
Electrocardiographic changes evoked by ajmaline in chronic chagas' disease without manifest...
7
Electrocardiographic Changes Evoked by Ajmaline in Chronic Chagas’ Disease Without Manifest Myocarditis PABLO A. CHIALE, MD JULIO PRZYBYLSKI, MD RUBEN A. LAIiiO, MD M. SUSANA HALPERN, MD RUBiN A. SANCHEZ, MD ALFRED0 GABRIELI, MD MARCEL0 V. ELIZARI, MD, FACC MAURICIO B. ROSENBAUM, MD, FACC Buenos Aires, Argentina From the Service of Cardiology and Department of Electrocardiography and Electrophysiology, Ramos Mejia Hospital, Buenos Aires, Argentina. This work was supported in part by the Fundacion de lnvestigaciones Cardiologicas Einthoven, Buenos Aires, Argentina, and the Subprograma National para el estudio de la enfermedad de Chagas. Manuscript received March 6, 1981; re- vised manuscript received June 16, 1981, ac- cepted June 22, 1981. Address for reprints: Mauricio 8. Rosenbaum, MD, Service of Cardiology, Ramos Mejia Hospital, Urquiza 609-1221 Buenos Aires, Argentina. Conversion from Chagas’ infection to chagasic myocarditis occurs slowly and the earliest signs of myocardial involvement are hard to define. To obtain new information on this difficult clinical problem, ajmaline was administered (1 mg/kg body weight intravenously) to 101 patients with Chagas’ Infection and to 46 patients without such infection (control group). In 3 patients in the control group left anterior hemiblock alone occurred whereas in the group with Chagas’ infection, ajmaline caused the oc- currence of right bundle branch block, left anterior hemiblock, or both, in 32 patients (31.6 percent), ventricular extrasystoles in 6 (7.9 percent) and ischemic ST-T changes in 7 (6.9 percent). Ajmaline may thus evoke the most typical electrocardiographic changes of chronic chagasic myocarditis in patients wtthout signs of myocardial involvement or only minor nonspecific signs. A posttive ajmaline test, defined in the present context as the occurrence of a fascicular block, ventricular arrhythmias or ischemic ST-T changes, may indicate the existence of localized areas of injured myocardial tissue, not enough to alter the electrocardiogram by itself, but able to give rise to severe abnormalities after exposure to the drug. The test may therefore be used as a nonspecific detector of myocardial damage, and thus may have a much broader scope of clinical application. In chronic Chagas’ infection, the ajmaline test is a relatively simple and apparently safe procedure that may serve to unveil the earliest signs of chagasic myocarditis. Chronic chagasic myocarditis occurs in 20 to 30 percent of patients in- fected by Trypanosoma cruzi. I92 During advanced stages, which may take 20 years to fully develop, right bundle branch block, left anterior hem- iblock, persistent ventricular arrhythmias and extensive T wave changes are commonly observed, whereas left bundle branch block is extremely rare.1,3-6 However, during earlier stages, patients may show only slight nonspecific changes or have a normal electrocardiogram, no symptoms and no cardiomegaly. Conversion from chronic infection to the slowly developing myocarditis is hard to define, posing a difficult problem when evaluation and prognosis of such patients are requested (for example, when they apply for a job). Noninvasive procedures7-lo have been used without proved success. A simple and reliable detector of the earliest signs of chronic chagasic myocarditis is needed, because millions of people in South America are known to have Chagas’ disease. Ajmaline is a strong conduction-depressing drug with a half-life no longer than 3 to 8 minutes. 11,12 In patients with suspected or partial in- traventricular or atrioventricular block, the drug has been shown to uncover or greatly enhance the conduction disturbance.13J4 Because conduction disturbances are so frequent in chronic chagasic myocarditis, we thought that ajmaline might eventually reveal latent conduction abnormalities in patients with Chagas’ disease and a normal electro- cardiogram. Initial studies proved this to be true in several patients, with the unforeseen dividend that ventricular arrhythmias and ST-T changes were also observed. Ajmaline was thus able to evoke all the typical 14 January 1982 The American Journal of CARDIOLOGY Volume 49
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Electrocardiographic changes evoked by ajmaline in chronic chagas' disease without manifest...

Electrocardiographic Changes Evoked by Ajmaline in
Chronic Chagas’ Disease Without Manifest Myocarditis
PABLO A. CHIALE, MD JULIO PRZYBYLSKI, MD RUBEN A. LAIiiO, MD M. SUSANA HALPERN, MD RUBiN A. SANCHEZ, MD ALFRED0 GABRIELI, MD MARCEL0 V. ELIZARI, MD, FACC MAURICIO B. ROSENBAUM, MD, FACC
Buenos Aires, Argentina
From the Service of Cardiology and Department of Electrocardiography and Electrophysiology, Ramos Mejia Hospital, Buenos Aires, Argentina. This work was supported in part by the Fundacion de lnvestigaciones Cardiologicas Einthoven, Buenos Aires, Argentina, and the Subprograma National para el estudio de la enfermedad de Chagas. Manuscript received March 6, 1981; re- vised manuscript received June 16, 1981, ac- cepted June 22, 1981.
Address for reprints: Mauricio 8. Rosenbaum, MD, Service of Cardiology, Ramos Mejia Hospital, Urquiza 609-1221 Buenos Aires, Argentina.
Conversion from Chagas’ infection to chagasic myocarditis occurs slowly and the earliest signs of myocardial involvement are hard to define. To obtain new information on this difficult clinical problem, ajmaline was administered (1 mg/kg body weight intravenously) to 101 patients with Chagas’ Infection and to 46 patients without such infection (control group). In 3 patients in the control group left anterior hemiblock alone occurred whereas in the group with Chagas’ infection, ajmaline caused the oc- currence of right bundle branch block, left anterior hemiblock, or both, in 32 patients (31.6 percent), ventricular extrasystoles in 6 (7.9 percent) and ischemic ST-T changes in 7 (6.9 percent). Ajmaline may thus evoke the most typical electrocardiographic changes of chronic chagasic myocarditis in patients wtthout signs of myocardial involvement or only minor nonspecific signs. A posttive ajmaline test, defined in the present context as the occurrence of a fascicular block, ventricular arrhythmias or ischemic ST-T changes, may indicate the existence of localized areas of injured myocardial tissue, not enough to alter the electrocardiogram by itself, but able to give rise to severe abnormalities after exposure to the drug. The test may therefore be used as a nonspecific detector of myocardial damage, and thus may have a much broader scope of clinical application. In chronic Chagas’ infection, the ajmaline test is a relatively simple and apparently safe procedure that may serve to unveil the earliest signs of chagasic myocarditis.
Chronic chagasic myocarditis occurs in 20 to 30 percent of patients in- fected by Trypanosoma cruzi. I92 During advanced stages, which may take 20 years to fully develop, right bundle branch block, left anterior hem- iblock, persistent ventricular arrhythmias and extensive T wave changes are commonly observed, whereas left bundle branch block is extremely rare.1,3-6 However, during earlier stages, patients may show only slight nonspecific changes or have a normal electrocardiogram, no symptoms and no cardiomegaly. Conversion from chronic infection to the slowly developing myocarditis is hard to define, posing a difficult problem when evaluation and prognosis of such patients are requested (for example, when they apply for a job). Noninvasive procedures7-lo have been used without proved success. A simple and reliable detector of the earliest signs of chronic chagasic myocarditis is needed, because millions of people in South America are known to have Chagas’ disease.
Ajmaline is a strong conduction-depressing drug with a half-life no longer than 3 to 8 minutes. 11,12 In patients with suspected or partial in- traventricular or atrioventricular block, the drug has been shown to uncover or greatly enhance the conduction disturbance.13J4 Because conduction disturbances are so frequent in chronic chagasic myocarditis, we thought that ajmaline might eventually reveal latent conduction abnormalities in patients with Chagas’ disease and a normal electro- cardiogram. Initial studies proved this to be true in several patients, with the unforeseen dividend that ventricular arrhythmias and ST-T changes were also observed. Ajmaline was thus able to evoke all the typical
14 January 1982 The American Journal of CARDIOLOGY Volume 49

TABLE I TABLE II
Electrocardiographic and Chest X-Ray Film Findings in 46 Normal Sublects and 101 Patlents With Chagas’ Disease
AJmallne lest In Patients Wlth and Without Chagas’ Disease
Chest Cases Electro- X-Ray
(n) cardiogram Film Age (yr)
Group A (control group: 46 patients without Chagas’ disease)
Slubgroup 30 Normal Normal 8-50 (m 31) il Ill
i0 IRBBB Normal 20-43 (m 29) 6 LAD (-30’) Normal 24-48 (m 44)
Group B: 10 1 Patients With Chagas’ Disease
srbgroup II Ill IV .
V
50 30
x
7
Zzl Normal 12-47 (m 28) Normal 10-43 (m 28) Normal 25-62 (m 32) L$;BFfOY Normal 25-59 (m 39)
LAD (-30”) 2 IRBBB 4 cardio- 28-61 (m 40) 1 LVH megaly; 1 LV 3 normal 2 Primary ST-T
changes 4 Abnormal Cl
waves
IRBBB = incomplete right bundle branch block; LAD = left axis de- viation: LV = low voltages; LVH = left ventricular hypertrophy; m = mean.
electrocardiographic changes of chronic chagasic myo- carditis. This raised the need to define specificity and sensitivity of the ajmdine test and prompted this more detailed study, in which the effects in patients with Chagas’ disease and no apparent myocarditis were shown to differ significantly from those occurring in normal subjects.
Methods
Study patients: The ajmaline test was performed on 147 patients classified into two groups: control (A) and chagasic (B), with the several subgroups listed in Table I. Although the initial purpose was to cbmpare patients with and without Chagas’ disease, both with normal electrocardiograms (subgroups AI and Br), the study was subsequently extended to patients having incomplete right bundle branch block or an electrical axis at -30“ (subgroups An, Brr and Am, Bm, respectively). Because these variants occur in persons with and without Chagas’ disease, we thought that ajmaline could be useful to evaluate their significance. The patients with Chagas’ disease alsoincluded two subgroups without equiv- alent in the control group: Brv consisted of patients showing incomplete right bundle branch block plus an electrical axis at -3O”, and Bv consisted of patients showing minor but combined changes excluding high grade fascicular blocks and ventricular arrhythmias, namely, those in whom the diagnosis of chagasic myocarditis was likely but inconclusive. All pa- tients had a normal-sized heart (except those in subgroup Bv), normal auscultation, normal blood pressure and total absence of symptoms. The diagnosis of Chagas’ disease was based on positivity of two serologic tests: complement fixation and hemagglutination. These tests are highly sensitive and spe- cific, and the incidence of both false positive and negative tests was statistically not significant.15
AJMALINE IN CHRONIC CHAGAS’ DISEASE-CHIALE ET AL
IV Conduction Disturbances lschemic Total
Cases ST-T Positive (n) RBBB LAH RBBB + LAH VE Changes Tests
Group A: 46 Patients Without Chagas’ Disease
Subgroup I 30 . . . . . .
111 10 . . . 1 6 . . : 1:: 1:: 1::
$
Group B: 101 Patients With Chagas’ Disease
S;bgroup 6 2 1 14
II :x : ! 1 2 7 Ill : 3 1 IV : ‘.. V 7 ‘i’ : 2”
: ; 1
z
&
IV = intraventricular; LAH = left anterior hemiblock; RBBB = right bundle branch block; VE = ventricular extrasystoles.
Ajmaline test: After all previous routine studies were performed, ajmaline aspartate* was administered intrave- nously in a dose of 1 mg/kg body weight in 90 seconds without exceeding 70 mg. Three simultaneous leads (I, II and VI) were continuously recorded during the first 150 seconds; thereafter 12 lead electrocardiograms were obtained every 2 minutes until the changes induced by the drug completely disappeared. Informed consent was obtained from each patient. The control electrocardiogram and the one showing the greatest changes were compared regarding duration of the P wave, P-R interval, QRS complex and corrected Q-T interval, electrical axis di- rection and morphologic changes of the QRS complex and ST-T waves.
Statistical analysis: In each group, the measurable drug- induced changes were compared and the significance of the changes tested with the t test for paiied data. Results from homologous subgroups were compared by using the t or 2 testa, both having similar statistical principles but applied to samples less than or more than 30 patients, respectively. The &i-square test was used in order to compare the incidence of bundle branch block, ventricular arrhythmias and ST-T changes in the patients with and without Chagas’ disease.
Results
Control Group A (Table IIA)
Subgroup AI: Figure 1 illustrates the changes pro- voked by ajmaline in 30 patients with a normal elec- trocardiogram without Chagas’ disease. The drug in- creased the heart rate and the duration of the P wave, P-R interval, QRS complex ar?d corrected Q-T interval. All these changes, which occurred within the first 1 to 2 minutes and gradually disappeared in 15 to 25 min- utes, were statistically significant (p <O.OOl), and oc- curred similarly in all the other subgroups (AI to Am and
l Kindly supplied by Craveri Laboratorios S.A.
January 1982 The American Journal of CARDIOLOGY Volume 49 15

AJMALINE IN CHRONlC CHAGAS’ DISEASE-CHIALE ET AL.
q msec 600 1
PR msec
Br to Bv). The T waves were unchanged in 21 patients but showed flattening and slight notching in 9 (Fig. 2). Analogous changes were observed in all other subgroups. The electrical axis-changed very little or not at all, and the QRS contour was unchanged in 15 pa- tients. Ajmaline caused a peculiar change in the elec- trocardiogram compatible with a slight or moderate slowing of conduction occurring or predominating at the base of the ventricles in the other 15 patients. Essen- tially, it had the appearance of slurred S waves in leads I, II, III, aVF and Vs, a small terminal slurred R wave in lead aVR, a smaller S wave in lead Vi and larger S waves in the remaining chest leads (Fig. 2). Vectocar- diograms recorded in several subjects showed slow terminal QRS forces oriented posteriorly, to the right
AJMAL INE 60 MG
FIGURE 2. Electrocardiographic changes induced by the administration of ajmaline in a normal 30 year old man (A,). Note widening of the P wave and QRS interval and prolongation of the P-R interval.
FIGURE 1. Effects of ajmaline on the heart rate (HR.) and duration of the P wave, P-R, QRS and corrected Q-T intervals in 30 normal persons (Group A). A = ajmaline; C G control values; d = mean difference.
and superiorly. In addition, a change in the initial QRS forces, consisting of smaller R waves in leads Vi and VZ, were seen in seven patients.
Subgroup AII: In 9 of 10 patients with incomplete right bundle branch block (rSr in lead Vi) as an isolated finding, ajmaline caused (in addition to the approximate 20 ms widening of the QRS complex common to all studies) a very small increase in R wave voltage. The QRS complex never exceeded 100 ms and complete or high grade right bundle branch block was not observed. One of these nine patients (an 18 year old woman) had a typical left anterior hemiblock.
I Cf PATIENTS
50
45 -
40 -
35 -
n HAlMslc PATENTS mo) 30 .
oNOM OtlAOASIc PATIENTS (N:30)
25 .
20 .
15 .
so -
5.
I 1 I I I
150 140 130 120 110 ml 90 80 70 60
DEGREES OF t&S DEVIATION
llh 120’30 40 Fiii?
FfGURE 3. Changes of the electrical axis direction provpked by ajmaline in 50 patients with and 30 patients without Chagas’ disease with a normal electrocardiogram.
16 January 1962 The American Journal of CARDIOLOGY Volume 49

AJMALINE IN CHRONIC CHAGAS’ DISEASE-CHIALE ET AL.
FIGURE 4. Right bundle branch block and left anterior hemiblock in- duced by the administration of ajmaline in a 27 year old woman with chronic Chagas’ infection and a normal electrocardiogram (group Br). No other evidence of myocardial involvement was apparent.
Subgroup A*u: In two of the six patients showing an electrical axis of -3O”, ajmaline shifted the axis to -50°, suggesting the possible presence of left anterior hemi- block. No arrhythmias occurred in any of the 46 patients in the control group.
Group B (Chagas’ disease) (Table MB) Subgroup Bt (50 patients with a normal electro-
cardiogram): Ajmaline provoked greater shifts of the electrical axis in group BI than in group Ar (Fig. 3). Whereas only 7 percent of the patients in group Ar had a maximal axis shift of 30” to the left, 11 patients (22 percent) in group Br had an axis shift of 40 to 150’ to the left or superiorly, or both, and all these shifts were re- lated to the development of fascicular block. The right axis shift of 10 to 40° that occurred in eight patients was more difficult to interpret and probably less significant. Table IIB shows that 13 patients in this subgroup (26 percent) had right bundle branch block or left anterior hemiblock, or both. The electrocardiogram of one such patient is shown in Figure 4. Two patients showed fre- quent ventricular extrasystoles that in one were asso- ciated with left anterior hemiblock and in the other with S-T segment elevation and T wave inversion (ischemic ST-T changes) in leads VI to Vs.
Subgroup Bti (30 patients with incomplete right bundle branch block): Six patients had high grade right bundle branch block, left anterior hemiblock, or both, and one had frequent multiform ventricular ex- trasystoles. Two patients exhibited ischemic ST-T changes in leads Vi to V:i that were associated with right bundle branch block in one and with right bundle branch block plus left anterior hemiblock in the other.
Subgroup Bin (eight patients with axis of -30”): Three patients had right bundle branch block plus left anterior hemiblock (one with ventricular extrasystoles), one had left anterior hemiblock alone and one had left anterior hemiblock plus ischemic ST-T changes over the anteroseptal region.
Subgroup Btv (six patients with incomplete right bundle branch block and axis of -30”): Three pa- tients had high grade right bundle branch block and typical left anterior hemiblock (associated with ischemic ST-T changes and ventricular extrasystoles in one); one patient had left anterior hemiblock alone and another only ischemic ST-T changes.
Subgroup Bv (seven patients with combined nonspecific changes): Two patients had right bundle branch block plus left anterior hemiblock (associated with ventricular extrasystoles in one), one had right bundle branch block and ventricular extrasystoles and one had left anterior hemiblock, ischemic ST-T changes and frequent ventricular extrasystoles. Two studies of this subgroup are illustrated in Figures 5 and 6.
Summary of electrocardiographic changes pro- voked by ajmaline in the group with Chagas’ dis- ease (Table IIB): Thirty-two (31.6 percent) of the 101 patients had extensive intraventricular conduction defects, sometimes accompanied by ventricular extra- systoles or ischemic ST-T changes over the right-sided chest leads, or both. All the changes induced by the drug
CONTROL
FIGURE 5. Effects of the administration of ajmaline in a 48 year old woman with chronic Chagas’ infection, nonspecific electrocardio- graphic changes and slight cardiomegaly (group Bv). The control tracing shows low voltage and abnormal T waves. Right bundle branch block and frequent ventricular ectopic beats occurred 1 minute after injection of the drug. Fifteen minutes later (bottom strip), the right bundle branch block was intermittent.
January 1982 The American Journal of CARDIOLOGY Volume 49 17
AJMALINE IN CHRONIC CHAGAS’ DISEASE-CHIALE ET AL.
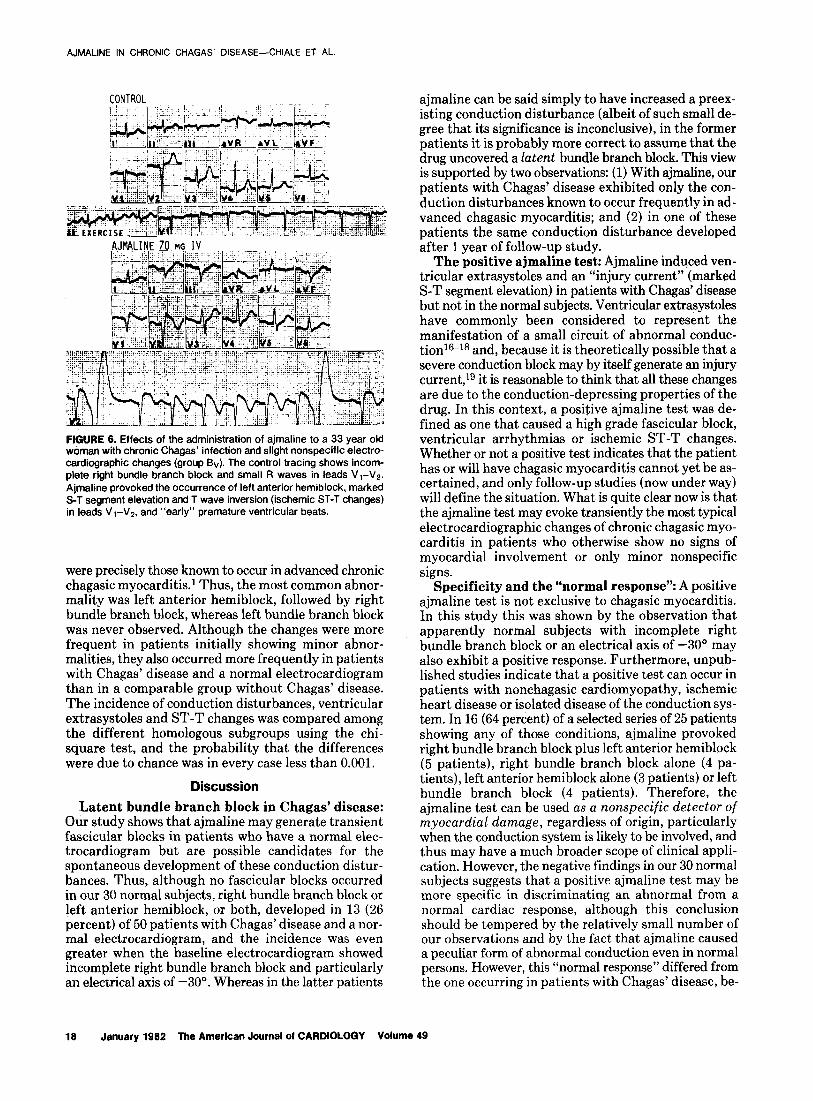
FIGURE 6. Effects of the administration of ajmaline to a 33 year old woman with chronic Chagas’ infection and slight nonspecific electro- cardiographic changes (group Bv). The control tracing shows incom- plete right bundle branch block and small R waves in leads VI-Vs. Ajmaline provoked the occurrence of left anterior hemiblock, marked S-T segment elevation and T wave inversion (ischemic ST-T changes) in leads VI-VP. and “early” premature ventricular beats.
were precisely those known to occur in advanced chronic chagasic myocarditisl Thus, the most common abnor- mality was left anterior hemiblock, followed by right bundle branch block, whereas left bundle branch block was never observed. Although the changes were more frequent in patients initially showing minor abnor- malities, they also occurred more frequently in patients with Chagas’ disease and a normal electrocardiogram than in a comparable group without Chagas’ disease. The incidence of conduction disturbances, ventricular extrasystoles and ST-T changes was compared among the different homologous subgroups using the chi- square test, and the probability that the differences were due to chance was in every case less than 0.001.
Discussion
Latent bundle branch block in Chagas’ disease: Our study shows that ajmaline may generate transient fascicular blocks in patients who have a normal elec- trocardiogram but are possible candidates for the spontaneous development of these conduction distur- bances. Thus, although no fascicular blocks occurred in our 30 normal subjects, right bundle branch block or left anterior hemiblock, or both, developed in 13 (26 percent) of 50 patients with Chagas’ disease and a nor- mal electrocardiogram, and the incidence was even greater when the baseline electrocardiogram showed incomplete right bundle branch block and particularly an electrical axis of -30”. Whereas in the latter patients
ajmaline can be said simply to have increased a preex- isting conduction disturbance (albeit of such small de- gree that its significance is inconclusive), in the former patients it is probably more correct to assume that the drug uncovered a latent bundle branch block. This view is supported by two observations: (1) With ajmaline, our patients with Chagas’ disease exhibited only the con- duction disturbances known to occur frequently in ad- vanced chagasic myocarditis; and (2) in one of these patients the same conduction disturbance developed after 1 year of follow-up study.
The positive ajmaline test: Ajmaline induced ven- tricular extrasystoles and an “injury current” (marked S-T segment elevation) in patients with Chagas’ disease but not in the normal subjects. Ventricular extrasystoles have commonly been considered to represent the manifestation of a small circuit of abnormal conduc- tion16-18 and, because it is theoretically possible that a severe conduction block may by itself generate an injury current,lg it is reasonable to think that all these changes are due to the conduction-depressing properties of the drug. In this context, a positive ajmaline test was de- fined as one that caused a high grade fascicular block, ventricular arrhythmias or ischemic ST-T changes. Whether or not a positive test indicates that the patient has or will have chagasic myocarditis cannot yet be as- certained, and only follow-up studies (now under way) will define the situation. What is quite clear now is that the ajmaline test may evoke transiently the most typical electrocardiographic changes of chronic chagasic myo- carditis in patients who otherwise show no signs of myocardial involvement or only minor nonspecific signs.
Specificity and the “normal response”: A positive ajmaline test is not exclusive to chagasic myocarditis. In this study this was shown by the observation that apparently normal subjects with incomplete right bundle branch block or an electrical axis of -30“ may also exhibit a positive response. Furthermore, unpub- lished studies indicate that a positive test can occur in patients with nonchagasic cardiomyopathy, ischemic heart disease or isolated disease of the conduction sys- tem. In 16 (64 percent) of a selected series of 25 patients showing any of those conditions, ajmaline provoked right bundle branch block plus left anterior hemiblock (5 patients), right bundle branch block alone (4 pa- tients), left anterior hemiblock alone (3 patients) or left bundle branch block (4 patients). Therefore, the ajmaline test can be used as a nonspecific detector of myocardial damage, regardless of origin, particularly when the conduction system is likely to be involved, and thus may have a much broader scope of clinical appli- cation. However, the negative findings in our 30 normal subjects suggests that a positive ajmaline test may be more specific in discriminating an abnormal from a normal cardiac response, although this conclusion should be tempered by the relatively small number of our observations and by the fact that ajmaline caused a peculiar form of abnormal conduction even in normal persons. However, this “normal response” differed from the one occurring in patients with Chagas’ disease, be-
16 January 1962 The American Journal of CARDIOLOGY Volume 49

cause fascicular blocks, ventricular arrhythmias and ST-T changes were never observed.
It is difficult to understand why, in some normal subjects, ajmaline generates terminal QRS forces ori- ented posteriorly, superiorly and to the right. To explain this pattern, we suggest that the effects of ajmaline are greater in regions of the heart where Purkinje tissue is scarce or absent, such as the base of the ventricles. Al- though this hypothesis is based mainly on the direc- tional change of the QRS forces, it may also explain some changes that occur whenever intraventricular conduction is diffusely depressed. In fact, a similar pattern may occur in hyperkalemia20 and in quinidine intoxication.21J2
Sensitivity of the ajmaline test compared with other diagnostic procedures: In a series of 12 patients with an apparently transient bundle branch block, the ajmaline test was clearly much more sensitive than atrial stimulation at rapid rates or the extrastimulus method in uncovering the conduction disturbance.23 Further- more, in a series of 21 patients with Chagas’ disease with a normal electrocardiogram, the M mode echocardio- gram was normal in all and thus was unable to distin- guish those in whom the ajmaline test was positive (6 patients) from those in which it was negative (15 pa- tients) (unpublished observations). Exercise te~ts~,~ and radionuclide studiesz4 have been used, but such studies included cases of Chagas’ disease with and without es- tablished myocarditis, in such a way that it is difficult to evaluate the real usefulness of such procedures. The overall sensitivity of the ajmaline test for detecting early myocarditis in patients with Chagas’ disease cannot be defined until a sufficiently long follow-up study of the patients with a positive ajmaline test and a complete comparison with other available diagnostic methods are carried out. Such studies are now under way in our laboratory.
Mechanism of the positive ajmaline test: Ajmaline depresses membrane responsiveness and the rate of depolarization in normal ventricular and Purkinje fi- bers.25,26 This may explain the QRS widening and pe- culiar QRS changes observed in normal persons, but it is not clear why ajmaline should cause bundle branch block, ventricular extrasystoles or ST-T changes in the anteroseptal region. The drug effect may be “potenti- ated” when acting on injured cardiac tissue, as also shown by other antiarrhythmic agents.27 In patients with intermittent bundle branch block, ajmaline causes a much greater deterioration of conduction in the af-
AJMALINE IN CHRONIC CHAGAS’ DISEASE--CulALE ET A_
fected fascicle.13 The best explanation for this effect IS probably the one provided by studies performed with other excitable tissues such as nerve and striated mus- c1e.2s-31 In such studies, it was demonstrated that small degrees of depolarization (induced by clamping) enor- mously increase the blocking action of ajmaline (as well as other local anesthetic agents) on sodium channel conduction. Furthermore, the partial inactivation that results from depolarization favors penetration and trapping of the drug in the sodium channel, in such a way that not only intensity but also duration of the drug action is enhanced. As stated by Hille,31 “depolarization would potentiate block of sodium channels by the drug and thus would selectiuely lower the excitability in these regions.” In light of these observations, a positive ajmaline test may indicate the existence of localized areas of injured tissue, not enough to alter the electro- cardiogram by itself, but able to give rise to severe ab- normalities after exposure to the drug.
Implications: The ajmaline test is a relatively simple procedure that may serve to unveil the earliest signs of chagasic myocarditis and thus benefit the evaluation of patients with Chagas’ disease and improve our knowledge of the natural course of the disease. This is particularly important for a condition affecting a large number of patients that may be at high risk of sudden death.1y2y32 The test may also open new ways of identi- fying myocardial damage in other types of cardiomy- opathy, ischemic heart disease and primary or secon- dary disease of the conduction system. Other conduc- tion-depressing drugs may possibly serve a similar purpose, but the extremely short half-life of ajmaline may have a definite advantage.
Despite the safety of the test during our study, the occurrence of ventricular extrasystoles and S-T segment elevation makes it advisable that the test be performed only in a setting in which there are available procedures for cardiopulmonary resuscitation and insertion of a standby pacemaker (complete heart block may even- tually occur in a patient with a subclinical lesion of the His bundle). However, because the development of complete atrioventricular block may be considered an extremely infrequent risk in patients without sponta- neous advanced intraventricular block, the placement of an electrode catheter in the right ventricle is not. necessary. As with other new diagnostic tools, the ajmaline test requires a much wider experience before its real usefulness, limitations and adverse effects can be properly assessed.
References
1. Rosenbaum MB. Ghagasic myocardiopathy. Prog Cardiovasc Dis 1964;7:199-224.
chagssica. Tesis doctoral. Caracas, 1961. 6. Ansaimi A, Hernhnder Pieretti 0. Contribution al estudio del
2. Porio CC. Prognostic0 e complicacoes da doenp de Chagas. Rev Goilnia Med 1959;5:87-99.
electrocardiograma en las miocarditis chag&icas. Rev Policlinica 1955;23:193-204.
3. Rassi A, Carnelro 0, Estudo clinico, electrocardiografico e ra- diologico da cardiopatia chagasica crbnica. Analise de 106 cases. Rev Goilnia Med 1956;2:287-307.
4. Rosenbaum MB, Alvarez AJ. The electrocardiogram in chronic chagasic myocarditis. Am Heart J 1955;50:492-527.
5. Hernandez Pieretti 0. El electrocardiograma en la cardiopatia
7. Farla CAF, Dlas JCP, Cintra ML, Rodrlguer LO. Chagas’ disease and work: Abstracts, Congress0 International sobre doenqa de Chagas. Rio de Janeiro. Brasil, 1979.
8. Baiiini AJ, Nicoiau JC, Biiaqul A, el al. Prova de esforqo na forma subckica da doenea de Chagas (abstr). In: Ref 7.
9. Moreyra E, Amuchirskgui LM, iosa D, et al. Estudio ecocardi-
January 1982 The American Journal of CARDIOLOGY Volume 49 19

AJb’ALINE IN CHRONIC CHAGAS’ DISEASE-CHIALE ET AL.
10
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
ografico en la enfermedad de Chagas. Medicina (Bs. As.) 1977; 37525-6. Caeiro TF, Amuchastegui LM, Moreyra E, losa D, Palmer0 H. Valoracion ecocardiogrtifica de la funcion ventricular en la en- fermedad de Chagas cronica. Rev Argent Cardioi 1980;48: 147-55. Kleinsorge M, Gaida P. Verhalten des Serumspiegels nach intra- venoser lnjektion von Ajmalin. Klin Wochenschr 1962;40:149- 58. Kleinsorge M, Gaida P. Ausscheinchengsmengen und Ges- chwinding-keinten des Rawolfia Alkaloids Ajmalin nach verschi- edersen Applikation formen. Arzneim Forsch 1961;11:2-11. Chiale PA, Przybylski J, Halpern, MS, et al. Comparative effects of ajmaline on intermittent bundle branch block and the Wolff- Parkinson-White syndrome. Am J Cardiol 1977;39:651-7. Guerot C, Caste A, VaPre PB, Tricot R. L’Bpreuve d I’ajmaline dans le diagnostic du bloc auriculo-ventriculaire paroxystique. Arch Mal Coeur 1973;66:1241-53. Camargo ME. Serologic diagnosis of Chagas’ disease. In: American Trypanosomiasis Research. Washington, DC, Pan American Health Organization, 1976:207-l 1. Cranefield PF, Wit AL, Hoffman BF. Genesis of cardiac arrhyth- mias. Circulation 1973;47: 190-204. Sasyniuk B, Mendez C. A mechanism for reentry in canine ven- tricular muscle. Circ Res 1971;28:3-15. Moe GK. Evidence for reentry as a mechanism of cardiac ar- rhythmias. Rev Physiol Biochem Pharmacol 1975;72:55-81. Sodi Pallares D. New Basis of Electrocardiography. St. Louis: CV Mosby, 1958:178. Merrill P, Levine HD, Somervllle W, Smith S. Clinical recognition and treatment of acute potassium intoxication. Ann Intern Med 1950;33:797-830. Heissenbuttel RH, Bigger JT. The effect of oral quinidine on in- traventricular conduction in man: correlation of plasma quinidine with changes in QRS duration. Am Heart J 1978;80:453-62.
22.
23.
24.
25.
28.
27.
Dick HLH, McCawley EL, Voiss DV, Krueger JD. Electrocardio- graphic evaluation on quinidine induced changes in myocardial conduction. Am Heart J 1958;56:396-404. Chlale PA, Przybylskl J, Laiiio RA, et al. Usefulness of the ajmaline test in patients with latent bundle branch block. Am J Cardiol 1982;49:21-6. Rotondaro D, Castellettl LJ, Rios V, et al. Cambios en las ima- genes de per!usion miocardica con Talio 201, en pacientes con miocardiopatra chagasica cronica, despues del tratamiento con dipiridamol. Rev Argent Cardiol 1979;47:130-7. Pillat B, Heitracher P. Elektrophysiologische Unterschungen uber die Wirkung von Ajmalin auf Reizleitungsfasern. Naunyn Schmiedebergs Arch Pharmacol 1964;246:375-88. BoJorges R, Pastelin G, Sanchez Perez S, Mender R, Kabela E. The effects of ajmaline in experimental and clinical arrhythmias and their relation to some electrophysiological parameters of the heart. J Pharmacol Exp Ther 1975;193:183-93. Kuppersmith J, Antman EM, Hoffman BF. In vivo electrophysio- logical effects of lidocaine in canine acute myocardial infarction. Circ Res 1975;36:84-91.
28. Helslracher P. Mechanism of action of antifibrillatory drugs. Naunyn Schmiedebergs Arch Pharmacol 1971;269:199-212.
29. Stricharlz GR. The inhibition of sodium currents in myelinated nerve by quaternary derivatives of lidocaine. J Gen Physiol 1973;62: 37-57.
30. Hille B. Local anesthetics: hydrophilic and hydrophobic pathways for the drug-receptor reaction. J Gen Physiol 1977;69:497-515.
31. Hille B. Local anesthetic action on inactivation of the Na channel in nerve and skeletal muscle: possible mechanism for antiar- rhythmic agents. In: Morad M, ed. Biophysiological Aspects of Cardiac Muscle. New York: Academic Press, 197855-74.
32. Lopes ER, Chapadelro E, Almelda HO, Rocha A de. Contribuicao ao estudio da anatomia patologica dos coragoes de chagasicos falecidos subitamente. Rev Sot Bras Med Trop 1975;9:269-82.
20 January 1982 The American Journal of CARDIOLOGY Volume 49




















