No evidence for protective erythropoietin alpha signalling in rat hepatocytes
Upload
independentCategory
view
1download
0
Erythropoietin Stimulates Normal Endothelial ProgenitorCell-Mediated Endothelial Turnover, but Attributesto Neovascularization Only in the Presence of Local Ischemia
B. Daan Westenbrink & Hisko Oeseburg & Lennaert Kleijn &
Pim van der Harst & Anne M. S. Belonje & Adriaan A. Voors &
Regien G. Schoemaker & Rudolf A. de Boer &
Dirk J. van Veldhuisen & Wiek H. van Gilst
Published online: 11 March 2008# Springer Science + Business Media, LLC 2008
AbstractPurpose We aimed to evaluate whether ischemia is re-quired for erythropoietin (EPO) induced stimulation ofendothelial progenitor cells (EPCs) and their related effectson endothelial and cardiac function.Methods Bone marrow of rats was replaced by transgeniccells to allow tracking of EPCs. Ischemic heart failure wasinduced by left coronary artery ligation to induce myocar-dial infarction (MI) and control rats received a shamprocedure. Three weeks after surgery, rats were randomizedto receive EPO (darbepoetin alfa 40 μg/kg per 3 weeks) orvehicle and were sacrificed 9 weeks after surgery.Results In all treated groups, EPO significantly increasedcirculating EPCs and their incorporation into the endothe-lium of the ischemic and non-ischemic hearts as well as inthe control organs; kidney and liver. This was associatedwith significantly improved endothelial function, whichwas strongly correlated with circulating EPCs (R=0.7, p<0.01). However, additional EPCs preferentially homed tothe ischemic MI borderzone (p<0.01) resulting in specificEPO-induced improvement of cardiac microvascularizationand performance only in ischemic hearts (all p<0.05). Thedifferential stimulation of neovascularization by EPO wasassociated with increased EPO-receptor and VEGF expres-sion in ischemic hearts only.
Conclusions In general, EPO stimulates normal endothelialprogenitor cell-mediated endothelial turnover, but improvescardiac microvascularization and function only in thepresence of ischemia.
Key words erythropoietin . endothelial function .
heart failure . endothelial progenitor cells
Introduction
Erythropoietin (EPO) improves cardiac function and in-duces neovascularization in experimental models of chronicmyocardial dysfunction and is currently evaluated inpatients with chronic heart failure [1–7]. EPO-inducedneovascularization is related to increased mobilization andincorporation of bone marrow derived endothelial progen-itor cells (EPCs) and augmented expression of angiogenicfactors in the myocardium [8]. These effects of EPO havealso been demonstrated in the endothelium of otherischemic organs, such as the brain and ischemic limbs [9–12]. In addition to new vessel formation, EPCs replaceinjured endothelium and thereby maintain the integrity ofthe endothelial monolayer [13]. Since endothelial dysfunc-tion has been recognized as one of the earliest events inatherosclerotic cardiovascular disease [14], stimulation ofEPC-mediated endothelial repair by EPO might be oftherapeutic interest.
However, the beneficial effects of EPO on endothelialrepair and new vessel formation have only been demonstratedin ischemic organs. It is therefore unknown whether theseeffects are attributable to the presence of ischemia or representa general phenomenon. We therefore aimed to evaluatewhether ischemia is required for erythropoietin (EPO) induces
Cardiovasc Drugs Ther (2008) 22:265–274DOI 10.1007/s10557-008-6094-y
B. D. Westenbrink (*) :H. Oeseburg : L. Kleijn :P. van der Harst :A. M. S. Belonje :A. A. Voors :R. G. Schoemaker :R. A. de Boer :D. J. van Veldhuisen :W. H. van GilstDepartment of Cardiology, Thoraxcenter,University Medical Center Groningen,Hanzeplein 1, P.O. Box 30001, 9700 RB Groningen,The Netherlandse-mail: [email protected]

stimulation of endothelial progenitor cells (EPCs) and theirrelated effects on endothelial and cardiac function.
Methods
Animals and bone marrow labeling
For bone marrow transplantation experiments we used maleFischer F344 rats (n=75) weighing 200–230 g (CharlesRivers, France) as recipients and R26-hPAP donor rats (n=10, F344 background, ubiquitously expressing humanplacental alkaline phosphatase, hPAP) [15]. Details ontransplantation have been described in detail previously[8]. Briefly, whole R26-hPAP bone marrow cells weretransfused to Fischer F344 recipients after total bodyirradiation and left to reconstitute for 5 weeks. Leucocytechimerism was assessed by FACS and rats with chimerism>80% were included in the experimental protocol. Animalswere fed and housed, according to institutional rules andregulations. The experimental protocol was approved by theAnimal Ethical Committee of the University of Groningen.Results of endothelial function were confirmed in maleSprague–Dawley rats weighing 270–320 g.
Experimental protocol
MI was induced by ligating the left coronary artery [6].Sham operated rats were used to control for surgery andpost-operation inflammation. In sham operated rats, thesame surgery was performed without closing the ligature.Three weeks after surgery, rats were randomly assigned totreatment with the long-acting EPO analogue darbepoetinalfa (40 μg/kg, Aranesp, Amgen Inc., Thousand Oaks, CA,USA) or vehicle; once every 3 weeks, at week 3 and week6. After 9 weeks, hemodynamic measurements wereperformed with a microtip pressure transducer (Millar Instr.Inc., Houston, Texas, USA) as described previously. Heartrate (HR), left ventricular systolic pressure (LVSP), and leftventricular end-diastolic pressure (LVEDP) were measured.The maximal rates of increase and decrease in LVP (dP/dtmax and dP/dtmin) were determined. Thereafter hearts wererapidly excised and weighed. Myocardial tissue wasdissected transversally and processed for immunohisto-chemistry or snap frozen for Western blot analysis.
Circulating endothelial progenitor cells
Circulating EPCs were enumerated as previously described[8]. Mononuclear cells were isolated from whole blood bydensity centrifugation and seeded onto fibronectin-precoated24-well plates (1×106 cells per well) in EndoCult medium(StemCell Technologies, London, UK) as described previ-
ously. After 6 days of culture, adherent cells were incubatedwith 1,1′-dioctadecyl-3,3,3′,3′-tetramethylindocarbocyanineabeled acetylated-LDL (DiL-AcLDL) for 12 hours, fixedwith 1% paraformaldehyde and counterstained withfluorescein- labeled isolectin B4. Cells double positive forDiI-AcLDL and lectin staining were considered EPCs andcounted in five high-power fields, by blinded observers.
Histology
Infarct size and capillary density were determined asdescribed in detail previously [6]. Briefly, infarct size wasdetermined at the mid-papillary level in transverse slices onpicrosirius red/fast green-stained sections. Endothelial cellswere stained with GSL-Lectin and image analysis was usedto measure capillary density and calculated as the numberof capillaries per tissue area (mm2). Cryosections werestained for hPAP (rabbit anti-hPAP, serotec, London, UKfollowed by FITC labeled goat anti-rabbit-IgG) and ratendothelial cell antigen (RECA; mouse anti-rat His52; akind gift from Dr. J.L. Hillebrands, followed by TRITC-labeled goat anti-mouse-IgG-isotype). DAPI was used fornuclear counterstaining. hPAP positive cells were consid-ered bone marrow derived cells (BMDC) and cells doublepositive for hPAP and His-52 were considered bonemarrow derived endothelial like cells (BMDEC). Cells infive random high power fields of the non-infracted leftventricular free wall were counted independently by twoblinded observers.
EPO-receptor and VEGF expression
The expression of EPO-receptor, Vascular EndothelialGrowth Factor (VEGF) and GAPDH was determined intissue homogenates of the viable left ventricular free wall(non infarcted area) by standard Western blotting tech-niques [8]. Antibodies were purchased from Santa CruzBiotechnology (EPO-receptor M-20, 1:500, VEGF C1,1:250, (recognizes all splice variants of VEGF), andFitzgerald Industries (GAPDH 6c5, 1:10,000). Horseradishperoxidase conjugated anti-mouse or anti-rabbit IgG wereused as secondary antibodies.
Organ bath studies with isolated aortic rings
Vascular measurements were performed as describedpreviously [16]. In brief, thoracic aortic rings wereconnected to an isotonic displacement transducer and afterstabilization rings were checked for viability by stimula-tion with phenylephrine (1 mmol/l). The endothelium-dependent vasodilatation was assessed by a cumulativedose of metacholine (10−9 to 10−5 mmol/l). In parallelrings, endothelium-independent vasodilatation was assessed
266 Cardiovasc Drugs Ther (2008) 22:265–274

in the presence of NG-Methyl-L-arginine acetate salt(L-NMMA, 10−5 mol/l) a nonspecific NOS blocker, or inthe presence of indomethacine (10−4 mol/l) a nonspecificprostaglandin inhibitor, and finally in the presence of bothL-NMMA and indomethacine. Drugs were purchased fromSigma-Aldrich.
Statistical methods
Data are expressed as means±SEM. Statistical analysisamong groups was performed by ANOVA. Differences invascular dose-response curves between groups were testedby ANCOVA for repeated measurements. Correlations wereassessed with Spearman’s correlation test. All p-valueswere two-tailed, and a p-value of <0.05 was consideredstatistically significant. All analyses were performed usingSPSS version 12.0 software (SPSS, Chicago, IL, USA).
Results
Two sham rats were excluded due to accidental proceduraldamage to a coronary artery. Mortality after MI was 32%.Hematocrit levels increased from 41±0.5% to 57±0.5% inEPO treated rats. No differences in hematocrit wereobserved between sham and MI. At sacrifice, body weightwas similar among groups, but heart weight/body weightratio was significantly increased in the MI groups comparedto shams (p<0.01). EPO treatment reduced the hyper-trophic response after MI (heart weight/body weight ratio,4.1±1 in MI vs 3.6±2 in MI-EPO p=0.04).
Effects of EPO on circulating EPCs number
In sham rats MI resulted in an almost 60% increase in thenumber of circulating EPCs (52±6 vs 83±12 per high-powered field in sham vs sham-EPO, p<0.01). MI wasassociated with significantly decreased numbers of circu-lating EPCs (31±7 in MI, p<0.01 vs sham). Treatment withEPO resulted in a substantially more pronounced increasein number of circulating EPCs (31±7 vs 115±22 in MI vsMI-EPO, Fig. 1a, p<0.01). Circulating EPC-numbers didnot differ significantly between EPO-treated groups.
Effect of EPO on incorporation of EPCs into the ischemicand non-ischemic myocardium
We determined the number of BMDEC in the viable leftventricular free wall, distant from the infarcted area, and inthe viable borderzone directly adjacent to the infracted areaif applicable. In the left ventricular free wall, the number ofBMDEC was comparable between sham and MI rats (3.2±0.6 vs 3.8±0.3 BMDEC per high-powered field, p=0.5,Fig. 1b). EPO treatment almost doubled the number ofBMDEC after MI in the left ventricular free wall, but to asimilar extent after sham operation (5.8±0.9 in MI-EPOand 5.0±0.9 in sham-EPO both p<0.05, Fig. 1b). Thenumber of BMDEC in the borderzone was significantlyhigher compared to the left ventricular free wall in both MIgroups (3.8±0.3 vs 10±0.6 in MI and 5.8±0.9 vs 15±1.7 inMI EPO, both p<0.01 Fig. 2), indicating preferentialhoming of EPCs into the ischemic myocardium. Ischemia-induced homing of EPCs to the MI-borderzone was also
EP
C/ h
igh
po
wer
fie
ld
0
50
100
150
200
BM
DE
C /
Fie
ld(V
iab
le L
V)
0
4
6
8
*#
*# *#
*#
Circulating EPC Cardiac EPCa
c
*
b
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
Fig. 1 Effect of EPO on circu-lating and cardiac EPCs.a Graphic representation of thenumber of circulating EPCs.b Bar graph representing thenumber of bone marrow derivedendothelial cells (BMDEC, cellsstaining double positive for hPAPand His 52) in the viable leftventricular free wall distant fromthe infarct (if applicable).c Typical BMDEC, myocardialsection stained with hPAP(green), His 52 (endothelium,red) and DAPI (nucleus, blue).The three panels display respec-tively nuclei, endothelium, bonemarrow derived cells and theoverlay of the three channels,where BMDEC appearyellow. *p<0.05 vs sham,#p<0.05 vs MI
Cardiovasc Drugs Ther (2008) 22:265–274 267267
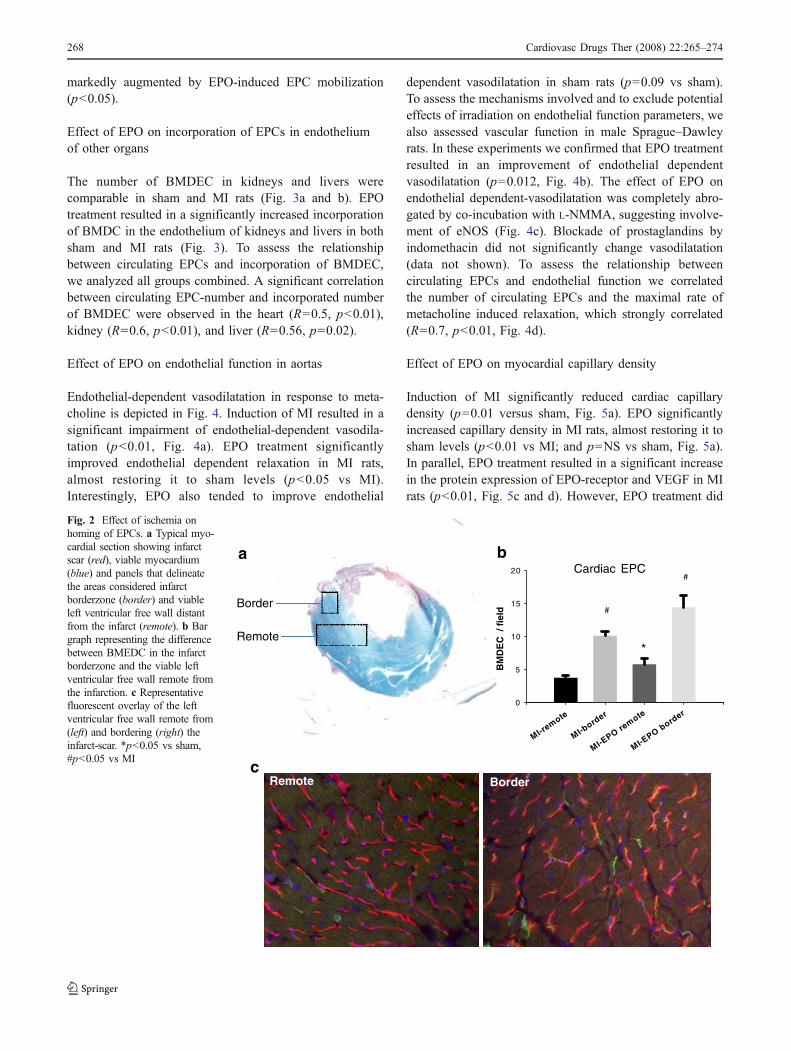
markedly augmented by EPO-induced EPC mobilization(p<0.05).
Effect of EPO on incorporation of EPCs in endotheliumof other organs
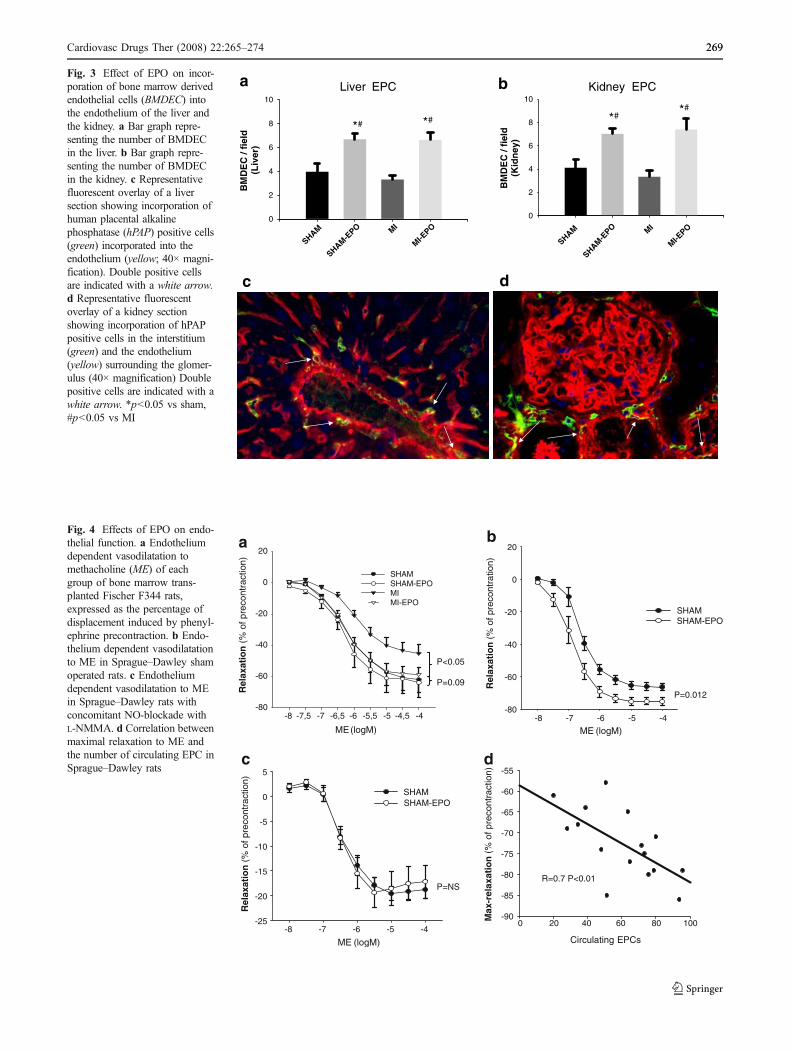
The number of BMDEC in kidneys and livers werecomparable in sham and MI rats (Fig. 3a and b). EPOtreatment resulted in a significantly increased incorporationof BMDC in the endothelium of kidneys and livers in bothsham and MI rats (Fig. 3). To assess the relationshipbetween circulating EPCs and incorporation of BMDEC,we analyzed all groups combined. A significant correlationbetween circulating EPC-number and incorporated numberof BMDEC were observed in the heart (R=0.5, p<0.01),kidney (R=0.6, p<0.01), and liver (R=0.56, p=0.02).
Effect of EPO on endothelial function in aortas
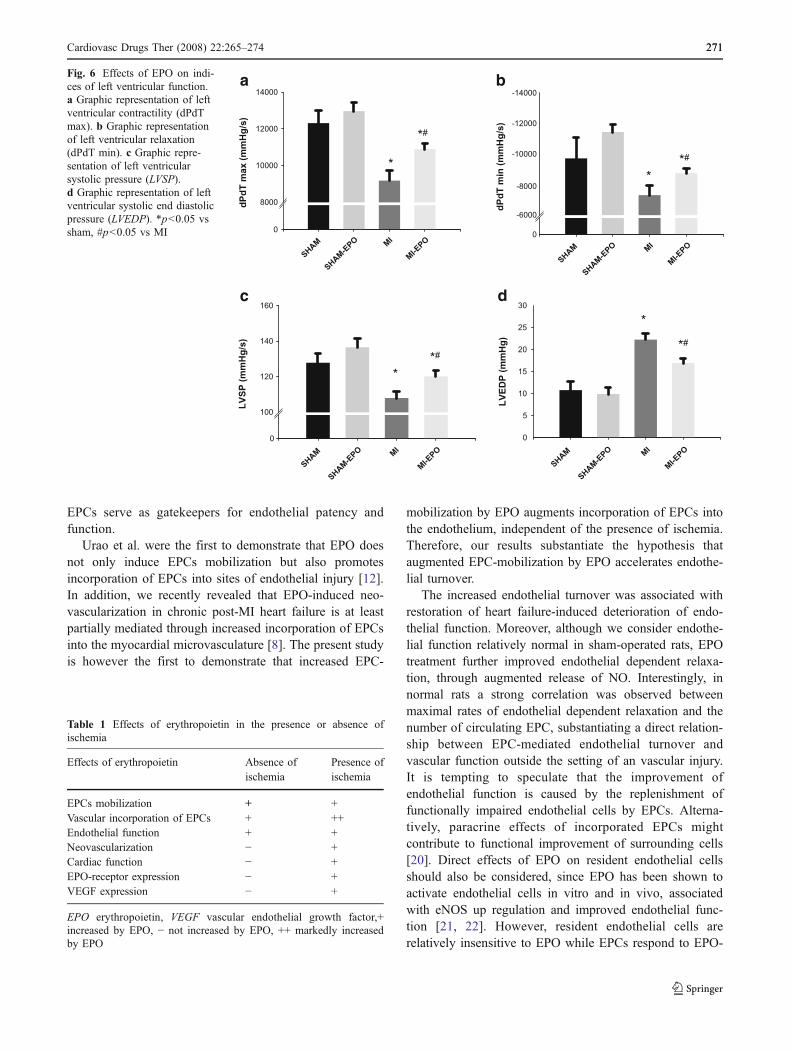
Endothelial-dependent vasodilatation in response to meta-choline is depicted in Fig. 4. Induction of MI resulted in asignificant impairment of endothelial-dependent vasodila-tation (p<0.01, Fig. 4a). EPO treatment significantlyimproved endothelial dependent relaxation in MI rats,almost restoring it to sham levels (p<0.05 vs MI).Interestingly, EPO also tended to improve endothelial
dependent vasodilatation in sham rats (p=0.09 vs sham).To assess the mechanisms involved and to exclude potentialeffects of irradiation on endothelial function parameters, wealso assessed vascular function in male Sprague–Dawleyrats. In these experiments we confirmed that EPO treatmentresulted in an improvement of endothelial dependentvasodilatation (p=0.012, Fig. 4b). The effect of EPO onendothelial dependent-vasodilatation was completely abro-gated by co-incubation with L-NMMA, suggesting involve-ment of eNOS (Fig. 4c). Blockade of prostaglandins byindomethacin did not significantly change vasodilatation(data not shown). To assess the relationship betweencirculating EPCs and endothelial function we correlatedthe number of circulating EPCs and the maximal rate ofmetacholine induced relaxation, which strongly correlated(R=0.7, p<0.01, Fig. 4d).
Effect of EPO on myocardial capillary density
Induction of MI significantly reduced cardiac capillarydensity (p=0.01 versus sham, Fig. 5a). EPO significantlyincreased capillary density in MI rats, almost restoring it tosham levels (p<0.01 vs MI; and p=NS vs sham, Fig. 5a).In parallel, EPO treatment resulted in a significant increasein the protein expression of EPO-receptor and VEGF in MIrats (p<0.01, Fig. 5c and d). However, EPO treatment did
MI-remote
MI-bord
er
MI-EPO re
mote
MI-EPO bord
er0
5
10
15
20#
#
Cardiac EPCa
cRemote Border
Border
Remote*
BM
DE
C /
fie
ld
b
Fig. 2 Effect of ischemia onhoming of EPCs. a Typical myo-cardial section showing infarctscar (red), viable myocardium(blue) and panels that delineatethe areas considered infarctborderzone (border) and viableleft ventricular free wall distantfrom the infarct (remote). b Bargraph representing the differencebetween BMEDC in the infarctborderzone and the viable leftventricular free wall remote fromthe infarction. c Representativefluorescent overlay of the leftventricular free wall remote from(left) and bordering (right) theinfarct-scar. *p<0.05 vs sham,#p<0.05 vs MI
268 Cardiovasc Drugs Ther (2008) 22:265–274
BM
DE
C /
fiel
d(L
iver
)
0
2
4
6
8
10
BM
DE
C /
fiel
d(K
idn
ey)
0
2
4
6
8
10
a
c
*# *# *#
*#
Kidney EPCLiver EPC
d
b
SHAM
SHAM-E
PO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
Fig. 3 Effect of EPO on incor-poration of bone marrow derivedendothelial cells (BMDEC) intothe endothelium of the liver andthe kidney. a Bar graph repre-senting the number of BMDECin the liver. b Bar graph repre-senting the number of BMDECin the kidney. c Representativefluorescent overlay of a liversection showing incorporation ofhuman placental alkalinephosphatase (hPAP) positive cells(green) incorporated into theendothelium (yellow; 40× magni-fication). Double positive cellsare indicated with a white arrow.d Representative fluorescentoverlay of a kidney sectionshowing incorporation of hPAPpositive cells in the interstitium(green) and the endothelium(yellow) surrounding the glomer-ulus (40× magnification) Doublepositive cells are indicated with awhite arrow. *p<0.05 vs sham,#p<0.05 vs MI
0 20 40 60 80 100Max
-rel
axat
ion
(%
of p
reco
ntra
ctio
n)
-90
-85
-80
-75
-70
-65
-60
-55
-8 -7 -6 -5 -4
Rel
axat
ion
(%
of p
reco
ntra
ctio
n)
-25
-20
-15
-10
-5
0
5
SHAM
-8 -7 -6 -5 -4
Rel
axat
ion
(%
of p
reco
ntra
tion)
-80
-60
-40
-20
0
20
SHAMSHAM-EPO
-8 -7,5 -7 -6,5 -6 -5,5 -5 -4,5 -4
Rel
axat
ion
(%
of p
reco
ntra
ctio
n)
-80
-60
-40
-20
0
20
SHAMSHAM-EPOMIMI-EPO
a
c
b
P<0.05
P=0.012
P=NS
d
R=0.7 P<0.01
P=0.09
Circulating EPCs ME (logM)
ME (logM) ME (logM)
SHAM-EPO
Fig. 4 Effects of EPO on endo-thelial function. a Endotheliumdependent vasodilatation tomethacholine (ME) of eachgroup of bone marrow trans-planted Fischer F344 rats,expressed as the percentage ofdisplacement induced by phenyl-ephrine precontraction. b Endo-thelium dependent vasodilatationto ME in Sprague–Dawley shamoperated rats. c Endotheliumdependent vasodilatation to MEin Sprague–Dawley rats withconcomitant NO-blockade withL-NMMA. d Correlation betweenmaximal relaxation to ME andthe number of circulating EPC inSprague–Dawley rats
Cardiovasc Drugs Ther (2008) 22:265–274 269269

not affect myocardial capillary density, EPO-receptor orVEGF expression in sham rats.
Effect of EPO on cardiac function
Cardiac function was significantly reduced in MI groupscompared to sham (all p<0.05, Fig. 6). EPO treatmentsignificantly increased myocardial contractility, relaxationand LVESP and a decrease in LVEDP in MI rats, but notin shams (Fig. 6).
Discussion
In the present study we demonstrate for the first time thatthe regenerative effects of EPO in chronic heart failure aredependent on the presence of ischemia. EPO stimulatedmobilization of EPCs from the bone marrow whichindiscriminately incorporated in the endothelium of ische-mic and non-ischemic tissues and significantly improvedendothelial function. However, EPO stimulated neovascu-larization and improved cardiac function only in ischemichearts, which was possibly driven by augmented localVEGF and EPO-receptor expression. These results suggestthat EPO regulates normal endothelial progenitor cell-
mediated endothelial turnover, but improves microvascula-rization and cardiac function only in the presence ofischemia. The differential effects of EPO in the presenceand absence of ischemia are summarized in Table 1.
EPO augments EPC-mediated endothelial turnover
The endothelium is recognized to play a crucial role inatherogenesis and considered to be involved early in thepathophysiology of cardiovascular disease [14]. In patientswith essential hypertension and documented coronaryartery disease, endothelial dysfunction appears a markerfor future cardiovascular events [17]. Moreover, chronicheart failure is associated with endothelial dysfunctionwhich promotes cardiac remodeling through increasedperipheral resistance, eventually reducing prognosis [18].Maintaining a vital endothelial monolayer is thereforeof pivotal importance in the prevention and treatment ofcardiovascular disease. Endothelial turnover can be facil-itated through migration and proliferation of neighboringendothelial cells, although the rate of endothelial-cellproliferation in arteries is relatively low [19]. In contrast,EPCs rapidly repopulate denuded arteries, associatedwith an immediate improvement of endothelial function[20]. Thus in addition to their role in neovascularization,
VE
GF
exp
ress
ion
/G
AP
DH
0,0
0,5
1,0
1,5
2,0
EP
OR
exp
ress
ion
/ G
AP
DH
Cap
illar
y d
ensi
ty
(no
/mm
2)
0
2000
3000
4000
5000a
dc
#
*
*#*#
SHAM SHAM-EPO
MI-EPOMI
b
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
0,0
0,5
1,0
1,5
2,0
Fig. 5 Effects of EPO on neo-vascularization and expressionof pro-angiogenic factors in is-chemic and non-ischemic hearts.a Measurements of capillarydensity expresses as the numberof capillaries per mm2. b Typicalexamples of capillary density inthe experimental groups. c Pro-tein expression of VEGF cor-rected for GAPDH in the leftventricular free wall. d Proteinexpression of EPO-receptor cor-rected for GAPDH in the leftventricular free wall. *p<0.05vs sham, #p<0.05 vs MI
270 Cardiovasc Drugs Ther (2008) 22:265–274
EPCs serve as gatekeepers for endothelial patency andfunction.
Urao et al. were the first to demonstrate that EPO doesnot only induce EPCs mobilization but also promotesincorporation of EPCs into sites of endothelial injury [12].In addition, we recently revealed that EPO-induced neo-vascularization in chronic post-MI heart failure is at leastpartially mediated through increased incorporation of EPCsinto the myocardial microvasculature [8]. The present studyis however the first to demonstrate that increased EPC-
mobilization by EPO augments incorporation of EPCs intothe endothelium, independent of the presence of ischemia.Therefore, our results substantiate the hypothesis thataugmented EPC-mobilization by EPO accelerates endothe-lial turnover.
The increased endothelial turnover was associated withrestoration of heart failure-induced deterioration of endo-thelial function. Moreover, although we consider endothe-lial function relatively normal in sham-operated rats, EPOtreatment further improved endothelial dependent relaxa-tion, through augmented release of NO. Interestingly, innormal rats a strong correlation was observed betweenmaximal rates of endothelial dependent relaxation and thenumber of circulating EPC, substantiating a direct relation-ship between EPC-mediated endothelial turnover andvascular function outside the setting of an vascular injury.It is tempting to speculate that the improvement ofendothelial function is caused by the replenishment offunctionally impaired endothelial cells by EPCs. Alterna-tively, paracrine effects of incorporated EPCs mightcontribute to functional improvement of surrounding cells[20]. Direct effects of EPO on resident endothelial cellsshould also be considered, since EPO has been shown toactivate endothelial cells in vitro and in vivo, associatedwith eNOS up regulation and improved endothelial func-tion [21, 22]. However, resident endothelial cells arerelatively insensitive to EPO while EPCs respond to EPO-
LV
ED
P (
mm
Hg
)
0
5
10
15
20
25
30
dP
dT
max
(m
mH
g/s
)0
8000
10000
12000
14000
dP
dT
min
(m
mH
g/s
)
-14000
-12000
-10000
0L
VS
P (
mm
Hg
/s)
0
100
120
140
160
*
*#
*#
*
**#
*
*#
a
c
b
d
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
SHAM
SHAM-EPO MI
MI-EPO
-8000
-6000
Fig. 6 Effects of EPO on indi-ces of left ventricular function.a Graphic representation of leftventricular contractility (dPdTmax). b Graphic representationof left ventricular relaxation(dPdT min). c Graphic repre-sentation of left ventricularsystolic pressure (LVSP).d Graphic representation of leftventricular systolic end diastolicpressure (LVEDP). *p<0.05 vssham, #p<0.05 vs MI
Table 1 Effects of erythropoietin in the presence or absence ofischemia
Effects of erythropoietin Absence ofischemia
Presence ofischemia
EPCs mobilization + +Vascular incorporation of EPCs + ++Endothelial function + +Neovascularization − +Cardiac function − +EPO-receptor expression − +VEGF expression − +
EPO erythropoietin, VEGF vascular endothelial growth factor,+increased by EPO, − not increased by EPO, ++ markedly increasedby EPO
Cardiovasc Drugs Ther (2008) 22:265–274 271271

doses that are insufficient to activate erythropoietic cells [9,23]. Future studies are required to differentiate betweendirect and indirect effects of EPO on endothelial function.
EPCs switch from endothelial turnover to EPO-inducedneovascularization in the presence of ischemia
After MI, perfusion of the remaining vital myocardium willbecome insufficient due to disproportionate cardiomyocytehypertrophy relative to (micro) vascular growth, resulting inischemia and up regulation of hypoxia inducible factors[24, 25]. Although non-specific incorporation of EPCs intothe systemic endothelium was observed, EPCs preferential-ly homed to ischemic hearts and even more specifically tothe regions with the most profound perfusion insufficiency.The specific homing of EPCs into ischemic myocardiumwas associated with differential induction of neovasculari-zation, only in rats with ischemia due to post-MI heartfailure. Hence, the presence of ischemia seems necessary toswitch from vascular “maintenance” to EPO-induced neo-vascularization.
VEGF levels were slightly increased in the untreated MIgroup, but EPO treatment augmented VEGF expressionfourfold. This effect of EPO could not be extended to shamoperated rats without cardiac ischemia. Upregulation ofVEGF at sites of EPO-induced neovascularization inischemic tissues has been substantiated in other reports[11, 26]. Moreover, in mice that lack EPO-receptorexpression in the vasculature, VEGF upregulation in theischemic hind limb is markedly attenuated and associatedwith significantly reduced neovascularization and homingof EPCs [27]. VEGF is a potent angiogenic factor thatstimulates in situ proliferation of endothelial cells and hasimportant chemotactic effects on EPCs [28]. Therefore,EPO-induced expression of VEGF might mediate thepreferential homing of EPCs into the ischemic tissue, thusfacilitating EPCs-mediated neovascularization. However,the increased VEGF expression might also stimulateresident endothelial cells and thereby induce neovasculari-zation through EPC-independent mechanisms.
EPO-induced VEGF upregulation is mediated throughEPOR signaling pathways [26, 27, 29]. In addition toVEGF upregulation, EPO was associated with augmentedEPOR expression in the MI but not in the sham group,which confirms similar findings by others [30]. Extra-hematopoietic tissues are relatively insensitive to EPO, andbinding affinities for EPO are 10-fold lower in endothelialcells compared to erythropoietic progenitors [23]. Thecombined presence of hypoxia and ischemia howeversignificantly augments sensitivity to EPO through anexponential increase in EPO-receptor expression [30].Separately these factors exert minute effects. Therefore,the absence of EPO-induced VEGF expression and neo-
vascularization might in part be explained through absenceof ischemia-induced sensitization to EPO.
Clinical implications
In the present study, we demonstrate that EPO treatmentmight reverse endothelial dysfunction in the early stages ofcardiovascular disease and thereby prevent the progressioninto cardiovascular events. This important role for EPO inthe regulation of endothelial cell turnover and endothelialfunction, might in part explain the high incidence ofvascular events in patients with EPO deficiency due tochronic kidney disease. The beneficial effects of EPOtreatment in these patients may not only result from thecorrection of anemia but from an improved endothelialfunction as well. Moreover, restoration of endothelialdysfunction in patients with heart failure will decreaseperipheral resistance and thereby reduce cardiac afterloadand possibly improve outcome as well. The improvementof endothelial function in our study was mediated throughaugmented endothelial NO-production. In addition tovasodilatation, augmented NO-production has been identi-fied as an important compensatory mechanism against thepro-thrombotic effects of EPO [21]. A possible therapeuticrole for EPO in its present form in non-anemic patients ishowever complicated by the unrestricted elevation ofhematocrit. The safety of which is currently also questionedin patients with chronic kidney disease and cancer [31, 32].Recently we have demonstrated that cardiac function inpost-MI heart failure can be augmented with an EPO dosethat does not increase hematocrit levels. This might suggestthat even non-erythropoeitic doses of EPO will benefitpatients [33]. Ideally, a minimally effective dose should beestablished which exerts optimal benefit with little or noeffects on hematocrit. In addition, non-erythropoietic EPOderivatives have emerged [34]. These strategies mightprovide us with tools to revitalize the endothelium ofpatients at risk of major cardiovascular events. Care shouldhowever be taken not to over stimulate the bone marrow asthis may lead to functional exhaustion the bone-marrowstem cell population [35, 36].
Conclusions
In general, EPO stimulates normal endothelial progenitorcell-mediated endothelial turnover. However, EPO attrib-utes to neovascularization and improves cardiac functiononly in the presence of local ischemia.
Acknowledgements We thank Bianca Meijeringh and Jan Roggeveldfor expert technical assistance. Dr. Westenbrink and dr. van der Harstare supported by the Netherlands Organisation for Scientific Research
272 Cardiovasc Drugs Ther (2008) 22:265–274

and dr. Belonje is supported by the Netherlands heart foundation. H.Oeseburg is supported by GUIDE. Dr. van Veldhuisen and Dr. Voors areestablished investigators of the Netherlands Heart Foundation (grantD97-017 and grant 2006T037 respectively).
References
1. Hamed S, Barshack I, Luboshits G, Wexler D, Deutsch V, KerenG, George J. Erythropoietin improves myocardial performance indoxorubicin-induced cardiomyopathy. Eur Heart J. 2006;27:1876–83.
2. Hirata A, Minamino T, Asanuma H, Fujita M, Wakeno M,Myoishi M, et al. Erythropoietin enhances neovascularization ofischemic myocardium and improves left ventricular dysfunctionafter myocardial infarction in dogs. J Am Coll Cardiol.2006;48:176–84.
3. Li L, Takemura G, Li Y, Miyata S, Esaki M, Okada H, et al.Preventive effect of erythropoietin on cardiac dysfunction indoxorubicin-induced cardiomyopathy. Circulation. 2006;113:535–43.
4. Li Y, Takemura G, Okada H, Miyata S, Maruyama R, Li L,Higuchi M, et al. Reduction of inflammatory cytokine expressionand oxidative damage by erythropoietin in chronic heart failure.Cardiovasc Res. 2006;71:684–94.
5. Prunier F, Pfister O, Hadri L, Liang L, Del MF, Liao R, et al.Delayed erythropoietin therapy reduces post-MI cardiac remodel-ing only at a dose that mobilizes endothelial progenitor cells. AmJ Physiol Heart Circ Physiol. 2007;292:H522–529.
6. van der Meer P, Lipsic E, Henning RH, Boddeus K, van derVelden J, Voors AA, van Veldhuisen DJ, van Gilst WH, Schoe-maker RG. Erythropoietin induces neovascularization andimproves cardiac function in rats with heart failure aftermyocardial infarction. J Am Coll Cardiol. 2005;46:125–33.
7. van Veldhuisen DJ, Dickstein K, Cohen-Solal A, Lok DJ,Wasserman SM, Baker N, et al. Randomized, double-blind,placebo-controlled study to evaluate the effect of two dosingregimens of darbepoetin alfa in patients with heart failure andanaemia. Eur Heart J 2007;28:2208–16.
8. Westenbrink BD, Lipsic E, van der Meer P, van der Harst P,Oeseburg H, Du Marchie Sarvaas GJ, et al. Erythropoietinimproves cardiac function through endothelial progenitor celland vascular endothelial growth factor mediated neovasculariza-tion. Eur Heart J. 2007;28:2018–27.
9. Bahlmann FH, Song R, Boehm SM, Mengel M, von WR,Lindschau C, et al. Low-dose therapy with the long-actingerythropoietin analogue darbepoetin alpha persistently activatesendothelial Akt and attenuates progressive organ failure. Circula-tion. 2004;110:1006–12.
10. Heeschen C, Aicher A, Lehmann R, Fichtlscherer S, Vasa M,Urbich C, et al. Erythropoietin is a potent physiologic stimulusfor endothelial progenitor cell mobilization. Blood. 2003;102:1340–6.
11. Imamura R, Moriyama T, Isaka Y, Namba Y, Ichimaru N,Takahara S, et al. Erythropoietin protects the kidneys againstischemia reperfusion injury by activating hypoxia induciblefactor-1alpha. Transplantation. 2007;83:1371–9.
12. Urao N, Okigaki M, Yamada H, Aadachi Y, Matsuno K, MatsuiA, et al. Erythropoietin-mobilized endothelial progenitors enhancereendothelialization via Akt-endothelial nitric oxide synthaseactivation and prevent neointimal hyperplasia. Circ Res. 2006;98:1405–13.
13. Dimmeler S, Zeiher AM. Vascular repair by circulating endothe-lial progenitor cells: the missing link in atherosclerosis? J MolMed. 2004;82:671–7.
14. Ross R. The pathogenesis of atherosclerosis—an update. N Engl JMed. 1986;314:488–500.
15. Kisseberth WC, Brettingen NT, Lohse JK, Sandgren EP. Ubiqui-tous expression of marker transgenes in mice and rats. Dev Biol.1999;214:128–38.
16. van der Harst P, Smilde TD, Buikema H, Voors AA, Navis G, vanVeldhuisen DJ, van Gilst WH. Vascular function and mild renalimpairment in stable coronary artery disease. Arterioscler ThrombVasc Biol. 2006;26:379–84.
17. Perticone F, Ceravolo R, Pujia A, Ventura G, Iacopino S,Scozzafava A, et al. Prognostic significance of endothelialdysfunction in hypertensive patients. Circulation. 2001;104:191–6.
18. Treasure CB, Vita JA, Cox DA, Fish RD, Gordon JB, Mudge GH,et al. Endothelium-dependent dilation of the coronary microvas-culature is impaired in dilated cardiomyopathy. Circulation.1990;81:772–9.
19. Dimmeler S, Zeiher AM, Schneider MD. Unchain my heart: thescientific foundations of cardiac repair. J Clin Invest.2005;115:572–83.
20. Santhanam AV, Smith LA, He T, Nath KA, Katusic ZS.Endothelial progenitor cells stimulate cerebrovascular productionof prostacyclin by paracrine activation of cyclooxygenase-2. CircRes. 2007;100:1379–88.
21. Lindenblatt N, Menger MD, Klar E, Vollmar B. Darbepoetin-alpha does not promote microvascular thrombus formation inmice: role of eNOS-dependent protection through platelet andendothelial cell deactivation. Arterioscler Thromb Vasc Biol.2007;27:1191–8.
22. d’Uscio LV, Smith LA, Santhanam AV, Richardson D, Nath KA,Katusic ZS. Essential role of endothelial nitric oxide synthasein vascular effects of erythropoietin. Hypertension. 2007;49:1142–8.
23. Brines M, Cerami A. Emerging biological roles for erythropoietinin the nervous system. Nat Rev Neurosci. 2005;6:484–94.
24. Kalkman EA, Bilgin YM, van der Harst P, van Suylen RJ, SaxenaPR, Schoemaker RG. Determinants of coronary reserve in ratssubjected to coronary artery ligation or aortic banding. CardiovascRes. 1996;32:1088–95.
25. Sano M, Minamino T, Toko H, Miyauchi H, Orimo M, Qin Y, etal. p53-induced inhibition of Hif-1 causes cardiac dysfunctionduring pressure overload. Nature. 2007;446:444–8.
26. Wang L, Zhang Z, Wang Y, Zhang R, Chopp M. Treatment ofstroke with erythropoietin enhances neurogenesis and angiogen-esis and improves neurological function in rats. Stroke.2004;35:1732–7.
27. Nakano M, Satoh K, Fukumoto Y, Ito Y, Kagaya Y, Ishii N, et al.Important role of erythropoietin receptor to promote VEGFexpression and angiogenesis in peripheral ischemia in mice. CircRes. 2007;100:662–9.
28. Zentilin L, Tafuro S, Zacchigna S, Arsic N, Pattarini L, SinigagliaM, et al. Bone marrow mononuclear cells are recruited to the sitesof VEGF-induced neovascularization but are not incorporated intothe newly formed vessels. Blood. 2006;107:3546–54.
29. Nitta K, Uchida K, Kimata N, Honda K, Kobayashi H,Kawashima A, et al. Recombinant human erythropoietin stim-ulates vascular endothelial growth factor release by glomerularendothelial cells. Eur J Pharmacol. 1999;373:121–4.
30. Beleslin-Cokic BB, Cokic VP, Yu X, Weksler BB, Schechter AN,Noguchi CT. Erythropoietin and hypoxia stimulate erythropoietinreceptor and nitric oxide production by endothelial cells. Blood.2004;104:2073–80.
31. Drueke TB, Locatelli F, Clyne N, Eckardt KU, Macdougall IC,Tsakiris D, et al. Normalization of hemoglobin level in patientswith chronic kidney disease and anemia. N Engl J Med. 2006;355:2071–84.
Cardiovasc Drugs Ther (2008) 22:265–274 273273

32. Steinbrook R. Erythropoietin, the FDA, and oncology. N Engl JMed. 2007;356:2448–51.
33. Lipsic E, Westenbrink BD, van der Meer P, van der Harst P, VoorsAA, van Veldhuisen DJ, et al. Low-dose erythropoietin improvescardiac function in experimental heart failure without increasinghaematocrit. Eur J Heart Fail. 2008;10:22–9.
34. Leist M, Ghezzi P, Grasso G, Bianchi R, Villa P, Fratelli M, et al.Derivatives of erythropoietin that are tissue protective but noterythropoietic. Science. 2004;305:239–42.
35. Kissel CK, Lehmann R, Assmus B, Aicher A, Honold J,Fischer-Rasokat U, et al. Selective functional exhaustion ofhematopoietic progenitor cells in the bone marrow of patientswith postinfarction heart failure. J Am Coll Cardiol. 2007;49:2341–9.
36. van der Harst P, van der Steege G, de Boer RA, Voors AA, HallAS, Mulder MJ, et al. Telomere length of circulating leukocytes isdecreased in patients with chronic heart failure. J Am CollCardiol. 2007;49:1459–64.
274 Cardiovasc Drugs Ther (2008) 22:265–274
Copyright © 2022 FDOKUMEN