What's in a Name: Exposing Gender Bias in Student Ratings of Teaching
Ethics of Asking Trauma-Related Questionsand Exposing Participants
to Arousal-Inducing Stimuli
Robin M. Carter-Visscher, MAAmy E. Naugle, PhDKathryn M. Bell, MA
Michael K. Suvak, MA
ABSTRACT. This study examined ethical concerns related to exposingparticipants with childhood victimization histories to both trauma-spe-cific and non-trauma-specific stimuli. We asked participants questionsabout childhood victimization experiences and exposed participants to anegatively-arousing experimental condition. Following each of theseprocedures and at a one-week follow-up session, participants completeda measure designed to asses their reactions to participation. The measureincluded several questions to assess reactions including questions aboutdistress, benefit, and willingness to participate in the study again. Over-all, participants reported low levels of distress and described their partic-ipation experience as interesting, enjoyable, and somewhat beneficial.Participants also indicated that they would be willing to participate in thestudy again with the knowledge of what participation was actually like.
Robin M. Carter-Visscher, Amy E. Naugle, and Kathryn M. Bell are affiliated withthe Department of Psychology, Western Michigan University, Kalamazoo, MI. Mi-chael K. Suvak is affiliated with the Department of Psychology, Boston University,Boston, MA.
Address correspondence to: Amy E. Naugle, Department of Psychology, 1903 WestMichigan Avenue, Western Michigan University, Kalamazoo, MI 49008-5439(E-mail: [email protected]).
Portions of these data were presented at the 2004 annual meeting of the Associationfor the Advancement of Behavior Therapy.
Journal of Trauma & Dissociation, Vol. 8(3) 2007Available online at http://jtd.haworthpress.com
© 2007 by The Haworth Press, Inc. All rights reserved.doi:10.1300/J229v08n03_03 27

Participants with childhood trauma histories and PTSD symptoms re-ported more distress during the childhood maltreatment screening com-pared to other participants. However, the level of distress theyexperienced was mild and transitory. Our findings add to the emergingdata indicating that individuals find their participation in trauma-relatedresearch to be a positive experience overall, rather than a harmful one.doi:10.1300/J229v08n03_03 [Article copies available for a fee from TheHaworth Document Delivery Service: 1-800-HAWORTH. E-mail address:<[email protected]> Website: <http://www.HaworthPress.com>© 2007 by The Haworth Press, Inc. All rights reserved.]
KEYWORDS. Trauma research, ethics, human subjects, childhood,abuse, maltreatment, participant reaction
Research in the area of trauma has proliferated over the past two de-cades and has advanced our knowledge regarding the impact thattrauma exposure can have on survivors. Furthermore, it has called intoquestion the ethical implications of conducting research with individu-als who have experienced horrific events, particularly when the re-search focuses specifically on the impact of those events. Although bothfederal regulations and ethical codes, guided by the principles of theBelmont Report (National Commission for the Protection of HumanSubjects of Biomedical and Behavioral Research, 1979), have been putforth to protect research participants, researchers had not empirically in-vestigated the ethical implications of conducting trauma-related re-search until recent years. Ethical concerns of trauma research include(1) whether participants with trauma histories are a particularly vulnera-ble population, (2) whether participants can fully provide informedconsent, and (3) what unique risks and benefits may be related to partic-ipation. In the absence of objective data, Institutional Review Boards(IRBs) and researchers have historically made decisions about the eth-ics of research protocols based upon subjective data, personal opinionand speculation about the potential risks of conducting research with aspecific population. Such a strategy leaves room for assumptions andbiases to influence decisions about measures researchers are asked tomake regarding protection of participants. In recent years, researchershave made strides to empirically investigate ethical implications oftrauma research, specifically with respect to potential risks associatedwith research participation.
28 JOURNAL OF TRAUMA & DISSOCIATION

The issue of participant vulnerability relates to all three basic ethicalprinciples outlined in the Belmont Report, which include (1) respect forpersons, (2) beneficence, and (3) justice and should, therefore, be exam-ined by researchers. As Levine (2004) notes, no legal definition of vul-nerability exists to guide the decision making process. Rather, theBelmont Report lists children, prisoners, pregnant women, fetuses, andneonates as “particularly vulnerable populations.” IRBs and investiga-tors have been left to judge whether populations other than those listedshould be considered vulnerable and if so, in what unique ways theyshould be protected. Some have questioned whether research partici-pants who have been exposed to traumatic events constitute a vulnera-ble population. When reviewing the literature examining consequencesof childhood maltreatment on adult survivors, one can readily under-stand why the emotional vulnerability of this trauma-exposed popu-lation has been questioned. Research indicates that childhoodmaltreatment is related to low self-esteem, substance abuse, sexual vic-timization, dissociation, posttraumatic stress disorder (PTSD), depres-sion, and borderline personality disorder, among other problems (Gold,1986; Lang, Stein, Kennedy, & Foy, 2004; Malinosky-Rummell &Hansen, 1993; Sanders & Moore, 1999). Based upon Levine’s observa-tion that “the concept of vulnerability is an extraordinarily elastic con-cept, capable of being stretched to cover almost any person, group, orsituation, and then of being snapped back to describe a narrow range ofcharacteristics” (p. 398), individuals exposed to trauma may be consid-ered vulnerable. However, depending upon how one defines vulnerabil-ity, almost anyone could be considered vulnerable, which leaves theconcept of vulnerability nearly meaningless (Levine, 2004). Ratherthan basing decisions regarding the ethical implications of a particularresearch protocol upon opinions and subjective judgment, researchmust be conducted to provide objective data to guide these decisions.
The ability of participants to provide fully informed consent is re-lated to the basic ethical principle of respect for persons and has beenstudied in trauma-exposed populations. One way to investigate whetherparticipants were fully informed about the study when they gave theirconsent to participate is to retrospectively examine whether individualsunderestimated the level of upset they would experience given the de-scription of the research protocol, and whether they regret participatingwith knowledge of what the experience of participating was actuallylike. Walker, Newman, Koss, and Bernstein (1997) examined thesequestions with 500 women enrolled in an HMO who answered ques-tions regarding their childhood victimization experiences and found
Carter-Visscher et al. 29

most women to report the research experience as positive. Only 13% ofthe participants found the experience more upsetting than they had ex-pected and 1% of these women stated that they would not have partici-pated in the study had they known in advance how they would feelwhile completing the survey. In all, 76% reported that they would stillparticipate and only 5% regretted completing the survey. Another studyexamined these questions with 1,174 women enrolled in an HMO whowere administered a trauma-focused health survey in either question-naire or interview format (Newman, Walker, & Gefland, 1999). Thisstudy found 5% of participants responding to the survey in question-naire format to regret participation and only one participant respondingusing the interview format to regret participation. After 48 hours, noparticipants reported regret and nearly three-quarters of the sample en-dorsed benefit. Although the mean levels of upset for all groups werelow, significantly higher levels of PTSD symptomatology were re-ported for women experiencing unexpected upset compared to thosewho did not report this. Unexpected upset was also reported most fre-quently by women with sexual maltreatment histories followed bywomen with nonsexual maltreatment histories. Only 10.5% of the par-ticipants completing the questionnaire reported unexpected upset andonly 1% of these participants reported regret. Nineteen percent of par-ticipants completing the interview reported unexpected upset and onlyone participant reported regret. The authors of both studies concludethat these results suggest that, overall, the informed consent proceduresused were adequate, and most trauma survivors appear capable ofanticipating the level of risk involved such that participants do not feelcoerced into participation.
The assessment of risks and benefits of research participation is an-other example of the application of the general ethical principles to theconduct of research. Researchers have examined risks and benefits intrauma research in recent years. Investigations of the ethical implica-tions of trauma research suggest that although participants may experi-ence emotional discomfort or distress while responding to questionsabout their traumas, most report a positive reaction toward participa-tion. A study examining distress associated with asking Vietnam veter-ans with PTSD to recall details of their trauma found that 75% ofparticipants with current PTSD reported experiencing distress follow-ing the interview compared to 20% of participants with no PTSD his-tory (Parslow, Jorm, O’Toole, Marshall, & Grayson, 2000). However,participants’ level of distress was neither associated with withdrawalfrom the study nor with increased medical service usage. Additionally,
30 JOURNAL OF TRAUMA & DISSOCIATION

no long-term negative effects of participation were reported. While par-ticipants attributed their level of distress to the interview, the authorsstate that they cannot conclude that the interview caused distress sinceno control condition was incorporated to measure distress outside theinterview.
DePrince and Freyd (2006) investigated how the experience of par-ticipating in trauma research compares to distress experienced inday-to-day life by asking 528 undergraduate and community partici-pants to compare the level of distress experienced while completing aself-report trauma survey to distress experienced in everyday life. Fewparticipants (37%) rated the experience of completing the questionnaireas more distressing than other experiences of day-to-day life. Of theseparticipants, 99% rated the importance and goodness of the research asoutweighing the relative distress. Cromer, Freyd, Binder, DePrince, andBecker-Blease (in press) examined participants’ reactions to beingasked personal questions that were not trauma-related (e.g., GPA andSAT scores, body image, sexual orientation) compared to their reac-tions to being asked questions about trauma histories. Participants re-ported that answering questions about trauma was not more distressingthan answering other personal questions. Further, participants rated thetrauma-related questions as more important and beneficial to askcompared to the other personal questions.
Although participants may experience some level of distress whenanswering questions regarding traumatic experiences, many partici-pants report that their participation in trauma research benefited them insome way (Brabin & Berah, 1995; Griffin, Resick, Waldrop, & Me-chanic, 2003; Ruzek & Zatzick, 2000). Carlson, Newman, Daniels,Armstrong, Roth, and Loewenstein (2003) examined the degree of dis-tress and usefulness psychiatric inpatients perceived when asked ques-tions regarding PTSD symptoms and childhood abuse. Seventy percentof participants reported low levels of distress and 51% reported the in-terview as useful. These results indicate that even participants with highdegrees of psychological distress, a population that would likely be con-sidered quite vulnerable, report a stable cost/benefit ratio in response toparticipating in trauma research.
Investigators have used a variety of procedures to examine the effectsof trauma (Newman & Kaloupek, 2004). However, most research onthe ethics of trauma-related research has not examined the use of proce-dures other than those that ask participants to answer questions abouttheir past traumatic experiences. As Levine (2004) suggests, research-ers need to explore the ethics of implementing procedures that differ
Carter-Visscher et al. 31

from those already investigated because these protocols have uncertainrisk-benefit ratios. In addition, these protocols should be examinedmore rigorously in order to maximize benefits and minimize risks. Thecurrent study examines the ethics of exposing participants with child-hood maltreatment histories to two different research procedures. Thefirst procedure asked participants to answer questions about their trau-matic childhood experiences, and the second procedure exposed partici-pants to an arousal-inducing experimental condition using stimuliunrelated to participants’ childhood maltreatment histories. Past re-search has not examined the ethics of exposing participants with traumahistories to physiologically arousing stimuli that are not related to thetype of trauma participants experienced, a procedure that would likelyact as a red flag for IRBs. Moreover, research has not examined theeffects of participating in a project that includes both types ofmethodologies.
PRIMARY RESEARCH PROJECT
This investigation was conducted as follow-up research to a study in-vestigating the relationship between childhood interpersonal victimiza-tion experiences and facial recognition skills under an arousal-inducingexperimental procedure. The following provides information regardingthe primary research project in order to clarify the methodology of thecurrent study. The primary research project consisted of a screeningsession (Session 1), an experimental session (Session 2), and a one-week follow-up session (Session 3). For the purpose of this study, par-ticipants completed a follow-up measure assessing their reactions toparticipation at the end of each session. All sessions were conductedindividually.
Session 1 screened participants for childhood victimization histories.Participants meeting childhood physical abuse only, sexual abuse only,combined physical and sexual abuse, dysfunctional family environmentand no abuse/maltreatment histories met inclusion criteria for the exper-imental session. However, in order to prevent more participants fromcompleting the experimental session than were needed to complete thestudy, participants were screened out as the groups were filled, per IRBguidelines. Therefore, all participants completed Session 1 while fewerparticipants completed Sessions 2 and 3. Potential participants were ex-cluded from the primary study if they were under the age of 18 or male.Exclusion criteria also included factors related to abuse perpetration
32 JOURNAL OF TRAUMA & DISSOCIATION

and victimization such as reporting that they were the perpetrator ofphysical and/or sexual abuse before the age of 14, experiencing abuseby a peer less than 5 years older than the participant (e.g., extreme bully-ing), and/or experiencing emotional abuse/neglect by non-family mem-bers (e.g., babysitters) and they did not meet the criteria for childhoodphysical and or sexual abuse. Finally, participants were excluded if thegroup they qualified for was closed to new recruits because it had beenfilled.
All participants completed the Childhood Trauma Questionnaire(CTQ; Bernstein et al., 1994) and Personal Data Survey (PDS; Naugle,1999) during Session 1 to gather childhood abuse and demographic in-formation. For privacy, the researcher stepped out of the room while theparticipant completed the measures. The researcher scored the CTQwhile the participant completed the PDS. If participants met initial in-clusion criteria for the experimental group based upon the CTQ mea-sure, the researcher asked the participant to complete the ChildhoodMaltreatment Interview Schedule (CMIS; Briere, 1992) to providemore information about the childhood experiences reported on theCTQ. This information was used to make further decisions about whichgroups the participants qualified for and which participants met the ex-clusion criteria. (See Measures for psychometric data.)
Session 2 exposed participants to the experimental procedure. Theinvestigators used JACFEE and JACNeuF slides (Matsumoto &Ekman, 1988), presented as part of a computer program, as stimuli forthe experimental procedure. These slides consist of photographs of in-dividuals displaying a variety of emotions including surprise, disgust,anger, happiness, sadness, fear, contempt, and neutral expressions.While the package includes Caucasian and Japanese models, only Cau-casian ones were included in this study because the majority of partici-pants and individuals in this region share this ethnicity. Photographs ofboth males and females were included in the study. JACFEE slides havedemonstrated strong internal consistency (alpha = .94) and concurrentvalidity with the Diagnostic Analysis of Nonverbal Accuracy (DANV;McIntire, Danforth, & Schneider, 1999; Nowicki & Duke, 1994). Ques-tions developed for the primary study, which measured participants’ re-actions to the facial expressions (i.e., how they would label the facialexpressions, their confidence in the label they provided, their behav-ioral responses to the facial expressions, and their desire to change theirreaction to each photograph), followed the presentation of each photo-graph. The Self Assessment Manikin (SAM; Bradley & Lang, 1994)was presented after every 3-4 facial expression photographs to assess
Carter-Visscher et al. 33

participants current valence and arousal levels with regard to the facialstimuli. Finally, unpleasant, arousal-inducing visual and auditory stim-uli designed to elicit affective responses at varying degrees of arousal,were dispersed throughout the program to sustain participants’ in-creased level of arousal throughout the experimental procedure. Pic-tures and sounds were selected from the International Affective PictureSystem (IAPS; Center for the Study of Emotion and Attention[CSEA-NIMH], 1999) and International Affective Digitized SoundsSystem (IADS; Bradley & Lang, 2000) for arousal-inducing stimuli.Seven negatively valenced, high arousal pictures (e.g., mutilated bod-ies, guns, burn victims), four positively valenced, high arousal pictures(e.g., sexually arousing), and three IADS sounds (i.e., car crash, alarm,and siren) were included. While these stimuli may be related to sometrauma-specific experiences, stimuli related to childhood interpersonalvictimization experiences were not included in this study. Physiologicalarousal was monitored using a heart rate monitor throughout theexperimental session.
Participants completed preparatory steps before beginning the exper-iment, which included putting on a heart monitor and completing apractice trial of the computer program to familiarize them with the ex-perimental procedure. They also completed seven questionnaires in-cluding the Modified PTSD Symptom Scale (MPSS-SR; Falsetti,Resnick, Resick, & Kilpatrick, 1993). Participants then engaged in theexperimental portion of the primary research project. After completingthe experimental computer program, participants removed the heart ratemonitor and were asked to stay in the laboratory for at least ten minutesto engage in a relaxing activity (e.g., looking at magazines, listening torelaxing music, viewing a presentation of pleasant pictures from theIAPS package) before leaving. Session 3 checked participants for theirreactions to participation one week after they engaged in the experimen-tal procedure. Participants attended this session to complete thefollow-up measure for a final time.
METHOD
Participants
Of the 203 female undergraduate students recruited to participate inthe primary research project, 79 completed all three sessions. Only theparticipants that completed all three sessions are included in the analy-
34 JOURNAL OF TRAUMA & DISSOCIATION

ses for this study. These participants ranged in age from 18 to 44 years(M = 20.7, SD = 4.1) and were primarily Caucasian (86%) with a smallproportion of African Americans (6%), Asians (3%) and other ethnicgroups (5%). The mean score on the CTQ was 40.2 (SD = 12.2). The to-tal mean MPSS-SR score was 19.4 (SD = 21.1) with mean PTSD symp-tom severity of 11 (SD = 12.9) and frequency of 8.6 (SD = 8.8).Participants whose course instructors offered extra credit for researchparticipation received extra credit while others chose to participatewithout compensation.
Measures
Follow-Up Questionnaire. For the purposes of this study, we devel-oped a follow-up questionnaire to assess a variety of reactions to partici-pation. Most items on the questionnaire consisted of items used inprevious research on the ethics of trauma-related research. Items mea-suring interest, difficulty, emotional reaction, and willingness to partici-pate again were modified versions of questions used by Griffin et al.(2003). Items measuring upset, benefit, and inconvenience were alsobased upon items used in past research (Walker et al., 1997; Newman etal., 1999; Ruzek & Zatzick, 2000). We also included items measuringthe level of bother and enjoyment reported by participants. In additionto providing a rating for bother and benefit, participants had the optionof answering open-ended questions to provide data about what wasbothersome and beneficial.
We were interested in examining participants’ reactions about thepositive and negative aspects of participating in this trauma-related re-search in addition to how willing these participants would be to partici-pate again with the knowledge of what participation was actually like.In order to create variables to be included in the final analyses, we statis-tically examined the relationship among follow-up items. Since therewere not enough data to run confirmatory factor analyses, we conductedinter-item correlations among all of the follow-up scaled items andmade statistical decisions to determine if certain follow-up items couldbe combined into specific composite scores measuring a single con-struct. We used George and Mallery’s (2003) guidelines for determin-ing the acceptability of the alpha values, and Gleim and Gliem’s (2003)recommendation of using Cronbach’s alpha of .8 as a reasonable goalfor a scale. A distress composite score was created by summing togetherthe follow-up items with an overall Cronbach’s alpha � .80. Distresscomposite scores for each participant were recoded into z-scores to con-
Carter-Visscher et al. 35
trol for scaling differences in the individual follow-up items. Thedistress composite included the following items:
1. Right now, rate how upsetting participating in this study has beenfor you (1 = not at all upsetting, 6 = very upsetting).
2. Right now, rate how difficult participating in this study has beenfor you (1 = not at all difficult, 6 = very difficult).
3. Right now, rate how bothered you are by thoughts about aspectsof this study (1 = not at all bothered, 6 = very bothered)
4. Right now, rate your emotional reactions to participating in thisstudy (1 = did not experience any feelings, 2 = felt minimal feel-ings, 3 = some feelings but not strong, 4 = some strong feelings,5 = felt very strong feelings).
The items referring to positive aspects of the study (i.e., interest, bene-fit, and enjoyment) did not have good internal consistency (Cronbach’salpha < .8) across sessions. Therefore, we chose to use single follow-upitems to examine the outcome variables of benefit and willingness toparticipate again. The following items measured these variables:
1. Right now, rate how beneficial it has been for you to participate inthis study (1 = not at all beneficial, 6 = very beneficial).
2. Right now, knowing what you do about this study, rate how will-ing you would be to participate again (1 = definitely not willing,2 = don’t think I am willing, 3 = might be willing, 4 = quite will-ing).
Personal Data Survey (PDS). The PDS is a self-report inventory de-signed to gather standard demographic information such as age, ethnic-ity, relationship status, and current dating and sexual practices (Naugle,1999). The PDS also includes questions from Wyatt Sexual HistoryQuestionnaire (Wyatt, 1985; Wyatt & Newcomb, 1990), the Sexual Ex-periences Survey (Koss & Oros, 1982) and National Women’s StudyVictimization Screening (Resnick, Kilpatrick, Dansky, Saunders, &Best, 1993) regarding the participants’ sexual experiences prior to andafter the age of 14.
Childhood Trauma Questionnaire (CTQ). The CTQ was used to ex-amine participants’ histories of childhood abuse and neglect using fourfactors identified to assess physical and emotional abuse, sexual abuse,physical neglect, and emotional neglect. The CTQ (Bernstein et al.,1994) is a 28-item, self-report screening tool that has participants rate
36 JOURNAL OF TRAUMA & DISSOCIATION

the frequency with which certain events occurred throughout theirchildhood using a 5-point Likert scale ranging from “never true” to“very often true.” The measure has demonstrated high internal consis-tency for each of the four factors, with Cronbach’s alphas ranging from.79 to .94, and good test-retest reliability across 2- and 6-month periodsfor each of the factors and for the total CTQ score, with correlationsranging from .80 to .88. The CTQ has also demonstrated good conver-gent and discriminant validity.
Childhood Maltreatment Interview Schedule (CMIS). The CMIS(Briere, 1992) is a retrospective, semi-structured interview designed toassess childhood maltreatment in both clinical and research settings.The interview includes nine sections assessing parental physical avail-ability, parental disorders, parental psychological availability, psycho-logical abuse, physical abuse, emotional abuse, sexual abuse, ritualisticabuse, and perceptions of abuse status. Eight sections of the CMIS wereused to obtain more detailed information regarding the type(s) of abuseexperienced, perpetrator(s) involved, age(s) at which participants expe-rienced abuse, and injuries obtained as result of abuse. The section as-sessing ritualistic abuse was not included in this study due to the lack ofempirical evidence supporting this construct (Ellis, 2000; McGrath,2002; Sherman, 1997). Information from the CMIS was used alongwith CTQ data to make decisions about which groups participantsshould be placed in, according to their childhood maltreatmenthistories, for the primary research project. Group data were not used forthe current study.
Modified PTSD Symptom Scale (MPSS-SR). The MPSS-SR (Falsettiet al., 1993) is a two-part scale that allows for a more continuous mea-surement of PTSD symptoms by using a cutoff score that can be used toindicate whether an individual is PTSD positive. The first part of thescale includes 17 items to assess PTSD criterion A, based onDSM-III-R diagnostic criteria, to measure the degree to which partici-pants have been exposed to traumatic events. The second part of thescale includes 17 items to assess whether or not individuals meet PTSDcriteria B through D over the two-week period prior to assessment. Thispart of the MPSS-SR uses frequency and severity measurements ofPTSD symptoms and is an extension of the PTSD Symptom Scale(PSS; Foa, Riggs, Dancu, & Rothbaum, 1993). The scale has beennormed on both clinical and community samples and has demonstratedstrong internal consistency for both samples, with alphas of .96 and .97,respectively. This measure also has demonstrated good concurrent va-lidity with the SCID PTSD Module. We used data from the MPSS-SR
Carter-Visscher et al. 37

to investigate whether PTSD symptomatology affects participants’responses to follow-up questions across Sessions 1, 2, and 3.
Procedures
We obtained data on the ethics of exposing participants with child-hood interpersonal victimization histories to procedures directly relatedto personal trauma experiences and to an arousal-inducing procedureunrelated to individual trauma experiences by asking participants to re-spond to follow-up questions about their experiences participating inthe primary research project. Participants were asked to complete thefollow-up questionnaire on three separate occasions during the study:(1) following the childhood victimization screening, (2) following theexperimental procedure, and (3) at a one-week follow-up. Each time thefollow-up measure was administered, participants were asked to com-plete it with regard to their current reactions to participating in thestudy. All procedures were conducted in accordance with IRB guide-lines.
Participants were recruited through oral recruitment conducted inclasses and recruitment flyers posted throughout campus. Both recruit-ment strategies stated that the study examines how individuals with dif-ferent types of childhood experiences react to and interpret facialexpressions under arousal-inducing situations. Students interested inparticipating contacted us via telephone or e-mail and scheduled anappointment for the first session.
During the first session, we informed participants about the details ofthe study. Each participant then provided written consent to participate.Participants completed the childhood victimization screening proce-dures, explained above. Participants that did not complete the CMISwere excluded from this study. Therefore, all participants in this studycompleted the same screening procedures, which included the CTQ,PDS, and CMIS. Participants then completed the follow-up question-naire. At the conclusion of the first session, all participants received areferral list containing information regarding local psychological ser-vices and a booklet providing tips for safe dating practices. Participantsalso provided their contact information and scheduled a tentative ap-pointment for either the experimental or final follow-up session, de-pending upon whether or not they met the inclusion criteria for theexperimental segment of the study. During Session 2, participants com-pleted the experimental procedure and the follow-up questionnaire. Be-fore leaving, participants scheduled a follow-up appointment for the
38 JOURNAL OF TRAUMA & DISSOCIATION

following week. Those that returned completed the follow-up question-naire for a third time in order to examine reactions to participation oneweek after completing the experiment.
Doctoral-level student therapists acted as research assistants duringthe first session and the primary investigator of the study, also trained asa doctoral-level student therapist, was available during all sessions. Wereminded participants during each session that they could discontinueparticipation at any time without repercussion. A specific protocol wasin place to manage participants’ distress should that become necessary.Two participants ended Session 2 prematurely. One of these partici-pants had a childhood victimization history while the other did not.Both participants stayed and completed the relaxation phase until theyreported that they were comfortable enough to go home. Before leaving,the investigator of the primary research project met with them to assesstheir emotional status and to determine whether further interventionwas needed. Further intervention was not needed in either case. Bothparticipants were reminded of the referral list for psychological servicesthat they received during Session 1 and were offered an additional copy.Both participants attended the follow-up session and their emotionalstatus was again assessed at this time. Both reported no lasting negativeeffects from their research experience. We excluded these participants’data from this study, as they did not fully complete Session 2.
Statistical Analysis Procedure
We plotted the follow-up questionnaire data for each session to testfor potential skewness and outliers prior to conducting analyses. Asdata were not found to be moderately to severely skewed, non-trans-formed data were retained for the following analyses.
Change across sessions and its relationship to childhood trauma andPTSD scores in the distress, beneficial, and willingness to participateoutcome variables was examined from a multilevel regression frame-work using the HLM 6 software package (Raudenbush, Bryk, Cheong,& Congdon, 2004). This approach to analyzing longitudinal data is be-ing increasingly utilized because of its numerous advantages over moretraditional techniques such as ordinary least squares (OLS) regressionand repeated measure analysis of variance (ANOVA). These advan-tages include handling missing observations and unbalanced designsmore efficiently (i.e., does not require listwise deletion of individualswho are missing one repeated measures observation), producing moreefficient estimates and more powerful tests, and increased flexibility al-
Carter-Visscher et al. 39

lowing for the inclusion of both fixed and time-varying, continuous andcategorical predictors and outcomes (see Singer & Willett, 2003). Forthe current analyses, session status (i.e., Session 1, 2, or 3) was includedby using dummy coded variables producing statistical models analo-gous to repeated measures analyses of variance that include the advan-tages of a multilevel regression framework.
Interaction (product) terms were computed between moderator vari-ables (i.e., history of childhood abuse and PTSD symptoms) anddummy coded session variables. As recommended by Cohen, Cohen,West and Aiken (2003), the moderator variables were mean centeredbefore the computation of the interaction terms. The interaction termswere (separately) entered into the level-two component of the modelalong with variables assessing the main effects of session condition(i.e., dummy coded variables) and the moderator variable. To assess thesignificance of three-way interactions, the goodness of fit of each modelwith main effects and two-way interactions was compared to the modelwith main effects, two-way interactions, and three-way interactionterms. Full maximum likelihood estimation was used, and a significantimprovement in model fit (as assessed by the change in the deviance[Δdev] statistic that has an approximate chi-square distribution with thedegrees of freedom equal to the difference in parameters estimated inthe two models) was used to determine the presence of significantthree-way interactions (Raudenbush & Bryk, 2002).
RESULTS
Follow-Up Descriptive Data
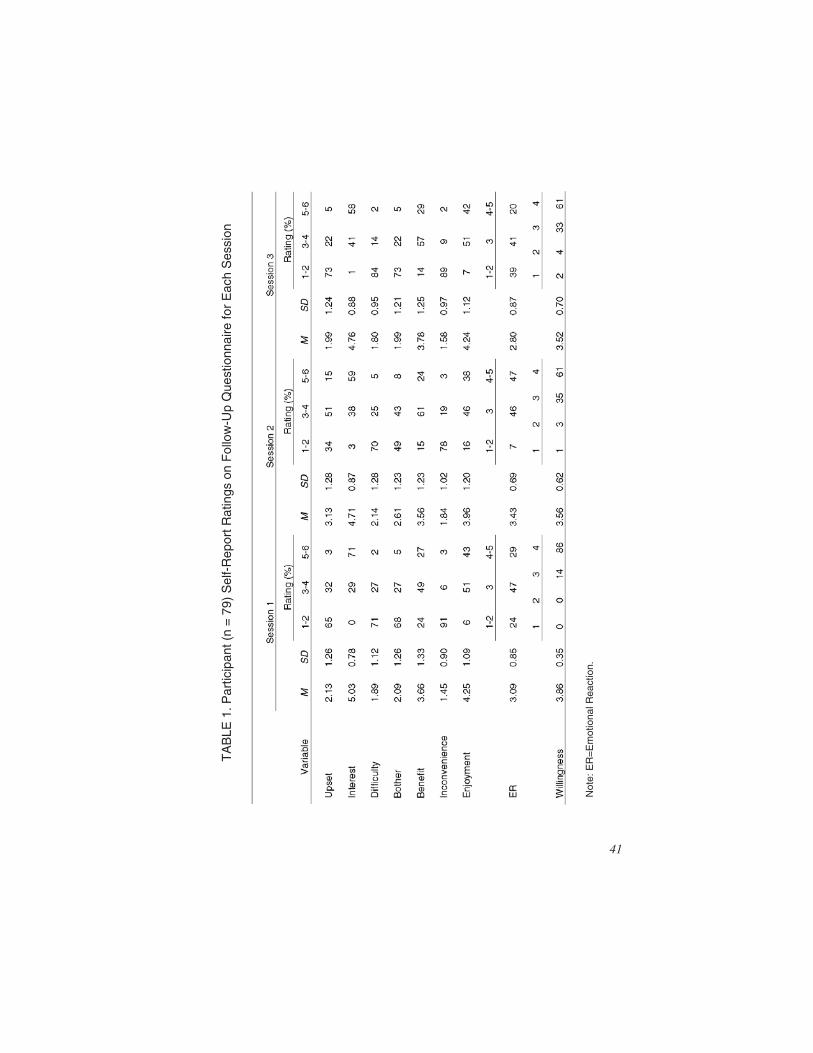
Table 1 provides overall mean, standard deviation, and frequencydata for participants’ ratings of the follow-up items for each session.Mean ratings of three on all 6-point scales indicate responses of “some-what” with regard to the given outcome variable. Upset at Session 2 hada mean rating of 3.13 while all other ratings for upset, difficulty, andbother had ratings of less than three. Most participants’ reported theiremotional reaction to participating in the study as experiencing somefeelings, but not strong ones, as indicated by means of about three foreach of the sessions. Participants also indicated that their experienceswith the study were positive overall. Mean ratings for interest, benefit,and enjoyment were above three for each session. In addition, 100% of
40 JOURNAL OF TRAUMA & DISSOCIATION
TA
BLE
1.P
artic
ipan
t(n
=79
)S
elf-
Rep
ortR
atin
gson
Fol
low
-Up
Que
stio
nnai
refo
rE
ach
Ses
sion
Not
e:E
R=
Em
otio
nalR
eact
ion.
41

the participants rated Session 1 as somewhat interesting or more andover 95% rated Sessions 2 and 3 that way. Over 75% rated all three ses-sions as somewhat beneficial and enjoyable or more. Finally, no partici-pants stated that they would be unwilling to participate again followingSession 1 while only 4% and 6% stated that they would be unwillingafter Sessions 2 and 3, respectively.
Level One–Change Across Sessions
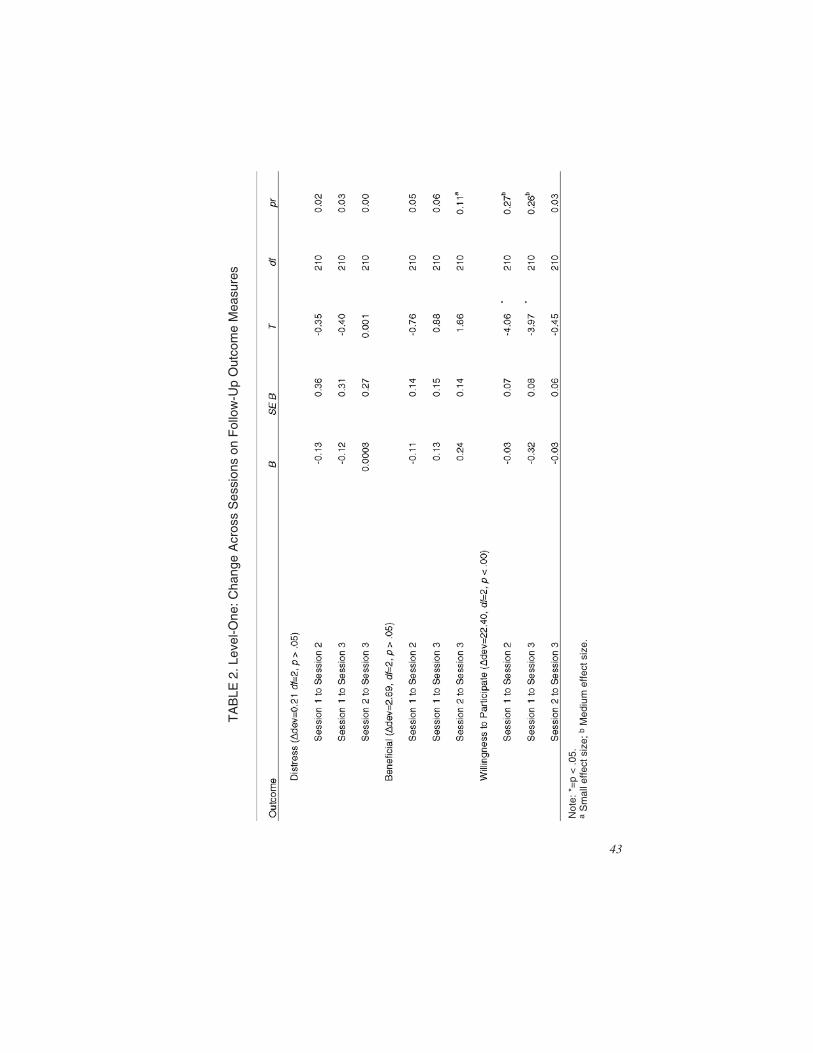
To examine initial status and change over time of the outcome vari-ables across the three sessions, we entered session status as a level-onepredictor variable with no level-two variables in the model. Table 2 pro-vides a summary of the level-one analyses examining Change AcrossSessions on the three follow-up outcome variables, including estimatedeffect sizes based on criteria defined by Kirk (1996). Change AcrossSessions was not statistically significant for the Distress or Beneficialoutcome variables (Δdev = 0.21, df = 2, p > .05; Δdev = 2.69, df = 2, p >.05). Change Across Sessions was statistically significant for the Will-ingness to Participate outcome variable, Δdev = 22.40, df = 2, p < .00.Willingness to participate significantly decreased from both Session 1to Session 2 and from Session 1 to Session 3 (B = �.03, p < .05; B =�.32, p < .05, respectively) while Willingness to Participate reported atSession 2 did not significantly differ from Willingness reported at Ses-sion 3 (B = �.03, p > .05).
Two-Way Interactions
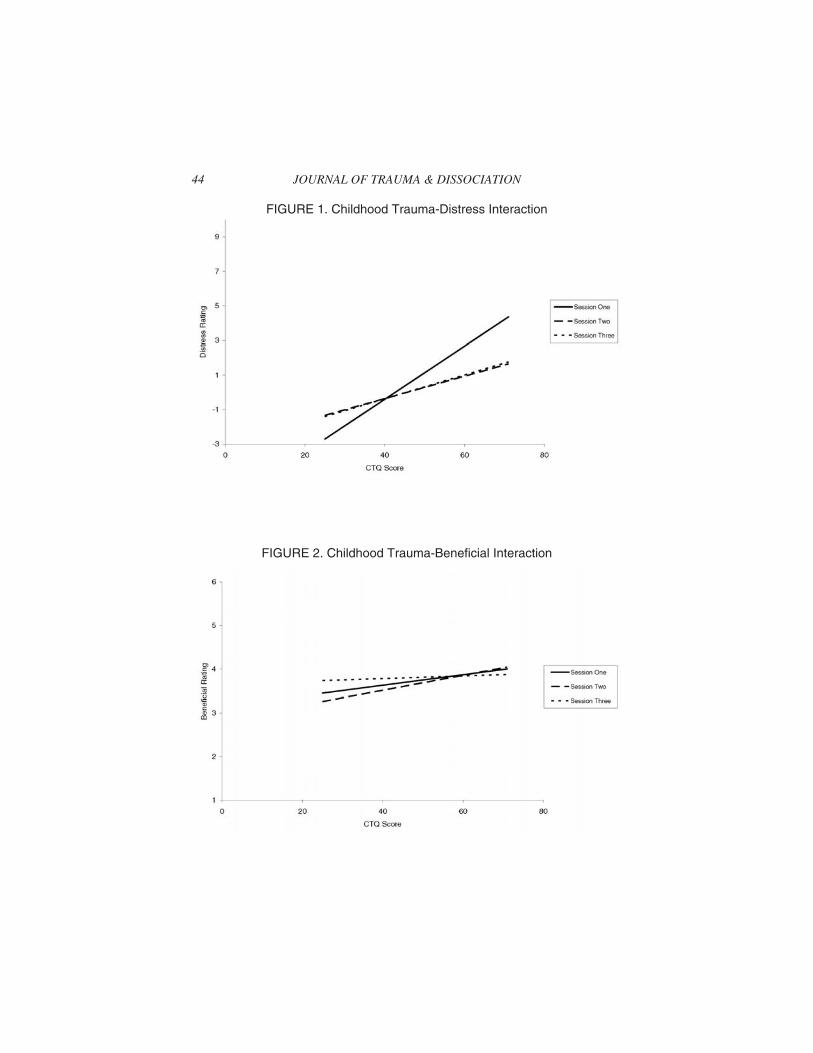
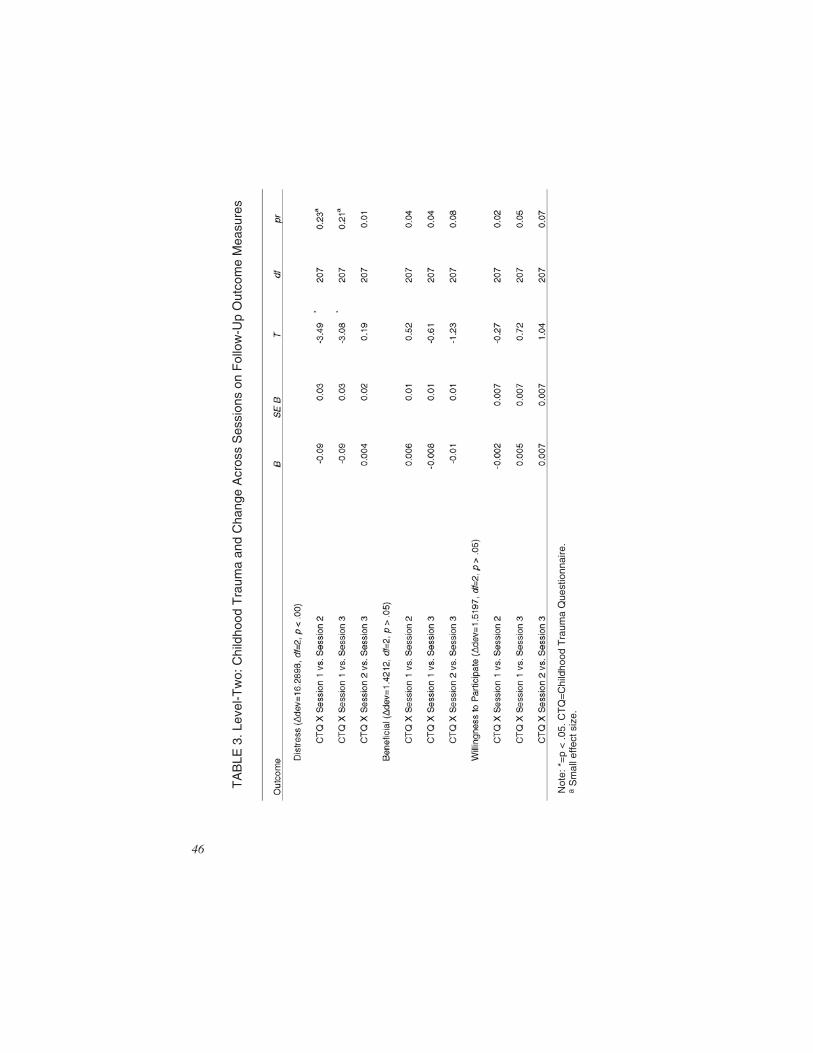
Figures 1-3 show the relationship between Change Across Sessionsand CTQ scores for each of the three outcome variables and Table 3provides a summary of these findings, including estimated effect sizesbased on criteria defined by Kirk (1996). As noted in Table 3, there wasa significant two-way CTQ and Change Across Sessions interaction forthe Distress outcome variable (Δdev = 16.29, df = 2, p < .00), suggestingthat session effects on distress levels varied as a function of childhoodtrauma. As depicted in Figure 1, the relationship between childhoodabuse (CTQ) and distress varied across Sessions. A history of childhoodabuse exhibited a stronger, positive association with Session 1 distressthan Session 2 (B = �0.09, p < .05) or Session 3 (B = �0.09, p < .05)distress suggesting that individuals reporting higher levels of childhoodabuse were impacted more by Session 1 than individuals reporting
42 JOURNAL OF TRAUMA & DISSOCIATION
TA
BLE
2.Le
vel-O
ne:C
hang
eA
cros
sS
essi
ons
onF
ollo
w-U
pO
utco
me
Mea
sure
s
Not
e:*=
p<
.05.
aS
mal
leffe
ctsi
ze;b
Med
ium
effe
ctsi
ze.
43
44 JOURNAL OF TRAUMA & DISSOCIATION
FIGURE 1. Childhood Trauma-Distress Interaction
FIGURE 2. Childhood Trauma-Beneficial Interaction
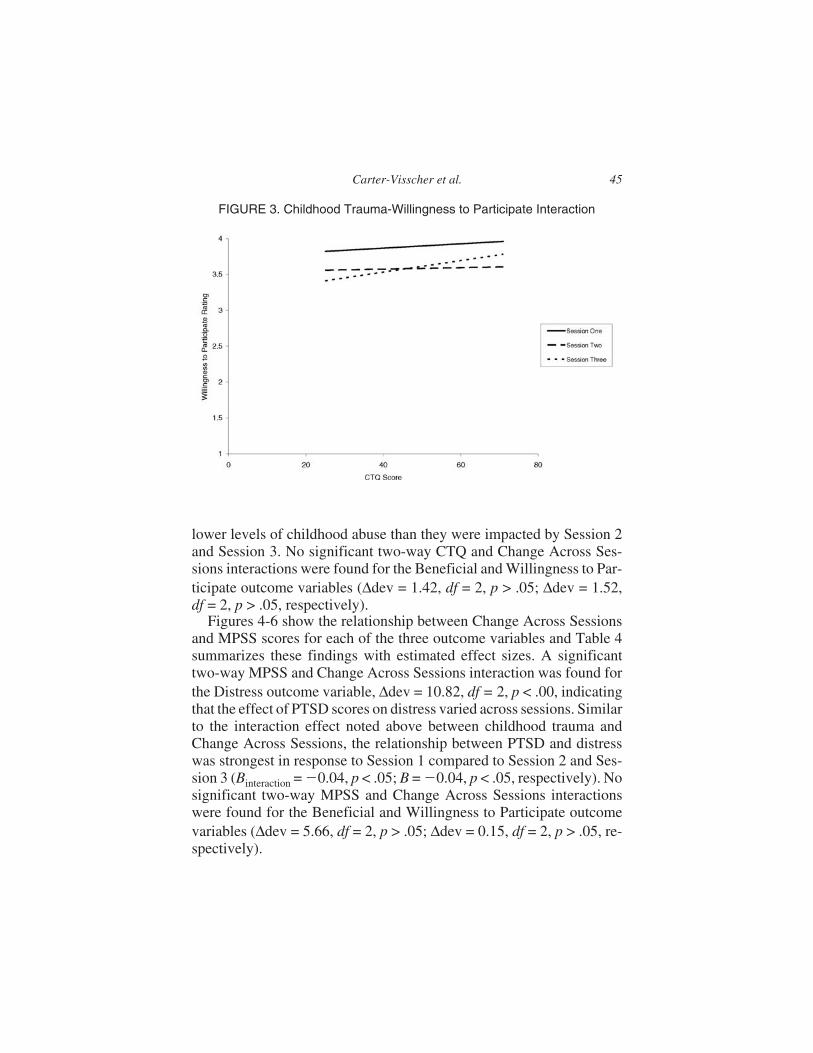
lower levels of childhood abuse than they were impacted by Session 2and Session 3. No significant two-way CTQ and Change Across Ses-sions interactions were found for the Beneficial and Willingness to Par-ticipate outcome variables (Δdev = 1.42, df = 2, p > .05; Δdev = 1.52,df = 2, p > .05, respectively).
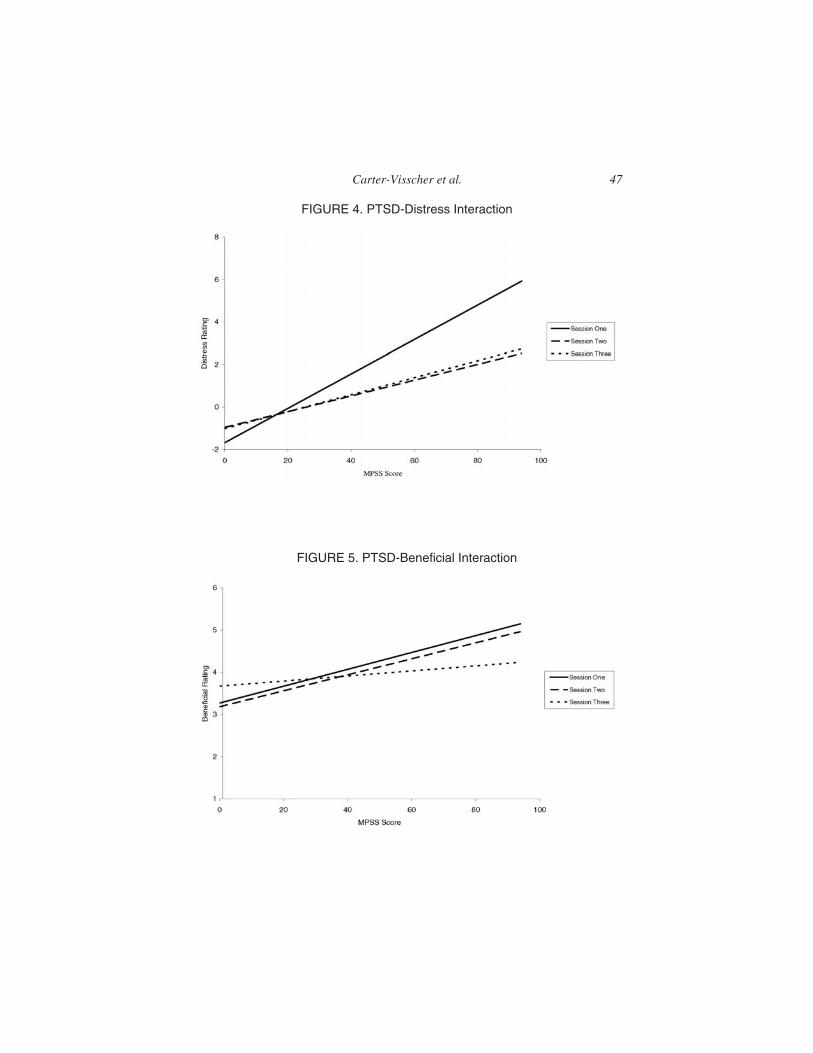
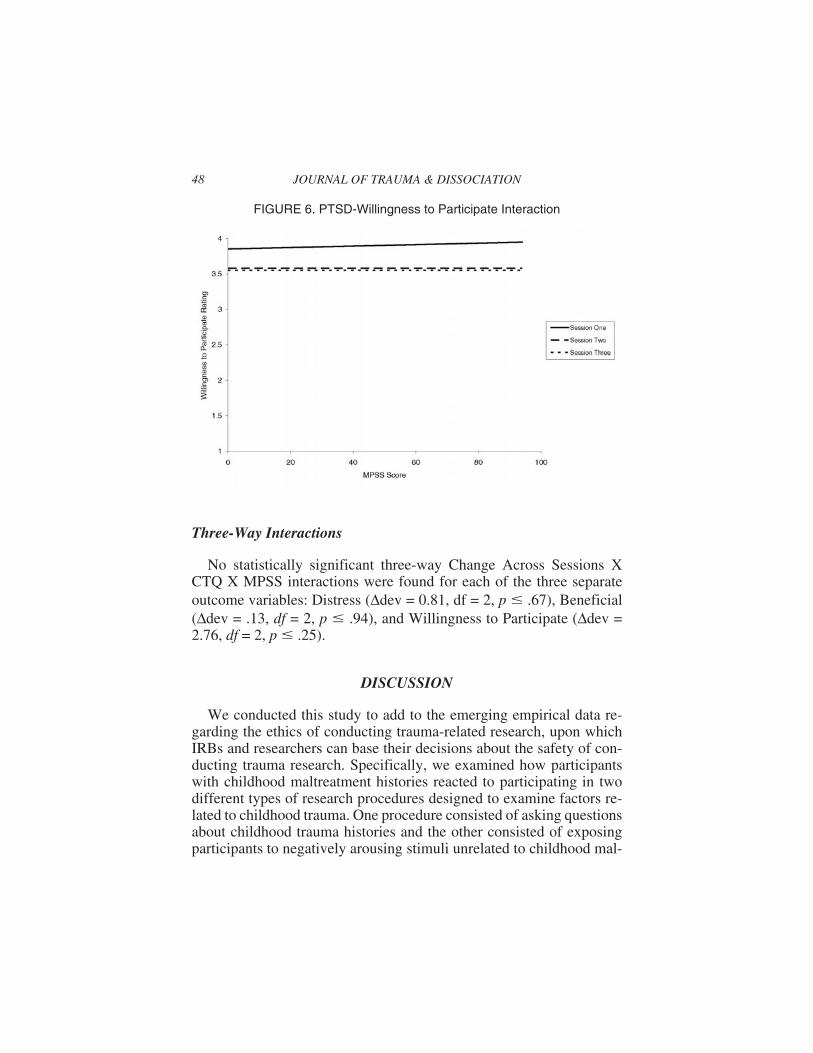
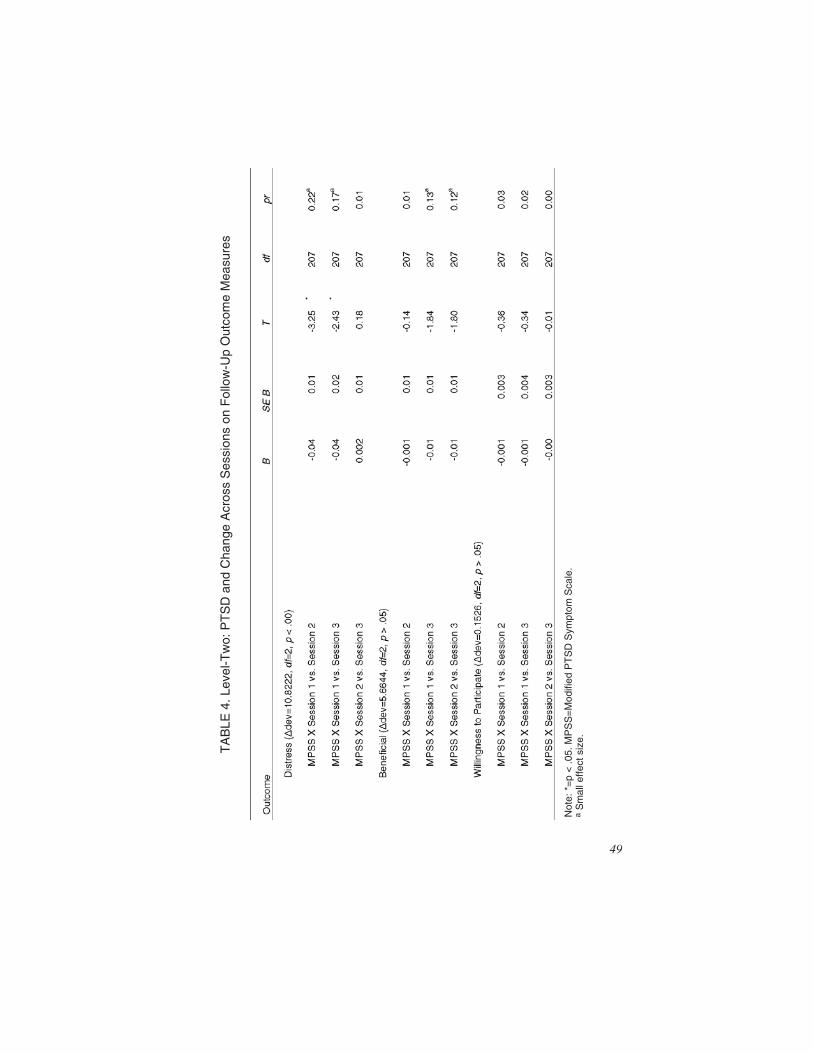
Figures 4-6 show the relationship between Change Across Sessionsand MPSS scores for each of the three outcome variables and Table 4summarizes these findings with estimated effect sizes. A significanttwo-way MPSS and Change Across Sessions interaction was found forthe Distress outcome variable, Δdev = 10.82, df = 2, p < .00, indicatingthat the effect of PTSD scores on distress varied across sessions. Similarto the interaction effect noted above between childhood trauma andChange Across Sessions, the relationship between PTSD and distresswas strongest in response to Session 1 compared to Session 2 and Ses-sion 3 (Binteraction = �0.04, p < .05; B = �0.04, p < .05, respectively). Nosignificant two-way MPSS and Change Across Sessions interactionswere found for the Beneficial and Willingness to Participate outcomevariables (Δdev = 5.66, df = 2, p > .05; Δdev = 0.15, df = 2, p > .05, re-spectively).
Carter-Visscher et al. 45
FIGURE 3. Childhood Trauma-Willingness to Participate Interaction
TA
BLE
3.Le
vel-T
wo:
Chi
ldho
odT
raum
aan
dC
hang
eA
cros
sS
essi
ons
onF
ollo
w-U
pO
utco
me
Mea
sure
s
Not
e:*=
p<
.05.
CT
Q=
Chi
ldho
odT
raum
aQ
uest
ionn
aire
.a
Sm
alle
ffect
size
.
46
Carter-Visscher et al. 47
FIGURE 4. PTSD-Distress Interaction
FIGURE 5. PTSD-Beneficial Interaction
Three-Way Interactions
No statistically significant three-way Change Across Sessions XCTQ X MPSS interactions were found for each of the three separateoutcome variables: Distress (Δdev = 0.81, df = 2, p � .67), Beneficial(Δdev = .13, df = 2, p � .94), and Willingness to Participate (Δdev =2.76, df = 2, p � .25).
DISCUSSION
We conducted this study to add to the emerging empirical data re-garding the ethics of conducting trauma-related research, upon whichIRBs and researchers can base their decisions about the safety of con-ducting trauma research. Specifically, we examined how participantswith childhood maltreatment histories reacted to participating in twodifferent types of research procedures designed to examine factors re-lated to childhood trauma. One procedure consisted of asking questionsabout childhood trauma histories and the other consisted of exposingparticipants to negatively arousing stimuli unrelated to childhood mal-
48 JOURNAL OF TRAUMA & DISSOCIATION
FIGURE 6. PTSD-Willingness to Participate Interaction
49
TA
BLE
4.Le
vel-T
wo:
PT
SD
and
Cha
nge
Acr
oss
Ses
sion
son
Fol
low
-Up
Out
com
eM
easu
res
Not
e:*=
p<
.05.
MP
SS
=M
odifi
edP
TS
DS
ympt
omS
cale
.a
Sm
alle
ffect
size
.

treatment. We also consider how our findings relate to the ethical con-cerns of vulnerability, informed consent, and unique risks and benefits.
Overall, participants reported low levels of distress and describedtheir participation experience as interesting, enjoyable, and somewhatbeneficial. Participants also indicated that they would be willing to par-ticipate in the study again with the knowledge of what participation wasactually like. One week after participants completed the experimentalsession, 61% of participants reported that they would be “quite willing”to participate in the study again and only 6% reported that they were un-willing to participate again. Willingness to participate decreased fromSession 1 to Session 2 and from Session 1 to Session 3. However, levelof willingness ranged from “quite willing” to “may be willing to partici-pate,” indicating that although willingness decreased, participants werenot unwilling to participate. Neither childhood maltreatment history norPTSD symptomatology significantly impacted willingness to partici-pant ratings across sessions. This suggests that factors other than child-hood maltreatment and PTSD influenced participant ratings ofwillingness from Session 1 to Session 3. Given that the nature of the pri-mary study did not allow for us to counterbalance the order of the ses-sions, it is difficult to determine what specific variables account for thischange in participants’ willingness ratings across sessions. Futureresearch should examine why participants’ willingness to engage in theresearch project again changes over the course of a study.
Individuals with a history of childhood trauma and those with PTSDwere more distressed than participants without that history after dis-cussing their childhood trauma (as indicated by significant childhoodmaltreatment x Session and PTSD X Session interactions), while therewere no differences in distress following Session 2 when participantswere exposed to potentially distressing stimuli not directly related totheir personal traumatic experiences. These results suggest that distressexperienced by individuals with trauma histories or PTSD symptoms intrauma-related research is more likely related to asking participants tofocus attention on trauma-specific stimuli than to participating innon-trauma-specific negatively arousing conditions. We assert that thisis a natural and expected response because individuals who have en-countered a greater degree of childhood maltreatment likely had moreto reflect upon and disclose when asked questions about those types ofpersonal experiences than participants with less traumatic histories ofnegative childhood experiences. Trauma-related research asks partici-pants to remember aspects of their lives that are likely upsetting and inturn, may create low level distress upon recalling these experiences.
50 JOURNAL OF TRAUMA & DISSOCIATION

However, experiencing upset is not the same as causing participantsharm (Becker-Blease & Freyd, 2006), especially if participants reportlow levels of upset as they did in this study and in previous trauma-re-lated research. Even though participants with more severe childhoodmaltreatment histories or PTSD symptoms reported a greater reaction toanswering questions about their life experiences, their reactions werenot strong. Becker-Blease and Freyd point out that when participantsare reminded of upsetting events, this is not always overwhelming orundesirable. Participants in this study reported experiencing both lowlevel distress and greater levels of enjoyment and interest in addition tosome benefit. Likewise, DePrince and Freyd (2006) found most partici-pants to rate the experience of answering questions about trauma historyas neutral compared to other experiences of everyday life and stated thatthe importance and goodness of the research outweighed the distressthat they experienced while participating.
What do these findings indicate about the ethical concerns oftrauma-related research? With regard to the ethical concern of partici-pant vulnerability, our results and the findings of past research do notindicate that participants with trauma histories belong to a particularlyvulnerable population that need unique protections put forth in order tosafely participate in trauma-related research. The presence of a child-hood abuse history did account for higher levels of distress after re-sponding to questions about this history, although these levels were stilllow, overall. This is not to say, however, that trauma survivors areunique in experiencing some level of distress during research participa-tion, particularly if the research requires them to focus on difficult lifeexperiences. Researchers should continue to examine the ethics of con-ducting psychological research outside the domain of trauma. We mayfind that many types of psychological research produce some level ofdistress and that trauma-related research is no exception. The findingthat PTSD symptomatology also accounted for higher levels of distressduring research participation indicates that the presence of a trauma his-tory does not solely account for higher levels of distress but that emo-tional status of participants can also play a role. Investigators shouldexamine how reactions of individuals with PTSD symptoms compare tothose of individuals experiencing other types of psychological distress.
As for the ethical concern of providing informed consent, the datasuggest that most participants experienced low level distress, equal orgreater levels of benefit and conclude that they would be quite willing toparticipate in the study again with the knowledge of what participationwas actually like. This judgment reflects rational and reasonable deci-
Carter-Visscher et al. 51

sion-making skills. Therefore, participants with a trauma history appearcapable of providing fully informed consent to participate. Researchersshould continue to examine this issue.
Considering the ethical concern of unique risks and benefits, ourfindings, along with the findings of past research, do not suggest thattrauma-related research presents unique risks that cause participantsharm. Participants may experience mild upset related to discussing pasttraumatic experiences, but exposure to negative emotions alone doesnot equal harm and does not necessarily warrant unique protection(Becker-Blease & Freyd, 2006). Investigators do need to be prepared toprovide crisis counseling and/or assist participants with finding mentalhealth services should that become necessary. However, taking this pre-caution is not unique to trauma-related research. Investigators shouldmonitor ethical concerns of all research throughout the data collectionphase and alter procedures as needed in order to make them as benefi-cial and risk-free as possible (Newman & Kaloupek, 2004). Future re-search should examine what participants find beneficial abouttrauma-related research and other research to examine whether or notthis type of research presents unique benefits.
The data produced by this study can guide IRBs and researchers tomake objective decisions about future trauma-related research proto-cols. The evidence indicates that participants with traumatic childhoodmaltreatment experiences and low levels of PTSD symptomatology donot warrant exclusion from experimental research protocols, even if theprotocol includes stimuli that may seem particularly upsetting for indi-viduals with these characteristics. Given that PTSD symptomatologyincludes hypervigilance and an exaggerated startle response, one caneasily understand why IRBs might assume that this type of researchprotocol may be too upsetting for participants with trauma histories whomay be experiencing PTSD symptoms. Contrary to this assumption, theobjective data indicate that although participants may experience dis-tress, the overall level of distress is low. Moreover, although distresswas higher during Session 1 for those with a childhood trauma, distressdecreased over time (Session 2 to Session 3) even for these participants.So, participants may have experienced some immediate, expected dis-tress from answering trauma-specific questions, but there does not ap-pear to be residual, longer lasting effects from asking those questions.Trauma-related research protocols often raise a red flag for IRBs. How-ever, our findings add to the existing literature suggesting that upset ex-perienced in trauma research is a transitory state, and individuals find
52 JOURNAL OF TRAUMA & DISSOCIATION

their participation in trauma-related research to be a positive experienceoverall, rather than a harmful one.
Investigators have made strides to increase the availability of datathat can guide decisions about the level of risk involved in trauma re-search so IRBs and researchers can modify higher risk protocols todecrease risk and put forth safeguards to better protect research partici-pants. Researchers should continue to collect data about the ethicalimplications of trauma-related research protocols, especially uniqueprotocols with uncertain cost/benefit ratios, in order to ensure thatsound empirical data guide the decision-making process so protocolswith the greatest benefit and least risk possible are developed and im-plemented (Levine, 2004). Likewise, future research should examinewhether participants consider the safeguards effective so that IRBs andresearchers can base these decisions upon objective data as well.
REFERENCES
Becker-Blease, K.A., & Freyd, J.J. (2006). Research participants telling the truth abouttheir lives: The ethics of asking and not asking about abuse. American Psychologist,61, 218-226.
Bernstein, D.P., Fink, L., Handelsman, L., Foote, J., Lovejoy, M., Wenzel, K., et al.(1994). Initial reliability and validity of a new retrospective measure of childhoodabuse and neglect. American Journal of Psychiatry, 151(8), 1132-1136.
Brabin, P.J., & Berah, E.F. (1995). Dredging up past traumas: Harmful or helpful? Psy-chiatry, Psychology, and Law, 2, 165-171.
Bradley, M.M., & Lang, P.J. (1994). Measuring emotion: The Self-Assessment Mani-kin and the semantic differential. Journal of Behavior Therapy & ExperimentalPsychiatry, 25, 49-59.
Bradley, M.M., & Lang, P.J. (2000). Affective reactions to acoustic stimuli.Psychophysiology, 37, 204-215.
Briere, J.N. (1992). Child abuse trauma: Theory and treatment of the lasting effects.Thousand Oaks, CA: Sage Publications.
Carlson, E.B., Newman, E., Daniels, J.W., Armstrong, J., Roth, D., & Loewenstein, R.(2003). Distress in response to and perceived usefulness of trauma research inter-views. Journal of Trauma & Dissociation, 4, 131-142.
Center for the Study of Emotion and Attention [CSEA-NIMH], (1999). The interna-tional affective picture system [CD-ROM]. Gainesville, FL: The Center for Re-search in Psychophysiology, University of Florida.
Cohen, J., Cohen, P., West, S.G., & Aiken, L.S. (2003). Applied multiple regression/correlation analysis for the behavioral sciences, 3rd ed. Mahwah, NJ: LawrenceErlbaum Associates.
Cromer, L.D., Freyd, J.J., Binder, A.K., DePrince, A.P., & Becker-Blease (in press).What’s the risk in asking? Participant reaction to trauma history questions com-pared with other personal questions. Ethics & Behavior.
Carter-Visscher et al. 53

DePrince, A.P., & Freyd, J.J. (2006). Costs and benefits of being asked about traumahistory. Journal of Trauma Practice, 3, 23-35.
Ellis, B. (2000). Raising the devil. Lexington, KY: University Press of Kentucky.Falsetti, S.A., Resnick, H.S., Resick, P.A., & Kilpatrick, D.G. (1993). The Modified
PTSD Symptom Scale: A brief self-report measure of posttraumatic stress disorder.The Behavior Therapist, 16, 161-162.
Foa, E.B., Riggs, D.S., Dancu, C.V., & Rothbaum, B.O. (1993). Reliability and valid-ity of a brief instrument for assessing posttraumatic stress disorder. Journal of Trau-matic Stress, 6, 459-473.
George, D., & Mallery, P. (2003). SPSS for Windows step by step: A simple guide andreference (4th ed.). Boston: Allyn & Bacon.
Gliem, J.A., & Gliem, R.R. (2003). Calculating, interpreting, and reporting Cronbach’salpha reliability coefficient for Likert-type scales. In 2003 Midwest Research toPractice Conference in Adult, Continuing, and Community Education (pp. 82-88).Columbus, OH.
Gold, E.R. (1986). Long-term effects of sexual victimization in childhood: Anattributional approach. Journal of Consulting and Clinical Psychology, 54,471-475.
Griffin, M.G., Resick, P.A., Waldrop, A.E., & Mechanic, M.B. (2003). Participation intrauma research: Is there evidence of harm? Journal of Traumatic Stress, 16,221-227.
Kirk, R.E. (1996). Practical significance: A concept whose time has come. Educationaland Psychological Measurement, 56(5), 746-759.
Koss, M.P., & Oros, C.J. (1982). Sexual experiences survey: A research instrument in-vestigating sexual aggression and victimization. Journal of Consulting and ClinicalPsychology, 50, 455-457.
Lang, A.J., Stein, M.B., Kennedy, C.M., & Foy, D.W. (2004). Adult psychopathologyand intimate partner violence among survivors of childhood maltreatment. Journalof Interpersonal Violence, 19, 1102-1118.
Levine, C. (2004). The concept of vulnerability in disaster research. Journal of Trau-matic Stress, 17, 395-402.
Malinosky-Rummell, R., & Hansen, D.J. (1993). Long-term consequences of child-hood physical abuse. Psychological Bulletin, 114, 68-79.
Matsumoto, D., & Ekman, P. (1988). Japanese and Caucasian Facial Expressions ofEmotion (JACFEE) and Neutral Faces (JACNeuF) [CD-ROM]. San Francisco,CA: Department of Psychology, San Francisco University.
McGrath, M. (2002). Demons of the modern world. Amherst, NY: Prometheus Books.McIntire, K.A., Danforth, M.M., & Schneider, H.G. (1999). Measuring cue perception:
Assessment of reliability and validity. North American Journal of Psychology, 1,261-266.
National Commission for the Protection of Human Subjects of Biomedical and Behav-ioral Research. (1979). The Belmont Report: Ethical principles and guidelines forthe protection of human subjects of research. Retrieved May 8, 2005, from http://www.hhs.gov/ohrp/humansubjects/guidance/belmont.htm
Naugle, A.E. (1999). Identifying behavioral risk factors for repeated victimization us-ing video-taped stimulus materials. Unpublished doctoral dissertation, Universityof Nevada, Reno.
54 JOURNAL OF TRAUMA & DISSOCIATION

Newman, E., & Kaloupek, D.G. (2004). The risks and benefits of participating intrauma-focused research studies. Journal of Traumatic Stress, 17, 383-394.
Newman, E., Walker, E.A., & Gefland, A. (1999). Assessing the ethical costs and ben-efits of trauma-focused research. General Hospital Psychiatry, 21, 187-196.
Nowicki, S.J., & Duke, M.P. (1994). Individual differences in the nonverbal communi-cation of affect: The Diagnostic Analysis of Nonverbal Accuracy Scale. Journal ofNonverbal Behavior, 18, 9-35.
Parslow, R.A., Jorm, A.F., O’Toole, B.I., Marshall, R.P., & Grayson, D.A. (2000). Dis-tress experienced by participants during an epidemiological survey of posttraumaticstress disorder. Journal of Traumatic Stress, 13, 465-471.
Raudenbush, S.W., & Bryk, A.S. (2002). Hierarchical linear models: Applicationsand data analysis methods (2nd ed.). Thousand Oaks, CA: Sage.
Raudenbush, S.W., Bryk, A.S., Cheong, Y.F., & Congdon, R. (2004). HLM 6: Hierar-chical linear and nonlinear modeling. Lincolnwood, IL: Scientific Software Inter-national.
Resnick, H.S., Kilpatrick, D.G., Dansky, B.S., Saunders, B.E., & Best, C.L. (1993).Prevalence of civilian trauma and posttraumatic stress disorder in a representativenational sample of women. Journal of Consulting and Clinical Psychology, 61,984-991.
Ruzek, J.I., & Zatzick, D.F. (2000). Ethical considerations in research participationamong acutely injured trauma survivors: An empirical investigation. General Hos-pital Psychiatry, 22, 27-36.
Sanders, B., & Moore, D.L. (1999). Childhood maltreatment and date rape. Journal ofInterpersonal Violence, 14, 115-124.
Sherman, M. (1997). Why people believe weird things: Pseudoscience, superstition,and other confusions of our times. New York: WH Freeman and Company.
Singer, J.D., & Willett, J.B. (2003). Applied longitudinal data analysis: Modelingchange and event occurrence. New York: Oxford University Press.
Walker, E.A., Newman, E., Koss, M., & Bernstein, D. (1997). Does the study of vic-timization revictimize the victims? General Hospital Psychiatry, 19, 403-410.
Wyatt, G.E. (1985). The sexual abuse of Afro-American and White-American womenin childhood. Child Abuse and Neglect, 9, 507-519.
Wyatt, G.E., & Newcomb, M. (1990). Internal and external mediators of women’s sex-ual abuse in childhood. Journal of Consulting and Clinical Psychology, 58,758-767.
RECEIVED: 08/04/06REVISED: 09/15/06
ACCEPTED: 09/18/06
doi:10.1300/J229v08n03_03
Carter-Visscher et al. 55

Copyright © 2022 FDOKUMEN