and evaluated (10). During validation, the study found that being of small stature and having at least one deceased parent had significant associations for identifying children living with HIV. A paediatric screening tool used in India, a low HIV prevalence setting, found that parental factors [having a chronically ill parent, prolonged separation of parents, a parent who is a member of a key population group, or one or both parents deceased] are effective for identifying children for HTS (16). In adult women in high prevalence settings, age <25, being unmarried or not living with a primary partner, and having a curable STI at baseline were the strongest predictors of HIV acquisition on the screening tool (26). In Malawi, the most sensitive (71%) and specific (44%) question on an adult facility-based screening tool was whether the patient received any health services in past month. In Zambia, the He2ro analysis showed that using an algorithm based on the date of last HIV test had a higher HIV positive yield (12%) compared to targeted testing based on other factors (10.4%). Individual questions were also assessed on an adult screening tool in a low prevalence setting in Nigeria, finding the most sensitive question (76%) was whether the client had unprotected sex with a regular partner in the last three months. In a tool from Ukraine, the questions which significantly predicted HIV were having more than one sexual partner, injecting drugs, having sex with a PWID, having anal sex, having a HIV-positive sexual partner and ever being in prison.
Time required for screening Only one study in Spain reported on the time required for administering screening tools (38). This study reported it took individuals three minutes on average to complete a series of 21 self-administered questions on an electronic tablet. No provider-administered tools were assessed for length of time to implement. Cost-effectiveness of HTS screening implementation Three included studies assessed cost-effectiveness of screening for HTS. In a study in France, the incremental cost-effectiveness ratio of the targeted screening compared to non-targeted was EUR 1324 (estimated USD 1476) per new HIV diagnosis. In Spain, the cost of universal HIV testing (USD 4176 per person diagnosed) was higher compared to using a screening tool based on risk behaviours (USD 894) or HIV indicator conditions (USD 542) (37). In India, it was also found that screening-in all TB patients for HIV testing would be cost-effective, increasing life expectancy by 16.91 years with an ICER of USD 730 per year of life saved, compared to selectively screening-in for HTS based on regional HIV prevalence (40). Screening tool performance outcomes Sensitivity and/or specificity of screening tools were reported in a subset of the included records (n=17) (Fig. 3.). Sensitivity among children and adolescents (n=5) ranged from 56-100% and specificity ranged from 40-81%. Tools for adults (n=9) performed between 75-100% sensitivity and 25-61% specificity. For tools reporting performance among key populations (n=3), sensitivity ranged from 83-86% and specificity from 43-45%.
173
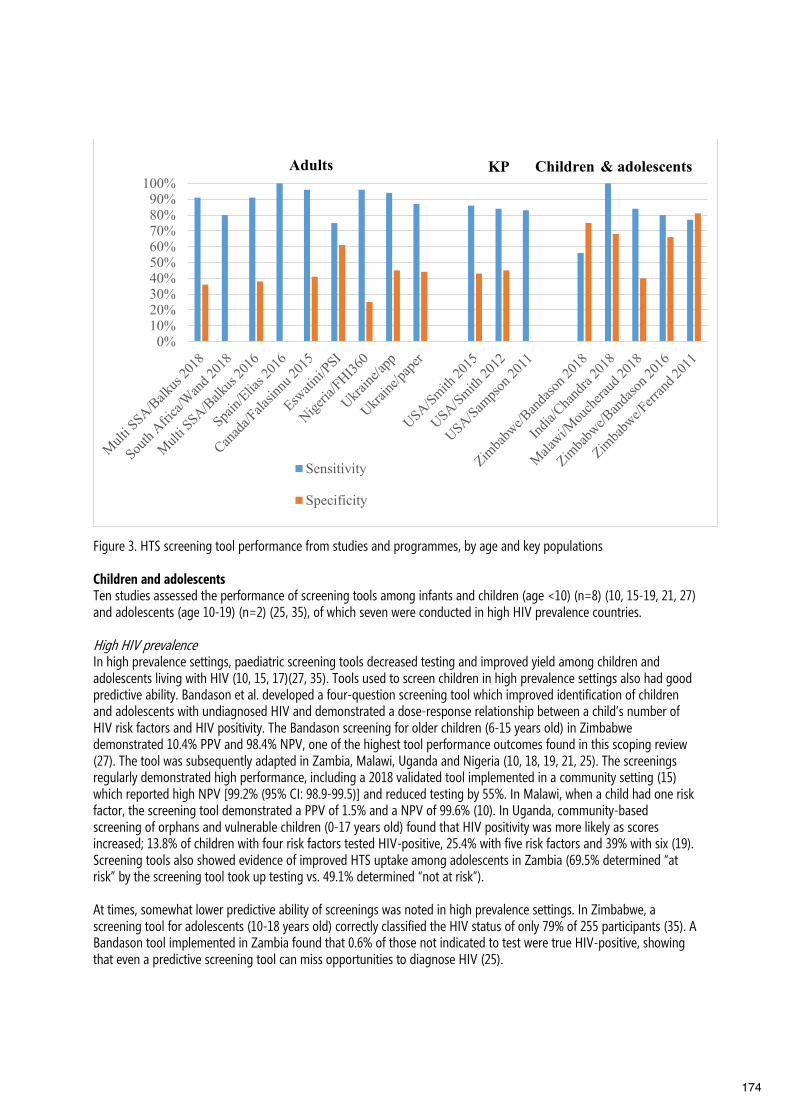
Figure 3. HTS screening tool performance from studies and programmes, by age and key populations Children and adolescents Ten studies assessed the performance of screening tools among infants and children (age <10) (n=8) (10, 15-19, 21, 27) and adolescents (age 10-19) (n=2) (25, 35), of which seven were conducted in high HIV prevalence countries. High HIV prevalence In high prevalence settings, paediatric screening tools decreased testing and improved yield among children and adolescents living with HIV (10, 15, 17)(27, 35). Tools used to screen children in high prevalence settings also had good predictive ability. Bandason et al. developed a four-question screening tool which improved identification of children and adolescents with undiagnosed HIV and demonstrated a dose-response relationship between a child’s number of HIV risk factors and HIV positivity. The Bandason screening for older children (6-15 years old) in Zimbabwe demonstrated 10.4% PPV and 98.4% NPV, one of the highest tool performance outcomes found in this scoping review (27). The tool was subsequently adapted in Zambia, Malawi, Uganda and Nigeria (10, 18, 19, 21, 25). The screenings regularly demonstrated high performance, including a 2018 validated tool implemented in a community setting (15) which reported high NPV [99.2% (95% CI: 98.9-99.5)] and reduced testing by 55%. In Malawi, when a child had one risk factor, the screening tool demonstrated a PPV of 1.5% and a NPV of 99.6% (10). In Uganda, community-based screening of orphans and vulnerable children (0-17 years old) found that HIV positivity was more likely as scores increased; 13.8% of children with four risk factors tested HIV-positive, 25.4% with five risk factors and 39% with six (19). Screening tools also showed evidence of improved HTS uptake among adolescents in Zambia (69.5% determined “at risk” by the screening tool took up testing vs. 49.1% determined “not at risk”). At times, somewhat lower predictive ability of screenings was noted in high prevalence settings. In Zimbabwe, a screening tool for adolescents (10-18 years old) correctly classified the HIV status of only 79% of 255 participants (35). A Bandason tool implemented in Zambia found that 0.6% of those not indicated to test were true HIV-positive, showing that even a predictive screening tool can miss opportunities to diagnose HIV (25).
0%10%20%30%40%50%60%70%80%90%100%
Sensitivity
Specificity
KP Children & adolescentsAdults
174

Low HIV prevalence Two studies adapted the paediatric Bandason tool to a low HIV prevalence, facility-based setting in Nigeria (18, 21). These resulted in higher coverage of HTS among children and adolescents (27%) and increased diagnoses (36%) (21). As in high prevalence settings, there was a dose-response relationship between increased risk scores and HIV positivity. HIV positivity grew significantly from 1.3% among those scoring one on the screening tool to 25% among those scoring four (p<0.001) (18). An additional study in a paediatric facility in India found PPV increased from 2% to 5.86% when testing was offered for children who had either two clinical signs of HIV and at least one parental factor or three clinical signs of HIV. In this validated screening, no children with undiagnosed HIV were missed (NPV=100%). (16). Key populations Four studies were specifically among key populations [two for MSM (23, 34), one for PWID (30) and one for people in prisons (36)]. All included studies with HIV screenings of key populations were conducted in very low HIV prevalence settings. Low HIV prevalence A risk scoring model among MSM in the United States resulted in 1.9% PPV and 99.5% NPV among MSM with risk scores ≥10 (34). Likewise, a model in China performed with a sensitivity of 86.2% and a specificity of 42.5% in PWID scoring ≥46 out of 100 (30). Another HIV screening was developed for use in prisons in the United States which scored prisoners based on age, race/ethnicity, date of last HIV test and having a male sexual partner (36). This screening tool reduced excess testing by 50% with a sensitivity of 82.6% (95% CI: 71.2%-94.0%) for individuals scoring ≥3 out of 6. General population adults Three records from peer-reviewed literature and four programmatic tools in high HIV prevalence settings focused on the use of HTS screening tools for general population adults; six additional studies were in low HIV prevalence settings. High HIV prevalence All three records from peer-reviewed literature in high prevalence settings focused on screening women (22, 24, 26). The risk-based algorithms to prioritise high HIV risk women for HTS had 83% and 91% sensitivity. One algorithm showed modest predictive ability, in which women scoring ≥3 had a HIV incidence of 5.21% (95% CI 4.22-6.44) compared to 0.98% (95% CI 0.51-1.88) among women scoring <3 (26).
Overall, the programme data for male and female adults in high prevalence settings shows screening tools can reduce overall testing and increase yields, but also miss some opportunities to test PLHIV. In Eswatini, Population Services International (PSI) validated a screening tool with 93% sensitivity, 31% specificity, 7% PPV and 99% NPV. Screening indicated an HIV test for 70% of patients and increased yield from 5.1% to 6.7%. However, out of 80 new diagnoses, 6 (8%) would have been missed by the tool. In Tanzania, an implemented screening tool also increased yield from 2.6% to 4.2%, yet 1.5% of clients not at risk according to the screening were true HIV-positive, representing some missed diagnoses.
Low HIV prevalence Four validated studies from the United States and Canada evaluated the Denver HIV risk score (29, 31-33), which demonstrated the utility of screening general population adults in low prevalence settings. The model showed good discrimination between patients with and without HIV in clinical settings (full: AUC=0.86, 95% CI: 0.84-0.88; abbreviated: AUC=0.75, 95% CI: 0.71–0.79) (31, 33). In 2016, the algorithm was validated in community settings where it identified 90% of all HIV infections (based on scoring ≥30) which represented only 63% of the total cohort (29). Another evaluation found a large reduction in the number of HIV tests (10% identified for testing with screening tool vs. 62% in non-targeted strategy) along with better HIV testing uptake and greater yield (32).
175

Two additional non-validated studies amongst general population adults were conducted in Spain and France, showing high acceptability and improved yield with the use of screening tools. In Spain, a self-administered tool in a primary care had high acceptability among health providers (100%, n=14) because they felt it reminded them to offer an HIV test (86%, n=12) and normalized HIV testing (79%, n=11) (14). In France, a trial in eight EDs using a short screening tool identified a significantly higher proportion of new HIV diagnoses during periods of targeted HIV screening compared to non-targeted control periods (RR=3.7; 95% CI 1.4 to 9.8) (20). Programmes in Nigeria and Ukraine highlighted the drawbacks of screening tools that reduce testing and miss people living with undiagnosed HIV. In Nigeria, a tool reduced testing by nearly 77%. Although 5.6% of those tested were positive, true HIV positivity inclusive of people screened out of testing was 8.7%, indicating missed diagnoses. In Ukraine, a programme conducting paper-based and self- or provider-administered app-based tools adapted eligibility to address missed diagnoses. By offering HTS to individuals at medium and high HIV risk, yield increased from 2% to 3% [87% sensitivity, 44% specificity] on the paper tool and from 2% to 4% [94% sensitivity, 45% specificity] on the app. Two individuals with HIV were missed using the paper-based tool (n=2/803) and one using the app (n=1/794). Following these results, programme implementers adjusted the risk classification so that females aged 40-49 years who reported multiple partners and condomless sex in Kyiv were eligible for testing, and subsequently, the screening tool became more effective [100% sensitivity, 40% specificity] with no missed diagnoses (n=0/793).
Discussion This review found that while evidence on accuracy, effectiveness and feasibility of HIV screening tools is limited, their routine use is increasing. We identified 47 screening tools, many non-validated, that are actively being used by programmes and implementers, mostly in high HIV prevalence settings. Across the tools reviewed, there appears to be benefit for increased coverage of HTS and identification of PLHIV when applying screening tools in low HIV prevalence settings where HIV testing is not routinely offered and among certain populations where coverage may be low, such as children and adolescents. However, application of these tools in high HIV prevalence settings and among key populations, where the standard of care is routine testing to all individuals presenting in clinical settings, has limited evidence especially in terms of feasibility, quality, cost and public health impact. HIV positivity and prevalence among children is very low and declining globally. In all HIV prevalence settings, there appears to be a rationale in applying screening tools to increase testing and identification of HIV infections in children and adolescents who would otherwise be missed, particularly in settings where sick and hospitalized children and adolescents are not routinely offered HTS. Previous studies have reported low testing coverage in entry points where sick and hospitalized children present (42), in addition to low provider willingness to test children in many settings (43, 44). In Nigeria, where very few children with HIV are enrolled in ART, application of a screening tool increased overall testing coverage by 27% and identified 36% more children with HIV (21). Likewise, in high HIV prevalence settings such as Malawi, Zambia, Zimbabwe and Uganda, screening tools increased yield and reduced the overall number of children and adolescents needed to be tested to identify a child with HIV. In accordance with national guidelines in high prevalence settings, all children should have been tested but in practice many are missed during prevention of mother-to-child transmission of HIV (PMTCT). The most commonly used paediatric screening identified in this review (27) focused on asking four questions which were well accepted and taken up. The tool was adapted to local contexts in five additional countries with high sensitivity and specificity. While not all tools for children were validated, the vast majority drew from and adapted validated tools. Further piloting and research on the implementation of these tools are needed, particularly within different child and adolescent age bands. Many of the tools reviewed covered a wide range of ages with different risk factors, which may require additional screening questions, such as STI symptoms and sexual activity among adolescents. Sensitive questions on sexual risk behaviours for adolescents should be further examined and assessed.
176

Low prevalence settings using validated screening tools, while few, generally reported strong benefits related to efficiency and increased offers of HIV testing in settings where routine offer of HIV testing is not practiced. Such settings may benefit from prioritization efforts such as testing guided by screening for HIV indicator conditions and risk behaviours. For adults, however, screening tools with evidence in high HIV burden settings were limited, but suggested that there was a substantial trade off of missing PLHIV who do not know their status in order to reduce testing and increase HIV positivity yield. Increasing yield may reduce resource use for testing, but should be considered cautiously as it may miss opportunities to test a high number of people living with undiagnosed HIV and there is not available evidence to assess effects on patient flow or provider time required to conduct screenings. Evidence from this review demonstrated that many programmes are using screening tools without validating the tool’s accuracy for identifying people at higher risk of HIV. It is imperative that validation studies be conducted so tools can be improved to reduce missed opportunities to test and treat PLHIV. A standard protocol for validating screening tools would be beneficial. In the absence of validation, simple tools in alignment with WHO’s existing recommendations on frequency of retesting, such as a question on whether someone has ever tested for HIV or whether they tested for HIV in past 3-6 months, may be considered but must also be evaluated in pilots and monitored closely. Across all settings, important issues related to acceptability, feasibility, cost and potential unintended effects emerged. Only one study (14) assessed acceptability of screening tools. While this study reported high patient and provider acceptability, it is far from representative of various populations, settings and contexts. Feasibility was not formally assessed in any study or programmatic tool, but potential challenges were identified particularly with the use of longer questionnaires, provider- versus patient-administered tools and the appropriateness of questions included. Tools included a wide range of questions – with as many as 23 questions being asked – which may impact the cost, time and feasibility of implementing screening systematically. Shorter and simpler screening tools would likely be preferable, though limited data was available on time or staffing required. Only two screening tools were self-administered by clients, but this approach has potential to conserve time and resources in busy testing environments, as well as address privacy concerns. By its nature, HIV screening tools ask sensitive questions to determine HIV risk, thus, mindfulness of confidentiality is necessary when implementing such screenings. Special consideration needs to be given to the acceptability of these questionnaires, particularly among vulnerable and key populations who may be deterred from seeking testing. Some programmes have worked to reduce stigma in the screening procedure by grouping the behavioural risk questions together such that the client does not specify which exact behaviour they engaged in, yet their overall HIV risk can still be assessed. Developing other best practices for ensuring privacy with provider-administered screenings should also include reflection on when and where screenings are conducted. In this review, only three studies reported on cost-effectiveness and all three were from low HIV prevalence settings (20, 37, 40). The findings indicated lower costs and greater efficiencies, though the overall public health impact of HTS screening tools and their role in achieving national and global targets is still uncertain. More cost-related evidence is needed, particularly for higher prevalence settings where more people require screening and testing; and the cost of missing a person with undiagnosed HIV may be higher (45-47). This review was intended to broadly scope the literature and identify programmatic tools and data to assess evidence for the use of HTS screening tools. Scoping reviews are distinct from systematic reviews in the absence of a priori article criteria; although, we comprehensively searched literature published since 2010 and focused exclusively on studies reporting information on HIV risk screening and study outcomes. However, because this was not a systematic review, it is possible that due to the targeted search criteria and single reviewer, relevant articles could have been missed. Furthermore, some articles were only available as conference abstracts and detailed methods or outcomes were unknown. Another limitation is the variation in validation methods which limited the comparability of included studies.
177

Few studies were validated – and some only described the development and validation of the tool and did not administer an actual screening tool. In these cases, actual implementation of the screening is unknown, and factors related to acceptability, time, cost, and screening efficiency in a real world setting could not be provided. Despite substantial efforts, it is highly likely that other screening tools in use were missed, yet our engagement with experts and programme implementers to share tools and unpublished information was an asset to this review.
Conclusions Our review shows that programmatic use of screening tools is increasing, with many non-validated tools in use. Use of validated screening tools may offer benefits in identification of additional HIV infections in settings where HIV testing is not routinely offered, such as low prevalence settings and amongst subpopulations with very low HIV prevalence, such as children and adolescents. In high prevalence settings, screening tools generally reduce the number of HIV tests conducted and increased positivity rate. Greater caution is needed with routine use of screening tools in these settings where people with HIV in need of testing and treatment may be missed. Robust assessment of the benefits and risks of screening tools is warranted before they are considered for wider implementation, including further research on acceptability and feasibility of screening tools in a range of settings and service delivery approaches.
Acknowledgements We acknowledge and appreciate collaboration from programmes and funding agencies which shared programme tools for this review, including the United States’ President’s Emergency Plan for AIDS Relief (PEPFAR), Population Services International (PSI), AIDSFree, Elizabeth Glaser Pediatric AIDS Foundation (EGPAF), the Bill and Melinda Gates Foundation (BMGF) and Bukoba Combination Prevention Evaluation (BCPE).
178

References 1. Communities at the centre: defending rights, breaking barriers, reaching people with HIV services. Geneva:
Joint United Nations Programme on HIV/AIDS; 2019 16 July 2019.
2. Fast-Track - Ending the AIDS epidemic by 2030. Geneva: Joint United Nations Programme on HIV and AIDS;
2014.
3. WHO encourages countries to adapt HIV testing strategies in response to changing epidemic. Geneva: World
Health Organization; 2019.
4. Differentiated service delivery for HIV: a decision framework for HIV testing services. Geneva: World Health
Organization; 2018.
5. Evaluating the impact of PEPFAR’s geographic prioritization on health facilities transitioning to central support
in Uganda. The U.S. President’s Emergency Plan for AIDS Relief (PEPFAR); 2019 Jan 7. 6. Elías MJP, Gómez-Ayerbe C, Elías PP, Muriel A, de Santiago AD, Martinez-Colubi M, et al. Development and
Validation of an HIV Risk Exposure and Indicator Conditions Questionnaire to Support Targeted HIV Screening.
Medicine. 2016;95(5):e2612-e.
7. Sanders EJ, Wahome E, Powers KA, Werner L, Fegan G, Lavreys L, et al. Targeted screening of at-risk adults for
acute HIV-1 infection in sub-Saharan Africa. AIDS. 2015;29 Suppl 3(0 3):S221-S30.
8. Pintye J, Drake AL, Kinuthia J, Unger JA, Matemo D, Heffron RA, et al. A Risk Assessment Tool for Identifying
Pregnant and Postpartum Women Who May Benefit From Preexposure Prophylaxis. Clinical Infectious Diseases.
2017;64(6):751-8.
9. Wahome E, Thiong'o AN, Mwashigadi G, Chirro O, Mohamed K, Gichuru E, et al. An Empiric Risk Score to
Guide PrEP Targeting Among MSM in Coastal Kenya. AIDS and behavior. 2018.
10. Moucheraud C, Chasweka D, Nyirenda M, Schooley A, Dovel K, Hoffman RM. Simple Screening Tool to Help
Identify High-Risk Children for Targeted HIV Testing in Malawian Inpatient Wards. Journal of acquired immune
deficiency syndromes (1999). 2018;79(3):352-7.
11. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. International Journal of Social
Research Methodology. 2005;8(1):19-32.
12. Studying the Organisation and Delivery of Health Services: Research Methods. Fulop N, Allen P, Clarke A, Black
N, editors. London: Routledge; 2001.
13. UNAIDS. AIDSInfo Geneva2018 [Available from: http://aidsinfo.unaids.org/.
14. Agusti C, Martin-Rabadan M, Zarco J, Aguado C, Carrillo R, Codinach R, et al. Early diagnosis of HIV in Primary
Care in Spain. Results of a pilot study based on targeted screening based on indicator conditions, behavioral criteria and
region of origin. Atencion primaria. 2018;50(3):159-65.
15. Bandason T, Dauya E, Dakshina S, McHugh G, Chonzi P, Munyati S, et al. Screening tool to identify adolescents
living with HIV in a community setting in Zimbabwe: A validation study. PloS one. 2018;13(10):e0204891.
16. Chandra J, Sahi PK, Gupta S, Gupta RA, Dutta R, Sherwal BL, et al. Addition of Questions on Parental Factors to
the WHO (Integrated Management of Childhood Illnesses) IMCI-HIV Algorithm Improves the Utility of the Algorithm for
Diagnosis of HIV Infection in Children. Journal of tropical pediatrics. 2018.
17. Dunlop J, Untiedt S, Makura C, Levin L, editors. Screening tools to identify children and adolescents living with
HIV: Increasing case finding in high HIV prevalence settings. International AIDS Conference; 2018 23-27 July 2018;
Amsterdam, The Netherlands.
18. Kunle K, Khamofu H, Obiora-Okafo C, Obanubi C, Adedokun O, Oladele E, et al. How Well Does the Bandason
HIV Risk Screening Tool Perform in the Nigerian Setting? Findings From a Large-scale Field Implementation. AIDS
research and human retroviruses. 2018;34:151-.
19. Kamwesigye N, editor Community-based HIV screening tool identifies children at high risk of testing positive
to HIV. International AIDS Conference; 2018 23-27 July 2018; Amsterdam, The Netherlands.
20. Leblanc J, Hejblum G, Costagliola D, Durand-Zaleski I, Lert F, de Truchis P, et al. Targeted HIV Screening in
Eight Emergency Departments: The DICI-VIH Cluster-Randomized Two-Period Crossover Trial. Annals of emergency
medicine. 2018;72(1):41-53.e9.
179

21. Olatoregun O, Banigbe B, Njoku K, Okonkwo P, Jolayemi T, Olaitan R, et al., editors. Improvements in pediatric HIV case identification across 17 health facilities in Lagos, Nigeria: a quality improvement collaborative approach. International AIDS Conference; 2018 23-27 July 2018. 22. Wand H, Reddy T, Naidoo S, Moonsamy S, Siva S, Morar NS, et al. A Simple Risk Prediction Algorithm for HIV Transmission: Results from HIV Prevention Trials in KwaZulu Natal, South Africa (2002-2012). AIDS and behavior. 2018;22(1):325-36. 23. Yin L, Zhao Y, Peratikos MB, Song L, Zhang X, Xin R, et al. Risk Prediction Score for HIV Infection: Development and Internal Validation with Cross-Sectional Data from Men Who Have Sex with Men in China. AIDS and behavior. 2018;22(7):2267-76. 24. Balkus JE, Brown E, Palanee T, Nair G, Gafoor Z, Zhang JY, et al. An Empiric HIV Risk Scoring Tool to Predict HIV-1 Acquisition in African Women. Jaids-Journal of Acquired Immune Deficiency Syndromes. 2016;72(3):333-43. 25. Chaila M, Macleod D, Schaap A, Floyd S, Thornicroft M, Hoddinott G, et al., editors. A primary care level algorithm increases yield of HIV-positive adolescents in a community intervention: HPTN071 (PopART) Study, Zambia. International AIDS Society Conference; 2017; Paris, France. 26. Balkus JE, Brown ER, Palanee-Phillips T, Kiweewa FM, Mgodi N, Naidoo L, et al. Performance of a Validated Risk Score to Predict HIV-1 Acquisition Among African Women Participating in a Trial of the Dapivirine Vaginal Ring. Jaids-Journal of Acquired Immune Deficiency Syndromes. 2018;77(1):E8-E10. 27. Bandason T, McHugh G, Dauya E, Mungofa S, Munyati SM, Weiss HA, et al. Validation of a screening tool to identify older children living with HIV in primary care facilities in high HIV prevalence settings. AIDS. 2016;30(5):779-85. 28. Falasinnu T, Gustafson P, Gilbert M, Shoveller J. Validation of the Denver HIV risk score for targeting HIV screening in Vancouver, British Columbia. Sexually transmitted infections. 2015;91:A63-A. 29. Haukoos J, Hopkins E, Bucossi M, Lyons M, Rothman R, White D, et al. Validation of a quantitative HIV risk prediction tool using a national HIV testing cohort. Journal of acquired immune deficiency syndromes (1999). 2015;68(5):599-603. 30. Smith DK, Pan Y, Rose CE, Pals SL, Mehta SH, Kirk GD, et al. A Brief Screening Tool to Assess the Risk of Contracting HIV Infection Among Active Injection Drug Users. Journal of addiction medicine. 2015;9(3):226-32. 31. Hsieh YH, Haukoos JS, Rothman RE. Validation of an abbreviated version of the Denver HIV Risk Score for prediction of HIV infection in an urban ED. American Journal of Emergency Medicine. 2014;32(7):775-9. 32. Haukoos JS, Hopkins E, Bender B, Sasson C, Al-Tayyib AA, Thrun MW, et al. Comparison of Enhanced Targeted Rapid HIV Screening Using the Denver HIV Risk Score to Nontargeted Rapid HIV Screening in the Emergency Department. Annals of emergency medicine. 2013;61(3):353-61. 33. Haukoos JS, Lyons MS, Lindsell CJ, Hopkins E, Bender B, Rothman RE, et al. Derivation and Validation of the Denver Human Immunodeficiency Virus (HIV) Risk Score for Targeted HIV Screening. American journal of epidemiology. 2012;175(8):838-46. 34. Smith DK, Pals SL, Herbst JH, Shinde S, Carey JW. Development of a Clinical Screening Index Predictive of Incident HIV Infection Among Men Who Have Sex With Men in the United States. Jaids-Journal of Acquired Immune Deficiency Syndromes. 2012;60(4):421-7. 35. Ferrand R, Weiss H, Nathoo K, Ndhlovu C, Mungofa S, Munyati S, et al. A primary care level algorithm for identifying HIV-infected adolescents in populations at high risk through mother-to-child transmission. Tropical medicine & international health : TM & IH. 2011;16(3):349²55. 36. Sampson LA, Miller WC, Leone PA. Evaluation of risk score algorithms for the detection of HIV infection and syphilis in North Carolina county jails. Sexually transmitted infections. 2011;87:A210-A. 37. Castañeda MP. Indicator condition, risk-based and universal offer in Primary Care in Madrid ESTVIH Project. [Presentation]. In press. 38. Elias MJ, Gomez-Ayerbe C, Elias PP, Muriel A, de Santiago AD, Martinez-Colubi M, et al. Development and Validation of an HIV Risk Exposure and Indicator Conditions Questionnaire to Support Targeted HIV Screening. Medicine (Baltimore). 2016;95(5):e2612. 39. Joseph R, Musingila PK, Miruka F, Ng'ang'a L, Muttai H, De Cock KM, et al. Expanded HIV testing eligibility increases detection of HIV infections, Western Kenya. Conference on Rotovirus and Opportunitistic Infections; March 4-7; Boston, MA2018.
180

40. Uhler LM, Kumarasamy N, Mayer KH, Saxena A, Losina E, Muniyandi M, et al. Cost-effectiveness of HIV testing referral strategies among tuberculosis patients in India. PloS one. 2010;5(9). 41. Zeng G, Lu F, Luo X, Zhou QF, Liu W, Huang AL, et al. [Comparison of effectiveness between two HIV screening strategies in outpatient setting]. Zhonghua yu fang yi xue za zhi [Chinese journal of preventive medicine]. 2013;47(11):1010-3. 42. Cohn J, Whitehouse K, Tuttle J, Lueck K, Tran T. Paediatric HIV testing beyond the context of prevention of mother-to-child transmission: a systematic review and meta-analysis. The Lancet HIV. 2016;3(10):e473-e81. 43. Mutambo C, Hlongwana K. Healthcare Workers' Perspectives on the Barriers to Providing HIV Services to Children in Sub-Saharan Africa. AIDS research and treatment. 2019;2019:8056382-. 44. Sibanda EL, Hatzold K, Mugurungi O, Ncube G, Dupwa B, Siraha P, et al. An assessment of the Zimbabwe ministry of health and child welfare provider initiated HIV testing and counselling programme. BMC health services research. 2012;12(1):131. 45. Dowdy DW, Rodriguez RM, Hare CB, Kaplan B. Cost-effectiveness of targeted human immunodeficiency virus screening in an urban emergency department. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2011;18(7):745-53. 46. Gomez-Ayerbe C, Elias MJ, Muriel A, Elias PP, Cano A, Diaz A, et al. Incremental cost per newly diagnosed HIV infection (NDHI): routine (RTS), targeted (TTS), and current clinical practice testing strategies (CPTS). Journal of the International AIDS Society. 2014;17(4 Suppl 3):19606. 47. Venkatesh KK, Becker JE, Kumarasamy N, Nakamura YM, Mayer KH, Losina E, et al. Clinical impact and cost-effectiveness of expanded voluntary HIV testing in India. PloS one. 2013;8(5):e64604.
181

www.thelancet.com/lancetgh Vol 8 February 2020
Articles
E!ect of facility-based HIV self-testing on uptake of testing among outpatients in Malawi: a cluster-randomised trialKathryn Dovel, Frackson Shaba, O Agatha O!orjebe, Kelvin Balakasi, Mike Nyirenda, Khumbo Phiri, Sundeep K Gupta, Vincent Wong, Chi-Hong Tseng, Brooke E Nichols, Refiloe Cele, Eric Lungu, Tobias Masina, Thomas J Coates, Risa M Ho!man
SummaryBackground HIV self-testing increases testing uptake in sub-Saharan Africa but scale-up is challenging because of resource constraints. We evaluated an HIV self-testing intervention integrated into high-burden outpatient departments in Malawi.
Methods In this cluster-randomised trial, we recruited participants aged 15 years or older from 15 outpatient departments at high-burden health facilities (including health centres, mission hospitals, and district hospitals) in central and southern Malawi. The trial was clustered at the health facility level. We used constrained randomisation to allocate each cluster (1:1:1) to one of the following groups: standard provider-initiated testing and counselling with no intervention (provider o!ered during consultations), optimised provider-initiated testing and counselling (with additional provider training and morning HIV testing), and facility-based HIV self-testing (Oraquick HIV self-test, group demonstration and distribution, and private spaces for interpretation and counselling). The primary outcome was the proportion of outpatients tested for HIV on the day of enrolment, measured through exit surveys with a sample of outpatients. Analyses were on an intention-to-treat basis. The trial is registered with ClinicalTrials.gov, NCT03271307, and Pan African Clinical Trials, PACTR201711002697316.
Findings Between Sept 12, 2017, and Feb 23, 2018, 5885 outpatients completed an exit survey—2097 in the HIV self-testing group, 1951 in the standard provider-initiated testing and counselling group, and 1837 in the optimised provider-initiated testing and counselling group. 1063 (51%) of 2097 patients in the HIV self-testing group had HIV testing on the same day as enrolment, compared with 248 (13%) of 1951 in the standard provider-initiated testing and counselling group and 261 (14%) of 1837 in the optimised provider-initiated testing and counselling group. The odds of same-day HIV testing were significantly higher in the facility-based HIV self-testing group compared with either standard provider-initiated testing and counselling (adjusted odds ratio 8·52, 95% CI 3·98–18·24) or optimised provider-initiated testing and counselling (6·29, 2·96–13·38). Around 4% of those tested in the standard provider-initiated testing and counselling and optimised provider-initiated testing and counselling groups felt coerced to test, and around 1% felt coerced to share test results. No coercion was reported in the facility-based HIV self-testing group.
Interpretation Facility-based HIV self-testing increased HIV testing among outpatients in Malawi, with a minimal risk of adverse events. Facility-based HIV self-testing should be considered for scale-up in settings with a high unmet need for HIV testing.
Funding United States Agency for International Development.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
IntroductionHIV testing is crucial for the UNAIDS 90-90-90 goals to be reached,1 yet only 76% of HIV-positive individuals in countries in east and southern Africa are aware of their status.2 HIV self-testing, whereby individuals perform and interpret their own HIV test, is an e!ective strategy to improve HIV testing coverage, especially among hard-to-reach populations such as men and adolescents.3–6 Current HIV self-testing strategies have focused on community-based distribution modalities, resulting in a high uptake of testing because of the private and convenient nature of self-testing.7 However, there is an urgent push to scale up HIV self-testing strategies
throughout the region,8 with nearly all countries in east and southern Africa developing or recently adopting HIV self-testing policies.
Scale-up of HIV self-testing in low-resource settings is challenging because of insu"cient infra structure and human capital throughout the region, challenges with monitoring and evaluation of HIV self-test use, and low antiretroviral therapy (ART) initiation among people who test positive through HIV self-testing strategies.9 Incorporating HIV self-testing into existing facility-based health services might be an important additional strategy to facilitate scale-up. Facility-based HIV self-testing could improve the e"ciency of facility-based
Lancet Glob Health 2020; 8: e276–87
This online publication has been corrected. The corrected version first appeared at thelancet.com/lancetgh on January 23, 2020
Division of Infectious Diseases (K Dovel PhD, S K Gupta MD Prof T J Coates PhD, R M Hoffman MD) and Division of General Internal Medicine and Health Services Research (C-H Tseng PhD), Department of Medicine and David Geffen School of Medicine (O A Offorjebe MD), University of California Los Angeles, Los Angeles, CA, USA; Partners in Hope, Lilongwe, Malawi (K Dovel, F Shaba MPH, K Balakasi BA, M Nyirenda MD, K Phiri MPH, E Lungu BA); School of Medicine, Charles R Drew University of Medicine and Science, Los Angeles, CA, USA (O A Offorjebe); USAID Global Health Bureau, Washington, DC, USA (V Wong MSc); Health Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa (B E Nichols PhD, R Cele MSc); Department of Global Health, School of Public Health, Boston University, Boston, MA, USA (B E Nichols); and Malawi Ministry of Health, HIV/AIDS Unit, Lilongwe, Malawi (T Masina BA)
Correspondence to: Dr Kathryn Dovel, Division of Infectious Diseases, Department of Medicine, University of California Los Angeles, Los Angeles, CA 90095, USA [email protected]
For more on HIV self-testing policies see www.HIVST.org
182

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
testing services, as patients can use HIV self-testing while waiting for other health services; improve ART initiation, as users are already at the facility and can easily access additional services; promote quality assurance, as users have direct access to trained HIV testing providers at the facility; and reduce costs associated with HIV self-testing through distribution that can be easily incorporated into the routine tasks of facility-based sta!.
Facility-based HIV self-testing might be particularly useful in high-burden outpatient departments, which are often overcrowded and understa!ed, where patients can experience considerable wait times; in Malawi, the median wait time to see a health-care provider is 4 hours.10 Furthermore, traditional provider-initiated testing and counselling in outpatient department settings is scarce, with low testing coverage.11–13 Barriers to testing in outpatient department settings include a paucity of HIV testing sta! available for individual testing and counselling, little availability of private spaces, and insu"cient integration of care, whereby outpatients referred for HIV testing must actively seek services in a separate HIV department.11 Facility-based HIV self-testing might be a critical addition to provider-initiated testing and counselling strategies and might overcome traditional barriers to testing by allowing outpatients to test themselves while waiting for routine services.
We aimed to assess the e"cacy, acceptability, and cost of facility-based HIV self-testing among outpatients in Malawi compared with standard and optimised provider-initiated testing and counselling. This study adds to the growing number of trials on HIV self-testing in
sub-Saharan Africa and, to our knowledge, provides a novel perspective by examining whether HIV self-testing can be integrated alongside facility-based health services in high-burden outpatient departments.
MethodsStudy design and participantsIn this cluster-randomised trial, we recruited participants from 15 outpatient departments at high-burden health facilities (including district hospitals, mission hospitals, and health centres) in central and southern Malawi. In outpatient departments, services are o!ered for adults with either acute illnesses or non-communicable diseases (NCDs). Typical acute illnesses include febrile syndromes, cough, diarrhoea, dehydration, and minor injuries. Common NCDs include hypertension and diabetes. Services for pregnant women, children younger than 5 years, and emergency or inpatients were provided in di!erent departments and therefore these individuals were not included in our study. Outpatients were encouraged to opt out of facility-based HIV self-testing if they met any of the following exclusion criteria: ever tested positive for HIV, tested negative for HIV in the past month, felt uncomfortable using HIV self-testing in the outpatient department, and were younger than 15 years. The intervention was designed to o!er multiple reasons for opting out to avoid inadvertent status disclosure of those who declined to take an HIV self-testing kit. This study was approved by the National Health and Sciences Research Committee in Malawi and the Institutional Review Board at the University of California Los Angeles, Los Angeles (CA, USA).
Research in context
Evidence before this studyInadequate HIV testing coverage remains the biggest barrier to reaching UNAIDS 90-90-90 goals. HIV self-testing is an e!ective strategy to improve HIV testing coverage, especially among hard-to-reach populations, such as men and adolescents. However, evidence-based, low-cost strategies to scale up HIV self-testing remain scarce. Facility-based distribution of HIV self-testing could be one strategy to increase access with minimal resource use. This strategy could be particularly beneficial in outpatient departments, where HIV testing coverage has been historically low. We searched PubMed for studies published from Jan 1, 2000, up to Nov 20, 2018, with the search terms “HIV” and “self-test” or “self-testing” and “outpatient departments” or “health facility”, with no language restrictions. Our search did not identify any evaluations of facility-based HIV self-testing up to the search end date.
Added value of this studyOur study adds to the literature on HIV self-testing and, to our knowledge, is unique in evaluating this strategy in busy
outpatient facilities in resource-limited settings. We found that facility-based HIV self-testing in the outpatient department significantly increased the proportion of outpatients tested for HIV, with 51% of all outpatients tested compared with 13% for standard provider-initiated testing and counselling. Our strategy markedly improved testing coverage for men and adolescents and, overall, more than doubled the absolute number of individuals newly diagnosed with HIV. To our knowledge, our study documents one of the first HIV self-test strategies to show high rates of antiretroviral therapy initiation (70% compared with the reported 29–45% in most HIV self-test studies).
Implications of all the available evidenceWe found that facility-based HIV self-testing in the outpatient department is an e!ective strategy for increasing testing coverage among outpatients in resource-limited settings, such as Malawi. Facility-based HIV self-testing might provide the greatest benefit in congested, high-burden health facilities, where human resource constraints limit the reach of traditional provider-initiated testing.
183

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
Randomisation and maskingThe trial was clustered at the health facility level. We used constrained randomisation to allocate each cluster (1:1:1) to one of the following groups: standard provider-initiated testing and counselling with no intervention, optimised provider-initiated testing and counselling, whereby additional training and job aids were provided to health workers to improve testing and counselling implemen tation and early morning HIV testing was o!ered to patients within the outpatient department, and facility-based HIV self-testing, whereby OraQuick ADVANCE HIV I/II self-testing kits (OraSure Tech-nologies; Bethlehem, PA, USA) were distributed to outpatients to use in clinic waiting spaces. Clusters were constrained by the following covariates: facility type (hospital or health facility), ownership (government or mission), and region (central or southern; appendix p 1). Random assignment was done by the project statistician using a computer-generated sequence of random
numbers, and outputs were shared with the Ministry of Health of Malawi, district-level governance, and medical providers at participating sites.
ProceduresFigure 1 shows the procedures for each study group. Although HIV testing is recommended for all outpatients in Malawi, as per national guidelines, referrals for testing are based on provider discretion. In the standard provider-initiated testing and counselling group, no additional support was provided. Outpatients were referred to a separate HIV department for HIV testing. All HIV tests were done according to national guidelines by a certified HIV testing counsellor with a fingerstick blood sample and Determine 1/2 (Abbott Laboratories; Chicago, IL, USA) tests. Positive tests were confirmed using Uni-Gold (Trinity Biotech; Bray, Ireland). Counselling was provided before and after testing. Confirmed HIV-positive individuals were referred to the facility’s ART clinic,
See Online for appendix
Figure !: Study procedures by interventionART=antiretroviral therapy.
Facility randomisation
Exit surveys conducted with a subset of outpatients (!15 years)
Medical chart reviews at 3 months to assess ART initiation
Standard provider-initiated testing and counselling
Step 1—outpatients gather in waiting spaces to access general outpatient services
Step 2—outpatients receive one-on-one communications for general outpatient services
Step 4—all referrals are to a separate HIV testing department
Step 5—HIV-positive clients confirmed as HIV-positive (Determine 1/2 and Uni-Gold) are o"ered same-day ART initiation at the ART department
Step 3—during outpatient services health workers use their own discretion to refer outpatients to HIV testing services (Determine 1/2 and Uni-Gold) o"ered at the HIV department
Optimised provider-initiated testing and counselling
Step 1—outpatients gather in waiting spaces to access general outpatient services
Step 2—health workers provide HIV education
Step 4—outpatients receive one-on-one consultations for general outpatient services
Step 5—HIV-positive clients confirmed as HIV-positive (Determine 1/2 and Uni-Gold) are o"ered same-day ART initiation at the ART department
Step 3—health workers o"er standard one-on-one HIV testing services (Determine 1/2 and Uni-Gold) while clients wait for routine outpatient services
Facility-based HIV self-testing
Step 1—outpatients gather in waiting spaces to access general outpatient services
Step 2—health workers provide HIV education
Step 4—outpatients receive one-on-one consultations for general outpatient services
Step 5—HIV-positive clients who present after testing HIV-positive receive HIV tests (Determine 1/2 and Uni-Gold), confirmatory testing (simultaneous Determine 1/2 and Uni-Gold), and are o"ered same-day ART initiation at the ART department
Step 3—one study sta" member provides group HIV self-testing demonstrations and distribution; private booths are placed in outpatient waiting spaces for HIV self-test interpretation before outpatients receive routine outpatient services
184

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
where they received additional verification testing for quality control (parallel Determine 1/2 and Uni-Gold tests) and were o!ered same-day ART initiation.
The aim of the optimised provider-initiated testing and counselling group was to improve implementation of provider-initiated testing and counselling in the out-patient department. Refresher provider-initiated testing and counselling training and job aids were provided to outpatient health-care workers at these facilities. HIV testing was integrated within the outpatient department and o!ered in the mornings before consultations began by certified HIV testing counsellors. One or two counsellors and one or two private spaces were available for morning testing. Services included a 10 min group health talk about the importance of HIV testing and one-on-one counselling before and after HIV testing. Standard procedures for HIV testing (Determine 1/2 and Uni-Gold) were used. HIV-positive clients received confirmatory HIV testing and were o!ered same-day ART initiation.
The facility-based HIV self-testing intervention included the following five components: a 10 min health talk to all outpatients about the importance of HIV testing; a 15 min Oraquick HIV self-testing demon-stration, including group pre-counselling; HIV self-test distribution for use in outpatient department waiting spaces and, if needed, assistance from a trained study sta! member with a background equivalent to a typical Malawian HIV diagnostic assistant; private spaces (temporary cardboard standing booths) for interpretation of HIV self-test results before receiving routine heath consultations; and optional post-test counselling and referral to additional HIV services for those who chose to disclose their HIV self-testing result.
One study sta! member demonstrated, distributed, and assisted with the use of HIV self-testing kits in outpatient department waiting spaces. Group HIV self-testing demonstrations occurred when there were large groups of outpatients in the waiting space, supplemented by small group talks when there were fewer people, allowing one health worker to distribute HIV self-testing kits to a large number of people in a small amount of time.
Pre-counselling and the need for confirmatory HIV testing was explained during the health talk before kit distribution. Disclosure of HIV self-test results was voluntary, but outpatients were encouraged to discuss their result with the health-care provider during routine outpatient services. Outpatients who tested HIV-positive with HIV self-testing and disclosed their status entered the national testing algorithm (Determine 1/2 followed by Uni-Gold, and confirmatory testing before ART initiation). Those who disclosed their HIV self-test result and were confirmed to be HIV-positive were o!ered same-day ART initiation.
Locked boxes were available at all exit points of the outpatient departments for disposal of self-test kits. Outpatients were instructed not to take unused test kits
home. Those who accepted a kit but decided not to use it could drop the unused kit into the locked box. Meetings with local community leaders and stakeholders were held before implementation of the intervention to familiarise them with the HIV self-testing kits and avoid confusion and misconceptions about the kits.
Cost analysisWe used a microcosting (bottom-up) approach from the provider perspective to assess study cost in each trial group using the HIV Counselling and Testing costing tool developed by the Health Economics and Epidemiology Research O"ce in South Africa.14 All resources used for HIV testing services were captured from five repre-sentative health facilities. Resource costs included testing consumables and equipment, sta! costs, sta! training, shared costs (eg, cleaning, stock taking, data capturing, HIV counselling, and testing sta! scheduling), and overhead costs (including building maintenance and utilities). We then averaged HIV counselling and testing costs across all five facilities and reported SDs around these costs (appendix p 2). Additional information about the composition of consumables can be found in the appendix (p 3). To estimate the additional cost per test of the optimised provider-initiated testing and counselling group, we divided the total additional training costs incurred and divided this by the number of people tested during the study period. In the HIV self-testing group, the cost of research assistants providing demonstrations was factored into the personnel time and divided by the total number of people who tested with an HIV self-test. The costs of training, community sensitisation, and cardboard booths were also divided by the total number of people who tested with an HIV self-test in this study. These study-related costs (training, sta! members, booth, and HIV self-test kits) were determined from service provider reports and research study procurement records and added to the cost of the standard HIV testing and counselling algorithm.
In the standard provider-initiated testing and counselling and optimised provider-initiated testing and counselling group, we assumed confirmatory testing and costs related to confirmatory testing for those who tested positive. Since HIV self-testing is considered a screening tool, those who screen positive are assumed to go through the full facility-based testing algorithm (two HIV tests—Determine 1/2 and Uni-Gold—followed by confirmatory testing for those who tested positive) and incur the related costs. We did not assume overhead costs for those who tested negative in the HIV self-test group as the testing space would be occupied by the same individuals regardless of the presence of HIV. We did assume overhead costs for those who tested positive and underwent the standard HIV testing algorithm within the facility. The cost of ART initiation itself was not included in the final production cost or the total cost to initiate one new client on ART. Total testing-related costs per test completed, per newly diagnosed HIV-positive individual,
185
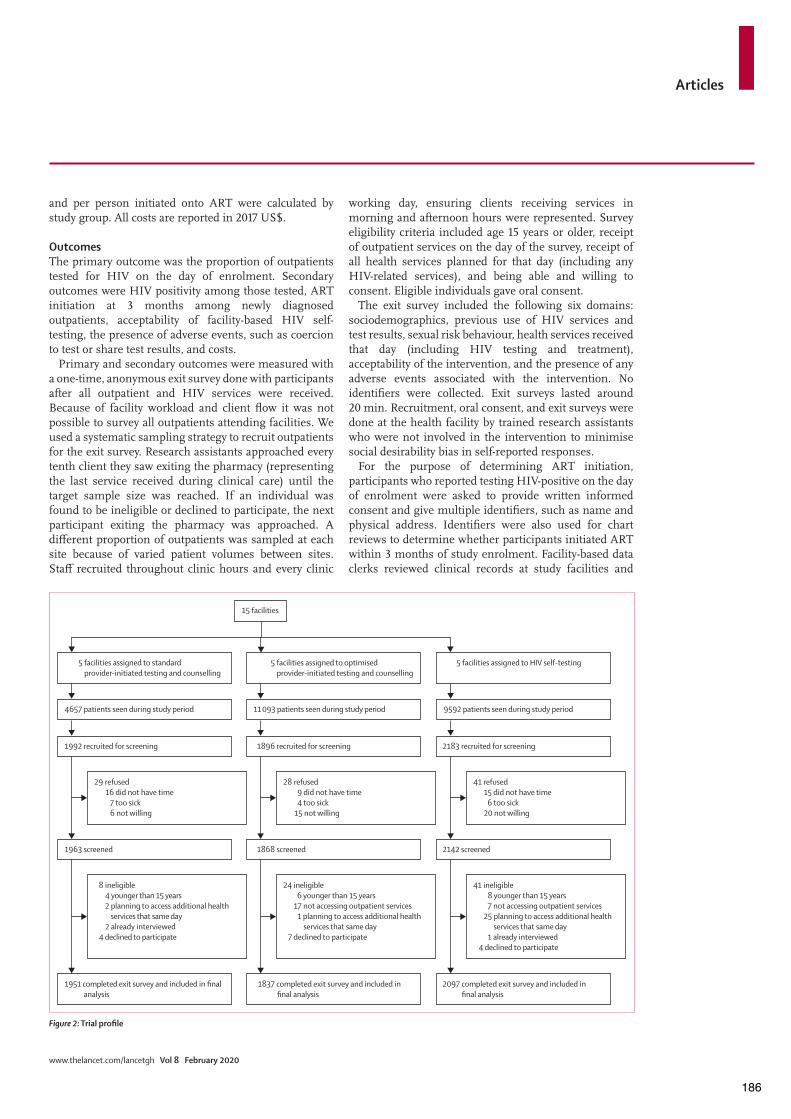
Articles
www.thelancet.com/lancetgh Vol 8 February 2020
and per person initiated onto ART were calculated by study group. All costs are reported in 2017 US$.
OutcomesThe primary outcome was the proportion of outpatients tested for HIV on the day of enrolment. Secondary outcomes were HIV positivity among those tested, ART initiation at 3 months among newly diagnosed outpatients, acceptability of facility-based HIV self-testing, the presence of adverse events, such as coercion to test or share test results, and costs.
Primary and secondary outcomes were measured with a one-time, anonymous exit survey done with participants after all outpatient and HIV services were received. Because of facility workload and client flow it was not possible to survey all outpatients attending facilities. We used a systematic sampling strategy to recruit outpatients for the exit survey. Research assistants approached every tenth client they saw exiting the pharmacy (representing the last service received during clinical care) until the target sample size was reached. If an individual was found to be ineligible or declined to participate, the next participant exiting the pharmacy was approached. A di!erent proportion of outpatients was sampled at each site because of varied patient volumes between sites. Sta! recruited throughout clinic hours and every clinic
working day, ensuring clients receiving services in morning and afternoon hours were represented. Survey eligibility criteria included age 15 years or older, receipt of outpatient services on the day of the survey, receipt of all health services planned for that day (including any HIV-related services), and being able and willing to consent. Eligible individuals gave oral consent.
The exit survey included the following six domains: sociodemographics, previous use of HIV services and test results, sexual risk behaviour, health services received that day (including HIV testing and treatment), acceptability of the intervention, and the presence of any adverse events associated with the intervention. No identifiers were collected. Exit surveys lasted around 20 min. Recruitment, oral consent, and exit surveys were done at the health facility by trained research assistants who were not involved in the intervention to minimise social desirability bias in self-reported responses.
For the purpose of determining ART initiation, participants who reported testing HIV-positive on the day of enrolment were asked to provide written informed consent and give multiple identifiers, such as name and physical address. Identifiers were also used for chart reviews to determine whether participants initiated ART within 3 months of study enrolment. Facility-based data clerks reviewed clinical records at study facilities and
Figure ": Trial profile
15 facilities
5 facilities assigned to standard provider-initiated testing and counselling
4657 patients seen during study period
1992 recruited for screening
1963 screened
1951 completed exit survey and included in final analysis
29 refused16 did not have time
7 too sick6 not willing
8 ineligible4 younger than 15 years2 planning to access additional health
services that same day2 already interviewed
4 declined to participate
5 facilities assigned to optimised provider-initiated testing and counselling
11 093 patients seen during study period
1896 recruited for screening
1868 screened
1837 completed exit survey and included in final analysis
28 refused9 did not have time4 too sick
15 not willing
24 ineligible6 younger than 15 years
17 not accessing outpatient services1 planning to access additional health
services that same day7 declined to participate
5 facilities assigned to HIV self-testing
9592 patients seen during study period
2183 recruited for screening
2142 screened
2097 completed exit survey and included in final analysis
41 refused15 did not have time
6 too sick20 not willing
41 ineligible8 younger than 15 years7 not accessing outpatient services
25 planning to access additional health services that same day
1 already interviewed4 declined to participate
186
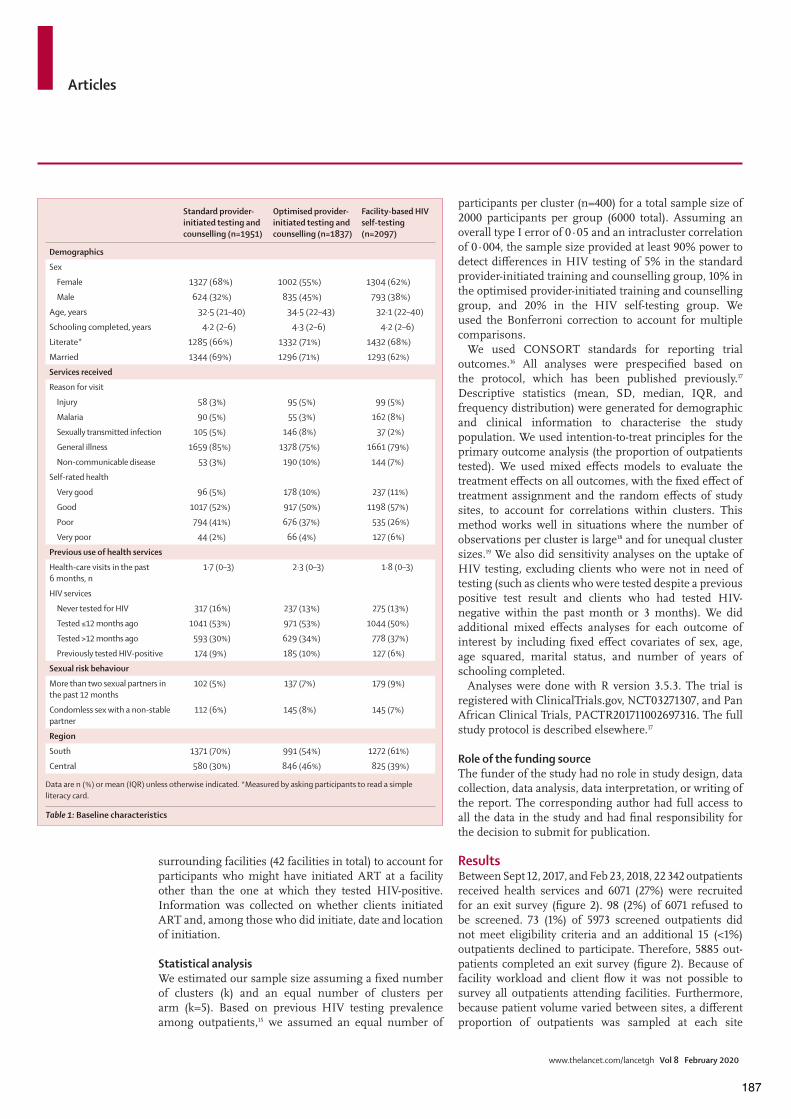
Articles
www.thelancet.com/lancetgh Vol 8 February 2020
surrounding facilities (42 facilities in total) to account for participants who might have initiated ART at a facility other than the one at which they tested HIV-positive. Information was collected on whether clients initiated ART and, among those who did initiate, date and location of initiation.
Statistical analysisWe estimated our sample size assuming a fixed number of clusters (k) and an equal number of clusters per arm (k=5). Based on previous HIV testing prevalence among outpatients,15 we assumed an equal number of
participants per cluster (n=400) for a total sample size of 2000 participants per group (6000 total). Assuming an overall type I error of 0·05 and an intracluster correlation of 0·004, the sample size provided at least 90% power to detect di!erences in HIV testing of 5% in the standard provider-initiated training and counselling group, 10% in the optimised provider-initiated training and counselling group, and 20% in the HIV self-testing group. We used the Bonferroni correction to account for multiple comparisons.
We used CONSORT standards for reporting trial outcomes.16 All analyses were prespecified based on the protocol, which has been published previously.17 Descriptive statistics (mean, SD, median, IQR, and frequency distribution) were generated for demographic and clinical information to characterise the study population. We used intention-to-treat principles for the primary outcome analysis (the proportion of outpatients tested). We used mixed e!ects models to evaluate the treatment e!ects on all outcomes, with the fixed e!ect of treatment assignment and the random e!ects of study sites, to account for correlations within clusters. This method works well in situations where the number of observations per cluster is large18 and for unequal cluster sizes.19 We also did sensitivity analyses on the uptake of HIV testing, excluding clients who were not in need of testing (such as clients who were tested despite a previous positive test result and clients who had tested HIV-negative within the past month or 3 months). We did additional mixed e!ects analyses for each outcome of interest by including fixed e!ect covariates of sex, age, age squared, marital status, and number of years of schooling completed.
Analyses were done with R version 3.5.3. The trial is registered with ClinicalTrials.gov, NCT03271307, and Pan African Clinical Trials, PACTR201711002697316. The full study protocol is described elsewhere.17
Role of the funding sourceThe funder of the study had no role in study design, data collection, data analysis, data inter pretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
ResultsBetween Sept 12, 2017, and Feb 23, 2018, 22 342 outpatients received health services and 6071 (27%) were recruited for an exit survey (figure 2). 98 (2%) of 6071 refused to be screened. 73 (1%) of 5973 screened outpatients did not meet eligibility criteria and an additional 15 (<1%) outpatients declined to participate. Therefore, 5885 out -patients completed an exit survey (figure 2). Because of facility workload and client flow it was not possible to survey all outpatients attending facilities. Furthermore, because patient volume varied between sites, a di!erent proportion of outpatients was sampled at each site
Standard provider-initiated testing and counselling (n=1951)
Optimised provider-initiated testing and counselling (n=1837)
Facility-based HIV self-testing (n=2097)
Demographics
Sex
Female 1327 (68%) 1002 (55%) 1304 (62%)
Male 624 (32%) 835 (45%) 793 (38%)
Age, years 32·5 (21–40) 34·5 (22–43) 32·1 (22–40)
Schooling completed, years 4·2 (2–6) 4·3 (2–6) 4·2 (2–6)
Literate* 1285 (66%) 1332 (71%) 1432 (68%)
Married 1344 (69%) 1296 (71%) 1293 (62%)
Services received
Reason for visit
Injury 58 (3%) 95 (5%) 99 (5%)
Malaria 90 (5%) 55 (3%) 162 (8%)
Sexually transmitted infection 105 (5%) 146 (8%) 37 (2%)
General illness 1659 (85%) 1378 (75%) 1661 (79%)
Non-communicable disease 53 (3%) 190 (10%) 144 (7%)
Self-rated health
Very good 96 (5%) 178 (10%) 237 (11%)
Good 1017 (52%) 917 (50%) 1198 (57%)
Poor 794 (41%) 676 (37%) 535 (26%)
Very poor 44 (2%) 66 (4%) 127 (6%)
Previous use of health services
Health-care visits in the past 6 months, n
1·7 (0–3) 2·3 (0–3) 1·8 (0–3)
HIV services
Never tested for HIV 317 (16%) 237 (13%) 275 (13%)
Tested "12 months ago 1041 (53%) 971 (53%) 1044 (50%)
Tested >12 months ago 593 (30%) 629 (34%) 778 (37%)
Previously tested HIV-positive 174 (9%) 185 (10%) 127 (6%)
Sexual risk behaviour
More than two sexual partners in the past 12 months
102 (5%) 137 (7%) 179 (9%)
Condomless sex with a non-stable partner
112 (6%) 145 (8%) 145 (7%)
Region
South 1371 (70%) 991 (54%) 1272 (61%)
Central 580 (30%) 846 (46%) 825 (39%)
Data are n (%) or mean (IQR) unless otherwise indicated. *Measured by asking participants to read a simple literacy card.
Table !: Baseline characteristics
187

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
depending on the number of clients seen in a given day. A similar number of outpatients per site completed the exit survey.
3633 (62%) exit survey respondents were female, representing the gendered composition of outpatients in Malawi (table 1). The median respondent age was 33 years (IQR 22–41). 5056 (86%) outpatients had been tested for HIV before, with 3056 (52%) tested within the past 12 months. 127 (6%) respondents in the HIV self-testing group reported previously testing HIV-positive before the study, compared with 174 (9%) in the standard provider-initiated testing and counselling group and 185 (10%) in the optimised provider-initiated testing and counselling group.
1063 (51%) of 2097 patients in the HIV self-testing group had HIV testing on the same day as enrolment, compared with 248 (13%) of 1951 in the standard provider-initiated testing and counselling group and 261 (14%) of 1837 in the optimised provider-initiated testing and counselling group (table 2). The odds of same-day HIV testing were significantly higher in the facility-based HIV self-testing group compared with either standard provider-initiated testing and counselling (adjusted odds ratio [OR] 8·52, 95% CI 3·98–18·24) or optimised provider-initiated testing and counselling (6·29, 2·96–13·38). Findings were similar across age and sex categories (figure 3), with adolescents showing the greatest benefit from facility-based HIV self-testing compared with standard provider-initiated testing and counselling (table 2).
Across all study groups, HIV testing was highest among those who reported risky sexual behaviour in the past 12 months (more than two sexual partners or condomless sex with a non-stable partner; table 2). Among those with risky sexual behaviour, 181 (56%) of 324 participants were tested in the HIV self-testing group, 49 (23%) of 214 participants were tested in the standard provider-initiated testing and counselling group, and 53 (19%) of 282 participants were tested in the optimised provider-initiated testing and counselling group. 145 (53%) of 275 patients who had never been tested for HIV before were tested in the HIV self-testing group, compared with 40 (13%) of 317 in the standard provider-initiated testing and counselling group and
Standard provider-initiated testing and counselling
Optimised provider-initiated testing and counselling
Facility-based HIV self-testing
Facility-based HIV self-testing vs standard provider-initiated testing and counselling
Facility-based HIV self-testing vs optimised provider-initiated testing and counselling
Adjusted OR (95% CI)* Adjusted OR (95% CI)† Adjusted OR (95% CI)* Adjusted OR (95% CI)†
Tested for HIV on day of enrolment
248/1951 (13%) 261/1837 (14%) 1063/2097 (51%) 8·89 (4·17–18·94) 8·52 (3·98–18·24) 6·85 (3·23–14·52) 6·29 (2·96–13·38)
Subset analysis by demographics
Male adult (#25 years) 57/417 (14%) 87/583 (15%) 230/493 (47%) 7·90 (3·62–17·27) 7·46 (3·35–16·59) 5·91 (2·85–12·29) 5·57 (2·64–11·75)
Female adult (#25 years) 105/792 (13%) 79/672 (12%) 452/838 (54%) 8·81 (3·80–20·46) 7·74 (3·09–19·39) 10·88 (4·62–25·63) 9·75 (3·84–24·74)
Adolescent (15–24 years) 86/742 (12%) 95/582 (16%) 381/766 (50%) 9·35 (4·01–21·82) 9·42 (4·15–21·38) 5·42 (2·36–12·46) 5·33 (2·38–11·92)
Subset analysis by testing history
Never tested HIV-positive and tested >3 months ago
148/849 (17%) 175/930 (19%) 797/1382 (58%) 10·01 (3·83–26·18) 9·29 (3·42–25·19) 6·97 (2·70–17·99) 6·77 (2·53–18·12)
Never tested for HIV 40/317 (13%) 38/237 (16%) 145/275 (53%) 11·05 (3·87–31·55) 10·91 (3·78–31·50) 7·17 (2·52–20·39) 5·41 (1·91–15·33)
Tested >12 months ago 124/910 (14%) 134/866 (15%) 550/1053 (52%) 10·00 (3·73–26·79) 9·27 (3·45–24·92) 6·66 (2·52–17·60) 5·90 (2·23–15·62)
Previously tested HIV-positive 0/174 2/185 (1%) 11/127 (9%) ·· ·· 8·68 (1·89–39·85) 8·51 (1·57–46·24)
Subset analysis by sexual risk behaviour
More than two sexual partners in past 12 months
23/102 (23%) 26/137 (19%) 96/179 (54%) 4·30 (1·90–9·71) 5·36 (2·45–11·74) 5·25 (2·43–11·36) 5·45 (2·63–11·32)
Condomless sex with a non-stable partner in past 12 months
26/112 (23%) 27/145 (19%) 85/145 (59%) 5·26 (2·29–12·06) 4·99 (2·25–11·07) 6·78 (3·14–14·64) 6·41 (3·02–13·60)
Data are n/N (%) unless otherwise indicated. OR=odds ratio. *Models with site as a random e!ect. †Models adjusted for facility, sex, age, age squared, currently married, and number of years of school completed, with site as a random e!ect.
Table ": Uptake of HIV testing on the day of enrolment
Figure #: HIV testing coverage by sex and age across trial groups (n=5885)
Total Female adult(!25 years)
Male adult(!25 years)
Adolescent(15–24 years)
0
10
20
30
40
50
60
100
HIV
test
ing
cove
rage
(%)
Standard provider-initiated training and counsellingOptimised provider-initiated training and counsellingFacility-based HIV self-testing
188
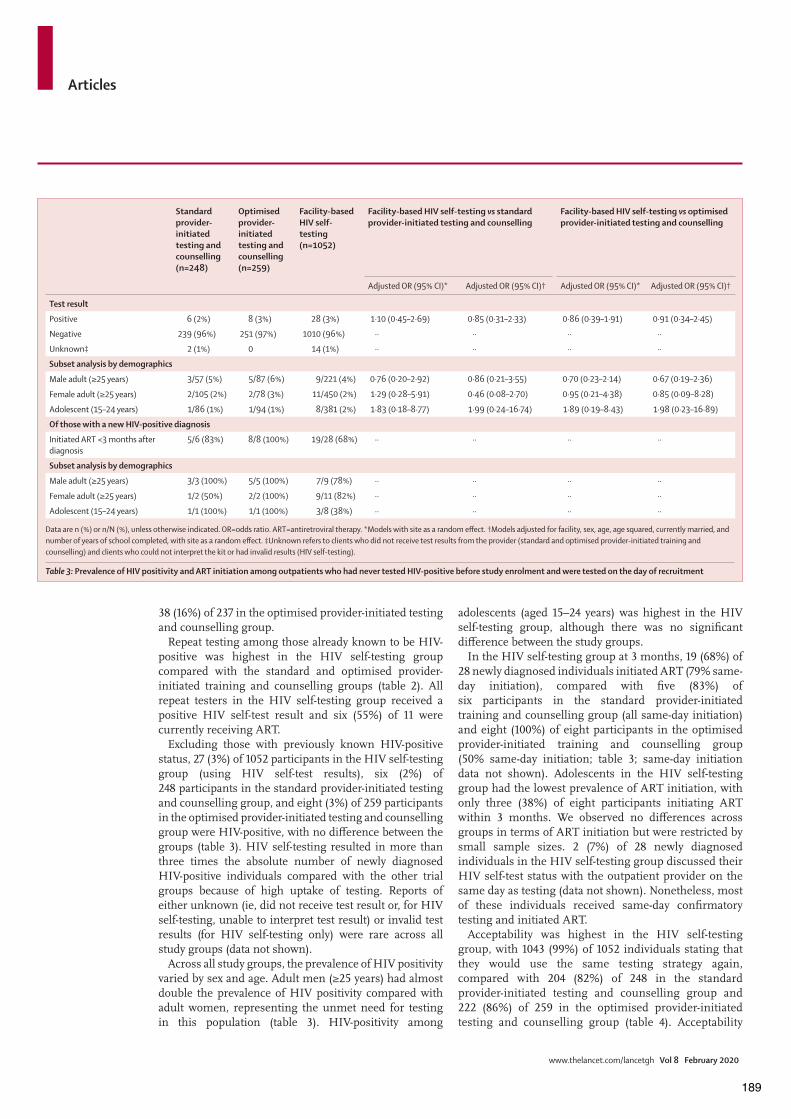
Articles
www.thelancet.com/lancetgh Vol 8 February 2020
38 (16%) of 237 in the optimised provider-initiated testing and counselling group.
Repeat testing among those already known to be HIV-positive was highest in the HIV self-testing group compared with the standard and optimised provider-initiated training and counselling groups (table 2). All repeat testers in the HIV self-testing group received a positive HIV self-test result and six (55%) of 11 were currently receiving ART.
Excluding those with previously known HIV-positive status, 27 (3%) of 1052 participants in the HIV self-testing group (using HIV self-test results), six (2%) of 248 participants in the standard provider-initiated testing and counselling group, and eight (3%) of 259 participants in the optimised provider-initiated testing and counselling group were HIV-positive, with no di!erence between the groups (table 3). HIV self-testing resulted in more than three times the absolute number of newly diagnosed HIV-positive individuals compared with the other trial groups because of high uptake of testing. Reports of either unknown (ie, did not receive test result or, for HIV self-testing, unable to interpret test result) or invalid test results (for HIV self-testing only) were rare across all study groups (data not shown).
Across all study groups, the prevalence of HIV positivity varied by sex and age. Adult men (#25 years) had almost double the prevalence of HIV positivity compared with adult women, representing the unmet need for testing in this population (table 3). HIV-positivity among
adolescents (aged 15–24 years) was highest in the HIV self-testing group, although there was no significant di!erence between the study groups.
In the HIV self-testing group at 3 months, 19 (68%) of 28 newly diagnosed individuals initiated ART (79% same-day initiation), compared with five (83%) of six participants in the standard provider-initiated training and counselling group (all same-day initiation) and eight (100%) of eight participants in the optimised provider-initiated training and counselling group (50% same-day initiation; table 3; same-day initiation data not shown). Adolescents in the HIV self-testing group had the lowest prevalence of ART initiation, with only three (38%) of eight participants initiating ART within 3 months. We observed no di!erences across groups in terms of ART initiation but were restricted by small sample sizes. 2 (7%) of 28 newly diagnosed individuals in the HIV self-testing group discussed their HIV self-test status with the outpatient provider on the same day as testing (data not shown). Nonetheless, most of these individuals received same-day confirmatory testing and initiated ART.
Acceptability was highest in the HIV self-testing group, with 1043 (99%) of 1052 individuals stating that they would use the same testing strategy again, compared with 204 (82%) of 248 in the standard provider-initiated testing and counselling group and 222 (86%) of 259 in the optimised provider-initiated testing and counselling group (table 4). Acceptability
Standard provider-initiated testing and counselling (n=248)
Optimised provider-initiated testing and counselling (n=259)
Facility-based HIV self-testing (n=1052)
Facility-based HIV self-testing vs standard provider-initiated testing and counselling
Facility-based HIV self-testing vs optimised provider-initiated testing and counselling
Adjusted OR (95% CI)* Adjusted OR (95% CI)† Adjusted OR (95% CI)* Adjusted OR (95% CI)†
Test result
Positive 6 (2%) 8 (3%) 28 (3%) 1·10 (0·45–2·69) 0·85 (0·31–2·33) 0·86 (0·39–1·91) 0·91 (0·34–2·45)
Negative 239 (96%) 251 (97%) 1010 (96%) ·· ·· ·· ··
Unknown‡ 2 (1%) 0 14 (1%) ·· ·· ·· ··
Subset analysis by demographics
Male adult (#25 years) 3/57 (5%) 5/87 (6%) 9/221 (4%) 0·76 (0·20–2·92) 0·86 (0·21–3·55) 0·70 (0·23–2·14) 0·67 (0·19–2·36)
Female adult (#25 years) 2/105 (2%) 2/78 (3%) 11/450 (2%) 1·29 (0·28–5·91) 0·46 (0·08–2·70) 0·95 (0·21–4·38) 0·85 (0·09–8·28)
Adolescent (15–24 years) 1/86 (1%) 1/94 (1%) 8/381 (2%) 1·83 (0·18–8·77) 1·99 (0·24–16·74) 1·89 (0·19–8·43) 1·98 (0·23–16·89)
Of those with a new HIV-positive diagnosis
Initiated ART <3 months after diagnosis
5/6 (83%) 8/8 (100%) 19/28 (68%) ·· ·· ·· ··
Subset analysis by demographics
Male adult (#25 years) 3/3 (100%) 5/5 (100%) 7/9 (78%) ·· ·· ·· ··
Female adult (#25 years) 1/2 (50%) 2/2 (100%) 9/11 (82%) ·· ·· ·· ··
Adolescent (15–24 years) 1/1 (100%) 1/1 (100%) 3/8 (38%) ·· ·· ·· ··
Data are n (%) or n/N (%), unless otherwise indicated. OR=odds ratio. ART=antiretroviral therapy. *Models with site as a random e!ect. †Models adjusted for facility, sex, age, age squared, currently married, and number of years of school completed, with site as a random e!ect. ‡Unknown refers to clients who did not receive test results from the provider (standard and optimised provider-initiated training and counselling) and clients who could not interpret the kit or had invalid results (HIV self-testing).
Table #: Prevalence of HIV positivity and ART initiation among outpatients who had never tested HIV-positive before study enrolment and were tested on the day of recruitment
189
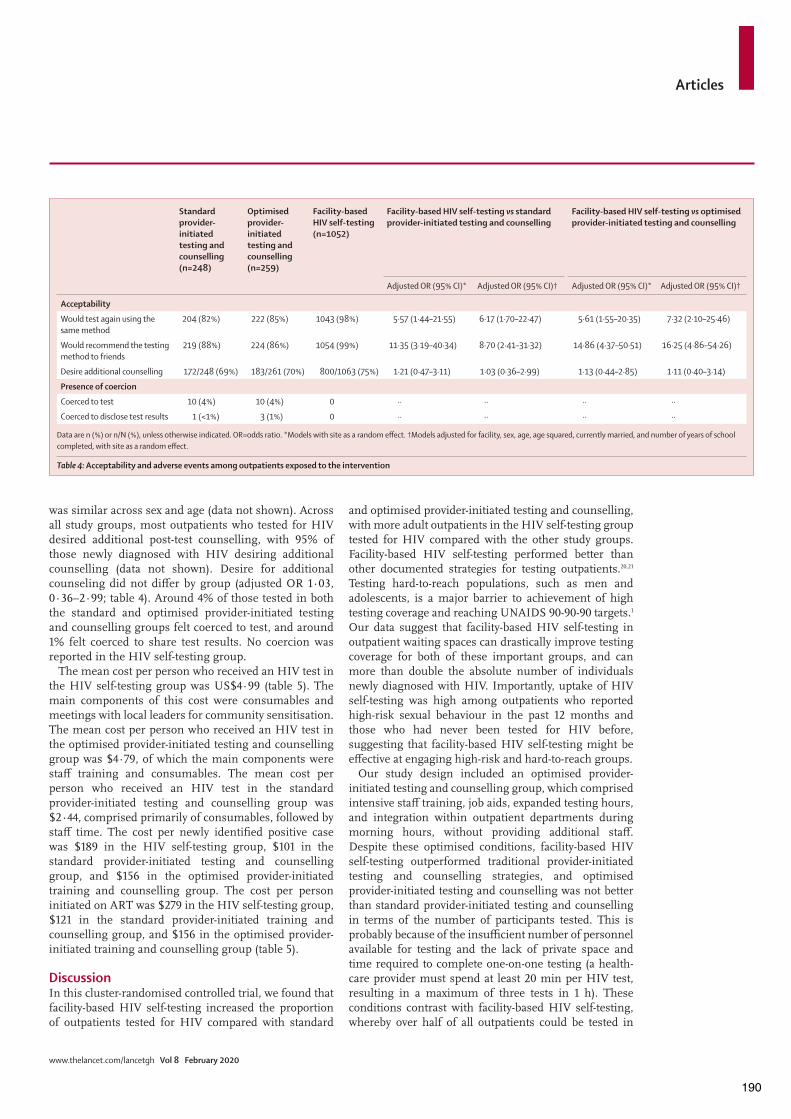
Articles
www.thelancet.com/lancetgh Vol 8 February 2020
was similar across sex and age (data not shown). Across all study groups, most outpatients who tested for HIV desired additional post-test counselling, with 95% of those newly diagnosed with HIV desiring additional counselling (data not shown). Desire for additional counseling did not di!er by group (adjusted OR 1·03, 0·36–2·99; table 4). Around 4% of those tested in both the standard and optimised provider-initiated testing and counselling groups felt coerced to test, and around 1% felt coerced to share test results. No coercion was reported in the HIV self-testing group.
The mean cost per person who received an HIV test in the HIV self-testing group was US$4·99 (table 5). The main components of this cost were consumables and meetings with local leaders for community sensitisation. The mean cost per person who received an HIV test in the optimised provider-initiated testing and counselling group was $4·79, of which the main components were sta! training and consumables. The mean cost per person who received an HIV test in the standard provider-initiated testing and counselling group was $2·44, comprised primarily of consumables, followed by sta! time. The cost per newly identified positive case was $189 in the HIV self-testing group, $101 in the standard provider-initiated testing and counselling group, and $156 in the optimised provider-initiated training and counselling group. The cost per person initiated on ART was $279 in the HIV self-testing group, $121 in the standard provider-initiated training and counselling group, and $156 in the optimised provider-initiated training and counselling group (table 5).
DiscussionIn this cluster-randomised controlled trial, we found that facility-based HIV self-testing increased the proportion of outpatients tested for HIV compared with standard
and optimised provider-initiated testing and counselling, with more adult outpatients in the HIV self-testing group tested for HIV compared with the other study groups. Facility-based HIV self-testing performed better than other documented strategies for testing outpatients.20,21 Testing hard-to-reach populations, such as men and adolescents, is a major barrier to achievement of high testing coverage and reaching UNAIDS 90-90-90 targets.1 Our data suggest that facility-based HIV self-testing in outpatient waiting spaces can drastically improve testing coverage for both of these important groups, and can more than double the absolute number of individuals newly diagnosed with HIV. Importantly, uptake of HIV self-testing was high among outpatients who reported high-risk sexual behaviour in the past 12 months and those who had never been tested for HIV before, suggesting that facility-based HIV self-testing might be e!ective at engaging high-risk and hard-to-reach groups.
Our study design included an optimised provider-initiated testing and counselling group, which comprised intensive sta! training, job aids, expanded testing hours, and integration within outpatient departments during morning hours, without providing additional sta!. Despite these optimised conditions, facility-based HIV self-testing outperformed traditional provider-initiated testing and counselling strategies, and optimised provider-initiated testing and counselling was not better than standard provider-initiated testing and counselling in terms of the number of participants tested. This is probably because of the insu"cient number of personnel available for testing and the lack of private space and time required to complete one-on-one testing (a health-care provider must spend at least 20 min per HIV test, resulting in a maximum of three tests in 1 h). These conditions contrast with facility-based HIV self-testing, whereby over half of all outpatients could be tested in
Standard provider-initiated testing and counselling (n=248)
Optimised provider-initiated testing and counselling (n=259)
Facility-based HIV self-testing (n=1052)
Facility-based HIV self-testing vs standard provider-initiated testing and counselling
Facility-based HIV self-testing vs optimised provider-initiated testing and counselling
Adjusted OR (95% CI)* Adjusted OR (95% CI)† Adjusted OR (95% CI)* Adjusted OR (95% CI)†
Acceptability
Would test again using the same method
204 (82%) 222 (85%) 1043 (98%) 5·57 (1·44–21·55) 6·17 (1·70–22·47) 5·61 (1·55–20·35) 7·32 (2·10–25·46)
Would recommend the testing method to friends
219 (88%) 224 (86%) 1054 (99%) 11·35 (3·19–40·34) 8·70 (2·41–31·32) 14·86 (4·37–50·51) 16·25 (4·86–54·26)
Desire additional counselling 172/248 (69%) 183/261 (70%) 800/1063 (75%) 1·21 (0·47–3·11) 1·03 (0·36–2·99) 1·13 (0·44–2·85) 1·11 (0·40–3·14)
Presence of coercion
Coerced to test 10 (4%) 10 (4%) 0 ·· ·· ·· ··
Coerced to disclose test results 1 (<1%) 3 (1%) 0 ·· ·· ·· ··
Data are n (%) or n/N (%), unless otherwise indicated. OR=odds ratio. *Models with site as a random e!ect. †Models adjusted for facility, sex, age, age squared, currently married, and number of years of school completed, with site as a random e!ect.
Table $: Acceptability and adverse events among outpatients exposed to the intervention
190

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
several hours with the assistance of one dedicated sta! member. Only one or two HIV testing counsellors were needed to demonstrate and administer HIV self-testing kits to an entire outpatient clinic. These HIV testing counsellors were readily available to assist individuals struggling with the HIV self-testing process. Private booths were placed throughout outpatient department waiting spaces for patients to interpret test results, addressing infrastructure limitations common for traditional provider-initiated testing and counselling strategies. Given the simplicity and low sta"ng requirements of facility-based HIV self-testing, along with high client acceptability and low risk for adverse events, this strategy has tremendous promise for scale-up across similar settings in sub-Saharan Africa. HIV self-testing might be particularly beneficial in other settings with high HIV prevalence, where facility-based HIV testing coverage is low.
Outpatients in all study groups desired additional post-test counselling, regardless of their HIV test result. Those who tested HIV-negative wanted information on how to remain uninfected, and those who tested positive desired more information about HIV. These findings suggest that improved counselling after HIV testing might be needed for all facility-based testing strategies. Post-test counselling could be particularly challenging for HIV self-test users since disclosure is voluntary. Options to improve post-test counselling in facility-based HIV self-testing could include generic group post-test counselling for HIV self-test users (providing simultaneous counselling for both negative and positive results) or o!ering opt-out one-on-one counselling after HIV testing to outpatients exiting private booths for HIV self-test interpretation. The latter strategy would increase cost but might also improve linkage to care for those who test positive, increase HIV prevention benefits of
testing for those who are negative, and improve post-test counselling satisfaction for all testers.
ART initiation in the HIV self-testing group was lower than in both provider-initiated training and counselling groups, although HIV self-testing resulted in more than double the absolute number of new initiators compared with the other study groups. Adolescents in the HIV self-testing group had a particularly low prevalence of ART initiation and warrant further study. Nonetheless, HIV self-testing linkage rates in our study were substantially higher than those reported in previous community-based HIV self-testing studies, where rates have been reported to be 29–45%.10,22–24 Higher prevalence of ART initiation with facility-based HIV self-testing compared with community-based strategies might be due to reduced barriers to ART initiation—individuals were already at health facilities, removing the time and financial costs usually required to access HIV services. Outpatients might also represent individuals who are ready and able to use facility-based health services.
Most newly diagnosed HIV-positive individuals in the HIV self-testing group initiated ART without discussing their HIV self-test result with the outpatient department provider. HIV-positive individuals either sought out ART initiation through their own initiative or disclosed to the study sta! distributing HIV self-test kits in the outpatient department waiting space, but not to the outpatient department provider. When developing the trial design, we hypothesised that providing HIV self-testing before an outpatient consultation would better facilitate integration of outpatient department and HIV services by giving outpatients and their providers the opportunity to have a one-on-one discussion about the HIV self-test result, post-test counselling, and referrals to additional HIV services. Our study findings show that under the strained conditions of busy health facilities and overworked providers, integration in routine outpatient consultations remains a challenge. Other studies showed that outpatient services are rushed, with little time for holistic care.16,25 Clients rarely feel comfortable asking unprompted questions to a health-care provider and often believe their concerns are not heard.26,27 As the strained environment of outpatient department clinics is unlikely to change, future interventions should focus on making HIV counsellors and strategies for linkage to additional services readily available in outpatient department waiting spaces before clients reach the providers.
Our costing analysis showed that the cost of providing one HIV self-test under study conditions is slightly more than the cost of providing one test through optimised provider-initiated testing and counselling and more than $2 more than the cost of one test with standard provider-initiated testing and counselling. The cost of HIV self-testing increased substantially between the cost per newly diagnosed positive case and cost per ART initiated because of a lower linkage rate with HIV self-testing
Standard provider-initiated testing and counselling (n=248)
Optimised provider-initiated testing and counselling (n=261)
Facility-based HIV self-testing (n=1063)
Sta!* 0·95 0·95 1·22
Equipment† 0·08 0·08 0·26
Consumables‡ 1·37 1·37 2·07
Facility overheads§ 0·03 0·03 0·00
Training 0·01 2·36 0·31
Community sensitisation 0·00 0·00 1·14
Total cost 2·44 4·79 4·99
Cost per newly identified positive case 100·85 156·27 189·44
Cost per person initiated on ART 121·02 156·27 279·18
All costs in 2017 US$. Does not include cost of ART. ART=antiretroviral therapy. *Depending on group, costs include HIV counsellors, outpatient department providers, and study sta! who conducted the HIV self-testing intervention. †Includes all facility-based equipment for standard and optimised provider-initiated testing and counselling, including testing booths for those in the HIV self-test group and facility-based equipment for those who were screened positive and went through the testing algorithm at the facility. ‡Depending on group, costs include HIV self-testing kits and standard-of-care testing supplies. §Includes building maintenance and utilities.
Table %: Cost analysis—cost per test provided, by cost category, total cost, and cost per outcome
191

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
compared with both standard and optimised provider-initiated testing and counselling. Reducing the cost of the HIV self-test kit, use of government HIV testing and counselling sta! (compared with research sta! used in our study), and improved ART initiation could reduce the cost per ART initiation using facility-based HIV self-testing. Our costs of facility-based HIV testing are lower than those previously reported in community-based studies ($4·92 in Malawi28 compared to our mean of $2·44). This di!erence was driven by di!erences in personnel costs, which could stem from di!erences in assumed compensation or duration of time sta! spend on di!erent activities. If our provider-initiated testing and counselling costing had yielded high costs similar to other studies, the relative di!erence between standard provider-initiated testing and counselling and HIV self-testing would decrease markedly, also making facility-based HIV self-testing more economically attractive. Further research is needed to assess whether facility-based HIV self-testing could have e"ciency e!ects for provider time among those responsible for HIV testing and e!ects on testing e"ciency (unit costs).
This trial has several limitations. First, it was not possible to survey all outpatients in high-burden sites because of infrastructure constraints; our study therefore relied on a sample of outpatients obtained by recruiting every tenth patient exiting the clinic. Although e!orts were taken to ensure systematic selection of survey participants, our sampling method was approximate and we might have missed clients who left from a separate entrance. Although a small number of clients declined to participate or were ineligible (allowing for strict adherence to the sampling strategy), there could be unmeasured biases resulting from our sampling methods. Second, HIV testing and test results were based on self-reports and might result in under-reporting of newly diagnosed HIV-positive individuals if outpatients felt uncomfortable sharing their test result. However, we do not anticipate di!erences in social desirability bias across study groups and reported HIV-positivity prevalence was similar to national averages within outpatient settings. Third, we were unable to mask the interventions from research assistants who did the exit surveys. Although these research assistants did not implement the interventions, they could have biased surveys toward a positive response. We attempted to minimise this risk by emphasising the importance of all study groups during the training of research assistants. Finally, ART initiation was assessed at 3 months after HIV testing, and some individuals might have initiated ART after the 3-month period. Underestimations of ART initiation would probably a!ect the HIV self-testing group and might have resulted in underestimation of the e!ects of facility-based HIV self-testing on ART initiation. The study was not powered to evaluate ART linkage, which is a critical step in the HIV test and treatment cascade.
In conclusion, facility-based HIV self-testing in outpatient department waiting spaces increased HIV
testing and the identification of HIV-infected individuals compared with standard and optimised provider-initiated testing and counselling, with no evidence of adverse events. HIV self-testing was easily integrated into routine outpatient services and drastically reduced provider workload related to HIV testing while increasing testing coverage, including coverage among high-risk and hard-to-reach individuals. Facility-based HIV self-testing provided privacy and autonomy for HIV testing and improved the e"ciency of testing by overcoming bottlenecks created by limitations in trained personnel and facility space. Additionally, facility-based HIV self-testing addressed several challenges faced during HIV self-testing scale-up, including decreased barriers to ART initiation and improved opportunities for quality assurance and monitoring and evaluation. More research is needed into ART linkage within facility-based HIV self-testing, particularly for adolescents, who had a low prevalence of ART initiation in this study. Further research is also needed into which high-risk populations might be missed through facility-based HIV self-testing and the best strategies to reach these individuals to achieve epidemic control.ContributorsKD and RMH conceived the study. KD, FS, KB, KP, VW, BEN, MN, TM, and RMH contributed to study design. KD, FS, OAO, KB, KP, and EL developed the guideline and training. KB and EL prepared and cleaned the data. KD and C-HT analysed the data. FS, OAO, RC, and BEN collected the cost data. RC and BEN analysed the cost data. SKG, VW, TJC, and RMH provided substantial scientific input into the statistical methods and interpretation of the results. KD, FS, and OAO did the literature reviews. FS, OAO, KB, KP, MN, and EL implemented the study. KD took the lead in drafting the report. FS, OAO, SKG, VW, BEN, RC, and RMH provided substantial comments to improve the draft. All authors contributed to the collection or interpretation of data, provided critical revisions to the report, and approved the final draft. KD and RMH are the guarantors of the study.
Declaration of interestsWe declare no competing interests.
Data sharingAll primary outcome data files are available upon request. Those interested in the dataset can contact Kathryn Dovel ([email protected]). Access will be granted after a signed data access agreement is attained. Available data include job aids, consent forms, data dictionary, and deidentified primary outcome data. The study protocol and statistical analysis plan have been published elsewhere and are freely available.
AcknowledgmentsThis study was funded by United States Agency for International Development under cooperative agreement AID-OAA-A-15-00070. KD is funded by the National Institute of Health Fogarty International Center (K01-TW011484-01). KD and RMH receive support from the University of California Los Angeles (UCLA) Center for AIDS (research grant AI028697) and the UCLA AIDS Institute. The views contained in this Article are those of the authors and do not necessarily reflect the views of the US President’s Emergency Plan for AIDS Relief, the US Agency for International Development, or the US Government. We thank the research assistants who were essential to data collection, outpatients who participated in the study, and health facility sta! for their dedicated contribution to study implementation.
References1 UNAIDS. Fast-track—ending the AIDS Epidemic by 2030.
Geneva: Joint United Nations Programme on HIV/AIDS, 2014.
192

Articles
www.thelancet.com/lancetgh Vol 8 February 2020
2 UNAIDS. Global HIV and AIDS statistics—2018 fact sheet. Geneva: Joint United Nations Programme on HIV/AIDS, 2018.
3 Pant Pai N, Sharma J, Shivkumar S, et al. Supervised and unsupervised self-testing for HIV in high- and low-risk populations: a systematic review. PLoS Med 2013; 10: e1001414.
4 Sharma M, Barnabas RV, Celum C. Community-based strategies to strengthen men’s engagement in the HIV care cascade in sub-Saharan Africa. PLoS Med 2017; 14: e1002262.
5 Choko AT, MacPherson P, Webb EL, et al. Uptake, accuracy, safety, and linkage into care over two years of promoting annual self-testing for HIV in Blantyre, Malawi: a community-based prospective study. PLoS Med 2015; 12: e1001873.
6 Masters SH, Agot K, Obonyo B, Napierala Mavedzenge S, Maman S, Thirumurthy H. Promoting partner testing and couples testing through secondary distribution of HIV self-tests: a randomized clinical trial. PLoS Med 2016; 13: e1002166.
7 WHO. Guidelines on HIV self-testing and partner notification. Geneva: World Health Organization, 2016.
8 WHO. Number of countries adopting HIV self-testing policies rises sharply. July 25, 2017. https://www.who.int/hiv/mediacentre/news/hiv-self-testing-increases/en/ (accessed Nov 8, 2019).
9 Sharma M, Ying R, Tarr G, Barnabas R. Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature 2015; 528: S77–85.
10 Yeatman S, Chamberlin S, Dovel K. Women’s (health) work: a population-based, cross-sectional study of gender di!erences in time spent seeking health care in Malawi. PLoS One 2018; 13: e0209586.
11 Mabuto T, Hansoti B, Charalambous S, Ho!mann C. Understanding the dynamics of HIV testing services in South African primary care facilities: Project SOAR results brief. Washington, DC: Population Council, 2018.
12 Roura M, Watson-Jones D, Kahawita TM, Ferguson L, Ross DA. Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational implementation. AIDS 2013; 27: 617–26.
13 Church K, Machiyama K, Todd J, et al. Identifying gaps in HIV service delivery across the diagnosis-to-treatment cascade: findings from health facility surveys in six sub-Saharan countries. J Int AIDS Soc 2017; 20: 21188.
14 van Rensburg C, Mandimika C, Mayer-Rath C, Long L. The HIV counselling and testing (HCT) costing tool. April 23, 2019. http://www.heroza.org/researchtools/the-hiv-counselling-and-testing-hct-costing-tool (accessed Nov 11, 2019).
15 Dovel K, Shaba F, Nyirenda M, et al. Evaluating the integration of HIV self-testing into low-resource health systems: study protocol for a cluster-randomized control trial from EQUIP Innovations. Trials 2018; 19: 498.
16 MacPherson P, Lalloo DG, Choko AT, et al. Suboptimal patterns of provider initiated HIV testing and counselling, antiretroviral therapy eligibility assessment and referral in primary health clinic attendees in Blantyre, Malawi. Trop Med Int Health 2012; 17: 507–17.
17 Begg C, Cho M, Eastwood S, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 1996; 276: 637–39.
18 Heo M, Leon AC. Comparison of statistical methods for analysis of clustered binary observations. Stat Med 2005; 24: 911–23.
19 Heo M, Leon AC. Performance of a mixed e!ects logistic regression model for binary outcomes with unequal cluster size. J Biopharm Stat 2005; 15: 513–26.
20 Ogbo FA, Mogaji A, Ogeleka P, et al. Assessment of provider-initiated HIV screening in Nigeria with sub-Saharan African comparison. BMC Health Serv Res 2017; 17: 188.
21 Franse CB, Kayigamba FR, Bakker MI, et al. Linkage to HIV care before and after the introduction of provider-initiated testing and counselling in six Rwandan health facilities. AIDS Care 2017; 29: 326–34.
22 Ortblad K, Kibuuka Musoke D, Ngabirano T, et al. Direct provision versus facility collection of HIV self-tests among female sex workers in Uganda: a cluster-randomized controlled health systems trial. PLoS Med 2017; 14: e1002458.
23 MacPherson P, Lalloo DG, Webb EL, et al. E!ect of optional home initiation of HIV care following HIV self-testing on antiretroviral therapy initiation among adults in Malawi: a randomized clinical trial. JAMA 2014; 312: 372–79.
24 Sibanda E, Neuman M, Tumushime M, et al. Linkage to care after HIV self-testing in Zimbabwe: a cluster-randomised trial. Conference on retroviruses and opportunistic infections; Boston, MA, USA; March 4–7, 2018 (abstr 150LB).
25 Dovel K. Shifting focus from individuals to institutions: the role of gendered health institutions on men’s use of HIV services. May 29, 2016. http://digital.auraria.edu/content/AA/00/00/58/88/00001/Dovel_ucdenver_0765D_10714.pdf (accessed Nov 8, 2019).
26 Lau SR, Christensen ST, Andreasen JT. Patients’ preferences for patient-centered communication: a survey from an outpatient department in rural Sierra Leone. Patient Educ Couns 2013; 93: 312–18.
27 WHO. Promote or discourage: how providers can influence service use. Social determinants of sexual and reproductive health: informing future research and programme implementation. Geneva: World Health Organization, 2010.
28 Mwenge L, Sande L, Mangenah C, et al. Costs of facility-based HIV testing in Malawi, Zambia and Zimbabwe. PLoS One 2017; 12: e0185740.
193

Volume 22, Supplement 3, July 2019
The power of partners: Experiences from implementing and scaling-up HIV partner notifi cation and index testing servicesGuest Editors: David A Katz, Vincent J Wong, Amy M Medley, Rachel C BaggaleySupplement Editors: Marlène Bras, Elisa de Castro Alvarez
194
EDITORIAL
The power of partners: positively engaging networks of peoplewith HIV in testing, treatment and preventionDavid A Katz1§, Vincent J Wong2, Amy M Medley3, Cheryl C Johnson4, Peter K Cherutich5, Kimberly E Green6,Phan Huong7 and Rachel C Baggaley4
§Corresponding author: David A Katz, Harborview Medical Center, 325 Ninth Avenue, Box 359931, Seattle, WA 98104, USA. Tel: +1 (206) 744 5877. ([email protected])
Keywords: HIV testing; partner notification; index testing; people with HIV; low and middle income countries; key populations
Received 23 April 2019; Accepted 15 May 2019
Copyright © 2019 World Health Organization; licensed by IAS.This is an open access article distributed under the terms of the Creative Commons Attribution IGO License https://creativecommons.org/licenses/by/3.0/igo/legalcode which permits unrestricted use, distribution and reproduction in any medium, provided that the original work is properly cited. In any reproduction of this articlethere should not be any suggestion that WHO or the article endorse any specific organization or products. The use of the WHO logo is not permitted. This noticeshould be preserved along with the article’s URL.
When HIV diagnostic tests first became available in 1985,HIV testing was offered with caution. No treatment was avail-able, prevention options were limited, and stigma and discrimi-nation against people with HIV was pervasive. Concerns aboutpreventing breaches of confidentiality and forced or manda-tory testing, especially among groups at high risk for HIVinfection, were dominant in early guidance released by theWorld Health Organization (WHO). An offer of an HIV testrequired extensive counselling both before and after the testto ensure the individual was able to cope with a possible reac-tive result. Then the development of point of care rapid HIVtests in 1987 offered the opportunity for immediate results inclinical and community settings [1]. When antiretroviral ther-apy (ART) became available globally in the early 2000s, WHOlaunched its “3 9 5” Initiative to provide 3 million people inlow and middle-income countries (LMIC) with ART by 2005.Scale-up of HIV testing through client-initiated approachesusing rapid test kits to provide same day results was a corecomponent to the success of this Initiative [2,3].Yet by 2007, HIV testing coverage was still low. Surveys in
sub-Saharan Africa showed that a median of 12% of men and10% of women had been tested for HIV and received theirresults [4]. In an effort to increase testing coverage, WHOreleased its Provider-Initiated Testing and Counselling Guideli-nes [5], recommending a routine offer of HIV testing byhealthcare providers in clinical settings. These guidelines sug-gest the benefits of HIV status disclosure and partner testingand recommended providers to discuss possible disclosure ofthe result, when and how this may happen and to whom and toencourage and offer referral for testing and counselling of partnersand children as part of post-test counselling. However, littleemphasis was given to partner testing in practice. Thus, whileHIV testing coverage increased enormously over the next fiveyears in clinical settings, especially among pregnant women aspart of a push to prevent HIV transmission from mothers totheir infants, the vast majority of HIV tests were conducted
on people who tested as individuals. Early efforts at partnerHIV testing and disclosure were documented, but thisapproach was rarely implemented and never successfullyscaled [6].Evidence for the benefits of partner testing and disclosure,
however, was growing. In addition, population-based surveysand surveillance efforts indicated that many people with HIVwere unaware that they were living in sero-discordant couples[7], leaving the HIV-negative partner at high risk for HIVacquisition. This led WHO to recommend partner and coupleHIV testing for all adults with HIV in all epidemic contextsand for HIV uninfected individuals living in high HIV burdensettings in 2012 [8]. The preventive benefits of ART [9] andthe effectiveness of HIV pre-exposure prophylaxis (PrEP) [10]in preventing HIV acquisition added to the motivation toscale-up partner and couple HIV testing.Over the four years following the release of these guideli-
nes partner testing services were not widely adopted orscaled in most LMICs. However, there were notable excep-tions: Cameroon adopted an ambitious partner notificationprogramme in 2007 [11]; while Kenya, Malawi and Tanzaniaundertook pivotal implementation studies of partner HIV test-ing services [12-14]. Rwanda supported male partner involve-ment and testing at the first antenatal care visit and reported87% of male partners attending this first visit by 2010 [15].To accelerate uptake of partner testing, WHO released
additional guidelines in 2016 on the implementation andscale-up of ethical, effective, acceptable and evidence-basedapproaches to assisted HIV partner notification services (PNS)[16]. This guidance was based on a review of available evi-dence and included the recommendation that voluntaryassisted PNS be offered as part of a comprehensive packageof testing and care offered to people with HIV. Since itslaunch, the number of countries including PNS in theirnational testing policies and guidelines has increased from 77in 2016 to 111 by the end of 2017 (C Johnson, personal
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
195

communication), although many countries were not yet imple-menting PNS at scale.PNS, or “index testing” as it is referred to in the 2019 Presi-
dent’s Emergency Plan for AIDS Relief (PEPFAR) CountryOperational Plan Guidance (see A Note on Terminology) arealso now prioritized as a major HIV case finding strategy in all37 PEPFAR-supported countries and regions. PEPFAR pro-grammes have been actively supporting and expanding indextesting approaches since 2016. This expansion has been aidedby the development of training materials for index partner andfamily testing that include information on approaches and stepsfor conducting PNS, how to screen for intimate partner vio-lence (IPV), brief motivational interviewing as a strategy forpartner elicitation, and documentation and monitoring of PNS.PEPFAR also provides technical support to country pro-grammes to assist implementing partners to deliver and moni-tor PNS [17]. In addition, WHO and PEPFAR have supportedthe development of the AIDSFree HIV Testing Knowledge Baseas a publicly available, online resource library of high qualitytools (e.g. training materials, standard operating procedures,data collection forms) to support PNS programme developmentand implementation [18]. As a result of this support, implemen-tation of PNS within PEPFAR-supported programmes has con-tinued to expand. For example, Jhpiego undertook anoperational research pilot in Njombe, Tanzania, in 2016 to inte-grate a free-choice PNS intervention into health centres whichled to successful outcomes at reaching partners [19].As PNS has expanded, it has also undergone differentiation
based on population needs and preferences, ranging from mod-els that centre on assisted PNS provided by healthcare work-ers, to those that include secondary distribution of HIV self-testing as part of PNS, to lay providers from key populationsusing social media and other online tools to trace listed part-ners. Ongoing challenges to assisted PNS scale-up include thelarge amount of human and financial resources needed to sup-port these services, such as the time needed to trace and test
partners, particularly if they live outside the jurisdiction of thehealth facility or community organization. In addition, assistedPNS is not allowed under the laws and policies of many coun-tries. Continued advocacy is needed to modify these policies sothat index clients are able to choose the best approach to noti-fying their partners based on their life circumstances.Some countries have also been considering or adopting
newer HIV testing strategies to increase detection of acuteand recent HIV infections. The United States’ Ending the HIVEpidemic: A Plan for America suggests that mapping clusters ofnew HIV infections and offering rapid PNS, ART, and preven-tion services within identified transmission clusters could dis-rupt onward transmission [20]. As more data and experiencefrom using HIV diagnostics that can detect acute and recentHIV infections in LMICs as part of testing services becomeavailable, their acceptability, impact and cost-effectiveness willguide future recommendations on their role and use.An indicator for monitoring partner testing cascades has
been integrated into PEPFAR’s list of required indicators since2019. This indicator measures both the reach and positivity ofindex testing offered to the sexual and needle-sharing partner(s) and biological child(ren) of people with HIV. These datanow present partner testing cascades that incorporate theoffer of PNS, number of partners and children (i.e. contacts)elicited per index client and downstream uptake and positivityof contacts tested. Examination of these cascades can supportimprovements to programmes for this new approach by iden-tifying bottlenecks to service delivery. Figure 1 provides anillustration of these partner testing cascades.Another important metric to measure is the proportion of
partners who report testing as a result of notification byeither sex partners or healthcare workers. This will allow pro-grammes to determine the scale and effectiveness of PNS atencouraging partners to seek HIV testing. In Kenya, a PNSsurveillance system was created from HIV registries to deter-mine the proportion of individuals who sought HIV testing
Index Testing O ered
Index Testing O ered
Index Testing
Accepted
Index Testing
Accepted
Number of Contacts
Number Tested and
Results
Number of Contacts
Number Tested and
Results
Tota
l Num
ber
of In
divi
dual
s
Community-based Index Approaches Facility-based Index Approaches
Figure 1. Illustrative adult partner notification and index testing cascade for community- and facility-based services.Cascades such as this can be created from data routinely collected by President’s Emergency Plan for AIDS Relief programmes. Note that, as cur-rently collected, index client outcomes (index testing offered and accepted) and the total number of contacts are counted where the index clientreceives services, whereas the number of contacts tested and their results are counted where the contact receives services. As a result, the num-ber of contacts tested and their results may not be counted in the same setting as the index clients who named them, which limits the interpreta-tion of these data as a true “cascade.” For example, index clients receiving services at a facility may indicate partners who are found and tested inthe community, and vice versa.
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
196

because they were notified of potential HIV exposure by asexual partner, by a health provider or some other source.This system allowed the Ministry of Health to determine thecoverage of assisted PNS and is now being used to identifypopulations and areas in need of targeted scale-up [21].The articles in this supplement represent a diversity of pro-
grammatic experiences, research, and community, provider,and client perspectives on PNS and index testing from 11countries across sub-Saharan Africa and Asia. Together, theyprovide new evidence to support the global focus on PNS asan effective, efficient and safe strategy for achieving the first90 of the UNAIDS 90-90-90 targets, to ensure that 90% ofpeople with HIV are aware of their status [22]. The articlesalso offer practical guidance for implementing PNS in a rangeof populations and settings and describe new strategies forenhancing PNS delivery. They highlight the need to provideservices that meet the WHO minimum standards for HIVtesting – consent, confidentiality, counselling, connection toservices, and correct test results (the 5C’s) [23] – and avoidsocial harms. Of note, Ayala and colleagues [24] emphasizethe importance of involving communities during programmedevelopment so that the benefits of PNS are understood andservices are provided in an ethical and inclusive way thatrespects individual choice and human rights.
1 | PROGRAMMATIC EVIDENCE OFASSISTED PNS EFFECTIVENESS
PNS are an increasingly prioritized HIV testing strategyglobally because of their potential to improve testing cover-age and efficiently identify people with undiagnosed HIVinfection [16]. In this supplement, evaluations of fiveassisted PNS programmes provide further evidence for theacceptability, sustained effectiveness, and high positivity ofnew HIV diagnoses among contacts across diverse popula-tions, programme types and settings. HIV positivity ratesamong contacts (i.e. proportion of contacts tested for HIVwho are newly diagnosed as HIV positive) in these pro-grammes ranged from 6% to 15% in Central and SouthAsia [25,26] to 29% to 52% in sub-Saharan Africa [27,28]and 42% in Southeast Asia [29].As with any intervention, however, the effectiveness of
assisted PNS may depend on the setting or client characteris-tics, and subgroup analyses have the potential to inform prior-itization of PNS when resources are scarce or duringprogramme scale-up. Masyuko et al. [30] present subgroupanalyses of a landmark cluster randomized controlled trial ofassisted PNS in Kenya [14], finding that assisted PNS weremore effective at increasing partner testing in a region withhigher HIV prevalence, in rural and peri-urban settings withless access to HIV testing services (HTS) and for female indexclients. Similarly, an evaluation of a community-based PNS pro-gramme in Zimbabwe found greater test positivity among con-tacts aged 35 to 49, sexual partners (vs. children and otherhousehold members), and female contacts and differences intest positivity by region of the country [27]. These results sug-gest that local differences in HIV prevalence and access toHTS or differences in testing behaviours or HIV incidence bygender and age may be useful for prioritizing limitedresources for PNS.
2 | CLIENT, COMMUNITY ANDPROVIDER PERSPECTIVES ON PNS
Understanding the perspectives of communities affected byHIV, potential clients and their partners, and healthcare work-ers who are or will be performing PNS is necessary for thedevelopment and implementation of effective, safe and scal-able programmes. Articles from this supplement provide newperspectives on PNS for key and vulnerable populations [24]and pregnant and postpartum women [31] as well as howPNS can be integrated into both HIV care and prevention pro-grammes [32,33].Global leaders and advocates from diverse communities
affected by HIV provide practical guidance on how to engagetheir communities and maintain a focus on human rights todeliver ethical and effective PNS, particularly for key popula-tions [24]. Odoyo et al. [32] discuss perspectives and experi-ences from HIV care providers in Kenya, who found that PNSand PrEP have the potential to be synergistic in the HIV caresetting. PNS was seen as an opportunity to increase uptake ofcouple-based prevention, including offering PrEP to negativepartners and retaining partners with HIV in ART services.Availability of PrEP within HIV treatment services alsoincreased the motivation of providers to offer PNS and of cli-ents with HIV to accept PNS and share their status with theirpartners. Also from the Kenyan HIV care setting, Monroe-Wise et al. [33] found that barriers to PNS among people withestablished HIV infection and on treatment revolved primarilyaround fear of repercussions stemming from sharing HIV diag-noses with their partners, particularly when the client had notshared their status with the partner immediately after diagno-sis. Providers and clients were able to identify multiple strate-gies for addressing these concerns and employ PNS safelyand effectively. Finally, pregnant women, their male partners,healthcare workers and policymakers from Zambia and Malawiconsidered multiple options for testing male partners of preg-nant women [31]. As no single approach was overwhelminglypreferred within or across stakeholder groups and all had mul-tiple pros and cons, the authors concluded that a choice-basedapproach may result in greatest uptake of these services andenhance their impact. Taken together, these perspectives cansupport the development of new strategies and best practicesto ensure the safe and effective delivery of PNS to all peoplewith HIV on an ongoing basis as recommended by WHO andPEPFAR guidelines.
3 | PNS FOR KEY POPULATIONS
To date, most of the evidence for the effectiveness and safetyof PNS in LMICs has come from programmes and studies inthe general population. There are concerns that this evidencemay not be generalizable to key populations in rights-con-strained settings where criminalization and stigma are preva-lent, confidentiality is frequently breached, and there is limitedaccess to rights-based and culturally sensitive services. Takentogether, these concerns may affect the acceptability, effec-tiveness and potential social harms associated with assistedand passive partner notification strategies. Additionally, differ-ences in partnership types (e.g. transactional partnerships ordrug-sharing contacts) and community norms across
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
197

populations may further influence the acceptability and deliv-ery of PNS. Formative evidence indicates that PNS may beacceptable to some members of key populations in LMIC [16],but may be challenging in others [34,35]. Encouragingly, PNSapproaches have also been successfully provided to gay, bisex-ual, and other men who have sex with men (MSM) and peoplewho inject drugs (PWID) in several high-income countries formany years and lessons learned from these programmes mayinform scale-up in LMICs.This supplement includes three articles describing the
implementation of PNS programmes serving key populations.From Vietnam, Nguyen et al. [29] describe assisted PNSwithin a community-led, peer educator-delivered HTS pro-gramme that serves MSM, PWID, female sex workers andtransgender people. Uptake of PNS was high (81%) and theHIV positivity rate among contacts was 42%, greater than therate from HTS delivered by lay providers and HIV self-testing.From Pakistan, Malik et al. [26] report on an assisted partnernotification strategy for reaching spouses of PWID with ongo-ing HIV testing, prevention and care services through fieldoutreach and sensitization of heads of family (often mothers-in-law) to overcome barriers related to local culture and familystructures. This programme reached the spouses of 71% ofmarried index clients but had relatively low positivity (9%).Finally, Little et al. [27] describe the integration of assistedPNS into three types of activities within PWID-focused pro-grammes in Kazakhstan, the Kyrgyz Republic and Tajikistan.These activities include: (1) HTS for people newly diagnosedwith HIV; (2) tracing of individuals with HIV who were lost-to-follow-up in order to re-engage them in HIV care and (3) HIVcare for individuals with HIV who are receiving HIV care ser-vices but are not yet taking ART. Compared to a period withpassive referral only, implementation of assisted PNSincreased the number of partners tested and newly diagnosedwith HIV per index client, significantly improving the efficiencyof HTS. Overall, these evaluations provide additional evidenceof the acceptability and potential effectiveness of PNS for keypopulations. They also provide examples of how PNS can betailored to the local context and populations being served. TheVietnam programme, in particular, highlights the role thatengaging affected communities can have in the developmentand implementation of successful PNS programmes, a messageconsistent with one of the key recommendations from theviewpoint by members of affected communities [24].
4 | SOCIAL HARMS FOLLOWING PNS
A key concern raised by advocates and providers alike aboutPNS implementation and scale-up, particularly around the provi-der referral method, is the potential for social harms, such asIPV, relationship dissolution and breaches of confidentiality.New results from the Cameroon Baptist Convention HealthServices’ PNS programme [28,36] add to previous evidencefrom research studies and programme evaluations[11-14,37,38] that facility-based assisted PNS for the generalpopulation result in few adverse events, even in settings withhigh background rates of gender-based violence. However, asdescribed in the previous section and in-depth in the communityviewpoint [24], it has not been clear to what extent these find-ings can be applied to PNS programmes serving key populations
in rights-constrained settings, where the consequences of PNSmay be complicated by structural and sociocultural factorsaffecting the lives and partnerships of these groups. Encourag-ingly, in this supplement, an evaluation of a community-led HTSprogramme with integrated assisted PNS for key populations inVietnam – primarily MSM and PWID – found no evidence ofsocial harms related to partner notification [29].To mitigate the risk of social harms, it will be critical for
PNS programmes to continue to screen for IPV prior to offer-ing PNS to index clients. Options for clients who report IPV inthe current relationship include partner notification (whichdoes not require disclosure to the partner and can be con-ducted anonymously) or a delay in participating in PNS untilthe safety of the index client can be assured. In addition, allindex clients who report IPV should be actively linked to gen-der-based violence services to get the care and support theyneed. HIV testing programmes should also monitor socialharms resulting from participation in PNS to ensure that pro-tections have been put in place to protect the safety of indexclients and their partner(s). Additional research is needed toensure the safety of PNS among key populations in differentprogramme models and settings. Articles by Ayala et al. [24]and Wamuti et al. [36] in this supplement present direct, prac-tical recommendations for ensuring safe, respectful and effec-tive delivery of PNS.
5 | TRAINING IS CRITICAL
Effective, culturally competent training for health workers andlay providers is critical to the successful and ethical implemen-tation of PNS programmes. As outlined by Han et al. [39] inthis supplement, successful training programmes for PNS typi-cally incorporate a combination of didactic and active skills-based learning with on-the-job mentorship, monitoring andevaluation and refresher trainings. This article also presentscommon topics of PNS training, from the rationale and princi-ples of PNS to counselling and communication skills to ethicalissues, as well as strategies for implementing and sustaininghigh-quality training programmes. Equally important are theselection criteria used to determine which healthcare workersshould provide PNS. Ideally, PNS providers should be experi-enced counsellors with at least one year of experience con-ducting HTS and should have the psychologic composure tooffer PNS in a tactful, patient and open-minded manner. Sup-portive supervision and mentoring for newly trained PNS pro-viders are also key for sharing best practices and avoidingburn-out.Tembo et al. [40] demonstrate the potential effectiveness of
a one-day behavioural skills-building training for improving thedelivery of a client referral model for partner testing in Malawi.Although WHO recommends assisted PNS, many index clientsselect client referral as their preferred strategy for notifyingpartner(s), and some programmes continue to rely exclusivelyor primarily on client referral strategies due to national policies,lack of programme capacity to offer assisted referral, and otherconcerns. Strategies for improving the effectiveness of passivereferral are therefore needed. In a pre/post evaluation, Temboand colleagues found that a one-day training to improve healthworker skills in offering and supporting clients in delivering fam-ily referral slips resulted in significant increases in the recorded
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
198
number of contacts that were elicited, received HIV testing, andwere diagnosed as HIV positive. This study suggests that a briefskills-based training has the potential to increase the effective-ness of passive referral, although further study will be neces-sary to assess its potential value within PNS programmesoffering assisted referral.
6 | CONCLUSIONS
Everyone with HIV benefits from early diagnosis and linkageto ART for their own health and to prevent transmission touninfected partners and infants. As countries reach theUNAIDS 90-90-90 targets – the first being 90% of peoplewith HIV knowing their status and the second linking to andtaking ART [22] – there remain significant gaps, and newapproaches are needed to address these gaps. Men and keypopulations, in particular, continue to have less access to HIVtesting and treatment services. Articles in this supplementcontribute to the growing evidence demonstrating that PNScan be a successful strategy in reaching undiagnosed popula-tions more efficiently and effectively.As with all testing approaches, PNS must be delivered in a
way that avoids social harms. Proper training of providers onhow to safely provide PNS and support for the index clientswho receive PNS services are therefore critical. For example,how do we do provide PNS safely to index clients in abusiverelationships? Articles in this supplement have provided somebest practices for mitigating the risk of social harms. Pro-grammes should also consider using WHO guidance onassessing IPV risk [41] and continue to monitor the experi-ence of social harms following PNS to ensure that these ser-vices are offered in ways that respects the human rights ofindex clients and their partner(s) and preserves their safety.Huge advances in HIV prevention, testing and treatment have
been made in the 35 years since the HIV epidemic began. HIVshould now be considered a manageable chronic condition, andHIV transmission should be easily preventable by supportingpeople with HIV to achieve viral suppression and engaging peo-ple at risk in the increasing options for HIV prevention. How-ever, HIV epidemic control cannot be achieved unless peoplewith HIV are diagnosed early, rapidly linked to HIV treatmentservices and have HIV prevention services readily availabilityfor their HIV-negative at-risk partners. By improving HIV test-ing coverage among underserved populations and those most atrisk for HIV infection, PNS can play a key role in achieving theseobjectives and, ultimately, HIV epidemic control.
AUTHORS ’ AFF I L IAT IONS1Department of Global Health, University of Washington, Seattle, WA, USA;2Global Health Bureau, Office of HIV/AIDS, United States Agency for Interna-tional Development (USAID), Washington, DC, USA; 3Division of Global HIV andTB, Center for Global Health, U.S. Centers for Disease Control and Prevention(CDC), Atlanta, GA, USA; 4HIV Department, World Health Organization (WHO),Geneva, Switzerland; 5National AIDS/Sexually Transmitted Diseases ControlProgramme, Ministry of Health, Nairobi, Kenya; 6HIV & TB Program, PATH,Hanoi, Vietnam; 7Vietnam Authority of HIV/AIDS Control, Ministry of Health,Hanoi, Vietnam
COMPET ING INTERESTS
The authors have no competing interests to declare.
AUTHORS ’ CONTR IBUT IONS
DK, VW and RB drafted the initial manuscript. All authors critically reviewedthe manuscript, suggested revisions and editorial changes, and approved thefinal version.
ACKNOWLEDGEMENTS
FUNDING
This supplement was made possible by funding from the United States Agencyfor International Development (USAID), project numbers: US-2015-0839 andUS-2016-940.
DISCLA IMER
The contents of this editorial are those of the authors and do not necessarilyrepresent the official views of the World Health Organization, U.S. PEPFAR, theU.S. Centers for Disease Control and Prevention, the U.S. Agency for Interna-tional Development, or the U.S. government.
A NOTE ON TERMINOLOGY
PNS, or contact tracing, is defined as a voluntary processwhereby a trained provider asks people diagnosed with HIVoften known as the “index case” about their sexual partnersand/or drug injecting partners and then, if the HIV-positiveclient agrees, offers these partners HTS. Partner notificationis provided using passive or assisted approaches.
Passive HIV PNS or “client referral” refer to when HIV-posi-tive clients are encouraged by a trained provider to disclosetheir HIV status to their sexual and/or drug injecting partnersby themselves, and to encourage their partner(s) to be testedfor HIV given their potential exposure to HIV infection.
Assisted HIV PNS refer to when consenting HIV-positiveclients are assisted by a trained provider to disclose theirstatus or to anonymously notify their sexual and/or druginjecting partner(s) of their potential exposure to HIV infec-tion. The provider then offers HIV testing to these partner(s). Assisted partner notification is done using contractreferral, provider referral or dual referral approaches.
! Contract referral: HIV-positive clients enter into a contractwith a trained provider and agree to disclose their statusand the potential HIV exposure to their partner(s) by them-selves and to refer their partner(s) to HTS within a specifictime period. If the partner(s) of the HIV-positive individualdoes not access HTS or contact the health provider withinthat period, then the provider will contact the partner(s)directly and offer voluntary HTS.
! Provider referral: With the consent of the HIV-positive cli-ent, a trained provider confidentially contacts the person’spartner(s) directly and offers the partner(s) voluntary HTS.
! Dual referral: A trained provider accompanies and providessupport to HIV-positive clients when they disclose their HIVstatus to their partner(s). The provider also offers voluntaryHTS to the partner(s).
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
199

Index testing usually refers more broadly to offering HIVtesting to all contacts of an index client including sexualand needle and syringe-sharing partners, biological children,and, in the case of an HIV-positive child, the mother andbiologic siblings.
Social network testing is where an HIV-positive client isasked to enlist people in their social networks who maybenefit from HIV testing to participate in HIV testing ser-vices [42,43]. These contacts can, in turn, recruit theirsocial contacts who are also at risk for HIV.
REFERENCES
1. Joint United Nations Programme on HIV/AIDS. Voluntary counseling andtesting: technical update. Geneva, Switzerland; 2000 [cited 2019 Apr 17]. Avail-able from: http://data.unaids.org/publications/irc-pub01/jc379-vct_en.pdf2. World Health Organization. The 3 by 5 initiative [Internet]. Geneva, Switzer-land. [cited 2019 Apr 17]. Available from: https://www.who.int/3by5/en/3. World Health Organization. Increasing access to HIV testing and counseling:report of a WHO consultation. Geneva, Switzerland; 2003 [cited 2019 Apr2017]. Available from: https://apps.who.int/iris/bitstream/handle/10665/42757/9241590904.pdf;jsessionid=A53C22DB68198AECE859BD83B3A84CB1?sequence=14. The Antiretroviral Therapy in Lower Income Countries (ART-LINC) Collabo-ration and ART Cohort Collaboration (ART-CC) Groups. Mortality of HIV-1-infected patients during the first year of antiretroviral therapy: comparisonbetween low-income and high-income countries. Lancet. 2006;367:817–24.5. World Health Organization. Guidance on provider-initiated HIV testing andcounselling in health facilities. Geneva, Switzerland; 2007 [cited 2019 Apr 17].Available from: https://www.who.int/hiv/pub/vct/pitc/en/6. Joint United Nations Programme on HIV/AIDS. Opening up the HIV/AIDSepidemic: guidance on encouraging beneficial disclosure, ethical partner counsel-ing & appropriate use of HIV case-reporting. Geneva, Switzerland; 2000 [cited2019 Apr 17]. Available from: http://www.unaids.org/sites/default/files/media_asset/jc-execsumm_en_0.pdf7. Eyawo O, de Walque D, Ford N, Gakii G, Lester RT, Mills EJ. HIV status indiscordant couples in sub-Saharan Africa: a systematic review and meta-analysis.Lancet Infect Dis. 2010;11(10):770–7.8. World Health Organization. Guidance on couples HIV testing and counselling- including antiretroviral therapy for treatment and prevention in serodiscordantcouples. Geneva, Switzerland; 2012 [cited 2019 Apr 17]. Available from: https://www.who.int/hiv/pub/guidelines/9789241501972/en9. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumara-samy N, et al. Prevention of HIV-1 infection with early antiretroviral therapy. NEngl J Med. 2011;365(6):493–505.10. Baeten JM, Donnell D, Ndase P, Mugo NR, Campbell JD, Wangisi J, et al.Antiretroviral prophylaxis for HIV prevention in heterosexual men and women.N Engl J Med. 2012;367(5):399–410.11. Henley C, Forgwei G, Welty T, Golden M, Adimora A, Shields R, et al.Scale-up and case-finding effectiveness of an HIV partner services program inCameroon: an innovative HIV prevention intervention for developing countries.Sex Transm Dis. 2013;40(12):909–14.12. Kahabuka C, Plotkin M, Christensen A, Brown C, Njozi M, Kisendi R, et al.Addressing the first 90: a highly effective partner notification approach reachespreviously undiagnosed sexual partners in Tanzania. AIDS Behav. 2017;21(8):2551–60.13. Brown LB, Miller WC, Kamanga G, Nyirenda N, Mmodzi P, Pettifor A, et al.HIV partner notification is effective and feasible in sub-Saharan Africa: opportu-nities for HIV treatment and prevention. J Acquir Immune Defic Syndr. 2011;56(5):437–42.14. Cherutich P, Golden MR, Wamuti B, Richardson BA, Asbjornsdottir KH,Otieno FA, et al. Assisted partner services for HIV in Kenya: a cluster random-ized controlled trial. Lancet HIV. 2017;4(2):e74–82.15. Jennings L, Na M, Cherewick M, Hindin M, Mullany B, Ahmed S. Women’sempowerment and male involvement in antenatal care: analyses of Demographicand Health Surveys (DHS) in selected African countries. BMC Pregnancy Child-birth. 2014;14:297.
16. World Health Organization. Guidelines on HIV self-testing and partner noti-fication. Geneva, Switzerland; 2016 [cited 2019 Apr 17]. Available from: https://www.who.int/hiv/pub/vct/hiv-self-testing-guidelines/en/17. U.S. President’s Emergency Plan for AIDS Relief. Partner and family-basedindex testing: a standard operating procedure. [cited 2019 Apr 17]. Availablefrom: https://aidsfree.usaid.gov/sites/default/files/pn_sop_slides.pdf18. U.S. Agency for International Development. U.S. President’s emergency planfor research, AIDSFree [Internet]. AIDSFree HIV testing services knowledge base.[cited 2019 Apr 17]. Available from: https://aidsfree.usaid.gov/resources/hts-kb19. Plotkin M, Kahabuka C, Christensen A, Ochola D, Betron M, Njozi M, et al.Outcomes and experiences of men and women with partner notification for HIVtesting in Tanzania: results from a mixed method study. AIDS Behav. 2018;22(1):102–16.20. Fauci AS, Redfield RR, Sigounas G. Ending the HIV epidemic: a plan for theUnited States. JAMA. 2019;321(9):844–5.21. Cherutich P, Golden M, Betz B, Wamuti B, Ng’ang’a A, Maingi P, et al.Surveillance of HIV assisted partner services using routine health informationsystems in Kenya. BMC Med Inform Decis Mak 2016;16:97.22. Joint United Nations Programme on HIV/AIDS. 90-90-90: an ambitioustreatment target to help end the AIDS epidemic. Geneva, Switzerland; 2014[cited 2019 Apr 17]. Available from: http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf23. World Health Organization. Consolidated guidelines on HIV testing ser-vices. Geneva, Switzerland; 2015 [cited 2019 Apr 17]. Available from: https://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/24. Ayala G, Bahati M, Balan E, Chang J, Do TD, Fokeerbux NA, et al. Partnernotification: a community viewpoint. J Int AIDS Soc. 2019;22(S3):e25291.25. Little KM, Kan M, Samoylova O, Rsaldinova A, Saliev D, Yaminova M,et al. Implementation experiences and insights from the scale-up of an HIVassisted partner notification intervention in Central Asia. J Int AIDS Soc.2019;22(S3):e25313.26. Malik M, Jamil MS, Johnson CC, Pasha MS, Hermez J, Qureshi S. Integrat-ing assisted partner notification within service package for people who injectdrugs in Pakistan. J Int AIDS Soc. 2019;22(S3):e25317.27. Mahachi N, Muchedzi A, Tafuma TA, Mawora P, Kariuki L, Sewo B, et al.Sustained high HIV case finding through index testing and partner notificationservices: experiences from three provinces in Zimbabwe. J Int AIDS Soc.2019;22(S3):e25321.28. Muffih PT, Temgbait Chimoun F, Khan EM, Nshom E, Nambu W, Shields R,et al. Assisted HIV partner notification services in resource-limited settings:experiences and achievements from Cameroon. J Int AIDS Soc. 2019;22(S3):e25310.29. Nguyen VTT, Huong PTT, Kato M, Thong NQ, Anh LAK, Son VH, et al.Community-led HIV testing services including HIV self-testing and assisted part-ner notification services: lessons from a pilot study in a concentrated epidemicsetting. J Int AIDS Soc. 2019;22(S3):e25301.30. Masyuko SJ, Cherutich PK, Contesse MG, Maingi PM, Wamuti BM,Macharia PM, et al. Index participant characteristics and HIV assisted partnerservices efficacy in Kenya: results of a cluster randomized trial. J Int AIDS Soc.2019;22(S3):e25305.31. Hershow RB, Zimba CC, Mweemba O, Chibwe K, Phanga T, Dunda W,et al. Perspectives on HIV partner notification, partner HIV self-testing, andpartner home-based HIV testing by pregnant and postpartum women in antena-tal settings: a qualitative analysis in Malawi and Zambia. J Int AIDS Soc.2019;22(S3):e25293.32. Odoyo JB, Morton JF, Ngure K, O’Malley G, Mugwanya K, Irungu E, et al.Integrating PrEP into HIV care clinics may improve partner testing services andreinforce mutual support among couples: experiences from a PrEP implementa-tion project in Kenya. J Int AIDS Soc. 2019;22(S3):e25303.33. Monroe-Wise A, Maingi P, Kimani H, Moraa H, Bukusi D, Farquhar C.Assisted partner notification services for patients receiving HIV care and treat-ment in an HIV clinic in Nairobi, Kenya: a qualitative assessment of barriers andopportunities for scale-up. J Int AIDS Soc. 2019;22(S3):e25315.34. Clark JL, Perez-Brumer A, Salazar X. “Manejar la Situacion”: partner notifica-tion, partner management, and conceptual frameworks for HIV/STI control andMSM in Peru. AIDS Behav. 2015;19(12):2245–54.35. Semple SJ, Pines HA, Strathdee SA, Vera AH, Rangel G, Magis-Rodriguez C,et al. Uptake of a partner notification model for HIV among men who have sex withmen and transgender women in Tijuana, Mexico. AIDS Behav. 2018;22(7):2042–55.36. Wamuti B, Welty T, Nambu W, Shields R, Temgbait Chimoun F, Golden M,et al. Low risk of adverse outcomes in an HIV assisted partner services programin Cameroon. J Int AIDS Soc. 2019;22(S3):e25308.37. Myers RS, Feldacker C, Cesar F, Paredes Z, Augusto G, Muluana C, et al.Acceptability and effectiveness of assisted human immunodeficiency virus
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
200

partner services in mozambique: results from a pilot program in a public, urbanclinic. Sex Transm Dis. 2016;43(11):690–5.38. Rosenberg NE, Mtande TK, Saldi F, Stanley C, Jere E, Paile L, et al. Recruit-ing male partners for couple HIV testing and counselling in Malawi’s option B+programme: an unblinded randomised controlled trial. Lancet HIV. 2015;2(11):e483–91.39. Han H, Myers S, Khan EM, Masyuko S, Paredes Z, Temgbait Chimoun F,et al. Assisted HIV partner services (aPS) training in three Sub-Saharan AfricanCountries: facilitators and barriers to sustainable approaches. J Int AIDS Soc.2019;22(S3):e25307.40. Tembo TA, Kim MH, Simon KR, Ahmed S, Beyene T, Wezel E, et al. Enhanc-ing an HIV index case testing passive referral model through a behavioral skills-
building training for health care providers: a pre-/post- assessment in MangochiDistrict, Malawi. J Int AIDS Soc. 2019;22(S3):e25292.41. World Health Organization. Responding to intimate partner violence andviolence against women: WHO clinical and policy guidelines. Geneva, Switzer-land; 2013 [cited 2019 Apr 17]. Available from: https://www.who.int/reproductivehealth/publications/violence/9789241548595/en/42. Latkin CA, Davey-Rothwell MA, Knowlton AR, Alexander KA, Williams CT, Boo-dram B. Social network approaches to recruitment, HIV prevention, medical care, andmedication adherence. J Acquir Immune Defic Syndr. 2013;63 Suppl 1:S54–8.43. U.S. Centers for Disease Control and Prevention. Social network strategy(SNS) for HIV testing recruitment. Atlanta, GA: U.S. Centers for Disease Controland Prevention.
Katz DA et al. Journal of the International AIDS Society 2019, 22(S3):e25314http://onlinelibrary.wiley.com/doi/10.1002/jia2.25314/full | https://doi.org/10.1002/jia2.25314
201

Vol.:(0123456789)1 3
AIDS and Behavior https://doi.org/10.1007/s10461-019-02552-2
ORIGINAL PAPER
Use and!Acceptability of!HIV Self-Testing Among First-Time Testers at!Risk for!HIV in!Senegal
Carrie!E.!Lyons1 !· Karleen!Coly1!· Anna!L.!Bowring1!· Benjamin!Liestman1!· Daouda!Diouf2!· Vincent!J.!Wong3!· Gnilane!Turpin1!· Delivette!Castor3!· Penda!Dieng2!· Oluwasolape!Olawore1!· Scott!Geibel6!· Sosthenes!Ketende1!· Cheikh!Ndour4!· Sa"atou!Thiam5!· Coumba!Touré-Kane7!· Stefan!D.!Baral1
© The Author(s) 2019
AbstractHIV Self-Testing (HIVST) aims to increase HIV testing coverage and can facilitate reaching the UNAIDS 90-90-90 targets. In Senegal, key populations bear a disproportionate burden of HIV and report limited uptake of HIV testing given pervasive stigma and criminalization. In these contexts, HIVST may represent a complementary approach to reach populations reporting barriers to engagement with existing and routine HIV testing services. In this study, 1839 HIVST kits were distributed in Sen-egal, with 1149 individuals participating in a pre-test questionnaire and 817 participating in a post-test questionnaire. Overall, 46.9% (536/1144) were first-time testers and 26.2% (300/1144) had tested within the last year; 94.3% (768/814) reported using the HIVST, and 2.9% (19/651) reported a reactive result which was associated with first-time testers (p = 0.024). HIVST represents an approach that reached first-time testers and those who had not tested recently. Implementation indicators sug-gest the importance of leveraging existing community structures and programs for distribution.
Keywords HIV!· Self-Testing!· Key populations!· Senegal!· Sub-Saharan Africa
ResumenEl autodiagnóstico del VIH (ADVIH) busca incrementar la cobertura de las pruebas del VIH y puede facilitar el alcance de los objetivos 90-90-90 de ONUSIDA. En Senegal, los grupos de población clave soportan una carga desproporcionada del VIH y reportan una utilización limitada de las pruebas del VIH, dada la generalización del estigma y la criminalización. En este contexto, el ADVIH puede servir como enfoque complementario para alcanzar a las poblaciones que reportan barreras al compromiso con los servicios de pruebas del VIH existentes y de rutina. En este estudio se distribuyeron 1839 ADVIH en Senegal, donde 1149 individuos participaron en una encuesta antes de recibir la prueba y 817 participaron en!una encuesta después de recibir la prueba. En general, el 46.9% (536/1144) se realizó la prueba por primera vez y el 26.2% (300/1144)
* Carrie E. Lyons [email protected] Department of!Epidemiology, Center for!Public Health
and!Human Rights, Johns Hopkins School of!Public Health, 615!N Wolfe St., Baltimore, MD!21205, USA
2 Enda Sante, Dakar, Senegal3 O"ce of!HIV/AIDS, Bureau for!Global Health, USAID,
Arlington, VA, USA4 Division de La Lutte Contre Le Sida et Les IST, Ministry
of!Health, Dakar, Senegal5 Conseil National de Lutte contre le Sida, Dakar, Senegal6 Population Council, Washington, DC, USA7 Laboratoire de Bacteriologie-Virologie, CHU Aristide Le
Dantec, Dakar, Senegal
202

AIDS and Behavior
1 3
se habían realizado una prueba en el último año; el 94.3% (768/814) reportó utilizar el ADVIH y el 2.9% (19/651) reportó un resultado reactivo asociado con realizar la prueba por primera vez (p = 0.024). El ADVIH representa un enfoque que alcanzó a las personas que realizaron la prueba por primera vez y a quienes no se!habían realizado la prueba recientemente. Los indicadores de implementación sugieren la importancia de aprovechar las estructuras comunitarias y los programas de distribución existentes.
Introduction
Increasing coverage of HIV testing and early detection of seroconversion among people living with HIV is essential for e#ectively responding to the HIV pandemic. Early detec-tion of HIV and initiation of antiretroviral therapy (ART) significantly reduces HIV-related morbidity and mortality, and can improve the quality of life for people living with HIV while also eliminating the risk of onward HIV trans-mission [1–3]. Similarly, awareness of one’s negative HIV serostatus is important for prioritizing prevention strate-gies especially in the context of increasing availability of pre-exposure prophylaxis (PrEP) [4, 5]. HIV self-testing (HIVST) is emerging as an important tool to potentially increase the uptake and the frequency of HIV testing in populations at increased risk for acquiring HIV such as key populations who may avoid HIV testing services because of stigma and criminalization of their sexual practices, orienta-tion, or occupation, or even the criminalization of HIV trans-mission [6]. Approximately 48 countries have established an HIVST supportive policy and far more countries have policies under development, including several across sub-Saharan African [7, 8]. Given the rapid adoption of HIVST globally, WHO guidelines have been developed to support the implementation and scale-up of ethical, e#ective, accept-able, and evidence-based approaches to HIVST [9].
HIVST can potentially overcome barriers to HIV test-ing uptake and accessibility by placing the locus of control of testing on the individual, increasing confidentiality, and allowing members of marginalized and stigmatized groups to test in settings of privacy, safety, and with dignity [10]. Oral HIVST has been shown to improve HIV testing cover-age and to be acceptable among diverse populations across varied settings [11–16]. However, there is currently limited evidence on acceptability of HIVST across Western and Central Africa despite the need to understand the accept-ability and strategies for e#ective implementation across the region [8].
The West African country of Senegal is one of the coun-tries in sub-Saharan Africa where an HIVST policy is cur-rently under development [8]. Senegal has a concentrated HIV epidemic with a prevalence among adults of reproduc-tive age consistently under 1%, and a high burden among specific key populations [17]. In Senegal, HIV dispropor-tionately a#ects men who have sex with men (MSM), female sex workers (FSW) and people who inject drugs (PWID)
with prevalence estimates of 23.5%, 3.3%, 10.2%, respec-tively [18, 19]. In Senegal, same-sex practices are criminal-ized and sex work for cisgender women is legal but highly regulated [20]. Stigma has been shown to be a barrier to uptake of HIV testing and accessing other HIV prevention and treatment services. In many places, there is stigma spe-cifically associated with seeking HIV testing [21, 22]. Fre-quent or regular HIV testing may be perceived by healthcare providers as disclosing a stigmatized behavior, and stigma relating to access to health services among key populations has been reported to be high [18]. Low rates of testing may be a#ecting Senegal’s progress towards epidemic control among key populations and achieving the UNAIDS 90-90-90 targets for all [23]. While available data are limited, UNAIDS estimates that only 71% of adults living with HIV know their status, of which only 58% are receiving ART [24.] However, uptake of HIV services has been shown to be lower among key populations, with a recent study estimating that only 13% of MSM and 55% of FSW living with HIV reported to be aware of their seropositive status [18].
Given the HIV epidemic profile in Senegal and the lim-ited uptake of HIV prevention and treatment services among key populations in the country, HIVST may represent an impactful strategy for increasing the uptake and coverage of HIV testing and accelerating progress towards achieving 90-90-90 goals. This study aimed to assess the acceptability of HIVST for key populations and people in their social and sexual networks and secondly, to assess the e#ectiveness of HIVST in reaching first-time testers. These results will inform appropriately scaled implementation of HIVST in Senegal and across West Africa.
Methods
This is a pilot study which distributed HIVST kits through targeted venues and recruited individuals through conveni-ence sampling to participate in pre and post HIVST socio-behavioral questionnaires.
HIVST Distribution
OraQuick HIV Self-Test Kits (Orasure Technologies, Inc) were distributed to individuals in Dakar and Ziguinchor through venue and social network-based distribution. The HIVST kits included an OraQuick test device, written and
203

AIDS and Behavior
1 3
pictorial step-by-step instructions, supplementary informa-tion on the test and HIV, and a referral card with information for confirmatory testing sites and study contacts. Instructions and supplementary information were provided in French and Wolof and adapted to the Senegalese context.
HIVST kit distribution and participant recruitment was led by study partner, Enda Santé, and aimed to reach popu-lations with increased vulnerability of HIV acquisition and high levels of health care related stigma, including MSM, FSW, PWID, and clients of FSW. [20].
The venue-based approach for distribution and recruit-ment utilized directly assisted distribution of HIVST and was conducted through outreach to sex work venues, bars, nightclubs, hot spots, and mobile clinics, as well as health facilities that provide services to key populations. Venues were selected based on recommendations of community partners with previous experience in the communities, and leveraged existing programmatic activities. Directly assisted distribution of HIVST followed the WHO definition [9] and was led by trained distributors who provided pre-test instruc-tions, test information, demonstration of proper HIVST use, and education on the importance for confirmatory testing, irrespective of a test reactivity. When possible, the partici-pant was given the choice to either self-administer in a pri-vate space on-site with a peer educator available, or to take their HIVST kit away with them to test later.
A small sample of additional HIVST kits were distributed through social network-based unassisted distribution. The social network-based approach was focused on providing a primary recipient with one HIVST kit for themselves and two additional kits to distribute to individuals within their network. Social network-based distribution leveraged venue-based distribution to engage the primary HIVST recipient, who received the HIVST kits directly from the trained dis-tributor. The primary recipient then distributed to secondary recipients through indirect, unassisted distribution as defined by WHO [9.] Secondary recipients only received written instructions and information contained within the HIVST kit.
Data Collection
Convenience sampling was used to recruit individuals into the study at the time of HIVST kit distribution. Individuals receiving the HIVST kits through directly assisted venue-based distribution were asked if they wished to participate in a pre- and post-test survey. Data from social network-based distribution were only obtained from the primary recipient as follow up was not possible for the network-based HIVST kit recipients. Participants were eligible if they reported being 18!years of age or older; capable of and willing to provide informed consent; agreed to use the HIVST; and spoke Wolof and/or French. Participation
was voluntary, and individuals could receive an HIVST kit regardless of survey participation. All pre- and post-test surveys were administered to eligible participants by trained interviewers. Among consenting participants, an interviewer administered pre-test surveys at the distribu-tion site before HIVST utilization. Pre-test surveys cap-tured information on demographic characteristics, HIV risk behaviors, HIV testing history, and motivation for testing.
Among individuals who opted to test at the HIVST dis-tribution sites, the HIVST was collected through a test disposal box after self-administration and was read imme-diately. The result was logged to track the overall results observed, but not connected to the individual participant. This approach was used to compare aggregate level results to those self-reported in the post-tests. Post-test surveys assessing self-reported HIVST use and acceptability were conducted by phone two weeks after the HIVST kit distri-bution. Data were not obtained from secondary recipients.
Ethical review and approval were provided by the National Research Ethics Committee in Senegal and the Johns Hopkins School of Public Health Institutional Review Board.
Measures
Key population characteristics were self-reported. Sex worker was defined as reporting exchanging sex for money or goods, and with more than half of income being from selling sex in the past 6!months. Male sex workers (MSW) were defined as sex workers above, as well as being assigned male sex at birth; and FSW were defined as sex workers as above and assigned female sex at birth. MSM was defined as being assigned the male sex at birth and ever having oral or anal sex with another man. Transgen-der women were defined using a two-step gender assess-ment of reporting male sex assigned at birth and gender identification as a woman. PWID were defined as ever having injected illicit drugs. Key population categories were not mutually exclusive. Key population was defined as meeting the criteria of at least one of the six key popu-lation categories.
First-time testers were defined as individuals who self-reported never having received an HIV test prior to the pre-test questionnaire. HIVST reactivity results were col-lected in two ways: 1. Results collected from used HIVST at the distribution sites; and 2. Self-reported HIVST results from those who participated in the post-test phone survey. Acceptability measures were informed by The Society for Implementation Research and Collaboration Indictor Review, however, have not yet been validated [25.]
204

AIDS and Behavior
1 3
Statistical Analyses
Demographic characteristics and HIV testing history were determined from pre-test questionnaires. Logistic regres-sion was used to assess the crude relationship between HIV testing history (first-time vs. previous testers), demographic characteristics, and HIV risk behaviors. Multiple multivari-able logistic regression models were developed to separately assess each demographic characteristic, HIV testing history, HIV risk behaviors as primary predictors of first-time test-ers and adjusted for a priori demographic characteristics. Pearson’s Chi squared tests were used to assess the crude relationships between first-time testers and HIVST use and acceptability, as well as the relationships between self-reported HIVST result and use and demographic charac-teristics. A significance value of p < 0.05 was used for all analyses.
Results
Distribution and!Study Participation
A total of 1839 HIVST kits were distributed between April 2017 to June 2018, and 62.5% (1149/1839) of recipients participated in the pre-test questionnaire before receiv-ing the HIVST (Table!1). Among pre-test participants, 71.1% (817/1149) participated in the follow up post-test questionnaire.
Among post-test respondents, 5.9% (48/810) had received additional HIVST kits for secondary, unassisted distribution, of which 80.0% (36/45) distributed the additional HIVST kits. Among individuals not provided additional HIVST kits for unassisted distribution, 1.2% (9/730) gave their HIVST kit to someone else.
Demographic Characteristics
Among participants who completed the pre-test, 47.9% (539/1125) were in Dakar and 52.1% (586/1125) were in Ziguinchor (Table!2). Among pre-test participants, 25.3%
(286/1130) were aged 18–24!years of age, 32.7% (370/1130) were 25–30!years, and 42.0 (474/1130) were 31!years and older. Overall, 52.9% (607/1148) reported female and 47.1% (541/1148) reported male sex at birth. Demographic char-acteristics of individuals who participated in the post-test questionnaire did not di#er from the pre-test, except for region (p = 0.011).
Key Populations
Among pre-test respondents, 32.2% (370/1149) self-reported membership of a key population group with 18.8% (204/1085) sex workers specifically, 14.3% (155/1085) FSW and 4.4% (48/1085) MSW; 15.1% (174/1149) MSM; 3.7% (42/1131) PWID; and 1.7% (20/1148) transgender women.
First-Time Testers
Among pre-test respondents, 46.9% (536/1144) of partici-pants were first-time testers, 26.9% (308/1144) had ever tested for HIV but not within the last 12!months, and 26.2% (300/1144) had tested within the last 12!months.
Among key populations, 36.8% (136/370) were first-time testers (Table!3). Among sex workers of all genders, 26.5% (54/204) were first time testers. Among FSW, 20.7% (32/155) were first-time testers, 27.7% (43/155) had tested but not in the last 12!months, and 51.6% (80/155) had tested in the last 12!months. Among MSW, 45.8% (22/48) were first-time testers. Overall, 46.0% (80/174) of MSM, 59.5% (25/42) of PWID, and 55.0% (11/20) of transgender women were first-time testers.
Among participants in Dakar, 42.2% (227/538) were first-time testers, and in Ziguinchor 52.6% (306/582) were first-time testers (Table!4). Among participants 18 to 24!years old, 62.8% (179/285) were first-time testers. Among partici-pants ages 25–30, 46.0% (169/367) were first-time testers, and 38.0% (171/444) were first-time testers among those 31!years and older. Among participants assigned female sex at birth, 38.6% (233/604) were first-time testers compared to 56.2% (303/539) of participants assigned male sex at birth.
Table 1 HIVST distribution and data collection summary in Senegal
n/N %
HIVST kits distributed 1839 100Pre-test participants 1149/1839 62.5Post-test participants among those who participated in the pre-test 817/1149 71.1Received additional HIVST for secondary distribution among post-test respondents 48/810 5.9Distributed HIVST for secondary distribution among post-test respondents 36/45 80.0Gave HIVST to someone else, although did not receive additional HIVST for second-
ary distribution9/730 1.2
HIVST results with positive reactivity among those collected at the distribution sites 76/1407 5.4
205

AIDS and Behavior
1 3
Table 2 Demographic characteristics of individuals who participated in pre- and post- HIVST questionnaires
a Not mutually exclusive
Pre-test participants Post-test participants X2 p value to compare samples
N = 1149 N = 817Demographic characteristics n/N % n/N %
Region 0.011!Dakar 539/1125 47.9 437/813 53.7!Ziguinchor 586/1125 52.1 376/813 46.3
Age 0.947!18–24 286/1130 25.3 207/803 25.8!25–30 370/1130 32.7 265/803 33.0!31+ 474/1130 42.0 331/803 41.2
Sex at birth 0.226!Female 607/1148 52.9 454/816 55.6!Male 541/1148 47.1 362/816 44.4
Key populationsa
Key population (any) 0.451!Yes 370/1149 32.2 250/817 30.6!No 779/1149 67.8 567/817 69.4
Sex worker (all genders) 0.841!Yes 204/1085 18.8 148/772 19.2!No 881/1085 81.2 624/772 80.8
Female sex worker 0.772!Yes 155/1085 14.3 114/772 14.8!No 994/1085 85.7 658/772 85.2
Male sex worker 0.877!Yes 48/1085 4.4 33/772 4.3!No 1101/1085 95.6 739/772 95.7
Men who have sex with men 0.417!Yes 174/1149 15.1 113/817 13.8!No 975/1149 84.9 704/817 86.2
People who inject drugs 0.230!Yes 42/1131 3.7 22/807 2.7!No 1089/1131 96.3 785/807 97.3
Transgender women 0.800!Yes 20/1148 1.7 13/816 1.6!No 1128/1148 98.3 803/816 98.4
HIV testing historyRecent testing for HIV 0.435!Never 536/1144 46.9 358/814 44.0!Yes, but not in the last 12!months 308/1144 26.9 227/814 27.9!Yes, within the last 12!months 300/1144 26.2 229/814 28.1
First time testers 0.208!Yes 536/1144 46.9 358/814 44.0!No 608/1144 53.1 456/814 56.0
206

AIDS and Behavior
1 3
Demographic Characteristics, HIV Testing History and!HIV Risk Behaviors, and!Associations with!First-Time Testers
When adjusting for sex and age, region was associated with HIV testing history, with an increased odds of being a first-time tester in Ziguinchor (aOR: 1.99; 95%CI: 1.53, 2.59; p value: < 0.001) compared to Dakar (Table!4). Age was associated with HIV testing history with an increased odds of being a first-time tester among those 18 to 24!years old compared to 31 + (aOR: 2.84; 95CI!%: 2.07, 3.90; p-value: < 0.001). Participants assigned male sex at birth had an increased odds of being a first-time tester compared to those assigned female sex (aOR: 2.71; 95CI!%: 2.08, 3.52; p-value: < 0.001).
Among pre-test participants, 79.5% (837/1053) had been worried about their HIV status, which was nega-tively associated with being a first-time tester (aOR: 0.68; 95%CI: 0.49, 0.94; p-value: 0.021) (Table!4). A sexual partner (aOR: 1.92; 95%CI: 1.06, 3.49; p-value: 0.032) or a family member (aOR: 2.61; 95%CI: 1.01, 6.69; p-value: 0.047) suggesting getting tested for HIV were associ-ated with reaching first-time testers compared to ‘other’
people suggesting. The reported primary reason for doing the HIV test was engagement in risky behavior (41.8%; 402/961), sexual partner engagement in risk behavior (7.4%; 71/961), had sex with someone who they thought or knew to be living with HIV (4.7%;45/961), condom failure (7.0%; 67/961), someone suggested to get tested (20.7%; 199/961), and part of a regular testing routine (17.2%; 165/961).
Use of!HIVST
Among post-test survey respondents, 94.3% (768/814) reported using the HIVST of which 43.5% (333/765) were first-time testers (Table!5). In total, 54.3% (363/668) used the HIVST at the distribution site and 45.7% (305/668) used the HIVST at home; and 88.9% (595/669) used the HIVST within 2!days. Among those who used the HIVST, 2.9% (19/651) reported a reactive result, and 2.0% (13/651) had an invalid result. Self-reported reactivity was associated with first-time testers (p = 0.024), and among those with a reac-tive result 63.2% (12/19) were first-time testers. Reported location of receiving the HIVST was associated with HIV testing history (p-value: < 0.001). Overall 10.3% (48/466)
Table 3 HIV testing history among self-reported key populations in Senegal
a Not mutually exclusive
Total HIV testing historySelf-reported key populationa First-time tester Yes, but not in the last
12!monthsYes, within the last 12!months
n/N % n/N % n/N % n/N % P value
Key population (any) <0.001!Yes 370/1149 32.2 136/370 36.8 103/325 27.8 131/325 35.4!No 779/1149 67.8 400/774 51.7 205/774 26.5 169/774 21.8
Sex worker (all genders) <0.001!Yes 204/1085 18.8 54/204 26.5 53/204 26.0 97/204 47.6!No 881/1085 81.2 450/878 51.3 240/878 27.3 188/878 21.4
Female sex worker <0.001!Yes 155/1085 14.3 32/155 20.7 43/155 27.7 80/155 51.6!No 930/1085 85.7 472/927 50.9 250/927 27.0 205/927 22.1
Male sex worker 0.239!Yes 48/1085 4.4 22/48 45.8 9/48 18.8 17/48 35.4!No 1037/1085 95.6 482/1034 46.6 284/1034 27.5 268/1034 25.9
Men who have sex with men 0.923!Yes 174/1149 15.1 80/174 46.0 49/174 28.2 45/174 25.9!No 975/1149 84.9 456/970 47.0 259/970 26.7 255/970 26.3
People who inject drugs 0.184!Yes 42/1131 3.7 25/42 59.5 7/42 16.7 10/42 23.8!No 1089/1131 96.3 500/1084 46.1 297/1084 27.4 287/1084 26.5
Transgender women 0.242!Yes 20/1048 1.7 11/20 55.0 7/20 35.0 2/20 10.0!No 1128/1148 98.3 525/1123 46.8 300/1123 26.7 298/1123 26.5
207

AIDS and Behavior
1 3
of those who reporting using the HIVST reported seeking follow up testing.
Acceptability of!HIVST
Overall, 74.5% (496/666) participants reported being com-fortable using the HIVST. In total, 86.1% (576/669) found the instructions easy to follow, and 94.4% (638/676) thought their family of friends would use the HIVST. After receiv-ing the HIVST, 30.6% (244/797) discussed HIV testing
with a sexual partner or friend. Among participants 78.5% (307/391) would be comfortable asking a primary sexual partner to use an HIVST, and 65.8% (150/228) would be comfortable asking a casual sexual partner to use an HIVST.
HIVST Reactivity
Among post-test respondents reporting a reactive result, 42.1% (8/19) used the test on site, and 57.9% (11/19) used the HIVST at home (Table!6). Among those with a reactive HIVST, 57.9% (11/19) went for confirmatory testing and
Table 4 Demographic characteristics, HIV testing history, motivation for HIV test use and associations with first-time testers in Senegal
*adjusted for other demographic characteristics presented in this table**adjusted for age, sex, and region
Characteristics Total HIV testing history X2 p value OR aOR* 95% CI P valueFirst-time tester
Individuals with testing history
n/N % n/N % n/N %
Region 0.001!Dakar 539/1125 47.9 227/538 42.2 311/538 57.8 Ref Ref!Ziguinchor 586/1125 52.1 306/582 52.6 276/582 47.4 1.52 1.99 1.53,2.59 <0.001
Age <0.001!18–24 286/1130 25.3 179/285 62.8 106/285 37.2 2.75 2.84 2.07,3.90 <0.001!25–30 370/1130 32.7 169/367 46.0 198/367 54.0 1.39 1.32 1.00,1.76 0.063!31+ 474/1130 42.0 171/444 38.0 293/473 62.0 Ref Ref
Sex at birth <0.001!Female 607/1148 52.9 233/604 38.6 371/604 61.4 Ref Ref!Male 541/1148 47.1 303/539 56.2 236/539 43.8 2.04 2.71 2.08,3.52 <0.001
HIV testing history n/N % n/N % n/N % P value OR aOR** 95% CI P value
Who suggested you get an HIV test? 0.056!Sexual partner 66/1134 5.8 42/66 63.6 24/66 36.6 2.13 1.92 1.06, 3.49 0.032!Peer educator 359/1134 31.7 164/357 45.9 193/357 54.1 1.03 1.09 0.76, 1.54 0.648!Doctor 226/1134 19.9 101/224 45.1 123/206 54.9 1.00 1.01 0.68, 1.49 0.979!Family member 22/1134 1.9 14/22 63.6 8/22 36.4 2.13 2.61 1.01, 6.69 0.047!Friend 213/1134 18.7 97/213 45.5 116/213 54.5 1.01 0.95 0.63, 1.42 0.793!Other 248/1134 21.9 112/248 45.2 136/248 54.8 Ref Ref
In the last 12!months, worried about HIV 0.065!Yes 837/1053 79.5 368/834 44.1 466/834 55.9 0.75 0.68 0.49, 0.94 0.021!No 216/1053 19.6 110/215 51.2 105/215 48.8 Ref
Main reason for doing the HIVST today <0.001!Engaged in risky behavior 402/961 41.8 156/401 38.9 245/401 61.1 3.74 4.11 2.46.6.86 <0.001!Sex partner engaged in risky behavior 71/961 7.4 48/71 67.6 23/71 32.4 12.26 10.92 5.38, 22.17 <0.001!Had sex with someone knew/thought to
be living with HIV45/961 4.7 27/45 60.0 18/45 40.0 8.81 8.16 3.70, 17.98 <0.001
!Condom broke or slipped 67/961 7.0 47/66 71.2 19/66 28.8 14.53 12.70 6.09, 26.51 <0.001!Someone suggested I get tested 199/961 20.7 116/197 58.9 81/197 41.1 8.41 9.32 5.33, 16.28 <0.001!Part of my regular testing pattern 165/961 17.2 24/165 14.6 141/165 85.5 Ref Ref!Other 12/840 1.3 5/12 41.7 7/12 58.3 4.20 1.28 0.24, 6.96 0.776
208
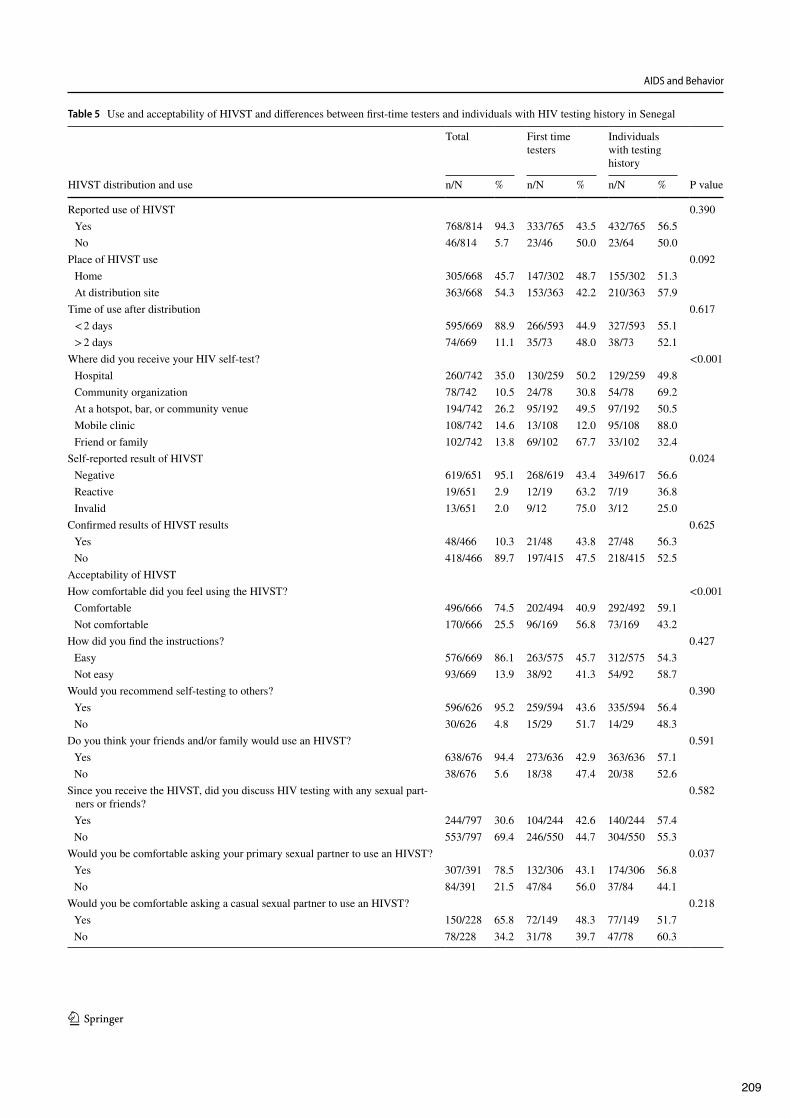
AIDS and Behavior
1 3
Table 5 Use and acceptability of HIVST and di#erences between first-time testers and individuals with HIV testing history in Senegal
Total First time testers
Individuals with testing history
HIVST distribution and use n/N % n/N % n/N % P value
Reported use of HIVST 0.390!Yes 768/814 94.3 333/765 43.5 432/765 56.5!No 46/814 5.7 23/46 50.0 23/64 50.0
Place of HIVST use 0.092!Home 305/668 45.7 147/302 48.7 155/302 51.3!At distribution site 363/668 54.3 153/363 42.2 210/363 57.9
Time of use after distribution 0.617!< 2!days 595/669 88.9 266/593 44.9 327/593 55.1!> 2!days 74/669 11.1 35/73 48.0 38/73 52.1
Where did you receive your HIV self-test? <0.001!Hospital 260/742 35.0 130/259 50.2 129/259 49.8!Community organization 78/742 10.5 24/78 30.8 54/78 69.2!At a hotspot, bar, or community venue 194/742 26.2 95/192 49.5 97/192 50.5!Mobile clinic 108/742 14.6 13/108 12.0 95/108 88.0!Friend or family 102/742 13.8 69/102 67.7 33/102 32.4
Self-reported result of HIVST 0.024!Negative 619/651 95.1 268/619 43.4 349/617 56.6!Reactive 19/651 2.9 12/19 63.2 7/19 36.8!Invalid 13/651 2.0 9/12 75.0 3/12 25.0
Confirmed results of HIVST results 0.625!Yes 48/466 10.3 21/48 43.8 27/48 56.3!No 418/466 89.7 197/415 47.5 218/415 52.5
Acceptability of HIVSTHow comfortable did you feel using the HIVST? <0.001!Comfortable 496/666 74.5 202/494 40.9 292/492 59.1!Not comfortable 170/666 25.5 96/169 56.8 73/169 43.2
How did you find the instructions? 0.427!Easy 576/669 86.1 263/575 45.7 312/575 54.3!Not easy 93/669 13.9 38/92 41.3 54/92 58.7
Would you recommend self-testing to others? 0.390!Yes 596/626 95.2 259/594 43.6 335/594 56.4!No 30/626 4.8 15/29 51.7 14/29 48.3
Do you think your friends and/or family would use an HIVST? 0.591!Yes 638/676 94.4 273/636 42.9 363/636 57.1!No 38/676 5.6 18/38 47.4 20/38 52.6
Since you receive the HIVST, did you discuss HIV testing with any sexual part-ners or friends?
0.582
!Yes 244/797 30.6 104/244 42.6 140/244 57.4!No 553/797 69.4 246/550 44.7 304/550 55.3
Would you be comfortable asking your primary sexual partner to use an HIVST? 0.037!Yes 307/391 78.5 132/306 43.1 174/306 56.8!No 84/391 21.5 47/84 56.0 37/84 44.1
Would you be comfortable asking a casual sexual partner to use an HIVST? 0.218!Yes 150/228 65.8 72/149 48.3 77/149 51.7!No 78/228 34.2 31/78 39.7 47/78 60.3
209
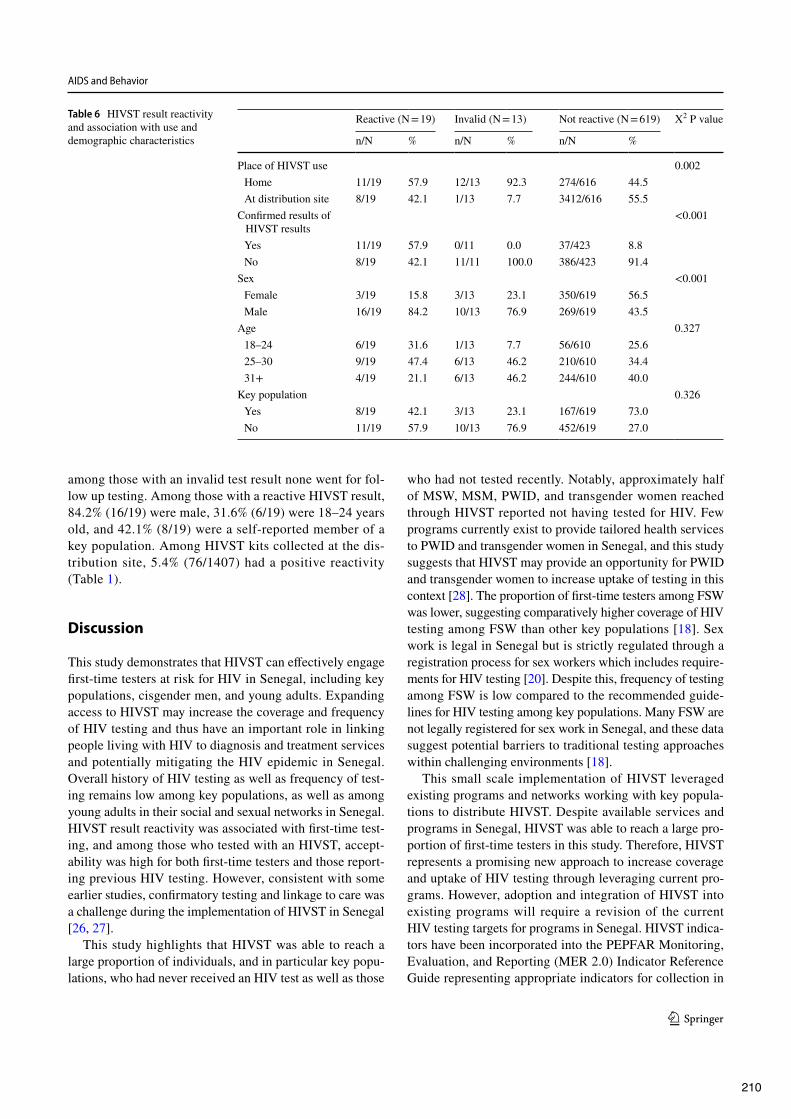
AIDS and Behavior
1 3
among those with an invalid test result none went for fol-low up testing. Among those with a reactive HIVST result, 84.2% (16/19) were male, 31.6% (6/19) were 18–24!years old, and 42.1% (8/19) were a self-reported member of a key population. Among HIVST kits collected at the dis-tribution site, 5.4% (76/1407) had a positive reactivity (Table!1).
Discussion
This study demonstrates that HIVST can e#ectively engage first-time testers at risk for HIV in Senegal, including key populations, cisgender men, and young adults. Expanding access to HIVST may increase the coverage and frequency of HIV testing and thus have an important role in linking people living with HIV to diagnosis and treatment services and potentially mitigating the HIV epidemic in Senegal. Overall history of HIV testing as well as frequency of test-ing remains low among key populations, as well as among young adults in their social and sexual networks in Senegal. HIVST result reactivity was associated with first-time test-ing, and among those who tested with an HIVST, accept-ability was high for both first-time testers and those report-ing previous HIV testing. However, consistent with some earlier studies, confirmatory testing and linkage to care was a challenge during the implementation of HIVST in Senegal [26, 27].
This study highlights that HIVST was able to reach a large proportion of individuals, and in particular key popu-lations, who had never received an HIV test as well as those
who had not tested recently. Notably, approximately half of MSW, MSM, PWID, and transgender women reached through HIVST reported not having tested for HIV. Few programs currently exist to provide tailored health services to PWID and transgender women in Senegal, and this study suggests that HIVST may provide an opportunity for PWID and transgender women to increase uptake of testing in this context [28]. The proportion of first-time testers among FSW was lower, suggesting comparatively higher coverage of HIV testing among FSW than other key populations [18]. Sex work is legal in Senegal but is strictly regulated through a registration process for sex workers which includes require-ments for HIV testing [20]. Despite this, frequency of testing among FSW is low compared to the recommended guide-lines for HIV testing among key populations. Many FSW are not legally registered for sex work in Senegal, and these data suggest potential barriers to traditional testing approaches within challenging environments [18].
This small scale implementation of HIVST leveraged existing programs and networks working with key popula-tions to distribute HIVST. Despite available services and programs in Senegal, HIVST was able to reach a large pro-portion of first-time testers in this study. Therefore, HIVST represents a promising new approach to increase coverage and uptake of HIV testing through leveraging current pro-grams. However, adoption and integration of HIVST into existing programs will require a revision of the current HIV testing targets for programs in Senegal. HIVST indica-tors have been incorporated into the PEPFAR Monitoring, Evaluation, and Reporting (MER 2.0) Indicator Reference Guide representing appropriate indicators for collection in
Table 6 HIVST result reactivity and association with use and demographic characteristics
Reactive (N = 19) Invalid (N = 13) Not reactive (N = 619) X2 P valuen/N % n/N % n/N %
Place of HIVST use 0.002!Home 11/19 57.9 12/13 92.3 274/616 44.5!At distribution site 8/19 42.1 1/13 7.7 3412/616 55.5
Confirmed results of HIVST results
<0.001
!Yes 11/19 57.9 0/11 0.0 37/423 8.8!No 8/19 42.1 11/11 100.0 386/423 91.4
Sex <0.001!Female 3/19 15.8 3/13 23.1 350/619 56.5!Male 16/19 84.2 10/13 76.9 269/619 43.5
Age 0.327!18–24 6/19 31.6 1/13 7.7 56/610 25.6!25–30 9/19 47.4 6/13 46.2 210/610 34.4!31+ 4/19 21.1 6/13 46.2 244/610 40.0
Key population 0.326!Yes 8/19 42.1 3/13 23.1 167/619 73.0!No 11/19 57.9 10/13 76.9 452/619 27.0
210

AIDS and Behavior
1 3
HIV testing programs [29]. Notably, the HIV testing yield for programs may decrease if HIVST are included though there will be a lower cost per test o#ered [30].
First-time testers were associated with HIVST result reactivity in this study, with the majority of self-reported reactive results being among first-time testers. These findings suggest the potential e#ectiveness of HIVST in increasing HIV diagnosis among those living with HIV in Senegal and not accessing traditional testing services. Additionally, acceptability was overall high among indi-viduals who participated in the post-test survey, as shown in other settings [16, 31, 32]. However, one quarter of participants reported that they were not comfortable using the HIVST, which highlights the need to better understand how to improve comfort during testing. Use and accept-ability of HIVST was overall not significantly di#erent between first-time testers and those with a testing his-tory for most measures in this study. These results sug-gest potential for sustained uptake among both new and returning users. Contrarily, other studies have found that acceptability was influenced by prior HIV testing [33].
Although acceptability of HIVST has been high in other studies, consistent evidence on confirmatory testing and linkage to care similarly remain sub-optimal [26, 27]. In this study, confirmatory testing was low, with approxi-mately two-thirds of those with reactive results, and none with invalid results reporting confirmatory testing. A recent study in Zambia found that individuals who had not previously tested for HIV were negatively associated with intention to linkage to care after HIVST [33]. Therefore, there is a need to better understand implementation strat-egies for linkage to care, especially for first-time testers. Preferred methods for follow up have varied across stud-ies [33, 34]. Community-based confirmation testing was preferred to facility-based testing in Zambia and Malawi [35]. Some studies have shown success in linkage to care through active follow up, however another study found active support for linkage was less important to individu-als than other attributes of confirmation testing locations [35]. HIVST strategies in Senegal may require more active mechanisms for follow up and support to improve linkage to confirmatory testing and care. Notably, young adults in this study had a higher odds of being first-time testers, suggesting traditional testing services are not currently reaching this group in Senegal. HIV incidence among ado-lescents and young adults is high globally, however uptake of HIV services is low [36]. In particular, HIV incidence is generally highest among young MSM in countries with age-disaggregated incidence data [37–39]. The emergence of social media and technology to engage young adults and though social and sexual networks may provide an avenue for increasing uptake of HIV testing services for these populations [40]. Mobile phone apps have also been shown
to be acceptable among young MSM in other settings and have been used to assess risk and coordinate HIVST dis-tribution [41–43]. HIVST web-based delivery has been acceptable across settings, including sub-Saharan Africa, and may provide further opportunity to increase uptake and frequency of testing among young MSM [41–43]. Mobile technology may also be an opportunity to reach individuals in rural areas where program coverage and access to services is less, such as the region of Ziguinchor [44].
Several limitations should be considered in this study. Participation in the pre- and post-test questionnaires was voluntary and may not represent the full sample of indi-viduals who participated in HIVST distribution. The results may therefore be subject to bias. Participants who received HIVST through network distribution were not captured in data collection and are not represented in this analysis. Dis-closure of key population status as well as positive reactiv-ity from the HIVST were low in self-reported measures of this study. The distribution strategy prioritized members of key populations and worked closely with existing programs providing services to these populations. However, only one-third of the study sample self-reported key population status. Therefore, it may be that HIVST reached individuals who may not currently be at high risk of HIV, in which case there is a need to consider strategies to more e#ectively target key populations. Alternatively, key population status may have been underreported, in which case HIVST was able to reach individuals unwilling to disclose their key population-related behavior and less integrated into the key population net-works [45]. Additionally, there was a discrepancy between the proportion of reactive HIVST collected at the distribu-tion sites and those who self-reported reactive results dur-ing posttest questionnaire. Although these figures cannot be linked or compared directly, it may suggest either under-reporting of reactive test results, or possibly greater loss to follow up for posttest questionnaire among individuals with a reactive HIVST.
Conclusions
In Senegal, key populations bear a disproportionate burden of HIV, and report limited uptake of existing HIV testing services given pervasive stigma and criminalization. In these contexts, HIVST may represent a complementary approach to reach populations reporting barriers to engagement with existing and routine HIV testing services. These data suggest the potential impact that HIVST could have in complement-ing existing HIV testing services by reaching a diverse group of first-time HIV-testers as well as those who have not tested recently in Senegal. This small-scale implementation further
211

AIDS and Behavior
1 3
suggested the importance of leveraging existing structures and programs for distribution. Moreover, since HIVST has the potential to disrupt traditional testing approaches, sus-tained engagement with government and community stake-holders is needed to inform optimal implementation strate-gies of HIVST.
Acknowledgements We would like to thank the study participants for donating their time to contribute to this research. Thank you to the study sta#, partners, and government support for making this study possible. Thank you to Amrita Rao for support throughout study imple-mentation and manuscript development. Thank you to Maria Garcia Quesada and Pedro Saa!for supporting translation. Thank you to Johns Hopkins University Center for AIDS Research (P30AI094189). This study was made possible by the generous support of the American people through the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) with the U.S. Agency for International Development (USAID) under the Cooperative Agreement Project SOAR (Support-ing Operational AIDS Research), number AID-OAA-14-00060. The information provided does not necessarily reflect the views of USAID or the United States Government, and the contents of this manuscript are the sole responsibility of Project SOAR, the Population Council, and the authors.
Compliance with Ethical Standards
Conflict of interest The authors declares that they have no conflicts of interest.
Ethical Approval Ethical review and approval were provided by the National Research Ethics Committee in Senegal and the Johns Hopkins School of Public Health Institutional Review Board.
Informed Consent Informed consent was obtained from all individual participants included in the study.
Open Access This article is distributed under the terms of the Crea-tive Commons Attribution 4.0 International License (http://creat iveco mmons .org/licen ses/by/4.0/), which permits unrestricted use, distribu-tion, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
References
1. Cohen MS, Chen YQ, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, et!al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011;365(6):493–505.
2. Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, Sharma S, et!al. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373(9):795–807.
3. Anglemyer A, Rutherford GW, Easterbrook PJ, Horvath T, Vito-ria M, Jan M, et!al. Early initiation of antiretroviral therapy in HIV-infected adults and adolescents: a systematic review. AIDS. 2014;28(Suppl 2):S105–18.
4. Grant RM, Lama JR, Anderson PL, McMahan V, Liu AY, Vargas L, et!al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363(27):2587–99.
5. McCormack S, Dunn DT, Desai M, Dolling DI, Gafos M, Gil-son R, et!al. Pre-exposure prophylaxis to prevent the acquisition
of HIV-1 infection (PROUD): effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet. 2016;387(10013):53–60.
6. Organization WH. Consolidated guidelines on HIV prevention, diagnosis, treatment and care for key populations. Geneva: WHO; 2014.
7. Venter F, Majam M, Jankelowitz L, Adams S, Moorhouse M. South African HIV self-testing policy and guidance considera-tions. Southern Afr J HIV Med. 2017;18(1):775.
8. HIVST.org HIV self-testing policy hub 2018 [Available from: http://hivst .org/.
9. WHO. Guidelines on HIV Self Testing and Partner Notification World Health Organization; 2016.
10. Wirtz AL, Clouse E, Veronese V, Thu KH, Naing S, Baral SD, et!al. New HIV testing technologies in the context of a con-centrated epidemic and evolving HIV prevention: qualitative research on HIV self-testing among men who have sex with men and transgender women in Yangon, Myanmar. J Int AIDS Soc. 2017;20(1):21796.
11. Chanda MM, Ortblad KF. HIV self-testing among female sex workers in Zambia: a cluster randomized controlled trial. PLoS Med. 2017;14(11):e1002442.
12. Stevens DR, Vrana CJ, Dlin RE, Korte JE. A global review of HIV self-testing: themes and implications. BMJ Open. 2018;22(2):497–512.
13. Jamil MS, Prestage G, Fairley CK, Grulich AE, Smith KS, Chen M, et!al. E#ect of availability of HIV self-testing on HIV test-ing frequency in gay and bisexual men at high risk of infection (FORTH): a waiting-list randomised controlled trial. Lancet HIV. 2017;4(6):e241–50.
14. Masters SH, Agot K. Promoting partner testing and couples testing through secondary distribution of HIV self-tests: a ran-domized clinical trial. PLoS Med. 2016;13(11):e1002166.
15. Johnston LG, McFarland W, Sabin ML, Prybylski D, Sabin K, Baral S, et!al. Measuring self-reported HIV status in bio-behav-ioural surveys. Bull World Health Organ. 2015;93(5):287.
16. Lippman SA, Lane T, Rabede O, Gilmore H, Chen YH, Mlot-shwa N, et!al. High acceptability and increased HIV-testing frequency after introduction of HIV self-testing and network distribution among South African MSM. J Acquir Immune Defic Syndr. 1999;77(3):279–87.
17. UNAIDS. Senegal 2016 [Available from: http://www.unaid s.org/en/regio nscou ntrie s/count ries/seneg al.
18. Lyons CE, Ketende S, Diouf D, Drame FM, Liestman B, Coly K, et!al. Potential impact of integrated stigma mitigation inter-ventions in improving hiv/aids service delivery and uptake for key populations in Senegal. J Acquir Immune Defic Syndr. 1999;2017(74 Suppl 1):S52.
19. UNAIDS. Senegal 2015 [cited 2016. Available from: http://www.unaid s.org/en/regio nscou ntrie s/count ries/seneg al.
20. Foley EE. Regulating sex work: subjectivity and stigma in Sen-egal. Cult Health Sex. 2017;19(1):50–63.
21. Knox J, Sandfort T, Yi H, Reddy V, Maimane S. Social vulner-ability and HIV testing among South African men who have sex with men. Int J STD AIDS. 2011;22(12):709–13.
22. Hu Y, Lu H, Raymond HF, Sun Y, Sun J, Jia Y, et!al. Measures of condom and safer sex social norms and stigma towards HIV/AIDS among Beijing MSM. AIDS Behav. 2014;18(6):1068–74.
23. UNAIDS. 90–90–90 - An ambitious treatment target to help end the AIDS epidemic. 2017.
24. UNAIDS. Senegal. 2017. 25. Lewis CC, Mettert KD, Dorsey CN, Martinez RG, Weiner BJ,
Nolen E, et!al. An updated protocol for a systematic review of implementation-related measures. Syst Rev. 2018;7(1):66.
26. Choko AT, MacPherson P, Webb EL, Willey BA, Feasy H, Sambakunsi R, et!al. Uptake, accuracy, safety, and linkage into
212

AIDS and Behavior
1 3
care over two years of promoting annual self-testing for HIV in Blantyre, Malawi: a community-based prospective study. PLoS Med. 2015;12(9):e1001873.
27. Choko AT, Desmond N, Webb EL, Chavula K, Napierala-Mavedzenge S, Gaydos CA, et!al. The uptake and accuracy of oral kits for HIV self-testing in high HIV prevalence setting: a cross-sectional feasibility study in Blantyre, Malawi. PLoS Med. 2011;8(10):e1001102.
28. MacDonell K, Naar-King S, Huszti H, Belzer M. Barriers to medication adherence in behaviorally and perinatally infected youth living with HIV. AIDS Behav. 2013;17(1):86–93.
29. PEPFAR Monitoring, Evaluation, and Reporting (MER 2.0) Indicator Reference Guide. 2017.
30. Cambiano V, Ford D, Mabugu T, Napierala Mavedzenge S, Min-ers A, Mugurungi O, et!al. Assessment of the potential impact and cost-e#ectiveness of self-testing for hiv in low-income countries. J Infect Dis. 2015;212(4):570–7.
31. Harichund C, Moshabela M. Acceptability of HIV self-testing in sub-saharan Africa: scoping study. AIDS Behav. 2018;22(2):560–8.
32. Thirumurthy H. Acceptability and feasibility of a novel approach to promote HIV testing in sexual and social networks using HIV self-tests. 8th IAS Conferenve on HIV Pathogensis, Treatment, & Prevention 19-22 July, 2015; Vancouver2015.
33. Chipungu J. Understanding linkage to care with HIV self-test approach in Lusaka, Zambia - A mixed method approach. PLoS Med. 2017;12(11):e0187998.
34. Green K. VNB, Phan Thi Thu H.,Tran Hung M, Vo Hai S., Ngo Van H., Doan H.A., Dang Hong L. How acceptable and feasible is HIV self-testing among key populations in Vietnam? Preliminary results from an intervention evaluation study. 9th IAS Conference on HIV Science (IAS 2017); Paris, France2017.
35. d’Elbee M, Indravudh PP, Mwenge L, Kumwenda MM, Simwinga M, Choko AT, et!al. Preferences for linkage to HIV care services following a reactive self-test: discrete choice experiments in Malawi and Zambia. AIDS. 2018;32(14):2043–9.
36. Kim SH, Gerver SM, Fidler S, Ward H. Adherence to antiretrovi-ral therapy in adolescents living with HIV: systematic review and meta-analysis. AIDS. 2014;28(13):1945–56.
37. Baral SD, Grosso A, Holland C, Papworth E. The epidemiology of HIV among men who have sex with men in countries with gener-alized HIV epidemics. Curr Opin HIV AIDS. 2014;9(2):156–67.
38. Garofalo R, Hotton AL, Kuhns LM, Gratzer B, Mustanski B. Inci-dence of HIV infection and sexually transmitted infections and related risk factors among very young men who have sex with men. J Acquir Immune Defic Syndr. 1999;72(1):79–86.
39. Bedoya CA, Mimiaga MJ, Beauchamp G, Donnell D, Mayer KH, Safren SA. Predictors of HIV transmission risk behavior and sero-conversion among Latino men who have sex with men in Project EXPLORE. AIDS Behav. 2012;16(3):608–17.
40. Perrin A. Social Networking Usage. Pew Research Center. 2015. 41. Sullivan PS, Driggers R. Usability and acceptability of a mobile
comprehensive hiv prevention app for men who have sex with men: a pilot study. JMIR mHealth uHealth. 2017;5(3):e26.
42. De Boni R.B. VVG, Fernandes N., Lessa F.,Girad R., Cruz M., Oliveira J., Lentine N., Miranda R., Bingham T, Barbosa A., Grinsztejn B. Online HIV self-testing: a tool to expand first HIV testing for young high-risk MSM in Brazil. 9th IAS Conference on HIV Science (IAS 2017); Paris, France2017.
43. Smith P. MR, Atujuna M., Madubela N., Bekker L.-G.. “I can do this myself”: investigating the acceptability of a web-based, HIV self-testing service in South Africa. 9th IAS Conference on HIV Science (IAS 2017); Paris, France2017.
44. Sullivan PS, Grey JA, Simon Rosser BR. Emerging technologies for HIV prevention for MSM: what we have learned, and ways forward. J Acquir Immune Defic Syndr. 1999;2013(63 Suppl 1):S102–7.
45. Rao A, Stahlman S. Sampling Key Populations for HIV Sur-veillance: Results From Eight Cross-Sectional Studies Using Respondent-Driven Sampling and Venue-Based Snowball Sam-pling. JMIR Public Health Surveill. 2017;3(4):e72.
Publisher’s Note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional a"liations.
213

Shedding light on a HIV blind spot: Factors associated with men’sHIV testing in !ve African countriesPaul J. Fleming a, Joseph G. Rosenb, Vincent J. Wongb and Maria Augusta Carrascob
aDepartment of Health Behavior and Health Education, University of Michigan School of Public Health, Ann Arbor,MI, USA; bO!ce of HIV/AIDS, United States Agency for International Development, Washington, DC, USA
ABSTRACTMen’s relatively low rates of HIV testing has been termed the ‘HIV blindspot’ and recently declared by UNAIDS as a top priority. This study usesdata from !ve nationally representative Demographic and HealthSurveys in Kenya, Malawi, Mozambique, Zambia, and Zimbabwe toexplore factors associated with men’s lifetime HIV testing. Between29.3% and 34.9% of men ages 15–49 in these countries had nevertested for HIV and men who held accepting attitudes towards gender-based violence, who lacked HIV knowledge, and who held stigmatisingviews of HIV were more likely to report never testing for HIV. Findingsare interpreted, including a discussion of the possible unintendedconsequences of current 90-90-90 targets on men’s relatively low testingrates. The results point to possible intervention opportunities to increaseHIV testing among men in high-HIV prevalence settings in Eastern andSouthern Africa and emphasise the importance of changing men’sperceptions related to stigma and gender norms.
ARTICLE HISTORYReceived 2 October 2018Accepted 2 February 2019
KEYWORDSHIV testing; men; Africa;violence; HIV knowledge
Introduction
HIV testing is a critical entry-point into HIV care and treatment, which reduce mortality and stemongoing HIV transmission (Cohen et al., 2011). Men living with HIV in Southern and Eastern Africa– the regions of the world with the highest HIV prevalence – are much less likely to receive HIV careand/or treatment and achieve viral suppression when compared with women, partially due to genderdisparities in HIV testing (Auld et al., 2015; Bor et al., 2015; Cornell et al., 2012; Muula et al., 2007).African men are less likely to test for HIV than women and more likely to be living with HIV butundiagnosed (Dovel, Yeatman, Watkins, & Poulin, 2015; Kigozi et al., 2009; Novitsky et al., 2015;Schell et al., 2016). Compared to women in sub-Saharan Africa, men living with HIV are 20%less likely to know their HIV status and 27% less likely to be accessing HIV care or treatment(UNAIDS, 2017).
This low HIV testing contributes to overall AIDS-related mortality on the continent. AIDS-related mortality in Africa is higher for men than for women, despite women having higher overallHIV prevalence (Barnighausen, Herbst, Tanser, Newell, & Bor, 2014; Dovel et al., 2015; Mills, Beyrer,Birungi, & Dybul, 2012). One recent estimate of HIV/AIDS-related deaths in South Africa documen-ted 2.5 million deaths among men from 2004 to 2015, compared with 1.2 million for women (Millset al., 2012). Additionally, South African men are less likely to get tested for HIV than women: 32%of men living with HIV are undiagnosed compared to 19% of women (Johnson, Rehle, Jooste, & Bek-ker, 2015). These suboptimal HIV testing and treatment-related outcomes have been termed the
© 2019 Informa UK Limited, trading as Taylor & Francis Group
CONTACT Paul J. Fleming [email protected] @FlemingPaulJ
GLOBAL PUBLIC HEALTH2019, VOL. 14, NO. 9, 1241–1251https://doi.org/10.1080/17441692.2019.1583266
214
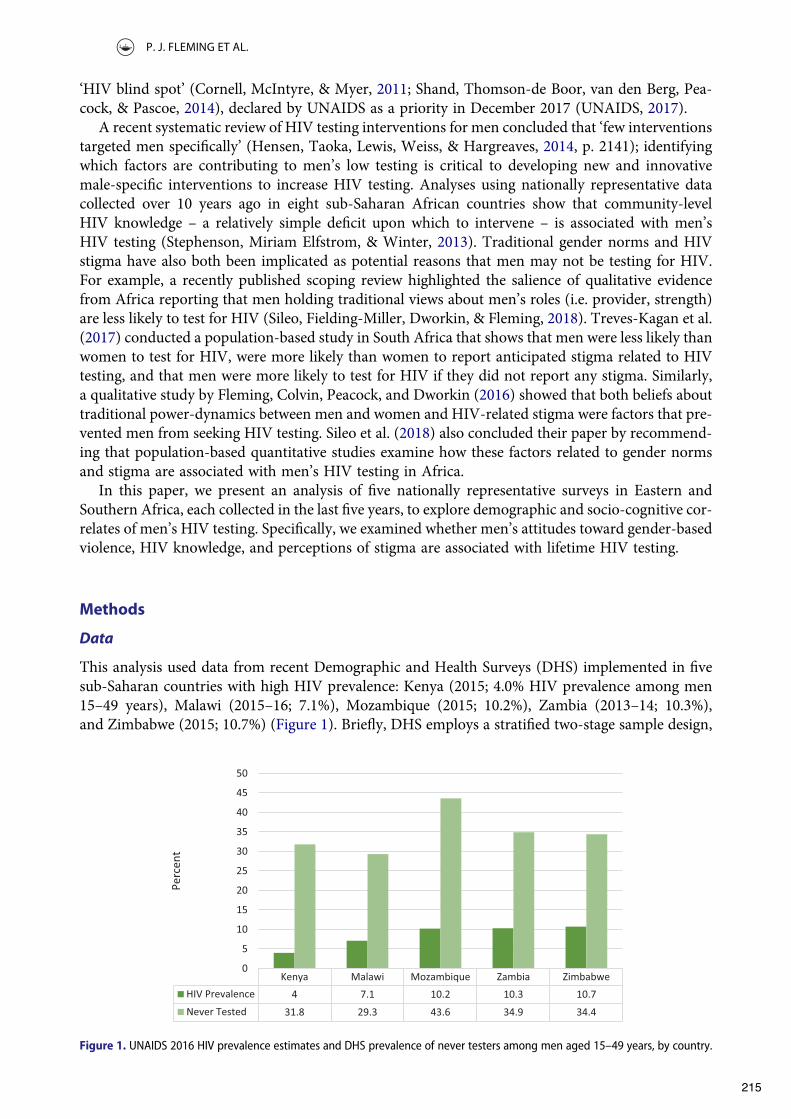
‘HIV blind spot’ (Cornell, McIntyre, & Myer, 2011; Shand, Thomson-de Boor, van den Berg, Pea-cock, & Pascoe, 2014), declared by UNAIDS as a priority in December 2017 (UNAIDS, 2017).
A recent systematic review of HIV testing interventions for men concluded that ‘few interventionstargeted men speci!cally’ (Hensen, Taoka, Lewis, Weiss, & Hargreaves, 2014, p. 2141); identifyingwhich factors are contributing to men’s low testing is critical to developing new and innovativemale-speci!c interventions to increase HIV testing. Analyses using nationally representative datacollected over 10 years ago in eight sub-Saharan African countries show that community-levelHIV knowledge – a relatively simple de!cit upon which to intervene – is associated with men’sHIV testing (Stephenson, Miriam Elfstrom, & Winter, 2013). Traditional gender norms and HIVstigma have also both been implicated as potential reasons that men may not be testing for HIV.For example, a recently published scoping review highlighted the salience of qualitative evidencefrom Africa reporting that men holding traditional views about men’s roles (i.e. provider, strength)are less likely to test for HIV (Sileo, Fielding-Miller, Dworkin, & Fleming, 2018). Treves-Kagan et al.(2017) conducted a population-based study in South Africa that shows that men were less likely thanwomen to test for HIV, were more likely than women to report anticipated stigma related to HIVtesting, and that men were more likely to test for HIV if they did not report any stigma. Similarly,a qualitative study by Fleming, Colvin, Peacock, and Dworkin (2016) showed that both beliefs abouttraditional power-dynamics between men and women and HIV-related stigma were factors that pre-vented men from seeking HIV testing. Sileo et al. (2018) also concluded their paper by recommend-ing that population-based quantitative studies examine how these factors related to gender normsand stigma are associated with men’s HIV testing in Africa.
In this paper, we present an analysis of !ve nationally representative surveys in Eastern andSouthern Africa, each collected in the last !ve years, to explore demographic and socio-cognitive cor-relates of men’s HIV testing. Speci!cally, we examined whether men’s attitudes toward gender-basedviolence, HIV knowledge, and perceptions of stigma are associated with lifetime HIV testing.
Methods
Data
This analysis used data from recent Demographic and Health Surveys (DHS) implemented in !vesub-Saharan countries with high HIV prevalence: Kenya (2015; 4.0% HIV prevalence among men15–49 years), Malawi (2015–16; 7.1%), Mozambique (2015; 10.2%), Zambia (2013–14; 10.3%),and Zimbabwe (2015; 10.7%) (Figure 1). Brie"y, DHS employs a strati!ed two-stage sample design,
Kenya Malawi Mozambique Zambia Zimbabwe
HIV Prevalence 4 7.1 10.2 10.3 10.7
Never Tested 31.8 29.3 43.6 34.9 34.4
0
5
10
15
20
25
30
35
40
45
50
Perc
ent
Figure 1. UNAIDS 2016 HIV prevalence estimates and DHS prevalence of never testers among men aged 15–49 years, by country.
P. J. FLEMING ET AL.
215

with a representative sample of male and female participants drawn from census-based enumerationareas and subsequently from households. Eligible male participants were between 15–59 years-oldand lived in every other household approached by surveyors. This analysis drew from 48,541male survey records across countries with a response on the HIV testing question (Kenya: n =12,793; Malawi: n = 7,472; Mozambique: n = 5,232; Zambia: n = 14,657; Zimbabwe: n = 8,387).
Measures
Outcome variableThe primary dependent variable of interest was never receiving an HIV test. This was measured byasking respondents if they had ever been tested for HIV. Respondents who did not provide an answerto the question were excluded from analysis.
Socio-cognitive variablesThe three socio-cognitive variables assessed were correct HIV prevention knowledge (HIV knowl-edge), accepting attitudes towards gender-based violence (GBV acceptance), and prejudice towardsPLHIV (stigma). An HIV knowledge index was constructed from three survey items assessing basicknowledge of HIV prevention (i.e. had heard about HIV, knew that to reduce risk of contracting HIVa person must always use condoms during sex, and that to reduce risk of contracting HIV a personmust have sex with only one sex partner who does not have other sex partners) and then dichoto-mised to demonstrate full knowledge or someone who lacks some knowledge. A GBV acceptanceindex was similarly developed from a battery of survey items and measured as a binary variable.Respondents reporting accepting attitudes towards hitting or beating spouses in at least one of!ve scenarios (i.e. wife goes out without telling the husband, wife neglects the children, wife argueswith husband, wife refuses to have sex with husband, wife burns food) were classi!ed as GBV accep-tors. This is how the scale is commonly treated in research by GBV experts (Heise & Kotsadam,2015). Lastly, respondents agreeing with or expressing ambiguity (i.e. responded ‘don’t know’)towards at least one of two survey items addressing HIV prejudice (i.e. they would not buy vegetablesfrom a vendor with HIV, and they would not be willing to care for a relative with AIDS) were con-sidered as prejudiced. For Malawi and Zimbabwe datasets, a proxy stigma item (i.e. respondentswould be ashamed if someone in their family had HIV/AIDS) was used in substitute of the willing-ness to provide care index item, as this question was not posed to respondents in either of thosenational surveys.
Socio-demographic variableSocio-demographic indicators included age quintiles (15–24, 25–34, 35–44, 45–54, 55–59), residence(urban or rural), educational attainment (none/primary, secondary or higher), religion (Catholic/Christian, Other, or none), and marital status (never in union, married/living with partners, orwidowed/divorced/separated).
Data management and analysisDescriptive statistics were generated for all covariates, which were inspected for completeness priorto regression analysis. Bivariate analysis was conducted to identify associations between never testedfor HIV and socio-demographic characteristics and HIV socio-cognitive variables. Multivariatelogistic regressions models were developed to identify associations between never tested for HIVand socio-cognitive variables, controlling for socio-demographic variables. Sample weights wereapplied prior to statistical analysis. Covariate selection during model-building was informed by exist-ing literature describing factors associated HIV testing.(Auld et al., 2015; Bor et al., 2015; Cornellet al., 2012; Muula et al., 2007; Sileo et al., 2018; Stephenson et al., 2013) Data were managed andanalysed in Stata 13 (College Station, Texas, USA).
GLOBAL PUBLIC HEALTH
216

Results
Descriptive statistics for each of the !ve samples are presented in Table 1. Mozambique had the high-est proportion of men reporting never testing for HIV (56.4%), while Malawi had the lowest percen-tage of men who had never tested (29.3%).
For the socio-cognitive variables of interest, there was a range across the study settings. GBVacceptance was relatively low in Malawi and Mozambique (12.3% and 15.1%, respectively) comparedto Kenya (38.4%), Zambia (32.1%), and Zimbabwe (31.4%). Men with comprehensive HIV preven-tion knowledge accounted for over 80% of respondents in Kenya, Zambia, and Zimbabwe but only69.4% in Malawi and 59.8% in Mozambique. Finally, the percentage of men in each country sampleharbouring stigmatising attitudes towards people living with HIV ranged from 18.3% in Zambia to28.3% in Zimbabwe.
For socio-demographic characteristics, men in Zambia and Zimbabwe had the highest levels ofeducational attainment among surveyed countries. The majority of men in each country reportedChristianity as their religion, but a substantial number of men in Kenya, Malawi, and Mozambiqueself-identi!ed as belonging to another unspeci!ed religion (most commonly Islam). In Zimbabwe,17.6% of men reported having no religion, but the percentage of men reporting no religion in theothers countries was less than 5%.
For our bivariate results (Table 2), we found that GBV acceptance, HIV knowledge, and HIVstigma were signi!cantly associated (p < 0.001) with never testing for HIV in each country. Menwho believed GBV was acceptable in at least one instance had between 1.22 (Kenya) and 2.17(Malawi) times the odds of never testing for HIV compared to men who did not !nd GBV acceptablein any situation. Men who answered all HIV knowledge questions correctly were signi!cantly less
Table 1. Weighted descriptive statistics for adult men sampled across Demographic and Health Surveys (DHS) in Kenya, Malawi,Mozambique, Zambia, and Zimbabwe.
Kenya Malawi Mozambique Zambia Zimbabwe
Observations 12,819 7,478 5,283 14,773 8,396
Dependent Variable n % n % n % n % n %
Never tested 4,070 31.75 2,192 29.31 2,997 56.35 5,148 34.85 2,899 34.41Socio-cognitive variablesViolence† 4,920 38.38 917 12.26 800 15.14 4,745 32.12 2,637 31.41HIV knowledge†† 10,472 81.69 5,193 69.44 3,158 59.78 12,218 82.70 7,136 84.99HIV stigma ††† 2,636 20.56 1,912 25.57 1,200 22.71 2,698 18.26 2,379 28.33Socio-demographic variablesResidenceUrban 4,915 38.34 1,661 22.21 2,696 51.03 6,828 46.22 3,456 41.16Rural 7,904 61.66 5,817 77.79 2,587 48.97 7,945 53.78 4,940 58.84AgeAge 15–24 4,792 37.38 3,226 43.14 2,117 40.07 5,650 38.25 3,441 40.98Age 25–34 3,643 28.42 1,975 26.41 1,347 25.50 3,828 25.91 2,270 27.04Age 35–44 2,684 20.94 1,485 19.86 893 16.90 3,058 20.70 1,729 20.59Age 45–54 1,700 13.26 792 10.59 679 12.85 1,714 11.60 956 11.39Age 55–59 247 4.68 523 3.54
Educational attainment†No education-Primary 7,316 57.07 4,651 62.20 3,159 59.80 6,535 44.27 1,912 22.77Secondary-Higher 5,503 42.93 2,827 37.80 2,124 40.20 8,228 55.73 6,484 77.23ReligionChristian 10,712 83.56 6,560 87.72 3,178 60.16 14,451 97.82 6,634 79.01Other religion 1,621 12.65 737 9.86 2,045 38.71 109 0.74 283 3.37No religion 482 3.76 181 2.42 56 1.06 156 1.06 1,479 17.62Marital StatusNever in union 5,400 42.12 2,932 39.21 1,806 34.19 5,924 40.10 3,619 43.10Married/living with partner 6,693 52.21 4,284 57.29 3,146 59.55 8,225 55.68 4,337 51.66Widowed/divorced/separated 726 5.66 262 3.50 331 6.27 624 4.22 440 5.24
† Men who said that beating a women is acceptable in at least 1 of 5 situations; †† Men who answered all 3 HIV prevention knowl-edge questions correctly; ††† Men who responded ‘yes’ or ‘don’t know’ to two stigma questions.
P. J. FLEMING ET AL.
217
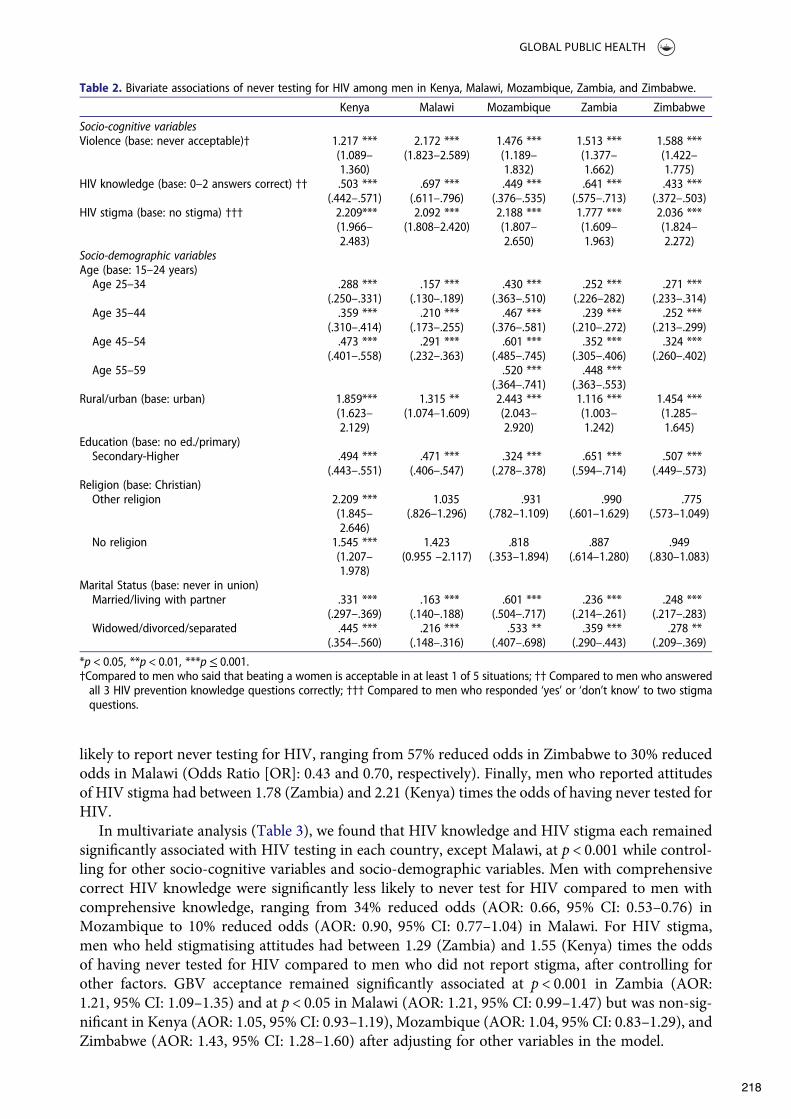
likely to report never testing for HIV, ranging from 57% reduced odds in Zimbabwe to 30% reducedodds in Malawi (Odds Ratio [OR]: 0.43 and 0.70, respectively). Finally, men who reported attitudesof HIV stigma had between 1.78 (Zambia) and 2.21 (Kenya) times the odds of having never tested forHIV.
In multivariate analysis (Table 3), we found that HIV knowledge and HIV stigma each remainedsigni!cantly associated with HIV testing in each country, except Malawi, at p < 0.001 while control-ling for other socio-cognitive variables and socio-demographic variables. Men with comprehensivecorrect HIV knowledge were signi!cantly less likely to never test for HIV compared to men withcomprehensive knowledge, ranging from 34% reduced odds (AOR: 0.66, 95% CI: 0.53–0.76) inMozambique to 10% reduced odds (AOR: 0.90, 95% CI: 0.77–1.04) in Malawi. For HIV stigma,men who held stigmatising attitudes had between 1.29 (Zambia) and 1.55 (Kenya) times the oddsof having never tested for HIV compared to men who did not report stigma, after controlling forother factors. GBV acceptance remained signi!cantly associated at p < 0.001 in Zambia (AOR:1.21, 95% CI: 1.09–1.35) and at p < 0.05 in Malawi (AOR: 1.21, 95% CI: 0.99–1.47) but was non-sig-ni!cant in Kenya (AOR: 1.05, 95% CI: 0.93–1.19), Mozambique (AOR: 1.04, 95% CI: 0.83–1.29), andZimbabwe (AOR: 1.43, 95% CI: 1.28–1.60) after adjusting for other variables in the model.
Table 2. Bivariate associations of never testing for HIV among men in Kenya, Malawi, Mozambique, Zambia, and Zimbabwe.
Kenya Malawi Mozambique Zambia Zimbabwe
Socio-cognitive variablesViolence (base: never acceptable)† 1.217 ***
(1.089–1.360)
2.172 ***(1.823–2.589)
1.476 ***(1.189–1.832)
1.513 ***(1.377–1.662)
1.588 ***(1.422–1.775)
HIV knowledge (base: 0–2 answers correct) †† .503 ***(.442–.571)
.697 ***(.611–.796)
.449 ***(.376–.535)
.641 ***(.575–.713)
.433 ***(.372–.503)
HIV stigma (base: no stigma) ††† 2.209***(1.966–2.483)
2.092 ***(1.808–2.420)
2.188 ***(1.807–2.650)
1.777 ***(1.609–1.963)
2.036 ***(1.824–2.272)
Socio-demographic variablesAge (base: 15–24 years)Age 25–34 .288 ***
(.250–.331).157 ***
(.130–.189).430 ***
(.363–.510).252 ***
(.226–282).271 ***
(.233–.314)Age 35–44 .359 ***
(.310–.414).210 ***
(.173–.255).467 ***
(.376–.581).239 ***
(.210–.272).252 ***
(.213–.299)Age 45–54 .473 ***
(.401–.558).291 ***
(.232–.363).601 ***
(.485–.745).352 ***
(.305–.406).324 ***
(.260–.402)Age 55–59 .520 ***
(.364–.741).448 ***
(.363–.553)Rural/urban (base: urban) 1.859***
(1.623–2.129)
1.315 **(1.074–1.609)
2.443 ***(2.043–2.920)
1.116 ***(1.003–1.242)
1.454 ***(1.285–1.645)
Education (base: no ed./primary)Secondary-Higher .494 ***
(.443–.551).471 ***
(.406–.547).324 ***
(.278–.378).651 ***
(.594–.714).507 ***
(.449–.573)Religion (base: Christian)Other religion 2.209 ***
(1.845–2.646)
1.035(.826–1.296)
.931(.782–1.109)
.990(.601–1.629)
.775(.573–1.049)
No religion 1.545 ***(1.207–1.978)
1.423(0.955 –2.117)
.818(.353–1.894)
.887(.614–1.280)
.949(.830–1.083)
Marital Status (base: never in union)Married/living with partner .331 ***
(.297–.369).163 ***
(.140–.188).601 ***
(.504–.717).236 ***
(.214–.261).248 ***
(.217–.283)Widowed/divorced/separated .445 ***
(.354–.560).216 ***
(.148–.316).533 **
(.407–.698).359 ***
(.290–.443).278 **
(.209–.369)
*p < 0.05, **p < 0.01, ***p! 0.001.†Compared to men who said that beating a women is acceptable in at least 1 of 5 situations; †† Compared to men who answeredall 3 HIV prevention knowledge questions correctly; ††† Compared to men who responded ‘yes’ or ‘don’t know’ to two stigmaquestions.
GLOBAL PUBLIC HEALTH
218

Discussion
We examined data from !ve sub-Saharan African countries to assess men’s HIV testing and its cor-relates. We found that between 29.3% and 34.9% of men had never tested for HIV and that men whoheld accepting attitudes towards GBV, who lacked HIV knowledge, and who held stigmatising viewsof HIV were more likely to report never testing for HIV. In this section, we !rst contextualise speci!c!ndings and then highlight the potential unintended consequences of the 90-90-90 goals for men’sHIV testing in Africa.
Men who lacked basic HIV knowledge were less likely to have tested for HIV. Other studies havelinked HIV knowledge to men’s HIV testing (Carrasco, Fleming, Wagman, & Wong, 2018; Mall,Middelkoop, Mark, Wood, & Bekker, 2013; Stephenson et al., 2013). In terms of intervention oppor-tunities, increasing men’s HIV knowledge may be achieved relatively simply by disseminating HIVinformation through community HIV prevention programmes and HIV testing demand creationactivities that speci!cally engage men.
Our !ndings related to men’s attitudes towards GBV echo prior qualitative !ndings that linkmen’s attitudes related to gender norms to HIV testing (DiCarlo et al., 2014; Sileo et al., 2018;Siu, Seeley, & Wight, 2013; Siu, Wight, & Seeley, 2014; Skovdal et al., 2011). Men’s attitudes thatare accepting of GBV may indicate that the man subscribes to traditional notions of masculinitywhere the man should be dominant. The recent systematic review of masculine norms and HIV test-ing shows that these types of attitudes can inhibit men from testing for HIV because, for example,
Table 3. Multivariable logistic regression model of never testing for HIV among men in Kenya, Malawi, Mozambique, Zambia, andZimbabwe, adjusting for socio-demographic characteristics and other highlighted socio-cognitive variables.
Kenya Malawi Mozambique Zambia Zimbabwe
Observations 12,654 7,330 4,942 14,470 8,241Socio-cognitive variablesViolence (base: never acceptable)† 1.054
(0.930–1.194)1.206 *
(0.992–1.466)1.036
(0.832–1.291)1.212 ***
(1.089–1.350)1.080
(0.952– 1.225)HIV knowledge (base: 0–2 answers correct) †† 0.739 ***
(0.644–0.849)0.895
(0.770–1.039)0.663 ***
(0.528–0.760)0.774 ***
(0.681–0.880)0.667 ***
(0.568–0.784)HIV stigma (base: no stigma) ††† 1.552 ***
(1.353–1.780)1.352 ***
(1.150–1.589)1.545 ***
(1.269–1.881)1.291 ***
(1.164–1.433)1.443 ***
(1.270–1.639)Socio-demographic variablesAge (base: 15–24)25–34 0.531***
(0.451–0.624)0.454***
(0.367–0.561)0.472***
(0.359–0.621)0.587***
(0.504–0.682)0.587***
(0.485–0.710)35–44 0.807***
(0.667–0.976)0.732***
(0.561–0.954)0.409***
(0.300–0.558)0.695***
(0.584–0.827)0.699***
(0.553–0.884)45–54 1.06
(0.846–1.327)0.902
(0.680–1.196)0.530***
(0.395–0.711)1.061
(0.871–1.294)0.895
(0.690–1.160)55–59 0.435***
(0.279–0.678)1.335**
(1.023–1.742)Residence – urban (base: rural) 1.460***
(1.268–1.682)0.988
(0.768–1.272)1.916***
(1.563–2.350)0.994
(0.875–1.129)1.11
(0.964–1.280)Education – secondary or higher (base: no ed/primary) 0.526***
(0.465–0.595)0.412***
(0.345–0.492)0.332***
(0.274–0.402)0.512***
(0.45–0.575)0.545***
(0.473–0.627)Religion (base: Catholic/Christian)Other religion 1.892***
(1.550–2.310)0.928
(0.731–1.179)1.045
(0.866–1.260)1.525
(0.802–2.899)1.041
(0.771–1.405)No religion 1.205
(0.924–1.572)1.315
(0.904–1.911)1.069
(0.459–2.487)1.059
(0.713–1.572)0.974
(0.835–1.135)Marital status (base: never in union)Married/living with partner 0.367***
(0.314–0.429)0.209***
(0.167–0.262)0.558***
(0.437–0.711)0.253***
(0.217–0.296)0.344***
(0.288–0.411)Widowed/divorced/separated 0.434***
(0.332–0.569)0.266***
(0.175–0.406)0.607***
(0.427–0.865)0.395***
(0.305–0.512)0.362***
(0.264–0.496)
*p < 0.05, **p < 0.01, ***p < 0.001; †Compared to men who said that beating a women is acceptable in at least 1 of 5 situations;††Compared to men who answered all 3 HIV prevention knowledge questions correctly; †††Compared to men who responded‘yes’ or ‘don’t know’ to two stigma questions.
P. J. FLEMING ET AL.
219

men feared that HIV would compromise their ability to work and be a provider (DiCarlo et al., 2014;Sileo et al., 2018; Wyrod, 2011). Men with traditional gender attitudes also perceive clinics as spacesfor women and, thus, may not feel comfortable going for HIV testing. These !ndings point to the factthat certain types of traditional masculinities can facilitate GBV and discourage HIV testing. Toincrease HIV testing uptake among men, it is critical to address the underlying gender normsthat drive men’s HIV testing behaviours.
For HIV stigma, some research suggests that HIV stigma and traditional gender attitudes mayinteract to prevent HIV testing. While stigma also a#ects women, some research shows that menavoid testing because men are stereotyped as having risky sexual behaviours and they are concernedthey will be blamed for spreading HIV in their community (Siu et al., 2013; Siu et al., 2014; Skovdalet al., 2011). This suggests that men may experience or perceive HIV stigma di#erently than womenand thus an intervention may need to address it di#erently. Additionally, while our study was unableto explore this dimension, men are not homogenous and men with di#erent identities or character-istics (i.e. age, sexual orientation, ethnicity) are likely to experience this intersection of stigma andmasculine norms di#erently.
These !ndings point to possible intervention opportunities to increase HIV testing among men inhigh-HIV prevalence settings in Eastern and Southern Africa. A recent systematic review of strat-egies to increase men’s HIV testing in Africa showed that few interventions targeted men speci!cally(Hensen et al., 2014). Most intervention strategies to improve HIV testing target entire communities,but evidence shows that many of these intervention strategies are less e#ective with men than theyare with women because they are not addressing male-speci!c barriers to testing. From 2010 to 2011,South Africa conducted a national multi-sectoral testing campaign; while HIV testing increasedoverall between 2010 and 2012, nationally representative data from 2012 indicated that, comparedto men, women were twice as likely as men to test for the !rst time because of the campaign(Maughan-Brown, Lloyd, Bor, & Venkataramani, 2016).
Given our !ndings related to attitudes towards GBV and stigma, interventions that speci!callyaddress underlying gender norms and the ways in which stigma manifests for men may be particularlyfruitful. One study showed that a gender-transformative intervention using principles of critical con-sciousness with South African men to challenge traditional gender norms was e#ective at increasingmen’s HIV testing (Dworkin, Fleming, & Colvin, 2015; Fleming, Colvin et al. 2016). Speci!cally, theintervention changed men’s views about gender equity and reduced HIV stigma since they no longerperceived HIV as a threat to their masculinity (Fleming, Colvin et al. 2016). This e#ect on both atti-tudes towards traditional gender norms and stigma emphasise the link between these two factors andthe importance of addressing them together within an intervention. These types of approaches may beparticularly promising since numerous studies have shown the link between masculine norms andavoiding HIV testing (Shand et al., 2014; Siu et al., 2014; Skovdal et al., 2011; Wyrod, 2011).
Another consideration for interventions is the fact that men who do not test may be more likely tobe perpetrating GBV. Ample evidence demonstrates that men’s attitudes towards GBV is associatedwith his perpetration of GBV (Fleming et al., 2015). Given that UNAIDS is implementing a plan toidentify non-testers, care should be taken to not instigate any GBV against men’s female partners.Men predisposed to GBV perpetration who newly test and subsequently identi!ed as HIV-infectedmay blame their female partner(s) and respond violently. Incorporating couples’ testing andsu$cient counselling that includes GBV prevention may present a viable opportunity to increasethe identi!cation of men living with HIV while monitoring and controlling for violence againstfemale partners.
Finally, our !ndings – as well as those in the UNAIDS ‘Blind Spot’ report – document men’s rela-tively low rates of HIV testing and emphasise the need to examine the overall global strategy for HIVtesting (UNAIDS, 2017). Seeking to attain UNAIDS 90-90-90 targets, which indicate that 90% ofpeople living with HIV should be tested, 90% linked to care, and 90% have suppressed viral loadsby 2020, has helped to get countries closer to epidemic control and enhance health outcomes forpeople living with HIV (UNAIDS, 2014). However, such an approach has also inadvertently has
GLOBAL PUBLIC HEALTH
220

led to linking HIV testing primarily with ‘case-!nding’ (Agolory et al., 2018; Dalal et al., 2017). Whilethis is not necessarily negative, an over-emphasis on case-!nding takes agency away from men byconceptualising them primarily as patients in need of assistance and diagnosis. Such surveillance-based approach renders them as docile bodies entering into a system of control where men (ifHIV positive) are required to follow certain rules of behaviour and time tables within the HIV treat-ment paradigm (Lopez, 2010). These men are required to leave life as they know it and assume a newidentity: that of a chronic disease patient who must live under the restraints and controls of biome-dicine to preserve their life.
Presented with the prospect of potential loss of power and sense of masculinity in case of a posi-tive diagnosis, it should not be surprising that men are accessing HIV testing less than women. Asdetailed by Sileo and colleagues, one barrier to HIV testing is that some African men do not feel com-fortable as a patient or being directed by health professionals (DiCarlo et al., 2014; Sileo et al., 2018).Indeed, framing HIV testing as strategy to enhance a man’s strength or independence has beenshown to be a facilitator to men’s testing (Barnabas Njozing, Edin, & Hurtig, 2010; Sileo et al.,2018). Aligning HIV testing strategies for men with dominant norms of masculinity (i.e. strength,independence) will likely help these strategies be more accepted and resonate with men in these pri-ority countries.
Increasing men’s HIV testing in the region may not only require this framing but also adoptingmore of a health promotion approach to HIV testing; one that empowers men whether HIV posi-tive or negative. Empowerment approaches (Wallerstein & Bernstein, 1988) for HIV testing andprevention are often focused on women and have rarely been applied to African men (Kerriganet al., 2015; Kerrigan et al., 2017; Pulerwitz, Mathur, & Woznica, 2018). But, what we see fromthe literature is that gender norms are constraining men’s ability to choose HIV testing (Sileoet al., 2018) and strategies are needed to help men break free of these limitations. Empoweringnegative men should entail providing them access to the HIV prevention information and servicesthat maximises their agency and helps them maintain their HIV negative status. This type ofapproach would give men the opportunity to choose HIV testing while ful!lling commonnorms of masculinity that emphasise independence and decision-making (Fleming, DiClemente,& Barrington, 2016; Sileo et al., 2018). Thus, better engaging men in HIV testing may necessitatean empowerment-based approach that balances treatment and prevention as the ethos underlyingHIV testing.
Limitations
While our study has many strengths, our !ndings should be interpreted with several limitations inmind. First, our data is cross-sectional and thus we are unable to make claims of causality. Longi-tudinal research would be needed to better understand whether our independent variables causedmen to avoid HIV testing. Second, measures of HIV knowledge – including the ones use in ourstudy – have been shown to have limited utility as reliable indicators of knowledge (Burke, Flem-ing, & Guest, 2014). We were limited to a standard battery of survey items included in the DHSand relied on these measures to construct knowledge indices for analysis. Finally, we only used !vecountries and thus caution should be used before applying these results to other settings withinAfrica.
Conclusions
Men are the ‘blind spot’ for e#orts to increase HIV testing in Africa. Our !ndings emphasise theimportance of changing men’s perceptions related to stigma and gender norms, as well as simplyincreasing men’s HIV knowledge with interventions that are designed to engage them. Indeed, tostem ongoing HIV transmission, it is essential that we speci!cally intervene with male-speci!c inter-ventions to increase HIV testing.
P. J. FLEMING ET AL.
221

Disclosure statement
No potential con"ict of interest was reported by the authors.
Disclaimer
The views in this publication do not necessarily re"ect the views of the U.S. Agency for InternationalDevelopment (USAID), the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), or the Uni-ted States Government.
Data availability statement
The data that support the !ndings of this study are available in at the Demographic and Health Sur-vey website: https://dhsprogram.com.
ORCID
Paul J. Fleming http://orcid.org/0000-0001-9150-1254
References
Agolory, S., de Klerk, M., Baughman, A. L., Sawadogo, S., Mutenda, N., Pentikainen, N.,…Medley, A. (2018). Low case!nding among men and poor viral load suppression among adolescents are impeding Namibia’s ability to achieveUNAIDS 90-90-90 targets. Open Forum Infections Diseases, 5(9), ofy200. doi:10.1093/o!d/ofy200
Auld, A. F., Shiraishi, R. W., Mbofana, F., Couto, A., Fetogang, E. B., El-Halabi, S.,… Ellerbrock, T. V. (2015). Lowerlevels of antiretroviral therapy enrollment among men with HIV compared with women – 12 countries, 2002–2013.Morbidity and Mortality Weekly Report, 64(46), 1281–1286. doi:10.15585/mmwr.mm6446a2
Barnabas Njozing, N., Edin, K. E., & Hurtig, A. K. (2010). ‘When I get better I will do the test’: Facilitators and barriersto HIV testing in Northwest region of Cameroon with implications for TB and HIV/AIDS control programmes.SAHARA-J: Journal of Social Aspects of HIV/AIDS, 7(4), 24–32. doi:10.1080/17290376.2010.9724974
Barnighausen, T., Herbst, A. J., Tanser, F., Newell, M.-L., & Bor, J. (2014). 150 unequal bene!ts from ART: A growingmale disadvantage in life expectancy in rural South Africa.
Bor, J., Rosen, S., Chimbindi, N., Haber, N., Herbst, K., Mutevedzi, T.,… Barnighausen, T. (2015). Mass HIV treatmentand sex disparities in life expectancy: Demographic surveillance in rural South Africa. PLoS Medicine, 12(11),e1001905; discussion e1001905. doi:10.1371/journal.pmed.1001905
Burke, H. M., Fleming, P. J., & Guest, G. (2014). Assessment of the psychometric properties of HIV knowledge itemsacross !ve countries. AIDS Education and Prevention, 26(6), 577–587. doi:10.1521/aeap.2014.26.6.577
Carrasco, M. A., Fleming, P., Wagman, J., & Wong, V. (2018). Toward 90-90-90: Identifying those who have neverbeen tested for HIV and di#erences by sex in Lesotho. AIDS Care, 30(3), 284–288. doi:10.1080/09540121.2017.1372559
Cohen, M. S., Chen, Y. Q., McCauley, M., Gamble, T., Hosseinipour, M. C., Kumarasamy, N.,… Team, H. S. (2011).Prevention of HIV-1 infection with early antiretroviral therapy. New England Journal of Medicine, 365(6), 493–505.doi:10.1056/NEJMoa1105243
Cornell, M., McIntyre, J., & Myer, L. (2011). Men and antiretroviral therapy in Africa: Our blind spot. TropicalMedicine & International Health, 16(7), 828–829. doi:10.1111/j.1365-3156.2011.02767.x
Cornell, M., Schomaker, M., Garone, D. B., Giddy, J., Ho#mann, C. J., Lessells, R.,… for the InternationalEpidemiologic Databases to Evaluate, A. S. A. C (2012). Gender di#erences in survival among adult patients startingantiretroviral therapy in South Africa: A multicentre cohort study. PLoS Medicine, 9(9), e1001304. doi:10.1371/journal.pmed.1001304
Dalal, S., Johnson, C., Fonner, V., Kennedy, C. E., Siegfried, N., Figueroa, C., & Baggaley, R. (2017). Improving HIV testuptake and case !nding with assisted partner noti!cation services. Aids, 31(13), 1867–1876. doi:10.1097/qad.0000000000001555
DiCarlo, A. L., Mantell, J. E., Remien, R. H., Zerbe, A., Morris, D., Pitt, B.,… El-Sadr, W. M. (2014). ‘Men usually saythat HIV testing is for women’: Gender dynamics and perceptions of HIV testing in Lesotho. Culture, Health &Sexuality, 16(8), 867–882. doi:10.1080/13691058.2014.913812
Dovel, K., Yeatman, S., Watkins, S., & Poulin, M. (2015). Men’s heightened risk of AIDS-related death: The legacy ofgendered HIV testing and treatment strategies. AIDS, 29(10), 1123–1125. doi:10.1097/QAD.0000000000000655
GLOBAL PUBLIC HEALTH
222

Dworkin, S. L., Fleming, P. J., & Colvin, C. J. (2015). The promises and limitations of gender-transformative healthprogramming with men: Critical re"ections from the !eld. Culture, Health & Sexuality, 17(sup2), 128–143.doi:1035751doi:10.1080/13691058.2015.1035751
Fleming, P. J., Colvin, C., Peacock, D., & Dworkin, S. L. (2016). What role can gender-transformative programming formen play in increasing men’s HIV testing and engagement in HIV care and treatment in South Africa? Culture,Health & Sexuality, 18(11), 1251–1264. doi:10.1080/13691058.2016.1183045
Fleming, P. J., DiClemente, R. J., & Barrington, C. (2016). Masculinity and HIV: Dimensions of masculine norms thatcontribute to men’s HIV-related sexual behaviors. AIDS and Behavior, 20(4), 788–798. doi:10.1007/s10461-015-1264-y
Fleming, P. J., McCleary-Sills, J., Morton, M., Levtov, R., Heilman, B., & Barker, G. (2015). Risk factors for men’s life-time perpetration of physical violence against intimate partners: Results from the international men and genderequality survey (IMAGES) in eight countries. PLoS One, 10(3), e0118639. doi:10.1371/journal.pone.0118639
Heise, L. L., & Kotsadam, A. (2015). Cross-national and multilevel correlates of partner violence: An analysis of datafrom population-based surveys. The Lancet Global Health, 3(6), e332–e340. doi:10.1016/S2214-109X(15)00013-3
Hensen, B., Taoka, S., Lewis, J. J., Weiss, H. A., & Hargreaves, J. (2014). Systematic review of strategies to increasemen’s HIV-testing in sub-Saharan Africa. Aids, 28(14), 2133–2145. doi:10.1097/qad.0000000000000395
Johnson, L. F., Rehle, T. M., Jooste, S., & Bekker, L. G. (2015). Rates of HIV testing and diagnosis in South Africa:Successes and challenges. Aids, 29(11), 1401–1409. doi:10.1097/qad.0000000000000721
Kerrigan, D., Kennedy, C. E., Morgan-Thomas, R., Reza-Paul, S., Mwangi, P., Win, K. T.,… Butler, J. (2015). A com-munity empowerment approach to the HIV response among sex workers: E#ectiveness, challenges, and consider-ations for implementation and scale-up. The Lancet, 385(9963), 172–185. doi:10.1016/S0140-6736(14)60973-9
Kerrigan, D., Mbwambo, J., Likindikoki, S., Beckham, S., Mwampashi, A., Shembilu, C.,…Galai, N. (2017). ProjectShikamana: Baseline !ndings from a community empowerment–based combination HIV prevention trial amongfemale sex workers in iringa. Tanzania. Journal of Acquired Immune De!ciciency Syndromes, 74(Suppl 1), S60.doi:10.1097/QAI.0000000000001203
Kigozi, I. M., Dobkin, L. M., Martin, J. N., Geng, E. H., Muyindike, W., Emenyonu, N. I.,…Hahn, J. A. (2009). Late-disease stage at presentation to an HIV clinic in the era of free antiretroviral therapy in Sub-Saharan Africa. Journalof Acquired Immune De!ciency Syndromes, 52(2), 280–289. doi:10.1097/QAI.0b013e3181ab6eab
Lopez, G. (2010). Forging a biomedical paradigm: Politics and illness in rural Mexico. Journal of ContemporaryAnthropology, 1(1), 22–32.
Mall, S., Middelkoop, K., Mark, D., Wood, R., & Bekker, L.-G. (2013). Changing patterns in HIV/AIDS stigma anduptake of voluntary counselling and testing services: The results of two consecutive community surveys conductedin the Western Cape, South Africa. AIDS Care, 25(2), 194–201. doi:10.1080/09540121.2012.689810
Maughan-Brown, B., Lloyd, N., Bor, J., & Venkataramani, A. S. (2016). Changes in self-reported HIV testing duringSouth Africa’s 2010/2011 national testing campaign: Gains and shortfalls. Journal of the International AIDS Society,19(1), 20658. doi:10.7448/ias.19.1.20658
Mills, E. J., Beyrer, C., Birungi, J., & Dybul, M. R. (2012). Engaging men in prevention and care for HIV/AIDS in Africa.PLoS Medicine, 9(2), e1001167. doi:10.1371/journal.pmed.1001167
Muula, A. S., Ngulube, T. J., Siziya, S., Makupe, C. M., Umar, E., Prozesky, H. W.,…Mataya, R. H. (2007). Genderdistribution of adult patients on highly active antiretroviral therapy (HAART) in Southern Africa: A systematicreview. BMC Public Health, 7(1), doi:10.1186/1471-2458-7-63
Novitsky, V., Bussmann, H., Okui, L., Logan, A., Moyo, S., van Widenfelt, E.,… Essex, M. (2015). Estimated age andgender pro!le of individuals missed by a home-based HIV testing and counselling campaign in a Botswana com-munity. Journal of the International AIDS Society, 18(1), 19918. doi:10.7448/IAS.18.1.19918
Pulerwitz, J., Mathur, S., & Woznica, D. (2018). How empowered are girls/young women in their sexual relationships?Relationship power, HIV risk, and partner violence in Kenya. PLoS One, 13(7), e0199733. doi:10.1371/journal.pone.0199733
Schell, E. S., Geo#roy, E., Phiri, M., Bvumbwe, A., Weinstein, J., & Jere, J. M. (2016). Cracking the code: Getting mentested in rural Africa. Aids, 30(2), 331–332. doi:10.1097/qad.0000000000000913
Shand, T., Thomson-de Boor, H., van den Berg, W., Peacock, D., & Pascoe, L. (2014). The HIV blind spot: men andHIV testing. Treatment and Care in Sub-Saharan Africa. Ids Bulletin-Institute of Development Studies, 45(1), 53–60.doi:10.1111/1759-5436.12068
Sileo, K. M., Fielding-Miller, R., Dworkin, S. L., & Fleming, P. J. (2018). What role do masculine norms play in men’sHIV testing in Sub-Saharan Africa?: A scoping review. AIDS and Behavior, 22(8), 2468–2479. doi:10.1007/s10461-018-2160-z
Siu, G. E., Seeley, J., & Wight, D. (2013). Dividuality, masculine respectability and reputation: How masculinity a#ectsmen’s uptake of HIV treatment in rural eastern Uganda. Social Science & Medicine, 89, 45–52. doi:10.1016/j.socscimed.2013.04.025
Siu, G. E., Wight, D., & Seeley, J. A. (2014). Masculinity, social context and HIV testing: An ethnographic study of menin Busia district, rural eastern Uganda. BMC Public Health, 14(1), doi:10.1186/1471-2458-14-33
P. J. FLEMING ET AL.
223
Skovdal, M., Campbell, C., Madanhire, C., Mupambireyi, Z., Nyamukapa, C., & Gregson, S. (2011). Masculinity as abarrier to men’s use of HIV services in Zimbabwe. Globalization and Health, 7(1), 13. doi:10.1186/1744-8603-7-13
Stephenson, R., Miriam Elfstrom, K., & Winter, A. (2013). Community in"uences on married men’s uptake of HIVtesting in eight African countries. AIDS and Behavior, 17(7), 2352–2366. doi:10.1007/s10461-012-0223-0
Treves-Kagan, S., El Ayadi, A. M., Pettifor, A., MacPhail, C., Twine, R., Maman, S.,… Lippman, S. A. (2017). Gender,HIV testing and stigma: The association of HIV testing behaviors and community-level and individual-level stigmain rural South Africa di#er for men and women. AIDS and Behavior, 21(9), 2579–2588. doi:10.1007/s10461-016-1671-8
UNAIDS. (2014, October). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Retrieved fromhttp://www.unaids.org/sites/default/!les/media_asset/90-90-90_en.pdf
UNAIDS. (2017). Reaching out to men and boys: Addressing a blind spot in the response to HIV. Retrieved fromhttp://www.unaids.org/sites/default/!les/media_asset/blind_spot_en.pdf
Wallerstein, N., & Bernstein, E. (1988). Empowerment education: Freire’s ideas adapted to health education. HealthEducation Quarterly, 15(4), 379–394. doi:10.1177/109019818801500402
Wyrod, R. (2011). Masculinity and the persistence of AIDS stigma. Culture, Health & Sexuality, 13(4), 443–456. doi:10.1080/13691058.2010.542565
GLOBAL PUBLIC HEALTH
224

Volume 22, Supplement 1, March 2019
Realizing the potential of HIV self-testing for Africa: lessons learned from the STAR projectGuest Editors: Vincent J Wong, Nathan Ford, Kawango AgotSupplement Editor: Anna Grimsrud
225

EDITORIAL
To thine own test be true: HIV self-testing and the global reachfor the undiagnosedVincent Wong1§ , Erin Jenkins1, Nathan Ford2 and Heather Ingold3
Corresponding author: United States Agency for International Development (USAID), Global Health Bureau, Office of HIV/AIDS, Prevention Care and TreatmentDivision, United States. Tel: +1 (571) 309 1273. ([email protected])
Keywords: HIV self-testing; HIV policy; VCT; PITC; HIV diagnosis
Received 18 January 2019; Accepted 24 January 2019
Copyright © 2019 World Health Organization; licensed by IAS. This is an open access article distributed under the terms of the Creative Commons Attribution IGOLicense https://creativecommons.org/licenses/by/3.0/igo/legalcode which permits unrestricted use, distribution and reproduction in any medium, provided that theoriginal work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or the article endorse any specific organization orproducts. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s URL.
Globally, we are at an inflection point in achieving UNAIDS’ 95-95-95 goals for 2030. A recent Lancet editorial observed that“the last big shared challenge remaining is testing—in everyregion the number of undiagnosed HIV infections remains asubstantial barrier to achieving UNAIDS targets and endingAIDS by 2030” [1]. While UNAIDS estimates we are at 75%diagnostic coverage globally, within this figure is great variation:between men and women, younger and older individuals, ruraland urban populations, among key populations and betweencountries [2,3]. After 18 years of expansive programming in glo-bal health for HIV testing through a multitude of modalities incommunities and facilities, reaching the remaining undiagnosedindividuals with flat-lined donor funding will require new efforts[3]. Many of the remaining undiagnosed individuals are presum-ably not engaging with HIV services, and novel avenues to HIVtesting services (HTS) that overcome both stigma and struc-tural barriers are needed: a new HIV testing paradigm isurgently needed to reach these remaining undiagnosed individ-uals and effectively link them to treatment.HIV self-testing (HIVST) has developed substantially in
recent years and is now considered a new and critical HIVresponse strategy in controlling the epidemic. In 2012, the USFDA approved the OraQuick® HIV Self-Test Kit introducingthe first HIV rapid test kit intended for use by the generalpopulation and available for purchase over-the-counter in theUnited States. Building on a history of public health interven-tions aimed at self-screening for health conditions thatincludes home pregnancy tests, breast self-examinations forcancer screening and blood-glucose monitoring, access toHIVST permits individuals perceiving themselves to be at-riskof infection to test independently and privately. Global atten-tion to the potential of HIVST took root in 2013 following theOraQuick FDA approval, with UNAIDS and the World HealthOrganization (WHO) holding an initial consultation on the eth-ical and public health implications of HIVST. At that time, noHIVST kits were publicly available in low- and middle-incomecountries (LMIC) (outside a small number of studies and “grey
market” test kits), no normative guidelines had been estab-lished and only a small body of LMIC-focused evidence aroundHIVST existed. Within a year, a full HIVST journal supplementhad been published exploring early issues in HIVST introduc-tion: regulation and policy, optimal product profiles, ethicalconsiderations and both positive and negative potentialimpacts of rollout [4-6]. This led, in 2015, to Unitaid’s catalyticinvestment in the five-year HIV Self-Testing Africa (STAR)initiative. The first two-year phase, which included Malawi,Zambia and Zimbabwe, aimed to generate evidence on thefeasibility and acceptability of HIVST as well as how to dis-tribute self-test products effectively, ethically and efficiently,with adequate post-test support. Evidence from this phasesupported country policy development, and studied impactsand cost-effectiveness of various delivery models, addressedstructural barriers and assessed consumer demand. Findingsfrom these and other studies led to the WHO guidance onHIVST in 2016 (also strategically paired with the HTS) Part-ner Notification guidelines [7]. A separate but concurrent pro-cess resulted OraQuick being the first WHO prequalifiedHIVST kit. In 2017, the Bill and Melinda Gates Foundationprovided financial support to bring the unit cost of theOraQuick self-test kit down to US$2 in selected sub-SaharanAfrican and other low-income countries, removing a criticalcost barrier to HIVST expansion [8].These initial supportive efforts established the foundation
needed for HIVST expansion across countries. The secondthree-year phase of STAR added Lesotho, Eswatini and SouthAfrica, and aimed to create a market for HIVST and evaluateoptimal distribution models for increasing access to testingamong those unwilling or unable to utilize traditional testingvenues and ensuring linkage from a preliminary positiveHIVST result to confirmatory testing and treatment. By theend of the programme, Unitaid, the STAR programme’s com-modities funder, will have provided five million HIVST kits tothe six project countries. Building on STAR’s momentum andtheir own smaller scale pilot programmes in 2016, PEPFAR
Wong V et al. Journal of the International AIDS Society 2019, 22(S1):e25256http://onlinelibrary.wiley.com/doi/10.1002/jia2.25256/full | https://doi.org/10.1002/jia2.25256
226
expanded its HIVST programming and will have delivered2.3 million HIVST kits across 11 countries in 2017 to 2018.Similarly, the Global Fund is expanding HIVST support across18 countries, estimated to cover about 12% of the globalHIVST volume [9]. With 59 countries having, or developing,national HIVST policies, there is global acceleration towardsthe expansion of HIVST access and programmes and, withgood linkage, increased diagnostic coverage [9]. However,these numbers remain small relative to the overall number ofpeople tested; PEPFAR alone accounted for roughly 85 millionHIV tests in 2017 [10]. But HIVST deployed strategicallywithin programmes, and made available through multipleavenues, is anticipated to amplify the impact of current HIVprogramming by reaching the critical remaining at-risk popula-tions with needed testing and treatment.The articles collected for this Supplement present a diverse
range of the key findings from the first phase of STAR, andprovide a basis for needed programmatic action to accelerateexpansion. Presently, in sub-Saharan Africa, there are 15 coun-tries that have HIVST policies in place or under considerationand multiple products available with some type of certification[9,11]. However, products of unknown quality have been avail-able on the unregulated market, posing risks and underscoringthe need for further quality and consumer protection regula-tions [6,11]. Dacombe et al. explore the regulatory environ-ment in Malawi, Zambia and Zimbabwe [12]. Using keyinformant interviews which included laboratory staff and poli-cymakers, they consulted 66 individuals from the three coun-tries. Interviews showed that in these countries, there was aneed for regulation of in vitro diagnostic tests in general, andHIVST kits were no exception. The authors call for a regionalcollaboration to spread the regulatory burden across countriesand facilitate the passing of required legislation to supportmore codified regulation of diagnostics.WHO prequalified test kits have gone through quality
assurance evaluations aimed at ensuring “global standards ofquality, safety and efficacy” to support Ministries of Healthand the introduction of quality diagnostics [13]. However, pro-duct performance includes not just quality standards of thetest kit itself, but also usability by the target population andthe successful insertion of HIVST into the clinical cascade.Early studies showed some challenges in following instructionsfor use (IFU) [5,14], but as kits have been refined, resultshave improved. A recent review demonstrated general agree-ment between results of HIVST kits and facility testing algo-rithms [15]. However, challenges relating to literacy remain,underscoring the need for clear and simple language in pack-age inserts [15-17] and IFUs that are adapted to local con-texts. In this Supplement, Simwinga et al. present findings fromMalawi and Zambia evaluating an IFU translated into the locallanguage and evaluated for clarity and ease of use [18]. Inves-tigators used feedback from testers to optimize the IFU, con-curring with previous findings that the educational level of thetester correlates to the ability to follow the IFU. In response,they suggest that in certain contexts community demonstra-tions of how to use HIVST kits could overcome this barrier.In another study, given that programmes have proposed late
reading of returned kits to determine HIV positivity, Watsonet al. evaluated the OraQuick HIV-1/2 antibody test kits forresult stability post-testing. They showed that while stronglyreactive HIVST remained stable, 29% of initially non-reactive
kits converting to be weakly reactive false positive when readat least four days later, countering previous work which indi-cated OraQuick test kits were stable for up to a year [19,20].Re-reading may be problematic and result in artificiallyinflated positivity rates; this finding led the WHO to recom-mend against any delayed readings of kits [21].Eaton et al. model how HIVST and other “test for triage”
strategies might impact national algorithm performance [22].Considering modelled high- and low-prevalence scenarios, aswell as using data from Malawi, a high-prevalence country withhigh rates of diagnosis [23], the authors show that the additionof triage testing before the national algorithm increases thepositive predictive value and decreases the number of false-positive diagnoses, possibly eliminating the need for verificationtesting at initiation of antiretroviral therapy (ART).Methodologies for HIVST distribution will be a critical aspect
of programme effectiveness. Various delivery modes have beenconsidered: vending machines, over-the-counter at pharmacies,secondary distribution when an HIVST is distributed to oneperson for use by another, and facility- and community-baseddistribution [11,15,24-26]. In this Supplement, Sibanda et al.began with the clients, investigating preferences for access toHIVST in rural Zimbabwe through discrete choice assessments,finding respondent preferences for door-to-door distribution,kits free-of-charge, access by telephone to help in using kitsand linkage to confirmatory testing, and that programmes usepatient reminders and outreach to enhance effectiveness [27].For confirmatory testing and ART initiation, respondents alsopreferred these to be free, located near their home and thatART could be initiated immediately [27]. This study supportsprevious findings on user preferences emphasizing ease ofaccess, usability and privacy [11].Also in this Supplement, Hatzold et al. reviewed STAR data
from Malawi, Zambia and Zimbabwe that assessed the integra-tion of HIVST tools into HIV programming [28]. They found thatby having clients perform HIVST in outpatient settings, theywere able to decongest clinical testing facilities because health-care workers could focus only on those that screened positive.They also demonstrated the ability to reach men through com-munity distribution and in particular workplaces, and exploredmale attitudes to HIVST, noting that the briefer counsellingmessages, privacy and convenience appealed to them [28].Advantages of HIVST, such as the ability to test privately,
may also be misused or abused and potential social harmsshould not be ignored. Previously in Kenya, low rates of physi-cal and verbal abuse have been reported with the introductionof HIVST kits by women for their male partners to test them-selves [29]. In this Supplement, Kumwenda et al. provide newevidence on social harms from projects in Malawi, summariz-ing data from six HIVST projects from 2011 to 2017 where acombination of qualitative and quantitative methods wereused [30]. Coercion was reframed to have both negative andpositive aspects, and the concept of compassionate coercionwas introduced to describe instances when family membersencourage a member who is ill to test. Overall, they report 25serious adverse events through the active reporting systemsfrom all six studies with a total of 178,833 self-tests dis-tributed. The most common event was marriage breakdown inserodiscordant relationships though verbal abuse, and physicaland economic intimate partner violence were infrequently alsoobserved [30]. The potential for social harms is not unique to
Wong V et al. Journal of the International AIDS Society 2019, 22(S1):e25256http://onlinelibrary.wiley.com/doi/10.1002/jia2.25256/full | https://doi.org/10.1002/jia2.25256
227

HIVST, but the present work elucidates the need for intimatepartner violence screening when considering HIVST secondarydistribution and partner testing, and the need for ongoingmonitoring of social harms within existing systems.In the context of HIVST, linkage to care refers not just to the
initiation of ART, but first to confirmatory testing after a posi-tive HIVST [31]. Since using an HIVST kit in private is oftenpreferred by testers, the onus to link to care is firmly placed inthe hands of the tester. As such, linking testers to care andestimating linkage rates can be a challenge. Some HIVSTresearch studies have estimated linkage rates to be between36% and 78% with a variety of methodologies as there is nostandard process to measure linkage [24,29,31,32]. In this Sup-plement, Neuman et al. reflect on the difficulties in estimatinglinkage as HIVST is brought to scale [33]. They note the limitedmetrics available – HIVST kit distribution totals and self-reported data, neither of which is optimal to estimate linkagerates accurately [33]. The investigators present a summary ofstudy protocols estimating linkage from published STAR stud-ies. These estimate HIVST linkage by using ecological indicatorssuch as comparisons of ART initiation rates in areas with HIVSTcampaigns versus in areas without HIVST campaigns. Taken onits own, it is only correlative; however, when considered inaddition to other information it can be used to create a body ofevidence regarding linkage to care.Costing HTS is highly contextual with considerable variation,
but important to programme planning and bringing HIVST toscale. In this Supplement, Mangenah et al. performed a costanalysis of community HIVST kit distribution in Malawi, Zam-bia and Zimbabwe as well as a sensitivity and scenario analy-sis to project future costs [34]. The average cost per kitdistributed (i.e. not only the commodity cost) ranged from US$ 7.23 to US$ 14.58 with variation by site location, but stillcomparable to previously published values [35]. In a secondarticle, Cambiano et al. use this data to present a modellinganalysis comparing community distribution to three prioritypopulations in Zimbabwe and Malawi: women having transac-tional sex (WTS), youth and adult men [36]. The model showedthat distribution to men averted the most deaths, but distribu-tion to WTS was the most efficient as measured in number oftests per death averted. Cambiano et al. have added to cost-effectiveness research, considering the trade-offs betweeninvesting in HIVST and other HIV programmes, they estimatethat HIVST is cost-effective when the mean cost per disabilityadjusted life year averted is below US$ 500. According totheir models, this occurs when HIVST kits were distributed toWTS and men but not to youth.Offering commentary on the use of HIVST, Ingold et al.
focus on the broader policy environment in LMIC, marketdevelopment for HIVST kits, the STAR programme experienceand its positioning for HIVST scale-up [37]. As part of theintervention, the STAR programme engaged with manufac-tures and stakeholders at the country and multilateral levelsto create demand, assess viability of HIVST as a route to diag-nosis and research delivery methods. The overall goal being topave the way for increased access to quality HIVST kits tomobilize more people living with HIV to know their status.The authors highlight the progress that has been made inaddressing these barriers, including amassing a sufficient evi-dence base for WHO guidance and a more enabling policyenvironment in general, prequalification of two types of HIVST
kits and a more robust product pipeline. Pilot studies havedemonstrated the ability of HIVST to reach populations thathave traditionally been refractory to other testing strategiesand viability for priority populations. Ingold et al. also touch onoutstanding challenges to be addressed and present a call toaction to maintain momentum in bringing HIVST to scale [37].Since 2012, substantial progress has been made on HIVST
programmes, policy and products – but few countries areimplementing HIVST at scale, with many still conducting smal-ler volume pilot programmes. Recent HIV response framingshave declared that “what got us here won’t get us there” [38];for HIV testing, the rapid expansion of voluntary counsellingand testing, provider-initiated approaches and community-based campaigns have achieved a global 75% diagnosis rate.The final reach to the remaining undiagnosed individuals,including early diagnosis of decreasing numbers of newlyinfected persons, will depend critically on an evolution of newapproaches: HIVST, expansions of index testing and partnernotification as a new minimum standard of care, and program-matic improvements of existing HTS access points. The evi-dence to date has demonstrated the potential of HIVST toreach both the unreached and those at high risk, which is keyin achieving the 95-95-95 goals and controlling the epidemic.However, operational questions remain. Intentional misuse,
accuracy and performance of secondary distribution, moreeffective leveraging of public–private sector collaborations toreach high-risk populations, programmatic use of blood-basedHIVST kits, use of HIVST as a demand generation tool for Pre-exposure prophylaxis (PrEP), volume procurement approachesto reduce unit pricing and the use of mobile technology andother methods to estimate linkage post-HIVST, could all benefitfrom more operations research to guide programming.The body of evidence produced in this Supplement adds signifi-
cantly to the field of HTS, exemplifying the potential public healthrole of this new technology to critically increase coverage. Still,HIVST access will not reach the scale needed to impact the epi-demic without both leveraging existing health programmes anddeveloping new and innovative avenues of access. The integrationof HIVST should work to amplify existing HIV programming toachieve multiple purposes that serve public health goals: reachingunreached and high-risk individuals at an early disease stage,reducing testing burdens on taxed health systems, and criticallyidentifying the most effective avenues to linking persons screeningpositive to onward testing and treating or linking persons screen-ing negative to prevention services. All are outcomes of criticalimportance to controlling the HIV epidemic. And novel avenuessuch as private sector delivery will continue to need to beexplored.While we find ourselves at the “last big shared challenge”of HIV testing, in the race towards control of the HIV epidemic,this Supplement strongly illustrates that a new testing paradigmbased in part on HIVST is key to the next decade of the HIVresponse and achieving 95% diagnosis rates everywhere.
AUTHORS ’ AFF I L IAT IONS1United States Agency for International Development (USAID), Global HealthBureau, Office of HIV/AIDS, Prevention Care and Treatment Division; 2HIV/AIDS Department, Organisation mondiale de la Sante, Geneva, Switzerland;3Unitaid, Geneva, Switzerland
COMPET ING INTERESTS
VW, EJ, NF and HI declare no competing interests.
Wong V et al. Journal of the International AIDS Society 2019, 22(S1):e25256http://onlinelibrary.wiley.com/doi/10.1002/jia2.25256/full | https://doi.org/10.1002/jia2.25256
228

AUTHORS ’ CONTR IBUT IONS
VW and EJ drafted the initial manuscript. All authors critically reviewed the manu-script, suggested revisions and editorial changes, and approved the final version.
VW is a member of the Unitaid HIVSTAR Technical Advisory Group.
ACKNOWLEDGEMENTS
The authors thank Dr. Kawango Agot for providing comments to the manu-script.
FUNDING
The STAR Initiative is made possible thanks to Unitaid’s funding and support.Unitaid accelerates access to innovative health products and lays the founda-tions for their scale-up by countries and partners. Unitaid is a hosted partner-ship of the World Health Organization.
DISCLA IMER
The contents in this article are those of the authors and do not necessarilyreflect the view of the U.S. President’s Emergency Plan for AIDS Relief, the U.S.Agency for International Development or the U.S. Government.
REFERENCES
1. The Lancet HIV. Divergent paths to the end of AIDS. Lancet HIV. 2017[cited 2019 January 11];4(9):e375. Available from: http://linkinghub.elsevier.com/retrieve/pii/S23523018173015712. PHIA. PHIA Project: A drop that counts [Internet]. 2018 [cited 2019 January11] ICAP at Columbia University. Available from: https://phia.icap.columbia.edu/3. UNAIDS. Global AIDS Update 2018: Miles To Go Closing Gaps BreakingBarriers Righting Injustices [Internet]. 2018[cited 2019 January 11]. Availablefrom: http://www.unaids.org/sites/default/files/media_asset/miles-to-go_en.pdf4. Brown AN, Djimeu EW, Cameron DB. A review of the evidence of harmfrom self-tests. AIDS Behav. 2014;18 Suppl 4:S445–9.5. Peck RB, Lim JM, Van Rooyen H, Mukoma W, Chepuka L, Bansil P, et al.What Should the Ideal HIV self-test look like? A usability study of test proto-types in unsupervised HIV self-testing in Kenya, Malawi, and South Africa. AIDSBehav. 2014;18 Suppl 4:S422–32.6. Wong V, Johnson C, Cowan E, Rosenthal M, Peeling R, Miralles M, et al. HIVself-testing in resource-limited settings: regulatory and policy considerations.AIDS Behav. 2014;18 Suppl 4:S415–21.7. WHO. Guidelines on HIV Self-Testing and Partner Notification. 2016.8. Orasure. OraQuick HIV Self-test [Internet]. 2017 [cited 2019 January 11].Available from: http://www.orasure.com/products-infectious/products-infectious-oraquick-self-test.asp9. WHO/UNITAID. HIV rapid diagnostic tests for HIV self-testing. 2018.10. PEPFAR. PEPFAR 2017 Annual Report to Congress. 2017.11. Indravudh PP, Choko AT, Corbett EL. Scaling up HIV self-testing in sub-Saharan Africa: a review of technology, policy and evidence. Curr Opin InfectDis. 2018;31(1):14–24.12. Dacombe R, Watson V, Nyirenda L, Madanhire C, Simwinga M, Chepuka L,et al. Regulation of HIV self-testing in Malawi, Zambia and Zimbabwe: a qualita-tive study with key stakeholders. J Int AIDS Soc. 2019;22(S1):e25229.13. WHO. Prequalification of in vitro diagnostics [Internet]. In vitro diagnosticsand laboratory technology. 2018 [cited 2018 Apr 9]. Available from: http://www.who.int/diagnostics_laboratory/evaluations/en/14. Pant Pai N, Sharma J, Shivkumar S, Pillay S, Vadnais C, Joseph L, et al.Supervised and unsupervised self-testing for HIV in high- and low-risk popula-tions: a systematic review. PLoS Med. 2013;10(4):e1001414.15. Figueroa C, Johnson C, Ford N, Sands A, Dalal S, Meurant R, et al. Reliability ofHIV rapid diagnostic tests for self-testing compared with testing by health-care work-ers: a systematic review and meta-analysis. Lancet HIV. 2018 [cited 2019 January11];5(6):e277–90. Available from: https://doi.org/10.1016/s2352-3018(18)30044-416. Gr!esenguet G, de Longo J D, Tonen-Wolyec S, Mboumba Bouassa R-S,Belec L. Acceptability and usability evaluation of finger-stick whole blood HIVself-test as an HIV screening tool adapted to the general public inthe Central African Republic. Open AIDS J. 2017[cited 2019 January 11];11(33):101–18. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29290887%0Ahttp://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=PMC573095617. Tonen-Wolyec S, Batina-Agasa S, Muwonga J, N’kulu FF, Bouassa RSM,B!elec L. Evaluation of the practicability and virological performance of finger-stick whole-blood HIV self-testing in French-speaking sub-Saharan Africa. PLoSOne. 2018;13(1):1–22.
18. Simwinga M, Kumwenda MKRD, Kayira L, Muzumara A, Johnson C, Indra-vudh P, et al. Ability to understand and correctly follow HIV self-test kit instruc-tions for use: applying the cognitive interview technique in Malawi and Zambia.J Int AIDS Soc. 2019;22(S1):e25253.19. Choko AT, Taegtmeyer M, Macpherson P, Cocker D, Khundi M, Thindwa D,et al. Initial accuracy of HIV Rapid test kits stored in suboptimal conditions andvalidity of delayed reading of oral fluid tests. PLoS One. 2016;11(6):6–13.20. Watson V, Dacombe RJ, Williams C, Edwards T, Adams ER, Johnson C, et al.Re-reading of OraQuick HIV-1/2 rapid antibody test results: quality assuranceimplications for HIV self-testing programmes. J Int AIDS Soc. 2019;22(S1):e25234.21. WHO. HIV Self-Testing Strategic Framework a Guide for Planning, Intro-ducing and Scaling Up. Geneva; 2018.22. Eaton JW, Terris-Prestholt F, Cambiano V, Sands A, Baggaley R, Hatzold K,et al. Optimizing HIV testing services in sub-Saharan Africa: cost and perfor-mance of verification testing with HIV self-tests and tests for triage. J Int AIDSSoc. 2019;22(S1):e25237.23. ONUSIDA. Unaids Data 2018. 2018 [cited 2019 January 11];370. Availablefrom: http://www.unaids.org/sites/default/files/media_asset/unaids-data-2018_en.pdf24. Choko AT, MacPherson P, Webb EL, Willey BA, Feasy H, Sambakunsi R,et al. Uptake, accuracy, safety, and linkage into care over two years of promot-ing annual self-testing for HIV in Blantyre, Malawi: a community-based prospec-tive study. PLoS Med. 2015;12(9):e1001873.25. Kojima N, Klausner JD. Accelerating epidemic control: the role of HIV self-testing. Lancet HIV. [cited 2019 January 11];2018;5(6):e266–7.26. Choko AT, Kumwenda MK, Johnson CC, Sakala DW, Chikalipo MC, FieldingK, et al. Acceptability of woman-delivered HIV self-testing to the male partner,and additional interventions: a qualitative study of antenatal care participants inMalawi. J Int AIDS Soc. 2017;20(1):1–10.27. Sibanda EL, D’Elb!ee M, Maringwa G, Ruhode N, Tumushime M, MadanhireC, et al. Applying user preferences to optimize the contribution of HIV self-test-ing to reaching the “first 90” target of UNAIDS Fast-track strategy: results fromdiscrete choice experiments in Zimbabwe. J Int AIDS Soc. 2019;22(S1):e25245.28. Hatzold K, Gudukeya S, Mutseta M, Chilongosi R, Nalubamba M, NkhomaC, et al. HIV self-testing: breaking the barriers to uptake of testing among menand adolescents in sub-Saharan Africa, experiences from STAR demonstrationprojects in Malawi, Zambia and Zimbabwe. J Int AIDS Soc. 2019;22(S1):e25244.29. Thirumurthy H, Masters SH, Mavedzenge SN, Maman S, Omanga E, AgotK. Promoting male partner HIV testing and safer sexual decision makingthrough secondary distribution of self-tests by HIV-negative female sex workersand women receiving antenatal and post-partum care in Kenya: a cohort study.Lancet HIV [Internet]. 2016 [cited 2019 January 11];3(6):e266–74. Availablefrom: https://doi.org/10.1016/s2352-3018(16)00041-230. Kumwenda M, Johnson C, Choko A, Lora W, Sibande W, Sakala D, et al.Exploring social harms during distribution of HIV self-testing kits using mixed-methods approaches in Malawi. J Int AIDS Soc. 2019;22(S1):e25251.31. Cambiano V, Mavedzenge SN, Phillips A. Modelling the potential populationimpact and cost-effectiveness of self-testing for HIV: evaluation of data require-ments. AIDS Behav. 2014;18 Suppl 4:S450–8.32. Macpherson P, Lalloo DG, Webb EL, Choko AT, Makombe SD, Anthony E, et al.Effect of optional home initiation of HIV care following HIV self- testing on antiretro-viral therapy initiation among adults in Malawi. JAMA. 2014;312(95):372–9.33. Neuman M, Taegtmeyer M, Hatzold K, Johnson C, Weiss HA, Fielding K.Challenges in measurement of linkage following HIV self-testing: examples fromthe STAR Project. J Int AIDS Soc. 2019;22(S1):e25238.34. Mangenah C, Lawrence M, Sande L, Ahmed N, D’Elbee M, Chiwawa P, et al.Economic cost analysis of door-to-door community-based distribution of HIVself-test kits in Malawi, Zambia and Zimbabwe. J Int AIDS Soc. 2019;22(S1):e25255.35. Maheswaran H, Petrou S, MacPherson P, Choko AT, Kumwenda F, LallooDG, et al. Cost and quality of life analysis of HIV self-testing and facility-basedHIV testing and counselling in Blantyre. Malawi. BMC Med [Internet]. 2016[cited 2019 January 11];14(1):1–12. Available from: https://doi.org/10.1186/s12916-016-0577-736. Cambiano V, Johnson C, Hatzold K, Fern T-P, Maheswaran H, ThirumurthyH, et al. The impact and cost-effectiveness of community-based HIV self-testingin sub-Saharan Africa: a health economic and modelling analysis. J Int AIDS Soc.2019;22(S1):e25243.37. Ingold H, Mwerinde O, Ross AL, Ross L, Corbett E, Hatzold K, et al. The Self-Testing AfRica (STAR) Initiative: accelerating global access and scale-up of HIVself-testing. J Int AIDS Soc. 2019;22(S1):e25249.38. El-Sadr WM, Harripersaud K, Rabkin M. Reaching global HIV/AIDS goals: whatgot us here, won’t get us there. PLoS Med. 2017 [cited 2019 January 11];14(11):e1002421. Available from: http://dx.plos.org/10.1371/journal.pmed.1002421
Wong V et al. Journal of the International AIDS Society 2019, 22(S1):e25256http://onlinelibrary.wiley.com/doi/10.1002/jia2.25256/full | https://doi.org/10.1002/jia2.25256
229

Review article
To err is human, to correct is public health: asystematic review examining poor quality testing andmisdiagnosis of HIV statusCheryl C. Johnson1,2§, Virginia Fonner3, Anita Sands4, Nathan Ford1, Carla Mahklouf Obermeyer5, Sharon Tsui6,Vincent Wong7 and Rachel Baggaley1
§Corresponding author: Cheryl C. Johnson, Department of HIV, World Health Organization, 20 Avenue Appia, Geneva, 1201, Switzerland. ([email protected])
AbstractIntroduction: In accordance with global testing and treatment targets, many countries are seeking ways to reach the “90-90-90” goals, starting with diagnosing 90% of all people with HIV. Quality HIV testing services are needed to enable people withHIV to be diagnosed and linked to treatment as early as possible. It is essential that opportunities to reach people withundiagnosed HIV are not missed, diagnoses are correct and HIV-negative individuals are not inadvertently initiated on life-long treatment. We conducted this systematic review to assess the magnitude of misdiagnosis and to describe poor HIVtesting practices using rapid diagnostic tests.Methods: We systematically searched peer-reviewed articles, abstracts and grey literature published from 1 January 1990 to19 April 2017. Studies were included if they used at least two rapid diagnostic tests and reported on HIV misdiagnosis, factorsrelated to potential misdiagnosis or described quality issues and errors related to HIV testing.Results: Sixty-four studies were included in this review. A small proportion of false positive (median 3.1%, interquartile range(IQR): 0.4-5.2%) and false negative (median: 0.4%, IQR: 0-3.9%) diagnoses were identified. Suboptimal testing strategies werethe most common factor in studies reporting misdiagnoses, particularly false positive diagnoses due to using a “tiebreaker”test to resolve discrepant test results. A substantial proportion of false negative diagnoses were related to retesting amongpeople on antiretroviral therapy.Conclusions: HIV testing errors and poor practices, particularly those resulting in false positive or false negative diagnoses, dooccur but are preventable. Efforts to accelerate HIV diagnosis and linkage to treatment should be complemented by effortsto improve the quality of HIV testing services and strengthen the quality management systems, particularly the use ofvalidated testing algorithms and strategies, retesting people diagnosed with HIV before initiating treatment and providingclear messages to people with HIV on treatment on the risk of a “false negative” test result.
Keywords: HIV; HIV testing; misdiagnosis; misclassification; diagnostic error; false positive; healthcare; patient safety
To access the supplementary material to this article please see Supplementary Files under Article Tools online.
Received 16 December 2016; Accepted 07 March 2017; Published 29 August 2017Copyright: © 2017 World Health Organization; licensee IAS. This is an open access article distributed under the terms of the Creative Commons Attribution IGOLicense (http://creativecommons.org/licenses/by/3.0/igo/legalcode), which permits unrestricted use, distribution, and reproduction in any medium, provided theoriginal work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organisation orproducts. The use of the WHO logo is not permitted.
IntroductionIn the last decade, HIV testing services have been scaled-upsubstantially. In 2005, it was estimated that only 12% ofpeople who wanted an HIV test were able to access test-ing; and that only 10% of people with HIV in Africa knewtheir status [1]. In contrast, between 2010 and 2014, morethan 600 million people in 122 low- and middle-income coun-tries received HIV testing [2], and as of 2015, approximately60% of people with HIV were aware of their status [3]. Suchscale-up has been possible through the expansion of provider-initiated testing and counselling and community-based testing
programmes, which have routinized HIV testing and extendedservices to many people.
Rapid diagnostic tests (RDTs) have been instrumental to thescale-up of HIV testing, particularly in resource-limited set-tings where access to laboratory services is poor. RDTs havebeen shown to be highly accurate and can often provide asame-day diagnosis when used within a validated testingstrategy (i.e. the order in which the tests are performed)and algorithm (i.e. the exact tests used within the testingstrategy) according to high (!5%) and low HIV prevalence(<5%), as recommended by the World Health Organization
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
7
230

(WHO) [4–6]. Recent reports, however, have shown that HIVtesting is not always conducted appropriately [7,8], and insome countries, quality systems have not kept pace withtesting scale-up. According to a review of national HIV testingpolicies, less than 20% of testing strategies were consistentwithWHO guidance, and only two included recommendationson retesting prior to the initiation of antiretroviral therapy(ART) [9]. In some cases, poor-quality testing has resulted inincorrect test results and the misdiagnosis of HIV status[10–14].
HIV misdiagnosis refers to any testing event where a diag-nosis is missed, inappropriately delayed or incorrect (eitherfalse positive or false negative) [15]. Poor-quality HIV testingand misdiagnosis have negative consequences for individuals,families, communities, health workers and health services.False negative diagnoses represent missed opportunities toidentify an HIV infection and link people to early treatment.False positive diagnosesmay cause social and emotional harmand create mistrust of health workers and the test results theydeliver. Without addressing HIV testing quality, new guidanceoffering same-day treatment to all people diagnosed with HIV[16] could lead to inappropriate ART initiation [11]. Onceindividuals are on treatment, because ART reduces antibodyproduction and can cause seroreversion, for example, falsenegative test results, determining a person’s true HIV statuscan be especially challenging [17,18].
We conducted this systematic review to assess the mag-nitude of misdiagnosis and to identify and describe poorHIV testing practices using RDTs, including those which mayhave led to incorrect test results and misdiagnosis.
MethodsWe systematically searched for peer-reviewed articles pub-lished from 1 January 1990 to 19 April 2017 using a predefinedsearch strategy in the following electronic databases: PubMed,CINAHL and EMBASE. All conferences of the International AIDSSociety were searched from July 2001 through July 2016; themost recent Conference on Retroviruses and OpportunisticInfections (2014–2017) database were searched because pastconference abstracts were unavailable. Conferences of theAfrican Society of Laboratory Medicine (ASLM) were searched2012–2016, as well as the ASLM website and other key globalhealth websites (see supplementary information). Wesearched reference lists to identify additional literature. Thisprocess was repeated until no new citations were identified.Experts were also contacted to identify additional reports. Nogeographic restrictions were placed on the search, but thereview was limited to studies published in English.
Studies were eligible if they used at least two RDTs andreported on HIV misdiagnosis, factors related to potentialmisdiagnosis or described quality issues and related to HIVtesting error.
Initial titles were screened by one investigator (VF) todetermine eligibility. A second and a third screening wasthen carried out (VF, ST and CJ). All differences wereresolved through consensus. Data from all sources wereextracted and placed into standardized forms and verified
in duplicate (VF and ST). CJ and NF assessed study quality(see supplementary data).
Potential factors relating to misdiagnosis wereextracted from studies using defined categories: (a) cle-rical error (error in documenting and reporting informa-tion essential to a correct status); (b) user error(operator error collecting specimen, performing an HIVRDT or interpreting the result); (c) suboptimal testingstrategy (errors related to the order in which specificRDTs are used, also known as a testing strategy); (d)poor management and supervision (lack of active qualitymanagement systems); (e) weak reactive results (faintlines appearing on test strips); and (f) additional factorsincluding cross-reactivity, acute/early infection and test-ing among people on ART.
Other summary measures included: misdiagnosis rates (totalnumber of false positive diagnoses reported over the totalnumber of HIV-positive tests retested and reported using aspecific testing algorithm and the total number of false negativediagnoses reported over the number of HIV-negative testsretested and reported using a specific testing algorithm). Forstudies exclusively among people diagnosedwith HIV, reportingon false positive statuses, the total study population was usedas the denominator.
For each study, rates of diagnostic error and misdiagnosisand corresponding 95% confidence intervals (CIs) werecalculated, using Wilson’s approach, and this was displayedgraphically using forest plots [19–21]. All statistical analyseswere conducted in STATA v13.0.
ResultsSixty-four studies reporting on misdiagnosis of HIV andfactors potentially related to misdiagnosis were includedin this review (Figure 1 and Table 1).
Most studies were carried out in Africa (n = 48) [5,7,10–14,16,22–25,29,30,32–34,36,37,39,41,43,44,46,47,49,51,52,54–59,61–65,67–72,74,75], followed by in the Americas(n = 7) [28,31,42,50,53,60,66], Asia (n = 4) [8,35,45,73]and Europe (n = 1) [48]. There were also four multi-coun-try/regional studies [26,27,38,40]. Samples varied by sizeand unit of measurement, including clients (n = 38 studies,range: 303,010 to 1 clients), specimens (n = 15 studies,range: 9419 to 16 specimens), health workers performingHIV tests (n = 5 studies, range: 3835 to 39 personnel) andsites where HIV testing was performed (n = 12 studies,range: 602 to 4 sites). Nine studies reported more thanone unit of measure, and three studies did not specifysample size (see supplementary information). The majorityof studies occurred in a facility-based setting; studies car-ried out in community settings included the workplace(n = 1) [57], home-based testing (n = 2) [14,39] and amobile setting (n = 1) [32].
Factors related to the quality of HIV testing and potentialmisdiagnosisSeveral factors, including HIV testing errors, were reportedfrequently (n = 131 times) across all included studies (seeTable 2).
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
8
231
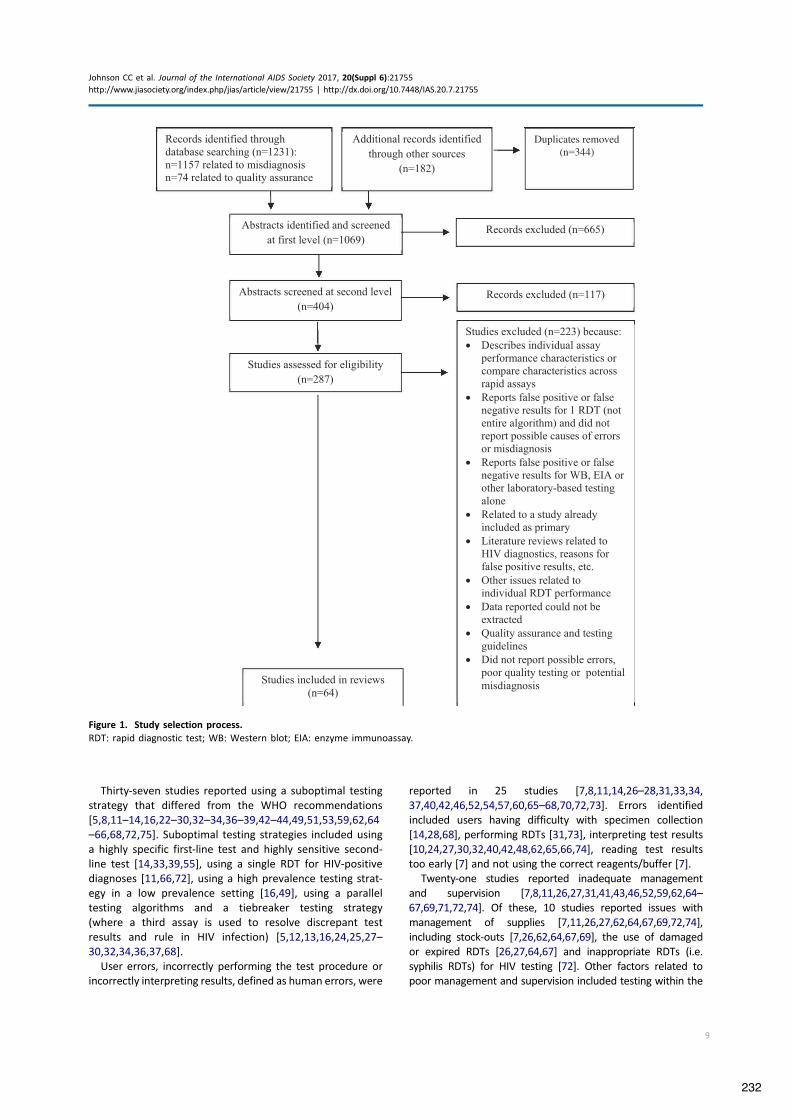
Thirty-seven studies reported using a suboptimal testingstrategy that differed from the WHO recommendations[5,8,11–14,16,22–30,32–34,36–39,42–44,49,51,53,59,62,64–66,68,72,75]. Suboptimal testing strategies included usinga highly specific first-line test and highly sensitive second-line test [14,33,39,55], using a single RDT for HIV-positivediagnoses [11,66,72], using a high prevalence testing strat-egy in a low prevalence setting [16,49], using a paralleltesting algorithms and a tiebreaker testing strategy(where a third assay is used to resolve discrepant testresults and rule in HIV infection) [5,12,13,16,24,25,27–30,32,34,36,37,68].
User errors, incorrectly performing the test procedure orincorrectly interpreting results, defined as human errors, were
reported in 25 studies [7,8,11,14,26–28,31,33,34,37,40,42,46,52,54,57,60,65–68,70,72,73]. Errors identifiedincluded users having difficulty with specimen collection[14,28,68], performing RDTs [31,73], interpreting test results[10,24,27,30,32,40,42,48,62,65,66,74], reading test resultstoo early [7] and not using the correct reagents/buffer [7].
Twenty-one studies reported inadequate managementand supervision [7,8,11,26,27,31,41,43,46,52,59,62,64–67,69,71,72,74]. Of these, 10 studies reported issues withmanagement of supplies [7,11,26,27,62,64,67,69,72,74],including stock-outs [7,26,62,64,67,69], the use of damagedor expired RDTs [26,27,64,67] and inappropriate RDTs (i.e.syphilis RDTs) for HIV testing [72]. Other factors related topoor management and supervision included testing within the
Figure 1. Study selection process.RDT: rapid diagnostic test; WB: Western blot; EIA: enzyme immunoassay.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
9
232
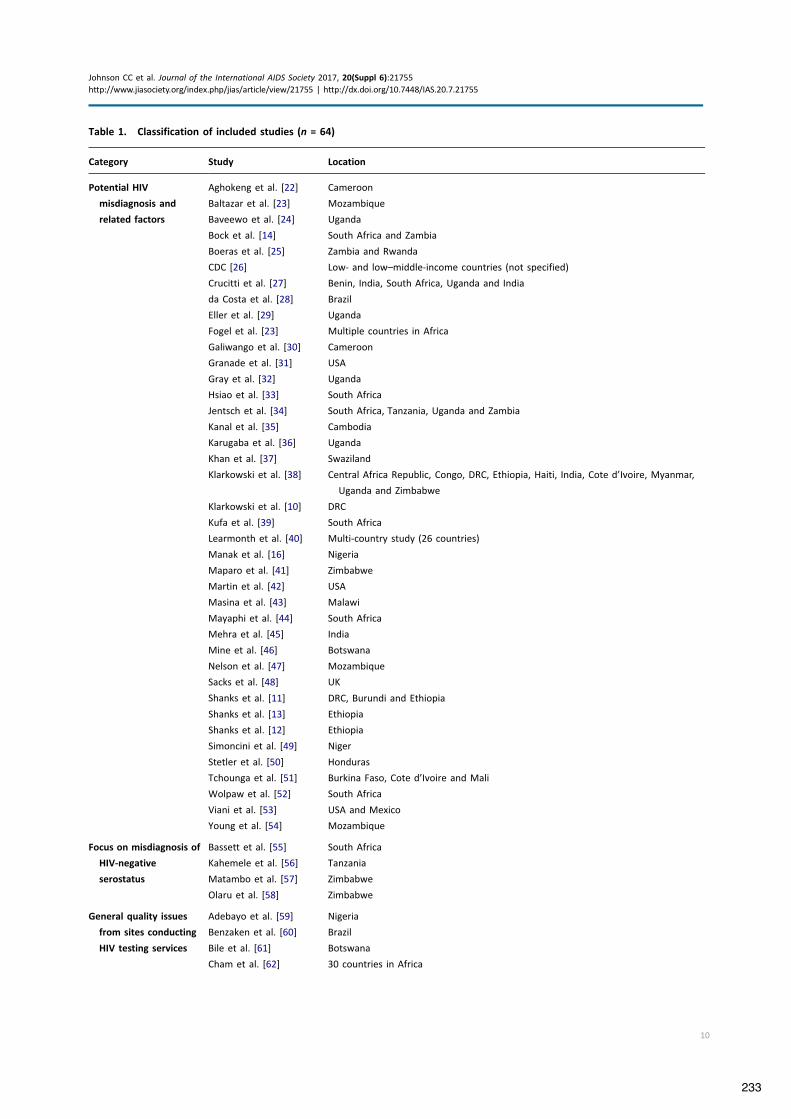
Table 1. Classification of included studies (n = 64)
Category Study Location
Potential HIV
misdiagnosis and
related factors
Aghokeng et al. [22] Cameroon
Baltazar et al. [23] Mozambique
Baveewo et al. [24] Uganda
Bock et al. [14] South Africa and Zambia
Boeras et al. [25] Zambia and Rwanda
CDC [26] Low- and low–middle-income countries (not specified)
Crucitti et al. [27] Benin, India, South Africa, Uganda and India
da Costa et al. [28] Brazil
Eller et al. [29] Uganda
Fogel et al. [23] Multiple countries in Africa
Galiwango et al. [30] Cameroon
Granade et al. [31] USA
Gray et al. [32] Uganda
Hsiao et al. [33] South Africa
Jentsch et al. [34] South Africa, Tanzania, Uganda and Zambia
Kanal et al. [35] Cambodia
Karugaba et al. [36] Uganda
Khan et al. [37] Swaziland
Klarkowski et al. [38] Central Africa Republic, Congo, DRC, Ethiopia, Haiti, India, Cote d’Ivoire, Myanmar,
Uganda and Zimbabwe
Klarkowski et al. [10] DRC
Kufa et al. [39] South Africa
Learmonth et al. [40] Multi-country study (26 countries)
Manak et al. [16] Nigeria
Maparo et al. [41] Zimbabwe
Martin et al. [42] USA
Masina et al. [43] Malawi
Mayaphi et al. [44] South Africa
Mehra et al. [45] India
Mine et al. [46] Botswana
Nelson et al. [47] Mozambique
Sacks et al. [48] UK
Shanks et al. [11] DRC, Burundi and Ethiopia
Shanks et al. [13] Ethiopia
Shanks et al. [12] Ethiopia
Simoncini et al. [49] Niger
Stetler et al. [50] Honduras
Tchounga et al. [51] Burkina Faso, Cote d’Ivoire and Mali
Wolpaw et al. [52] South Africa
Viani et al. [53] USA and Mexico
Young et al. [54] Mozambique
Focus on misdiagnosis of
HIV-negative
serostatus
Bassett et al. [55] South Africa
Kahemele et al. [56] Tanzania
Matambo et al. [57] Zimbabwe
Olaru et al. [58] Zimbabwe
General quality issues
from sites conducting
HIV testing services
Adebayo et al. [59] Nigeria
Benzaken et al. [60] Brazil
Bile et al. [61] Botswana
Cham et al. [62] 30 countries in Africa
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
10
233

window period without referring clients for retesting [32,45],HIV testing performed by undertrained or ineligible staff[7,31,59,64,72], low levels of retesting to verify diagnosisbefore ART initiation [43], poor participation in external qualityassessment (EQA) schemes [62], poor site-level supervision [65]and poor adherence to standard operating procedures[7,35,52,59,67,69].
Sixteen studies reported clerical errors [8,11,26,28,29,31,34,35,45,50,63–65,67,73,75]. Errors included poorrecord-keeping [35], data reporting problems, labellingand transcription mistakes [73] and specimen mix-ups.Poor record-keeping, according to one study, resulted innearly 30% of errors leading to incorrect status [67]. Clerical
errors were not always clearly defined and may not havealways led to misdiagnosis [28].
Fourteen studies reported challenges related to weakreactive test results, particularly difficulty with interpreta-tion [8,10,24,27,30,32,36,38,40,42,44,48,62,74]. A study,which assessed the proficiency of laboratory technicians,found that specimens with very weak levels of HIV-1/2antibodies were less accurately reported [40]. In Uganda,two studies found that the majority of false reactive resultscame from weak reactive RDTs [32,36]. A study from the UKthat assessed the visual depiction of false reactive and truepositive readings reported that most false reactive speci-mens had a fainter test line than true positive specimens
Table 1. (Continued)
Category Study Location
General quality issues Iwe et al. [63] Nigeria
from sites conducting Kalou et al. [64] Uganda and Tanzania
HIV testing services Kitheka et al. [65] Kenya
(Continued) Kyaw et al. [8] Myanmar
Louis et al. [66] Haiti
Lali et al. [67] Uganda
Manyazewal et al. [68] Ethiopia
Mashauri et al. [69] Tanzania
Mwangala et al. [70] Zambia
Ntim et al. [71] Ghana
Ocheng et al. [72] Tanzania
Plate et al. [5] 11 countries in Africa
SEAD [7] South Africa
Sushi et al. [73] India
Tegbaru et al. [74] Ethiopia
DRC: Democratic Republic of Congo.
Table 2. Reported HIV testing errors and factors potentially related to misdiagnosis
Category No. of Studies
Incorrect/suboptimal testing strategy or algorithm (e.g. testing strategies not aligned to the World Health Organization
recommendations, such as a tiebreaker or parallel testing strategies, use of a single RDT to make an HIV-positive
diagnosis)
37
User error (e.g. errors performing RDT or interpreting results, misapplication of buffer, inaccurate reading time and other
human errors)
25
Poor or inadequate management and supervision (e.g. work load stress, staff shortages, lack of training, poor adherence
to testing strategy or testing algorithm, substandard operating procedures, testing in window period)
21
Other factors (e.g. acute infection, cross-reactivity, known HIV status/on ART) 18
Clerical/technical errors (e.g. mislabelling, poor record-keeping and clerical mistakes) 16
Weak reactive test results (e.g. faint or ghost lines appearing on test strip) 14
RDT: rapid diagnostic test; ART: antiretroviral therapy.Table includes 63 reporting studies. One study (Bile et al. 2017) did not report a specific factor or error related to misdiagnosis. Some studiesreported multiple factors related to poor quality testing and factors that could be related to potential misdiagnosis.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
11
234

[48]. Two studies reported incorrect reading of weak reac-tive bands contributed to the misdiagnosis [10,11].
Eighteen studies reported on several other testing errorsand factors potentially related to misdiagnosis. Nine ofthese studies reported cross-reactivity either betweenRDTs within an algorithm or with population and individualcharacteristics [10,22,24,25,27,32,38,56,60]. One study sug-gested that cross-reactivity between assays used within analgorithm resulted in false positive statuses [27]. Anotherhypothesized that cross-reactivity may present as weakreactive lines and thereby cause misdiagnosis [32]. Sixstudies [10,11,25,38,56,60] reported potential issues withRDTs interacting with characteristics of individuals under-going testing [10,11,38], including having low levels of HIV-1/2 antibodies due to late stage HIV infection [56,60] andexposure of assays to adverse environmental conditionsduring storage and use [25,38].
Additionally, six studies reported that a proportion offalse negative diagnoses were among people with aknown HIV status who were on ART [14,16,39,44,47,58];one of these studies was among children on ART retestedusing an oral fluid-based HIV RDT [58]. And three studiesreported false negative results were due to patients testingin the window period [45] or with acute or early infection[16,44]. For instance, in South Africa, 0.04% (95% CI: 0.0–0.001) and 0.3% (95% CI: 0.1–0.4) of clients with a falsenegative diagnosis using serology tests were later found tohave acute or early HIV infection after retesting withnucleic acid testing technologies [44].
False positive diagnostic errors and misdiagnosis ratesThirty studies reported on false positive diagnostic errors(43 reports; n = 16,777 total positive diagnoses). In general,error rates were small (median: 3.1%; IQR: 0.4%-5.2%)with the exception of a few studies where a tiebreakertest was used to resolve discrepant results [10–14,23,32,33,37,39,41,44,46,47,75] (Figure 2). Of these, six stu-dies (eight reports) exclusively among people with HIV enrolledin care or ART reported that between 0.1% (95% CI: 0–0.3) and6.6% (95% CI: 4.5–9.6) of people were misdiagnosed (median:1.6%, IQR: 0.3–4.7%) [10–13,33,37,39,41,47] (Table 3).In studies reporting false positive diagnoses, nearly all
reported the use of a suboptimal testing strategy [11–13,33,39,49,75]. Sixteen studies reported the use of a tie-breaker testing strategy were related to false positive HIVdiagnoses [5,12,13,16,24,25,27,29,30,32,34,36,37,68]. In oneof these studies, 95% (123/129) of false positive statusesresulted specifically from using a tiebreaker test [32].Additionally, one study which reported misdiagnosis rates inBurundi, Democratic Republic of Congo (DRC) and Ethiopiareported some clients may have been provided an HIV-positivediagnosis based on a single HIV RDT [11].
False negative diagnostic errors and misdiagnosis ratesTwenty-eight studies reported on false negative diagnoses(40 reports, total negatives = 55,626) (median: 0.4%, IQR0–3.9%) (Figure 3) [10,12,13,37,39,47,55–57]. The studiesreporting the highest proportions, for example, Olaru et al.,which was designed to assess how ART impacts test
performance [58], of false negative diagnoses were exclu-sively among people with HIV on ART who were retestedusing an HIV RDT-based algorithm.
Nearly all studies reporting false negative diagnoses alsoreported using a suboptimal testing strategy. Four studies inSouth Africa reporting false negative diagnoses reportedthat HIV testing was conducted with an algorithm using afirst-line test with high specificity and poorer sensitivity[14,33,39,55]. According to one of these studies [14],between 2014 and 2016, the testing algorithm changedfour times in an effort to address the high proportion offalse negative diagnoses resulting from these algorithms.
Clerical and user errors [57], early/acute infection[16,44,45], presentation late in disease stage [56] and indi-viduals with known HIV status on ART who sought retesting,or were retested using oral fluid-based RDTs [58], were alsoreported as factors contributing to false negative diagnosticerrors [14,16,39,44,47]. In Zimbabwe, all the reported falsenegative diagnoses were among children on ART who wereretested with an oral fluid-based HIV RDT [58]. In SouthAfrica and Zambia, individuals on ART comprised 44% (26/59) and 14% (5/38) of false negative diagnoses, respectively[14]. In Mozambique, 88% (21/24) of all true HIV-positiveclients with a false negative test result were confirmed toknow their HIV status and 62% (13/21) were reportedly onART [47]; reasons for retesting in study reportedly includedusers misunderstanding the question or hoping to receivehealth services and emotional or mental health issues.
DiscussionThis review identified and described a number of diagnosticerrors and poor HIV testing practices that may lead tomisdiagnosis. Data on the magnitude of misdiagnosis wasidentified but limited, and no study could determine orquantify the exact cause(s) of misdiagnosis. Although nostudies could determine and quantify the exact cause(s) ofmisdiagnosis, several identified the following factors tohave strongly contributed: (1) suboptimal testing strategies,(2) poor management of supplies, (3) user errors includingdifficulty interpreting weak reactive lines and (4) retestingamong people with known HIV status on ART.
No assay is perfect. False reactive and false non-reactiveresults are inevitable when using a single RDT and should beanticipated. However, the risk of misdiagnosis should be verylow when a validated testing algorithm for high (!5%) or low(<5%) prevalence settings is used [76]. In this review, we iden-tified that many studies reporting diagnostic errors - both falsepositive and false negative - utilized suboptimal testing strate-gies which were not aligned to international guidance. Studiesreviewed clearly showed the use of a tiebreaker strategy torule-in HIV infection increases the likelihood of false positivestatuses and possible misdiagnosis. This is concerning becausea third of national testing strategies reviewed in 2015 recom-mended using a tiebreaker testing strategy [9].
In addition to adopting a proven testing strategy, nationalor regional validation is critical to determine which RDTs,and in which order, perform the best as a complete algo-rithm. As previously reported [38,77–83], tests and
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
12
235

algorithm performance vary across settings, often due tocross-reactivity caused by HIV subtypes, co-infections,comorbidities and possible environmental or populationcharacteristics. Without validating a testing algorithm at acountry or regional level, it would not be possible to fullyunderstand the causes of poor performance. Furthermore,to ensure correct diagnoses, it is important to retest peoplediagnosed HIV positive before they enrol in care and ART.This is a cost-effective approach [84] which is increasinglycritical as more people with HIV are being offered immedi-ate treatment.
To ensure correct results, all staff providing HIV testingmust be trained, certified and provided ongoing supportand supervision. In several studies, this was not the case,
and untrained and uncertified providers were performingHIV testing [7,72]. Training, including pre-service, in-serviceand periodic refresher training, is important to maintainand improve the quality of services. Participation in EQAschemes is another way to monitor performance andimprove testing services. Several studies also reporteduser and clerical errors resulted from inadequate support,demanding workloads, burnout and high levels of stress[11,62,64,66]. Adequate support and supervision are criticalto reduce stock outs which may contribute to the use ofdamaged or expired test kits, incorrect test kits and buffer.Sites should routinely assess and manage their supplies andhuman resource planning to prevent or reduce thesecircumstances.
Boeras et al. 2011Gray et al. 2007Fogel et al. 2015cSacks et al. 2012Fogel et al. 2015dFogel et al. 2015aBock et al. 2017 SAFogel et al. 2015bKanal et al. 2005Mehra et al. 2014 aMine et al. 2015bMehra et al. 2014 bJentsch et al. 2012Crucitti et al. 2011Aghokeng et al.. 2009bShanks et al. 2015 (VL)Shanks et al. 2015Bock et al. 2017 ZAMEller et al. 2007Klarkowski et al.. 2009Shanks et al. 2015 (No VL)Kufa et al. 2017Shanks et al. 2013 cShanks et al. 2013 bGranade et al. 2004aGranade et al. 2004bViani et al. 2013Shanks et al. 2013 aMine et al. 2015aAghokeng et al.. 2009aStetler et al. 1997Baveewo et al. 2012Manak et al. 2015 (HP)Baltazar et al. 2014bKhan et al. 2017Martin et al. 2011Hsiao et al. 2017Maparo et al. 2015Baltazar et al. 2014aNelson et al. 2016Manak et al. 2015 (LP)Bassett et al. 2011Mayaphi et al. 2016
Study
45.95 (31.04, 61.62)43.73 (38.18, 49.43)38.64 (25.72, 53.38)34.62 (19.41, 53.78)33.33 (21.01, 48.45)33.33 (9.68, 70.00)32.78 (27.16, 38.94)22.22 (6.32, 54.74)18.18 (5.14, 47.70)12.20 (5.32, 25.54)11.11 (4.41, 25.31)10.26 (4.06, 23.58)10.24 (7.95, 13.10)8.70 (3.43, 20.32)8.26 (4.40, 14.95)7.84 (3.09, 18.50)7.31 (4.55, 11.54)7.02 (5.84, 8.43)6.58 (3.43, 20.32)6.58 (4.46, 9.60)6.54 (3.94, 10.68)6.00 (2.00, 24.00)4.81 (3.61, 6.40)4.70 (2.29, 9.38)4.21 (1.65, 10.33)4.11 (1.41, 11.40)4.00 (0.71, 19.54)2.56 (0.71, 8.88)2.43 (1.28, 4.56)1.96 (0.54, 6.87)1.61 (0.44, 5.69)1.38 (0.83, 2.31)1.16 (0.21, 6.30)0.78 (0.30, 1.96)0.55 (0.33, 0.93)0.54 (0.15, 1.95)0.32 (0.11, 0.92)0.28 (0.11, 0.71)0.19 (0.03, 1.09)0.09 (0.03, 0.28)0.00 (0.00, 1.59)0.00 (0.00, 27.75)0.00 (0.00, 6.31)
positive (95% CI)Proportion false
C, FC, E, FA, CEA, CA, CB, C, FA, CAA, FB, DA, FA,B,CB, C, D, E, FC, FC, FCB, C, FA, CC, E, FCC, FB, D, CB, D, CA, B, D, FA, B, D, FCB, D, CB, DC, FAC, EC, FC, FB, CB, C, EB, CDC, FFC, FCE, F
Factors
0 100
Figure 2. Rates of false positive diagnostic error rates diagnosis (n = 30 studies, 43 reports).LP: low prevalence; HP: high prevalence; ZAM: Zambia; VL: visceral Leishmaniasis; Data reported include reports of misdiagnosis of HIV-positive statuses. False positive diagnoses were reported in 30 studies (43 reports), total positive diagnoses n = 16,777. Kufa et al. 2017reported proportion misdiagnosed by did not report full sample size. In studies where all participants were known to be HIV positive and/oron ART at the beginning of the study, the full study population was used as the denominator.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
13
236

Table 3. Rates of false positive diagnosis rates among people diagnosed with HIV and/or enrolled in care or antiretroviral therapy(ART)
Study/author Sample size Total no. of retested No. of false positives Percentage of false positive diagnoses
Klarkowski et al. 2009 365 229 24 6.6
Shanks et al. 2013c 914 54 44 4.8
Shanks et al. 2013b 149 149 7 4.7
Shanks et al. 2013a 78 78 2 2.6
Khan et al. 2017 2533 88 14 0.55
Hsiao et al. 2017 952 37 3 0.3
Maparo et al. 2015 1447 1447 4 0.28
Nelson et al. 2016 3160 3146 3 0.1
Olaru et al. 2017 (blood)Olaru et al. 2017 (oral)Khan et al. 2017Fogel et al. 2015aFogel et al. 2015bMartin et al. 2011Kufa et al. 2017Granade et al. 2004bGranade et al. 2004aAghokeng et al.. 2009aNelson et al. 2016Mehra et al. 2014 bFogel et al. 2015cBoeras et al. 2011Mine et al. 2015aBock et al. 2017 SABassett et al. 2011Mayaphi et al. 2016Fogel et al. 2015dKanal et al. 2005Baltazar et al. 2014aGray et al. 2007Bock et al. 2017 ZAMManak et al. 2015 (LP)Manak et al. 2015 (HP)Matambo et al. 2006Baltazar et al. 2014bEller et al. 2007Mehra et al. 2014 aShanks et al. 2015Sacks et al. 2012Crucitti et al. 2011Shanks et al. 2015 (No VL)Shanks et al. 2015 (VL)Aghokeng et al.. 2009bStetler et al. 1997Jentsch et al. 2012Mine et al. 2015bViani et al. 2013Baveewo et al. 2012
Study
100.00 (20.65, 100.00)100.00 (74.12, 100.00)82.35 (58.97, 93.81)18.18 (12.32, 26.00)13.41 (9.03, 19.48)12.50 (4.97, 28.07)8.30 (5.70, 11.90)7.32 (2.52, 19.43)6.00 (2.06, 16.22)5.66 (2.62, 11.00)3.33 (0.59, 16.67)2.28 (1.21, 4.28)1.55 (0.43, 5.48)1.49 (0.58, 3.76)1.39 (0.67, 2.83)1.09 (0.85, 1.42)1.02 (0.55, 1.86)0.82 (0.64, 1.07)0.76 (0.13, 4.20)0.36 (0.10, 1.31)0.34 (0.13, 0.88)0.33 (0.13, 0.84)0.25 (0.18, 0.34)0.23 (0.08, 0.69)0.19 (0.06, 0.55)0.18 (0.03, 1.03)0.09 (0.02, 0.49)0.02 (0.00, 0.11)0.00 (0.00, 48.99)0.00 (0.00, 1.80)0.00 (0.00, 11.35)0.00 (0.00, 0.07)0.00 (0.00, 1.97)0.00 (0.00, 9.18)0.00 (0.00, 3.70)0.00 (0.00, 1.36)0.00 (0.00, 0.69)0.00 (0.00, 1.45)0.00 (0.00, 0.11)0.00 (0.00, 0.16)
negative (95% CI)Proportion false
FFB, CA,CA,CB,C,EC,FA, B, D, FA, B, D, FC,FFA, FA,CC, FB, DB, C, FCE,FA,CAC,FC, E, FB, C, FC,FC,FB,CC,FA,CA, FCEB, C, D, E, FCC, FC,FAA,B,CB,DCC,E
Factors
0 100
Figure 3. False negative diagnostic error rates (n = 28 studies, 40 reports).LP: low prevalence; HP: high prevalence; SA: South Africa, discrepant results; ZAM: Zambia, discrepant results; VL: visceral Leishmaniasis;Data reported includes reports of misdiagnosis of HIV-negative statuses. Misdiagnoses of HIV-negative statuses were reported 28 studies (40reports), total negative = 55, 626. Kufa et al. 2017 reported proportion misdiagnosed but did not report full sample size information.Note Olaru et al. was exclusively among people with HIV on ART, accounting for the high rate of false negative diagnoses.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
14
237

User error interpreting weak reactive lines was a com-mon challenge which contributed to false positive results.To address this, specialized training for health workers andsite-level standard operating procedures including the useof a “second-reader” to validate the correct interpretationof test results may be needed, as well as work with man-ufacturers to improve RDTs and instructions on how tointerpret faint lines and weak control lines. Several studieshypothesized that weak reactive lines may be caused byother user errors, for example, misapplication of buffer andreading test results too early and cross-reactivity. Furtherinvestigation into the cause of weak reactive and otherfaint lines, and how they can be prevented, is needed.
False negative test results among people with HIV andon ART were observed and contributed to a substantialproportion of misdiagnoses [14,16,39,44,47]. While it isunclear why people on ART would seek retesting, somereports suggest it may be due to wanting to “check” or“confirm” one’s HIV status and religious beliefs aboutbeing “cured” [85], as well as misunderstandings andemotional or mental health issues [47]. It is importantfor programmes and users to be aware of the potentialrisk of false negative results, as the presence of ART canlead to confusing test results and could result in indivi-duals unnecessarily stopping treatment which could havedire individual and public health implications. As “treat all”policies are rolled out, it will be increasingly critical forprogrammes to address this issue and ensure clients andhealth workers are aware that testing individuals on ART isnot recommended [76].
Strengths and limitationsThis analysis is the first to bring together a diverse set ofstudies with the aim of identifying and describing subopti-mal HIV testing practices and misdiagnosis. The resultsindicate the problem of misdiagnosis deserves attention.However, there are several limitations to this review.
As with all literature reviews, publication bias may bean issue and for this topic is inevitable and informationon misdiagnosis is often unreported. This review was alsolimited to reports in English and may have missed reportsin other languages. The majority of reports are fromAfrica and may not be representative of other geogra-phies. Because the review was designed to identifyreports of misdiagnosis, it is possible studies reportingerrors and quality of HIV testing may have been missed.
Due to both the paucity and heterogeneity of data, it wasnot possible to conduct more quantitative analyses. Studiesincluded were generally not designed to determine theexact cause or causes of misdiagnoses, a weakness citedacross research on diagnostic errors [86].
This review focused on human errors and quality systemfailures. While we did identify some reports of cross-reac-tivity [10,22,24,25,27,32,38,56,60], reports did not provideconclusive information on what exactly caused cross-reac-tivity. Possible biological factors due to antibodies frominter-current infections, adverse environmental exposureto assay components, HIV subtype or shared false cross-
reactivity in RDTs within an algorithm may be issues requir-ing further investigation.
Acute and early infection did not appear to be a signifi-cant cause of false negative diagnoses; however, few stu-dies identified reported on acute infection. Retestingamong HIV-positive individuals taking ART did emerge as akey factor contributing to a substantial proportion of falsenegative diagnostic errors and misdiagnoses. Furtherresearch is needed to understand how ART, as well as theuse of antiretroviral drugs for prevention, for example, pre-exposure prophylaxis, may impact the performance of HIVRDTs, as well as how frequently people previously diag-nosed with HIV and on ART retest.
ConclusionsOur review has identified a number of factors and practicesthat may contribute to diagnostic error and HIV misdiagno-sis. Although no study could fully determine and quantifythe exact cause(s) of misdiagnosis, our review elucidatedfour key factors: (1) suboptimal testing strategies, primarilythe use of a tiebreaker testing strategy to rule in HIVinfection, (2) user errors including interpretation of weakreactive lines, (3) inadequate management and supervisionof testers and (4) retesting among people with HIV on ART.Most, if not all, are avoidable with appropriate guidelines,training and supervision. The consequences of misdiag-noses are serious at an individual and public health level.With the momentum to scale-up HIV diagnosis and linkageto ART, a parallel push to improve the quality of HIV testingservices and prevent misdiagnosis is essential.
Authors’ affiliations1Department of HIV, World Health Organization, Geneva, Switzerland;2Department of Clinical Research, London School of Hygiene and TropicalMedicine, London, UK; 3Department of Psychiatry and Behavioral Sciences,Medical University of South Carolina, Charleston, SC, USA; 4Department ofEssential Medicines and Health Products, World Health Organization,Geneva, Switzerland; 5Department of Epidemiology and Population Health,American University of Beirut, Beirut, Lebanon; 6Department of InternationalHealth, Johns Hopkins University, Bloomberg School of Public Health,Baltimore, MD, USA; 7US Agency for International Development,Washington, DC, USA
Competing interestsThe authors declare no completing interests. The authors alone are respon-sible for the views expressed in this article and they do not necessarilyrepresent the views, decisions or policies of the institutions with which theyare affiliated.
Authors’ contributionsRB, CMO, CJ and AS conceived of and provided overall guidance to the study.VF and ST conducted the primary literature review and drafted the initialreport. VF and CJ conducted the update of the literature review and dataextraction. CJ primarily drafted the manuscript, performed quality assess-ment and data analyses and undertook supplementary literature reviews. NFand CJ conducted the analyses. All authors have contributed to the concep-tualization of the study, contributed to the development of drafts and readand approved the final version.
FundingThis publication was supported in part by a grant from the US NationalInstitutes of Health (NIH; 5 R01 HD053268), Carla Makhlouf Obermeyer, PI,
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
15
238

and the U.S. Agency for International Development (USAID), with supportfrom the U.S. President’s Emergency Plan for AIDS Relief. The content of thissupplement is solely the responsibility of the authors and does not necessa-rily represent the official views of the USA Government or the World HealthOrganization.
DisclaimerThe funders of the study had no role in study design, data collection, dataanalysis, data interpretation or writing of the report. The correspondingauthor had full access to all the data in the study and had final responsibilityfor the decision to submit for publication.
References
1. WHO. Towards universal access by 2010: how WHO is working withcountries to scale-up HIV prevention, treatment, care and support.Geneva:World Health Organization;2006.2. WHO. Factsheet to the WHO consolidated guidelines on HIV testingservices. Geneva:World Health Organization;2015.3. UNAIDS. Get on the fast-track: the life cycle approach to HIV. Geneva:JointUnited Nations Programme on HIV/AIDS;2016.4. Molesworth AM, Ndhlovu R, Banda E, Saul J, Ngwira B, Glynn JR, et al.High accuracy of home-based community rapid HIV testing in rural Malawi. JAcquir Immune Defic Syndr. 2010;55(5):625–30.5. Plate, DK, Group, RHIVTEW. Evaluation and implementation of rapid HIVtests: the experience in 11 African countries. AIDS Res Hum Retroviruses.2007;23(12):1491–98.6. Lyamuya EF, Aboud S, Urassa WK, Sufi J, Mbwana J, Ndugulile F, et al.Evaluation of simple rapid HIV assays and development of national rapid HIVtest algorithms in Dar es Salaam, Tanzania. BMC Inf Dis. 2009;9.7. SEAD. Analysis of POCT/VCT performed at South African primary healthcare clinics 2010 [cited 2014 July 14]. Available from: http://www.sead.co.za/downloads/POCT-clinics-2011.pdf8. Kyaw LL, Nozaki I, Wada K, Oo KY, Tin HH, Yoshihara N. Ensuring accuratetesting for human immunodeficiency virus in Myanmar. Bull World HealthOrg. 2015;93(1):42–46.9. Flynn D, Johnson C, Sands A, Wong V, Baggaley R. Annex 2. An analysis of48 national HIV testing and counselling policies. Geneva:World HealthOrganization;2015.10. Klarkowski DB, Wazome JM, Lokuge KM, Shanks L, Mills CF, O’Brien DP.The evaluation of a rapid in situ HIV confirmation test in a programme with ahigh failure rate of the WHO HIV two-test diagnostic algorithm. PloS One.2009;4(2).11. Shanks L, Klarkowski D, O’Brien DP. False positive HIV diagnoses inresource limited settings: operational lessons learned for HIV programmes.PloS One. 2013;8(3).12. Shanks L, Ritmeijer K, Piriou E, Siddiqui MR, Kliescikova J, Pearce N, et al.Accounting for false positive HIV tests: is visceral Leishmaniasis responsible?PloS One. 2015;10(7):e0132422.13. Shanks L, Siddiqui MR, Kliescikova J, Pearce N, Ariti C, Muluneh L, et al.Evaluation of HIV testing algorithms in Ethiopia: the role of the tie-breakeralgorithm and weakly reacting test lines in contributing to a high rate of falsepositive HIV diagnoses. BMC Infect Dis. 2015;15:39.14. Bock P, Phiri C, Piwowar Manning E, Kosloff B, Mandla N, Young A, et al.Understanding low sensitivity of community-based HIV rapid testing: experi-ences from the HPTN 071 (PopART) trial in Zambia and South Africa. J IntAIDS Soc. 2017;20(Suppl 6):21780.15. WHO. Diagnostic errors: technical series on safer primary care. Geneva:World Health Organization;2016.16. Manak MM, Njoku OS, Shutt A, Malia J, Jagodzinski LL, Milazzo M, et al.Evaluation of performance of two rapid tests for detection of HIV-1 and "2 inhigh- and low-prevalence populations in Nigeria. J Clin Microbiol. 2015;53(11):3501–06.17. Jaspard M, Le Moal G, Saberan-Roncato M, Plainchamp D, Langlois A,Camps P, et al. Finger-stick whole blood HIV-1/-2 home-use tests are moresensitive than oral fluid-based in-home HIV tests. PloS One. 2014;9(6):e101148.18. O’Connell RJ, Merritt TM, Malia JA, VanCott TC, Dolan MJ, Zahwa H, et al.Performance of the OraQuick rapid antibody test for diagnosis of human
immunodeficiency virus type 1 infection in patients with various levels ofexposure to highly active antiretroviral therapy. J Clin Microbiol. 2003;41(5):2153–55.19. Freeman MF, Tukey JW. Transformations related to the angular and thesquare root. Ann Math Stat. 1950;21:607–11.20. Miller J. The inverse of the Freeman-Tukey double arcsine transforma-tion. Amer Stat. 1978;32(4):138.21. Brown L, Cat T, DasGupta A. Interval estimation for a proportion. Stat Sci.2001;16:101–33.22. Aghokeng AF, Mpoudi-Ngole E, Dimodi H, Atem-Tambe A, Tongo M,Butel C, et al. Inaccurate diagnosis of HIV-1 group M and O is a key challengefor ongoing universal access to antiretroviral treatment and HIV preventionin Cameroon. PloS One. 2009;4(11).23. Baltazar CS, Raposo C, Jani IV, Shodell D, Correia D, Da Silva CG, et al.Evaluation of performance and acceptability of two rapid oral fluid tests forHIV detection in Mozambique. J Clin Micr. 2014;52(10):3544–48.24. Baveewo S, Kamya MR, Mayanja-Kizza H, Fatch R, Bangsberg DR, CoatesT, et al. Potential for false positive HIV test results with the serial rapid HIVtesting algorithm. BMC Res Not. 2012;5:154.25. Boeras DI, Luisi N, Karita E, McKinney S, Sharkey T, Keeling M, et al.Indeterminate and discrepant rapid HIV test results in couples’ HIV testingand counselling centres in Africa. J Int AIDS Soc. 2011;14(1):18.26. CDC. HIV testing for surveillance: evidence from assessments of routinediagnostic testing in ANC. Presented at: WHO HIV testing and counsellingconsultation; 2014 Sep 10-12; Geneva, Switzerland.27. Crucitti T, Taylor D, Beelaert G, Fransen K, Van Damme L. Performance ofa rapid and simple HIV testing algorithm in a multicenter phase III micro-bicide clinical trial. Clin Vac Immun. 2011;18(9):1480–85.28. Da Costa Ferreira JO, Ferreira C, Riedel M, Widolin V, Ito S, Westman S,et al. Field evaluation of an HIV rapid test algorithm for the rapid diagnosisof HIV infection in Brazil. Presented at: HIV Pathogenesis, Treatment andPrevention; 2007 July 22-25 Sydney, Australia.29. Eller LA, Eller MA, Ouma BJ, Kataaha P, Bagaya BS, Olemukan RL, et al.Large-scale human immunodeficiency virus rapid test evaluation in a low-prevalence Ugandan blood bank population. J Clin Microbiol. 2007;45(10):3281–85.30. Galiwango RM, Musoke R, Lubyayi L, Ssekubugu R, Kalibbala S,Ssekweyama V, et al. Evaluation of current rapid HIV test algorithms inRakai, Uganda. J Virol Methods. 2013;192(1–2):25–27.31. Granade TC, Parekh BS, Phillips SK, McDougal JS. Performance of theOraQuick and Hema-Strip rapid HIV antibody detection assays by non-labor-atorians. J Clin Virol. 2004;30(3):229–32.32. Gray RH, Makumbi F, Serwadda D, Lutalo T, Nalugoda F, Opendi P, et al.Limitations of rapid HIV-1 tests during screening for trials in Uganda: diag-nostic test accuracy study. BMJ Open. 2007;335(7612):188.33. Hsiao N, Zerbe A, Phillips T,Myer L, Abrams E.Misdiagnosed HIV infection inpregnant women initiating universal ART in South Africa. J Int AIDS Soc. 2017;20(Suppl 6):21758.34. Jentsch U, Lunga P, Lacey C, Weber J, Cairns J, Pinheiro G, et al. Theimplementation and appraisal of a novel confirmatory HIV-1 testing algo-rithm in the Microbicides Development Programme 301 Trial (MDP301). PloSOne. 2012;7(9).35. Kanal K, Chou TL, Sovann L, Morikawa Y, Mukoyama Y, Kakimoto K.Evaluation of the proficiency of trained non-laboratory health staffs andlaboratory technicians using a rapid and simple HIV antibody test. AIDS ResTher. 2005;2:5.36. Karugaba P, Elbireer A, Nansamba A, Amukele T Weakly reactive HIVrapid diagnostic test kits shouldn’t be reported as positive. Presented at:Conference on Retroviruses and Opportunistic Infections; 2016 Feb 22–25;Boston, USA.37. Khan S, Mafara E, PasipamireM, SpiegelmanM, S;M, Ntshalintshali N, et al.Identification of misdiagnosed HIV clients in an early access to ART for allimplementation study in Swaziland. J Int AIDS Soc. 2017;20(Suppl 6):21756.38. Klarkowski D, Glass K, O’Brien D, Lokuge K, Piriou E, Shanks L. Variationin specificity of HIV rapid diagnostic tests over place and time: an analysis ofdiscordancy data using a bayesian approach. PloS One. 2013;8(11).39. Kufa T, Kharsany A, Cawood C, Khanyile D, Lewis L, Grobler A, et al.Misdiagnosis of HIV infection during a South African community-based sur-vey: implications for rapid HIV testing. J Int AIDS Soc. 2017;20(Suppl6):21753.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
16
239

40. Learmonth KM, McPhee DA, Jardine DK, Walker SK, Aye TT, Dax EM.Assessing proficiency of interpretation of rapid human immunodeficiencyvirus assays in nonlaboratory settings: ensuring quality of testing. J ClinMicr. 2008;46(5):1692–97.41. Maparo T, Arhem J, Harrison R, Matimba M, Belaye AK, Bara H, et al. Anevaluation of false positive HIV results due to testing errors. Presented at:International Conference on AIDS and STIs in Africa; 29 Nov 2015 Dec 4;Harare, Zimbabwe.42. Martin EG, Salaru G, Paul SM, Cadoff EM. Use of a rapid HIV testingalgorithm to improve linkage to care. J Clin Vir. 2011;52(Suppl. 1):S11–S5.43. Masina T. Implementing HTS quality systems and retesting before ART initia-tion. Lilongwe:Ministry of Health Malawi;2017.44. Mayaphi SH, Martin DJ, Quinn TC, Laeyendecker O, Olorunju SA, TintingerGR, et al. Detection of acute and early HIV-1 infections in an HIV hyper-endemic area with limited resources. PloS One. 2016;11(10):e0164943.45. Mehra B, Bhattar S, Bhalla P, Rawat D. Rapid tests versus ELISA forscreening of HIV infection: our experience from a voluntary counsellingand testing facility of a tertiary care centre in North India. Isrn Aids.2014;2014:296840.46. Mine M, Chishala S, Makhaola K, Tafuma TA, Bolebantswe J, MerriganMB. Performance of rapid HIV testing by lay counselors in the field duringthe behavioral and biological surveillance survey among female sex workersand men who have sex with men in Botswana. J Acquir Immune Defic Syndr.2015;68(3):365–68.47. Nelson R, MacKellar D, Thompson R, De Almeida M, Bonzela J, MugabeD, et al. Low prevalence of false prior HIV diagnoses in Chokwe district,Mozambique. Presented at: Conference on Retroviruses and OpportunisticInfections; 2016Feb 22-25; Boston, USA.48. Sacks R, Omodele-Lucien A, Whitbread N, Muir D, Smith A. Rapid HIVtesting using Determine HIV 1/2 antibody tests: is there a differencebetween the visual appearance of true- and false-positive tests? Int J STDAIDS. 2012;23(9):644–46.49. Simoncini GM, Megill M, Berg-Wolf MV. Reducing false-positive HIVdiagnosis in Niger: a women’s issue. J Int Assoc Provid AIDS Care. 2015;15(1):15–8.50. Stetler HC, Granade TC, Nunez CA, Meza R, Terrell S, Amador L, et al.Field evaluation of rapid HIV serologic tests for screening and confirmingHIV-1 infection in Honduras. Aids. 1997;11(3):369–75.51. Tchounga BK, Inwoley A, Coffie PA, Minta D, Messou E, Bado G, et al. Re-testing and misclassification of HIV-2 and HIV-1&2 dually reactive patientsamong the HIV-2 cohort of the West African Database to evaluate AIDScollaboration. J Int AIDS Soc. 2014;17(1):19064.52. Wolpaw BJ, Mathews C, Chopra M, Hardie D, De Azevedo V, Jennings K,et al. The failure of routine rapid HIV testing: a case study of improving lowsensitivity in the field. BMC Health Serv Res. 2010;10:73.53. Viani RM, Araneta MRG, Spector SA. Parallel rapid HIV testing in preg-nant women at Tijuana General Hospital, Baja California, Mexico. AIDS ResHum Retro. 2013;29(3):429–34.54. Young PW, Mahomed M, Horth RZ, Shiraishi RW, Jani IV. Routine datafrom prevention of mother-to-child transmission (PMTCT) HIV testing not yetready for HIV surveillance in Mozambique: a retrospective analysis ofmatched test results. BMC Infec Dis. 2013;13(1).55. Bassett IV, Chetty S, Giddy J, Reddy S, Bishop K, Lu Z, et al. Screening foracute HIV infection in South Africa: finding acute and chronic disease. HIVMed. 2011;12(1):46–53.56. Kahemele NJ, Lyyaruu E, Mayeye M. HIV infection diagnostic uncertai-nity, a field experience.. Presented at: AIDS 2008 - XVII International AIDSConference; 2008 3-8 August; Mexico City, Mexico.57. Matambo R, Dauya E, Mutswanga J, Makanza E, Chandiwana S, MasonPR, et al. Voluntary counseling and testing by nurse counselors: what is therole of routine repeated testing after a negative result?. Clin Infect Dis.2006;42(4):569–71.58. Olaru I, McHugh G, Dakshina S, Majonga E, Dauya E, Bandason T, et al.False negative HIV tests using oral fluid tests in children taking antiretroviraltherapy from Harare, Zimbabwe. J Int AIDS Soc. 2017.59. Adebayo A, Olufemi A, Adekunle B, Louisa O A Limited survey on HIV-testing knowledge and practice of laboratory personnel at some point-of-care services in Abuja, Federal Capital Territory (FCT), Nigeria. Presented at:African Society of Laboratory Medicine; Cape Town, South Africa. Oral Posteron Wednesday, Dec. 5 2012 2012.
60. Benzaken AS, Bazzo ML, Galban E, Pinto ICP, Nogueira CL, Golfetto L,et al. External quality assurance with dried tube specimens (DTS) for point-of-care syphilis and HIV tests: experience in an indigenous populationsscreening programme in the Brazilian Amazon. Sex Trans Inf. 2014;90(1):14–18.61. Bile E, Bachanas P, Maurice F, Modise S, Chebani L, Makovore V, et al.Accuracy of HIV and CD4 field testing in the Botswana combination preven-tion project. Presented at: Conference on Retroviruses and OpportunisticInfections; 13-16 February 2017; Seattle, USA.62. Cham F, Maleka M, Masango M, Goetsch E, Belabbes EH, Singh B, et al.The World Health Organization African region external quality assessmentscheme for anti-HIV serology. Afr J Lab Med. 2012;1(1). Art. 39.63. Iwe E, Livinus I, Omoregbe E, Okoye B, Nwuba C, Mbanefo A et al.Preparation and use of dry tube specimens (DTS) method by laboratoriansand non- laboratorians for quality assurance of HIV services (HCT) in MSHsupported sites, Niger State, North-Central Nigeria. Presented at: 6th IASConference on HIV Pathogenesis and Treatment; 2001 17-21 July; Rome,Italy.64. Kalou M, Mosha F, Ndlovu N, Jackson K, Mwassekage M, Ngoi M, et al.Implementation of a proficiency testing program using dried tube specimen(DTS) approach to improve the quality of HIV rapid testing in testing sites inUganda and Tanzania. Presented at: First International Conference of theAfrican Society for Laboratory Medicine; 2012 5 December 2012; Cape Town,South Africa.65. Kitheka F, Umuro M, Mwa S, editors. Implementing rapid HIV proficiencytesting program in Kenya: key findings from corrective actions following theswitch from facility-based to individual-based proficiency testing. FirstInternational Conference of the African Society for Laboratory Medicine;2012 5 December 2012; Cape Town, South Africa.66. Louis FJ, Anselme R, Ndongmo C, Buteau J, Boncy J, Dahourou G, et al.Evaluation of an external quality assessment program for HIV testing in Haiti,2006-2011. Am J Clin Pathol. 2013;140(6):867–71.67. Lali W, Guma G, Awongo P, Akol Z, Kajumbula H, Namupijja P, et al.Challenges of implementation of integrated national laboratory qualityimprovement in Uganda. Presented at: AIDS 2010 - XVIII International AIDSConference; 2008 18–23 July; Vienna, Austria.68. Manyazewal T, Paterniti AD, Redfield RR, Marinucci F. Role of secondarylevel laboratories in strengthening quality at primary level health facilities’laboratories: an innovative approach to ensure accurate HIV, tuberculosis,and malaria test results in resource-limited settings. Diagn Microbiol InfectDis. 2013;75(1):55–59.69. Mashauri FM, Siza JE, Temu MM, Mngara JT, Kishamawe C, ChangaluchaJM. Assessment of quality assurance in HIV testing in health facilities in LakeVictoria zone, Tanzania. Tanzan Health Res Bull. 2007;9(2):110–14.70. Mwangala SM, Musonda K, Monze M, Musukwa K, Fylkesnes K. Accuracyin HIV rapid testing among laboratory and non-laboratory personnel inZambia: observations from the National HIV Proficiency Testing System. IntJ Inf Dis. 2014;21:129.71. Ntim NAA, Nyarko KM. Quality audit of rapid HIV diagnostic processesand outcomes in selected health facilities in the central region of Ghana. Int JInf Dis. 2014;21:132.72. Ocheng D, Mattaro S, Msilama L, Msauka A, Khama M, Mshanga N, et al.Establishing competence in HIV rapid testing among non-laboratory healthprofessional is key to tasking: preliminary results from ten regions ofTanzania. Presented at: 19th International AIDS Conference; 2012 22-27July; Washington, DC.73. Sushi K, Saraminijacob G, Thatchinamoorthy G External quality assurancescheme in a national reference laboratory for HIV testing in resource limitedsettings, India. Presented at: 6th IAS Conference on HIV Pathogenesis andTreatment; 2001 17-21 July; Rome, Italy.74. Tegbaru B, Wolday D, Messele T, Meless H, Kassa D, Tesema D, et al.Assessment of the implementation of HIV-rapid test kits at differentlevels of health institutions in Ethiopia. Ethiop Med J. 2007;45(3):293–99.75. Fogel JM, Piwowar-Manning E, Donohue K, Cummings V, Marzinke MA,Clarke W, et al. Determination of HIV status in African adults with discordantHIV rapid tests. J Acquir Immune Defic Syndr. 2015;69(4):430–38.76. WHO. Consolidated guidelines on HIV testing services. Geneva:WorldHealth Organization;2015.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
17
240

77. Lejon V, Ngoyi DM, Ilunga M, Beelaert G, Maes I, Buscher P, et al. Lowspecificities of HIV diagnostic tests caused by Trypanosoma brucei gambiensesleeping sickness. J Clin Microbiol. 2010;48(8):2836–39.78. Esteva MH, Blasini AM, Ogly D, Rodriguez MA. False positive results forantibody to HIV in two men with systemic lupus erythematosus. Ann RheumDis. 1992;51(9):1071–73.79. Riberio T, Brites C, Moreira EJ, Siller K, Silva N, Johnson WJ, et al.Serologic validation of HIV infection in a tropical area. J Acquir ImmuneDefic Syndr. 1993;6(3):319–22.80. Everett DB, Baisely KJ, McNerney R, Hambleton I, Chirwa T, Ross DA,et al. Association of schistosomiasis with false-positive HIV test results in anAfrican adolescent population. J Clin Micr. 2010;48(5):1570–77.81. Salinas A, Górgolas M, Fernández-Guerrero M. Refrain from telling badnews: patients with Leishmaniasis can have false-positive HIV test results.Clin Inf Dis. 2007;45(1):139–40.
82. Klarkowski D, O’Brien DP, Shanks L, Singh KP. Causes of false-positiveHIV rapid diagnostic test results. Exp Rev Anti Inf Ther. 2014;12(1):49–62.83. Kosack CS, Page AL, Beelaert G, Benson T, SavaneA, Ng’ang’a A, et al. Towardsmore accurate HIV testing in sub-Saharan Africa: a multi-site evaluation of HIVRDTs and risk factors for false positives. J Int AIDS Soc. 2017;19(1):1–12.84. Eaton J, Johnson C, Gregson S. The cost of not retesting: human immu-nodeficiency virus misdiagnosis in the antiretroviral therapy “test-and-offer”era. Clin Infect Dis. 2017;cix341.85. Kumwenda M, Munthali A, Phiri M, Mwale D, Gutteberg T, MacPhersonE, et al. Factors shaping initial decision-making to self-test amongst coha-biting couples in urban Blantyre, Malawi. AIDS Behav. 2014;373(26):2491–2493.86. Khullar D, Jha A, Jena A. Reducing diagnostic errors – why now? N Eng JMed. 2015:2491–93.
Johnson CC et al. Journal of the International AIDS Society 2017, 20(Suppl 6):21755http://www.jiasociety.org/index.php/jias/article/view/21755 | http://dx.doi.org/10.7448/IAS.20.7.21755
18
241
Vol:.(1234567890)
AIDS Behav (2018) 22:102–116https://doi.org/10.1007/s10461-017-1936-x
1 3
ORIGINAL PAPER
Outcomes and!Experiences of!Men and!Women with!Partner Notification for!HIV Testing in!Tanzania: Results from!a!Mixed Method StudyMarya!Plotkin1 !· Catherine!Kahabuka2!· Alice!Christensen1!· Denice!Ochola3!· Myra!Betron4!· Mustafa!Njozi1!· Werner!Maokola5!· Renatus!Kisendy5!· Erick!Mlanga6!· Kelly!Curran4,7!· Mary!Drake1!· Eusebi!Kessy8!· Vincent!Wong9!
Published online: 31 October 2017 © The Author(s) 2017. This article is an open access publication
noted disease symptoms as a motivating factor for HIV test-ing. Female index clients mentioned gender-specific chal-lenges to successful referral. Women may need additional support to overcome challenges in the partner notification process. In addition to reducing barriers to partner notifica-tion specific to women, a programmatic emphasis on social strengths of males in successfully referring partners should be considered.
Keywords HIV testing!· Partner notification!· Index clients!· Gender!· Tanzania
Abstract A growing evidence base supports expansion of partner notification in HIV testing services (HTS) in sub-Saharan Africa. In 2015, a cross-sectional study was con-ducted in Njombe region, Tanzania, to evaluate partner noti-fication within facility-based HTS. Men and women newly diagnosed with HIV were enrolled as index clients and asked to list current or past sexual partners for referral to HTS. Successful partner referral was 2.5 times more likely among married compared to unmarried index clients and 2.2 times more likely among male compared to female index clients. In qualitative analysis, male as well as female index clients mentioned di"culties notifying past or casual partners, and
* Marya Plotkin [email protected] Catherine Kahabuka [email protected] Alice Christensen [email protected] Denice Ochola [email protected] Myra Betron [email protected] Mustafa Njozi [email protected] Werner Maokola [email protected] Renatus Kisendy [email protected] Erick Mlanga [email protected] Kelly Curran [email protected] Mary Drake [email protected]
Eusebi Kessy [email protected] Vincent Wong [email protected]
1 Jhpiego Tanzania, Dar!es!Salaam, Tanzania2 CSK Research Solutions Ltd., Dar!es!Salaam, Tanzania3 Jhpiego, Consultant, Baltimore, MD, USA4 Jhpiego Baltimore, Baltimore, MD, USA5 National AIDS Control Programme, Ministry of!Health,
Community Development, Gender, Elderly and!Children, Dar!es!Salaam, Tanzania
6 USAID Tanzania, Dar!es!Salaam, Tanzania7 Johns Hopkins Bloomberg School of!Public Health,
Baltimore, MD, USA8 Ministry of!Health, Community Development, Gender,
Elderly and!Children, Njombe, Tanzania9 USAID Washington, Washington, DC, USA
242

AIDS Behav (2018) 22:102–116
1 3
Introduction
According to the 2016 UNAIDS Global AIDS Update, there are an estimated 36.7 million people living with HIV, 54% of whom are not accessing life-saving treatment [1]. E#ec-tive approaches to HIV testing are needed to reach undiag-nosed people and link them to HIV care and treatment. As part of the UNAIDS 90-90-90 goals, 90% of HIV-infected individuals will know their HIV status by the year 2020. However, few HIV testing approaches are highly e#ective in reaching undiagnosed HIV-infected people. A review drawn from Demographic and Health Surveys (DHS) from 2003 to 2011 noted that, in 16 of 25 countries studied, the majority of HIV-positive men and women have never been tested [2]. In Tanzania, 33% of women and 50% of men report never having been tested [3].
HIV testing services (HTS) in sub-Saharan African (SSA) countries have evolved as HIV prevention, care, and treat-ment interventions have changed. Between 2005 and 2007, most SSA countries began massive scale-up of HTS, and in 2007 the World Health Organization issued guidelines supporting provider-initiated testing and counseling (PITC), which recommended routine HIV testing in clinical settings [3]. By 2010, PITC policies were in place in a majority of SSA countries, with specific emphasis on testing within antenatal care services as prevention of mother-to-child transmission (PMTCT) services were rolled out [4]. How-ever, HTS expansion in SSA has not been even. The mas-sive scale-up of PMTCT services dramatically increased the number of women who learned their HIV status. A review of 29 SSA country DHS findings confirms that women are much more likely than men to have ever been tested [2]. Reaching men with HTS is thus a priority. A systematic review of strategies to increase the uptake of HIV testing among men noted that increased uptake of HTS by men is possible, and has been achieved, most notably through mobile and home-based HTS [5].
Partner notification, in which sexual partners of those recently diagnosed with HIV are notified of their exposure and referred to HIV testing, has shown promise in reach-ing previously undiagnosed individuals [6, 7] and has been shown to be well regarded by communities served by HIV testing services [8]. HIV partner notification is described in the 2015 World Health Organization (WHO) Consolidated Guidelines on HIV Testing Services, as a process in which persons newly diagnosed with HIV are enrolled as index clients, and then o#ered options for notifying and linking their sexual partners to HTS [9]. This was followed by WHO guidance released in 2016 which strongly recommended the o#er of assisted HIV partner notification for all HIV-positive persons as part of HTS [10].
A growing base of evidence supports an expanded use of partner notification for HTS in SSA, where the
majority of people living with undiagnosed HIV infection reside [11]. HIV partner notification has been shown to be e#ective in multiple countries. In Malawi, a randomized controlled trial compared passive, provider and contract referral to HIV testing of newly diagnosed HIV positive individuals, with an overall testing rate of 35% of partners (range 24–51%), of whom 64% were HIV positive [12]. An evaluation of a large scale partner services program in Cameroon found that 67% of partners tested, and 50% of them were HIV positive [13]. In Mozambique, there was a 99% acceptance rate of partner notification from com-munity health workers, and only 2.5 index partners were needed to receive assisted partner notification in order to identify a previously undiagnosed partner with HIV [14]. In a cluster randomized trial in Kenya, 67% of partners had tested at 6!weeks after the index partners had enrolled in immediate partner notification services [15]. A recent meta-analysis concluded that partner notification improved partner testing and diagnosis of HIV positive partners, with few harmful consequences [7].
Multiple studies have shown that gender norms and roles have an impact on decisions people!make around testing, partner notification of exposure, disclosure of HIV status and referral to HTS in sub-Saharan Africa [16–18]. While women‘s exposure to antenatal care services makes them more likely to be tested, they face a host of other barriers to HIV testing, status disclosure and/or partner notification that derive from gender roles and inequalities in relation-ships. These barriers may include lack of resources or ability to get to services; lack of education; and fear of violence, abandonment, or other abuse arising from partner notifica-tion [18–20].
For men, HIV testing and disclosure, particularly in SSA, may be inhibited by stigma and by social roles prescribing that men should be strong, dominant, and healthy. Multiple studies in Zimbabwe described men’s discomfort with test-ing, based on pressures related to gender roles and stereo-types [21, 22], and in Lesotho and Uganda, men described their fear of testing as a fear of showing weakness [23, 24]. A study in Zambia showed that gender determinants, including tolerant attitudes about intimate partner violence (IPV) and unequal power dynamics within relationships, had marked e#ects for men and for women, on the decision to seek HIV testing [16]. Studies have also found that men, compared to women, underestimate their level of risk of HIV infection [25]. However, once they have tested, men may be more likely to disclose their HIV status. A study of HIV-positive men and women in Burkina Faso showed that twice as many men as women reported having disclosed their HIV infection to their sexual partners, with some men indicating that they felt their role as the family’s breadwinner protected them against rejection when revealing their HIV-positive status following testing [26].
243

AIDS Behav (2018) 22:102–116
1 3
Di#erential outcomes of male versus female index cli-ents in successfully referring partners to HTS in the con-text of partner notification in SSA have not been previously described in the literature. Further, although a recent publi-cation addressed men and women’s experiences with disclo-sure of HIV status in South Africa [18], men and women’s experiences associated with partner notification has not been described. As partner notification for HTS is scaled up in SSA, gender and sex-related dimensions must be taken into account in implementation strategies, in order for partner notification and referral to HTS programs to achieve maxi-mum impact.
This paper uses findings from a study in Tanzania to explore the research question: do male and female index clients have di#erent outcomes in getting their sexual part-ners to come in for HIV testing following referral through the partner notification? The paper describes the success of men and women in referring their sexual partners to HTS in a partner notification study conducted in Tanzania, as well as describing barriers and experiences arising for index clients and their partners during the process of partner notification for HTS.
Methods
Study Design
A mixed-methods, cross-sectional study on partner notifica-tion for HIV testing was conducted in three hospitals in the Njombe region of Tanzania between June and September 2015. The overview results of the study, which looked at the e#ectiveness of partner notification in getting sexual part-ners to come to the facility for HIV testing, are described in a previous publication [27]. The current analysis examines referral outcomes among male versus female index clients. The main quantitative outcome of interest for this analysis was di#erences in success of referral for HTS among male versus female and between married and non-married index clients. The study also qualitatively explored men and wom-en’s views on barriers and other experiences!arising during the partner notification process, from both the index client and the sexual partner perspective.
Study Setting
Njombe is Tanzania’s highest HIV prevalence region, with 14.8% of the adult population infected with HIV [3]. Study facilities included peri-urban Kibena Regional Hospital, urban Makambako Town Hospital, and the rural, faith-based Ilembula Designated District Hospital. Each facility had a dedicated, on-site voluntary counseling and testing (VCT)
center, and o#ered PITC to inpatients and to outpatients. These three facilities were selected in consultation with regional authorities because of their high testing volume.
Study Population and!Eligibility Criteria
The study population comprised 390 index clients (men and women at the study facilities who had been diagnosed with HIV on the same day of testing, through either PITC or VCT) and 249 sexual partners of index clients (partners who had been listed by index clients and had come to the health facility for HIV testing). Eligibility criteria for study enrollment as an index client included the following: newly diagnosed with HIV; 18!years or older; not pregnant; had a sexual partner currently or in the past 24!months. Eligi-bility criteria for enrollment as a sexual partner was that the partner was 18!years of age or older. Pregnant women were excluded from enrolling in the study as index clients since a di#erent form of partner notification exists in Tan-zania within antenatal care services: pregnant women are encouraged to bring their partner into the health facility to be tested.
The 46 participants in the qualitative component of the study were selected on a convenience basis from the index clients and sexual partners enrolled in the study. The index clients were selected in equal number from male and female index clients who successfully referred a sexual partner and those who were not successful in referring a sexual partner, and the male and female sexual partners were selected in a roughly equal number according to whether they tested positive or negative for the virus. Index clients and partners were selected by study sta# for par-ticipating in an in-depth interview (IDI) on a convenience basis. A rough quota was given to each facility, balancing out male and female participants, and those index clients or partners who were invited to participate and agreed and consented were interviewed.
Sampling
The sample size for the study was calculated to answer the main study objectives, which was the successful referral of sexual partners of the index clients. The sample size cal-culation for the original research question was based on an assumption that index clients would list an average of one sexual partner, and that 51% of partners would come to the facility following notification, as seen in a study con-ducted in the hospital setting in Malawi [12]. Based on these assumptions, a sample size of 384 index clients was needed to detect a similar rate of attendance among sexual partners with 85% power ($!=!0·05, two-sided test). The design e#ect
244

AIDS Behav (2018) 22:102–116
1 3
(DEFF) was set at 1.0 because we expected minimal varia-tion between facilities. The sample size formula was:
The current analysis utilized this sampling framework. The di#erences between sex and marital status were thus not sampled for, but strongly emerged from the analysis.
Study Procedures
Partner Notification
Potentially eligible men and women (diagnosed with HIV through PITC or VCT at the study facilities) were referred to onsite researchers at the time of their diagnosis. Study sta#—who were trained HIV counselors—screened poten-tial participants for study eligibility for enrollment as an index client (eligibility criteria detailed above). Written informed consent was obtained from interested and eligible people before enrolling them as index clients. Index clients wrote down names and contact information for sexual part-ners in a log, and these partners are referred to in this study as “listed sexual partners.” Enrolled index clients were inter-viewed using a questionnaire that collected demographic information and contained questions to flag individuals with a history of IPV. Index clients were asked to list current or past (within 24!months) sexual partners, provide loca-tor information (most relevant being phone number), and decide how the partner was to be contacted for the referral to HTS. During partner listing, the index client was asked questions designed to identify listed sexual partners to whom disclosure or the referral to HTS might cause a risk of IPV. Any sexual partners the index client felt might react with violence were excluded from the notification process. Index clients could elect to contact the partner themselves (pas-sive referral), have the study sta# contact the partner (pro-vider referral), or attempt to contact the partner themselves, with the understanding that the study sta# would contact the partner should the index client fail (contract referral). A second written consent, was filled in before the index client listed partners, or before the study sta# followed up with a partner. Index clients were requested to list as many partners as they could, with locator information, indicating the type (married, unmarried, casual partner, boyfriend or girlfriend), duration, and status (past or current) of the relationship for each partner. Index clients were given a choice as to whether or not they wanted a written referral card to take to their partner.
Sexual partners were referred back to the facility in which the index client tested (these referred partners are now no longer “listed sexual partners” and are referred to here as
n =1.962p (1 ! p) (DEFF)
d2=
1.962 " 0.51 (1 ! 0.51) (1.0)
(0.05)2= 384
“sexual partners” or “partners”). Partners were given the name and room number of the counselor who had conducted the index client testing, and were o#ered HIV testing by the same counselor or another study counselor. This pro-cess both made it clear to the partner where to go as well as allowing the study sta# to link the partner with the index client. Sexual partners who decided to seek testing at another facility, or who decided to come in for testing but did not identify themselves to the study sta#, were not successfully referred partners in this study.
In this study, “successful referral” is defined as the part-ner coming to the health facility following referral (passive, contract or provider) whether or not the partner tested at the facility. A very small number of partners (n!=!10) came to the facility but did not test due to being previously diagnosed HIV positive. These are counted as successfully referred since they came to the facility following referral.
Qualitative Interviews
IDI participants returned to the study site for the interview, and were reimbursed for their transport costs. Interviews were conducted in Kiswahili by a trained study sta# member using a standardized interview guide. Interviews were audio recorded, transcribed into Kiswahili transcripts, and then translated into English.
Data Management and!Analysis
Quantitative data were collected either manually, using paper forms, or electronically, using tablets. Paper-based data were entered into ODK data files that had field checks for data quality. Data collected using tablets were uploaded immediately to a server in Dar es Salaam. Data were cleaned by running queries and reports using STATA version 14.0 and correcting discrepancies. Data were extracted and ana-lyzed using SPSS version 23. Qualitative data were in the form of audio files, which were transcribed and translated, entered as English transcripts, which was then uploaded into MAXQDA (VERBI Software—Consult—Sozialforschung GmbH 2014).
Descriptive statistics were performed to describe the background characteristics of index clients and success-fully referred sexual partners. Analysis entailed simple fre-quencies of the main study outcomes and cross-tabulations with Chi square tests to determine if there were significant di#erences in the success of referral for HTS among male and female index clients based on their background char-acteristics. Key analyses included di#erences in successful referral and listing of multiple partners by sex. Bivariate and multivariate logistic regressions were run to identify index client and partner characteristics associated with success-ful partner referral, including sex and marital/relationship
245

AIDS Behav (2018) 22:102–116
1 3
status. Backward elimination was used to determine the final logistic model. Covariates were included in the model if 1) they had a p value!<!0.25; and/or 2) were known to a#ect the outcome of interest from previously published studies. The main study outcomes in regression models were “listing more than one sexual partner” and “referring at least one sexual partner” for index clients (Table!2), and for sexual partners “being successful referred for HTS” and “having a positive HIV diagnosis” (Table!4). The covariates that were included in the model were age, sex, education and marital status.
For the qualitative data, a codebook was developed by a team of three researchers (DO, CK, MP) incorporating themes that corresponded to study interview guides. Eng-lish transcripts were reviewed and uploaded into MAXQDA qualitative analysis software where the data were tagged using previously identified codes as well as codes that emerged from the data, in the Grounded Theory tradition [28]. One researcher applied cross-case analysis to organize the transcript data into themes and provided relevant narra-tives and quotations illustrating each theme [29].
In analysis of qualitative data, we adapted Weinstein et!al.’s Precaution Adoption Process Model (PAPM) [30] to categorize the stages through which a partner might pass through in the decision of whether or not to come in for test-ing following a referral. The PAPM describes stages of pre-caution-taking, and seeks to elaborate the stages that people go through to commence a health-protective behavior [30].
This model, with some adaptations reflecting this study, can be seen in Fig.!1.
Ethical Oversight
The study was conducted with ethical oversight from the Institutional Review Boards (IRB) of the Johns Hopkins Bloomberg School of Public Health (IRB 00006116) and the Tanzanian National Institute of Medical Research (NIMR) IRB (NIMR/HQ/R.8a/vol.1x/1914) with support from the Njombe Regional Medical Authorities.
Results
Results: Quantitative
Overview of!Study Outcomes
Figure!2 depicts the number of HIV-positive individuals approached, enrolled index clients, and listed and success-fully referred sexual partners by sex. Of the 653 newly diag-nosed HIV-positive men and women, 390 (46.9% males and 53.1% females) were enrolled as index clients. The enrolled clients listed 439 sexual partners (224 female partners and 215 male partners). No index clients listed same-sex sexual partners. Of the listed partners, 249 (56.7%) were success-fully referred (i.e., came to a study facility following the
Partner unaware of exposure to HIV
(Stage 1)
Partner unengaged in decision to test
for HIV(Stage 2)
Partner undecided about going to
health facility for tes!ng
(Stage 3)
Partner decided to get tested(Stage 5)
Partner successfully
referred to health facility for HTC
(Stage 6)
Partner decided not to get tested
(Stage 4)
Referral to HTS from index client
Barriers to deciding to test:fear of loss of rela!onship or income; fear of s!gma; denial of risk
Barrier to engaging in decision to test: percep!on that lack of symptoms of opportunis!c infec!ons indicates no infec!on
Outcomes or experiences based on decision to test
Nega!ve outcomes: end of rela!onships; arguments, stress, depression, physical illness, anger
Posi!ve outcomes: linkage to care and treatment, sense of responsibility and caring in rela!onship
Fig. 1 PAPM model with reference to partner notification process. Text in blue is based on findings from the current study (Color figure online).Adapted from Ref. [30]
246

AIDS Behav (2018) 22:102–116
1 3
notification). Overall, 63.4% of the female partners and 49.8% of the male partners were successfully referred. Among partners who were successfully referred to the facil-ity, testing was close to universal for both female and male partners (96.5% and 95.3%, respectively).
Enrollment and!Eligibility
Enrollment and eligibility information is presented to aug-ment understanding of the type of client seen in a typical service delivery setting who may or may not be interested or eligible for partner notification. Of the 653 HIV-positive individuals who were screened, 31 were ineligible since they were under 18!years of age, and 232 did not enroll in the study for other various reasons. The most frequently reported reason for non-enrollment was not having had a partner in the past 24!months (n!=!167), followed by being distraught or decline to participate (n!=!36), or other reasons (n!=!13) (Fig.!3).
Table!1 presents demographic information on the 390 (enrolled) index clients and on the 232 newly diagnosed HIV-positive people above the age of 18 who did not enroll.
Married people were much more likely to enroll in the study than unmarried people (76.2% vs. 24.8%).
Type of!Referral and!Relationship Status
Almost all index clients (91.6%) chose passive referral, meaning that they contacted their listed sexual partners themselves (data not shown). Table!2 shows the tendency of index clients to list multiple partners and success of part-ner referral, by sex and marital status of the index clients. Among index clients, 47 listed more than one sexual partner: in multivariate analysis, male index clients were 6.2 times more likely to list more than one sexual partner than female index clients. In multivariate analysis, male index clients were 2.2 times more likely than female index clients to be successful in referring at least one partner. In multivariate analysis, married index clients were 2.5 times more likely than unmarried index clients to be successful in referring at least one partner.
Newly diagnosed HIV+ individuals
653
Male275 (42.1%)
Enrolled 183 (66.5%)
Listed partners (Females)
224
Successfully referred
142 (63.4%)
Tested for HIV137 (96.5%)
Posi!ve 91 (66.4%)
Nega!ve46 (33.6%)
Did not test for HIV5 (3.5%)
Not successfully referred
82 (36.6%)
Not enrolled92 (33.5%)
Female 378 (57.9%)
Enrolled207 (54.8%)
Listed partners (Males)
215
Not successfully referred
108 (50.2%)
Successfully referred
107 (49.8%)
Did not test for HIV5 (4.7%)
Tested for HIV102 (95.3%)
Nega!ve45 (44.1%)
Posi!ve57 (55.9%)
Not enrolled171 (45.2%)
Fig. 2 Overview, partner notification study enrollment, listing, referral and testing by sex, June–September 2015
247

AIDS Behav (2018) 22:102–116
1 3
63.0%11.4%
13.6%
4.2%
2.3%4.9%
No partner in past 24 months (n=167)
**Other reasons: partner on ART (n=4), partner deceased (n=1), partner is geographically distant (n=1), fear of IPV (1), and unspecified (n=6)
Under 18 years of age (n=30)Distraught or declined for other reason (n=36) Insufficient contact information available (n=11)Pregnant (n=6) Other** (n=13)
Fig. 3 Reasons for non-enrollment in Tanzania partner notification study, June–Sep-tember 2015
Table 1 Demographic factors of HIV-positive, non-enrolled individuals and index clients
NA information was not collected for the non-enrolled
Demographic factors HIV positive, non-enrolled in study (n!=!232) Index clients (n!=!390)MalesN (%)
FemalesN (%)
TotalN (%)
P-value MalesN (%)
FemalesN (%)
TotalN (%)
p value
Age group 0.011 0.000NA NA NA
!18–24 4 (5.2) 31 (20.0) 35 (15.1) 13 (7.1) 49 (23.7) 62 (15.9)!25–34 31 (40.3) 66 (42.6) 97 (41.8) 74 (40.4) 100 (48.3) 174 (44.6)!35–44 25 (32.4) 33 (21.3) 58 (25.0) 61 (33.3) 41 (19.8) 102 (26.2)!45 and above 17 (22.1) 25 (16.1) 42 (18.1) 35 (19.1) 17 (8.2) 52 (13.3)
Education 0.757 0.541!No formal education 17 (22.1) 35 (22.6) 52 (22.4) 24 (13.1) 34 (16.4) 58 (14.9)!Primary education 56 (72.7) 108 (69.7) 164 (70.7) 138 (75.4) 146 (70.5) 284 (72.8)!Secondary and above 4 (5.2) 12 (7.7) 16 (6.9) 21 (11.5) 27 (13.0) 48 (12.3)
Marital Status 0.375 0.000!Single 27 (35.1) 52 (33.5) 79 (34.1) 21 (11.5) 52 (25.1) 73 (18.7)!Married 22 (28.6) 42 (27.2) 64 (27.6) 156 (85.2) 141 (68.1) 297 (76.2)!Divorced 17 (22.1) 25 (16.1) 42 (18.1) 6 (3.3) 8 (3.9) 14 (3.6)!Widowed 11 (14.2) 36 (23.2) 47 (20.2) 0 (0.0) 6 (2.9) 6 (1.5)
Main economic activity 0.000!Housewife NA NA NA 0 (0.0) 6 (2.9) 6 (1.5)!Farmer 105 (57.4) 113 (54.6) 218 (55.9)!Small scale business 39 (21.3) 72 (34.8) 111 (28.5)!Formally employed 26 (14.2) 14 (6.8) 40 (10.3)!Other 13 (7.1) 2 (1.0) 15 (3.8)
Total 77 (100.0) 155 (100.0) 232 (100.0) 183 (100.0) 207 (100.0) 390 (100.0)
248

AIDS Behav (2018) 22:102–116
1 3
Characteristics of!Sexual Partners
Table!3 presents demographic information on the 249 suc-cessfully referred sexual partners. Successfully referred male
partners tended to be older than female partners (27% vs. 9.2% were 45!years and above) (p!<!0.00). While the major-ity of all partners (66.3%) had primary education, more male partners (73.8%) had completed primary education
Table 2 Successful referral and multiple partner listing by sex and marital status of index clients
CI confidence interval* p!<!0.001a Adjusted for age, education, sex and marital status
Study outcome Index clients (N!=!390)YesN (%)
NoN (%)
TotalN (%)
BivariateOdds Ratio (CI)
MultivariateOdds Ratio (CI)a
Index client listed more than one sexual partner!Female 10 (4.8) 197 (95.2) 207 (100.0) Reference Reference!Male 37 (20.2) 146 (79.8) 183 (100.0) 5.0 (2.4–10.4)* 6.2 (2.7–14.1)*
Index client listed more than one sexual partner!Not married 11 (11.8) 82 (88.2) 93 (100.0) Reference Reference!Married 36 (12.1) 261 (87.9) 297 (100.0) 1.0 (0.5–2.1) 0.6 (0.3–1.3)
Index client referred at least one listed sexual partner!Female 107 (51.7) 100 (48.3) 207 (100.0) Reference Reference!Male 130 (71.0) 53 (29.0) 183 (100.0) 2.3 (1.5–3.5)* 2.2 (1.4–3.5)*
Index client referred at least one listed sexual partner by marital status!Not married 39 (41.9) 54 (58.1) 93 (100.0) Reference Reference!Married 198 (66.7) 99 (33.3) 297 (100.0) 2.7 (1.7–4.5)* 2.5 (1.5–4.2)*
Table 3 Demographic characteristics of successfully referred sexual partners by sex
Demographic factors Successfully referred sexual partners (n!=!249) p valueMalesN (%)
FemalesN (%)
TotalN (%)
Age group 0.000!18–24 11 (10.3) 30 (21.1) 41 (16.5)!25–34 35 (32.7) 61 (43.0) 96 (38.6)!35–44 32 (29.9) 38 (26.8) 70 (28.1)!45 and above 29 (27.1) 13 (9.2) 42 (16.9)
Education 0.012!No formal education 14 (13.1) 41 (28.9) 55 (22.1)!Primary education 79 (73.8) 86 (60.6) 165 (66.3)!Secondary and above 14 (13.1) 15 (10.6) 29 (11.6)
Marital Status (missing information!=!1) 0.124!Single 14 (13.2) 8 (5.6) 22 (8.9)!Married/living together 89 (84.0) 131 (92.3) 220 (88.7)!Divorced/separated 2 (1.9) 3 (2.1) 5 (2.0)!Widowed 1 (0.9) 0 (0.0) 1 (0.4)
Main economic activity 0.000!Housewife 0 (0.0) 3 (2.1) 3 (1.2)!Farmer 61 (57.0) 102 (71.8) 163 (65.5)!Small scale business/trader 21 (19.6) 30 (21.1) 51 (20.5)!Formally employed 15 (14.0) 3 (2.1) 18 (7.2)!Other 10 (9.3) 4 (2.8) 14 (5.6)
Total 107 (100.0) 142 (100.0) 249 (100.0)
249

AIDS Behav (2018) 22:102–116
1 3
than female partners (60.6%) (p!=!0.012). More of the male partners were formally employed than female partners (14% vs. 2.1%) (p!<!0.000).
Table!4 presents successful referral and HIV status of listed sexual partners by the sex, marital status, and relation-ship status of the listed sexual partners. In multivariate anal-ysis, female sexual partners were 1.5 times more likely to be successfully referred than male sexual partners, and mar-ried partners 3.7 times more likely than unmarried. Partners who were listed as being a girlfriend/boyfriend or casual sex partner were less likely to be successfully referred: 30.4% of boyfriends/girlfriends and 33.9% of casual partners were successfully referred, compared to 72.5% wives and 54.7% of husbands.
Results: Qualitative
A total of 46 participants (26 index clients and 20 sexual partners) were interviewed as part of the IDI’s. Half were male and half female. Table!5 presents demographic char-acteristics of the IDI participants.
Language Used in!Notifying Partner
Many of the index clients interviewed chose to use indirect language (i.e., avoided direct reference to HIV testing or avoided disclosing that they had been tested) when notify-ing and referring their partner. Multiple male index clients interviewed told their partners that the health care provider would not reveal their test results unless the partner came
Table 4 Successful referral and HIV status by sex, marital status, and relationship status of sexual partners
CI confidence interval* p!<!0.05** p!<!0.01*** p!<!0.001a Adjusted for age, sex, education and marital status
Study outcome YesN (%)
NoN (%)
Total Bivariate Odds Ratio (CI) Multivariate Odds Ratio (CI)a
Partner successfully referred to HTS (n!=!439 listed sexual partners)!Sex!!Male sexual partner 108 (49.8) 109 (50.2) 217 (100.0) Reference Reference!!Female sexual partner 141 (63.5) 81 (36.5) 222 (100.0) 1.7 (1.2–2.5)** 1.5 (1.0-2.2)*
!Marital status (missing!=!4)!!Unmarried 37 (32.2) 78 (67.8) 115 (100.0) Reference Reference!!Married 208 (65.0) 112 (35.0) 320 (100.0) 3.9 (2.5–6.2)*** 3.7 (2.3-5.8)***
!Relationship status (missing!=!5)!!Casual sexual partner 20 (33.9) 39 (66.1) 59 (100.0) Reference Reference!!Husband 75 (54.7) 62 (45.3) 137 (100.0) 2.4 (1.3–4.5)** 1.8 (0.9–3.6)!!Wife 132 (72.5) 50 (27.5) 182 (100.0) 5.1 (2.7–9.7)*** 7.4 (3.3–16.3)***!!Girlfriend/boyfriend 17 (30.4) 39 (69.6) 56 (100.0) 0.9 (0.4–1.7) 1.9 (0.9–4.4)
Partner diagnosed with HIV infection (n!=!239 partners tested for HIV)!Sex!!Male 57 (55.3) 46 (44.7) 103 (100.0) Reference Reference!!Female 91 (66.9) 45 (33.1) 136 (100.0) 1.6 (1.0–2.8) 1.7 (0.9–3.3)
!Marital status (missing!=!5)!!Not married 17 (44.7) 21 (55.3) 38 (100.0) Reference Reference!!Married 129 (65.8) 67 (34.2) 196 (100.0) 2.6 (1.3–5.4) * 1.5 (0.6–3.6)
!Relationship status (missing!=!5)!!Casual sexual partner 13 (65.0) 7 (35.0) 20 (100.0) Reference Reference!!Husband 42 (60.0) 28 (40.0) 70 (100.0) 0.8 (0.3–2.3) 0.3 (0.1–1.6)!!Wife 88 (69.3) 39 (30.7) 127 (100.0) 1.2 (0.5–3.3) 0.5 (0.1–3.1)!!Girlfriend/boyfriend 3 (17.6) 14 (82.4) 17 (100.0) 0.1 (0.0–0.5)** 0.1 (0.0–0.5)**
250
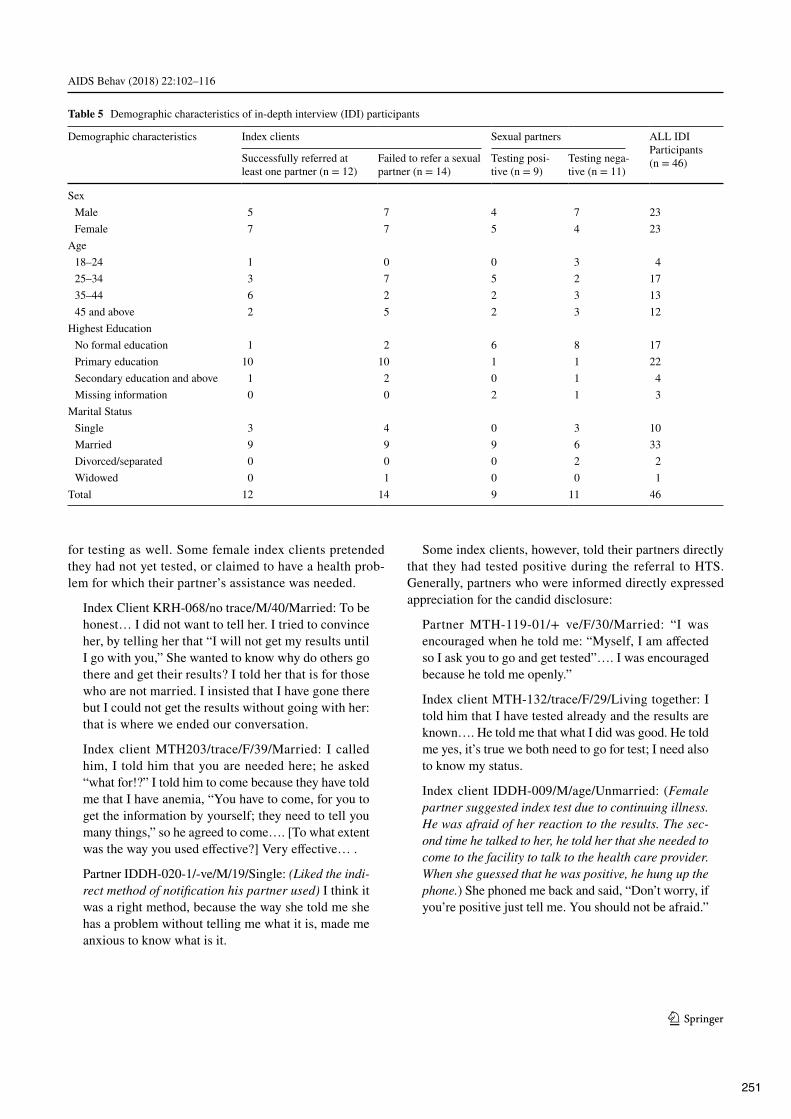
AIDS Behav (2018) 22:102–116
1 3
for testing as well. Some female index clients pretended they had not yet tested, or claimed to have a health prob-lem for which their partner’s assistance was needed.
Index Client KRH-068/no trace/M/40/Married: To be honest… I did not want to tell her. I tried to convince her, by telling her that “I will not get my results until I go with you,” She wanted to know why do others go there and get their results? I told her that is for those who are not married. I insisted that I have gone there but I could not get the results without going with her: that is where we ended our conversation.Index client MTH203/trace/F/39/Married: I called him, I told him that you are needed here; he asked “what for!?” I told him to come because they have told me that I have anemia, “You have to come, for you to get the information by yourself; they need to tell you many things,” so he agreed to come…. [To what extent was the way you used e#ective?] Very e#ective… .Partner IDDH-020-1/-ve/M/19/Single: (Liked the indi-rect method of notification his partner used) I think it was a right method, because the way she told me she has a problem without telling me what it is, made me anxious to know what is it.
Some index clients, however, told their partners directly that they had tested positive during the referral to HTS. Generally, partners who were informed directly expressed appreciation for the candid disclosure:
Partner MTH-119-01/+! ve/F/30/Married: “I was encouraged when he told me: “Myself, I am a#ected so I ask you to go and get tested”…. I was encouraged because he told me openly.”Index client MTH-132/trace/F/29/Living together: I told him that I have tested already and the results are known…. He told me that what I did was good. He told me yes, it’s true we both need to go for test; I need also to know my status.Index client IDDH-009/M/age/Unmarried: (Female partner suggested index test due to continuing illness. He was afraid of her reaction to the results. The sec-ond time he talked to her, he told her that she needed to come to the facility to talk to the health care provider. When she guessed that he was positive, he hung up the phone.) She phoned me back and said, “Don’t worry, if you’re positive just tell me. You should not be afraid.”
Table 5 Demographic characteristics of in-depth interview (IDI) participants
Demographic characteristics Index clients Sexual partners ALL IDI Participants (n!=!46)Successfully referred at
least one partner (n!=!12)Failed to refer a sexual partner (n!=!14)
Testing posi-tive (n!=!9)
Testing nega-tive (n!=!11)
Sex!Male 5 7 4 7 23!Female 7 7 5 4 23
Age!18–24 1 0 0 3 4!25–34 3 7 5 2 17!35–44 6 2 2 3 13!45 and above 2 5 2 3 12
Highest Education!No formal education 1 2 6 8 17!Primary education 10 10 1 1 22!Secondary education and above 1 2 0 1 4!Missing information 0 0 2 1 3
Marital Status!Single 3 4 0 3 10!Married 9 9 9 6 33!Divorced/separated 0 0 0 2 2!Widowed 0 1 0 0 1
Total 12 14 9 11 46
251

AIDS Behav (2018) 22:102–116
1 3
Barriers to!Referral of!Partners for!Testing or!Partner Notification
Time/Distance as! a! Barrier Many index clients made contact with their partners over the phone. Index clients—those who were successful in referring partners as well as those who were not—mentioned barriers involving time and geographical distance.
Index client MTH122/trace/M/42/Married: [Why were you not able to remember most of your part-ners?] Because these people, I was with them in a far o# location from here, I think I got this problem [HIV infection] not here, but there in Madibira. That’s why I was not able to remember all of them.Some female index clients noted that male partners whose
jobs required frequent travel were particularly di"cult to locate and/or refer.
Bad End or!Long Duration of!Separation as!a!Barrier Male as well as female index clients were reluctant to get in touch with former partners who were suspected, or were known, to have married, or with whom the relationship had ended poorly.
Index client KRH-042/trace/F/43/Married: [For the partner you could not convince to come for testing, what do you think was a major obstacle?] I could not, because those [relationships] are from a long time ago, since the year before last year. Would you call someone who you had broken up with? The person has a wife or wives and you broke up with a fight. You do not call each other! Why would you call such a person?!Index client IDDH-009/trace/M/36/Married: As I told you earlier we separated, not in a peaceful way, it wasn’t in a manner that we could later look for one another. She moved on and got married, and had a child with someone else.
Absence of! Symptoms as! a! Barrier Many index clients reported that either they or their partners did not feel they should test for HIV because of a lack of symptoms of oppor-tunistic!infections. In some cases, the presence of symptoms prompted testing-seeking behavior in the partner; in some cases it motivated the index client to seek testing. Alterna-tively, the absence of symptoms served as justification for the decision not to test, for male partners in particular.
Index client MTH-107 no trace/F/26/Married (bar worker): They [my partners] have refused; I am still in the process of mobilizing them to come [for testing]…. Both replied that they are not ready…. The first one said he is confident that he is healthy, and the other one… he is not ready to test until he gets sick.
Symptoms were mentioned in numerous cases as the rea-son that the index client sought HIV testing.
Index client MTH-148/no trace/M/54/Married: So those diseases were troubling us, she was complain-ing sometimes about back pain, sometimes stomach ache. Sometimes we feel hungry, she cooks but we can’t eat…. She said, “My husband, when you go there you should check this [HIV].”Index client IDDH-007/trace/F/37/Married: I got that courage because I was sick… and it seems this was the root cause. That is why I had the courage to talk to him. I said I can’t keep on being afraid, as am already infected and I am the one su#ering.
Type of!Relationship and!Success in!Referral
When index clients discussed casual or multiple concur-rent partners, they characterized this as di"cult for partner notification or expressed reluctance to engage in partner notification:
Index client MTH-090/no trace/F/28/Single: [Were you able to remember all of the partners you had within 24!months?] Really I can’t recall them…. Even if I recall them it won’t be easy for me to give them this information… because others have their own families already. We just met as “friends for a day.” You can meet someone when traveling or at work. If you met someone just for a day, do you think you can tell him this matter?Index client MTH-060/no trace/M/30/Married: So I told them [my partners] that I have checked and I have been found with problems, please you must also go for a checkup. One of them said you have told me a very important thing. But another one felt I did something wrong. [What did she say?] She said what is yours is yours and what is mine is mine…. [Are you living with one of those three or they are just sex partners?] These are my sex partners, apart from my wife. I told my wife, but she did not say anything.Multiple women brought up the issue of having a child
with their partner. If a woman did not have a child with her male partner, this was often presented as a less serious rela-tionship or as a problematic relationship with poorer success at partner notification. The theme in this quote was echoed in multiple other female index clients’ quotes:
Index client IDDH-011/no trace/F/29/Single: [What stopped him from coming into test?] Maybe he wasn’t interested in me…. He once told me the way I am sick, “I’m tired of spending my money, because you mean nothing,” because I didn’t bear him a child…. [There-
252

AIDS Behav (2018) 22:102–116
1 3
fore, the main reason is a child.] Yes, he said he can’t take care of me every time because I don’t have a child.Two female index clients indicated that they were
engaged in commercial sex as a livelihood, one married and one unmarried. These women suggested that commercial sex work made partner notification very di"cult.
Index client MTH-107/no trace/F/26/Married: [Do you think you can remember all of your partners within the past 24!months?] No, I can’t remember them. [Why?] Because of my working environment… in a bar. There are those you see them once and never see them again. Up until now I only have two whom I have here with me.
Negative Outcomes to!Partner Notification
None of the index clients or partners interviewed reported being physically hurt as a result of their participation in the notification or referral process, and none of the partici-pants in the qualitative assessment reported cases of IPV. However, four of the interviewed female index clients (one married and three unmarried) mentioned, at the time of the interview, that the HIV diagnosis resulted in the end of the relationship.
KRH-053/trace/F/23/Single (engaged): We entered in the counseling room and had a health checkup. Then he tested and my partner was found clean, while on my side there was a problem. After that we decided to have a meeting…. I told him finally, I’m ready to break up and you are free to marry another woman if you decide…. And that was the end of the relationship.MTH-090/no trace/F/28/Single: I don’t know what he is thinking but what I know is one day he will go to test voluntarily. Right now is like I am forcing him. He is rude. Since I told him about going to test we are not in good terms, we are not close anymore, we don’t see each other, it’s like he is not around. He doesn’t call me… just because I told him about testing.Only one male index client (MTH122/trace/M/42/Mar-
ried) noted strong negative feedback, and this was from his in-laws rather than his sexual partner.
Female as well as male sexual partners interviewed expe-rienced stress-related physical and/or psychological distress after being notified of their potential HIV exposure.
Partner MTH-076-1/-ve/M/42/Married: It was di"-cult… for sure you cannot feel good… you feel as if you don’t deserve to live.Partner KRH-001-1/+ve/F/35/Married: I got stom-ach problems since I was shocked to the extent that I
experienced diarrhea…. But I was encouraged later. I continued to recover…. I reached a point where I had to encourage myself that I should persevere. I will be treated… .
Precaution Adoption Process Model (PAPM) for!Partner Notification
When applying the (PAPM) (Fig.!1) [30] to the process of partner notification evaluated in this study, we found that the equivalent to Stage 1 was when the!partner notification pro-cess made!sexual partners aware of their exposure to HIV. Following notification, many partners reported a period of shock or distress, during which they were unable or unwill-ing to contemplate getting tested (Stage 2). For partners who did not test, it is unclear whether they stayed at Stage 2, unengaged in the decision of whether to test for HIV, or if they went through the decision-making process and ended up at Stage 4 (decided not to test). We were not able to interview any partners who did not come in for testing. Our analysis centered around those partners who reached Stage 6, successful referral. The quantitative and qualita-tive data both show that the decision to test (Stage 5) and successful referral (Stage 6) were heavily influenced by the relationship between index clients and their sexual partners (specifically whether or not they were married), with mar-ried partners as the group most likely to reach Stage 6. The PAPM highlighted the decision-making process around test-ing for HIV!faced by partners, influenced by barriers and facilitators, some sex and gender-related, some of which were described to us by participants in the study.
Discussion
In this model of partner notification (integrated into routine HIV testing, high prevalence HIV region) index clients’ abil-ity to successfully refer partners to testing significantly var-ied based on marital status and sex of the index client. Mar-ried index clients were 2.5 times more likely than unmarried index clients to be successful in referring at least one sexual partner, and male index clients were 2.2 times more likely than female index clients to get at least one sexual partner to come in for HIV testing. Although not a predictor of suc-cess, it is notable that male index clients were 6.2 times more likely to list more than one sexual partner.
Many of the stated barriers to successfully referring part-ners for testing were not specific to sex or gender-related. These included geography (meaning partners were remote or traveled for work) and the absence of symptoms in part-ners. Past partners, multiple/casual partners, and partners in relationships that ended badly were all mentioned by both
253

AIDS Behav (2018) 22:102–116
1 3
male and female index clients as people whom the index cli-ent would be reluctant, or unable, to contact. Both male and female sexual partners discussed experiencing anger, depres-sion, physical ailments such as nausea and lack of appetite, stress and exhaustion around the HIV testing.
Some barriers to partner notification appeared to impact women more heavily than men. Experiences mentioned only by women included being abandoned or the ending of the relationship because HIV status was disclosed; being undervalued for not having a child; and having di"culty in notifying partners when her livelihood was sex work. These findings, which point to gender barriers which women dis-proportionately face, echo findings from other studies. In a study from South Africa, unequal and gendered dynamics in relationships caused di#erent likelihood of HIV status disclosure when comparing men to women [18].
Globally, men are less likely than women to engage in each stage of the testing and treatment cascade [31]. How-ever, our findings also showed that men had more success in referring partners. Sex and gender power di#erentials have long been associated with HIV-related risk factors, decision-making, including around testing, and consequences associ-ated with status disclosure. In Uganda, a study showed that men may be more susceptible to perceptions about commu-nity norms for testing for HIV than women, since men’s per-ceptions that testing was “not normal” was associated with never testing [32]. Multiple reviews have shown that, for women, fear or experience of physical or emotional violence or abandonment upon disclosure of HIV status are very real concerns, and these concerns may impact women’s deci-sions regarding testing [19, 20]. Qualitative findings from this study indicate that for some participants these were also concerns. This study did not measure or analyze male or female gender norms, attitudes or power dynamics in rela-tionships as they relate to willingness to test or ability to refer partners. However, other studies have found evidence for these impacting HIV care-seeking, treatment and dis-closure [21, 33].
Based on study findings, a targeted e#ort to introduce men to HIV testing and increase their engagement in partner referral may have tremendous potential for find-ing previously undiagnosed people with!HIV infection. Such e#orts will require working against social and health system patterns in which women attend health services much more than men, and also against male social norms that undermine testing [33]. However, evidence suggests that interventions which challenge masculine norms and promote gender equality (gender-transformative interven-tions) can foster greater willingness to be tested for HIV and initiate care and treatment for those testing positive [33]. Supportive social networks can also increase a man’s likelihood to test: a recent study in Tanzania found that men who thought at least one close friend in their social
network had ever tested were 2.7 times more likely to have ever been tested for HIV themselves [34]. A study in Uganda suggested that billboards or radio messages that disseminate information on true HIV testing uptake in communities could a#ect uptake of HTS by men [32]. Fur-ther research is needed to understand how best to attract men to testing services or reach them in communities. Helpful suggestions, including multi-session interven-tions and interventions focused on trustful communica-tion between couples, were made in a recent study on HIV status disclosure in South Africa [18]. Di#erent strategies may be needed for notifying partners who are considered hard to reach, such as former partners or partners of index clients who have multiple casual partners. According to a study in Uganda which included sex workers, provider assisted approaches may be more acceptable to people who have multiple casual partners, such as female sex workers or fishermen [8].
In our study, no index clients or partners reported physi-cal abuse. Partners as well as index clients described nega-tive consequences such as sadness, anger, disturbance in sleep, anxiety, headaches, diarrhea, not being able to eat, and in the case of four female index clients, the dissolution of marriages or relationships. This is consistent with a recent systematic review of partner notification approaches, which showed very few cases of harm, leading to WHO’s 2016 recommendation to include assisted partner notification in HIV testing and care services [32].
This study did have some limitations. Our sample for the qualitative component of this study was a conveni-ence sample and thus may not represent the experiences of all the index clients and partners involved in this study. Although the qualitative findings highlighted both di#er-ences and similarities in experience between male and female participants in the partner notification process, it was not designed to elicit in-depth findings around gen-der roles and norms in relation to partner notification. In regards to the high number of HIV-positive individuals ineligible because they did not have a partner in the last 24!months, we feel that it is quite likely that some HIV-positive individuals may have been using this response as a way to politely opt out of the partner notification process. Despite this, the acceptance rate is consistent with findings from the region: in our sample, 25.6% of the HIV-positive people approached indicated they had not had a sexual partner in the past 24!months, while in the 2011–2012 Tanzania HIV/AIDS and Malaria Indicator Survey, 75.2% of male and 72.1% of female respondents in Njombe region indicated that they had a sexual partner in the last 12!months [3]. An amendment to the eligibil-ity criteria for partners occurred after the first month of fieldwork. At that time, we extended the criteria for eligi-bility from a sexual partner within the last 12!months to
254

AIDS Behav (2018) 22:102–116
1 3
a sexual partner within the last 24!months, because many participants indicated that they had partners within the last 24 but not 12!months. This may have a#ected roughly 20% of our index clients’ listing and notification choices, and may have had the e#ect of slightly limiting number of index clients participating and number of partners listed in the initial month of the study. Additionally, this study was not designed to capture testing which occurred outside of the three study facilities. If partners went to another facil-ity to test following referral or if they went to the same facility but did not identify themselves to study sta#, we would not know about that partner’s decision to test. This could mean that our estimates of the successful referrals in the study are lower than the actual. Finally, our study was not designed to assess the safety of the partner notifi-cation approach in regard to IPV. We recognize that even though no cases of IPV were reported, unreported cases may have occurred.
Our findings on the sex-related di#erences that create bar-riers for partner notification and HIV sero-status disclosure underscore the importance of principles described in the World Health Organization tool for integrating gender into HIV/AIDS programs in the health sector [35]. Programs scal-ing up partner notification should consult this tool closely. For example, by discussing the benefits and potential disad-vantages of disclosure, programs can help women disclose their HIV status safely. Programs can also help those at risk of violence with safety planning and mediated disclosure [35].
Conclusion
Partner notification integrated into routine facility HIV testing, in this high HIV-prevalence setting in Tanzania, was an e#ective way to reach previously undiagnosed HIV-infected individuals. Marital status was a huge deter-minant of success in referral, with married index clients 2.5 times more likely to be successful in referring their sexual partners to HTS. Success at referral to HTS varied by sex, with men being 2.2 times more likely to succeed in referring at least one sexual partner. Major barriers were both non-sex and gender-specific (being reluctant to contact a previous partner who is in another relationship, having a short-term relationship and being uncomfortable contacting the partner) and sex and gender–specific (feel-ing undervalued in a relationship because of the absence of childbearing, fear of dissolution of the relationship, which were greater concerns for females). It is clear that partner notification is deeply entrenched in roles and norms related to sex of the index client as well as norms related to mari-tal status. Programs which scale up partner notification for HTS should take these factors into consideration in
development of messages for clients in partner notifica-tion services. Formative studies of gender dynamics and gender-related barriers and facilitators of partner notifica-tion for men compared to women, including studies of both attitudes to and experiences with IPV, are recommended either before partner notification programs are rolled out or associated with rollout. Monitoring systems should be designed to capture successful referral to HTS by sex, age, marital status, so as to give useful feedback on these dif-ferent characteristics to program planners. Additionally, partner notification service planners and implementers should be aware that reaching non-marital partners, and supporting female index clients to refer their sexual part-ners to HTS, may require additional investment of time and resources.
Acknowledgements The described study was a collaboration of Tan-zania’s Ministry of Health, Community Development, Gender, Elderly and Children (MOHCDGEC), Jhpiego, and the United States Agency for International Development (USAID). Special thanks to the District O"ces of Makambako, Njombe district and Njombe town council, and the facility sta# and leadership of Kibena, Makambako, and Ilembula Hospitals, and to the HIV testing services clients and their partners who participated in the study. Without them, the learning derived from this study would not have been possible. This manuscript was edited by Chris Merriman and reviewed by Jason Reed.
Funding This publication is made possible by the generous support of the American people through the United States Agency for Interna-tional Development (USAID) and through PEPFAR under the terms of Cooperative Agreement #AID OAA-A-11-00050. The contents are the responsibility of the authors!and do not necessarily reflect the views of USAID, PEPFAR, or the U.S. Government.
Authors’ contributions MP and CK drafted the article. CK and MN conducted the statistics for the article and DO, MP and CK conducted the qualitative analysis. MB, AC and MD assisted drafting the qualita-tive analysis. EK and MN reviewed findings for accuracy in fieldwork. MB, AC, RK, WM, VW, EM and KC drafted and reviewed sections of the article.
Compliance with Ethical Standards
Conflict of interest The authors have no competing interests to de-clare.
Ethical Approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual partici-pants included in the study.
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://crea-tivecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appro-priate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
255

AIDS Behav (2018) 22:102–116
1 3
References 1. UNAIDS. Global AIDS Update 2016. 2016. http://www.unaids.
org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf. Accessed June 7, 2017.
2. Staveteig S, Wang S, Head SK, Bradley SEK, Nybro E. Demo-graphic patterns of HIV testing uptake in sub-Saharan Africa. Demogr Patterns HIV Test Uptake Sub-Saharan Africa DHS Comp Reports No 30. 2013:81. http://dhsprogram.com/pubs/pdf/CR30/CR30.pdf.
3. Tanzania Commission forAIDS, (TACAIDS), (ZAC) ZAC, (NBS) NB of S, (OCGS) O of the CGS, International I. Tanzania HIV/AIDS and Malaria Indicator Survey 2011–12. Dar es Salaam; 2013.
4. Baggaley R, Hensen B, Ajose O, et!al. From caution to urgency: the evolution of HIV testing and counselling in Africa. Bull World Health Organ. 2012;90(9):652B–8B. doi:10.2471/BLT.11.100818.
5. Hensen B, Taoka S, Lewis JJ, Weiss HA, Hargreaves J. Sys-tematic review of strategies to increase men’s HIV-testing in sub-Saharan Africa. AIDS. 2014:15–17. doi:10.1097/QAD.0000000000000395.
6. Hosseinipour MC, Rosenberg NE. HIV partner notification: possible and essential. Sex Transm Dis. 2013;40(12):915–6. doi:10.1097/OLQ.0000000000000060.HIV.
7. Dalal S, Johnson C, Fonner V, et!al. Improving HIV test uptake and case finding with assisted partner notification services. Aids. 2017;31(13):1867–76. doi:10.1097/QAD.0000000000001555.
8. Payne C, Nakyanjo N, Ddaaki W, et!al. HIV partner notification values and preferences in Rakai, Uganda: a qualitative study. Ann Glob Health. 2017;83(1):162. doi:10.1016/j.aogh.2017.03.363.
9. WHO. Consolidated guidelines on hiv testing services. Geneva, Switzerland; 2015.
10. WHO. Guidelines on HIV self-testing and partner noti-fication. Geneva; 2016. http://apps.who.int/ir is/bitstream/10665/251655/1/9789241549868-eng.pdf?ua=1. Accessed 10 May 2017.
11. United Nations Joint Programme on AIDS. the Gap Report. 2014:422. ISBN: 978-92-9253-062-4.
12. Brown LB, Miller WC, Kamanga G, et!al. HIV partner notifica-tion is e#ective and feasible in sub-Saharan Africa: opportunities for HIV treatment and prevention. J Acquir Immune Defic Syndr. 2011;56(5):437–42. doi:10.1097/QAI.0b013e318202bf7d.
13. Henley C, Forgwei G, Welty T, et!al. Scale-up and case-find-ing e#ectiveness of an HIV partner services program in cam-eroon: an innovative HIV prevention intervention for developing countries. Sex Transm Dis. 2013;40(12):909–14. doi:10.1097/OLQ.0000000000000032.
14. Myers RS, Feldacker C, Cesár F, et!al. Acceptability and e#ec-tiveness of assisted human immunodeficiency virus partner services in Mozambique. Sex Transm Dis. 2016;43(11):690–5. doi:10.1097/OLQ.0000000000000529.
15. Cherutich P, Golden MR, Wamuti B, et!al. Assisted partner ser-vices for HIV in Kenya: a cluster randomised controlled trial. Lan-cet HIV. 2017;4(2):e74–82. doi:10.1016/S2352-3018(16)30214-4.
16. Gari S, Malungo JRS, Martin-Hilber A, Musheke M, Schindler C, Merten S. HIV testing and tolerance to gender based vio-lence: a cross-sectional study in Zambia. PLoS ONE. 2013;8(8). doi:10.1371/journal.pone.0071922.
17. Dovel K, Yeatman S, Watkins S, Poulin M. Men’s heightened risk of AIDS-related death: the legacy of gendered HIV testing and treatment strategies. AIDS. 2015;29(10):1123–5. doi:10.1097/QAD.0000000000000655.
18. Bhatia DS, Harrison AD, Kubeka M, et!al. The role of rela-tionship dynamics and gender inequalities as barriers to HIV-serostatus disclosure: qualitative study among women and men
living with HIV in Durban, South Africa. Front Public Health. 2017;5(July):1–9. doi:10.3389/fpubh.2017.00188.
19. Obermeyer C, Osborn M. The utilization of testing and counseling for HIV: a review of the social and behavioural evidence. Am J Public Health. 2007;97(10):1762–74.
20. World Health Organization. HIV status disclosure to sexual part-ners: rates, barriers, and outcomes for women. Geneva; 2003. http://apps.who.int/iris/bitstream/10665/42717/1/9241590734.pdf. Accessed 2 June 2017.
21. O’Brien S, Broom A. Gender, culture and changing atti-tudes: experiences of HIV in Zimbabwe. Cult Health Sex. 2013;15(5):583–97. doi:10.1080/13691058.2013.776111.
22. Skovdal M, Campbell C, Madanhire C, Mupambireyi Z, Nyamukapa C, Gregson S. Masculinity as a barrier to men’s use of HIV services in Zimbabwe. Glob Health. 2011;7(1):13. doi:10.1186/1744-8603-7-13.
23. Siu GE, Wight D, Seeley JA. Masculinity, social context and HIV testing: an ethnographic study of men in Busia district, rural eastern Uganda. BMC Public Health. 2014;14(1):33. doi:10.1186/1471-2458-14-33.
24. DiCarlo AL, Mantell JE, Remien RH, et!al. “Men usually say that HIV testing is for women”: gender dynamics and perceptions of HIV testing in Lesotho. Cult Health Sex. 2014;16(8):867–82. doi:10.1080/13691058.2014.913812.
25. Obermeyer C, Osborn M. The utilization of testing and counseling for HIV: a review of the social and behavioral evidence. Am J Public Health. 2007;97(10):1762–74.
26. Obermeyer CM, Sankara A, Bastien V, Parsons M. Gender and HIV testing in Burkina Faso: an exploratory study. Soc Sci Med. 2009;69(6):877–84. doi:10.1016/j.socscimed.2009.07.003.
27. Kahabuka C, Plotkin M, Christensen A, et!al. Addressing the First 90: a highly e#ective partner notification approach reaches pre-viously undiagnosed sexual partners in Tanzania. AIDS Behav. 2017;. doi:10.1007/s10461-017-1750-5.
28. Charmaz K. Constructing grounded theory: a practical guide through qualitative analysis. London: SAGE; 2006.
29. Miles M, Huberman A. Qualitative data analysis: an expanded sourcebook. London: SAGE; 1994.
30. Weinstein N, Sandman P, Blalock S. The precaution adoption process model. In: Glanz K, Rimer BK, Viswanath KE, editors. Health behavior and health education. 4th ed. San Francisco, CA: Jossey-Bass; 2008.
31. Underwood C, Hendrickson Z, Van Lith L, Lengwe Kunda J, Mallalieu E. Role of community-level factors across the treat-ment cascade: a critical review. J Acquir Immune Defic Syndr. 2014;66(Suppl 3):S311–8.
32. Perkins JM, Nyakato VN, Kakuhikire B, et!al. Actual versus per-ceived HIV testing norms, and personal HIV testing uptake: a cross-sectional, population-based study in rural Uganda. AIDS Behav. 2017:1–13. doi:10.1007/s10461-017-1691-z.
33. Fleming P, Colvin C, Peacock D, Dworkin S. What role can gen-der-transformative programming for men play in increasing men’s HIV testing and engagement in HIV care and treatment in South Africa? Cult Health Sex. 2016;18(11):1251–64.
34. Yamanis T, Dervisevic E, Mulawa M, et!al. Social network influ-ence on HIV testing among urban men in Tanzania. AIDS Behav. 2017;21:1171–82.
35. WHO. Integrating gender into HIV/AIDS programmes in the health sector: tool to improve responsiveness to women’s needs. Geneva, Switzerland; 2009.
256
Flynn et al. BMC Res Notes (2017) 10:20 DOI 10.1186/s13104-016-2339-1
RESEARCH ARTICLE
Can trained lay providers perform HIV testing services? A review of!national HIV testing policiesDavid E. Flynn1,5*, Cheryl Johnson2, Anita Sands3, Vincent Wong4, Carmen Figueroa2 and Rachel Baggaley2
Abstract Background: Only an estimated 54% of people living with HIV are aware of their status. Despite progress scaling up HIV testing services (HTS), a testing gap remains. Delivery of HTS by lay providers may help close this testing gap, while also increasing uptake and acceptability of HIV testing among key populations and other priority groups.
Methods: 50 National HIV testing policies were collated from WHO country intelligence databases, contacts and testing program websites. Data regarding lay provider use for HTS was extracted and collated. Our search had no geo-graphical or language restrictions. This data was then compared with reported data from the Global AIDS Response Progress Reporting (GARPR) from July 2015.
Results: Forty-two percent of countries permit lay providers to perform HIV testing and 56% permit lay providers to administer pre-and post-test counseling. Comparative analysis with GARPR found that less than half (46%) of reported data from countries were consistent with their corresponding national HIV testing policy.
Conclusions: Given the low uptake of lay provider use globally and their proven use in increasing HIV testing, coun-tries should consider revising policies to support lay provider testing using rapid diagnostic tests.
Keywords: HIV testing, Lay providers, Community health workers, HIV policy
© The Author(s) 2017. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
BackgroundDespite achievements and expansion of HIV testing ser-vices (HTS) to date, presently only 54% of people living with HIV are aware of their serostatus [1]. It is estimated that there are approximately 2 million new infections annually, half of which are among key populations who often have poor access to HTS, and when they do test, they test late in their infection [2]. Additional and more focused HTS approaches are critical to reach the United Nations “90-90-90” global targets which aims to diagnose 90% of all people living with HIV by 2020, have 90% of those diagnosed receiving sustained antiretroviral ther-apy (ART) and aiming to have 90% of those on ART to be virally suppressed [3]. To reach this testing target of 90%, it is critical to address the existing gaps in service
provision, including health worker shortages and the lack of community-based HTS, which limit the expansion and e!ectiveness of HTS in many resource-limited settings [4–6].
Testing for HIV infection is a crucial part of HTS. His-torically, HIV testing involved lengthy laboratory testing of blood collected by venipuncture for HIV antibodies involving specialist equipment and specialist sta!. Rapid diagnostic tests (RDTs) for HIV were introduced in the early 2000’s and allow for testing of fingerstick whole blood or oral fluid, with a result established in under an hour. Due to their low cost, reliability, ease of use and speed, they are now widely used as a diagnostic means (within a testing algorithm) by low resource countries. Testing with RDTs (both fingerstick blood and oral fluid rapid tests) is possible with adequately trained lay provid-ers. Trained lay providers have been delivering HTS for decades and in many settings [7] across the Americas [8], Europe [9, 10], sub-Saharan Africa [11–17] and Asia [18].
Open Access
BMC Research Notes
*Correspondence: [email protected] 5 8 Bellevue St, Chatswood West, NSW 2067, AustraliaFull list of author information is available at the end of the article
257

Flynn et al. BMC Res Notes (2017) 10:20
Task-sharing—the rational redistribution of tasks from “higher-level” cadres of health professionals to trained lay provider cadres—can expand HTS more broadly, has been shown to increase uptake of HIV testing [8, 12, 19], and can facilitate testing in community based and out-reach services, especially for key populations [20]. Lay providers have been shown to provide high quality ser-vices, provide accurate HIV test results [11, 18], and may also be lower in cost than services performed by other health providers.
Since 2008 the World Health Organization (WHO) has recommended task-sharing clinical services within the HIV continuum of diagnosis, prevention, care and treat-ment [21]. In particular, WHO recommends that pro-grams increase the scope of work of trained lay providers and introduce task-sharing across professional cadres [22]. "is task-sharing involves providing clinical ser-vices, counseling and referrals to HIV specialist services. However, in many settings lay provider HTS has not been utilized and suboptimal HTS coverage persists.
Global AIDS Response Progress Reporting (GARPR) (WHO, UNAIDS, UNICEF) is an annual initiative that allows representatives from government health depart-ments to voluntarily report information such as epidemi-ological statistics as well as current clinical HIV testing practices within their country. "is information is based upon the clinical practices within the country. Accord-ing to data from the 2015 Global AIDS Response Pro-gress Reporting (GARPR) (WHO, UNAIDS, UNICEF), only 52% (n#=#65/124) of reporting countries said that lay providers were allowed to perform HIV rapid diagnostic tests (RDTs) [23]. With this low reported uptake of lay provider use, there is no data regarding the role of HIV national health policies in lay provider utilisation and as a result these policies could be a key barrier to lay provider delivered HTS.
Within this paper we analyzed national HIV testing policies from a range of countries to determine the role of lay providers in delivering HIV testing (through the use of RDTs) as well as pre and post-test counselling. In doing so, we sought to investigate whether national health policy permitted trained lay providers to perform HTS (specifically RDTs and counselling) and compare this to the GARPR reported data to determine whether the national HIV health policy reflects what happens in HIV healthcare systems.
MethodsPolicy criteriaWe collected national policy documents from WHO country intelligence databases, national HIV testing pro-gram websites and comprehensive web-based search-ing through databases and national health department
websites. "e search and analysis of national HIV policies took place from November 1, 2014 to December 21, 2014. Our search had no geographical or language restrictions. We selected the most recent HIV national testing policies and, when not available, national policy statements on who can perform HTS. We excluded HTS standards and protocols developed by nongovernmental organizations, donors or other technical agencies.
Policy analysisWe reviewed the policies in full text, extracting three pieces of information: whether trained lay providers can perform HIV rapid tests using finger stick blood, whether trained lay providers can perform HIV rapid tests using oral fluid and whether trained lay providers can perform pre and post-test counselling (which includes the deliver-ing of results). Six researchers (VW, CB, AS, RB, CJ and DF) developed the data extraction form. One reviewer (DF) extracted data, two other reviewers (RB and CJ) evaluated and approved the extracted data. Disagree-ments between reviewers (RB, CJ and DF) were resolved through discussion and consensus. Our results were then compared with data reported by countries to GARPR (WHO, UNAIDS, UNICEF) as of July 1, 2015, based on the policy and programmatic indicator that asks whether current HIV testing guidelines recommend that RDTs can be performed by lay providers [24].
Global AIDS response progress reporting (GARPR) data"e GARPR online reporting tool is a method of collec-tion of clinical data and epidemiological statics from a variety of countries on various indicators of global HIV response. Primarily low- and middle-income countries report this data to WHO, UNAIDS and UNICEF. "ese indicators include epidemiological HIV data as well as a variety of questions regarding HIV practices. Specifically, there are four primary questions about national HIV test-ing in the GARPR online reporting tool, of which lay pro-vider testing with RDTs is a sub-question. "e data is a reflection of the clinical activities that occur within that country (i.e. a reflection of what occurs ‘on the ground’), which should ideally be reflected in national HIV poli-cies, however sometimes this is not the case.
National representatives from reporting countries are responsible for providing this information according to the guidance provided by WHO, UNAIDS and UNICEF [24]. "ese representatives are designated individuals from governmental health departments or government HIV-specific programs
Data regarding whether lay providers can administer HTS in each country was collected in July 2015 and com-pared to the same information extracted from their cor-responding national HIV testing policies.
258

Flynn et al. BMC Res Notes (2017) 10:20
"e type of HIV testing allowed (i.e. fingerstick or oral fluid based) to be performed by lay providers was not specified in the question the GARPR data collection tool.
ResultsWe identified HIV policies from 61 countries and excluded policies from 11 countries because they did not include su$cient information, were not o$cial documents or were not able to be translated. "us, we included a total of 50 national testing polices in this review: 25 countries were from the WHO African region, four countries from the WHO American region, nine from the WHO Eastern-Mediterranean region, three from the WHO European region, three from the WHO Southeast Asia region, and six from the WHO Western Pacific region.
Analysis of!RDTs (using "ngerstick blood) use by!lay providersTwenty-one of 50 national policies allow lay providers to use RDTs using fingerstick blood and 15 of 50 country policies explicitly prohibit lay providers from perform-ing them. Fourteen of 50 countries do not specify a role for lay providers in HIV testing with fingerstick RDTs (Fig.#1).
Analysis of!RDTs (using oral #uid) use by!lay providersNine out of the 50 countries had policies allowing lay providers to use RDTs using oral fluid while ten coun-tries specifically did not permit lay providers to use oral fluid RDTs. "e majority of countries (n#=#31/50) did not specify if lay providers could use RDTs using oral fluid or not.
Analysis of!"ngerstick blood vs oral #uid RDT use by!lay providersCountries that do not permit lay provider RDT testing (with finger stick blood) either do not allow oral fluid testing as well or do not specify if they can perform oral fluid based RDTs. "e number of countries that did not allow lay providers to perform either type of RDT was evenly spread across all geographical areas, with no obvi-ous predisposing factor as to why those countries do not permit lay provider testing. Reasons behind the non-use of lay providers were not addressed within the national policies.
Analysis of!pre and!post-test counselling by!lay providersTwenty-eight of 50 countries permit lay providers to pro-vide pre- and post-test counseling, 12 of 50 countries prohibit lay providers from performing counseling and
Fig. 1 Distributional map showing whether national HIV testing policies permit lay providers to perform RDTs using fingerstick/whole blood (n = 50)
259
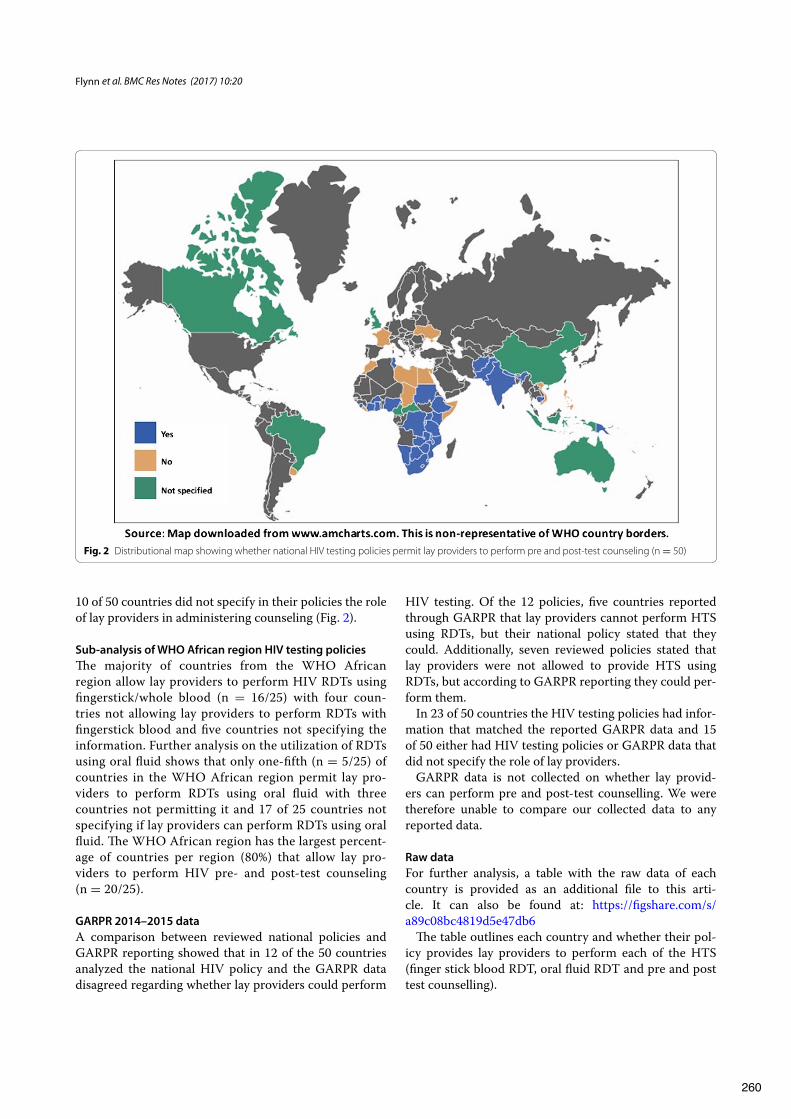
Flynn et al. BMC Res Notes (2017) 10:20
10 of 50 countries did not specify in their policies the role of lay providers in administering counseling (Fig.#2).
Sub-analysis of!WHO African region HIV testing policies"e majority of countries from the WHO African region allow lay providers to perform HIV RDTs using fingerstick/whole blood (n# =# 16/25) with four coun-tries not allowing lay providers to perform RDTs with fingerstick blood and five countries not specifying the information. Further analysis on the utilization of RDTs using oral fluid shows that only one-fifth (n#=#5/25) of countries in the WHO African region permit lay pro-viders to perform RDTs using oral fluid with three countries not permitting it and 17 of 25 countries not specifying if lay providers can perform RDTs using oral fluid. "e WHO African region has the largest percent-age of countries per region (80%) that allow lay pro-viders to perform HIV pre- and post-test counseling (n#=#20/25).
GARPR 2014–2015 dataA comparison between reviewed national policies and GARPR reporting showed that in 12 of the 50 countries analyzed the national HIV policy and the GARPR data disagreed regarding whether lay providers could perform
HIV testing. Of the 12 policies, five countries reported through GARPR that lay providers cannot perform HTS using RDTs, but their national policy stated that they could. Additionally, seven reviewed policies stated that lay providers were not allowed to provide HTS using RDTs, but according to GARPR reporting they could per-form them.
In 23 of 50 countries the HIV testing policies had infor-mation that matched the reported GARPR data and 15 of 50 either had HIV testing policies or GARPR data that did not specify the role of lay providers.
GARPR data is not collected on whether lay provid-ers can perform pre and post-test counselling. We were therefore unable to compare our collected data to any reported data.
Raw dataFor further analysis, a table with the raw data of each country is provided as an additional file to this arti-cle. It can also be found at: https://figshare.com/s/a89c08bc4819d5e47db6
"e table outlines each country and whether their pol-icy provides lay providers to perform each of the HTS (finger stick blood RDT, oral fluid RDT and pre and post test counselling).
Fig. 2 Distributional map showing whether national HIV testing policies permit lay providers to perform pre and post-test counseling (n = 50)
260

Flynn et al. BMC Res Notes (2017) 10:20
Discussion"is is the first review of national policies on HTS for inclusion of lay providers. Similar reviews have been undertaken on HIV policy regarding self-testing [25], but to date there is no information regarding the role of lay providers in national HIV policies.
"is review revealed that of the 50 countries analyzed, 58% either do not permit lay providers to perform HIV RDTs using fingerstick blood (the most common type of HIV RDT) or do not specify if they can, while 44% do not permit or do not specify whether lay providers can perform HIV pre- and post-test counseling. "e regional comparison analysis showed that the WHO African region had the highest proportion of countries in which lay testing is permitted.
"irteen of the 50 reviewed policies did not specify or explicitly outline the role of lay providers in providing HTS. While some of these countries may have provisions that allow lay providers to perform HIV testing and pre- and/or post-test counseling, the lack of explicit reference to the role of lay providers may introduce misunderstand-ings or misinterpretations by providers and national pro-gram managers. Furthermore, if lay testing is not explicitly sanctioned, systems to support training, supervision and provide quality assurance of lay testing may not be rou-tinely and consistently applied. Countries should regularly review their national HIV testing policy to make sure it contains correct information, reflects national practice as well as lay provider training, testing and quality assurance.
"e di!erence between reported GARPR data and that extracted from o$cial HIV testing policies may be due to several reasons such as policies that had not been updated to account for lay provider use, incorrect information from the national representative regarding lay provider use in their country, or the policy may not have been clear regarding the role of lay providers in HIV testing.
GARPR data only asks if lay providers are permitted to perform RDTs in general and does not specify whether lay providers are permitted to perform the di!erent types of RDTs (i.e. fingerstick whole blood or oral fluid). "is specific information would have helped to give greater clarity on the role of lay providers and aided in our com-parison of GARPR data to national HIV policy.
Of the 12 countries with di!ering information, half (n#=#6/12) of them were from African nations. "is dif-ference demonstrates a disparity between reported data and national policy information. Greater care must be taken when reporting GARPR data to make sure it cor-relates with approved practice. It is suggested that in a bid to increase accuracy, the reporting of GARPR data could be accompanied by policy documents to support their reported data and help catalyze regular reviewing of national policy documents.
"rough task-sharing, lay provider HTS have been widely implemented throughout Africa. Sub-analysis of data from the WHO African region suggests that there is a more supportive policy environment for lay provider HTS compared to other global regions. Task sharing to increase the scope of work for lay providers is important to scaling up HTS, as recent reviews have shown that it is acceptable, can be low cost and can increase uptake of HTS, particularly among key populations who are gen-erally underserved [26]. "us, based on the review of existing evidence, WHO recommends that trained lay providers can perform RDTs safely and e!ectively [26].
LimitationsAlthough we reviewed the most currently available HTS policies, some may be out of date or in the process of being updated. As we collected and analyzed national testing policies, it is possible that some information on lay provider testing was not specified in these, but instead included in national PMTCT guidelines, treatment guidelines or other national guidelines.
Although 50 national policies were collected, this did not match the number of countries reported in GARPR data (n#=# 124). A greater number of HIV testing poli-cies would have made for a greater comparison and stronger analysis however this di!erence was explained by the di$culty in obtaining formal HIV policies, the lack of formal HIV policies from a number of the reporting countries and the time limitations that were placed on the analysis.
Data on whether lay providers are permitted to perform pre and post-test counseling was not collected as a part of the 2014–2015 GARPR reporting cycle. "erefore, we could not compare information from reviewed national policies with GARPR reports. Inconsistencies identified between national policies and GARPR reports highlight that the term lay provider may need further definition. It is possible that errors in reporting or missing information may have occurred because of di!erences in terminology.
ConclusionTo increase access to and e!ectiveness of HTS, WHO supports the use of trained lay providers for HIV testing. Trained lay testers can have an important role in provid-ing services in communities to people who do not attend health facilities. Many countries continue to prohibit testing by trained lay testers, and this may be a barrier to reaching those most vulnerable to HIV who do not access existing services.
For countries to increase reach of their HTS, task shar-ing to lay providers must be a part of a country’s testing protocol and should be included in national HIV test-ing guidelines. Lay provider use is an important way to
261

Flynn et al. BMC Res Notes (2017) 10:20
provide acceptable services to key populations, and those other populations who might not present for testing using traditional laboratory-based HTS. Ensuring that RDTs using oral fluid and fingerstick whole blood can be conducted by lay providers will remain the cornerstone of HTS and will be necessary to promote the expansion and uptake of HIV testing.
National representatives must also take greater care when reporting on national HIV testing practices, ensur-ing that the data reported is up-to-date and reflected in national policies. Regular updating of policies with regards to all aspects of HTC is encouraged.
Increased e!orts are needed to accelerate policy adap-tation and implementation of the new 2015 WHO Con-solidated guidelines on HTS, to help expand HIV testing coverage in areas and among populations with the great-est need.
AbbreviationsHTS: HIV testing services; GARPR: global AIDS response progress reporting; WHO: World Health Organisation; UNAIDS: The Joint United Nations Pro-gramme on HIV and AIDS; UNICEF: The United Nations Children’s Fund; RDT: rapid diagnostic test.
Authors’ contributionsDF undertook the primary analysis of the national policies, collated the data and aided in a raw draft and final manuscript of the piece. CJ helped to design the study, collate national policies, helped to clarify data and results which were not agreed on by the primary reviewer and helped to write the raw draft of the study with particular emphasis on the literature review. AS was integral in developing the data collection tool as well as the statistical analysis and approving the final draft. VW helped to retrieve national policies and worked on the primary analysis of the policies. CF helped with the statistical analysis of the results, double-checked the results and provided feedback on drafts through the review process. RB conceived the study and coordinated the authors in their various roles. She was instrumental in collecting policies from contacts and reviewed the final set of manuscripts for publication. All authors read and approved the final manuscript.
Authors’ informationDF is a medical student who undertook an unpaid internship at the World Health Organisation to work collaboratively with members of the Key Popula-tion and Prevention team within HIV department (working collaboratively with associate Vincent Wong from USAID) to undertake this project.
Author details1 Gri!th University School of Medicine, Gri!th University, Gold Coast, QLD, Australia. 2 HIV Department, World Health Organization (WHO), Geneva, Swit-zerland. 3 Essential Medicines and Health Products, World Health Organiza-tion (WHO), Geneva, Switzerland. 4 Global Health Bureau: O!ce of HIV/AIDS, United States Agency for International Development (USAID), Washington, DC, USA. 5 8 Bellevue St, Chatswood West, NSW 2067, Australia.
AcknowledgementsPermission was granted by ‘amCharts’ (www.amcharts.com) for the use and alternation of their world map for the use of Figs. 1 and 2.
Additional !le
Additional !le"1. Annex 1: Overview of the roles of lay providers accord-ing to national HIV testing. Description of Data: A table demonstrating each individual countries use of lay providers in HIV testing for di"erent modalities and HIV pre and post test counselling.
Competing InterestsDEF The author declares that they have no competing interests. CJ Employee of the World Health Organisation (WHO) where this research was undertaken. The WHO will be financing the article processing charge. The organisation does not stand to gain financially or non-financially from this re
search. AS Employee of the World Health Organisation (WHO) where this research was undertaken. The WHO will be financing the article processing charge. The organisation does not stand to gain financially or non-financially from this research. VW The author declares that they have no competing interests. CF Employee of the World Health Organisation (WHO) where this research was undertaken. The WHO will #be financing the article processing charge. The organisation does not stand to gain financially or non-financially from this research. RB Employee of the World Health Organisation (WHO) where this research was undertaken. The WHO will be financing the article processing charge. The organisation does not stand to gain financially or non-financially from this research.
Availability of data and materialsRaw data is provided as an additional file to this paper, titled: ‘Annex 1: Over-view of the roles of lay providers according to national HIV testing’. It can also be accessed via figshare at: https://figshare.com/s/a89c08bc4819d5e47db6. GARPR data is not publically available in tabulated form, but is available from the UNADIS website: http://www.unaids.org/AIDSReporting. Alternatively, contact [email protected] for additional support.
DatabasesAll databases within the research paper are publically available with the exception of the World Health Organisation Country (WHO) Intelligence Data-bases and GARPR Data. Both the WHO Country Intelligence Databases and GARPR data is not publically available. Permission to access both databases/data was given by Ms Cheryl Johnson (Technical O!cer in the Department for HIV at the WHO and co-author of the paper) and overseen by Dr. Rachel Baggaley (Coordinator of HIV Key Population and Prevention unit at the WHO and co-author of this paper).
Ethics approval and consent to participateAs determined by the WHO Ethics Review Committee, this study did not require ethics approval as it is a policy review and does not contain any human data.
FundingDF undertook this project as an unpaid intern and did not receive any grants/funding for this project. CJ, AS, CF and RB are all employees of the World Health Organisation, while VW is an employee of The United States Agency for International Development (USAID). No grants/external funds were acquired for this research.
Received: 11 February 2016 Accepted: 13 December 2016
References 1. The Joint United Nations Programme on HIV/AIDS (UNAIDS). How AIDS
changed everything—MDG6: 15 years, 15 lessons of hope from the AIDS response. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2015.
2. The Joint United Nations Programme on HIV/AIDS (UNAIDS). AIDS by the numbers. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2013.
3. The Joint United Nations Programme on HIV/AIDS (UNAIDS). 90-90-90: An ambitious treatment target to help end the AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014.
4. Samb B, Celletti F, Holloway J, Van Damme W, De Cock K, Dybul M. Rapid expansion of the health workforce in response to the HIV epidemic. N Engl J Med. 2007;357(24):2510–4.
5. Zachariah R, Ford N, Philips M, Lynch S, Massaquoi M, Janssens V, et al. Task shifting in HIV/AIDS: opportunities, challenges and pro-posed actions for sub-Saharan Africa. Trans R Soc Trop Med Hyg. 2009;103(6):549–58.
262

Flynn et al. BMC Res Notes (2017) 10:20
• We accept pre-submission inquiries • Our selector tool helps you to find the most relevant journal• We provide round the clock customer support • Convenient online submission• Thorough peer review• Inclusion in PubMed and all major indexing services • Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
6. Parekh B, Kalou M, Alemnji G, Ou C-Y, Gershy-Damet G-M, Nkengasong J. Scaling up HIV rapid testing in developing countries comprehen-sive approach for implementing quality assurance. Am J Clin Pathol. 2010;134(4):573–84.
7. Walsh A, Ndubani P, Simbaya J, Dicker P, Brugha R. Task sharing in Zambia: HIV service scale-up compounds the human resource crisis. BMC Health Serv Res. 2010;10(1):272.
8. Walensky R, Reichmann W, Arbelaez C, Wright E, Katz J, Seage I, et al. Counselor-versus provider-based HIV screening in the emergency department: results from the universal screening for HIV Infection in the Emergency Room (USHER) randomized controlled trial. Ann Emerg Med. 2011;58(1):126–32.
9. Champenois K, Le Gall J, Jacquemin C, Jean S, Martin C, Rios L, et al. ANRS-COM’TEST: description of a community-based HIV testing interven-tion in non-medical settings for men who have sex with men. BMJ Open. 2012;2(2):693.
10. Lorente N, Preau M, Vernay-Vaisse C, Mora M, Blanche J, Otis J. Expanding access to non-medicalized community-based rapid testing to men who have sex with men: an urgent HIV prevention intervention (the ANRS-DRAG study). PLoS ONE. 2013;8(4):e61225.
11. Molesworth A, Ndhlovu R, Banda E, Ngwira B, Glynn J, Crampin A, et al. High accuracy of home-based community rapid HIV testing in rural Malawi. J Acquir Immune Defic Syndr. 2010;55(5):625–30.
12. Bemelmans M, Van den Akker T, Ford N, Philips M, Zachariah R, Harries A, et al. Providing universal access to antiretroviral therapy in Thyolo, Malawi through task shifting and decentralization of HIV/AIDS care. Trop Med Int Health. 2010;15(12):1413–20.
13. Jackson D, Naik R, Tabana H, Pillay M, Madurai S, Zembe W, et al. Quality of home-based rapid HIV testing by community lay counsellors in a rural district of South Africa. J Int AIDS Soc. 2013;16(1):18744.
14. Fylkesnes K, Sandoy I, Jurgensen M, Chipimo P, Mwangala S, Michelo C. Strong e"ects of home-based voluntary HIV counselling and testing on acceptance and equity: a cluster randomised trial in Zambia. Soc Sci Med. 2013;86:9–16.
15. Iwu E, Holzemer W. Task shifting of HIV management from doctors to nurses in Africa: clinical outcomes and evidence on nurse self-e!cacy and job satisfaction. AIDS Care. 2014;26(1):42–52.
16. Jurgensen M, Sandoy I, Michelo C, Fylkesnes K. E"ects of home-based Voluntary Counselling and Testing on HIV-related stigma: findings from a cluster-randomized trial in Zambia. Soc Sci Med. 2013;81:18–25.
17. Leon N, Naidoo P, Mathews C, Lewin S, Lombard C. The impact of provider-initiated (opt-out) HIV testing and counseling of patients with sexually transmitted infection in Cape Town, South Africa: a controlled trial. Implement Sci. 2010;5(8):11.
18. Kanal K, Chou T, Sovann L, Morikawa Y, Mukoyama Y, Kakimoto K. Evaluation of the proficiency of trained non-laboratory health sta" and laboratory technicians using a rapid and simple HIV antibody test. AIDS Res Ther. 2005;2(1):5.
19. Mathews R, Johnson C, Verster A, Baggaley R. Annex 11: a systematic review of community-based HIV testing and counselling among key populations. In: Consolidated guidelines on HIV testing services: 5Cs: con-sent, confidentiality, counselling, correct results and connection. Geneva: World Health Organisation; 2015. http://www.ncbi.nlm.nih.gov/books/NBK316038/.
20. World Health Organisation. Annex 3: global examples of HIV test-ing servies. In: Consolidated guidelines on HIV testing services. Geneva: World Health Organisation; 2015. http://apps.who.int/iris/bit-stream/10665/180212/1/WHO_HIV_2015.22_eng.pdf. Accessed 12 June 2015.
21. World Health Organisation. Optimizing health worker roles to improve access to key maternal and newborn health interventions through task-shifting. Geneva: World Health Organization; 2014.
22. World Health Organisation. Global recommendations and guidelines on task shifting. Geneva: World Health Organization; 2007. http://www.who.int/workforcealliance/knowledge/resources/taskshifting_guidelines/en/. Accessed June 15 2015.
23. World Health Organisation. Fact sheet to the WHO consolidated guide-lines on HIV testing services. Geneva: World Health Organisation; 2015. http://www.who.int/hiv/topics/vct/fact_sheet/en/. Accessed July 17 2015.
24. World Health Organisation. Global AIDS response progress reporting 2015. Geneva: World Health Organisation and UNAIDS; 2015.
25. Mavedzenge SN, Baggaley R, Corbett EL. A review of self-testing for HIV: research and policy priorities in a new era of HIV prevention. Clin Infect Dis. 2013;57(1):126–38.
26. World Health Organisation. Consolidated guidelines on HIV testing services. Geneva: World Health Organisation; 2015. http://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/. Accessed July 15 2015.
263

Toward 90-90-90: identifying those who have never been tested for HIV anddifferences by sex in LesothoMaria Augusta Carrasco a, Paul Flemingb, Jocelyn Wagmana and Vincent Wonga
aUnited States Agency for International Development, Washington, DC, USA; bDepartment of Health Behavior and Health Education,University of Michigan School of Public Health, Ann Arbor, MI, USA
ABSTRACTTo reach HIV epidemic control it is important to ensure that those who have never been tested accessHIV testing and counseling (HTC) particularly in the context of a generalized HIV epidemic. Using datafrom the2014 LesothoDemographicHealth Surveybivariate andmultivariate logistic regressionswereconducted to determine the associations between never tested for HIV and key socio-cognitivecharacteristics by sex. Marginal probabilities at the means were calculated for the socio-cognitivevariables for men and women to ascertain the magnitude of the differences in the likelihood ofnever being tested by sex. We stratified by gender and controlled for age, education, religion,marital status, place of residence, and years circumcised (for men only). Results indicate that moremen than women have never been tested (!2= 461.16, p < 0.001); and, among men, acceptance ofgender based violence (Odds ratio [OR]: 1.44, p < 0.001), holding discriminatory attitudes (OR: 1.50,p < 0.001), and not having basic HIV prevention knowledge (OR: 1.53, p < 0.001) were significantlyassociated with never being tested. The likelihood of never being tested among those who hadthese three socio-cognitive characteristics was much higher among men (0.56, p < 0.001) thanwomen (0.20, p < 0.001). Given the strong sex differential, there is an urgent need for strategiesspecifically targeting men in order to effectively promote HTC uptake among them. Additionally,results suggest that those strategies should integrate strategies to address GBV acceptance, HIVprevention knowledge, and HIV discrimination or link men to programs addressing these.
ARTICLE HISTORYReceived 13 December 2016Accepted 22 August 2017
KEYWORDSHIV testing and counseling;sex; HIV prevention; 90-90-90goals; Lesotho
Background
Lesotho has one of the highest HIV burdens in the world(adult prevalence: 25%), with higher prevalence amongwomen than men (Ministry of Health & ICF Inter-national, 2016). Ensuring that people access HIV testingand counseling (HTC) and know their status has becomeessential to reach HIV epidemic control. A crucial step toimprove HTC access is to identify those who have neverbeen tested for HIV to devise targeted social and behav-ior change (SBC) strategies to promote HTC uptake. Pre-vious campaigns by the Lesotho government have fallenfar short of testing targets (Coburn, Okano, & Blower,2013). As of 2014, 83.6% of women and 62.9% of menages 12 and older report having ever tested for HIVand received their results (Ministry of Health & ICFInternational, 2016). Despite this fairly high testing cov-erage, a significant proportion of men who are HIV posi-tive remain undiagnosed (Camlin et al., 2016).
Numerous studies in sub-Saharan Africa (SSA) haveused population-based surveys such as the DemographicHealth Survey (DHS) to analyze factors associated withHIV testing, including Ethiopia (Godif, Assefa, Ale-mayehu, & Terefe, 2015), South Africa (Hutchinson &
Mahlalela, 2006), Cote D’Ivoire (Jean, Anglaret, Moh,Lert, & Dray-Spira, 2012), Kenya (Ng’ang’a et al., 2014;Waruiru et al., 2014; Ziraba et al., 2011), and across fourcountries (Asaolu et al., 2016). A study conducted inLesotho with DHS data collected in 2004 and 2009found that men and women with stigmatizing beliefswere less likely to be tested (Corno & de Walque, 2013).Other factors that significantly associated with greatertesting formenwere age, secondary education (comparedto no education), and being Catholic (compared to beingMuslim); only agewas significant for women (Corno&deWalque, 2013). The purpose of this study is to analyzedata from the most recent Demographic Health Survey(DHS) conducted in Lesotho in 2014 to determinesocio-cognitive characteristics around HIV knowledge,gender based violence (GBV), and HIV discrimination,of men and women who have never been tested for HIV.
Methods
Data
We used data from the 2014 Lesotho DHS survey, whichis a representative sample of men and women of
© 2017 Informa UK Limited, trading as Taylor & Francis Group
CONTACT Maria Augusta Carrasco [email protected], [email protected] United States Agency for International Development, 2100 Crystal Drive,Arlington, VA 22202, USA
AIDS CARE, 2017https://doi.org/10.1080/09540121.2017.1372559
Dow
nloa
ded
by [J
H L
ibra
ries]
at 0
5:33
06
Sept
embe
r 201
7
264
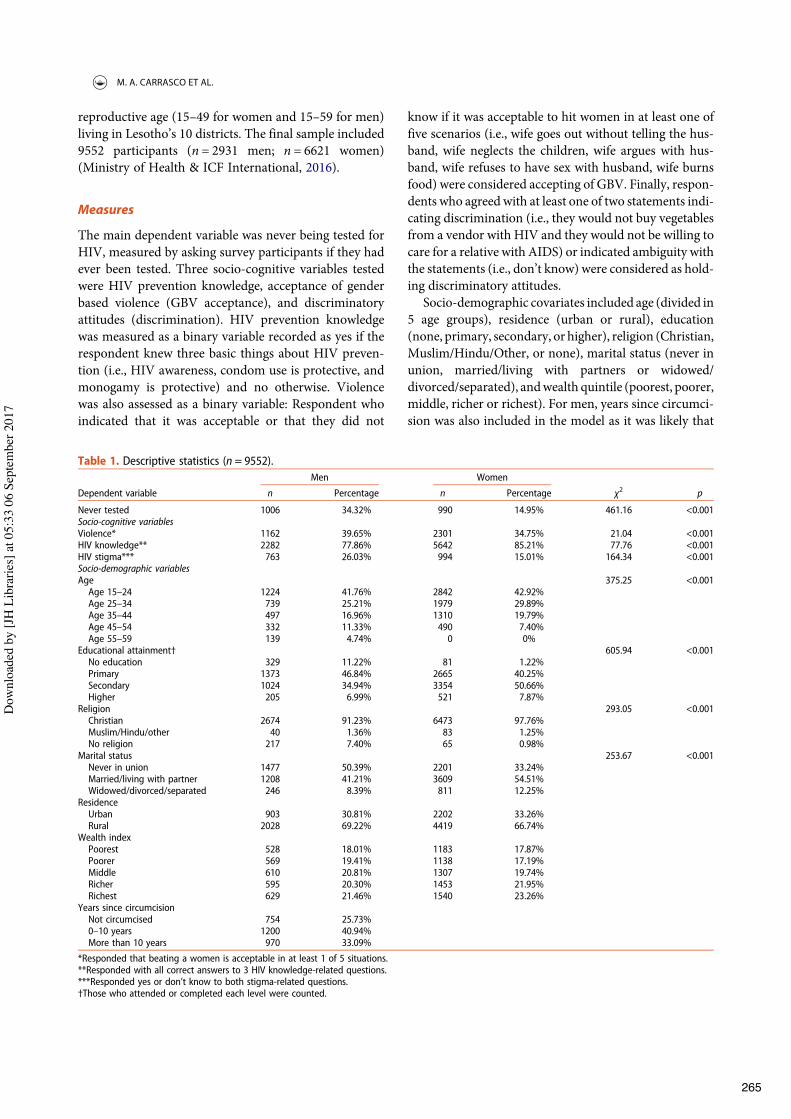
reproductive age (15–49 for women and 15–59 for men)living in Lesotho’s 10 districts. The final sample included9552 participants (n = 2931 men; n = 6621 women)(Ministry of Health & ICF International, 2016).
Measures
The main dependent variable was never being tested forHIV, measured by asking survey participants if they hadever been tested. Three socio-cognitive variables testedwere HIV prevention knowledge, acceptance of genderbased violence (GBV acceptance), and discriminatoryattitudes (discrimination). HIV prevention knowledgewas measured as a binary variable recorded as yes if therespondent knew three basic things about HIV preven-tion (i.e., HIV awareness, condom use is protective, andmonogamy is protective) and no otherwise. Violencewas also assessed as a binary variable: Respondent whoindicated that it was acceptable or that they did not
know if it was acceptable to hit women in at least one offive scenarios (i.e., wife goes out without telling the hus-band, wife neglects the children, wife argues with hus-band, wife refuses to have sex with husband, wife burnsfood) were considered accepting of GBV. Finally, respon-dents who agreed with at least one of two statements indi-cating discrimination (i.e., they would not buy vegetablesfrom a vendor with HIV and they would not be willing tocare for a relative with AIDS) or indicated ambiguity withthe statements (i.e., don’t know) were considered as hold-ing discriminatory attitudes.
Socio-demographic covariates included age (divided in5 age groups), residence (urban or rural), education(none, primary, secondary, or higher), religion (Christian,Muslim/Hindu/Other, or none), marital status (never inunion, married/living with partners or widowed/divorced/separated), andwealth quintile (poorest, poorer,middle, richer or richest). For men, years since circumci-sion was also included in the model as it was likely that
Table 1. Descriptive statistics (n = 9552).Men Women
Dependent variable n Percentage n Percentage !2 p
Never tested 1006 34.32% 990 14.95% 461.16 <0.001Socio-cognitive variablesViolence* 1162 39.65% 2301 34.75% 21.04 <0.001HIV knowledge** 2282 77.86% 5642 85.21% 77.76 <0.001HIV stigma*** 763 26.03% 994 15.01% 164.34 <0.001Socio-demographic variablesAge 375.25 <0.001Age 15–24 1224 41.76% 2842 42.92%Age 25–34 739 25.21% 1979 29.89%Age 35–44 497 16.96% 1310 19.79%Age 45–54 332 11.33% 490 7.40%Age 55–59 139 4.74% 0 0%
Educational attainment† 605.94 <0.001No education 329 11.22% 81 1.22%Primary 1373 46.84% 2665 40.25%Secondary 1024 34.94% 3354 50.66%Higher 205 6.99% 521 7.87%
Religion 293.05 <0.001Christian 2674 91.23% 6473 97.76%Muslim/Hindu/other 40 1.36% 83 1.25%No religion 217 7.40% 65 0.98%
Marital status 253.67 <0.001Never in union 1477 50.39% 2201 33.24%Married/living with partner 1208 41.21% 3609 54.51%Widowed/divorced/separated 246 8.39% 811 12.25%
ResidenceUrban 903 30.81% 2202 33.26%Rural 2028 69.22% 4419 66.74%
Wealth indexPoorest 528 18.01% 1183 17.87%Poorer 569 19.41% 1138 17.19%Middle 610 20.81% 1307 19.74%Richer 595 20.30% 1453 21.95%Richest 629 21.46% 1540 23.26%
Years since circumcisionNot circumcised 754 25.73%0–10 years 1200 40.94%More than 10 years 970 33.09%
*Responded that beating a women is acceptable in at least 1 of 5 situations.**Responded with all correct answers to 3 HIV knowledge-related questions.***Responded yes or don’t know to both stigma-related questions.†Those who attended or completed each level were counted.
M. A. CARRASCO ET AL.
Dow
nloa
ded
by [J
H L
ibra
ries]
at 0
5:33
06
Sept
embe
r 201
7
265

men who have been medically circumcised have beentested for HIV (not circumcised, less than 10 years, ormore than 10 years).
Data analysis
Proportions are reported for all variables. The distri-bution of age and years circumcised was inspected andthe variables were converted into categorical variablessince they were highly skewed. Chi square tests indicatedsignificant differences between men and women; thus,subsequent statistical analyses were stratified by sexand weighted using sample weights provided by DHS.Bivariate and multivariate logistic regressions wereused to determine the associations between never testedfor HIV and socio-cognitive and socio-demographicvariables. The choice of covariates was informed by pre-vious literature on factors influencing testing for HIV.Wealth quintile was originally included in the multi-variate models for men and women but it was droppedfrom both models as it was not significant in either. Mar-ginal probabilities at the means were calculated for thesocio-cognitive variables for men and women to ascer-tain the magnitude of the differences by sex. Data wereanalyzed using Stata version 13 (College Station, Texas).
Results
Table 1 provides summary statistics. A total of 34.32%of the men and 14.95% of the women surveyed reportednever being tested for HIV (!2 = 461.16, p < 0.001).Compared to women, men reported greater GBV accep-tance (39.65% vs. 34.75%) and HIV discrimination(26.03% vs. 15.01%). Women had more HIV preventionknowledge than men (85.21% vs. 77.86%). The socio-cognitive variables were significant for men andwomen in unadjusted analysis (Table 2). For thesocio-cognitive variables in adjusted analysis (Table 3)GBV acceptance was not significant among women(Adjusted OR [AOR] = 1.10, p > 0.05) but it was signifi-cant among men (AOR = 1.44, p < 0.05). In adjustedanalysis, HIV knowledge and stigma were significantamong men (AOR = 0.53, p < 0.001; AOR = 1.50, p <0.05) and women (AOR = 0.49, p < 0.001; AOR = 1.59,p < 0.001). Table 4 presents the marginal probability(at the means) of never being tested. Lacking basicHIV knowledge, and holding HIV discriminatorybeliefs increased the likelihood of never being testedby 56% among men and 20% among women. Amongmen, the likelihood of never being tested increased by36% for those with GBV acceptance, 43% for men with-out basic HIV knowledge and 38% for with stigmatizingbeliefs. Among women, the marginal probabilities were
much lower than men (see Table 4). All marginal prob-abilities were significant (p < 0.001).
Discussion
More men (compared to women) in Lesotho have neverbeen tested. Researchers in other settings in SSA havefound similar HIV testing disparities between men andwomen (Bila & Egrot, 2009; Gari, Martin-Hilber, Mal-ungo, Musheke, & Merten, 2014; Parrott et al., 2011).While women are routinely tested during prenatal care,men’s primary point of entry to HIV services is voluntarymedical male circumcision (VMMC). But, as of 2014,Lesotho had only reached 23% of their VMMC target(WHO, 2015).
Across SSA, current intervention strategies to increasemen’s HIV testing are lacking. A recent systematic
Table 2. Bivariate associations of never testing for HIV amongmen and women in Lesotho.
Men WomenNever tested Never tested
OR OR
Socio-cognitive variablesGBV acceptance (base: never acceptable) † 1.95*** 1.52***
(1.64–2.32) (1.28–1.80)HIV knowledge (base: 0–2 answers correct) †† 0.45*** 0.39***
(0.36–0.56) (0.31–0.44)HIV stigma (base: no stigma) ††† 2.19*** 2.27***
(1.82–2.63) (1.85–2.80)Socio-demographic variablesEducational attainment (base: no education)Primary 1.11 0.53
(0.80–1.52) (0.25–1.13)Secondary 0.68* 0.79
(0.50–0.94) (0.38–1.67)Higher 0.30*** 0.47
(0.18–0.50) (0.18–1.22)Age (base: 15–24 years)25–34 0.39*** 0.11***
(0.31–0.49) (0.08–0.15)35–44 0.30*** 0.18***
(0.22–0.41) (0.13–0.24)45–54 0.32*** 0.23***
(0.23–0.45) (0.15–0.36)55–59 0.34*** –
(0.23–0.52)Marital status (base: never in union)Married/living with partner 0.344*** 0.09***
(0.28–0.42) (0.07–0.12)Widowed/divorced/separated 0.41*** 0.08***
(0.30–0.59) (0.05–0.12)Rural/urban (base: urban) 2.12*** 0.91
(1.72–2.78) (0.74–1.13)Religion (base: Christian)Muslim/other 1.23 2.4
(0.49–3.11) (0.81–7.14)No religion 2.52*** 0.66
(1.80–3.52) (0.25–1.73)Observations 2931 6621
*p < 0.05, **p < 0.01, ***p < 0.001,†Compared to men who said that beating a women is acceptable in at least 1of 5 situations.
††Compared to men who answered all 3 HIV prevention knowledge questionscorrectly.
†††Compared to men who responded “yes” or “don’t know” to two stigmaquestions.
AIDS CARE
Dow
nloa
ded
by [J
H L
ibra
ries]
at 0
5:33
06
Sept
embe
r 201
7
266
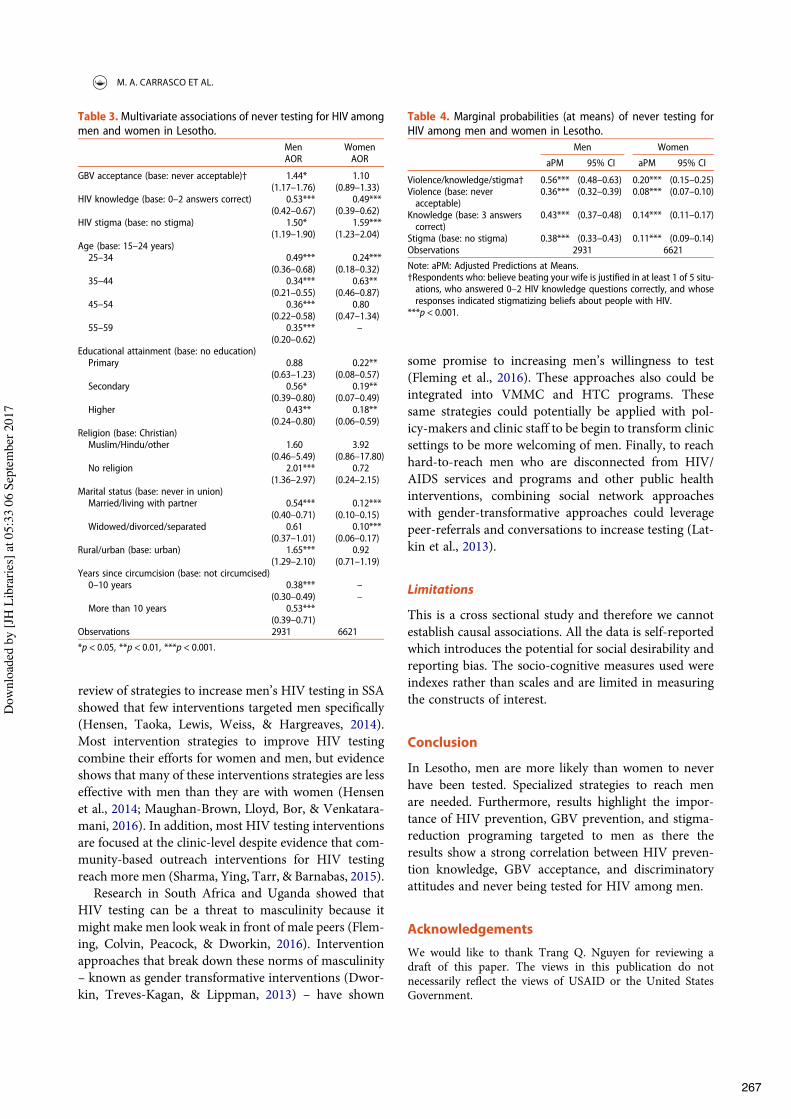
review of strategies to increase men’s HIV testing in SSAshowed that few interventions targeted men specifically(Hensen, Taoka, Lewis, Weiss, & Hargreaves, 2014).Most intervention strategies to improve HIV testingcombine their efforts for women and men, but evidenceshows that many of these interventions strategies are lesseffective with men than they are with women (Hensenet al., 2014; Maughan-Brown, Lloyd, Bor, & Venkatara-mani, 2016). In addition, most HIV testing interventionsare focused at the clinic-level despite evidence that com-munity-based outreach interventions for HIV testingreach more men (Sharma, Ying, Tarr, & Barnabas, 2015).
Research in South Africa and Uganda showed thatHIV testing can be a threat to masculinity because itmight make men look weak in front of male peers (Flem-ing, Colvin, Peacock, & Dworkin, 2016). Interventionapproaches that break down these norms of masculinity– known as gender transformative interventions (Dwor-kin, Treves-Kagan, & Lippman, 2013) – have shown
some promise to increasing men’s willingness to test(Fleming et al., 2016). These approaches also could beintegrated into VMMC and HTC programs. Thesesame strategies could potentially be applied with pol-icy-makers and clinic staff to be begin to transform clinicsettings to be more welcoming of men. Finally, to reachhard-to-reach men who are disconnected from HIV/AIDS services and programs and other public healthinterventions, combining social network approacheswith gender-transformative approaches could leveragepeer-referrals and conversations to increase testing (Lat-kin et al., 2013).
Limitations
This is a cross sectional study and therefore we cannotestablish causal associations. All the data is self-reportedwhich introduces the potential for social desirability andreporting bias. The socio-cognitive measures used wereindexes rather than scales and are limited in measuringthe constructs of interest.
Conclusion
In Lesotho, men are more likely than women to neverhave been tested. Specialized strategies to reach menare needed. Furthermore, results highlight the impor-tance of HIV prevention, GBV prevention, and stigma-reduction programing targeted to men as there theresults show a strong correlation between HIV preven-tion knowledge, GBV acceptance, and discriminatoryattitudes and never being tested for HIV among men.
Acknowledgements
We would like to thank Trang Q. Nguyen for reviewing adraft of this paper. The views in this publication do notnecessarily reflect the views of USAID or the United StatesGovernment.
Table 3. Multivariate associations of never testing for HIV amongmen and women in Lesotho.
Men WomenAOR AOR
GBV acceptance (base: never acceptable)† 1.44* 1.10(1.17–1.76) (0.89–1.33)
HIV knowledge (base: 0–2 answers correct) 0.53*** 0.49***(0.42–0.67) (0.39–0.62)
HIV stigma (base: no stigma) 1.50* 1.59***(1.19–1.90) (1.23–2.04)
Age (base: 15–24 years)25–34 0.49*** 0.24***
(0.36–0.68) (0.18–0.32)35–44 0.34*** 0.63**
(0.21–0.55) (0.46–0.87)45–54 0.36*** 0.80
(0.22–0.58) (0.47–1.34)55–59 0.35*** –
(0.20–0.62)Educational attainment (base: no education)Primary 0.88 0.22**
(0.63–1.23) (0.08–0.57)Secondary 0.56* 0.19**
(0.39–0.80) (0.07–0.49)Higher 0.43** 0.18**
(0.24–0.80) (0.06–0.59)Religion (base: Christian)Muslim/Hindu/other 1.60 3.92
(0.46–5.49) (0.86–17.80)No religion 2.01*** 0.72
(1.36–2.97) (0.24–2.15)Marital status (base: never in union)Married/living with partner 0.54*** 0.12***
(0.40–0.71) (0.10–0.15)Widowed/divorced/separated 0.61 0.10***
(0.37–1.01) (0.06–0.17)Rural/urban (base: urban) 1.65*** 0.92
(1.29–2.10) (0.71–1.19)Years since circumcision (base: not circumcised)0–10 years 0.38*** –
(0.30–0.49) –More than 10 years 0.53***
(0.39–0.71)Observations 2931 6621
*p < 0.05, **p < 0.01, ***p < 0.001.
Table 4. Marginal probabilities (at means) of never testing forHIV among men and women in Lesotho.
Men Women
aPM 95% CI aPM 95% CI
Violence/knowledge/stigma† 0.56*** (0.48–0.63) 0.20*** (0.15–0.25)Violence (base: neveracceptable)
0.36*** (0.32–0.39) 0.08*** (0.07–0.10)
Knowledge (base: 3 answerscorrect)
0.43*** (0.37–0.48) 0.14*** (0.11–0.17)
Stigma (base: no stigma) 0.38*** (0.33–0.43) 0.11*** (0.09–0.14)Observations 2931 6621
Note: aPM: Adjusted Predictions at Means.†Respondents who: believe beating your wife is justified in at least 1 of 5 situ-ations, who answered 0–2 HIV knowledge questions correctly, and whoseresponses indicated stigmatizing beliefs about people with HIV.
***p < 0.001.
M. A. CARRASCO ET AL.
Dow
nloa
ded
by [J
H L
ibra
ries]
at 0
5:33
06
Sept
embe
r 201
7
267

Disclosure statement
No potential conflict of interest was reported by the authors.
Ethical approval
All procedures performed in studies involving human partici-pants were in accordance with the ethical standards of theinstitutional and/or national research committee and withthe 1964 Helsinki declaration and its later amendments orcomparable ethical standards.
Informed consent
Informed consent was obtained from all individual partici-pants included in the study.
ORCID
Maria Augusta Carrasco http://orcid.org/0000-0002-7053-2462
References
Asaolu, I. O., Gunn, J. K., Center, K. E., Koss, M. P.,Iwelunmor, J. I., & Ehiri, J. E. (2016). Predictors of HIVtesting among youth in Sub-saharan Africa: A cross-sec-tional study. PloS one, 11(10), e0164052. doi:10.1371/journal.pone.0164052
Bila, B., & Egrot, M. (2009). Gender asymmetry in healthcare-facility attendance of people living with HIV/AIDS inBurkina Faso. Social Science & Medicine, 69(6), 854–861.doi:10.1016/j.socscimed.2009.05.035
Camlin, C. S., Ssemmondo, E., Chamie, G., El Ayadi, A. M.,Kwarisiima, D., Sang, N., … Clark, T. D. (2016). Men“missing” from population-based HIV testing: Insightsfrom qualitative research. AIDS Care, 28(sup3), 67–73.doi:10.1080/09540121.2016.1164806
Coburn, B. J., Okano, J. T., &Blower, S. (2013). Current driversand geographic patterns of HIV in Lesotho: Implications fortreatment and prevention in Sub-saharan Africa. BMCMedicine, 11(1), e3729. doi:10.1186/1741-7015-11-224
Corno, L.,&deWalque, D. (2013). Socioeconomicdeterminantsof stigmatization and HIV testing in Lesotho. AIDS Care, 25(sup1), S108–113. doi:10.1080/09540121.2012.736937
Dworkin, S. L., Treves-Kagan, S., & Lippman, S. A. (2013).Gender-Transformative interventions to reduce HIV risksand violence with heterosexually-active Men: A review ofthe global evidence. AIDS and Behavior, 17, 2845–2863.doi:10.1007/s10461-013-0565-2
Fleming, P. J., Colvin, C., Peacock, D., & Dworkin, S. L.(2016). What role can gender-transformative programmingfor men play in increasing South African men’s HIV testingand engagement in HIV care and treatment? Culture,Health & Sexuality, 18, 1251–1264. doi:10.1080/13691058.2016.1183045
Gari, S., Martin-Hilber, A., Malungo, J. R., Musheke, M., &Merten, S. (2014). Sex differentials in the uptake of antire-troviral treatment in Zambia. AIDS Care, 26(10), 1258–1262. doi:10.1080/09540121.2014.897911
Godif, M., Assefa, H., Alemayehu, M., & Terefe, W. (2015).Factors associated with HIV counseling and testing amongmales and females in Ethiopia: Evidence from Ethiopiandemographic and health survey data. Journal of AIDS &Clinical Research, 6, 429. doi:10.4172/2155-6113.1000429
Hensen, B., Taoka, S., Lewis, J. J., Weiss, H. A., & Hargreaves,J. (2014). Systematic review of strategies to increase men’sHIV-testing in sub-saharan Africa. Aids (london, England),28(14), 2133–2145. doi:10.1097/qad.0000000000000395
Hutchinson, P., & Mahlalela, X. (2006). Utilization of volun-tary counseling and testing services in the eastern cape,South Africa. AIDS Care, 18(5), 446–455. doi:10.1080/09540120500213511
Jean, K., Anglaret, X., Moh, R., Lert, F., & Dray-Spira, R.(2012). Barriers to HIV testing in côte d’Ivoire: The roleof individual characteristics and testing modalities. PLoSOne, 7(7), e41353. doi:10.1371/journal.pone.0041353
Latkin, C. A., Davey-Rothwell, M. A., Knowlton, A. R.,Alexander, K. A., Williams, C. T., & Boodram, B.(2013). Social network approaches to recruitment, HIV pre-vention, medical care, and medication adherence. JAIDSJournal of Acquired Immune Deficiency Syndromes, 63(Suppl 1), S54–58. doi:10.1097/QAI.0b013e3182928e2a
Maughan-Brown, B., Lloyd, N., Bor, J., & Venkataramani, A.S. (2016). Changes in self-reported HIV testing duringSouth Africa’s 2010/2011 national testing campaign: Gainsand shortfalls. Journal of the International AIDS Society,19(1), 20658. doi:10.7448/ias.19.1.20658
Ministry of Health & ICF International. (2016). Lesotho demo-graphic and health survey 2014. Maseru: The Ministry ofHealth & ICF International.
Ng’ang’a, A., Waruiru, W., Ngare, C., Ssempijja, V., Gachuki,T., Njoroge, I., … Group, f. t. K. S. (2014). The Status ofHIVtesting and counseling in Kenya: Results from a nationallyrepresentative population-based survey. JAIDS Journal ofAcquired Immune Deficiency Syndromes, 66, S27–S36.doi:10.1097/qai.0000000000000102
Parrott, F. R., Mwafulirwa, C., Ngwira, B., Nkhwazi, S.,Floyd, S., Houben, R. M., … French, N. (2011).Combining qualitative and quantitative evidence to deter-mine factors leading to late presentation for antiretroviraltherapy in Malawi. PLoS One, 6(11), e27917. doi:10.1371/journal.pone.0027917
Sharma, M., Ying, R., Tarr, G., & Barnabas, R. (2015).Systematic review and meta-analysis of community andfacility-based HIV testing to address linkage to care gapsin sub-saharan Africa. Nature, 528(7580), S77–85. doi:10.1038/nature16044
Waruiru, W., Ngare, C., Ssempijja, V., Gachuki, T., Njoroge,I., Oluoch, P., … Kim, A. A. (2014). The status of HIV test-ing and counseling inKenya: Results from a nationally repre-sentative population-based survey. Journal of AcquiredImmune Deficiency Syndromes (1999), 66(Suppl 1), S27.
WHO. (2015).Voluntarymedicalmale circumcision forHIV pre-vention in 14 priority countries in east and Southern Africa.Retrieved from http://apps.who.int/iris/bitstream/10665/179933/1/WHO_HIV_2015.21_eng.pdf?ua = 1&ua = 1
Ziraba, A. K., Madise, N. J., Kimani, J. K., Oti, S., Mgomella,G., Matilu, M., & Ezeh, A. (2011). Determinants for HIVtesting and counselling in Nairobi urban informal settle-ments. BMC Public Health, 11(1), 749. doi:10.1186/1471-2458-11-663
AIDS CARE
Dow
nloa
ded
by [J
H L
ibra
ries]
at 0
5:33
06
Sept
embe
r 201
7
268

ORIGINAL PAPER
Addressing the First 90: A Highly Effective Partner NotificationApproach Reaches Previously Undiagnosed Sexual Partnersin Tanzania
Catherine Kahabuka1 • Marya Plotkin1,7 • Alice Christensen1 • Charlene Brown2 •
Mustafa Njozi1 • Renatus Kisendi3 • Werner Maokola3 • Erick Mlanga4 •
Ruth Lemwayi1 • Kelly Curran5,6 • Vincent Wong2
Published online: 15 March 2017! The Author(s) 2017. This article is published with open access at Springerlink.com
Abstract To meet UNAIDS’ 90–90–90 treatment goals,effective approaches to HIV testing services (HTSs) are
urgently needed. In 2015, a cross-sectional study was
conducted to evaluate effectiveness and feasibility ofpartner notification for HTS in Tanzania. Men and women
newly diagnosed with HIV were enrolled as index clients,
listed sexual partners, and given options to notify and linktheir partners to HTS. Of 653 newly diagnosed individuals,
390 index clients were enrolled, listed 438 sexual partners,
of whom 249 (56.8%) were successfully referred. Of 249partners reaching the facilities, 96% tested for HIV, 148
(61.9%) tested HIV? (all newly diagnosed), and 104
(70.3%) of partners testing positive were enrolled into HIV
care and treatment. Results showed good acceptability,feasibility and effectiveness, as evidenced by high uptake
of partner notification among newly diagnosed individuals,
over half of listed partners successfully referred, and a veryhigh positivity rate among referred sexual partners.
Keywords Partner notification ! HIV testing services !Index clients ! Undiagnosed HIV ! Tanzania
AbbreviationsART Antiretroviral therapy
HTS HIV testing servicesIPV Intimate partner violence
PITC Provider initiated testing and counseling
STI Sexually transmitted infectionsVCT Voluntary counseling and testingCatherine Kahabuka and Marya Plotkin have contributed equally to
the work.
& Marya [email protected]
Catherine [email protected]
Alice [email protected]
Charlene [email protected]
Mustafa [email protected]
Renatus [email protected]
Werner [email protected]
Erick [email protected]
Ruth [email protected]
Kelly [email protected]
Vincent [email protected]
1 Jhpiego Tanzania, Dar es Salaam, Tanzania
2 USAID Washington, Washington, DC, USA
3 National AIDS Control Programme, Ministry of Health,Community Development, Gender, Elderly and Children,Dar es Salaam, Tanzania
4 USAID Tanzania, Dar es Salaam, Tanzania
5 Jhpiego Baltimore, Baltimore, USA
6 Johns Hopkins Bloomberg School of Public Health,Baltimore, USA
7 1660 Thames Street, Baltimore, MD 21231, USA
123
AIDS Behav (2017) 21:2551–2560
DOI 10.1007/s10461-017-1750-5
269

Background
The proportion of people living with HIV (PLHIV) who
know their status in sub-Saharan Africa (SSA) has risenfrom an estimated 10% in 2004 to 45% in 2015 [1, 2].
Effective approaches are urgently needed to find and
diagnose the remaining 55% and link them to care andtreatment, in support of UNAIDS’ 90–90–90 by 2020 goals
[3]. In light of the clinical and prevention benefits of early
initiation of treatment, the World Health Organization(WHO) now recommends early HIV case identification and
early initiation of antiretroviral therapy (ART), regardless
of CD4 count [4]. Partner notification—when partners ofthose recently diagnosed are notified of their exposure to a
communicable disease—is an effective strategy to identify
undiagnosed PLHIV and serodiscordant couples [5]. As anHIV testing services (HTSs) strategy, partner notification
may contribute to prevention of onward HIV transmission,
reduce HIV-related morbidity and mortality, and supportepidemic control, particularly when combined with a ‘‘test
and start’’ approach to ART in which all persons living
with HIV are eligible to start treatment immediately [6].With roots in sexually transmitted infection (STI) con-
trol and contact tracing, HIV partner notification is a pro-
cess in which a person newly diagnosed with HIV, referredto as the ‘‘index client,’’ either contacts or has a health care
provider contact his or her sexual partners to inform themof their HIV exposure and advise HIV testing. When health
care providers conduct the notification, the provider noti-
fies the partner of possible exposure without divulging theidentity of the index client. If positive, partners are linked
to HIV treatment services [7]. If negative, these partners
may be at high risk of HIV infection and require additionalprevention interventions if they remain in partnership with
the index client. Partner notification is featured in the
WHO 2015 consolidated guidelines on HTSs [8] and hasbeen proven effective in identifying persons with undiag-
nosed HIV infection [9–11] but has been underutilized in
SSA.The following methods of partner notification described
in the literature are relevant to this study:
• With passive referral, health workers encourage index
clients to notify and refer their partners for HTS on
their own (simple) [12], or with an invitation card oradditional information (enhanced).
• Under contract referral, health workers encourage index
clients to refer their partners for HIV testing, with theunderstanding that a health worker will contact partners
who do not visit the site by an agreed-upon date.
• With provider referral, a trained health worker locatesand notifies partners immediately and directly, while
maintaining the anonymity of the index client
[9, 13, 14].
Although HIV partner notification has long been estab-lished in the US and Europe [9, 15, 16], it has not been
widely implemented in SSA [10, 11], and is not the stan-
dard of care in Tanzania. However, a growing evidencebase supports its feasibility and effectiveness via facility-
and community-based HTS programs [17], including pre-
vention of mother-to-child transmission services [18] andSTI clinics [10]. Recent HIV partner notification studies
conducted in Malawi [10], Cameroon [11], and Mozam-
bique [17] have consolidated the evidence supporting thefeasibility [19] and acceptability of the passive, contract,
and provider referral approaches to partner notification. A
cluster-randomized trial in Kenya has also provided strongevidence for the success of provider-assisted partner noti-
fication [20].
The current study provides a unique contribution to theexisting evidence on partner notification by examining the
approach in the ‘‘real world’’ setting of routine, facility-
based HTS in Tanzania. Our index clients presented at thehealth facility for voluntary counseling and testing (VCT)
or were tested through provider-initiated testing and
counseling (PITC). We gave index clients a choice ofreferral method, allowing us to document client preference
with regard to partner notification, and test key outcomeswith an eye to feasibility in the Tanzanian public health
system. In this cross-sectional study, we assessed accept-
ability and measured effectiveness of partner notification in(a) locating and reaching high-risk sexual partners of index
clients, (b) reaching a high proportion of undiagnosed
HIV? persons, (c) achieving successful linkage to treat-ment for HIV? partners not currently in care, and
(d) identifying serodiscordant couples.
Methods
Study Design and Setting
A cross-sectional study was conducted in three hospitals inNjombe region, Tanzania between June and September
2015. Njombe is Tanzania’s highest prevalence region
where 14.8% of adults are infected with HIV [21]. Studyfacilities included peri-urban Kibena Regional Hospital,
urban Makambako Town Hospital, and the rural, Faith-
Based Ilembula Designated District Hospital. Each facilityhad a dedicated, onsite VCT center, and offered PITC to
inpatients and outpatients. These three facilities were
selected because of their high testing volume, in consul-tation with regional authorities.
AIDS Behav (2017) 21:2551–2560
123
270

Study Population and Eligibility Criteria
Men and women newly diagnosed with HIV through VCT orPITC at the three study sites were screened for study eligi-
bility. Eligibility criteria for index clients were: newly
diagnosed with HIV, 18 years or older, not pregnant, hadcurrent sexual partner or had partner in the past 24 months.
Pregnant women were excluded from the study since a form
of partner services already exists within antenatal care ser-vices in Tanzania—pregnant women are requested to bring
their sexual partner in for HIV testing. Referred sexual
partners were enrolled in this study if they met the eligibilitycriteria for the study: 18 years or older, were listed as having
been a sexual partner within the last 24 months, and had
locator information, and consented to participate.
Sample Size
We based our sample size calculation on an assumption that
index clients would list an average of one sexual partner, and
that 51% of partners would come to the facility followingnotification, as seen in theMalawi study [10]. Based on these
assumptions, a sample size of 384 index clients was needed
to detect a similar rate of attendance among sexual partnerswith 85% power (a = 0.05, two-sided test). The design
effect (DEFF) was set at 1.0 because we expected minimal
variation between facilities. The sample size formula for asingle cross-sectional survey was:
n " 1:962p#1$ p%#DEFF%d2
" 1:962 & 0:51#1$ 0:51%#1:0%#0:05%2
" 384:
Study Procedures
Individuals newly diagnosed with HIV through PITC or
VCT were referred to onsite researchers, who were alsoHIV counselors, and screened for study eligibility. Written
informed consent was obtained from interested and eligible
participants, referred to as ‘‘index clients.’’ Enrolled indexclients first answered a brief questionnaire that collected
demographic information, general sexual history, history of
intimate partner violence (IPV), and then were asked to listcurrent or past (within 24 months) sexual partners. Clients
with a history of IPV were noted, so that study staff could
provide appropriate counseling. Written consent, separatefrom participation in the study, was obtained before the
index client listed partners. Index clients were asked to list
as many partners as they could, with locator information,duration, status (past or current) and type of relationship for
each partner.
The study team member then informed the index client
about the three types of partner notification (passive, con-tract, and provider) and the index client selected the pre-
ferred approach to notify each of the listed sexual partners.
Partner notification by study staff was only initiated afterobtaining consent from the index client. For passive
referral, the study staff and the client agreed on a timeline
when the index client would bring in or refer listed part-ners. Index clients received a pre-printed study referral card
to give to partners, if they chose. If index clients did notbring in partners by the agreed date, study staff contacted
the index client by phone to encourage him or her to
complete the referral. For contract referral, the study staffinitiated partner notification if after 2 weeks the index
client had failed to bring in the sexual partner. For provider
referral, the study staff contacted partners directly by phonewithin 24 h, and read pre-scripted information from the
referral card, requesting partners to come for HTS. No
information on the identity of the index client was providedto the partner. Study staff contacted partners three to five
times before they were declared lost to follow-up (unless
the partner declined the referral). Index clients were linkedto partners using an ID code. Partners who came for ser-
vices without the index client had been contacted in
advance by the study team member and told where to comein the health facility, so the study team member was able to
link the partner to the index client.
During partner listing, the study staff assisted indexclients to assess the risk of IPV specific to each listed
sexual partner, using a standardized set of questions. Any
sexual partners the index client indicated might react withviolence were excluded from the notification process.
Partners coming for HTS were informed of the study,
consented, linked to the index client’s ID, and recorded assuccessful referrals. Unless already enrolled in an HIV
Care and Treatment Centre (CTC), as verified by self-re-
port or a CTC card, all sexual partners were offered HTSfollowing the Ministry of Health, Community Develop-
ment, Gender, Elderly and Children HIV testing protocols.
Partners testing positive for HIV were referred to theirchosen CTC using a referral form with a detachable portion
which the client could return to the site of the original
referral.Three methods were used to verify study participants’
enrollment at the CTC; (1) returned note signed by CTC
staff as confirmation of enrollment, (2) study staff checkingCTC registers at the study facilities and at nearby facilities
for the names and addresses of those who did not return the
referral note, and (3) study staff contacting participants byphone and asking them whether they were already enrolled
into CTC (self-report).
AIDS Behav (2017) 21:2551–2560
123
271

Data Management and Analysis
Data were collected using both paper forms and electronictablets. Paper-based data were entered into ODK data files
that had field checks for data quality. Data collected using
tablets were uploaded immediately to a server located inDar es Salaam. Data were cleaned by running queries and
reports using STATA version 14.0 and correcting dis-
crepancies. Data were extracted and analyzed using SPSSversion 23.
Descriptive statistics were performed to describe the
background characteristics of index clients and success-fully referred partners. Partners were considered success-
fully referred if they came to the respective facilities as a
result of any notification method, whether or not theytested for HIV. Assessment of differences between sites
was conducted and no major differences were seen on
study outcome variables. Univariate and multivariatelogistic regressions were run to identify predictors of par-
ticipation in the study among newly diagnosed individuals,
and success of referral among listed sexual partners.Backward elimination was used to establish the final
logistic model. Covariates were included into the final
model if they had a p value\0.25 and/or were known toaffect the outcome of interest in previously published
studies. Variables dropped out of the original model
include: occupation, duration of relationship, and whethersexual partner is a current partner. Table 2 depicts vari-
ables that were retained in the final multivariate model and
their effect on the study outcome.
Ethical Considerations
The study was conducted with ethical oversight from the
Institutional Review Boards (IRBs) of the Johns Hopkins
University Bloomberg School of Public Health (IRB00006116) and the Tanzania National Institute for Medical
Research (NIMR/HQ/R.8a/vol.1x/1914) with support from
the Njombe regional medical authorities.
Results
Study Overview
Of the 653 individuals newly diagnosed with HIV who were
approached about participation in the study, a total of 390
index clients were enrolled in the study (Fig. 1). A total of263 (40.3%) newly diagnosed HIV? individuals contacted
for the study were not enrolled. The most common reason to
not enroll in the study was the individual not having a sexualpartner in the last 24 months (n = 167, 63.5%), followed by
distraught or declined for other reason (n = 36, 13.6%),
being under 18 years of age (n = 30, 11.4%), having
insufficient contact information for partner (n = 11, 4.2%),being pregnant (n = 6, 2.3%), or other reasons (n = 13,
4.9%). The mean age of non-enrolled HIV? individuals was
similar to the mean age of enrolled index clients (32.2 vs.33.2 years, respectively); however, the proportion of eligible
males enrolled compared to females was higher (66.5% of
males vs. 54.8% of females, p = 0.002), and the proportionof HIV? individuals reporting they were single compared to
those married was much lower (39.9% single vs. 82.3%married, p\ 0.001; Table 1).
The 390 index clients listed 439 sexual partners (average
of 1.1 per index client). Initially, index clients chose pas-sive referral for 402 (91.6%) partners, provider referral for
14 (3.2%) partners, and contract referral for 2 (0.5%)
partners. Index clients refused partner notification servicesfor 17 (3.9%) listed partners, and information on the
selected referral approach was missing for four listed
partners. In all but three cases, the approach the indexclient chose for the partner initially was successful in
bringing in the partner for HTS: in two cases index clients
chose provider referral but ended up bringing their partnersthemselves, and one client chose passive referral but then
requested provider assistance.
Of the 439 listed sexual partners, 249 (56.7%) weresuccessfully referred (came to the health facility); 242
(97.2%) through passive referral, 6 (2.4%) through provi-
der, and 1 (0.4%) through contract referral. Of the suc-cessfully referred sexual partners, 239 (96.0%) were tested
for HIV, of whom 148 (61.9%) tested HIV?. All of the
partners testing HIV? were newly diagnosed.The 10 partners who came to the facility but were not
tested had a previously confirmed HIV diagnosis, of which
the index client was unaware. These 10 came to the facilitywith the index client and informed the client of their HIV
status at the facility instead of testing. Of the HIV? sexual
partners, 104 (70.3%) were enrolled in HIV care andtreatment by the end of the 3-month data collection period.
Information on partner CTC enrollment was obtained
through returned referral slip for 70 (67.3%), self-reportover the phone for 24 (23.1%) and study staff checking
area CTC registers for 10 (9.6%) of the sexual partners.
Characteristics of Index Clients Who were Ableto Successfully Refer at Least One Partner
Among index clients, nearly half (46.9%) were males and
76.2% were married (Table 1). Most index clients (70.3%)
had completed primary education and 55.9% were farmers.Index clients successfully referred 206 (82.7%) sexual
partners who were spouses, 18 (7.2%) who were
boyfriend/girlfriend, and 20 (8.0%) who were casual
AIDS Behav (2017) 21:2551–2560
123
272

partners. Among successfully referred sexual partners,43.0% were males and 88.4% were married/cohabiting.
The mean age was 33.2 years for index clients and
35.5 years for sexual partners (Table 1). Married indexclients were 2.7 times more likely (CI 1.5–4.8) to suc-
cessfully refer their sexual partners compared with
unmarried index clients (Table 2). Women were less likely(OR 0.5, CI 0.3–0.7) to successfully refer at least one
partner compared to men.
HIV Testing, HIV Sero-discordance, and IPV
Among the tested sexual partners, women tested positive ata higher rate than men (67.2% women vs. 54.9% men,
p = 0.036; Table 3). The highest HIV infection rate was
seen among wives (69.3%), followed by casual partners(both male and female, 65.0%). Out of 233 couples who
reported being in a current partnership, 88 were serodis-cordant couples, i.e., the partner tested negative for HIV.
No relationship was found between HIV positivity and
relationship duration.All 88 partners testing HIV- were described by the
index clients as current sexual partners, meaning that the
partner notification process found serodiscordant couples.Of the 71 HIV- current sexual partners whose information
on condom use was recorded, 50 (70.4%) reported not
using condoms at all, 16 (22.5%) reported using condomsinconsistently while only 5 (7.0%) said they used condoms
consistently with the index clients during sex in the past
12 months (Table 3).While six index clients indicated a general history of
IPV in the index client interview form, no index clients
indicated a perceived risk of IPV from a particular listedsexual partner (which would have disqualified that partner
from notification; data not shown).
Self-reported via phone call
24 (23.1%)Confirmed80 (76.9%)
NOT enrolled into CTC/ information missing
44 (29.7%)
Enrolled into care and treatment (CTC)
104 (70.3%)
Tested negative91 (38.2%)
Tested positive148 (61.8%)
Partners not tested for HIV
10 (4%)
Partners tested for HIV
239 (96.0%)
Partners who did not come in following referral
190 (43.4%)
Partners who came in following referral
249 (56.6%)
Listed sexual partners439
Enrolled as index client
390 (59.7%)
Newly diagnosed HIV infected individuals
653
Not enrolled as index client
263 (40.3%)
Returned referral slip
70 (67.3)
Checked CTC register
10 (9.6%)
Fig. 1 Overview of HTC partner notification study, Njombe, Tanzania, June–September 2015
AIDS Behav (2017) 21:2551–2560
123
273
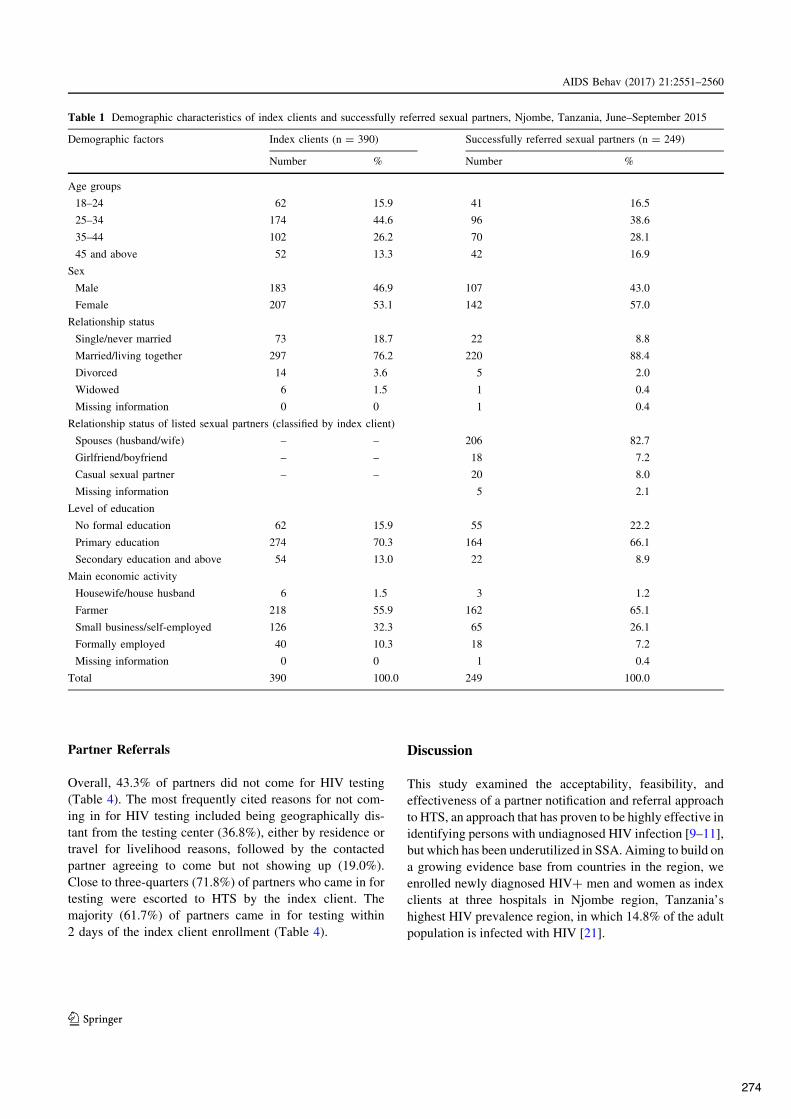
Partner Referrals
Overall, 43.3% of partners did not come for HIV testing(Table 4). The most frequently cited reasons for not com-
ing in for HIV testing included being geographically dis-
tant from the testing center (36.8%), either by residence ortravel for livelihood reasons, followed by the contacted
partner agreeing to come but not showing up (19.0%).
Close to three-quarters (71.8%) of partners who came in fortesting were escorted to HTS by the index client. The
majority (61.7%) of partners came in for testing within
2 days of the index client enrollment (Table 4).
Discussion
This study examined the acceptability, feasibility, andeffectiveness of a partner notification and referral approach
to HTS, an approach that has proven to be highly effective in
identifying persons with undiagnosed HIV infection [9–11],but which has been underutilized in SSA. Aiming to build on
a growing evidence base from countries in the region, we
enrolled newly diagnosed HIV? men and women as indexclients at three hospitals in Njombe region, Tanzania’s
highest HIV prevalence region, in which 14.8% of the adult
population is infected with HIV [21].
Table 1 Demographic characteristics of index clients and successfully referred sexual partners, Njombe, Tanzania, June–September 2015
Demographic factors Index clients (n = 390) Successfully referred sexual partners (n = 249)
Number % Number %
Age groups
18–24 62 15.9 41 16.5
25–34 174 44.6 96 38.6
35–44 102 26.2 70 28.1
45 and above 52 13.3 42 16.9
Sex
Male 183 46.9 107 43.0
Female 207 53.1 142 57.0
Relationship status
Single/never married 73 18.7 22 8.8
Married/living together 297 76.2 220 88.4
Divorced 14 3.6 5 2.0
Widowed 6 1.5 1 0.4
Missing information 0 0 1 0.4
Relationship status of listed sexual partners (classified by index client)
Spouses (husband/wife) – – 206 82.7
Girlfriend/boyfriend – – 18 7.2
Casual sexual partner – – 20 8.0
Missing information 5 2.1
Level of education
No formal education 62 15.9 55 22.2
Primary education 274 70.3 164 66.1
Secondary education and above 54 13.0 22 8.9
Main economic activity
Housewife/house husband 6 1.5 3 1.2
Farmer 218 55.9 162 65.1
Small business/self-employed 126 32.3 65 26.1
Formally employed 40 10.3 18 7.2
Missing information 0 0 1 0.4
Total 390 100.0 249 100.0
AIDS Behav (2017) 21:2551–2560
123
274

The current study demonstrated high acceptability, fea-
sibility, and effectiveness of this approach in the ‘‘realworld’’ setting of routine facility-based HTS in Tanzania.
High acceptability was evidenced by high uptake of the
passive notification and referral process service amongeligible index clients. A high level of feasibility was
demonstrated, with more than half of listed sexual partners
(56.6%) coming in for testing. The approach also proved tobe effective; nearly 62% of successfully referred sexual
partners were found to be HIV?, and of these, all werenewly diagnosed. More than 70% of the HIV? partners
were linked to care and treatment. Our study found partner
notification to be particularly effective in bringing currentsexual partners in stable relationships (marriage or cohab-
itation) to the facility for testing. No cases of notification-
related violence were reported in this study.Our findings underscore the need for a good counseling
and prevention package to be provided for serodiscordant
couples as part of a partner notification program. Over one-third (36.2%) of the partners tested, all of whom indicated
that they were in current partnership with the index client,
tested negative. In our study, these couples were offered
the standard of care in Tanzania during this time period,
which included prevention counseling and condoms. Pro-gram and policy implementers should consider offering an
effective prevention package for serodiscordant couples
identified through partner notification approaches. Thismay include immediate initiation of ART for HIV? part-
ners. Additionally, pre-exposure prophylaxis (PrEP) for
negative partners, where negative partners can come offPrEP if their positive partner is virally suppressed and they
don’t have any other HIV risk, could be an important partof a serodiscordant couple package.
This study reinforces an emerging evidence base that in
Africa, partner notification yields high rates of successfulreferral and high HIV positivity. In Kenya, in the first
cluster randomized trial of partner notification in SSA,
index clients were provided with an immediate provider-assisted partner notification service and 76% of their sexual
partners were successfully referred to HTS [20]. Studies in
Malawi and Cameroon have shown high HIV positivityrates among partners (64 and 50%, respectively), and as in
Tanzania, the listed partner was generally a spouse or the
main sexual partner of the index client [10, 11]. In a pilot
Table 2 Index clients who successfully referred at least one sexual partner, by background characteristics, Njombe, Tanzania, June–September2015
Demographic factors Index clients OR (95% CI)
Total index clients(n = 390)
% successfully referred at least onepartner
Univariate Multivariate
Sex
Male 183 71.0 Reference
Female 207 51.7 0.4 (0.3–0.7)*** 0.5 (0.3–0.7)**
Age (years)
18–24 62 58.1 Reference
25–34 174 58.0 1.0 (0.6–1.8) 0.6 (0.3–1.2)
35–44 102 62.7 1.2 (0.6–2.3) 0.6 (0.3–1.3)
45 and above 52 69.2 1.6 (0.7–3.5) 0.7 (0.3–1.7)
Marital status
Single 73 41.1 Reference
Married 297 66.7 2.9 (1.7–4.8)*** 2.7 (1.5–4.8)**
Divorced 14 50.0 1.4 (0.5–4.5) 1.6 (0.5–5.2)
Widowed 6 33.3 0.7 (0.1–4.2) 0.8 (0.1–4.8)
Education levels
No formal education 62 74.2 Reference
Primary education 274 59.5 0.5 (0.3–0.9)* 0.5 (0.2–0.9)*
Secondary education or above 54 51.9 0.4 (0.2–0.8)* 0.4 (0.2–0.8)*
OR odds ratio, CI confidence interval
* p\ 0.05, ** p\ 0.01, *** p\ 0.001
AIDS Behav (2017) 21:2551–2560
123
275

study in Mozambique [17], community health workers
provided assisted partner notification via contract referralto people newly diagnosed with HIV, and 54% of sexual
partners were HIV?.
By assessing feasibility as well as effectiveness, thisstudy offers unique insights into the application of partner
notification in facility settings. Because index clients were
offered a choice of referral method, rather than beingrandomized into a referral approach, we were able to assess
index client preferences. The findings—that index clientsoverwhelmingly preferred passive referral and predomi-
nantly chose to list and notify a spouse—have important
implications for the application and rollout of partnernotification. There is clearly room for success in applica-
tion of both client and provider initiated approaches to
partner notification. In Kenya, 67% of sexual partnerscontacted using via provider-assisted partner notification
came in for testing, when offered the service early [20].
Passive referral had not been highlighted as a promisingapproach in other studies: only 6.7% of partners in the
Cameroon study were notified by passive referral [11]; in
the Malawi study, passive referral had a comparativelypoor uptake of 24% compared to 51% in the provider-
assisted arms [10]. Our study was not designed to assess
uptake of or otherwise make comparisons between referralmethods, but rather to evaluate the effectiveness of a
partner notification intervention implemented by providing
a choice of referral by the index client. This would reflect a
real world application of increasing focus on voluntarypartner services into PITC/VCT contexts. Our index clients
showed a much higher preference for passive referral.
Relative to the Malawi study, the higher success of passivereferral may be due to the fact that index clients were
allowed to choose—rather than being randomized into—a
notification approach; however, in the Cameroon study,index clients were allowed to choose their referral method
and only a small proportion chose passive referral. Thechoices made by participants in our study suggest that, in
Njombe, the majority of index clients were comfort-
able with passive referral, and viewed the role of thecounselor as someone who could assist with facilitated
disclosure of their status to their primary, current partner
once the index client had convinced the partner to come fortesting. Given the different results seen in this study and
other studies in the region, implementers of partner noti-
fication approaches in SSA may wish to conduct formativeresearch to explore preferences around provider-assisted
versus passive referral, to create the most effective service
delivery option.Roughly 60% of the newly diagnosed individuals
approached for enrollment in this study met eligibility
criteria and elected to enroll. The most common reason forexclusion (n = 167, 65%) was not having a sexual partner
in the last 24 months. In reality this may have been a
Table 3 HIV sero-statusamong tested sexual partners,Njombe, Tanzania, June–September 2015
Demographic factors HIV sero-status of tested sexual partners n = 239 Total n (%) p values
HIV? = 148n (%)
HIV- = 91n (%)
Sex
Male 56 (54.9) 46 (45.1) 102 (100.0)
Female 92 (67.2) 45 (32.8) 137 (100.0) 0.036*
Relationship type (missing information = 5)
Husband 42 (60.0) 28 (40.0) 70 (100.0)
Wife 88 (69.3) 39 (30.7) 127 (100.0)
Boyfriend/girlfriend 3 (17.6) 14 (82.4) 17 (100.0)
Casual sexual partner 13 (65.0) 7 (35.0) 20 (100.0) 0.001*
Relationship duration (missing information = 5)
Less than a year 22 (50.0) 22 (50.0) 44 (100.0)
1–5 years 51 (63.7) 29 (36.3) 80 (100.0)
6–10 years 29 (65.9) 15 (34.1) 44 (100.0)
More than 10 years 44 (66.7) 22 (33.3) 66 (100.0) 0.297
Current sexual partner (missing information = 5)
Yes 145 (62.2) 88 (37.8) 233 (100.0)
No 1 (100.0) 0 (0.0) 1 (100.0) 0.624
Self-reported condom use in past 12 months among current sexual partners (missing information = 139)
None 75 (60.0) 50 (40.0) 125 (100.0)
Inconsistently 40 (71.4) 16 (28.6) 56 (100.0) 0.333
Consistently 8 (61.5) 5 (38.5) 13 (100.0)
AIDS Behav (2017) 21:2551–2560
123
276

response which allowed people who were anxious about
partner notification to opt out of the process without statingtheir reluctance; this should be further investigated in
future studies. These findings may differ in settings where
HIV prevalence is lower, which may result in more stigmafor HIV? individuals and more reluctance to disclose
status to partners. One limitation of the study was that we
did not actively follow index clients or partners for IPVreporting. We were only able to ask about IPV from 20
index clients and 20 sexual partners who were interviewed
2–4 weeks following the partner notification process.
Conclusions
Reaching the first 90 requires efficient and effective HIV
testing strategies. As the proportion of PLHIV who remainundiagnosed decreases, reaching thosewho are asymptomatic
and not engaged with the health system is a critical challenge.
Our study confirms that partner notification could dra-matically increase the number of previously undiagnosed
PLHIV who learn their status and are linked to care.
Offering partner notification from within existing facility
HTS settings could—with limited additional burden on thehealth system—greatly expand access to testing and link-
age to care among people at very high risk of infection.
Allowing index clients to choose their preferred referralmethod may have led to increased success in the referral
process, resulting in more partners being tested. We found
a clear preference for passive referral, especially to notify aspouse, among index clients in our study.
We recommend partner notification as a priority HIV
testing strategy, and that provision of a package for pre-vention for serodiscordant couples be included as part of
the service. Because of the heterogeneity in the successes
and preferences associated with partner notification indifferent studies, no single partner notification strategy
stands out as the recommended approach. However, our
findings suggest that offering index clients options forpassive or provider-facilitated notification and referral may
result in a high uptake of passive referral. Further research
is needed to evaluate whether or not partner notificationstrategies, tailored differently, could be more successful in
reaching multiple or casual partners.
Table 4 Partner follow-upoutcomes and process, Njombe,Tanzania, June–September 2015
Referral factors n %
Outcome of partner notification out of listed sexual partners
Successfully referred 249 56.7
Not successfully referred 190 43.3
Total 439 100.0
Reasons for failure of referral
Partner geographically distant (travel or residence) 70 36.8
Partner agreed to come but did not show up 36 19.0
Partner was not reached 29 15.3
Partner refused upon contact 18 9.5
Partner too busy to come in (farming/business/work) 9 4.7
Other reasons 28 14.7
Total 190 100.0
Partner escorted by index client (missing information = 1)
Yes 178 71.8
No 60 24.2
Total 238 100.0
Days taken to successful referral (missing information = 1)
Partner came to facility by day 2 153 61.7
Partner came to the facility within days 3–7 19 7.7
Partner came to the facility within days 8–14 27 10.9
Partner came to the facility 15? days 49 19.7
Total 248 100.0
Average number of contacts to partners (missing information = 1) Mean [range]
Successfully referred (n = 248) 2 [1–5]
Not successfully referred (n = 190) 1 [1–4]
AIDS Behav (2017) 21:2551–2560
123
277

Acknowledgements The authors thank the regional health authoritiesof Njombe for their tireless efforts to combat HIV infection and supportHIV? people in their region, with special recognition to Dr. EusebiusKessy, who provided critical leadership to this study. YusuphKulindwacreated themap for this manuscript. Dr.Mbaraka Amuri provided studyleadership. The management of Kibena Hospital, Ilembula Hospital,and Makambako Hospital are gratefully acknowledged for their activesupport of the study and thoughtful consideration of how HTS mightreach more people in need of services. Linda Fogarty, Jason Reed, andElizabeth Manfredini reviewed, and Chris Merriman edited the article.
Funding This study was funded by the United States President’sEmergency Plan for AIDS Relief (PEPFAR) through the United StatesAgency for International Development’s (USAID’s) Technologies forHealth/Accelovate Program under Cooperative Agreement # AID-OAA-A-11-00050. The opinions herein are those of the authors and donot necessarily reflect the views of USAID or of PEPFAR.
Author contributions CK and MP drafted the article. CK and MNconducted the statistics for the article. RL and MN reviewed findingsfor accuracy in fieldwork. RK, WM, AC, VW, CB, EM and KCdrafted and reviewed sections of the article.
Compliance with Ethical Standards
Conflict of interest Catherine Kahabuka declares that she has noconflict of interest. Marya Plotkin declares that she has no conflict ofinterest. Alice Christensen declares that she has no conflict of interest.Charlene Brown declares that she has no conflict of interest. MustafaNjozi declares that he has no conflict of interest. Renatus Kisendideclares that he has no conflict of interest. Werner Maokola declaresthat he has no conflict of interest. Eric Mlanga declares that he has noconflict of interest. Ruth Lemwayi declares that she has no conflict ofinterest. Kelly Curran declares that she has no conflict of interest.Vincent Wong declares that he has no conflict of interest.
Ethical approval All procedures performed in studies involvinghuman participantswere in accordancewith the Ethical Standards of theInstitutional and/or National Research Committees of Johns HopkinsUniversity and the National Institute of Medical Research of Tanzania.
Informed consent Informed consent was obtained from all individ-ual participants included in the study.
Open Access This article is distributed under the terms of the CreativeCommons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distri-bution, and reproduction in anymedium, provided you give appropriatecredit to the original author(s) and the source, provide a link to theCreative Commons license, and indicate if changes were made.
References
1. World Health Organization (WHO). 3 by 5 Progress reportDecember 2003 through June 2004. Geneva: WHO; 2004.
2. UNAIDS. The gap report. Geneva: UNAIDS; 2014. http://www.unaids.org/sites/default/files/en/media/unaids/contentassets/documents/unaidspublication/2014/UNAIDS_Gap_report_en.pdf Acces-sed 4 Jan 2017.
3. UNAIDS. 90–90–90 An ambitious treatment target to help endthe AIDS epidemic. Geneva: UNAIDS; 2014.
4. World Health Organization (WHO). Guidelines: guideline onwhen to start antiretroviral therapy and on pre-exposure pro-phylaxis for HIV. Geneva: WHO; 2015. http://apps.who.int/iris/
bitstream/10665/186275/1/9789241509565_eng.pdf?ua=1. Acces-sed 4 Jan 2017.
5. Hosseinipour MC, Rosenberg NE. HIV partner notification:possible and essential. Sex Transm Dis. 2013;40(12):915–6.doi:10.1097/OLQ.0000000000000060.
6. Tanser F, Barnighausen T, Grapsa E, Zaidi J, Newell M-L. Highcoverage of ART associated with decline in risk of HIV acqui-sition in rural KwaZulu-Natal, South Africa. Science.2013;339:966–71. doi:10.1126/science.1228160.
7. Mathews C, Coetzee N, Zwarenstein M, Lombard C, GuttmacherS, Oxman A, et al. A systematic review of strategies for partnernotification for sexually transmitted diseases, including HIV/AIDS. Int J STD AIDS. 2002;13:285–300.
8. World Health Organization (WHO). Guidelines: consolidatedguidelines on HIV testing services. Geneva: WHO; 2015.
9. Hogben M, McNally T, McPheeters M, Hutchinson AB, TaskForce on Community Preventive Services. The effectiveness ofHIV partner counseling and referral services in increasing iden-tification of HIV-positive individuals: a systematic review. Am JPrev Med. 2007;33(2S):S89–100.
10. Brown LB, Miller WC, Kamanga G, Nyirenda N, Mmodzi P,Pettifor A, et al. HIV partner notification is effective and feasiblein sub-Saharan Africa: opportunities for HIV treatment and pre-vention. J Acquir Immune Defic Syndr. 2011;56(5):437–42.doi:10.1097/QAI.0b013e318202bf7d.
11. Henley C, Forgwei G, Welty T, Golden M, Adimora A, ShieldsR, et al. Scale-up and case-finding effectiveness of an HIVpartner services program in Cameroon: an innovative HIV pre-vention intervention for developing countries. Sex Transm Dis.2013;40(12):909–14. doi:10.1097/OLQ.0000000000000032.
12. Ward H, Bell G. Partner notification. Medicine. 2014;42(6):314–7.13. Ferreira A, Young T, Mathews C, Zunza M, Low N. Strategies
for partner notification for sexually transmitted infections,including HIV. Cochrane Database Syst Rev. 2013;10:CD002843. doi:10.1002/14651858.CD002843.pub2.
14. Adams OP, Carter AO, Redwood-Campbell L. Understandingattitudes, barriers and challenges in a small island nation to dis-ease and partner notification for HIV and other sexually trans-mitted infections: a qualitative study. BMC Public Health.2015;15:455. doi:10.1186/s12889-015-1794-2.
15. Macke BA, Maher JE. Partner notification in the United States:an evidence-based review. Am J Prev Med. 1999;17(3):230–42.
16. Dehne KL, Riedner G, Neckermann C, Mykyev O, Ndowa FJ,Laukamm-Josten U. A survey of STI policies and programmes inEurope: preliminary results. Sex Transm Infect. 2002;78:380–4.doi:10.1136/sti.78.5.380.
17. Feldacker C, Myers S, Cesar F, Paredes Z, Augusto G, MuluanaX, et al. Who benefits from partner services in Mozambique?Results from a pilot program in a public, urban clinic. Poster:Assisted Partner Services; IAS 2015.
18. Rosenberg NE, Mtande TK, Saidi F, Stanley C, Jere E, Paile L,et al. Recruiting male partners for couple HIV testing andcounselling in Malawi’s option B? programme: an unblindedrandomised controlled trial. Lancet HIV. 2015;2(11):e483–91.doi:10.1016/S2352-3018(15)00182-4.
19. Rutstein SE, Brown LB, Biddle AK, Wheeler SB, Kamanga G,Mmodzi P, et al. Cost-effectiveness of provider-based HIVpartner notification in urban Malawi. Health Policy Plan.2014;29:115–26. doi:10.1093/heapol/czs140.
20. Cherutich P, Golden MR, Wamuti B, Richardson BA, Asb-jornsdottir KH, Otieno FA, et al. Assisted partner services forHIV in Kenya: a cluster randomised controlled trial. Lancet HIV.2016;. doi:10.1016/S2352-3018(16)30214-4.
21. Tanzania Commission for AIDS (TACAIDS). National HIV andAIDS response report 2012: Tanzania mainland. Dar es Salaam:TACAIDS; 2013.
AIDS Behav (2017) 21:2551–2560
123
278
'RZ
QORDGHGIURP
KWWSV���MRXUQDOV�OZZ�FRP
�DLGVRQOLQHE\
%K'0I�H3+
.DY�](RXP�W4
I1�D�N-/K(=JEV,+
R�;0L�K&
\Z&;�$:
Q<4S�,O4
U+'�0
*�QM(M+
*WYR�FP
T[:''&RVO\XS1
=���&]&
D/O[R4�SZ
%/Q�FQ+9QJ
RQ����������
'RZQORDGHGIURPKWWSV���MRXUQDOV�OZZ�FRP�DLGVRQOLQHE\%K'0I�H3+.DY�](RXP�W4I1�D�N-/K(=JEV,+R�;0L�K&\Z&;�$:Q<4S�,O4U+'�0*�QM(M+*WYR�FPT[:''&RVO\XS1=���&]&D/O[R4�SZ%/Q�FQ+9QJ RQ����������
Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved.
EDITORIAL
Adolescents, young people, and the 90–90–90 goals:a call to improve HIV testing and linkage to treatment
Vincent J. Wonga, Kate R. Murrayb, B. Ryan Phelpsa,
Sten H. Vermundc and Donna R. McCarraherb
The current low rates of HIV diagnosis and treatment initiation among adolescents andyoung people ages 15–24 continues to present a significant challenge to the epidemiccontrol of HIV. With a ‘business as usual’ approach to HIV testing and linkage totreatment, new infections among adolescents and youth will likely increase, with theburden compounded by the increasing number of youth in Africa, expected to reach293 million by 2025. Recent studies reveal significant gaps in the HIV clinical cascadeamong young people as the global community pursues the Joint United NationsProgramme on HIV and AIDS 90–90–90 targets. This AIDS supplement was commis-sioned with the goal of informing program planners, researchers, policymakers, andfunding agencies about the development and design of effective adolescent and youthprograms, policies, and strategies for improving the first two 90s among adolescentsand youth: HIV testing and diagnosis and linkage to care and treatment. Emergingevidence should inform efforts to better target the youth and adolescents who are mostat risk, aiming for early diagnosis and treatment initiation for those who are HIVpositive, while also ensuring appropriate primary prevention so that those identified asHIV negative remain so.
Copyright ! 2017 The Author(s). Published by Wolters Kluwer Health, Inc.
AIDS 2017, 31 (Suppl 3):S191–S194
Keywords: adolescents, HIV, linkage, pediatrics, provider-initiated testing andcounseling, testing, voluntary counseling and testing, youth
The good news in global health includes the tremendousgains made in prevention of mother-to-child transmissionservices, which now reach 80% of pregnant women livingwith HIV in 21 priority countries, and toward the boldnew goal of eliminating HIV among infants [1,2].However, the troubling news remains the current lowrates of HIV diagnosis and treatment initiation amongyoung people ages 15–24 which continue to present asignificant challenge to epidemic control. In theUnited States, 59% of adolescents and young adults ages13–29 who are living with HIV remain undiagnosed [3].In Sub-Saharan Africa, where most young people and
adolescents living with HIV (ALHIV) reside, only one infive HIV-positive adolescent girls know her HIV status.Moreover, globally an estimated one-third of all newinfections occurs in those 15–24 demonstrates theimportance of an HIV response targeting these agegroups [4]. The prevention of mother-to-child trans-mission gains that have reduced infant infection ratescould be reversed if high rates of HIV transmission persistamong adolescents and youth. With a ‘business as usual’approach to HIV testing and treatment, new infectionsamong adolescents and youth will likely increase, with theburden compounded by the increasing number of youth
aUSAID, Office of HIV/AIDS, Arlington, Virginia, bFHI 360, Durham, North Carolina, and cYale Schools of Public Health andMedicine, New Haven, Connecticut, USA.Correspondence to Vincent J. Wong, MSc, USAID, Office of HIV/AIDS, 2100 Crystal Drive. Box 9044, Arlington, VA 22202, USA.Tel: +1 15713091273; e-mail: [email protected]: 3 May 2017; accepted: 3 May 2017.
DOI:10.1097/QAD.0000000000001539ISSN 0269-9370 Written work prepared by employees of the Federal Government as part of their official duties is, under the U.S. Copyright Act, a ‘‘work ofthe United States Government’’ for which copyright protection under Title 17 of the United States Code is not available. As such, copyright does not extendto the contributions of employees of the Federal Government. S191
279

Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved.
in Africa, expected to reach 293 million by 2025 and 535million by 2065 [5]. Furthermore, a recent modes oftransmission study in South Africa continues to highlightthe fact that adolescent girls are primarily infected byolder males, putting them at particular risk of earlierinfection [6]. In 2015, 250 000 ALHIV were newlyinfected, and two out of three resided in Sub-SaharanAfrica [2]. As we look to the years ahead, constant (orincreased) incidence with this growing population,combined with limited access to or uptake of HIVservices will inevitably lead to a substantially higherHIV burden.
In a dire complement to these statistics, results fromrecent studies reveal significant gaps in the HIV clinicalcascade among young people in terms of reaching the90–90–90 targets set by Joint United Nations Pro-gramme on HIV and AIDS [7–10]. Combined resultsfrom population-based HIV surveys conducted in 2016to measure HIV incidence in Malawi, Zambia, andZimbabwe showed that 46% of people ages 15–24 wereaware of their HIV status, and of those who were aware,only 82% were on treatment and 79% of these were virallysuppressed [11–14]. In these countries, older adults arefaring much better with 78% reporting they were awareof their HIV status, 90% of those diagnosed were ontreatment, and 90% of those on treatment were virallysuppressed [14]. Even when adolescents seek healthservices for HIV-related illnesses, openings are lost toengage them in care. Health facilities have reported lowrates of testing coverage, representing critical missedopportunities to diagnose ALHIV, improve adolescenthealth and reduce onward transmission. One studyfrom Zimbabwe suggests that primary healthcare providersoften do not recognize HIV infection among adolescents,many of whom reported likely infection at birth, but someof whom may have acquired HIV sexually [15].
The evidence on successful efforts to get adolescents andyoung people into HIV testing and link them to treatmentis also insufficient. A recent systematic review of theuptake and positivity rate of HIV testing services amongchildren and adolescents (ages 5–19) reported thatapproaches evaluated to date have not been tailored toneeds of this age group [16]. Rather, they replicatestrategies for adults and do not consider the specificbarriers that adolescents face [17]. Once diagnosed,multiple factors have been reported as thwartingsuccessful linkage to care; providers lack ‘friendliness,’and adolescents’ developmental stage makes managingtheir illness challenging [18]. Another systematic reviewthat described key factors affecting linkage to care forALHIV found that most work has focused on addressingindividual barriers and not adequately addressed otherbarriers such as structural and health system issues [19].For both HIV testing and linkage to treatment, most newapproaches that have been vetted are based on smallstudies with methodological constraints; new approaches
developed with scale-up in mind are sorely needed tomeet the needs of adolescents and young people [19].
Despite the gaps in evidence, the importance ofimproving HIV testing and linkage to care has beenrecognized by the global health community. For example,a WHO values and preferences study revealed that keybarriers to HIV testing and counseling includedunfriendly services and adolescents’ concerns aboutconfidentiality [20]. Subsequently, WHO released its‘Guidance for HIV Testing and Counselling and Care forALHIV’ and a complementary online tool (http://apps.who.int/adolescent/hiv-testing-treatment/) [21] inorder to guide countries as they modify existing programsand develop new ones. A key policy barrier that manycountries must address to improve access and coverage isadolescents’ ability to provide legal informed consent forHIV services, including testing and care [17].
This AIDS supplement was commissioned with the goalof providing new evidence and insights to programplanners, researchers, policy makers, and funding agencieswho are seeking to improve or develop HIV testing,diagnosis, linkage to care and treatment programs,policies, and strategies for adolescents and youth. Sevenof the nine articles focus on Sub-Saharan Africa,reflecting the continent’s burden of the global HIVepidemic; two articles highlight challenges in the UnitedStates in addressing adolescent key populations, who havespecific barriers to accessing services. Together, thesestudies not only identify key gaps in access andacceptability of services, but highlight a range ofpromising programmatic responses.
With a focus on at-risk adolescents accessing HIVservices, the Metropolitan Atlanta community adolescentrapid testing initiative study by Camacho-Gonzalez et al.[22] identified an intervention that provided venue-basedtesting, motivational interviewing and case managementto adolescents and youth. Wilson et al. [23] highlight thatadolescents value caregiver support and positive inter-actions with healthcare workers, and that they desiremaking autonomous decisions regarding HIV diagnosisand disclosure. Denison et al. [24] detail the process andimportance of engaging youth in programs and researchdesigned to meet their needs.
Community-based approaches demonstrate successes inincreasing access and uptake: Indravudh et al. [25] assessedHIV self-testing in Malawi and Zimbabwe, and Shanaubeet al. [26] describe the benefits of a combination HIVprevention package in Zambia that included universalHIV testing and linkage to treatment.
Among adolescent MSM in the United States, Maranoet al. [27] found variable, but overall low, reach bycommunity-based HIV testing services, as well as lowrates of linkage to treatment, illustrating the need to
AIDS 2017, Vol 31 (Suppl 3)
280

Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved.
identify barriers to HIV diagnosis, especially among Blackand Hispanic adolescent MSM populations. Ruria et al.[28] found that active youth engagement, efforts topromote links between facilities and schools, and youth-friendly programming for newly diagnosed adolescentsand youth were associated with increased retention in care.
Kaufman et al. [29] found that despite the scale-up ofvoluntary male circumcision programs to prevent HIVtransmission, opportunities are being missed to deliverHIV prevention messaging and counseling to both infectedand uninfected youth. Finally, Wagner et al. [30] assess theuse of continuous quality improvement to improveadolescents’ satisfaction with HIV testing services, theirHIV knowledge, and their intentions to retest in the future.
Several important themes emerge when we consider theexisting evidence alongside the research presented in thissupplement. The combination of demographic shifts,high-HIV prevalence, and incidence rates, and compara-tively low rates of treatment coverage and viralsuppression in adolescents and young people highlightsa serious programmatic gap that threatens the global gainsmade against the HIV pandemic. These disconnectsrequire attention in both programs and policies. To reachthe first two 90s and attain primary prevention amongHIV-uninfected adolescents (including key populations),there are multiple needs to be addressed. Consent policiesand laws must be changed to respect the autonomy ofadolescents and youth and to take into consideration thecrucial support they receive from caregivers andhealthcare workers. We need to develop and evaluatenew programmatic and policy innovations that areinformed by the adolescents and youth they are intendedto serve [31,32]. Program data must guide implementa-tion and, along with survey data, may serve to identify90–90–90 gaps among younger age bands. Finally, ourefforts must target those who are most at risk –diagnosing them early and immediately treating thosewho are HIV positive, and ensuring through appropriateprimary prevention efforts that those identified HIVnegative are empowered to remain so.
Acknowledgements
Conflicts of interestThere are no conflicts of interest.
References
1. WHO. Progress Report 2016: Prevent HIV, Test and Treat All.Geneva, Switzerland: World Health Organization; 2016.
2. United Nations Children’s Fund. For Every Child, End AIDS –Seventh Stocktaking Report. New York: UNICEF; 2016.
3. Zanoni BC, Mayer KH. The adolescent and young adult HIVcascade of care in the United States: exaggerated healthdisparities. AIDS Patient Care STDS 2014; 28:128–135.
4. United Nations Children’s Fund. Towards an AIDS-free Gen-eration-Children and AIDS: Sixth Stocktaking Report. New York,NY: UNICEF; 2013.
5. Economic Commission for Africa. The Demographic Profil ofAfrican Countries.Addis Ababa, Ethiopia; 2016.
6. de Oliveira T, Kharsany A, Graf T, Cawood C, Khanyile D,Grobler A, et al. Transmission networks and risk of HIV infec-tion in KwaZulu-Natal, South Africa: a community-wide phy-logenetic study. Lancet HIV 2017; 4:e41–e50.
7. UNAIDS. 90–90–90: an ambitious treatment target to help endthe AIDS epidemic.UNAIDS; 2014.
8. Philbin MM, Tanner AE, DuVal A, Ellen JM, Xu J, Kapogiannis B,et al. Factors affecting linkage to care and engagement in carefor newly diagnosed HIV-positive adolescents within fifteenadolescent medicine clinics in the United States. AIDS Behav2014; 18:1501–1510.
9. Fox MP, Rosen S. Systematic review of retention of pediatricpatients on HIV treatment in low and middle-income countries2008–2013. AIDS 2015; 29:493–502.
10. Kim SH, Gerver SM, Fidler S, Ward H. Adherence to antire-troviral therapy in adolescents living with HIV: systematicreview and meta-analysis. AIDS 2014; 28:1945–1956.
11. ICAP. Summary Sheet: Preliminary Findings: Zimbabwe popu-lation-based HIV impact assessment ZIMPHIA 2015–2016. In;2016.
12. ICAP. Summary Sheet: Preliminary Findings: Malawi popula-tion-based HIV impact assessment MPHIA 2015–2016. In;2016.
13. ICAP. Summary Sheet: Preliminary Findings: Zambia popula-tion-based HIV impact assessment ZAMPHIA 2015–2016. In;2016.
14. Justman J. Real Progress in the HIV epidemic: PHIA findingsfrom Zimbabwe, Malawi, and Zambia. Seattle, WA: CROI;2017.
15. Ferrand R, Munaiwa L, Matsekete J, Bandason T, Nathoo K,Ndhlovu C, et al. Undiagnosed HIV infection among adoles-cents seeking primary healthcare in Zimbabwe. Clin Infect Dis2010; 51:844–851.
16. Govindasamy D, Ferrand RA, Wilmore SM, Ford N, Ahmed S,Afnan-Holmes H, et al. Uptake and yield of HIV testingand counselling among children and adolescents in sub-Saharan Africa: a systematic review. J Int AIDS Soc 2015;18:20182.
17. Fox K, Ferguson J, Ajose W, Singh J, Marum E, Baggaley R. HIVand adolescents: guidance for HIV testing and counselling andcare for adolescents living with HIV: Annex 15: Adolescentconsent to testing: a review of current policies and issues inSub-Saharan Africa.World Health Organization; 2013.
18. Philbin MM, Tanner AE, Duval A, Ellen J, Kapogiannis B,Fortenberry JD. Linking HIV-positive adolescents to care in15 different clinics across the United States: creating solutionsto address structural barriers for linkage to care. AIDS Care2014; 26:12–19.
19. MacPherson P, Munthali C, Ferguson J, Armstrong A, Kranzer K,Ferrand RA, et al. Service delivery interventions to improveadolescents’ linkage, retention and adherence to antiretro-viral therapy and HIV care. Trop Med Int Health 2015;20:1015–1032.
20. Armstrong A, Baggaley R, Ferguson J, Van der Kwaak A,Wolmarans L. The Voices Values and Preference of Adolescentson HIV Testing and Counselling: Consultation for the Devel-opment of the World Health Organization HIV Testing andCounselling Guidelines for Adolescents In. Edited by WHO2013.
21. HIV and adolescents: guidance for HIV testing and counsellingand care for adolescents living with HIV: recommendations for apublic health approach and considerations for policy-makersand managers. Geneva, Switzerland: World Health Organiza-tion; 2013.
22. Camacho-Gonzalez AF, Gillespie SE, Thomas-Seaton L, FriesonK, Hussen SA, Murray A, et al. The Metropolitan Atlantacommunity adolescent rapid testing initiative study: closingthe gaps in HIV care among youth in Atlanta, Georgia, USA.AIDS 2017; 31 (Suppl 3):S267–S275.
23. Wilson KS, Beima-Sofie KM, Moraa H, Wagner AD, Mugo C,Mutiti PM. ‘‘At our age, we would like to do things the way wewant:’’ a qualitative study of adolescent HIV testing services inKenya. AIDS 2017; 31 (Suppl 3):S213–S220.
Adolescents, young people, and the 90–90–90 goals Wong et al.
281

Copyright © 2017 Wolters Kluwer Health, Inc. All rights reserved.
24. Denison JA, Pettifor A, Mofenson LM, Kasedde S, Marcus R,Konayuma KJ, et al. Youth engagement in developing animplementation science research agenda on adolescent HIVtesting and care linkages in sub-Saharan Africa. AIDS 2017; 31(Suppl 3):S195–S201.
25. Indravudh PP, Sibanda EL, d’Elbee M, Kumwenda MK,Ringwald B, Maringwa G, et al. ‘I will choose when to test,where I want to test’: investigating young people’s preferencesfor HIV self-testing in Malawi and Zimbabwe. AIDS 2017; 31(Suppl 3):S203–S212.
26. Shanaube K, Schaap A, Chaila MJ, Floyd S, Mackworth-YoungC, Hoddinott G, et al., on behalf of the HPTN 071 (PopART)Study Team. Community intervention improves knowledgeof HIV status of adolescents in Zambia: findings fromHPTN 071-PopART for youth study. AIDS 2017; 31 (Suppl 3):S221–S232.
27. Marano MR, Stein R, Williams WO, Wang G, Xu S, Uhl G, et al.HIV testing in nonhealthcare facilities among adolescent MSM.AIDS 2017; 31 (Suppl 3):S261–S265.
28. Ruria EC, Masaba R, Kose J, Woelk G, Mwangi E, Matu L, et al.Optimizing linkage to care and initiation and retention ontreatment of adolescents with newly diagnosed HIV infection.AIDS 2017; 31 (Suppl 3):S253–S260.
29. Kaufman MR, Dam KH, Van Lith LM, Hatzold K, Mavhu W,Kahabuka C, et al. Voluntary medical male circumcision amongadolescents: a missed opportunity for HIV behavioral inter-ventions. AIDS 2017; 31 (Suppl 3): S233–S241.
30. Wagner AD, Mugo C, Bluemer-Miroite S, Mutiti PM, WamalwaDC, Bukusi D, et al. Continuous quality improvement inter-vention for adolescent and young adult HIV testing services inKenya improves HIV knowledge. AIDS 2017; 31 (Suppl 3):S243–S252.
31. Villa-Torres L, Svanemyr J. Ensuring youth’s right to participa-tion and promotion of youth leadership in the development ofsexual and reproductive health policies and programs. J Ado-lesc Health 2015; 56 (1 Suppl):S51–S57.
32. Youth in development policy: realizing the demographicopportunity. Washington, DC: USAID; 2012..
AIDS 2017, Vol 31 (Suppl 3)
282

Research article
Assessment of linkages from HIV testing to enrolment andretention in HIV care in Central MozambiqueCelso Azarias Inguane§,*,1,2, Stephen Gloyd*,2,3, Joao Luis Manuel4, Charlene Brown5, Vincent Wong5,Orvalho Augusto2,3,6,7, Wisal Mustafa Hassan2,3, Lucia Vieira4, Pires Afonso2, Mehol Jamnadas4, Jama Joy Bernard2,James Cowan2, Samuel Kalibala8 and James Pfeiffer2,3
§Corresponding author: Celso Azarias Inguane, University of Washington, Box 353100, Seattle, WA 98195, USA. Tel: !001 206 596 1634. ([email protected])*These authors have contributed equally to the work.
AbstractIntroduction: Effectiveness of the rapid expansion of antiretroviral therapy (ART) throughout sub-Saharan Africa is highly
dependent on adequate enrolment and retention in HIV care. However, the measurement of both has been challenging in thesesettings. This study aimed to assess enrolment and retention in HIV care (pre-ART and ART) among HIV-positive adults in CentralMozambique, including identification of barriers and facilitators.Methods: We assessed linkages to and retention in HIV care using a mixed quantitative and qualitative approach in six districts
of Manica and Sofala provinces. We analyzed routine district and health facility monthly reports and HIV care registries fromApril 2012 to March 2013 and used single imputation and trimmed means to adjust for missing values. In eight health facilities inthe same districts and period, we assessed retention in HIV care among 795 randomly selected adult patient charts (15 years and
older). We also conducted 25 focus group discussions and 53 in-depth interviews with HIV-positive adults, healthcare providersand community members to identify facilitators and barriers to enrolment and retention in HIV care.Results: Overall, 46% of the monthly HIV testing reports expected at the district level were missing, compared to 6.4% of the
pre-ART registry reports. After adjustment for missing values, we estimated that the aggregate numbers of adults registered inpre-ART was 75% of the number of persons tested HIV-positive in the six districts. In the eight health facilities, 40% of the patientcharts for adults enrolled in pre-ART and 44% in ART were missing. Of those on ART for whom charts were found, retention in
treatment within 90 and 60 days prior to the study team visit was 34 and 25%, respectively. Combining these multiple datasources, the overall estimated retention was 18% in our sample. Individual-level factors were perceived to be key influences toenrolment in HIV care, while health facility and structural-level factors were perceived to be key influences of retention.Conclusions: Efforts to increase linkages to and retention in HIV care should address individual, health facility, and structural-
level factors in Central Mozambique. However, their outcomes cannot be reliably assessed without improving the quality ofroutine health information systems.
Keywords: linkages; retention; HIV care; treatment; Mozambique.
To access the supplementary material to this article please see Supplementary Files under Article Tools online.
Received 27 November 2015; Revised 22 April 2016; Accepted 2 May 2016; Published 20 July 2016
Copyright: – 2016 Inguane CA et al; licensee International AIDS Society. This is an Open Access article distributed under the terms of the Creative Commons
Attribution 3.0 Unported (CC BY 3.0) License (http://creativecommons.org/licenses/by/3.0/), which permits unrestricted use, distribution, and reproduction in any
medium, provided the original work is properly cited.
IntroductionIn the past decade, Mozambique has expanded access to
HIV testing services and antiretroviral therapy (ART) and has
integrated them into the primary healthcare system [1"4].Still, the proportion of people with an HIV-positive diagnosis
who have been linked to and retained in HIV care has been
reported to be low [5,6], similar to much of sub-Saharan
Africa [7,8]. The Mozambique Ministry of Health reported
in 2015 that ART coverage was only 59% of the estimated
treatment needs [9], and, as in other countries in the region,
the proportion of those retained in pre-ART care and ART in
Mozambique tends to decrease over time [8"10]. This poseschallenges to reaching the ambitious 90-90-90 goals of the
Joint United Nations Programme on HIV/AIDS’ (UNAIDS)
[11,12]. The new WHO guidelines on early initiation of ART
[13] may contribute to achieving those goals, but only if
people who are diagnosed HIV-positive are enrolled and
retained in care. Moreover, accurate monitoring of enrol-
ment and retention with reliable information about the
HIV cascade [14] is critical for making progress in HIV care.
Nevertheless, poor HIV data quality from both routine sources
and international implementing partners [9,15] remains a
challenge to understanding the cascade.A study aimed to identify and measure loss to follow-up in
the HIV care cascade in Manica and Sofala provinces, Central
Mozambique, using adjusted routine health systems data and
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
1
283

patient charts to estimate the proportion of people with anHIV-positive diagnosis who were linked to and retained inpre-ART care and ART. The study also aimed to identify
perceived barriers and facilitators of enrolment and retentionin pre-ART care and ART.
MethodsStudy setting and designWe conducted this mixed methods study in six districts: Beira,
Buzi and Dondo in Sofala Province; and Barue, Chimoio andManica in Manica Province. Beira and Chimoio are the capitalcities of Sofala and Manica provinces, respectively. The otherfour districts are rural. We selected these six districts because
of their rural-urban mix, their mix of different levels of healthservices, and their security. These districts are mostly con-tiguous and cover most of the major health facilities in Central
Mozambique. Self-referral to health facilities inside or outsidethis six-district regionwould likely have been infrequent. At thetime of the study, HIV testing, pre-ARTcare and ART were free
and widely available throughout the country.To obtain an overview of HIV testing and HIV care
enrolment at the district level, we examined routine monthlyreports from all (87) health facilities that provided HIV testing
or treatment in those districts. To obtain an in-depth assess-ment of enrolment, patient flow and retention in pre-ARTcare and ART at the health facility level, we selected eight of
the 87 facilities for further study. The eight facilities wereamong the 34 facilities that provided ART during the studyperiod; four were the main referral health facilities in rural
districts and four were moderate to large patient volumefacilities in urban areas.
District overview assessment
We collected and analyzed routine district and health facilitymonthly reports of HIV testing and HIV testing registries (pre-ART, ART) in each of the six districts from April 2012 to March2013 (the study period). The study start date corresponds
with a major revision of HIV data collection and monitoringregistries, including new patient forms, registry books andreporting templates, that had been introduced in Mozambi-
que in early 2012. We also collected data directly from HIVregistries at district-level health offices, from pharmacyrecords of tests distributed and reported positive and from
the national electronic health information system, locallyknown as the Modulo Basico.We conducted descriptive analyses such as frequency for
HIV tests, pre-ART and ART registrants, and for missing valuesin the routine data set. We examined missing value patternsover time and by health facility, and tested several imputationmethods to substitute missing values: (1) single imputation
using mean, trimmed means (replacing values above 50% ofthe mean for facilities that had less than five months data) andmedian, (2) Poisson generalized linear modelling and (3)
iterative singular value decomposition (SVD) method (speci-fically rank-1 SVD approximation). None of these methodsyielded consistently higher or lower imputed values than the
other methods.We finally used the single imputation methodbecause it gave the most conservative values. We performedthe imputations in R (version 3.2) and analysis in Stata 13.1.
Health facility quantitative assessmentAt each of the eight health facilities, we abstracted enrol-
ment data from the pre-ART and ART registry books and
retention data from patient charts and pharmacy records.
Mozambique Ministry of Health policy stipulates that (1) all
newly diagnosed HIV-positive patients be first registered in
pre-ART registry books (even those who are eligible for ART)
and (2) patient charts be created for all pre-ART and ART
patients. The pre-ART and ART registry books included dates
of HIV-positive and CD4 tests and the dates of ART initiation.
We conducted a stratified random sample of registrants from
the pre-ART and ART registries separately (using random.org)
to obtain 100 charts of patients older than 15 years from
each facility, excluding women in prevention of mother-
to-child transmission of HIV (PMTCT) programmes. We
searched for the selected patient charts in archives, con-
sultation rooms and other parts of the health facilities. Data
abstracted from patient charts included demographic
characteristics, site of testing, and dates for ordering CD4
tests, receipt of CD4 results, enrolment into care, ART
initiation, consultations, ART pickups, and the date of the
study team visit. Data were entered into study computers
using EPIDATA 3.2 and exported for cleaning and analysis in
Stata 13.1.
To construct the overall HIV cascade, we used different
data sources for enrolment and retention. Enrolment propor-
tions were measured in two steps: first, by the number of
people, district-wide, registered in pre-ART divided by the
estimated (adjusted) number of newly diagnosed HIV positive
in each district during the study period; and second, by the
proportion of charts found among the selected people
registered on pre-ART and ART at each of the eight health
facilities. Retention rates were measured by the proportion
of patient charts with evidence of an ART clinic visit or
antiretroviral (ARV) pickup by patient charts or individual
pharmacy records within 30, 60 or 90 days prior to the study
team visit to the facility. Retention was examined separately
for pre-ART and ART patients.
Health facility qualitative assessment
At each of the eight facilities and their surrounding areas,
we conducted in-depth interviews (IDIs) with health facility
directors and with people living with HIV who (1) enrolled in
pre-ART care within 30 days of their HIV-positive test result,
(2) enrolled after 30 days from their HIV-positive test result,
(3) enrolled but eventually dropped out of pre-ART care and
(4) never enrolled in HIV care. In each facility, we had aimed
to include at least one person living with HIV from each of
the four categories, and adolescents (18"19 years old).
Participants were at least 18 years old. Study interviewers
contacted and obtained informed consent directly from
facility directors before conducting an IDI. During health
facility visits, healthcare providers informed people living
with HIV eligible for study participation about the study and
gave them the option of contacting study interviewers for
informed consent if they were interested in participating in
the study. In health facility surrounding areas, facility-based
outreach workers provided information about the study to
people who had dropped out of care or who had never
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
2
284

enrolled in care, and gave them the option of contactingstudy interviewers for informed consent if they were in-terested in participating in the study. Study interviewers also
conducted focus group discussions (FGDs) with healthcareproviders, community outreach workers, and members ofpatient-support groups at the health facility. They conducted
FGDs with community leaders in community meeting rooms.IDIs and FGDs focused on people’s experience with HIVtesting and HIV care, barriers and facilitators of enrolment
and retention in pre-ART care and ART, and on visualizingthose experiences, barriers and facilitators through develop-ing patient flow maps in each facility.Study interviewers took notes and audio-recorded IDIs and
FGDs to expand notes and improve reliability. We coded andanalyzed notes using ATLAS.ti 7TM (www.atlasti.com/). Thispaper reports only on the main facilitators and barriers for
linkages and retention in pre-ART care and ART, that is, thosementioned by at least three out of the four types of peopleliving with HIV, and in at least four out of the eight study
sites. More in-depth analysis of the qualitative data isplanned for future publication.
Ethical considerationsThe Institutional Review Boards of the Population Council,United States, and the Mozambique National Institute of
Health (CIBS-INS) approved the study. All participants pro-vided written informed consent. In the published figures andtables, we replaced actual names of health facilities with
anonymous alphabetical codes to avoid adverse events thatmight result from reporting on low performance.
ResultsAt the district level, we analyzed all available reports fromthe 87 facilities providing HIV testing and the 34 facilities
providing ART. At the eight health facilities providing ART, weabstracted information from 795 patient charts (430 pre-ARTand 365 ART) and we conducted 25 FGDs (comprising 248
participants) and 53 IDIs. We excluded three low-qualityIDIs from analysis, leaving 23 IDIs with people who enro-lled within 30 days of being diagnosed HIV-positive, seven
with people who had enrolled 30 days or more after their
HIV-positive test result, 10 with people who had enrolled incare and dropped out and two with HIV-positive people whonever enrolled in care. We also conducted eight IDIs with
health facility directors.
District-level HIV testing and enrolment in careMonthly reports submitted at the district level indicated thatslightly more people tested HIV-positive than the number of
people newly registered in pre-ART care (Table 1). Beira andManica districts reported fewer people who tested HIV-positive than those registered in pre-ART. Overall, 46% (range25"65% among districts) of the 1944 monthly reports for HIV
testing that were expected from the 87 facilities were missing,compared to 6.4% (range 2"15%) of the 312 expectedmonthlyreports for registry in pre-ART and ART. Missing values were
more frequent from the electronic health information system,including three districts without reports for any HIV testingdata during the study period. After imputation adjustment, the
proportional increase from raw totals was 35% for peopletested HIV-positive and only 4.2% for those registered in pre-ART care. With the adjustment, the overall proportion of HIV-positive people who enrolled in pre-ARTcare in the six districts
was 75% (range 46"92%).
Enrolment in HIV care in the eight ART facilities
The overall mean proportion of pre-ART and ART registrantswhose charts were located at the health facilities was 60 and66%, respectively, with a high variation between the facilities
(range 31"85% for ART and 7"64% for pre-ART). Patientdemographics abstracted from the charts were not signifi-cantly different between pre-ART and ART patients (Supple-
mentary Table 1). Pre-ART and ART samples from the eighthealth facilities had similarly high proportions of women(62% pre-ART and 55% ART). Patients were mostly between15 and 49 years old (91% pre-ART and 92% ART), and most
had primary and secondary level of education (68% pre-ARTand 69% ART). The socio-demographic profiles of HIV-positivepersons interviewed were similar to those whose charts were
reviewed: 95% were between 20 and 49 years of age, 61%were women, 57% reported completing primary and 31%reported completing secondary or higher education level.
Thirty-eight percent of interviewees reported being married
Table 1. Monthly reported and adjusted numbers and percentages of people with HIV-positive diagnosis and enrolled in pre-ART
between April 2012 and March 2013 in six districts in Manica and Sofala provinces
Number of people with HIV-
positive diagnosis
Number of people with HIV-positive
diagnosis enrolled in pre-ART
Proportion of people with HIV-
positive diagnosis enrolled in pre-ART
Districts Reported Adjusted Reported Adjusted Reported (%) Adjusted (%)
Buzi 2104 3363 1549 1658 74 46
Dondo 2898 2757 1681 2681 58 56
Beira 8143 12,040 11,061 11,061 136 92
Manica 2404 3498 2660 2660 111 76
Barue 2096 2164 1194 1194 57 55
Chimoio 7032 7406 5675 5675 81 77
Total 24,677 33,228 23,820 24,820 97 75
Note: Adjusted numbers combined reported values for reported months and imputed values for missing months.
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
3
285

or in marital union, 21% widowed and 77% reported having
children. Regarding occupations, 33% reported being domes-
tic workers, 24% small business owners and 15% workers in
agriculture/fishing.Patient chart data demonstrated a large variation between
the health facilities in time from HIV-positive test to first
clinical consultation (overall mean 13.3 days; IQR 0.0"12.0days; range 0.0"13.3 months) and in time from HIV diagnosis
to ART initiation (overall mean 1.8 months; IQR 0.7"2.1months; range 0.1"12.2 months) (Figure 1).
Retention in ART in the eight ART facilitiesAmong the 346 ART charts found, the median time from the
initiation of treatment until study team visit was 18.6
months. Overall, 34, 27 and 8% of these ART charts had
evidence of a clinic visit or ARV pickup within 90, 60 or 30
days of the study team visit, with a wide variation among the
eight health facilities (Figure 2). We found that the number of
days for which ARVs were dispensed was frequently missing.
However, during IDIs and FGDs, health providers consistently
reported that ARVs were usually dispensed for 60 days oroccasionally for 90 days when patients were clinically stable.Crude and adjusted logistic regression did not show
differences in retention rates between males and females.However, retention (evidence of ARV pickup within 90 daysof study visit) in Manica Province was significantly greater
than in Sofala Province (Supplementary Table 2).
Overall HIV care cascadeWe constructed an overall HIV care cascade (Figure 3) using
the following sources of data: (1) district-level proportions ofestimated HIV-positive people who were registered in pre-ART, (2) proportions of patients registered in ART in the eight
health facilities whose charts were found and (3) proportionsof those patient charts with any evidence of clinic visit or ARVpick up within 90 days of our study team review visit. The
calculations suggest that, in aggregate, 18% of the HIV-positivepatients diagnosed in health facilities during the study periodwere retained in treatment one to two years later.
Figure 1. Months from HIV-positive diagnosis to first consultation
among pre-ART patients (a), and time from HIV-positive diagnosis
to ART initiation among ART patients (b), in eight health facilities in
Manica and Sofala provinces.
Figure 2. Proportion of ART patient charts with evidence of
clinical visit or ARV pickup, 30, 60 and 90 days before study visit in
eight health facilities of Manica and Sofala provinces.
Figure 3. Overall HIV cascade " from HIV testing to enrolment to
charts located to retention " aggregate data from eight health
facilities in Manica and Sofala provinces. Note: Each bar represents
the proportion of the original total of people tested HIV-positive,
for example, 50% of HIV-positive charts found #66% charts found
times 75% registered. Adjusted numbers combined reported values
with imputed values for missing months.
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
4
286

Perceived facilitators and barriers to HIV testing, enrolmentand retentionMost respondents from both the IDIs and FGDs said that
they preferred to be tested at sites that provided ART and
near their places of residence. Both men and women who
enrolled early in HIV care said that the main reason for
obtaining an HIV test " and for enrolling in HIV care " was
the presence of symptoms of sickness. Conversely, the main
perceived barrier for enrolment was lack of symptoms of
sickness. Some women who enrolled early mentioned their
desire to protect their children from vertical transmission and
wishing to live longer to raise their children.
Only early enrollers in HIV care mentioned a facilitator of
retention, living near the health facility where one receives
HIV care. Perceived barriers for retention included: (1) the
perception of poor and disrespectful service at the health
facility, especially for people on ART who were late to their
ARV pickup appointments and (2) lack of money for food and
for transportation.Table 2 summarizes facilitators and barriers to enrolment
and retention in HIV care that were mentioned during IDIs and
FGDs.Healthcare providers described how HIV-positive patients
could be lost at different steps along the HIV continuum of care
through a variety of delays and loss to follow-up in patient flow
that varied by site. For example, losses were especially common
in the intervals between patients receiving their HIV-positive
result and creating the chart, or between having their blood
drawn for laboratory tests and receiving those results. Inter-
viewees also mentioned that, at all eight health facilities, charts
were not created in the same room where HIV tests were done
and results disclosed. In some health facilities, patients were
sent to queue at the health facility reception to have their charts
created when frequently charts were not created at all. At other
facilities, providers said they took the patient’s test results and
went to create the chart themselves at the reception. When
blood samples were sent to other health facilities to obtain CD4
counts, the results often took several weeks to be returned to
patients.
We constructed Figure 4 that shows an idealized flow map
for HIV-positive patients in ART, based on the Mozambique
2014 national ART guidelines. The information gathered from
our eight FGDs with 74 healthcare providers at the eight
study health facilities suggested specific points in the flowmap
where patients were typically lost to follow-up (LTFU), noted
with black downward-pointing arrows with an LTFU label.
DiscussionThis study demonstrated substantial losses to follow-up of
HIV-positive persons at all points along the HIV care
and treatment cascade in Central Mozambique. Moreover,
our findings suggest that the routine HIV information, as
reported, grossly overestimates both the true enrolment and
retention in HIV care. Our findings also suggest that HIV-positive
patients experienced major facilitators and barriers for
enrolment and retention in HIV care, including individual,
health system and structural factors.Our estimate of the proportion of people diagnosed with
HIV who are registered in pre-ART care was slightly
higher than other estimates in sub-Saharan Africa [8]. Our
overall retention estimates are much lower than nationally
reported retention estimates in Mozambique for 2014
(67% at 12 months after ART initiation, and 56% at 24 months)
[9,12]. Our low retention estimates are, however, not sub-
stantially different than other carefully conducted studies in
sub-Saharan Africa [7,11,12]. Our facilitators for enrolment in
pre-ART and ART care (e.g. proximity to ART services and
severity of illness) were similar to studies elsewhere [16,17].
Yet, in contrast to those studies, facilitators for enrolment and
retention in our study seemed to only help those who enrolled
early in care (within 30 days of their HIV diagnosis). Our
barriers for retention (e.g., lack of symptoms, perceived poor
quality of healthcare) were consistent with other studies in
sub-Saharan Africa [16"18].The large variations in patient flow patterns, in observance
of national norms, and LTFU found among the eight ART faci-
lities suggest that targeted health systems change, including
simplification of patient flow, improved patient information
and improving health worker behaviour, might substantially
improve performance. The data also suggest that there is an
urgent need for strategies to re-link patients into HIV care in
Mozambique, using lessons learned from the country and
other low-resource settings [19]. Strategies might include
having healthcare workers, with whom many patients have
developed close relationships, contact patients who have
dropped out and understand reasons why they dropped out
[19]. Judgemental attitudes or threatening patients is not
helpful, as has been reported in other sub-Saharan African
Table 2. Perceived facilitators and barriers to enrolment and retention in HIV care in eight health facilities in Manic and Sofala
provinces
Facilitators Mentioned by Barriers Mentioned by
Enrolment in
HIV care
Presence of
symptoms
Early enrollers
Community leaders
Lack of symptoms Late enrolment, never enrolled, dropouts, patient-
support group and healthcare providers
Retention in
HIV care
Proximity to
health facility
Early enrollers Disrespect by health workers,
poor quality of healthcare
Lack of money for food and
transport
Early enrolment, late enrolment, dropouts, patient-
support group, healthcare providers and outreach
workers
Early enrolment, late enrolment and dropouts
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
5
287

contexts [20]. However, in Mozambique, many of these health-care workers battle with work overload [21,22] or lack of
motivation because they feel ‘‘exploited and ultimatelyabandoned’’ by the nature of global HIV interventions [23].
Working conditions need to be addressed to complementtraining. Improving workforce morale, understanding indivi-
dual patient circumstances (including reasons beyond their
control) and bearing in mind that missing visits are inevitableover the lifelong course of HIV care can help in the process of
re-linking patients into care [20]. Another strategy, based onour results, would be to simplify algorithms of patient care
and confusing patient flow patterns, and to address chal-
lenges with patient chart management.Our finding that a large proportion of those who register in
pre-ART (who are thus considered ‘‘linked’’ to HIV care) have
no evidence of subsequent encounters with the health
system is disturbing. The finding raises serious concernsabout using registration at ART facilities as an indicator for
effective enrolment. Measuring retention is also a challenge.If retention is measured only among those with patient
charts or pharmacy records, the results will overestimate the
true retention of the people originally tested HIV-positive inthe health system. On the other hand, incomplete recording
of visits or ARV pickup in patient charts may underestimatetrue retention of those in care with charts. Follow-up of
pharmacy records can complement data on patient retention
if the pharmacy records are adequately filled out. Allenrolment and retention estimates, however, will be mean-
ingful only when they are based on an accurate denominator
of the total numbers of people tested HIV-positive in the
health system.TheMozambiqueMinistry of Health has acknowledged poor
HIV data quality nationally [9,15] and data concerns have been
well documented through ethnographic research in Mozam-
bique [21]. Authors concerned about data quality in other
countries have called for the use of multiple measures of
linkages to HIV care and retention in HIV care and treatment
[24"26]. Other lower resolution proxy measures (e.g. viral
load) may provide broader generalizability for the measure-
ment of trends in linkage to care over time [27].We hope that
our research will contribute to a deeper understanding of how
to use proxy measures of linkage to HIV care and treatment to
match the desired programmatic or clinical outcomes.
LimitationsThe poor quality of reported data was both a principal find-
ing of the study and a limitation. Although our imputation
methods were designed to supplement routine data to
obtain more accurate estimates, we cannot be certain that
the adjusted estimates reflect the true picture of registry and
enrolment in care. Patients may have received effective ART
without adequate evidence of their treatment in patient
charts. We noted earlier that the data systems in Mozambi-
que did not allow for analysis of individual linkages of people
tested HIV-positive to HIV care, since no codes were used
Counseling roomVCT/PICT
Results disclosure
Create patient chartPsychosocial assessment
HIV+
HIV-
Clinical consult. 1Staging, lab, CTZ
Psychosocial assessment
ART eligible
Clinical consult.2ARV prescription
Counseling
Assessment:Prepared to start ART ?
No
ARV pickupAdherence counseling
Clinical consult. 3ARV pickup
Adhere. counseling
Yes
Non-ART eligible
PRE-ART
Clinical consult.4
ARV pickup ARV pickup
Clinical consult.6
ARV pickup
ARV pickup
Clinical consult.7
ARV pickup
Clinical consult.8Clinical consult.9
Every 6 months thereafter
ARV pickup
AZT+3TC+NVP
30thday60thday
3rd month
6th month9th month12th month
15th day after
starting ART
Adhere. counselling
ARV pickupEvery 3 months thereafter
Adhere. counselling Adhere. counselling Adhere. counselling Thereafter -whenever
needed
ARV pickup
5th month
4th month
Referral to support groups
LTF
U
LTF
U
LTF
U
LTF
U
LTF
U
Figure 4. Patient flow map showing loss to follow up along the HIV continuum of care in eight health facilities of Manica and Sofala
provinces. ART: antiretroviral therapy; AZT!3TC!NVP: zidovudine! stavudine!niverapine; CTZ: cotrimoxazole; HIV+: HIV-positive; PICT:
provider initiated counselling and testing; LTFU: lost to follow-up; VCT: voluntary counselling and testing.
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
6
288

for testing, and as a result testing could not be linked toregistries in the ART sites. Thus, it was not possible toascertain the extent to which people tested HIV-positive
might be obtaining care from elsewhere, including outsidethe study districts. Since transfers of patients were rarelyregistered, our estimates of retention likely underestimated
the true retention of our sample HIV-positive registrants.The qualitative assessment was limited by the small
numbers of HIV-positive people who enrolled late, dropped
out or never enrolled in care that we were able to interview.Moreover, the findings related to health systems barriers canonly represent the practices at these eight facilities. Otherfacilities might have presented substantially different quali-
tative (and quantitative) findings. Nevertheless, our diversesample that included perspectives of people living withHIV, health providers, and community outreach workers and
members provided wide-ranging perceptions.
ConclusionsOur findings suggest that these districts in Central Mozambique
face serious challenges to effectively enrol and retain peoplewho are tested HIV-positive in the health system. The poorquality of routine reported data, especially regarding HIV
testing, is a major barrier to identifying these bottlenecks.More attention needs to be focused on improving thequality and analysis of routine data regarding all steps ofthe HIV cascade at each health facility. We think that our
careful utilization of routine health system information, whichincluded data quality assessment, triangulation of data fromother sources, adjustment by imputation for missing data, and
patient chart review, provided a reasonably high-resolutionmeasure of linkage to care. The HIV care cascade model thatwe constructed provided health facility-specific detail on
critical bottlenecks from which tailored interventions can bedeveloped. Our study results also suggest that health system,individual and structural factors were important perceived
barriers to enrolment and retention in care. Modifying thesefactors and assessing their impact with reliable data shouldsubstantially improve linkages to enrolment and retention inHIV care and enhance global efforts to address HIV.
Authors’ affiliations1Department of Anthropology, University of Washington, Seattle, WA,
USA; 2Health Alliance International, Seattle, WA, USA; 3Department of Global
Health, University of Washington, Seattle, WA, USA; 4Centro de Investigacao
Operacional de Beira (CIOB), Ministry of Health, Beira, Mozambique; 5Office
of HIV/AIDS, USA, Agency for International Development, Washington,
DC, USA; 6Faculdade de Medicina, Universidade Eduardo Mondlane, Maputo,
Mozambique; 7Manhica Research Center (CISM), Manhica, Mozambique;8HIVCore/Population Council, Washington, DC, USA
Competing interests
None.
Authors’ contributions
CI, SG, JM, CB, JB, SC and JP conceived the study and contributed to the study
design. CI, SG, OA, LV and WM analysed the data. CI and SG drafted the
manuscript. JM, CB, VW, OA, LV, PA, MJ, WM, JB, JC, SC and JP revised the
manuscript. All authors read and approved the final draft.
Acknowledgements and funding
This study was made possible through support provided by the President’s
Emergency Plan for AIDS Relief and theU.S. Agency for International Development
(USAID) via HIVCore, a Task Order funded by USAID under the Project SEARCH
indefinite quantity contract (Contract No. AID-OAA-TO-11-00060). The Task Order
is led by the Population Council in partnership with the Elizabeth Glaser Pediatric
AIDS Foundation, Palladium and the University of Washington. The research was
also supported by NIAID, NCI, NIMH, NIDA, NICHD, NHLBI, NIA, NIGMS and NIDDK
of the National Institutes of Health under award number AI027757.
Disclaimer
The authors’ views expressed in this manuscript do not necessarily reflect the
views of USAID, NIH or the US government.
References
1. Pfeiffer J, Montoya P, Baptista AJ, Karagianis M, de Morais Pugas M, Micek
M, et al. Integration of HIV/AIDS services into African primary health care:
lessons learned for health system strengthening in Mozambique " A case
study. J Int AIDS Soc. 2010;13(1):3.
2. Lambdin BH, Micek M, Sherr K, Gimbel S, Karagianis M, Lara J, et al.
Integration of HIV care and treatment in primary health care centers and
patient retention in central Mozambique: a retrospective cohort study. J Acquir
Immune Defic Syndr. 2013;62(5):e146"52.3. MISAU, DNAM. Directriz Nacional para Implementacao do Aconselhamento
e Testagem em Saude. Maputo City, Mozambique: MISAU; 2015.
4. MISAU, DNAM. Guia de Tratamento Antiretroviral e Infeccoes Oportunistas
no Adulto, Crianca, Adolescente e Gravida, 2013. Maputo City, Mozambique:
MISAU; 2014.
5. Micek MA, Gimbel-Sherr K, Baptista AJ, Matediana E, Montoya P, Pfeiffer J,
et al. Loss to follow-up of adults in public HIV care systems in Mozambique:
identifying obstacles to treatment. J Acquir Immune Defic Syndr. 2009;52(3):
397"405.6. Pearson CR, Micek MA, Pfeiffer J, Montoya P, Matediane E, Jonasse T, et al.
One year after ART initiation: psychosocial factors associated with stigma
among HIV-positive Mozambicans. AIDS Behav. 2009;13(6):1189"96.7. Brennan A, Browne JP, Horgan M. A systematic review of health service
interventions to improve linkage with or retention in HIV care. AIDS Care.
2014;26(7):804"12.8. Rosen S, Fox MP. Retention in HIV care between testing and treatment in
sub-Saharan Africa: a systematic review. PLoS Med. 2011;8(7):e1001056.
9. MISAU. Relatorio Anual. Relatorio anual das actividades referentes ao HIV/
SIDA. Maputo, Mozambique: MISAU; 2015.
10. Auld AF, Mbofana F, Shiraishi RW, Sanchez M, Alfredo C, Nelson LJ, et al.
Four-year treatment outcomes of adult patients enrolled in Mozambique’s
rapidly expanding antiretroviral therapy program. PLoS One. 2011;6(4):e18453.
11. UNAIDS. Ambitious treatment targets: writing the final chapter of the AIDS
epidemic [Internet]. Geneva, Switzerland: UNAIDS; 2014. [cited 2015 Nov 1].
Available from: http://www.unaids.org/en/resources/documents/2014/90-90-90
12. US Department of State office of the US Global AIDS Coordinator.
PEPFAR 3.0: controlling the epidemic: delivering on the promise of an AIDS-
free generation. [Internet]. 2014 [cited 2015 Nov 1]. Available from: http://
www.pepfar.gov/documents/organization/234744.pdf
13. World Health Organization, Department of HIV/AIDS. Guideline on when to
start antiretroviral therapy and on pre-exposure prophylaxis for HIV. [Internet].
2015. [cited 2015 Nov 6]. Available from: http://apps.who.int/iris/bitstream/
10665/186275/1/9789241509565_eng.pdf
14. World Health Organization, Department of HIV/AIDS. Consolidated strate-
gic information guidelines for HIV in the health sector: HIV strategic informa-
tion for impact. [Internet]. 2015 [cited 2015 Nov 6]. Available from: http://
www.ncbi.nlm.nih.gov/books/NBK299486/
15. MISAU. Relatorio AQD-HIV 2014 Relatorio da Ronda Piloto Nacional da
Avaliacao da Qualidade de Dados. Cidade de Maputo: MISAU; 2015. p. 53.
16. Govindasamy D, Ford N, Kranzer K. Risk factors, barriers and facilitators for
linkage to antiretroviral therapy care: a systematic review. AIDS. 2012;26(16):
2059"67.17. Tomori C, Kennedy CE, Brahmbhatt H, Wagman JA, Mbwambo JK,
Likindikoki S, et al. Barriers and facilitators of retention in HIV care and
treatment services in Iringa, Tanzania: the importance of socioeconomic and
sociocultural factors. AIDS Care. 2014;26(7):907"13.18. Roura M, Busza J, Wringe A, Mbata D, Urassa M, Zaba B. Barriers to
sustaining antiretroviral treatment in Kisesa, Tanzania: a follow-up study to
understand attrition from the antiretroviral program. AIDS Patient Care STDS.
2009;23(3):203"10.19. Raper JL. Going the extra mile for retention and re-engagement in care:
nurses make a difference. J Assoc Nurses AIDS Care. 2014;25(2):108"11.
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
7
289

20. Ware NC, Wyatt MA, Geng EH, Kaaya SF, Agbaji OO, Muyindike WR, et al.
Toward an understanding of disengagement from HIV treatment and care in
sub-Saharan Africa: a qualitative study. PLoS Med. 2013;10(1):e1001369.
21. McKay R. Documentary disorders: managing medical multiplicity in
Maputo, Mozambique. Am Ethnol. 2012;39(3):545"61.22. Pfeiffer J, Chapman R. An anthropology of aid in Africa. Lancet. 2015;
385(9983):2144"5.23. Kalofonos I. ‘‘All they do is pray’’: community labour and the narrowing of
‘‘care’’ during Mozambique’s HIV scale-up. Glob Public Health. 2014;9(1"2):7"24.24. Firth CL, Schafer SD, Greene K. Monitoring retention in care: using multiple
laboratory tests as an indicator for HIV medical care. AIDS Care. 2014;26(12):
1546"9.
25. Kelly JD, Hartman C, Graham J, Kallen MA, Giordano TP. Social support
as a predictor of early diagnosis, linkage, retention, and adherence to HIV
care: results from the steps study. J Assoc Nurses AIDS Care. 2014;25(5):
405"13.26. Mugavero MJ, Westfall AO, Zinski A, Davila J, Drainoni M-L, Gardner L,
et al. Measuring retention in HIV care: the elusive gold standard. J Acquir
Immune Defic Syndr. 2012;61(5):574"80.27. Das M, Christopoulos KA, Geckeler D, Huriaux E, Cohen SE, Philip S, et al.
Linkage to HIV care in San Francisco: implications of measure selection.
J Acquir Immune Defic Syndr. 2013;64(1):S27.
Inguane CA et al. Journal of the International AIDS Society 2016, 19(Suppl 4):20846
http://www.jiasociety.org/index.php/jias/article/view/20846 | http://dx.doi.org/10.7448/IAS.19.5.20846
8
290

Strengthening HIV Test Access and Treatment Uptake Study (Project STATUS): A Randomized Trial of HIV Testing and Counseling Interventions
A. D. McNaghten, PhD, MHSA*, Allison Schilsky Mneimneh, MPH†, Thato Farirai, BSW‡, Nafuna Wamai, MBCHB, MPH§, Marylad Ntiro, MD, MPHᒭ, Jennifer Sabatier, MS†, Nondumiso Makhunga-Ramfolo, MBChB, MSc¶, Salli Mwanasalli, DDS#, Anna Awor, MSc§, Jan Moore, PhD†, and the Project STATUS Study Team
*Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, GA †Division of Global HIV/AIDS, Centers for Disease Control and Prevention, Atlanta, GA ‡Centers for Disease Control and Prevention, Pretoria, South Africa §Division of Global HIV/AIDS, Centers for Disease Control and Prevention, Entebbe, Uganda ᒭMinistry of Health and Social Welfare, Dar es Salaam, Tanzania ¶University Research Co., LLC, Pretoria, South Africa #Centers for Disease Control and Prevention, Dar es Salaam, Tanzania
AbstractObjective—To determine which of 3 HIV testing and counseling (HTC) models in outpatient departments (OPDs) increases HIV testing and entry of newly identified HIV-infected patients into care.
Design—Randomized trial of HTC interventions.
Methods—Thirty-six OPDs in South Africa, Tanzania, and Uganda were randomly assigned to 3 different HTC models: (A) health care providers referred eligible patients (aged 18–49, not tested in the past year, not known HIV positive) to on-site voluntary counseling and testing for HTC offered and provided by voluntary counseling and testing counselors after clinical consultation; (B) health care providers offered and provided HTC to eligible patients during clinical consultation; and (C) nurse or lay counselors offered and provided HTC to eligible patients before clinical consultation. Data were collected from October 2011 to September 2012. We describe testing eligibility and acceptance, HIV prevalence, and referral and entry into care. Chi-square analyses were conducted to examine differences by model.
Correspondence to: A. D. McNaghten, PhD, MHSA, Department of Epidemiology, Rollins School of Public Health, Emory University, 1518 Clifton Road NE, Atlanta, GA 30322 ([email protected]).Members of the Project STATUS Study Team are listed in Appendix 1.Presented at the 20th Conference on Retroviruses and Opportunistic Illnesses, March 4, 2013, Atlanta, GA.The authors have no conflicts of interest to disclose.A.D.M. and A.S.M. wrote the article; J.S. conducted the analyses; T.F., N.W., M.N., N.M.-R., S.M., and A.A. were involved in implementation; and J.M. was involved in the conception and design of Project STATUS. All authors commented on drafts of the article.The findings and conclusions of this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
HHS Public AccessAuthor manuscriptJ Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Published in final edited form as:J Acquir Immune Defic Syndr. 2015 December 1; 70(4): e140–e146. doi:10.1097/QAI.0000000000000785.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
291
Results—Of 79,910 patients, 45% were age eligible and 16,099 (45%) age eligibles were tested. Ten percent tested HIV positive. Significant differences were found in percent tested by model. The proportion of age eligible patients tested by Project STATUS was highest for model C (54.1%, 95% confidence interval [CI]: 42.4 to 65.9), followed by model A (41.7%, 95% CI: 30.7 to 52.8), and then model B (33.9%, 95% CI: 25.7 to 42.1). Of the 1596 newly identified HIV positive patients, 94% were referred to care (96.1% in model A, 94.7% in model B, and 94.9% in model C), and 58% entered on-site care (74.4% in model A, 54.8% in model B, and 55.6% in model C) with no significant differences in referrals or care entry by model.
Conclusions—Model C resulted in the highest proportion of all age-eligible patients receiving a test. Although 94% of STATUS patients with a positive test result were referred to care, only 58% entered care. We found no differences in patients entering care by HTC model. Routine HTC in OPDs is acceptable to patients and effective for identifying HIV-infected persons, but additional efforts are needed to increase entry to care.
Keywordscounseling/methods; HIV infections/diagnosis; sero-prevalence; South Africa; Tanzania; Uganda
INTRODUCTIONHIV testing and counseling (HTC) is an important entry point to HIV prevention, care, and treatment, and an integral component of efforts to achieve universal access to HIV services. Identifying HIV positive persons and linking them to care and treatment can improve health outcomes1–5 and decrease HIV transmission through viral load suppression.5,6
To improve access to HIV prevention, care, and treatment services in developing countries, the World Health Organization and the Joint United Nations Programme on HIV/AIDS published guidance in 2007 calling for the scale-up of HTC in health facilities worldwide.7,8
For countries with generalized HIV epidemics, this guidance recommends that in addition to client-initiated HTC, health care providers should recommend HTC as part of routine care, regardless of whether the patient shows signs and symptoms of HIV infection, or their reason for attending the health facility.7 More than 42 countries have adopted policies on HIV testing in a variety of health care settings including inpatient and outpatient departments (OPDs), antenatal care (ANC) and tuberculosis (TB) clinics, and emergency and surgical departments.9
Routine HTC is being successfully implemented in inpatient wards and in TB, sexually transmitted infection, and ANC clinics in many countries. Among countries receiving financial and technical assistance through the President’s Emergency Plan for AIDS Relief, HIV testing in some ANC clinics has exceeded 50% of attendees, with some testing more than 80%.10,11 HIV testing in TB clinics has also increased, reaching over 50% of patients in several countries.12 A review of studies of HTC implementation in clinical settings reports even higher levels of testing under controlled study conditions.13 These successes indicate that in appropriately resourced contexts, implementation of routine HTC is achievable.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
292
Several studies have reported feasibility and uptake of HIV testing in OPDs, showing that testing in OPDs is achievable,14–16 but rates of testing are relatively low compared with other clinical venues.13 As a primary source of health care for many people in developing countries, OPDs provide a venue for accessing large numbers of people from the general population. Although we do not know how many people accessing OPDs know their HIV status, OPDs may offer the opportunity to efficiently diagnose many infected persons before they develop life-threatening illness. Assessing the outcomes of HIV testing in OPDs would provide valuable information about the importance and feasibility of HIV testing in this setting and could inform policy-makers about how and why various HTC models may or may not be effective. Furthermore, determining whether different models of HTC delivery in the OPD vary in the number of HIV infected persons identified and linked to care and treatment services would be valuable information for decision makers trying to stretch HTC resources while assuring the greatest public health impact.
We present the findings of Project STATUS, a randomized trial of HTC interventions in OPDs in primary health care centers and district-level hospitals in South Africa, Tanzania, and Uganda. The primary objective of this evaluation was to compare 3 models of HTC in OPDs to determine which model results in the highest percentage of eligible outpatients receiving an HIV test and the highest percentage of HIV infected persons newly identified in the OPD who enter HIV care and treatment services.
METHODSStudy Design
Thirty-six OPDs in South Africa, Tanzania, and Uganda participated in Project STATUS. Each country selected a convenience sample of 12 OPDs in primary health care centers or district-level hospitals for inclusion in the study. Facilities varied in the size of their patient population but were comparable in the services offered and met the following inclusion criteria: OPD located at a district-level hospital or health care center in which less than 5% of outpatients were receiving routine HTC; provider-to-patient ratio of 1 health care provider providing care to 25–35 patients per day; on-site voluntary counseling and testing (VCT) center or services; space to conduct private HTC sessions; provision of HIV care and treatment services at the health facility; and ability to determine CD4 T-lymphocyte counts on-site or by sending blood samples to an off-site laboratory. Block randomization was used to assign the 12 OPDs in each country to one of 3 HTC models, resulting in 4 OPDs per model in each country or 12 OPDs per model across all 3 countries. Institutional review boards at the Centers for Disease Control and Prevention and in each country approved the study protocol.
In addition, patient interviews were conducted at all participating OPDs, 2 randomly selected OPDs per model per country conducted a time motion study, and 1 conveniently selected OPD per model per country participated in provider focus group discussions after the data collection period. These data are not reported in this article.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
293
Data CollectionAt each participating health facility, health care providers, HTC nurse or lay counselors, and other relevant persons in the OPD were trained to deliver the HTC model to which their facility was randomized. Providers were trained on data collection procedures and the use of data collection tools. After a 2-month pilot study, data collection for HTC and HIV care entry was conducted for a 3-month study period (between October 2011 and September 2012). STATUS participants who entered HIV care were followed for 4 months after care entry to determine whether they returned to care.
HIV Testing and Counseling—All patients attending a STATUS OPD during the study period were registered in a study log, in which age and sex were documented, and a unique study identifier was assigned. All OPD patients were given a packet containing a patient enumeration form (PEF) and referral cards, all marked with the patient’s unique study identifier (PEF number). Study staff documented patients’ age and sex on the PEF and requested that patients carry the packet with them throughout their visit. Patients in all models were eligible for HTC as part of Project STATUS if they were
• attending the OPD for a consultation with a health care provider for any routine or acute medical condition (excluding emergency cases),
• age eligible (18–49 years),
• test eligible (no documentation in patient records of having an HIV test in the past year or of ever testing HIV positive),
• able to provide informed consent for HIV testing.
The age of 18 was selected as the lower limit for study eligibility because it is the age of majority in the 3 participating countries; thus, patients 18 and older could legally provide verbal consent for HIV testing. The upper limit of 49 was selected to target persons at risk for HIV infection. OPDs typically see a high percentage of older patients, particularly the elderly, who would likely be at lower risk for HIV infection.
STATUS participants who tested HIV positive in all models were given a Project STATUS Care and Treatment Referral Card and encouraged to access on-site HIV care. The 3 HTC models are described below.
Model A: Health care providers referred eligible patients to on-site VCT services after clinical consultation. For age eligible patients, test eligibility was determined by the health care provider during the consultation. Test eligibility and referral to VCT were documented on the PEF by the provider, who referred test-eligible patients to VCT at the end of the consultation. For patients who went to VCT after their consultation, the VCT counselor documented whether they offered the patient HTC, whether they tested the patient, and the result. Patients testing HIV positive were referred to onsite HIV care by the VCT counselor, who also recorded referral data on the PEF.
Model B: All OPD patients in the waiting area heard a group talk that included HIV information. Eligible patients were offered HTC during clinical consultation. Test eligibility
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
294
of age eligible patients was determined by the health care provider, who also recommended and provided HTC during the consultation. The provider referred HIV positive patients to on-site HIV care and documented all testing and referral data on the PEF.
Model C: Eligible patients were offered and provided HTC before clinical consultation. Age eligible patients were sent to a waiting area separate from non–age eligible patients, where the age eligible patients heard a group talk about HIV. These patients were encouraged to be tested for HIV by a nurse or lay counselor before their clinical consultation and assured they would not lose their place in the queue to see the provider. Patients who chose to see the counselor had test eligibility determined by the counselor and were offered and provided HTC by the counselor before their consultation. Persons who tested HIV positive were informed of their result by the counselor, who documented all eligibility and testing data on the PEF. The OPD provider reviewed patients’ PEFs during the clinical consultation and referred HIV positive patients to on-site HIV care after the consultation. The provider documented referral data on the PEF.
OPD patients who did not meet STATUS age or test eligibility criteria, but wanted to receive a test, were provided testing; testing and referral data for these patients were not documented on their PEFs.
Entry Into HIV Care—Each model included referring all patients who tested HIV positive to on-site HIV care. Entry into HIV care was defined as having the patient’s information documented in the facility’s HIV care and treatment register and/or patient’s medical record. Project STATUS Care and Treatment Referral Cards included a peel-off sticker printed with the patient’s PEF number, which was affixed in the HIV care and treatment register to identify STATUS patients. Study staff were not able to assess care entry at non-STATUS HIV care and treatment facilities.
AnalysesWe describe a cascade including age eligibility, test eligibility, receipt of HIV test, HIV prevalence, and referral to and entry into HIV care, in which each step in the cascade is dependent on the previous step. Rao Scott modified ů2 tests were conducted to examine differences by model for HIV test eligibility, testing rates, referral, and care entry. Analyses were conducted using SAS version 9.3.2 (SAS Institute, Cary, NC). All analyses, both descriptive and inferential, accounted for the study design by including the clustering within facility and stratification by country in the estimation of variances and 95% confidence intervals. In addition, because random selection of patients was not possible and the number of patients attending each OPD varied, there were unequal sampling rates across OPDs; therefore, sampling weights were used. These weights were created using the population size of the OPD during the study, the number of participants eligible for each outcome, and the number sampled. Therefore, different weights were used for estimating each outcome.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
295

RESULTSTest Eligibility and Outcomes Among All OPD Attendees
During the 3-month study period, a total of 79,910 patients were registered in the 36 study OPDs. Forty-five percent of registered patients were age eligible, with a mean age of 29 years. Seventy-four percent of age eligible patients were women. Sixty-one percent (n = 22,034) of age eligible patients were determined to be test eligible (62% of all age-eligible women and 73% of all age eligible men). Providers determined 9987 age eligible patients were ineligible for testing; 6320 had documentation of a nonreactive test in the past 12 months; and 3605 had documentation of a previous reactive test (patients could have both documentation of a nonreactive test in the past 12 months and of a previous reactive test). Of the age eligible patients, 16,132 (45%) were tested with an overall prevalence of 10% (women 10.0% and men 9.5%). HIV prevalence for STATUS patients was higher in South Africa (22%) than in Tanzania and Uganda (6% each). Ninety-four percent of the 1596 newly diagnosed HIV-positive patients from the OPD were referred to HIV care, and fifty-eight percent (n = 932) of those referred had documentation of registering at the on-site care and treatment clinic. We identified an additional 23 STATUS patients with documentation of entering care but no documentation of being referred to care.
Cascade of Testing Uptake, Referral to Care, and Care Entry by ModelIn model A, 6564 (67%) age eligible participants were determined by the OPD provider to be test eligible during the clinical consultation (Fig. 1A). Eighty-three percent (n = 5448) of the 6564 eligible patients were referred to VCT, and 84% of all eligible patients actually went to VCT. Of those who went to VCT, 99% were offered testing, and 93% of patients offered testing accepted. Of the 445 persons who tested HIV positive, 95% were referred to care, and 75% of those who were referred entered care.
In model B, 57% of the age eligible participants were determined by the OPD provider to be test eligible during the clinical consultation (Fig. 1B). Model B providers indicated that they offered testing to 99% of test-eligible patients, and 65% accepted. Of the 520 persons who tested HIV positive, 94% were referred to care, and 57% of those who were referred entered care.
In model C, 9004 (80%) age eligible patients went to the HTC counselor before their clinical consultation (Fig. 1C). Seventy-eight percent were determined by the counselor to be test eligible, 99% of test-eligible patients were offered testing, and 92% accepted. Of the 631 persons who tested HIV positive, 94% were referred to care, and 57% of those who were referred entered care.
Differences in Testing Rates, Referrals, and Care Entry by ModelNo significant differences were found among models in the percentage of total patients attending the OPD or the percentage of patients who were age eligible or test eligible (Table 1). When we examined the percentage of patients who were tested in the OPD among those who were age eligible, we found a significant difference by model (Table 2). The proportion of all age eligible patients who were tested was highest for model C (54.1%), followed by
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
296

model A (41.7%), and then model B (33.9%). When we examined the percentage of patients tested among those determined to be test eligible, we also found a significant difference by model with higher testing rates in model A (93.0%) and model C (91.9%) than in model B (65.5%) (Table 1). There were no significant differences by model in the percentage of patients found to be HIV positive or in the percentage of patients referred to care (96.1% in model A, 94.7% in model B, and 94.9% in model C). The percentage of referred patients who entered care was highest for model A (74.4%) compared with model B (54.8%) and model C (55.6%); however, this finding was not statistically significant. An additional analysis was conducted including those patients who entered care without documentation of referral, which also found no significant difference in care entry by model (data not shown).
DISCUSSIONImplementing HTC as Standard of Care
Despite World Health Organization’s recommendation that HTC be offered as a standard part of medical care in countries with generalized HIV epidemics7 and an increase in the implementation of HIV testing in sub-Saharan Africa (SSA),11,17 nationwide routine HTC in OPDs is still not a common practice. The benefits of implementing a policy of routine opt-out HIV testing in SSA, including the potential for earlier antiretroviral therapy initiation and ultimately increased survival of persons with HIV, must be considered alongside the possible drawbacks of this approach such as patients thinking they cannot refuse or the stigma associated with a positive test result.18–21 Project STATUS demonstrated that it is feasible to routinely offer HTC to OPD patients and have substantial testing uptake, identify many undiagnosed HIV-infected persons, and have a substantial proportion enter HIV care soon after diagnosis.
Testing UptakeSTATUS resulted in high testing uptake with more than 81% of all persons offered testing accepting a test (16,132/19,953). Other studies have shown that routine HIV testing in health care settings is acceptable to patients and an effective method for increasing HTC uptake.15,22–24 For example, a study conducted in Zambian primary care clinics reported that 75% of patients with no proof of their HIV status who were offered HTC accepted under a model C–type arrangement.15
Patients were lost at different points in the cascade of each model. In model A, 16% of patients were never referred to VCT by the OPD provider, and not all who were referred went. Of those who went to VCT, 93% were tested. In model B, almost all test-eligible patients were offered HTC, but 35% declined. In model C, similar to model A, 20% of patients chose not to go to the area of the OPD where HTC was being offered, thereby essentially “opting out.” Of those who went, 92% were tested.
Given that patients in model C who “opted out” by not going to testing did not have their test eligibility determined, we compared testing rates by model among all age eligible patients rather than just test-eligible patients. The percentage of age eligible patients receiving a test was highest in model C. There are several possible reasons for this finding.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
297

Model C OPDs had a separate waiting area for HTC located near the main waiting area and close to where testing was provided, allowing patients to conveniently test before their OPD consultation without worrying about losing their place in the queue to see the provider. Model C had designated staff trained and tasked to provide HTC, making the process quick. Unlike model A, there was no additional waiting time to receive HTC in model C; the waiting time to see the nurse or lay counselor for testing occurred during, not in addition to, the waiting time to see the OPD health care provider. Age eligible patients in model C OPDs also received a health talk from the OPD staff reinforcing the importance of knowing their HIV status and informing them that HIV care was available on-site for anyone with a positive result. Although model C resulted in the highest testing uptake, it also required substantial changes to OPDs’ standard operating procedures. Countries and OPDs considering implementation of this model must consider how changes to patient flow can be operationalized and how the additional staff needed to provide HTC before the OPD consultation can be effectively integrated.
The various methods currently being used in SSA have both strengths and limitations. Before the recommendation that health care providers routinely offer testing to all patients,7
the most common practice in OPDs was provider referral to a VCT site within the health facility, similar to STATUS’ model A. This model is successful at identifying persons with HIV, as patients who perceive themselves to be at risk may be more motivated to test. However, those who perceive themselves to be at low risk may choose not to access VCT or to accept a test. Others may choose not to access services at the VCT because of the additional time required. In addition, previous studies have shown that uptake of HTC in a model A–type arrangement is lower among those experiencing poverty,25 who fear or have experienced stigma and discrimination,25,26 and who have lower education levels.27
STATUS’ model B was modeled after the diagnostic testing approach used in some OPDs, in which health care providers offer and provide HTC during the clinical consultation to patients suspected of having HIV. Although implementing this model routinely can result in a high proportion of patients offered and receiving testing, its success depends largely on the actions and attitudes of the provider. Rather than conducting routine HTC, the provider may use clinical judgment to determine who may be HIV infected or at risk, resulting in patients who are asymptomatic or whom the provider perceives as having no risk not receiving HTC.7 A study by Dalal et al16 involving provider-initiated testing and counseling (PITC) under a model B–type arrangement identified increased workload and concerns regarding confidentiality as concerns of providers delivering this model. It is possible that providers in Project STATUS OPDs assigned to model B did not actually offer all eligible patients HTC because of the increased workload, confidentiality concerns, or other reasons, but indicated on the PEF that HTC was offered and the patient declined. Other studies have reported success with testing strategies similar to STATUS’ model C. A study in a South African OPD assessed a routine voluntary HIV testing intervention compared with the standard-of-care provider-referral to a VCT site located in the same hospital complex as the OPD. Offering pretest information and HIV testing while patients waited to see the provider, the routine HTC intervention resulted in a 10-fold increase in HIV tests completed and over 4 times as many HIV positive persons identified.14 A Zambian study that introduced PITC delivered by lay counselors in 9 urban primary care facilities tested twice as many patients
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
298

than when conducting VCT alone.15 The high acceptance of routine PITC in these studies and in Project STATUS may be due in-part to making HTC a standard feature of attending a health facility.7,15
Identification of HIV-Infected Persons, Referral to and Entry Into CareSystematically offering HTC to all patients who visit the health facility increases the identification of HIV-infected patients.14 In Project STATUS across all 3 countries, 10% of patients who tested were newly identified with HIV. HIV prevalence rates in the STATUS OPDs were similar to estimates reported for the same period in the areas where the STATUS OPDs were located in South Africa (22% versus 24.7% in KwaZulu-Natal Province)28 and Uganda (6% versus 8.2% in Mid-Western Region).29 In Tanzania, rates in the STATUS OPDs were higher (6% versus 3.2% and 2.4% in Arusha and Tanga regions, respectively).30
Although HIV case finding rates are higher in other health care settings,15,23,31 providing HTC in OPDs seems to be an effective method for identifying HIV positive individuals who are unaware of their status.
A goal of PITC is to link newly identified HIV-infected patients to care.7 Although 94% of the 1596 newly HIV-diagnosed patients from Project STATUS were referred, only 58% of them entered care at the STATUS facility. Although not significant, the highest percentage entering care by model came from model A, in which VCT counselors referred patients to care.
Referral to and entry into care for patients with newly diagnosed HIV remains an issue.32 A recent review of the operational implementation of PITC in SSA found linkage of newly identified HIV-infected patients to care was generally poor.13 Given that HIV care is easier to access from OPDs than other testing venues, we would expect higher rates of linkage. STATUS patients may have accessed care at other facilities. Clearly, additional research is needed to understand linkage patterns and determine how to motivate patients or to offer them the support needed to access care.
LimitationsOur study had several limitations. Across all models, the performance of the model was dependent on participation by facility staff and fidelity to the assigned model, which varied by facility. Since documentation of previous HIV testing is generally limited, persons who had already been tested in the past 12 months may have been tested again as part of Project STATUS because previous testing was not documented. Estimates of care entry are likely conservative. As we followed a cascade of study activities, STATUS patients who were not documented as being referred to care were excluded from the care entry analysis. Patients who did not enter care the day diagnosed but returned at a later date may not have returned with their Care and Treatment Referral Card and therefore were not identified as STATUS patients in the care and treatment register. Data were not collected at non-STATUS facilities, so patients who entered care at a different facility were not documented.
Project STATUS demonstrated that routine HIV testing in OPDs is acceptable to patients and an effective method for identifying HIV-infected persons, but additional efforts are needed to increase entry to care. Model C, in which nurse or lay counselors offered and
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
299

provided HTC to eligible patients before their clinical consultation, had the highest percentage of all patients aged 18–49 years receiving a test. Model C was convenient; there was no additional waiting time to receive HTC, and HTC was provided by staff specifically trained and tasked to conduct HTC. This study demonstrates an important venue and model that could increase access to life-saving HIV-related services.
AcknowledgmentsThe authors gratefully acknowledge the guidance, input, and commitment of their respected and cherished colleague, Dr. Gilly Arthur, in the design and implementation of Project STATUS. Dr. Arthur, an outstanding champion for HIV prevention in East Africa, passed away in June 2014.
Supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention (CDC). This study was a joint endeavor of the US government PEPFAR programs in South Africa, Tanzania, Uganda, the CDC in Atlanta, and the US Agency for International Development (USAID) in Washington, DC; the Ministries of Health in the participating countries; and implementing partners working in each country. Funding for Project STATUS was provided by the Department of State, Office of the Global AIDS Coordinator (OGAC).
REFERENCES1. Palella FJ Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients
with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998; 338:853–860. [PubMed: 9516219]
2. Egger M, May M, Chene G, et al. Prognosis of HIV-1 infected patients starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002; 360:119–129. [PubMed: 12126821]
3. Walensky RP, Paltiel AD, Losina E, et al. The survival benefits of AIDS treatment in the United States. J Infect Dis. 2006; 194:11–19. [PubMed: 16741877]
4. Cain LE, Logan R, Robins JM, et al. HIV-CAUSAL Collaboration. When to initiate combined antiretroviral therapy to reduce mortality and AIDS defining illness in HIV-infected persons in developed countries: an observational study. Ann Intern Med. 2011; 154:509–515. [PubMed: 21502648]
5. Cohen MS, Chen YQ, McCauley M, et al. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med. 2011; 365:493–505. [PubMed: 21767103]
6. Donnell, D.; Kiairie, J.; Thomas, K., et al. ART and risk of heterosexual HIV-1 transmission in HIV-1 serodiscordant African couples: a multinational prospective study. Paper Presented at 17th Conference on Retroviruses and Opportunistic Infections; February 16–19, 2010; San Francisco CA..
7. World Health Organization/UNAIDS. Guidance on Provider-Initiated HIV Testing and Counselling in Health Facilities. Geneva, Switzerland: World Health Organization; 2007. Available at: http://www.who.int/hiv/topics/vct/en/index.html [Accessed January 9, 2012]
8. World Health Organization. Towards Universal Access: Progress Report. Geneva, Switzerland: World Health Organization; 2008. Available at: http://www.who.int/hiv/pub/towards_universal_access_report_2008.pdf [Accessed January 9, 2012]
9. Baggaley R, Hensen B, Ajose O, et al. From caution to urgency: the evolution of HIV testing and counselling in Africa. Bull World Health Organ. 2012; 90:652–658. [PubMed: 22984309]
10. Office of the U.S. Global AIDS Coordinator. Celebrating Life: Latest PEPFAR Results. President’s Emergency Plan for AIDS Relief. Washington, D.C.: Available at: http://www.pepfar.gov/documents/organization/115411.pdf [Accessed January 9, 2012]
11. World Health Organization. Global HIV/AIDS Response: Epidemic Update and Health Sector Progress towards Universal Access: Progress Report 2011. Geneva, Switzerland: World Health Organization; 2011. Available at: http://whqlibdoc.who.int/publications/2011/9789241502986_eng.pdf [Accessed January 9, 2012]
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
300

12. WHO. Global Update on the Health Sector Response to HIV, 2014. Geneva, Switzerland: WHO; 2014. Available at: http://apps.who.int/iris/bitstream/10665/128494/1/9789241507585_eng.pdf?ua=1 [Accessed December 12, 2014]
13. Roura M, Watson-Jones D, Kahawita TM, et al. Provider-initiated testing and counselling programmes in sub-Saharan Africa: a systematic review of their operational implementation. AIDS. 2013; 27:617–626. [PubMed: 23364442]
14. Bassett IV, Giddy J, Nkera J, et al. Routine voluntary HIV testing in Durban, South Africa: the experience from an outpatient department. J Acquir Immune Defic Syndr. 2007; 46:181–186. [PubMed: 17667332]
15. Topp SM, Chipukuma JM, Chiko MM, et al. Opt-out provider-initiated HIV testing and counseling in primary care outpatient clinics in Zambia. Bull World Health Organ. 2011; 89:328–335A. [PubMed: 21556300]
16. Dalal S, Lee CW, Farirai T, et al. Provider-initiated HIV testing and counseling: increased uptake in two public community health centers in South Africa and implications for scale-up. PLoS One. 2011; 6:e27293. [PubMed: 22114668]
17. WHO. Service Delivery Approaches to HIV Testing and Counselling (HTC): A Strategic HTC Policy Framework. Geneva, Switzerland: World Health Organization; 2012. Available at: http://www.who.int/hiv/pub/vct/htc_framework/en/ [Accessed January 9, 2012]
18. Obermeyer CM, Verhulst C, Asmar K, et al. Could you have said no? A mixed-methods investigation of consent to HIV tests in four African countries. J Int AIDS Soc. 2014; 17:18898. [PubMed: 24647205]
19. April MD. Rethinking HIV exceptionalism: the ethics of opt-out HIV testing in sub-Saharan Africa. Bull World Health Organ. 2010; 88:703–708. [PubMed: 20865076]
20. Monjok E, Smesny A, Mgbere O, et al. Routine HIV testing in health care settings: the deterrent factors to maximal implementation in sub- Saharan Africa. J Int Assoc Physicians AIDS Care (Chic). 2010; 9:23–29. [PubMed: 20071594]
21. Gruskin S, Ahmed S, Ferguson L. Provider-initiated HIV testing and counseling in health facilities—what does this mean for the health and human rights of pregnant women? Dev World Bioeth. 2007; 8:23–32. [PubMed: 18315722]
22. Kennedy CE, Fonner VA, Sweat MD, et al. Provider-initiated HIV testing and counseling in low- and middle-income countries: a systematic review. AIDS Behav. 2013; 17:1571–1590. [PubMed: 22752501]
23. Wanyenze RK, Nawavvu C, Namale AS, et al. Acceptability of routine HIV counselling and testing, and HIV seroprevalence in Ugandan hospitals. Bull World Health Organ. 2008; 86:302–309. [PubMed: 18438519]
24. Nakanjako D, Kamya M, Mayanja-Kizza H, et al. Acceptance of routine testing for HIV among adult patients at the medical emergency unit at a national referral hospital in Kampala, Uganda. AIDS Behav. 2007; 11:753–758. [PubMed: 17096199]
25. Yahaya LA, Jimoh AAG, Balogun OR. Factors hindering acceptance of HIV/AIDS voluntary counseling and testing (VCT) among youth in Kwara State, Nigeria. Afr J Reprod Health. 2010; 14:159–164. [PubMed: 21495608]
26. Leta TH, Sandøy IF, Fylkesnes K. Factors affecting voluntary HIV counselling and testing among men in Ethiopia: a cross-sectional survey. BMC Public Health. 2012; 12:438. [PubMed: 22703550]
27. Karau PB, Winnie MS, Geoffrey M, et al. Responsiveness to HIV education and VCT services among Kenyan rural women: a community-based survey. J Reprod Health. 2010; 14:165–169.
28. National Department of Health. The 2011 National Antenatal Sentinel HIV & Syphilis Prevalence Survey in South Africa. Pretoria, South Africa: National Department of Health; 2012. Available at: http://www.health.gov.za/docs/reports/2013/Antenatal_survey_report_2012_web_optimized.pdf [Accessed April 15, 2013]
29. Ministry of Health and ICF International. 2011 Uganda AIDS Indicator Survey. Entebbe: Ministry of Health; 2012. Available at: http://health.go.ug/docs/UAIS_2011_REPORT.pdf [Accessed April 15, 2013]
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
301

30. Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF International. Tanzania HIV/AIDS and Malaria Indicator Survey 2011–12. Dar es Salaam: TACAIDS, ZAC, NBS, OCGS, and ICF International; 2013. Available at: http://dhsprogram.com/pubs/pdf/AIS11/AIS11.pdf [Accessed April 15, 2013]
31. Wanyenze, RK.; Kamya, MR.; Fatch, R., et al. A factorial randomized trial of abbreviated HIV counseling and testing and enhanced referral to care in Uganda. Presented at 7th IAS Conference on HIV Pathogenesis, Treatment and Prevention; June 30 – July 3, 2013; Kuala Lumpur, Malaysia.
32. Bassett IV, Giddy J, Wang B, et al. Routine, voluntary HIV testing in Durban, South Africa: correlates of HIV infection. HIV Med. 2008; 9:863–867. [PubMed: 18754802]
APPENDIX 1. THE PROJECT STATUS STUDY TEAM
South AfricaAmajuba Department of Health, Ladysmith, South Africa: Ntombi Phakathi. Centers for Disease Control and Prevention, South Africa: Thurma Goldman, Sara Hersey, Tembeka Sonkwele, and Carlos Toledo. KwaZulu Natal Department of Health, Pietermaritzburg, South Africa: Themba Ndabandaba. National Department of Health, Pretoria, South Africa: Thato Chidarikire. University Research Co., Pretoria, South Africa: Brighton Khumalo, Ishmael Khumalo, Refiloe Matji, and Sibongile Mkhize. Uthukela Department of Health, Newcastle, South Africa: Gabisile Maths.
UgandaCenters for Disease Control and Prevention, Uganda: David Katuntu and Felix Ocom. Infectious Diseases Institute, Kampala, Uganda: Vincent Kawooya, Timothy Kiyemba, Michael Makuba, Norbert Mubiru, Alex Muganzi, and Catherine Mwebaze. Ministry of Health, Kampala, Uganda: Jane Nabalonzi and Benson Tumwesigye.
TanzaniaCenters for Disease Control and Prevention, Tanzania: Gilly Arthur, Irene Benech, Hannah Godlove, Colleen Scott, and Rachel Weber. Intra- Health International, Dar es Salaam, Tanzania: Ruth Lemwayi, Zaynab Lweno, and Lucy Mphuru. Jhpiego, Dar es Salaam, Tanzania: Fatma Kabole, Rita Mutayoba, Lusekelo Njonge, and Marya Plotkin. Ministry of Health and Social Welfare, Dar es Salaam, Tanzania: Joseph Hokororo, D.W. Mmbando, Angela Ramadhani, and Peris Urasa. National Institute for Medical Research, Mwanza, Tanzania: Jonas Aswile.
United StatesCenters for Disease Control and Prevention, Atlanta, GA: Gillian Anderson, Stephanie Behel, Wei Fang, Jonathan Grund, Catherine Nichols, and Ray Ransom. ICF Macro: Sonal Pathak. US Agency for International Development, Washington, DC: Alison Surdo Cheng and Vincent Wong.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
302

FIGURE 1. Cascade of Testing Uptake, Referral to Care, and Care Entry by Model.
McNaghten et al.
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
303
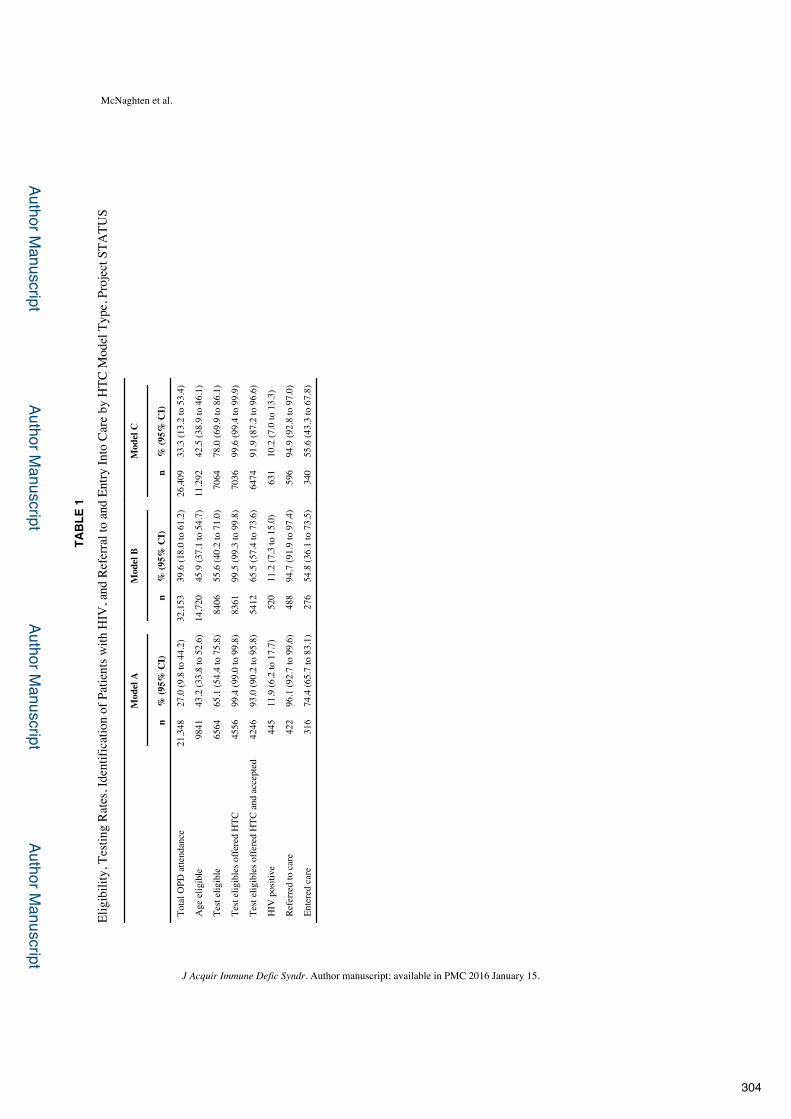
Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
McNaghten et al.
TAB
LE 1
Elig
ibili
ty, T
estin
g Ra
tes,
Iden
tific
atio
n of
Pat
ient
s with
HIV
, and
Ref
erra
l to
and
Entry
Into
Car
e by
HTC
Mod
el T
ype,
Pro
ject
STA
TUS
Mod
el A
Mod
el B
Mod
el C
n%
(95%
CI)
n%
(95%
CI)
n%
(95%
CI)
Tota
l OPD
atte
ndan
ce21
,348
27.0
(9.8
to 4
4.2)
32,1
5339
.6 (1
8.0
to 6
1.2)
26,4
0933
.3 (1
3.2
to 5
3.4)
Age
elig
ible
9841
43.2
(33.
8 to
52.
6)14
,720
45.9
(37.
1 to
54.
7)11
,292
42.5
(38.
9 to
46.
1)
Test
elig
ible
6564
65.1
(54.
4 to
75.
8)84
0655
.6 (4
0.2
to 7
1.0)
7064
78.0
(69.
9 to
86.
1)
Test
elig
ible
s offe
red
HTC
4556
99.4
(99.
0 to
99.
8)83
6199
.5 (9
9.3
to 9
9.8)
7036
99.6
(99.
4 to
99.
9)
Test
elig
ible
s offe
red
HTC
and
acc
epte
d42
4693
.0 (9
0.2
to 9
5.8)
5412
65.5
(57.
4 to
73.
6)64
7491
.9 (8
7.2
to 9
6.6)
HIV
pos
itive
445
11.9
(6.2
to 1
7.7)
520
11.2
(7.3
to 1
5.0)
631
10.2
(7.0
to 1
3.3)
Refe
rred
to c
are
422
96.1
(92.
7 to
99.
6)48
894
.7 (9
1.9
to 9
7.4)
596
94.9
(92.
8 to
97.
0)
Ente
red
care
316
74.4
(65.
7 to
83.
1)27
654
.8 (3
6.1
to 7
3.5)
340
55.6
(43.
3 to
67.
8)
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
304

Author Manuscript
Author Manuscript
Author Manuscript
Author Manuscript
McNaghten et al.
TAB
LE 2
Perc
enta
ge o
f All
Age
Elig
ible
Pat
ient
s Rec
eivi
ng H
TC b
y M
odel
, Pro
ject
STA
TUS
Mod
el A
Mod
el B
Mod
el C
n%
(95%
CI)
n%
(95%
CI)
n%
(95%
CI)
P
Tota
l age
elig
ible
s tes
ted
4246
41.7
(30.
7 to
52.
8)54
1233
.9 (2
5.7
to 4
2.1)
6474
54.1
(42.
4 to
65.
9)0.
0433
J Acquir Immune Defic Syndr. Author manuscript; available in PMC 2016 January 15.
305

GUIDELINES
CONSOLIDATED GUIDELINES ON
HIV
TEST
ING
SERV
ICES
ISBN 978 92 4 150892 6
For more information, contact:
World Health Organization Department of HIV 20, avenue Appia 1211 Geneva 27 Switzerland
E-mail: [email protected]
http://www.who.int/hiv/pub/guidelines/keypopulations/
JULY 2015
HIV TESTING SERVICES
5Cs: CONSENT, CONFIDENTIALITY, COUNSELLING, CORRECT RESULTS AND CONNECTION
CON
SOLID
ATED
GU
IDELIN
ES ON
HIV TESTIN
G SERV
ICES, 5Cs: CON
SENT, CO
NFID
ENTIA
LITY, COU
NSELLIN
G, CO
RRECT RESULTS A
ND
CON
NECTIO
N
306

vi Consolidated guidelines on HIV testing services
ACKNOWLEDGEMENTS
Guideline Development Group Jamila Taiseer Al-Abri (Department of Family and Community Health, Ministry of Health, Oman), Kathleen Charters (UK Civil Society Advisory Board, United Kingdom), Martin Choo (Global Network of People Living with HIV/AIDS, Malaysia), Elizabeth Corbett (London School of Hygiene & Tropical Medicine, Malawi), Neeraj Dhingra (Ministry of Health and Family Welfare, India), Miriam Franchini (Ministry of Health, Brazil), Mehdi Karkouri (Centre Hospitalier Universitaire, Ibn, Morocco), Segundo Leon (Universidad Nacional Mayor de San Marcos, Peru), Joseph Tak Fai Lau (Chinese University of Hong Kong, Hong Kong SAR, China), Gertrude Ncube (Ministry of Health, Zimbabwe), Lisa Nelson (Global Fund to Fight Tuberculosis, HIV/AIDS and Malaria, Switzerland), Anne Ng’ang’a (National AIDS Control Programme, Kenya), Carla Obermeyer (American University of Beirut, Lebanon), Midnight Poonkasetwattana (Asia Pacific Coalition on Male Sexual Health, Thailand), Jennifer Stuart-Dixon (University of the West Indies, Jamaica), Miriam Taegtmeyer (Liverpool School of Tropical Medicine, United Kingdom), Johnny Tohme (Arab Foundation for Freedoms and Equality, Lebanon), Coumba Toure-Kane (Laboratoire de Bacteriologie, CHU Le Dantec, Senegal) and Vincent Wong (United States Agency for International Development (USAID), USA).
Contributors to the GRADE systematic reviewCaitlin Kennedy and Virginia Fonner (Johns Hopkins Bloomberg School of Public Health, USA); Nandi Siegfried (independent clinical epidemiologist, South Africa) was the methodologist.
Contributors to supporting evidenceRuanne Barnabas° and Monisha Sharma° (University of Washington, USA), Lynae Darbes, Gail Kennedy, Ryan Keating and Hilary Spindler (University of California at San Francisco, USA), Jeffrey Eaton° (Imperial College of London, UK), Carmen Figueroa (Instituto de Salud Carlos III, Madrid, Spain), David Flynn (Griffith University, Australia), Virginia Fonner, Caitlin Kennedy and Sharon Tsui (Johns Hopkins Bloomberg School of Public Health, USA), Daniel Hogan (World Health Organization (WHO), Health Statistics and Information Systems), Naoko Ishikawa° (WHO Regional Office for the Western Pacific), Rebecca Mathews and Gretchen Parrott° (consultant, WHO Department of HIV), Carla Obermeyer (American University of Beirut, Lebanon) and Vincent Wong (USAID, USA).
Special thanks to all the contributors of the case examples.
° Peer reviewer+ Steering committee member and peer reviewer
307

WHO/HIV/2015.33 © World Health Organization 2015
ANNEX 14. A report on the misdiagnosis of HIV status Authors: Johnson C1, Fonner V2, Sands A3, Tsui S2, Ford N1, Wong V4, Obermeyer C5, Baggaley R1
14.1 Purpose and introduction
Between 2010 and 2014 nearly 600 million adults (ages 15+) reportedly received HIV testing services in 122 low- and middle-income countries in this period. In 2014 alone, approximately 150 million children and adults men and women across 129 low- and middle-income countries received HIV testing and their test results.6 Such scale-up has been possible partly through the use of rapid diagnostic tests (RDTs) which have been critical for expanding HTS, particularly in resource-limited settings where access to laboratory services is limited. RDTs that have been prequalified by the World Health Organization (WHO) have at least a diagnostic and clinical sensitivity of 99% and a specificity of 98% (1). The performance of such RDTs within a WHO recommended testing strategy and a validated national testing algorithm has been shown to be highly reliable (2-4). Despite this, in many countries quality management systems have not kept pace with the scale-up of HTS and have not utilized WHO prequalified RDTs or implemented WHO recommended testing strategies. According to a recent analysis of 48 country HIV testing policies, only 20% of testing strategies followed current WHO recommendations (5). There are a growing number of reports indicating poor quality HIV testing, some of which result in the misdiagnosis of HIV status. Misdiagnosis of HIV status refers to an incorrectly reported outcome of a testing process, i.e. incorrectly identifying someone who is HIV-infected as HIV-uninfected or vice versa. According to audits in some settings there a substantial level of false-positive diagnoses (6, 7). Misdiagnosis of HIV can result from limitations of the assay itself, operator-related factors, facility-related factors such as inappropriate storage of reagents and selection of inappropriate testing strategies, and suboptimal national testing algorithms. Workload can also contribute to misdiagnosis – either through high client volume resulting in overburden, with low client volumes resulting in poor proficiency; inadequate training and lack of supportive supervision can further contribute to operator error (7, 8). In many countries errors that occur may be missed and go without correction due to the lack of comprehensive quality management systems or adequate external quality assessment. The consequences of such misdiagnoses are serious. A false-negative HIV status is a failure to correctly diagnosis a client, link them to prevention, treatment and care services; and to also prevent ongoing HIV transmission. A false-positive HIV diagnosis can result in the unnecessary initiation of life-long antiretroviral therapy (ART) and the potential for stigma, discrimination, criminalization; it limits the full offer of interventions to prevent HIV infection; it may also harm community and family relationships, and if the results are subsequently found to be incorrect may reduce the credibility of test results and the trust in health services. Incorrectly initiating ART wastes scarce resources, including stocks of medicines, clinic and staff time, and ART monitoring by viral load and other laboratory tests. This is particularly troubling in settings where after receiving a HIV-positive result clients are offered ART immediately regardless of CD4 count or clinical assessment. Left unaddressed, such quality issues and misdiagnoses could undermine the HIV response and make it difficult to reach new global targets, including to correctly diagnose 90% of people with HIV by 2020 (9), prevent new HIV infections and provide treatment to people with HIV. We conducted this systematic literature review to assess the causes and extent of misdiagnosis in different settings.
1 WHO, HIV/AIDS Department, Geneva, Switzerland 2 Johns Hopkins University, Bloomberg School of Public Health, Baltimore, USA 3 WHO, Essential Medicines and Health Products, Geneva, Switzerland 4 USAID, Global Health Bureau, Office of HIV/AIDS, Washington, DC 5 American University of Beirut, Beirut, Lebanon 6 Global AIDS Response Progress Reporting (GARPR) (WHO, UNAIDS, UNICEF) 6 July 2015.
308

WHO/HIV/2015.33 © World Health Organization 2015
14.2. Methods We systematically searched for peer-reviewed articles published from January 1990 to July 2014 using a pre-defined set of search terms in the several electronic databases (see Table 14.1A): International AIDS Conference (IAC) and IAS conference abstracts were searched from July 2001 through July 2013. At the time of the search, only the most recent CROI conference (2014) database was searched because abstracts from past conferences were not electronically available. For ASLM, only 2012 conference abstracts were searched because at the time the 2014 meeting had not yet occurred and previous conferences were not electronically available. We also searched reference lists to identify additional relevant literature. This process was repeated iteratively until no new citations were identified. Experts were also contacted to identify additional articles and gray literature reports. No geographic restrictions were placed on the search, but the review was limited to documents in English. Table 14.1A Search strategy and search terms Search strategy 1. Database searching: PubMed, CINAHL, and EMBASE will be searching from January 1, 1990-July 9 2014 to
identify relevant scientific articles.
2. Conference abstracts: International AIDS Conference (IAC), Conference on HIV Pathogenesis, Treatment, and Prevention (IAS), and Conference on Retroviruses and Opportunistic Infections (CROI) websites to identify conference abstracts. The IAC and IAS conference abstracts will be searched from 2001-present. For CROI, only the most recent conference (2014) will be searched as past conferences are inaccessible.
3. Government and NGO websites: Médecins Sans Frontières, USAID, UNAIDS, WHO, CDC, AMREF, SEAD, ASLM, FHI360, CHAI, JHPIEGO, PSI and ICAP
Search Terms 1. (misclassif* OR error* OR “false positive” OR “false positives” OR “false negative” OR “false negatives” OR
misdiagnos*) AND (test* or algorithm* or screen* OR diagnos*) AND (rapid OR “point of care” OR POC OR RDT) AND (“HIV” OR “Human Immunodeficiency Virus”)
For searching electronic databases related to proficiency testing and external quality assessment of HIV testing
algorithms involving RDTs, the following set of search terms will be used:
(“proficiency testing” OR “external quality assessment”) AND (rapid OR “point of care” OR POC OR RDT) AND (HIV OR “Human Immunodeficiency Virus”)
2. For conference abstract searching, more simplified search terms will be used due to the basic search capacity
of databases. Multiple searches will take place, including searches on “misclassification,” “misdiagnosis” and other terms related to misclassification of HIV status. Additionally, abstracts will be searched using terms
related to poor quality testing, quality assurance, and proficiency testing failure.
3. For website searches, all available publications will be searched for reports, abstracts, studies, or articles related
to HIV status misclassification, factors related to potential misclassification, and quality of HIV testing occurring
in programmatic settings.
Studies were eligible for inclusion if they included rates of HIV status misdiagnosis using algorithms involving at least two RDTs, reported factors related to potential misdiagnosis, or described issues related to the quality of HIV testing being implemented in programmatic settings (facility, laboratory or community-based) as well as sites reporting on results of external quality assessment schemes, such as proficiency testing. Potential causes of
309

WHO/HIV/2015.33 © World Health Organization 2015
misdiagnosis were extracted from studies using the following categories: test kits, operator error, testing strategy or algorithm, population characteristics, and testing sites. The primary summary of measure was the count of studies which reported one of the following errors: (1) clerical/technical error (defined as operator error in documenting and reporting information essential to a correct test result), (2) user error (defined as operator error collecting specimen, performing an HIV RDT or interpreting the test result), (3) cross-reactivity (defined as characteristics of the HIV RDT, of the population or of the geographic location that are related to incorrect test results); (4) incorrect/suboptimal testing strategy (defined as errors related to the order in which specific RDTs are used, also known as a testing strategy); and (5) poor management and supervision (defined as lack of active quality management systems). Secondary summary measures include: HIV-positive misdiagnosis rates (number of false-positive tests reported over the number of HIV-positive tests reported and retested to confirm HIV status reports), (2) HIV-negative misdiagnosis rates (number of false-negative tests reported over the number of HIV-negative tests reported); and (3) sensitivity and specificity of the reporting testing algorithm (see full Tables 4a-4f and Table 5). We followed PRISMA reporting standards (see annex). The full electronic search strategy is available in the review protocol (see annex). Initial titles were screened by one investigator (VF) to determine eligibility. A second screening was then carried out by two reviewers (VF and ST). Final inclusion was determined by CJ, AS, and RB. All differences were resolved through consensus with VF, AS, CJ and RB. Data from all sources were extracted and placed into standardized forms by one reviewer (VF). A second reviewer (ST) verified data extracted. CJ and AS independently reviewed and finalized data for inclusion.
14.3. Results Forty-two studies that addressed and reported factors potentially related to misdiagnosis were identified and included in this review (see Figure 14.1A, Table 14.2A and Table 14.3A). Studies were carried out in Brazil (n=2) (10, 11), Cameroon (n=2) (12, 13), Cambodia (n=1) (14), the Democratic Republic of Congo (DRC) (n=1) (6), Ethiopia (n=2) (15, 16), Honduras (n=1) (17), Haiti (n=1), India (n=1), Kenya (n=1) (18), Malawi (n=2)(19, 20), Mozambique (n=1) (21), Nigeria (n=2) (22, 23), South Africa (n=3) (24-26), Tanzania (n=3) (27-29), Uganda (n=4) (30-33), United Kingdom (n=1), USA (n=2), Zimbabwe (n=1) (34), and multi-country studies (n=13) (3, 8, 35-44). Sample sizes varied in unit of measure, including clients (n=20 range: 106 035 to 3), specimens (n=14, range: 9 419 to 34), health workers performing HIV testing (n=4 range: 3 835 to 39 personnel), sites where HIV testing was performed (n=8 range: 602 to 38 sites) and six studies reported more than one unit of measure (see Supplementary Tables 3a-f and Table 14.4A). Forty-two studies occurred in a facility-based setting; the other two studies took place in the workplace (n=1) (34) in a field-based mobile-testing service (n=1) (32). Misdiagnosis of HIV-positive status Two studies, which evaluated the same HTS programme, conducted a retrospective audit to assess misdiagnosis of HIV status among individuals in HIV care and treatment programmes (6, 35). The first study, conducted in DRC, Burundi and Ethiopia reported multiple reasons which may have caused misdiagnosis including providers not following standard operating procedures, high workload and stress on testing providers, damaged test kits (i.e. “ruptured test kits”) and incorrect diagnosed using the result of a single assay (RDT or enzyme immunosassay (EIA)) rather than a full recommended testing strategy (35). Overall the rate of false-positive diagnoses was 2.6% in Burundi, 4.8% DRC—which was 10.3% in the first 5 months of retesting with a parallel testing strategy—and 4.7% in Ethiopia (35). The second study, conducted in DRC by the same group but over a different time period, reported a false-positive diagnosis rate of 10.5% in the first five months of re-testing and average of 10.3% misdiagnosis rate by the study end (6). The testing strategy used in this study consisted of two HIV RDTs conducted in parallel (6). Potential causes of misdiagnosis reported include the over-interpretation of weak reactive test results and possible cross reactivity due to HLA class II antigens directly modulating the immune response, on-with specific polyclonal B-lymphocyte antibodies (6). Misdiagnosis HIV-negative status Three studies reported rates of missed HIV infection where testing algorithms incorrectly identified HIV-positive individuals as HIV-negative (24, 27, 34). One study in South Africa, reported that 2% of patients who were later found to be HIV-positive (and not recently infected) had previously been diagnosed HIV-negative or HIV-
310

WHO/HIV/2015.33 © World Health Organization 2015
inconclusive (with discrepant HIV test results) (24). The reported cause of these misdiagnoses was the testing strategy: the study used both serial and parallel two-assay testing strategies and the testing algorithm (24). A second study, from Zimbabwe, reported 81% (547/674) of participants who were tested for HIV were HIV-negative; one of which was false-negative (34). It was reported that the cause of this false-negative was “user error” attributed to “slowly reactive” specimens both times the RDT was performed (34). The third study, from Tanzania, reported three false-negative cases, including a single case of a woman who was experiencing symptoms associated with HIV and several opportunistic infections and who tested HIV-negative but was in fact HIV-positive (27). The cause of this misdiagnosis, reported by the authors, was late-stage HIV infection which can result in low levels of antibodies (27). Figure 14.1A Study selection process
Records identified through database searching (n=958): n=902 related to misdiagnosis n=56 related to quality assurance
Additional records identified through other sources
(n=172)
Abstracts identified and screened at first level (n=841)
Abstracts screened at second level (n=292)
Records excluded (n=549)
Studies assessed for eligibility (n=269)
Studies excluded (n=225) because: xDescribes individual assay
performance characteristics or compare characteristics across rapid assays
xReports false positive or false negative results for 1 RDT (not entire algorithm) and did not report possible causes of errors or misdiagnosis.
xRelated to a study already included as primary
xLiterature reviews related to HIV diagnostics, reasons for false positive test results, etc.
xOther issues related to RDTs (e.g., cross-reactivity)
xQuality assurance and testing guidelines
x Did not report possible errors, poor quality testing or actual or potential misdiagnosis.
Records excluded (n=23)
Studies included in reviews (n=44)
Duplicates removed (n=289)
311
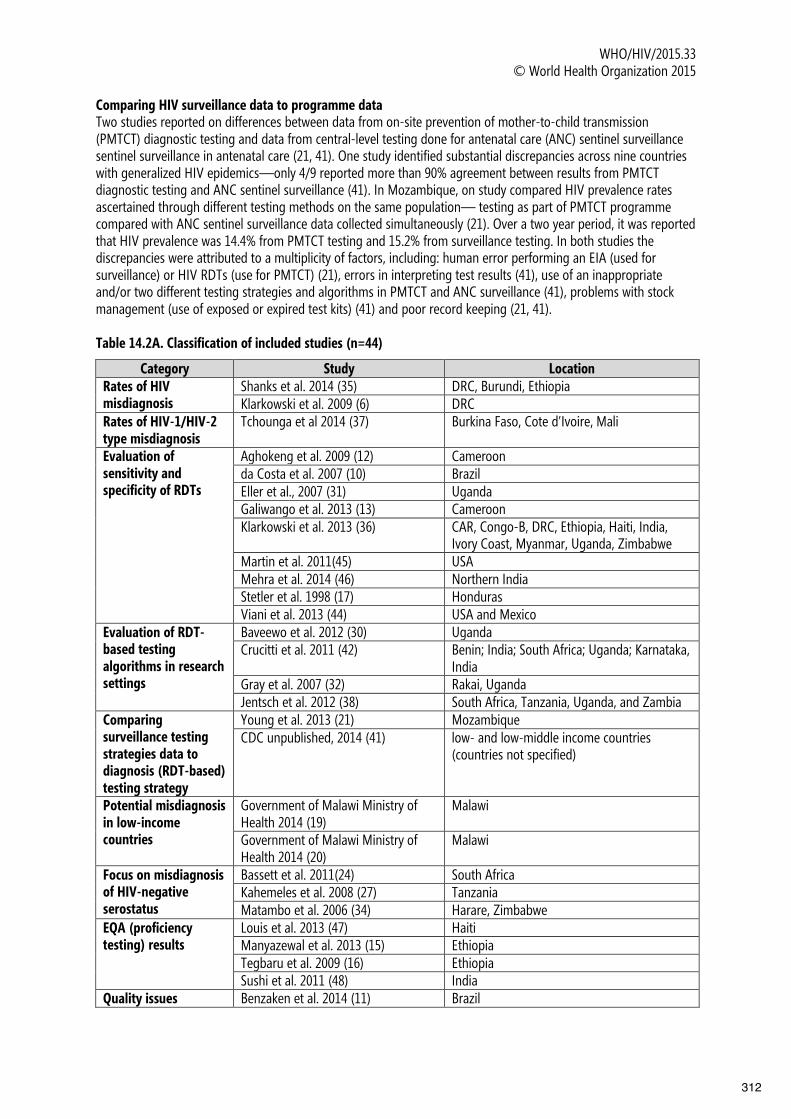
WHO/HIV/2015.33 © World Health Organization 2015
Comparing HIV surveillance data to programme data Two studies reported on differences between data from on-site prevention of mother-to-child transmission (PMTCT) diagnostic testing and data from central-level testing done for antenatal care (ANC) sentinel surveillance sentinel surveillance in antenatal care (21, 41). One study identified substantial discrepancies across nine countries with generalized HIV epidemics—only 4/9 reported more than 90% agreement between results from PMTCT diagnostic testing and ANC sentinel surveillance (41). In Mozambique, on study compared HIV prevalence rates ascertained through different testing methods on the same population— testing as part of PMTCT programme compared with ANC sentinel surveillance data collected simultaneously (21). Over a two year period, it was reported that HIV prevalence was 14.4% from PMTCT testing and 15.2% from surveillance testing. In both studies the discrepancies were attributed to a multiplicity of factors, including: human error performing an EIA (used for surveillance) or HIV RDTs (use for PMTCT) (21), errors in interpreting test results (41), use of an inappropriate and/or two different testing strategies and algorithms in PMTCT and ANC surveillance (41), problems with stock management (use of exposed or expired test kits) (41) and poor record keeping (21, 41). Table 14.2A. Classification of included studies (n=44)
Category Study Location Rates of HIV misdiagnosis
Shanks et al. 2014 (35) DRC, Burundi, Ethiopia Klarkowski et al. 2009 (6) DRC
Rates of HIV-1/HIV-2 type misdiagnosis
Tchounga et al 2014 (37) Burkina Faso, Cote d’Ivoire, Mali
Evaluation of sensitivity and specificity of RDTs
Aghokeng et al. 2009 (12) Cameroon da Costa et al. 2007 (10) Brazil Eller et al., 2007 (31) Uganda Galiwango et al. 2013 (13) Cameroon Klarkowski et al. 2013 (36) CAR, Congo-B, DRC, Ethiopia, Haiti, India,
Ivory Coast, Myanmar, Uganda, Zimbabwe Martin et al. 2011(45) USA Mehra et al. 2014 (46) Northern India Stetler et al. 1998 (17) Honduras Viani et al. 2013 (44) USA and Mexico
Evaluation of RDT-based testing algorithms in research settings
Baveewo et al. 2012 (30) Uganda Crucitti et al. 2011 (42) Benin; India; South Africa; Uganda; Karnataka,
India Gray et al. 2007 (32) Rakai, Uganda Jentsch et al. 2012 (38) South Africa, Tanzania, Uganda, and Zambia
Comparing surveillance testing strategies data to diagnosis (RDT-based) testing strategy
Young et al. 2013 (21) Mozambique CDC unpublished, 2014 (41) low- and low-middle income countries
(countries not specified)
Potential misdiagnosis in low-income countries
Government of Malawi Ministry of Health 2014 (19)
Malawi
Government of Malawi Ministry of Health 2014 (20)
Malawi
Focus on misdiagnosis of HIV-negative serostatus
Bassett et al. 2011(24) South Africa Kahemeles et al. 2008 (27) Tanzania Matambo et al. 2006 (34) Harare, Zimbabwe
EQA (proficiency testing) results
Louis et al. 2013 (47) Haiti Manyazewal et al. 2013 (15) Ethiopia Tegbaru et al. 2009 (16) Ethiopia Sushi et al. 2011 (48) India
Quality issues Benzaken et al. 2014 (11) Brazil
312

WHO/HIV/2015.33 © World Health Organization 2015
Category Study Location
discovered from EQA Cham et al. 2012 (39) 30 countries in Africa Plate et al. 2007 (3) 11 countries in Africa Iwe et al. 2011 (22) Nigeria Kalou et al. 2012 (8) Uganda and Tanzania Kitheka et al. 2012 (18) Kenya Lali et al. 2010 (33) Uganda Ocheng et al. 2012 (28) Tanzania
Factors related to potential misdiagnosis
Boeras et al. 2011 (40) Lusaka, Zambia and Rwanda Granade et al. 2004 (49) USA Kanal et al. 2005 (14) Cambodia Learmonth et al. 2008 (43) 26 countries Sacks et al. 2012 (50) UK Wolpaw et al. 2010 (25) South Africa
General quality issues from sites conducting HTS
Adebayo et al. 2012 (23) Nigeria Mashauri et al. 2007 (29) Tanzania SEAD 2010 (26) South Africa
Programme data In Malawi, following the retesting of people diagnosed HIV-positive before they enrolled in care or treatment, 7.7% (534/7,007) could not be conclusively diagnosed (19). A follow-up study also reported 4.3% (346/8,017) of individuals previously diagnosed HIV-positive could not be conclusively diagnosed (20). At the time of both studies it was reported that many sites where ART is initiated did implement retesting routinely (19, 20). Results from proficiency testing/external quality assessment schemes Three articles (15, 16, 47) reported results from external quality assessment (EQA) schemes (also known as proficiency testing) that compared with the assigned value (expected reference results). One study, from Haiti, reported that between across a six year period 92.0% (242/263) of laboratories participated in proficiency testing and that concordance ranged from 88% to 90% in 2006 and 2011 respectively. Declines in concordance of results were noted in 2008 and 2010 and were linked to health worker shortages that resulted from natural disasters (47). Two studies from Ethiopia reported good performance within proficiency testing schemes (15, 16). Overall agreement was high (between 95% and 100%)(15, 16). However, one study reported the concordance of results was lower in health centres than in district hospitals when HIV RDTs using capillary whole blood specimens were tested, 87.5% (14/16) 93.8% (15/16) respectively (15). Other errors that caused incorrect results include the use of a tiebreaker strategy (15), health workers having difficulty interpreting weakly reactive test lines and stock-outs of reagents (16). Clerical errors Fourteen studies reported on clerical errors (8, 10, 14, 17, 18, 21, 22, 31, 33, 38, 41, 46, 48, 49). These did not always lead to misdiagnosis but report that errors did occur, such as poor recordkeeping including writing reports (14), data reporting problems, labelling and transcription mistakes (48) and specimen mix-ups could have result in misdiagnosis of HIV status. Poor record keeping, according to one study, resulted in nearly 30% of errors resulting in incorrect test status (33). Clerical errors were not always clearly defined in the studies reviewed, but noted as possible causes of incorrect test results and therefore HIV status (10). User error User error was reported as a potential cause of misdiagnosis in 21 studies (6, 10, 11, 13, 15, 16, 18, 26, 30, 32, 34, 35, 39, 42, 43, 45, 47-50). User errors were defined as human errors by the operator such as incorrectly performing the test procedure or incorrectly interpreting test results, incorrect buffer volume, not following reading times, inaccurate reading time stated in the instructions for use and non-adherence to standard operating procedures (6, 13, 16, 30, 32, 39, 42, 43, 48, 50). In some provinces in South Africa, it was reported that the average turnaround time for an HIV testing visit was four minutes whereas the first assay of the testing algorithm had a recommended minimum reading time of 15 minutes (26); other errors identified include users having difficulty performing the RDT
313
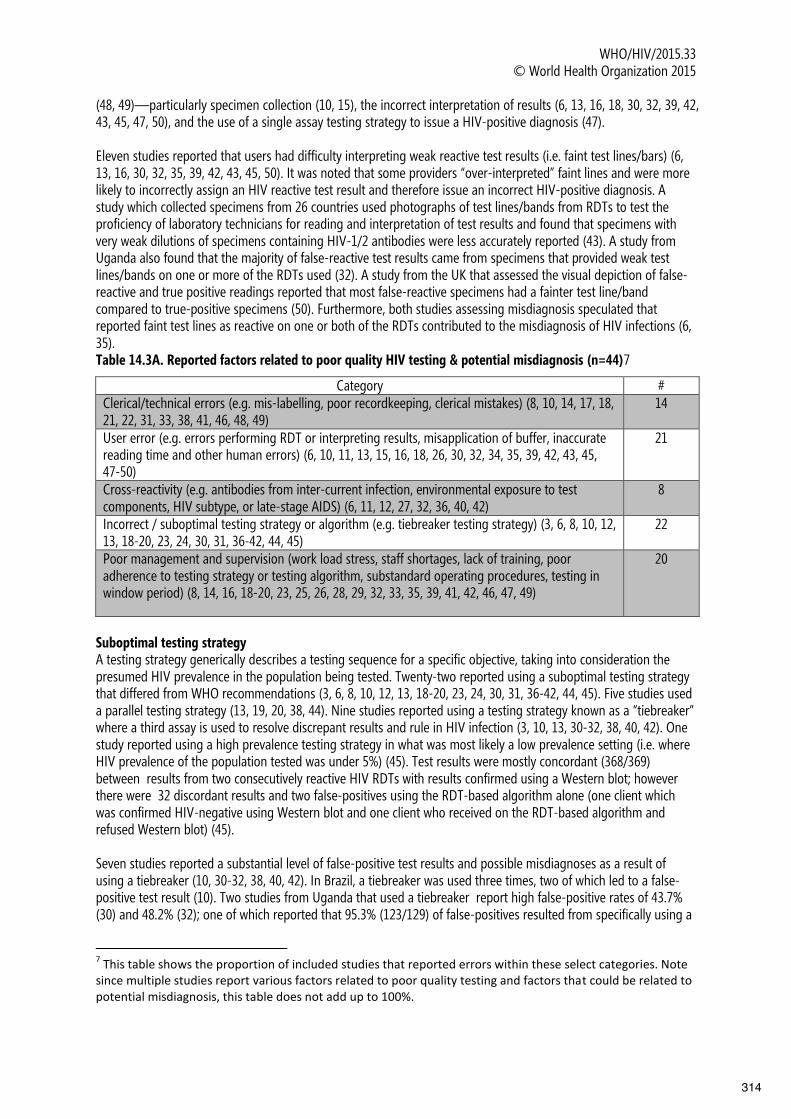
WHO/HIV/2015.33 © World Health Organization 2015
(48, 49)—particularly specimen collection (10, 15), the incorrect interpretation of results (6, 13, 16, 18, 30, 32, 39, 42, 43, 45, 47, 50), and the use of a single assay testing strategy to issue a HIV-positive diagnosis (47). Eleven studies reported that users had difficulty interpreting weak reactive test results (i.e. faint test lines/bars) (6, 13, 16, 30, 32, 35, 39, 42, 43, 45, 50). It was noted that some providers “over-interpreted” faint lines and were more likely to incorrectly assign an HIV reactive test result and therefore issue an incorrect HIV-positive diagnosis. A study which collected specimens from 26 countries used photographs of test lines/bands from RDTs to test the proficiency of laboratory technicians for reading and interpretation of test results and found that specimens with very weak dilutions of specimens containing HIV-1/2 antibodies were less accurately reported (43). A study from Uganda also found that the majority of false-reactive test results came from specimens that provided weak test lines/bands on one or more of the RDTs used (32). A study from the UK that assessed the visual depiction of false-reactive and true positive readings reported that most false-reactive specimens had a fainter test line/band compared to true-positive specimens (50). Furthermore, both studies assessing misdiagnosis speculated that reported faint test lines as reactive on one or both of the RDTs contributed to the misdiagnosis of HIV infections (6, 35). Table 14.3A. Reported factors related to poor quality HIV testing & potential misdiagnosis (n=44)7
Category # Clerical/technical errors (e.g. mis-labelling, poor recordkeeping, clerical mistakes) (8, 10, 14, 17, 18, 21, 22, 31, 33, 38, 41, 46, 48, 49)
14
User error (e.g. errors performing RDT or interpreting results, misapplication of buffer, inaccurate reading time and other human errors) (6, 10, 11, 13, 15, 16, 18, 26, 30, 32, 34, 35, 39, 42, 43, 45, 47-50)
21
Cross-reactivity (e.g. antibodies from inter-current infection, environmental exposure to test components, HIV subtype, or late-stage AIDS) (6, 11, 12, 27, 32, 36, 40, 42)
8
Incorrect / suboptimal testing strategy or algorithm (e.g. tiebreaker testing strategy) (3, 6, 8, 10, 12, 13, 18-20, 23, 24, 30, 31, 36-42, 44, 45)
22
Poor management and supervision (work load stress, staff shortages, lack of training, poor adherence to testing strategy or testing algorithm, substandard operating procedures, testing in window period) (8, 14, 16, 18-20, 23, 25, 26, 28, 29, 32, 33, 35, 39, 41, 42, 46, 47, 49)
20
Suboptimal testing strategy A testing strategy generically describes a testing sequence for a specific objective, taking into consideration the presumed HIV prevalence in the population being tested. Twenty-two reported using a suboptimal testing strategy that differed from WHO recommendations (3, 6, 8, 10, 12, 13, 18-20, 23, 24, 30, 31, 36-42, 44, 45). Five studies used a parallel testing strategy (13, 19, 20, 38, 44). Nine studies reported using a testing strategy known as a “tiebreaker” where a third assay is used to resolve discrepant results and rule in HIV infection (3, 10, 13, 30-32, 38, 40, 42). One study reported using a high prevalence testing strategy in what was most likely a low prevalence setting (i.e. where HIV prevalence of the population tested was under 5%) (45). Test results were mostly concordant (368/369) between results from two consecutively reactive HIV RDTs with results confirmed using a Western blot; however there were 32 discordant results and two false-positives using the RDT-based algorithm alone (one client which was confirmed HIV-negative using Western blot and one client who received on the RDT-based algorithm and refused Western blot) (45). Seven studies reported a substantial level of false-positive test results and possible misdiagnoses as a result of using a tiebreaker (10, 30-32, 38, 40, 42). In Brazil, a tiebreaker was used three times, two of which led to a false-positive test result (10). Two studies from Uganda that used a tiebreaker report high false-positive rates of 43.7% (30) and 48.2% (32); one of which reported that 95.3% (123/129) of false-positives resulted from specifically using a
7 This table shows the proportion of included studies that reported errors within these select categories. Note since multiple studies report various factors related to poor quality testing and factors that could be related to potential misdiagnosis, this table does not add up to 100%.
314

WHO/HIV/2015.33 © World Health Organization 2015
tiebreaker (32). Three multi-country studies report false-positive rates of 8.7% (4/46) (42), 10.2% (55/537) (38) and 45.9% (17/37) (40) when participants were incorrectly diagnosed HIV-positive using a tiebreaker. Cross-reactivity and characteristics of the individual undergoing testing Cross-reactivity related issues based on population and individual characteristics were reported in nine studies (6, 11, 12, 27, 32, 36, 40, 42). Results for potential interactions could be biological due to antibodies from inter-current infections, adverse environmental exposure to assay components, HIV subtype, or interactions between test kits in an algorithm. One study suggested cross-reactivity between test kits within an algorithm led to final false-positive result (42).One study hypothesized that cross-reactivity may cause weak reactive test results (32). Six studies (6, 11, 27, 35, 36, 40) reported potential issues with RDTs interacting with particular characteristics of the individual undergoing testing (6, 35, 36) including individuals with low levels of HIV-1/2 antibodies (11, 27)—particularly due to late stage HIV infection (27), and potential cross-reactivity or environmental exposure to test kits components
(36, 40). Poor management and supervision Twenty studies reported poor management and supervision practices related to poor quality testing and potential misdiagnosis of HIV status (8, 14, 16, 18-20, 23, 25, 26, 28, 29, 32, 33, 35, 39, 41, 42, 46, 47, 49). Of these, 10 studies specifically reported on improper practices for management of supplies (8, 16, 26, 28, 29, 33, 35, 39, 41, 42). Errors that were specifically linked to misdiagnosis included the use of damaged RDT test kits (35); the use of damaged or expired kits (8, 33, 41, 42); stock outs (8, 26, 29, 33, 39, 41); the use of wrong RDT for HIV testing (28); and not using a timer nor the correct reagent with RDT selected (26). According to one study from Tanzania, an assessment of non-laboratory personnel competency identified that a syphilis RDT was being used incorrectly to test for an HIV infection (28). Errors related to poor management and supervision also include clients receiving HIV testing within the window period (32, 46), HIV testing performed by under-trained or ineligible staff (8, 23, 26, 28, 49), poor quality instructions for use (32), low levels of re-testing before ART initiation (19, 20), poor participation in EQA schemes (39), poor site-level supervision (18), lack of and poor adherence to standard operating procedures (14, 23, 25, 26, 29, 33). Four studies also reported that user and/or clerical errors were linked to high workload and stress (8, 35, 39, 47). An EQA scheme in Nigeria reported that over 40% of laboratory respondents had no training on HIV testing and only 33.3% of sites used an approved national testing algorithm (23). In South Africa, an assessment of 38 facilities reported that compliance to standard operating procedures was very low and that out of all HIV testing events observed (n=265) only 3.4% were performed correctly (26). They reported common causes for incorrectly performing processes included: a deviation of staff roles; lack of necessary equipment, or lack of useable equipment; and inadequate training (26).
14.4. Discussion This review found limited data on the magnitude of misdiagnosis of HIV status. The review only identified two studies that specifically reported the number of individuals who were actually HIV-negative but who had been misdiagnosed and enrolled in HIV-related care and treatment (6, 35). In both studies substantial loss to follow-up was documented and not all clients diagnosed HIV-positive were retested. Thus, it is possible that these rates are under-estimates and the actual level of misdiagnosis may be even higher than what was reported. Although none of the reviewed studies were able to determine and quantify the exact cause(s) of misdiagnosis, several provided hypotheses that attributed misdiagnosis to various factors. Three key factors emerged in this review: (1) poor management of supplies including the use of inappropriate, damaged or expired test kits, (2) user errors interpreting weak reactive test results and (3) the use of a “tiebreaker” testing strategy. Poor management of supplies appears in half (10/20) of studies reporting poor management and supervision. To ensure correct results, all staff providing HIV testing must be adequately trained and certified. In several studies this was not the case and ineligible providers were performing HIV testing services (26, 28). Training, including pre-service, in-service and periodic refresher training is important to maintain and improve the quality of services, as well as participation in proficiency testing schemes. In this review the studies that participated in such programmes were able to monitor and track their performance and identify issues, including difficulty interpreting faint lines and health worker shortages that needed to be addressed to improve the quality of HIV testing. In addition to training
315

WHO/HIV/2015.33 © World Health Organization 2015
personnel and participating in external quality assurance, overarching management and supervision of sites is essential. Several studies reported user and clerical errors were a result of demanding workloads, burnout and high levels of stress (8, 35, 39, 47). Sites should routinely assess and manage their human resource planning to prevent and reduce staff shortages as much as possible. User error interpreting faint lines and weak reactive test results was also a common challenge identified, often leading to substantial levels of false-positive results. This issue has been reported and evaluated previously. Historically this issue has been well-documented and evaluated in the literature (32, 50); however the challenges and errors with over-interpretation persist. To address this issue specialized training for health workers may be needed, as well as work with manufacturers to improve instructions for use on the interpretation of faint lines and site-level standard operating procedures to guide health workers on how to handle faint lines when they occur. No assay or testing algorithm is perfect and false-positive and false-negative test results do occur and should be anticipated. However, this review highlights errors and practices that compromise the reliability test results; in particular the use of a tiebreaker testing strategy. Based on the studies reviewed, it appeared that a tiebreaker increases the likelihood of false-positive test results and possible misdiagnosis. Although our review did not examine possible cross-reactivity between assays used within an algorithm, this also may have contributed to false-positive results. Since our search was completed, two more studies reported on the use of a tiebreaker strategy. In Ethiopia, a tiebreaker testing strategy resulted in 16 false positive diagnoses (PPV 92.7%, 95% CI: 88.4%-95.8%), compared to a serial testing strategy with 1 false positive diagnosis (PPV of 99.5% (95% CI 97.3%-100%)) (51). In a multi-country study among African adults, using a tiebreaker testing strategy with RDTs resulted in a poor sensitivity within the algorithm, ranging from 8.3%-43% (52). These results are concerning because out of 48 recent national policies reviewed, 30% recommend using a tiebreaker testing strategy (5). It is important that national programmes and policy makers select and use an appropriate testing strategy and validated testing algorithm. A tiebreaker testing strategy has never been recommended by WHO, but it appears to be common practice in many settings. To ensure that test results and HIV status are reported correctly it is important WHO recommendations emphasize re-testing people diagnosed HIV-positive before they enrol in care and/or treatment. This is increasingly critical as more people are being offered immediate treatment without being clinically assessed.
14.5. Limitations This review suffers from publication bias as it focused on identifying studies related to the misdiagnosis of HIV status in the published and gray literature, including information from programme evaluations. However, this information is often not publically available. To find additional information to corroborate the concerns regarding misdiagnosis we also reviewed available data external quality assessment (proficiency testing and on-site supervision) and studies reporting sensitivity and specificity HIV testing algorithms which also reported on causes of false-positive and false-negative results. Nevertheless, there are several limitations to this review. This review was limited to the English language and therefore may have missed reports in other languages. Because of the heterogeneity of studies we were unable to assess the quality of studies more rigorously, as reports were all observational and no the primary outcome for most studies reviewed. Likewise, because the review was designed to identify reports on misdiagnosis it is possible that studies only reporting on errors and quality of HIV testing may have been missed. While some reports of cross-reactivity were identified in this review, we focus on human errors and quality system failures. Other reviews exist and provide more details information on such issues (53). Furthermore, we did not identify or examine reports of incorrect test results or misdiagnosis of HIV status due to testing people exposed to ARV drugs, e.g. ART, pre-exposure prophylaxis or post-exposure prophylaxis.
14.6. Conclusion The paucity of data regarding the magnitude of misdiagnosis within HIV testing programmes does not make it possible to determine whether misdiagnosis is not reported because it is negligible or because it is not monitored. Nevertheless, our review suggests that there are many potential factors and practices which could contribute to misdiagnosis and insufficient attention is given to quality assurance in many settings. The consequences of misdiagnoses are serious on an individual and public health level. Ensuring the quality of HIV testing services and that HIV diagnoses are correct is an urgent priority. Any site providing HIV testing must have
316
WHO/HIV/2015.33 © World Health Organization 2015
quality management systems to minimize the risk of incorrect test results and to identify and correct misdiagnoses if they occur. Without such provisions there is a risk the many successes of national programmes and the HIV response as a whole could be compromised and undermined. With the momentum to increase diagnosis of people with HIV and link them to care and treatment, a parallel push to improve quality and prevent misdiagnosis is essential.
References 1. Annex 6. Diagnostics for HIV diagnosis of the Consolidated Guidelines on HIV testing services. Geneva: World Health Organization; 2015. 2. Molesworth AM, Ndhlovu R, Banda E, Saul J, Ngwira B, Glynn JR, et al. High accuracy of home-based community rapid HIV testing in rural Malawi. J Acquir Immune Defic Syndr. 2010 Dec 15;55(5):625-30. 3. Plate DK, Rapid HIVTEWG. Evaluation and implementation of rapid HIV tests: the experience in 11 African countries. AIDS Res Hum Retroviruses. 2007 Dec;23(12):1491-8. 4. Lyamuya EF, Aboud S, Urassa WK, Sufi J, Mbwana J, Ndugulile F, et al. Evaluation of simple rapid HIV assays and development of national rapid HIV test algorithms in Dar es Salaam, Tanzania. BMC Infectious Diseases. 2009;9. 5. Flynn D, Johnson C, Sands A, Wong V, Baggaley R. An analysis of the role of lay providers in HIV testing and counseling in 48 countries. In press unpublished data. 6. Klarkowski DB, Wazome JM, Lokuge KM, Shanks L, Mills CF, O'Brien DP. The evaluation of a rapid in situ HIV confirmation test in a programme with a high failure rate of the WHO HIV two-test diagnostic algorithm. PLoS ONE. 2009;4(2). 7. Shanks L, Klarkowski D, O'Brien DP. False positive HIV diagnoses in resource limited settings: operational lessons learned for HIV programmes. PLoS One. 2013;8(3):e59906. 8. Kalou M, Mosha F, Ndlovu N, Jackson K, Mwassekage M, Ngoi M, et al. Implementation of a Proficiency Testing Program Using Dried Tube Specimen (DTS) Approach to Improve the Quality of HIV Rapid Testing in Testing Sites in Uganda and Tanzania. First International Conference of the African Society for Laboratory Medicine (ASLM); 2012; Cape Town, South Africa. Abstract No. 69. 2012. 9. 90-90-90 Ambitious treatment targets: writing the final chapter of the AIDS epidemic - a discussion paper. Geneva: Joint United Nations Programme on HIV/AIDS; 2014. 10. da Costa Ferreira Junior O, Ferreira C, Riedel M., Visinoni Widolin, Sasazawa Ito, Westman S, et al. Field evaluation of an HIV rapid test algorithm for the rapid diagnosis of HIV infection in Brazil. HIV Pathogenesis, Treatment and Prevention; 2007; Sydney, Australia. 2007. 11. Benzaken AS, Bazzo ML, Galban E, Pinto ICP, Nogueira CL, Golfetto L, et al. External quality assurance with dried tube specimens (DTS) for point-of-care syphilis and HIV tests: Experience in an indigenous populations screening programme in the Brazilian Amazon. Sexually Transmitted Infections. 2014;90(1):14-8. 12. Aghokeng AF, Mpoudi-Ngole E, Dimodi H, Atem-Tambe A, Tongo M, Butel C, et al. Inaccurate diagnosis of HIV-1 group M and O is a key challenge for ongoing universal access to antiretroviral treatment and HIV prevention in Cameroon. PLoS ONE. 2009;4(11). 13. Galiwango RM, Musoke R, Lubyayi L, Ssekubugu R, Kalibbala S, Ssekweyama V, et al. Evaluation of current rapid HIV test algorithms in Rakai, Uganda. J Virol Methods. 2013 Sep;192(1-2):25-7. 14. Kanal K, Chou TL, Sovann L, Morikawa Y, Mukoyama Y, Kakimoto K. Evaluation of the proficiency of trained non-laboratory health staffs and laboratory technicians using a rapid and simple HIV antibody test. AIDS Research and Therapy. 2005;2(1). 15. Manyazewal T, Paterniti AD, Redfield RR, Marinucci F. Role of secondary level laboratories in strengthening quality at primary level health facilities' laboratories: an innovative approach to ensure accurate HIV, tuberculosis, and malaria test results in resource-limited settings. Diagn Microbiol Infect Dis. 2013 Jan;75(1):55-9. 16. Tegbaru B, Wolday D, Messele T, Meless H, Kassa D, Tesema D, et al. Assessment of the implementation of HIV-rapid test kits at different levels of health institutions in Ethiopia. Ethiop Med J. 2007 Jul;45(3):293-9. 17. Stetler HC, Granade TC, Nunez CA, Meza R, Terrell S, Amador L, et al. Field evaluation of rapid HIV serologic tests for screening and confirming HIV-1 infection in Honduras. AIDS. 1997;11(3):369-75. 18. F. Kitheka, M. Umuro, S. Mwa, editors. Implementing Rapid HIV Proficiency Testing Program in Kenya: Key Findings from Corrective Actions Following the Switch from Facility-Based to Individual-Based Proficiency Testing. First International Conference of the African Society for Laboratory Medicine (ASLM); 2012; Cape Town, South Africa. Oral Poster on Wednesday, Dec. 5 2012.
317

WHO/HIV/2015.33 © World Health Organization 2015
19. Malawi Go. Integrated HIV program report January - March 2014. In: Health Mo, editor. Malawi; 2014. 20. Malawi Go. Integrated HIV program report April-June 2014. Malawi: Ministry of Health; 2014. 21. Young PW, Mahomed M, Horth RZ, Shiraishi RW, Jani IV. Routine data from prevention of mother-to-child transmission (PMTCT) HIV testing not yet ready for HIV surveillance in Mozambique: A retrospective analysis of matched test results. BMC Infectious Diseases. 2013;13(1). 22. E. Iwe, I. Livinus, E. Omoregbe, B. Okoye, C. Nwuba, A. Mbanefo, et al. Preparation and use of dry tube specimens (DTS) method by laboratorians and non- laboratorians for quality assurance of HIV services (HCT) in MSH supported sites, Niger State, North-Central Nigeria. 6th IAS Conference on HIV Pathogenesis and Treatment; 2011; Rome, Italy. Abstract no. CDD076. 2011. 23. A. Adebayo, A. Olufemi, B. Adekunle, O. Louisa. A Limited survey on HIV-testing knowledge and practice of laboraty personnel at some point-of-care services in Abuja, Federal Capital Territory (FCT), Nigeria. A Limited survey on HIV-testing knowledge and practice of laboraty personnel at some point-of-care services in Abuja, Federal Capital Territory (FCT), Nigeria; 2012; Cape Town, South Africa. Oral Poster on Wednesday, Dec. 5 2012. 2012. 24. Bassett IV, Chetty S, Giddy J, Reddy S, Bishop K, Lu Z, et al. Screening for acute HIV infection in South Africa: Finding acute and chronic disease. HIV Medicine. 2011;12(1):46-53. 25. Wolpaw BJ, Mathews C, Chopra M, Hardie D, de Azevedo V, Jennings K, et al. The failure of routine rapid HIV testing: a case study of improving low sensitivity in the field. BMC health services research. 2010;10:73. 26. SEAD. Analysis of POCT/VCT performed at South African primary health care clinics. 2010 [updated 2010; cited 2014 July 14]; Available from: http://www.sead.co.za/downloads/POCT-clinics-2011.pdf 27. Kahemele N.J., et al. HIV infection diagnostic uncertainity, a field experience. AIDS 2008 - XVII International AIDS Conference; 2008; Mexico City, Mexico. Abstract no. CDB0362. 2008. 28. D. Ocheng, S. Mattaro, L. Msilama, A. Msauka, M. Khama, N. Mshanga, et al. Establishing competence in HIV rapid testing among non-laboratory health professional is key to tasking: preliminary results from ten regions of Tanzania. 19th International AIDS Conference; 2012; Washington, DC. Abstract no. MOPE682. 2012. 29. Mashauri FM, Siza JE, Temu MM, Mngara JT, Kishamawe C, Changalucha JM. Assessment of quality assurance in HIV testing in health facilities in Lake Victoria zone, Tanzania. Tanzania health research bulletin. 2007 May;9(2):110-4. 30. Baveewo S, Kamya MR, Mayanja-Kizza H, Fatch R, Bangsberg DR, Coates T, et al. Potential for false positive HIV test results with the serial rapid HIV testing algorithm. BMC research notes. 2012;5:154. 31. Eller LA, Eller MA, Ouma BJ, Kataaha P, Bagaya BS, Olemukan RL, et al. Large-scale human immunodeficiency virus rapid test evaluation in a low-prevalence ugandan blood bank population. Journal of clinical microbiology. 2007 Oct;45(10):3281-5. 32. Gray RH, Makumbi F, Serwadda D, Lutalo T, Nalugoda F, Opendi P, et al. Limitations of rapid HIV-1 tests during screening for trials in Uganda: diagnostic test accuracy study. 2007. 33. W. Lali, G. Guma, P. Awongo, Z. Akol, H. Kajumbula, P. Namupijja, et al. Challenges of implementation of integrated national laboratory quality improvement in Uganda. AIDS 2010 - XVIII International AIDS Conference 2010; Vienna, Austria. Abstract No. LBPE43 2010. 34. Matambo R, Dauya E, Mutswanga J, Makanza E, Chandiwana S, Mason PR, et al. Voluntary counseling and testing by nurse counselors: What is the role of routine repeated testing after a negative result? Clinical Infectious Diseases. 2006;42(4):569-71. 35. Shanks L, Klarkowski D, O'Brien DP. False Positive HIV Diagnoses in Resource Limited Settings: Operational Lessons Learned for HIV Programmes. PLoS ONE. 2013;8(3). 36. Klarkowski D, Glass K, O'Brien D, Lokuge K, Piriou E, Shanks L. Variation in specificity of HIV rapid diagnostic tests over place and time: An analysis of discordancy data using a bayesian approach. PLoS ONE. 2013;8(11). 37. Tchounga BK, Inwoley A, Coffie PA, Minta D, Messou E, Bado G, et al. Re-testing and misclassification of HIV-2 and HIV-1&2 dually reactive patients among the HIV-2 cohort of The West African Database to evaluate AIDS collaboration. J Int AIDS Soc. 2014;17(1):19064. 38. Jentsch U, Lunga P, Lacey C, Weber J, Cairns J, Pinheiro G, et al. The Implementation and Appraisal of a Novel Confirmatory HIV-1 Testing Algorithm in the Microbicides Development Programme 301 Trial (MDP301). PLoS ONE. 2012;7(9).
318

WHO/HIV/2015.33 © World Health Organization 2015
39. Cham F, Maleka M, Masango M, Goetsch E, Belabbes EH, Singh B, et al. The World Health Organization African region external quality assessment scheme for anti-HIV serology. African Journal of Laboratory Medicine. 2012;1(1). 40. Boeras DI, Luisi N, Karita E, McKinney S, Sharkey T, Keeling M, et al. Indeterminate and discrepant rapid HIV test results in couples' HIV testing and counselling centres in Africa. Journal of the International AIDS Society. 2011;14(1). 41. CDC. HIV testing for surveillance: Evidence from assessments of routine diagnostic testing in ANC. WHO HIV testing and counselling consultation. In press 2014. 42. Crucitti T, Taylor D, Beelaert G, Fransen K, Van Damme L. Performance of a rapid and simple HIV testing algorithm in a multicenter phase III microbicide clinical trial. Clinical and Vaccine Immunology. 2011;18(9):1480-5. 43. Learmonth KM, McPhee DA, Jardine DK, Walker SK, Aye TT, Dax EM. Assessing proficiency of interpretation of rapid human immunodeficiency virus assays in nonlaboratory settings: Ensuring quality of testing. Journal of Clinical Microbiology. 2008;46(5):1692-7. 44. Viani RM, Araneta MRG, Spector SA. Parallel rapid HIV testing in pregnant women at Tijuana General Hospital, Baja California, Mexico. AIDS Research and Human Retroviruses. 2013;29(3):429-34. 45. Martin EG, Salaru G, Paul SM, Cadoff EM. Use of a rapid HIV testing algorithm to improve linkage to care. Journal of Clinical Virology. 2011;52(SUPPL. 1):S11-S5. 46. Mehra B, Bhattar S, Bhalla P, Rawat D. Rapid Tests versus ELISA for Screening of HIV Infection: Our Experience from a Voluntary Counselling and Testing Facility of a Tertiary Care Centre in North India. Isrn Aids. 2014;2014:296840. 47. Louis FJ, Anselme R, Ndongmo C, Buteau J, Boncy J, Dahourou G, et al. Evaluation of an external quality assessment program for HIV testing in Haiti, 2006-2011. Am J Clin Pathol. 2013 Dec;140(6):867-71. 48. K.M. Sushi, G. Saraminijacob, G. Thatchinamoorthy. External quality assurance scheme in a national reference laboratory for HIV testing in resource limited settings, India. 6th IAS Conference on HIV Pathogenesis and Treatment; 2011; Rome, Italy. Abstract no. CDD032. 2011. 49. Granade TC, Parekh BS, Phillips SK, McDougal JS. Performance of the OraQuick and Hema-Strip rapid HIV antibody detection assays by non-laboratorians. Journal of clinical virology : the official publication of the Pan American Society for Clinical Virology. 2004 Jul;30(3):229-32. 50. Sacks R., Omodele-Lucien A., Whitbread N., Muir D., Smith A. Rapid HIV testing using Determine HIV 1/2 antibody tests: is there a difference between the visual appearance of true- and false-positive tests? International journal of STD & AIDS. 2012 Sep;23(9):644-6. 51. Shanks L, Siddiqui MR, Kliescikova J, Pearce N, Ariti C, Muluneh L, et al. Evaluation of HIV testing algorithms in Ethiopia: the role of the tie-breaker algorithm and weakly reacting test lines in contributing to a high rate of false positive HIV diagnoses. BMC Infect Dis. 2015;15(1):39. 52. Fogel JM, Piwowar-Manning E, Donohue K, Cummings V, Marzinke MA, Clarke W, et al. Determination of HIV status in African adults with discordant HIV rapid tests. J Acquir Immune Defic Syndr. 2015 Mar 27. 53. Klarkowski D, O'Brien DP, Shanks L, Singh KP. Causes of false-positive HIV rapid diagnostic test results. Expert Review of Anti-Infective Therapy. 2014;12(1):49-62.
319

ORIGINAL PAPER
HIV Self-Testing in Resource-Limited Settings: Regulatoryand Policy Considerations
Vincent Wong • Cheryl Johnson • Elliot Cowan •
Matthew Rosenthal • Rosanna Peeling •
Maria Miralles • Anita Sands • Charlene Brown
Published online: 24 June 2014! Springer Science+Business Media New York (outside the USA) 2014
Abstract HIV self-testing (HIVST) is an emerging HIVtesting strategy intended to address challenges of increas-
ing access to preliminary knowledge of serostatus. It offers
the potential for tests and testing to reach more people thanpreviously possible, including those who do not seek test-
ing in facilities. With approval of an HIV self-test kit in the
USA, increasing evidence from public pilot programs insub-Saharan Africa showing high acceptability and feasi-
bility, and evidence of the informal sale of rapid HIV test
kits in the private sector, options for individuals to accessHIV self-testing, as well as consumer-demand, appear to be
increasing. More recently WHO and UNAIDS have
explored self-testing as an option to achieving greater HIVtesting coverage to support global treatment targets.
However, for resource-limited settings, technological
development, diagnostic device regulation and qualityassurance policies are lagging behind. This commentary
will examine regulatory and policy issues with HIVST,
given its increased prominence as a potential part of theglobal HIV/AIDS response.
Keywords HIV ! Testing ! Self testing ! VCT ! Policy !Regulation ! Diagnostics ! Rapid test ! HTC
HIV Self-Testing: Policy Context and Use
Increasing access to HIV testing and counselling (HTC)
remains a priority for global HIV programming, critical formeeting prevention and treatment targets [1–3]. Through a
combination of facility- and community-based approaches,
an estimated 118 million people tested for HIV across 124low- and middle-income countries in 2012 [4]. Still, fewer
than half of people living with HIV (PLHIV) in Africa are
aware of their status; with two million new infectionsyearly, many remain undiagnosed and at increased risk for
morbidity, mortality and onward transmission [4]. RapidHIV diagnostic tests (RDTs) are critical tools for increasing
access to testing and knowledge of HIV sero-status, which
many countries have utilized to scale-up HTC access anduptake. The use of RDTs by individuals who want to test
themselves and interpret their results in private, through
HIV self-testing (HIVST), is an emerging strategy thatoffers the potential to reach more people than previously
possible, including those who do not present at health or
community facilities for HIV testing [5]. While non-HIVself-testing has been introduced successfully for other dis-
eases and conditions [6], HIVST in resource-limited set-
tings presents some unique potential challenges and risks, aswell as substantial opportunities for testing expansion.
V. Wong (&) ! C. BrownOffice of HIV/AIDS, USAID, Washington, DC 20004, USAe-mail: [email protected]
C. JohnsonHIV Department, WHO, Geneva, Switzerland
E. CowanPartners in Diagnostics, LLC, Rockville, MD, USA
M. RosenthalUSAID Namibia, Windhoek, Namibia
R. PeelingDepartment of Clinical Research, London School of Hygieneand Tropical Medicine, London, UK
M. MirallesOffice of Health Systems, USAID, Washington, DC, USA
A. SandsDepartment of Essential Medicines and Health Products, WorldHealth Organization, Geneva, Switzerland
123
AIDS Behav (2014) 18:S415–S421
DOI 10.1007/s10461-014-0825-9
Author's personal copy
320

Currently most HIV RDTs are intended for use only by
trained healthcare providers. Because results provided bythese diagnostic devices have both serious individual and
public health implications, and potential for harm due to
false results (e.g. increased transmission, unnecessarytreatment through false or unconfirmed positive results,
non-access to treatment), HIV RDTs have been classified
as ‘‘high risk devices’’. As such, they must meet minimumperformance standards, and diagnoses are made only
through validated, multi-test algorithms [2, 7]. Neverthe-less, benefits of HIVST within specific settings and popu-
lations have now been documented in literature reviews [8–
10], pilot studies [11–13], meeting reports [14], technicalupdates [15], and interim data and research [16–18].
Governments and policy makers must now play a key
role in considering both the potential benefits and harmsthat may result from HIVST; and where HIVST is adopted,
develop systems to monitor and regulate the sale, distri-
bution and use of diagnostics intended for HIVST. Thesuccess of HIV self-testing efforts will require maximizing
benefits while minimizing harm, and involve regulations
stemming from legal systems that establish diagnosticstandards and provide authority and context to imple-
ment responsible policies; and national health policies
which, within the confines of medical device regulation,should guide and inform HIV self-testing implementation
in both the public and private sectors (see Table 1).
HIVST policies and HIVST RDT regulation will clearlybe informed by the increasing evidence-base. Pilot studies
in Malawi and Kenya have demonstrated generally high
acceptability among health workers and the general popu-lations [11, 12], along with high accuracy of self-testing
with HIV RDTs that use oral fluid, when combined with a
demonstration step and illustrated instructions [11, 16, 17].In the USA, France and Australia, acceptability of targeted
HIVST is reportedly high among men who have sex with
men [19–21]. There have been only limited studies onunsupervised HIVST in resource-limited settings [8, 12].
One South African study of unsupervised/uninstructed self-
testing among health care workers found low sensitivity(66.7 %) [22]. Another South African study reported high
accuracy using a fingerstick HIVST kit with tailored
instructions for use among rural and urban men and womenwith minimal education in KwaZuluNatal, where 99 % of
participants received a valid result, with a sensitivity of
97.4 % (95 % CI 86.47–99.57 %) [23]. The positive find-ings of many of these studies will lead to increasing calls
for implementation; as technologies come online, testing
regulation and policies will need to be adapted.At present, self-testing and self-tests mean different
things in different countries. Implementation approaches to
HIVST and existing policies are diverse. Access to RDTsvaries, with some countries having no policies or legal/
regulatory uncertainty on how policies apply to HIVST, to
others with open access to consumers in the private sector,
such as the USA (see Table 2) [14]. Increasingly, self-testing is also occurring through the private sector in
resource-limited countries, where professional-use RDTs
are varyingly packaged and sold directly to consumers[24]. This corresponds with high-utilization of private-
sector HIV services for HIV testing and treatment [25, 26].
However, these services are often unregulated and notcovered within national HIV policies, and the ability of
governments to ensure appropriate, quality RDTs is lim-
ited. Despite or because of this absence of regulation, RDTdistribution continues through pharmacies, Internet sales,
groceries and other businesses [24, 27–29]. With this cross-
section of studies, pilot programs and reports of informalself-testing, HIVST implementation, interest and access
appear to be expanding. As countries explore the benefits
and risks of these multiple approaches to HIVST, dueconsideration should be given to the availability of quality
RDTs and HIVST kits that meet international and national
standards for testing in the intended populations in con-junction with any proposals of HIVST policy.
Regulatory and Policy Issues with HIVST: BalancingRisks and Benefits
HIV self-testing was recently defined by WHO as a process
in which individuals being tested conduct the testing pro-
cess, collect the specimen, run the test, and read andinterpret the result [14, 15]. And for medical devices
generally, WHO has articulated seven principles for
effective regulation [30], all equally relevant for HIV self-testing devices, including: protection of public heath and
safety; assurance to access to valuable new technologies;science-based regulatory decision-making; effective rule of
Table 1 Definitions: regulatory authority and health policy
Regulatory authority is a government body or other entity thatexercises a legal right to control the use or sale of medicaldevices within its jurisdiction, and that may take enforcementaction to ensure that medical products marketed within itsjurisdiction comply with legal requirements [7, 49]
Regulatory capacity may be considered a given country’s ability tocontrol the quality, safety and efficacy of medicines and medicaldevices circulating on their markets or passing through theirterritories [50]
Health policy refers to decisions, plans, and actions that areundertaken to achieve specific health care goals within a society.An explicit health policy can achieve several things: it defines avision for the future which in turn helps to establish targets andpoints of reference for the short and medium term. It outlinespriorities and the expected roles of different groups; and it buildsconsensus and informs people [51]
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
321

law; government prescribed rules; assurance of device
safety; and communication of information on risks.
Country contexts, including its prevalence, will influencegovernments’ determinations about enacting effective
regulation of HIVST devices. Australia and the US provide
two contrasting regulatory examples. In Australia, acountry with a sophisticated regulatory environment, HIV
self-testing is not currently legally supported as any HIV
testing requires ‘‘appropriate level of interaction (with) asuitably qualified health professional’’ [31]. By contrast, an
HIVST kit was made available in the United States in 2012
with the U.S. Food and Drug Administration (FDA)’sapproval of the OraQuick" In-Home HIV Test [32, 33].
This was the first complete, over-the-counter diagnostic
test system for an infectious disease approved in the USAfor consumer-use [34, 35]. A key aspect of the approval
process was a risk–benefit model, finding that 4,000 newinfections could be averted and 44,000 people would learn
their HIV status in the first year of introduction [32, 33]. A
similar approach was implemented in 2014 in the UnitedKingdom and is planned for France [36, 37].
The FDA approval has generated interest globally in
making similar devices available in resource-limited set-tings. However, this approval was based on a test specifi-
cally designed for consumer-use in a U.S. market, with its
design and performance validation based on U.S. popula-tion studies. Thus, the safety and effectiveness of this RDT
in populations outside the US needs to be determined, and
risk–benefit profiles would likely differ in resource-limitedsettings and those with higher HIV prevalence rates.
Moreover, regulatory systems for diagnostics in many
African countries tend to be weak and not every country hasa regulatory body overseeing medical devices [38–41]. A
2002 WHO survey found that 42 out of 86 resource-limited
countries surveyed reported having medical device regula-tions, and 11 out of 15 African countries had no regulatory
structure for diagnostic devices [42]. Still, millions of rapid
HIV tests are conducted through the public health sectorannually within existing national policy frameworks, often
supported by quality mechanisms such as WHO diagnostic
pre-qualification and Ministry of Health validation of testkits [2, 4]. For countries considering the approach, HIVST
will benefit from clear regulations and policies that ensure
appropriate test kits are brought to market and quality willbe ensured. And although HIVST regulatory efforts and
policies in most resource-constrained countries are nascent,
country activities around HIVST is evident:
• In Kenya, responding to demand and informal use of
HIV RDTs for self-testing among healthcare workersand increasing availability of oral fluid RDTs, the 2008
National HTC guidelines incorporated a policy specific
to HIV self-testing [43]. Criteria for approval of RDTsfor self-testing include: (1) evaluation and approval of
the test in Kenya; (2) storage and quality control
standards; (3) pharmacist training and approval todispense, counsel, and demonstrate use to clients; and
(4) making accessible follow-up and referral services,
including services for confirming positive test results.Despite inclusion of HIVST in policy for the general
Table 2 Selected country policies on HIV self-testing
Country HIV self-testing policy,guidance or law
Access restrictions
Australia [52] Currently not legal Explicitly restricted useto only healthprofessionals
Botswana Currently not legal—stated in Sept 2013policy
Public Health Bill 2013restricts use to healthprofessionals
Kenya [43] Legal since 2008;included in NationalHTC Policy
Nationally approvedtests only; vendortraining and instructionare required
Hong Kong[53]
Currently legal Only the US FDAapproved kit isapproved; thegovernment providesinformation on self-testing and informationon a general freehotline
Namibia [24,28]
No specific guidelines,laws or policies,although RDTs areregulated as medicaldevices. Private sectorappears unregulated
Private sector appearsunregulated
France [37] Legal to purchaseapproved HIV self-testkits planned in 2014
National regulatoryapproval of self-testkits;
UnitedKingdom[36]
Legal to purchaseapproved HIV self-testkits
National regulatoryapproval of self-testkits; not availableHIVST kits in themarket
United States[32, 35]
Legal to purchaseapproved HIV self-testkits since July 2012
National regulatoryapproval of self-testkits; Currentlyapproved kit is for age17 and over
South Africa[27]
Currently legal forHIVST kits to beaccessed through somestores and the internetbut not in pharmacies
No clear regulatorypolicies on the qualityof available HIVSTkits
Multilateral—WHO [21,54]
Currently no normativeguidelines and noRDTs intended forself-testing have beenpre-qualified
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
322

population, implementation in the pubic sector has been
limited.
• In South Africa, national policies permit HIV RDTs tobe sold over the internet and in some stores, but not in
pharmacies, and effective regulation of RDTs is
difficult [27]. Concerns exist regarding informal HIV-ST and questions around the accuracy, interpretability,
usability, and quality of available HIV RDTs designed
for professionals but sold to consumers for HIV self-testing. Such limitations have solicited response and
advocacy from the South African HIV Clinician’s
Society, which in 2012 requested that policy limitingthe sale of HIV RDTs over-the-counter be amended
[44]. South Africa is currently reviewing their existing
policies and may develop additional policies andregulations to support sale in pharmacies.
• In Namibia, there is evidence of demand and sale of
clinical-use HIV RDTs in private sector pharmacies atlow levels relative to overall numbers tested, neverthe-
less, sales volumes may be expanding; two distributors
reported increased RDT volumes sold between 2011and 2012 (45 and 72 % increases, respectively) [5].
While HIV self-testing is not addressed in the National
HIV Strategic Framework, there are legal frameworksthat regulate diagnostic devices. However, these are not
currently applied to the private sector. Currently the
Government of Namibia is working to develop specificpolicies addressing HIVST.
Future Directions: HIV Rapid Diagnostics and Self-Testing
The WHO has emphasized that ‘‘the use of rapid tests for
HIVST requires a regulatory framework that ensures
quality diagnostics that give accurate results in the hands ofthe intended user(s)’’ and that while HIVST shows much
promise, regulations and policies still require adaptation [5,
14]. Regulatory processes will need updating for newtechnologies and expansions of intended-use. Strengthen-
ing regulatory infrastructures and assisting with policy
development and decision-making related to the evalua-tion, sale or introduction of HIV rapid diagnostic tests
intended for use by consumers should be a priority [42].The US FDA provides one example for regulation of
self-testing technology, where diagnostics are legally reg-
ulated in both public and private sectors. While the medicaldevice regulatory infrastructures of many resource-limited
countries remains weak, effective regulatory frameworks
may yet be established to guide policy development relatedto the use HIV RDTs for self-testing and contribute to an
environment where appropriate testing platforms intended
for consumer use are made available [42]. Given the high
acceptability, increasing global interest, and potential
public health benefit in expanding HIVST, there are spe-cific regulatory and policy domains that should be
addressed globally and at the country level:
Regulatory Oversight
To support the quality of HIVST and associated RDTscountries should, based on WHO frameworks, consider
supporting the following elements [45]:
• Ensure that all importation, exportation, wholesale and
distribution establishments for RDTs are licensed
• Before HIVST RDTs are marketed or programmed,consider and assess their quality, safety and efficacy for
their intended-use
• Monitor the quality and safety of diagnostics on themarket to prevent harmful, substandard and counterfeit
devices from reaching the public• Monitor advertising and promotion of these devices,
and provide independent information on their rational
use to the public and professionals• Post-marketing surveillance to monitor the ongoing
quality of tests sold, and laws that prevent low quality
tests from entering the market• Develop policies and systems for corrective action
For countries with limited capacity to control the qual-
ity, safety and efficacy of HIVST, assessments of themedical device regulatory systems may identify gaps and
needed frameworks to regulate the use and sale of HIVST
in the public and private sectors. Countries should worktowards consistent implementation of essential regulatory
functions, based on the key provisions of the existing legal
frameworks, addressing regulatory system strengtheningneeded to support HIVST. Efforts at strengthening man-
agement structures, technical regulatory expertise and
physical resources may be needed, in addition to moni-toring mechanisms of OTC sale of test kits. There is also a
role for regional regulatory-strengthening initiatives that
support regulation of diagnostics, and international anddonor quality assurance processes that inform procurement
decisions in evaluating self-testing RDTs [46–48].
Diagnostic Technology Assessment and Policy
Development
National disease control programs should assess RDTs for
self-testing as intended for implementation (e.g. throughsupervised self-testing, or open access) and consider their
strategic placement to maximize the health-impacts and
minimize risks. HIVST policy development will depend onconsiderations that include effectiveness, and since HIV
self-test kits may have different performance characteristics
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
323
in different populations, validation of RDTs may be needed
for diverse groups of ‘‘intended users’’ within countries,regions and even settings, and both public and private
sectors should be considered. Risk–benefit modeling may
be an important component of an evaluation, informingwhat test performance is acceptable. Policies should clarify
where and by whom an HIV test can be performed or
interpreted, requirements for face-to-face counseling, andhow HIVST relates to national algorithms. Developing
national models to estimate these parameters are importantpriorities. Additionally, considerations will include deter-
mining whether the HIV self-tests are made formally
available through the private sector or restricted to HIVprograms with integrated counselling and self-test training/
instruction.
Implementation
Building on a national policy/regulatory framework devel-oped establishing HIVST, implementation will involve the
development of training modules for the public and private
sectors, establishment of quality assurance systems, moni-toring and evaluation (including of adverse outcomes), and
support for linkage to additional testing, care and treatment.
Additional implementation issues include:
• Building an evidence-base on optimal operational
approaches and use to include feasibility studies andimpact evaluations to inform approaches that maximize
benefit and minimize harm [55]
• Increased numbers of preliminary reactive self-testresults may increase demand for HTC and care/
treatment; health systems must accommodate increased
utilization• Ethical issues that accompany HIV self-testing require
attention, including coercive testing
• The role of public/private partnerships in sustainableapproaches to HIV programs should be clarified
• Opportunity to leverage expertise and experience of
other countries in the region on these and related issues• Potential replacement of HTC with HIVST could lead
to increased prevalence in certain populations and
settings, from false-negative results [56]
Industry Engagement
Efforts are needed to engage the HIV diagnostics industry
and other stakeholders to establish optimal target productprofiles and minimum performance characteristics for
RDTs intended for self-testing use in resource-limited
countries. Harmonizing ‘‘minimum standards’’ of self-testdevices for diverse populations will be critical, as well as
engaging with manufacturers in optimizing HIV self-test
kit design to meet these minimum performance standards
for intended populations.
Conclusion
HIVST offers the opportunity to expand HIV testing,
allowing individuals to test themselves and providingpreliminary knowledge of HIV sero-status. HIV RDTs are
considered ‘‘high-risk’’ diagnostic devices and resultsobtained by intended users can have significant implica-
tions for an individual’s health and HIV transmission.
Broadly, it’s recognized that increased access to testing cancontribute to attaining public health goals, and HIV self-
testing is an innovative strategy to expanding access. Pilot
studies globally have documented high HIVST accept-ability. Additionally, there is demonstrated demand for
access to RDTs for self-testing in the private sector. If
HIVST is to expand, regulatory frameworks supportingappropriate HIVST devices and self-testing implementa-
tion policies are both needed, and equally important.
Device regulation and clear policies should precedeimplementation. As countries consider the risks, benefits,
feasibility and acceptability of introducing HIVST, ensur-
ing appropriate, safe, and effective diagnostics that meetdefined standards in the hands of intended users should
ensure maximal benefit and minimal risk to public and
individual health. For self-testing devices, the regulatoryprocesses needed to achieve these aims may leverage
existing systems regulating devices and/or require further
systems, development, and investment. Policies guidingHIVST implementation should be harmonized with diag-
nostic device regulation. Evidence and experience around
non-HIV home diagnostics that have proven effective(while for conditions and diseases more benign than HIV)
may help inform approaches to policies, regulation,
research and evaluation. Short-term strategies that includebroad stakeholder engagement to ensure appropriate and
quality tests, and quality assurance processes that support
HIVST should be complemented with country readinessassessments around the conditions of their possible intro-
duction. Longer-term strategies for strengthening country
regulatory capacity for HIV diagnostics, including self-testRDTs continue to be needed. While questions remain
regarding the programmatic implementation of HIV self-
testing and its impacts, the approach has a great potential—with safeguards in place—to significantly increase access
to HIV testing, and support global goals around
HIV treatment, care and prevention.
Acknowledgments We thank Brad Corner (USAID, Namibia), El-isabeth Ludeman (USAID, Washington DC, Office of Health Sys-tems) and Cheryl Dietrich (USAID, Washington DC, Office of HIV/AIDS) for their reviews and contributions to this article.
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
324

References
1. U.S. Department of State. PEPFAR blueprint: creating and AIDS-free generation. Washington DC, 2012.
2. WHO. Service delivery approaches to HIV testing and counseling(HTC): a strategic HTC programme framework. Geneva, 2012.
3. WHO. Handbook for improving HIV testing and counselingservices. Geneva. 2011.
4. WHO. Global update on HIV treatment 2013: results, impact andopportunities. Geneva, 2013.
5. WHO. Supplement to the 2013 consolidated guidelines on the useof antiretroviral drugs for treating and preventing HIV infection:recommendations for a public health approach. 2014.
6. Ibitoye M, Frasca T, Giguere R, Carballo-Dieguez A. Hometesting past, present and future: lessons learned and implicationsfor HIV home tests. AIDS Behav. 2014;18(5):933–49.
7. Global Harmonization Task Force. Principles of in vitro diag-nostic (IVD) medical devices classification. Available fromhttp://www.imdrf.org/docs/ghtf/archived/sg1/technical-docs/ghtf-sg1-n045r12-invitro-diagnostic-classification-070209.pdf (2007).Accessed 18 April 2014.
8. Pant Pai N, Sharma J, Shivkumar S, et al. Supervised andunsupervised self-testing for HIV in high- and low-risk popula-tions: a systematic review. PLoS Med. 2013;10(4):e1001414.
9. Napierala-Mavedzenge S, Baggeley R, Lo R, Corbett EL. HIVself-testing among health workers: a review of the literature anddiscussion of current practices, issues and options for increasingaccess to HIV testing in sub-Saharan Africa, 2011.
10. Krause K, Subklew-Sehume F, Kenyon C, Colebunders R.Acceptability of HIV self-testing: a systematic literature review.BMC Public Health. 2013;13:735.
11. Choko A, Desmond N, Webb EL, Chavula K, Napierala-Mav-edzenge S, Gaydos CA, Makombe SD, Chunda T, Squire SB,French N, Mwapasa V, Corbett EL. The uptake and accuracy oforal kits for HIV self-testing in high HIV prevalence setting: across-sectional feasibility study in Blantyre, Malawi. PLoS Med.2011;8(10):e1001102.
12. Kalibala S, Tun W, Muraah W, et al. ‘Knowing myself first’:feasibility of self-testing among health workers in Kenya. Nai-robi: Population Council; 2011.
13. el Fuente L, Rosales-Statkus ME, Hoyos J, et al. Are participants ina street-based HIV testing program able to perform their own rapidtest and interpret the results? PLoS ONE. 2012;7(10):e46555.
14. WHO. Report on the first international symposium on self-testingfor HIV: the legal, ethical, gender, human rights and public healthimplications of self-testing scale-up. Geneva, 2013. http://who.int/hiv/pub/vct/self_test/en/index.html.
15. WHO. 2014. Draft Technical update: self-testing for HIV(forthcoming).
16. MacPherson P, Lalloo D, Choko A, van Oosterhaut J, Thindwa D,Webb E, Squire B, Makombe S, Hayes R, Corbett E. Homeassessment and initiation of ART following HIV self-testing: acluster randomised trial to improve linkage to ART in Blantyre,Malawi. 20th Conference of Retroviruses and OpportunisticInfections (CROI). Oral LB95. 2013 Mar 3–6. Atlanta, Georgia.
17. Corbett E. Accuracy of self-testing and linkage to care andtreatment. Presented at: first international symposium on self-testing for HIV, 8–9 April 2013, Brocher Foundation, Geneva,Switzerland.
18. Kumwenda M. Partnership dynamics and care-seeking trajecto-ries among couples after HIV self-testing in Blantyre. Presentedat: first international symposium on self-testing for HIV, 8–9April 2013, Brocher Foundation, Geneva, Switzerland.
19. Carballo-Dieguez A, Frasca T, Balan I, Ibitoye M, Dolezal C.Use of a rapid HIV home test prevents HIV exposure in a high
risk sample of men who have sex with men. AIDS Behav.2012;16(7):1753–60.
20. Bavinton BR, Brown G, Hurley M, Bradley J, Keen P, ConwayDP, Guy R, Grulich AE, Prestage G. Which gay men wouldincrease their frequency of HIV testing with home self-testing?AIDS Behav. 2013;17(6):2084–92.
21. Greacen T, Friboulet D, Blachier A, Fugon L, Hefez S, LorenteN, Spire B. Internet-using men who have sex with men would beinterested in accessing authorised HIV self-tests available forpurchase online. AIDS Care. 2013;25(1):49–54.
22. Pant Pai N, Behlim T, Abrahams L, Vadnais C, Shivkumar S,et al. Will an unsupervised self-testing strategy for HIV work inhealth care workers of South Africa? a cross sectional pilot fea-sibility study. PLoS ONE. 2013;8(11):e79772.
23. Dong M, Regina R, Hlongwane S, Ghebremichael M, Wilson D,Dong K. Can laypersons in high-prevalence South Africa perform anHIV self-test accurately? 20th International AIDS Conference, 2014July 20–25, Melbourne, Australia. Abstract No. A-641-0087-10374.
24. Nersesian P, Hulsmann M, Cloutier S, and Chintalova-Dallas R.Assessment of over-the-Counter HIV rapid test kits in Namibia.Arlington, VA. USAID AIDS Support and Technical AssistanceResources, AIDSTAR-One, Task Order 1. 2013. Available from:http://www.aidstar-one.com/sites/default/files/AIDSTAR-One_Report_Namibia_OTC_Rapid_Test_Kits.pdf.
25. Strengthening Health Outcomes through the Private Sector. HIVtesting by private health providers: evidence from 18 countries.Washington DC. Available from: http://www.shopsproject.org/resource-center/hiv-testing-by-private-health-providers-evidence-from-18-countries (2012). Accessed 4 Nov 2013.
26. Sargent J, Johnson, J, Majorowski, M, Friedman, N, and Blazer, C.Private sector involvement in HIV service provision. Arlington,VA: USAID AIDS Support and Technical Assistance Resources,AIDSTAR-One Project, Task Order 1. Available from: http://www.aidstar-one.com/sites/default/files/AIDSTAR-One_Private_Sector_Tech_Brief_rev.pdf (2009). Accessed 4 Nov 2013.
27. Richter M, Venter FD, Gray A. Home self-testing for HIV: AIDSexceptionalism gone wrong. South African Medical Journal.2010;100(10).
28. Muraranganda E. Govt probes HIV self-test kits. Namibian Sun.Available from: http://www.namibiansun.com/health/govt-probes-hiv-self-test-kits.54388 (2013). Accessed 26 June 2013.
29. Anonymous. Home-testing kits for HIV now available amidconcern. The Star. Available from: http://www.hst.org.za/news/home-testing-kits-hiv-now-available-amid-concern (2000).Accessed 4 Nov 2013.
30. WHO, Pan-American Health Organization. A model regulatoryprogram for medical devices: an international guide. Geneva,2001. Available from: http://www1.paho.org/English/HSP/HSE/medical_devices.pdf. Accessed Nov 4, 2013.
31. Australasian Society for HIV Medicine. 2012 National HIVtesting policy v1.2. Surry Hills, Australia. 2012. http://testingportal.ashm.org.au/hiv/home-based-testing-in-australia.
32. United States Food and Drug Administration. OraQuick" In-home hiv test summary of safety and effectiveness. WashingtonDC. 2012. Available from: http://www.fda.gov/downloads/BiologicsBloodVaccines/BloodBloodProducts/ApprovedProducts/PremarketApprovalsPMAs/UCM312534.pdf. Accessed Nov 4, 2013.
33. Oraquick Technologies. Final advisory committee briefingmaterials: OraQuick" In-Home HIV test. Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/BloodVaccinesandOtherBiologics/BloodProductsAdvisoryCommittee/UCM303652.pdf (2012). Accessed 4 Nov2013.
34. CDC. HIV surveillance—United States, 1981–2008. Morb Mor-tal Weekly Rep. 2011;60(21):689–693.
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
325

35. US FDA. First rapid home-use HIV kit approved for self-testing.Available from: http://www.fda.gov/forconsumers/consumerupdates/ucm310545.htm (2013). Accessed 4 Nov 2013.
36. Department of Public Health. Modernisation of HIV rules tobetter protect public. London. Available from: https://www.gov.uk/government/news/modernisation-of-hiv-rules-to-better-protect-public (2013). Accessed 4 Nov 2013.
37. NY Daily News. France OKs home tests for HIV. Availablefrom: http://www.nydailynews.com/life-style/health/france-oks-home-tests-hiv-article-1.1510008 (2013). Accessed 31 Jan 2014.
38. WHO. Medical device regulation—global overview and guidingprinciples. Geneva, 2003.
39. Peeling R. Update on regulatory harmonization of in vitro diag-nostics in Africa. Presented at: Global HIV Diagnostics WorkingGroup Meeting. Sep 2013, Geneva, Switzerland.
40. Preston C, Valdez ML, Bond K. Strengthening medical productregulation in low and middle income countries. PloS Med.2012;9(10):e1001327.
41. WHO. National regulatory agency for medical devices (map).Available from: http://gamapserver.who.int/mapLibrary/Files/Maps/Global_DIM_Indicator3_20110211.PNG (2011). Accessed4 Nov 2013.
42. WHO. Increasing access to diagnostics through technologytransfer and local production. Geneva, 2011.
43. National AIDS and STD Control Programme. National guidelinesfor HIV testing and counseling in Kenya. Nairobi. Availablefrom: http://www.ilo.org/wcmsp5/groups/public/—ed_protect/—protrav/—ilo_aids/documents/legaldocument/wcms_127533.pdf(2008). Accessed 31 Oct 2013.
44. South African HIV Clinicians Society, Treatment Action Cam-paign. Joint statement on HIV testing and counselling, Johan-nesburg. Available from: http://www.sahivsoc.org/newsroom/society-news (2012). Accessed 31 Oct 2013.
45. WHO. Effective medicines regulation: ensuring safety, efficacyand quality. Policy Perspectives on Medicines No. 7. Availablefrom: http://whqlibdoc.who.int/hq/2003/WHO_EDM_2003.2.pdf(2003). Accessed 4 Nov 2013.
46. Pan African Harmonization Working Party on Medical Devicesand Diagnostics. Available from: http://pahwp.org/index.html(2014). Accessed 18 April 2018.
47. WHO. WHO Prequalification of Diagnostics Programme.Available from: http://www.who.int/diagnostics_laboratory/evaluations/en/ (2014). Accessed 18 April 2014
48. USAID. HIV rapid test kits approval and technical guidance.Available from: http://www.usaid.gov/sites/default/files/documents/1864/GuidanceHIVRTKs.pdf (2013). Accessed 18 April2014.
49. Study Group 1, Global Harmonization Task Force. Principles ofconformity assessment for medical devices. Available from:http://www.imdrf.org/docs/ghtf/final/sg1/technical-docs/ghtf-sg1-n78-2012-conformity-assessment-medical-devices-121102.pdf(2012). Accessed 31 Jan 2014.
50. WHO. Assessment of medicines regulatory systems in sub-Sah-aran African countries. Available from: http://www.who.int/healthsystems/Assessment26African_countries.pdf (2010). Accessed14 April 2014.
51. WHO. Health Policy. Available from: http://www.who.int/topics/health_policy/en/ (2013). Accessed 14 April 2014.
52. Australian Government Department of Health and Aging.National HIV testing policy: home based testing in Australia.Available from: http://testingportal.ashm.org.au/hiv/home-based-testing-in-australia (2012). Accessed 18 April 2014.
53. Hong Kong Department of Health. Knowing about HIV AntibodyTest. Available from: http://www.info.gov.hk/aids/english/hotline/testing_question.htm#d2 (2013). Accessed 31 Jan 2014.
54. WHO, UNAIDS, UNICEF. Global HIV response epidemic:update and health sector progress towards Universal Access,Progress Report. Geneva, 2011.
55. Napierala-Mavedzenge S, Baggaley R, Corbett EL. A review ofself-testing for HIV: research and policy priorities in a new era ofHIV prevention. Clin Infect Dis. 2013;57(1):126–38.
56. Katz D, Cassels S, Stekler J. Replacing clinic-based tests withhome-use tests may increase HIV prevalence among Seattle menwho have sex with men: evidence from a mathematical model.Sex Transm Dis. 2014;41(1):2–9.
AIDS Behav (2014) 18:S415–S421
123
Author's personal copy
326

Towards Universal Voluntary HIV Testing andCounselling: A Systematic Review and Meta-Analysis ofCommunity-Based ApproachesAmitabh B. Suthar1*, Nathan Ford1, Pamela J. Bachanas2, Vincent J. Wong3, Jay S. Rajan4,
Alex K. Saltzman5, Olawale Ajose6, Ade O. Fakoya7, Reuben M. Granich8, Eyerusalem K. Negussie1,
Rachel C. Baggaley1
1 Department of HIV/AIDS, World Health Organization, Geneva, Switzerland, 2 Global AIDS Program, Centers for Disease Control and Prevention, Atlanta, Georgia, United
States of America, 3 Office of HIV/AIDS, United States Agency for International Development, Washington, District of Columbia, United States of America, 4 School of
Medicine, University of California at San Francisco, San Francisco, California, United States of America, 5 School of Medicine, Cornell University, New York, New York, United
States of America, 6 Clinton Health Access Initiative, Boston, Massachusetts, United States of America, 7 The Global Fund to Fight AIDS, Tuberculosis and Malaria, Geneva,
Switzerland, 8 Joint United Nations Programme on HIV/AIDS, Geneva, Switzerland
Abstract
Background: Effective national and global HIV responses require a significant expansion of HIV testing and counselling(HTC) to expand access to prevention and care. Facility-based HTC, while essential, is unlikely to meet national and globaltargets on its own. This article systematically reviews the evidence for community-based HTC.
Methods and Findings: PubMed was searched on 4 March 2013, clinical trial registries were searched on 3 September 2012,and Embase and the World Health Organization Global Index Medicus were searched on 10 April 2012 for studies includingcommunity-based HTC (i.e., HTC outside of health facilities). Randomised controlled trials, and observational studies wereeligible if they included a community-based testing approach and reported one or more of the following outcomes: uptake,proportion receiving their first HIV test, CD4 value at diagnosis, linkage to care, HIV positivity rate, HTC coverage, HIVincidence, or cost per person tested (outcomes are defined fully in the text). The following community-based HTCapproaches were reviewed: (1) door-to-door testing (systematically offering HTC to homes in a catchment area), (2) mobiletesting for the general population (offering HTC via a mobile HTC service), (3) index testing (offering HTC to householdmembers of people with HIV and persons who may have been exposed to HIV), (4) mobile testing for men who have sexwith men, (5) mobile testing for people who inject drugs, (6) mobile testing for female sex workers, (7) mobile testing foradolescents, (8) self-testing, (9) workplace HTC, (10) church-based HTC, and (11) school-based HTC. The Newcastle-OttawaQuality Assessment Scale and the Cochrane Collaboration’s ‘‘risk of bias’’ tool were used to assess the risk of bias in studieswith a comparator arm included in pooled estimates.
117 studies, including 864,651 participants completing HTC, met the inclusion criteria. The percentage of people offeredcommunity-based HTC who accepted HTC was as follows: index testing, 88% of 12,052 participants; self-testing, 87% of1,839 participants; mobile testing, 87% of 79,475 participants; door-to-door testing, 80% of 555,267 participants; workplacetesting, 67% of 62,406 participants; and school-based testing, 62% of 2,593 participants. Mobile HTC uptake among keypopulations (men who have sex with men, people who inject drugs, female sex workers, and adolescents) ranged from 9%to 100% (among 41,110 participants across studies), with heterogeneity related to how testing was offered. Community-based approaches increased HTC uptake (relative risk [RR] 10.65, 95% confidence interval [CI] 6.27–18.08), the proportion offirst-time testers (RR 1.23, 95% CI 1.06–1.42), and the proportion of participants with CD4 counts above 350 cells/ml (RR 1.42,95% CI 1.16–1.74), and obtained a lower positivity rate (RR 0.59, 95% CI 0.37–0.96), relative to facility-based approaches. 80%(95% CI 75%–85%) of 5,832 community-based HTC participants obtained a CD4 measurement following HIV diagnosis, and73% (95% CI 61%–85%) of 527 community-based HTC participants initiated antiretroviral therapy following a CD4measurement indicating eligibility. The data on linking participants without HIV to prevention services were limited. In low-and middle-income countries, the cost per person tested ranged from US$2–US$126. At the population level, community-based HTC increased HTC coverage (RR 7.07, 95% CI 3.52–14.22) and reduced HIV incidence (RR 0.86, 95% CI 0.73–1.02),although the incidence reduction lacked statistical significance. No studies reported any harm arising as a result of havingbeen tested.
Conclusions: Community-based HTC achieved high rates of HTC uptake, reached people with high CD4 counts, and linkedpeople to care. It also obtained a lower HIV positivity rate relative to facility-based approaches. Further research is needed tofurther improve acceptability of community-based HTC for key populations. HIV programmes should offer community-based HTC linked to prevention and care, in addition to facility-based HTC, to support increased access to HIV prevention,care, and treatment.
Review Registration: International Prospective Register of Systematic Reviews CRD42012002554
Please see later in the article for the Editors’ Summary.
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
327

Citation: Suthar AB, Ford N, Bachanas PJ, Wong VJ, Rajan JS, et al. (2013) Towards Universal Voluntary HIV Testing and Counselling: A Systematic Review andMeta-Analysis of Community-Based Approaches. PLoS Med 10(8): e1001496. doi:10.1371/journal.pmed.1001496
Academic Editor: Stephanie L. Sansom, Centers for Disease Control and Prevention, United States of America
Received December 5, 2012; Accepted June 27, 2013; Published August 13, 2013
Copyright: ! 2013 Suthar et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: The authors were personally salaried by their institutions during the period of writing. No specific funding was received for this study. No fundingbodies had any role in the study design, data collection, data analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist. The opinions and statements in this article are those of the authors and donot necessarily represent the official policy, endorsement, or views of their organisations.
Abbreviations: ART, antiretroviral therapy: CI, confidence interval; FSW, female sex workers; HTC, HIV testing and counselling; MSM, men who have sex withmen; PWID, people who inject drugs; RR, relative risk; WHO, World Health Organization
* E-mail: [email protected]
Introduction
HIV is a leading cause of morbidity and mortality globally [1].Despite considerable progress in controlling the epidemic, therewere approximately 2.2 million new HIV infections, 1.7 millionHIV-related deaths, and 34.2 million people with HIVworldwide in 2011; 1.5 million of these new HIV infections,1.2 million of the HIV deaths, and 23.5 million of the peopleliving with HIV were in Africa [2]. Given the urgency to act onthe epidemic, all United Nations member states agreed toachieve the following HIV targets by 2015: (1) reduce sexual andparenteral HIV transmission by 50%, (2) eliminate vertical HIVtransmission, (3) reduce tuberculosis deaths among people withHIV by 50%, and (4) deliver antiretroviral therapy (ART) to 15million people [3]. Achieving these targets will require people atrisk of HIV to learn their status and link to prevention and careservices.
In an effort to expand access to prevention and care services,World Health Organization (WHO) guidelines recommendprovider-initiated HIV testing and counselling (HTC) for allpeople seen in all health facilities in generalised epidemics (i.e.,antenatal HIV prevalence $1%) and in specific facilities inconcentrated epidemics [4]. While provider-initiated HTC pro-grammes have been successful in identifying previously undiag-nosed individuals in generalised epidemics, they may not reach allpeople at risk of HIV acquisition [5,6]. Indeed, the latestDemographic and Health Surveys from 29 sub-Saharan Africancountries, representing approximately half of the global burden ofHIV, indicate that only 15% of adults received results from anHIV test in the previous year [7]. This low coverage is recognisedas a critical barrier to scaling up HIV prevention and careinterventions. Furthermore, people living with HIV are oftendiagnosed late in the course of their disease, resulting in avoidablemorbidity, mortality, and transmission of the virus. [8].
The reasons for the current low coverage of HTC are variousand include service, patient, and demographic barriers [9,10].For example, in generalised epidemics women have higher ratesof testing than men and adolescents, perhaps because of theircontact with reproductive and antenatal health services [7].Implementation of provider-initiated HTC guidance remains apriority for countries. However, because many people havelimited contact with healthcare providers, HTC provision inhealth facilities alone is insufficient to achieve national and globaltargets. Although previous research has reviewed home-basedHTC [11,12], the impact of all community-based HTCapproaches has not been systematically reviewed. The objectiveof this study was to systematically review all community-based HTC approaches to inform global and national HIVprogramming.
Methods
Conduct of Systematic ReviewThis systematic review was conducted in accordance with the
PRISMA statement using a pre-defined protocol (InternationalProspective Register of Systematic Reviews identification num-ber: CRD42012002554; Text S1 and Protocol S1) [13,14]. ThePubMed database was searched on 4 March 2013, and Embaseand WHO Global Index Medicus were systematically searchedon 10 April 2012, without language, geographic, publication,date, or any other restrictions. In addition, the WHO Interna-tional Clinical Trials Registry Platform, the Cochrane CentralRegister of Controlled Trials, the International StandardRandomised Controlled Trial Number Register, and Clinical-Trials.gov were systematically searched without language, pub-lication, or date restrictions on 3 September 2012. Experts in thefield were contacted to identify unpublished research andongoing studies, and bibliographies of relevant studies werescreened.
Study DefinitionsCommunity-based HTC was defined as HTC outside of health
facilities. Facility-based HTC approaches were defined as those inhealthcare sites (e.g., health facilities, hospitals, and fixed, stand-alone voluntary counselling and testing sites). Eleven differentcommunity-based HTC approaches were reviewed in this study:(1) door-to-door testing (systematically offering HTC to homes in acatchment area), (2) mobile testing for the general population(offering HTC via a mobile HTC service in areas visited by thegeneral public, such as shopping centres, transport hubs, orroadside restaurants), (3) index testing (offering HTC to householdmembers of people with HIV and persons who may have beenexposed to HIV such as spouses, sexual partners, or children ofpeople with HIV); (4) mobile testing for men who have sex withmen (MSM), (5) mobile testing for people who inject drugs(PWID), (6) mobile testing for female sex workers (FSW), (7)mobile testing for adolescents, (8) self-testing, (9) workplace HTC,(10) church-based HTC, and (11) school-based HTC.
Several outcomes were analysed in this study. Uptake wascalculated by dividing the number of individuals accepting HTCby the number of individuals offered HTC. The proportion offirst-time testers was calculated by dividing the number of peoplereporting receiving their first HIV test by the total number ofpeople tested. The proportion of participants with a CD4 countgreater than 350 cells/ml was calculated among participants withHIV who had their CD4 count measured. Two steps of theretention continuum were assessed: (1) CD4 measurement(among all participants found to have HIV) and (2) initiation ofART (among participants eligible per national guidelines). In
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
328

studies with a comparator arm, the HIV positivity rate wascalculated by dividing the number of individuals found to be HIVpositive by the number of individuals tested. HTC coverage wascalculated by dividing the number of people tested by the totalnumber of people living in the catchment area for thecommunity-based HTC approach. HIV incidence was calculat-ed by dividing the risk of infection in communities with access tocommunity- and facility-based HTC by the risk of infection incommunities with access to only facility-based HTC. Some of theoutcomes were not independent. For example, the number ofpeople tested was the denominator for the HIV positivity rateand first-time testers and also the numerator for HTC coverage.Moreover, the number of people living with HIV was thenumerator for the HIV positivity rate and also the denominatorfor calculating the first step of the retention continuum (CD4measurement). The cost per person tested was approximated bydividing the economic costs incurred during HTC in studies bythe total number of people tested. Costs were adjusted forinflation from the year the costs were estimated to 2012 United
Ta
ble
1.
Sum
mar
yo
fst
ud
yp
arti
cip
ants
and
met
ho
ds.
Te
stin
gM
od
el
Nu
mb
er
of
Stu
die
sT
ota
lN
um
be
rT
est
ed
Me
dia
nY
ea
rS
tud
yC
on
du
cte
d(I
QR
)aN
um
be
ro
fM
ale
s(P
erc
en
t)b
Nu
mb
er
of
Stu
die
sw
ith
aD
em
an
dC
rea
tio
nC
om
po
ne
nt
(Pe
rce
nt)
Nu
mb
er
of
Stu
die
sP
rov
idin
gIn
cen
tiv
es
(Pe
rce
nt)
Nu
mb
er
of
Stu
die
sw
ith
aM
ult
i-D
ise
ase
Co
mp
on
en
t(P
erc
en
t)
Nu
mb
er
of
Stu
die
sL
ink
ing
Pe
op
lew
ith
HIV
toC
are
(Pe
rce
nt)
Ind
ex8
12,4
0020
05(2
004
to20
06)
5,55
6(4
5.3)
0(0
)1
(12.
5)2
(25.
0)5
(62.
5)
Do
or-
to-d
oo
r33
595,
389
2008
(200
4to
2009
)24
7,43
9(4
5.9)
11(3
3.3)
2(6
.1)
8(2
4.2)
19(5
7.6)
Mo
bile
3419
3,60
220
08(2
005
to20
09)
86,9
89(4
4.9)
20(6
0.6)
7(2
0.6)
15(4
4.1)
16(4
7.1)
Key
po
pu
lati
on
s29
41,4
5120
05(2
002
to20
08)
12,8
66(6
1.9)
10(3
4.5)
15(5
1.7)
9(3
1.0)
16(5
5.2)
Self
31,
779
2006
(200
2to
2008
)1,
113
(62.
6)1
(33.
3)2
(66.
7)0
(0.0
)1
(33.
3)
Wo
rkp
lace
617
,352
2004
(200
3to
2009
)9,
817
(67.
0)2
(33.
3)1
(16.
7)4
(66.
7)3
(50.
0)
Sch
oo
l4
2,67
820
09(2
005
to20
09)
957
(42.
2)2
(50.
0)0
(0.0
)2
(50.
0)3
(75.
0)
aTh
em
idp
oin
tw
asu
sed
for
stu
die
sth
atto
ok
pla
ceo
ver
seve
ral
year
s.b
Am
on
gst
ud
ies
that
incl
ud
edg
end
erd
ata.
IQR
,in
terq
uar
tile
ran
ge.
do
i:10.
1371
/jo
urn
al.p
me
d.1
0014
96.t
001
Figure 1. Flow of information through different phases of thereview.doi:10.1371/journal.pmed.1001496.g001
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
329

States dollars using the US Bureau of Labor Statistics’ inflationcalculator [15].
Search Strategy and Selection CriteriaThe search strategies (Table S1) were designed with the
assistance of a librarian to identify studies including community-based HTC. Following recommendations from PRISMA,eligibility criteria were based on key study characteristics:population, intervention, comparator, outcome, and design[13]. Specifically, studies were included when (1) the studypopulation included people in generalised, concentrated, or low-level HIV epidemics; (2) the intervention was community-basedHTC offered in combination with a background of facility-basedHTC; (3) the comparator was facility-based HTC; (4) theoutcome(s) included uptake, proportion of people reportingreceiving their first HIV test, CD4 value at diagnosis, rates oflinkage to care, HIV positivity rate, HTC coverage, HIV
incidence, or cost per person tested; and (5) the study design wasa randomised trial or observational cohort study. Given the lackof comparative studies for community-based HTC, studieswithout a comparator arm were also included if they met theremaining eligibility criteria.
A. B. S., N. F., and O. A. independently screened the abstractsof all articles identified via the literature database searches andthen compared the full texts of all articles selected during screeningagainst the inclusion criteria. Disagreements were resolved bydiscussion. J. S. R. and A. K. S. repeated the same process for theclinical trial registries.
Data ExtractionA. B. S., J. S. R., and A. K. S. completed the data extraction of
characteristics of study participants, community-based testingapproaches, outcomes, and quality assessment using a standard-ised extraction form.
Table 2. Percentage of clients received as couples in community-wide testing efforts.
Study (Testing Approach) Country YearNumber Tested as aCouple
NumberTested
Percent Tested asa Couple
Sweat (facility-based) [23] Thailand 2007 1,472 2,721 54.1%
Sweat (mobile) [23] Thailand 2007 2,574 10,464 24.6%
Tumwesigye (door-to-door) [74] Uganda 2007 35,634 264,966 13.4%
Sweat (facility-based) [23] Zimbabwe 2007 61 610 10.0%
Naik (door-to-door) [70] South Africa 2010 458 5,086 9.1%
Lugada (mobile) [56] Kenya 2008 3,296 47,173 7.0%
Sweat (facility-based) [23] Tanzania 2007 24 685 3.5%
Sweat (mobile) [23] Zimbabwe 2007 223 6,579 3.4%
Sweat (mobile) [23] Tanzania 2007 54 2,832 1.9%
doi:10.1371/journal.pmed.1001496.t002
Figure 2. Pooled uptake of community-based HTC approaches. Bars indicate 95% CIs.doi:10.1371/journal.pmed.1001496.g002
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
330

Quality AssessmentThe Newcastle-Ottawa Quality Assessment Scale was used to
assess bias in studies with a comparator arm included in pooledanalyses [16]. This scale rates studies based on eight criteria inthree sources of bias. We modified this scale to remove onecriterion, demonstration that the outcome of interest was notpresent at the start of study, since a previous HIV test may not
affect all the outcomes analysed in this article. The CochraneCollaboration’s ‘‘risk of bias’’ tool was used to assess bias inrandomised trials with a comparator arm [17].
Statistical AnalysesOutcome proportions from studies meeting inclusion criteria
were stabilised using the Freeman-Tukey-type arcsine square-roottransformation and then pooled to summarise the proportion of
Figure 3. Uptake of index HTC.doi:10.1371/journal.pmed.1001496.g003
Figure 4. Uptake of self-testing.doi:10.1371/journal.pmed.1001496.g004
Figure 5. Uptake of mobile HTC.doi:10.1371/journal.pmed.1001496.g005
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
331
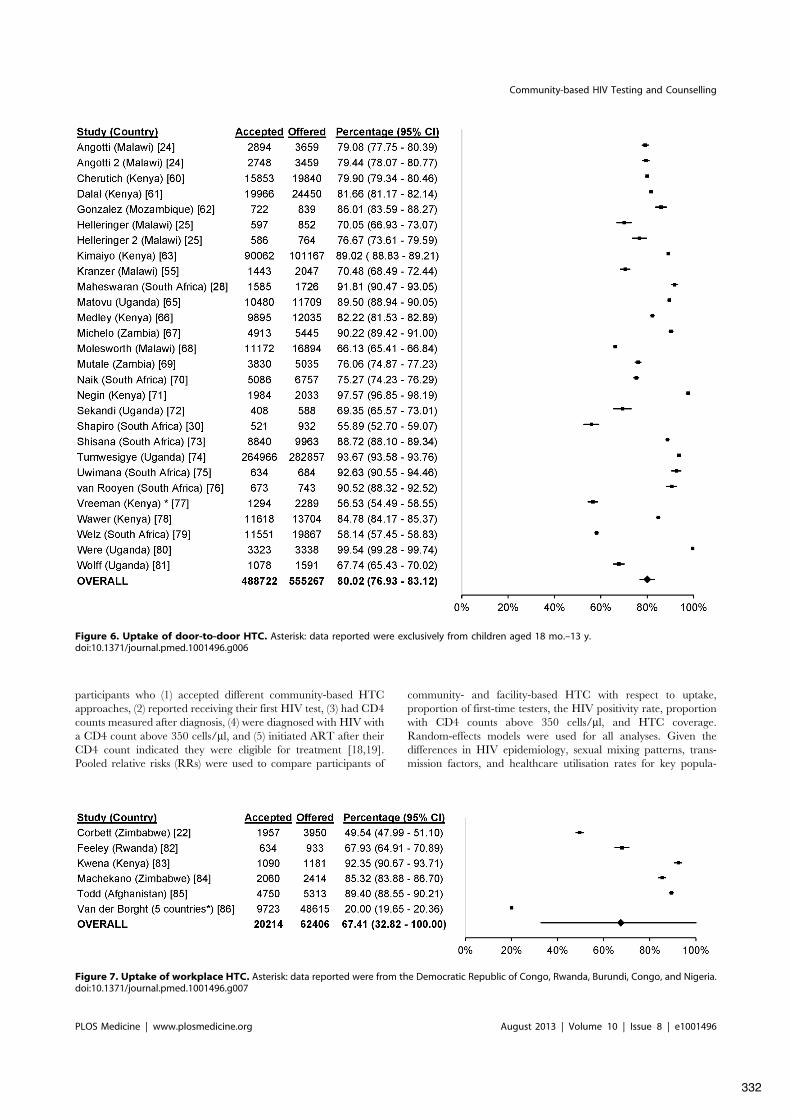
participants who (1) accepted different community-based HTCapproaches, (2) reported receiving their first HIV test, (3) had CD4counts measured after diagnosis, (4) were diagnosed with HIV witha CD4 count above 350 cells/ml, and (5) initiated ART after theirCD4 count indicated they were eligible for treatment [18,19].Pooled relative risks (RRs) were used to compare participants of
community- and facility-based HTC with respect to uptake,proportion of first-time testers, the HIV positivity rate, proportionwith CD4 counts above 350 cells/ml, and HTC coverage.Random-effects models were used for all analyses. Given thedifferences in HIV epidemiology, sexual mixing patterns, trans-mission factors, and healthcare utilisation rates for key popula-
Figure 6. Uptake of door-to-door HTC. Asterisk: data reported were exclusively from children aged 18 mo.–13 y.doi:10.1371/journal.pmed.1001496.g006
Figure 7. Uptake of workplace HTC. Asterisk: data reported were from the Democratic Republic of Congo, Rwanda, Burundi, Congo, and Nigeria.doi:10.1371/journal.pmed.1001496.g007
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
332

tions, key population outcome data were reported individually andnot pooled. I2 statistics were used to measure heterogeneity [20]. I2
statistics near 25% indicate low heterogeneity, values near 50%indicate moderate heterogeneity, and those above 75% indicatehigh heterogeneity [21]. All analyses were completed in STATAversion 12.0.
Results
Search Results108 articles, describing studies conducted from 1987 to 2012
and including 864,651 participants completing HTC, met theeligibility criteria (Table 1; Figure 1). Two articles wererandomised trials [22,23], and the rest were observational indesign. Data from one multi-centre cluster-randomised trial werestratified into three studies (based on the country where the testingwas offered) [23], data from three articles were stratified based onthe year community-based HTC was offered [24–26], and datafrom four articles were stratified based on the community-basedHTC approach used [27–30]. Given that 108 articles provideddata from 108 studies and there were nine additional studies afterstratification, there were a total of 117 studies included (Table S4).76 studies were from Africa, 28 were from North America(excluding Central America), six were from Asia, four were fromCentral and South America, three were from Europe, and one wasfrom Australia. The clinical trial registers identified ten ongoingtrials: one on index testing [31], one on mobile testing [32], five ondoor-to-door testing [33–37], one on self-testing [38], and two oncommunity-based testing for key populations [39,40].
The percentage of participants who were male was 45.3% forindex testing, 45.9% for door-to-door testing, 44.9% for mobiletesting, 62.6% for self-testing, 67.0% for workplace testing, and42.2% for school-based testing (Table 1). Excluding studiesincluding only MSM or only FSW, 62.9% of testers were malein mobile testing for key populations (Table 1). Population-levelHTC efforts found that implementation of community-basedHTC increases the number of couples receiving testing (Table 2).
Uptake61 studies reported uptake of different community-based testing
approaches among 713,632 participants: seven studies evaluatedindex testing among 12,052 participants [29,30,41–46], threeevaluated self-testing among 1,839 participants [47–49], 14evaluated mobile HTC among 79,475 participants [26,28,50–59], 28 evaluated door-to-door testing among 555,267 participants[24,25,28,30,60–81], six evaluated workplace HTC among 62,406participants [22,82–86], and three evaluated school-based HTCamong 2,593 participants [87–89] (Figure 2). The percentage ofparticipants accepting HTC was 88.2% for index testing (95%confidence interval [CI] 80.5%–95.9%; I2 99.7%, 95% CI 99.7%–99.8%; Figure 3), 87.1% for self-testing (95% CI 85.1%–89.0%; I2
28.8%, 95% CI 0%–92.6%; Figure 4), 86.8% for mobile HTC
(95% CI 85.6%–88.1%; I2 99.9%, 95% CI 99.9%–99.9%;Figure 5), 80.0% for door-to-door HTC (95% CI 76.9%–83.1%;I2 99.9%, 95% CI 99.9%–99.9%; Figure 6), 67.4% for workplaceHTC (95% CI 32.8%–100.0%; I2 100%, 100.0%–100.0%;Figure 7), and 62.1% for school-based HTC (95% CI 39.6%–84.5%; I2 99.0%, 95% CI 98.5%–99.4%; Figure 8). Uptake washigher in community-based HTC compared to providing vouchersto participants for facility-based HTC (RR 10.65, 95% CI 6.27–18.08; I2 96.1%; Figure 9) [22,43].
19 studies reported uptake among 41,110 participants in keypopulations, including 16,725 MSM [90–97], 4,681 PWID[92,98–100], 81 FSW [101], 13,240 adolescents [102,103], and6,383 individuals from combinations of key populations. Thepercentage accepting HTC was 99.7% among FSW, ranged from13.7% to 94.5% among PWID, ranged from 9.4% to 95.0%among MSM, and ranged from 33.9% to 96.6% amongadolescents (Figure 10). One study reported an uptake percentageof 95.2% among PWID and FSW [104], another reported anuptake percentage of 75.1% among PWID, FSW, and MSM[105], and another reported an uptake percentage of 60.0%among PWID and MSM [106]. Uptake was higher for commu-nity-based testing than for facility-based testing among FSW (RR1.10, 95% CI 1.03–1.17) [101] and MSM (RR 1.53, 95% CI1.42–1.65) [96] (Figure 11).
First-Time Testers33 studies reported the HTC history among 597,016 partic-
ipants in community-based HTC approaches [23,25,27–29,44,47,51,53–55,58–61,63,64,69,70,72,74,83,107–112]. 62.2%(95% CI 58.0%–66.4%; I2 99.9%, 95% CI 99.9%–99.9%;Figure 12) of participants at community-based HTC sitesreported receiving their first HIV test. In the nine studies witha facility-based comparator arm, a larger proportion of partic-ipants reported receiving their first HIV test at community-basedHTC than at facility-based HTC (RR 1.23, 95% CI 1.06–1.42; I2
99.8%, 95% CI 99.8%–99.9%; Figure 9) [23,27,29,107,108,111].17 studies reported the HTC history of 25,311 participants from
key populations receiving community-based HTC [27,90,92,94,96,98,105,108,113–118]. 9% to 79% of participants reportedreceiving their first HIV test (Figure 13). Five of these studiesincluded a facility-based comparator arm (Figure 11). There weremore first-time testers in community-based HTC than facility-based HTC for two study populations of MSM (RR 2.24, 95% CI1.27–3.93 [113] and RR 1.37, 95% CI 1.18–1.59 [108]); however,there were fewer first-time testers in community-based HTC for adifferent study population of MSM (RR 0.33, 95% CI 0.26–0.43[96]). There were more first-time testers in community-basedHTC than facility-based HTC for a study population includingPWID and MSM (RR 1.10, 95% CI 1.08–1.13 [116]); however,there was no difference in the proportion of first-time testers for astudy population of FSW (RR 0.97, 95% CI 0.72–1.30 [108]).
Figure 8. Uptake of school-based HTC.doi:10.1371/journal.pmed.1001496.g008
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
333
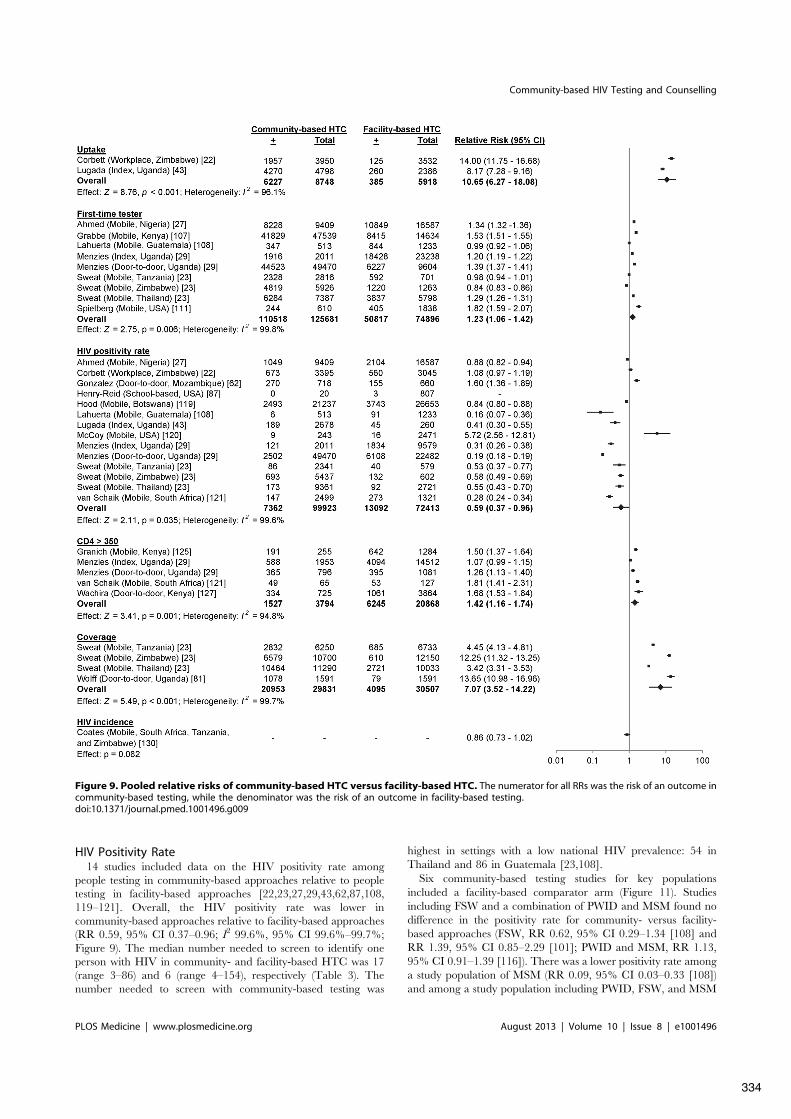
HIV Positivity Rate14 studies included data on the HIV positivity rate among
people testing in community-based approaches relative to peopletesting in facility-based approaches [22,23,27,29,43,62,87,108,119–121]. Overall, the HIV positivity rate was lower incommunity-based approaches relative to facility-based approaches(RR 0.59, 95% CI 0.37–0.96; I2 99.6%, 95% CI 99.6%–99.7%;Figure 9). The median number needed to screen to identify oneperson with HIV in community- and facility-based HTC was 17(range 3–86) and 6 (range 4–154), respectively (Table 3). Thenumber needed to screen with community-based testing was
highest in settings with a low national HIV prevalence: 54 inThailand and 86 in Guatemala [23,108].
Six community-based testing studies for key populationsincluded a facility-based comparator arm (Figure 11). Studiesincluding FSW and a combination of PWID and MSM found nodifference in the positivity rate for community- versus facility-based approaches (FSW, RR 0.62, 95% CI 0.29–1.34 [108] andRR 1.39, 95% CI 0.85–2.29 [101]; PWID and MSM, RR 1.13,95% CI 0.91–1.39 [116]). There was a lower positivity rate amonga study population of MSM (RR 0.09, 95% CI 0.03–0.33 [108])and among a study population including PWID, FSW, and MSM
Figure 9. Pooled relative risks of community-based HTC versus facility-based HTC. The numerator for all RRs was the risk of an outcome incommunity-based testing, while the denominator was the risk of an outcome in facility-based testing.doi:10.1371/journal.pmed.1001496.g009
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
334

(RR 0.51, 95% CI 0.28–0.94 [122]). There was also a higherpositivity rate among a study population of MSM (RR 2.37, 95%CI 1.35–4.15 [123]). The number needed to screen to identify oneperson with HIV varied depending on the key population andstudy setting (Table 4).
CD4 Counts18 studies reported the CD4 counts of 8,993 participants found
to be HIV-positive using point-of-care or standard lab diagnostics[29,30,51,55,56,60,61,74,76,82,110,121,124–127]. 56.7% (95%CI 49.6%–63.9%; I2 97.6%, 95% CI 97.0%–98.1%; Figure 14)of participants testing positive had CD4 counts above 350 cells/ml.In the five studies with a facility-based HTC comparator arm,more participants in community-based HTC approaches hadCD4 counts above 350 cells/ml than in facility-based approaches
(RR 1.42, 95% CI 1.16–1.74; I2 94.8%, 95% CI 90.5%–97.1%;Figure 9) [29,121,125,127].
Two studies reported the CD4 counts of participants found tobe HIV-positive in a key population. Using standard labdiagnostics these studies reported a median CD4 count of 550cells/ml among MSM [115] and 385 cells/ml among MSM,PWID, and FSW [105].
Linkage to Care17 studies, including 5,852 participants with HIV, reported
linkage to care from HIV diagnosis to CD4 measurement[30,51,55,60,61,76,82,86,89,110,124–126,128,129]. Overall,80.1% of participants had their CD4 count measured after HIVdiagnosis (95% CI 74.8%–85.4%; I2 99.5%, 95% CI 99.4%–99.5%; Figure 15). Nine studies with 527 participants reported
Figure 10. Uptake of community-based HTC approaches among key populations.doi:10.1371/journal.pmed.1001496.g010
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
335
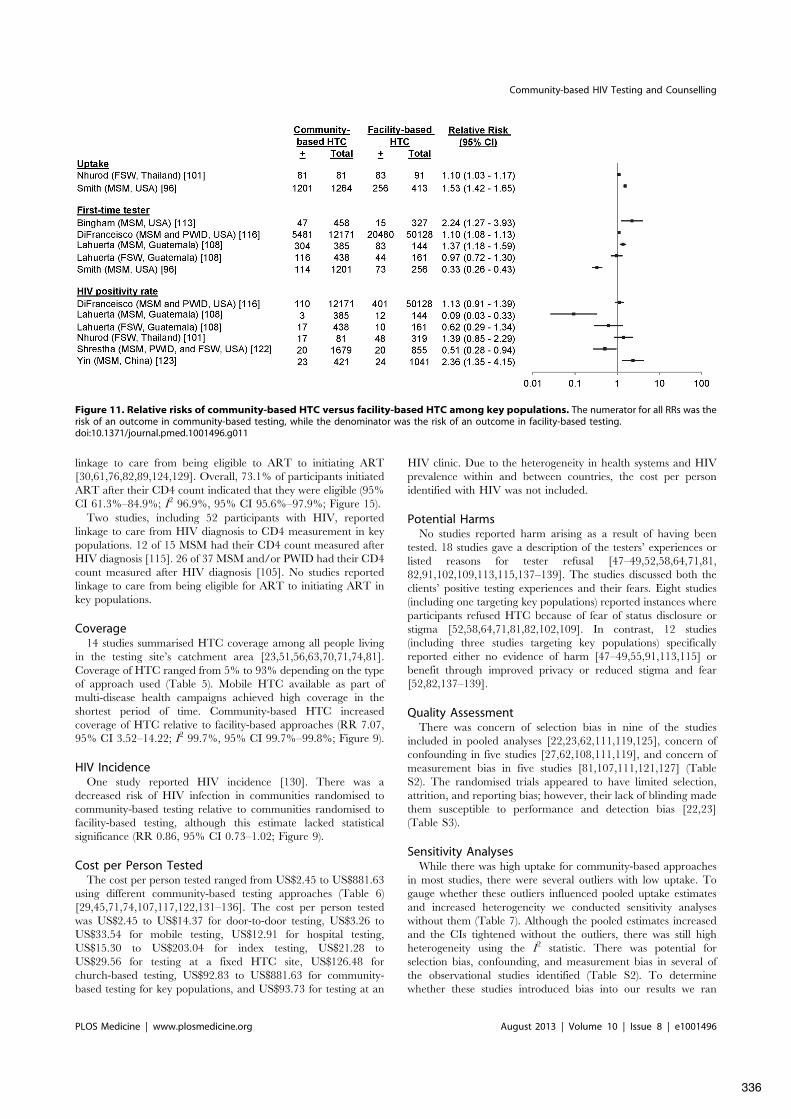
linkage to care from being eligible to ART to initiating ART[30,61,76,82,89,124,129]. Overall, 73.1% of participants initiatedART after their CD4 count indicated that they were eligible (95%CI 61.3%–84.9%; I2 96.9%, 95% CI 95.6%–97.9%; Figure 15).
Two studies, including 52 participants with HIV, reportedlinkage to care from HIV diagnosis to CD4 measurement in keypopulations. 12 of 15 MSM had their CD4 count measured afterHIV diagnosis [115]. 26 of 37 MSM and/or PWID had their CD4count measured after HIV diagnosis [105]. No studies reportedlinkage to care from being eligible for ART to initiating ART inkey populations.
Coverage14 studies summarised HTC coverage among all people living
in the testing site’s catchment area [23,51,56,63,70,71,74,81].Coverage of HTC ranged from 5% to 93% depending on the typeof approach used (Table 5). Mobile HTC available as part ofmulti-disease health campaigns achieved high coverage in theshortest period of time. Community-based HTC increasedcoverage of HTC relative to facility-based approaches (RR 7.07,95% CI 3.52–14.22; I2 99.7%, 95% CI 99.7%–99.8%; Figure 9).
HIV IncidenceOne study reported HIV incidence [130]. There was a
decreased risk of HIV infection in communities randomised tocommunity-based testing relative to communities randomised tofacility-based testing, although this estimate lacked statisticalsignificance (RR 0.86, 95% CI 0.73–1.02; Figure 9).
Cost per Person TestedThe cost per person tested ranged from US$2.45 to US$881.63
using different community-based testing approaches (Table 6)[29,45,71,74,107,117,122,131–136]. The cost per person testedwas US$2.45 to US$14.37 for door-to-door testing, US$3.26 toUS$33.54 for mobile testing, US$12.91 for hospital testing,US$15.30 to US$203.04 for index testing, US$21.28 toUS$29.56 for testing at a fixed HTC site, US$126.48 forchurch-based testing, US$92.83 to US$881.63 for community-based testing for key populations, and US$93.73 for testing at an
HIV clinic. Due to the heterogeneity in health systems and HIVprevalence within and between countries, the cost per personidentified with HIV was not included.
Potential HarmsNo studies reported harm arising as a result of having been
tested. 18 studies gave a description of the testers’ experiences orlisted reasons for tester refusal [47–49,52,58,64,71,81,82,91,102,109,113,115,137–139]. The studies discussed both theclients’ positive testing experiences and their fears. Eight studies(including one targeting key populations) reported instances whereparticipants refused HTC because of fear of status disclosure orstigma [52,58,64,71,81,82,102,109]. In contrast, 12 studies(including three studies targeting key populations) specificallyreported either no evidence of harm [47–49,55,91,113,115] orbenefit through improved privacy or reduced stigma and fear[52,82,137–139].
Quality AssessmentThere was concern of selection bias in nine of the studies
included in pooled analyses [22,23,62,111,119,125], concern ofconfounding in five studies [27,62,108,111,119], and concern ofmeasurement bias in five studies [81,107,111,121,127] (TableS2). The randomised trials appeared to have limited selection,attrition, and reporting bias; however, their lack of blinding madethem susceptible to performance and detection bias [22,23](Table S3).
Sensitivity AnalysesWhile there was high uptake for community-based approaches
in most studies, there were several outliers with low uptake. Togauge whether these outliers influenced pooled uptake estimatesand increased heterogeneity we conducted sensitivity analyseswithout them (Table 7). Although the pooled estimates increasedand the CIs tightened without the outliers, there was still highheterogeneity using the I2 statistic. There was potential forselection bias, confounding, and measurement bias in several ofthe observational studies identified (Table S2). To determinewhether these studies introduced bias into our results we ran
Figure 11. Relative risks of community-based HTC versus facility-based HTC among key populations. The numerator for all RRs was therisk of an outcome in community-based testing, while the denominator was the risk of an outcome in facility-based testing.doi:10.1371/journal.pmed.1001496.g011
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
336

Figure 12. First-time testers in community-based testing approaches.doi:10.1371/journal.pmed.1001496.g012
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
337

sensitivity analyses without them and found the results to besimilar (Table 8).
Discussion
This systematic review found that community-based HTCapproaches were successful in reaching populations early in thecourse of HIV infection. The studies with facility-based compar-ator arms further suggest that community-based HTC reachedpopulations earlier in the course of HIV infection than facility-based HTC. Earlier HIV diagnosis supports timely access to ART,which could improve life expectancy and reduce HIV transmission[140–142]. Earlier HIV diagnosis linked to ART may also haveimportant socioeconomic effects at the population level, including(1) reducing the number of orphans [143], (2) improving educationand employment outcomes [144,145], and (3) increasing the sizeof workforces [146,147].
The HIV positivity rate among participants in community-based HTC approaches was generally lower than that amongparticipants in facility-based HTC. This could be because (1)symptomatic people with HIV are more likely to visit healthfacilities, (2) healthcare workers are more likely to offer HTC topatients with symptoms that might be associated with HIV, and (3)
the positivity rate of participants in community-based HTC ismore likely to be representative of the general population. Whileobtaining a lower positivity rate may immediately be associatedwith increased numbers needing to be tested to identify peoplewith HIV, community-based HTC increased the number of newlydiagnosed people with HIV 4-fold in a randomised controlled trial,has the potential to decrease HIV stigma by normalising HIVtesting, and is an opportunity to provide prevention interventionsfor HIV and other diseases to asymptomatic populations[23,52,82,137–139]. The HIV positivity rate among key popula-tions utilising community-based testing varied relative to the HIVpositivity rate among key populations utilising facility-based HTCand requires further examination within different epidemiologicalcontexts. Although few comparative cost data exist on the variousHTC approaches, the reported estimates indicate that severalcommunity-based testing approaches are cheaper or similarlypriced compared to facility-based HTC (Table 6).
Because many settings lack universal health coverage, otherdisease control strategies—such as the guinea worm eradicationcampaign [148], eradication campaigns against polio and measles[149,150], and efforts to eliminate preventable blindness [151]—are built upon community-based elements for broader reach.Since community outreach efforts for these disease control
Figure 13. First time testers in community-based testing approaches for key populations.doi:10.1371/journal.pmed.1001496.g013
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
338
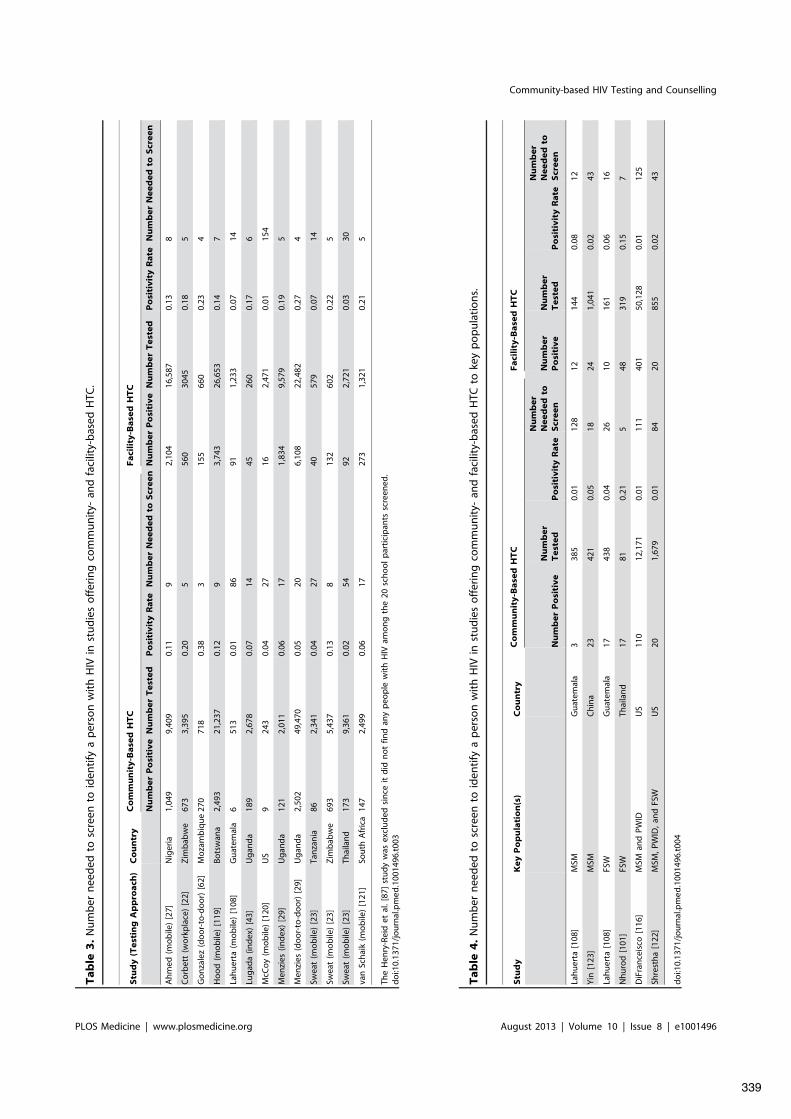
Ta
ble
3.
Nu
mb
ern
eed
edto
scre
ento
iden
tify
ap
erso
nw
ith
HIV
inst
ud
ies
off
erin
gco
mm
un
ity-
and
faci
lity-
bas
edH
TC.
Stu
dy
(Te
stin
gA
pp
roa
ch)
Co
un
try
Co
mm
un
ity
-Ba
sed
HT
CF
aci
lity
-Ba
sed
HT
C
Nu
mb
er
Po
siti
ve
Nu
mb
er
Te
ste
dP
osi
tiv
ity
Ra
teN
um
be
rN
ee
de
dto
Scr
ee
nN
um
be
rP
osi
tiv
eN
um
be
rT
est
ed
Po
siti
vit
yR
ate
Nu
mb
er
Ne
ed
ed
toS
cre
en
Ah
med
(mo
bile
)[2
7]N
iger
ia1,
049
9,40
90.
119
2,10
416
,587
0.13
8
Co
rbet
t(w
ork
pla
ce)
[22]
Zim
bab
we
673
3,39
50.
205
560
3045
0.18
5
Go
nza
lez
(do
or-
to-d
oo
r)[6
2]M
oza
mb
iqu
e27
071
80.
383
155
660
0.23
4
Ho
od
(mo
bile
)[1
19]
Bo
tsw
ana
2,49
321
,237
0.12
93,
743
26,6
530.
147
Lah
uer
ta(m
ob
ile)
[108
]G
uat
emal
a6
513
0.01
8691
1,23
30.
0714
Lug
ada
(ind
ex)
[43]
Ug
and
a18
92,
678
0.07
1445
260
0.17
6
McC
oy
(mo
bile
)[1
20]
US
924
30.
0427
162,
471
0.01
154
Men
zies
(ind
ex)
[29]
Ug
and
a12
12,
011
0.06
171,
834
9,57
90.
195
Men
zies
(do
or-
to-d
oo
r)[2
9]U
gan
da
2,50
249
,470
0.05
206,
108
22,4
820.
274
Swea
t(m
ob
ile)
[23]
Tan
zan
ia86
2,34
10.
0427
4057
90.
0714
Swea
t(m
ob
ile)
[23]
Zim
bab
we
693
5,43
70.
138
132
602
0.22
5
Swea
t(m
ob
ile)
[23]
Thai
lan
d17
39,
361
0.02
5492
2,72
10.
0330
van
Sch
aik
(mo
bile
)[1
21]
Sou
thA
fric
a14
72,
499
0.06
1727
31,
321
0.21
5
The
Hen
ry-R
eid
etal
.[8
7]st
ud
yw
asex
clu
ded
sin
ceit
did
no
tfin
dan
yp
eop
lew
ith
HIV
amo
ng
the
20sc
ho
ol
par
tici
pan
tssc
reen
ed.
do
i:10.
1371
/jo
urn
al.p
me
d.1
0014
96.t
003
Ta
ble
4.
Nu
mb
ern
eed
edto
scre
ento
iden
tify
ap
erso
nw
ith
HIV
inst
ud
ies
off
erin
gco
mm
un
ity-
and
faci
lity-
bas
edH
TCto
key
po
pu
lati
on
s.
Stu
dy
Ke
yP
op
ula
tio
n(s
)C
ou
ntr
yC
om
mu
nit
y-B
ase
dH
TC
Fa
cili
ty-B
ase
dH
TC
Nu
mb
er
Po
siti
ve
Nu
mb
er
Te
ste
dP
osi
tiv
ity
Ra
te
Nu
mb
er
Ne
ed
ed
toS
cre
en
Nu
mb
er
Po
siti
ve
Nu
mb
er
Te
ste
dP
osi
tiv
ity
Ra
te
Nu
mb
er
Ne
ed
ed
toS
cre
en
Lah
uer
ta[1
08]
MSM
Gu
atem
ala
338
50.
0112
812
144
0.08
12
Yin
[123
]M
SMC
hin
a23
421
0.05
1824
1,04
10.
0243
Lah
uer
ta[1
08]
FSW
Gu
atem
ala
1743
80.
0426
1016
10.
0616
Nh
uro
d[1
01]
FSW
Thai
lan
d17
810.
215
4831
90.
157
DiF
ran
ceis
co[1
16]
MSM
and
PW
IDU
S11
012
,171
0.01
111
401
50,1
280.
0112
5
Shre
sth
a[1
22]
MSM
,P
WID
,an
dFS
WU
S20
1,67
90.
0184
2085
50.
0243
do
i:10.
1371
/jo
urn
al.p
me
d.1
0014
96.t
004
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
339

strategies have largely been vertical in nature, some have suggestedleveraging community-based HTC as a conduit for deliveringother public health activities based on national burden of disease[152]. Multi-disease approaches may include the provision ofvaccines, water filters, and malaria bed nets and screening forcardiovascular disease, diabetes, and pulmonary disease [153].Settings implementing recent WHO guidance on community-based screening for tuberculosis and malaria could also considermulti-disease frameworks to improve efficiency [154,155]. Includ-ing other public health activities based on national epidemiology,such as family planning and viral hepatitis screening andtreatment, may also be appropriate. Indeed, 40 of the 117 studiesmeeting this review’s eligibility criteria (34%) had a multi-diseasecomponent. Broadening community-based HTC to includepreventive interventions and screening for other diseases couldfurther improve cost-effectiveness [156].
In the studies reviewed, HTC uptake exceeded 80% in themobile, index, self, and door-to-door testing approaches. Whileworkplace and school-based testing could be an importantapproach in some settings, the uptake of these approaches waslower than that of other community-based approaches. Furtherresearch may improve their acceptability and could evaluate theirimpact on employment and education outcomes. Although therewas no evidence of any harm resulting from being tested incommunity-based HTC approaches, there were reports of fear ofstatus disclosure or stigma. Moreover, a recent report highlightsthe possibility of false positive diagnoses in settings (1) lacking aconfirmation HIV test, (2) with poor training and supervision ofcommunity health workers, and (3) with insufficient qualitycontrol procedures [157]. These findings highlight the continuingneed to adhere to validated testing algorithms and to addresslegal and human rights issues, and for the 5 Cs of good testing
Figure 14. Pooled percentage of community-based HTC participants with CD4 counts above 350 cells/ml.doi:10.1371/journal.pmed.1001496.g014
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
340

practices—informed consent, confidentiality, counselling, correcttest results, and connection to prevention and care—to always bepresent [10].
There was variable uptake for community-based testing amongkey populations. The heterogeneity between studies likely relatesto differences in the way HTC was offered. For example, thestudies with the lowest uptake among key populations offeredHTC only in combination with extensive behavioural surveys[92,95]. The findings from this small number of studies cannot begeneralised widely. Moreover, there were limited CD4 count andART linkage data from these studies, indicating that caution maybe needed when providing HTC to key populations in settingswhere they remain marginalised and stigmatised and where thereare inadequate linkages to prevention and care services. It is alsoimportant to safeguard confidentiality and prevent possible
coercion, discrimination, and other adverse consequences for keypopulations being offered HTC in community settings. Furtheroperational research on community-based testing for key popula-tions, including mobile peer-based models [120,133,158,159],within this human rights framework is needed.
One of the benefits of community-based testing, especially door-to-door testing, is allowing couples and families to be counselledabout their HIV status, behaviour change, ART, and preventioninterventions together [160,161]. Review of population-level HTCefforts suggest that implementation of community-based HTCcould increase the number of couples receiving testing (Table 2).There were relatively limited data on HTC approaches for infants,children and adolescents. The door-to-door, mobile, school, andindex community-based approaches have promise for these youngpopulations, but further research could improve their operationa-
Figure 15. Linkage to care with community-based approaches to HTC. Asterisk: study included 14 workplace sites in the DemocraticRepublic of Congo, Rwanda, Burundi, Congo, and Nigeria.doi:10.1371/journal.pmed.1001496.g015
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
341

lisation [43,44,87–89,102,103,128]. In addition to implementingprovider-initiated HTC in all health facilities in generalisedepidemics, introducing HIV testing at scheduled immunisationvisits may facilitate earlier diagnosis linked to care [162].
Offering community-based HTC in addition to facility-basedHTC increased knowledge of HIV status approximately 7-fold atthe population level. Providing near universal knowledge of HIVstatus linked to prevention and care may impact HIV transmissionnetworks through increased coverage of ART, increased malecircumcision prevalence, increased utilisation of needle exchangeprogrammes, increased utilisation of condoms, increased utilisa-tion of pre-exposure prophylaxis, behavioural change, andincreased coverage of opiate substitution therapy. A cluster-randomised trial detected a statistically non-significant 14%reduction in population incidence in communities where commu-nity-based HTC was available [130]. Since community-basedHTC wasn’t directly linked to prevention and care services in thistrial, achieving and maintaining high levels of HTC coverage andmaximising linkage to ART and other components of combinationprevention could lead to more substantial reductions in populationincidence [163–165].
Incidence reductions depend on high coverage of repeat testingamong people at risk of HIV infection. WHO recommends thatHIV-negative individuals with ongoing sexual behaviour and/orwho inject drugs with partners of positive or unknown HIV statusshould be tested at least annually [166]. A high percentage ofpeople reported being first-time testers with community-basedapproaches, and overall there was a higher proportion of first-timetesters in community-based approaches than in facility-basedapproaches. In effective HTC programmes, the proportion ofpeople reporting receiving their first test should decrease over timeas a result of implementing WHO repeat testing recommendations[25]. Several studies assessed uptake in the context of repeattesting. In several generalised epidemic settings, uptake remainedhigh among the general population [24,25]. Conversely, uptakedecreased among the general population in a concentratedepidemic, suggesting that HTC may need to be targeted to keypopulations on an ongoing basis in these settings [26].
This review found that 80% of participants in the community-based HTC studies where CD4 measurement was offered hadtheir CD4 count measured after HIV diagnosis. CD4 measure-ment was facilitated by (1) point-of-care CD4 diagnostics, (2)collection of blood samples at the time of diagnosis, and (3)workplace programmes that had regular contact with participantsbecause of their work schedules. This percentage was similar to thepercentages reported in two systematic reviews evaluating CD4measurement from facility-based testing (59%–72%) [167,168],and supports the notion that high uptake of CD4 measurementcan be achieved outside of health facilities when it is offered incombination with testing results. This review also found that 73%of participants initiated ART after their CD4 counts indicatedthat they were eligible. This proportion was comparable toprevious estimates from two systematic reviews evaluating ARTinitiation rates from healthcare facilities (62%–68%) [167,168].Linkage from community-based HTC approaches to community-based treatment programmes could improve ART access anduptake and merits further exploration [169–171]. The data onlinkage to prevention services, including linking men withnegative results to male circumcision [57], were very limited.These linkages will be required to maximise the populationbenefits of community-based testing. Additional data on linkageto prevention services are urgently needed. Because self-testingachieves anonymous knowledge of status, no studies have beenable to provide data on rates of linkage to care or prevention forpeople using this testing approach [172]. Nonetheless, self-testingmay provide programmatic advantages in some settings andrequires further research [173].
There are some methodological limitations that need to beconsidered when evaluating the impact of community-basedHTC. One of the outcomes, first-time tester proportion, haspotential for recall bias since it relies on participants to recall theirhistory of HIV testing. Since all of the studies that included afacility-based HTC comparator arm did not indicate whetherHTC was provider- or client-initiated, comparisons were made tofacility-based HTC approaches irrespective of who initiated theinteraction. Therefore, this review may not provide conclusive
Table 5. Community coverage of voluntary HTC.
Study (Testing Approach) Duration (Months) Country Year Number Tested Number EligiblePercentCoverage
Sweat (mobile) [23] 42 Thailand 2007 10,464 11,290 93%
Lugada (mobile) [56] 0.23 Kenya 2008 47,173 51,178 92%
Chamie (mobile) [51] 0.16 Uganda 2007 4,343 6,300 69%
Wolff (door-to-door) [81] 1 Uganda 2001 1,078 1,591 68%
Naik (door-to-door) [70] 16 South Africa 2010 5,086 7,614 67%
Kimaiyo (door-to-door) [63] 7 Kenya 2009 90,062 143,284 63%
Negin (door-to-door) [71] — Kenya 2008 1,984 3,180 62%
Sweat (mobile) [23] 42 Zimbabwe 2007 6,579 10,700 61%
Tumwesigye (door-to-door) [74] 30 Uganda 2007 264,966 — 52%
Sweat (mobile) [23] 37 Tanzania 2007 2,832 6,250 45%
Sweat (facility-based) [23] 42 Thailand 2007 2,721 10,033 27%
Sweat (facility-based) [23] 37 Tanzania 2007 685 6,733 10%
Sweat (facility-based) [23] 42 Zimbabwe 2007 610 12,150 5%
Wolff (facility-based) [81] 12 Uganda 2000 79 1,591 5%
—, data not reported.doi:10.1371/journal.pmed.1001496.t005
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
342
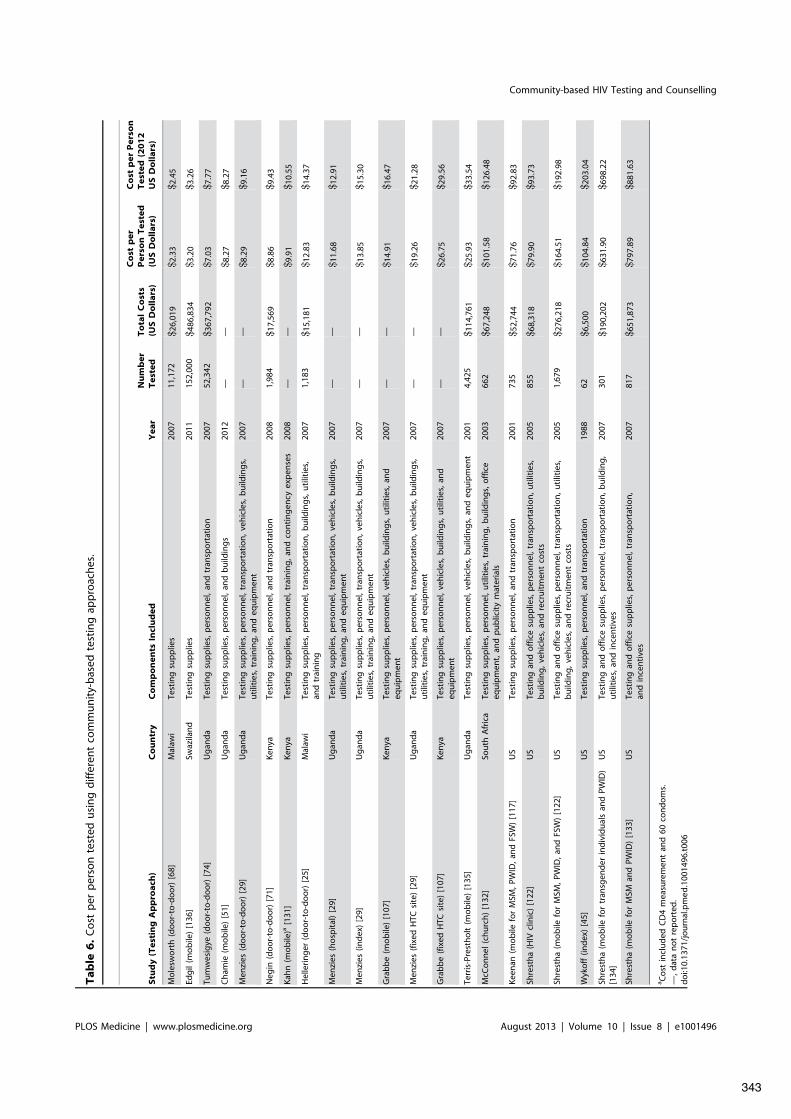
Ta
ble
6.
Co
stp
erp
erso
nte
sted
usi
ng
diff
eren
tco
mm
un
ity-
bas
edte
stin
gap
pro
ach
es.
Stu
dy
(Te
stin
gA
pp
roa
ch)
Co
un
try
Co
mp
on
en
tsIn
clu
de
dY
ea
rN
um
be
rT
est
ed
To
tal
Co
sts
(US
Do
lla
rs)
Co
stp
er
Pe
rso
nT
est
ed
(US
Do
lla
rs)
Co
stp
er
Pe
rso
nT
est
ed
(20
12
US
Do
lla
rs)
Mo
lesw
ort
h(d
oo
r-to
-do
or)
[68]
Mal
awi
Test
ing
sup
plie
s20
0711
,172
$26,
019
$2.3
3$2
.45
Edg
il(m
ob
ile)
[136
]Sw
azila
nd
Test
ing
sup
plie
s20
1115
2,00
0$4
86,8
34$3
.20
$3.2
6
Tum
wes
igye
(do
or-
to-d
oo
r)[7
4]U
gan
da
Test
ing
sup
plie
s,p
erso
nn
el,
and
tran
spo
rtat
ion
2007
52,3
42$3
67,7
92$7
.03
$7.7
7
Ch
amie
(mo
bile
)[5
1]U
gan
da
Test
ing
sup
plie
s,p
erso
nn
el,
and
bu
ildin
gs
2012
——
$8.2
7$8
.27
Men
zies
(do
or-
to-d
oo
r)[2
9]U
gan
da
Test
ing
sup
plie
s,p
erso
nn
el,
tran
spo
rtat
ion
,ve
hic
les,
bu
ildin
gs,
uti
litie
s,tr
ain
ing
,an
deq
uip
men
t20
07—
—$8
.29
$9.1
6
Neg
in(d
oo
r-to
-do
or)
[71]
Ken
yaTe
stin
gsu
pp
lies,
per
son
nel
,an
dtr
ansp
ort
atio
n20
081,
984
$17,
569
$8.8
6$9
.43
Kah
n(m
ob
ile)a
[131
]K
enya
Test
ing
sup
plie
s,p
erso
nn
el,
trai
nin
g,
and
con
tin
gen
cyex
pen
ses
2008
——
$9.9
1$1
0.55
Hel
leri
ng
er(d
oo
r-to
-do
or)
[25]
Mal
awi
Test
ing
sup
plie
s,p
erso
nn
el,
tran
spo
rtat
ion
,b
uild
ing
s,u
tilit
ies,
and
trai
nin
g20
071,
183
$15,
181
$12.
83$1
4.37
Men
zies
(ho
spit
al)
[29]
Ug
and
aTe
stin
gsu
pp
lies,
per
son
nel
,tr
ansp
ort
atio
n,
veh
icle
s,b
uild
ing
s,u
tilit
ies,
trai
nin
g,
and
equ
ipm
ent
2007
——
$11.
68$1
2.91
Men
zies
(ind
ex)
[29]
Ug
and
aTe
stin
gsu
pp
lies,
per
son
nel
,tr
ansp
ort
atio
n,
veh
icle
s,b
uild
ing
s,u
tilit
ies,
trai
nin
g,
and
equ
ipm
ent
2007
——
$13.
85$1
5.30
Gra
bb
e(m
ob
ile)
[107
]K
enya
Test
ing
sup
plie
s,p
erso
nn
el,
veh
icle
s,b
uild
ing
s,u
tilit
ies,
and
equ
ipm
ent
2007
——
$14.
91$1
6.47
Men
zies
(fix
edH
TCsi
te)
[29]
Ug
and
aTe
stin
gsu
pp
lies,
per
son
nel
,tr
ansp
ort
atio
n,
veh
icle
s,b
uild
ing
s,u
tilit
ies,
trai
nin
g,
and
equ
ipm
ent
2007
——
$19.
26$2
1.28
Gra
bb
e(f
ixed
HTC
site
)[1
07]
Ken
yaTe
stin
gsu
pp
lies,
per
son
nel
,ve
hic
les,
bu
ildin
gs,
uti
litie
s,an
deq
uip
men
t20
07—
—$2
6.75
$29.
56
Terr
is-P
rest
ho
lt(m
ob
ile)
[135
]U
gan
da
Test
ing
sup
plie
s,p
erso
nn
el,
veh
icle
s,b
uild
ing
s,an
deq
uip
men
t20
014,
425
$114
,761
$25.
93$3
3.54
McC
on
nel
(ch
urc
h)
[132
]So
uth
Afr
ica
Test
ing
sup
plie
s,p
erso
nn
el,
uti
litie
s,tr
ain
ing
,b
uild
ing
s,o
ffic
eeq
uip
men
t,an
dp
ub
licit
ym
ater
ials
2003
662
$67,
248
$101
.58
$126
.48
Kee
nan
(mo
bile
for
MSM
,P
WID
,an
dFS
W)
[117
]U
STe
stin
gsu
pp
lies,
per
son
nel
,an
dtr
ansp
ort
atio
n20
0173
5$5
2,74
4$7
1.76
$92.
83
Shre
sth
a(H
IVcl
inic
)[1
22]
US
Test
ing
and
off
ice
sup
plie
s,p
erso
nn
el,
tran
spo
rtat
ion
,u
tilit
ies,
bu
ildin
g,
veh
icle
s,an
dre
cru
itm
ent
cost
s20
0585
5$6
8,31
8$7
9.90
$93.
73
Shre
sth
a(m
ob
ilefo
rM
SM,
PW
ID,
and
FSW
)[1
22]
US
Test
ing
and
off
ice
sup
plie
s,p
erso
nn
el,
tran
spo
rtat
ion
,u
tilit
ies,
bu
ildin
g,
veh
icle
s,an
dre
cru
itm
ent
cost
s20
051,
679
$276
,218
$164
.51
$192
.98
Wyk
off
(ind
ex)
[45]
US
Test
ing
sup
plie
s,p
erso
nn
el,
and
tran
spo
rtat
ion
1988
62$6
,500
$104
.84
$203
.04
Shre
sth
a(m
ob
ilefo
rtr
ansg
end
erin
div
idu
als
and
PW
ID)
[134
]U
STe
stin
gan
do
ffic
esu
pp
lies,
per
son
nel
,tr
ansp
ort
atio
n,
bu
ildin
g,
uti
litie
s,an
din
cen
tive
s20
0730
1$1
90,2
02$6
31.9
0$6
98.2
2
Shre
sth
a(m
ob
ilefo
rM
SMan
dP
WID
)[1
33]
US
Test
ing
and
off
ice
sup
plie
s,p
erso
nn
el,
tran
spo
rtat
ion
,an
din
cen
tive
s20
0781
7$6
51,8
73$7
97.8
9$8
81.6
3
aC
ost
incl
ud
edC
D4
mea
sure
men
tan
d60
con
do
ms.
—,
dat
an
ot
rep
ort
ed.
do
i:10.
1371
/jo
urn
al.p
me
d.1
0014
96.t
006
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
343

evidence of community-based HTC relative to provider-initiatedHTC. While 73% of participants initiated ART after their CD4count indicated they were eligible, all of the studies providing thesedata did not provide information on the timing of this outcome.Understanding how soon after diagnosis participants were able toinitiate ART could help establish the efficiency of linkage systems.While this review summarises information from different commu-nity-based testing approaches globally, only six of the 117 studiesidentified were from Asia, indicating a need to expand commu-nity-based HTC research efforts in this region. Finally, given thecomplexity and expense of conducting cluster-randomised con-trolled trials, most of the studies meeting the eligibility criteriawere observational. Although our analyses included data fromrandomised controlled trials, the potential for unmeasuredconfounding in observational studies makes attempts to establishcausal effect more difficult.
The meta-analyses may have limitations in the statisticalmethodology used. Using the I2 statistic, there was highheterogeneity for most meta-analyses. All analyses should beinterpreted with respect to local epidemiology, social and culturalcontext, and the health systems organisation of the studiescontributing data. Publication bias was not formally assessed, asanalytical methods to test for publication bias, such as funnel plotsand funnel plot asymmetry tests, may not be appropriate forobservational data [174]. Multiple study estimates and standard-ised variable definitions are required to explore the contributors ofheterogeneity for pooled estimates. Given that the same variableswere not collected systematically in all studies, this assessment wasnot undertaken for this review.
In conclusion, many community-based approaches achievedhigh uptake of HTC. Costs and linkage to care appeared similarto those of facility-based HTC approaches. The lower yield ofpeople with HIV relative to facility-based HTC approaches
appears to be offset by increasing knowledge of status at thepopulation level, which, combined with timely linkage totreatment and prevention services, could have population effectson life expectancy and HIV transmission. As countries developtheir new national strategic plans and investment cases based onWHO and Joint United Nations Programme on HIV/AIDSstrategic guidance [175], consideration should be given toincreasing the proportion of people with HIV who know theirstatus, with linkages to prevention and care, by offeringcommunity-based testing in addition to facility-based testing[176].
Supporting Information
Protocol S1 Systematic review protocol.(PDF)
Table S1 Search strategy for all databases.(PDF)
Table S2 Newcastle-Ottawa Quality Assessment Scale.*Given that the distribution of possible confounders in randomisedcontrolled trials is related to chance alone, randomised controlledtrials were not assessed for confounding.(PDF)
Table S3 Bias assessment for randomised controlledtrials.(PDF)
Table S4 Characteristics of studies meeting inclusioncriteria. CE model, cost-effectiveness model; N/A, not applica-ble (e.g., gender data was not calculated for community-basedtesting only for MSM or FSW); N/R, not reported; OS,observational study; RCT, randomised controlled trial; STD,
Table 7. Pooled relative risks of community- versus facility-based HTC sensitivity analyses.
Outcome Pooled RR (95% CI) I2 StatisticObservational StudiesRemoved
Revised PooledEstimate (95% CI)
Revised I2
Statistic
Uptake 10.65 (6.27–18.08) 96.1% [43] 13.99 (11.75–16.68) N/A
Proportion of first-time testers 1.23 (1.06–1.42) 99.8% [27,29,107,108,111] 1.12 (0.91–1.38) 99.9%
HIV positivity rate 0.59 (0.37–0.96) 99.6% [27,29,43,62,87,108,119–121] 0.47 (0.22–1.02) 99.6%
Coverage 7.07 (3.52–14.22) 99.7% [81] 5.71 (2.63–12.40) 99.8%
N/A, not applicable.doi:10.1371/journal.pmed.1001496.t007
Table 8. Pooled uptake proportion sensitivity analyses.
HTC Approach Pooled Estimate (95% CI) I2 Statistic Outliers RemovedRevised PooledEstimate (95% CI)
Revised I2
Statistic
Index 88.2 (80.5–95.9) 99.7% [30] 93.5 (89.1–97.9) 99.0%
Mobile 86.8 (85.6–88.1) 99.9% [26,52,53] 97.9 (97.6–98.3) 98.5%
Door-to-door 80.0 (76.9–83.1) 99.9% [30,68,77,79,81] 84.2 (81.8–86.6) 99.9%
Workplace 67.4 (32.8–100.0) 100% [86] 76.9 (61.8–92.0) 99.8%
School 62.1 (39.6–84.5) 99.0% [87] 71.9 (46.4–97.3) 99.4%
Outliers were defined as study estimates more than one standard deviation away from the pooled estimate.doi:10.1371/journal.pmed.1001496.t008
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
344

sexually transmitted disease; TB, tuberculosis; VCT, voluntarycounselling and testing.(PDF)
Text S1 PRISMA checklist.(DOC)
Acknowledgments
We thank Elizabeth Marum for helpful advice, investigators from severalstudies for providing additional data, and members of the Operational and
Service Delivery Guideline Development Group for discussing criticalissues.
Author Contributions
Conceived and designed the experiments: ABS NF EKN RCB. Performedthe experiments: ABS NF JSR AKS OA. Analyzed the data: ABS NF.Wrote the first draft of the manuscript: ABS. Contributed to the writing ofthe manuscript: ABS NF PJB VJW JSR AKS OA AOF RMG EKN RCB.ICMJE criteria for authorship read and met: ABS NF PJB VJW JSR AKSOA AOF RMG EKN RCB. Agree with manuscript results andconclusions: ABS NF PJB VJW JSR AKS OA AOF RMG EKN RCB.
References
1. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, et al. (2012)Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21regions, 1990–2010: a systematic analysis for the Global Burden of DiseaseStudy 2010. Lancet 380: 2197–2223.
2. Joint United Nations Programme on HIV/AIDS (2012) UNAIDS report onthe global AIDS epidemic. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/epidemiology/2012/gr2012/20121120_UNAIDS_Global_Report_2012_en.pdf. Accessed 25 July 2013.
3. United Nations General Assembly (2011) Political declaration on HIV/AIDS:intensifying our efforts to eliminate HIV/AIDS. Available: http://www.unaids.org/en/media/unaids/contentassets/documents/document/2011/06/20110610_un_a-res-65-277_en.pdf. Accessed 1 July 2013.
4. World Health Organization (2007) Guidance on provider-initiated HIV testingand counselling in health facilities. Available: http://whqlibdoc.who.int/publications/2007/9789241595568_eng.pdf. Accessed 1 July 2013.
5. Roura M, Watson-Jones D, Kahawita TM, Ferguson L, Ross DA (2013)Provider-initiated testing and counselling programmes in sub-Saharan Africa: asystematic review of their operational implementation. AIDS 27: 617–626.
6. Hensen B, Baggaley R, Wong VJ, Grabbe KL, Shaffer N, et al. (2012)Universal voluntary HIV testing in antenatal care settings: a review of thecontribution of provider-initiated testing & counselling. Trop Med Int Health17: 59–70.
7. Staveteig S, Wang S, Head SK, Bradley SEK, Nybro E (2013) Demographicpatterns of HIV testing uptake in Sub-Saharan Africa. Available: http://www.measuredhs.com/pubs/pdf/CR30/CR30.pdf. Accessed 1 July 2013.
8. Egger M, The IDEA and ART cohort collaborations (2013) Immunodeficiencyat the start of combination antiretroviral therapy in low-, middle- and high-income countries. J Acquir Immune Defic Syndr. E-pub ahead of print.
9. Matovu JK, Makumbi FE (2007) Expanding access to voluntary HIVcounselling and testing in sub-Saharan Africa: alternative approaches forimproving uptake, 2001–2007. Trop Med Int Health 12: 1315–1322.
10. World Health Organization (2012) Service delivery approaches to HIV testingand counselling (HTC): a strategic policy framework. Available: http://apps.who.int/iris/bitstream/10665/75206/1/9789241593877_eng.pdf. Accessed 1July 2013.
11. Bateganya MH, Abdulwadud OA, Kiene SM (2007) Home-based HIVvoluntary counseling and testing in developing countries. Cochrane DatabaseSyst Rev 2007: CD006493.
12. Sabapathy K, Van den Bergh R, Fidler S, Hayes R, Ford N (2012) Uptake ofhome-based voluntary HIV testing in sub-Saharan Africa: a systematic reviewand meta-analysis. PLoS Med 9: e1001351. doi:10.1371/jour-nal.pmed.1001351
13. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, et al. (2009) ThePRISMA statement for reporting systematic reviews and meta-analyses ofstudies that evaluate health care interventions: explanation and elaboration.PLoS Med 6: e1000100. doi:10.1371/journal.pmed.1000100
14. Suthar AB (2012) Towards universal voluntary HIV testing and counselling: asystematic review of community-based approaches. Available: http://www.crd.york.ac.uk/PROSPEROFILES/2554_PROTOCOL_20120527.pdf. Accessed1 July 2013.
15. United States Department of Labor Bureau of Labor Statistics (2012) CPIinflation calculator [database]. Available: http://www.bls.gov/data/inflation_calculator.htm. Accessed 1 July 2013.
16. Wells G, Shea B, O’Connell D, Peterson J, Welch V, et al. (2011) TheNewcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomisedstudies in meta-analyses. Available: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 1 July 2013.
17. The Cochrane Collaboration (2011) Cochrane handbook for systematicreviews of interventions, version 5.1.0. Available: http://www.cochrane-handbook.org/. Accessed 1 July 2013.
18. Freeman M, Tukey J (1950) Transformations related to the angular and thesquare root. Ann Math Stat 21: 607–611.
19. Newcombe RG (1998) Interval estimation for the difference betweenindependent proportions: comparison of eleven methods. Stat Med 17: 873–890.
20. Higgins JP, Thompson SG (2002) Quantifying heterogeneity in a meta-analysis. Stat Med 21: 1539–1558.
21. Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuringinconsistency in meta-analyses. BMJ 327: 557–560.
22. Corbett EL, Dauya E, Matambo R, Cheung YB, Makamure B, et al. (2006)Uptake of workplace HIV counselling and testing: a cluster-randomised trial inZimbabwe. PLoS Med 3: e238. doi:10.1371/journal.pmed.0030238
23. Sweat M, Morin S, Celentano D, Mulawa M, Singh B, et al. (2011)Community-based intervention to increase HIV testing and case detection inpeople aged 16-32 years in Tanzania, Zimbabwe, and Thailand (NIMHProject Accept, HPTN 043): a randomised study. Lancet Infect Dis 11: 525–532.
24. Angotti N, Bula A, Gaydosh L, Kimchi EZ, Thornton RL, et al. (2009)Increasing the acceptability of HIV counseling and testing with three C’s:convenience, confidentiality and credibility. Soc Sci Med 68: 2263–2270.
25. Helleringer S, Mkandawire J, Reniers G, Kalilani-Phiri L, Kohler HP (2012)Should home-based HIV testing and counseling services be offered periodicallyin programs of ARV treatment as prevention? A case study in Likoma(Malawi). AIDS Behav 17: 2100–2108.
26. Slesak G, Inthalad S, Kim JH, Manhpadit S, Somsavad S, et al. (2012) HighHIV vulnerability of ethnic minorities after a trans-Asian highway constructionin remote northern Laos. Int J STD AIDS 23: 570–575.
27. Ahmed S, Delaney K, Villalba-Diebold P, Aliyu G, Constantine N, et al. (2013)HIV counseling and testing and access-to-care needs of populations most-at-risk for HIV in Nigeria. AIDS Care 25: 85–94.
28. Maheswaran H, Thulare H, Stanistreet D, Tanser F, Newell ML (2012)Starting a home and mobile HIV testing service in a rural area of South Africa.J Acquir Immune Defic Syndr 59: e43–e46.
29. Menzies N, Abang B, Wanyenze R, Nuwaha F, Mugisha B, et al. (2009) Thecosts and effectiveness of four HIV counseling and testing strategies in Uganda.AIDS 23: 395–401.
30. Shapiro AE, Variava E, Rakgokong MH, Moodley N, Luke B, et al. (2012)Community-based targeted case finding for tuberculosis and HIV in householdcontacts of patients with tuberculosis in South Africa. Am J Respir Crit CareMed 185: 1110–1116.
31. University of Washington (2012) Home-based versus partner-friendly clinictesting to enhance male partner HIV-1 testing during pregnancy. Available:http://clinicaltrials.gov/ct2/show/NCT01620073. Accessed 1 July 2013.
32. National Institute of Allergy and Infectious Diseases (2010) A pilot semi-factorial cluster-randomized trial to estimate the effect size of communitymobilization and VCT vans on the adoption of voluntary counseling andtesting (VCT) services in Andhra Pradesh, India: the MCVCT Study.Available: http://clinicaltrials.gov/ct2/show/NCT01160575. Accessed 1 July2013.
33. Liverpool School of Tropical Medicine (2011) Home assessment and initiationof antiretroviral therapy for HIV in Malawi (CONDA-YAPA). Available:http://clinicaltrials.gov/ct2/show/NCT01414413. Accessed 1 July 2013.
34. SolidarMed (2011) Comparison of door-to-door versus community gathering toprovide HIV counseling and testing services in rural Lesotho (DoDoPi).Available: http://clinicaltrials.gov/ct2/show/record/NCT01459120. Ac-cessed 1 July 2013.
35. University of Zambia (2009) Home-based voluntary human immunodeficiencyvirus (HIV) counselling and testing in Zambia. Available: http://www.controlled-trials.com/ISRCTN53353725. Accessed 1 July 2013.
36. Stellenbosch University (2008) Is it possible to develop a home based package ofinterventions delivered by community based women that will improve levels ofmaternal, newborn, child and HIV care in a disadvantaged community inSouth Afr i ca? Ava i lab le : h t tp ://www.cont ro l l ed - t r i a l s . com/ISRCTN41046462. Accessed 1 July 2013.
37. London School of Hygiene and Tropical Medicine (2012) Intensified HIV/TBprevention linking home-based HIV testing, including the option of self-testing,with HIV care: a cluster-randomised trial in Blantyre, Malawi. Available:http://www.controlled-trials.com/ISRCTN02004005. Accessed 1 July 2013.
38. University of Washington (2010) Home self-testing for HIV to increase HIVtesting frequency in men who have sex with men (the iTest Study). Available:http://clinicaltrials.gov/ct2/show/study/NCT01161446. Accessed 1 July2013.
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
345

39. New York University (2012) Testing and linkage to care for injecting drug usersin Kenya (TLC-IDU Kenya). Available: http://clinicaltrials.gov/ct2/show/NCT01557998. Accessed 1 July 2013.
40. University of California at Los Angeles (2010) Using incentives to improveparolee participation and attendance in community treatment (PIP). Available:http://clinicaltrials.gov/ct2/show/NCT01090245. Accessed 1 July 2013.
41. Armbruster B, Helleringer S, Kalilani-Phiri L, Mkandawire J, Kohler HP(2011) Exploring the relative costs of contact tracing for increasing HIV casefinding in sub-Saharan countries. J Acquir Immune Defic Syndr 58: e29–e36.
42. Colindres P, Mermin J, Ezati E, Kambabazi S, Buyungo P, et al. (2008)Utilization of a basic care and prevention package by HIV-infected persons inUganda. AIDS Care 20: 139–145.
43. Lugada E, Levin J, Abang B, Mermin J, Mugalanzi E, et al. (2010) Comparisonof home and clinic-based HIV testing among household members of personstaking antiretroviral therapy in Uganda: results from a randomized trial.J Acquir Immune Defic Syndr 55: 245–252.
44. Were WA, Mermin JH, Wamai N, Awor AC, Bechange S, et al. (2006)Undiagnosed HIV infection and couple HIV discordance among householdmembers of HIV-infected people receiving antiretroviral therapy in Uganda.J Acquir Immune Defic Syndr 43: 91–95.
45. Wykoff RF, Heath CW Jr, Hollis SL, Leonard ST, Quiller CB, et al. (1988)Contact tracing to identify human immunodeficiency virus infection in a ruralcommunity. JAMA 259: 3563–3566.
46. Nelson AK, Caldas A, Sebastian JL, Munoz M, Bonilla C, et al. (2012)Community-based rapid oral human immunodeficiency virus testing fortuberculosis patients in Lima, Peru. Am J Trop Med Hyg 87: 399–406.
47. Choko AT, Desmond N, Webb EL, Chavula K, Napierala-Mavedzenge S,et al. (2011) The uptake and accuracy of oral kits for HIV self-testing in highHIV prevalence setting: a cross-sectional feasibility study in Blantyre, Malawi.PLoS Med 8: e1001102. doi:10.1371/journal.pmed.1001102
48. Frank AP, Wandell MG, Headings MD, Conant MA, Woody GE, et al. (1997)Anonymous HIV testing using home collection and telemedicine counseling. Amulticenter evaluation. Arch Intern Med 157: 309–314.
49. Spielberg F, Critchlow C, Vittinghoff E, Coletti AS, Sheppard H, et al. (2000)Home collection for frequent HIV testing: acceptability of oral fluids, driedblood spots and telephone results. HIV Early Detection Study Group. AIDS14: 1819–1828.
50. Bahwere P, Piwoz E, Joshua MC, Sadler K, Grobler-Tanner CH, et al. (2008)Uptake of HIV testing and outcomes within a community-based therapeuticcare (CTC) programme to treat severe acute malnutrition in Malawi: adescriptive study. BMC Infect Dis 8: 106.
51. Chamie G, Kwarisiima D, Clark TD, Kabami J, Jain V, et al. (2012)Leveraging rapid community-based HIV testing campaigns for non-commu-nicable diseases in rural Uganda. PLoS ONE 7: e43400. doi:10.1371/journal.pone.0043400
52. Chirawu P, Langhaug L, Mavhu W, Pascoe S, Dirawo J, et al. (2010)Acceptability and challenges of implementing voluntary counselling and testing(VCT) in rural Zimbabwe: evidence from the Regai Dzive Shiri Project. AIDSCare 22: 81–88.
53. Darling KE, Diserens EA, N’Garambe C, Ansermet-Pagot A, Masserey E, etal. (2012) A cross-sectional survey of attitudes to HIV risk and rapid HIVtesting among clients of sex workers in Switzerland. Sex Transm Infect 88:462–464.
54. Kawichai S, Celentano DD, Chariyalertsak S, Visrutaratna S, Short O, et al.(2007) Community-based voluntary counseling and testing services in ruralcommunities of Chiang Mai Province, Northern Thailand. AIDS Behav 11:770–777.
55. Kranzer K, Govindasamy D, van Schaik N, Thebus E, Davies N, et al. (2012)Incentivized recruitment of a population sample to a mobile HIV testingservice increases the yield of newly diagnosed cases, including those in need ofantiretroviral therapy. HIV Med 13: 132–137.
56. Lugada E, Millar D, Haskew J, Grabowsky M, Garg N, et al. (2010) Rapidimplementation of an integrated large-scale HIV counseling and testing,malaria, and diarrhea prevention campaign in rural Kenya. PLoS ONE 5:e12435. doi:10.1371/journal.pone.0012435
57. Mahler HR, Kileo B, Curran K, Plotkin M, Adamu T, et al. (2011) Voluntarymedical male circumcision: matching demand and supply with quality andefficiency in a high-volume campaign in Iringa Region, Tanzania. PLoS Med8: e1001131. doi:10.1371/journal.pmed.1001131
58. Ostermann J, Reddy EA, Shorter MM, Muiruri C, Mtalo A, et al. (2011) Whotests, who doesn’t, and why? Uptake of mobile HIV counseling and testing inthe Kilimanjaro Region of Tanzania. PLoS ONE 6: e16488. doi:10.1371/journal.pone.0016488
59. van Rooyen H, McGrath N, Chirowodza A, Joseph P, Fiamma A, et al. (2012)Mobile VCT: reaching men and young people in urban and rural SouthAfrican pilot studies (NIMH Project Accept, HPTN 043). AIDS Behav. E-pubahead of print. doi:10.1007/s10461-012-0368-x
60. Cherutich P, Kaiser R, Galbraith J, Williamson J, Shiraishi RW, et al. (2012)Lack of knowledge of HIV status a major barrier to HIV prevention, care andtreatment efforts in Kenya: results from a nationally representative study. PLoSONE 7: e36797. doi:10.1371/journal.pone.0036797
61. Dalal W, Feikin DR, Amolloh M, Ransom R, Burke H, et al. (2013) Home-based HIV testing and counseling in rural and urban Kenyan communities.J Acquir Immune Defic Syndr 62: e47–e54.
62. Gonzalez R, Munguambe K, Aponte J, Bavo C, Nhalungo D, et al. (2012)High HIV prevalence in a southern semi-rural area of Mozambique: acommunity-based survey. HIV Med 13: 581–588.
63. Kimaiyo S, Were MC, Shen C, Ndege S, Braitstein P, et al. (2010) Home-based HIV counselling and testing in western Kenya. East Afr Med J 87: 100–108.
64. Kranzer K, McGrath N, Saul J, Crampin AC, Jahn A, et al. (2008) Individual,household and community factors associated with HIV test refusal in ruralMalawi. Trop Med Int Health 13: 1341–1350.
65. Matovu JK, Kigozi G, Nalugoda F, Wabwire-Mangen F, Gray RH (2002) TheRakai Project counselling programme experience. Trop Med Int Health 7:1064–1067.
66. Medley A, Ackers M, Amolloh M, Owuor P, Muttai H, et al. (2013) Earlyuptake of HIV clinical care after testing HIV-positive during home-basedtesting and counseling in western Kenya. AIDS Behav 17: 224–234.
67. Michelo C, Sandoy IF, Dzekedzeke K, Siziya S, Fylkesnes K (2006) Steep HIVprevalence declines among young people in selected Zambian communities:population-based observations (1995–2003). BMC Public Health 6: 279.
68. Molesworth AM, Ndhlovu R, Banda E, Saul J, Ngwira B, et al. (2010) Highaccuracy of home-based community rapid HIV testing in rural Malawi.J Acquir Immune Defic Syndr 55: 625–630.
69. Mutale W, Michelo C, Jurgensen M, Fylkesnes K (2010) Home-basedvoluntary HIV counselling and testing found highly acceptable and to reduceinequalities. BMC Public Health 10: 347.
70. Naik R, Tabana H, Doherty T, Zembe W, Jackson D (2012) Clientcharacteristics and acceptability of a home-based HIV counselling and testingintervention in rural South Africa. BMC Public Health 12: 824.
71. Negin J, Wariero J, Mutuo P, Jan S, Pronyk P (2009) Feasibility, acceptabilityand cost of home-based HIV testing in rural Kenya. Trop Med Int Health 14:849–855.
72. Sekandi JN, Sempeera H, List J, Mugerwa MA, Asiimwe S, et al. (2011) Highacceptance of home-based HIV counseling and testing in an urban communitysetting in Uganda. BMC Public Health 11: 730.
73. Shisana O, Stoker D, Simbayi LC, Orkin M, Bezuidenhout F, et al. (2004)South African national household survey of HIV/AIDS prevalence, behav-ioural risks and mass media impact—detailed methodology and response rateresults. S Afr Med J 94: 283–288.
74. Tumwesigye E, Wana G, Kasasa S, Muganzi E, Nuwaha F (2010) High uptakeof home-based, district-wide, HIV counseling and testing in Uganda. AIDSPatient Care STDS 24: 735–741.
75. Uwimana J, Zarowsky C, Hausler H, Jackson D (2012) Training communitycare workers to provide comprehensive TB/HIV/PMTCT integrated care inKwaZulu-Natal: lessons learnt. Trop Med Int Health 17: 488–496.
76. van Rooyen H, Phakathi Z, Krows M, Hong T, Barnabas R, et al. (2012) Hightesting uptake and linkages to HIV treatment through home-based HIVcounseling and testing and facilitated referral: KwaZulu-Natal, South Africa[abstract]. 19th Conference on Retroviruses and Opportunistic Infections; 5–8March 2012; Seattle, Washington, US.
77. Vreeman RC, Nyandiko WM, Braitstein P, Were MC, Ayaya SO, et al. (2010)Acceptance of HIV testing for children ages 18 months to 13 years identifiedthrough voluntary, home-based HIV counseling and testing in western Kenya.J Acquir Immune Defic Syndr 55: e3–e10.
78. Wawer MJ, Gray RH, Sewankambo NK, Serwadda D, Paxton L, et al. (1998)A randomized, community trial of intensive sexually transmitted disease controlfor AIDS prevention, Rakai, Uganda. AIDS 12: 1211–1225.
79. Welz T, Hosegood V, Jaffar S, Batzing-Feigenbaum J, Herbst K, et al. (2007)Continued very high prevalence of HIV infection in rural KwaZulu-Natal,South Africa: a population-based longitudinal study. AIDS 21: 1467–1472.
80. Were W, Mermin J, Bunnell R, Ekwaru JP, Kaharuza F (2003) Home-basedmodel for HIV voluntary counselling and testing. Lancet 361: 1569.
81. Wolff B, Nyanzi B, Katongole G, Ssesanga D, Ruberantwari A, et al. (2005)Evaluation of a home-based voluntary counselling and testing intervention inrural Uganda. Health Policy Plan 20: 109–116.
82. Feeley FG, Collier AC, Richards SC, Van der Borght SF, Rinke de Wit T(2007) A successful workplace program for voluntary counseling and testing andtreatment of HIV/AIDS at Heineken, Rwanda. Int J Occup Environ Health13: 99–106.
83. Kwena ZA, Camlin CS, Shisanya CA, Mwanzo I, Bukusi EA (2013) Short-term mobility and the risk of HIV infection among married couples in thefishing communities along Lake Victoria, Kenya. PLoS ONE 8: e54523.doi:10.1371/journal.pone.0054523
84. Machekano R, McFarland W, Mbizvo MT, Bassett MT, Katzenstein D, et al.(1998) Impact of HIV counselling and testing on HIV seroconversion andreported STD incidence among male factory workers in Harare, Zimbabwe.Cent Afr J Med 44: 98–102.
85. Todd CS, Nasir A, Mansoor GF, Sahibzada SM, Jagodzinski LL, et al. (2012)Cross-sectional assessment of prevalence and correlates of blood-borne andsexually-transmitted infections among Afghan National Army recruits. BMCInfect Dis 12: 196.
86. Van der Borght SF, Schim van der Loeff MF, Clevenbergh P, Kabarega JP,Kamo E, et al. (2010) Long-term voluntary counseling and testing (VCT)uptake dynamics in a multicountry HIV workplace program in sub-SaharanAfrica. AIDS Care 22: 195–205.
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
346

87. Henry-Reid LM, Rodriguez F, Bell MA, Martinez J, Peera A (1998) Youthcounseled for HIV testing at school- and hospital-based clinics. J Natl MedAssoc 90: 287–292.
88. Kharsany AB, Mlotshwa M, Frohlich JA, Yende Zuma N, Samsunder N, et al.(2012) HIV prevalence among high school learners—opportunities for schools-based HIV testing programmes and sexual reproductive health services. BMCPublic Health 12: 231.
89. Patel D, Matyanga P, Nyamundaya T, Chimedza D, Webb K, et al. (2012)Facilitating HIV testing, care and treatment for orphans and vulnerablechildren aged five years and younger through community-based earlychildhood development playcentres in rural Zimbabwe. J Int AIDS Soc 15(Suppl 2): 17404.
90. Lister NA, Smith A, Tabrizi SN, Garland S, Hayes P, et al. (2005)Comprehensive clinical care on-site in men-only saunas: confidential STI/HIV screening outreach clinic. Int J STD AIDS 16: 794–798.
91. Outlaw AY, Naar-King S, Parsons JT, Green-Jones M, Janisse H, et al. (2010)Using motivational interviewing in HIV field outreach with young AfricanAmerican men who have sex with men: a randomized clinical trial. Am J PublicHealth 100 (Suppl 1): S146–S151.
92. Spielberg F, Branson BM, Goldbaum GM, Lockhart D, Kurth A, et al. (2005)Choosing HIV counseling and testing strategies for outreach settings: arandomized trial. J Acquir Immune Defic Syndr 38: 348–355.
93. Centers for Disease Control and Prevention (2007) Rapid HIV testing amongracial/ethnic minority men at gay pride events—nine U.S. cities, 2004-2006.MMWR Morb Mortal Wkly Rep 56: 602–604.
94. Balaji AB, Bowles KE, Le BC, Paz-Bailey G, Oster AM (2013) High HIVincidence and prevalence and associated factors among young MSM, 2008.AIDS 27: 269–278.
95. Galvan FH, Bluthenthal RN, Ani C, Bing EG (2006) Increasing HIV testingamong latinos by bundling HIV testing with other tests. J Urban Health 83:849–859.
96. Smith LV, Rudy ET, Javanbakht M, Uniyal A, Sy LS, et al. (2006) Clientsatisfaction with rapid HIV testing: comparison between an urban sexuallytransmitted disease clinic and a community-based testing center. AIDS PatientCare STDS 20: 693–700.
97. Sy FS, Rhodes SD, Choi ST, Drociuk D, Laurent AA, et al. (1998) Theacceptability of oral fluid testing for HIV antibodies. A pilot study in gay bars ina predominantly rural state. Sex Transm Dis 25: 211–215.
98. Centers for Disease Control and Prevention (1997) Community-based HIVprevention in presumably underserved populations—Colorado Springs,Colorado, July-September 1995. MMWR Morb Mortal Wkly Rep 46: 152–155.
99. Gelberg L, Robertson MJ, Arangua L, Leake BD, Sumner G, et al. (2012)Prevalence, distribution, and correlates of hepatitis C virus infection amonghomeless adults in Los Angeles. Public Health Rep 127: 407–421.
100. O’Connor CA, Patsdaughter CA, Grindel CG, Taveira PF, Steinberg JL (1998)A mobile HIV education and testing program: bringing services to hard-to-reach populations. AIDS Patient Care STDS 12: 931–937.
101. Nhurod P, Bollen LJ, Smutraprapoot P, Suksripanich O, Siangphoe U, et al.(2010) Access to HIV testing for sex workers in Bangkok, Thailand: a highprevalence of HIV among street-based sex workers. Southeast Asian J TropMed Public Health 41: 153–162.
102. Bell DN, Martinez J, Botwinick G, Shaw K, Walker LE, et al. (2003) Casefinding for HIV-positive youth: a special type of hidden population. J AdolescHealth 33: 10–22.
103. Robbins CL, Zapata L, Kissin DM, Shevchenko N, Yorick R, et al. (2010)Multicity HIV seroprevalence in street youth, Ukraine. Int J STD AIDS 21:489–496.
104. Liang TS, Erbelding E, Jacob CA, Wicker H, Christmyer C, et al. (2005) RapidHIV testing of clients of a mobile STD/HIV clinic. AIDS Patient Care STDS19: 253–257.
105. Bucher JB, Thomas KM, Guzman D, Riley E, Dela Cruz N, et al. (2007)Community-based rapid HIV testing in homeless and marginally housed adultsin San Francisco. HIV Med 8: 28–31.
106. Bowles KE, Clark HA, Tai E, Sullivan PS, Song B, et al. (2008) Implementingrapid HIV testing in outreach and community settings: results from anadvancing HIV prevention demonstration project conducted in seven U.S.cities. Public Health Rep 123 (Suppl 3): 78–85.
107. Grabbe KL, Menzies N, Taegtmeyer M, Emukule G, Angala P, et al. (2010)Increasing access to HIV counseling and testing through mobile services inKenya: strategies, utilization, and cost-effectiveness. J Acquir Immune DeficSyndr 54: 317–323.
108. Lahuerta M, Sabido M, Giardina F, Hernandez G, Palacios JF, et al. (2011)Comparison of users of an HIV/syphilis screening community-based mobilevan and traditional voluntary counselling and testing sites in Guatemala. SexTransm Infect 87: 136–140.
109. Morin SF, Khumalo-Sakutukwa G, Charlebois ED, Routh J, Fritz K, et al.(2006) Removing barriers to knowing HIV status: same-day mobile HIV testingin Zimbabwe. J Acquir Immune Defic Syndr 41: 218–224.
110. Nglazi MD, van Schaik N, Kranzer K, Lawn SD, Wood R, et al. (2012) Anincentivized HIV counseling and testing program targeting hard-to-reachunemployed men in Cape Town, South Africa. J Acquir Immune Defic Syndr59: e28–e34.
111. Spielberg F, Kurth A, Reidy W, McKnight T, Dikobe W, et al. (2011) Iterativeevaluation in a mobile counseling and testing program to reach people of colorat risk for HIV—new strategies improve program acceptability, effectiveness,and evaluation capabilities. AIDS Educ Prev 23: 110–116.
112. Truong HM, Fritz K, McFarland W, Hartogensis W, Fiamma A, et al. (2011)Recent HIV type 1 infection among participants in a same-day mobile testingpilot study in Zimbabwe. AIDS Res Hum Retroviruses 27: 593–595.
113. Bingham TA, Secura GM, Behel SK, Bunch JG, Simon PA, et al. (2008) HIVrisk factors reported by two samples of male bathhouse attendees in LosAngeles, California, 2001–2002. Sex Transm Dis 35: 631–636.
114. Bungay V, Kolar K, Thindal S, Remple VP, Johnston CL, et al. (2013)Community-based HIV and STI prevention in women working in indoor sexmarkets. Health Promot Pract 14: 247–255.
115. Champenois K, Le Gall JM, Jacquemin C, Jean S, Martin C, et al. (2012)ANRS-COM’TEST: description of a community-based HIV testing interven-tion in non-medical settings for men who have sex with men. BMJ Open 2:e000693.
116. DiFranceisco W, Holtgrave DR, Hoxie N, Reiser WJ, Resenhoeft R, et al.(1998) HIV seropositivity rates in outreach-based counseling and testingservices: program evaluation. J Acquir Immune Defic Syndr Hum Retrovirol19: 282–288.
117. Keenan PA, Keenan JM (2001) Rapid HIV testing in urban outreach: astrategy for improving posttest counseling rates. AIDS Educ Prev 13: 541–550.
118. Stein R, Green K, Bell K, Toledo CA, Uhl G, et al. (2011) Provision of HIVcounseling and testing services at five community-based organizations amongyoung men of color who have sex with men. AIDS Behav 15: 743–750.
119. Hood JE, MacKellar D, Spaulding A, Nelson R, Mosiakgabo B, et al. (2012)Client characteristics and gender-specific correlates of testing HIV positive: acomparison of standalone center versus mobile outreach HIV testing andcounseling in Botswana. AIDS Behav 16: 1902–1916.
120. McCoy SI, Shiu K, Martz TE, Smith CD, Mattox L, et al. (2013) Improvingthe efficiency of HIV testing with peer recruitment, financial incentives, and theinvolvement of persons living with HIV infection. J Acquir Immune DeficSyndr 63: e56–e63.
121. van Schaik N, Kranzer K, Wood R, Bekker LG (2010) Earlier HIV diagnosis—are mobile services the answer? S Afr Med J 100: 671–674.
122. Shrestha RK, Clark HA, Sansom SL, Song B, Buckendahl H, et al. (2008)Cost-effectiveness of finding new HIV diagnoses using rapid HIV testing incommunity-based organizations. Public Health Rep 123 (Suppl 3): 94–100.
123. Yin YP, Chen SC, Wang HC, Wei WH, Wang QQ, et al. (2012) Prevalenceand risk factors of HSV-2 infection and HSV-2/HIV coinfection in men whohave sex with men in China: a multisite cross-sectional study. Sex Transm Dis39: 354–358.
124. Govindasamy D, van Schaik N, Kranzer K, Wood R, Mathews C, et al. (2011)Linkage to HIV care from a mobile testing unit in South Africa by differentCD4 count strata. J Acquir Immune Defic Syndr 58: 344–352.
125. Granich R, Muraguri N, Doyen A, Garg N, Williams BG (2012) Achievinguniversal access for human immunodeficiency virus and tuberculosis: potentialprevention impact of an integrated multi-disease prevention campaign inkenya. AIDS Res Treat 2012: 412643.
126. Larson BA, Schnippel K, Ndibongo B, Xulu T, Brennan A, et al. (2012) Rapidpoint-of-care CD4 testing at mobile HIV testing sites to increase linkage tocare: an evaluation of a pilot program in South Africa. J Acquir Immune DeficSyndr 61: e13–e17.
127. Wachira J, Kimaiyo S, Ndege S, Mamlin J, Braitstein P (2012) What is theimpact of home-based HIV counseling and testing on the clinical status ofnewly enrolled adults in a large HIV care program in western Kenya? ClinInfect Dis 54: 275–281.
128. Naughton J, Hughes H, Wilkinson L, Boyles T (2011) HIV counselling andtesting in South African schools. Lancet 377: 1748.
129. Wringe A, Floyd S, Kazooba P, Mushati P, Baisley K, et al. (2012)Antiretroviral therapy uptake and coverage in four HIV community cohortstudies in sub-Saharan Africa. Trop Med Int Health 17: e38–e48.
130. Coates T, Eshleman S, Chariyalertsak S, Chingono A, Gray G, et al. (2013)Community-level reductions in estimated HIV incidence: HIV PreventionTrials Network 043, Project Accept [abstract]. 20th Conference onRetroviruses and Opportunistic Infections; 3–6 March 2013; Atlanta, Georgia,US.
131. Kahn JG, Harris B, Mermin JH, Clasen T, Lugada E, et al. (2011) Cost ofcommunity integrated prevention campaign for malaria, HIV, and diarrhea inrural Kenya. BMC Health Serv Res 11: 346.
132. McConnel CE, Stanley N, du Plessis JA, Pitter CS, Abdulla F, et al. (2005) Thecost of a rapid-test VCT clinic in South Africa. S Afr Med J 95: 968–971.
133. Shrestha RK, Sansom SL, Kimbrough L, Hutchinson AB, Daltry D, et al.(2010) Cost-effectiveness of using social networks to identify undiagnosed HIVinfection among minority populations. J Public Health Manag Pract 16: 457–464.
134. Shrestha RK, Sansom SL, Schulden JD, Song B, Smith LC, et al. (2011) Costsand effectiveness of finding new HIV diagnoses by using rapid testing intransgender communities. AIDS Educ Prev 23: 49–57.
135. Terris-Prestholt F, Kumaranayake L, Foster S, Kamali A, Kinsman J, et al.(2006) The role of community acceptance over time for costs of HIV and STIprevention interventions: analysis of the Masaka Intervention Trial, Uganda,1996–1999. Sex Transm Dis 33: S111–S116.
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
347
136. Edgil D, Stankard P, Forsythe S, Rech D, Chrouser K, et al. (2011) Voluntarymedical male circumcision: logistics, commodities, and waste managementrequirements for scale-up of services. PLoS Med 8: e1001128. doi:10.1371/journal.pmed.1001128
137. Jurgensen M, Sandoy IF, Michelo C, Fylkesnes K (2013) Effects of home-basedvoluntary counselling and testing on HIV-related stigma: findings from acluster-randomized trial in Zambia. Soc Sci Med 81: 18–25.
138. Kyaddondo D, Wanyenze RK, Kinsman J, Hardon A (2012) Home-basedHIV counseling and testing: client experiences and perceptions in EasternUganda. BMC Public Health 12: 966.
139. Nuwaha F, Kasasa S, Wana G, Muganzi E, Tumwesigye E (2012) Effect ofhome-based HIV counselling and testing on stigma and risky sexualbehaviours: serial cross-sectional studies in Uganda. J Int AIDS Soc 15: 17423.
140. Tanser F, Barnighausen T, Grapsa E, Zaidi J, Newell ML (2013) Highcoverage of ART associated with decline in risk of HIV acquisition in ruralKwaZulu-Natal, South Africa. Science 339: 966–971.
141. Fonner VA, Denison J, Kennedy CE, O’Reilly K, Sweat M (2012) Voluntarycounseling and testing (VCT) for changing HIV-related risk behavior indeveloping countries. Cochrane Database Syst Rev: CD001224.
142. Bor J, Herbst AJ, Newell ML, Barnighausen T, et al. (2013) Increases in adultlife expectancy in rural South Africa: valuing the scale-up of HIV treatment.Science 339: 961–965.
143. Anema A, Au-Yeung CG, Joffres M, Kaida A, Vasarhelyi K, et al. (2011)Estimating the impact of expanded access to antiretroviral therapy onmaternal, paternal and double orphans in sub-Saharan Africa, 2009–2020.AIDS Res Ther 8: 13.
144. Thirumurthy H, Chamie G, Jain V, Kabami J, Kwarisiima D, et al. (2013)Improved employment and education outcomes in households of HIV-infectedadults with high CD4 cell counts: evidence from a community health campaignin Uganda. AIDS 27: 627–634.
145. Bor J, Tanser F, Newell ML, Barnighausen T (2012) In a study of a populationcohort in South Africa, HIV patients on antiretrovirals had nearly full recoveryof employment. Health Aff (Millwood) 31: 1459–1469.
146. Risley CL, Drake LJ, Bundy DA (2012) Economic impact of HIV andantiretroviral therapy on education supply in high prevalence regions. PLoSONE 7: e42909. doi:10.1371/journal.pone.0042909
147. Ventelou B, Arrighi Y, Greener R, Lamontagne E, Carrieri P, et al. (2012) Themacroeconomic consequences of renouncing to universal access to antiretro-viral treatment for HIV in Africa: a micro-simulation model. PLoS ONE 7:e34101. doi:10.1371/journal.pone.0034101
148. Hopkins DR (1998) The Guinea worm eradication effort: lessons for the future.Emerg Infect Dis 4: 414–415.
149. de Quadros CA, Andrus JK, Olive JM, Guerra de Macedo C, Henderson DA(1992) Polio eradication from the Western Hemisphere. Annu Rev PublicHealth 13: 239–252.
150. de Quadros CA, Olive JM, Hersh BS, Strassburg MA, Henderson DA, et al.(1996) Measles elimination in the Americas. Evolving strategies. JAMA 275:224–229.
151. Natchiar G, Robin AL, Thulasiraj RD, Krishnaswamy S (1994) Attacking thebacklog of India’s curable blind. The Aravind Eye Hospital model. ArchOphthalmol 112: 987–993.
152. Suthar AB, Klinkenberg E, Ramsay A, Garg N, Bennett R, et al. (2012)Community-based multi-disease prevention campaigns for controlling humanimmunodeficiency virus-associated tuberculosis. Int J Tuberc Lung Dis 16:430–436.
153. World Health Organization (2012) Prevention and control of NCDs: guidelinesfor primary health care in low-resource settings. Available: http://apps.who.int/iris/bitstream/10665/76173/1/9789241548397_eng.pdf. Accessed 1 July2013.
154. World Health Organization (2012) Disease surveillance for malaria elimina-tion: an operational manual. Available: http://whqlibdoc.who.int/publications/2012/9789241503334_eng.pdf. Accessed 1 July 2013.
155. World Health Organization (2013) Systematic screening for active tuberculosis:principles and recommendations. Available: http://www.who.int/tb/publications/Final_TB_Screening_guidelines.pdf. Accessed 1 July 2013.
156. Kahn JG, Muraguri N, Harris B, Lugada E, Clasen T, et al. (2012) IntegratedHIV testing, malaria, and diarrhea prevention campaign in Kenya: modeledhealth impact and cost-effectiveness. PLoS ONE 7: e31316. doi:10.1371/journal.pone.0031316
157. Shanks L, Klarkowski D, O’Brien DP (2013) False positive HIV diagnoses inresource limited settings: operational lessons learned for HIV programmes.PLoS ONE 8: e59906. doi:10.1371/journal.pone.0059906
158. Kimbrough LW, Fisher HE, Jones KT, Johnson W, Thadiparthi S, et al. (2009)Accessing social networks with high rates of undiagnosed HIV infection: thesocial networks demonstration project. Am J Public Health 99: 1093–1099.
159. Ti L, Hayashi K, Kaplan K, Suwannawong P, Wood E, et al. (2013)Willingness to access peer-delivered HIV testing and counseling among peoplewho inject drugs in Bangkok, Thailand. J Community Health 38: 427–433.
160. World Health Organization (2012) Guidance on couples HIV testing andcounselling including antiretroviral therapy for treatment and prevention inserodiscordant couples. Available: http://whqlibdoc.who.int/publications/2012/9789241501972_eng.pdf. Accessed 1 July 2013.
161. World Health Organization (2012) Planning, implementing and monitoringhome-based HIV testing. Available: http://apps.who.int/iris/bitstream/10665/75366/1/9789241504317_eng.pdf. Accessed 1 July 2013.
162. Binagwaho A, Mugwaneza P, Irakoze AA, Nsanzimana S, Agbonyitor M, et al.(2013) Scaling up early infant diagnosis of HIV in Rwanda, 2008-2010. J PublicHealth Policy 34: 2–16.
163. Granich RM, Gilks CF, Dye C, De Cock KM, Williams BG (2009) Universalvoluntary HIV testing with immediate antiretroviral therapy as a strategy forelimination of HIV transmission: a mathematical model. Lancet 373: 48–57.
164. Kato M, Granich R, Duc Bui D, Vu Tran H, Nadol P, et al. (2013) Thepotential impact of expanding antiretroviral therapy and combinationprevention in Vietnam: towards elimination of HIV transmission. J AcquirImmune Defic Syndr. E-pub ahead of print. doi: 10.1097/QAI.0-b013e31829b535b
165. Granich R, Gupta S, Suthar AB, Smyth C, Hoos D, et al. (2011) Antiretroviraltherapy in prevention of HIV and TB: update on current research efforts. CurrHIV Res 9: 446–469.
166. World Health Organization (2010) Delivering HIV test results and messages forre-testing and counseling in adults. Available: http://whqlibdoc.who.int/publications/2010/9789241599115_eng.pdf. Accessed 1 July 2013.
167. Mugglin C, Estill J, Wandeler G, Bender N, Egger M, et al. (2012) Loss toprogramme between HIV diagnosis and initiation of antiretroviral therapy insub-Saharan Africa: systematic review and meta-analysis. Trop Med IntHealth. E-pub ahead of print. doi: 10.1111/j.1365-3156.2012.03089.x.
168. Rosen S, Fox MP (2011) Retention in HIV care between testing and treatmentin sub-Saharan Africa: a systematic review. PLoS Med 8: e1001056.doi:10.1371/journal.pmed.1001056
169. Jaffar S, Amuron B, Foster S, Birungi J, Levin J, et al. (2009) Rates ofvirological failure in patients treated in a home-based versus a facility-basedHIV-care model in Jinja, southeast Uganda: a cluster-randomised equivalencetrial. Lancet 374: 2080–2089.
170. Kipp W, Konde-Lule J, Saunders LD, Alibhai A, Houston S, et al. (2010)Results of a community-based antiretroviral treatment program for HIV-1infection in Western Uganda. Curr HIV Res 8: 179–185.
171. Selke HM, Kimaiyo S, Sidle JE, Vedanthan R, Tierney WM, et al. (2010)Task-shifting of antiretroviral delivery from health care workers to personsliving with HIV/AIDS: clinical outcomes of a community-based program inKenya. J Acquir Immune Defic Syndr 55: 483–490.
172. Pant Pai N, Sharma J, Shivkumar S, Pillay S, Vadnais C, et al. (2013)Supervised and unsupervised self-testing for HIV in high- and low-riskpopulations: a systematic review. PLoS Med 10: e1001414. doi:10.1371/journal.pmed.1001414
173. World Health Organization (2013) Report on the first international symposiumon self-testing for HIV: the legal, ethical, gender, human rights and publichealth implication of HIV self-testing scale-up. Available: http://apps.who.int/iris/bitstream/10665/85267/1/9789241505628_eng.pdf. Accessed 1 July2013.
174. Tang JL, Liu JL (2000) Misleading funnel plot for detection of bias in meta-analysis. J Clin Epidemiol 53: 477–484.
175. Schwartlander B, Stover J, Hallett T, Atun R, Avila C, et al. (2011) Towards animproved investment approach for an effective response to HIV/AIDS. Lancet377: 2031–2041.
176. World Health Organization (2013) Consolidated guidelines on the use ofantiretroviral drugs for treating and preventing HIV infection: recommenda-tions for a public health approach. Available: http://www.who.int/hiv/pub/guidelines/arv2013/. Accessed 1 July 2013.
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
348
Editors’ Summary
Background. Three decades into the AIDS epidemic, about34 million people (most living in resource-limited countries)are infected with HIV, the virus that causes AIDS. Every yearanother 2.2 million people become infected with HIV, usuallythrough unprotected sex with an infected partner, and about1.7 million people die. Infection with HIV, which graduallydestroys the CD4 lymphocytes and other immune systemcells that provide protection from life-threatening infections,is usually diagnosed by looking for antibodies to HIV in theblood or saliva. Disease progression is subsequently moni-tored in HIV-positive individuals by counting the CD4 cells intheir blood. Initiation of antiretroviral drug therapy—acombination of drugs that keeps HIV replication in checkbut that does not cure the infection—is recommended whenan individual’s CD4 count falls below 500 cells/ml of blood orwhen he or she develops signs of severe or advanceddisease, such as unusual infections.
Why Was This Study Done? As part of intensified effortsto eliminate HIV/AIDS, United Nations member statesrecently set several HIV-related targets to be achieved by2015, including reduced transmission of HIV and increaseddelivery of antiretroviral therapy. These targets can only beachieved if there is a large expansion in HIV testing andcounseling (HTC) and increased access to HIV prevention andcare services. The World Health Organization currentlyrecommends that everyone attending a healthcare facilityin regions where there is a generalized HIV epidemic(defined as when 1% or more of the general population isHIV-positive) should be offered HTC. However, many peoplerarely visit healthcare facilities, and others refuse ‘‘facility-based’’ HTC because they fear stigmatization and discrimi-nation. Thus, facility-based HTC alone is unlikely to besufficient to enable national and global HIV targets to bereached. In this systematic review and meta-analysis, theresearchers evaluate the performance of community-basedHTC approaches such as index testing (offering HTC to thesexual and injecting partners and household members ofpeople with HIV), mobile testing (offering HTC through aservice that visits shopping centers and other publicfacilities), and door-to-door testing (systematically offeringHTC to homes in a catchment area). A systematic review usespredefined criteria to identify all the research on a giventopic; meta-analysis combines the results of several studies.
What Did the Researchers Do and Find? The researchersidentified 117 studies (most undertaken in Africa and NorthAmerica) involving 864,651 participants that evaluatedcommunity-based HTC approaches. Among these studies,the percentage of people offered community-based HTCwho accepted it (HTC uptake) was 88% for index testing,87% for self-testing, 80% for door-to-door testing, 67% forworkplace testing, and 62% for school-based testing.Compared to facility-based approaches, community-basedapproaches increased the chances of an individual’s CD4count being above 350 cells/ml at diagnosis (an importantobservation because early diagnosis improves subsequentoutcomes) but had a lower positivity rate, possibly becausepeople with symptoms of HIV are more likely to visit
healthcare facilities than healthy individuals. Importantly,80% of participants in the community-based HTC studieshad their CD4 count measured after HIV diagnosis, and 73%of the participants initiated antiretroviral therapy after theirCD4 count fell below national eligibility criteria; both theseobservations suggest that community-based HTC success-fully linked people to care. Finally, offering community-based HTC approaches in addition to facility-based ap-proaches increased HTC coverage seven-fold at the popu-lation level.
What Do These Findings Mean? These findings showthat community-based HTC can achieve high HTC uptakerates and can reach HIV-positive individuals earlier, whenthey still have high CD4 counts. Importantly, they alsosuggest that the level of linkage to care of community-basedHTC is similar to that of facility-based HTC. Although thelower positivity rate of community-based HTC approachesmeans that more people need to be tested with theseapproaches than with facility-based HTC to identify the samenumber of HIV-positive individuals, this downside of com-munity-based HTC is likely to be offset by the earlieridentification of HIV-positive individuals, which shouldimprove life expectancy and reduce HIV transmission atthe population level. Although further studies are needed toevaluate community-based HTC in other regions of theworld, these findings suggest that offering community-based HTC in HIV programs in addition to facility-basedtesting should support the increased access to HIV preven-tion and care that is required for the intensification of HIV/AIDS elimination efforts.
Additional Information. Please access these websites viathe online version of this summary at http://dx.doi.org/10.1371/journal.pmed.1001496.
N The World Health Organization provides information on allaspects of HIV/AIDS, including information on counselingand testing (in several languages)
N Information is available from the US National Institute ofAllergy and Infectious Diseases on HIV infection and AIDS
N NAM/aidsmap provides basic information about HIV/AIDSand summaries of recent research findings on HIV care andtreatment
N Information is available from Avert, an international AIDScharity, on many aspects of HIV/AIDS, including informa-tion on the global HIV/AIDS epidemic, on HIV testing, andon HIV transmission and testing (in English and Spanish)
N The UK National Health Service Choices website providesinformation (including personal stories) about HIV andAIDS
N The World AIDS Day Report 2012 provides up-to-dateinformation about the AIDS epidemic and efforts to halt it
N Patient stories about living with HIV/AIDS are availablethrough Avert; the nonprofit website Healthtalkonline alsoprovides personal stories about living with HIV, includingstories about getting a diagnosis
Community-based HIV Testing and Counselling
PLOS Medicine | www.plosmedicine.org August 2013 | Volume 10 | Issue 8 | e1001496
349

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
Research
From caution to urgency: the evolution of HIV testing and counselling in AfricaR Baggaley,a B Hensen,b O Ajose,c KL Grabbe,d VJ Wong,e A Schilsky,d Y-R Lo,a F Lule,f R Granicha & J Hargreavesb
BackgroundSince the !rst antibody tests for human immunode!ciency virus (HIV) infection became available, public health orga-nizations and human rights activists have debated the best approach to HIV testing and counselling (HTC).1 At a time when there was no e"ective treatment and HIV-infected indi-viduals faced widespread discrimination and stigmatization,1 many argued that HTC was inappropriate because it provided little bene!t to the individual.1,2 Conversely, others believed that testing was the key to promoting a change in behaviour.1,3 #ese two concerns framed early debates about HTC.4
Initially, there was general support for a cautious response to HTC and HIV infection, although this was considered “exceptional” compared with responses to other infectious diseases.1,5 For example, in 1987, the World Health Organiza-tion (WHO) emphasized caution in extending routine HIV testing beyond blood donors.1 At that time, standards for HTC, which were based on an international consensus reached by WHO and other stakeholders, emphasized voluntarism and gave rise to the adoption of voluntary counselling and test-ing.1 #is approach consisted of three primary components: counselling before and a$er an HIV test, which included an individualized risk-reduction plan based on the test results; informed written consent; and con!dentiality.1
As evidence emerged that antiretroviral therapy (ART) could signi!cantly reduce mother-to-child HIV transmission and “alter the clinical course” of HIV infection, the HTC debate changed.1,3,6 Clinicians and public health professionals now argued that an exceptional approach to HTC was no longer
appropriate. #e view was that HTC should be standard clini-cal practice in settings where patients present with symptoms of an HIV infection and where ART is available.1,2
At !rst, however, ART was not universally available. In 2003, only 1% of individuals in need of ART had access to treatment and WHO declared a global health emergency.7 #is declaration gave rise to a series of initiatives for expanding access to ART in developing countries, including the 2003 WHO 3-by-5 initiative and #e World Bank’s Multi-Country HIV/AIDS Program.7–9 In the same year, increased funding for extending treatment became available through the United States President’s Emergency Plan for AIDS Relief and the Global Fund to Fight AIDS, Tuberculosis and Malaria. In addition, the political climate changed and increased access to prevention and treatment of HIV infection was endorsed. #ese developments profoundly in%uenced the debate on HTC at a time when fewer than 10% of those infected with HIV were aware of their status10 and most were diagnosed at the end stage of the disease, when immune suppression made ART less e"ective.11,12 Consequently, voluntary counselling and testing was no longer seen as su&cient for enabling people to become aware of their HIV status. In the era of ART, alterna-tive approaches to HTC were required.1,2
One development was the emergence of provider-initiated HIV testing and counselling (PITC).1 In 2003, only 52% of pregnant women in Botswana knew their HIV status.13 To increase the knowledge of HIV status, the government insti-tuted a policy of “routine” PITC in various clinical settings in 2004.14 Similarly, Uganda implemented PITC in referral hospitals in 2005 and Zambia implemented it in tuberculosis
Objective To describe recent changes in policy on provider-initiated testing and counselling (PITC) for human immunodeficiency virus (HIV) infection in African countries and to investigate patients’ experiences of and views about PITC.Methods A review of the published literature and of national HIV testing policies, strategic frameworks, plans and other relevant documents was carried out.Findings Of the African countries reviewed, 42 (79.2%) had adopted a PITC policy. Of the 42, all recommended PITC for the prevention of mother-to-child HIV transmission, 66.7% recommended it for tuberculosis clinics and patients, and 45.2% for sexually transmitted infection clinics. Moreover, 43.6% adopted PITC in 2005 or 2006. The literature search identified 11 studies on patients’ experiences of and views about PITC in clinical settings in Africa. The clear majority regarded PITC as acceptable. However, women in antenatal clinics were not always aware that they had the right to decline an HIV test.Conclusion Policy and practice on HIV testing and counselling in Africa has shifted from a cautious approach that emphasizes confidentiality to greater acceptance of the routine o!er of HIV testing. The introduction of PITC in clinical settings has contributed to increased HIV testing in several of these settings. Most patients regard PITC as acceptable. However, other approaches are needed to reach people who do not consult health-care services.
a HIV/AIDS Department, World Health Organization, Geneva, Switzerland.b Department of Infectious Disease Epidemiology, London School of Hygiene and Tropical Medicine, Keppel Street, London WC1E 7HT, England.c Clinton Health Access Initiative, Dar es Salaam, United Republic of Tanzania.d Division of Global HIV/AIDS, Centers for Disease Control and Prevention, Atlanta, United States of America (USA).e O"ce of HIV/AIDS, United States Agency for International Development, Washington, USA.f Communicable Diseases, World Health Organization Regional O"ce for Africa, Brazzaville, Congo.Correspondence to B Hensen (e-mail: [email protected]).(Submitted: 5 December 2011 – Revised version received: 9 May 2012 – Accepted: 11 May 2012 – Published online: 27 June 2012 )
350

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in AfricaR Baggaley et al.
clinics in 2004.15,16 In 2006, the United States Centers for Disease Control and Prevention recommended that PITC be o"ered to adults aged 13 to 64 years in all health-care settings, with consent be-ing assumed unless the patient explicitly declined.1,17 As treatment was scaled up, routine HTC gained traction and several countries introduced PITC in clinical settings. Early results demonstrated an increase in HTC uptake.18–20 With the implementation of PITC expanding globally, WHO recognized the need for guidance. In 2007, WHO and the United Nations Programme on HIV/AIDS issued a document on PITC in health-care facilities. #e !nal document was an extensive revision of an initial 2006 dra$ and took into account concerns about coercion, human rights and the de!nition of the word “routine”.1,7
#e primary aim of this study was to review how policy in African countries has changed in response to the growing recognition that health-care providers should o"er more HTC. #e rationale for focusing on HTC policy in Africa was, !rst, that 68% of the estimated 34 million people with HIV infections worldwide at the end of 2010 resided in sub-Saharan Africa, a region with only 12% of the global population,21 and, second, that it was important to examine policy responses in settings where there was an urgent need to ad-dress low HTC coverage, for example, to prevent mother-to-child HIV trans-mission or to identify individuals with HIV infections who could bene!t from ART. Additional aims were to investigate patients’ perceptions of PITC and their experience of the process of PITC, with particular reference to informed consent and counselling.
MethodsNational policy documents, strategies, plans, frameworks, guidelines and re-ports on HIV testing or HIV prevention and treatment were identi!ed by search-ing the WHO Library Information Sys-tem, Google Scholar and the knowledge base repositories of organizations and institutions, including the International Labour Organization, the United States Agency for International Development (the AIDSTAR One project), the Uni-versity of California in San Francisco (the HIVInSite knowledge base) and Harvard University. #e Evidence to Ac-tion HIV and AIDS Data Hub was also
searched. Where information was not readily available or further clari!cation was required, WHO country represen-tatives were contacted. In addition, the review also considered documents that did not focus on HIV prevention alone but covered relevant broad issues, such as maternal and child health, human rights, tuberculosis and opportunistic infections.
Identi!ed documents were grouped into three categories according to their overall objectives:r� guidelines, manuals, protocols, legis-
lation and policy;r� national strategic plans, strate-
gic frameworks and multisectoral frameworks;
r� other literature, including published and unpublished reviews.
#e date assumed for the adoption of a policy depended largely on the type of documents identi!ed and the strength of the evidence available, with further con!rmation being obtained from WHO country representatives. Since the date of publication of legislation, policy, guidelines, manuals and protocols (i.e. the !rst document category) explicitly indicated the date on which a policy was adopted, this date was used in preference to the dates of other documents. When these documents were not available, the publication date of a strategic plan (i.e. the second document category) was used. However, when the only docu-ments identi!ed belonged to the third category, the date on which a policy was adopted was determined by consultation with WHO country representatives.
To obtain information on patients’ experiences of and views about PITC, we searched the MEDLINE, EMBASE, International Bibliography of the Social Sciences, PsychINFO and Global Health databases for relevant documents pub-lished in 2000 or later using the follow-ing terms: provider-initiated, routine, diagnostic, opt-out, HIV, human im-munode!ciency virus, AIDS, acquired immune de!ciency syndrome, coun-selling, testing, screening, experience, personal experience, opinion, attitude, acceptability and informed consent. We considered publications from a range of disciplines, with a focus on quantitative and qualitative studies of PITC. Reports of studies were reviewed if the studies: (i) involved the routine o"er of HTC in an African country; (ii) were conducted in a clinical setting a$er HTC had been
o"ered to patients or involved patients who were recruited in a clinical setting and had experience of PITC in that clinical setting; or (iii) assessed the ac-ceptability of PITC to patients or their experience with components of the PITC process, particularly the acquisi-tion of informed consent; and (iv) were published in English. Data on the ac-ceptability of PITC and on patients’ experiences of PITC were extracted separately.
ResultsThe policies, guidelines or strategic plans on PITC from 52 African coun-tries were reviewed. Documents for one country could not be retrieved and Western Sahara was not included in the review. There was evidence that a policy had been adopted by 42 (79.2%) of 53 countries (Table 1), whereas 10 (18.9%) had not adopted a policy: Algeria, Angola, Chad, Egypt, Libya, Morocco, the Niger, Sao Tome and Principe and Tunisia (Fig. 1). Documents could not be retrieved for the Gambia. A large proportion of countries (n = 17; 43.6%) adopted a PITC policy between 2005 and 2006, whereas 10 (25.6%) adopted a policy between 2003 and 2004 and 10 (25.6%), including the Comoros, the Congo, the Democratic Republic of the Congo and South Africa, adopted a policy between 2007 and 2008. The Central African Republic and Equatorial Guinea were the last of the 42 countries to adopt PITC, in 2009 and 2010, respectively (Table 1).
Clinical settings and target populations
All 42 countries that adopted a PITC policy recommended that pregnant women should be covered either in an-tenatal clinics or in services provided for the prevention of mother-to-child HIV transmission. In addition, 73.8% of the 42 countries adopted a policy of univer-sal PITC, which was de!ned as o"ering HTC to all patients or adults visiting a health-care facility. Documents for 66.7% of countries recommended PITC for either tuberculosis patients or clin-ics, 45.2% recommended it for patients with sexually transmitted infections, 14.3% for family planning clinics, 7.1% for most-at-risk populations and 7.1% for individuals attending out-patient departments (Table 1).
351

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in Africa R Baggaley et al.
Patient’s perspectives and experience
#e literature search identi!ed over 2000 publications, of which 11 were considered eligible for inclusion in the review (Table 2 and Table 3, avail-able at: http://www.who.int/bulletin/volumes/90/9/11-100818). #e ma9-jority were observational studies; 8 investigated the acceptability of PITC to women or their experiences of it in antenatal clinics, whereas the remaining 3 involved tuberculosis patients, women attending immunization clinics with their infants and patients attending a medical emergency unit.
Overall, the large majority of in-dividuals who received PITC found it acceptable (Table 2). For example, in Uganda 98.5% of women who were at-tending an antenatal clinic for the !rst
time considered the routine o"er of HTC during pregnancy “good” or “very good”.26 In South Africa, 93% of women o"ered HTC while attending midwife obstetric units agreed that all pregnant women should be tested for HIV.22 Among pregnant women who opted for HTC in a study from Zimbabwe, 89% stated that the routine o"er of HTC was helpful and empowering and enabled women to make an informed decision about the prevention of mother-to-child HIV transmission and infant feeding.24
In addition, experience of PITC was generally regarded as good (Table 3). For example, in Zimbabwe, 98% of pregnant women stated they were satis!ed with the information they received on routine HTC.24 In South Africa, 52% of pregnant women who had been tested for HIV felt they had made an informed choice
and had a positive experience, whereas 28% felt that their choice had been “less clear” and 20% that their voluntariness had been compromised.31
Discussion#is review of HTC policy in Africa illus-trates the changing response to HTC that has taken place in the last decade. Before WHO issued guidance on PITC in 2007, approximately 50% of African coun-tries had adopted PITC in health-care facilities.3,33,34 Subsequently, the number of countries that included PITC in their HIV policies or strategies increased and, by the time of writing, 42 African coun-tries had elected to recommend PITC in health-care facilities, with a large propor-tion adopting such a policy between 2005 and 2006. With evidence that ART can reduce mother-to-child HIV transmis-sion, all these countries recommended PITC in antenatal clinics. In addition, more than half recommended universal coverage for all adults and coverage for tuberculosis clinics and patients.
Previous studies of the acceptability of PITC have used the uptake of test-ing as an indicator of acceptability.35,36 Although they provided evidence of the feasibility of PITC, these studies did not re%ect patients’ experiences of or views about PITC. Our review of the published literature suggests that PITC is generally acceptable to patients. Studies reported that more than 75% regarded PITC as acceptable, particularly in antenatal clinics.22 However, !ndings from studies of pregnant women may not be general-izable to other population groups since these women may be more willing to un-dergo HIV testing because they believe it will bene!t their children.37 Patients in other clinical settings may !nd PITC less acceptable, perhaps because of their perceived risk of infection or fear.37 In our review, evidence from four studies, the majority involving small groups of pregnant women, indicated that patients were not always aware they had the right to decline HTC in antenatal clinics, perhaps because of the power balance between patients and health-care pro-viders.29,31 However, studies in other regions suggest that women may !nd the routine o"er of HTC acceptable because it “normalizes” the process of HTC.38
Our review has several limitations. It was di&cult to retrieve all the docu-ments required to understand national PITC policy fully. Although we con-
Table 1. Provider-initiated HIV testing and counselling in African countries, 2003–2010
Details of PITC policy Countries
No. (%)
Policy adoptedYes 42 (79.2)No 10 (18.9)No information 1 (1.9)Total 53 (100)Year policy adopteda
2003 or 2004 10 (25.6)2005 or 2006 17 (43.6)2007 or 2008 10 (25.6)2009 or 2010 2 (5.1)Total 39 (100)Document detailing PITC policyNational policy document 35 (83.3)National strategic plan (excluding national policy documents) 7 (16.7)Total 42 (100)Clinical services or settings in which PITC was o!eredb
Pregnant women attending antenatal clinics or PMTCT services 42 (100)All patients or all adults visiting a health-care facility 31 (73.8)Tuberculosis clinics or patients 28 (66.7)Sexually transmitted infection clinics or patients 19 (45.2)Family planning services 6 (14.3)Inpatients (adult or paediatric) 4 (9.5)Infants of HIV-positive mothers 4 (9.5)Most-at-risk populations (e.g. men who have sex with men, injecting drug users, female sex workers and commercial sex workers)
3 (7.1)
Outpatient departments 3 (7.1)Therapeutic feeding centres or children with malnutrition 2 (4.8)Psychiatric services 1 (2.4)Male circumcision services 1 (2.4)
HIV, human immunodeficiency virus; PITC, provider-initiated HIV testing and counselling; PMTCT, prevention of mother-to-child HIV transmission.a The date the policy was adopted could not be determined for three countries.b The total exceeds 100% as some countries adopted PITC for more than one target population.
352

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in AfricaR Baggaley et al.
tacted WHO country o&ces, it was not possible to obtain information for some countries and, for others, the date on which policy was adopted was unknown. In addition, the ambiguous language of some documents made it di&cult to determine when and in which settings policies were adopted. Consequently, our data on the years in which PITC policies were adopted may be inaccurate. We minimized this inaccuracy by asking two reviewers to determine indepen-dently the date of policy adoption using the available evidence. Our review of patients’ experiences of and views about PITC also has several limitations and the !ndings must be interpreted with caution. First, our review was subject to a language bias and a publication bias. Second, the majority of studies included took place in antenatal clinics and there may be studies from other clinical settings that we did not identify. Some studies that reported on the ac-ceptability of PITC included only small samples of women and did not involve interviews with women who declined an
o"er of HTC.28,31,32 In addition, the stud-ies included in our review are subject to their own limitations: the majority were nonrandomized studies and the di&culty of reporting and synthesizing evidence from nonrandomized studies is well documented.39 Moreover, studies were subject to acquiescence bias40 and, as the questions posed to patients were di"erent in each study, it was di&cult to compare their !ndings.
In general, the evidence suggests that the introduction of PITC in ante-natal clinics has been associated with an increase in HIV testing rates. A 2010 WHO report on universal access stated that the testing rate in eastern and south-ern Africa rose from 48% in 2008 to 50% in 2009.10 Moreover, with the increased uptake of HTC and the better access to ART that followed from the introduc-tion of PITC,13 mother-to-child HIV transmission has been virtually elimi-nated in some countries:13,24 in 2009, four of the 25 countries with the highest HIV disease burden achieved the target set by the United Nations General As-
sembly Special Session on HIV/AIDS of providing at least 80% of HIV-infected pregnant women with ART.10 In addi-tion, one literature review found that the introduction of PITC in antenatal clinics contributed to the achievement of universal HTC in pregnant women.41 Moreover, the results of the seven Afri-can-based studies included in our review indicate that implementation of PITC led to an increase in the uptake of HTC by pregnant women that ranged from 9.9% in Malawi to 65.6% in Uganda, with more than 75% of women accepting PITC across all seven studies.41
#e implementation of PITC has also led to a high rate of HIV testing among individuals visiting tuberculo-sis and sexually transmitted infection clinics.15,42–44 A cluster randomized trial conducted in tuberculosis clinics in South Africa in 2005 found that the introduction of opt-out PITC increased the uptake of HIV testing by 13.7%, from 6.5% when HIV testing was carried out on an opt-in basis to 20.2% with opt-out PITC.45 #e 2011 WHO report on global tuberculosis control stated that HTC is now standard for tuberculosis patients in many countries, especially in Africa. In 2010, more than 75% of tuberculosis patients knew their HIV status in 68 countries and territories, including 22 countries in the WHO African Region.46 Further e"orts are still needed globally, however, since only 34% of 6.2 million tuberculosis patients were aware of their HIV status in 2010.
Despite the availability of e"ective therapy and the increase in HIV testing, population-based surveys conducted be-tween 2007 and 2009 in 10 sub-Saharan African countries indicated that the me-dian proportion of people with an HIV infection who are aware of their status was under 40%.10,47 Moreover, although PITC can contribute to increased test-ing in clinical settings,41 the adoption of PITC alone will not achieve universal access to HTC. Other approaches that enable people not attending health-care services to access HIV testing should be developed in parallel to ensure that access to testing is equitable and that in-dividuals with HIV infections are diag-nosed before they become symptomatic. In 2011, the HIV Prevention Trials Net-work study 52 (HPTN052) con!rmed that ART was e"ective for preventing the transmission of HIV in serodiscordant
Fig. 1. Adoption of a policy on provider-initiated HIV testing and counselling, Africa, 2003–2010
2003–20042005–20062007–20082009–2010Date of PITC policy adoption not identifiedPITC policy not adoptedData not available
Year PITC policy was adopted
HIV, human immunodeficiency virus; PITC, provider-initiated HIV testing and counselling.
353
Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in Africa R Baggaley et al.
couples.48 #ere is a rationale, therefore, for considering and evaluating house-hold or community-based testing in addition to expanding PITC.49 Data on these alternative approaches would help
identify the most e"ective and appropri-ate way of implementing HIV testing in speci!c local contexts, while taking into account the resources available and social constraints. !
AcknowledgementsWe would like to thank Chris Grundy for Fig. 1.
Competing interests: None declared.
摘要从谨慎到紧迫:非洲的艾滋病检测咨询的演变目的 描述非洲各国最近在艾滋病毒(HIV)感染的医务人员主动提供检测咨询(PITC)政策方面的变化,并调查病人有关PITC的体验和看法。方法 审查已发表的文献和国家HIV检测的政策、战略框架、计划和其他有关文件。结果 在审查的个非洲国家中,有42 个(79.2%)国家已经采用了PITC政策。在这42 个国家当中,所有国家都推荐PITC用于预防母婴HIV传播,66.7%的国家推荐用于结核病诊所和患者,45.2%的国家推荐用于性传播感染诊所。此外,43.6%的国家在2005 年或2006 年采用PITC。文
献检索确定了11 项有关病人对非洲诊所背景中PITC的体验和看法的研究。绝大多数人认为PITC是可接受的。然而,在产前诊所的妇女并不总是知道她们有拒绝接受HIV检测的权利。结论 非洲HIV检测咨询的政策和实践已经从强调保密的谨慎态度转变为具有更大接受程度的常规HIV检测。在诊所背景中引进PITC有利于在多个这样的背景中增加HIV检测。大多数患者认为PITC是可以接受的。然而,还需要其他方法让没到医院看病的人也能被覆盖到。
Résumé
De la prudence à l’urgence: l’évolution des activités de conseil et de dépistage du VIH en AfriqueObjectif Décrire les changements récents dans la politique d’activités de conseil et de dépistage à l’initiative du fournisseur (PITC), du virus de l’immunodéficience humaine (VIH) dans les pays africains, et enquêter sur les expériences et opinions des patients relatives à la PITC.Méthodes Les publications, ainsi que les politiques nationales, les cadres stratégiques, les plans et autres documents pertinents relatifs au dépistage du VIH ont été étudiés.Résultats Sur les pays africains passés en revue, 42 d’entre eux (79.2%) avaient adopté une PITC. Sur ces 42 pays, tous recommandaient la PITC pour la prévention de la transmission mère-enfant du VIH, 66,7% pour les cliniques soignant la tuberculose et les patients a!ectés par cette maladie, et 45,2%, pour les cliniques soignant les infections sexuellement transmissibles. En outre, 43,6% des pays avaient adopté la PITC en 2005 ou 2006. L’examen des publications a permis d’identifier 11 études
sur les expériences des patients et leur opinion relatives à la PITC dans les environnements cliniques en Afrique. La grande majorité considérait la PITC comme étant acceptable. Cependant, les femmes en consultations prénatales n’étaient pas toujours conscientes du fait qu’elles avaient le droit de refuser un dépistage du VIH.Conclusion La politique et la pratique relatives aux activités de conseil et de dépistage du VIH en Afrique sont passées d’une approche prudente, mettant l’accent sur la confidentialité, à une plus grande acceptation de l’o!re systématique de dépistage du VIH. L’introduction de la PITC dans les milieux cliniques a contribué à augmenter le dépistage du VIH dans plusieurs de ces environnements. La plupart des patients considèrent la PITC comme étant acceptable. Toutefois, d’autres approches sont nécessaires pour atteindre les personnes qui ne font pas appel aux services de santé.
��cXmgaw|QÎ�9�ïO�TÐ��KmeBÐ�Û�^TÐ�ÜíDQ�ëiY<�ogK��TÐí�Úm��AøÐ�Ú�\=��o�cBÐ�o?m"Ð�NÎ�Ú{"Ð��X
�Ún��Bøn= �pÉn#Ð �pHnh�UÐ �: �ÒEBúÐ �ÓÐE`�UÐ ��Éí �ß|_TÐ�îí{L �ëjZ= ��PITC� �ÓnY{#Ð ��Y{bY ��Y �ÒÚØn�e= �phL��UÐí�ï}Ļí�phbx}RúÐ�ëÐ{d�UÐ�:��HIV��ïP�UÐ��LnfCÐ�Û�_UÐ�ÜíER��Y{bY��Y�ÒÚØn�e=�phL��UÐí�Ún��BøÐ�é�A��}CÐ�ÊÐÚËí�ÑÚn9
�ÓnY{#Ð�phfJ�UÐ �ÓnHnh�UÐí �ÒÚ�ZfCÐ �ØÐ�edU �p_@Ð}Y �ÊÐ}@Î ��> �oaw|\TÐ�ºph�h>ÐGHüÐ�}JúÐí�ºïP�UÐ��LnfCÐ�Û�_UÐ�ÜíER�ÓÐÚn��Bø
�pd[UÐ�ÓÐÙ�î}BúÐ�ÓÐ{f��CÐí��]#Ðí�Ð ð{d=�42�{e�LÐ�ºßÐ}_�HĆU�q_\B�nðhbx}RÌ�Ð ð{d=�N=��Y�rým�eTÐ��ÓnY{#Ð��Y{bY��Y�ÒÚØn�e=�phL��UÐí�Ún��BøÐ�pHnhH��79.2%(�phL��UÐí �Ún��Bøn= �ngdT �N_=ÚúÐí �Nf?øÐ �ëÐ{d�UÐ �qÉíÌ �{Sí�Û�_UÐ �ÜíER �énb�iÐ ��fC ��UÙí �ÓnY{#Ð ��Y{bY ��Y �ÒÚØn�e=�ngfY�·�66.7 �p��i�qÉíÌí�º�a]UÐ�OÎ�êúÐ��Y�ïP�UÐ��LnfCÐ % 45.2 �p��i �qÉíÌí �º��UÐ ��}Yí �ÓÐØnh_U �pHnh�UÐ �ì|)�º�UÙ�DL�ÒíĆL��ðnh�f@�pU�bfCÐ�îí{_UÐ�ÓÐØnhL��Y�ngYÐ{��Hn=��Y{bY ��Y �ÒÚØn�e= �phL��UÐí �Ún��BøÐ �· �43.6 �p��i �Ó{e�LÐ
�ØÐ�CÐ �: �r��UÐ �Ø{Aí ��2006 �íÌ �2005 ��YnL �: �ÓnY{#Ð�Ún��BøÐ �ëjZ= ��}CÐ �ÊÐÚËí �ÑÚn9 �é�A �pHÐÚØ �11 �ÒÚ�ZfCÐ�: �ÓÐØnh_UÐ ��SÐ�Y �: �ÓnY{#Ð ��Y{bY ��Y �ÒÚØn�e= �phL��UÐí�ÒÚØn�e=�phL��UÐí�Ún��BøÐ�ëÌ�p��Ðí�ph�dQÌ�ÓF�LÐ�{Sí��nhbx}RÎ�ÓÐØnhL �: �Ên�fUÐ �ëlR �º�UÙ ��Yí ��é��bY �ÓnY{#Ð ��Y{bY ��Y�Ún��BÐ�ÊÐ}@Î��RÚ�:��gb�=�pxÐÚØ�DL� ð5ýÐØ� ö�cx�3��e"Ð�pxnLÚ
�ïP�UÐ��LnfCÐ�Û�_UÐ�ÜíER�phL��UÐí �Ún��Bøn= �pÉn#Ð �pHÚ5CÐí �pHnh�UÐ �qU�Ļ �Õm�e�GøÐ�{Tkx�Ú|A�s¹��Y�nhbx}RÎ�:�ïP�UÐ��LnfCÐ�Û�_UÐ�ÜíER�ëjZ=�ÜíER�Ún��BÐ�ÊÐ}@ü�ïØnh�LøÐ�sgfdU�FTÌ�é��S�OÎ�px�UÐ�DL�ÒÚØn�e=�phL��UÐí�Ún��BøÐ��x{b>��wnH�{Sí��ïP�UÐ��LnfCÐ�Û�_UÐ�ÓÐÚn��BÐ �Ø{L�ÒØnxÛ�:�ÓÐØnh_UÐ ��SÐ�Y�:�ÓnY{#Ð��Y{bY��Y�F�LÐí ���SÐ�CÐ �ì|w��Y�{x{_UÐ �:�ïP�UÐ ��LnfCÐ �Û�_UÐ �ÜíER�ÓnY{#Ð��Y{bY��Y�ÒÚØn�e=�phL��UÐí�Ún��BøÐ�ëÌ��}CÐ��^_Y�OÎ �é�É�dU �î}BÌ �s ô¹ �OÎ �p@nA�ènfw �º�UÙ ��Yí ��é��bY �}YÌ
�ph�[UÐ�pxnL}UÐ�ÓnY{B�OÎ�ë�þ�dx�ø��x|UÐ�Þn�IúÐ
354

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in AfricaR Baggaley et al.
"#$%&#
'( )*#+,)*#-+#./0 1 .#2342+/&25(/: *6$7/(/# 12.5,89(/*276./0 / (#5(/*276./0 .6 :;< 7 =>*/1#?6+6@6 !"#$%&' ()*%+(#) #,-)()(#. + $&/%&)0## &)$&#/1+%(#. # 21($34'&#/1+%(#. "1 #(5)26## +#/3$% #--3(1*)5#6#&% 7)41+)2% (89:), "/1+1*#-101 "1 #(#6#%&#+) -)*#6#($2#; /%<1&(#21+ (PITC) + %5/#2%($2#; $&/%(%;, # #$$4)*1+%&' 1"=& # 1&(1>)(#) "%6#)(&1+ 2 PITC.A#(2+B ?=4 "/1+)*)( 1<,1/ 1"3<4#21+%((1@ 4#&)/%&3/= # (%6#1(%4'(=; $&/%&)0#@ &)$&#/1+%(#. (% 89:, 1$(1+(=; $;)- 1")/%&#+(1@ *).&)4'(1$&#, "4%(1+ # */30#; $11&+)&$&+3AB#; *123-)(&1+."#$,89(6(B 9, /%$$-1&/)((=; %5/#2%($2#; $&/%(, + 42 (79.2%) $&/%(%; <=4% "/#(.&% $&/%&)0#. PITC. 9, 42 $&/%(, +$)-# /)21-)(*1+%(% PITC *4. "/15#4%2# ")/)*%7# 89: 1& -%&)/# 2 /)<)(23, 66,7% /)21-)(*1+%4# $&/%&)0#A *4. &3<)/234),(=; <14'(#6 # "%6#)(&1+, $&/%*%AB#; &3<)/234),1-, # 45,2% - *4. <14'(#6, $")6#%4#,#/3AB#;$. (% #(5)26#1((=; ,%<14)+%(#.;, ")/)*%AB#;$. "141+=- "3&)-. C/1-) &101, 43,6% "/#(.4#
PITC + 2005-2006 00. ?4%01*%/. #(51/-%6#1((1-3 "1#$23, <=41 1"/)*)4)(1 11 #$$4)*1+%(#@, "1$+.B)((=; 1"=&3 # 1&(1>)(#A "%6#)(&1+ 2 PITC + 3$41+#.; 24#(#7)$21@ "/%2# + D5/#2). E+(1) <14'>#($&+1 $7#&%41 PITC "/#)-4)-1@. 8"/17)-, F)(B#(= + 24#(#2%; *1/1*1+101 (%<4A*)(#. () +1 +$); $437%.; ,(%4# 1 $+1)- "/%+) (% ()"/1;1F*)(#) &)$&% (% 89:.:B72+ G&/%&)0#. # "/%2% "1 21($34'&#/1+%(#A # &)$&#/1+%(#A (% 89: + D5/#2) #,-)(#4%$' $ "/1*3-%((101 "1*;1*%, %26)(&#/1+%((101 (% 21(5#*)(6#%4'(1$&#, 2 <14'>)-3 "/#(.&#A "/)*41F)(#@ 1 &)$&#/1+%(## (% 89: + 6)4.; "/15#4%2#. 8()*/)(#) PITC + 24#(#7)$23A "/%2 "/#+)41 2 3+)4#7)(#A 7#$4% &)$&1+ (% 89: + ()21&1/=; 37/)F*)(#.;. ?14'>#($&+1 "%6#)(&1+ $7#&%A& PITC "/#)-4)-1@. !*(%21 ()1<;1*#-1 +=/%<1&%&' */30#) "1*;1*= *4. 4A*)@, 21&1/=) () "14',3A&$. 3$430%-# ,*/%+11;/%()(#..
Resumen
De la cautela a la urgencia: La evolución de las pruebas de detección del VIH y el asesoramiento en ÁfricaObjetivo Describir los cambios recientes en la estrategia sobre la realización de pruebas de detección del virus de la inmunodeficiencia humana (VIH) y el asesoramiento emprendidos por los proveedores (PITC) en países africanos e investigar las experiencias de los pacientes y sus opiniones acerca de la PITC.Métodos Se llevó a cabo un examen de las publicaciones y de estrategias de detección del VIH nacionales, convenios estratégicos, planes y otros documentos importantes.Resultados De los países africanos examinados, 42 (79,2%) había adoptado la estrategia PITC. De esos 42, todos recomendaban la PITC para prevenir la transmisión maternoinfantil del VIH, el 66,7% la recomendaba a las clínicas y pacientes con tuberculosis y el 42,5% a las clínicas de tratamiento de infecciones de transmisión sexual. Además, el 43,6% adoptó la PITC en el año 2005 o 2006. La búsqueda bibliográfica
identificó 11 estudios sobre las experiencias de los pacientes y sus opiniones acerca de la PITC en entornos clínicos de África. Una mayoría clara consideró la PICT aceptable. Sin embargo, las mujeres en las clínicas de atención prenatal no siempre fueron conscientes de que tenían el derecho a rechazar las pruebas de detección del VIH.Conclusión La estrategia y práctica de las pruebas de detección del VIH y el asesoramiento en África han cambiado desde un enfoque cauteloso que enfatiza la confidencialidad a una mayor aceptación de la oferta sistemática de pruebas de detección del VIH. La introducción de la PITC en los entornos clínicos ha contribuido a incrementar el número de pruebas de detección del VIH en muchos de esos entornos. La mayoría de pacientes considera la PTIC aceptable. No obstante, se necesitan otros enfoques para llegar a aquellas personas que no acuden a los servicios sanitarios.
References1. Bayer R, Edington C. HIV testing, human rights, and the global AIDS policy:
exceptionalism and its discontents. J Health Polit Policy Law 2009;34:301–23. doi:10.1215/03616878-2009-002 PMID:19451406
2. De Cock KM, Mbori-Ngacha D, Marum E. Shadow on the continent: public health and HIV/AIDS in Africa in the 21st century. Lancet 2002;360:67–72. doi:10.1016/S0140-6736(02)09337-6 PMID:12114058
3. Branson BM. To screen or not to screen: is that really the question? Ann Intern Med 2006;145:857–9. PMID:17146069
4. Gruskin S, Tarantola D. HIV/AIDS and human rights revisited. Can HIV AIDS Policy Law Rev 2001;6:24–9. PMID:11837018
5. Bayer R. Changing the paradigm for HIV testing – the end of exceptionalism. N Engl J Med 2006;355:647–9. doi:10.1056/NEJMp068153 PMID:16914699
6. De Cock KM. HIV testing in the era of treatment scale up. Health Hum Rights 2005;8:31–5. doi:10.2307/4065331 PMID:17136900
7. Jurgens R. “Routinizing” HIV testing in low- and middle-income countries. New York: Public Health Program Open Society Institute; 2007.
8. Macklin R. Scaling up HIV testing: ethical issues. Health Hum Rights 2005;8:27–30. doi:10.2307/4065330 PMID:17136899
9. The right to know: new approaches to HIV testing and counselling. Geneva: World Health Organization; 2003.
10. Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Geneva: World Health Organization; 2006.
11. Becker J, Tsague L, Sahabo R, Twyman P. Provider-initiated testing and counseling (PITC) for HIV in resource-limited clinical settings: important questions unanswered. Pan Afr Med J 2009;3:4. PMID:21532713
12. Klein D, Hurley LB, Merrill D, Quesenberry CP Jr; Consortium for HIV/AIDS Interregional Research. Review of medical encounters in the 5 years before a diagnosis of HIV-1 infection: implications for early detection. J Acquir Immune Defic Syndr 2003;32:143–52. doi:10.1097/00126334-200302010-00005 PMID:12571523
13. Centers for Disease Control and Prevention (CDC). Introduction of routine HIV testing in prenatal care – Botswana, 2004. MMWR Morb Mortal Wkly Rep 2004;53:1083–6. PMID:15565017
14. Weiser SD, Heisler M, Leiter K, Percy-de Korte F, Tlou S, DeMonner S et al. Routine HIV testing in Botswana: a population-based study on attitudes, practices, and human rights concerns. PLoS Med 2006;3:e261. doi:10.1371/journal.pmed.0030261 PMID:16834458
15. Centers for Disease Control and Prevention. Provider-initiated HIV testing and counseling of TB patients – Livingstone District, Zambia, September 2004-December 2006. MMWR Morb Mortal Wkly Rep 2008;57:285–9. PMID:18354372
16. Wanyenze RK, Nawavvu C, Namale AS, Mayanja B, Bunnell R, Abang B et al. Acceptability of routine HIV counselling and testing, and HIV seroprevalence in Ugandan hospitals. Bull World Health Organ 2008;86:302–9. doi:10.2471/BLT.07.042580 PMID:18438519
17. Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss SB et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Morb Mortal Wkly Rep 2006;55:1–17.
355
Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in Africa R Baggaley et al.
18. Wanyenze R, Kamya M, Liechty CA, Ronald A, Guzman DJ, Wabwire-Mangen F et al. HIV counseling and testing practices at an urban hospital in Kampala, Uganda. AIDS Behav 2006;10:361–7. doi:10.1007/s10461-005-9035-9 PMID:16395619
19. Guidance on provider-initiated HIV testing and counselling in health facilities. Geneva: World Health Organization and Joint United Nations Programme on HIV/AIDS; 2007.
20. Homsy J, Kalamya JN, Obonyo J, Ojwang J, Mugumya R, Opio C et al. Routine intrapartum HIV counseling and testing for prevention of mother-to-child transmission of HIV in a rural Ugandan hospital. J Acquir Immune Defic Syndr 2006;42:149–54. doi:10.1097/01.qai.0000225032.52766.c2 PMID:16760796
21. UNAIDS World AIDS Day Report. Geneva: World Health Organization and Joint United Nations Programme on HIV/AIDS; 2011.
22. Etiebet MA, Fransman D, Forsyth B, Coetzee N, Hussey G. Integrating prevention of mother-to-child HIV transmission into antenatal care: learning from the experiences of women in South Africa. AIDS Care 2004;16:37–46. doi:10.1080/09540120310001633958 PMID:14660142
23. Nakanjako D, Kamya M, Daniel K, Mayanja-Kizza H, Freers J, Whalen C et al. Acceptance of routine testing for HIV among adult patients at the medical emergency unit at a national referral hospital in Kampala, Uganda. AIDS Behav 2007;11:753–8. doi:10.1007/s10461-006-9180-9 PMID:17096199
24. Chandisarewa W, Stranix-Chibanda L, Chirapa E, Miller A, Simoyi M, Mahomva A et al. Routine o!er of antenatal HIV testing (“opt-out” approach) to prevent mother-to-child transmission of HIV in urban Zimbabwe. Bull World Health Organ 2007;85:843–50. PMID:18038074
25. Corneli A, Jarrett NM, Sabue M, Duvall S, Bahati E, Behets F et al. Patient and provider perspectives on implementation models of HIV counseling and testing for patients with TB. Int J Tuberc Lung Dis 2008;12(Suppl 1):79–84. PMID:18302828
26. Byamugisha R, Tumwine JK, Ndeezi G, Karamagi CA, Tylleskär T. Attitudes to routine HIV counselling and testing, and knowledge about prevention of mother to child transmission of HIV in eastern Uganda: a cross-sectional survey among antenatal attendees. J Int AIDS Soc 2010;13:52. doi:10.1186/1758-2652-13-52 PMID:21144037
27. Rollins N, Mzolo S, Moodley T, Esterhuizen T, van Rooyen H. Universal HIV testing of infants at immunization clinics: an acceptable and feasible approach for early infant diagnosis in high HIV prevalence settings. AIDS 2009;23:1851–7. doi:10.1097/QAD.0b013e32832d84fd PMID:19491653
28. Angotti N, Dionne KY, Gaydosh L. An o!er you can’t refuse? Provider-initiated HIV testing in antenatal clinics in rural Malawi. Health Policy Plan 2011;26:307–15. doi:10.1093/heapol/czq066 PMID:21047809
29. Larsson EC, Thorson A, Pariyo G, Conrad P, Arinaitwe M, Kemigisa M et al. Opt-out HIV testing during antenatal care: experiences of pregnant women in rural Uganda. Health Policy Plan 2012;27:69–75. doi:10.1093/heapol/czr009 PMID:21292708
30. Mugore L, Engelsman B, Ndoro T, Dabis F, Perez F. An assessment of the understanding of the o!er of routine HIV testing among pregnant women in rural Zimbabwe. AIDS Care 2008;20:660–6. doi:10.1097/QAI.0b013e318030!a9 PMID:17211281
31. Groves AK, Maman S, Msomi S, Makhanya N, Moodley D. The complexity of consent: women’s experiences testing for HIV at an antenatal clinic in Durban, South Africa. AIDS Care 2010;22:538–44. doi:10.1080/09540120903311508 PMID:20229376
32. Ujiji OA, Rubenson B, Ilako F, Marrone G, Wamalwa D, Wangalwa G et al. Is ‘opt-out HIV testing’ a real option among pregnant women in rural districts in Kenya? BMC Public Health 2011;11:151. doi:10.1186/1471-2458-11-151 PMID:21385423
33. Creek TL, Ntumy R, Seipone K, Smith M, Mogodi M, Smit M et al. Successful introduction of routine opt-out HIV testing in antenatal care in Botswana. J Acquir Immune Defic Syndr 2007;45:102–7. doi:10.1097/QAI.0b013e318047df88 PMID:17460473
34. Fenton KA. Sustaining HIV prevention: HIV testing in health care settings. Top HIV Med 2007;15:146–9. PMID:18073449
35. Perez F, Zvandaziva C, Engelsmann B, Dabis F. Acceptability of routine HIV testing (“opt-out”) in antenatal services in two rural districts of Zimbabwe. J Acquir Immune Defic Syndr 2006;41:514–20. doi:10.1097/01.qai.0000191285.70331.a0 PMID:16652062
36. Jerene D, Endale A, Lindtjorn B. Acceptability of HIV counselling and testing among tuberculosis patients in south Ethiopia. BMC Int Health Hum Rights 2007;7:4. doi:10.1186/1472-698X-7-4 PMID:17537265
37. Obermeyer CM, Osborn M. The utilization of testing and counseling for HIV: a review of the social and behavioral evidence. Am J Public Health 2007;97:1762–74. doi:10.2105/AJPH.2006.096263 PMID:17761565
38. Oosterho! P, Hardon AP, Nguyen TA, Pham NY, Wright P. Dealing with a positive result: routine HIV testing of pregnant women in Vietnam. AIDS Care 2008;20:654–9. doi:10.1080/09540120701687026 PMID:18576166
39. Deeks JJ, Dinnes J, D’Amico R, Sowden AJ, Sakarovitch C, Song F et al.; International Stroke Trial Collaborative Group, European Carotid Surgery Trial Collaborative Group. Evaluating non-randomised intervention studies. Health Technol Assess 2003;7:iii–x, 1-173. PMID:14499048
40. Novick G. Women’s experience of prenatal care: an integrative review. J Midwifery Womens Health 2009;54:226–37. doi:10.1016/j.jmwh.2009.02.003 PMID:19410215
41. Hensen B, Baggaley R, Wong VJ, Grabbe KL, Sha!er N, Lo YR et al. Universal voluntary HIV testing in antenatal care settings: a review of the contribution of provider-initiated testing and counselling. Trop Med Int Health 2011. Epub ahead of print PMID:22032300
42. Harris JB, Hatwiinda SM, Randels KM, Chi BH, Kancheya NG, Jham MA et al. Early lessons from the integration of tuberculosis and HIV services in primary care centers in Lusaka, Zambia. Int J Tuberc Lung Dis 2008;12:773–9. PMID:18544203
43. Sherr L, Fox Z, Lipton M, Whyte P, Jones P, Harrison U; Camden and Islington Steering Group. Sustaining HIV testing in pregnancy - evaluation of routine o!er of HIV testing in three London hospitals over 2 years. AIDS Care 2006;18:183–8. doi:10.1080/09540120500456599 PMID:16615201
44. Haukoos JS, Hopkins E, Conroy AA, Silverman M, Byyny RL, Eisert S et al.; Denver Emergency Department HIV Opt-Out Study Group. Routine opt-out rapid HIV screening and detection of HIV infection in emergency department patients. JAMA 2010;304:284–92. doi:10.1001/jama.2010.953 PMID:20639562
45. Pope DS, Deluca AN, Kali P, Hausler H, Sheard C, Hoosain E et al. A cluster-randomized trial of provider-initiated (opt-out) HIV counseling and testing of tuberculosis patients in South Africa. J Acquir Immune Defic Syndr 2008;48:190–5. doi:10.1097/QAI.0b013e3181775926 PMID:18520677
46. Global tuberculosis control. Geneva: World Health Organization; 2011.47. April MD. Rethinking HIV exceptionalism: the ethics of opt-out HIV testing
in sub-Saharan Africa. Bull World Health Organ 2010;88:703–8. doi:10.2471/BLT.09.073049 PMID:20865076
48. Cohen MS, McCauley M, Gamble T, Hosseinipour MC, Kumarasamy N, Hakim JG et al.; HPTN 052 Study Team. Prevention of HIV-1 infection with early antiretroviral therapy. N Engl J Med 2011;365:493–505. doi:10.1056/NEJMoa1105243 PMID:21767103
49. Grabbe KL, Menzies N, Taegtmeyer M, Emukule G, Angala P, Mwega I et al. Increasing access to HIV counseling and testing through mobile services in Kenya: strategies, utilization, and cost-e!ectiveness. J Acquir Immune Defic Syndr 2010;54:317–23. doi:10.1097/QAI.0b013e3181ced126 PMID:20453819
356

Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in AfricaR Baggaley et al.
Table 2. Acceptability of provider-initiated HIV testing and counselling, Africa, 1999–2009
Publication (Author, year)
Country Primary objective Sample size Population group
Acceptability
Etiebet, 200422 South Africa Knowledge, attitude and practices survey of women receiving prenatal or postnatal care
264 Women attending midwife obstetric units
(i) 93% agreed that all pregnant women should be tested for HIV; (ii) 98% agreed they would recommend attendance at a clinic that routinely o!ers HIV testing to a friend or sister
Nakanjako, 200723 Uganda To determine whether patients would accept a routine o!er of HIV testing in a medical emergency setting
233 Adult patients (i) 99% expressed a need to integrate routine HTC into medical care at the emergency unit; (ii) 86% believed routine testing would help link HIV-positive patients to HIV care services
Chandisarewa, 200724
Zimbabwe To assess the impact of routine ANC testing for PMTCT
221 Follow-up survey with pregnant women
(i) 89.1% stated that o!ering routine testing was helpful as it empowers women to “exercise their rights and responsibilities” with regard to accessing relevant information and making informed choices about PMTCT; (ii) 10.9% stated that the o!er of routine antenatal testing was not helpful
Corneli, 200825 Democratic Republic of the Congo
To identify an acceptable approach to HIV testing for tuberculosis patients based on the views of patients and health-care workers
88 Tuberculosis patients
(i) 99% supported the incorporation of HIV testing into routine care for tuberculosis patients; (ii) 99% expressed the view that HIV testing should be o!ered at the start of tuberculosis treatment; (iii) 68% preferred HIV testing to be o!ered by a tuberculosis nurse (including 93% of tuberculosis patients who were tested in this way); (iv) 24% preferred referral to on-site HIV testing; (v) 8% preferred referral to a freestanding voluntary HTC site
Byamugisha, 200926
Uganda To assess attitudes towards routine HIV testing among new ANC attendees
388 First-time ANC attendees
Question posed: “Nowadays in this clinic all mothers are tested for HIV unless they say no, what do you think about this system?” 98.5% responded “good” or “very good (helps them know their HIV status and thus plan for their future and that of their baby)”; 1.5% responded “fair”, “bad” or “very bad”
Rollins, 200927 South Africa To determine the acceptability and feasibility of universal HIV testing of 6-week-old infants attending immunization clinics
646 Women with infants
(i) Question posed: “How did you feel when o!ered the opportunity of HIV testing?” (for infants). Response: 77.9% comfortable; 11% surprised; 4.5% frightened; 3.4% shocked; 1.5% anxious; 0.3% preferred not to answer; 0.2% other; (ii) 89.8% would recommend HTC to “others”
Angotti, 201028 Malawi To determine local perceptions of routine HIV testing and the potential consequences
18 (12 from an ANC
attendee sample)
Women who had been o!ered HTC in an ANC and accepted
Interviewees made “favourable” comments about the routine o!er of HTC and generally accepted its implementation in an ANC
Larsson, 201129 Uganda To explore women’s experiences of, and views on, the opt-out testing policy and associated HIV testing in an ANC
18 Pregnant women attending an ANC
Some women viewed the opt-out testing policy as positive as it could benefit their child and themselves
ANC, antenatal clinic; HIV, human immunodeficiency virus; HTC, HIV testing and counselling; PMTCT, prevention of mother-to-child HIV transmission.
357
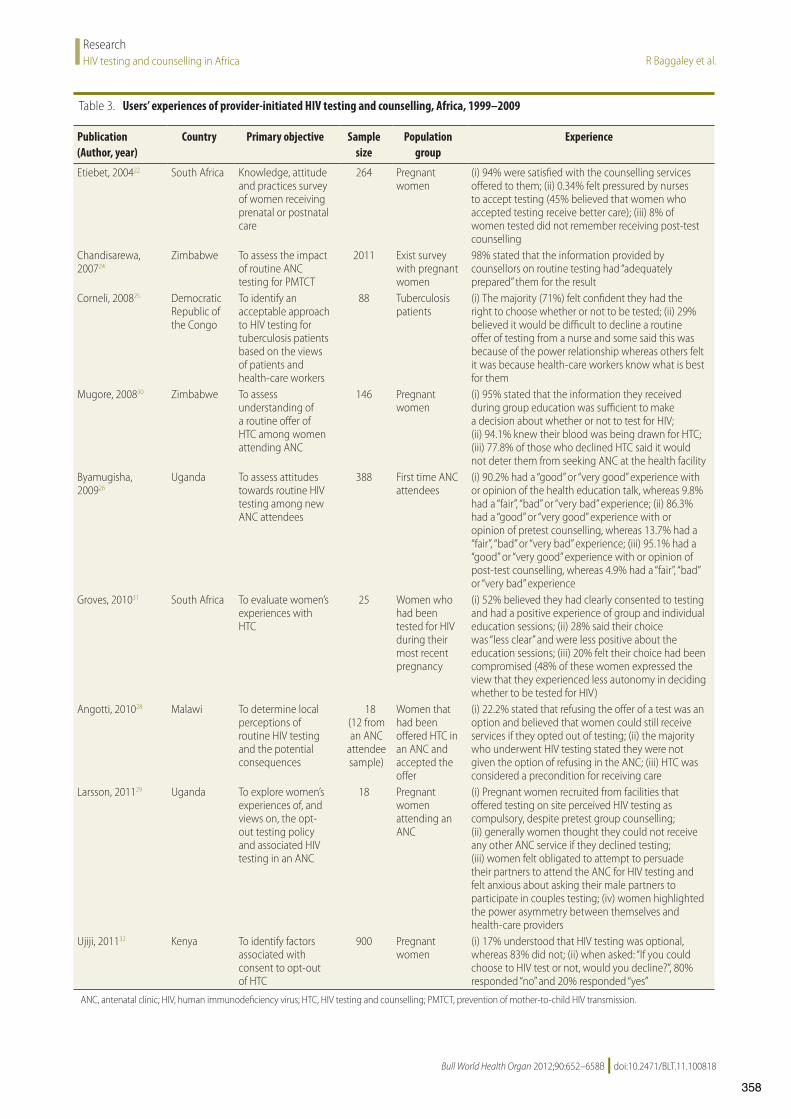
Bull World Health Organ 2012;90:652–658B | doi:10.2471/BLT.11.100818
ResearchHIV testing and counselling in Africa R Baggaley et al.
Table 3. Users’ experiences of provider-initiated HIV testing and counselling, Africa, 1999–2009
Publication (Author, year)
Country Primary objective Sample size
Population group
Experience
Etiebet, 200422 South Africa Knowledge, attitude and practices survey of women receiving prenatal or postnatal care
264 Pregnant women
(i) 94% were satisfied with the counselling services o!ered to them; (ii) 0.34% felt pressured by nurses to accept testing (45% believed that women who accepted testing receive better care); (iii) 8% of women tested did not remember receiving post-test counselling
Chandisarewa, 200724
Zimbabwe To assess the impact of routine ANC testing for PMTCT
2011 Exist survey with pregnant women
98% stated that the information provided by counsellors on routine testing had “adequately prepared” them for the result
Corneli, 200825 Democratic Republic of the Congo
To identify an acceptable approach to HIV testing for tuberculosis patients based on the views of patients and health-care workers
88 Tuberculosis patients
(i) The majority (71%) felt confident they had the right to choose whether or not to be tested; (ii) 29% believed it would be di"cult to decline a routine o!er of testing from a nurse and some said this was because of the power relationship whereas others felt it was because health-care workers know what is best for them
Mugore, 200830 Zimbabwe To assess understanding of a routine o!er of HTC among women attending ANC
146 Pregnant women
(i) 95% stated that the information they received during group education was su"cient to make a decision about whether or not to test for HIV; (ii) 94.1% knew their blood was being drawn for HTC; (iii) 77.8% of those who declined HTC said it would not deter them from seeking ANC at the health facility
Byamugisha, 200926
Uganda To assess attitudes towards routine HIV testing among new ANC attendees
388 First time ANC attendees
(i) 90.2% had a “good” or “very good” experience with or opinion of the health education talk, whereas 9.8% had a “fair”, “bad” or “very bad” experience; (ii) 86.3% had a “good” or “very good” experience with or opinion of pretest counselling, whereas 13.7% had a “fair”, “bad” or “very bad” experience; (iii) 95.1% had a “good” or “very good” experience with or opinion of post-test counselling, whereas 4.9% had a “fair”, “bad” or “very bad” experience
Groves, 201031 South Africa To evaluate women’s experiences with HTC
25 Women who had been tested for HIV during their most recent pregnancy
(i) 52% believed they had clearly consented to testing and had a positive experience of group and individual education sessions; (ii) 28% said their choice was “less clear” and were less positive about the education sessions; (iii) 20% felt their choice had been compromised (48% of these women expressed the view that they experienced less autonomy in deciding whether to be tested for HIV)
Angotti, 201028 Malawi To determine local perceptions of routine HIV testing and the potential consequences
18 (12 from an ANC
attendee sample)
Women that had been o!ered HTC in an ANC and accepted the o!er
(i) 22.2% stated that refusing the o!er of a test was an option and believed that women could still receive services if they opted out of testing; (ii) the majority who underwent HIV testing stated they were not given the option of refusing in the ANC; (iii) HTC was considered a precondition for receiving care
Larsson, 201129 Uganda To explore women’s experiences of, and views on, the opt-out testing policy and associated HIV testing in an ANC
18 Pregnant women attending an ANC
(i) Pregnant women recruited from facilities that o!ered testing on site perceived HIV testing as compulsory, despite pretest group counselling; (ii) generally women thought they could not receive any other ANC service if they declined testing; (iii) women felt obligated to attempt to persuade their partners to attend the ANC for HIV testing and felt anxious about asking their male partners to participate in couples testing; (iv) women highlighted the power asymmetry between themselves and health-care providers
Ujiji, 201132 Kenya To identify factors associated with consent to opt-out of HTC
900 Pregnant women
(i) 17% understood that HIV testing was optional, whereas 83% did not; (ii) when asked: “If you could choose to HIV test or not, would you decline?”, 80% responded “no” and 20% responded “yes”
ANC, antenatal clinic; HIV, human immunodeficiency virus; HTC, HIV testing and counselling; PMTCT, prevention of mother-to-child HIV transmission.
358
Universal voluntary HIV testing in antenatal care settings:
a review of the contribution of provider-initiated testing &
counselling
Bernadette Hensen1, Rachel Baggaley2, Vincent J. Wong3, Kristina L. Grabbe4, Nathan Shaffer2,
Ying-Ru Jacqueline Lo2 and James Hargreaves5
1 Faculty of Infectious Diseases, London School of Hygiene and Tropical Medicine, London, UK2 World Health Organization, HIV Department, Geneva, Switzerland3 USAID, Office of HIV ⁄ AIDS, Washington, DC, USA4 Division of Global HIV ⁄ AIDS, Center for Global Health, US Centers for Disease Control, Atlanta, GA, USA5 Faculty of Epidemiology and Population Health, London School of Hygiene and Tropical Medicine, London, UK
Abstract objective To assess the contribution of provider-initiated testing and counselling (PITC) to achievinguniversal testing of pregnant women and, from available data on components of PITC, assess whetherPITC adoption adheres to pre-test information, post-test counselling procedures and linkage totreatment.methods Systematic review of published literature. Findings were collated and data extracted on HIVtesting uptake before and after the adoption of a PITC model. Data on pre- and post-test counsellinguptake and linkage to anti-retrovirals, where available, were also extracted.results Ten eligible studies were identified. Pre-intervention testing uptake ranged from 5.5% to78.7%. Following PITC introduction, testing uptake increased by a range of 9.9% to 65.6%, withtesting uptake ‡85% in eight studies. Where reported, pre-test information was provided to between91.5% and 100% and post-test counselling to between 82% and 99.8% of pregnant women. Linkage toARVs for prevention of mother to child transmission (PMTCT) was reported in five studies and rangedfrom 53.7% to 77.2%. Where reported, PITC was considered acceptable by ANC attendees.conclusion Our review provides evidence that the adoption of PITC within ANC can facilitateprogress towards universal voluntary testing of pregnant women. This is necessary to increase thecoverage of PMTCT services and facilitate access to treatment and prevention interventions. We foundsome evidence that PITC adoption does not undermine processes inherent to good conduct of testing,with high levels of pre-test information and post-test counselling, and two studies suggesting that PITC isacceptable to ANC attendees.
keywords human immunodeficiency virus, pregnant women, prevention of mother to childtransmission, diagnostic tests – routine, infection transmission – vertical
Introduction
HIV testing is a ‘critical gateway’ to treatment, care andsupport services. Knowledge of HIV status can empowerindividuals and couples to take measures to prevent HIVacquisition or onward transmission. For those alreadyinfected, a positive test result is necessary to accesstreatment and, in the case of pregnant women, to accessprevention of mother to child transmission (PMTCT)services (Higgins et al. 1991, Coates et al. 2000; WHO2003). Across communities, normalising awareness of HIVstatus through increasing testing could reduce HIV-relatedstigma and discrimination (WHO 2003).
However, progress towards universal knowledge of HIVstatus is inadequate (Granich et al. 2009). In 10 popula-tion-based surveys conducted in sub-Saharan Africa in2007–2009, the median percentage of people living withHIV who knew their status was <40% (WHO 2010). InAfrica, the estimated percentage of people who know theirHIV status ranges from <10% in Sierra Leone, DRC andLiberia to 40–56% in Kenya and South Africa (WHO2010). In 2009, an estimated 50% of pregnant women inEastern and Southern Africa received an HIV test, up from43% in 2008(WHO 2010).
For many years, HIV testing was delivered througha voluntary counselling and testing (VCT) model. A
Tropical Medicine and International Health doi:10.1111/j.1365-3156.2011.02893.x
volume 00 no 00
ª 2011 Blackwell Publishing Ltd
359

client-initiated approach, VCT guidelines stressed theimportance of confidentiality, expressed voluntarism andwritten informed consent. VCT relied on personal moti-vation to seek testing, which is influenced by a number offactors that might act as barriers to widespread testing(Leon et al. 2010b). With <10% of key populations in low-and middle-income countries who may have been exposedto HIV accessing VCT and with evidence that manyopportunities to diagnose patients with HIV were lost(Seipone 2004; Fetene & Feleke 2010), VCT was increas-ingly seen as inadequate (Nieburg et al. 2005; Fetene &Feleke 2010).
To address this problem in 2007 WHO issued guidancerecommending the routine offer of HIV testing in clinicalsettings. Termed ‘provider-initiated testing and counsel-ling’ (PITC), this model supports recommending testing toall patients attending health facilities, including antenatalservices, in countries with generalised epidemics and forthose attending, for example, antenatal, tuberculosis andsexually transmitted infection services in non-generalisedepidemiological contexts (WHO 2007). PITC eliminatesthe need for lengthy pre-test counselling, replacing it withpre-test information that meets the minimum standard forinformed consent (WHO 2007). Opt-out PITC is recom-mended; however, the guidance suggests that opt-in PITCshould be considered for ‘highly vulnerable populations’(WHO 2007). PITC proponents highlight its potentialimpact on universal knowledge of HIV status, thereby itspotential to reduce mother-to-child transmission (MTCT),HIV-related morbidity and mortality (Bayer & Edington2009), and its capacity to ‘normalise’ HIV testing (Leonet al. 2010a). However, others have concerns that remov-ing extensive pre-test counselling and written informedconsent could lead to coercion and thus threatens the ethicsand human rights of HIV testing (Gruskin et al. 2008;Bayer & Edington 2009). Prior to the WHO guidance,numerous countries had adopted the models of PITC inclinical settings, particularly in antenatal clinics (ANC) inresponse to evidence of the effectiveness of antiretrovirals(ARV) in reducing MTCT and the urgent need to provideaccess to PMTCT services to pregnant women with HIV(Seipone 2004; Centers for Disease Control & Prevention2008).
Growing evidence suggests that adopting PITC inANC reduces lost opportunities to test pregnant womenfor HIV and increases PMTCT uptake and coverage(Kharsany et al. 2010, Amornwichet et al. 2002, Weigelet al. 2009; Chersich & Luchters 2008). The aim ofthis systematic review was to determine the extent to whichthe adoption of guidelines for a PITC-related model inANC contributes to achieving the goal of universalvoluntary testing of pregnant women and increases the
coverage of PMTCT, treatment and care services. Wealso aimed to assess whether PITC adheres to thestandards inherent to good conduct of HIV testing, namelythat it provides pre-test information and post-testcounselling.
Methods
We conducted a systematic review of published literature.We searched Medline, Embase and Global Health using thefollowing search terms: provider-initiated, routine, diag-nostic, opt-out, HIV, human immunodeficiency virus,AIDS, acquired immune deficiency syndrome, counselling,counseling, testing and screening, antenatal, PMTCT,vertical transmission and prenatal care. The final fullsearch was conducted in December 2010. BH conductedthe literature search and, with support from DB and MK,determined whether full references extracted were eligiblefor inclusion. Studies were considered eligible for inclusionif they were conducted in ANC settings and reported on theimpact of adopting a model of PITC on the primaryoutcome: HIV testing uptake, and were English languagestudies. We included randomised controlled trials (RCT)and non-randomised studies (NRS) with >1 site per arm aslong as they collected both pre- and post-intervention datafor each facility. We also included time series studiesconducted in one facility if they had collected pre- andpost-intervention data. We excluded studies conducted atpopulation level as they provide limited information ofchanges within individual facilities, thus imposing greaterchallenges in inferring causation. Our review identifiedthree types of intervention ⁄ comparison conditions thatsatisfied these criteria (Table 1).
Data extraction
BH extracted data into two data extraction forms, one forstudy design (Table 2) and one for data relating to HIVtesting uptake and adjusted odds ratios, where reported.We also collated data on counselling and linkage to ARV.We critically appraised the quality of studies using aquality assessment tool adapted from the Effective PublicHealth Practice Project (EPHPP1). The tool included 22questions that allowed for yes, no and cannot tellresponses. Studies were not excluded on the basis ofquality, but given a weak, moderate or strong qualityrating (weak n = 2, moderate n = 7 and strong n = 1).
1http://www.ephpp.ca/PDF/Quality%20Assessment%20Tool_2010_2.pdf
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
360

Defining PITC and lost opportunities
For the purpose of this review, we defined PITC as theroutine offer of HIV testing, regardless of whether theemphasis of consent was opt-in or opt-out, by healthcareproviders to pregnant women attending ANC settings as astandard component of clinical practice. Lost opportunitiesto test for HIV were defined as the difference betweenthe reported proportion of women accepting testing anduniversal (100%) testing uptake. Although achieving100% uptake of testing is an ambitious goal, universaltesting is defined as such – the universal uptake of HIVtesting to achieve universal knowledge of HIV status. Weexpected studies to report increased uptake of HIV testing
after implementation of PITC; however, our primaryresearch question was to determine the ability of PITC toachieve universal (100%; 0% lost opportunities) HIVtesting in ANC. We restricted this review to studiesconducted in ANC settings as the majority of studies onPITC were conducted in ANC and the majority of PITCprogrammes were initially implemented in ANC.
Results
We retrieved 1009 references, of which 831 were excludedfollowing title review. Of the remaining 178, a further 158were excluded following abstract review or retrieval ofthe full paper as they did not meet the inclusion criteria(Figure 1). Of the remaining 20 studies, ten targeted thepopulation of interest (Table 2).
Studies that met the inclusion criteria
Tables 2 and 3 present the details and characteristics ofthe included studies. The majority were NRS (90%)comparing the period before the introduction of a routinetesting guideline, implemented either through an interven-tion at specific clinics or through a national policy change,to the period after. We identified only one RCT (Simpsonet al. 1998). In the studies, the number of clinics variedfrom 1 to 52 and sample sizes varied from 1456 to 54 429women. Seven studies were conducted in Africa (van’t
Table 1 Comparison and intervention conditions consideredeligible for inclusion
Comparison HIVtesting model
Intervention HIVtesting model
A VCT Routine offer of testingB Diagnostic testing Routine offer of testingC Routine offer of
opt-in testingRoutine offer ofopt-out testing*
*These models were defined as those where the emphasis of con-sent changed from one where, following a routine offer of testing,a patient explicity opted-in to a testing model where the patienthad to opt-out should they choose not to test.
1009 references retrieved fromelectronic database search
831 references excluded
81 references excluded
from title review
178 references
after abstract review77 references excluded based on study
design–majority were cross sectional studies
20 references
10 excluded based on target population
10 references considered eligible for review
Figure 1 Inclusion flow diagram.
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
361

Tab
le2
Det
ails
of
studie
sin
cluded
inth
ere
view
Sett
ing
Yea
rof
study
Study
des
ign
Study
of
apoli
cy
chan
geor
PIT
C
trai
nin
gin
terv
enti
on
Com
par
ison
group
Per
iod
of
follow
-up
Fac
ilit
y
sett
ing
Num
.of
faci
liti
esPopula
tion
Popula
tion
size
Urb
an⁄
Rura
lO
utc
om
e(s)
Scotl
and
(Sim
pso
net
al.
1998)
1996–1
997
RC
TR
CT
com
par
ing
VC
Tto
4m
odel
s
of
routi
ne
test
ing
Ran
dom
lyse
lect
ed
VC
Tco
ntr
ol
10
month
sH
osp
ital
AN
C1
Pre
gnan
t
wom
en
3024
UU
pta
ke
and
acce
pta
bilit
y
of
HIV
test
ing,
wom
en’s
know
ledge
,sa
tisf
acti
on
and
anxie
ty
Scotl
and
(Sim
pso
net
al.
1999)
1998
BA
Policy
chan
ge10
month
spri
or
to
opt-
out
test
ing
3m
onth
sPre
gnan
t
wom
en
2954
UU
pta
ke
and
acce
pta
bilit
yof
HIV
test
ing,
test
ing-
rela
ted
anxie
ty
USA
(Str
inge
ret
al.
2001)
1998–2
000
BA
Tra
inin
g&
poli
cych
ange
Dat
afr
om
year
bef
ore
policy
chan
ge
2ye
ars
AN
C8
Pre
gnan
t
wom
en
7193
UU
pta
ke
of
opt-
out
test
ing
on
HIV
test
ing
rate
s
Ken
ya(v
an’t
Hoog
etal
.
2005)
2001–2
003
RB
AIm
ple
men
tati
on
of
pil
ot
pro
ject
Yea
rpri
or
to
pil
ot
pro
ject
2ye
ars
Hosp
ital
AN
C1
(6publi
c
hea
lth
centr
es)
Pre
gnan
t
wom
en
8231
UU
pta
ke
of
counse
llin
g,
test
ing
and
nev
irap
ine
Bots
wan
a
(Cre
eket
al.
2007)
2003–2
004
BA
Tra
inin
g&
poli
cych
ange
Las
t5
month
s
of
VC
T
1ye
arA
NC
4Pre
gnan
t
wom
en
1456
UH
IVte
stin
gupta
ke,
PM
TC
Tin
terv
enti
on
rate
s,an
dra
tes
of
AN
Cat
tendan
ce
Zim
bab
we
(Chan
dis
arew
aet
al.
2007)
2004–2
005
BA
Tra
inin
g&
poli
cych
ange
Las
t6
month
s
of
opt-
in
1ye
arA
NC
4Pre
gnan
t
wom
en
&th
eir
par
tner
s
9423
UH
IVte
stin
gupta
ke,
mat
ernal
HIV
stat
us;
per
cepti
ons
of
routi
ne
test
ing
Mal
awi
(Mose
set
al.
2008,
Zim
ba
etal
.2006*)
2002–2
006
TS
Policy
chan
geL
ast
9m
onth
s
of
opt-
in
18
month
sA
NC
4Pre
gnan
t
wom
en
30
092
UR
ate
HIV
counse
lled
,
HIV
test
ing
upta
ke
and
HIV
posi
tivi
ty
Uga
nda
(Bya
mugi
sha
etal
.2010)
2002–2
009
TS
Tra
inin
g&
Poli
cych
ange
His
tori
cal
contr
ol
–hosp
ital
reco
rds
pre
⁄post
poli
cych
ange
7ye
ars
Ref
erra
l
Hosp
ital
1Pre
gnan
t
wom
en
&th
eir
par
tner
s
54
429
UN
um
ber
of
new
AN
C
atte
ndan
ces
⁄yea
r,
num
ber
of
AN
C
pat
ients
counse
lled
and
test
ed,
num
ber
that
obta
ined
a
posi
tive
resu
lt,
num
ber
of
mal
e
par
tner
sco
unse
lled
and
test
edan
d
obta
ined
posi
tive
resu
lt,
HIV
-posi
tive
moth
ers
and
infa
nts
that
rece
ived
AR
T
pro
phyl
axis
Eth
iopia
(Mir
kuzi
eet
al.
2010)
2004–2
009
TS
Policy
chan
ge
His
tori
cal
contr
ol
–
PM
TC
Tre
port
s
5ye
ars!
Publi
can
d
pri
vate
faci
liti
es
52 (2
5pri
vate
)
Pre
gnan
t
wom
en
and
thei
r
par
tner
s
663
603
(fro
m2004
to2009)
UPro
port
ion
of
wom
enre
ceiv
ing
pre
-tes
tco
unse
llin
g,
HIV
test
ing
and
post
-tes
tco
unse
llin
g;
pro
port
ion
of
wom
en
and
bab
ies
who
rece
ived
AR
Vpro
phyl
axis
Mal
awi
(Kas
enga
etal
.
2009)"
2005–2
007
TS
Policy
chan
ge
His
tori
cal
contr
ol
–hosp
ital
reco
rds
pre
⁄post
poli
cych
ange
2ye
ars
Hosp
ital
AN
C
1Pre
gnan
t
wom
en
2055
RD
eman
dfo
rA
NC
,H
IV
test
ing
upta
ke
and
hosp
ital
del
iver
y
*U
npublish
edre
sult
sfr
om
confe
rence
abst
ract
san
dpre
senta
tions
pro
vided
det
ails
of
the
study,
incl
udin
gnum
ber
of
wom
enre
ached
,fo
rth
eper
iod
2004–2
005.
Res
ult
sonly
incl
ude
dat
afr
om
thes
eye
ars.
!Alt
hough
2004–2
009
resu
lts
are
avai
lable
,only
2007–2
009
are
incl
uded
inth
ere
view
asin
2007
pri
vate
faci
liti
es,
whic
har
ein
cluded
in2009
dat
a,st
arte
dPM
TC
T.
"Res
ult
sonly
pre
sente
dfo
rper
iod
Mar
ch–D
ecem
ber
2005,
when
test
ing
was
opt-
in,
wit
hJa
nuar
y–D
ecem
ber
2006,
bef
ore
the
imple
men
tati
on
of
free
serv
ices
.
RC
T,
random
ised
contr
oll
edtr
ial;
BA
,bef
ore
⁄aft
erst
udy;
RB
A,
retr
osp
ecti
ve(b
efore
⁄aft
er)
study;
TS,
tim
ese
ries
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
362

Hoog et al. 2005; Chandisarewa et al. 2007; Creek et al.2007; Moses et al. 2008; Kasenga et al. 2009; Byamugishaet al. 2010; Mirkuzie et al. 2010), two in Europe (Simpsonet al. 1998, 1999) and one in the USA (Stringer et al.2001). The outcome of HIV testing uptake was reported inall studies (Table 2).
Intervention heterogeneity
The PITC interventions under study varied in a number ofways. Some studies reported extensive healthcare workertraining prior to the implementation of PITC (Chandis-arewa et al. 2007; Creek et al. 2007; Byamugisha et al.2010), whilst others did not report on this (Kasenga et al.2009). Some studies were the evaluations of interventionsimplemented in facilities, whilst others evaluated theinfluence of policy change on activities at facility level(Table 2). The information provided to women throughpre-test education also varied: one study reported extensivecommunity mobilisation (Chandisarewa et al. 2007),whilst two reported provision of leaflets (Simpson et al.1998, 1999) (Table 4).
Missed opportunities for testing
Table 5 presents data on HIV testing uptake. Prior to theimplementation of PITC, lost opportunities for testingranged from 94.5% in Scotland (Simpson et al. 1998) to21.3% in a study from Malawi (Kasenga et al. 2009).Following implementation of PITC, lost opportunitiesdecreased substantially in all settings (Figure 2). Despite asignificant decrease in lost opportunities, in Scotland,where the aim of the study was to determine uptake andacceptability of different methods of a universal offer oftesting, the lost opportunities amongst women in inter-vention groups remained high at 65.2% (P < 0.001)(Simpson et al. 1998). The adoption of opt-out PITCfurther reduced missed opportunities to 11.7% (Simpsonet al. 1999). In rural Malawi, implementation of opt-outtesting reduced lost opportunities to test by 9.9%; theintroduction of free maternity services in October 2006reduced lost opportunities further to 1.2% (testing uptake98.8% (n = 2,249 ⁄ 2,277);Kasenga et al. 2009). The lowestproportion of lost opportunities for testing was reported inZimbabwe, where <0.1% of opportunities to test womenwere lost (P < 0.001) (Chandisarewa et al. 2007).
Components of the PITC process
Four studies presented results for the proportion of womenprovided pre-test counselling ⁄ information (van’t Hooget al. 2005; Chandisarewa et al. 2007; Byamugisha et al.
2010; Mirkuzie et al. 2010) (Table 6). Followingimplementation of PITC, pre-test counselling ⁄ informationranged from 91.5% in a study from Kenya (van’t Hooget al. 2005) to 100% in Zimbabwe (Chandisarewa et al.2007). These four studies also presented results on theproportion of women tested and subsequently post-testcounselled or received test results (van’t Hoog et al. 2005;Chandisarewa et al. 2007; Creek et al. 2007; Mirkuzieet al. 2010). Prior to the implementation of revised PITCmodels the proportion of women receiving post-testcounselling and test results ranged from 72% who receivedtest results in Botswana (Creek et al. 2007) to 96.9% inZimbabwe (Chandisarewa et al. 2007). Following imple-mentation of revised PITC models post-test counselling ⁄
Table 3 Study characteristics
Study characteristics Frequency (n)
Study designNon-randomised study 9Randomised controlled trial 1
Year of study initiation1995–1996 11997–1998 21999–2000 02001–2002 22003–2004 42005–2006 1
Study directionProspective 5Retrospective 5
Inclusion and exclusion criteria (individuals)Reported 1Not reported 9
Reason for selection of clinic(s)Reported 1Not reported 9
Results assessors blinded during interpretationReported 0Not reported 10
Intervention groupRoutine offer of testing vs. VCT 4Routine offer of opt-out testing vs.
routine offer opt-in testing6*
Comparison groupBefore intervention comparison 6Historical comparison 3Controlled comparison 1
Study typology (Table 1)Group A 4Group B 0Group C 6
*For the study conducted in Ethiopia, public facilities adoptedopt-out testing but private facilities adopted opt-in testing afterVCT.
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
363
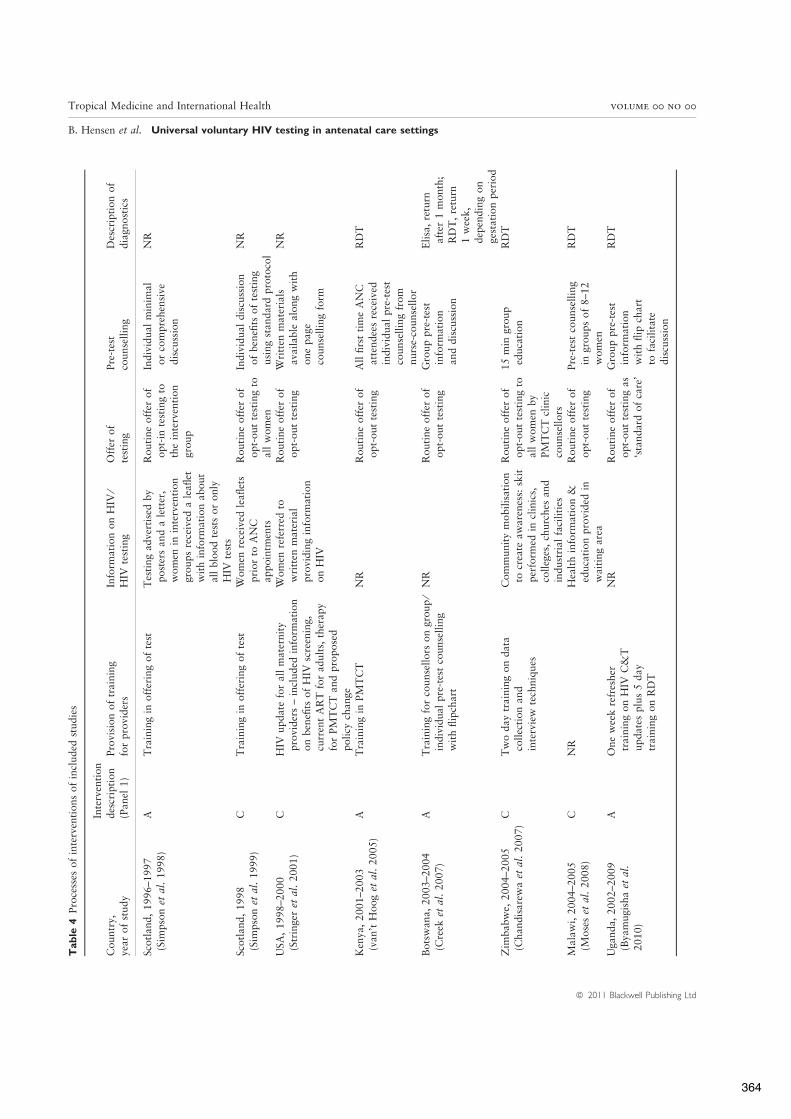
Tab
le4
Pro
cess
esof
inte
rven
tions
of
incl
uded
studie
s
Countr
y,ye
arof
study
Inte
rven
tion
des
crip
tion
(Pan
el1)
Pro
visi
on
of
trai
nin
gfo
rpro
vider
sIn
form
atio
non
HIV
⁄H
IVte
stin
gO
ffer
of
test
ing
Pre
-tes
tco
unse
llin
gD
escr
ipti
on
of
dia
gnost
ics
Scotl
and,
1996–1
997
(Sim
pso
net
al.
1998)
AT
rain
ing
inoff
erin
gof
test
Tes
ting
adve
rtis
edby
post
ers
and
ale
tter
,w
om
enin
inte
rven
tion
groups
rece
ived
ale
aflet
wit
hin
form
atio
nab
out
all
blo
od
test
sor
only
HIV
test
s
Routi
ne
off
erof
opt-
inte
stin
gto
the
inte
rven
tion
group
Indiv
idual
min
imal
or
com
pre
hen
sive
dis
cuss
ion
NR
Scotl
and,
1998
(Sim
pso
net
al.
1999)
CT
rain
ing
inoff
erin
gof
test
Wom
enre
ceiv
edle
aflet
spri
or
toA
NC
appoin
tmen
ts
Routi
ne
off
erof
opt-
out
test
ing
toal
lw
om
en
Indiv
idual
dis
cuss
ion
of
ben
efits
of
test
ing
usi
ng
stan
dar
dpro
toco
l
NR
USA
,1998–2
000
(Str
inge
ret
al.
2001)
CH
IVupdat
efo
ral
lm
ater
nit
ypro
vider
s–
incl
uded
info
rmat
ion
on
ben
efits
of
HIV
scre
enin
g,cu
rren
tA
RT
for
adult
s,th
erap
yfo
rPM
TC
Tan
dpro
pose
dpoli
cych
ange
Wom
enre
ferr
edto
wri
tten
mat
eria
lpro
vidin
gin
form
atio
non
HIV
Routi
ne
off
erof
opt-
out
test
ing
Wri
tten
mat
eria
lsav
aila
ble
along
wit
hone
pag
eco
unse
llin
gfo
rm
NR
Ken
ya,
2001–2
003
(van
’tH
oog
etal
.2005)
AT
rain
ing
inPM
TC
TN
RR
outi
ne
off
erof
opt-
out
test
ing
All
firs
tti
me
AN
Cat
tendee
sre
ceiv
edin
div
idual
pre
-tes
tco
unse
llin
gfr
om
nurs
e-co
unse
llor
RD
T
Bots
wan
a,2003–2
004
(Cre
eket
al.
2007)
AT
rain
ing
for
counse
llors
on
group
⁄in
div
idual
pre
-tes
tco
unse
llin
gw
ith
flip
char
t
NR
Routi
ne
off
erof
opt-
out
test
ing
Gro
up
pre
-tes
tin
form
atio
nan
ddis
cuss
ion
Eli
sa,
retu
rnaf
ter
1m
onth
;R
DT
,re
turn
1w
eek,
dep
endin
gon
gest
atio
nper
iod
Zim
bab
we,
2004–2
005
(Chan
dis
arew
aet
al.
2007)
CT
wo
day
trai
nin
gon
dat
aco
llec
tion
and
inte
rvie
wte
chniq
ues
Com
munit
ym
obil
isat
ion
tocr
eate
awar
enes
s:sk
itper
form
edin
clin
ics,
colleg
es,
churc
hes
and
indust
rial
faci
liti
es
Routi
ne
off
erof
opt-
out
test
ing
toal
lw
om
enby
PM
TC
Tcl
inic
counse
llors
15
min
group
educa
tion
RD
T
Mal
awi,
2004–2
005
(Mose
set
al.
2008)
CN
RH
ealt
hin
form
atio
n&
educa
tion
pro
vided
inw
aiti
ng
area
Routi
ne
off
erof
opt-
out
test
ing
Pre
-tes
tco
unse
llin
gin
groups
of
8–1
2w
om
en
RD
T
Uga
nda,
2002–2
009
(Bya
mugi
sha
etal
.2010)
AO
ne
wee
kre
fres
her
trai
nin
gon
HIV
C&
Tupdat
esplu
s5
day
trai
nin
gon
RD
T
NR
Routi
ne
off
erof
opt-
out
test
ing
as‘s
tandar
dof
care
’
Gro
up
pre
-tes
tin
form
atio
nw
ith
flip
char
tto
faci
lita
tedis
cuss
ion
RD
T
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
364
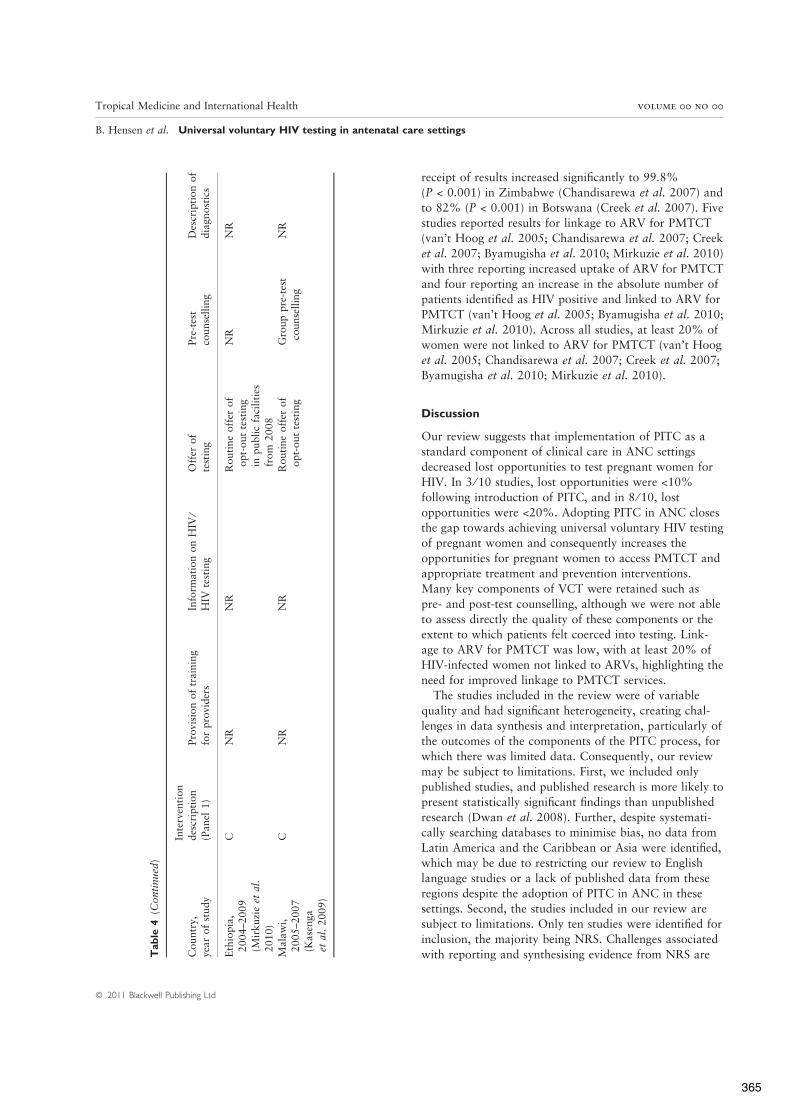
receipt of results increased significantly to 99.8%(P < 0.001) in Zimbabwe (Chandisarewa et al. 2007) andto 82% (P < 0.001) in Botswana (Creek et al. 2007). Fivestudies reported results for linkage to ARV for PMTCT(van’t Hoog et al. 2005; Chandisarewa et al. 2007; Creeket al. 2007; Byamugisha et al. 2010; Mirkuzie et al. 2010)with three reporting increased uptake of ARV for PMTCTand four reporting an increase in the absolute number ofpatients identified as HIV positive and linked to ARV forPMTCT (van’t Hoog et al. 2005; Byamugisha et al. 2010;Mirkuzie et al. 2010). Across all studies, at least 20% ofwomen were not linked to ARV for PMTCT (van’t Hooget al. 2005; Chandisarewa et al. 2007; Creek et al. 2007;Byamugisha et al. 2010; Mirkuzie et al. 2010).
Discussion
Our review suggests that implementation of PITC as astandard component of clinical care in ANC settingsdecreased lost opportunities to test pregnant women forHIV. In 3 ⁄ 10 studies, lost opportunities were <10%following introduction of PITC, and in 8 ⁄ 10, lostopportunities were <20%. Adopting PITC in ANC closesthe gap towards achieving universal voluntary HIV testingof pregnant women and consequently increases theopportunities for pregnant women to access PMTCT andappropriate treatment and prevention interventions.Many key components of VCT were retained such aspre- and post-test counselling, although we were not ableto assess directly the quality of these components or theextent to which patients felt coerced into testing. Link-age to ARV for PMTCT was low, with at least 20% ofHIV-infected women not linked to ARVs, highlighting theneed for improved linkage to PMTCT services.
The studies included in the review were of variablequality and had significant heterogeneity, creating chal-lenges in data synthesis and interpretation, particularly ofthe outcomes of the components of the PITC process, forwhich there was limited data. Consequently, our reviewmay be subject to limitations. First, we included onlypublished studies, and published research is more likely topresent statistically significant findings than unpublishedresearch (Dwan et al. 2008). Further, despite systemati-cally searching databases to minimise bias, no data fromLatin America and the Caribbean or Asia were identified,which may be due to restricting our review to Englishlanguage studies or a lack of published data from theseregions despite the adoption of PITC in ANC in thesesettings. Second, the studies included in our review aresubject to limitations. Only ten studies were identified forinclusion, the majority being NRS. Challenges associatedwith reporting and synthesising evidence from NRS areT
ab
le4
(Conti
nued
)
Countr
y,ye
arof
study
Inte
rven
tion
des
crip
tion
(Pan
el1)
Pro
visi
on
of
trai
nin
gfo
rpro
vider
sIn
form
atio
non
HIV
⁄H
IVte
stin
gO
ffer
of
test
ing
Pre
-tes
tco
unse
llin
gD
escr
ipti
on
of
dia
gnost
ics
Eth
iopia
,2004–2
009
(Mir
kuzi
eet
al.
2010)
CN
RN
RR
outi
ne
off
erof
opt-
out
test
ing
inpublic
faci
liti
esfr
om
2008
NR
NR
Mal
awi,
2005–2
007
(Kas
enga
etal
.2009)
CN
RN
RR
outi
ne
off
erof
opt-
out
test
ing
Gro
up
pre
-tes
tco
unse
llin
gN
R
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
365
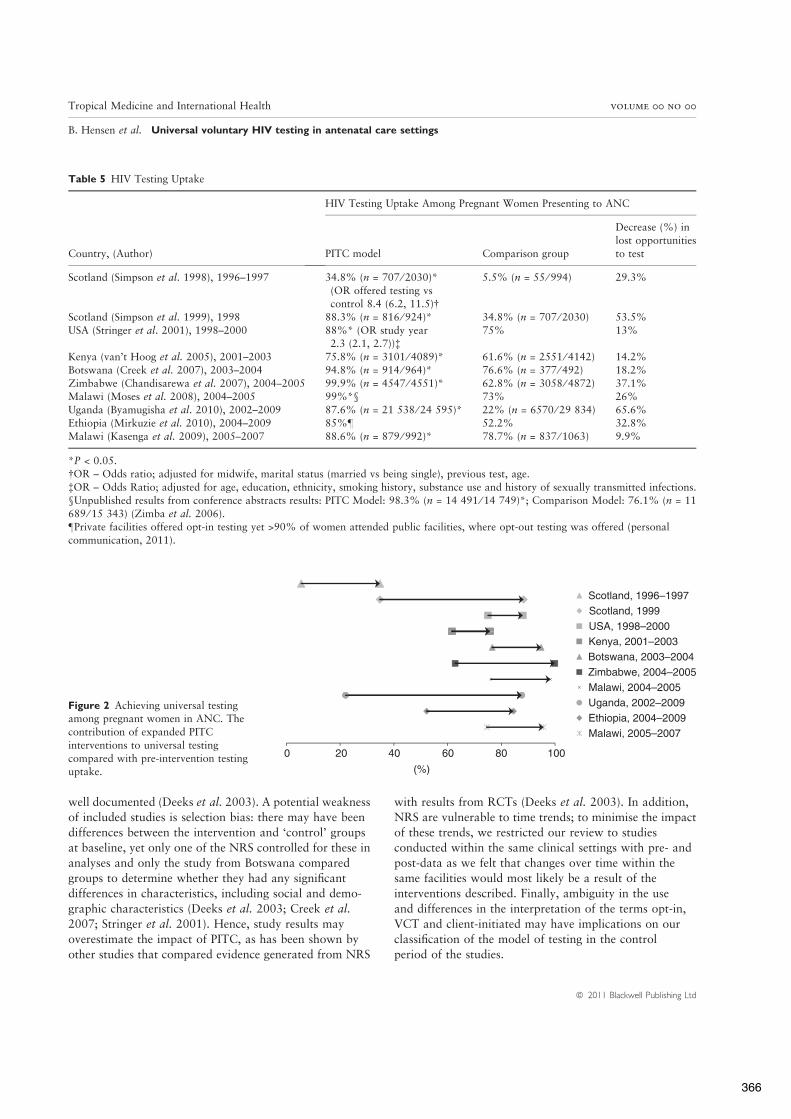
well documented (Deeks et al. 2003). A potential weaknessof included studies is selection bias: there may have beendifferences between the intervention and ‘control’ groupsat baseline, yet only one of the NRS controlled for these inanalyses and only the study from Botswana comparedgroups to determine whether they had any significantdifferences in characteristics, including social and demo-graphic characteristics (Deeks et al. 2003; Creek et al.2007; Stringer et al. 2001). Hence, study results mayoverestimate the impact of PITC, as has been shown byother studies that compared evidence generated from NRS
with results from RCTs (Deeks et al. 2003). In addition,NRS are vulnerable to time trends; to minimise the impactof these trends, we restricted our review to studiesconducted within the same clinical settings with pre- andpost-data as we felt that changes over time within thesame facilities would most likely be a result of theinterventions described. Finally, ambiguity in the useand differences in the interpretation of the terms opt-in,VCT and client-initiated may have implications on ourclassification of the model of testing in the controlperiod of the studies.
Table 5 HIV Testing Uptake
Country, (Author)
HIV Testing Uptake Among Pregnant Women Presenting to ANC
PITC model Comparison group
Decrease (%) inlost opportunitiesto test
Scotland (Simpson et al. 1998), 1996–1997 34.8% (n = 707 ⁄ 2030)*(OR offered testing vscontrol 8.4 (6.2, 11.5)!
5.5% (n = 55 ⁄ 994) 29.3%
Scotland (Simpson et al. 1999), 1998 88.3% (n = 816 ⁄ 924)* 34.8% (n = 707 ⁄ 2030) 53.5%USA (Stringer et al. 2001), 1998–2000 88%* (OR study year
2.3 (2.1, 2.7))"75% 13%
Kenya (van’t Hoog et al. 2005), 2001–2003 75.8% (n = 3101 ⁄ 4089)* 61.6% (n = 2551 ⁄ 4142) 14.2%Botswana (Creek et al. 2007), 2003–2004 94.8% (n = 914 ⁄ 964)* 76.6% (n = 377 ⁄ 492) 18.2%Zimbabwe (Chandisarewa et al. 2007), 2004–2005 99.9% (n = 4547 ⁄ 4551)* 62.8% (n = 3058 ⁄ 4872) 37.1%Malawi (Moses et al. 2008), 2004–2005 99%*§ 73% 26%Uganda (Byamugisha et al. 2010), 2002–2009 87.6% (n = 21 538 ⁄ 24 595)* 22% (n = 6570 ⁄ 29 834) 65.6%Ethiopia (Mirkuzie et al. 2010), 2004–2009 85%– 52.2% 32.8%Malawi (Kasenga et al. 2009), 2005–2007 88.6% (n = 879 ⁄ 992)* 78.7% (n = 837 ⁄ 1063) 9.9%
*P < 0.05.!OR – Odds ratio; adjusted for midwife, marital status (married vs being single), previous test, age."OR – Odds Ratio; adjusted for age, education, ethnicity, smoking history, substance use and history of sexually transmitted infections.§Unpublished results from conference abstracts results: PITC Model: 98.3% (n = 14 491 ⁄ 14 749)*; Comparison Model: 76.1% (n = 11689 ⁄ 15 343) (Zimba et al. 2006).–Private facilities offered opt-in testing yet >90% of women attended public facilities, where opt-out testing was offered (personalcommunication, 2011).
Scotland, 1996–1997Scotland, 1999USA, 1998–2000Kenya, 2001–2003Botswana, 2003–2004Zimbabwe, 2004–2005Malawi, 2004–2005
0 20 40 60 80 100
Uganda, 2002–2009Ethiopia, 2004–2009Malawi, 2005–2007
(%)
Figure 2 Achieving universal testingamong pregnant women in ANC. Thecontribution of expanded PITCinterventions to universal testingcompared with pre-intervention testinguptake.
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
366

Notwithstanding these limitations, we attempted tosynthesis the findings of studies on similar primaryoutcomes assessed through similar study designs and insimilar (ANC) settings. Most studies were from Africancountries with generalised epidemics. The overall direc-tion and size of the effect provide evidence of the impactof this strategy on universal voluntary testing in ANC insimilar contexts. National testing figures report substan-tial increases in HIV testing coverage where the testingmodel is PITC (WHO 2008, 2009, 2010): WHO 2010Universal Access Report documents high coverage of HIVtesting amongst pregnant women in Europe and CentralAsia at 75% and in Latin America and the Caribbean at57% (WHO 2010). In Eastern and Southern Africa, theregion with the highest HIV prevalence, HIV testingamongst pregnant women reached over 50%, an increasefrom 43% in 2008 (WHO 2010). In Western and CentralAfrica, coverage increased from 16% to 21% between2008 and 2009, with 54% [40–84%] of pregnant womenwith HIV in sub-Saharan Africa receiving ARVs forPMTCT compared with 45% [37–58%] in 2008 (WHO2010). Consequently, although attributing reduced lostopportunities for testing to PITC is challenging in theabsence of RCTs, as testing uptake is likely to beinfluenced by multiple correlated factors including theavailability of rapid testing kits, increased availability ofART, healthcare providers expectations and attitudes, andthe introduction of free services (Moses et al. 2008; Aprilet al. 2009), the consistency and strength of association
suggest that these results are reliable in terms of directionand magnitude.
A number of important questions remain. Reports ofhigh HIV testing coverage and a reduction in lost oppor-tunities where testing is routinely offered have been metwith caution by some as concerns remain that, in theabsence of written informed consent following individualpre-test information, intentional and unintentional coer-cion may confound patient choice (Gruskin et al. 2008;Becker et al. 2009). The process by which individualsdecide to undergo testing is complex, being influenced notonly by available information, but also by cultural, societaland individual beliefs and values and the potentialindividual and social implications of a positive test result(Gruskin et al. 2008). The routine offer of HIV testing inANC settings might, however, simplify the decision-mak-ing process, through the normalisation of testing byremoving fear of stigma, discrimination and moral judg-ements where testing is client-initiated (Oosterhoff et al.2008). PITC has also raised ethical and human rightsconcerns in relation to testing and counselling and concernsregarding potential psychological consequences of apositive result in the absence of extensive pre-test coun-selling (Koo et al. 2006). Concerns exist that PITC will failto adhere to the principles of consent, confidentiality andcounselling inherent to VCT. Yet, anecdotal evidencesuggests that where the testing strategy is VCT, pre- and ⁄ orpost-test counselling is sometimes of poor quality orlacking (Paxton et al. 1999; Ayarza & Reyes 2002, Chopra
Table 6 Outcomes of the PITC components
Pre-test counselled ⁄ information PITC model Comparison group
Kenya (van’t Hoog et al. 2005) 91.5% (n = 3743 ⁄ 4089)* 77.4% (n = 3206 ⁄ 4142)Uganda (Byamugisha et al. 2010) 98.3% (n = 24 171 ⁄ 24 595)* 62.3% (n = 18 583 ⁄ 29 834)Zimbabwe(Chandisarewa et al. 2007)
100% (n = 4551 ⁄ 4551) 100% (n = 4872 ⁄ 4872)
Ethiopia (Mirkuzie et al. 2010) 94% 71.9%Patients post-test counselled
Kenya (van’t Hoog et al. 2005) 90.3% (n = 2799 ⁄ 3101) 89.3% (n = 2278 ⁄ 2551)Botswana (Creek et al. 2007) 82% (n = 753 ⁄ 914)* 72% (n = 272 ⁄ 377)Zimbabwe
(Chandisarewa et al. 2007)99.8% (n = 4538 ⁄ 4547)* 96.9% (n = 2964 ⁄ 3058)
Ethiopia (Mirkuzie et al. 2010) 84.5% 50.7%Linkage to PMTCT for womenwith positive resultsKenya (van’t Hoog et al. 2005) 70% (n = 471 ⁄ 673)* 56.6% (n = 302 ⁄ 534)Botswana (Creek et al. 2007) 66% (n = 144 ⁄ 220) 70% (n = 87 ⁄ 125)Zimbabwe
(Chandisarewa et al. 2007)73% (n = 663 ⁄ 908) 76.3% (n = 372 ⁄ 487)
Uganda (Byamugisha et al. 2010) 77.2% (n = 885 ⁄ 1147)* 55.8% (n = 316 ⁄ 566)Ethiopia (Mirkuzie et al. 2010) 53.7% 33.8%
*P < 0.05.
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
367

et al. 2005). In our review, we found that opt-out PITCadhered to the standards inherent to counselling andtesting, with data indicating that women who were testedalso receive pre-test counselling ⁄ information and that amajority of the women tested receive post-test counselling.The quality of these components was, however, notassessed, and additional research of the quality of the PITCcomponents is warranted.
Although PITC closes the gap towards universal testing,a minority of women continue to refuse testing. Anincreased understanding of the factors associated with opt-out, such as age, ethnicity and ‡12 years of education inthe USA (Stringer et al. 2001), and marital status inScotland (Simpson et al. 1998), as suggested by evidencefrom studies included in our review, would ensure oppor-tunities to test specific subpopulations within ANC settingsare addressed (Homsy et al. 2007). Similarly, furtherresearch regarding the acceptability of services within ANCsettings is required as, although we present evidence of theadherence to the standards inherent to good HIV testingconduct, our review provides limited evidence of women’sperception and acceptability of the strategy. Studiesincluded in our review suggest that the routine offer oftesting is ‘helpful’ to women in Zimbabwe, with a majorityof women in Scotland in favour of the availability of testingto all pregnant women (Simpson et al. 1998; Chandis-arewa et al. 2007). In-depth personal perceptions regard-ing PITC processes were, however, not examined in thestudies identified, and additional research is warranted.
Despite evidence that implementation of a PITC inter-vention may improve linkage to ARVs for PMTCT, at least20% of women testing positive across five studies failed toaccess ARVs for PMTCT; in two studies conducted inBotswana and Zimbabwe, the proportion of women linkedto ARVs for PMTCT decreased, albeit insignificantly. Thereis limited current published evidence of why a largeproportion of women fail to be linked to ARV for PMTCTand of the effectiveness of linkage to ART, and subsequentadherence to ART regimens, for the management of themother’s infection for women testing in ANC and requiringtreatment for their own health. The benefits of testing, in theabsence of effective linkage to PMTCT, treatment and careservices, are limited. Understanding these linkages, andtheir weaknesses, is crucial to ensuring the benefits of testingare maximised. The studies included in this review focusprimarily on HIV testing uptake. The majority are earlyPITC studies, conducted during a transitional period whencommunity and political support and healthcare providerconfidence in conducting PITC may have been limited.Additional research of recent studies, which focus on PITCand the effectiveness of linkages to ARVs and ART in theera of ART scale-up and of increased support for PITC,
through the availability of WHO guidance and nationalpolicies recommending PITC, is required. In addition, thecosts associated with the introduction of PITC need to beassessed alongside assessments of any impact PITC has onoverburdened services and service providers. For individu-als accepting the offer of testing, sexual behavioursfollowing a negative test result also need to be monitoredand researched as concerns exist that a negative result mayresult in sexual disinhibition (Kiene et al. 2009). Finally,our review was restricted to the contribution of PITC touniversal voluntary testing for pregnant women in ANCsettings; additional research is needed to better understandhow PITC might contribute to universal voluntary testingamongst different populations within different clinicalcontexts.
Acknowledgements
We thank Dr. Delia Boccia and Dr. Mishal Khan who wereinvolved in determining eligibility and critically appraisingstudies identified for review. This study was funded byWHO and CDC.
References
Amornwichet P, Teeraratkul A, Simonds RJ et al. (2002)Preventing mother-to-child transmission. The first year ofThailand’s national program. JAMA 288, 245–248.
April M, Walensky R, Chang Y et al. (2009) HIV testing rates andoutcomes in a South African community, 2001–2006: implica-tions for expanded screening policies. Journal of AcquiredImmune Deficiency Syndrome 51, 310–316.
Ayarza R & Reyes B (2002) Changes in quality of life of peopleliving with HIV ⁄ AIDS in Ecuador. XIV International AIDSConference. Barcelona, Spain.
Bayer R & Edington C (2009) HIV testing, human rights, and theglobal AIDS policy: exceptionalism and its discontents. Journalof Health Politics, Policy and Law 34, 301–323.
Becker J, Tsague L, Sahabo R & Twyman P (2009) ProviderInitiated Testing and Counseling (PITC) for HIV in resource-limited clinical settings: important questions unanswered.Pan African Medical Journal 3, 1–5.
Byamugisha R, Tylleskar T, Kagawa MN, OnyangoS, Karamagi CA& Tumwine JK (2010) Dramatic and sustained increase in HIV-testing rates among antenatal attendees in Eastern Uganda after apolicy change from voluntary counselling and testing to routinecounsellingandtesting forHIV:aretrospectiveanalysisofhospitalrecords, 2002–2009. BMC Health Services Research 10, 290.
Centers for Disease Control & Prevention. (2008) Provider-initiated HIV testing and counseling of TB patients – Living-stone District, Zambia, September 2004–December 2006.MMWR – Morbidity & Mortality Weekly Report 57, 285–289.
Chandisarewa W, Stranix-Chibanda L, Chirapa E et al. (2007)Routine offer of antenatal HIV testing (‘‘opt-out’’ approach)
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
368

to prevent mother-to-child transmission of HIV in urbanZimbabwe. Bulletin of the World Health Organization 85,843–850.
Chersich M, Luchters SMF, Othigo MJ et al. (2008) HIV testingand counselling for women attending child health clinics: anopportunity for entry to prevent mother-to-child transmissionand HIV treatment. International Journal of STD & AIDS 19,42–46.
Chopra M, Doherty T, Jackson D & Ashworth A (2005)Preventing HIV transmission to children: quality ofcounselling of mothers in South Africa. Acta Paediatrica 94,357–363.
Coates T, Grinstead O, Gregorich S et al. (2000) Efficacy of vol-untary HIV-1 counselling and testing in individuals and couplesin Kenya, Tanzania, and Trinidad: a randomised trial. TheVoluntary HIV-1 Counseling and Testing Efficacy Study Group.The Lancet 8, 103–112.
Creek TL, Ntumy R, Seipone K et al. (2007) Successful intro-duction of routine opt-out HIV testing in antenatal care inBotswana. Journal of Acquired Immune Deficiency Syndromes45, 102–107.
Deeks J, Dinnes J, D’Amico R et al. (2003) Evaluatingnon-randomised intervention studies. Health TechnologyAssessment 7, 1–173.
Dwan K, Altman DG, Arnaiz JA et al. (2008) Systematic review ofthe empirical evidence of study publication bias and outcomereporting bias. PLoS ONE 3, e3081.
Fetene NW & Feleke AD (2010) Missed opportunities forearlier HIV testing and diagnosis at the health facilities ofDessie town, North East Ethiopia. BMC Public Health 10,362.
Granich R, Gilks C, Dye C, De Cock K & Williams B (2009)Universal voluntary HIV testing with immediate antiretroviraltherapy as a strategy for elimination of HIV transmission: amathematical model. The Lancet. 373, 48–57.
Gruskin S, Ahmed S & Ferguson L (2008) Provider-initiated HIVtesting and counseling in health facilities – what does this meanfor the health and human rights of pregnant women? Devel-oping World Bioethics 8, 23–32.
Higgins DL, Galavotti C, O’Reilly KR et al. (1991) Evidence forthe effects of HIV antibody counseling and testing on riskbehaviors. JAMA 266, 2419–2429.
Homsy J, King R, Malamba S et al. (2007) The need for partnerconsent is a main reason for opting out of routine HIV testingfor prevention of mother-to-child transmission in a ruralUgandan hospital. Journal of Acquired Immune DeficiencySyndromes 44, 366–369.
Kasenga F, Byass P, Emmelin M & Hurtig A-K (2009) Theimplications of policy changes on the uptake of a PMTCTprogramme in rural Malawi: first three years of experience.Global Health Action 2, 1–7.
Kharsany ABM, Karim QA & Karim SSA (2010) Uptake ofprovider-initiated HIV testing and counseling among womenattending an urban sexually transmitted disease clinic in SouthAfrica – missed opportunities for early diagnosis of HIVinfection. AIDS Care 22, 533–537.
Kiene S, Bateganya M, Wanyenze R et al. (2009) Provider-initiatedHIV testing in health care settings: should it be client-centeredcounselling? Journal des Sociaux du VIH/SIDA 6, 115–119.
Koo DJ, Begier EM, Henn MH, Sepkowitz KA & Kellerman SE(2006) HIV counseling and testing: less targeting, more testing.American Journal of Public Health 96, 962–964.
Leon N, Colvin CJ, Lewin S, Mathews C & Jennings K (2010a)Provider-initiated testing and counselling for HIV – fromdebate to implementation. South African Medical Journal 100,220–221.
Leon N, Naidoo P, Mathews C, Lewin S & Lombard C (2010b)The impact of provider-initiated (opt-out) HIV testing andcounseling of patients with sexually transmitted infection inCape Town, South Africa: a controlled trial. ImplementationScience 5, 8.
Mirkuzie AH, Hinderaker SG & Morkve O (2010) Promisingoutcomes of a national programme for the prevention ofmother-to-child HIV transmission in Addis Ababa: aretrospective study. BMC Health Services Research 10, 267.
Moses A, Zimba C, Kamanga E et al. (2008) Prevention ofmother-to-child transmission: program changes and the effecton uptake of the HIVNET 012 regimen in Malawi. AIDS22, 83–87.
Nieburg P, Cannell T & Morrison J (2005) Expanded HIVTesting: Critical Gateway to HIV Treatment and PreventionRequires Major Resources, Effective Protections. The Center forStrategic International Studies, Washington D.C.
Oosterhoff P, Hardon AP, Nguyen TA, Pham NY & Wright P(2008) Dealing with a positive result: routine HIV testing ofpregnant women in Vietnam. AIDS Care 20, 654–659.
Paxton S, Diaz J, Junga R, Pillai A & Thomas J (1999) APN+Human Rights Initiative: participatory research into HIV ⁄ AIDS-related human rights violations in 10 Asian countries. 5thInternational Congress on HIV ⁄ AIDS in Asia and the Pacific.Malaysia.
Seipone K (2004) Introduction of routine HIV testing in prenatalcare – Botswana, 2004. MMWR. Morbidity and MortalityWeekly Report 53, 1083–1086.
Simpson WM, Johnstone FD, Boyd FM, Goldberg DJ, Hart GJ &Prescott RJ (1998) Uptake and acceptability of antenatal HIVtesting: randomised controlled trial of different methods ofoffering the test. BMJ 316, 262–267.
Simpson WM, Johnstone FD, Goldberg DJ, Gormley SM &Hart GJ (1999) Antenatal HIV testing: assessment of a routinevoluntary approach. BMJ 318, 1660–1661.
Stringer EM, Stringer JS, Cliver SP, Goldenberg RL & GoepfertAR (2001) Evaluation of a new testing policy for humanimmunodeficiency virus to improve screening rates. Obstetricsand Gynecology 98, 1104–1108.
van’t Hoog AH, Mbori-Ngacha DA, Marum LH et al. (2005)Preventing mother-to-child transmission of HIV in WesternKenya: operational issues. Journal of Acquired ImmuneDeficiency Syndromes 40, 344–349.
Weigel R, Kamthunzi P, Mwansambo C, Phiri S & Kazembe PN(2009) Effect of provider-initiated testing and counselling andintegration of ART services on access to HIV diagnosis and
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
369

treatment for children in Lilongwe, Malawi: a pre- postcomparison. BMC Pediatrics 9, 80.
WHO. (2003) The Right to Know. New Approaches to HIVTesting and Counselling. WHO, Geneva.
WHO. (2008) Towards Universal Access: Scaling Up PriorityHIV ⁄ AIDS Interventions in the Health Sector. WHO, Geneva.
WHO. (2009). Towards Universal Access: Scaling Up PriorityHIV ⁄ AIDS Interventions in the Health Sector. WHO, Geneva.
WHO. (2010). Towards Universal Access: Scaling Up PriorityHIV ⁄ AIDS Interventions in the Health Sector. WHO, Geneva.
WHO, UNAIDS. (2007) Guidance on Provider-Initiated HIVTesting and Counselling in Health Facilities. WHO, UNAIDS,Geneva.
Zimba C, Kamanga E, Chilongozi D et al. (2006) Impact ofroutine HIV counseling and testing with an opt-out strategycompared to voluntary counseling and testing in theimplementation of PMTCT services, Lilongwe,Malawi 16th International AIDS Conference. Toronto,Canada.
Zimba C, Kamanga E, Chilongozi D et al. (2010) The Impact ofRoutine Counseling and Testing With an Opt-Out StrategyCompared to Voluntary Counseling and Testing in the Imple-mentation of PMTCT Services in Lilongwe, Malawi. UNCProject, Lilongwe.
Corresponding Author Bernadette Hensen, Faculty of Epidemiology and Population Health, London School of Hygiene and TropicalMedicine, London, UK. E-mail: [email protected]
Tropical Medicine and International Health volume 00 no 00
B. Hensen et al. Universal voluntary HIV testing in antenatal care settings
ª 2011 Blackwell Publishing Ltd
370

Journal of HIV/AIDS & Social Services, 12:49–62, 2013Copyright © Taylor & Francis Group, LLCISSN: 1538-1501 print/1538-151X onlineDOI: 10.1080/15381501.2012.749818
Foundation for the Future: Meeting the Psychosocial Needs of Children Living With HIV in South Africa and Uganda
JENNIFER MCCLEARY-SILLS, PhD, MPH and ANJALA KANESATHASAN, MPH
International Center for Research on Women, Washington, DC, USA
JONATHAN BRAKARSH, PhD, MA Independent Consultant, Harare, Zimbabwe
MARNIE VUJOVIC, PhD, MA and KGETHI DLAMINI, MeD Independent Consultant, Johannesburg, South Africa
EVE NAMISANGO, MSc and ROSE NASABA, MA Independent Consultant, Kampala, Uganda
KATHERINE FRITZ, PhD, MPH International Center for Research on Women, Washington, DC, USA
VINCENT J. WONG, MSc U.S. Agency for International Development (USAID), Office of HIV/AIDS,
Washington, DC, USA
SARA BOWSKY, RN, MPH U.S. Agency for International Development (USAID), Mozambique
Successes in diagnosing and treating pediatric HIV have necessi-tated care that extends beyond basic medical needs. However, capacity for providing childhood psychosocial support (PSS) remains limited. Programmatic research with young PLHIV, care providers and parents in Uganda and South Africa explored chal-lenges in meeting the psychosocial needs of HIV-positive children. Three areas for childhood PSS were examined: disclosure, stigma, and grief/bereavement. This research identified programming gaps, strategies and good practices in five focal areas: providing
Address correspondence to Vincent J. Wong, MSc, United States Agency for International Development (USAID), Office of HIV/AIDS, Division of Technical Leadership and Research, 1201 Pennsylvania Avenue, Suite 200, Washington, DC 20004, USA. E-mail: [email protected]
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
371

J. McCleary-Sills et al.
immediate postdiagnosis support, stigma reduction, capacity building, addressing grief, and promoting peer support. Recom-mendations are presented for enhancing PSS for HIV-positive chil-dren in resource-limited settings.
KEYWORDS adolescents, AIDS, care, children, counseling, HIV, psychosocial, testing
INTRODUCTION
Increased efforts to diagnose HIV in infants and provide antiretroviral ther-apy (ART) have contributed to reductions in HIV-related deaths among chil-dren under age 15. While many infections in children still go undiagnosed, these recent advances enable a new generation of children to live longer, healthier lives (Ferrand et! al.. 2010; Sopena, Evangeli, Dodge, & Melvin, 2010). As HIV management shifts toward a chronic disease model, address-ing the psychosocial concerns of people living with HIV (PLHIV)— especially children—becomes a pressing priority for ensuring their long-term well-being (Gutmann & Fullem, 2009; Rochat, Mitchell, & Richter, 2008).
Children with HIV are likely to experience more psychological prob-lems than are their uninfected peers (Gaughan et!al., 2004; Gosling, Burns, & Hirst, 2004). Therefore, good psychosocial support (PSS) is especially criti-cal, creating the foundation from which children can establish their identity and place in society, manage their care and live positively, cope with chal-lenges, and plan for their future (Regional Psychosocial Support Initiative [REPSSI], 2003; Rochat, Mitchell, & Richter 2008). PSS for children entails meeting their emotional, mental, and social needs, often through counseling, cognitive behavior therapy, and play groups (Clay, Bond, & Nyblade, 2003; Richter, Foster, & Sherr, 2006). For most children with HIV, the first line of support is family caregivers who also face HIV-related stressors, including their own HIV status, challenges with disclosure, and social isolation due to stigma (Brown & Lourie, 2000; King, De Silva, Stein, & Patel, 2009). Such stresses can render these adults less capable of providing much-needed sup-port to the children in their care (Abasiubong, Bassey, Ogunsemi, & Udobang, 2011; Murphy, Marelich, Armistead, Herbeck, & Payne, 2010). Despite these findings, few studies have explored how programs equip parents, caregivers, and service providers to meet the psychosocial needs of children with HIV.
This article presents findings about PSS for children based on a litera-ture review and data collection including expert informants, parents, chil-dren, and caregivers. Interviews with experts in pediatric HIV identified three key threats to the psychosocial well-being of children with HIV: mis-handling of disclosure, stigma, and grief and bereavement (Instone, 2000; Lin et!al., 2010). Qualitative field research then explored how these challenges
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
372

Children With HIV in South Africa and Uganda
are currently addressed by parents, caregivers, and professionals providing PSS to 0- to 12-year-old children with HIV in Uganda and South Africa. The research also identified promising practices in bridging the gap between children’s psychosocial needs and the capacity of those who care for them.
METHODS
Data Collection
Investigators conducted interviews with global HIV program experts in gov-ernment and civil society to explore strengths and gaps in providing care for children with HIV. These background interviews informed a desk survey of peer-reviewed and gray literature on the psychosocial needs of children with HIV and current programming responses. Through this review and in con-sultation with a Technical Advisory Group (TAG), the research team nar-rowed the study focus to three core themes of disclosure, stigma, and grief and bereavement, and developed the research protocol. Semistructured in-depth interview (IDI) and focus group discussion (FGD) guides were designed for three groups of research participants: pediatric care providers, parents/family caregivers of children with HIV from birth to 12, and perina-tally infected young people aged 15 to 18 years. The guide for the third group was designed to help young people reflect on how their psychosocial needs were met or could have been better addressed.
Through these conversations, the study team sought to understand cur-rent approaches and persistent gaps in providing support to children with HIV and their caregivers as they navigate the disclosure process, encounter stigma, and experience grief and bereavement. With the project’s TAG and U.S. government stakeholders in Washington, DC, Johannesburg, and Kampala, eight programs (four each in South Africa and Uganda) were selected to participate. Field visits occurred between May and November 2010. Parents/caregivers and young people living with HIV were invited by program staff to participate in FGDs if support groups already existed on-site; otherwise, they were invited to take part in IDIs. Providers were identi-fied by the program leadership and invited to participate in FGDs or IDIs, based on their availability and scheduling preferences.
The research protocol was reviewed by the Institutional Review Board of the International Center for Research on Women and received ethical approval from three in-country ethics committees: Uganda National Council for Science and Technology, University of Witwatersrand (South Africa), and Hospice Palliative Care Association (South Africa). Written informed consent was obtained from all participants before each interview or focus group using the language preferred by the participant: Luganda or Runyankole in Uganda, Xhosa or Sotho in South Africa, and English in both countries.
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
373

J. McCleary-Sills et al.
Participants unable to read the documents were asked to provide verbal consent before beginning the interview or focus group. The voluntary nature of participation was emphasized at the recruitment phase, when reviewing the consent forms, and during the interview process to ensure that participants understood their participation would in no way affect their receipt of benefits from the service provider. Members of the research team facilitated discussions in English ( J.M.S., A.K., J.B., M.V.) and in local lan-guages (K.D., E.N., R.N.), and information was recorded through hand-written notes.
Analysis
Qualitative data were collected through selective transcription of quotes and topics within each of the three key themes. Notes from FGDs and IDIs were recorded by multiple team members using a standardized data collec-tion matrix to ensure consistency and data quality. The research team com-pared matrices at the end of each day to assess the extent to which key themes had been addressed, and the degree of agreement within and across participant groups. If gaps in responses relevant to a particular theme were identified, this domain was prioritized for the remaining ses-sions at that site. When the team agreed that saturation had been reached on a topic, this line of inquiry was de-prioritized in subsequent interviews. This triangulation helped identify consistency across the three perspec-tives: young people with HIV, caregivers of children with HIV, and service providers. This process allowed for iterative validation of data within and across discussions as well as program sites. Once all data had been col-lected for each country, the research team conducted cross-program analy-ses to identify common themes, promising practices, and emerging recommendations. After data collection ended, additional thematic com-parisons were conducted to identify divergences and consistencies across the two country contexts.
RESULTS
Sample Description
A total of 216 parents/caregivers, service providers, and young people with HIV participated in this study. These included 128 individuals in Uganda: FGDs with 49 young PLHIV (30 female participants), 39 parents/caregivers (33 female participants), and 22 service providers (16 female participants). Some of this latter group also participated in IDIs, in addition to 18 other providers. In South Africa, a total of 88 people participated: FGDs with 15 young adult PLHIV (all female participants), 22 parents/caregivers of children
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
374

Children With HIV in South Africa and Uganda
living with HIV (21 female participants), and IDIs with 51 service providers (43 female participants). Three-quarters (n = 165; 76%) of all participants were female. One South African ethics committee restricted recruitment to partici-pants over 18; thus, Ugandan youth participants were perinatally infected 15- to 18-year-olds, while in South Africa they were behaviorally infected 18- to 25-year-olds.
Findings
This research revealed some important commonalities in the experiences of parents, caregivers, and providers in supporting children who are living with HIV, as well as in the experiences of the young people themselves. Findings related to three key areas (disclosure, stigma and discrimination, grief and bereavement) are presented next, with illustrative quotes about the chal-lenges in meeting children’s psychosocial needs at key points in the diagno-sis and treatment processes.
Disclosure
The necessity of catering to children’s psychosocial needs and disclosure-related concerns begins at the time of initial HIV testing and counselling. Many young people interviewed revealed that they had been lied to during the testing and counselling about the reason for giving a blood sample. They recalled being upset by the adults’ decision not to tell them the true reason for their test.
I was hurt. They did not tell me they were taking off the blood sample for HIV testing. (Youth, Uganda)
Participants highlighted the period immediately following a child’s initial diagnosis as a time during which children’s needs are often inadequately addressed. Young people again expressed frustration and anger over being lied to about their diagnosis.
Doctors lied to me. They gave it a funny name, told me it was malaria. They gave my father the results, not me. (Youth, Uganda)
While this was a commonly cited practice, young people overwhelmingly did not support the decision to lie to children. Many instead suggested grad-ual, partial disclosure based on children’s readiness to comprehend the information.
You need to tell the character of the kid. Do you tell him fast or slow? Do you hit him in the face with it and teach him later or teach first, then hit him with the truth? (Youth, Uganda)
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
375
J. McCleary-Sills et al.
Many providers also promoted partial disclosure, citing age and develop-mental readiness as important criteria for determining whether and how to inform a child that he has HIV.
I tell a little child that he’s sick and needs to take his medicine so he can be strong and play like other kids, but I don’t tell him that he is HIV-positive unless he’s old enough to understand and handle the news. (Provider, Uganda)
Providers in both countries expressed concern about the impact that a fam-ily’s decision to not tell a child has on overall well-being and adherence to life-saving medication.
Every time a child takes a drug without knowing its purpose, adherence becomes a challenge. (Provider, Uganda)
Participants noted that lack of willingness to disclose is often dictated by fac-tors not related to the child’s own readiness. Rather, the willingness of par-ents and family caregivers and their level of comfort are very influential in determining when a child learns of his HIV-positive status.
Mums are not happy to disclose. They are scared. (Provider, South Africa)
He is asking, why must I take my pills? I don’t know how to answer him and I am hoping this will be done by our nurses at hospice. (Caregiver, South Africa)
Programs use a number of approaches to address the PSS needs of children during the pre- and post-test periods, such as by assigning individ-ual counselors to accompany children through the testing process.
We try to create a friendship with the children from the first moment we meet them in pre-test counseling. We escort them to the lab and stay with them during the test if they want us to be there. (Provider, Uganda)
Other programs also work with and provide support to parents who are navigating decisions around partial, full, and third-party disclosure about their children’s status.
We train childcare workers to help mum disclose the child’s status to him or her as early as possible so that the child can take responsibility for himself or herself. (Provider, South Africa)
Stigma and Discrimination
In addition to parents’ feeling unprepared to answer their children’s ques-tions, they also fear their children will experience stigma and discrimination if others find out they are living with HIV.
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
376

Children With HIV in South Africa and Uganda
Parents don’t tell because they’re protecting their children. Children can be cruel, and parents don’t want people to be mean to their children. (Provider, South Africa)
Concerns about stigma infused all the conversations and were consistently linked to participants’ decisions about informing a child of his status and disclosing to third parties. Parents, providers, and young people all under-scored the pervasiveness of HIV-related stigma in their communities, and expressed concerns about how experiences with externalized and internal-ized stigma can harm children’s well-being.
Children need a constant loving presence because they can often be iso-lated from others because of stigma. (Youth, Uganda)
Many adult participants emphasized the importance of helping children with HIV feel special and giving them extra attention, saying that such efforts were important to ensuring the self-esteem and well-being of children who struggle to accept the need for medication and special diets.
I don’t want her to feel bad about having to take medicine and eat differ-ent foods than the other children. I tell her that she gets to have those things because she’s special. (Caregiver, Uganda)
Young people, however, felt that special treatment could make others view them as different, and therefore lead to discrimination. Many expressed a desire to have the same household chores and responsibilities as their siblings.
We don’t want to feel like we are special. We want to feel like every other child. (Youth, Uganda)
Youth respondents were proponents of support groups as sources of a peer network and role models, and felt that such support should be available to children immediately after they learn of their seropositive status.
You should go into peer support. Maybe it’s hard for you to talk about, but so many people are talking so freely about it, you can talk. (Youth, Uganda)
Both support groups and individual counseling were mentioned as useful in helping young people fend off internalized stigma.
My counselor helped me see that whatever they said, I had the power to take it in or not, let it affect my life or not. (Youth, Uganda)
Programs also attempted to address stigma experienced within children’s social environments, especially in their communities and at school.
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
377

J. McCleary-Sills et al.
We have had problems with teachers ostracizing our children in school, so now we go to the schools and engage with the teachers. (Provider, South Africa)
Grief and Bereavement
In both countries, the need for addressing children’s grief, particularly help-ing them cope with the loss of a parent or caregiver, was strongly expressed. Providers and parents felt that cultural prohibitions keep children from receiving bereavement support.
We have many kids who don’t want to talk about loss. The cultural situ-ation is that children are not part of death. Children don’t even go to the graveside. They don’t have closure. (Provider, South Africa)
Even a child of three years old can know that someone has died, but we don’t talk to them about it. (Caregiver, Uganda)
While most programs struggled to actively address children’s grief, several had introduced activities to stimulate dialogue about illness and dying.
We really need to be talking about death, dying, and health. For this reason, our social workers come into class and read stories about kids who get sick. (Provider, South Africa)
A few of the programs used books, recreational therapy, and tailored activi-ties to encourage children and their caregivers to talk about a loved one who has died.
That Memory Box … helps us a lot. When we think about the mother, we open the box, look at the photographs and feel comforted and accept that she has passed away. (Caregiver, South Africa)
DISCUSSION
Across the focus group discussions and in-depth interviews, participants consistently revealed that children with HIV and those who care for them experience multiple challenges related to disclosure, stigma, and grief and bereavement. Improving the management of these processes is critical to supporting children’s psychosocial well-being (Gosling et!al., 2004; Rochat et!al., 2008). As programs expand their services to incorporate PSS within their continuum of HIV care, concentrated efforts are necessary to build the capacity of caregivers to meet the psychosocial needs of children (Brouwer, Lok, Wolffers, & Sebagalls, 2000). Many studies have found that enhancing
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
378

Children With HIV in South Africa and Uganda
the coping strategies and minimizing the stress of caregivers are necessary elements of PSS for children (Palattiyil & Chakrabarti, 2008; Van Winghem et!al., 2008). Several studies also suggest that the psychosocial well-being of children and their caregivers can improve adherence to ART and other clini-cal outcomes (Bikaako-Kajura et! al., 2006; Brouwer et! al., 2000; Mellins, Brackis-Cott, Dolezal, & Abrams, 2004; Williams et!al., 2006).
Participants recognized that disclosure is not a single event but rather a process that occurs over the course of a child’s life (Nabilek, 2009; Wiener, Mellins, Marhefka, & Battles, 2007). While they understood that many factors influence why, how, and when disclosures occur, there was consensus that such decisions should be based on a child’s developmental and emotional maturity. Although this concept was accepted across the projects and partici-pant groups, there was little evidence of tools to guide such assessments of children’s readiness, which instead was often dependent on an individual provider’s perception of a child’s understanding and maturity level. Similarly, while stigma was viewed as a substantial obstacle to disclosure and the receipt of appropriate PSS, programs lacked clear strategies to proactively prevent and address stigma at the institutional or community level. The impact of grief and bereavement on children’s psychosocial development was also recognized by all programs, though few had ongoing or systematic activities or services to help children through their bereavement. The two most significant obstacles faced by all programs were limited resources and lack of targeted training on providing PSS to children. These challenges held true for programs centered on both biomedical models and social service models.
While this study included a large number of participants, some method-ological limitations inhibit cross-programmatic and cross-context compari-sons. First, the South African youth interviewed were not able to discuss the PSS needs of children with HIV from first-hand experience. However, many of these participants were raising children living with HIV and were able to share their opinions on how to meet the needs of children with HIV. Second, while every effort was made to include male and female participants, most caregivers and providers interviewed were female. Finally, the study incor-porates findings from only a small number of the many programs working throughout Sub-Saharan Africa addressing these issues. Despite these limita-tions, this review illustrates some promising practices that enhance the psy-chosocial well-being of children living with HIV.
Recognizing that parents, caregivers, providers, and program staff are often overburdened and under-resourced, the following five recommenda-tions are offered for improving capacity to meet the psychosocial needs of children aged 0 to 12 years living with HIV. Many of these recommendations should not require significant resources to implement, especially those that emphasize the role of caregivers, parents, community members, and/or chil-dren and adolescents in programming. Where staffing, technical capacity,
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
379

J. McCleary-Sills et al.
time, and financial resources are limited, programs can select those pieces that best address current priorities or complement existing programs.
1. Focus on the period immediately following a child’s HIV diagnosis.
Parents and caregivers identified the time after HIV testing as being critical to their own psychosocial well-being and to effective planning for care of the child. This is also an important stage to build support and prevent/address stigma within the household. Programs should prioritize resources that maxi-mize this opportunity to provide the information and support that families need. This should include three key elements: (a) strengthening providers’ capacity in child and family counseling and communication, and allowing adequate time for these initial conversations; (b) helping the family develop care plans that consider the disclosure process, medical treatment and adher-ence, on-going psychosocial well-being (including access to education and other social interactions) and planning for bereavement, grief, and family transitions (such as succession planning); and (c) providing systematic post-test follow-up through clinic- or home-based visits to meet the needs of children and their parents/caregivers (e.g., for couples testing and counsel-ing) and support family adjustments to providing on-going care (e.g., skill-building of family members, facilitation of discussions and disclosure among family members).
2. Reduce stigma within children’s “circles of care.”
The intersecting spheres in which children are socialized include house-holds, clinics, schools, and communities. Stigma can be experienced in any of these circles, and often several at once. Programs should proactively aim to reduce stigma by (a) building awareness and understanding of stigma within all program staff and partners through trainings and values-analysis, (b) reducing fear and value-driven stigma in households and communities through on-going screening (e.g., during routine clinic or home visits) and targeted outreach (e.g., intervening at schools where stigma has emerged as a problem), and (c) promoting peer or community-led stigma reduction activities through outreach activities, mentoring, and role modeling. Such efforts should be integrated into PSS programs from the start to optimize outcomes for children and limit the potential harm of program activities such as unintended disclosure.
3. Build the capacity of caregivers and children to meet their own PSS needs.
By building the capacity of caregivers and children to provide PSS to them-selves and each other, programs can encourage more responsive, sustainable models extending beyond the clinic or program activities. While trainings or
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
380

Children With HIV in South Africa and Uganda
workshops can be one approach, emphasis should be placed on developing simple forms of support within the home, such as one-on-one skill building, mentoring, and facilitated communications. Such skills-transfer can be inte-grated into all interactions between trained providers and caregivers and/or children at little additional cost. Three specific areas emerge: (a) building capacity of parents and primary caregivers in listening and communication skills, as well as in creating opportunities for play and/or other interactions with their children; (b) developing skills of children with HIV to manage their own care, including issues of managing disclosure and stigma; and (c) cultivating the ability of older children or youth living with HIV to provide peer support or mentoring for younger children through structured activities (e.g., during clinic visits, support groups, camps) or more informal interac-tions in the home, school or community.
4. Address grief as a process.
Addressing grief is critical to building the PSS capacity of caregivers and chil-dren. Programs should acknowledge grief and bereavement as long-term influences on psychosocial health rather than a discrete event. Programs should help children and their parents discuss and plan for death before it happens and process grief after. Many programs use culturally appropriate strategies for encouraging family and/or parent–child preparation for a death, including planning for succession and continuous child care, will writing, and creating memory boxes, books, and family trees. Several approaches can be used throughout the grief process, including play ther-apy, reading stories about illness and loss, and peer support groups for chil-dren and caregivers.
5. Create forums for interaction and peer support.
Programs with limited resources can create structured and unstructured opportunities for children and caregivers to interact with peers, providing important ways to share experiences and learning. Activities that are decen-tralized from a program/clinic setting and led by young people or caregivers can cultivate a sense of leadership, shared experience, and support. These can include peer support and counseling groups, performance troupes, sports teams or events, livelihoods-based groups, and interactive educational sessions about important themes such as the nutritional needs of children with HIV and living positively. It is also important for programs and provid-ers to consider fostering opportunities for children living with HIV to interact with peers who are not known to be HIV-positive. While it is important to ensure that these exchanges be carefully facilitated to avoid unintentional disclosure of HIV status and exposure to stigma and discrimination, such opportunities can promote a greater sense of common ground and mutual
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
381

J. McCleary-Sills et al.
understanding in the long term. More deliberate efforts to offer and integrate these forms of interaction into the core services and support provided for children living with HIV during initial stages of their HIV care may help build a set of resources to provide ongoing social capital and build resilience and capacity for children to manage their psychosocial well-being into the future.
CONCLUSION
This study of eight programs in South Africa and Uganda offers opportunities for other programs to learn about promising approaches for providing psy-chosocial support to children with HIV. As the pendulum of HIV program-ming and funding swings back toward a more biomedical focus, program resources will be even more constrained and less able to address the critical PSS needs of these children and their families. Thus, it is recommended that program staff, planners, and funders dedicate their limited resources for non-medical care to the five strategies outlined here to best meet the PSS needs of the children they serve and to improve their chances for long, healthy lives.
ACKNOWLEDGMENTS
USAID Colleagues: Seyoum Dejene, Julius Kalamya, USAID, Uganda; Dr. Ryan Phelps, Alison Cheng, Dr. Linda Sussman, USAID, Washington; and Anita Sampson, USAID, South Africa.
Technical Advisory Group: Amelia Jones, Community Chest, South Africa; Dr. Janet Kayita, UNICEF, Nigeria; F. Amolo Okero, World Health Organization, Switzerland; Marie Parks, University of Maryland Department of Pediatric Immunology, USA; Dr. Lineo Thahane, Baylor College of Medicine Children’s Foundation, Lesotho.
Programs Participating in Technical Reviews
South Africa
• St. Nicholas Bana Pele Network, Free State• Butterfly House, Drakenstein Palliative Hospice, Western Cape• Cotlands, Western Cape• National Association of Child Care Workers, Eastern Cape
Uganda
• Baylor Uganda, Kampala• Joint Clinical Research Center ( JCRC), Mbarara
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
382

Children With HIV in South Africa and Uganda
• Mildmay Uganda supported-site, Naggalama Hospital, Mukono• The AIDS Support Organization (TASO), Masaka
The views and opinions expressed in this article are solely those of the authors and do not necessarily reflect those of the U.S. Agency for International Development or the U.S. Government.
REFERENCES
Abasiubong, F., Bassey, E. A., Ogunsemi, O. O., & Udobang, J. A. (2011). Assessing the psychological well-being of caregivers of people living with HIV/AIDS in Niger Delta region, Nigeria. AIDS Care, 23(4), 494–500.
Bikaako-Kajura, W., Luyirika, E., Purcell, D. W., Downing, J., Kaharuza, F., Mermin, J., … Bunnell, R. (2006). Disclosure of HIV status and adherence to daily drug regimens among HIV-infected children in Uganda. AIDS and Behavior, 10(4!Suppl), S85–S93.
Brouwer, C. N. M., Lok, C. L., Wolffers, I., & Sebagalls, S. (2000). Psychosocial and economic aspects of HIV/AIDS and counselling of caretakers of HIV-infected children in Uganda. AIDS Care, 12(5), 535–540.
Brown, L. K., & Lourie, K. J. (2000). Children and adolescents living with HIV and AIDS: A review. Journal of Child Psychology and Psychiatry, 41(1), 81–96.
Clay, S., Bond, V., & Nyblade, L. (2003). We can tell them AIDS doesn’t come through being together: Children’s experience of HIV and AIDS related stigma in Zambia 2002-2003. Lusaka, Zambia: ZAMBART Project, The School of Medicine, University Teaching Hospital.
Ferrand, R. A., Munaiwa, L., Matsekete, J., Bandason, T., Nathoo, K., Ndhlovu, C.!E., … Corbett, E. (2010). Undiagnosed HIV infection among adolescents seeking primary health care in Zimbabwe. Clinical Infectious Diseases, 51(7), 844–851.
Gaughan, D. M., Hughes, M. D., Oleske, J. M., Malee, K., Gore, C. A., & Nachman, S. (2004). Psychiatric hospitalizations among children and youths with human immunodeficiency virus infection. Pediatrics, 113(6), e544–e551.
Gosling, A. S., Burns, J., & Hirst, F. (2004). Children with HIV in the UK: A longitu-dinal study of adaptive and cognitive functioning. Clinical Child Psychology and Psychiatry, 9(1), 25–37.
Gutmann, M., & Fullem, A. (2009). Mental health and HIV/AIDS. Arlington, VA: USAID, AIDSTAR-One.
Instone, S. L. (2000). Perceptions of children with HIV infection when not told for so long: Implications for diagnosis disclosure. Journal of Pediatric Health Care, 14(5), 235–243.
King, E., De Silva, M., Stein, A., & Patel, V. (2009). Interventions for improving the psy-chosocial well-being of children affected by HIV and AIDS. Cochrane Database of Systematic Reviews, 2, CD006733. doi:10.1002/14651858.CD006733.pub2
Lin, X., Zhao, G., Li, X., Stanton, B., Zhang, L., Hong, Y., … Fang, X. (2010). Perceived HIV stigma among children in a high HIV-prevalence area in central China: Beyond the parental HIV-related illness and death. AIDS Care: Psychological and Socio-medical Aspects of AIDS/HIV, 22, 545–555.
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
383

J. McCleary-Sills et al.
Mellins, C. A., Brackis-Cott, E., Dolezal, C., & Abrams, E. J. (2004). The role of psy-chosocial and family factors in adherence to antiretroviral treatment in human immunodeficiency virus-infected children. The Pediatric Infectious Disease Journal, 23, 1035–1041.
Murphy, D. A., Marelich, W. D., Armistead, L., Herbeck, D. M., & Payne, D. L. (2010). Anxiety/stress among mothers living with HIV: Effects on parenting skills and child outcomes. AIDS Care, 22, 1449–1458.
Nabilek, Z. (2009). HIV stigma and disclosure. Can social support help? Positively Aware, 20, 37–38.
Nyblade, L., Hong, K. T., Anh, N. V., Ogden, J., Jain, A., Stangl, A., … Ashburn, K. (2008). Communities confront HIV stigma in Viet Nam: Participatory interven-tions reduce HIV-related stigma in two provinces. Washington, DC/Hanoi, Vietnam: International Center for Research on Women (ICRW); Institute for Social Development Studies (ISDS).
Palattiyil, G., & Chakrabarti, M. (2008). Coping strategies of families in HIV/AIDS care: some exploratory data from two developmental contexts. AIDS Care, 20, 881–885.
Regional Psychosocial Support Initiative (REPSSI). (2003). Mainstreaming psychoso-cial care and support within paediatric HIV and AIDS treatment. Randburg, South Africa: REPSSI.
Richter, L., Foster, G., & Sherr, L. (2006). Where the heart is: Meeting the psychosocial needs of young children in the context of HIV/AIDS. The Hague, Netherlands: Bernard van Leer Foundation.
Rochat, T., Mitchell, C., & Richter, L. (2008). The psychological, social and develop-ment needs of babies and young children and their caregivers living with HIV and AIDS. Pretoria, South Africa: National Department of Health.
Sopena, S., Evangeli, M., Dodge, J., & Melvin, D. (2010). Coping and psychological adjustment in adolescents with vertically acquired HIV. AIDS Care, 22, 1252–1258.
Van Winghem, J., Telfer, B., Reid, T., Ouko, J., Mutunga, A., Jama, Z., … Vakil, S. (2008). Implementation of a comprehensive program including psycho-social and treatment literacy activities to improve adherence to HIV care and treat-ment for a pediatric population in Kenya. BMC Pediatrics, 8, 52.
Wiener, L., Mellins, C. A., Marhefka, S., & Battles, H. B. (2007). Disclosure of an HIV diagnosis to children: History, current research, and future directions. Journal of Development and Behavioral Pediatrics, 28, 155–166.
Williams, P. L., Storm, D., Montepiedra, G., Nichols, S., Kammerer, B., Sirois, P.!A., … Malee, K. (2006). Predictors of adherence to antiretroviral medications in children and adolescents with HIV infection. Pediatrics, 118, e1745–e1757.
Dow
nloa
ded
by [V
ince
nt J.
Won
g] a
t 15:
27 1
3 M
arch
201
3
384

Vulnerable Children and Youth Studies, April 2006; 1(1): 47–58
ISSN 1745-0128 print/ISSN 1745-0136 online ! 2006 Taylor & FrancisDOI: 10.1080/17450120600700004
RVCH1745-01281745-0136Vulnerable Childern and Youth Studies, Vol. 1, No. 1, March 2006: pp. 0–0Vulnerable Children and Youth StudiesThe lost children of universal access – issues in scaling-up HIV testing and counselling
Issues in scaling-up HIV testing and counsellingV. Wong et al.V. WONG, I. MACLEOD, C. GILKS, D. HIGGINS, & S. CROWLEY
Department of HIV/AIDS, World Health Organization, Geneva, Switzerland
AbstractThis descriptive study is based upon information and data gathered from a convenience sample andreview of national human immunodeficiency virus (HIV)/voluntary counselling and testing (VCT)policies; a review of existing recommended or selected tools and guidance; and informants workingwith HIV testing and counselling (HTC) and children at an implementation or policy level selectedthrough purposive, snowball sampling. Questionnaires captured data on problems, strategies andlegal frameworks on HTC provision to children in multiple countries and regions. The policy reviewof 20 high-prevalence countries revealed that while 84% distinguished identified children as a specificsubgroup affected by HIV, only 35% of national policies offered details on HTC and children. Fifty-seven key informants (53% implementers, 48% policy-level) from 25 countries in four regionsresponded; 93% stated problems existed in the area of HTC and children and further specific guid-ance was needed on children in the following issues: informed consent (63.2% of respondents), child-counselling (54.4%), discrimination/stigma/child’s rights (42.1%), diagnosis/laboratory issues(38.6%), disclosure (33.3%), service delivery (31%), access (29.8%), policy (23%) and confidential-ity (21%). No geographic differences were found. Eighty guidance publications were reviewed thatcovered some of these issues. While some guidance, policies, strategies and tools have been developedaround HTC and children, findings suggest that in many countries significant gaps and correspond-ing needs exist if children are to benefit from the move to Universal Access. Policy makers, program-mers, implementers and monitoring efforts need to better directed. National policies must beupdated to specify and reflect the technical and policy needs relating to diagnosis of HIV in children,and offer implementers specific directives related to consent, confidentiality and counselling needs.Stakeholders at international and country levels need to work to improve and update existing guid-ance; implementers must be updated in current best practices.
Keywords: HIV testing and counselling, Children, consent, VCT
Introduction
At the end of 2005, there were an estimated 2.3 million children living with HIV; in 2004there were 15 million orphans due to AIDS worldwide (UNAIDS, 2004b, 2005). Daily,1400 children die of an AIDS-related illness and 1800 are newly infected (UNICEF,2005). Regions with the highest prevalences are disproportionately affected. The majorityof children infected and affected by HIV are located in sub-Saharan Africa (UNAIDS,2004b) and most new infections occur in resource-poor regions. These children are affected
Correspondence: Siobhan Crowley, Department of HIV/AIDS, World Health Organization, CH-1211, Geneva 27, Switzerland.Tel: 41 (0) 22 791 1609. Fax: 41 (0) 22 791 4834. E-mail: [email protected]
385

V. Wong et al.
in multiple ways beyond the infection itself: as orphans and/or child-heads of households,by stigma and discrimination, through economic hardship, loss of educational opportuni-ties and increased vulnerability to infection (UNICEF, 2003). The United Nations (UN)Convention on the Right of the Child (CRC), ratified by all but one country, provides animportant framework to guide any response to HIV/AIDS prevention, care and support ofchildren and young people. The CRC, along with other human rights instruments, recog-nizes that children are rights-holders, not merely beneficiaries of protective measures, andis based on four principles:
• Best interests of the child (article 3)• Right to non-discrimination (article 2)• Right to life, survival and development (article 6)• Right to have views respected (articles 12–13)
The CRC and the Declaration of Commitment on HIV/AIDS (DCHA) affirm ‘the right ofthe child to the enjoyment of the highest attainable standard of health’. The CRC is sup-ported by the DCHA which states that, by 2005, national policies should be implementedto provide a ‘supportive environment’ for children infected and affected by HIV/AIDS,including counselling and access to health services as well as protection from discrimina-tion (UN, 2001, 2003). Commitments to scaling-up treatment and prevention in childrenhave been made by the World Health Organization (WHO) in ‘providing policy and tech-nical guidance in implementing key interventions for preventing HIV transmission towomen, infants and young children and for the care and support of those already infectedor exposed and as commitments to achieving 3 " 5 targets’ (WHO, 2004b). The UnitedNations Children’s Fund (UNICEF) has also set goals for the provision of paediatricantiretroviral therapy (ART) for 80% of children in need by 2010 (UNICEF, 2005). How-ever, universal access to treatment and prevention for children is far from reality; significantobstacles remain to be overcome and gaps exist in both national policies and technicalguidance. UNICEF has reported that less that 10% of mothers are being offered access toprevention of mother-to-child transmission (PMTCT) services and UNICEF and 3 " 5progress reports suggest that only 5% of children requiring ARV therapy are receiving it(UNICEF, 2005). UNAIDS revealed ‘39% of countries with generalized epidemics haveno national policy… to provide essential support to children orphaned or made vulnerableby HIV/AIDS’ (UNAIDS, 2003). These data lie in stark contrast to the fact that 16.7% ofAIDS-related deaths occur in children and that there were an estimated 700 000 new childinfections in 2005 (UNAIDS, 2005; UNICEF, 2005).
HIV testing and counselling (HTC) is understood as an essential gateway to treatment,care, support and prevention, as is the importance of a rights-based approach grounded inthe so-called ‘three C’s’ of consent, counselling and confidentiality (GHPWG, 2004;Miller et al., 2004; UNAIDS, 2002, 2004; WHO, 2004a). Accordingly, the Global HIVPrevention Working Group has recommended the expansion of HTC wherever ART exists(GHPWG, 2004). Timely provision of treatment and care to HIV-infected children inneed will be predicated on their identification through proper testing and diagnosis; effect-ive prevention measures depend on identifying those uninfected. There is an urgent corre-sponding need to increase access to HTC services for both the care and prevention oftransmission and infection. Although PMTCT interventions can lower the risk of transmis-sion to 2%, low levels of coverage allow for up to 35% of infants born to HIV-positivemothers to be infected (CDC, 2004; UNAIDS, 2002). Even with use of ARV duringlabour, delivery and the immediate postpartum period, postpartum transmission leads toabout 50–60% of transmitted cases. Roughly half of these infants who are infected will
386

Issues in scaling-up HIV testing and counselling
survive the first 2 years of life and their symptoms may not arise for 3 or more years(National Department of Health South Africa, 2005; NIAID-NIH, 2004). Importantly, amajority of infants are HIV-negative and need access to prevention interventions to facili-tate remaining uninfected. Given the low rates of MTCT possible, each child born withHIV can be considered a failure of prevention. Determination of an infant’s infection statuswill assist in making informed decisions regarding infant feeding, the need for cotrimoxazoleprophylaxis and identifying children who are uninfected (UNAIDS, WHO, UNICEF,2004). This also saves resources and increases orphans’ chances of adoption (M. Meiring,personal communication). Timely access to testing is also of concern in countries where childsexual assaults are increasing, as HIV post-exposure prophylaxis following rape is often contin-gent upon testing (HRW, 2003, 2004; National Department of Health South Africa, 2005).
However, HTC for infants and children poses challenges that differ from those associ-ated with standard VCT services targeting adolescents or adults (UNAIDS, 2004).UNAIDS has outlined complexities of balancing the rights and responsibilities of states,parents and children with human rights. HTC in children is best framed in two CRC prin-ciples: the child’s best interest and a child’s right to participate in decisions affecting his/herwell-being based on evolving capacities. Additionally, ‘laws, policies, and social normsmay… facilitate or impede access to testing and eventually treatment for children’(UNAIDS, 2004). A balance of increasing access and child’s rights protections is necessaryand the ‘Three Cs’ must apply to children of any age. Consent must be given (by the childand/or by the parent/caretaker). Notably, there are often discrepancies between the medianage of first sex, marriage and the age of consent for medical procedures. Consent has alsobeen reported as an obstacle for minor’s access to HIV testing (McCauley, 2004). Coun-selling must be available for the child and the parent/caretaker and confidentiality must bemaintained. Another consideration is that children are tested primarily within provider-initiated (or parent/caretaker-initiated) rather than client-initiated contexts. These includePMTCT programmes, antenatal care facilities, hospitals/clinics, formal or informalorphanages, childcare centres and outreach programmes. Those children requiring accessto testing services include infants of HIV-positive or potentially HIV-infected parents,infants post-PMTCT, child-survivors of sexual assault, street children, orphans due toHIV/AIDS, children exposed to HIV through contaminated needles or blood supplies andchildren with clinical symptoms suggesting an HIV infection or STI (UNAIDS, 2004).Abandoned babies are also at risk and present similar challenges if past-exposure prophylaxis(PEP) is indicated (M. Meiring, personal communication). Children may be with or with-out a legal parent/guardian and issues of consent, disclosure, confidentiality and counsel-ling present unique problems. Furthermore, technical obstacles exist surrounding earlyinfant diagnosis. Although strategies have been proposed, early diagnosis with nucleic acidtesting remains too costly for most resource-constrained providers (Sherman et al., 2005a,2005b). This paper seeks to explore issues surrounding HTC provision for infants and chil-dren and identify problems, strategies, tools and needs in multiple countries and regions.
Problem statement
Problems exist with respect to providing HTV to infants and children and there are gaps incurrent tools and guidance. Many national policies remain unclear in their recommenda-tions on how to provide HIV testing services to infants and children. The overall objectiveof this study is to explore issues and strategies surrounding HTC provision to infants andchildren. Specific goals are to better define issues and needs confronting implementers andpolicy-makers in resource-limited countries and regions of either concentrated or generalized
387

V. Wong et al.
epidemics and to make an initial assessment as to whether informants know of specific pol-icy or programme responses or implementation measures for increasing access to HTC forinfants or children in their countries. Selected national policies will be evaluated for theirrelevance to HTC and children/infants. Gaps in existing guidance will be evaluated.
Methodology
This descriptive study is based upon information gathered from three sources: national pol-icies, tools and guidance relating to HTC provision to children and informants workingwith children at an implementation or policy level.
A preliminary review of national HIV/AIDS or VCT policies or strategic frameworks wasundertaken to evaluate whether they specifically address HTC and related issues for childrenor infants. A convenience sample of 3 " 5 focus countries was used and all policies availablein English at the WHO in Geneva were reviewed. Queries included whether they distin-guished among youth, children or infants, and whether testing, consent, confidentiality, dis-closure or counselling were addressed specifically with respect to children or infants. Thereview included visual scanning and using search terms in Microsoft Word 2003 or AdobeAcrobat 5.0 including: infant, child, children, orphans and other vulnerable children (OVC),youth, young, adolescent, test, consent, counsel, disclosure, confidentiality, PMTCT.
Published guidance considered useful for the implementation of HIV testing services andchildren were collected through both informant recommendations and internet searchesand categorized as: guiding principles; monitoring and evaluation; operational guidance;background, policy and advocacy; or websites and additional resources. Journal and aca-demic articles were generally not included. The documents obtained were nominally evalu-ated by visual and key word searches for relevancy to infants or children and informedconsent, counselling, confidentiality, disclosure, testing and child’s rights.
Roughly 150 key informants involved in the policy on and/or management/provision ofHTC for infants or children believed by the authors to be well-placed to inform on thetopic from WHO/UN-partner regional and country offices, international and local non-governmental organizations (NGOs), ministries of health and implementing organizationswere contacted through e-mailed questionnaires or interviewed directly. ‘Snowball sam-pling’ was used and other informants referred or recommended by the initial respondentswere subsequently invited or contacted for inclusion in the study. The questionnaires uti-lized open and closed questions to collect qualitative and semi-quantitative data on prob-lems and obstacles, existing services, approaches and strategies, key tools andimplementation/policy measures and existing legal frameworks relating to the provision ofHTC to infants and children. Data were entered, coded, checked and evaluated usingHyper Research version 2.6 and Microsoft Excel version X.
Results
Overview of respondents
In total, 57 respondents (in five cases, groups of respondents from multiple agencies) tookpart in the study and included 30 implementers (52.6%) and 27 individuals working at apolicy level (47.4%). Geographically, 25 countries were represented (including 41% of the3 " 5 high-burden countries). Twenty-four respondents were from sub-Saharan Africa(42%), 19 from Southeast Asia (33%), five from Europe (9%) and 16% were from otherregions or working at an international level (16%).
388

Issues in scaling-up HIV testing and counselling
Policy review
An initial review of selected national HIV/AIDS policies, strategic frameworks and/ornational VCT guidelines for 20 of the 49 3 " 5 focus countries was undertaken (40.8%),including 53% of high burden countries (WHO, 2004). The Africa region accounted for65% of the policies studied; other regions included Eastern Mediterranean, European,South East Asian and Western Pacific regions. A majority of the documents distinguishedbetween both youth and children (both 84%) as specific subgroups affected by HIV. How-ever, fewer documents addressed specifically the topics of children and HIV testing, con-sent, confidentiality/disclosure or counselling for OVCs. Seven documents (35%)specifically addressed the issue of HIV testing and children. Five documents (25%) men-tioned children and consent and five documents addressed OVC counselling. Two of thesemade allowances for ‘mature’ or ‘emancipated’ minors (minors who were married, preg-nant, child-heads of households or at increased risk of infection due to sexual activity) whowere then able to consent for themselves. One set of VCT guidelines offered contradictoryinformation on consent, stating that minors should have access to HIV testing based upontheir capacities, but only with parental consent. Fifteen per cent addressed the importanceof maintaining the confidentiality of a child’s HIV status. These findings suggest that whilecurrent policies on HIV/AIDS and HTC generally acknowledge that youth and childrenrequire interventions addressing their particular needs, they do not address specific issuessurrounding the provision of testing services to children; consent, confidentiality, disclos-ure and counselling are frequently not described clearly, as they are for adult populations.Findings reflect the need to include children in national policies dealing with HIV andHTC. Additionally, 47% of 49 applicable country respondents stated that, to their know-ledge, there was no policy or legal framework for dealing with HIV testing and children orinfants. Responses came from both implementers and policy-makers from all regions; noregional differences were seen in the data collected.
Review of guidance, tools and resources
Eighty-three documents were either recommended by informants (n = 15) or selected bythe authors (n = 68) that were considered relevant for HTC provision for infants or chil-dren. Five of these documents (6%) were considered to be guiding principles, including theCRC and the DCHA. Thirty-seven documents (45%) could be classified as ‘operationalguidance’, offering child-specific guidelines on testing processes, consent, confidentiality/disclosure, counselling and testing in emergencies. Four operational guidance documentsoffered specific guidelines on counselling children. Although general guidelines on consent,disclosure and confidentiality for children were also found, specific guidelines for imple-menters were limited. Technical information on testing processes was well covered in manyof the clinical guidelines. Thirty documents (36%) were categorized thematically as ‘back-ground, policy and advocacy’. These included publications on relevant backgroundinformation, case examples, children’s rights and issues of consent and strategic frame-works. Four documents (5%) were relevant for monitoring and evaluation. Seven ‘docu-ments’ (8%) were websites focusing on infants and children and/or HTC were includedand offered a range of publications in this area (including: http://www.ovcsupport.net;http://www.savethechildren.org/technical/resources.asp; http://womenchildrenhiv.org; andhttp://who.arvkit.net/tc/en/index.jsp). Of the total, 30 were authored by WHO and UNpartners and were considered broadly relevant to the topic. Gaps in the literature reviewedare discussed below.
389

V. Wong et al.
Feedback from respondents
Barriers, obstacles, problems, needs. Not unexpectedly, responses indicated that problemsand needs relating to the provision of HTC to infants, children, orphans or other childrenat risk were evident among both policy makers and implementers from all the regions rep-resented. A total of 93% (n = 53) of respondents stated they had encountered problems;90% stated that they felt further guidance was needed in this area. The obstacles and guid-ance needs are outlined below and have been organized broadly into the following thematicgroups: advocacy/discrimination/stigma/rights; confidentiality; consent; counselling; diag-nosis/laboratory issues; disclosure; HIV/AIDS/VCT policies; other access issues; andservice delivery.
The most common concerns arose in the area of informed consent for children (63.2%;n = 36); 47.4% stated that increased guidance was needed in this area and 29.8% statedthat the age of consent was either too high or unclear in their country. The age of consentgiven by respondents for an HIV test ranged from 12 to 21 years, with a mode of 18 yearsin 11 countries. In two countries it was lower than 14. Respondents from nine countriesstated that, to their knowledge, the age of consent for an HIV test was not specified. Fur-thermore, a related and equally complex problem impacting access was parental or guard-ian refusal to give consent (12.3%; n = 7). Some of the specific areas of guidance requestedincluded determining the optimal age of consent; how best to deal with unaccompaniedminors or vulnerable children such as orphans or street children; determining maturityrequired to give consent; and how to deal with testing if the parents or guardians refuse toallow it. Other issues raised included how to deal with abandoned babies (particularly withregard to testing for PEP if it is a newborn) and the need for simpler consent forms.
Issues on counselling were the next frequently mentioned problem area; 54.4% said coun-selling presented challenges to HTC provision in children. Respondents felt a guidance needprimarily for specialized counselling for children (38.6%; n = 22). One implementer statedconcisely that resources were needed for the development of skills necessary ‘to communicatewith children, to seek their consent, to empower them for decision[-making] and to respecttheir feelings’. Additional issues raised included counselling for parents (particularly thosewho refuse to have their children tested), behaviour change communication for children,nutrition counselling for children and the need for better PMTCT counselling.
Problems and needs around discrimination, stigma, child rights and advocacy werestated for 24 cases (42.1%). Some of the main areas of concern included: denial of HIVtesting services due to lack of consenting parent or guardian in four countries (n = 6); prob-lems related to stigma and discrimination (n = 7); low public knowledge of HIV/AIDS (n =5); testing for exclusion to other services (n = 3); the occurrence of obligatory or mandatorytesting (n = 3); and assumptions of HIV infection (n = 2). Guidance needs were stated inareas of discrimination/stigma (n = 3) and child’s rights (n = 2).
Twenty-two respondents (38.6%) described problems relating to HIV diagnosis in chil-dren or laboratory issues. These included a lack of laboratory capacity (e.g. access to PCR)(n = 14) and the late diagnosis of children (n = 10). Needs stated included general guid-ance on children and HIV testing (n = 9) and access to PCR for early diagnosis (n = 4).
Nineteen respondents (33.3%) stated that disclosure presented problems and felt thatguidance on disclosure of HIV status to children was needed. The issue of parents/guardiansnot wanting to disclose to their children was also raised and correspondingly, how health-careworkers can best disclose to parents and support them in disclosing, and also how best forparents disclose to their child. Disclosure of a child’s status may help to improve adherence(Blasini et al., 2004; Hammami et al., 2004), increase access to care and peer support groups
390

Issues in scaling-up HIV testing and counselling
and minimize psychological problems (Gerson et al., 2001). Interviews with counsellors atone clinic and one children’s home in South Africa suggested that disclosure does help facili-tate treatment adherence. Closely related to the issue of disclosure was the issue of confiden-tiality. Twelve respondents (21.1%) raised problems around confidentiality. Frequentviolations of children’s confidentiality are said to occur. Respondents raised issues of betterdefining the limits of confidentiality in children and methods of minimizing breaches of con-fidentiality. One respondent felt that perceptions of a lack of confidentiality had the effect ofdecreasing uptake of HTC on the part of the parents and caretakers.
Seventeen respondents (29.8%) mentioned problems related to access to services. Lossto follow-up both for children and in the context of PMTCT was the most frequent issue(n = 12; 21.1%). Others included health-care workers’ reluctance to test children (n = 3),limited access to HTC for children in general (n = 1), problems of access to PMTCT serv-ices (n = 1) and access to testing services for rural communities (n = 1). Needs statedincluded outreach workers for HTC for children (n = 2).
Issues were also raised by 13 respondents (22.8%) around policies relating to or affectingHTC provision in children. In four cases, respondents stated that children were notaddressed in national HIV policies. Others stated that no HTC guidelines existed specifi-cally for children (n = 4). Accordingly, respondents felt that needs included the drafting ofguidelines addressing these issues. Some emphasized that such guidelines should be coun-try-specific and based upon expert consultations. Additionally, there is a need for increasedpublicity and awareness campaigns for new and/or relevant laws affecting the provision ofHTC to children.
Lastly, 31% of respondents raised a variety of general issues and needs surrounding ser-vice delivery including more child-friendly facilities (n = 7); comprehensive guidance onHIV treatment, care, prevention and support for children (n = 3); general training in work-ing with children (n = 3); and increased cooperation between HIV and child health pro-grammes (n = 2). Other issues raised included increased quality assurance and theimportance of the routine offer of testing in reproductive and child health services.
Implementation measures and strategies for increasing access to HTC
Respondents from 11 countries stated that specific implementation measures had beenundertaken to increase access to HIV testing for infants and children. In both South Africaand India, legal actions in combination with advocacy work (media campaigns, workshops,lobbying, etc.) are being pursued to amend legislation to lower the age of consent andbroaden the role of informal caretakers in their ability to give consent for children. The lat-ter is particularly important for children who live with extended family or are in informalcare settings. This should result in increased access to HTC services. Recent legislativedevelopments in South Africa have also worked to develop a clearer definition of ‘bestinterests’ with respect to children. Uganda has reportedly lowered the age of consent to 12and has undertaken a programme for sensitizing communities and incorporating child par-ticipation to increase access to testing for children below 12 years. Efforts are being under-taken to revise the national HIV testing policy to better reflect the needs of children (IrinNews, 2004). In Guyana, whose age of consent for medical procedures is 18, alternativelaws are applied to VCT services that govern the termination of pregnancy and non-dis-crimination of pregnant women, effectively allowing people younger than 18 to access HIVtesting without requiring a parent’s consent or notification. The Romanian Ministry ofHealth has worked to set out clear guidelines on the criteria for HIV testing in children. Sixcountries are reported to have implemented policies regulating PMTCT programmes.
391

V. Wong et al.
Three countries were reportedly developing specific child-focused policies for either OVCsor child-focused VCT.
The number of stated strategies for implementers confronting obstacles to increase accesswere fewer. The most common related to informed consent. Seven respondents from threecountries reported that either legal or extralegal consent was taken from a health-careworker, caretaker or NGO if no parent/guardian was present. In two other countries, consentwas reportedly obtained from local government, although this was found to be impracticaland inefficient. Two respondents stated that testing was undertaken without consent.Regarding PEP, two doctors working with MSF reported that HIV testing was not a require-ment for access. One respondent reported testing without consent in emergency cases. InSouth Africa, attempts are being made to change the policy requiring HIV testing beforeaccess to PEP. Steps to address confidentiality issues have also been undertaken by oneIndian NGO, who produced a confidentiality handbook for staff and conducted workshopson appropriate handling of patient/client information. Lastly, one potential strategy forincreasing access to confirmatory PCR testing receiving increased attention in South Africa isthe use of testing dried blood spots which can be transported easily to central laboratories.
Discussion
A spectrum of problems and obstacles are confronting implementers, managers and policy-makers in multiple regions and countries in their efforts to initiate and/or provide HTCservices to infants and children. Many of these issues are exacerbated by the general lack ofclear and specific national and international policies and guidance. Critically, it is clear thatmany individual countries’ policies on HIV/AIDS and HIV testing need to be amended tooffer more specific guidance for providing testing to infants and children. Approaches willneed to be country-specific, taking into account HIV prevalence; global or regional guid-ance should therefore reflect the different needs of high- and low-burden countries. Incountries with concentrated epidemics, additional efforts will be needed to minimizestigma and discrimination among high-risk and marginalized populations. Internationaland country-specific legal and policy guidance would be beneficial in confronting many ofthe obstacles facing providers and offer a basis for the fulfilment and the protection ofchild’s rights. Additionally, while a certain number of tools and guidelines do exist,responses suggest they are not widely distributed or known among implementers and pol-icy-makers. The limited resources specifically aimed at providing HTC to infants and pre-adolescent children found in this study suggests that guidance has largely been adult- andadolescent-focused at both international and country levels.
The results of this exploratory study illustrate some of the key issues that need to beaddressed and articulated if access to HIV testing, a key entry-point to ART and a criticalcomponent of prevention, is to be increased and internationally accepted goals, includingthe Millenium Development Goals (MDGs), are to be met. With respect to HTC provi-sion, children’s needs must be considered and defined and a rights-based approach to HIVtesting is necessary focusing on a child’s right to have access to prevention and care inter-ventions and to accept or decline testing (WHO, 2001). Prevention and treatment inter-ventions must be undertaken with this rights-focus to ensure that the best interests of theinfant or child are met. However, applying the ‘three Cs’ framework to infants/children poseschallenges illustrated by the needs articulated by the informants. Cases in this study have pro-vided anecdotal evidence of services being denied to children as a result of reservations anduncertainties on the part of health-care workers in the face of these challenges. Based uponthe respondents’ feedback and the review of guidance, clearer, widely available guidelines
392

Issues in scaling-up HIV testing and counselling
and operational tools for providing HTC to infants and young children are needed in thefollowing areas:
• Informed consent – guidance is needed on the age of consent; how and by whom consentmay be given, particularly in cases of unaccompanied minors; what informed consentmeans in the case of children. Legal frameworks are often contradictory, unclear or silenton the matter or stipulate ages of consent that do not correspond to country needs.Broadening the ‘rules of consent’ for children will also require careful consideration ofcorresponding protection mechanisms to ensure consent is given with and for a child orinfant’s best interest. How providers can deal with a parent/guardian’s refusal to consentmust also be addressed. The testing of a child is frequently equivalent to testing themother; reservations may stem from both their fear of learning their status as well as theirchild’s.
• Counselling – specialized counselling techniques are important for both children and par-ents/caretakers; they should include methods for effectively counselling parents/caretak-ers who refuse testing on behalf of their children.
• Confidentiality – guidance on confidentiality in children should be given and includemechanisms for ensuring that a child’s HIV status is handled appropriately and parame-ters for dealing with unaccompanied children are well defined.
• Disclosure – disclosure processes need to be better described and elaborated. How, whenand to whom should a child’s HIV status be given? Benefits should be emphasized asshould ways of minimizing/compensating for risks and involving the child in the process.Disclosure may occur at a variety of levels including health-care worker to parent/care-taker or child, from parent/caretaker to child and from child to others (friends, family,community, etc). Articulation and guidance on disclosure at these different levels isneeded.
• Technical aspects of testing – proper testing algorithms to be used for infants and childrenneed to be emphasized; greater use of antibody testing in children is needed, as is theexpansion of capacity for early infant diagnosis.
Among the UN publications, the preceding resource gaps would be well-served by fur-ther WHO/UN partner guidance in accelerating HTC for infants and children. In additionthe following were considered to be other areas where gaps exist:
• monitoring and evaluation tools for child/OVC-focused HTC programmes, including qual-itative evaluation tools for counselling children and other indicators for ‘child-friendliness’;
• a strategic framework for increasing access to and acceptability of HTC services foryoung children.
The published literature, tools and approaches collected for this study offer a basis fromwhich best practices and guidance can be further developed. Measures undertaken anddescribed in this study may be applicable and adaptable to other regions or countries strug-gling with similar issues. Documentation of these examples could also be beneficial. Othercontroversial interventions such as testing without consent would also be discouraged withclearer guidance. Strategies to raise awareness and equip and train health-care providers toprovide HIV-related services to children and their caregivers must also be undertaken.Lastly, research is needed to help to inform and shape guidance and explore ways ofincreasing access:
• What are the factors/barriers affecting:
the ‘late diagnosis’ of children
393

V. Wong et al.
health-care workers initiating HIV testing in children/infantsa parent/caretaker’s decision to test or not to test an child/infanthow could these be overcome?
• How can technical/logistical obstacles to the testing of infants in resource-poor settingsbe overcome?
• Role of confidentiality and disclosure in adherence to HIV care including follow-up cotri-moxazole and ART
• How can follow-up rates be improved with PMTCT and other child testing pro-grammes?
Limitations of the study
The policy review was limited in scope. Documents were drawn from a small conveniencesample and those evaluated sometimes differed among countries (strategic frameworks ornational HIV or VCT policies, depending upon availability). This limited comparability.The sample size and methods limit the generalizeability of the study’s findings and the abil-ity to distinguish differences among regional/country subgroups. The review of resourceswas not exhaustive and based upon informant recommendations and searches performedby the authors.
Conclusion
Children and infants are increasingly being infected and affected by HIV worldwide. Inter-nationally accepted goals have been set to try and mitigate the epidemic in infants and chil-dren by scaling up both HIV treatment and prevention. Access to HIV testing andcounselling is an essential prerequisite for increasing access to both treatment and care forthose who are positive and to prevention measures for uninfected infants. However, signi-ficant obstacles to providing HTC to infants and children exist. This study aimed toexplore problems, strategies and tools associated with HTC and infants/children. Whilesome policies and strategies have been developed around HTC and children, findings sug-gest that in countries around the world, significant gaps and corresponding needs exist forfurther specific policies, guidance and tools. National policies must be updated to betterreflect the needs of infant and child diagnosis of HIV and offer implementers specific,country-level guidance. Issues including consent, counselling, confidentiality, disclosureand child’s rights need to be addressed by experts and stakeholders at both an internationaland country level to provide better guidance and best practice examples. There remain sig-nificant problems in resource-limited settings to be overcome, including a lack of labora-tory capacity, poor follow-up rates and late diagnosis. Strategies must be explored thatincrease access while ensuring that a child’s rights and best interests are met. Many currentapproaches employed by implementers and policy-makers such as the lowering the age ofconsent for an HIV test, the consideration of ‘mature minors’, broadening the legal role ofcaretakers, specialized counselling for children and parents, approaches to maintainingconfidentiality and appropriate methods of disclosure will help lead the way as possibleexamples of best practices. These should inform developing national and internationalguidance. While further areas of research are essential, existing resources and guidance andthe present expertise in the field offer a good basis from which to begin to developframeworks that facilitate access to HTC for infants and children. UN partners, nationalbodies and international organizations urgently need to take steps to develop and establish
394

Issues in scaling-up HIV testing and counselling
child-focused frameworks, policies and guidelines reflecting current situations and help toincrease children’s access to essential treatment and prevention interventions.
References
Blasini, I., Chantry, C., Cruz, C., et al. (2004). Disclosure model for pediatric patients living with HIV in PuertoRico: Design, implementation, and evaluation. Journal of Developmental and Behavioral Pediatrics, 25, 181–189.
Centers for Disease Control and Prevention (CDC) (2004). Routine prenatal testing: The opt-out approach. Availableat www.cdc.gov/hiv/projects/perinatal/materials/OptOutNew3-2.htm. Accessed April 20 April 2006
Gerson, A., Joyner, M., Fosarelli, P., et al. (2001). Disclosure of HIV diagnosis to children: When, where, why,and how? Journal of Pediatric Health Care, 15, 161–167.
Global HIV Prevention Working Group (GHPWG) (2004). HIV prevention in the era of expanded treatment access.Bill & Melinda Gates Foundation and the Kaiser Family Foundation.
Hammami, N., Nostlinger, C., Hoeree, T., Lefevre, P., Jonckheer, T., & Kolsteren, P. (2004). Integrating adherenceto highly active antiretroviral therapy into children’s daily lives: A qualitative study. Pediatrics, 114, e591–e597.
Human Rights Watch (HRW) (2003). South Africa: Safeguarding children’s rights to medical care. New York:Human Rights Watch.
Human Rights Watch (HRW) (2004). Deadly delay: South Africa’s efforts to prevent HIV in survivors of sexual violence.New York: Human Rights Watch.
Irin News (2004). Uganda: Policy on HIV testing for children being formulated. UNOCHA, 8 October, 2004. McCauley, A. (2004). Equitable access to HIV counseling and testing for youth in developing countries: A review of cur-
rent practices. Horizons Report. Washington DC: Population Council.Meiring, M. (2005), Personal communication. Children’s Homes Outreach Medical Programme, Johannesburg,
South Africa, 7 November 2005.Miller, D., Bitalabeho, A., Shakow, A., et al. (2004). The gateway to treatment: An increased role for provider-initiated
HIV testing and counselling in resource-poor settings. Geneva: World Health Organization.National Department of Health South Africa (2005). Guidelines for the managementof HIV-infected children. Pretoria:
National Department of Health South Africa.National Institute of Allergy and Infectious Diseases (2004). HIV infection in infants and children. National Insti-
tutes of Health, US Department of Health and Human Services. Available at: www.thebody.com/niaid/pediatri.html. Accessed 20 April 2006.
Sherman, G. G., Matsebula, T., & Jones, S. (2005). Is early HIV testing of infants in poorly resourced preventionof mother to child transmission programmes unaffordable? Tropical Medicine and International Health, 10,1108–1113.
Sherman, G. G., Stevens, G., Jones, S., Horsfield, P., & Stevens, W. (2005). Dried blood spots improve access toHIV diagnosis and care for infants in low-resource settings. Journal of Acquired Immune Deficiency Syndrome,38, 615–617.
United Nations (UN) (1989). Convention on the Rights of the Child. Geneva: United Nations General AssemblyDocument.
United Nations (UN) (2001). Declaration of Commitment on HIV/AIDS. Geneva: United Nations General Assem-bly Document.
United Nations (UN) (2002). HIV/AIDS and Human Rights: International Guidelines Revised Guideline 6: Access toPrevention Treatment, Care and Support. Geneva: United Nations Publication.
United Nations (UN) (2003). Convention on the Rights of the Child: General Comment No. 3: HIV/AIDS and therights of the child. United Nations Committee on the Rights of the Child, 32nd Session, 13–31 January 2003,Geneva.
United Nations Children’s Fund (UNICEF) (2003). Children on the brink. New York: United Nations Children’sFund.
United Nations Children’s Fund (UNICEF) (2005). A call to action – Children: the missing face of AIDS. Joint United Nations Programme on HIV/AIDS (UNAIDS) (2002a). HIV voluntary counselling and testing: A gate-
way to prevention and care. Geneva: UNAIDS.Joint United Nations Programme on HIV/AIDS (UNAIDS) (2002b). Paediatric HIV infection and AIDS. Geneva:
UNAIDS.Joint United Nations Programme on HIV/AIDS (UNAIDS) (2003). Progress report on the global response to the HIV/
AIDS epidemic. Geneva: UNAIDS.Joint United Nations Programme on HIV/AIDS (UNAIDS) (2004a). Issue paper: HIV testing of specific popula-
tions: children and adolescents. UNAIDS global reference group on HIV/AIDS and human rights, 3rd meeting,Geneva, 28–30 January 2004. Geneva: UNAIDS.
395

V. Wong et al.
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2004b). Report on the Global AIDS Epidemic: 4thGlobal Report. Geneva: UNAIDS.
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2005). AIDS epidemic update. Geneva: UNAIDS.Joint United Nations Programme on HIV/AIDS (UNAIDS) and World Health Organization (WHO) (2004).
Policy statement on HIV testing. Geneva: UNAIDS and WHO.Joint United Nations Programme on HIV/AIDS (UNAIDS), World Health Organization (WHO), United
Nations Children’s Fund (UNICEF) (2004). Joint UNAIDS/WHO/UNICEF statement on use of cotrimoxa-zole as prophylaxis in HIV-exposed and HIV-infected children. Geneva: UNAIDS, WHO, UNICEF.
World Health Organization (WHO) (2004a). Increasing access to HIV testing and counselling. Geneva: WHO.World Health Organization (WHO) (2004b). Investing in a comprehensive health sector response to HIV/AIDS – scal-
ing up treatment and accelerating prevention. Geneva: WHO.World Health Organization (WHO). Regional Office for South-East Asia (2001). Towards a better tomorrow: child’s
rights and health. New Delhi: WHO.
396
Appendix 2: Selected Co-authored Conference Posters and Abstracts
397

www.cdc.gov | Contact CDC at: 1-800-CDC-INFO or www.cdc.gov/info The !ndings and conclusions in this report are those of the authors and do not necessarily represent the of!cial position of the Centers for Disease Control and Prevention. CS-315363-A
Optimizing Testing Increases Yield in HIV Case Finding in 24 Countries, 2018–2019Shahul H. Ebrahim1, Arielle Lasry1, Randy Yee1, Wayne A Duffus1, John Abellera1, Shane T Diekman1, Jacqueline Rurangirwa1, Bakary Drammeh1, Tiffany Aholou1, Michael Grillo2, Vincent Wong3, Stephanie Behel1
1Center for Disease Control and Prevention (CDC), Atlanta; 2Defense Health Agency, San Diego; 3United States Agency for International Development, Washington, DC
BACKGROUND RESULTS cont’d
Shahul H. Ebrahim [email protected]
Contact Info
In 2018, U.S. President’s Emergency Plan for AIDS Relief (PEFPAR) supported programs conducted over 95 million HIV tests resulting in 3.4% positive tests (yield). In 2019, to reduce test volume and increase yield, PEPFAR prioritized HIV testing (1) notably symptom or risk- based testing in provider -initiated testing and counseling services (PITC), and (2) strengthening of active contact testing to increase case !nding.
METHODS
We compared HIV test data from 2018 and 2019 and calculated the number of HIV tests and the yield by test modality (method or location of testing) in 24 countries that reported at least 2000 positive HIV tests per quarter. We also present data on contact testing among adults (age 15+ years), Quarter 4, 2019.
RESULTS
Overall, between 2018 and 2019, HIV test volume decreased by 16% (92 million to 77 million), whereas yield increased by 12% (3.4% to 3.9%) (Table 1). The yield was 4.3% in Quarter 4, 2019 (Figure 1). Among adults, PITC in Out Patient Departments (OPD)s contributed to the largest volume of HIV-positive results (2018, 55%; 2019, 47%), due to high volume of testing.
Among adults, contact testing had the highest yield (increased from 12.1% to 22.0%), and the second highest contribution to HIV case !nding, despite a very low-test volume (3% in 2019). Compared to contact testing, the changes in yield and contribution to case !nding were smaller in all other modalities. Total positive HIV tests decreased by 6% between 2018 and 2019 (3,174,631 to 2,997,241).
2019 Tests in Millions
2019 Tests in Millions (% of
total tests)
Change in number
of tests2018 Yield
(%)2019 Yield
(%)Change in
Yield
Overall 92.2 77.4 (85) -16% 3.4 3.9 12%
Adults age (!15 years) 76.9 65.5 (85) -15% 3.9 4.3 10%
Men 27.6 22.7 (35) -18% 3.9 4.6 18%
Women 47.2 41.1 (65) -13% 3.8 4.0 87%
Testing Modalities, Adults
PITC in OPDs* 43.7 33.8 (52) -23% 83.8 83.8 81%
Antenatal clinics 10.0 89.7 (15) 8-3% 82.4 82.6 87%
Voluntary testing 11.5 87.2 (11) -37% 84.0 84.7 85%
Mobile clinics 85.4 84.8 8(7) -13% 84.0 847 16%
Contact testing 82.0 82.1 8(3) 84% 12.1 22.0 69%
All other** 85.1 88.8 (13) 72% 83.9 83.4 -12%
CONCLUSIONS
Among these 24 PEPFAR-funded countries, testing volume has decreased while the positivity rate has increased, largely owing to the increase in contact testing and the reduction in PITC. Given the high contact test acceptance rates in most countries, strengthening of contact testing may help further improve case !nding. Annual volume of positive HIV tests decreased by 6%. Both yield and absolute number of positive tests should be considered in assessing the impact of changes in HTS strategies.
https://www.state.gov/pepfar
Table 1. HIV Tests and Yield, 2018 and 2019, 24 Countries
*OPD= outpatient departments, **includes TB, STI, inpatient, emergency, antenatal clinics, pediatrics.
3525
Figure 1. Quarterly Trend in Number of HIV Tests and Positive Tests, All Ages, and Yield in 24 PEPFAR Countries†, 2018-2019*
Recent data from Quarter 4 of 2019 showed high rates of acceptance of contact testing (85%) (Table 2), and 19 of the 24 countries achieved >70% acceptance rate. Men elicited more contacts than women. Also, the contribution to HIV case !nding from contacts was greater among men.
% accepting contact
elicitation (range)
Average number contacts
elicited (range)
% yield among contacts (range)
Contribution of contact testing to HIV cases found
(range)
Adults 85(41-97)
1.4(0.7-3.5)
24.4(5-38)
16%(5-31)
Men 85(42-98)
1.9(1.0-4.2)
22.8(4-31)
20%(7-36)
Women 85(40-97)
1.1(0.5-6.6)
26.7(6-46)
15%(4-35)
Table 2. HIV Contact Testing Among Adults, 24 Countries, Q4, 2019
697,059 780,027 763,566 933,979 666,234 730,978 706,405 894,124
19.9M
23.3M
22.5M
26.5M
19.6M 19.1M17.8M
20.9M
3.5%
3.3%
3.4% 3.5% 3.4% 3.8%
4.0%
0.0%
0.5%
1.0%
1.5%
2.0%
2.5%
3.0%
3.5%
4.0%
4.5%
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
2018 Qtr1 2018 Qtr2 2018 Qtr3 2018 Qtr4 2019 Qtr1 2019 Qtr2 2019 Qtr3 2019 Qtr4
PosƟve tests Total Tests Yield
4.3%
†Angola, Botswana, Burundi, Cameroon, Cote d’Ivore, DRC, Ewatini, Ethiopia, Ghana, Haiti, Kenya, Lesotho, Malawi, Mozambique, Namibia, Nigeria, Rwanda, South Africa, Tanzania, Uganda, Ukraine, Vietnam, Zambia, Zimbabwe
*Due to multiple tests among some individuals, number of tests or positives do not equal number of persons
• In PEPFAR countries, optimization of HIV testing in PITC with contact testing helped decrease test volume and increase yield.
• Contact testing offers the highest yield from HIV testing, and the second largest contribution to HIV case finding.
• Increase yield and scale of contact testing was insufficient to compensate the decrease in volume of positive tests.
398
E!ective, High-Yield HIV Testing for Partners of Newly Diagnosed Persons in Tanzaniaby: Marya Plotkin1, Catherine Kahabuka2, Mbaraka Amuri1, Mustafa Njozi1, Werner Maokola3, Erick Mlanga4, Mary Drake1, Kelly Curran1,5, Charlene Brown4, and Vincent J. Wong4
a!liate: 1Jhpiego; 2CSK Research Solutions; 3National AIDS Control Programme; 4United States Agency for International Development (USAID); 5Johns Hopkins Bloomberg School of Public Health
Methods��Cross-sectional, hospital-based, mixed-methods study
conducted in 3 hospitals from June to September 2015 LQ�7DQ]DQLD·V�KLJKHVW�+,9�SUHYDOHQFH�UHJLRQ��1MRPEH��DGXOW�SUHYDOHQFHV���������7+0,6��������
��1HZO\�+,9�GLDJQRVHG�PHQ�DQG�ZRPHQ��YLD�SURYLGHU�LQLWLDWHG�+,9�WHVWLQJ�DQG�FRXQVHOLQJ�>3,7&@�RU�YROXQWDU\�FRXQVHOLQJ�DQG�WHVWLQJ�>9&7@��HQUROOHG�DV�LQGH[�FOLHQWV��DQG�ZDV�D�RIIHUHG�FKRLFH�RI�UHIHUUDO�PHWKRGV�
��(OLJLELOLW\�FULWHULD������\HDUV�RI�DJH��KDG�VH[XDO�SDUWQHU�ZLWKLQ�ODVW����
PRQWKV���1RQ�SUHJQDQW��ZDV�ZLOOLQJ�WR�OLVW�SDUWQHUV�IRU�UHIHUUDO�
��,QGH[�FOLHQWV�ZHUH�UHTXHVWHG�WR�OLVW�DOO�SDUWQHUV�ZLWKLQ�SDVW�������PRQWKV�
��,QWLPDWH�SDUWQHU�YLROHQFH��,39��VFUHHQLQJ�DW�WZR�VWDJHV��GXULQJ�LQLWLDO�LQWHUYLHZ�ZLWK�LQGH[�DQG�DW�SDUWQHU�OLVWLQJ�
Results��,QGH[�FOLHQWV��Q� �������
��������PDOHV�DQG�������IHPDOHV��$YHUDJH�DJH� �����UDQJH���²�����������PDUULHG��(QUROOHG�IURP�9&7�������DQG�3,7&������
��/HDGLQJ�UHDVRQ�IRU�QRQ�HQUROOPHQW�LQ�WKH�VWXG\��QR�VH[XDO�SDUWQHU�ZLWKLQ�WKH�ODVW���²���PRQWKV��Q �����
��3 potential index clients successfully screened out IRU�,39
5HIHUUDO�2XWFRPHV�2YHUYLHZ
,QGH[�FOLHQWV���
Partners who did not come in following referral
190 (43.4%)
3DUWQHUV�ZKR�FDme in IROORZLQJ�UHIHUUDO
�����������
3DUWQHUV� WHVWHG�IRU�+,9
�����������
Partners not tested for HIV
10 (4.1%)
Tested SRVLWLYH�����������
Tested negative91 (38.2%)
Enrolled in care and treatment
�&7�����������
Self-report: not
enrolled in CT
11 (7.5%)
Un-known
43 (29.2%)
9HULÀHG�����������
1RW� YHULÀHG����������
Listed sexual partners���
5HVXOWV��FRQW��/LVWHG�DQG�6XFFHVVIXOO\�5HIHUUHG�6H[XDO�3DUWQHUV
0
100
200
300
400
Husband/Wife
Freq
uenc
y
Type of Sexual Partner
Boyfriend/Girlfriend
Casual Sexual Partner
318
57 59
+76�DQG�(QUROOPHQW�LQWR�&DUH�DQG�7UHDWPHQW���2I�WKH�����SDUWQHUV�VXFFHVVIXOO\�UHIHUUHG��������������
XQGHUZHQW�+76����������������IRXQG�WR�EH�+,9�SRVLWLYH
��0DOH�SDUWQHUV� ��������)HPDOH�SDUWQHUV� ������
������RI�WKH�SDUWQHUV�ZHUH�+,9�QHJDWLYH�����VHUR�����GLVFRUGDQW�FRXSOHV��
��������RI�+,9�SRVLWLYH�SDUWQHUV�ZHUH�HQUROOHG�LQWR�&7
Listed partnersn = 438
Passive referral402 (92.6%)
Provider referral14 (3.2%)
Contact referral2 (0.5%)
Passive referral237 (56.6%)
Provider referral10 (2.6%)
Contact referral2 (0.5%)
Partners who came to facility
following referraln = 248
Average: 1.01 partner listed per index client (range 1–4)
12 index clients successfully referred more than 1 sexual partner��$YHUDJH�������SDUWQHU�OLVWHG�SHU�LQGH[�FOLHQW��UDQJH��²����12 index clients successfully referred more than 1 sexual
partner
7\SHV�RI�6H[XDO�3DUWQHU�/LVWHG�$FFRUGLQJ�WR�,QGH[�&OLHQW
DXUDWLRQ�EHWZHHQ�3DUWQHU�5HIHUUDO�DQG�+76:LWKLQ��²��GD\V �����������
:LWKLQ��²��GD\V ���������
:LWKLQ��²���GD\V ����������0RUH�WKDQ����GD\V ��������Other ����������
5HVXOWV��FRQW��7LPH�WR�6XFFHVVIXO�+76�5HIHUUDO
Conclusions��This study demonstrated feasibility, acceptability and
HIIHFWLYHQHVV�RI�SDUWQHU�QRWLILFDWLRQ�UHIHUUDO�LQ�WKH�FRQWH[W�RI�IDFLOLW\�EDVHG�+76�LQ�7DQ]DQLD��
��1RWLÀFDWLRQ�DQG�UHIHUUDO�ZHUH�SULPDULO\�SDVVLYH�DQG�WHQGHG�WRZDUG�D�VLQJOH�SDUWQHU��JHQHUDOO\�D�VSRXVH�
��7KH�ILQGLQJV�SUHVHQW�VWURQJ�HYLGHQFH�IRU�LQWHJUDWLQJ�SDUWQHU�QRWLILFDWLRQ�DQG�WHVWLQJ�LQWR�IDFLOLW\�EDVHG�+7&�VHUYLFHV�LQ�7DQ]DQLD�DQG�VLPLODU�VHWWLQJV�LQ�66$���6KRXOG�SDUWQHU�QRWLÀFDWLRQ�UHIHUUDO�EH�UROOHG�RXW�
ZLWK�HQKDQFHG�HQUROOPHQW�LQWR�FDUH��WUHDWPHQW�DQG�SUHYHQWLRQ�IRU�VHUR�GLVFRUGDQW�FRXSOHV�
ReferencesBrown LB, Miller WC, Kamanga G, et al. 2011. HIV partner notification is effective and feasible in sub-Saharan Africa: Opportunities for HIV treatment and prevention. J Acquire Immune Defic Syndr. 56:437.
Henley C, Forgwei G, Welty T, et al. 2013. Scale-up and case-finding effectiveness of an HIV partner services program in Cameroon: An innovative HIV prevention intervention for developing countries. Sex Transm Dis. 40:909-14.
Tanzania Commission for AIDS (TACAIDS), Zanzibar AIDS Commission (ZAC), National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF International. 2013. Tanzania HIV/AIDS and Malaria Indicator Survey 2011²12. Dar es Salaam, Tanzania: TACAIDS, ZAC, NBS, OCGS, and ICF International.
WHO. 2015. Fact sheet N°360. http://www.who.int/mediacentre/factsheets/fs360/en/. Updated November 2015.
%DFNJURXQG���$Q�HVWLPDWHG�����RI�SHRSOH�OLYLQJ�ZLWK�+,9�LQIHFWLRQ�GR�
QRW�NQRZ�WKHLU�VWDWXV��:RUOG�+HDOWK�2UJDQL]DWLRQ��������7R�UHDFK�WKH�´ILUVW���µ�RI�81$,'6·V����������VWUDWHJ\��KLJK�\LHOG�DSSURDFKHV�WR�+,9�WHVWLQJ�VHUYLFHV��+76��DUH�FULWLFDO��
��3DUWQHU�QRWLILFDWLRQ��VH[XDO�SDUWQHUV�RI�+,9�GLDJQRVHG�clients are contacted by their partner or a health SURYLGHU��LV�HIIHFWLYH�LQ�LGHQWLI\LQJ�SHUVRQV�ZLWK�XQGLDJQRVHG�+,9�LQIHFWLRQV�����$�0DODZL�VWXG\��%URZQ�HW�DO���IRXQG�D�����LQIHFWLRQ�
UDWH�DPRQJ�SDUWQHUV�RI�LQGH[�FOLHQWV���,Q�D�&DPHURRQ�VWXG\��+HQOH\�HW�DO����������ZHUH�
LQIHFWHG�����$OWKRXJK�SDUWQHU�QRWLILFDWLRQ�KDV�EHHQ�KLJKO\�XWLOL]HG�
LQ�WKH�8QLWHG�6WDWHV�DQG�(XURSH��LW�LV�DQ�XQGHUXWLOL]HG�DSSURDFK�LQ�VXE�6DKDUDQ�$IULFD��66$���
6WXG\�2EMHFWLYH�7R�HYDOXDWH�WKH�feasibility, acceptability and HIIHFWLYH-ness�RI�D�SDUWQHU�QRWLÀFDWLRQ�DQG�UHIHUUDO�DSSURDFK�WR�+76�LQ�WKH�FRQWH[W�RI�URXWLQH��IDFLOLW\�EDVHG�+76�LQ�Tanzania
7KLV�SRVWHU�LV�PDGH�SRVVLEOH�E\�WKH�JHQHURXV�VXSSRUW�RI�WKH�3UHVLGHQW�V�(PHUJHQF\�3ODQ�IRU�$,'6�5HOLHI��3(3)$5��DQG�86$,'��XQGHU�WKH�WHUPV�RI�WKH�7HFKQRORJLHV�IRU�+HDOWK�$,'�2$$�$�����������7KH�FRQWHQWV�DUH�WKH�UHVSRQVLELOLW\�RI�WKH�DXWKRUV�DQG�GR�QRW�QHFHVVDULO\�UHIOHFW�WKH�YLHZV�RI�3(3)$5��86$,'�RU�WKH�8QLWHG�6WDWHV�*RYHUQPHQW�
TA NZ A NIA NS A ND AME RIC A NSIN PA RTN E RSHIP TO FIG HT HIV/AIDS
THE UNITED REPUBLIC OF TANZANIAMinistry of Health, Community Development,
Gender, Seniors and Children
1RWLÀFDWLRQ�DQG�5HIHUUDO�$SSURDFKHV�1HZO\�+,9�'LDJQRVHG�0HQ�DQG�:RPHQThree methods of sexual partner notification and UHIHUUDO�ZHUH�RIIHUHG�WR�LQGH[�FOLHQWV����3DVVLYH�UHIHUUDO��,QGH[�FOLHQW�QRWLÀHV�UHIHUV�
SDUWQHU�V��WR�+76���3URYLGHU�UHIHUUDO��+HDOWK�FDUH�SURYLGHU�
DQRQ\PRXVO\�QRWLÀHV�UHIHUV�SDUWQHU�V��WR�+76���&RQWUDFW�UHIHUUDO��,QGH[�FOLHQW�DWWHPSWV�
QRWLÀFDWLRQ�UHIHUUDO�RI�SDUWQHU�V��WR�+76�ZLWK�DJUHHPHQW�WKDW�KHDOWK�FDUH�SURYLGHU�ZLOO�FRQWDFW�SDUWQHU�LI�LQGH[�LV�QRW�DEOH�WR�EULQJ�LQ�SDUWQHU�E\�DQ�DJUHHG�XSRQ�GDWH��
��3DUWQHUV�SUHVHQWLQJ�WR�WKH�IDFLOLW\�ZHUH�RIIHUHG�+76�DQG�UHIHUUHG�LQWR�+,9�FDUH�DQG�WUHDWPHQW�LI�IRXQG�+,9�SRVLWLYH�
��2XWFRPH�PHDVXUHV����3HUFHQWDJH�RI�SDUWQHUV�VXFFHVVIXOO\�UHIHUUHG�
WR�+76���3HUFHQWDJH�RI�+,9�SRVLWLYH�SDUWQHUV�ZLWK�
XQGLDJQRVHG�+,9�LQIHFWLRQ���3HUFHQWDJH�RI�SDUWQHUV�DQG�LQGH[�FOLHQWV�
HQUROOHG�LQ�+,9�FDUH�DQG�WUHDWPHQW�
����ZLWKLQ���GD\V������ZLWKLQ���GD\V������ZLWKLQ����GD\V
399

© 2021 - International AIDS Society
Partner notification for HIV testing services (HTS) approach inTanzania underscores need for discordant couple package
Background: With UNAIDS''s 90-90-90 goal, approaches to HIV testing which yield high positivity rates are critical for sub-Saharan Africa.Partner notification, where sexual partners of newly-diagnosed clients are contacted by their partner or a provider, is effective, but underutilized,in identifying undiagnosed individuals. Successful applications of this approach have been documented in Malawi and Cameroon. Identification ofserodiscordant couples presents a critical HIV prevention opportunity given high risk of the uninfected partner. This study evaluated feasibility,acceptability and effectiveness of partner notification in facility-based HIV testing services (HTS) in Tanzania.Methods: The study was conducted in 3 hospitals in Njombe (Tanzania''s highest HIV prevalence region), June - September 2015. Individualsdiagnosed with HIV in PITC or VCT were enrolled as index clients, and offered passive, contract or provider referral to HTS at the same facility:partners testing positive were referred into HIV care and treatment. Serodiscordant couples were defined as those in which the sexual partnerindicated that they were in a current partnership with the index client.Results: 390 individuals (53.1% female) enrolled as index clients and 248 of their named sexual partners were successfully referred, in all but onecase via passive referral. 238 partners tested for HIV, 61.8% testing positive. More female partners tested positive (67.9% vs. 53.5% for male). 88sero-discordant couples were identified, 87 of which were reached through passive referral - the remaining one through provider referral. 76.1%of discordant couples were husbands or wives, 15.9% were boyfriends/girlfriends and 8% were casual partners.Conclusions: Tanzanian facility-based HTS settings are a feasible venue for high-positivity rate partner notification programs, includingidentification of sero-discordant couples. A social preference for partner notification as a means to disclose serostatus to the main partner wasseen in the study, making the intervention in many cases a facilitated disclosure intervention by the HTS counselor. Given the number of sero-discordant couples identified, we recommend that partner notification programs are rolled out with a comprehensive prevention package fordiscordant couples, including risk reduction counseling, provision of condoms, immediate provision of ART for the index partner and PreP for theHIV uninfected partner as appropriate.
M. Plotkin , C. Kahabuka , R. Kisendi , A. Christensen , E. Mlanga , K. Curran , C. Brown , V. WongJhpiego, Monitoring, Evaluation and Research, Baltimore, United States, CSK Research Associates, Dar es Salaam, Tanzania, United Republic of,Ministry of Health and Social Welfare, National AIDS Control Programme, Dar es Salaam, Tanzania, United Republic of, Jhpiego Tanzania, Dar es
Salaam, Tanzania, United Republic of, USAID Tanzania, Dar es Salaam, Tanzania, United Republic of, Jhpiego, Baltimore, United States, USAIDWashington, Washington, United States
ABSTRACT ARCHIVE
1 2 3 4 5 6 7 7
1 2
3 4
5 6 7
Abstract Archive https://www.abstract-archive.org/Abstract/Share/72992
1 of 1 8/19/21, 3:31 PM
400
� VHT records show 647 client visits for HTC between January and March 2013 � Men were tested in 80.0% of visits, and women in 49.6% of visits � 27% of surveyed clients who accepted a test were first time testers for HIV � Three surveyed clients tested HIV+ with the VHT - all reported functional linkages to care � 93.5% of surveyed clients who tested HIV- with the VHT intend to get tested again and would like to get their next test from the VHT � External Quality Assessment conducted in April-June 2012 quarter as part of program implementation: Proficiency Testing panels sent by National Lab
through districts � 29 VHTs participated in exercise � 85% of participating staff had 100% concordance with the national lab
� 3 staff failed due to recording problems � 2 staff failed due to technical factors
Community Delivery of integrated family planning/HIV testing and counseling services by VHTs in Uganda Aurélie Brunie1, Alison Cheng5, Patricia WamalaMucheri2, Jane H. Namwebya3, Tricia Petruney4, Benson Tumwesigye6, Sarah Mercer4, Victor D. Afayo3, Angela Akol3, Vincent J. Wong5
1. FHI 360, Washington DC, 2. Clinton Health Access Initiative, Kampala, UGANDA; 3. FHI 360, Kampala, UGANDA, 4. FHI 360, Durham, NC, 5. USAID, Office of HIV/AIDS, 1200 Pennsylvania Ave, Wash DC, 6. Ugandan Ministry of Health, National HTC Coordinator, Kampala, UGANDA.
%$&.*5281'�� In Uganda, HIV prevalence is rising and yet HIV testing rates remain low � Family Planning (FP) clients are simultaneously at risk of unintended pregnancy and HIV infection � Community and home-based HIV testing and counseling (HTC) provision has potential to increase access and uptake � Village Health Teams (VHTs) are a nationwide government-supported platform for community-based health programming. � VHTs have established relationships with communities and already provide FP services, including DMPA, in many areas � This study integrated HTC into FP service delivery by VHT, seeking health system efficiency while meeting comprehensive reproductive and sexual
health needs � New, innovative model with potential to reduce access barriers to HTC and increase range of services available to FP clients .
Table 2: Surveyed clients’ perspectives on HTC services within intervention group (n=110)
5(68/76�
0(7+2'6�
� Challenges and recommendations by VHTs (n=36): Reported supply challenges (47%); 50% are very concerned about contracting HIV through testing, 16.7% are somewhat concerned; 61% wanted transport assistance/financial incentives; 44% desired more training
5(68/76�
/,0,7$7,216�
� Recall and reporting bias � Reliability of record data � Interim analysis has only included the evaluation of the intervention group � Small number of units of randomization limits ability to match health centers
&21&/86,216�
� Noting the need to ensure adequate supporting mechanisms and quality assurance and improvement processes, overall, this integrated model appeared feasible to implement and client acceptability was high, suggesting this approach could be used to offer comprehensive sexual and reproductive health services at the community level.
� The small number of newly diagnosed HIV positive clients in the study sample suggests limited overall contribution to enrollment into HIV care and treatment in this target population. However, a number of clients received HIV testing for the first time.
� In an era of reduced resources for community-based HIV prevention and HTC services, an integrated FP/HTC approach that takes advantage of the existing community FP system could be more efficient and sustainable.
� Programs should consider the specifics of the context to determine the potential added value of this model. The effectiveness of similar integrated approaches should consider rates of HIV positivity in target populations.
CROI 2014 Abstract Number: 2175
Table 3: VHT workload and satisfaction (n=36)
Table 1: VHT Profile
� To evaluate the extent to which trained VHTs can safely provide quality HTC services in addition to their FP work; � To examine acceptance of community-based FP/HTC integrated services and the specific factors contributing to acceptance of testing by VHTs; � To assess effectiveness in modifying HIV testing attitudes and practices; � To characterize the effect of HTC/FP integration on VHTs’ client loads and perceived workloads; and � To examine the effect of HTC/FP integration on FP uptake and clients’ perceptions of the quality of the base FP service
2%-(&7,9(6�
INTERVENTION ELEMENTS � 38 VHTs already providing FP, with six months experience offering DMPA injections � Training with 8 days of classroom training and 4 days of practicum � Community mobilization meetings as follow-on practicum � Adaptation of mechanisms for FP supervision, quality assurance, commodity management and record keeping � Collaboration between the Ministry of Health and FHI 360
Busia (N=18)
Kanungu (N=18)
Total (N=36)
Mean age (years) 45.5 41.9 43.7 Mean years of experience providing pills and condoms 5.5 6.9 6.2
Mean years of experience providing injectables 4.2 5.1 4.6
Sex (%) Female Male
77.8 22.2
83.3 16.7
80.6 19.4
Highest level of school attended (%) Primary Secondary or higher
11.1 88.9
44.4 55.6
27.8 72.2
Prior experience with HIV counseling (%) 38. 9 66. 7 52.8
Prior experience with HIV testing (%) 11.1 0 5.6
Figure 1: Intervention Schema
%
Fingerpricking technique No problem with fingerpricking site at last test
100
Counseling content What client can do to avoid getting infected/infecting others FP methods that protect against both HIV and pregnancy Condoms
90.9 90.9 94.6
Rapport with VHT Comfortable discussing HIV with VHT Satisfied with explanations about test results Trusted VHT with private information Satisfied with HTC services received overall
95.5 99.1 99.1 99.1
%
Change in overall monthly number of clients More now than prior to HTC service provision Same number of clients Fewer clients now
83.3 13.9 2.8
Workload Easy to manage Somewhat difficult to manage
91.7 8.3
Change in overall quality of work Better now than prior to HTC service provision About the same Not as good now
91.7 5.6 2.8
Change in work satisfaction as VHT More satisfied now than prior to HTC service provision Equally as satisfied
91.7 8.3
Wish to continue HTC service provision 100
SITES AND SERVICES � 8 randomly selected health centers III were assigned to intervention or control (matched pairs) in two districts: Busia and Kanungu � VHTs in the intervention arm offered FP and HTC services; only FP services were provided in the control arm DATA SOURCES � Survey of all trained VHTs and survey of 256 FP clients in the intervention and control groups 10 months after implementation � Service statistics
3RVW�7HVW�&RXQVHOLQJ���,1',9,'8$/�
1(*��
3UH�WHVW�&RXQVHOLQJ��$'8/7�&283/(6�
�
3UH�WHVW�&RXQVHOLQJ�,1',9,'8$/�$'8/7�
�
5DSLG�+,9�7HVWLQJ���6WDQGDUG�6HULDO�$OJRULWKP�
�
+,9�%DVLF�,QIRUPDWLRQ�DQG�.H\�0HVVDJH�'HOLYHU\�DQG�FKRLFH�RI�9+70�WHVW�RU�UHIHUUDO�WR�+&�
�
0HVVDJHV�RQ�)3�IRU�3/:+$��6DIHU�3UHJQDQF\��RU�307&7�
��'LVFORVXUH�6XSSRUW��
5()(55$/6��7HVWLQJ�QHJDWLYH�WR�UHSHDW�WHVW�LQ���PR¶V��WHVWLQJ�SRVLWLYH�IRU�OLQN�WR�FDUH�WUHDWPHQW��FRQILUPDWRU\�WHVW��DQG�RWKHUV�DV�QHHGHG��HJ�FKLOG�WHVWLQJ��SHHU�JURXSV���
�
&OLHQW�GHFOLQHV�WHVW��
%RWK�FOLHQWV�
GHFOLQH�WHVW��
3RVW�WHVW�&RXQVHOLQJ�
&283/(�%27+�1(*��
3RVW�WHVW�&RXQVHOLQJ�,1',9,'8$/�
326��
3RVW�WHVW�&RXQVHOLQJ�&283/(�
326��1(*��
3RVW�WHVW�&RXQVHOLQJ�&283/(�%27+�326�
�
&RPSOHWH�5HFRUG�)RUPV��
VHTMs visit Health Centers once per month for supportive supervision, records submission, and material re-supply
For quality assurance, VHTMs will be observed in a counseling session for a clinic-based client and given a prepared Dried Tube Specimen panel for testing. As needed, VHTMs will receive OTJ and/or refresher support.
VHTM Community Mobilization FP Clients of VHTM
Corresponding Author: Vincent J. Wong, USAID Washington, Office of HIV/AIDS, [email protected]
401

Out of the clinic and into the home Development of WHO/PEPFAR Home-Based HIV Testing and Counseling Support Tools
Miriam Taegtmeyer,1 Cassandra Blazer,2 Maria Claudia Escobar,2 Kristina Grabbe,3 Vincent J. Wong,4 and Rachel Baggaley5
1 Liverpool School of Tropical Medicine, Liverpool, 2 BroadReach Healthcare, Arlington, VA, 3 U.S. Centers for Disease Control and Prevention, Atlanta, GA, 4 U.S. Agency for International Development, Office of HIV/AIDS, Washington, DC, 5 World Health Organization, Geneva
Methods
• Structured questionnaires were sent to 35 PEPFAR-supported countries with generalized epidemics in sub-Saharan Africa, Latin America and the Caribbean, Asia and the Pacific, Central Asia, Southeast Asia, and Russia and Ukraine; 18 surveys were completed.
• Identified and summarized existing home-based HTC materials, best practices, and challenges.
• Observed home-based HTC programs and practices in Kenya, Uganda, Swaziland, Mozambique, and Ethiopia.
• Conducted individual and group discussions with program managers and staff.
Results
10 out of 35 countries had active home-based HTC programs of varying size and scope; 5 countries had home-based HTC materials available for review (3 guidelines, 2 operational manuals). Program observations identified key elements necessary for successful home-based HTC programs which include:
• Advance planning and geographical mapping to reduce program overlap and estimate population size for coverage
• Community mobilization and engagement to facilitate home entry • Ensuring provider safety • Advance logistical planning to ensure smooth programmatic operations.
Critical steps in planning community entry for home-based HTC (with corresponding section in the WHO/PEPFAR Practical Handbook for Planning, Implementing and Monitoring HBHTC)
Background on Home-based HTC Home-based HIV testing and counseling (HTC) is used throughout sub-Saharan Africa—varying contexts, common approaches. Models of home-based HTC:
• Door-to-door: offering HTC to every household in a given geographical area or region.
• Index patient: offering HTC to family members of a patient enrolled in HIV treatment or care (or the “index client”)
• Integrated: offering HTC as the primary service while including additional educational or screening interventions (i.e., tuberculosis screening and sputum collection, de-worming, and/or distribution of bed nets); this approach may also be integrated into home-based or community-based care.
Results (continued)
Practical Tools Developed
Home-based HTC best practices identified include: • Engaging local leadership • Delivering an integrated approach which may include tuberculosis
screening or family planning education • Setting appointments with households to maximize couples/partner
HTC • Maintaining strong supportive supervision to ensure quality
services • Ensuring national coordination.
Objectives To address the gap in guidance, an assessment was conducted in countries with generalized epidemics to help inform the development of two practical home-based HTC support tools:
1. World Health Organization (WHO)/U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) Practical Handbook for Planning, Implementing and Monitoring HBHTC
2. AIDSTAR-One Case Study: Getting in the Door: Home-based HTC in Kenya
Steps Planning Rationale
Ensure in line with national strategy
(3.2)
Involve stakeholders
(5.2)
Involve district administration
(5.2)
Involve local area administration
(6.1)
Attend community meetings
(6.1)
Community sensitization and mobilization (6.3)
Allows areas to be appropriately prioritized for home-based HTC and helps avoid duplication of efforts.
Involvement of a wide range of stakeholders at the regional level ensures buy-in and correct communication. It is an opportunity to clarify program objectives and methods.
Support from district officials facilitates buy-in from village chiefs and local leaders. Obtaining information or maps of other organizations providing services in the testing area creates comprehensive referral directories for each area.
Program managers meet with local chiefs to explain their purpose and obtain approval to move forward.
Community meetings organized by local leaders helps sensitize the community to home-based HTC, allows people to ask questions, and may identify potential community mobilizers.
Door-to-door sensitization increases awareness. Community health workers/mobilizers set up appointments with households. Strategies such as radio and public announcements, fliers, and T-shirts, supplement door-to-door sensitization.
WHO/PEPFAR Practical Handbook for Planning, Implementing and Monitoring HBHTC
Chapter Key Points Coordination at the national level
• Coordinate at the national level to reduce duplication of efforts and ensure quality service delivery
• Authorize organizations and certifying providers to conduct home-based HTC
Personnel • Personnel varies according to setting and home-based HTC model (door-to-door, index, integrated)
• Personnel generally consists of: program manager to oversee and coordinate all home-based HTC efforts and supervisors; 2-4 providers who conduct home-based HTC; laboratory staff to ensure quality HIV testing procedures; and community liaison officers and community mobilizers to ensure buy-in and community support
Program planning
• Work with national, regional, and local authorities to identify appropriate and priority locations for home-based HTC services
• Work in areas that can provide ART with capacity to enroll new patients • Conduct geographic mapping to ensure services are provided systematically and to
establish coverage area • Obtain detailed knowledge of follow-up services and develop referral directory • Develop policy for return visits • Identify and address security issues and provide viable transportation
Community and home entry
see figure for detailed steps
Populations tested
• Clearly define who is to be tested (i.e., who qualifies as family versus who is present at the residence at the time of visit)
• Family and couples testing is an aim of home-based HTC programs • Children and adolescent testing is conducted in an age appropriate manner and age of
consent follows local guidance and norms • A table of age considerations for testing and consent is provided
Protocol for home-based HTC
• Protocol steps cover: introduction to session, consent, pre-test, testing, post-test, and disclosure
• Guiding principles of “4 C’s” are upheld (consent, confidentiality, counselling, and correct HIV testing procedures)
Referral and linkages
• Mapping of referral points takes place before program begins • Indications for referral and where to refer to are provided • Strategies to ensure successful linkage are provided
Data and M&E • Types of data to collect are provided • Indicators to include are: coverage, refusal, testing rates, and successful linkage
Quality assurance
QA elements for counselling and testing include: quality control; external quality assessment; proper documentation and recordkeeping; and supervisory visits and observed practice
Special circumstances
Suggestions are provided for addressing: alcohol; violence; sexual abuse; and most at-risk populations
Leaving an area • Identify when to move on from an area based on objectives and coverage rates • Determine if linkages were successful • Community feedback meetings provide critical information which can shape program
efforts and address issues
AIDSTAR-One Case Study: Getting in the Door: Home-based HTC in Kenya
Focus on: • Community mobilization • Home-based HTC implementation issues • Ensuring quality in HIV testing and counseling • Linkages with appropriate treatment, care and support, and prevention
services
Common challenges: • Couples and partner HTC • Disclosure (to partners and
children) • Consent and refusal to test • Religious and cultural beliefs pose
barriers to testing and referral to treatment
• Counselor burnout • Safety and security • Child consent (lack of experience in
age appropriate counseling; consent issues)
• Alcohol use and abuse • Partner violence
Acknowledgments This research has been supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) through the U.S.
Agency for International Development under the terms of contract no. GHH-I-00–07–00059–00.
No international guidance exists and few countries have national operational guidance. Limited guidance may: 1) potentially impact the quality, acceptability, and impact of home-based HTC, and 2) lead to duplication of efforts by various programs.
Key challenges across programs include: • Ensuring acceptable and effective HTC services and accuracy of
test results, with appropriate strategy to confirm all positive results • Implementing quality control of counseling and external quality
assurance of testing • Facilitating and monitoring linkage to care to a range of services
(i.e., HIV treatment, care, and support and other medical and support services for individuals and families)
• Lacking guidance for challenges (e.g., violence, clients with alcohol issues, counseling for test refusal, and counseling and testing of children based on developmental stage).
www.aidstar-one.com
402

Key Findings � Unit costs for HTC delivery vary greatly in Botswana, from US$8 to US$314.
� HIV prevalence also varies widely, depending on the service delivery modality, from 3 percent for PITC to 49 percent for TB.
� The cost per HIV infection identified appears to be lowest for mobile service provision through NGOs (US$93) and highest for PITC (US$11,018).
� One of the main cost drivers is human resources. As a result, any effort to reduce the cost of HTC in Botswana would need to focus on staffing issues (e.g., task shifting, more staff at higher volume sites, etc.)
� While HTC service delivery is likely to continue through a combination of modalities in Botswana, development partners and the government of Botswana may wish to emphasize mobile and VCT testing (through the public sector and NGOs) to identify the largest number of infections at the lowest possible cost.
The Costing Of HIV Testing and Counseling in Botswana: Capturing Cost and Effectiveness Data for Multiple Service Delivery Models
Authors: P. M. Stegman1, W. Mosime1, S. Forsythe1, S. Alkenbrack2, R. Lebelonyane3, and V. Wong4
1Futures Institute; 2Futures Group; 3Ministry of Health, Botswana; 4USAID Washington, DC
Presented at the International Conference on AIDS and STIs in Africa; December 7-11, 2013; Cape Town, South Africa
IntroductionThe USAID | Health Policy Initiative Costing Task Order assisted the government of Botswana to better understand the costs and cost drivers of HIV testing and counseling (HTC) service delivery. In addition to understanding the costs of HTC in Botswana, the project was asked to develop an HTC Costing Model that could be used to estimate the costs of different types of HTC service delivery modalities.
The objectives were threefold:
1. To examine the unit costs of various HTC service delivery modalities;
2. To examine the cost effectiveness of HTC service delivery, defined in this case as the cost per infection detected; and
3. To identify possible strategies to scale-up and increase access to HTC.
MethodsA sample of 38 sites (both public and nongovernmental) were selected to include all service delivery modalities (stand-alone, integrated, and mobile), as well as geographical disparities, rural/urban split, volume of service delivery, and the level of (public) facilities (hospital, clinic, health post).
An ingredients approach to the costing analysis was used whereby all the inputs, direct and indirect, were listed and their contribution to the overall cost tallied. The direct and indirect costs for each facility providing HTC services were computed separately, and a median unit cost for fixed/integrated and mobile services was obtained based on the unit cost per facility.
DiscussionFor VCT and mobile provision, costs in Botswana do not differ much from other countries. However, integrated HTC service delivery costs are much higher. This is largely due to the high human resource and infrastructure costs in Botswana.
HTC delivery through campaigns and mobile/outreach (both in public facilities and NGOs) provide good value and can target hard-to-reach clients.
ConclusionsThe study suggests that the future of HTC service delivery will likely involve a combination of facility-based and mobile testing. However, to initiate people on treatment earlier, mobile service delivery, especially through NGOs, may be a priority.
Further research into cost effectiveness and linking clients to early treatment initiation is needed when the Ministry of Health’s monitoring and evaluation structures are strengthened.
References1. Ministry of Health (Botswana). (2010) National Guidelines
for HIV Testing and Counseling, Gaborone: Government of Botswana.
2. Menzies, et al. (2009) “The costs and effectiveness of four HIV counseling and testing strategies in Uganda.” AIDS 23: 395–401
3. Marseille, et al. (2007) “HIV prevention costs and program scale: data from the PANCEA project in five low and middle-income countries.” BMC Health Services Research 7: 108
4. Forsythe, et al. (2002) “Assessing the cost and willingness to pay for voluntary HIV counseling and testing in Kenya.” Health Policy and Planning 17(2): 187–195
5. World Health Organization. (2011) Global Health Sector Strategy on HIV/AIDS 2011–2015. Geneva: World Health Organization.
ContactHealth Policy Initiative, Costing Task Order
Futures Group One Thomas Circle, NW, Suite 200
Washington, DC 20005 USA
Tel: (202) 775-9680 Fax: (202) 775-9694
http://ghiqc.usaid.gov http://www.healthpolicyinitiative/costing.
com
� Sampled nongovernmental organization (NGO) sites had administered >20,000 tests in the previous 12 months, more than any other delivery modality.
� Indirect costs are high for stand-alone voluntary counseling and testing (VCT), but insignificant for mobile services.
� Overhead and management costs contributed the most to indirect costs of service provision.
� Unit costs for HTC in the Public Sector vary widely from US$7.85 for mobile service delivery to US$314.03 through the tuberculosis (TB) program.
� Direct costs contribute the most to the cost per client tested.
� Human resource costs were the most expensive cost input to Public Sector HTC service delivery.
� PITC had the highest cost per HIV infection identified: more than US$11,000.
� The most cost-effective HTC service delivery modality was mobile service provision through NGOs, which cost approximately US$92 per HIV infection identified.
� “Integrated” service delivery (PMTCT and TB) were less cost-effective at US$635 and US$734, respectively.
� TB had the highest HIV prevalence by volume (due to high rates of co-morbidity), but also had the lowest testing volume.
� Provider-initiated testing and counseling (PITC) had lower HIV prevalence than any other delivery modality.
� VCT provided by NGOs had a high HIV prevalence and very high volume, demonstrating the public preference for testing outside of the public sector.
Results
050
100150200250300350
Indirect CostsDirect Costs
MobilePITCVCTTBPMTCT
Indirect Costs
Direct Costs
30.73
34.51
66.53
247.75
11.46
21.6
16.73
259.47
0.35
7.5
0
10
20
30
40
50
PMTC
T TB
VCT P
ub. S
ector
)
MSP
(Pub
. Sec
tor)
PITC
VCT (
NGO
)
MSP
(NGO
)
Camp
aign
01020304050607080
Indirect CostsDirect Costs
MobileVCT
Indirect Costs
Direct Costs
39.52
27.73
0.15
7.23
0
2,000
4,000
6,000
8,000
10,000
12,000
PMTC
T TB
VCT P
ub. S
ector
)
MSP
(Pub
. Sec
tor)
PITC
VCT (
NG
O)
MSP
(NG
O)
Camp
aign
View publication statsView publication stats
403

© 2021 - International AIDS Society
Examining reporting of quality elements in a provider-initiated HIVtesting and counseling and implications for rights-basedapproaches: a literature review
Background: Provider-initiated HIV testing and counseling (PITC) was first adopted by Botswana and Kenya in 2004. In 2007, WHO/UNAIDSresponded to country-level operational guidance with its publication: Provider initiated HIV testing and counselling in health facilities. In 2009,WHO commissioned a literature review to map-out implementation successes and challenges and define areas for further study.Methods: This review through PubMed and conference abstracts returned 147 studies (including 80 journal articles) from 1/2003-7/2009describing PITC implementation in developing countries. Search terms combined “HIV testing” with “provider-initiated”, “routine” or “opt-out”.Studies were coded with 1-3 emergent themes. If available, testing acceptance, HIV-seroprevalence and return/post-test counselling rates wererecorded. Publications were sorted categorically and analyzed for convergent/divergent themes.Results: Among all developing countries, 75% of studies were based in sub-Saharan Africa. Key themes included: 1)PITC increases testinguptake and is widely acceptable (n=67; 55% had >90% acceptance; range:31.5-99.9%); 2)results are returned to the majority of testers (n=13;mean return-rate: 87%; range:49-99%); 3)Studies examining informed consent are limited (n=3). 4)Absence of pre-test information and “forced”testing are reported(n=4). Patient-refusal due to fear, perceptions of non-confidentiality, low-risk and providers not offering testing can be factorsin patients declining testing (n=15); 5)Loss to post-test follow-up, particularly in PMTCT-contexts remains challenging (n=14, mean PMTCTenrollment=51.2%; range:14.9-86%); 6)Poor quality or no counseling/pre-test information is reported; 7)Low rates of partner testing/involvementand disclosure reported (n=3).Conclusions: As countries expand PITC, it remains critical that all patients are recommended quality HIV testing and counselling, and informedconsent must be clearly communicated., In the spirit of the WHO guidance, PITC programs should address adequate counseling/information,confidentiality/privacy, loss-to-follow up, and increasing partner involvement/disclosure. Future studies assessing these and other aspects ofimplementation can help inform programs, improve PITC delivery, and ensure due attention is paid to human rights in HIV testing.
V. Wong , M. SabinWorld Health Organisation, Department of HIV/AIDS, Geneva, Switzerland, US Agency for International Development, Office of HIV/AIDS,
Washington, United States
ABSTRACT ARCHIVE
1,2 1
1 2
Abstract Archive https://www.abstract-archive.org/Abstract/Share/2884
1 of 1 8/19/21, 3:26 PM
404

To determine what materials and content were most appropriate to meet this need, FHI !"#, on behalf of USAID’s Interagency Youth Working Group (IYWG), created a technical advisory group of $% global experts, conducted a desk review, and worked with partners to survey &' ALHIV in !( countries and conduct informal focus groups in three countries.
Positive Connections: Leading Information and Support Groups for Adolescents Living with HIVJoy Cunningham!, Suzanne Fischer!, Vincent Wong"
www.fhi#$%.org
Young people (ages $% to )*) accounted for an estimated *$ percent of new HIV infections worldwide in )##&. Also, with the success of pediatric antiretroviral therapy, many more infants who were born HIV positive are growing up into adolescents and young adults living with HIV. Adolescence is often when young people begin having sex, so there are increased chances that adolescents who are living with HIV (ALHIV) might pass the infection to partners who are HIV negative. Another concern is that girls living with HIV will become pregnant and, if they do not know about or do not have access to services for the prevention of mother-to-child transmission, might pass the infection to their babies.
The U.S. Agency for International Development (USAID) and FHI !"# identified a need for ongoing HIV-related support and education, beyond counseling and testing, for ALHIV.
BACKGROUND
METHODS
AUTHOR AFFILIATIONS$ FHI !"#, Global Health, Population, and Nutrition;
Research Triangle Park, NC) U.S. Agency for International Development, Office of HIV/AIDS;
Washington, DC
From this assessment, we learned that:
ʳ� � -4#��**�#*1#ʓ��"-*#1!#,21�5&-��0#�*'4',%�5'2&�� ��are first and foremost adolescents — who want the same information about sex and reproductive health as all young people do.
“I might have HIV, but I still want to have a boyfriend.…get married one day. The nurses won’t tell me about contraception because they think I shouldn’t be having sex.” (Survey respondent)
ʳ� �'1!*-130#ʓ�12'%+�ʓ��,"��"�#,!#�2-��,2'0#20-4'0�*�therapy (ART) were major areas of concern among ALHIV.
“I am living with high pressure. I want to tell my friends [about my HIV status], but I am afraid that after knowing the truth they will not be friends with me anymore. I have to ignore this and nobody should know about it. That is the strategy I choose 2-�$-**-5ʒʢ�ʴʰ7#�0ʰ-*"�%'0*�',��'#2,�+ʵ
ʳ� ��,7���� ��5#0#��5�0#�-$�.0-2#!2'4#� #&�4'-01�but felt peer pressure against adopting them.
RESULTS
Based on the findings, the IYWG developed Positive Connections: Leading Information and Support Groups for Adolescents Living with HIV, a guide for adults who lead post-test information and support groups for ALHIV. The guide’s main goals are to help ALHIV:
$. Understand their HIV diagnosis and participate in the management of their care and treatment.
). Learn that many young people live healthy and productive lives while living with HIV.
!. Identify strategies for positive living including eating right, exercising, avoiding drugs and alcohol, and most importantly adhering to their treatment regimen.
CONCLUSIONS
ʒ���)#�',$-0+#"�"#!'1'-,1�� -32�2&#'0�1#63�*��,"�reproductive health, especially about how to prevent the transmission of HIV to others; avoid re-infection; consistently use family planning to prevent unintended pregnancy; and, if or when they wish to start a family, learn how to avoid infecting their babies.
%. Develop life skills such as understanding their emotions, communicating effectively, dealing with stigma and discrimination, making decisions about their future, and improving their quality of life.
We are developing a targeted utilization plan for this guide to be rolled out initially in two countries.
ʳ� ��,7���� ��!'2#"�0#!#'4',%�*'22*#�',$-0+�2'-,�-0�emotional support after learning about their status.
“The key issue for me is that there was exceptionally minimal support offered when I found out I was positive and a long waiting period to see a specialist. Accordingly, I was in a precarious emotional situation but was simply given a few pamphlets by the STI clinic...There should #� $-**-5ʰ3.ʒ� 2� 1&-3*"� ,-2� #� �,� -,31�upon youth to simply engage with resources for HIV. That kind of mindset does not exist right after you test positive.” (Survey respondent)
ʳ� �,�-,ʰ%-',%�13..-02�%0-3.�5-3*"� #���%--"�venue for ALHIV to get evidence-based information as well as support from a trusted adult and peers.
“Before joining the club you think you’re the only young person living with HIV. Coming to a group of people with whom you can disclose and talk freely about your status makes a huge difference.” (Botswana focus group participant)
High school students attend a DramAidE forum theater performance at a high school in Kwazulu Natal, a province in South Africa with the highest HIV/AIDS prevalence.
����
�����
����
ʓ�����
���
�����
���
����
405

© 2021 - International AIDS Society
A descriptive study of VCT implementation in the AccraMetropolitan District, Ghana
Background: In Accra, Ghana VCT is a key prevention intervention and includes components outlined in national and international guidelines,including consent, counseling, confidentiality and testing algorithms. This study’s objective was to describe VCT services within the district andcompare findings to the WHO/UNAIDS-endorsed national guidelines.Methods: This descriptive study used quota sampling of 269 potential VCT sites: public and private hospitals/clinics, laboratories and NGOs.Direct observations and questionnaire-based interviews were undertaken with two counselors/staff per site. Variables captured characteristics oftesting services derived from national guidelines.Results: VCT was provided by 42% (N=79) from all sectors. An estimate of utilization (290 tests/month) demonstrated demand. Of the 33 sitesoffering HIV testing: guidelines were used at 33%; the average fee was €5; regarding confidentiality, testing was always performed out of sight;76% used a private counseling room; most staff received confidentiality guidance; consent forms were used at 21%; staff at 30% stated testingwithout consent occurred; counseling was performed primarily by nurses and available at 88%; pre-test counseling was offered at 76%; post-testat 85%; counseling protocols were utilized at 18%; ARV therapy was available as fee-for-service at seven facilities; condoms were distributed at49%; anonymous testing was available at 21%; for screening, 48% used ELISA or external laboratories; 52% used rapid tests; two sitesperformed no confirmatory testing; 61% used rapid tests for confirmation; rapid tests used were of adequate sensitivity/specificity. An index wasgenerated contrasting guidelines and variables; a range of differences of facilities’ compliance was found.Conclusions: Findings gave an initial picture of VCT implementation in the district. Regarding compliance to guideline indicators, VCT servicesshowed a range of differences with no detectable differences among subgroups. Facilities from all sectors and types complied with manyminimum standards. Current standards are theoretically attainable. However, many VCT facilities in each sector didn´t meet the minimumstandards.
V. WongHumboldt University, Institute for Tropical Medicine, Berlin, Germany
ABSTRACT ARCHIVE
Abstract Archive https://www.abstract-archive.org/Abstract/Share/49937
1 of 1 8/19/21, 3:52 PM
406
Appendix 3: Research Ethics Review Checklist
407
UPR16 – April 2018
FORM UPR16 Research Ethics Review Checklist
Please include this completed form as an appendix to your thesis (see the Research Degrees Operational Handbook for more information
Postgraduate Research Student (PGRS) Information
Student ID:
PGRS Name:
Department:
First Supervisor:
Start Date: (or progression date for Prof Doc students)
Study Mode and Route:
Part-time�
Full-time
�
MPhil
PhD
MD
Professional Doctorate
Title of Thesis:
Thesis Word Count: (excluding ancillary data)
If you are unsure about any of the following, please contact the local representative on your Faculty Ethics Committee for advice. Please note that it is your responsibility to follow the University’s Ethics Policy and any relevant University, academic or professional guidelines in the conduct of your study
Although the Ethics Committee may have given your study a favourable opinion, the final responsibility for the ethical conduct of this work lies with the researcher(s).
UKRIO Finished Research Checklist: (If you would like to know more about the checklist, please see your Faculty or Departmental Ethics Committee rep or see the online version of the full checklist at: http://www.ukrio.org/what-we-do/code-of-practice-for-research/)
a) Have all of your research and findings been reported accurately, honestly and within a reasonable time frame?
YES NO
b) Have all contributions to knowledge been acknowledged?
YES NO
c) Have you complied with all agreements relating to intellectual property, publication and authorship?
YES NO
d) Has your research data been retained in a secure and accessible form and will it remain so for the required duration?
YES NO
e) Does your research comply with all legal, ethical, and contractual requirements?
YES NO
Candidate Statement:
I have considered the ethical dimensions of the above named research project, and have successfully obtained the necessary ethical approval(s)
Ethical review number(s) from Faculty Ethics Committee (or from NRES/SCREC):
If you have not submitted your work for ethical review, and/or you have answered ‘No’ to one or more of questions a) to e), please explain below why this is so:
Signed (PGRS):
Date:
Vincent Joseph Wong
XX
Oct 1, 2020
School of Health and Care Professions
PhD by Publication; All included research and publications have been approved by relevant institutional ethics committees or review boards.
X
X
X
X
X
Evolution and scale up of global HIV testing service approaches: 2000-2020
Main Commentary to PhD by Publication: 11,586 words; Total with Introduction: 14,348
Prof. Sasee Pallikadavath
UP 2044605
Sept 5, 2021
N/A
408
Copyright © 2022 FDOKUMEN