Barriers to Women's Entrepreneurship: SME Sector in Sri Lanka


Barriers to access to tes+ng in Central and Eastern Europe
Tamás Bereczky European AIDS Treatment Group –
EATG [email protected]
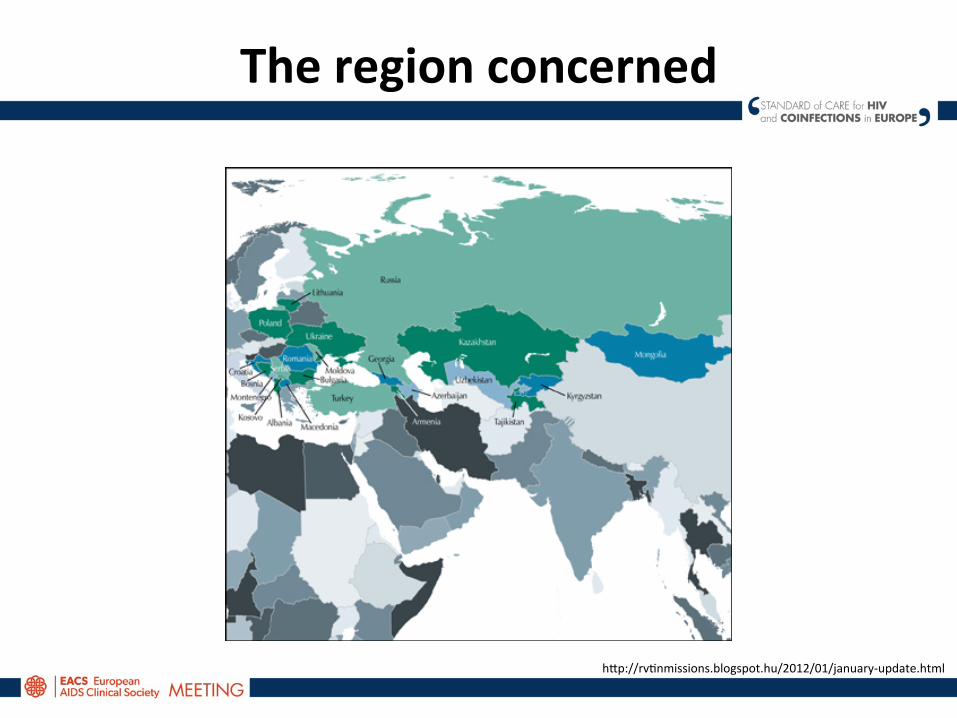
The region concerned
h=p://rvAnmissions.blogspot.hu/2012/01/january-‐update.html
What differences vs. the West?
• Historical – Ethnic diversity – Religious diversity – Differences in the development trajectories – A history of dependency on the state/sovereign
• Cultural • Structural
While there are huge differences within the region, there are also some common points
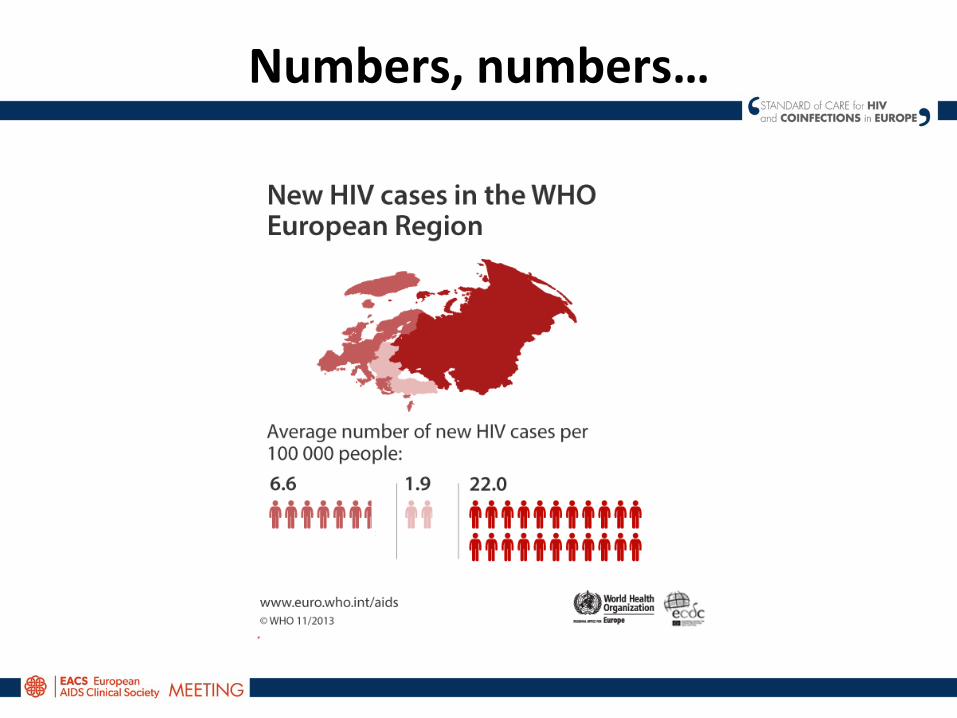
Numbers, numbers…
More numbers!
• App. 1.4 million people in Russia, Eastern Europe and Central Asia living with HIV at the end of 2011*
• Rate of new infecAons increasing – MSM and IDU drive the epidemic* • 21% increase in AIDS related deaths 2005-‐2011* • Russia (8%-‐1.4% prevalence) and Ukraine (0.8% prevalence) face the
largest problems* • Some of the countries in the region and pracAcally invisible to surveillance • Late presenters: “55% saAsfied the widest definiAon of being a late
presenter between the years 2002 and 2005: by 2008 to 2010, this had reduced to 48%. The proporAon with CD4 counts under 200 cells/mm3 had shrunk from 34 to 27% and who had AIDS upon diagnosis from 16 to 12%.”** (BUT excluding Russia and a few other countries.)
• Prevalence in Sub-‐Saharan Africa dropped from 5.8% to 5% between 2005 and 2011*
• * h=p://www.avert.org/hiv-‐aids-‐russia-‐eastern-‐europe-‐central-‐asia.htm • ** h=p://www.aidsmap.com/Late-‐tesAng-‐rates-‐declining-‐in-‐Europe-‐but-‐largely-‐in-‐gay-‐men/page/2783456/
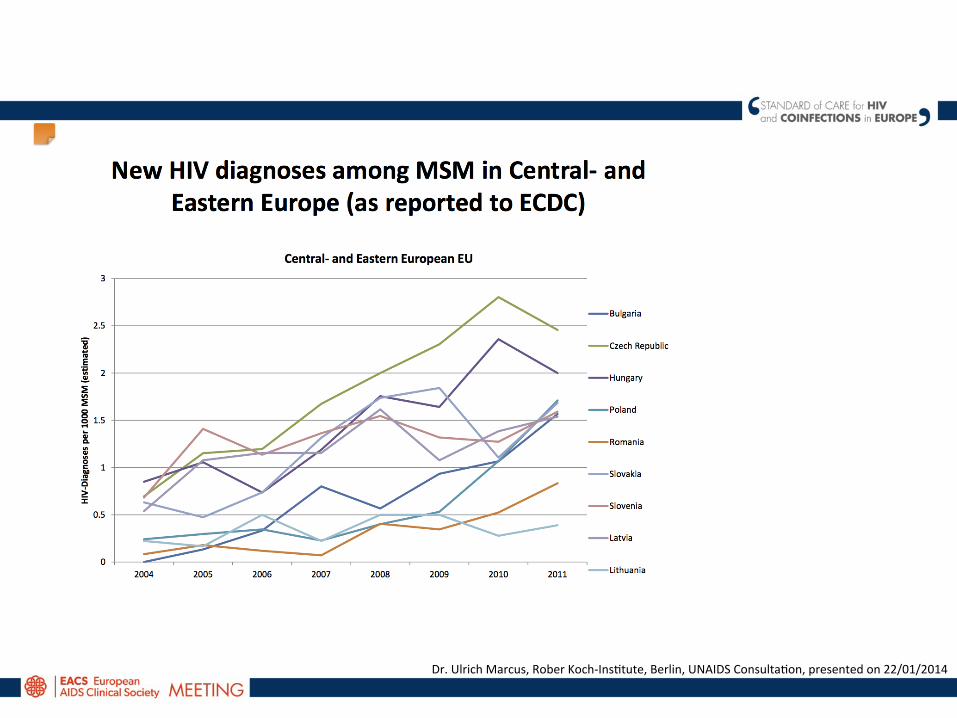
Dr. Ulrich Marcus, Rober Koch-‐InsAtute, Berlin, UNAIDS ConsultaAon, presented on 22/01/2014
Specific problems
• MedicalisaAon of tesAng • PoliAcal climate/disincenAve • SAgma and discriminaAon • Unawareness of “the big picture”, and synergisAc epidemics
• Lack of informaAon • Lack of civil society acAvity • Low prevalence – low interest • Economic/financial hardship
The ECDC categories
• Barriers on an individual level – Low percepAon of risk (general populaAon) – Fear (of death, sAgma, discriminaAon, rejecAon – Lack of informaAon (about health and health care) – ConfidenAality
• Barriers at the healthcare provider level – Lack of and gaps in knowledge – DiscriminaAon against PLH – Lack of money and Ame – CorrupAon
• Barriers at the ins+tu+onal level – CorrupAon – Lack of policies – PoliAcal pressure – Low prevalence – li=le a=enAon – Lack of capaciAes – Very weak NGO sector
h=p://ecdc.europa.eu/en/publicaAons/PublicaAons/101129_TER_HIV_tesAng_evidence.pdf
Community based tes+ng? – Not yet!
• “The main barrier in Lithuania is that rapid HIV test can be performed only in medical insAtuAons. It is because rapid tests need capillary blood and it can be taken by perforaAng the skin. All procedures with perforaAng the skin belong to medical manipulaAons in special premises, etc. And discussions to reduce the threshold for rapid HIV test for risk groups All now was unsuccessful. And we need to use different cooperaAon models with friendly medical insAtuAons for IDUs, MSM tesAng.” (Loreta Stoneiné, HIV acAvist)
• “June 2013, WHO published the ‘Clinical guidelines for HIV diagnosis and ARV drugs for HIV prevenAon’. This doc provides a summary of exisAng and new evidence-‐based clinical recommendaAons outlining a public health approach to diagnosing HIV infecAon with a focus on seqngs with limited health system capacity and resources. The use of rapid HIV diagnosAc tests using blood from a finger-‐prick sample taken by trained lay counselors and community health workers has facilitated the expansion of HIV tesAng and counseling in community seqngs including homes, transport staAons, religious faciliAes, schools, universiAes, workplaces and venues frequented by key populaAons. (CrisAna Torró, HIV policy acAvist)

Legal barriers to conduct rapid tests in Europe and Central Asia
Community survey
Overcoming the barriers
• Mass media campaigns can have an impact on tesAng behavior in the short term. • Reducing sAgma around HIV tesAng and diagnosis can be addressed at the
insAtuAonal level through ‘normalizaAon’ of the tesAng procedure and the introducAon of a universal offer of tesAng.
• Training healthcare providers can effecAvely increase HIV tesAng rates and improve healthcare providers’ aqtudes towards HIV and confidence in conducAng a test.
• Wri=en informed consent has been idenAfied as a barrier to tesAng, and verbal informed consent is acceptable alternaAve and results in higher tesAng uptake.
• Brief post-‐test informaAon may be given to those tesAng negaAve in place of counseling in innovaAve ways.
• Raise awareness of HIV and moAvaAon to test. • OpAmal frequency of tesAng. • Ensuring access to care and follow up ater HIV diagnosis. • TesAng approaches by seqng – local strategies work be=er • Community based tesAng should be part of an overall, reasonable tesAng strategy
h=p://ecdc.europa.eu/en/publicaAons/PublicaAons/101129_TER_HIV_tesAng_evidence.pdf
What can be done?
• Set more realisAc objecAves • Raise awareness • Local approaches instead of exporAng models from the West
• EducaAon and empowerment of the local PLH communiAes In order to retain people in the cascade of care, you need to establish the cascade of
care first.
Copyright © 2022 FDOKUMEN