Effects of low level laser therapy (808 nm) on physical strength training in humans
12
1 23 Lasers in Medical Science ISSN 0268-8921 Volume 26 Number 3 Lasers Med Sci (2011) 26:349-358 DOI 10.1007/ s10103-010-0855-0 Effects of low level laser therapy (808 nm) on physical strength training in humans
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Effects of low level laser therapy (808 nm) on physical strength training in humans
1 23
Lasers in Medical Science ISSN 0268-8921Volume 26Number 3 Lasers Med Sci (2011)26:349-358DOI 10.1007/s10103-010-0855-0
Effects of low level laser therapy (808 nm)on physical strength training in humans

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer-Verlag
London Ltd. This e-offprint is for personal
use only and shall not be self-archived in
electronic repositories. If you wish to self-
archive your work, please use the accepted
author’s version for posting to your own
website or your institution’s repository. You
may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

ORIGINAL ARTICLE
Effects of low level laser therapy (808 nm) on physicalstrength training in humans
Cleber Ferraresi & Taysa de Brito Oliveira & Leonardo de Oliveira Zafalon &
Rodrigo Bezerra de Menezes Reiff & Vilmar Baldissera &
Sérgio Eduardo de Andrade Perez & Euclides Matheucci Júnior &
Nivaldo Antônio Parizotto
Received: 3 August 2010 /Accepted: 21 October 2010 /Published online: 18 November 2010# Springer-Verlag London Ltd 2010
Abstract Recent studies have investigated whether lowlevel laser therapy (LLLT) can optimize human muscleperformance in physical exercise. This study tested theeffect of LLLT on muscle performance in physical strengthtraining in humans compared with strength training only.The study involved 36 men (20.8±2.2 years old), clinicallyhealthy, with a beginner and/or moderate physical activitytraining pattern. The subjects were randomly distributedinto three groups: TLG (training with LLLT), TG (trainingonly) and CG (control). The training for TG and TLGsubjects involved the leg-press exercise with a load equal to80% of one repetition maximum (1RM) in the leg-press testover 12 consecutive weeks. The LLLT was applied to thequadriceps muscle of both lower limbs of the TLG subjects
immediately after the end of each training session. Using aninfrared laser device (808 nm) with six diodes of 60 mWeach a total energy of 50.4 J of LLLT was administeredover 140 s. Muscle strength was assessed using the 1RMleg-press test and the isokinetic dynamometer test. Themuscle volume of the thigh of the dominant limb wasassessed by thigh perimetry. The TLG subjects showed anincrease of 55% in the 1RM leg-press test, which wassignificantly higher than the increases in the TG subjects(26%, P=0.033) and in the CG subjects (0.27%, P<0.001).The TLG was the only group to show an increase in muscleperformance in the isokinetic dynamometry test comparedwith baseline. The increases in thigh perimeter in the TLGsubjects and TG subjects were not significantly different(4.52% and 2.75%, respectively; P=0.775). Strengthtraining associated with LLLT can increase muscle perfor-mance compared with strength training only.
Keywords Low level laser therapy (LLLT) . High-intensityexercise . Isokinetic Dynamometer . Leg press .
One-repetition maximum test
Introduction
Strength training, mainly high-intensity exercises, usesenergy from anaerobic metabolism and promotes changesin the contractile characteristics of the muscle fibersinvolving a transition from type I and type IIx to type IIa.An increase in fiber recruitment, and the timing and firingfrequency of motor units also occurs with this kind ofexercise [1, 2]. In addition, strength training increasesmuscle cross-sectional area (hypertrophy), which is associ-ated with neural adaptation of muscle recruitment, increas-ing muscle strength and performance [1, 2].
C. Ferraresi (*) : T. de Brito Oliveira : L. de Oliveira Zafalon :N. A. ParizottoLaboratory of Electrothermophototherapy,Department of Physical Therapy,Federal University of São Carlos,Rodovia Washington Luís, km 235,13565-905, São Carlos, SP, Brazile-mail: [email protected]
C. Ferraresi : E. M. JúniorDepartment of Biotechnology, Federal University of São Carlos,São Carlos, SP, Brazil
R. B. de Menezes ReiffDepartment of Orthopedics and Traumatology,University of São Paulo,Cerqueira César, SP, Brazil
V. Baldissera : S. E. de Andrade PerezLaboratory of Physiology of Exercise,Department of Physiological Sciences, Federal University of SãoCarlos,São Carlos, SP, Brazil
Lasers Med Sci (2011) 26:349–358DOI 10.1007/s10103-010-0855-0
Author's personal copy

In general, exercises can be carried out in two ways:closed kinetic chain (CKC) and open kinetic chain (OKC)[3, 4]. CKC exercises involve multiple articulations withbody weight or random loads being unloaded on a distalbody segment that is fixed to the ground or another base,such as in squats or leg-press exercises. OKC exercisesgenerally involve movement in only one articulation, andhave the workload fixed on a distal extremity of the bodysegment that is free to move, such as in knee extensionfitness equipment [5].
The measurement of muscle performance in CKC andOKC exercises usually involves isotonic tests includingthe one-repetition maximum leg-press (1RMleg) test(CKC) and isokinetic muscle performance in isokineticdynamometry (MPID), especially in activities involvingknee extension (OKC) [6, 7]. These tests allow morecomplete evaluations and assist in directing trainingprograms [8].
The desire to increase and/or accelerate the gains inphysical performance, such as muscle hypertrophy andenhancement of aerobic and anaerobic capacities, oftenleads athletes and sportsmen to improve their nutrition [9].Androgenic substances can also can be used but they maypose risks to health [10]. The potential of low level lasertherapy (LLLT) for improving performance in exercises,such as strength and resistance to fatigue has been tested[11, 12].
LLLT is mainly used for local pain control and tissuerepair [13, 14]. It interacts with the cellular mitochondria,promoting structural changes (appearance of giant mito-chondria) and metabolic changes (increased oxidativeenzyme activity), increasing energy synthesis (ATP) formetabolic processes [15, 16]. Thus, the few recent studieswith laser therapy in men during physical exercise haveconcentrated on investigating fatigue and muscle damageafter acute exercise of high intensity, and have involved thedetermination of the concentrations and kinetics of bio-chemical markers such as lactate and muscle creatine kinase[12, 17, 18]. However, some studies reported in theliterature are divergent as to the effectiveness of LLLT inincreasing muscle performance in humans [11, 18]. In thesestudies, LLLT parameters such as dose and wavelength aredefined in terms of the depth of tissue reached by theenergy and consequently its attenuation, which directlyinfluences the therapeutic effect in the target tissue [13].Furthermore, infrared laser radiation seems to be better forstimulating muscle tissue because it can penetrate the skinlayers and reach greater depths without significant loss ofenergy [13].
The purpose of this study was to determine whetherLLLT is able to optimize the effects of chronic strengthtraining. It was hypothesized that a chronic strength trainingprogram associated with LLLT would promote a greater
increase in muscle performance than strength trainingalone. The study was a randomized controlled clinical trialwith three tools to measure muscle performance: (1)1RMleg test, (2) MPID test (knee torque extensor), and(3) thigh perimetry as a measure of changes in thighvolume.
Materials and methods
This study was designed as a randomized controlled clinicaltrial. All procedures were approved by the Ethics in HumanResearch Committee of the Federal University of SãoCarlos (approval no. 342/2008) and the study was regis-tered with NIH ClinicalTrials (NCT01113021). The sub-jects were recruited from among graduate students at theuniversity. All volunteers were informed about the studypurposes and procedures. After inclusion in the trial, allsubjects signed a consent form.
Subjects
The study participants were 36 male subjects who reportedbeing clinically healthy.
Inclusion criteria
The inclusion criteria were: healthy males aged between 18and 28 years with a body mass index (BMI) equal to or lessthan 26 kg/m2, and with a beginner or moderately trainedpattern of physical activity, i.e. performed some physicalactivity with a noncompetitive aim one to three times aweek, in accordance with previous studies [7, 19].
Exclusion criteria
The exclusion criteria were: previous injury to the femoralquadriceps or hamstring muscles (within 6 months prior tostudy), osseous or articular disorder in the lower limbs,cardiovascular system disorders, systemic disease, andtaking prescription medicines or using dietary supplements(such as muscle mass builders).
After entering the study, subjects who did not complyproperly with the training routine, missed two consecutivetraining sessions or developed any osseous or muscle orarticular injuries were excluded.
Randomization
Randomization was performed by a simple drawingprocedure and the subjects were distributed equally intothree groups: training with LLLT group (TLG), trainingalone group (TG) and control group (CG).
350 Lasers Med Sci (2011) 26:349–358
Author's personal copy

Study groups
TG and TLG subjects were submitted to a dynamic strengthtraining program involving the leg-press exercise twice aweek for 12 consecutive weeks. Soon after the end of eachsession, the TLG subjects underwent LLLT to both femoralquadriceps muscles. CG subjects did not carry out any formof intervention and did not receive any treatment. Thus, thisgroup was evaluated only at the beginning and at the end ofthe study.
Instruments
The following instruments were used: a 45° leg press(ReForce, São Paulo, Brazil) for the 1RMleg test; agoniometer (ISP, São Paulo Institute, São Paulo, Brazil) todetermine knee flexion angle in the 1RMleg test; a digitalQwik Time QT5 metronome to standardize the timing ofconcentric and eccentric muscle contractions during training;a computerized isokinetic dynamometer (Multi-Joint System3; Biodex, NewYork, NY) to record the isokinetic variables inthe MPID test; and a metric tape (3M, model Sanny, Brazil) tomeasure the thigh perimeter of the subjects.
Procedures
The baseline assessments were carried out in the morningand consisted primarily of recording the subjects’ thighperimeter, followed by the MPID test. The MPID testrecorded the values for PT.ext. (knee peak torque extensorof two series of evaluation) and Avg.PT.ext. (knee peaktorque extensor, average of two evaluation series). Theafternoon of the same day the 1RMleg test was performed.The results of these muscle performance assessments werenormalized to the individual body mass (BM) and multi-plied by 100, following the procedure described previously[20]. All subjects were instructed not to change their usualphysical routine or eating habits during the study, not toingest alcohol, and to sleep well (both in quantity andquality).
A pilot study was also conducted to establish thereliability of the 1RMleg test, the MPID test and thighperimetry. The two tests were applied by the sameinvestigator randomly to six subjects who were not part ofthe study on two separate occasions and separated by a 5-day interval. The intraclass correlation coefficient (ICC 3,1)was used to assess intraexaminer reliability and the standarderror of measurement (SEM) to describe measurementaccuracy. The results were: ICC 0.92, SEM (5.00 Nm/BM)×100, for Avg.PT.ext.; ICC 0.93, SEM (5.17 Nm/BM)×100, for PT.ext.; ICC 0.99, SEM (0.71 kg/BM)×100,for the 1RMleg test; and ICC 0.99, SEM 0.01 cm, forthigh perimetry.
Protocols for assessments, training and LLLT
All protocols for muscle performance assessments andworkload adjustment were performed by the same evalu-ator. It is important to note that the assessment at baselineand after 12 weeks were conducted on different trainingdays and that the assessment results were normalized bysubject BM at both the beginning and the end of the study.
Protocol I (thigh perimetry) The thigh perimeter wasmeasured midway between the anterior/superior iliac spineand the base of the patella of the subject’s dominant lowerlimb. The dominant lower limb was determined as that usedto kick a ball with greater accuracy. This assessment wasperformed in orthostatic position and with the thighmuscles relaxed. The thigh perimeter was measured onlyat baseline and after 12 weeks of strength training.
Protocol II (isokinetic dynamometry) A brief 5-min warm-up was carried out on a cycle ergometer (Ergo 167 Cycle;Ergo-FIT, Pirmasens, Germany) with a load of 100 W and aspeed in the range 60–70 rpm. Next, the subjects werepositioned on the isokinetic dynamometer which had beenpreviously calibrated. The subjects stood properly alignedand stabilized with straps in order to avoid possiblecompensatory movements, in accordance with the guide-lines for the device. The evaluation was performed only onthe subject’s dominant lower limb, and the dynamometerrotation axis was adjusted to the knee axis of the subjectbeing assessed (at the lateral epicondyle of the femur;Fig. 1a). The hip was stabilized in 80° flexion and the leverarm of the equipment was set approximately 1 cm abovethe tibial malleolus. Parameters such as chair height,backrest distance, seat level and dynamometer base wereadjusted for each subject.
Before starting the recording of isokinetic variables,there was a familiarization period with the apparatus thatconsisted of three submaximal voluntary concentric musclecontractions in the full range of standardized and preprog-rammed motion (90–20°), with a constant angular velocityof 60°/s. After a 3-min rest, the test began with two sets(separated by a 3-min interval) of five maximal voluntaryconcentric and reciprocal quadriceps and hamstring con-tractions in all ranges of standardized and preprogrammedknee motion in flexion and extension (Fig. 1b). Thesubjects were encouraged verbally and visually to achievemaximum effort. This evaluation was performed only at thebaseline and after 12 weeks of strength training. Only thosefindings with a coefficient of variation less than 10% wereaccepted [21].
Protocol III (1RMleg test) There was a brief warm-upperiod of 5 min on a cycle ergometer (Ergo 167 Cycle;
Lasers Med Sci (2011) 26:349–358 351
Author's personal copy

Ergo-FIT, Pirmasens, Germany) with a load of 100 W and aspeed in the range 60–70 rpm. Next, the load-liftingtechnique was demonstrated by the evaluator. The test wasstandardized by defining the subject’s lower limb extension,identifying 90° knee flexion (using the goniometer) andmarking the position (in centimeters) corresponding to thisangle on the leg-press machine. The proposed range of motionwas 0° (full knee extension, start) to 90° (finish). Theanatomical references for the identification of the desiredangle were the greater trochanter of the femur, lateralepicondyle of the femur and the malleolus of the fibula ofthe same lower limb (Fig. 1c). Before beginning the test,there was a familiarization period with the apparatusconsisting of ten repetitions with a load estimated less than60% of 1RM. This subjective load was identified inaccordance with the level of physical effort by the subjectduring the familiarization period, following the OMNI scale(0 equal extremely easy and 10 equal extremely hard) [22].The load increments for identifying the 1RMleg were interms of percentage of the load in the familiarization period,and depended on the subject's score on the OMNI scale. Theload choices were limited to five attempts, separated by 5-min intervals to avoid metabolic disorders and impairment oftest quality. The subjects were encouraged verbally toachieve maximum effort.
Protocol IV (training) TG and TLG subjects began thestrength training program based on specific scientific datain the literature [23, 24] after 2 days of baseline assess-ments. The training program consisted of twice-weeklytraining sessions for the leg-press exercise at 45° onnonconsecutive days. The total training period was 12consecutive weeks (3 months), giving a total of 24sessions. The training intensity was always 80% andthe training volume was 50 repetitions divided into fivesets of ten repetitions each. If the subject could not
complete ten repetitions in each set, he would continueuntil concentric muscle failure and then rest. The restinterval between sets was 2 min and the exercise speedwas governed by the metronome: 2 s eccentric muscleaction for each second of concentric action [23]. Duringall training sessions (the leg-press exercise and the1RMleg test) the heart rate of subjects and the range ofmotion of the lower limbs were monitored to validate thetraining and load in the 1RMleg test. The room temper-ature was maintained between 23°C and 26°C. Adjust-ments in workload were made by retesting the 1RMlegevery eight sessions during normal training (thus replacingthe session). Two days after the 24th session, subjectsunderwent a final thigh perimetry assessment, followed byfinal MPID and the 1RMleg test.
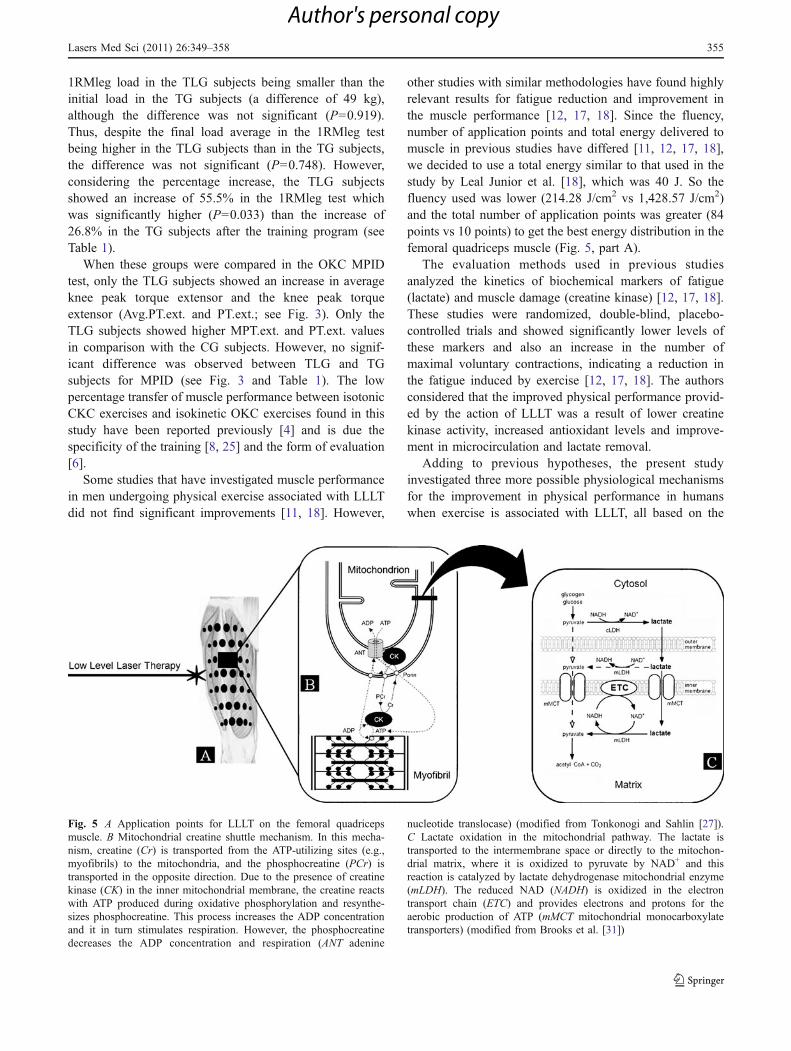
Protocol V (LLLT) TLG subjects underwent a LLLTprotocol immediately after each training session. A contacttechnique was used for the infrared laser treatment. Thebeam was kept stationary and perpendicular to the skinduring the 24 sessions in seven areas distributed over thebelly of the femoral quadriceps muscle of each subject inpreviously demarcated areas. The first area was 10 cmbelow the superior-anterior iliac spine and the others wereevery 5 cm below the initial marks (Fig. 5, part A). Thepattern in each areas was recorded to make the laserapplications uniform between sessions. A near-infraredlaser device (GaAlAs, 808 nm) with six obliquely arrangeddiodes of 60 mW power each was used operating incontinuous mode with the following parameters: beam area0.0028 cm2; energy per point (diode) 0.6 J; per-session totalenergy in each lower limb 25.2 J (for a total of 50.4 J);application points 42 (for a total of 84 points); diode energydensity (fluency) 214.28 J/cm2; diode power density21.42 W/cm2; and an application time in each lower limbof 70 s (for a total time of 140 s, both lower limbs).
Fig. 1 a Subject positioning for the MPID test. b Range of motion developed in the MPID test. c Subject positioning in the 1RMleg test anddefinition of knee angle flexion
352 Lasers Med Sci (2011) 26:349–358
Author's personal copy

Statistical analysis
The normality of the data distribution was analyzed usingthe Shapiro-Wilk test and the homogeneity of variancesusing Levene’s test. The effects of training on 1RMleg,MPID and thigh perimetry were evaluated by two-wayanalysis of variance (ANOVA) with repeated measures onlyon one factor. The independent factors were group (withthree levels: TLG, TG and CG) and time (with two levels;baseline and after 12 weeks), which was also considered asa repeated measurement. When significant differences werefound, Tukey’s post-hoc test was applied. The training effectwas also analyzed in terms of the percentage change in thevariables studied in relation to baseline (considered 100%)and was compared among the groups by the Kruskal-WallisANOVA test. Significance was set at P<0.05.
Results
The study began with 36 male subjects who met all theinclusion criteria and signed a consent form. However, sixsubjects were excluded during the study for the followingreasons: one subject did not agree with the group to whichhe was randomly allocated, three were injured duringtraining and two CG subjects began a physical trainingprogram during the study. Thus, our final sample size was 30subjects, ten in each group. TLG subjects had a mean age of19.7±0.8 years, a mean weight 76.6±11.5 kg, a mean height of1.78±0.06 m and a BMI of 23.3±2.1 kg/m2. TG subjects hada mean age of 21.2±2.5 years, a body weight of 75.7±6.3 kg,a mean height of 1.78±0.05 m and a BMI of 23.7±1.9 kg/m2.CG subjects had a mean age 21.8±2.1 years, a body weightof 77.1±13.5 kg, a mean height of 1.80±0.05 m and a BMIof 22.4±3.1 kg/m2.
The baseline 1RMleg, MPID and thigh perimetryassessments were compared among the three groups toidentify any statistically significant differences. No signif-icant difference was observed in any variable (P>0.05) atbaseline. BM used for muscle performance normalizationof the 1RMleg and MPID test results changed after thetraining program, but not significantly (P>0.05). The TLGsubjects showed an increase in BM of 1.30%, the TGsubjects an increase of 1.50% and the CG subjects anincrease of 0.12%. The TLG and TG subjects showedsignificant increases (P<0.001) in the 1RMleg after thestrength training program. The 1RMleg in the TLG subjectswas higher (P<0.001) than that in the CG subjects and notsignificantly different from that in the TG subjects (P=0.748). The TG subjects had a higher 1RMleg (P=0.008)than the CG subjects. In terms of average percentage, the1RMleg in the TLG subjects increased by 55.59%, in theTG subjects by 26.83% and in the CG subjects by 0.27%.
Comparing the groups, the TLG subjects had a higherpercentage gain than the TG subjects (P=0.033) and theCG subjects (P<0.001). The TG subjects had a higherpercentage gain than the CG subjects (P=0.033). Thesechanges in the load in 1RMleg test are summarized inFig. 2 and the percentages in Table 1.
The MPID test results were higher in the TLG and TGsubjects after the strength training program but only theTLG subjects showed statistically significant increases inAvg.PT.ext. (P=0.003) and PT.ext. (P=0.036). The com-parison among the groups did not identify significantdifferences (P>0.05). In terms of percentages, the TLGsubjects showed an increase in Avg.PT.ext. of 7.38% and inPT.ext. of 4.67%. In terms of percentage comparisons, thevalues of Avg.PT.ext. and PT.ext. in the TLG subjects weresignificantly higher than the values in the CG subjects(P<0.001, P=0.001, respectively). There were no significantdifferences (P>0.05) between the TLG and TG subjects orbetween the TG and CG subjects. These changes in theMPID test results are summarized in Fig. 3 and thepercentages are shown in Table 1.
The thigh perimeter of the dominant lower limbincreased significantly in TLG and TG subjects (P<0.001). CG subjects showed a decrease in thigh perimeterwithout statistical significance (P=0.999). In terms ofpercentage change in thigh perimeter, the TLG subjectsshowed an increase of 4.52%, the TG subjects an increaseof 2.75% and the CG subjects a decrease of 0.53%.Comparing these percentages among groups, the thighperimeter in the TLG subjects was significantly higher thanin the CG subjects (P<0.001) but not significantly differentfrom that in the TG subjects (P=0.775). The thighperimeter in the TG subjects was significantly higher thanin the CG subjects (P=0.006). These changes in the thigh
Fig. 2 Loads in the 1RMleg test in the three study groups at baselineand after 12 weeks of strength training (TLG training and LLLT group,TG training only group, CG control group; BM body mass; *P<0.05)
Lasers Med Sci (2011) 26:349–358 353
Author's personal copy
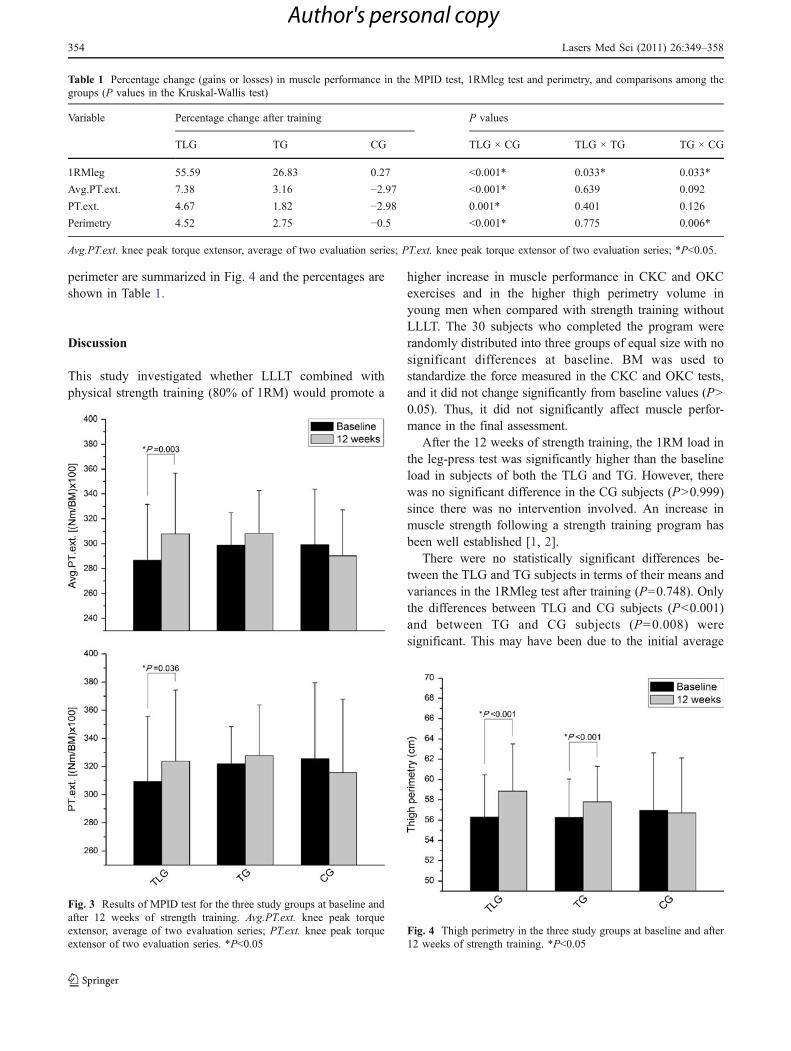
perimeter are summarized in Fig. 4 and the percentages areshown in Table 1.
Discussion
This study investigated whether LLLT combined withphysical strength training (80% of 1RM) would promote a
higher increase in muscle performance in CKC and OKCexercises and in the higher thigh perimetry volume inyoung men when compared with strength training withoutLLLT. The 30 subjects who completed the program wererandomly distributed into three groups of equal size with nosignificant differences at baseline. BM was used tostandardize the force measured in the CKC and OKC tests,and it did not change significantly from baseline values (P>0.05). Thus, it did not significantly affect muscle perfor-mance in the final assessment.
After the 12 weeks of strength training, the 1RM load inthe leg-press test was significantly higher than the baselineload in subjects of both the TLG and TG. However, therewas no significant difference in the CG subjects (P>0.999)since there was no intervention involved. An increase inmuscle strength following a strength training program hasbeen well established [1, 2].
There were no statistically significant differences be-tween the TLG and TG subjects in terms of their means andvariances in the 1RMleg test after training (P=0.748). Onlythe differences between TLG and CG subjects (P<0.001)and between TG and CG subjects (P=0.008) weresignificant. This may have been due to the initial average
Fig. 4 Thigh perimetry in the three study groups at baseline and after12 weeks of strength training. *P<0.05
Fig. 3 Results of MPID test for the three study groups at baseline andafter 12 weeks of strength training. Avg.PT.ext. knee peak torqueextensor, average of two evaluation series; PT.ext. knee peak torqueextensor of two evaluation series. *P<0.05
Table 1 Percentage change (gains or losses) in muscle performance in the MPID test, 1RMleg test and perimetry, and comparisons among thegroups (P values in the Kruskal-Wallis test)
Variable Percentage change after training P values
TLG TG CG TLG × CG TLG × TG TG × CG
1RMleg 55.59 26.83 0.27 <0.001* 0.033* 0.033*
Avg.PT.ext. 7.38 3.16 −2.97 <0.001* 0.639 0.092
PT.ext. 4.67 1.82 −2.98 0.001* 0.401 0.126
Perimetry 4.52 2.75 −0.5 <0.001* 0.775 0.006*
Avg.PT.ext. knee peak torque extensor, average of two evaluation series; PT.ext. knee peak torque extensor of two evaluation series; *P<0.05.
354 Lasers Med Sci (2011) 26:349–358
Author's personal copy
1RMleg load in the TLG subjects being smaller than theinitial load in the TG subjects (a difference of 49 kg),although the difference was not significant (P=0.919).Thus, despite the final load average in the 1RMleg testbeing higher in the TLG subjects than in the TG subjects,the difference was not significant (P=0.748). However,considering the percentage increase, the TLG subjectsshowed an increase of 55.5% in the 1RMleg test whichwas significantly higher (P=0.033) than the increase of26.8% in the TG subjects after the training program (seeTable 1).
When these groups were compared in the OKC MPIDtest, only the TLG subjects showed an increase in averageknee peak torque extensor and the knee peak torqueextensor (Avg.PT.ext. and PT.ext.; see Fig. 3). Only theTLG subjects showed higher MPT.ext. and PT.ext. valuesin comparison with the CG subjects. However, no signif-icant difference was observed between TLG and TGsubjects for MPID (see Fig. 3 and Table 1). The lowpercentage transfer of muscle performance between isotonicCKC exercises and isokinetic OKC exercises found in thisstudy have been reported previously [4] and is due thespecificity of the training [8, 25] and the form of evaluation[6].
Some studies that have investigated muscle performancein men undergoing physical exercise associated with LLLTdid not find significant improvements [11, 18]. However,
other studies with similar methodologies have found highlyrelevant results for fatigue reduction and improvement inthe muscle performance [12, 17, 18]. Since the fluency,number of application points and total energy delivered tomuscle in previous studies have differed [11, 12, 17, 18],we decided to use a total energy similar to that used in thestudy by Leal Junior et al. [18], which was 40 J. So thefluency used was lower (214.28 J/cm2 vs 1,428.57 J/cm2)and the total number of application points was greater (84points vs 10 points) to get the best energy distribution in thefemoral quadriceps muscle (Fig. 5, part A).
The evaluation methods used in previous studiesanalyzed the kinetics of biochemical markers of fatigue(lactate) and muscle damage (creatine kinase) [12, 17, 18].These studies were randomized, double-blind, placebo-controlled trials and showed significantly lower levels ofthese markers and also an increase in the number ofmaximal voluntary contractions, indicating a reduction inthe fatigue induced by exercise [12, 17, 18]. The authorsconsidered that the improved physical performance provid-ed by the action of LLLT was a result of lower creatinekinase activity, increased antioxidant levels and improve-ment in microcirculation and lactate removal.
Adding to previous hypotheses, the present studyinvestigated three more possible physiological mechanismsfor the improvement in physical performance in humanswhen exercise is associated with LLLT, all based on the
Fig. 5 A Application points for LLLT on the femoral quadricepsmuscle. B Mitochondrial creatine shuttle mechanism. In this mecha-nism, creatine (Cr) is transported from the ATP-utilizing sites (e.g.,myofibrils) to the mitochondria, and the phosphocreatine (PCr) istransported in the opposite direction. Due to the presence of creatinekinase (CK) in the inner mitochondrial membrane, the creatine reactswith ATP produced during oxidative phosphorylation and resynthe-sizes phosphocreatine. This process increases the ADP concentrationand it in turn stimulates respiration. However, the phosphocreatinedecreases the ADP concentration and respiration (ANT adenine
nucleotide translocase) (modified from Tonkonogi and Sahlin [27]).C Lactate oxidation in the mitochondrial pathway. The lactate istransported to the intermembrane space or directly to the mitochon-drial matrix, where it is oxidized to pyruvate by NAD+ and thisreaction is catalyzed by lactate dehydrogenase mitochondrial enzyme(mLDH). The reduced NAD (NADH) is oxidized in the electrontransport chain (ETC) and provides electrons and protons for theaerobic production of ATP (mMCT mitochondrial monocarboxylatetransporters) (modified from Brooks et al. [31])
Lasers Med Sci (2011) 26:349–358 355
Author's personal copy

importance of the cellular mitochondria in energy produc-tion. There is strong evidence in the scientific literature thatLLLT has a close relationship with the mitochondria,promoting their growth and/or fusion of smaller mitochon-dria to form giant mitochondria consequently increasing themitochondrial density in the tissues [15, 16]. Greatermitochondria have been associated with higher enzymaticmachinery for aerobic ATP production [15, 16]. Althoughthese organelles play a fundamental role in the energyproduction necessary in endurance training and in low-intensity exercise [26–28], they may also contribute to thegreater energy availability in high-intensity exercise, suchas that investigated in the present study. This is based onthe hierarchical and ramp recruitment of the muscle fibers.It has been found that in increasing exercise intensity, theorder of muscle fiber recruitment necessarily follows thefollowing order: type I (oxidative), type II (glycolytic andoxidative), and finally type IIx (glycolytic) [29]. Therefore,aerobic energy production (oxidative) is supplemented byanaerobic energy production (glycolytic) as exercisebecomes more intense [30].
The second hypothesis for the muscle performanceimprovement in the TLG subjects is the integration betweenthe aerobic and anaerobic ATP production described byTonkonogi and Sahlin [27]. This mechanism involvesphosphocreatine resynthesis which is dependent on theshuttling of mitochondrial creatine in the greatest quantitiesinto muscle fibers with oxidative characteristics [27]. Thecreatine shuttle system captures ADP and inorganicphosphorus that result from the use of ATP in musclecontraction, and transports them to the mitochondrialmatrix through the inner membrane organelle by means ofadenine nucleotide translocase. The ATP produced byoxidative phosphorylation takes the same route, althoughin the opposite direction, providing energy for the phos-phocreatine resynthesis reaction in the active muscle. Thisreaction is catalyzed by muscle creatine kinase. Concom-itantly, the use of phosphocreatine energy generates musclecreatine, ADP and inorganic phosphorus. While the ADPand inorganic phosphorus follow the above-mentionedpath, creatine is transported to the mitochondrial intermem-brane spaces of the muscle, and then mitochondrial creatinekinase catalyzes the phosphocreatine resynthesis reaction,also using ATP produced through oxidative phosphoryla-tion. Ultimately, the phosphocreatine is transported to themuscle contraction site, supplies the energy necessary tocontinue the contractile activity and increases the ATP/ADPratio [27] (Fig. 5, part B).
Considering the effects of LLLT on mitochondria, andthe greater mitochondrial density and/or the enzymaticmachinery for ATP production [15, 16], a bigger phospho-creatine re-synthesis possibly must be occurs. Phosphocre-atine resynthesis, that mainly occurs in the rest intervals
during high-intensity exercise, would be able to supplysome of the necessary energy for the next series of musclecontractions, by providing the resynthesis of the ATP usedduring session training or during maximal CKC and OKCtests.
The third hypothesis for the muscle performanceimprovement on the TLG subjects is the removal andoxidation of lactic acid produced anaerobically duringexercise, because metabolic acidosis may induce musclefatigue [31, 32]. Lactic acid formation in the cytosol ofmuscle fibers is due to the reduction of the pyruvate tolactate, which is catalyzed by cytosolic lactate dehydroge-nase, and occurs mainly in anaerobic and strength exer-cises. Next, lactate is transported to the mitochondrialmatrix via monocarboxylic acid transporters and, by meansof the NAD+ and mitochondrial lactate dehydrogenase, isoxidized to pyruvate. The reduced NAD (NADH) isoxidized in the electron transport chain and provides thenecessary electrons and protons for the aerobic productionof ATP. The pyruvate in turn is oxidized to acetyl-CoA and,in the Krebs cycle, it continues to be oxidized to produceATP aerobically through the electron transport chain [31,32] (Fig. 5, part C).
Regarding the thigh perimetry results in the TLG, TGand CG subjects, only the TLG and TG subjects showed asignificant increase in thigh perimeter after the trainingprogram. However, the change in thigh perimeter was notsignificantly different among all groups when comparedwith their the mean and variances. With regard to thepercentage changes in thigh perimeter, TLG and TGsubjects showed a greater increase than the CG subjects(see Table 1).
Numerous studies have shown increases in cross-sectional area of muscle tissue following physical strengthtraining (for review see references [2, 8, 23]). A hypothesisthat could explain this physiological adaptation to strengthtraining is the association between the degree of muscleinjury and the possible greater activation of muscle satellitecells, i.e. situations where microdamage occurring in themuscle structure needs repair [33–35]. Microdamagestimulates mononuclear inflammatory cells (neutrophilsand macrophages), attracts satellite cells to the injury sitethrough chemotactic mechanisms and activates their prolif-eration and differentiation through molecular mechanisms[36–38]. After cell differentiation, satellite cells are calledmyotubes and can fuse with damaged muscle fibers, ororiginate new contractile proteins [36–38]. In this process,LLLT seems to modulate satellite cell metabolism, thusdirectly influencing muscle tissue regeneration [39–41].
We suggest that future work should investigate thepossible action of LLLT on gene expression in humans.The main genes that specifically encode transcriptionfactors for satellite cells in the quiescent state include
356 Lasers Med Sci (2011) 26:349–358
Author's personal copy

Pax7 (paired box 7) and c-met (hepatocyte growth factorreceptor), and in the activated (proliferative) state formyoblast formation include Myf-5 (myogenic factor 5),and for myoblast differentiation into myotubes includemyogenin (myogenic factor 4), MyoD (myogenic differen-tiation) and MRF4 (muscle-specific regulatory factor 4),which is known as Myf-6 (myogenic factor 6) [36–38]. Inaddition, the gene for expression of myostatin (GDF-8)may be modulated by LLLT, since this gene is a majoratrophy marker and acts against the process of muscleregeneration, leading to an inhibition of satellite cellproliferation and less hypertrophy [36]. Furthermore, in thecontext of gene expression, LLLTcould alter the expression ofgenes for muscular hypertrophy, such as mTOR (mechanistictarget of rapamycin) and/or the genes responsible formitochondrial biogenesis, including NRF-1, NRF-2 (nuclearrespiratory factor 1 and 2), Tfam (transcription factor A,mitochondrial) and PCG-1α (peroxisome proliferator-activated receptor gamma, coactivator 1 alpha) [42, 43].
Conclusion
The results of this study suggest that strength trainingcombined with LLLT may be superior to strength trainingonly. We emphasize that care is needed in generalizing theresults. Further studies, especially those involving LLLTand gene expression, are necessary to elucidate theinteraction between laser radiation and the molecularmechanisms of recovery and muscle performance.
Acknowledgments The authors would like to thank the Depart-ments of Physical Therapy and Physiological Sciences of the FederalUniversity of São Carlos for assistance with this study, the researchsubjects, and also the Conselho Nacional de DesenvolvimentoCientífico e Tecnológico (CNPq) for partial funding of the research.
References
1. Folland JP, Williams AG (2007) The adaptations to strength training:morphological and neurological contributions to increased strength.Sports Med 37(2):145–168. doi:3724
2. Fry AC (2004) The role of resistance exercise intensity on musclefibre adaptations. Sports Med 34(10):663–679
3. Tagesson S, Oberg B, Good L, Kvist J (2008) A comprehensiverehabilitation program with quadriceps strengthening in closedversus open kinetic chain exercise in patients with anteriorcruciate ligament deficiency: a randomized clinical trial evaluatingdynamic tibial translation and muscle function. Am J Sports Med36(2):298–307. doi:10.1177/0363546507307867
4. Augustsson J, Esko A, Thomee R, Svantesson U (1998) Weighttraining of the thigh muscles using closed vs. open kinetic chainexercises: a comparison of performance enhancement. J OrthopSports Phys Ther 27(1):3–8
5. Stensdotter AK, Hodges PW, Mellor R, Sundelin G, Hager-RossC (2003) Quadriceps activation in closed and in open kinetic
chain exercise. Med Sci Sports Exerc 35(12):2043–2047.doi:10.1249/01.MSS.0000099107.03704.AE
6. Verdijk LB, van Loon L, Meijer K, Savelberg HH (2009) One-repetition maximum strength test represents a valid means toassess leg strength in vivo in humans. J Sports Sci 27(1):59–68.doi:10.1080/02640410802428089
7. Wawrzyniak JR, Tracy JE, Catizone PV, Storrow RR (1996)Effect of closed chain exercise on quadriceps femoris peak torqueand functional performance. J Athl Train 31(4):335–340
8. Harris N, Cronin J, Keogh J (2007) Contraction force specificityand its relationship to functional performance. J Sports Sci 25(2):201–212. doi:10.1080/02640410600630910
9. Rodriguez NR, Di Marco NM, Langley S (2009) AmericanCollege of Sports Medicine position stand. Nutrition and athleticperformance. Med Sci Sports Exerc 41(3):709–731. doi:10.1249/MSS.0b013e31890eb86
10. Hoffman JR, Kraemer WJ, Bhasin S, Storer T, Ratamess NA, HaffGG, Willoughby DS, Rogol AD (2009) Position stand onandrogen and human growth hormone use. J Strength Cond Res23(5 Suppl):S1–S59. doi:10.1519/JSC.0b013e31819df2e6
11. Gorgey AS, Wadee AN, Sobhi NN (2008) The effect of low-level laser therapy on electrically induced muscle fatigue: apilot study. Photomed Laser Surg 26(5):501–506. doi:10.1089/pho.2007.2161
12. Leal Junior EC, Lopes-Martins RA, Vanin AA, Baroni BM,Grosselli D, De Marchi T, Iversen VV, Bjordal JM (2009) Effectof 830 nm low-level laser therapy in exercise-induced skeletalmuscle fatigue in humans. Lasers Med Sci 24(3):425–431.doi:10.1007/s10103-008-0592-9
13. Enwemeka CS (2009) Intricacies of dose in laser phototherapy fortissue repair and pain relief. Photomed Laser Surg 27(3):387–393.doi:10.1089/pho.2009.2503
14. Enwemeka CS, Parker JC, Dowdy DS, Harkness EE, Sanford LE,Woodruff LD (2004) The efficacy of low-power lasers in tissuerepair and pain control: a meta-analysis study. Photomed LaserSurg 22(4):323–329. doi:10.1089/1549541041797841
15. Bakeeva LE, Manteifel VM, Rodichev EB, Karu TI (1993)Formation of gigantic mitochondria in human blood lymphocytesunder the effect of an He-Ne laser. Mol Biol (Mosk) 27(3):608–617
16. Manteifel VM, Karu TI (2005) Structure of mitochondria andactivity of their respiratory chain in subsequent generations ofyeast cells exposed to He-Ne laser light. Izv Akad Nauk Ser Biol6:672–683
17. Leal Junior EC, Lopes-Martins RA, Dalan F, Ferrari M, SbaboFM, Generosi RA, Baroni BM, Penna SC, Iversen VV, BjordalJM (2008) Effect of 655-nm low-level laser therapy on exercise-induced skeletal muscle fatigue in humans. Photomed Laser Surg26(5):419–424. doi:10.1089/pho.2007.2160
18. Leal Junior EC, Lopes-Martins RA, Baroni BM, De Marchi T,Taufer D, Manfro DS, Rech M, Danna V, Grosselli D, GenerosiRA, Marcos RL, Ramos L, Bjordal JM (2009) Effect of 830 nmlow-level laser therapy applied before high-intensity exercises onskeletal muscle recovery in athletes. Lasers Med Sci 24(6):857–863. doi:10.1007/s10103-008-0633-4
19. Caspersen CJ, Pereira MA, Curran KM (2000) Changes inphysical activity patterns in the United States, by sex and cross-sectional age. Med Sci Sports Exerc 32(9):1601–1609
20. Nakagawa TH, Muniz TB, Baldon Rde M, Dias Maciel C, deMenezes Reiff RB, Serrao FV (2008) The effect of additionalstrengthening of hip abductor and lateral rotator muscles inpatellofemoral pain syndrome: a randomized controlled pilotstudy. Clin Rehabil 22(12):1051–1060
21. Gulick DT, Chiappa JJ, Crowley KR, Schade ME, Wescott SR(1998) Predicting 1-RM isotonic knee extension strength utilizingisokinetic dynamometry. Isokinet Exerc Sci 7(4):145–149
Lasers Med Sci (2011) 26:349–358 357
Author's personal copy

22. Irving BA, Rutkowski J, Brock DW, Davis CK, Barrett EJ, GaesserGA, Weltman A (2006) Comparison of Borg- and OMNI-RPE asmarkers of the blood lactate response to exercise. Med Sci SportsExerc 38(7):1348–1352. doi:10.1249/01.mss.0000227322.61964.d2
23. Wernbom M, Augustsson J, Thomee R (2007) The influence offrequency, intensity, volume and mode of strength training onwhole muscle cross-sectional area in humans. Sports Med 37(3):225–264
24. American College of Sports Medicine (2009) American Collegeof Sports Medicine position stand. Progression models resistancetraining healthy adults. Med Sci Sports Exerc 41(3):687–708.doi:10.1249/MSS.0b013e3181915670
25. Stone M, Plisk S, Collins D (2002) Training principles: evaluationof modes and methods of resistance training – a coachingperspective. Sports Biomech 1(1):79–103
26. Tonkonogi M, Walsh B, Svensson M, Sahlin K (2000) Mitochon-drial function and antioxidative defence in human muscle: effectsof endurance training and oxidative stress. J Physiol 528(Pt2):379–388
27. Tonkonogi M, Sahlin K (2002) Physical exercise and mitochon-drial function in human skeletal muscle. Exerc Sport Sci Rev 30(3):129–137
28. Sahlin K, Mogensen M, Bagger M, Fernstrom M, Pedersen PK(2007) The potential for mitochondrial fat oxidation in humanskeletal muscle influences whole body fat oxidation during low-intensity exercise. Am J Physiol Endocrinol Metab 292(1):E223–E230
29. Hodson-Tole EF, Wakeling JM (2009) Motor unit recruitment fordynamic tasks: current understanding and future directions. JComp Physiol B 179(1):57–66. doi:10.1007/s00360-008-0289-1
30. Goreham C, Green HJ, Ball-Burnett M, Ranney D (1999) High-resistance training and muscle metabolism during prolongedexercise. Am J Physiol 276(3 Pt 1):E489–E496
31. Brooks GA, Dubouchaud H, Brown M, Sicurello JP, Butz CE(1999) Role of mitochondrial lactate dehydrogenase and lactateoxidation in the intracellular lactate shuttle. Proc Natl Acad Sci US A 96(3):1129–1134
32. Hashimoto T, Hussien R, Brooks GA (2006) Colocalization ofMCT1, CD147, and LDH in mitochondrial inner membrane of L6muscle cells: evidence of a mitochondrial lactate oxidationcomplex. Am J Physiol Endocrinol Metab 290(6):E1237–E1244
33. Harridge SD (2007) Plasticity of human skeletal muscle: geneexpression to in vivo function. Exp Physiol 92(5):783–797. doi:expphysiol.2006.036525
34. Vierck J, O’Reilly B, Hossner K, Antonio J, Byrne K, Bucci L,Dodson M (2000) Satellite cell regulation following myotraumacaused by resistance exercise. Cell Biol Int 24(5):263–272.doi:10.1006/cbir.2000.0499
35. Petrella JK, Kim JS, Mayhew DL, Cross JM, Bamman MM(2008) Potent myofiber hypertrophy during resistance training inhumans is associated with satellite cell-mediated myonuclearaddition: a cluster analysis. J Appl Physiol 104(6):1736–1742
36. Charge SB, Rudnicki MA (2004) Cellular and molecularregulation of muscle regeneration. Physiol Rev 84(1):209–238.doi:10.1152/physrev.00019.2003
37. Hawke TJ, Garry DJ (2001) Myogenic satellite cells: physiologyto molecular biology. J Appl Physiol 91(2):534–551
38. Holterman CE, Rudnicki MA (2005) Molecular regulation ofsatellite cell function. Semin Cell Dev Biol 16(4-5):575–584
39. Weiss N, Oron U (1992) Enhancement of muscle regeneration inthe rat gastrocnemius muscle by low energy laser irradiation. AnatEmbryol (Berl) 186(5):497–503
40. Shefer G, Partridge TA, Heslop L, Gross JG, Oron U, Halevy O(2002) Low-energy laser irradiation promotes the survival and cellcycle entry of skeletal muscle satellite cells. J Cell Sci 115(Pt7):1461–1469
41. Ben-Dov N, Shefer G, Irintchev A, Wernig A, Oron U, Halevy O(1999) Low-energy laser irradiation affects satellite cell proliferationand differentiation in vitro. Biochim Biophys Acta 1448(3):372–380
42. Coffey VG, Hawley JA (2007) The molecular bases of trainingadaptation. Sports Med 37(9):737–763
43. Hawley JA (2009) Molecular responses to strength and endurancetraining: are they incompatible? Appl Physiol Nutr Metab 34(3):355–361
358 Lasers Med Sci (2011) 26:349–358
Author's personal copy




















