Diclofenac phonophoresis in human volunteers
7
Ultrasound in Med. & Biol., Vol. 31 No. 3 pp. 337-343, 2005 Copyright © World Federation for Ultrasound in Medicine & Biology Printed in the USA. 0301-56291O5/$-see front matter doi: 10.1 0161j.ultrasmedbio.2004.11.012 .Original Contribution DICLOFENAC PHONOPHORESIS IN HUMAN VOLUNTEERS GIOVANA C. ROSIM, * CLÁUDIO HENRIQUE BARBIERI, * FERNANDO MAURO LANÇAS, and Nilton Mazzer* *Department of Biomechanics, Medicine and Rehabilitation of the Locomotor Apparatus, Ribeirão Preto School of Medicine, São Paulo University, Ribeirão Preto (SP), Brazil; and tDepartment of Analytic Chemistry, São Carlos Institute of Chemistry, São Paulo University, São Carlos (SP), Brazil (Received 28 June 2004; revised 9 November 2004; in final form 18 November 2004) Abstract-A quantitative study of sodium diclofenac (Voltaren Emulgel®, Novartis) phonophoresis was undertaken in humans. Fourteen healthy human volunteers were submitted to ultrasound irradiation ou two 225cm² areas on the dorsum (group A), foUowed by the application or the medication gel, and the plasma diclofenac mass was measured at 1,2 and 3h later by high performance liquid chromatography. The same procedure was repeated one month later with the same volunteers but with the ultrasound equipment switched off for the control group (group B). The plasma diclofenac mass was significantly higher in group A than in group B at 1 h (0.0987 µg/mL as opposed to 0.0389 µg/mL; p= 0.01) and 2 h (0.0724 µg/mL as opposed to 0.0529µg/mL; p = 0.01), but not at 3 h (0.0864 µg/mL as opposed to 0.0683 µg/mL; p=0.16). The authors couclude that previously applied therapeutic ultrasound irradiation enhances the percutaneous penetration of the topical diclofenac gel, although the mechanism remains nuclear. (E-mail: [email protected] ) © 2005 World Federation for Ultrasound in Medicine & Biology. Key Words: Therapeutic ultrasound, Phonophoresis, Transdermal penetration, Sodium diclofenac, Plasma mass, High performance liquid chromatography. INTRODUCTION Therapeutic ultrasound is widely used in the daily prac-tice of physiotherapy and sports medicine for the treat-ment of a variety of acquired and traumatic conditions affecting the locomotor apparatus, its beneficial effects including the healing of varicose ulcers (Dyson and Suckding 1978), tendon repair (Enwemeka 1989; Jackson et al. 1991; Gan et al. 1995) and stretched skeletal muscle repair (Menezes et al. 1999) and the regeneration of peripheral nerves (Hong et al. 1988). It has also been used to enhance transdermal penetration of medications, the so-called phonophoresis, specifically with a cortico-steroid (Byl et alo 1993), methyl-nicotinate (McElnay et al. 1993), protein (Mitragotri et al. 1995), indomethacin (Asano et alo 1997) and large size molecules as poly I-Iysine (Weimann and Wu 2002). Phonophoresis is defined as the enhancement of penetration of any medication through the normal skin Address correspondence to: Cláudio Henrique Barbieri, Departamento de Biomecânica, Medicina e Reabilitação do Aparelho Locomotor. Faculdade de Medicina de Ribeirão Preto-USP, Campus Universitário. 14049-900 Ribeirão Preto SP Brazil. E-mail: chbarbie@ fmrp.usp.br by ultrasound irradiation. It can be obtained with the medication gel or cream either used as a coupling me-dium for the ultrasound head or with previous irradiation with any regular coupling gel, the actual medication gel or cream being applied on the irradiated area immediately thereafter. To use a medication gel or cream as coupling medium, it is necessary to determine that it actually is a good ultrasound conductor, otherwise the treatment will be ineffective (Low and Reed 2001). Actually, many variations have been found in the transmis-sion properties of different medications, some of them having been demonstrated to be poor ultrasound trans-mitters (Bensonand McElnay 1994). The efficacy of phonophoresis of medication gels has been investigated in humans using the regular coupling gel for control (El-Hadidi and El-Garf 1991; Klaiman et al. 1998). However, the results are not em-tirely reliable, since the evaluation criteria include ex-cessively subjective parameters, such as pain on pressure and motion, although measured with a pain analogical scale. So far, no demonstration has been produced that phonophoresis results in satisfactory or effective blood concentration of diclofenac gel, one of the tropical anti-
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Diclofenac phonophoresis in human volunteers

Ultrasound in Med. & Biol., Vol. 31 No. 3 pp. 337-343, 2005Copyright © World Federation for Ultrasound in Medicine & Biology
Printed in the USA.0301-56291O5/$-see front matter
doi: 10.1 0161j.ultrasmedbio.2004.11.012.Original Contribution
DICLOFENAC PHONOPHORESIS IN HUMAN VOLUNTEERS
GIOVANA C. ROSIM, * CLÁUDIO HENRIQUE BARBIERI, * FERNANDO MAURO LANÇAS, and Nilton Mazzer*
*Department of Biomechanics, Medicine and Rehabilitation of the Locomotor Apparatus, Ribeirão Preto School of Medicine, São Paulo University, Ribeirão Preto (SP), Brazil; and tDepartment of Analytic Chemistry, São Carlos Institute of Chemistry, São Paulo University, São Carlos (SP), Brazil
(Received 28 June 2004; revised 9 November 2004; in final form 18 November 2004)
Abstract-A quantitative study of sodium diclofenac (Voltaren Emulgel®, Novartis) phonophoresis was undertaken in humans. Fourteen healthy human volunteers were submitted to ultrasound irradiation ou two 225cm² areas on the dorsum (group A), foUowed by the application or the medication gel, and the plasma diclofenac mass was measured at 1,2 and 3h later by high performance liquid chromatography. The same procedure was repeated one month later with the same volunteers but with the ultrasound equipment switched off for the control group (group B). The plasma diclofenac mass was significantly higher in group A than in group B at 1 h (0.0987 µg/mL as opposed to 0.0389 µg/mL; p= 0.01) and 2 h (0.0724 µg/mL as opposed to 0.0529µg/mL; p = 0.01), but not at 3 h (0.0864 µg/mL as opposed to 0.0683 µg/mL; p=0.16). The authors couclude that previously applied therapeutic ultrasound irradiation enhances the percutaneous penetration of the topical diclofenac gel, although the mechanism remains nuclear. (E-mail: [email protected]) © 2005 World Federation for Ultrasound in Medicine & Biology.
Key Words: Therapeutic ultrasound, Phonophoresis, Transdermal penetration, Sodium diclofenac, Plasma mass, High performance liquid chromatography.
INTRODUCTION
Therapeutic ultrasound is widely used in the daily prac-tice of physiotherapy and sports medicine for the treat-ment of a variety of acquired and traumatic conditions affecting the locomotor apparatus, its beneficial effects including the healing of varicose ulcers (Dyson and Suckding 1978), tendon repair (Enwemeka 1989; Jackson et al. 1991; Gan et al. 1995) and stretched skeletal muscle repair (Menezes et al. 1999) and the regeneration of peripheral nerves (Hong et al. 1988). It has also been used to enhance transdermal penetration of medications, the so-called phonophoresis, specifically with a cortico-steroid (Byl et alo 1993), methyl-nicotinate (McElnay et al. 1993), protein (Mitragotri et al. 1995), indomethacin (Asano et alo 1997) and large size molecules as poly I-Iysine (Weimann and Wu 2002).
Phonophoresis is defined as the enhancement of penetration of any medication through the normal skin
Address correspondence to: Cláudio Henrique Barbieri, Departamento de Biomecânica, Medicina e Reabilitação do Aparelho Locomotor. Faculdade de Medicina de Ribeirão Preto-USP, Campus Universitário. 14049-900 Ribeirão Preto SP Brazil. E-mail: chbarbie@ fmrp.usp.br
by ultrasound irradiation. It can be obtained with the medication gel or cream either used as a coupling me-dium for the ultrasound head or with previous irradiation with any regular coupling gel, the actual medication gel or cream being applied on the irradiated area immediately thereafter. To use a medication gel or cream as coupling medium, it is necessary to determine that it actually is a good ultrasound conductor, otherwise the treatment will be ineffective (Low and Reed 2001). Actually, many variations have been found in the transmis-sion properties of different medications, some of them having been demonstrated to be poor ultrasound trans-mitters (Bensonand McElnay 1994).
The efficacy of phonophoresis of medication gels has been investigated in humans using the regular coupling gel for control (El-Hadidi and El-Garf 1991; Klaiman et al. 1998). However, the results are not em-tirely reliable, since the evaluation criteria include ex-cessively subjective parameters, such as pain on pressure and motion, although measured with a pain analogical scale.
So far, no demonstration has been produced that phonophoresis results in satisfactory or effective blood concentration of diclofenac gel, one of the tropical anti-

338 Ultrasound in Medicine and Biology
inflammatory medieations most extensively used in physiotherapy and sports medicine practice, also as a coupling gel for ultrasound irradiation. Therefore, it was the purpose of the present investigation to quantify in humans the transdermal absorption of sodium diclofenac as a topical gel following therapeutic ultrasound irradiation, by measuring its plasma mass by high performance liquid chromatography.
MA TERIALS AND METHODS
The present investigation was approved by the Ethics in Research Committee of the University Hospital, Ribeirão Preto School of Medicine. All potential volunteers were adequately instrueted about the nature and purpose of the investigation, warned about potential risks to their health and warranted freedom to quit at any time of their own free will. All were submitted to a questionnaire about their previous known health situation regarding possible heart, liver, kidney, lung, gastrointestinal, hematologie, neurologic problems and any hypersensitivity to medication, particularly antinflammatories; women were also questioned about a possible pregnancy and were submitted to a pregnaney test. Candidates with a single positive record of a previous health problem, smokers and suspeeted drug addicts were excluded. All candidates were examined for skin problems, particularly in the area to be treated (dorsum). Fourteen human volunteers were selected, including 10 women and 4 meu aged on average 26.4 y (range: 19 to 50 y), with an average weight of 62 kg (range: 50 to 80 kg) and an average height of 1.7 m (range: 1.6 to 1.9 m). All selected volunteers signed an informed consent form and were wamed not do drink any alcohol for at least one week before treatment.
Ultrasound equipment and irradiation: Diclofenac gel application
Conventional 1 MHz microprocessed therapeutic ultrasound equipment adjusted for continuous wave of 0.5 W/cm² intensity (SATA) was used (Pro Seven 977 to 2000 model, Quark Produtos Médicos, Brazil). It was certified that the equipment was in accordance with general IEC 601 and ultrasound specific IEC 601 to 2-5 safety roles.
The entire dorsum of the volunteers was carefully washed with neutral bath soap and a soft sponge and dried. Two 225 cm² (15x15 cm) square areas were then drawn, one on each side of the dorsum, and irradiated for 5 min, one immediately after the other, using a regular coupling gel. Immediately following irradiation of the second area,
Volume 31, Number 3, 2005
a total amount of 5g of a commercially available diclofenac gel (Voltaren Emulgel®, Novartis) was applied to the irradiated arcas (2.5g on each area) and left to dry for at least 1h before the volunteers were allowed to put their clothes back on. According to the producer, Voltaren Emulgel is an oil-based emulsion in an aqueous gel and contains 1g of sodium diclofenac per 100g of the gel, so that each volunteer received a total dose of 0.05g of the therapeutic agent.
To minimize possible errors doe to different skin texture, all volunteers were submitted to the same treatment twice, the first with the ultrasound equipment switched on (effective irradiation, group A) and the second, one month later, with the equipment switched off (placebo effect, group B).
Blood samples (2 rnL each) were collected from a forearm superficial vein of each volunteer with a sterile syringe and needle (Abbocath®, Abbot) and transferred into tubes with an anticoagulant (EDTA, 10mg) immediately before and 1, 2 and 3h after the application of the diclofenac gel to the irradiated areas. The samples were then centrifuged at 3000 rpm for 10 min to separate the plasma, which was stored in a freezer at -20°C until the day of the chromatographic analysis (one week on average), when it was taken from the freezer and defrosted at roam temperature (23°C on average) for 6h.
Chromatographic analysisPlasma concentration (mass) of the absorbed di-
clofenac was measured by high performance liquid chromatography (HPLC) with an equipment (Shimadzu®) consisting of a pump (model LC-l0AD), a 278 nm ultraviolet detector (UV 278 nm), a 20 µl, injector, a 250mm x 4.6mm chromatographic separation column (C-18, 5µm, Maeherey-Nagel) and a recorder. The recorder was linked to an integrator able to supply the exact value of the area under the curve (AVC) and convert it into concentration (or mass, in µg min/mL) of the analyzed substance. Chromatographic extraction was dane at a l-mLlmin flow using a mobile phase composed of a mixture of acetonitrile and sodium acetate (35:65, 0.1 mol/L) adjusted to pH 6.3 with glacial acetic acid. Under such eonditions, extraction of sodium diclofenac took about 15 min.
Before analysis of the volunteers' plasma, the equipment was calibrated with plasma solutions of the sodium diclofenac of known concentrations, which were prepared according to the method proposed by Giagoudakis and Markantonis (1998), as follows:
1. Preparation of a 1µg/mL stock solution (permanently kept in a refrigerator at 6°C) by the dilution of the sodium diclofenac analytical standard kindly donated by the producer (Novartis Pharma, Brazil) in ethanol;
2. Preparation of solutions of growing concentration (0.0125, 0.025, 0.05, 0.1, 0.2 and 0.3 µg/rnL) by the addition of enough volume of the analytical standard

Diclofenac phonophoresis in humans
stock solution to 225 µl of blank plasma from the vol-unteers themselves (obtained from the blood collected immediately before treatment), with the solution being kept in individual tubes until analysis;
3. Addition of 500 µl of orthophosphoric acid (2.5 mol/L) to each tube and vigorous shaking for 20s using a mixer (LabLine, model Mistral 1190);
4. Addition of 1.5 mL of a mixture of hexane and isopropylic alcohols (80:20) and vigorous shaking for 2.5 min;
5. Centrifuging at 3000 rpm for 10 min, the organic layer being then transferred to a 1.5 mL Eppendorf tube and submitted to evaporation under a nitrogen flow and the residue being rediluted in 250 µl of the mobile phase (described above), for manual injection into the chro-matographer at the rate of 1mL/min.
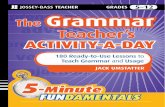
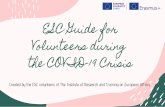
A chromatogram was obtained for each preparation of known concentration, the diclofenac extraction peak being identified in comparison with the chromatogram of blank plasma, where it was regularly absent (Fig. 1). The integrator automatically supplied the diclofenac peak area (µg min/mL) for every chromatogram. The procedure was repeated twice and an average value was calculated for each solution of known concentration. A standard curve (known-concentration vs. mass) was then plotted and later used to calculate the concentration of the absorbed diclofenac in the volunteers' blood plasma (Fig. 2). The coefficient of correlation between known concentration standard plasma solutions and diclofenac mass measured was 0.999566, meaning an almost absolute linearity, and
Fig. 1. Chromatograms obtained before and 2 h after treatment. (a) Without diclofenac. (b) Showing the diclofenac absorption
peak around the 15-min mark of extraction (arrow).
● G. DE CASSIA ROSIM et al. 339
Fig. 2. The diclofenac extraction (x) standard curve of the known-concentration solutions (y) showing the almost absolute linearity and the linear equation (y = 102.79x + 0.9505) used
to calculate the diclofenac mass in the volunteers' plasma.
the linear equation was y = 102.79x + 0.9505. Sensitivity of the extraction method was of 0.001 µg/mL.
The volunteers' plasma obtained at 1,2 and 3 h after treatment with diclofenac gel was submitted to the same extraction procedures as described in steps 3 through 5 for injection into the chromatographer. Again, the procedure was repeated twice and an average of the two values of the diclofenac mass was obtained for each volunteer, the actual plasma diclofenac concentration (mass) being calculated with the linear equation mentioned above.
Statistical analysis of the results (the median was preferred instead of the mean values due to the wide variety between extremes) was done separately in group A and group B to evaluate the temporal evolution of the diclofenac absorption curve using Friedman's non-parametric test at the 5% level of significance (p≤ 0.05). The temporal comparison between groups A and B was done by Wilcoxon's nonparametric test also at the 5% level of significance (p ≤ 0.05).
RESULTSNo volunteers presented any complication of any kind
nor did they report any discomfort with the treatment at any time, all of them resuming normal life immediately after the end of treatment Apart from slight redness and a temperature increase on touch, no sign of local irritation was detected by macroscopic inspection of the irradiated areas.
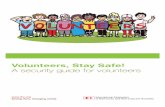
In group A, the median sodium dic10fenac plasma mass was 0.0987 µg/mL, 0.0724 µg/mL and 0.0864 µg/mL at 1, 2 and 3h after irradiation and topical application of the diclofenac gel, respectively. In group B, it was 0389 µg/mL, 0.0529 µg/mL and 0.0683 µg/mL at the same time points, respectively (Fig. 3). There was a significant difference between the values of the diclofenac plasma mass at 1h (p = 0.01) and 2h (p = 0.01), but

340 Ultrasound in Medicine and Biology
Fig. 3. (a) Box plot graphic of the dic1ofenac mass in groups A and B at 1h, showing median (internal full line), first and third quartile (upper and lower box limits), minimum and maximum values obtained (upper and
lower brackets) and 1.5 times the first and third quartile (upper and lower isolated lines). (b) Box plot graphic of the dic1ofenac mass in groups A
and B at 2 h. (c) Box plot graphic of the dic1ofenac mass in groups A and B at 3 h.
not at 3 h (p = 0.16). Within each group, there was no significant difference between the values of the diclofenac mass measured according to time (p = 0.11 in group A and p = 0.22 in group B).
Volume 31, Number 3,2005
The enhancement factor, defined as the average quotient between the values of the diclofenac plasma mass in groups A and B according to timing, was 2.5,1.4 and 1.3, at 1, 2 and 3 h after irradiation and application of the diclofenac gel, respectively.
DISCUSSION
Phonophoresis and systemic nonsteroidal antiin-flammatory drugs are quite effective for the treatment of a variety of acquired and traumatic conditions of the locomotor apparatus. Used either separately-or in com-bination, they generally produce beneficial effects. How-ever, the systemic (oral or parenteral) use of antiinflam-matory drugs like diclofenac is associated with a variable incidence of undesirable side effects such as gastritis or gastric and duodenal ulcers (Muller et al. 1997), this being the reason why topical formulations as gel, cream or ointment have been developed. These, however, are of more difficult absorption through the skin and do not present the same effect as obtained with the systemic use.
The concomitant use of ultrasound and a topic an-tiinflammatory gel or cream to replace the regular cou-pling gel by rehabilitation professionals is quite common, under the allegation that ultrasound stimulates the transdermal penetration of the medication, in an almost entirely empirical belief, since there is no conclusive laboratory demonstration of such a fact nor of the mech-anism involved. Actually, phonophoresis can be applied with the medication gel or cream as a coupling medium for the ultrasound head, provided the medication is known to be a good and resistant ultrasound conductor (Low and Reed 2001). Benson and McElnay (1994) investigated ultrasound transmission through commercially available topical products containing nonsteroidal antiinflammatory drugs and demonstrated that gel preparations conduct ultrasound more efficiently than do cream preparations and that gel preparations act as efficient coupling agents for ultrasound transmission at high frequencies but do not show the same efficiency at low frequencies. Therefore, according to these authors, ultrasound attenuation depends on the frequency of irradiation and "it is possible that high frequency ultrasound irradiation causes some breakdown of the polymer chains of the viscosity-inducing agents used in the topical formulations. This would have the effect of partially fluidizing the formulation structure, thereby reducing its ability to attenuate the ultrasound energy", thus hindering or preventing the transdermal penetration of the medication and making the treatment useless. The ultra-sound equipment producers themselves warn that viscous medication gels do not transmit ultrasound adequately, because they reflect a part of the ultrasound waves with consequent overheating and possible damage

Diclofenac phonophoresis in humans
to the ultrasound head (Quark Produtos Medicos, Brazil). On the other hand, ultrasound waves produce defects in the skin structure, which remain after the ultrasound irradiation is discontinued and through which substances from the external environment could penetrate, as will be discussed later. Therefore, it was our option to irradiate. the skin areas chosen for the experiment before the application of the diclofenac gel, which was then applied immediately thereafter.
Sodium diclofenac (molecular weight 318.13, as obtained at http://www.drugs.com) was chosen for the experiment for being a well-known and widely used nonsteroidal antiinflammatory drug whose analgesic ef-fects manifest quickly after administration (El-Hadidi and El-Garf 1991). Also, the use of human volunteers has obvious advantages in comparison with animals, whose skin does not have the same histologic structure or transdermal absorption properties. Furthermore, in the present investigation, the same volunteers formed both the experimental and control groups, in two separate treatment sessions, which is an effective way to minimize individal skin and general constitution variability.The ultrasound parameters chosen (continuous, I MHz frequency, 0.5 W/cm² intensity, 5 min irradiation) are of common use in rehabilitation programs and almost certainly do not produce any harm to the skin, as demonstrated by Asano et al. (1997), who found significantly increased skin temperature and tissue necrosis with 1 W/cm² intensity, but not with 0.5 W/cm², after a 10-min continuous irradiation in rats. Similarly, Frenkel et al. (1999, 2000) observed that the first signs of skin damage begin with a 0.75 W/cm² continuous irradiation and do not occur with 0.5 W/cm², although this was in fish, whose skin substantially differs from human skin.
The mechanism by which ultrasound enhances the transdermal penetration of substances is not entirely clear. One could think of the vasodilation observed on macroscopic examination, but this would certainly not be enough on its own, since it does not imply any change of the waterproof keratin layer of the skin, which should necessarily be altered. However, Wu et al. (1998) dem-onstrated, in human cadaver skin, that underwater ultra-sound irradiation (168 MHz, 12 W/cm², 15 min) signif-icantly disturbs superficial skin structure by forming large gaps of up to 20 µm in width and deranging the highly organized lipid layers between the keratinocytes, responsible for skin impermeability. Furthermore, Frenkel et al. (1999, 2000) demonstrated, in fish skin, that the intercellular spaces of the most superficial skin cell layer widened to, form gaps and dissociations of 0.3 µm in width that extended horizontally and sometimes also vertically between desmosomes with 1.7 W/cm² perpendicular ultrasound (3 MHz) irradiation for 90 s; the gaps increased to 1 to 3 µm in width with 2.2 W/cm² perpen-
● G. DE CASSIA ROSIM et al. 341
dicular irradiation for 30 s, with actual cell separation being observed with 90 s irradiation. Vertical gaps increased with 45° irradiation, reaching the fourth and fifth cell layer. Despite such a derangement of the superficial skin structure, skin cells were not damaged, but the horizontal and vertical gaps and spaces could actually interfere with skin permeability.
The same phenomenon can possibly happen in human skin, since Weimann and Wu (2002), based on the results obtained in their in vitro study, considered that "experimental results from transdermal flux kinetics, and confocal microscopic cross-sectional and optical images (as obtained by them), suggested that the formation of pores in the stratum corneum, whose size varies with skin samples, may be in the range of 1 to 100 µm . The confocal images also suggest the formation of µm-size pathways in epidermis during ultrasound exposure". Actually, it seems obvious to us that the opening of pores or gaps in the skin is the only possible way by which the trans dermal transfer of large molecules can occur.
Sundaram et al. (2003) studied the influence of low-frequency ultrasound irradiation on cell membrane permeability, using 3T3 mouse cell suspension and an-alyzing viability and cellular uptake of calcein, after exposure to varying acoustic energy doses at four different frequencies (between 20 and 100 kHz). It was dem-onstrated that cell viability decreases with increasing acoustic energy, while calcein uptake was maximum at an intermediate dose. According to their results, there is enough evidence that ultrasound irradiation changes cell membrane permeability and that this would be an effect of cavitation, with bubble expansion, collapse and subsequent shock waves, which may even cause disruption of cell membrane. The changes in permeability would be reversible or irreversible, according to the volume of the bubbles. A theoretical model was developed to relate the reversible and irreversible changes in membrane perme-ability to the number of transient cavitation events, thus allowing for predictions. In a way, these findings support the idea that cavitation is also responsible for the forma-tion of pores and gaps between skin cells, thus establish-ing a passageway for transdermal transmission of med-ications like diclofenac.Therefore, although still to be proved, the mechanism of phonophoresis would be twofold: 1) the opening of a passageway through the waterproof layers of the skin to permit the substance to diffuse into the intercellular space and to reach the deeper blood vessels and 2) blood vessel dilation to permit absorption and to carry the substance into the circulation.The high performance liquid chromatography method used in the present investigation was the same as proposed by Giagoudakis and Markantonis (1998) and permitted a quite accurate and reliable quantification of the

342 Ultrasound in Medicine and Biology
Fig. 4. Simplified graphic representation of the behavior of the diclofenac plasma mass in group A compared with group B at all times.
sodium diclofenac mass in the volunteers' plasma by comparison with the values obtained from the analysis of the plasma solutions of known concentration and with the standard absorption curve. The diclofenac mass in the volunteers' plasma was increased after ultrasound irra-diation (group A), being 2.5 times higher than in group B at 1 h, 1.4 times at 2 h and 1.3 times at 3 h, the difference between groups being significant at 1 and 2 h, but not at 3 h. So, the diclofenac plasma mass decreased with time in group A (0.0987 µg/mL, 0.0724 I µg/mL and 0.0864 µg/mL, at 1, 2 and 3 h, respectively) and increased in group B (0.0389 µg/mL, 0.0529 µg/mL and 0.0683 µg/mL, at 1,2 and 3 h, respectively), but, interestingly, the differ-ences with time in both groups were nonsignificant (Fig. 4). The mechanism by which the diclofenac plasma mass increased so much during the first hour, decreasing during the second hour and increasing again during the third hour in group A was not perfectly understood, but it is a possibility that a portion of the twofold mechanism that permits such a high transdermal absorption during the first hour quickly ceases. This would probably be vasodilation, which is a physiological phenomenon of easier regression, and not the gaps between skin cells, which are structural defects that take longer to regress. Actually, the failures would remain for enough time to explain the increased absorption during the third hour, when vasodilation was virtually absent.
Whether the sodium diclofenac plasma mass en-hanced by previous ultrasound irradiation is enough to obtain general therapeutic effects is difficult to know. Giagoudakis and Markantonis (1998) measured the sodium diclofenac plasma mass after oral administration of 50 mg of the medication (Voltaren®) and found that the maximal concentration obtained was 743 ng/mL, that is, about five times as high as the highest concentration measured in the
Volume 31, Number 3, 2005
present investigation, of the order of 150 ng/mL (0.15 µg/mL). According to Radermacher et al. (1991), sodium diclofenac is a potent drug and a plasma concentration of about 100 ng/mL is already enough to produce therapeutic effects.
The authors conclude that previously applied therapeutic ultrasound irradiation with the parameters used significantly enhances transdermal penetration of sodium diclofenac in the first 2 h following application of the medication gel and, since it does not seem to have any deleterious local or systemic side effect, it can be used in clinical situations as an adjunct treatment.
Acknowledgments-The authors acknowledge Prof. Antônio Dorival Campos, mathematician from the Department of Social Medicine, for his kind statistical study and assistance on the interpretation of the results.
REFERENCES
Asano J, Suisha F, Takada M, Kawasaki N, Miyazaki S. Effect of pulsed output ultrasound on the transderrna1 absorption of indomethacin from an ointment in rats. BioI Phann Bull 1997;20:288-291.
Benson HAE, McElnay JC. Topical non-steroidal anti-inflammatory products as ultrasound couplants: their potential in phonophoresis. Physiotherapy 1994;80:74-76.
Byl N, McKenzie A, Hamday B, Wong T, O'Connell J. The effects of phonophoresis with corticosteroids: a controlled pilot study. J Orthop Sports Phys Ther 1993;18:590-600.
Dyson M, Suckling 1. Stimulation of tissue repair by ultrasound: a survey of mechanisms involved. Physiotherapy 1978;64:105-108.
El-Hadidi T, El-Garf A. Double-blind study comparing the use of Voltaren Emulgel versus regular gel during ultrasonic sessions in the treatment of localized traumatic and rheumatic painful conditions. J Intern Med Res 1991;19:219-227.
Enwemeka CS. The effects of therapeutic ultrasound on tendon healing: a biomechanical study. Am J Phys Med Rehab 1989;68:283-287.
Frenkel V, Kimmel E, Iger Y. Ultrasound-induced cavitation damage to external epithelia of fish skin. Ultrasound Med BioI 1999;25: 1295-1303.
Frenkel V, Kimmel E, 1ger Y. Ultrasound-induced intercellular space widening in fish epidermis. Ultrasound Med BioI 2000;26:473-480.
Gan BS, Sherebrin MH, Scilley CG. The effects of ultrasound treatment on flexor tendon healing in the chicken limb. J Hand Surg 1995;20:809-814.
Giagoudakis G, Markantonis. SL. An alternative high-performance liquid-chromatographic method for the determination of diclofenac and flurbiprofen in plasma. J Pharmac Biomed Anal 1998;17:897-901.
Hong Cz, Liu HH, Yu 1. Ultrasound thermotherapy effect on the recovery of nerve conduction in experimental compression neuropathy. Arch Phys Med Rehab 1988;69:410-414.
. Jackson BA, Schwane JA, Starcher BC. Effects of ultrasound therapy on the repair of Achilles tendon injuries in rats. Moo Sc Sports Exere 1991;23:171-176.
Klaiman MD, Shrader JA, Danoff N, Hicks IE, Pesce WJ, Ferland J. Phonophoresis versus ultrasound in the treatment of common musculoskeletal conditions. Med Sci Sports Exerc 1998;30(9):1349-1355.
Low J, Reed A. Therapeutic Ultrasound, in: Electrotherapy explained principles and practice (3m Ed.). Butterworth Heinemann, Oxford, 1999, P 172.
McElnay JC, Benson RAE, Harland R, Hadgraft J. Phonophoresis of methyl-nicotinate: A preliminary study to elucidate the mechanism of action. Pharm Res 1993;10:1726-1731.
Menezes DF. Volpon JB, Shimano AC. Aplicações de ultra-som terapeutico em lesão muscular experimental aguda (Therapeutic ultrasound application in acute experimental muscle lesion). Rev Bras Fisiot 1999;4:27-31.
Mitragotri S. Blankschtein D. Langer R. Ultrasound-mediated transdermal protein delivery. Science 1995;269:850-853.

Diclofenac phonophoresis in humans
Müller M. Mascher H, Kikuta C. Schafer S. Brunner S, Domer G.Eichler H. Diclofenac concentrations in defined tissue layers after topical administration. Clin Pharmacol Therap 1997;62:293-299.
Radermacher I, Ientsch D. Scholl MA, Lustinetz T. Frolich IC. Diclofenac concentrations in synovial fluid and plasma after cutaneous application in inflammatory and degenerative joint disease. Br J Clin Pharmacol 1991;31:537-541.
● G. DE CASSIA ROSIM et al. 343
Sundaram J, Mellein BR, Mitragotri S. An experimental and theoretical analysis of untrasound-induced permeabilization of cell membranes. Biophysical J 2003;84:3087-3101.
Weimann L. Wu 1. Transderma1 delivery of poly-I-lysine by sonomacroporation. Ultrasound Med Biol 2002;28(9):1173-1180.
Wu I. Chappelow I. Yang I, Weimann L. Defects generated in human tratum corneum specimens by ultrasound. Ultrasound Med Biol 1998;24:705-710.