Effect of Magnetic Resonance Imaging Field Strength on Delineation and Signal Intensity of Alar...
6
DIAGNOSTICS SPINE Volume 37, Number 17, pp E1062–E1067 ©2012, Lippincott Williams & Wilkins E1062 www.spinejournal.com August 2012 Effect of Magnetic Resonance Imaging Field Strength on Delineation and Signal Intensity of Alar Ligaments in Healthy Volunteers Nina Lummel, MD,* Veronika Schöpf, Dipl.Ing,† Harro Bitterling, MD,‡ Christian Zeif, MD,* Andrea Kloetzer, MD ,* Hartmut Brückmann, MD,* and Jennifer Linn, MD* Study Design. A prospective study of healthy volunteers. Objective. To evaluate the influence of magnetic resonance imaging (MRI) field strength on the delineation and signal intensity of alar ligaments (AL) in healthy volunteers. Summary of Background Data. The fact that AL physiologically show morphologic variabilities is well established. However, presence and etiology of high-signal intensities within the AL as well as the influence of the MRI field strength on the signal characteristics of AL are still not completely understood. Methods. Coronal and sagittal 2-mm proton-density weighted sequences were acquired in 50 healthy volunteers using different MRI field strengths (1 T, 1.5 T, 3 T). Delineation and signal characteristics of AL were evaluated by 2 neuroradiologists independently. Differences concerning delineation and signal intensity between the MRI scanners, inter rater reliability between the 2 readers, and intrarater reliability at different time points were calculated. Results. Delineation of AL was significantly better both on 3 T and 1.5 T than on 1 T ( P = 0.05) in sagittal as well as in coronal view. In coronal view delineation was significantly better on 3 T than on 1.5 T, whereas in sagittal view no significant difference was evident when comparing 1.5 T and 3 T. Concerning signal intensity of AL in sagittal view, there was no significant difference between the 3 different field strengths. Inter-rater and intrarater agreements were fair to moderate with respect to delineation as well as signal intensity of AL. Conclusion. 1.5 T and 3 T significantly improve the delineation of AL when compared with lower field strength (1 T), but signal intensity of the AL in healthy volunteers is not influenced by the field A lar ligaments (AL) connect the dens axis to the occipital condyles and play an important role in the movement and stability of the craniocervical junction. 1 ,2 Because of their suggested involvement in whiplash-associated disor- der after head or neck trauma, extensive in vivo and postmor- tem investigations have been performed on AL anatomy and signal characteristics on magnetic resonance imaging (MRI) since the 1990s. Imaging studies showed that the upper cervi- cal ligaments, including AL, can be adequately evaluated on MRI, 3 –7 especially using thin proton-density (PD)-weighted sequences. 8 Data consistently showed a high anatomic vari- ability of AL in the craniocaudal as well as in the anterodor- sal orientation, frequently with an asymmetric appearance. 4 ,7 ,8 Still not conclusively resolved is the presence and etiology of hyperintense signal alterations within AL. MRI-investigations using low-field magnetic strength (0.2 T–0.5 T) 4 ,5 ,9 –11 as well as using higher-field magnetic strength (1.5 T) 7 ,12 ,13 are incon- sistent on whether high-signal intensities in the AL account for anatomic variances or whether they should be interpreted as pathological findings indicative of AL trauma. As signal- to-noise ratio changes with the use of different magnetic field strengths, an influence of the field strength on the delineation and signal characteristics of AL is probable, however, it has not been systematically investigated to date. For this reason, we conducted this study to evaluate the influence of MRI field strength on the delineation and signal intensity of AL in healthy volunteers. MATERIALS AND METHODS Subjects This study was approved by the regional ethics committee. Volunteers were recruited by a notice in our hospital entrance From the *Department of Neuroradiology, University of Munich, Munich, Germany; †MR Centre of Excellence, Medical University Vienna, Vienna, Austria; and ‡Sygehus Sønderjyll, Sønderborg, Danmark. Acknowledgment date: September 6, 2011. First revision: December 2, 2011. Second revision date: January 25, 2012. Third revision date: March 13, 2012. Acceptance date: March 16, 2012. The manuscript submitted does not contain information about medical device(s)/drug(s). No funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript. Address correspondence and reprint requests to Nina Lummel, MD, Department of Neuroradiology, University of Munich, Grosshadern, Marchioninistrasse 15, 81377 Munich, Germany; E-mail: nina.lummel@med. uni.muenchen.de strength. Increased signal is present in asymptomatic subjects on both low- and high-field magnetic resonance systems. Accordingly, the pathologic relevance of increased signal intensity of the AL, regardless of field strength, may not be indicative of traumatic AL injury. Key words: alar ligaments, delineation, signal characteristics, magnetic resonance imaging, field strength, Tesla. Spine 2012;17:E1062–E1067 DOI: 10.1097/BRS.0b013e31825831ca Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Effect of Magnetic Resonance Imaging Field Strength on Delineation and Signal Intensity of Alar...

DIAGNOSTICS
SPINE Volume 37, Number 17, pp E1062–E1067©2012, Lippincott Williams & Wilkins
E1062 www.spinejournal.com August 2012
Effect of Magnetic Resonance Imaging Field Strength on Delineation and Signal Intensity of Alar Ligaments in Healthy Volunteers
Nina Lummel , MD , * Veronika Schöpf , Dipl.Ing , † Harro Bitterling , MD , ‡ Christian Zeif , MD , * Andrea Kloetzer , MD , * Hartmut Brückmann , MD , * and Jennifer Linn , MD *
Study Design. A prospective study of healthy volunteers. Objective. To evaluate the infl uence of magnetic resonance imaging (MRI) fi eld strength on the delineation and signal intensity of alar ligaments (AL) in healthy volunteers. Summary of Background Data. The fact that AL physiologically show morphologic variabilities is well established. However, presence and etiology of high-signal intensities within the AL as well as the infl uence of the MRI fi eld strength on the signal characteristics of AL are still not completely understood. Methods. Coronal and sagittal 2-mm proton-density weighted sequences were acquired in 50 healthy volunteers using different MRI fi eld strengths (1 T, 1.5 T, 3 T). Delineation and signal characteristics of AL were evaluated by 2 neuroradiologists independently. Differences concerning delineation and signal intensity between the MRI scanners, inter rater reliability between the 2 readers, and intrarater reliability at different time points were calculated. Results. Delineation of AL was signifi cantly better both on 3 T and 1.5 T than on 1 T ( P = 0.05) in sagittal as well as in coronal view. In coronal view delineation was signifi cantly better on 3 T than on 1.5 T, whereas in sagittal view no signifi cant difference was evident when comparing 1.5 T and 3 T. Concerning signal intensity of AL in sagittal view, there was no signifi cant difference between the 3 different fi eld strengths. Inter-rater and intrarater agreements were fair to moderate with respect to delineation as well as signal intensity of AL. Conclusion. 1.5 T and 3 T signifi cantly improve the delineation of AL when compared with lower fi eld strength (1 T), but signal intensity of the AL in healthy volunteers is not infl uenced by the fi eld
Alar ligaments (AL) connect the dens axis to the occipital condyles and play an important role in the movement and stability of the craniocervical junction. 1 , 2 Because
of their suggested involvement in whiplash-associated disor-der after head or neck trauma, extensive in vivo and postmor-tem investigations have been performed on AL anatomy and signal characteristics on magnetic resonance imaging (MRI) since the 1990s. Imaging studies showed that the upper cervi-cal ligaments, including AL, can be adequately evaluated on MRI, 3 – 7 especially using thin proton-density (PD)-weighted sequences. 8 Data consistently showed a high anatomic vari-ability of AL in the craniocaudal as well as in the anterodor-sal orientation, frequently with an asymmetric appearance. 4 , 7 , 8 Still not conclusively resolved is the presence and etiology of hyperintense signal alterations within AL. MRI-investigations using low-fi eld magnetic strength (0.2 T–0.5 T) 4 , 5 , 9 – 11 as well as using higher-fi eld magnetic strength (1.5 T) 7 , 12 , 13 are incon-sistent on whether high-signal intensities in the AL account for anatomic variances or whether they should be interpreted as pathological fi ndings indicative of AL trauma. As signal-to-noise ratio changes with the use of different magnetic fi eld strengths, an infl uence of the fi eld strength on the delineation and signal characteristics of AL is probable, however, it has not been systematically investigated to date.
For this reason, we conducted this study to evaluate the infl uence of MRI fi eld strength on the delineation and signal intensity of AL in healthy volunteers.
MATERIALS AND METHODS
Subjects This study was approved by the regional ethics committee. Volunteers were recruited by a notice in our hospital entrance
From the * Department of Neuroradiology, University of Munich, Munich, Germany ; † MR Centre of Excellence, Medical University Vienna, Vienna, Austria ; and ‡ Sygehus Sønderjyll, Sønderborg, Danmark .
Acknowledgment date: September 6, 2011. First revision: December 2, 2011. Second revision date: January 25, 2012. Third revision date: March 13, 2012. Acceptance date: March 16, 2012.
The manuscript submitted does not contain information about medical device(s)/drug(s). No funds were received in support of this work.
No benefi ts in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Address correspondence and reprint requests to Nina Lummel, MD, Department of Neuroradiology, University of Munich, Grosshadern, Marchioninistrasse 15, 81377 Munich, Germany; E-mail: [email protected]
strength. Increased signal is present in asymptomatic subjects on both low- and high-fi eld magnetic resonance systems. Accordingly, the pathologic relevance of increased signal intensity of the AL, regardless of fi eld strength, may not be indicative of traumatic AL injury. Key words: alar ligaments , delineation , signal characteristics , magnetic resonance imaging , fi eld strength , Tesla . Spine 2012 ; 17 : E1062 – E1067
DOI: 10.1097/BRS.0b013e31825831ca
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1062BRS205053.indd E1062 01/07/12 12:16 AM01/07/12 12:16 AM

DIAGNOSTICS Alar Ligaments at Different MRI Field Strengths • Lummel et al
Spine www.spinejournal.com E1063
hall summarizing the course of the study as well as exclusion criteria, namely (1) involvement in any car accident or case history of any head or neck trauma, (2) chronic neck pain with or without restricted mobility of the cervical spine, (3) malignant disease or disease with potential affection of the cervical spine and craniocervical junction ( e.g. , chronic poly-arthritis, rheumatic arthritis, or juvenile arthritis). Prior to the onset of the study, each volunteer was interviewed in detail regarding the exclusion criteria, using a standard question-naire. Fifty healthy volunteers (23 men, 27 women; mean age = 24.1 yr; range = 20–31 yr; SD ± 2.7) provided their written informed consent and were included in the study.
MRI Protocol All volunteers were investigated on 3 different MRI scanners: a 1.0-tesla (T) scanner (Magnetom Harmony Siemens Medical Solutions, Erlangen, Germany), a 1.5-T scanner (Magnetom Vision or Symphony; Siemens Medical Solutions, Erlangen, Germany), and a 3-T scanner (Signa HDx; GE Healthcare, Milwaukee). Standard head coils were used on all 3 scanners, and all images were obtained with the subject’s head and neck in a neutral position. Neutral position was standardized by looking at a visual target attached to the head coil`s center. In this position, the head was fi xed by bilateral pads throughout the examination. PD-weighted fast spin-echo images with a slice thickness of 2 mm were obtained in coronal and sagittal planes. Imaging parameters are summarized in Table 1 .
Image Evaluation Image interpretation was performed on a standard PACS workstation (Magic View VE42; Siemens Medical Solutions). All MRI examinations were independently evaluated by 2 experienced neuroradiologists to calculate the inter-rater reli-ability.
On PD-weighted sequences, delineations of AL were evalu-ated in the sagittal and coronal planes for the “whole” liga-ment on a number of contiguous slices and classifi ed into 4 groups—not defi nable (0), poor (1), moderate (2), and good (3) delineation. 7 Signal intensities of AL were evaluated in the sagittal view on 1 single slice in the midsection of the ligament and rated on a 4-point grading scale proposed by Krakenes et al . 12 Low signal throughout the entire cross-sectional area of the alar ligament was graded as 0, high signal in less than one-third of the cross section was graded as 1, high signal in one-third to two-thirds of the cross section was graded as 2, and high signal in more than two-thirds of the cross section was graded as 3.
To determine the intrarater reliability, one of the readers performed a second reading at least 4 weeks apart from the fi rst one. There, he re-evaluated 20 randomly chosen cases (40 ligaments) concerning signal intensity in the sagittal view for all 3 MRI scanners.
Statistics A Wilcoxon signed rank test was performed to analyze differ-ences between the 3 different MRI fi eld strengths concerning the delineation of AL in the coronal and sagittal planes. A P value of less than 0.05 was considered to indicate a statistically signifi cant difference ( P = 0.05). Cohen kappa coeffi cients 14 were used to evaluate the inter-rater agreement between the 2 neuroradiologists with respect to delineation in coronal and sagittal views as well as signal intensity in sagittal view for each scanner. Intrarater agreement concerning signal intensity using different MRI fi eld strengths was likewise analyzed with kappa coeffi cients. Furthermore, a Kruskal-Wallis test was performed to test for differences of the 3 scanners (1 T, 1.5 T, 3 T) concerning signal intensity in sagittal view. Statistical analyses were performed using the Statistical Package for the Social Sciences version 17.0 (SPSS, Chicago, IL).
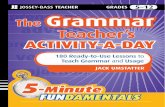
RESULTS Delineation of AL in coronal and sagittal views at the differ-ent fi eld strengths is detailed in Table 2 . Delineation of AL in the coronal view was signifi cantly better at 3 T than at lower fi eld strengths (1 T vs . 1.5 T: P = 0.005; 1 T vs . 3 T: P = 0.000; 1.5 T vs . 3 T: P = 0.013) ( Figure 1 ). In the sagittal view, AL were signifi cantly better delineated on 3 T than on 1 T ( P = 0.000) as well as on 1.5 T than on 1 T ( P = 0.000) ( Figure 2 ). There was no signifi cant difference concerning the delineation of AL in the sagittal view when comparing 3 T and 1.5 T ( P = 0.871).
The inter-rater agreement in terms of kappa with respect to delineation in the coronal and sagittal views was kappa ( κ ) = 0.27 and 0.49 for 1 T, κ = 0.32 and 0.4 for 1.5 T, and κ = 0.35 and 0.36 for 3 T, all numbers indicating fair to moderate agreement. 15
Signal intensities in the left and right AL of all volun-teers in the sagittal plane at the different fi eld strengths are detailed in Table 2 . The inter-rater agreement regarding the signal intensity was κ = 0.31 for 1 T, κ = 0.31 for 1.5 T, and κ = 0.39 for 3 T, indicating likewise fair agreement. The
TABLE 1. Imaging Parameters of the Different Proton-Density–Weighted Sequences
1 T 1.5 T 3 T
TR (ms) 3000 3200 3220
TE (ms) 14 14 7.9
Number of slices
19 19 19
Slice thickness (mm)
2 2 2
Voxel size (mm) 0.7 × 0.7 × 2 0.6 × 0.6 × 2 0.4 × 0.4 × 2
FOV (mm) 139 × 139 120 × 120 110 × 110
Matrix size 192 × 192 192 × 192 256 × 256
Interslice gap 0 0 0
Acquisition time (min:s)
4:54 4:32 4:14
T indicates Tesla; TR, repetition time; TE, echo time; FOV, fi eld of view.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1063BRS205053.indd E1063 01/07/12 12:16 AM01/07/12 12:16 AM

DIAGNOSTICS Alar Ligaments at Different MRI Field Strengths • Lummel et al
E1064 www.spinejournal.com August 2012
intrarater agreement with respect to signal intensity in the sagittal view was κ = 0.31 for 1 T, κ = 0.47 for 1.5 T, and κ = 0.38 for 3 T, indicating again fair to moderate agreement.
There was no signifi cant difference between the 3 different MRI scanners concerning signal intensity in the sagittal view (H (2) = 1.79, P = 0.41), with a mean rank of 288.01 for 1 T, 300.60 for 1.5 T, and 279.79 for 3 T ( Figure 3 ).
DISCUSSION This study assessed the infl uence of the MRI fi eld strength on the delineation and signal intensity of AL in healthy volunteers.
AL connect the lateral part of the dens and the medial inferior aspect of the occipital condyles. 16 The ligaments have a length of about 10 mm, with a general variation of 2 mm
Figure 1. Proton density–weighted magnetic resonance images of alar ligaments ( arrows ) in coronal plane acquired in the same healthy volunteer at 1 T (A), 1.5 T (B), and 3 T (C). At 1 T (A) delineation was rated poor (grade 1) on the left and moderate (grade 2) on the right by both readers. At 1.5T, delineation was rated moderate (grade 2) on the left by both readers and poor (grade 1) by 1 reader and moderate (grade 2) by 1 reader on the right. At 3 T, delineation was rated good (grade 3) on both sides by both readers.
TABLE 2. Summary of Imaging Findings Regarding Delineation and Signal of AL 1 T 1.5 T 3 T
Delineation of AL in sagittal plane
Good (grade 3) 7 (3.5%) 24 (12%) 33 (16.5%)
Moderate (grade 2) 63 (31.5%) 80 (40%) 66 (33%)
Poor (grade 1) 109 (54.5%) 95 (47.5%) 98 (49%)
Not defi nable (grade 0) 21 (40.5%) 1 (0.5%) 3 (1.5%)
Inter-rater agreement (kappa) 0.27 0.32 0.35
Delineation of AL in coronal plane
Good (grade 3) 19 (9.5%) 34 (17%) 50 (25%)
Moderate (grade 2) 101 (50.5%) 101 (50.5%) 99 (49.5%)
Poor (grade 1) 75 (37.5%) 64 (32%) 51 (25.5%)
Not defi nable (grade 0) 5 (2.5%) 1 (0.5%) 0 (0%)
Inter-rater agreement (kappa) 0.49 0.4 0.36
Signal intensity of AL in sagittal plane
Low signal throughout entire c.s. (0) 19 (9.5%) 34 (17%) 50 (25%)
High signal in 1/3 or less of c.s. (1) 101 (50.5%) 101 (50.5%) 99 (49.5%)
High signal in 1/3–2/3 of c.s. (2) 75 (37.5%) 64 (32%) 51 (25.5%)
High signal in 2/3 or more of c.s. (3) 5 (2.5%) 1 (0.5%) 0 (0%)
Inter-rater agreement (kappa) 0.31 0.31 0.39
Total of 200 ligaments (50 volunteers, i.e. , 100 ligaments, evaluated by 2 readers independently).
T indicates Tesla; AL, alar ligaments; c.s., cross section.
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1064BRS205053.indd E1064 01/07/12 12:16 AM01/07/12 12:16 AM

DIAGNOSTICS Alar Ligaments at Different MRI Field Strengths • Lummel et al
Spine www.spinejournal.com E1065
should be better visualized at higher fi eld strengths because of the improved spatial resolution. 19 – 21 Appositely, we found a signifi cantly better delineation of AL at 1.5 T and 3 T than at 1 T in the sagittal view. Delineation of the AL in the coronal view was enhanced with MR fi eld strength.
Although higher fi eld strengths were benefi cial to a cer-tain regard for the delineation of AL, we found no signifi -cant differences between the 3 different MRI fi eld strengths with regard to their signal intensity, which was graded on a 4-point scale as introduced by Krakenes et al . 8 In this investi-gation, signal intensities of AL were evaluated in sagittal view as signal characteristics of AL are controversially discussed in the literature, and the sagittal view is a representative plane to classify their appearance. In our group of healthy volun-teers, we found various degrees of hyperintense signal altera-tions in the cross section of AL at all MRI fi eld strengths. For AL signal intensity, the inter- and intrarater agreements were only fair to moderate for each of the addressed fi eld strength. Concerning this matter, our results go along with previous studies showing a likewise fair to moderate inter-rater agree-ment for the evaluation of the signal intensity of AL. 4,6,7,12,18
The variable signal intensities of AL may be due to par-tial volume effects from high-signal intensity tissues such as
and a diameter varying from 2.9 ± 0.9 mm, 17 and show a high degree of morphologic variability, frequently with an asymmet-ric appearance. 4 , 7 , 8 Their main assignment is the limitation of the axial rotation in the upper cervical spine (mainly C1–C2) by the contralateral alar ligament, respectively. 2 Supporting structures in this connection are the transverse ligament, apical odontoid ligament, the posterior longitudinal ligament, and the tectorial membrane.
Various reports have shown that AL can be clearly detected using MRI. 3 – 8 , 18 An early study by Krakenes et al 8 investi-gated various MRI parameters and concluded that detailed structural information of ligaments and membranes in the craniocervical region was best obtained with high-resolution PD-weighted images with 2-mm slice thickness. This type of imaging sequence was also applied in this study. However, up-to-date data concerning the infl uence of the MRI fi eld strength on the visualization of AL are rare. Initial reports have shown a good visual resolution of the ligaments and membranes of the craniocervical junction at 3 T. 19 , 20 To our knowledge, there is little, if any, evidence that AL signal intensities differ across MRI fi eld strengths.
As signal-to-noise ratio improves linearly as the strength of the main magnetic fi eld increases, small structures like AL
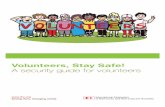
Figure 2. Proton density–weighted magnetic resonance images of alar ligaments in coronal (1) and sagittal (2) planes acquired in 1 healthy volunteer at 1 T (A), 1.5 T (B), and 3 T (C). The dashed lines in A1-3 indicate the orientation of the respective sagittal slice in B1-3. Delineation of the left alar ligament in sagittal plane ( arrows ) was rated poor (grade 1) at 1 T (A2), moderate (grade 2) at 1.5 T (B2), and good (grade 3) at 3 T (C2).
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1065BRS205053.indd E1065 01/07/12 12:16 AM01/07/12 12:16 AM

DIAGNOSTICS Alar Ligaments at Different MRI Field Strengths • Lummel et al
E1066 www.spinejournal.com August 2012
majority of biomechanical experiments with special focus on injuries of the upper cervical spine and craniocervical junc-tion could not verify such a vulnerability of AL. 28 – 30 The poor reliability (inter- and intrarater values) in the assessment of AL found in our study indicates that observer variation may infl uence the interpretation of the examinations and query the clinical application of the rating scale if not the signifi cance of the examination itself in connection with chronic whiplash-associated disorders.
Taken together our results and all available data, there is clear evidence that signal inhomogeneities or hyperintensities within AL are normal variations. 31 They are frequently found in healthy persons and should not be misinterpreted as patho-logical fi ndings as a consequence of whiplash trauma.
There are some study limitations to this study. First, the average age of the population in this investigation is fairly young, with a limited age range. In order to evaluate a correla-tion between hyperintense signal of AL and interspersed fatty tissue due to degeneration, it would be of interest to correlate signal intensity with age. In addition, histopathologic corre-lations would be helpful. Furthermore, we did not correlate our results with a group of patients with whiplash-associated disorder in this investigation.
bone marrow and fatty tissues. The application of a thin slice thickness (2 mm) in more than 1 plane reduces this partial volume effect. Nevertheless, misinterpretation of partial volume effects from surrounding anatomical tissues cannot be eliminated. In addition, anatomic variances in the connec-tive fi ber density may also infl uence the imaging appearance of AL. If the ligament has high-fi ber density, it will appear hypointense on MRI, whereas a ligament with loose fi ber den-sity and interspersed fatty tissue will appear with high-signal intensity. Age-dependent degeneration and interspersed fatty tissue in tendons and ligaments of other localizations are also known to cause high-signal MRI changes. 22 – 25 Theoretically, a similar effect could be true for AL. However, a recent study could not demonstrate an association between frequency of alar ligament hyperintensities and patient’s age. 26 In 2008, Koch 27 examined specimens of the upper cervical spine after fatal head trauma. Signifi cant inter- and intraindividual differ-ences of interspersed fatty tissue in the AL were noted and a strong correlation between histological samples and the MR signal was observed.
Because of their function and their structure with an extremely high proportion of collagen streaks, AL have a cer-tain vulnerability in a traumatic whiplash event. However, the
Figure 3. Sagittal proton density–weighted magnetic resonance images of 2 alar ligaments acquired in 2 healthy volunteers at 1 T (1), 1.5 T (2), and 3 T (3). One ligament (A1–A3) shows a hypointense signal in the entire cross section (grade 0) at all fi eld strengths (arrows in A1 to A3). The other ligament (B1–B3) was classifi ed as grade 2 (hyperintense signal in 1/3–2/3 of the cross section) by both readers at all fi eld strengths (short arrows in B1–B3).
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1066BRS205053.indd E1066 01/07/12 12:16 AM01/07/12 12:16 AM

DIAGNOSTICS Alar Ligaments at Different MRI Field Strengths • Lummel et al
Spine www.spinejournal.com E1067
CONCLUSION In recent years, attention has been drawn toward imaging of the ligaments and membranes in the craniocervical junction after whiplash trauma. Using magnetic resonance imaging, these structures can be well visualized. In this study, we could verify that high-fi eld MRI (1.5 T, 3 T) possesses a signifi cant superiority compared with low-fi eld MRI (1 T) in the delin-eation of AL. An infl uence of the MRI fi eld strength on the signal intensity of AL was not detectable. Hyperintense signal alterations of AL were present in healthy volunteers at high- and low- fi eld strengths and thus have per se no pathologic relevance.
➢ Key Points
The upper cervical ligaments, including AL, can be adequately evaluated on MRI, especially using 2-mm PD-weighted sequences.
In the delineation of AL, high-fi eld MRI (1.5 T, 3 T) pro-vides a signifi cant benefi t compared with low-fi eld MRI (1 T).
Signal intensity of AL is not aff ected by the MRI fi eld strength.
Hyperintense signal alterations of AL are present in healthy volunteers on both high- and low-fi eld magnetic resonance images, and thus, have per se no pathologic relevance.
References 1. Williams PL , Warwick R . Gray’s Anatomy: The Anatomical Basis
of Medicine and Surgery . 39th ed . New York : Churchill-Lining-stone ; 2004 .
2. Dvorak J , Panjabi MM . Functional anatomy of the alar ligaments . Spine 1987 ; 12 : 183 – 89 .
3. Krakenes J , Kaale BR . Magnetic resonance imaging assessment of craniovertebral ligaments and membranes after whiplash trauma . Spine 2006 ; 31 : 2820 – 26 .
4. Pfi rrmann CW , Binkert CA , Zanetti M , et al. MR morphology of alar ligaments and occipitoatlantoaxial joints: study in 50 asymp-tomatic subjects . Radiology 2001 ; 218 : 133 – 37 .
5. Willauschus WG , Kladny B , Beyer WF , et al. Lesions of the alar ligaments. In vivo and in vitro studies with magnetic resonance imaging . Spine 1995 ; 20 : 2493 – 98 .
6. Myran R , Kvistad KA , Nygaard OP , et al. Magnetic resonance imaging assessment of the alar ligaments in whiplash injuries: a case-control study . Spine 2008 ; 33 : 2012 – 16 .
7. Lummel N , Zeif C , Kloetzer A , et al. Variability of morphology and signal intensity of alar ligaments in healthy volunteers using MR imaging . AJNR Am J Neuroradiol 2010 ; 32 : 125 – 30 .
8. Krakenes J , Kaale BR , Rorvik J , et al. MRI assessment of normal ligamentous structures in the craniovertebral junction . Neuroradi-ology 2001 ; 43 : 1089 – 97 .
9. Wilmink JT , Patijn J . MR imaging of alar ligament in whiplash associated disorders: an observer study . Neuroradiology 2001 ; 43 : 859 – 63 .
10. Roy S , Hol PK , Laerum LT , et al. Pitfalls of magnetic resonance imaging of alar ligament . Neuroradiology 2004 ; 46 : 392 – 98 .
11. Volle E , Montazem A . MRI video diagnosis and surgical therapy of soft tissue trauma to the craniocervical junction . Ear Nose Throat J 2001 ; 80 : 41 – 4 , 46 – 8 .
12. Krakenes J , Kaale BR , Moen G , et al. MRI assessment of the alar ligaments in the late stage of whiplash injury-a study of struc-tural abnormalities and observer agreement . Neuroradiology 2002 ; 44 : 617 – 24 .
13. Kim HJ , Jun BY , Kim WH , et al. MR imaging of the alar ligament: morphologic changes during axial rotation of the head in asymp-tomatic young adults . Skeletal Radiol 2002 ; 31 : 637 – 42 .
14. Cohen J. A coeffi cient of agreement for nominal scales . Edu Psychol Meas 1960 ; 20 : 213 – 20 .
15. Landis JR , Koch GG . The measurement of observer agreement for categorical data . Biometrics 1977 ; 33 : 159 – 74 .
16. Daniels DL , Williams AL , Haughton VM . Computed tomogra-phy of the articulations and ligaments at the occipito-atlantoaxial region . Radiology 1983 ; 146 : 709 – 16 .
17. Cattrysse E , Barbero M , Kool P , et al. 3D morphometry of the transverse and alar ligaments in the occipito-atlanto-axial complex: an in vitro analysis . Clin Anat 2007 ; 20 : 892 – 98 .
18. Dullerud R , Gjertsen O , Server A . Magnetic resonance imaging of ligaments and membranes in the craniocervical junction in whip-lash-associated injury and in healthy control subjects . Acta Radiol 2010 ; 51 : 207 – 12 .
19. Yuksel M , Heiserman JE , Sonntag VK . Magnetic resonance imag-ing of the craniocervical junction at 3-T: observation of the acces-sory atlantoaxial ligaments . Neurosurgery 2006 ; 59 : 888 – 92 .
20. Yuksel KZ , Yuksel M , Gonzalez LF , et al. Occipitocervical verti-cal distraction injuries: anatomical biomechanical, and 3-tesla magnetic resonance imaging investigation . Spine (Phila Pa 1976) 2008 ; 33 : 2066 – 73 .
21. Saupe N , Prussmann KP , Luechinger R , et al. MR imaging of the wrist: comparison between 1.5- and 3-T MR imaging—preliminary experience . Radiology 2005 ; 234 : 256 – 64 .
22. el-Khoury GY , Wira RL , Berbaum KS , et al. MR imaging of patellar tendinitis . Radiology 1992 ; 184 : 849 – 54 .
23. Hodler J , Haghighi P , Trudell D , et al. The cruciate ligaments of the knee: correlation between MR appearance and gross and his-tologic fi ndings in cadaveric specimens . AJR Am J Roentgenol 1992 ; 159 : 357 – 60 .
24. Kjellin I , Ho CP , Cervilla V , et al. Alterations in the supraspinatus tendon at MR imaging: correlation with histopathologic fi ndings in cadavers . Radiology 1991 ; 181 : 837 – 41 .
25. Schweitzer ME , Mitchell DG , Ehrlich SM . The patellar tendon: thickening, internal signal buckling, and other MR variants . Skeletal Radiol 1993 ; 22 : 411 – 16 .
26. Vetti N , Krakenes J , Eide GE , et al. MRI of the alar and transverse ligaments in whiplash-associated disorders (WAD) grades 1–2: high-signal changes by age, gender, event and time since trauma . Neuroradiology 2009 ; 51 : 227 – 35 .
27. Koch S. Magnetresonanztomographische, pathoanatomische und histologische Korrelation von Ligamenta alaria an humanen Präparaten nach gewaltsamem Tod [dissertation] . Munich, Germany: University of Munich, LMU ; 2008 .
28. Panjabi MM , Cholewicki J , Nibu K , et al. [Biomechanics of whip-lash injury] . Orthopade 1998 ; 27 : 813 – 19 .
29. Panjabi MM , Cholewicki J , Nibu K , et al. Mechanism of whiplash injury . Clin Biomech (Bristol, Avon) 1998 ; 13 : 239 – 49 .
30. Panjabi MM , Cholewicki J , Nibu K , et al. Simulation of whip-lash trauma using whole cervical spine specimens . Spine 1998 ; 23 : 17 – 24 .
31. Vetti N , Krakenes J , Eide GE , et al. Are MRI high-signal changes of alar and transverse ligaments in acute whiplash injury related to outcome? BMC Musculoskelet Disord 2010 ; 11 : 260 .
Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BRS205053.indd E1067BRS205053.indd E1067 01/07/12 12:16 AM01/07/12 12:16 AM