
Establishing an epidemiologic al field laboratory in rural areas - potentials for public health...
47
Establishing an epidemiological field laboratory 1 Establishing an epidemiological field laboratory in rural areas - potentials for public health research and interventions The Butajira Rural Health Programme 1987-1999 Yemane Berhane 1,2 , Stig Wall 2 , Derege Kebede 1 , Anders Emmelin 2 , Fikre Enquselassie 1 , Peter Byass 2,3 , Lulu Muhe 4 , Tobias Andersson 2 , Negussie Deyessa 1 , Ulf Högberg 2 , Yegomawork Gossaye 1 , Atalay Alem 1,5 , Kjerstin Dahlblom 2 1. B ACKGROUND Basic health care and essential health research need an epidemio- logical perspective. This requires local data on the health situation of the whole community. Such an approach must not be solely a method of counting heads, but must also relate to cultural patterns and values. When fed back to the people who are the source of the information, epidemiological data may "talk", and increase our understanding of causes and needs. A valid health information system is also a prerequisite for the analysis of secular trends and for their delineation from societal interventions. For low-income countries there is also a demand for timely vital statis- tics. Epidemiological surveillance re- presents on-going systems for the collection, analysis and interpretation of health data, which are essential to the planning, implementation and evaluation of health programmes. An effective surveillance system also implies timely dissemination of its data to those who need to know. The final link in the surveillance chain is the application of these data to prevention and disease control. Epidemiological surveillance activities are usually included as part of the health in- formation systems of governmental institutions that have responsibility for health care. Basic epidemiological know-how can be gathered through formal courses or textbooks, but practical experiences can only be learnt through research out in the field. Within the so-called sandwich model of research training, most of the trainees’ time is spent on the job, researching questions that relate to local 1 Dept Community Health, Medical Faculty, Addis Ababa University, Ethiopia 2 Epidemiology, Dept Public Health and Clinical Medicine, Umeå University, Sweden 3 School of Community Health Sciences, University of Nottingham, UK 4 Dept Paediatrics, Medical Faculty, Addis Ababa University, Ethiopia 5 Dept Psychiatry, Medical Faculty, Addis Ababa University, Ethiopia
-
Upload
addiscontinental -
Category
Documents
-
view
2 -
download
0
Transcript of Establishing an epidemiologic al field laboratory in rural areas - potentials for public health...
Establishing an epidemiological field laboratory 1
Establishing an epidemiological field laboratoryin rural areas - potentials for public healthresearch and interventions
The Butajira Rural Health Programme 1987-1999
Yemane Berhane1,2, Stig Wall2, Derege Kebede1, Anders Emmelin2, FikreEnquselassie1, Peter Byass2,3, Lulu Muhe4, Tobias Andersson2, NegussieDeyessa1, Ulf Högberg2, Yegomawork Gossaye1, Atalay Alem1,5, KjerstinDahlblom2
1. BACKGROUNDBasic health care and essential
health research need an epidemio-logical perspective. This requires localdata on the health situation of thewhole community. Such an approachmust not be solely a method ofcounting heads, but must also relate tocultural patterns and values. When fedback to the people who are the sourceof the information, epidemiologicaldata may "talk", and increase ourunderstanding of causes and needs. Avalid health information system is alsoa prerequisite for the analysis ofsecular trends and for their delineationfrom societal interventions.
For low-income countries there isalso a demand for timely vital statis-tics. Epidemiological surveillance re-presents on-going systems for thecollection, analysis and interpretationof health data, which are essential tothe planning, implementation andevaluation of health programmes. Aneffective surveillance system alsoimplies timely dissemination of its datato those who need to know. The finallink in the surveillance chain is theapplication of these data to preventionand disease control. Epidemiologicalsurveillance activities are usuallyincluded as part of the health in-formation systems of governmentalinstitutions that have responsibility forhealth care.
Basic epidemiological know-howcan be gathered through formalcourses or textbooks, but practicalexperiences can only be learnt throughresearch out in the field. Within theso-called sandwich model of researchtraining, most of the trainees’ time isspent on the job, researchingquestions that relate to local
1Dept Community Health, Medical Faculty, Addis Ababa University, Ethiopia2Epidemiology, Dept Public Health and Clinical Medicine, Umeå University, Sweden3School of Community Health Sciences, University of Nottingham, UK4Dept Paediatrics, Medical Faculty, Addis Ababa University, Ethiopia5Dept Psychiatry, Medical Faculty, Addis Ababa University, Ethiopia

2 Ethiop. J. Health Dev.
situations. Technology also has a partto play here; telephone, fax and e-mail, even to some of the world’smost remote communities, havedeveloped appreciably over the lastfew years. Fieldwork is no longerconstrained by computer facilities.Field- and process-oriented teachingof epidemiology and public healthalso increases awareness of thecommunity perspective amongmedical personnel who previouslywere only clinically oriented.
In developing countries, adequateand reliable health information is oftenlacking. There is usually nosystematically organised registrationof vital events. Also, national figuresare of limited use for health planningat regional levels. Population studiesare therefore needed.
The overall objectives of theButajira "field laboratory" were todevelop and evaluate a system forcontinuous registration of births anddeaths, to generate valid data onfertility and mortality and to provide apopulation and study base foressential health research and inter-vention in the area. The ultimate aimof the project was therefore toprovide a current epidemiologicalsurveillance system at district level.
Specifically, this aimed to enablethe assessment of fertility and mor-tality trends, the analysis of publichealth and health behavioural deter-minants of mortality and morbidity aswell as the assessment of coverageand utilisation of health services in thearea in relation to health needs of thepeople.
When establishing the study basein the Butajira district it was essentialto get the support of the governmentofficials and mass organisationsconcerned. Letters were written byhigher authorities to all thoseconcerned requesting their supportand co-operation. Close links wereestablished with government officialsand mass organisations, local leadersand members of the community.Often, open-air meetings were heldwith members of peasants’associations, as well as with mosqueand church leaders in the villages, toexplain further the purpose of theproject. A considerable amount of co-operation was solicited from theparticipants, especially theirwillingness to accept and respond tointerviewers who would be going intotheir houses and asking a number ofquestions for months and years tocome. Informed consent andparticipation was sought from theonset through community leaders [1].
This report is an attempt to shareexperiences from the first thirteenyears of the Butajira Rural Health Pro-gramme (BRHP), to present somebasic data on demography, to sum-marise results from specific applic-ations of its epidemiological labora-tory and to suggest and outlineresearch and intervention activitiesdeparting from the major findings sofar.

Establishing an epidemiological field laboratory 3
2. SETTING THE SCENE
2.1 GeographyThe Butajira Rural Health Pro-
gramme (BRHP) is located in Meskanand Mareko District, Gurage Zone, inthe Southern Nations, Nationalitiesand Peoples Regional State(SNNPRG) in Ethiopia. Historicallythe District was part of what wasknown as "Gurageland". The Districtacquired its present name in 1954.
At the same time Butajira becamethe capital town of the District. TheDistrict borders the Silti District to thesouth, the Adamitulu District to theeast, the Sabat-Bet Gurage to the westand the Sodo District to the north.The estimated size of the District is797 km2, of which Butajira towncovers approximately 9 km2.
A view from the rural village
Location of the study sites in the district
4 Ethiop. J. Health Dev.
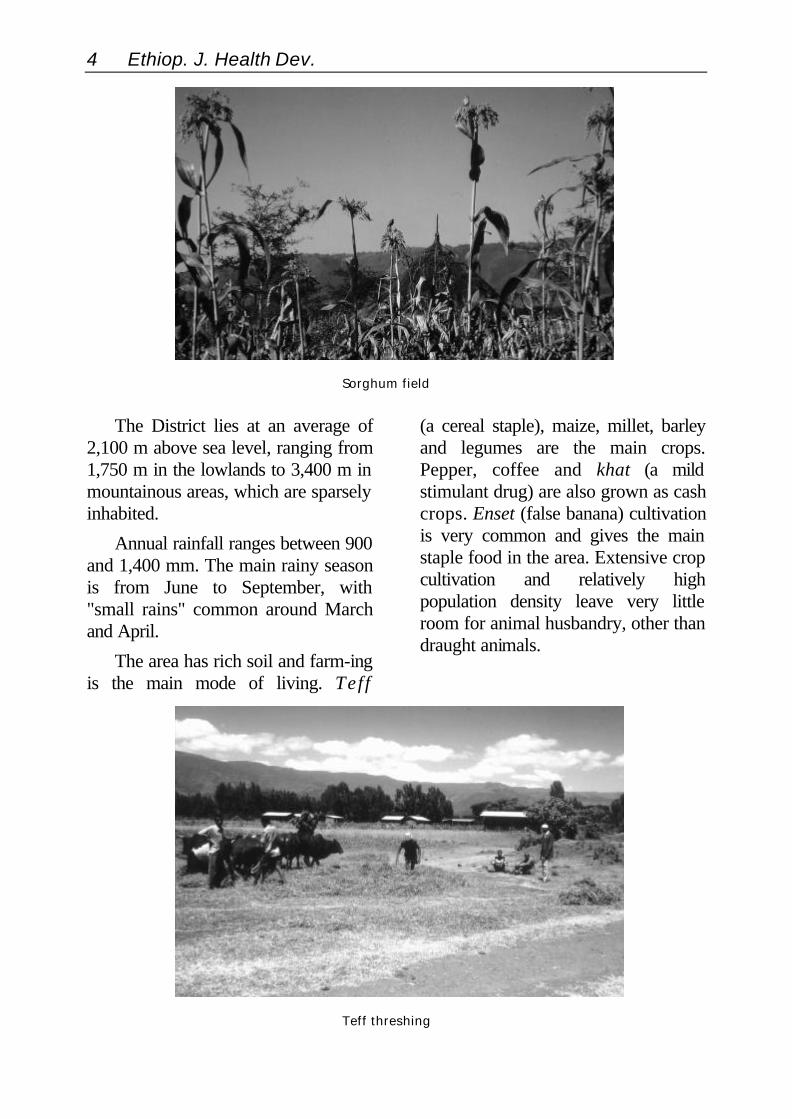
The District lies at an average of2,100 m above sea level, ranging from1,750 m in the lowlands to 3,400 m inmountainous areas, which are sparselyinhabited.
Annual rainfall ranges between 900and 1,400 mm. The main rainy seasonis from June to September, with"small rains" common around Marchand April.
The area has rich soil and farm-ingis the main mode of living. Teff
(a cereal staple), maize, millet, barleyand legumes are the main crops.Pepper, coffee and khat (a mildstimulant drug) are also grown as cashcrops. Enset (false banana) cultivationis very common and gives the mainstaple food in the area. Extensive cropcultivation and relatively highpopulation density leave very littleroom for animal husbandry, other thandraught animals.
Sorghum field
Teff threshing

Establishing an epidemiological field laboratory 5
2.2 PeopleThe Gurage people migrated from
the northern part of Ethiopia in theninth century with the expansion ofthe Christian kingdom southwards.Since then they have been livingtogether with the Kushitic and Omoticpeople who were previously in thearea. The Meskan, Mareko, Sodo,Siliti and Dobi tribal groups dominate.The Mareko are predominantlyKushitic. They were also the first tocome into the area and they occupy agreater part of the land compared tothe other tribes. The Siliti group,though Semitic in origin, migrated tothe area from the eastern part ofEthiopia (Harar) in the sixteenthcentury. Several clans are identifiedwithin each tribal group.
The population of the district wasgiven as 182,000 during the 1984census and on the basis of the 1994census is estimated to have grown to257,000 by 1999. The Butajira townpopulation has grown from about13,000 in 1984 to 25,000 by 1999.The population structure shows atypical developing country pattern.The proportion of children under 14years is 46% and that of people 65years and older is 1.3% [2, 3].
The vast majority of the Districtpopulation follow the Christian andIslamic religions. Currently Islamdominates, being followed by two-thirds of the District population.
Well in a lowland village

6 Ethiop. J. Health Dev.
Islam started to expand exten-sively in the area after the AhmedGragn invasion in the sixteenthcentury and subsequently through theexpansion of Islamic education byvery influential and feared religiousleaders [4]. Sodo and Dobi tribes arepredominantly Orthodox Christianswhile others are predominantlyMoslem.
The predominant language, Gur-agigna, belongs to the Ethio-semiticlanguage group, resembling thenorthern Ethiopian languages but in-fluenced by the Kushitic language ofthe surroundings. The people havedeveloped a variety of dialects ofGuragigna within their clans. TheMareko group, however, have a dis-tinct language, Marekogna, that moreclosely resembles the Kushiticlanguage spoken by their neighbours,the Hadiyas.
2.3 Traditional systemsUntil recently, the tribes have
depended on their own traditionalsystems of administration to keeporder and settle disputes. Clans arethe basis for defining power. Theirtraditional rules are influenced byreligion and culture, and thus differfrom tribe to tribe. The establishmentof a central authority in Ethiopia at thebeginning of the nineteenth centurystarted to gradually erode the powerof the clan administration. The centralauthority commonly appointed menfrom other areas as governors, thoughsometimes were chosen. Currently,traditional rules have very limitedinfluence and people are largelygoverned by the law of the country.As the national government structuredeveloped during the twentiethcentury, local people have becomemore and more involved in the
Enset (false banana plant) processing
Establishing an epidemiological field laboratory 7
government system rather thanobserving traditional practices.
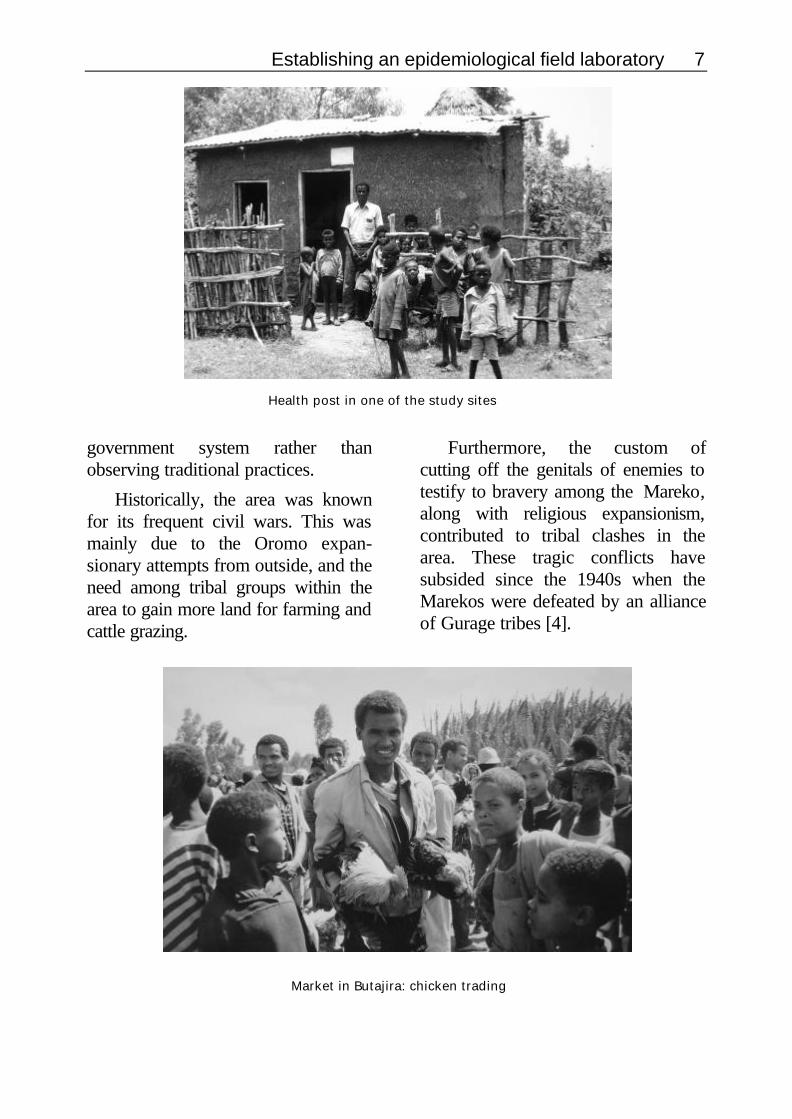
Historically, the area was knownfor its frequent civil wars. This wasmainly due to the Oromo expan-sionary attempts from outside, and theneed among tribal groups within thearea to gain more land for farming andcattle grazing.
Furthermore, the custom ofcutting off the genitals of enemies totestify to bravery among the Mareko,along with religious expansionism,contributed to tribal clashes in thearea. These tragic conflicts havesubsided since the 1940s when theMarekos were defeated by an allianceof Gurage tribes [4].
Health post in one of the study sites
Market in Butajira: chicken trading

8 Ethiop. J. Health Dev.
2.4 Butajira townThe town is located at 2,100 m
above sea level. The municipalityadministers 9 km2 of land to belong tothe town. The town has a temperate(woyna-dega) climate which favourshuman habitation and a wide range ofcultivation. It is located 130 km southof Addis Ababa and 50 km to thewest of Zway town in the Rift Valley.
Butajira town has grown from asmall settlement that was establishedby the Shoan military forces - theNaftegna - over hundred years ago.The soldiers were known as Kita-Balas they were paid only in kind. Theofficial establishment of Butajira townis dated as 1929. The town area wasearlier occupied by the Mareko tribebut subsequently annexed by theMeskan tribe after they conquered theMarekos in war [4].
The existence of the River Eresha inthe north of the town along the roadto Zway and the River Rinzaf to thesouth made the location suitable forsettlement because of the supply ofwater. This strategic location of thetown and its service as market area forsurrounding communities contributedto its growth.
The growth of the town wasmarked by the appearance of a clusterof thatched roof huts. The marketthen was very small and was usedonly by the local people. The mainform of trade was barter and usingamole - a type of rock salt.Improvements in road communi-cations and the production of cropslike teff and pepper encouraged theexpansion of the market and thus ofthe town.
Main road in Butajira town
Establishing an epidemiological field laboratory 9
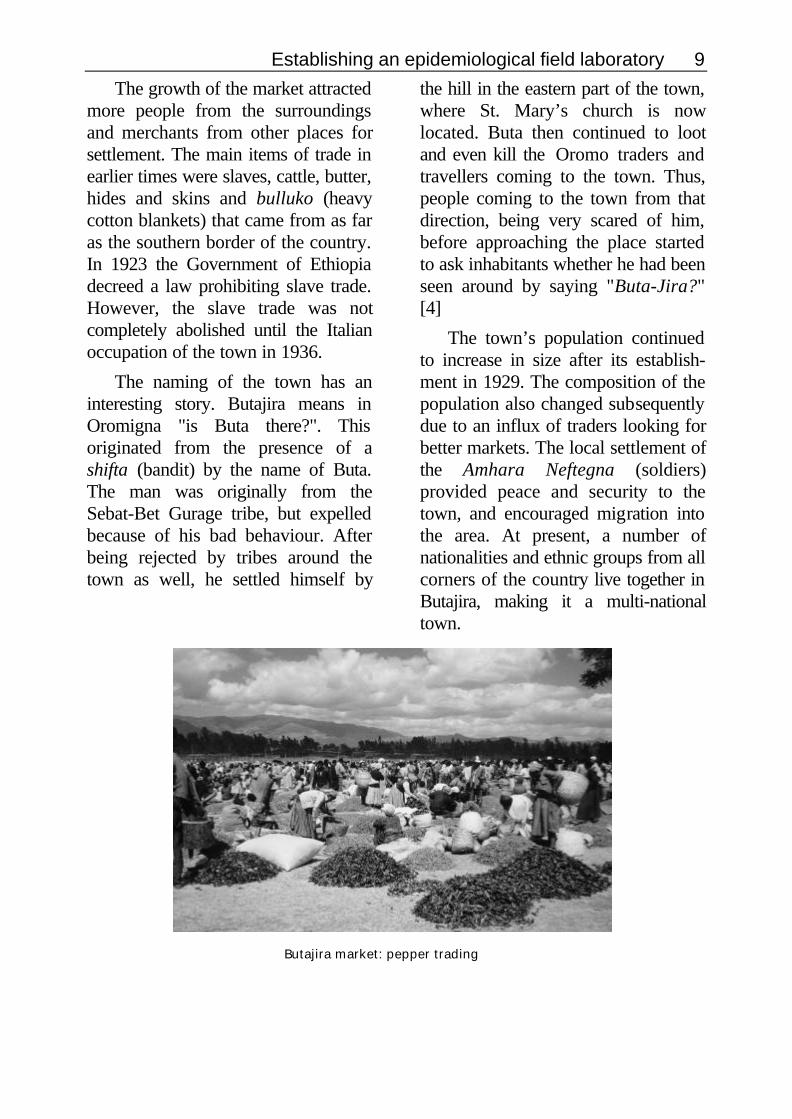
The growth of the market attractedmore people from the surroundingsand merchants from other places forsettlement. The main items of trade inearlier times were slaves, cattle, butter,hides and skins and bulluko (heavycotton blankets) that came from as faras the southern border of the country.In 1923 the Government of Ethiopiadecreed a law prohibiting slave trade.However, the slave trade was notcompletely abolished until the Italianoccupation of the town in 1936.
The naming of the town has aninteresting story. Butajira means inOromigna "is Buta there?". Thisoriginated from the presence of ashifta (bandit) by the name of Buta.The man was originally from theSebat-Bet Gurage tribe, but expelledbecause of his bad behaviour. Afterbeing rejected by tribes around thetown as well, he settled himself by
the hill in the eastern part of the town,where St. Mary’s church is nowlocated. Buta then continued to lootand even kill the Oromo traders andtravellers coming to the town. Thus,people coming to the town from thatdirection, being very scared of him,before approaching the place startedto ask inhabitants whether he had beenseen around by saying "Buta-Jira?"[4]
The town’s population continuedto increase in size after its establish-ment in 1929. The composition of thepopulation also changed subsequentlydue to an influx of traders looking forbetter markets. The local settlement ofthe Amhara Neftegna (soldiers)provided peace and security to thetown, and encouraged migration intothe area. At present, a number ofnationalities and ethnic groups from allcorners of the country live together inButajira, making it a multi-nationaltown.
Butajira market: pepper trading
10 Ethiop. J. Health Dev.
Butajira was occupied by theItalian army in April 1936. The Italianstook control of the town, abolishedexisting rules and replaced them withtheir own rule. During this time, newtraders including Arabs came into thetown. They brought goods likefabricated textiles, salt, sugar,kerosene, needles and blades into themarkets. At the same time the numberof local bars (tej bet, tella bet andarake bet) increased. The MariaTheresa thaler was the main currencyat that time.
The Italians also introduced theconstruction of modern residentialhouses in the town. Those houseswere used later as the governmentoffices after the Italians left. TheItalians also improved the road fromAddis Ababa and cleared it furthersouth. They constructed a new roadbetween Butajira and Zway. TheItalians left the town defeated in April1941. Following liberation, the growthof the town accelerated when Butajirabecame the capital of the Gurage andMareko awraja (province) in 1954.The municipality of Butajira town wasestablished in 1945 by proclamationof the Government of Ethiopia. Thisproclamation gave 133 towns in thecountry legal status.
After Butajira became the capitaltown of the district in 1954, publicservices like schools, clinics andhotels started to flourish. The townwas surveyed for the first time in 1958by experts from the Ministry of theInterior with the aim of expanding itsterritory. The expansion failedbecause of the unwillingness of the
landlords occupying the area. Becauseof that the governor changed his seatto Adami-Tulu town on the Awassaroad in 1960, then to Zway in 1962, asa result of which Butajira lost its statusof being provincial capital. Butajirabecame the capital of Meskan andMareko District under a new provincecalled Haikoch and Butajira. The sizeof Butajira town did not increasefurther until after the 1974 popularrevolution in the country [4].
A master plan for the town wasprepared in 1967. Based on this plan,the municipality constructed the firstroads in the town in 1972. Thenumber of houses registered by themunicipality in 1956 was 1,616. 976 ofthose houses were made of wood andmud, with corrugated iron roofs. Theremaining were traditional round huts.Later in 1967, a survey revealed thatabout 70% of the houses in the townwere in bad hygienic condition.
The population, according tosome official reports, increased from3,451 in 1962 to 6,600 in 1971. Thesestatistics also showed that there was ahigher proportion of females thanmales in the town.
2.5 Social servicesEducation was started in the town
early in the twentieth century byreligious groups in the mosque andchurches, with the establishment of aQuranic school and Yeqes TimihirtBet (church school), for Moslem andChristian inhabitants respectively. Thefirst modern school was established intown in 1947 with two teachers in

Establishing an epidemiological field laboratory 11
private premises. In 1954 the schoolwas giving education up to gradethree. It was upgraded to teach up tograde 5 in 1955 and then to grade 8 in1956. In 1957, the students numbered200, with eight teachers. The schoolexpanded to accommodate morestudents in 1964 with a female:malestudent ratio of 1:6. In 1967, theschool was named Ras Desta DamtewJunior Secondary School.
At present, there is one technicalschool, one high school, 14 juniorsecondary schools and 14 primaryschools in the district. The total stud-ent number is estimated to be 14,738,with a female to male ratio of 1:3.5.About 77% of the district populationare illiterate and less than 2% of thepopulation have education beyondjunior secondary school.
Medical services were started byEuropean missionaries that lived inButajira between 1957 and 1964.These missionaries came with theSudan Interior Mission (SIM) on atemporary basis. The Health Centre inthe town was established in 1976-7.On establishment, the Health Centrewas staffed by three health workers: ahealth officer, a nurse and a juniorhealth assistant. In the first 3-4 yearsof its work the Health Centre waslimited to providing only curativehealth services. The number of staffand the services rendered wereprogressively expanded to meetpublic demand [5]. Currently itprovides an integrated curative andpreventive health service and has atotal of 31 staff, comprising 26 healthpersonnel and 5 administrators. Theannual budget of the Health Centre isnow 540,000 Birr (approximately US$8,000), of which about 76% isaccounted for by salaries.
Health centre in Butajira

12 Ethiop. J. Health Dev.
At present, in addition to ButajiraHealth Centre, there are two govern-ment health stations, 11 private clinics(5 of which are in Butajira town), 11functional health posts (5 of which arein BRHP surveillance areas) and 8private drug vendors (5 in Butajiratown) in the District, together servingsome quarter of a million people. Fournew health posts are also underconstruction.
Butajira Health Centre has nocapacity to manage surgical andobstetric emergencies. The nearestreferral centre is 100 km south ofButajira town, at Hosanna. There is noefficient transport facility to thereferral centre and the road is often inbad condition. To overcome these
shortcomings, the population of theDistrict and the surroundings, incollaboration with non-governmentalorganisations (NGOs) have completedthe construction of a hospital inButajira town, although it is not yetequipped and staffed. When thehospital starts to function, it isintended to provide a wider range ofmedical services that are badly neededin the area.
The rivers around Butajira townwere the main source of water until1980. At that time the municipalityafter very hard struggles through theyears managed to pipe water to thetown population from two wells. Thesource wells for this tap water aretested twice a year and the distributiontanks are cleaned regularly.
The new hospital in Butajira town under construction

Establishing an epidemiological field laboratory 13
2.6 EconomyThe backbone of the economy in
the district is the agricultural sector.Pepper, coffee and khat are the maincash crops produced in the area. Teffis also mainly produced for sale. Intown most people are engaged incommercial activities. Shops, foodand drink establishments, carpentry,and flour mills dominate the town’scommercial activities. These are alsothe main source of revenue for thetown municipality.
2.7 Communication and powerThe all-weather road that connects
Butajira town with Addis Ababa wasbuilt in 1966. The town is also con-nected to the Rift Valley town ofZway by an all-weather road. Thevillages in the district with fewexceptions are connected to the townonly by dry-weather roads.
The completion of the all-weatherroad to Addis Ababa heralded thestart of postal service in town. Thepost office serves five other sur-rounding districts. It has a capacity of150 private boxes. A telephoneservice was started in the 1970s.Currently an automatic dialling serviceis provided within the town, butoutside calls are made through theoperator. Plans are being carried outto provide a fully automatic digitalservice to the town. There are cur-rently 186 customers for telecom-munication services, which do notextend outside the urban area.
An electricity supply was startedfor the first time by an Arab merchantin 1956 from a diesel generator. The
supply of electricity to the towncontinued to be supplied by a groupof Arab merchants until the 1974revolution. Currently a 24 hour serviceis available from the Kokahydroelectric power plant.
3. PLANNING AND ORGANISING
THE FIELD WORK
3.1 The project designThe objectives of the BRHP,
when initiated in 1986, were togenerate health-related information, toestablish and maintain an epi-demiologic research laboratory, tobuild and strengthen research cap-ability and to develop local capacity inthe prevention and control of disease.
The Study district is administra-tively located in Gurage zone,Southern Nations, Nationalities andPeoples Regional State (SNNPRG).The District is divided for admini-strative purposes into a total of 82Peasants' Associations (PAs) in therural areas and 4 Urban DwellersAssociations (UDAs) in Butajira town.The study has been conducted in a setof nine randomly selected PAs (usingthe probability proportionate to sizetechnique) and one UDA. In line withits objectives, the initial tasks for theBRHP during 1986-87 were toperform a census of the population inthe selected villages to obtain thebaseline population and to establish asystem of demographic surveillancewith continuous registration of vitaland migratory events at a householdlevel (Appendix IV). Events registeredby the BRHP are birth, death,marriage, new household, out-

14 Ethiop. J. Health Dev.
migration, in-migration and internalmove (migration within the BRHP sur-veillance villages).
Data are collected monthly byvisiting each household. Each house-hold is identified by a unique numberwithin its village, and each individualwithin their household.
Individuals can thus be charac-terised by a unique identity numberwithin the entire surveillance system.This unique identity number is tencharacters long and is composed ofthe village number, the house-hold
number and the individual numberwithin the household. Once anindividual is allocated a unique identitynumber in this way, it is permanentlyassociated with that individual, even ifthey move to a new location (thedetails of which are separatelyrecorded).
Any adult of the household abovethe age of 15 years is eligible torespond to the monthly householdevent collection interviews. The statusof each individual is checked duringthe monthly visit and recorded on ademographic surveillance sheet. Basicdemographic, social, housingconditions and health care utilisationcharacteristics are recorded for eachhousehold at entry into thesurveillance system and during any re-census process.
Household included in the demographic surveillance

Establishing an epidemiological field laboratory 15
The surveillance system operateson an open cohort system and isdynamic. Individuals enter and leavethe system any time. Since individualmovements are tracked regularly, anindividual’s overall time contributionto the study base can easily becalculated. The individual person-times calculated can then providedenominators for calculation of, forexample, mortality and fertility rateswithin the study base (Figure 1).
Each vital event is registered on aseparate form at the household level.Each form contains several questionsthat are pertinent to adequatelycharacterise the event. The householdinterviews are conducted by village-based enumerators (enumerators whothemselves live in the study villages).Village based enumerators have had atleast 10 years of formal education.They were trained at recruitment onthe use of the surveillance forms, onhow to conduct interviews and ondata management in the field. Inaddition, they receive periodicrefresher training on the same
subjects. Job descriptions andinterview guides are provided to thefield staff to clearly indicate theirduties and responsibilities. Datacollection is usually undertaken in themorning (0700-1300). Each village isdivided into four zones for the sake ofsimplicity. The enumerator in thevillage will spend one week in eachzone and is not allowed to continueonto the next zone before the allottedtime even on completing one zone.This is to ensure that each householdis visited at monthly intervals.Completed questionnaires aresubmitted by the enumerators to theirfield supervisors on a weekly basis.
Data quality assurance mechan-isms have been instituted at severalpoints. The most critical of these isthe field supervision. Field super-visors (4 persons) each designated to2-3 villages and a project coordi-natorat Butajira perform the immediatesupervision of data procedures on adaily basis. These people have servedthe project from its inception and arevital organs of
Figure 1: S t u d y d e s i g n – p r o s p e c t i v e s u r v e i l l a n c e o f v i t a l S t u d y d e s i g n – p r o s p e c t i v e s u r v e i l l a n c e o f v i t a le ven t s .e ven t s .
January 1987
Death Out-migration
Birth In-migration
Census Dynamic cohort

16 Ethiop. J. Health Dev.
Figure 2: S c h e m e o f s u p e r v i s i o n . S c h e m e o f s u p e r v i s i o n .
the surveillance system. Their tasksinclude checking of each and everycompleted surveillance form andvisiting a randomly selected 5% ofhouseholds each month on a weeklydistributed time table. The next levelof supervision is performed by theBRHP research assistants (1-2 per-sons). Research assistants have hadpublic health training at Masters' level.They are responsible for the overallsupervision of the surveillance systemfrom the household level to thecomputer system. They also performactual data checking at a field leveland randomly check on somehouseholds every fifteen days.
The highest level of supervision isperformed by the researchers them-selves (Figure 2).
Data entry is performed at theDepartment of Community Health inAddis Ababa. Specially developedcomputer software, using the dBaseIV platform, is used to facilitate
automatic data checking at entry. Eachevent form is entered in a separatetransaction file by data entry clerks.The transfer of data from thetransaction files to the main databaseis done by the researchers using amonthly updating function. Datarecords rejected by the computer forvarious reasons are returned to thefield supervisors for appropriatemeasures through the researchassistant (Figure 3). The introductionof this computer software hassubstantially improved data qualityand management. Efficientmanagement of such a dynamic studybase was not possible to achieve withthe use of commercially availablesoftware. Ideally the data processingshould be done at the field level butlogistic reasons have precluded theimplementation of this so far.Unreliability in the electricity supply,lack of appropriately trained computerpersonnel and unreliablecommunication systems (telephoneand transport) in Butajira were themain reasons keeping the dataprocessing away from Butajira.
The overall field work planning is theresponsibility of the Department ofCommunity Health. Field plans aremade by a management teamcomposed of the Ethiopian re-searchers and research assistantschaired by the Head of Department.Administrative matters and requiredlogistics are arranged through the
Enumerators(At least one for each kebele/PA)
Field Supervisors(Long serving high school
graduates for 2-3 sites)
Field coordinator(Senior nurse)
Research Assistants(Two public health specialists)
Researchers(Multidisciplinary team)
Supervisionand feedback
Quality control

Establishing an epidemiological field laboratory 17
administrative assistant in Addis
Figure 3: D a t a s y s t e m . D a t a s y s t e m .
Ababa and the field co-ordinator inButajira. At the field level feedback isgiven to enumerators and fieldsupervisors on an individual basisweekly or as otherwise appropriate.Short meetings are held monthly wheneverybody gathers to collect theirmonthly salaries. Overall feedback forfield staff is given during thesequarterly meetings, which all field staffare required to attend. That also givesthem the opportunity to learn fromeach others’ experiences.
3.2 Organisational structureThe Butajira Board, composed of
all Ethiopian researchers from all pro-jects operating in the study base and arepresentative from the local healthauthority, meet occasionally. TheBoard is meant to oversee the overallco-ordination of research projects andto maintain ethical standards. Thismay be seen as a safety valve to avoidduplication of efforts and violation ofthe rights of the study population.
On scientific grounds periodiccensuses are necessary to check onthe validity of the surveillance systemand to detect any missed events. Asecond census was done inNovember 1995 in all study villages.Since the interval between the twocensuses was felt to be too long, athird census took place in November1999. The extent of similarity betweenthe census and the surveillancedatabase illustrates the quality of thecontinuous registration system.
The BRHP field office in Butajiraprovides a very good workingenvironment. It was constructed in1995. Before that the project washoused in a very small room sharedwith the local Kebele 04 administrationin Butajira.
The field compound located be-hind Butajira Health Centre hasoffices, computing equipment andguest rooms. The facilities are suffi-cient to carry out the surveillanceactivities and potentially to establish adata management centre closer to thefield.
Though not yet extensively de-livered, some medical benefits haveaccrued to the populations in thestudy villages. Many of the surveysconducted within the study base haveoffered treatment for locally endemicdiseases at the time of the interview.Intervention studies such as the ARIstudy and the indoor air
Raw data
Monthly updating
Data entry intotransaction files
Back to field
Main data base
Data not acceptedto the main data base
Error identified
Correcteddata

18 Ethiop. J. Health Dev.
pollution study (see below) haveprovided complete treatment for thespecific diseases targeted in the study.
These projects support theestablishment and maintenance ofhealth posts in all rural villages and thetraining of community health workers.A mental health study (one of theaffiliated research projects)established a psychiatric clinic at Bu-tajira Health Centre and assisted in thetraining of psychiatric nurses.
The study base is now wellestablished and is being utilised forother more focused studies on es-sential health problems of the countryusing quantitative as well as qualitativeresearch methods. So far research inthe area of childhood respiratoryillnesses, reproductive health, mentalhealth and other infectious diseaseshave been conducted utilising thestudy base infrastructure.
Many of these projects have been partof doctoral studies for Ethiopiancandidates as well as for Swedishpartners.
3.3 The trainingBRHP has contributed to human
resource development and the build-ing of research capacity at the Facultyof Medicine, Addis Ababa University.Nine doctoral study projects havebeen carried out in the study base. Sofar, four have been completed anddefended. The remaining five areongoing projects to be completed inthe coming 1-2 years. These doctoralstudies are mainly registered andsupervised by Umeå University andother Swedish Institutions. Three ofthe nine doctoral studies are forSwedish researchers. The training isconducted in a sandwich model thatallows doctoral researchers to stayclose to
The BRHP field office

Establishing an epidemiological field laboratory 19
their mother institution and carry ontheir routine teaching and otherresponsibilities. The sandwich modelof training also significantly reducesthe risk of the brain drain that mayoccur when people are sent for long-term training abroad. The Departmentof Community Health has witnessedthat with only one out of four staffreturning from long-term studies inNorth America.
Research capacity was alsoenhanced through the short-termtraining programme offered by UmeåUniversity. Seven academic staff ofthe Faculty of Medicine have attendedthe summer course on field researchmethods in Umeå. The Department ofCommunity Health also offered aresearch methodology course forpublic health workers in Ethiopia.Over ten health professionalsrepresenting all but two RegionalHealth Bureaux in Ethiopia haveattended a research methodologycourse in Nazareth, Ethiopia.
This training is one of the directoutputs of the BRHP in bothcollaborating institutions. It is also anincentive for collaborating Ethiopianresearchers to receive further andadditional training on recent advancesin research methodology.
3.4 The collaborationThe BRHP is a collaborative
research undertaking between theDepartment of Community Health,Faculty of Medicine, Addis AbabaUniversity in Ethiopia, and theDepartment of Epidemiology andPublic Health (now Department ofPublic Health and Clinical Medicine),University of Umeå, Sweden. Thecollaboration is based on mutualunderstanding and interest on bothsides.
The collaboration started as anindividual doctoral study project. Asenvisaged from the beginning, it grewinto departmental collaboration alongwith the development of the studybase infrastructure.
Part of the BRHP team at the computer in the field
20 Ethiop. J. Health Dev.
The intensity and diversity of theresearch activities also necessitated awider participation of multidisciplinaryresearchers. At present, the Butajirastudy base has proved that it is in agood position for undertakingscientifically rigorous studies on majorpublic health problems in a developingcountry setting. Thus, thecollaboration is expanding its scopeto involve more departments andinstitutes in the collaborating and othercountries. This growing collaborationwill facilitate the maximum utilisationof the study base and improve on thequality of the research output.
The BRHP study base has re-quired a tremendous amount of per-sonal and institutional investment. Thegenerous and continuous financialsupport from Sida/SAREC has beenvery crucial throughout its long life.However, the strong professionalcommitment of collaboratingresearchers on both sides has beenthe major driving force. The EthiopianScience and Technology Commissionand Addis Ababa University,particularly the Faculty of Medicine,have nurtured the collaboration overthe entire period of the base’sexistence.
4. BASIC DEMOGRAPHY
4.1 The baseline populationThe initial aim of the Butajira
project was to study disease occur-rence in terms of mortality. It is thusnatural to start by describing thebaseline population as of 1st of Janu-ary 1987, the starting date for thedocumentation of cases of death,migration and person-time of follow-up.
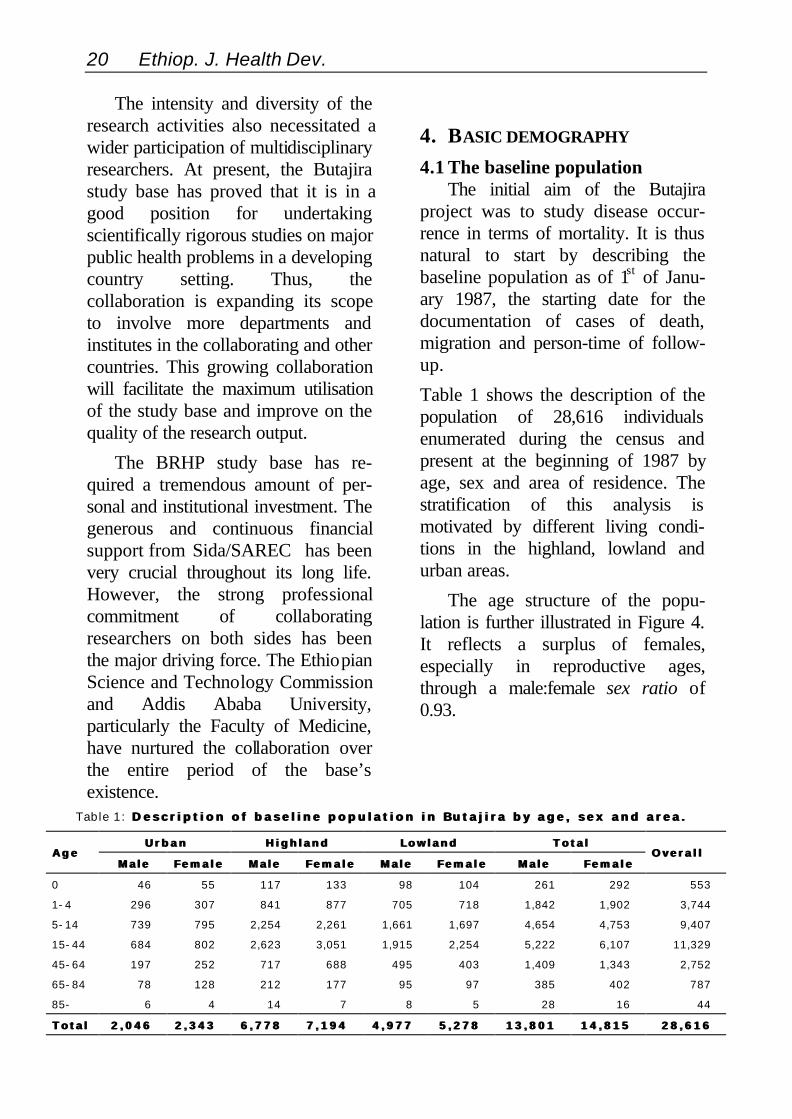
Table 1 shows the description of thepopulation of 28,616 individualsenumerated during the census andpresent at the beginning of 1987 byage, sex and area of residence. Thestratification of this analysis ismotivated by different living condi-tions in the highland, lowland andurban areas.
The age structure of the popu-lation is further illustrated in Figure 4.It reflects a surplus of females,especially in reproductive ages,through a male:female sex ratio of0.93.
Table 1: D e s c r i p t i o n o f b a s e l i n e p o p u l a t i o n i n B u t a j i r a b y a g e , s e x a n d a r e a . D e s c r i p t i o n o f b a s e l i n e p o p u l a t i o n i n B u t a j i r a b y a g e , s e x a n d a r e a .
U r b a nU r b a n H i g h l a n dH i g h l a n d L o w l a n dL o w l a n d T o t a lT o t a lA g eA g e
M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l eO v e r a l lO v e r a l l
0 46 55 117 133 98 104 261 292 553
1-4 296 307 841 877 705 718 1,842 1,902 3,744
5-14 739 795 2,254 2,261 1,661 1,697 4,654 4,753 9,407
15-44 684 802 2,623 3,051 1,915 2,254 5,222 6,107 11,329
45-64 197 252 717 688 495 403 1,409 1,343 2,752
65-84 78 128 212 177 95 97 385 402 787
85- 6 4 14 7 8 5 28 16 44
T o t a lT o t a l 2 , 0 4 62 , 0 4 6 2 , 3 4 32 , 3 4 3 6 , 7 7 86 , 7 7 8 7 , 1 9 47 , 1 9 4 4 , 9 7 74 , 9 7 7 5 , 2 7 85 , 2 7 8 1 3 , 8 0 11 3 , 8 0 1 1 4 , 8 1 51 4 , 8 1 5 2 8 , 6 1 62 8 , 6 1 6

Establishing an epidemiological field laboratory 21
Of all women, 41% are in 15-44 yearage group. The broad-baseddistribution includes 48% childrenunder fifteen and 15% under-fives.Three percent of the population are 65and above. The distribution may becharacterised through a dependencyratio of 1.03, implying that there areequally many outside ("dependants")as within the 15-64 age group("supporters").
These indicators may also be used tocompare the different peasants' asso-ciations (PAs) within the three areas(Table 2).
Table 2 shows that there is asurplus of females in all the studypopulations, particularly so in Butajiratown. The urban area also dis-
plays the highest dependency ratio,reflecting an ageing population andpossibly also the absenteeism of menin productive ages. The proportion ofwomen in reproductive ages is alsolowest in the town.
Figure 4: S t r u c t u r e o f t h e b a s e l i n e S t r u c t u r e o f t h e b a s e l i n ep o p u l a t i o n i n 1 9 8 7 .p o p u l a t i o n i n 1 9 8 7 .
A family in one the study sites in front of their house
0 1000 2000 3000 4000 5000
< 10
10-19
20-29
30-39
40-49
50-59
60-69
70-79
80 +
MalesFemales

22 Ethiop. J. Health Dev.
Table 2: B a s i c d e m o g r a p h i c i n d i c a t o r s o f t h e t e n s t u d y p o p u l a t i o n s . B a s i c d e m o g r a p h i c i n d i c a t o r s o f t h e t e n s t u d y p o p u l a t i o n s .
A r e aA r e a P A p o p u l a t i o nP A p o p u l a t i o nS e xS e x
r a t i or a t i o
D e p e n d -D e p e n d -e n c ye n c yr a t i or a t i o
W o m e n o fW o m e n o fr e p r o d u c -r e p r o d u c -
t i v e a g et i v e a g e
P r o p o r t i o nP r o p o r t i o no f c h i l d r e no f c h i l d r e n
u n d e r 1 5u n d e r 1 5
P r o p o r t i o nP r o p o r t i o no f c h i l d r e no f c h i l d r e nu n d e r f i v eu n d e r f i v e
Urban Butajira 4 (4,389) 0.87 1.27 0.34 0.51 0.16
Mmeskan (2,769) 0.95 0.96 0.43 0.46 0.15Bido (1,824) 0.92 1.05 0.39 0.46 0.14Dirama (2,073) 0.96 1.07 0.42 0.50 0.15Yeteker (3,634) 0.92 0.99 0.41 0.46 0.14
Highland
Wrib (3,663) 0.96 0.89 0.46 0.45 0.13
Mjarda (1,802) 0.94 1.12 0.40 0.51 0.15Bati (2,835) 0.92 1.09 0.40 0.50 0.15Dobena (3,257) 0.96 0.96 0.45 0.47 0.16Lowland
Hobe (2,361) 0.95 0.98 0.44 0.48 0.17
Table 3: B a s i c s o c i a l , e n v i r o n m e n t a l a n d c u l t u r a l c h a r a c t e r i s t i c s o f t h e b a s e l i n e B a s i c s o c i a l , e n v i r o n m e n t a l a n d c u l t u r a l c h a r a c t e r i s t i c s o f t h e b a s e l i n ep o p u l a t i o n .p o p u l a t i o n .
C h a r a c t e r i s t i cC h a r a c t e r i s t i c C a t e g o r yC a t e g o r y U r b a n %U r b a n % H i g h l a n d %H i g h l a n d % L o w l a n d %L o w l a n d % nn
Moslem 64.7 81.5 72.7 20,417religion Christian 35.3 18.5 27.3 6,532
Sodo 6.6 15.7 2.3 2,367Dobi 12.5 4.0 0.7 983Meskan 71.3 63.7 33.8 13,225Mareko 0.0 0.5 32.4 2,853
ethnicity
Silti 9.6 16.2 30.9 4,993
literate 52.3 10.7 19.9 3,505read only 6.8 4.4 9.3 1,131literacy*illiterate 40.9 84.8 70.9 12,857
literate adults 79.5 23.1 36.4 10,027household literacy none 20.5 76.9 63.6 17,480
both literate 36.6 6.3 14.3 2,620head only 33.2 14.4 21.4 3,865spouse only 5.8 1.2 1.2 359
literacycomparisonbetween head andspouse neither 24.4 78.1 63.1 13,073
mean 5.69 5.21 5.22householdmembers s.d. 2.60 2.34 2.27
health system 92.7 93.6 19.3 17,225pharmacy 4.6 3.2 75.9 7,569traditional 1.4 2.2 3.6 664healthcare source
self-treatment 1.3 1.0 1.3 298
river 10.7 80.4 22.0 12,095well 2.7 19.2 78.0 9,352source of waterurban supply 86.6 0.3 0 3,239
thatched 9.5 95.2 95.7 20,621roof of house corrugated iron 90.5 4.8 4.3 4,310
yes 13.8 90.1 87.8 19,234livestock in house
no 86.2 9.9 12.2 5,466
* 9,218 individuals (32.2%) were too young to be literate
Establishing an epidemiological field laboratory 23
The aim of the census was toenumerate the study population (i.e. toget a baseline for the continuoussurveillance) and also to get somebackground information about thepopulation. Information collectionwas based on a structured question-naire containing questions concerningbasic demographic characteristics,cultural patterns, household structure,environmental conditions, health careutilisation and recall of vital events.
Table 3 compares the three areasin terms of these basic characteristics.It shows that this is a predominantlyMuslim community, especially in therural area. There is ethnic variety,although there is one major ethnicgroup in the urban and highland areas.Illiteracy is very high, with two out ofthree house-holds in the rural areahaving no literate adults in thehousehold while, in the town, 80% ofthe households have at least oneliterate household member. Asexpected, there is inequity in thehousehold with regard to literacy, withmainly the head of the householdbeing literate. Urban households tendto be somewhat larger than ruralfamilies.
Socio-economic conditions areillustrated from water supply, houseroofing and the presence of livestockin the house. While there is a pipedwater system in the town, highlandhouseholds mainly utilise river waterand lowland households have wells.Typically the houses in the town havecorrugated iron roofs and the tukuls inthe rural areas have thatched roofs.The latter usually goes with keepinglivestock in the house.
4.2 Population development 1987-96
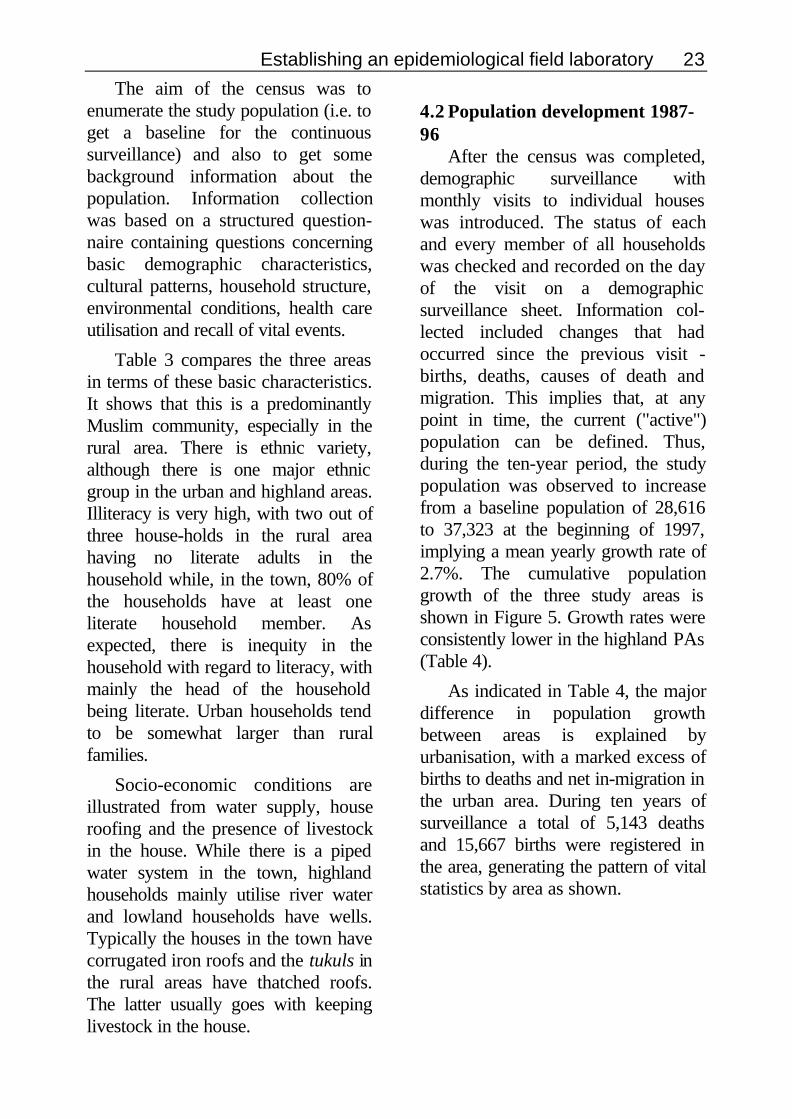
After the census was completed,demographic surveillance withmonthly visits to individual houseswas introduced. The status of eachand every member of all householdswas checked and recorded on the dayof the visit on a demographicsurveillance sheet. Information col-lected included changes that hadoccurred since the previous visit -births, deaths, causes of death andmigration. This implies that, at anypoint in time, the current ("active")population can be defined. Thus,during the ten-year period, the studypopulation was observed to increasefrom a baseline population of 28,616to 37,323 at the beginning of 1997,implying a mean yearly growth rate of2.7%. The cumulative populationgrowth of the three study areas isshown in Figure 5. Growth rates wereconsistently lower in the highland PAs(Table 4).
As indicated in Table 4, the majordifference in population growthbetween areas is explained byurbanisation, with a marked excess ofbirths to deaths and net in-migration inthe urban area. During ten years ofsurveillance a total of 5,143 deathsand 15,667 births were registered inthe area, generating the pattern of vitalstatistics by area as shown.

24 Ethiop. J. Health Dev.
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
Highland
Lowland
Urban
1987 -88 -89 -90 -97-91 -92 -93 -94 -95 -96
Figure 5: P o p u l a t i o n d e v e l o p m e n t i n P o p u l a t i o n d e v e l o p m e n t i nt h e t h r e e s t u d y a r e a s 1 9 8 7 - 9 6 .t h e t h r e e s t u d y a r e a s 1 9 8 7 - 9 6 .
4.3 Overall mortality patternDuring the ten years of sur-
veillance, a total of 336,074 person-years of follow-up were generated.Thus, by relating the observed totalnumber of deaths to this study base,we get a crude mortality rate of5,143/336,076 = 15.30 per 1,000person-years. Based on the Poissondistribution, the 95% confidenceinterval for this estimate is 14.9 to15.7.
From Table 5 we may concludethat there are major differences inmortality between areas and con-sistently higher mortality amongmales.
To provide information about age-specific mortality patterns, Table 6shows the overall infant, childhoodand adult mortality rates by area andsex.
A sex-specific graphical illustra-tion of mortality patterns in the threeareas over age is shown in Figure 6.
Figure 6: S e x - s p e c i f i c m o r t a l i t y S e x - s p e c i f i c m o r t a l i t yr a t e s b y a r e a .r a t e s b y a r e a .
These "bath-tub" curves show thehigher mortality in the lowlands forboth males and females.
An interesting pattern nowemerges where the excess male tofemale mortality still holds in the urbanarea for all age groups while, in thelowlands, there is a shift to thedisadvantage of females above 45years of age.
Age in years
Rate per 1000
Infan
ts
1-4
5-1
4
15
-44
45
-64
65
-
Infan
ts
1-4
5-1
4
15
-44
45
-64
65
-
0
50
100
150
LowlandHighlandUrban
Males Females
Establishing an epidemiological field laboratory 25
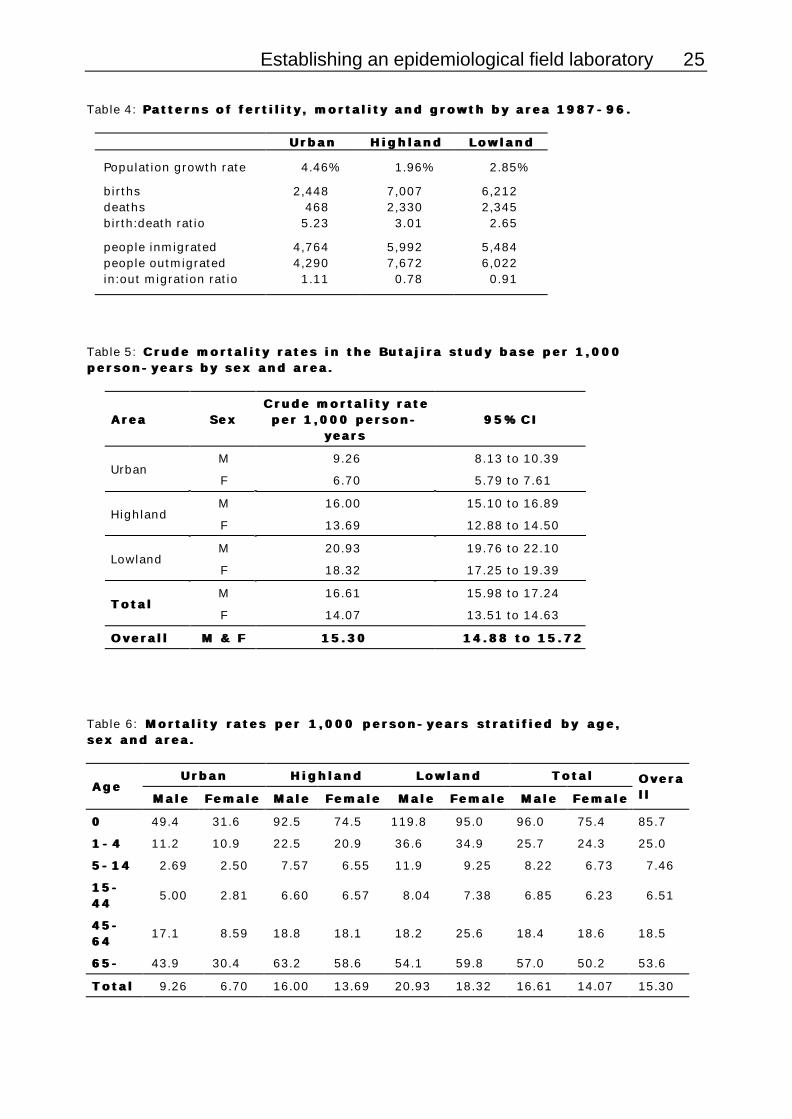
Table 4: P a t t e r n s o f f e r t i l i t y , m o r t a l i t y a n d g r o w t h b y a r e a 1 9 8 7 - 9 6 . P a t t e r n s o f f e r t i l i t y , m o r t a l i t y a n d g r o w t h b y a r e a 1 9 8 7 - 9 6 .
U r b a nU r b a n H i g h l a n dH i g h l a n d L o w l a n dL o w l a n d
Population growth rate 4.46% 1.96% 2.85%
births 2,448 7,007 6,212deaths 468 2,330 2,345birth:death ratio 5.23 3.01 2.65
people inmigrated 4,764 5,992 5,484people outmigrated 4,290 7,672 6,022in:out migration ratio 1.11 0.78 0.91
Table 5: C r u d e m o r t a l i t y r a t e s i n t h e B u t a j i r a s t u d y b a s e p e r 1 , 0 0 0 C r u d e m o r t a l i t y r a t e s i n t h e B u t a j i r a s t u d y b a s e p e r 1 , 0 0 0p e r s o n - y e a r s b y s e x a n d a r e a .p e r s o n - y e a r s b y s e x a n d a r e a .
A r e aA r e a S e xS e xC r u d e m o r t a l i t y r a t eC r u d e m o r t a l i t y r a t e
p e r 1 , 0 0 0 p e r s o n -p e r 1 , 0 0 0 p e r s o n -y e a r sy e a r s
9 5 % C I9 5 % C I
M 9.26 8.13 to 10.39Urban
F 6.70 5.79 to 7.61
M 16.00 15.10 to 16.89Highland
F 13.69 12.88 to 14.50
M 20.93 19.76 to 22.10Lowland
F 18.32 17.25 to 19.39
M 16.61 15.98 to 17.24T o t a lT o t a l
F 14.07 13.51 to 14.63
O v e r a l lO v e r a l l M & FM & F 1 5 . 3 01 5 . 3 0 1 4 . 8 8 t o 1 5 . 7 21 4 . 8 8 t o 1 5 . 7 2
Table 6: M o r t a l i t y r a t e s p e r 1 , 0 0 0 p e r s o n - y e a r s s t r a t i f i e d b y a g e , M o r t a l i t y r a t e s p e r 1 , 0 0 0 p e r s o n - y e a r s s t r a t i f i e d b y a g e ,s e x a n d a r e a .s e x a n d a r e a .
U r b a nU r b a n H i g h l a n dH i g h l a n d L o w l a n dL o w l a n d T o t a lT o t a lA g eA g e
M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l e M a l eM a l e F e m a l eF e m a l e
O v e r aO v e r al ll l
00 49.4 31.6 92.5 74.5 119.8 95.0 96.0 75.4 85.7
1 - 41 - 4 11.2 10.9 22.5 20.9 36.6 34.9 25.7 24.3 25.0
5 - 1 45 - 1 4 2.69 2.50 7.57 6.55 11.9 9.25 8.22 6.73 7.46
1 5 -1 5 -4 44 4
5.00 2.81 6.60 6.57 8.04 7.38 6.85 6.23 6.51
4 5 -4 5 -6 46 4
17.1 8.59 18.8 18.1 18.2 25.6 18.4 18.6 18.5
6 5 -6 5 - 43.9 30.4 63.2 58.6 54.1 59.8 57.0 50.2 53.6
T o t a lT o t a l 9.26 6.70 16.00 13.69 20.93 18.32 16.61 14.07 15.30

26 Ethiop. J. Health Dev.
The highland area seems to be inan intermediate position with regard tothis "transition" (Figure 7).
Figure 7: C o m p a r i n g l i f e - s p a n C o m p a r i n g l i f e - s p a nm o r t a l i t y b e t w e e n s e x e s b y m e a n sm o r t a l i t y b e t w e e n s e x e s b y m e a n so f f e m a l e t o m a l e m o r t a l i t y r a t i o so f f e m a l e t o m a l e m o r t a l i t y r a t i o sf o r t h e t h r e e a r e a s .f o r t h e t h r e e a r e a s .
The rural to urban mortalitydifferentials are somewhat more pro-nounced for females, especially foradults.
Figure 8, again, illustrates thedisadvantageous situation of ruralwomen while, for men, there is only arather small excess mortality in ruralareas. The most marked areadifferences in mortality occur amongchildren.
The 2,456 under-five deathsrepresent nearly 50% of all deaths.
Female to malemortality rate
Infants 1-4 5-14 15-44 45-64 65+0,0
0,5
1,0
1,5
Lowland
Highland
Urban
Figure 8: C o m p a r i n g l i f e - s p a n m o r t a l i t y b e t w e e n a r e a s f o r m a l e s a n d f e m a l e s . C o m p a r i n g l i f e - s p a n m o r t a l i t y b e t w e e n a r e a s f o r m a l e s a n d f e m a l e s .
Mortality rates relative to urban area
Infants 1-4 5-14 15-44 45-64 65+0
1
2
3
4
Lowland to urban
Highland to urban
MalesMales
Infants 1-4 5-14 15-44 45-64 65+0
1
2
3
4
Lowland to urban
Highland to urban
FemalesFemales
Establishing an epidemiological field laboratory 27
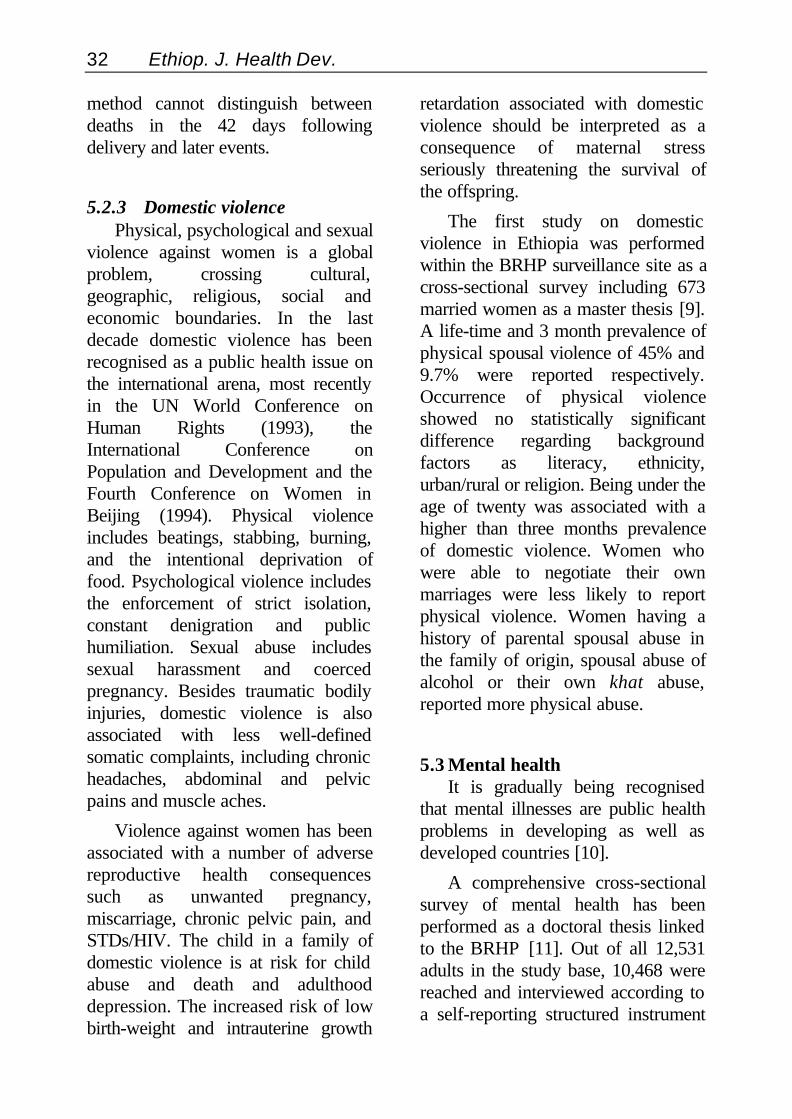
Half of the under-five deathsoccurred during the first year of life,half of which fell below 2 months ofage. From the age-specific mortalityrates we can estimate the cumulativemortality throughout life. Thus, amonglive births 4.2% are estimated to dieduring the first two months of life,8.0% before one year, 16.6% before 5years, 36% before 15 years, and 56%before 65 years. There weresubstantial variations between areasalso with regard to under-fivemortality ranging from 80 per 1,000person-years in the urban area to 219per 1,000 person-years in thelowlands (Figure 9).
Figure 9: C u m u l a t i v e u n d e r - f i v e C u m u l a t i v e u n d e r - f i v em o r t a l i t y r a t e b y a r e a i n B u t a j i r am o r t a l i t y r a t e b y a r e a i n B u t a j i r ad u r i n g 1 9 8 7 - 9 6 .d u r i n g 1 9 8 7 - 9 6 .
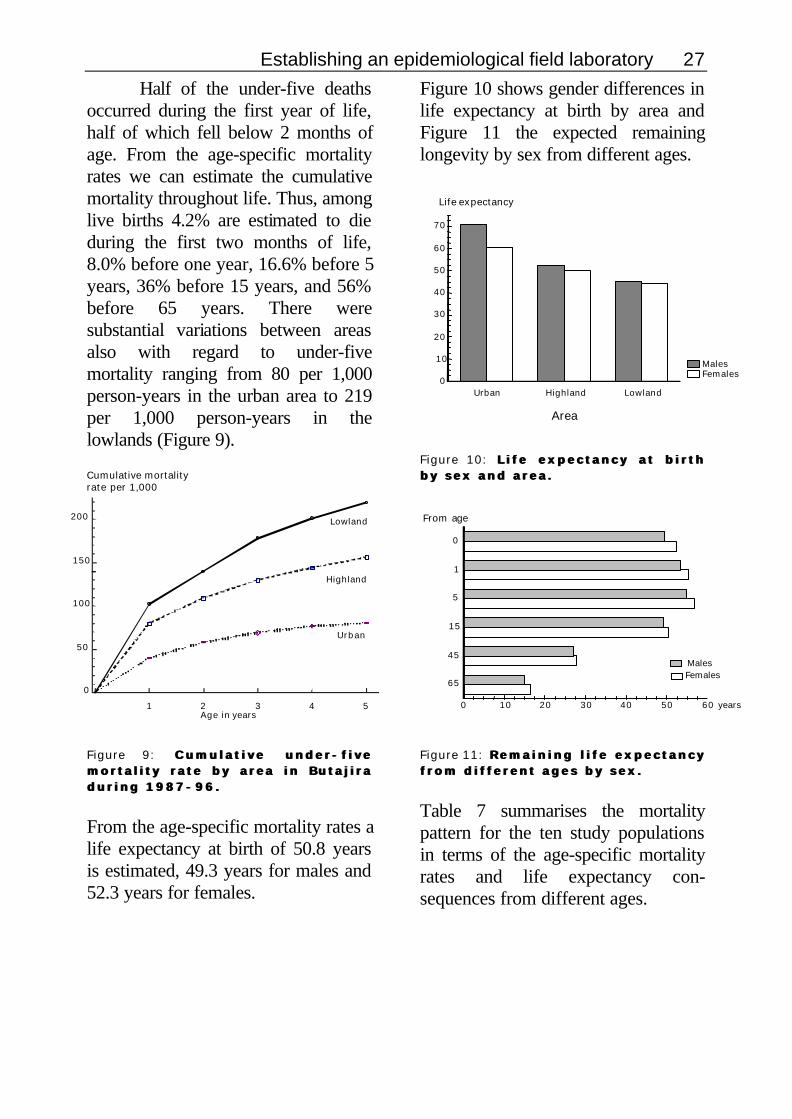
From the age-specific mortality rates alife expectancy at birth of 50.8 yearsis estimated, 49.3 years for males and52.3 years for females.
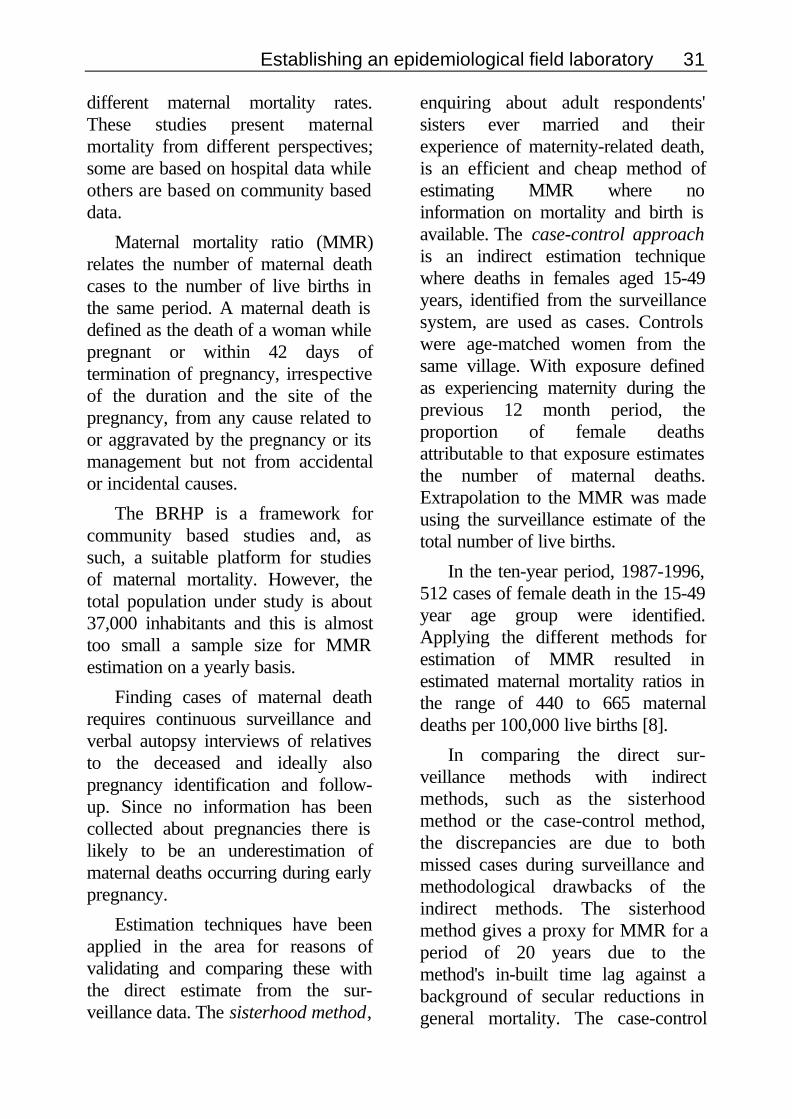
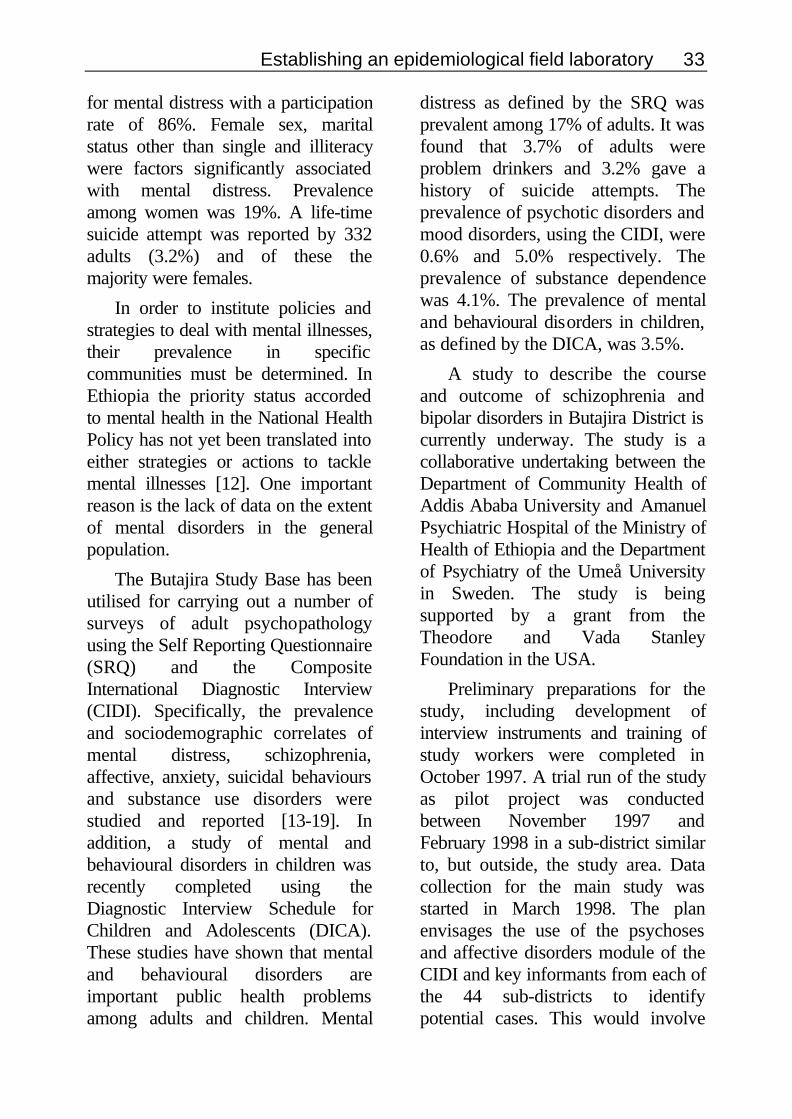
Figure 10 shows gender differences inlife expectancy at birth by area andFigure 11 the expected remaininglongevity by sex from different ages.
Figure 10: L i f e e x p e c t a n c y a t b i r t h L i f e e x p e c t a n c y a t b i r t hb y s e x a n d a r e a .b y s e x a n d a r e a .
Figure 11: R e m a i n i n g l i f e e x p e c t a n c y R e m a i n i n g l i f e e x p e c t a n c yf r o m d i f f e r e n t a g e s b y s e x .f r o m d i f f e r e n t a g e s b y s e x .
Table 7 summarises the mortalitypattern for the ten study populationsin terms of the age-specific mortalityrates and life expectancy con-sequences from different ages.
Area
Life expectancy
Urban Highland Lowland0
10
20
30
40
50
60
70
FemalesMales
0
1
5
15
45
65
0 10 20 30 40 50 60
Females Males
From age
yearsAge in years
Cumulative mortalityrate per 1,000
1 2 3 4 5
0
50
100
150
200
Urban
Highland
Lowland

28 Ethiop. J. Health Dev.
Table 7 : M o r t a l i t y c h a r a c t e r i s t i c s o f e a c h o f t h e t e n d i f f e r e n t s t u d y: M o r t a l i t y c h a r a c t e r i s t i c s o f e a c h o f t h e t e n d i f f e r e n t s t u d yp o p u l a t i o n s .p o p u l a t i o n s .
A g e - s p e c i f i c m o r t a l i t y r a t e s / 1 , 0 0 0A g e - s p e c i f i c m o r t a l i t y r a t e s / 1 , 0 0 0p e r s o n - y e a r sp e r s o n - y e a r s
L i f eL i f ee x p e c t a ne x p e c t a nc yc yA r e aA r e a P AP A
00 1 - 41 - 4 5 - 1 45 - 1 41 5 -1 5 -4 44 4
4 5 -4 5 -6 46 4
6 5 +6 5 +
A l lA l la g e sa g e s
a t b i r t ha t b i r t h
Urban Butajira 40.5 11.1 2.59 3.83 12.3 35.4 7.91 69.2
Mmeskan 71.8 18.8 6.23 6.52 18.6 67.6 13.8 55.1Bido 97.8 27.2 11.20 9.52 17.9 55.2 19.9 48.4Dirama 96.6 29.3 8.75 7.31 15.5 91.2 16.6 49.8Yeteker 64.9 19.8 6.76 6.22 17.4 58.7 13.5 56.2
Highland
Wrib 95.5 19.6 5.23 5.46 21.2 51.7 13.8 55.4
Mjarda 100.3 32.8 10.10 9.12 21.6 54.7 18.4 47.2Bati 114.4 37.5 11.50 9.28 22.2 51.1 20.6 45.2Dobena 128.2 42.4 11.10 7.40 22.8 64.9 21.8 44.4
Lowland
Hobe 83.2 28.4 9.23 5.24 18.5 54.2 16.5 53.2
T o t a lT o t a l A l l A l l P A sP A s 8 5 . 78 5 . 7 2 5 . 02 5 . 0 7 . 4 67 . 4 6 6 . 5 16 . 5 1 1 8 . 51 8 . 5 5 3 . 65 3 . 6 1 5 . 31 5 . 3 5 0 . 85 0 . 8
5. APPLYING THE STUDY BASE
TO SPECIFIC STUDIES
5.1 Acute respiratory infectionsamong children
From various ARI studies, severalreports have been completed and anew study is at the planning and fieldstaff recruitment stage. All of thesestudies have been nested in thedemographic surveillance system,using its output - the populationdatabase - as a sampling frame foridentifying specific study populationsand utilising the monthly routinesurveillance to follow the studysubjects. The existing infrastructure ofthe BRHP field organisation has beenused for co-ordination of projectactivities, supplemented by extra staffwho have been specially trained forthe data
collection activities of each specificproject. This also has meant that overthe years a pool of trained field staff,enumerators, has grown to become aresource for new activities.
A variety of study designs,focussing on different aspects of ARIepidemiology, have been used to givea broader view of the problem area, asshown in Figure 12. After an initialcohort study using the routinesurveillance to follow the population,there was a cross-sectional prevalencestudy, a nested case-referent study, across-sectional survey, a prospectivecohort study and a step-wedge designintervention study. The new study isto be a cohort and nested case-referent study.

Establishing an epidemiological field laboratory 29
..
The ultimate objective of the ARIstudies has been the design of aneffective and appropriate casemanagement protocol for pneumoniain children under 5 years of age at thecommunity level. Existing datasuggested that up to 35% of infantand child mortality in Ethiopia isassociated with pneumonia. Thus theARI component of the BRHP aimedat identifying major deficiencies andobstacles in health care delivery,reviewing mothers' perceptions andpractices in the care of children withARI and characterising aetiologicagents and risk factors. A carriershipstudy showed that 85% of children inthe project area carried Haemophilusinfluenzae, 83% Moraxellacatarrhalis and 90% Streptococcuspneumoniae in the nasopharynx.
5.1.1 MortalityAn early application of the BRHP
study base grew out of the findingsfrom the verbal autopsy data of thefirst two years (1987-88) of thedemographic surveillance. As in manydeveloping country settings, acuterespiratory infections (ARI) werefound to constitute the majoridentifiable cause of death amonginfants and children up to five years ofage, exceeding the mortality fromdiarrhoeal diseases in all the ruralareas in the study base [6]. Therewere also shown marked differencesin both ARI mortality and all-causesmortality among under-fives betweendifferent parts of the study area,highest in the rural lowland and lowestin the urban sub-population of thestudy base.
Figure 12: S t u d y d e s i g n s a n d d i f f e r e n t c o m p o n e n t s o f s t u d i e s o f a c u t e S t u d y d e s i g n s a n d d i f f e r e n t c o m p o n e n t s o f s t u d i e s o f a c u t er e s p i r a t o r y i n f e c t i o n s .r e s p i r a t o r y i n f e c t i o n s .
Prevalence study ofpotential respiratorydisease bacteria inchildren under five
Mothers’ perceptionsof illness and practices
in care of children with ARI
Prospective study ofmorbidity patterns in
under-fives
Initial study of causeof death pattern in
under-fives
Nested study ofdeterminants of
under-five mortality
Step-wedge designcase management
intervention
Cross-sectional Cohort Case-referent
Nested study of ALRIand indoor air
pollution
Prospective exposureassessment for indoor
air pollution

30 Ethiop. J. Health Dev.
ARI mortality was particularlyaffected by parental factors, includingilliteracy of the father, andenvironmental factors, including lackof windows in the house, and less soby breast-feeding, milk, and proteinsupplementation, which insteadsignificantly affected diarrhoealmortality [7].
5.1.2 MorbidityThe prospective morbidity study
was based on weekly home-visits. Acohort of 1,315 children under the ageof 5 years were followed weekly,including the use of a recall card, overa one-year period. The recall card wasa simple calendar with a photographof the child, on which mothersrecorded perceived illness on a dailybasis. The weekly interviews collectedthis information as well as limitedclinical observations made by the fieldworkers, who were specifically trainedfor this. The results of the dailyreported morbidity were assembledand used to define episodes ofdisease entities such as ARI,diarrhoeal disease and febrile illness.Incidence of disease episodes werethen related to individual risk factorsin a multivariate Poisson regressionmodel.
5.1.3 InterventionIntervention strategies to reduce
ARI mortality and morbidity werereviewed. The implementation of anARI intervention package consistingof health posts, community healthagents and a handful of inexpensive
drugs to reduce mortality from ARIwas a logical follow up. Such apackage is affordable and sustainablein a poor country like Ethiopia. Beforelaunching the intervention, it wasimportant to talk to leaders ofcommunities on the aims, processesand advantages including responsi-bilities of the communities. Theimpact of the intervention can beevaluated almost continuously by themonthly surveillance in terms ofunder-five or infant mortality rates orcause-specific mortality ratescomparing intervention areas withprevious years and with control areas.
5.2 Women’s health5.2.1 Maternal mortality
Maternal mortality is difficult toestimate from rural populations inlow-income countries due to therelative rarity of the event and lack ofofficial birth and death registration.Hospitals are scarce and means ofreaching hospital from rural areas aredifficult or impossible. Several studiesfrom Ethiopia have reported quite
Establishing an epidemiological field laboratory 31
different maternal mortality rates.These studies present maternalmortality from different perspectives;some are based on hospital data whileothers are based on community baseddata.
Maternal mortality ratio (MMR)relates the number of maternal deathcases to the number of live births inthe same period. A maternal death isdefined as the death of a woman whilepregnant or within 42 days oftermination of pregnancy, irrespectiveof the duration and the site of thepregnancy, from any cause related toor aggravated by the pregnancy or itsmanagement but not from accidentalor incidental causes.
The BRHP is a framework forcommunity based studies and, assuch, a suitable platform for studiesof maternal mortality. However, thetotal population under study is about37,000 inhabitants and this is almosttoo small a sample size for MMRestimation on a yearly basis.
Finding cases of maternal deathrequires continuous surveillance andverbal autopsy interviews of relativesto the deceased and ideally alsopregnancy identification and follow-up. Since no information has beencollected about pregnancies there islikely to be an underestimation ofmaternal deaths occurring during earlypregnancy.
Estimation techniques have beenapplied in the area for reasons ofvalidating and comparing these withthe direct estimate from the sur-veillance data. The sisterhood method,
enquiring about adult respondents'sisters ever married and theirexperience of maternity-related death,is an efficient and cheap method ofestimating MMR where noinformation on mortality and birth isavailable. The case-control approachis an indirect estimation techniquewhere deaths in females aged 15-49years, identified from the surveillancesystem, are used as cases. Controlswere age-matched women from thesame village. With exposure definedas experiencing maternity during theprevious 12 month period, theproportion of female deathsattributable to that exposure estimatesthe number of maternal deaths.Extrapolation to the MMR was madeusing the surveillance estimate of thetotal number of live births.
In the ten-year period, 1987-1996,512 cases of female death in the 15-49year age group were identified.Applying the different methods forestimation of MMR resulted inestimated maternal mortality ratios inthe range of 440 to 665 maternaldeaths per 100,000 live births [8].
In comparing the direct sur-veillance methods with indirectmethods, such as the sisterhoodmethod or the case-control method,the discrepancies are due to bothmissed cases during surveillance andmethodological drawbacks of theindirect methods. The sisterhoodmethod gives a proxy for MMR for aperiod of 20 years due to themethod's in-built time lag against abackground of secular reductions ingeneral mortality. The case-control
32 Ethiop. J. Health Dev.
method cannot distinguish betweendeaths in the 42 days followingdelivery and later events.
5.2.3 Domestic violencePhysical, psychological and sexual
violence against women is a globalproblem, crossing cultural,geographic, religious, social andeconomic boundaries. In the lastdecade domestic violence has beenrecognised as a public health issue onthe international arena, most recentlyin the UN World Conference onHuman Rights (1993), theInternational Conference onPopulation and Development and theFourth Conference on Women inBeijing (1994). Physical violenceincludes beatings, stabbing, burning,and the intentional deprivation offood. Psychological violence includesthe enforcement of strict isolation,constant denigration and publichumiliation. Sexual abuse includessexual harassment and coercedpregnancy. Besides traumatic bodilyinjuries, domestic violence is alsoassociated with less well-definedsomatic complaints, including chronicheadaches, abdominal and pelvicpains and muscle aches.
Violence against women has beenassociated with a number of adversereproductive health consequencessuch as unwanted pregnancy,miscarriage, chronic pelvic pain, andSTDs/HIV. The child in a family ofdomestic violence is at risk for childabuse and death and adulthooddepression. The increased risk of lowbirth-weight and intrauterine growth
retardation associated with domesticviolence should be interpreted as aconsequence of maternal stressseriously threatening the survival ofthe offspring.
The first study on domesticviolence in Ethiopia was performedwithin the BRHP surveillance site as across-sectional survey including 673married women as a master thesis [9].A life-time and 3 month prevalence ofphysical spousal violence of 45% and9.7% were reported respectively.Occurrence of physical violenceshowed no statistically significantdifference regarding backgroundfactors as literacy, ethnicity,urban/rural or religion. Being under theage of twenty was associated with ahigher than three months prevalenceof domestic violence. Women whowere able to negotiate their ownmarriages were less likely to reportphysical violence. Women having ahistory of parental spousal abuse inthe family of origin, spousal abuse ofalcohol or their own khat abuse,reported more physical abuse.
5.3 Mental healthIt is gradually being recognised
that mental illnesses are public healthproblems in developing as well asdeveloped countries [10].
A comprehensive cross-sectionalsurvey of mental health has beenperformed as a doctoral thesis linkedto the BRHP [11]. Out of all 12,531adults in the study base, 10,468 werereached and interviewed according toa self-reporting structured instrument
Establishing an epidemiological field laboratory 33
for mental distress with a participationrate of 86%. Female sex, maritalstatus other than single and illiteracywere factors significantly associatedwith mental distress. Prevalenceamong women was 19%. A life-timesuicide attempt was reported by 332adults (3.2%) and of these themajority were females.
In order to institute policies andstrategies to deal with mental illnesses,their prevalence in specificcommunities must be determined. InEthiopia the priority status accordedto mental health in the National HealthPolicy has not yet been translated intoeither strategies or actions to tacklemental illnesses [12]. One importantreason is the lack of data on the extentof mental disorders in the generalpopulation.
The Butajira Study Base has beenutilised for carrying out a number ofsurveys of adult psychopathologyusing the Self Reporting Questionnaire(SRQ) and the CompositeInternational Diagnostic Interview(CIDI). Specifically, the prevalenceand sociodemographic correlates ofmental distress, schizophrenia,affective, anxiety, suicidal behavioursand substance use disorders werestudied and reported [13-19]. Inaddition, a study of mental andbehavioural disorders in children wasrecently completed using theDiagnostic Interview Schedule forChildren and Adolescents (DICA).These studies have shown that mentaland behavioural disorders areimportant public health problemsamong adults and children. Mental
distress as defined by the SRQ wasprevalent among 17% of adults. It wasfound that 3.7% of adults wereproblem drinkers and 3.2% gave ahistory of suicide attempts. Theprevalence of psychotic disorders andmood disorders, using the CIDI, were0.6% and 5.0% respectively. Theprevalence of substance dependencewas 4.1%. The prevalence of mentaland behavioural disorders in children,as defined by the DICA, was 3.5%.
A study to describe the courseand outcome of schizophrenia andbipolar disorders in Butajira District iscurrently underway. The study is acollaborative undertaking between theDepartment of Community Health ofAddis Ababa University and AmanuelPsychiatric Hospital of the Ministry ofHealth of Ethiopia and the Departmentof Psychiatry of the Umeå Universityin Sweden. The study is beingsupported by a grant from theTheodore and Vada StanleyFoundation in the USA.
Preliminary preparations for thestudy, including development ofinterview instruments and training ofstudy workers were completed inOctober 1997. A trial run of the studyas pilot project was conductedbetween November 1997 andFebruary 1998 in a sub-district similarto, but outside, the study area. Datacollection for the main study wasstarted in March 1998. The planenvisages the use of the psychosesand affective disorders module of theCIDI and key informants from each ofthe 44 sub-districts to identifypotential cases. This would involve
34 Ethiop. J. Health Dev.
the application of the CIDI to theentire district population 15-49 yearsof age (estimated to be over 100,000).A total of over 32,000 adults betweenthe ages of 15 and 49 have so far beeninterviewed in 27 sub-districts(kebeles).
5.4 Master of Public HealthStudies
The Department of CommunityHealth has been running a Master ofPublic Health programme since 1984.The training consists of coursework,residency attachment programmes andresearch work. The Butajira studybase has provided a continuous forumfor research and residency work forthese MPH students. Masters’students take research areas that arebeing developed by researchers in thedepartment to avoid over-burdeningthe study population.
Besides enhancing the efficientutilisation of resources and personnelin the study base, the Masters’ studieshave made significant scientificcontributions. Areas of Masters’studies include the following broadsubjects: child feeding and nutrition,drug utilisation patterns, domesticviolence, migration, reproductivehealth, mental health and healthservices assessment. To date theBRHP has involved 15 Masters’students from the Department.(Appendix I). The Ethiopiancollaborating researchers were able totake heavy loads of Masters’ studiessupervision since students are comingto an established study base and
working in line with existing researchinterests.
6. MAJOR FINDINGS SO FAR
6.1 The public health of Butajira1987-96
The Butajira project has docu-mented high under-five and infantmortality in rural Ethiopian com-munities. Under-five mortality ac-counted for 50% of all deaths. ARIcontributed one fifth of the under-fivemortality and one third of the infantmortality. ARI was more commonthan diarrhoea as a cause of deathamong infants.
Based on the first ten years ofsurveillance cumulative mortalitythroughout life has been estimated.Thus, among live births 17% areestimated to die before 5 years, 36%before 15 years and 56% before 65years. The overall life expectancy hasbeen 49.3 years for males and 52.3years for females.
The Butajira study base was alsoused to perform a one-year pro-spective morbidity study based onweekly home-visits. Overall, illnesswas reported in 5.8% of 11,216person-years among the under-fives.ARI and acute diarrhoea were thecommonest conditions. ARI wasresponsible for 48% of the under-fiveillness load and 5.7% of all ARI wereacute lower respiratory tractinfections. ARI mortality was parti-cularly affected by parental factors,including illiteracy of the father, andenvironmental factors, including lackof window in the house. Parental
Establishing an epidemiological field laboratory 35
factors, such as illiteracy were alsolinked to morbidity. In summary,housing factors mainly affectedmortality while sanitation, healthbehaviour and reproductive healthfactors mainly affected morbidity.Urban/rural residence and parentalfactors affected both mortality andmorbidity.
The extension of health services tothe underserved rural population hasbeen an explicit goal in nationaldevelopment plans in Ethiopia overthe last decade. The number of healthunits and health personnel in ruralareas and small towns has indeedincreased. But has this also meant animproved access to the services? Thisstudy illustrates that the outreach ofhealth services within a rural districtcan be very limited and that largeinequalities exist. Over 70% of thepopulation in the small town ofButajira used the health care inconnection with reported illnesswhereas less than 30% of the peopleoutside the town did so. Themagnitude of this problem is shownby the fact that the population ofpeasants is about 20 times that of thetown population and that they report2-5 times more illness. The perceivedmorbidity in the urban area, the ruralhighland and the rural lowland couldbe contrasted with the mortality ratesas recorded in the continuous sur-veillance of vital events during thesame year. A high rate of reportedillness was associated with highmortality rates, whereas the pro-portion of clinic users was highestamong those with the lowest rate of
reported illness and with the lowestmortality, i.e. in the urban area.
The differences in access to andutilisation of preventive services areeven more dramatic. Whereas 70% ofmothers in the town used the antenatalservices, less than 20% of the mothersin the peasant households did so. Thevaccination programmes reach thetown children but practically none ofthe children in the rural areas nearby[1].
It is also obvious that this ruralcommunity is a society in transitionand urbanisation. Over the ten-yearperiod the overall growth rate hasbeen 2.7% per year on average and ashigh as 4.5% in Butajira town. Therural to urban mortality differentialsare most marked for children, and tothe disadvantage of rural women.While, for instance, female mortality45-54 years in the town is half thatamong males, it is well above that ofmales in the rural lowlands.
In summary, this project highlightsa gross discrepancy between needsfor and access to organised healthcare at district level, where availablehealth services also seem to workbelow capacity. Equity in health careis far from having been achieved. Nodoubt improvements can be madewithin existing limited resourcesthrough better organisation and moreattention to outreach programmes andthrough developing ways to work withthe people, empowering them toengage in solving their own healthproblems and demanding their ownshare of health resources.

36 Ethiop. J. Health Dev.
6.2 Methodological experiencesSince the basic raison d'être for
this type of population based sur-veillance arises out of a lack of civilregistration infrastructure, it followsthat appropriate methodologies haveto be implemented from first prin-ciples. Thus in many ways the BRHPhas pioneered methods ofepidemiological and demographicsurveillance that can be appropriatelyapplied in this kind of setting.
When the Butajira project startedin the late 1980s, personal computerswere still in early stages ofdevelopment and there was very littleexperience of their use in sub-SaharanAfrica, particularly in remote locationssuch as this [20]. Initially therefore itwas unrealistic to think of com-puterisation of the data on-site, andeven at Addis Ababa Universityfacilities for handling the data werelimited at this stage. Records wereoriginally entered as plain text stringsusing a simple text editor. Whilst thisserved a useful function for lateranalysis, it did not facilitate easyinteraction with the data, nor permittedreal-time error checking and qualityassurance procedures. As well as thebasic requirements for processing thiskind of data, a special issue arose inthe Ethiopian context because of theunique calendar system in use, inwhich the year starts in mid-September, has 13 months (12 of 30days and one of 5 or 6) and runs2,809 days behind the international(Gregorian) system. Since fieldworkers were much more conversant
with the local Ethiopian system, thisas used for dates in the field, whichwere then converted as part of thedata entry process. In the initialphases of the project, when data entrywas in text strings, this conversionprocess added further difficulties.
Following a decision in 1993 that are-census of the entire studypopulation was called for in order tovalidate and update the study base,new forms for the census itself andcontinuing vital event surveillancethereafter were developed. These weretranslated into the common locallanguage, Amharic, and field tested. Asample of the Birth Registration form(English and Amharic versions) areappended. Experience shows that,given the basic educational level ofmost field staff, the extra time andeffort involved in using locallanguages (and also in this case thelocal calendar) is well spent in termsof data quality.

Establishing an epidemiological field laboratory 37
Prior to the 1995 re-census, and inthe light of developments in computerhardware and software in themeantime, a new software system fordata entry and storage was developedusing a relational database approach[21]. The basic design of this systemis shown in Figure 13.
Within the data checking part ofthis system, implemented under dBaseIV, it was possible to include a routinefor automatic conversion of datevariables from the Ethiopian format onentry. The development of this newsystem involved a considerableamount of effort and difficulty, notleast as a result of the relative scarcityof computer trained personnel inEthiopia at the time. Much of thetechnical support was provided fromcollaboration with Sweden, thoughthis in itself was not an ideal solution.It also transpired that in previousyears a considerable backlog of dataerrors had accumulated in the absenceof checking facilities, particularly inrespect of the date variables. Forexample, it emerged that a proportionof dates of birth had been enteredunconverted, resulting in some
individuals being recorded as someseven years too old, and giving a verydistorted age/sex distribution asshown in Figure 14.
Figure 14: D i s t o r t e d a g e - s e x D i s t o r t e d a g e - s e xp y r a m i d a s a c o n s e q u e n c e o f s o m ep y r a m i d a s a c o n s e q u e n c e o f s o m ew r o n g l y c o d e d d a t e s o f b i r t hw r o n g l y c o d e d d a t e s o f b i r t h
Simultaneously implementing thenew software, undertaking the re-census and trying to trace ac-cumulated errors led to a difficultperiod in the life of the project whichtook several years to work through.
The intention from the census of1995 was to localise data processingat the office in Butajira, so that formswould not need to be transported toAddis Ababa and real-time errordetection and enquiry processescould be implemented much closer tothe field. However, serious problemswith the local power supply andtelecommunications services made itnecessary to revert to handling data inAddis Ababa, although the goal oflocalising it in Butajira remains, and
85 -80 - 8475 - 7970 - 7465 - 6960 - 6455 - 5950 - 5445 - 4940 - 4435 - 3930 - 3425 - 2920 - 2415 - 1910 - 14
5 - 90 - 4
3000 2000 1000 0 1000 2000 3000
FemalesMales
Age group
Newhousehold
register
Mainhouseholddatabase
Main individualdatabase
Maritalstatus
register
Internal move
register
Outmigrationregister
In migrationregister
Deathregister
New birthregister
updating
EntryEntry of vital of vital events events
F i g u r e 1 3 :F i g u r e 1 3 : Conceptual design of theBRHP software system.
38 Ethiop. J. Health Dev.
looks more feasible as the localinfrastructure improves.
Following the extensive datacleaning processes between 1995 and1998, it proved possible, thanks tofurther technological advances, tocommit the definitive version of thedatabase for the first 10 years'surveillance (1987 to 1996) to a CD-ROM. This relatively simple step hasproved to be very helpful to theinternational group of collaboratorsworking on the analysis of this largeset of data, since all were assured ofhaving exactly the same unmodifiabledataset to work with.
7. OUTLINING THE ANALYSIS
AND DISCUSSING RESEARCH
AND INTERVENTION PRIOR-ITIES
7.1 The continued surveillanceMonthly surveillance has been
carried out since January 1987. Thecollection of data has been performedby enumerators, who were initiallytrained for the task. They havecontinuously been exposed to re-training in specific and/or new areasof work.
Vital events have been made easyfor the enumerator to record. Eachevent is recorded on a uniquelycoloured sheet. All forms arecollected daily by supervisors andchecked for inconsistencies anderrors before they are sent to the fieldoffice.
Further attempts are being madeto decentralise the processing ofinterview forms to the field office inButajira town. The potential benefitsof doing this are several, includingcloser co-operation between differenttypes of staff. Thus, the interviewerswill find it easier to discuss items withthe data entry clerks. The dataprocessing will be easier to superviseand validity and quality controlprocesses should be more effectivecloser to the field. Some of thedrawbacks of this decentralisationmay be that electric power can beunstable and sometimes interrupted,causing a lot of computer down-time.Also, qualified researchers are notalways present to supervise.
During 1999 quarterly surveillancewas introduced on a pilot basis inselected areas. The purpose is toreduce the interview load on thepopulation and to keep costs low,with minimal consequences for dataquality. This pilot scheme will becarefully evaluated in the light of thethird re-census, scheduled for late1999, to compare the relative rates ofmissed events and other surveillanceerrors.

Establishing an epidemiological field laboratory 39
7.2 Reproductive healthIn establishing the study base, the
potential for reproductive healthresearch was one envisaged appli-cation, for example in pregnancysurveillance and studies of femalehealth and reproductive outcome.
Building on the basic populationdata, specific studies are beingundertaken to evaluate and assess riskfactors and other parameters whichare associated with, or cause, poorreproductive outcomes. A prerequisitefor well-designed interventions is thefacility to assess morbidity, perceivedhealth needs and social support.Focus group discussions, in-depthinterviews and key informant studiesare important tools. Results ofquantitative multivariate riskassessments will be interpreted inconjunction with qualitative findings.Following the Safe MotherhoodInitiative, providing efficient maternalhealth care in order to reduce maternalmorbidity and mortality is a highpriority. The Population Conferencein Cairo in 1994 underlined women'sdecision making ability, propertyrights and literacy as importantfactors, thus widening the genderaspects of health. Achieving accept-able patterns of reproduction meanspromoting people's own choices anddecisions regarding fertility, sexualityand control over reproduction in aculturally acceptable way, combinedwith effective strategies for reducingmortality and morbidity for womenand children.
The planned project will seek toincrease understanding of these inter-
related social, cultural and healthissues within sub-Saharan Africa, aswell as implementing and evaluatingoperational strategies forimprovements in health care. The aimof the project is to develop anddemonstrate approaches for sustain-able, long-term maternal and childhealth programmes, promoting safe,effective and acceptable methods ofreproduction. It is envisaged that theexperience gained from the projectwould be applicable elsewhere inEthiopia and provide a basis for anintegrated approach that could beimplemented more widely in sub-Saharan Africa.
The purpose of a proposedintervention study in reproductivehealth is to evaluate the imple-mentation and effectiveness ofspecific strategies for developmentand aid within the reproductive healthfield. The aim of the interventions is toprevent bad outcomes of pregnancy.Pre- and post-intervention studies onoutcomes, facilitated by the step-wedge approach, will besupplemented with cost-benefitanalyses of the intervention packages.The intervention will be evaluated bydifferent approaches, outcomeresearch and process-based research,and using both quantitative andqualitative methodologies. Theoutcome research will assess theefficiency of referral by linkage of thedifferent data records: radio calls,ambulance journeys and hospitalnotes. The utilisation of the referralsystem will be evaluated bycomparing numbers of mothers from
40 Ethiop. J. Health Dev.
the study area with the remainingpopulation in the district. Thisprocess-based research is concernedto evaluate strengths and weaknessesof the chain of obstetric services, howparturients are brought into the serviceand how they progress through it andthe interaction between staff and theparturients and their relatives as wellas traditional birth attendants.Evaluation of the interventions willinclude the acceptance, quality andefficiency of health care. Theinterviews with professionals andparturients will be done usingqualitative methods for evaluation.Further, social support, continuity ofhealth care support, and women'sopinions on health care will beconsidered. Sub-optimal care will bedetected by continuous audit(including cases and controls) and byin-depth interviews following maternaland perinatal deaths as well as "nearmiss" episodes of, for example, life-threatening obstructed labour andpostpartum haemorrhage. Thecontinuous registration of surveillancedata before and after the intervention(stillbirths, neonatal, infant, andmaternal deaths), as well as using astep-wedge study design will enableevaluation of the programme’s impactin the study area. It is expected thatperinatal deaths could be the bestproxy to evaluate the intervention. Theintervention is planned to go on for a3-year period, and the problems ofsustainability and applicability forother African settings will also beconsidered.
7.3 ARI and indoor-air pollutionBeginning in 1999, a new applied
study on Acute Lower RespiratoryInfections (ALRI) and indoor airpollution is under way. Indoor airpollution has been suspected as oneof several factors that affect theincidence of or mortality fromrespiratory infections, since in manydeveloping countries open, unventedfireplaces are commonly used forboth cooking and heating. In the fewstudies that report actualmeasurements of pollutants (mainlynitrogen dioxide and respirableparticulate matter) concentrations havefar exceeded threshold limit values forthe working environment in mostindustrial countries, which in turn areconsiderably higher than therecommended concentration limits forthe general environment [22, 23]. Theepidemiologic data on indoor airpollution as a risk factor for ARImorbidity and mortality amongchildren are ambiguous. Fromdeveloping countries, several studiesusing proxy measures of air pollution,report an effect on ARI morbidity ormortality [6, 24-28], whereas a study,where pollution measurements areused, shows no such relation [22].
The specific background of theplanned study is the finding byShamebo, Muhe et al of ARI as oneof the major causes of death amongchildren in Butajira District [6] and thefindings that among the factors thatare most strongly related to totalunder-five mortality are lack ofwindows in the home (odds ratio 1.6),living in a traditional hut (tukul) and
Establishing an epidemiological field laboratory 41
having cooking fires in the house [7].These factors would all be directlyrelated to exposure to indoor airpollution, but also indirectly to otherrisk factors. Among children dyingfrom ARI, the odds ratio for "havingno window" is 1.8, in a logistic re-gression model also including factorssuch as ethnicity and literacy. Thecorresponding odds ratio for infantsonly is approximately 5.
The study is planned as aspecialised project within the ButajiraRural Health Project. The new studyis performed in collaboration with theresearchers at the Community HealthDepartment in Addis AbabaUniversity and the ChemistryDepartment of the Science Faculty ofthe Addis Ababa University.
In 1995 a pilot study of indoor airpollution exposure was performed.The aim of the study was to make asmall series of pollutant measurementsin order to find the range of indoorconcentrations and to study theexposure-time patterns of the children.Nitrogen dioxide, NO2, was measuredas an indicator of indoor air pollutionthat can be easily quantified underfield conditions. Samples arecollected passively on a diffusionsampler, which precludes the need foran electric pump. Ten households intwo different villages were visited forsample collection. Samples werecollected in three overlapping timeseries, 16, 24 and 40 hours res-pectively. The results showed littledifference between the two villages inaverage NO2 concentration, butsubstantial between-household vari-
ation. Average concentrations rangedbetween 23 µg m-3 and 258 µg m-3.Conclusions from the pilot studymeasurements are that the between-household variation is sufficient toshow differences in the children’sexposure and that many of thechildren in Butajira are exposed tolevels of NO2 well above currentEuropean 24-hour limit values forurban air.
The exposure-time patterns of thechildren were studied in March 1996,by observations made by high-schoolstudents in their own homes. 120students with siblings under five yearsof age, from all communities includedin the study base of the Butajira RuralHealth Project (BRHP) were recruitedand equipped with digital watches.For three days running, they recordedthe hours when a fire was burning onthe hearth, and the times when siblingswere indoors (hour and minute ofentering and leaving the house). Thenumber of hours the fire was burningand the total time per day of thechildren’s smoke exposure wascalculated. The number of hours perday of keeping the fire burning variedbetween less than 1 and more than 23,with a median value of 9 hours. Theexposure times of the children variedbetween less than one hour (5%) andmore than 15 hours (5%). The medianexposure time was 5 hours. As withthe NO2 measurements, the resultsindicate a sufficient variation inexposure, to allow a meaningfulepidemiologic study.
The study will use a case-referentdesign, where cases of ALRI among

42 Ethiop. J. Health Dev.
under-fives will be compared to thenon-case referent sample with respectto indoor smoke exposure andpossible confounding factors. Expo-sure will be surveyed prospectively(sampling and chemical analysis plusinterviews) in all households withchildren under five at three monthintervals, as well as retrospectively(interviews) at the time of diagnosisfor the case and its referents. Caseswill be identified by specially trainedvillage based health workers, who willalso provide treatment for thechildren.
Exposure assessment will be bothprospective and retrospective. In theprospective part, air pollution will bechemically measured and informationon fire, cooking and children’smovements will be collected ininterviews. The aim of the prospectiveexposure survey, which will cover allhouseholds with children under five, isto characterise the household withrespect to the cooking habits and toallow classification of households intogroups with respect to averagepollution concentrations. This will bedone at three-month intervalsthroughout the study. Retrospectiveexposure assessment at diagnosis isrestricted to
the households of the cases and thechildren in the referent sample. Onidentifying a case, the project healthworker notifies the village basedproject assistant who selects referentsfrom the BRHP population registerand performs the interviews aboutcooking (cooking hours, what wascooked, choice of fuels) and thechild’s movements during cooking(indoor/outdoor). The questionnaire isbeing developed in collaboration withthe Ethiopian researchers and will betested in a field trial before the actualdata collection starts.
In view of the enormous impact ofALRI on child health and mortality indeveloping countries, a contributionto primary prevention could havegreat value. In the more immediatefuture, results indicating an effect ofair pollution exposure on ALRIincidence or mortality should beutilised in an intervention study inEthiopia. Since the study is dependenton information from the householdson exposure and the children’sillnesses, it is planned to give a serviceback to the surveyed communities inthe form of basic health care and asimple drug supply. The caseidentification method of having villagebased trained health workers toprovide treatment for the children’srespiratory infections will be extendedto supply certain other drugs such aschloroquine and paracetamol to allages.

Establishing an epidemiological field laboratory 43
7.4 Mental health and domesticviolence
Effects of domestic violence onwomen’s mental health have been wellrecognised. Victims of intimatepartner violence often exhibit a varietyof symptoms, including tendencies forsuicide, cognitive disturbances, highavoidance or depression behavioursand high arousal or anxietydisturbances which has beenconceptualised as battered womansyndrome, and which meets the dia-gnostic criteria for post-traumaticstress disorder (PTSD). Domesticviolence should be viewed as a long-term, chronic condition with long-lasting emotional and psychologicalconsequences as depression andinsomnia. Gender differences ofpsychiatric disorders have consist-ently been found. A primary exampleis depression, which is a major threatto health and one of the mostcommon psychiatric disorders at thecommunity level. Gender differenceshave been well documented, withpoint prevalence, 12-monthprevalence and lifetime prevalence ofmajor depression all found in greaterfrequency in women than in men.
To date, population based re-search on mental health has notexplored the extent to which domesticviolence may contribute to genderdifferentials in depression. Epi-demiological research with moreaccurate diagnostic techniques isneeded in order to establish, at thecommunity level, the effects ofdomestic violence on women’s mental
health. The general objective shouldbe to study the magnitude andcharacteristics of both domesticviolence and depression amongwomen of childbearing age within theButajira research area.
Specific objectives will includeexamining the cultural context inwhich violence against women occurs,by identifying the most commonbeliefs and attitudes of both men andwomen regarding domestic violence;estimating the prevalence of domesticviolence and depression/dysthymiaamong women of child bearing age;analysing the association betweendomestic violence anddepression/dysthymia; determininghow much violence contributes tomental health problems; and assessingthe reproductive outcomes of womenexposed to domestic violence.
The design of the study addres-sing the objectives will be populationbased, starting with formativequalitative research, followed by across-sectional survey among women,a nested case-referent study, andfinally linkage of the offspring to thedemographic surveillance.
7.5 Other plansThe BRHP is a continuous source
of information for planning andevaluating public health interventionsand a very suitable platform forresearch training in a developingcountry. The collaboratinginstitutions, inspired by theachievements so far, are committed tomaintaining the study base in the

44 Ethiop. J. Health Dev.
future. Further objectives for theBRHP will be to strengthen evidence-based approaches to major publichealth problems in the country. It willpromote and facilitate the use ofresearch findings for planning publichealth interventions through timely andregular publications.
Opportunities for extending re-search training to the doctoral level inthe Department of Community Healthin Addis Ababa will be explored. Thecurrent sandwich programme fordoctoral studies in Sweden constitutesa good precedent for any suchundertaking in the Department ofCommunity Health. The School ofPublic Health envisaged by AddisAbaba University could greatly benefitfrom the existence of such a wellmaintained "population laboratory" asthe BRHP.
8. CONCLUDING REMARKSThe quality of research in Butajira
can only be maintained through acollaborative undertaking that involvesexperienced and qualified researchersfrom both the quantitative andqualitative arenas in sufficient number.The collaboration
that has survived for the last 15 yearsbetween the Department ofCommunity Health in Addis Ababaand the Department of Epidemiologyand Public Health in Umeå, Sweden,is highly valued. However, there is aneed to expand this collaboration inorder to examine the widely diversehealth problems in the country, and toexpand training opportunities invarious specialised field such asnutrition and health education. One ofthe major priority areas for newresearch is to study the epidemiologyof HIV/AIDS in rural setting and thespread of infection from urban to ruralsettings.
The major challenge for sustainingthis study base would be to getcontinuous funding for its activities.Plans for sustainability include de-veloping a cost-sharing scheme (inwhich projects served by the studybase contribute a certain proportionof their budget), diversifying fundingfrom external sources, and solicitinglocal funding.
In conclusion, the BRHP is anational asset that can provide scien-tifically sound information for use inpublic health planning, policy makingand evaluation. It also provides afertile platform for training inepidemiology and public health for thecountry.

Establishing an epidemiological field laboratory 45
9. ACKNOWLEDGEMENTSThe Butajira Rural Health Pro-
gramme is very grateful to the peoplein the study areas for continuous andunfailing generous co-operation andfor their kind hospitality. TheEthiopian Science and TechnologyCommission (ESTC) and the SwedishAgency for Research Cooperationwith Developing Countries (SAREC),now Sida/ SAREC, are gratefullyacknowledged for the financialsupport.
Special thanks go to the entirefield staff in Butajira, computer datamanagers, administrative staff and toAto Yemiru Teka, the field co-ordinator in Butajira.
Addis Ababa University in generaland the Research and PublicationsOffice and Faculty of Medicine inparticular are also greatlyacknowledged for their kind allrounded assistance since inception.
46 Ethiop. J. Health Dev.
10. REFERENCES1. Shamebo D. Epidemiology for public health
research and action in a developing society:the Butajira Rural Health Project in Ethiopia[dissertation], Umeå: Umeå University,Department of Epidemiology and PublicHealth; 1993.
2. Census 1994. The 1994 Population andHousing Census of Ethiopia. Results atcountry level. Statistical report, 1998.Office of Population and Housing CensusCommission, Central Statistical Authority:Addis Ababa, Ethiopia.
3. Census 1984. The 1984 Population andHousing Census of Ethiopia. 1990. Officeof Population and Housing CensusCommission, Central Statistical Authority:Addis Ababa, Ethiopia.
4. Shimelis B. The history of Butajira townto 1974 [Senior essay]. Addis Ababa:Department of History, Addis AbabaUniversity; 1990.
5. Adege A. Utilization of Butajira HealthCentre: A study in medical geography[Senior essay]. Addis Ababa: Departmentof Geography, Addis Ababa University;1991.
6. Shamebo D, Muhe L, Sandström A, WallS. The Butajira rural health project inEthiopia: mortality pattern of the underfives. J Trop Pediatr 1991; 37:254-61.
7. Shamebo D, Sandström A, Muhe L, et al.The Butajira project in Ethiopia: a nestedcase-referent study of under- five mortalityand its public health determinants. BullWorld Health Organ 1993;71:389-96.
8. Berhane Y, Andersson T, Wall S, HögbergU, Byass P. Aims, options and outcome inmeasuring maternal mortality in developingsocieties. Submitted manuscript 1999.
9. Deyessa N, Kassaye M, Demeke B, TaffaN. Magnitude, type and outcomes ofphysical violence against married women inButajira, southern Ethiopia. Ethiop Med J1998;36:83-92.
10. Desjarlais R, Eisenberg L, Good B,Kleinman A. World mental health:Problems and properties in low-incomecountries. Oxford: Oxford UniversityPress; 1995.
11. Alem A. Mental health in rural Ethiopia:Studies on mental distress, suicidalbehaviour and use of khat and alcohol[dissertation]. Umeå: Umeå University,Department of Psychiatry; 1997.
12. TGE. National Health Policy of Ethiopia.1992, Transitional Government of Ethiopia:Addis Ababa.
13. Alem A, Kebede D, Kullgren G. Theprevalence and socio-demographic cor-relates of khat chewing in Butajira,Ethiopia. Acta Psychiatr Scand Suppl1999;397:84-91.
14. Alem A, Kebede D, Kullgren G. Theepidemiology of problem drinking inButajira, Ethiopia. Acta Psychiatr ScandSuppl 1999;397:77-83.
15. Alem A, Kebede D, Jacobsson L, KullgrenG. Suicide attempts among adults inButajira, Ethiopia. Acta Psychiatr ScandSuppl 1999;397:70-6.
16. Alem A, Jacobsson L, Kebede D, KullgrenG. Awareness and attitudes of a ruralEthiopian community toward suicidalbehaviour. A key informant study inButajira, Ethiopia. Acta Psychiatr ScandSuppl 1999;397:65-9.
17. Alem A, Kebede D, Woldesemiat G,Jacobsson L, Kullgren G. The prevalenceand socio-demographic correlates ofmental distress in Butajira, Ethiopia. ActaPsychiatr Scand Suppl 1999;397:48-55.
Establishing an epidemiological field laboratory 47
18. Alem A, Jacobsson L, Araya M, KebedeD, Kullgren G. How are mental disordersseen and where is help sought in a ruralEthiopian community? A key informantstudy in Butajira, Ethiopia. Acta PsychiatrScand Suppl 1999; 397:40-7.
19. Awas M, Kebede D, Alem A. Majormental disorders in Butajira, southernEthiopia. Acta Psychiatr Scand Suppl1999;397:56-64.
20. Byass P. Computers in Africa - appropriatetechnology? Computer Bulletin1987;3:17.
21. Stephens J, Alonso PL, Byass P, SnowRW. Tropical epidemiology: a system forcontinuous demographic monitoring of astudy population. Methods Inf Med1989;28:155-9.
22. Boleij J, Ruigewaard P, Hoek F, et al.Domestic air pollution from biomassburning in Kenya. Atmosph environ1989;23:1677-81.
23. Pandey MR, Boleij JS, Smith KR, WafulaEM. Indoor air pollution in developingcountries and acute respiratory infection inchildren. Lancet 1989;1:427-9.
24. Anderson HR. Respiratory abnormalities inPapua New Guinea children: the effects oflocality and domestic wood smokepollution. Int J Epidemiol 1978;7:63-72.
25. Kossove D. Smoke-filled rooms and lowerrespiratory disease in infants. S Afr Med J1982;61:622-4.
26. Campbell H, Armstrong JR, Byass P.Indoor air pollution in developing countriesand acute respiratory infection in children[letter]. Lancet 1989; 1:1012.
27. Pandey MR, Regmi HN, Neupane RP,Gautam A, Bhandari DP. Domestic smokepollution and respiratory function in ruralNepal. Tokai J Exp Clin Med1985;10:471-81.
28. Armstrong JR , Campbell H. Indoor airpollution exposure and lower respiratoryinfections in young Gambian children. Int JEpidemiol 1991;20:424-9.




















