
Epidemiology and determinants of blood glucose self-monitoring in clinical practice
11
Diabetes Research and Clinical Practice 34 (1996) 1155 125 Epidemiology and determinants of blood glucose self-monitoring in clinical practice’ N. Scorpiglione”,“, M. El-Shazlyb, M. Abdel-Fattahb, M. Belfiglio”, D. Cavaliere”, F. Carinc?, D. Labbrozzi”, E. Mari”, M. Massi Benedetti”, G. Tognoni”, A. Nicolucci” aDepartment of Clinical Pharmacology and Epidemiology, Consorzio Mario Negri Sud, 66030 S. Maria Imbaro (Chieti), Italy ‘Medical Statistics and Clinical Epidemiology Department, Medical Research Institute, Alexandria University, Alexandria, Egypt “Institute of Internal Medicine, Endocrine and Metabolic Science, University of Perugia, Perugia, Italy Received 20 May 1996; revised 5 September 1996; accepted 4 October 1996 * Corresponding author. Tel.: + 39 872 570260; fax: + 39 872 578240. ’ This study was undertaken on behalf of the Italian Study Group for the Implementation of the St. Vincent Declaration (Coordinator: M. Massi Benedetti; Scientific committee; F. Capani, Q. Carta, E. De Feo, C. Taboga, G. Tognoni; Coordinating Center: M. El-Shazly, M. Abdel-Fattah, M. Belfiglio, D. Cavaliere, F. Carinci, D. Labbrozzi, E. Mari, A. Nicolucci, L. Scorpiglione). The participating clinicians were: Diabetes clinics: S. Ponzano (Alessandria); P. Fumelli, P. Sorichetti (Ancona); G.M. Nardelli, A. D’Alessandro (Bari); F. Farci (Cagliari); A. Aiello, M.R. Cristofaro (Campobasso); C. Giarrocco, D. Rotundo (Casoli); R. Biagioli, C. Santini (Cesena); E. Moratti, V. Rotolo (Cividale del Friuli); C. Ruffino (Finale Ligure); S. Pocciati (Foligno); C. Bordone (Genova); M. Tagliaferri (Larino); G. Brusco, E. Caruso (Lauria); A. Venezia (Matera); M.E. De Feo, P. Guerriero, G. Corigliano, D. Vitale (Napoli); M. Trovati, C. Ponziani (Orbassano); E. Secchi (Ozieri); E. Savagnone (Palermo); C. Coscelli (Parma); M. Massi Benedetti, R. Norgiolini (Perugia); F. Capani, G. La Penna (Pescara); D. Giorgi Pierfranceschi (Piacenza); G. Seghieri (Pistoia); L. Pappalardo, V. Travaglio (Portici); R. Amoretti, G. Ghirlanda, G. Marra (Roma); G. Monesi, E. Cecchetto (Rovigo); S. De Cosmo, S. Bacci (S. Giovanni Rotondo); G. Pipicelli, A. Mosca (Soverato); S. Albano, C. Spinelli (Taranto); Q. Carta, G. Petraroli, M. Porta, M. Tomalino (Torino); C. Taboga (Udine); G. Erle, L. Lora (Vicenza). General Practitioners: M. Cappelletti(Alessandria); R. Giaretta (Altavilla Vicentina); E. Mossuto (Arqua Polesine); A. Spina (Avellino); V. D’Alessandro (Bari); F. Richeri (Calice Ligure); L. Pascali (Camerano); L. Puddu (Cagliari); G. Ragazzi (Camisano); M. Fusco (Cardito); V. Biagini, I. Garavina (Cesena); F. Magini, C. Polidori (Citta di Castello); S. Previato (Crespino); G.M. Masazza (Finale Ligure); L. Tomain (Fontecchio); A. Bragiotto (Frassinelle); M. Lioniello (Frattaminore); G. Di Menza (Fubine); E. Mazzoccato (Isola Vicentina); F. Gesualdi (Latronico); G. Capozza, F. Morelli, R. Tataranni (Matera); E. Saffi Giustini (Montale); E. Magliani, G. Sampaolo (Osimo); L. Galvano, L. Spicola (Palermo); E. Goracci, S. Sbrenna (Perugia); G. Meucci (Pistoia); S. Porru (Quartu S. Elena); A. Briganti, C.A. Belli (Recco); A. Benedetto, S. Burzacca (Rivalta di Torino); E. De Bella, A. Di Carluccio, E. Fantini, P. Pietravalle, M. Turato (Roma); S. Mella, F. Paparella (Rovigo); M. Bertone, M. Zoppi (Torino); G. Cabri (Vicenza); E. Maragnamo (Villadose). 0168-8227/96/$15.00 Copyright 0 1996 Elsevier Science Ireland Ltd. All rights reserved PIISO168-8227(96)01343-5
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Epidemiology and determinants of blood glucose self-monitoring in clinical practice

Diabetes Research and Clinical Practice 34 (1996) 1155 125
Epidemiology and determinants of blood glucose self-monitoring in clinical practice’
N. Scorpiglione”,“, M. El-Shazlyb, M. Abdel-Fattahb, M. Belfiglio”, D. Cavaliere”, F. Carinc?, D. Labbrozzi”, E. Mari”, M. Massi Benedetti”, G. Tognoni”,
A. Nicolucci” aDepartment of Clinical Pharmacology and Epidemiology, Consorzio Mario Negri Sud, 66030 S. Maria Imbaro (Chieti), Italy
‘Medical Statistics and Clinical Epidemiology Department, Medical Research Institute, Alexandria University, Alexandria, Egypt “Institute of Internal Medicine, Endocrine and Metabolic Science, University of Perugia, Perugia, Italy
Received 20 May 1996; revised 5 September 1996; accepted 4 October 1996
* Corresponding author. Tel.: + 39 872 570260; fax: + 39 872 578240. ’ This study was undertaken on behalf of the Italian Study Group for the Implementation of the St. Vincent Declaration
(Coordinator: M. Massi Benedetti; Scientific committee; F. Capani, Q. Carta, E. De Feo, C. Taboga, G. Tognoni; Coordinating Center: M. El-Shazly, M. Abdel-Fattah, M. Belfiglio, D. Cavaliere, F. Carinci, D. Labbrozzi, E. Mari, A. Nicolucci, L. Scorpiglione).
The participating clinicians were: Diabetes clinics: S. Ponzano (Alessandria); P. Fumelli, P. Sorichetti (Ancona); G.M. Nardelli, A. D’Alessandro (Bari); F. Farci
(Cagliari); A. Aiello, M.R. Cristofaro (Campobasso); C. Giarrocco, D. Rotundo (Casoli); R. Biagioli, C. Santini (Cesena); E. Moratti, V. Rotolo (Cividale del Friuli); C. Ruffino (Finale Ligure); S. Pocciati (Foligno); C. Bordone (Genova); M. Tagliaferri (Larino); G. Brusco, E. Caruso (Lauria); A. Venezia (Matera); M.E. De Feo, P. Guerriero, G. Corigliano, D. Vitale (Napoli); M. Trovati, C. Ponziani (Orbassano); E. Secchi (Ozieri); E. Savagnone (Palermo); C. Coscelli (Parma); M. Massi Benedetti, R. Norgiolini (Perugia); F. Capani, G. La Penna (Pescara); D. Giorgi Pierfranceschi (Piacenza); G. Seghieri (Pistoia); L. Pappalardo, V. Travaglio (Portici); R. Amoretti, G. Ghirlanda, G. Marra (Roma); G. Monesi, E. Cecchetto (Rovigo); S. De Cosmo, S. Bacci (S. Giovanni Rotondo); G. Pipicelli, A. Mosca (Soverato); S. Albano, C. Spinelli (Taranto); Q. Carta, G. Petraroli, M. Porta, M. Tomalino (Torino); C. Taboga (Udine); G. Erle, L. Lora (Vicenza).
General Practitioners: M. Cappelletti(Alessandria); R. Giaretta (Altavilla Vicentina); E. Mossuto (Arqua Polesine); A. Spina (Avellino); V. D’Alessandro (Bari); F. Richeri (Calice Ligure); L. Pascali (Camerano); L. Puddu (Cagliari); G. Ragazzi (Camisano); M. Fusco (Cardito); V. Biagini, I. Garavina (Cesena); F. Magini, C. Polidori (Citta di Castello); S. Previato (Crespino); G.M. Masazza (Finale Ligure); L. Tomain (Fontecchio); A. Bragiotto (Frassinelle); M. Lioniello (Frattaminore); G. Di Menza (Fubine); E. Mazzoccato (Isola Vicentina); F. Gesualdi (Latronico); G. Capozza, F. Morelli, R. Tataranni (Matera); E. Saffi Giustini (Montale); E. Magliani, G. Sampaolo (Osimo); L. Galvano, L. Spicola (Palermo); E. Goracci, S. Sbrenna (Perugia); G. Meucci (Pistoia); S. Porru (Quartu S. Elena); A. Briganti, C.A. Belli (Recco); A. Benedetto, S. Burzacca (Rivalta di Torino); E. De Bella, A. Di Carluccio, E. Fantini, P. Pietravalle, M. Turato (Roma); S. Mella, F. Paparella (Rovigo); M. Bertone, M. Zoppi (Torino); G. Cabri (Vicenza); E. Maragnamo (Villadose).
0168-8227/96/$15.00 Copyright 0 1996 Elsevier Science Ireland Ltd. All rights reserved PIISO168-8227(96)01343-5

116 N. Scorpiglione et al, /Diabetes Research and Clinical Practice 34 (1996) 115-125
Abstract
The aim of this study was to describe the epidemiology of self-monitoring of blood glucose and to identify specific characteristics of those subgroups of diabetic patients treated with insulin that are most likely to monitor their blood glucose according to medical recommendations. Data were collected on 1384 insulin-treated patients, enrolled from 35 diabetic outpatient clinics and 49 general practitioners’ offices between December 1993 and June 1994. Seventeen Italian regions out of 20 were included in the study. Our data show that 418 (31%) diabetic patients treated with insulin had never practised blood glucose self-monitoring. In addition, only 242 patients (18.2%) self-monitored their glycemia with a mean frequency of at least once a day (29.7% among insulin-dependent diabetes mellitus (IDDM) and 13.9% among insulin-treated non-insulin-dependent diabetes mellitus (NIDDM-IT) patients). Patients’ characteristics associated with a higher probability of practising blood glucose self-monitoring were age below 50 years, being treated at a diabetic outpatient clinic, hypertension, need of three or more insulin injections per day, history of hypoglycemic episodes, ability to self-manage insulin doses. Our study calls for vigorous efforts aimed at promoting the incorporation of clearly-defined educational programs at each level of care, in order to improve the motivation and self-care of diabetic patients. Furthermore, studies are necessary to identify subgroups of diabetic patients that truly need to self-monitor blood glycemia, and to assess the efficacy of the practice of self-monitoring of blood glucose in improving metabolic control and reducing acute and long-term diabetic complications. Copyright 0 1996 Elsevier Science Ireland Ltd.
Keywords: Insulin-dependent diabetes mellitus; Non-insulin-dependent diabetes mellitus; Insulin treated; Blood glucose self-monitoring
1. Introduction
Self-monitoring of blood glucose (SMBG) is widely considered as an important component of diabetes care to achieve both short-term and long- term goals. Among the former are self-adjusting insulin dose, controlling hypoglycemic episodes, and providing the clinician with an updated profile of blood glucose levels. Long-term benefits are also expected, on the assumption that SMBG can help avoid the more disabling diabetic com- plications by reducing the severity and frequency of both hyperglycemic and hypoglycemic episodes. While the short-term benefits of SMBG in insulin-treated patients have been investigated in the context of several randomized trials [l-3], leading to controversial results, its long-term im- pact is still unknown.
In non-insulin-dependent diabetes mellitus (NIDDM) patients not treated with insulin, sev- eral studies of SMBG found no difference in glycemic control between those who monitored their blood glucose and those who did not [4-71.
The lack of any clear evidence on the relative benefits of different SMBG schedules is reflected in the existing practice guideline, where SMBG is
formally recommended, but with different modali- ties. As a matter of fact, the recommended fre- quency for SMBG ranges from a minimal policy of once daily to four tests a day or more. Indica- tions also vary for different subgroups of patients depending on their current level of metabolic con- trol [8-lo].
Given the lack of information on the epidemiol- ogy of SMBG in Italy, we decided to investigate the frequency and the factors associated with the practice of SMBG by adults with insulin-treated diabetes.
2. Materials and methods
The material for our study was recruited from a wide case-control study aimed at assessing the avoidability of long-term diabetic complications (eye, kidney, lower limb complications), which was carried out in Italy between December 1993 and June 1994. Design of that study is reported in detail elsewhere [ll]. Briefly, patients were re- cruited from 35 diabetic clinics (DOCs) and 49 general practitioners’ offices (GPs) in 17 out of the 20 Italian regions. For each diabetic clinic, at

N. Scorpiglione et al. /Diabetes Research and Clinical Practice 34 (1996) 115-125 117
least two general practitioners from the same health district were involved. Both DOCs and GPs were selected on the basis of their willingness to participate. In DOCs, patients with diabetic complications were identified among all subjects seen during the study period. In GPs’ offices, subjects with complications were identified among all diabetic patients in the practice. In DOCs, a random sample of patients without complications was recruited, while in GPs’ offices, all diabetic patients without complications were enrolled. Pa- tients were considered controlled by a specialist if they declared that were usually treated by one. The distinction between type 1 and type 2 dia- betes was made on the basis of clinical diagnosis and this information was abstracted directly from medical records. Minimal criteria for classifying patients according to the type of diabetes were reported in the protocol. According to these crite- ria, patients were classified as having type 1 dia- betes if their age at diagnosis was below 30 years and insulin was used continuously from the time of diagnosis, and they were classified as type 2 if their age at onset of diabetes was above 30 years with no evidence of ketonuria. All patients en- rolled had a diabetes duration of at least 5 years. A pretested questionnaire was used for collection of data. Data were collected by trained physicians who interviewed patients and by searching medi- cal records for relevant information. Questions included focused on demographic, socio-eco- nomic, clinical and self-care characteristics. The frequency of performing blood glucose self-tests refers to the last month before the patient’s inter- view. Since normal ranges for glycated hemoglobin varied in the different centers, the percentage change with respect to the upper nor- mal values (actual value/upper normal limit x 100) was utilized.
Glycosylated hemoglobin was considered good, acceptable and bad if the percentage change with respect to the upper normal limit was less than or equal to lo%, between 11 and 30%, and over 30%, respectively. For all clinical variables, the last value in the past 12 months was requested.
All patients with insulin-dependent diabetes mellitus (IDDM) or non-insulin-dependent dia- betes mellitus treated with insulin (NIDDM-IT)
were considered eligible for entry in the present study. Patients were considered as practising SMBG if the mean frequency of blood glucose tests was at least once a day.
2.1. Statistical analysis
Analysis was initially carried out based on a series of univariate comparisons. The x2 test was used to detect association between patients’ char- acteristics and frequency of practising blood glu- cose self-testing. When more than two levels of a variable were considered, x2 represents the x2 value of heterogeneity among the different levels. In order to control simultaneously for the possible confounding effects of the different variables, a multiple logistic regression analysis with stepwise variable selection was utilized to evaluate factors related with SMBG practice [12].
The variables entered into the logistic regres- sion analysis were the following: (rc = reference category): Age ( < 50 (rc), 50-70, > 70); setting of care (GPs (rc), DOCs, specialists); hypertension (No (rc), Yes controlled, Yes uncontrolled); num- ber of insulin injections per day ( < 3/day (rc), 2 3/day); hypoglycemic episodes (No (rc), Yes); self-management of insulin doses (No (rc), Yes); sex (males (rc), female); education ( I 5 years (rc), > 5 years); occupation (professional/managerial (rc), technical/clerical, skilled worker, unskilled worker, other); type of diabetes (IDDM (rc), NIDDM insulin treated); duration of diabetes ( I 10 years (rc), lo-20 years, > 20 years); major diabetic complications (No (rc), Yes); cardiocere- bra1 diseases (No (rc), Yes); compliance with visit scheduling (No (t-c), Yes); living alone (Yes (rc), No); smoking habit (No (rc), current, ex-smoker); alcohol consumption (No (rc), l-3 cups/day, > 3 cups/day); compliance with dietary recommenda- tions (No (rc), Yes); glycated hemoglobin (good/ acceptable (rc), bad). The significance level for covariates entering and staying in the logistic model was 0.1. Both in univariate and multivari- ate analyses, the association between exposures and outcome are thus expressed in terms of odds ratios (OR) together with their 95% confidence intervals (95% CI).

118 N. Scorpiglione et al. /Diabetes Research and Clinical Practice 34 (1996) 115-125
3. Results
3.1. General characteristics of the study population
A total number of 1384 patients treated with insulin was considered eligible for the present analysis (379 as IDDM and 1005 as NIDDM-IT). Table 1 represents the clinical and socio-demo- graphic characteristics of patients with respect to frequency of self-testing of blood glucose levels. Overall, only 242 patients (18%) practised SMBG, 418 (31%) had never performed any kind of self- monitoring of blood glucose, and 674 (50%) de- clared that they tested their glycemic level with a mean frequency ranging from less than once daily to less than once per week. This overall frequency was observed in both males and females with no difference between the sexes. The same general pattern was followed by patients whether their glycated hemoglobin was within normal level or not. Patients with diabetic complications did not deviate from this pattern. In cases with uncon- trolled hypertension, 43.6% had never performed any type of self-testing of blood glucose. The proportion of SMBG was 17.7% and 18% in cases with and without hypertension, respectively.
blood glucose was observed in IDDM patients (29.7%) compared with NIDDM-IT cases (13.9%). Among IDDM, only 15.1% had never self-checked their glycemic state, compared with 37.3% in NIDDM-IT. When looking at the set- ting of care, it emerged that patients treated by general practitioners had the lowest percentage of SMBG (5.9%), compared with 21.4 and 15.4% in those who were treated at diabetic outpatient clinics or by specialists.
Out of patients who needed less than three daily injections of insulin, 12.6% performed SMBG, whereas 23.3% of those receiving more than three injections per day performed it. An average of at least one test per day was more common among patients capable of adjusting in- sulin doses (30.4%), with respect to those who declared they were not capable of self-modifying insulin treatment (8.3%), a high proportion of whom had never self-checked blood glucose (46.5%).
Only 13.8% of patients with diabetes for less than 10 years declared that they practiced SMBG and 35.2% had never performed blood testing. In patients with a longer duration of diabetes, the corresponding figures were 19.4 and 32.8% in those with diabetes for lo-20 years, and 18.9 and 27.9% in those with diabetes over 20 years.
The probability of SMBG was higher among patients who were compliant with the visit scheduling at clinics (20.7%) than those who were not (8.5%). The proportion of patients practising SMBG was higher among those who suffered from hypoglycemia with respect to those who did not (26.6 versus 16.1%). The clinical and socio-de- mographic characteristics of patients with respect to practising SMBG and the results of univariate analysis are reported in Table 2.
3.2. Results of the logistic regression analysis
Patients over 50 years of age practised self-test- Results of the logistic regression are summa- ing of blood glucose less frequently. The propor- rized in Table 3. There was a greater probability tion of patients practising SMBG in the 51-70 of testing blood glucose at least once per day for and over 70 years age groups were 15.5 and patients treated at DOCs (OR = 2.73, 95% CI = 13.4%, respectively, compared with 35.9% in cases 1.57-4.74); with either controlled (OR = 1.56, under the age of 50. The percentages of those who 95% CI = 1.10-2.20) or uncontrolled hyperten- had never self-performed blood glucose testing sion (OR = i.88, 95% CI = 1.08-3.25); who were 31.9 and 41%, compared with 8.5% in the needed three or more insulin injections per day corresponding age groups. Patients with a higher (OR = 1.50, 95% CI = 1.09-2.08); who had a pre- level of education were more liable to perform vious history of hypoglycemic episodes (OR = blood glucose testing than those with a lower level 1.47, 95% CI = 1.03-2.09); and were able to (24.3% practised SMBG versus 14.3% and only self-adjust insulin doses (OR = 2.77, 95% CI = 18.8% had never performed blood testing versus 1.94-3.98). Patients who were over 50 years of 39.1%). Increased frequency of self-monitoring of age were less likely to practice SMBG (51-70

Tabl
e 1
Dis
tribu
tion
of
case
s by
fre
quen
cy
of
prac
ticin
g bl
ood
gluc
ose
self-
test
ing
and
patie
nts
char
acte
ristic
s
Varia
ble
Bloo
d gl
ucos
e se
lf-te
stin
g
> 1 /
day
-c 1
/day
- 1 /
wee
k <
1 /w
eek
Nev
er
Subt
otal
x2
val
ue
No.
no
t To
tal
(n =
242
) %
(n
= 4
27)
%
(n =
247
) %
(n
=418
) %
10
0%
m
asse
ssab
le
no.
Gen
der
Fem
ale
Mal
es
Age
(yea
rs)
50
51-7
0 >7
0 Ed
ucat
ion
(yea
rs)
5 15
Ty
pe
of
diab
etes
ID
DM
N
IDD
M-IT
D
iabe
tes
dura
tion
(yea
rs)
<lO
10-2
0 >2
0 Se
tting
of
car
e G
P D
OC
Sp
ecia
list
Dia
bete
s co
mpl
icat
ions
Ab
sent
Pr
esen
t H
yper
tens
ion
No Ye
s, c
ontro
lled
Yes,
un
cont
rolle
d Ty
pe
of
treat
men
t In
sulin
In
sulin
+
OAA
” In
sulin
in
ject
ions
(/d
ay)
1 2 3 4 Not
kn
own
11.1
30
.2
20.0
32
.1
707
18.7
34
.0
16.9
30
.4
627
35.9
45
.7
9.9
8.5
223
15.5
33
.0
19.6
31
.9
418
13.4
24
.5
21.1
41
.0
493
14.3
25
.9
20.7
39
.1
523
24.3
41
.9
15.0
18
.8
511
29.7
44
.5
10.7
15
.1
351
13.9
27
.4
21.4
31
.3
977
13.8
29
.7
21.3
35
.2
239
19.4
30
.6
17.2
32
.8
540
18.9
34
.6
18.6
27
.9
555
5.9
22.3
36
.1
35.7
26
9 21
.4
35.5
13
.6
30.5
10
26
15.4
33
.3
28.2
23
.1
39
17.2
31
.4
17.7
33
.1
646
19.0
32
.6
19.3
29
.1
688
17.7
34
.6
17.7
30
.0
746
18.9
29
.9
21.3
29
.9
136
18.1
24
.8
13.5
43
.6
133
18.7
34
.1
18.7
28
.5
1051
15
.9
24
17.7
42
.4
283
8.7
21.3
21
.8
48.2
20
6 14
.4
33.4
16
.7
35.5
43
7 23
.6
34.5
18
.6
23.3
61
7 33
.3
44.5
11
.1
11.1
21
12
.7
25.5
23
.4
38.4
47
3.54
(0.
315)
131.
91 (
<O.O
Ol)
89.2
7 (<
O.O
Ol)
116.
95 (
<O.O
Ol)
10.1
(0.
121)
101.
37 (
<O.O
Ol)
3.60
(0.
308)
15.6
5 (0
.016
)
22.3
2 (<
O.O
Ol)
77.3
6 (iO
.001
)
28
735
22
649
17
240
23
641
10
503
21
844
29
540
22
379
28
1005
7 24
6 18
55
8 25
58
0
4 27
3 46
10
72
0 39
28
674
22
710
31
18 1
717
473
134
4 10
96
1.7
288
2.8
212
2.8
450
4. I
644
10
30
2 48

Table
1
(con
tinue
d)
Varia
ble
Bloo
d gl
ucos
e se
lf-te
stin
g
> l/d
ay
i l/d
ay-
l/wee
k <
1 /we
ek
Nev
er
Subt
otal
x2
val
ue
(n =
242
) %
(n
= 4
27)
%
(n =
247
) %
(n
=418
) %
, 10
0%
(P)
No.
not
asse
ssab
le
Tota
l 2 a
tl0.
r-
Hyp
ogly
cem
ic
episo
des
No
16.1
30
.1
Yes
26.6
39
.8
Glyc
ated
hem
oglob
in G
ood-
acce
ptab
le
19.7
32
.3
Bad
24.7
34
.9
Not
asse
ssab
le
Self-
man
agem
ent
of in
sulin
do
ses
No
8.3
22.2
Ye
s 30
.4
44.1
Co
mpl
ianc
e wi
th
visi
t sc
hedu
ling
No
8.5
23.7
Ye
s 20
.7
34.3
Tota
l 18
.2
32.0
19.7
34
.1
1078
13
.7
19.9
25
6
19.3
15
.9
23.0
46
.5
738
12.9
12
.6
596
26.1
41
.7
283
16.5
28
.5
1051
18.5
31
.3
1334
28.7
50
2 24
.5
384
448
35.6
4 (<
O.O
Ol)
5.82
(0.
12)
277.
33 (
<O.O
Ol)
49.8
8 (<
O.o
ol)
45 5 21
18
11
12
38 4 46
50
$ $ 11
23
1123
B B F F
261
261
; ; 52
3 52
3 iz iz
402
402
z- z- 45
9 45
9 9 9 iL iL 0 0 =r
=r
s‘
. s‘
. 75
0 75
0 i: i:
634
634
rp
rp
R R R.
R.
m
m
287
287
L.i
L.i
1097
10
97
A A 2 2 13
84
1384
%
%
9 9
a OAA
, O
ral
antid
iabe
tic
agen
ts.
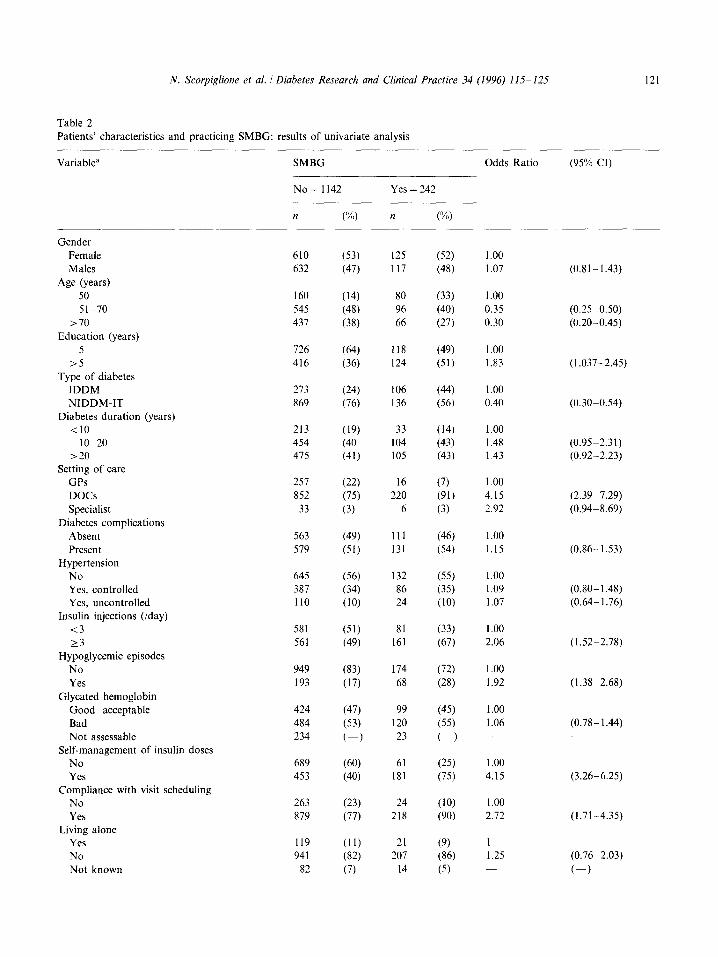
Table 2
N. Scorpiglione et al. / Diabetes Research and Clinical Practice 34 (1996) 115-125 121
Patients’ characteristics and practicing SMBG: results of univariate analysis
Variable” SMBG Odds Ratio (95%) CI)
Gender Female Males
Age (years) 50 51-70
>70 Education (years)
>5 Type of diabetes
IDDM NIDDM-IT
Diabetes duration (years) <lO
IO-20 >20
Setting of care GPs DOCs Specialist
Diabetes complications Absent Present
Hypertension No Yes, controlled Yes, uncontrolled
Insulin injections (/day) <3
23 Hypoglycemic episodes
No Yes
Glycated hemoglobin Gooddacceptable Bad Not assessable
Self-management of insulin doses No Yes
Compliance with visit scheduling No Yes
Living alone Yes No Not known
No= 1142 Yes = 242
n (‘1%) n (oh)
610 (53) 125 (52) 1.00 632 (47) 117 (48) 1.07
160 (14) 80 (33) 1 .oo 545 (48) 96 (40) 0.35 437 (38) 66 (27) 0.30
726 (64) 118 (49) 1 .oo 416 (36) 124 (51) 1.83
273 (24) 106 (9 1.00 869 (76) 136 (56) 0.40
213 (19) 33 (14) 1.00 454 (40 104 (43) 1.48 475 (41) 105 (43) 1.43
257 (22) 16 (7) 1 .oo 852 (75) 220 (91) 4.15
33 (3) 6 (3) 2.92
563 (49) 111 (46) 1 .oo 579 (51) 131 (54) 1.15
645 (56) 132 (55) 1.00 387 (34) 86 (35) 1.09 110 (10) 24 (10) 1.07
581 (51) 81 (33) I .oo 561 (49) 161 (67) 2.06
949 (83) 174 (72) 1.00 193 (17) 68 (28) 1.92
424 (47) 99 484 (53) 120 234 C-1 23
689 (60) 61 453 (40) 181
263 (23) 24 879 (77) 218
119 (11) 21 941 (82) 207
82 (7) 14
(45) (55) (-1
(25) (75)
(10) (90)
(9) (86) (5)
1.00 1.06
1 .oo 4.15
1.00 2.72
I 1.25
(0.81-1.43)
(0.25-0.50) (0.20-0.45)
(1.037-2.45)
(0.30-0.54)
(0.9552.31) (0.92-2.23)
(2.3997.29) (0.9448.69)
(0.86-1.53)
(0.80- 1.48) (0.66 1.76)
(1.52-2.78)
(1.38-2.68)
(0.78- 1.44)
(3.26-6.25)
(1.71-4.35)
(0.7662.03)
C-J

122 N. Scorpiglione et al. /Diabetes Research and Clinical Practice 34 (1996) 115-125
Table 2 (continued)
Variable” SMBG
No= 1142 Yes = 242
n (%) n (‘%)
Odds Ratio (95% Cl)
Occupation Professional Clerical Skilled workers Unskilled workers Other works Not known
Compliance with dietary recommendations Yes No Not known
Smoking habits Never Current Ex-smoker Not known
Alcohol consumption None l-3 cups/day > 3 cups/day
55 (5) 8 (3) 193 (17) 48 (20) 236 (21) 56 (23) 444 (39) 80 (33) 203 (17) 44 (18)
11 (1) 6 (3)
381 (34) 646 (57) 108 (9)
701 (61) 199 (17) 241 (22)
1 C-1
128 (64) 168 361 (32) 68 53 (4) 6
59 (25) 166 (69)
14 (6)
140 43 59
(58) (18) (24) C-1
1 1.08 1.23
(69) 1 (28) 0.82 (3) 0.49
1 1.71 1.63 1.24 1.49
1 1.66
(0.76-3.83) (0.7663.62) (0.5772.70) (0.6663.35) C-1
(1.20-2.29) C-1
(0.74- 1.58) (0.87-l .72) C-1
(0.60-1.11) (0.2lLl.16)
a First category is the reference one.
years: OR= 0.61, 95% CI = 0.41-0.92; > 70 years: OR = 0.81, 95% CI = 0.51-1.28).
Variables not related to SMBG practice in- cluded sex, years of education, living status, occu- pation, smoking, alcohol consumption, type of diabetes, diabetes duration, glycated hemoglobin, major diabetic complications, compliance with clinical visit schedules, and compliance with di- etary recommendations.
In order to evaluate the impact of the afore- mentioned factors among IDDM and NIDDM- IT patients and among patients with or without major complications, four additional logistic re- gression analyses were run. Variables associated with SMBG practice and the magnitude of the risks in the four subgroups of patients were con- sistent with those found in the main analysis.
4. Discussion
Little information is available on the frequency of self-monitoring in clinical practice. A national survey conducted in 1989 in the United States on a sample of 2405 subjects over 18 years of age showed that the proportion of patients practising SMBG varied from 79% among IDDM subjects to 53% among those with insulin-treated NIDDM[13].
Our data show that one-third of the insulin- treated diabetic patients in our sample had never tested their blood glucose. In addition, only a minority self-monitored their glycemia once or more per day. The low frequency of self-monitor- ing in a considerable proportion of the study population may reflect the lack of any clear evi-

N. Scorpiglione et al. /Diabetes Research and Clinical Practice 34 (1996) 115-125 123
dence of the benefits of intensive monitoring for patients treated with insulin. Considering the variables influencing SMBG practice, several fac- tors related to patients’ characteristics, clinical variables and the delivery of care were found to be associated with the current use of the proce- dure.
It is not surprising that factors related to in- tensive insulin therapy such as three or more insulin injections per day, ability to adjust in- sulin doses and suffering from episodes of hypo- glycemia were strong predictors of practicing self-monitoring. On the contrary, the association
Table 3 Factors affecting SMBG practice: result of stepwise logistic regression analysis
Variable Odds Ratio
Age (years) 50 51-70
>70
1.00 0.61 0.81
Setting of care GPs DOCs Specialist
1 .oo 2.13 1.63
Hypertension No Yes, controlled Yes, uncontrolled
1 .oo 1.56 1.88
Insulin injections (/day) 13 23
1 .oo 1.50
Hypoglycemic episodes No Yes
1 .oo 1.47
Self-management of insulin doses No Yes
1 .oo 2.17
(95% CI)
(0.41-0.92) (0.51l1.28)
(1.57-4.74) (0.57-4.70)
(1.10-2.20) (1.08-3.25)
(1.09-2.08)
(1.03-2.09)
(1.94-3.98)
List of the variables included in the logistic model (rc = refer- ence category): age, setting of care, hypertension, number of insulin injections per day, hypoglycemic episodes, self-manage- ment of insulin doses, sex, education, occupation, type of diabetes, duration of diabetes, major diabetic complications, cardiocerebral diseases, compliance with visits scheduling, liv- ing alone, smoking habit, alcohol consumption, compliance with dietary recommendations, glycated hemoglobin.
between SMBG and hypertension is more difficult to interpret. One possible explanation is that greater attention is devoted to patients with hypertension, who are particularly exposed to the risk of developing major complications. It should be noted that the lack of association be- tween hypertension and SMBG in the univariate analysis is related to the confounding effect ex- erted by patients’ age. In fact, when the associa- tion was evaluated within each age strata, it consistently emerged that SMBG was practised more frequently among patients with hyperten- sion.
Advanced age was associated with a low probability of practising SMBG. It is apparent that SMBG is not usually utilized in an appro- priate manner by the elderly because of their decreased visual acuity, lack of appropriate co- ordination in performing the test and deteriora- tion of memory. Recent reports indicate that urine glucose testing may be used as a substitute for SMBG in the management of NIDDM since it is simple, non-invasive and less expensive [14- 161. Nevertheless, urine glucose testing is insuffi- cient for detecting hypoglycemia and can also be difficult to perform for elderly patients.
The association between the use of self-moni- toring and setting of care showed that patients treated by general practitioners were those less likely to practice self-monitoring. This finding is consistent with several studies conducted in other countries which have already suggested that primary-care physicians are less likely to recommend SMBG [ 17,181.
On the other hand, the difference observed between DOCs and GPs (21.4 versus 5.9%) may be at least partially related to the fact that pa- tients with major problems in metabolic control, who are more likely to benefit from SMBG, are generally referred to DOCK The lack of ade- quate continuous education by GPs and the pro- motion of patient motivation by DOCs thus seem to be the main explanatory factors for this observation. Furthermore, patients cared for by GPs were older and probably less likely to pur- sue self-care practices with respect to those who chose to be cared for by DOCs.
124 N. Scorpiglione et al. /Diabetes Research and Clinical Practice 34 (1996) 115-125
Nevertheless, even among patients who were below 50 years and who declared that they self- managed insulin treatment, only one-third prac- tised SMBG with a mean frequency of one test per day or more. Similarly, among patients treated with more intensive regimens ( > 3/day) and those more exposed to the risk of hypo- glycemia, less than one-quarter practised self- monitoring with a mean frequency of one test per day or more. While a decrease in the fre- quency of monitoring to less than four times a day has been shown to result in poorer glycemic control in one study [l], more recent data has failed to demonstrate any significant difference in metabolic control according to the frequency of blood glucose monitoring [2].
The practice of SMBG does not appear asso- ciated with other socio-demographic characteris- tics (e.g. gender, occupation, level of education). It is worth mentioning that the financial aspect cannot be considered as a possible limiting fac- tor, since in Italy devices for monitoring blood glycemia at home are dispensed by the National Health Service free of charge.
Studies have found that home monitoring of blood glucose in patients with non-insulin- treated type 2 diabetes does not affect glycemic control [4-71. Our results seem to confirm the lack of association between glycated hemoglobin levels and SMBG practice also for type 2 in- sulin-treated patients.
Similarly, suffering from a major diabetic complication or having a previous history of cardiac or cerebrovascular disease were not pre- dictors of self-monitoring.
These data suggest that, among Italian doc- tors, the prevailing attitude is to consider inten- sive SMBG for short-term purposes (e.g. as a guide to self-managing insulin treatment and to controlling hypoglycemic episodes), while its role as a tool for improving metabolic control in high-risk patients (high glycated hemoglobin lev- els, presence of major complications) appears not to have entered the clinical practice.
As a final point, some possible limitations of our study need to be discussed.
First, patients were selected in the framework of a case-control study, thus leading to a popu-
lation with an over-representation of compli- cated patients. Although this could, in principle, undermine the generalization of the results, the multivariate analyses showed that the presence of major complications is not, per se, an inde- pendent predictor of SMBG practice. Further- more, two separate logistic models performed for patients with and without major complica- tions showed that the same factors have a pre- dictive role in the two populations.
Second, we classified patients as practising SMBG on the basis of the average number of blood glucose measurements per day, with no possibility of identifying the true timing and scheduling of blood glucose tests. Nevertheless, it is hard to believe that more strict criteria re- garding SMBG practice would have improved the overall picture emerging from our data.
Finally, both DOCs and GPs were selected on the basis of their willingness to participate. Non- participants could thus be even less likely to rec- ommend SMBG practice.
Overall, we believe that, because of the large number of DOCs and GPs involved, reflecting different settings of care and practice styles, this study represents a realistic picture of the true prevalence of practice of self-monitored glycemia in the Italian diabetic population.
5. Conclusions
Considering the inconsistency of the currently available guidelines, SMBG seems to be utilized mainly for controlling short-term diabetic compli- cations.
Only a minority of Italian patients practice intensive self-monitoring, particularly those who are treated intensively, more prone to hypo- glycemia and capable of adjusting insulin doses. The majority of subjects treated with insulin, even in the presence of very poor metabolic control or of major diabetic complications, either test blood glucose with a lower than recommended fre- quency or not at all. The main reasons for not practising SMBG seem to be the lack of adequate information for patients treated by GPs and poor

N. Scorpiglione et al. 1 Diabetes Research and Clinical Practice 34 (1996) 11% 125 125
compliance with medical recommendations for those attending DOCs. The lack of clear evidence from the literature may also play an important role.
Furthermore, additional scientific research will be needed for the identification of subgroups of patients that truly need to monitor their blood glucose, to better understand the optimal timing and frequency of SMBG and set up more effective clinical practice guidelines on this component of diabetic care. We also recommend that these guidelines should be differentiated according to diabetes type and treatment, where the frequency of SMBG performed within each category could be clearly defined according to the number of daily injections and the presence of stable or unstable disease.
Acknowledgements
This study was supported by Pfizer Italiana S.p.A. and by the Italian National Research Council (CNR, Rome) contract No. 94.00989.04. We also thank Barbara Di Nardo, Elisa Sasso and Loredana Sacco for their assistance in data handling and study coordination, and Maria Pia De Simone for revision of the English text.
References
[2] Gordon, D., Semple, C.G. and Paterson, K.R. (1991) Do different frequencies of self-monitoring of blood glucose influence control in type I diabetic patients? Diabetic Med. 8, 6799682.
[l] Schiffrin, A. and Belmonte, M. (1982) Multiple daily self-glucose monitoring: its essential role in long-term glucose control in insulin-dependent diabetic patients treated with pump and multiple subcutaneous injections. Diabetes Care 5, 479-484.
(31 Worth, R., Home, P.D., Johnston, D.G. et al. (1982) Intensive attention improves glycaemic control in insulin- dependent diabetes without further advantage from home blood glucose monitoring: results of a controlled trial. Br. Med. J. 285, 123331240.
[4] Patrick, A.W., Gill, G.V., MacFarlane, LA., Cullen, A., Power, E. and Wallymahmed, M. (1994) Home glucose
151
PI
[71
181
[91
HOI
1111
1121
monitoring in type 2 diabetes: is it a waste of time? Diabetic Med. 11, 62-65. Wing, R.R., Epstein, L.H., Nowalk, M.P., Scott, N., Koeske, R. and Hagg, S. (1986) Does self-monitoring of blood glucose levels improve dietary compliance for obese patients with type 2 diabetes? Am. J. Med. 81, 830-836. Allen, B.T., DeLong, E.R. and Feussner, J.R. (1990) Impact of glucose self-monitoring on non-insulin-treated patients with type II diabetes mellitus. Randomized con- trolled trial comparing blood and urine testing. Diabetes Care 13, 10441050. Fontbonne, A., Billaut, B. and Acosta, M. (1989) Is glucose self-monitoring beneficial in non-insulin-treated diabetic patients? Results of a randomized comparative trial. Diabete Metab. 25, 2555260. European IDDM Policy Group (1993) Consensus guideli- nes for the management of insulin-dependent diabetes. Medicom Europe, Bussum, The Netherlands. European NIDDM Policy Group (1993) A desktop guide for the management of non-insulin-dependent diabetes mellitus (NIDDM). International Diabetes Federation, Brussels, Belgium, pp. 14- 15. Consensus Development Panel (1994) Consensus state- ment on self-monitoring of blood glucose. Diabetes Care 17, 81-86. Nicolucci, A., Cavaliere, D., Belfiglio, M. et al. (1993) A case-control study on risk factors for development of some long-term diabetic complications: design and feasi- bility. Diabetes Nutr. Metab. 6, 357-360. Hosmer. D.W. and Lemeshow, S. (1989) Applied logistic regression. Wiley, New York.
[13] Harris, M.I., Cowie, CC. and Howie, L.J. (1993) Self- monitoring of blood glucose by adults with diabetes in the United States population. Diabetes Care 16, 1116- 1123.
[14] Newman, W.P., Laqua, D. and Engelbrecht, D. (1990) Impact of glucose self-monitoring on glycohemoglobin values in a veteran population. Arch. Intern. Med. 150, 107.
[16] Allen, B.T., DeLong, E.R. and Feussner, J.R. (1990) Impact of glucose self-monitoring on non-insulin-treated patients with type II diabetes mellitus. Diabetes Care 13, 1044.
[I51 Albisser, A.M., Sozzi, S. and Strack, T.R. (1990) Blood or urine glucose-based insulin therapy and control of glycaemia: computer-stimulation study. Diabetes Care 13, 393.
[l7] Adamson, T.E. and Gullion, D.S. (1986) Assessment of diabetes continuing medical education. Diabetes Care 9, 11-16.
[18] Jacques, C.H.M., Jones, R.L., Houts, P. et al. (1991) Reported practice behaviors for medical care of patients with diabetes mellitus by primary-care physicians in Penn- sylvania. Diabetes Care 14, 712-717.




















