er: diagnosis and treatment Advanced breast canc - NICE
146
DRAFT FOR CONSULTATION 1 2 3 Clinical Guideline 4 5 er: 6 diagnosis and treatment 7 8 9 10 11 Full Guideline 12 13 14 Draft for consultation 15 Advanced breast canc Advanced breast cancer: full guideline DRAFT (August 2008) Page 1 of 146
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of er: diagnosis and treatment Advanced breast canc - NICE
DRAFT FOR CONSULTATION
1
2
3
Clinical Guideline 4
5
er: 6
diagnosis and treatment 7
8
9
10
11
Full Guideline 12
13
14
Draft for consultation 15
Advanced breast canc
Advanced breast cancer: full guideline DRAFT (August 2008) Page 1 of 146

DRAFT FOR CONSULTATION
Contents 1 .............3 2 .............5 3 .............6 4 ...........18 5 ...........23 6 .............23 7 .............23 8
1.3 .............26 9 England 10
.............28 11
...........31 12
.............31 13
.............34 14
...........40 15
...........44 16
.............45 17
.............50 18
.............58 19
.............61 20
...........71 21
.............71 22
.............72 23
...........75 24
.............75 25 .........................77 26
.............79 27
.............80 28
.............83 29 e 30
............93 31 .........122 32
Appendix 3 - Glossary..................................................................................123 33 Appendix 4 - Guideline Scope .....................................................................127 34 Appendix 5 - List of Topics Covered by Each Chapter.................................132 35 Appendix 6 - People and Organisations Involved in Production of the 36
Guideline ................................................................................................134 37 38
Key priorities ................................................................................... ...................
....w .......................................................
................for ...........
Key research recommendations ..................................................... ..Methodology .................................................................................. ..Algorithms...................................................................................... ..1 Epidemiology ............................................................................ ..
1.1 Introduction ................................................................................ ..1.2 Availability of Routine Data ...........................................................
Epidemiology of Advanced Breast Cancer ........................... ..1.4 Summary of findings from breast cancer teams peer revie in
2004–2007 ............................................................................... ..2 Presentation and Diagnosis...................................................... ..
2.1 Making a diagnosis................................................................... ..2.2 Monitoring disease progress................................................... ..
3 Providing Information and Support for Decision Making........... ..4 Systemic Disease-Modifying Therapy ...................................... ..
4.1 Endocrine Therapy ................................................................... ..4.2 Chemotherapy........................................................................... ..4.3 Biological Response Modifiers ............................................... ..4.4 No systemic disease-modifying treatment ............................ ..
5 Community-based Treatment and Supportive Care ................. ..5.1 Community-based treatment .................................................. ..
.5.2 Supportive Care ....... ................................................................ ..6 Management of Specific Problems........................................... ..
6.1 Lymphoedema .......................................................................... ..6.2 Cancer-related Fatigue ......................................................6.3 Uncontrolled local disease ...................................................... ..6.4 Bone metastases .................................................................... ..6.5 Brain Metastases .................................................................... ..
Appendix 1 - A cost-utility analysis of chemotherapy sequences th.......treatment of patients with advanced breast cancer .........
Appendix 2 - Abbreviations .......................................................... ..
Advanced breast cancer: full guideline DRAFT (August 2008) Page 2 of 146

DRAFT FOR CONSULTATION
Key priorities 1
of metastases for whose imaging is suspicious but not
5
ssed at me of
tumour recurrence. In the absence of any tumour tissue from the primary 9 le.
ositive advanced breast cancer, e is a clinical
yclines or first-line metastatic therapy should be
el, 20 e,
ichever was
24 not
utside the
advanced rovision of
in breast 32 d palliative 33
wo 34 35
cal, ld be 37
s diagnosis at commencement, 38 when death is
continuity of care, which might include the nomination of a person to take on the role 42 of 'key worker' for individual patients.’ 43
44 7. A breast cancer multidisciplinary team should assess all patients 45
presenting with uncontrolled local disease and discuss the therapeutic 46 options for controlling the disease and relieving symptoms. 47
48
2 1. PET-CT should only be used to make a new diagnosis 3
patients with breast cancer 4 diagnostic of metastatic disease.
6 2. If receptor status (oestrogen receptor and HER2) was not asse7
the time of initial diagnosis, then it should be assessed at the ti8
tumour a biopsy of a metastasis should be obtained if feasib10 11
3. For patients with hormone receptor-p12 offer endocrine therapy as first-line treatment unless ther13 need to achieve a rapid tumour response. 14
15 4. For patients with advanced breast cancer who are not suitable for 16
anthracyclines (adjuvant anthrac17 anthracyclines, or contraindicated), systemic chemo18 offered in the following sequence: 19 - first line: single-agent docetax- second line: single-agent vinorelbine or capecitabin21 - third line: single-agent capecitabine or vinorelbine (wh22
not used as second-line treatment). 23
5. Patients who are receiving treatment with trastuzumab should25 continue trastuzumab at the time of disease progression o26 central nervous system. 27
28 6. Healthcare professionals involved in the care of patients with29
breast cancer should ensure that the organisation and p30 supportive care services comply with the recommendations made in 31 previous NICE guidance documents (‘Improving outcomescancer: Manual opdate [2002] and ‘Improving supportive ancare for adults with cancer [2004]), in particular the following trecommendations: - ‘Assessment and discussion of patients’ needs for physi36
psychological, social, spiritual and financial support shouundertaken at key points such aduring, and at the end of treatment; at relapse; and39 approaching.’ 40
- ‘Mechanisms should be developed to promote41
Advanced breast cancer: full guideline DRAFT (August 2008) Page 3 of 146

DRAFT FOR CONSULTATION
8. Offer bisphosphonates to patients newly diagnosed with b1 one metastases, to prevent skeletal-related events and to reduce pain. 2
a single fraction of 8Gy to treat 5
s who have etastases, a
e no or well-controlled other metastatic disease. 10
3 9. Use external beam radiotherapy in4
patients with bone metastases and pain. 6 10. Offer surgery followed by whole brain radiotherapy to patient7
a single or small number of potentially resectable brain m8 good performance status and who hav9
Advanced breast cancer: full guideline DRAFT (August 2008) Page 4 of 146

DRAFT FOR CONSULTATION
Key research recommendations 1
docrine positive
s who progress on treatment with a third-generation aromatase
effectiveness of different sequences of chemotherapy for advanced 9
3. The use of continued trastuzumab in patients with progressive metastatic 12 ed trial.
trolled trials are needed to assess whether patients who 15 cal
5. The relevant research organisations should be encouraged to address 19 the topic of uncontrolled local disease and devise appropriate research 20 studies. This might include development of a national register. 21
22
2 1. Clinical trials are needed to investigate the most effective en3
therapy for post-menopausal women with oestrogen receptor4 tumour5 inhibitor. 6
7 2. Randomised clinical trials should evaluate the clinical and cost 8
breast cancer. 10 11
disease should be investigated as part of a randomised controll13 14 4. Randomised con
have had adjuvant trastuzumab should receive further biologi16 response modifiers. 17
18
Advanced breast cancer: full guideline DRAFT (August 2008) Page 5 of 146

DRAFT FOR CONSULTATION
Methodology 1 Introduction 2
3 ic clinical 4 to 5 E clinical 6
ost 7 nd patients 8
formed choices about appropriate healthcare. While guidelines assist 9 the practice of healthcare professionals, they do not replace their knowledge 10
11
land are 12 (DH). 13 whether 14 cal 15
rofessional 16 en 17
to produce 18 ent and 19 ealth 20
ntre for 21 003 as 22
NICE’s ninth wave work programme. Because of the size of this topic, 23 the NCC-C used 2 guideline slots (early breast cancer and advanced breast 24
25 ble at the 26
27
28 tail of the 29
tead we have tried to 30 focus on those areas of clinical practice that are (i) known to be controversial 31
iii) where there 32 likely to 33 ed later in 34
35
thcare professionals who come into 36 advanced breast cancer, as well as to the patients 37
ill be of 38 d secondary 39
to deliver appropriate care 40 to this group of patients. 41
The Remit of the Guideline 42 Guideline topics selected by the DH identify the main areas to be covered by 43 the guideline in a specific remit. The following remit for this guideline was 44 received as part of NICE’s ninth wave programme of work: 45
What is a Clinical Guideline? Guidelines are recommendations for the care of individuals in specifconditions or circumstances – from prevention and self-care throughprimary and secondary care and onto more specialised services. NICguidelines are based on the best available evidence of clinical and ceffectiveness, and are produced to help healthcare professionals amake in
and skills.
Clinical guidelines for the NHS in England, Wales and Northern Ireproduced as a response to a request from the Department of HealthThey approve topics for guideline development and before decidingto refer a particular topic to the National Institute for Health and CliniExcellence (NICE) they consult with the relevant patient bodies, porganisations and companies. Once a topic is referred, NICE thcommissions one of seven National Collaborating Centres (NCCs)a guideline. The Collaborating Centres are independent of governmcomprise partnerships between a variety of academic institutions, hprofession bodies and patient groups. The National Collaborating CeCancer (NCC-C) was referred the topic of breast cancer in October 2part of
cancer) to fulfil this remit. However, the guideline development process began officially on 22-23 June 2006 when sufficient capacity became availaNCC-C.
Who is the Guideline Intended For? This guideline does not include recommendations covering every dediagnosis and treatment of advanced breast cancer. Ins
or uncertain; (ii) where there is identifiable practice variation; (is a lack of high quality evidence; or (iv) where NICE guidelines arehave most impact. More detail on how this was achieved is presentthe section on ‘Developing Clinical Evidence Based Questions’.
This guideline is relevant to all healcontact with patients withthemselves and their carers. It is also expected that the guideline wvalue to those involved in clinical governance in both primary ancare to help ensure that arrangements are in place
Advanced breast cancer: full guideline DRAFT (August 2008) Page 6 of 146

DRAFT FOR CONSULTATION
‘To prepare a guideline for the NHS in England and Wales on the cmanagement of brea
linical 1 st cancer, to supplement existing service guidance. The 2
hormonal treatments hosphonates.’ 6
7 8
into a scope document by the Guideline 9 he NCC-C.
11 and exclude
13 clear
by NICE
• inform the development of the clinical questions and search strategy 17 nt of the 18
19
, the scope 20 nce with 21 l’ (NICE, 2005, 22
ing the 23 e 24
older 25 nd the NICE Guideline Review Panel (GRP). Further 26
can also be found on the NICE website. The NCC-27 d the 28 posted on 29
30
31 fessional 32
of this 33 nd on the NICE website or in the ‘NICE guidelines manual’ 34
rief, their contribution involves commenting on the draft 35 t version of 36
keholder 37 uideline can be 38
39
40 ment process the NCC-C invited specialist 41
registrars to undertake a needs assessment (see Appendix 6.3). The needs 42 assessment aims to describe the burden of disease and current service 43 provision for patients with breast cancer in England and Wales, which 44 informed the development of the guideline. This document forms a 45 supplement to the full guideline and will also appear on the accompanying 46 CD-ROM to this guideline. 47
guideline should cover: 3
• the key diagnostic and staging procedures 4 • the main treatment modalities including5 • the role of tumour-specific bisp
What the Guideline Covers - The Scope The remit was then translatedDevelopment Group (GDG) Chair and Lead Clinician and staff at t10 The purpose of the scope was to:
• provide an overview of what the guideline would include12 identify the key aspects of care that must be included
• set the boundaries of the development work and provide a 14 framework to enable work to stay within the priorities agreed15 and the NCC-C and the remit 16
• inform professionals and the public about the expected conteguideline.
Prior to the commencement of the guideline development processwas subject to a four week stakeholder consultation in accordaprocesses established by NICE in the ‘NICE guidelines manuaNICE 2006, NICE 2007). The full scope is shown in Appendix 4. Durconsultation period, the scope was posted on the NICE websit(www.nice.org.uk). Comments were invited from registered stakehorganisations ainformation about the GRPC and NICE reviewed the scope in light of comments received, anrevised scope was reviewed by the GRP; signed off by NICE and the NICE website.
Involvement of Stakeholders Key to the development of all NICE guidelines are the relevant proand patient/carer organisations that register as stakeholders. Detailsprocess can be fou(NICE 2007). In bscope, submitting relevant evidence and commenting on the drafthe guideline during the end consultation period. A full list of all staorganisations who registered for the advanced breast cancer gfound in Appendix 6.2.
Needs Assessment As part of the guideline develop
Advanced breast cancer: full guideline DRAFT (August 2008) Page 7 of 146

DRAFT FOR CONSULTATION
Assessment of the effectiveness of interventions is not included in thassessment, and was undertaken sep
e needs 1 arately by researchers in the NCC-C as 2
part of the guideline development process. 3
s presented 4 stages of 5
meet the 6 ormation needs of the GDG during the course of guideline 7
8
9 10
11 ned by the 12 resentatives 13
14 from the NCC-C staff, undertook the development of this clinical guideline. 15
d and 17
which sets the parameters of the
t group
ce h economic evidence
•25 26 27 28
29 h the existing 30
t step was to 31 d for both 32
red the 33 list of 34
r 35 patient 36
rs were 37 n, based on 38
stakeholder 39 organisation. The guideline development process was supported by staff from 40 the NCC-C, who undertook the clinical and health economics literature 41 searches, reviewed and presented the evidence to the GDG, managed the 42 process and contributed to drafting the guideline. At the start of the guideline 43 development process all GDG members’ interests were recorded on a 44 standard declaration form that covered consultancies, fee-paid work, share-45
The information included in the needs assessment document wato the GDG. Most of the information was presented early in theguideline development, and other information was included toevolving infdevelopment.
The Process of Guideline Development – Who Develops the Guideline?
Overview The development of this guideline was based upon methods outli‘NICE guidelines manual’. A team of health professionals, lay repand technical experts known as the GDG (see Appendix 6.1), with support
The basic steps in the process of developing a guideline are liste16 discussed below:
• using the remit, defined 18 the scope guideline 19
• forming the guideline developmen20 • developing clinical questions 21
r the evidence • systematically searching fo22 • critically appraising the eviden23 • incorporating healt24 distilling and synthesising the evidence and writing recommendations • agreeing the recommendations • structuring and writing the guideline • updating the guideline.
The Guideline Development Group (GDG) The Advanced Breast Cancer GDG was recruited in line witNICE protocol as set out in the ‘NICE guidelines manual’. The firsappoint a Chair and a Lead Clinician. Advertisements were placeposts and candidates were informally interviewed prior to being offerole. The NCC-C Director, GDG Chair and Lead Clinician identified aspecialties that needed to be represented on the GDG. Requests fonominations were sent to the main stakeholder organisations andorganisations/charities (see Appendix 6.2). Individual GDG membeselected by the NCC-C Director, GDG Chair and Lead Cliniciatheir application forms, following nomination from their respective
Advanced breast cancer: full guideline DRAFT (August 2008) Page 8 of 146

DRAFT FOR CONSULTATION
holdings, fellowships and support from the healthcare industry.subsequent GDG meetings, members declared ne
At all 1 w, arising conflicts of 2
interest which were always recorded (see Appendix 6.1). 3
4 and 2 July 5 clinical 6 sed and 7
8 item. 9
llocating specific 10 ub-11
12 viewed by 13 o 14 by a GDG 15
the 16 lthcare professionals). The GDG subgroups often helped refine the clinical 17
treatments. They also assisted the 18 pecific 19
20
21 s gave an 22
ess. The 23 ient/carer representatives. They contributed as full 24
ng the clinical questions, helping to ensure that the 25 ensitive issues 26
esearch 27 28
29 During the development phase of the guideline the GDG identified areas 30
list clinical 31 duction of a 32 had been 33
d via the relevant registered stakeholder organisation. 34
e guideline can be found 35 x 6.4. All relevant position papers are presented as part of the 36
M to this 37 38
vidence-Based Questions 39
Background 40 The scope, as described in Appendix 4, needs to be very clear about which 41 patient groups are included and which areas of clinical care should be 42 considered. But within these boundaries it does not usually specify which 43 topics are considered a priority. 44
Guideline Development Group Meetings Fourteen GDG meetings were held between 22 and 23 June 2006 2008. During each GDG meeting (either held over one or two days) questions and clinical and economic evidence were reviewed, assesrecommendations formulated. At each meeting patient/carer and service-user concerns were routinely discussed as part of a standing agenda
NCC-C project managers divided the GDG workload by aclinical questions, relevant to their area of clinical practice, to small sgroups of the GDG in order to simplify and speed up the guideline development process. These groups considered the evidence, as rethe researcher, and synthesised it into draft recommendations prior tpresenting it to the GDG as a whole. Each clinical question was led member with expert knowledge of the clinical area (usually one of heaquestions and the clinical definitions ofNCC-C team in drafting the section of the guideline relevant to their stopic.
Patient/Carer Representatives Individuals with direct experience of advanced breast cancer serviceintegral user focus to the GDG and the guideline development procGDG included three patGDG members to writievidence addressed their views and preferences, highlighting sand terminology relevant to the guideline and bringing service-user rto the attention of the GDG.
Expert Advisers
where there was a requirement for expert input on particular speciaquestions. The clinical questions were addressed by either the proposition paper or a formal presentation by a recognised expert whoidentifie
A full list of recognised experts who contributed to thin Appendievidence review and will also appear on the accompanying CD-ROguideline.
Developing Clinical E
Advanced breast cancer: full guideline DRAFT (August 2008) Page 9 of 146

DRAFT FOR CONSULTATION
It was recognised by the NCC-C at an early stage that in order to cothe guideline development work to an appropriate standard theto restrict its work to approximately 30 clinical questions. Previously prioritisation would have been carried out by the GDG at its first tbut it was clear from some guidelines already published that this ap
mplete 1 GDG needed 2
this 3 wo meetings 4
proach 5 ddressed. 6
d should 7 endations 8
herefore felt 9 as that 10
ertain, where there was identifiable 11 12
13 14
ian in 15 y teams 16
17
dents to 18 ow or high 19
ld be rating the 20 a clinical guideline to be published in 21
suggest any 22 23 24
visory 25 England and Wales with a request for a 4-26
Cancer 27 a the 28
levant 29 30
questionnaire were aggregated by NCC-C 31 32
GDG at its 33 ionnaire 34
ults to agree their 35 36
k was used. 37 38
tions (what is being 39 done - I), the comparisons (other main treatment options - C) and the 40 outcomes (the measures of how effective the interventions have been - O). 41 Where appropriate, the clinical questions were refined once the evidence had 42 been searched and, where necessary, sub-questions were generated. 43
The final list of clinical questions can be found in Appendix 5. 44
had resulted in a much larger number of questions than 30 being a
Clinical guidelines should be aimed at changing clinical practice anavoid ending up as ‘evidence-based textbooks’ or making recommon topics where there is already agreed clinical practice. It was timportant that the 30 clinical questions should be prioritised into arewere known to be controversial or uncpractice variation, or where NICE guidelines were likely to have most impact.
Method An extensive list of potential topics for the guideline to investigate was compiled by the NCC-C Director and GDG Chair and Lead Clinicconsultation with a small number of breast cancer multidisciplinaracross England and Wales.
This list was incorporated into a questionnaire which asked responrate each topic as low, medium or high clinical priority as well as leconomic priority. It was made clear that respondents woupriority for each topic to be included in two years’ time. The questionnaire also asked respondents toadditional topics they would like to see included with an equivalent assessment of their priority.
Questionnaires were subsequently sent to the Breast Cancer AdGroups of all 37 cancer networks inweek turnaround. (A list of all cancer networks can be found on theAction Team website at the DH). Questionnaires were also sent viPatient and Public Involvement Programme (PPIP) at NICE to all repatient/ carer stakeholder organisations.
The scores from each completed staff and ranked. These results together with information on identifiable practice variation (see needs assessment) were presented to thefirst meeting. The list of prioritised topics produced via the questsurvey was in no way definitive and the GDG used these resfinal priorities for the clinical questions.
For clinical questions about interventions, the PICO frameworThis structured approach divides each question into four components: the patients (the population under study - P), the interven
Advanced breast cancer: full guideline DRAFT (August 2008) Page 10 of 146
DRAFT FOR CONSULTATION
Care Pathway Early in the development process the GDG drafted an outline care(or algorithm) in order to explore ho
1 pathway 2
w patients with advanced breast cancer 3 4
5 were 6
rnational) 7 8
organisations were invited to submit evidence for consideration by the GDG, 9 10
t developed 11 linical and 12
agreed in 13 14
detailed health economic work, for 15 mic 16
17
viewed 18 hose to identify 19
s) were 20 nguage restrictions 21
h; however, foreign language papers were not lar importance to that question).
ochrane Library 25
wards Cinahl) 1982
rds
chinfo 1806 onwards 32 ards. [specifically Science Citation Index
d Social Sciences Citation Index (SSCI)] LE) 1980–36
37 38
• National Research Register (NRR) 39 • Current Controlled Trials. 40
From this list the information specialist sifted and removed any irrelevant 41 material based on the title or abstract before passing to the researcher. All the 42 remaining articles were then stored in a Reference Manager electronic library. 43
might access and be treated by the NHS.
Review of Clinical Literature At the beginning of the development phase, initial scoping searchescarried out to identify any relevant guidelines (local, national or inteproduced by other groups or institutions. Additionally, stakeholder
provided it was relevant to the agreed list of clinical questions.
In order to answer each question the NCC-C information specialisa search strategy to identify relevant published evidence for both ccost effectiveness. Key words and terms for the search were collaboration with the GDG. When required, the health economist searched for supplementary papers to inform example modelling (see section on ‘Incorporating Health EconoEvidence’).
Papers that were published or accepted for publication in peer-rejournals were considered as evidence. Search filters, such as tsystematic reviews (SRs) and randomised controlled trials (RCTapplied to the search strategies when necessary. No lawere applied to the searc22 requested or reviewed (unless of particu23
The following databases were included in the literature search: 24 • The C• Medline and Premedline 1950 onwards 26 • Excerpta Medica (Embase) 1980 on27 • Cumulative Index to Nursing and Allied Health Literature (28
onwards 29 • Allied & Complementary Medicine (AMED) 1985 onwa30 • British Nursing Index (BNI) 1994 onwards 31 • Psy• Web of Science 1970 onw33
Expanded 34 • (SCI-EXPANDED) an35 • System for Information on Grey Literature In Europe (SIG
2005 • Biomed Central 1997 onwards
Advanced breast cancer: full guideline DRAFT (August 2008) Page 11 of 146

DRAFT FOR CONSULTATION
Searches were updated and re-run 6–8 weeks before the stakeholdeconsultation, thereby ensuring that the latest relevant publishedincluded in the database. Any evidence published after this date wasincluded. For the purposes of updating this guideline,
r 1 evidence was 2
not 3 30 June 2008 should be 4
5
logical filters 6 view (and will also appear on the 7 line). 8
9 scanned the 10
lications 11 re was 12
. The 13 o 14
15 stion and the 16
ed. 17
18 ook the 19
20
to the 21 ndomised 22 s 23
ied using this established hierarchical system. However this checklist is 24 cy. In the 25 gests levels of 26
unt the factors likely to affect the validity of these 27 28
: ‘NICE 29 guideli30
evel
considered the starting point for searching for new evidence.
Further details of the search strategies, including the methodoused, are provided in the evidence reaccompanying CD-ROM to this guide
Critical Appraisal and Evidence Grading Following the literature search one researcher independentlytitles and abstracts of every article for each question, and full pubwere obtained for any studies considered relevant or where theinsufficient information from the title and abstract to make a decisionresearcher then individually applied the inclusion/exclusion criteria tdetermine which studies would be relevant for inclusion and subsequent appraisal. Lists of excluded papers were generated for each querationale for the exclusion was presented to the GDG when requir
The researcher then critically appraised the full papers. Critical appraisal checklists were compiled for each paper and one researcher undertcritical appraisal and data extraction.
The researcher assessed the quality of eligible studies by referring SIGN quality checklist for systematic reviews/meta-analyses and racontrol trials (Table A). Evidence relating to clinical effectiveness waclassifless appropriate for studies reporting diagnostic tests of accuraabsence of a validated hierarchy for this type of test, NICE sug
oevidence that take into accstudies.
Table A Levels of evidence for intervention studies. Data sourcenes manual’ (NICE 2007).
L Source of evidence 31 32
ias 33 1+ CTs or 34
35 − ith a high 36
37 2++ ematic reviews of case–control or cohort studies; 38
risk of 39 the 40
relationship is causal 41 2+ Well-conducted case–control or cohort studies with a low risk of 42
confounding, bias or chance and a moderate probability that the 43 relationship is causal 44
2− Case–control or cohort studies with a high risk of confounding, bias 45 or chance and a significant risk that the relationship is not causal 46
1++ High-quality meta-analyses, systematic reviews of randomised controlled trials (RCTs) or RCTs with a very low risk of bWell-conducted meta-analyses, systematic reviews of RRCTs with a low risk of bias
1 Meta-analyses, systematic reviews of RCTs or RCTs wrisk of bias High-quality systhigh-quality case–control or cohort studies with a very lowconfounding, bias or chance and a high probability that
Advanced breast cancer: full guideline DRAFT (August 2008) Page 12 of 146

DRAFT FOR CONSULTATION
3 1 4 Expert opinion, formal consensus
Non-analytical studies (for example case reports, case series) 2
data on the 3 ICO) was 4
y 5 ll the evidence was considered 6
7
All procedures were fully compliant with NICE methodology as detailed in the 8 9
h authors; however, there were ad 10 etails. 11
12 13
potential economic issues relating to advanced breast cancer. It is important 14 d cost 15
16
ithin the 17 ailable 18
necessary, conducting economic analysis. 19 tified that addressed 20
ngside the 21 22
priority topic, a 23 onducted. 24
similar 25 e 26
inclusion of a health economics and quality of life filter. 27
esigned to find any applied study estimating the of the topic under consideration. A health economist
red for appraisal.
ned from a variety of sources: 31 32 33 34 35
36 In addition to the review of the relevant clinical evidence, the GDG were 37 required to determine whether or not the cost-effectiveness of each of the 38 individual clinical questions should be investigated. After the clinical questions 39 were decided, the GDG agreed which topics were an ‘economic priority’ for 40 modelling. These ‘economic priorities’ were chosen on the basis of the 41 following criteria, in broad accordance with the ‘NICE guidelines manual: 42
For all the relevant appraised studies for a particular question,type of population, intervention, comparator and outcomes (Precorded in evidence tables and an accompanying evidence summarprepared for the GDG (see evidence review). Acarefully by the GDG for accuracy and completeness.
‘NICE guidelines manual’.
In general, no formal contact was made withoc occasions when this was required in order to clarify specific d
Incorporating Health Economics Evidence The aim of the economic input into the guideline was to inform the GDG of
to investigate whether health services are both clinically effective aneffective, i.e. are they ‘value for money’.
The health economist helped the GDG by identifying priority topics wguideline that might benefit from economic analysis, reviewing the aveconomic evidence and, whereWhere published economic evaluation studies were identhe economic issues for a clinical question, these are presented aloclinical evidence wherever possible.
In order to assess the cost-effectiveness of eachcomprehensive systematic review of the economic literature was cFor those clinical areas reviewed, the information specialists used a search strategy as used for the review of clinical evidence but with th
Each search strategy was d28 cost or cost effectiveness 29 reviewed abstracts and relevant papers were orde30
Published economic evidence was obtai• Medline 1966 onwards • Embase 1980 onwards • NHS Economic Evaluations Database (NHS EED) • EconLit 1969 onwards.
Economic Modelling
Advanced breast cancer: full guideline DRAFT (August 2008) Page 13 of 146

DRAFT FOR CONSULTATION
O ev rall Relevance of the Topic • The number of patients affected: interventions affecting rela
numbers of patients
1 tively large 2
were given a higher economic priority than those 3
5 oth survival and
financial 8 to
s 10 changing clinical practice: priority was given to topics that 11
to represent a significant change to existing 12 13
14 s given to 15 sidered 16
ss. Low priority 17 implied a
ess ratio, 19 ng 20
ty with further analyses (feasibility 21 veness of 22 tion for an 23
24
next task 25 s literature. When 26
ufficient 27 or that 28
t cost-effectiveness evidence was 29 ality, 30
his decision 31 vidence 32
33
ired, the 34 obtain 35 s were 36
s, and they 37 38
The clinical questions in this guideline selected for modelling was chosen 39 because at the time it was considered likely that the recommendations under 40 consideration could substantially change clinical practice in the NHS and have 41 important consequences for resource use. The details of the model are 42 presented in the evidence review and Appendix 1. During the modelling 43 process the following general principles were adhered to: 44
affecting fewer patients 4 • The health benefits to the patient: interventions that that were
considered to have a potentially significant impact on b6 quality of life were given a higher economic priority 7
• The per patient cost: interventions with potentially high(cost/savings) implications were given high priority compared9 interventions expected to have lower financial implication
• Likelihood ofwere considered likelyclinical practice.
Uncertainty • High level of existing uncertainty: higher economic priority wa
clinical questions in which further economic analysis was conlikely to reduce current uncertainty over cost-effectivenewas given to clinical questions when the current literature18 clearly ‘attractive’ or ‘unattractive’ incremental cost-effectivenwhich was regarded as generalisable to a UK healthcare setti
• Likelihood of reducing uncertainissues): when there was poor evidence for the clinical effectian intervention, then there was considered to be less justificaeconomic analysis to be undertaken.
Once the economic priority clinical questions had been chosen, thewas to perform a systematic review of the cost-effectivenesrelevant published evidence was identified and considered to be of squality, this information was used to inform the recommendation fspecific clinical question. When no relevanidentified, or when it was not considered to be of reasonable quconsideration was given to building a de novo economic model. Twas made by the GDG based on an assessment of the available erequired to populate a potential economic model.
For those clinical questions where an economic model was requinformation specialist performed supplemental literature searches toadditional data for modelling. Assumptions and designs of the modelexplained to and agreed by the GDG members during meetingcommented on subsequent revisions.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 14 of 146

DRAFT FOR CONSULTATION
• the GDG Chair and Clinical Lead were consulted during the 1
the systematic review
lts were subject to thorough sensitivity analysis and limitations 5
rom a health services perspective. 7
8 of the 9
from the 10 were able to 11
dations. The link between the evidence and the 12 aking each recommendation is made explicit in the 13
14
15 ope for 16
ion from the 17 nical and cost-effectiveness. To make this process more 18
easily 19 king each 20
21
evidence about benefits and harms for the intervention 24 25 26
ealth 27 28
29 nsus. Shortly before the consultation 30
period, ten key priorities and five key research recommendations were 31 patient algorithms were 32
ion that 33 ion, NICE 34
35
36
staff in partnership with the 37 GDG Chair and Lead Clinician. This was then discussed and agreed with the 38 GDG and subsequently forwarded to NICE for consultation with stakeholders. 39 Registered stakeholders (see Appendix 6.2) had one opportunity to comment 40 on the draft guideline and this was posted on the NICE website between 13 41 August 2008 and 8 October 2008. The GRP also reviewed the guideline and 42 checked that stakeholder comments had been addressed. 43
construction and interpretation of the model 2 • the model was based on the best evidence from 3 • model assumptions were reported fully and transparently 4 • the resu
discussed 6 • costs were calculated f
Agreeing the Recommendations For each clinical question the GDG were presented with a summaryclinical evidence, and where appropriate economic evidence, derivedstudies reviewed and appraised. From this information the GDGderive the guideline recommenview of the GDG in maccompanying qualifying statement.
Qualifying Statements As clinical guidelines are currently formatted, there is limited scexpressing how and why a GDG made a particular recommendatevidence of clitransparent to the reader, the NCC-C felt the need for an explicit,understood and consistent way of expressing the reasons for mar oec mmendation.
The way we have chosen to do this is by writing a ‘qualifying statement’ to 22 accompany every recommendation and will usually cover: 23
• the strength ofbeing considered
• the degree of consensus within the GDG • the costs and cost-effectiveness (if formally assessed by the h
economics team).
Where evidence was weak or lacking the GDG agreed the final recommendations through informal conse
selected by the GDG for implementation and theagreed (see pages 18-22 for algorithms). To avoid giving the impresshigher grade recommendations are of higher priority for implementatno longer assigns grades to recommendations.
Consultation and Validation of the Guideline
The draft of the guideline was prepared by NCC-C
Advanced breast cancer: full guideline DRAFT (August 2008) Page 15 of 146

DRAFT FOR CONSULTATION
Following the consultation period the GDG finalised the recommendathe NCC-C produced the final document. This was then submitted tapproval and publication on their website. The other versions of the(see below)
tions and 1 o NICE for 2 guideline 3
were also discussed and approved by the GDG and published at 4 5
6
oad free of charge from 7 the NICE website (www.nice.org.uk) and the NCC-C website 8
9
ncer guideline 11
line, s and all
14 main
ies, phone 16 g.uk 17
guideline 18 nts with 19
t may also be useful for family members, 20 who care for patients with advanced breast cancer. 21
publications on 0845 003 7783 or 22 23
24
the end of 25 ed 26
l consider 27 28
Two years after publication of the guideline, NICE will commission a National 29 ating Centre to determine whether the evidence base has progressed 30
early 31 fter 32
33
Funding 34
by NICE to 35 36
Disclaimer 37
The GDG assumes that healthcare professionals will use clinical judgment, 38 knowledge and expertise when deciding whether it is appropriate to apply 39 these guidelines. The recommendations cited here are a guide and may not 40 be appropriate for use in all situations. The decision to adopt any of the 41
the same time.
Other Versions of the Guideline
This full version of the guideline is available to downl
(www.wales.nhs.uk/nccc).
NICE also produces three versions of the advanced breast ca10 which are available from the NICE website:
• the NICE guideline, which is a shorter version of this guide12 containing the key priorities, key research recommendation13 other recommendations
• the Quick Reference Guide (QRG), which is a summary of the15 recommendations in the NICE guideline. For printed copNICE publications on 0845 003 7783 or email [email protected]
• ‘Understanding NICE Guidance’ (‘UNG’), which describes theusing non-technical language. It is written chiefly for patieadvanced breast cancer buadvocates or thoseFor printed copies, phone NICE email [email protected]
Updating the Guideline
Literature searches were repeated for all of the clinical questions atthe GDG development process, allowing any relevant papers publishbefore 30 June 2008 to be considered. Future guideline updates wilevidence published after this cut-off date.
Collaborsignificantly to alter the guideline recommendations and warrant anupdate. If not, the guideline will be updated approximately 4 years apublication.
The National Collaborating Centre for Cancer was commissioneddevelop this guideline.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 16 of 146

DRAFT FOR CONSULTATION
recommendations cited here must be made by the practitioner individu
in light of 1 al patient circumstances, the wishes of the patient and clinical 2
expertise. 3
ut of the use or 4 of these guidelines and the literature used in support of these 5
6
7
National Institute for Health and Clinical Excellence (2005) The guidelines 8 nce. 9
uidelines 10 e. 11
National Institute for Health and Clinical Excellence (2007) The guidelines 12 manual. London: National Institute for Health and Clinical Excellence. 13
The NCC-C disclaims any responsibility for damages arising onon-use guidelines.
References
manual. London: National Institute for Health and Clinical Excelle
National Institute for Health and Clinical Excellence (2006) The gmanual. London: National Institute for Health and Clinical Excellenc
Advanced breast cancer: full guideline DRAFT (August 2008) Page 17 of 146

DRAFT FOR CONSULTATION
Algorithms 1 Overview of pathway 2
3 4
Patient presenting with suspected advanced breast cancer
Assessment
Sequential systemic therapy
Systemic anti-cancer therapy stopped
Decision support
5 6
7
Advanced breast cancer: full guideline DRAFT (August 2008) Page 18 of 146

DRAFT FOR CONSULTATION
Diagnosing Advanced Breast Cancer 1 2
Imaging assessment 3 4
Patient presents with suspected advanced breast cancer
Assess for visceral metastases:CT/MRI, plain X-rays, US Assess for bone metastases
Axial skeleton:CT scan or MRI or bone
scintigrapy
Proximal limb bones:Bone scintigrapy or plain X-rays
MRI
Y
PET-CT
Y
Imaging equivocal but high suspicion of
metastases
Equivocal images or concern about spinal
canal
N N
Diagnosis of advanced breast cancer confirmed, extent of metastases known?
Treatment
Y
Not covered by this guidelineN
Imaging results
5 6
Advanced breast cancer: full guideline DRAFT (August 2008) Page 19 of 146

DRAFT FOR CONSULTATION
Assessing receptor status 1 2
Patient presents with suspected advanced breast cancer
Take tissue biopsy and assess for ER and HER2
No further biopsy
Assess for ER and HER2
Take tissue biopsy and assess for ER and HER2
Receptor status known
Y
N
Y
N
N
Y
First presentation?
Previous tumours assessed for ER/
HER2?
Tumour sample
available?
3 4
Advanced breast cancer: full guideline DRAFT (August 2008) Page 20 of 146

DRAFT FOR CONSULTATION
Endocrine therapy 1 2
3 4 5 * for ER positive men with advanced breast cancer offer tamoxifen as the first-line treatment 6
Advanced breast cancer: full guideline DRAFT (August 2008) Page 21 of 146

DRAFT FOR CONSULTATION
Chemotherapy 1 2
Patients requiring chemotherapy
Offer anthracyclines
Disease progression
N
N
HER2 +ve
Trastuzumab + taxane
Extracranial disease
progression
Stop trastuzumab
N
Research requiredY
1st line single agent docetaxel *
2nd line single agent vinorelbine or capecitabine
3rd line single agent
capecitabine or vinorelbine
HER2 -ve
Previous anthracyclines
?
Contra-indication to anthracyclines?
Y
HER2 status?
Patient previously treated with trastuzumab
Y
3 4 * Consider combination therapy for patients in whom a greater probability of response is important and who 5 understand/are likely to tolerate the additional toxicity 6 7
Advanced breast cancer: full guideline DRAFT (August 2008) Page 22 of 146

DRAFT FOR CONSULTATION
1 Epidemiology 1 2 3
t 4 r regionally, 5
r this 6 se 7
g whether variation in epidemiology or service utilisation 8 9
10 d is available 11
the same in 12 lates to 13
ith 14 ptoms, 15
16 quality of life. The process of producing this summary has highlighted the lack 17
e burden of advanced breast cancer on 18 individuals, society and the NHS. 19
20 21 22 23
r for the 24 published by the Office of National Statistics (UK Statistics Authority 25
2007). It is based on data collated by 11 registries covering Northern Ireland, 26 f Health 27
28 29 30
parent at 31 ome data 32
e of primary 33 ence and 34
ary diagnosis. 35 cer 36 reast cancer 37
easons that 38 rmation relate to various problems of 39
mongst the 40 in other 41
f Cancer 42 rce 43
2007). 44 45 One implication of this is that population level data for describing the 46 epidemiology of secondary breast cancer are relatively sparse. The data 47 available tend to be framed in terms of the start and end of the illness. The 48 argument has been made that such data are more descriptive for women with 49
1.1 Introduction The following needs assessment provides a summary of the curreninformation available regarding the epidemiology of breast cancenationally and internationally. Its purpose is to provide the context foguideline, providing an overview of the size of the problem and diseaburden, and assessinexists. The full report covers both early and advanced breast cancer anas a supplement to the full guidelines. Although the disease is both cases, the issues differ markedly. This executive summary readvanced breast cancer, breast cancer with metastases. For those wadvanced breast cancer the focus is inevitably upon palliation of symdealing with the longer term side effects of treatment and improving the
of routine data available to assess th
1.2 Availability of Routine Data
Cancer registries Information on the incidence, mortality and survival of breast canceUK is
Scotland, Wales and 8 regional registries in England (Department o2008). The registries are the only source of reliable population level data for the UK. Most registries are designed to record information about cancers apthe time of diagnosis of the primary neoplasm. Whereas there are savailable on the occurrence of secondary breast cancer at the timdiagnosis, most registries do not collect information on the occurrdistribution of secondary breast cancer occurring after the primA recent survey found that only one registry (West Midlands CanIntelligence Unit) collects information on all cases of secondary bwithin their area (Secondary Breast Cancer Taskforce 2007). Rother registries do not collect this infosystems, process and capacity – both within registries and ainstitutions from which they collect data. Similar problems exist countries, including those contributing to the European Network oRegistries, Australia, and the USA (Secondary Breast Cancer Taskfo
Advanced breast cancer: full guideline DRAFT (August 2008) Page 23 of 146

DRAFT FOR CONSULTATION
early stage breast cancer than they are for women with secondarycancer (Musa 2004). The lack of data available regarding secondcancers (cancers which occur after the initial diagnosis) has receraised as an issue by the Secondary Breast Cancer Taskforce and Cancer Care (2007) These data are not collected nationally or and thi
breast 1 ary breast 2 ntly been 3
Breast 4 internationally 5
s leads to great difficulties in estimating the burden of secondary 6 7 8
y be 9 ical 10
han 11 nagement of 12
OM 2007). In some instances, 13 regional data provide the best indicator of the national position. Data on 14
ast cancers are a good example of this. 15 16
17 e NHS, 18 are 19
nt Episode 20 duals and 21 ther early 22
ata are 23 us errors, 24
ing these data 25 within 26
as a 27 d breast 28 ntly 29
er way to combine the HES data with the cancer registry data in England. 30 ssessment 31
on of a 32 r Intelligence 33
34 35
36 with the 37 ta have 38
39 40 41
ronic 42 main 43
available sources tailored to collect 44 monitoring information for a specific purpose. An example is the monitoring of 45 disease registers and treatment of individuals with certain health conditions 46 through QOF (Quality and Outcomes Framework). Breast cancer is not a 47 condition monitored through the QOF system. The second main source is a 48 group of primary care research databases that represent a sample of practice 49 activity but are not routinely accessible. 50
disease. Where there is a lack of comprehensive national data, there maalternative sources available. For example, the Breast Cancer ClinOutcome Measures (BCCOM) project has audited a cohort of more t16,000 individuals diagnosed in 2004, providing data on the masymptomatic breast cancer across the UK (BCC
secondary bre Hospital activity Information regarding every hospital admission commissioned by thincluding details of the patient, diagnosis and procedures performedrecorded in England (Hospital Episode Statistics) and Wales (PatieDatabase Wales). This relates to episodes of care rather than indivialso relates to procedures performed rather than the indication, wheor advanced breast cancer, or the outcome of treatment. These dprocessed and ‘cleaned’ nationally, removing duplicates and obvioto provide the most robust data possible. The purpose of includin the full report is to give an estimate of the level of inpatient activitysecondary care, and so emphasise the importance of breast cancerresource issue. However, as these data are not relevant to advancecancer it has not been included in this summary. There is work curreundThis will enable analysis at an individual level and also allow the aof repeat procedures and outcomes. This work will be an extensiprevious cohort analysis performed by the West Midlands CanceUnit.
Outpatient data have also been collected through the hospital activity data since 2003. However, these data record the speciality associatedappointment but not the diagnosis or reason for referral. These datherefore not been examined for this assessment. Primary care The majority of contacts in primary care are now recorded on electsystems. There are several sources of these data, which fall into twogroups. The first are the routinely
Advanced breast cancer: full guideline DRAFT (August 2008) Page 24 of 146

DRAFT FOR CONSULTATION
There are issues regarding how primary care contacts are recordedfor patient contacts may be coded with the reason for attendance, udiagnosis or left uncoded. A survey in 2003, of practice information sfound that although 96% of paper and 94% of computerised recorthe reason for a patient contact episode in primary care, only 48%records and 34% of computerised records contained a diagnosis (HCox et al. 2003). Systems will also not detect contacts which are rebreast cancer, for example psychological
1 , entries 2 nderlying 3 ystems, 4
ds recorded 5 of paper 6
ippisley-7 lated to 8
problems related to a diagnosis or 9 10 11
provide 12 Morbidity survey 13
le from the Royal College of General Practitioners 14 15 16 17
e literature 18 gett et al. 2007). 19 easures, place 20
which 21 onstructed by 22
cultures, for example 23 wding may be a choice rather than a sign of poverty in some cultures 24
25 26 27 28
or cancer 29 ountry of 30
eath 31 t ethnicity 32
but the 33 recording remains incomplete and the use of the ‘not known’ category 34
gh. The Quality and Outcomes Framework (QOF) has begun to 35 s with a practice. 36
available, 37 cer guideline. 38
39 40
T 41 le to make 42 rticular 43
d are not 44 allocated to individual patients or to the diagnosis or reason for prescription. 45 46 National data are not available for hospital based prescribing. However, the 47 National Cancer Director (2004) published an audit of the usage of cancer 48 drugs approved by NICE. The data used for the audit were taken from the 49 IMS Health Hospital Pharmacy Audit, collected in 2005 from hospitals 50
treatment, unless specifically coded. Surveys of the population have been conducted in the past to information on the level of activity in primary care. information is availabAnnual Prevalence Report (2007) and has been included. Socioeconomic status Information regarding socioeconomic status was obtained from thas it is not routinely available from cancer registry data (SlogStudies have examined socioeconomic status by individual mof residence or country of residence. Status is defined by indicatorsmark material deprivation. These markers are socially cjudgements which may not be appropriate for all overcro(Farooq et al. 2005). There are also difficulties in assessing the socioeconomic status of women (Coleman et al. 2001). Ethnicity Ethnicity is poorly recorded in NHS data. It is part of the dataset fregistries (Farooq et al. 2005) but remains an optional field and cbirth, not ethnicity, is currently the method of recording used in UK dregistrations (Wild et al. 2006). NHS providers are required to collecmonitoring data for outpatients and inpatients (Farooq et al. 2005),
remains hiencourage recording of ethnicity but only for new registrationInformation was obtained from the literature as no routine data arebut there were no specific findings for the advanced breast can Prescribing Primary care prescribing data are collected nationally, through PAC(Prescribing Analysis and Cost) by prescriber, but it is not possibconclusions relating to breast cancer from the prescriptions of pamedications. The data are collected for budgetary reasons an
Advanced breast cancer: full guideline DRAFT (August 2008) Page 25 of 146

DRAFT FOR CONSULTATION
covering 93% of acute beds in the UK. The audit reviewed the use for cancers that included breast cancer, and for trastuzamab ucancer alone. These data indicate the presence of variation across country, but do not include information regarding the type of cdisease,
of 6 drugs 1 sed for breast 2
the 3 ancer, stage of 4
particularly if early or advanced breast cancer, or outcome of 5 6 7 8
of 9 ivered, but 10
n for 11 se data, but the 12
d in the 13 nd 14
rting for radiotherapy data which will enable separation of 15 ble at the 16
17 18
y the National Cancer Services Analysis Team 19 (NATCANSAT) to examine travel distances to radiotherapy centres. These 20
cal issues that impact 21 upon patient access to treatment. 22
23 24 25
ncer. 26 dicate that 27
1992 28 ondary 29
her 35% of 30 in the 10 31
he number 32 time period. 33
34 cidence of 35
icate an 36 there are 37
rtality from 38 treatment, 39
icular 40 year cannot be related to the incidence of new cases in that year, as those 41
42 43
breast cancer follows the same socioeconomic gradient as 44 incidence (Gage et al 1997; Faggiano et al 1997). Women in higher 45 socioeconomic groups are more likely to have breast cancer recorded as their 46
treatment. Radiotherapy Radiotherapy centres currently collect information regarding the sitetreatment and the dose and number of fractions of radiotherapy delthis may not include the primary site of the cancer or the indicatiotreatment. There has been voluntary national reporting of thecompleteness and quality is questionable and so this is not includereport. Agreement has been reached to introduce a core data set amandatory repodoses given for treatment and for palliation, but this was not availatime of this report. Work has been undertaken b
data are included to highlight some of the geographi
1.3 Epidemiology of Advanced Breast Cancer There are no national data on the incidence1 of advanced breast caRegional data from the West Midlands Cancer Intelligence Unit inabout 5% of women and men diagnosed with breast cancer betweenand 1994 had metastases at the time of their primary diagnosis (SecBreast Cancer Taskforce 2007). The data also suggest that a furtall those with a primary diagnosis went on to develop metastasesyears following diagnosis. Currently there are few data to quantify tof cases of secondary breast cancer developing after the 10-year Mortality2 data may be considered as a proxy measure for the inadvanced breast cancer. For example, a trend in mortality may indunderlying trend in incidence of advanced breast cancer. However,important cautions to consider in making these assumptions. Mobreast cancer may include those who die from complications of rather than advanced metastatic disease. Also the mortality in a part
who die from breast cancer will have been diagnosed over a range of years. Mortality from
1 Incidence – the number of new cases occurring in a period of time in a defined population. 2 Mortality - the number of deaths attributed to breast cancer in a specified period of time in a defined population.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 26 of 146

DRAFT FOR CONSULTATION
cause of death than those in lower socioeconomic groups. Howsurvival
ever, the 1 of the disease 2
ower 3 with more 4
re 5 more 6
et al. 1998). 7 likely to 8
2006). 9 10
historical 11 approximately 12
number 13 cidence and 14
d in the UK since the early 1990s. The proportion of these 15 ). 16
17 18
h a current 19 physical 20
s social and 21 pport. Survey estimates reveal that an average practice of 22
ients who consult their GP regarding 23 24 25 26 27
Cancer 28 sumed to 29
reast cancer as the 30 se in early breast cancer. Although there 31
Trusts across 32 on in 2003. A 33
34 35 36
uity of 37 early 38
required to 39 d as a 40
n distance 41 es not 42
t gives 43 affected by the 44
availability of public transport in the area and the time to travel on these 45
3 in more deprived groups is worse at every stage (Garvican et al. 1998). Studies have shown that women from lsocioeconomic backgrounds are more likely to be diagnosedadvanced disease (Downing et al. 2007), with differences being mopronounced in the 50-69 age group (Schrijvers et al. 1995), and arelikely to have a poorer prognosis4 than affluent women (GarvicanThis relates to the fact that women from deprived groups are lesshave their breast tumours diagnosed by screening (Robinson et al. Based on numbers of women diagnosed up to the end of 1992, andsurvival patterns it has been estimated that in 2003 there were 172,000 women in the UK who have a history of breast cancer. Thisis likely to be an underestimate in view of the increases in insurvival experienceliving with advanced breast cancer is not known (Micheli et al. 2002 Primary Care Activity Primary care provides a great deal of healthcare to individuals witdiagnosis or past history of breast cancer. This includes contacts for problems associated with the cancer and its treatment, plupsychological su10,000 will have around 25 registered pattheir breast cancer diagnosis each year (Royal college of General Practitioners 2007). Variation in Use of Chemotherapeutic Drugs The audit of the use of NICE approved cancer drugs by the NationalDirector (2004) included the use of trastuzamab. These data are asapply mainly to the use of trastuzamab in advanced breview was prior to the start of its uwas a nearly threefold difference in the level of its use by AcuteEngland in 2005, this had reduced from an over fourfold variatisimilar pattern was seen for the other cancer drugs reviewed. Distance from Radiotherapy Centres Distance from radiotherapy centres is a significant factor in the eqprovision of radiotherapy services. It has a more marked impact inbreast cancer with this particular therapy as patients are often travel daily for treatment. Palliative radiotherapy is usually deliveresingle dose, but several visits may be required, and the variation ito travel will still impact upon patients and carers. Pure distance docapture all the variables which affect equity of access in this case buone method of assessing the access. This may also be
3 Survival – in this case refers to relative survival - the proportion of people diagnosed with breast cancer who are living at the end of a defined period of time (for example, after five or ten years) when compared to similar people of the same age who do not have breast cancer. This measure takes into account deaths from other causes. 4 Prognosis - a prediction of the probable course and outcome of a disease.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 27 of 146

DRAFT FOR CONSULTATION
roads. There are large areas that are over 50km by road from theiradiotherapy centre. These are rural areas with low levels of populat7% of the population of England and Wales do live more than 50kmradiotherapy centre
r local 1 ion, but 2 from their 3
. 15% of the Welsh population live more than 50km away 4 5 6 7
er. Up to 8 isease 9
eans that we have very little information with which to 10 plan services for the future or to estimate resource use and better information 11
12 13
ver, 14 nomic 15 oups. 16
17 for advanced breast cancer, but evidence shows that access to NICE 18
es vary across 19 the 20 21
ms peer 22 23 24
ng 25 outcomes in breast cancer’ (NICE 2002) a process was put in place in 26
rom NICE or 27 g the 28 mended. 29
30 eams 31 n the first 32
n reviewed 33 34 35
gland and 36 e reviewed by a team of clinical 37
his 2004-38 ship in 39
though 40 pdated guidance requirement (NICE 2002) to 41
have two core members in all the key disciplines. 42 43 For breast cancer teams alone, core members are required to spend at least 44 half of their clinical time on breast cancer management. Only half of the teams 45 reviewed complied with this measure, the most frequent source of non-46 compliance being histopathologists. 47 48
from their local centre. Summary There is little information available regarding advanced breast canc40% of those diagnosed with breast cancer will develop advanced dwithin 10 years. This m
is needed for this purpose. Variation in outcomes does not appear to vary geographically. Howemortality from breast cancer is highest in those from higher socioecogroups, and survival is poorest in those from lower socioeconomic grInformation is insufficient to assess variations in most treatments and services
approved drugs and physical access to radiotherapy centres docountry.
1.4 Summary of findings from breast cancer teareview in England 2004–2007
Following the publication of the updated NICE guidance on ‘Improvi
England (as for other cancer sites covered by service guidance fthe Department of Health) to monitor progress made in implementinchanges in service organisation and delivery which had been recom Breast cancer care was the first to be managed by multidisciplinary t(MDTs), starting in the early 1990s. All these MDTs were reviewed iround of cancer peer review carried out in 2001 and many had beein predecessor systems too. Between November 2004 and May 2007 each cancer network in Enall the designated breast cancer MDTs werpeers. A total of 174 breast cancer MDTs were included as part of t2007 peer review round. Of these, 88% had a full core team memberplace (a figure exceeded only by specialist urology cancer teams) alonly half of the teams met the u
Advanced breast cancer: full guideline DRAFT (August 2008) Page 28 of 146

DRAFT FOR CONSULTATION
Compliance to attend MDT meetings (at the 50% minimum attendawas high at 77% a
nce level) 1 nd exceeded only by specialist teams in gynaecological 2
and urological cancer. 3 4
(after 5 ree years. A 6 l others, 7
llowed. 8 nd 9
es with symptomatic services. Less than half of 10 the cancer networks had carried out the required review and only a third had 11
12 13
igh compliance with patient experience measures (e.g. patient 14 located a 15
16 17
As many as 16 (9%) of the breast cancer teams had workload volumes of less 18 mpliance 19
20 21
ancer measures by breast cancer teams was 22 is amongst the highest for all cancer sites (exceeded only by 23
d total 24 25 26 27
sis of the 28 Year 29
07. 30
31 Wales. Cancer. 32
33
stem. 34
2007) 35 stage at diagnosis, treatment and 36
): 836-40. 37
iano F. Partanen T. Kogevinas M. Boffetta P. (1997) Socioeconomic 38 differences in cancer incidence and mortality. IARC Scientific Publications 39 (138): 65-176. 40
Farooq S. Coleman MP. (2005) Breast cancer survival in South Asian women 41 in England and Wales. Journal of Epidemiology & Community Health 59(5): 42 402-6. 43
The extant NICE Guidance (2002) requires hospital-based follow-uptreatment of early breast cancer) to be limited to a maximum of thtotal of 40% of cancer networks did not consent to this and severadespite having guidelines to that effect, did not expect them to be foThe 2002 guidance also seeks movement towards harmonisation aalignment of screening servic
actually developed an action plan. There is hsurveys) in most breast cancer teams but only 69% of teams were alkey worker.
than 100 patients a year. Most of these teams had low overall colevels with all breast cancer measures. Overall compliance with all c77% whichspecialist gynaecological cancer teams). However, 5% of teams hacompliance levels of under 50%. References Breast Cancer Clinical Outcome Measures Project. BCCOM: Analymanagement of symptomatic breast cancers diagnosed in 2004, 3rd
Report December 20
Coleman M.P. Babb P. Sloggett A. Quinn M. De Stavola B. (2001) Socioeconomic inequalities in cancer survival in England and 91(1 SUPPL.): 208-216.
Department of Health (2008). The national cancer registration sy
Downing A. Prakash K. Gilthorpe MS. Mikeljevic JS. Forman D. (Socioeconomic background in relation tosurvival in women with breast cancer. British Journal of Cancer 96(5
Fagg
Advanced breast cancer: full guideline DRAFT (August 2008) Page 29 of 146

DRAFT FOR CONSULTATION
Gage H. Fouquet R. (1997) Explaining breast cancer mortality in Engeffect of socioeconomic fact
land: the 1 ors and health care services. European Journal of 2
Cancer Prevention 6(4): 341-50. 3
-4 en-detected and symptomatic cases of breast cancer. 5
6
7 439-43. 8
ogh V, Quinn MJ, Coleman M, Hakulinen T, et al. 9 Annals 10
11
d outcomes for high-risk and metastatic breast 12 : California 13
ram. 14
approved by 15 16
proving 17 tional 18
. 19
of 20 ancer presenting to a District General Hospital breast 21
22
it. Annual 23 e Report. 2006 24
(1995) 25 urvival from breast cancer. British Journal of Cancer 72(3): 26
27
ted: The need for 28 t cancer and survival. 29
30
Sloggett A. Young H. Grundy E. (2007) The association of cancer survival 31 er 32
33
Statistics Authority. Cancer statistics registrations: registrations of cancer 34 diagnosed in 2004, England. Series MB1 No. 35. 2007. London, 2007. 35
Wild SH. Fischbacher CM. Brock A. Griffiths C. Bhopal R. (2006) Mortality 36 from all cancers and lung, colorectal, breast and prostate cancer by country of 37 birth in England and Wales,2001-2003 British Journal of Cancer 94(7): 1079-38 85. 39
Garvican L. Littlejohns P. (1998) Comparison of prognostic and socioeconomic factors in screPublic Health 112(1): 15-20.
Hippisley-Cox J. et al. (2003) The electronic patient record in primary care- regression or progression? A cross sectional study. BMJ 326: 1
Micheli A, Mugno E, Kr(2002) Cancer prevalence in European registry areas.[see comment]. of Oncology 13(6): 840-65.
Musa M. (2004) Treatment ancancer in California: an inquiry into disparities and research needsBreast Cancer Research Prog
National Cancer Director. Variations in usage of cancer drugsNICE. Department of Health 2006.
National Institute for Health and Clinical Excellence (2002). Imoutcomes in breast cancer. Cancer service guidance. London: NaInstitute for Health and Clinical Excellence
Robinson D, Bell J, Moller H, Salman A. (2006) A 13-year follow-uppatients with breast cunit in southeast England. Breast 15(2): 173-80.
Royal College of General Practitioners – Birmingham Research UnPrevalenc
Schrijvers CT. Mackenbach JP. Lutz JM. Quinn MJ. Coleman MP.Deprivation and s738-743.
Secondary Breast Cancer Taskforce. Stand up and be counthe collection of data on incidence of secondary breasBreast Cancer Care.
with four socioeconomic indicators: A longitudinal study of the oldpopulation of England and Wales 1981-2000. BMC Cancer 7.
UK
Advanced breast cancer: full guideline DRAFT (August 2008) Page 30 of 146

DRAFT FOR CONSULTATION
2 Presentation and Diagnosis 1 2
2.1 Making a diagnosis 3 4 5 6
atients 7 ent with 8
such as bone pain, dyspnoea, nausea, abdominal discomfort and 9 general malaise. Occasionally metastatic disease may be suspected at first 10
11 12
stance a 13 to assess 14
s 15 to confirm 16
with more 17 ment of 18
A variety of 19 ging techniques are available: plain radiography, ultrasound, bone 20
aging (MRI), 21 phy (PET-22
23 24
ormation by 25 sitron 26
nant tumours have a higher glucose metabolism 27 than normal tissue, take up more FDG than the surrounding tissue and emit 28
ased 29 ation can be
Imaging A new diagnosis of advanced breast cancer may be suspected in pwho have previously been treated for breast cancer, and who pressymptoms
presentation. The initial investigation depends on the presenting symptoms, for inchest radiograph performed to investigate dyspnoea or radiographslocalised bone pain. Once a diagnosis of advanced breast cancer isuspected either clinically or on initial imaging, it is routine practice the diagnosis and to assess the extent of metastatic disease imaging (commonly referred to as staging). This may include assessthe commoner sites of metastasis including lung, liver and bone. imascintigraphy, computed tomography (CT), magnetic resonance imand positron emission tomography fused with computed tomograCT). Unlike imaging with X-rays or MRI, PET provides functional infusing 18F-deoxyglucose (FDG), a glucose analogue labelled with poemitting fluorine. Most malig
more positrons, so areas of malignancy show up as areas of increactivity on the scan. When PET is fused with CT functional inform30 accurately located anatomically. 31 32 Recommendations 33 • Assess visceral metastases using an appropriate combination of plain 34
radiography, ultrasound, CT scan and MRI. 35 • Use either bone windows on a CT scan, MRI or bone scintigraphy to 36
assess the presence and extent of metastases in the bones of the axial 37 skeleton. 38
• Assess proximal limb bones in patients with evidence of bone 39 metastases elsewhere, for the risk of pathological fracture using either 40 bone scintigraphy and/or plain radiographs. 41
• Use MRI to assess bony metastases if other imaging is equivocal for 42 metastatic disease or if more information is needed (for example lytic 43 metastases encroaching on the spinal canal). 44
• PET-CT should only be used to make a new diagnosis of metastases for 45 patients with breast cancer whose imaging is suspicious but not 46 diagnostic of metastatic disease. 47
Advanced breast cancer: full guideline DRAFT (August 2008) Page 31 of 146

DRAFT FOR CONSULTATION
Qualifying statement: There was insufficient evidence to support the choice 1 s that of one imaging modality over another but there was GDG consensu2
imaging should still be used to assess the extent of advanced breast cancer. 3 4
Clinical Evidence 5 d fifteen Two systematic reviews (Isasi et al., 2005 and Shie et al., 2008) an6 fer et al., small comparative studies or case series (Abe et al., 2005, Altehoe7
, Engelhard 2001, Bradley et al., 2000, Bristow et al., 2008, Cook et al., 19988 et al., 2005, et al., 2004, Eubank et al., 2001, Eubank et al., 2004, Fueger 9 005, Haubold-Reuter et al., 1993, Kamby et al., 1987, Nakai et al., 210 ., 2006) Schirrmeister et al., 1999, Schmidt et al., 2008 and Ternier et al11
on imaging to determine disease 12 formed the evidence base for the topic 13 extent. Other than the reviews, papers were generally of poor to medium 14 quality and many were retrospective studies.
15 ing MRI and FDG-PET were equal to or better than scintigraphy in visualis16
y MRI was bone metastases, other than osteoblastic lesions, but whole bod17 particularly in abdominal better than FDG-PET at detecting distant metastases 18
organs, brain and bone. MRI also detected previously unidentified 19 udy, the 20 metastases, including those that were non-skeletal and, in one st
21 treatment plan was changed accordingly in ~43% of patients. 22
alue in detecting local breast cancer recurrence CT had a high diagnostic v23 higher and, when the field was extended to include the pelvis, also had a 24
tigraphy. diagnostic accuracy in detecting bone metastases than scin25 26
conomic Evaluation Health E27 The GDG did not consider this topic as a health economic priority; therefore 28
ewed. the cost-effectiveness literature on this topic has not been revi29 30 31 32 33
the origin, but sometimes is 35
r lesion not 37 tic of metastatic disease. 38
t origin 39 40 41
may be 42 43 44
The treatment of patients with advanced breast cancer is guided by a number 45 of factors including the hormone receptor (oestrogen and progesterone 46 receptor) status and the expression of HER2 of the primary tumour or the 47 metastases. Current practice in some centres is to establish oestrogen and 48 progesterone receptor and HER 2 status on all newly diagnosed breast 49 cancers. However there is no evidence that assessing progesterone receptor 50
Pathology Histological verification of metastatic disease is not needed routinely in patients who have a history of previous breast cancer and in whom34 pattern of metastatic disease is consistent with breastappropriate. For example: 36
• If the imaging findings are equivocal such as a solitary livediagnos
• If a patient presents with metastatic cancer of possible breaswithout a history of a previous primary breast cancer.
• If patients have a history of more than one different primary cancer in the past and therefore the source of the metastatic diseaseuncertain.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 32 of 146

DRAFT FOR CONSULTATION
status adds significant information to oestrogen receptor status in presponse to hormone treatment (see Chapter 4 of the NICE full gEarly Breast Cancer: diagnosis and treatment). It is not routine prareassess receptor status on recurrence. If the receptor status of the ptumour is unknown and fur
redicting 1 uideline on 2
ctice to 3 rimary 4
ther analysis is not possible, it may be necessary to 5 6 7
biopsy the metastatic disease. Recommendations 8 • Patients with tumours of known oestrogen receptor status whose disease 9
10 recurs should not have a further biopsy to reassess oestrogen receptor status. 11
ervational Qualifying statement: Although there is some evidence from obs12 at oestrogen receptor status can change on recurrence, there was 13 studies th
14 GDG consensus that there are few clinical situations in which re-biopsy can be justified. 15 16
curs • Patients with tumours of known HER2 status whose disease re17 not have a further biopsy to reassess HER2 status should18
Qualifying statement: The evidence about change in HER2 status was poor 19 a change and there was no evidence about how to manage patients in whom20
was detected. 21 22
• If receptor status (oestrogen receptor and HER2) was not assessed at 23 at the time of the time of initial diagnosis then it should be assessed24
r recurrence. In the absence of any tumour tissue from the primary tumou25 tumour a biopsy of a metastasis should be obtained if feasible. 26
ement: This recommendation is based on the GDG Qualifying stat27 28 consensus that knowledge of receptor status will significantly affect
29 30
management. Clinical Evidence 31
l studies The evidence for this topic was provided by seventeen observationa32 eedle all of which compared paired (from the same patient) biopsy or fine n33
ur tissue. aspirate samples from primary and locoregional or metastatic tumo34 t al., 2002, Her2 (Niehans et al., 1993, Shimizu et al., 2000, Gancberg e35
idan et al., Carlsson et al., 2004, Regitnig et al., 2004, Gong et al., 2005, Z36 006, Rom et al., 2006, Pectasides et al., 2006, Tapia et 2005, Lorincz et al., 237
Spataro et al., al., 2007 and Santinelli et al., 2008) and/or endocrine receptor (38 himizu et 1992, Johnston et al., 1995, Lower et al., 2005, Rom et al., 2006, S39
by al., 2000 and Brankovic-Magic et al., 2002) status was determined40 ants had 41 immunohistochemistry or in situ hybridisation. All study particip
42 advanced breast cancer. 43 The majority of papers were concerned with identifying the rate of status 44 change but did not address overall survival, time to progression or quality of 45 life. Approximately 15% of patients showed a change in endocrine receptor 46 status, from positive to negative, comparing primary with locoregional or 47 metastatic tumour samples. 93% of patients tested for HER2 status showed 48 no change between paired samples. 49 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 33 of 146

DRAFT FOR CONSULTATION
Health Economic Evaluation 1 riority; therefore The GDG did not consider this topic as a health economic p2
the cost-effectiveness literature on this topic has not been reviewed. 3 4
2.2 Monitoring disease progress 5 6
ent. The choice 7 ing technique will depend on the site of the patient’s metastatic 8
9 10
breast 11 olytic 12
essing lytic 13 ed before a 14 is laid 15
of sclerosis 16 tastases. It is 17
ot always possible to say whether new sclerotic lesions in bone 18 indicate healing and a response to treatment, or disease progression. 19
on plain 20 21 22
s bony 23 e of the 24
cting 25 not 26
h between healing of previously lytic disease and progression of 27 osteoblastic disease. If a bone scintigram is done early in treatment, a so-28
he degree 29 blastic 30
31 32
but is 33 r variability, 34 s such as 35
36 37
an be used 38 progress. PET-CT has the potential to provide additional 39
ing fluorine (FES)
elpful in indicating 42 py. 43
44 Recommendations
Imaging is useful in assessing how patients respond to treatmof imagdisease. The progress of bone metastases is difficult to assess. Those due tocancer may be either osteolytic, osteoblastic (sclerotic) or mixed osteand osteoblastic. Plain radiographs are relatively insensitive in assbony metastases because 50% of the bone matrix may be destroylucency is visualised. When osteolytic metastases heal, new bonedown and the lesion then appears sclerotic; however new areas could also be due to the development of new osteoblastic metherefore n
Osteoblastic bony metastases are regarded as unassessable radiographs. There can also be problems with bone scintigraphy which detectmetastases by the osteoblastic response excited by the presenctumour. This means that bone scintigraphy is more sensitive for deteosteoblastic than lytic metastases but, like plain radiographs, candistinguis
called ‘flare reaction’ may be seen in which there is an increase in tof abnormal activity on the bone scintigram due to the healing osteoresponse. Ultrasound can be used to monitor the progress of liver metastasesaffected by factors such as patient body habitus and inter-operatoand is much less reproducible than other cross-sectional techniqueCT. CT and MRI are reproducible cross-sectional techniques which cto assess diseasefunctional information. Estradiol labelled with positron emitt40 has been used as an alternative to 18F-deoxyglucose (FDG) in breast cancer 41 patients who are oestrogen receptor positive and may be hwhether the metastatic disease is likely to respond to endocrine thera
45 • Do not use bone scintigraphy to monitor the response of bone 46
metastases to treatment. 47 Qualifying statement There is a poor evidence base with a single 48 prospective study. There is no evidence that bone scintigraphy can be used to 49 assess the response to treatment. 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 34 of 146

DRAFT FOR CONSULTATION
• Do not use PET-CT for monitoring patients with advanced breast cancer 1 ET-CT Qualifying statement: There is no evidence that monitoring with P2
mpared to standard imaging modalities in patients improves management co3 with advanced breast cancer. 4
5 Clinical Evidence 6
ies, five The evidence for this topic was limited comprising six small case ser7 6, Huber et of which were retrospective (Ciray et al., 2001, Couturier et al., 2008
et al., 2006) al., 2002, Stafford et al., 2002, Mortimer et al., 1996 and Linden 9 aging methods. All patients had locally and describing four different im10
advanced or metastatic breast cancer which in most papers was stated to 11 12 have been bone dominant disease.
13 cho-time-inversion images were superior to T1-MRI fat-suppressed-long-e14
to the 15 weighted-sequence images in accurately assessing the response16 treatment of bone metastases.
17 Radiography detected treatment responses to any form of cancer therapy 18
regression 19 within three months in 80% of cases and differentiated between 20 and progression of disease.
21 ith the Fluorodeoxyglucose-PET (FDG-PET) scans correlated positively w22
in the 23 levels of tumour markers and clinical category suggesting efficacyassessment of tumour response. Semi-quantitative analysis of scan data 24
nd, after three cycles of treatment, correlated with predicted overall survival a25 iol, PET the short term response to chemotherapy. Coupled to fluoroestrad26
y. 27 scans accurately reflected the response to endocrine therap 28
nomic Evaluation Health Eco29 erefore The GDG did not consider this topic as a health economic priority; th30
wed. the cost-effectiveness literature on this topic has not been revie31 32
References 33 ., Takahashi N 34
DP 35 breast 36
573-579. 37
). 38 y of 39 breast 40
41
agee B (2000). 42 Accuracy of axillary MR imaging in treated breast cancer for distinguishing 43 between recurrent tumour and treatment effects: does intravenous Gd-DTPA 44 enhancement help in cases of diagnostic dilemma? Clin Radiol 55: 921-928. 45
Brankovic-Magic MV., Nikolic-Vukosavljevic DB., Neskovic-Konstantinovic 46 ZB., Kanjer KS and Spuzic IV (1992) Variations in the content of steroid 47
Abe K., Sasaki M., Kuwabara Y., Koga H., Baba S., Hayashi Kand Honda H (2005). Comparison of 18FDG-PET with 99mTc-HMscintigraphy for the detection of bone metastases in patients withcancer. Ann Nucl Med 19:
Altehoefer C., Ghanem N., Hogerle S., Moser E and Langer M (2001Comparative detectability of bone metastases and impact on therapmagnetic resonance imaging and bone scintigraphy in patients withcancer. Eur J Radiol 40: 16-23.
Bradley AJ., Carrington BM., Hammond CL., Swindell R and M
Advanced breast cancer: full guideline DRAFT (August 2008) Page 35 of 146

DRAFT FOR CONSULTATION
receptors in breast cancer. Comparison between primary tumors and 1 metastatic lesions. Acta Oncol 31: 629-633. 2
e scintigraphy 3 e metastases from breast cancer? A prospective study. 4
5
son NO., 6 sion in breast 7
cancer primary tumours and corresponding metastases. Original data and 8 9
., Bergh J and Ahlstrom KH (2001) Early 10 evaluated with 11
12
13 Detection of bone metastases in breast cancer by (18) FDG PET: Differing 14
col 16: 3375-15 16
O., Jerusalem G., N'Guyen JM and Hustinx R (2006) Sequential 17 or monitoring 18
er Res 12: 19 20
Engelhard K., Hollenbach HP., Wohlfart K., von IE and Fellner FA (2004). 21 ique and 22
with breast 23 24
Vesselle H., Eary JF., Shanley TJ., 25 M., 26
itron 27 etastases 28
29
llis G., 30 G PET on 31
recurrent 32 or metastatic breast cancer. AJR Am J Roentgenol 183: 479-486. 33
Halpern 34 -deoxy-2-[F-35
and integrated PET/CT in 36 restaged breast cancer patients. Mol Imaging Biol 7: 369-376. 37
Gancberg D., Di LA., Cardoso F., Rouas G., Pedrocchi M., Paesmans M., 38 Verhest A., Bernard-Marty C., Piccart MJ and Larsimont D (2002) Comparison 39 of HER-2 status between primary breast cancer and corresponding distant 40 metastatic sites.[see comment]. Ann Oncol 13: 1036-1043. 41
Bristow AR (2008) Can computerised tomography replace bonin detecting bonBreast 17: 98-103.
Carlsson J., Nordgren H., Sjostrom J., Wester K., Villman K., BengtsOstenstad B., Lundqvist H and Blomqvist C (2004) HER2 expres
literature review. [Review] [38 refs]. Br J Cancer 90: 2344-2348.
Ciray I., Lindman H., Astrom KGOresponse of breast cancer bone metastases to chemotherapyMR imaging. Acta Radiol 42: 198-206.
Cook GJ., Houston S., Rubens R., Maisey MN and Fogelman I (1998).
metabolic activity in osteoblastic and osteolytic lesions. J Clin On3379.
Couturierpositron emission tomography using [F-18] fluorodeoxyglucose fresponse to chemotherapy in metastatic breast cancer. Clin Canc6437-6443.
Comparison of whole-body MRI with automatic moving table technbone scintigraphy for screening for bone metastases in patientscancer. Eur Radiol 14: 99-105.
Eubank WB., Mankoff DA., Takasugi J.,Gralow JR., Charlop A., Ellis GK., Lindsley KL., ustin-Seymour MFunkhouser CP and Livingston RB (2001) 18fluorodeoxyglucose posemission tomography to detect mediastinal or internal mammary min breast cancer. J Clin Oncol 19: 3516-3523.
Eubank WB., Mankoff D., Bhattacharya M., Gralow J., Linden H., ELindsley S., ustin-Seymour M and Livingston R (2004) Impact of FDdefining the extent of disease and on the treatment of patients with
Fueger BJ., Weber WA., Quon A., Crawford TL., len-Auerbach MS., BS., Ratib O., Phelps ME and Czernin J (2005) Performance of 218]fluoro-D-glucose positron emission tomography
Advanced breast cancer: full guideline DRAFT (August 2008) Page 36 of 146

DRAFT FOR CONSULTATION
Gong Y., Booser DJ and Sneige N (2005) Comparison of HER-2determined by fluorescence in situ hy
status 1 bridization in primary and metastatic 2
breast carcinoma. Cancer 103: 1763-1769. 3
von 4 ow 5 aging of 6
malignant solid tumours: a prospective study. Eur J Nucl Med 7 8
oderhold G and Czembirek H (2002) 9 10 11
meta-analysis of FDG-PET 12 ARE 13
14
Jotti G., Smith IE., Salter J., Newby J., Coppen M., 15 16
cancer. 17 18
by C., Dirksen H., Vejborg I., Daugaard S., Guldhammer B., Rossing N 19 the 20
ncer 59: 1524-21 22
va SA., Link JM., Gralow JR., Livingston RB., Ellis GK., 23 and 24
ography 25 26
Oncol 24: 2793-2799. 27
R-2/neu 28 ay change in bone metastasis. Pathol Oncol Res 29
30
Impact 31 survival. 32
: 65-70. 33
sso P 34 2-[F-18]fluoro-2-35
deoxy-D-glucose and 16 alpha-[F-18]fluoro-17 beta-estradiol in breast cancer: 36 Correlation with estrogen receptor status and response to systemic therapy. 37 Clin Cancer Res 2: 933-939. 38
Nakai T., Okuyama C., Kubota T., Yamada K., Ushijima Y., Taniike K., Suzuki 39 T and Nishimura T (2005) Pitfalls of FDG-PET for the diagnosis of 40
Haubold-Reuter BG., Duewell S., Schilcher BR., Marincek B andSchulthess GK (1993) The value of bone scintigraphy, bone marrscintigraphy and fast spin-echo magnetic resonance imaging in stpatients with20: 1063-1069.
Huber S., Ulsperger E., Gomar C., KOsseous metastases in breast cancer: Radiographic monitoring of therapeutic response. Anticancer Res 22: 1279-1288.
Isasi CR., Moadel RM and Blaufox MD (2005) A for the evaluation of breast cancer recurrence and metastases (Dstructured abstract). Breast Cancer Res Tr 90: 105-112.
Johnston SR., Saccani-Ebbs SR and Dowsett M (1995) Changes in estrogen receptor, progesterone receptor, and pS2 expression in tamoxifen-resistant human breastCancer Res 55: 3331-3338.
Kamand Mouridsen HT (1987) Incidence and methodologic aspects ofoccurrence of liver metastases in recurrent breast cancer. Ca1529.
Linden HM., StekhoPetra PH., Peterson LM., Schubert EK., Dunnwald LK., Krohn KA Mankoff DA (2006) Quantitative fluoroestradiol positron emission tomimaging predicts response to endocrine treatment in breast cancer. J Clin
Lorincz T., Toth J., Badalian G., Timar J and Szendroi M (2006) HEgenotype of breast cancer m12: 149-152.
Lower EE., Glass EL., Bradley DA., Blau R and Heffelfinger S (2005)of metastatic estrogen receptor and progesterone receptor status onBreast Cancer Res Tr 90
Mortimer JE., Dehdashti F., Siegel BA., Katzenellenbogen JA., Fracaand Welch MJ (1996) Positron emission tomography with
Advanced breast cancer: full guideline DRAFT (August 2008) Page 37 of 146

DRAFT FOR CONSULTATION
osteoblastic bone metastases in patients with breast cancer. Eur J Nuc Med 1 Mol Imaging 32: 1253-1258. 2
y of HER-3 sion over time and at multiple metastatic sites. J Natl Cancer Inst 4
5
nis C., 6 7
cancer and 8 corresponding metastatic sites in patients with advanced breast cancer 9
53. 10
ndbauer M., Samonigg H and Lax SF (2004) 11 ses from breast 12
13
Rom J., Aulmann S., Schneeweiss A., Sohn C and Sinn HP (2006) 14 st cancers and 15
5-130. 16
-2 status 17 es. Impact on 18
19
hn T., 20 enberg R., Messer P., Nussle K., Elsner K., Glatting G., Trager H., 21
Neumaier B., Diederichs C and Reske SN (1999) Early detection and 22 cancer 23 : 2381-24
25
rfeind I., Reiser 26 currence 27
T compared to 28 29
e-30 n of bone 31
Clin Nucl Med 33: 97-101. 32
T., 33 34
urg Oncol 35 36
Spataro V., Price K., Goldhirsch A., Cavalli F., Simoncini E., Castiglione M., 37 Rudenstam CM., Collins J., Lindtner J and Gelber RD (1992) Sequential 38 estrogen receptor determinations from primary breast cancer and at relapse: 39 prognostic and therapeutic relevance. The International Breast Cancer Study 40 Group (formerly Ludwig Group). Ann Oncol 3: 733-740. 41
Niehans GA., Singleton TP., Dykoski D and Kiang DT (1993) Stabilit2/neu expres85: 1230-1235.
Pectasides D., Gaglia A., rapantoni-Dadioti P., Bobota A., ValavaKostopoulou V., Mylonakis N., Karabelis A., Pectasides M and Economopoulos T (2006) HER-2/neu status of primary breast
treated with trastuzumab-based therapy. Anticancer Res 26: 647-6
Regitnig P., Schippinger W., LiChange of HER-2/neu status in a subset of distant metastacarcinomas. J Pathol 203: 918-926.
Comparison of immunohistological parameters in primary breacorresponding locoregional recurrences. Pathol Res Pract 202: 12
Santinelli A., Pisa E., Stramazzotti D and Fabris G (2008) HERdiscrepancy between primary breast cancer and metastatic sittarget therapy. Int J Cancer 122: 999-1004.
Schirrmeister H., Guhlmann A., Kotzerke J., Santjohanser C., KuKrei
accurate description of extent of metastatic bone disease in breast with fluoride ion and positron emission tomography. J Clin Oncol 172389.
Schmidt GP., Baur-Melnyk A., Haug A., Heinemann V., BaueMF and Schoenberg SO (2008) Comprehensive imaging of tumor rein breast cancer patients using whole-body MRI at 1.5 and 3FDG-PET-CT. Eur J Radiol 65: 47-58.
Shie P (2008) Meta-analysis: Comparison of F-18 fluorodeoxyglucospositron emission tomography and bone scintigraphy in the detectiometastases in patients with breast cancer.
Shimizu C., Fukutomi T., Tsuda H., kashi-Tanaka S., WatanabeNanasawa T and Sugihara K (2000) c-erbB-2 protein overexpression and p53immunoreaction in primary and recurrent breast cancer tissues. J S73: 17-20.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 38 of 146

DRAFT FOR CONSULTATION
Stafford SE., Gralow JR., Schubert EK., Rinn KJ., Dunnwald LK., LRB and Mankoff DA (2002) Use of serial FDG PET to measu
ivingston 1 re the response 2
of bone-dominant breast cancer to therapy. Acad Radiol 9: 913-921. 3
erzog M., 4 d 5
mary breast cancers and matched 6 7
n D., Brunelle 8 S and Stefano DD (2006) Computed tomography in suspected local breast 9
-254. 10
k B and Geiger X (2006) Concordance of HER2 and hormone receptor 11 es Tr 94: 12
13
rman C., Basher W., Cozacov C and Hadary A 14 (2005) Comparison of HER-2 overexpression in primary breast cancer and 15 metastatic sites and its effect on biological targeting therapy of metastatic 16 disease. Br J Cancer 93: 552-556. 17
Tapia C., Savic S., Wagner U., Schonegg R., Novotny H., Grilli B., HBarascud AD., Zlobec I., Cathomas G., Terracciano L., Feichter G anBubendorf L (2007) HER2 gene status in pridistant metastases. Breast Cancer Research 9 (3).
Ternier F., Houvenaeghel G., Lecrivain F., Brigand BL., Margai
cancer recurrence. Breast Cancer Research & Treatment 100: 247
Wirexpression in primary and recurrent breast cancer. Breast Cancer RS89.
Zidan J., Dashkovsky I., Staye
Advanced breast cancer: full guideline DRAFT (August 2008) Page 39 of 146

DRAFT FOR CONSULTATION
3 Providing Information and SuppoDecision Makin
rt for 1
g 2 3
ly recently. 4 lex 5 tment of 6
n of patients 7 8
. 9 10
eed to 11 t options. High 12
ental to 13 nt 14
es for 15 ge over time 16
f 17 be given 18 e provided 19
terial, use of which can be tailored 20 l attainment or mental capacity5. Patients 21
22
The treatment of advanced breast cancer has changed considerabAn increase in the treatment options available has led to more compdecisions for both healthcare professionals and patients. The DeparHealth has developed policies that encourage greater participatioin decision-making about their own healthcare and provide individuals with more choice about how, when and where they receive treatment In order to make decisions, patients with advanced breast cancer nunderstand their diagnosis and the reasoning behind treatmenquality information in a language understood by the patient is fundamdecision making and ultimately the patients’ satisfaction with treatmechoices. However, individual patients will have different preferencquantity, completeness and format of information which may chanand over the course of their illness. Some may wish to receive a lot oinformation from the point of diagnosis, while others will prefer toinformation gradually as treatment progresses. Information can bface-to-face or as written or audio-visual mafor different levels of educationaneed to feel confident that they have understood the information they are given and have the opportunity to ask questions. 23 24 Recommendations 25 • Assess the patient’s individual preference for the level and type of 26
information, and reassess this as circumstances change 27 t, offer consistent, relevant information and • On the basis of this assessmen28
29 clear explanations, and provide opportunities for patients to discuss issues and ask questions. 30
moderate-Qualifying statement: These recommendations are based on31 32 quality evidence from randomised trials.
33 The level of involvement that individuals want in making decisions about their 34 treatment and care will vary and this needs to be considered by the 35 healthcare professionals involved in their care. Treatment choices often 36 involve complex issues such as balancing the possible adverse effect of 37 treatment with quality of life, and incorporating the views of family, cultural and 38 religious beliefs and social circumstances. Decision making can increase 39 anxiety in patients who want to be certain they are making the right choice. 40 Individuals will need sufficient time to make their decision as well as support 41 from the health professionals involved in their care, family, friends and people 42 who have experienced similar situations. 43 44 Decision aids, interventions which help people make specific and deliberate 45 choices, are available. These include tape recordings of consultations, 46 question prompt sheets, face to face counselling and interactive computer 47 5 Mental capacity act, 2005
Advanced breast cancer: full guideline DRAFT (August 2008) Page 40 of 146

DRAFT FOR CONSULTATION
programmes. Such aids should at least provide information on the options and 1 potential outcomes relevant to that person’s health status. 2
3 Recommendations 4 • Assess the patient’s individual preference for how much they wish to be 5
involved in decision making, and reassess this as circumstances change. 6 • Help patients make difficult decisions about their treatment. Be aware of 7
8 the range and value of decision aids available and make the most appropriate aid available to the patient. 9
Qualifying statement: These recommendations are based on moderate-10 from randomised trials 11
12 quality evidence Clinical Evidence 13 Information Provision 14
iew The evidence on patient information comprised one systematic rev15 03, Jones et (Gaston and Mitchell, 2005) and five RCTs (Winzelberg et al., 2016
al., 2006, Williams and Schreier, 2005, Aranda et al., 2006 and Walker and 17 on to 18 Podbilewicz-Schuller, 2005). RCT evidence focused broadly on pers
19 person interventions, written information or audiovisual aids. 20
d as much The review found that patients with advanced disease often require21 but the information from their clinician as patients with early breast cancer 22 as desire for involvement with treatment decisions sometimes declined23 ctive but disease progressed. The review found consultation tapes to be effe24
ved, occasionally caused general information tapes, although well recei25 confusion. Written information was only effective if pitched at the appropriate 26
l and educational level for the patient. Question prompt sheets were usefu27 ation to 28 resulted in better consultations whilst giving the patient written inform
29 take home improved communication with the family. 30
ion, stress A web-based support group significantly reduced levels of depress31 h controls. However, a nurse-led and anxiety in users when compared wit32
th provision of intervention of active listening, empathy and support together wi33 g in self-care, information cards tailored to the patient’s need and coachin34
men with high 35 stress reduction and communication was only effective for wo36 initial psychological needs.
37 atient’s own clinical information Information booklets supplemented by a p38
ere were thought more likely to tell the patient something new and w39 let. considered less limited in scope when compared to a generic book40
r literature Patients found an automatically selected range of breast cance41 -selected 42 more informative and less overwhelming than a number of self
43 booklets chosen from a computer generated list. 44 An audio tape of education about exercise and relaxation as a means to 45 combat anxiety, fatigue and sleep problems associated with chemotherapy, 46 together with a self-care diary, reduced the increase in patient-reported 47 anxiety as treatment progressed when compared with standard care. A 48 videotape plus a list of basic questions to be asked at a multi-disciplinary 49 team consultation, when added to standard written information, made no 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 41 of 146

DRAFT FOR CONSULTATION
significant impact on depression, patient anxiety, quality of life or feelings of 1 helplessness/hopelessness. 2
3 Decision Making 4
l., 2002) and Two systematic reviews (O’Brien et al., 2002 and O’Connor et a5 rovided two RCTs (Siminoff et al., 2006 & Davison and Degner, 2002) p6
t papers and of high 7 evidence for the use of decision aids. All were recen8 quality. The majority of study participants had breast cancer.
9 in their The reviews showed that decision aids were effective for patients10
ledge and decision making, better than standard care for patients to gain know11 decision, realistic expectations and better than standard care in reducing in12
ignificant difference conflict and passivity. However, decisions aids made no s13 ad no 14 to patients’ satisfaction with their decisions or treatment choice and h
15 effect on health related outcomes such as anxiety or quality of life 16
Good evidence showed that giving patients the choice of assuming a passive, 17 active or co-operative role in making treatment decisions with their clinician 18
ices 19 had a greater influence on treatment outcomes than the actual cho20 themselves.
21 d software tool (Adjuvant!) giving breast cancer patients A personally tailore22
pending on case history and choice of adjuvant their 10-year prognosis, de23 a generic 24 therapy, was significantly more influential on decision making than
pamphlet without data. 25 26
nomic Evaluation Health Eco27 ; therefore The GDG did not consider this topic as a health economic priority28 d. the cost-effectiveness literature on this topic has not been reviewe29
30 31
(2006) 32 ds of women with advanced breast 33
cancer: a randomised controlled trial. Br J Cancer 95: 667-673 34
assisted 35 vention to enhance the way women with breast cancer communicate with 36
37
-making in 38 A systematic review. Soc Sci Med 61: 2252-39
40
J., White CA 41 and Gilmour WH (2006) Effect of different forms of information produced for 42 cancer patients on their use of the information, social support, and anxiety: 43 randomised trial. BMJ 332: 942-948. 44
O'Brien MA., Villias-Keever M., Robinson P., Skye A., Gafni A., Brouwers M., 45 Charles C., Baldassarre F and Gauld M (2002) Impact of Cancer-Related 46
References Aranda S., Schofield P., Weih L., Milne D., Yates P and Faulkner R Meeting the support and information nee
Davison BJ and Degner LF (2002) Feasibility of using a computer-intertheir physicians. Cancer Nursing 25: 417-424.
Gaston CM and Mitchell G (2005) Information giving and decisionpatients with advanced cancer: 2264.
Jones RB., Pearson J., Cawsey AJ., Bental D., Barrett A., White
Advanced breast cancer: full guideline DRAFT (August 2008) Page 42 of 146
DRAFT FOR CONSULTATION
Decision Aids. Evidence Report/Technology Assessment Number (Prepared by McMaster University under Contract No. 290-97-0017.Publica
46. 1 ) AHRQ 2
tion No. 02-E004, Rockville, MD: Agency for Healthcare Research and 3 4
ner D., 5 es J. (2003) 6
eatment or screening decisions. 7 8
and Podbilewicz-Schuller Y (2005) Video preparation for breast 9 10 11
ewlett J., De 12 d trial of a 13
t!" to present tailored prognostic 14 Res Tr 64: 15
16
g 17 herapy for 18
19
Winzelberg AJ., Classen C., Alpers GW., Roberts H., Koopman C., Adams 20 RE., Ernst H., Dev P and Taylor CB (2003) Evaluation of an internet support 21 group for women with primary breast cancer. Cancer 97: 1164-1173. 22
Quality.
O'Connor AM., Stacey D., Entwistle V., Llewellyn-Thomas H., RovHolmes-Rovner M., Tait V., Tetroe J., Fiset V., Barry M and JonDecision aids for people facing health trCochrane Database.Syst. Rev (2):CD001431.
Walker MScancer treatment planning: results of a randomized clinical trial. Psycho-Oncol 14: 408-420.
Siminoff LA., Ravdin PM., Peele P., Silverman P., Mercer MB., HLos SL., Parker HL and Gordon N (2000) Results of a randomizecomputerized decision aid "Adjuvaninformation to stage I-III breast cancer patients. Breast Cancer 129.
Williams SA and Schreier AM (2005) The role of education in managinfatigue, anxiety, and sleep disorders in women undergoing chemotbreast cancer. Appl Nurs Res 18: 138-147.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 43 of 146
DRAFT FOR CONSULTATION
4 Systemic Disease-Modifying The rapy 1 2
ex. When 3 life, the risks 4
toms, 5 standing by 6
ffered. 7 about 8 n will be 9
ances and their 10 or absence of 11
erformance status, the site and 12 te at 13
14
y – endocrine 15 is also the 16 palliative 17
care will be needed by all patients along with the active treatments. 18 d of or 19 deline. 20
21 breast 22 . Endocrine 23
as 24 and 25
ffered 26 use is 27 f of cancer 28 needs to 29
30 less toxic than chemotherapy, response to treatment tends 31
to be slower in onset. In addition a number of new chemotherapeutic drugs 32 w years
ividuals.
The management of patients with advanced breast cancer is complmaking treatment choices there is a trade off between quality of of toxicity and the probabilities of benefit in terms of improving symp
rquality of life or survival. Decisions need to be based on an undethe patient of the effectiveness and side effects of the treatments oMany factors will influence treatment choices. Ultimately, the choice what treatment to have will be made by the patient, and their decisioinfluenced by their beliefs, values, goals, social/family circumstquality of life. Clinical advice will take into account the presencecomorbidities, treatment effectiveness, pextent of disease, the presence or absence of symptoms, and the rawhich the disease appears to be progressing.
There are three categories of systemic disease-modifying theraptherapy, chemotherapy and biological response modifiers. Thereoption of having no disease-modifying treatment. Supportive and
Complementary therapies are also chosen by some patients insteatogether with active treatment. Their use is not discussed in this gui Endocrine therapy has been used to treat patients with advancedcancer for over 100 years and chemotherapy for several decadestherapy is only effective in hormone receptor positive disease wherechemotherapy can be effective in both hormone receptor negativepositive disease. Only patients with a HER2 positive cancer will be otreatment with trastuzumab. The decision about which treatment to based on an assessment of the likelihood of tumour response, relierelated symptoms, improvement in quality of life and survival. This be balanced against the risks of side effects of treatment. Although endocrine therapy is usually
with different side effect profiles have become available in the last fe33 so that uncertainties remain about the best treatment for certain ind34
Recommendations 35
• For patients with hormone receptor-positive advanced breast cancer, offer 36 endocrine therapy as first-line treatment unless there is a clinical need to 37 achieve a rapid tumour response. 38
• For patients with hormone receptor-positive advanced breast cancer 39 whose disease is imminently life-threatening or requires early relief of 40
f significant visceral organ involvement, offer symptoms because o41 chemotherapy as first-line treatment if they are fit enough and are 42 prepared to accept the toxicity. 43
• For patients with hormone receptor-positive advanced breast cancer, offer 44 endocrine therapy following chemotherapy. 45
Qualifying statement: These recommendations are based on one systematic 46 review and GDG consensus. 47
Advanced breast cancer: full guideline DRAFT (August 2008) Page 44 of 146
DRAFT FOR CONSULTATION
1
Clinical Evidence 2 matic review Only one paper was appraised for this topic. A high quality syste3
s endocrine (Wilcken et al., 2006) examined ten RCTs of chemotherapy v4 en though therapy, the most recent of which was published in 1995 (ev5
6 Cochrane databases were searched as recently as October 2006). 7
antage in Neither chemotherapy nor endocrine therapy demonstrated an adv8 s. No data overall survival and tumour response was variable between studie9
in narrative were presented for quality of life (QOL) or adverse events but, 10 y had form, the reviewers stated that in the majority of studies chemotherap11
of toxicity (predominantly nausea, vomiting and resulted in higher levels12 ection QOL had been affected as 13 alopecia) but that it was not clear in which dir
14 the results were conflicting. 15 Health Economic Evaluation 16 The GDG did not consider this topic as a health economic priority; therefore 17
re on this topic has not been reviewed. the cost-effectiveness literatu18 19
20 21
d breast 22 any patients 23
ss. 24 f patients who 25
st cancer. It has no role in the 26 cer. 27
erapy is 28 , 29
gh high-quality evidence to justify this is lacking. 30
breast cancer 31 used as 32 ced breast 33
34
ith either 35 developing 36 hem. There 37
endocrine treatment for 38 39
re-menopausal 40 women and fulvestrant for postmenopausal women. Older, less often used 41 therapies include progestogens, androgens, stilboestrol and trilostane, the 42 latter two are licensed for postmenopausal women only. 43
The factors that need to be taken into account when considering what 44 endocrine therapy is appropriate for a particular patient include: 45
4.1 Endocrine Therapy Hormonal therapies are widely used in the management of advancecancer. A range of different treatment options is available and mwill be treated with several of these during the course of their illneEndocrine therapy is appropriate for the approximately 70% ohave hormone receptor positive advanced breamanagement of patients with hormone receptor negative breast canAlthough not used in combination with chemotherapy, endocrine thcombined in certain circumstances with biological response modifiersalthou
Tamoxifen was the first line endocrine treatment for advanced for many years. More recently aromatase inhibitors (AIs) have beenfirst line endocrine treatment in postmenopausal women with advancancer.
Many patients will have received adjuvant endocrine therapy wtamoxifen or an AI (NICE, 2006) for primary breast cancer prior toadvanced breast cancer and some may relapse while still taking tis currently no evidence on the most appropriate patients who have received prior treatment with an AI.
Other endocrine therapies include ovarian ablation for p
Advanced breast cancer: full guideline DRAFT (August 2008) Page 45 of 146

DRAFT FOR CONSULTATION
• Whether or not they have had previous endocrine therapy (including as 1
ration of any previous response to endocrine therapy 5
nsidering 6 is only 7 ; in pre-8 els. In the 9
ausal if one 10 f any other 11 ary and 12 ndocrine 13 on. There 14
r more than one year 15 inhibitors and 16
y becoming pregnant. 17
on the
hould be he has previously had
replacement my), and provided
given
sed since
sal given above d before introducing
ibitors
ctomy), or 32 ith HRT that includes a monthly 33
ed, should be over 55 before being considered 34
ul adjunct 37
Recommendations
an adjuvant) 2 • If so, which agent 3 • The extent and du4 • Menopausal status.
Definition of the menopause is a particularly difficult topic when cothe endocrine therapy of breast cancer. Aromatase inhibitor therapy effective in suppressing oestrogen levels in postmenopausal womenmenopausal women it can actually result in elevation of estradiol levUK a woman is usually regarded by gynaecologists as postmenopyear has elapsed since the last menstrual period, in the absence ocause (e.g. pregnancy). A number of the therapies used in the primadjuvant treatment of breast cancer, including chemotherapy and etherapy with tamoxifen, can result in a temporary lack of menstruatiare reports of women who had been amenorrhoeic fofollowing adjuvant chemotherapy being treated with aromatase then subsequentl
In the light of these uncertainties our recommendations are based 18 following definitions: 19
• A woman who has been amenorrhoeic for more than one year s20 regarded as being postmenopausal unless s21 chemotherapy, endocrine therapy with tamoxifen, hormone 22 therapy or a hysterectomy (without bilateral oophorecto23 there is no other obvious cause such as pregnancy. 24
• A woman who does not meet the definition of postmenopausal 25 above before starting chemotherapy, should not be considered 26 postmenopausal until two years without menstruation have elap27 completing that treatment. 28
• If a woman does not meet the definition of postmenopau29 before starting tamoxifen, caution should be exercise30 aromatase inh31
• Women who have had a hysterectomy (without bilateral oophorewomen who have been treated wwithdrawal blepostmenopausal 35
Measurement of serum FSH, LH and estradiol levels may be a usef36 to clinical evaluation in some situations.
38 • Offer a third-generation aromatase inhibitor (either non-steroidal or 39
steroidal) to: 40 - postmenopausal women with hormone receptor-positive breast cancer 41
and no prior history of endocrine therapy 42
Advanced breast cancer: full guideline DRAFT (August 2008) Page 46 of 146

DRAFT FOR CONSULTATION
- postmenopausal women with hormone receptor-positive breast cancer 1 who have previously been treated with tamoxifen. 2
quality Qualifying statement: these recommendations are based on high3 . There is not enough evidence to 4 evidence of clinical and cost effectiveness
recommend any particular aromatase inhibitor. 5
• Offer tamoxifen as first-line treatment to pre-menopausal and peri-6 menopausal women with hormone receptor-positive advanced breast 7 cancer not previously treated with tamoxifen. 8
• Offer ovarian suppression to pre-menopausal and peri-menopausal 9 10 women who have responded to tamoxifen and then develop progressive
disease. 11 evidence of Qualifying statement: these recommendations are based on12
ic review of randomised clinical effectiveness from one high-quality systemat13 at peri-trials in pre-menopausal women. There was GDG consensus th14
menopausal women should be treated in the same manner. 15
• Offer tamoxifen as first-line treatment to men with oestrogen receptor-16 ncer. positive advanced breast ca17
Qualifying statement: This recommendation is based on evidence from two 18 ive case series and GDG consensus that this was an 19 small retrospect
20 appropriate and effective treatment.
Clinical Evidence 21 Women 22
en et al., The evidence base for this question comprises one guideline (Eis23 007; Ferretti 2004), four systematic reviews (Mauri et al., 2006; Gibson et al., 224 , Mouridsen et al., 2006 and Crump et al., 1997), three RCTs (Chia et al. 200825
007) and a small, low quality comparative study et al. 2007 and Goss et al. 226 ded 30,500 (Catania et al. 2007a). The number of study participants excee27
breast women, the majority of whom were post-menopausal with metastatic28 ine did 29 cancer. Most of the papers were of high quality, although the guidel
30 review non-published abstracts. 31 Pre-menopausal women with metastatic breast cancer experienced no 32
ablation significant difference in tumour response or survival between ovarian33 st line and tamoxifen as first line therapy. Atamestane and toremifine as fir34 l 35 combination therapy resulted in similar tumour response and surviva
36 compared with letrozole alone. 37
en that had Fulvestrant and exemestane showed equal clinical benefit for wom38 d breast previously received non-steroidal AIs for the treatment of advance39
red short term cancer. Limited evidence also suggested that fulvestrant confer40 stponing benefit to heavily pre-treated women with metastatic disease by po41
the requirement for chemotherapy. 42 43 Good evidence showed that there was significant clinical benefit, increased 44 progression-free survival and ~13% reduction in the risk of death with third 45 generation AIs compared with standard endocrine therapy (the analyses 46 included all treatment lines). No individual AI was better than another in this 47
Advanced breast cancer: full guideline DRAFT (August 2008) Page 47 of 146

DRAFT FOR CONSULTATION
regard. Very limited evidence suggested that there was no significant 1 eported quality of difference between the AIs and standard therapy in patient r2
life. However, more gastro-intestinal symptoms and hot flushes were3 ndard endocrine therapy but were 4 associated with AI therapy compared to sta
5 fewer reports of blood clots and vaginal bleeding. 6
Men 7 t al. 1985a) Three papers (Kantarjian et al. 1983, Patel et al. 1984 and Lopez e8
f endocrine presented case series of men who had received a great variety o9 y. None of the treatments were highlighted for therapies, including surger10
specific analysis and the numbers of each patient sub-group are too low to 11 12 make a summary of any value.
13 ui 2002, Otherwise, there were eight retrospective case series (El Omari-Alao14 t al. 1980 Giordano 2002, Harris et al. 1986, Lopez 1985b & 1993, Patterson e15 le and Ribeiro 1976 & 1983) which reviewed data from case files of ma16 decades patients treated for breast cancer. The papers spanned nearly three17
and involved 321 males - four papers were from the United Kingdom. None of 18 resent probably 19 the studies were comparative and, although of low quality, rep
20 the best available evidence on this topic. 21
ay be Very limited evidence (n=5) suggested that aminoglutethimide m22 ancer who have been suitable therapy for men with advanced breast c23
for men previously orchidectomised. Diethylstilboestrol therapy was effective24 nse in 25 with soft tissue disease but failed to elicit a significant tumour respo
26 those with more widespread metastatic breast cancer. 27
y in some Limited evidence suggests that cyproterone was an effective therap28 and the men but there were no factors by which response could be predicted29
mpotence and loss of libido for many patients. Androgen treatment resulted in i30 ut may blockade with buserelin did not appear to enhance the response b31
howed that have prevented response flare. A very limited case series (n=5) s32 males with 33 anastrazole therapy did not result in a positive response in ER +ve
34 metastatic breast cancer. 35
or quality studies reviewed data on treatment with tamoxifen. Some Two po36 ies. The authors reported objective patients were included in both stud37
month to 5 response rates from 37.5% to 48% and response duration from 1 38 roup was years. Where endocrine status was known, only the ER +ve sub-g39
re 40 associated with favourable tumour response. Few adverse events we41 reported. 42
Health Economic Evaluation 43 criteria This question yielded a relatively large evidence base so the review44
were tightened to include those studies that were most relevant to the 45 decision problem; thus only studies taken from the perspective of the UK NHS 46 were reviewed. A total of five studies met the stricter inclusion criteria from an 47 initial search which identified 358 papers. No additional papers were identified 48 in an update search. None of the economic evaluations compared hormone 49 therapy with a ‘do-nothing’ alternative, probably due to the fact that hormone 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 48 of 146

DRAFT FOR CONSULTATION
therapy in postmenopausal women with advanced breast cancer is standard 1 ny of the evaluations compare all the relevant clinical practice. Neither did a2
interventions against each other. 3 4
tase inhibitors The three older studies evaluate various third-generation aroma5 dard (AIs) against Megestol as second-line treatment which was the stan6 ozole hormone therapy at the time. The more recent studies evaluate Letr7
t Tamoxifen as e line with current clinical practice. agains first-lin treatment, in8 9
Linetherapy
rventio mparison Study of Inte n Co
Karnon and Jones2003
, first fen Letrozole Tamoxi
Karnon and Jet al, 2003
ohns t ole (then ifen)
amoxifen (then trozole)
002 co mestan egestrol Drummond et al, second Anastrozole Megestrol
strol
ton firs Letrotamox
z Tle
Lindgren et al 2 se nd Exe e M
1999 Nuijten et al, 1999 second Letrozole Mege
All studies presented cost-effectiveness analyses (results in terms olife years gained) and the two Karnon papers also presen
10 f cost per 11
ted cost-utility 12 e 13 ced breast 14
15 16
m over a 17 efits 18 orm the 19
n and 20 as more 21
allowing 22 xpert 23
studies. 24 n of 3.5% for 25
l discount 26 y using a lower discount rate for health benefits these studies will 27
28 n reported. 29
yet never 30 s from the 31
32 33
strozole and 34 Tamoxifen were below £5,075 per life year gained and £9,200 per QALY. 35 Similar results were obtained for Letrozole, Anastrozole or Exemestane 36 versus Megestrol with a maximum ICER of £9,667 per life year. All of these 37 results were tested to varying degrees of sophistication with sensitivity 38 analysis and were robust to all scenarios presented. However a major 39 limitation of the studies was that all were supported by the pharmaceutical 40
analyses (results in terms of cost per QALYs gained). Since we arinvestigating the use of AIs in the treatment of patients with advancancer, a consideration of quality of life is particularly important. All studies used modelling techniques to model the decision problelifelong time horizon. This meant including the costs and health benassociated with subsequent treatment. All papers used RCTs to infclinical data and costs from nationally published sources. The KarnoJones and the Nuijten analysis used a similar model structure that wcomprehensive than the other models, using a Markov process andfor various clinical pathways subsequent to hormone treatment. Eopinion was ascertained using formal methods of elicitation in these None of the studies used the current discounting recommendatioboth health benefits and costs; many of the studies used differentiarates. Bhave overestimated future health benefits of the interventions which would result in higher incremental cost effectiveness ratios than have beeHowever since the time horizon is not long (lifetime perspective more than 6 years) this effect is not likely to change the conclusionstudies. All baseline ICERs for the comparison between Letrozole or Ana
Advanced breast cancer: full guideline DRAFT (August 2008) Page 49 of 146

DRAFT FOR CONSULTATION
industry. Since not all assumptions were tested, bias from this sourbe ruled out. In addition none of the studies compared third-generaaromatase inhibitors against each other, so there is no ev
ce cannot 1 tion 2
idence as to which 3 AI is most cost-effective, in either the first- or second- line setting. 4
5 indirect 6
inst each 7 s guideline 8 r new AIs 9
in first- or second-line fall within an acceptable level of cost-effectiveness; 10 g on this topic was not considered a high priority. 11
An independent analysis would be useful, especially if it incorporatedcomparison methods to compare all the interventions of interest agaother. This was not undertaken as part of the economic work for thisince it was felt that the evidence showed all the baseline ICERs fo
thus independent modellin 12 Research recommendations 13 • Clinical trials are needed to investigate the most effective endocrine 14
therapy for postmenopausal women with oestrogen receptor-positive 15 tumours who progress on treatment with a third-generation aromatase 16 inhibitor. 17
• Clinical trials are need to investigate the effectiveness of ovarian 18 suppression in combination with an aromatase inhibitor compared with that 19 of tamoxifen in pre-menopausal women with oestrogen receptor-positive 20 tumours. 21
• All randomised controlled trials of treatment after failure of all available 22 good quality evidence exists should either contain a 23 treatments for which
placebo arm, or provide a valid justification for not doing so. 24 25 26 27
ositive and 28 f toxicity 29 l mean that 30
of different 31 racyclines 32
abine, 33 mide, and 34
35 36
as single agents 37 used in combinations. As more effective agents have been 38
agents ractice
v nts and 41 w ation chemotherapy. 42 43 Recommendations
4.2 Chemotherapy Chemotherapy is used in the treatment of both hormone receptor pnegative patients with advanced breast cancer. Despite the risks othe benefits in terms of symptom control, quality of life and survivait is an appropriate option for many patients. A numberchemotherapy drugs, or classes of drug, are active, including anth(doxorubicin, epirubicin), taxanes (docetaxel and paclitaxel), capecitvinorelbine, gemcitabine, alkylating agents such as cyclophosphaplatinum-based drugs such as carboplatin. First generation cytotoxic drugs were relatively ineffectiveand so were oftendeveloped, they have more often been used sequentially as single 39 rather than in combination. However there are uncertainties (and p40 ariation) about whether this is an appropriate policy for all patiehether some should be treated with combin
44 • Use sequential single agents on disease progression to treat the majority 45
of patients with advanced breast cancer who require chemotherapy. 46 Qualifying statement: These recommendations are based on limited 47 randomised trial evidence and GDG consensus. 48
49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 50 of 146

DRAFT FOR CONSULTATION
• Consider using combination chemotherapy to treat patients with advanced 1 breast cancer for whom a greater probability of response is important and 2 who understand and are likely to tolerate the additional toxicity 3
zed trial Qualifying statement: this recommendation is based on randomi4 mbination evidence confirming increased response rate and toxicity from co5
er overall survival benefit compared with chemotherapy and uncertainty ov6 e agent chemotherapy. 7
8 sequential singl Clinical Evidence 9 Combination versus sequential chemotherapy 10
otherapy Evidence for comparing single chemotherapy with sequential chem11 979, Sledge et comprised five RCTs (Creech et al., 1979, Chlebowski et al., 112
y et al., 1976 and Baker et al., 1974) and one observational al., 2003, Smalle13 lways very 14 study (Chlebowski et al., 1989). The older studies were not a
15 stringently reported. 16
mour Two small, poor quality trials found no significant difference in tu17 al when response, response duration, time to progression or overall surviv18
e chemotherapy agents were given together or sequentially (on diseas19 nalysis of their data 20 progression). Two other studies and a retrospective a
showed that whilst combined therapy resulted in superior tumour response 21 revealed 22 and apparently significantly longer median overall survival, follow-up
23 that long term survival was no different between study arms. 24 One large RCT demonstrated that combining anthracycline and taxane, rather 25
tumour than giving the drugs sequentially in either order, resulted in a better 26 edian overall response and superior time to progression but did not improve m27
l. 28 surviva 29
ted as being Consistently, adverse events due to combined therapy were repor30 single 31 more numerous or of greater severity than those experienced with
32 agents. 33
Combined versus single chemotherapy regimes 34 otherapy 35 Evidence for comparing single chemotherapy with combined chem
comprised one very high quality systematic review (n > 7,000 study 36 ew (Takeda participants) (Carrick et al., 2005) a more modest systematic revi37
d Martin et al., 2007) three RCTs (Eijertsen et al. 2004, Pacilio et al., 2006 an38 al by et al., 2007) and two post-study papers published from the pivotal tri39
l., 2004). 40 O’Shaughnessy et al., 2002) (Leonard et al., 2006 and Miles et a 41
hat the relative risk of death was significantly Good evidence suggests t42 reduced for patients given combined chemotherapy agents compared with 43 single drugs as first or second line treatment. The advantage was greatest for 44 combinations which did not include their comparator. Combined therapies 45 containing anthracyclines or alkylating agents were significantly better at 46 reducing the relative risk of death whereas taxanes did not improve survival 47 as part of a combined therapy. 48 49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 51 of 146

DRAFT FOR CONSULTATION
RCT evidence from three trials showed that first line treatment with combined 1 e same therapies including an anthracycline and/or taxane compared with th2 ssociated anthracycline or taxane, provided no survival advantages but were a3 quivocal. with higher levels of adverse events. Quality of life outcomes were e4 erapy of Similarly, a small RCT compared second line (or higher) combined th5
no significant vinorelbine and gemcitabine with vinorelbine alone and reported6 nts with difference in overall survival between arms but more adverse eve7
atient combined therapy. In contrast, a post-study analyses of long term p8 s DOC outcomes from a trial of capecitabine (CAP) and docetaxel (DOC) v9
alone showed that either combined or sequential therapy with the two agents 10 ne. 11 was significantly better in terms of survival than receiving DOC alo
12 atic reviews about Although considerable data were published within system13
quality of life between combined and 14 comparison of adverse events and 15 single agent regimes the findings were equivocal across studies.
16 Recommendation 17 • For patients with advanced breast cancer who are not suitable for 18
anthracyclines (adjuvant anthracyclines or first-line metastatic 19 anthracyclines, or contraindicated), systemic chemotherapy should be 20 offered in the following sequence: 21
22 - first line: single-agent docetaxel, - second line: single-agent vinorelbine or capecitabine, 23
ever was not 24 - third line: single-agent capecitabine or vinorelbine (whichused as second-line treatment). 25
atement: This recommendation was based on the findings of a Qualifying st26 health economic analysis that compared the cost-effectiveness of various 27
gimens, for sequences of single-agent and combination chemotherapy re28 herapy is 29 patients who are anthracycline resistant or for whom anthracycline t
30 contraindicated. 31
ring While it was acknowledged that there is no direct evidence compa32 native chemotherapy sequences, the GDG considered it important to alter33
explore the cost effectiveness of plausible sequences using the best available 34 mportant data. An indirect treatment comparison methodology was an i35
lative component of this, but it was restricted to an assessment of the re36 ble RCT 37 effectiveness of alternative first-line treatments based on the availa
38 data. 39
The base case analysis showed that the most cost-effective treatment 40 sequence based on a threshold of £30,000 per QALY was docetaxel 41
itabine monotherapy followed by vinorelbine monotherapy followed by capec42 660 per monotherapy. The ICER for this sequence was estimated to be £23,43 ost-QALY. When applying a threshold of £20,000 per QALY, the most c44
effective sequence was docetaxel monotherapy followed by capecitabine 45 monotherapy, followed by no further chemotherapy. 46 47 The GDG however acknowledged that the economic analysis was subject to a 48 level of uncertainty that would make distinguishing between certain strategies 49 difficult. In addition, it was the GDG’s view that the benefit from three lines of 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 52 of 146

DRAFT FOR CONSULTATION
therapy was potentially underestimated in the analysis leading to ICERs that 1 ce were too high. The GDG noted that the there was no strong eviden2
tions (including underpinning the effectiveness estimates of third-line interven3 red. The ‘no chemotherapy’) in any of the alternative strategies conside4
tegy difference in expected benefits and costs between the optimal stra5 itabine-beneath a threshold of £30,000 and the sequence docetaxel-capec6
It was the vinorelbine (dominated in the base-case analysis) was very small. 7 alent and that GDG’s view that essentially these two alternatives were equiv8
norelbine would also be a cost 9 the sequence docetaxel-capecitabine-vi10 effective option.
11 price The GDG acknowledged that the existence of nationally agreed12
f the discounts for paclitaxel can significantly alter the cost effectiveness o13 elief of the sequences examined in the analysis. While it was the strong b14
elbine-capecitabine is cost-effective in GDG that the sequence docetaxel-vinor15 nt the 16 most instances, the choice of taxane should also take into accou
17 existence of any nationally agreed discounts. 18
(for example While there is evidence to suggest that combination therapy 19 o improved when capecitabine is used concurrently with docetaxel) may lead t20
file. survival, this can be associated with an unacceptable side-effect pro21 n However, the GDG considered that there will be circumstances whe22
r example, combination therapy would be appropriate and cost-effective. Fo23 portant to patients may consider that a greater probability of response is im24
ware of the them. Under these circumstances, patients should be made fully a25 l toxicity. 26 expected side effect profile and be likely to tolerate the additiona
27 nology appraisal The recommendations contained in the recent NICE tech28
ination of guidance 116 are being incorporated into this guideline. The comb29 cetaxel gemcitabine and paclitaxel is only recommended as an option if do30
ine would also be monotherapy or the combination of docetaxel and capecitab31 appropriate. However, the GDG considered that in the majority of 32
patients should start treatment with taxane monotherapy circumstances, 33 ly docetaxel) followed by vinorelbine or capecitabine monotherapy (preferab34
. 35 second line then capecitabine or vinorelbine monotherapy third line 36
37 38 39
elbine (VIN) as a monotherapy or in 40 r agents is generally of very poor quality consisting 41
all RCTs. 42 caution. 43 ine 44
therapy. 45 46 Vinorelbine monotherapy
Clinical Evidence Vinorelbine The level of evidence on the use of vinorcombination with othemainly of low patient number, non-comparative phase II trials or smAs such, the findings from these studies should be interpreted with The majority of patients were believed to have had prior anthracycl
47 One small, statistically underpowered RCT (Pajk et al. 2008) compared VIN 48 with capecitabine (CAP) in a small number of heavily pre-treated women and 49 reported no significant difference in response or survival outcomes but more 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 53 of 146

DRAFT FOR CONSULTATION
adverse events (particularly neutropenia) in the VIN group. Two pophase II studies evaluated VIN for women with metastatic disease (al., 2000 and Zelek et al., 2001) finding that as second or third lresponse rates of up to 41%, response
or quality 1 Udom et 2
ine treatment 3 duration of 4 months and time to 4
5 6
progression of ~2.75 months were reported. Vinorelbine combined therapy Two poor to moderate quality RCTs tested VIN in combination fluorouracil (5´-FU) vs docetaxel (DOC) - Bonneterre et al., 2002) or gemcitabine (GEM) vs VIN - Martin et al., 2007). VIN + 5´-FU comresulted in similar treatment outcomes as DOC monotherapy but incidence of neutropen
7 with 5’-8
9 bined 10
with a higher 11 ia. VIN + GEM resulted in superior progression-free 12
13 14 15
s 16 , 2003, Chan 17 et al., 2007 18
, DOC 19 ), GEM (Ardavanis et al., 2007 and Colomer et al. 20
21 followed 22
23 24
rates ranged 25 esponse 26
duration from 2.6-17.5 months, median time to progression (reported in two 27 m 6.6-8.6 months and median progression-free survival (reported 28
dverse 29 alopecia. 30
31 32
The level of evidence on the use of capecitabine (CAP) as a monotherapy or 33 etaxel (DOC) is generally of poor quality consisting 34
ith one good 35 nterpreted 36
37 38
survival, but not significantly different overall survival or response duration, compared with VIN alone. Thirteen poor to moderate quality phase II, non-comparative, studiedescribed VIN combined with: trastuzumab (TRZ) (Burstein et al.et al., 2006, Jahanzeb et al., 2002, Bartsch et al., 2007, De Maio and Catania et al., 2007), CAP (Ghosn et al., 2006 and Davis, 2007)(Mayordomo et al., 20042006), 5’-FU (Stuart, 2008), mitozantrone (MTZ) (Onyenadum et al. 2007), cisplatin (CIS) followed by DOC (Shamseddine et al. 2006) and CAPby DOC (Ghosn et al. 2008). For all phase II combination studies, the overall tumour response from 33-75%, median overall survival from 13-35.8 months, median r
studies) froin two studies) from 9.6-9.9 months. The most commonly reported aevents attributed to VIN were neutropenia, nausea and vomiting and Capecitabine
in combination with docmainly of low patient number, non-comparative phase II studies wphase III RCT. As such, the findings from these studies should be iwith caution. Capecitabine monotherapy 39
al., 2004, 40 l., 2004, 41
one 42 he majority 43
line and taxane. 44 45 Across all studies, the overall tumour response rates ranged from 10-42%, 46 median overall survival from 9.4-18.1 months, median response duration from 47 3.8-15.4 months and median time to progression from 3.5-6.6 months. The 48 most commonly reported adverse event was hand-foot syndrome which at 49 grade 3/4 occurred in up to 21% of patients. 50
Nine phase II studies (El Helw and Coleman, 2005, Fumoleau et Lee et al., 2004, Pierga et al., 2004, Reichardt et al., 2003, Wist et aSezgin et al. 2007, Venturini et al. 2007 and Yap et al. 2007) and retrospective case series (Leonard et al., 2002) were identified. Tof patients are believed to have been treated with anthracyc
Advanced breast cancer: full guideline DRAFT (August 2008) Page 54 of 146

DRAFT FOR CONSULTATION
1 Capecitabine combined therapy 2
one phase The evidence for combined therapy with CAP and DOC comprised3 ilva et al. III RCT (Chan, 2005) three phase II studies (Mackey et al., 2004, S4
k et al. 2006) and a retrospective analysis of post-study data 5 2008 and Mroze6 (Miles et al., 2004).
7 significant The RCT compared CAP + DOC with gemcitabine and reported no8 e to difference between study arms in overall response rate, median tim9
of hand-foot treatment failure or response duration. There were higher levels10 offered syndrome and diarrhoea in the CAP and DOC arm. Phase II studies11
DOC poor quality and conflicting evidence on reduced doses of CAP and12 n overall reporting overall tumour response rates ranged from 44-50%, media13 months survival of ~19 months (1 study), median response duration of ~ 9.114
(1 study). A 15 (1 study) months and median time to progression of ~5.5 monthspost study analysis of a pivotal RCT (O’Shaughnessy et al., 2002) confirmed 16
val advantage with CAP and DOC, either combined or sequentially, 17 a survi18 when compared with either agent as monotherapy. 19
Taxanes 20 econd line There was good quality evidence on the use of taxanes as first or s21 are monotherapy or in combination, comprising a high quality Cancer C22
s (Ghersi Ontario guideline (Verma et al., 2003), two good systematic review23 Cassier et et al., 2005 and Bria et al., 2005) and three RCTs (Lin et al. 2003, 24
ded 14,800. 25 al. 2008 and Jones et al., 2005). The total patient number excee 26
paclitaxel (PAC) Anthracycline naïve women did not derive any benefit from 27 matic review as first line monotherapy compared with controls. A large syste28
dded to found that for anthracycline naïve patients, when taxanes were a29 time to anthracycline based regimes, there were no significant differences in30
31 progression (TTP) or overall survival (OS) but tumour response wassignificantly improved. However, PAC and doxorubicin (DOX) combined 32
ith therapy resulted in superior median OS and TTP compared w33 gest a cyclophosphamide, 5´-FU and DOX. There was no evidence to sug34 either was 35 significant difference in quality of life between DOC and PAC when
36 combined with anthracycline as first line therapy. 37
, tumour Meta-analysis demonstrated significant improvements in TTP38 containing regimes response and time to treatment failure in favour of taxane 39
antage in compared with non-taxane containing regimes and a borderline adv40 n only first OS. However, statistical significance for OS and TTP was lost whe41
ne-containing line therapy with taxanes was considered. Taxanes and taxa42 nd regimes were reported to have a higher incidence of neurotoxicity a43
leukopenia but fewer cases of nausea and vomiting than controls. 44 45 PAC monotherapy was preferable to mitomycin in terms of TTP but not other 46 outcomes. DOC monotherapy correlated with improved OS (compared with 47 combined mitomycin and vinblastine) and improved TTP and tumour 48 response compared with several other multi-agent therapies. Good RCT data 49 demonstrated a significant advantage in OS, TTP and response duration for 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 55 of 146

DRAFT FOR CONSULTATION
patients on DOC versus PAC monotherapy although the tumour responses 1 y or were similar. Another RCT found no significant differences in efficac2
AC and DOC as first-line therapy combined with survival outcomes between P3 DOX then given as monotherapy. 4
5 Health Economic Evaluation (see also Appendix 1) 6 Introduction 7
th The choice of chemotherapy regimens with which to treat patients wi8 luations. advanced breast cancer has been the subject of many economic eva9
tic review of Despite this, none of the economic studies identified by a systema10 wer the these topics provided a comprehensive analysis with which to ans11
sequential review question. The guideline development group identified that12 te has use of chemotherapy agents was an important comparator that to da13 of the not been evaluated against combination therapies. In addition none 14
ntions. An 15 economic evaluations compared more than three different interveindependent modelling exercise was conducted to address these concerns. In 16
rect treatment comparison was also the absence of direct evidence, an indi17 ted on first-line treatment options to make use of all the data from 18 conduc
19 available randomised controlled trials. 20 Methods 21
e therapies Four first-line therapies, two second-line therapies and two third-lin22 pment group were considered in the analysis. In addition the guideline develo23 palliative thought a ‘no chemotherapy’ option consisting of supportive and24
therapy care was an important and relevant comparator to the active chemo25 knowledged no data were available on this options, although it was ac26
‘intervention’ so expert opinion was used to inform the parameters. It was 27 ence of assumed a chemotherapy agent cannot be reused later in a sequ28
h other in 29 therapy so in total seventeen strategies were evaluated against eac30 a decision analytic framework.
31 vice in line The perspective adopted was that of the UK National Health Ser32
en the nature of with the NICE Reference Case for economic evaluations. Giv33 lity of life was considered a particularly important metastatic disease, qua34
outcome. As such a cost-utility analysis was undertaken with quality adjusted 35 ated life years (QALYs) as the primary health outcome. QALYs were estim36 t al. using published utility values derived from oncology nurses (Cooper e37
health outcomes assessed were life years and 38 2003). The secondary39 progression-free life years.
40 ences of A decision tree was constructed to represent the seventeen sequ41 s or not 42 chemotherapy agents, and the potential for encountering toxicitie
43 responding to treatment. 44 The clinical evidence required to populate the model was obtained from a 45 number of different sources. An indirect treatment comparison was conducted 46 to synthesise data from eight RCTs investigating first line (post-anthracycline) 47 chemotherapy for advanced breast cancer. This provided consistent data on 48 the probabilities of toxic death, discontinuing treatment due to toxicity, 49 response or disease stabilisation and progression-free survival estimates 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 56 of 146

DRAFT FOR CONSULTATION
associated with each intervention. Second-line data for vinorelbine were 1 lation (in estimated from an RCT (Martin et al, 2007) with a mixed patient popu2 ecitabine terms of line of treatment received) and second-line data for cap3 hird-line from a non-randomised retrospective study (Pierga et al, 2004). T4 ent. No treatment was assumed to be as effective as second-line treatm5
rt opinion evidence was available for the ‘no chemotherapy’ option, so expe6 available was sought from the guideline development group. No evidence was7 sumed to on overall survival resulting from any of the strategies, so this was as8 ent, plus be equal to the sum of time to progression from each line of treatm9
the time lag between ending one treatment and starting another (1 month), 10 11 plus the time from progression to death (estimated to be 5 months).
12 HS, and The costs considered in the analysis were those relevant to the N13
ment and included drug acquisition costs, administration costs, cost of assess14 palliative follow-up, cost of treating adverse events, cost of supportive and 15 iterature, care. Costs were based on NHS Reference Costs or taken from the l16 e uplifted and were estimated using 2006-7 prices. When necessary, costs wer17 es Index using the Hospitals and Community Health Services Pay and Pric18 osts nor (PSSRU, 2007). Discounting was not carried out; neither on c19 ime) was benefits. However, since the time horizon of the decision model (lifet20 at can be short, this limitation is unlikely to affect the results or conclusions th21
s of one-way deterministic sensitivity drawn from the analysis. A serie22 nducted to assess the robustness of the study results by analyses were co23
variables 24 varying the values of relevant parameters in order to identify those 25 that had the biggest impact on the results. 26
Summary of results 27 ranged The results of the base-case analysis showed that the total QALYs28 ated to from 0.36 to 1.19 per patient, whilst total costs per patient were estim29 ertaken range from £14,000 up to £31,500. An incremental analysis was und30
) against on the results, comparing each strategy (or sequence of therapies31 trategies the next best alternative after first removing any dominated s32
er QALY, (highlighted in grey in table 1). Using a threshold value of £20,000 p33 by no strategy 14 (docetaxel followed by capecitabine followed 34
es health chemotherapy) was shown to be most cost-effective since it maximis35 elopment benefits given the budget constraint. However the guideline dev36 at which group considered a higher threshold value of £30,000 per QALY, 37 e) would strategy 15 (docetaxel followed by vinorelbine and then capecitabin38 e to the be considered most cost-effective since it maximises QALYs. Du39
in the analysis, the results need careful interpretation. multitude of strategies40 Since there is very little difference between strategies 13 (docetaxel followed 41 by capecitabine followed by vinorelbine) and 15, in terms of QALYs, and given 42 the uncertainty surrounding these point estimates, it is not clear which 43 strategy is dominated and thus which should be excluded from the 44 incremental analysis. 45
Advanced breast cancer: full guideline DRAFT (August 2008) Page 57 of 146

DRAFT FOR CONSULTATION
1 Table 1: Results of the base-case analysis 2 Strategy T1 T2 T3 ot
ExpQA
Total EC
ICER T al ected
LYs xpected osts
3 O CAP 1.18 £3 £160,748 GEM+D C VIN 96 1,479 5 GEM+DO VIN CAP 1.18 £30,859 £40,959 C 57 6 GEM+DOC VIN No Chemo 0.8230 £27,124 13 DOC CAP VIN 1.0738 £26,442 4 GEM+DOC CAP No Chemo 0.9734 £25,882 15 DOC VIN 1.05 £25,675 £23,660 CAP 92 8 PAC CAP VIN 0.9739 £24,521 10 PAC VIN CAP 0.9642 £23,872 16 DOC VIN No Chemo 0.6997 £21,962 1 DOC+CAP VIN No Chemo 0.7694 £21,406 7 GEM+DOC No Chemo 0.5827 £21,056 14 OC No C 0.85 £20,727 £19,072 D CAP hemo 00 11 PAC VIN No Chemo 0.6009 £20,119 9 AC No C 0.75 £18,871 £16,119 P CAP hemo 27 17 DOC No Chemo 0.4718 £15,928 2 DOC+CAP No Chemo 0.5452 £15,526 £8,325 12 PAC No Chemo 0.3645 £14,022 GEM = gemcitabine; DOC = docetaxel; CAP = capecitabine; VIN = vinorelbinpaclitaxel A number of scenarios were considered using one-way detsensitivity analysis. These showed the results to be sensitive discount
e; PAC = 3 4 5
erministic 6 to price 7
s available on paclitaxel and the effectiveness of third-line therapy. 8 ited and was taken into 9
account by the guideline development group when deliberating over the 10 11
R 16)
However this approach to sensitivity analysis is lim
evidence. 12 For the full report of the economic analysis see Appendix 1. 13 14
ecommendations (from NICE technology appraisal guidance 115 • ication, is Gemcitabine in combination with paclitaxel, within its licensed ind16
ast cancer recommended as an option for the treatment of metastatic bre17 plus capecitabine are also only when docetaxel monotherapy or docetaxel 18
considered appropriate. 19 t: This recommendation is from ‘Gemcitabine for the Qualifying statemen20
y appraisal treatment of metastatic breast cancer’, NICE technolog21 guidance 116 (2007). It has been incorporated into this guideline in line 22 with NICE procedures for developing clinical guidelines. 23
Research recommendation
24 25
cost • Randomised clinical trials should evaluate the clinical and 26 vanced breast 27 effectiveness of different sequences of chemotherapy for ad
cancer. 28 29 4.3 Biological Response Modifiers 30 31 Over the last 10 to 15 years the identification of some of the molecular 32 processes occurring in breast cancer has led to the development of new 33 treatment possibilities using agents which can be directed specifically at these 34
Advanced breast cancer: full guideline DRAFT (August 2008) Page 58 of 146

DRAFT FOR CONSULTATION
molecular processes. The term "biological response modifiers" isdescribe such treatments. They
used to 1 may be used alone or in combination with 2
chemotherapy or endocrine therapy. 3
in patients 4 atinib. 5
ected to gain a licence for 6 7 8
n 9 surface of the 10
nts whose 11 ion as 12 patients 13
tumours that overexpress HER2. Because 14 ting metastatic 15
16 17
th of 18 sels. Lapatinib is an oral agent which affects tumour growth 19
eceptor and the 20 a NICE 21
22 23 24
s the only one of these agents approved for use in the 25 NHS in England and Wales, for patients with advanced breast cancer, in 26
actice variation 27 nged at the 28
29 30
with 31 e only 32
re of 33 and 34 d which 35
ited data 36 , it was not 37
op a robust health economic model and so the GDG could 38 tuzumab tand and
mbination.
There are currently three main biological response modifiers usedwith advanced breast cancer – trastuzumab, bevacizumab and lapMany more biological response modifiers are expthe treatment of breast cancer over the next few years. Trastuzumab is a recombinant humanised monoclonal antibody, giveintravenously, that attaches to the HER2 receptor protein on the cancer cell and affects its growth. Trastuzumab is only used in patietumours have either HER2 overexpression or HER2 gene amplificatdetermined by an accurate and validated test. Approximately 25% ofwith advanced breast cancer haveit does not cross the blood-brain barrier it is not effective in treadisease of the central nervous system. Bevacizumab is a similar monoclonal antibody that affects the growtumour blood vesby switching off the metabolic pathways of the HER2 repidermal growth factor receptor (EGFR). Lapatinib is the subject of technology appraisal (www.nice.org.uk/guidance/index.jsp?action=byID&o=11731). Currently, trastuzumab i
combination with chemotherapy. There is controversy and prabout continuing its use when chemotherapy is stopped or chatime of disease progression. Trastuzumab was approved by NICE in 2002 for treating womenadvanced breast cancer solely in combination with paclitaxel, thcombination licensed at that time (NICE 2002). The GDG was awawidespread adoption in the UK of the combination of trastuzumab docetaxel, which has been licensed since the original appraisal anwas considered to be more clinically effective. Because of the limavailable from the one published trial on this new combinationpossible to develmake no recommendation about the use of the combination of tras39 with docetaxel. As a result the recommendations from TA 34 still s40 the GDG have recommended that a technology appraisal is conducted to 41 investigate the clinical and cost-effectiveness of this new co42
Recommendations 43 • Trastuzumab in combination with paclitaxel (combination trastuzumab is 44
currently only licensed for use with paclitaxel) is recommended as an 45 option for people with tumours expressing human epidermal growth factor 46 receptor 2 (HER2) scored at levels of 3+ who have not received 47
Advanced breast cancer: full guideline DRAFT (August 2008) Page 59 of 146

DRAFT FOR CONSULTATION
chemotherapy for metastatic breast cancer and in whom anthracycline 1 treatment is inappropriate. 2
• Trastuzumab monotherapy is recommended as an option for people with 3 tumours expressing HER2 scored at levels of 3+ who have received at 4 least two chemotherapy regimens for metastatic breast cancer. Prior 5 chemotherapy must have included at least an anthracycline and a taxane 6 where these treatments are appropriate. It should also have included 7 hormonal therapy in suitable oestrogen receptor positive patients. 8
• HER2 levels should be scored using validated immunohistochemical 9 techniques and in accordance with published guidelines. Laboratories 10 offering tissue sample immunocytochemical or other predictive tests for 11 therapy response should use validated standardised assay methods and 12 participate in and demonstrate satisfactory performance in a 13 recognised external quality assurance scheme.’ 14
inical Qualifying statement: These recommendations are from ‘The cl15 ’, effectiveness and cost effectiveness of trastuzumab for breast cancer16
NICE technology appraisal guidance 34 (2005).They have been 17 eveloping incorporated into this guideline in line with NICE procedures for d18
clinical guidelines. 19 20
• Patients who are receiving treatment with trastuzumab should not continue 21 de the central nervous 22 trastuzumab at the time of disease progression outsi
system. 23 bsence of Qualifying statement: This recommendation is based on the a24
ome. 25 evidence that continuing trastuzumab leads to a better outc
Clinical Evidence 26 ho 27 For patients undergoing therapy with a biological response modifier w
experience disease progression there was only limited evidence on 28 which comprised a RCT (von Minckwitz et al. 2008) a trastuzumab (TRZ)29
case prospective post RCT study (Tripathy et al., 2004) five retrospective 30 al., 2005, series (Fountzilas et al., 2003, Gelmon et al., 2004, Garcia-Saenz et31
e II study 32 Montemurro et al., 2006 and Stemmler et al., 2005) and a phas33 (Bartsch et al., 2006).
34 ements in Limited data from a post-RCT analysis showed no significant improv35 TRZ safety or efficacy for women with disease progression who continued36
different chemotherapies when compared with women in combined with 37 d on whom TRZ was given for the first time after their disease progresse38 support chemotherapy alone. Most case series also offered little evidence in39
ant of continuing TRZ therapy beyond progression since, where relev40 r survival, 41 comparisons were made, no significant improvements were found fo
42 efficacy or safety. 43 One retrospective case series demonstrated a significant survival advantage 44 for women who had received both first and second line therapy with TRZ but, 45 taken from a non-randomised study, the data was open to strong selection 46 bias. Weak phase II evidence showed no significant difference in the length of 47 time to progression between first, second or further lines of TRZ therapy 48 which was interpreted as support for TRZ continuation. 49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 60 of 146

DRAFT FOR CONSULTATION
1 fficacy of 2
e who 3 The response 4
ival were all 5 uperior for the combined therapy and with no 6 ity. 7
A very recent, unpublished RCT showed that TRZ improved the esecond line capecitabine in Her2 +ve patients with metastatic diseashad previously received TRZ in the adjuvant or first line setting. rate, clinical benefit rate, time to progression and overall survstatistically significantly sadditional significant toxic 8 Research Recommendation 9 • The use of continued trastuzumab in patients with progressive metastatic 10
disease should be investigated as part of a randomised controlled trial. 11 • Randomised controlled trials are needed to assess whether patients who 12
13 have had adjuvant trastuzumab should receive further biological response modifiers. 14
15 16 17
The decision not to have a systemic disease-modifying treatment is an active 18 ssibility of 19
20
ept 21 althcare 22
not prevent 23 tients with 24
veral 25 uch treatments 26
patient 27 -modifying 28
at any point, and although it is important to explore the reasons for 29 majority of 30
he most 31 g 32
33
34 st cancer. 35 roughout 36
37
38 Basioukas S., 39
s G (2007) Gemcitabine and oral 40 vinorelbine as salvage treatment in patients with advanced anthracycline- and 41 taxane-pretreated breast cancer. Anticancer Res 27: 2989-2992 42
Baker LH., Vaughn CB and Al SM (1974) Evaluation of combination vs. 43 sequential cytotoxic chemotherapy in the treatment of advanced breast 44 cancer. Cancer (Philad) 33(2): 513-518 45
4.4 No systemic disease-modifying treatment
one. Ultimately there will come a point when there is no realistic pobenefit from further systemic disease-modifying treatment.
Where active intervention may be appropriate the decision to acctreatment or not is made by the patient after discussion with their heprofessional. It is a decision that needs to be supported, and doesa later decision to receive an active treatment. For example, pahormone receptor negative, HER2 negative cancers may receive sedifferent courses of chemotherapy, with intervals in between sduring which they receive no active disease-modifying treatment. Amay, when fully informed, opt not to receive systemic diseasetreatmentsuch a choice, it is one that needs to be respected. For thepatients with advanced breast cancer, there will come a point when tappropriate choice is to receive no further systemic disease-modifyintreatments.
The provision of supportive and palliative care must be an essential consideration in the management of individuals with advanced breaSupportive and palliative care needs should be assessed and met ththe patient journey, whatever treatment choices are made.
References Ardavanis A., Kountourakis P., Maliou S., Vassilakopoulou M.,Kyriakou F., Koumna S and Rigato
Advanced breast cancer: full guideline DRAFT (August 2008) Page 61 of 146

DRAFT FOR CONSULTATION
Bartsch R., Wenzel C., Altorjai G., Pluschnig U., Bachleitner-HoffmaLocker GJ., Rudas M., Mader R., Zielinski CC and Steger GG (2007from an observational trial with oral vinorelbine and trastuz
nn T., 1 ) Results 2
umab in advanced 3 4
er W., 5 ) Analysis 6
r the failure 7 cer 6. 8
eot P and 9 ian S (2002) Docetaxel vs 5-fluorouracil plus vinorelbine in 10
ncer. 87: 11 12
. Cuppone F., 13 line 14
-679 15
in K., Overmoyer 16 D., Ellis 17 d Winer 18
rst-line therapy for HER2-19 l with clinical 20
nd cardiac 21 22
Wilcken N., Ghersi D., Marzo M and Simes J (2005) 23 24
ous 25 ter (UK): 26
27
Cassier PA., Chabaud S., Trillet-Lenoir V., Peaud PY., Tigaud JD., Cure H., 28 lla JP., 29
nd docetaxel 30 ults of the 31
32
ceschelli L., 33 07) 34
ncer: 35 e centre. Breast Cancer 36
Res Treat 106: 97-103. 37
Catania C., Medici M., Magni E., Munzone E., Cardinale D., Adamoli L., 38 Sanna G., Minchella I., Radice D., Goldhirsch A and Nole F (2007) Optimizing 39 clinical care of patients with metastatic breast cancer: a new oral vinorelbine 40 plus trastuzumab combination. Ann Oncol 18: 1969-1975 41
breast cancer. Breast Cancer Research & Treatment 102: 375-381
Bartsch R., Wenzel C., Hussian D., Pluschnig U., Sevelda U., KoestlAltorjai G., Locker GJ., Mader R., Zielinski CC and Steger GG (2006of trastuzumab and chemotherapy in advanced breast cancer afteof at least one earlier combination: An observational study. BMC Can
Bonneterre J., Roché H., Monnier A., Guastalla JP., Namer M., FargAssadourmetastatic breast cancer after anthracycline therapy failure. Brit J Ca1210-1215.
Bria E., Giannarelli D., Felici A., Peters WP., Nistico C., Vanni BCognetti F and Terzoli E (2005) Taxanes with anthracyclines as first-chemotherapy for metastatic breast carcinoma. Cancer 103(4): 672
Burstein HJ., Harris LN., Marcom PK., Lambert-Falls R., HavlB., Friedlander RJ., Jr.., Gargiulo J., Strenger R., Vogel CL., Ryan PMJ., Nunes RA., Bunnell CA., Campos SM., Hallor M., Gelman R anEP (2003) Trastuzumab and vinorelbine as fioverexpressing metastatic breast cancer: multicenter phase II triaoutcomes, analysis of serum tumor markers as predictive factors, asurveillance algorithm. J Clin Oncol 21: 2889-2895.
Carrick S., Parker S.,Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database of Systematic Reviews: Reviews. In: AnonymCochrane Database of Systematic Reviews 2005 Issue 2. ChichesJohn Wiley & Sons, Ltd.
Orfeuvre H., Salles B., Martin C., Jacquin JP., Agostini C., GuastaPerol D and Bachelot T (2008) A phase-III trial of doxorubicin aversus doxorubicin and paclitaxel in metastatic breast cancer: resERASME 3 study. Breast Cancer Res Treat 109: 343-350
Catania C., Ascione G., Adamoli L., De Pas T., Medici M., FranVerri E., Magni E., Sanna G., Torrisi R., Goldhirsch A and Nole F (20Fulvestrant in heavily pre-treated patients with advanced breast caresults from a single compassionate use programm
Advanced breast cancer: full guideline DRAFT (August 2008) Page 62 of 146

DRAFT FOR CONSULTATION
Chan S (2005) Gemcitabine plus docetaxel versus capecitabdocetaxel for patients with anthracycline-pretreated metastatic breaa
ine plus 1 st cancer: 2
review of the results of a European Phase III trial. Ejc Supplements 3: 17-3 4
wicz M., 5 Pawlicki 6
7 8
therapy for HER 2-positive metastatic breast cancer patients: an international 9 10
Fein L., 11 ., Rennie P., 12
d placebo 13 14
herapy in postmenopausal women with 15 EFECT 19 16
17
ski RT., Irwin LE., Pugh RP., Sadoff L., Hestorff R., Wiener JM and 18 19
es 39(11): 20 21
artolucci AA and 22 Bateman JR (1989) Combination versus sequential single agent 23
tatic sites 24 25 26
27 B., Ciruelos E., Hornedo J., Vicente D and Cortes-Funes H (2006) Biweekly 28
: efficacy and 29 ational Oncology: 30
tes & of the 31 exico 8: 896-902 32
to Markov 33 n 34
ty Series A-35 -405. 36
Creech RH., Catalano RB., Harris DT., Engstrom PF and Grotzinger PJ 37 (1979) Low dose chemotherapy of metastatic breast cancer with 38 cyclophosphamide., adriamycin., methotrexate., 5-fluorouracil (CAMF) versus 39 sequential cyclophosphamide., methotrexate., 5-fluorouracil (CMF) and 40 adriamycin. Cancer 43(1): 51-59 41
21.
Chan A, Martin M., Untch M., Gil MG., Guillem-Porta V., WojtukieKellokumpu-Lehtinen P., Sommer HL., Georgoulias V., Battelli N.,M., Aubert D., Bourlard T., Gasmi J., Villanova G., Petruzelka L andNavelbine HP (2006) Vinorelbine plus trastuzumab combination as first-line
phase II trial. Brit J Cancer 95: 788-793.
Chia S., Gradishar W., Mauriac L., Bines J., Amant F., Federico M., Romieu G., Buzdar A., Robertson JFR., Brufsky A., Possinger KSapunar F., Lowe E and Piccart M (2008) Double-blind, Randomizecontrolled trial of fulvestrant compared with exemestane after prior nonsteroidal aromatase inhibitor thormone receptor-positive, advanced breast cancer: Results from 28. J Clin Oncol 26: 1664-1670.
ChlebowBateman JR (1979) Survival of patients with metastatic breast cancer treated with either combination or sequential chemotherapy. Cancer R4503-4506
Chlebowski RT., Smalley RV., Weiner JM., Irwin LE., B
chemotherapy in advanced breast cancer: associations with metasand long-term survival. The Western Cancer Study Group and The Southeastern Cancer Study Group. Br J Cancer 59(2): 227-230
Colomer R., Llombart-Cussac A., Tusquets I., Rifa J., Mayordomo JI., Ojeda
gemcitabine plus vinorelbine in first-line metastatic breast cancercorrelation with HER2 extracellular domain. Clinical & TranslOfficial Publication of the Federation of Spanish Oncology SocieNational Cancer Institute of M
Cooper, N. J., K. R. Abrams, et al. (2003). " Bayesian approachmodelling in cost-effectiveness analyses: application to taxane use iadvanced breast cancer. Journal of the Royal Statistical SocieStatistics in Society 166: 389
Advanced breast cancer: full guideline DRAFT (August 2008) Page 63 of 146

DRAFT FOR CONSULTATION
Crump M., Sawka CA., DeBoer G., Buchanan RB., Ingle JN., ForbMeakin JW., Shelley W and Pritchard KI (1997) An individual pameta-analysis of tamoxifen versus ovarian ablation as first line etherapy for premenopausal women with metastatic b
es J., 1 tient-based 2 ndocrine 3
reast cancer (DARE 4 5
herapy with 6 d 7 3: 37-43 8
onia V., Landi 9 P., Formichelli 10
R., 11 G., Perrone F and de MA (2007) Vinorelbine plus 3-weekly 12
rial. BMC 13 14
Drummond M, Thompson E, Howell A, Jonat W, Buzdar A, Brown J. (1999) 15 zole in the 16
s 2: 33-43. 17
18 ic breast 19
20
T., Langkjer ST., Andersen J., Sjöström J., Kjaer M 21 and Scandinavian Breast Group (2004). Phase III study of intravenous 22
atients 23 G9403). 24
ol (12): 2313-2320 25
2005) Reduced dose capecitabine is an effective 26 and well-tolerated treatment in patients with metastatic breast cancer. Breast 27
28
of 71 cases. 29 30
i A., Papaldo P., Fabi A., Di CS., 31 r A., Nuzzo C., 32
neration 33 usal 34
ed trials. 35 36
Fountzilas G., Razis E., Tsavdaridis D., Karina M., Labropoulos S., 37 Christodoulou C., Mavroudis D., Gogas H., Georgoulias V and Skarlos D 38 (2003) Continuation of trastuzumab beyond disease progression is feasible 39 and safe in patients with metastatic breast cancer: a retrospective analysis of 40 80 cases by the Hellenic Cooperative Oncology Group. Clin Breast Cancer 4: 41 120-125. 42
structured abstract). Breast Cancer Res Treat 44: 201-210.
Davis AJ (2007) Multicenter phase II study of combination chemotcapecitabine and intravenous vinorelbine in patients with pretreatemetastatic breast cancer. Asia-Pacific Journal of Clinical Oncology
De Maio ME., Pacilio C., Gravina A., Morabito A., Di RF., LabG., Nuzzo F., Rossi E., Silvestro P., Botti G., Di BM., Curcio MF., La VF., Staiano M., Maurea N., D'Aiuto G., D'Aiuto M., ThomasSignoriello trastuzumab in metastatic breast cancer: a single-centre phase 2 tCancer 7: 50-
Cost-effectiveness implications of increased survival with anastrotreatment of advanced breast cancer. Journal of Medical Economic
Eisen A., Pritchard K., Johnston M and Oliver T (2004) Role of aromatase inhibitors in the treatment of postmenopausal women with metastatcancer. Curr Oncol 11(2): 41-52.
Ejlertsen B., Mouridsen H
vinorelbine in combination with epirubicin versus epirubicin alone in pwith advanced breast cancer: a Scandinavian Breast Group Trial (SBJ Clin Onc
El-Helw L and Coleman RE (
14: 368-374.
El Omari-Alaoui H (2002) Male breast cancer. A report Cancer/Radiotherapie 6: 349-351
Ferretti G., Bria E., Giannarelli D., FelicRuggeri EM., Milella M., Ciccarese M., Cecere FL., GelibteCognetti F., Terzoli E and Carlini P (2006) Second- and third-gearomatase inhibitors as first-line endocrine therapy in postmenopametastatic breast cancer patients: a pooled analysis of the randomisBr J Cancer 94(12): 1789-1796.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 64 of 146

DRAFT FOR CONSULTATION
Fumoleau P., Largillier R., Clippe C., Dieras V., Orfeuvre H., LesCuline S., Audhuy B., Serin D., Cure H., Vuillemin E., Morere J-F., MF., Mouri Z and Namer M (2004) Multicentre, phase II study capecitabine monotherapy in patients with anthra
imple T., 1 ontestruc 2
evaluating 3 cycline- and taxane-4
. 5
do A., 6 ciated with 7
8 9
nn N., Klimo P., 10 ich B., 11
(2004) Use of trastuzumab beyond disease 12 ries. Clin 13
14
d Donoghue E (2005) Taxane containing 15 regimens for metastatic breast cancer. Cochrane Database of Systematic 16
sue 2. 17 18
se II trial of 19 tic breast 20
21
Ghosn M., Kattan J., Farhat F., Younes F., Nasr F., Moukadem W., Gasmi J 22 owed by 23
se II trial. 24 25
ase 26 al women. 27
Cochrane Database of Systematic Reviews: Reviews Cochrane Database of 28 y & Sons, Ltd. 29
. American 30 31
, Miller WH., 32 d, controlled trial of 33
atamestane plus toremifene compared with letrozole in postmenopausal 34 : official 35 36
Harris AL., Dowsett M., Stuart-Harris R and Smith IE (1986) Role of 37 aminoglutethimide in male breast cancer. Br J Cancer 54: 657-660 38
Jahanzeb M., Mortimer JE., Yunus F., Irwin DH., Speyer J., Koletsky AJ., 39 Klein P., Sabir T and Kronish L (2002) Phase II trial of weekly vinorelbine and 40
pretreated metastatic breast cancer. Eur J Cancer 40: 536-542
Garcia-Saenz JA., Martin M., Puente J., Lopez-Tarruella S., CasaMoreno F., Grande E and az-Rubio E (2005) Trastuzumab assosuccessive cytotoxic therapies beyond disease progression in metastatic breast cancer. Clin Breast Cancer 6: 325-329.
Gelmon KA., Mackey J., Verma S., Gertler SZ., BangemaSchneeweiss A., Bremer K., Soulieres D., Tonkin K., Bell R., HeinrGrenier D and Dias Rprogression: observations from a retrospective review of case histoBreast Cancer 5: 52-58.
Ghersi D., Wilcken N., Simes J an
Reviews: Reviews. In: Cochrane Database of Systematic Reviews IsChichester (UK): John Wiley & Sons Ltd.
Ghosn M., Kattan J., Farhat F., Younes F and Gasmi J (2006) Phacapecitabine and vinorelbine as first-line chemotherapy for metastacancer patients. Anticancer Res 26: 2451-2456.
and Chahine G (2008) Sequential vinorelbine-capecitabine folldocetaxel in advanced breast cancer: long-term results of a pilot phaCancer Chemother Pharmacol 62: 11-18
Gibson LJ., Dawson CL., Lawrence DJ and Bliss JM (2007) Aromatinhibitors for treatment of advanced breast cancer in postmenopaus
Systematic Reviews 2007 Issue 1. Chichester (UK): John Wile
Giordano SH (2002) Efficacy of anastrozole in male breast cancerJournal of Clinical Oncology: Cancer Clinical Trials 25: 235-237
Goss P., Bondarenko IN., Manikhas GN., Pendergrass KB.Langecker P and Blanchett D (2007) Phase III, double-blin
women with advanced receptor-positive breast cancer. J Clin Oncoljournal of the American Society of Clinical Oncology 25: 4961-4966.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 65 of 146

DRAFT FOR CONSULTATION
trastuzumab as first-line therapy in patients with HER2(+) metastatic breast 1 cancer. The Oncologist 7: 410-417. 2
E., 3 ards D., 4 I study of 5
red with paclitaxel in metastatic breast cancer. J Clin Oncol 6 7
ian H., Yap HY., Hortobagyi G., Buzdar A and Blumenschein G (1983) 8 Hormonal therapy for metastatic male breast cancer. Arch Intern Med 143: 9
10
ed cost-11 analysis of letrozole followed by tamoxifen versus tamoxifen 12
er. Ann Oncol 13 14
Karnon J, Jones T. (2003b) A stochastic economic evaluation of letrozole 15 t cancer 16
17
, Nam E., Park JO., Kim 18 K and Im YH 19
d taxane-20 21
Chan-Navarro 22 23
l: can 24 25 26
., Salazar R 27 e for patients 28 er 38: 2020-29
24. 30
007) A 31 tatic 32
Breast Cancer after Anthracycline: A Final Analysis. Jpn J Oncol 37 (1): 23-33 34
35 ast cancer - 36
omics 20(2): 101-108. 37
Lopez M (1985a) Cyproterone acetate in the treatment of metastatic cancer of 38 the male breast. Cancer 55 2334-2336 39
Lopez M., Di LL., Lazzaro B and Papaldo P (1985b) Hormonal treatment of 40 disseminated male breast cancer. Oncology 42: 345-349 41
Jones SE., Erban J., Overmoyer B., Budd GT., Hutchins L., LowerLaufman L., Sundaram S., Urba WJ., Pritchard KI., Mennel R., RichOlsen S. Meyers ML and Ravdin PM (2005) Randomized phase IIdocetaxel compa23 (24): 5542-5551
Kantarj
237-240.
Karnon J, Johnston SR, Jones T, Glendenning A. (2003a) A trial-baseffectiveness followed by letrozole for postmenopausal advanced breast canc14(11): 1629-33.
versus tamoxifen as a firstline hormonal therapy: For advanced breasin postmenopausal patients. Pharmacoeconomics 21(7): 513-525.
Lee SH., Lee J., Park J., Park SH., Lee KE., Lee SI.K., Jung CW., Park YS., Yoon SS., Kang WK., Lee MH., Park (2004) Capecitabine monotherapy in patients with anthracycline- anpretreated metastatic breast cancer. Med Oncol 21: 223-231.
Leonard R., O'Shaughnessy J., Vukelja S., Gorbounova V.,CA., Maraninchi D., Barak-Wigler N., McKendrick JJ., Harker WG., Bexon AS and Twelves C (2006) Detailed analysis of a randomized phase III triathe tolerability of capecitabine plus docetaxel be improved without compromising its survival advantage? Ann Oncol 17 (9): 1379-1385
Leonard RC., Twelves C., Breddy J., Chaturvedi A., Hutcheon Aand Cameron D (2002) Capecitabine named-patient programmwith advanced breast cancer. The UK experience. Eur J Canc20
Lin YC. Chang HK., Chen JS., Wang HM., Yang TS and Liaw CC (2Phase II Randomized Study of Two Taxanes and Cisplatin for Metas
29.
Lindgren P, Jonsson B, Redaelli A, Radice D. (2002) Cost-effectiveness analysis of exemestane compared with Megestrol in advanced breA model for Europe and Australia. Pharmacoecon
Advanced breast cancer: full guideline DRAFT (August 2008) Page 66 of 146

DRAFT FOR CONSULTATION
Lopez M (1993) Combined treatment with buserelin and cyproterone acetate 1 in metastatic male breast cancer. Cancer 72: 502-505 2
AA., Au 3 phase II 4 abine in 5
ycline-pretreated metastatic breast cancer. Clinical Breast Cancer 5: 6 7
rrasco E., 8 ., Jara C., 9
., Adrover 10 citabine 11
metastatic 12 treated with anthracyclines and taxanes: final results 13
AM) trial. 14 15
ri D., Pavlidis N., Polyzos NP and Ioannidis JP (2006) Survival with 16 aromatase inhibitors and inactivators versus standard hormonal therapy in 17
1285-18 19
20 lo MA and 21
ne chemotherapy 22 23
24 ith 25
y in a 26 27
Montemurro F., Donadio M., Clavarezza M., Redana S., Jacomuzzi ME., 28 i M and 29
s with HER2-positive advanced breast 30 ist 11: 318-31
32
25 trial. 33 Breast Cancer Res Treat 105(1): 19-29. 34
K., Allen J., 35 ona-Calero M 36
iro CL (2006) Phase II study of weekly docetaxel and capecitabine 37 in patients with metastatic breast cancer. Clinical Breast Cancer 7: 141-145 38
National Institute for Health and Clinical Excellence (2002) Guidance on the 39 use of trastuzumab for the treatment of advanced breast cancer. NICE 40 technology appraisal 34. London: National Institute for Health and Clinical 41 Excellence. 42
Mackey JR., Tonkin KS., Koski SL., Scarfe AG., Smylie MGB., JoyH., Bodnar DM., Soulieres D and Smith SW. (2004) Final results of aclinical trial of weekly docetaxel in combination with capecitanthrac287-292,
Martín M., Ruiz A., Muñoz M., Balil A., García-Mata J., Calvo L., CaMahillo E., Casado A., García-Saenz JA., Escudero MJ., Guillem VRibelles N., Salas F., Soto C., Morales-Vasquez F., Rodríguez CAE., Mel JR and Spanish Breast Cancer Research Group (2007) Gemplus vinorelbine versus vinorelbine monotherapy in patients withbreast cancer previouslyof the phase III Spanish Breast Cancer Research Group (GEICLancet Oncol 8 (3): 219-225
Mau
advanced breast cancer: meta-analysis. J Natl Cancer Inst 98 (18):1291.
Mayordomo JI., Milla A., Morales S., Yubero A., Lorenzo A., Baena JM., Modolell A., Sanz J., Illarramendi J., Garcia MJ., Machengs I., BurilTres A (2004) Biweekly docetaxel and vinorelbine as first-liin metastatic breast cancer. Clin Breast Cancer 5: 131-135.
Miles D., Vukelja S., Moiseyenko V., Cervantes G., Mauriac L., Van HG., Liu WY., Ayoub JP and O'Shaughnessy JA (2004) Survival benefit wcapecitabine/docetaxel versus docetaxel alone: analysis of theraprandomized phase III trial. Clin Breast Cancer 5 (4): 273-278
Valabrega G., Danese S., Vietti-Ramus G., Durando A., VenturinAglietta M (2006) Outcome of patientcancer progressing during trastuzumab-based therapy. Oncolog324.
Mouridsen HT (2007) Letrozole in advanced breast cancer: the PO
Mrozek E., Ramaswamy B., Young D., Rhoades CA., Kendra Moore T., Hauger M., Watson H., Merriman N., Nadella P., Villaland Shap
Advanced breast cancer: full guideline DRAFT (August 2008) Page 67 of 146

DRAFT FOR CONSULTATION
National Institute for Health and Clinical Excellence (2006) Hortherapies for the adjuvant treatment of early oestrogen-receptor-pobreast cancer. NICE techn
monal 1 sitive 2
ology appraisal 112. London: National Institute for 3 4
f letrozole 5 cancer in postmenopausal women in the 6
7
vantinos G., 8 tsoris T., 9 ine in 10 582-589 11
12 ves C., Van 13
14 docetaxel combination therapy in anthracycline-pretreated patients with 15
: 2812-16 17
di G., Rossi E., 18 allo C., Perrone 19
herapy of 20 ant 21
36. 22
n D., Blot E., Vermorken J., 23 24
racycline- 25 ndings from the EORTC 26
27
Patel JK., Nemoto T and Dao TL (1984) Metastatic breast cancer in males. 28 29
30 31
oudier 32 amer M., Chollet P., Sutherland W and 33
Barats JC (2004) Efficacy and safety of single agent capecitabine in 34 assionate 35
7-129. 36
PSSRU Unit Costs of Health and Social Care (2007) 37 www.pssru.ac.uk/uc/uc2007contents.htm 38
Ribeiro GG (1976) The results of diethylstilboestrol therapy for recurrent and 39 metastatic carcinoma of the male breast. Br J Cancer 33: 465-467 40
Health and Clinical Excellence.
Nuijten M, Meester L, Waibel F, Wait S. (1999) Cost effectiveness oin the treatment of advanced breast UK. Pharmacoeconomics 16(4): 379-397.
Onyenadum A., Gogas H., Markopoulos C., Bafaloukos D., AraMantzourani M., Koutras A., Tzorakoelefterakis E., Xiros N., MakaFountzilas G and Kalofonos HP (2007) Mitozantrone plus vinorelbpretreated patients with metastatic breast cancer. J Chemother 19:
O'Shaughnessy J., Miles D., Vukelja S., Moiseyenko V., Ayoub JP.,Cervantes G., Fumoleau P., Jones S., Lui WY., Mauriac L., TwelHG., Verma S and Leonard R (2002) Superior survival with capecitabine plus
advanced breast cancer: phase III trial results. J Clin Oncol 20 (12)2823
Pacilio C., Morabito A., Nuzzo F., Gravina A., Labonia V., LanDe Maio M., D’Aiuto G., Botti G Normanno N., Chiodini P., GF., de Matteis A (2006). Is epirubicin effective in first-line chemotmetastatic breast cancer (MBC) after an epirubicin-containing adjuvtreatment? A single centre phase III trial. Br J Cancer 94: 1233-12
Pajk B., Cufer T., Canney P., Ellis P., CameroColeman R., Marreaud S., Bogaerts J., Basaran G and Piccart M (2008) Anti-tumor activity of capecitabine and vinorelbine in patients with anthand taxane-pretreated metastatic breast cancer: Fi10001 randomized phase II trial. Breast 17: 180-185
Assessment of endocrine therapy. Cancer 53: 1344-1346
Patterson JS., Battersby LA and Bach BK (1980) Use of tamoxifen in advanced male breast cancer. Cancer Treat Rep 64: 801-804
Pierga JY., Fumoleau P., Brewer Y., Zelek L., Martin D., Turpin FL., GMJ., Gil-Delgado M., Baticle JL., N
pretreated metastatic breast cancer patients from the French compuse program. Breast Cancer Research & Treatment 88: 11
Advanced breast cancer: full guideline DRAFT (August 2008) Page 68 of 146

DRAFT FOR CONSULTATION
Ribeiro GG (1983) Tamoxifen in the treatment of male breast carcinoma. Clin 1 Radiol 34: 625-628 2
nicke F., 3 and Luck 4 n patients 5
ing after treatment with a taxane-6 7
r E 8 cacy of lower dose capecitabine in patients with metastatic breast 9
South Med 10 11
afeddine M., 12 shi A., 13 non-14
anthracycline sequential combination of cisplatin-vinorelbine followed by 15 gy 70: 16
17
., Abdullah 18 k S (2008) 19
taxel and low-dose capecitabine: A 20 nts with 21
ancer 8: 162-22 23
dge GW., Neuberg D., Bernardo P., Ingle JN., Martino S., Rowinsky EK 24 xel., and the 25 otherapy for 26 Oncol (4): 588-27
28
(1976) 29 tic 30
ma of the breast. Cancer Res 36 (11 Pt 1): 3911-3916 31
einemann 32 33
east 15: 34 35
Vinorelbine and Infusional 5-fluorouracil in Anthracycline 36 and Taxane Pre-treated Metastatic Breast Cancer. Clin Oncol 20: 152-156 37
Takeda AL., Jones J., Loveman E., Tan SC and Clegg AJ (2007) The clinical 38 effectiveness and cost-effectiveness of gemcitabine for metastatic breast 39 cancer: a systematic review and economic evaluation. Health Technol 40 Assess 11 (19): iii-ixi 41
Reichardt P., von MG., Thuss-Patience PC., Jonat W., Kolbl H., JaKieback DG., Kuhn W., Schindler AE., Mohrmann S., Kaufmann M HJ (2003) Multicenter phase II study of oral capecitabine (Xeloda) iwith metastatic breast cancer relapscontaining therapy. Ann Oncol 14: 1227-1233.
Sezgin C., Kurt E., Evrensel T., Ozdemir N., Manavoglu O and Goke(2007) Efficancer and factors influencing therapeutic response and outcome. J 100: 27-32
Shamseddine AI., Otrock ZK., Khalifeh MJ., Yassine HR., Charbdel-Khalek Z., Chehal A., Bitar N., Jalloul R., Dheiny M., DandaWehbeh M and El-Saghir NS (2006) A clinical phase II study of a
docetaxel as first-line treatment in metastatic breast cancer. Oncolo330-338
Silva O., Lopes G., Morgenzstern D., Lobo C., Doliny P., Santos ES., Gautam U., Reis I., Welsh C., Slingerland J., Hurley J and GlucA phase II trial of split, low-dose docetolerable and efficacious regimen in the first-line treatment of patieHER2/neu-negative metastatic breast cancer. Clinical Breast C167
Sleand Wood WC (2003) Phase III trial of doxorubicin., paclitacombination of doxorubicin and paclitaxel as front-line chemmetastatic breast cancer: an intergroup trial (E1193). J Clin 592
Smalley RV., Murphy S., Huguley CM., Jr and Bartolucci AACombination versus sequential five-drug chemotherapy in metastacarcino
Stemmler HJ., Kahlert S., Siekiera W., Untch M., Heinrich B and HV (2006) Characteristics of patients with brain metastases receiving trastuzumab for HER2 overexpressing metastatic breast cancer. Br219-225
Stuart NSA (2008)
Advanced breast cancer: full guideline DRAFT (August 2008) Page 69 of 146

DRAFT FOR CONSULTATION
Tripathy D., Slamon DJ., Cobleigh M., Arnold A., Saleh M., MortiMurphy M and Stewart SJ (2004) Safety of treatment of metastatic canc
mer JE., 1 breast 2
er with trastuzumab beyond disease progression. J Clin Oncol 22: 1063-3 4
oombes 5 ve 6
rior chemotherapy regimes for advanced breast cancer. 7 8
rtier JW., 9 007) An open-label, multicenter study 10
eated 11 12
ancer 13 iative Breast Cancer Disease Site Group 14
ast cancer. Curr 15 16
chmidt M., 17 ufman M., 18 19
itive metastatic breast cancer 20 dy 21
ology in 22 t 1025. 23
versus 24 chrane Database of 25
26
jaaland I 27 eated 28
29
nd 30 otherapy in 31
low can you go? Breast 16: 420-424 32
Zelek L., Barthier S., Riofrio M., Fizazi K., Rixe O., Delord JP., Le CA and 33 Spielmann M (2001) Weekly vinorelbine is an effective palliative regimen after 34 failure with anthracyclines and taxanes in metastatic breast carcinoma. [see 35 comment]. Cancer 92: 2267-2272. 36
1070.
Udom DI., Vigushin DM., Linardou H., Graham H., Palmieri C and CRC (2000) Two weekly vinorelbine: administration in patients who hareceived at least two pEur J Cancer 36: 177-182.
Venturini M., Paridaens R., Rossner D., Vaslamatzis MM., NoSalzberg M., Rodrigues H and Bell R (2of outpatient capecitabine monotherapy in 631 patients with pretradvanced breast cancer. Oncology 72: 51-57
Verma S., Trudeau M., Pritchard K., Oliver T., Robinson P and the CCare Ontario Practice Guidelines Init(2003). Role of taxanes in the management of metastatic breOncol 10(2): 68-83.
Von Minckwitz G., Zielinski C., Maartense E., du Bois A., SEidtmann H., Cufer T., De Jongh FE., Andersson M., Stein R., KaNekljudovas V and Loibl S (2008). Capecitabine vs capecitabine +trastuzumab in patients with Her2 posprogressing during trastuzumab treatment – the TBP phase III stu(GBG26/BIG 3-05). Annual Meeting of the American Society of OncChicago, IL (USA) abstrac
Wilcken N., Hornbuckle J and Ghersi D (2006) Chemotherapy aloneendocrine therapy alone for metastatic breast cancer. CoSystematic Reviews: Reviews.
Wist EA., Sommer HH., Ostenstad B., Risberg T., Bremnes Y and M(2004) Oral capecitabine in anthracycline- and taxane-pretradvanced/metastatic breast cancer. Acta Oncol 43: 186-189.
Yap YS., Kendall A., Walsh G., Banerji U., Johnston SR., Smith IE aO'Brien M (2007) Clinical efficacy of capecitabine as first-line chemmetastatic breast cancer--how
Advanced breast cancer: full guideline DRAFT (August 2008) Page 70 of 146

DRAFT FOR CONSULTATION
5 Community-based Treatment anSupportive Ca
d 1
re 2 3
4 5
atients 6 ng-7 y patients 8 d, with 9 ave been 10
. For many, 11 condition. Although the number of patients 12
vention 13 14 15
ver, with 16 its, some 17 nity. This 18 t sector. 19 nhanced 20
available in the 21 lation to 22 f interval 23 . 24
25 hallenges 26 and care 27
nding of 28 with all 29 h as the 30 to where 31 of empty 32
for the 33 needed. 34 omes ill 35 ary care 36
onal. Clinical guidance for primary care professionals (and A&E staff) 37 eed care 38 e risk of 39 careful 40
avoid depletion of skilled chemotherapy nurses from centres 41 and units. 42 43 While some treatments may be deliverable in the community, the issue of 44 patient choice and satisfaction needs to be considered. Some patients may 45 feel more secure in a hospital setting; others may wish to remain at home 46 wherever possible. 47 48
5.1 Community-based treatment Primary care and community services are a first point of contact for pand families. Patients place high value on the relationships, often loestablished, with the professionals in their Primary Care Team. Manwith advanced breast cancer will have had a long illness pathway anthe greater part of their cancer journey being spent at home, often haccompanied on their journey by their GP and/or community nursebreast cancer becomes a chronicwith advanced breast cancer is probably decreasing the level of interand care required is likely to increase. Cancer treatments have traditionally been delivered in hospital. Howethe increasing volume of treatment activity at cancer centres and unservices are beginning to develop treatment provision in the commuincludes some chemotherapy provided at home by the independenSome community nursing services are developing teams with eclinical skills to extend the range of treatments and care community and decrease the need for hospital admission. In readvanced breast cancer care, this may include the monitoring obloods and care of central lines with support from hospital colleagues Consideration of community-based treatments raises considerable cincluding the development of quality assured clinical protocols pathways, enhanced clinical skills in the community, a clear understaclinical governance responsibilities and active communication concerned including out of hours providers. Logistical challenges suctiming of pharmacy preparation of regimens, safe physical delivery the treatment is to be administered (transport) and safe disposal containers are additional considerations. Clear arrangements management of chemotherapy complications would also be Irrespective of where treatment is administered, the patient who becneeds to know what to do, whom to contact first, as does the primprofession recognising an ill patient after chemotherapy together with agrpathways devised by oncology and primary care would minimise thadverse events. Economic and workforce implications requireconsideration to
Advanced breast cancer: full guideline DRAFT (August 2008) Page 71 of 146

DRAFT FOR CONSULTATION
Choice and Supportive and Palliative Care Patients with advanced breast cancer have complex physpsychosocial needs. Holistic care that aims to maximise quality ofrequires disease management and this is best achieved where osupportive and palliative care services are integrated. Achieving a stransition from active treatment to supportive and palliative care difficult. When the options for active treatment become limited patients’ insight into their poor prognosis develops, they will nee
1 ical and 2 life also 3 ncology, 4 eamless 5 may be 6 and the 7
d support in 8 iding their preferred place of care. 9
10 planning for end of life care, including dec Clinical Evidence 11
all RCTs One moderate quality but dated RCT (Mor et al., 1988), three sm12 one high (Hall and Lloyd, 2008, Smith et al., 1994 and Majid et al., 1989) and13 logies et quality Canadian systematic review (Agence d'Evaluation des Techno14
eral forms of home des Modes d'Intervention en Sante, 2004) looked at sev15 ne paper 16 therapy vs in-patient treatment for patients with cancer. Only o
17 specifically looked at breast cancer patients (Hall and Lloyd, 2008). 18
egard to None of the studies identified a significant clinical advantage with r19 there a treatment in the community compared with the hospital nor was20
f life, as measured by standard scales. However, difference in patient quality o21 ent across studies that patient satisfaction was there was broad agreem22
red with 23 considerably higher with treatment in the home or community compa24 the hospital in-patient experience.
25 Health Economic Evaluation 26
s originally considered a priority for economic Although this topic wa27 to make a evaluation, the lack of clinical evidence meant it was not possible 28
urther. recommendation. Therefore the economics were not investigated f29 30
Research Recommendation
31
plore whether patients with advanced breast cancer Research is needed to ex32 would prefer intravenous therapies to be delivered at home, near home or in 33 the hospital setting. 34
35
36 37
atient and 38 y. People 39
ve complex 40 t needs. 41
ed by family and social circumstances 42 for example individuals caring for young children or elderly parents may need 43 support to care for their dependents during treatment. Regular assessment of 44 such needs may help to ensure they are met and that people are signposted 45 to appropriate support. Access to supportive and palliative care can improve 46 the patient’s experience, but patients often report that they were unaware of 47 the psychosocial support services available. 48
5.2 Supportive Care A diagnosis of advanced breast cancer can be devastating for the ptheir family and carers leading to anxiety, depression and uncertaintwith advanced breast cancer and their families and carers often haand changing psychosocial, physical, spiritual and financial supporPsychosocial needs are often influenc
Advanced breast cancer: full guideline DRAFT (August 2008) Page 72 of 146

DRAFT FOR CONSULTATION
Patients with advanced breast cancer frequently report differences insupport available compared to when they were diagnosed with primacancer. In particular there appears to be less good access to ain many centres the breast care nurses’ role ends with the diagnosis advanced disease. Acc
the 1 ry breast 2
key worker, as 3 of 4
ess to a key worker has been shown to be beneficial to 5 6
solated. 7 the 8
ge of local 9 s, 10 forums. 11
to help them 12 the family. 13
their families and carers will 14 estions 15
16
cuments 17 anual Update 18
ults with 19 care nurse 20
d access to 21 practical support. The latter (which of course has a wider 22
n of care 23 for 24
25
A particular concern is the provision of care and support for younger patients 26 ortunately there is insufficient evidence to make a specific 27
patients and their families. A diagnosis of advanced breast cancer may leave patients feeling iThey may want to contact others with a similar diagnosis or to haveopportunity to talk about their emotions and fears. There are a ranand national support services available including counselling servicepsychologists, support groups, peer support, help lines and internet Families may also need access to psychosocial support servicescope with the impact of a diagnosis of advanced breast cancer onAt a later stage in the treatment, patients andhave to make choices about end of life preferences and will have quabout the type of palliative care services available. All these issues have been addressed in previous NICE guidance doon Cancer Services, ‘Improving Outcomes in Breast Cancer: M(NICE 2002) and Improving Supportive and Palliative Care for AdCancer (NICE 2004). The former emphasises the role of the breastin ensuring patient-centred care, effective communication anpsychosocial andfocus) also makes specific recommendations about the co-ordinatioand the ‘nomination of a person to take on the role of ‘key worker’individual patients’.
with families. Unfrecommendation for this group. 28
29
Recommendations 30 • Healthcare professionals involved in the care of patients with advanced 31
breast cancer should ensure that the organisation and provision of 32 supportive care services comply with the recommendations made in 33 previous NICE guidance documents (‘Improving outcomes in breast 34
lliative cancer: Manual update’ [2002] and ‘Improving supportive and pa35 llowing two 36 care for adults with cancer’ [2004]), in particular the fo
recommendations: 37 - ‘Assessment and discussion of patients’ needs for physical, 38
itual and financial support should be psychological, social, spir39 undertaken at key points such as diagnosis at commencement, during, 40 and at the end of treatment; at relapse; and when death is 41 approaching.’ 42
- ‘Mechanisms should be developed to promote continuity of care, which 43 might include the nomination of a person to take on the role of 'key 44 worker' for individual patients.’ 45
Advanced breast cancer: full guideline DRAFT (August 2008) Page 73 of 146

DRAFT FOR CONSULTATION
Qualifying statement: These recommendations are based on anecdotal 1 evidence and experience of GDG members that previous NICE guidance 2 has not been fully implemented and GDG consensus that implementation 3 would improve patients’ experience. 4
5 6
periences of home and 7 8
ling SM., 9 ndomized study of inpatient 10
11 12
ty AM., 13 Day hospital as an alternative to 14
in Epidemiol 15 16
y S., Andrews CD., Baister ER., Bilbrough C., 17 ital care in 18
al journal 19 20
21 (AETMIS)., Boothroyd L and Lehoux P (2004) Home-based chemotherapy for 22 cancer: issues for patients, caregivers and the health care system 13100. 23 ISBN: 2-550-42584-7 (French: 2-550-42578-2): xvi; 77p. 24
References Hall M and Lloyd H (2008). Evaluating patients' exhospital chemotherapy. Cancer Nursing Practice 7: 35-38
Magid DM., Vokes EE., Schilsky RL., Guarnieri CM., WhaWeichselbaum RR and Panje WR (1989) A raversus outpatient continuous intravenous infusion chemotherapy: psychosocial aspects. Sel Cancer Ther 5: 137-145.
Mor V., Stalker MZ., Gralla R., Scher HI., Cimma C., Park D., FlaherKiss M., Nelson P and Laliberte L (1988) inpatient care for cancer patients: a random assignment trial. J Cl41: 771-785.
Smith AG., Soutar RL., ScheConnelly M., Joyce A and Child JA (2004) Home care versus hosppatients with multiple myeloma treated with pamidronate. Internationof palliative nursing 10: 144-149.
Agence d'evaluation des technologies et des modes d'intervention en sante
Advanced breast cancer: full guideline DRAFT (August 2008) Page 74 of 146

DRAFT FOR CONSULTATION
6 Management of Specific Probl ems 1 2
6.1 Lymphoedema 3 4
lymphatic 5 side of the 6 ulting in 7
infections 8 e axilla it can 9
cal 10 lti-professional team 11
including allied health professionals, clinical psychologists and tissue viability 12 13 14
because of 15 16
isease. 17 disease 18
nt during the illness, when it may be a sign of loco-19 20
ase, are 21 22 23
t there are 24 25 26
Complex Decongestive Therapy (CDT6) is the recognised conservative 27 setting 28 ed or 29
30
tensive period of ays per week) for up to six weeks delivered by a
healthcare professional trained in its use. It includes: 34 35
aging (MLLB) 36
rages the transfer of care from professional to patient/carers and includes: 41
• provision and use of compression/containment garments 42 43
• self skin care and exercise programme 44 • nocturnal bandaging in some circumstances. 45
Lymphoedema is a swelling of body tissue caused by failure of thesystem. In patients with breast cancer it is usually the arm on theoriginal breast cancer that is affected. It is a chronic condition resdiscomfort, pain, functional limitation, increased risk of recurrentand psychological distress. In combination with disease in thincrease pressure over the brachial plexus compromising neurologifunction. Patients may need access to a wide mu
services as well as dedicated lymphoedema therapists. Patients with advanced breast cancer may develop lymphoedema damage to the lymph nodes and vessels following surgery or radiotherapy, or by the pathological changes associated with progressive localised dLymphoedema can be present at the time of diagnosis of advancedor develop at any poiregional disease progression. It is important that potential underlying causes such as axillary thrombosis, extensive axillary or supraclavicular diseinvestigated and treated. Early identification and management of the swelling is important, buno agreed diagnostic tests and assessment methods.
management of lymphoedema (Rockson et al. 1998). In the palliativetreatment modifications may be required and outcomes may be reducd iciff ult to maintain. 31
f two main phases. The initial phase is an inCDT consists o32 daily treatment (five d33
• manual lymphatic drainage (MLD) • multi-layer lymphoedema band• skin care 37
38 • remedial exercise. 39 The second, a maintenance phase, encou40
• simple lymph drainage (self/carer administered)
6 Complex decongestive therapy (CDT) is also known as Decongestive Lymphatic Therapy (DLT) and Complex Physical Therapy (CPT)
Advanced breast cancer: full guideline DRAFT (August 2008) Page 75 of 146

DRAFT FOR CONSULTATION
Lymphoedema is a chronic condition and the patient will need regular check-1 ups (and further intensive treatment if needed) for the rest of their life. 2
3 he patient with 4
5 6
, manual 7 may cause spread of the tumour but there is no 8
9 10
uidelines 11 eness in 12 ce about 13
such as radiotherapy to obstructing tumour 14 cellulitis 15
16 17
ema in 18 an be modified to fit 19
the needs of specific patients but this will require input from a lymphoedema 20 e recommendations are equally appropriate for the 21
cer.
It may however not be clinically appropriate or acceptable to tadvanced breast cancer to participate in such an extensive programme. Concerns have been raised that the massage component of CDTlymphatic drainage (MLD)evidence to support this belief. Although CDT is widely used, there are currently no national gabouts its use, and very little reliable evidence about its effectivpatients with advanced breast cancer. Equally there is little evidenthe use of other interventions masses or bulk reduction surgery. It is also very uncertain howshould be managed in these patients. The recommendations below apply to the management of lymphoedpatients with advanced breast cancer. These treatments c
specialist. Thesmanagement of lymphoedema in patients with early breast can22 23 Recommendations 24 • Assess patients with advanced breast cancer and lymphoedema for 25
treatable underlying factors before starting any lymphoedema 26 management programme. 27
• Offer all patients with lymphoedema related to advanced breast cancer 28 complex decongestive therapy (CDT) as the first form of lymphoedema 29 management. 30
• Consider using multi-layer lymphoedema bandaging (MLLB) for volume 31 reduction, as a first treatment option before compression hosiery. 32
• Provide patients with advanced breast cancer and lymphoedema with at 33 least two suitable compression garments. These should be of the 34
olours should be 35 appropriate class and size, and a choice of fabrics and cavailable. 36
nts with advanced breast cancer and lymphoedema with the • Provide patie37 ils of local and national lymphoedema support groups. 38 contact deta
39 G Qualifying statement: these recommendations are based on GD40 tients with 41 consensus and extrapolation of evidence of the management of pa
42 43
early breast cancer. Clinical Evidence 44 Fourteen papers addressed the topic of lymphoedema management 45 comprising a guideline (Harris et al., 2001) one very high quality systematic 46 review (Moseley et al., 2007) two systematic reviews of less quality (Kligman 47 et al., 2004 and Rinehart-Ayres et al., 2007) four randomised trials (Didem et 48 al., 2005, Irdesel et al., 2007, Badger et al., 2004 and Johansson et al., 2005) 49 and five case series or phase II studies (Vignes et al., 2007; Hamner and 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 76 of 146

DRAFT FOR CONSULTATION
Fleming, 2007; Sitzia et al., 2002, Kim et al., 2007, Koul et al., 2007 and 1 management Fiaschi et al. 1998). These papers all addressed lymphoedema 2
active in women who had been treated for breast cancer but did not have3 er. The disease and, as such, the evidence only related to early breast canc4
(CDT), manual treatments evaluated included complex decongestive therapy5 D), pneumatic compression bandaging/garments, 6 lymph drainage (ML
7 massage and exercise. 8
rapists and Intensive treatments, such as CDT and MLD, given by trained the9 aintenance other health professionals, yielded better results than simpler m10
home. treatments performed by the patient, carer or family member in the 11 ema reduction and 12 Patients given CDT experienced significant lymphoed
13 improvement in quality of life outcomes but an association between variables 14 could not be proved definitively by a non-randomised study. 15
Pneumatic compression therapy was not significantly better at reducing limb 16 , when volume when compared with no treatment, education or MLD but17 girth. 18 added to MLD, significantly improved oedema reduction and limb
19 Multi-layer bandaging with hosiery was significantly better at reducing limb 20
21 volume when compared with hosiery alone, an improvement still significant 22 after six months.
23 ation Health Economic Evalu24
ic priority; therefore The GDG did not consider this topic as a health econom25 the cost-effectiveness literature on this topic has not been reviewed. 26 27 Research recommendation 28 • Research is needed to compare the effectiveness of complex 29
s intensive interventions in patients with 30 decongestive therapy with les31 advanced breast cancer. The research should incorporate both objective
and quality of life measures. 32 33 34 35
gue (CRF) is a symptom of advanced cancer. Patient 36 37
ctive sense of 38 sual 39
ality of life over 40 41 42
g the 43 cancer treatment itself, anaemia, nutritional factors, psychological factors, 44 cognitive factors, sleep disorders, inactivity and medications. Many advanced 45 breast cancer patients may have co-existing chronic illness which may 46 increase the severity of fatigue and complicate its management. As the 47 disease progresses the experience of fatigue tends to intensify. The 48 relationship between internal factors, both physiological and psychological, 49
6.2 Cancer-related Fatigue
Cancer-related fatiadvocates report that it frequently goes unrecognised. CRF is defined by the National Comprehensive Cancer Network as “a persistent, subjetiredness related to cancer or cancer treatment that interferes with ufunctioning”. If unrelieved the symptoms of CRF can impair qua long period of time. There are a variety of factors thought to contribute to CRF includin
Advanced breast cancer: full guideline DRAFT (August 2008) Page 77 of 146

DRAFT FOR CONSULTATION
and external environmental factors, as causal, modifying, or associated 1 factors in CRF has not been fully investigated. 2
3 en identified 4
gs that 5 ssants 6
7 ication, cognitive behavioural therapies, exercise and complementary 8
9
Once treatable factors such as anaemia and depression have beand treated, the current management of CRF is unsatisfactory. Druhave been used include glucocorticoids, psychostimulants, antidepreand erythropoietin. Non-pharmacological interventions include communtherapies. 10 Recommendations 11 • Offer all patients with advanced breast cancer for whom fatigue is a 12
significant problem an assessment to identify any treatable causative 13 factors and offer appropriate management as necessary. 14
tions that offer • Provide clear, written information about fatigue, organisa15 16 psychosocial support and patient-led groups.
17 Qualifying Statement: These recommendations are based on GDG18
consensus and very poor quality evidence. 19 20 • Provide information about and timely access to an exercise programme for 21
ast cancer experiencing cancer-related 22 all patients with advanced brefatigue. 23
ality Qualifying statement: This recommendation is based on a high-qu24 25 26
systematic review and meta-analysis. Clinical Evidence 27
ement of cancer-related fatigue (CRF) comprised two 28 Evidence on the managsystematic reviews (Minton et al., 2007 and Cramp & Daniel, 2008) one on 29
30 drug therapies and one on exercise regimes, together with two RCTs31 (Headley et al., 2004 and Bordeleau et al., 2003) and a poor quality case 32 series (Carson et al., 2007).
33 roids, Good evidence showed no significant effect of progestational ste34
t of CRF. 35 including megesterol acetate, compared with placebo in the treatmen 36
t effect of Meta-analysis of data from 28 RCTs showed a highly significan37 r patients exercise compared with controls on fatigue reduction both in cance38 eview as a whole and in a large sub-group with breast cancer. Since the r39
on could not 40 included all forms of exercise, a specific regime, intensity or duratibe recommended. 41 42 There were no positive outcomes from a yoga program, seated exercise 43 activity or weekly support group meetings with respect to improving levels of 44 fatigue as assessed by standard measurement tools. No papers were 45 identified to determine the effectiveness of cognitive behavioural therapy or 46 psychotherapy in patients with advanced breast cancer. 47 48
Advanced breast cancer: full guideline DRAFT (August 2008) Page 78 of 146

DRAFT FOR CONSULTATION
Health Economic Evaluation 1 riority; therefore The GDG did not consider this topic as a health economic p2
the cost-effectiveness literature on this topic has not been reviewed. 3 4
Research recommendation 5 • Randomised controlled trials are needed to assess the value of 6
psychological interventions in the management of fatigue in patients with 7 advanced breast cancer. Both short- and long-term outcomes should be 8 evaluated. An appropriate validated tool to measure fatigue should be 9 used. 10
• Further research is required into which excercise programmes are most 11 12 effective for patients with advanced breast cancer and to identify the most
efficient way to deliver these in an NHS service. 13 14 15 16
with skin 17 anable to 18 patients 19 sease. A 20 d causing 21 ns are a 22
rom both 23 24
it repulsive and difficult to deal with, both physically and emotionally, and this 25 may not 26
y or healthcare 27
nsider including: tion and its associated consequences such as
33 34 35 36
eeding 37 38
individualised and h is therefore ologists and
Recommendations
6.3 Uncontrolled local disease Patients with advanced breast cancer may develop local disease ulceration involving the chest wall and axilla which is initially amesystemic treatments, radiotherapy or surgery. Ultimately, in somethese options may be exhausted, resulting in uncontrolled local difungating tumour may bleed, exude a discharge and become infectepain and an unpleasant smell. For the patient the symptoms and sigvisible reminder of their illness and may lead to social isolation ffriends and close relatives, and further psychological distress. Carers may find
may exacerbate physical and social isolation. Sometimes patientseven disclose the existence of a fungating tumour to their familprofessionals until it has become well established. 28 29 Uncontrolled local disease is a d30 ifficult clinical condition either to eradicate or to palliate. There are a number of important issues to co31
• Control of infe32 unpleasant smell
c
• Management of the wound • Management of social and psychological consequences • Management of pain • Control of bl
The management of uncontrolled local disease needs to be39 will usually involve a combination of treatments. A team approac40 very important and will include nurses, surgeons, onc41 psychological support. 42 43
44 • A breast cancer multidisciplinary team should assess all patients 45
presenting with uncontrolled local disease and discuss the therapeutic 46 options for controlling the disease and relieving symptoms. 47
• A wound care team should see all patients with fungating tumours to plan 48 a dressing regimen and supervise management with the breast care team. 49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 79 of 146

DRAFT FOR CONSULTATION
• A palliative care team should assess all patients with uncontrolled local 1 disease and their families in order to plan a symptom management 2 strategy and to provide psychological support. 3
ns are based on poor quality Qualifying statement: These recommendatio4 evidence, expert position papers and GDG consensus. 5
6 Clinical Evidence 7
sease was The standard of publications on the topic of uncontrolled local di8 r et al., very poor comprising seven low patient number case series (Bowe9
1987; 1992; Kuge et al., 1996; Lund-Nielsen et al., 2005; Kumar et al., 10 005), the Kolodziejski et al., 2005, Faneyte et al.. 1997 and Pameijer et al., 211
cerned women majority of which were retrospective. Whilst the studies con12 classified as fungating, others with breast cancer, some with wounds clearly 13
chest wall, the evidence was considered 14 with local recurrence in the15 inadequate and a position paper was commissioned.
16 Health Economic Evaluation 17
r this topic as a health economic priority; therefore The GDG did not conside18 the cost-effectiveness literature on this topic has not been reviewed.19
20 Research Recommendation 21 • The relevant research organisations should be encouraged to address the 22
al disease and devise appropriate research topic of uncontrolled loc23 ter. studies. This might include development of a national regis24
25
reast 29 30 31
nal cord 32 33 34
A variety of different treatments including bisphosphonates, external beam 35 actions), radionuclide therapy 36
Although bisphosphonates are frequently 37 38
40 41 42
dations
6.4 Bone metastases 26 27 Modern systemic anti-cancer treatment means that patients with b28 cancer may live with bone metastases for a long time. Management involves:
• trying to prevent skeletal events • controlling pain • treating complications such as fractures, immobility, and spi
compression.
radiotherapy (given in a single or with multiple frand surgical fixation are available.used, it is not clear whether oral or intravenous therapy is better or which bisphosphonate is the most effective. 39 Rehabilitation may also be important for these patients. Recommen43 • Offer bisphosphonates to patients newly diagnosed with bone metastases, 44
to prevent skeletal-related events and to reduce pain. 45 Qualifying statement: This recommendation is based on strong evidence of 46 clinical effectiveness in reducing skeletal related events and pain, and 47 reasonable evidence of cost effectiveness for the NHS in preventing skeletal 48 related events. 49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 80 of 146

DRAFT FOR CONSULTATION
1 • The choice of which bisphosphonate to use for patients with bone 2
metastases should be a local decision, taking into account patient 3 preference and limited to preparations licensed for this indication. 4
consensus Qualifying statement: This recommendation was based on GDG5 e clinical effectiveness and 6 that there was no strong evidence of comparativ
conflicting evidence of comparative cost effectiveness. 7 8 • Use external beam radiotherapy in a single fraction of 8 Gy to treat 9
bone metastases and pain patients with10 Qualifying statement: This recommendation was based on evidence from 11 randomised trials. 12 13 • An orthopaedic surgeon should assess all patients at risk of a long bone 14
onsider prophylactic surgery. fracture, to c15 DG consensus. Qualifying statement: This recommendation was based on G16
17 Clinical Evidence 18
included a The evidence base on the management of bone metastases 19 02), five RCTs systematic review (Sze et al., 2002), a guideline (Warr et al., 2020
rdley et al., (Tripathy et al., 2004, Hartsell et al., 2005, Salazar et al., 2001, Wa21 s 22 2005 and Rasmussen et al., 1995), two comparative or cohort studie
(Weinfurt et al., 2004 and Pecherstorfer et al., 2006) and six case series 23 Gristina et al., 1983, Scarantino et (Broos et al.,1993, Gerszten et al., 2005,24
were no papers al., 1996, Borojevic et al., 1999 and Durr et al., 2002). There 25 as part of 26 dealing specifically with solitary bone metastases, bone metastases
27 wider metastatic disease or rehabilitation. 28
hilst Good evidence, including a treatment guideline, suggested that w29 reduce pain bisphosphonates made little impact on overall survival, they could30
e to and the occurrence of skeletal events. There was no comparative evidenc31 respect. A suggest that one bisphosphonate was better than others in any32
ate and meta-analysis found no significant difference between oral clodron33 isease-34 placebo or no treatment in terms of bone metastasis-free survival, d
35 free survival or non-skeletal metastasis-free survival. 36
ysis, High quality evidence, including a systematic review with meta-anal37 ere equally demonstrated that single and multiple fractions of radiotherapy w38
rong evidence that single fractions effective at relieving pain. There was no st39 ression. resulted in a higher rate of subsequent fracture or spinal cord comp40
ce in outcomes between stereotactic radiosurgery as salvage An equivalen41 therapy after disease progression with conventional radiotherapy and upfront 42
viously external beam radiotherapy suggested a possible treatment for pre43 tment options left. irradiated patients with few trea44
45 The evidence on the use of radiotherapy to prevent skeletally related events 46 was equivocal. 47 48 Four observational studies provided limited evidence suggesting a potential 49 role for surgery in giving pain relief. 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 81 of 146

DRAFT FOR CONSULTATION
1 Health Economic Evaluation 2
dentified from Six papers were selected from the original list of 959 papers i3 s the search of economic evidence. Despite the numerous intervention4 onates in identified for this topic, all six papers referred to the use of bisphosph5
idence on the prevention of skeletal related events. There was no economic ev6 ared all the use of bisphosphonates for pain relief. None of the studies comp7 ividually the bisphosphonates against each other; instead they were either ind8
er of compared against no treatment or compared against a limited numb9 alternatives. All presented cost-utility analyses, four of which were undertaken 10
11 in a UK setting, the other two in America and Canada. 12
ent report One of the six papers in the review is a Health Technology Assessm13 then) (Ross et al, 2004). This report presents an economic review of the (14
ffectiveness published literature, and also a model which estimates the cost-e15 skeletal of pamidronate in the treatment of hypercalcaemia and prevention of16
ally, it morbidity. Although the report is not limited to breast cancer specific17 does report findings in patients with breast cancer separately, and on that 18
e that it is an basis is included in this review. The HTA report has the advantag19 rs. 20 independent analysis, unlike the other three UK economic pape
21 s from The model built for the HTA report (Ross et al, 2004) considers cost22 t the both a hospital and social care perspective. The report indicates tha23 erable community care costs associated with fracture care might be consid24
ess of and if omitted might substantially underestimate the cost-effectiven25 te is highly bisphosphonates. The authors conclude that the use of pamidrona26 prevention cost-effective (£1,300 per QALY compared to no treatment) in the 27
metastases, of skeletal morbidity in patients with breast cancer and skeletal 28 r variables are and that it may be cost-saving when fracture care, and/or othe29
ourably low taken into account. Despite the basecase analysis yielding a fav30 igh degree incremental cost-effectiveness ratio, the results are subject to a h31
ult is of uncertainty. In their analysis the base case cost-effectiveness res32 o sensitive to bisphosphonate cost, event rate and events costs but n33
y do sensitivity analysis on the cost-utility analysis is made explicit. The34 one-way sensitivity analysis on the cost-effectiveness analysis present a35
showing the worst case scenario ranges from cost-saving to a incremental 36 r than the cost per skeletal related event per patient averted is 53 times highe37 f £1,380 baseline result. If we apply this to the baseline cost-utility estimate o38 73,140 39 per QALY, bisphosphonates could range from being cost-saving to £
40 per QALY. 41
ptions 42 The most recent study, Botteman et al 2006, uses many of the assumemployed by Ross et al 2004, but updates the costs used and incorporates 43 results of a recent zoledronic acid vs. placebo trial. The authors conclude that 44 zoledronic acid dominates other bisphosphonates (it is both less costly and 45 more effective), although it should be noted that this study includes authors 46 employed by the manufacturers of zoledronic acid. De Cock et al on the other 47 hand, in their two papers (chemotherapy treated patients 2005a, and hormone 48 therapy patients 2005b) both of which include authors from the manufacturer 49
Advanced breast cancer: full guideline DRAFT (August 2008) Page 82 of 146

DRAFT FOR CONSULTATION
of ibandronate, infer that oral ibandronate dominates i.v. zoledronic acid and 1 i.v. pamidronate. 2
3 The North American studies reported very different levels of cost-4
. These ratios effectiveness (range CAN$18,000 to US$305,000 per QALY)5 t be cost effective compared to no 6 imply that bisphosphonates may no
7 treatment in a North American context. 8
ctive The economic modelling from a UK NHS and social services perspe9 of conducted in the studies included in this review indicates that use 10
reast cancer bisphosphonates in the management of bone metastases from b11 nflicting appears to be cost-effective. However the papers reviewed show co12
st cost-effective. Since evidence over which of the bisphosphonates is mo13 s of drugs seem to be highly cost-effective, further bisphosphonates as a clas14 not considered a high priority. independent analysis was 15
16 17 18
tic brain 19 in 20 ause the 21
er prevents access of most chemotherapy or targeted drugs 22 mprovements in 23
ervous 24
ses can have profound physical and ) because of:
29 30 31
iotherapy and 32 33 34 35 36 37
ave a 38 tases; this 39 for 40
immediate symptom relief but only reduce the inflammatory oedema with no 41 rm because of 42
t patients will 43 then also have whole brain radiotherapy (WBRT) which may improve their 44 symptoms and function and allow the dose of corticosteroids to gradually be 45 reduced. Systemic therapies may also be effective treatment. 46 47 Any treatment decision needs to take into account that the chances of a 48 clinical benefit are reduced by poor performance status, increased age, 49
6.5 Brain Metastases Some patients with advanced breast cancer will develop symptomametastases, usually at multiple sites. The highest incidence of brametastases is in women with HER2-overexpressing tumours. Becblood–brain barriprescribed for treatment of primary or metastatic disease, isystemic treatment may lead to an increasing incidence of central nsystem metastases. 25 26 The diagnosis of brain metasta27 psychological effects on the patient (and their family and carers28
• Loss of independence, • Physical deterioration • Communication difficulties • Issues with body image (such as hair loss from rad
weight gain from corticosteroids). Further distress can result from the patient realising that they have progressive disease and a particularly poor prognosis. The three main treatment options are surgery, corticosteroids and radiotherapy. Surgery is usually only considered for patients who hsolitary metastasis or occasionally a limited number of brain metasapplies to the minority of patients. Corticosteroids are usually given
direct effect on the tumour. High doses cannot be given long tesignificant side effects and eventual disease progression. Mos
Advanced breast cancer: full guideline DRAFT (August 2008) Page 83 of 146

DRAFT FOR CONSULTATION
multiple lobes of the brain being affected and having uncontrolled metastases 1 elsewhere. 2
3 ored to 4 tive care; 5
and input 6 sts; social care; psychological support and 7
choose place of care. 8
Whether or not active intervention is offered, full supportive care tailthe individual will be required for all patients. This may include palliarehabilitation with physiotherapy, occupational therapy assessmentfrom speech and language therapithe opportunity to 9 Recommendations 10 • Offer surgery followed by whole brain radiotherapy to patients who have a 11
single or small number of potentially resectable brain metastases, a good 12 performance status and who have no or well-controlled other metastatic 13 disease. 14
• Offer whole brain radiotherapy to patients for whom surgery is not 15 appropriate, unless they have a very poor prognosis. 16
• Offer active rehabilitation to patients who have surgery and/or whole brain 17 radiotherapy 18
active treatment for brain metastases would be • Patients for whom 19 inappropriate should be referred for specialist palliative care. 20
These recommendations are based on evidence from Qualifying statement: 21 22 23
retrospective case series. Clinical Evidence 24
mainly The papers addressing the management of brain metastases were25 retrospective case series none of which were of particularly good quality. 26
27 Most studies did not differentiate between single, multiple or solitary metastases. Two papers specifically addressed the treatment of 28
1996). 29 leptomeningeal metastases (Rudnicka et al., 2007 and Fizazi et al., 30
et al., 1997) Papers were reviewed on surgery (Pieper et al., 1997 and Wroski31 stereotactic radiosurgery (Comb et al., 2004, Lederman et al., 2001,32
urek et al., Amendola et al., 2000, Firlik et al., 2000, Levin et al., 2002, Aky33 t al., 2006, Rosner et 2007 and Muacevic et al., 2004) chemotherapy (Rivera e34
al., 1986, Boogerd et al., 1992, Franciosi et al., 1999, Oberhoff et al., 2001, 35 WBRT) Lassman, 2006 and Trudeau, 2006) and whole brain radiotherapy (36
Szpytma 1987, (Bartsch et al., 2006, Fokstuen et al., 2000, Korzeniowski and37 ahmoud-38 Lenztsch et al., 1999, Liu et al., 2006, Ogura et al., 2003 and M
39 Ahmed et al., 2002, Viani et al., 2007 and Johansen et al., 2008). 40
between 41 WBRT of cerebral metastases resulted in median overall survival ofapproximately 4 and 7 months. Patients who received whole brain 42
ry had improved survival with a median overall radiotherapy after surge43 survival of approximately 15 to 16 months. However, where measured, 44 performance status did not improve as a result of surgery. Recursive partition 45 analyses of retrospective WBRT data by one group identified prior surgery, 46 absence of extracranial metastases and RPA class I as significant prognostic 47 factors for survival. A much smaller study found only single vs multiple brain 48 metastases of significance. 49 50
Advanced breast cancer: full guideline DRAFT (August 2008) Page 84 of 146

DRAFT FOR CONSULTATION
Treatment with stereotactic radiosurgery (SRS) resulted in median overall 1 ients with survival ranging from 7.5 to 15 months. Of those receiving SRS, pat2
better survival smaller tumours seemed to fare better. Most studies predicted3 First-line for younger patients and those with good performance status. 4
esponse and survival to 5 therapy with SRS was comparable in terms of r6 salvage therapy after WBRT in one poor quality study.
7 reported The studies analysing data on a variety of chemotherapeutic agents8 ers were extremely variable response and survival data and, as patient numb9
red to be low in each study, no one agent or combination of agents appea10 stases. Response rates of better than any other in the treatment of brain meta11
up to 64% were reported with median overall survival to a maximum of 61 12 13 months in one study. The standard of evidence was weak.
14 study, Chemotherapy, including high dose intravenous methotrexate in one15
es and 16 appeared to be crucial in the treatment of leptomeningeal metastasboth intrathecal and intravenous chemotherapy improved patient survival. 17
wn in other studies to have improved quality of life 18 WBRT may have been sho19 but had a questionable effect on survival for these patients.
20 Health Economic Evaluation 21 The GDG did not consider this topic as a health economic priority; therefore 22
wed. the cost-effectiveness literature on this topic has not been revie23 24
Research Recommendation 25 ised controlled trial is needed to compare stereotactic • A random26
anced radiotherapy with whole brain radiotherapy in patients with adv27 astases. breast cancer and solitary or a limited number of brain met28
29 ces 30
athews 31 gical 32
cancer. Am J Clin Oncol 33 34
Gamma 35 brain 36
rcinoma of the breast. Cancer J 6, 88-92. 37
d, controlled, 38 by hosiery 39
a of the limb. 40 41
Bartsch R., Fromm S., Rudas M., Wenzel C., Harbauer S., Roessler K., Kitz 42 K., Steger GG., Weitmann HD., Poetter R., Zielinski CC and Dieckmann K 43 (2006) Intensified local treatment and systemic therapy significantly increase 44 survival in patients with brain metastases from advanced breast cancer - a 45 retrospective analysis Rad Oncol 80, 313-317. 46
ReferenAkyurek S., Chang EL., Mahajan A., Hassenbusch SJ., Allen PK., MLA., Shiu AS., Maor MH and Woo SY (2007) Stereotactic radiosurtreatment of cerebral metastases arising from breast 30: 310-314
Amendola BE., Wolf AL., Coy SR., Amendola M and Bloch L (2000) knife radiosurgery in the treatment of patients with single and multiplemetastases from ca
Badger CMA., Peacock JL and Mortimer PS (2000) A randomizeparallel-group clinical trial comparing multilayer bandaging followedversus hosiery alone in the treatment of patients with lymphedemCancer 88: 2832-2837.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 85 of 146

DRAFT FOR CONSULTATION
Boogerd W., Dalesio O., Bais EM and van der Sande JJ (1992). Rebrain m
sponse of 1 etastases from breast cancer to systemic chemotherapy. Cancer 69: 2
972-980. 3
., Doll R., 4 lewellyn-5
6 ancer: 7
J Clin 8 9
Radosevic L (1999) Bone metastases in 10 erent fractionation 11
12
6). "Cost effectiveness of 13 bone 14
15
16 tment of 17
18
ical 19 of life. 20
21
iller JM (2007) 22 pilot study 134. 23
33: 331-341. 24
004). 25 Treatment of cerebral metastases from breast cancer with stereotactic 26
27
t of cancer-related 28 atic Reviews: Reviews. 29
andronate 30 dronate in 31
ts with metastatic bone disease undergoing i.v. 32 chemotherapy." Support Care Cancer 13(12): 975-986. 33
ibandronate 34 ne metastases in patients 35
receiving oral hormonal therapy for breast cancer in the United Kingdom. Clin 36 Ther 27(8): 1295-1310. 37
Didem K., Ufuk YS., Serdar S and Zümre A (2005) The comparison of two 38 different physiotherapy methods in treatment of lymphedema after breast 39 surgery. Breast cancer research and treatment 93: 49-54. 40
Bordeleau L., Szalai JP., Ennis M., Leszcz M., Speca M., Sela RChochinov HM., Navarro M., Arnold A., Pritchard KI., Bezjak A., LThomas HA., Sawka CA and Goodwin PJ (2003) Quality of life in a randomized trial of group psychosocial support in metastatic breast coverall effects of the intervention and an exploration of missing data 34. Oncol 21: 1944-1951.
Borojevic N., Golubicic I and Jelic-breast cancer patients: Efficacy of radiotherapy with diffschedules 669. Journal of B 4: 167-172.
Botteman, M., V. Barghout, et al. (200bisphosphonates in the management of breast cancer patients with metastases." Ann Oncol 17(7): 1072-1082.
Bower M., Stein R., Evans TR., Hedley A., Pert P and Coombes RC (1992) A double-blind study of the efficacy of metronidazole gel in the treamalodorous fungating tumours 57. Eur J Cancer 28A: 888-889.
Broos P., Reynders P., van den BW and Vanderschot P (1993) Surgtreatment of metastatic fracture of the femur improvement of qualityActa Orthop Belg 59 Suppl 1: 52-56.
Carson JW., Carson KM., Porter LS., Keefe FJ., Shaw H and MYoga for women with metastatic breast cancer: results from aJournal of Pain & Symptom Management
Combs SE., Schulz-Ertner D., Thilmann C., Edler L and Debus J (2
radiosurgery. Strahlenther Onkol 180: 590-596.
Cramp F and Daniel J (2008) Exercise for the managemenfatigue in adults. Cochrane Database of System
De Cock E., J. Hutton, et al. (2005a). "Cost-effectiveness of oral ibcompared with intravenous (i.v.) zoledronic acid or i.v. generic pamibreast cancer patien
De Cock E., J. Hutton, et al. (2005b). Cost-effectiveness of oral versus IV zoledronic acid or IV pamidronate for bo
Advanced breast cancer: full guideline DRAFT (August 2008) Page 86 of 146

DRAFT FOR CONSULTATION
Durr HR., Muller PE., Lenz T., Baur A., Jansson V and Refior HJSurgical treatment of bone metastases in pat
(2002) 1 ients with breast cancer 614. 2
Clinical Orthopaedics & Related Research 191-196. 3
section in 4 east carcinoma - Indications and outcome 5
6
7 Manual lymphatic drainage for chronic post-mastectomy lymphoedema 8
9
S., Kondziolka D., Flickinger JC and Lunsford LD (2000). Stereotactic 10 col 7: 11
12
Palangie T., 13 zeboc P., Dorval T and Pouillart P (1996). Meningeal carcinomatosis in 14
patients with breast carcinoma. Clinical features, prognostic factors, and 15 7: 1315-16
17
mklao T 18 f brain 19
6. 20
V., Cocconi G., Michiara M., Di CF., Fosser V., Tonato M., Carlini 21 P., Boni C and Di SS (1999). Front-line chemotherapy with cisplatin and 22
inoma, nonsmall 23 udy Cancer 85: 24
25
BC., 26 C and Vogel WJ (2005) Single-fraction radiosurgery for the 27
28
breast 29 atment with internal fixation and study of survival 522. Ann Surg 30
31
leming MD (2007) Lymphedema therapy reduces the 32 volume of edema and pain in patients with breast cancer. Ann Surg Oncol 14: 33
34
ractice 35 guidelines for the care and treatment of breast cancer: 11. Lymphoedema. 36 CMAJ 164: 191-199. 37
Hartsell WF., Scott CB., Bruner DW., Scarantino CW., Ivker RA., Roach M., 38 Suh JH., Demas WF., Movsas B., Petersen IA., Konski AA., Cleeland CS., 39 Janjan NA and DeSilvio M (2005) Randomized trial of short- versus long-40
Faneyte IF., Rutgers EJT and Zoetmulder FAN (1997) Chest wall rethe treatment of locally recurrent brfor 44 patients 325. Cancer 80: 886-891.
Fiaschi E., Francesconi G., Fiumicelli S., Nicolini A and Camici M (1998)
treatment. Panminerva Med 40: 48-50.
Firlik Kradiosurgery for brain metastases from breast cancer. Ann Surg On333-338.
Fizazi K., Asselain B., Vincent-Salomon A., Jouve M., Dieras V.,Beu
results of a high-dose intrathecal methotrexate regimen. Cancer 71323.
Fokstuen T., Wilking N., Rutqvist LE., Wolke J., Liedberg A., Signoand Fernberg JO (2000). Radiation therapy in the management ometastases from breast cancer. Breast Cancer Res Treat 62: 211-21
Franciosi
etoposide for patients with brain metastases from breast carccell lung carcinoma, or malignant melanoma: a prospective st1599-1605.
Gerszten PC., Burton SA., Welch WC., Brufsky AM., Lembersky Ozhasoglu treatment of spinal breast metastases 46. Cancer 104: 2244-2254.
Gristina AG., Adair DM and Spurr CL (1983) Intraosseous metastaticcancer tre197: 128-134.
Hamner JB and F
1904-1908.
Harris SR., Hugi MR., Olivotto IA and Levine M (2001) Clinical p
Advanced breast cancer: full guideline DRAFT (August 2008) Page 87 of 146

DRAFT FOR CONSULTATION
course radiotherapy for palliation of painful bone metastases 1043. J Natl 1 Cancer Inst 97: 798-804. 2
xercise on 3 ty of life in women with advanced breast cancer. Oncol Nurs 4
5
6 lated lymphedema. 7
8
C (2005) Low intensity 9 10 11
e of 12 7: 261-266 13
Kim SJ., Yi CH and Kwon OY (2007) Effect of complex decongestive therapy 14 teral 15
16
treatment of 17 ence 18
(Review) (30 refs). Support Care Cancer 12: 421-431. 19
ickness 20 st Journal 21
22
Patients 23 e 8: 25-30. 24
XY and Cooke AL 25 nual lymphatic 26
tional 27 y Biology Physics 67: 841-846 28
., 29 30 31 32
Kumar A., Shah LL., Khanna S and Khanna NN (1987) Preoperative 33 chemotherapy for fungating breast cancer 147 12723. J Surg Oncol 36: 295-34 298. 35
Lassman AB (2006) Systemic high-dose intravenous methotrexate for central 36 nervous system metastases. J Neurooncol 78: 255-260 37
Headley JA., Ownby KK and John LD (2004) The effect of seated efatigue and qualiForum 31: 977-983.
Irdesel J and Kahraman CS (2007) Effectiveness of exercise and compression garments in the treatment of breast cancer reFtr - Turkiye Fiziksel Tip Ve Rehabilitasyon Dergisi 53: 16-21.
Johansson K., Tibe K., Weibull A and Newton Rresistance exercise for breast cancer patients with arm lymphedema with or without compression sleeve. Lymphology 38: 167-180.
Johansen R., Westin AA., Bofin AM and Lundgren S (2008) Outcomwhole-brain irradiation for breast cancer patients. Acta Oncol 4
on edema and the quality of life in breast cancer patients with unilalymphedema. Lymphology 40: 143-151
Kligman L., Wong RK., Johnston M and Laetsch NS (2004) Thelymphedema related to breast cancer: a systematic review and evidsummary.
Kolodziejski LS., Wysocki WM and Komorowski AL (2005) Full-thchest wall resection for recurrence of breast malignancy 277. Brea11: 273-277.
Korzeniowski S and Szpytma T (1987) Survival of Breast-Cancerwith Brain Metastases Treated by Irradiation. J Eur Radiotherapi
Koul R., Dufan T., Russell C., Guenther W., Nugent Z., Sun(2007) Efficacy of complete decongestive therapy and madrainage on treatment-related lymphedema in breast cancer. InternaJournal of Radiation Oncolog
Kuge S., Tokuda Y., Ohta M., Okumura A., Kubota M., Ninomiya SSawamura S., Makuuchi H., Tajima T and Mitomi T (1996) Use of metronidazole gel to control malodor in advanced and recurrent breast cancer 86. Jpn J Clin Oncol 26: 207-210.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 88 of 146

DRAFT FOR CONSULTATION
Lederman G., Wronski M and Fine M (2001) Fractionated radiosubrain metastase
rgery for 1 s in 43 patients with breast carcinoma. Breast Cancer Res 2
Treat 65: 145-154. 3
1999) Brain 4 ast cancer: prognostic factors and management. Eur J 5
6
orano L 7 (2002) Gamma knife radiosurgery in patients with advanced breast cancer 8
9
CC., Huang CY 10 in 11
12
2005) Qualitative and quantitative 13 h advanced 14
15
ud-Ahmed AS., Suh JH., Lee SY., Crownover RL and Barnett GH 16 rain metastases 17
iol Phys 54: 18 19
McNeely ML., Campbell KL., Rowe BH., Klassen TP., Mackey JR and 20 ts and 21
n 22 l 175: 34-41. 23
) Drug 24 25
Systematic Reviews: Reviews. 26
of common 27 herapies for arm lymphoedema secondary to breast cancer 28
29
reotactic 30 rcinoma. Cancer 31
100: 1705-1711. 32
C., 33 b HJ and Schindler AE (2001) 34
Topotecan chemotherapy in patients with breast cancer and brain 35 metastases: results of a pilot study. Onkologie 24: 256-260. 36
Ogura M., Mitsumori M., Okumura S., Yamauchi C., Kawamura S., Oya N., 37 Nagata Y and Hiraoka M (2003) Radiation therapy for brain metastases from 38 breast cancer. Breast Cancer 10: 349-355. 39
Lentzsch S., Reichardt P., Weber F., Budach V and Dorken B (metastases in breCancer 35: 580-585.
Levin KJ., Youssef EF., Sloan AE., Patel R., Zabad RK and Zam
undergoing bone marrow transplant. J Neurosurg 97: 663-665.
Liu MT., Hsieh CY., Wang AY., Chang TH., Pi CP., Huang and Liou CH (2006). Prognostic factors affecting the outcome of brametastases from breast cancer. Support Care Cancer 14: 936-942.
Lund-Nielsen B., Muller K and Adamsen L (evaluation of a new regimen for malignant wounds in women witbreast cancer. 6412725. J Wound Care 14: 69-73.
Mahmo(2002). Results of whole brain radiotherapy in patients with bfrom breast cancer: a retrospective study. Int J Radiat Oncol B810-817.
Courneya KS (2006) Effects of exercise on breast cancer patiensurvivors: a systematic review and meta-analysis 58. CMAJ CanadiaMedical Association Journa
Minton O., Stone P., Richardson A., Sharpe M and Hotopf M (2008therapy for the management of cancer related fatigue. Cochrane Database of
Moseley AL., Carati CJ and Piller NB (2007) A systematic reviewconservative ttreatment. Ann Oncol 18: 639-646.
Muacevic A., Kreth FW., Tonn JC and Wowra B (2004). Steradiosurgery for multiple brain metastases from breast ca
Oberhoff C., Kieback DG., Wurstlein R., Deertz H., Sehouli J., van SHilfrich J., Mesrogli M., von MG., Staa
Advanced breast cancer: full guideline DRAFT (August 2008) Page 89 of 146

DRAFT FOR CONSULTATION
Pameijer CR., Smith D., McCahill LE., Bimston DN., Wagman LD Ellenhorn JD (2005) Full-thickness chest wall resection for recurrecar
and 1 nt breast 2
cinoma: an institutional review and meta-analysis 371. Am Surg 71: 711-3 4
006) Long-5 metastatic 6
2. 7
per DR., Hess KR and Sawaya RE (1997) Role of surgery in the treatment 8 of brain metastases in patients with breast cancer. Ann Surg Oncol 4: 481-9
10
., 11 tion of bone 12
omized study with 1 year follow-13 an Society for 14
15
art-Ayres ME., Fish K., Lapp K., Nagle C and Rucker B (2007) 16 17
ncology 18 19
un B., Broglio K., 20 citabine 21
h brain 22 23
Casley-Smith JR, Foldi E, Foldi 24 er PS, Norman 25
ancer 26 Society Lymphoedema Workshop. Work group III: Diagnosis and 27
28
er D., Nemoto T and Lane WW (1986) Chemotherapy Induces 29 ancer 58: 832-839. 30
le 31 phonates in metastatic disease. Health Technology Assessment 8(4): 32
33
34 J Neurooncol 35
84: 57-62 36
Salazar OM., Sandhu T., da Motta NW., Escutia MA., Lanzós-Gonzales E., 37 Mouelle-Sone A., Moscol A., Zaharia M and Zaman S (2001) Fractionated 38 half-body irradiation (HBI) for the rapid palliation of widespread, symptomatic, 39 metastatic bone disease: a randomized Phase III trial of the International 40
715.
Pecherstorfer M., Rivkin S., Body JJ., Diel I and Bergstrom B (2term safety of intravenous ibandronic acid for up to 4 years in breast cancer - An open-label trial 1095. Clin Drug Invest 26: 315-32
Pie
490.
Rasmusson B., Vejborg I., Jensen AB., Andersson M., Banning AMHoffmann T., Pfeiffer P., Nielsen HK and Sjøgren P (1995) Irradiametastases in breast cancer patients: a randup 1031. Radiotherapy and Oncology: Journal of the EuropeTherapeutic Radiology and Oncology 34: 179-184.
RinehSystematic review of the use of compression pumps for upper extremity lymphedema following treatment for breast cancer. Rehabilitation O25: 25-
Rivera E., Meyers C., Groves M., Valero V., Francis D., ArYin G., Hortobagyi GN and Buchholz T (2006) Phase I study of capein combination with temozolomide in the treatment of patients witmetastases from breast carcinoma. Cancer 107: 1348-1354.
Rockson SG, Miller LT, Senie R, Brennan MJ, M, Gamble GL, Kasseroller RG, Leduc A, Lerner R, MortimSA, Plotkin CL, Rinehart-Ayres ME, Walder AL (1998) American C
management of lymphoedema Cancer 83: 2882-2885
RosnRegression of Brain Metastases in Breast-Carcinoma. C
Ross, J. R., Y. Saunders, et al. (2004). A systematic review of the robisphosiii-139.
Rudnicka H., Niwinska A and Murawska M (2007) Breast cancer leptomeningeal metastasis--the role of multimodality treatment.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 90 of 146

DRAFT FOR CONSULTATION
Atomic Energy Agency (IAEA) 1025. International Journal of Radiation 1 Oncology, Biology, Physics 50: 765-775. 2
and Delrowe 3 hemibody 4 2 1009. 5
s 36: 37-48. 6
7 compared with simple lymphatic drainage in the treatment of post-mastectomy 8
9
(2002) Palliation of metastatic 10 chrane 11
12
aedt J., 13 Group. (2004) Oral ibandronate for the 14
treatment of metastatic bone disease in breast cancer: efficacy and safety 15 e 16
17
): A 18 19 20
Viani GA., Castilho MS., Salvajoli JV., Pellizzon AC., Novaes PE., Guimarães 21 brain 22
two stratification 23 24
management 25 26
5-290. 27
Wardley A., Davidson N., Barrett-Lee P., Hong A., Mansi J., Dodwell D., 28 ntly 29 bone 30
mised, crossover study of community vs hospital 31 32
Use of 33 n with breast cancer: practice guideline report #1-11 34
(Version 2.2002) 11741 35
Weinfurt KP., Castel LD., Li Y., Timbie JW., Glendenning GA and Schulman 36 KA (2004) Health-related quality of life among patients with breast cancer 37 receiving zoledronic acid or pamidronate disodium for metastatic bone lesions 38 1026. Med Care 42: 164-175. 39
Scarantino CW., Caplan R., Rotman M., Coughlin C., Demas W J (1996) A phase I/II study to evaluate the effect of fractionatedirradiation in the treatment of osseous metastases--RTOG 88-2International Journal of Radiation Oncology, Biology, Physic
Sitzia J., Sobrido L and Harlow W (2002) Manual lymphatic drainage
lymphoedema. Physiotherapy 88: 99-107.
Sze WM., Shelley M., Held I and Mason Mbone pain: single fraction versus multifraction radiotherapy. CoDatabase of Systematic Reviews: Reviews 988.
Tripathy D., Lichinitzer M., Lazarev A., MacLachlan SA., ApffelstBudde M., Bergstrom B and Study
results from a randomized, double-blind, placebo-controlled trial. [secomment] 123. Ann Oncol 15: 743-750.
Trudeau ME (2006) Temozolomide in metastatic breast cancer (MBCphase II trial of the National Cancer Institute of Canada - Clinical Trials Group (NCIC-CTG). Ann Oncol 17: 952-956
FS., Conte MA and Fogaroli RC (2007) Whole brain radiotherapy formetastases from breast cancer: estimation of survival usingsystems. BMC cancer 7: 53-
Vignes S., Porcher R., Arrault M and Dupuy A (2007) Long-termof breast cancer-related lymphedema after intensive decongestivephysiotherapy. Breast Cancer Research & Treatment 101: 28
Murphy R., Mason T and Cameron D (2005) Zoledronic acid significaimproves pain scores and quality of life in breast cancer patients withmetastases: a randobisphosphonate administration 1053. Bri J Cancer 92: 1869-1876.
Warr D., Johnston M and Breast Cancer Disease Site Group (2002) bisphosphonates in wome
Advanced breast cancer: full guideline DRAFT (August 2008) Page 91 of 146

DRAFT FOR CONSULTATION
Wroski M., Arbit E and McCormick B (1997) Surgical treatment of 7with brain metastases from breast carcinoma. [Erratum appears in Cancer
0 patients 1 2
1998 Feb 15, 82(4)] Cancer 80: 1746-1754. 3
Advanced breast cancer: full guideline DRAFT (August 2008) Page 92 of 146

DRAFT FOR CONSULTATION
Appendix 1 1 2
es for 3 the treatment of patients with advanced breast cancer 4
5 6 7
lives during 8 9
supportive and palliative care is of great importance. However the economic 10 alanced. 11
12 ecitabine 13 ast 14
4 (2002); 15 in the guideline 16
al evidence it 17 re re-18 een 19 equential 20
arator to combination therapies in previous technology 21 Appraisal Committee of the recent 22 Advanced Breast Cancer Guideline 23
24 25 26 27
ting the 28 patients 29 original 30
31 the 32 h, 2003; Li 33
osts of third-line 34 herapy was published in 1999 but was not included in the previous 35
reviews since third-line therapy was not part of the inclusion criteria. The main 36 limitations of these studies are that none compare more than three types of 37 therapy, nor do they consider more than one line of therapy. This highlights 38 the need for de novo economic modelling to directly answer the review 39 question. 40 41
A cost-utility analysis of chemotherapy sequenc
INTRODUCTION Since metastatic breast cancer is incurable, the quality of patients’ the final stages of life with various forms of active chemotherapy and
cost of this treatment and care to the NHS must be considered and b NICE has previously issued guidance on the use of the taxanes, capand vinorelbine for use in the treatment of patients with advanced brecancer in the form of three technology appraisals (TA30 (2001); TA5TA62 (2003)). These appraisals are now being updated withfor the treatment of advanced breast cancer. In light of new clinicis important that the economics of these chemotherapy agents aexamined. In addition, the sequencing of these agents has not bconsidered in the economic literature to date and the neglect of stherapy as a compappraisals was a concern to both theGemcitabine STA (TA 116) and to theDevelopment Group. EXISTING ECONOMIC EVIDENCE There are a number of good quality economic evaluations investigacost-effectiveness of first and second-line chemotherapy regimes in with metastatic breast cancer, most of which were appraised for the technology appraisals (summarised below). Four new full economic evaluations have been published since the review undertaken for appraisals (Verma et al, 2005; Cooper et al, 2003; Verma & Ilersicet al 2001). One partial economic evaluation considering the cchemot
Advanced breast cancer: full guideline DRAFT (August 2008) Page 93 of 146

DRAFT FOR CONSULTATION
TA30 – Taxanes In the original appraisal no economic evaluations for the first line treabreast cancer with a taxane were identified. For second-line treatmeeconomic evaluations were identified and reviewed. One comparewith mitomycin but was submitted in confidence to NICE andnot published in the subsequent HTA report. The other six comppaclitaxel and docetaxel in cost-utility analyses where the range of incremental QALYs gained was £1990-£2431
1 tment7 of 2
nt8, seven 3 d paclitaxel 4
therefore was 5 ared 6
7 alyses 8
ut in the UK 9 £14,050. 10
xane was 11 ne treatment of breast cancer, despite the evidence 12
13 14 15 16
for the 17 er other 18
-line 19 s much less 20
d a useful 21 of the RCT 22 id not 23
24 ated the 25 orelbine in 26 e reviews 27
ination 28 notherapy 29 ung et al, 30 ovided little 31
or cost-32 NHS 33
S and 34 g the cost-35
effectiveness of vinorelbine, paclitaxel and docetaxel, one economic 36 evaluation reported that vinorelbine was more effective and less costly than 37
xpensive 38 be less 39 2). In 40
9. In addition three ancompared docetaxel and vinorelbine - one of which was carried oand yielded a cost-utility ratio for incremental QALYs gained wasThe original guidance did not give any indication as to which tapreferred for second-lishowing that docetaxel has a highly favourable cost-effectiveness ratio compared with paclitaxel. TA54 – Vinorelbine Evidence at the time of TA54 was scarce. The evidence reviewed appraisal showed no clinical benefit of vinorelbine monotherapy ovtherapies as first-line treatment. Vinorelbine monotherapy as secondtreatment was slightly less effective than taxane therapy but watoxic. For a sub-group of patients (e.g. elderly) this was consideretreatment option and was backed up by economic evidence. None data favoured vinorelbine combinations and the case-series data dprovide a robust alternative interpretation. The economics involved in the original appraisal comprised of two literature reviews (one investiguse of vinorelbine as a single agent and the other investigated vincombination with other agents), with no independent modelling. Thfound no economic evaluations investigating vinorelbine as combtherapy, and identified four economic analyses for vinorelbine mo(Brown et al, 2001; Silberman et al, 1999; Launois et al, 1996; Le1999), though one of these was in abstract form and therefore prdetail. Three of these were fairly well conducted cost-effectivenessutility analyses, one of which was carried out in a UK setting from anperspective (the remaining three were undertaken in Canada, the UFrance). However they gave conflicting results, "when comparin
taxane therapy, one found vinorelbine to be less effective and less ethan either of the taxanes and a third evaluation found vinorelbine toeffective and more expensive than taxane therapy" (Lewis et al, 200
f patients in port refers to
the first therapy received by a patient with advanced disease for which anthracycline therapy is not suitable. 8 Similarly, ‘second-line treatment’ as referred to here is later referred to as ‘first-line treatment’ in the rest of this appendix. 9 The accepted threshold for evaluating the cost-effectiveness of any given treatment in the context of the UK is around £20,000-£30,000 per QALY. As such the range of £1,990-£2,431 per QALY shows docetaxel therapy to be very cost-effective compared to paclitaxel therapy.
7 It is important to note that the term ‘first-line treatment’ is used here to describe treatment given to patients who are not anthracycline-resistant or failing. Since the number othis category is now very small, the term ‘first-line treatment’ in the rest of this re
Advanced breast cancer: full guideline DRAFT (August 2008) Page 94 of 146

DRAFT FOR CONSULTATION
addition none of the studies adequately addressed the uncertainty 1 surrounding their results. 2
3 4
al was one 5 e 6
ination with 7 ther of these models has since been published in a peer-8 al. 9
10 11 12
ral 13 sted below), as well as 14
breast cancer 15 16 17
es of 18 ffective from an NHS perspective. 19
20 the economic analysis, an indirect treatment comparison will be 21
rst-line treatment. 22 23
METHODS 24 25 26
27 ls, the 28 ancer 29 ve been 30
e breast 31 norm’, and 32 at is 33
and anthracycline therapy (Jones et al, 2001). 34 35
icit distinction is made, it is assumed patients in whom the 36 ive alternative/additional treatment. 37
f these patients is 38 39 40 41
42 ): 43
Capecitabine + docetaxel combination therapy (‘T1: CAP + DOC’) 44 Gemcitabine + docetaxel combination therapy (‘T1: DOC + GEM’) 45 Paclitaxel monotherapy (‘T1: PAC’) 46 Docetaxel monotherapy (‘T1: DOC’) 47 48 Second-line therapy options (T2): 49
TA 62 - Capecitabine The only economic evidence available at the time of the appraisabstract (not reviewed) and the economic model submitted by thmanufacturer for both capecitabine monotherapy and in combdocetaxel. Neireviewed journ OBJECTIVES This economic evaluation will assess the cost-effectiveness of sevesequences of the main chemotherapy regimes (lisupportive and palliative care, that are used to treat metastaticpatients who have received prior anthracycline therapy. A secondary objective is to rule out certain strategies (i.e. sequenctherapy) that are likely not to be cost-e
To facilitatecarried out on RCTs for fi
Study Population In contrast to the populations considered in the technology appraisapopulation of interest in this study is patients with metastatic breast cwho have previously received anthracycline treatment which may hagiven as adjuvant treatment. Aggressive treatment of early stagcancer has led to the presentation of such patients becoming the ‘increasingly patients are even presenting with advanced disease thresistant to or has failed taxane
Whilst no expldisease is hormone responsive will receThe clinical and economic evidence for the management oexplored elsewhere in the guideline. Interventions
First-line therapy options (T1
Advanced breast cancer: full guideline DRAFT (August 2008) Page 95 of 146

DRAFT FOR CONSULTATION
Capecitabine monotherapy (‘T2: CAP’) 1 2
Supportive and Palliative Care only (‘T2: No Chemo’) 3 4
: 5 6 7
emo’) 8 9
Table 1: Standard dosages assumed by the model 10 11
1 e 2
Vinorelbine monotherapy (‘T2: VIN’)
Third-line therapy options (T3)Capecitabine monotherapy (‘T3:CAP’) Vinorelbine monotherapy (‘T3: VIN’) Supportive and Palliative Care only (‘T3: No Ch
Dosage DosagCapecit
eabine
taxe twice 1 - 14
2 on day 1 + doc l daily on days
1250mg/m2 75 mg/m
Gemcitabine taxe
1250mg/m on days
75 mg/m2 on day 1
l rap
2 on day 1 -
l rap
n day 1 -
bine g/m2 twice daily on days 1 - 14
-
30 mg/m2, days 1 -
+ docePaclitaxe
l 1 and 82
monothexe
y 175 mg/m
2 oDocetamonotheCapecita
y 100 mg/m
1250mmonotherapy Vinorelbinemonotherapy and 8
Structure of the Model A decision tree w
12 13 14
as constructed to represent all the possible consequences 15 resulting from a sequence of treatment. A total of 724 branches were 16
herapy, listed below in 17 table 2. It was assumed that a chem18 the sam ence19 20 Table 2: T seven tegies idered in model 21 22
trategy First-line (T1) cond-line (T2 (T3)
estimated for seventeen different sequences of chemototherapy agent could not be used twice in
e s ueq .
he teen stra cons the
S Se ) Third-line 1 DOC+CAP VIN No Chemo 2 DOC+CAP Chemo 3 OC CAP VIN 4 GEM+DOC CAP No Chemo 5 OC VIN CAP 6 OC VIN No Chemo 7 GEM+DOC No Chemo 8 PAC (3-weekly) CAP VIN 9 PAC (3-weekly) CAP No Chemo
10 PAC (3-weekly VIN CAP 11 PAC (3-weekly) VIN No Chemo 12 PAC (3-weekly) No Chemo 13 DOC CAP VIN 14 DOC CAP No Chemo 15 DOC VIN CAP 16 DOC VIN No Chemo 17 DOC No Chemo
NoGEM+D
GEM+DGEM+D
)
Advanced breast cancer: full guideline DRAFT (August 2008) Page 96 of 146

DRAFT FOR CONSULTATION
1 2
Figure 1: decision tree (for first 28 branches) 3 4
5 st cancer (who 6
have received prior anthracycline therapy). The first decision is which first-line 7 treatment to offer the patient. The decision tree shows explicitly all the 8 possible decisions that could be taken (given the confines of our decision 9 problem) and all the possible consequences resulting from this first decision 10 (again we have limited these). Four first-line treatments are considered. Time 11 is not made explicit in a decision tree model, but we assume the patient 12
The model begins by considering patients with metastatic brea
Advanced breast cancer: full guideline DRAFT (August 2008) Page 97 of 146
DRAFT FOR CONSULTATION
receives one cycle of the first line therapy. At this point, there is a pthat the patient might die of a toxic death. If the patient dies of a toxthat is the end of the possible outcomes associated with the treatmen
ossibility 1 ic death, 2
t. It has 3 been assumed that a toxic death can only occur after the first cycle of therapy. 4
5 two more 6 e patient 7 ance 8
f the current 9 cessarily 10
another 11 12
ting on 13 he will 14
py. At this point it is assumed that response can be 15 apy, of 16
17 18
r partial 19 ients go 20 dian 21 (in the 22 sponse is 23
e or their 24 r treatment. 25
nt or not, 26 sion will be 27
s) he faces 28 th only results 29
gressive disease or toxicity; the possibility of death from other causes 30 or prognosis of 31
nomic 32 ine 33
34 35
At this decision node, there may be two or three possible second-line 36 as been 37 s first-38
idered as 39 above. 40
41 first-line 42 ading to 43 second-44
line therapy is discontinued or progression has been reached after completing 45 the full course of second-line treatment, the patient continues onto third-line 46 therapy. In Figure 1 this decision has only one possible option thus is not 47 depicted with a decision node. Since both capecitabine and vinorelbine have 48 been used by this point, the only treatment option left for this patient is 49 Supportive and Palliative Care (‘No Chemotherapy’). There is only one 50
If that patient survives the risk of toxic death, (s) he will then receivecycles of therapy. This brings the total number of cycles of therapy thhas received at this point to three. The patient then faces another chevent of experiencing toxicity that will lead to the discontinuation ofirst-line treatment (no chance or decision to be taken here, this nefollows on from experiencing major toxicity). At this point we facedecision node, the choice of which second-line treatment to take. There is a time-lag of 1 month between discontinuing first-line therapy and starsecond-line therapy. If the patient didn’t experience toxicity, (s)continue on first-line theraassessed, so the patient faces a probability of responding to therhaving stable disease or not. For the purposes of the model, response is defined as complete otumour response to the first-line therapy. Responders and stable paton to receive additional cycles of treatment, receiving in total the menumber of cycles as reported in the RCTs investigating that therapy case of all the interventions in the mode, this was six cycles). Non-redefined as patients who are classified as having progressive diseastumour was non-assessable. These patients do not receive furtheRegardless of whether the patient has responded to first-line treatmeprogression is an inevitable outcome. However the time to progresdifferent. Once the patient is experiencing progressive disease, (the probability of dying from progressive disease. Indeed deafrom prowas not considered to be relevant to the model due to the pothese patients. This approach is consistent with other published ecoevaluations. If the patient survives, (s) he will continue to second-ltreatment.
therapies. This is because it has been assumed that if capecitabine hused as first-line treatment, or a part of a combination therapy given aline treatment (e.g. capecitabine + docetaxel), then it cannot be consa second-line therapy option. This is the scenario depicted in figure 1 The patient then experiences the same chance events as withtreatment (chance of toxic death, chance of experiencing toxicity lediscontinuation, chance of responding to second-line therapy). Once
Advanced breast cancer: full guideline DRAFT (August 2008) Page 98 of 146

DRAFT FOR CONSULTATION
possible outcome from the ‘No Chemotherapy’ option, so thisterminates. If third-line treatment is a chemotherapy regime, the samevents as with first-line and second-line treatment may occur (the ctoxic death, chance of experiencing toxici
branch 1 e chance 2 hance of 3
ty leading to discontinuation, chance 4 cond-line therapy). 5
6 7
8 of interest 9
iques this 10 each trial. It 11
uced into clinical practice before 12 other 13
14 15
on on each intervention 16 would cause a number of methodological problems. Not only would this not 17
lose the effect of 18 19 20 21
nomic 22 eline are based 23
24 e to C. The main 25
t the 26 27
C would be the same as the 28 d 29 in cost-30 variety of 31
32 33
appraisal was 34 topics. As 35 cancer 36 of trials 37
pdate 38 matic 39
l search aiming to identify trials that may have been excluded from the 40 clinical review (due to stricter inclusion criteria). Randomised controlled trials 41
d in the 42 lines of 43
therapy, no RCTs were identified for second- or third-line therapy. Thus, the 44 indirect treatment comparison was only carried out on first-line treatment 45 options. 46 47 The indirect comparison was undertaken using two separate statistical models 48 using the statistical computer software, WinBUGS. The first describes the 49
of responding to se Clinical Evidence
First-Line Treatment – An indirect treatment comparison An RCT or a meta-analysis of RCTs comparing all the interventionsto this analysis is not available. Indeed using conventional technwould not be possible due to the different comparisons made by is common for new therapies to be introdformal treatment comparisons with the current standard approach or new agents have been planned or carried out. Using just one arm of one RCT to give us informati
make use of all the available evidence, it would also randomization which is what gives the RCT its gold standard. In the absence of direct comparative evidence, an indirect treatment comparison has been performed to inform the parameters of the ecomodel and ultimately ensure the recommendations in the guidon all available evidence. Indirect comparisons use evidence from A vs. B and A vs. C trials to draw conclusions about the effect of B relativassumption made using this approach to evidence synthesis is thaevidence is consistent. That is, the treatment effect of B relative to Cestimated by a real trial comparing B vs.treatment effect estimated by the A vs. B and A vs. C trials if they haincluded C and B arms respectively. This assumption is also impliciteffectiveness analysis, since evidence is routinely combined from a sources, thus consistency has to be assumed. The clinical evidence review for the update of each technologyperformed separately, which informed the search strategy for thesesuch a full systematic search for all treatments for metastatic breastwas not undertaken. The network of RCT evidence is thus made upthat were identified for the original appraisals, from the individual usearches for the three technology appraisals and from an unsystemanua
that involved one or more of the interventions of interest were includenetwork of evidence. Whilst the economic model assesses three
Advanced breast cancer: full guideline DRAFT (August 2008) Page 99 of 146

DRAFT FOR CONSULTATION
relationship between toxic deaths and discontinuation due to toxicthe second links the response rate, progression rates and mortnetworks of RCT evidence for each statistical model are depicted(figures 2 and 3); each line represents one RCT and the shadinginterventions highlights those that are of interest in our decision prOther interventions are included to add to the information we can the interventions that are of interest, through indirect comparisons.evidence structure is presented below the diagram in table 3. If all reported all the data that was needed, all trials would have been inboth the indirect treatment comparisons. Since there were gaps inthree of the trials (Sjostrom 1998, Bonneterre 2002 and Monnierexcluded from the analysis of progression and sur
ity, whilst 1 ality. The 2
below 3 of certain 4
oblem. 5 obtain on 6 The 7 the trials 8 cluded in 9 the data, 10
1998) were 11 vival. Whilst the analysis 12
was undertaken from a Bayesian framework, flat priors were used in both 13 ct on the results. 14
15 16 Figure 2: RCT network for toxicity model 17
18
19 20
21
22
statistical models and thus did not impa
Figure 3: RCT network for survival model
Docetaxel(DOC)
Paclitaxel (PAC)
CAP + DOC DOC +
GEM
MV304 Study: Nabholtz
(1997)
Chan (2005) O’Shaughnessy
(2002)
Jones (2005)
JHQG trial: Albain (2004)
GEM + PAC
Docetaxel(DOC)
FUN
MtF
CAP + DOC DOC +
GEM
MV304 Study: Nabholtz
(
Paclitaxel (PAC)
Chan (2005) ghnessy
(2002)
Jon(2005)
Bonneterre (2002)
JHQG trial: Albain (2004)
Scand: Sjostrom 1997) (1998)
es
O’Shau
Monnier (1998) GEM + PAC
Advanced breast cancer: full guideline DRAFT (August 2008) Page 100 of 146

DRAFT FOR CONSULTATION
1 able 3: ev ctu2
Study m to
deaths
e
ue to xicity
mresp
Dus
responders)
e to p on (for all)
n rall
s ival (for all)
Log hazard ratio
T idencNuof
e struber xic
Numbdiscontinuing
re r Nu
dto
ber of onders re
(for
ration of ponse
M dian timerogressi
Mediaoveurv
Jones 2005
O'Shaughnessy 2002
7
998 onneterre 2002
Albain 2004
Chan 2005
Nabholtz 199
Sjostrom 1BMonnier 1998
The text that follows is a simple description of thindirect treatment compa
3 e methods used for the 4
risons. The WinBUGS code is not presented here but 5 om the author on request (please contact 6 is available fr
[email protected]). Toxicity model A number of assumptions were made in order to get the most out of Firstly, it was assumed that the toxic death rate did not vary by studyfixed effects model was used. Secondly, the two measures of toxicity (toxic death and discontinuation due to toxicity) are related by a constantwhich was allowed to vary by study (from a random effects model). Thirdly the
7 8 9
the data. 10 , so a 11
12 , beta, 13
14 baseline probability of toxic death (to which all the relative effects are 15
this case the probability of toxic death for docetaxel) was 16 ls involving 17
18 19 20
l, it is 21 22
(s), with progressive disease (pd), or non-assessable (na). There is data on 23 the split between these groups from mo24 reports whether a responder, stable or not, and one study only reports 25
n categories 26 follow a multinomial distribution: 27 28
29 30 We model the effect of treatment using multinomial logistic regression. Let 31
, )−32
compared, in estimated by a random effects model of the arms of the three triadocetaxel. Survival model In line with the assumptions made in structuring the economic modeassumed that patients are categorised at 9 weeks as responders (r), stable
st studies, although one study only
whether a responder or not. It was assumed that the split betwee
( , , , ) ~ Multinomial(( , , , ), )r s pd na r s pd nan n n n p p p p N
,1 ,
,2 , ,
,3 , ,
( )( | ) / (1 )( . | , ) / (1
1
i i r
i i s i r
i i pd i r i s
na r s pd
q p responder pq p stable non responder p pq p prog disease non responder non stable p p p
p p p p
= =
= − = −
= − − = −
= − − −
Advanced breast cancer: full guideline DRAFT (August 2008) Page 101 of 146

DRAFT FOR CONSULTATION
We assume the following model for the conditiona q: 1
m sd
m sd
l probabilities, ,1 ( ) ( ),1 ( ),1
2,2 ( ) ( ) ( ),2 ( ),2 j
2,3 ( ) ( ) ( ),3 ( ),3 j
logit( ) ( )
logit( ) ( ); ~ ( , )
logit( ) ( ); ~ ( , )
i s i t i b i
i s i s i t i b i
i s i s i t i b i
q
q N
q Nζ ζ
γ γ
ϕ θ θ
ϕ ζ θ θ ζ
ϕ γ θ θ γ
= + −
= + + −
= + + −
2
3 4
atment effects which differ for different conditional outcomes: 6 og.disease|{non-responder &
9 on-10
ease|{non-responder & non-stable} differ from 11 me from 12
13 14
for all. 15 n in responders 16
and non-responders with rates λr and λnr respectively. We therefore needed a 17 model for the progression rate for responders, λr, and non-responders, λnr. We 18 put a log-linear model on the progression rate in responders and stable: 19 20
Key assumptions: 5
o Fixed treresponders; stable|non-responder; and pr7 non-stable}. 8
o The proportion of responders depends on study. o The baseline log-odds of the conditional outcomes stable|n
responder; and prog.disthat for responders by study specific terms ζj and γj which corandom effects distributions.
Most studies reported median time to progression for responders andWe assume exponential distributions for the time to progressio
( )log( )r s i ( ) ( )t i b i( )d dλ α= +2
( ) ( ) ( ) ( )log( ) ( ); ~ ( , )s s i s i t i b i jd d N m sdη ηλ α η η= + + −
− 21
22 Key assumptions: 23
24 der 25
e for responders 26 and stable individuals. 27
28 The mean progression time in non-responders is a weighted average of mean 29 progression time for stable, non-assessable, and progressive disease 30 patients, giving progression rate in non-responders of: 31
32
o Study specific baselines for responders o Random effects model for log-hazard ratio for stable vs respono Fixed treatment effect across studies, which is the sam
1
1.5)nr ppλ =
+ 33
((1 ) (1 )
pdna s
s r r
pp pλ
⎛ ⎞+⎜ ⎟− −⎝ ⎠
34 35
se with 36 progressive disease. 37
o Non-assessable patients have the same progression rate as 38 progressive patients. 39
40 Most studies reported median time to mortality for all patients. If we assume a 41 constant term linking progression rates with mortality rates, then we can 42
Key assumptions: o Time to progression is 4.5 weeks (1.125 months) for tho
Advanced breast cancer: full guideline DRAFT (August 2008) Page 102 of 146

DRAFT FOR CONSULTATION
model mortality in exactly the same way as for progression. However, we do not know the mortality rate (1
1 /μ) for those with progressive disease, and so 2
this was estimated from the data. 3 4
ponders 5 e need a 6 , μnr. We 7 e, which 8
9 assumed to come from a random effects distribution: 10 11
We assume exponential distributions for the time to mortality in resand non-responders with rates μr and μnr respectively. We thereformodel for the mortality rate for responders, μr, and non-respondersput a log-linear model on the mortality rate in responders and stabldiffer from log progression rates by a constant, which depends on study, but
2( )log( ) ( ) ; ~ ( , )r r s i jlog N m sd
( )log( ) ( )s s s ilogβ βμ λ β β= +
μ λ β= +
The mean survival time in non-responders is
12
13 a weighted average of mean 14
survival time for stable, non-assessable, and progressive disease patients, 15 giving mortality rate in non-responders of: 16 17
1(nr
nap p⎛ + ) pds pμ
κ=
⎞ 18
o βj) of mortality relative to progression 22
al time λ for those with progressive disease. 23 gressive 24
25 26 27
studies 28 rt the 29
30 31
e 32 h the GDG since the 33
(patients received vinorelbine as first-, 34 35
k 2001; 36 s considered 37
38 39
40 Five non-randomised studies were identified for capecitabine monotherapy as 41 second-line treatment (Fumoleau et al. 2004; Lee et al. 2004; Pierga et al. 42 2004; Reichardt et al. 2003; Wist et al. 2004). Whilst all were considered 43 acceptable in terms of being able to provide reasonably robust evidence, not 44 all trials provided data on the same parameters. Pierga et al 2004 provided 45
(1 ) (1 )s r rp pμ+⎜ ⎟− −⎝ ⎠
19 Key assumptions: 20
Random effects model on the log-hazard ratio’s (21
o Fixed mean survivo Non-assessable patients have the same mortality rate as pro
patients. Second-line Treatment There is one randomised controlled trial and seven non-randomisedinvestigating second-line therapy. No evidence was found to repoeffectiveness of the ‘No chemotherapy’ intervention. The Martin et al (2007) RCT was used to provide data on vinorelbinmonotherapy as second-line treatment by agreement wittrial has a mixed patient populationsecond- and third- line treatment). Although there were two other observational studies investigating vinorelbine monotherapy (ZeleUdom 2000) they were both small trials and the Martin RCT waby the GDG subgroup to provide the best estimate of vinorelbine monotherapy in the second-line setting.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 103 of 146

DRAFT FOR CONSULTATION
data on response duration, duration of stable disease and time to prfor all. As such this trial was used to provide in
ogression 1 formation for the model on 2
capecitabine monotherapy as second-line treatment. 3 4
motherapy’ 5 lt in no 6
rvival and 5 months survival with progressive disease. 7 8 9
10 s third-line 11
ata for 12 e 13
receiving the 14 15
although the effect of reducing the survival estimates by 16 will be explored in the sensitivity analysis. 17
18 Health Benefits 19
20 21 22
to toxicity 23 The toxicity 24
data for second and third-line treatment are shown in table 5. 25 26 Table 4 abilities estimated by the indirect trea nt comparison 27
rvention Toxic death rate Discontinuation due to toxicity
No evidence was found to report the effectiveness of the ‘No cheintervention. It was assumed that ‘No Chemotherapy’ would resuprogression-free su Third-line treatment No evidence for capecitabine or vinorelbine monotherapy atreatment was identified. It was therefore assumed that the same dsecond-line treatment would provide a suitable estimate of third-lintreatment, since the patient populations included some patients study therapy as third-line. In the base-case analysis, no adjustments to the data were madevarying degrees
Probabilities The probabilities of toxic death and of discontinuing treatment dueshown i e d odel. n table 4 w re all estimate via the ITC statistical m
: prob tmeInte
T1:DOC+CAP 0.020 0.337 T1:GEM+DOC 0.008 0.201
0.003 0.116 .014 0.278
T1:PAC T1: DOC 0
28 Table 5: probabilities for second and third-line treatment 29
ation icity
Intervention Source Toxic death rate
Discontinudue to tox
T2 and T3: VIN Martin et al, 2007 0.008 0.048 T2 and T3: CAP Pierga et al, 2004 0.000 0.162
30 T ies of re , st tion ase, dise ogression 31 an ssability estim via the second ITC statistical model, 32 sh table 6 below33 34 Table 6: probabilities estimated by the indirect treatment comparison 35
Intervention Response Stable Progression Non-assessable
he probabilit sponse abilisa of dise ase prd non-asse were atedown in :
T1:DOC+CAP 0.4070 0.3427 0.1244 0.1258 T1:GEM+DOC 0.4023 0.4209 0.1148 0.0620 T1:PAC 0.2316 0.3911 0.3234 0.0539 T1: DOC 0.2899 0.3841 0.2200 0.1060
36
Advanced breast cancer: full guideline DRAFT (August 2008) Page 104 of 146

DRAFT FOR CONSULTATION
For the economic model, it was assumed that non-assessable patients were 1 the same as patients with progressive disease. 2
3 Ta babiliti secon ird- ea4
ion nse Stable n-response
ble 7: pro es for d and th line tr tment
Intervent Source Respo NoT2 and T3: VIN l 2007 0.2 0.25 0.484 Martin et a 62 4T2 and T3: CAP Pierga et al 2004 0.152 0.335 0.513
5 6 7
gression 8 t2), TTP 9
to death 10 emotherapy 11
ever the 12 ment. 13
14 from the 15
n survival and are reported below in table 8. It is assumed 16 that time to progression for patients with progressive disease reported as their 17
le) is 1.125 18 .5 wee19
20 Table 8: Survival d ta estima y the indirect treatment comparison 21 (in months) 22
tion TTP - esponder
TTP – Stable
Survival Overall survival (OS) was assumed to be the sum of time to pro(TTPt1) of first-line treatment, TTP from second-line treatment (TTPfrom third-line treatment (TTPt3) and the period from progression(assumed to be 5 months). This assumption implies that chimpacts on time to progression, and through that overall survival. Howtime from (final) progression to death is fixed regardless of prior treat Mean ‘progression-free’ survival times (in months) were estimated statistical model o
best response to treatment (or if the tumour was not assessabmonths (4 ks).
a ted b
IntervenR s
mean mean T1:DOC+CAP 12.19 7.53 T1:GEM+DOC 11.08 6.84 T1:PAC 5.63 3.47 T1: DOC 10.27 6.34
Mean values are used for
23 the economic evaluation since they are a more 24
appropriate measure of the average at a population level. Since only median 25 values were reported in th 2007 and Pierga 2004 trials, it was 26
exponential 27 s. Median values were then converted to mean values by 28
29 h = -ln (0.5)/30
31 wh line ard; tm ediansurvival tim ean=mean 32 survival tim33 34 Table 9: Survival data for second and third-line treatment (in months) 35
Intervention Source TTP - Responders
TTP - Stable
TTP - Progression
e Martin assumed that survival and time to progression followed distributioncalculating the baseline hazard:
tmed . tmean=1/h
ere, h=base absolute haz ed=m e; tme
T2 and T3: VIN Martin et al 2007 5.77 5.77 1.13 T2 and T3: CAP Pierga et al 2003 12.84 9.52 3.45
36
Advanced breast cancer: full guideline DRAFT (August 2008) Page 105 of 146

DRAFT FOR CONSULTATION
Utilities
1 2 3
pathway 4 calculate 5 gressive 6 gressed 7
ed utility 8 dies that 9
The most 10 oncology 11 oper and 12 the utility 13 tility with 14 response 15 , 0.65, to 16
17 by definition the disease is not yet progressive); and time before toxicities 18
assume utility associated with 19 pr isease, 0.45). 20 21 Ta al (2003)22
Utility weights were linked to the time spent at different points of the(not strictly health states since we did not use a Markov process) to QALYs. No trials reported utility losses due to toxicity or to prodisease, so the proportion of patients in each arm of an RCT that proor discontinued treatment due to toxicity were relevant publishweights to estimate the overall utility. There are a number of stureport utility weights in the treatment of advanced breast cancer. recent pooling of utilities from different sources (all derived from nurses using the Standard Gamble technique) was published by Coco-workers (2003). A number of assumptions had to be made about associated with time spent between treatment (we assume uprogressive disease, 0.45); the time spent on treatment before could be assessed (we assume utility associated with stable diseaseensure consistency with the indirect treatment comparison since at this stage
identified after 3 cycles of treatment (weogressive d
ble 10: utility values from Cooper etHealth state
Pooled utilities
Response 0.81 StaStable dise
ble disease 0.65 ase and febrile neutropenia or infection 0.44
sease 0.45 with hospitalisation Progressive diProgressive disease with toxicity (assumption) 0.35 Death 0
Cost Estimation The costs considered in this analysis are only those relevant to the UK NHS,
23 24
25 in accordance with the perspective taken by the NICE Reference Case for 26
es. Where costs 27 rom sources using a different price year, they have been
Community Health Services Pay and Prices
costs considered in the model: 32 ent 33
o Cost of assessment/ follow-up 34 35 36 37
38 Cost of treatment 39 40 The average dose for each regime was presented in table 1. The possibility of 41 reducing the dose (in response to an adverse event) was not allowed for in 42 the model. The drug acquisition cost per cycle were calculated for each 43
economic evaluations. Costs were estimated in 2006-7 prichave been taken f28 inflated using the Hospital and29 Index (PSSRU, 2007). 30 31 There are broadly five categories ofo Cost of treatm
o Cost of treating adverse events o Cost of supportive and palliative care o Costs associated with death
Advanced breast cancer: full guideline DRAFT (August 2008) Page 106 of 146

DRAFT FOR CONSULTATION
chemotherapy regime based on an average dose per patient (standa1.75m2), the average number of doses per cycle and the averagmg. Whilst it is recognised that discounts are available on some of drugs, the list price was used in the base case as recommended Reference Case. The effect of these drug discounts will be esensitivity analysis. Where the price is given for b
rd 1 e list price per 2
these 3 in the NICE 4
xplored in the 5 oth the generic and 6
used in the base-case. 7 8
11: Dru i os9 Vino el Docetaxel
proprietary drug, the cheapest is Table g acqu sition c ts (1)
Drug relbine PaclitaxBrand name (generic) Navelbine (gene Taxol Taxotere ric) Manufacturer n/a abre n/a Bristol-
Myers Squibb
Sanofi-Aventis
List pr NF 54, Se
ial 162.75 32.95 29.75
534.75 153.98 139 11 116.05
l vial 333.91 347.82 ml vial 500.86 521.73 ml vial 1001.72 1043.46
e ml)
10 10
30 75 se .5 52.5 306.25 306.2 131.25
per 3.12 2.83 3.36 3.50 6.98 6.98
ost 3.56 148 102 107 1 915.47
tion 2.56 2.56
2 1 1 1 1
age drug cost )
3 97.03 28.17 1071.01 8 918.02
F
ices, £ (Bpt 2007):
0 ml v 1 ml vial 2 ml vial 5 ml vial .98 1.41
16.7 m25 50
i.v. concentrat(mg/
6 6 40
Dose (mg/m2) 30 175 175 100 Average doAverage cost
52 5 175
mg (£) Average drug cper dose (£) Premedica
16 .51 8.17 1.01 220.63
cost per dose (£) Number of doses 2 per cycle Averper cycle (£
27.13 2 10 1223.1
10 Table 12: Drug acquisition costs (2) 11
ection (powder) Orally administered Inj Drug Capecita emcitabine bine Drug GBr Xeloda emzar
Roche facturer i Lilly
32.55 n 2150 1g vial 162.76
ired st per mg 0.16 500mg tablets re d Dose (mg/m2) 1250
k (60 tab)
Average dose 2187.5
Cost per 150mg tablet 0.741166667 Average cost per dose Cost per 500mg pack (120 tab)
295.06 356.03
Cost per 500mg tablet 2.458833333 Number of doses per cycle
2
Cost per administration 10.5765
and name Brand name GManufacturer Manu El
Dose (mg/m2) Dose per administratio
1250 200mg vial
150mg tablets requ 1 Average co4 quire
Cost per 150mg pac 44.47
Advanced breast cancer: full guideline DRAFT (August 2008) Page 107 of 146

DRAFT FOR CONSULTATION
No of doses per cycle 28 Average drug cost per cycle 2 Average drug cost per
cycle 712.0677083 96.142
In addition to the drug acquisition costs, the cost of administewas estimated from the NHS National Reference Costs. For theradministered by i.v. or injection (gemcitabine), the cost used was £outpatient delivery of complex perenteral chemotherapy and subseelements. This cost includes hospital overheads, the administrachemotherapy and clinical time, but does not, for example, distingbetween different i.v. infusion times of paclitaxel vs. docetaadministered orally (capecitabine) the administration costsusing the outpatient tariff, £209 for first attendance and then £82 forsubsequent attendances. It has been assumed that one outpatient appointment would be required per cycle of therapy (one every threeIn the case of combination therapy it has been assumed that two dbe administered at one time, thus requiring the cost of only one admto be conside
1 ring the drug 2
apies 3 293 for 4 quent 5
tion costs of 6 uish 7
xel. For drugs 8 were estimated 9
10 11
weeks). 12 rugs can 13
inistration 14 red. In addition to the drug acquisition and drug administration 15
costs, it has been assumed that a consultation with an oncologist (£209 for 16 ence Costs 2006-7) would be necessary at the 17
starting cycle. 18 19 20 21
cycles of 22 treatment was used as a proxy for the cost of assessing response (NHS 23
nders, 24 nature of 25
26 27
e there 28 29
ncluded in 30 on with specialist 31
ths after treatment has finished (£105 per month, NHS Reference 32 costs 2006-7) is used as a proxy for follow-up costs. 33
34 35 36 37 38 39 40
The cost of treating major toxicities (which necessarily lead to the 41 discontinuation of treatment) was estimated as £804, the mean of two costs 42 from the literature; from the cost of treating severe infection or febrile 43 neutropenia in hospital £1,281 (Cooper et al, 2003) and the cost of treating a 44 severe infection or febrile neutropenia at home £328 (Cooper et al, 2003), 45 both reported here already inflated to 2006-7 prices. This cost was used 46
first attendance, National Refer
Cost of assessment/ follow-up The cost of taking one CT scan (2 areas, with contrast) every three
Reference Costs, 2006-7). This is equivalent to £125 for non-respo£250 for responders. This is an attempt to capture the continuousassessing response. Once the patient has finished chemotherapy and achieves a responswill still be a cost associated with the contact the patient receives from her consultant. (The cost of contact with other health professionals is isupportive care package 1 below). Cost of one consultatievery 2 mon
Response is not assessed when first-line chemotherapy ends so the cost of one CT scan is included before the patient begins the next line of chemotherapy. Cost of treating adverse events
Advanced breast cancer: full guideline DRAFT (August 2008) Page 108 of 146

DRAFT FOR CONSULTATION
across all treatments, so was not specific to the type of toxicity that leads to 1 discontinuation which we know does vary by therapy. 2
3 Cost of supportive and palliative care 4
5 s’ of care 6
d below for patients at different points along the care pathway. 8 9
care a 10 rom the time of 11
ich point 12 e, this 13
ven to a patient until they begin the ‘no chemotherapy’ 14 ategies this package of care will be given for the whole 15
16 17 18
Community nurse: home visit 20m, £24.00, 1 per fortnight (PSSRU, 2007) 19 isit £34.00 every month (PSSRU, 2007) 20
PSSRU, 2007) 21 22
ated elements: £34.00 24
25 26 27
portive and 28 tion might be 29
o weeks of life. This package of care is 30 follows the strategies in the model with three 31
o weeks 32 care 33
34 35
ents (weekly costs): 36
SSRU, 2007) 38 39 40 41
o Package 3 42 43
as 44 attributable to all patients dying in the model, it would be superfluous to the 45 analysis since we are interested solely in incremental costs and incremental 46 benefits. This package of care is not however given to patients who die in the 47
Due to the nature of supportive and palliative, three likely ‘packageare describe7 o Package 1 The first package of care describes an average level of supportivepatient receiving chemotherapy might be expected to receive ffirst cycle of treatment until the onset of progressive disease at whthe next line of chemotherapy is started. Given the model structurpackage of care is gioption. For some strtime spent in the model. Time-related elements:
GP contact: 1 surgery vClinical nurse specialist 1hr contact time, £74.00, 1 per month ( Time non-rel23 Social worker: 1hr client-related work but not direct contact time, (PSSRU, 2007)
o Package 2 The second package of care describes an average level of suppalliative care a patient receiving the ‘no chemotherapy’ intervenexpected to receive until the last twalso included for the patient that lines of chemotherapy, from the time of progression until the twbefore death. Unlike the care given in package 1, all elements of thedelivered in package 2 are time-related. Time-related elemCommunity nurse: home visit 20m, 37 £24.00, 1 per week (PSSRU, 2007) Clinical nurse specialist: 1hr contact time, £74.00, 1 per week (PGP contact: 1 home visit, £27.50, every fortnight (PSSRU, 2007) Therapist10: 1 hour, £20.00, every fortnight (PSSRU, 2007)
The third package of supportive and palliative care is a cost for the more intensive needs of patients in the final two weeks of life. If this cost w
10 The type of therapist was not made explicit. The unit cost of all therapists listed in the PSSRU costs was £40 per hour. This was roughly the same for an hour of home visiting time.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 109 of 146

DRAFT FOR CONSULTATION
model from toxic death. Since the toxic death varies (albeit not between the interventions compared in the model, the cos
greatly) 1 t of package 3 2
supportive and palliative care does need to be taken into account. 3 4
in the 5 into the cost of dying at home (inflated as 6
p7 8 9
10 occurring in 11
ing in a hospice and the remaining 50% of deaths 12 st two weeks of care was therefore 13
14 15 16 17
t 18 th. No 19
e published 20 f toxic death. A 21
re; from the 22 tropenia 23
t al, 2001) and the cost of treating a severe infection in 24 ooper et al 2003), both reported here already inflated to 25
model is £2,287. 26 27 28 29 30
expect 31 sults of the model since many of 32
through the model are associated with survival of less 33 ition the majority of the costs for pathways that do 34
evenly 35 36 37 38 39
preferred 40 patients 41
ectiveness analysis was 42 conducted after ranking the alternative strategies from the most to the least 43 cost-effective and excluding any dominated strategies (i.e. those strategies 44 achieving lower effectiveness and incurring higher costs when compared to 45 any other, highlighted in table 14 in light grey, or those which are ruled out if 46 they achieve lower effectiveness and higher costs than a combination of two 47 other strategies, highlighted in table 14 in dark grey). 48 49
The cost used was a weighted average of the three costs reportedM rt arie Curie commissioned repo
reviously described to 2006/7 prices). last 14 days - in hospital, £4,706 last 14 days - in Marie Curie hospice, £5,867 last 14 days - at home (with community support), £2,428
The weights applied to calculate this average were 40% deathshospital, 10% occurroccurring at home. The cost of the laestimated to be £3,418. Costs associated with death Apart from package 3 of supportive and palliative care, the other cosassociated with death included in the model is the cost of toxic deacosts related to toxic deaths were reported explicitly for any of theconomic evaluations, despite all papers considering the risk oproxy was used by way of the mean of two costs from the literatucost of 7 days hospitalisation and treatment of severe febrile neu£3,586 (Brown ehospital £988 (C2006-7 prices. In total the cost of toxic death used in the DISCOUNTING Discounting was not conducted, so the results that follow are the undiscounted costs and health outcomes. However we would not discounting to have much impact on the rethe possible pathwaysthan 24 months. In addresult in a longer survival, come at the beginning rather than spreadacross the year. TYPE OF ANALYSIS A cost-utility analysis was performed given that the health outcomeby NICE is the QALY and quality of life is of particular importance towith metastatic cancer. An incremental cost-eff
Advanced breast cancer: full guideline DRAFT (August 2008) Page 110 of 146
DRAFT FOR CONSULTATION
SENSITIVITY ANALYSIS 1 2
ucted to 3 lysis’ 4 nalysing 5
the model analysed to see if this parameter influences any of the 6 7 8
surrounding 9 on the 10
fectiveness of third-line 11 therapy, possible price discounts and the calculation of overall survival. A 12
14 15
(pooled by 16 ncerned about 17
nts may 18 values 19 ility 20
21 se value of 0.44 22
toxicity). 23 24
o Effectiveness of capecitabine monotherapy 25 ion associated with capecitabine
one third 27 28 29 30
y, so both 31 rk as well as 32
e fact that the data used to 33 inform the second-line therapy parameters in the model came from trials with 34
ulations which included patients who were receiving the nd disease 36 to 37
38 39 40
el and 41 e. However there is not one 42
single agreed price discount available for either agent that is applicable 43 d Wales. Therefore a number of different price
discounts for paclitaxel were investigated (50%, 60%, 70%, 80%, 90%) as 45 well as the effect of a price reduction also available for vinorelbine, vinorelbine 46 45% discount, paclitaxel 90% discount (current price discounts suggested by 47 the Purchasing and Supply Agency database, eMIT). 48 49 o Calculation of overall survival 50
A series of one-way deterministic sensitivity analyses were condassess the robustness of the study results. ‘One-way sensitivity anadescribes the process of changing one parameter in the model and athe results ofoverall results. Five sources were thought to contribute most to the uncertainty the analysis; the utility values used in the analysis, the data usedeffectiveness of capecitabine monotherapy, the ef
number of scen13 arios were investigated as outlined below: o Utility values Although the most current utility values were used in the analysis Cooper et al, 2003), the guideline development group were cothe validity of values ascribed to the different health states patieexperience. An arbitrary 10% increase and decrease in all the utilityused in the model was explored. The effect of just increasing the utascribed to progressive disease by 10% was tested. In addition the utility ascribed to patients with toxicity was varied from the base-cato 0.35 (to equal the utility associated with progressive disease with
It was noted that the time to progress26 monotherapy was high. Therefore these estimates were reduced byin this scenario. o Effectiveness of third-line treatment No evidence was available for the effectiveness of third-line therapcapecitabine and vinorelbine monotherapies were assumed to wofor second-line therapy. This was justified by th
mixed patient pop35 study therapy as third-line. The effect of reducing the response astabilisation rates by one third, and separately reducing the time progression estimates by one third was investigated. o Price discounts Price discounts are available across England and Wales on paclitaxvinorelbine since generic versions are availabl
across the whole of England an44
Advanced breast cancer: full guideline DRAFT (August 2008) Page 111 of 146

DRAFT FOR CONSULTATION
Whilst it was acknowledged the calculation of overall survival was uncertainty, this assumption was inherent to the structure of the mowas not tested in the sensitivity analysis. However the time from proto death (as
subject to 1 del and 2 gression 3
sumed to be 5 months in the base-case analysis) was varied from 4 5 6
ey are more 7 ch allows 8
ich are then 9 planned to be 10
undertaken during the consultation period for this guideline. This should 11 etter picture of the uncertainty surrounding the analysis. 12
13 14 15 16 17
below. There 18 ival, quality 19
y ranges 20 8.5 21
(strategy 12: PAC, No Chemo). Strategy 3 yields the highest number 22 of QALYs (1.1896) compared to 0.3645 for strategy 12. Total costs for each 23 strategy ranged from £14,000 (strategy 12) to over double that for strategy 3, 24 £31,500. 25
4 – 6 months. However these scenarios are unlikely to happen independently; thlikely to occur concurrently. A probabilistic sensitivity analysis, whimultiple parameters to vary over specified distributions from whsampled at random many times, was not conducted but is
provide a b
RESULTS Base-case results The base-case results are shown listed by strategy, in table 13is a considerable difference between the strategies in terms of survof life and associated costs. The overall survival from each strategfrom just over 23 months (strategy 5: GEM+DOC, VIN, CAP) to justmonths
Advanced breast cancer: full guideline DRAFT (August 2008) Page 112 of 146

DRAFT FOR CONSULTATION
1 le as ategy2
Strategy First line Second line ThiExpe Pfyears
TE LYs
ed QALYs
Total Expected Costs
Tab 13: b e-case results, by strrd line Total
cted
otal xpected
Total Expect
1 DOC+CAP N Chemo
0.7833 1.2643 0.7694 £21,406 VIN o
2 A No Chemo 0.5009 0.9283 0.5452 £15,526 3 O CAP VIN 1.3392 1.9352 1.1896 £31,479 4 GEM+DO CAP No
Chemo 1.0600 1.5768 0.9734 £25,882
5 O C P 1.3422 1.9405 1.1857 £30,859 6 GEM+DO VIN No
Chemo 0.8306 1.3390 0.8230 £27,124
7 O No Chemo 0.5443 0.9691 0.5827 £21,056 AC CAP VIN 1.0 1 £24,521 AC CAP No
Chemo 0.7716 1.2763 0.7527 £18,871
10 CAP 1.0551 1.6377 0.9642 £23,872 VIN No
Chemo 0.5411 1.0359 0.6009 £20,119
2 AC No Chemo 0.2534 0.6754 0.3645 £14,022 3 OC CAP VIN 1.2043 1.7680 1.0738 £26,442 4 OC N
Chemo 0.9197 1.4150 0.8500 £20,727
1.0592 £25,675 16 DOC VIN No 0.6916 1.1771 0.6997 £21,962
0.4069 0.8337 0.4718 £15,928
DOC+C P GEM+D C
C
GEM+D C VIN AC
GEM+D C 8 P 532 .6240 0.9739 9 P
PAC VIN 11 PAC
1 P 1 D1 D CAP o
15 DOC VIN CAP 1.2002 1.7726
Chemo 17 DOC No Chemo
PFyears = progression-free years, LYs = life years, QALYs = quality adjusted Incremental cost-effectiveness analysis Using QALYs as the outcome measure, an incremental cost-effectianalysis was performed by first ranking the strategies according to per patient (highest to lowest). This allowed the dominated strategidentified and ruled out of the incremental analysis. Any strategies fewer QALYs and incurring higher cos
life years 3 4 5 6
veness 7 the cost 8
ies to be 9 achieving 10
ts when compared to any other are 11 ruled out by simple dominance (highlighted in table 14 in light grey), and any 12 stategies that achieve fewer QALYs and higher costs than a combination of 13 two other strategies are ruled out via extended dominance (highlighted in 14 table 14 in dark grey). This left seven remaining strategies (2, 3, 5, 9, 12, 14 15 and 15) which are labelled in figure 3 below. 16
Advanced breast cancer: full guideline DRAFT (August 2008) Page 113 of 146
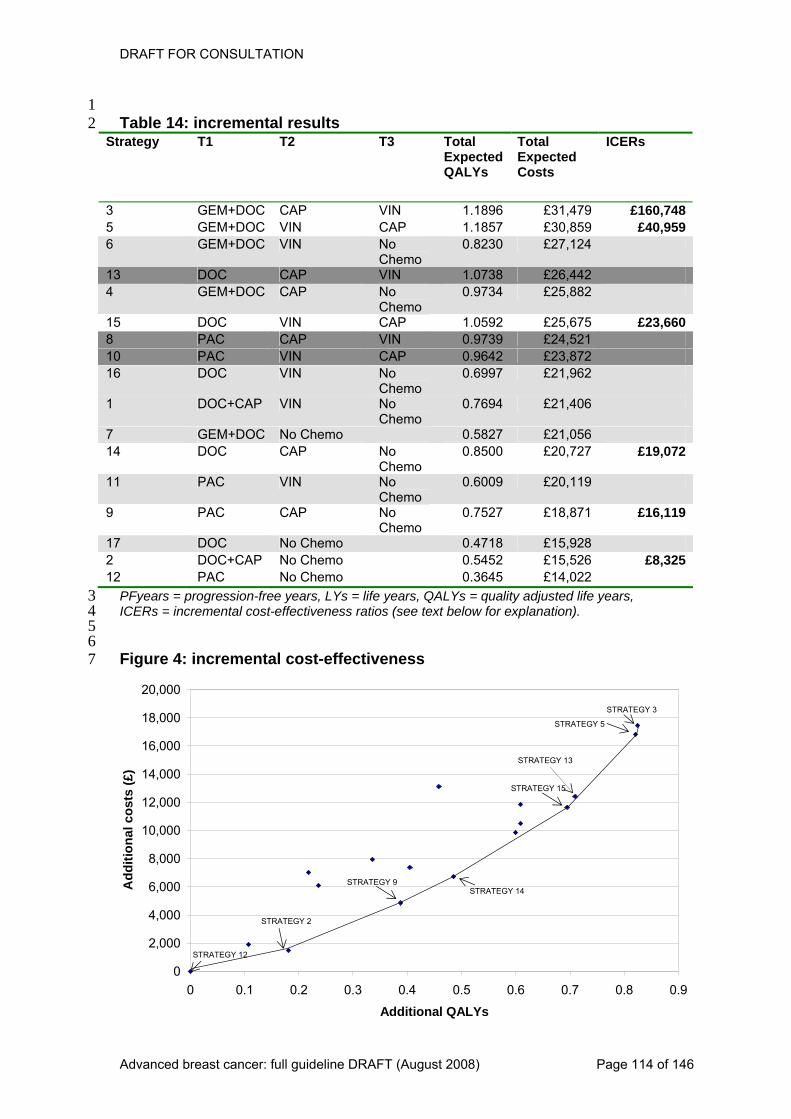
DRAFT FOR CONSULTATION
1 le 1 ncrem al results2
Strategy T1 T2 T3 oExpected QALYs
Total Expected Costs
ICERs Tab 4: i ent
T tal
3 CAP VIN 1.1 £31 £160,748GEM+DOC 896 ,479 5 GEM+DO VIN 1.1857 £30,859 £40,959C CAP 6 GEM+DOC VIN No
Chemo 0.8230 £27,124
13 DOC CAP VIN 1.0738 £26,442 4 GEM+DOC CAP No
Chemo 0.9734 £25,882
15 OC VIN CAP 1.0 £25,675 £23,660D 5928 PAC CAP VIN 0.9739 £24,521 10 PAC VIN CAP 0.9642 £23,872 16 DOC VIN No
Chemo 0.6997 £21,962
1 DOC+CAP VIN No Chemo
0.7694 £21,406
7 GEM+DOC No Chemo 0.5827 £21,056 14 DOC CAP No
o 0.8 £20 £19,072
Chem500 ,727
11 PAC VIN No Chemo
0.6009 £20,119
AC No 0.7 £18,871 £16,1199 P CAP 527Chemo
17 DOC No Chemo 0.4718 £15,928 DOC+CAP No Chemo 0.5452 £15,526 £8,325
0.3645 £14,022 212 PAC No Chemo
PFyears = progression-free years, LYs = life years, QALYs = quality adjusted life years, 3 ICERs = incremental cost-effectiveness ratios (see text below for explanation). 4 5 6 Figure 4: incremental cost-effectiveness 7
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
Additional QALYs
Add
ition
al c
osts
(£)
STRATEGY 15
STRATEGY 13
STRATEGY 3
STRATEGY 5
STRATEGY 14
STRATEGY 2
STRATEGY 9
STRATEGY 12
Advanced breast cancer: full guideline DRAFT (August 2008) Page 114 of 146

DRAFT FOR CONSULTATION
The seven unshaded strategies in table 14 above (strategieand 15) are non-dominated strategies which were considered in tincremental analysis. All the other strategies are considered not toeffective so would never be chosen on the basis of cost-effectiveneincremental cost-effectiveness ratios (ICERs) shown in the last columtable 14 are the ratios of cost and health benefit for each strategy coto the next best strategy. NICE recommends the use of a thresper QALY. Using a threshold value of £20,000 per QALY, strategy (docetaxel followed by capecitabine followed by no chemotherapshown to be most cost-effective since it maximises health benefitsbudget constraint. However there may be compelling reasons slightly higher ICER of up to £30,000 per QALY which would make s15 (docetaxel followed by vinorelbine and then capecitabine) moeffective since it maximises QALYs below this threshold. Due to thof strategies in the analysis, the results need careful interpretationthere is very little difference between strategies 13 (docetaxecapecitabine follow
1 s 2, 3, 5, 6, 12, 14 2
he 3 be cost-4 ss. The 5
n of 6 mpared 7
hold of £20,000 8 14 9
y) was 10 given the 11
to accept a 12 trategy 13
st cost-14 e multitude 15 . Since 16
l followed by 17 ed by vinorelbine) and 15, in terms of QALYs, and given 18
the uncertainty surrounding these point estimates, it is not clear which 19 the 20
21 22
an be 23 es 3 and 5 24
would be ruled out since their ICERs of £160,748 and £40,959 respectively, 25 imum threshold NICE recommends; the additional 26
0.1265 is judged to not be worth the extra £5,184, nor is the 0.1302 QALYs 27 28 29 30 31 32
e utility values used in the analysis, the data used on the hird-line 34
ll survival. A 35 elow: 36
37 38
d in the 39 re 40
ffectiveness. At 41 xel, vinorelbine, 42
Rs 43 ncreased (due 44
to higher QALYs) to £26,250 when the utility values were decreased. At a 45 willingness to pay of £20,000 strategy 14 remained most cost effective when 46 utilities increased (with an ICER of £21,000) but when the utilities were 47 reduced, strategy 9 (paclitaxel, capecitabine, no chemo) had the most 48 favourable ICER at £17,923. When the utility ascribed to patients with toxicity 49 was varied from the base-case value of 0.44 to 0.35 (to equal the utility 50
strategy is dominated and thus which should be excluded from incremental analysis. Strategies 2, 9, 12 and 14 would be ruled out since more QALYs cachieved given the maximum willingness to pay. Similarly strategi
are far above the max
for the extra £5,804. Sensitivity Analysis Five sources were thought to contribute most to the uncertainty surrounding the analysis; th33 effectiveness of capecitabine monotherapy, the effectiveness of ttherapy, possible price discounts and the calculation of overanumber of scenarios were investigated and the results are outlined b o Utility values An arbitrary 10% increase and decrease in all the utility values usemodel were tested and made no difference to the strategies that wedominated or to the ranking of the strategies in terms of cost-ea willingness to pay of £30,000 per QALY, strategy 15 (docetacapecitabine) was still the most cost-effective strategy, with the ICEranging from roughly £21,500 when all the utility values were i
Advanced breast cancer: full guideline DRAFT (August 2008) Page 115 of 146

DRAFT FOR CONSULTATION
associated with progressive disease with toxicity), this made little difthe base-case results. Total QALYs (per patient) w
ference to 1 ere slighted reduced with 2
strategy 15 but it still had a favourable ICER of £23,687. 3
5 abine 6 is 7 en it had 8
00 strategy 9 eshold and 10
orelbine) 11 12
cetaxel + capecitabine, then no chemo) 13 14 15 16
in the 17 time spent 18 -19
hem by one 20 was no 21
f strategies. 22 ffective 23 £30,000 per 24
. The survival estimates 25 proved to have more impact, since strategy 15 (docetaxel, vinorelbine, 26
dominated. Strategy 13 was associated with an ICER of bine, no 28
29 30 31
tigated (50%, 32 ase results. 33
therapy, but 34 s did not 35
0 36 er 37
then no chemotherapy yielded 38 14,250 and would be most cost-effective
n both 40 an even 41
effective at a 42 43
44 o Time from progression to death 45 The time from progression to death (assumed to be 5 months in the base-46 case analysis) was varied from 4 – 6 months. This change, in either direction, 47 had little effect on the base-case results serving to increase (6 months) or 48 decrease (4 months) both the health benefits and the costs. Depending on the 49
4 o Effectiveness of capecitabine monotherapy The time spent without progressive disease having received capecitmonotherapy was reduced by one third in the sensitivity analysis. Thresulted in strategy 13 being included in the incremental analysis, whbeen dominated in the base case. Using a threshold value of £30,015 was still most cost-effective, maximising QALYs given the thrwith an ICER of £25,359. Strategy 13 (docetaxel, capecitabine, vinwas associated with an ICER of £32,445. If a stricter threshold value was applied, say £20,000, strategy 2 (Dowas most cost-effective with an ICER of £8,325. o Effectiveness of third-line treatment Two ‘effectiveness’ parameters for third-line treatment were variedsensitivity analysis; the response and disease stabilisation, and thefree of progressive disease for responders, stable patients and nonresponders. Both parameters were separately tested, reducing tthird. When the response and stabilisation rates were reduced there change to the strategies that were dominated, or to the ranking oThe conclusions from the base-case held, but the two most cost-estrategies (when examining two different thresholds, £20,000 andQALY) were associated with slightly higher ICERs
capecitabine) was27 £34,878 but the best strategy was strategy 14 (docetaxel, capecitachemo) with an ICER of slightly over £19,000 per QALY. o Price discounts A number of different price discounts for paclitaxel were inves60%, 70%, 80%, and 90%) and, as expected, changed the base-cPaclitaxel replaced docetaxel as the most cost-effective starting after this the preferred sequences in terms of cost-effectiveneschange from the base case. The ICERs associated with strategy 1(paclitaxel, vinorelbine, capecitabine) ranged from £19,000 to just ov£21,000. Paclitaxel followed by capecitabineICERs ranging from £16,300 to £39 given a £20,000 per ICER threshold. A likely discount available opaclitaxel (90%) and vinorelbine (45%) showed strategy 10 to have more favourable ICER (£18,666 per QALY), making it most cost-threshold of both £20,000 and £30,000 per QALY.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 116 of 146

DRAFT FOR CONSULTATION
threshold value, either strategy 15 or strategy 14 would be considered most 1 cost-effective. 2
3 ase were 4 s resulted 5 el as the 6 the 7 l resulting 8
9 different strategies being dominated and thus excluded from the incremental 10 results. 11
12 13
14 15 16
y show that 17 18
ies but those 19 ness. 20
21 ategy 22 the use of 23
y accept 24 first by vinorelbine 25
lity-adjusted 26 sults need 27 el followed 28
29 y a tiny 30
these 31 which 32
should be excluded from the incremental analysis. If strategy 15 was 33 egy 13 would 34
. On these 35 is always 36
37 38
out in terms of cost-effectiveness 39 s to pay. 40 £160,748 41
CE 42 the extra £5,184, 43
44 45 The sensitivity analysis show there may however be circumstances in which 46 the base-case results do not hold true. The presence of substantial discounts 47 available nationally for paclitaxel show that if this discount is maintained and 48 is available across England and Wales, the taxane of choice would be 49 paclitaxel rather than docetaxel, since these strategies yielded more 50
Overall the sensitivity analyses showed that the results of the base creasonably robust to the parameters investigated. The main changefrom big potential price discounts, substituting docetaxel for paclitaxpreferred starting therapy. Other changes were noted when alteringeffectiveness of third-line therapy and the ‘progression-free’ survivafrom capecitabine, which was due to small differences in QALYs leading to
DISCUSSION The base-case results of this analysis provide a clear message for recommendations on this topic, in terms of cost-effectiveness. Thedocetaxel as a single agent therapy dominates the other taxane, paclitaxel, and any combination therapy involving gemcitabine, so all strategstarting with first-line docetaxel are ruled out in terms of cost-effectiveUsing the threshold of £20,000, the most cost-effective strategy wasdocetaxel followed by capecitabine and then no further treatment (str14). The GDG may consider there to be circumstances which justify a higher threshold by which to judge cost-effectiveness and therebstrategy 15 which also starts with docetaxel but is followed and then capecitabine. This strategy is associated with higher quasurvival. Due to the multitude of strategies in the analysis, the recareful interpretation. There is one strategy, strategy 13 (docetaxby capecitabine then vinorelbine) that is narrowly excluded from theincremental analysis on the basis of extended dominance, but only bdifference in total QALYs, 0.015. Given the uncertainty surroundingpoint estimates, it is not clear which strategy is dominated and thus
dominated, leaving strategy 13 in the incremental analysis, stratbe associated with a favourable ICER of below £30,000 per QALYgrounds the analysis does not provide clear evidence on whether it preferable to give vinorelbine first followed by capecitabine. Strategies 2, 9, 12 and 14 can be ruled since more QALYs can be achieved given the maximum willingnesSimilarly strategies 3 and 5 would be ruled out since their ICERs of and £40,959 respectively, are far above the maximum threshold NIrecommends; the additional 0.1265 is judged to not be worth nor is the 0.1302 QALYs for the extra £5,804.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 117 of 146

DRAFT FOR CONSULTATION
favourable ratios of costs and health benefits. In response to doubtvalidity of the utility value for progressive disease, a 10% increasevalue w
s over the 1 in this 2
as tested and it was found that the results were not sensitive to this 3 increase. 4
5 g was 6
y. 7 e the 8
to costs 9 nsitivity 10 h does not 11 e of the 12 pact on 13
idered in 14 were not exhaustive and whilst the most common sequences were 15
ded from 16 17 18
sistent data on 19 many 20
ferent 21 t 22
poorer for 23 erapy 24
sults 25 26
ticular this was 27 ted with any quality of life increase from the published utility values 28
29 lored in the 30
e 31 32 33
re and 34 ferences between the different therapies, for 35
instance the differences in i.v. times were not captured by costs (or utilities). It 36 ith 37 f the 38
ed, which 39 40 41
some 42 e in its 43
pic. Single 44 agent taxane (either docetaxel or paclitaxel depending on the price discounts 45 available) is the most cost-effective starting therapy. The combination 46 therapies are much less cost-effective primarily due to the fact repetition of a 47 chemotherapy agent later in the sequence was not allowed in this analytical 48 model. Three lines of chemotherapy were shown to deliver more QALYs than 49 one or two lines. The choice of which order to deliver capecitabine and 50
There are a number of limitations to this analysis. No discountinundertaken on either the costs or benefits attributed to each strategHowever this is unlikely to have a major bearing on the results sincpatients live for a short time and treatment is the biggest contributor which fall at the beginning rather than throughout the year. The seanalyses conducted was rather limited and using an approach whicfully capture the uncertainty surrounding the model. In addition somstrong structural assumptions were not tested, and therefore their imthe conclusions of the analysis is unknown. The interventions consthe model included, there may be relevant comparators that have been excluthe analysis. Whilst a great deal of effort has been spent on obtaining confirst-line treatment, by undertaking an indirect treatment comparison,strong assumptions had to be made to combine evidence from difsources to inform the model on the relative effect of the full treatmensequences. Evidence on second-line treatment was poor, and eventhird-line treatment. The survival estimates from capecitabine monothseem very high, higher even than first line treatment; although the reseem to be robust to a reduction in these by a third in the sensitivity analysis. No evidence existed for the ‘No Chemotherapy’ option, in parnot associafor progressive disease. Expert opinion from the guideline development group was used to fill in gaps in the data, but this has not been fully expsensitivity analysis and some concerns remain as to the validity of thassumptions. The costs used were often proxies for costs that were hard to captumay not fully capture the dif
was also assumed that combination therapy was not associated wadditional administration times, thus biasing the results in favour ocombination therapies. In addition it was no vial sharing was assummay not reflect clinical practice. Despite these acknowledged limitations, this analysis does provideuseful information for which the guideline development group can usdeliberations over the recommendations to be made on this to
Advanced breast cancer: full guideline DRAFT (August 2008) Page 118 of 146

DRAFT FOR CONSULTATION
vinorelbine is not as clear cut, and although the results show vinorela more cost-effective second line treatment than capecitabine, the dibetween the two strategies (13 and 15) is so sma
bine to be 1 fference 2
ll, the guideline development 3 group should interpret this particular result with caution. 4
5 6 7
bine plus 8 paclitaxel (GT) vs. paclitaxel (T) as frontline therapy for metastatic breast 9
S. 10 11 12 13 14 15
ost-utility model comparing docetaxel 16 ct)." Anti
References Albain KS, Nag S, et al. (2004) Global phase III study of gemcita
cancer (MBC): first report of overall survival. J Clin Oncol 22:5 Bonneterre, J., H. Roch‚, et al. (2002). "Docetaxel vs 5-fluorouracil plus vinorelbine in metastatic breast cancer after anthracycline therapy failure." British journal of cancer 87(11): 1210-1215. Brown, R. E. and J. Hutton (1998). "Cand paclitaxel in advanced breast cancer patients (Structured abstra17
18 19
Brown, R. E., J. Hutton, et al. (2001). "Cost effectiveness of treatment options 20 21 22 23
etaxel versus capecitabine plus 24 ast cancer: 25
an Journal of 26 27 28 29
in 30 y Series A-31
32 33
99) “Costs of palliative care in the community, in 34 hospitals and in hospices in the UK”. Crit Rev Oncol Hematol, 32: 71-85. 35
36 37
sandstatistics/Publications/PublicationsP
Cancer Drugs 9(10): 899-907.
in advanced breast cancer in the UK. [Review] [27 refs]." Pharmacoeconomics 19(11): 1091-1102. Chan, S. (2005). "Gemcitabine plus docdocetaxel for patients with anthracycline-pretreated metastatic breA review of the results of a European Phase III trial." EuropeCancer Supplement 1990 3(5): 17-21. Cooper, N. J., K. R. Abrams, et al. (2003). "A Bayesian approach to Markov modelling in cost-effectiveness analyses: application to taxane useadvanced breast cancer." Journal of the Royal Statistical SocietStatistics in Society 166: 389-405. Coyle D, Small N, et al. (19
Department of Health. National Reference Costs 2006/07 (http://www.dh.gov.uk/en/Publication38 olicyAndGuidance/DH_082571) Dieras V, Marty M, Tubiana N, Corette L, Mo
39 40
rvan F, Serin D, et al. (1995) 41 Phase II randomized study of paclitaxel versus mitomycin in advanced breast 42
43 44
Frasci, G., R. Comella, et al. (2000). "Weekly docetaxel plus gemcitabine or 45 vinorelbine in refractory advanced breast cancer patients: A parallel dose-46 finding study." Annals of Oncology 11(3): 367-371. 47 48 Jones, S. E., J. Erban, et al. (2005). "Randomized phase III study of docetaxel 49 compared with paclitaxel in metastatic breast cancer." Journal of clinical 50
cancer. Semin Oncol 22(4 Suppl 8):33–9.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 119 of 146

DRAFT FOR CONSULTATION
oncology : official journal of the American Society of Clinical Oncology. 1 23(24): 5542-5551. 2
3 linical 4
cally 5 tatic breast cancer." Health Technology Assessment 6
7 8 9
10 11
ost-utility 12 13
04–21. 14 15 16
el, or vinorelbine for patients with 17 )." Journal of Clinical 18
19 20
is, R. Bagnall, A-M. (2002) The clinical effectiveness and cost-21 and 22
England) 23 24
25 analysis comparing second-line 26
er. Anti-Cancer 27 28 29 30
C1-42C5-31 32
33 P, et al. 34
avelbine 35 ) as 2nd line 36
37 38
L, Douma 39 ycline-40
tant metastatic breast cancer. Oncology 11(8 Suppl 8):25–30. 41 42
apecitabine 43 ents with 44
advanced breast cancer: phase III trial results. Journal of clinical oncology : 45 official journal of the American Society of Clinical Oncology. 20(12): 2812-46 2823. 47 48 Pierga, J. Y., P. Fumoleau, et al. (2004). Efficacy and safety of single agent 49 capecitabine in pretreated metastatic breast cancer patients from the French 50
Jones, L., N. Hawkins, et al. (2001) "Systematic review of the ceffectiveness and cost-effectiveness of capecitabine (Xeloda) for loadvanced and/or metas(Winchester, England) 8(5) Launois, R. (2003). "Economic assessment, a field between clinical research and observational studies." Bulletin du Cancer 90(1): 97-104. Launois R, Reboul Marty J, Henry B, Bonneterre J. (1996) “A canalysis of second-line chemotherapy in metastatic breast cancer: docetaxel versus paclitaxel versus vinorelbine.” Pharmacoeconomics;10:5 Leung, P. P., I. F. Tannock, et al. (1999). "Cost-utility analysis of chemotherapy using paclitaxel, docetaxanthracycline-resistant breast cancer (Structured abstractOncology 17(10): 3082-3090. Leweffectiveness of vinorelbine for breast cancer: a systematic review economic evaluation. Health Technology Assessment (Winchester, 6(14)
Li, N., A. M. van, et al. (2001). A cost--utilitychemotherapy schemes in patients with metastatic breast cancDrugs 12(6): 533-540. Marie Curie report Valuing Choice: Dying at Home (http://campaign.mariecurie.org.uk/NR/rdonlyres/646C31D0-498BFE-D1A8F3F3A499/0/campaign_valuing_choice.pdf)
Monnier A, Bonneterre J, Roche H, Fargeot P, Namer M, Gustalla J(1998) Phase III study: taxotere (TXT) versus 5-fluorouracil + N(FUN) in patients (pts) with metastatic breast cancer (MBCchemotherapy (CT) (preliminary results). Ann Oncol ;9 Suppl 4:12. Nabholtz J, Thuerlimann B, Bezwoda W, Melnychuk D, DeschenesJ, et al. (1997) Docetaxel vs mitomycin plus vinblastine in anthracresis
O'Shaughnessy, J., D. Miles, et al. (2002). Superior survival with cplus docetaxel combination therapy in anthracycline-pretreated pati
Advanced breast cancer: full guideline DRAFT (August 2008) Page 120 of 146

DRAFT FOR CONSULTATION
compassionate use program. Breast Cancer Research & Treatment 88(2): 1 117-129. 2
3 Care (2007). 4
5 6
ral 7 psing after 8
ne-containing therapy. Annals of Oncology 14(8): 1227-9 10 11
t-12 ine and 13
ng abstract]. 14 edings of the 35th Annual Meeting of the American Society of Clinical 15
ria, VA: ASCO; 16 17 18
rsus 19 methotrexate–5-fluorourocil in patients with advanced anthracycline resistant 20
tudy by the 21 1. 22
23 al. (2002). Randomised, phase II trial 24
25 ines. British 26
PSSRU, Unit Costs of Health and Socialhttp://www.pssru.ac.uk/uc/uc2007contents.htm Reichardt, P., M. G. von, et al. (2003). Multicenter phase II study of ocapecitabine (Xeloda) in patients with metastatic breast cancer relatreatment with a taxa1233. Silberman G, Gupta S, Berkowitz N, Leyland Jones B. (1999) Coseffectiveness of capecitabine, continuous infusion 5-FU, gemcitabvinorelbine in the treatment of metastatic breast cancer [meetiProceOncology; 1999 May 15–18; Atlanta, GA, USA. AlexandA1629. Sjostrom J, Mouridsen H, Pluzanska A. (1998) Taxotere ve
breast cancer: preliminary results of a randomised Phase III sScandinavian Breast Cancer Group [abstract]. Proc ASCO 17:11 Talbot, D. C., V. Moiseyenko, etcomparing oral capecitabine (Xeloda) with paclitaxel in patients withmetastatic/advanced breast cancer pretreated with anthracycljournal of cancer. 86(9): 1367-1372. Verma, S, Verma
27 28
, S. Maraninchi D, O’Shaughnessy J, Jameison C, Jones S, 29 2005) 30 ess in 31 Cancer 32
(12): 2455-2465. 33 34 Verma, S. and A. L. Ilersich (2003). Population-based pharmacoeconomic 35 model for adopting capecitabine/docetaxel combination treatment for 36 anthracycline-pretreated metastatic breast cancer. The oncologist.
Martin M, McKendrick J, Miles D, Twelves C and Hornberger J, (Capecitabine plus docetaxel combination therapy: Cost-effectivenpatients with anthracycline-pretreated advanced breast carcinoma.103
8(3): 232-37 240. 38 39
Advanced breast cancer: full guideline DRAFT (August 2008) Page 121 of 146

DRAFT FOR CONSULTATION
Appendix 2 1
2 Abbreviations 3
4 5 6 7 8
or 9 10 11
2 tor receptor 2 12 13 14 15 16
CT tomography fused with computed 17 tomography 18
RCT randomised controlled trial 19 WBRT whole brain radiotherapy 20
AI aromatase inhibitor CDT complex decongestive therapy
CRF cancer-related fatigue CT computed tomography EGFR epidermal growth factor receptER oestrogen receptor FDG 18F-deoxyglucose HER human epidermal growth facMLD manual lymphatic drainage
MLLB multi-layer lymphoedema bandaging MRI magnetic resonance imaging PET positron emission tomography PET- positron emission
Advanced breast cancer: full guideline DRAFT (August 2008) Page 122 of 146

DRAFT FOR CONSULTATION
Appendix 3 1 2
Glossary 3 4 5
d to remove any microscopic 6 may have been left behind. 7
8 9
s, travelling 10 h the bloodstream or lymphatic system (locally advanced breast cancer 11
12 13 14 15
oestrogen in postmenopausal women by 16 e, a key enzyme which helps to form oestrogen from other 17
18 19
20 21 22
isease 23 t or above 24
25 26
onse modifier 27 r to inhibit 28
29 30 31
A group of drugs used to treat or prevent osteoporosis and to treat the bone 32 d by some types of cancer. 33
34 35 36 37 38
urrounds the cells. 39 40 41
based on the detection of radiation emitted by 42 a radioactive tracer injected into the body that targets abnormal areas of 43 bone. 44 45 Brachial plexus 46 A network of nerves in the neck and armpit that conducts signals from the 47 spine to the shoulder, arm and hand. 48 49
Adjuvant therapy Treatment as a follow-up to surgery designetraces of tumour which Advanced breast cancer Disease that has spread from the breast to other body systemthrougis disease that has spread to large parts of the breast or nearby lymph nodes). Aromatase inhibitor Drugs that reduce the blood levels ofblocking aromatassteroids.
Axillary thrombosis A blood clot in the large vein under the arm. Axillary/supraclavicular dSpread of (breast cancer) disease to the lymph nodes in the armpithe collar bone.
Biological respA substance which aids the body’s natural defence system in ordethe growth of a tumour. Bisphosphonates
pain cause Body habitus The size and shape of a person's body. Bone matrix The major constituent of bone tissue which s Bone scintigraphy A diagnostic imaging technique
Advanced breast cancer: full guideline DRAFT (August 2008) Page 123 of 146

DRAFT FOR CONSULTATION
Chemotherapy 1 A chemical that specifically binds to and kills tumour cells. 2
3 4
inside of the chest, taken using X-rays. Most often used 5 ngs. 6
7 8 9
d an intervention with a similar group of people that did not. 10 11
ity 12 ion in an individual at 13
14 15 16
ovide mild compression in order to increase the flow 17 18 19
Computed tomography (CT) 20 21 22 23
aids 24 sources which can help patients participate in decisions about 25
their health e.g. information booklet, CD-ROM. 26 27 28 29 30 31
down or 32 the growth of a tumour. 33
34 35
Open to more than one interpretation and therefore of uncertain significance. 36 37 38
encodes a growth-promoting protein which helps to control how 39 selves. 40
41 42
describe the variation in the ways in which several people carry out 43 the same task. 44 45 Magnetic resonance imaging 46 A diagnostic imaging technique that uses powerful electromagnets, radio 47 waves and a computer to produce well-defined images of the body’s internal 48 structures. 49 50
Chest radiograph An image of theto show the lu Cohort studies Observational studies in which outcomes are compared in a group of patients that receive Co-morbidThe presence of more than one disease or health condita given time. Compression/containment garment Items of clothing which prof blood to and from specific muscle groups.
A diagnostic imaging technique that uses X-rays and a computer to produce a detailed picture of a cross section of the body DecisionA variety of re
Dyspnoea Breathlessness. Endocrine therapy Treatment that adds, blocks, or removes hormones in order to slowstop Equivocal
HER2 A gene that cells divide and repair them Inter-operator variability A term to
Advanced breast cancer: full guideline DRAFT (August 2008) Page 124 of 146

DRAFT FOR CONSULTATION
Manual lymphatic drainage A massage technique that uses a gentle pumping technique to stimulate the
1 2
lymphatic system and improve lymph drainage. 3 4 5
earch by reviewing and combining the 6 number of different clinical trials. 7
8 9
Spread of cancer away from the primary site to somewhere else via the 10 m. 11
12 g 13
dage around a limb to apply graduated pressure 14 15 16
stases 17 growth. 18
19 etastases 20
n. 21 22
ession 23 tioning of the 24
ies and significantly reduces oestrogen levels in the blood. 25 26
27 gion of the 28
29 30 31 32
increased tissue metabolism. 33 34 35
the arms and legs which are nearest to the main 36 37 38 39 40
rays) to prevent cell growth. 41 42 43
A clinical trial in which subjects are randomized to different groups for the 44 purpose of studying the effect of a new intervention, for example a drug or 45 other therapy. 46 47 Simple lymph drainage 48 Gentle massage to move excess lymph fluid away from a swollen area. 49 50
Meta-analysis A method of summarizing previous resresults of a Metastases
bloodstream or the lymphatic syste Multi-layer lymphoedema bandaginUsing multiple layers of banand reduce swelling due to lymphoedema. Osteoblastic bone metaCancer that has spread to the bone causing disorganised new
Osteolytic bone mCancer that has spread to the bone causing areas of bone destructio Ovarian supprSurgery, radiation therapy or drug treatment which stops the funcovar
Plain radiograph A diagnostic image obtained by directing X-rays to a specific rebody. Positron emission tomography A diagnostic imaging technique using a radio-active tracer which shows
Proximal limb bones Bones in those parts of trunk. Radiotherapy A treatment for cancer that uses high energy ionising radiation (usually X-
Randomised controlled trials (RCTs)
Advanced breast cancer: full guideline DRAFT (August 2008) Page 125 of 146

DRAFT FOR CONSULTATION
Stereotactic radiosurgery A radiation therapy that uses special equipment to position the ppreci
1 atient and 2
sely deliver a large radiation dose to a tumour while avoiding normal 3 tissue. 4
5 6
address a defined 7 and using quantitative methods to summarize the results. 8
9 oxifen 10
An anti-cancer drug that blocks the effects of the hormone oestrogen in the 11 12 13 14
An imaging method in which high-frequency sound waves are used to outline 15 a part of the body. 16 17
Systematic review A systematic review of the literature carried out in order to question Tam
body. Ultrasound
Advanced breast cancer: full guideline DRAFT (August 2008) Page 126 of 146

DRAFT FOR CONSULTATION
Appendix 4 1 2
Guideline Scope 3
5
breast cancer: diagnosis and treatment
7
ast cancer
9
the 10 ancer to 11 cancer 12 topic by 13
ppendix 14 cer will be developed 15
his document is the scope for the recommendations on advanced 16 d practice 17
18 19
ational 20 ects of care where a Framework has 21
22 s and 23 en issued 24
25
‘NHS 26 ‘Manual of 27
d’ and the ‘Wales Cancer Standards’. 28 29
‘Improving 30 al guideline 31
elines for suspected cancer’. 32
NICE clinical guidelines support the role of healthcare professionals in 33 providing care in partnership with patients, taking account of their individual 34 needs and preferences, and ensuring that patients (and their carers and 35 families, where appropriate) can make informed decisions about their care 36 and treatment. 37
4
Guideline title Advanced 6
Short title Advanced bre8
Background The National Institute for Health and Clinical Excellence (‘NICE’ or ‘Institute’) has commissioned the National Collaborating Centre for Cdevelop a clinical guideline on the diagnosis and treatment of breast for use in the NHS in England and Wales. This follows referral of thethe Department of Health and Welsh Assembly Government (see aA). Recommendations on early and advanced breast canin parallel. Tbreast cancer. The guideline will provide recommendations for goothat are based on the best available evidence of clinical and cost effectiveness.
The Institute’s clinical guidelines will support the implementation of NService Frameworks (NSFs) in those aspbeen published. The statements in each NSF reflect the evidence that was used at the time the Framework was prepared. The clinical guidelinetechnology appraisals published by the Institute after an NSF has bewill have the effect of updating the Framework.
This guideline will support current national initiatives outlined in the Cancer Plan’, the ‘Calman-Hine Report’, the ‘Cameron Report’, the Cancer Service Standards for EnglanThe guidelines will also refer to the
NICE service guidance ‘Improving outcomes in breast cancer’ andsupportive and palliative care for adults with cancer’ and the clinic‘Referral guid
Advanced breast cancer: full guideline DRAFT (August 2008) Page 127 of 146

DRAFT FOR CONSULTATION
Clinical need for the guide1 line Breast cancer is the most common cancer for women in England anwith about 37,000 new cases diagnosed
d Wales, 2 ecorded in 3
ut 270 4 r. Of these 5 vanced 6
or to other 7 men who 8
ently develop 9 ave been 10
se 11 agents. 12
e country and of patchy 13 ertain treatments and procedures. A clinical guideline will help e issues and offer guidance on best practice.
16
n two publications 17 ’). ‘The 18
public and 19 become involved in the 20
ation for 21 dvice on 22
23
This document is the scope. It defines exactly what this guideline will (and will 24 scope is 25 embly 26
27
the basis on which the work of a guideline development 28 group (GDG) is planned and should be very clear about which patient groups 29
and which areas of clinical care will be considered.
ressed by the guideline are described in the
Population 33
34
t of clinical 35 c disease). 36
1112 and 11,000 deaths13 rEngland and Wales each year. In men breast cancer is rare, with abocases diagnosed1,2 and 70 deaths3 in England and Wales each yeanew cases in women and men, around 10% are diagnosed in the adstages, when the tumour has spread significantly within the breastorgans of the body. In addition, there is a significant number of wohave been previously treated with curative intent who subsequeither a local recurrence or metastases. Over recent years there himportant developments in the investigation and management of thepatients including new chemotherapy, and biological and hormonalThere is some evidence of practice variation across thavailability of c14 to address thes15
The guideline The guideline development process is described in detail iwhich are available from the NICE website (see ‘Further informationguideline development process: an overview for stakeholders, thethe NHS’ describes how organisations candevelopment of a guideline. ‘Guideline development methods: informnational collaborating centres and guideline developers’ provides athe technical aspects of guideline development.
not) examine, and what the guideline developers will consider. Thebased on the referral from the Department of Health and Welsh AssGovernment (see appendix).
The scope forms
are included30
The areas that will be add31 following sections. 32
Groups that will be covered • Women and men with invasive adenocarcinoma of the breas
stage 4 (i.e. with known metastati
11 Office for National Statistics (2005) Cancer statistics registrations: registrations of cancer diagnosed in 2002, England. Series MB1 number 33. London: National Statistics. 12 Welsh Cancer Intelligence and Surveillance Unit (2005) Cancer incidence in Wales 1992−2002. Cardiff: Welsh Cancer Intelligence and Surveillance Unit. 13 Office for National Statistics (2003) Mortality statistics: cause. England and Wales 2003. London: The Stationery Office.
Advanced breast cancer: full guideline DRAFT (August 2008) Page 128 of 146

DRAFT FOR CONSULTATION
G1 roups that will not be covered • Women and men with invasive adenocarcinoma of the breas2
stages 1, 2 and 3 (this will be covere3 t of clinical
d by the NICE guideline on ‘Early
rcoma,
• Women and men with benign breast tumours (for example, fibroadenoma, 9 tumours).
d and opportunistic screening.
cialist breast cancer teams. ces
agement
• Bisphosphonates 23 agement of lymphoedema
tient information and communication pportive and palliative care
28
n of the scope.
of the guideline recommendations will begin in June 2006.
32
Published guidance 34
The following guidance will be cross referred to in the advanced breast cancer 35 guideline as appropriate: 36
• Referral guidelines for suspected cancer. NICE clinical guideline no. 27 37 (2005). Available from: www.nice.org.uk/CG027 38
breast cancer: diagnosis and treatment’). 4 • Women and men with metastases to the breast from other primary 5
tumours. 6 • Women and men with rare breast tumours (for example, angiosa7
lymphoma) 8
benign phyllodes10
Healthcare sett11 ing • Primary care − excluding population-base12 • Secondary care. 13 • Tertiary care by spe14
re servi• Palliative ca15
Clinical man16
• Investigation 17 • Surgery 18 • Radiotherapy 19 • Hormonal therapy 20 • Chemotherapy 21
r targeted therapies • Biological agents and othe22
• Man24 • Pa25 • Su26
Status 27
Scope This is the final versio29
Guideline 30
The development31
Further information
Related NICE guidance 33
Advanced breast cancer: full guideline DRAFT (August 2008) Page 129 of 146
DRAFT FOR CONSULTATION
• Familial breast cancer: the classification and care of women at ris1 familial breast cancer in primary, secondary and tertiary 2
k of care. NICE clinical
14 ancer. Cancer
sp
one
evention of osteoporotic fragility fractures in postmenopausal women. NICE technology appraisal no. 87 (2005). 11
w.nice.org.uk/TA087
13
guideline
advanced o. 62 (2003).
.nice.org.uk/TA062 ced breast
le from:
ed breast logy appraisal no. 54 (2002). Available from:
www.nice.org.uk/TA054 24 se of taxanes for the treatment of breast cancer. NICE al no. 30 (2001). Available from:
27 28
e in development 29
praisal
guideline no. 14 (2004). Available from: www.nice.org.uk/CG03 • Improving supportive and palliative care for adults with c4
service guidance (2004). Available from: www.nice.org.uk/csg5 • Improving outcomes in breast cancer – manual update. Cancer service 6
guidance (2002). Available from: www.nice.org.uk/csgbc 7 • Bisphosphonates (alendronate, etidronate, risedronate), selective8
oestrogen receptor modulators (raloxifene) and parathyroid horm9 (teriparatide) for the secondary pr10
Available from: ww12
Guidance to be updated The following NICE technology appraisals will be updated within this14 and withdrawn when the guideline is published: 15
• Guidance on the use of capecitabine for the treatment of locally 16 or metastatic breast cancer. NICE technology appraisal n17 Available from: www18
• Guidance on the use of trastuzumab for the treatment of advan19 cancer. NICE technology appraisal no. 34 (2002). Availab20 www.nice.org.uk/TA034 21
• Guidance on the use of vinorelbine for the treatment of advanc22 cancer. NICE techno23
• Guidance on the u25 technology apprais26 www.nice.org.uk/TA030
GuidancNICE is in the process of developing the following technology ap30 (details available from www.nice.org.uk). Recommendations from th31 technology appraisa
is l will be incorporated in the advanced breast cancer 32
33
tic breast 34 expected October 35
eloping the following guidance (details available from www.nice.org.uk
guideline:
• Gemcitabine for the treatment of locally advanced or metastacancer. NICE single technology appraisal. (Publication2006.) 36
37 NICE is also in the process of dev38
) and these will be cross referred to in the 39 advanced breast cancer guideline as appropriate: 40
• Osteoporosis: assessment of fracture risk and the prevention of 41 osteoporotic fractures in individuals at high risk. NICE clinical guideline. 42 (Publication date to be confirmed.) 43
Advanced breast cancer: full guideline DRAFT (August 2008) Page 130 of 146

DRAFT FOR CONSULTATION
• Alendronate, etidronate, risedronate, raloxifene and strontium ran1 the primary prevention of osteoporotic fragility fractures in pos2
elate for tmenopausal ril 2006.)
te and gility fractures
l women. NICE technology appraisal. (Publication expected April 2006.) 7
9
ers, the 12
onal Collaborating 13 14 15
These booklets are available as PDF files from the NICE website 16 ation on the progress of the
18
Referral from the Department of Health 19
the 20 21
n the clinical
• the key diagnostic and staging procedures 25 • the main treatment modalities including hormonal treatments 26 • the role of tumour-specific bisphosphonates.’ 27 28
women. NICE technology appraisal. (Publication expected Ap3 • Alendronate, etidronate, risedronate, raloxifene, strontium ranela4
teriparatide for the secondary prevention of osteoporotic fra5 in postmenopausa6
8
Guideline development process Information on the guideline development process is provided in: 10
• ‘The guideline development process: an overview for stakehold11 public and the NHS’
• ‘Guideline development methods: information for NatiCentres and guideline developers’.
(www.nice.org.uk/guidelinesprocess). Inform17 guideline will also be available from the website.
The Department of Health and Welsh Assembly Government askedInstitute:
‘To prepare a guideline for the NHS in England and Wales o22 existing service guidance. The management of breast cancer, to supplement23
guideline should cover: 24
Advanced breast cancer: full guideline DRAFT (August 2008) Page 131 of 146

DRAFT FOR CONSULTATION
Appendix 5 1 2
List of Topics Covered by Each Chapter 3 4
oring the phy (PET) 7 gression 8
10 • The use of (1) decision aids and (2) information tools to improve 11
12
tastatic
and (2) 17 18
(ii) single chemotherapy regimes: 19 static breast 20
ingle-agent
etastatic
relbine for 26
citabine for 28
t of 30
E
ior anthracycline (or 33 where anthracycline was inappropriate) what is the best chemotherapy 34
35 cancer who
39 t and Supportive Care 40
vanced breast cancer patients in the community setting 42
• What are the effective interventions used to support young families in 43 which a parent has advanced breast cancer. 44
45 Chapter 6 – Management of Specific Problems 46 • The management of lymphoedema in: 47
Chapter 2 – Presentation and Diagnosis 5 • it Investigations for (1) assessing disease extent and (2) mon6
response to treatment, including positron emission tomogra• Reassessment of endocrine and Her2 status on disease pro 9 Chapter 3 – Providing Information and Support for Decision Making
treatment outcomes and quality of life 13 Chapter 4 – Systemic Disease-Modifying Therapy 14 • What is the choice of 1st line treatment for patients with me15
breast cancer, endocrine therapy or chemotherapy? 16 • What is the most effective hormone treatment for (1) women
men with metastatic breast cancer? • Combination vs (i) sequential or
- Which is most effective at treating patients with metacancer – combination chemotherapy or sequential s21 chemotherapy 22
- Which is the most effective at treating patients with m23 breast cancer – single vs combination chemotherapy24
• The clinical effectiveness and cost effectiveness of vino25 breast cancer (update of TA 54)
• The clinical effectiveness and cost effectiveness of cape27 breast cancer (update of TA 62)
• The clinical and cost effectiveness of taxanes in the treatmen29 advanced breast cancer (update of TA 30)
• Gemcitabine for the treatment of metastatic breast cancer. NIC31 technology appraisal guidance 116 (2007) 32
• For patients taking Herceptin that relapsed with pr
regimen (update of TA 34) • The management of patients with metastatic HER2+ breast36
have had (i) no previous treatment with (ii) previous treatment with or 37 (iii) ongoing treatment with a biological response modifier. 38
Chapter 5 – Community-based Treatmen• The ongoing management of ad41
Advanced breast cancer: full guideline DRAFT (August 2008) Page 132 of 146

DRAFT FOR CONSULTATION
- Patients who have completed their primary treatment and have no 1 2
ients who have advanced breast cancer (inc. disease of the 3
ed breast 5
in the
onates, 10
tastatic brain and meningeal disease (surgery, 11 stereotactic radiotherapy, external beam radiotherapy, intrathecal 12 chemotherapy, rehabilitation) 13
14
active disease - Pat
axilla) 4 • The role of cancer-related fatigue management in advanc
cancer patients 6 • The management of patients with uncontrolled local disease7
presence of metastases or following primary treatment 8 • The management of metastatic bone disease (inc. bisphosph9
samarium, radiotherapy, surgery and rehabilitation) • The management of me
Advanced breast cancer: full guideline DRAFT (August 2008) Page 133 of 146

DRAFT FOR CONSULTATION
Advanced breast cancer: full guideline DRAFT (August 2008) Page 134 of 146
6 1 2
and Organisations Involved in Production of the 3 Guideline 4
5 6
17 2 ent 8
eviews and complementary work 9 6.4 Expert advisers to the Guideline Development Group 10 6.5 Members of the Guideline Review Panel 11
Appendix People
6. Members of the Guideline Development Group
e developm6. Organisations invited to comment on guidelin6.3 Individuals carrying out literature r

DRAFT FOR CONSULTATION
Appendix 6.1 1 2
Members of the Guideline Development Group (GDG) 3 4 5 6
tanley , Royal Bolton Hospital1 7 Medical Director, InHealth2 8
9 GDG Lead Clinicia10 Dr Nick Murray nsultant 11
Medical Oncologist, Cancer Research UK 12 13 14
ers 15 16
ust 17 Dr Helen Burrell University 18
19 dicine/ Network 20
th West Wales 21 t 22
23 24
avison d 25 y Cancer 26
27 28
ne t Unit4 29 aettig ull and East 30
Group 31 in l ast City 32
33 Mrs Claire Ryan ead Research Nurse Oncology Clinical Trials, 34
Kent Oncology Research Centre5 35 Mr John Winstanley Consultant Surgeon, Royal Bolton Hospital6 36 Mrs Netta Wooles Patient/carer representative 37 Miss Anna Wood Head of Policy and Campaigns, Breast Cancer 38
Care7 39
GDG ChairsMr John Wins Consultant Surgeon
Dr Sarah Wilson
n Senior Lecturer and Honorary Co
Clinical Centre, University of Southampton Group MembDr Murray Brunt Consultant Clinical Oncologist, University
Hospital of North Staffordshire NHS TrConsultant Radiologist, NottinghamHospitals NHS Trust
Dr Susan Closs Lead Consultant in Palliative MeChair in Palliative Care (SouCancer Network), Swansea NHS Trus
Mrs Debbie Collins Macmillan Radiotherapy Specialist, Kent Oncology Centre
Dr Dermott D GP, County Antrim, Northern IrelanDr Chris Gaffne Consultant Clinical Oncologist, Velindre
Centre, Cardiff3 Mrs Kathleen Jenkins Retired Clinical Nurse Specialist Mrs Mary Mil Nurse Consultant, The Parapet BreasMrs Susan R Patient/carer representative, Chair, H
Riding Cancer Patient Involvementk therapist, Be fMiss Jane Ran Lead Cancer Physio
Hospital L
1 From February 2008 – February 2009 2 From June 2006 to February 2008 3 From September 2007 – February 2009 4 From June 2006 to July 2007 5 From November 2007 to February 2009 6 From June 2006 to February 2008 7 From June 2006 to May 2008
Advanced breast cancer: full guideline DRAFT (August 2008) Page 135 of 146

DRAFT FOR CONSULTATION
1 2
possible 3 with their work on the guideline. 4
5 6
e e of sions Taken
Declarations of interest The Guideline Development Group were asked to declare any conflicts of interest which could interfere The interests that were declared are as follows:
GDG Memb r Interest Declared Typ Interest DeciDr Nick Murra N ZIC
oledronic acid in metastatic breast cancer to bone.
Non-perpecuniaspecific
re and must raw from
ions on all
sphonates as entions
y Co-chief investigator of NCRof ibandronic acid versus z
E trial
Roche are providing drug support
sonal ry,
Declawithddiscusstopics that include bisphointerv
phase ne + carboplatin in
metastatic breast cancer. Lilly are providing drug support
Non-perpecuniaspecific
re and must raw from
iscussions on all at include
y as ventions.
rson's action at can be asked
cific technical stions about
otherapy topics.
Chief investigator of NCRNof biweekly gemcitabi
II trial sonal ry,
Declawithddtopics thchemotherapinterChairpetaken thspequechem
Received reagent and equipment support from Becamn Coulter for tumour marker study in breast cancer
Non-perpecuniaspecific
nd can te in
cussions on all s as interventions
cluded in the trial are eing investigated guideline
sonal ry, non-
Declare aparticipadistopicinnot bby the
Chief investigator for phase II trial of metasta
ing
Non-perpecunia
ific
clare and must draw from
cussions on all s that include
s an tion.1
sunitinib in triple negativebreast cancer. Pfizer are providand per patient support
tic set up spec
sonal Dery, with
distopicsunitinib ainterven
ce dinas
Personania
can icipate in
ssions on all the expenses
not beyond ble amounts.
Received travel and subsistenexpenses from Roche for attenacademic meeting on bone dise
g an e
pecuspecific
l ry, non-
Declare and partdiscutopics as werereasona
Received travel expenses from Sanofi Aventis for attending the European Breast Cancer Conference in April 2008
Personal pecuniary, non-specific
Declare and can participate in discussions on all topics as the expenses were not beyond reasonable amounts.
1 Sunitinib was not included as an intervention in any of the topics investigated by the guideline and was therefore not discussed by the GDG
Advanced breast cancer: full guideline DRAFT (August 2008) Page 136 of 146

DRAFT FOR CONSULTATION
Dr Murray Bru pding an a
board on adjuvant exemestane
ersonapecuniaspecific
eclare and must raw from ssions on all
at include tane as an
ention until July
nt Received honorarium from Pfizertravel expenses for atten
lus dvisory
P l ry,
Dwithddiscutopics thexemesinterv2007
om AstraZfor attending advisory board on fulvestrant in the EFECT trial
Personapecuniaspecific
re and must raw from
ussions on all cs that include strant as an ention until
r 2007
Received honorarium fr eneca l ry,
DeclawithddisctopifulveintervNovembe
enewn choice of
subject. Cancelled by GPs at short notice by fee still payable for preparation
Personapecuniaspecific
must from
ssion on all topics at include
rventions made by eneca until
008
Received honorarium from AstraZto give lecture to GPs on o
ca l ry,
Declare and withdrawdiscuthinteAstraZJanuary 2
sistence and registration fee expenses from
r
Personapecuniaspecific
nd can te in
ssions on all s as the expenses
eyond mounts.
Received travel, sub
AstraZeneca to attend St Gallen bmeeting in March 07
east
l ry, non-
Declare aparticipadiscutopicwere not breasonable a
Commissioned by HealthEd agency to produce 2 case reports on trastuzumab
Personapecuniaspecific
re and must draw from
ssion on all topics include
ab as an ion until
tember 2008
for advanced breast cancer
l ry,
Declawithdiscuthat trastuzuminterventSep
Received an honorarium from Roche is
Personapecunia
must raw from ssion on all topics
e tamoxifen s an
ention until ust 2008
Diagnostics for attending an advboard on tamoxifen modifiers
ory specific
l Declare and ry, withd
discuthat includmodifiers aintervAug
che fo Personaniaific
lare and must draw from
ssion on all topics de ab as an
vention until September 2008
Received an honorarium from Rochairing an advisory board on trastuzumab
r pecuspec
l Decry, with
discuthat inclutrastuzuminter
Received an honorarium from Cephalon for chairing an educational meeting where 2 palliative care physicians gave talks
Personal pecuniary, non-specific
Declare and can participate in discussions on all topics as meeting was not specific to advanced breast cancer
Advanced breast cancer: full guideline DRAFT (August 2008) Page 137 of 146
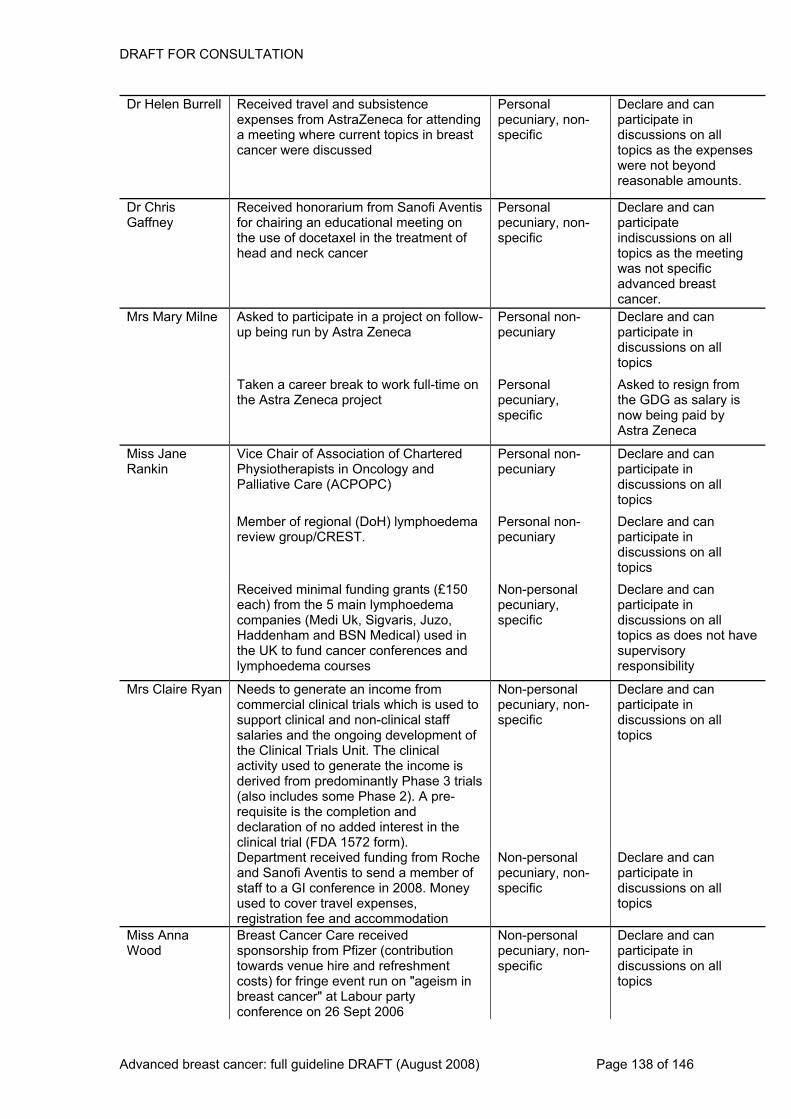
DRAFT FOR CONSULTATION
Dr Helen Burrat
current topics in breast cancer were discussed
onapecuniaspecific
clare and can ipate in
ns on all s the expenses t beyond
onable amounts.
ell Received travel and subsistence expenses from AstraZeneca for a meeting where
tending Pers l
ry, non-Departicdiscussiotopics awere noreas
Dr Chris Gaffney
ofi ducational meeting on
the use of docetaxel in the treatment of head and neck cancer
onapecuniaspecific
e and can te
scussions on all s as the meeting
was not specific anced breast er.
Received honorarium from Sanfor chairing an e
Aventis Pers l ry, non-
Declarparticipainditopic
advcanc
Mrs Mary Milne Asked to participate in a project on follow- Personapecunia
can ate in ions on all
up being run by Astra Zeneca l non- Declare and ry particip
discusstopics
Taken a career break to work full-time on Personaunia
specific
sked to resign from GDG as salary is
eing paid by Zeneca
the Astra Zeneca project l A
pec ry, the now bAstra
Miss Jane Rankin
te
C)
sonaunia
can icipate in
ssions on all
Vice Chair of Association of CharPhysiotherapists in Oncology andPalliative Care (ACPOP
red Perpec
l non-ry
Declare and partdiscutopics
ho sona can pate in
s on all
Member of regional (DoH) lympreview group/CREST.
edema Perpecunia
l non-ry
Declare and particidiscussiontopics
l funding grants (£150 hoedem
zal) us
es and
Non-peruniaific
clare and can icipate in ussions on all s as does not have
supervisory responsibility
Received minimaeach) from the 5 main lympcompanies (Medi Uk, Sigvaris, JuHaddenham and BSN Medicthe UK to fund cancer conferenclymphoedema courses
a o, ed in
pecspec
sonal Dery, part
disctopic
Mrs Claire Ry h is used to
-clinical staff lopment of
al m
se
d d interest in
Non-personal pecuniary, non-specific
Declare and can participate in discussions on all topics
an Needs to generate an income fromcommercial clinical trials whicsupport clinical and nonsalaries and the ongoing devethe Clinical Trials Unit. The clinicactivity used to generate the incoderived from predominantly Pha(also includes some Phase 2). A pre-requisite is the completion an
e is 3 trials
declaration of no addeclinical trial (FDA 1572 form).
the
frommber of
in 2008. Money xpenses,
registration fee and accommodation
Non-perpecunia -specific
re and can participate in discussions on all topics
Department received fundingand Sanofi Aventis to send a mestaff to a GI conferenceused to cover travel e
Roche sonal ry, non
Decla
Miss Anna Wood
Breast Cancer Care received sponsorship from Pfizer (contribution towards venue hire and refreshment costs) for fringe event run on "ageism in breast cancer" at Labour party conference on 26 Sept 2006
Non-personal pecuniary, non-specific
Declare and can participate in discussions on all topics
Advanced breast cancer: full guideline DRAFT (August 2008) Page 138 of 146

DRAFT FOR CONSULTATION
tributi
ent "ageism in
vative party
perpecuniaspecific
clare and can ipate in
discussions on all topics
Breast Cancer Care receivedsponsorship from Pfizer (contowards venue hire and refreshmcosts) for fringe event run onbreast cancer" at Co
on Non-
nserconference on 3 Oct 2006
sonal ry, non-
Departic
d
ment of registration fee to attend the San Antonio Breast Cancer Conference
onapecuniaspecific
re and can in
ussions on all s the expenses
e not beyond sonable amounts.
Received travel and subsistenceexpenses from Astra Zeneca anpay
in 2006
Pers l ry, non-
Declaparticipatedisctopics awerrea
t Cancer organisation) to NICE
technology appraisals of Gemcitabine and Lapatinib in ABC
Personapecunia
re and can participate in discussions on all topics
Responded on behalf of BreasCare (consultee
l non-ry
Decla
1
Advanced breast cancer: full guideline DRAFT (August 2008) Page 139 of 146

DRAFT FOR CONSULTATION
Advanced breast cancer: full guideline DRAFT (August 2008) Page 140 of 146
.2 1 2
ns Invited to Comment on Guideline 3 Development 4
5 6 7
9 ncer Network10
ad roup 12 tories Ltd )
oncern England 19 rust
l Enu
ealth 26
rk rk 28 t 29
ed
ive 33 34
urgeons
Britishls Indus
td
• Barnsley Acute Trust 42 • Barnsley PCT 43 • Bath and North East 44
Somerset PCT 45 • Baxter Healthcare Ltd 46 • Bayer Healthcare PLC 47
dfordshire & Hertfordshire rategic Health
T cer Network
l Trials
rust Local Health
im Ltd oole
irdale PCT Breast Cancer
are b
ticals Ltd sociation for
Cognitive s (BABCP) for
ounselling and
ion of Art - 2nd contact
of Plastic
Association ritish Geriatrics Society
eopathic ociation
• British Lymphology Society 81 • British Menopause Society 82 • British Nuclear Medicine 83
Society 84 • British Oncological 85
Association 86
Appendix 6 Organisatio
The following stakeholders registered with NICE and were invited to comment on the scope and8 • 3 Countries Ca
the draft version of this guideline.
• Be48 Palliative Care Le11 Clinicians G
• Abbott Laborall14
13 (BASF/Kno
• Abbott Molecular15 • Abraxis Oncology 16 • Afiya Trust, The17 • Age Concern Cymru 18 • Age C• Airedale NHS T20 • All About Nocturna
Team 22 resis
Board 58 5921
• Almac Diagnostics 23 • Amgen UK Ltd 24 • Anglesey Local H25
Board • Anglia Cancer Netwo27 • Arden Cancer Netwo• Association of Breas
Surgery at BASO 30 • Association of Charter31
Physiotherapists in32 Oncology and PalliatCare
• Association of S35 of • British Associat73 Grea36 t Britain and Ireland
n of the37 • Associatio •Pharmaceutica38 (ABPI) 39
try Surgeons 76
• AstraZeneca UK L40 • Bard Ltd 41
NHS St49 Authority 50
• Bedfordshire PC51 • Birmingham Can52 • Birmingham Clinica53
Unit 54 • Birmingham Heartlands & 55
Solihull NHS T56 • Blaenau Gwent57
• Boehringer Ingelhe th and P• Bournemou60
PCT 61 • Bradford & A62 • Breakthrough63 • Breast Cancer C64 • Bristol-Myers Squib65
Pharmaceu66 • British As67
Behavioural &68 Psychotherapie69
• British Association70 C71 Psychotherapy 72
Therapists74 British Association75
• British Dietetic 77 • B78 • British Hom79
Ass80

DRAFT FOR CONSULTATION
• British Oncology Pharm1 acy
hological 3
iety for Cance
bridge University 10 HS Founda
12
s Forum earch UK
s
erBACUP
s
of
26 dge Centre for
st 29
lerapists 33
ial Care n 35
alth 37
y ion
ster dation
• Craven, Harrogate & Rural 44 District PCT 45
• Cytyc UK Ltd 46 • DakoCytomation Ltd 47 • David Lewis Centre, The 48 • Department of Health 49
n Cancer rk
oncaster PCT
mpany Ltd Network
blic Health ctice and
oSmithKline UK re Hospitals
rust ster &
cer Network ories Ltd
s NHS
& Isle of Wight lth Authority
d District NHS rust
mission ces
nd Yorkshire Network
t Ltd care
isory Service Tech Healthcare Ltd
nson Medical Hospital NHS
ees PCT e UK
stics Ltd
ospitals st
re onshire and ncer Network
Hospital
• Long Term Medical 94 Conditions Alliance 95
• Luton and Dunstable 96 Hospital NHS Trust 97
• Macclesfield District General 98 Hospital 99
•Association 2
• British PsycSociety, The 4
• British S oc5 enetics6
r • Eli Lilly and C54 G
• Bromley PCT7 • BUPA 8 • Calderdale PCT 9 • Cam
Hospitals N11 Trust
tion • Gloucestershi60
• Cancer Network 13 Pharmacist14
• Cancer Res15 • Cancer Service16
tiveCollabora17 • Canc18 • Cancer Black Care19 • Cancer Voice20 • CASPE 21
al Liverpool PCT• Centr22 • Cephalon UK Ltd 23 • Chartered Society 24
Physiotherapy25 • CIS’ters • Clatterbri27
Oncology NHS Tru28 • Clinical K nowledge
Summaries (CKS) 30 • Clinovia Ltd 31 • College of Occupationa32
Th •
• Commission for Soc34 Inspectio
• Connecting for He36 • Conwy & Denbighshire NHS
Trust 38 • Co-operative Pharmac39
Associat40 • Countess of Che41
Hospital NHS Foun42 Trust 43
Derby-Burto50 Netwo51
• D52 • Eisai Ltd 53
o• Essex Canc• Faculty of Pu56
er 55
• General Pra57 Primary Care 58
• Glax59
NHS Trust 61 • Good Hope NHS T 62
e63 • Greater Manch Cheshire Can64
• Guerbet Laborat65 • Guys & St Thoma66
Trust 67 • Hampshire68
Strategic Hea69 • Harrogate70 an
Foundation T71 m• Healthcare Co72
• Help the Hospi73 • Humber a74
Coast Cancer 75 • Imaging Equipmen76 • Independent Health77
Adv78 a-• Intr79
• Johnson & Joh80 's College King81
Trust 82 • Kirkl83 • L'Arch84 • Launch Diagno85 • Leeds PCT 86• Leeds Teaching H87
NHS Tru88 • Leicestershi89
Northampt90 Rutland Ca91
• Liverpool Women’s92 NHS Trust 93
Advanced breast cancer: full guideline DRAFT (August 2008) Page 141 of 146

DRAFT FOR CONSULTATION
• Macmillan Cancer Re1 • Maidstone and
lief Tunbridg2
cer Car
e Innovati
althca9 ory
ticals 12 enerust 15
tion of al
18
or20 rou21 earical
24 rust25
l for eople, Blac27
nic alities) 29 r
osis
tient Safety cy
lth 37
eening 41
ge aries Service 44
• NHS Direct 45 • NHS Health and Social Care 46
Information Centre 47 • North Bradford PCT 48 • North East London Cancer 49
Network 50
Strategic ty
North Eastern Derbyshire
lnshire PCT T
d York T
don Hospitals S Trust
althcare
Hospital
itals NHS Trust Pharmaceuticals
tron B.V. ety
aboratories Ltd
ction Ltd
ach la Clinical Genetics
are Ltd
armacists’
dra Hospital
izabeth Hospital st oria Hospital
ation Trust l Public Health
Roche Diagnostics
rham General Hospitals NHS Trust 95
• Rotherham PCT 96 • Royal Bolton Hospitals NHS 97
Trust 98 • Royal College of General 99
Practitioners 100
e Health Authori52 • 53 Wells NHS Trust 3
• Marie Curie Can4 e PCT 54 • Medeus Pharma Ltd 5 • Medical Devic6
7 ons 56
Ltd • Medical Solutions 8 • Medicines and He re • North Yorkshire an59
PC60 Products Regulat10 Agency 11
• Merck Pharmaceu• Mid Staffordshir13 e G
Hospitals NHS Tr14 • Milton Keynes PCT
al • Northumbria He63
• National Associa16 Assistants in Surgic17 Practice
• National Audit Office 19 • National Cancer Netw
Clinical Dirk • Nucle70
ectors Gr Res22
p • Nutrition Soci71 • National Cance
Institute (NCRI) Clin23 Studies Group
• National Childbirth T
ch Organon L72
•• National Counci26
Disabled P k, • Peninsu77 Minority and Eth28 Community (Equ
• National Council fo30 Palliative Care 31
• National Osteopor32 Society 33
• National Pa34 Agen35
• National Public Hea36 Service – Wales
• Newcastle PCT 38 PCT • Newham39
• NCCHTA 40 • NHS Cancer Scr
Programme 42 • NHS Clinical Knowled43
Summ
• North East London51
• North Linco55 • North Sheffield PC
57 • North Tees PCT • North Trent Cancer network 58
• Northwest Lon61 NH62
NHS Trust 64 • Nottingham City65 • Nottingham University 66
Hosp67 • Novartis68
UK Ltd 69
• • Ortho Biotech 73 • Ovarian Cancer A74 Oxford Nutrition 75 • Pe76
Service 78 • PERI GON Healthc79 • Pfizer Ltd 80 • Pierre Fabre Ltd81 • Primary Care Ph82
Association 83 • Princess Alexan84
NHS Trust 85 • Queen El86
NHS Tru87 • Queen Vict88
NHS Found89 • Regiona90
Group – London 91 • 92 • Roche Ltd 93 • Rothe94
Advanced breast cancer: full guideline DRAFT (August 2008) Page 142 of 146
DRAFT FOR CONSULTATION
Advanced breast cancer: full guideline DRAFT (August 2008) Page 143 of 146
neral
wiv College of Nursing 4
of 6 s &
gists
gists 10 of Physicians
12 of
icinal United Hospital Bath 18
ust ussex Trust,
21 T West
spitals
ntis 27 d
or29 t
Wrekin PCT 33
West PCT Hosp
ation Trust36 Solutions
Ltd
f
Central 44 Huddersfield PCT 45
• South East Sheffield PCT 46 • South West Kent PCT 47 • South West London SHA 48 • South East Wales Cancer 49
Network 50
r Network ssop HS Trust
Glossop PCT Medical
Cancer
es Valley Strategic rity
ord PCT undation
Screening ee College London NHS Trust
l S st
itals rwickshire
t Birmingham,
ment of Primary l Practice
rust hing PCT
ic Advisory C)
r Trust ancer
ire PCT ertfordshire Hospitals
Cancer Research ional
• Wyeth Laboratories 95 • Wyeth Pharmaceuticals 96 • York NHS Trust 97 • Yorkshire and the Humber 98
Specialised 99 Commissioning Group 100
• Royal College of Ge1 Practitioners Wales 2
• Royal College of Mid3 • Royal
es • Stockport PCT 53
(RCN) 5 • Royal College
nObstetricia7 Gynaecolo8
• Royal College of 9 Patholo
• Royal College11 of London
• Royal College13 Psychiatrists 14
• Royal College of 15 Radiologists 16
• Royal Society of Med17 • Roy
e • UK Anaemia 67 • UK National68
NHS Tr19 • Royal West S20
The • Salford PC22 • Sandwell &23
Birmingham Ho24 NHS Trust 25
• Sandwell PCT 26 • sanofi-ave• Schering-Plough Lt28 • Scotland Cancer Ne tw
30 k Depart79
• Scottish Executive HealDepartment 31
h Care & Genera80 • Velindre NHS T81
• Shropshire County and32 Telford &
• Sheffield South34 • Sheffield Teaching35
NHS Founditals • Welsh Scientif85 C
• Siemens Medical37 Diagnostics38
• Sigvaris Britain 39 • Society and College o40
Radiographers 41 • Society for Academic42
Primary Care 43 • South &
• Staffordshire Moorlands 51 PCT 52
• Sussex Cance54 • Tameside and Glo 55
ces N56 Acute Servi• Tameside and57 • Taunton Road58
Centre 59 • Thames Valley60
Network61 • Tham62
Health Autho63 • Traff64 • UCLH NHS Fo65
Trust 66
Committ69 • University 70
Hospital 71 • University Hospita72
Birmingham NH73 Foundation Tru74
• University Hosp75 Coventry & Wa76 NHS Trus77
• University of 78
• Walsall Teac82 • Welsh Assembly 83
Government 84
ommittee (WSA86 • Wessex Cance87 • West London C88
Network 89 • Western Chesh90 • West H91
Trust 92 • World93
Fund Internat94

DRAFT FOR CONSULTATION
Appendix 6.3 1 2
g out Literature Reviews and 3 Work 4
5 6
r Cancer, 7 8
Dr Andrew Champion Centre Manager, National Collaborating Centre for 9 Cancer, Cardiff 10
11 Project Manager 12
nnett Assistant Centre Manager, National Collaborating 13 14 15 16
Francis r, Cardiff 17 18
n Spec19 ardiff 20
se cer, Cardiff 21 Anne Cleves Wales Library, Velindre NHS 22
Trust 23 s dre NHS 24
25 26
Health Economis27 Research Assistant, London School of Hygiene 28
29 it of Primary 30
31 32
33 Dr Robyn Dewis by City 34
rimary Care Trust 35 Jonathan Gribbin Specialist Trainee in Public Health, Derbyshire 36
County Primary Care Trust 37 Prof Mark Baker22 Medical Director for Oncology and Surgery and 38
Lead Cancer Clinician, Leeds Teaching Hospitals, 39 Leeds 40
41
Individuals CarryinComplementary Overall Co-ordinators Dr Fergus Macbeth Director, National Collaborating Centre fo
Cardiff
Angela BeCentre for Cancer, Cardiff
Researcher Dr Karen National Collaborating Centre for Cance Informatio ialists
NationaElise Collins l Collaborating Centre for Cancer, CSabine Berend National Collaborating Centre for Can
Cancer Research
Bernadet Cancer Research Wales Library, VelinTrust
te Cole
ts
Sarah Willis and Tropical Medicine, London
Nicky Welton Senior Research Fellow, Academic UnHealth Care, University of Bristol
Needs Assessment Specialist Registrar in Public Health, DerP
22 Provided peer review data
C:\Documents and Settings\bhendry\Local Settings\Temporary Internet Files\ABC full guideline for consultation 120808.doc Page 144 of 146

DRAFT FOR CONSULTATION
Appendix 6.4 1 2
Expert Advisers to the Guideline Development Group 3 4
Professor Robert J. Grie ist, Arden 5 itals 6
7 Mrs Samantha Holloway 8
School of Medicine, Cardiff University 9 10
ve Consultant Clinical Oncolog
Cancer Centre, University HospCoventry & Warwickshire Lecturer, Department of Wound Healing,
C:\Documents and Settings\bhendry\Local Settings\Temporary Internet Files\ABC full guideline for consultation 120808.doc Page 145 of 146

DRAFT FOR CONSULTATION
C:\Documents and Settings\bhendry\Local Settings\Temporary Internet Files\ABC full guideline for consultation 120808.doc Page 146 of 146
.5 1 2
Members of the Guideline Review Panel 3 4
rsees the 5 itoring its 6
quality. The members of the Guideline Review Panel were as follows: 7 8
Dr John Hyslop - Chair 9 t Radiologist, Royal Cornwall Hospital NHS Trust 10
11 12
Professor Liam Smeeth 13 inical Epidemiology, London School of Hygiene and 14
edicine 15
16 17
Mr Jonathan Hopper 18 Medical Director (Northern Europe), ConvaTec Ltd 19
Appendix 6
The Guideline Review Panel is an independent panel that ovedevelopment of the guideline and takes responsibility for mon
Consultan
Dr Ash Paul Deputy Medical Director, Health Commission Wales
Professor of ClTropical M
Mr Peter Gosling Lay member









![Saugu[!] Asmundar, er kalladur er Kappabani :](https://static.fdokumen.com/doc/165x107/63264a17051fac18490dae0e/saugu-asmundar-er-kalladur-er-kappabani-.jpg)